User login
Risk of Perioperative Morbidity, Post-Op Mortality Higher for Current Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day postoperative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10–1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51–1.81 vs. OR 1.20; CI, 1.09–1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40–1.51 vs. OR, 1.13; CI, 1.08–1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease postoperative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013;148:755-762.
Reviews of Reseach on Perioperative Morbidity, Capnography with Diabetic Ketoacidosis in the ED, Mortality Rate for Elective Surgeries
In This Edition
Literature At A Glance
A guide to this month’s studies
- Early treatment with intravenous tPA for acute stroke
- Perioperative morbidity, mortality for current smokers
- Statins associated with musculoskeletal conditions
- Antithrombotic medications in patients with history of stroke
- Extended prophylaxis with aspirin for patients after total hip arthroplasty
- Prognosis for symptomatic subsegmental pulmonary embolism
- Video-based educational workshops for academic hospitalists
- Increased mortality for elective surgeries on Fridays, weekends
- Basal plus correction insulin regimen and Type 2 diabetes
- Capnography to diagnose diabetic ketoacidosis in the ED
- How publicly reported mortality rates correlate with hospitals’ overall mortality
- Cost savings and preventable acute-care visits for Medicare patients
Early tPA in Acute Stroke Is Associated with Better Short-Term Outcomes in Routine Clinical Practice
Clinical question: Does early treatment with intravenous (IV) tissue plasminogen activator (tPA) result in better outcomes among patients with acute ischemic stroke in routine clinical practice?
Background: IV tPA for acute ischemic stroke is beneficial if given in the first 4.5 hours after symptom onset. However, pooled data from clinical trials have been limited in characterizing the extent to which onset-to-treatment (OTT) with IV tPA influences outcomes and how effective tPA is in routine clinical practice.
Study design: Data analysis from a stroke registry.
Setting: One thousand three hundred ninety-five U.S. hospitals participating in the Get with the Guidelines—Stroke Program.
Synopsis: Data were analyzed from 58,353 tPA-treated patients within 4.5 hours of symptom onset. Clinical outcomes were compared among patients treated in the 0-90-, 91-180-, and 181-270-minute OTT windows. Patient factors strongly associated with shorter OTT were greater stroke severity (odds ratio [OR] 2.8; 95% confidence interval [CI], 2.5-3.1 per five-point increase), arrival by ambulance (OR 5.9; 95% CI, 4.5-7.3), and arrival during regular hours (OR 4.6; 95% CI, 3.8-5.4). Faster OTT, in 15-minute increments, was associated with reduced in-hospital mortality (OR 0.96; 95% CI, 0.95-0.98; P<.001), reduced symptomatic intracranial hemorrhage (OR 0.96; 95% CI, 0.95-0.98; P<.001), increased achievement of independent ambulation at discharge (OR 1.04; 95% CI, 1.03-1.05; P<.001), and increased discharge to home (OR 1.03; 95% CI, 1.02-1.04; P<.001).
Data collected were dependent on the accuracy and completeness of the chart abstraction, and only short-term outcomes were reported. Although no post-discharge outcomes were reported, previous studies have shown that functional status at discharge strongly correlates with three-month disability outcomes.
Bottom line: In routine clinical practice, earlier tPA for acute ischemic strokes results in better short-term clinical outcomes.
Citation: Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309:2480-2488.
Current Smokers Have Higher Perioperative Morbidity and Mortality Compared to Past Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day post-operative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10-1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51-1.81 vs. OR 1.20; CI, 1.09-1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40-1.51 vs. OR, 1.13; CI, 1.08-1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease post-operative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013 Jun 19:1-8. doi: 10.1001/jamasurg.2013.2360 [Epub ahead of print].
Statins Associated with Several Musculoskeletal Conditions
Clinical question: Is statin use associated with musculoskeletal adverse events, including arthropathy and injury, in physically active individuals?
Background: Statin-induced musculoskeletal adverse events (AEs) include myalgias, muscle weakness, cramps, rhabdomyolysis, and tendinous disease. The full spectrum of AEs is unknown because randomized clinical trials have not been powered to detect uncommon AEs.
Study design: Retrospective cohort study with propensity score matching.
Setting: San Antonio military area.
Synopsis: A total of 46,249 patients aged 30 to 85 years who met study criteria were propensity-matched into 6,967 statin users and 6,967 nonusers. The occurrence of musculoskeletal conditions were categorized using ICD-9 codes: Msk1, all musculoskeletal diseases; Msk1a, arthropathies and related diseases; Msk1b, injury-related diseases; and Msk2, drug-associated musculoskeletal pain. Of these, statin users had a higher odds ratio (OR) for Msk1 (OR 1.19; 95% CI, 1.08-1.30), Msk1b (1.13; 1.05-1.21), and Msk2 (1.09; 1.02-1.18). Msk1b (arthropathies) had an OR of 1.07 (0.9-1.16, P=0.07). Simvastatin was used by 73.5% of patients, and years of simvastatin use was not a significant predictor of any of the outcome measures. Secondary and sensitivity analyses showed higher adjusted ORs for statin users in all groups. This study was limited by the use of ICD-9-CM codes for identification of baseline characteristics, and the musculoskeletal diagnosis groups used were not validated.
Bottom line: Statin use is associated with an increased likelihood of musculoskeletal conditions, arthropathies, injuries, and pain.
Citation: Mansi I, Frei CR, Pugh M, Makris U, Mortensen EM. Statins and musculoskeletal conditions, arthropathies, and injuries. JAMA Intern Med. 2013;173:1318-1326.
Evidence-Based Guidelines on Periprocedural Management of Antithrombotic Medications in Patients with History of Stroke
Clinical question: What is the evidence for the periprocedural management of antithrombotics in patients with ischemic cerebrovascular accidents (CVAs)?
Background: Evidence-based guidelines are needed to help clinicians determine the thromboembolic risk of temporary discontinuation of antithrombotic medications, the perioperative bleeding risks of continuing antithrombotic agents, whether bridging therapy should be used, and the appropriate timing of antithrombotic agent discontinuation.
Study design: Systematic literature review with practice recommendations.
Setting: American Academy of Neurology Guideline Development Subcommittee convened an expert panel to review and provide recommendations.
Synopsis: Researchers analyzed 133 literature reviews via MEDLINE and EMBASE. Aspirin in stroke patients:
- Should routinely be continued for dental procedures (Level A);
- Should probably be continued for invasive ocular anesthesia, cataract surgery, dermatologic procedures, transrectal ultrasound-guided prostate biopsy, spinal/epidural procedures, and carpal tunnel surgery (Level B); and
- Should possibly be continued for vitreoretinal surgery, electromyogram (EMG), transbronchial lung biopsy, colonoscopic polypectomy, upper endoscopy and biopsy/sphincterotomy, and abdominal ultrasound-guided biopsies (Level C).
Warfarin in stroke patients:
- Should routinely be continued for dental procedures (Level A); and
- Should possibly continued for dermatologic procedures (Level B) and EMG, prostate procedures, inguinal hemiorrhaphy, and endothermal ablation of great saphenous vein (Level C).
- There is a lack of evidence on warfarin for ophthalmologic procedures, with the exception of ocular anesthesia, where it probably does not increase clinically significant bleeding (Level B).
There was not enough evidence to support or refute a recommendation regarding heparin bridge therapy in reducing thromboembolism in chronically anticoagulated patients (Level B).
Bottom line: These are the most up-to-date guidelines for anticoagulant and antiplatelet agents in patients with transient ischemic attacks and strokes undergoing procedures, but further research is needed in many areas.
Citation: Armstrong MJ, Gronseth G Anderson DC, et al. Summary of evidence-based guideline: periprocedural management of antithrombotic medications in patients with ischemic cerebrovascular disease: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2065-2069.
Extended Prophylaxis with Aspirin Was Noninferior to Extended Prophylaxis with Low-Molecular-Weight Heparin
Clinical question: Is aspirin as effective as low-molecular-weight heparin (LMWH) for the extended prophylaxis of venous thromboembolism (VTE) after total hip arthroplasty (THA)?
Background: Deep vein thrombosis (DVT) and pulmonary embolism (PE) are common complications after THA. After initial prophylaxis, LMWH given for up to 30 days has been shown to reduce VTE compared with placebo. However, LMWH is costly and may increase the risk of minor bleeding. Aspirin is a potentially simple, low-cost alternative.
Study design: Randomized, placebo-controlled trial.
Setting: Twelve university-affiliated orthopedic hospitals in Canada.
Synopsis: Patients undergoing elective THA without hip fracture, metastatic cancer, or bleeding precluding anticoagulants were eligible. All patients received dalteparin for 10 days and were then randomized to aspirin 81 mg daily or to continue dalteparin. The primary outcome was symptomatic proximal DVT or PE during 90 days’ follow-up. The study was terminated early due to slow enrollment. At that time, 2,364 patients had been enrolled, and an analysis by an independent data safety and monitoring board determined that continuing the study was unlikely to alter the main findings. Extended prophylaxis with aspirin was noninferior to LMWH for the primary outcome, which occurred in 0.3% vs. 1.3%, respectively (95% CI, -0.5% to 2.5%, P<.001 for noninferiority). There were no significant differences in major or minor bleeding.
Though the early termination is a concern, the sample size was large and the results do not suggest inadequate power as a reason for lack of superiority for LMWH. Also, all patients received 10 days of LMWH, which indicates a period of LMWH after discharge will still be needed for most patients prior to initiating aspirin.
Bottom line: After initial LMWH prophylaxis for 10 days, extended prophylaxis with aspirin can be considered, particularly for patients for whom LMWH may not be feasible.
Citation: Anderson DR, Dunbar MJ, Bohm ER, et al. Aspirin versus low-molecular-weight heparin for extended venous thromboembolism prophylaxis after total hip arthroplasty: a randomized trial. Ann Intern Med. 2013;158:800-806.
Symptomatic Subsegmental Pulmonary Embolism (PE) Has a Prognosis Similar to Proximal PE
Clinical question: Is the prognosis of a symptomatic subsegmental pulmonary embolism (PE) similar to that of a more proximal PE?
Background: The use of multidetector computed tomography angiography (CTA) has allowed for better assessment of the pulmonary vasculature and increased detection of distal emboli. Prior studies have raised questions on the clinical importance of subsegmental PE but have been limited by small size or retrospective design.
Study design: Combined data from two prospective trials of management of suspected PE.
Setting: Twelve hospitals in the Netherlands and four tertiary-care emergency departments in Canada.
Synopsis: The study cohort consisted of 3,769 patients with suspected PE, of which 2,688 underwent CTA. Of patients diagnosed with PE, 15.5% had isolated subsegmental emboli. All patients were treated with anticoagulation. During three months of follow-up, the incidence of symptomatic recurrence for subsegmental PE was similar to patients with proximal PE (3.6% vs. 2.5%, respectively). The mortality rates for patients with subsegmental and proximal PE were also similar (10.3% vs. 6.3%, respectively).
The study may have been underpowered to detect small differences in event rates; however, there was no trend suggesting that subsegmental PE had better outcomes than more proximal PE. Also, the study did not specifically investigate whether any management strategy is preferred based on thrombus location on CTA.
Bottom line: Clinicians should continue to anticoagulate patients with subsegmental PE as the prognosis is similar to those with proximal PE.
Citation: Den Exter PL, van Es J, Klok FA, et al. Risk profile and clinical outcome of symptomatic subsegmental pulmonary embolism. Blood. 2013;122:1144-1149.
Video-Based Educational Workshop for Academic Hospitalists and House Staff May Improve Professionalism
Clinical question: Can video-based education promote professionalism among academic hospitalists and house staff?
Background: Unprofessional behavior by academic hospitalists and residents can negatively impact the learning environment and patient safety. This behavior increases throughout training, and faculty behavior can be influential. There is a paucity of educational materials to train hospitalists and house staff to recognize and ameliorate unprofessional behaviors.
Study design: Educational survey study.
Setting: University of Chicago, Northwestern University, and NorthShore University Health System teaching hospitals.
Synopsis: Three videos were developed displaying three types of unprofessional behavior: disparaging other physicians, “blocking” admissions, and misrepresenting tests to expedite their completion. There were 44 hospitalists and 244 house staff who received a 60-minute workshop in which they watched the videos using a viewing tool and discussed the videos in small groups.
For all three videos, more than three-quarters of both hospitalists and house staff felt the behavior was unprofessional or somewhat unprofessional. Hospitalists and house staff found the workshop useful and effective (65.9% and 77.1%, respectively) and would change their behavior as a result of the workshop (65.9% and 67.2%, respectively). Those who perceived the videos as “very realistic” were more likely to report intent to change behavior (93% vs. 53%, P=0.01).
This study is limited by its small sample size and possible selection bias. Those interested or concerned about unprofessional behavior may have been more likely to attend the workshop.
Bottom line: Video-based professionalism education is a feasible and well-received way to educate hospitalists and residents about unprofessional behavior and may even affect their future behavior.
Citation: Farnan JM, O’Leary KJ, Didwania A, et al. Promoting professionalism via a video-based educational workshop for academic hospitalists and housestaff. J Hosp Med. 2013;8:386-389.
Friday and Weekend Elective Surgeries Have Increased Mortality
Clinical question: How can the association between mortality and the day of elective surgical procedures be assessed?
Background: Several studies have described the “weekend effect” for both surgical and medical patients, with higher mortality and length of stay in patients admitted on the weekend compared to weekdays. Two potential explanations are poorer quality of care being delivered on the weekend or more severely ill patients being operated on or admitted on the weekend.
Study design: Retrospective analysis of national hospital administrative data.
Setting: All acute-care and specialist hospitals in England from 2008 to 2011.
Synopsis: There were 4,133,346 elective, inpatient surgical procedures studied. Friday surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.44 [95% CI, 1.39-1.50] and 1.42 [95% CI, 1.26-1.60], respectively, when compared with Monday. Weekend surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.82 [95% CI, 1.71-1.94] and 2.67 [95% CI, 2.30-3.09], respectively, when compared with Monday. There were significant trends toward higher mortality at the end of the workweek and weekends for four high-risk procedures: esophagus and/or stomach excision, colon and/or rectum excisions, coronary artery bypass graft, and lung excision. For lower-risk procedures, there was a significant increase in mortality for Friday surgeries but not weekend surgeries. As with all studies using administrative data, inherent selection biases could not be adjusted for Friday or weekend procedures.
Bottom line: Elective surgeries that occur on the weekend and later in the week have an increased risk of mortality, implying that the weekend effect is due to poorer quality of care during weekends, rather than higher-acuity patients presenting on weekends.
Citation: Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A. Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
Basal Plus Correction Insulin Regimen Is Effective in Hospitalized Patients with Type 2 Diabetes
Clinical question: Does a basal plus correction insulin regimen (as needed with meals) result in similar glycemic control and lower rates of hypoglycemia compared to a basal-bolus regimen?
Background: Basal bolus is the preferred insulin regimen for non-critically-ill hospitalized patients as per clinical guidelines. But use is limited due to the complexity of the regimen and the fear of inducing hypoglycemia. A less complex, easier-to-implement basal plus correction insulin regimen may be an effective alternative.
Study design: Multicenter, prospective, open-label, randomized study.
Setting: Six hospitals in the U.S.
Synopsis: A group of 375 medical and surgical patients with Type 2 diabetes treated with diet, oral anti-diabetic agents, or low-dose insulin (≤ 0.4 units/kg/day) were randomized to:
- Basal-bolus insulin regimen with glargine once daily and fixed doses of glusiline before meals;
- Basal plus correction insulin (“basal plus”) regimen with glargine once daily and glusiline sliding scale insulin (SSI) before meals; or
- Regular SSI alone.
After the first day of therapy, treatment with basal-bolus and basal-plus regimens resulted in similar improvements in daily blood glucose (BG) (P=0.16), and both were superior to SSI alone (P=0.04). Both regimens also resulted in less treatment failure (defined as mean daily BG of >240 mg/dl or >2 consecutive BG >240 mg/dl) than did treatment with SSI. Hypoglycemia (BG <70 mg/dl) occurred in 16%, 13%, and 3% of patients in the basal-bolus, basal-plus, and SSI groups, respectively (P=0.02). There were no between-group differences in the frequency of severe hypoglycemia (<40 mg/dl; P=0.76).
The study was not powered to evaluate hospital complications (infection, mortality, hospital stay, and readmissions) across groups.
Bottom line: The basal-plus regimen resulted in glycemic control similar to standard basal-bolus regimen and is an effective alternative for the initial management of hyperglycemia in general medical and surgical patients with Type 2 diabetes.
Citation: Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: Basal plus trial. Diabetes Care. 2013;36:2169-2174.
Capnography Can Help Diagnose Diabetic Ketoacidosis in the ED
Clinical question: Can capnography be used as a screening tool to identify patients with diabetic ketoacidosis (DKA)?
Background: Metabolic acidosis is a major criterion for diagnosing DKA. Previous studies have shown that end-tidal carbon dioxide (ETCO2) measurement by capnography can provide an accurate estimation of arterial carbon dioxide tension (PaCO2) and may be a noninvasive, fast, inexpensive measurement of acidosis in DKA. However, those studies were in pediatric patients and had small sample sizes.
Study design: Cross-sectional, prospective descriptive-analytic study.
Setting: The ED of Imam Reza Medical Research and Training Hospital, Tabriz, East Azarbaijan, Iran.
Synopsis: A total of 181 adult patients older than 18 with suspected DKA and blood sugar >250 mg/dl were included in the study. Simultaneous capnography and arterial blood gas (ABG) were obtained on all patients. Urine ketones, complete blood count, serum levels of potassium, urea, and creatinine were collected. Sixty-two patients were found to have DKA, while 119 had other conditions associated with metabolic acidosis. There was a significant linear relationship between pH and ETCO2 (P>0.0001, relative risk (R)=0.253), PaCO2 and ETCO2 (P>0.0001, R=0.572), and bicarbonate (HCO3) and ETCO2 (P>0.0001, R=0.730). ETCO2 values >24.5 mmHg had a sensitivity and specificity of 0.90 for ruling out DKA. No cutoff point could be determined for ruling in DKA.
The study was open to selection bias as patient collection was only done during the day, so eligible subjects may have been missed. Moreover, though the study suggests that capnography has a role in ruling out DKA, the exact cutoff value is unclear. Other studies found that higher values were needed to exclude diagnosis.
Bottom line: Using ETCO2 values >24.5 mmHg, capnography can help exclude the diagnosis of DKA in adult patients with elevated BG.
Citation: Soleimanour H, Taghizadieh A, Niafar M, Rahmani F, Golzari S, Esfanjani RM. Predictive value of capnography for diagnosis in patients with suspected diabetic ketoacidosis in the emergency department. West J Emerg Med. 2013. doi: 10.5811/westjem.2013.4.14296.
Publicly Reported Mortality Correlates with Overall Mortality
Clinical question: Are publicly reported mortality rates associated with a hospital’s overall medical and surgical mortality rate?
Background: Public reporting of mortality has become an important strategy in Medicare’s quality-improvement initiative. However, the mortality rate for only three conditions, acute myocardial infarction, congestive heart failure, and pneumonia are reported. It is unclear if these rates correlate to a hospital’s overall mortality rate.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Using 2008-2009 data from 2,322 acute-care hospitals with 6.7 million admissions, an aggregate mortality rate for the three publicly reported conditions, a standardized 30-day mortality rate for selected medical and surgical conditions, and an overall average composite mortality score was calculated for each hospital. Based on their mortality for the three publicly reported conditions, hospitals were grouped into quartiles from highest (top-performing hospitals) to lowest mortality (poor-performing hospitals).
Top-performing hospitals had a 3.6% (9.4%vs 13.0%; P<.001) lower mortality rate than poor-performing hospitals and an odds ratio >5 of being a top performer in overall mortality (OR 5.3; 95% CI, 4.3-6.5). They also had an 81% lower chance of being in the worst-performing quartile in overall mortality (OR 0.19; 95% CI, 0.14-0.27). Conversely, poor-performing hospitals had a 4.5 times higher risk of being in the lowest quartile in overall mortality. The study is limited by the use of administrative data, which limits the ability to adjust for severity of illness, overall health, and socioeconomic status of each hospital’s population.
Bottom line: A hospital’s mortality performance on the three publicly reported conditions may predict mortality rates across a wide range of medical and surgical conditions.
Citation: McCrum ML, Joynt KE, Orav EJ, Gawande AA, Jha AK. Mortality for publicly reported conditions and overall hospital mortality rates. JAMA Intern Med. 2013;173:1351-1357.
Cost Savings in Decreasing Preventable Acute-Care Visits Are Limited among High-Cost Medicare Utilizers
Clinical question: What role do preventable acute-care visits play in the overall costs of care for the highest Medicare utilizers?
Background: Some 10% of Medicare patients account for more than half the costs. Interventions targeted at decreasing acute-care costs (ED visits and inpatient hospitalizations) for this high-cost population are widespread, but it is unknown what impact they can have.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Standardized total costs were created for fee-for-service Medicare patients for 2009 and 2010 in order to identify high-cost and persistently high-cost patients. Algorithms were used to identify preventable ED visits and hospitalizations in both the high-cost and non-high-cost cohorts.
Of the more than 1 million patients in the sample Medicare population, as many as 113,341 were high-cost. As much as 73% of acute-care spending was attributable to this cohort. Overall, 10% of acute-care costs were felt to be preventable in the high-cost group, 13.5% in the persistently high-cost group, and 19% in the non-high-cost group for 2010. The most common reasons for preventable acute care in the high-cost cohort were heart failure, bacterial pneumonia, and chronic obstructive pulmonary disease. Catastrophic events (myocardial infarction, stroke, sepsis), cancer, and orthopedic procedures drove overall inpatient costs in the high-cost group.
Preventable costs were higher per capita in areas with higher numbers of primary-care and specialist physicians, but it’s unclear if this was a supply or demand issue. The study also used algorithms that possibly overestimate the amount of preventable acute care.
Bottom line: In the highest Medicare utilizers, cost savings aimed at preventable acute care may be limited and might be better targeted at efficiency during acute-care episodes.
Citation: Joynt KE, Gawande AA, Orav EJ, Jha AK. Contribution of preventable acute care spending to total spending for high-cost Medicare patients. JAMA. 2013;309:2572-2578.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Early treatment with intravenous tPA for acute stroke
- Perioperative morbidity, mortality for current smokers
- Statins associated with musculoskeletal conditions
- Antithrombotic medications in patients with history of stroke
- Extended prophylaxis with aspirin for patients after total hip arthroplasty
- Prognosis for symptomatic subsegmental pulmonary embolism
- Video-based educational workshops for academic hospitalists
- Increased mortality for elective surgeries on Fridays, weekends
- Basal plus correction insulin regimen and Type 2 diabetes
- Capnography to diagnose diabetic ketoacidosis in the ED
- How publicly reported mortality rates correlate with hospitals’ overall mortality
- Cost savings and preventable acute-care visits for Medicare patients
Early tPA in Acute Stroke Is Associated with Better Short-Term Outcomes in Routine Clinical Practice
Clinical question: Does early treatment with intravenous (IV) tissue plasminogen activator (tPA) result in better outcomes among patients with acute ischemic stroke in routine clinical practice?
Background: IV tPA for acute ischemic stroke is beneficial if given in the first 4.5 hours after symptom onset. However, pooled data from clinical trials have been limited in characterizing the extent to which onset-to-treatment (OTT) with IV tPA influences outcomes and how effective tPA is in routine clinical practice.
Study design: Data analysis from a stroke registry.
Setting: One thousand three hundred ninety-five U.S. hospitals participating in the Get with the Guidelines—Stroke Program.
Synopsis: Data were analyzed from 58,353 tPA-treated patients within 4.5 hours of symptom onset. Clinical outcomes were compared among patients treated in the 0-90-, 91-180-, and 181-270-minute OTT windows. Patient factors strongly associated with shorter OTT were greater stroke severity (odds ratio [OR] 2.8; 95% confidence interval [CI], 2.5-3.1 per five-point increase), arrival by ambulance (OR 5.9; 95% CI, 4.5-7.3), and arrival during regular hours (OR 4.6; 95% CI, 3.8-5.4). Faster OTT, in 15-minute increments, was associated with reduced in-hospital mortality (OR 0.96; 95% CI, 0.95-0.98; P<.001), reduced symptomatic intracranial hemorrhage (OR 0.96; 95% CI, 0.95-0.98; P<.001), increased achievement of independent ambulation at discharge (OR 1.04; 95% CI, 1.03-1.05; P<.001), and increased discharge to home (OR 1.03; 95% CI, 1.02-1.04; P<.001).
Data collected were dependent on the accuracy and completeness of the chart abstraction, and only short-term outcomes were reported. Although no post-discharge outcomes were reported, previous studies have shown that functional status at discharge strongly correlates with three-month disability outcomes.
Bottom line: In routine clinical practice, earlier tPA for acute ischemic strokes results in better short-term clinical outcomes.
Citation: Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309:2480-2488.
Current Smokers Have Higher Perioperative Morbidity and Mortality Compared to Past Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day post-operative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10-1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51-1.81 vs. OR 1.20; CI, 1.09-1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40-1.51 vs. OR, 1.13; CI, 1.08-1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease post-operative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013 Jun 19:1-8. doi: 10.1001/jamasurg.2013.2360 [Epub ahead of print].
Statins Associated with Several Musculoskeletal Conditions
Clinical question: Is statin use associated with musculoskeletal adverse events, including arthropathy and injury, in physically active individuals?
Background: Statin-induced musculoskeletal adverse events (AEs) include myalgias, muscle weakness, cramps, rhabdomyolysis, and tendinous disease. The full spectrum of AEs is unknown because randomized clinical trials have not been powered to detect uncommon AEs.
Study design: Retrospective cohort study with propensity score matching.
Setting: San Antonio military area.
Synopsis: A total of 46,249 patients aged 30 to 85 years who met study criteria were propensity-matched into 6,967 statin users and 6,967 nonusers. The occurrence of musculoskeletal conditions were categorized using ICD-9 codes: Msk1, all musculoskeletal diseases; Msk1a, arthropathies and related diseases; Msk1b, injury-related diseases; and Msk2, drug-associated musculoskeletal pain. Of these, statin users had a higher odds ratio (OR) for Msk1 (OR 1.19; 95% CI, 1.08-1.30), Msk1b (1.13; 1.05-1.21), and Msk2 (1.09; 1.02-1.18). Msk1b (arthropathies) had an OR of 1.07 (0.9-1.16, P=0.07). Simvastatin was used by 73.5% of patients, and years of simvastatin use was not a significant predictor of any of the outcome measures. Secondary and sensitivity analyses showed higher adjusted ORs for statin users in all groups. This study was limited by the use of ICD-9-CM codes for identification of baseline characteristics, and the musculoskeletal diagnosis groups used were not validated.
Bottom line: Statin use is associated with an increased likelihood of musculoskeletal conditions, arthropathies, injuries, and pain.
Citation: Mansi I, Frei CR, Pugh M, Makris U, Mortensen EM. Statins and musculoskeletal conditions, arthropathies, and injuries. JAMA Intern Med. 2013;173:1318-1326.
Evidence-Based Guidelines on Periprocedural Management of Antithrombotic Medications in Patients with History of Stroke
Clinical question: What is the evidence for the periprocedural management of antithrombotics in patients with ischemic cerebrovascular accidents (CVAs)?
Background: Evidence-based guidelines are needed to help clinicians determine the thromboembolic risk of temporary discontinuation of antithrombotic medications, the perioperative bleeding risks of continuing antithrombotic agents, whether bridging therapy should be used, and the appropriate timing of antithrombotic agent discontinuation.
Study design: Systematic literature review with practice recommendations.
Setting: American Academy of Neurology Guideline Development Subcommittee convened an expert panel to review and provide recommendations.
Synopsis: Researchers analyzed 133 literature reviews via MEDLINE and EMBASE. Aspirin in stroke patients:
- Should routinely be continued for dental procedures (Level A);
- Should probably be continued for invasive ocular anesthesia, cataract surgery, dermatologic procedures, transrectal ultrasound-guided prostate biopsy, spinal/epidural procedures, and carpal tunnel surgery (Level B); and
- Should possibly be continued for vitreoretinal surgery, electromyogram (EMG), transbronchial lung biopsy, colonoscopic polypectomy, upper endoscopy and biopsy/sphincterotomy, and abdominal ultrasound-guided biopsies (Level C).
Warfarin in stroke patients:
- Should routinely be continued for dental procedures (Level A); and
- Should possibly continued for dermatologic procedures (Level B) and EMG, prostate procedures, inguinal hemiorrhaphy, and endothermal ablation of great saphenous vein (Level C).
- There is a lack of evidence on warfarin for ophthalmologic procedures, with the exception of ocular anesthesia, where it probably does not increase clinically significant bleeding (Level B).
There was not enough evidence to support or refute a recommendation regarding heparin bridge therapy in reducing thromboembolism in chronically anticoagulated patients (Level B).
Bottom line: These are the most up-to-date guidelines for anticoagulant and antiplatelet agents in patients with transient ischemic attacks and strokes undergoing procedures, but further research is needed in many areas.
Citation: Armstrong MJ, Gronseth G Anderson DC, et al. Summary of evidence-based guideline: periprocedural management of antithrombotic medications in patients with ischemic cerebrovascular disease: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2065-2069.
Extended Prophylaxis with Aspirin Was Noninferior to Extended Prophylaxis with Low-Molecular-Weight Heparin
Clinical question: Is aspirin as effective as low-molecular-weight heparin (LMWH) for the extended prophylaxis of venous thromboembolism (VTE) after total hip arthroplasty (THA)?
Background: Deep vein thrombosis (DVT) and pulmonary embolism (PE) are common complications after THA. After initial prophylaxis, LMWH given for up to 30 days has been shown to reduce VTE compared with placebo. However, LMWH is costly and may increase the risk of minor bleeding. Aspirin is a potentially simple, low-cost alternative.
Study design: Randomized, placebo-controlled trial.
Setting: Twelve university-affiliated orthopedic hospitals in Canada.
Synopsis: Patients undergoing elective THA without hip fracture, metastatic cancer, or bleeding precluding anticoagulants were eligible. All patients received dalteparin for 10 days and were then randomized to aspirin 81 mg daily or to continue dalteparin. The primary outcome was symptomatic proximal DVT or PE during 90 days’ follow-up. The study was terminated early due to slow enrollment. At that time, 2,364 patients had been enrolled, and an analysis by an independent data safety and monitoring board determined that continuing the study was unlikely to alter the main findings. Extended prophylaxis with aspirin was noninferior to LMWH for the primary outcome, which occurred in 0.3% vs. 1.3%, respectively (95% CI, -0.5% to 2.5%, P<.001 for noninferiority). There were no significant differences in major or minor bleeding.
Though the early termination is a concern, the sample size was large and the results do not suggest inadequate power as a reason for lack of superiority for LMWH. Also, all patients received 10 days of LMWH, which indicates a period of LMWH after discharge will still be needed for most patients prior to initiating aspirin.
Bottom line: After initial LMWH prophylaxis for 10 days, extended prophylaxis with aspirin can be considered, particularly for patients for whom LMWH may not be feasible.
Citation: Anderson DR, Dunbar MJ, Bohm ER, et al. Aspirin versus low-molecular-weight heparin for extended venous thromboembolism prophylaxis after total hip arthroplasty: a randomized trial. Ann Intern Med. 2013;158:800-806.
Symptomatic Subsegmental Pulmonary Embolism (PE) Has a Prognosis Similar to Proximal PE
Clinical question: Is the prognosis of a symptomatic subsegmental pulmonary embolism (PE) similar to that of a more proximal PE?
Background: The use of multidetector computed tomography angiography (CTA) has allowed for better assessment of the pulmonary vasculature and increased detection of distal emboli. Prior studies have raised questions on the clinical importance of subsegmental PE but have been limited by small size or retrospective design.
Study design: Combined data from two prospective trials of management of suspected PE.
Setting: Twelve hospitals in the Netherlands and four tertiary-care emergency departments in Canada.
Synopsis: The study cohort consisted of 3,769 patients with suspected PE, of which 2,688 underwent CTA. Of patients diagnosed with PE, 15.5% had isolated subsegmental emboli. All patients were treated with anticoagulation. During three months of follow-up, the incidence of symptomatic recurrence for subsegmental PE was similar to patients with proximal PE (3.6% vs. 2.5%, respectively). The mortality rates for patients with subsegmental and proximal PE were also similar (10.3% vs. 6.3%, respectively).
The study may have been underpowered to detect small differences in event rates; however, there was no trend suggesting that subsegmental PE had better outcomes than more proximal PE. Also, the study did not specifically investigate whether any management strategy is preferred based on thrombus location on CTA.
Bottom line: Clinicians should continue to anticoagulate patients with subsegmental PE as the prognosis is similar to those with proximal PE.
Citation: Den Exter PL, van Es J, Klok FA, et al. Risk profile and clinical outcome of symptomatic subsegmental pulmonary embolism. Blood. 2013;122:1144-1149.
Video-Based Educational Workshop for Academic Hospitalists and House Staff May Improve Professionalism
Clinical question: Can video-based education promote professionalism among academic hospitalists and house staff?
Background: Unprofessional behavior by academic hospitalists and residents can negatively impact the learning environment and patient safety. This behavior increases throughout training, and faculty behavior can be influential. There is a paucity of educational materials to train hospitalists and house staff to recognize and ameliorate unprofessional behaviors.
Study design: Educational survey study.
Setting: University of Chicago, Northwestern University, and NorthShore University Health System teaching hospitals.
Synopsis: Three videos were developed displaying three types of unprofessional behavior: disparaging other physicians, “blocking” admissions, and misrepresenting tests to expedite their completion. There were 44 hospitalists and 244 house staff who received a 60-minute workshop in which they watched the videos using a viewing tool and discussed the videos in small groups.
For all three videos, more than three-quarters of both hospitalists and house staff felt the behavior was unprofessional or somewhat unprofessional. Hospitalists and house staff found the workshop useful and effective (65.9% and 77.1%, respectively) and would change their behavior as a result of the workshop (65.9% and 67.2%, respectively). Those who perceived the videos as “very realistic” were more likely to report intent to change behavior (93% vs. 53%, P=0.01).
This study is limited by its small sample size and possible selection bias. Those interested or concerned about unprofessional behavior may have been more likely to attend the workshop.
Bottom line: Video-based professionalism education is a feasible and well-received way to educate hospitalists and residents about unprofessional behavior and may even affect their future behavior.
Citation: Farnan JM, O’Leary KJ, Didwania A, et al. Promoting professionalism via a video-based educational workshop for academic hospitalists and housestaff. J Hosp Med. 2013;8:386-389.
Friday and Weekend Elective Surgeries Have Increased Mortality
Clinical question: How can the association between mortality and the day of elective surgical procedures be assessed?
Background: Several studies have described the “weekend effect” for both surgical and medical patients, with higher mortality and length of stay in patients admitted on the weekend compared to weekdays. Two potential explanations are poorer quality of care being delivered on the weekend or more severely ill patients being operated on or admitted on the weekend.
Study design: Retrospective analysis of national hospital administrative data.
Setting: All acute-care and specialist hospitals in England from 2008 to 2011.
Synopsis: There were 4,133,346 elective, inpatient surgical procedures studied. Friday surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.44 [95% CI, 1.39-1.50] and 1.42 [95% CI, 1.26-1.60], respectively, when compared with Monday. Weekend surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.82 [95% CI, 1.71-1.94] and 2.67 [95% CI, 2.30-3.09], respectively, when compared with Monday. There were significant trends toward higher mortality at the end of the workweek and weekends for four high-risk procedures: esophagus and/or stomach excision, colon and/or rectum excisions, coronary artery bypass graft, and lung excision. For lower-risk procedures, there was a significant increase in mortality for Friday surgeries but not weekend surgeries. As with all studies using administrative data, inherent selection biases could not be adjusted for Friday or weekend procedures.
Bottom line: Elective surgeries that occur on the weekend and later in the week have an increased risk of mortality, implying that the weekend effect is due to poorer quality of care during weekends, rather than higher-acuity patients presenting on weekends.
Citation: Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A. Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
Basal Plus Correction Insulin Regimen Is Effective in Hospitalized Patients with Type 2 Diabetes
Clinical question: Does a basal plus correction insulin regimen (as needed with meals) result in similar glycemic control and lower rates of hypoglycemia compared to a basal-bolus regimen?
Background: Basal bolus is the preferred insulin regimen for non-critically-ill hospitalized patients as per clinical guidelines. But use is limited due to the complexity of the regimen and the fear of inducing hypoglycemia. A less complex, easier-to-implement basal plus correction insulin regimen may be an effective alternative.
Study design: Multicenter, prospective, open-label, randomized study.
Setting: Six hospitals in the U.S.
Synopsis: A group of 375 medical and surgical patients with Type 2 diabetes treated with diet, oral anti-diabetic agents, or low-dose insulin (≤ 0.4 units/kg/day) were randomized to:
- Basal-bolus insulin regimen with glargine once daily and fixed doses of glusiline before meals;
- Basal plus correction insulin (“basal plus”) regimen with glargine once daily and glusiline sliding scale insulin (SSI) before meals; or
- Regular SSI alone.
After the first day of therapy, treatment with basal-bolus and basal-plus regimens resulted in similar improvements in daily blood glucose (BG) (P=0.16), and both were superior to SSI alone (P=0.04). Both regimens also resulted in less treatment failure (defined as mean daily BG of >240 mg/dl or >2 consecutive BG >240 mg/dl) than did treatment with SSI. Hypoglycemia (BG <70 mg/dl) occurred in 16%, 13%, and 3% of patients in the basal-bolus, basal-plus, and SSI groups, respectively (P=0.02). There were no between-group differences in the frequency of severe hypoglycemia (<40 mg/dl; P=0.76).
The study was not powered to evaluate hospital complications (infection, mortality, hospital stay, and readmissions) across groups.
Bottom line: The basal-plus regimen resulted in glycemic control similar to standard basal-bolus regimen and is an effective alternative for the initial management of hyperglycemia in general medical and surgical patients with Type 2 diabetes.
Citation: Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: Basal plus trial. Diabetes Care. 2013;36:2169-2174.
Capnography Can Help Diagnose Diabetic Ketoacidosis in the ED
Clinical question: Can capnography be used as a screening tool to identify patients with diabetic ketoacidosis (DKA)?
Background: Metabolic acidosis is a major criterion for diagnosing DKA. Previous studies have shown that end-tidal carbon dioxide (ETCO2) measurement by capnography can provide an accurate estimation of arterial carbon dioxide tension (PaCO2) and may be a noninvasive, fast, inexpensive measurement of acidosis in DKA. However, those studies were in pediatric patients and had small sample sizes.
Study design: Cross-sectional, prospective descriptive-analytic study.
Setting: The ED of Imam Reza Medical Research and Training Hospital, Tabriz, East Azarbaijan, Iran.
Synopsis: A total of 181 adult patients older than 18 with suspected DKA and blood sugar >250 mg/dl were included in the study. Simultaneous capnography and arterial blood gas (ABG) were obtained on all patients. Urine ketones, complete blood count, serum levels of potassium, urea, and creatinine were collected. Sixty-two patients were found to have DKA, while 119 had other conditions associated with metabolic acidosis. There was a significant linear relationship between pH and ETCO2 (P>0.0001, relative risk (R)=0.253), PaCO2 and ETCO2 (P>0.0001, R=0.572), and bicarbonate (HCO3) and ETCO2 (P>0.0001, R=0.730). ETCO2 values >24.5 mmHg had a sensitivity and specificity of 0.90 for ruling out DKA. No cutoff point could be determined for ruling in DKA.
The study was open to selection bias as patient collection was only done during the day, so eligible subjects may have been missed. Moreover, though the study suggests that capnography has a role in ruling out DKA, the exact cutoff value is unclear. Other studies found that higher values were needed to exclude diagnosis.
Bottom line: Using ETCO2 values >24.5 mmHg, capnography can help exclude the diagnosis of DKA in adult patients with elevated BG.
Citation: Soleimanour H, Taghizadieh A, Niafar M, Rahmani F, Golzari S, Esfanjani RM. Predictive value of capnography for diagnosis in patients with suspected diabetic ketoacidosis in the emergency department. West J Emerg Med. 2013. doi: 10.5811/westjem.2013.4.14296.
Publicly Reported Mortality Correlates with Overall Mortality
Clinical question: Are publicly reported mortality rates associated with a hospital’s overall medical and surgical mortality rate?
Background: Public reporting of mortality has become an important strategy in Medicare’s quality-improvement initiative. However, the mortality rate for only three conditions, acute myocardial infarction, congestive heart failure, and pneumonia are reported. It is unclear if these rates correlate to a hospital’s overall mortality rate.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Using 2008-2009 data from 2,322 acute-care hospitals with 6.7 million admissions, an aggregate mortality rate for the three publicly reported conditions, a standardized 30-day mortality rate for selected medical and surgical conditions, and an overall average composite mortality score was calculated for each hospital. Based on their mortality for the three publicly reported conditions, hospitals were grouped into quartiles from highest (top-performing hospitals) to lowest mortality (poor-performing hospitals).
Top-performing hospitals had a 3.6% (9.4%vs 13.0%; P<.001) lower mortality rate than poor-performing hospitals and an odds ratio >5 of being a top performer in overall mortality (OR 5.3; 95% CI, 4.3-6.5). They also had an 81% lower chance of being in the worst-performing quartile in overall mortality (OR 0.19; 95% CI, 0.14-0.27). Conversely, poor-performing hospitals had a 4.5 times higher risk of being in the lowest quartile in overall mortality. The study is limited by the use of administrative data, which limits the ability to adjust for severity of illness, overall health, and socioeconomic status of each hospital’s population.
Bottom line: A hospital’s mortality performance on the three publicly reported conditions may predict mortality rates across a wide range of medical and surgical conditions.
Citation: McCrum ML, Joynt KE, Orav EJ, Gawande AA, Jha AK. Mortality for publicly reported conditions and overall hospital mortality rates. JAMA Intern Med. 2013;173:1351-1357.
Cost Savings in Decreasing Preventable Acute-Care Visits Are Limited among High-Cost Medicare Utilizers
Clinical question: What role do preventable acute-care visits play in the overall costs of care for the highest Medicare utilizers?
Background: Some 10% of Medicare patients account for more than half the costs. Interventions targeted at decreasing acute-care costs (ED visits and inpatient hospitalizations) for this high-cost population are widespread, but it is unknown what impact they can have.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Standardized total costs were created for fee-for-service Medicare patients for 2009 and 2010 in order to identify high-cost and persistently high-cost patients. Algorithms were used to identify preventable ED visits and hospitalizations in both the high-cost and non-high-cost cohorts.
Of the more than 1 million patients in the sample Medicare population, as many as 113,341 were high-cost. As much as 73% of acute-care spending was attributable to this cohort. Overall, 10% of acute-care costs were felt to be preventable in the high-cost group, 13.5% in the persistently high-cost group, and 19% in the non-high-cost group for 2010. The most common reasons for preventable acute care in the high-cost cohort were heart failure, bacterial pneumonia, and chronic obstructive pulmonary disease. Catastrophic events (myocardial infarction, stroke, sepsis), cancer, and orthopedic procedures drove overall inpatient costs in the high-cost group.
Preventable costs were higher per capita in areas with higher numbers of primary-care and specialist physicians, but it’s unclear if this was a supply or demand issue. The study also used algorithms that possibly overestimate the amount of preventable acute care.
Bottom line: In the highest Medicare utilizers, cost savings aimed at preventable acute care may be limited and might be better targeted at efficiency during acute-care episodes.
Citation: Joynt KE, Gawande AA, Orav EJ, Jha AK. Contribution of preventable acute care spending to total spending for high-cost Medicare patients. JAMA. 2013;309:2572-2578.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Early treatment with intravenous tPA for acute stroke
- Perioperative morbidity, mortality for current smokers
- Statins associated with musculoskeletal conditions
- Antithrombotic medications in patients with history of stroke
- Extended prophylaxis with aspirin for patients after total hip arthroplasty
- Prognosis for symptomatic subsegmental pulmonary embolism
- Video-based educational workshops for academic hospitalists
- Increased mortality for elective surgeries on Fridays, weekends
- Basal plus correction insulin regimen and Type 2 diabetes
- Capnography to diagnose diabetic ketoacidosis in the ED
- How publicly reported mortality rates correlate with hospitals’ overall mortality
- Cost savings and preventable acute-care visits for Medicare patients
Early tPA in Acute Stroke Is Associated with Better Short-Term Outcomes in Routine Clinical Practice
Clinical question: Does early treatment with intravenous (IV) tissue plasminogen activator (tPA) result in better outcomes among patients with acute ischemic stroke in routine clinical practice?
Background: IV tPA for acute ischemic stroke is beneficial if given in the first 4.5 hours after symptom onset. However, pooled data from clinical trials have been limited in characterizing the extent to which onset-to-treatment (OTT) with IV tPA influences outcomes and how effective tPA is in routine clinical practice.
Study design: Data analysis from a stroke registry.
Setting: One thousand three hundred ninety-five U.S. hospitals participating in the Get with the Guidelines—Stroke Program.
Synopsis: Data were analyzed from 58,353 tPA-treated patients within 4.5 hours of symptom onset. Clinical outcomes were compared among patients treated in the 0-90-, 91-180-, and 181-270-minute OTT windows. Patient factors strongly associated with shorter OTT were greater stroke severity (odds ratio [OR] 2.8; 95% confidence interval [CI], 2.5-3.1 per five-point increase), arrival by ambulance (OR 5.9; 95% CI, 4.5-7.3), and arrival during regular hours (OR 4.6; 95% CI, 3.8-5.4). Faster OTT, in 15-minute increments, was associated with reduced in-hospital mortality (OR 0.96; 95% CI, 0.95-0.98; P<.001), reduced symptomatic intracranial hemorrhage (OR 0.96; 95% CI, 0.95-0.98; P<.001), increased achievement of independent ambulation at discharge (OR 1.04; 95% CI, 1.03-1.05; P<.001), and increased discharge to home (OR 1.03; 95% CI, 1.02-1.04; P<.001).
Data collected were dependent on the accuracy and completeness of the chart abstraction, and only short-term outcomes were reported. Although no post-discharge outcomes were reported, previous studies have shown that functional status at discharge strongly correlates with three-month disability outcomes.
Bottom line: In routine clinical practice, earlier tPA for acute ischemic strokes results in better short-term clinical outcomes.
Citation: Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. 2013;309:2480-2488.
Current Smokers Have Higher Perioperative Morbidity and Mortality Compared to Past Smokers
Clinical question: Is there an association between current and past smoking on outcomes among patients having major surgery?
Background: Smoking is associated with adverse postoperative outcomes, but it is not known whether the associations are dose-dependent or limited to patients with smoking-related diseases. Smoking-related effects on postoperative events among patients having major surgery are also not well established.
Study design: Retrospective cohort study.
Setting: Four hundred forty-eight non-VA hospitals across the U.S., Canada, Lebanon, and the United Arab Emirates.
Synopsis: Data from 607,558 adult patients undergoing major surgery were obtained from the American College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP) database. After adjusting for confounders (cardiopulmonary diseases and cancer), the effects of current and past smoking (quit >1 year prior) on 30-day post-operative outcomes were measured.
There were 125,192 (21%) current smokers and 78,763 (13%) past smokers. Increased odds of post-op mortality were noted in current smokers only (odds ratio [OR] 1.17; 95% CI, 1.10-1.24). The adjusted odds ratios were higher for arterial and respiratory events among current smokers compared with past smokers (OR 1.65; 95% CI, 1.51-1.81 vs. OR 1.20; CI, 1.09-1.31 for arterial events, respectively) and (OR, 1.45; CI, 1.40-1.51 vs. OR, 1.13; CI, 1.08-1.18, for respiratory events, respectively). No significant effects on venous events were observed.
There was an increased adjusted odds of mortality for current smokers with <10 pack-years, while the effects on arterial and respiratory events increased incrementally with increased pack-years. Smoking was associated with adverse post-op outcomes regardless of smoking-related diseases. Variability in hospital quality or surgical strategies may have confounded the results.
Bottom line: Among patients undergoing major surgery, current but not past smoking was associated with higher mortality; smoking cessation for at least a year prior to surgery may decrease post-operative adverse events.
Citation: Musallam KM, Rosendaal FR, Zaatari G, et al. Smoking and the risk of mortality and vascular and respiratory events in patients undergoing major surgery. JAMA Surg. 2013 Jun 19:1-8. doi: 10.1001/jamasurg.2013.2360 [Epub ahead of print].
Statins Associated with Several Musculoskeletal Conditions
Clinical question: Is statin use associated with musculoskeletal adverse events, including arthropathy and injury, in physically active individuals?
Background: Statin-induced musculoskeletal adverse events (AEs) include myalgias, muscle weakness, cramps, rhabdomyolysis, and tendinous disease. The full spectrum of AEs is unknown because randomized clinical trials have not been powered to detect uncommon AEs.
Study design: Retrospective cohort study with propensity score matching.
Setting: San Antonio military area.
Synopsis: A total of 46,249 patients aged 30 to 85 years who met study criteria were propensity-matched into 6,967 statin users and 6,967 nonusers. The occurrence of musculoskeletal conditions were categorized using ICD-9 codes: Msk1, all musculoskeletal diseases; Msk1a, arthropathies and related diseases; Msk1b, injury-related diseases; and Msk2, drug-associated musculoskeletal pain. Of these, statin users had a higher odds ratio (OR) for Msk1 (OR 1.19; 95% CI, 1.08-1.30), Msk1b (1.13; 1.05-1.21), and Msk2 (1.09; 1.02-1.18). Msk1b (arthropathies) had an OR of 1.07 (0.9-1.16, P=0.07). Simvastatin was used by 73.5% of patients, and years of simvastatin use was not a significant predictor of any of the outcome measures. Secondary and sensitivity analyses showed higher adjusted ORs for statin users in all groups. This study was limited by the use of ICD-9-CM codes for identification of baseline characteristics, and the musculoskeletal diagnosis groups used were not validated.
Bottom line: Statin use is associated with an increased likelihood of musculoskeletal conditions, arthropathies, injuries, and pain.
Citation: Mansi I, Frei CR, Pugh M, Makris U, Mortensen EM. Statins and musculoskeletal conditions, arthropathies, and injuries. JAMA Intern Med. 2013;173:1318-1326.
Evidence-Based Guidelines on Periprocedural Management of Antithrombotic Medications in Patients with History of Stroke
Clinical question: What is the evidence for the periprocedural management of antithrombotics in patients with ischemic cerebrovascular accidents (CVAs)?
Background: Evidence-based guidelines are needed to help clinicians determine the thromboembolic risk of temporary discontinuation of antithrombotic medications, the perioperative bleeding risks of continuing antithrombotic agents, whether bridging therapy should be used, and the appropriate timing of antithrombotic agent discontinuation.
Study design: Systematic literature review with practice recommendations.
Setting: American Academy of Neurology Guideline Development Subcommittee convened an expert panel to review and provide recommendations.
Synopsis: Researchers analyzed 133 literature reviews via MEDLINE and EMBASE. Aspirin in stroke patients:
- Should routinely be continued for dental procedures (Level A);
- Should probably be continued for invasive ocular anesthesia, cataract surgery, dermatologic procedures, transrectal ultrasound-guided prostate biopsy, spinal/epidural procedures, and carpal tunnel surgery (Level B); and
- Should possibly be continued for vitreoretinal surgery, electromyogram (EMG), transbronchial lung biopsy, colonoscopic polypectomy, upper endoscopy and biopsy/sphincterotomy, and abdominal ultrasound-guided biopsies (Level C).
Warfarin in stroke patients:
- Should routinely be continued for dental procedures (Level A); and
- Should possibly continued for dermatologic procedures (Level B) and EMG, prostate procedures, inguinal hemiorrhaphy, and endothermal ablation of great saphenous vein (Level C).
- There is a lack of evidence on warfarin for ophthalmologic procedures, with the exception of ocular anesthesia, where it probably does not increase clinically significant bleeding (Level B).
There was not enough evidence to support or refute a recommendation regarding heparin bridge therapy in reducing thromboembolism in chronically anticoagulated patients (Level B).
Bottom line: These are the most up-to-date guidelines for anticoagulant and antiplatelet agents in patients with transient ischemic attacks and strokes undergoing procedures, but further research is needed in many areas.
Citation: Armstrong MJ, Gronseth G Anderson DC, et al. Summary of evidence-based guideline: periprocedural management of antithrombotic medications in patients with ischemic cerebrovascular disease: Report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;80:2065-2069.
Extended Prophylaxis with Aspirin Was Noninferior to Extended Prophylaxis with Low-Molecular-Weight Heparin
Clinical question: Is aspirin as effective as low-molecular-weight heparin (LMWH) for the extended prophylaxis of venous thromboembolism (VTE) after total hip arthroplasty (THA)?
Background: Deep vein thrombosis (DVT) and pulmonary embolism (PE) are common complications after THA. After initial prophylaxis, LMWH given for up to 30 days has been shown to reduce VTE compared with placebo. However, LMWH is costly and may increase the risk of minor bleeding. Aspirin is a potentially simple, low-cost alternative.
Study design: Randomized, placebo-controlled trial.
Setting: Twelve university-affiliated orthopedic hospitals in Canada.
Synopsis: Patients undergoing elective THA without hip fracture, metastatic cancer, or bleeding precluding anticoagulants were eligible. All patients received dalteparin for 10 days and were then randomized to aspirin 81 mg daily or to continue dalteparin. The primary outcome was symptomatic proximal DVT or PE during 90 days’ follow-up. The study was terminated early due to slow enrollment. At that time, 2,364 patients had been enrolled, and an analysis by an independent data safety and monitoring board determined that continuing the study was unlikely to alter the main findings. Extended prophylaxis with aspirin was noninferior to LMWH for the primary outcome, which occurred in 0.3% vs. 1.3%, respectively (95% CI, -0.5% to 2.5%, P<.001 for noninferiority). There were no significant differences in major or minor bleeding.
Though the early termination is a concern, the sample size was large and the results do not suggest inadequate power as a reason for lack of superiority for LMWH. Also, all patients received 10 days of LMWH, which indicates a period of LMWH after discharge will still be needed for most patients prior to initiating aspirin.
Bottom line: After initial LMWH prophylaxis for 10 days, extended prophylaxis with aspirin can be considered, particularly for patients for whom LMWH may not be feasible.
Citation: Anderson DR, Dunbar MJ, Bohm ER, et al. Aspirin versus low-molecular-weight heparin for extended venous thromboembolism prophylaxis after total hip arthroplasty: a randomized trial. Ann Intern Med. 2013;158:800-806.
Symptomatic Subsegmental Pulmonary Embolism (PE) Has a Prognosis Similar to Proximal PE
Clinical question: Is the prognosis of a symptomatic subsegmental pulmonary embolism (PE) similar to that of a more proximal PE?
Background: The use of multidetector computed tomography angiography (CTA) has allowed for better assessment of the pulmonary vasculature and increased detection of distal emboli. Prior studies have raised questions on the clinical importance of subsegmental PE but have been limited by small size or retrospective design.
Study design: Combined data from two prospective trials of management of suspected PE.
Setting: Twelve hospitals in the Netherlands and four tertiary-care emergency departments in Canada.
Synopsis: The study cohort consisted of 3,769 patients with suspected PE, of which 2,688 underwent CTA. Of patients diagnosed with PE, 15.5% had isolated subsegmental emboli. All patients were treated with anticoagulation. During three months of follow-up, the incidence of symptomatic recurrence for subsegmental PE was similar to patients with proximal PE (3.6% vs. 2.5%, respectively). The mortality rates for patients with subsegmental and proximal PE were also similar (10.3% vs. 6.3%, respectively).
The study may have been underpowered to detect small differences in event rates; however, there was no trend suggesting that subsegmental PE had better outcomes than more proximal PE. Also, the study did not specifically investigate whether any management strategy is preferred based on thrombus location on CTA.
Bottom line: Clinicians should continue to anticoagulate patients with subsegmental PE as the prognosis is similar to those with proximal PE.
Citation: Den Exter PL, van Es J, Klok FA, et al. Risk profile and clinical outcome of symptomatic subsegmental pulmonary embolism. Blood. 2013;122:1144-1149.
Video-Based Educational Workshop for Academic Hospitalists and House Staff May Improve Professionalism
Clinical question: Can video-based education promote professionalism among academic hospitalists and house staff?
Background: Unprofessional behavior by academic hospitalists and residents can negatively impact the learning environment and patient safety. This behavior increases throughout training, and faculty behavior can be influential. There is a paucity of educational materials to train hospitalists and house staff to recognize and ameliorate unprofessional behaviors.
Study design: Educational survey study.
Setting: University of Chicago, Northwestern University, and NorthShore University Health System teaching hospitals.
Synopsis: Three videos were developed displaying three types of unprofessional behavior: disparaging other physicians, “blocking” admissions, and misrepresenting tests to expedite their completion. There were 44 hospitalists and 244 house staff who received a 60-minute workshop in which they watched the videos using a viewing tool and discussed the videos in small groups.
For all three videos, more than three-quarters of both hospitalists and house staff felt the behavior was unprofessional or somewhat unprofessional. Hospitalists and house staff found the workshop useful and effective (65.9% and 77.1%, respectively) and would change their behavior as a result of the workshop (65.9% and 67.2%, respectively). Those who perceived the videos as “very realistic” were more likely to report intent to change behavior (93% vs. 53%, P=0.01).
This study is limited by its small sample size and possible selection bias. Those interested or concerned about unprofessional behavior may have been more likely to attend the workshop.
Bottom line: Video-based professionalism education is a feasible and well-received way to educate hospitalists and residents about unprofessional behavior and may even affect their future behavior.
Citation: Farnan JM, O’Leary KJ, Didwania A, et al. Promoting professionalism via a video-based educational workshop for academic hospitalists and housestaff. J Hosp Med. 2013;8:386-389.
Friday and Weekend Elective Surgeries Have Increased Mortality
Clinical question: How can the association between mortality and the day of elective surgical procedures be assessed?
Background: Several studies have described the “weekend effect” for both surgical and medical patients, with higher mortality and length of stay in patients admitted on the weekend compared to weekdays. Two potential explanations are poorer quality of care being delivered on the weekend or more severely ill patients being operated on or admitted on the weekend.
Study design: Retrospective analysis of national hospital administrative data.
Setting: All acute-care and specialist hospitals in England from 2008 to 2011.
Synopsis: There were 4,133,346 elective, inpatient surgical procedures studied. Friday surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.44 [95% CI, 1.39-1.50] and 1.42 [95% CI, 1.26-1.60], respectively, when compared with Monday. Weekend surgeries had an adjusted odds ratio of death within 30 days and within two days of 1.82 [95% CI, 1.71-1.94] and 2.67 [95% CI, 2.30-3.09], respectively, when compared with Monday. There were significant trends toward higher mortality at the end of the workweek and weekends for four high-risk procedures: esophagus and/or stomach excision, colon and/or rectum excisions, coronary artery bypass graft, and lung excision. For lower-risk procedures, there was a significant increase in mortality for Friday surgeries but not weekend surgeries. As with all studies using administrative data, inherent selection biases could not be adjusted for Friday or weekend procedures.
Bottom line: Elective surgeries that occur on the weekend and later in the week have an increased risk of mortality, implying that the weekend effect is due to poorer quality of care during weekends, rather than higher-acuity patients presenting on weekends.
Citation: Aylin P, Alexandrescu R, Jen MH, Mayer EK, Bottle A. Day of week of procedure and 30 day mortality for elective surgery: retrospective analysis of hospital episode statistics. BMJ. 2013;346:f2424.
Basal Plus Correction Insulin Regimen Is Effective in Hospitalized Patients with Type 2 Diabetes
Clinical question: Does a basal plus correction insulin regimen (as needed with meals) result in similar glycemic control and lower rates of hypoglycemia compared to a basal-bolus regimen?
Background: Basal bolus is the preferred insulin regimen for non-critically-ill hospitalized patients as per clinical guidelines. But use is limited due to the complexity of the regimen and the fear of inducing hypoglycemia. A less complex, easier-to-implement basal plus correction insulin regimen may be an effective alternative.
Study design: Multicenter, prospective, open-label, randomized study.
Setting: Six hospitals in the U.S.
Synopsis: A group of 375 medical and surgical patients with Type 2 diabetes treated with diet, oral anti-diabetic agents, or low-dose insulin (≤ 0.4 units/kg/day) were randomized to:
- Basal-bolus insulin regimen with glargine once daily and fixed doses of glusiline before meals;
- Basal plus correction insulin (“basal plus”) regimen with glargine once daily and glusiline sliding scale insulin (SSI) before meals; or
- Regular SSI alone.
After the first day of therapy, treatment with basal-bolus and basal-plus regimens resulted in similar improvements in daily blood glucose (BG) (P=0.16), and both were superior to SSI alone (P=0.04). Both regimens also resulted in less treatment failure (defined as mean daily BG of >240 mg/dl or >2 consecutive BG >240 mg/dl) than did treatment with SSI. Hypoglycemia (BG <70 mg/dl) occurred in 16%, 13%, and 3% of patients in the basal-bolus, basal-plus, and SSI groups, respectively (P=0.02). There were no between-group differences in the frequency of severe hypoglycemia (<40 mg/dl; P=0.76).
The study was not powered to evaluate hospital complications (infection, mortality, hospital stay, and readmissions) across groups.
Bottom line: The basal-plus regimen resulted in glycemic control similar to standard basal-bolus regimen and is an effective alternative for the initial management of hyperglycemia in general medical and surgical patients with Type 2 diabetes.
Citation: Umpierrez GE, Smiley D, Hermayer K, et al. Randomized study comparing a basal-bolus with a basal plus correction insulin regimen for the hospital management of medical and surgical patients with type 2 diabetes: Basal plus trial. Diabetes Care. 2013;36:2169-2174.
Capnography Can Help Diagnose Diabetic Ketoacidosis in the ED
Clinical question: Can capnography be used as a screening tool to identify patients with diabetic ketoacidosis (DKA)?
Background: Metabolic acidosis is a major criterion for diagnosing DKA. Previous studies have shown that end-tidal carbon dioxide (ETCO2) measurement by capnography can provide an accurate estimation of arterial carbon dioxide tension (PaCO2) and may be a noninvasive, fast, inexpensive measurement of acidosis in DKA. However, those studies were in pediatric patients and had small sample sizes.
Study design: Cross-sectional, prospective descriptive-analytic study.
Setting: The ED of Imam Reza Medical Research and Training Hospital, Tabriz, East Azarbaijan, Iran.
Synopsis: A total of 181 adult patients older than 18 with suspected DKA and blood sugar >250 mg/dl were included in the study. Simultaneous capnography and arterial blood gas (ABG) were obtained on all patients. Urine ketones, complete blood count, serum levels of potassium, urea, and creatinine were collected. Sixty-two patients were found to have DKA, while 119 had other conditions associated with metabolic acidosis. There was a significant linear relationship between pH and ETCO2 (P>0.0001, relative risk (R)=0.253), PaCO2 and ETCO2 (P>0.0001, R=0.572), and bicarbonate (HCO3) and ETCO2 (P>0.0001, R=0.730). ETCO2 values >24.5 mmHg had a sensitivity and specificity of 0.90 for ruling out DKA. No cutoff point could be determined for ruling in DKA.
The study was open to selection bias as patient collection was only done during the day, so eligible subjects may have been missed. Moreover, though the study suggests that capnography has a role in ruling out DKA, the exact cutoff value is unclear. Other studies found that higher values were needed to exclude diagnosis.
Bottom line: Using ETCO2 values >24.5 mmHg, capnography can help exclude the diagnosis of DKA in adult patients with elevated BG.
Citation: Soleimanour H, Taghizadieh A, Niafar M, Rahmani F, Golzari S, Esfanjani RM. Predictive value of capnography for diagnosis in patients with suspected diabetic ketoacidosis in the emergency department. West J Emerg Med. 2013. doi: 10.5811/westjem.2013.4.14296.
Publicly Reported Mortality Correlates with Overall Mortality
Clinical question: Are publicly reported mortality rates associated with a hospital’s overall medical and surgical mortality rate?
Background: Public reporting of mortality has become an important strategy in Medicare’s quality-improvement initiative. However, the mortality rate for only three conditions, acute myocardial infarction, congestive heart failure, and pneumonia are reported. It is unclear if these rates correlate to a hospital’s overall mortality rate.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Using 2008-2009 data from 2,322 acute-care hospitals with 6.7 million admissions, an aggregate mortality rate for the three publicly reported conditions, a standardized 30-day mortality rate for selected medical and surgical conditions, and an overall average composite mortality score was calculated for each hospital. Based on their mortality for the three publicly reported conditions, hospitals were grouped into quartiles from highest (top-performing hospitals) to lowest mortality (poor-performing hospitals).
Top-performing hospitals had a 3.6% (9.4%vs 13.0%; P<.001) lower mortality rate than poor-performing hospitals and an odds ratio >5 of being a top performer in overall mortality (OR 5.3; 95% CI, 4.3-6.5). They also had an 81% lower chance of being in the worst-performing quartile in overall mortality (OR 0.19; 95% CI, 0.14-0.27). Conversely, poor-performing hospitals had a 4.5 times higher risk of being in the lowest quartile in overall mortality. The study is limited by the use of administrative data, which limits the ability to adjust for severity of illness, overall health, and socioeconomic status of each hospital’s population.
Bottom line: A hospital’s mortality performance on the three publicly reported conditions may predict mortality rates across a wide range of medical and surgical conditions.
Citation: McCrum ML, Joynt KE, Orav EJ, Gawande AA, Jha AK. Mortality for publicly reported conditions and overall hospital mortality rates. JAMA Intern Med. 2013;173:1351-1357.
Cost Savings in Decreasing Preventable Acute-Care Visits Are Limited among High-Cost Medicare Utilizers
Clinical question: What role do preventable acute-care visits play in the overall costs of care for the highest Medicare utilizers?
Background: Some 10% of Medicare patients account for more than half the costs. Interventions targeted at decreasing acute-care costs (ED visits and inpatient hospitalizations) for this high-cost population are widespread, but it is unknown what impact they can have.
Study design: Retrospective cohort.
Setting: National Medicare fee-for-service population.
Synopsis: Standardized total costs were created for fee-for-service Medicare patients for 2009 and 2010 in order to identify high-cost and persistently high-cost patients. Algorithms were used to identify preventable ED visits and hospitalizations in both the high-cost and non-high-cost cohorts.
Of the more than 1 million patients in the sample Medicare population, as many as 113,341 were high-cost. As much as 73% of acute-care spending was attributable to this cohort. Overall, 10% of acute-care costs were felt to be preventable in the high-cost group, 13.5% in the persistently high-cost group, and 19% in the non-high-cost group for 2010. The most common reasons for preventable acute care in the high-cost cohort were heart failure, bacterial pneumonia, and chronic obstructive pulmonary disease. Catastrophic events (myocardial infarction, stroke, sepsis), cancer, and orthopedic procedures drove overall inpatient costs in the high-cost group.
Preventable costs were higher per capita in areas with higher numbers of primary-care and specialist physicians, but it’s unclear if this was a supply or demand issue. The study also used algorithms that possibly overestimate the amount of preventable acute care.
Bottom line: In the highest Medicare utilizers, cost savings aimed at preventable acute care may be limited and might be better targeted at efficiency during acute-care episodes.
Citation: Joynt KE, Gawande AA, Orav EJ, Jha AK. Contribution of preventable acute care spending to total spending for high-cost Medicare patients. JAMA. 2013;309:2572-2578.
Physician Reviews of HM-Related Research
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: Three hundred four patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: Three hundred four patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
Visit our website for more physician reviews of recent HM-relevant literature.
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: Three hundred four patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
Visit our website for more physician reviews of recent HM-relevant literature.
Surviving Sepsis Campaign 2012 Guidelines: Updates For the Hospitalist
Background
Sepsis is a clinical syndrome with systemic effects that can progress to severe sepsis and/or septic shock. The incidence of severe sepsis and septic shock is rising in the United States, and these syndromes are associated with significant morbidity and a mortality rate as high as 25% to 35%.1 In fact, sepsis is one of the 10 leading causes of death in the U.S., accounting for 2% of hospital admissions but 17% of in-hospital deaths.1
The main principles of effective treatment for severe sepsis and septic shock are timely recognition and early aggressive therapy. Launched in 2002, the Surviving Sepsis Campaign (SSC) was the result of a collaboration of three professional societies. The goal of the SSC collaborative was to reduce mortality from severe sepsis and septic shock by 25%. To that end, the SSC convened representatives from several international societies to develop a set of evidence-based guidelines as a means of guiding clinicians in optimizing management of patients with severe sepsis and septic shock. Since the original publication of the SSC guidelines in 2004, there have been two updates—one in 2008 and one in February 2013.2
Guideline Updates
Quantitative, protocol-driven initial resuscitation in the first six hours for patients with severe sepsis and septic shock remains a high-level recommendation, but SSC has added normalization of the lactate level as a resuscitation goal. This new suggestion is based on two studies published since the 2008 SCC guidelines that showed noninferiority to previously established goals and absolute mortality benefit.3,4
There is a new focus on screening for sepsis and the use of hospital-based performance-improvement programs, which were not previously addressed in the 2008 SCC guidelines. Patients with suspected infections and who are seriously ill should be screened in order to identify sepsis early during the hospital course. Additionally, it is recommended that hospitals implement performance-improvement measures by which multidisciplinary teams can address treatment of sepsis by improving compliance with the SSC bundles, citing their own data as the model but ultimately leaving this recommendation as ungradable in regards to the quality of available supporting evidence.5
Cultures drawn before antibiotics and early imaging to confirm potential sources are still recommended, but the committee has added the use of one: 3 beta D-glucan and the mannan antigen and anti-mannan antibody assays when considering invasive candidiasis as your infective agent. They do note the known risk of false positive results with these assays and warn that they should be used with caution.
Early, broad-spectrum antibiotic administration within the first hour of presentation was upgraded for severe sepsis and downgraded for septic shock. The decision to initiate double coverage for suspected gram-negative infection is not recommended specifically but can be considered in situations when highly antibiotic resistant pathogens are potentially present. Daily assessment of the appropriate antibiotic regimen remains an important tenet, and the use of low procalcitonin levels as a tool to assist in the decision to discontinue antibiotics has been introduced. Source control is still strongly recommended in the first 12 hours of treatment.
The SSC 2012 guidelines specifically address the rate of fluid administered and the type of fluid that should be used. It is now recommended that a fluid challenge of 30 mL/kg be used for initial resuscitation, but the guidelines leave it up to the clinician to give more fluid if needed. There is a strong push for use of crystalloids rather than colloids during initial resuscitation and thereafter. Disfavor for colloids stemmed from trials showing increased mortality when comparing resuscitation with hydroxyethyl starch versus crystalloid for patients in septic shock.6,7 Albumin, on the other hand, is recommended to resuscitate patients with severe sepsis and septic shock in cases for which large amounts of crystalloid are required.
The 2012 SSC guidelines recommend norepinephrine (NE) alone as the first-line vasopressor in sepsis and no longer include dopamine in this category. In fact, the use of dopamine in septic shock has been downgraded and should only to be considered in patients at low risk of tachyarrhythmia and in bradycardia syndromes. Epinephrine is now favored as the second agent or as a substitute to NE. Phenylephrine is no longer recommended unless there is contraindication to using NE, the patient has a high cardiac output, or it is used as a salvage therapy. Vasopressin is considered only an adjunctive agent to NE and should never be used alone.
Recommendations regarding corticosteroid therapy remain largely unchanged from 2008 SCC guidelines, which only support their use when adequate volume resuscitation and vasopressor support has failed to achieve hemodynamic stability. Glucose control is recommended but at the new target of achieving a level of <180 mg/dL, up from a previous target of <150 mg/dL.
Notably, recombinant human activated protein C was completely omitted from the 2012 guidelines, prompted by the voluntary removal of the drug by the manufacturer after failing to show benefit. Use of selenium and intravenous immunoglobulin received comment, but there is insufficient evidence supporting their benefit at the current time. They also encourage clinicians to incorporate goals of care and end-of-life issues into the treatment plan and discuss this with patients and/or surrogates early in treatment.
Guideline Analysis
Prior versions of the SSC guidelines have been met with a fair amount of skepticism.8 Much of the criticism is based on the industry sponsorship of the 2004 version, the lack of transparency regarding potential conflicts of interest of the committee members, and that the bundle recommendations largely were based on only one trial and, therefore, not evidenced-based.9 The 2012 SSC committee seems to have addressed these issues as the guidelines are free of commercial sponsorship in the 2008 and current versions. They also rigorously applied the GRADE system to methodically assess the strength and quality of supporting evidence. The result is a set of guidelines that are partially evidence-based and partially based on expert opinion, but this is clearly delineated in these newest guidelines. This provides clinicians with a clear and concise recommended approach to the patient with severe sepsis and septic shock.
The guidelines continue to place a heavy emphasis on three- and six-hour treatment bundles, and with the assistance of the Institute for Health Care Improvement efforts to improve implementation of the bundle, they are already are widespread with an eye to expand across the country. The components of the three-hour treatment bundle (lactate measurement, blood cultures prior to initiation of antibiotics, broad-spectrum antibiotics, and IV crystalloids for hypotension or for a lactate of >4 mmol/L) recommended by the SSC have not changed substantially since 2008. The one exception is the rate at which IV crystalloid should be administered of 30 mL/kg, which is up from 20 mL/kg. Only time will tell how this change will affect bundle compliance or reduce mortality. But this does pose a significant challenge to quality and performance improvement groups accustomed to tracking compliance with IV fluid administration under the old standard and the educational campaigns associated with a change.
It appears that the SSC is here to stay, now in its third iteration. The lasting legacy of the SSC guidelines might not rest with the content of the guidelines, per se, but in raising awareness of severe sepsis and septic shock in a way that had not previously been considered.
HM Takeaways
The revised 2012 SCC updates bring some new tools to the clinician for early recognition and effective management of patients with sepsis. The push for institutions to adopt screening and performance measures reflects a general trend in health care to create high-performance systems. As these new guidelines are put into practice, there are several changes that might require augmentation of quality metrics being tracked at institutions nationally and internationally.
Dr. Pendharker is assistant professor of medicine in the division of hospital medicine at the University of California San Francisco and San Francisco General Hospital. Dr. Gomez is assistant professor of medicine in the division of pulmonary and critical care medicine at UCSF and San Francisco General Hospital.
References
- Hall MJ, Williams SN, DeFrances CJ, et al. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011:1-8.
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580-637.
- Jansen TC, van Bommel J, Schoonderbeek FJ, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752-761.
- Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA. 2010;303:739-746.
- Levy MM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367-374.
- Guidet B, Martinet O, Boulain T, et al. Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care. 2012;16:R94.
- Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367:124-134.
- Marik PE. Surviving sepsis: going beyond the guidelines. Ann Intensive Care. 2011;1:17.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
Background
Sepsis is a clinical syndrome with systemic effects that can progress to severe sepsis and/or septic shock. The incidence of severe sepsis and septic shock is rising in the United States, and these syndromes are associated with significant morbidity and a mortality rate as high as 25% to 35%.1 In fact, sepsis is one of the 10 leading causes of death in the U.S., accounting for 2% of hospital admissions but 17% of in-hospital deaths.1
The main principles of effective treatment for severe sepsis and septic shock are timely recognition and early aggressive therapy. Launched in 2002, the Surviving Sepsis Campaign (SSC) was the result of a collaboration of three professional societies. The goal of the SSC collaborative was to reduce mortality from severe sepsis and septic shock by 25%. To that end, the SSC convened representatives from several international societies to develop a set of evidence-based guidelines as a means of guiding clinicians in optimizing management of patients with severe sepsis and septic shock. Since the original publication of the SSC guidelines in 2004, there have been two updates—one in 2008 and one in February 2013.2
Guideline Updates
Quantitative, protocol-driven initial resuscitation in the first six hours for patients with severe sepsis and septic shock remains a high-level recommendation, but SSC has added normalization of the lactate level as a resuscitation goal. This new suggestion is based on two studies published since the 2008 SCC guidelines that showed noninferiority to previously established goals and absolute mortality benefit.3,4
There is a new focus on screening for sepsis and the use of hospital-based performance-improvement programs, which were not previously addressed in the 2008 SCC guidelines. Patients with suspected infections and who are seriously ill should be screened in order to identify sepsis early during the hospital course. Additionally, it is recommended that hospitals implement performance-improvement measures by which multidisciplinary teams can address treatment of sepsis by improving compliance with the SSC bundles, citing their own data as the model but ultimately leaving this recommendation as ungradable in regards to the quality of available supporting evidence.5
Cultures drawn before antibiotics and early imaging to confirm potential sources are still recommended, but the committee has added the use of one: 3 beta D-glucan and the mannan antigen and anti-mannan antibody assays when considering invasive candidiasis as your infective agent. They do note the known risk of false positive results with these assays and warn that they should be used with caution.
Early, broad-spectrum antibiotic administration within the first hour of presentation was upgraded for severe sepsis and downgraded for septic shock. The decision to initiate double coverage for suspected gram-negative infection is not recommended specifically but can be considered in situations when highly antibiotic resistant pathogens are potentially present. Daily assessment of the appropriate antibiotic regimen remains an important tenet, and the use of low procalcitonin levels as a tool to assist in the decision to discontinue antibiotics has been introduced. Source control is still strongly recommended in the first 12 hours of treatment.
The SSC 2012 guidelines specifically address the rate of fluid administered and the type of fluid that should be used. It is now recommended that a fluid challenge of 30 mL/kg be used for initial resuscitation, but the guidelines leave it up to the clinician to give more fluid if needed. There is a strong push for use of crystalloids rather than colloids during initial resuscitation and thereafter. Disfavor for colloids stemmed from trials showing increased mortality when comparing resuscitation with hydroxyethyl starch versus crystalloid for patients in septic shock.6,7 Albumin, on the other hand, is recommended to resuscitate patients with severe sepsis and septic shock in cases for which large amounts of crystalloid are required.
The 2012 SSC guidelines recommend norepinephrine (NE) alone as the first-line vasopressor in sepsis and no longer include dopamine in this category. In fact, the use of dopamine in septic shock has been downgraded and should only to be considered in patients at low risk of tachyarrhythmia and in bradycardia syndromes. Epinephrine is now favored as the second agent or as a substitute to NE. Phenylephrine is no longer recommended unless there is contraindication to using NE, the patient has a high cardiac output, or it is used as a salvage therapy. Vasopressin is considered only an adjunctive agent to NE and should never be used alone.
Recommendations regarding corticosteroid therapy remain largely unchanged from 2008 SCC guidelines, which only support their use when adequate volume resuscitation and vasopressor support has failed to achieve hemodynamic stability. Glucose control is recommended but at the new target of achieving a level of <180 mg/dL, up from a previous target of <150 mg/dL.
Notably, recombinant human activated protein C was completely omitted from the 2012 guidelines, prompted by the voluntary removal of the drug by the manufacturer after failing to show benefit. Use of selenium and intravenous immunoglobulin received comment, but there is insufficient evidence supporting their benefit at the current time. They also encourage clinicians to incorporate goals of care and end-of-life issues into the treatment plan and discuss this with patients and/or surrogates early in treatment.
Guideline Analysis
Prior versions of the SSC guidelines have been met with a fair amount of skepticism.8 Much of the criticism is based on the industry sponsorship of the 2004 version, the lack of transparency regarding potential conflicts of interest of the committee members, and that the bundle recommendations largely were based on only one trial and, therefore, not evidenced-based.9 The 2012 SSC committee seems to have addressed these issues as the guidelines are free of commercial sponsorship in the 2008 and current versions. They also rigorously applied the GRADE system to methodically assess the strength and quality of supporting evidence. The result is a set of guidelines that are partially evidence-based and partially based on expert opinion, but this is clearly delineated in these newest guidelines. This provides clinicians with a clear and concise recommended approach to the patient with severe sepsis and septic shock.
The guidelines continue to place a heavy emphasis on three- and six-hour treatment bundles, and with the assistance of the Institute for Health Care Improvement efforts to improve implementation of the bundle, they are already are widespread with an eye to expand across the country. The components of the three-hour treatment bundle (lactate measurement, blood cultures prior to initiation of antibiotics, broad-spectrum antibiotics, and IV crystalloids for hypotension or for a lactate of >4 mmol/L) recommended by the SSC have not changed substantially since 2008. The one exception is the rate at which IV crystalloid should be administered of 30 mL/kg, which is up from 20 mL/kg. Only time will tell how this change will affect bundle compliance or reduce mortality. But this does pose a significant challenge to quality and performance improvement groups accustomed to tracking compliance with IV fluid administration under the old standard and the educational campaigns associated with a change.
It appears that the SSC is here to stay, now in its third iteration. The lasting legacy of the SSC guidelines might not rest with the content of the guidelines, per se, but in raising awareness of severe sepsis and septic shock in a way that had not previously been considered.
HM Takeaways
The revised 2012 SCC updates bring some new tools to the clinician for early recognition and effective management of patients with sepsis. The push for institutions to adopt screening and performance measures reflects a general trend in health care to create high-performance systems. As these new guidelines are put into practice, there are several changes that might require augmentation of quality metrics being tracked at institutions nationally and internationally.
Dr. Pendharker is assistant professor of medicine in the division of hospital medicine at the University of California San Francisco and San Francisco General Hospital. Dr. Gomez is assistant professor of medicine in the division of pulmonary and critical care medicine at UCSF and San Francisco General Hospital.
References
- Hall MJ, Williams SN, DeFrances CJ, et al. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011:1-8.
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580-637.
- Jansen TC, van Bommel J, Schoonderbeek FJ, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752-761.
- Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA. 2010;303:739-746.
- Levy MM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367-374.
- Guidet B, Martinet O, Boulain T, et al. Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care. 2012;16:R94.
- Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367:124-134.
- Marik PE. Surviving sepsis: going beyond the guidelines. Ann Intensive Care. 2011;1:17.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
Background
Sepsis is a clinical syndrome with systemic effects that can progress to severe sepsis and/or septic shock. The incidence of severe sepsis and septic shock is rising in the United States, and these syndromes are associated with significant morbidity and a mortality rate as high as 25% to 35%.1 In fact, sepsis is one of the 10 leading causes of death in the U.S., accounting for 2% of hospital admissions but 17% of in-hospital deaths.1
The main principles of effective treatment for severe sepsis and septic shock are timely recognition and early aggressive therapy. Launched in 2002, the Surviving Sepsis Campaign (SSC) was the result of a collaboration of three professional societies. The goal of the SSC collaborative was to reduce mortality from severe sepsis and septic shock by 25%. To that end, the SSC convened representatives from several international societies to develop a set of evidence-based guidelines as a means of guiding clinicians in optimizing management of patients with severe sepsis and septic shock. Since the original publication of the SSC guidelines in 2004, there have been two updates—one in 2008 and one in February 2013.2
Guideline Updates
Quantitative, protocol-driven initial resuscitation in the first six hours for patients with severe sepsis and septic shock remains a high-level recommendation, but SSC has added normalization of the lactate level as a resuscitation goal. This new suggestion is based on two studies published since the 2008 SCC guidelines that showed noninferiority to previously established goals and absolute mortality benefit.3,4
There is a new focus on screening for sepsis and the use of hospital-based performance-improvement programs, which were not previously addressed in the 2008 SCC guidelines. Patients with suspected infections and who are seriously ill should be screened in order to identify sepsis early during the hospital course. Additionally, it is recommended that hospitals implement performance-improvement measures by which multidisciplinary teams can address treatment of sepsis by improving compliance with the SSC bundles, citing their own data as the model but ultimately leaving this recommendation as ungradable in regards to the quality of available supporting evidence.5
Cultures drawn before antibiotics and early imaging to confirm potential sources are still recommended, but the committee has added the use of one: 3 beta D-glucan and the mannan antigen and anti-mannan antibody assays when considering invasive candidiasis as your infective agent. They do note the known risk of false positive results with these assays and warn that they should be used with caution.
Early, broad-spectrum antibiotic administration within the first hour of presentation was upgraded for severe sepsis and downgraded for septic shock. The decision to initiate double coverage for suspected gram-negative infection is not recommended specifically but can be considered in situations when highly antibiotic resistant pathogens are potentially present. Daily assessment of the appropriate antibiotic regimen remains an important tenet, and the use of low procalcitonin levels as a tool to assist in the decision to discontinue antibiotics has been introduced. Source control is still strongly recommended in the first 12 hours of treatment.
The SSC 2012 guidelines specifically address the rate of fluid administered and the type of fluid that should be used. It is now recommended that a fluid challenge of 30 mL/kg be used for initial resuscitation, but the guidelines leave it up to the clinician to give more fluid if needed. There is a strong push for use of crystalloids rather than colloids during initial resuscitation and thereafter. Disfavor for colloids stemmed from trials showing increased mortality when comparing resuscitation with hydroxyethyl starch versus crystalloid for patients in septic shock.6,7 Albumin, on the other hand, is recommended to resuscitate patients with severe sepsis and septic shock in cases for which large amounts of crystalloid are required.
The 2012 SSC guidelines recommend norepinephrine (NE) alone as the first-line vasopressor in sepsis and no longer include dopamine in this category. In fact, the use of dopamine in septic shock has been downgraded and should only to be considered in patients at low risk of tachyarrhythmia and in bradycardia syndromes. Epinephrine is now favored as the second agent or as a substitute to NE. Phenylephrine is no longer recommended unless there is contraindication to using NE, the patient has a high cardiac output, or it is used as a salvage therapy. Vasopressin is considered only an adjunctive agent to NE and should never be used alone.
Recommendations regarding corticosteroid therapy remain largely unchanged from 2008 SCC guidelines, which only support their use when adequate volume resuscitation and vasopressor support has failed to achieve hemodynamic stability. Glucose control is recommended but at the new target of achieving a level of <180 mg/dL, up from a previous target of <150 mg/dL.
Notably, recombinant human activated protein C was completely omitted from the 2012 guidelines, prompted by the voluntary removal of the drug by the manufacturer after failing to show benefit. Use of selenium and intravenous immunoglobulin received comment, but there is insufficient evidence supporting their benefit at the current time. They also encourage clinicians to incorporate goals of care and end-of-life issues into the treatment plan and discuss this with patients and/or surrogates early in treatment.
Guideline Analysis
Prior versions of the SSC guidelines have been met with a fair amount of skepticism.8 Much of the criticism is based on the industry sponsorship of the 2004 version, the lack of transparency regarding potential conflicts of interest of the committee members, and that the bundle recommendations largely were based on only one trial and, therefore, not evidenced-based.9 The 2012 SSC committee seems to have addressed these issues as the guidelines are free of commercial sponsorship in the 2008 and current versions. They also rigorously applied the GRADE system to methodically assess the strength and quality of supporting evidence. The result is a set of guidelines that are partially evidence-based and partially based on expert opinion, but this is clearly delineated in these newest guidelines. This provides clinicians with a clear and concise recommended approach to the patient with severe sepsis and septic shock.
The guidelines continue to place a heavy emphasis on three- and six-hour treatment bundles, and with the assistance of the Institute for Health Care Improvement efforts to improve implementation of the bundle, they are already are widespread with an eye to expand across the country. The components of the three-hour treatment bundle (lactate measurement, blood cultures prior to initiation of antibiotics, broad-spectrum antibiotics, and IV crystalloids for hypotension or for a lactate of >4 mmol/L) recommended by the SSC have not changed substantially since 2008. The one exception is the rate at which IV crystalloid should be administered of 30 mL/kg, which is up from 20 mL/kg. Only time will tell how this change will affect bundle compliance or reduce mortality. But this does pose a significant challenge to quality and performance improvement groups accustomed to tracking compliance with IV fluid administration under the old standard and the educational campaigns associated with a change.
It appears that the SSC is here to stay, now in its third iteration. The lasting legacy of the SSC guidelines might not rest with the content of the guidelines, per se, but in raising awareness of severe sepsis and septic shock in a way that had not previously been considered.
HM Takeaways
The revised 2012 SCC updates bring some new tools to the clinician for early recognition and effective management of patients with sepsis. The push for institutions to adopt screening and performance measures reflects a general trend in health care to create high-performance systems. As these new guidelines are put into practice, there are several changes that might require augmentation of quality metrics being tracked at institutions nationally and internationally.
Dr. Pendharker is assistant professor of medicine in the division of hospital medicine at the University of California San Francisco and San Francisco General Hospital. Dr. Gomez is assistant professor of medicine in the division of pulmonary and critical care medicine at UCSF and San Francisco General Hospital.
References
- Hall MJ, Williams SN, DeFrances CJ, et al. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011:1-8.
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580-637.
- Jansen TC, van Bommel J, Schoonderbeek FJ, et al. Early lactate-guided therapy in intensive care unit patients: a multicenter, open-label, randomized controlled trial. Am J Respir Crit Care Med. 2010;182:752-761.
- Jones AE, Shapiro NI, Trzeciak S, et al. Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial. JAMA. 2010;303:739-746.
- Levy MM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: results of an international guideline-based performance improvement program targeting severe sepsis. Crit Care Med. 2010;38:367-374.
- Guidet B, Martinet O, Boulain T, et al. Assessment of hemodynamic efficacy and safety of 6% hydroxyethylstarch 130/0.4 vs. 0.9% NaCl fluid replacement in patients with severe sepsis: The CRYSTMAS study. Crit Care. 2012;16:R94.
- Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.42 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367:124-134.
- Marik PE. Surviving sepsis: going beyond the guidelines. Ann Intensive Care. 2011;1:17.
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368-1377.
Physician Reviews of Hospital Medicine-Related Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- BNP-driven fluid management to improve ventilator weaning
- Examining 30-day readmission patterns to reduce repeat hospitalizations
- Impact of hospitalists’ workload on patient safety, care
- Permanent atrial fibrillation is best controlled by diltiazem
- Low-dose thrombolysis effective for pulmonary embolism
- High mortality rate seen in surgical patients requiring CPR
- ED visits common for acute-care patients post-discharge
- Restrictive transfusion strategies effective for upper GI bleeding
- Need for non-ICU acid suppression may be predictable
- Recommended changes for adult immunizations
BNP-Driven Fluid Management Improves Ventilator Weaning
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: In a multicenter randomized controlled trial, 304 patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
30-Day Readmission Patterns for MI, Heart Failure, Pneumonia
Clinical question: Do patterns exist among patients readmitted within 30 days of discharge for acute myocardial infarction (AMI), heart failure, or pneumonia that could provide insight for improving strategies aimed at reducing readmission rates?
Background: Examining readmission timing, diagnoses, and patient demographics might provide information to better guide post-discharge programs aimed at reducing overall readmissions.
Study design: Retrospective review of Centers for Medicare & Medicaid Services (CMS) data.
Setting: Acute-care hospitals.
Synopsis: Using CMS hospitalization data for principal diagnoses of AMI, heart failure, or pneumonia from 2007 through 2009, the authors examined the percentage of 30-day readmissions occurring on each day after discharge; the most common readmission diagnoses; the median time to readmission for common readmission diagnoses; and the relationship between patient demographic characteristics, readmission diagnoses, and timing. They found total readmission rates of 24.8% for heart failure, 19.9% for AMI, and 18.3% for pneumonia. Approximately two-thirds of 30-day readmissions occurred within the first 15 days after discharge for each cohort. Neither readmission diagnoses nor timing varied by patient age, sex, or race.
Although the majority of readmissions do occur soon after discharge, it is important to note that about one-third of all readmissions occur 16 to 30 days after discharge. There also was a diverse spectrum of readmission diagnoses that were not associated with patient demographic characteristics. These findings suggest that current post-discharge strategies aimed at specific diseases or time periods might only address a fraction of the patients at risk for readmission.
Bottom line: Among Medicare patients hospitalized for heart failure, AMI, or pneumonia, 30-day readmissions were frequent throughout the entire period, and readmission diagnoses or timing did not vary by patient age, sex, or race.
Citation: Dharmarajan K, Hsich AF, Lin Z, et al. Diagnosis and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
Workload Might Impact Patient Safety and Quality of Care
Clinical question: Do hospitalists’ workloads affect patient quality of care and safety?
Background: Preventable medical errors contribute to a large number of patient deaths each year. It is unclear if a hospitalist’s clinical workload affects rates of medical errors or patient harm.
Study design: Cross-sectional cohort study.
Setting: Hospitalists enrolled in online physician community QuantiaMD.com.
Synopsis: There has been limited research evaluating the correlation between physician workload and patient safety. An online survey compared the responses of 506 out of 890 enrolled physicians on the impact of average patient census and several outcome measures of quality of care. Some 40% reported that their patient census exceeded their personal safe workload at least once a month. They also reported that less time for patient evaluations led to fewer discussions with patients and family members, more unnecessary medical work-ups, and lower patient satisfaction.
A limitation of this study is that this electronic survey had the potential for selection bias. It also only measured perceptions of safety and quality, and only used standard daytime shifts (excluding night, cross-cover, weekend, and holiday shifts), which might have been associated with significantly different conclusions.
Bottom line: Increase in workload has a negative perceived impact on patient safety and quality of care for attending hospitalists.
Citation: Michtalik HJ, Yeh HC, Pronovost P, et. al. Impact of attending physician workload on patient care: a survey of hospitalists. JAMA Intern Med. 2013;173(5):375-377.
Permanent Atrial Fibrillation Best Controlled by Diltiazem
Clinical question: Is there a difference between beta-blockers and calcium channel blockers for ventricular rate control and arrhythmia-related symptoms in patients with permanent atrial fibrillation?
Background: Rate control with beta-blockers or calcium channel blockers is recommended for the initial therapy of atrial fibrillation. However, studies comparing those drug classes or drugs within them are lacking.
Study design: Prospective, randomized, investigator-blind crossover study.
Setting: Majority of patients from an atrial fibrillation outpatient clinic at Baerum Hospital in Norway.
Synopsis: The RATe Control in Atrial Fibrillation (RATAF) study included 60 participants with permanent atrial fibrillation. The goal of the study was to compare the efficacy of diltiazem at 360 mg/day, verapamil at 240 mg/day, metoprolol at 100 mg/day, and carvedilol at 25mg/day on ventricular heart rate and related symptoms in atrial fibrillation. Patients had a mean age of 71, atrial fibrillation for more than three months, and mean heart rate of 96 beats/minute. Exclusion criteria included the presence of congestive heart failure or ischemic heart disease with the need for other medications that could compromise the study.
From this study, diltiazem was shown to have the greatest effect in lowering heart rate, and those patients taking this medication had decreased symptoms related to atrial fibrillation. Hospitalists should not rely solely on this study for their treatment choice in all atrial fibrillation patients, but in certain populations, they should consider diltiazem as their first-line drug.
Bottom line: Diltiazem was shown to have the greatest reduction in heart rate and symptoms related to permanent atrial fibrillation.
Citation: Ulimoen SR, Enger S, Carlson J, et al. Comparison of four single-drug regimens on ventricular rate and arrhythmia-related symptoms in patients with permanent atrial fibrillation. Am J Cardiol. 2013:111(2):225-230.
Low-Dose Thrombolysis Effective in Moderate Pulmonary Embolism
Clinical question: Can low-dose tissue plasminogen activator (tPA) help reduce pulmonary artery pressure in those with moderate pulmonary embolism (PE)?
Background: Studies have shown full-dose thrombolysis can effectively decrease pulmonary artery pressure in patients with massive PE. However, there are limited data regarding low-dose or “safe dose” thrombolytic therapy and its effect on pulmonary artery pressure.
Study design: Prospective, controlled, randomized study.
Setting: Single center.
Synopsis: The Moderate Pulmonary Embolism Treated with Thrombolysis (MOPETT) study enrolled patients with moderate PE, defined as signs and symptoms of PE plus computed tomographic pulmonary angiographic involvement of > 70% involvement of thrombus in ≥2 lobar or left/right main pulmonary arteries or high probability ventilation/perfusion scan (mismatch in ≥2 lobes). Patients in the thrombolysis group (n=61) were given low-dose tPA (100 mg tPA) and anticoagulation vs. the control group (n=60), which received only anticoagulation.
The study ran for 22 months, and the primary end points were pulmonary hypertension and recurrent PE. After analysis, low-dose thrombolysis was shown to significantly decrease pulmonary artery pressure and occurrence of recurrent PE compared to the control group.
This study demonstrates that, while the decision to use thrombolytics should always be made cautiously, hospitalists can consider low-dose thrombolysis in patients with moderate PE.
Bottom line: Low-dose thrombolysis, in addition to anticoagulation, in patients with moderate PE decreases pulmonary hypertension and recurrent PE.
Citation: Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” trial). Am J Cardiol. 2013;111(2):273-277.
High Mortality in Surgical Patients Requiring CPR
Clinical question: What are the incidence, characteristics, and 30-day-outcomes of CPR in surgical patients?
Background: Most studies of CPR are based on the medical population, and little is known about the utilization, risk factors, and outcomes of CPR in surgical patients.
Study design: Retrospective cohort study.
Setting: Two hundred fifty U.S. hospitals in the American College of Surgeons’ National Surgical Quality Improvement Program.
Synopsis: A total of 1.3 million surgical cases were studied in the data set. The overall incidence was 1 event per 203 cases. Most patients (77.6%) experienced a complication and did so on or before the day of CPR in three-fourths of cases. The incidence of CPR was the highest for cardiac surgery patients. Patients who received CPR had a mortality rate of 71.6%. Mortality rates of CPR patients increased with more comorbidities.
Additionally, older age and an American Society of Anesthesiologists (ASA) class of 5 was associated with higher mortality.
Limitations of this study included coding flaws in data collection, lack of capture of resuscitation-related injuries, and failure to account for changes in DNR orders.
Hospitalists should be mindful of risk factors contributing to CPR in surgical patients when performing perioperative evaluations.
Bottom line: Surgical patients who experience CPR have a high mortality rate, but many of these patients have pre-arrest complications that can be preventable.
Citation: Kazaure HS, Roman SA, Rosenthal RA, Sosa, JA. Cardiac arrest among surgical patients. JAMA Surg. 2013;148(1):14-21.
Emergency Department Visits are Frequent Post-Discharge
Clinical question: What role do ED visits contribute to the overall use of acute-care services within 30 days of hospital discharge?
Background: Hospital readmissions within 30 days of discharge are a marker of the quality of care and reflect the effectiveness of the discharge process. ED visits are also a marker of hospital-based acute care following discharge, but little is known about the role of the ED during the post-discharge period.
Study design: Prospective study.
Setting: Acute-care hospitals in California, Florida, and Nebraska.
Synopsis: Using the Healthcare Cost and Utilization Project state inpatient and ED databases, all discharges between July 1, 2008, and Sept. 31, 2009, were evaluated for residents aged 18 years or older from three hospitals in three states. After exclusions, 5 million index hospitalizations among 4 million unique patients were studied.
Approximately 40% of the more than 1 million post-discharge acute-care encounters involved a visit to the ED.
Limitations of this study include that the data was derived from only three states, and only hospital-based acute-care visits were measured (i.e. visits to physician offices were not included). As hospitalists, we are responsible for discharges and care transitions. Being sensitive to the common medical conditions resulting in post-discharge ED encounters might improve care transitions.
Bottom line: Hospital readmission rates underestimate ED use following discharge.
Citation: Vashi AA, Fox JP, Carr BG, et al. Use of hospital-based acute care among patients recently discharged from the hospital. JAMA. 2013;309(4):364-371.
Restrictive Transfusion Strategy Beneficial in Upper GI Bleeding
Clinical question: What is the hemoglobin threshold for transfusion of red cells in patients with acute upper GI bleeding?
Background: Controlled trials have shown that restrictive transfusion strategies (Hgb<7) are as effective as liberal transfusion strategies (Hgb<9) in critically ill patients. These studies have excluded patients with GI bleeding. In cases for which GI is not severe, the safest transfusion strategy is controversial.
Study design: Single-center study at Hospital de la Santa Creu i Sant Pau, Barcelona, Spain.
Synopsis: A total of 921 adult patients with acute upper GI bleeding were enrolled and assigned: 461 to a restrictive transfusion strategy (hemoglobin<7) and 460 to a liberal strategy (hemoglobin<9). Patients with massive exsanguinating bleeding, acute coronary syndrome, peripheral vasculopathy, stroke, transient ischemic attack, lower GI bleed, recent trauma or surgery, or low risk of rebleeding were excluded. The primary outcome measure was the rate of death from any cause within the first 45 days.
Secondary outcomes included the rate of further bleeding and the rate of in-hospital complications.
Statistically significant benefit in following a restrictive versus liberal strategy was demonstrated in all major outcomes: mortality (5% vs, 9%, P=0.02), rate of further bleeding (10% vs 18%, P=0.01), and rate of complications (40% vs. 48%, P=0.02).
The study is limited by its inability to be generalized to all patients with acute GI bleeding, as patients with massive exsanguinating bleeds and those with low risk of rebleeding were excluded.
Bottom line: Restrictive transfusion (Hgb<7) significantly improved outcomes for patients with acute upper GI bleeding.
Citation: Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11-21.
Need for Non-ICU Acid Suppression Might Be Predictable
Clinical question: What are the risk factors for nosocomial bleeding in non-critically-ill patients?
Background: Acid-suppressive medication has been shown to reduce the incidence of nosocomial GI bleed in the ICU, but current guidelines recommend against its use in non-critically-ill patients. However, a subgroup of these patients might possess a high enough risk for GI bleed that prophylaxis is warranted.
Study design: Cohort study.
Setting: Academic medical center in Boston.
Synopsis: A total of 75,723 admissions of adult patients hospitalized for three or more days were included. Exclusion criteria included primary discharge diagnosis of GI bleed; principal procedure code of cardiac catheterization; and bleeding episodes occurring while in the ICU or within 48 hours of transfer out of the ICU. The primary outcome was nosocomial GI bleed (>24 hours after admission) occurring outside the ICU.
Nosocomial GI bleeding occurred in 203 patients (0.27%). Independent risk factors for bleeding included age >60, male sex, liver disease, acute renal failure, sepsis, being on a medicine service, prophylactic anticoagulation, and coagulopathy. Based on the data, a scoring system was created that identified a high-risk group in whom the number needed to treat with acid-suppressive medication to prevent one bleed was 48.
The major limitations of this study are its observational nature and the need for validation of the proposed scoring system.
Bottom line: Risk for nosocomial GI bleeding appears predictable and supports the selective use of prophylactic acid suppression in non-critically-ill patients.
Citation: Herzig SJ, Rothberg MB, Feinbloom DB, et al. Risk factors for nosocomial gastrointestinal bleeding and use of acid-suppressive medication in non-critically ill patients. J Gen Intern Med. 2013; January 5. [Epub ahead of print].
Additions, Modifications, and Clarifications Regarding Adult Immunization
Clinical question: What are the changes to the recommended Adult Immunization Schedule for 2013?
Background: Despite the known public health benefits of immunization, adult vaccination rates remain low. The positive impact of strong provider recommendations regarding vaccines underscores the importance of provider awareness of vaccine schedules, precautions, and contraindications.
Study design: Annual Advisory Committee on Immunization Practices (ACIP) review.
Setting: Data from 2011 National Health Interview Survey.
Synopsis: Highlighted changes include: 1) a single dose of pneumococcal 13-valent conjugate (PCV13) vaccine is now recommended for all individuals over the age of 19 with qualifying conditions; 2) clarification regarding pneumococcal polysaccharide (PPSV23) vaccine illustrates that high-risk individuals will receive up to three doses (one or two doses prior to age 65, plus an additional dose after the age of 65); 3) one dose of tetanus, diphtheria, and acellular pertussis (Tdap) vaccine is now recommended for all adults, including individuals age >65; 4) pregnant woman are advised to receive Tdap between 27 and 36 weeks’ gestation, with each pregnancy to provide protection to their newborn in the first months of life; 5) quadrivalent formulations of the live attenuated influenza vaccine (LAIV) and most likely the inactivated influenza vaccine (IIV) will be available in the 2013-2014 influenza season to increase cross-reactive protection against influenza B; and 6) both injection and noninjection illicit drug users are recommended to receive hepatitis A vaccine.
Bottom line: Expanded recommendations for adult immunization provide more opportunities for the practicing hospitalist to improve vaccine capture.
Citation: Advisory Committee on Immunization Practices. Recommended adult immunization schedule: United States, 2013. Ann Int Med. 2013;158(3):191-199.
In This Edition
Literature At A Glance
A guide to this month’s studies
- BNP-driven fluid management to improve ventilator weaning
- Examining 30-day readmission patterns to reduce repeat hospitalizations
- Impact of hospitalists’ workload on patient safety, care
- Permanent atrial fibrillation is best controlled by diltiazem
- Low-dose thrombolysis effective for pulmonary embolism
- High mortality rate seen in surgical patients requiring CPR
- ED visits common for acute-care patients post-discharge
- Restrictive transfusion strategies effective for upper GI bleeding
- Need for non-ICU acid suppression may be predictable
- Recommended changes for adult immunizations
BNP-Driven Fluid Management Improves Ventilator Weaning
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: In a multicenter randomized controlled trial, 304 patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
30-Day Readmission Patterns for MI, Heart Failure, Pneumonia
Clinical question: Do patterns exist among patients readmitted within 30 days of discharge for acute myocardial infarction (AMI), heart failure, or pneumonia that could provide insight for improving strategies aimed at reducing readmission rates?
Background: Examining readmission timing, diagnoses, and patient demographics might provide information to better guide post-discharge programs aimed at reducing overall readmissions.
Study design: Retrospective review of Centers for Medicare & Medicaid Services (CMS) data.
Setting: Acute-care hospitals.
Synopsis: Using CMS hospitalization data for principal diagnoses of AMI, heart failure, or pneumonia from 2007 through 2009, the authors examined the percentage of 30-day readmissions occurring on each day after discharge; the most common readmission diagnoses; the median time to readmission for common readmission diagnoses; and the relationship between patient demographic characteristics, readmission diagnoses, and timing. They found total readmission rates of 24.8% for heart failure, 19.9% for AMI, and 18.3% for pneumonia. Approximately two-thirds of 30-day readmissions occurred within the first 15 days after discharge for each cohort. Neither readmission diagnoses nor timing varied by patient age, sex, or race.
Although the majority of readmissions do occur soon after discharge, it is important to note that about one-third of all readmissions occur 16 to 30 days after discharge. There also was a diverse spectrum of readmission diagnoses that were not associated with patient demographic characteristics. These findings suggest that current post-discharge strategies aimed at specific diseases or time periods might only address a fraction of the patients at risk for readmission.
Bottom line: Among Medicare patients hospitalized for heart failure, AMI, or pneumonia, 30-day readmissions were frequent throughout the entire period, and readmission diagnoses or timing did not vary by patient age, sex, or race.
Citation: Dharmarajan K, Hsich AF, Lin Z, et al. Diagnosis and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
Workload Might Impact Patient Safety and Quality of Care
Clinical question: Do hospitalists’ workloads affect patient quality of care and safety?
Background: Preventable medical errors contribute to a large number of patient deaths each year. It is unclear if a hospitalist’s clinical workload affects rates of medical errors or patient harm.
Study design: Cross-sectional cohort study.
Setting: Hospitalists enrolled in online physician community QuantiaMD.com.
Synopsis: There has been limited research evaluating the correlation between physician workload and patient safety. An online survey compared the responses of 506 out of 890 enrolled physicians on the impact of average patient census and several outcome measures of quality of care. Some 40% reported that their patient census exceeded their personal safe workload at least once a month. They also reported that less time for patient evaluations led to fewer discussions with patients and family members, more unnecessary medical work-ups, and lower patient satisfaction.
A limitation of this study is that this electronic survey had the potential for selection bias. It also only measured perceptions of safety and quality, and only used standard daytime shifts (excluding night, cross-cover, weekend, and holiday shifts), which might have been associated with significantly different conclusions.
Bottom line: Increase in workload has a negative perceived impact on patient safety and quality of care for attending hospitalists.
Citation: Michtalik HJ, Yeh HC, Pronovost P, et. al. Impact of attending physician workload on patient care: a survey of hospitalists. JAMA Intern Med. 2013;173(5):375-377.
Permanent Atrial Fibrillation Best Controlled by Diltiazem
Clinical question: Is there a difference between beta-blockers and calcium channel blockers for ventricular rate control and arrhythmia-related symptoms in patients with permanent atrial fibrillation?
Background: Rate control with beta-blockers or calcium channel blockers is recommended for the initial therapy of atrial fibrillation. However, studies comparing those drug classes or drugs within them are lacking.
Study design: Prospective, randomized, investigator-blind crossover study.
Setting: Majority of patients from an atrial fibrillation outpatient clinic at Baerum Hospital in Norway.
Synopsis: The RATe Control in Atrial Fibrillation (RATAF) study included 60 participants with permanent atrial fibrillation. The goal of the study was to compare the efficacy of diltiazem at 360 mg/day, verapamil at 240 mg/day, metoprolol at 100 mg/day, and carvedilol at 25mg/day on ventricular heart rate and related symptoms in atrial fibrillation. Patients had a mean age of 71, atrial fibrillation for more than three months, and mean heart rate of 96 beats/minute. Exclusion criteria included the presence of congestive heart failure or ischemic heart disease with the need for other medications that could compromise the study.
From this study, diltiazem was shown to have the greatest effect in lowering heart rate, and those patients taking this medication had decreased symptoms related to atrial fibrillation. Hospitalists should not rely solely on this study for their treatment choice in all atrial fibrillation patients, but in certain populations, they should consider diltiazem as their first-line drug.
Bottom line: Diltiazem was shown to have the greatest reduction in heart rate and symptoms related to permanent atrial fibrillation.
Citation: Ulimoen SR, Enger S, Carlson J, et al. Comparison of four single-drug regimens on ventricular rate and arrhythmia-related symptoms in patients with permanent atrial fibrillation. Am J Cardiol. 2013:111(2):225-230.
Low-Dose Thrombolysis Effective in Moderate Pulmonary Embolism
Clinical question: Can low-dose tissue plasminogen activator (tPA) help reduce pulmonary artery pressure in those with moderate pulmonary embolism (PE)?
Background: Studies have shown full-dose thrombolysis can effectively decrease pulmonary artery pressure in patients with massive PE. However, there are limited data regarding low-dose or “safe dose” thrombolytic therapy and its effect on pulmonary artery pressure.
Study design: Prospective, controlled, randomized study.
Setting: Single center.
Synopsis: The Moderate Pulmonary Embolism Treated with Thrombolysis (MOPETT) study enrolled patients with moderate PE, defined as signs and symptoms of PE plus computed tomographic pulmonary angiographic involvement of > 70% involvement of thrombus in ≥2 lobar or left/right main pulmonary arteries or high probability ventilation/perfusion scan (mismatch in ≥2 lobes). Patients in the thrombolysis group (n=61) were given low-dose tPA (100 mg tPA) and anticoagulation vs. the control group (n=60), which received only anticoagulation.
The study ran for 22 months, and the primary end points were pulmonary hypertension and recurrent PE. After analysis, low-dose thrombolysis was shown to significantly decrease pulmonary artery pressure and occurrence of recurrent PE compared to the control group.
This study demonstrates that, while the decision to use thrombolytics should always be made cautiously, hospitalists can consider low-dose thrombolysis in patients with moderate PE.
Bottom line: Low-dose thrombolysis, in addition to anticoagulation, in patients with moderate PE decreases pulmonary hypertension and recurrent PE.
Citation: Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” trial). Am J Cardiol. 2013;111(2):273-277.
High Mortality in Surgical Patients Requiring CPR
Clinical question: What are the incidence, characteristics, and 30-day-outcomes of CPR in surgical patients?
Background: Most studies of CPR are based on the medical population, and little is known about the utilization, risk factors, and outcomes of CPR in surgical patients.
Study design: Retrospective cohort study.
Setting: Two hundred fifty U.S. hospitals in the American College of Surgeons’ National Surgical Quality Improvement Program.
Synopsis: A total of 1.3 million surgical cases were studied in the data set. The overall incidence was 1 event per 203 cases. Most patients (77.6%) experienced a complication and did so on or before the day of CPR in three-fourths of cases. The incidence of CPR was the highest for cardiac surgery patients. Patients who received CPR had a mortality rate of 71.6%. Mortality rates of CPR patients increased with more comorbidities.
Additionally, older age and an American Society of Anesthesiologists (ASA) class of 5 was associated with higher mortality.
Limitations of this study included coding flaws in data collection, lack of capture of resuscitation-related injuries, and failure to account for changes in DNR orders.
Hospitalists should be mindful of risk factors contributing to CPR in surgical patients when performing perioperative evaluations.
Bottom line: Surgical patients who experience CPR have a high mortality rate, but many of these patients have pre-arrest complications that can be preventable.
Citation: Kazaure HS, Roman SA, Rosenthal RA, Sosa, JA. Cardiac arrest among surgical patients. JAMA Surg. 2013;148(1):14-21.
Emergency Department Visits are Frequent Post-Discharge
Clinical question: What role do ED visits contribute to the overall use of acute-care services within 30 days of hospital discharge?
Background: Hospital readmissions within 30 days of discharge are a marker of the quality of care and reflect the effectiveness of the discharge process. ED visits are also a marker of hospital-based acute care following discharge, but little is known about the role of the ED during the post-discharge period.
Study design: Prospective study.
Setting: Acute-care hospitals in California, Florida, and Nebraska.
Synopsis: Using the Healthcare Cost and Utilization Project state inpatient and ED databases, all discharges between July 1, 2008, and Sept. 31, 2009, were evaluated for residents aged 18 years or older from three hospitals in three states. After exclusions, 5 million index hospitalizations among 4 million unique patients were studied.
Approximately 40% of the more than 1 million post-discharge acute-care encounters involved a visit to the ED.
Limitations of this study include that the data was derived from only three states, and only hospital-based acute-care visits were measured (i.e. visits to physician offices were not included). As hospitalists, we are responsible for discharges and care transitions. Being sensitive to the common medical conditions resulting in post-discharge ED encounters might improve care transitions.
Bottom line: Hospital readmission rates underestimate ED use following discharge.
Citation: Vashi AA, Fox JP, Carr BG, et al. Use of hospital-based acute care among patients recently discharged from the hospital. JAMA. 2013;309(4):364-371.
Restrictive Transfusion Strategy Beneficial in Upper GI Bleeding
Clinical question: What is the hemoglobin threshold for transfusion of red cells in patients with acute upper GI bleeding?
Background: Controlled trials have shown that restrictive transfusion strategies (Hgb<7) are as effective as liberal transfusion strategies (Hgb<9) in critically ill patients. These studies have excluded patients with GI bleeding. In cases for which GI is not severe, the safest transfusion strategy is controversial.
Study design: Single-center study at Hospital de la Santa Creu i Sant Pau, Barcelona, Spain.
Synopsis: A total of 921 adult patients with acute upper GI bleeding were enrolled and assigned: 461 to a restrictive transfusion strategy (hemoglobin<7) and 460 to a liberal strategy (hemoglobin<9). Patients with massive exsanguinating bleeding, acute coronary syndrome, peripheral vasculopathy, stroke, transient ischemic attack, lower GI bleed, recent trauma or surgery, or low risk of rebleeding were excluded. The primary outcome measure was the rate of death from any cause within the first 45 days.
Secondary outcomes included the rate of further bleeding and the rate of in-hospital complications.
Statistically significant benefit in following a restrictive versus liberal strategy was demonstrated in all major outcomes: mortality (5% vs, 9%, P=0.02), rate of further bleeding (10% vs 18%, P=0.01), and rate of complications (40% vs. 48%, P=0.02).
The study is limited by its inability to be generalized to all patients with acute GI bleeding, as patients with massive exsanguinating bleeds and those with low risk of rebleeding were excluded.
Bottom line: Restrictive transfusion (Hgb<7) significantly improved outcomes for patients with acute upper GI bleeding.
Citation: Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11-21.
Need for Non-ICU Acid Suppression Might Be Predictable
Clinical question: What are the risk factors for nosocomial bleeding in non-critically-ill patients?
Background: Acid-suppressive medication has been shown to reduce the incidence of nosocomial GI bleed in the ICU, but current guidelines recommend against its use in non-critically-ill patients. However, a subgroup of these patients might possess a high enough risk for GI bleed that prophylaxis is warranted.
Study design: Cohort study.
Setting: Academic medical center in Boston.
Synopsis: A total of 75,723 admissions of adult patients hospitalized for three or more days were included. Exclusion criteria included primary discharge diagnosis of GI bleed; principal procedure code of cardiac catheterization; and bleeding episodes occurring while in the ICU or within 48 hours of transfer out of the ICU. The primary outcome was nosocomial GI bleed (>24 hours after admission) occurring outside the ICU.
Nosocomial GI bleeding occurred in 203 patients (0.27%). Independent risk factors for bleeding included age >60, male sex, liver disease, acute renal failure, sepsis, being on a medicine service, prophylactic anticoagulation, and coagulopathy. Based on the data, a scoring system was created that identified a high-risk group in whom the number needed to treat with acid-suppressive medication to prevent one bleed was 48.
The major limitations of this study are its observational nature and the need for validation of the proposed scoring system.
Bottom line: Risk for nosocomial GI bleeding appears predictable and supports the selective use of prophylactic acid suppression in non-critically-ill patients.
Citation: Herzig SJ, Rothberg MB, Feinbloom DB, et al. Risk factors for nosocomial gastrointestinal bleeding and use of acid-suppressive medication in non-critically ill patients. J Gen Intern Med. 2013; January 5. [Epub ahead of print].
Additions, Modifications, and Clarifications Regarding Adult Immunization
Clinical question: What are the changes to the recommended Adult Immunization Schedule for 2013?
Background: Despite the known public health benefits of immunization, adult vaccination rates remain low. The positive impact of strong provider recommendations regarding vaccines underscores the importance of provider awareness of vaccine schedules, precautions, and contraindications.
Study design: Annual Advisory Committee on Immunization Practices (ACIP) review.
Setting: Data from 2011 National Health Interview Survey.
Synopsis: Highlighted changes include: 1) a single dose of pneumococcal 13-valent conjugate (PCV13) vaccine is now recommended for all individuals over the age of 19 with qualifying conditions; 2) clarification regarding pneumococcal polysaccharide (PPSV23) vaccine illustrates that high-risk individuals will receive up to three doses (one or two doses prior to age 65, plus an additional dose after the age of 65); 3) one dose of tetanus, diphtheria, and acellular pertussis (Tdap) vaccine is now recommended for all adults, including individuals age >65; 4) pregnant woman are advised to receive Tdap between 27 and 36 weeks’ gestation, with each pregnancy to provide protection to their newborn in the first months of life; 5) quadrivalent formulations of the live attenuated influenza vaccine (LAIV) and most likely the inactivated influenza vaccine (IIV) will be available in the 2013-2014 influenza season to increase cross-reactive protection against influenza B; and 6) both injection and noninjection illicit drug users are recommended to receive hepatitis A vaccine.
Bottom line: Expanded recommendations for adult immunization provide more opportunities for the practicing hospitalist to improve vaccine capture.
Citation: Advisory Committee on Immunization Practices. Recommended adult immunization schedule: United States, 2013. Ann Int Med. 2013;158(3):191-199.
In This Edition
Literature At A Glance
A guide to this month’s studies
- BNP-driven fluid management to improve ventilator weaning
- Examining 30-day readmission patterns to reduce repeat hospitalizations
- Impact of hospitalists’ workload on patient safety, care
- Permanent atrial fibrillation is best controlled by diltiazem
- Low-dose thrombolysis effective for pulmonary embolism
- High mortality rate seen in surgical patients requiring CPR
- ED visits common for acute-care patients post-discharge
- Restrictive transfusion strategies effective for upper GI bleeding
- Need for non-ICU acid suppression may be predictable
- Recommended changes for adult immunizations
BNP-Driven Fluid Management Improves Ventilator Weaning
Clinical question: Does fluid management guided by daily plasma natriuretic peptide-driven (BNP) levels in mechanically ventilated patients improve weaning outcomes compared with usual therapy dictated by clinical acumen?
Background: Ventilator weaning contributes at least 40% of the total duration of mechanical ventilation; strategies aimed at optimizing this process could provide substantial benefit. Previous studies have demonstrated that BNP levels prior to ventilator weaning independently predict weaning failure. No current objective practical guide to fluid management during ventilator weaning exists.
Study design: Randomized controlled trial.
Setting: Multiple international centers.
Synopsis: In a multicenter randomized controlled trial, 304 patients who met specific inclusion and exclusion criteria were randomized to either a BNP-driven or physician-guided strategy for fluid management during ventilator weaning. Patients with renal failure were excluded because of the influence of renal function on BNP levels.
All patients in both groups were ventilated with an automatic computer-driven weaning system to standardize the weaning process. In the BNP-driven group, diuretic use was higher, resulting in a more negative fluid balance and significantly shorter time to successful extubation (58.6 hours vs. 42.2 hours, P=0.03). The effect on weaning time was strongest in patients with left ventricular systolic dysfunction, whereas those with COPD seemed less likely to benefit. The two groups did not differ in baseline characteristics, length of stay, mortality, or development of adverse outcomes of renal failure, shock, or electrolyte disturbances.
Bottom line: Compared with physician-guided fluid management, a BNP-driven fluid management protocol decreased duration of ventilator weaning without significant differences in adverse events, mortality rate, or length of stay between the two groups.
Citation: Dessap AM, Roche-Campo F, Kouatchet A, et al. Natriuretic peptide-driven fluid management during ventilator weaning. Am J Respir Crit Care Med. 2012;186(12):1256-1263.
30-Day Readmission Patterns for MI, Heart Failure, Pneumonia
Clinical question: Do patterns exist among patients readmitted within 30 days of discharge for acute myocardial infarction (AMI), heart failure, or pneumonia that could provide insight for improving strategies aimed at reducing readmission rates?
Background: Examining readmission timing, diagnoses, and patient demographics might provide information to better guide post-discharge programs aimed at reducing overall readmissions.
Study design: Retrospective review of Centers for Medicare & Medicaid Services (CMS) data.
Setting: Acute-care hospitals.
Synopsis: Using CMS hospitalization data for principal diagnoses of AMI, heart failure, or pneumonia from 2007 through 2009, the authors examined the percentage of 30-day readmissions occurring on each day after discharge; the most common readmission diagnoses; the median time to readmission for common readmission diagnoses; and the relationship between patient demographic characteristics, readmission diagnoses, and timing. They found total readmission rates of 24.8% for heart failure, 19.9% for AMI, and 18.3% for pneumonia. Approximately two-thirds of 30-day readmissions occurred within the first 15 days after discharge for each cohort. Neither readmission diagnoses nor timing varied by patient age, sex, or race.
Although the majority of readmissions do occur soon after discharge, it is important to note that about one-third of all readmissions occur 16 to 30 days after discharge. There also was a diverse spectrum of readmission diagnoses that were not associated with patient demographic characteristics. These findings suggest that current post-discharge strategies aimed at specific diseases or time periods might only address a fraction of the patients at risk for readmission.
Bottom line: Among Medicare patients hospitalized for heart failure, AMI, or pneumonia, 30-day readmissions were frequent throughout the entire period, and readmission diagnoses or timing did not vary by patient age, sex, or race.
Citation: Dharmarajan K, Hsich AF, Lin Z, et al. Diagnosis and timing of 30-day readmissions after hospitalization for heart failure, acute myocardial infarction, or pneumonia. JAMA. 2013;309(4):355-363.
Workload Might Impact Patient Safety and Quality of Care
Clinical question: Do hospitalists’ workloads affect patient quality of care and safety?
Background: Preventable medical errors contribute to a large number of patient deaths each year. It is unclear if a hospitalist’s clinical workload affects rates of medical errors or patient harm.
Study design: Cross-sectional cohort study.
Setting: Hospitalists enrolled in online physician community QuantiaMD.com.
Synopsis: There has been limited research evaluating the correlation between physician workload and patient safety. An online survey compared the responses of 506 out of 890 enrolled physicians on the impact of average patient census and several outcome measures of quality of care. Some 40% reported that their patient census exceeded their personal safe workload at least once a month. They also reported that less time for patient evaluations led to fewer discussions with patients and family members, more unnecessary medical work-ups, and lower patient satisfaction.
A limitation of this study is that this electronic survey had the potential for selection bias. It also only measured perceptions of safety and quality, and only used standard daytime shifts (excluding night, cross-cover, weekend, and holiday shifts), which might have been associated with significantly different conclusions.
Bottom line: Increase in workload has a negative perceived impact on patient safety and quality of care for attending hospitalists.
Citation: Michtalik HJ, Yeh HC, Pronovost P, et. al. Impact of attending physician workload on patient care: a survey of hospitalists. JAMA Intern Med. 2013;173(5):375-377.
Permanent Atrial Fibrillation Best Controlled by Diltiazem
Clinical question: Is there a difference between beta-blockers and calcium channel blockers for ventricular rate control and arrhythmia-related symptoms in patients with permanent atrial fibrillation?
Background: Rate control with beta-blockers or calcium channel blockers is recommended for the initial therapy of atrial fibrillation. However, studies comparing those drug classes or drugs within them are lacking.
Study design: Prospective, randomized, investigator-blind crossover study.
Setting: Majority of patients from an atrial fibrillation outpatient clinic at Baerum Hospital in Norway.
Synopsis: The RATe Control in Atrial Fibrillation (RATAF) study included 60 participants with permanent atrial fibrillation. The goal of the study was to compare the efficacy of diltiazem at 360 mg/day, verapamil at 240 mg/day, metoprolol at 100 mg/day, and carvedilol at 25mg/day on ventricular heart rate and related symptoms in atrial fibrillation. Patients had a mean age of 71, atrial fibrillation for more than three months, and mean heart rate of 96 beats/minute. Exclusion criteria included the presence of congestive heart failure or ischemic heart disease with the need for other medications that could compromise the study.
From this study, diltiazem was shown to have the greatest effect in lowering heart rate, and those patients taking this medication had decreased symptoms related to atrial fibrillation. Hospitalists should not rely solely on this study for their treatment choice in all atrial fibrillation patients, but in certain populations, they should consider diltiazem as their first-line drug.
Bottom line: Diltiazem was shown to have the greatest reduction in heart rate and symptoms related to permanent atrial fibrillation.
Citation: Ulimoen SR, Enger S, Carlson J, et al. Comparison of four single-drug regimens on ventricular rate and arrhythmia-related symptoms in patients with permanent atrial fibrillation. Am J Cardiol. 2013:111(2):225-230.
Low-Dose Thrombolysis Effective in Moderate Pulmonary Embolism
Clinical question: Can low-dose tissue plasminogen activator (tPA) help reduce pulmonary artery pressure in those with moderate pulmonary embolism (PE)?
Background: Studies have shown full-dose thrombolysis can effectively decrease pulmonary artery pressure in patients with massive PE. However, there are limited data regarding low-dose or “safe dose” thrombolytic therapy and its effect on pulmonary artery pressure.
Study design: Prospective, controlled, randomized study.
Setting: Single center.
Synopsis: The Moderate Pulmonary Embolism Treated with Thrombolysis (MOPETT) study enrolled patients with moderate PE, defined as signs and symptoms of PE plus computed tomographic pulmonary angiographic involvement of > 70% involvement of thrombus in ≥2 lobar or left/right main pulmonary arteries or high probability ventilation/perfusion scan (mismatch in ≥2 lobes). Patients in the thrombolysis group (n=61) were given low-dose tPA (100 mg tPA) and anticoagulation vs. the control group (n=60), which received only anticoagulation.
The study ran for 22 months, and the primary end points were pulmonary hypertension and recurrent PE. After analysis, low-dose thrombolysis was shown to significantly decrease pulmonary artery pressure and occurrence of recurrent PE compared to the control group.
This study demonstrates that, while the decision to use thrombolytics should always be made cautiously, hospitalists can consider low-dose thrombolysis in patients with moderate PE.
Bottom line: Low-dose thrombolysis, in addition to anticoagulation, in patients with moderate PE decreases pulmonary hypertension and recurrent PE.
Citation: Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” trial). Am J Cardiol. 2013;111(2):273-277.
High Mortality in Surgical Patients Requiring CPR
Clinical question: What are the incidence, characteristics, and 30-day-outcomes of CPR in surgical patients?
Background: Most studies of CPR are based on the medical population, and little is known about the utilization, risk factors, and outcomes of CPR in surgical patients.
Study design: Retrospective cohort study.
Setting: Two hundred fifty U.S. hospitals in the American College of Surgeons’ National Surgical Quality Improvement Program.
Synopsis: A total of 1.3 million surgical cases were studied in the data set. The overall incidence was 1 event per 203 cases. Most patients (77.6%) experienced a complication and did so on or before the day of CPR in three-fourths of cases. The incidence of CPR was the highest for cardiac surgery patients. Patients who received CPR had a mortality rate of 71.6%. Mortality rates of CPR patients increased with more comorbidities.
Additionally, older age and an American Society of Anesthesiologists (ASA) class of 5 was associated with higher mortality.
Limitations of this study included coding flaws in data collection, lack of capture of resuscitation-related injuries, and failure to account for changes in DNR orders.
Hospitalists should be mindful of risk factors contributing to CPR in surgical patients when performing perioperative evaluations.
Bottom line: Surgical patients who experience CPR have a high mortality rate, but many of these patients have pre-arrest complications that can be preventable.
Citation: Kazaure HS, Roman SA, Rosenthal RA, Sosa, JA. Cardiac arrest among surgical patients. JAMA Surg. 2013;148(1):14-21.
Emergency Department Visits are Frequent Post-Discharge
Clinical question: What role do ED visits contribute to the overall use of acute-care services within 30 days of hospital discharge?
Background: Hospital readmissions within 30 days of discharge are a marker of the quality of care and reflect the effectiveness of the discharge process. ED visits are also a marker of hospital-based acute care following discharge, but little is known about the role of the ED during the post-discharge period.
Study design: Prospective study.
Setting: Acute-care hospitals in California, Florida, and Nebraska.
Synopsis: Using the Healthcare Cost and Utilization Project state inpatient and ED databases, all discharges between July 1, 2008, and Sept. 31, 2009, were evaluated for residents aged 18 years or older from three hospitals in three states. After exclusions, 5 million index hospitalizations among 4 million unique patients were studied.
Approximately 40% of the more than 1 million post-discharge acute-care encounters involved a visit to the ED.
Limitations of this study include that the data was derived from only three states, and only hospital-based acute-care visits were measured (i.e. visits to physician offices were not included). As hospitalists, we are responsible for discharges and care transitions. Being sensitive to the common medical conditions resulting in post-discharge ED encounters might improve care transitions.
Bottom line: Hospital readmission rates underestimate ED use following discharge.
Citation: Vashi AA, Fox JP, Carr BG, et al. Use of hospital-based acute care among patients recently discharged from the hospital. JAMA. 2013;309(4):364-371.
Restrictive Transfusion Strategy Beneficial in Upper GI Bleeding
Clinical question: What is the hemoglobin threshold for transfusion of red cells in patients with acute upper GI bleeding?
Background: Controlled trials have shown that restrictive transfusion strategies (Hgb<7) are as effective as liberal transfusion strategies (Hgb<9) in critically ill patients. These studies have excluded patients with GI bleeding. In cases for which GI is not severe, the safest transfusion strategy is controversial.
Study design: Single-center study at Hospital de la Santa Creu i Sant Pau, Barcelona, Spain.
Synopsis: A total of 921 adult patients with acute upper GI bleeding were enrolled and assigned: 461 to a restrictive transfusion strategy (hemoglobin<7) and 460 to a liberal strategy (hemoglobin<9). Patients with massive exsanguinating bleeding, acute coronary syndrome, peripheral vasculopathy, stroke, transient ischemic attack, lower GI bleed, recent trauma or surgery, or low risk of rebleeding were excluded. The primary outcome measure was the rate of death from any cause within the first 45 days.
Secondary outcomes included the rate of further bleeding and the rate of in-hospital complications.
Statistically significant benefit in following a restrictive versus liberal strategy was demonstrated in all major outcomes: mortality (5% vs, 9%, P=0.02), rate of further bleeding (10% vs 18%, P=0.01), and rate of complications (40% vs. 48%, P=0.02).
The study is limited by its inability to be generalized to all patients with acute GI bleeding, as patients with massive exsanguinating bleeds and those with low risk of rebleeding were excluded.
Bottom line: Restrictive transfusion (Hgb<7) significantly improved outcomes for patients with acute upper GI bleeding.
Citation: Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11-21.
Need for Non-ICU Acid Suppression Might Be Predictable
Clinical question: What are the risk factors for nosocomial bleeding in non-critically-ill patients?
Background: Acid-suppressive medication has been shown to reduce the incidence of nosocomial GI bleed in the ICU, but current guidelines recommend against its use in non-critically-ill patients. However, a subgroup of these patients might possess a high enough risk for GI bleed that prophylaxis is warranted.
Study design: Cohort study.
Setting: Academic medical center in Boston.
Synopsis: A total of 75,723 admissions of adult patients hospitalized for three or more days were included. Exclusion criteria included primary discharge diagnosis of GI bleed; principal procedure code of cardiac catheterization; and bleeding episodes occurring while in the ICU or within 48 hours of transfer out of the ICU. The primary outcome was nosocomial GI bleed (>24 hours after admission) occurring outside the ICU.
Nosocomial GI bleeding occurred in 203 patients (0.27%). Independent risk factors for bleeding included age >60, male sex, liver disease, acute renal failure, sepsis, being on a medicine service, prophylactic anticoagulation, and coagulopathy. Based on the data, a scoring system was created that identified a high-risk group in whom the number needed to treat with acid-suppressive medication to prevent one bleed was 48.
The major limitations of this study are its observational nature and the need for validation of the proposed scoring system.
Bottom line: Risk for nosocomial GI bleeding appears predictable and supports the selective use of prophylactic acid suppression in non-critically-ill patients.
Citation: Herzig SJ, Rothberg MB, Feinbloom DB, et al. Risk factors for nosocomial gastrointestinal bleeding and use of acid-suppressive medication in non-critically ill patients. J Gen Intern Med. 2013; January 5. [Epub ahead of print].
Additions, Modifications, and Clarifications Regarding Adult Immunization
Clinical question: What are the changes to the recommended Adult Immunization Schedule for 2013?
Background: Despite the known public health benefits of immunization, adult vaccination rates remain low. The positive impact of strong provider recommendations regarding vaccines underscores the importance of provider awareness of vaccine schedules, precautions, and contraindications.
Study design: Annual Advisory Committee on Immunization Practices (ACIP) review.
Setting: Data from 2011 National Health Interview Survey.
Synopsis: Highlighted changes include: 1) a single dose of pneumococcal 13-valent conjugate (PCV13) vaccine is now recommended for all individuals over the age of 19 with qualifying conditions; 2) clarification regarding pneumococcal polysaccharide (PPSV23) vaccine illustrates that high-risk individuals will receive up to three doses (one or two doses prior to age 65, plus an additional dose after the age of 65); 3) one dose of tetanus, diphtheria, and acellular pertussis (Tdap) vaccine is now recommended for all adults, including individuals age >65; 4) pregnant woman are advised to receive Tdap between 27 and 36 weeks’ gestation, with each pregnancy to provide protection to their newborn in the first months of life; 5) quadrivalent formulations of the live attenuated influenza vaccine (LAIV) and most likely the inactivated influenza vaccine (IIV) will be available in the 2013-2014 influenza season to increase cross-reactive protection against influenza B; and 6) both injection and noninjection illicit drug users are recommended to receive hepatitis A vaccine.
Bottom line: Expanded recommendations for adult immunization provide more opportunities for the practicing hospitalist to improve vaccine capture.
Citation: Advisory Committee on Immunization Practices. Recommended adult immunization schedule: United States, 2013. Ann Int Med. 2013;158(3):191-199.
How Should Acute Alcoholic Hepatitis be Treated?
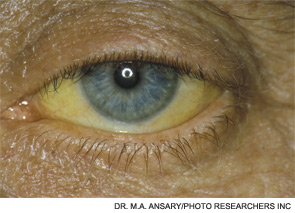
Case
A 53-year-old man with a history of daily alcohol use presents with one week of jaundice. His blood pressure is 95/60 mmHg, pulse 105/minute, and temperature 38.0°C. Examination discloses icterus, ascites, and an enlarged, tender liver. His bilirubin is 9 mg/dl, AST 250 IU/dL, ALT 115 IU/dL, prothromin time 22 seconds, INR 2.7, creatinine 0.9 mg/dL, and leukocyte count 15,000/cu mm with 70% neutrophils. He is admitted with a diagnosis of acute alcoholic hepatitis. How should he be treated?
Background
Hospitalists frequently encounter patients who use alcohol and have abnormal liver tests. Regular, heavy alcohol consumption is associated with a variety of forms of liver disease, including fatty liver, inflammation, hepatic fibrosis, and cirrhosis. The term “alcoholic hepatitis” describes a more severe form of alcohol-related liver disease associated with significant short-term mortality.
Alcoholic hepatitis typically occurs after more than 10 years of regular heavy alcohol use; average consumption in one study was 100 g/day (the equivalent of 10 drinks per day).1 The typical patient presents with recent onset of jaundice, ascites, and proximal muscle loss. Fever and leukocytosis also are common but should prompt an evaluation for infection, especially spontaneous bacterial peritonitis. Liver biopsy in these patients shows steatosis, swollen hepatocytes containing eosinophilic inclusion (Mallory) bodies, and a prominent neutrophilic inflammatory cell infiltrate. Because of the accuracy of clinical diagnosis, biopsy is rarely required, relying instead on clinical and laboratory features for diagnosis (see Table 1, below).
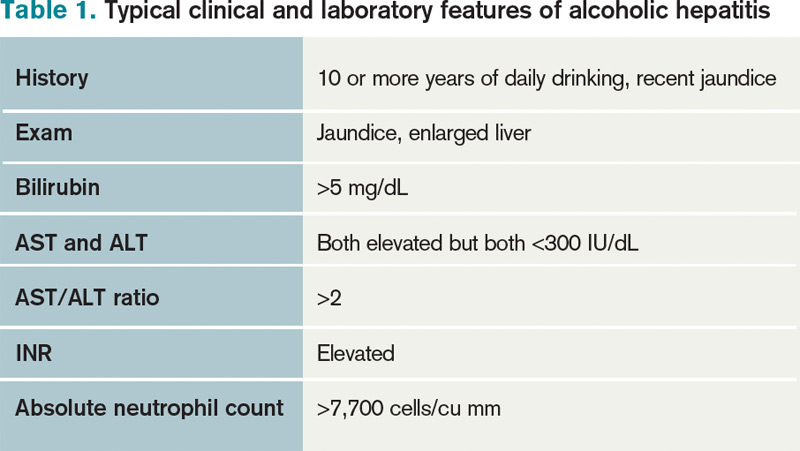
Prognosis can be determined with prediction models. The most common are Model for End-Stage Liver Disease (MELD) and Maddrey’s discriminate score (see Table 2). Several websites allow quick calculation of these scores and provide estimated 30-day or 90-day mortality. These scores can be used to guide therapy.

Review of the Data
How should hospitalists treat this serious illness? The evidence-based literature supporting the efficacy of treatments for alcoholic hepatitis is limited, and expert opinions sometimes conflict.
Abstinence has been shown to improve survival in all stages of alcohol-related liver disease.2 This can be accomplished by admitting this patient population to the hospital. A number of interventions and therapies are available to increase the chance of continued abstinence following discharge (see Table 3).
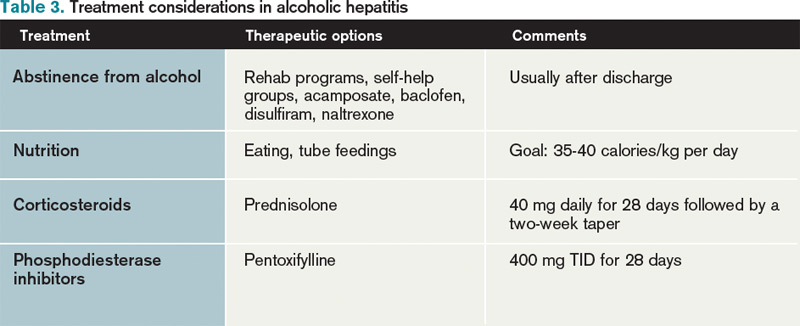
Nutritional support. Protein-calorie malnutrition is seen in up to 90% of patients with cirrhosis.3 The cause of malnutrition in these patients includes decreased caloric intake, metabolic derangements that accompany liver disease, and micronutrient and vitamin deficiencies. Many of these patients rely almost solely on alcohol for caloric intake; this contributes to potassium depletion, which is frequently seen. After admission, these patients are often evaluated for other conditions (such as gastrointestinal bleeding and altered mental status) that require them to be NPO overnight, thus further confounding their malnutrition. Enteral nutritional support was shown in a multicenter study to be associated with reduced infectious complications and improved one-year mortality.4
Little clinical data support specific recommendations for the amount of nutritional support. The American College of Gastroenterology (ACG) recommends 35 calories/kg to 40 calories/kg of body weight per day and a protein intake of 1.2 g/kg to 1.5g/kg per day.5 In an average, 70-kg patient, this is 2,450 to 2,800 calories a day. For patients who are not able to meet these nutritional needs by mouth, enteral feeding with a small-bore (Dobhoff) feeding tube can be used, even in patients with known esophageal varices.
Most of these patients have anorexia and nausea and do not meet these caloric recommendations by eating. Nutritional support is a low-risk intervention that can be provided on almost all inpatient medical care areas. Hospitalists should be attentive to nutritional support early in the hospitalization of these patients.
Corticosteroid therapy is recommended by the ACG for patients with alcoholic hepatitis and a Maddrey’s discriminant function greater than 32.5 There is much debate about this recommendation, as conflicting data about efficacy exist.

A 2008 Cochrane review included clinical trials published before July 2007 that examined corticosteroid use in patients with alcoholic hepatitis. A total of 15 trials with 721 randomized patients were included. The review concluded that corticosteroids did not statistically reduce mortality compared with placebo or no intervention; however, mortality was reduced in the subgroup of patients with Maddrey’s scores greater than 32 and hepatic encephalopathy.6 The review concluded that current evidence does not support the use of corticosteroids in alcoholic hepatitis, and more randomized trials were needed.
Another meta-analysis demonstrated a mortality benefit when the largest studies, which included 221 patients with high Maddrey’s scores, were analyzed separately.7 Contraindications to corticosteroid treatment include active infection, gastrointestinal bleeding, acute pancreatitis, and renal failure. Other concerns about corticosteroids include potential adverse reactions (hyperglycemia) and increased risk of infection. Prednisolone is preferred over prednisone because it is the active drug. The recommended dosage is 40 mg/day for 28 days followed by a taper (20 mg/day for one week, then 10 mg/day for one week).
Some data suggest that if patients on corticosteroid therapy do not demonstrate a decrease in their bilirubin levels by Day 7, they are at higher risk of developing infections, have a poorer prognosis, and that corticosteroid therapy should be stopped.8 Some experts use the Lille model to decide whether to continue corticosteroids. In one study, patients who did not respond to prednisolone did not improve when switched to pentoxifyline.9
Patients discharged on corticosteroids require very careful coordination with outpatient providers as prolonged corticosteroid treatment courses can lead to serious complications and death. Critics of corticosteroid therapy in these patients often cite problems related to prolonged steroid use, especially in patients who do not respond to therapy.10
Pentoxifylline, an oral phosphodiesterase inhibitor, is recommended by the ACG, especially if corticosteroids are contraindicated.5 In 2008, 101 patients with alcoholic hepatitis were enrolled in a double-blind, placebo-controlled trial comparing pentoxifylline and placebo. This study demonstrated that patients who received pentoxifylline had decreased 28-day mortality (24.6% versus 46% receiving placebo). Of those patients who died during the study, only 50% (versus 91% in the placebo group) developed hepatorenal syndrome.11 However, a Cochrane review of all studies with pentoxifylline concluded that no firm conclusions could be drawn.12
One small, randomized trial comparing pentoxifylline with prednisolone demonstrated that pentoxifylline was superior.13 Pentoxifylline can be prescribed to patients who have contraindications to corticosteroid use (infection or gastrointestinal bleeding). The recommended dose is 400 mg orally three times daily (TID) for four weeks. Common side effects are nausea and vomiting. Pentoxifylline cannot be administered by nasogastric tubes and should not be used in patients with recent cerebral or retinal hemorrhage.
Other therapies. Several studies have examined vitamin E, N-acetylcystine, and other antioxidants as treatment for alcoholic hepatitis. No clear benefit has been demonstrated for any of these drugs. Tumor necrosis factor (TNF)-alpha inhibitors (e.g. infliximab) have been studied, but increased mortality was demonstrated and these studies were discontinued. Patients are not usually considered for liver transplantation until they have at least six months of abstinence from alcohol as recommended by the American Society of Transplantation.14
Discharge considerations. No clinical trials have studied optimal timing of discharge. Expert opinion based on clinical experience recommends that patients be kept in the hospital until they are eating, signs of alcohol withdrawal and encephalopathy are absent, and bilirubin is less than 10 mg/dL.14 These patients often are quite sick and hospitalization frequently exceeds 10 days. Careful outpatient follow-up and assistance with continued abstinence is very important.
Back to the Case
The patient fits the typical clinical picture of alcoholic hepatitis. Cessation of alcohol consumption is the most important treatment and is accomplished by admission to the hospital. Because of his daily alcohol consumption, folate, thiamine, multivitamins, and oral vitamin K are ordered. Though he has no symptoms of alcohol withdrawal, a note is added about potential withdrawal to the handoff report.
An infectious workup is completed by ordering blood and urine cultures, a chest X-ray, and performing paracentesis to exclude spontaneous bacterial peritonitis. A dietary consult with calorie count is given, along with a plan to discuss with the patient the importance of consuming at least 2,500 calories a day is made. Tube feedings will be considered if the patient does not meet this goal in 48 hours. Clinical calculators determine his Maddrey’s and MELD scores (50 and 25, respectively). If he is actively bleeding or infected, pentoxifylline (400 mg TID for 28 days) is favored due to its lower-side-effect profile.
His MELD score predicts a 90-day mortality of 43%; a meeting is planned to discuss code status and end-of-life issues with the patient and his family. Due to the severity of his illness, a gastroenterology consultation is recommended.
Bottom Line
Alcoholic hepatitis is a serious disease with significant short-term mortality. Treatment options are limited but include abstinence from alcohol, supplemental nutrition, and, for select patients, pentoxifylline or corticosteroids. Because most transplant centers require six months of abstinence, these patients usually are not eligible for urgent liver transplantation.
Dr. Parada is a clinical instructor and chief medical resident in the Department of Internal Medicine at the University of New Mexico School of Medicine and the University of New Mexico Hospital, Albuquerque. Dr. Pierce is associate professor in the Division of Hospital Medicine at the University of New Mexico School of Medicine and the University of New Mexico Hospital.
References
- Naveau S, Giraud V, Borotto E, Aubert A, Capron F, Chaput JC. Excess weight risk factor for alcoholic liver disease. Hepatology. 1997;25:108-111.
- Pessione F, Ramond MJ, Peters L, et al. Five-year survival predictive factors in patients with excessive alcohol intake and cirrhosis. Effect of alcoholic hepatitis, smoking and abstinence. Liver Int. 2003;23:45-53.
- Mendenhall CL, Anderson S, Weesner RE, Goldberg SJ, Crolic KA. Protein-calorie malnutrition associated with alcoholic hepatitis. Veterans Administration Cooperative Study Group on alcoholic hepatitis. Am J Med. 1984;76:211-222.
- Cabre E, Rodriguez-Iglesias P, Caballeria J, et al. Short- and long-term outcome of severe alcohol-induced hepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology. 2000;32:36-42.
- O’Shea RS, Dasarathy S, McCullough AJ, Practice Guideline Committee of the American Association for the Study of Liver Diseases, Practice Parameters Committee of the American College of Gastroenterology. Alcoholic liver disease. Hepatology. 2010;51:307-328.
- Rambaldi A, Saconato HH, Christensen E, Thorlund K, Wetterslev J, Gluud C. Systematic review: Glucocorticosteroids for alcoholic hepatitis—a Cochrane hepato-biliary group systematic review with meta-analyses and trial sequential analyses of randomized clinical trials. Aliment Pharmacol Ther. 2008;27:1167-1178.
- Mathurin P, Mendenhall CL, Carithers RL Jr., et al. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis (AH): individual data analysis of the last three randomized placebo controlled double blind trials of corticosteroids in severe AH. J Hepatol. 2002;36:480-487.
- Louvet A, Naveau S, Abdelnour M, et al. The Lille model: A new tool for therapeutic strategy in patients with severe alcoholic hepatitis treated with steroids. Hepatology. 2007;45:1348-1354.
- Louvet A, Diaz E, Dharancy S, et al. Early switch topentoxifylline in patients with severe alcoholic hepatitis is inefficient in non-responders to corticosteroids. J Hepatol. 2008;48:465-470.
- Amini M, Runyon BA. Alcoholic hepatitis 2010: A clinician’s guide to diagnosis and therapy. World J Gastroenterol. 2010;16:4905-4912.
- Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil O. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: A double-blind, placebo-controlled trial. Gastroenterology. 2000;119:1637-1648.
- Whitfield K, Rambaldi A, Wetterslev J, Gluud C. Pentoxifylline for alcoholic hepatitis. Cochrane Database Syst Rev. 2009;(4):CD007339.
- De BK, Gangopadhyay S, Dutta D, Baksi SD, Pani A, Ghosh P. Pentoxifylline versus prednisolone for severe alcoholic hepatitis: A randomized controlled trial. World J Gastroenterol. 2009;15:1613-1619.
- Lucey MR, Brown KA, Everson GT, et al. Minimal criteria for placement of adults on the liver transplant waiting list: a report of a national conference organized by the American Society of Transplant Physicians and the American Association for the Study of Liver Diseases. Liver Transpl Surg. 1997;3:628-637.
Case
A 53-year-old man with a history of daily alcohol use presents with one week of jaundice. His blood pressure is 95/60 mmHg, pulse 105/minute, and temperature 38.0°C. Examination discloses icterus, ascites, and an enlarged, tender liver. His bilirubin is 9 mg/dl, AST 250 IU/dL, ALT 115 IU/dL, prothromin time 22 seconds, INR 2.7, creatinine 0.9 mg/dL, and leukocyte count 15,000/cu mm with 70% neutrophils. He is admitted with a diagnosis of acute alcoholic hepatitis. How should he be treated?
Background
Hospitalists frequently encounter patients who use alcohol and have abnormal liver tests. Regular, heavy alcohol consumption is associated with a variety of forms of liver disease, including fatty liver, inflammation, hepatic fibrosis, and cirrhosis. The term “alcoholic hepatitis” describes a more severe form of alcohol-related liver disease associated with significant short-term mortality.
Alcoholic hepatitis typically occurs after more than 10 years of regular heavy alcohol use; average consumption in one study was 100 g/day (the equivalent of 10 drinks per day).1 The typical patient presents with recent onset of jaundice, ascites, and proximal muscle loss. Fever and leukocytosis also are common but should prompt an evaluation for infection, especially spontaneous bacterial peritonitis. Liver biopsy in these patients shows steatosis, swollen hepatocytes containing eosinophilic inclusion (Mallory) bodies, and a prominent neutrophilic inflammatory cell infiltrate. Because of the accuracy of clinical diagnosis, biopsy is rarely required, relying instead on clinical and laboratory features for diagnosis (see Table 1, below).
Prognosis can be determined with prediction models. The most common are Model for End-Stage Liver Disease (MELD) and Maddrey’s discriminate score (see Table 2). Several websites allow quick calculation of these scores and provide estimated 30-day or 90-day mortality. These scores can be used to guide therapy.
Review of the Data
How should hospitalists treat this serious illness? The evidence-based literature supporting the efficacy of treatments for alcoholic hepatitis is limited, and expert opinions sometimes conflict.
Abstinence has been shown to improve survival in all stages of alcohol-related liver disease.2 This can be accomplished by admitting this patient population to the hospital. A number of interventions and therapies are available to increase the chance of continued abstinence following discharge (see Table 3).
Nutritional support. Protein-calorie malnutrition is seen in up to 90% of patients with cirrhosis.3 The cause of malnutrition in these patients includes decreased caloric intake, metabolic derangements that accompany liver disease, and micronutrient and vitamin deficiencies. Many of these patients rely almost solely on alcohol for caloric intake; this contributes to potassium depletion, which is frequently seen. After admission, these patients are often evaluated for other conditions (such as gastrointestinal bleeding and altered mental status) that require them to be NPO overnight, thus further confounding their malnutrition. Enteral nutritional support was shown in a multicenter study to be associated with reduced infectious complications and improved one-year mortality.4
Little clinical data support specific recommendations for the amount of nutritional support. The American College of Gastroenterology (ACG) recommends 35 calories/kg to 40 calories/kg of body weight per day and a protein intake of 1.2 g/kg to 1.5g/kg per day.5 In an average, 70-kg patient, this is 2,450 to 2,800 calories a day. For patients who are not able to meet these nutritional needs by mouth, enteral feeding with a small-bore (Dobhoff) feeding tube can be used, even in patients with known esophageal varices.
Most of these patients have anorexia and nausea and do not meet these caloric recommendations by eating. Nutritional support is a low-risk intervention that can be provided on almost all inpatient medical care areas. Hospitalists should be attentive to nutritional support early in the hospitalization of these patients.
Corticosteroid therapy is recommended by the ACG for patients with alcoholic hepatitis and a Maddrey’s discriminant function greater than 32.5 There is much debate about this recommendation, as conflicting data about efficacy exist.
A 2008 Cochrane review included clinical trials published before July 2007 that examined corticosteroid use in patients with alcoholic hepatitis. A total of 15 trials with 721 randomized patients were included. The review concluded that corticosteroids did not statistically reduce mortality compared with placebo or no intervention; however, mortality was reduced in the subgroup of patients with Maddrey’s scores greater than 32 and hepatic encephalopathy.6 The review concluded that current evidence does not support the use of corticosteroids in alcoholic hepatitis, and more randomized trials were needed.
Another meta-analysis demonstrated a mortality benefit when the largest studies, which included 221 patients with high Maddrey’s scores, were analyzed separately.7 Contraindications to corticosteroid treatment include active infection, gastrointestinal bleeding, acute pancreatitis, and renal failure. Other concerns about corticosteroids include potential adverse reactions (hyperglycemia) and increased risk of infection. Prednisolone is preferred over prednisone because it is the active drug. The recommended dosage is 40 mg/day for 28 days followed by a taper (20 mg/day for one week, then 10 mg/day for one week).
Some data suggest that if patients on corticosteroid therapy do not demonstrate a decrease in their bilirubin levels by Day 7, they are at higher risk of developing infections, have a poorer prognosis, and that corticosteroid therapy should be stopped.8 Some experts use the Lille model to decide whether to continue corticosteroids. In one study, patients who did not respond to prednisolone did not improve when switched to pentoxifyline.9
Patients discharged on corticosteroids require very careful coordination with outpatient providers as prolonged corticosteroid treatment courses can lead to serious complications and death. Critics of corticosteroid therapy in these patients often cite problems related to prolonged steroid use, especially in patients who do not respond to therapy.10
Pentoxifylline, an oral phosphodiesterase inhibitor, is recommended by the ACG, especially if corticosteroids are contraindicated.5 In 2008, 101 patients with alcoholic hepatitis were enrolled in a double-blind, placebo-controlled trial comparing pentoxifylline and placebo. This study demonstrated that patients who received pentoxifylline had decreased 28-day mortality (24.6% versus 46% receiving placebo). Of those patients who died during the study, only 50% (versus 91% in the placebo group) developed hepatorenal syndrome.11 However, a Cochrane review of all studies with pentoxifylline concluded that no firm conclusions could be drawn.12
One small, randomized trial comparing pentoxifylline with prednisolone demonstrated that pentoxifylline was superior.13 Pentoxifylline can be prescribed to patients who have contraindications to corticosteroid use (infection or gastrointestinal bleeding). The recommended dose is 400 mg orally three times daily (TID) for four weeks. Common side effects are nausea and vomiting. Pentoxifylline cannot be administered by nasogastric tubes and should not be used in patients with recent cerebral or retinal hemorrhage.
Other therapies. Several studies have examined vitamin E, N-acetylcystine, and other antioxidants as treatment for alcoholic hepatitis. No clear benefit has been demonstrated for any of these drugs. Tumor necrosis factor (TNF)-alpha inhibitors (e.g. infliximab) have been studied, but increased mortality was demonstrated and these studies were discontinued. Patients are not usually considered for liver transplantation until they have at least six months of abstinence from alcohol as recommended by the American Society of Transplantation.14
Discharge considerations. No clinical trials have studied optimal timing of discharge. Expert opinion based on clinical experience recommends that patients be kept in the hospital until they are eating, signs of alcohol withdrawal and encephalopathy are absent, and bilirubin is less than 10 mg/dL.14 These patients often are quite sick and hospitalization frequently exceeds 10 days. Careful outpatient follow-up and assistance with continued abstinence is very important.
Back to the Case
The patient fits the typical clinical picture of alcoholic hepatitis. Cessation of alcohol consumption is the most important treatment and is accomplished by admission to the hospital. Because of his daily alcohol consumption, folate, thiamine, multivitamins, and oral vitamin K are ordered. Though he has no symptoms of alcohol withdrawal, a note is added about potential withdrawal to the handoff report.
An infectious workup is completed by ordering blood and urine cultures, a chest X-ray, and performing paracentesis to exclude spontaneous bacterial peritonitis. A dietary consult with calorie count is given, along with a plan to discuss with the patient the importance of consuming at least 2,500 calories a day is made. Tube feedings will be considered if the patient does not meet this goal in 48 hours. Clinical calculators determine his Maddrey’s and MELD scores (50 and 25, respectively). If he is actively bleeding or infected, pentoxifylline (400 mg TID for 28 days) is favored due to its lower-side-effect profile.
His MELD score predicts a 90-day mortality of 43%; a meeting is planned to discuss code status and end-of-life issues with the patient and his family. Due to the severity of his illness, a gastroenterology consultation is recommended.
Bottom Line
Alcoholic hepatitis is a serious disease with significant short-term mortality. Treatment options are limited but include abstinence from alcohol, supplemental nutrition, and, for select patients, pentoxifylline or corticosteroids. Because most transplant centers require six months of abstinence, these patients usually are not eligible for urgent liver transplantation.
Dr. Parada is a clinical instructor and chief medical resident in the Department of Internal Medicine at the University of New Mexico School of Medicine and the University of New Mexico Hospital, Albuquerque. Dr. Pierce is associate professor in the Division of Hospital Medicine at the University of New Mexico School of Medicine and the University of New Mexico Hospital.
References
- Naveau S, Giraud V, Borotto E, Aubert A, Capron F, Chaput JC. Excess weight risk factor for alcoholic liver disease. Hepatology. 1997;25:108-111.
- Pessione F, Ramond MJ, Peters L, et al. Five-year survival predictive factors in patients with excessive alcohol intake and cirrhosis. Effect of alcoholic hepatitis, smoking and abstinence. Liver Int. 2003;23:45-53.
- Mendenhall CL, Anderson S, Weesner RE, Goldberg SJ, Crolic KA. Protein-calorie malnutrition associated with alcoholic hepatitis. Veterans Administration Cooperative Study Group on alcoholic hepatitis. Am J Med. 1984;76:211-222.
- Cabre E, Rodriguez-Iglesias P, Caballeria J, et al. Short- and long-term outcome of severe alcohol-induced hepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology. 2000;32:36-42.
- O’Shea RS, Dasarathy S, McCullough AJ, Practice Guideline Committee of the American Association for the Study of Liver Diseases, Practice Parameters Committee of the American College of Gastroenterology. Alcoholic liver disease. Hepatology. 2010;51:307-328.
- Rambaldi A, Saconato HH, Christensen E, Thorlund K, Wetterslev J, Gluud C. Systematic review: Glucocorticosteroids for alcoholic hepatitis—a Cochrane hepato-biliary group systematic review with meta-analyses and trial sequential analyses of randomized clinical trials. Aliment Pharmacol Ther. 2008;27:1167-1178.
- Mathurin P, Mendenhall CL, Carithers RL Jr., et al. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis (AH): individual data analysis of the last three randomized placebo controlled double blind trials of corticosteroids in severe AH. J Hepatol. 2002;36:480-487.
- Louvet A, Naveau S, Abdelnour M, et al. The Lille model: A new tool for therapeutic strategy in patients with severe alcoholic hepatitis treated with steroids. Hepatology. 2007;45:1348-1354.
- Louvet A, Diaz E, Dharancy S, et al. Early switch topentoxifylline in patients with severe alcoholic hepatitis is inefficient in non-responders to corticosteroids. J Hepatol. 2008;48:465-470.
- Amini M, Runyon BA. Alcoholic hepatitis 2010: A clinician’s guide to diagnosis and therapy. World J Gastroenterol. 2010;16:4905-4912.
- Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil O. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: A double-blind, placebo-controlled trial. Gastroenterology. 2000;119:1637-1648.
- Whitfield K, Rambaldi A, Wetterslev J, Gluud C. Pentoxifylline for alcoholic hepatitis. Cochrane Database Syst Rev. 2009;(4):CD007339.
- De BK, Gangopadhyay S, Dutta D, Baksi SD, Pani A, Ghosh P. Pentoxifylline versus prednisolone for severe alcoholic hepatitis: A randomized controlled trial. World J Gastroenterol. 2009;15:1613-1619.
- Lucey MR, Brown KA, Everson GT, et al. Minimal criteria for placement of adults on the liver transplant waiting list: a report of a national conference organized by the American Society of Transplant Physicians and the American Association for the Study of Liver Diseases. Liver Transpl Surg. 1997;3:628-637.
Case
A 53-year-old man with a history of daily alcohol use presents with one week of jaundice. His blood pressure is 95/60 mmHg, pulse 105/minute, and temperature 38.0°C. Examination discloses icterus, ascites, and an enlarged, tender liver. His bilirubin is 9 mg/dl, AST 250 IU/dL, ALT 115 IU/dL, prothromin time 22 seconds, INR 2.7, creatinine 0.9 mg/dL, and leukocyte count 15,000/cu mm with 70% neutrophils. He is admitted with a diagnosis of acute alcoholic hepatitis. How should he be treated?
Background
Hospitalists frequently encounter patients who use alcohol and have abnormal liver tests. Regular, heavy alcohol consumption is associated with a variety of forms of liver disease, including fatty liver, inflammation, hepatic fibrosis, and cirrhosis. The term “alcoholic hepatitis” describes a more severe form of alcohol-related liver disease associated with significant short-term mortality.
Alcoholic hepatitis typically occurs after more than 10 years of regular heavy alcohol use; average consumption in one study was 100 g/day (the equivalent of 10 drinks per day).1 The typical patient presents with recent onset of jaundice, ascites, and proximal muscle loss. Fever and leukocytosis also are common but should prompt an evaluation for infection, especially spontaneous bacterial peritonitis. Liver biopsy in these patients shows steatosis, swollen hepatocytes containing eosinophilic inclusion (Mallory) bodies, and a prominent neutrophilic inflammatory cell infiltrate. Because of the accuracy of clinical diagnosis, biopsy is rarely required, relying instead on clinical and laboratory features for diagnosis (see Table 1, below).
Prognosis can be determined with prediction models. The most common are Model for End-Stage Liver Disease (MELD) and Maddrey’s discriminate score (see Table 2). Several websites allow quick calculation of these scores and provide estimated 30-day or 90-day mortality. These scores can be used to guide therapy.
Review of the Data
How should hospitalists treat this serious illness? The evidence-based literature supporting the efficacy of treatments for alcoholic hepatitis is limited, and expert opinions sometimes conflict.
Abstinence has been shown to improve survival in all stages of alcohol-related liver disease.2 This can be accomplished by admitting this patient population to the hospital. A number of interventions and therapies are available to increase the chance of continued abstinence following discharge (see Table 3).
Nutritional support. Protein-calorie malnutrition is seen in up to 90% of patients with cirrhosis.3 The cause of malnutrition in these patients includes decreased caloric intake, metabolic derangements that accompany liver disease, and micronutrient and vitamin deficiencies. Many of these patients rely almost solely on alcohol for caloric intake; this contributes to potassium depletion, which is frequently seen. After admission, these patients are often evaluated for other conditions (such as gastrointestinal bleeding and altered mental status) that require them to be NPO overnight, thus further confounding their malnutrition. Enteral nutritional support was shown in a multicenter study to be associated with reduced infectious complications and improved one-year mortality.4
Little clinical data support specific recommendations for the amount of nutritional support. The American College of Gastroenterology (ACG) recommends 35 calories/kg to 40 calories/kg of body weight per day and a protein intake of 1.2 g/kg to 1.5g/kg per day.5 In an average, 70-kg patient, this is 2,450 to 2,800 calories a day. For patients who are not able to meet these nutritional needs by mouth, enteral feeding with a small-bore (Dobhoff) feeding tube can be used, even in patients with known esophageal varices.
Most of these patients have anorexia and nausea and do not meet these caloric recommendations by eating. Nutritional support is a low-risk intervention that can be provided on almost all inpatient medical care areas. Hospitalists should be attentive to nutritional support early in the hospitalization of these patients.
Corticosteroid therapy is recommended by the ACG for patients with alcoholic hepatitis and a Maddrey’s discriminant function greater than 32.5 There is much debate about this recommendation, as conflicting data about efficacy exist.
A 2008 Cochrane review included clinical trials published before July 2007 that examined corticosteroid use in patients with alcoholic hepatitis. A total of 15 trials with 721 randomized patients were included. The review concluded that corticosteroids did not statistically reduce mortality compared with placebo or no intervention; however, mortality was reduced in the subgroup of patients with Maddrey’s scores greater than 32 and hepatic encephalopathy.6 The review concluded that current evidence does not support the use of corticosteroids in alcoholic hepatitis, and more randomized trials were needed.
Another meta-analysis demonstrated a mortality benefit when the largest studies, which included 221 patients with high Maddrey’s scores, were analyzed separately.7 Contraindications to corticosteroid treatment include active infection, gastrointestinal bleeding, acute pancreatitis, and renal failure. Other concerns about corticosteroids include potential adverse reactions (hyperglycemia) and increased risk of infection. Prednisolone is preferred over prednisone because it is the active drug. The recommended dosage is 40 mg/day for 28 days followed by a taper (20 mg/day for one week, then 10 mg/day for one week).
Some data suggest that if patients on corticosteroid therapy do not demonstrate a decrease in their bilirubin levels by Day 7, they are at higher risk of developing infections, have a poorer prognosis, and that corticosteroid therapy should be stopped.8 Some experts use the Lille model to decide whether to continue corticosteroids. In one study, patients who did not respond to prednisolone did not improve when switched to pentoxifyline.9
Patients discharged on corticosteroids require very careful coordination with outpatient providers as prolonged corticosteroid treatment courses can lead to serious complications and death. Critics of corticosteroid therapy in these patients often cite problems related to prolonged steroid use, especially in patients who do not respond to therapy.10
Pentoxifylline, an oral phosphodiesterase inhibitor, is recommended by the ACG, especially if corticosteroids are contraindicated.5 In 2008, 101 patients with alcoholic hepatitis were enrolled in a double-blind, placebo-controlled trial comparing pentoxifylline and placebo. This study demonstrated that patients who received pentoxifylline had decreased 28-day mortality (24.6% versus 46% receiving placebo). Of those patients who died during the study, only 50% (versus 91% in the placebo group) developed hepatorenal syndrome.11 However, a Cochrane review of all studies with pentoxifylline concluded that no firm conclusions could be drawn.12
One small, randomized trial comparing pentoxifylline with prednisolone demonstrated that pentoxifylline was superior.13 Pentoxifylline can be prescribed to patients who have contraindications to corticosteroid use (infection or gastrointestinal bleeding). The recommended dose is 400 mg orally three times daily (TID) for four weeks. Common side effects are nausea and vomiting. Pentoxifylline cannot be administered by nasogastric tubes and should not be used in patients with recent cerebral or retinal hemorrhage.
Other therapies. Several studies have examined vitamin E, N-acetylcystine, and other antioxidants as treatment for alcoholic hepatitis. No clear benefit has been demonstrated for any of these drugs. Tumor necrosis factor (TNF)-alpha inhibitors (e.g. infliximab) have been studied, but increased mortality was demonstrated and these studies were discontinued. Patients are not usually considered for liver transplantation until they have at least six months of abstinence from alcohol as recommended by the American Society of Transplantation.14
Discharge considerations. No clinical trials have studied optimal timing of discharge. Expert opinion based on clinical experience recommends that patients be kept in the hospital until they are eating, signs of alcohol withdrawal and encephalopathy are absent, and bilirubin is less than 10 mg/dL.14 These patients often are quite sick and hospitalization frequently exceeds 10 days. Careful outpatient follow-up and assistance with continued abstinence is very important.
Back to the Case
The patient fits the typical clinical picture of alcoholic hepatitis. Cessation of alcohol consumption is the most important treatment and is accomplished by admission to the hospital. Because of his daily alcohol consumption, folate, thiamine, multivitamins, and oral vitamin K are ordered. Though he has no symptoms of alcohol withdrawal, a note is added about potential withdrawal to the handoff report.
An infectious workup is completed by ordering blood and urine cultures, a chest X-ray, and performing paracentesis to exclude spontaneous bacterial peritonitis. A dietary consult with calorie count is given, along with a plan to discuss with the patient the importance of consuming at least 2,500 calories a day is made. Tube feedings will be considered if the patient does not meet this goal in 48 hours. Clinical calculators determine his Maddrey’s and MELD scores (50 and 25, respectively). If he is actively bleeding or infected, pentoxifylline (400 mg TID for 28 days) is favored due to its lower-side-effect profile.
His MELD score predicts a 90-day mortality of 43%; a meeting is planned to discuss code status and end-of-life issues with the patient and his family. Due to the severity of his illness, a gastroenterology consultation is recommended.
Bottom Line
Alcoholic hepatitis is a serious disease with significant short-term mortality. Treatment options are limited but include abstinence from alcohol, supplemental nutrition, and, for select patients, pentoxifylline or corticosteroids. Because most transplant centers require six months of abstinence, these patients usually are not eligible for urgent liver transplantation.
Dr. Parada is a clinical instructor and chief medical resident in the Department of Internal Medicine at the University of New Mexico School of Medicine and the University of New Mexico Hospital, Albuquerque. Dr. Pierce is associate professor in the Division of Hospital Medicine at the University of New Mexico School of Medicine and the University of New Mexico Hospital.
References
- Naveau S, Giraud V, Borotto E, Aubert A, Capron F, Chaput JC. Excess weight risk factor for alcoholic liver disease. Hepatology. 1997;25:108-111.
- Pessione F, Ramond MJ, Peters L, et al. Five-year survival predictive factors in patients with excessive alcohol intake and cirrhosis. Effect of alcoholic hepatitis, smoking and abstinence. Liver Int. 2003;23:45-53.
- Mendenhall CL, Anderson S, Weesner RE, Goldberg SJ, Crolic KA. Protein-calorie malnutrition associated with alcoholic hepatitis. Veterans Administration Cooperative Study Group on alcoholic hepatitis. Am J Med. 1984;76:211-222.
- Cabre E, Rodriguez-Iglesias P, Caballeria J, et al. Short- and long-term outcome of severe alcohol-induced hepatitis treated with steroids or enteral nutrition: a multicenter randomized trial. Hepatology. 2000;32:36-42.
- O’Shea RS, Dasarathy S, McCullough AJ, Practice Guideline Committee of the American Association for the Study of Liver Diseases, Practice Parameters Committee of the American College of Gastroenterology. Alcoholic liver disease. Hepatology. 2010;51:307-328.
- Rambaldi A, Saconato HH, Christensen E, Thorlund K, Wetterslev J, Gluud C. Systematic review: Glucocorticosteroids for alcoholic hepatitis—a Cochrane hepato-biliary group systematic review with meta-analyses and trial sequential analyses of randomized clinical trials. Aliment Pharmacol Ther. 2008;27:1167-1178.
- Mathurin P, Mendenhall CL, Carithers RL Jr., et al. Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis (AH): individual data analysis of the last three randomized placebo controlled double blind trials of corticosteroids in severe AH. J Hepatol. 2002;36:480-487.
- Louvet A, Naveau S, Abdelnour M, et al. The Lille model: A new tool for therapeutic strategy in patients with severe alcoholic hepatitis treated with steroids. Hepatology. 2007;45:1348-1354.
- Louvet A, Diaz E, Dharancy S, et al. Early switch topentoxifylline in patients with severe alcoholic hepatitis is inefficient in non-responders to corticosteroids. J Hepatol. 2008;48:465-470.
- Amini M, Runyon BA. Alcoholic hepatitis 2010: A clinician’s guide to diagnosis and therapy. World J Gastroenterol. 2010;16:4905-4912.
- Akriviadis E, Botla R, Briggs W, Han S, Reynolds T, Shakil O. Pentoxifylline improves short-term survival in severe acute alcoholic hepatitis: A double-blind, placebo-controlled trial. Gastroenterology. 2000;119:1637-1648.
- Whitfield K, Rambaldi A, Wetterslev J, Gluud C. Pentoxifylline for alcoholic hepatitis. Cochrane Database Syst Rev. 2009;(4):CD007339.
- De BK, Gangopadhyay S, Dutta D, Baksi SD, Pani A, Ghosh P. Pentoxifylline versus prednisolone for severe alcoholic hepatitis: A randomized controlled trial. World J Gastroenterol. 2009;15:1613-1619.
- Lucey MR, Brown KA, Everson GT, et al. Minimal criteria for placement of adults on the liver transplant waiting list: a report of a national conference organized by the American Society of Transplant Physicians and the American Association for the Study of Liver Diseases. Liver Transpl Surg. 1997;3:628-637.
What Is the Best Approach to Medical Therapy for Patients with Ischemic Stroke?
Case
A 58-year-old woman with diabetes mellitus and hypertension presents with dysarthria and weakness on the right side of her body starting six hours prior to presentation. She is afebrile and has a blood pressure of 162/84 mmHg. Exam reveals the absence of a heart murmur and no lower-extremity swelling or calf tenderness. There is weakness of the right side of the body on exam with diminished proprioception. A noncontrast head CT shows no intracranial hemorrhage. She is admitted to the hospital with the diagnosis of acute ischemic stroke. What anticlotting or antiplatelet medications should she receive?
Overview
Stroke remains a significant cause of morbidity and mortality in the U.S. and around the world. The majority of strokes are ischemic in etiology. Although thrombolytic therapy is the most effective way to salvage ischemic brain tissue that has not yet infarcted, there is a narrow window for the use of thrombolytics in the treatment of acute ischemic stroke. As a result, many patients will not be eligible for thrombolysis. Outside of 4.5 hours from symptom onset, evidence suggests that the risk outweighs the benefit of using the thrombolytic alteplase. For patients ineligible for thrombolytic therapy, antiplatelet therapy remains the best choice for treatment.
Medications that prevent blood from coagulating or clotting are used to treat and prevent a recurring or second stroke. Typically, an antiplatelet agent (most often aspirin) is initiated within 48 hours of an ischemic stroke and continued in low doses as maintenance. Multiple studies suggest that antiplatelet therapy can reduce the risk for a second stroke by 25%. Specific anticlotting agents might be warranted in some patients with high-risk conditions for a stroke.
Review of Data
Early initiation of aspirin has shown benefit in the treatment of an acute ischemic stroke. Two major trials—the International Stroke Trial (IST) and the Chinese Acute Stroke Trial (CAST)— evaluated the role of aspirin (see Table 1, p. 15).1,2 The IST and CAST trials showed that roughly nine nonfatal strokes were avoided per every 1,000 early treatments. Taking the endpoint of death, as well as focal deficits, the two trials confirmed a rate of reduction of 13 per 1,000 patients.
Overall, the consensus was that initiating aspirin within 48 hours of a presumed ischemic cerebrovascular accident posed no major risk of hemorrhagic complication and improved the long-term outcomes.
Along with aspirin, other antiplatelet agents have been studied, most commonly dipyridamole and clopidrogel. The EARLY trial demonstrated no significant differences in the aspirin and dipyridamole groups at 90 days.3
Another large trial, which focused on clopidrogel and aspirin, looked at aspirin plus clopidrogel or aspirin alone. The FASTER trial enrolled mostly patients with mild cerebrovasular accidents (CVA) or transient ischemic attacks (TIA), and there was no difference in outcome measures between the groups.4 However, the MATCH trial found that aspirin and clopidrogel did not provide improved stroke preventions versus clopidogrel alone but had a larger risk of hemorrhagic/bleeding complications.5
Aspirin dosage is somewhat controversial. Fewer side effects occur with lower doses. Combining the trials, consensus treatment includes early aspirin dosing (325 mg initially, then 150 mg-325 mg daily) given to patients with ischemic stroke. Early aspirin should be avoided in those patients who qualify for and are receiving alteplase, heparin, or oral warfarin therapy.
There are other antiplatelet agents for long-term management of ischemic stroke. Whereas aspirin alone is used in the early management of acute ischemic stroke in those ineligible for thrombolytic therapy, many patients are transitioned to other antiplatelet strategies for secondary prevention long-term. The number needed to treat for aspirin to reduce one future stroke, myocardial infarction (MI), or vascular death when compared to placebo is quite high at 33. However, the combination of aspirin and dipyradimole does not prevent MI, vascular death, or the combined endpoint of either stroke or death.
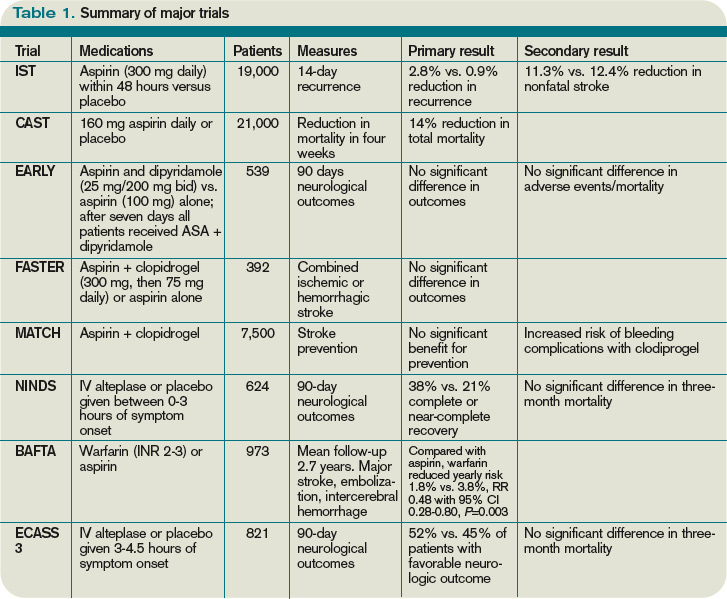
Clopidogrel is more effective than aspirin in preventing a combined endpoint of ischemic stroke, MI, or vascular death, but it is not superior to aspirin in preventing recurrent stroke in TIA or stroke patients. The effects of clopidrogel are greater in patients with peripheral arterial disease, previous coronary artery bypass grafting, insulin-dependent diabetes, or recurrent vascular events.
There is a substantially high cost of treatment and long-term disability associated with stroke. Costs can vary from 3% to 5% of the annual healthcare budget. The newer antiplatelet agents are more expensive than aspirin, and overall cost-effectiveness is difficult to estimate. Yet, from an economic standpoint, the combination of aspirin and dipyradimole can be recommended as an alternative for secondary stroke prevention in patients without major comorbidities. In those patients with higher risk factors and/or comorbidities, clopidogrel might be more cost-effective than aspirin alone. Furthermore, in patients with aspirin intolerance, clopidogrel is a useful, but expensive, alternative.
Thrombolytic therapy. Restora-tion of blood flow with thrombolytic therapy is the most effective way of salvaging ischemic brain tissue that has not already infarcted. The window for use of the thrombolytic alteplase is narrow; studies suggest that its benefit diminishes with increasing time to treatment. Indeed, after 4.5 hours from the onset of symptoms, evidence suggests that the harm might outweigh the benefit, so the determination of who is eligible for its use has to be made quickly.
Guidelines published by the American Heart Association/American Stoke Association stroke council outline strict inclusion and exclusion criteria for the use of alteplase in the management of acute ischemic stroke.6 Obtaining informed consent and emergent neuroimaging are vital in preventing delays in alteplase administration.
Two major trials that illustrate the benefit of alteplase in the treatment of acute ischemic stroke are the NINDS trial and the ECASS 3 trial. NINDS showed that when intravenous alteplase was used within three hours of symptom onset, patients had improved functional outcome at three months.7 The ECASS 3 trial showed that intravenous alteplase has benefit when given up to 4.5 hours after symptom onset.8 Treatment with intravenous alteplase from three-4.5 hours in the ECASS 3 trial showed a modest improvement in patient outcomes at three months, with a number needed to treat of 14 for a favorable outcome.
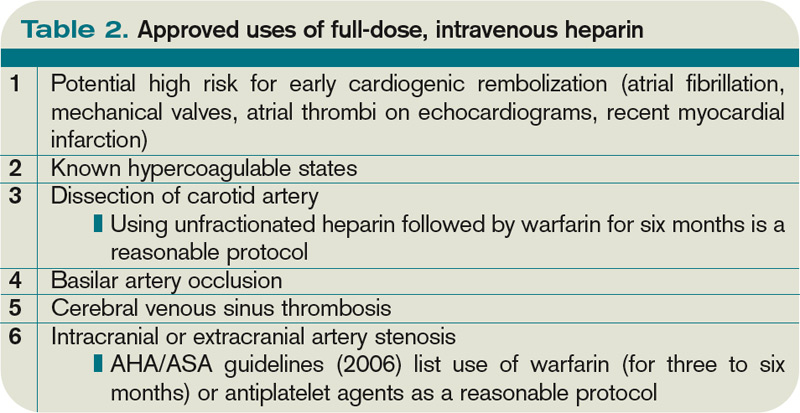
A 2010 meta-analysis looked specifically at outcomes in stroke based on time to treat with alteplase using pooled data from the NINDS, ATLANTIS, ECASS (1, 2, and 3), and EPITHET trials.9 It showed that the number needed to treat for a favorable outcome at three months increased steadily when time to treatment was delayed. It also showed that the risk of death after alteplase administration increased significantly after 4.5 hours. Thus, after 4.5 hours, it suggests that harm might exceed the benefits of treatment.
Anticoagulant use in ischemic stroke. Clinical trials have not been effective in demonstrating the use of heparin and low-molecular-weight heparins (LMWHs). A 2008 systematic review of 24 trials (approximately 24,000 patients) demonstrated:
- Anticoagulant therapy did not reduce odds of death;
- Therapy was associated with nine fewer recurrent ischemic strokes per 1,000 patients, but also showed a similar increase in symptomatic intracranial hemorrhages; and
- Overall, researchers could not specify a particular anticoagulant mode or regimen that had an overall net patient benefit.
The use of heparin in atrial fibrillation and stroke has generated controversy in recent years. Review of the data, however, indicates that early treatment with heparin might cause more harm than benefit. A 2007 meta-analysis did not support the use of early anticoagulant therapy. Seven trials (4,200 patients) compared heparin or LMWH started within 48 hours to other treatments (aspirin, placebo). The study authors found:
- Nonsignificant reduction in recurrent ischemic stroke within seven to 14 days;
- Statistically significant increase in symptomatic intracranial hemorrhages; and
- Similar rates of death/disability at final follow-up of studies.
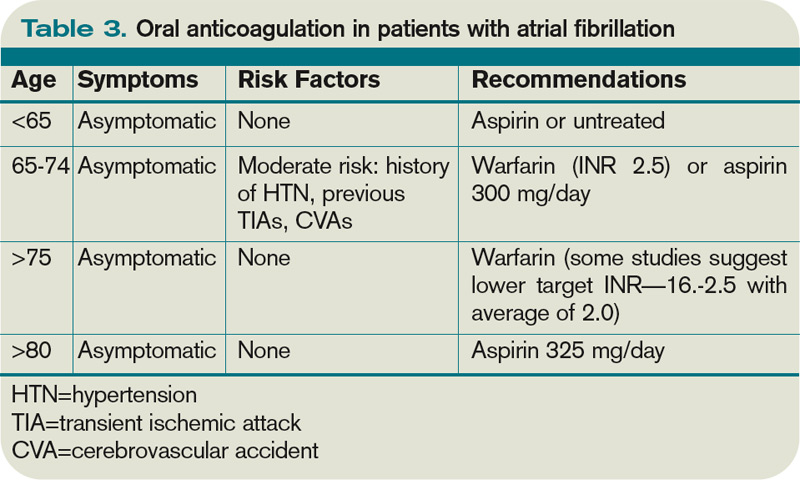
For those patients who continue to demonstrate neurological deterioration, heparin and LMWH use did not appear to improve outcomes. Therefore, based on a consensus of national guidelines, the use of full-dose anticoagulation with heparin or LMWH is not recommended.
The data suggest that in patients with stroke secondary to:
- Dissection of cervical or intracranial arteries;
- Intracardiac thrombus and valvular disease; and
- Mechanical heart valves, full-dose anticoagulation can be initiated. However, the benefit is unproven.
Back to the Case
Our patient with acute ischemic stroke with right-sided weakness on exam presented outside of the window within which alteplase could be administered safely. She was started on aspirin 325 mg daily. There was no indication for full anticoagulation with intravenous heparin or warfarin. Her weakness showed slight improvement on exam during the hospitalization. As an insulin-dependent diabetic, she was thought to be at high risk for recurrent stroke. As such, she was transitioned to a combination of aspirin and clopidogrel prior to her discharge to an acute inpatient rehabilitation hospital.
Bottom Line
Early aspirin therapy (within 48 hours) is recommended (initial dose 325 mg, then 150 mg-325 mg daily) for patients with ischemic stroke who are not candidates for alteplase, IV heparin, or oral anticoagulants.10 Aspirin is the only antiplatelet agent that has been shown to be effective for the early treatment of acute ischemic stroke. In patients without contraindications, aspirin, the combination of aspirin-dipyradimole, or clopidogrel is appropriate for secondary prevention.
The subset of patients at high risk of recurrent stroke should be transitioned to clopidogrel or aspirin/clopidogrel, unless otherwise contraindicated. TH
Dr. Chaturvedi is an instructor in the Division of Hospital Medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and medical director of HM at Northwestern Lake Forest Hospital. Dr. Abraham is an instructor in the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine.
References
- The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19,435 patients with acute ischemic stroke. International Stroke Trial Collaborative Group. Lancet. 1997;349:1569-1581.
- CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet. 1997;349:1641-1649.
- Dengler R, Diener HC, Schwartz A, et al. Early treatment with aspirin plus extended-release dipyridamole for transient ischaemic attack or ischaemic stroke within 24 h of symptom onset (EARLY trial): a randomised, open-label, blinded-endpoint trial. Lancet Neurol. 2010;9:159-166.
- Kennedy J, Hill MD, Ryckborst KJ, et al. Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial. Lancet Neurol. 2007;6:961-969.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364:331-337.
- Adams HP Jr, del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38:1655-1711.
- Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695-1703.
- Hacke W, Kaste M, Bluhmki E, et al. Thombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317-1329.
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581-1587.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133:630S-669S.
Case
A 58-year-old woman with diabetes mellitus and hypertension presents with dysarthria and weakness on the right side of her body starting six hours prior to presentation. She is afebrile and has a blood pressure of 162/84 mmHg. Exam reveals the absence of a heart murmur and no lower-extremity swelling or calf tenderness. There is weakness of the right side of the body on exam with diminished proprioception. A noncontrast head CT shows no intracranial hemorrhage. She is admitted to the hospital with the diagnosis of acute ischemic stroke. What anticlotting or antiplatelet medications should she receive?
Overview
Stroke remains a significant cause of morbidity and mortality in the U.S. and around the world. The majority of strokes are ischemic in etiology. Although thrombolytic therapy is the most effective way to salvage ischemic brain tissue that has not yet infarcted, there is a narrow window for the use of thrombolytics in the treatment of acute ischemic stroke. As a result, many patients will not be eligible for thrombolysis. Outside of 4.5 hours from symptom onset, evidence suggests that the risk outweighs the benefit of using the thrombolytic alteplase. For patients ineligible for thrombolytic therapy, antiplatelet therapy remains the best choice for treatment.
Medications that prevent blood from coagulating or clotting are used to treat and prevent a recurring or second stroke. Typically, an antiplatelet agent (most often aspirin) is initiated within 48 hours of an ischemic stroke and continued in low doses as maintenance. Multiple studies suggest that antiplatelet therapy can reduce the risk for a second stroke by 25%. Specific anticlotting agents might be warranted in some patients with high-risk conditions for a stroke.
Review of Data
Early initiation of aspirin has shown benefit in the treatment of an acute ischemic stroke. Two major trials—the International Stroke Trial (IST) and the Chinese Acute Stroke Trial (CAST)— evaluated the role of aspirin (see Table 1, p. 15).1,2 The IST and CAST trials showed that roughly nine nonfatal strokes were avoided per every 1,000 early treatments. Taking the endpoint of death, as well as focal deficits, the two trials confirmed a rate of reduction of 13 per 1,000 patients.
Overall, the consensus was that initiating aspirin within 48 hours of a presumed ischemic cerebrovascular accident posed no major risk of hemorrhagic complication and improved the long-term outcomes.
Along with aspirin, other antiplatelet agents have been studied, most commonly dipyridamole and clopidrogel. The EARLY trial demonstrated no significant differences in the aspirin and dipyridamole groups at 90 days.3
Another large trial, which focused on clopidrogel and aspirin, looked at aspirin plus clopidrogel or aspirin alone. The FASTER trial enrolled mostly patients with mild cerebrovasular accidents (CVA) or transient ischemic attacks (TIA), and there was no difference in outcome measures between the groups.4 However, the MATCH trial found that aspirin and clopidrogel did not provide improved stroke preventions versus clopidogrel alone but had a larger risk of hemorrhagic/bleeding complications.5
Aspirin dosage is somewhat controversial. Fewer side effects occur with lower doses. Combining the trials, consensus treatment includes early aspirin dosing (325 mg initially, then 150 mg-325 mg daily) given to patients with ischemic stroke. Early aspirin should be avoided in those patients who qualify for and are receiving alteplase, heparin, or oral warfarin therapy.
There are other antiplatelet agents for long-term management of ischemic stroke. Whereas aspirin alone is used in the early management of acute ischemic stroke in those ineligible for thrombolytic therapy, many patients are transitioned to other antiplatelet strategies for secondary prevention long-term. The number needed to treat for aspirin to reduce one future stroke, myocardial infarction (MI), or vascular death when compared to placebo is quite high at 33. However, the combination of aspirin and dipyradimole does not prevent MI, vascular death, or the combined endpoint of either stroke or death.
Clopidogrel is more effective than aspirin in preventing a combined endpoint of ischemic stroke, MI, or vascular death, but it is not superior to aspirin in preventing recurrent stroke in TIA or stroke patients. The effects of clopidrogel are greater in patients with peripheral arterial disease, previous coronary artery bypass grafting, insulin-dependent diabetes, or recurrent vascular events.
There is a substantially high cost of treatment and long-term disability associated with stroke. Costs can vary from 3% to 5% of the annual healthcare budget. The newer antiplatelet agents are more expensive than aspirin, and overall cost-effectiveness is difficult to estimate. Yet, from an economic standpoint, the combination of aspirin and dipyradimole can be recommended as an alternative for secondary stroke prevention in patients without major comorbidities. In those patients with higher risk factors and/or comorbidities, clopidogrel might be more cost-effective than aspirin alone. Furthermore, in patients with aspirin intolerance, clopidogrel is a useful, but expensive, alternative.
Thrombolytic therapy. Restora-tion of blood flow with thrombolytic therapy is the most effective way of salvaging ischemic brain tissue that has not already infarcted. The window for use of the thrombolytic alteplase is narrow; studies suggest that its benefit diminishes with increasing time to treatment. Indeed, after 4.5 hours from the onset of symptoms, evidence suggests that the harm might outweigh the benefit, so the determination of who is eligible for its use has to be made quickly.
Guidelines published by the American Heart Association/American Stoke Association stroke council outline strict inclusion and exclusion criteria for the use of alteplase in the management of acute ischemic stroke.6 Obtaining informed consent and emergent neuroimaging are vital in preventing delays in alteplase administration.
Two major trials that illustrate the benefit of alteplase in the treatment of acute ischemic stroke are the NINDS trial and the ECASS 3 trial. NINDS showed that when intravenous alteplase was used within three hours of symptom onset, patients had improved functional outcome at three months.7 The ECASS 3 trial showed that intravenous alteplase has benefit when given up to 4.5 hours after symptom onset.8 Treatment with intravenous alteplase from three-4.5 hours in the ECASS 3 trial showed a modest improvement in patient outcomes at three months, with a number needed to treat of 14 for a favorable outcome.
A 2010 meta-analysis looked specifically at outcomes in stroke based on time to treat with alteplase using pooled data from the NINDS, ATLANTIS, ECASS (1, 2, and 3), and EPITHET trials.9 It showed that the number needed to treat for a favorable outcome at three months increased steadily when time to treatment was delayed. It also showed that the risk of death after alteplase administration increased significantly after 4.5 hours. Thus, after 4.5 hours, it suggests that harm might exceed the benefits of treatment.
Anticoagulant use in ischemic stroke. Clinical trials have not been effective in demonstrating the use of heparin and low-molecular-weight heparins (LMWHs). A 2008 systematic review of 24 trials (approximately 24,000 patients) demonstrated:
- Anticoagulant therapy did not reduce odds of death;
- Therapy was associated with nine fewer recurrent ischemic strokes per 1,000 patients, but also showed a similar increase in symptomatic intracranial hemorrhages; and
- Overall, researchers could not specify a particular anticoagulant mode or regimen that had an overall net patient benefit.
The use of heparin in atrial fibrillation and stroke has generated controversy in recent years. Review of the data, however, indicates that early treatment with heparin might cause more harm than benefit. A 2007 meta-analysis did not support the use of early anticoagulant therapy. Seven trials (4,200 patients) compared heparin or LMWH started within 48 hours to other treatments (aspirin, placebo). The study authors found:
- Nonsignificant reduction in recurrent ischemic stroke within seven to 14 days;
- Statistically significant increase in symptomatic intracranial hemorrhages; and
- Similar rates of death/disability at final follow-up of studies.
For those patients who continue to demonstrate neurological deterioration, heparin and LMWH use did not appear to improve outcomes. Therefore, based on a consensus of national guidelines, the use of full-dose anticoagulation with heparin or LMWH is not recommended.
The data suggest that in patients with stroke secondary to:
- Dissection of cervical or intracranial arteries;
- Intracardiac thrombus and valvular disease; and
- Mechanical heart valves, full-dose anticoagulation can be initiated. However, the benefit is unproven.
Back to the Case
Our patient with acute ischemic stroke with right-sided weakness on exam presented outside of the window within which alteplase could be administered safely. She was started on aspirin 325 mg daily. There was no indication for full anticoagulation with intravenous heparin or warfarin. Her weakness showed slight improvement on exam during the hospitalization. As an insulin-dependent diabetic, she was thought to be at high risk for recurrent stroke. As such, she was transitioned to a combination of aspirin and clopidogrel prior to her discharge to an acute inpatient rehabilitation hospital.
Bottom Line
Early aspirin therapy (within 48 hours) is recommended (initial dose 325 mg, then 150 mg-325 mg daily) for patients with ischemic stroke who are not candidates for alteplase, IV heparin, or oral anticoagulants.10 Aspirin is the only antiplatelet agent that has been shown to be effective for the early treatment of acute ischemic stroke. In patients without contraindications, aspirin, the combination of aspirin-dipyradimole, or clopidogrel is appropriate for secondary prevention.
The subset of patients at high risk of recurrent stroke should be transitioned to clopidogrel or aspirin/clopidogrel, unless otherwise contraindicated. TH
Dr. Chaturvedi is an instructor in the Division of Hospital Medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and medical director of HM at Northwestern Lake Forest Hospital. Dr. Abraham is an instructor in the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine.
References
- The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19,435 patients with acute ischemic stroke. International Stroke Trial Collaborative Group. Lancet. 1997;349:1569-1581.
- CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet. 1997;349:1641-1649.
- Dengler R, Diener HC, Schwartz A, et al. Early treatment with aspirin plus extended-release dipyridamole for transient ischaemic attack or ischaemic stroke within 24 h of symptom onset (EARLY trial): a randomised, open-label, blinded-endpoint trial. Lancet Neurol. 2010;9:159-166.
- Kennedy J, Hill MD, Ryckborst KJ, et al. Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial. Lancet Neurol. 2007;6:961-969.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364:331-337.
- Adams HP Jr, del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38:1655-1711.
- Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695-1703.
- Hacke W, Kaste M, Bluhmki E, et al. Thombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317-1329.
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581-1587.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133:630S-669S.
Case
A 58-year-old woman with diabetes mellitus and hypertension presents with dysarthria and weakness on the right side of her body starting six hours prior to presentation. She is afebrile and has a blood pressure of 162/84 mmHg. Exam reveals the absence of a heart murmur and no lower-extremity swelling or calf tenderness. There is weakness of the right side of the body on exam with diminished proprioception. A noncontrast head CT shows no intracranial hemorrhage. She is admitted to the hospital with the diagnosis of acute ischemic stroke. What anticlotting or antiplatelet medications should she receive?
Overview
Stroke remains a significant cause of morbidity and mortality in the U.S. and around the world. The majority of strokes are ischemic in etiology. Although thrombolytic therapy is the most effective way to salvage ischemic brain tissue that has not yet infarcted, there is a narrow window for the use of thrombolytics in the treatment of acute ischemic stroke. As a result, many patients will not be eligible for thrombolysis. Outside of 4.5 hours from symptom onset, evidence suggests that the risk outweighs the benefit of using the thrombolytic alteplase. For patients ineligible for thrombolytic therapy, antiplatelet therapy remains the best choice for treatment.
Medications that prevent blood from coagulating or clotting are used to treat and prevent a recurring or second stroke. Typically, an antiplatelet agent (most often aspirin) is initiated within 48 hours of an ischemic stroke and continued in low doses as maintenance. Multiple studies suggest that antiplatelet therapy can reduce the risk for a second stroke by 25%. Specific anticlotting agents might be warranted in some patients with high-risk conditions for a stroke.
Review of Data
Early initiation of aspirin has shown benefit in the treatment of an acute ischemic stroke. Two major trials—the International Stroke Trial (IST) and the Chinese Acute Stroke Trial (CAST)— evaluated the role of aspirin (see Table 1, p. 15).1,2 The IST and CAST trials showed that roughly nine nonfatal strokes were avoided per every 1,000 early treatments. Taking the endpoint of death, as well as focal deficits, the two trials confirmed a rate of reduction of 13 per 1,000 patients.
Overall, the consensus was that initiating aspirin within 48 hours of a presumed ischemic cerebrovascular accident posed no major risk of hemorrhagic complication and improved the long-term outcomes.
Along with aspirin, other antiplatelet agents have been studied, most commonly dipyridamole and clopidrogel. The EARLY trial demonstrated no significant differences in the aspirin and dipyridamole groups at 90 days.3
Another large trial, which focused on clopidrogel and aspirin, looked at aspirin plus clopidrogel or aspirin alone. The FASTER trial enrolled mostly patients with mild cerebrovasular accidents (CVA) or transient ischemic attacks (TIA), and there was no difference in outcome measures between the groups.4 However, the MATCH trial found that aspirin and clopidrogel did not provide improved stroke preventions versus clopidogrel alone but had a larger risk of hemorrhagic/bleeding complications.5
Aspirin dosage is somewhat controversial. Fewer side effects occur with lower doses. Combining the trials, consensus treatment includes early aspirin dosing (325 mg initially, then 150 mg-325 mg daily) given to patients with ischemic stroke. Early aspirin should be avoided in those patients who qualify for and are receiving alteplase, heparin, or oral warfarin therapy.
There are other antiplatelet agents for long-term management of ischemic stroke. Whereas aspirin alone is used in the early management of acute ischemic stroke in those ineligible for thrombolytic therapy, many patients are transitioned to other antiplatelet strategies for secondary prevention long-term. The number needed to treat for aspirin to reduce one future stroke, myocardial infarction (MI), or vascular death when compared to placebo is quite high at 33. However, the combination of aspirin and dipyradimole does not prevent MI, vascular death, or the combined endpoint of either stroke or death.
Clopidogrel is more effective than aspirin in preventing a combined endpoint of ischemic stroke, MI, or vascular death, but it is not superior to aspirin in preventing recurrent stroke in TIA or stroke patients. The effects of clopidrogel are greater in patients with peripheral arterial disease, previous coronary artery bypass grafting, insulin-dependent diabetes, or recurrent vascular events.
There is a substantially high cost of treatment and long-term disability associated with stroke. Costs can vary from 3% to 5% of the annual healthcare budget. The newer antiplatelet agents are more expensive than aspirin, and overall cost-effectiveness is difficult to estimate. Yet, from an economic standpoint, the combination of aspirin and dipyradimole can be recommended as an alternative for secondary stroke prevention in patients without major comorbidities. In those patients with higher risk factors and/or comorbidities, clopidogrel might be more cost-effective than aspirin alone. Furthermore, in patients with aspirin intolerance, clopidogrel is a useful, but expensive, alternative.
Thrombolytic therapy. Restora-tion of blood flow with thrombolytic therapy is the most effective way of salvaging ischemic brain tissue that has not already infarcted. The window for use of the thrombolytic alteplase is narrow; studies suggest that its benefit diminishes with increasing time to treatment. Indeed, after 4.5 hours from the onset of symptoms, evidence suggests that the harm might outweigh the benefit, so the determination of who is eligible for its use has to be made quickly.
Guidelines published by the American Heart Association/American Stoke Association stroke council outline strict inclusion and exclusion criteria for the use of alteplase in the management of acute ischemic stroke.6 Obtaining informed consent and emergent neuroimaging are vital in preventing delays in alteplase administration.
Two major trials that illustrate the benefit of alteplase in the treatment of acute ischemic stroke are the NINDS trial and the ECASS 3 trial. NINDS showed that when intravenous alteplase was used within three hours of symptom onset, patients had improved functional outcome at three months.7 The ECASS 3 trial showed that intravenous alteplase has benefit when given up to 4.5 hours after symptom onset.8 Treatment with intravenous alteplase from three-4.5 hours in the ECASS 3 trial showed a modest improvement in patient outcomes at three months, with a number needed to treat of 14 for a favorable outcome.
A 2010 meta-analysis looked specifically at outcomes in stroke based on time to treat with alteplase using pooled data from the NINDS, ATLANTIS, ECASS (1, 2, and 3), and EPITHET trials.9 It showed that the number needed to treat for a favorable outcome at three months increased steadily when time to treatment was delayed. It also showed that the risk of death after alteplase administration increased significantly after 4.5 hours. Thus, after 4.5 hours, it suggests that harm might exceed the benefits of treatment.
Anticoagulant use in ischemic stroke. Clinical trials have not been effective in demonstrating the use of heparin and low-molecular-weight heparins (LMWHs). A 2008 systematic review of 24 trials (approximately 24,000 patients) demonstrated:
- Anticoagulant therapy did not reduce odds of death;
- Therapy was associated with nine fewer recurrent ischemic strokes per 1,000 patients, but also showed a similar increase in symptomatic intracranial hemorrhages; and
- Overall, researchers could not specify a particular anticoagulant mode or regimen that had an overall net patient benefit.
The use of heparin in atrial fibrillation and stroke has generated controversy in recent years. Review of the data, however, indicates that early treatment with heparin might cause more harm than benefit. A 2007 meta-analysis did not support the use of early anticoagulant therapy. Seven trials (4,200 patients) compared heparin or LMWH started within 48 hours to other treatments (aspirin, placebo). The study authors found:
- Nonsignificant reduction in recurrent ischemic stroke within seven to 14 days;
- Statistically significant increase in symptomatic intracranial hemorrhages; and
- Similar rates of death/disability at final follow-up of studies.
For those patients who continue to demonstrate neurological deterioration, heparin and LMWH use did not appear to improve outcomes. Therefore, based on a consensus of national guidelines, the use of full-dose anticoagulation with heparin or LMWH is not recommended.
The data suggest that in patients with stroke secondary to:
- Dissection of cervical or intracranial arteries;
- Intracardiac thrombus and valvular disease; and
- Mechanical heart valves, full-dose anticoagulation can be initiated. However, the benefit is unproven.
Back to the Case
Our patient with acute ischemic stroke with right-sided weakness on exam presented outside of the window within which alteplase could be administered safely. She was started on aspirin 325 mg daily. There was no indication for full anticoagulation with intravenous heparin or warfarin. Her weakness showed slight improvement on exam during the hospitalization. As an insulin-dependent diabetic, she was thought to be at high risk for recurrent stroke. As such, she was transitioned to a combination of aspirin and clopidogrel prior to her discharge to an acute inpatient rehabilitation hospital.
Bottom Line
Early aspirin therapy (within 48 hours) is recommended (initial dose 325 mg, then 150 mg-325 mg daily) for patients with ischemic stroke who are not candidates for alteplase, IV heparin, or oral anticoagulants.10 Aspirin is the only antiplatelet agent that has been shown to be effective for the early treatment of acute ischemic stroke. In patients without contraindications, aspirin, the combination of aspirin-dipyradimole, or clopidogrel is appropriate for secondary prevention.
The subset of patients at high risk of recurrent stroke should be transitioned to clopidogrel or aspirin/clopidogrel, unless otherwise contraindicated. TH
Dr. Chaturvedi is an instructor in the Division of Hospital Medicine at Northwestern University’s Feinberg School of Medicine in Chicago, and medical director of HM at Northwestern Lake Forest Hospital. Dr. Abraham is an instructor in the Division of Hospital Medicine at Northwestern University Feinberg School of Medicine.
References
- The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19,435 patients with acute ischemic stroke. International Stroke Trial Collaborative Group. Lancet. 1997;349:1569-1581.
- CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. CAST (Chinese Acute Stroke Trial) Collaborative Group. Lancet. 1997;349:1641-1649.
- Dengler R, Diener HC, Schwartz A, et al. Early treatment with aspirin plus extended-release dipyridamole for transient ischaemic attack or ischaemic stroke within 24 h of symptom onset (EARLY trial): a randomised, open-label, blinded-endpoint trial. Lancet Neurol. 2010;9:159-166.
- Kennedy J, Hill MD, Ryckborst KJ, et al. Fast assessment of stroke and transient ischaemic attack to prevent early recurrence (FASTER): a randomised controlled pilot trial. Lancet Neurol. 2007;6:961-969.
- Diener HC, Bogousslavsky J, Brass LM, et al. Aspirin and clopidogrel compared with clopidogrel alone after recent ischaemic stroke or transient ischaemic attack in high-risk patients (MATCH): randomised, double-blind, placebo-controlled trial. Lancet. 2004;364:331-337.
- Adams HP Jr, del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke. 2007;38:1655-1711.
- Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375:1695-1703.
- Hacke W, Kaste M, Bluhmki E, et al. Thombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317-1329.
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581-1587.
- Albers GW, Amarenco P, Easton JD, et al. Antithrombotic and thrombolytic therapy for ischemic stroke: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133:630S-669S.
In the Literature: Research You Need to Know
Clinical question: What is the in-hospital mortality risk associated with hospital-acquired Clostridium difficile infection after accounting for time to infection and baseline mortality risk at admission?
Background: Hospital-acquired C. diff infection (CDI) has been shown to be associated with a higher mortality rate and longer length of stay and cost. Previous studies have demonstrated an independent association of mortality with CDI, but have not incorporated time to infection and baseline mortality risk in the analyses.
Study design: Retrospective observational study.
Setting: Single-center, tertiary-care teaching hospital.
Synopsis: Patients who were hospitalized for more than three days were eligible. A baseline in-hospital mortality risk was estimated for each patient using an internally validated tool. A total of 136,877 admissions were identified. Mean baseline mortality risk was 1.8%. Overall rate of CDI was 1.02%.
Patients in the highest decile of baseline mortality risk had a higher rate of CDI than patients in the lowest decile (2.6% vs. 0.2%). Median time to diagnosis was 12 days. CDI was associated with an unadjusted fourfold higher risk of in-hospital death. When baseline mortality risk was included, the RR of death with CDI was 1.99 (95% CI 1.81-2.19).
Patients in the lowest decile of mortality risk had the highest risk of death (RR 45.70, 95% CI 11.35-183.98) compared with those in the highest decile (RR 1.29, 95% CI 1.11-1.50). Cox modeling estimated a threefold increase in death.
This study is limited by being single-site and the mortality risk model has not been validated externally. Results are also estimated from a small number of cases in the lower deciles.
Bottom line: CDI is associated with threefold higher in-hospital mortality. Patients with higher baseline mortality risk have a higher risk of CDI but have a lesser risk of dying compared with patients with lower baseline mortality risk. Hospitals should continue their efforts to reduce rates of CDI.
Citation: Oake N, Taljaard M, van Walraven C, Wilson K, Roth V, Forster AJ. The effect of hospital-acquired C. diff infection on in-hospital mortality. Arch Intern Med. 2010;170(20):1804-1810.
For more physician reviews of HM-related research, visit our website.
Clinical question: What is the in-hospital mortality risk associated with hospital-acquired Clostridium difficile infection after accounting for time to infection and baseline mortality risk at admission?
Background: Hospital-acquired C. diff infection (CDI) has been shown to be associated with a higher mortality rate and longer length of stay and cost. Previous studies have demonstrated an independent association of mortality with CDI, but have not incorporated time to infection and baseline mortality risk in the analyses.
Study design: Retrospective observational study.
Setting: Single-center, tertiary-care teaching hospital.
Synopsis: Patients who were hospitalized for more than three days were eligible. A baseline in-hospital mortality risk was estimated for each patient using an internally validated tool. A total of 136,877 admissions were identified. Mean baseline mortality risk was 1.8%. Overall rate of CDI was 1.02%.
Patients in the highest decile of baseline mortality risk had a higher rate of CDI than patients in the lowest decile (2.6% vs. 0.2%). Median time to diagnosis was 12 days. CDI was associated with an unadjusted fourfold higher risk of in-hospital death. When baseline mortality risk was included, the RR of death with CDI was 1.99 (95% CI 1.81-2.19).
Patients in the lowest decile of mortality risk had the highest risk of death (RR 45.70, 95% CI 11.35-183.98) compared with those in the highest decile (RR 1.29, 95% CI 1.11-1.50). Cox modeling estimated a threefold increase in death.
This study is limited by being single-site and the mortality risk model has not been validated externally. Results are also estimated from a small number of cases in the lower deciles.
Bottom line: CDI is associated with threefold higher in-hospital mortality. Patients with higher baseline mortality risk have a higher risk of CDI but have a lesser risk of dying compared with patients with lower baseline mortality risk. Hospitals should continue their efforts to reduce rates of CDI.
Citation: Oake N, Taljaard M, van Walraven C, Wilson K, Roth V, Forster AJ. The effect of hospital-acquired C. diff infection on in-hospital mortality. Arch Intern Med. 2010;170(20):1804-1810.
For more physician reviews of HM-related research, visit our website.
Clinical question: What is the in-hospital mortality risk associated with hospital-acquired Clostridium difficile infection after accounting for time to infection and baseline mortality risk at admission?
Background: Hospital-acquired C. diff infection (CDI) has been shown to be associated with a higher mortality rate and longer length of stay and cost. Previous studies have demonstrated an independent association of mortality with CDI, but have not incorporated time to infection and baseline mortality risk in the analyses.
Study design: Retrospective observational study.
Setting: Single-center, tertiary-care teaching hospital.
Synopsis: Patients who were hospitalized for more than three days were eligible. A baseline in-hospital mortality risk was estimated for each patient using an internally validated tool. A total of 136,877 admissions were identified. Mean baseline mortality risk was 1.8%. Overall rate of CDI was 1.02%.
Patients in the highest decile of baseline mortality risk had a higher rate of CDI than patients in the lowest decile (2.6% vs. 0.2%). Median time to diagnosis was 12 days. CDI was associated with an unadjusted fourfold higher risk of in-hospital death. When baseline mortality risk was included, the RR of death with CDI was 1.99 (95% CI 1.81-2.19).
Patients in the lowest decile of mortality risk had the highest risk of death (RR 45.70, 95% CI 11.35-183.98) compared with those in the highest decile (RR 1.29, 95% CI 1.11-1.50). Cox modeling estimated a threefold increase in death.
This study is limited by being single-site and the mortality risk model has not been validated externally. Results are also estimated from a small number of cases in the lower deciles.
Bottom line: CDI is associated with threefold higher in-hospital mortality. Patients with higher baseline mortality risk have a higher risk of CDI but have a lesser risk of dying compared with patients with lower baseline mortality risk. Hospitals should continue their efforts to reduce rates of CDI.
Citation: Oake N, Taljaard M, van Walraven C, Wilson K, Roth V, Forster AJ. The effect of hospital-acquired C. diff infection on in-hospital mortality. Arch Intern Med. 2010;170(20):1804-1810.
For more physician reviews of HM-related research, visit our website.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children

Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children
Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Early ambulation and LOS in geriatric patients
- Patient-safety movement and hospital harm rates
- Lifestyle modification and weight loss
- Outcomes of transcatheter aortic-valve implantation
- Tool for predicting mortality in advanced dementia
- Residents’ opinion of new duty-hour regulations
- Renal ultrasound predictor for acute kidney injury
- Romiplostim use in immune thrombocytopenia
Increasing Ambulation within 48 Hours of Admission Decreases LOS by Two Days
Clinical question: Is there an association between an early increase in ambulation and length of stay (LOS) in geriatric patients admitted with an acute illness?
Background: Early ambulation leading to better recovery in such illnesses as pneumonia and myocardial infarction is well known, as is early ambulation after hip fracture surgery to prevent complications. However, no specific guidelines exist in regard to ambulation in older patients.
Study design: Prospective, nonblinded study.
Setting: Acute-care geriatric unit in an academic medical center.
Synopsis: A total of 162 patients 65 or older were studied. Data were collected during a four-month period in 2009. A Step Activity Monitor (SAM) was placed on admission. Patients were instructed to walk as usual. Investigators measured the number of steps taken per day and change in steps between the first and second day.
Patients averaged 662.1 steps per day, with a mean step change of 196.5 steps. The adjusted mean difference in LOS for patients who increased their total steps by 600 or more between the first and second day was 2.13 days (95% CI, 1.05-3.97). Patients who had low or negative changes in steps had longer LOS. The 32 patients who walked more than 600 steps were more likely to be men (P=0.02), independently ambulate (P<0.01), and have admitting orders of “ambulate with assist” (P=0.03).
One limitation of this study is that patients who walked more might have been less ill or very functional on admission.
Bottom line: Increasing ambulation early in a hospitalization (first two days) is associated with a decreased LOS in an elderly population.
Citation: Fisher SR, Kuo YF, Graham JE, Ottenbacher KJ, Ostir GV. Early ambulation and length of stay in older adults hospitalized for acute illness. Arch Intern Med. 2010;170(21):1942-1943.
Despite Efforts to Improve Patient Safety in Hospitals, No Reduction in Longitudinal Rates of Harm
Clinical question: As hospitals focus more on programs to improve patient safety, has the rate of harms decreased?
Background: Since the Institute of Medicine published a groundbreaking report (To Err is Human) a little more than a decade ago, policymakers, hospitals, and healthcare organizations have focused more on efforts to improve patient safety with the goal of reducing harms. It is not clear if these efforts have reduced harms.
Study design: Retrospective chart review.
Setting: Ten hospitals in North Carolina.
Synopsis: Ten charts per quarter were randomly selected from each hospital from January 2002 through December 2007. Internal and external reviewers used the IHI Global Trigger Tool for Measuring Adverse Events to identify rates of harm. Harms were classified into categories of severity and assessed for preventability.
Kappa scores were generally higher for internal reviewers, indicating higher reliability for internal reviewers. Internal reviewers identified 588 harms for 10,415 patient days (25.1 harms per 100 patient days), which occurred in 423 unique patients (18.1%). A majority (63.1%) of harms were considered preventable. Forty-one percent of harms were temporary and required intervention; 2.4% caused or contributed to a patient’s death.
There was no significant change over time in the rate of harms (regardless of reviewer type) even after adjusting for demographics.
This study is limited because it is based only in North Carolina hospitals. It was not powered to evaluate change in individual hospitals. There might have been unmeasurable improvements that were not accounted for by the trigger tool.
Bottom line: Despite a higher focus on patient safety, investigators did not find a decrease in the rate of harms. A majority of the harms were preventable. This study should not preclude efforts to continue to improve patient safety.
Citation: Landrigan CP, Parry GJ, Bones CB, Hackbarth AD, Goldmann DA, Sharek PJ. Temporal trends in rates of patient harm resulting from medical care. N Engl J Med. 2010;363(22):2124-2134.
Intensive Lifestyle Modification Improves Weight Loss in Severely Obese Individuals
Clinical question: Does the combination of diet modification and increased physical activity lead to weight loss and improve health risks in severely obese patients?
Background: Obesity is at epidemic proportions, but there are no evidence-based treatment guidelines for severe obesity.
Study design: Randomized, single-blind trial.
Setting: Community volunteers.
Synopsis: A total of 130 individuals with a body mass index (BMI) of ≥35 were randomized to receive lifestyle interventions consisting of diet and initial physical activity for 12 months, or diet for six months and delayed physical activity for the remainder of the year.
The initial-physical-activity group demonstrated greater weight loss at six months, but the overall weight loss did not differ between the two groups. At 12 months, the initial physical activity group lost 12.1 kg and the delayed-physical-activity group lost 9.87 kg. Both groups demonstrated significantly reduced blood pressure, reduced serum liver enzymes, and improved insulin resistance.
Candidates with a history of coronary artery disease, uncontrolled blood pressure, or diabetes were excluded. Participants were provided with prepackaged meal replacements for the first six months and received financial compensation for participation in the study.
This study is limited by the fact that a majority of the participants were female (85.1%). Providing meals to the participants also limits the application of this program to the general public.
Bottom line: The results of this study reflect the importance of diet and exercise on weight loss in obese individuals. However, adherence to the goals of the study required multiple individual and group meetings throughout the year, the provision of prepackaged meals, and some financial incentive for compliance.
Citation: Goodpaster GH, Delany JP, Otto AD, et al. Effects of diet and physical activity interventions on weight loss and cardiometabolic risk factors in severely obese adults: a randomized trial. JAMA. 2010;304 (16):1795-1802.
Transcatheter Aortic-Valve Implantation Is Superior to Standard Nonoperative Therapy for Symptomatic Aortic Stenosis
Clinical question: Is there a mortality benefit to transcatheter valve implantation over standard therapy in nonsurgical candidates with severe aortic stenosis (AS)?
Background: Untreated, symptomatic AS has a high rate of death, but a significant proportion of patients with severe aortic stenosis are poor surgical candidates. Available since 2002, transcatheter aortic-valve implantation (TAVI) is a promising, nonsurgical treatment option for severe AS. However, to date, TAVI has lacked rigorous clinical data.
Study design: Prospective, multicenter, randomized, active-treatment-controlled clinical trial.
Setting: Twenty-one centers, 17 of which were in the U.S.
Synopsis: A total of 358 patients with severe AS who were considered nonsurgical candidates were randomized to either TAVI or standard therapy. A majority (83.8%) of the patients in the standard group underwent balloon aortic valvuloplasty.
Researchers found a significant reduction (HR 0.55, 95% CI 0.40 to 0.74, P<0.001) in all-cause mortality at one year in those patients undergoing TAVI (30.7%) vs. standard therapy (50.7%). Additional benefits included lower rates of the composite endpoints of death from any cause or repeat hospitalization (42.5% vs. 71.6%, P<0.001) and NYHA Functional Class III or IV symptoms (25.2% vs. 58.0%, P<0.001) at one year. However, higher incidences of major strokes (5.0% vs. 1.6%, P=0.06) and major vascular complications (16.2% vs. 1.1%, P<0.001) were seen.
While the one-year mortality benefit of TAVI over standard nonoperative therapy was clearly demonstrated by this study, hospitalists should interpret these data cautiously with respect to their inpatient populations as exclusion criteria were extensive, including bicuspid or noncalcified aortic valve, LVEF less than 20%, and severe renal insufficiency. Additionally, the entity of standard therapy was poorly delineated.
Bottom line: TAVI should be considered in patients with severe aortic stenosis who are not suitable surgical candidates.
Citation: Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-1607.
ADEPT Score Better Predicts Six-Month Mortality in Nursing Home Residents with Advanced Dementia
Clinical question: Are current Medicare hospice eligibility guidelines accurate enough to predict six-month survival in nursing home residents with dementia when compared with the Advanced Dementia Prognostic Tool (ADEPT)?
Background: Incorrectly estimating the life expectancy in almost 5 million nursing home residents with dementia prevents enrollment to palliative care and hospice for those who would benefit most. Creating and validating a mortality risk score would allow increased services to these residents.
Study design: Prospective cohort study.
Setting: Twenty-one nursing homes in Boston.
Synopsis: A total of 606 nursing home residents with advanced dementia were recruited for this study. Each resident was assessed for Medicare hospice eligibility and assigned an ADEPT score. Mortality rate was determined six months later. These two assessment tools were compared regarding their ability to predict six-month mortality.
The mean ADEPT score was 10.1 (range of 1.0-32.5), with a higher score meaning worse prognosis. Sixty-five residents (10.7%) met Medicare hospice eligibility guidelines. A total of 111 residents (18.3%) died.
The ADEPT score was more sensitive (90% vs. 20%) but less specific (28.3% vs. 89%) than Medicare guidelines. The area under the receiver operating characteristic (AUROC) curve was 0.67 (95% CI, 0.62-0.72) for ADEPT and 0.55 (95% CI, 0.51-0.59) for Medicare.
ADEPT was slightly better than hospice guidelines in predicting six-month mortality.
This study was limited in that the resident data were collected at a single random time point and might not reflect reality, as with palliative care and hospice, there usually is a decline in status that stimulates the referrals.
Bottom line: The ADEPT score might better estimate the six-month mortality in nursing home residents with dementia, which can help expand the enrollment of palliative care and hospice for these residents.
Citation: Mitchell SL, Miller SC, Teno JM, Kiely DK, Davis RB, Shaffer ML. Prediction of 6-month survival of nursing home residents with advanced dementia using ADEPT vs hospice eligibility guidelines. JAMA. 2010;304(17):1929-1935.
Residents Concerned about How New ACGME Duty-Hour Restrictions Will Impact Patient Care and Education
Clinical question: How do residents believe the forthcoming revised ACGME Rules for Supervision and Duty Hours will impact their residency?
Background: On July 1, revised ACGME duty-hour rules go into effect, limiting PGY-1 residents to 16-hour duty periods and PGY-2 and above to 28 hours. The effect these recommendations will have on patient care and resident education is unknown.
Study design: Twenty-question electronic, anonymous survey.
Setting: Twenty-three medical centers in the U.S., including residents from all disciplines and years in training.
Synopsis: Twenty-two percent of residents responded to the survey (n=2,521). Overall, 48% of residents disagreed with this statement: “Overall the changes will have a positive effect on education,” while only 26% agreed. Approximately half of those surveyed agreed that the revisions would improve their quality of life, but the same percentage also believed the revisions would increase the length of their residencies.
Residents reacted negatively to the idea that the proposed changes would improve patient safety and quality of care delivered, promote education over service obligations, and prepare them to assume senior roles. In free-text comments, residents expressed concerns about an increased number of handoffs and decreased continuity of care.
While the sample size is large and diverse, results of this survey can be affected by voluntary response bias and, therefore, could be skewed toward more extreme responses (in this case, more negative responses). The wide distribution of the responses suggests this might not be the case.
Bottom line: Residents do not believe the new requirements—though they could improve their quality of life—will positively impact patient care and education.
Citation: Drolet BC, Spalluto LB, Fischer SA. Residents’ perspectives on ACGME regulation of supervision and duty hours—a national survey. N Engl J Med. 2010;363(23):e34(1)-e34.
Decision Rule Might Help Clinicians Decide When to Order Renal Ultrasound to Evaluate Hospitalized Patients with Acute Kidney Injury
Clinical question: Can a clinical prediction rule aid clinicians in deciding when to order a renal ultrasound (RUS) in hospitalized patients with acute kidney injury?
Background: RUS routinely is obtained in patients admitted with acute kidney injury (AKI) to rule out obstruction as a cause of AKI. It is not known if this test adds any additional information in the routine evaluation of AKI and if obtaining the test is cost-effective.
Study design: Cross-sectional study.
Setting: Yale-New Haven Hospital in Connecticut.
Synopsis: This study evaluated 997 inpatients with AKI who underwent RUS. Outcome events were RUS identification of hydronephrosis (HN) or hydronephrosis requiring intervention (HNRI). The patients were divided into two samples: 200 in derivation sample and 797 in validation sample. The derivation sample was used to identify specific factors associated with HN. Seven clinical variables were identified and were used to create three risk groups: low, medium, and high.
In the validation sample, 10.6% of patients had HN and 3.3% had HNRI. The negative predictive value for HN was 96.9%, sensitivity 91.8%, and negative likelihood ratio 0.27. The number needed to screen (NNS) low-risk patients for HN was 32 and 223 for HNRI. Based on their findings, if the patient was classified low-risk, clinicians might be able to delay or avoid ordering RUS.
The major limitation of this study was that it was based at a single institution. This study only evaluated RUS obtained in patients who were hospitalized and might not be applicable to outpatients.
Bottom line: RUS was not found to change clinical management in patients with AKI and classified as low-risk for HN. Limiting RUS to patients who are high-risk for obstruction will increase the chance of finding useful clinical information that can change management decisions and limit cost of unnecessary testing.
Citation: Licurse A, Kim MC, Dziura J, et al. Renal ultrasonography in the evaluation of acute kidney injury: developing a risk stratification framework. Arch Intern Med. 2010;170(21):1900-1907.
Romiplostim Has Higher Rate of Platelet Response and Fewer Adverse Events in Patients with Immune Thrombocytopenia
Clinical question: Does the use of romiplostim lead to increased platelet counts and lower rates of splenectomy and other adverse events when compared with standard therapy in patients with immune thrombocytopenia?
Background: Romiplostim is a thrombopoetin mimetic used to increase platelet counts in immune thrombocytopenia. Initial treatments for this disease involve glucocorticoids or intravenous immune globulin. Most patients require second-line medical or surgical therapies, including splenectomy.
Study design: Randomized, open-label controlled trial.
Setting: Eighty-five medical centers in North America, Europe, and Australia.
Synopsis: A total of 234 patients were randomized in a 2:1 ratio to receive either romiplostim or the medical standard of care. Co-primary endpoints were the incidence of treatment failure and the incidence of splenectomy; secondary endpoints included time to splenectomy, platelet count, platelet response, and quality of life. Treatment failure was defined as a platelet count of 20x109 per liter or lower for four weeks, or a major bleeding event.
At the end of 52 weeks, patients receiving romiplostim had higher platelet counts, fewer bleeding events, less need for splenectomy (9% vs. 36%), and a better quality of life.
The short-term use of romiplostim in this study was not associated with an increase in adverse events when compared with standard therapy. However, maintenance of the elevated platelet count, which results from romiplostim treatment, requires continuous use of the drug; the long-term effects are unknown.
Bottom line: In patients with immune thrombocytopenia, romiplostim leads to increased platelet counts, decreased bleeding events, and decreased need for splenectomy compared to standard of care. However, the cost of the medication, when compared with current therapies, could be prohibitive.
Citation: Kuter DJ, Rummel M, Boccia R, et al. Romiplostim or standard of care in patients with immune thrombocytopenia. N Engl J Med. 2010;363(20):1889-1899. TH
Pediatric HM Literature
Parental History Portends Persistent Chronic Abdominal Pain in Children
Clinical question: What is the quality of the current evidence for potential prognostic factors of persistent chronic abdominal pain in children?
Background: Chronic abdominal pain (CAP) is a prevalent condition in childhood that might be associated with increased healthcare costs, including hospital admission. Retrospective studies have implicated psychosocial factors as being of prognostic relevance, but these are unable to offer greater insight into the relationship given the complex nature of this chronic illness.
Study design: Systematic review of literature.
Setting: MEDLINE, EMBASE, and PsycINFO.
Synopsis: The databases were searched through June 2008 for articles that focused on children 4 to 18 years of age; used criteria for CAP as defined by Apley and Naish, von Baeyer and Walker, or the Rome Committee; and demonstrated prospective determination of outcomes. Eight studies were included in the final review, and the levels of evidence were graded based on assessment of risk for bias.
Female sex and severity of baseline abdominal pain did not predict persistence of CAP, although there was conflicting evidence as to the role of psychological factors. There was moderate evidence that having a parent with functional gastrointestinal (GI) symptoms predicted persistence of CAP in children, and there was weak evidence that having parents who eschew psychological factors in favor of searching for an organic explanation predicted persistence of CAP.
Due to a limited number of studies or conflicting associations, conclusions regarding the following factors could not be drawn: age, educational level, duration of CAP, associated symptoms, socioeconomic status, and history of two or more surgical operations.
In addition, the univariate analysis used by the included studies might not be appropriate for such a multifactorially complex disease. Nevertheless, this study challenges the conventional wisdom that psychological factors predict persistence of pain and should remind clinicians to assess for parental functional GI disorders in this patient population.
Bottom line: Parental history of functional GI disorders predicts persistence of CAP in children.
Citation: Gieteling MJ, Bierma-Zeinstra SM, van Leeuwen Y, Passchier J, Berger MY. Prognostic factors for persistence of chronic abdominal pain in children. J Pediatr Gastroenterol Nutr. 2011;52(2):154-161.
In the Literature: HM-Related Research You Need to Know
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effects of extended VTE prophylaxis in medical patients
- Outcomes with and without preprocedural statins
- Association of subclinical hypothyroidism and CHD
- BP treatment after intracerebral hemorrhage
- Outcomes of ICD therapy in the elderly
- Systems delays and outcomes of STEMI
- D-dimer to predict recurrent VTE
- Stocking height and risk of post-stroke DVT
Extending Anticoagulant Prophylaxis after Medical Hospitalization Decreases VTE, Increases Major Bleeding
Clinical question: For patients with acute medical illness, does extending low-molecular-weight heparin (LMWH) administration for up to 28 days after discharge reduce the incidence of venous thromboembolism (VTE)?
Background: DVT and pulmonary embolism (PE) are common hospital-acquired complications. LMWH has been shown to reduce VTE for medical and surgical patients, and extended-duration LMWH reduces VTE in high-risk surgical patients. Whether extending anticoagulant prophylaxis after discharge for acutely ill medical patients with reduced mobility improves outcomes is unknown.
Study design: Randomized, placebo-controlled trial.
Setting: Three hundred seventy hospitals in 20 countries.
Synopsis: Eligible patients were >40 years old, hospitalized with acute medical illness, and had reduced mobility for ≥3 days. Patients received enoxaparin 40 mg SC daily prophylaxis while hospitalized and were then randomized to an additional 28±4 days of enoxaparin or placebo. Patients received a screening ultrasound to assess for asymptomatic DVT. The primary outcome was a composite of asymptomatic proximal DVT, symptomatic DVT or PE, or fatal PE during the period of extended prophylaxis.
An interim analysis indicated that extended prophylaxis was ineffective; at that time, the protocol was amended to target patients with severe immobility or with moderate immobility plus an additional risk factor (e.g. cancer, prior VTE, or age >75).
The study found that extended prophylaxis decreased the composite VTE outcome (2.5% vs 4.0%, P<0.05) and symptomatic VTE (0.2% vs 1.0%, P<0.05). The incidence of major bleeding was increased in the extended prophylaxis group (0.8% vs 0.3%, P<0.05). There was no difference in mortality.
The unplanned, midstudy protocol amendment to target higher-risk patients is a concern, though the final analyses included patients pre- and post-amendment.
Bottom line: Extending LMWH beyond hospitalization for patients admitted with acute medical illness and decreased mobility decreases VTE, but increases major bleeding.
Citation: Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153(1);8-18.
Preprocedural Statin Therapy Reduces Postprocedural Myocardial Infarction
Clinical question: Does statin therapy reduce periprocedural cardiovascular events?
Background: Myocardial infarction (MI) and death are inherent risks of invasive procedures. Reduction of these risks in certain patient populations has been shown with the use of a beta blockade. Statins have shown promise during acute coronary syndrome. Questions remain about the role of statin therapy before invasive procedures in reducing adverse cardiovascular events.
Study design: Meta-analysis of randomized controlled trials.
Setting: Twenty-one studies involving 4,805 patients, published from inception of MEDLINE, Cochrane, and Clinicaltrials to February 2010.
Synopsis: The use of statins one to seven days preprocedure significantly reduced post-procedural MI in percutaneous coronary interventions (PCI) (P<0.0001). Statins given approximately four weeks in advance of noncardiac surgical procedures also significantly reduced postprocedural MI (P=0.004). An absolute risk reduction of 5.8% for postprocedural MI was found after PCI and 4.1% in noncardiac surgical procedures.
Statins did not show a significant reduction in postprocedural MI (P=0.40) or all-cause mortality (P=0.15) in coronary artery bypass graft surgery (CABG). However, statins did reduce post-CABG atrial fibrillation (P<0.0001).
The 21 studies used a variety of drugs and doses. However, the PCI studies favored atorvastatin 40 mg; more than half the CABG studies used atorvastatin 20 mg; and 91% of the noncardiac surgical studies used fluvastatin 80 mg. Dedicated trials are needed to demonstrate optimal statin agent, dose, and timing of therapy.
Bottom line: Preprocedural statin therapy reduces postprocedural MI after both PCI and noncardiac procedures but not after CABG.
Citation: Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy: a meta-analysis of randomized trials. J Am Coll Cardiol. 2010;56(19); 1099-1109.
Subclinical Hypothyroidism Increases the Risk of Coronary Heart Disease and Mortality
Clinical question: What are the risks of coronary heart disease (CHD) and mortality among adults with subclinical hypothyroidism?
Background: Subclinical hypo-thyroidism is defined as an elevated serum thyroid stimulating hormone (TSH) level with a normal T4 concentration. Controversy exists regarding the treatment of subclinical hypothyroidism. Because of the association with hyperlipidemia and atherosclerosis, treatment of subclinical hypothyroidism is thought to be beneficial. Previous data from large prospective cohort studies regarding this association are conflicting.
Study design: Study-level meta-analysis of prospective cohort studies.
Setting: Eleven prospective cohorts in the U.S., Europe, Australia, Brazil, and Japan from 1972 to 2007.
Synopsis: Among 55,287 adults, 3,450 (6.2%) had subclinical hypothyroidism and 51,837 were euthyroid. Using Cox proportional hazard models, the association of subclinical hypothyroidism with CHD and mortality were determined for each cohort.
The risk of CHD events and CHD mortality increased with higher TSH concentrations.
In age- and sex-adjusted analyses, the hazard ratio (HR) for CHD events were as follows: HR=1.0 (TSH=4.5-6.9 mIU/L); HR=1.17 (TSH=7-9.9 mIU/L), and HR=1.89 (TSH=10-19.9 mIU/L). Similarly, HRs for CHD mortality showed an increasing trend: 1.09, 1.42, and 1.58, respectively.
Although the association is clearly established here, randomized controlled trials are needed to address whether thyroxine replacement can prevent CHD and the TSH threshold that will provide the most clinical benefit.
Bottom line: Subclinical hypo-thyroidism is associated with an increased risk for CHD events and mortality, primarily in patients with TSH concentrations of 10 mIU/L or higher.
Citation: Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12): 1365-1374.
Reduction in Hematoma Growth after Acute Intracerebral Hemorrhage Associated with Lower Blood Pressure
Clinical question: Does intensive systolic blood pressure (SBP) <140 mmHg within one hour reduce hematoma growth after acute intracerebral bleeding?
Background: Early elevation of blood pressure after an acute intracerebral bleed is strongly associated with hematoma growth and worse outcomes. The pilot phase of the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) showed that early intensive blood pressure lowering reduced hematoma growth within six hours after onset of intracerebral hemorrhage.
Study design: Randomized controlled trial in which patients received an early intensive blood-pressure-lowering treatment (goal SBP<140 mmHg within one hour) or the AHA recommended best practice guidelines (goal SBP <180 mmHg), which were published in 1999.
Setting: Network of hospitals in China, South Korea, and Australia.
Synopsis: From 2005 to 2007, the study examined 404 patients with computed-tomography (CT) evidence of intracerebral hemorrhage, elevated SBP (150 mmHg-220 mmHg), and ability to commence BP lowering treatment within six hours of onset. Hematoma volumes were measured in the intensive treatment and guideline groups based on CT scans done at baseline and after 24 hours.
No significant association was found between the baseline SBP and the absolute or proportional growth of the hematoma. However, in the intensively treated patients who achieved target SBP within the first 24 hours, a significant association was found with the absolute and proportional hematoma growth.
Maximum reduction of hematoma growth occurred in the group with a median SBP of 135 mmHg.
This single-observational study did not include patients with severe intracranial bleeding who died or required surgical evacuation within the first 24 hours.
Hematoma size reduction did not improve survival or outcomes.
Bottom line: Intensive SBP lowering from 140 mmHg to 130 mmHg within one hour reduces hematoma growth after an intracranial hemorrhage.
Citation: Arima H, Anderson CS, Wang JG, et al. Lower treatment blood pressure is associated with the greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension. 2010;56(5):852-858.
Implantable Cardioverter-Defibrillator (ICD) Therapy for Primary Prevention of Sudden Cardiac Death Might Not Provide Survival Benefit to Elderly
Clinical question: Does ICD therapy for primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction improve survival in elderly patients?
Background: Several clinical trials of select individuals with severe left ventricular dysfunction (EF <40%) have demonstrated that ICD therapy is associated with a reduction in overall mortality. Given the costs and risks associated with ICD placement, it is important to assess how this therapy affects survival in younger versus older individuals.
Study design: Meta-analysis of five randomized controlled trials.
Setting: Five trials (MADIT-II, DEFINITE, DINAMIT, SCDHeFT, and IRIS).
Synopsis: All included studies compared ICD therapy to standard medical care in the primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction. Elderly patients comprised 44% of the 5,783 patients included in the study; elderly patients were defined as >65 in three studies, and >60 in two studies. Pooled analysis of the three trials examining ICD use for primary prevention found a nonsignificant reduction in all-cause mortality compared with medical therapy in elderly patients (HR 0.81 [95% CI 0.62 to 1.05], P=0.11). The two remaining studies involving post-MI patients showed no statistically significant reduction in mortality in elderly patients.
In contrast, pooled data from younger patients in the five trials showed that prophylactic ICD therapy reduced all-cause mortality.
None of the selected trials demonstrated evidence of selection, performance, detection, or attrition bias. Only a small number of studies were included, and four potentially relevant trials were not included because mortality data by age group were not available.
Trials including cardiac resynchronization therapy (CRT) were excluded from this meta-analysis, and elderly patients meeting criteria for CRT comprise an important group that must be considered separately.
Bottom line: There is no definitive reduction in mortality with prophylactic ICD therapy in elderly patients with severe left ventricular dysfunction.
Citation: Santangeli P, Di Biase L, Dello Russo A, et al. Meta-analysis: age and effectiveness of prophylactic implantable cardioverter-defibrillators. Ann Intern Med. 2010;153(9):592-599.
System Delay Is Mortality Marker in STEMI Patients Treated with Primary PCI
Clinical question: What is the relationship between system delays to reperfusion therapy and mortality in patients with ST-segment-elevation myocardial infarction (STEMI)?
Background: In patients with STEMI, an early reperfusion strategy is often sought, and several studies have focused on the association between door-to-balloon delay and outcomes. Focusing more broadly on the time from first contact with the healthcare system to the initiation of reperfusion therapy (system delay) might be a more relevant approach.
Study design: Historical follow-up study.
Setting: Three high-volume PCI centers in Denmark.
Synopsis: Using population-based medical registries of 6,209 Danish patients treated for STEMI with percutaneous coronary intervention (PCI), the authors examined the association between delays in reperfusion therapy and mortality. System delay encompassed the entire time from first contact with the healthcare system to the initiation of reperfusion therapy.
Overall, shorter system delay was associated with significantly decreased mortality, as were the individual components of system delay (prehospital delay and door-to-balloon delay). The shortest delays (0-60 minutes) corresponded to a mortality rate of 15%, and the longest delays (181-360 minutes) corresponded to a mortality rate of 31%. Patients were followed for a median of 3.4 years.
This study is unique, as it is the first to look at the association between system delay and outcomes in patients with STEMI transported by EMS and treated with primary PCI. The study highlights the harmful impact of longer system delays on mortality. Limitations of this study include possible underestimation of system delay and challenges surrounding the right marker for reperfusion.
Bottom line: System delay might serve as a broad, comprehensive marker for predicting mortality in patients with STEMI treated with primary PCI.
Citation: Terkelsen CJ, Sorensen JT, Maeng M, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA. 2010;304(7): 763-771.
D-Dimer Is Effective in Determining the Risk of VTE Recurrence after First Unprovoked Event
Clinical question: Does the timing, patient age, or cut point level affect the predictive value of a D-dimer in predicting VTE recurrence after a first unprovoked event?
Background: Anticoagulation duration after a first unprovoked VTE is at least three months, but it can be indefinite in patients with stable anticoagulation and low bleeding risk. Measuring a D-dimer level after discontinuation of anticoagulation is helpful in determining which patients might benefit from prolonged anticoagulation. However, several unanswered questions remain regarding D-dimer testing.
Study design: Patient-level meta-analysis.
Setting: Pooled patient-level data from seven prospective studies.
Synopsis: Patient-level data were obtained for all patients enrolled using post-treatment D-dimer measurement to predict recurrent VTE in patients with a first unprovoked VTE who had completed at least three months of anticoagulation therapy. The mean length of follow-up was 30 months. Patients with a positive D-dimer had recurrent VTE at a rate of 8.8 per 100 patient-years while those with a negative D-dimer had a rate of 3.7 per 100 patient-years.
Univariate analysis revealed an HR of 2.59 for patients with a positive versus a negative test result. The analysis also showed that the timing of the test, the age of the patient, and the actual cut points used for the various D-dimer tests did not affect the analysis significantly.
These studies’ strength is their large sample sizes and the use of prospective studies. The weaknesses include a mostly white patient population and incomplete data on all patients.
Bottom line: D-dimer testing is useful in predicting VTE recurrence after treatment for a first unprovoked event regardless of patient age, post-treatment timing, or the assay cut point used.
Citation: Douketis J, Tosetto A, Marcucci M, et al. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med. 2010;153(8): 523-531.
Thigh-High Stockings Are Better than Knee-High Stockings for Post-Stroke DVT Prophylaxis
Clinical question: Are thigh-high compression stockings better then knee-high stockings in immobilized acute-stroke patients?
Background: DVT is common in hospitalized stroke patients with immobility. Graduated compression stockings are often used for DVT prophylaxis, but the CLOTS-1 trial recently found that thigh-high stockings were ineffective after acute stroke. It is unclear if the more commonly used knee-high stockings are more effective than thigh-high stockings.
Study design: Parallel-group trial (the CLOTS-2 trial).
Setting: One hundred twelve hospitals in nine countries.
Synopsis: More than 3,100 patients with acute stroke and immobilization were recruited from January 2002 to May 2009. Patients were randomized to receive thigh-high or knee-high stockings. Patients also received usual care, including anticoagulants and a screening ultrasound for asymptomatic proximal DVT at seven to 10 days. Approximately 640 patients in each group also underwent ultrasound at 25-30 days.
Overall, 6.3% of patients in the thigh-high group had DVT, compared with 8.8% in the knee-high group (P=0.007). There were no significant differences in the secondary outcomes of pulmonary embolism or death. The thigh-high stockings had a higher number of adverse skin events. Enrollment was stopped early when the CLOTS-1 trial showed no difference in DVT rates between thigh-high stockings and no stockings.
Bottom line: Knee-high graduated compression stockings lead to worse outcomes than thigh-high stockings for DVT prophylaxis in immobilized acute-stroke patients.
Citation: CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration. Thigh-length versus below-knee stockings for deep venous thrombosis prophylaxis after stroke: a randomized trial. Ann Intern Med. 2010;153(9):553-562. TH
Pediatric HM Literature
Co-Infection with Pertussis in Infants Hospitalized for Bronchiolitis

Clinical question: How often are infants admitted with bronchiolitis co-infected with Bordatella pertussis?
Background: Infants admitted for bronchiolitis have previously been reported to have co-infection with B. pertussis. Given the nonspecific symptoms associated with early B. pertussis infection, as well as the epidemiology of ongoing outbreaks, it might be useful to better define the risk of co-infection in the seasonal surge of acute bronchiolitis.
Study design: Retrospective cohort study.
Setting: One university hospital in Finland.
Synopsis: A prior study had generated nasopharyngeal aspirate samples for viral antigen detection from 205 healthy, full-term infants younger than 6 months hospitalized for bronchiolitis from 2001 to 2004. Of these samples, 142 (69%) were of quality sufficient for B. pertussis PCR testing in 2009.
Twelve (8.5%) of the 142 infants admitted with bronchiolitis were found to have B. pertussis. Eleven of the 12 infants were co-infected with at least one other virus (RSV in eight of them). Infants who tested positive for pertussis were more often found to have coughing spells (41.7% vs. 14.6% in those who tested negative).
The reported rate of co-infection in this study is higher than other recent reports from the U.S., likely due to the fact that samples were collected during a time period when the incidence of pertussis was relatively high in Finland.
Nevertheless, given the magnitude of a recent pertussis outbreak in California, it might be useful to consider co-infection in young infants admitted for bronchiolitis in areas with a relatively higher incidence of pertussis.
Although the retrospective nature of this study and the lack of a reported definition of coughing spells make further conclusions difficult to draw, cough might deserve further scrutiny during bronchiolitis season.
Bottom line: Consider co-infection with pertussis in young infants admitted with bronchiolitis.
Citation: Nuolivirta K, Koponen P, He Q, et al. Bordatella pertussis infection is common in nonvaccinated infants admitted for bronchiolitis. Pediatr Infect Dis J. 2010;29(11):1013-1015.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effects of extended VTE prophylaxis in medical patients
- Outcomes with and without preprocedural statins
- Association of subclinical hypothyroidism and CHD
- BP treatment after intracerebral hemorrhage
- Outcomes of ICD therapy in the elderly
- Systems delays and outcomes of STEMI
- D-dimer to predict recurrent VTE
- Stocking height and risk of post-stroke DVT
Extending Anticoagulant Prophylaxis after Medical Hospitalization Decreases VTE, Increases Major Bleeding
Clinical question: For patients with acute medical illness, does extending low-molecular-weight heparin (LMWH) administration for up to 28 days after discharge reduce the incidence of venous thromboembolism (VTE)?
Background: DVT and pulmonary embolism (PE) are common hospital-acquired complications. LMWH has been shown to reduce VTE for medical and surgical patients, and extended-duration LMWH reduces VTE in high-risk surgical patients. Whether extending anticoagulant prophylaxis after discharge for acutely ill medical patients with reduced mobility improves outcomes is unknown.
Study design: Randomized, placebo-controlled trial.
Setting: Three hundred seventy hospitals in 20 countries.
Synopsis: Eligible patients were >40 years old, hospitalized with acute medical illness, and had reduced mobility for ≥3 days. Patients received enoxaparin 40 mg SC daily prophylaxis while hospitalized and were then randomized to an additional 28±4 days of enoxaparin or placebo. Patients received a screening ultrasound to assess for asymptomatic DVT. The primary outcome was a composite of asymptomatic proximal DVT, symptomatic DVT or PE, or fatal PE during the period of extended prophylaxis.
An interim analysis indicated that extended prophylaxis was ineffective; at that time, the protocol was amended to target patients with severe immobility or with moderate immobility plus an additional risk factor (e.g. cancer, prior VTE, or age >75).
The study found that extended prophylaxis decreased the composite VTE outcome (2.5% vs 4.0%, P<0.05) and symptomatic VTE (0.2% vs 1.0%, P<0.05). The incidence of major bleeding was increased in the extended prophylaxis group (0.8% vs 0.3%, P<0.05). There was no difference in mortality.
The unplanned, midstudy protocol amendment to target higher-risk patients is a concern, though the final analyses included patients pre- and post-amendment.
Bottom line: Extending LMWH beyond hospitalization for patients admitted with acute medical illness and decreased mobility decreases VTE, but increases major bleeding.
Citation: Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153(1);8-18.
Preprocedural Statin Therapy Reduces Postprocedural Myocardial Infarction
Clinical question: Does statin therapy reduce periprocedural cardiovascular events?
Background: Myocardial infarction (MI) and death are inherent risks of invasive procedures. Reduction of these risks in certain patient populations has been shown with the use of a beta blockade. Statins have shown promise during acute coronary syndrome. Questions remain about the role of statin therapy before invasive procedures in reducing adverse cardiovascular events.
Study design: Meta-analysis of randomized controlled trials.
Setting: Twenty-one studies involving 4,805 patients, published from inception of MEDLINE, Cochrane, and Clinicaltrials to February 2010.
Synopsis: The use of statins one to seven days preprocedure significantly reduced post-procedural MI in percutaneous coronary interventions (PCI) (P<0.0001). Statins given approximately four weeks in advance of noncardiac surgical procedures also significantly reduced postprocedural MI (P=0.004). An absolute risk reduction of 5.8% for postprocedural MI was found after PCI and 4.1% in noncardiac surgical procedures.
Statins did not show a significant reduction in postprocedural MI (P=0.40) or all-cause mortality (P=0.15) in coronary artery bypass graft surgery (CABG). However, statins did reduce post-CABG atrial fibrillation (P<0.0001).
The 21 studies used a variety of drugs and doses. However, the PCI studies favored atorvastatin 40 mg; more than half the CABG studies used atorvastatin 20 mg; and 91% of the noncardiac surgical studies used fluvastatin 80 mg. Dedicated trials are needed to demonstrate optimal statin agent, dose, and timing of therapy.
Bottom line: Preprocedural statin therapy reduces postprocedural MI after both PCI and noncardiac procedures but not after CABG.
Citation: Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy: a meta-analysis of randomized trials. J Am Coll Cardiol. 2010;56(19); 1099-1109.
Subclinical Hypothyroidism Increases the Risk of Coronary Heart Disease and Mortality
Clinical question: What are the risks of coronary heart disease (CHD) and mortality among adults with subclinical hypothyroidism?
Background: Subclinical hypo-thyroidism is defined as an elevated serum thyroid stimulating hormone (TSH) level with a normal T4 concentration. Controversy exists regarding the treatment of subclinical hypothyroidism. Because of the association with hyperlipidemia and atherosclerosis, treatment of subclinical hypothyroidism is thought to be beneficial. Previous data from large prospective cohort studies regarding this association are conflicting.
Study design: Study-level meta-analysis of prospective cohort studies.
Setting: Eleven prospective cohorts in the U.S., Europe, Australia, Brazil, and Japan from 1972 to 2007.
Synopsis: Among 55,287 adults, 3,450 (6.2%) had subclinical hypothyroidism and 51,837 were euthyroid. Using Cox proportional hazard models, the association of subclinical hypothyroidism with CHD and mortality were determined for each cohort.
The risk of CHD events and CHD mortality increased with higher TSH concentrations.
In age- and sex-adjusted analyses, the hazard ratio (HR) for CHD events were as follows: HR=1.0 (TSH=4.5-6.9 mIU/L); HR=1.17 (TSH=7-9.9 mIU/L), and HR=1.89 (TSH=10-19.9 mIU/L). Similarly, HRs for CHD mortality showed an increasing trend: 1.09, 1.42, and 1.58, respectively.
Although the association is clearly established here, randomized controlled trials are needed to address whether thyroxine replacement can prevent CHD and the TSH threshold that will provide the most clinical benefit.
Bottom line: Subclinical hypo-thyroidism is associated with an increased risk for CHD events and mortality, primarily in patients with TSH concentrations of 10 mIU/L or higher.
Citation: Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12): 1365-1374.
Reduction in Hematoma Growth after Acute Intracerebral Hemorrhage Associated with Lower Blood Pressure
Clinical question: Does intensive systolic blood pressure (SBP) <140 mmHg within one hour reduce hematoma growth after acute intracerebral bleeding?
Background: Early elevation of blood pressure after an acute intracerebral bleed is strongly associated with hematoma growth and worse outcomes. The pilot phase of the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) showed that early intensive blood pressure lowering reduced hematoma growth within six hours after onset of intracerebral hemorrhage.
Study design: Randomized controlled trial in which patients received an early intensive blood-pressure-lowering treatment (goal SBP<140 mmHg within one hour) or the AHA recommended best practice guidelines (goal SBP <180 mmHg), which were published in 1999.
Setting: Network of hospitals in China, South Korea, and Australia.
Synopsis: From 2005 to 2007, the study examined 404 patients with computed-tomography (CT) evidence of intracerebral hemorrhage, elevated SBP (150 mmHg-220 mmHg), and ability to commence BP lowering treatment within six hours of onset. Hematoma volumes were measured in the intensive treatment and guideline groups based on CT scans done at baseline and after 24 hours.
No significant association was found between the baseline SBP and the absolute or proportional growth of the hematoma. However, in the intensively treated patients who achieved target SBP within the first 24 hours, a significant association was found with the absolute and proportional hematoma growth.
Maximum reduction of hematoma growth occurred in the group with a median SBP of 135 mmHg.
This single-observational study did not include patients with severe intracranial bleeding who died or required surgical evacuation within the first 24 hours.
Hematoma size reduction did not improve survival or outcomes.
Bottom line: Intensive SBP lowering from 140 mmHg to 130 mmHg within one hour reduces hematoma growth after an intracranial hemorrhage.
Citation: Arima H, Anderson CS, Wang JG, et al. Lower treatment blood pressure is associated with the greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension. 2010;56(5):852-858.
Implantable Cardioverter-Defibrillator (ICD) Therapy for Primary Prevention of Sudden Cardiac Death Might Not Provide Survival Benefit to Elderly
Clinical question: Does ICD therapy for primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction improve survival in elderly patients?
Background: Several clinical trials of select individuals with severe left ventricular dysfunction (EF <40%) have demonstrated that ICD therapy is associated with a reduction in overall mortality. Given the costs and risks associated with ICD placement, it is important to assess how this therapy affects survival in younger versus older individuals.
Study design: Meta-analysis of five randomized controlled trials.
Setting: Five trials (MADIT-II, DEFINITE, DINAMIT, SCDHeFT, and IRIS).
Synopsis: All included studies compared ICD therapy to standard medical care in the primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction. Elderly patients comprised 44% of the 5,783 patients included in the study; elderly patients were defined as >65 in three studies, and >60 in two studies. Pooled analysis of the three trials examining ICD use for primary prevention found a nonsignificant reduction in all-cause mortality compared with medical therapy in elderly patients (HR 0.81 [95% CI 0.62 to 1.05], P=0.11). The two remaining studies involving post-MI patients showed no statistically significant reduction in mortality in elderly patients.
In contrast, pooled data from younger patients in the five trials showed that prophylactic ICD therapy reduced all-cause mortality.
None of the selected trials demonstrated evidence of selection, performance, detection, or attrition bias. Only a small number of studies were included, and four potentially relevant trials were not included because mortality data by age group were not available.
Trials including cardiac resynchronization therapy (CRT) were excluded from this meta-analysis, and elderly patients meeting criteria for CRT comprise an important group that must be considered separately.
Bottom line: There is no definitive reduction in mortality with prophylactic ICD therapy in elderly patients with severe left ventricular dysfunction.
Citation: Santangeli P, Di Biase L, Dello Russo A, et al. Meta-analysis: age and effectiveness of prophylactic implantable cardioverter-defibrillators. Ann Intern Med. 2010;153(9):592-599.
System Delay Is Mortality Marker in STEMI Patients Treated with Primary PCI
Clinical question: What is the relationship between system delays to reperfusion therapy and mortality in patients with ST-segment-elevation myocardial infarction (STEMI)?
Background: In patients with STEMI, an early reperfusion strategy is often sought, and several studies have focused on the association between door-to-balloon delay and outcomes. Focusing more broadly on the time from first contact with the healthcare system to the initiation of reperfusion therapy (system delay) might be a more relevant approach.
Study design: Historical follow-up study.
Setting: Three high-volume PCI centers in Denmark.
Synopsis: Using population-based medical registries of 6,209 Danish patients treated for STEMI with percutaneous coronary intervention (PCI), the authors examined the association between delays in reperfusion therapy and mortality. System delay encompassed the entire time from first contact with the healthcare system to the initiation of reperfusion therapy.
Overall, shorter system delay was associated with significantly decreased mortality, as were the individual components of system delay (prehospital delay and door-to-balloon delay). The shortest delays (0-60 minutes) corresponded to a mortality rate of 15%, and the longest delays (181-360 minutes) corresponded to a mortality rate of 31%. Patients were followed for a median of 3.4 years.
This study is unique, as it is the first to look at the association between system delay and outcomes in patients with STEMI transported by EMS and treated with primary PCI. The study highlights the harmful impact of longer system delays on mortality. Limitations of this study include possible underestimation of system delay and challenges surrounding the right marker for reperfusion.
Bottom line: System delay might serve as a broad, comprehensive marker for predicting mortality in patients with STEMI treated with primary PCI.
Citation: Terkelsen CJ, Sorensen JT, Maeng M, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA. 2010;304(7): 763-771.
D-Dimer Is Effective in Determining the Risk of VTE Recurrence after First Unprovoked Event
Clinical question: Does the timing, patient age, or cut point level affect the predictive value of a D-dimer in predicting VTE recurrence after a first unprovoked event?
Background: Anticoagulation duration after a first unprovoked VTE is at least three months, but it can be indefinite in patients with stable anticoagulation and low bleeding risk. Measuring a D-dimer level after discontinuation of anticoagulation is helpful in determining which patients might benefit from prolonged anticoagulation. However, several unanswered questions remain regarding D-dimer testing.
Study design: Patient-level meta-analysis.
Setting: Pooled patient-level data from seven prospective studies.
Synopsis: Patient-level data were obtained for all patients enrolled using post-treatment D-dimer measurement to predict recurrent VTE in patients with a first unprovoked VTE who had completed at least three months of anticoagulation therapy. The mean length of follow-up was 30 months. Patients with a positive D-dimer had recurrent VTE at a rate of 8.8 per 100 patient-years while those with a negative D-dimer had a rate of 3.7 per 100 patient-years.
Univariate analysis revealed an HR of 2.59 for patients with a positive versus a negative test result. The analysis also showed that the timing of the test, the age of the patient, and the actual cut points used for the various D-dimer tests did not affect the analysis significantly.
These studies’ strength is their large sample sizes and the use of prospective studies. The weaknesses include a mostly white patient population and incomplete data on all patients.
Bottom line: D-dimer testing is useful in predicting VTE recurrence after treatment for a first unprovoked event regardless of patient age, post-treatment timing, or the assay cut point used.
Citation: Douketis J, Tosetto A, Marcucci M, et al. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med. 2010;153(8): 523-531.
Thigh-High Stockings Are Better than Knee-High Stockings for Post-Stroke DVT Prophylaxis
Clinical question: Are thigh-high compression stockings better then knee-high stockings in immobilized acute-stroke patients?
Background: DVT is common in hospitalized stroke patients with immobility. Graduated compression stockings are often used for DVT prophylaxis, but the CLOTS-1 trial recently found that thigh-high stockings were ineffective after acute stroke. It is unclear if the more commonly used knee-high stockings are more effective than thigh-high stockings.
Study design: Parallel-group trial (the CLOTS-2 trial).
Setting: One hundred twelve hospitals in nine countries.
Synopsis: More than 3,100 patients with acute stroke and immobilization were recruited from January 2002 to May 2009. Patients were randomized to receive thigh-high or knee-high stockings. Patients also received usual care, including anticoagulants and a screening ultrasound for asymptomatic proximal DVT at seven to 10 days. Approximately 640 patients in each group also underwent ultrasound at 25-30 days.
Overall, 6.3% of patients in the thigh-high group had DVT, compared with 8.8% in the knee-high group (P=0.007). There were no significant differences in the secondary outcomes of pulmonary embolism or death. The thigh-high stockings had a higher number of adverse skin events. Enrollment was stopped early when the CLOTS-1 trial showed no difference in DVT rates between thigh-high stockings and no stockings.
Bottom line: Knee-high graduated compression stockings lead to worse outcomes than thigh-high stockings for DVT prophylaxis in immobilized acute-stroke patients.
Citation: CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration. Thigh-length versus below-knee stockings for deep venous thrombosis prophylaxis after stroke: a randomized trial. Ann Intern Med. 2010;153(9):553-562. TH
Pediatric HM Literature
Co-Infection with Pertussis in Infants Hospitalized for Bronchiolitis
Clinical question: How often are infants admitted with bronchiolitis co-infected with Bordatella pertussis?
Background: Infants admitted for bronchiolitis have previously been reported to have co-infection with B. pertussis. Given the nonspecific symptoms associated with early B. pertussis infection, as well as the epidemiology of ongoing outbreaks, it might be useful to better define the risk of co-infection in the seasonal surge of acute bronchiolitis.
Study design: Retrospective cohort study.
Setting: One university hospital in Finland.
Synopsis: A prior study had generated nasopharyngeal aspirate samples for viral antigen detection from 205 healthy, full-term infants younger than 6 months hospitalized for bronchiolitis from 2001 to 2004. Of these samples, 142 (69%) were of quality sufficient for B. pertussis PCR testing in 2009.
Twelve (8.5%) of the 142 infants admitted with bronchiolitis were found to have B. pertussis. Eleven of the 12 infants were co-infected with at least one other virus (RSV in eight of them). Infants who tested positive for pertussis were more often found to have coughing spells (41.7% vs. 14.6% in those who tested negative).
The reported rate of co-infection in this study is higher than other recent reports from the U.S., likely due to the fact that samples were collected during a time period when the incidence of pertussis was relatively high in Finland.
Nevertheless, given the magnitude of a recent pertussis outbreak in California, it might be useful to consider co-infection in young infants admitted for bronchiolitis in areas with a relatively higher incidence of pertussis.
Although the retrospective nature of this study and the lack of a reported definition of coughing spells make further conclusions difficult to draw, cough might deserve further scrutiny during bronchiolitis season.
Bottom line: Consider co-infection with pertussis in young infants admitted with bronchiolitis.
Citation: Nuolivirta K, Koponen P, He Q, et al. Bordatella pertussis infection is common in nonvaccinated infants admitted for bronchiolitis. Pediatr Infect Dis J. 2010;29(11):1013-1015.
In This Edition
Literature at a Glance
A guide to this month’s studies
- Effects of extended VTE prophylaxis in medical patients
- Outcomes with and without preprocedural statins
- Association of subclinical hypothyroidism and CHD
- BP treatment after intracerebral hemorrhage
- Outcomes of ICD therapy in the elderly
- Systems delays and outcomes of STEMI
- D-dimer to predict recurrent VTE
- Stocking height and risk of post-stroke DVT
Extending Anticoagulant Prophylaxis after Medical Hospitalization Decreases VTE, Increases Major Bleeding
Clinical question: For patients with acute medical illness, does extending low-molecular-weight heparin (LMWH) administration for up to 28 days after discharge reduce the incidence of venous thromboembolism (VTE)?
Background: DVT and pulmonary embolism (PE) are common hospital-acquired complications. LMWH has been shown to reduce VTE for medical and surgical patients, and extended-duration LMWH reduces VTE in high-risk surgical patients. Whether extending anticoagulant prophylaxis after discharge for acutely ill medical patients with reduced mobility improves outcomes is unknown.
Study design: Randomized, placebo-controlled trial.
Setting: Three hundred seventy hospitals in 20 countries.
Synopsis: Eligible patients were >40 years old, hospitalized with acute medical illness, and had reduced mobility for ≥3 days. Patients received enoxaparin 40 mg SC daily prophylaxis while hospitalized and were then randomized to an additional 28±4 days of enoxaparin or placebo. Patients received a screening ultrasound to assess for asymptomatic DVT. The primary outcome was a composite of asymptomatic proximal DVT, symptomatic DVT or PE, or fatal PE during the period of extended prophylaxis.
An interim analysis indicated that extended prophylaxis was ineffective; at that time, the protocol was amended to target patients with severe immobility or with moderate immobility plus an additional risk factor (e.g. cancer, prior VTE, or age >75).
The study found that extended prophylaxis decreased the composite VTE outcome (2.5% vs 4.0%, P<0.05) and symptomatic VTE (0.2% vs 1.0%, P<0.05). The incidence of major bleeding was increased in the extended prophylaxis group (0.8% vs 0.3%, P<0.05). There was no difference in mortality.
The unplanned, midstudy protocol amendment to target higher-risk patients is a concern, though the final analyses included patients pre- and post-amendment.
Bottom line: Extending LMWH beyond hospitalization for patients admitted with acute medical illness and decreased mobility decreases VTE, but increases major bleeding.
Citation: Hull RD, Schellong SM, Tapson VF, et al. Extended-duration venous thromboembolism prophylaxis in acutely ill medical patients with recently reduced mobility: a randomized trial. Ann Intern Med. 2010;153(1);8-18.
Preprocedural Statin Therapy Reduces Postprocedural Myocardial Infarction
Clinical question: Does statin therapy reduce periprocedural cardiovascular events?
Background: Myocardial infarction (MI) and death are inherent risks of invasive procedures. Reduction of these risks in certain patient populations has been shown with the use of a beta blockade. Statins have shown promise during acute coronary syndrome. Questions remain about the role of statin therapy before invasive procedures in reducing adverse cardiovascular events.
Study design: Meta-analysis of randomized controlled trials.
Setting: Twenty-one studies involving 4,805 patients, published from inception of MEDLINE, Cochrane, and Clinicaltrials to February 2010.
Synopsis: The use of statins one to seven days preprocedure significantly reduced post-procedural MI in percutaneous coronary interventions (PCI) (P<0.0001). Statins given approximately four weeks in advance of noncardiac surgical procedures also significantly reduced postprocedural MI (P=0.004). An absolute risk reduction of 5.8% for postprocedural MI was found after PCI and 4.1% in noncardiac surgical procedures.
Statins did not show a significant reduction in postprocedural MI (P=0.40) or all-cause mortality (P=0.15) in coronary artery bypass graft surgery (CABG). However, statins did reduce post-CABG atrial fibrillation (P<0.0001).
The 21 studies used a variety of drugs and doses. However, the PCI studies favored atorvastatin 40 mg; more than half the CABG studies used atorvastatin 20 mg; and 91% of the noncardiac surgical studies used fluvastatin 80 mg. Dedicated trials are needed to demonstrate optimal statin agent, dose, and timing of therapy.
Bottom line: Preprocedural statin therapy reduces postprocedural MI after both PCI and noncardiac procedures but not after CABG.
Citation: Winchester DE, Wen X, Xie L, Bavry AA. Evidence of pre-procedural statin therapy: a meta-analysis of randomized trials. J Am Coll Cardiol. 2010;56(19); 1099-1109.
Subclinical Hypothyroidism Increases the Risk of Coronary Heart Disease and Mortality
Clinical question: What are the risks of coronary heart disease (CHD) and mortality among adults with subclinical hypothyroidism?
Background: Subclinical hypo-thyroidism is defined as an elevated serum thyroid stimulating hormone (TSH) level with a normal T4 concentration. Controversy exists regarding the treatment of subclinical hypothyroidism. Because of the association with hyperlipidemia and atherosclerosis, treatment of subclinical hypothyroidism is thought to be beneficial. Previous data from large prospective cohort studies regarding this association are conflicting.
Study design: Study-level meta-analysis of prospective cohort studies.
Setting: Eleven prospective cohorts in the U.S., Europe, Australia, Brazil, and Japan from 1972 to 2007.
Synopsis: Among 55,287 adults, 3,450 (6.2%) had subclinical hypothyroidism and 51,837 were euthyroid. Using Cox proportional hazard models, the association of subclinical hypothyroidism with CHD and mortality were determined for each cohort.
The risk of CHD events and CHD mortality increased with higher TSH concentrations.
In age- and sex-adjusted analyses, the hazard ratio (HR) for CHD events were as follows: HR=1.0 (TSH=4.5-6.9 mIU/L); HR=1.17 (TSH=7-9.9 mIU/L), and HR=1.89 (TSH=10-19.9 mIU/L). Similarly, HRs for CHD mortality showed an increasing trend: 1.09, 1.42, and 1.58, respectively.
Although the association is clearly established here, randomized controlled trials are needed to address whether thyroxine replacement can prevent CHD and the TSH threshold that will provide the most clinical benefit.
Bottom line: Subclinical hypo-thyroidism is associated with an increased risk for CHD events and mortality, primarily in patients with TSH concentrations of 10 mIU/L or higher.
Citation: Rodondi N, den Elzen WP, Bauer DC, et al. Subclinical hypothyroidism and the risk of coronary heart disease and mortality. JAMA. 2010;304(12): 1365-1374.
Reduction in Hematoma Growth after Acute Intracerebral Hemorrhage Associated with Lower Blood Pressure
Clinical question: Does intensive systolic blood pressure (SBP) <140 mmHg within one hour reduce hematoma growth after acute intracerebral bleeding?
Background: Early elevation of blood pressure after an acute intracerebral bleed is strongly associated with hematoma growth and worse outcomes. The pilot phase of the Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) showed that early intensive blood pressure lowering reduced hematoma growth within six hours after onset of intracerebral hemorrhage.
Study design: Randomized controlled trial in which patients received an early intensive blood-pressure-lowering treatment (goal SBP<140 mmHg within one hour) or the AHA recommended best practice guidelines (goal SBP <180 mmHg), which were published in 1999.
Setting: Network of hospitals in China, South Korea, and Australia.
Synopsis: From 2005 to 2007, the study examined 404 patients with computed-tomography (CT) evidence of intracerebral hemorrhage, elevated SBP (150 mmHg-220 mmHg), and ability to commence BP lowering treatment within six hours of onset. Hematoma volumes were measured in the intensive treatment and guideline groups based on CT scans done at baseline and after 24 hours.
No significant association was found between the baseline SBP and the absolute or proportional growth of the hematoma. However, in the intensively treated patients who achieved target SBP within the first 24 hours, a significant association was found with the absolute and proportional hematoma growth.
Maximum reduction of hematoma growth occurred in the group with a median SBP of 135 mmHg.
This single-observational study did not include patients with severe intracranial bleeding who died or required surgical evacuation within the first 24 hours.
Hematoma size reduction did not improve survival or outcomes.
Bottom line: Intensive SBP lowering from 140 mmHg to 130 mmHg within one hour reduces hematoma growth after an intracranial hemorrhage.
Citation: Arima H, Anderson CS, Wang JG, et al. Lower treatment blood pressure is associated with the greatest reduction in hematoma growth after acute intracerebral hemorrhage. Hypertension. 2010;56(5):852-858.
Implantable Cardioverter-Defibrillator (ICD) Therapy for Primary Prevention of Sudden Cardiac Death Might Not Provide Survival Benefit to Elderly
Clinical question: Does ICD therapy for primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction improve survival in elderly patients?
Background: Several clinical trials of select individuals with severe left ventricular dysfunction (EF <40%) have demonstrated that ICD therapy is associated with a reduction in overall mortality. Given the costs and risks associated with ICD placement, it is important to assess how this therapy affects survival in younger versus older individuals.
Study design: Meta-analysis of five randomized controlled trials.
Setting: Five trials (MADIT-II, DEFINITE, DINAMIT, SCDHeFT, and IRIS).
Synopsis: All included studies compared ICD therapy to standard medical care in the primary prevention of sudden cardiac death in individuals with severe left ventricular dysfunction. Elderly patients comprised 44% of the 5,783 patients included in the study; elderly patients were defined as >65 in three studies, and >60 in two studies. Pooled analysis of the three trials examining ICD use for primary prevention found a nonsignificant reduction in all-cause mortality compared with medical therapy in elderly patients (HR 0.81 [95% CI 0.62 to 1.05], P=0.11). The two remaining studies involving post-MI patients showed no statistically significant reduction in mortality in elderly patients.
In contrast, pooled data from younger patients in the five trials showed that prophylactic ICD therapy reduced all-cause mortality.
None of the selected trials demonstrated evidence of selection, performance, detection, or attrition bias. Only a small number of studies were included, and four potentially relevant trials were not included because mortality data by age group were not available.
Trials including cardiac resynchronization therapy (CRT) were excluded from this meta-analysis, and elderly patients meeting criteria for CRT comprise an important group that must be considered separately.
Bottom line: There is no definitive reduction in mortality with prophylactic ICD therapy in elderly patients with severe left ventricular dysfunction.
Citation: Santangeli P, Di Biase L, Dello Russo A, et al. Meta-analysis: age and effectiveness of prophylactic implantable cardioverter-defibrillators. Ann Intern Med. 2010;153(9):592-599.
System Delay Is Mortality Marker in STEMI Patients Treated with Primary PCI
Clinical question: What is the relationship between system delays to reperfusion therapy and mortality in patients with ST-segment-elevation myocardial infarction (STEMI)?
Background: In patients with STEMI, an early reperfusion strategy is often sought, and several studies have focused on the association between door-to-balloon delay and outcomes. Focusing more broadly on the time from first contact with the healthcare system to the initiation of reperfusion therapy (system delay) might be a more relevant approach.
Study design: Historical follow-up study.
Setting: Three high-volume PCI centers in Denmark.
Synopsis: Using population-based medical registries of 6,209 Danish patients treated for STEMI with percutaneous coronary intervention (PCI), the authors examined the association between delays in reperfusion therapy and mortality. System delay encompassed the entire time from first contact with the healthcare system to the initiation of reperfusion therapy.
Overall, shorter system delay was associated with significantly decreased mortality, as were the individual components of system delay (prehospital delay and door-to-balloon delay). The shortest delays (0-60 minutes) corresponded to a mortality rate of 15%, and the longest delays (181-360 minutes) corresponded to a mortality rate of 31%. Patients were followed for a median of 3.4 years.
This study is unique, as it is the first to look at the association between system delay and outcomes in patients with STEMI transported by EMS and treated with primary PCI. The study highlights the harmful impact of longer system delays on mortality. Limitations of this study include possible underestimation of system delay and challenges surrounding the right marker for reperfusion.
Bottom line: System delay might serve as a broad, comprehensive marker for predicting mortality in patients with STEMI treated with primary PCI.
Citation: Terkelsen CJ, Sorensen JT, Maeng M, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA. 2010;304(7): 763-771.
D-Dimer Is Effective in Determining the Risk of VTE Recurrence after First Unprovoked Event
Clinical question: Does the timing, patient age, or cut point level affect the predictive value of a D-dimer in predicting VTE recurrence after a first unprovoked event?
Background: Anticoagulation duration after a first unprovoked VTE is at least three months, but it can be indefinite in patients with stable anticoagulation and low bleeding risk. Measuring a D-dimer level after discontinuation of anticoagulation is helpful in determining which patients might benefit from prolonged anticoagulation. However, several unanswered questions remain regarding D-dimer testing.
Study design: Patient-level meta-analysis.
Setting: Pooled patient-level data from seven prospective studies.
Synopsis: Patient-level data were obtained for all patients enrolled using post-treatment D-dimer measurement to predict recurrent VTE in patients with a first unprovoked VTE who had completed at least three months of anticoagulation therapy. The mean length of follow-up was 30 months. Patients with a positive D-dimer had recurrent VTE at a rate of 8.8 per 100 patient-years while those with a negative D-dimer had a rate of 3.7 per 100 patient-years.
Univariate analysis revealed an HR of 2.59 for patients with a positive versus a negative test result. The analysis also showed that the timing of the test, the age of the patient, and the actual cut points used for the various D-dimer tests did not affect the analysis significantly.
These studies’ strength is their large sample sizes and the use of prospective studies. The weaknesses include a mostly white patient population and incomplete data on all patients.
Bottom line: D-dimer testing is useful in predicting VTE recurrence after treatment for a first unprovoked event regardless of patient age, post-treatment timing, or the assay cut point used.
Citation: Douketis J, Tosetto A, Marcucci M, et al. Patient-level meta-analysis: effect of measurement timing, threshold, and patient age on ability of D-dimer testing to assess recurrence risk after unprovoked venous thromboembolism. Ann Intern Med. 2010;153(8): 523-531.
Thigh-High Stockings Are Better than Knee-High Stockings for Post-Stroke DVT Prophylaxis
Clinical question: Are thigh-high compression stockings better then knee-high stockings in immobilized acute-stroke patients?
Background: DVT is common in hospitalized stroke patients with immobility. Graduated compression stockings are often used for DVT prophylaxis, but the CLOTS-1 trial recently found that thigh-high stockings were ineffective after acute stroke. It is unclear if the more commonly used knee-high stockings are more effective than thigh-high stockings.
Study design: Parallel-group trial (the CLOTS-2 trial).
Setting: One hundred twelve hospitals in nine countries.
Synopsis: More than 3,100 patients with acute stroke and immobilization were recruited from January 2002 to May 2009. Patients were randomized to receive thigh-high or knee-high stockings. Patients also received usual care, including anticoagulants and a screening ultrasound for asymptomatic proximal DVT at seven to 10 days. Approximately 640 patients in each group also underwent ultrasound at 25-30 days.
Overall, 6.3% of patients in the thigh-high group had DVT, compared with 8.8% in the knee-high group (P=0.007). There were no significant differences in the secondary outcomes of pulmonary embolism or death. The thigh-high stockings had a higher number of adverse skin events. Enrollment was stopped early when the CLOTS-1 trial showed no difference in DVT rates between thigh-high stockings and no stockings.
Bottom line: Knee-high graduated compression stockings lead to worse outcomes than thigh-high stockings for DVT prophylaxis in immobilized acute-stroke patients.
Citation: CLOTS (Clots in Legs Or sTockings after Stroke) Trial Collaboration. Thigh-length versus below-knee stockings for deep venous thrombosis prophylaxis after stroke: a randomized trial. Ann Intern Med. 2010;153(9):553-562. TH
Pediatric HM Literature
Co-Infection with Pertussis in Infants Hospitalized for Bronchiolitis
Clinical question: How often are infants admitted with bronchiolitis co-infected with Bordatella pertussis?
Background: Infants admitted for bronchiolitis have previously been reported to have co-infection with B. pertussis. Given the nonspecific symptoms associated with early B. pertussis infection, as well as the epidemiology of ongoing outbreaks, it might be useful to better define the risk of co-infection in the seasonal surge of acute bronchiolitis.
Study design: Retrospective cohort study.
Setting: One university hospital in Finland.
Synopsis: A prior study had generated nasopharyngeal aspirate samples for viral antigen detection from 205 healthy, full-term infants younger than 6 months hospitalized for bronchiolitis from 2001 to 2004. Of these samples, 142 (69%) were of quality sufficient for B. pertussis PCR testing in 2009.
Twelve (8.5%) of the 142 infants admitted with bronchiolitis were found to have B. pertussis. Eleven of the 12 infants were co-infected with at least one other virus (RSV in eight of them). Infants who tested positive for pertussis were more often found to have coughing spells (41.7% vs. 14.6% in those who tested negative).
The reported rate of co-infection in this study is higher than other recent reports from the U.S., likely due to the fact that samples were collected during a time period when the incidence of pertussis was relatively high in Finland.
Nevertheless, given the magnitude of a recent pertussis outbreak in California, it might be useful to consider co-infection in young infants admitted for bronchiolitis in areas with a relatively higher incidence of pertussis.
Although the retrospective nature of this study and the lack of a reported definition of coughing spells make further conclusions difficult to draw, cough might deserve further scrutiny during bronchiolitis season.
Bottom line: Consider co-infection with pertussis in young infants admitted with bronchiolitis.
Citation: Nuolivirta K, Koponen P, He Q, et al. Bordatella pertussis infection is common in nonvaccinated infants admitted for bronchiolitis. Pediatr Infect Dis J. 2010;29(11):1013-1015.