User login
Myasthenia gravis drug gets FDA nod
, the drug’s manufacturer, UCB, has announced.

Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3 MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported last month in Lancet Neurology, rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
“There is a significant need for new, innovative treatment options to reduce the day-to-day burden of gMG,” lead investigator Vera Bril, MD, professor of medicine (neurology), University of Toronto, said in a news release.
Rozanolixizumab is “a new treatment option, targeting one of the mechanisms of disease to provide symptom improvement in patient- and physician-reported outcomes at day 43,” Dr. Bril added.
The most common adverse reactions (reported in at least 10% of patients treated with rozanolixizumab) were headache, infections, diarrhea, pyrexia, hypersensitivity reactions, and nausea.
The company expects rozanolixizumab to be available in the United States during the third quarter of 2023.
The FDA granted the application for rozanolixizumab in gMG priority review.
A version of this article first appeared on Medscape.com.
, the drug’s manufacturer, UCB, has announced.
Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3 MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported last month in Lancet Neurology, rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
“There is a significant need for new, innovative treatment options to reduce the day-to-day burden of gMG,” lead investigator Vera Bril, MD, professor of medicine (neurology), University of Toronto, said in a news release.
Rozanolixizumab is “a new treatment option, targeting one of the mechanisms of disease to provide symptom improvement in patient- and physician-reported outcomes at day 43,” Dr. Bril added.
The most common adverse reactions (reported in at least 10% of patients treated with rozanolixizumab) were headache, infections, diarrhea, pyrexia, hypersensitivity reactions, and nausea.
The company expects rozanolixizumab to be available in the United States during the third quarter of 2023.
The FDA granted the application for rozanolixizumab in gMG priority review.
A version of this article first appeared on Medscape.com.
, the drug’s manufacturer, UCB, has announced.
Rozanolixizumab is a subcutaneous-infused humanized IgG4 monoclonal antibody that binds to the neonatal Fc receptor (FcRn), reducing the concentration of pathogenic IgG autoantibodies.
U.S. approval is based on results of the phase 3 MycarinG study involving 200 patients with AChR or MuSK autoantibody-positive gMG. Patients were randomly assigned to one of two rozanolixizumab groups (7 mg/kg or 10 mg/kg) or placebo for 6 weeks.
As reported last month in Lancet Neurology, rozanolixizumab led to statistically significant improvements in gMG-specific outcomes, including everyday activities such as breathing, talking, swallowing, and being able to rise from a chair.
“There is a significant need for new, innovative treatment options to reduce the day-to-day burden of gMG,” lead investigator Vera Bril, MD, professor of medicine (neurology), University of Toronto, said in a news release.
Rozanolixizumab is “a new treatment option, targeting one of the mechanisms of disease to provide symptom improvement in patient- and physician-reported outcomes at day 43,” Dr. Bril added.
The most common adverse reactions (reported in at least 10% of patients treated with rozanolixizumab) were headache, infections, diarrhea, pyrexia, hypersensitivity reactions, and nausea.
The company expects rozanolixizumab to be available in the United States during the third quarter of 2023.
The FDA granted the application for rozanolixizumab in gMG priority review.
A version of this article first appeared on Medscape.com.
FDA clears new biomarker assays for early Alzheimer’s detection
The Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys total-tau CSF assays (tTau) (used as a tTau/Abeta42 ratio) are for use in adults ages 55 and older being evaluated for AD.
They join the Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys phospho-tau (181P) CSF (pTau181) assays (used as a pTau181/Abeta42 ratio) that received FDA 510(k) clearance in 2022.
“An early and accurate diagnosis can help patients, caregivers and physicians determine a path forward, and the Elecsys CSF assays support diagnosis at early disease stages, when treatment is most effective,” Brad Moore, president and CEO of Roche Diagnostics North America, said in a statement.
Appropriate use recommendations for new and emerging AD drugs call for confirmation of amyloid pathology. Currently, the only FDA-cleared methods to confirm amyloid pathology are CSF tests and PET scans.
“The Elecsys AD CSF assays are concordant with amyloid PET scan imaging and have the potential to provide a more affordable and accessible routine option to confirm the presence of amyloid pathology in the brain,” Roche said.
“They also offer detection of both amyloid and tau biomarkers from one draw, with no radiation and potential to detect Alzheimer’s pathology in early stages of disease,” the company added.
The previously approved Elecsys pTau181/Abeta42 ratio is currently available and the newly approved Elecsys tTau/Abeta42 ratio will be available in the fourth quarter of 2023.
A version of this article first appeared on Medscape.com.
The Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys total-tau CSF assays (tTau) (used as a tTau/Abeta42 ratio) are for use in adults ages 55 and older being evaluated for AD.
They join the Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys phospho-tau (181P) CSF (pTau181) assays (used as a pTau181/Abeta42 ratio) that received FDA 510(k) clearance in 2022.
“An early and accurate diagnosis can help patients, caregivers and physicians determine a path forward, and the Elecsys CSF assays support diagnosis at early disease stages, when treatment is most effective,” Brad Moore, president and CEO of Roche Diagnostics North America, said in a statement.
Appropriate use recommendations for new and emerging AD drugs call for confirmation of amyloid pathology. Currently, the only FDA-cleared methods to confirm amyloid pathology are CSF tests and PET scans.
“The Elecsys AD CSF assays are concordant with amyloid PET scan imaging and have the potential to provide a more affordable and accessible routine option to confirm the presence of amyloid pathology in the brain,” Roche said.
“They also offer detection of both amyloid and tau biomarkers from one draw, with no radiation and potential to detect Alzheimer’s pathology in early stages of disease,” the company added.
The previously approved Elecsys pTau181/Abeta42 ratio is currently available and the newly approved Elecsys tTau/Abeta42 ratio will be available in the fourth quarter of 2023.
A version of this article first appeared on Medscape.com.
The Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys total-tau CSF assays (tTau) (used as a tTau/Abeta42 ratio) are for use in adults ages 55 and older being evaluated for AD.
They join the Elecsys beta-amyloid (1-42) CSF II (Abeta42) and Elecsys phospho-tau (181P) CSF (pTau181) assays (used as a pTau181/Abeta42 ratio) that received FDA 510(k) clearance in 2022.
“An early and accurate diagnosis can help patients, caregivers and physicians determine a path forward, and the Elecsys CSF assays support diagnosis at early disease stages, when treatment is most effective,” Brad Moore, president and CEO of Roche Diagnostics North America, said in a statement.
Appropriate use recommendations for new and emerging AD drugs call for confirmation of amyloid pathology. Currently, the only FDA-cleared methods to confirm amyloid pathology are CSF tests and PET scans.
“The Elecsys AD CSF assays are concordant with amyloid PET scan imaging and have the potential to provide a more affordable and accessible routine option to confirm the presence of amyloid pathology in the brain,” Roche said.
“They also offer detection of both amyloid and tau biomarkers from one draw, with no radiation and potential to detect Alzheimer’s pathology in early stages of disease,” the company added.
The previously approved Elecsys pTau181/Abeta42 ratio is currently available and the newly approved Elecsys tTau/Abeta42 ratio will be available in the fourth quarter of 2023.
A version of this article first appeared on Medscape.com.
New DEA CME mandate affects 2 million prescribers
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.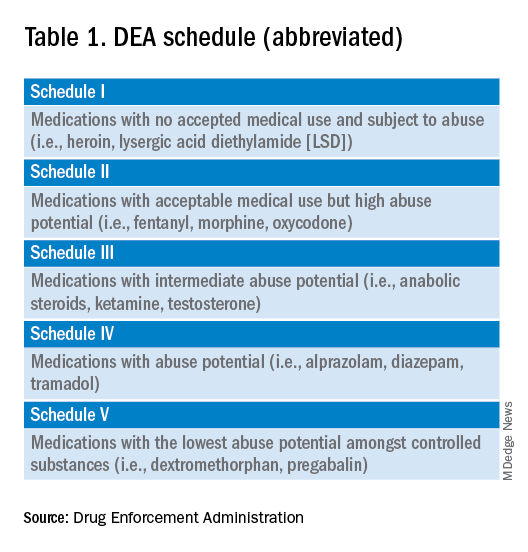
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements. 
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
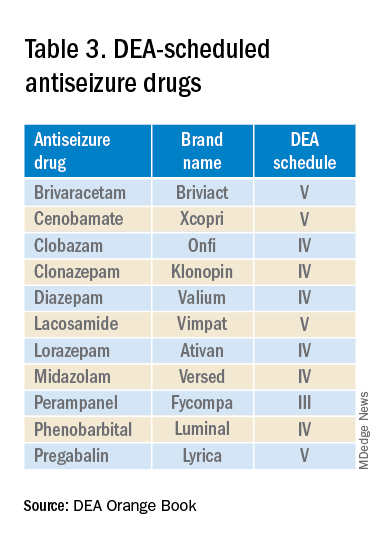
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
The Consolidated Appropriations Act of 2023 mandates that all Drug Enforcement Administration–registered physicians and health care providers complete a one-time, 8-hour CME training on managing and treating opioid and other substance abuse disorders. This requirement goes into effect on June 27, 2023. New DEA registrants must also comply. Veterinarians are exempt.
A DEA registration is required to prescribe any controlled substance. The DEA categorizes these as Schedule I-V, with V being the least likely to be abused (Table 1). For example, opioids like fentanyl, oxycodone, and morphine are Schedule II. Medications without abuse potential are not scheduled.
Will 16 million hours of opioid education save lives?
One should not underestimate the sweeping scope of this new federal requirement. DEA registrants include physicians and other health care providers such as nurse practitioners, physician assistants, and dentists. That is 8 hours per provider x 2 million providers: 16 million hours of CME!
Many states already require 1 or more hours of opioid training and pain management as part of their relicensure requirements (Table 2). To avoid redundancy, the DEA-mandated 8-hour training satisfies the various states’ requirements.
An uncompensated mandate
Physicians are no strangers to lifelong learning and most eagerly pursue educational opportunities. Though some physicians may have CME time and stipends allocated by their employers, many others, such as the approximately 50,000 locum tenens doctors, do not. However, as enthusiastic as these physicians may be about this new CME course, they will likely lose a day of seeing patients (and income) to comply with this new obligation.
Not just pain doctors
The mandate’s broad brush includes many health care providers who hold DEA certificates but do not prescribe opioids. For example, as a general neurologist and epileptologist, I do not treat patients with chronic pain and cannot remember the last time I wrote an opioid prescription. However, I frequently prescribe lacosamide, a Schedule V drug. A surprisingly large number of antiseizure drugs are Schedule III, IV, or V drugs (Table 3).
Real-world abuse?
How often scheduled antiseizure drugs are diverted or abused in an epilepsy population is unknown but appears to be infrequent. For example, perampanel abuse has not been reported despite its classification as a Schedule III drug. Anecdotally, in more than 40 years of clinical practice, I have never known a patient with epilepsy to abuse their antiseizure medications.
Take the course
Many organizations are happy to charge for the new 8-hour course. For example, the Tennessee Medical Association offers the training for $299 online or $400 in person. Materials from Elite Learning satisfy the 8-hour requirement for $80. However, NEJM Knowledge+ provides a complimentary 10-hour DEA-compliant course.
I recently completed the NEJM course. The information was thorough and took the whole 10 hours to finish. As excellent as it was, the content was only tangentially relevant to my clinical practice.
Conclusions
To obtain or renew a DEA certificate, neurologists, epilepsy specialists, and many other health care providers must comply with the new 8-hour CME opioid training mandate. Because the course requires 1 day to complete, health care providers would be prudent to obtain their CME well before their DEA certificate expires.
Though efforts to control the morbidity and mortality of the opioid epidemic are laudatory, perhaps the training should be more targeted to physicians who actually prescribe opioids rather than every DEA registrant. In the meantime, whether 16 million CME hours will save lives remains to be seen.
Dr. Wilner is professor of neurology at the University of Tennessee Health Science Center, Memphis. He reported a conflict of interest with Accordant Health Services.
A version of this article first appeared on Medscape.com.
HPV rates skyrocket despite safe, effective vaccine
An epidemic of sexually transmitted HPV is now swirling around the United States and the United Kingdom, with some serious cases leading to oropharyngeal cancer, which can affect the back of the throat, tonsils, and tongue.
HPV is the leading cause (70%) of this oropharyngeal cancer, according to the CDC. It is the most common sexually transmitted disease in the nation, and around 3.6% of women and 10% of men report oral HPV specifically. But over the past decade, oropharyngeal cases have been steadily falling a little under 4% and 2%, respectively, according to the National Cancer Institute.
HPV is often undetectable and can clear up within a few months. But unfortunately for some, serious disease, such as throat cancer, can develop.
Studies show the HPV vaccine to be extremely effective in lowering sexually transmitted HPV cases. Yet, only 54.5% of young people aged 13-15 have taken the recommended two to three doses, according to the National Cancer Institute.
Why aren’t more young people taking the vaccine?
Low public awareness of the dangers of HPV may be behind young people’s poor vaccination rates, according to Teresa Lee, MD, of the Fox Chase Cancer Center in Philadelphia. “For example, while the link with head and neck cancers has been well-studied, the FDA labeling was not changed to reflect this as an indication until 2020,” she said.
Other reasons can include one’s socioeconomic background, poor health literacy, cultural or religious stigmas around vaccines, and lack of quality, low-cost health care, says Emmanuel Aguh, MD, a board-certified family medicine physician. “Some individuals and families are still resistant to vaccines and the noted lack of uptake.”
Doctors and other health care professionals should also be sure to tell patients of all ages about the risks of HPV infection and how well the vaccine works, Dr. Lee said. “Not everyone who is now eligible may have been offered the vaccine as a child, and the first time young adults may receive counseling on this subject may not be until they are entering a very busy period of their lives with many responsibilities – when it may be hard to fit in things like health maintenance.”
How safe is the HPV vaccine?
The Food and Drug Administration and Centers for Disease Control and Prevention have studied the HPV vaccine for years to find out how safe it is and how well it works, Dr. Aguh said. No major side effects have been reported, and the most common side effect is soreness where you get the shot (which is normal after most vaccines). Some dizziness and fainting in adolescents can also occur, so young people are usually asked to sit or lie down during the shot and for 15 minutes afterward, he said.
“Serious adverse events have not been reported at higher rates than expected following HPV vaccination, meaning there is no clear evidence they are related to the vaccine,” Dr. Lee said. “The vaccine is highly effective in decreasing rates of detectable infection with the high-risk HPV strains responsible for HPV-associated cancers.”
The HPV vaccine is largely recommended for people aged 9-26, and sometimes up to age 45, depending on the individual, Dr. Aguh said. If you are over 26, talk to your doctor about whether you should consider getting the vaccine.
“It is usually given in two doses for complete protection if taken before the 15th birthday,” Dr. Aguh said. “If taken afterward, or in those with a weak immune system, they might require three doses to be fully protected.”
The vaccine produces antibodies that can stop HPV from infecting cells and lowers your chances of catching an HPV-related cancer, such as throat cancer or cancer of the cervix, he said.
While the vaccine is not guaranteed to protect you from the more than 100 strains of HPV, it can protect you from HPV 16 and HPV 18 – two high-risk strains that cause around 70% of cervical cancers.
What is fueling the rise of HPV cases?
A misconception that oral sex is somehow a “safe and risk-free” alternative to anal or vaginal sex could be one reason, Dr. Aguh said.
“It is important to know that, with oral sex, you are exposed to many of the risks associated with vaginal intercourse, especially if you do not take any measures to protect yourself and/or your partner,” Dr. Aguh said. “[With oral sex] it is possible to end up contracting an infection like chlamydia, gonorrhea, and even HPV, leading to an increased risk of HPV-associated oropharyngeal cancers.”
A lack of public awareness of what can cause throat cancer could also explain this phenomenon. The number of people you have oral sex with, along with the age you begin sexual activity, can greatly determine your risk of the disease, according to Dr. Lee. She echoes a report by Hisham Mehanna, PhD, in The Conversation.
“For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex,” wrote Dr. Mehanna, a professor at the Institute of Cancer and Genomic Sciences at the University of Birmingham (England). “Those with six or more lifetime oral-sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practice oral sex.”
What are symptoms of oropharyngeal cancer?
Labored breathing or swallowing, a cough that won’t go away, and crackling or hoarseness of your voice could all be signs of throat cancer. Other symptoms include earaches, swelling of the head or neck, and enlarged lymph nodes, among others, Dr. Aguh said.
“The signs and symptoms of HPV-related throat cancers can be difficult to identify and recognize, as they can be vague and are also associated with other medical conditions. Sometimes, there are no signs at all, or they are not easily noticeable due to the location,” he said.
You should go see your doctor if you have any of these ailments for an extended period.
How to reduce your risk
In addition to having six or more oral-sex partners, smoking and drinking heavily could also raise your risk of throat cancer, said Dr. Lee. Proper dental health – like seeing your dentist regularly and practicing proper oral hygiene – can also shave your risk.
“[Good dental health] can help not just with head and neck cancer risk, but with many other inflammation-related diseases,” Dr. Lee said.
Using dental dams and condoms can also be a good method of protection, Dr. Aguh said. A dental dam is a stretchy sheet of latex, or polyurethane plastic, in the shape of a square that is made for blocking body fluid to lower your risk of contracting an STD via oral sex.
Keep in mind: Even with these protections, make sure you and your partner discuss each other’s sexual history, any prior or current STDs and their preferred protection from STDs, said Dr. Aguh.
If you or your partner is being treated for an STD, consider opting out of oral sex and consulting a doctor.
The HPV vaccine is another common method of protection. The shot is “approved for prevention of nine of the most high-risk strains of HPV,” or those that are most commonly linked to cancer, according to Dr. Lee. The vaccine “reduces the frequency of infection” with these viruses, which can ultimately lower the risk of cancers linked to HPV, including cervical, anal, and vulvar and vaginal cancers, she said.
“The best time to receive treatment for prevention of disease is prior to onset of sexual intercourse,” said Dr. Lee.
To get your HPV vaccine, head to your family doctor, school- or community-based health center, or state health department, suggests the CDC.
A version of this article originally appeared on WebMD.com.
An epidemic of sexually transmitted HPV is now swirling around the United States and the United Kingdom, with some serious cases leading to oropharyngeal cancer, which can affect the back of the throat, tonsils, and tongue.
HPV is the leading cause (70%) of this oropharyngeal cancer, according to the CDC. It is the most common sexually transmitted disease in the nation, and around 3.6% of women and 10% of men report oral HPV specifically. But over the past decade, oropharyngeal cases have been steadily falling a little under 4% and 2%, respectively, according to the National Cancer Institute.
HPV is often undetectable and can clear up within a few months. But unfortunately for some, serious disease, such as throat cancer, can develop.
Studies show the HPV vaccine to be extremely effective in lowering sexually transmitted HPV cases. Yet, only 54.5% of young people aged 13-15 have taken the recommended two to three doses, according to the National Cancer Institute.
Why aren’t more young people taking the vaccine?
Low public awareness of the dangers of HPV may be behind young people’s poor vaccination rates, according to Teresa Lee, MD, of the Fox Chase Cancer Center in Philadelphia. “For example, while the link with head and neck cancers has been well-studied, the FDA labeling was not changed to reflect this as an indication until 2020,” she said.
Other reasons can include one’s socioeconomic background, poor health literacy, cultural or religious stigmas around vaccines, and lack of quality, low-cost health care, says Emmanuel Aguh, MD, a board-certified family medicine physician. “Some individuals and families are still resistant to vaccines and the noted lack of uptake.”
Doctors and other health care professionals should also be sure to tell patients of all ages about the risks of HPV infection and how well the vaccine works, Dr. Lee said. “Not everyone who is now eligible may have been offered the vaccine as a child, and the first time young adults may receive counseling on this subject may not be until they are entering a very busy period of their lives with many responsibilities – when it may be hard to fit in things like health maintenance.”
How safe is the HPV vaccine?
The Food and Drug Administration and Centers for Disease Control and Prevention have studied the HPV vaccine for years to find out how safe it is and how well it works, Dr. Aguh said. No major side effects have been reported, and the most common side effect is soreness where you get the shot (which is normal after most vaccines). Some dizziness and fainting in adolescents can also occur, so young people are usually asked to sit or lie down during the shot and for 15 minutes afterward, he said.
“Serious adverse events have not been reported at higher rates than expected following HPV vaccination, meaning there is no clear evidence they are related to the vaccine,” Dr. Lee said. “The vaccine is highly effective in decreasing rates of detectable infection with the high-risk HPV strains responsible for HPV-associated cancers.”
The HPV vaccine is largely recommended for people aged 9-26, and sometimes up to age 45, depending on the individual, Dr. Aguh said. If you are over 26, talk to your doctor about whether you should consider getting the vaccine.
“It is usually given in two doses for complete protection if taken before the 15th birthday,” Dr. Aguh said. “If taken afterward, or in those with a weak immune system, they might require three doses to be fully protected.”
The vaccine produces antibodies that can stop HPV from infecting cells and lowers your chances of catching an HPV-related cancer, such as throat cancer or cancer of the cervix, he said.
While the vaccine is not guaranteed to protect you from the more than 100 strains of HPV, it can protect you from HPV 16 and HPV 18 – two high-risk strains that cause around 70% of cervical cancers.
What is fueling the rise of HPV cases?
A misconception that oral sex is somehow a “safe and risk-free” alternative to anal or vaginal sex could be one reason, Dr. Aguh said.
“It is important to know that, with oral sex, you are exposed to many of the risks associated with vaginal intercourse, especially if you do not take any measures to protect yourself and/or your partner,” Dr. Aguh said. “[With oral sex] it is possible to end up contracting an infection like chlamydia, gonorrhea, and even HPV, leading to an increased risk of HPV-associated oropharyngeal cancers.”
A lack of public awareness of what can cause throat cancer could also explain this phenomenon. The number of people you have oral sex with, along with the age you begin sexual activity, can greatly determine your risk of the disease, according to Dr. Lee. She echoes a report by Hisham Mehanna, PhD, in The Conversation.
“For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex,” wrote Dr. Mehanna, a professor at the Institute of Cancer and Genomic Sciences at the University of Birmingham (England). “Those with six or more lifetime oral-sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practice oral sex.”
What are symptoms of oropharyngeal cancer?
Labored breathing or swallowing, a cough that won’t go away, and crackling or hoarseness of your voice could all be signs of throat cancer. Other symptoms include earaches, swelling of the head or neck, and enlarged lymph nodes, among others, Dr. Aguh said.
“The signs and symptoms of HPV-related throat cancers can be difficult to identify and recognize, as they can be vague and are also associated with other medical conditions. Sometimes, there are no signs at all, or they are not easily noticeable due to the location,” he said.
You should go see your doctor if you have any of these ailments for an extended period.
How to reduce your risk
In addition to having six or more oral-sex partners, smoking and drinking heavily could also raise your risk of throat cancer, said Dr. Lee. Proper dental health – like seeing your dentist regularly and practicing proper oral hygiene – can also shave your risk.
“[Good dental health] can help not just with head and neck cancer risk, but with many other inflammation-related diseases,” Dr. Lee said.
Using dental dams and condoms can also be a good method of protection, Dr. Aguh said. A dental dam is a stretchy sheet of latex, or polyurethane plastic, in the shape of a square that is made for blocking body fluid to lower your risk of contracting an STD via oral sex.
Keep in mind: Even with these protections, make sure you and your partner discuss each other’s sexual history, any prior or current STDs and their preferred protection from STDs, said Dr. Aguh.
If you or your partner is being treated for an STD, consider opting out of oral sex and consulting a doctor.
The HPV vaccine is another common method of protection. The shot is “approved for prevention of nine of the most high-risk strains of HPV,” or those that are most commonly linked to cancer, according to Dr. Lee. The vaccine “reduces the frequency of infection” with these viruses, which can ultimately lower the risk of cancers linked to HPV, including cervical, anal, and vulvar and vaginal cancers, she said.
“The best time to receive treatment for prevention of disease is prior to onset of sexual intercourse,” said Dr. Lee.
To get your HPV vaccine, head to your family doctor, school- or community-based health center, or state health department, suggests the CDC.
A version of this article originally appeared on WebMD.com.
An epidemic of sexually transmitted HPV is now swirling around the United States and the United Kingdom, with some serious cases leading to oropharyngeal cancer, which can affect the back of the throat, tonsils, and tongue.
HPV is the leading cause (70%) of this oropharyngeal cancer, according to the CDC. It is the most common sexually transmitted disease in the nation, and around 3.6% of women and 10% of men report oral HPV specifically. But over the past decade, oropharyngeal cases have been steadily falling a little under 4% and 2%, respectively, according to the National Cancer Institute.
HPV is often undetectable and can clear up within a few months. But unfortunately for some, serious disease, such as throat cancer, can develop.
Studies show the HPV vaccine to be extremely effective in lowering sexually transmitted HPV cases. Yet, only 54.5% of young people aged 13-15 have taken the recommended two to three doses, according to the National Cancer Institute.
Why aren’t more young people taking the vaccine?
Low public awareness of the dangers of HPV may be behind young people’s poor vaccination rates, according to Teresa Lee, MD, of the Fox Chase Cancer Center in Philadelphia. “For example, while the link with head and neck cancers has been well-studied, the FDA labeling was not changed to reflect this as an indication until 2020,” she said.
Other reasons can include one’s socioeconomic background, poor health literacy, cultural or religious stigmas around vaccines, and lack of quality, low-cost health care, says Emmanuel Aguh, MD, a board-certified family medicine physician. “Some individuals and families are still resistant to vaccines and the noted lack of uptake.”
Doctors and other health care professionals should also be sure to tell patients of all ages about the risks of HPV infection and how well the vaccine works, Dr. Lee said. “Not everyone who is now eligible may have been offered the vaccine as a child, and the first time young adults may receive counseling on this subject may not be until they are entering a very busy period of their lives with many responsibilities – when it may be hard to fit in things like health maintenance.”
How safe is the HPV vaccine?
The Food and Drug Administration and Centers for Disease Control and Prevention have studied the HPV vaccine for years to find out how safe it is and how well it works, Dr. Aguh said. No major side effects have been reported, and the most common side effect is soreness where you get the shot (which is normal after most vaccines). Some dizziness and fainting in adolescents can also occur, so young people are usually asked to sit or lie down during the shot and for 15 minutes afterward, he said.
“Serious adverse events have not been reported at higher rates than expected following HPV vaccination, meaning there is no clear evidence they are related to the vaccine,” Dr. Lee said. “The vaccine is highly effective in decreasing rates of detectable infection with the high-risk HPV strains responsible for HPV-associated cancers.”
The HPV vaccine is largely recommended for people aged 9-26, and sometimes up to age 45, depending on the individual, Dr. Aguh said. If you are over 26, talk to your doctor about whether you should consider getting the vaccine.
“It is usually given in two doses for complete protection if taken before the 15th birthday,” Dr. Aguh said. “If taken afterward, or in those with a weak immune system, they might require three doses to be fully protected.”
The vaccine produces antibodies that can stop HPV from infecting cells and lowers your chances of catching an HPV-related cancer, such as throat cancer or cancer of the cervix, he said.
While the vaccine is not guaranteed to protect you from the more than 100 strains of HPV, it can protect you from HPV 16 and HPV 18 – two high-risk strains that cause around 70% of cervical cancers.
What is fueling the rise of HPV cases?
A misconception that oral sex is somehow a “safe and risk-free” alternative to anal or vaginal sex could be one reason, Dr. Aguh said.
“It is important to know that, with oral sex, you are exposed to many of the risks associated with vaginal intercourse, especially if you do not take any measures to protect yourself and/or your partner,” Dr. Aguh said. “[With oral sex] it is possible to end up contracting an infection like chlamydia, gonorrhea, and even HPV, leading to an increased risk of HPV-associated oropharyngeal cancers.”
A lack of public awareness of what can cause throat cancer could also explain this phenomenon. The number of people you have oral sex with, along with the age you begin sexual activity, can greatly determine your risk of the disease, according to Dr. Lee. She echoes a report by Hisham Mehanna, PhD, in The Conversation.
“For oropharyngeal cancer, the main risk factor is the number of lifetime sexual partners, especially oral sex,” wrote Dr. Mehanna, a professor at the Institute of Cancer and Genomic Sciences at the University of Birmingham (England). “Those with six or more lifetime oral-sex partners are 8.5 times more likely to develop oropharyngeal cancer than those who do not practice oral sex.”
What are symptoms of oropharyngeal cancer?
Labored breathing or swallowing, a cough that won’t go away, and crackling or hoarseness of your voice could all be signs of throat cancer. Other symptoms include earaches, swelling of the head or neck, and enlarged lymph nodes, among others, Dr. Aguh said.
“The signs and symptoms of HPV-related throat cancers can be difficult to identify and recognize, as they can be vague and are also associated with other medical conditions. Sometimes, there are no signs at all, or they are not easily noticeable due to the location,” he said.
You should go see your doctor if you have any of these ailments for an extended period.
How to reduce your risk
In addition to having six or more oral-sex partners, smoking and drinking heavily could also raise your risk of throat cancer, said Dr. Lee. Proper dental health – like seeing your dentist regularly and practicing proper oral hygiene – can also shave your risk.
“[Good dental health] can help not just with head and neck cancer risk, but with many other inflammation-related diseases,” Dr. Lee said.
Using dental dams and condoms can also be a good method of protection, Dr. Aguh said. A dental dam is a stretchy sheet of latex, or polyurethane plastic, in the shape of a square that is made for blocking body fluid to lower your risk of contracting an STD via oral sex.
Keep in mind: Even with these protections, make sure you and your partner discuss each other’s sexual history, any prior or current STDs and their preferred protection from STDs, said Dr. Aguh.
If you or your partner is being treated for an STD, consider opting out of oral sex and consulting a doctor.
The HPV vaccine is another common method of protection. The shot is “approved for prevention of nine of the most high-risk strains of HPV,” or those that are most commonly linked to cancer, according to Dr. Lee. The vaccine “reduces the frequency of infection” with these viruses, which can ultimately lower the risk of cancers linked to HPV, including cervical, anal, and vulvar and vaginal cancers, she said.
“The best time to receive treatment for prevention of disease is prior to onset of sexual intercourse,” said Dr. Lee.
To get your HPV vaccine, head to your family doctor, school- or community-based health center, or state health department, suggests the CDC.
A version of this article originally appeared on WebMD.com.
Once-weekly basal insulin nears market for type 2 diabetes
SAN DIEGO – results from two new phase 3a studies suggest.
Data from Novo Nordisk’s ONWARDS 1, comparing once-weekly icodec with once-daily glargine, and ONWARDS 3, comparing once-weekly icodec with daily degludec (Tresiba, Novo Nordisk), both in insulin-naive patients with type 2 diabetes, were presented at the annual scientific sessions of the American Diabetes Association.
In both trials, primary endpoints of superiority and noninferiority in A1c reduction were achieved, and in ONWARDS 1, patients spent more time in target blood glucose range.
“I feel that weekly insulins have the potential to become transformational as preferred options for basal insulin replacement in people with type 2 diabetes in need of initiation of insulin therapy,” said Julio Rosenstock, MD, the lead author of ONWARDS 1.
Asked to comment, independent diabetes industry consultant Charles Alexander, MD, said: “The data certainly support approval of Icodec.”
Dr. Alexander said that an ideal candidate for once-weekly insulin “is someone who’s already on once-weekly [glucagon-like peptide-1 (GLP-1) agonist]. Then, taking your GLP-1 [agonist] and your basal insulin at the same time once a week makes a lot of sense ... Since they’re taking a weekly injection anyway, it’s relatively easy for a person to remember ‘When I take my weekly GLP-1 [agonist], I’ll take my weekly basal insulin.’ ”
However, he also pointed out: “Payers may say they don’t care about the convenience of once-weekly and they prefer to pay for the cheaper daily basal [insulin] ... I think a lot of people will continue to use [insulin] glargine because it is cheaper than either degludec or icodec.”
The data from ONWARDS 1 was published in the New England Journal of Medicine, and the data from ONWARDS 3 was published in JAMA.
Six ONWARDS trials make up Novo Nordisk’s phase 3a clinical development program comparing the efficacy and safety of once-weekly insulin icodec with once-daily basal insulin comparators.
Previously, findings from ONWARDS 2, in which patients with type 2 diabetes taking basal insulin had improved A1c after being switched to once-weekly icodec or once-daily degludec, were presented at the annual meeting of the European Association for the Study of Diabetes.
Insulin icodec has been submitted for regulatory review in the United States, Canada, Europe, China, Australia, Switzerland, and Brazil, with decisions anticipated starting in the first half of 2024.
Hypoglycemia: Is the slight increase clinically significant?
One concern about the once-weekly insulins is that they might result in higher rates of hypoglycemia because they stay active in the body for so long.
Differences in rates of combined level 2 (clinically significant) and level 3 (severe) hypoglycemia were increased with borderline significance in ONWARDS 1.
In ONWARDS 3 there was a threefold significant difference, but the overall risk was still low, equating to one episode per patient per 3 years, said Ildiko Lingvay, MD, of University of Texas Southwestern Medical Center, Dallas, who is lead author for ONWARDS 1 and a co-author for ONWARDS 3.

“Insulin is insulin. When we use insulin there will always be hypoglycemia. But we only have less than one event per year,” added Dr. Rosenstock, of Velocity Clinical Research at Medical City, Dallas.
Dr. Alexander pointed out that in ONWARDS 3 just under half of both groups were taking a sulfonylurea, although the trial design allowed for cutting the dose in half when the basal insulin was added.
In ONWARDS 1, in contrast, sulfonylureas and glinides were stopped at the time of randomization. “That’s not definitive, but I would argue that’s the explanation, to be proven by formal testing.”
Indeed, an audience member asked about that during the discussion, and Dr. Lingvay said they were still analyzing those data. “We’re working on that. It’s very important.”
Dr. Alexander noted, “I think the message here is don’t continue sulfonylureas or glinides in someone you’re giving insulin to because you’re going to get hypoglycemia.”
Better glycemic control, with fewer injections
ONWARDS 1 was a 78-week, randomized, open-label, treat-to-target trial, with a main 52-week phase and a 26-week extension phase. A total of 984 patients with type 2 diabetes and A1c 7%-11% with no prior insulin treatment were randomized 1:1 to once-weekly icodec or daily insulin glargine. All baseline medications except sulfonylureas and glinides were continued.
The primary endpoint was change in A1c from baseline to week 52, and this dropped from 8.5% to 6.9% with icodec, versus 8.4% to 7.1% with glargine, a significant difference, confirming both noninferiority (P < .001) and superiority (P = .02) of icodec, Dr. Rosenstock said.
The percentage of time in blood glucose range (70-180 mg/dL) was also significantly higher with icodec than glargine (71.9% vs. 66.9%; P < .001), also confirming superiority.
Rates of combined clinically significant or severe hypoglycemia at 83 weeks were 0.30 versus 0.16 events per person-year of exposure at week 83 (P = .043). No new safety signals were identified, and incidences of adverse events were similar in the two groups.
A significantly higher proportion of participants achieved an A1c of less than 7% without clinically significant or severe hypoglycemia with once-weekly basal insulin icodec versus once-daily basal insulin glargine (52.6% vs. 42.6%).
ONWARDS 3 randomized 588 patients each to once-weekly insulin icodec plus once-weekly placebo or once-daily insulin degludec plus once-weekly placebo. The primary endpoint, change in A1c from baseline to week 26, fell from 8.6% to 7.0% with icodec and from 8.5% to 7.2% with degludec, confirming both noninferiority (P < .001) and superiority (P = .002).
There were no significant differences between the two insulins in change in fasting plasma glucose, mean weekly insulin dose, or body weight.
Combined level 2 or 3 hypoglycemia rates were numerically higher in the icodec group than in the degludec group from week 0 to 31 (0.31 vs. 0.15 events per patient-year exposure; P = .11) and statistically higher in the icodec group from week 0 to 26 (0.35 vs. 0.12 events per patient-year exposure; P = .01).
The percentage of patients achieving an A1c of less than 7% without level 2 or 3 hypoglycemia was 52.1% with icodec versus 39.9% with degludec.
Dr. Lingvay and Dr. Rosenstock have reported financial relationships with multiple companies.
A version of this article originally appeared on Medscape.com.
SAN DIEGO – results from two new phase 3a studies suggest.
Data from Novo Nordisk’s ONWARDS 1, comparing once-weekly icodec with once-daily glargine, and ONWARDS 3, comparing once-weekly icodec with daily degludec (Tresiba, Novo Nordisk), both in insulin-naive patients with type 2 diabetes, were presented at the annual scientific sessions of the American Diabetes Association.
In both trials, primary endpoints of superiority and noninferiority in A1c reduction were achieved, and in ONWARDS 1, patients spent more time in target blood glucose range.
“I feel that weekly insulins have the potential to become transformational as preferred options for basal insulin replacement in people with type 2 diabetes in need of initiation of insulin therapy,” said Julio Rosenstock, MD, the lead author of ONWARDS 1.
Asked to comment, independent diabetes industry consultant Charles Alexander, MD, said: “The data certainly support approval of Icodec.”
Dr. Alexander said that an ideal candidate for once-weekly insulin “is someone who’s already on once-weekly [glucagon-like peptide-1 (GLP-1) agonist]. Then, taking your GLP-1 [agonist] and your basal insulin at the same time once a week makes a lot of sense ... Since they’re taking a weekly injection anyway, it’s relatively easy for a person to remember ‘When I take my weekly GLP-1 [agonist], I’ll take my weekly basal insulin.’ ”
However, he also pointed out: “Payers may say they don’t care about the convenience of once-weekly and they prefer to pay for the cheaper daily basal [insulin] ... I think a lot of people will continue to use [insulin] glargine because it is cheaper than either degludec or icodec.”
The data from ONWARDS 1 was published in the New England Journal of Medicine, and the data from ONWARDS 3 was published in JAMA.
Six ONWARDS trials make up Novo Nordisk’s phase 3a clinical development program comparing the efficacy and safety of once-weekly insulin icodec with once-daily basal insulin comparators.
Previously, findings from ONWARDS 2, in which patients with type 2 diabetes taking basal insulin had improved A1c after being switched to once-weekly icodec or once-daily degludec, were presented at the annual meeting of the European Association for the Study of Diabetes.
Insulin icodec has been submitted for regulatory review in the United States, Canada, Europe, China, Australia, Switzerland, and Brazil, with decisions anticipated starting in the first half of 2024.
Hypoglycemia: Is the slight increase clinically significant?
One concern about the once-weekly insulins is that they might result in higher rates of hypoglycemia because they stay active in the body for so long.
Differences in rates of combined level 2 (clinically significant) and level 3 (severe) hypoglycemia were increased with borderline significance in ONWARDS 1.
In ONWARDS 3 there was a threefold significant difference, but the overall risk was still low, equating to one episode per patient per 3 years, said Ildiko Lingvay, MD, of University of Texas Southwestern Medical Center, Dallas, who is lead author for ONWARDS 1 and a co-author for ONWARDS 3.
“Insulin is insulin. When we use insulin there will always be hypoglycemia. But we only have less than one event per year,” added Dr. Rosenstock, of Velocity Clinical Research at Medical City, Dallas.
Dr. Alexander pointed out that in ONWARDS 3 just under half of both groups were taking a sulfonylurea, although the trial design allowed for cutting the dose in half when the basal insulin was added.
In ONWARDS 1, in contrast, sulfonylureas and glinides were stopped at the time of randomization. “That’s not definitive, but I would argue that’s the explanation, to be proven by formal testing.”
Indeed, an audience member asked about that during the discussion, and Dr. Lingvay said they were still analyzing those data. “We’re working on that. It’s very important.”
Dr. Alexander noted, “I think the message here is don’t continue sulfonylureas or glinides in someone you’re giving insulin to because you’re going to get hypoglycemia.”
Better glycemic control, with fewer injections
ONWARDS 1 was a 78-week, randomized, open-label, treat-to-target trial, with a main 52-week phase and a 26-week extension phase. A total of 984 patients with type 2 diabetes and A1c 7%-11% with no prior insulin treatment were randomized 1:1 to once-weekly icodec or daily insulin glargine. All baseline medications except sulfonylureas and glinides were continued.
The primary endpoint was change in A1c from baseline to week 52, and this dropped from 8.5% to 6.9% with icodec, versus 8.4% to 7.1% with glargine, a significant difference, confirming both noninferiority (P < .001) and superiority (P = .02) of icodec, Dr. Rosenstock said.
The percentage of time in blood glucose range (70-180 mg/dL) was also significantly higher with icodec than glargine (71.9% vs. 66.9%; P < .001), also confirming superiority.
Rates of combined clinically significant or severe hypoglycemia at 83 weeks were 0.30 versus 0.16 events per person-year of exposure at week 83 (P = .043). No new safety signals were identified, and incidences of adverse events were similar in the two groups.
A significantly higher proportion of participants achieved an A1c of less than 7% without clinically significant or severe hypoglycemia with once-weekly basal insulin icodec versus once-daily basal insulin glargine (52.6% vs. 42.6%).
ONWARDS 3 randomized 588 patients each to once-weekly insulin icodec plus once-weekly placebo or once-daily insulin degludec plus once-weekly placebo. The primary endpoint, change in A1c from baseline to week 26, fell from 8.6% to 7.0% with icodec and from 8.5% to 7.2% with degludec, confirming both noninferiority (P < .001) and superiority (P = .002).
There were no significant differences between the two insulins in change in fasting plasma glucose, mean weekly insulin dose, or body weight.
Combined level 2 or 3 hypoglycemia rates were numerically higher in the icodec group than in the degludec group from week 0 to 31 (0.31 vs. 0.15 events per patient-year exposure; P = .11) and statistically higher in the icodec group from week 0 to 26 (0.35 vs. 0.12 events per patient-year exposure; P = .01).
The percentage of patients achieving an A1c of less than 7% without level 2 or 3 hypoglycemia was 52.1% with icodec versus 39.9% with degludec.
Dr. Lingvay and Dr. Rosenstock have reported financial relationships with multiple companies.
A version of this article originally appeared on Medscape.com.
SAN DIEGO – results from two new phase 3a studies suggest.
Data from Novo Nordisk’s ONWARDS 1, comparing once-weekly icodec with once-daily glargine, and ONWARDS 3, comparing once-weekly icodec with daily degludec (Tresiba, Novo Nordisk), both in insulin-naive patients with type 2 diabetes, were presented at the annual scientific sessions of the American Diabetes Association.
In both trials, primary endpoints of superiority and noninferiority in A1c reduction were achieved, and in ONWARDS 1, patients spent more time in target blood glucose range.
“I feel that weekly insulins have the potential to become transformational as preferred options for basal insulin replacement in people with type 2 diabetes in need of initiation of insulin therapy,” said Julio Rosenstock, MD, the lead author of ONWARDS 1.
Asked to comment, independent diabetes industry consultant Charles Alexander, MD, said: “The data certainly support approval of Icodec.”
Dr. Alexander said that an ideal candidate for once-weekly insulin “is someone who’s already on once-weekly [glucagon-like peptide-1 (GLP-1) agonist]. Then, taking your GLP-1 [agonist] and your basal insulin at the same time once a week makes a lot of sense ... Since they’re taking a weekly injection anyway, it’s relatively easy for a person to remember ‘When I take my weekly GLP-1 [agonist], I’ll take my weekly basal insulin.’ ”
However, he also pointed out: “Payers may say they don’t care about the convenience of once-weekly and they prefer to pay for the cheaper daily basal [insulin] ... I think a lot of people will continue to use [insulin] glargine because it is cheaper than either degludec or icodec.”
The data from ONWARDS 1 was published in the New England Journal of Medicine, and the data from ONWARDS 3 was published in JAMA.
Six ONWARDS trials make up Novo Nordisk’s phase 3a clinical development program comparing the efficacy and safety of once-weekly insulin icodec with once-daily basal insulin comparators.
Previously, findings from ONWARDS 2, in which patients with type 2 diabetes taking basal insulin had improved A1c after being switched to once-weekly icodec or once-daily degludec, were presented at the annual meeting of the European Association for the Study of Diabetes.
Insulin icodec has been submitted for regulatory review in the United States, Canada, Europe, China, Australia, Switzerland, and Brazil, with decisions anticipated starting in the first half of 2024.
Hypoglycemia: Is the slight increase clinically significant?
One concern about the once-weekly insulins is that they might result in higher rates of hypoglycemia because they stay active in the body for so long.
Differences in rates of combined level 2 (clinically significant) and level 3 (severe) hypoglycemia were increased with borderline significance in ONWARDS 1.
In ONWARDS 3 there was a threefold significant difference, but the overall risk was still low, equating to one episode per patient per 3 years, said Ildiko Lingvay, MD, of University of Texas Southwestern Medical Center, Dallas, who is lead author for ONWARDS 1 and a co-author for ONWARDS 3.
“Insulin is insulin. When we use insulin there will always be hypoglycemia. But we only have less than one event per year,” added Dr. Rosenstock, of Velocity Clinical Research at Medical City, Dallas.
Dr. Alexander pointed out that in ONWARDS 3 just under half of both groups were taking a sulfonylurea, although the trial design allowed for cutting the dose in half when the basal insulin was added.
In ONWARDS 1, in contrast, sulfonylureas and glinides were stopped at the time of randomization. “That’s not definitive, but I would argue that’s the explanation, to be proven by formal testing.”
Indeed, an audience member asked about that during the discussion, and Dr. Lingvay said they were still analyzing those data. “We’re working on that. It’s very important.”
Dr. Alexander noted, “I think the message here is don’t continue sulfonylureas or glinides in someone you’re giving insulin to because you’re going to get hypoglycemia.”
Better glycemic control, with fewer injections
ONWARDS 1 was a 78-week, randomized, open-label, treat-to-target trial, with a main 52-week phase and a 26-week extension phase. A total of 984 patients with type 2 diabetes and A1c 7%-11% with no prior insulin treatment were randomized 1:1 to once-weekly icodec or daily insulin glargine. All baseline medications except sulfonylureas and glinides were continued.
The primary endpoint was change in A1c from baseline to week 52, and this dropped from 8.5% to 6.9% with icodec, versus 8.4% to 7.1% with glargine, a significant difference, confirming both noninferiority (P < .001) and superiority (P = .02) of icodec, Dr. Rosenstock said.
The percentage of time in blood glucose range (70-180 mg/dL) was also significantly higher with icodec than glargine (71.9% vs. 66.9%; P < .001), also confirming superiority.
Rates of combined clinically significant or severe hypoglycemia at 83 weeks were 0.30 versus 0.16 events per person-year of exposure at week 83 (P = .043). No new safety signals were identified, and incidences of adverse events were similar in the two groups.
A significantly higher proportion of participants achieved an A1c of less than 7% without clinically significant or severe hypoglycemia with once-weekly basal insulin icodec versus once-daily basal insulin glargine (52.6% vs. 42.6%).
ONWARDS 3 randomized 588 patients each to once-weekly insulin icodec plus once-weekly placebo or once-daily insulin degludec plus once-weekly placebo. The primary endpoint, change in A1c from baseline to week 26, fell from 8.6% to 7.0% with icodec and from 8.5% to 7.2% with degludec, confirming both noninferiority (P < .001) and superiority (P = .002).
There were no significant differences between the two insulins in change in fasting plasma glucose, mean weekly insulin dose, or body weight.
Combined level 2 or 3 hypoglycemia rates were numerically higher in the icodec group than in the degludec group from week 0 to 31 (0.31 vs. 0.15 events per patient-year exposure; P = .11) and statistically higher in the icodec group from week 0 to 26 (0.35 vs. 0.12 events per patient-year exposure; P = .01).
The percentage of patients achieving an A1c of less than 7% without level 2 or 3 hypoglycemia was 52.1% with icodec versus 39.9% with degludec.
Dr. Lingvay and Dr. Rosenstock have reported financial relationships with multiple companies.
A version of this article originally appeared on Medscape.com.
AT ADA 2023
No link between heartburn meds and dementia
A new study provides reassurance about the safety of long-term proton pump inhibitor (PPIs) and histamine-2 receptor antagonist (H2RA) use in older adults, finding no increased risk for dementia or cognitive changes.
It was published online in Gastroenterology.
The post hoc observational study was led by Raaj Mehta, MD, PhD, with Massachusetts General Hospital and Harvard Medical School in Boston.
The researchers analyzed results from the Aspirin in Reducing Events in the Elderly clinical trial. The randomized trial of aspirin included 18,934 adults aged 65 and older from the United States and Australia. Patients’ use of PPI and H2RA was tracked, along with dementia incidence and cognitive changes.
The results showed that there was no link to new dementia diagnoses in patients who used PPIs (25%) and H2RA (2%) at baseline, versus those who did not use either heartburn medication.
Limitations of prior studies are referenced, including the potential for residual confounding and underestimation of PPI and H2RA use, the lack of data on medication dose and duration, and the absence of apo E4 allele status.
The study was funded by grants from the National Institute on Aging, the National Cancer Institute, and other institutions. Dr. Mehta has disclosed no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
A new study provides reassurance about the safety of long-term proton pump inhibitor (PPIs) and histamine-2 receptor antagonist (H2RA) use in older adults, finding no increased risk for dementia or cognitive changes.
It was published online in Gastroenterology.
The post hoc observational study was led by Raaj Mehta, MD, PhD, with Massachusetts General Hospital and Harvard Medical School in Boston.
The researchers analyzed results from the Aspirin in Reducing Events in the Elderly clinical trial. The randomized trial of aspirin included 18,934 adults aged 65 and older from the United States and Australia. Patients’ use of PPI and H2RA was tracked, along with dementia incidence and cognitive changes.
The results showed that there was no link to new dementia diagnoses in patients who used PPIs (25%) and H2RA (2%) at baseline, versus those who did not use either heartburn medication.
Limitations of prior studies are referenced, including the potential for residual confounding and underestimation of PPI and H2RA use, the lack of data on medication dose and duration, and the absence of apo E4 allele status.
The study was funded by grants from the National Institute on Aging, the National Cancer Institute, and other institutions. Dr. Mehta has disclosed no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
A new study provides reassurance about the safety of long-term proton pump inhibitor (PPIs) and histamine-2 receptor antagonist (H2RA) use in older adults, finding no increased risk for dementia or cognitive changes.
It was published online in Gastroenterology.
The post hoc observational study was led by Raaj Mehta, MD, PhD, with Massachusetts General Hospital and Harvard Medical School in Boston.
The researchers analyzed results from the Aspirin in Reducing Events in the Elderly clinical trial. The randomized trial of aspirin included 18,934 adults aged 65 and older from the United States and Australia. Patients’ use of PPI and H2RA was tracked, along with dementia incidence and cognitive changes.
The results showed that there was no link to new dementia diagnoses in patients who used PPIs (25%) and H2RA (2%) at baseline, versus those who did not use either heartburn medication.
Limitations of prior studies are referenced, including the potential for residual confounding and underestimation of PPI and H2RA use, the lack of data on medication dose and duration, and the absence of apo E4 allele status.
The study was funded by grants from the National Institute on Aging, the National Cancer Institute, and other institutions. Dr. Mehta has disclosed no relevant conflicts of interest.
A version of this article originally appeared on Medscape.com.
FROM GASTROENTEROLOGY
ADA: Screen all with type 2 diabetes for fatty liver disease
SAN DIEGO – and provides new recommendations for management in those with the condition or who are at risk for it.
Liver disease affects up to 70% of people with type 2 diabetes and is common in people with prediabetes and in those with type 1 diabetes who also have obesity. Non-alcoholic fatty liver disease (NAFLD) is the most common form of liver disease in people with diabetes. It can lead to cirrhosis and liver cancer and is associated with an increased risk for cardiovascular disease and death. The condition includes non-alcoholic steatohepatitis (NASH).
“The ADA has recognized that this has become a big problem for their patients because NASH is becoming the number one cause of cirrhosis in people with type 2 diabetes and the number one cause of liver transplantation in the United States, so we have to do something about it,” Kenneth Cusi, MD, who presented a summary of the new guidance at the annual scientific sessions of the American Diabetes Association, said in an interview.
The new ADA guidance was published as a mid-year update to the ADA’s Standards of Care in Diabetes–2023 in the section on “Comprehensive Medical Evaluation and Assessment of Comorbidities.”
Asked to comment, Atlanta endocrinologist Scott Isaacs, MD, said, “It is wonderful to see that the ADA has recognized NAFLD ... as the hepatic complication of type 2 diabetes and has updated the Standards of Care reflecting the current knowledge and evidence of this ubiquitous and often silent disease.”
The new ADA guidance aligns with those of other professional societies, including the American Association for the Study of Liver Diseases, the American Gastroenterological Society, and the American Association of Clinical Endocrinology.
Dr. Isaacs, who chaired the AACE guidance writing panel, noted, “The ADA update essentially repeats the same guidance in the AACE and AASLD documents. It is excellent to see this type of alignment of guidance among the major organizations.”
FIB-4: Easy calculation in the EHR
The ADA now advises screening all adults with type 2 diabetes or prediabetes, particularly those with obesity or cardiometabolic risk factors or established cardiovascular disease – even those with normal liver enzyme levels. People with type 1 diabetes who have obesity and/or cardiovascular risk factors are also to be screened for NAFLD.
The recommended screening tool is the fibrosis-4 index (FIB-4), a calculation that includes the patient’s age, liver enzyme levels, and platelet counts. A score of 1.3 or higher is considered high risk for clinically significant fibrosis and above 2.6 is very high-risk.
Dr. Cusi noted, “The reason we advise using the FIB-4 ... instead of liver enzymes as ADA advised in the past, is that now we know that 70% of people with type 2 diabetes have steatosis already and about one in five have fibrosis, but if you go by liver enzymes you will miss most of them. Liver enzymes are ineffective as a screening tool.”
The FIB-4 is “a simple tool we already have in our electronic health records (EHR) but we’re just simply not using it,” noted Dr. Cusi, chief of endocrinology, diabetes, and metabolism at the University of Florida, Gainesville.
Indeed, Dr. Isaacs said, “The FIB-4 is a simple ... great screening test because it is essentially free.” But he cautioned that it has some limitations.
“It is a good test for ruling out advanced liver disease but can have false positives and false negatives. The FIB-4 cutoffs need to be adjusted for persons over 65 years old and [should] not to be used for persons under 30 years old.”
Dr. Isaacs also pointed out that, while the calculation can be done from a website, “even this adds time to a clinician’s busy day. Ideally, the FIB-4 should be automatically calculated in the EHR or on the lab report, similar to the [estimated glomerular filtration rate] calculation [for kidney function] and flagged if greater than 1.3.”
The ADA update also provides guidance on follow-up for patients flagged with the FIB-4, including when referral to a gastroenterologist or hepatologist is appropriate.
Treatment: Lifestyle modification plus GLP-1 agonists or pioglitazone
Lifestyle modification is recommended for all adults with diabetes or prediabetes and NAFLD, particularly those with overweight or obesity.
In addition, the ADA now advises consideration of a using a glucagonlike peptide–1 (GLP-1) agonist with demonstrated benefits in NAFLD as adjunctive therapy to lifestyle interventions for weight loss in those with type 2 diabetes, particularly with overweight/obesity.
And for those with biopsy-proven NASH or who are identified with clinically significant liver fibrosis using non-invasive tests, either a GLP-1 agonist or pioglitazone are the “preferred treatments.”
However, insulin is the preferred treatment for hyperglycemia in adults with type 2 diabetes who have decompensated cirrhosis.
Dr. Isaacs commented, “Pioglitazone has so many benefits and a few known risks ... it is an underused medication. It is very inexpensive. Pioglitazone should be considered as a first line treatment for patients with type 2 diabetes and NAFLD.”
The ADA update also advises statin therapy for people with type 2 diabetes and NAFLD, given their increased cardiovascular risk. However, statins are not recommended for people with decompensated cirrhosis because of limited safety and efficacy data.
Dr. Cusi noted that he has been advocating for fatty liver screening in people with type 2 diabetes for over a decade.
“Doctors have already been adopting it, but ADA as an organization in diabetes care has a big impact. I dreamed many years ago that the day would come when we would screen all people with type 2 diabetes, and that day is today.”
Dr. Cusi is a consultant for Altimmune, Akero, Arrowhead, AstraZeneca, 89Bio, BMS, Coherus, Intercept, Lilly, Madrigal, Merck, Novo Nordisk, Quest, Sagimet, Sonic Incytes, Terns, Thera Technologies, and MSD. Dr. Isaacs reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – and provides new recommendations for management in those with the condition or who are at risk for it.
Liver disease affects up to 70% of people with type 2 diabetes and is common in people with prediabetes and in those with type 1 diabetes who also have obesity. Non-alcoholic fatty liver disease (NAFLD) is the most common form of liver disease in people with diabetes. It can lead to cirrhosis and liver cancer and is associated with an increased risk for cardiovascular disease and death. The condition includes non-alcoholic steatohepatitis (NASH).
“The ADA has recognized that this has become a big problem for their patients because NASH is becoming the number one cause of cirrhosis in people with type 2 diabetes and the number one cause of liver transplantation in the United States, so we have to do something about it,” Kenneth Cusi, MD, who presented a summary of the new guidance at the annual scientific sessions of the American Diabetes Association, said in an interview.
The new ADA guidance was published as a mid-year update to the ADA’s Standards of Care in Diabetes–2023 in the section on “Comprehensive Medical Evaluation and Assessment of Comorbidities.”
Asked to comment, Atlanta endocrinologist Scott Isaacs, MD, said, “It is wonderful to see that the ADA has recognized NAFLD ... as the hepatic complication of type 2 diabetes and has updated the Standards of Care reflecting the current knowledge and evidence of this ubiquitous and often silent disease.”
The new ADA guidance aligns with those of other professional societies, including the American Association for the Study of Liver Diseases, the American Gastroenterological Society, and the American Association of Clinical Endocrinology.
Dr. Isaacs, who chaired the AACE guidance writing panel, noted, “The ADA update essentially repeats the same guidance in the AACE and AASLD documents. It is excellent to see this type of alignment of guidance among the major organizations.”
FIB-4: Easy calculation in the EHR
The ADA now advises screening all adults with type 2 diabetes or prediabetes, particularly those with obesity or cardiometabolic risk factors or established cardiovascular disease – even those with normal liver enzyme levels. People with type 1 diabetes who have obesity and/or cardiovascular risk factors are also to be screened for NAFLD.
The recommended screening tool is the fibrosis-4 index (FIB-4), a calculation that includes the patient’s age, liver enzyme levels, and platelet counts. A score of 1.3 or higher is considered high risk for clinically significant fibrosis and above 2.6 is very high-risk.
Dr. Cusi noted, “The reason we advise using the FIB-4 ... instead of liver enzymes as ADA advised in the past, is that now we know that 70% of people with type 2 diabetes have steatosis already and about one in five have fibrosis, but if you go by liver enzymes you will miss most of them. Liver enzymes are ineffective as a screening tool.”
The FIB-4 is “a simple tool we already have in our electronic health records (EHR) but we’re just simply not using it,” noted Dr. Cusi, chief of endocrinology, diabetes, and metabolism at the University of Florida, Gainesville.
Indeed, Dr. Isaacs said, “The FIB-4 is a simple ... great screening test because it is essentially free.” But he cautioned that it has some limitations.
“It is a good test for ruling out advanced liver disease but can have false positives and false negatives. The FIB-4 cutoffs need to be adjusted for persons over 65 years old and [should] not to be used for persons under 30 years old.”
Dr. Isaacs also pointed out that, while the calculation can be done from a website, “even this adds time to a clinician’s busy day. Ideally, the FIB-4 should be automatically calculated in the EHR or on the lab report, similar to the [estimated glomerular filtration rate] calculation [for kidney function] and flagged if greater than 1.3.”
The ADA update also provides guidance on follow-up for patients flagged with the FIB-4, including when referral to a gastroenterologist or hepatologist is appropriate.
Treatment: Lifestyle modification plus GLP-1 agonists or pioglitazone
Lifestyle modification is recommended for all adults with diabetes or prediabetes and NAFLD, particularly those with overweight or obesity.
In addition, the ADA now advises consideration of a using a glucagonlike peptide–1 (GLP-1) agonist with demonstrated benefits in NAFLD as adjunctive therapy to lifestyle interventions for weight loss in those with type 2 diabetes, particularly with overweight/obesity.
And for those with biopsy-proven NASH or who are identified with clinically significant liver fibrosis using non-invasive tests, either a GLP-1 agonist or pioglitazone are the “preferred treatments.”
However, insulin is the preferred treatment for hyperglycemia in adults with type 2 diabetes who have decompensated cirrhosis.
Dr. Isaacs commented, “Pioglitazone has so many benefits and a few known risks ... it is an underused medication. It is very inexpensive. Pioglitazone should be considered as a first line treatment for patients with type 2 diabetes and NAFLD.”
The ADA update also advises statin therapy for people with type 2 diabetes and NAFLD, given their increased cardiovascular risk. However, statins are not recommended for people with decompensated cirrhosis because of limited safety and efficacy data.
Dr. Cusi noted that he has been advocating for fatty liver screening in people with type 2 diabetes for over a decade.
“Doctors have already been adopting it, but ADA as an organization in diabetes care has a big impact. I dreamed many years ago that the day would come when we would screen all people with type 2 diabetes, and that day is today.”
Dr. Cusi is a consultant for Altimmune, Akero, Arrowhead, AstraZeneca, 89Bio, BMS, Coherus, Intercept, Lilly, Madrigal, Merck, Novo Nordisk, Quest, Sagimet, Sonic Incytes, Terns, Thera Technologies, and MSD. Dr. Isaacs reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
SAN DIEGO – and provides new recommendations for management in those with the condition or who are at risk for it.
Liver disease affects up to 70% of people with type 2 diabetes and is common in people with prediabetes and in those with type 1 diabetes who also have obesity. Non-alcoholic fatty liver disease (NAFLD) is the most common form of liver disease in people with diabetes. It can lead to cirrhosis and liver cancer and is associated with an increased risk for cardiovascular disease and death. The condition includes non-alcoholic steatohepatitis (NASH).
“The ADA has recognized that this has become a big problem for their patients because NASH is becoming the number one cause of cirrhosis in people with type 2 diabetes and the number one cause of liver transplantation in the United States, so we have to do something about it,” Kenneth Cusi, MD, who presented a summary of the new guidance at the annual scientific sessions of the American Diabetes Association, said in an interview.
The new ADA guidance was published as a mid-year update to the ADA’s Standards of Care in Diabetes–2023 in the section on “Comprehensive Medical Evaluation and Assessment of Comorbidities.”
Asked to comment, Atlanta endocrinologist Scott Isaacs, MD, said, “It is wonderful to see that the ADA has recognized NAFLD ... as the hepatic complication of type 2 diabetes and has updated the Standards of Care reflecting the current knowledge and evidence of this ubiquitous and often silent disease.”
The new ADA guidance aligns with those of other professional societies, including the American Association for the Study of Liver Diseases, the American Gastroenterological Society, and the American Association of Clinical Endocrinology.
Dr. Isaacs, who chaired the AACE guidance writing panel, noted, “The ADA update essentially repeats the same guidance in the AACE and AASLD documents. It is excellent to see this type of alignment of guidance among the major organizations.”
FIB-4: Easy calculation in the EHR
The ADA now advises screening all adults with type 2 diabetes or prediabetes, particularly those with obesity or cardiometabolic risk factors or established cardiovascular disease – even those with normal liver enzyme levels. People with type 1 diabetes who have obesity and/or cardiovascular risk factors are also to be screened for NAFLD.
The recommended screening tool is the fibrosis-4 index (FIB-4), a calculation that includes the patient’s age, liver enzyme levels, and platelet counts. A score of 1.3 or higher is considered high risk for clinically significant fibrosis and above 2.6 is very high-risk.
Dr. Cusi noted, “The reason we advise using the FIB-4 ... instead of liver enzymes as ADA advised in the past, is that now we know that 70% of people with type 2 diabetes have steatosis already and about one in five have fibrosis, but if you go by liver enzymes you will miss most of them. Liver enzymes are ineffective as a screening tool.”
The FIB-4 is “a simple tool we already have in our electronic health records (EHR) but we’re just simply not using it,” noted Dr. Cusi, chief of endocrinology, diabetes, and metabolism at the University of Florida, Gainesville.
Indeed, Dr. Isaacs said, “The FIB-4 is a simple ... great screening test because it is essentially free.” But he cautioned that it has some limitations.
“It is a good test for ruling out advanced liver disease but can have false positives and false negatives. The FIB-4 cutoffs need to be adjusted for persons over 65 years old and [should] not to be used for persons under 30 years old.”
Dr. Isaacs also pointed out that, while the calculation can be done from a website, “even this adds time to a clinician’s busy day. Ideally, the FIB-4 should be automatically calculated in the EHR or on the lab report, similar to the [estimated glomerular filtration rate] calculation [for kidney function] and flagged if greater than 1.3.”
The ADA update also provides guidance on follow-up for patients flagged with the FIB-4, including when referral to a gastroenterologist or hepatologist is appropriate.
Treatment: Lifestyle modification plus GLP-1 agonists or pioglitazone
Lifestyle modification is recommended for all adults with diabetes or prediabetes and NAFLD, particularly those with overweight or obesity.
In addition, the ADA now advises consideration of a using a glucagonlike peptide–1 (GLP-1) agonist with demonstrated benefits in NAFLD as adjunctive therapy to lifestyle interventions for weight loss in those with type 2 diabetes, particularly with overweight/obesity.
And for those with biopsy-proven NASH or who are identified with clinically significant liver fibrosis using non-invasive tests, either a GLP-1 agonist or pioglitazone are the “preferred treatments.”
However, insulin is the preferred treatment for hyperglycemia in adults with type 2 diabetes who have decompensated cirrhosis.
Dr. Isaacs commented, “Pioglitazone has so many benefits and a few known risks ... it is an underused medication. It is very inexpensive. Pioglitazone should be considered as a first line treatment for patients with type 2 diabetes and NAFLD.”
The ADA update also advises statin therapy for people with type 2 diabetes and NAFLD, given their increased cardiovascular risk. However, statins are not recommended for people with decompensated cirrhosis because of limited safety and efficacy data.
Dr. Cusi noted that he has been advocating for fatty liver screening in people with type 2 diabetes for over a decade.
“Doctors have already been adopting it, but ADA as an organization in diabetes care has a big impact. I dreamed many years ago that the day would come when we would screen all people with type 2 diabetes, and that day is today.”
Dr. Cusi is a consultant for Altimmune, Akero, Arrowhead, AstraZeneca, 89Bio, BMS, Coherus, Intercept, Lilly, Madrigal, Merck, Novo Nordisk, Quest, Sagimet, Sonic Incytes, Terns, Thera Technologies, and MSD. Dr. Isaacs reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ADA 2023
Intermittent fasting, cutting calories give same weight loss
a new study published online in Annals of Internal Medicine has found. The small, unblinded study compared weight loss in 77 participants who either intermittently fasted, adhered to a calorie-restricted diet, or were in a control group with no eating restrictions.
Compared with the control group, absolute weight loss for people in the intermittent fasting group was about 4.6 kg (10 lb), compared with 5.4 kg (12 lb) for those in the calorie-restriction group, after 12 months, with no significant difference between the intervention groups.
Intermittent fasting, or time-restricted eating, relies on the idea that the time you eat is more important for weight loss than what or how much you eat. The term is a catch-all for eating patterns that could include several full days of fasting per week or time-restricted eating during the day.
The effect of having less time to eat is thought to lead to the consumption of fewer calories, thought to be the main reason the approach works. Indeed, this trial found the intermittent fasting group ate 425 fewer calories per day, compared with 405 fewer calories per day in the calorie-restricted group.
“Time-restricted eating is undoubtedly an attractive approach to weight loss in that it does not require the purchase of expensive food products, allows persons to continue consuming familiar foods, and omits complicated calorie tracking,” Shuhao Lin, RD, University of Illinois at Chicago, and colleagues write.
During the trial, participants were in a weight-loss phase for 6 months. The intermittent fasting group could eat anything they wanted to between 12 p.m. and 8 p.m., and didn’t have to count calories. The later time window is on par with the eating pattern of most people in the United States who fast.
The calorie-restriction group had to cut 25% of their daily calorie intake based on their total energy expenditure. They were also told to fill half of every plate with fruits or vegetables, and consume about half their energy as carbohydrates, 30% as fat, and 20% as protein.
The weight-loss phase was followed by a 6-month weight-maintenance phase. During this phase, the window for eating was extended from 10 a.m. to 8 p.m. for the intermittent fasting group, and the calorie-restriction group was told to match their energy needs, which overall, had reduced by about 15%, compared with baseline.
Most participants were women with a mean body weight of about 100 kg (220 pounds) at baseline.
Both the time-restricted eating and calorie-restriction groups regularly met with dietitians, which the authors of an accompanying editorial say could have made the intermittent fasting more effective than in previous trials.
An earlier, shorter trial found about 0.9 kg (2 lb) weight loss after 12 weeks of adhering to a similar eating window, a more modest result, compared with the 4 kg (9 lb) weight loss at 6 months in this trial.
“The difference in outcomes between these two trials is likely attributable to differences in dietary counseling,” write the editorialists, Adam Gilden, MD, and Victoria Catenacci, MD, from University of Colorado at Denver, Aurora.
Previous studies of intermittent fasting have been short and showed similar findings, compared with a calorie-restricted diet.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
a new study published online in Annals of Internal Medicine has found. The small, unblinded study compared weight loss in 77 participants who either intermittently fasted, adhered to a calorie-restricted diet, or were in a control group with no eating restrictions.
Compared with the control group, absolute weight loss for people in the intermittent fasting group was about 4.6 kg (10 lb), compared with 5.4 kg (12 lb) for those in the calorie-restriction group, after 12 months, with no significant difference between the intervention groups.
Intermittent fasting, or time-restricted eating, relies on the idea that the time you eat is more important for weight loss than what or how much you eat. The term is a catch-all for eating patterns that could include several full days of fasting per week or time-restricted eating during the day.
The effect of having less time to eat is thought to lead to the consumption of fewer calories, thought to be the main reason the approach works. Indeed, this trial found the intermittent fasting group ate 425 fewer calories per day, compared with 405 fewer calories per day in the calorie-restricted group.
“Time-restricted eating is undoubtedly an attractive approach to weight loss in that it does not require the purchase of expensive food products, allows persons to continue consuming familiar foods, and omits complicated calorie tracking,” Shuhao Lin, RD, University of Illinois at Chicago, and colleagues write.
During the trial, participants were in a weight-loss phase for 6 months. The intermittent fasting group could eat anything they wanted to between 12 p.m. and 8 p.m., and didn’t have to count calories. The later time window is on par with the eating pattern of most people in the United States who fast.
The calorie-restriction group had to cut 25% of their daily calorie intake based on their total energy expenditure. They were also told to fill half of every plate with fruits or vegetables, and consume about half their energy as carbohydrates, 30% as fat, and 20% as protein.
The weight-loss phase was followed by a 6-month weight-maintenance phase. During this phase, the window for eating was extended from 10 a.m. to 8 p.m. for the intermittent fasting group, and the calorie-restriction group was told to match their energy needs, which overall, had reduced by about 15%, compared with baseline.
Most participants were women with a mean body weight of about 100 kg (220 pounds) at baseline.
Both the time-restricted eating and calorie-restriction groups regularly met with dietitians, which the authors of an accompanying editorial say could have made the intermittent fasting more effective than in previous trials.
An earlier, shorter trial found about 0.9 kg (2 lb) weight loss after 12 weeks of adhering to a similar eating window, a more modest result, compared with the 4 kg (9 lb) weight loss at 6 months in this trial.
“The difference in outcomes between these two trials is likely attributable to differences in dietary counseling,” write the editorialists, Adam Gilden, MD, and Victoria Catenacci, MD, from University of Colorado at Denver, Aurora.
Previous studies of intermittent fasting have been short and showed similar findings, compared with a calorie-restricted diet.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
a new study published online in Annals of Internal Medicine has found. The small, unblinded study compared weight loss in 77 participants who either intermittently fasted, adhered to a calorie-restricted diet, or were in a control group with no eating restrictions.
Compared with the control group, absolute weight loss for people in the intermittent fasting group was about 4.6 kg (10 lb), compared with 5.4 kg (12 lb) for those in the calorie-restriction group, after 12 months, with no significant difference between the intervention groups.
Intermittent fasting, or time-restricted eating, relies on the idea that the time you eat is more important for weight loss than what or how much you eat. The term is a catch-all for eating patterns that could include several full days of fasting per week or time-restricted eating during the day.
The effect of having less time to eat is thought to lead to the consumption of fewer calories, thought to be the main reason the approach works. Indeed, this trial found the intermittent fasting group ate 425 fewer calories per day, compared with 405 fewer calories per day in the calorie-restricted group.
“Time-restricted eating is undoubtedly an attractive approach to weight loss in that it does not require the purchase of expensive food products, allows persons to continue consuming familiar foods, and omits complicated calorie tracking,” Shuhao Lin, RD, University of Illinois at Chicago, and colleagues write.
During the trial, participants were in a weight-loss phase for 6 months. The intermittent fasting group could eat anything they wanted to between 12 p.m. and 8 p.m., and didn’t have to count calories. The later time window is on par with the eating pattern of most people in the United States who fast.
The calorie-restriction group had to cut 25% of their daily calorie intake based on their total energy expenditure. They were also told to fill half of every plate with fruits or vegetables, and consume about half their energy as carbohydrates, 30% as fat, and 20% as protein.
The weight-loss phase was followed by a 6-month weight-maintenance phase. During this phase, the window for eating was extended from 10 a.m. to 8 p.m. for the intermittent fasting group, and the calorie-restriction group was told to match their energy needs, which overall, had reduced by about 15%, compared with baseline.
Most participants were women with a mean body weight of about 100 kg (220 pounds) at baseline.
Both the time-restricted eating and calorie-restriction groups regularly met with dietitians, which the authors of an accompanying editorial say could have made the intermittent fasting more effective than in previous trials.
An earlier, shorter trial found about 0.9 kg (2 lb) weight loss after 12 weeks of adhering to a similar eating window, a more modest result, compared with the 4 kg (9 lb) weight loss at 6 months in this trial.
“The difference in outcomes between these two trials is likely attributable to differences in dietary counseling,” write the editorialists, Adam Gilden, MD, and Victoria Catenacci, MD, from University of Colorado at Denver, Aurora.
Previous studies of intermittent fasting have been short and showed similar findings, compared with a calorie-restricted diet.
The study was funded by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Triple-agonist retatrutide hits new weight loss highs
SAN DIEGO – New designer molecules that target weight loss via multiple mechanisms continue to raise the bar of how many pounds people with overweight or obesity can lose.
Retatrutide (Eli Lilly), an investigational agent that combines agonism to three key hormones that influence eating and metabolism into a single molecule, safely produced weight loss at levels never seen before in a pair of phase 2 studies that together randomized more than 600 people with overweight or obesity, with or without type 2 diabetes.
Among 338 randomized people with overweight or obesity and no type 2 diabetes,
Among 281 randomized people with overweight or obesity and type 2 diabetes, the same dose of retatrutide produced a nearly 17% cut in weight from baseline after 36 weeks of treatment.
Never before seen weight loss
“I have never seen weight loss at this level” after nearly 1 year of treatment, Ania M. Jastreboff, MD, PhD, who led the obesity study, said during a press briefing at the annual scientific sessions of the American Diabetes Association.

The average weight loss by study participants taking high-dose retatrutide in the two studies “is really impressive, way beyond my wildest dreams,” said Carel le Roux, MBChB, PhD, an obesity and diabetes researcher at University College Dublin, Ireland, who was not involved with the retatrutide studies.
And Robert A. Gabbay, MD, chief scientific and medical officer of the ADA, called the results “stunning,” and added, “we are now witnessing the first triple-hormone combination being highly effective for not only weight loss but liver disease and diabetes.”

A prespecified subgroup analysis of the obesity study showed that at both 8-mg and 12-mg weekly doses, 24 weeks of retatrutide produced complete resolution of excess liver fat (hepatic steatosis) in about 80% of the people eligible for the analysis (those with at least 10% of their liver volume as fat at study entry); that figure increased to about 90% of people on these doses after 48 weeks, Lee M. Kaplan, MD, reported during a separate presentation at the meeting.
Adding glucagon agonism ups liver-fat clearance
“When you add glucagon activity,” one of the three agonist actions of retatrutide, “liver-fat clearance goes up tremendously,” said Dr. Kaplan, director of the Obesity, Metabolism and Nutrition Institute at Massachusetts General Hospital in Boston.

“To my knowledge, no mono-agonist of the glucagon-like peptide-1 (GLP-1) receptor [such as semaglutide or liraglutide] produces more than 50% clearance of liver fat,” added Dr. Kaplan.
The separate, randomized study of people with type 2 diabetes showed that in addition to producing an unprecedented average level of weight loss at the highest retatrutide dose, the agent also produced an average reduction from baseline levels of A1c of about 2 percentage points, an efficacy roughly comparable to maximum doses of the most potent GLP-1 mono-agonist semaglutide (Ozempic, Novo Nordisk), as well as by tirzepatide (Mounjaro, Eli Lilly), a dual agonist for the GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors.
“No other medication has shown an average 17% reduction from baseline bodyweight after 36 weeks in people with type 2 diabetes,” said Julio Rosenstock, MD, director of the Dallas Diabetes Research Center at Medical City, Texas, who presented the results from the type 2 diabetes study of retatrutide.
For the obesity study, people with a body mass index of 27-50 kg/m2 and no diabetes were randomized to placebo or any of four retatrutide target dosages using specified dose-escalation protocols. Participants were an average of 48 years old, and by design, 52% were men. (The study sought to enroll roughly equal numbers of men and women.) Average BMI at study entry was 37 kg/m2.
Weight loss levels after 24 and 48 weeks of retatrutide treatment followed a clear dose-related pattern. (Weight loss averaged about 2% among the 70 controls who received placebo.)
Twenty-six percent without diabetes lost at least 30% of body weight
Every person who escalated to receive the 8-mg or 12-mg weekly dose of retatrutide lost at least 5% of their bodyweight after 48 weeks, 83% of those taking the 12-mg dose lost at least 15%, 63% of those on the 12-mg dose lost at least 20%, and 26% of those on the highest dose lost at least 30% of their starting bodyweight, reported Dr. Jastreboff, director of the Yale Obesity Research Center of Yale University in New Haven, Conn.
The highest dose was also associated with an average 40% relative reduction in triglyceride levels from baseline and an average 22% relative drop in LDL cholesterol levels.
The results were simultaneously published online in the New England Journal of Medicine.
The incidence of serious adverse events with retatrutide was low, similar to the rate in those who received placebo, and showed no dose relationship.
The most common adverse events were gastrointestinal, in as many as 16% of those on the highest dose; these were mild to moderate in severity and usually occurred during dose escalation. In general, adverse events were comparable to what is seen with a GLP-1 agonist or the dual agonist tirzepatide, Dr. Jastreboff said.
A1c normalization in 26% at the highest dose
A similar safety pattern occurred in the study of people with type 2 diabetes, which randomized people with an average A1c of 8.3% and an average BMI of 35.0 kg/m2. After 36 weeks of treatment, the 12-mg weekly dose of retatrutide led to normalization of A1c < 5.7% in 27% of people and A1c ≤ 6.5% in 77%.
“The number of people we were able to revert to a normal A1c was impressive,” said Dr. Rosenstock. These results were simultaneously published online in The Lancet.
The additional findings on liver-fat mobilization in people without diabetes enrolled in the obesity study are notable because no agent currently has labeling from the Food and Drug Administration for the indication of reducing excess liver fat, said Dr. Kaplan.
The researchers measured liver fat at baseline and then during treatment using MRI.
“With the level of fat clearance from the liver that we see with retatrutide it is highly likely that we’ll also see improvements in liver fibrosis” in retatrutide-treated patients, Dr. Kaplan predicted.
Next up for retatrutide is testing in pivotal trials, including the TRIUMPH-3 trial that will enroll about 1,800 people with severe obesity and cardiovascular disease, with findings expected toward the end of 2025.
The retatrutide studies are sponsored by Eli Lilly. Dr. Jastreboff, Dr. Rosenstock, Dr. Kaplan, and Dr. Le Roux have reported financial relationships with Eli Lilly as well as other companies.
A version of this article first appeared on Medscape.com.
SAN DIEGO – New designer molecules that target weight loss via multiple mechanisms continue to raise the bar of how many pounds people with overweight or obesity can lose.
Retatrutide (Eli Lilly), an investigational agent that combines agonism to three key hormones that influence eating and metabolism into a single molecule, safely produced weight loss at levels never seen before in a pair of phase 2 studies that together randomized more than 600 people with overweight or obesity, with or without type 2 diabetes.
Among 338 randomized people with overweight or obesity and no type 2 diabetes,
Among 281 randomized people with overweight or obesity and type 2 diabetes, the same dose of retatrutide produced a nearly 17% cut in weight from baseline after 36 weeks of treatment.
Never before seen weight loss
“I have never seen weight loss at this level” after nearly 1 year of treatment, Ania M. Jastreboff, MD, PhD, who led the obesity study, said during a press briefing at the annual scientific sessions of the American Diabetes Association.
The average weight loss by study participants taking high-dose retatrutide in the two studies “is really impressive, way beyond my wildest dreams,” said Carel le Roux, MBChB, PhD, an obesity and diabetes researcher at University College Dublin, Ireland, who was not involved with the retatrutide studies.
And Robert A. Gabbay, MD, chief scientific and medical officer of the ADA, called the results “stunning,” and added, “we are now witnessing the first triple-hormone combination being highly effective for not only weight loss but liver disease and diabetes.”
A prespecified subgroup analysis of the obesity study showed that at both 8-mg and 12-mg weekly doses, 24 weeks of retatrutide produced complete resolution of excess liver fat (hepatic steatosis) in about 80% of the people eligible for the analysis (those with at least 10% of their liver volume as fat at study entry); that figure increased to about 90% of people on these doses after 48 weeks, Lee M. Kaplan, MD, reported during a separate presentation at the meeting.
Adding glucagon agonism ups liver-fat clearance
“When you add glucagon activity,” one of the three agonist actions of retatrutide, “liver-fat clearance goes up tremendously,” said Dr. Kaplan, director of the Obesity, Metabolism and Nutrition Institute at Massachusetts General Hospital in Boston.
“To my knowledge, no mono-agonist of the glucagon-like peptide-1 (GLP-1) receptor [such as semaglutide or liraglutide] produces more than 50% clearance of liver fat,” added Dr. Kaplan.
The separate, randomized study of people with type 2 diabetes showed that in addition to producing an unprecedented average level of weight loss at the highest retatrutide dose, the agent also produced an average reduction from baseline levels of A1c of about 2 percentage points, an efficacy roughly comparable to maximum doses of the most potent GLP-1 mono-agonist semaglutide (Ozempic, Novo Nordisk), as well as by tirzepatide (Mounjaro, Eli Lilly), a dual agonist for the GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors.
“No other medication has shown an average 17% reduction from baseline bodyweight after 36 weeks in people with type 2 diabetes,” said Julio Rosenstock, MD, director of the Dallas Diabetes Research Center at Medical City, Texas, who presented the results from the type 2 diabetes study of retatrutide.
For the obesity study, people with a body mass index of 27-50 kg/m2 and no diabetes were randomized to placebo or any of four retatrutide target dosages using specified dose-escalation protocols. Participants were an average of 48 years old, and by design, 52% were men. (The study sought to enroll roughly equal numbers of men and women.) Average BMI at study entry was 37 kg/m2.
Weight loss levels after 24 and 48 weeks of retatrutide treatment followed a clear dose-related pattern. (Weight loss averaged about 2% among the 70 controls who received placebo.)
Twenty-six percent without diabetes lost at least 30% of body weight
Every person who escalated to receive the 8-mg or 12-mg weekly dose of retatrutide lost at least 5% of their bodyweight after 48 weeks, 83% of those taking the 12-mg dose lost at least 15%, 63% of those on the 12-mg dose lost at least 20%, and 26% of those on the highest dose lost at least 30% of their starting bodyweight, reported Dr. Jastreboff, director of the Yale Obesity Research Center of Yale University in New Haven, Conn.
The highest dose was also associated with an average 40% relative reduction in triglyceride levels from baseline and an average 22% relative drop in LDL cholesterol levels.
The results were simultaneously published online in the New England Journal of Medicine.
The incidence of serious adverse events with retatrutide was low, similar to the rate in those who received placebo, and showed no dose relationship.
The most common adverse events were gastrointestinal, in as many as 16% of those on the highest dose; these were mild to moderate in severity and usually occurred during dose escalation. In general, adverse events were comparable to what is seen with a GLP-1 agonist or the dual agonist tirzepatide, Dr. Jastreboff said.
A1c normalization in 26% at the highest dose
A similar safety pattern occurred in the study of people with type 2 diabetes, which randomized people with an average A1c of 8.3% and an average BMI of 35.0 kg/m2. After 36 weeks of treatment, the 12-mg weekly dose of retatrutide led to normalization of A1c < 5.7% in 27% of people and A1c ≤ 6.5% in 77%.
“The number of people we were able to revert to a normal A1c was impressive,” said Dr. Rosenstock. These results were simultaneously published online in The Lancet.
The additional findings on liver-fat mobilization in people without diabetes enrolled in the obesity study are notable because no agent currently has labeling from the Food and Drug Administration for the indication of reducing excess liver fat, said Dr. Kaplan.
The researchers measured liver fat at baseline and then during treatment using MRI.
“With the level of fat clearance from the liver that we see with retatrutide it is highly likely that we’ll also see improvements in liver fibrosis” in retatrutide-treated patients, Dr. Kaplan predicted.
Next up for retatrutide is testing in pivotal trials, including the TRIUMPH-3 trial that will enroll about 1,800 people with severe obesity and cardiovascular disease, with findings expected toward the end of 2025.
The retatrutide studies are sponsored by Eli Lilly. Dr. Jastreboff, Dr. Rosenstock, Dr. Kaplan, and Dr. Le Roux have reported financial relationships with Eli Lilly as well as other companies.
A version of this article first appeared on Medscape.com.
SAN DIEGO – New designer molecules that target weight loss via multiple mechanisms continue to raise the bar of how many pounds people with overweight or obesity can lose.
Retatrutide (Eli Lilly), an investigational agent that combines agonism to three key hormones that influence eating and metabolism into a single molecule, safely produced weight loss at levels never seen before in a pair of phase 2 studies that together randomized more than 600 people with overweight or obesity, with or without type 2 diabetes.
Among 338 randomized people with overweight or obesity and no type 2 diabetes,
Among 281 randomized people with overweight or obesity and type 2 diabetes, the same dose of retatrutide produced a nearly 17% cut in weight from baseline after 36 weeks of treatment.
Never before seen weight loss
“I have never seen weight loss at this level” after nearly 1 year of treatment, Ania M. Jastreboff, MD, PhD, who led the obesity study, said during a press briefing at the annual scientific sessions of the American Diabetes Association.
The average weight loss by study participants taking high-dose retatrutide in the two studies “is really impressive, way beyond my wildest dreams,” said Carel le Roux, MBChB, PhD, an obesity and diabetes researcher at University College Dublin, Ireland, who was not involved with the retatrutide studies.
And Robert A. Gabbay, MD, chief scientific and medical officer of the ADA, called the results “stunning,” and added, “we are now witnessing the first triple-hormone combination being highly effective for not only weight loss but liver disease and diabetes.”
A prespecified subgroup analysis of the obesity study showed that at both 8-mg and 12-mg weekly doses, 24 weeks of retatrutide produced complete resolution of excess liver fat (hepatic steatosis) in about 80% of the people eligible for the analysis (those with at least 10% of their liver volume as fat at study entry); that figure increased to about 90% of people on these doses after 48 weeks, Lee M. Kaplan, MD, reported during a separate presentation at the meeting.
Adding glucagon agonism ups liver-fat clearance
“When you add glucagon activity,” one of the three agonist actions of retatrutide, “liver-fat clearance goes up tremendously,” said Dr. Kaplan, director of the Obesity, Metabolism and Nutrition Institute at Massachusetts General Hospital in Boston.
“To my knowledge, no mono-agonist of the glucagon-like peptide-1 (GLP-1) receptor [such as semaglutide or liraglutide] produces more than 50% clearance of liver fat,” added Dr. Kaplan.
The separate, randomized study of people with type 2 diabetes showed that in addition to producing an unprecedented average level of weight loss at the highest retatrutide dose, the agent also produced an average reduction from baseline levels of A1c of about 2 percentage points, an efficacy roughly comparable to maximum doses of the most potent GLP-1 mono-agonist semaglutide (Ozempic, Novo Nordisk), as well as by tirzepatide (Mounjaro, Eli Lilly), a dual agonist for the GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors.
“No other medication has shown an average 17% reduction from baseline bodyweight after 36 weeks in people with type 2 diabetes,” said Julio Rosenstock, MD, director of the Dallas Diabetes Research Center at Medical City, Texas, who presented the results from the type 2 diabetes study of retatrutide.
For the obesity study, people with a body mass index of 27-50 kg/m2 and no diabetes were randomized to placebo or any of four retatrutide target dosages using specified dose-escalation protocols. Participants were an average of 48 years old, and by design, 52% were men. (The study sought to enroll roughly equal numbers of men and women.) Average BMI at study entry was 37 kg/m2.
Weight loss levels after 24 and 48 weeks of retatrutide treatment followed a clear dose-related pattern. (Weight loss averaged about 2% among the 70 controls who received placebo.)
Twenty-six percent without diabetes lost at least 30% of body weight
Every person who escalated to receive the 8-mg or 12-mg weekly dose of retatrutide lost at least 5% of their bodyweight after 48 weeks, 83% of those taking the 12-mg dose lost at least 15%, 63% of those on the 12-mg dose lost at least 20%, and 26% of those on the highest dose lost at least 30% of their starting bodyweight, reported Dr. Jastreboff, director of the Yale Obesity Research Center of Yale University in New Haven, Conn.
The highest dose was also associated with an average 40% relative reduction in triglyceride levels from baseline and an average 22% relative drop in LDL cholesterol levels.
The results were simultaneously published online in the New England Journal of Medicine.
The incidence of serious adverse events with retatrutide was low, similar to the rate in those who received placebo, and showed no dose relationship.
The most common adverse events were gastrointestinal, in as many as 16% of those on the highest dose; these were mild to moderate in severity and usually occurred during dose escalation. In general, adverse events were comparable to what is seen with a GLP-1 agonist or the dual agonist tirzepatide, Dr. Jastreboff said.
A1c normalization in 26% at the highest dose
A similar safety pattern occurred in the study of people with type 2 diabetes, which randomized people with an average A1c of 8.3% and an average BMI of 35.0 kg/m2. After 36 weeks of treatment, the 12-mg weekly dose of retatrutide led to normalization of A1c < 5.7% in 27% of people and A1c ≤ 6.5% in 77%.
“The number of people we were able to revert to a normal A1c was impressive,” said Dr. Rosenstock. These results were simultaneously published online in The Lancet.
The additional findings on liver-fat mobilization in people without diabetes enrolled in the obesity study are notable because no agent currently has labeling from the Food and Drug Administration for the indication of reducing excess liver fat, said Dr. Kaplan.
The researchers measured liver fat at baseline and then during treatment using MRI.
“With the level of fat clearance from the liver that we see with retatrutide it is highly likely that we’ll also see improvements in liver fibrosis” in retatrutide-treated patients, Dr. Kaplan predicted.
Next up for retatrutide is testing in pivotal trials, including the TRIUMPH-3 trial that will enroll about 1,800 people with severe obesity and cardiovascular disease, with findings expected toward the end of 2025.
The retatrutide studies are sponsored by Eli Lilly. Dr. Jastreboff, Dr. Rosenstock, Dr. Kaplan, and Dr. Le Roux have reported financial relationships with Eli Lilly as well as other companies.
A version of this article first appeared on Medscape.com.
AT ADA 2023
Vaginal microbiota transfer may affect neurodevelopment in cesarean infants
Previous studies have shown that gut microbiota in infancy could affect neurodevelopment, and infants delivered by cesarean are not exposed to potentially helpful microbes acquired by infants during vaginal delivery, wrote Lepeng Zhou, MD, of Southern Medical University, Guangdong, China, and colleagues.
“Infants delivered by C-section start life with very different bacteria than those born vaginally,” corresponding author Jose Clemente, PhD, of Icahn School of Medicine at Mount Sinai, New York, said in an interview. “Because this is the first time the newborn is exposed to microbes, we and others have hypothesized for some time that this ‘first encounter’ might be significant to shape the development of the baby,” he said.
“A few years ago, we demonstrated that it is possible to change the microbiome of C-section–delivered infants using an intervention that makes their microbiome more similar to that of a vaginally-delivered infant,” Dr. Clemente told this news organization. “In this study just published, we show that this procedure not only changes the microbiome of C-section infants, but it also modifies a health outcome (in this case, neurodevelopment). This is highly significant because it opens the way to reduce the risk that C-section infants have for certain conditions through a very simple microbial intervention,” he said.
‘Significantly higher’ ASQ-3 scores
In the current study, published in Cell Host & Microbe, the researchers examined the impact of vaginal microbiota transfer (VMT) on the neurodevelopment of cesarean-delivered infants. They randomized 35 women scheduled for cesarean delivery with a single infant to VMT and 41 to a control intervention of saline gauze for their infants immediately after delivery.
The primary outcome of infant neurodevelopment was assessed using the Ages and Stages Questionnaire (ASQ-3) score at 6 months. The researchers also collected fecal samples and assessed safety outcomes for the infants at 3, 7, 30, and 42 days after birth. The final analysis comprised 32 infants in the VMT group and 36 in the control group. The mean age of the mothers was 32 years; the mean gestational age of the infants was 39 weeks, but the difference was significant and slightly less in the VMT group compared with the controls (38.38 weeks vs. 39.13 weeks, P = .007). A group of 33 vaginally-delivered infants (VD) underwent ASQ-3 testing to serve as a reference group.
At 6 months, ASQ-3 scores were significantly higher (10.09%, P = .014) with VMT compared with controls, and the difference remained significant after adjustment for multiple factors including gestational age.
ASQ-3 total scores at 6 months were not significantly different between the VMT group and the VD reference group (mean difference of 8.84 VMT to VD, P = .346); scores between these groups also were similar at 3 months (mean difference of –1.48 VMT to VD, P = .900) and no significant differences appeared in ASQ-3 subdomains between these groups at either time period.
An examination of gut metabolites in stool showed significant differences in fecal metabolites and metabolic function, signs of gut microbiota maturation, the researchers noted.
“Interestingly, all the genera and metabolites that exhibited positive correlations with neurodevelopmental scores were upregulated in the VMT group, whereas the only negative correlation of Klebsiella was downregulated, indicating that VMT may impact neurodevelopment through the modulation of specific gut microbial genera and metabolites,” the researchers wrote.
No serious adverse events occurred in either group during the study period. Nine adverse events were reported; 4 in the VMT group and 5 in the control group. The most common AEs were mild skin disorders, including papules, pustules, and erythema.
The findings were limited by several factors including the potential for transfer not only of vaginal microbiota, but also vaginal metabolites, mycobiome, and virome, which blurs the potential mechanism of VMT, the researchers noted. Other limitations were the relatively short study period, small sample size, and cervical HPV screening within the past 5 years, not during pregnancy, they wrote.
However, the results suggest that VMT is safe, and may help improve the fecal microbiome in cesarean-delivered infants, and the long-term effects merit further studies in larger populations, they concluded.
Limitations and outlook
Dr. Clemente said in an interview that the researchers were “hopeful that the study would demonstrate a health benefit, as it does with some limitations.” The current study findings confirm some previous results showing that modification of the microbiomes of C-section infants is possible through a transfer of maternal vaginal microbes, he said.
“There is also an important aspect that was confirmed here: The lack of serious adverse events associated with the procedure, and the fact that transferring vaginal microbes did not increase the risk of adverse events compared to the control group or to vaginally-delivered infants. This is fundamental to establish that using rigorous exclusion criteria we can perform this procedure safely for infants and mothers,” he added.
“We are at very early stages yet to talk about clinical implications,” said Dr. Clemente. “This is one of the first studies to demonstrate a benefit to the transfer of microbes from mothers to infants, and as such it opens the way for future trials that confirm these findings. The clinical application is still in the future, but this is an important first step towards that goal.”
Interest in restoring gut microbiota to potentially benefit infants persists, but a recent study published in Frontiers and Cellular and Infection Microbiology contradicted the potential association between maternal vaginal microbiome and an infant’s gut microbiome based on an analysis of infant stool.
“There are many reasons why different studies might reach different conclusions: The experimental procedures, the analytical methods, the cohort under study,” Dr. Clemente said when asked to comment on the Frontiers study. “Further studies are needed to establish whether this procedure is equally effective under all conditions and whether health benefits are generalizable or specific to particular populations.”
Several research gaps remain, Dr. Clemente said. “First, neurodevelopment was measured through a questionnaire that captures various aspects such as communication, motor skills, or problem solving. While this is a standard way to establish that an infant is in the correct neurodevelopmental pathway, it is not a ‘hard’ measure of cellular or biochemical processes being impacted by the intervention. Some of our results suggest that there is a change in the metabolome of this infants, particularly an enrichment in GABA, a neurotransmitter, but the exact mechanisms by which the intervention is resulting in a health benefit still remains to be explored,” he said.
“We have an ongoing study here at Mount Sinai to test whether this microbial intervention can be effective in lowering the risk of developing food allergies in newborns who are at high risk, so that is another important future question: What other conditions could benefit from this approach,” said Dr. Clemente.
A third research goal, he added, is “determining what microbes precisely are responsible for the health benefits; this study uses a full microbial community to colonize infants. We show that this is effective and, importantly, that there were no significant adverse events in the treated infants,” he noted. “However, identifying what specific microbes are beneficial would further lower the risk of any potential side effects, while facilitating the development of drugs based on defined microbial consortia,” he said.
Safety and efficacy support further studies
“It is widely accepted that the gut microbiome of neonates varies based on mode of delivery,” Anna K. Knight, PhD, assistant professor of gynecology and obstetrics at Emory University, Atlanta, said in an interview.
“C-sections have been associated with increased risk of asthma and metabolic disease, and have been associated with differences in the development of the immune system,” said Dr. Knight, who was not involved in the study. “There have been small pilot studies examining the use of vaginal microbiome transplants to shift the gut microbiome of neonates born by C-section to be more like the gut microbiome of neonates born via vaginal delivery, but the safety and efficacy of this treatment has not been well established. This study examines both, while also evaluating potential changes in the metabolome and neurodevelopmental trajectories.”
The current study confirmed the impact of the neonatal gut microbe on neurodevelopmental outcomes during a sensitive period, said Dr. Knight. “The fact that these differences persisted at 6 months suggests that even if the microbiome composition between vaginally-delivered and preterm infants converged at 1-2 years old, there may be lasting impacts of mode of delivery,” she said.
“The results of this study suggest that vaginal microbiome transplant may be a safe and effective way to mitigate the negative impacts of C-section delivery on the neonatal gut microbiome, and may be protective for neurodevelopment,” she added.
Regarding the Frontiers in Medicine study, Dr. Knight noted that it examined a very different population, with Zhou and colleagues focusing on Chinese infants, while Dos Santos and colleagues focused on Canadian infants.
“There was also a substantial difference in sample size between the two studies, with Dos Santos and colleagues examining > 500 more infants,” she said. “Additionally, the two studies differed in the sequencing technology used, sample collection methods, and antibiotic exposure, which can all impact microbiome study results.”
Since the current study showed efficacy and safety of VMT in a small clinical trial, larger trials with more diverse participants are needed to further examine the impact of VMT, said Dr. Knight. “The risks of vaginal microbiome transplant in mothers with infections should also be considered, and the mechanisms by which the neonatal gut microbiome impacts neurodevelopment need further investigation,” she said.
The study was funded by the National Key R&D Program of China, the Canadian Institute of Health Research, the National Natural Science Foundation of China, the Clinical Research Startup Program of Southern Medical University, China, and the Top Talent Program of Foshan Women and Children Hospital, China. The researchers and Dr. Knight had no financial conflicts to disclose.
Previous studies have shown that gut microbiota in infancy could affect neurodevelopment, and infants delivered by cesarean are not exposed to potentially helpful microbes acquired by infants during vaginal delivery, wrote Lepeng Zhou, MD, of Southern Medical University, Guangdong, China, and colleagues.
“Infants delivered by C-section start life with very different bacteria than those born vaginally,” corresponding author Jose Clemente, PhD, of Icahn School of Medicine at Mount Sinai, New York, said in an interview. “Because this is the first time the newborn is exposed to microbes, we and others have hypothesized for some time that this ‘first encounter’ might be significant to shape the development of the baby,” he said.
“A few years ago, we demonstrated that it is possible to change the microbiome of C-section–delivered infants using an intervention that makes their microbiome more similar to that of a vaginally-delivered infant,” Dr. Clemente told this news organization. “In this study just published, we show that this procedure not only changes the microbiome of C-section infants, but it also modifies a health outcome (in this case, neurodevelopment). This is highly significant because it opens the way to reduce the risk that C-section infants have for certain conditions through a very simple microbial intervention,” he said.
‘Significantly higher’ ASQ-3 scores
In the current study, published in Cell Host & Microbe, the researchers examined the impact of vaginal microbiota transfer (VMT) on the neurodevelopment of cesarean-delivered infants. They randomized 35 women scheduled for cesarean delivery with a single infant to VMT and 41 to a control intervention of saline gauze for their infants immediately after delivery.
The primary outcome of infant neurodevelopment was assessed using the Ages and Stages Questionnaire (ASQ-3) score at 6 months. The researchers also collected fecal samples and assessed safety outcomes for the infants at 3, 7, 30, and 42 days after birth. The final analysis comprised 32 infants in the VMT group and 36 in the control group. The mean age of the mothers was 32 years; the mean gestational age of the infants was 39 weeks, but the difference was significant and slightly less in the VMT group compared with the controls (38.38 weeks vs. 39.13 weeks, P = .007). A group of 33 vaginally-delivered infants (VD) underwent ASQ-3 testing to serve as a reference group.
At 6 months, ASQ-3 scores were significantly higher (10.09%, P = .014) with VMT compared with controls, and the difference remained significant after adjustment for multiple factors including gestational age.
ASQ-3 total scores at 6 months were not significantly different between the VMT group and the VD reference group (mean difference of 8.84 VMT to VD, P = .346); scores between these groups also were similar at 3 months (mean difference of –1.48 VMT to VD, P = .900) and no significant differences appeared in ASQ-3 subdomains between these groups at either time period.
An examination of gut metabolites in stool showed significant differences in fecal metabolites and metabolic function, signs of gut microbiota maturation, the researchers noted.
“Interestingly, all the genera and metabolites that exhibited positive correlations with neurodevelopmental scores were upregulated in the VMT group, whereas the only negative correlation of Klebsiella was downregulated, indicating that VMT may impact neurodevelopment through the modulation of specific gut microbial genera and metabolites,” the researchers wrote.
No serious adverse events occurred in either group during the study period. Nine adverse events were reported; 4 in the VMT group and 5 in the control group. The most common AEs were mild skin disorders, including papules, pustules, and erythema.
The findings were limited by several factors including the potential for transfer not only of vaginal microbiota, but also vaginal metabolites, mycobiome, and virome, which blurs the potential mechanism of VMT, the researchers noted. Other limitations were the relatively short study period, small sample size, and cervical HPV screening within the past 5 years, not during pregnancy, they wrote.
However, the results suggest that VMT is safe, and may help improve the fecal microbiome in cesarean-delivered infants, and the long-term effects merit further studies in larger populations, they concluded.
Limitations and outlook
Dr. Clemente said in an interview that the researchers were “hopeful that the study would demonstrate a health benefit, as it does with some limitations.” The current study findings confirm some previous results showing that modification of the microbiomes of C-section infants is possible through a transfer of maternal vaginal microbes, he said.
“There is also an important aspect that was confirmed here: The lack of serious adverse events associated with the procedure, and the fact that transferring vaginal microbes did not increase the risk of adverse events compared to the control group or to vaginally-delivered infants. This is fundamental to establish that using rigorous exclusion criteria we can perform this procedure safely for infants and mothers,” he added.
“We are at very early stages yet to talk about clinical implications,” said Dr. Clemente. “This is one of the first studies to demonstrate a benefit to the transfer of microbes from mothers to infants, and as such it opens the way for future trials that confirm these findings. The clinical application is still in the future, but this is an important first step towards that goal.”
Interest in restoring gut microbiota to potentially benefit infants persists, but a recent study published in Frontiers and Cellular and Infection Microbiology contradicted the potential association between maternal vaginal microbiome and an infant’s gut microbiome based on an analysis of infant stool.
“There are many reasons why different studies might reach different conclusions: The experimental procedures, the analytical methods, the cohort under study,” Dr. Clemente said when asked to comment on the Frontiers study. “Further studies are needed to establish whether this procedure is equally effective under all conditions and whether health benefits are generalizable or specific to particular populations.”
Several research gaps remain, Dr. Clemente said. “First, neurodevelopment was measured through a questionnaire that captures various aspects such as communication, motor skills, or problem solving. While this is a standard way to establish that an infant is in the correct neurodevelopmental pathway, it is not a ‘hard’ measure of cellular or biochemical processes being impacted by the intervention. Some of our results suggest that there is a change in the metabolome of this infants, particularly an enrichment in GABA, a neurotransmitter, but the exact mechanisms by which the intervention is resulting in a health benefit still remains to be explored,” he said.
“We have an ongoing study here at Mount Sinai to test whether this microbial intervention can be effective in lowering the risk of developing food allergies in newborns who are at high risk, so that is another important future question: What other conditions could benefit from this approach,” said Dr. Clemente.
A third research goal, he added, is “determining what microbes precisely are responsible for the health benefits; this study uses a full microbial community to colonize infants. We show that this is effective and, importantly, that there were no significant adverse events in the treated infants,” he noted. “However, identifying what specific microbes are beneficial would further lower the risk of any potential side effects, while facilitating the development of drugs based on defined microbial consortia,” he said.
Safety and efficacy support further studies
“It is widely accepted that the gut microbiome of neonates varies based on mode of delivery,” Anna K. Knight, PhD, assistant professor of gynecology and obstetrics at Emory University, Atlanta, said in an interview.
“C-sections have been associated with increased risk of asthma and metabolic disease, and have been associated with differences in the development of the immune system,” said Dr. Knight, who was not involved in the study. “There have been small pilot studies examining the use of vaginal microbiome transplants to shift the gut microbiome of neonates born by C-section to be more like the gut microbiome of neonates born via vaginal delivery, but the safety and efficacy of this treatment has not been well established. This study examines both, while also evaluating potential changes in the metabolome and neurodevelopmental trajectories.”
The current study confirmed the impact of the neonatal gut microbe on neurodevelopmental outcomes during a sensitive period, said Dr. Knight. “The fact that these differences persisted at 6 months suggests that even if the microbiome composition between vaginally-delivered and preterm infants converged at 1-2 years old, there may be lasting impacts of mode of delivery,” she said.
“The results of this study suggest that vaginal microbiome transplant may be a safe and effective way to mitigate the negative impacts of C-section delivery on the neonatal gut microbiome, and may be protective for neurodevelopment,” she added.
Regarding the Frontiers in Medicine study, Dr. Knight noted that it examined a very different population, with Zhou and colleagues focusing on Chinese infants, while Dos Santos and colleagues focused on Canadian infants.
“There was also a substantial difference in sample size between the two studies, with Dos Santos and colleagues examining > 500 more infants,” she said. “Additionally, the two studies differed in the sequencing technology used, sample collection methods, and antibiotic exposure, which can all impact microbiome study results.”
Since the current study showed efficacy and safety of VMT in a small clinical trial, larger trials with more diverse participants are needed to further examine the impact of VMT, said Dr. Knight. “The risks of vaginal microbiome transplant in mothers with infections should also be considered, and the mechanisms by which the neonatal gut microbiome impacts neurodevelopment need further investigation,” she said.
The study was funded by the National Key R&D Program of China, the Canadian Institute of Health Research, the National Natural Science Foundation of China, the Clinical Research Startup Program of Southern Medical University, China, and the Top Talent Program of Foshan Women and Children Hospital, China. The researchers and Dr. Knight had no financial conflicts to disclose.
Previous studies have shown that gut microbiota in infancy could affect neurodevelopment, and infants delivered by cesarean are not exposed to potentially helpful microbes acquired by infants during vaginal delivery, wrote Lepeng Zhou, MD, of Southern Medical University, Guangdong, China, and colleagues.
“Infants delivered by C-section start life with very different bacteria than those born vaginally,” corresponding author Jose Clemente, PhD, of Icahn School of Medicine at Mount Sinai, New York, said in an interview. “Because this is the first time the newborn is exposed to microbes, we and others have hypothesized for some time that this ‘first encounter’ might be significant to shape the development of the baby,” he said.
“A few years ago, we demonstrated that it is possible to change the microbiome of C-section–delivered infants using an intervention that makes their microbiome more similar to that of a vaginally-delivered infant,” Dr. Clemente told this news organization. “In this study just published, we show that this procedure not only changes the microbiome of C-section infants, but it also modifies a health outcome (in this case, neurodevelopment). This is highly significant because it opens the way to reduce the risk that C-section infants have for certain conditions through a very simple microbial intervention,” he said.
‘Significantly higher’ ASQ-3 scores
In the current study, published in Cell Host & Microbe, the researchers examined the impact of vaginal microbiota transfer (VMT) on the neurodevelopment of cesarean-delivered infants. They randomized 35 women scheduled for cesarean delivery with a single infant to VMT and 41 to a control intervention of saline gauze for their infants immediately after delivery.
The primary outcome of infant neurodevelopment was assessed using the Ages and Stages Questionnaire (ASQ-3) score at 6 months. The researchers also collected fecal samples and assessed safety outcomes for the infants at 3, 7, 30, and 42 days after birth. The final analysis comprised 32 infants in the VMT group and 36 in the control group. The mean age of the mothers was 32 years; the mean gestational age of the infants was 39 weeks, but the difference was significant and slightly less in the VMT group compared with the controls (38.38 weeks vs. 39.13 weeks, P = .007). A group of 33 vaginally-delivered infants (VD) underwent ASQ-3 testing to serve as a reference group.
At 6 months, ASQ-3 scores were significantly higher (10.09%, P = .014) with VMT compared with controls, and the difference remained significant after adjustment for multiple factors including gestational age.
ASQ-3 total scores at 6 months were not significantly different between the VMT group and the VD reference group (mean difference of 8.84 VMT to VD, P = .346); scores between these groups also were similar at 3 months (mean difference of –1.48 VMT to VD, P = .900) and no significant differences appeared in ASQ-3 subdomains between these groups at either time period.
An examination of gut metabolites in stool showed significant differences in fecal metabolites and metabolic function, signs of gut microbiota maturation, the researchers noted.
“Interestingly, all the genera and metabolites that exhibited positive correlations with neurodevelopmental scores were upregulated in the VMT group, whereas the only negative correlation of Klebsiella was downregulated, indicating that VMT may impact neurodevelopment through the modulation of specific gut microbial genera and metabolites,” the researchers wrote.
No serious adverse events occurred in either group during the study period. Nine adverse events were reported; 4 in the VMT group and 5 in the control group. The most common AEs were mild skin disorders, including papules, pustules, and erythema.
The findings were limited by several factors including the potential for transfer not only of vaginal microbiota, but also vaginal metabolites, mycobiome, and virome, which blurs the potential mechanism of VMT, the researchers noted. Other limitations were the relatively short study period, small sample size, and cervical HPV screening within the past 5 years, not during pregnancy, they wrote.
However, the results suggest that VMT is safe, and may help improve the fecal microbiome in cesarean-delivered infants, and the long-term effects merit further studies in larger populations, they concluded.
Limitations and outlook
Dr. Clemente said in an interview that the researchers were “hopeful that the study would demonstrate a health benefit, as it does with some limitations.” The current study findings confirm some previous results showing that modification of the microbiomes of C-section infants is possible through a transfer of maternal vaginal microbes, he said.
“There is also an important aspect that was confirmed here: The lack of serious adverse events associated with the procedure, and the fact that transferring vaginal microbes did not increase the risk of adverse events compared to the control group or to vaginally-delivered infants. This is fundamental to establish that using rigorous exclusion criteria we can perform this procedure safely for infants and mothers,” he added.
“We are at very early stages yet to talk about clinical implications,” said Dr. Clemente. “This is one of the first studies to demonstrate a benefit to the transfer of microbes from mothers to infants, and as such it opens the way for future trials that confirm these findings. The clinical application is still in the future, but this is an important first step towards that goal.”
Interest in restoring gut microbiota to potentially benefit infants persists, but a recent study published in Frontiers and Cellular and Infection Microbiology contradicted the potential association between maternal vaginal microbiome and an infant’s gut microbiome based on an analysis of infant stool.
“There are many reasons why different studies might reach different conclusions: The experimental procedures, the analytical methods, the cohort under study,” Dr. Clemente said when asked to comment on the Frontiers study. “Further studies are needed to establish whether this procedure is equally effective under all conditions and whether health benefits are generalizable or specific to particular populations.”
Several research gaps remain, Dr. Clemente said. “First, neurodevelopment was measured through a questionnaire that captures various aspects such as communication, motor skills, or problem solving. While this is a standard way to establish that an infant is in the correct neurodevelopmental pathway, it is not a ‘hard’ measure of cellular or biochemical processes being impacted by the intervention. Some of our results suggest that there is a change in the metabolome of this infants, particularly an enrichment in GABA, a neurotransmitter, but the exact mechanisms by which the intervention is resulting in a health benefit still remains to be explored,” he said.
“We have an ongoing study here at Mount Sinai to test whether this microbial intervention can be effective in lowering the risk of developing food allergies in newborns who are at high risk, so that is another important future question: What other conditions could benefit from this approach,” said Dr. Clemente.
A third research goal, he added, is “determining what microbes precisely are responsible for the health benefits; this study uses a full microbial community to colonize infants. We show that this is effective and, importantly, that there were no significant adverse events in the treated infants,” he noted. “However, identifying what specific microbes are beneficial would further lower the risk of any potential side effects, while facilitating the development of drugs based on defined microbial consortia,” he said.
Safety and efficacy support further studies
“It is widely accepted that the gut microbiome of neonates varies based on mode of delivery,” Anna K. Knight, PhD, assistant professor of gynecology and obstetrics at Emory University, Atlanta, said in an interview.
“C-sections have been associated with increased risk of asthma and metabolic disease, and have been associated with differences in the development of the immune system,” said Dr. Knight, who was not involved in the study. “There have been small pilot studies examining the use of vaginal microbiome transplants to shift the gut microbiome of neonates born by C-section to be more like the gut microbiome of neonates born via vaginal delivery, but the safety and efficacy of this treatment has not been well established. This study examines both, while also evaluating potential changes in the metabolome and neurodevelopmental trajectories.”
The current study confirmed the impact of the neonatal gut microbe on neurodevelopmental outcomes during a sensitive period, said Dr. Knight. “The fact that these differences persisted at 6 months suggests that even if the microbiome composition between vaginally-delivered and preterm infants converged at 1-2 years old, there may be lasting impacts of mode of delivery,” she said.
“The results of this study suggest that vaginal microbiome transplant may be a safe and effective way to mitigate the negative impacts of C-section delivery on the neonatal gut microbiome, and may be protective for neurodevelopment,” she added.
Regarding the Frontiers in Medicine study, Dr. Knight noted that it examined a very different population, with Zhou and colleagues focusing on Chinese infants, while Dos Santos and colleagues focused on Canadian infants.
“There was also a substantial difference in sample size between the two studies, with Dos Santos and colleagues examining > 500 more infants,” she said. “Additionally, the two studies differed in the sequencing technology used, sample collection methods, and antibiotic exposure, which can all impact microbiome study results.”
Since the current study showed efficacy and safety of VMT in a small clinical trial, larger trials with more diverse participants are needed to further examine the impact of VMT, said Dr. Knight. “The risks of vaginal microbiome transplant in mothers with infections should also be considered, and the mechanisms by which the neonatal gut microbiome impacts neurodevelopment need further investigation,” she said.
The study was funded by the National Key R&D Program of China, the Canadian Institute of Health Research, the National Natural Science Foundation of China, the Clinical Research Startup Program of Southern Medical University, China, and the Top Talent Program of Foshan Women and Children Hospital, China. The researchers and Dr. Knight had no financial conflicts to disclose.
FROM CELL HOST & MICROBE