User login
Accountable Care Organizations (ACO) Gain Popularity with Physicians in Wake of Added Incentives, Revised Federal Rules
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
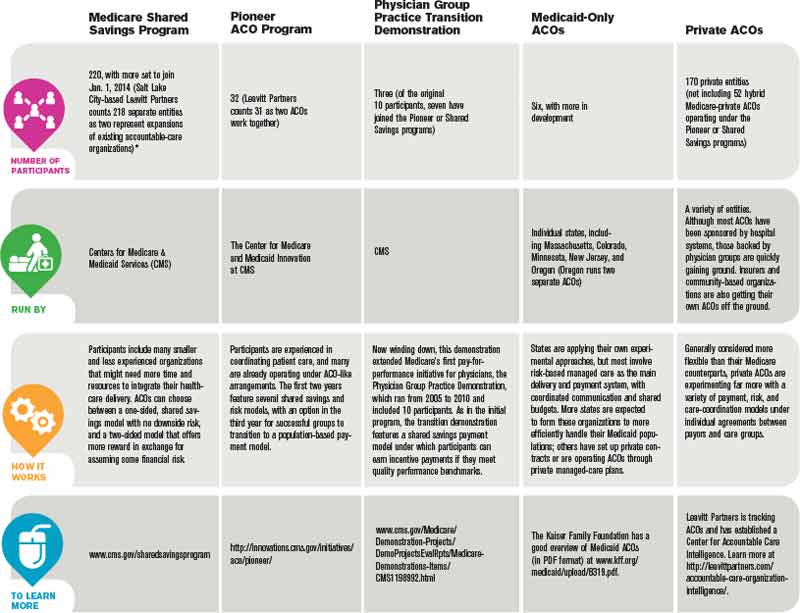
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.

—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”

Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.

—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.

Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.
—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”
Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.
—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.
Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
Throughout much of 2011, ambivalence plagued efforts by the Centers for Medicare & Medicaid Services (CMS) to expand the federal government’s reach into integrated care delivery to help improve patient outcomes while lowering costs. Critics panned the initial draft of regulations for a large accountable-care demonstration project called the Shared Savings Program, and prominent medical groups announced their intention to sit on the sidelines.
At the start of 2013, the atmosphere couldn’t be more different. CMS won over most of its critics with a well-received final version of the rules that provided more incentives for groups to form accountable-care organizations (ACOs), and the presidential election provided more clarity about the future of healthcare reform. Medical groups around the country are readily jumping on the ACO bandwagon, with its emphasis on shared responsibility among provider groups for a defined pool of patients.
Few medical groups have enough data to suggest whether their varied approaches to managing patient populations will lead to better-quality care that’s also more affordable; the first batch of Medicare ACO data isn’t expected until later this spring. And healthcare experts differ on which models and components are likely to make the biggest long-term impact; even the precise definition of an ACO remains a moving target. But industry observers say they’re surprised and encouraged not only by the speed with which the movement has taken off, but also by the breadth of models being investigated, the strong engagement of the private sector, and a spreading sense of cautious optimism.
“This is actually moving faster than I thought—faster than I think anybody thought,” says SHM Public Policy Committee chair Ron Greeno, MD, FCCP, MHM.
Although CMS still is in the beginning stages of its work and has focused most of its efforts on reviewing applications and providing feedback on organizations’ historical expenditure and utilization patterns, agency officials say the ACO initiative has not encountered any unexpected setbacks. “As with any new program, there are bumps along the way, but I don’t think we’ve experienced anything that is out of the ordinary,” says John Pilotte, director of Performance-Based Payment Policy in the Center for Medicare. “We’re pretty happy with where we are with the program.”
The Shared Savings Program, which Pilotte describes as “an easier on-ramp” to population management for providers and offers low financial risk in exchange for a modest level of shared cost savings, is proving especially popular. Combined, several hundred organizations submitted applications for the program’s second and third rounds, which began July 1, 2012, and Jan. 1, 2013, respectively.
“Two hundred twenty ACOs are currently up and running, and we expect to continue to add ACOs to the program annually,” Pilotte says.
—David Muhlestein, analyst, Leavitt Partners
Last January, another 32 groups joined Medicare’s Pioneer ACO program, designed for more experienced organizations with more resources. The groups assume more risk, and in return are more handsomely rewarded if they meet benchmarks.
All told, the tally of confirmed ACOs in the U.S. reached 428 by the end of January, according to Leavitt Partners, a Salt Lake City-based healthcare consulting firm that is tracking the growth of accountable care (see “A Sampling of Significant ACO Programs,” below). David Muhlestein, an analyst with Leavitt Partners, says private ACOs now account for roughly half of that total, a trend driven by their ability to experiment with different approaches and more easily track costs through clearly defined patient populations.
The central role for hospitalists within most ACOs is rooted in the reality that hospital care is the most expensive part of healthcare. Successfully implementing a plan to coordinate care and prevent hospital readmissions might not correlate directly with improved quality metrics, but it can lead to significant savings.
The diverse ACO models now being tested, however, could result in varying responsibilities for hospitalists, depending on the focal points of the sponsoring entities. After patients have been admitted to a hospital, for example, many hospitalists assume responsibility for managing inpatient care and the inpatient-outpatient handoff. A main goal of a physician-owned medical group, such as an independent practice association (IPA), by contrast, is to keep patients out of the hospital altogether, placing more of the focus on primary and specialty care. An IPA that forms an ACO, Muhlestein says, might hire its own hospitalists to monitor the care of patients in affiliated hospitals while using the association’s approach to limiting costs.
ACO participants also have varied widely in the effort expended to get up to speed. “Some people have said they haven’t had to make any major changes to their organization, while some people have had to drastically think how they provide care,” Muhlestein says. In general, many of the former have had the luxury of working within relatively integrated facilities and building upon existing frameworks, whereas many of the latter previously toiled away in silos and are now scrambling to establish more cohesive working relationships from scratch.
Optimism Abounds
Though many ACOs have only limited data so far, Muhlestein says most are generally optimistic that their early results will be positive. Even so, Dr. Greeno says, he fully expects the Pioneer ACOs to produce the best results among the Medicare demonstration projects. Those organizations already have successful track records in managing patient populations, and the Pioneer model’s incentives are stronger because the groups are assuming more risk. If the Pioneer ACO results are eclipsed by those of the Shared Savings Program, he says, “I’d fall out of my chair.”
The Beth Israel Deaconess Physician Organization (BIDPO) now has four global payment contracts, including its Pioneer ACO arrangement with CMS that serves 33,000 beneficiaries in the Boston metropolitan region. “The decision-making around joining was a recognition that the fee-for-service model is highly dysfunctional,” says Richard Parker, MD, BIDPO’s medical director. “Our organization and our leadership believed that most of the country, both private payor and governmental payor, would be moving toward global payment and that it would be to our advantage to get in early.”
Despite the complicated rollout and delays in receiving Medicare data on patients from CMS, Dr. Parker says, the feedback from both providers and patients has been mostly positive. “I would say, anecdotally, that the doctors seem appreciative that we’re trying to fix some of these gaps in care that we all know have existed for some time,” he says. “And, anecdotally from the patients, we get appreciation that we’re trying to take better care of them.”
Chris Coleman, chief financial officer for Phoenix-based Banner Health Network, another Pioneer ACO participant, says the project fits in well with his company’s decision “to transform itself into more of a value-based, performance-based provider.” Banner’s ACO, which serves about 50,000 beneficiaries, is still setting up needed systems, including a consistent platform for electronic medical records throughout the entire provider network. Even during the building phase, however, Coleman says company officials have been pleasantly surprised by the ACO’s positive effect on utilization, patient care, and apparent savings.
Although the company has only a partial year of Medicare claims to go by, Coleman says the data look “pretty good” so far and suggest the ACO is on track for modest savings of perhaps 3% or 4%. Like BIDPO, Banner has other shared-risk agreements in place, including one for a Medicare Advantage population and another with a private payor. So far, Coleman says, those arrangements also seem to be “performing positively.”
Dr. Greeno and other experts see the best ACO results coming from such rapidly growing private arrangements, and early published data have been generally encouraging.1 The ability to more narrowly define patient groups and assume more control over payments, he says, has allowed private ACOs to keep better track of costs and implement innovative population health interventions.
—Ron Greeno, MD, FCCP, MHM, SHM Public Policy Committee chair
Built to Last?
Whether public, private, or a hybrid between the two, some ACOs are trying to manage the care of their entire patient pool and look at everything that might help them accrue cost savings. Others are focusing only on the sickest patients to reach their quality improvement (QI) and savings goals, and targeting specific parameters, such as blood pressure or medication adherence, for patients with myocardial infarction.
Joane Goodroe, an Atlanta-based healthcare consultant, favors the latter approach, at least for new ACOs. Goodroe recommends adopting a streamlined strategy that will get an ACO up and running, then allow the group to gradually add to it, rather than waiting until all of the right pieces fall into place. Her own data analysis of Medicare patients, for example, suggests that a diabetic who’s been an inpatient can average $50,000 in yearly costs, compared with $2,400 for a diabetic who has never been admitted to a hospital.
Setting up a system to manage every diabetic patient from the start, she says, would require too much time and money. “If you try to build the perfect ACO structure, it’s going to be too expensive for the results you initially get back,” she says, making it seem like the ACO is an unsustainable failure. “You’ve got to figure out how to build a cost-effective infrastructure while you’re also improving the care of the patients, and the best place to go is to target your sickest patients first.”
CMS’ Advance Payment ACO Model is designed to help by providing upfront payments to smaller ACO organizations that might lack capital, giving them an advance on potential shared savings so they can install the infrastructure and support structures necessary to redesign care.
To maximize the overall chances of success, Dr. Parker says, ACO leadership should be fully engaged, and each organization should have enough resources to address its own care management and information technology needs. “My goal as medical director is to improve the quality of care of the patients and, hopefully, also improve the working life of the doctors and staff,” he says. “And my belief and expectation is that if we do that, the cost of care will ultimately go down.”
Bryn Nelson is a freelance medical writer in Seattle.
Reference
20 Things Psychiatrists Think Hospitalists Need to Know
20 Things At A Glance
- Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
- Secure patient consent before consulting a psychiatrist.
- Present the psychiatrist’s anticipated insight as a benefit to the patient.
- Ask the patient if it’s all right to discuss their health status and needs with family members.
- Recognize that psychiatric illness is real, not imaginary.
- Realize that not all sadness constitutes depression.
- Don’t gloss over the possibility of delirium.
- Take the time to really listen.
- Always remain conscious of alcohol and substance abuse.
- Monitor patients’ vital signs for autonomic instability.
- Avoid arguments and power struggles with difficult or demanding patients.
- Adapt your vocabulary to the patient’s and family’s level of understanding.
- Be mindful of your nonverbal cues.
- Always take suicide risk seriously.
- Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
- Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
- Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
- Listen to your instincts.
- Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
- Extend genuine compassion to your patients.
Patients can be hospitalized with chest pain, a kidney infection, pneumonia, or myriad other medical conditions. Hospital stays on occasion upend a patient’s mental state, with upcoming tests, surgery, or other procedures triggering anxiety or other conditions.
That doesn’t mean these patients have psychiatric or psychological problems, but some of them might. Hospitalists walk a fine line in deciding when to consult a psychiatrist in certain cases.

“A common mistake, when it comes to psychiatry, for hospitalists is to either think they know too much or they know too little,” says Philip R. Muskin, MD, professor of clinical psychiatry at Columbia University College of Physicians & Surgeons in New York City. “Sometimes they’re too quick to call a psychiatrist, and sometimes they’re too slow to call a specialist because they don’t think it’s a psychiatric problem.”
The Hospitalist asked more than half a dozen specialists in psychiatry and hospital medicine to shed light on when to seek additional expertise—and how to inform patients about your request to do so. “If I say, ‘You need to see a psychiatrist,’ it carries some stigma,” says Dr. Muskin, who is the chief of consultation for liaison psychiatry at New York-Presbyterian Medical Center’s Columbia campus. “We have to be sensitive to that.”
So how can you more comfortably approach psychiatric or psychological issues in the hospital setting?
1. Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
“Because of the overwhelming comorbidity between psychiatric illness and medical illness, it’s important to have some communication between the emergency room, caregiver, the hospitalist, and the psychiatrist,” says Ken Duckworth, MD, medical director of the National Alliance on Mental Illness (NAMI) and an assistant clinical professor of psychiatry at Harvard Medical School in Boston. “We know that people with mental health vulnerabilities consume a much higher amount of medical services. That’s a well-known phenomenon.”
2. Secure patient consent before consulting a psychiatrist.

“You need the patient’s permission,” Dr. Duckworth says. “That’s an important piece of the equation.” There are exceptions in emergencies, and the laws pertaining to this vary by state. Verbal consent may suffice if written authorization is already on file. If a patient declines, a hospitalist has to respect those wishes.
3. Present the psychiatrist’s anticipated insight as a benefit to the patient.

Physicians sometimes are uncomfortable informing their patients that they’re asking for a psychiatric consultation. They fear a bad reaction, such as “You think I’m crazy?” The consultation will be more useful if the patient is open and accepting of the process. For example, tell your patient at the outset: “I’d really like you to talk to one of my colleagues, whom I trust a great deal. He/she is an expert in the overlapping area between the body and the brain. I need their help so that I can take better care of you,’” says Linda L.M. Worley, MD, FAPM, professor of psychiatry and obstetrics and gynecology at the University of Arkansas for Medical Sciences in Little Rock.
4. Ask the patient if it’s all right to discuss their health status and needs with family members.
Get to know their names. Identify the medical expert in the family and be certain to involve them in overall discussions and the decision-making process, Dr. Worley says.
5. Recognize that psychiatric illness is real, not imaginary.
The illness “should be placed in exactly the same arena as other medical problems,” Dr. Muskin says. Patients with psychiatric conditions are “not weak. They’re not dumb. It’s not all in their head.” Their mental health “deserves the same attention as their heart, stomach, or kidneys.”
6. Realize that not all sadness constitutes depression.

“There are many reasons why people cry or feel down, and most are not psychiatric illnesses. Depression is often overdiagnosed, leading to wasted time and inappropriate medications,” says Robert Boland, MD, professor of psychiatry and human behavior at Brown University’s Warren Alpert School of Medicine in Providence, R.I. “Unfortunately, the opposite is also true. Depression is often missed in the hospital.”
So how does a hospitalist reconcile those extremes? First, consider depression in any patient who is predisposed, then rely on a consistent way of working it up. The Diagnostic and Statistical Manual of Mental Disorders (DSM, http://www.dsm5.org) offers a conservative approach, so you usually can’t go wrong by following it.
7. Don’t gloss over the possibility of delirium.
It is probably the most frequently missed diagnosis in the general hospital. “We usually recognize it when patients are agitated, but most patients aren’t,” Dr. Boland says. “If anything, they are hypoactive or change throughout the day. When a patient seems confused, we want to find a cause, but that cause isn’t always obvious.”
These situations are particularly true in fragile patients (e.g. the very old or those with dementia). Sometimes medical problems that seem very minor can “push them over the edge,” he adds. When you do expect dementia, the main treatments revolve around medically stabilizing the patient, and psychiatric medications are a minor part of the management, if at all.
8. Take the time to really listen.
Patients’ biggest complaint is that physicians don’t listen. “The best doctors in any specialty know how to communicate with patients,” Dr. Boland says. “It doesn’t take longer—in fact, good communication usually saves time. But it does take attention and focus to let the patient try and explain what is going on with them. It always pays off in the end.”
9. Always remain conscious of alcohol and substance abuse.
Although it might not be the reason patients are hospitalized, it is one of the more common underlying causes. When this is the case, don’t be nihilistic. Many patients improve with treatment, and some get better simply because a physician explained how damaging substance abuse can be to their health, Dr. Boland says.
For those in complete remission from a past addiction to alcohol, benzodiazepines, opiates, or a combination thereof, beware that prescribing certain medications puts them at substantially increased risk for relapse. Use alternative treatments whenever possible; if clinically indicated, be certain that these patients have a safety net to prevent relapse. Patients with severe pain need effective relief.
“If a patient has been exposed to significant dosages of pain medications in the past, their neurotransmitters will have physically adapted,” says Dr. Worley, president-elect of the Academy of Psychosomatic Medicine. “They will require higher doses than normal for effective pain relief.”

—Gregory Ruhnke, MD, assistant professor in the section of hospital medicine, University of Chicago Pritzker School of Medicine
10. Monitor patients’ vital signs for autonomic instability.
“Patients in withdrawal from physiologically addictive medications may have forgotten to tell you that they were taking these medications,” Dr. Worley says. “Abrupt discontinuation can cause incapacitating anxiety and life-threatening delirium.”
11. Avoid arguments and power struggles with difficult or demanding patients.
Put on your thick skin. Don’t take insults or slights personally. And resist the urge to flee or counterattack. Instead, Dr. Worley suggests hospitalists stay calm and focused on providing the best medical care that they can. “Chronically noncompliant patients can be excruciatingly frustrating to care for when they don’t follow through on what they are repeatedly advised to do, but lecturing more vigorously at them won’t help,” she says. “It only makes them shut down more and feel more helpless and you more exhausted. Shift to more of a listening mode and inquire about what they hope to accomplish by coming to you for help.”
12. Adapt your vocabulary to the patient’s and family’s level of understanding.
After your explanation, ask them, “Do me a favor and explain back to me in your words what I said. I want to be sure I got across what I wanted to say.” Then ask whether they have any questions. Also know that all too often patients are so anxious and upset that they are “emotionally flooded” and unable to hear much of what you communicated. You can save a lot of time if they understand you in the first place.
13. Be mindful of your nonverbal cues.
A majority of communication is nonverbal, and your facial expressions, gestures, and body posture speak volumes to patients and family members. “The innocent tilt of a chin upwards while peering through bifocals can be misperceived as arrogance,” Dr. Worley says. “The thoughtful furled brow of contemplation may be misconstrued as irritability or disapproval.”
14. Always take suicide risk seriously.
It’s better to call a psychiatrist unnecessarily than to overlook a patient at risk for suicide. Benzodiazepines, alcohol, or a combination of the two might reduce inhibition and increase the likelihood of a suicide attempt. Be sure to assess suicidal ideation, intent, and lethality of suicide attempt.
“Hopelessness about the future correlates with completed suicide,” says Gregory Ruhnke, MD, assistant professor in the section of hospital medicine at the University of Chicago Pritzker School of Medicine. “Additionally, it is helpful to ask about the four H’s: Hate, humiliation, hostility, handguns.”
15. Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
“The patient may become angry and engage in splitting, whereby he or she emphatically expresses the view that certain caregivers are all good or all bad. This may reflect such [a] patient’s desire to divide the caregivers into opposing factions. It’s a maladaptive way of coping,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the Pritzker School of Medicine. This can be very time-consuming, and it can breed hostility among colleagues. “Communication between caregivers is really important in creating a unified treatment plan that is coherently presented to the patient in a single voice.”
Fortunately, she says, “even though these situations can arise, they are the exception rather than the rule.”

—Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist, University of Chicago Pritzker School of Medicine
16. Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
For example, Dr. Ruhnke says, if a patient complains of hemoptysis and hematochezia with negative endoscopies, talk to the nurse about the patient’s diet, and be suspicious if it includes only red foods and liquids. The most common symptoms among patients who come to medical attention because of factitious disorders are diarrhea, fever of unknown origin, gastrointestinal bleeding, hematuria, seizures, and hypoglycemia.
17. Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
A patient with schizophrenia or bipolar disorder could experience a severe psychiatric episode without psychiatric medication. An appropriate alternative, perhaps administered intravenously if necessary, “can make all the difference in the world,” says Christopher Dobbelstein, MD, assistant professor of psychiatry at the University of Pittsburgh School of Medicine.
18. Listen to your instincts.
Medical teams can handle many psychiatric issues. Straightforward delirium is a good example. The bigger question, which takes experience and confidence, is to recognize when a line has been crossed. “The decision to consult psychiatry is not formulaic,” Dr. Dobbelstein says.
Sometimes a patient is acting strangely, and the team can’t explain why a psychiatrist could offer sound advice. “That’s when they should trust their instincts and consult us,” he says, “because the patient likely does have something more complex going on.”
19. Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
Sometimes psychiatric medications are started without good oversight. Suicide risk is highest during the weeks following an inpatient psychiatric admission, so a patient should see an outpatient mental health provider within seven days after hospital discharge, says NAMI’s Dr. Duckworth.
20. Extend genuine compassion to your patients.
“This is the secret to achieving a lifelong rewarding career in medicine,” Dr. Worley says, “and is the most important ingredient in positive outcomes.”
Susan Kreimer is a freelance writer in New York.
Survival Tips
- Pull up a chair and sit down.
- Ask what name your patient likes to go by. Be respectful and use correct titles when appropriate. One size doesn’t fit all. “Mrs. X” might be a mother-in-law.
- Appreciate how terrifying it can be as a patient—ill, in pain, having no control, with a loss of privacy and at times dignity.
- Remember that any one of us in the role of a patient regresses and copes in different ways. Some become demanding and express a strong need for control, while others want and need information from their physician.
- Privacy is important. Close the door. Don’t ask sensitive questions within earshot of other patients or visitors.
20 Things At A Glance
- Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
- Secure patient consent before consulting a psychiatrist.
- Present the psychiatrist’s anticipated insight as a benefit to the patient.
- Ask the patient if it’s all right to discuss their health status and needs with family members.
- Recognize that psychiatric illness is real, not imaginary.
- Realize that not all sadness constitutes depression.
- Don’t gloss over the possibility of delirium.
- Take the time to really listen.
- Always remain conscious of alcohol and substance abuse.
- Monitor patients’ vital signs for autonomic instability.
- Avoid arguments and power struggles with difficult or demanding patients.
- Adapt your vocabulary to the patient’s and family’s level of understanding.
- Be mindful of your nonverbal cues.
- Always take suicide risk seriously.
- Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
- Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
- Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
- Listen to your instincts.
- Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
- Extend genuine compassion to your patients.
Patients can be hospitalized with chest pain, a kidney infection, pneumonia, or myriad other medical conditions. Hospital stays on occasion upend a patient’s mental state, with upcoming tests, surgery, or other procedures triggering anxiety or other conditions.
That doesn’t mean these patients have psychiatric or psychological problems, but some of them might. Hospitalists walk a fine line in deciding when to consult a psychiatrist in certain cases.
“A common mistake, when it comes to psychiatry, for hospitalists is to either think they know too much or they know too little,” says Philip R. Muskin, MD, professor of clinical psychiatry at Columbia University College of Physicians & Surgeons in New York City. “Sometimes they’re too quick to call a psychiatrist, and sometimes they’re too slow to call a specialist because they don’t think it’s a psychiatric problem.”
The Hospitalist asked more than half a dozen specialists in psychiatry and hospital medicine to shed light on when to seek additional expertise—and how to inform patients about your request to do so. “If I say, ‘You need to see a psychiatrist,’ it carries some stigma,” says Dr. Muskin, who is the chief of consultation for liaison psychiatry at New York-Presbyterian Medical Center’s Columbia campus. “We have to be sensitive to that.”
So how can you more comfortably approach psychiatric or psychological issues in the hospital setting?
1. Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
“Because of the overwhelming comorbidity between psychiatric illness and medical illness, it’s important to have some communication between the emergency room, caregiver, the hospitalist, and the psychiatrist,” says Ken Duckworth, MD, medical director of the National Alliance on Mental Illness (NAMI) and an assistant clinical professor of psychiatry at Harvard Medical School in Boston. “We know that people with mental health vulnerabilities consume a much higher amount of medical services. That’s a well-known phenomenon.”
2. Secure patient consent before consulting a psychiatrist.
“You need the patient’s permission,” Dr. Duckworth says. “That’s an important piece of the equation.” There are exceptions in emergencies, and the laws pertaining to this vary by state. Verbal consent may suffice if written authorization is already on file. If a patient declines, a hospitalist has to respect those wishes.
3. Present the psychiatrist’s anticipated insight as a benefit to the patient.
Physicians sometimes are uncomfortable informing their patients that they’re asking for a psychiatric consultation. They fear a bad reaction, such as “You think I’m crazy?” The consultation will be more useful if the patient is open and accepting of the process. For example, tell your patient at the outset: “I’d really like you to talk to one of my colleagues, whom I trust a great deal. He/she is an expert in the overlapping area between the body and the brain. I need their help so that I can take better care of you,’” says Linda L.M. Worley, MD, FAPM, professor of psychiatry and obstetrics and gynecology at the University of Arkansas for Medical Sciences in Little Rock.
4. Ask the patient if it’s all right to discuss their health status and needs with family members.
Get to know their names. Identify the medical expert in the family and be certain to involve them in overall discussions and the decision-making process, Dr. Worley says.
5. Recognize that psychiatric illness is real, not imaginary.
The illness “should be placed in exactly the same arena as other medical problems,” Dr. Muskin says. Patients with psychiatric conditions are “not weak. They’re not dumb. It’s not all in their head.” Their mental health “deserves the same attention as their heart, stomach, or kidneys.”
6. Realize that not all sadness constitutes depression.
“There are many reasons why people cry or feel down, and most are not psychiatric illnesses. Depression is often overdiagnosed, leading to wasted time and inappropriate medications,” says Robert Boland, MD, professor of psychiatry and human behavior at Brown University’s Warren Alpert School of Medicine in Providence, R.I. “Unfortunately, the opposite is also true. Depression is often missed in the hospital.”
So how does a hospitalist reconcile those extremes? First, consider depression in any patient who is predisposed, then rely on a consistent way of working it up. The Diagnostic and Statistical Manual of Mental Disorders (DSM, http://www.dsm5.org) offers a conservative approach, so you usually can’t go wrong by following it.
7. Don’t gloss over the possibility of delirium.
It is probably the most frequently missed diagnosis in the general hospital. “We usually recognize it when patients are agitated, but most patients aren’t,” Dr. Boland says. “If anything, they are hypoactive or change throughout the day. When a patient seems confused, we want to find a cause, but that cause isn’t always obvious.”
These situations are particularly true in fragile patients (e.g. the very old or those with dementia). Sometimes medical problems that seem very minor can “push them over the edge,” he adds. When you do expect dementia, the main treatments revolve around medically stabilizing the patient, and psychiatric medications are a minor part of the management, if at all.
8. Take the time to really listen.
Patients’ biggest complaint is that physicians don’t listen. “The best doctors in any specialty know how to communicate with patients,” Dr. Boland says. “It doesn’t take longer—in fact, good communication usually saves time. But it does take attention and focus to let the patient try and explain what is going on with them. It always pays off in the end.”
9. Always remain conscious of alcohol and substance abuse.
Although it might not be the reason patients are hospitalized, it is one of the more common underlying causes. When this is the case, don’t be nihilistic. Many patients improve with treatment, and some get better simply because a physician explained how damaging substance abuse can be to their health, Dr. Boland says.
For those in complete remission from a past addiction to alcohol, benzodiazepines, opiates, or a combination thereof, beware that prescribing certain medications puts them at substantially increased risk for relapse. Use alternative treatments whenever possible; if clinically indicated, be certain that these patients have a safety net to prevent relapse. Patients with severe pain need effective relief.
“If a patient has been exposed to significant dosages of pain medications in the past, their neurotransmitters will have physically adapted,” says Dr. Worley, president-elect of the Academy of Psychosomatic Medicine. “They will require higher doses than normal for effective pain relief.”
—Gregory Ruhnke, MD, assistant professor in the section of hospital medicine, University of Chicago Pritzker School of Medicine
10. Monitor patients’ vital signs for autonomic instability.
“Patients in withdrawal from physiologically addictive medications may have forgotten to tell you that they were taking these medications,” Dr. Worley says. “Abrupt discontinuation can cause incapacitating anxiety and life-threatening delirium.”
11. Avoid arguments and power struggles with difficult or demanding patients.
Put on your thick skin. Don’t take insults or slights personally. And resist the urge to flee or counterattack. Instead, Dr. Worley suggests hospitalists stay calm and focused on providing the best medical care that they can. “Chronically noncompliant patients can be excruciatingly frustrating to care for when they don’t follow through on what they are repeatedly advised to do, but lecturing more vigorously at them won’t help,” she says. “It only makes them shut down more and feel more helpless and you more exhausted. Shift to more of a listening mode and inquire about what they hope to accomplish by coming to you for help.”
12. Adapt your vocabulary to the patient’s and family’s level of understanding.
After your explanation, ask them, “Do me a favor and explain back to me in your words what I said. I want to be sure I got across what I wanted to say.” Then ask whether they have any questions. Also know that all too often patients are so anxious and upset that they are “emotionally flooded” and unable to hear much of what you communicated. You can save a lot of time if they understand you in the first place.
13. Be mindful of your nonverbal cues.
A majority of communication is nonverbal, and your facial expressions, gestures, and body posture speak volumes to patients and family members. “The innocent tilt of a chin upwards while peering through bifocals can be misperceived as arrogance,” Dr. Worley says. “The thoughtful furled brow of contemplation may be misconstrued as irritability or disapproval.”
14. Always take suicide risk seriously.
It’s better to call a psychiatrist unnecessarily than to overlook a patient at risk for suicide. Benzodiazepines, alcohol, or a combination of the two might reduce inhibition and increase the likelihood of a suicide attempt. Be sure to assess suicidal ideation, intent, and lethality of suicide attempt.
“Hopelessness about the future correlates with completed suicide,” says Gregory Ruhnke, MD, assistant professor in the section of hospital medicine at the University of Chicago Pritzker School of Medicine. “Additionally, it is helpful to ask about the four H’s: Hate, humiliation, hostility, handguns.”
15. Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
“The patient may become angry and engage in splitting, whereby he or she emphatically expresses the view that certain caregivers are all good or all bad. This may reflect such [a] patient’s desire to divide the caregivers into opposing factions. It’s a maladaptive way of coping,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the Pritzker School of Medicine. This can be very time-consuming, and it can breed hostility among colleagues. “Communication between caregivers is really important in creating a unified treatment plan that is coherently presented to the patient in a single voice.”
Fortunately, she says, “even though these situations can arise, they are the exception rather than the rule.”
—Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist, University of Chicago Pritzker School of Medicine
16. Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
For example, Dr. Ruhnke says, if a patient complains of hemoptysis and hematochezia with negative endoscopies, talk to the nurse about the patient’s diet, and be suspicious if it includes only red foods and liquids. The most common symptoms among patients who come to medical attention because of factitious disorders are diarrhea, fever of unknown origin, gastrointestinal bleeding, hematuria, seizures, and hypoglycemia.
17. Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
A patient with schizophrenia or bipolar disorder could experience a severe psychiatric episode without psychiatric medication. An appropriate alternative, perhaps administered intravenously if necessary, “can make all the difference in the world,” says Christopher Dobbelstein, MD, assistant professor of psychiatry at the University of Pittsburgh School of Medicine.
18. Listen to your instincts.
Medical teams can handle many psychiatric issues. Straightforward delirium is a good example. The bigger question, which takes experience and confidence, is to recognize when a line has been crossed. “The decision to consult psychiatry is not formulaic,” Dr. Dobbelstein says.
Sometimes a patient is acting strangely, and the team can’t explain why a psychiatrist could offer sound advice. “That’s when they should trust their instincts and consult us,” he says, “because the patient likely does have something more complex going on.”
19. Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
Sometimes psychiatric medications are started without good oversight. Suicide risk is highest during the weeks following an inpatient psychiatric admission, so a patient should see an outpatient mental health provider within seven days after hospital discharge, says NAMI’s Dr. Duckworth.
20. Extend genuine compassion to your patients.
“This is the secret to achieving a lifelong rewarding career in medicine,” Dr. Worley says, “and is the most important ingredient in positive outcomes.”
Susan Kreimer is a freelance writer in New York.
Survival Tips
- Pull up a chair and sit down.
- Ask what name your patient likes to go by. Be respectful and use correct titles when appropriate. One size doesn’t fit all. “Mrs. X” might be a mother-in-law.
- Appreciate how terrifying it can be as a patient—ill, in pain, having no control, with a loss of privacy and at times dignity.
- Remember that any one of us in the role of a patient regresses and copes in different ways. Some become demanding and express a strong need for control, while others want and need information from their physician.
- Privacy is important. Close the door. Don’t ask sensitive questions within earshot of other patients or visitors.
20 Things At A Glance
- Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
- Secure patient consent before consulting a psychiatrist.
- Present the psychiatrist’s anticipated insight as a benefit to the patient.
- Ask the patient if it’s all right to discuss their health status and needs with family members.
- Recognize that psychiatric illness is real, not imaginary.
- Realize that not all sadness constitutes depression.
- Don’t gloss over the possibility of delirium.
- Take the time to really listen.
- Always remain conscious of alcohol and substance abuse.
- Monitor patients’ vital signs for autonomic instability.
- Avoid arguments and power struggles with difficult or demanding patients.
- Adapt your vocabulary to the patient’s and family’s level of understanding.
- Be mindful of your nonverbal cues.
- Always take suicide risk seriously.
- Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
- Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
- Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
- Listen to your instincts.
- Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
- Extend genuine compassion to your patients.
Patients can be hospitalized with chest pain, a kidney infection, pneumonia, or myriad other medical conditions. Hospital stays on occasion upend a patient’s mental state, with upcoming tests, surgery, or other procedures triggering anxiety or other conditions.
That doesn’t mean these patients have psychiatric or psychological problems, but some of them might. Hospitalists walk a fine line in deciding when to consult a psychiatrist in certain cases.
“A common mistake, when it comes to psychiatry, for hospitalists is to either think they know too much or they know too little,” says Philip R. Muskin, MD, professor of clinical psychiatry at Columbia University College of Physicians & Surgeons in New York City. “Sometimes they’re too quick to call a psychiatrist, and sometimes they’re too slow to call a specialist because they don’t think it’s a psychiatric problem.”
The Hospitalist asked more than half a dozen specialists in psychiatry and hospital medicine to shed light on when to seek additional expertise—and how to inform patients about your request to do so. “If I say, ‘You need to see a psychiatrist,’ it carries some stigma,” says Dr. Muskin, who is the chief of consultation for liaison psychiatry at New York-Presbyterian Medical Center’s Columbia campus. “We have to be sensitive to that.”
So how can you more comfortably approach psychiatric or psychological issues in the hospital setting?
1. Acknowledge that collaboration between health professionals is important, even when schedules are hectic and reimbursement doesn’t cover these discussions.
“Because of the overwhelming comorbidity between psychiatric illness and medical illness, it’s important to have some communication between the emergency room, caregiver, the hospitalist, and the psychiatrist,” says Ken Duckworth, MD, medical director of the National Alliance on Mental Illness (NAMI) and an assistant clinical professor of psychiatry at Harvard Medical School in Boston. “We know that people with mental health vulnerabilities consume a much higher amount of medical services. That’s a well-known phenomenon.”
2. Secure patient consent before consulting a psychiatrist.
“You need the patient’s permission,” Dr. Duckworth says. “That’s an important piece of the equation.” There are exceptions in emergencies, and the laws pertaining to this vary by state. Verbal consent may suffice if written authorization is already on file. If a patient declines, a hospitalist has to respect those wishes.
3. Present the psychiatrist’s anticipated insight as a benefit to the patient.
Physicians sometimes are uncomfortable informing their patients that they’re asking for a psychiatric consultation. They fear a bad reaction, such as “You think I’m crazy?” The consultation will be more useful if the patient is open and accepting of the process. For example, tell your patient at the outset: “I’d really like you to talk to one of my colleagues, whom I trust a great deal. He/she is an expert in the overlapping area between the body and the brain. I need their help so that I can take better care of you,’” says Linda L.M. Worley, MD, FAPM, professor of psychiatry and obstetrics and gynecology at the University of Arkansas for Medical Sciences in Little Rock.
4. Ask the patient if it’s all right to discuss their health status and needs with family members.
Get to know their names. Identify the medical expert in the family and be certain to involve them in overall discussions and the decision-making process, Dr. Worley says.
5. Recognize that psychiatric illness is real, not imaginary.
The illness “should be placed in exactly the same arena as other medical problems,” Dr. Muskin says. Patients with psychiatric conditions are “not weak. They’re not dumb. It’s not all in their head.” Their mental health “deserves the same attention as their heart, stomach, or kidneys.”
6. Realize that not all sadness constitutes depression.
“There are many reasons why people cry or feel down, and most are not psychiatric illnesses. Depression is often overdiagnosed, leading to wasted time and inappropriate medications,” says Robert Boland, MD, professor of psychiatry and human behavior at Brown University’s Warren Alpert School of Medicine in Providence, R.I. “Unfortunately, the opposite is also true. Depression is often missed in the hospital.”
So how does a hospitalist reconcile those extremes? First, consider depression in any patient who is predisposed, then rely on a consistent way of working it up. The Diagnostic and Statistical Manual of Mental Disorders (DSM, http://www.dsm5.org) offers a conservative approach, so you usually can’t go wrong by following it.
7. Don’t gloss over the possibility of delirium.
It is probably the most frequently missed diagnosis in the general hospital. “We usually recognize it when patients are agitated, but most patients aren’t,” Dr. Boland says. “If anything, they are hypoactive or change throughout the day. When a patient seems confused, we want to find a cause, but that cause isn’t always obvious.”
These situations are particularly true in fragile patients (e.g. the very old or those with dementia). Sometimes medical problems that seem very minor can “push them over the edge,” he adds. When you do expect dementia, the main treatments revolve around medically stabilizing the patient, and psychiatric medications are a minor part of the management, if at all.
8. Take the time to really listen.
Patients’ biggest complaint is that physicians don’t listen. “The best doctors in any specialty know how to communicate with patients,” Dr. Boland says. “It doesn’t take longer—in fact, good communication usually saves time. But it does take attention and focus to let the patient try and explain what is going on with them. It always pays off in the end.”
9. Always remain conscious of alcohol and substance abuse.
Although it might not be the reason patients are hospitalized, it is one of the more common underlying causes. When this is the case, don’t be nihilistic. Many patients improve with treatment, and some get better simply because a physician explained how damaging substance abuse can be to their health, Dr. Boland says.
For those in complete remission from a past addiction to alcohol, benzodiazepines, opiates, or a combination thereof, beware that prescribing certain medications puts them at substantially increased risk for relapse. Use alternative treatments whenever possible; if clinically indicated, be certain that these patients have a safety net to prevent relapse. Patients with severe pain need effective relief.
“If a patient has been exposed to significant dosages of pain medications in the past, their neurotransmitters will have physically adapted,” says Dr. Worley, president-elect of the Academy of Psychosomatic Medicine. “They will require higher doses than normal for effective pain relief.”
—Gregory Ruhnke, MD, assistant professor in the section of hospital medicine, University of Chicago Pritzker School of Medicine
10. Monitor patients’ vital signs for autonomic instability.
“Patients in withdrawal from physiologically addictive medications may have forgotten to tell you that they were taking these medications,” Dr. Worley says. “Abrupt discontinuation can cause incapacitating anxiety and life-threatening delirium.”
11. Avoid arguments and power struggles with difficult or demanding patients.
Put on your thick skin. Don’t take insults or slights personally. And resist the urge to flee or counterattack. Instead, Dr. Worley suggests hospitalists stay calm and focused on providing the best medical care that they can. “Chronically noncompliant patients can be excruciatingly frustrating to care for when they don’t follow through on what they are repeatedly advised to do, but lecturing more vigorously at them won’t help,” she says. “It only makes them shut down more and feel more helpless and you more exhausted. Shift to more of a listening mode and inquire about what they hope to accomplish by coming to you for help.”
12. Adapt your vocabulary to the patient’s and family’s level of understanding.
After your explanation, ask them, “Do me a favor and explain back to me in your words what I said. I want to be sure I got across what I wanted to say.” Then ask whether they have any questions. Also know that all too often patients are so anxious and upset that they are “emotionally flooded” and unable to hear much of what you communicated. You can save a lot of time if they understand you in the first place.
13. Be mindful of your nonverbal cues.
A majority of communication is nonverbal, and your facial expressions, gestures, and body posture speak volumes to patients and family members. “The innocent tilt of a chin upwards while peering through bifocals can be misperceived as arrogance,” Dr. Worley says. “The thoughtful furled brow of contemplation may be misconstrued as irritability or disapproval.”
14. Always take suicide risk seriously.
It’s better to call a psychiatrist unnecessarily than to overlook a patient at risk for suicide. Benzodiazepines, alcohol, or a combination of the two might reduce inhibition and increase the likelihood of a suicide attempt. Be sure to assess suicidal ideation, intent, and lethality of suicide attempt.
“Hopelessness about the future correlates with completed suicide,” says Gregory Ruhnke, MD, assistant professor in the section of hospital medicine at the University of Chicago Pritzker School of Medicine. “Additionally, it is helpful to ask about the four H’s: Hate, humiliation, hostility, handguns.”
15. Beware of patients who exhibit attention-seeking behavior, which can have a negative impact on the healthcare team and the care provided to the patient.
“The patient may become angry and engage in splitting, whereby he or she emphatically expresses the view that certain caregivers are all good or all bad. This may reflect such [a] patient’s desire to divide the caregivers into opposing factions. It’s a maladaptive way of coping,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the Pritzker School of Medicine. This can be very time-consuming, and it can breed hostility among colleagues. “Communication between caregivers is really important in creating a unified treatment plan that is coherently presented to the patient in a single voice.”
Fortunately, she says, “even though these situations can arise, they are the exception rather than the rule.”
—Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist, University of Chicago Pritzker School of Medicine
16. Consider the possibility of a factitious disorder when there is a lack of objective evidence for pathology to explain a patient’s symptoms despite extensive evaluation.
For example, Dr. Ruhnke says, if a patient complains of hemoptysis and hematochezia with negative endoscopies, talk to the nurse about the patient’s diet, and be suspicious if it includes only red foods and liquids. The most common symptoms among patients who come to medical attention because of factitious disorders are diarrhea, fever of unknown origin, gastrointestinal bleeding, hematuria, seizures, and hypoglycemia.
17. Choose an intravenous psychiatric medication when a patient with severe and persistent mental illness should avoid oral medication for a procedure.
A patient with schizophrenia or bipolar disorder could experience a severe psychiatric episode without psychiatric medication. An appropriate alternative, perhaps administered intravenously if necessary, “can make all the difference in the world,” says Christopher Dobbelstein, MD, assistant professor of psychiatry at the University of Pittsburgh School of Medicine.
18. Listen to your instincts.
Medical teams can handle many psychiatric issues. Straightforward delirium is a good example. The bigger question, which takes experience and confidence, is to recognize when a line has been crossed. “The decision to consult psychiatry is not formulaic,” Dr. Dobbelstein says.
Sometimes a patient is acting strangely, and the team can’t explain why a psychiatrist could offer sound advice. “That’s when they should trust their instincts and consult us,” he says, “because the patient likely does have something more complex going on.”
19. Arrange for post-discharge follow-up with a primary-care physician or psychiatrist.
Sometimes psychiatric medications are started without good oversight. Suicide risk is highest during the weeks following an inpatient psychiatric admission, so a patient should see an outpatient mental health provider within seven days after hospital discharge, says NAMI’s Dr. Duckworth.
20. Extend genuine compassion to your patients.
“This is the secret to achieving a lifelong rewarding career in medicine,” Dr. Worley says, “and is the most important ingredient in positive outcomes.”
Susan Kreimer is a freelance writer in New York.
Survival Tips
- Pull up a chair and sit down.
- Ask what name your patient likes to go by. Be respectful and use correct titles when appropriate. One size doesn’t fit all. “Mrs. X” might be a mother-in-law.
- Appreciate how terrifying it can be as a patient—ill, in pain, having no control, with a loss of privacy and at times dignity.
- Remember that any one of us in the role of a patient regresses and copes in different ways. Some become demanding and express a strong need for control, while others want and need information from their physician.
- Privacy is important. Close the door. Don’t ask sensitive questions within earshot of other patients or visitors.
Keep an Eye Out for Factitious Disorders
Among the challenging psychiatric conditions hospitalists encounter are factitious disorders in which patients fabricate symptoms to draw attention, elicit empathy, and intentionally take on a sick role.
For example, at the University of Chicago, a patient in her 30s complained of blood in her urine, stool, and vomit. The staff performed an extensive evaluation, including laboratory analyses and upper and lower gastrointestinal endoscopies, but they found no source of the alleged bleeding, says Gregory Ruhnke, MD, MS, MPH, assistant professor in the section of hospital medicine at the university’s Pritzker School of Medicine.

In this instance, the patient’s objective was “to stay in the hospital,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the University of Chicago. “That’s the goal—to be taken care of as a patient.”
The staff later learned that the patient had engaged in similar tactics at other hospitals. When physicians wanted to obtain medical records from those facilities, the patient declined to grant permission.
“We do have to respect the patient’s confidentiality,” Dr. Tobin says. “If they refuse, we really can’t [obtain their records].”
Aside from previous records, “room searches can help confirm suspicions,” Dr. Ruhnke says. Security personnel should conduct a room search when necessary. This preserves the patient’s therapeutic rapport with healthcare providers. A search could uncover knives or needles, which a patient could use to inflict harm. More important, room searches can resolve inconsistencies and help hospitalists avoid ordering unjustified tests and procedures.
“It’s not a pleasant situation, but it is for safety,” Dr. Tobin says of investigations.
“These are people who can be at high risk to themselves.” TH
Susan Kreimer is a freelance writer in New York.
Among the challenging psychiatric conditions hospitalists encounter are factitious disorders in which patients fabricate symptoms to draw attention, elicit empathy, and intentionally take on a sick role.
For example, at the University of Chicago, a patient in her 30s complained of blood in her urine, stool, and vomit. The staff performed an extensive evaluation, including laboratory analyses and upper and lower gastrointestinal endoscopies, but they found no source of the alleged bleeding, says Gregory Ruhnke, MD, MS, MPH, assistant professor in the section of hospital medicine at the university’s Pritzker School of Medicine.
In this instance, the patient’s objective was “to stay in the hospital,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the University of Chicago. “That’s the goal—to be taken care of as a patient.”
The staff later learned that the patient had engaged in similar tactics at other hospitals. When physicians wanted to obtain medical records from those facilities, the patient declined to grant permission.
“We do have to respect the patient’s confidentiality,” Dr. Tobin says. “If they refuse, we really can’t [obtain their records].”
Aside from previous records, “room searches can help confirm suspicions,” Dr. Ruhnke says. Security personnel should conduct a room search when necessary. This preserves the patient’s therapeutic rapport with healthcare providers. A search could uncover knives or needles, which a patient could use to inflict harm. More important, room searches can resolve inconsistencies and help hospitalists avoid ordering unjustified tests and procedures.
“It’s not a pleasant situation, but it is for safety,” Dr. Tobin says of investigations.
“These are people who can be at high risk to themselves.” TH
Susan Kreimer is a freelance writer in New York.
Among the challenging psychiatric conditions hospitalists encounter are factitious disorders in which patients fabricate symptoms to draw attention, elicit empathy, and intentionally take on a sick role.
For example, at the University of Chicago, a patient in her 30s complained of blood in her urine, stool, and vomit. The staff performed an extensive evaluation, including laboratory analyses and upper and lower gastrointestinal endoscopies, but they found no source of the alleged bleeding, says Gregory Ruhnke, MD, MS, MPH, assistant professor in the section of hospital medicine at the university’s Pritzker School of Medicine.
In this instance, the patient’s objective was “to stay in the hospital,” says Marie Tobin, MD, associate professor of psychiatry and consult-liaison psychiatrist at the University of Chicago. “That’s the goal—to be taken care of as a patient.”
The staff later learned that the patient had engaged in similar tactics at other hospitals. When physicians wanted to obtain medical records from those facilities, the patient declined to grant permission.
“We do have to respect the patient’s confidentiality,” Dr. Tobin says. “If they refuse, we really can’t [obtain their records].”
Aside from previous records, “room searches can help confirm suspicions,” Dr. Ruhnke says. Security personnel should conduct a room search when necessary. This preserves the patient’s therapeutic rapport with healthcare providers. A search could uncover knives or needles, which a patient could use to inflict harm. More important, room searches can resolve inconsistencies and help hospitalists avoid ordering unjustified tests and procedures.
“It’s not a pleasant situation, but it is for safety,” Dr. Tobin says of investigations.
“These are people who can be at high risk to themselves.” TH
Susan Kreimer is a freelance writer in New York.

ONLINE EXCLUSIVE: The Medical Director of the National Alliance on Mental Illness Spotlights Hospitalist Communication, Attention to Discharge Details
Click here to listen to Dr. Duckworth
Click here to listen to Dr. Duckworth
Click here to listen to Dr. Duckworth
Conservative Management of Pediatric Pleural Empyema Results in Good Long-Term Outcomes

Clinical question: What are the long-term outcomes of pediatric pleural empyema?
Background: Hospitalizations for complicated pneumonia have increased in recent years. In the U.S., early intervention—commonly video-assisted thorascopic surgery (VATS)—has become popular. Although short-term outcomes appear cost-effective with this approach, long-term comparative-effectiveness outcomes are not entirely clear.
Study design: Prospective observational study.
Setting: Tertiary-care children's hospital.
Synopsis: Over a two-year period, 82 patients were enrolled and available for at least one follow-up visit in a 12-month period. Chest drain was used in 62% of children; fibrinolytics were used in 78% of those cases. All patients received antibiotics. Six patients (7%) were readmitted in the first month, with three patients requiring a chest drain. At 12 months, four patients (5%) had mildly abnormal spirometric or radiographic abnormalities but were asymptomatic with normal quality-of-life scores.
This prospective observational study is notable for the relatively conservative approach (antibiotics alone or chest drainage, without VATS) employed in all subjects. The results provide a comprehensive summary of outcomes at 12 months in this population. Unfortunately, comparative-effectiveness data for VATS are not available in a generalizable form. Nevertheless, this single-center snapshot suggests that long-term outcomes are good with a conservative approach.
Given these findings, and the low likelihood that significant advantages of VATS will be demonstrated in the absence of a large multicenter trial, better understanding of parental preferences will become critical to making the right decision for each patient.
Bottom line: Conservative management of pediatric pleural empyema yields good long-term outcomes.
Citation: Cohen E, Mahant S, Dell SD, et al. The long-term outcomes of pediatric pleural empyema: a prospective study. Arch Pediatr Adolesc Med. 2012;166(11):999-1004.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What are the long-term outcomes of pediatric pleural empyema?
Background: Hospitalizations for complicated pneumonia have increased in recent years. In the U.S., early intervention—commonly video-assisted thorascopic surgery (VATS)—has become popular. Although short-term outcomes appear cost-effective with this approach, long-term comparative-effectiveness outcomes are not entirely clear.
Study design: Prospective observational study.
Setting: Tertiary-care children's hospital.
Synopsis: Over a two-year period, 82 patients were enrolled and available for at least one follow-up visit in a 12-month period. Chest drain was used in 62% of children; fibrinolytics were used in 78% of those cases. All patients received antibiotics. Six patients (7%) were readmitted in the first month, with three patients requiring a chest drain. At 12 months, four patients (5%) had mildly abnormal spirometric or radiographic abnormalities but were asymptomatic with normal quality-of-life scores.
This prospective observational study is notable for the relatively conservative approach (antibiotics alone or chest drainage, without VATS) employed in all subjects. The results provide a comprehensive summary of outcomes at 12 months in this population. Unfortunately, comparative-effectiveness data for VATS are not available in a generalizable form. Nevertheless, this single-center snapshot suggests that long-term outcomes are good with a conservative approach.
Given these findings, and the low likelihood that significant advantages of VATS will be demonstrated in the absence of a large multicenter trial, better understanding of parental preferences will become critical to making the right decision for each patient.
Bottom line: Conservative management of pediatric pleural empyema yields good long-term outcomes.
Citation: Cohen E, Mahant S, Dell SD, et al. The long-term outcomes of pediatric pleural empyema: a prospective study. Arch Pediatr Adolesc Med. 2012;166(11):999-1004.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
Clinical question: What are the long-term outcomes of pediatric pleural empyema?
Background: Hospitalizations for complicated pneumonia have increased in recent years. In the U.S., early intervention—commonly video-assisted thorascopic surgery (VATS)—has become popular. Although short-term outcomes appear cost-effective with this approach, long-term comparative-effectiveness outcomes are not entirely clear.
Study design: Prospective observational study.
Setting: Tertiary-care children's hospital.
Synopsis: Over a two-year period, 82 patients were enrolled and available for at least one follow-up visit in a 12-month period. Chest drain was used in 62% of children; fibrinolytics were used in 78% of those cases. All patients received antibiotics. Six patients (7%) were readmitted in the first month, with three patients requiring a chest drain. At 12 months, four patients (5%) had mildly abnormal spirometric or radiographic abnormalities but were asymptomatic with normal quality-of-life scores.
This prospective observational study is notable for the relatively conservative approach (antibiotics alone or chest drainage, without VATS) employed in all subjects. The results provide a comprehensive summary of outcomes at 12 months in this population. Unfortunately, comparative-effectiveness data for VATS are not available in a generalizable form. Nevertheless, this single-center snapshot suggests that long-term outcomes are good with a conservative approach.
Given these findings, and the low likelihood that significant advantages of VATS will be demonstrated in the absence of a large multicenter trial, better understanding of parental preferences will become critical to making the right decision for each patient.
Bottom line: Conservative management of pediatric pleural empyema yields good long-term outcomes.
Citation: Cohen E, Mahant S, Dell SD, et al. The long-term outcomes of pediatric pleural empyema: a prospective study. Arch Pediatr Adolesc Med. 2012;166(11):999-1004.
Reviewed by Pediatric Editor Mark Shen, MD, SFHM, medical director of hospital medicine at Dell Children's Medical Center, Austin, Texas.
ITL: Physician Reviews of HM-Relevant Research
In This Edition
Literature At A Glance
A guide to this month’s studies
- Value of routine preoperative urine screening assessed
- Impact of hospitalist-led intermediate care on patient survival
- Risks of blood transfusion to treat upper GI bleeding
- Low-dose steroids and increased mortality in sepsis
- Reduced length of stay and hospital readmission rates
- Restrictive blood transfusion strategies better for acute myocardial infarction
- Trends in GI illnesses and their associated costs
- Apixaban as a stand-alone anticoagulant in patients with VTE
- Guidelines for upper endoscopy use in gastroesophageal reflux disease
Avoid Preoperative Urine Culture in Nonurologic Surgical Procedures
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Intermediate Care Staffed by Hospitalists: Impact on Mortality, Comanagement, and Teaching
Clinical question: Does a hospitalist-led intermediate-care unit improve patient survival?
Background: Hospitalized patients are complex, and institutions often have to balance matching patient acuity to either an ICU or a regular ward. However, an intermediate-care setting might be an attractive strategy to provide rational care according to patient needs while expanding comanagement and teaching services.
Study design: Retrospective observational study.
Setting: Intermediate-care unit of a single academic hospital.
Synopsis: In-hospital mortality in this intermediate-care unit was 20.6%, whereas the expected mortality was 23.2% based on Simplified Acute Physiology Score II (SAPS II) score. The correlation between SAPS II predicted and observed death rates was accurate and statistically significant (P<0.001). Comanagement was performed with several medical and surgical teams, with an increase in perioperative comanagement of 22.7% (P=0.014). The number of training residents in the intermediate-care unit increased to 30.4% from 4.3% (P=0.002).
Bottom line: An intermediate-care unit led by hospitalists showed encouraging results in patient mortality, as well as comanagement and teaching opportunities.
Citation: Lucena JF, Alegre F, Rodil R, et al. Results of a retrospective observational study of intermediate care staffed by hospitalists: impact on mortality, co-management, and teaching. J Hosp Med. 2012;7(5):411-415.
Blood Transfusion Associated with Increased Risk of Rebleeding in Patients with Nonvariceal Upper GI Bleeding
Clinical question: Does more liberal use of blood transfusions in the setting of nonvariceal upper GI bleeding result in patient harm?
Background: Randomized controlled trials have demonstrated that a more liberal approach to blood transfusions for patients in the medical intensive-care unit results in higher mortality. However, the potential harmful effect of blood transfusions in the setting of GI bleeding has not been demonstrated.
Study design: Retrospective cohort study.
Setting: Canadian hospitals.
Synopsis: Based on a retrospective analysis of the Canadian Registry of patients with Upper Gastrointestinal Bleeding and Endoscopy (RUGBE), the authors determined there was a statistically significant association between patients who received a blood transfusion for the management of nonvariceal upper GI bleeding and the risk of rebleeding. The rate of rebleeding in patients who received a blood transfusion was 23.6% compared with 11.3% in patients who were not transfused (P<0.01). There was no statistically significant difference in mortality.
Although this was a reasonably large observational study that included 1,677 patients with nonvariceal upper GI bleeding, it is vulnerable to confounding. It suggests the need to further study potential harm of blood transfusion in the setting of GI bleeding, but it should not result in a change in clinical practice at this time.
Bottom line: Prospective randomized studies are needed to determine if there are harmful effects of blood transfusions in the setting of GI bleeding and to better define a threshold for transfusion.
Citation: Restellini S, Kherad O, Jairath V, Martel M, Barkun AN. Red blood cell transfusion is associated with increased rebleeding in patients with nonvariceal upper gastrointestinal bleeding. Aliment Pharmacol Ther. 2013;37:316-322.
Low-Dose Steroids in Sepsis Associated with Increase in Mortality
Clinical question: What is the role of steroids in the treatment of adult patients with sepsis?
Background: The Surviving Sepsis Campaign guidelines have previously recommended administering steroids to patients with septic shock not responsive to fluid resuscitation and who require vasopressors. However, prior randomized clinical trials studying the use of steroids in these settings have produced conflicting results.
Study design: Retrospective cohort study.
Setting: Two hundred fifty-two hospitals in North America, South America, and Europe.
Synopsis: The Surviving Sepsis Campaign management bundle has been shown to reduce mortality in patients with sepsis. However, it is not known which particular elements of the management bundle result in improved mortality. The Surviving Sepsis Campaign database included 17,847 patients who required vasopressor therapy after adequate fluid resuscitation. This subgroup was analyzed to see if there was a difference in mortality between patients who received low-dose steroids versus those who did not receive steroids. The mortality rate among those who received steroids was statistically higher (with odds ratio of 1.18 and P<0.001) compared with those who did not receive steroids. This finding adds to the body of evidence that calls into question the commonplace practice of administrating steroids to septic patients on vasopressor therapy.
The most recent campaign guidelines recommend the use of steroids in septic patients only if both adequate fluid resuscitation and vasopressor therapy are not able to restore hemodynamic stability.
Bottom line: Further studies are needed to better define the role of steroids in the treatment of sepsis.
Citation: Casserly B, Gerlach H, Phillips GS, et al. Low-dose steroids in adult septic shock: results of the Surviving Sepsis Campaign. Intensive Care Med. 2012;38:1946-1954.
Link Between Length of Stay and Readmission Rates
Clinical question: How has reducing length of stay affected hospital readmission rates?
Background: There are ongoing concerns that improving a hospital’s efficiency by reducing length of stay (LOS) could be associated with higher hospital readmission rates. However, no studies evaluating the relationship between LOS and readmission rates have been done using recent data.
Study design: Retrospective observational study.
Setting: All acute-care Veterans Affairs (VA) hospitals in the U.S.
Synopsis: A total of 4,124,907 index admissions were included in the final sample from all acute medical admissions in 129 acute-care VA hospitals from October 1996 to September 2010. The primary outcomes were the hospital LOS and the 30-day readmission rate. Index admissions for heart failure, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (AMI), community-acquired pneumonia, and gastrointestinal hemorrhage were also analyzed separately.
The risk-adjusted analysis of LOS demonstrated significant reductions for all admissions over the 14-year period, to 3.98 days from 5.44 days, and for all of the individual conditions with reductions ranging from 1.40 days for gastrointestinal hemorrhage to 2.85 days for AMI. There were similar significant reductions in 30-day readmission rates for all admissions to 13.8% from 16.5% and within the individual conditions ranging from 0.9% in community-acquired pneumonia to 3.3% in COPD. These results show that the reductions in LOS did not increase the risk of readmissions. The major limitation of the study was that these data are only from a single healthcare system.
Bottom line: Data from VA hospitals show that reductions in LOS do not have adverse effects on 30-day readmission rates; instead, both LOS and readmission rates improved over the same time period.
Citation: Kaboli PJ, Go JT, Hockenberry J, et al. Associations between reduced hospital length of stay and 30-day readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Ann Intern Med. 2012;157:837-845.
Better to Restrict Blood Transfusions in Acute Myocardial Infarction
Clinical question: Is a liberal or restrictive blood transfusion strategy better in patients with anemia and acute myocardial infarction?
Background: Patients with acute myocardial infarction (AMI) are often given therapies that can increase their risk for bleeding and anemia, and it is known that AMI patients have a worse prognosis if they have concomitant anemia. No clear consensus exists on the benefit or harm of blood transfusions in AMI patients.
Study design: Systematic review and meta-analysis.
Setting: Ten articles included in the qualitative and quantitative analyses out of 729 screened articles from Jan. 1, 1966, to March 31, 2012, using the search terms “transfusion,” “myocardial infarction,” and “mortality” in English language.
Synopsis: A total of 203,665 study participants were identified from the 10 studies (one randomized and nine observational) that met the inclusion and exclusion criteria. All-cause mortality was significantly higher in AMI patients who received a blood transfusion compared with those who did not (18.2% vs. 10.2%). However, this difference was not statistically significant in patients that had a STEMI or in patients with a baseline hematocrit less than 30%. A multivariate meta-regression with several covariates, excluding demographics, also showed that blood transfusion was associated with higher mortality and higher risk for subsequent myocardial infarction. There was significant heterogeneity in all results, but no single study was found as the source of the heterogeneity, and no significant publication bias was identified. The major limitations to this study are that there is a paucity of randomized trials available that pertain to this specific topic and the authors did not have patient-level covariates to include in their analyses.
Bottom line: There appears to be an increased risk of mortality and subsequent myocardial infarction in AMI patients who receive blood transfusions versus those who do not.
Citation: Chatterjee S, Wetterslev J, Sharma A, Lichstein E, Mukherjee D. Association of blood transfusion with increased mortality in myocardial infarction: a meta-analysis and diversity-adjusted study sequential analysis. JAMA Intern Med. 2013;173(2):132-139.
Trends in GI Illnesses and Their Associated Costs
Clinical question: What are the new trends in GI illnesses and their associated costs?
Background: The frequency of illnesses and their treatment costs have changed over the last decade. In order to help healthcare providers focus their attention on these new trends, a new compilation of data is needed.
Study design: Epidemiological analysis.
Setting: Various governmental and private databases representing outpatient clinics, hospitals, and death certificates from multiple regions of the U.S.
Synopsis: The analysis was blinded to patient identifiers but represented multiple regions of the U.S. Symptoms were abstracted from patient surveys, and the rest of the data were collected from record review. The most common reported symptoms were abdominal pain, followed by nausea, vomiting, diarrhea, constipation, and heartburn. The most common clinic diagnoses were reflux, abdominal pain, enteritis/dyspepsia, and constipation. The most common inpatient discharge primary diagnoses included acute pancreatitis, cholecystitis, and diverticulitis. Impressive increases were seen in the number of morbidly obese, C. diff, and fatty liver diagnoses.
Colon cancer was the most common GI malignancy and had the highest mortality. C. diff was the ninth-leading cause of GI-related deaths. All types of scopes (except endoscopic retrograde cholangiopancreatography) were performed more commonly now than in the past, with colonoscopy being the most common. The most common indication for an upper endoscopy was reflux, which was also the most common outpatient GI diagnosis.
Bottom line: Healthcare providers need to be aware of new GI illness trends and their associated costs.
Citation: Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterol. 2012;143:1179-1187.
Is Apixaban a Good Stand-Alone Anticoagulant for Extended Treatment in VTE Patients?
Clinical question: Is apixaban an option for the extended treatment of VTE in a simple, fixed-dose regimen?
Background: Apixaban is an oral factor Xa inhibitor that is administered in fixed doses without the need for laboratory monitoring. In the Apixaban after the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy—Extended Treatment (AMPLIFY-EXT) study, investigators compared the efficacy and safety of two doses of apixaban (2.5 mg and 5 mg) with those of placebo in patients with VTE who had completed six to 12 months of anticoagulation therapy and for whom treating physicians were uncertain about continuing therapy. Additional aims of the study were to determine whether the lower dose of apixaban was effective and whether it was associated with less bleeding than the higher dose, and to examine the effect of treatment on arterial thrombotic outcomes.
Study design: Randomized, double-blind study.
Synopsis: A total of 2,486 patients underwent randomization, 2,482 of whom were included in the intention-to-treat analyses. Symptomatic recurrent VTE or death from VTE occurred in 73 of the 829 patients (8.8%) who were receiving placebo, compared with 14 of the 840 patients (1.7%) who were receiving 2.5 mg of apixaban (a difference of 7.2 percentage points; 95% confidence interval [CI], 5.0 to 9.3) and 14 of the 813 patients (1.7%) who were receiving 5 mg of apixaban (a difference of 7.0 percentage points; 95% CI, 4.9 to 9.1) (P<0.001 for both comparisons). The rates of major bleeding were 0.5% in the placebo group, 0.2% in the 2.5-mg apixaban group, and 0.1% in the 5-mg apixaban group. The rates of clinically relevant nonmajor bleeding were 2.3% in the placebo group, 3.0% in the 2.5-mg apixaban group, and 4.2% in the 5-mg apixaban group. The rate of death from any cause was 1.7% in the placebo group, compared with 0.8% in the 2.5-mg apixaban group and 0.5% in the 5-mg apixaban group.
Bottom line: Apixaban is a safe and effective anticoagulant for extended anticoagulation in patients with VTE initially treated with six to 12 months of warfarin.
Citation: Agnelli GM, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699-708.
ACP Guideline Review: Upper Endoscopy for Gastroesophageal Reflux Disease
Clinical question: What are the indications of upper endoscopy in the setting of gastroesophageal reflux disease (GERD)?
Background: GERD is a common condition. Upper endoscopy is widely available and routinely used for diagnosis and management of GERD and its complications. The indications for this procedure are not clearly defined. Overuse of upper endoscopy contributes to higher healthcare costs without improving patient outcomes.
Study design: Literature review and comparison of clinical guidelines from professional organizations by a team of general internists, gastroenterologists, and clinical epidemiologists. The document was not based on a formal systemic review but was intended to provide practical advice based on the best available evidence.
Synopsis: Best practice advice No. 1: Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).
Best practice advice No. 2: Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton-pump inhibitor therapy, severe erosive esophagitis after a two-month course of proton-pump inhibitor therapy to assess healing and rule out Barrett esophagus, and history of esophageal stricture who have recurrent symptoms of dysphagia.
Best practice advice No. 3: Upper endoscopy might be indicated in men older than 50 with chronic GERD symptoms (symptoms for more than five years) and additional risk factors (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat) to detect esophageal adenocarcinoma and Barrett esophagus. It might also be indicated for surveillance evaluation in men and women with a history of Barrett esophagus. In men and women with Barrett esophagus and no dysplasia, surveillance examinations should occur at intervals no more frequently than three to five years. More frequent intervals are indicated in patients with Barrett esophagus and dysplasia.
Bottom line: Use upper endoscopy selectively for patients with GERD.
Citation: Shaheen NJ, Weinberg DS, Denberg TD, et al. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2012;157(11):808-816.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Value of routine preoperative urine screening assessed
- Impact of hospitalist-led intermediate care on patient survival
- Risks of blood transfusion to treat upper GI bleeding
- Low-dose steroids and increased mortality in sepsis
- Reduced length of stay and hospital readmission rates
- Restrictive blood transfusion strategies better for acute myocardial infarction
- Trends in GI illnesses and their associated costs
- Apixaban as a stand-alone anticoagulant in patients with VTE
- Guidelines for upper endoscopy use in gastroesophageal reflux disease
Avoid Preoperative Urine Culture in Nonurologic Surgical Procedures
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Intermediate Care Staffed by Hospitalists: Impact on Mortality, Comanagement, and Teaching
Clinical question: Does a hospitalist-led intermediate-care unit improve patient survival?
Background: Hospitalized patients are complex, and institutions often have to balance matching patient acuity to either an ICU or a regular ward. However, an intermediate-care setting might be an attractive strategy to provide rational care according to patient needs while expanding comanagement and teaching services.
Study design: Retrospective observational study.
Setting: Intermediate-care unit of a single academic hospital.
Synopsis: In-hospital mortality in this intermediate-care unit was 20.6%, whereas the expected mortality was 23.2% based on Simplified Acute Physiology Score II (SAPS II) score. The correlation between SAPS II predicted and observed death rates was accurate and statistically significant (P<0.001). Comanagement was performed with several medical and surgical teams, with an increase in perioperative comanagement of 22.7% (P=0.014). The number of training residents in the intermediate-care unit increased to 30.4% from 4.3% (P=0.002).
Bottom line: An intermediate-care unit led by hospitalists showed encouraging results in patient mortality, as well as comanagement and teaching opportunities.
Citation: Lucena JF, Alegre F, Rodil R, et al. Results of a retrospective observational study of intermediate care staffed by hospitalists: impact on mortality, co-management, and teaching. J Hosp Med. 2012;7(5):411-415.
Blood Transfusion Associated with Increased Risk of Rebleeding in Patients with Nonvariceal Upper GI Bleeding
Clinical question: Does more liberal use of blood transfusions in the setting of nonvariceal upper GI bleeding result in patient harm?
Background: Randomized controlled trials have demonstrated that a more liberal approach to blood transfusions for patients in the medical intensive-care unit results in higher mortality. However, the potential harmful effect of blood transfusions in the setting of GI bleeding has not been demonstrated.
Study design: Retrospective cohort study.
Setting: Canadian hospitals.
Synopsis: Based on a retrospective analysis of the Canadian Registry of patients with Upper Gastrointestinal Bleeding and Endoscopy (RUGBE), the authors determined there was a statistically significant association between patients who received a blood transfusion for the management of nonvariceal upper GI bleeding and the risk of rebleeding. The rate of rebleeding in patients who received a blood transfusion was 23.6% compared with 11.3% in patients who were not transfused (P<0.01). There was no statistically significant difference in mortality.
Although this was a reasonably large observational study that included 1,677 patients with nonvariceal upper GI bleeding, it is vulnerable to confounding. It suggests the need to further study potential harm of blood transfusion in the setting of GI bleeding, but it should not result in a change in clinical practice at this time.
Bottom line: Prospective randomized studies are needed to determine if there are harmful effects of blood transfusions in the setting of GI bleeding and to better define a threshold for transfusion.
Citation: Restellini S, Kherad O, Jairath V, Martel M, Barkun AN. Red blood cell transfusion is associated with increased rebleeding in patients with nonvariceal upper gastrointestinal bleeding. Aliment Pharmacol Ther. 2013;37:316-322.
Low-Dose Steroids in Sepsis Associated with Increase in Mortality
Clinical question: What is the role of steroids in the treatment of adult patients with sepsis?
Background: The Surviving Sepsis Campaign guidelines have previously recommended administering steroids to patients with septic shock not responsive to fluid resuscitation and who require vasopressors. However, prior randomized clinical trials studying the use of steroids in these settings have produced conflicting results.
Study design: Retrospective cohort study.
Setting: Two hundred fifty-two hospitals in North America, South America, and Europe.
Synopsis: The Surviving Sepsis Campaign management bundle has been shown to reduce mortality in patients with sepsis. However, it is not known which particular elements of the management bundle result in improved mortality. The Surviving Sepsis Campaign database included 17,847 patients who required vasopressor therapy after adequate fluid resuscitation. This subgroup was analyzed to see if there was a difference in mortality between patients who received low-dose steroids versus those who did not receive steroids. The mortality rate among those who received steroids was statistically higher (with odds ratio of 1.18 and P<0.001) compared with those who did not receive steroids. This finding adds to the body of evidence that calls into question the commonplace practice of administrating steroids to septic patients on vasopressor therapy.
The most recent campaign guidelines recommend the use of steroids in septic patients only if both adequate fluid resuscitation and vasopressor therapy are not able to restore hemodynamic stability.
Bottom line: Further studies are needed to better define the role of steroids in the treatment of sepsis.
Citation: Casserly B, Gerlach H, Phillips GS, et al. Low-dose steroids in adult septic shock: results of the Surviving Sepsis Campaign. Intensive Care Med. 2012;38:1946-1954.
Link Between Length of Stay and Readmission Rates
Clinical question: How has reducing length of stay affected hospital readmission rates?
Background: There are ongoing concerns that improving a hospital’s efficiency by reducing length of stay (LOS) could be associated with higher hospital readmission rates. However, no studies evaluating the relationship between LOS and readmission rates have been done using recent data.
Study design: Retrospective observational study.
Setting: All acute-care Veterans Affairs (VA) hospitals in the U.S.
Synopsis: A total of 4,124,907 index admissions were included in the final sample from all acute medical admissions in 129 acute-care VA hospitals from October 1996 to September 2010. The primary outcomes were the hospital LOS and the 30-day readmission rate. Index admissions for heart failure, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (AMI), community-acquired pneumonia, and gastrointestinal hemorrhage were also analyzed separately.
The risk-adjusted analysis of LOS demonstrated significant reductions for all admissions over the 14-year period, to 3.98 days from 5.44 days, and for all of the individual conditions with reductions ranging from 1.40 days for gastrointestinal hemorrhage to 2.85 days for AMI. There were similar significant reductions in 30-day readmission rates for all admissions to 13.8% from 16.5% and within the individual conditions ranging from 0.9% in community-acquired pneumonia to 3.3% in COPD. These results show that the reductions in LOS did not increase the risk of readmissions. The major limitation of the study was that these data are only from a single healthcare system.
Bottom line: Data from VA hospitals show that reductions in LOS do not have adverse effects on 30-day readmission rates; instead, both LOS and readmission rates improved over the same time period.
Citation: Kaboli PJ, Go JT, Hockenberry J, et al. Associations between reduced hospital length of stay and 30-day readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Ann Intern Med. 2012;157:837-845.
Better to Restrict Blood Transfusions in Acute Myocardial Infarction
Clinical question: Is a liberal or restrictive blood transfusion strategy better in patients with anemia and acute myocardial infarction?
Background: Patients with acute myocardial infarction (AMI) are often given therapies that can increase their risk for bleeding and anemia, and it is known that AMI patients have a worse prognosis if they have concomitant anemia. No clear consensus exists on the benefit or harm of blood transfusions in AMI patients.
Study design: Systematic review and meta-analysis.
Setting: Ten articles included in the qualitative and quantitative analyses out of 729 screened articles from Jan. 1, 1966, to March 31, 2012, using the search terms “transfusion,” “myocardial infarction,” and “mortality” in English language.
Synopsis: A total of 203,665 study participants were identified from the 10 studies (one randomized and nine observational) that met the inclusion and exclusion criteria. All-cause mortality was significantly higher in AMI patients who received a blood transfusion compared with those who did not (18.2% vs. 10.2%). However, this difference was not statistically significant in patients that had a STEMI or in patients with a baseline hematocrit less than 30%. A multivariate meta-regression with several covariates, excluding demographics, also showed that blood transfusion was associated with higher mortality and higher risk for subsequent myocardial infarction. There was significant heterogeneity in all results, but no single study was found as the source of the heterogeneity, and no significant publication bias was identified. The major limitations to this study are that there is a paucity of randomized trials available that pertain to this specific topic and the authors did not have patient-level covariates to include in their analyses.
Bottom line: There appears to be an increased risk of mortality and subsequent myocardial infarction in AMI patients who receive blood transfusions versus those who do not.
Citation: Chatterjee S, Wetterslev J, Sharma A, Lichstein E, Mukherjee D. Association of blood transfusion with increased mortality in myocardial infarction: a meta-analysis and diversity-adjusted study sequential analysis. JAMA Intern Med. 2013;173(2):132-139.
Trends in GI Illnesses and Their Associated Costs
Clinical question: What are the new trends in GI illnesses and their associated costs?
Background: The frequency of illnesses and their treatment costs have changed over the last decade. In order to help healthcare providers focus their attention on these new trends, a new compilation of data is needed.
Study design: Epidemiological analysis.
Setting: Various governmental and private databases representing outpatient clinics, hospitals, and death certificates from multiple regions of the U.S.
Synopsis: The analysis was blinded to patient identifiers but represented multiple regions of the U.S. Symptoms were abstracted from patient surveys, and the rest of the data were collected from record review. The most common reported symptoms were abdominal pain, followed by nausea, vomiting, diarrhea, constipation, and heartburn. The most common clinic diagnoses were reflux, abdominal pain, enteritis/dyspepsia, and constipation. The most common inpatient discharge primary diagnoses included acute pancreatitis, cholecystitis, and diverticulitis. Impressive increases were seen in the number of morbidly obese, C. diff, and fatty liver diagnoses.
Colon cancer was the most common GI malignancy and had the highest mortality. C. diff was the ninth-leading cause of GI-related deaths. All types of scopes (except endoscopic retrograde cholangiopancreatography) were performed more commonly now than in the past, with colonoscopy being the most common. The most common indication for an upper endoscopy was reflux, which was also the most common outpatient GI diagnosis.
Bottom line: Healthcare providers need to be aware of new GI illness trends and their associated costs.
Citation: Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterol. 2012;143:1179-1187.
Is Apixaban a Good Stand-Alone Anticoagulant for Extended Treatment in VTE Patients?
Clinical question: Is apixaban an option for the extended treatment of VTE in a simple, fixed-dose regimen?
Background: Apixaban is an oral factor Xa inhibitor that is administered in fixed doses without the need for laboratory monitoring. In the Apixaban after the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy—Extended Treatment (AMPLIFY-EXT) study, investigators compared the efficacy and safety of two doses of apixaban (2.5 mg and 5 mg) with those of placebo in patients with VTE who had completed six to 12 months of anticoagulation therapy and for whom treating physicians were uncertain about continuing therapy. Additional aims of the study were to determine whether the lower dose of apixaban was effective and whether it was associated with less bleeding than the higher dose, and to examine the effect of treatment on arterial thrombotic outcomes.
Study design: Randomized, double-blind study.
Synopsis: A total of 2,486 patients underwent randomization, 2,482 of whom were included in the intention-to-treat analyses. Symptomatic recurrent VTE or death from VTE occurred in 73 of the 829 patients (8.8%) who were receiving placebo, compared with 14 of the 840 patients (1.7%) who were receiving 2.5 mg of apixaban (a difference of 7.2 percentage points; 95% confidence interval [CI], 5.0 to 9.3) and 14 of the 813 patients (1.7%) who were receiving 5 mg of apixaban (a difference of 7.0 percentage points; 95% CI, 4.9 to 9.1) (P<0.001 for both comparisons). The rates of major bleeding were 0.5% in the placebo group, 0.2% in the 2.5-mg apixaban group, and 0.1% in the 5-mg apixaban group. The rates of clinically relevant nonmajor bleeding were 2.3% in the placebo group, 3.0% in the 2.5-mg apixaban group, and 4.2% in the 5-mg apixaban group. The rate of death from any cause was 1.7% in the placebo group, compared with 0.8% in the 2.5-mg apixaban group and 0.5% in the 5-mg apixaban group.
Bottom line: Apixaban is a safe and effective anticoagulant for extended anticoagulation in patients with VTE initially treated with six to 12 months of warfarin.
Citation: Agnelli GM, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699-708.
ACP Guideline Review: Upper Endoscopy for Gastroesophageal Reflux Disease
Clinical question: What are the indications of upper endoscopy in the setting of gastroesophageal reflux disease (GERD)?
Background: GERD is a common condition. Upper endoscopy is widely available and routinely used for diagnosis and management of GERD and its complications. The indications for this procedure are not clearly defined. Overuse of upper endoscopy contributes to higher healthcare costs without improving patient outcomes.
Study design: Literature review and comparison of clinical guidelines from professional organizations by a team of general internists, gastroenterologists, and clinical epidemiologists. The document was not based on a formal systemic review but was intended to provide practical advice based on the best available evidence.
Synopsis: Best practice advice No. 1: Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).
Best practice advice No. 2: Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton-pump inhibitor therapy, severe erosive esophagitis after a two-month course of proton-pump inhibitor therapy to assess healing and rule out Barrett esophagus, and history of esophageal stricture who have recurrent symptoms of dysphagia.
Best practice advice No. 3: Upper endoscopy might be indicated in men older than 50 with chronic GERD symptoms (symptoms for more than five years) and additional risk factors (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat) to detect esophageal adenocarcinoma and Barrett esophagus. It might also be indicated for surveillance evaluation in men and women with a history of Barrett esophagus. In men and women with Barrett esophagus and no dysplasia, surveillance examinations should occur at intervals no more frequently than three to five years. More frequent intervals are indicated in patients with Barrett esophagus and dysplasia.
Bottom line: Use upper endoscopy selectively for patients with GERD.
Citation: Shaheen NJ, Weinberg DS, Denberg TD, et al. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2012;157(11):808-816.
In This Edition
Literature At A Glance
A guide to this month’s studies
- Value of routine preoperative urine screening assessed
- Impact of hospitalist-led intermediate care on patient survival
- Risks of blood transfusion to treat upper GI bleeding
- Low-dose steroids and increased mortality in sepsis
- Reduced length of stay and hospital readmission rates
- Restrictive blood transfusion strategies better for acute myocardial infarction
- Trends in GI illnesses and their associated costs
- Apixaban as a stand-alone anticoagulant in patients with VTE
- Guidelines for upper endoscopy use in gastroesophageal reflux disease
Avoid Preoperative Urine Culture in Nonurologic Surgical Procedures
Clinical question: Is routine preoperative urine screening beneficial?
Background: The value of preoperative urine screening is unproven, except before urologic procedures. Furthermore, treatment of asymptomatic bacteriuria may lead to adverse events, including diarrhea, allergic reactions, and Clostridium difficile infection (CDI).
Study design: Retrospective chart review.
Setting: Patients who underwent cardiothoracic, orthopedic, and vascular surgeries at the Minneapolis Veterans Affairs Medical Center in 2010.
Synopsis: A total of 1,934 procedures were performed on 1,699 patients, most of which were orthopedics procedures (1,291 in 1,115 patients). A urine culture was obtained before 25% of procedures with significant variation by service (cardiothoracic, 85%; vascular, 48%; orthopedic, 4%). Bacteriuria was detected in 11% of urine cultures (54 of 489), but antimicrobial drugs were dispensed to just 16 patients.
To identify correlates of preoperative urine culture use, patients with and without urine cultures were compared. The rate of surgical-site infection was similar for both groups. Postoperative UTI was more frequent among patients with bacteriuria. Rates of diarrhea, allergy, and CDI did not differ. Paradoxically, patients treated for preoperative UTI were more likely to develop surgical-site infections (45% vs. 14%; P=0.03). Postoperative UTI was also more frequent among treated patients versus untreated patients (18% vs. 7%).
Bottom line: This is the largest study to assess outcomes for routine preoperative urine cultures. These findings demonstrate that preoperative screening for, and treatment of, asymptomatic bacteriuria should be avoided in patients undergoing nonurologic surgical procedures.
Citation: Drekonja DM, Zarmbinski B, Johnson JR. Preoperative urine culture at a veterans affairs medical center. JAMA Intern Med. 2013;173(1):71-72.
Intermediate Care Staffed by Hospitalists: Impact on Mortality, Comanagement, and Teaching
Clinical question: Does a hospitalist-led intermediate-care unit improve patient survival?
Background: Hospitalized patients are complex, and institutions often have to balance matching patient acuity to either an ICU or a regular ward. However, an intermediate-care setting might be an attractive strategy to provide rational care according to patient needs while expanding comanagement and teaching services.
Study design: Retrospective observational study.
Setting: Intermediate-care unit of a single academic hospital.
Synopsis: In-hospital mortality in this intermediate-care unit was 20.6%, whereas the expected mortality was 23.2% based on Simplified Acute Physiology Score II (SAPS II) score. The correlation between SAPS II predicted and observed death rates was accurate and statistically significant (P<0.001). Comanagement was performed with several medical and surgical teams, with an increase in perioperative comanagement of 22.7% (P=0.014). The number of training residents in the intermediate-care unit increased to 30.4% from 4.3% (P=0.002).
Bottom line: An intermediate-care unit led by hospitalists showed encouraging results in patient mortality, as well as comanagement and teaching opportunities.
Citation: Lucena JF, Alegre F, Rodil R, et al. Results of a retrospective observational study of intermediate care staffed by hospitalists: impact on mortality, co-management, and teaching. J Hosp Med. 2012;7(5):411-415.
Blood Transfusion Associated with Increased Risk of Rebleeding in Patients with Nonvariceal Upper GI Bleeding
Clinical question: Does more liberal use of blood transfusions in the setting of nonvariceal upper GI bleeding result in patient harm?
Background: Randomized controlled trials have demonstrated that a more liberal approach to blood transfusions for patients in the medical intensive-care unit results in higher mortality. However, the potential harmful effect of blood transfusions in the setting of GI bleeding has not been demonstrated.
Study design: Retrospective cohort study.
Setting: Canadian hospitals.
Synopsis: Based on a retrospective analysis of the Canadian Registry of patients with Upper Gastrointestinal Bleeding and Endoscopy (RUGBE), the authors determined there was a statistically significant association between patients who received a blood transfusion for the management of nonvariceal upper GI bleeding and the risk of rebleeding. The rate of rebleeding in patients who received a blood transfusion was 23.6% compared with 11.3% in patients who were not transfused (P<0.01). There was no statistically significant difference in mortality.
Although this was a reasonably large observational study that included 1,677 patients with nonvariceal upper GI bleeding, it is vulnerable to confounding. It suggests the need to further study potential harm of blood transfusion in the setting of GI bleeding, but it should not result in a change in clinical practice at this time.
Bottom line: Prospective randomized studies are needed to determine if there are harmful effects of blood transfusions in the setting of GI bleeding and to better define a threshold for transfusion.
Citation: Restellini S, Kherad O, Jairath V, Martel M, Barkun AN. Red blood cell transfusion is associated with increased rebleeding in patients with nonvariceal upper gastrointestinal bleeding. Aliment Pharmacol Ther. 2013;37:316-322.
Low-Dose Steroids in Sepsis Associated with Increase in Mortality
Clinical question: What is the role of steroids in the treatment of adult patients with sepsis?
Background: The Surviving Sepsis Campaign guidelines have previously recommended administering steroids to patients with septic shock not responsive to fluid resuscitation and who require vasopressors. However, prior randomized clinical trials studying the use of steroids in these settings have produced conflicting results.
Study design: Retrospective cohort study.
Setting: Two hundred fifty-two hospitals in North America, South America, and Europe.
Synopsis: The Surviving Sepsis Campaign management bundle has been shown to reduce mortality in patients with sepsis. However, it is not known which particular elements of the management bundle result in improved mortality. The Surviving Sepsis Campaign database included 17,847 patients who required vasopressor therapy after adequate fluid resuscitation. This subgroup was analyzed to see if there was a difference in mortality between patients who received low-dose steroids versus those who did not receive steroids. The mortality rate among those who received steroids was statistically higher (with odds ratio of 1.18 and P<0.001) compared with those who did not receive steroids. This finding adds to the body of evidence that calls into question the commonplace practice of administrating steroids to septic patients on vasopressor therapy.
The most recent campaign guidelines recommend the use of steroids in septic patients only if both adequate fluid resuscitation and vasopressor therapy are not able to restore hemodynamic stability.
Bottom line: Further studies are needed to better define the role of steroids in the treatment of sepsis.
Citation: Casserly B, Gerlach H, Phillips GS, et al. Low-dose steroids in adult septic shock: results of the Surviving Sepsis Campaign. Intensive Care Med. 2012;38:1946-1954.
Link Between Length of Stay and Readmission Rates
Clinical question: How has reducing length of stay affected hospital readmission rates?
Background: There are ongoing concerns that improving a hospital’s efficiency by reducing length of stay (LOS) could be associated with higher hospital readmission rates. However, no studies evaluating the relationship between LOS and readmission rates have been done using recent data.
Study design: Retrospective observational study.
Setting: All acute-care Veterans Affairs (VA) hospitals in the U.S.
Synopsis: A total of 4,124,907 index admissions were included in the final sample from all acute medical admissions in 129 acute-care VA hospitals from October 1996 to September 2010. The primary outcomes were the hospital LOS and the 30-day readmission rate. Index admissions for heart failure, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (AMI), community-acquired pneumonia, and gastrointestinal hemorrhage were also analyzed separately.
The risk-adjusted analysis of LOS demonstrated significant reductions for all admissions over the 14-year period, to 3.98 days from 5.44 days, and for all of the individual conditions with reductions ranging from 1.40 days for gastrointestinal hemorrhage to 2.85 days for AMI. There were similar significant reductions in 30-day readmission rates for all admissions to 13.8% from 16.5% and within the individual conditions ranging from 0.9% in community-acquired pneumonia to 3.3% in COPD. These results show that the reductions in LOS did not increase the risk of readmissions. The major limitation of the study was that these data are only from a single healthcare system.
Bottom line: Data from VA hospitals show that reductions in LOS do not have adverse effects on 30-day readmission rates; instead, both LOS and readmission rates improved over the same time period.
Citation: Kaboli PJ, Go JT, Hockenberry J, et al. Associations between reduced hospital length of stay and 30-day readmission rate and mortality: 14-year experience in 129 Veterans Affairs hospitals. Ann Intern Med. 2012;157:837-845.
Better to Restrict Blood Transfusions in Acute Myocardial Infarction
Clinical question: Is a liberal or restrictive blood transfusion strategy better in patients with anemia and acute myocardial infarction?
Background: Patients with acute myocardial infarction (AMI) are often given therapies that can increase their risk for bleeding and anemia, and it is known that AMI patients have a worse prognosis if they have concomitant anemia. No clear consensus exists on the benefit or harm of blood transfusions in AMI patients.
Study design: Systematic review and meta-analysis.
Setting: Ten articles included in the qualitative and quantitative analyses out of 729 screened articles from Jan. 1, 1966, to March 31, 2012, using the search terms “transfusion,” “myocardial infarction,” and “mortality” in English language.
Synopsis: A total of 203,665 study participants were identified from the 10 studies (one randomized and nine observational) that met the inclusion and exclusion criteria. All-cause mortality was significantly higher in AMI patients who received a blood transfusion compared with those who did not (18.2% vs. 10.2%). However, this difference was not statistically significant in patients that had a STEMI or in patients with a baseline hematocrit less than 30%. A multivariate meta-regression with several covariates, excluding demographics, also showed that blood transfusion was associated with higher mortality and higher risk for subsequent myocardial infarction. There was significant heterogeneity in all results, but no single study was found as the source of the heterogeneity, and no significant publication bias was identified. The major limitations to this study are that there is a paucity of randomized trials available that pertain to this specific topic and the authors did not have patient-level covariates to include in their analyses.
Bottom line: There appears to be an increased risk of mortality and subsequent myocardial infarction in AMI patients who receive blood transfusions versus those who do not.
Citation: Chatterjee S, Wetterslev J, Sharma A, Lichstein E, Mukherjee D. Association of blood transfusion with increased mortality in myocardial infarction: a meta-analysis and diversity-adjusted study sequential analysis. JAMA Intern Med. 2013;173(2):132-139.
Trends in GI Illnesses and Their Associated Costs
Clinical question: What are the new trends in GI illnesses and their associated costs?
Background: The frequency of illnesses and their treatment costs have changed over the last decade. In order to help healthcare providers focus their attention on these new trends, a new compilation of data is needed.
Study design: Epidemiological analysis.
Setting: Various governmental and private databases representing outpatient clinics, hospitals, and death certificates from multiple regions of the U.S.
Synopsis: The analysis was blinded to patient identifiers but represented multiple regions of the U.S. Symptoms were abstracted from patient surveys, and the rest of the data were collected from record review. The most common reported symptoms were abdominal pain, followed by nausea, vomiting, diarrhea, constipation, and heartburn. The most common clinic diagnoses were reflux, abdominal pain, enteritis/dyspepsia, and constipation. The most common inpatient discharge primary diagnoses included acute pancreatitis, cholecystitis, and diverticulitis. Impressive increases were seen in the number of morbidly obese, C. diff, and fatty liver diagnoses.
Colon cancer was the most common GI malignancy and had the highest mortality. C. diff was the ninth-leading cause of GI-related deaths. All types of scopes (except endoscopic retrograde cholangiopancreatography) were performed more commonly now than in the past, with colonoscopy being the most common. The most common indication for an upper endoscopy was reflux, which was also the most common outpatient GI diagnosis.
Bottom line: Healthcare providers need to be aware of new GI illness trends and their associated costs.
Citation: Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterol. 2012;143:1179-1187.
Is Apixaban a Good Stand-Alone Anticoagulant for Extended Treatment in VTE Patients?
Clinical question: Is apixaban an option for the extended treatment of VTE in a simple, fixed-dose regimen?
Background: Apixaban is an oral factor Xa inhibitor that is administered in fixed doses without the need for laboratory monitoring. In the Apixaban after the Initial Management of Pulmonary Embolism and Deep Vein Thrombosis with First-Line Therapy—Extended Treatment (AMPLIFY-EXT) study, investigators compared the efficacy and safety of two doses of apixaban (2.5 mg and 5 mg) with those of placebo in patients with VTE who had completed six to 12 months of anticoagulation therapy and for whom treating physicians were uncertain about continuing therapy. Additional aims of the study were to determine whether the lower dose of apixaban was effective and whether it was associated with less bleeding than the higher dose, and to examine the effect of treatment on arterial thrombotic outcomes.
Study design: Randomized, double-blind study.
Synopsis: A total of 2,486 patients underwent randomization, 2,482 of whom were included in the intention-to-treat analyses. Symptomatic recurrent VTE or death from VTE occurred in 73 of the 829 patients (8.8%) who were receiving placebo, compared with 14 of the 840 patients (1.7%) who were receiving 2.5 mg of apixaban (a difference of 7.2 percentage points; 95% confidence interval [CI], 5.0 to 9.3) and 14 of the 813 patients (1.7%) who were receiving 5 mg of apixaban (a difference of 7.0 percentage points; 95% CI, 4.9 to 9.1) (P<0.001 for both comparisons). The rates of major bleeding were 0.5% in the placebo group, 0.2% in the 2.5-mg apixaban group, and 0.1% in the 5-mg apixaban group. The rates of clinically relevant nonmajor bleeding were 2.3% in the placebo group, 3.0% in the 2.5-mg apixaban group, and 4.2% in the 5-mg apixaban group. The rate of death from any cause was 1.7% in the placebo group, compared with 0.8% in the 2.5-mg apixaban group and 0.5% in the 5-mg apixaban group.
Bottom line: Apixaban is a safe and effective anticoagulant for extended anticoagulation in patients with VTE initially treated with six to 12 months of warfarin.
Citation: Agnelli GM, Buller HR, Cohen A, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med. 2013;368(8):699-708.
ACP Guideline Review: Upper Endoscopy for Gastroesophageal Reflux Disease
Clinical question: What are the indications of upper endoscopy in the setting of gastroesophageal reflux disease (GERD)?
Background: GERD is a common condition. Upper endoscopy is widely available and routinely used for diagnosis and management of GERD and its complications. The indications for this procedure are not clearly defined. Overuse of upper endoscopy contributes to higher healthcare costs without improving patient outcomes.
Study design: Literature review and comparison of clinical guidelines from professional organizations by a team of general internists, gastroenterologists, and clinical epidemiologists. The document was not based on a formal systemic review but was intended to provide practical advice based on the best available evidence.
Synopsis: Best practice advice No. 1: Upper endoscopy is indicated in men and women with heartburn and alarm symptoms (dysphagia, bleeding, anemia, weight loss, and recurrent vomiting).
Best practice advice No. 2: Upper endoscopy is indicated in men and women with typical GERD symptoms that persist despite a therapeutic trial of four to eight weeks of twice-daily proton-pump inhibitor therapy, severe erosive esophagitis after a two-month course of proton-pump inhibitor therapy to assess healing and rule out Barrett esophagus, and history of esophageal stricture who have recurrent symptoms of dysphagia.
Best practice advice No. 3: Upper endoscopy might be indicated in men older than 50 with chronic GERD symptoms (symptoms for more than five years) and additional risk factors (nocturnal reflux symptoms, hiatal hernia, elevated body mass index, tobacco use, and intra-abdominal distribution of fat) to detect esophageal adenocarcinoma and Barrett esophagus. It might also be indicated for surveillance evaluation in men and women with a history of Barrett esophagus. In men and women with Barrett esophagus and no dysplasia, surveillance examinations should occur at intervals no more frequently than three to five years. More frequent intervals are indicated in patients with Barrett esophagus and dysplasia.
Bottom line: Use upper endoscopy selectively for patients with GERD.
Citation: Shaheen NJ, Weinberg DS, Denberg TD, et al. Upper endoscopy for gastroesophageal reflux disease: best practice advice from the Clinical Guidelines Committee of the American College of Physicians. Ann Intern Med. 2012;157(11):808-816.
How Should a Patient with Cocaine-Associated Chest Pain be Treated?

Case
A 38-year-old man with a history of tobacco use presents to the emergency department complaining of constant substernal chest pain for three hours. His temperature is 37.7°C, his heart rate is 110 beats per minute, and his blood pressure is 155/95 mmHg. He appears anxious and diaphoretic but examination is otherwise unremarkable. He admits to cocaine use one hour before the onset of symptoms. What are the appropriate treatments for his condition?
Overview
Cocaine is the second-most-commonly used illicit drug in the U.S. and represents 31% of all ED visits related to substance abuse.1,2 According to recent survey results, 2.1 million people report recent cocaine use, and 1.6 million engage in cocaine abuse or dependence.2 Acute cardiopulmonary complaints are common in individuals who present to the ED after cocaine use, with chest pain being the most frequently reported symptom in 40%.3
Numerous etiologies for cocaine-associated chest pain (CACP) have been discovered, including musculoskeletal pain, pulmonary hypertension, cardiomyopathy, arrhythmias, and endocarditis.4 Only 0.5% of patients with aortic dissection over a four-year period had a recent history of cocaine use, making cocaine a rare cause of a rare condition.5 Cardiac chest pain remains the most frequent underlying etiology, resulting in the most common complication of myocardial infarction (MI) in up to 6% of patients.6,7
The ways in which cocaine use can cause myocardial ischemia and MI are multifactorial. A vigorous central sympathomimetic effect, coronary artery vasoconstriction, stimulation of platelets, and enhanced atherosclerosis all lead to a myocardial oxygen supply-demand imbalance.8 Other key interactions in the cardiovascular system are displayed in Figure 1. Understanding the role of these mechanisms in CACP is crucial to patient care.
Clinician goals in the management of CACP are to rapidly and accurately exclude life-threatening etiologies; assess the need for urgent acute coronary syndrome (ACS) evaluation; risk-stratify patients and ensure appropriate disposition; normalize the toxic effects of cocaine; treat resultant organ damage; and prevent long-term complications. An algorithm detailing this approach is provided in Figure 2.

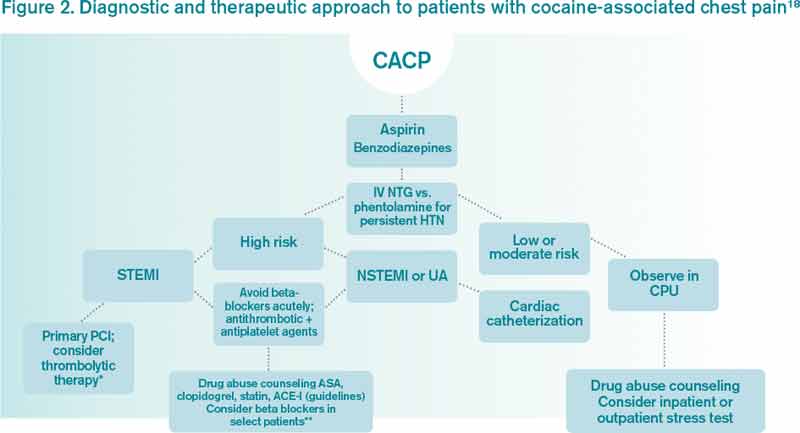
Review of the Data
Diagnostic evaluation. Given potential differences in treatment regimens, it is imperative to differentiate patients who present with CACP from those whose chest pain is not associated with cocaine either by direct questioning or by screening of urine for cocaine metabolites. Once the presence of cocaine has been confirmed, guideline-based evaluation for potential ACS with serial electrocardiograms (ECG), cardiac biomarkers, and close monitoring of cardiac rhythms and hemodynamics is largely similar to standard management of all patients presenting with chest pain, with a few caveats.
Interpretation of the ECG can be challenging in the setting of cocaine. Studies have shown “abnormal” ECGs in 56% to 84% of patients, with many representing early repolarization or left ventricular hypertrophy.9,10 Likewise, patients with MI are as likely to present with normal or nonspecific ECG findings as with ischemic findings.7,11 ECG interpretation to diagnose ischemia or infarction in patients with CACP yields a sensitivity of 36% and specificity of 90%.7
Creatine kinase (CK), CK-MB fraction, and myoglobin have low specificity for the diagnosis of ischemia, as cocaine can induce skeletal muscle injury and rhabdomyolysis.9,12 Cardiac troponins demonstrate a superior specificity compared to CK and CK-MB and are thus the preferred cardiac biomarkers in diagnosing cocaine-associated MI.12
Initial management and disposition. Patients at high risk for cardiovascular events are generally admitted to a monitored bed.13 Immediate reperfusion therapy with primary percutaneous coronary intervention is recommended in patients with ST-elevation MI (STEMI). Treatment with thrombolytic agents is associated with an increased risk of intracerebral hemorrhage and lacks documented efficacy in patients with CACP. Thrombolysis should therefore only be utilized if the diagnosis of STEMI is unequivocal and an experienced cardiac catheterization laboratory is unavailable.14,15
Patients with unstable angina (UA) or non-ST-elevation MI (NSTEMI) are at higher risk for further cardiac events in a similar manner to those with ACS unrelated to cocaine. These cases might benefit from early cardiac catheterization and revascularization.16 Because of the increased risk of stent thrombosis in cocaine-users, thought to be due to recidivism, a detailed risk-benefit analysis should be undertaken prior to the implantation of cardiac stents.
Other diagnostic tests, such as stress testing and myocardial imaging, have not shown significant accuracy in diagnosing MI in this setting; moreover, these patients are at low overall risk for cardiac events and mortality. Consequently, an extensive diagnostic evaluation might not be cost-effective.7,10,13,17 Patients who have CACP without MI have a very low frequency of delayed complications.3,17 As such, cost-effective evaluation strategies, such as nine- or 12-hour observation periods in a chest pain unit, are appropriate for many of these low- to moderate-risk patients.13 For all CACP patients, the most critical post-discharge interventions are cardiac risk modification and cocaine cessation.13
Normalizing the toxic effects of cocaine with medications.
Aspirin: While no specific study has been performed in patients with CACP and aspirin, CACP guidelines, based on data supporting ACS guidelines for all patients, recommend administration of full-dose aspirin given its associated reduction in morbidity and mortality.18,19 Furthermore, given the platelet-stimulating effects of cocaine, using aspirin in this setting seems very reasonable.
Benzodiazepines: CACP guidelines support the use of benzodiazepines early in management to indirectly combat the agitation, hypertension, and tachycardia resulting from the stimulatory effects of cocaine.18,20 These recommendations are based on several animal and human studies that demonstrate significant reduction in heart rate and systemic arterial pressure with the use of these agents.21,22
Nitroglycerin: Cardiac catheterization studies have shown reversal of vasoconstriction with administration of nitroglycerin. One study demonstrated a benefit of the drug in 49% of participants.23 Additional investigation into the benefit of benzodiazepine and nitroglycerin combination therapy revealed mixed results. In one study, lorazepam plus nitroglycerin was found to be more efficacious than nitroglycerin alone.24 In another, however, use of diazepam in combination with nitroglycerin did not show benefit when evaluating pain relief, cardiac dynamics, and left ventricular function.25
Phentolamine: Phentolamine administration has been studied much less in the literature. This nonselective alpha-adrenergic antagonist exerts a dose-dependent reversal of cocaine’s vasoconstrictive properties in monkeys and humans.26,27 International guidelines for Emergency Cardiovascular Care recommend its use in treatment of cocaine-associated ACS;27 however, the AHA recommends it less strongly.18
Calcium channel blockers: Calcium channel blockers (CCBs) have not shown promise as first-line agents. While catheterization studies demonstrate the vasodilatory properties of verapamil, larger studies looking at all-cause mortality conclude that CCBs might worsen mortality rates,28 and animal studies indicate an increased risk of seizures.29 At this time, CCBs are recommended only if cardiac symptoms continue after both benzodiazepines and nitroglycerin are administered.18
The beta-blocker controversy: The use of beta-blockers in patients with CACP remains controversial given the theoretical risk of unopposed alpha-adrenergic activation. Coronary vasospasm, decreased myocardial oxygen delivery, and increased systemic vascular resistance can result from their use.30
Propranolol, a nonselective beta-blocker, was shown in catheterization studies to potentiate the coronary vasoconstriction of cocaine.31 Labetalol, a combined alpha/beta-blocker, reduced mean arterial pressure after cocaine administration during cardiac catheterization but did not reverse coronary vasoconstriction.32 This was attributed to the predominating beta greater than alpha blockade at doses administered. The selective beta-1 antagonists esmolol and metoprolol have shown no benefit in CACP.33 Carvedilol, a combined alpha/beta-blocker with both peripheral and central nervous system activity, has potential to attenuate both physiologic and behavioral response to cocaine, but it has not been well studied in this patient subset.34
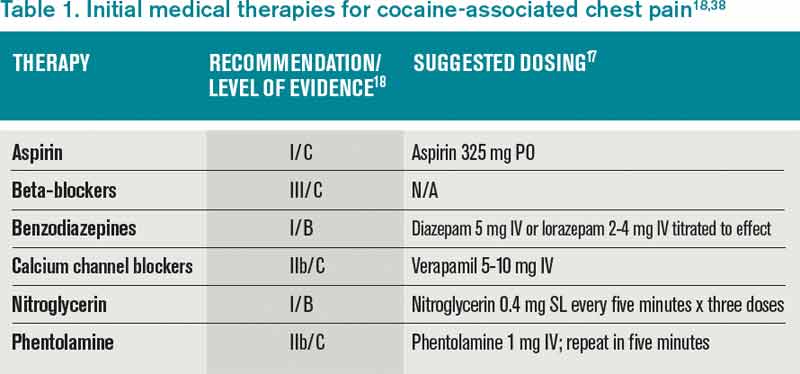
The 2005 ACC/AHA STEMI guidelines recommended against beta-blockers in the setting of STEMI precipitated by cocaine use due to the potential of exacerbating coronary vasoconstriction.35 The 2007 ACC/AHA UA/NSTEMI guidelines stated that the use of a combined alpha/beta-blocker in patients with cocaine-induced ACS may be reasonable for patients with hypertension or tachycardia if pre-treated with a vasodilator.19 The 2008 ACC/AHA guidelines on the management of cocaine-related chest pain and MI recommended against the use of beta-blockers in the acute setting given the low incidence of cocaine-related MI and death.18
In a more recent study, Dattilo et al showed that beta-blockers administered to patients admitted with positive urine toxicology for cocaine significantly reduced MI and in-hospital mortality. Reduction of MI was of borderline significance in those admitted with a chief complaint of chest pain.36 Limitations of this study include unknown time of cocaine ingestion, lack of follow-up on discharge mortality, and a small sample size of 348 patients lacking statistical power.
Another retrospective cohort study examined patients admitted with chest pain and urine toxicology positive for cocaine and found that beta-blocker administration during hospitalization was not associated with increased incident mortality. Further, after a mean follow-up of 2.5 years, there was a statistically significant decrease in cardiovascular death.37 Drawbacks of this study included an older patient population, greater proportion of coronary artery disease, and higher follow-up of cardiovascular mortality rates than in previous studies, suggesting this subset might have received greater benefit from beta-blockers as a result of these characteristics.
The 2008 ACC/AHA guidelines instruct individualized consideration of the risk/benefit ratio for beta-blocker use in patients with CACP given the high rate of recidivism in cocaine abusers. The strongest indication is given to those with documented MI, left ventricular systolic dysfunction, or ventricular arrhythmias.18
It is important to note that these recommendations are based on cardiac catheterization laboratory studies, case reports, retrospective analyses, and animal experiments. No prospective controlled trials evaluating the role of beta-blockers in CACP and MI exist, and no trials regarding therapies to improve outcomes of patients sustaining a cocaine-associated MI have been reported.18
Back to the Case
This patient was experiencing cocaine-associated chest pain, which was confirmed with positive urine toxicology. Initial diagnostic workup with basic laboratory studies and cardiac biomarkers showed mild elevation in CK with troponin levels within normal limits. His ECG showed changes consistent with left ventricular hypertrophy. Chest radiograph was unremarkable.
He received aspirin, benzodiazepines, and nitroglycerin with normalization of vital signs, as well as subjective improvement in chest pain and anxiety. He was deemed to be at low risk for potential cardiac complications; thus, further cardiac testing was not pursued. Rather, he was admitted to an overnight observation unit with telemetry monitoring, where his chest pain did not recur.
He was seen in consultation with social work staff who arranged for drug abuse counseling after discharge. Given the uncertainty of relapse to cocaine use, as well as lack of known cardiac risk factors, he was not discharged on any new medications.
Bottom Line
The treatment of CACP includes normalizing the toxic systemic effects of the drug and minimizing the direct ischemic damage to the myocardium. Management varies slightly from traditional chest pain algorithms and includes benzodiazepines as well as antiplatelet agents and vasodilators to achieve this goal. Initial therapy with beta-blockers remains undefined and is largely discouraged in the acute setting. The role of beta-blockade upon discharge, however, can be beneficial in specific populations, especially those found to have underlying coronary disease.
Dr. Houchens and Dr. Czarnik are clinical instructors and Dr. Mack is a clinical lecturer at the University of Michigan Health System in Ann Arbor.
References
- Hughes A, Sathe N, Spagnola K. State Estimates of Substance Use from the 2005-2006 National Surveys on Drug Use and Health. DHHS Publication No. SMA 08-4311, NSDUH Series H-33. Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2008.
- Volkow ND. Cocaine: Abuse and Addiction. National Institute on Drug Abuse. Washington, DC: U.S. Department of Health and Human Services; 2009.
- Brody SL, Slovis CM, Wrenn KD. Cocaine-related medical problems: consecutive series of 233 patients. Am J Med. 1990;88:325-331.
- Levis JT, Garmel GM. Cocaine-associated chest pain. Emerg Med Clin North Am. 2005;23:1083-1103.
- Eagle KA, Isselbacher EM, DeSanctis RW. Cocaine-related aortic dissection in perspective. Circulation. 2002;105:1529-1530.
- Feldman JA, Fish SS, Beshansky JR, Griffith JL, Woolard RH, Selker HP. Acute cardiac ischemia in patients with cocaine-associated complaints: results of a multicenter trial. Ann Emerg Med. 2000;36:469-476.
- Hollander JE, Hoffman RS, Gennis P, et al. Prospective multicenter evaluation of cocaine associated chest pain. Cocaine Associated Chest Pain (COCHPA) Study Group. Acad Emerg Med. 1994;1:330-339.
- Schwartz BG, Rezkalla S, Kloner RA. Cardiovascular effects of cocaine. Circulation. 2010;122:2558-2569.
- Gitter MJ, Goldsmith SR, Dunbar DN, et al. Cocaine and chest pain: clinical features and outcomes of patients hospitalized to rule out myocardial infarction. Ann Intern Med. 1991;115:277-282.
- Amin M, Gabelman G, Karpel J, et al. Acute myocardial infarction and chest pain syndromes after cocaine use. Am J Cardiol. 1990;66:1434-1437.
- Tokarski GF, Paganussi P, Urbanski R, et al. An evaluation of cocaine-induced chest pain. Ann Emerg Med. 1990;19:1088-1092.
- Hollander JE, Levitt MA, Young GP, Briglia E, Wetli CV, Gawad Y. Effect of recent cocaine use on the specificity of cardiac markers for diagnosis of acute myocardial infarction. Am Heart J. 1998;135(2 Pt 1):245-252.
- Weber JE, Shofer FS, Larkin GL, Kalaria AS, Hollander JE. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med. 2003;348:510-517.
- Hahn IH, Hoffman RS. Diagnosis and treatment of acute myocardial infarction: cocaine use and acute myocardial infarction. Emerg Med Clin North Am. 2001;19(2):1-18.
- Hoffman RS, Hollander JE. Evaluation of patients with chest pain after cocaine use. Crit Care Clin. 1997;13:809-828. Cannon CP, Weintraub WS, Demopoulos LA, et al.
- Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887.
- Hollander JE, Hoffman RS. Cocaine-induced myocardial infarction: an analysis and review of the literature. J Emerg Med. 1992;10:169-177.
- McCord J, Jneid H, Hollander JE, et al. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117:1897-1907.
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:E1-E157.
- Hollander JE. Management of cocaine-associated myocardial ischemia. N Engl J Med. 1995;333:1267-1272.
- Brubacher JR, Hoffman RS. Cocaine toxicity. Top Emerg Med. 1997;19(4):1-16.
- Catavas JD, Waters IW. Acute cocaine intoxication in the conscious dog: studies on the mechanism of lethality. J Pharmacol Exp Ther. 1981;217:350-356.
- Hollander JE, Hoffman RS, Gennis P, et al. Nitroglycerin in the treatment of cocaine associated chest pain—clinical safety and efficacy. J Toxicol Clin Toxicol. 1994;32(3): 243-256.
- Honderick T, Williams D, Seaberg D, Wears R. A prospective, randomized, controlled trial of benzodiazepines and nitroglycerin or nitroglycerin alone in the treatment of cocaine-associated acute coronary syndromes. Am J Emerg Med. 2003;21(1):39-42.
- Baumann BM, Perrone J, Hornig SE, Shofer FS, Hollander JE. Randomized, double-blind, placebo-controlled trial of diazepam, nitroglycerin, or both for treatment of patients with potential cocaine-associated acute coronary syndromes. Acad Emerg Med. 2000;7:878-885.
- Schindler CW, Tella SR, Goldberg SR. Adrenoceptor mechanisms in the cardiovascular effects of cocaine in conscious squirrel monkeys. Life Sci. 1992;51(9):653-660.
- Lange RA, Cigarroa RG, Yancy CW Jr., et al. Cocaine-induced coronary-artery vasoconstriction. N Engl J Med. 1989;321(23):1557-1562.
- Furberg CD, Psaty BM, Meyer JV. Nifedipine. Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995;92:1326-1331.
- Derlet RW, Albertson TE. Potentiation of cocaine toxicity with calcium channel blockers. Am J Emerg Med. 1989;7:464-468.
- Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351-358.
- Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade. Ann Intern Med. 1990;112:897-903.
- Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA. Influence of labetalol on cocaine-induced coronary vasoconstriction in humans. Am J Med. 1993;94:608-610.
- Sand IC, Brody SL, Wrenn KD, Slovis CM. Experience with esmolol for the treatment of cocaine-associated cardiovascular complications. Am J Emerg Med. 1991;9:161-163.
- Sofuoglo M, Brown S, Babb DA, Pentel PR, Hatsukami DK. Carvedilol affects the physiological and behavioral response to smoked cocaine in humans. Drug Alcohol Depend. 2000;60:69-76.
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force of Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44:E1-E211.
- Dattilo PB, Hailpern SM, Fearon K, Sohal D, Nordin C. Beta-blockers are associated with reduced risk of myocardial infarction after cocaine use. Ann Emerg Med. 2008;51:117-125.
- Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170:874-879.
Case
A 38-year-old man with a history of tobacco use presents to the emergency department complaining of constant substernal chest pain for three hours. His temperature is 37.7°C, his heart rate is 110 beats per minute, and his blood pressure is 155/95 mmHg. He appears anxious and diaphoretic but examination is otherwise unremarkable. He admits to cocaine use one hour before the onset of symptoms. What are the appropriate treatments for his condition?
Overview
Cocaine is the second-most-commonly used illicit drug in the U.S. and represents 31% of all ED visits related to substance abuse.1,2 According to recent survey results, 2.1 million people report recent cocaine use, and 1.6 million engage in cocaine abuse or dependence.2 Acute cardiopulmonary complaints are common in individuals who present to the ED after cocaine use, with chest pain being the most frequently reported symptom in 40%.3
Numerous etiologies for cocaine-associated chest pain (CACP) have been discovered, including musculoskeletal pain, pulmonary hypertension, cardiomyopathy, arrhythmias, and endocarditis.4 Only 0.5% of patients with aortic dissection over a four-year period had a recent history of cocaine use, making cocaine a rare cause of a rare condition.5 Cardiac chest pain remains the most frequent underlying etiology, resulting in the most common complication of myocardial infarction (MI) in up to 6% of patients.6,7
The ways in which cocaine use can cause myocardial ischemia and MI are multifactorial. A vigorous central sympathomimetic effect, coronary artery vasoconstriction, stimulation of platelets, and enhanced atherosclerosis all lead to a myocardial oxygen supply-demand imbalance.8 Other key interactions in the cardiovascular system are displayed in Figure 1. Understanding the role of these mechanisms in CACP is crucial to patient care.
Clinician goals in the management of CACP are to rapidly and accurately exclude life-threatening etiologies; assess the need for urgent acute coronary syndrome (ACS) evaluation; risk-stratify patients and ensure appropriate disposition; normalize the toxic effects of cocaine; treat resultant organ damage; and prevent long-term complications. An algorithm detailing this approach is provided in Figure 2.
Review of the Data
Diagnostic evaluation. Given potential differences in treatment regimens, it is imperative to differentiate patients who present with CACP from those whose chest pain is not associated with cocaine either by direct questioning or by screening of urine for cocaine metabolites. Once the presence of cocaine has been confirmed, guideline-based evaluation for potential ACS with serial electrocardiograms (ECG), cardiac biomarkers, and close monitoring of cardiac rhythms and hemodynamics is largely similar to standard management of all patients presenting with chest pain, with a few caveats.
Interpretation of the ECG can be challenging in the setting of cocaine. Studies have shown “abnormal” ECGs in 56% to 84% of patients, with many representing early repolarization or left ventricular hypertrophy.9,10 Likewise, patients with MI are as likely to present with normal or nonspecific ECG findings as with ischemic findings.7,11 ECG interpretation to diagnose ischemia or infarction in patients with CACP yields a sensitivity of 36% and specificity of 90%.7
Creatine kinase (CK), CK-MB fraction, and myoglobin have low specificity for the diagnosis of ischemia, as cocaine can induce skeletal muscle injury and rhabdomyolysis.9,12 Cardiac troponins demonstrate a superior specificity compared to CK and CK-MB and are thus the preferred cardiac biomarkers in diagnosing cocaine-associated MI.12
Initial management and disposition. Patients at high risk for cardiovascular events are generally admitted to a monitored bed.13 Immediate reperfusion therapy with primary percutaneous coronary intervention is recommended in patients with ST-elevation MI (STEMI). Treatment with thrombolytic agents is associated with an increased risk of intracerebral hemorrhage and lacks documented efficacy in patients with CACP. Thrombolysis should therefore only be utilized if the diagnosis of STEMI is unequivocal and an experienced cardiac catheterization laboratory is unavailable.14,15
Patients with unstable angina (UA) or non-ST-elevation MI (NSTEMI) are at higher risk for further cardiac events in a similar manner to those with ACS unrelated to cocaine. These cases might benefit from early cardiac catheterization and revascularization.16 Because of the increased risk of stent thrombosis in cocaine-users, thought to be due to recidivism, a detailed risk-benefit analysis should be undertaken prior to the implantation of cardiac stents.
Other diagnostic tests, such as stress testing and myocardial imaging, have not shown significant accuracy in diagnosing MI in this setting; moreover, these patients are at low overall risk for cardiac events and mortality. Consequently, an extensive diagnostic evaluation might not be cost-effective.7,10,13,17 Patients who have CACP without MI have a very low frequency of delayed complications.3,17 As such, cost-effective evaluation strategies, such as nine- or 12-hour observation periods in a chest pain unit, are appropriate for many of these low- to moderate-risk patients.13 For all CACP patients, the most critical post-discharge interventions are cardiac risk modification and cocaine cessation.13
Normalizing the toxic effects of cocaine with medications.
Aspirin: While no specific study has been performed in patients with CACP and aspirin, CACP guidelines, based on data supporting ACS guidelines for all patients, recommend administration of full-dose aspirin given its associated reduction in morbidity and mortality.18,19 Furthermore, given the platelet-stimulating effects of cocaine, using aspirin in this setting seems very reasonable.
Benzodiazepines: CACP guidelines support the use of benzodiazepines early in management to indirectly combat the agitation, hypertension, and tachycardia resulting from the stimulatory effects of cocaine.18,20 These recommendations are based on several animal and human studies that demonstrate significant reduction in heart rate and systemic arterial pressure with the use of these agents.21,22
Nitroglycerin: Cardiac catheterization studies have shown reversal of vasoconstriction with administration of nitroglycerin. One study demonstrated a benefit of the drug in 49% of participants.23 Additional investigation into the benefit of benzodiazepine and nitroglycerin combination therapy revealed mixed results. In one study, lorazepam plus nitroglycerin was found to be more efficacious than nitroglycerin alone.24 In another, however, use of diazepam in combination with nitroglycerin did not show benefit when evaluating pain relief, cardiac dynamics, and left ventricular function.25
Phentolamine: Phentolamine administration has been studied much less in the literature. This nonselective alpha-adrenergic antagonist exerts a dose-dependent reversal of cocaine’s vasoconstrictive properties in monkeys and humans.26,27 International guidelines for Emergency Cardiovascular Care recommend its use in treatment of cocaine-associated ACS;27 however, the AHA recommends it less strongly.18
Calcium channel blockers: Calcium channel blockers (CCBs) have not shown promise as first-line agents. While catheterization studies demonstrate the vasodilatory properties of verapamil, larger studies looking at all-cause mortality conclude that CCBs might worsen mortality rates,28 and animal studies indicate an increased risk of seizures.29 At this time, CCBs are recommended only if cardiac symptoms continue after both benzodiazepines and nitroglycerin are administered.18
The beta-blocker controversy: The use of beta-blockers in patients with CACP remains controversial given the theoretical risk of unopposed alpha-adrenergic activation. Coronary vasospasm, decreased myocardial oxygen delivery, and increased systemic vascular resistance can result from their use.30
Propranolol, a nonselective beta-blocker, was shown in catheterization studies to potentiate the coronary vasoconstriction of cocaine.31 Labetalol, a combined alpha/beta-blocker, reduced mean arterial pressure after cocaine administration during cardiac catheterization but did not reverse coronary vasoconstriction.32 This was attributed to the predominating beta greater than alpha blockade at doses administered. The selective beta-1 antagonists esmolol and metoprolol have shown no benefit in CACP.33 Carvedilol, a combined alpha/beta-blocker with both peripheral and central nervous system activity, has potential to attenuate both physiologic and behavioral response to cocaine, but it has not been well studied in this patient subset.34
The 2005 ACC/AHA STEMI guidelines recommended against beta-blockers in the setting of STEMI precipitated by cocaine use due to the potential of exacerbating coronary vasoconstriction.35 The 2007 ACC/AHA UA/NSTEMI guidelines stated that the use of a combined alpha/beta-blocker in patients with cocaine-induced ACS may be reasonable for patients with hypertension or tachycardia if pre-treated with a vasodilator.19 The 2008 ACC/AHA guidelines on the management of cocaine-related chest pain and MI recommended against the use of beta-blockers in the acute setting given the low incidence of cocaine-related MI and death.18
In a more recent study, Dattilo et al showed that beta-blockers administered to patients admitted with positive urine toxicology for cocaine significantly reduced MI and in-hospital mortality. Reduction of MI was of borderline significance in those admitted with a chief complaint of chest pain.36 Limitations of this study include unknown time of cocaine ingestion, lack of follow-up on discharge mortality, and a small sample size of 348 patients lacking statistical power.
Another retrospective cohort study examined patients admitted with chest pain and urine toxicology positive for cocaine and found that beta-blocker administration during hospitalization was not associated with increased incident mortality. Further, after a mean follow-up of 2.5 years, there was a statistically significant decrease in cardiovascular death.37 Drawbacks of this study included an older patient population, greater proportion of coronary artery disease, and higher follow-up of cardiovascular mortality rates than in previous studies, suggesting this subset might have received greater benefit from beta-blockers as a result of these characteristics.
The 2008 ACC/AHA guidelines instruct individualized consideration of the risk/benefit ratio for beta-blocker use in patients with CACP given the high rate of recidivism in cocaine abusers. The strongest indication is given to those with documented MI, left ventricular systolic dysfunction, or ventricular arrhythmias.18
It is important to note that these recommendations are based on cardiac catheterization laboratory studies, case reports, retrospective analyses, and animal experiments. No prospective controlled trials evaluating the role of beta-blockers in CACP and MI exist, and no trials regarding therapies to improve outcomes of patients sustaining a cocaine-associated MI have been reported.18
Back to the Case
This patient was experiencing cocaine-associated chest pain, which was confirmed with positive urine toxicology. Initial diagnostic workup with basic laboratory studies and cardiac biomarkers showed mild elevation in CK with troponin levels within normal limits. His ECG showed changes consistent with left ventricular hypertrophy. Chest radiograph was unremarkable.
He received aspirin, benzodiazepines, and nitroglycerin with normalization of vital signs, as well as subjective improvement in chest pain and anxiety. He was deemed to be at low risk for potential cardiac complications; thus, further cardiac testing was not pursued. Rather, he was admitted to an overnight observation unit with telemetry monitoring, where his chest pain did not recur.
He was seen in consultation with social work staff who arranged for drug abuse counseling after discharge. Given the uncertainty of relapse to cocaine use, as well as lack of known cardiac risk factors, he was not discharged on any new medications.
Bottom Line
The treatment of CACP includes normalizing the toxic systemic effects of the drug and minimizing the direct ischemic damage to the myocardium. Management varies slightly from traditional chest pain algorithms and includes benzodiazepines as well as antiplatelet agents and vasodilators to achieve this goal. Initial therapy with beta-blockers remains undefined and is largely discouraged in the acute setting. The role of beta-blockade upon discharge, however, can be beneficial in specific populations, especially those found to have underlying coronary disease.
Dr. Houchens and Dr. Czarnik are clinical instructors and Dr. Mack is a clinical lecturer at the University of Michigan Health System in Ann Arbor.
References
- Hughes A, Sathe N, Spagnola K. State Estimates of Substance Use from the 2005-2006 National Surveys on Drug Use and Health. DHHS Publication No. SMA 08-4311, NSDUH Series H-33. Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2008.
- Volkow ND. Cocaine: Abuse and Addiction. National Institute on Drug Abuse. Washington, DC: U.S. Department of Health and Human Services; 2009.
- Brody SL, Slovis CM, Wrenn KD. Cocaine-related medical problems: consecutive series of 233 patients. Am J Med. 1990;88:325-331.
- Levis JT, Garmel GM. Cocaine-associated chest pain. Emerg Med Clin North Am. 2005;23:1083-1103.
- Eagle KA, Isselbacher EM, DeSanctis RW. Cocaine-related aortic dissection in perspective. Circulation. 2002;105:1529-1530.
- Feldman JA, Fish SS, Beshansky JR, Griffith JL, Woolard RH, Selker HP. Acute cardiac ischemia in patients with cocaine-associated complaints: results of a multicenter trial. Ann Emerg Med. 2000;36:469-476.
- Hollander JE, Hoffman RS, Gennis P, et al. Prospective multicenter evaluation of cocaine associated chest pain. Cocaine Associated Chest Pain (COCHPA) Study Group. Acad Emerg Med. 1994;1:330-339.
- Schwartz BG, Rezkalla S, Kloner RA. Cardiovascular effects of cocaine. Circulation. 2010;122:2558-2569.
- Gitter MJ, Goldsmith SR, Dunbar DN, et al. Cocaine and chest pain: clinical features and outcomes of patients hospitalized to rule out myocardial infarction. Ann Intern Med. 1991;115:277-282.
- Amin M, Gabelman G, Karpel J, et al. Acute myocardial infarction and chest pain syndromes after cocaine use. Am J Cardiol. 1990;66:1434-1437.
- Tokarski GF, Paganussi P, Urbanski R, et al. An evaluation of cocaine-induced chest pain. Ann Emerg Med. 1990;19:1088-1092.
- Hollander JE, Levitt MA, Young GP, Briglia E, Wetli CV, Gawad Y. Effect of recent cocaine use on the specificity of cardiac markers for diagnosis of acute myocardial infarction. Am Heart J. 1998;135(2 Pt 1):245-252.
- Weber JE, Shofer FS, Larkin GL, Kalaria AS, Hollander JE. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med. 2003;348:510-517.
- Hahn IH, Hoffman RS. Diagnosis and treatment of acute myocardial infarction: cocaine use and acute myocardial infarction. Emerg Med Clin North Am. 2001;19(2):1-18.
- Hoffman RS, Hollander JE. Evaluation of patients with chest pain after cocaine use. Crit Care Clin. 1997;13:809-828. Cannon CP, Weintraub WS, Demopoulos LA, et al.
- Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887.
- Hollander JE, Hoffman RS. Cocaine-induced myocardial infarction: an analysis and review of the literature. J Emerg Med. 1992;10:169-177.
- McCord J, Jneid H, Hollander JE, et al. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117:1897-1907.
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:E1-E157.
- Hollander JE. Management of cocaine-associated myocardial ischemia. N Engl J Med. 1995;333:1267-1272.
- Brubacher JR, Hoffman RS. Cocaine toxicity. Top Emerg Med. 1997;19(4):1-16.
- Catavas JD, Waters IW. Acute cocaine intoxication in the conscious dog: studies on the mechanism of lethality. J Pharmacol Exp Ther. 1981;217:350-356.
- Hollander JE, Hoffman RS, Gennis P, et al. Nitroglycerin in the treatment of cocaine associated chest pain—clinical safety and efficacy. J Toxicol Clin Toxicol. 1994;32(3): 243-256.
- Honderick T, Williams D, Seaberg D, Wears R. A prospective, randomized, controlled trial of benzodiazepines and nitroglycerin or nitroglycerin alone in the treatment of cocaine-associated acute coronary syndromes. Am J Emerg Med. 2003;21(1):39-42.
- Baumann BM, Perrone J, Hornig SE, Shofer FS, Hollander JE. Randomized, double-blind, placebo-controlled trial of diazepam, nitroglycerin, or both for treatment of patients with potential cocaine-associated acute coronary syndromes. Acad Emerg Med. 2000;7:878-885.
- Schindler CW, Tella SR, Goldberg SR. Adrenoceptor mechanisms in the cardiovascular effects of cocaine in conscious squirrel monkeys. Life Sci. 1992;51(9):653-660.
- Lange RA, Cigarroa RG, Yancy CW Jr., et al. Cocaine-induced coronary-artery vasoconstriction. N Engl J Med. 1989;321(23):1557-1562.
- Furberg CD, Psaty BM, Meyer JV. Nifedipine. Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995;92:1326-1331.
- Derlet RW, Albertson TE. Potentiation of cocaine toxicity with calcium channel blockers. Am J Emerg Med. 1989;7:464-468.
- Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351-358.
- Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade. Ann Intern Med. 1990;112:897-903.
- Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA. Influence of labetalol on cocaine-induced coronary vasoconstriction in humans. Am J Med. 1993;94:608-610.
- Sand IC, Brody SL, Wrenn KD, Slovis CM. Experience with esmolol for the treatment of cocaine-associated cardiovascular complications. Am J Emerg Med. 1991;9:161-163.
- Sofuoglo M, Brown S, Babb DA, Pentel PR, Hatsukami DK. Carvedilol affects the physiological and behavioral response to smoked cocaine in humans. Drug Alcohol Depend. 2000;60:69-76.
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force of Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44:E1-E211.
- Dattilo PB, Hailpern SM, Fearon K, Sohal D, Nordin C. Beta-blockers are associated with reduced risk of myocardial infarction after cocaine use. Ann Emerg Med. 2008;51:117-125.
- Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170:874-879.
Case
A 38-year-old man with a history of tobacco use presents to the emergency department complaining of constant substernal chest pain for three hours. His temperature is 37.7°C, his heart rate is 110 beats per minute, and his blood pressure is 155/95 mmHg. He appears anxious and diaphoretic but examination is otherwise unremarkable. He admits to cocaine use one hour before the onset of symptoms. What are the appropriate treatments for his condition?
Overview
Cocaine is the second-most-commonly used illicit drug in the U.S. and represents 31% of all ED visits related to substance abuse.1,2 According to recent survey results, 2.1 million people report recent cocaine use, and 1.6 million engage in cocaine abuse or dependence.2 Acute cardiopulmonary complaints are common in individuals who present to the ED after cocaine use, with chest pain being the most frequently reported symptom in 40%.3
Numerous etiologies for cocaine-associated chest pain (CACP) have been discovered, including musculoskeletal pain, pulmonary hypertension, cardiomyopathy, arrhythmias, and endocarditis.4 Only 0.5% of patients with aortic dissection over a four-year period had a recent history of cocaine use, making cocaine a rare cause of a rare condition.5 Cardiac chest pain remains the most frequent underlying etiology, resulting in the most common complication of myocardial infarction (MI) in up to 6% of patients.6,7
The ways in which cocaine use can cause myocardial ischemia and MI are multifactorial. A vigorous central sympathomimetic effect, coronary artery vasoconstriction, stimulation of platelets, and enhanced atherosclerosis all lead to a myocardial oxygen supply-demand imbalance.8 Other key interactions in the cardiovascular system are displayed in Figure 1. Understanding the role of these mechanisms in CACP is crucial to patient care.
Clinician goals in the management of CACP are to rapidly and accurately exclude life-threatening etiologies; assess the need for urgent acute coronary syndrome (ACS) evaluation; risk-stratify patients and ensure appropriate disposition; normalize the toxic effects of cocaine; treat resultant organ damage; and prevent long-term complications. An algorithm detailing this approach is provided in Figure 2.
Review of the Data
Diagnostic evaluation. Given potential differences in treatment regimens, it is imperative to differentiate patients who present with CACP from those whose chest pain is not associated with cocaine either by direct questioning or by screening of urine for cocaine metabolites. Once the presence of cocaine has been confirmed, guideline-based evaluation for potential ACS with serial electrocardiograms (ECG), cardiac biomarkers, and close monitoring of cardiac rhythms and hemodynamics is largely similar to standard management of all patients presenting with chest pain, with a few caveats.
Interpretation of the ECG can be challenging in the setting of cocaine. Studies have shown “abnormal” ECGs in 56% to 84% of patients, with many representing early repolarization or left ventricular hypertrophy.9,10 Likewise, patients with MI are as likely to present with normal or nonspecific ECG findings as with ischemic findings.7,11 ECG interpretation to diagnose ischemia or infarction in patients with CACP yields a sensitivity of 36% and specificity of 90%.7
Creatine kinase (CK), CK-MB fraction, and myoglobin have low specificity for the diagnosis of ischemia, as cocaine can induce skeletal muscle injury and rhabdomyolysis.9,12 Cardiac troponins demonstrate a superior specificity compared to CK and CK-MB and are thus the preferred cardiac biomarkers in diagnosing cocaine-associated MI.12
Initial management and disposition. Patients at high risk for cardiovascular events are generally admitted to a monitored bed.13 Immediate reperfusion therapy with primary percutaneous coronary intervention is recommended in patients with ST-elevation MI (STEMI). Treatment with thrombolytic agents is associated with an increased risk of intracerebral hemorrhage and lacks documented efficacy in patients with CACP. Thrombolysis should therefore only be utilized if the diagnosis of STEMI is unequivocal and an experienced cardiac catheterization laboratory is unavailable.14,15
Patients with unstable angina (UA) or non-ST-elevation MI (NSTEMI) are at higher risk for further cardiac events in a similar manner to those with ACS unrelated to cocaine. These cases might benefit from early cardiac catheterization and revascularization.16 Because of the increased risk of stent thrombosis in cocaine-users, thought to be due to recidivism, a detailed risk-benefit analysis should be undertaken prior to the implantation of cardiac stents.
Other diagnostic tests, such as stress testing and myocardial imaging, have not shown significant accuracy in diagnosing MI in this setting; moreover, these patients are at low overall risk for cardiac events and mortality. Consequently, an extensive diagnostic evaluation might not be cost-effective.7,10,13,17 Patients who have CACP without MI have a very low frequency of delayed complications.3,17 As such, cost-effective evaluation strategies, such as nine- or 12-hour observation periods in a chest pain unit, are appropriate for many of these low- to moderate-risk patients.13 For all CACP patients, the most critical post-discharge interventions are cardiac risk modification and cocaine cessation.13
Normalizing the toxic effects of cocaine with medications.
Aspirin: While no specific study has been performed in patients with CACP and aspirin, CACP guidelines, based on data supporting ACS guidelines for all patients, recommend administration of full-dose aspirin given its associated reduction in morbidity and mortality.18,19 Furthermore, given the platelet-stimulating effects of cocaine, using aspirin in this setting seems very reasonable.
Benzodiazepines: CACP guidelines support the use of benzodiazepines early in management to indirectly combat the agitation, hypertension, and tachycardia resulting from the stimulatory effects of cocaine.18,20 These recommendations are based on several animal and human studies that demonstrate significant reduction in heart rate and systemic arterial pressure with the use of these agents.21,22
Nitroglycerin: Cardiac catheterization studies have shown reversal of vasoconstriction with administration of nitroglycerin. One study demonstrated a benefit of the drug in 49% of participants.23 Additional investigation into the benefit of benzodiazepine and nitroglycerin combination therapy revealed mixed results. In one study, lorazepam plus nitroglycerin was found to be more efficacious than nitroglycerin alone.24 In another, however, use of diazepam in combination with nitroglycerin did not show benefit when evaluating pain relief, cardiac dynamics, and left ventricular function.25
Phentolamine: Phentolamine administration has been studied much less in the literature. This nonselective alpha-adrenergic antagonist exerts a dose-dependent reversal of cocaine’s vasoconstrictive properties in monkeys and humans.26,27 International guidelines for Emergency Cardiovascular Care recommend its use in treatment of cocaine-associated ACS;27 however, the AHA recommends it less strongly.18
Calcium channel blockers: Calcium channel blockers (CCBs) have not shown promise as first-line agents. While catheterization studies demonstrate the vasodilatory properties of verapamil, larger studies looking at all-cause mortality conclude that CCBs might worsen mortality rates,28 and animal studies indicate an increased risk of seizures.29 At this time, CCBs are recommended only if cardiac symptoms continue after both benzodiazepines and nitroglycerin are administered.18
The beta-blocker controversy: The use of beta-blockers in patients with CACP remains controversial given the theoretical risk of unopposed alpha-adrenergic activation. Coronary vasospasm, decreased myocardial oxygen delivery, and increased systemic vascular resistance can result from their use.30
Propranolol, a nonselective beta-blocker, was shown in catheterization studies to potentiate the coronary vasoconstriction of cocaine.31 Labetalol, a combined alpha/beta-blocker, reduced mean arterial pressure after cocaine administration during cardiac catheterization but did not reverse coronary vasoconstriction.32 This was attributed to the predominating beta greater than alpha blockade at doses administered. The selective beta-1 antagonists esmolol and metoprolol have shown no benefit in CACP.33 Carvedilol, a combined alpha/beta-blocker with both peripheral and central nervous system activity, has potential to attenuate both physiologic and behavioral response to cocaine, but it has not been well studied in this patient subset.34
The 2005 ACC/AHA STEMI guidelines recommended against beta-blockers in the setting of STEMI precipitated by cocaine use due to the potential of exacerbating coronary vasoconstriction.35 The 2007 ACC/AHA UA/NSTEMI guidelines stated that the use of a combined alpha/beta-blocker in patients with cocaine-induced ACS may be reasonable for patients with hypertension or tachycardia if pre-treated with a vasodilator.19 The 2008 ACC/AHA guidelines on the management of cocaine-related chest pain and MI recommended against the use of beta-blockers in the acute setting given the low incidence of cocaine-related MI and death.18
In a more recent study, Dattilo et al showed that beta-blockers administered to patients admitted with positive urine toxicology for cocaine significantly reduced MI and in-hospital mortality. Reduction of MI was of borderline significance in those admitted with a chief complaint of chest pain.36 Limitations of this study include unknown time of cocaine ingestion, lack of follow-up on discharge mortality, and a small sample size of 348 patients lacking statistical power.
Another retrospective cohort study examined patients admitted with chest pain and urine toxicology positive for cocaine and found that beta-blocker administration during hospitalization was not associated with increased incident mortality. Further, after a mean follow-up of 2.5 years, there was a statistically significant decrease in cardiovascular death.37 Drawbacks of this study included an older patient population, greater proportion of coronary artery disease, and higher follow-up of cardiovascular mortality rates than in previous studies, suggesting this subset might have received greater benefit from beta-blockers as a result of these characteristics.
The 2008 ACC/AHA guidelines instruct individualized consideration of the risk/benefit ratio for beta-blocker use in patients with CACP given the high rate of recidivism in cocaine abusers. The strongest indication is given to those with documented MI, left ventricular systolic dysfunction, or ventricular arrhythmias.18
It is important to note that these recommendations are based on cardiac catheterization laboratory studies, case reports, retrospective analyses, and animal experiments. No prospective controlled trials evaluating the role of beta-blockers in CACP and MI exist, and no trials regarding therapies to improve outcomes of patients sustaining a cocaine-associated MI have been reported.18
Back to the Case
This patient was experiencing cocaine-associated chest pain, which was confirmed with positive urine toxicology. Initial diagnostic workup with basic laboratory studies and cardiac biomarkers showed mild elevation in CK with troponin levels within normal limits. His ECG showed changes consistent with left ventricular hypertrophy. Chest radiograph was unremarkable.
He received aspirin, benzodiazepines, and nitroglycerin with normalization of vital signs, as well as subjective improvement in chest pain and anxiety. He was deemed to be at low risk for potential cardiac complications; thus, further cardiac testing was not pursued. Rather, he was admitted to an overnight observation unit with telemetry monitoring, where his chest pain did not recur.
He was seen in consultation with social work staff who arranged for drug abuse counseling after discharge. Given the uncertainty of relapse to cocaine use, as well as lack of known cardiac risk factors, he was not discharged on any new medications.
Bottom Line
The treatment of CACP includes normalizing the toxic systemic effects of the drug and minimizing the direct ischemic damage to the myocardium. Management varies slightly from traditional chest pain algorithms and includes benzodiazepines as well as antiplatelet agents and vasodilators to achieve this goal. Initial therapy with beta-blockers remains undefined and is largely discouraged in the acute setting. The role of beta-blockade upon discharge, however, can be beneficial in specific populations, especially those found to have underlying coronary disease.
Dr. Houchens and Dr. Czarnik are clinical instructors and Dr. Mack is a clinical lecturer at the University of Michigan Health System in Ann Arbor.
References
- Hughes A, Sathe N, Spagnola K. State Estimates of Substance Use from the 2005-2006 National Surveys on Drug Use and Health. DHHS Publication No. SMA 08-4311, NSDUH Series H-33. Rockville, MD: Substance Abuse and Mental Health Services Administration, Office of Applied Studies; 2008.
- Volkow ND. Cocaine: Abuse and Addiction. National Institute on Drug Abuse. Washington, DC: U.S. Department of Health and Human Services; 2009.
- Brody SL, Slovis CM, Wrenn KD. Cocaine-related medical problems: consecutive series of 233 patients. Am J Med. 1990;88:325-331.
- Levis JT, Garmel GM. Cocaine-associated chest pain. Emerg Med Clin North Am. 2005;23:1083-1103.
- Eagle KA, Isselbacher EM, DeSanctis RW. Cocaine-related aortic dissection in perspective. Circulation. 2002;105:1529-1530.
- Feldman JA, Fish SS, Beshansky JR, Griffith JL, Woolard RH, Selker HP. Acute cardiac ischemia in patients with cocaine-associated complaints: results of a multicenter trial. Ann Emerg Med. 2000;36:469-476.
- Hollander JE, Hoffman RS, Gennis P, et al. Prospective multicenter evaluation of cocaine associated chest pain. Cocaine Associated Chest Pain (COCHPA) Study Group. Acad Emerg Med. 1994;1:330-339.
- Schwartz BG, Rezkalla S, Kloner RA. Cardiovascular effects of cocaine. Circulation. 2010;122:2558-2569.
- Gitter MJ, Goldsmith SR, Dunbar DN, et al. Cocaine and chest pain: clinical features and outcomes of patients hospitalized to rule out myocardial infarction. Ann Intern Med. 1991;115:277-282.
- Amin M, Gabelman G, Karpel J, et al. Acute myocardial infarction and chest pain syndromes after cocaine use. Am J Cardiol. 1990;66:1434-1437.
- Tokarski GF, Paganussi P, Urbanski R, et al. An evaluation of cocaine-induced chest pain. Ann Emerg Med. 1990;19:1088-1092.
- Hollander JE, Levitt MA, Young GP, Briglia E, Wetli CV, Gawad Y. Effect of recent cocaine use on the specificity of cardiac markers for diagnosis of acute myocardial infarction. Am Heart J. 1998;135(2 Pt 1):245-252.
- Weber JE, Shofer FS, Larkin GL, Kalaria AS, Hollander JE. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med. 2003;348:510-517.
- Hahn IH, Hoffman RS. Diagnosis and treatment of acute myocardial infarction: cocaine use and acute myocardial infarction. Emerg Med Clin North Am. 2001;19(2):1-18.
- Hoffman RS, Hollander JE. Evaluation of patients with chest pain after cocaine use. Crit Care Clin. 1997;13:809-828. Cannon CP, Weintraub WS, Demopoulos LA, et al.
- Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344:1879-1887.
- Hollander JE, Hoffman RS. Cocaine-induced myocardial infarction: an analysis and review of the literature. J Emerg Med. 1992;10:169-177.
- McCord J, Jneid H, Hollander JE, et al. Management of cocaine-associated chest pain and myocardial infarction: a scientific statement from the American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology. Circulation. 2008;117:1897-1907.
- Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. J Am Coll Cardiol. 2007;50:E1-E157.
- Hollander JE. Management of cocaine-associated myocardial ischemia. N Engl J Med. 1995;333:1267-1272.
- Brubacher JR, Hoffman RS. Cocaine toxicity. Top Emerg Med. 1997;19(4):1-16.
- Catavas JD, Waters IW. Acute cocaine intoxication in the conscious dog: studies on the mechanism of lethality. J Pharmacol Exp Ther. 1981;217:350-356.
- Hollander JE, Hoffman RS, Gennis P, et al. Nitroglycerin in the treatment of cocaine associated chest pain—clinical safety and efficacy. J Toxicol Clin Toxicol. 1994;32(3): 243-256.
- Honderick T, Williams D, Seaberg D, Wears R. A prospective, randomized, controlled trial of benzodiazepines and nitroglycerin or nitroglycerin alone in the treatment of cocaine-associated acute coronary syndromes. Am J Emerg Med. 2003;21(1):39-42.
- Baumann BM, Perrone J, Hornig SE, Shofer FS, Hollander JE. Randomized, double-blind, placebo-controlled trial of diazepam, nitroglycerin, or both for treatment of patients with potential cocaine-associated acute coronary syndromes. Acad Emerg Med. 2000;7:878-885.
- Schindler CW, Tella SR, Goldberg SR. Adrenoceptor mechanisms in the cardiovascular effects of cocaine in conscious squirrel monkeys. Life Sci. 1992;51(9):653-660.
- Lange RA, Cigarroa RG, Yancy CW Jr., et al. Cocaine-induced coronary-artery vasoconstriction. N Engl J Med. 1989;321(23):1557-1562.
- Furberg CD, Psaty BM, Meyer JV. Nifedipine. Dose-related increase in mortality in patients with coronary heart disease. Circulation. 1995;92:1326-1331.
- Derlet RW, Albertson TE. Potentiation of cocaine toxicity with calcium channel blockers. Am J Emerg Med. 1989;7:464-468.
- Lange RA, Hillis LD. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351-358.
- Lange RA, Cigarroa RG, Flores ED, et al. Potentiation of cocaine-induced coronary vasoconstriction by beta-adrenergic blockade. Ann Intern Med. 1990;112:897-903.
- Boehrer JD, Moliterno DJ, Willard JE, Hillis LD, Lange RA. Influence of labetalol on cocaine-induced coronary vasoconstriction in humans. Am J Med. 1993;94:608-610.
- Sand IC, Brody SL, Wrenn KD, Slovis CM. Experience with esmolol for the treatment of cocaine-associated cardiovascular complications. Am J Emerg Med. 1991;9:161-163.
- Sofuoglo M, Brown S, Babb DA, Pentel PR, Hatsukami DK. Carvedilol affects the physiological and behavioral response to smoked cocaine in humans. Drug Alcohol Depend. 2000;60:69-76.
- Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force of Practice Guidelines (Committee to Revise the 1999 Guidelines for the Management of patients with acute myocardial infarction). J Am Coll Cardiol. 2004;44:E1-E211.
- Dattilo PB, Hailpern SM, Fearon K, Sohal D, Nordin C. Beta-blockers are associated with reduced risk of myocardial infarction after cocaine use. Ann Emerg Med. 2008;51:117-125.
- Rangel C, Shu RG, Lazar LD, Vittinghoff E, Hsue PY, Marcus GM. Beta-blockers for chest pain associated with recent cocaine use. Arch Intern Med. 2010;170:874-879.
Clarifying the Role of Hospitalists Focused on Family Medicine in the ICU

Clarifying Family-Practice Hospitalists’ Value, Focused-Practice Opportunities
I am writing regarding the letter and your response in the January 2013 issue of The Hospitalist regarding hospitalists trained in family medicine and practice in critical-care units. I am the chair of the Family Medicine Committee for SHM, a practicing hospitalist, and an SHM member for over 10 years. There is an error in your reply, in that physicians who are board-certified through the American Board of Family Medicine (ABFM) are indeed eligible to take the examination for Recognition of Focused Practice in Hospital Medicine (RFPHM). This examination is administered by the American Board of Internal Medicine (ABIM), and is the same examination for all physicians, regardless of whether their residency was completed in family or internal medicine.
I am proud to be among the six family physicians who took and passed the first examination in October 2010. Through 2012, there have been 28 family physicians who have passed this exam, and attained RFPHM (verbal communication from ABFM). According to the ABIM website, there have been 267 total physicians who have taken the examination through 2011, which includes family-medicine-trained physicians. There are a number of Maintenance of Certification (MOC) modules offered through the ABIM that are available to hospitalists trained in family medicine.
A prior study showed that 66% of hospitalists trained in family medicine practice in critical-care units (McElrath et al). You are correct that there is no current pathway for HTFM to pursue a critical-care fellowship or attain board certification by the SCCM, as diplomats of the ABFM are excluded. However, there are many hospitalists trained in family medicine providing excellent care to patients in critical-care units. There are clearly not enough board certified intensivists to provide the care.
—Kevin Ahern, MD, SFHM, chief hospitalist, Sound Physicians, Urbana, Ohio
Dr. Hospitalist responds:
You are absolutely correct in your point of clarification regarding the Recognition of Focused Practice in Hospital Medicine from the ABFM. I was aware of this at the time of the article; however, in my efforts to outline the proposed path from RFPHM to ICU certification, I focused solely on the ABIM pathway without mentioning the additional recognition available to family-practice physicians. In no way was this meant to denigrate the efforts or contributions of family-practice physicians to HM and SHM, but I could have been much more clear on this point. Having hired and worked alongside family-practice hospitalists, I know just how valuable you are.
The overall picture is consistent with what you described in that there are “clearly not enough board-certified intensivists” to fully staff ICUs. However, it is evident that it will be an uphill battle to sanction an alternate pathway that lets any hospitalist gain certification as an ICU physician. Truth be told, there are fundamental differences in the amount of ICU exposure between internal-medicine and family-practice training programs. As a result, in the current proposal there is no overt discussion of the role for family-practice hospitalists in the ICU. I think that this will continue to remain a conscious omission for both political and practical reasons.
Clarifying Family-Practice Hospitalists’ Value, Focused-Practice Opportunities
I am writing regarding the letter and your response in the January 2013 issue of The Hospitalist regarding hospitalists trained in family medicine and practice in critical-care units. I am the chair of the Family Medicine Committee for SHM, a practicing hospitalist, and an SHM member for over 10 years. There is an error in your reply, in that physicians who are board-certified through the American Board of Family Medicine (ABFM) are indeed eligible to take the examination for Recognition of Focused Practice in Hospital Medicine (RFPHM). This examination is administered by the American Board of Internal Medicine (ABIM), and is the same examination for all physicians, regardless of whether their residency was completed in family or internal medicine.
I am proud to be among the six family physicians who took and passed the first examination in October 2010. Through 2012, there have been 28 family physicians who have passed this exam, and attained RFPHM (verbal communication from ABFM). According to the ABIM website, there have been 267 total physicians who have taken the examination through 2011, which includes family-medicine-trained physicians. There are a number of Maintenance of Certification (MOC) modules offered through the ABIM that are available to hospitalists trained in family medicine.
A prior study showed that 66% of hospitalists trained in family medicine practice in critical-care units (McElrath et al). You are correct that there is no current pathway for HTFM to pursue a critical-care fellowship or attain board certification by the SCCM, as diplomats of the ABFM are excluded. However, there are many hospitalists trained in family medicine providing excellent care to patients in critical-care units. There are clearly not enough board certified intensivists to provide the care.
—Kevin Ahern, MD, SFHM, chief hospitalist, Sound Physicians, Urbana, Ohio
Dr. Hospitalist responds:
You are absolutely correct in your point of clarification regarding the Recognition of Focused Practice in Hospital Medicine from the ABFM. I was aware of this at the time of the article; however, in my efforts to outline the proposed path from RFPHM to ICU certification, I focused solely on the ABIM pathway without mentioning the additional recognition available to family-practice physicians. In no way was this meant to denigrate the efforts or contributions of family-practice physicians to HM and SHM, but I could have been much more clear on this point. Having hired and worked alongside family-practice hospitalists, I know just how valuable you are.
The overall picture is consistent with what you described in that there are “clearly not enough board-certified intensivists” to fully staff ICUs. However, it is evident that it will be an uphill battle to sanction an alternate pathway that lets any hospitalist gain certification as an ICU physician. Truth be told, there are fundamental differences in the amount of ICU exposure between internal-medicine and family-practice training programs. As a result, in the current proposal there is no overt discussion of the role for family-practice hospitalists in the ICU. I think that this will continue to remain a conscious omission for both political and practical reasons.
Clarifying Family-Practice Hospitalists’ Value, Focused-Practice Opportunities
I am writing regarding the letter and your response in the January 2013 issue of The Hospitalist regarding hospitalists trained in family medicine and practice in critical-care units. I am the chair of the Family Medicine Committee for SHM, a practicing hospitalist, and an SHM member for over 10 years. There is an error in your reply, in that physicians who are board-certified through the American Board of Family Medicine (ABFM) are indeed eligible to take the examination for Recognition of Focused Practice in Hospital Medicine (RFPHM). This examination is administered by the American Board of Internal Medicine (ABIM), and is the same examination for all physicians, regardless of whether their residency was completed in family or internal medicine.
I am proud to be among the six family physicians who took and passed the first examination in October 2010. Through 2012, there have been 28 family physicians who have passed this exam, and attained RFPHM (verbal communication from ABFM). According to the ABIM website, there have been 267 total physicians who have taken the examination through 2011, which includes family-medicine-trained physicians. There are a number of Maintenance of Certification (MOC) modules offered through the ABIM that are available to hospitalists trained in family medicine.
A prior study showed that 66% of hospitalists trained in family medicine practice in critical-care units (McElrath et al). You are correct that there is no current pathway for HTFM to pursue a critical-care fellowship or attain board certification by the SCCM, as diplomats of the ABFM are excluded. However, there are many hospitalists trained in family medicine providing excellent care to patients in critical-care units. There are clearly not enough board certified intensivists to provide the care.
—Kevin Ahern, MD, SFHM, chief hospitalist, Sound Physicians, Urbana, Ohio
Dr. Hospitalist responds:
You are absolutely correct in your point of clarification regarding the Recognition of Focused Practice in Hospital Medicine from the ABFM. I was aware of this at the time of the article; however, in my efforts to outline the proposed path from RFPHM to ICU certification, I focused solely on the ABIM pathway without mentioning the additional recognition available to family-practice physicians. In no way was this meant to denigrate the efforts or contributions of family-practice physicians to HM and SHM, but I could have been much more clear on this point. Having hired and worked alongside family-practice hospitalists, I know just how valuable you are.
The overall picture is consistent with what you described in that there are “clearly not enough board-certified intensivists” to fully staff ICUs. However, it is evident that it will be an uphill battle to sanction an alternate pathway that lets any hospitalist gain certification as an ICU physician. Truth be told, there are fundamental differences in the amount of ICU exposure between internal-medicine and family-practice training programs. As a result, in the current proposal there is no overt discussion of the role for family-practice hospitalists in the ICU. I think that this will continue to remain a conscious omission for both political and practical reasons.
Record Number of Physicians Pass Hospice and Palliative Medicine Exam
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
Number of physicians who passed for the first time the most recent Hospice and Palliative Medicine (HPM) board-certifying exam given in October by the American Board of Internal Medicine (ABIM). This number, an 83% success rate, represents a major influx of mid-career physicians qualifying in HPM just ahead of the closure of an experiential pathway to HPM board certification. Starting in 2013, physicians must complete a full-time, yearlong fellowship in HPM in order to sit for its board exam. ABIM and nine other specialty societies are responsible for HPM board certification. The last experiential pathway exam for HPM, in osteopathy, will be in September.
Clinical Guidelines Updated for Surviving Sepsis in Hospitals
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.
Reference
The Surviving Sepsis Campaign (www.survivingsepsis.org) has updated its best clinical practices for patients with severe sepsis or septic shock.6 Sixty-eight international experts worked to update the campaign’s 2008 guidelines. For example, the update includes a strong recommendation for the use of crystalloids (e.g. normal saline) as the initial fluid resuscitation for patients with severe sepsis.
The campaign, a collaboration of the Society of Critical Care Medicine and the European Society of Intensive Care Medicine, estimates 400,000 lives could be saved per year worldwide if 10,000 hospitals were committed to its recommendations and if even half of eligible patients were treated in conformance with the campaign’s quality bundles. The campaign also tries to develop strategies for improving the care of septic patients in settings where healthcare resources are limited.
Larry Beresford is a freelance writer in Oakland, Calif.