User login
Patients with fibromyalgia often resist being referred to a psychiatrist because they fear being told their pain and other somatic symptoms are “all in their heads.” Evidence is mounting that they may be literally correct—the symptoms of fibromyalgia appear to have a physiologic connection with the central nervous system. Abnormal CNS activity, including sleep patterns, response to stress, pain processing, and neurotransmitter levels, has been documented in patients with fibromyalgia.
As psychiatrists, we can reassure these patients—and their primary care physicians and rheumatologists—that we are in a position to help because we:
- have expertise in assessing mood and anxiety disorders and in managing antidepressants, the medication physicians most commonly prescribe for fibromyalgia;
- are skilled in the use of the anticonvulsant gabapentin, which is being used in fibromyalgia for its analgesic and sedative effects;
- can offer much-needed support through psychotherapy, as chronic pain and other fibromyalgia-related symptoms create great stress in these patients’ lives.
Antidepressants are showing promise as an effective treatment for pain, fatigue, and depression in patients with fibromyalgia in studies by our group and others. The following information can help you stay current with the newest understandings of this ailment.
Table 1
CRITERIA FOR DIAGNOSING FIBROMYALGIA
| 1. | History of widespread pain |
| Definition Pain in the right and left side of the body, pain above and below the waist, axial skeletal pain (cervical spine or anterior chest or thoracic spine or low back). In this definition, shoulder and buttock pain is considered as pain for each involved side. “Low back” pain is considered lower segment pain. | |
| 2. | Pain in 11 of 18 tender point sites on digital palpation |
| Definition Pain, on digital palpation, must be present in at least 11 of the following 18 tender points: | |
| Occiput Bilateral, at the suboccipital muscle insertion | |
| Low cervical Bilateral, at the anterior aspects of the intertransverse spaces at C5-C7 | |
| Trapezius Bilateral, at the midpoint of the upper border | |
| Supraspinatus Bilateral, at origins, above the scapula spine near the medial border | |
| Second rib Bilateral, at the second costochondral junctions, just lateral to the junctions on upper surfaces | |
| Lateral epicondyle Bilateral, 2 cm distal to the epicondyles | |
| Gluteal Bilateral, in upper outer quadrants of buttocks in anterior fold of muscle | |
| Greater trochanter Bilateral, posterior to the trochanteric prominence | |
| Knee Bilateral, at the medial fat pad proximal to the joint line | |
| Digital palpation should be performed with an approximate force of 4 kg. For a tender point to be considered “positive” the patient must state that the palpation was painful. “Tender” is not to be considered “painful” Source: American College of Rheumatology1 | |
Figure 1 LOCATION OF FIBROMYALGIA TENDER POINTS
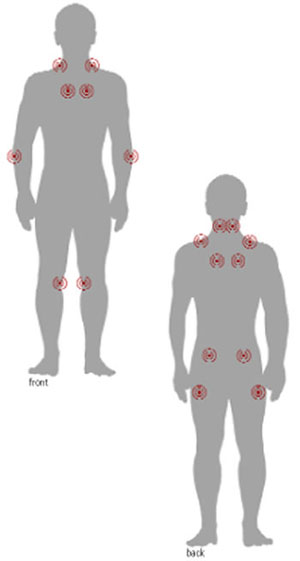
To palpate tender point sites, pressure is applied with the thumb pad perpendicularly to each site and the force increased by 1 kg per second until 4 kg of pressure is achieved. Whitening of the thumbnail bed usually occurs when applying the 4-kg force.
Mood disorders in fibromyalgia
A diagnosis of fibromyalgia requires the finding of widespread pain and tenderness at specific anatomic points (Table 1, Figure 1).1 Most patients also report fatigue, sleep disturbance, and morning stiffness (Box 1).2-5 American College of Rheumatology criteria do not require exclusionary tests such as radiographs and blood tests for the diagnosis.
Primary care physicians are increasingly making the diagnosis themselves and referring patients to rheumatologists only when conditions other than fibromyalgia are suspected. The differential diagnosis is broad, and other rheumatic and nonrheumatic disorders have similar symptoms, require different treatment, and affect fibromyalgia management (Table 2).6
Patients with fibromyalgia often report symptoms of major depressive disorder, such as depressed mood, anxiety, fatigue, and insomnia.7 Many psychological studies of such patients have documented increased rates of depressive symptoms.8 Depression and anxiety symptoms are common and frequently severe, even among individuals with fibromyalgia in the general population.9
Patients’ mood and anxiety disorders correlate highly with the number of medically unexplained symptoms and are associated with functional disability.10 The presence of psychological symptoms predicts persistent fibromyalgia symptoms,11 and psychological distress is strongly associated with symptom severity.12
Evidence for a CNS link
CNS mechanisms appear to contribute to the development of clinical findings in fibromyalgia.
Abnormal sleep A qualitative defect in sleep has been identified in patients with fibromyalgia.13 This sleep abnormality consists of inappropriate intrusion of alpha waves (normally seen during wakefulness or REM sleep) into deep sleep (usually characterized by delta waves).13 Some researchers believe alpha-delta sleep intrusion is associated with the chronic musculoskeletal pain and fatigue of fibromyalgia and, in turn, is mediated by an abnormality in central serotonergic neurotransmission.14 This sleep abnormality is not specific to fibromyalgia and can be found in other conditions, however.15 Debate continues regarding the role of sleep dysregulation in the pathophysiology of fibromyalgia.
Fibromyalgia is more common in women than men, with an estimated prevalence of 2% in the general population (3.4% in women and 0.5% in men). Its prevalence increases with age, rising sharply in middle age and then dropping off after age 80.2
Fibromyalgia is seen most often in women ages 50 and older.2 It occurs in 5% to 6% of patients presenting to general medical and family practice clinics and in 15% to 20% of patients presenting to rheumatologists, making it one of the most common diagnoses in office-based rheumatology practices.
American College of Rheumatology criteria may require only widespread pain and tenderness for a diagnosis of fibromyalgia, but most patients (73% to 85%) also report fatigue, sleep disturbance, and morning stiffness. Many (45% to 69%) report “pain all over,” paresthesias, headache, and anxiety. Co-occurring irritable bowel syndrome, sicca symptoms, and Raynaud’s phenomenon are less common (<35%).1 Patients with fibromyalgia also have high lifetime rates of other comorbid disorders, including migraine, chronic fatigue syndrome, and mood and anxiety disorders. Some patients report weakness, forgetfulness, difficulties in concentration, urinary frequency, history of dysmenorrhea, and restless legs.
Fibromyalgia is chronic, debilitating, and often leads to substantial functional impairment.3 Most patients with fibromyalgia do not display significant improvement over an average of 7 years of treatment.4 Patients with fibromyalgia report lower quality of well-being than patients with diagnoses of chronic obstructive pulmonary disease, rheumatoid arthritis, atrial fibrillation, advanced cancer, and several other chronic diseases.5
Stress response Stress appears to precipitate or exacerbate fibromyalgia symptoms in many patients.16 For example, fibromyalgia appears to be associated with victimization (adult and childhood sexual, physical, and emotional trauma), and this stress may trigger the development of fibromyalgia in some patients.17
Patients with fibromyalgia appear to develop disturbances in the two major stress-response systems: the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system.16 Although the interpretation of these disturbances is still debated, some researchers suggest that the available data point to reduction in CNS corticotropin releasing hormone (CRH), the key mediator in the HPA axis.18,19 CRH is also a behaviorally active peptide that leads to physiologic and behavioral arousal when administered centrally to animals.18 CRH reduction could contribute to the clinical features of fibromyalgia (e.g., fatigue) either directly or indirectly by causing a relative glucocorticoid deficiency.18,19
Table 2
DIFFERENTIAL DIAGNOSIS OF FIBROMYALGIA
| Rheumatic disorders | Nonrheumatic disorders |
|---|---|
| Rheumatoid arthritis | Hypothyroidism |
| Systemic lupus erythematosus | Sleep apnea |
| Polyarticular osteoarthritis | Hepatitis |
| Polymyalgia rheumatica | Cushing’s syndrome |
| Addison’s disease | |
| Hyperparathyroidism | |
| Adapted from Clauw DJ. Fibromyalgia syndrome: an update on current understanding and medical management. Rheumatol Grand Rds 2000;3:1-9. | |
Fibromyalgia is also associated with moderate basal hypocortisolism.18,19 A relative glucocorticoid deficiency could contribute to fibromyalgia’s characteristic fatigue, arthralgias, myalgias, and disturbances in mood and sleep.18 This deficiency may also cause some of the immunologic disturbances seen with fibromyalgia.18,19
Atypical depression, which shares such features of fibromyalgia as profound lethargy, is also associated with inappropriately normal or reduced activation of the HPA axis and a functional deficit in the release of hypothalamic CRH.18 The unifying feature of HPA axis activity in both atypical depression and fibromyalgia may be a shared hypofunctioning.18 A more complete understanding of the neuroendocrine changes in fibromyalgia awaits further study.
Pain processing Aberrant CNS processing of pain may also play a role in fibromyalgia.16,20 Fibromyalgia is sometimes precipitated by physical trauma.21 A traumatic injury may start a process in susceptible individuals that leads to an enhanced central processing of painful stimuli characteristic of central sensitization.22 Patients with fibromyalgia often develop an increased response to painful stimuli (hyeralgesia) and experience pain from normally nonnoxious stimuli (allodynia).20
Substance P, an important nociceptive neurotransmitter, may have a role in generating central sensitization.23 Elevated concentrations of substance P have been found in the cerebrospinal fluid (CSF) of individuals with fibromyalgia.24 Substance P also inhibits CRH release and may contribute to low CRH activity in fibromyalgia.16
Neurotransmitter defects A functional reduction in serotonergic activity has been demonstrated in patients with fibromyalgia. Schwarz et al25 found a strong negative correlation between serum concentrations of the primary serotonin metabolite, 5-hydroxyindoleacetic acid (5-HIAA), and substance P, pain, and insomnia. Evidence also exists of reduced concentrations of the primary norepinephrine metabolite, 3-methoxy-4-hydroxyphenethylene (MHPG), in the CSF of patients with fibromyalgia.26 Reduced serotonin and norepinephrine levels in descending pain-inhibitory pathways may cause the allodynia and hyperalgesia of fibromyalgia.
Pharmacologic treatment
Most studies of pharmacologic treatment of fibromyalgia have examined antidepressants for three reasons:
- There is evidence of the successful use of antidepressants in other chronic pain conditions.27
- These agents are effective for treating mood and anxiety disorders, which frequently occur in patients with fibromyalgia and may share a common physiologic abnormality.28
- Antidepressants might enhance the activity of neurotransmitters such as serotonin and norepinephrine in the descending inhibitory pain pathways, leading to reduced pain perception.29
Tricyclics In randomized, controlled trials, tricyclic medications (including the muscle relaxant cyclobenzaprine) appear to be moderately effective in improving fibromyalgia symptoms. Two meta-analyses of trials of tricyclic medications (amitriptyline, dothiepin, cyclobenzaprine, clomipramine, and maprotiline) have found similar results.30,31 Our group found the greatest effect on measures of sleep improvement, which may be due in part to tricyclics’ sedative properties.30 Many patients with fibromyalgia, however, cannot tolerate the sedative and other side effects associated with tricyclic agents, even though low dosages (e.g., 25 mg/d of amitriptyline) have typically been used in clinical trials.
SSRIs. Selective serotonin reuptake inhibitors, although likely to be better tolerated than tricyclics, have been examined in only five placebo-controlled trials in fibromyalgia: two with citalopram, and three with fluoxetine. One citalopram study found no significant differences in efficacy between citalopram and a placebo,32 but the other reported significant improvement in one measure of pain and a significant decrease in depressive symptoms compared with the placebo group.33 No significant differences were found between groups in the global assessment of improvement.
The initial fluoxetine trial in fibromyalgia treatment did not reveal a significant therapeutic effect over a placebo,34 although the study was limited by a high (57%) placebo dropout rate, small sample size (42 subjects), brief duration (3 to 6 weeks after treatment), and restriction of fluoxetine dosage to 20 mg/d. In the two other controlled trials, including one which we recently conducted, fluoxetine was superior to a placebo in reducing pain and other fibromyalgia-associated symptoms.35,36
In our 12-week investigation (a randomized, placebocontrolled, parallel-group, flexible-dose trial), 60 subjects with fibromyalgia received fluoxetine 20 to 80 mg/d or a placebo.36 Those receiving fluoxetine (mean dosage 45 ±25 mg/d) displayed significantly greater reduction in pain, fatigue, and depression compared with those receiving the placebo. The effect of fluoxetine on pain remained significant after we adjusted for change in depression.
Sertraline was evaluated in an open study of 47 fibromyalgia patients at dosages of 25 to 200 mg/d for 6 weeks. Nearly two-thirds (63%) assessed the efficacy of sertraline as good or very good in the treatment of their symptoms.37 Paroxetine effectively reduced fibromyalgia symptoms in a single-blind study at dosages of 20 mg/d for 3 months.38
SNRIs Venlafaxine, a dual serotonin and norepinephrine reuptake inhibitor, has shown promise in the treatment of fibromyalgia in a preliminary open trial conducted by our group.39 Venlafaxine at a mean dosage of 167 mg/d resulted in significant improvement in fibromyalgia symptoms and quality of life compared with baseline. Notably, lifetime comorbid depressive and anxiety disorders were common in this sample, and their presence predicted response of fibromyalgia symptoms to venlafaxine.
Gabapentin Although no studies have been published on fibromyalgia treatment with this anticonvulsant, gabapentin has been found to exert substantial analgesic effects in controlled studies of other kinds of pain, including diabetic neuropathy, post-herpetic neuralgia, and migraines.40-42 There are also anecdotal reports of its successful use in fibromyalgia.2
Nonpharmacologic treatment
Cardiovascular fitness training, regional sympathetic block, electromyographic biofeedback, hypnotherapy, and electroacupuncture have been reported to have modest efficacy for fibromyalgia symptoms in short-term, randomized controlled trials.43-46 Other studies, however, have not replicated the efficacy of these treatments.
Cognitive-behavioral therapy has shown promise in preliminary studies.47,48 Cognitive restructuring techniques that challenge negative thoughts and promote an active, positive, problem-solving approach to pain were found to be important components of fibromyalgia therapy, as were relaxation training, aerobic exercise and stretching, pacing of activities, and family education.47
Recommendations
Based on our group’s experience and the limited data available, the following are recommendations for the pharmacologic treatment of fibromyalgia:
- Consider a trial of antidepressant medication for patients with a history of mood (unipolar) or anxiety disorders. First try an SSRI or an SNRI because many patients do not tolerate tricyclics. Use antidepressant therapeutic dosages and an adequate duration of treatment (at least 6 weeks).
- If symptoms do not respond to an adequate trial of first-line medications, treatment with tricyclics appears warranted. Although studies have focused mostly on tertiary amine tricyclics (e.g., amitriptyline), secondary amine agents (e.g., nortriptyline) may be just as effective and better tolerated, allowing for titration to higher dosages.
- Consider combination therapy when needed. For example, in patients who experience relief of pain, fatigue, and depressed mood with fluoxetine but continue to have insomnia, gabapentin can be added at night. Begin with 100 mg/d and increase by 100 mg/d until you see improvement or intolerance. Another option is trazodone, beginning with 50 mg hs. If you add a low-dose tricyclic to an SSRI, be aware of pharmacokinetic interaction and monitor tricyclic levels.
- Gabapentin alone, although it has not been studied in controlled trials of fibromyalgia, may be an option for patients who do not respond to antidepressants. Other pain conditions treated with gabapentin have required dosages of 1,600 to 2,400 mg/d to achieve substantial analgesic effects.
Cardiovascular fitness training is a potentially important component of fibromyalgia treatment. Many patients, however, have difficulty getting started because of increased pain after exercise and disabling fatigue. Treatment with medications as recommended may provide enough relief for patients to start an exercise program. Remind patients to start slowly, increasing the frequency and intensity of exercise as their endurance improves.
Because stress and a history of psychological trauma contribute to the onset and exacerbation of symptoms in some patients, cognitive-behavioral therapy is recommended as an adjunctive treatment as appropriate.
Related resources
- American Fibromyalgia Syndrome Association, Inc. www.afsafund.org
- Arnold LM, et al. Antidepressant treatment of fibromyalgia. A metaanalysis and review. Psychosomatics 2000;41:104-13.
- Kranzler JD, Gendreau JF, Rao SG. The psychopharmacology of fibromyalgia: a drug development perspective. Psychopharmacol Bull 2002;36:165-213.
Drug brand names
- Amitriptyline • Elavil
- Citalopram • Celexa
- Clomipramine • Anafranil
- Cyclobenzaprine • Flexeril
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Maprotiline • Ludiomil
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
Disclosure
The author reports that she receives research support from Eli Lilly & Co. and Pfizer Inc. and serves as a consultant and member of the speakers’ bureaus for both of those companies.
1. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum 1990;33:160-72.
2. Wolfe F, Ross K, Anderson J, et al. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum 1995;38:19-28.
3. White KP, Speechley M, Harth M, et al. Comparing self-reported function and work disability in 100 community cases of fibromyalgia syndrome versus controls in London, Ontario. The London fibromyalgia epidemiology study. Arthritis Rheum 1999;42:76-83.
4. Wolfe F, Anderson J, Harkness D, et al. Health status and disease severity in fibromyalgia. Arthritis Rheum 1997;40:1571-9.
5. Kaplan RM, Schmidt SM, Cronan TA. Quality of well being in patients with fibromyalgia. J Rheumatol 2000;27:785-9.
6. Clauw DJ. Fibromyalgia syndrome: an update on current understanding and medical management. Rheumatol Grand Rds 2000;3:1-9.
7. Yunus MB, Masi AT, Aldag JC. A controlled study of primary fibromyalgia syndrome: Clinical features and association with other functional syndromes. J Rheumatol 1989;16:62-71.
8. Wolfe F, Cathey MA, Kleinheksel SM, et al. Psychological status in primary fibrositis and fibrositis associated with rheumatoid arthritis. J Rheumatol 1984;11:500-6.
9. White KP, Nielson WR, Harth M, et al. Chronic widespread musculoskeletal pain with or without fibromyalgia: Psychological distress in a representative community adult sample. J Rheumatol 2002;29:588-94.
10. Walker EA, Keegan D, Gardner G, et al. Psychosocial factors in fibromyalgia and rheumatoid arthritis: I. Psychiatric diagnoses and functional disability. Psychosomatic Med 1997;59:565-71.
11. MacFarlane GJ, Thomas E, Papageorgiou AC, et al. The natural history of chroninc pain in the community: A better prognosis than in the clinic? J Rheumatol 1996;23:1617-20.
12. Aaron LA, Bradley LA, Alarcón GS, et al. Psychiatric diagnoses in patients with fibromyalgia are related to health care-seeking behavior rather than to illness. Arthritis Rheum 1996;39:436-45.
13. Moldofsky H, Scarisbrick P, England R, et al. Musculoskeletal symptoms and non-REM sleep disturbance in patients with “fibrositis syndrome” and healthy subjects. Psychosom Med 1975;37:341-5.
14. Moldofsky H, Scarisbrick P. Induction of neurasthenic musculoskeletal pain syndrome by selective sleep stage deprivation. Psychosom Med 1975;38:35-44.
15. Schneider-Helmert D, Whitehouse I, Kumar A, et al. Insomnia and alpha sleep in chronic non-organic pain as compared to primary insomnia. Neuropsychobiology 2001;43:54-8.
16. Pillemer SR, Bradley LA, Crofford LJ, et al. The neuroscience and endocrinology of fibromyalgia. Arthritis Rheum 1997;40:1928-39.
17. Walker EA, Keegan D, Gardner G, et al. Psychosocial factors in fibromyalgia and rheumatoid arthritis: II. Sexual, physical, and emotional abuse and neglect. Psychosomatic Med 1997;59:572-7.
18. Demitrack MA, Crofford LJ. Hypothalamic-pituitary-adrenal axis dysregulation in fibromyalgia and chronic fatigue syndrome: An overview and hypothesis. J Musculoskeletal Pain 1995;3:67-73.
19. Heim C, Ehlert U, Hellhammer DH. The potential role of hypocortisolism in the pathophysiology of stress-related bodily disorders. Psychoneuroendocrinology 2000;25:1-35.
20. Bennett RM. Emerging concepts in the neurobiology of chronic pain: Evidence of abnormal sensory processing in fibromyalgia. Mayo Clin Proc 1999;74:385-98.
21. Weigent DA, Bradley LA, Blalock JE, et al. Current concepts in the pathophysiology of abnormal pain perception in fibromyalgia. Am J Med Sci 1998;315:405-12.
22. Baranauskas G, Nistri A. Sensitization of pain pathways in the spinal cord: cellular mechanisms. Prog Neurobiol 1998;7:309-38.
23. Watkins LR, Wiertelak EP, Furness LE, et al. Illness-induced hyperalgesia is mediated by spinal neuropeptides and excitatory amino acids. Brain Res 1994;664:17-24.
24. Russell IJ, Orr MD, Littman B, et al. Elevated cerebrospinal fluid levels of substance P in patients with fibromyalgia syndrome. Arthritis Rheum 1994;37:1593-1601.
25. Schwarz MJ, Spath M, Muller-Bardorff H, et al. Relationship of substance P, 5-hydroxyindole acetic acid and tryptophan in serum of fibromyalgia patients. Neurosci Lett 1999;259:196-8.
26. Russell IJ, Vaeroy H, Javors M, Nyberg F. Cerebrospinal fluid biogenic amine metabolites in fibromyalgia/fibrositis syndrome and rheumatoid arthritis. Arthrits Rheum 1993;35(5):550-6.
27. Fishbain D. Evidence-based data on pain relief with antidepressants. Ann Med 2000;32:305-16.
28. Hudson JI, Goldenberg DL, Pope HG, et al. Comorbidity of fibromyalgia with medical and psychiatric disorders. Am J Med 1992;92:363-7.
29. Basbaum AI, Fields HL. Endogenous pain control systems: Brainstem pathways and endorphin circuitry. Ann Rev Neurosci 1984;7:309-38.
30. Arnold LM, Keck PE, Jr, Welge JA. Antidepressant treatment of fibromyalgia. A meta-analysis and review. Psychosomatics 2000;41:104-13.
31. O’Malley PG, Balden E, Tomkins G, et al. Treatment of fibromyalgia with antidepressants. A meta-analysis. J Gen Intern Med 2000;15:659-66.
32. Nørregaard J, Volkmann H, Danneskiold-Samsø B. A randomized controlled trial of citalopram in the treatment of fibromyalgia. Pain 1995;61:445-9.
33. Anderberg UM, Marteinsdottir I, von Knokrring L. Citalopram in patients with fibromyalgia-A randomized, double-blind, placebo-controlled study. Eur J Pain 2000;4:27-35.
34. Wolfe F, Cathey MA, Hawley DJ. A double-blind placebo controlled trial of fluoxetine in fibromyalgia. Scand J Rheumatol 1994;23(5):255-9.
35. Goldenberg DL, Mayskiy M, Mossey C, et al. A randomized, double-blind crossover trial of fluoxetine and amitriptyline in the treatment of fibromyalgia. Arthritis Rheum 1996;39:1852-9.
36. Arnold LM, Hess EV, Hudson JI, et al. A randomized, placebo-controlled, double-blind, flexible-dose study of fluoxetine in the treatment of women with fibromyalgia. Am J Med 2002;112:191-7.
37. Syuertsen JO, Smedsrud T, Lane RM. An open study of sertraline in fibromyalgia syndrome. Eur Neuropsychopharmacol 1995;5:315.-
38. Giordano N, Geraci S, et al. Efficacy and tolerability of paroxetine in patients with fibromyalgia syndrome: A single blind study. Curr Ther Res 1999;60:696-702.
39. Dwight MM, Arnold LM, O’Brien H, et al. An open clinical trial of venlafaxine treatment of fibromyalgia. Psychosomatics 1998;39:14-17.
40. Backonja M, Beydoun A, Edwards KR, et al. Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: A randomized controlled trial. JAMA 1998;280:1831-6.
41. Rice AS, Maton S. Gabapentin in postherpetic neuralgia: A randomized, doubleblind, placebo controlled study. Pain 2001;94:215-24.
42. Mathew NT, Rapoport A, Saper J, et al. Efficacy of gabapentin in migraine prophylaxis. Headache 2001;41:119-28.
43. Ferraccioli G, Ghirelli L, Scita F, et al. EMG-biofeedback training in fibromyalgia syndrome. J Rheumatol 1987;14:820-5.
44. McCain GA, Bell DA, Mai FM, et al. A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis Rheum 1988;31:1135-41.
45. Haanen HCM, Hoenderdos HTW, van Romande LKJ, et al. Controlled trial of hypnotherapy in the treatment of refractory fibromyalgia. J Rheumatol 1991;18:72-5.
46. Deluze C, Bosia L, Irbs A, et al. Electroacupuncture in fibromyalgia: Results of a controlled trial. BMJ 1992;1249-52.
47. Nielson WR, Walker C, McCain GA. Cognitive behavioral treatment of fibromyalgia syndrome preliminary findings. J Rheumatol 1992;19:98-103.
Patients with fibromyalgia often resist being referred to a psychiatrist because they fear being told their pain and other somatic symptoms are “all in their heads.” Evidence is mounting that they may be literally correct—the symptoms of fibromyalgia appear to have a physiologic connection with the central nervous system. Abnormal CNS activity, including sleep patterns, response to stress, pain processing, and neurotransmitter levels, has been documented in patients with fibromyalgia.
As psychiatrists, we can reassure these patients—and their primary care physicians and rheumatologists—that we are in a position to help because we:
- have expertise in assessing mood and anxiety disorders and in managing antidepressants, the medication physicians most commonly prescribe for fibromyalgia;
- are skilled in the use of the anticonvulsant gabapentin, which is being used in fibromyalgia for its analgesic and sedative effects;
- can offer much-needed support through psychotherapy, as chronic pain and other fibromyalgia-related symptoms create great stress in these patients’ lives.
Antidepressants are showing promise as an effective treatment for pain, fatigue, and depression in patients with fibromyalgia in studies by our group and others. The following information can help you stay current with the newest understandings of this ailment.
Table 1
CRITERIA FOR DIAGNOSING FIBROMYALGIA
| 1. | History of widespread pain |
| Definition Pain in the right and left side of the body, pain above and below the waist, axial skeletal pain (cervical spine or anterior chest or thoracic spine or low back). In this definition, shoulder and buttock pain is considered as pain for each involved side. “Low back” pain is considered lower segment pain. | |
| 2. | Pain in 11 of 18 tender point sites on digital palpation |
| Definition Pain, on digital palpation, must be present in at least 11 of the following 18 tender points: | |
| Occiput Bilateral, at the suboccipital muscle insertion | |
| Low cervical Bilateral, at the anterior aspects of the intertransverse spaces at C5-C7 | |
| Trapezius Bilateral, at the midpoint of the upper border | |
| Supraspinatus Bilateral, at origins, above the scapula spine near the medial border | |
| Second rib Bilateral, at the second costochondral junctions, just lateral to the junctions on upper surfaces | |
| Lateral epicondyle Bilateral, 2 cm distal to the epicondyles | |
| Gluteal Bilateral, in upper outer quadrants of buttocks in anterior fold of muscle | |
| Greater trochanter Bilateral, posterior to the trochanteric prominence | |
| Knee Bilateral, at the medial fat pad proximal to the joint line | |
| Digital palpation should be performed with an approximate force of 4 kg. For a tender point to be considered “positive” the patient must state that the palpation was painful. “Tender” is not to be considered “painful” Source: American College of Rheumatology1 | |
Figure 1 LOCATION OF FIBROMYALGIA TENDER POINTS
To palpate tender point sites, pressure is applied with the thumb pad perpendicularly to each site and the force increased by 1 kg per second until 4 kg of pressure is achieved. Whitening of the thumbnail bed usually occurs when applying the 4-kg force.
Mood disorders in fibromyalgia
A diagnosis of fibromyalgia requires the finding of widespread pain and tenderness at specific anatomic points (Table 1, Figure 1).1 Most patients also report fatigue, sleep disturbance, and morning stiffness (Box 1).2-5 American College of Rheumatology criteria do not require exclusionary tests such as radiographs and blood tests for the diagnosis.
Primary care physicians are increasingly making the diagnosis themselves and referring patients to rheumatologists only when conditions other than fibromyalgia are suspected. The differential diagnosis is broad, and other rheumatic and nonrheumatic disorders have similar symptoms, require different treatment, and affect fibromyalgia management (Table 2).6
Patients with fibromyalgia often report symptoms of major depressive disorder, such as depressed mood, anxiety, fatigue, and insomnia.7 Many psychological studies of such patients have documented increased rates of depressive symptoms.8 Depression and anxiety symptoms are common and frequently severe, even among individuals with fibromyalgia in the general population.9
Patients’ mood and anxiety disorders correlate highly with the number of medically unexplained symptoms and are associated with functional disability.10 The presence of psychological symptoms predicts persistent fibromyalgia symptoms,11 and psychological distress is strongly associated with symptom severity.12
Evidence for a CNS link
CNS mechanisms appear to contribute to the development of clinical findings in fibromyalgia.
Abnormal sleep A qualitative defect in sleep has been identified in patients with fibromyalgia.13 This sleep abnormality consists of inappropriate intrusion of alpha waves (normally seen during wakefulness or REM sleep) into deep sleep (usually characterized by delta waves).13 Some researchers believe alpha-delta sleep intrusion is associated with the chronic musculoskeletal pain and fatigue of fibromyalgia and, in turn, is mediated by an abnormality in central serotonergic neurotransmission.14 This sleep abnormality is not specific to fibromyalgia and can be found in other conditions, however.15 Debate continues regarding the role of sleep dysregulation in the pathophysiology of fibromyalgia.
Fibromyalgia is more common in women than men, with an estimated prevalence of 2% in the general population (3.4% in women and 0.5% in men). Its prevalence increases with age, rising sharply in middle age and then dropping off after age 80.2
Fibromyalgia is seen most often in women ages 50 and older.2 It occurs in 5% to 6% of patients presenting to general medical and family practice clinics and in 15% to 20% of patients presenting to rheumatologists, making it one of the most common diagnoses in office-based rheumatology practices.
American College of Rheumatology criteria may require only widespread pain and tenderness for a diagnosis of fibromyalgia, but most patients (73% to 85%) also report fatigue, sleep disturbance, and morning stiffness. Many (45% to 69%) report “pain all over,” paresthesias, headache, and anxiety. Co-occurring irritable bowel syndrome, sicca symptoms, and Raynaud’s phenomenon are less common (<35%).1 Patients with fibromyalgia also have high lifetime rates of other comorbid disorders, including migraine, chronic fatigue syndrome, and mood and anxiety disorders. Some patients report weakness, forgetfulness, difficulties in concentration, urinary frequency, history of dysmenorrhea, and restless legs.
Fibromyalgia is chronic, debilitating, and often leads to substantial functional impairment.3 Most patients with fibromyalgia do not display significant improvement over an average of 7 years of treatment.4 Patients with fibromyalgia report lower quality of well-being than patients with diagnoses of chronic obstructive pulmonary disease, rheumatoid arthritis, atrial fibrillation, advanced cancer, and several other chronic diseases.5
Stress response Stress appears to precipitate or exacerbate fibromyalgia symptoms in many patients.16 For example, fibromyalgia appears to be associated with victimization (adult and childhood sexual, physical, and emotional trauma), and this stress may trigger the development of fibromyalgia in some patients.17
Patients with fibromyalgia appear to develop disturbances in the two major stress-response systems: the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system.16 Although the interpretation of these disturbances is still debated, some researchers suggest that the available data point to reduction in CNS corticotropin releasing hormone (CRH), the key mediator in the HPA axis.18,19 CRH is also a behaviorally active peptide that leads to physiologic and behavioral arousal when administered centrally to animals.18 CRH reduction could contribute to the clinical features of fibromyalgia (e.g., fatigue) either directly or indirectly by causing a relative glucocorticoid deficiency.18,19
Table 2
DIFFERENTIAL DIAGNOSIS OF FIBROMYALGIA
| Rheumatic disorders | Nonrheumatic disorders |
|---|---|
| Rheumatoid arthritis | Hypothyroidism |
| Systemic lupus erythematosus | Sleep apnea |
| Polyarticular osteoarthritis | Hepatitis |
| Polymyalgia rheumatica | Cushing’s syndrome |
| Addison’s disease | |
| Hyperparathyroidism | |
| Adapted from Clauw DJ. Fibromyalgia syndrome: an update on current understanding and medical management. Rheumatol Grand Rds 2000;3:1-9. | |
Fibromyalgia is also associated with moderate basal hypocortisolism.18,19 A relative glucocorticoid deficiency could contribute to fibromyalgia’s characteristic fatigue, arthralgias, myalgias, and disturbances in mood and sleep.18 This deficiency may also cause some of the immunologic disturbances seen with fibromyalgia.18,19
Atypical depression, which shares such features of fibromyalgia as profound lethargy, is also associated with inappropriately normal or reduced activation of the HPA axis and a functional deficit in the release of hypothalamic CRH.18 The unifying feature of HPA axis activity in both atypical depression and fibromyalgia may be a shared hypofunctioning.18 A more complete understanding of the neuroendocrine changes in fibromyalgia awaits further study.
Pain processing Aberrant CNS processing of pain may also play a role in fibromyalgia.16,20 Fibromyalgia is sometimes precipitated by physical trauma.21 A traumatic injury may start a process in susceptible individuals that leads to an enhanced central processing of painful stimuli characteristic of central sensitization.22 Patients with fibromyalgia often develop an increased response to painful stimuli (hyeralgesia) and experience pain from normally nonnoxious stimuli (allodynia).20
Substance P, an important nociceptive neurotransmitter, may have a role in generating central sensitization.23 Elevated concentrations of substance P have been found in the cerebrospinal fluid (CSF) of individuals with fibromyalgia.24 Substance P also inhibits CRH release and may contribute to low CRH activity in fibromyalgia.16
Neurotransmitter defects A functional reduction in serotonergic activity has been demonstrated in patients with fibromyalgia. Schwarz et al25 found a strong negative correlation between serum concentrations of the primary serotonin metabolite, 5-hydroxyindoleacetic acid (5-HIAA), and substance P, pain, and insomnia. Evidence also exists of reduced concentrations of the primary norepinephrine metabolite, 3-methoxy-4-hydroxyphenethylene (MHPG), in the CSF of patients with fibromyalgia.26 Reduced serotonin and norepinephrine levels in descending pain-inhibitory pathways may cause the allodynia and hyperalgesia of fibromyalgia.
Pharmacologic treatment
Most studies of pharmacologic treatment of fibromyalgia have examined antidepressants for three reasons:
- There is evidence of the successful use of antidepressants in other chronic pain conditions.27
- These agents are effective for treating mood and anxiety disorders, which frequently occur in patients with fibromyalgia and may share a common physiologic abnormality.28
- Antidepressants might enhance the activity of neurotransmitters such as serotonin and norepinephrine in the descending inhibitory pain pathways, leading to reduced pain perception.29
Tricyclics In randomized, controlled trials, tricyclic medications (including the muscle relaxant cyclobenzaprine) appear to be moderately effective in improving fibromyalgia symptoms. Two meta-analyses of trials of tricyclic medications (amitriptyline, dothiepin, cyclobenzaprine, clomipramine, and maprotiline) have found similar results.30,31 Our group found the greatest effect on measures of sleep improvement, which may be due in part to tricyclics’ sedative properties.30 Many patients with fibromyalgia, however, cannot tolerate the sedative and other side effects associated with tricyclic agents, even though low dosages (e.g., 25 mg/d of amitriptyline) have typically been used in clinical trials.
SSRIs. Selective serotonin reuptake inhibitors, although likely to be better tolerated than tricyclics, have been examined in only five placebo-controlled trials in fibromyalgia: two with citalopram, and three with fluoxetine. One citalopram study found no significant differences in efficacy between citalopram and a placebo,32 but the other reported significant improvement in one measure of pain and a significant decrease in depressive symptoms compared with the placebo group.33 No significant differences were found between groups in the global assessment of improvement.
The initial fluoxetine trial in fibromyalgia treatment did not reveal a significant therapeutic effect over a placebo,34 although the study was limited by a high (57%) placebo dropout rate, small sample size (42 subjects), brief duration (3 to 6 weeks after treatment), and restriction of fluoxetine dosage to 20 mg/d. In the two other controlled trials, including one which we recently conducted, fluoxetine was superior to a placebo in reducing pain and other fibromyalgia-associated symptoms.35,36
In our 12-week investigation (a randomized, placebocontrolled, parallel-group, flexible-dose trial), 60 subjects with fibromyalgia received fluoxetine 20 to 80 mg/d or a placebo.36 Those receiving fluoxetine (mean dosage 45 ±25 mg/d) displayed significantly greater reduction in pain, fatigue, and depression compared with those receiving the placebo. The effect of fluoxetine on pain remained significant after we adjusted for change in depression.
Sertraline was evaluated in an open study of 47 fibromyalgia patients at dosages of 25 to 200 mg/d for 6 weeks. Nearly two-thirds (63%) assessed the efficacy of sertraline as good or very good in the treatment of their symptoms.37 Paroxetine effectively reduced fibromyalgia symptoms in a single-blind study at dosages of 20 mg/d for 3 months.38
SNRIs Venlafaxine, a dual serotonin and norepinephrine reuptake inhibitor, has shown promise in the treatment of fibromyalgia in a preliminary open trial conducted by our group.39 Venlafaxine at a mean dosage of 167 mg/d resulted in significant improvement in fibromyalgia symptoms and quality of life compared with baseline. Notably, lifetime comorbid depressive and anxiety disorders were common in this sample, and their presence predicted response of fibromyalgia symptoms to venlafaxine.
Gabapentin Although no studies have been published on fibromyalgia treatment with this anticonvulsant, gabapentin has been found to exert substantial analgesic effects in controlled studies of other kinds of pain, including diabetic neuropathy, post-herpetic neuralgia, and migraines.40-42 There are also anecdotal reports of its successful use in fibromyalgia.2
Nonpharmacologic treatment
Cardiovascular fitness training, regional sympathetic block, electromyographic biofeedback, hypnotherapy, and electroacupuncture have been reported to have modest efficacy for fibromyalgia symptoms in short-term, randomized controlled trials.43-46 Other studies, however, have not replicated the efficacy of these treatments.
Cognitive-behavioral therapy has shown promise in preliminary studies.47,48 Cognitive restructuring techniques that challenge negative thoughts and promote an active, positive, problem-solving approach to pain were found to be important components of fibromyalgia therapy, as were relaxation training, aerobic exercise and stretching, pacing of activities, and family education.47
Recommendations
Based on our group’s experience and the limited data available, the following are recommendations for the pharmacologic treatment of fibromyalgia:
- Consider a trial of antidepressant medication for patients with a history of mood (unipolar) or anxiety disorders. First try an SSRI or an SNRI because many patients do not tolerate tricyclics. Use antidepressant therapeutic dosages and an adequate duration of treatment (at least 6 weeks).
- If symptoms do not respond to an adequate trial of first-line medications, treatment with tricyclics appears warranted. Although studies have focused mostly on tertiary amine tricyclics (e.g., amitriptyline), secondary amine agents (e.g., nortriptyline) may be just as effective and better tolerated, allowing for titration to higher dosages.
- Consider combination therapy when needed. For example, in patients who experience relief of pain, fatigue, and depressed mood with fluoxetine but continue to have insomnia, gabapentin can be added at night. Begin with 100 mg/d and increase by 100 mg/d until you see improvement or intolerance. Another option is trazodone, beginning with 50 mg hs. If you add a low-dose tricyclic to an SSRI, be aware of pharmacokinetic interaction and monitor tricyclic levels.
- Gabapentin alone, although it has not been studied in controlled trials of fibromyalgia, may be an option for patients who do not respond to antidepressants. Other pain conditions treated with gabapentin have required dosages of 1,600 to 2,400 mg/d to achieve substantial analgesic effects.
Cardiovascular fitness training is a potentially important component of fibromyalgia treatment. Many patients, however, have difficulty getting started because of increased pain after exercise and disabling fatigue. Treatment with medications as recommended may provide enough relief for patients to start an exercise program. Remind patients to start slowly, increasing the frequency and intensity of exercise as their endurance improves.
Because stress and a history of psychological trauma contribute to the onset and exacerbation of symptoms in some patients, cognitive-behavioral therapy is recommended as an adjunctive treatment as appropriate.
Related resources
- American Fibromyalgia Syndrome Association, Inc. www.afsafund.org
- Arnold LM, et al. Antidepressant treatment of fibromyalgia. A metaanalysis and review. Psychosomatics 2000;41:104-13.
- Kranzler JD, Gendreau JF, Rao SG. The psychopharmacology of fibromyalgia: a drug development perspective. Psychopharmacol Bull 2002;36:165-213.
Drug brand names
- Amitriptyline • Elavil
- Citalopram • Celexa
- Clomipramine • Anafranil
- Cyclobenzaprine • Flexeril
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Maprotiline • Ludiomil
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
Disclosure
The author reports that she receives research support from Eli Lilly & Co. and Pfizer Inc. and serves as a consultant and member of the speakers’ bureaus for both of those companies.
Patients with fibromyalgia often resist being referred to a psychiatrist because they fear being told their pain and other somatic symptoms are “all in their heads.” Evidence is mounting that they may be literally correct—the symptoms of fibromyalgia appear to have a physiologic connection with the central nervous system. Abnormal CNS activity, including sleep patterns, response to stress, pain processing, and neurotransmitter levels, has been documented in patients with fibromyalgia.
As psychiatrists, we can reassure these patients—and their primary care physicians and rheumatologists—that we are in a position to help because we:
- have expertise in assessing mood and anxiety disorders and in managing antidepressants, the medication physicians most commonly prescribe for fibromyalgia;
- are skilled in the use of the anticonvulsant gabapentin, which is being used in fibromyalgia for its analgesic and sedative effects;
- can offer much-needed support through psychotherapy, as chronic pain and other fibromyalgia-related symptoms create great stress in these patients’ lives.
Antidepressants are showing promise as an effective treatment for pain, fatigue, and depression in patients with fibromyalgia in studies by our group and others. The following information can help you stay current with the newest understandings of this ailment.
Table 1
CRITERIA FOR DIAGNOSING FIBROMYALGIA
| 1. | History of widespread pain |
| Definition Pain in the right and left side of the body, pain above and below the waist, axial skeletal pain (cervical spine or anterior chest or thoracic spine or low back). In this definition, shoulder and buttock pain is considered as pain for each involved side. “Low back” pain is considered lower segment pain. | |
| 2. | Pain in 11 of 18 tender point sites on digital palpation |
| Definition Pain, on digital palpation, must be present in at least 11 of the following 18 tender points: | |
| Occiput Bilateral, at the suboccipital muscle insertion | |
| Low cervical Bilateral, at the anterior aspects of the intertransverse spaces at C5-C7 | |
| Trapezius Bilateral, at the midpoint of the upper border | |
| Supraspinatus Bilateral, at origins, above the scapula spine near the medial border | |
| Second rib Bilateral, at the second costochondral junctions, just lateral to the junctions on upper surfaces | |
| Lateral epicondyle Bilateral, 2 cm distal to the epicondyles | |
| Gluteal Bilateral, in upper outer quadrants of buttocks in anterior fold of muscle | |
| Greater trochanter Bilateral, posterior to the trochanteric prominence | |
| Knee Bilateral, at the medial fat pad proximal to the joint line | |
| Digital palpation should be performed with an approximate force of 4 kg. For a tender point to be considered “positive” the patient must state that the palpation was painful. “Tender” is not to be considered “painful” Source: American College of Rheumatology1 | |
Figure 1 LOCATION OF FIBROMYALGIA TENDER POINTS
To palpate tender point sites, pressure is applied with the thumb pad perpendicularly to each site and the force increased by 1 kg per second until 4 kg of pressure is achieved. Whitening of the thumbnail bed usually occurs when applying the 4-kg force.
Mood disorders in fibromyalgia
A diagnosis of fibromyalgia requires the finding of widespread pain and tenderness at specific anatomic points (Table 1, Figure 1).1 Most patients also report fatigue, sleep disturbance, and morning stiffness (Box 1).2-5 American College of Rheumatology criteria do not require exclusionary tests such as radiographs and blood tests for the diagnosis.
Primary care physicians are increasingly making the diagnosis themselves and referring patients to rheumatologists only when conditions other than fibromyalgia are suspected. The differential diagnosis is broad, and other rheumatic and nonrheumatic disorders have similar symptoms, require different treatment, and affect fibromyalgia management (Table 2).6
Patients with fibromyalgia often report symptoms of major depressive disorder, such as depressed mood, anxiety, fatigue, and insomnia.7 Many psychological studies of such patients have documented increased rates of depressive symptoms.8 Depression and anxiety symptoms are common and frequently severe, even among individuals with fibromyalgia in the general population.9
Patients’ mood and anxiety disorders correlate highly with the number of medically unexplained symptoms and are associated with functional disability.10 The presence of psychological symptoms predicts persistent fibromyalgia symptoms,11 and psychological distress is strongly associated with symptom severity.12
Evidence for a CNS link
CNS mechanisms appear to contribute to the development of clinical findings in fibromyalgia.
Abnormal sleep A qualitative defect in sleep has been identified in patients with fibromyalgia.13 This sleep abnormality consists of inappropriate intrusion of alpha waves (normally seen during wakefulness or REM sleep) into deep sleep (usually characterized by delta waves).13 Some researchers believe alpha-delta sleep intrusion is associated with the chronic musculoskeletal pain and fatigue of fibromyalgia and, in turn, is mediated by an abnormality in central serotonergic neurotransmission.14 This sleep abnormality is not specific to fibromyalgia and can be found in other conditions, however.15 Debate continues regarding the role of sleep dysregulation in the pathophysiology of fibromyalgia.
Fibromyalgia is more common in women than men, with an estimated prevalence of 2% in the general population (3.4% in women and 0.5% in men). Its prevalence increases with age, rising sharply in middle age and then dropping off after age 80.2
Fibromyalgia is seen most often in women ages 50 and older.2 It occurs in 5% to 6% of patients presenting to general medical and family practice clinics and in 15% to 20% of patients presenting to rheumatologists, making it one of the most common diagnoses in office-based rheumatology practices.
American College of Rheumatology criteria may require only widespread pain and tenderness for a diagnosis of fibromyalgia, but most patients (73% to 85%) also report fatigue, sleep disturbance, and morning stiffness. Many (45% to 69%) report “pain all over,” paresthesias, headache, and anxiety. Co-occurring irritable bowel syndrome, sicca symptoms, and Raynaud’s phenomenon are less common (<35%).1 Patients with fibromyalgia also have high lifetime rates of other comorbid disorders, including migraine, chronic fatigue syndrome, and mood and anxiety disorders. Some patients report weakness, forgetfulness, difficulties in concentration, urinary frequency, history of dysmenorrhea, and restless legs.
Fibromyalgia is chronic, debilitating, and often leads to substantial functional impairment.3 Most patients with fibromyalgia do not display significant improvement over an average of 7 years of treatment.4 Patients with fibromyalgia report lower quality of well-being than patients with diagnoses of chronic obstructive pulmonary disease, rheumatoid arthritis, atrial fibrillation, advanced cancer, and several other chronic diseases.5
Stress response Stress appears to precipitate or exacerbate fibromyalgia symptoms in many patients.16 For example, fibromyalgia appears to be associated with victimization (adult and childhood sexual, physical, and emotional trauma), and this stress may trigger the development of fibromyalgia in some patients.17
Patients with fibromyalgia appear to develop disturbances in the two major stress-response systems: the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system.16 Although the interpretation of these disturbances is still debated, some researchers suggest that the available data point to reduction in CNS corticotropin releasing hormone (CRH), the key mediator in the HPA axis.18,19 CRH is also a behaviorally active peptide that leads to physiologic and behavioral arousal when administered centrally to animals.18 CRH reduction could contribute to the clinical features of fibromyalgia (e.g., fatigue) either directly or indirectly by causing a relative glucocorticoid deficiency.18,19
Table 2
DIFFERENTIAL DIAGNOSIS OF FIBROMYALGIA
| Rheumatic disorders | Nonrheumatic disorders |
|---|---|
| Rheumatoid arthritis | Hypothyroidism |
| Systemic lupus erythematosus | Sleep apnea |
| Polyarticular osteoarthritis | Hepatitis |
| Polymyalgia rheumatica | Cushing’s syndrome |
| Addison’s disease | |
| Hyperparathyroidism | |
| Adapted from Clauw DJ. Fibromyalgia syndrome: an update on current understanding and medical management. Rheumatol Grand Rds 2000;3:1-9. | |
Fibromyalgia is also associated with moderate basal hypocortisolism.18,19 A relative glucocorticoid deficiency could contribute to fibromyalgia’s characteristic fatigue, arthralgias, myalgias, and disturbances in mood and sleep.18 This deficiency may also cause some of the immunologic disturbances seen with fibromyalgia.18,19
Atypical depression, which shares such features of fibromyalgia as profound lethargy, is also associated with inappropriately normal or reduced activation of the HPA axis and a functional deficit in the release of hypothalamic CRH.18 The unifying feature of HPA axis activity in both atypical depression and fibromyalgia may be a shared hypofunctioning.18 A more complete understanding of the neuroendocrine changes in fibromyalgia awaits further study.
Pain processing Aberrant CNS processing of pain may also play a role in fibromyalgia.16,20 Fibromyalgia is sometimes precipitated by physical trauma.21 A traumatic injury may start a process in susceptible individuals that leads to an enhanced central processing of painful stimuli characteristic of central sensitization.22 Patients with fibromyalgia often develop an increased response to painful stimuli (hyeralgesia) and experience pain from normally nonnoxious stimuli (allodynia).20
Substance P, an important nociceptive neurotransmitter, may have a role in generating central sensitization.23 Elevated concentrations of substance P have been found in the cerebrospinal fluid (CSF) of individuals with fibromyalgia.24 Substance P also inhibits CRH release and may contribute to low CRH activity in fibromyalgia.16
Neurotransmitter defects A functional reduction in serotonergic activity has been demonstrated in patients with fibromyalgia. Schwarz et al25 found a strong negative correlation between serum concentrations of the primary serotonin metabolite, 5-hydroxyindoleacetic acid (5-HIAA), and substance P, pain, and insomnia. Evidence also exists of reduced concentrations of the primary norepinephrine metabolite, 3-methoxy-4-hydroxyphenethylene (MHPG), in the CSF of patients with fibromyalgia.26 Reduced serotonin and norepinephrine levels in descending pain-inhibitory pathways may cause the allodynia and hyperalgesia of fibromyalgia.
Pharmacologic treatment
Most studies of pharmacologic treatment of fibromyalgia have examined antidepressants for three reasons:
- There is evidence of the successful use of antidepressants in other chronic pain conditions.27
- These agents are effective for treating mood and anxiety disorders, which frequently occur in patients with fibromyalgia and may share a common physiologic abnormality.28
- Antidepressants might enhance the activity of neurotransmitters such as serotonin and norepinephrine in the descending inhibitory pain pathways, leading to reduced pain perception.29
Tricyclics In randomized, controlled trials, tricyclic medications (including the muscle relaxant cyclobenzaprine) appear to be moderately effective in improving fibromyalgia symptoms. Two meta-analyses of trials of tricyclic medications (amitriptyline, dothiepin, cyclobenzaprine, clomipramine, and maprotiline) have found similar results.30,31 Our group found the greatest effect on measures of sleep improvement, which may be due in part to tricyclics’ sedative properties.30 Many patients with fibromyalgia, however, cannot tolerate the sedative and other side effects associated with tricyclic agents, even though low dosages (e.g., 25 mg/d of amitriptyline) have typically been used in clinical trials.
SSRIs. Selective serotonin reuptake inhibitors, although likely to be better tolerated than tricyclics, have been examined in only five placebo-controlled trials in fibromyalgia: two with citalopram, and three with fluoxetine. One citalopram study found no significant differences in efficacy between citalopram and a placebo,32 but the other reported significant improvement in one measure of pain and a significant decrease in depressive symptoms compared with the placebo group.33 No significant differences were found between groups in the global assessment of improvement.
The initial fluoxetine trial in fibromyalgia treatment did not reveal a significant therapeutic effect over a placebo,34 although the study was limited by a high (57%) placebo dropout rate, small sample size (42 subjects), brief duration (3 to 6 weeks after treatment), and restriction of fluoxetine dosage to 20 mg/d. In the two other controlled trials, including one which we recently conducted, fluoxetine was superior to a placebo in reducing pain and other fibromyalgia-associated symptoms.35,36
In our 12-week investigation (a randomized, placebocontrolled, parallel-group, flexible-dose trial), 60 subjects with fibromyalgia received fluoxetine 20 to 80 mg/d or a placebo.36 Those receiving fluoxetine (mean dosage 45 ±25 mg/d) displayed significantly greater reduction in pain, fatigue, and depression compared with those receiving the placebo. The effect of fluoxetine on pain remained significant after we adjusted for change in depression.
Sertraline was evaluated in an open study of 47 fibromyalgia patients at dosages of 25 to 200 mg/d for 6 weeks. Nearly two-thirds (63%) assessed the efficacy of sertraline as good or very good in the treatment of their symptoms.37 Paroxetine effectively reduced fibromyalgia symptoms in a single-blind study at dosages of 20 mg/d for 3 months.38
SNRIs Venlafaxine, a dual serotonin and norepinephrine reuptake inhibitor, has shown promise in the treatment of fibromyalgia in a preliminary open trial conducted by our group.39 Venlafaxine at a mean dosage of 167 mg/d resulted in significant improvement in fibromyalgia symptoms and quality of life compared with baseline. Notably, lifetime comorbid depressive and anxiety disorders were common in this sample, and their presence predicted response of fibromyalgia symptoms to venlafaxine.
Gabapentin Although no studies have been published on fibromyalgia treatment with this anticonvulsant, gabapentin has been found to exert substantial analgesic effects in controlled studies of other kinds of pain, including diabetic neuropathy, post-herpetic neuralgia, and migraines.40-42 There are also anecdotal reports of its successful use in fibromyalgia.2
Nonpharmacologic treatment
Cardiovascular fitness training, regional sympathetic block, electromyographic biofeedback, hypnotherapy, and electroacupuncture have been reported to have modest efficacy for fibromyalgia symptoms in short-term, randomized controlled trials.43-46 Other studies, however, have not replicated the efficacy of these treatments.
Cognitive-behavioral therapy has shown promise in preliminary studies.47,48 Cognitive restructuring techniques that challenge negative thoughts and promote an active, positive, problem-solving approach to pain were found to be important components of fibromyalgia therapy, as were relaxation training, aerobic exercise and stretching, pacing of activities, and family education.47
Recommendations
Based on our group’s experience and the limited data available, the following are recommendations for the pharmacologic treatment of fibromyalgia:
- Consider a trial of antidepressant medication for patients with a history of mood (unipolar) or anxiety disorders. First try an SSRI or an SNRI because many patients do not tolerate tricyclics. Use antidepressant therapeutic dosages and an adequate duration of treatment (at least 6 weeks).
- If symptoms do not respond to an adequate trial of first-line medications, treatment with tricyclics appears warranted. Although studies have focused mostly on tertiary amine tricyclics (e.g., amitriptyline), secondary amine agents (e.g., nortriptyline) may be just as effective and better tolerated, allowing for titration to higher dosages.
- Consider combination therapy when needed. For example, in patients who experience relief of pain, fatigue, and depressed mood with fluoxetine but continue to have insomnia, gabapentin can be added at night. Begin with 100 mg/d and increase by 100 mg/d until you see improvement or intolerance. Another option is trazodone, beginning with 50 mg hs. If you add a low-dose tricyclic to an SSRI, be aware of pharmacokinetic interaction and monitor tricyclic levels.
- Gabapentin alone, although it has not been studied in controlled trials of fibromyalgia, may be an option for patients who do not respond to antidepressants. Other pain conditions treated with gabapentin have required dosages of 1,600 to 2,400 mg/d to achieve substantial analgesic effects.
Cardiovascular fitness training is a potentially important component of fibromyalgia treatment. Many patients, however, have difficulty getting started because of increased pain after exercise and disabling fatigue. Treatment with medications as recommended may provide enough relief for patients to start an exercise program. Remind patients to start slowly, increasing the frequency and intensity of exercise as their endurance improves.
Because stress and a history of psychological trauma contribute to the onset and exacerbation of symptoms in some patients, cognitive-behavioral therapy is recommended as an adjunctive treatment as appropriate.
Related resources
- American Fibromyalgia Syndrome Association, Inc. www.afsafund.org
- Arnold LM, et al. Antidepressant treatment of fibromyalgia. A metaanalysis and review. Psychosomatics 2000;41:104-13.
- Kranzler JD, Gendreau JF, Rao SG. The psychopharmacology of fibromyalgia: a drug development perspective. Psychopharmacol Bull 2002;36:165-213.
Drug brand names
- Amitriptyline • Elavil
- Citalopram • Celexa
- Clomipramine • Anafranil
- Cyclobenzaprine • Flexeril
- Fluoxetine • Prozac
- Gabapentin • Neurontin
- Maprotiline • Ludiomil
- Nortriptyline • Pamelor
- Paroxetine • Paxil
- Sertraline • Zoloft
- Trazodone • Desyrel
- Venlafaxine • Effexor
Disclosure
The author reports that she receives research support from Eli Lilly & Co. and Pfizer Inc. and serves as a consultant and member of the speakers’ bureaus for both of those companies.
1. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum 1990;33:160-72.
2. Wolfe F, Ross K, Anderson J, et al. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum 1995;38:19-28.
3. White KP, Speechley M, Harth M, et al. Comparing self-reported function and work disability in 100 community cases of fibromyalgia syndrome versus controls in London, Ontario. The London fibromyalgia epidemiology study. Arthritis Rheum 1999;42:76-83.
4. Wolfe F, Anderson J, Harkness D, et al. Health status and disease severity in fibromyalgia. Arthritis Rheum 1997;40:1571-9.
5. Kaplan RM, Schmidt SM, Cronan TA. Quality of well being in patients with fibromyalgia. J Rheumatol 2000;27:785-9.
6. Clauw DJ. Fibromyalgia syndrome: an update on current understanding and medical management. Rheumatol Grand Rds 2000;3:1-9.
7. Yunus MB, Masi AT, Aldag JC. A controlled study of primary fibromyalgia syndrome: Clinical features and association with other functional syndromes. J Rheumatol 1989;16:62-71.
8. Wolfe F, Cathey MA, Kleinheksel SM, et al. Psychological status in primary fibrositis and fibrositis associated with rheumatoid arthritis. J Rheumatol 1984;11:500-6.
9. White KP, Nielson WR, Harth M, et al. Chronic widespread musculoskeletal pain with or without fibromyalgia: Psychological distress in a representative community adult sample. J Rheumatol 2002;29:588-94.
10. Walker EA, Keegan D, Gardner G, et al. Psychosocial factors in fibromyalgia and rheumatoid arthritis: I. Psychiatric diagnoses and functional disability. Psychosomatic Med 1997;59:565-71.
11. MacFarlane GJ, Thomas E, Papageorgiou AC, et al. The natural history of chroninc pain in the community: A better prognosis than in the clinic? J Rheumatol 1996;23:1617-20.
12. Aaron LA, Bradley LA, Alarcón GS, et al. Psychiatric diagnoses in patients with fibromyalgia are related to health care-seeking behavior rather than to illness. Arthritis Rheum 1996;39:436-45.
13. Moldofsky H, Scarisbrick P, England R, et al. Musculoskeletal symptoms and non-REM sleep disturbance in patients with “fibrositis syndrome” and healthy subjects. Psychosom Med 1975;37:341-5.
14. Moldofsky H, Scarisbrick P. Induction of neurasthenic musculoskeletal pain syndrome by selective sleep stage deprivation. Psychosom Med 1975;38:35-44.
15. Schneider-Helmert D, Whitehouse I, Kumar A, et al. Insomnia and alpha sleep in chronic non-organic pain as compared to primary insomnia. Neuropsychobiology 2001;43:54-8.
16. Pillemer SR, Bradley LA, Crofford LJ, et al. The neuroscience and endocrinology of fibromyalgia. Arthritis Rheum 1997;40:1928-39.
17. Walker EA, Keegan D, Gardner G, et al. Psychosocial factors in fibromyalgia and rheumatoid arthritis: II. Sexual, physical, and emotional abuse and neglect. Psychosomatic Med 1997;59:572-7.
18. Demitrack MA, Crofford LJ. Hypothalamic-pituitary-adrenal axis dysregulation in fibromyalgia and chronic fatigue syndrome: An overview and hypothesis. J Musculoskeletal Pain 1995;3:67-73.
19. Heim C, Ehlert U, Hellhammer DH. The potential role of hypocortisolism in the pathophysiology of stress-related bodily disorders. Psychoneuroendocrinology 2000;25:1-35.
20. Bennett RM. Emerging concepts in the neurobiology of chronic pain: Evidence of abnormal sensory processing in fibromyalgia. Mayo Clin Proc 1999;74:385-98.
21. Weigent DA, Bradley LA, Blalock JE, et al. Current concepts in the pathophysiology of abnormal pain perception in fibromyalgia. Am J Med Sci 1998;315:405-12.
22. Baranauskas G, Nistri A. Sensitization of pain pathways in the spinal cord: cellular mechanisms. Prog Neurobiol 1998;7:309-38.
23. Watkins LR, Wiertelak EP, Furness LE, et al. Illness-induced hyperalgesia is mediated by spinal neuropeptides and excitatory amino acids. Brain Res 1994;664:17-24.
24. Russell IJ, Orr MD, Littman B, et al. Elevated cerebrospinal fluid levels of substance P in patients with fibromyalgia syndrome. Arthritis Rheum 1994;37:1593-1601.
25. Schwarz MJ, Spath M, Muller-Bardorff H, et al. Relationship of substance P, 5-hydroxyindole acetic acid and tryptophan in serum of fibromyalgia patients. Neurosci Lett 1999;259:196-8.
26. Russell IJ, Vaeroy H, Javors M, Nyberg F. Cerebrospinal fluid biogenic amine metabolites in fibromyalgia/fibrositis syndrome and rheumatoid arthritis. Arthrits Rheum 1993;35(5):550-6.
27. Fishbain D. Evidence-based data on pain relief with antidepressants. Ann Med 2000;32:305-16.
28. Hudson JI, Goldenberg DL, Pope HG, et al. Comorbidity of fibromyalgia with medical and psychiatric disorders. Am J Med 1992;92:363-7.
29. Basbaum AI, Fields HL. Endogenous pain control systems: Brainstem pathways and endorphin circuitry. Ann Rev Neurosci 1984;7:309-38.
30. Arnold LM, Keck PE, Jr, Welge JA. Antidepressant treatment of fibromyalgia. A meta-analysis and review. Psychosomatics 2000;41:104-13.
31. O’Malley PG, Balden E, Tomkins G, et al. Treatment of fibromyalgia with antidepressants. A meta-analysis. J Gen Intern Med 2000;15:659-66.
32. Nørregaard J, Volkmann H, Danneskiold-Samsø B. A randomized controlled trial of citalopram in the treatment of fibromyalgia. Pain 1995;61:445-9.
33. Anderberg UM, Marteinsdottir I, von Knokrring L. Citalopram in patients with fibromyalgia-A randomized, double-blind, placebo-controlled study. Eur J Pain 2000;4:27-35.
34. Wolfe F, Cathey MA, Hawley DJ. A double-blind placebo controlled trial of fluoxetine in fibromyalgia. Scand J Rheumatol 1994;23(5):255-9.
35. Goldenberg DL, Mayskiy M, Mossey C, et al. A randomized, double-blind crossover trial of fluoxetine and amitriptyline in the treatment of fibromyalgia. Arthritis Rheum 1996;39:1852-9.
36. Arnold LM, Hess EV, Hudson JI, et al. A randomized, placebo-controlled, double-blind, flexible-dose study of fluoxetine in the treatment of women with fibromyalgia. Am J Med 2002;112:191-7.
37. Syuertsen JO, Smedsrud T, Lane RM. An open study of sertraline in fibromyalgia syndrome. Eur Neuropsychopharmacol 1995;5:315.-
38. Giordano N, Geraci S, et al. Efficacy and tolerability of paroxetine in patients with fibromyalgia syndrome: A single blind study. Curr Ther Res 1999;60:696-702.
39. Dwight MM, Arnold LM, O’Brien H, et al. An open clinical trial of venlafaxine treatment of fibromyalgia. Psychosomatics 1998;39:14-17.
40. Backonja M, Beydoun A, Edwards KR, et al. Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: A randomized controlled trial. JAMA 1998;280:1831-6.
41. Rice AS, Maton S. Gabapentin in postherpetic neuralgia: A randomized, doubleblind, placebo controlled study. Pain 2001;94:215-24.
42. Mathew NT, Rapoport A, Saper J, et al. Efficacy of gabapentin in migraine prophylaxis. Headache 2001;41:119-28.
43. Ferraccioli G, Ghirelli L, Scita F, et al. EMG-biofeedback training in fibromyalgia syndrome. J Rheumatol 1987;14:820-5.
44. McCain GA, Bell DA, Mai FM, et al. A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis Rheum 1988;31:1135-41.
45. Haanen HCM, Hoenderdos HTW, van Romande LKJ, et al. Controlled trial of hypnotherapy in the treatment of refractory fibromyalgia. J Rheumatol 1991;18:72-5.
46. Deluze C, Bosia L, Irbs A, et al. Electroacupuncture in fibromyalgia: Results of a controlled trial. BMJ 1992;1249-52.
47. Nielson WR, Walker C, McCain GA. Cognitive behavioral treatment of fibromyalgia syndrome preliminary findings. J Rheumatol 1992;19:98-103.
1. Wolfe F, Smythe HA, Yunus MB, et al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum 1990;33:160-72.
2. Wolfe F, Ross K, Anderson J, et al. The prevalence and characteristics of fibromyalgia in the general population. Arthritis Rheum 1995;38:19-28.
3. White KP, Speechley M, Harth M, et al. Comparing self-reported function and work disability in 100 community cases of fibromyalgia syndrome versus controls in London, Ontario. The London fibromyalgia epidemiology study. Arthritis Rheum 1999;42:76-83.
4. Wolfe F, Anderson J, Harkness D, et al. Health status and disease severity in fibromyalgia. Arthritis Rheum 1997;40:1571-9.
5. Kaplan RM, Schmidt SM, Cronan TA. Quality of well being in patients with fibromyalgia. J Rheumatol 2000;27:785-9.
6. Clauw DJ. Fibromyalgia syndrome: an update on current understanding and medical management. Rheumatol Grand Rds 2000;3:1-9.
7. Yunus MB, Masi AT, Aldag JC. A controlled study of primary fibromyalgia syndrome: Clinical features and association with other functional syndromes. J Rheumatol 1989;16:62-71.
8. Wolfe F, Cathey MA, Kleinheksel SM, et al. Psychological status in primary fibrositis and fibrositis associated with rheumatoid arthritis. J Rheumatol 1984;11:500-6.
9. White KP, Nielson WR, Harth M, et al. Chronic widespread musculoskeletal pain with or without fibromyalgia: Psychological distress in a representative community adult sample. J Rheumatol 2002;29:588-94.
10. Walker EA, Keegan D, Gardner G, et al. Psychosocial factors in fibromyalgia and rheumatoid arthritis: I. Psychiatric diagnoses and functional disability. Psychosomatic Med 1997;59:565-71.
11. MacFarlane GJ, Thomas E, Papageorgiou AC, et al. The natural history of chroninc pain in the community: A better prognosis than in the clinic? J Rheumatol 1996;23:1617-20.
12. Aaron LA, Bradley LA, Alarcón GS, et al. Psychiatric diagnoses in patients with fibromyalgia are related to health care-seeking behavior rather than to illness. Arthritis Rheum 1996;39:436-45.
13. Moldofsky H, Scarisbrick P, England R, et al. Musculoskeletal symptoms and non-REM sleep disturbance in patients with “fibrositis syndrome” and healthy subjects. Psychosom Med 1975;37:341-5.
14. Moldofsky H, Scarisbrick P. Induction of neurasthenic musculoskeletal pain syndrome by selective sleep stage deprivation. Psychosom Med 1975;38:35-44.
15. Schneider-Helmert D, Whitehouse I, Kumar A, et al. Insomnia and alpha sleep in chronic non-organic pain as compared to primary insomnia. Neuropsychobiology 2001;43:54-8.
16. Pillemer SR, Bradley LA, Crofford LJ, et al. The neuroscience and endocrinology of fibromyalgia. Arthritis Rheum 1997;40:1928-39.
17. Walker EA, Keegan D, Gardner G, et al. Psychosocial factors in fibromyalgia and rheumatoid arthritis: II. Sexual, physical, and emotional abuse and neglect. Psychosomatic Med 1997;59:572-7.
18. Demitrack MA, Crofford LJ. Hypothalamic-pituitary-adrenal axis dysregulation in fibromyalgia and chronic fatigue syndrome: An overview and hypothesis. J Musculoskeletal Pain 1995;3:67-73.
19. Heim C, Ehlert U, Hellhammer DH. The potential role of hypocortisolism in the pathophysiology of stress-related bodily disorders. Psychoneuroendocrinology 2000;25:1-35.
20. Bennett RM. Emerging concepts in the neurobiology of chronic pain: Evidence of abnormal sensory processing in fibromyalgia. Mayo Clin Proc 1999;74:385-98.
21. Weigent DA, Bradley LA, Blalock JE, et al. Current concepts in the pathophysiology of abnormal pain perception in fibromyalgia. Am J Med Sci 1998;315:405-12.
22. Baranauskas G, Nistri A. Sensitization of pain pathways in the spinal cord: cellular mechanisms. Prog Neurobiol 1998;7:309-38.
23. Watkins LR, Wiertelak EP, Furness LE, et al. Illness-induced hyperalgesia is mediated by spinal neuropeptides and excitatory amino acids. Brain Res 1994;664:17-24.
24. Russell IJ, Orr MD, Littman B, et al. Elevated cerebrospinal fluid levels of substance P in patients with fibromyalgia syndrome. Arthritis Rheum 1994;37:1593-1601.
25. Schwarz MJ, Spath M, Muller-Bardorff H, et al. Relationship of substance P, 5-hydroxyindole acetic acid and tryptophan in serum of fibromyalgia patients. Neurosci Lett 1999;259:196-8.
26. Russell IJ, Vaeroy H, Javors M, Nyberg F. Cerebrospinal fluid biogenic amine metabolites in fibromyalgia/fibrositis syndrome and rheumatoid arthritis. Arthrits Rheum 1993;35(5):550-6.
27. Fishbain D. Evidence-based data on pain relief with antidepressants. Ann Med 2000;32:305-16.
28. Hudson JI, Goldenberg DL, Pope HG, et al. Comorbidity of fibromyalgia with medical and psychiatric disorders. Am J Med 1992;92:363-7.
29. Basbaum AI, Fields HL. Endogenous pain control systems: Brainstem pathways and endorphin circuitry. Ann Rev Neurosci 1984;7:309-38.
30. Arnold LM, Keck PE, Jr, Welge JA. Antidepressant treatment of fibromyalgia. A meta-analysis and review. Psychosomatics 2000;41:104-13.
31. O’Malley PG, Balden E, Tomkins G, et al. Treatment of fibromyalgia with antidepressants. A meta-analysis. J Gen Intern Med 2000;15:659-66.
32. Nørregaard J, Volkmann H, Danneskiold-Samsø B. A randomized controlled trial of citalopram in the treatment of fibromyalgia. Pain 1995;61:445-9.
33. Anderberg UM, Marteinsdottir I, von Knokrring L. Citalopram in patients with fibromyalgia-A randomized, double-blind, placebo-controlled study. Eur J Pain 2000;4:27-35.
34. Wolfe F, Cathey MA, Hawley DJ. A double-blind placebo controlled trial of fluoxetine in fibromyalgia. Scand J Rheumatol 1994;23(5):255-9.
35. Goldenberg DL, Mayskiy M, Mossey C, et al. A randomized, double-blind crossover trial of fluoxetine and amitriptyline in the treatment of fibromyalgia. Arthritis Rheum 1996;39:1852-9.
36. Arnold LM, Hess EV, Hudson JI, et al. A randomized, placebo-controlled, double-blind, flexible-dose study of fluoxetine in the treatment of women with fibromyalgia. Am J Med 2002;112:191-7.
37. Syuertsen JO, Smedsrud T, Lane RM. An open study of sertraline in fibromyalgia syndrome. Eur Neuropsychopharmacol 1995;5:315.-
38. Giordano N, Geraci S, et al. Efficacy and tolerability of paroxetine in patients with fibromyalgia syndrome: A single blind study. Curr Ther Res 1999;60:696-702.
39. Dwight MM, Arnold LM, O’Brien H, et al. An open clinical trial of venlafaxine treatment of fibromyalgia. Psychosomatics 1998;39:14-17.
40. Backonja M, Beydoun A, Edwards KR, et al. Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: A randomized controlled trial. JAMA 1998;280:1831-6.
41. Rice AS, Maton S. Gabapentin in postherpetic neuralgia: A randomized, doubleblind, placebo controlled study. Pain 2001;94:215-24.
42. Mathew NT, Rapoport A, Saper J, et al. Efficacy of gabapentin in migraine prophylaxis. Headache 2001;41:119-28.
43. Ferraccioli G, Ghirelli L, Scita F, et al. EMG-biofeedback training in fibromyalgia syndrome. J Rheumatol 1987;14:820-5.
44. McCain GA, Bell DA, Mai FM, et al. A controlled study of the effects of a supervised cardiovascular fitness training program on the manifestations of primary fibromyalgia. Arthritis Rheum 1988;31:1135-41.
45. Haanen HCM, Hoenderdos HTW, van Romande LKJ, et al. Controlled trial of hypnotherapy in the treatment of refractory fibromyalgia. J Rheumatol 1991;18:72-5.
46. Deluze C, Bosia L, Irbs A, et al. Electroacupuncture in fibromyalgia: Results of a controlled trial. BMJ 1992;1249-52.
47. Nielson WR, Walker C, McCain GA. Cognitive behavioral treatment of fibromyalgia syndrome preliminary findings. J Rheumatol 1992;19:98-103.