User login
Your patient comes in complaining of acute eye pain. Is it an ophthalmic emergency? Benign? Something in between?
The varying degrees of severity are reflected in the cases presented here, and in the multiple-choice quiz that follows. After selecting your answer to each of the questions, turn the page to find out if you were right.
CASE 1 A 74-year-old man presents with left eye pain that began when he lowered the shades in his bedroom to get ready for a nap. The pain worsened rapidly, he reports, and now—a half hour later—he has a headache, nausea, and blurred vision in the affected eye.
The patient has a history of hypertension, which is controlled with hydrochlorothiazide, but takes no other drugs. He denies any eye trauma. An eye exam reveals that the pupil is dilated and reacts poorly to light; you note corneal haziness and edema, as well ( FIGURE 1; vertical line is the slit lamp beam).
FIGURE 1
What’s your diagnosis?
- angle-closure glaucoma
- macular degeneration
- open-angle glaucoma
- retinal detachment.
CASE 2 A 20-year-old man was playing touch football while wearing contact lenses. Soon after, the game, he felt a stinging sensation in his right eye—”like sand under the eyelid,” he said. Exposure to sunlight also produced eye pain. The patient had tried flushing his eye with water, but experienced little pain relief.
An eye exam reveals a grayish-white spot in the line of vision ( FIGURE 2 ), with no sign of a penetrating injury.
FIGURE 2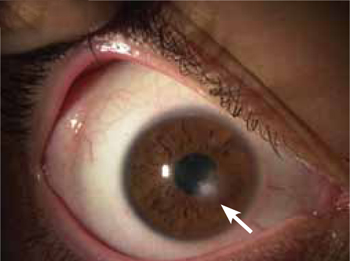
What’s your next step?
- Prescribe antibiotic eye drops and send the patient home.
- Provide an emergent ophthalmology referral for foreign body extraction.
- Send the patient home with an eye patch to relieve the photophobia.
- Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
CASE 3 A 17-year-old woman is brought in by her mother because of pain and vision loss in her right eye. The pain started as soon as she awoke; 2 hours later, the vision in the affected eye became blurry. Soon after, she saw spots of light, followed by complete loss of vision. She denies any trauma and says she has never experienced anything like this before.
The patient’s visual acuity is 20/200 in her right eye, and 20/40 in the left. You follow up with a funduscopic exam of the eye, which shows edema of the optic disc, blurring of the disc margins, and distended veins ( FIGURE 3 ).
FIGURE 3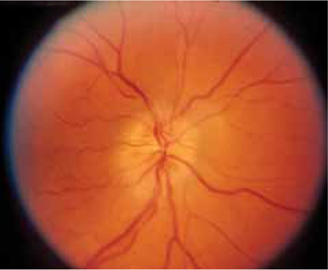
What diagnostic test should be next?
- fluorescein angiography
- intraocular pressure measurement
- magnetic resonance imaging (MRI) of the brain
- visual fields assessment.
CASE 4 A 31-year-old woman with a history of sarcoidosis comes in because of spontaneous redness ( FIGURE 4 ) and pain in her left eye, which began early that day. She denies any eye trauma, eye surgery, or recent cold, and has no discharge or crust around the eye.
FIGURE 4
What’s your diagnosis?
- anterior uveitis
- conjunctivitis
- corneal abrasion
- posterior uveitis.
CASE 5 A 21-year-old college student complains of pain in her left eye that started a day ago. She wears contact lenses and, upon questioning, tells you that she sometimes keeps them in all night.
The patient reports that she used a friend’s steroid eye drops twice yesterday, but the drops didn’t help. The pain is worse today. It feels as if there’s something in her eye, she says, and she finds it hard to open her eye. Penlight examination ( FIGURE 5 ) reveals a branching opacity on the cornea.
FIGURE 5
What’s your next step?
- Advise the patient to stop wearing her contact lenses overnight, give her a cycloplegic, and follow up in 2 days.
- Patch the patient’s left eye, prescribe antibiotics, and tell her to return tomorrow.
- Prescribe steroid eye drops and follow up in 2 days.
- Provide an urgent referral to an ophthalmologist.
CASE 1 The answer is A: angle-closure glaucoma.
Glaucoma is the world’s leading cause of blindness,1,2 and angle-closure glaucoma comprises 10% of cases.2 In this condition, the anterior chamber angle—formed by the iris and the cornea—is narrow. When the iris dilates in low light (eg, the darkened room in which the patient had planned to nap), it folds into the narrowed angle, preventing the flow of aqueous humor and leading to an increase in intraocular pressure.3
Signs and symptoms
Patients with acute angle-closure glaucoma often develop decreased vision, halos, headaches, severe eye pain, nausea, and vomiting. If the intraocular pressure increases quickly, symptoms can have an acute and dramatic onset; if pressure builds slowly, patients may have limited or no symptoms.4
Physical findings
An eye exam will reveal conjunctival erythema, corneal edema and cloudiness, iris irregularity, a shallow anterior chamber (visible with a slit lamp), a dilated pupil (4-6 mm) that reacts sluggishly to light, and increased ocular pressure. The cupping of the optic disc seen in this patient’s retinal exam ( FIGURE 6 ) is more commonly associated with chronic open-angle glaucoma.
FIGURE 6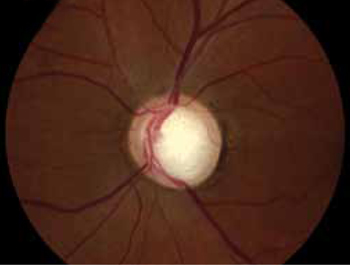
Management
Acute angle-closure glaucoma is an ophthalmologic emergency, and a referral to a specialist is crucial. If no ophthalmologist can see the patient within an hour of the presentation of symptoms, you’ll need to initiate topical treatment to reduce intraocular pressure and ensure that he or she is seen by a specialist as soon as possible.5 First-line treatments for acute angle-closure glaucoma are listed in TABLE 1 .5,6
In severe cases, topical therapy alone may be ineffective. If there are no contraindications, systemic medications such as acetazolamide, mannitol, glycerol, or isosorbide may be needed. Eye pressure should be checked 30 to 60 minutes after initiating systemic therapy and the patient closely monitored for adverse effects (eg, anaphylaxis, convulsions [acetazolamide]; hypotension [mannitol, isosorbide]).5
When the patient does see an ophthalmologist, the evaluation will include assessment of visual acuity, pupillary evaluation, measurement of intraocular pressure, slit lamp examination, gonioscopy to measure the angle of the anterior chamber, and a fundus exam without pupil dilation.5 Treatment may include a surgical procedure, such as paracentesis of the eye, peripheral iridotomy, or iridectomy, and chronic administration of topical medication.7
TABLE 1
Treatments for acute angle-closure glaucoma5,6
| Medication | Quantity |
|---|---|
| Topical | |
| 0.5% timolol maleate | 1 drop in affected eye 2x/d |
| 1% apraclonidine | 1-2 drops 3x/d |
| 2% pilocarpine | 1 drop 4x/d |
| Oral | |
| Acetazolamide | 500 mg 2x/d |
| Glycerol 50% solution | 1-1.8 g/kg |
| Isosorbide solution | 1.5 g/kg |
| Intravenous | |
| Acetazolamide | 250 mg 4x/d |
| Mannitol | 0.25-2 g/kg (one-time dose) |
CASE 2 The answer is D: Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
This patient likely has a corneal ulcer or abrasion caused by a contact lens. Corneal ulcers—which constitute a loss of the corneal epithelium—can be caused by trauma or a foreign body, or develop spontaneously.
Signs and symptoms
Because of the rich innervation of the corneal epithelium by the trigeminal nerve, the cornea is highly sensitive to pain. Patients with corneal abrasions typically experience eye pain, photophobia, tearing, a foreign body sensation, and discomfort when driving, working, or reading. If a patient has damage to the trigeminal nerve, however (eg, from trauma, a tumor, or a herpes infection), corneal injuries may be painless.8
In some cases, corneal abrasions may be so painful that patients become disruptive while waiting to be seen. Thus, any patient suspected of having a corneal ulcer or abrasion should be ushered into a quiet, dark room and instructed to keep his or her eyes closed until the examination.
The patient history should focus on recent trauma, type of work, and use of protective eyewear, which may provide clues to the development of penetrating injuries, retained foreign bodies, or abrasions caused by a foreign body. Ask about the use of contact lenses, as well; corneal injury caused by contacts is associated with specific bacterial infections, most commonly staphylococcal organisms and Pseudomonas.9
Physical findings
Attempt to test visual acuity without topical anesthetics. If the patient can’t tolerate the test, a single drop of topical anesthetic (proparacaine 0.5%) may help. Visual acuity provides clues to the location of the injury. If acuity is close to baseline, the corneal abrasion is likely peripheral to the visual axis. Decreased visual acuity indicates either that the abrasion involves the central axis area or that there is corneal edema.9
Evaluation of the pupillary reflex and optic fundus should follow. Reactive miosis may be present with corneal abrasions. A large, nonreactive pupil may be a sign of injury to the pupillary sphincter from blunt or penetrating injury—an ophthalmologic emergency that requires urgent referral. The eyelid should be flipped and examined for foreign bodies. 9
Some abrasions can be seen with the naked eye, so a penlight exam should be performed before applying fluorescein stain. If a corneal lesion is suspicious for herpesvirus infection ( SEE CASE 5 ), fluorescein should not be applied, as it can interfere with the antibody test.10 Refer the patient to an ophthalmologist instead.
If there’s no evidence of infection, apply fluorescein and examine the cornea with a Wood’s lamp. A thin line or several vertical lines are suggestive of a foreign body in the cornea or under the eyelid, whereas round defects are often due to contact lenses.9 Physical findings associated with specific types of corneal abrasions or ulcers are detailed in TABLE 2 .9,11,12
TABLE 2
Corneal abrasion or ulcers: The differential diagnosis9,11,12
| Diagnosis | Physical findings | Management |
|---|---|---|
| Penetrating trauma |
|
|
| Infected corneal abrasion | Grayish edge near abrasions or ulcers |
|
| Retained foreign body |
|
|
| Herpesvirus infection | Branching pattern |
|
| Spontaneous erosions |
|
|
| *Gel-like extrusion of ocular contents seen with fluorescein. †Ointment is preferable to drops. If a contact lens caused the abrasion, a solution that covers Pseudomonas should be used. | ||
Management
Patients with corneal abrasions or ulcers should receive topical antibiotics to prevent infection. Ointments (erythromycin ointment 4 times daily for 3-5 days) are preferable to drops, but may be harder to obtain.9 If a patient must use drops, sulfacetamide 10%, polymyxin/trimethoprim, ciprofloxacin, or ofloxacin can be used, with the same frequency and duration.
Aminoglycosides are toxic to the corneal epithelium and should be avoided, except in abrasions caused by contacts.9 Because of the likelihood of pseudomonal keratitis in cases involving contact lenses, antibiotics covering Pseudomonas, such as ofloxacin, ciprofloxacin, or tobramycin, should be used.9
Pain control is achieved with cycloplegics11 like cyclopentolate 0.5% to 1% or a one-day course of systemic opioids. For children, over-the-counter analgesics for mild pain and mild opioids for severe pain may be used.
Chronic use of topical anesthetics should be avoided in patients of any age. Although they relieve pain, frequent use can lead to delayed healing, ulcerations, perforations, scarring, or even blindness.8
Patching has not been found to improve healing or comfort;13 instead, it delays healing.14,15 The “pirate patch,” which hovers over the eye, does not keep the eyelid down and therefore is not recommended.9
Follow up within 24 hours of initiating treatment to assure that the abrasion is healing. If it appears to be getting worse or is simply not improving, an immediate referral to an ophthalmologist is needed. Abrasions caused by contact with potentially infected material (eg, farm equipment, tree branches, or soil) require daily monitoring until they heal.11
CASE 3 The answer is C: Order an MRI of the brain.
This patient has optic neuritis, caused by inflammation of the optic nerve and disruption of the nerve’s myelin sheath. It predominantly affects young adults, and is more common in women than in men.16 The incidence of optic neuritis is higher among Asians, black South Africans, and children under the age of 15.17,18
Signs and symptoms
Optic neuritis is characterized by monocular (90%) or binocular (10%) complete or partial vision loss, photopsia (flashes of light), and eye pain. Up to 60% of pediatric patients present with blurred vision, bilateral involvement,19 and no pain, while adults predominantly have pain and unilateral vision loss.20 Optic neuritis is often a presenting symptom of multiple sclerosis (MS).16
Physical findings
Physical exam findings in optic neuritis include a sluggish direct light reflex, loss of visual acuity and color vision, as well as acute eye pain.18 Ophthalmoscopic exam may reveal papillitis with edema of the optic disc.21 In the Optic Neuritis Treatment Trial (ONTT), however, only one-third of patients presented with papillitis and swelling of the optic disc.22
MRI of the brain with gadolinium contrast is generally used to confirm the diagnosis. On MRI, 95% of patients with optic neuritis have signs of inflammation of the optic nerve and/or white matter changes consistent with MS (periventricular and ovoid demyelination).23,24
Patients with evidence of demyelination should also be evaluated for MS and other demyelinating disorders. In the ONTT trial, the risk of developing MS within 15 years of an optic neuritis diagnosis was as low as 25% (95% confidence interval [CI], 18%-32%) for patients with no lesions on a baseline brain MRI and as high as 72% (95% CI, 63%-81%) for those with one or more lesions on a baseline MRI, according to the study’s final follow-up.22
Management
The recommended treatment for optic neuritis is intravenous (IV) methylprednisolone 250 mg every 6 hours for 3 to 5 days, followed by oral prednisone at 1 mg/kg/d for 7 to 10 days. Vision usually returns slowly over the course of several months to a year. Ophthalmology consultation should be considered to rule out other causes of optic neuritis.25
CASE 4 The answer is A: anterior uveitis.
Uveitis is often associated with systemic disease or infection, and diagnosis is typically suspected based on a history of conditions such as sarcoidosis, juvenile idiopathic arthritis, Kawasaki’s disease, Sjögren’s syndrome, toxoplasmosis, human immunodeficiency virus (HIV), tuberculosis (TB), syphilis, herpes simplex, and herpes zoster.26
Signs and symptoms
Signs and symptoms vary depending on the part of the uveal tract that’s involved. Anterior uveitis, or iritis, is associated with pain, photophobia, redness, and a varying degree of vision loss. Posterior and intermediate uveitis are less likely to be associated with pain, but can be accompanied by decreased visual acuity and floaters.27
Physical findings
Visual acuity in patients with uveitis can range from normal to varying degrees of vision loss. Redness around the iris can be seen; conjunctival infection is most marked around the circumference of the corneal limbus rather than more peripherally, as seen in conjunctivitis. On slit lamp examination, the beam of light can be seen in the aqueous humor due to protein and leukocyte accumulation—a phenomenon known as “flare.” The pupillary light reflex may be abnormal, and the pupillary opening may be irregular rather than round due to anterior and posterior synechia.28
Management
Patients should be referred to an ophthalmologist for management of the immediate condition and to prevent or treat complications such as vision loss, optic nerve damage, and glaucoma. Acute management includes topical steroids, such as prednisolone acetate ophthalmic 1% 2 to 4 times daily, as well as treatment of the underlying condition. Long-term management varies, depending on the cause of the uveitis.26,29
If the etiology is unknown, a workup should be considered to identify inflammatory and infectious disorders that might be causing uveitis. Chest radiograph is a good beginning to look for evidence of sarcoidosis or TB; serologic testing for syphilis, HIV, and lupus may also be considered.26,29
CASE 5 The answer is D: Provide an urgent referral to an ophthalmologist.
This patient has viral keratitis caused by herpes. While the pain and foreign body sensation are the same for bacterial and viral keratitis, herpesvirus is distinguishable by the branching opacity that develops on the cornea.
Varicella zoster is the most common cause of viral keratitis, although it can also be caused by herpes simplex and adeno-virus. Because a person who is infected with herpes has the virus for life, however, multiple attacks are possible. Reactivation is associated with stress and a weakened immune system, but may occur spontaneously, as well. Patients who wear contact lenses are no more likely than those who don’t to be infected with the herpesvirus.
Bacterial keratitis is often associated with contact lenses, particularly when they’re continually worn, but also with normal wear.30 Immunosuppression, dry ocular surfaces, and topical corticosteroid use may predispose patients to bacterial keratitis, as well.12 Staphylococcus aureus, Pseudomonas aeruginosa, coagulase-negative Staphylococcus, diphtheroids, and Streptococcus pneumoniae are the most common pathogens.31
Signs and symptoms
Patients with keratitis typically complain of eye pain, a sensation of having a foreign body in the eye, photophobia, tearing, and vision changes; a mucopurulent discharge is sometimes present, as well.3 The condition is easily distinguished from conjunctivitis, which typically does not involve eye pain or vision changes.
Physical findings
Visual acuity may be affected if the lesion or corneal edema involves the visual axis. Physical exam in a patient with bacterial keratitis sometimes shows a gray or white corneal opacity, along with corneal erythema. As already noted, a penlight exam will reveal a branching opacity in patients with herpes keratitis.30
Management
Patients with keratitis should be referred immediately to an ophthalmologist32 for a slit lamp evaluation, treatment, and close follow-up.
Corneal cultures can be difficult to obtain, but before prescribing antibiotics, an attempt to collect samples should be made. This can be done—after the administration of topical anesthesia—with a sterile calcium alginate swab. Gently swab the cornea and then inoculate the appropriate gels or mediums. Avoid contact with lashes and eyelids to prevent culture contamination.32
When herpesvirus is suspected, start the patient on an antiviral agent such as trifluridine ophthalmic (1%) 9 times a day, vidarabine ophthalmic (3%) 5 times daily, or 400 mg oral acyclovir 5 times a day. Patients with bacterial keratitis should be started on antibiotic eye drops with Pseudomonas coverage, such as ofloxacin (0.3%), ciprofloxacin (0.3%), or tobramycin (0.3%), 6 to 8 times a day.9
CORRESPONDENCE Uyen Michelle Le, MD, 967 Galindo Court, Milpitas, CA 95035; mlkala21@aol.com
1. Foster PJ, Johnson GJ. Glaucoma in China: how big is the problem? Br J Ophthalmol. 2001;85:1277-1282.
2. American Academy of Ophthalmology. Preferred Practice Pattern Guidelines. Primary angle closure PPP - October 2010. Available at: http://one.aao.org/CE/PracticeGuidelines/PPP_Content.aspx?cid=92bea8f6-5459-49a6-9233-4528343dc4c3. Accessed July 12, 2012.
3. Sau SM, Gazzard G, Friedman DS. Interventions for angle-closure glaucoma: an evidence-based update. Ophthalmology. 2003;110:1878-1879, 1930.
4. Leibowitz HM. The red eye. N Engl J Med. 2000;343:345-351.
5. Shields SR. Managing eye disease in primary care. Part 3. When to refer for ophthalmologic care. Postgrad Med. 2000;108:99-106.
6. Awasthi P. Srivastava SN. Role of oral glycerol in glaucoma. Br J Ophthalmol. 1965;49:660-666.
7. Quigley HA. Glaucoma. Lancet. 2011;377:1367-1377.
8. Peyman GA, Rahimy MH, Fenandes ML. Effects of morphine on corneal sensitivity and epithelial wound healing: implications for topical ophthalmic analgesia. Br J Ophthalmol. 1994;78:138-141.
9. Schein OD. Contact lens abrasions and the nonophthalmologist. Am J Emerg Med. 1993;11:606-608.
10. Goldschmidt P. Effects of topical anaesthetics and fluorescein on the real-time PCR used for the diagnosis of herpesviruses and acanthamoeba keratitis. Br J Ophthalmol. 2006;90:1354-1356.
11. Benson WH, Snyder IS, Granus V, et al. Tetanus prophylaxis following ocular injuries. J Emerg Med. 1993;11:677-683.
12. DeBroff BM, Donahue SP, Caputo BJ, et al. Clinical characteristics of corneal foreign bodies and their associated culture results. CLAO J. 1994;20:128-130.
13. Turner A, Rabiu M. Patching for corneal abrasion. Cochrane Database Syst Rev. 2006;(2):CD004764.-
14. Kaiser PK. A comparison of pressure patching versus no patching for corneal abrasions due to trauma or foreign body removal. Corneal Abrasion Patching Study Group. Ophthalmology. 1995;102:1936-1942.
15. Clemons CS, Cohen EJ, Arentset JJ, et al. Pseudomonas ulcers following patching of corneal abrasions associated with contact lens wear. CLAO J. 1987;13:161-164.
16. Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med. 2006;354:1273-1280.
17. De la Cruz J, Kupersmith MJ. Clinical profile of simultaneous bilateral optic neuritis in adults. Br J Ophthalmol. 2006;90:551-554.
18. Hwang JM, Lee YJ, Kim MK. Optic neuritis in Asian children. J Ped Ophthalmol Strabismus. 2002;39:26-32.
19. Lana-Peixoto MA, Andreade GC. The clinical profile of childhood optic neuritis. Arq Neuropsiquiatr. 2001;59(2-B):311-317.
20. Boomer JA, Siatkowski RM. Optic neuritis is adults and children. Semin Ophthalmol. 2003;18:174-180.
21. Lucchinetti CF, Kiers L, O’Duffy A, et al. Risk factors for developing multiple sclerosis after childhood optic neuritis. Neurology. 1997;49:1413-1418.
22. Optic Neuritis Study Group. Multiple sclerosis risk after optic neuritis: final optic neuritis treatment trial follow-up. Arch Neurol. 2008;65:727-732.
23. Wray SH. Optic neuritis. In: Principles and Practice of Ophthalmology. Albert DM, Jakobiec FA, eds. WB Saunders; Philadelphia, Pa: 1994.
24. Hickman SJ, Toosy AT, Miszkiel KA, et al. Visual recovery following acute optic neuritis—a clinical, electrophysiological and magnetic resonance imaging study. J Neurol. 2004;251:996-1005.
25. Sellebjerg F, Nielsen HS, Frederiksen JL, et al. A randomized, controlled trial of oral high-dose methylprednisolone in acute optic neuritis. Neurology. 1999;52:1479.-
26. Rosenbaum JT, Wernick R. The utility of routine screening of patients with uveitis for systemic lupus erythematosus or tuberculosis. A Bayesian analysis. Arch Ophthalmol. 1990;108:1291-1293.
27. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509-516.
28. Darrel RW, Wagener HP, Kurland LT. Epidemiology of uveitis. Incidence and prevalence in a small urban community. Arch Ophthalmol. 1962;68:502-514.
29. Rosenbaum JT, Rahn DW. Prevalence of Lyme disease among patients with uveitis. Am J Ophthalmol. 1991;112:462-463.
30. Limberg MB. A review of bacterial keratitis and bacterial conjunctivitis. Am J Ophthalmol. 1991;112(4 suppl):2S-9S.
31. Hindman HB, Patel SB, Jun AS. Rationale for adjunctive topical corticosteroids in bacterial keratitis. Arch Ophthalmol. 2009;127:97-102.
32. Kaye SB, Rao PG, Smith G, et al. Simplifying collection of corneal specimens in cases of suspected bacterial keratitis. J Clin Microbiol. 2003;41:3192-3197.
Your patient comes in complaining of acute eye pain. Is it an ophthalmic emergency? Benign? Something in between?
The varying degrees of severity are reflected in the cases presented here, and in the multiple-choice quiz that follows. After selecting your answer to each of the questions, turn the page to find out if you were right.
CASE 1 A 74-year-old man presents with left eye pain that began when he lowered the shades in his bedroom to get ready for a nap. The pain worsened rapidly, he reports, and now—a half hour later—he has a headache, nausea, and blurred vision in the affected eye.
The patient has a history of hypertension, which is controlled with hydrochlorothiazide, but takes no other drugs. He denies any eye trauma. An eye exam reveals that the pupil is dilated and reacts poorly to light; you note corneal haziness and edema, as well ( FIGURE 1; vertical line is the slit lamp beam).
FIGURE 1
What’s your diagnosis?
- angle-closure glaucoma
- macular degeneration
- open-angle glaucoma
- retinal detachment.
CASE 2 A 20-year-old man was playing touch football while wearing contact lenses. Soon after, the game, he felt a stinging sensation in his right eye—”like sand under the eyelid,” he said. Exposure to sunlight also produced eye pain. The patient had tried flushing his eye with water, but experienced little pain relief.
An eye exam reveals a grayish-white spot in the line of vision ( FIGURE 2 ), with no sign of a penetrating injury.
FIGURE 2
What’s your next step?
- Prescribe antibiotic eye drops and send the patient home.
- Provide an emergent ophthalmology referral for foreign body extraction.
- Send the patient home with an eye patch to relieve the photophobia.
- Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
CASE 3 A 17-year-old woman is brought in by her mother because of pain and vision loss in her right eye. The pain started as soon as she awoke; 2 hours later, the vision in the affected eye became blurry. Soon after, she saw spots of light, followed by complete loss of vision. She denies any trauma and says she has never experienced anything like this before.
The patient’s visual acuity is 20/200 in her right eye, and 20/40 in the left. You follow up with a funduscopic exam of the eye, which shows edema of the optic disc, blurring of the disc margins, and distended veins ( FIGURE 3 ).
FIGURE 3
What diagnostic test should be next?
- fluorescein angiography
- intraocular pressure measurement
- magnetic resonance imaging (MRI) of the brain
- visual fields assessment.
CASE 4 A 31-year-old woman with a history of sarcoidosis comes in because of spontaneous redness ( FIGURE 4 ) and pain in her left eye, which began early that day. She denies any eye trauma, eye surgery, or recent cold, and has no discharge or crust around the eye.
FIGURE 4
What’s your diagnosis?
- anterior uveitis
- conjunctivitis
- corneal abrasion
- posterior uveitis.
CASE 5 A 21-year-old college student complains of pain in her left eye that started a day ago. She wears contact lenses and, upon questioning, tells you that she sometimes keeps them in all night.
The patient reports that she used a friend’s steroid eye drops twice yesterday, but the drops didn’t help. The pain is worse today. It feels as if there’s something in her eye, she says, and she finds it hard to open her eye. Penlight examination ( FIGURE 5 ) reveals a branching opacity on the cornea.
FIGURE 5
What’s your next step?
- Advise the patient to stop wearing her contact lenses overnight, give her a cycloplegic, and follow up in 2 days.
- Patch the patient’s left eye, prescribe antibiotics, and tell her to return tomorrow.
- Prescribe steroid eye drops and follow up in 2 days.
- Provide an urgent referral to an ophthalmologist.
CASE 1 The answer is A: angle-closure glaucoma.
Glaucoma is the world’s leading cause of blindness,1,2 and angle-closure glaucoma comprises 10% of cases.2 In this condition, the anterior chamber angle—formed by the iris and the cornea—is narrow. When the iris dilates in low light (eg, the darkened room in which the patient had planned to nap), it folds into the narrowed angle, preventing the flow of aqueous humor and leading to an increase in intraocular pressure.3
Signs and symptoms
Patients with acute angle-closure glaucoma often develop decreased vision, halos, headaches, severe eye pain, nausea, and vomiting. If the intraocular pressure increases quickly, symptoms can have an acute and dramatic onset; if pressure builds slowly, patients may have limited or no symptoms.4
Physical findings
An eye exam will reveal conjunctival erythema, corneal edema and cloudiness, iris irregularity, a shallow anterior chamber (visible with a slit lamp), a dilated pupil (4-6 mm) that reacts sluggishly to light, and increased ocular pressure. The cupping of the optic disc seen in this patient’s retinal exam ( FIGURE 6 ) is more commonly associated with chronic open-angle glaucoma.
FIGURE 6
Management
Acute angle-closure glaucoma is an ophthalmologic emergency, and a referral to a specialist is crucial. If no ophthalmologist can see the patient within an hour of the presentation of symptoms, you’ll need to initiate topical treatment to reduce intraocular pressure and ensure that he or she is seen by a specialist as soon as possible.5 First-line treatments for acute angle-closure glaucoma are listed in TABLE 1 .5,6
In severe cases, topical therapy alone may be ineffective. If there are no contraindications, systemic medications such as acetazolamide, mannitol, glycerol, or isosorbide may be needed. Eye pressure should be checked 30 to 60 minutes after initiating systemic therapy and the patient closely monitored for adverse effects (eg, anaphylaxis, convulsions [acetazolamide]; hypotension [mannitol, isosorbide]).5
When the patient does see an ophthalmologist, the evaluation will include assessment of visual acuity, pupillary evaluation, measurement of intraocular pressure, slit lamp examination, gonioscopy to measure the angle of the anterior chamber, and a fundus exam without pupil dilation.5 Treatment may include a surgical procedure, such as paracentesis of the eye, peripheral iridotomy, or iridectomy, and chronic administration of topical medication.7
TABLE 1
Treatments for acute angle-closure glaucoma5,6
| Medication | Quantity |
|---|---|
| Topical | |
| 0.5% timolol maleate | 1 drop in affected eye 2x/d |
| 1% apraclonidine | 1-2 drops 3x/d |
| 2% pilocarpine | 1 drop 4x/d |
| Oral | |
| Acetazolamide | 500 mg 2x/d |
| Glycerol 50% solution | 1-1.8 g/kg |
| Isosorbide solution | 1.5 g/kg |
| Intravenous | |
| Acetazolamide | 250 mg 4x/d |
| Mannitol | 0.25-2 g/kg (one-time dose) |
CASE 2 The answer is D: Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
This patient likely has a corneal ulcer or abrasion caused by a contact lens. Corneal ulcers—which constitute a loss of the corneal epithelium—can be caused by trauma or a foreign body, or develop spontaneously.
Signs and symptoms
Because of the rich innervation of the corneal epithelium by the trigeminal nerve, the cornea is highly sensitive to pain. Patients with corneal abrasions typically experience eye pain, photophobia, tearing, a foreign body sensation, and discomfort when driving, working, or reading. If a patient has damage to the trigeminal nerve, however (eg, from trauma, a tumor, or a herpes infection), corneal injuries may be painless.8
In some cases, corneal abrasions may be so painful that patients become disruptive while waiting to be seen. Thus, any patient suspected of having a corneal ulcer or abrasion should be ushered into a quiet, dark room and instructed to keep his or her eyes closed until the examination.
The patient history should focus on recent trauma, type of work, and use of protective eyewear, which may provide clues to the development of penetrating injuries, retained foreign bodies, or abrasions caused by a foreign body. Ask about the use of contact lenses, as well; corneal injury caused by contacts is associated with specific bacterial infections, most commonly staphylococcal organisms and Pseudomonas.9
Physical findings
Attempt to test visual acuity without topical anesthetics. If the patient can’t tolerate the test, a single drop of topical anesthetic (proparacaine 0.5%) may help. Visual acuity provides clues to the location of the injury. If acuity is close to baseline, the corneal abrasion is likely peripheral to the visual axis. Decreased visual acuity indicates either that the abrasion involves the central axis area or that there is corneal edema.9
Evaluation of the pupillary reflex and optic fundus should follow. Reactive miosis may be present with corneal abrasions. A large, nonreactive pupil may be a sign of injury to the pupillary sphincter from blunt or penetrating injury—an ophthalmologic emergency that requires urgent referral. The eyelid should be flipped and examined for foreign bodies. 9
Some abrasions can be seen with the naked eye, so a penlight exam should be performed before applying fluorescein stain. If a corneal lesion is suspicious for herpesvirus infection ( SEE CASE 5 ), fluorescein should not be applied, as it can interfere with the antibody test.10 Refer the patient to an ophthalmologist instead.
If there’s no evidence of infection, apply fluorescein and examine the cornea with a Wood’s lamp. A thin line or several vertical lines are suggestive of a foreign body in the cornea or under the eyelid, whereas round defects are often due to contact lenses.9 Physical findings associated with specific types of corneal abrasions or ulcers are detailed in TABLE 2 .9,11,12
TABLE 2
Corneal abrasion or ulcers: The differential diagnosis9,11,12
| Diagnosis | Physical findings | Management |
|---|---|---|
| Penetrating trauma |
|
|
| Infected corneal abrasion | Grayish edge near abrasions or ulcers |
|
| Retained foreign body |
|
|
| Herpesvirus infection | Branching pattern |
|
| Spontaneous erosions |
|
|
| *Gel-like extrusion of ocular contents seen with fluorescein. †Ointment is preferable to drops. If a contact lens caused the abrasion, a solution that covers Pseudomonas should be used. | ||
Management
Patients with corneal abrasions or ulcers should receive topical antibiotics to prevent infection. Ointments (erythromycin ointment 4 times daily for 3-5 days) are preferable to drops, but may be harder to obtain.9 If a patient must use drops, sulfacetamide 10%, polymyxin/trimethoprim, ciprofloxacin, or ofloxacin can be used, with the same frequency and duration.
Aminoglycosides are toxic to the corneal epithelium and should be avoided, except in abrasions caused by contacts.9 Because of the likelihood of pseudomonal keratitis in cases involving contact lenses, antibiotics covering Pseudomonas, such as ofloxacin, ciprofloxacin, or tobramycin, should be used.9
Pain control is achieved with cycloplegics11 like cyclopentolate 0.5% to 1% or a one-day course of systemic opioids. For children, over-the-counter analgesics for mild pain and mild opioids for severe pain may be used.
Chronic use of topical anesthetics should be avoided in patients of any age. Although they relieve pain, frequent use can lead to delayed healing, ulcerations, perforations, scarring, or even blindness.8
Patching has not been found to improve healing or comfort;13 instead, it delays healing.14,15 The “pirate patch,” which hovers over the eye, does not keep the eyelid down and therefore is not recommended.9
Follow up within 24 hours of initiating treatment to assure that the abrasion is healing. If it appears to be getting worse or is simply not improving, an immediate referral to an ophthalmologist is needed. Abrasions caused by contact with potentially infected material (eg, farm equipment, tree branches, or soil) require daily monitoring until they heal.11
CASE 3 The answer is C: Order an MRI of the brain.
This patient has optic neuritis, caused by inflammation of the optic nerve and disruption of the nerve’s myelin sheath. It predominantly affects young adults, and is more common in women than in men.16 The incidence of optic neuritis is higher among Asians, black South Africans, and children under the age of 15.17,18
Signs and symptoms
Optic neuritis is characterized by monocular (90%) or binocular (10%) complete or partial vision loss, photopsia (flashes of light), and eye pain. Up to 60% of pediatric patients present with blurred vision, bilateral involvement,19 and no pain, while adults predominantly have pain and unilateral vision loss.20 Optic neuritis is often a presenting symptom of multiple sclerosis (MS).16
Physical findings
Physical exam findings in optic neuritis include a sluggish direct light reflex, loss of visual acuity and color vision, as well as acute eye pain.18 Ophthalmoscopic exam may reveal papillitis with edema of the optic disc.21 In the Optic Neuritis Treatment Trial (ONTT), however, only one-third of patients presented with papillitis and swelling of the optic disc.22
MRI of the brain with gadolinium contrast is generally used to confirm the diagnosis. On MRI, 95% of patients with optic neuritis have signs of inflammation of the optic nerve and/or white matter changes consistent with MS (periventricular and ovoid demyelination).23,24
Patients with evidence of demyelination should also be evaluated for MS and other demyelinating disorders. In the ONTT trial, the risk of developing MS within 15 years of an optic neuritis diagnosis was as low as 25% (95% confidence interval [CI], 18%-32%) for patients with no lesions on a baseline brain MRI and as high as 72% (95% CI, 63%-81%) for those with one or more lesions on a baseline MRI, according to the study’s final follow-up.22
Management
The recommended treatment for optic neuritis is intravenous (IV) methylprednisolone 250 mg every 6 hours for 3 to 5 days, followed by oral prednisone at 1 mg/kg/d for 7 to 10 days. Vision usually returns slowly over the course of several months to a year. Ophthalmology consultation should be considered to rule out other causes of optic neuritis.25
CASE 4 The answer is A: anterior uveitis.
Uveitis is often associated with systemic disease or infection, and diagnosis is typically suspected based on a history of conditions such as sarcoidosis, juvenile idiopathic arthritis, Kawasaki’s disease, Sjögren’s syndrome, toxoplasmosis, human immunodeficiency virus (HIV), tuberculosis (TB), syphilis, herpes simplex, and herpes zoster.26
Signs and symptoms
Signs and symptoms vary depending on the part of the uveal tract that’s involved. Anterior uveitis, or iritis, is associated with pain, photophobia, redness, and a varying degree of vision loss. Posterior and intermediate uveitis are less likely to be associated with pain, but can be accompanied by decreased visual acuity and floaters.27
Physical findings
Visual acuity in patients with uveitis can range from normal to varying degrees of vision loss. Redness around the iris can be seen; conjunctival infection is most marked around the circumference of the corneal limbus rather than more peripherally, as seen in conjunctivitis. On slit lamp examination, the beam of light can be seen in the aqueous humor due to protein and leukocyte accumulation—a phenomenon known as “flare.” The pupillary light reflex may be abnormal, and the pupillary opening may be irregular rather than round due to anterior and posterior synechia.28
Management
Patients should be referred to an ophthalmologist for management of the immediate condition and to prevent or treat complications such as vision loss, optic nerve damage, and glaucoma. Acute management includes topical steroids, such as prednisolone acetate ophthalmic 1% 2 to 4 times daily, as well as treatment of the underlying condition. Long-term management varies, depending on the cause of the uveitis.26,29
If the etiology is unknown, a workup should be considered to identify inflammatory and infectious disorders that might be causing uveitis. Chest radiograph is a good beginning to look for evidence of sarcoidosis or TB; serologic testing for syphilis, HIV, and lupus may also be considered.26,29
CASE 5 The answer is D: Provide an urgent referral to an ophthalmologist.
This patient has viral keratitis caused by herpes. While the pain and foreign body sensation are the same for bacterial and viral keratitis, herpesvirus is distinguishable by the branching opacity that develops on the cornea.
Varicella zoster is the most common cause of viral keratitis, although it can also be caused by herpes simplex and adeno-virus. Because a person who is infected with herpes has the virus for life, however, multiple attacks are possible. Reactivation is associated with stress and a weakened immune system, but may occur spontaneously, as well. Patients who wear contact lenses are no more likely than those who don’t to be infected with the herpesvirus.
Bacterial keratitis is often associated with contact lenses, particularly when they’re continually worn, but also with normal wear.30 Immunosuppression, dry ocular surfaces, and topical corticosteroid use may predispose patients to bacterial keratitis, as well.12 Staphylococcus aureus, Pseudomonas aeruginosa, coagulase-negative Staphylococcus, diphtheroids, and Streptococcus pneumoniae are the most common pathogens.31
Signs and symptoms
Patients with keratitis typically complain of eye pain, a sensation of having a foreign body in the eye, photophobia, tearing, and vision changes; a mucopurulent discharge is sometimes present, as well.3 The condition is easily distinguished from conjunctivitis, which typically does not involve eye pain or vision changes.
Physical findings
Visual acuity may be affected if the lesion or corneal edema involves the visual axis. Physical exam in a patient with bacterial keratitis sometimes shows a gray or white corneal opacity, along with corneal erythema. As already noted, a penlight exam will reveal a branching opacity in patients with herpes keratitis.30
Management
Patients with keratitis should be referred immediately to an ophthalmologist32 for a slit lamp evaluation, treatment, and close follow-up.
Corneal cultures can be difficult to obtain, but before prescribing antibiotics, an attempt to collect samples should be made. This can be done—after the administration of topical anesthesia—with a sterile calcium alginate swab. Gently swab the cornea and then inoculate the appropriate gels or mediums. Avoid contact with lashes and eyelids to prevent culture contamination.32
When herpesvirus is suspected, start the patient on an antiviral agent such as trifluridine ophthalmic (1%) 9 times a day, vidarabine ophthalmic (3%) 5 times daily, or 400 mg oral acyclovir 5 times a day. Patients with bacterial keratitis should be started on antibiotic eye drops with Pseudomonas coverage, such as ofloxacin (0.3%), ciprofloxacin (0.3%), or tobramycin (0.3%), 6 to 8 times a day.9
CORRESPONDENCE Uyen Michelle Le, MD, 967 Galindo Court, Milpitas, CA 95035; mlkala21@aol.com
Your patient comes in complaining of acute eye pain. Is it an ophthalmic emergency? Benign? Something in between?
The varying degrees of severity are reflected in the cases presented here, and in the multiple-choice quiz that follows. After selecting your answer to each of the questions, turn the page to find out if you were right.
CASE 1 A 74-year-old man presents with left eye pain that began when he lowered the shades in his bedroom to get ready for a nap. The pain worsened rapidly, he reports, and now—a half hour later—he has a headache, nausea, and blurred vision in the affected eye.
The patient has a history of hypertension, which is controlled with hydrochlorothiazide, but takes no other drugs. He denies any eye trauma. An eye exam reveals that the pupil is dilated and reacts poorly to light; you note corneal haziness and edema, as well ( FIGURE 1; vertical line is the slit lamp beam).
FIGURE 1
What’s your diagnosis?
- angle-closure glaucoma
- macular degeneration
- open-angle glaucoma
- retinal detachment.
CASE 2 A 20-year-old man was playing touch football while wearing contact lenses. Soon after, the game, he felt a stinging sensation in his right eye—”like sand under the eyelid,” he said. Exposure to sunlight also produced eye pain. The patient had tried flushing his eye with water, but experienced little pain relief.
An eye exam reveals a grayish-white spot in the line of vision ( FIGURE 2 ), with no sign of a penetrating injury.
FIGURE 2
What’s your next step?
- Prescribe antibiotic eye drops and send the patient home.
- Provide an emergent ophthalmology referral for foreign body extraction.
- Send the patient home with an eye patch to relieve the photophobia.
- Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
CASE 3 A 17-year-old woman is brought in by her mother because of pain and vision loss in her right eye. The pain started as soon as she awoke; 2 hours later, the vision in the affected eye became blurry. Soon after, she saw spots of light, followed by complete loss of vision. She denies any trauma and says she has never experienced anything like this before.
The patient’s visual acuity is 20/200 in her right eye, and 20/40 in the left. You follow up with a funduscopic exam of the eye, which shows edema of the optic disc, blurring of the disc margins, and distended veins ( FIGURE 3 ).
FIGURE 3
What diagnostic test should be next?
- fluorescein angiography
- intraocular pressure measurement
- magnetic resonance imaging (MRI) of the brain
- visual fields assessment.
CASE 4 A 31-year-old woman with a history of sarcoidosis comes in because of spontaneous redness ( FIGURE 4 ) and pain in her left eye, which began early that day. She denies any eye trauma, eye surgery, or recent cold, and has no discharge or crust around the eye.
FIGURE 4
What’s your diagnosis?
- anterior uveitis
- conjunctivitis
- corneal abrasion
- posterior uveitis.
CASE 5 A 21-year-old college student complains of pain in her left eye that started a day ago. She wears contact lenses and, upon questioning, tells you that she sometimes keeps them in all night.
The patient reports that she used a friend’s steroid eye drops twice yesterday, but the drops didn’t help. The pain is worse today. It feels as if there’s something in her eye, she says, and she finds it hard to open her eye. Penlight examination ( FIGURE 5 ) reveals a branching opacity on the cornea.
FIGURE 5
What’s your next step?
- Advise the patient to stop wearing her contact lenses overnight, give her a cycloplegic, and follow up in 2 days.
- Patch the patient’s left eye, prescribe antibiotics, and tell her to return tomorrow.
- Prescribe steroid eye drops and follow up in 2 days.
- Provide an urgent referral to an ophthalmologist.
CASE 1 The answer is A: angle-closure glaucoma.
Glaucoma is the world’s leading cause of blindness,1,2 and angle-closure glaucoma comprises 10% of cases.2 In this condition, the anterior chamber angle—formed by the iris and the cornea—is narrow. When the iris dilates in low light (eg, the darkened room in which the patient had planned to nap), it folds into the narrowed angle, preventing the flow of aqueous humor and leading to an increase in intraocular pressure.3
Signs and symptoms
Patients with acute angle-closure glaucoma often develop decreased vision, halos, headaches, severe eye pain, nausea, and vomiting. If the intraocular pressure increases quickly, symptoms can have an acute and dramatic onset; if pressure builds slowly, patients may have limited or no symptoms.4
Physical findings
An eye exam will reveal conjunctival erythema, corneal edema and cloudiness, iris irregularity, a shallow anterior chamber (visible with a slit lamp), a dilated pupil (4-6 mm) that reacts sluggishly to light, and increased ocular pressure. The cupping of the optic disc seen in this patient’s retinal exam ( FIGURE 6 ) is more commonly associated with chronic open-angle glaucoma.
FIGURE 6
Management
Acute angle-closure glaucoma is an ophthalmologic emergency, and a referral to a specialist is crucial. If no ophthalmologist can see the patient within an hour of the presentation of symptoms, you’ll need to initiate topical treatment to reduce intraocular pressure and ensure that he or she is seen by a specialist as soon as possible.5 First-line treatments for acute angle-closure glaucoma are listed in TABLE 1 .5,6
In severe cases, topical therapy alone may be ineffective. If there are no contraindications, systemic medications such as acetazolamide, mannitol, glycerol, or isosorbide may be needed. Eye pressure should be checked 30 to 60 minutes after initiating systemic therapy and the patient closely monitored for adverse effects (eg, anaphylaxis, convulsions [acetazolamide]; hypotension [mannitol, isosorbide]).5
When the patient does see an ophthalmologist, the evaluation will include assessment of visual acuity, pupillary evaluation, measurement of intraocular pressure, slit lamp examination, gonioscopy to measure the angle of the anterior chamber, and a fundus exam without pupil dilation.5 Treatment may include a surgical procedure, such as paracentesis of the eye, peripheral iridotomy, or iridectomy, and chronic administration of topical medication.7
TABLE 1
Treatments for acute angle-closure glaucoma5,6
| Medication | Quantity |
|---|---|
| Topical | |
| 0.5% timolol maleate | 1 drop in affected eye 2x/d |
| 1% apraclonidine | 1-2 drops 3x/d |
| 2% pilocarpine | 1 drop 4x/d |
| Oral | |
| Acetazolamide | 500 mg 2x/d |
| Glycerol 50% solution | 1-1.8 g/kg |
| Isosorbide solution | 1.5 g/kg |
| Intravenous | |
| Acetazolamide | 250 mg 4x/d |
| Mannitol | 0.25-2 g/kg (one-time dose) |
CASE 2 The answer is D: Attempt to conduct a visual acuity test and penlight exam without anesthetic; if necessary, apply anesthetic drops and fluorescein stain.
This patient likely has a corneal ulcer or abrasion caused by a contact lens. Corneal ulcers—which constitute a loss of the corneal epithelium—can be caused by trauma or a foreign body, or develop spontaneously.
Signs and symptoms
Because of the rich innervation of the corneal epithelium by the trigeminal nerve, the cornea is highly sensitive to pain. Patients with corneal abrasions typically experience eye pain, photophobia, tearing, a foreign body sensation, and discomfort when driving, working, or reading. If a patient has damage to the trigeminal nerve, however (eg, from trauma, a tumor, or a herpes infection), corneal injuries may be painless.8
In some cases, corneal abrasions may be so painful that patients become disruptive while waiting to be seen. Thus, any patient suspected of having a corneal ulcer or abrasion should be ushered into a quiet, dark room and instructed to keep his or her eyes closed until the examination.
The patient history should focus on recent trauma, type of work, and use of protective eyewear, which may provide clues to the development of penetrating injuries, retained foreign bodies, or abrasions caused by a foreign body. Ask about the use of contact lenses, as well; corneal injury caused by contacts is associated with specific bacterial infections, most commonly staphylococcal organisms and Pseudomonas.9
Physical findings
Attempt to test visual acuity without topical anesthetics. If the patient can’t tolerate the test, a single drop of topical anesthetic (proparacaine 0.5%) may help. Visual acuity provides clues to the location of the injury. If acuity is close to baseline, the corneal abrasion is likely peripheral to the visual axis. Decreased visual acuity indicates either that the abrasion involves the central axis area or that there is corneal edema.9
Evaluation of the pupillary reflex and optic fundus should follow. Reactive miosis may be present with corneal abrasions. A large, nonreactive pupil may be a sign of injury to the pupillary sphincter from blunt or penetrating injury—an ophthalmologic emergency that requires urgent referral. The eyelid should be flipped and examined for foreign bodies. 9
Some abrasions can be seen with the naked eye, so a penlight exam should be performed before applying fluorescein stain. If a corneal lesion is suspicious for herpesvirus infection ( SEE CASE 5 ), fluorescein should not be applied, as it can interfere with the antibody test.10 Refer the patient to an ophthalmologist instead.
If there’s no evidence of infection, apply fluorescein and examine the cornea with a Wood’s lamp. A thin line or several vertical lines are suggestive of a foreign body in the cornea or under the eyelid, whereas round defects are often due to contact lenses.9 Physical findings associated with specific types of corneal abrasions or ulcers are detailed in TABLE 2 .9,11,12
TABLE 2
Corneal abrasion or ulcers: The differential diagnosis9,11,12
| Diagnosis | Physical findings | Management |
|---|---|---|
| Penetrating trauma |
|
|
| Infected corneal abrasion | Grayish edge near abrasions or ulcers |
|
| Retained foreign body |
|
|
| Herpesvirus infection | Branching pattern |
|
| Spontaneous erosions |
|
|
| *Gel-like extrusion of ocular contents seen with fluorescein. †Ointment is preferable to drops. If a contact lens caused the abrasion, a solution that covers Pseudomonas should be used. | ||
Management
Patients with corneal abrasions or ulcers should receive topical antibiotics to prevent infection. Ointments (erythromycin ointment 4 times daily for 3-5 days) are preferable to drops, but may be harder to obtain.9 If a patient must use drops, sulfacetamide 10%, polymyxin/trimethoprim, ciprofloxacin, or ofloxacin can be used, with the same frequency and duration.
Aminoglycosides are toxic to the corneal epithelium and should be avoided, except in abrasions caused by contacts.9 Because of the likelihood of pseudomonal keratitis in cases involving contact lenses, antibiotics covering Pseudomonas, such as ofloxacin, ciprofloxacin, or tobramycin, should be used.9
Pain control is achieved with cycloplegics11 like cyclopentolate 0.5% to 1% or a one-day course of systemic opioids. For children, over-the-counter analgesics for mild pain and mild opioids for severe pain may be used.
Chronic use of topical anesthetics should be avoided in patients of any age. Although they relieve pain, frequent use can lead to delayed healing, ulcerations, perforations, scarring, or even blindness.8
Patching has not been found to improve healing or comfort;13 instead, it delays healing.14,15 The “pirate patch,” which hovers over the eye, does not keep the eyelid down and therefore is not recommended.9
Follow up within 24 hours of initiating treatment to assure that the abrasion is healing. If it appears to be getting worse or is simply not improving, an immediate referral to an ophthalmologist is needed. Abrasions caused by contact with potentially infected material (eg, farm equipment, tree branches, or soil) require daily monitoring until they heal.11
CASE 3 The answer is C: Order an MRI of the brain.
This patient has optic neuritis, caused by inflammation of the optic nerve and disruption of the nerve’s myelin sheath. It predominantly affects young adults, and is more common in women than in men.16 The incidence of optic neuritis is higher among Asians, black South Africans, and children under the age of 15.17,18
Signs and symptoms
Optic neuritis is characterized by monocular (90%) or binocular (10%) complete or partial vision loss, photopsia (flashes of light), and eye pain. Up to 60% of pediatric patients present with blurred vision, bilateral involvement,19 and no pain, while adults predominantly have pain and unilateral vision loss.20 Optic neuritis is often a presenting symptom of multiple sclerosis (MS).16
Physical findings
Physical exam findings in optic neuritis include a sluggish direct light reflex, loss of visual acuity and color vision, as well as acute eye pain.18 Ophthalmoscopic exam may reveal papillitis with edema of the optic disc.21 In the Optic Neuritis Treatment Trial (ONTT), however, only one-third of patients presented with papillitis and swelling of the optic disc.22
MRI of the brain with gadolinium contrast is generally used to confirm the diagnosis. On MRI, 95% of patients with optic neuritis have signs of inflammation of the optic nerve and/or white matter changes consistent with MS (periventricular and ovoid demyelination).23,24
Patients with evidence of demyelination should also be evaluated for MS and other demyelinating disorders. In the ONTT trial, the risk of developing MS within 15 years of an optic neuritis diagnosis was as low as 25% (95% confidence interval [CI], 18%-32%) for patients with no lesions on a baseline brain MRI and as high as 72% (95% CI, 63%-81%) for those with one or more lesions on a baseline MRI, according to the study’s final follow-up.22
Management
The recommended treatment for optic neuritis is intravenous (IV) methylprednisolone 250 mg every 6 hours for 3 to 5 days, followed by oral prednisone at 1 mg/kg/d for 7 to 10 days. Vision usually returns slowly over the course of several months to a year. Ophthalmology consultation should be considered to rule out other causes of optic neuritis.25
CASE 4 The answer is A: anterior uveitis.
Uveitis is often associated with systemic disease or infection, and diagnosis is typically suspected based on a history of conditions such as sarcoidosis, juvenile idiopathic arthritis, Kawasaki’s disease, Sjögren’s syndrome, toxoplasmosis, human immunodeficiency virus (HIV), tuberculosis (TB), syphilis, herpes simplex, and herpes zoster.26
Signs and symptoms
Signs and symptoms vary depending on the part of the uveal tract that’s involved. Anterior uveitis, or iritis, is associated with pain, photophobia, redness, and a varying degree of vision loss. Posterior and intermediate uveitis are less likely to be associated with pain, but can be accompanied by decreased visual acuity and floaters.27
Physical findings
Visual acuity in patients with uveitis can range from normal to varying degrees of vision loss. Redness around the iris can be seen; conjunctival infection is most marked around the circumference of the corneal limbus rather than more peripherally, as seen in conjunctivitis. On slit lamp examination, the beam of light can be seen in the aqueous humor due to protein and leukocyte accumulation—a phenomenon known as “flare.” The pupillary light reflex may be abnormal, and the pupillary opening may be irregular rather than round due to anterior and posterior synechia.28
Management
Patients should be referred to an ophthalmologist for management of the immediate condition and to prevent or treat complications such as vision loss, optic nerve damage, and glaucoma. Acute management includes topical steroids, such as prednisolone acetate ophthalmic 1% 2 to 4 times daily, as well as treatment of the underlying condition. Long-term management varies, depending on the cause of the uveitis.26,29
If the etiology is unknown, a workup should be considered to identify inflammatory and infectious disorders that might be causing uveitis. Chest radiograph is a good beginning to look for evidence of sarcoidosis or TB; serologic testing for syphilis, HIV, and lupus may also be considered.26,29
CASE 5 The answer is D: Provide an urgent referral to an ophthalmologist.
This patient has viral keratitis caused by herpes. While the pain and foreign body sensation are the same for bacterial and viral keratitis, herpesvirus is distinguishable by the branching opacity that develops on the cornea.
Varicella zoster is the most common cause of viral keratitis, although it can also be caused by herpes simplex and adeno-virus. Because a person who is infected with herpes has the virus for life, however, multiple attacks are possible. Reactivation is associated with stress and a weakened immune system, but may occur spontaneously, as well. Patients who wear contact lenses are no more likely than those who don’t to be infected with the herpesvirus.
Bacterial keratitis is often associated with contact lenses, particularly when they’re continually worn, but also with normal wear.30 Immunosuppression, dry ocular surfaces, and topical corticosteroid use may predispose patients to bacterial keratitis, as well.12 Staphylococcus aureus, Pseudomonas aeruginosa, coagulase-negative Staphylococcus, diphtheroids, and Streptococcus pneumoniae are the most common pathogens.31
Signs and symptoms
Patients with keratitis typically complain of eye pain, a sensation of having a foreign body in the eye, photophobia, tearing, and vision changes; a mucopurulent discharge is sometimes present, as well.3 The condition is easily distinguished from conjunctivitis, which typically does not involve eye pain or vision changes.
Physical findings
Visual acuity may be affected if the lesion or corneal edema involves the visual axis. Physical exam in a patient with bacterial keratitis sometimes shows a gray or white corneal opacity, along with corneal erythema. As already noted, a penlight exam will reveal a branching opacity in patients with herpes keratitis.30
Management
Patients with keratitis should be referred immediately to an ophthalmologist32 for a slit lamp evaluation, treatment, and close follow-up.
Corneal cultures can be difficult to obtain, but before prescribing antibiotics, an attempt to collect samples should be made. This can be done—after the administration of topical anesthesia—with a sterile calcium alginate swab. Gently swab the cornea and then inoculate the appropriate gels or mediums. Avoid contact with lashes and eyelids to prevent culture contamination.32
When herpesvirus is suspected, start the patient on an antiviral agent such as trifluridine ophthalmic (1%) 9 times a day, vidarabine ophthalmic (3%) 5 times daily, or 400 mg oral acyclovir 5 times a day. Patients with bacterial keratitis should be started on antibiotic eye drops with Pseudomonas coverage, such as ofloxacin (0.3%), ciprofloxacin (0.3%), or tobramycin (0.3%), 6 to 8 times a day.9
CORRESPONDENCE Uyen Michelle Le, MD, 967 Galindo Court, Milpitas, CA 95035; mlkala21@aol.com
1. Foster PJ, Johnson GJ. Glaucoma in China: how big is the problem? Br J Ophthalmol. 2001;85:1277-1282.
2. American Academy of Ophthalmology. Preferred Practice Pattern Guidelines. Primary angle closure PPP - October 2010. Available at: http://one.aao.org/CE/PracticeGuidelines/PPP_Content.aspx?cid=92bea8f6-5459-49a6-9233-4528343dc4c3. Accessed July 12, 2012.
3. Sau SM, Gazzard G, Friedman DS. Interventions for angle-closure glaucoma: an evidence-based update. Ophthalmology. 2003;110:1878-1879, 1930.
4. Leibowitz HM. The red eye. N Engl J Med. 2000;343:345-351.
5. Shields SR. Managing eye disease in primary care. Part 3. When to refer for ophthalmologic care. Postgrad Med. 2000;108:99-106.
6. Awasthi P. Srivastava SN. Role of oral glycerol in glaucoma. Br J Ophthalmol. 1965;49:660-666.
7. Quigley HA. Glaucoma. Lancet. 2011;377:1367-1377.
8. Peyman GA, Rahimy MH, Fenandes ML. Effects of morphine on corneal sensitivity and epithelial wound healing: implications for topical ophthalmic analgesia. Br J Ophthalmol. 1994;78:138-141.
9. Schein OD. Contact lens abrasions and the nonophthalmologist. Am J Emerg Med. 1993;11:606-608.
10. Goldschmidt P. Effects of topical anaesthetics and fluorescein on the real-time PCR used for the diagnosis of herpesviruses and acanthamoeba keratitis. Br J Ophthalmol. 2006;90:1354-1356.
11. Benson WH, Snyder IS, Granus V, et al. Tetanus prophylaxis following ocular injuries. J Emerg Med. 1993;11:677-683.
12. DeBroff BM, Donahue SP, Caputo BJ, et al. Clinical characteristics of corneal foreign bodies and their associated culture results. CLAO J. 1994;20:128-130.
13. Turner A, Rabiu M. Patching for corneal abrasion. Cochrane Database Syst Rev. 2006;(2):CD004764.-
14. Kaiser PK. A comparison of pressure patching versus no patching for corneal abrasions due to trauma or foreign body removal. Corneal Abrasion Patching Study Group. Ophthalmology. 1995;102:1936-1942.
15. Clemons CS, Cohen EJ, Arentset JJ, et al. Pseudomonas ulcers following patching of corneal abrasions associated with contact lens wear. CLAO J. 1987;13:161-164.
16. Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med. 2006;354:1273-1280.
17. De la Cruz J, Kupersmith MJ. Clinical profile of simultaneous bilateral optic neuritis in adults. Br J Ophthalmol. 2006;90:551-554.
18. Hwang JM, Lee YJ, Kim MK. Optic neuritis in Asian children. J Ped Ophthalmol Strabismus. 2002;39:26-32.
19. Lana-Peixoto MA, Andreade GC. The clinical profile of childhood optic neuritis. Arq Neuropsiquiatr. 2001;59(2-B):311-317.
20. Boomer JA, Siatkowski RM. Optic neuritis is adults and children. Semin Ophthalmol. 2003;18:174-180.
21. Lucchinetti CF, Kiers L, O’Duffy A, et al. Risk factors for developing multiple sclerosis after childhood optic neuritis. Neurology. 1997;49:1413-1418.
22. Optic Neuritis Study Group. Multiple sclerosis risk after optic neuritis: final optic neuritis treatment trial follow-up. Arch Neurol. 2008;65:727-732.
23. Wray SH. Optic neuritis. In: Principles and Practice of Ophthalmology. Albert DM, Jakobiec FA, eds. WB Saunders; Philadelphia, Pa: 1994.
24. Hickman SJ, Toosy AT, Miszkiel KA, et al. Visual recovery following acute optic neuritis—a clinical, electrophysiological and magnetic resonance imaging study. J Neurol. 2004;251:996-1005.
25. Sellebjerg F, Nielsen HS, Frederiksen JL, et al. A randomized, controlled trial of oral high-dose methylprednisolone in acute optic neuritis. Neurology. 1999;52:1479.-
26. Rosenbaum JT, Wernick R. The utility of routine screening of patients with uveitis for systemic lupus erythematosus or tuberculosis. A Bayesian analysis. Arch Ophthalmol. 1990;108:1291-1293.
27. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509-516.
28. Darrel RW, Wagener HP, Kurland LT. Epidemiology of uveitis. Incidence and prevalence in a small urban community. Arch Ophthalmol. 1962;68:502-514.
29. Rosenbaum JT, Rahn DW. Prevalence of Lyme disease among patients with uveitis. Am J Ophthalmol. 1991;112:462-463.
30. Limberg MB. A review of bacterial keratitis and bacterial conjunctivitis. Am J Ophthalmol. 1991;112(4 suppl):2S-9S.
31. Hindman HB, Patel SB, Jun AS. Rationale for adjunctive topical corticosteroids in bacterial keratitis. Arch Ophthalmol. 2009;127:97-102.
32. Kaye SB, Rao PG, Smith G, et al. Simplifying collection of corneal specimens in cases of suspected bacterial keratitis. J Clin Microbiol. 2003;41:3192-3197.
1. Foster PJ, Johnson GJ. Glaucoma in China: how big is the problem? Br J Ophthalmol. 2001;85:1277-1282.
2. American Academy of Ophthalmology. Preferred Practice Pattern Guidelines. Primary angle closure PPP - October 2010. Available at: http://one.aao.org/CE/PracticeGuidelines/PPP_Content.aspx?cid=92bea8f6-5459-49a6-9233-4528343dc4c3. Accessed July 12, 2012.
3. Sau SM, Gazzard G, Friedman DS. Interventions for angle-closure glaucoma: an evidence-based update. Ophthalmology. 2003;110:1878-1879, 1930.
4. Leibowitz HM. The red eye. N Engl J Med. 2000;343:345-351.
5. Shields SR. Managing eye disease in primary care. Part 3. When to refer for ophthalmologic care. Postgrad Med. 2000;108:99-106.
6. Awasthi P. Srivastava SN. Role of oral glycerol in glaucoma. Br J Ophthalmol. 1965;49:660-666.
7. Quigley HA. Glaucoma. Lancet. 2011;377:1367-1377.
8. Peyman GA, Rahimy MH, Fenandes ML. Effects of morphine on corneal sensitivity and epithelial wound healing: implications for topical ophthalmic analgesia. Br J Ophthalmol. 1994;78:138-141.
9. Schein OD. Contact lens abrasions and the nonophthalmologist. Am J Emerg Med. 1993;11:606-608.
10. Goldschmidt P. Effects of topical anaesthetics and fluorescein on the real-time PCR used for the diagnosis of herpesviruses and acanthamoeba keratitis. Br J Ophthalmol. 2006;90:1354-1356.
11. Benson WH, Snyder IS, Granus V, et al. Tetanus prophylaxis following ocular injuries. J Emerg Med. 1993;11:677-683.
12. DeBroff BM, Donahue SP, Caputo BJ, et al. Clinical characteristics of corneal foreign bodies and their associated culture results. CLAO J. 1994;20:128-130.
13. Turner A, Rabiu M. Patching for corneal abrasion. Cochrane Database Syst Rev. 2006;(2):CD004764.-
14. Kaiser PK. A comparison of pressure patching versus no patching for corneal abrasions due to trauma or foreign body removal. Corneal Abrasion Patching Study Group. Ophthalmology. 1995;102:1936-1942.
15. Clemons CS, Cohen EJ, Arentset JJ, et al. Pseudomonas ulcers following patching of corneal abrasions associated with contact lens wear. CLAO J. 1987;13:161-164.
16. Balcer LJ. Clinical practice. Optic neuritis. N Engl J Med. 2006;354:1273-1280.
17. De la Cruz J, Kupersmith MJ. Clinical profile of simultaneous bilateral optic neuritis in adults. Br J Ophthalmol. 2006;90:551-554.
18. Hwang JM, Lee YJ, Kim MK. Optic neuritis in Asian children. J Ped Ophthalmol Strabismus. 2002;39:26-32.
19. Lana-Peixoto MA, Andreade GC. The clinical profile of childhood optic neuritis. Arq Neuropsiquiatr. 2001;59(2-B):311-317.
20. Boomer JA, Siatkowski RM. Optic neuritis is adults and children. Semin Ophthalmol. 2003;18:174-180.
21. Lucchinetti CF, Kiers L, O’Duffy A, et al. Risk factors for developing multiple sclerosis after childhood optic neuritis. Neurology. 1997;49:1413-1418.
22. Optic Neuritis Study Group. Multiple sclerosis risk after optic neuritis: final optic neuritis treatment trial follow-up. Arch Neurol. 2008;65:727-732.
23. Wray SH. Optic neuritis. In: Principles and Practice of Ophthalmology. Albert DM, Jakobiec FA, eds. WB Saunders; Philadelphia, Pa: 1994.
24. Hickman SJ, Toosy AT, Miszkiel KA, et al. Visual recovery following acute optic neuritis—a clinical, electrophysiological and magnetic resonance imaging study. J Neurol. 2004;251:996-1005.
25. Sellebjerg F, Nielsen HS, Frederiksen JL, et al. A randomized, controlled trial of oral high-dose methylprednisolone in acute optic neuritis. Neurology. 1999;52:1479.-
26. Rosenbaum JT, Wernick R. The utility of routine screening of patients with uveitis for systemic lupus erythematosus or tuberculosis. A Bayesian analysis. Arch Ophthalmol. 1990;108:1291-1293.
27. Jabs DA, Nussenblatt RB, Rosenbaum JT. Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140:509-516.
28. Darrel RW, Wagener HP, Kurland LT. Epidemiology of uveitis. Incidence and prevalence in a small urban community. Arch Ophthalmol. 1962;68:502-514.
29. Rosenbaum JT, Rahn DW. Prevalence of Lyme disease among patients with uveitis. Am J Ophthalmol. 1991;112:462-463.
30. Limberg MB. A review of bacterial keratitis and bacterial conjunctivitis. Am J Ophthalmol. 1991;112(4 suppl):2S-9S.
31. Hindman HB, Patel SB, Jun AS. Rationale for adjunctive topical corticosteroids in bacterial keratitis. Arch Ophthalmol. 2009;127:97-102.
32. Kaye SB, Rao PG, Smith G, et al. Simplifying collection of corneal specimens in cases of suspected bacterial keratitis. J Clin Microbiol. 2003;41:3192-3197.