User login
Kate, age 14, is referred for follow-up treatment of depression after she impulsively swallowed a bottle of acetaminophen. She says she is in academic trouble and has no friends. Kate describes her childhood as mostly happy except for her parents’ arguments. Her medical history indicates she began developing breasts at age 10 and had her first menstrual period at age 12.
Her father is largely absent, traveling and working long hours. Her mother developed postpartum depression and stopped working after Kate’s younger brother was born.
Girls and boys show similar depression risks during childhood, but girls are twice as likely as boys to become clinically depressed after puberty. The key to treating depression in teen girls is to recognize that brain development and fluctuating hormones can influence behavior in ways that confuse them and the people around them. Successfully treating teen girls’ depression may require a gender-specific approach.
3 stages of brain development
Fetal differentiation. All brains start out with female-type brain circuits. At 8 weeks of fetal life, however, tiny testicles in the male begin to produce large amounts of testosterone, which changes the brain and body to male. Thus, sex-specific genes and hormones guide aspects of the first phase of brain development.1
Table 1
Female hormonal development: Gestation to puberty
| Stage/age | Hormonal events | Effect on female brain |
|---|---|---|
| Gestation | Components of reproductive axis form in early embryonic development; at 8 weeks, testosterone from fetal testicles begins to change female-type brain areas to male | Unperturbed by testosterone, brain continues to develop along female lines |
| Birth to age 24 months | Hormone-secreting placenta detaches at birth, dramatically increasing GnRH and LH/FSH and driving infant gonads to produce estrogen in girls or testosterone in boys (“infantile puberty”) | Abundant ovarian estrogen secretion enhances development of brain circuits, such as those associated with reproduction, maternal behavior, and social relatedness |
| Age 24 months to prepuberty | “Brakes” put on GnRH and LH/FSH pulsatile brain cells | “Juvenile pause” begins, with constant low estrogen secretion in girls by 24 months (in boys, “brakes” are on by 12 months) |
| Puberty | “Brakes” released on GnRH and LH/FSH neurons, reactivating reproductive axis | Ovary resumes estrogen production (“adolescent puberty”); increase in estrogen, progesterone, and testosterone stimulates brain circuit development; unipolar depression rates increase to 2:1 (female to male) by age 15 |
| GnRH: gonadotropin-releasing hormone; LH/FSH: luteinizing hormone/follicle-stimulating hormone | ||
| Source: References 4,5 | ||
Infantile puberty and the second phase of brain development begin in early childhood, as the ovaries and testicles start to produce large amounts of estrogen and testosterone soon after birth.
Puberty launches the final brain development phase. Up to 2 years before menstruation begins, pulsatile gonadotropin-releasing hormone cells in the hypothalamus wake up and start stimulating the ovaries to produce estrogen, thrusting the girl brain into puberty (Figure). The teen girl brain begins to experience not only estrogen surges from the ovary but progesterone and testosterone surges as well.
Although brain size and basic circuitry are mostly set by age 5, puberty stimulates new brain cells and increases myelin production.2 Faster myelinated connections between emotionally impulsive limbic brain areas such as the amygdala and sensible, cognitive areas such as the prefrontal cortex are not finished until the early 20s.3
Hormonal changes at puberty
The female brain is remodeled during puberty, leading to sexually dimorphic brain activation and development that further differentiates it from the male brain.4
Estrogen surges are associated with increased production of neurohormones and neurochemicals, such as:
- oxytocin, which reinforces social bonding and intimacy
- dopamine, which stimulates motivation and pleasure circuits in the brain.
Hormonal changes and brain development alter gene expression and affect neurodevelopment. These events may trigger a first depression in pubertal girls with a family history of mood disorder (Table 1).4,5 Although menarche has begun at an average age of 12 in the United States for decades, the most recent National Health and Examination Survey (NHANES) shows puberty onset in girls is occurring earlier (Table 2).6-9
Tanner stage—a measure of pubertal status—is a more accurate predictor of depression in teen girls than age.10 Pubertal transition to Tanner stage 3 (development of pubic and axillary hair and breast buds) is associated with a sharp increase in depression rates. Girls at stage 3 and higher are approximately 3 times more likely to be depressed than girls at stages 1 or 2.11
Pubic hair, breast development, and menstruation are markers for underlying hormonal changes (Table 3).4,5 The onset of estrogen, progesterone, and testosterone surges closely correlates with the difference in depression rates between pre- and postpubertal girls.12 After estrogen and progesterone surges begin at puberty, negative emotions exert an increased activating effect on the female brain,13 and social stressors more deeply affect girls than they do boys. This may explain why girls are more susceptible to depression when a friendship fails.14
CASE CONTINUED: Boy troubles
Kate tells you that in 9th grade she and her best friend, Ellen, would talk about boys for hours after school and try on sexually provocative outfits. They both liked Matt, a 10th grader, so when he asked Kate out, Ellen stopped speaking to her. Kate and Matt began some heavy petting, and Kate said she felt selfish and guilty about hurting Ellen. But when girls at school began spreading rumors that Kate was a “slut,” Kate blamed Ellen and told her, “I hate you!”
Soon after, Matt broke up with Kate. Distraught, she dreaded going to school and cried in her room at night for several weeks. She became chronically tired and had difficulty concentrating in class. She ruminated about losing Matt and worried that she was too fat, too ugly, or too flat-chested. She missed Ellen and felt no one liked her.
Table 2
Puberty’s developmental milestones in U.S. girls (averages)
| Correlate | African Americans | Whites | School grade* |
|---|---|---|---|
| Breast bud development | Age 9 | Age 10 | 4th to 5th |
| Girls with puberty onset by age 8 | 32% | 11% | 3rd |
| Girls with puberty onset by age 10 | 76% | 53% | 5th |
| Menarche onset | Age 12.1 | Age 12.6 | 7th |
| Tanner stage 5† onset | Age 13.9 | Age 15.5 | 8th to 9th |
| * Approximate grade level for age groups | |||
| † Pubic hair and breast development reach adult stage | |||
| Source: Data from references 6-9, including the Pediatric Research in Office Settings network and Third National Health and Nutrition Examination Survey, 1988-1994. | |||
Figure Hypothalamic-pituitary-ovarian axis: Turned on at puberty in girls
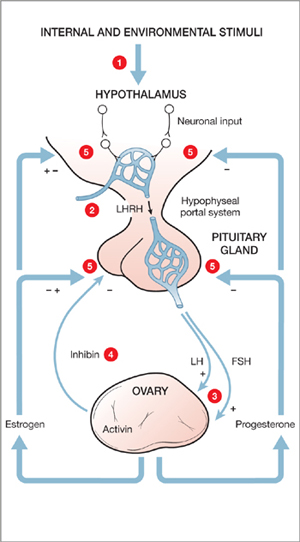
Puberty onset stimulates depression in genetically vulnerable girls; more likely after Tanner stage 3 (development of pubic and axillary hair and breast buds).
Male vs female teen brains
Depression after a relationship failure in teen girls often begins with ruminative thoughts about her flaws, mistakes, or appearance. These negative thoughts may preoccupy her day and night. Teen girls often feel confused by contradictory social pressures to look and dress provocatively but resist having sex. A sexual encounter can trigger shame and fear.
Although clinical and developmental studies indicate that teen girls respond more dramatically to relationship troubles than boys, the brain and hormone differences responsible for these effects remain unclear. Male hormones hugely increase in boys at puberty—up to 25-fold between ages 9 and 15—but do not cycle. Male brains do not have the same capacity as female brains to respond to cyclical hormonal activity because exposure to androgens during fetal development eliminates this ability. The fetal testosterone surge causes the area associated with sexual pursuit to double in the male brain.
Outside of fertility considerations, Baron-Cohen et al15 suggest that male brain circuits have been formed by fetal testosterone to focus more on systematization—which emphasizes figuring out how things work and performing tasks—rather than empathy and bonding in relationships. This difference has been shown in neuroimaging studies comparing the genders’ attentional systems.16,17 In contrast to the systematizing male brain, female brains are more likely to activate the mirror neuron system—the area required for empathizing.18
Female brains, of course, respond to cyclical hormonal activity. However, the regular monthly waves of estrogen and progesterone do not affect all female brains the same. A subset of women who experience premenstrual dysphoric disorder appear to have brains that trigger depressed moods and irritability during the last 2 weeks of the menstrual cycle.19 A genetic difference in these women is suspected as the culprit; these genes may affect the way their brains metabolize progesterone.
CASE CONTINUED: An overdose of stress
Kate’s poor concentration lingered, and her grades continued to drop. She tells you her parents were having marital problems and she did not want to bother them with her difficulties. Two days before her period was due, she learned she had failed 2 classes. That night, as she got some acetaminophen for a headache, she impulsively took the rest of the bottle.
After swallowing the pills, Kate panicked. She forced herself to vomit and tearfully told her parents what she had done. They took her to the emergency room, where she was medically stabilized, evaluated by a psychiatrist, and referred to you for outpatient treatment.
Treatment recommendations
A combination of factors—genetic, hormonal, and neurodevelopmental—probably contributed to Kate’s acute depressed mood and overdose. Thus, to treat depression in adolescent girls, emerging evidence supports:
- stabilizing hormonal fluctuations such as rapidly falling progesterone just before the start of menstrual periods with an extended-cycle contraceptive (we would try an ethinyl estradiol/levonorgestrel combination such as Seasonale®)
- treating depressive symptoms with a selective serotonin reuptake inhibitor such as citalopram, 10 mg once daily, with careful monitoring for suicidal thoughts or behavior
- providing tools to manage stress and impulsive behavior through weekly psychotherapy (such as cognitive-behavioral therapy, dialectical behavioral therapy, or supportive therapy).
Genetic factors. Kate’s mother’s history of postpartum depression suggests genetic risk for Kate. Studies have found that the expression of particular genes—such as the serotonin transporter (5-HTT) gene—may be associated with depression. Staley et al20 found that depressed women show a significantly greater decrease in 5-HTT availability in the diencephalon (forebrain region containing the thalamus, hypothalamus, and part of the pituitary gland) when compared with healthy women and depressed men.
Table 3
3 stages of girls’ gonadal development
| Stage | Timing | Developmental events |
|---|---|---|
| Adrenarche | Onset around age 6, peaks by age 20 | Rise in weak androgens (DHEA and DHEAS) from adrenal gland results in pubic and axillary hair and increases likelihood of acne |
| Gonadarche | Usually ~2 years before menarche | Pulses of GnRH, LH/FSH lead to increased estrogen, which stimulates breast development, widening of hips, and increased subcutaneous fat deposition |
| Menarche | Relatively late in puberty (usually not before Tanner stage 4) | “Monthly” cycle established; ovarian estrogen pulses in response to GnRH and FSH, the LH surge, and ovulation; progesterone produced after ovulation |
| DHEA: dehydroepiandrosterone; DHEAS: dehydroepiandrosterone sulfate; GnRH: gonadotropin-releasing hormone; | ||
| LH/FSH: luteinizing hormone/follicle-stimulating hormone | ||
| Tanner stage 4: pubic hair and breast development typical of middle to late adolescence (ages 12 to 17) | ||
| Source: References 4,5 | ||
Although men and women have the same 5-HTT gene, women may possess a gender-specific factor—such as estrogen or progesterone—that differentially alters this and other genes’ expression in women with depression. Individuals who carry a short version of the gene may be at particular risk of becoming depressed when exposed to stressful life events.
Caspi et al21 found a polymorphism in the 5-HTT gene on chromosome 17 that can manifest differentially based on environmental factors. In this study, individuals with 2 copies of the long version of this gene were relatively resistant to stressful life events, whereas those with 1 or 2 copies of the short version were highly sensitive to stressful life events. The depression rate in short-gene individuals was:
- 9% in those who had not experienced stressful life events
- nearly 40% in those who had experienced ≥4 stressful life events.
Hormonal and stress factors. Stress responsiveness becomes sexually dimorphic at puberty. Compared with men, women are:
- at greater risk after puberty for heightened stress responsiveness, which is associated with major depressive disorder
- 3 times more likely to develop depression after a stressful life event.22
Women’s and men’s different biological responses to stress might be related to the gender-specific hormones that emerge during puberty. Kate could be at increased risk for depression—especially immediately before her period—if she inherited a stress-sensitive gene and now has increased stress sensitivity triggered by the hormones of puberty.23
Neurodevelopmental factors. Dorsolateral prefrontal cortex circuits associated with making good decisions and weighing the consequences of actions are immature in the adolescent and the last part of the brain to undergo myelination.24-26 Teens are well-known for erratic, emotionally driven behaviors.27,28 Kate’s impulsive overdose exemplifies the consequences of emotional reactivity without the benefit of inhibitory mature brain connections.
Related resources
- Brizendine L. Teen girl brain. In: The female brain. New York: Morgan Road Books; 2006:31-56. www.thefemalebrain.com.
- Strauch B. The primal teen: what discoveries about the teenage brain tell us about our kids. New York: Doubleday; 2003.
- Harter S. Self and identity development. In: Feldman S, Elliott G, eds. At the threshold: the developing adolescent. Cambridge, MA: Harvard University Press; 1990:352-87.
Drug brand names
- Ethinyl estradiol/levonorgestrel • Seasonale
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Arnold AP. Sex chromosomes and brain gender. Nat Rev Neurosci 2004;5(9):701-8.
2. Giedd JN, Snell JW, Lange N, et al. Quantitative magnetic resonance imaging of human brain development: ages 4-18. Cereb Cortex 1996;6(4):551-60.
3. Yurgelun-Todd DA. Emotional and cognitive changes during adolescence. Curr Opin Neurobiol. In press.
4. Cameron J. Interrelationships between hormones, behavior, and affect during adolescence: understanding hormonal, physical, and brain changes occurring in association with pubertal activation of the reproductive axis. Ann NY Acad Sci 2004;1021:110-23.
5. Dahl R. Adolescent brain development: a period of vulnerabilities and opportunities. Ann NY Acad Sci 2004;1021:1-22.
6. Biro F, Huang B, Crawford P, et al. Pubertal correlates in black and white girls. J Pediatr 2006;148(2):234-40.
7. Herman-Giddens M, Kaplowitz P, Wasserman R. Navigating the recent articles on girls’ puberty in pediatrics: what do we know and where do we go from here? Pediatrics 2004;113(4):911-7.
8. Herman-Giddens M, Slora E, Wasserman R, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 1997;99(4):505-12.
9. Wu T, Mendola P, Buck G. Ethnic differences in the presence of secondary sex characteristics and menarche among US girls: the Third National Health and Nutrition Examination Survey, 1988-1994. Pediatrics 2002;110(4):752-7.
10. Rapkin A, Tsao J, Turk N, et al. Relationships among self-rated Tanner staging, hormones, and psychosocial factors in healthy female adolescents. J Pediatr Adolesc Gynecol 2006;19:181-7.
11. Angold A, Costello E, Worthman C. Puberty and depression: the roles of age, pubertal status and pubertal timing. Psychol Med 1998;28:51-61.
12. Angold A, Costello E, Erkanli A, Worthman C. Pubertal changes in hormone levels and depression in girls. Psychol Med 1999;29:1043-53.
13. Hofer A, Siedentopf CM, Ischebeck A, et al. Gender differences in regional cerebral activity during the perception of emotion: a functional MRI study. Neuroimage 2006;32(2):854-62.
14. McClure EB, Parrish JM, Nelson EE, et al. Responses to conflict and cooperation in adolescents with anxiety and mood disorders. J Abnorm Child Psychol. In press.
15. Baron-Cohen S, Richler J, Bisarya D, et al. The systemizing quotient: an investigation of adults with Asperger syndrome or high-functioning autism, and normal sex differences. Philos Trans R Soc Lond B Biol Sci 2003;358(1430):361-74.
16. Williams LM, Barton MJ, Kemp AH, et al. Distinct amygdala-autonomic arousal profiles in response to fear signals in healthy males and females. Neuroimage 2005;28(3):618-26.
17. Killgore WD, Yurgelun-Todd DA. Sex-related developmental differences in the lateralized activation of the prefrontal cortex and amygdala during perception of facial affect. Percept Mot Skills 2004;99(2):371-91.
18. Cheng YW, Tzeng OJ, Decety J, et al. Gender differences in the human mirror system: a magnetoencephalography study. Neuroreport 2006;17(11):1115-9.
19. Schmidt PJ, Nieman LK, Danaceau MA, et al. Differential behavioral effects of gonadal steroids in women with and those without premenstrual syndrome. N Engl J Med 1998;338(4):209-16.
20. Staley J, Sanacora G, Tamagnan G, et al. Sex differences in diencephalon serotonin transporter availability in major depression. Biol Psychiatry 2006;59:40-7.
21. Caspi A, Sugden K, Moffitt T, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 2003;301:386-9.
22. Maciejewski P, Prigerson H, Mazure C. Sex differences in event-related risk for major depression. Psychol Med 2001;31(4):593-604.
23. Seeman M. Psychopathology in women and men: focus on female hormones. Am J Psychiatry 1997;154(12):1641-7.
24. Kupfer D, Woodward H. Adolescent development and the regulation of behavior and emotion. Ann NY Acad Sci 2004;1021:320-2.
25. Kelley A, Schochet T, Landry C. Risk taking and novelty seeking in adolescence. Ann NY Acad Sci 2004;1021:27-32.
26. Ellis L, Rothbart M, Posner M. Individual differences in executive attention predict self-regulation and adolescent psychosocial behaviors. Ann NY Acad Sci 2004;1021:337-40.
27. Dahl R. Adolescent brain development: a period of vulnerabilities and opportunities. Ann NY Acad Sci 2004;1021:1-22.
28. Pelkonen M, Marttunen M. Child and adolescent suicide: epidemiology, risk factors, and approaches to prevention. Paediatr Drugs 2003;5(4):243-65.
Kate, age 14, is referred for follow-up treatment of depression after she impulsively swallowed a bottle of acetaminophen. She says she is in academic trouble and has no friends. Kate describes her childhood as mostly happy except for her parents’ arguments. Her medical history indicates she began developing breasts at age 10 and had her first menstrual period at age 12.
Her father is largely absent, traveling and working long hours. Her mother developed postpartum depression and stopped working after Kate’s younger brother was born.
Girls and boys show similar depression risks during childhood, but girls are twice as likely as boys to become clinically depressed after puberty. The key to treating depression in teen girls is to recognize that brain development and fluctuating hormones can influence behavior in ways that confuse them and the people around them. Successfully treating teen girls’ depression may require a gender-specific approach.
3 stages of brain development
Fetal differentiation. All brains start out with female-type brain circuits. At 8 weeks of fetal life, however, tiny testicles in the male begin to produce large amounts of testosterone, which changes the brain and body to male. Thus, sex-specific genes and hormones guide aspects of the first phase of brain development.1
Table 1
Female hormonal development: Gestation to puberty
| Stage/age | Hormonal events | Effect on female brain |
|---|---|---|
| Gestation | Components of reproductive axis form in early embryonic development; at 8 weeks, testosterone from fetal testicles begins to change female-type brain areas to male | Unperturbed by testosterone, brain continues to develop along female lines |
| Birth to age 24 months | Hormone-secreting placenta detaches at birth, dramatically increasing GnRH and LH/FSH and driving infant gonads to produce estrogen in girls or testosterone in boys (“infantile puberty”) | Abundant ovarian estrogen secretion enhances development of brain circuits, such as those associated with reproduction, maternal behavior, and social relatedness |
| Age 24 months to prepuberty | “Brakes” put on GnRH and LH/FSH pulsatile brain cells | “Juvenile pause” begins, with constant low estrogen secretion in girls by 24 months (in boys, “brakes” are on by 12 months) |
| Puberty | “Brakes” released on GnRH and LH/FSH neurons, reactivating reproductive axis | Ovary resumes estrogen production (“adolescent puberty”); increase in estrogen, progesterone, and testosterone stimulates brain circuit development; unipolar depression rates increase to 2:1 (female to male) by age 15 |
| GnRH: gonadotropin-releasing hormone; LH/FSH: luteinizing hormone/follicle-stimulating hormone | ||
| Source: References 4,5 | ||
Infantile puberty and the second phase of brain development begin in early childhood, as the ovaries and testicles start to produce large amounts of estrogen and testosterone soon after birth.
Puberty launches the final brain development phase. Up to 2 years before menstruation begins, pulsatile gonadotropin-releasing hormone cells in the hypothalamus wake up and start stimulating the ovaries to produce estrogen, thrusting the girl brain into puberty (Figure). The teen girl brain begins to experience not only estrogen surges from the ovary but progesterone and testosterone surges as well.
Although brain size and basic circuitry are mostly set by age 5, puberty stimulates new brain cells and increases myelin production.2 Faster myelinated connections between emotionally impulsive limbic brain areas such as the amygdala and sensible, cognitive areas such as the prefrontal cortex are not finished until the early 20s.3
Hormonal changes at puberty
The female brain is remodeled during puberty, leading to sexually dimorphic brain activation and development that further differentiates it from the male brain.4
Estrogen surges are associated with increased production of neurohormones and neurochemicals, such as:
- oxytocin, which reinforces social bonding and intimacy
- dopamine, which stimulates motivation and pleasure circuits in the brain.
Hormonal changes and brain development alter gene expression and affect neurodevelopment. These events may trigger a first depression in pubertal girls with a family history of mood disorder (Table 1).4,5 Although menarche has begun at an average age of 12 in the United States for decades, the most recent National Health and Examination Survey (NHANES) shows puberty onset in girls is occurring earlier (Table 2).6-9
Tanner stage—a measure of pubertal status—is a more accurate predictor of depression in teen girls than age.10 Pubertal transition to Tanner stage 3 (development of pubic and axillary hair and breast buds) is associated with a sharp increase in depression rates. Girls at stage 3 and higher are approximately 3 times more likely to be depressed than girls at stages 1 or 2.11
Pubic hair, breast development, and menstruation are markers for underlying hormonal changes (Table 3).4,5 The onset of estrogen, progesterone, and testosterone surges closely correlates with the difference in depression rates between pre- and postpubertal girls.12 After estrogen and progesterone surges begin at puberty, negative emotions exert an increased activating effect on the female brain,13 and social stressors more deeply affect girls than they do boys. This may explain why girls are more susceptible to depression when a friendship fails.14
CASE CONTINUED: Boy troubles
Kate tells you that in 9th grade she and her best friend, Ellen, would talk about boys for hours after school and try on sexually provocative outfits. They both liked Matt, a 10th grader, so when he asked Kate out, Ellen stopped speaking to her. Kate and Matt began some heavy petting, and Kate said she felt selfish and guilty about hurting Ellen. But when girls at school began spreading rumors that Kate was a “slut,” Kate blamed Ellen and told her, “I hate you!”
Soon after, Matt broke up with Kate. Distraught, she dreaded going to school and cried in her room at night for several weeks. She became chronically tired and had difficulty concentrating in class. She ruminated about losing Matt and worried that she was too fat, too ugly, or too flat-chested. She missed Ellen and felt no one liked her.
Table 2
Puberty’s developmental milestones in U.S. girls (averages)
| Correlate | African Americans | Whites | School grade* |
|---|---|---|---|
| Breast bud development | Age 9 | Age 10 | 4th to 5th |
| Girls with puberty onset by age 8 | 32% | 11% | 3rd |
| Girls with puberty onset by age 10 | 76% | 53% | 5th |
| Menarche onset | Age 12.1 | Age 12.6 | 7th |
| Tanner stage 5† onset | Age 13.9 | Age 15.5 | 8th to 9th |
| * Approximate grade level for age groups | |||
| † Pubic hair and breast development reach adult stage | |||
| Source: Data from references 6-9, including the Pediatric Research in Office Settings network and Third National Health and Nutrition Examination Survey, 1988-1994. | |||
Figure Hypothalamic-pituitary-ovarian axis: Turned on at puberty in girls
Puberty onset stimulates depression in genetically vulnerable girls; more likely after Tanner stage 3 (development of pubic and axillary hair and breast buds).
Male vs female teen brains
Depression after a relationship failure in teen girls often begins with ruminative thoughts about her flaws, mistakes, or appearance. These negative thoughts may preoccupy her day and night. Teen girls often feel confused by contradictory social pressures to look and dress provocatively but resist having sex. A sexual encounter can trigger shame and fear.
Although clinical and developmental studies indicate that teen girls respond more dramatically to relationship troubles than boys, the brain and hormone differences responsible for these effects remain unclear. Male hormones hugely increase in boys at puberty—up to 25-fold between ages 9 and 15—but do not cycle. Male brains do not have the same capacity as female brains to respond to cyclical hormonal activity because exposure to androgens during fetal development eliminates this ability. The fetal testosterone surge causes the area associated with sexual pursuit to double in the male brain.
Outside of fertility considerations, Baron-Cohen et al15 suggest that male brain circuits have been formed by fetal testosterone to focus more on systematization—which emphasizes figuring out how things work and performing tasks—rather than empathy and bonding in relationships. This difference has been shown in neuroimaging studies comparing the genders’ attentional systems.16,17 In contrast to the systematizing male brain, female brains are more likely to activate the mirror neuron system—the area required for empathizing.18
Female brains, of course, respond to cyclical hormonal activity. However, the regular monthly waves of estrogen and progesterone do not affect all female brains the same. A subset of women who experience premenstrual dysphoric disorder appear to have brains that trigger depressed moods and irritability during the last 2 weeks of the menstrual cycle.19 A genetic difference in these women is suspected as the culprit; these genes may affect the way their brains metabolize progesterone.
CASE CONTINUED: An overdose of stress
Kate’s poor concentration lingered, and her grades continued to drop. She tells you her parents were having marital problems and she did not want to bother them with her difficulties. Two days before her period was due, she learned she had failed 2 classes. That night, as she got some acetaminophen for a headache, she impulsively took the rest of the bottle.
After swallowing the pills, Kate panicked. She forced herself to vomit and tearfully told her parents what she had done. They took her to the emergency room, where she was medically stabilized, evaluated by a psychiatrist, and referred to you for outpatient treatment.
Treatment recommendations
A combination of factors—genetic, hormonal, and neurodevelopmental—probably contributed to Kate’s acute depressed mood and overdose. Thus, to treat depression in adolescent girls, emerging evidence supports:
- stabilizing hormonal fluctuations such as rapidly falling progesterone just before the start of menstrual periods with an extended-cycle contraceptive (we would try an ethinyl estradiol/levonorgestrel combination such as Seasonale®)
- treating depressive symptoms with a selective serotonin reuptake inhibitor such as citalopram, 10 mg once daily, with careful monitoring for suicidal thoughts or behavior
- providing tools to manage stress and impulsive behavior through weekly psychotherapy (such as cognitive-behavioral therapy, dialectical behavioral therapy, or supportive therapy).
Genetic factors. Kate’s mother’s history of postpartum depression suggests genetic risk for Kate. Studies have found that the expression of particular genes—such as the serotonin transporter (5-HTT) gene—may be associated with depression. Staley et al20 found that depressed women show a significantly greater decrease in 5-HTT availability in the diencephalon (forebrain region containing the thalamus, hypothalamus, and part of the pituitary gland) when compared with healthy women and depressed men.
Table 3
3 stages of girls’ gonadal development
| Stage | Timing | Developmental events |
|---|---|---|
| Adrenarche | Onset around age 6, peaks by age 20 | Rise in weak androgens (DHEA and DHEAS) from adrenal gland results in pubic and axillary hair and increases likelihood of acne |
| Gonadarche | Usually ~2 years before menarche | Pulses of GnRH, LH/FSH lead to increased estrogen, which stimulates breast development, widening of hips, and increased subcutaneous fat deposition |
| Menarche | Relatively late in puberty (usually not before Tanner stage 4) | “Monthly” cycle established; ovarian estrogen pulses in response to GnRH and FSH, the LH surge, and ovulation; progesterone produced after ovulation |
| DHEA: dehydroepiandrosterone; DHEAS: dehydroepiandrosterone sulfate; GnRH: gonadotropin-releasing hormone; | ||
| LH/FSH: luteinizing hormone/follicle-stimulating hormone | ||
| Tanner stage 4: pubic hair and breast development typical of middle to late adolescence (ages 12 to 17) | ||
| Source: References 4,5 | ||
Although men and women have the same 5-HTT gene, women may possess a gender-specific factor—such as estrogen or progesterone—that differentially alters this and other genes’ expression in women with depression. Individuals who carry a short version of the gene may be at particular risk of becoming depressed when exposed to stressful life events.
Caspi et al21 found a polymorphism in the 5-HTT gene on chromosome 17 that can manifest differentially based on environmental factors. In this study, individuals with 2 copies of the long version of this gene were relatively resistant to stressful life events, whereas those with 1 or 2 copies of the short version were highly sensitive to stressful life events. The depression rate in short-gene individuals was:
- 9% in those who had not experienced stressful life events
- nearly 40% in those who had experienced ≥4 stressful life events.
Hormonal and stress factors. Stress responsiveness becomes sexually dimorphic at puberty. Compared with men, women are:
- at greater risk after puberty for heightened stress responsiveness, which is associated with major depressive disorder
- 3 times more likely to develop depression after a stressful life event.22
Women’s and men’s different biological responses to stress might be related to the gender-specific hormones that emerge during puberty. Kate could be at increased risk for depression—especially immediately before her period—if she inherited a stress-sensitive gene and now has increased stress sensitivity triggered by the hormones of puberty.23
Neurodevelopmental factors. Dorsolateral prefrontal cortex circuits associated with making good decisions and weighing the consequences of actions are immature in the adolescent and the last part of the brain to undergo myelination.24-26 Teens are well-known for erratic, emotionally driven behaviors.27,28 Kate’s impulsive overdose exemplifies the consequences of emotional reactivity without the benefit of inhibitory mature brain connections.
Related resources
- Brizendine L. Teen girl brain. In: The female brain. New York: Morgan Road Books; 2006:31-56. www.thefemalebrain.com.
- Strauch B. The primal teen: what discoveries about the teenage brain tell us about our kids. New York: Doubleday; 2003.
- Harter S. Self and identity development. In: Feldman S, Elliott G, eds. At the threshold: the developing adolescent. Cambridge, MA: Harvard University Press; 1990:352-87.
Drug brand names
- Ethinyl estradiol/levonorgestrel • Seasonale
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Kate, age 14, is referred for follow-up treatment of depression after she impulsively swallowed a bottle of acetaminophen. She says she is in academic trouble and has no friends. Kate describes her childhood as mostly happy except for her parents’ arguments. Her medical history indicates she began developing breasts at age 10 and had her first menstrual period at age 12.
Her father is largely absent, traveling and working long hours. Her mother developed postpartum depression and stopped working after Kate’s younger brother was born.
Girls and boys show similar depression risks during childhood, but girls are twice as likely as boys to become clinically depressed after puberty. The key to treating depression in teen girls is to recognize that brain development and fluctuating hormones can influence behavior in ways that confuse them and the people around them. Successfully treating teen girls’ depression may require a gender-specific approach.
3 stages of brain development
Fetal differentiation. All brains start out with female-type brain circuits. At 8 weeks of fetal life, however, tiny testicles in the male begin to produce large amounts of testosterone, which changes the brain and body to male. Thus, sex-specific genes and hormones guide aspects of the first phase of brain development.1
Table 1
Female hormonal development: Gestation to puberty
| Stage/age | Hormonal events | Effect on female brain |
|---|---|---|
| Gestation | Components of reproductive axis form in early embryonic development; at 8 weeks, testosterone from fetal testicles begins to change female-type brain areas to male | Unperturbed by testosterone, brain continues to develop along female lines |
| Birth to age 24 months | Hormone-secreting placenta detaches at birth, dramatically increasing GnRH and LH/FSH and driving infant gonads to produce estrogen in girls or testosterone in boys (“infantile puberty”) | Abundant ovarian estrogen secretion enhances development of brain circuits, such as those associated with reproduction, maternal behavior, and social relatedness |
| Age 24 months to prepuberty | “Brakes” put on GnRH and LH/FSH pulsatile brain cells | “Juvenile pause” begins, with constant low estrogen secretion in girls by 24 months (in boys, “brakes” are on by 12 months) |
| Puberty | “Brakes” released on GnRH and LH/FSH neurons, reactivating reproductive axis | Ovary resumes estrogen production (“adolescent puberty”); increase in estrogen, progesterone, and testosterone stimulates brain circuit development; unipolar depression rates increase to 2:1 (female to male) by age 15 |
| GnRH: gonadotropin-releasing hormone; LH/FSH: luteinizing hormone/follicle-stimulating hormone | ||
| Source: References 4,5 | ||
Infantile puberty and the second phase of brain development begin in early childhood, as the ovaries and testicles start to produce large amounts of estrogen and testosterone soon after birth.
Puberty launches the final brain development phase. Up to 2 years before menstruation begins, pulsatile gonadotropin-releasing hormone cells in the hypothalamus wake up and start stimulating the ovaries to produce estrogen, thrusting the girl brain into puberty (Figure). The teen girl brain begins to experience not only estrogen surges from the ovary but progesterone and testosterone surges as well.
Although brain size and basic circuitry are mostly set by age 5, puberty stimulates new brain cells and increases myelin production.2 Faster myelinated connections between emotionally impulsive limbic brain areas such as the amygdala and sensible, cognitive areas such as the prefrontal cortex are not finished until the early 20s.3
Hormonal changes at puberty
The female brain is remodeled during puberty, leading to sexually dimorphic brain activation and development that further differentiates it from the male brain.4
Estrogen surges are associated with increased production of neurohormones and neurochemicals, such as:
- oxytocin, which reinforces social bonding and intimacy
- dopamine, which stimulates motivation and pleasure circuits in the brain.
Hormonal changes and brain development alter gene expression and affect neurodevelopment. These events may trigger a first depression in pubertal girls with a family history of mood disorder (Table 1).4,5 Although menarche has begun at an average age of 12 in the United States for decades, the most recent National Health and Examination Survey (NHANES) shows puberty onset in girls is occurring earlier (Table 2).6-9
Tanner stage—a measure of pubertal status—is a more accurate predictor of depression in teen girls than age.10 Pubertal transition to Tanner stage 3 (development of pubic and axillary hair and breast buds) is associated with a sharp increase in depression rates. Girls at stage 3 and higher are approximately 3 times more likely to be depressed than girls at stages 1 or 2.11
Pubic hair, breast development, and menstruation are markers for underlying hormonal changes (Table 3).4,5 The onset of estrogen, progesterone, and testosterone surges closely correlates with the difference in depression rates between pre- and postpubertal girls.12 After estrogen and progesterone surges begin at puberty, negative emotions exert an increased activating effect on the female brain,13 and social stressors more deeply affect girls than they do boys. This may explain why girls are more susceptible to depression when a friendship fails.14
CASE CONTINUED: Boy troubles
Kate tells you that in 9th grade she and her best friend, Ellen, would talk about boys for hours after school and try on sexually provocative outfits. They both liked Matt, a 10th grader, so when he asked Kate out, Ellen stopped speaking to her. Kate and Matt began some heavy petting, and Kate said she felt selfish and guilty about hurting Ellen. But when girls at school began spreading rumors that Kate was a “slut,” Kate blamed Ellen and told her, “I hate you!”
Soon after, Matt broke up with Kate. Distraught, she dreaded going to school and cried in her room at night for several weeks. She became chronically tired and had difficulty concentrating in class. She ruminated about losing Matt and worried that she was too fat, too ugly, or too flat-chested. She missed Ellen and felt no one liked her.
Table 2
Puberty’s developmental milestones in U.S. girls (averages)
| Correlate | African Americans | Whites | School grade* |
|---|---|---|---|
| Breast bud development | Age 9 | Age 10 | 4th to 5th |
| Girls with puberty onset by age 8 | 32% | 11% | 3rd |
| Girls with puberty onset by age 10 | 76% | 53% | 5th |
| Menarche onset | Age 12.1 | Age 12.6 | 7th |
| Tanner stage 5† onset | Age 13.9 | Age 15.5 | 8th to 9th |
| * Approximate grade level for age groups | |||
| † Pubic hair and breast development reach adult stage | |||
| Source: Data from references 6-9, including the Pediatric Research in Office Settings network and Third National Health and Nutrition Examination Survey, 1988-1994. | |||
Figure Hypothalamic-pituitary-ovarian axis: Turned on at puberty in girls
Puberty onset stimulates depression in genetically vulnerable girls; more likely after Tanner stage 3 (development of pubic and axillary hair and breast buds).
Male vs female teen brains
Depression after a relationship failure in teen girls often begins with ruminative thoughts about her flaws, mistakes, or appearance. These negative thoughts may preoccupy her day and night. Teen girls often feel confused by contradictory social pressures to look and dress provocatively but resist having sex. A sexual encounter can trigger shame and fear.
Although clinical and developmental studies indicate that teen girls respond more dramatically to relationship troubles than boys, the brain and hormone differences responsible for these effects remain unclear. Male hormones hugely increase in boys at puberty—up to 25-fold between ages 9 and 15—but do not cycle. Male brains do not have the same capacity as female brains to respond to cyclical hormonal activity because exposure to androgens during fetal development eliminates this ability. The fetal testosterone surge causes the area associated with sexual pursuit to double in the male brain.
Outside of fertility considerations, Baron-Cohen et al15 suggest that male brain circuits have been formed by fetal testosterone to focus more on systematization—which emphasizes figuring out how things work and performing tasks—rather than empathy and bonding in relationships. This difference has been shown in neuroimaging studies comparing the genders’ attentional systems.16,17 In contrast to the systematizing male brain, female brains are more likely to activate the mirror neuron system—the area required for empathizing.18
Female brains, of course, respond to cyclical hormonal activity. However, the regular monthly waves of estrogen and progesterone do not affect all female brains the same. A subset of women who experience premenstrual dysphoric disorder appear to have brains that trigger depressed moods and irritability during the last 2 weeks of the menstrual cycle.19 A genetic difference in these women is suspected as the culprit; these genes may affect the way their brains metabolize progesterone.
CASE CONTINUED: An overdose of stress
Kate’s poor concentration lingered, and her grades continued to drop. She tells you her parents were having marital problems and she did not want to bother them with her difficulties. Two days before her period was due, she learned she had failed 2 classes. That night, as she got some acetaminophen for a headache, she impulsively took the rest of the bottle.
After swallowing the pills, Kate panicked. She forced herself to vomit and tearfully told her parents what she had done. They took her to the emergency room, where she was medically stabilized, evaluated by a psychiatrist, and referred to you for outpatient treatment.
Treatment recommendations
A combination of factors—genetic, hormonal, and neurodevelopmental—probably contributed to Kate’s acute depressed mood and overdose. Thus, to treat depression in adolescent girls, emerging evidence supports:
- stabilizing hormonal fluctuations such as rapidly falling progesterone just before the start of menstrual periods with an extended-cycle contraceptive (we would try an ethinyl estradiol/levonorgestrel combination such as Seasonale®)
- treating depressive symptoms with a selective serotonin reuptake inhibitor such as citalopram, 10 mg once daily, with careful monitoring for suicidal thoughts or behavior
- providing tools to manage stress and impulsive behavior through weekly psychotherapy (such as cognitive-behavioral therapy, dialectical behavioral therapy, or supportive therapy).
Genetic factors. Kate’s mother’s history of postpartum depression suggests genetic risk for Kate. Studies have found that the expression of particular genes—such as the serotonin transporter (5-HTT) gene—may be associated with depression. Staley et al20 found that depressed women show a significantly greater decrease in 5-HTT availability in the diencephalon (forebrain region containing the thalamus, hypothalamus, and part of the pituitary gland) when compared with healthy women and depressed men.
Table 3
3 stages of girls’ gonadal development
| Stage | Timing | Developmental events |
|---|---|---|
| Adrenarche | Onset around age 6, peaks by age 20 | Rise in weak androgens (DHEA and DHEAS) from adrenal gland results in pubic and axillary hair and increases likelihood of acne |
| Gonadarche | Usually ~2 years before menarche | Pulses of GnRH, LH/FSH lead to increased estrogen, which stimulates breast development, widening of hips, and increased subcutaneous fat deposition |
| Menarche | Relatively late in puberty (usually not before Tanner stage 4) | “Monthly” cycle established; ovarian estrogen pulses in response to GnRH and FSH, the LH surge, and ovulation; progesterone produced after ovulation |
| DHEA: dehydroepiandrosterone; DHEAS: dehydroepiandrosterone sulfate; GnRH: gonadotropin-releasing hormone; | ||
| LH/FSH: luteinizing hormone/follicle-stimulating hormone | ||
| Tanner stage 4: pubic hair and breast development typical of middle to late adolescence (ages 12 to 17) | ||
| Source: References 4,5 | ||
Although men and women have the same 5-HTT gene, women may possess a gender-specific factor—such as estrogen or progesterone—that differentially alters this and other genes’ expression in women with depression. Individuals who carry a short version of the gene may be at particular risk of becoming depressed when exposed to stressful life events.
Caspi et al21 found a polymorphism in the 5-HTT gene on chromosome 17 that can manifest differentially based on environmental factors. In this study, individuals with 2 copies of the long version of this gene were relatively resistant to stressful life events, whereas those with 1 or 2 copies of the short version were highly sensitive to stressful life events. The depression rate in short-gene individuals was:
- 9% in those who had not experienced stressful life events
- nearly 40% in those who had experienced ≥4 stressful life events.
Hormonal and stress factors. Stress responsiveness becomes sexually dimorphic at puberty. Compared with men, women are:
- at greater risk after puberty for heightened stress responsiveness, which is associated with major depressive disorder
- 3 times more likely to develop depression after a stressful life event.22
Women’s and men’s different biological responses to stress might be related to the gender-specific hormones that emerge during puberty. Kate could be at increased risk for depression—especially immediately before her period—if she inherited a stress-sensitive gene and now has increased stress sensitivity triggered by the hormones of puberty.23
Neurodevelopmental factors. Dorsolateral prefrontal cortex circuits associated with making good decisions and weighing the consequences of actions are immature in the adolescent and the last part of the brain to undergo myelination.24-26 Teens are well-known for erratic, emotionally driven behaviors.27,28 Kate’s impulsive overdose exemplifies the consequences of emotional reactivity without the benefit of inhibitory mature brain connections.
Related resources
- Brizendine L. Teen girl brain. In: The female brain. New York: Morgan Road Books; 2006:31-56. www.thefemalebrain.com.
- Strauch B. The primal teen: what discoveries about the teenage brain tell us about our kids. New York: Doubleday; 2003.
- Harter S. Self and identity development. In: Feldman S, Elliott G, eds. At the threshold: the developing adolescent. Cambridge, MA: Harvard University Press; 1990:352-87.
Drug brand names
- Ethinyl estradiol/levonorgestrel • Seasonale
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Arnold AP. Sex chromosomes and brain gender. Nat Rev Neurosci 2004;5(9):701-8.
2. Giedd JN, Snell JW, Lange N, et al. Quantitative magnetic resonance imaging of human brain development: ages 4-18. Cereb Cortex 1996;6(4):551-60.
3. Yurgelun-Todd DA. Emotional and cognitive changes during adolescence. Curr Opin Neurobiol. In press.
4. Cameron J. Interrelationships between hormones, behavior, and affect during adolescence: understanding hormonal, physical, and brain changes occurring in association with pubertal activation of the reproductive axis. Ann NY Acad Sci 2004;1021:110-23.
5. Dahl R. Adolescent brain development: a period of vulnerabilities and opportunities. Ann NY Acad Sci 2004;1021:1-22.
6. Biro F, Huang B, Crawford P, et al. Pubertal correlates in black and white girls. J Pediatr 2006;148(2):234-40.
7. Herman-Giddens M, Kaplowitz P, Wasserman R. Navigating the recent articles on girls’ puberty in pediatrics: what do we know and where do we go from here? Pediatrics 2004;113(4):911-7.
8. Herman-Giddens M, Slora E, Wasserman R, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 1997;99(4):505-12.
9. Wu T, Mendola P, Buck G. Ethnic differences in the presence of secondary sex characteristics and menarche among US girls: the Third National Health and Nutrition Examination Survey, 1988-1994. Pediatrics 2002;110(4):752-7.
10. Rapkin A, Tsao J, Turk N, et al. Relationships among self-rated Tanner staging, hormones, and psychosocial factors in healthy female adolescents. J Pediatr Adolesc Gynecol 2006;19:181-7.
11. Angold A, Costello E, Worthman C. Puberty and depression: the roles of age, pubertal status and pubertal timing. Psychol Med 1998;28:51-61.
12. Angold A, Costello E, Erkanli A, Worthman C. Pubertal changes in hormone levels and depression in girls. Psychol Med 1999;29:1043-53.
13. Hofer A, Siedentopf CM, Ischebeck A, et al. Gender differences in regional cerebral activity during the perception of emotion: a functional MRI study. Neuroimage 2006;32(2):854-62.
14. McClure EB, Parrish JM, Nelson EE, et al. Responses to conflict and cooperation in adolescents with anxiety and mood disorders. J Abnorm Child Psychol. In press.
15. Baron-Cohen S, Richler J, Bisarya D, et al. The systemizing quotient: an investigation of adults with Asperger syndrome or high-functioning autism, and normal sex differences. Philos Trans R Soc Lond B Biol Sci 2003;358(1430):361-74.
16. Williams LM, Barton MJ, Kemp AH, et al. Distinct amygdala-autonomic arousal profiles in response to fear signals in healthy males and females. Neuroimage 2005;28(3):618-26.
17. Killgore WD, Yurgelun-Todd DA. Sex-related developmental differences in the lateralized activation of the prefrontal cortex and amygdala during perception of facial affect. Percept Mot Skills 2004;99(2):371-91.
18. Cheng YW, Tzeng OJ, Decety J, et al. Gender differences in the human mirror system: a magnetoencephalography study. Neuroreport 2006;17(11):1115-9.
19. Schmidt PJ, Nieman LK, Danaceau MA, et al. Differential behavioral effects of gonadal steroids in women with and those without premenstrual syndrome. N Engl J Med 1998;338(4):209-16.
20. Staley J, Sanacora G, Tamagnan G, et al. Sex differences in diencephalon serotonin transporter availability in major depression. Biol Psychiatry 2006;59:40-7.
21. Caspi A, Sugden K, Moffitt T, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 2003;301:386-9.
22. Maciejewski P, Prigerson H, Mazure C. Sex differences in event-related risk for major depression. Psychol Med 2001;31(4):593-604.
23. Seeman M. Psychopathology in women and men: focus on female hormones. Am J Psychiatry 1997;154(12):1641-7.
24. Kupfer D, Woodward H. Adolescent development and the regulation of behavior and emotion. Ann NY Acad Sci 2004;1021:320-2.
25. Kelley A, Schochet T, Landry C. Risk taking and novelty seeking in adolescence. Ann NY Acad Sci 2004;1021:27-32.
26. Ellis L, Rothbart M, Posner M. Individual differences in executive attention predict self-regulation and adolescent psychosocial behaviors. Ann NY Acad Sci 2004;1021:337-40.
27. Dahl R. Adolescent brain development: a period of vulnerabilities and opportunities. Ann NY Acad Sci 2004;1021:1-22.
28. Pelkonen M, Marttunen M. Child and adolescent suicide: epidemiology, risk factors, and approaches to prevention. Paediatr Drugs 2003;5(4):243-65.
1. Arnold AP. Sex chromosomes and brain gender. Nat Rev Neurosci 2004;5(9):701-8.
2. Giedd JN, Snell JW, Lange N, et al. Quantitative magnetic resonance imaging of human brain development: ages 4-18. Cereb Cortex 1996;6(4):551-60.
3. Yurgelun-Todd DA. Emotional and cognitive changes during adolescence. Curr Opin Neurobiol. In press.
4. Cameron J. Interrelationships between hormones, behavior, and affect during adolescence: understanding hormonal, physical, and brain changes occurring in association with pubertal activation of the reproductive axis. Ann NY Acad Sci 2004;1021:110-23.
5. Dahl R. Adolescent brain development: a period of vulnerabilities and opportunities. Ann NY Acad Sci 2004;1021:1-22.
6. Biro F, Huang B, Crawford P, et al. Pubertal correlates in black and white girls. J Pediatr 2006;148(2):234-40.
7. Herman-Giddens M, Kaplowitz P, Wasserman R. Navigating the recent articles on girls’ puberty in pediatrics: what do we know and where do we go from here? Pediatrics 2004;113(4):911-7.
8. Herman-Giddens M, Slora E, Wasserman R, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 1997;99(4):505-12.
9. Wu T, Mendola P, Buck G. Ethnic differences in the presence of secondary sex characteristics and menarche among US girls: the Third National Health and Nutrition Examination Survey, 1988-1994. Pediatrics 2002;110(4):752-7.
10. Rapkin A, Tsao J, Turk N, et al. Relationships among self-rated Tanner staging, hormones, and psychosocial factors in healthy female adolescents. J Pediatr Adolesc Gynecol 2006;19:181-7.
11. Angold A, Costello E, Worthman C. Puberty and depression: the roles of age, pubertal status and pubertal timing. Psychol Med 1998;28:51-61.
12. Angold A, Costello E, Erkanli A, Worthman C. Pubertal changes in hormone levels and depression in girls. Psychol Med 1999;29:1043-53.
13. Hofer A, Siedentopf CM, Ischebeck A, et al. Gender differences in regional cerebral activity during the perception of emotion: a functional MRI study. Neuroimage 2006;32(2):854-62.
14. McClure EB, Parrish JM, Nelson EE, et al. Responses to conflict and cooperation in adolescents with anxiety and mood disorders. J Abnorm Child Psychol. In press.
15. Baron-Cohen S, Richler J, Bisarya D, et al. The systemizing quotient: an investigation of adults with Asperger syndrome or high-functioning autism, and normal sex differences. Philos Trans R Soc Lond B Biol Sci 2003;358(1430):361-74.
16. Williams LM, Barton MJ, Kemp AH, et al. Distinct amygdala-autonomic arousal profiles in response to fear signals in healthy males and females. Neuroimage 2005;28(3):618-26.
17. Killgore WD, Yurgelun-Todd DA. Sex-related developmental differences in the lateralized activation of the prefrontal cortex and amygdala during perception of facial affect. Percept Mot Skills 2004;99(2):371-91.
18. Cheng YW, Tzeng OJ, Decety J, et al. Gender differences in the human mirror system: a magnetoencephalography study. Neuroreport 2006;17(11):1115-9.
19. Schmidt PJ, Nieman LK, Danaceau MA, et al. Differential behavioral effects of gonadal steroids in women with and those without premenstrual syndrome. N Engl J Med 1998;338(4):209-16.
20. Staley J, Sanacora G, Tamagnan G, et al. Sex differences in diencephalon serotonin transporter availability in major depression. Biol Psychiatry 2006;59:40-7.
21. Caspi A, Sugden K, Moffitt T, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science 2003;301:386-9.
22. Maciejewski P, Prigerson H, Mazure C. Sex differences in event-related risk for major depression. Psychol Med 2001;31(4):593-604.
23. Seeman M. Psychopathology in women and men: focus on female hormones. Am J Psychiatry 1997;154(12):1641-7.
24. Kupfer D, Woodward H. Adolescent development and the regulation of behavior and emotion. Ann NY Acad Sci 2004;1021:320-2.
25. Kelley A, Schochet T, Landry C. Risk taking and novelty seeking in adolescence. Ann NY Acad Sci 2004;1021:27-32.
26. Ellis L, Rothbart M, Posner M. Individual differences in executive attention predict self-regulation and adolescent psychosocial behaviors. Ann NY Acad Sci 2004;1021:337-40.
27. Dahl R. Adolescent brain development: a period of vulnerabilities and opportunities. Ann NY Acad Sci 2004;1021:1-22.
28. Pelkonen M, Marttunen M. Child and adolescent suicide: epidemiology, risk factors, and approaches to prevention. Paediatr Drugs 2003;5(4):243-65.