User login
Internists are experts in general medicine, skilled at mapping the few hundred ways the human body can go awry onto thousands of diagnoses, and managing the uncertainty inherent in that process. Generalists, almost by definition, consult specialists with their specialty-focused questions; but who does one call for a general consultation about diagnosis if a specific diagnosis remains elusive and the pathology does not fit cleanly into the purview of a consultant? Outside of sage advice from colleagues (usually senior), most medical centers lack a consultation service focused on diagnosis. There is no oracle to seek. In this perspective, we describe our institution’s answer to this problem: the creation of a service for difficult diagnosis based on Socratic principles, particularly the role of iterative hypothesis testing in the process of diagnosis.1
In 2015, Northwestern Medicine began the Socrates Project, a physician-to-physician consultation service that assists doctors working to diagnose conditions that have so far eluded detection. Our service’s goal is to improve patient care by providing an opinion to the referring physician on diagnostic possibilities for a particular case and ideas to reduce—or at least manage—diagnostic uncertainty.
Most patients referred to the Socrates Project have already undergone an extensive evaluation at top medical centers by experienced clinicians. It would be hubris to assume that we will find a definitive diagnosis in every case; indeed, because of the types of cases referred to our group, it is rare that we find a “Eureka!” diagnosis. When a colleague consults our group, we under-promise in hopes of over-delivering. Instead, we convey to referring physicians that we will conduct a thorough case review and explain our thinking in hopes of uncovering an additional diagnostic avenue, even if that avenue does not ultimately lead to a definitive diagnosis. In addition, the Socrates Project often serves as a broker between consulting services that are deadlocked because of differing diagnostic opinions. We also assist with cases in which a functional disorder is suspected, yet the referring physician is hesitant to diagnose a patient with such a disorder out of concern about missing an important (and possibly obscure) diagnosis.
PERSONNEL AND PROCESS
The Socrates Project receives approximately two consult requests per week, usually from general internists but also from specialists in nearly all disciplines. Around 80% of the referrals are for current inpatients. Our service model is similar to a tumor board, which exists as an interdisciplinary group operating in parallel to the clinical services, to provide consensus-based recommendations. As a result, we act as doctors for doctors, formalizing the curbside consultation. Our usual turnaround time is a week but can be faster for urgent cases. Currently, Socrates Project members, including the faculty leader, volunteer their time and effort at no cost, and there are no charges to patients when physicians consult our group. An overview of the Socrates Project’s personnel and process are outlined in the Figure.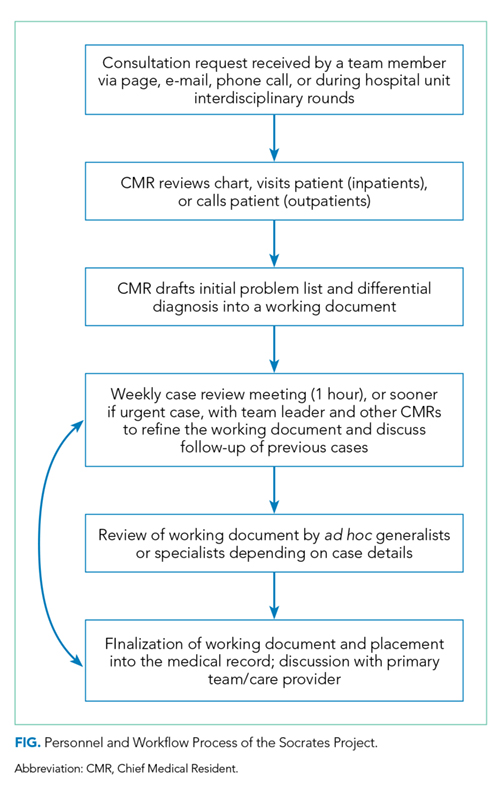
Northwestern’s Chief Medical Residents (CMRs) serve as the fellows for the service, and one of them assumes primary responsibility for each new consultation request the service receives. After obtaining the patient’s case history from the referring provider, the CMR then undertakes a thorough review of the electronic health record and any other available records from other institutions. In the inpatient setting, the CMR performs a new history and physical; phone calls or video conferencing permit history taking for outpatients. In contrast with the standard consultant note, we do not redocument the history, physical, and lab and imaging findings but instead construct a detailed problem list that synthesizes relevant findings into a useful working document.
The service’s faculty leader (BDS) then reviews the problem list with the CMRs to help refine the problem list and begin producing a differential diagnosis during a weekly hour-long meeting. As evidence supports team-based diagnostic collaborations,2 the problem list and preliminary differential diagnosis then becomes a shareable document that the CMR or team leader presents to ad hoc general internists, specialists, and the other CMRs. The presentation can be in person, by phone, or e-mail. These ad hoc members, approximately 20 in number and spanning from junior attending physicians to senior clinicians, have volunteered to help the Socrates Project by adding their thoughts on differential diagnoses that explain the problem list and how to move forward with further testing. The ad hoc members have self-identified as clinicians with an interest in medical diagnosis—including surgeons, neurologists, psychiatrists, radiologists, and pathologists—and range in expertise from general internists to subspecialists. Finally, we document our problem list, differential diagnosis, and recommendations in the medical record and discuss the case with the referring team. The service limits its scope of clinical recommendation to diagnosis and avoids commenting on management decisions outside of the use of therapies as empiric diagnostic tests. A sample note is provided as an online Appendix.
MOVING FORWARD WITH ONGOING UNCERTAINTY
Despite our process, we are often left without a satisfying diagnosis. We then are then faced with three possibilities: (1) The diagnosis is identifiable, just not by the physicians involved in the case—we did not think of the diagnosis in our deliberations; (2) The diagnosis is a described condition but without an available test—autoimmune limbic encephalitis associated with an unassayable or unknown auto-antibody, or the acuity of a critically ill patient makes diagnostic testing unreliable or not feasible; (3) The diagnosis has not yet been described by medical science—we are seeing a case of HIV infection in 1971.
With the personnel and process outlined above, we hope to provide recommendations that are useful in guiding a diagnostic workup regardless of which of these three scenarios is applicable. Our flexibility with involving the appropriate specialists in the Socrates Project should minimize the number of patients with a knowable diagnosis that is unknown to us. In the second scenario, our recommendations may rest upon the incorporation of a treatment as a diagnostic test. In the limbic encephalitis example above, a trial of steroids with rapid improvement in the patient’s condition may increase diagnostic certainty. The third scenario is the most difficult to identify. Pattern recognition of similarly presenting patients, keeping ourselves updated on pertinent primary literature, and consideration of advanced diagnostic testing such as exome sequencing and other next-generation sequencing strategies are essential in hoping to characterize a specific clinical syndrome that has yet to be described.
For situations in which our recommendations do not yield a diagnosis, we recognize the role for protocols such as genomic or metagenomic sequencing that assess multiple diagnostic possibilities in parallel without an a priori hypothesis.3,4 The utility of multi-omics testing in diagnostic workups has been detailed by the Undiagnosed Diseases Network (UDN), which has created a systematic approach to describing new syndromes with the aid of metabolomic and genomic profiling.5 It is important to note that even with the resources available to the UDN, the diagnosis rate is 35%, emphasizing that in the majority of diagnosis-refractory cases, a diagnosis will not be found. This low diagnosis rate underscores the need for continued inquiry and cataloging of cases and data for further review or synthesis as the body of medical knowledge continues to expand. For these reasons, we have a follow-up system in place, which involves the assigned CMR regularly reviewing the chart and reporting during our weekly meetings. We make phone calls to patients and providers for cases that appear to be lost to follow-up.
LIMITATIONS
We recognize several important limitations to our care model that may represent barriers to establishing, maintaining, and evaluating a similar service at other institutions. For example, there are limitations and benefits of the CMR as point person for managing our consultations. While they are admittedly junior colleagues with limited experience, CMRs tend to be among the best-read and up-to-date clinicians in the hospital by virtue of their recent general-medicine training and identification as a top clinician and leader. Moreover, in their role with the Socrates Project, CMRs have more time to think, talk with patients, and review the medical record than other clinicians, who may be under pressure to see an increasing number of patients while billing at higher levels. Indeed, the Socrates Project CMRs have, on a number of occasions, been the team members who find the piece of data that no one else thought relevant.
Another factor that may limit establishment of a similar team at other institutions is our volunteer-based model. The Socrates Project members volunteer because they love clinical medicine and serve on the team without remuneration for professional effort. With the CMR role as a notable exception, pressure from achieving relative value unit targets, obtaining grant funding, and publishing primary research publications in their field may limit this care model, particularly when shifting from a clinical-only activity to one that also formally investigates the service’s process and outcomes.
DISCOVERY AND FUTURE DIRECTIONS
Beyond our clinical objective, we hope that the Socrates Project will further the discovery and description of previously unrecognized disease processes. To that end, we are pursuing an institutional review board-approved protocol to perform a rigorous assessment of the Socrates Project’s process and outcomes, including a cataloging of case archetypes and the time to definitive diagnosis if a diagnosis is established. As we continue to collect data, increasing our referral network may also lead to refinement and improvement in diagnostic processes and outcomes. Over time, we expect that the diagnostic resources available to us will evolve. Utilizing collective intelligence has been shown to improve diagnostic accuracy,6 and emerging artificial intelligence technologies may improve diagnostic performance as well.7,8 Most importantly, through this endeavor, we hope to serve less as an oracle and more as a humble Socratic consultant for clinicians working to reduce diagnostic uncertainty for their patients.
Acknowledgments
The authors wish to thank the Northwestern University Chief Medical Residents, 2015-present, for their tireless efforts in support of the Socrates Project.
1. Cooper JM. Plato: Five dialogues : euthyphro, apology, crito, meno, phaedo. Hackett Publishing; 2002.
2. Hautz WE, Kammer JE, Schauber SK, Spies CD, Gaissmaier W. Diagnostic performance by medical students working individually or in teams. JAMA. 2015;313(3):303-304. https://doi.org/10.1001/jama.2014.15770.
3. Adams DR, Eng CM. Next-generation sequencing to diagnose suspected genetic disorders. N Engl J Med. 2018;379(14):1353-1362. https://doi.org/10.1056/NEJMra1711801.
4. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341-355. https://doi.org/10.1038/s41576-019-0113-7.
5. Splinter K, Adams DR, Bacino CA, et al. Effect of genetic diagnosis on patients with previously undiagnosed disease. N Engl J Med. 2018;379(22):2131-2139. https://doi.org/10.1056/NEJMoa1714458.
6. Barnett ML, Boddupalli D, Nundy S, Bates DW. Comparative accuracy of diagnosis by collective intelligence of multiple physicians vs individual physicians. JAMA Netw Open. 2019;2(3):e190096. https://doi.org/10.1001/jamanetworkopen.2019.0096.
7. Liang H, Tsui BY, Ni H, et al. Evaluation and accurate diagnoses of pediatric diseases using artificial intelligence. Nat Med. 2019;25(3):433-438. https://doi.org/10.1038/s41591-018-0335-9.
8. Rajkomar A, Dean J, Kohane I. Machine learning in medicine. N Engl J Med. 2019;380(14):1347-1358. https://doi.org/10.1056/NEJMra1814259.
Internists are experts in general medicine, skilled at mapping the few hundred ways the human body can go awry onto thousands of diagnoses, and managing the uncertainty inherent in that process. Generalists, almost by definition, consult specialists with their specialty-focused questions; but who does one call for a general consultation about diagnosis if a specific diagnosis remains elusive and the pathology does not fit cleanly into the purview of a consultant? Outside of sage advice from colleagues (usually senior), most medical centers lack a consultation service focused on diagnosis. There is no oracle to seek. In this perspective, we describe our institution’s answer to this problem: the creation of a service for difficult diagnosis based on Socratic principles, particularly the role of iterative hypothesis testing in the process of diagnosis.1
In 2015, Northwestern Medicine began the Socrates Project, a physician-to-physician consultation service that assists doctors working to diagnose conditions that have so far eluded detection. Our service’s goal is to improve patient care by providing an opinion to the referring physician on diagnostic possibilities for a particular case and ideas to reduce—or at least manage—diagnostic uncertainty.
Most patients referred to the Socrates Project have already undergone an extensive evaluation at top medical centers by experienced clinicians. It would be hubris to assume that we will find a definitive diagnosis in every case; indeed, because of the types of cases referred to our group, it is rare that we find a “Eureka!” diagnosis. When a colleague consults our group, we under-promise in hopes of over-delivering. Instead, we convey to referring physicians that we will conduct a thorough case review and explain our thinking in hopes of uncovering an additional diagnostic avenue, even if that avenue does not ultimately lead to a definitive diagnosis. In addition, the Socrates Project often serves as a broker between consulting services that are deadlocked because of differing diagnostic opinions. We also assist with cases in which a functional disorder is suspected, yet the referring physician is hesitant to diagnose a patient with such a disorder out of concern about missing an important (and possibly obscure) diagnosis.
PERSONNEL AND PROCESS
The Socrates Project receives approximately two consult requests per week, usually from general internists but also from specialists in nearly all disciplines. Around 80% of the referrals are for current inpatients. Our service model is similar to a tumor board, which exists as an interdisciplinary group operating in parallel to the clinical services, to provide consensus-based recommendations. As a result, we act as doctors for doctors, formalizing the curbside consultation. Our usual turnaround time is a week but can be faster for urgent cases. Currently, Socrates Project members, including the faculty leader, volunteer their time and effort at no cost, and there are no charges to patients when physicians consult our group. An overview of the Socrates Project’s personnel and process are outlined in the Figure.
Northwestern’s Chief Medical Residents (CMRs) serve as the fellows for the service, and one of them assumes primary responsibility for each new consultation request the service receives. After obtaining the patient’s case history from the referring provider, the CMR then undertakes a thorough review of the electronic health record and any other available records from other institutions. In the inpatient setting, the CMR performs a new history and physical; phone calls or video conferencing permit history taking for outpatients. In contrast with the standard consultant note, we do not redocument the history, physical, and lab and imaging findings but instead construct a detailed problem list that synthesizes relevant findings into a useful working document.
The service’s faculty leader (BDS) then reviews the problem list with the CMRs to help refine the problem list and begin producing a differential diagnosis during a weekly hour-long meeting. As evidence supports team-based diagnostic collaborations,2 the problem list and preliminary differential diagnosis then becomes a shareable document that the CMR or team leader presents to ad hoc general internists, specialists, and the other CMRs. The presentation can be in person, by phone, or e-mail. These ad hoc members, approximately 20 in number and spanning from junior attending physicians to senior clinicians, have volunteered to help the Socrates Project by adding their thoughts on differential diagnoses that explain the problem list and how to move forward with further testing. The ad hoc members have self-identified as clinicians with an interest in medical diagnosis—including surgeons, neurologists, psychiatrists, radiologists, and pathologists—and range in expertise from general internists to subspecialists. Finally, we document our problem list, differential diagnosis, and recommendations in the medical record and discuss the case with the referring team. The service limits its scope of clinical recommendation to diagnosis and avoids commenting on management decisions outside of the use of therapies as empiric diagnostic tests. A sample note is provided as an online Appendix.
MOVING FORWARD WITH ONGOING UNCERTAINTY
Despite our process, we are often left without a satisfying diagnosis. We then are then faced with three possibilities: (1) The diagnosis is identifiable, just not by the physicians involved in the case—we did not think of the diagnosis in our deliberations; (2) The diagnosis is a described condition but without an available test—autoimmune limbic encephalitis associated with an unassayable or unknown auto-antibody, or the acuity of a critically ill patient makes diagnostic testing unreliable or not feasible; (3) The diagnosis has not yet been described by medical science—we are seeing a case of HIV infection in 1971.
With the personnel and process outlined above, we hope to provide recommendations that are useful in guiding a diagnostic workup regardless of which of these three scenarios is applicable. Our flexibility with involving the appropriate specialists in the Socrates Project should minimize the number of patients with a knowable diagnosis that is unknown to us. In the second scenario, our recommendations may rest upon the incorporation of a treatment as a diagnostic test. In the limbic encephalitis example above, a trial of steroids with rapid improvement in the patient’s condition may increase diagnostic certainty. The third scenario is the most difficult to identify. Pattern recognition of similarly presenting patients, keeping ourselves updated on pertinent primary literature, and consideration of advanced diagnostic testing such as exome sequencing and other next-generation sequencing strategies are essential in hoping to characterize a specific clinical syndrome that has yet to be described.
For situations in which our recommendations do not yield a diagnosis, we recognize the role for protocols such as genomic or metagenomic sequencing that assess multiple diagnostic possibilities in parallel without an a priori hypothesis.3,4 The utility of multi-omics testing in diagnostic workups has been detailed by the Undiagnosed Diseases Network (UDN), which has created a systematic approach to describing new syndromes with the aid of metabolomic and genomic profiling.5 It is important to note that even with the resources available to the UDN, the diagnosis rate is 35%, emphasizing that in the majority of diagnosis-refractory cases, a diagnosis will not be found. This low diagnosis rate underscores the need for continued inquiry and cataloging of cases and data for further review or synthesis as the body of medical knowledge continues to expand. For these reasons, we have a follow-up system in place, which involves the assigned CMR regularly reviewing the chart and reporting during our weekly meetings. We make phone calls to patients and providers for cases that appear to be lost to follow-up.
LIMITATIONS
We recognize several important limitations to our care model that may represent barriers to establishing, maintaining, and evaluating a similar service at other institutions. For example, there are limitations and benefits of the CMR as point person for managing our consultations. While they are admittedly junior colleagues with limited experience, CMRs tend to be among the best-read and up-to-date clinicians in the hospital by virtue of their recent general-medicine training and identification as a top clinician and leader. Moreover, in their role with the Socrates Project, CMRs have more time to think, talk with patients, and review the medical record than other clinicians, who may be under pressure to see an increasing number of patients while billing at higher levels. Indeed, the Socrates Project CMRs have, on a number of occasions, been the team members who find the piece of data that no one else thought relevant.
Another factor that may limit establishment of a similar team at other institutions is our volunteer-based model. The Socrates Project members volunteer because they love clinical medicine and serve on the team without remuneration for professional effort. With the CMR role as a notable exception, pressure from achieving relative value unit targets, obtaining grant funding, and publishing primary research publications in their field may limit this care model, particularly when shifting from a clinical-only activity to one that also formally investigates the service’s process and outcomes.
DISCOVERY AND FUTURE DIRECTIONS
Beyond our clinical objective, we hope that the Socrates Project will further the discovery and description of previously unrecognized disease processes. To that end, we are pursuing an institutional review board-approved protocol to perform a rigorous assessment of the Socrates Project’s process and outcomes, including a cataloging of case archetypes and the time to definitive diagnosis if a diagnosis is established. As we continue to collect data, increasing our referral network may also lead to refinement and improvement in diagnostic processes and outcomes. Over time, we expect that the diagnostic resources available to us will evolve. Utilizing collective intelligence has been shown to improve diagnostic accuracy,6 and emerging artificial intelligence technologies may improve diagnostic performance as well.7,8 Most importantly, through this endeavor, we hope to serve less as an oracle and more as a humble Socratic consultant for clinicians working to reduce diagnostic uncertainty for their patients.
Acknowledgments
The authors wish to thank the Northwestern University Chief Medical Residents, 2015-present, for their tireless efforts in support of the Socrates Project.
Internists are experts in general medicine, skilled at mapping the few hundred ways the human body can go awry onto thousands of diagnoses, and managing the uncertainty inherent in that process. Generalists, almost by definition, consult specialists with their specialty-focused questions; but who does one call for a general consultation about diagnosis if a specific diagnosis remains elusive and the pathology does not fit cleanly into the purview of a consultant? Outside of sage advice from colleagues (usually senior), most medical centers lack a consultation service focused on diagnosis. There is no oracle to seek. In this perspective, we describe our institution’s answer to this problem: the creation of a service for difficult diagnosis based on Socratic principles, particularly the role of iterative hypothesis testing in the process of diagnosis.1
In 2015, Northwestern Medicine began the Socrates Project, a physician-to-physician consultation service that assists doctors working to diagnose conditions that have so far eluded detection. Our service’s goal is to improve patient care by providing an opinion to the referring physician on diagnostic possibilities for a particular case and ideas to reduce—or at least manage—diagnostic uncertainty.
Most patients referred to the Socrates Project have already undergone an extensive evaluation at top medical centers by experienced clinicians. It would be hubris to assume that we will find a definitive diagnosis in every case; indeed, because of the types of cases referred to our group, it is rare that we find a “Eureka!” diagnosis. When a colleague consults our group, we under-promise in hopes of over-delivering. Instead, we convey to referring physicians that we will conduct a thorough case review and explain our thinking in hopes of uncovering an additional diagnostic avenue, even if that avenue does not ultimately lead to a definitive diagnosis. In addition, the Socrates Project often serves as a broker between consulting services that are deadlocked because of differing diagnostic opinions. We also assist with cases in which a functional disorder is suspected, yet the referring physician is hesitant to diagnose a patient with such a disorder out of concern about missing an important (and possibly obscure) diagnosis.
PERSONNEL AND PROCESS
The Socrates Project receives approximately two consult requests per week, usually from general internists but also from specialists in nearly all disciplines. Around 80% of the referrals are for current inpatients. Our service model is similar to a tumor board, which exists as an interdisciplinary group operating in parallel to the clinical services, to provide consensus-based recommendations. As a result, we act as doctors for doctors, formalizing the curbside consultation. Our usual turnaround time is a week but can be faster for urgent cases. Currently, Socrates Project members, including the faculty leader, volunteer their time and effort at no cost, and there are no charges to patients when physicians consult our group. An overview of the Socrates Project’s personnel and process are outlined in the Figure.
Northwestern’s Chief Medical Residents (CMRs) serve as the fellows for the service, and one of them assumes primary responsibility for each new consultation request the service receives. After obtaining the patient’s case history from the referring provider, the CMR then undertakes a thorough review of the electronic health record and any other available records from other institutions. In the inpatient setting, the CMR performs a new history and physical; phone calls or video conferencing permit history taking for outpatients. In contrast with the standard consultant note, we do not redocument the history, physical, and lab and imaging findings but instead construct a detailed problem list that synthesizes relevant findings into a useful working document.
The service’s faculty leader (BDS) then reviews the problem list with the CMRs to help refine the problem list and begin producing a differential diagnosis during a weekly hour-long meeting. As evidence supports team-based diagnostic collaborations,2 the problem list and preliminary differential diagnosis then becomes a shareable document that the CMR or team leader presents to ad hoc general internists, specialists, and the other CMRs. The presentation can be in person, by phone, or e-mail. These ad hoc members, approximately 20 in number and spanning from junior attending physicians to senior clinicians, have volunteered to help the Socrates Project by adding their thoughts on differential diagnoses that explain the problem list and how to move forward with further testing. The ad hoc members have self-identified as clinicians with an interest in medical diagnosis—including surgeons, neurologists, psychiatrists, radiologists, and pathologists—and range in expertise from general internists to subspecialists. Finally, we document our problem list, differential diagnosis, and recommendations in the medical record and discuss the case with the referring team. The service limits its scope of clinical recommendation to diagnosis and avoids commenting on management decisions outside of the use of therapies as empiric diagnostic tests. A sample note is provided as an online Appendix.
MOVING FORWARD WITH ONGOING UNCERTAINTY
Despite our process, we are often left without a satisfying diagnosis. We then are then faced with three possibilities: (1) The diagnosis is identifiable, just not by the physicians involved in the case—we did not think of the diagnosis in our deliberations; (2) The diagnosis is a described condition but without an available test—autoimmune limbic encephalitis associated with an unassayable or unknown auto-antibody, or the acuity of a critically ill patient makes diagnostic testing unreliable or not feasible; (3) The diagnosis has not yet been described by medical science—we are seeing a case of HIV infection in 1971.
With the personnel and process outlined above, we hope to provide recommendations that are useful in guiding a diagnostic workup regardless of which of these three scenarios is applicable. Our flexibility with involving the appropriate specialists in the Socrates Project should minimize the number of patients with a knowable diagnosis that is unknown to us. In the second scenario, our recommendations may rest upon the incorporation of a treatment as a diagnostic test. In the limbic encephalitis example above, a trial of steroids with rapid improvement in the patient’s condition may increase diagnostic certainty. The third scenario is the most difficult to identify. Pattern recognition of similarly presenting patients, keeping ourselves updated on pertinent primary literature, and consideration of advanced diagnostic testing such as exome sequencing and other next-generation sequencing strategies are essential in hoping to characterize a specific clinical syndrome that has yet to be described.
For situations in which our recommendations do not yield a diagnosis, we recognize the role for protocols such as genomic or metagenomic sequencing that assess multiple diagnostic possibilities in parallel without an a priori hypothesis.3,4 The utility of multi-omics testing in diagnostic workups has been detailed by the Undiagnosed Diseases Network (UDN), which has created a systematic approach to describing new syndromes with the aid of metabolomic and genomic profiling.5 It is important to note that even with the resources available to the UDN, the diagnosis rate is 35%, emphasizing that in the majority of diagnosis-refractory cases, a diagnosis will not be found. This low diagnosis rate underscores the need for continued inquiry and cataloging of cases and data for further review or synthesis as the body of medical knowledge continues to expand. For these reasons, we have a follow-up system in place, which involves the assigned CMR regularly reviewing the chart and reporting during our weekly meetings. We make phone calls to patients and providers for cases that appear to be lost to follow-up.
LIMITATIONS
We recognize several important limitations to our care model that may represent barriers to establishing, maintaining, and evaluating a similar service at other institutions. For example, there are limitations and benefits of the CMR as point person for managing our consultations. While they are admittedly junior colleagues with limited experience, CMRs tend to be among the best-read and up-to-date clinicians in the hospital by virtue of their recent general-medicine training and identification as a top clinician and leader. Moreover, in their role with the Socrates Project, CMRs have more time to think, talk with patients, and review the medical record than other clinicians, who may be under pressure to see an increasing number of patients while billing at higher levels. Indeed, the Socrates Project CMRs have, on a number of occasions, been the team members who find the piece of data that no one else thought relevant.
Another factor that may limit establishment of a similar team at other institutions is our volunteer-based model. The Socrates Project members volunteer because they love clinical medicine and serve on the team without remuneration for professional effort. With the CMR role as a notable exception, pressure from achieving relative value unit targets, obtaining grant funding, and publishing primary research publications in their field may limit this care model, particularly when shifting from a clinical-only activity to one that also formally investigates the service’s process and outcomes.
DISCOVERY AND FUTURE DIRECTIONS
Beyond our clinical objective, we hope that the Socrates Project will further the discovery and description of previously unrecognized disease processes. To that end, we are pursuing an institutional review board-approved protocol to perform a rigorous assessment of the Socrates Project’s process and outcomes, including a cataloging of case archetypes and the time to definitive diagnosis if a diagnosis is established. As we continue to collect data, increasing our referral network may also lead to refinement and improvement in diagnostic processes and outcomes. Over time, we expect that the diagnostic resources available to us will evolve. Utilizing collective intelligence has been shown to improve diagnostic accuracy,6 and emerging artificial intelligence technologies may improve diagnostic performance as well.7,8 Most importantly, through this endeavor, we hope to serve less as an oracle and more as a humble Socratic consultant for clinicians working to reduce diagnostic uncertainty for their patients.
Acknowledgments
The authors wish to thank the Northwestern University Chief Medical Residents, 2015-present, for their tireless efforts in support of the Socrates Project.
1. Cooper JM. Plato: Five dialogues : euthyphro, apology, crito, meno, phaedo. Hackett Publishing; 2002.
2. Hautz WE, Kammer JE, Schauber SK, Spies CD, Gaissmaier W. Diagnostic performance by medical students working individually or in teams. JAMA. 2015;313(3):303-304. https://doi.org/10.1001/jama.2014.15770.
3. Adams DR, Eng CM. Next-generation sequencing to diagnose suspected genetic disorders. N Engl J Med. 2018;379(14):1353-1362. https://doi.org/10.1056/NEJMra1711801.
4. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341-355. https://doi.org/10.1038/s41576-019-0113-7.
5. Splinter K, Adams DR, Bacino CA, et al. Effect of genetic diagnosis on patients with previously undiagnosed disease. N Engl J Med. 2018;379(22):2131-2139. https://doi.org/10.1056/NEJMoa1714458.
6. Barnett ML, Boddupalli D, Nundy S, Bates DW. Comparative accuracy of diagnosis by collective intelligence of multiple physicians vs individual physicians. JAMA Netw Open. 2019;2(3):e190096. https://doi.org/10.1001/jamanetworkopen.2019.0096.
7. Liang H, Tsui BY, Ni H, et al. Evaluation and accurate diagnoses of pediatric diseases using artificial intelligence. Nat Med. 2019;25(3):433-438. https://doi.org/10.1038/s41591-018-0335-9.
8. Rajkomar A, Dean J, Kohane I. Machine learning in medicine. N Engl J Med. 2019;380(14):1347-1358. https://doi.org/10.1056/NEJMra1814259.
1. Cooper JM. Plato: Five dialogues : euthyphro, apology, crito, meno, phaedo. Hackett Publishing; 2002.
2. Hautz WE, Kammer JE, Schauber SK, Spies CD, Gaissmaier W. Diagnostic performance by medical students working individually or in teams. JAMA. 2015;313(3):303-304. https://doi.org/10.1001/jama.2014.15770.
3. Adams DR, Eng CM. Next-generation sequencing to diagnose suspected genetic disorders. N Engl J Med. 2018;379(14):1353-1362. https://doi.org/10.1056/NEJMra1711801.
4. Chiu CY, Miller SA. Clinical metagenomics. Nat Rev Genet. 2019;20(6):341-355. https://doi.org/10.1038/s41576-019-0113-7.
5. Splinter K, Adams DR, Bacino CA, et al. Effect of genetic diagnosis on patients with previously undiagnosed disease. N Engl J Med. 2018;379(22):2131-2139. https://doi.org/10.1056/NEJMoa1714458.
6. Barnett ML, Boddupalli D, Nundy S, Bates DW. Comparative accuracy of diagnosis by collective intelligence of multiple physicians vs individual physicians. JAMA Netw Open. 2019;2(3):e190096. https://doi.org/10.1001/jamanetworkopen.2019.0096.
7. Liang H, Tsui BY, Ni H, et al. Evaluation and accurate diagnoses of pediatric diseases using artificial intelligence. Nat Med. 2019;25(3):433-438. https://doi.org/10.1038/s41591-018-0335-9.
8. Rajkomar A, Dean J, Kohane I. Machine learning in medicine. N Engl J Med. 2019;380(14):1347-1358. https://doi.org/10.1056/NEJMra1814259.
© 2019 Society of Hospital Medicine