User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
Personalized nutrition therapy promotes diabetes remission
LEIPZIG, GERMANY — For patients newly diagnosed with type 2 diabetes, nutrition therapy is highly effective at achieving remission. “The greater the reduction in body weight, the higher the chances that blood sugar levels will normalize,” Diana Rubin, MD, said at the fall press conference of the German Diabetes Society (DDG). Dr. Rubin is conference president and chief physician of the Center for Nutritional Medicine and Diabetology at Vivantes Humboldt Hospital and the Spandau Hospital, Berlin, Germany.
Because of the development of modern medicines, nutrition therapy has increasingly been pushed into the background over the past 50 years. However, nutrition therapy and weight reduction can effectively delay diabetes for years, said Dr. Rubin. The patients are healthy, without being healed.
Nevertheless, the remission is rarely permanent. Most of the patients develop type 2 diabetes again after 5 years.
Personalized Nutrition Therapy
It is not just developments in medicine that have pushed nutrition therapy into the background. Another contributing factor is that statutory health insurance companies do not cover personalized nutrition counseling as standard, said Dr. Rubin.
Modern research in nutrition therapy has shown that patients with diabetes should receive personalized treatment. However, this idea is not taken into consideration in current diabetes training programs, which are the only forms of nutrition therapy covered by statutory health insurance companies.
Instead, nutrition information is mostly conveyed through group training sessions. Individuals do not necessarily find each other again. What’s more, these sessions are seldom led by nutrition experts. “It is rarely helpful to use a ‘one size fits all’ approach, as is often the case with these group training sessions,” said Dr. Rubin.
The DiRECT study, in which patients reduced their weight by 15 kg and achieved remission rates of almost 90%, is an example of how nutrition therapy can be highly effective. This is especially true if the aims and methods are determined on an individual basis and if there is frequent contact with a therapist. German and international guidelines, including the DDG’s best practice guides from 2022, highlight the importance of personalized nutrition therapy.
Telemedicine Encourages Adherence
“It is very important to consider the current living situation of the person concerned,” said Dr. Rubin. “It is important to set small objectives that can also be implemented in everyday life.” This can only succeed with a professional face-to-face consultation. “Achieving this objective then also becomes realistic — i.e., losing 10% to 15% body weight and maintaining this loss,” she said. “Long-term monitoring is needed to maintain this weight.”
Weight reduction methods should generally be determined according to the preferences of the person concerned, since dietary habits and environments are personal. For example, reducing the intake of carbohydrates and fats, intermittent fasting, or using meal replacement drinks can all be considered.
New data also show that digital apps available on prescription (DiGA) can be helpful for support; this idea is reflected in the DDG’s nutrition best practice guides for patients with type 2 diabetes.
“Studies show that adherence is highly dependent on the amount of contact with therapists and the long-term nature of the treatment,” said Dr. Rubin. She referred to the need for long-term monitoring, during which the patient can be repeatedly reminded of the therapeutic objective. “In this respect, I see a lot of potential in digital apps, and also in telemedicine, to cater to the short-term contact with the person concerned.”
A 2015 meta-analysis of 92 studies revealed a significant reduction in A1c for patients with type 1 or type 2 diabetes when using telemedicine nutrition therapy. Dr. Rubin frequently prescribes DiGAs, which are approved for obesity, “simply because I can recognize it makes it easier for many patients to stick to their goals.”
Dr. Rubin also recommends connecting with sport groups and self-help groups. “Maintaining the weight is a long-term project.”
Abdominal Fat Decisive
Prediabetes is a precursor to type 2 diabetes and entails an increased risk of heart attack, kidney and eye diseases, and various kinds of cancer. To date, physicians have tried to delay the onset of type 2 diabetes by aiming to reduce the weight of patients with prediabetes. However, scientists at the German Center for Diabetes Research showed with the Prediabetes Lifestyle Intervention Study that abdominal fat plays an important role in the remission of prediabetes.
The 1-year program with a healthy diet and increased physical activity was followed by 1105 patients with prediabetes. When every subject lost at least 5% of their weight, it turned out that some achieved remission, and others did not.
People who achieved remission exhibited better insulin sensitivity and had lost more visceral abdominal fat. Visceral abdominal fat can influence insulin sensitivity, not least by an inflammatory reaction in the fatty tissue.
Reducing visceral abdominal fat is clearly crucially important in achieving prediabetes remission. Subjects who achieved remission in the study had a strongly reduced risk for type 2 diabetes for up to 2 years after the end of the program. They had improved kidney function, and their blood vessels were in better condition.
Waist Circumference
According to the new results, the chances of remission increase if body weight is reduced by 5% and waist circumference is reduced by around 4 cm in women and 7 cm in men.
“Based on the new data, remission should be the new therapeutic objective in people with prediabetes. This could potentially change clinical practice and minimize the complication rate for our patients, both male and female,” said author Reiner Jumpertz-von Schwartzenberg, MD, a researcher at the Tübingen University Hospital in Germany.
Prediabetes remission can be assumed if the fasting blood glucose falls below 100 mg/dL (5.6 mmol/L), the 2-hour glucose below 140 mg/dL (7.8 mmol/L), and the A1c value below 5.7%. From the new findings, it can be seen that the chances of remission increase the more the body weight decreases.
Dr. Jumpertz-von Schwartzenberg and his colleagues want to investigate whether this strategy is cost-effective so that the support of payers can also be ensured.
This article was translated from the Medscape German edition.
A version of this article appeared on Medscape.com.
LEIPZIG, GERMANY — For patients newly diagnosed with type 2 diabetes, nutrition therapy is highly effective at achieving remission. “The greater the reduction in body weight, the higher the chances that blood sugar levels will normalize,” Diana Rubin, MD, said at the fall press conference of the German Diabetes Society (DDG). Dr. Rubin is conference president and chief physician of the Center for Nutritional Medicine and Diabetology at Vivantes Humboldt Hospital and the Spandau Hospital, Berlin, Germany.
Because of the development of modern medicines, nutrition therapy has increasingly been pushed into the background over the past 50 years. However, nutrition therapy and weight reduction can effectively delay diabetes for years, said Dr. Rubin. The patients are healthy, without being healed.
Nevertheless, the remission is rarely permanent. Most of the patients develop type 2 diabetes again after 5 years.
Personalized Nutrition Therapy
It is not just developments in medicine that have pushed nutrition therapy into the background. Another contributing factor is that statutory health insurance companies do not cover personalized nutrition counseling as standard, said Dr. Rubin.
Modern research in nutrition therapy has shown that patients with diabetes should receive personalized treatment. However, this idea is not taken into consideration in current diabetes training programs, which are the only forms of nutrition therapy covered by statutory health insurance companies.
Instead, nutrition information is mostly conveyed through group training sessions. Individuals do not necessarily find each other again. What’s more, these sessions are seldom led by nutrition experts. “It is rarely helpful to use a ‘one size fits all’ approach, as is often the case with these group training sessions,” said Dr. Rubin.
The DiRECT study, in which patients reduced their weight by 15 kg and achieved remission rates of almost 90%, is an example of how nutrition therapy can be highly effective. This is especially true if the aims and methods are determined on an individual basis and if there is frequent contact with a therapist. German and international guidelines, including the DDG’s best practice guides from 2022, highlight the importance of personalized nutrition therapy.
Telemedicine Encourages Adherence
“It is very important to consider the current living situation of the person concerned,” said Dr. Rubin. “It is important to set small objectives that can also be implemented in everyday life.” This can only succeed with a professional face-to-face consultation. “Achieving this objective then also becomes realistic — i.e., losing 10% to 15% body weight and maintaining this loss,” she said. “Long-term monitoring is needed to maintain this weight.”
Weight reduction methods should generally be determined according to the preferences of the person concerned, since dietary habits and environments are personal. For example, reducing the intake of carbohydrates and fats, intermittent fasting, or using meal replacement drinks can all be considered.
New data also show that digital apps available on prescription (DiGA) can be helpful for support; this idea is reflected in the DDG’s nutrition best practice guides for patients with type 2 diabetes.
“Studies show that adherence is highly dependent on the amount of contact with therapists and the long-term nature of the treatment,” said Dr. Rubin. She referred to the need for long-term monitoring, during which the patient can be repeatedly reminded of the therapeutic objective. “In this respect, I see a lot of potential in digital apps, and also in telemedicine, to cater to the short-term contact with the person concerned.”
A 2015 meta-analysis of 92 studies revealed a significant reduction in A1c for patients with type 1 or type 2 diabetes when using telemedicine nutrition therapy. Dr. Rubin frequently prescribes DiGAs, which are approved for obesity, “simply because I can recognize it makes it easier for many patients to stick to their goals.”
Dr. Rubin also recommends connecting with sport groups and self-help groups. “Maintaining the weight is a long-term project.”
Abdominal Fat Decisive
Prediabetes is a precursor to type 2 diabetes and entails an increased risk of heart attack, kidney and eye diseases, and various kinds of cancer. To date, physicians have tried to delay the onset of type 2 diabetes by aiming to reduce the weight of patients with prediabetes. However, scientists at the German Center for Diabetes Research showed with the Prediabetes Lifestyle Intervention Study that abdominal fat plays an important role in the remission of prediabetes.
The 1-year program with a healthy diet and increased physical activity was followed by 1105 patients with prediabetes. When every subject lost at least 5% of their weight, it turned out that some achieved remission, and others did not.
People who achieved remission exhibited better insulin sensitivity and had lost more visceral abdominal fat. Visceral abdominal fat can influence insulin sensitivity, not least by an inflammatory reaction in the fatty tissue.
Reducing visceral abdominal fat is clearly crucially important in achieving prediabetes remission. Subjects who achieved remission in the study had a strongly reduced risk for type 2 diabetes for up to 2 years after the end of the program. They had improved kidney function, and their blood vessels were in better condition.
Waist Circumference
According to the new results, the chances of remission increase if body weight is reduced by 5% and waist circumference is reduced by around 4 cm in women and 7 cm in men.
“Based on the new data, remission should be the new therapeutic objective in people with prediabetes. This could potentially change clinical practice and minimize the complication rate for our patients, both male and female,” said author Reiner Jumpertz-von Schwartzenberg, MD, a researcher at the Tübingen University Hospital in Germany.
Prediabetes remission can be assumed if the fasting blood glucose falls below 100 mg/dL (5.6 mmol/L), the 2-hour glucose below 140 mg/dL (7.8 mmol/L), and the A1c value below 5.7%. From the new findings, it can be seen that the chances of remission increase the more the body weight decreases.
Dr. Jumpertz-von Schwartzenberg and his colleagues want to investigate whether this strategy is cost-effective so that the support of payers can also be ensured.
This article was translated from the Medscape German edition.
A version of this article appeared on Medscape.com.
LEIPZIG, GERMANY — For patients newly diagnosed with type 2 diabetes, nutrition therapy is highly effective at achieving remission. “The greater the reduction in body weight, the higher the chances that blood sugar levels will normalize,” Diana Rubin, MD, said at the fall press conference of the German Diabetes Society (DDG). Dr. Rubin is conference president and chief physician of the Center for Nutritional Medicine and Diabetology at Vivantes Humboldt Hospital and the Spandau Hospital, Berlin, Germany.
Because of the development of modern medicines, nutrition therapy has increasingly been pushed into the background over the past 50 years. However, nutrition therapy and weight reduction can effectively delay diabetes for years, said Dr. Rubin. The patients are healthy, without being healed.
Nevertheless, the remission is rarely permanent. Most of the patients develop type 2 diabetes again after 5 years.
Personalized Nutrition Therapy
It is not just developments in medicine that have pushed nutrition therapy into the background. Another contributing factor is that statutory health insurance companies do not cover personalized nutrition counseling as standard, said Dr. Rubin.
Modern research in nutrition therapy has shown that patients with diabetes should receive personalized treatment. However, this idea is not taken into consideration in current diabetes training programs, which are the only forms of nutrition therapy covered by statutory health insurance companies.
Instead, nutrition information is mostly conveyed through group training sessions. Individuals do not necessarily find each other again. What’s more, these sessions are seldom led by nutrition experts. “It is rarely helpful to use a ‘one size fits all’ approach, as is often the case with these group training sessions,” said Dr. Rubin.
The DiRECT study, in which patients reduced their weight by 15 kg and achieved remission rates of almost 90%, is an example of how nutrition therapy can be highly effective. This is especially true if the aims and methods are determined on an individual basis and if there is frequent contact with a therapist. German and international guidelines, including the DDG’s best practice guides from 2022, highlight the importance of personalized nutrition therapy.
Telemedicine Encourages Adherence
“It is very important to consider the current living situation of the person concerned,” said Dr. Rubin. “It is important to set small objectives that can also be implemented in everyday life.” This can only succeed with a professional face-to-face consultation. “Achieving this objective then also becomes realistic — i.e., losing 10% to 15% body weight and maintaining this loss,” she said. “Long-term monitoring is needed to maintain this weight.”
Weight reduction methods should generally be determined according to the preferences of the person concerned, since dietary habits and environments are personal. For example, reducing the intake of carbohydrates and fats, intermittent fasting, or using meal replacement drinks can all be considered.
New data also show that digital apps available on prescription (DiGA) can be helpful for support; this idea is reflected in the DDG’s nutrition best practice guides for patients with type 2 diabetes.
“Studies show that adherence is highly dependent on the amount of contact with therapists and the long-term nature of the treatment,” said Dr. Rubin. She referred to the need for long-term monitoring, during which the patient can be repeatedly reminded of the therapeutic objective. “In this respect, I see a lot of potential in digital apps, and also in telemedicine, to cater to the short-term contact with the person concerned.”
A 2015 meta-analysis of 92 studies revealed a significant reduction in A1c for patients with type 1 or type 2 diabetes when using telemedicine nutrition therapy. Dr. Rubin frequently prescribes DiGAs, which are approved for obesity, “simply because I can recognize it makes it easier for many patients to stick to their goals.”
Dr. Rubin also recommends connecting with sport groups and self-help groups. “Maintaining the weight is a long-term project.”
Abdominal Fat Decisive
Prediabetes is a precursor to type 2 diabetes and entails an increased risk of heart attack, kidney and eye diseases, and various kinds of cancer. To date, physicians have tried to delay the onset of type 2 diabetes by aiming to reduce the weight of patients with prediabetes. However, scientists at the German Center for Diabetes Research showed with the Prediabetes Lifestyle Intervention Study that abdominal fat plays an important role in the remission of prediabetes.
The 1-year program with a healthy diet and increased physical activity was followed by 1105 patients with prediabetes. When every subject lost at least 5% of their weight, it turned out that some achieved remission, and others did not.
People who achieved remission exhibited better insulin sensitivity and had lost more visceral abdominal fat. Visceral abdominal fat can influence insulin sensitivity, not least by an inflammatory reaction in the fatty tissue.
Reducing visceral abdominal fat is clearly crucially important in achieving prediabetes remission. Subjects who achieved remission in the study had a strongly reduced risk for type 2 diabetes for up to 2 years after the end of the program. They had improved kidney function, and their blood vessels were in better condition.
Waist Circumference
According to the new results, the chances of remission increase if body weight is reduced by 5% and waist circumference is reduced by around 4 cm in women and 7 cm in men.
“Based on the new data, remission should be the new therapeutic objective in people with prediabetes. This could potentially change clinical practice and minimize the complication rate for our patients, both male and female,” said author Reiner Jumpertz-von Schwartzenberg, MD, a researcher at the Tübingen University Hospital in Germany.
Prediabetes remission can be assumed if the fasting blood glucose falls below 100 mg/dL (5.6 mmol/L), the 2-hour glucose below 140 mg/dL (7.8 mmol/L), and the A1c value below 5.7%. From the new findings, it can be seen that the chances of remission increase the more the body weight decreases.
Dr. Jumpertz-von Schwartzenberg and his colleagues want to investigate whether this strategy is cost-effective so that the support of payers can also be ensured.
This article was translated from the Medscape German edition.
A version of this article appeared on Medscape.com.
New cardiology certification board: What’s the plan?
The proposal by the major cardiovascular societies in the US to form a new board of cardiovascular medicine to manage initial and ongoing certification of cardiologists represents something of a revolution in the field of continuing medical education and assessment of competency.
Five US cardiovascular societies — the American College of Cardiology (ACC), the American Heart Association (AHA), the Heart Failure Society of America (HFSA), the Heart Rhythm Society (HRS), and the Society for Cardiovascular Angiography & Interventions (SCAI) — have now joined forces to propose a new professional certification board for cardiovascular medicine, to be known as the American Board of Cardiovascular Medicine (ABCVM).
The ABCVM would be independent of the American Board of Internal Medicine (ABIM), the current organization providing maintenance of certification for cardiologists as well as many other internal medicine subspecialties. The ABIM’s maintenance of certification process has been widely criticized for many years and has been described as “needlessly burdensome and expensive.”
, according to Jeffrey Kuvin, MD, a trustee of the ACC, who has been heading up the working group to develop this plan.
Dr. Kuvin, who is chair of the cardiology at Northwell Health, Manhasset, New York, a large academic healthcare system, explained that maintenance of certification has been a topic of discussion across the cardiovascular community for many years, and the ACC has a working group focused on the next steps for evaluation of competency, which he chairs.
“The topic of evaluation of competence has been on the mind of the ACC for many years and hence a work group was developed to focus on this,” Dr. Kuvin noted. “A lot of evolution of the concepts and next steps have been drawn out of this working group. And now other cardiovascular societies have joined to show unification across the house of cardiology and that this is indeed the way that the cardiovascular profession should move.”
“Time to Separate from Internal Medicine”
The general concept behind the new cardiology board is to separate cardiology from the ABIM.
“This is rooted from the concept that cardiology has evolved so much over the last few decades into such a large multidimensional specialty that it really does demarcate itself from internal medicine, and as such, it deserves a separate board governed by cardiologists with collaboration across the entirely of cardiology,” Dr. Kuvin said.
Cardiology has had significant growth and expansion of technology, tools, medications, and the approach to patients in many specialities and subspecialties, he added. “We have defined training programs in many different areas within cardiology; we have our own guidelines, our own competency statements, and in many cases, cardiology exists as its own department outside of medicine in many institutions. It’s just time to separate cardiology from the umbrella of internal medicine.”
The new cardiology board would be separate from, and not report to, the ABIM; rather, it would report directly to the American Board of Medical Specialties (ABMS), the only recognized medical certification body in the US.
What Are the Proposed Changes
Under the present system, managed by the ABIM, clinicians must undergo two stages of certification to be a cardiologist. First, they have to pass the initial certification exam in general cardiology, and then exams in one of four subspecialties if they plan to enter one of these, including interventional cardiology, electrophysiology, advanced heart failure or adult congenital heart disease.
Next, clinicians enter the maintenance of certification phase, which can take three different forms: 1) taking another recertification exam every 10 years; 2) the collaborative maintenance pathway — a collaboration between ACC and ABIM, which includes evaluation, learning and a certified exam each year; or 3) longitudinal knowledge and assessment — in which the program interacts with the clinician on an ongoing basis, sending secured questions regularly.
All three of these pathways for maintenance of certification involve high stakes questions and a set bar for passing or failing.
Under the proposed new cardiology board, an initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured, with the new approach taking the form of continuous learning and assessment of competency.
“This is an iterative process, but we envision with a new American Board of Cardiovascular Medicine, we will pick up where the ABIM left off,” Dr. Kuvin notes. “That includes an initial certifying examination for the five areas that already exist under the ABIM system but with the opportunities to expand that to further specialties as well.”
He points out that there are several areas in cardiology that are currently not represented by these five areas that warrant some discussion, including multimodality imaging, vascular heart disease, and cardio-oncology.
“At present, everybody has to pass the general cardiology exam and then some may wish to further train and get certified in one of the other four other specific areas. But one topic that has been discussed over many years is how do we maintain competency in the areas in which clinicians practice over their lifetime as a cardiologist,” Dr. Kuvin commented.
He said the proposed cardiology board would like to adhere to some basic principles that are fundamental to the practice of medicine.
“We want to make sure that we are practicing medicine so that our patients derive the most benefit from seeing a cardiologist,” he said. “We also want to make sure, however, that this is a supportive process, supporting cardiologists to learn what they know and more importantly what they don’t know; to identify knowledge gaps in specific area; to help the cardiologist fill those knowledge gaps; to acknowledge those gaps have been filled; and then move on to another area of interest. This will be the focus of this new and improved model of continuous competency.”
The proposed new board also says it wants to make sure this is appropriate to the area in which the clinician is practicing.
“To take a closed book certified exam every 10 years on the world of cardiology as happens at the current time – or the assessments conducted in the other two pathways – is often meaningless to the cardiologist,” Dr. Kuvin says. “All three current pathways involve high stakes questions that are often irrelevant to one’s clinical practice.”
Lifelong Learning
“The crux of the changes we are proposing will be away from the focus of passing a test towards a model of helping the individual with their competency, with continuous learning and evaluation of competency to help the clinician fill in their knowledge gaps,” he explains.
He described the new approach as “lifelong learning,” adding that, instead of it being “a punitive pass/fail environment with no feedback, which causes a lot of discontent among clinicians,” it will be a supportive process, where a clinician will be helped in filling their knowledge gaps.
“I think this would be a welcome change not just for cardiology but across medical specialties,” Dr. Kuvin said.
He also pointed out the ABMS itself is considering a continuous competency approach, and the proposed new cardiology board aims to work with the ABMS to make sure that their goals of continuous competency assessment are matched.
“The world has changed. The ability to access information has changed. It is no longer imperative for a clinician to have every piece of knowledge in their brain, but rather to know how to get knowledge and to incorporate that knowledge into clinical practice,” Dr. Kuvin noted. “Competency should not involve knowledge alone as in a closed book exam. It is more about understanding the world that we live in, how to synthesize information, where we need to improve knowledge and how to do that.”
Dr. Kuvin acknowledged that asking clinicians questions is a very helpful tool to identify their knowledge base and their knowledge gaps. “But we believe the clinician needs to be given resources — that could be a conference, an article, a simulation — to fill that knowledge gap. Then we could ask clinicians some different questions and if they get those right then we have provided a service.”
Tactile skills for cardiologists needing to perform procedures – such as interventionalists or electrophysiologists may be incorporated by simulation in a technology-based scenario.
On how often these assessments would take place, Dr. Kuvin said that hadn’t been decided for sure.
“We certainly do not think an assessment every 10 years is appropriate. We envision, instead of an episodic model, it will be rather a lifelong journey of education and competency. This will involve frequent contact and making sure knowledge gaps are being filled. There are criteria being set out by the ABMS that there should be a certain number of touch points with individuals on an annual as well as a 5-year basis to make sure cardiologists are staying within specific guardrails. The exact nature of these is yet to be determined,” he said.
Dr. Kuvin added that it was not known yet what sort of hours would be required but added that “this will not be a significant time burden.”
What is the Timeframe?
The application to the ABMS for a separate cardiology board is still ongoing and has not yet received formal acceptance. Representatives from the five US cardiovascular societies are in the initial stages of formulating a transition board.
“The submission to the ABMS will take time for them to review. This could take up to a year or so,” Dr. Kuvin estimates.
This is the first time the ABMS has entertained the concept of a new board in many years, he noted. “It will be a paradigm shift for the whole country. I think that cardiology is really at the forefront and in a position where we can actually do this. If cardiovascular medicine is granted a new board, I think this will help change the approach of how physicians are assessed in terms of continuous competency not just in cardiology but across all specialties of medicine.”
He added: “We are confident that we can work within the construct of the ABMS guidelines that have been revised to be much more holistic in the approach of continuous competence across the board. This includes thinking beyond rote medical knowledge and thinking about the clinician as a whole and their abilities to communicate, act professionally, work within a complex medical system, utilize medical resources effectively. These all have to be part of continuous competence.”
How Much Will This Cost?
Noting that the ABIM has received criticism over the costs of the certification process, Dr. Kuvin said they intend to make this “as lean a machine as possible with the focus on reducing the financial [burden] as well as the time burden for cardiologists. It is very important that this is not cumbersome, that it is woven into clinical practice, and that it is not costly.”
But he pointed out that building a new board will have significant costs.
“We have to think about developing initial board certification examinations as well as changing the paradigm on continuous certification,” he said. “This will take some up-front costs, and our society partners have decided that they are willing to provide some start-up funds for this. We anticipate the initial certification will remain somewhat similar in price, but the cost of ongoing continuous competency assessment will be significantly reduced compared to today’s models.”
Dr. Kuvin said the collaboration of the five participating US cardiovascular societies was unprecedented. But he noted that while the transition board is beginning with representatives of these individual societies, it will ultimately be independent from these societies and have its own board of directors.
He suggested that other societies representing other parts of cardiology are also interested. “Cardiology has recognized how important this is,” he said. “Everybody is excited about this.”
A version of this article appeared on Medscape.com.
The proposal by the major cardiovascular societies in the US to form a new board of cardiovascular medicine to manage initial and ongoing certification of cardiologists represents something of a revolution in the field of continuing medical education and assessment of competency.
Five US cardiovascular societies — the American College of Cardiology (ACC), the American Heart Association (AHA), the Heart Failure Society of America (HFSA), the Heart Rhythm Society (HRS), and the Society for Cardiovascular Angiography & Interventions (SCAI) — have now joined forces to propose a new professional certification board for cardiovascular medicine, to be known as the American Board of Cardiovascular Medicine (ABCVM).
The ABCVM would be independent of the American Board of Internal Medicine (ABIM), the current organization providing maintenance of certification for cardiologists as well as many other internal medicine subspecialties. The ABIM’s maintenance of certification process has been widely criticized for many years and has been described as “needlessly burdensome and expensive.”
, according to Jeffrey Kuvin, MD, a trustee of the ACC, who has been heading up the working group to develop this plan.
Dr. Kuvin, who is chair of the cardiology at Northwell Health, Manhasset, New York, a large academic healthcare system, explained that maintenance of certification has been a topic of discussion across the cardiovascular community for many years, and the ACC has a working group focused on the next steps for evaluation of competency, which he chairs.
“The topic of evaluation of competence has been on the mind of the ACC for many years and hence a work group was developed to focus on this,” Dr. Kuvin noted. “A lot of evolution of the concepts and next steps have been drawn out of this working group. And now other cardiovascular societies have joined to show unification across the house of cardiology and that this is indeed the way that the cardiovascular profession should move.”
“Time to Separate from Internal Medicine”
The general concept behind the new cardiology board is to separate cardiology from the ABIM.
“This is rooted from the concept that cardiology has evolved so much over the last few decades into such a large multidimensional specialty that it really does demarcate itself from internal medicine, and as such, it deserves a separate board governed by cardiologists with collaboration across the entirely of cardiology,” Dr. Kuvin said.
Cardiology has had significant growth and expansion of technology, tools, medications, and the approach to patients in many specialities and subspecialties, he added. “We have defined training programs in many different areas within cardiology; we have our own guidelines, our own competency statements, and in many cases, cardiology exists as its own department outside of medicine in many institutions. It’s just time to separate cardiology from the umbrella of internal medicine.”
The new cardiology board would be separate from, and not report to, the ABIM; rather, it would report directly to the American Board of Medical Specialties (ABMS), the only recognized medical certification body in the US.
What Are the Proposed Changes
Under the present system, managed by the ABIM, clinicians must undergo two stages of certification to be a cardiologist. First, they have to pass the initial certification exam in general cardiology, and then exams in one of four subspecialties if they plan to enter one of these, including interventional cardiology, electrophysiology, advanced heart failure or adult congenital heart disease.
Next, clinicians enter the maintenance of certification phase, which can take three different forms: 1) taking another recertification exam every 10 years; 2) the collaborative maintenance pathway — a collaboration between ACC and ABIM, which includes evaluation, learning and a certified exam each year; or 3) longitudinal knowledge and assessment — in which the program interacts with the clinician on an ongoing basis, sending secured questions regularly.
All three of these pathways for maintenance of certification involve high stakes questions and a set bar for passing or failing.
Under the proposed new cardiology board, an initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured, with the new approach taking the form of continuous learning and assessment of competency.
“This is an iterative process, but we envision with a new American Board of Cardiovascular Medicine, we will pick up where the ABIM left off,” Dr. Kuvin notes. “That includes an initial certifying examination for the five areas that already exist under the ABIM system but with the opportunities to expand that to further specialties as well.”
He points out that there are several areas in cardiology that are currently not represented by these five areas that warrant some discussion, including multimodality imaging, vascular heart disease, and cardio-oncology.
“At present, everybody has to pass the general cardiology exam and then some may wish to further train and get certified in one of the other four other specific areas. But one topic that has been discussed over many years is how do we maintain competency in the areas in which clinicians practice over their lifetime as a cardiologist,” Dr. Kuvin commented.
He said the proposed cardiology board would like to adhere to some basic principles that are fundamental to the practice of medicine.
“We want to make sure that we are practicing medicine so that our patients derive the most benefit from seeing a cardiologist,” he said. “We also want to make sure, however, that this is a supportive process, supporting cardiologists to learn what they know and more importantly what they don’t know; to identify knowledge gaps in specific area; to help the cardiologist fill those knowledge gaps; to acknowledge those gaps have been filled; and then move on to another area of interest. This will be the focus of this new and improved model of continuous competency.”
The proposed new board also says it wants to make sure this is appropriate to the area in which the clinician is practicing.
“To take a closed book certified exam every 10 years on the world of cardiology as happens at the current time – or the assessments conducted in the other two pathways – is often meaningless to the cardiologist,” Dr. Kuvin says. “All three current pathways involve high stakes questions that are often irrelevant to one’s clinical practice.”
Lifelong Learning
“The crux of the changes we are proposing will be away from the focus of passing a test towards a model of helping the individual with their competency, with continuous learning and evaluation of competency to help the clinician fill in their knowledge gaps,” he explains.
He described the new approach as “lifelong learning,” adding that, instead of it being “a punitive pass/fail environment with no feedback, which causes a lot of discontent among clinicians,” it will be a supportive process, where a clinician will be helped in filling their knowledge gaps.
“I think this would be a welcome change not just for cardiology but across medical specialties,” Dr. Kuvin said.
He also pointed out the ABMS itself is considering a continuous competency approach, and the proposed new cardiology board aims to work with the ABMS to make sure that their goals of continuous competency assessment are matched.
“The world has changed. The ability to access information has changed. It is no longer imperative for a clinician to have every piece of knowledge in their brain, but rather to know how to get knowledge and to incorporate that knowledge into clinical practice,” Dr. Kuvin noted. “Competency should not involve knowledge alone as in a closed book exam. It is more about understanding the world that we live in, how to synthesize information, where we need to improve knowledge and how to do that.”
Dr. Kuvin acknowledged that asking clinicians questions is a very helpful tool to identify their knowledge base and their knowledge gaps. “But we believe the clinician needs to be given resources — that could be a conference, an article, a simulation — to fill that knowledge gap. Then we could ask clinicians some different questions and if they get those right then we have provided a service.”
Tactile skills for cardiologists needing to perform procedures – such as interventionalists or electrophysiologists may be incorporated by simulation in a technology-based scenario.
On how often these assessments would take place, Dr. Kuvin said that hadn’t been decided for sure.
“We certainly do not think an assessment every 10 years is appropriate. We envision, instead of an episodic model, it will be rather a lifelong journey of education and competency. This will involve frequent contact and making sure knowledge gaps are being filled. There are criteria being set out by the ABMS that there should be a certain number of touch points with individuals on an annual as well as a 5-year basis to make sure cardiologists are staying within specific guardrails. The exact nature of these is yet to be determined,” he said.
Dr. Kuvin added that it was not known yet what sort of hours would be required but added that “this will not be a significant time burden.”
What is the Timeframe?
The application to the ABMS for a separate cardiology board is still ongoing and has not yet received formal acceptance. Representatives from the five US cardiovascular societies are in the initial stages of formulating a transition board.
“The submission to the ABMS will take time for them to review. This could take up to a year or so,” Dr. Kuvin estimates.
This is the first time the ABMS has entertained the concept of a new board in many years, he noted. “It will be a paradigm shift for the whole country. I think that cardiology is really at the forefront and in a position where we can actually do this. If cardiovascular medicine is granted a new board, I think this will help change the approach of how physicians are assessed in terms of continuous competency not just in cardiology but across all specialties of medicine.”
He added: “We are confident that we can work within the construct of the ABMS guidelines that have been revised to be much more holistic in the approach of continuous competence across the board. This includes thinking beyond rote medical knowledge and thinking about the clinician as a whole and their abilities to communicate, act professionally, work within a complex medical system, utilize medical resources effectively. These all have to be part of continuous competence.”
How Much Will This Cost?
Noting that the ABIM has received criticism over the costs of the certification process, Dr. Kuvin said they intend to make this “as lean a machine as possible with the focus on reducing the financial [burden] as well as the time burden for cardiologists. It is very important that this is not cumbersome, that it is woven into clinical practice, and that it is not costly.”
But he pointed out that building a new board will have significant costs.
“We have to think about developing initial board certification examinations as well as changing the paradigm on continuous certification,” he said. “This will take some up-front costs, and our society partners have decided that they are willing to provide some start-up funds for this. We anticipate the initial certification will remain somewhat similar in price, but the cost of ongoing continuous competency assessment will be significantly reduced compared to today’s models.”
Dr. Kuvin said the collaboration of the five participating US cardiovascular societies was unprecedented. But he noted that while the transition board is beginning with representatives of these individual societies, it will ultimately be independent from these societies and have its own board of directors.
He suggested that other societies representing other parts of cardiology are also interested. “Cardiology has recognized how important this is,” he said. “Everybody is excited about this.”
A version of this article appeared on Medscape.com.
The proposal by the major cardiovascular societies in the US to form a new board of cardiovascular medicine to manage initial and ongoing certification of cardiologists represents something of a revolution in the field of continuing medical education and assessment of competency.
Five US cardiovascular societies — the American College of Cardiology (ACC), the American Heart Association (AHA), the Heart Failure Society of America (HFSA), the Heart Rhythm Society (HRS), and the Society for Cardiovascular Angiography & Interventions (SCAI) — have now joined forces to propose a new professional certification board for cardiovascular medicine, to be known as the American Board of Cardiovascular Medicine (ABCVM).
The ABCVM would be independent of the American Board of Internal Medicine (ABIM), the current organization providing maintenance of certification for cardiologists as well as many other internal medicine subspecialties. The ABIM’s maintenance of certification process has been widely criticized for many years and has been described as “needlessly burdensome and expensive.”
, according to Jeffrey Kuvin, MD, a trustee of the ACC, who has been heading up the working group to develop this plan.
Dr. Kuvin, who is chair of the cardiology at Northwell Health, Manhasset, New York, a large academic healthcare system, explained that maintenance of certification has been a topic of discussion across the cardiovascular community for many years, and the ACC has a working group focused on the next steps for evaluation of competency, which he chairs.
“The topic of evaluation of competence has been on the mind of the ACC for many years and hence a work group was developed to focus on this,” Dr. Kuvin noted. “A lot of evolution of the concepts and next steps have been drawn out of this working group. And now other cardiovascular societies have joined to show unification across the house of cardiology and that this is indeed the way that the cardiovascular profession should move.”
“Time to Separate from Internal Medicine”
The general concept behind the new cardiology board is to separate cardiology from the ABIM.
“This is rooted from the concept that cardiology has evolved so much over the last few decades into such a large multidimensional specialty that it really does demarcate itself from internal medicine, and as such, it deserves a separate board governed by cardiologists with collaboration across the entirely of cardiology,” Dr. Kuvin said.
Cardiology has had significant growth and expansion of technology, tools, medications, and the approach to patients in many specialities and subspecialties, he added. “We have defined training programs in many different areas within cardiology; we have our own guidelines, our own competency statements, and in many cases, cardiology exists as its own department outside of medicine in many institutions. It’s just time to separate cardiology from the umbrella of internal medicine.”
The new cardiology board would be separate from, and not report to, the ABIM; rather, it would report directly to the American Board of Medical Specialties (ABMS), the only recognized medical certification body in the US.
What Are the Proposed Changes
Under the present system, managed by the ABIM, clinicians must undergo two stages of certification to be a cardiologist. First, they have to pass the initial certification exam in general cardiology, and then exams in one of four subspecialties if they plan to enter one of these, including interventional cardiology, electrophysiology, advanced heart failure or adult congenital heart disease.
Next, clinicians enter the maintenance of certification phase, which can take three different forms: 1) taking another recertification exam every 10 years; 2) the collaborative maintenance pathway — a collaboration between ACC and ABIM, which includes evaluation, learning and a certified exam each year; or 3) longitudinal knowledge and assessment — in which the program interacts with the clinician on an ongoing basis, sending secured questions regularly.
All three of these pathways for maintenance of certification involve high stakes questions and a set bar for passing or failing.
Under the proposed new cardiology board, an initial certification exam would still be required after fellowship training, but the maintenance of certification process would be completely restructured, with the new approach taking the form of continuous learning and assessment of competency.
“This is an iterative process, but we envision with a new American Board of Cardiovascular Medicine, we will pick up where the ABIM left off,” Dr. Kuvin notes. “That includes an initial certifying examination for the five areas that already exist under the ABIM system but with the opportunities to expand that to further specialties as well.”
He points out that there are several areas in cardiology that are currently not represented by these five areas that warrant some discussion, including multimodality imaging, vascular heart disease, and cardio-oncology.
“At present, everybody has to pass the general cardiology exam and then some may wish to further train and get certified in one of the other four other specific areas. But one topic that has been discussed over many years is how do we maintain competency in the areas in which clinicians practice over their lifetime as a cardiologist,” Dr. Kuvin commented.
He said the proposed cardiology board would like to adhere to some basic principles that are fundamental to the practice of medicine.
“We want to make sure that we are practicing medicine so that our patients derive the most benefit from seeing a cardiologist,” he said. “We also want to make sure, however, that this is a supportive process, supporting cardiologists to learn what they know and more importantly what they don’t know; to identify knowledge gaps in specific area; to help the cardiologist fill those knowledge gaps; to acknowledge those gaps have been filled; and then move on to another area of interest. This will be the focus of this new and improved model of continuous competency.”
The proposed new board also says it wants to make sure this is appropriate to the area in which the clinician is practicing.
“To take a closed book certified exam every 10 years on the world of cardiology as happens at the current time – or the assessments conducted in the other two pathways – is often meaningless to the cardiologist,” Dr. Kuvin says. “All three current pathways involve high stakes questions that are often irrelevant to one’s clinical practice.”
Lifelong Learning
“The crux of the changes we are proposing will be away from the focus of passing a test towards a model of helping the individual with their competency, with continuous learning and evaluation of competency to help the clinician fill in their knowledge gaps,” he explains.
He described the new approach as “lifelong learning,” adding that, instead of it being “a punitive pass/fail environment with no feedback, which causes a lot of discontent among clinicians,” it will be a supportive process, where a clinician will be helped in filling their knowledge gaps.
“I think this would be a welcome change not just for cardiology but across medical specialties,” Dr. Kuvin said.
He also pointed out the ABMS itself is considering a continuous competency approach, and the proposed new cardiology board aims to work with the ABMS to make sure that their goals of continuous competency assessment are matched.
“The world has changed. The ability to access information has changed. It is no longer imperative for a clinician to have every piece of knowledge in their brain, but rather to know how to get knowledge and to incorporate that knowledge into clinical practice,” Dr. Kuvin noted. “Competency should not involve knowledge alone as in a closed book exam. It is more about understanding the world that we live in, how to synthesize information, where we need to improve knowledge and how to do that.”
Dr. Kuvin acknowledged that asking clinicians questions is a very helpful tool to identify their knowledge base and their knowledge gaps. “But we believe the clinician needs to be given resources — that could be a conference, an article, a simulation — to fill that knowledge gap. Then we could ask clinicians some different questions and if they get those right then we have provided a service.”
Tactile skills for cardiologists needing to perform procedures – such as interventionalists or electrophysiologists may be incorporated by simulation in a technology-based scenario.
On how often these assessments would take place, Dr. Kuvin said that hadn’t been decided for sure.
“We certainly do not think an assessment every 10 years is appropriate. We envision, instead of an episodic model, it will be rather a lifelong journey of education and competency. This will involve frequent contact and making sure knowledge gaps are being filled. There are criteria being set out by the ABMS that there should be a certain number of touch points with individuals on an annual as well as a 5-year basis to make sure cardiologists are staying within specific guardrails. The exact nature of these is yet to be determined,” he said.
Dr. Kuvin added that it was not known yet what sort of hours would be required but added that “this will not be a significant time burden.”
What is the Timeframe?
The application to the ABMS for a separate cardiology board is still ongoing and has not yet received formal acceptance. Representatives from the five US cardiovascular societies are in the initial stages of formulating a transition board.
“The submission to the ABMS will take time for them to review. This could take up to a year or so,” Dr. Kuvin estimates.
This is the first time the ABMS has entertained the concept of a new board in many years, he noted. “It will be a paradigm shift for the whole country. I think that cardiology is really at the forefront and in a position where we can actually do this. If cardiovascular medicine is granted a new board, I think this will help change the approach of how physicians are assessed in terms of continuous competency not just in cardiology but across all specialties of medicine.”
He added: “We are confident that we can work within the construct of the ABMS guidelines that have been revised to be much more holistic in the approach of continuous competence across the board. This includes thinking beyond rote medical knowledge and thinking about the clinician as a whole and their abilities to communicate, act professionally, work within a complex medical system, utilize medical resources effectively. These all have to be part of continuous competence.”
How Much Will This Cost?
Noting that the ABIM has received criticism over the costs of the certification process, Dr. Kuvin said they intend to make this “as lean a machine as possible with the focus on reducing the financial [burden] as well as the time burden for cardiologists. It is very important that this is not cumbersome, that it is woven into clinical practice, and that it is not costly.”
But he pointed out that building a new board will have significant costs.
“We have to think about developing initial board certification examinations as well as changing the paradigm on continuous certification,” he said. “This will take some up-front costs, and our society partners have decided that they are willing to provide some start-up funds for this. We anticipate the initial certification will remain somewhat similar in price, but the cost of ongoing continuous competency assessment will be significantly reduced compared to today’s models.”
Dr. Kuvin said the collaboration of the five participating US cardiovascular societies was unprecedented. But he noted that while the transition board is beginning with representatives of these individual societies, it will ultimately be independent from these societies and have its own board of directors.
He suggested that other societies representing other parts of cardiology are also interested. “Cardiology has recognized how important this is,” he said. “Everybody is excited about this.”
A version of this article appeared on Medscape.com.
Antihypertensives show similar long-term mortality rates
Long-term data showed negligible differences in mortality among hypertensive adults treated with thiazide-type diuretics, calcium channel blockers, or angiotensin-converting enzyme inhibitors in a review of nearly 33,000 individuals published in JAMA Network Open.
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) study was designed to compare initial antihypertensive treatments with a calcium channel blocker (CCB; amlodipine), an angiotensin-converting enzyme (ACE) inhibitor (lisinopril) or an alpha-blocker (doxazosin), and a thiazide-type diuretic (chlorthalidone).
The composite primary outcome was fatal coronary heart disease (CHD) or nonfatal myocardial infarction (MI), but long-term data were lacking, wrote Jose-Miguel Yamal, PhD, of University of Texas Health Science Center at Houston, and colleagues. A previous study with 8-13 years of follow-up showed no significant differences in mortality between the treatment groups, the researchers noted.
In the current study, a prespecified secondary analysis of ALLHAT, the researchers added 11 more years of data for a total of 19-24 years of follow-up after randomization.
In the original ALLHAT, 32,804 adults aged 55 years and older with a diagnosis of hypertension and at least one additional coronary heart disease risk factor were followed for 4-8 years for all-cause mortality. A subgroup of 22,754 were followed for fatal or nonfatal cardiovascular disease (CVD) for a mean of 13.7 years, with a maximum of 23.9 years.
The study occurred from Feb. 23, 1994, to Dec. 31, 2017. The participants were randomized to receive a thiazide-type diuretic (15,002 patients), a CCB (8,898 patients), or an ACE inhibitor (8,904 patients).
The primary outcome was CVD mortality; secondary outcomes included all-cause mortality, combined fatal and nonfatal CVD (CVD morbidity), and both morbidity and mortality for coronary heart disease, stroke, heart failure, end-stage renal disease, and cancer.
At 23 years, CVD mortality rates per 100 persons were 23.7, 21.6, and 23.8 in the diuretic, CCB, and ACE inhibitor groups, respectively. The adjusted hazard ratios were 0.97 for CCB vs. diuretics and 1.06 for ACE inhibitors vs. diuretics.
Although the risk of stroke mortality and of combined fatal and nonfatal hospitalized stroke was higher in the ACE inhibitor group compared with the diuretic group (adjusted hazard ratios 1.19 and 1.11, respectively), this increase was no longer significant after adjustment for multiple comparisons. “In contrast to the in-trial and 8-year to 13-year analyses, we now observed that the lisinopril group had an increased risk of kidney disease mortality that emerged after approximately 13 years after randomization, but this effect was attenuated after adjustment for baseline variables,” the researchers wrote in their discussion.
The findings were limited by several factors including the potential effect of unblinding if participants stopped the randomized drug, and by the lack of morbidity and mortality data on Canadian participants, Veterans Affairs participants, and those with no Medicare number, the researchers noted. Other limitations included the lack of data on posttrial medication use, blood pressure, and laboratory findings, they said.
However, the results over the follow-up period of up to 23 years supported those of the larger ALLHAT study, with similar outcomes among the drugs, and with 11 years of passive follow-up, “the results for lisinopril vs. chlorthalidone for stroke and stroke mortality are almost the same,” they concluded.
Findings support current practice, but new drug data are needed
The current study was important to determine whether there was a significant difference in long-term morbidity and mortality between patients treated with thiazide diuretics, calcium channel blockers and ACE inhibitors, Noel Deep, MD, said in an interview.
“Previously reported data had indicated no significant differences between patients randomized to one of these three classes of antihypertensive medications during the trial period or at 8-13 years post trial,” said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep is chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
“This study reinforces the previously noted benefits of the three classes of antihypertensive medications, as well as the higher rates of cardiovascular disease and stroke in the ACE inhibitor arm,” he said.
In clinical practice, the results suggest that thiazide diuretics should be considered first-line agents for management of hypertension based on their noninferiority compared with ACE inhibitors and CCBs, and lower risk of stroke compared with ACE inhibitors, Dr. Deep said in an interview. “All three classes of antihypertensive medications are equally efficacious in blood pressure control and preventing all-cause mortality,” he said.
More research is needed in the wake of the introduction of other classes of antihypertensives since the original ALLHAT trial, Dr. Deep said. “It would be beneficial to assess the relative benefit/risks of those medications compared to the thiazide diuretics, and I would also look at studies comparing beta blockers to the thiazide diuretics,” he said. The question remains as to whether outcomes were affected by patients’ use of other classes of antihypertensives after the trial period, he said.
The study was supported by the National Institute on Aging of the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the editorial advisory board of Internal Medicine News.
Long-term data showed negligible differences in mortality among hypertensive adults treated with thiazide-type diuretics, calcium channel blockers, or angiotensin-converting enzyme inhibitors in a review of nearly 33,000 individuals published in JAMA Network Open.
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) study was designed to compare initial antihypertensive treatments with a calcium channel blocker (CCB; amlodipine), an angiotensin-converting enzyme (ACE) inhibitor (lisinopril) or an alpha-blocker (doxazosin), and a thiazide-type diuretic (chlorthalidone).
The composite primary outcome was fatal coronary heart disease (CHD) or nonfatal myocardial infarction (MI), but long-term data were lacking, wrote Jose-Miguel Yamal, PhD, of University of Texas Health Science Center at Houston, and colleagues. A previous study with 8-13 years of follow-up showed no significant differences in mortality between the treatment groups, the researchers noted.
In the current study, a prespecified secondary analysis of ALLHAT, the researchers added 11 more years of data for a total of 19-24 years of follow-up after randomization.
In the original ALLHAT, 32,804 adults aged 55 years and older with a diagnosis of hypertension and at least one additional coronary heart disease risk factor were followed for 4-8 years for all-cause mortality. A subgroup of 22,754 were followed for fatal or nonfatal cardiovascular disease (CVD) for a mean of 13.7 years, with a maximum of 23.9 years.
The study occurred from Feb. 23, 1994, to Dec. 31, 2017. The participants were randomized to receive a thiazide-type diuretic (15,002 patients), a CCB (8,898 patients), or an ACE inhibitor (8,904 patients).
The primary outcome was CVD mortality; secondary outcomes included all-cause mortality, combined fatal and nonfatal CVD (CVD morbidity), and both morbidity and mortality for coronary heart disease, stroke, heart failure, end-stage renal disease, and cancer.
At 23 years, CVD mortality rates per 100 persons were 23.7, 21.6, and 23.8 in the diuretic, CCB, and ACE inhibitor groups, respectively. The adjusted hazard ratios were 0.97 for CCB vs. diuretics and 1.06 for ACE inhibitors vs. diuretics.
Although the risk of stroke mortality and of combined fatal and nonfatal hospitalized stroke was higher in the ACE inhibitor group compared with the diuretic group (adjusted hazard ratios 1.19 and 1.11, respectively), this increase was no longer significant after adjustment for multiple comparisons. “In contrast to the in-trial and 8-year to 13-year analyses, we now observed that the lisinopril group had an increased risk of kidney disease mortality that emerged after approximately 13 years after randomization, but this effect was attenuated after adjustment for baseline variables,” the researchers wrote in their discussion.
The findings were limited by several factors including the potential effect of unblinding if participants stopped the randomized drug, and by the lack of morbidity and mortality data on Canadian participants, Veterans Affairs participants, and those with no Medicare number, the researchers noted. Other limitations included the lack of data on posttrial medication use, blood pressure, and laboratory findings, they said.
However, the results over the follow-up period of up to 23 years supported those of the larger ALLHAT study, with similar outcomes among the drugs, and with 11 years of passive follow-up, “the results for lisinopril vs. chlorthalidone for stroke and stroke mortality are almost the same,” they concluded.
Findings support current practice, but new drug data are needed
The current study was important to determine whether there was a significant difference in long-term morbidity and mortality between patients treated with thiazide diuretics, calcium channel blockers and ACE inhibitors, Noel Deep, MD, said in an interview.
“Previously reported data had indicated no significant differences between patients randomized to one of these three classes of antihypertensive medications during the trial period or at 8-13 years post trial,” said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep is chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
“This study reinforces the previously noted benefits of the three classes of antihypertensive medications, as well as the higher rates of cardiovascular disease and stroke in the ACE inhibitor arm,” he said.
In clinical practice, the results suggest that thiazide diuretics should be considered first-line agents for management of hypertension based on their noninferiority compared with ACE inhibitors and CCBs, and lower risk of stroke compared with ACE inhibitors, Dr. Deep said in an interview. “All three classes of antihypertensive medications are equally efficacious in blood pressure control and preventing all-cause mortality,” he said.
More research is needed in the wake of the introduction of other classes of antihypertensives since the original ALLHAT trial, Dr. Deep said. “It would be beneficial to assess the relative benefit/risks of those medications compared to the thiazide diuretics, and I would also look at studies comparing beta blockers to the thiazide diuretics,” he said. The question remains as to whether outcomes were affected by patients’ use of other classes of antihypertensives after the trial period, he said.
The study was supported by the National Institute on Aging of the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the editorial advisory board of Internal Medicine News.
Long-term data showed negligible differences in mortality among hypertensive adults treated with thiazide-type diuretics, calcium channel blockers, or angiotensin-converting enzyme inhibitors in a review of nearly 33,000 individuals published in JAMA Network Open.
The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT) study was designed to compare initial antihypertensive treatments with a calcium channel blocker (CCB; amlodipine), an angiotensin-converting enzyme (ACE) inhibitor (lisinopril) or an alpha-blocker (doxazosin), and a thiazide-type diuretic (chlorthalidone).
The composite primary outcome was fatal coronary heart disease (CHD) or nonfatal myocardial infarction (MI), but long-term data were lacking, wrote Jose-Miguel Yamal, PhD, of University of Texas Health Science Center at Houston, and colleagues. A previous study with 8-13 years of follow-up showed no significant differences in mortality between the treatment groups, the researchers noted.
In the current study, a prespecified secondary analysis of ALLHAT, the researchers added 11 more years of data for a total of 19-24 years of follow-up after randomization.
In the original ALLHAT, 32,804 adults aged 55 years and older with a diagnosis of hypertension and at least one additional coronary heart disease risk factor were followed for 4-8 years for all-cause mortality. A subgroup of 22,754 were followed for fatal or nonfatal cardiovascular disease (CVD) for a mean of 13.7 years, with a maximum of 23.9 years.
The study occurred from Feb. 23, 1994, to Dec. 31, 2017. The participants were randomized to receive a thiazide-type diuretic (15,002 patients), a CCB (8,898 patients), or an ACE inhibitor (8,904 patients).
The primary outcome was CVD mortality; secondary outcomes included all-cause mortality, combined fatal and nonfatal CVD (CVD morbidity), and both morbidity and mortality for coronary heart disease, stroke, heart failure, end-stage renal disease, and cancer.
At 23 years, CVD mortality rates per 100 persons were 23.7, 21.6, and 23.8 in the diuretic, CCB, and ACE inhibitor groups, respectively. The adjusted hazard ratios were 0.97 for CCB vs. diuretics and 1.06 for ACE inhibitors vs. diuretics.
Although the risk of stroke mortality and of combined fatal and nonfatal hospitalized stroke was higher in the ACE inhibitor group compared with the diuretic group (adjusted hazard ratios 1.19 and 1.11, respectively), this increase was no longer significant after adjustment for multiple comparisons. “In contrast to the in-trial and 8-year to 13-year analyses, we now observed that the lisinopril group had an increased risk of kidney disease mortality that emerged after approximately 13 years after randomization, but this effect was attenuated after adjustment for baseline variables,” the researchers wrote in their discussion.
The findings were limited by several factors including the potential effect of unblinding if participants stopped the randomized drug, and by the lack of morbidity and mortality data on Canadian participants, Veterans Affairs participants, and those with no Medicare number, the researchers noted. Other limitations included the lack of data on posttrial medication use, blood pressure, and laboratory findings, they said.
However, the results over the follow-up period of up to 23 years supported those of the larger ALLHAT study, with similar outcomes among the drugs, and with 11 years of passive follow-up, “the results for lisinopril vs. chlorthalidone for stroke and stroke mortality are almost the same,” they concluded.
Findings support current practice, but new drug data are needed
The current study was important to determine whether there was a significant difference in long-term morbidity and mortality between patients treated with thiazide diuretics, calcium channel blockers and ACE inhibitors, Noel Deep, MD, said in an interview.
“Previously reported data had indicated no significant differences between patients randomized to one of these three classes of antihypertensive medications during the trial period or at 8-13 years post trial,” said Dr. Deep, a general internist in private practice in Antigo, Wisc., who was not involved in the study. Dr. Deep is chief medical officer and a staff physician at Aspirus Langlade Hospital in Antigo.
“This study reinforces the previously noted benefits of the three classes of antihypertensive medications, as well as the higher rates of cardiovascular disease and stroke in the ACE inhibitor arm,” he said.
In clinical practice, the results suggest that thiazide diuretics should be considered first-line agents for management of hypertension based on their noninferiority compared with ACE inhibitors and CCBs, and lower risk of stroke compared with ACE inhibitors, Dr. Deep said in an interview. “All three classes of antihypertensive medications are equally efficacious in blood pressure control and preventing all-cause mortality,” he said.
More research is needed in the wake of the introduction of other classes of antihypertensives since the original ALLHAT trial, Dr. Deep said. “It would be beneficial to assess the relative benefit/risks of those medications compared to the thiazide diuretics, and I would also look at studies comparing beta blockers to the thiazide diuretics,” he said. The question remains as to whether outcomes were affected by patients’ use of other classes of antihypertensives after the trial period, he said.
The study was supported by the National Institute on Aging of the National Institutes of Health. The researchers had no financial conflicts to disclose. Dr. Deep had no financial conflicts to disclose and serves on the editorial advisory board of Internal Medicine News.
FROM JAMA NETWORK OPEN
Vegan diet confers cardiometabolic benefits
TOPLINE:
Compared with a healthy omnivore diet, low-density lipoprotein cholesterol (LDL-C) as well as fasting insulin and weight loss in a randomized controlled trial of identical twins.
METHODOLOGY:
- Researchers randomly assigned 22 pairs of healthy adult identical twins (34 women, mean age 39 years, mean body mass index 25.9) to a healthy vegan or omnivore diet (1 twin per pair) for 8 weeks.
- For the first 4 weeks, diet-specific meals were provided via a meal delivery service. For the final 4 weeks, participants prepared their own diet-appropriate meals/snacks.
- The primary outcome was change in LDL-C; secondary outcomes included changes in body weight and fasting insulin.
TAKEAWAY:
- After 8 weeks, twins eating a vegan diet showed a significant mean decrease of 13.9 mg/dL in LDL-C compared with twins eating an omnivorous diet.
- The vegan diet also led to a significant mean decrease of 2.9 Times New RomanμIU/mL in fasting insulin and 1.9 kg in body weight after 8 weeks compared with the omnivore diet, although weight loss was observed in both diet groups.
- The vegan diet group also had a larger but nonsignificant absolute median decrease in fasting HDL-C triglycerides, vitamin B12, glucose, and trimethylamine N-oxide levels at 8 weeks.
IN PRACTICE:
“Our results corroborate a previous finding showing that eating a vegan diet can improve cardiovascular health. Clinicians may consider recommending plant-based diets to reduce cardiometabolic risk factors, as well as aligning with environmental benefits,” the researchers concluded.
SOURCE:
The study, with first author Matthew J. Landry, PhD, RDN, Stanford Prevention Research Center, Stanford University School of Medicine, California, was published online November 30 in JAMA Network Open.
LIMITATIONS:
The adult twin population was generally healthy and findings may not be generalizable to other populations. The sample size was small, and the duration of intervention was short and there was no follow-up period, which limits insights on stability and sustainability of the diets.
DISCLOSURES:
Funding was provided by the Vogt Foundation, and grants from Stanford University and the National Heart, Lung, and Blood Institute. Dr. Landry has no relevant disclosures. One author reported receiving funding from Beyond Meat outside of this study.
A version of this article appeared on Medscape.com.
TOPLINE:
Compared with a healthy omnivore diet, low-density lipoprotein cholesterol (LDL-C) as well as fasting insulin and weight loss in a randomized controlled trial of identical twins.
METHODOLOGY:
- Researchers randomly assigned 22 pairs of healthy adult identical twins (34 women, mean age 39 years, mean body mass index 25.9) to a healthy vegan or omnivore diet (1 twin per pair) for 8 weeks.
- For the first 4 weeks, diet-specific meals were provided via a meal delivery service. For the final 4 weeks, participants prepared their own diet-appropriate meals/snacks.
- The primary outcome was change in LDL-C; secondary outcomes included changes in body weight and fasting insulin.
TAKEAWAY:
- After 8 weeks, twins eating a vegan diet showed a significant mean decrease of 13.9 mg/dL in LDL-C compared with twins eating an omnivorous diet.
- The vegan diet also led to a significant mean decrease of 2.9 Times New RomanμIU/mL in fasting insulin and 1.9 kg in body weight after 8 weeks compared with the omnivore diet, although weight loss was observed in both diet groups.
- The vegan diet group also had a larger but nonsignificant absolute median decrease in fasting HDL-C triglycerides, vitamin B12, glucose, and trimethylamine N-oxide levels at 8 weeks.
IN PRACTICE:
“Our results corroborate a previous finding showing that eating a vegan diet can improve cardiovascular health. Clinicians may consider recommending plant-based diets to reduce cardiometabolic risk factors, as well as aligning with environmental benefits,” the researchers concluded.
SOURCE:
The study, with first author Matthew J. Landry, PhD, RDN, Stanford Prevention Research Center, Stanford University School of Medicine, California, was published online November 30 in JAMA Network Open.
LIMITATIONS:
The adult twin population was generally healthy and findings may not be generalizable to other populations. The sample size was small, and the duration of intervention was short and there was no follow-up period, which limits insights on stability and sustainability of the diets.
DISCLOSURES:
Funding was provided by the Vogt Foundation, and grants from Stanford University and the National Heart, Lung, and Blood Institute. Dr. Landry has no relevant disclosures. One author reported receiving funding from Beyond Meat outside of this study.
A version of this article appeared on Medscape.com.
TOPLINE:
Compared with a healthy omnivore diet, low-density lipoprotein cholesterol (LDL-C) as well as fasting insulin and weight loss in a randomized controlled trial of identical twins.
METHODOLOGY:
- Researchers randomly assigned 22 pairs of healthy adult identical twins (34 women, mean age 39 years, mean body mass index 25.9) to a healthy vegan or omnivore diet (1 twin per pair) for 8 weeks.
- For the first 4 weeks, diet-specific meals were provided via a meal delivery service. For the final 4 weeks, participants prepared their own diet-appropriate meals/snacks.
- The primary outcome was change in LDL-C; secondary outcomes included changes in body weight and fasting insulin.
TAKEAWAY:
- After 8 weeks, twins eating a vegan diet showed a significant mean decrease of 13.9 mg/dL in LDL-C compared with twins eating an omnivorous diet.
- The vegan diet also led to a significant mean decrease of 2.9 Times New RomanμIU/mL in fasting insulin and 1.9 kg in body weight after 8 weeks compared with the omnivore diet, although weight loss was observed in both diet groups.
- The vegan diet group also had a larger but nonsignificant absolute median decrease in fasting HDL-C triglycerides, vitamin B12, glucose, and trimethylamine N-oxide levels at 8 weeks.
IN PRACTICE:
“Our results corroborate a previous finding showing that eating a vegan diet can improve cardiovascular health. Clinicians may consider recommending plant-based diets to reduce cardiometabolic risk factors, as well as aligning with environmental benefits,” the researchers concluded.
SOURCE:
The study, with first author Matthew J. Landry, PhD, RDN, Stanford Prevention Research Center, Stanford University School of Medicine, California, was published online November 30 in JAMA Network Open.
LIMITATIONS:
The adult twin population was generally healthy and findings may not be generalizable to other populations. The sample size was small, and the duration of intervention was short and there was no follow-up period, which limits insights on stability and sustainability of the diets.
DISCLOSURES:
Funding was provided by the Vogt Foundation, and grants from Stanford University and the National Heart, Lung, and Blood Institute. Dr. Landry has no relevant disclosures. One author reported receiving funding from Beyond Meat outside of this study.
A version of this article appeared on Medscape.com.
Pulmonary arterial hypertension: Promising results for investigational agents and catheter-based denervation
PHILADELPHIA — Promise that the unmet need for more effective pulmonary artery hypertension treatments may soon be met was in strong evidence in research into three strategies presented at this year’s recent American Heart Association scientific sessions; one was based on an ancient Chinese herb epimedium (yin yang huo or horny goat weed) commonly used for treating sexual dysfunction and directly related to the phosphodiesterase inhibitors sildenafil, vardenafil, and tadalafil (sold as Viagra, Levitra, and Cialis). A second studied sotatercept, an investigational, potential first-in-class activin signaling inhibitor biologic, and a third evaluated physically ablating the baroreceptor nerves that stimulate vasoconstriction of the pulmonary artery via catheter-based techniques.
Until as recently as the late 1970s, a pulmonary arterial hypertension diagnosis was a uniformly fatal one.1 While associated with pulmonary and right ventricle remodeling, and leads toward heart failure and death. The complex underlying pathogenesis was divided into six groups by the 6th World Symposium on Pulmonary Hypertension (WSPH) in 2018, and includes as its most common features pulmonary artery endothelial cell dysfunction, pulmonary artery smooth muscle cell proliferation and migration, and dysregulated fibroblast activity leading to dysregulated vasoconstriction, micro and in-situ vascular thrombosis, vascular fibrosis and pathogenic remodeling of pulmonary vessels.1 The threshold mean arterial pressure (mPAP) for pulmonary arterial hypertension was defined by the 6th [WSPH] at mPAP ≥ 20 mm Hg, twice the upper limit of a normal mPAP of 14.0 ± 3.3 mm Hg as reported by Kovacs et al. in 2018.2
Pathways for current therapies
Current drugs for pulmonary arterial hypertension focus on three signaling pathways, including the endothelin receptor, prostacyclin and nitric oxide pathways, stated Zhi-Cheng Jing, MD, professor of medicine, head of the cardiology department at Peking Union Medical College Hospital, Peking, China. While the phosphodiesterase 5 inhibitors sildenafil and tadalafil, which target the nitric oxide pathway, came into wide use after Food and Drug Administration approval, the need for higher PDE5-selectivity remains, Dr. Jing said. Structurally modified from the active ingredient in epimedium, TPN171H is an investigational PDE5 inhibitor which has shown several favorable features: a greater PDE5 selectivity than both sildenafil and tadalafil in vitro, an ability to decrease right ventricular systolic pressure and alleviate arterial remodeling in animal studies, and safety and tolerability in healthy human subjects.
The current randomized, double-blind, placebo-and active-controlled phase IIa study assessed the hemodynamic impact of a single oral dose of TPN171H in 60 pulmonary arterial hypertension patients (mean age ~34 years, 83.3% female), all with negative vasodilation test results and in WHO class 2 or 3. Only patients aged 18-75 years with group 1 pulmonary arterial hypertension of idiopathic, connective tissue disorder, or repaired congenital heart defects etiology were included. Patients were divided into six groups: placebo, TPN171H at 2.5, 5, and 10 milligrams, and tadalafil at 20 and 40 milligrams.
For the primary endpoint of maximum decrease in pulmonary vascular resistance (PVR), significant reductions vs. placebo were found only for the TPN171H 5-mg group (–41.2% vs. –24.4%; P = .008) and for the 20-mg (–39.8%) and 40-mg (–37.6%) tadalafil groups (both P < .05). What was not seen in the tadalafil groups, but was evident in the TPN171H 5-mg group, was a significant reduction in the secondary endpoint of PVR/SVR (systolic vascular resistance) at 2, 3, and 5 hours (all P < .05). “As we know,” Dr. Jing said in an interview, “the PDE5 inhibitor functions as a vasodilator, having an impact on both pulmonary circulation and systemic circulation. So, to evaluate the selectivity for pulmonary circulation is crucial when exploring a novel drug for pulmonary arterial hypertension. The change of PVR/SVR ratio from baseline is an indicator for selectivity for pulmonary circulation and implies that TPN171H has good PDE5 selectivity in the pulmonary vasculature,” Dr. Jing said.
TPN171H was well tolerated with no serious adverse effects (vomiting 10% and headache 10% were most common with no discontinuations).
TGF-signaling pathway
A meta-analysis of randomized controlled trials of sotatercept, an investigational fusion protein under priority FDA review that modulates the TGF-beta superfamily signaling pathway, looked at PVR, pulmonary arterial pressure (PAP), right arterial pressure (RAP) and N-terminal pro-brain natriuretic peptide (NT-proBNP). A literature search by corresponding author Vamsikalyan Borra, MD, Knapp Medical Center, Weslaco, Texas, and colleagues identified two trials (STELLAR and PULSAR) comprising 429 patients with pulmonary arterial hypertension. The experimental arms (sotatercept) had 237 patients (mean age ~49 years, ~82% female) and the placebo arm had 192 patients (mean age ~47 years, ~80% female).
A pooled analysis showed significant reductions with sotatercept in PVR (standardization mean difference [SMD] = –1.00, 95% confidence interval [CI] = –1.2, –.79, P < .001), PAP (SMD = –1.34, 95% CI = 1.6, –1.08, P < .001), RAP (SMD = –0.66, 95% CI = –0.93, –0.39, P < .001), and the levels of NT-proBNP (SMD = –0.64, 95% CI = –1.01, –0.27, P < .001) at 24 weeks from baseline. The sotatercept safety profile was favorable, with lower overall incidence of adverse events (84.8% vs. 87.5%) and fewer adverse events leading to death (0.4% vs. 3.1%) compared with placebo. Further investigation is needed, however, according to Dr. Borra, into the higher frequency of reported thrombocytopenia (71.7% vs. 20.8%) with sotatercept. “Our findings,” Dr. Borra said in a poster session, “suggest that sotatercept is an effective treatment option for pulmonary arterial hypertension, with the potential to improve both pulmonary and cardiac function.”
Denervation technique
Catheter-based ablation techniques, most commonly using thermal energy, target the afferent and efferent fibers of the baroreceptor reflex in the main pulmonary artery trunk and bifurcation involved in elevated pulmonary artery pressure. Mounica Vorla, MD, Carle Foundation Hospital, Urbana, Illinois, and colleagues conducted an updated systematic review and meta-analysis of the safety and efficacy of pulmonary artery denervation (PADN) for pulmonary arterial hypertension in seven clinical trials with 506 patients with moderate-severe pulmonary arterial hypertension conducted from 2013 to 2022.
Compared with placebo, PADN treatment was associated with a significant reduction in mean pulmonary artery pressure (weighted mean difference [WMD] = –6.9 mm Hg; 95% CI = –9.7, –4.1; P < .01; I2 = 61) and pulmonary vascular resistance (WMD = –3.2; 95% CI = –5.4, –0.9; P = .005). PADN improvements in cardiac output were also statistically significant (WMD = 0.3; 95% CI = 0.07, 0.6; P = .012), with numerical improvement in 6-minute walking distance (WMD = 67.7; 95% CI = –3.73, 139.2; P = .06) in the PADN group. Side effects were less common in the PADN group as compared with the placebo group, Dr. Vorla reported. She concluded, “This updated meta-analysis supports PADN as a safe and efficacious therapy for severe pulmonary arterial hypertension.” The authors noted limitations imposed by the small sample size, large data heterogeneity, and medium-quality literature. Larger randomized, controlled trials with clinical endpoints comparing PADN with optimal medical therapy are needed, they stated.
References
1. Shah AJ et al. New Drugs and Therapies in Pulmonary Arterial Hypertension. Int J Mol Sci. 2023 Mar 19;24(6):5850. doi: 10.3390/ijms24065850. PMID: 36982922; PMCID: PMC10058689.
2. Kovacs G et al. Pulmonary Vascular Involvement in Chronic Obstructive Pulmonary Disease. Is There a Pulmonary Vascular Phenotype? Am J Respir Crit Care Med. 2018 Oct 15;198(8):1000-11. doi: 10.1164/rccm.201801-0095PP. PMID: 29746142.
PHILADELPHIA — Promise that the unmet need for more effective pulmonary artery hypertension treatments may soon be met was in strong evidence in research into three strategies presented at this year’s recent American Heart Association scientific sessions; one was based on an ancient Chinese herb epimedium (yin yang huo or horny goat weed) commonly used for treating sexual dysfunction and directly related to the phosphodiesterase inhibitors sildenafil, vardenafil, and tadalafil (sold as Viagra, Levitra, and Cialis). A second studied sotatercept, an investigational, potential first-in-class activin signaling inhibitor biologic, and a third evaluated physically ablating the baroreceptor nerves that stimulate vasoconstriction of the pulmonary artery via catheter-based techniques.
Until as recently as the late 1970s, a pulmonary arterial hypertension diagnosis was a uniformly fatal one.1 While associated with pulmonary and right ventricle remodeling, and leads toward heart failure and death. The complex underlying pathogenesis was divided into six groups by the 6th World Symposium on Pulmonary Hypertension (WSPH) in 2018, and includes as its most common features pulmonary artery endothelial cell dysfunction, pulmonary artery smooth muscle cell proliferation and migration, and dysregulated fibroblast activity leading to dysregulated vasoconstriction, micro and in-situ vascular thrombosis, vascular fibrosis and pathogenic remodeling of pulmonary vessels.1 The threshold mean arterial pressure (mPAP) for pulmonary arterial hypertension was defined by the 6th [WSPH] at mPAP ≥ 20 mm Hg, twice the upper limit of a normal mPAP of 14.0 ± 3.3 mm Hg as reported by Kovacs et al. in 2018.2
Pathways for current therapies
Current drugs for pulmonary arterial hypertension focus on three signaling pathways, including the endothelin receptor, prostacyclin and nitric oxide pathways, stated Zhi-Cheng Jing, MD, professor of medicine, head of the cardiology department at Peking Union Medical College Hospital, Peking, China. While the phosphodiesterase 5 inhibitors sildenafil and tadalafil, which target the nitric oxide pathway, came into wide use after Food and Drug Administration approval, the need for higher PDE5-selectivity remains, Dr. Jing said. Structurally modified from the active ingredient in epimedium, TPN171H is an investigational PDE5 inhibitor which has shown several favorable features: a greater PDE5 selectivity than both sildenafil and tadalafil in vitro, an ability to decrease right ventricular systolic pressure and alleviate arterial remodeling in animal studies, and safety and tolerability in healthy human subjects.
The current randomized, double-blind, placebo-and active-controlled phase IIa study assessed the hemodynamic impact of a single oral dose of TPN171H in 60 pulmonary arterial hypertension patients (mean age ~34 years, 83.3% female), all with negative vasodilation test results and in WHO class 2 or 3. Only patients aged 18-75 years with group 1 pulmonary arterial hypertension of idiopathic, connective tissue disorder, or repaired congenital heart defects etiology were included. Patients were divided into six groups: placebo, TPN171H at 2.5, 5, and 10 milligrams, and tadalafil at 20 and 40 milligrams.
For the primary endpoint of maximum decrease in pulmonary vascular resistance (PVR), significant reductions vs. placebo were found only for the TPN171H 5-mg group (–41.2% vs. –24.4%; P = .008) and for the 20-mg (–39.8%) and 40-mg (–37.6%) tadalafil groups (both P < .05). What was not seen in the tadalafil groups, but was evident in the TPN171H 5-mg group, was a significant reduction in the secondary endpoint of PVR/SVR (systolic vascular resistance) at 2, 3, and 5 hours (all P < .05). “As we know,” Dr. Jing said in an interview, “the PDE5 inhibitor functions as a vasodilator, having an impact on both pulmonary circulation and systemic circulation. So, to evaluate the selectivity for pulmonary circulation is crucial when exploring a novel drug for pulmonary arterial hypertension. The change of PVR/SVR ratio from baseline is an indicator for selectivity for pulmonary circulation and implies that TPN171H has good PDE5 selectivity in the pulmonary vasculature,” Dr. Jing said.
TPN171H was well tolerated with no serious adverse effects (vomiting 10% and headache 10% were most common with no discontinuations).
TGF-signaling pathway
A meta-analysis of randomized controlled trials of sotatercept, an investigational fusion protein under priority FDA review that modulates the TGF-beta superfamily signaling pathway, looked at PVR, pulmonary arterial pressure (PAP), right arterial pressure (RAP) and N-terminal pro-brain natriuretic peptide (NT-proBNP). A literature search by corresponding author Vamsikalyan Borra, MD, Knapp Medical Center, Weslaco, Texas, and colleagues identified two trials (STELLAR and PULSAR) comprising 429 patients with pulmonary arterial hypertension. The experimental arms (sotatercept) had 237 patients (mean age ~49 years, ~82% female) and the placebo arm had 192 patients (mean age ~47 years, ~80% female).
A pooled analysis showed significant reductions with sotatercept in PVR (standardization mean difference [SMD] = –1.00, 95% confidence interval [CI] = –1.2, –.79, P < .001), PAP (SMD = –1.34, 95% CI = 1.6, –1.08, P < .001), RAP (SMD = –0.66, 95% CI = –0.93, –0.39, P < .001), and the levels of NT-proBNP (SMD = –0.64, 95% CI = –1.01, –0.27, P < .001) at 24 weeks from baseline. The sotatercept safety profile was favorable, with lower overall incidence of adverse events (84.8% vs. 87.5%) and fewer adverse events leading to death (0.4% vs. 3.1%) compared with placebo. Further investigation is needed, however, according to Dr. Borra, into the higher frequency of reported thrombocytopenia (71.7% vs. 20.8%) with sotatercept. “Our findings,” Dr. Borra said in a poster session, “suggest that sotatercept is an effective treatment option for pulmonary arterial hypertension, with the potential to improve both pulmonary and cardiac function.”
Denervation technique
Catheter-based ablation techniques, most commonly using thermal energy, target the afferent and efferent fibers of the baroreceptor reflex in the main pulmonary artery trunk and bifurcation involved in elevated pulmonary artery pressure. Mounica Vorla, MD, Carle Foundation Hospital, Urbana, Illinois, and colleagues conducted an updated systematic review and meta-analysis of the safety and efficacy of pulmonary artery denervation (PADN) for pulmonary arterial hypertension in seven clinical trials with 506 patients with moderate-severe pulmonary arterial hypertension conducted from 2013 to 2022.
Compared with placebo, PADN treatment was associated with a significant reduction in mean pulmonary artery pressure (weighted mean difference [WMD] = –6.9 mm Hg; 95% CI = –9.7, –4.1; P < .01; I2 = 61) and pulmonary vascular resistance (WMD = –3.2; 95% CI = –5.4, –0.9; P = .005). PADN improvements in cardiac output were also statistically significant (WMD = 0.3; 95% CI = 0.07, 0.6; P = .012), with numerical improvement in 6-minute walking distance (WMD = 67.7; 95% CI = –3.73, 139.2; P = .06) in the PADN group. Side effects were less common in the PADN group as compared with the placebo group, Dr. Vorla reported. She concluded, “This updated meta-analysis supports PADN as a safe and efficacious therapy for severe pulmonary arterial hypertension.” The authors noted limitations imposed by the small sample size, large data heterogeneity, and medium-quality literature. Larger randomized, controlled trials with clinical endpoints comparing PADN with optimal medical therapy are needed, they stated.
References
1. Shah AJ et al. New Drugs and Therapies in Pulmonary Arterial Hypertension. Int J Mol Sci. 2023 Mar 19;24(6):5850. doi: 10.3390/ijms24065850. PMID: 36982922; PMCID: PMC10058689.
2. Kovacs G et al. Pulmonary Vascular Involvement in Chronic Obstructive Pulmonary Disease. Is There a Pulmonary Vascular Phenotype? Am J Respir Crit Care Med. 2018 Oct 15;198(8):1000-11. doi: 10.1164/rccm.201801-0095PP. PMID: 29746142.
PHILADELPHIA — Promise that the unmet need for more effective pulmonary artery hypertension treatments may soon be met was in strong evidence in research into three strategies presented at this year’s recent American Heart Association scientific sessions; one was based on an ancient Chinese herb epimedium (yin yang huo or horny goat weed) commonly used for treating sexual dysfunction and directly related to the phosphodiesterase inhibitors sildenafil, vardenafil, and tadalafil (sold as Viagra, Levitra, and Cialis). A second studied sotatercept, an investigational, potential first-in-class activin signaling inhibitor biologic, and a third evaluated physically ablating the baroreceptor nerves that stimulate vasoconstriction of the pulmonary artery via catheter-based techniques.
Until as recently as the late 1970s, a pulmonary arterial hypertension diagnosis was a uniformly fatal one.1 While associated with pulmonary and right ventricle remodeling, and leads toward heart failure and death. The complex underlying pathogenesis was divided into six groups by the 6th World Symposium on Pulmonary Hypertension (WSPH) in 2018, and includes as its most common features pulmonary artery endothelial cell dysfunction, pulmonary artery smooth muscle cell proliferation and migration, and dysregulated fibroblast activity leading to dysregulated vasoconstriction, micro and in-situ vascular thrombosis, vascular fibrosis and pathogenic remodeling of pulmonary vessels.1 The threshold mean arterial pressure (mPAP) for pulmonary arterial hypertension was defined by the 6th [WSPH] at mPAP ≥ 20 mm Hg, twice the upper limit of a normal mPAP of 14.0 ± 3.3 mm Hg as reported by Kovacs et al. in 2018.2
Pathways for current therapies
Current drugs for pulmonary arterial hypertension focus on three signaling pathways, including the endothelin receptor, prostacyclin and nitric oxide pathways, stated Zhi-Cheng Jing, MD, professor of medicine, head of the cardiology department at Peking Union Medical College Hospital, Peking, China. While the phosphodiesterase 5 inhibitors sildenafil and tadalafil, which target the nitric oxide pathway, came into wide use after Food and Drug Administration approval, the need for higher PDE5-selectivity remains, Dr. Jing said. Structurally modified from the active ingredient in epimedium, TPN171H is an investigational PDE5 inhibitor which has shown several favorable features: a greater PDE5 selectivity than both sildenafil and tadalafil in vitro, an ability to decrease right ventricular systolic pressure and alleviate arterial remodeling in animal studies, and safety and tolerability in healthy human subjects.
The current randomized, double-blind, placebo-and active-controlled phase IIa study assessed the hemodynamic impact of a single oral dose of TPN171H in 60 pulmonary arterial hypertension patients (mean age ~34 years, 83.3% female), all with negative vasodilation test results and in WHO class 2 or 3. Only patients aged 18-75 years with group 1 pulmonary arterial hypertension of idiopathic, connective tissue disorder, or repaired congenital heart defects etiology were included. Patients were divided into six groups: placebo, TPN171H at 2.5, 5, and 10 milligrams, and tadalafil at 20 and 40 milligrams.
For the primary endpoint of maximum decrease in pulmonary vascular resistance (PVR), significant reductions vs. placebo were found only for the TPN171H 5-mg group (–41.2% vs. –24.4%; P = .008) and for the 20-mg (–39.8%) and 40-mg (–37.6%) tadalafil groups (both P < .05). What was not seen in the tadalafil groups, but was evident in the TPN171H 5-mg group, was a significant reduction in the secondary endpoint of PVR/SVR (systolic vascular resistance) at 2, 3, and 5 hours (all P < .05). “As we know,” Dr. Jing said in an interview, “the PDE5 inhibitor functions as a vasodilator, having an impact on both pulmonary circulation and systemic circulation. So, to evaluate the selectivity for pulmonary circulation is crucial when exploring a novel drug for pulmonary arterial hypertension. The change of PVR/SVR ratio from baseline is an indicator for selectivity for pulmonary circulation and implies that TPN171H has good PDE5 selectivity in the pulmonary vasculature,” Dr. Jing said.
TPN171H was well tolerated with no serious adverse effects (vomiting 10% and headache 10% were most common with no discontinuations).
TGF-signaling pathway
A meta-analysis of randomized controlled trials of sotatercept, an investigational fusion protein under priority FDA review that modulates the TGF-beta superfamily signaling pathway, looked at PVR, pulmonary arterial pressure (PAP), right arterial pressure (RAP) and N-terminal pro-brain natriuretic peptide (NT-proBNP). A literature search by corresponding author Vamsikalyan Borra, MD, Knapp Medical Center, Weslaco, Texas, and colleagues identified two trials (STELLAR and PULSAR) comprising 429 patients with pulmonary arterial hypertension. The experimental arms (sotatercept) had 237 patients (mean age ~49 years, ~82% female) and the placebo arm had 192 patients (mean age ~47 years, ~80% female).
A pooled analysis showed significant reductions with sotatercept in PVR (standardization mean difference [SMD] = –1.00, 95% confidence interval [CI] = –1.2, –.79, P < .001), PAP (SMD = –1.34, 95% CI = 1.6, –1.08, P < .001), RAP (SMD = –0.66, 95% CI = –0.93, –0.39, P < .001), and the levels of NT-proBNP (SMD = –0.64, 95% CI = –1.01, –0.27, P < .001) at 24 weeks from baseline. The sotatercept safety profile was favorable, with lower overall incidence of adverse events (84.8% vs. 87.5%) and fewer adverse events leading to death (0.4% vs. 3.1%) compared with placebo. Further investigation is needed, however, according to Dr. Borra, into the higher frequency of reported thrombocytopenia (71.7% vs. 20.8%) with sotatercept. “Our findings,” Dr. Borra said in a poster session, “suggest that sotatercept is an effective treatment option for pulmonary arterial hypertension, with the potential to improve both pulmonary and cardiac function.”
Denervation technique
Catheter-based ablation techniques, most commonly using thermal energy, target the afferent and efferent fibers of the baroreceptor reflex in the main pulmonary artery trunk and bifurcation involved in elevated pulmonary artery pressure. Mounica Vorla, MD, Carle Foundation Hospital, Urbana, Illinois, and colleagues conducted an updated systematic review and meta-analysis of the safety and efficacy of pulmonary artery denervation (PADN) for pulmonary arterial hypertension in seven clinical trials with 506 patients with moderate-severe pulmonary arterial hypertension conducted from 2013 to 2022.
Compared with placebo, PADN treatment was associated with a significant reduction in mean pulmonary artery pressure (weighted mean difference [WMD] = –6.9 mm Hg; 95% CI = –9.7, –4.1; P < .01; I2 = 61) and pulmonary vascular resistance (WMD = –3.2; 95% CI = –5.4, –0.9; P = .005). PADN improvements in cardiac output were also statistically significant (WMD = 0.3; 95% CI = 0.07, 0.6; P = .012), with numerical improvement in 6-minute walking distance (WMD = 67.7; 95% CI = –3.73, 139.2; P = .06) in the PADN group. Side effects were less common in the PADN group as compared with the placebo group, Dr. Vorla reported. She concluded, “This updated meta-analysis supports PADN as a safe and efficacious therapy for severe pulmonary arterial hypertension.” The authors noted limitations imposed by the small sample size, large data heterogeneity, and medium-quality literature. Larger randomized, controlled trials with clinical endpoints comparing PADN with optimal medical therapy are needed, they stated.
References
1. Shah AJ et al. New Drugs and Therapies in Pulmonary Arterial Hypertension. Int J Mol Sci. 2023 Mar 19;24(6):5850. doi: 10.3390/ijms24065850. PMID: 36982922; PMCID: PMC10058689.
2. Kovacs G et al. Pulmonary Vascular Involvement in Chronic Obstructive Pulmonary Disease. Is There a Pulmonary Vascular Phenotype? Am J Respir Crit Care Med. 2018 Oct 15;198(8):1000-11. doi: 10.1164/rccm.201801-0095PP. PMID: 29746142.
FROM AHA 2023
Are you sure your patient is alive?
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.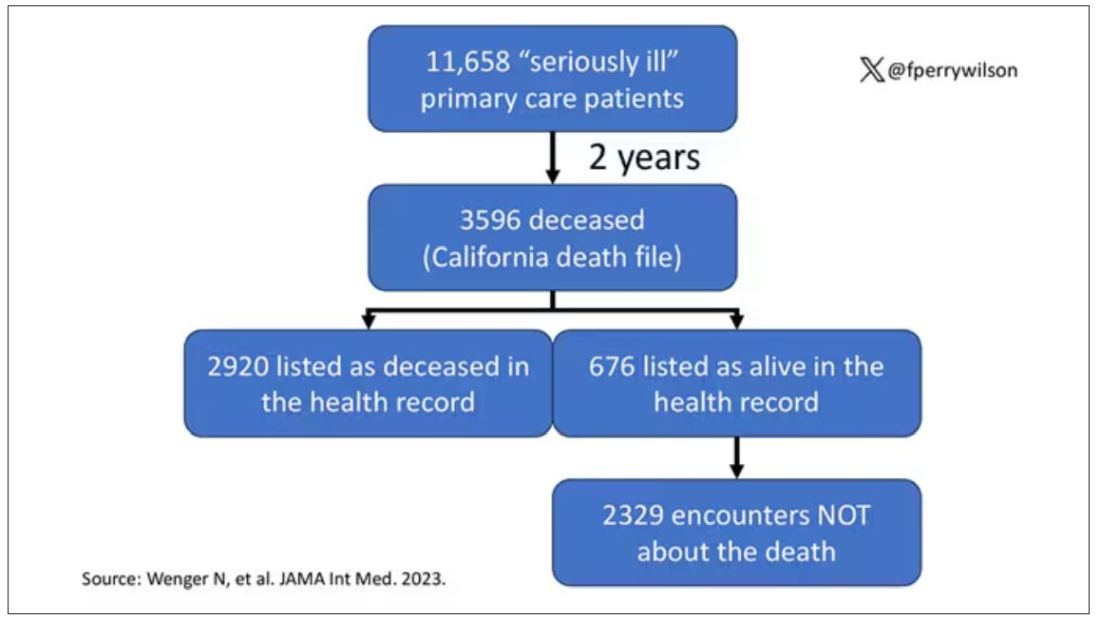
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.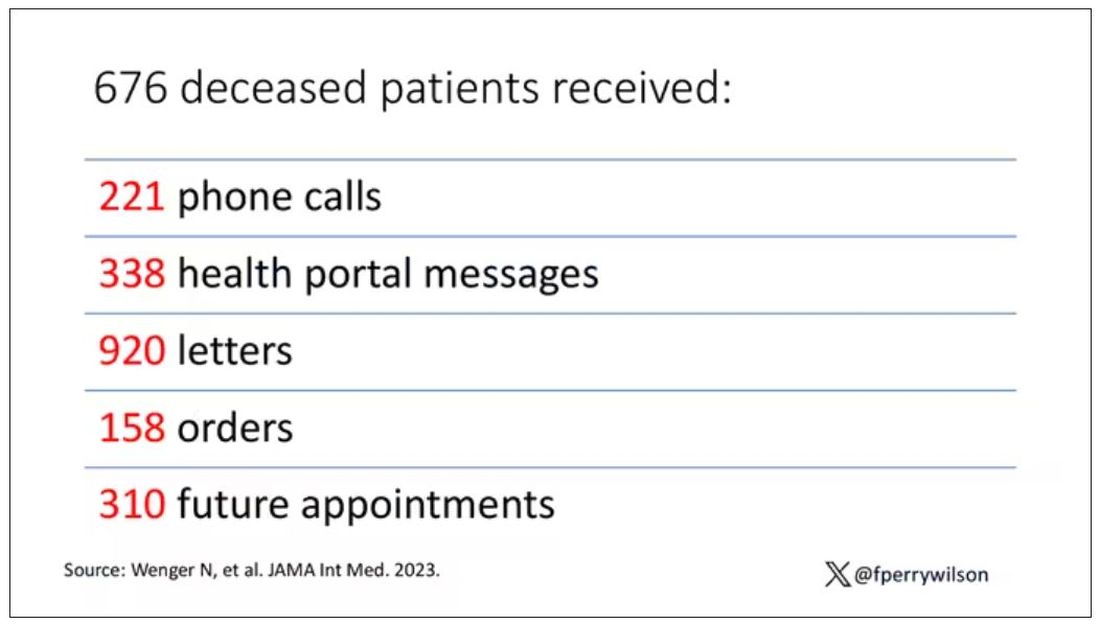
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
This transcript has been edited for clarity.
Much of my research focuses on what is known as clinical decision support — prompts and messages to providers to help them make good decisions for their patients. I know that these things can be annoying, which is exactly why I study them — to figure out which ones actually help.
When I got started on this about 10 years ago, we were learning a lot about how best to message providers about their patients. My team had developed a simple alert for acute kidney injury (AKI). We knew that providers often missed the diagnosis, so maybe letting them know would improve patient outcomes.
As we tested the alert, we got feedback, and I have kept an email from an ICU doctor from those early days. It read:
Dear Dr. Wilson: Thank you for the automated alert informing me that my patient had AKI. Regrettably, the alert fired about an hour after the patient had died. I feel that the information is less than actionable at this time.
Our early system had neglected to add a conditional flag ensuring that the patient was still alive at the time it sent the alert message. A small oversight, but one that had very large implications. Future studies would show that “false positive” alerts like this seriously degrade physician confidence in the system. And why wouldn’t they?
Not knowing the vital status of a patient can have major consequences.
Health systems send messages to their patients all the time: reminders of appointments, reminders for preventive care, reminders for vaccinations, and so on.
But what if the patient being reminded has died? It’s a waste of resources, of course, but more than that, it can be painful for their families and reflects poorly on the health care system. Of all the people who should know whether someone is alive or dead, shouldn’t their doctor be at the top of the list?
A new study in JAMA Internal Medicine quantifies this very phenomenon.
Researchers examined 11,658 primary care patients in their health system who met the criteria of being “seriously ill” and followed them for 2 years. During that period of time, 25% were recorded as deceased in the electronic health record. But 30.8% had died. That left 676 patients who had died, but were not known to have died, left in the system.
And those 676 were not left to rest in peace. They received 221 telephone and 338 health portal messages not related to death, and 920 letters reminding them about unmet primary care metrics like flu shots and cancer screening. Orders were entered into the health record for things like vaccines and routine screenings for 158 patients, and 310 future appointments — destined to be no-shows — were still on the books. One can only imagine the frustration of families checking their mail and finding yet another letter reminding their deceased loved one to get a mammogram.
How did the researchers figure out who had died? It turns out it’s not that hard. California keeps a record of all deaths in the state; they simply had to search it. Like all state death records, they tend to lag a bit so it’s not clinically terribly useful, but it works. California and most other states also have a very accurate and up-to-date death file which can only be used by law enforcement to investigate criminal activity and fraud; health care is left in the lurch.
Nationwide, there is the real-time fact of death service, supported by the National Association for Public Health Statistics and Information Systems. This allows employers to verify, in real time, whether the person applying for a job is alive. Healthcare systems are not allowed to use it.
Let’s also remember that very few people die in this country without some health care agency knowing about it and recording it. But sharing of medical information is so poor in the United States that your patient could die in a hospital one city away from you and you might not find out until you’re calling them to see why they missed a scheduled follow-up appointment.
These events — the embarrassing lack of knowledge about the very vital status of our patients — highlight a huge problem with health care in our country. The fragmented health care system is terrible at data sharing, in part because of poor protocols, in part because of unfounded concerns about patient privacy, and in part because of a tendency to hoard data that might be valuable in the future. It has to stop. We need to know how our patients are doing even when they are not sitting in front of us. When it comes to life and death, the knowledge is out there; we just can’t access it. Seems like a pretty easy fix.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com .
Meet the newest acronym in primary care: CKM
The advisory, published recently in Circulation introduces the concept of CKM health and reevaluates the relationships between obesity, diabetes, kidney disease, and cardiovascular disease (CVD).
“This approach not only raises awareness, it also empowers PCPs to diagnose and treat these conditions more holistically,” Salim Hayek, MD, associate professor of cardiovascular disease and internal medicine, and medical director of the Frankel Cardiovascular Center Clinics at the University of Michigan in Ann Arbor, said in an interview.
New CKM Staging, Testing, and Care Strategies
The advisory introduces a new scoring system that ranges from stage 0 (patients with no risk factors for CKM) through stage 4 (patients with clinical CVD in CKM syndrome). Each stage requires specific management strategies and may include screening starting at age 30 years for diabetes, hypertension, and heart failure.
“Stage 0 CKM is usually found in young people, and CKM risk factors and scores typically increase as people age,” said Sean M. Drake, MD, a primary care physician at Henry Ford Health in Sterling Heights, Michigan.
Dr. Drake advised PCPs to encourage patients who are at stage 0 to maintain ideal cardiovascular health and to monitor those at risk of progressing through the stages.
While PCPs already perform many of the tests the advisory recommends, the conditions overlap and an abnormality in one system should prompt more testing for other conditions. Additional tests, such as urine albumin-creatinine ratio, and more frequent glomerular filtration rate and lipid profile are advised, according to Dr. Drake.
“There also appears to be a role for additional cardiac testing, including echocardiograms and coronary CT scans, and for liver fibrosis screening,” Dr. Drake said. “Medications such as SGLT2 inhibitors, GLP-1 receptor agonists, and ACE inhibitors, beyond current routine use, are emphasized.”
To better characterize body composition and help diagnose metabolic syndrome, the advisory also recommends measuring waist circumference, which is not routine practice, noted Joshua J. Joseph, MD, MPH, an associate professor of endocrinology, diabetes, and metabolism at The Ohio State University Wexner Medical Center in Columbus, and a co-author of the advisory.
Recognizing the interconnected nature of cardiac, kidney, and metabolic diseases encourages a shift in mindset for clinicians, according to Neha Pagidipati, MD, MPH, a cardiologist at Duke Health in Durham, North Carolina.
“We have often been trained to focus on the specific problem in front of us,” Dr. Pagidipati said. “We need to be hyper-aware that many patients we see are at risk for multiple CKM entities. We need to be proactive about screening for and treating these when appropriate.”
The advisory emphasizes the need for CKM coordinators to support teams of clinicians from primary care, cardiology, endocrinology, nephrology, nursing, and pharmacy, as well as social workers, care navigators, or community health workers, Dr. Joseph said.
“The advisory repositions the PCP at the forefront of CKM care coordination, marking a departure from the traditional model where subspecialists primarily manage complications,” Dr. Hayek added.
Changes to Payment
The new recommendations are consistent with current management guidelines for obesity, hypertriglyceridemia, hypertension, type 2 diabetes, and chronic kidney disease.
“The advisory provides integrated algorithms for cardiovascular prevention and management, with specific therapeutic guidance tied to CKM stages, bringing together the current evidence for best practices from the various guidelines and filling gaps in a unified approach,” Dr. Joseph said.
In addition, the advisory draws attention to the care of younger patients, who may be at increased risk for cardiovascular disease due to lifestyle factors, according to Nishant Shah, MD, assistant professor of medicine at Duke.
“It considers barriers to care that prevent people from optimizing their cardiovascular health,” Dr. Shah said.
Although the advisory does not specify proposed payment changes to support the new care model, the move towards value-based care may require billing practices that accommodate integrated care as well as more frequent and more specialized testing, Dr. Hayek said.
“The advisory is an empowering tool for PCPs, underscoring their critical role in healthcare,” Dr. Hayek said. “It encourages PCPs to advocate for integrated care within their practices and to consider workflow adjustments that enhance the identification and initiation of preventive care for at-risk patients.”
Funding information was not provided.
Dr. Joseph reports no relevant financial involvements; several advisory co-authors report financial involvements with pharmaceutical companies. Dr. Pagidipati reports relevant financial involvement with pharmaceutical companies. Dr. Hayek, Dr. Drake, and Dr. Shah report no relevant financial involvements. Dr. Joseph is an author of the advisory. Dr. Pagidipati, Dr. Hayek, Dr. Drake, and Dr. Shah were not involved in the writing of the advisory.
A version of this article appeared on Medscape.com.
The advisory, published recently in Circulation introduces the concept of CKM health and reevaluates the relationships between obesity, diabetes, kidney disease, and cardiovascular disease (CVD).
“This approach not only raises awareness, it also empowers PCPs to diagnose and treat these conditions more holistically,” Salim Hayek, MD, associate professor of cardiovascular disease and internal medicine, and medical director of the Frankel Cardiovascular Center Clinics at the University of Michigan in Ann Arbor, said in an interview.
New CKM Staging, Testing, and Care Strategies
The advisory introduces a new scoring system that ranges from stage 0 (patients with no risk factors for CKM) through stage 4 (patients with clinical CVD in CKM syndrome). Each stage requires specific management strategies and may include screening starting at age 30 years for diabetes, hypertension, and heart failure.
“Stage 0 CKM is usually found in young people, and CKM risk factors and scores typically increase as people age,” said Sean M. Drake, MD, a primary care physician at Henry Ford Health in Sterling Heights, Michigan.
Dr. Drake advised PCPs to encourage patients who are at stage 0 to maintain ideal cardiovascular health and to monitor those at risk of progressing through the stages.
While PCPs already perform many of the tests the advisory recommends, the conditions overlap and an abnormality in one system should prompt more testing for other conditions. Additional tests, such as urine albumin-creatinine ratio, and more frequent glomerular filtration rate and lipid profile are advised, according to Dr. Drake.
“There also appears to be a role for additional cardiac testing, including echocardiograms and coronary CT scans, and for liver fibrosis screening,” Dr. Drake said. “Medications such as SGLT2 inhibitors, GLP-1 receptor agonists, and ACE inhibitors, beyond current routine use, are emphasized.”
To better characterize body composition and help diagnose metabolic syndrome, the advisory also recommends measuring waist circumference, which is not routine practice, noted Joshua J. Joseph, MD, MPH, an associate professor of endocrinology, diabetes, and metabolism at The Ohio State University Wexner Medical Center in Columbus, and a co-author of the advisory.
Recognizing the interconnected nature of cardiac, kidney, and metabolic diseases encourages a shift in mindset for clinicians, according to Neha Pagidipati, MD, MPH, a cardiologist at Duke Health in Durham, North Carolina.
“We have often been trained to focus on the specific problem in front of us,” Dr. Pagidipati said. “We need to be hyper-aware that many patients we see are at risk for multiple CKM entities. We need to be proactive about screening for and treating these when appropriate.”
The advisory emphasizes the need for CKM coordinators to support teams of clinicians from primary care, cardiology, endocrinology, nephrology, nursing, and pharmacy, as well as social workers, care navigators, or community health workers, Dr. Joseph said.
“The advisory repositions the PCP at the forefront of CKM care coordination, marking a departure from the traditional model where subspecialists primarily manage complications,” Dr. Hayek added.
Changes to Payment
The new recommendations are consistent with current management guidelines for obesity, hypertriglyceridemia, hypertension, type 2 diabetes, and chronic kidney disease.
“The advisory provides integrated algorithms for cardiovascular prevention and management, with specific therapeutic guidance tied to CKM stages, bringing together the current evidence for best practices from the various guidelines and filling gaps in a unified approach,” Dr. Joseph said.
In addition, the advisory draws attention to the care of younger patients, who may be at increased risk for cardiovascular disease due to lifestyle factors, according to Nishant Shah, MD, assistant professor of medicine at Duke.
“It considers barriers to care that prevent people from optimizing their cardiovascular health,” Dr. Shah said.
Although the advisory does not specify proposed payment changes to support the new care model, the move towards value-based care may require billing practices that accommodate integrated care as well as more frequent and more specialized testing, Dr. Hayek said.
“The advisory is an empowering tool for PCPs, underscoring their critical role in healthcare,” Dr. Hayek said. “It encourages PCPs to advocate for integrated care within their practices and to consider workflow adjustments that enhance the identification and initiation of preventive care for at-risk patients.”
Funding information was not provided.
Dr. Joseph reports no relevant financial involvements; several advisory co-authors report financial involvements with pharmaceutical companies. Dr. Pagidipati reports relevant financial involvement with pharmaceutical companies. Dr. Hayek, Dr. Drake, and Dr. Shah report no relevant financial involvements. Dr. Joseph is an author of the advisory. Dr. Pagidipati, Dr. Hayek, Dr. Drake, and Dr. Shah were not involved in the writing of the advisory.
A version of this article appeared on Medscape.com.
The advisory, published recently in Circulation introduces the concept of CKM health and reevaluates the relationships between obesity, diabetes, kidney disease, and cardiovascular disease (CVD).
“This approach not only raises awareness, it also empowers PCPs to diagnose and treat these conditions more holistically,” Salim Hayek, MD, associate professor of cardiovascular disease and internal medicine, and medical director of the Frankel Cardiovascular Center Clinics at the University of Michigan in Ann Arbor, said in an interview.
New CKM Staging, Testing, and Care Strategies
The advisory introduces a new scoring system that ranges from stage 0 (patients with no risk factors for CKM) through stage 4 (patients with clinical CVD in CKM syndrome). Each stage requires specific management strategies and may include screening starting at age 30 years for diabetes, hypertension, and heart failure.
“Stage 0 CKM is usually found in young people, and CKM risk factors and scores typically increase as people age,” said Sean M. Drake, MD, a primary care physician at Henry Ford Health in Sterling Heights, Michigan.
Dr. Drake advised PCPs to encourage patients who are at stage 0 to maintain ideal cardiovascular health and to monitor those at risk of progressing through the stages.
While PCPs already perform many of the tests the advisory recommends, the conditions overlap and an abnormality in one system should prompt more testing for other conditions. Additional tests, such as urine albumin-creatinine ratio, and more frequent glomerular filtration rate and lipid profile are advised, according to Dr. Drake.
“There also appears to be a role for additional cardiac testing, including echocardiograms and coronary CT scans, and for liver fibrosis screening,” Dr. Drake said. “Medications such as SGLT2 inhibitors, GLP-1 receptor agonists, and ACE inhibitors, beyond current routine use, are emphasized.”
To better characterize body composition and help diagnose metabolic syndrome, the advisory also recommends measuring waist circumference, which is not routine practice, noted Joshua J. Joseph, MD, MPH, an associate professor of endocrinology, diabetes, and metabolism at The Ohio State University Wexner Medical Center in Columbus, and a co-author of the advisory.
Recognizing the interconnected nature of cardiac, kidney, and metabolic diseases encourages a shift in mindset for clinicians, according to Neha Pagidipati, MD, MPH, a cardiologist at Duke Health in Durham, North Carolina.
“We have often been trained to focus on the specific problem in front of us,” Dr. Pagidipati said. “We need to be hyper-aware that many patients we see are at risk for multiple CKM entities. We need to be proactive about screening for and treating these when appropriate.”
The advisory emphasizes the need for CKM coordinators to support teams of clinicians from primary care, cardiology, endocrinology, nephrology, nursing, and pharmacy, as well as social workers, care navigators, or community health workers, Dr. Joseph said.
“The advisory repositions the PCP at the forefront of CKM care coordination, marking a departure from the traditional model where subspecialists primarily manage complications,” Dr. Hayek added.
Changes to Payment
The new recommendations are consistent with current management guidelines for obesity, hypertriglyceridemia, hypertension, type 2 diabetes, and chronic kidney disease.
“The advisory provides integrated algorithms for cardiovascular prevention and management, with specific therapeutic guidance tied to CKM stages, bringing together the current evidence for best practices from the various guidelines and filling gaps in a unified approach,” Dr. Joseph said.
In addition, the advisory draws attention to the care of younger patients, who may be at increased risk for cardiovascular disease due to lifestyle factors, according to Nishant Shah, MD, assistant professor of medicine at Duke.
“It considers barriers to care that prevent people from optimizing their cardiovascular health,” Dr. Shah said.
Although the advisory does not specify proposed payment changes to support the new care model, the move towards value-based care may require billing practices that accommodate integrated care as well as more frequent and more specialized testing, Dr. Hayek said.
“The advisory is an empowering tool for PCPs, underscoring their critical role in healthcare,” Dr. Hayek said. “It encourages PCPs to advocate for integrated care within their practices and to consider workflow adjustments that enhance the identification and initiation of preventive care for at-risk patients.”
Funding information was not provided.
Dr. Joseph reports no relevant financial involvements; several advisory co-authors report financial involvements with pharmaceutical companies. Dr. Pagidipati reports relevant financial involvement with pharmaceutical companies. Dr. Hayek, Dr. Drake, and Dr. Shah report no relevant financial involvements. Dr. Joseph is an author of the advisory. Dr. Pagidipati, Dr. Hayek, Dr. Drake, and Dr. Shah were not involved in the writing of the advisory.
A version of this article appeared on Medscape.com.
FROM CIRCULATION
Statin use remains low for at-risk patients
TOPLINE:
Changes in statin prescribing guidelines in 2013 had little effect on statin use for patients who are at risk for atherosclerotic cardiovascular disease (ASCVD), according to a study published Dec. 5 in the Annals of Internal Medicine.
METHODOLOGY:
- Statins lower cholesterol and can reduce the risk for heart and circulatory disease.
- In 2013, the American College of Cardiology and the American Heart Association (ACC/AHA) expanded indications for which clinicians could prescribe statins to adults for primary prevention, including risk scores for ASCVD above a certain threshold.
- Researchers studied trends in statin use between 1999 and 2018 using National Health and Nutrition Examination Survey data for 21,961 adults older than 20 years who did not have ASCVD.
- They analyzed data from before and after implementation of the 2013 guidelines.
TAKEAWAY:
- Statin usage increased since 1999 but peaked at 35% in 2013 despite the expanded ACC/AHA guidelines.
- No changes in usage were observed for the proportion of adults who were newly eligible for statins.
- Statin use among patients with diabetes increased by 31.1 percentage points between 1999 and 2014 but then remained stagnant from 2014 to 2018.
- Statin use among those with ASCVD risk of more than 20% increased by 23.1 percentage points between 1999 and 2013 but did not increase between 2013 and 2018.
IN PRACTICE:
“Although the ACC/AHA guidelines expanded indications for primary prevention, they also increased decision-making complexity, requiring new multistep risk calculation… Many clinicians do not routinely use cardiovascular risk calculators because of a lack of time, input availability, or buy-in. Electronic health record tools that calculate ASCVD risks show promise, but they are not routinely implemented and do not address other barriers, such as competing patient priorities and limited time for shared decision-making.“
SOURCE:
The study was led by Timothy S. Anderson, MD, MAS, Division of General Internal Medicine, at the University of Pittsburgh. The research was funded by the National Institute on Aging of the National Institutes of Health.
LIMITATIONS:
Data on whether patients had previously been offered and declined statins were not available. Risk score data for baseline ASCVD, which affects risk classification, were also not available.
DISCLOSURES:
The authors report no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
Changes in statin prescribing guidelines in 2013 had little effect on statin use for patients who are at risk for atherosclerotic cardiovascular disease (ASCVD), according to a study published Dec. 5 in the Annals of Internal Medicine.
METHODOLOGY:
- Statins lower cholesterol and can reduce the risk for heart and circulatory disease.
- In 2013, the American College of Cardiology and the American Heart Association (ACC/AHA) expanded indications for which clinicians could prescribe statins to adults for primary prevention, including risk scores for ASCVD above a certain threshold.
- Researchers studied trends in statin use between 1999 and 2018 using National Health and Nutrition Examination Survey data for 21,961 adults older than 20 years who did not have ASCVD.
- They analyzed data from before and after implementation of the 2013 guidelines.
TAKEAWAY:
- Statin usage increased since 1999 but peaked at 35% in 2013 despite the expanded ACC/AHA guidelines.
- No changes in usage were observed for the proportion of adults who were newly eligible for statins.
- Statin use among patients with diabetes increased by 31.1 percentage points between 1999 and 2014 but then remained stagnant from 2014 to 2018.
- Statin use among those with ASCVD risk of more than 20% increased by 23.1 percentage points between 1999 and 2013 but did not increase between 2013 and 2018.
IN PRACTICE:
“Although the ACC/AHA guidelines expanded indications for primary prevention, they also increased decision-making complexity, requiring new multistep risk calculation… Many clinicians do not routinely use cardiovascular risk calculators because of a lack of time, input availability, or buy-in. Electronic health record tools that calculate ASCVD risks show promise, but they are not routinely implemented and do not address other barriers, such as competing patient priorities and limited time for shared decision-making.“
SOURCE:
The study was led by Timothy S. Anderson, MD, MAS, Division of General Internal Medicine, at the University of Pittsburgh. The research was funded by the National Institute on Aging of the National Institutes of Health.
LIMITATIONS:
Data on whether patients had previously been offered and declined statins were not available. Risk score data for baseline ASCVD, which affects risk classification, were also not available.
DISCLOSURES:
The authors report no disclosures.
A version of this article appeared on Medscape.com.
TOPLINE:
Changes in statin prescribing guidelines in 2013 had little effect on statin use for patients who are at risk for atherosclerotic cardiovascular disease (ASCVD), according to a study published Dec. 5 in the Annals of Internal Medicine.
METHODOLOGY:
- Statins lower cholesterol and can reduce the risk for heart and circulatory disease.
- In 2013, the American College of Cardiology and the American Heart Association (ACC/AHA) expanded indications for which clinicians could prescribe statins to adults for primary prevention, including risk scores for ASCVD above a certain threshold.
- Researchers studied trends in statin use between 1999 and 2018 using National Health and Nutrition Examination Survey data for 21,961 adults older than 20 years who did not have ASCVD.
- They analyzed data from before and after implementation of the 2013 guidelines.
TAKEAWAY:
- Statin usage increased since 1999 but peaked at 35% in 2013 despite the expanded ACC/AHA guidelines.
- No changes in usage were observed for the proportion of adults who were newly eligible for statins.
- Statin use among patients with diabetes increased by 31.1 percentage points between 1999 and 2014 but then remained stagnant from 2014 to 2018.
- Statin use among those with ASCVD risk of more than 20% increased by 23.1 percentage points between 1999 and 2013 but did not increase between 2013 and 2018.
IN PRACTICE:
“Although the ACC/AHA guidelines expanded indications for primary prevention, they also increased decision-making complexity, requiring new multistep risk calculation… Many clinicians do not routinely use cardiovascular risk calculators because of a lack of time, input availability, or buy-in. Electronic health record tools that calculate ASCVD risks show promise, but they are not routinely implemented and do not address other barriers, such as competing patient priorities and limited time for shared decision-making.“
SOURCE:
The study was led by Timothy S. Anderson, MD, MAS, Division of General Internal Medicine, at the University of Pittsburgh. The research was funded by the National Institute on Aging of the National Institutes of Health.
LIMITATIONS:
Data on whether patients had previously been offered and declined statins were not available. Risk score data for baseline ASCVD, which affects risk classification, were also not available.
DISCLOSURES:
The authors report no disclosures.
A version of this article appeared on Medscape.com.
Reducing albumin improves kidney and heart function in people with type 2 diabetes
TOPLINE:
Reducing the urine albumin-to-creatinine ratio (UACR) significantly reduces kidney risk in people with type 2 diabetes, per new research in the Annals of Internal Medicine.
METHODOLOGY:
- Post hoc retrospective analysis of two phase 3 double-blind trials of finerenone in people with type 2 diabetes and chronic kidney disease
- Quantify the long-term health effects of reducing UACR within 4 months of taking finerenone by examining the records of 12,512 participants with an equal chance of receiving finerenone or placebo
- Isolate the impact of UACR reduction on kidney function and cardiovascular function by tracking health indicators related to the kidneys and the heart in participants for up to 4 years
TAKEAWAY:
- Over half of participants who received finerenone had reduced UACR by at least 30% from the baseline of 514 mg/g at the 4-month point after starting treatment, and the median UACR reduction in this group was 33%.
- By 4 months, a little over a quarter of participants who received the placebo had reduced their UACR levels by at least 30%, and the median UACR reduction in this group was 2.6%.
- A UACR reduction of at least 30% reduced kidney risk by 64%, as measured by reductions in kidney failure, sufficient glomerular filtration, and death from kidney disease.
- A UACR reduction of at least 30% reduced cardiovascular risk by 26%, as measured by fewer incidences of cardiovascular death, nonfatal infarction or stroke, and hospitalization for heart failure.
IN PRACTICE:
“Achieving early UACR reduction can lead to tangible benefits for kidney and cardiovascular health,” the authors note.
SOURCE:
The study was published in the Annals of Internal Medicine; the lead author is Rajiv Agarwal, MD, MS.
LIMITATIONS:
The study pertains only to finerenone, so the findings cannot be extrapolated to other drugs with different mechanisms of action.
DISCLOSURES:
Bayer AG Pharmaceuticals, which manufactures finerenone, was the primary funder of the study. The US National Institutes of Health and Veterans Administration also provided funding. Some study authors are full-time employees of Bayer AG. Many authors report consulting relationships with various pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
Reducing the urine albumin-to-creatinine ratio (UACR) significantly reduces kidney risk in people with type 2 diabetes, per new research in the Annals of Internal Medicine.
METHODOLOGY:
- Post hoc retrospective analysis of two phase 3 double-blind trials of finerenone in people with type 2 diabetes and chronic kidney disease
- Quantify the long-term health effects of reducing UACR within 4 months of taking finerenone by examining the records of 12,512 participants with an equal chance of receiving finerenone or placebo
- Isolate the impact of UACR reduction on kidney function and cardiovascular function by tracking health indicators related to the kidneys and the heart in participants for up to 4 years
TAKEAWAY:
- Over half of participants who received finerenone had reduced UACR by at least 30% from the baseline of 514 mg/g at the 4-month point after starting treatment, and the median UACR reduction in this group was 33%.
- By 4 months, a little over a quarter of participants who received the placebo had reduced their UACR levels by at least 30%, and the median UACR reduction in this group was 2.6%.
- A UACR reduction of at least 30% reduced kidney risk by 64%, as measured by reductions in kidney failure, sufficient glomerular filtration, and death from kidney disease.
- A UACR reduction of at least 30% reduced cardiovascular risk by 26%, as measured by fewer incidences of cardiovascular death, nonfatal infarction or stroke, and hospitalization for heart failure.
IN PRACTICE:
“Achieving early UACR reduction can lead to tangible benefits for kidney and cardiovascular health,” the authors note.
SOURCE:
The study was published in the Annals of Internal Medicine; the lead author is Rajiv Agarwal, MD, MS.
LIMITATIONS:
The study pertains only to finerenone, so the findings cannot be extrapolated to other drugs with different mechanisms of action.
DISCLOSURES:
Bayer AG Pharmaceuticals, which manufactures finerenone, was the primary funder of the study. The US National Institutes of Health and Veterans Administration also provided funding. Some study authors are full-time employees of Bayer AG. Many authors report consulting relationships with various pharmaceutical companies.
A version of this article appeared on Medscape.com.
TOPLINE:
Reducing the urine albumin-to-creatinine ratio (UACR) significantly reduces kidney risk in people with type 2 diabetes, per new research in the Annals of Internal Medicine.
METHODOLOGY:
- Post hoc retrospective analysis of two phase 3 double-blind trials of finerenone in people with type 2 diabetes and chronic kidney disease
- Quantify the long-term health effects of reducing UACR within 4 months of taking finerenone by examining the records of 12,512 participants with an equal chance of receiving finerenone or placebo
- Isolate the impact of UACR reduction on kidney function and cardiovascular function by tracking health indicators related to the kidneys and the heart in participants for up to 4 years
TAKEAWAY:
- Over half of participants who received finerenone had reduced UACR by at least 30% from the baseline of 514 mg/g at the 4-month point after starting treatment, and the median UACR reduction in this group was 33%.
- By 4 months, a little over a quarter of participants who received the placebo had reduced their UACR levels by at least 30%, and the median UACR reduction in this group was 2.6%.
- A UACR reduction of at least 30% reduced kidney risk by 64%, as measured by reductions in kidney failure, sufficient glomerular filtration, and death from kidney disease.
- A UACR reduction of at least 30% reduced cardiovascular risk by 26%, as measured by fewer incidences of cardiovascular death, nonfatal infarction or stroke, and hospitalization for heart failure.
IN PRACTICE:
“Achieving early UACR reduction can lead to tangible benefits for kidney and cardiovascular health,” the authors note.
SOURCE:
The study was published in the Annals of Internal Medicine; the lead author is Rajiv Agarwal, MD, MS.
LIMITATIONS:
The study pertains only to finerenone, so the findings cannot be extrapolated to other drugs with different mechanisms of action.
DISCLOSURES:
Bayer AG Pharmaceuticals, which manufactures finerenone, was the primary funder of the study. The US National Institutes of Health and Veterans Administration also provided funding. Some study authors are full-time employees of Bayer AG. Many authors report consulting relationships with various pharmaceutical companies.
A version of this article appeared on Medscape.com.
Smoking alters salivary microbiota in potential path to disease risk
TOPLINE:
Salivary microbiota changes caused by cigarette smoking may affect metabolic pathways and increase disease risk.
METHODOLOGY:
The researchers analyzed health information and data on the composition of salivary microbiota from 1601 adult participants in the Cooperative Health Research in South Tyrol (CHRIS) microbiome study (CHRISMB); CHRIS is an ongoing study in Italy.
The average age of the study population was 45 years; 53% were female, and 45% were current or former smokers.
The researchers hypothesized that changes in salivary microbial composition would be associated with smoking, with more nitrate-reducing bacteria present, and that nitrate reduction pathways would be reduced in smokers.
TAKEAWAY:
The researchers identified 44 genera that differed in the salivary microbiota of current smokers and nonsmokers. In smokers, seven genera in the phylum Proteobacteria were decreased and six in the phylum Actinobacteria were increased compared with nonsmokers; these phyla contain primarily aerobic and anaerobic taxa, respectively.
Some microbiota changes were significantly associated with daily smoking intensity; genera from the classes Betaproteobacteria (Lautropia or Neisseria), Gammaproteobacteria (Cardiobacterium), and Flavobacteriia (Capnocytophaga) decreased significantly with increased grams of tobacco smoked per day, measured in 5-g increments.
Smoking was associated with changes in the salivary microbiota; the nitrate reduction pathway was significantly lower in smokers compared with nonsmokers, and these decreases were consistent with previous studies of decreased cardiovascular events in former smokers.
However, the salivary microbiota of smokers who had quit for at least 5 years resembled that of individuals who had never smoked.
IN PRACTICE:
“Decreased microbial nitrate reduction pathway abundance in smokers may provide an additional explanation for the effect of smoking on cardiovascular and periodontal diseases risk, a hypothesis which should be tested in future studies,” the researchers wrote.
SOURCE:
The lead author of the study was Giacomo Antonello, MD, of Eurac Research, Affiliated Institute of the University of Lübeck, Bolzano, Italy. The study was published online in Scientific Reports (a Nature journal) on November 2, 2023.
LIMITATIONS:
The cross-sectional design and lack of professional assessment of tooth and gum health were limiting factors, as were potential confounding factors including medication use, diet, and alcohol intake.
DISCLOSURES:
The study was supported by the Department of Innovation, Research and University of the Autonomous Province of Bolzano-South Tyrol and by the European Regional Development Fund. The CHRISMB microbiota data generation was funded by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
TOPLINE:
Salivary microbiota changes caused by cigarette smoking may affect metabolic pathways and increase disease risk.
METHODOLOGY:
The researchers analyzed health information and data on the composition of salivary microbiota from 1601 adult participants in the Cooperative Health Research in South Tyrol (CHRIS) microbiome study (CHRISMB); CHRIS is an ongoing study in Italy.
The average age of the study population was 45 years; 53% were female, and 45% were current or former smokers.
The researchers hypothesized that changes in salivary microbial composition would be associated with smoking, with more nitrate-reducing bacteria present, and that nitrate reduction pathways would be reduced in smokers.
TAKEAWAY:
The researchers identified 44 genera that differed in the salivary microbiota of current smokers and nonsmokers. In smokers, seven genera in the phylum Proteobacteria were decreased and six in the phylum Actinobacteria were increased compared with nonsmokers; these phyla contain primarily aerobic and anaerobic taxa, respectively.
Some microbiota changes were significantly associated with daily smoking intensity; genera from the classes Betaproteobacteria (Lautropia or Neisseria), Gammaproteobacteria (Cardiobacterium), and Flavobacteriia (Capnocytophaga) decreased significantly with increased grams of tobacco smoked per day, measured in 5-g increments.
Smoking was associated with changes in the salivary microbiota; the nitrate reduction pathway was significantly lower in smokers compared with nonsmokers, and these decreases were consistent with previous studies of decreased cardiovascular events in former smokers.
However, the salivary microbiota of smokers who had quit for at least 5 years resembled that of individuals who had never smoked.
IN PRACTICE:
“Decreased microbial nitrate reduction pathway abundance in smokers may provide an additional explanation for the effect of smoking on cardiovascular and periodontal diseases risk, a hypothesis which should be tested in future studies,” the researchers wrote.
SOURCE:
The lead author of the study was Giacomo Antonello, MD, of Eurac Research, Affiliated Institute of the University of Lübeck, Bolzano, Italy. The study was published online in Scientific Reports (a Nature journal) on November 2, 2023.
LIMITATIONS:
The cross-sectional design and lack of professional assessment of tooth and gum health were limiting factors, as were potential confounding factors including medication use, diet, and alcohol intake.
DISCLOSURES:
The study was supported by the Department of Innovation, Research and University of the Autonomous Province of Bolzano-South Tyrol and by the European Regional Development Fund. The CHRISMB microbiota data generation was funded by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
TOPLINE:
Salivary microbiota changes caused by cigarette smoking may affect metabolic pathways and increase disease risk.
METHODOLOGY:
The researchers analyzed health information and data on the composition of salivary microbiota from 1601 adult participants in the Cooperative Health Research in South Tyrol (CHRIS) microbiome study (CHRISMB); CHRIS is an ongoing study in Italy.
The average age of the study population was 45 years; 53% were female, and 45% were current or former smokers.
The researchers hypothesized that changes in salivary microbial composition would be associated with smoking, with more nitrate-reducing bacteria present, and that nitrate reduction pathways would be reduced in smokers.
TAKEAWAY:
The researchers identified 44 genera that differed in the salivary microbiota of current smokers and nonsmokers. In smokers, seven genera in the phylum Proteobacteria were decreased and six in the phylum Actinobacteria were increased compared with nonsmokers; these phyla contain primarily aerobic and anaerobic taxa, respectively.
Some microbiota changes were significantly associated with daily smoking intensity; genera from the classes Betaproteobacteria (Lautropia or Neisseria), Gammaproteobacteria (Cardiobacterium), and Flavobacteriia (Capnocytophaga) decreased significantly with increased grams of tobacco smoked per day, measured in 5-g increments.
Smoking was associated with changes in the salivary microbiota; the nitrate reduction pathway was significantly lower in smokers compared with nonsmokers, and these decreases were consistent with previous studies of decreased cardiovascular events in former smokers.
However, the salivary microbiota of smokers who had quit for at least 5 years resembled that of individuals who had never smoked.
IN PRACTICE:
“Decreased microbial nitrate reduction pathway abundance in smokers may provide an additional explanation for the effect of smoking on cardiovascular and periodontal diseases risk, a hypothesis which should be tested in future studies,” the researchers wrote.
SOURCE:
The lead author of the study was Giacomo Antonello, MD, of Eurac Research, Affiliated Institute of the University of Lübeck, Bolzano, Italy. The study was published online in Scientific Reports (a Nature journal) on November 2, 2023.
LIMITATIONS:
The cross-sectional design and lack of professional assessment of tooth and gum health were limiting factors, as were potential confounding factors including medication use, diet, and alcohol intake.
DISCLOSURES:
The study was supported by the Department of Innovation, Research and University of the Autonomous Province of Bolzano-South Tyrol and by the European Regional Development Fund. The CHRISMB microbiota data generation was funded by the National Institute of Dental and Craniofacial Research. The researchers had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.