User login
A 58-year-old patient came into the office complaining of sinus congestion with sinus pressure, sore throat, and postnasal drip that had been getting progressively worse over the past week. He had tried over-the-counter decongestants, but his symptoms were not resolving. He told the physician’s assistant (DR) that he’d had sinus infections in the past and that he thought he had one now.
When asked about his general health, the patient indicated that he vaguely remembered being told years ago that his cholesterol was elevated, but at the time, declined any medical treatment. He indicated that he hadn’t had a physical examination in years. He said that he only went to the doctor when he was “sick.”
The patient was a cigarette smoker and had smoked a pack a day for 35 years. He said that while he smoked mostly cigarettes, he would also have an occasional cigar. He said that he had never smoked tobacco through a pipe. He also indicated that he drank 3 to 4 beers daily.
While inspecting his pharynx during the physical examination, DR noted a lesion on the posterior hard palate that extended to the soft palate (FIGURE 1). It appeared macular and erythematous, and had an eroded surface. The borders of the lesion were diffuse and irregular, measuring approximately 2 cm Ø 3 cm. During palpation, the lesion was mildly painful, but there was no firmness along the soft palate, buccal mucosa, or tongue. The patient had poor oral hygiene, multiple missing and carious teeth, and a removable partial denture. All other mucosal surfaces were within normal limits.
As the patient suspected, he did have a sinus infection. He left the office with a prescription for an antibiotic. He also left with a referral to an oral maxillofacial surgeon for further evaluation of the lesion.
FIGURE 1
Lesion on the hard palate
What is your diagnosis?
How would you manage this condition?
Diagnosis: Perianal streptococcal dermatitis
The oral maxillofacial surgeon (TAC) concurred with the previous examination findings. He was concerned by the appearance of the lesion and the history of tobacco use and performed a biopsy of the lesion. The pathology report revealed that the patient had nicotine stomatitis with a concomitant candidiasis infection.
Nicotine stomatitis is a common mucosal keratosis caused by smoking tobacco. It is localized to the hard palate of the mouth, but can extend to the soft palate. The mucosa of the hard palate becomes white and thickened due to hyperkeratosis of the tissue.1 Thin red lines of normal mucosa can be seen throughout the lesion. Red dots or papules can appear in the center of the lesion, which represent irritated salivary glands with inflamed duct openings (FIGURE 2).2
Our patient’s lesion had an atypical presentation. Classically the lesions are whiter, but in this case, the patient’s lesion was more erythematous. The reason: A super-infection of candidiasis caused an atrophic form of the condition.
FIGURE 2
Classic presentation of nicotine stomatitis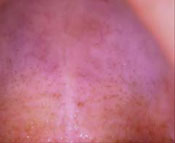
Differential Dx includes squamous cell carcinoma
The differential diagnosis in a case of nicotine stomatitis includes:
- irritation from dental appliances
- trauma from hot liquids
- squamous cell carcinoma
- atrophic candidiasis.
ill-fitting dentures can cause erythematous lesions along the hard palate and gingiva. The erythema from dentures is usually uniform in color without ulceration and follows the outline or shape of the oral appliance. In contrast, nicotine stomatitis will typically present on exposed areas of the palate and not follow any specific pattern. Most lesions caused by irritations or trauma resolve within 2 weeks of removal of the offending agent.
In the case of burns from food or liquids, the patient will tell you that he drank or ate something hot, and he’ll have a red lesion on the tongue or roof of his mouth.
Squamous cell carcinoma of the hard palate is part of the differential diagnosis because smoking increases a patient’s risk of this form of oral cancer. Squamous cell carcinoma of the palate accounts for 5% to 15% of intraoral carcinomas, depending on whether it is on the hard or soft palate.1 The lesions are typically red or red/white in color and have ulcerated and/or necrotic surfaces. The lesions can become exophytic if left untreated. In comparison, nicotine stomatitis does not ulcerate unless there is a concomitant disease process, which should prompt the clinician to perform further diagnostics tests.
Atrophic candidiasis is also part of the differential, and in the case of our patient, it was a concomitant infection. Candidiasis has a variable presentation, but typically presents with plaques in the oral cavity—commonly referred to as thrush. In the case of atrophic candidiasis, the lesion is usually raised and erythematous, giving a red velvety appearance of the oral mucosa.1 It is caused by the invasion of the candidal organism into the mucosal surface. Oral candidiasis presents in patients who are immunocompromised, taking long-term corticosteroids, and using antibiotics. It is also seen in infants.2 Our patient likely developed candidiasis because of his poor oral hygiene.
Pipe smoking is the usual red flag
Nicotine stomatitis is commonly seen in middle-age men who have a history of tobacco use.2 It is most commonly seen in pipe smokers, but can occur in cigar and cigarette smokers, as well. The intense heat in the oral cavity generated by smoking causes changes in the oral mucosa—typically on the hard palate. The stem of the pipe increases the amount of heat directed at the hard palate, resulting in a higher incidence of nicotine stomatitis in pipe smokers.3,4 The severity and extent of the lesion is directly proportional to the frequency of tobacco inhalation. Interestingly, the chemicals in the tobacco are not responsible for the mucosal changes, therefore there is no pre-malignant potential.
The risk of malignancy does, however, come into play if your patient does something called reverse smoking. Members of some Asian cultures practice this form of smoking, in which the lit end of the cigarette is placed in the mouth. This practice raises the risk of malignancy. Any patient with nicotine stomatitis who practices reverse smoking should have a biopsy of the lesion done.5
Our approach to the Dx differed from the norm
Typically, you’ll make the diagnosis of nicotine stomatitis clinically, since few lesions resemble its appearance.1 The atypical nature of our patient’s lesion, however, is what prompted a biopsy. You may also do a biopsy if there is any suspicion of cancer or if a lesion is still present after the patient stops smoking.
In our patient’s case, the pathology report revealed a thickened epithelial layer with no evidence of atypia or dysplasia. The minor salivary glands showed chronic inflammatory cells consistent with nicotine stomatitis. The area biopsied also contained a large amount of hyphae, consistent with candidiasis.
Treatment hinges on smoking cessation
Primary treatment for nicotine stomatitis is for the patient to stop smoking. Most lesions will resolve within several months of smoking cessation.1 The lesion is indicative of heavy tobacco use and other mucosal tissues of the oralpharyngeal tract may have similar damage. Therefore, the oropharyngeal cavity should be thoroughly evaluated for dysplastic or malignant lesions.
Our patient received counseling on tobacco cessation and oral hygiene practices. He also received clotrimazole troches for the Candida infection. Two weeks after he started taking the anti-fungal medication, and after he began smoking cessation efforts, the lesion significantly improved. The patient did not return for additional follow-up visits, so we do not know whether the lesion resolved completely.
Correspondence
Denise Rizzolo, PA-C, MS, 348 East Main street, First Floor, Somerville, NJ 08876; rizzoloden@aol.com
1. Mark RE, Stern D. Oral and Maxillofacial Pathology: A Rational for Diagnosis and Treatment. Carol stream, Ill: Quintessence Publishing Co, Inc; 2003: chap 7.
2. Regezi JA, Sciubba J, Jordan RCK. Oral Pathology: Clinical Pathologic Conditions. 4rd ed. Philadelphia, Pa: WB saunders Co; 2003.
3. Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin 2002;52:195-215.
4. Taybos G. Oral changes associated with tobacco use. Am J Med Sci 2003;326:179-182.
5. Ramulu C, Raju MVS, Reddy CRRM. Nicotine stomatitis and its relation to carcinoma of the hard palate in reverse smokers of chuttas. J Dent Res 1973;52:711-718.
A 58-year-old patient came into the office complaining of sinus congestion with sinus pressure, sore throat, and postnasal drip that had been getting progressively worse over the past week. He had tried over-the-counter decongestants, but his symptoms were not resolving. He told the physician’s assistant (DR) that he’d had sinus infections in the past and that he thought he had one now.
When asked about his general health, the patient indicated that he vaguely remembered being told years ago that his cholesterol was elevated, but at the time, declined any medical treatment. He indicated that he hadn’t had a physical examination in years. He said that he only went to the doctor when he was “sick.”
The patient was a cigarette smoker and had smoked a pack a day for 35 years. He said that while he smoked mostly cigarettes, he would also have an occasional cigar. He said that he had never smoked tobacco through a pipe. He also indicated that he drank 3 to 4 beers daily.
While inspecting his pharynx during the physical examination, DR noted a lesion on the posterior hard palate that extended to the soft palate (FIGURE 1). It appeared macular and erythematous, and had an eroded surface. The borders of the lesion were diffuse and irregular, measuring approximately 2 cm Ø 3 cm. During palpation, the lesion was mildly painful, but there was no firmness along the soft palate, buccal mucosa, or tongue. The patient had poor oral hygiene, multiple missing and carious teeth, and a removable partial denture. All other mucosal surfaces were within normal limits.
As the patient suspected, he did have a sinus infection. He left the office with a prescription for an antibiotic. He also left with a referral to an oral maxillofacial surgeon for further evaluation of the lesion.
FIGURE 1
Lesion on the hard palate
What is your diagnosis?
How would you manage this condition?
Diagnosis: Perianal streptococcal dermatitis
The oral maxillofacial surgeon (TAC) concurred with the previous examination findings. He was concerned by the appearance of the lesion and the history of tobacco use and performed a biopsy of the lesion. The pathology report revealed that the patient had nicotine stomatitis with a concomitant candidiasis infection.
Nicotine stomatitis is a common mucosal keratosis caused by smoking tobacco. It is localized to the hard palate of the mouth, but can extend to the soft palate. The mucosa of the hard palate becomes white and thickened due to hyperkeratosis of the tissue.1 Thin red lines of normal mucosa can be seen throughout the lesion. Red dots or papules can appear in the center of the lesion, which represent irritated salivary glands with inflamed duct openings (FIGURE 2).2
Our patient’s lesion had an atypical presentation. Classically the lesions are whiter, but in this case, the patient’s lesion was more erythematous. The reason: A super-infection of candidiasis caused an atrophic form of the condition.
FIGURE 2
Classic presentation of nicotine stomatitis
Differential Dx includes squamous cell carcinoma
The differential diagnosis in a case of nicotine stomatitis includes:
- irritation from dental appliances
- trauma from hot liquids
- squamous cell carcinoma
- atrophic candidiasis.
ill-fitting dentures can cause erythematous lesions along the hard palate and gingiva. The erythema from dentures is usually uniform in color without ulceration and follows the outline or shape of the oral appliance. In contrast, nicotine stomatitis will typically present on exposed areas of the palate and not follow any specific pattern. Most lesions caused by irritations or trauma resolve within 2 weeks of removal of the offending agent.
In the case of burns from food or liquids, the patient will tell you that he drank or ate something hot, and he’ll have a red lesion on the tongue or roof of his mouth.
Squamous cell carcinoma of the hard palate is part of the differential diagnosis because smoking increases a patient’s risk of this form of oral cancer. Squamous cell carcinoma of the palate accounts for 5% to 15% of intraoral carcinomas, depending on whether it is on the hard or soft palate.1 The lesions are typically red or red/white in color and have ulcerated and/or necrotic surfaces. The lesions can become exophytic if left untreated. In comparison, nicotine stomatitis does not ulcerate unless there is a concomitant disease process, which should prompt the clinician to perform further diagnostics tests.
Atrophic candidiasis is also part of the differential, and in the case of our patient, it was a concomitant infection. Candidiasis has a variable presentation, but typically presents with plaques in the oral cavity—commonly referred to as thrush. In the case of atrophic candidiasis, the lesion is usually raised and erythematous, giving a red velvety appearance of the oral mucosa.1 It is caused by the invasion of the candidal organism into the mucosal surface. Oral candidiasis presents in patients who are immunocompromised, taking long-term corticosteroids, and using antibiotics. It is also seen in infants.2 Our patient likely developed candidiasis because of his poor oral hygiene.
Pipe smoking is the usual red flag
Nicotine stomatitis is commonly seen in middle-age men who have a history of tobacco use.2 It is most commonly seen in pipe smokers, but can occur in cigar and cigarette smokers, as well. The intense heat in the oral cavity generated by smoking causes changes in the oral mucosa—typically on the hard palate. The stem of the pipe increases the amount of heat directed at the hard palate, resulting in a higher incidence of nicotine stomatitis in pipe smokers.3,4 The severity and extent of the lesion is directly proportional to the frequency of tobacco inhalation. Interestingly, the chemicals in the tobacco are not responsible for the mucosal changes, therefore there is no pre-malignant potential.
The risk of malignancy does, however, come into play if your patient does something called reverse smoking. Members of some Asian cultures practice this form of smoking, in which the lit end of the cigarette is placed in the mouth. This practice raises the risk of malignancy. Any patient with nicotine stomatitis who practices reverse smoking should have a biopsy of the lesion done.5
Our approach to the Dx differed from the norm
Typically, you’ll make the diagnosis of nicotine stomatitis clinically, since few lesions resemble its appearance.1 The atypical nature of our patient’s lesion, however, is what prompted a biopsy. You may also do a biopsy if there is any suspicion of cancer or if a lesion is still present after the patient stops smoking.
In our patient’s case, the pathology report revealed a thickened epithelial layer with no evidence of atypia or dysplasia. The minor salivary glands showed chronic inflammatory cells consistent with nicotine stomatitis. The area biopsied also contained a large amount of hyphae, consistent with candidiasis.
Treatment hinges on smoking cessation
Primary treatment for nicotine stomatitis is for the patient to stop smoking. Most lesions will resolve within several months of smoking cessation.1 The lesion is indicative of heavy tobacco use and other mucosal tissues of the oralpharyngeal tract may have similar damage. Therefore, the oropharyngeal cavity should be thoroughly evaluated for dysplastic or malignant lesions.
Our patient received counseling on tobacco cessation and oral hygiene practices. He also received clotrimazole troches for the Candida infection. Two weeks after he started taking the anti-fungal medication, and after he began smoking cessation efforts, the lesion significantly improved. The patient did not return for additional follow-up visits, so we do not know whether the lesion resolved completely.
Correspondence
Denise Rizzolo, PA-C, MS, 348 East Main street, First Floor, Somerville, NJ 08876; rizzoloden@aol.com
A 58-year-old patient came into the office complaining of sinus congestion with sinus pressure, sore throat, and postnasal drip that had been getting progressively worse over the past week. He had tried over-the-counter decongestants, but his symptoms were not resolving. He told the physician’s assistant (DR) that he’d had sinus infections in the past and that he thought he had one now.
When asked about his general health, the patient indicated that he vaguely remembered being told years ago that his cholesterol was elevated, but at the time, declined any medical treatment. He indicated that he hadn’t had a physical examination in years. He said that he only went to the doctor when he was “sick.”
The patient was a cigarette smoker and had smoked a pack a day for 35 years. He said that while he smoked mostly cigarettes, he would also have an occasional cigar. He said that he had never smoked tobacco through a pipe. He also indicated that he drank 3 to 4 beers daily.
While inspecting his pharynx during the physical examination, DR noted a lesion on the posterior hard palate that extended to the soft palate (FIGURE 1). It appeared macular and erythematous, and had an eroded surface. The borders of the lesion were diffuse and irregular, measuring approximately 2 cm Ø 3 cm. During palpation, the lesion was mildly painful, but there was no firmness along the soft palate, buccal mucosa, or tongue. The patient had poor oral hygiene, multiple missing and carious teeth, and a removable partial denture. All other mucosal surfaces were within normal limits.
As the patient suspected, he did have a sinus infection. He left the office with a prescription for an antibiotic. He also left with a referral to an oral maxillofacial surgeon for further evaluation of the lesion.
FIGURE 1
Lesion on the hard palate
What is your diagnosis?
How would you manage this condition?
Diagnosis: Perianal streptococcal dermatitis
The oral maxillofacial surgeon (TAC) concurred with the previous examination findings. He was concerned by the appearance of the lesion and the history of tobacco use and performed a biopsy of the lesion. The pathology report revealed that the patient had nicotine stomatitis with a concomitant candidiasis infection.
Nicotine stomatitis is a common mucosal keratosis caused by smoking tobacco. It is localized to the hard palate of the mouth, but can extend to the soft palate. The mucosa of the hard palate becomes white and thickened due to hyperkeratosis of the tissue.1 Thin red lines of normal mucosa can be seen throughout the lesion. Red dots or papules can appear in the center of the lesion, which represent irritated salivary glands with inflamed duct openings (FIGURE 2).2
Our patient’s lesion had an atypical presentation. Classically the lesions are whiter, but in this case, the patient’s lesion was more erythematous. The reason: A super-infection of candidiasis caused an atrophic form of the condition.
FIGURE 2
Classic presentation of nicotine stomatitis
Differential Dx includes squamous cell carcinoma
The differential diagnosis in a case of nicotine stomatitis includes:
- irritation from dental appliances
- trauma from hot liquids
- squamous cell carcinoma
- atrophic candidiasis.
ill-fitting dentures can cause erythematous lesions along the hard palate and gingiva. The erythema from dentures is usually uniform in color without ulceration and follows the outline or shape of the oral appliance. In contrast, nicotine stomatitis will typically present on exposed areas of the palate and not follow any specific pattern. Most lesions caused by irritations or trauma resolve within 2 weeks of removal of the offending agent.
In the case of burns from food or liquids, the patient will tell you that he drank or ate something hot, and he’ll have a red lesion on the tongue or roof of his mouth.
Squamous cell carcinoma of the hard palate is part of the differential diagnosis because smoking increases a patient’s risk of this form of oral cancer. Squamous cell carcinoma of the palate accounts for 5% to 15% of intraoral carcinomas, depending on whether it is on the hard or soft palate.1 The lesions are typically red or red/white in color and have ulcerated and/or necrotic surfaces. The lesions can become exophytic if left untreated. In comparison, nicotine stomatitis does not ulcerate unless there is a concomitant disease process, which should prompt the clinician to perform further diagnostics tests.
Atrophic candidiasis is also part of the differential, and in the case of our patient, it was a concomitant infection. Candidiasis has a variable presentation, but typically presents with plaques in the oral cavity—commonly referred to as thrush. In the case of atrophic candidiasis, the lesion is usually raised and erythematous, giving a red velvety appearance of the oral mucosa.1 It is caused by the invasion of the candidal organism into the mucosal surface. Oral candidiasis presents in patients who are immunocompromised, taking long-term corticosteroids, and using antibiotics. It is also seen in infants.2 Our patient likely developed candidiasis because of his poor oral hygiene.
Pipe smoking is the usual red flag
Nicotine stomatitis is commonly seen in middle-age men who have a history of tobacco use.2 It is most commonly seen in pipe smokers, but can occur in cigar and cigarette smokers, as well. The intense heat in the oral cavity generated by smoking causes changes in the oral mucosa—typically on the hard palate. The stem of the pipe increases the amount of heat directed at the hard palate, resulting in a higher incidence of nicotine stomatitis in pipe smokers.3,4 The severity and extent of the lesion is directly proportional to the frequency of tobacco inhalation. Interestingly, the chemicals in the tobacco are not responsible for the mucosal changes, therefore there is no pre-malignant potential.
The risk of malignancy does, however, come into play if your patient does something called reverse smoking. Members of some Asian cultures practice this form of smoking, in which the lit end of the cigarette is placed in the mouth. This practice raises the risk of malignancy. Any patient with nicotine stomatitis who practices reverse smoking should have a biopsy of the lesion done.5
Our approach to the Dx differed from the norm
Typically, you’ll make the diagnosis of nicotine stomatitis clinically, since few lesions resemble its appearance.1 The atypical nature of our patient’s lesion, however, is what prompted a biopsy. You may also do a biopsy if there is any suspicion of cancer or if a lesion is still present after the patient stops smoking.
In our patient’s case, the pathology report revealed a thickened epithelial layer with no evidence of atypia or dysplasia. The minor salivary glands showed chronic inflammatory cells consistent with nicotine stomatitis. The area biopsied also contained a large amount of hyphae, consistent with candidiasis.
Treatment hinges on smoking cessation
Primary treatment for nicotine stomatitis is for the patient to stop smoking. Most lesions will resolve within several months of smoking cessation.1 The lesion is indicative of heavy tobacco use and other mucosal tissues of the oralpharyngeal tract may have similar damage. Therefore, the oropharyngeal cavity should be thoroughly evaluated for dysplastic or malignant lesions.
Our patient received counseling on tobacco cessation and oral hygiene practices. He also received clotrimazole troches for the Candida infection. Two weeks after he started taking the anti-fungal medication, and after he began smoking cessation efforts, the lesion significantly improved. The patient did not return for additional follow-up visits, so we do not know whether the lesion resolved completely.
Correspondence
Denise Rizzolo, PA-C, MS, 348 East Main street, First Floor, Somerville, NJ 08876; rizzoloden@aol.com
1. Mark RE, Stern D. Oral and Maxillofacial Pathology: A Rational for Diagnosis and Treatment. Carol stream, Ill: Quintessence Publishing Co, Inc; 2003: chap 7.
2. Regezi JA, Sciubba J, Jordan RCK. Oral Pathology: Clinical Pathologic Conditions. 4rd ed. Philadelphia, Pa: WB saunders Co; 2003.
3. Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin 2002;52:195-215.
4. Taybos G. Oral changes associated with tobacco use. Am J Med Sci 2003;326:179-182.
5. Ramulu C, Raju MVS, Reddy CRRM. Nicotine stomatitis and its relation to carcinoma of the hard palate in reverse smokers of chuttas. J Dent Res 1973;52:711-718.
1. Mark RE, Stern D. Oral and Maxillofacial Pathology: A Rational for Diagnosis and Treatment. Carol stream, Ill: Quintessence Publishing Co, Inc; 2003: chap 7.
2. Regezi JA, Sciubba J, Jordan RCK. Oral Pathology: Clinical Pathologic Conditions. 4rd ed. Philadelphia, Pa: WB saunders Co; 2003.
3. Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin 2002;52:195-215.
4. Taybos G. Oral changes associated with tobacco use. Am J Med Sci 2003;326:179-182.
5. Ramulu C, Raju MVS, Reddy CRRM. Nicotine stomatitis and its relation to carcinoma of the hard palate in reverse smokers of chuttas. J Dent Res 1973;52:711-718.