User login
DVT, PE Risk Increased in Surgery Patients with IBD
Patients with inflammatory bowel disease who undergo surgery have a twofold increase in the risk of deep vein thrombosis or pulmonary embolism, compared with those without IBD, and the risk is even greater among those with IBD who undergo nonintestinal surgery, according to findings from the American College of Surgeons National Surgical Quality Improvement Program.
In a retrospective cohort study of nearly 269,000 patients from the National Surgical Quality Improvement Program (NSQIP) 2008, 2,249 (0.8%) had IBD. Deep vein thrombosis (DVT) or pulmonary embolism (PE) occurred in 1% of those without IBD, in 2.5% of those with IBD, and in 5% of those with IBD who underwent nonintestinal surgery.
Dr. Andrea Merrill of Massachusetts General Hospital and Dr. Frederick Millham of Newton Wellesley Hospital, both in Boston, reported the research online in the Oct. 17 issue of Archives of Surgery. The findings suggest that the standard DVT and PE prophylaxis for patients undergoing surgery should be reconsidered for those with IBD, they concluded.
After adjustment for more than 30 possible confounders available in the NSQIP that add to the power to predict DVT or PE, a significant association remained between IBD and DVT or PE overall (odds ratio, 2.03) and among those undergoing nonintestinal surgery (OR, 4.45), the investigators found (Arch. Surg. 2011 Oct. 17 [doi:10.1001/archsurg.2011.297]).
No difference was seen between the patients with and without IBD in regard to the occurrence of cerebrovascular accident or myocardial infarction, with 0.4% of patients in both groups experiencing such events.
Although IBD has long been known to be associated with an increased risk of thromboembolic events, data on those undergoing surgery has been scarce, and standard DVT and PE prophylaxis guidelines in the IBD population have not been adjusted to include enhanced prophylaxis.
In light of one recent study suggesting a very high risk of postoperative DVT in those undergoing surgery, the investigators sought to evaluate the risk among IBD patients in the NSQIP, which collected data from 170 hospitals in 2008, resulting in a Participant Use Data File (PUF). The de-identified research database is made available to the participating hospitals.
"As such, the NSQIP PUF data set presents an opportunity to examine the relationship of DVT and PE with IBD in a large group of patients for whom data on comorbid conditions and other potential confounding variables are available and well defined. Furthermore, hospitals participating in the NSQIP, having invested in quality improvement, might be expected to treat patients with best practices, at least with respect to DVT prophylaxis," the investigators said, explaining that this would reduce the opportunity for treatment bias between centers.
The finding of an increased risk of DVT or PE in IBD patients was consistent with others in both surgical and nonsurgical IBD patients, they found.
An exception is with the lethality of DVT or PE in the setting of IBD. One prior study demonstrated an increased risk of death among IBD patients with DVT or PE, but the investigators of the current study found no support for this finding. Mortality occurred in 8.6% and 8.8% of those without IBD who had DVT or PE, and those with IBD who had DVT or PE, respectively.
They also found no support for one prior study’s finding of an increased risk of arterial thromboembolic events in patients with IBD, but they noted that the current study may have been limited by the lack of data on arterial thrombotic events not involving the coronary or cerebral vessels.
"It may be that if arterial thromboembolism were a reported NSQIP complication, such a relationship would appear," they said.
Although this study is limited by the fact that the NSQIP was designed to compare overall outcomes across many hospitals rather than to answer specific research questions regarding specific diseases or procedures, its strengths – namely the fact that the data were gathered by specially trained nurses who were accountable to a rigid quality-assurance program, and who were working from a well-defined data dictionary – likely outweigh any potential sources of bias, they said.
The authors reported that they had no disclosures.
Patients with inflammatory bowel disease who undergo surgery have a twofold increase in the risk of deep vein thrombosis or pulmonary embolism, compared with those without IBD, and the risk is even greater among those with IBD who undergo nonintestinal surgery, according to findings from the American College of Surgeons National Surgical Quality Improvement Program.
In a retrospective cohort study of nearly 269,000 patients from the National Surgical Quality Improvement Program (NSQIP) 2008, 2,249 (0.8%) had IBD. Deep vein thrombosis (DVT) or pulmonary embolism (PE) occurred in 1% of those without IBD, in 2.5% of those with IBD, and in 5% of those with IBD who underwent nonintestinal surgery.
Dr. Andrea Merrill of Massachusetts General Hospital and Dr. Frederick Millham of Newton Wellesley Hospital, both in Boston, reported the research online in the Oct. 17 issue of Archives of Surgery. The findings suggest that the standard DVT and PE prophylaxis for patients undergoing surgery should be reconsidered for those with IBD, they concluded.
After adjustment for more than 30 possible confounders available in the NSQIP that add to the power to predict DVT or PE, a significant association remained between IBD and DVT or PE overall (odds ratio, 2.03) and among those undergoing nonintestinal surgery (OR, 4.45), the investigators found (Arch. Surg. 2011 Oct. 17 [doi:10.1001/archsurg.2011.297]).
No difference was seen between the patients with and without IBD in regard to the occurrence of cerebrovascular accident or myocardial infarction, with 0.4% of patients in both groups experiencing such events.
Although IBD has long been known to be associated with an increased risk of thromboembolic events, data on those undergoing surgery has been scarce, and standard DVT and PE prophylaxis guidelines in the IBD population have not been adjusted to include enhanced prophylaxis.
In light of one recent study suggesting a very high risk of postoperative DVT in those undergoing surgery, the investigators sought to evaluate the risk among IBD patients in the NSQIP, which collected data from 170 hospitals in 2008, resulting in a Participant Use Data File (PUF). The de-identified research database is made available to the participating hospitals.
"As such, the NSQIP PUF data set presents an opportunity to examine the relationship of DVT and PE with IBD in a large group of patients for whom data on comorbid conditions and other potential confounding variables are available and well defined. Furthermore, hospitals participating in the NSQIP, having invested in quality improvement, might be expected to treat patients with best practices, at least with respect to DVT prophylaxis," the investigators said, explaining that this would reduce the opportunity for treatment bias between centers.
The finding of an increased risk of DVT or PE in IBD patients was consistent with others in both surgical and nonsurgical IBD patients, they found.
An exception is with the lethality of DVT or PE in the setting of IBD. One prior study demonstrated an increased risk of death among IBD patients with DVT or PE, but the investigators of the current study found no support for this finding. Mortality occurred in 8.6% and 8.8% of those without IBD who had DVT or PE, and those with IBD who had DVT or PE, respectively.
They also found no support for one prior study’s finding of an increased risk of arterial thromboembolic events in patients with IBD, but they noted that the current study may have been limited by the lack of data on arterial thrombotic events not involving the coronary or cerebral vessels.
"It may be that if arterial thromboembolism were a reported NSQIP complication, such a relationship would appear," they said.
Although this study is limited by the fact that the NSQIP was designed to compare overall outcomes across many hospitals rather than to answer specific research questions regarding specific diseases or procedures, its strengths – namely the fact that the data were gathered by specially trained nurses who were accountable to a rigid quality-assurance program, and who were working from a well-defined data dictionary – likely outweigh any potential sources of bias, they said.
The authors reported that they had no disclosures.
Patients with inflammatory bowel disease who undergo surgery have a twofold increase in the risk of deep vein thrombosis or pulmonary embolism, compared with those without IBD, and the risk is even greater among those with IBD who undergo nonintestinal surgery, according to findings from the American College of Surgeons National Surgical Quality Improvement Program.
In a retrospective cohort study of nearly 269,000 patients from the National Surgical Quality Improvement Program (NSQIP) 2008, 2,249 (0.8%) had IBD. Deep vein thrombosis (DVT) or pulmonary embolism (PE) occurred in 1% of those without IBD, in 2.5% of those with IBD, and in 5% of those with IBD who underwent nonintestinal surgery.
Dr. Andrea Merrill of Massachusetts General Hospital and Dr. Frederick Millham of Newton Wellesley Hospital, both in Boston, reported the research online in the Oct. 17 issue of Archives of Surgery. The findings suggest that the standard DVT and PE prophylaxis for patients undergoing surgery should be reconsidered for those with IBD, they concluded.
After adjustment for more than 30 possible confounders available in the NSQIP that add to the power to predict DVT or PE, a significant association remained between IBD and DVT or PE overall (odds ratio, 2.03) and among those undergoing nonintestinal surgery (OR, 4.45), the investigators found (Arch. Surg. 2011 Oct. 17 [doi:10.1001/archsurg.2011.297]).
No difference was seen between the patients with and without IBD in regard to the occurrence of cerebrovascular accident or myocardial infarction, with 0.4% of patients in both groups experiencing such events.
Although IBD has long been known to be associated with an increased risk of thromboembolic events, data on those undergoing surgery has been scarce, and standard DVT and PE prophylaxis guidelines in the IBD population have not been adjusted to include enhanced prophylaxis.
In light of one recent study suggesting a very high risk of postoperative DVT in those undergoing surgery, the investigators sought to evaluate the risk among IBD patients in the NSQIP, which collected data from 170 hospitals in 2008, resulting in a Participant Use Data File (PUF). The de-identified research database is made available to the participating hospitals.
"As such, the NSQIP PUF data set presents an opportunity to examine the relationship of DVT and PE with IBD in a large group of patients for whom data on comorbid conditions and other potential confounding variables are available and well defined. Furthermore, hospitals participating in the NSQIP, having invested in quality improvement, might be expected to treat patients with best practices, at least with respect to DVT prophylaxis," the investigators said, explaining that this would reduce the opportunity for treatment bias between centers.
The finding of an increased risk of DVT or PE in IBD patients was consistent with others in both surgical and nonsurgical IBD patients, they found.
An exception is with the lethality of DVT or PE in the setting of IBD. One prior study demonstrated an increased risk of death among IBD patients with DVT or PE, but the investigators of the current study found no support for this finding. Mortality occurred in 8.6% and 8.8% of those without IBD who had DVT or PE, and those with IBD who had DVT or PE, respectively.
They also found no support for one prior study’s finding of an increased risk of arterial thromboembolic events in patients with IBD, but they noted that the current study may have been limited by the lack of data on arterial thrombotic events not involving the coronary or cerebral vessels.
"It may be that if arterial thromboembolism were a reported NSQIP complication, such a relationship would appear," they said.
Although this study is limited by the fact that the NSQIP was designed to compare overall outcomes across many hospitals rather than to answer specific research questions regarding specific diseases or procedures, its strengths – namely the fact that the data were gathered by specially trained nurses who were accountable to a rigid quality-assurance program, and who were working from a well-defined data dictionary – likely outweigh any potential sources of bias, they said.
The authors reported that they had no disclosures.
FROM ARCHIVES OF SURGERY
Major Finding: After adjustment for more than 30 possible confounders available in the NSQIP that add to the power to predict DVT or PE, a significant association remained between IBD and DVT or PE overall (OR, 2.03) and among those undergoing nonintestinal surgery (OR, 4.45).
Data Source: A large retrospective cohort study.
Disclosures: The authors had no disclosures.
CMS Considers Coverage of Laparoscopic Sleeve Gastrectomy
The Centers for Medicare and Medicaid Services said on Sept. 30 that it is soliciting comments on a proposal to cover laparoscopic sleeve gastrectomy for Medicare patients.
Currently, that procedure is not covered by the federal health program. In its solicitation, the agency said it is asking the public "whether there is adequate evidence, including clinical trials, for evaluating health outcomes of laparoscopic sleeve gastrectomy (LSG) for the indications listed in the current Bariatric Surgery for the Treatment of Morbid Obesity National Coverage Determination."
LSG is a procedure in which the vast majority of the stomach is removed, leaving a tube or sleeve. It may be a first step before a gastric bypass, or it may be the primary procedure. It is an option for patients with a very high body mass index (BMI) who cannot tolerate a bypass procedure. Postoperatively, patients do not experience dumping or malabsorption of nutrients. However, if weight is regained, the decision about what to do next is not easy (World J. Gastroenterol. 2008;14:821-7).
Medicare has covered three bariatric procedures since 2006: open and laparoscopic Roux-en-Y gastric bypass; laparoscopic adjustable gastric banding; and open and laparoscopic biliopancreatic diversion with duodenal switch.
The procedures are reimbursed only for Medicare beneficiaries who have a BMI of 35 kg/m2 or greater; who have at least one obesity-related comorbidity, such as cardiovascular disease, chronic obstructive pulmonary disease, or type 2 diabetes mellitus; and who have not been successfully treated otherwise.
In order to be covered, the procedures must be performed at facilities certified either by the American College of Surgeons (ACS) as a level I bariatric surgery center or by the American Society for Metabolic and Bariatric Surgery as a bariatric surgery center of excellence (BSCOE).
Open vertical banded gastroplasty, laparoscopic vertical banded gastroplasty, open sleeve gastrectomy, and open adjustable gastric banding are among the bariatric procedures that are not currently covered.
A recent observational study presented at the annual meeting of the American Surgical Association found that at 1 year after surgery, LSG was associated with morbidity and effectiveness rates that fell between those of laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y bypass procedures.
The absolute reduction in BMI at 1 year was smallest in the laparoscopic adjustable gastric banding group at about 6, greatest with open or laparoscopic Roux-en-Y gastric bypass at about 15, and intermediate at close to 12 with LSG.
The study, based on prospective, longitudinal, standardized data from 109 hospitals, was the first to come out of the ACS Bariatric Surgery Center Network accreditation program. Additional years of follow-up are planned, according to Dr. Matthew M. Hutter, an ACS Fellow with Massachusetts General Hospital, Boston.
Dr. Hutter reported no financial conflicts.
CMS will seek public comment until Oct. 30. The agency plans to issue a proposed decision by March 30, 2012, and to make a final decision by June 30.
The Centers for Medicare and Medicaid Services said on Sept. 30 that it is soliciting comments on a proposal to cover laparoscopic sleeve gastrectomy for Medicare patients.
Currently, that procedure is not covered by the federal health program. In its solicitation, the agency said it is asking the public "whether there is adequate evidence, including clinical trials, for evaluating health outcomes of laparoscopic sleeve gastrectomy (LSG) for the indications listed in the current Bariatric Surgery for the Treatment of Morbid Obesity National Coverage Determination."
LSG is a procedure in which the vast majority of the stomach is removed, leaving a tube or sleeve. It may be a first step before a gastric bypass, or it may be the primary procedure. It is an option for patients with a very high body mass index (BMI) who cannot tolerate a bypass procedure. Postoperatively, patients do not experience dumping or malabsorption of nutrients. However, if weight is regained, the decision about what to do next is not easy (World J. Gastroenterol. 2008;14:821-7).
Medicare has covered three bariatric procedures since 2006: open and laparoscopic Roux-en-Y gastric bypass; laparoscopic adjustable gastric banding; and open and laparoscopic biliopancreatic diversion with duodenal switch.
The procedures are reimbursed only for Medicare beneficiaries who have a BMI of 35 kg/m2 or greater; who have at least one obesity-related comorbidity, such as cardiovascular disease, chronic obstructive pulmonary disease, or type 2 diabetes mellitus; and who have not been successfully treated otherwise.
In order to be covered, the procedures must be performed at facilities certified either by the American College of Surgeons (ACS) as a level I bariatric surgery center or by the American Society for Metabolic and Bariatric Surgery as a bariatric surgery center of excellence (BSCOE).
Open vertical banded gastroplasty, laparoscopic vertical banded gastroplasty, open sleeve gastrectomy, and open adjustable gastric banding are among the bariatric procedures that are not currently covered.
A recent observational study presented at the annual meeting of the American Surgical Association found that at 1 year after surgery, LSG was associated with morbidity and effectiveness rates that fell between those of laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y bypass procedures.
The absolute reduction in BMI at 1 year was smallest in the laparoscopic adjustable gastric banding group at about 6, greatest with open or laparoscopic Roux-en-Y gastric bypass at about 15, and intermediate at close to 12 with LSG.
The study, based on prospective, longitudinal, standardized data from 109 hospitals, was the first to come out of the ACS Bariatric Surgery Center Network accreditation program. Additional years of follow-up are planned, according to Dr. Matthew M. Hutter, an ACS Fellow with Massachusetts General Hospital, Boston.
Dr. Hutter reported no financial conflicts.
CMS will seek public comment until Oct. 30. The agency plans to issue a proposed decision by March 30, 2012, and to make a final decision by June 30.
The Centers for Medicare and Medicaid Services said on Sept. 30 that it is soliciting comments on a proposal to cover laparoscopic sleeve gastrectomy for Medicare patients.
Currently, that procedure is not covered by the federal health program. In its solicitation, the agency said it is asking the public "whether there is adequate evidence, including clinical trials, for evaluating health outcomes of laparoscopic sleeve gastrectomy (LSG) for the indications listed in the current Bariatric Surgery for the Treatment of Morbid Obesity National Coverage Determination."
LSG is a procedure in which the vast majority of the stomach is removed, leaving a tube or sleeve. It may be a first step before a gastric bypass, or it may be the primary procedure. It is an option for patients with a very high body mass index (BMI) who cannot tolerate a bypass procedure. Postoperatively, patients do not experience dumping or malabsorption of nutrients. However, if weight is regained, the decision about what to do next is not easy (World J. Gastroenterol. 2008;14:821-7).
Medicare has covered three bariatric procedures since 2006: open and laparoscopic Roux-en-Y gastric bypass; laparoscopic adjustable gastric banding; and open and laparoscopic biliopancreatic diversion with duodenal switch.
The procedures are reimbursed only for Medicare beneficiaries who have a BMI of 35 kg/m2 or greater; who have at least one obesity-related comorbidity, such as cardiovascular disease, chronic obstructive pulmonary disease, or type 2 diabetes mellitus; and who have not been successfully treated otherwise.
In order to be covered, the procedures must be performed at facilities certified either by the American College of Surgeons (ACS) as a level I bariatric surgery center or by the American Society for Metabolic and Bariatric Surgery as a bariatric surgery center of excellence (BSCOE).
Open vertical banded gastroplasty, laparoscopic vertical banded gastroplasty, open sleeve gastrectomy, and open adjustable gastric banding are among the bariatric procedures that are not currently covered.
A recent observational study presented at the annual meeting of the American Surgical Association found that at 1 year after surgery, LSG was associated with morbidity and effectiveness rates that fell between those of laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y bypass procedures.
The absolute reduction in BMI at 1 year was smallest in the laparoscopic adjustable gastric banding group at about 6, greatest with open or laparoscopic Roux-en-Y gastric bypass at about 15, and intermediate at close to 12 with LSG.
The study, based on prospective, longitudinal, standardized data from 109 hospitals, was the first to come out of the ACS Bariatric Surgery Center Network accreditation program. Additional years of follow-up are planned, according to Dr. Matthew M. Hutter, an ACS Fellow with Massachusetts General Hospital, Boston.
Dr. Hutter reported no financial conflicts.
CMS will seek public comment until Oct. 30. The agency plans to issue a proposed decision by March 30, 2012, and to make a final decision by June 30.
Standard Beats Anesthesia EEG Technique for Preventing Surgery Awareness
A method of administering general anesthesia while monitoring EEG activity to track the patient’s level of consciousness proved to be no better than the standard anesthesia technique at preventing episodes of patient awareness during surgery, according to a study published in the Aug. 18 issue of the New England Journal of Medicine.
"The overall incidence of awareness was lower than anticipated, suggesting that both protocols were likely to have had efficacy, but the finding of fewer cases [with the standard approach than with the EEG method] was contrary to the expected result," said Dr. Michael S. Avidan of the department of anesthesiology at Washington University, St. Louis, and his associates.
"Notwithstanding major advances in our understanding of consciousness and anesthesia, until we clarify fully the mechanisms and measurement of anesthetic-induced unconsciousness and amnesia, some patients are still likely to have this complication," the researchers noted.
Unintended intraoperative awareness (defined as the experience and explicit recall of sensory perceptions during surgery) is estimated to occur in approximately 1% of at-risk patients, and can lead to posttraumatic stress disorder. Approximately 20,000-40,000 U.S. patients each year are estimated to experience such awareness while under general anesthesia.
Some factors that appear to raise the risk of unintended awareness while under general anesthesia are a history of the condition during previous surgery, aortic stenosis, pulmonary hypertension, end-stage lung disease, anticipation of difficult intubation, poor exercise tolerance, impaired cardiac ejection fraction, excess alcohol intake, and the use of benzodiazepines, opiates, or anticonvulsants.
The current standard method for monitoring intraoperative patient awareness doesn’t measure consciousness itself, but instead ensures that "enough" anesthetic is used by tracking the end-tidal anesthetic-agent concentration (ETAC). Maintaining this at 0.7 MAC (minimum alveolar concentration) or higher is thought to decrease the incidence of awareness during surgery.
An alternative method is the bispectral index (BIS), which uses a single EEG signal from a sensor on the patient’s forehead to calculate brain activity and produces a numerical readout on a scale from 0 (indicating the suppression of all brain activity) to 100 (indicating a fully awake state). Maintaining a target range of 40-60 on this scale is thought to both prevent awareness and allow reductions in the dose of anesthetic.
Two previous clinical trials comparing the two techniques have yielded conflicting results.
Dr. Avidan and his colleagues conducted the BAG-RECALL (BIS or Anesthetic Gas to Reduce Explicit Recall) clinical trial to determine whether the BIS method is superior to standard ETAC in at-risk surgical patients.
They randomly assigned 6,041 adults undergoing elective surgery during a 2-year period at three medical centers in the United States and Canada to one or the other technique. In the BIS group, an alarm sounded when the BIS value exceeded 60 or fell below 40. In the ETAC group, an alarm sounded if the ETAC fell below 0.7 or exceeded 1.3 MAC.
In both study groups, a sign was attached to the anesthesia machines reminding clinicians to check these values and consider whether the patient might be aware. In addition, these values were recorded electronically at 1-minute intervals; manual records were kept of anesthesia; and photographs of trends on the monitors were taken and stored digitally.
There were no important differences between the two groups in doses of sedative, hypnotic, opioid, analgesic, or neuromuscular-blocking drugs given, nor in the amount of anesthetic given; the rate of adverse postoperative outcomes including mortality; the median length of stay in intensive care; or the median length of hospital stay.
Patients’ intraoperative awareness was assessed via a questionnaire within 72 hours after surgery and at 30 days after extubation. A total of 49 patients reported some degree of awareness at some time when they were undergoing surgery, Dr. Avidan and his associates said (N. Engl. J. Med. 2011;365:591-600).
All patients who reported that they had memories of the period between "going to sleep" and "waking up" from anesthesia were further evaluated in more detail and were offered referral to a psychologist for counseling.
Contrary to expectations, there were fewer cases of definite intraoperative awareness in the ETAC group (0.07%) than in the BIS group (0.24%). Similarly, there were fewer cases of possible or definite intraoperative awareness in the ETAC group (0.28%) than in the BIS group (0.66%).
Thus, BIS was not superior in preventing intraoperative awareness.
This study was supported by the Foundation for Anesthesia Education and Research, the American Society of Anesthesiologists, the Winnipeg Regional Health Authority, and the departments of anesthesia at the University of Manitoba, Washington University, and the University of Chicago. The researchers reported no financial conflicts of interest.
The findings by Dr. Avidan and colleagues are "disappointing but not surprising," given that the tools available to assess consciousness, memory, and general anesthesia are rudimentary, said Dr. Gregory Crosby.
Today, "brain functioning is judged clinically much as it was 165 years ago, with the use of bodily signs and responses [such as blood pressure, heart rate, and movement] that are, at best, loosely related to higher brain function," he noted.
In this study, despite what could be considered optimal management, 49 patients experienced definite or possible awareness during surgery. "Moreover, 41% of the cases occurred when the ETAC or BIS values were in the target ranges." It thus appears that many such cases are not preventable with any monitoring method now available, Dr. Crosby said.
Dr. Crosby is with the department of anesthesiology and perioperative and pain medicine at Brigham and Women’s Hospital, Boston. He reported no relevant financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Avidan’s report (N. Engl. J. Med. 2011;365:660-1).
The findings by Dr. Avidan and colleagues are "disappointing but not surprising," given that the tools available to assess consciousness, memory, and general anesthesia are rudimentary, said Dr. Gregory Crosby.
Today, "brain functioning is judged clinically much as it was 165 years ago, with the use of bodily signs and responses [such as blood pressure, heart rate, and movement] that are, at best, loosely related to higher brain function," he noted.
In this study, despite what could be considered optimal management, 49 patients experienced definite or possible awareness during surgery. "Moreover, 41% of the cases occurred when the ETAC or BIS values were in the target ranges." It thus appears that many such cases are not preventable with any monitoring method now available, Dr. Crosby said.
Dr. Crosby is with the department of anesthesiology and perioperative and pain medicine at Brigham and Women’s Hospital, Boston. He reported no relevant financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Avidan’s report (N. Engl. J. Med. 2011;365:660-1).
The findings by Dr. Avidan and colleagues are "disappointing but not surprising," given that the tools available to assess consciousness, memory, and general anesthesia are rudimentary, said Dr. Gregory Crosby.
Today, "brain functioning is judged clinically much as it was 165 years ago, with the use of bodily signs and responses [such as blood pressure, heart rate, and movement] that are, at best, loosely related to higher brain function," he noted.
In this study, despite what could be considered optimal management, 49 patients experienced definite or possible awareness during surgery. "Moreover, 41% of the cases occurred when the ETAC or BIS values were in the target ranges." It thus appears that many such cases are not preventable with any monitoring method now available, Dr. Crosby said.
Dr. Crosby is with the department of anesthesiology and perioperative and pain medicine at Brigham and Women’s Hospital, Boston. He reported no relevant financial conflicts of interest. These remarks were taken from his editorial accompanying Dr. Avidan’s report (N. Engl. J. Med. 2011;365:660-1).
A method of administering general anesthesia while monitoring EEG activity to track the patient’s level of consciousness proved to be no better than the standard anesthesia technique at preventing episodes of patient awareness during surgery, according to a study published in the Aug. 18 issue of the New England Journal of Medicine.
"The overall incidence of awareness was lower than anticipated, suggesting that both protocols were likely to have had efficacy, but the finding of fewer cases [with the standard approach than with the EEG method] was contrary to the expected result," said Dr. Michael S. Avidan of the department of anesthesiology at Washington University, St. Louis, and his associates.
"Notwithstanding major advances in our understanding of consciousness and anesthesia, until we clarify fully the mechanisms and measurement of anesthetic-induced unconsciousness and amnesia, some patients are still likely to have this complication," the researchers noted.
Unintended intraoperative awareness (defined as the experience and explicit recall of sensory perceptions during surgery) is estimated to occur in approximately 1% of at-risk patients, and can lead to posttraumatic stress disorder. Approximately 20,000-40,000 U.S. patients each year are estimated to experience such awareness while under general anesthesia.
Some factors that appear to raise the risk of unintended awareness while under general anesthesia are a history of the condition during previous surgery, aortic stenosis, pulmonary hypertension, end-stage lung disease, anticipation of difficult intubation, poor exercise tolerance, impaired cardiac ejection fraction, excess alcohol intake, and the use of benzodiazepines, opiates, or anticonvulsants.
The current standard method for monitoring intraoperative patient awareness doesn’t measure consciousness itself, but instead ensures that "enough" anesthetic is used by tracking the end-tidal anesthetic-agent concentration (ETAC). Maintaining this at 0.7 MAC (minimum alveolar concentration) or higher is thought to decrease the incidence of awareness during surgery.
An alternative method is the bispectral index (BIS), which uses a single EEG signal from a sensor on the patient’s forehead to calculate brain activity and produces a numerical readout on a scale from 0 (indicating the suppression of all brain activity) to 100 (indicating a fully awake state). Maintaining a target range of 40-60 on this scale is thought to both prevent awareness and allow reductions in the dose of anesthetic.
Two previous clinical trials comparing the two techniques have yielded conflicting results.
Dr. Avidan and his colleagues conducted the BAG-RECALL (BIS or Anesthetic Gas to Reduce Explicit Recall) clinical trial to determine whether the BIS method is superior to standard ETAC in at-risk surgical patients.
They randomly assigned 6,041 adults undergoing elective surgery during a 2-year period at three medical centers in the United States and Canada to one or the other technique. In the BIS group, an alarm sounded when the BIS value exceeded 60 or fell below 40. In the ETAC group, an alarm sounded if the ETAC fell below 0.7 or exceeded 1.3 MAC.
In both study groups, a sign was attached to the anesthesia machines reminding clinicians to check these values and consider whether the patient might be aware. In addition, these values were recorded electronically at 1-minute intervals; manual records were kept of anesthesia; and photographs of trends on the monitors were taken and stored digitally.
There were no important differences between the two groups in doses of sedative, hypnotic, opioid, analgesic, or neuromuscular-blocking drugs given, nor in the amount of anesthetic given; the rate of adverse postoperative outcomes including mortality; the median length of stay in intensive care; or the median length of hospital stay.
Patients’ intraoperative awareness was assessed via a questionnaire within 72 hours after surgery and at 30 days after extubation. A total of 49 patients reported some degree of awareness at some time when they were undergoing surgery, Dr. Avidan and his associates said (N. Engl. J. Med. 2011;365:591-600).
All patients who reported that they had memories of the period between "going to sleep" and "waking up" from anesthesia were further evaluated in more detail and were offered referral to a psychologist for counseling.
Contrary to expectations, there were fewer cases of definite intraoperative awareness in the ETAC group (0.07%) than in the BIS group (0.24%). Similarly, there were fewer cases of possible or definite intraoperative awareness in the ETAC group (0.28%) than in the BIS group (0.66%).
Thus, BIS was not superior in preventing intraoperative awareness.
This study was supported by the Foundation for Anesthesia Education and Research, the American Society of Anesthesiologists, the Winnipeg Regional Health Authority, and the departments of anesthesia at the University of Manitoba, Washington University, and the University of Chicago. The researchers reported no financial conflicts of interest.
A method of administering general anesthesia while monitoring EEG activity to track the patient’s level of consciousness proved to be no better than the standard anesthesia technique at preventing episodes of patient awareness during surgery, according to a study published in the Aug. 18 issue of the New England Journal of Medicine.
"The overall incidence of awareness was lower than anticipated, suggesting that both protocols were likely to have had efficacy, but the finding of fewer cases [with the standard approach than with the EEG method] was contrary to the expected result," said Dr. Michael S. Avidan of the department of anesthesiology at Washington University, St. Louis, and his associates.
"Notwithstanding major advances in our understanding of consciousness and anesthesia, until we clarify fully the mechanisms and measurement of anesthetic-induced unconsciousness and amnesia, some patients are still likely to have this complication," the researchers noted.
Unintended intraoperative awareness (defined as the experience and explicit recall of sensory perceptions during surgery) is estimated to occur in approximately 1% of at-risk patients, and can lead to posttraumatic stress disorder. Approximately 20,000-40,000 U.S. patients each year are estimated to experience such awareness while under general anesthesia.
Some factors that appear to raise the risk of unintended awareness while under general anesthesia are a history of the condition during previous surgery, aortic stenosis, pulmonary hypertension, end-stage lung disease, anticipation of difficult intubation, poor exercise tolerance, impaired cardiac ejection fraction, excess alcohol intake, and the use of benzodiazepines, opiates, or anticonvulsants.
The current standard method for monitoring intraoperative patient awareness doesn’t measure consciousness itself, but instead ensures that "enough" anesthetic is used by tracking the end-tidal anesthetic-agent concentration (ETAC). Maintaining this at 0.7 MAC (minimum alveolar concentration) or higher is thought to decrease the incidence of awareness during surgery.
An alternative method is the bispectral index (BIS), which uses a single EEG signal from a sensor on the patient’s forehead to calculate brain activity and produces a numerical readout on a scale from 0 (indicating the suppression of all brain activity) to 100 (indicating a fully awake state). Maintaining a target range of 40-60 on this scale is thought to both prevent awareness and allow reductions in the dose of anesthetic.
Two previous clinical trials comparing the two techniques have yielded conflicting results.
Dr. Avidan and his colleagues conducted the BAG-RECALL (BIS or Anesthetic Gas to Reduce Explicit Recall) clinical trial to determine whether the BIS method is superior to standard ETAC in at-risk surgical patients.
They randomly assigned 6,041 adults undergoing elective surgery during a 2-year period at three medical centers in the United States and Canada to one or the other technique. In the BIS group, an alarm sounded when the BIS value exceeded 60 or fell below 40. In the ETAC group, an alarm sounded if the ETAC fell below 0.7 or exceeded 1.3 MAC.
In both study groups, a sign was attached to the anesthesia machines reminding clinicians to check these values and consider whether the patient might be aware. In addition, these values were recorded electronically at 1-minute intervals; manual records were kept of anesthesia; and photographs of trends on the monitors were taken and stored digitally.
There were no important differences between the two groups in doses of sedative, hypnotic, opioid, analgesic, or neuromuscular-blocking drugs given, nor in the amount of anesthetic given; the rate of adverse postoperative outcomes including mortality; the median length of stay in intensive care; or the median length of hospital stay.
Patients’ intraoperative awareness was assessed via a questionnaire within 72 hours after surgery and at 30 days after extubation. A total of 49 patients reported some degree of awareness at some time when they were undergoing surgery, Dr. Avidan and his associates said (N. Engl. J. Med. 2011;365:591-600).
All patients who reported that they had memories of the period between "going to sleep" and "waking up" from anesthesia were further evaluated in more detail and were offered referral to a psychologist for counseling.
Contrary to expectations, there were fewer cases of definite intraoperative awareness in the ETAC group (0.07%) than in the BIS group (0.24%). Similarly, there were fewer cases of possible or definite intraoperative awareness in the ETAC group (0.28%) than in the BIS group (0.66%).
Thus, BIS was not superior in preventing intraoperative awareness.
This study was supported by the Foundation for Anesthesia Education and Research, the American Society of Anesthesiologists, the Winnipeg Regional Health Authority, and the departments of anesthesia at the University of Manitoba, Washington University, and the University of Chicago. The researchers reported no financial conflicts of interest.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: There were fewer cases of definite intraoperative awareness with the standard anesthesia technique (0.07%) than with the EEG technique (0.24%), and there were fewer cases of possible or definite intraoperative awareness with the standard anesthesia technique (0.28%) than with the EEG technique (0.66%).
Data Source: A randomized, prospective, blinded clinical trial comparing standard anesthesia techniques with an EEG-derived bispectral index method of monitoring consciousness in 6,041 adults during surgery at three medical centers over a 2-year period.
Disclosures: This study was supported by the Foundation for Anesthesia Education and Research, the American Society of Anesthesiologists, the Winnipeg Regional Health Authority, and the departments of anesthesia at the University of Manitoba, Washington University, and the University of Chicago. No financial conflicts of interest were reported.
Data Analysis Favors Laparoscopic Abdominal Wall Hernia Repair
BOCA RATON, FLA. – Laparoscopic repair of anterior abdominal wall hernia was associated with significantly less morbidity, a shorter hospitalization stay, and lower mortality than was open repair in a study of more than 71,000 patients in the American College of Surgeons’ National Surgical Quality Improvement Program database.
"Laparoscopic repair is underutilized," Dr. Rodney J. Mason said, noting that only 17% of the repairs in the study were performed laparoscopically.

The laparoscopic and open-repair patients were quite different in terms of baseline characteristics, so he and his coinvestigators performed two separate analyses of the NSQIP data. The first incorporated the full 71,026 patients; a second matched-pair analysis involved a subgroup comprising 7,060 open-repair patients and 7,069 similar patients with laparoscopic repair, Dr. Mason explained at the annual meeting of the American Surgical Association.
He and his colleagues turned to the NSQIP database because adverse-event rates associated with anterior abdominal wall hernia repair are so low that a definitive, randomized, controlled trial would require more than 100,000 patients in each study arm, according to Dr. Mason of the University of Southern California in Los Angeles.
In the matched-pair analysis, the 30-day overall morbidity rate was significantly lower in the laparoscopic repair group (2.83%) than in the patients undergoing open repair (5.14%). The serious complication rate was also significantly less (0.99% vs. 1.71% with open repair). Pulmonary embolism, sepsis, wound infection, and urinary tract infection were among the serious complications that were significantly less frequent with laparoscopic repair. In contrast, 30-day mortality rates weren’t significantly different (0.08% with laparoscopic and 0.06% with open repair).
However, in the full analysis of 71,026 patients, mortality was significantly lower in the laparoscopic repair group at 0.18%, which was roughly half the 0.33% rate with open repair. Similarly, the laparoscopic repair group’s 1.57% serious complication rate was significantly better than the 2.54% rate with open repair. Overall complication rates were 3.8% for laparoscopic repair vs. 6.02% for open repair.
Overall and serious morbidity rates were significantly lower with laparoscopic repair of nearly all types of abdominal wall hernias, including umbilical, incisional, ventral, incarcerated, strangulated, recurrent, and reducible hernias. In fact, the only setting in which there was no significant difference in complications between the two surgical approaches was in repair of initial primary hernias.
The average length of hospital stay was 2.71 days with laparoscopic repair in the matched-pair comparison – significantly shorter than the 3.36 days with open repair. The margin of difference was larger in the full analysis (3.25 days with laparoscopic vs. 4.43 days for open repair).
The new analysis of NSQIP data is particularly timely in light of a recent Cochrane review that concluded that laparoscopic repair hasn’t been shown to be superior to open repair in terms of complications, Dr. Mason observed (Cochrane Database Syst. Rev. 2011 [doi:10.1002/14651858.CD007781.pub2]).
Discussant Dr. Hobart W. Harris commented that with more than 400,000 incisional and ventral hernia repairs being performed annually, the incidence of this problem rivals that of acute appendicitis. Yet to date, no standardized hernia classification systems or evidence-based treatment guidelines exist.
"This is a common yet inadequately studied condition that adds several billion dollars to our annual health care expenditures," said Dr. Harris, professor of surgery and chief of the division of general surgery at the University of California, San Francisco.
He offered some tough love for Dr. Mason and his coinvestigators: "Enthusiasm must not overshadow the evidence or lack thereof. Due to the limitations of the ACS NSQIP data, my respected colleagues are unable to comment on postoperative pain or recovery time, let alone operating room time or costs, or – perhaps most importantly – the recurrence rates for the two techniques," Dr. Harris pointed out.
Although the NSQIP analysis demonstrated statistically significant differences favoring laparoscopic repair, these differences are arguably too small to be clinically meaningful, in his view.
"In the absence of equivalent or superior long-term recurrence rate data, I fear that the jury is still out. And I am not alone in that view, given that only one in five of these hernias were repaired using laparoscopic techniques," Dr. Harris said.
Dr. John M. Kellum Jr. cautioned Dr. Mason against making sweeping declarations regarding the superiority of laparoscopic repair.
"I have a concern that the message from your study will be that if you don’t do a laparoscopic incisional hernia repair, you’re lacking in testosterone," said Dr. Kellum, professor of surgery at Virginia Commonwealth University, Richmond.
Dr. Kellum said that he likes doing laparoscopic hernia repairs, but if the CT scan of a large hernia shows significant adhesions of intestine to the abdominal wall, an open repair is probably the best way to go.
Dr. Mason declared having no financial conflicts.
BOCA RATON, FLA. – Laparoscopic repair of anterior abdominal wall hernia was associated with significantly less morbidity, a shorter hospitalization stay, and lower mortality than was open repair in a study of more than 71,000 patients in the American College of Surgeons’ National Surgical Quality Improvement Program database.
"Laparoscopic repair is underutilized," Dr. Rodney J. Mason said, noting that only 17% of the repairs in the study were performed laparoscopically.
The laparoscopic and open-repair patients were quite different in terms of baseline characteristics, so he and his coinvestigators performed two separate analyses of the NSQIP data. The first incorporated the full 71,026 patients; a second matched-pair analysis involved a subgroup comprising 7,060 open-repair patients and 7,069 similar patients with laparoscopic repair, Dr. Mason explained at the annual meeting of the American Surgical Association.
He and his colleagues turned to the NSQIP database because adverse-event rates associated with anterior abdominal wall hernia repair are so low that a definitive, randomized, controlled trial would require more than 100,000 patients in each study arm, according to Dr. Mason of the University of Southern California in Los Angeles.
In the matched-pair analysis, the 30-day overall morbidity rate was significantly lower in the laparoscopic repair group (2.83%) than in the patients undergoing open repair (5.14%). The serious complication rate was also significantly less (0.99% vs. 1.71% with open repair). Pulmonary embolism, sepsis, wound infection, and urinary tract infection were among the serious complications that were significantly less frequent with laparoscopic repair. In contrast, 30-day mortality rates weren’t significantly different (0.08% with laparoscopic and 0.06% with open repair).
However, in the full analysis of 71,026 patients, mortality was significantly lower in the laparoscopic repair group at 0.18%, which was roughly half the 0.33% rate with open repair. Similarly, the laparoscopic repair group’s 1.57% serious complication rate was significantly better than the 2.54% rate with open repair. Overall complication rates were 3.8% for laparoscopic repair vs. 6.02% for open repair.
Overall and serious morbidity rates were significantly lower with laparoscopic repair of nearly all types of abdominal wall hernias, including umbilical, incisional, ventral, incarcerated, strangulated, recurrent, and reducible hernias. In fact, the only setting in which there was no significant difference in complications between the two surgical approaches was in repair of initial primary hernias.
The average length of hospital stay was 2.71 days with laparoscopic repair in the matched-pair comparison – significantly shorter than the 3.36 days with open repair. The margin of difference was larger in the full analysis (3.25 days with laparoscopic vs. 4.43 days for open repair).
The new analysis of NSQIP data is particularly timely in light of a recent Cochrane review that concluded that laparoscopic repair hasn’t been shown to be superior to open repair in terms of complications, Dr. Mason observed (Cochrane Database Syst. Rev. 2011 [doi:10.1002/14651858.CD007781.pub2]).
Discussant Dr. Hobart W. Harris commented that with more than 400,000 incisional and ventral hernia repairs being performed annually, the incidence of this problem rivals that of acute appendicitis. Yet to date, no standardized hernia classification systems or evidence-based treatment guidelines exist.
"This is a common yet inadequately studied condition that adds several billion dollars to our annual health care expenditures," said Dr. Harris, professor of surgery and chief of the division of general surgery at the University of California, San Francisco.
He offered some tough love for Dr. Mason and his coinvestigators: "Enthusiasm must not overshadow the evidence or lack thereof. Due to the limitations of the ACS NSQIP data, my respected colleagues are unable to comment on postoperative pain or recovery time, let alone operating room time or costs, or – perhaps most importantly – the recurrence rates for the two techniques," Dr. Harris pointed out.
Although the NSQIP analysis demonstrated statistically significant differences favoring laparoscopic repair, these differences are arguably too small to be clinically meaningful, in his view.
"In the absence of equivalent or superior long-term recurrence rate data, I fear that the jury is still out. And I am not alone in that view, given that only one in five of these hernias were repaired using laparoscopic techniques," Dr. Harris said.
Dr. John M. Kellum Jr. cautioned Dr. Mason against making sweeping declarations regarding the superiority of laparoscopic repair.
"I have a concern that the message from your study will be that if you don’t do a laparoscopic incisional hernia repair, you’re lacking in testosterone," said Dr. Kellum, professor of surgery at Virginia Commonwealth University, Richmond.
Dr. Kellum said that he likes doing laparoscopic hernia repairs, but if the CT scan of a large hernia shows significant adhesions of intestine to the abdominal wall, an open repair is probably the best way to go.
Dr. Mason declared having no financial conflicts.
BOCA RATON, FLA. – Laparoscopic repair of anterior abdominal wall hernia was associated with significantly less morbidity, a shorter hospitalization stay, and lower mortality than was open repair in a study of more than 71,000 patients in the American College of Surgeons’ National Surgical Quality Improvement Program database.
"Laparoscopic repair is underutilized," Dr. Rodney J. Mason said, noting that only 17% of the repairs in the study were performed laparoscopically.
The laparoscopic and open-repair patients were quite different in terms of baseline characteristics, so he and his coinvestigators performed two separate analyses of the NSQIP data. The first incorporated the full 71,026 patients; a second matched-pair analysis involved a subgroup comprising 7,060 open-repair patients and 7,069 similar patients with laparoscopic repair, Dr. Mason explained at the annual meeting of the American Surgical Association.
He and his colleagues turned to the NSQIP database because adverse-event rates associated with anterior abdominal wall hernia repair are so low that a definitive, randomized, controlled trial would require more than 100,000 patients in each study arm, according to Dr. Mason of the University of Southern California in Los Angeles.
In the matched-pair analysis, the 30-day overall morbidity rate was significantly lower in the laparoscopic repair group (2.83%) than in the patients undergoing open repair (5.14%). The serious complication rate was also significantly less (0.99% vs. 1.71% with open repair). Pulmonary embolism, sepsis, wound infection, and urinary tract infection were among the serious complications that were significantly less frequent with laparoscopic repair. In contrast, 30-day mortality rates weren’t significantly different (0.08% with laparoscopic and 0.06% with open repair).
However, in the full analysis of 71,026 patients, mortality was significantly lower in the laparoscopic repair group at 0.18%, which was roughly half the 0.33% rate with open repair. Similarly, the laparoscopic repair group’s 1.57% serious complication rate was significantly better than the 2.54% rate with open repair. Overall complication rates were 3.8% for laparoscopic repair vs. 6.02% for open repair.
Overall and serious morbidity rates were significantly lower with laparoscopic repair of nearly all types of abdominal wall hernias, including umbilical, incisional, ventral, incarcerated, strangulated, recurrent, and reducible hernias. In fact, the only setting in which there was no significant difference in complications between the two surgical approaches was in repair of initial primary hernias.
The average length of hospital stay was 2.71 days with laparoscopic repair in the matched-pair comparison – significantly shorter than the 3.36 days with open repair. The margin of difference was larger in the full analysis (3.25 days with laparoscopic vs. 4.43 days for open repair).
The new analysis of NSQIP data is particularly timely in light of a recent Cochrane review that concluded that laparoscopic repair hasn’t been shown to be superior to open repair in terms of complications, Dr. Mason observed (Cochrane Database Syst. Rev. 2011 [doi:10.1002/14651858.CD007781.pub2]).
Discussant Dr. Hobart W. Harris commented that with more than 400,000 incisional and ventral hernia repairs being performed annually, the incidence of this problem rivals that of acute appendicitis. Yet to date, no standardized hernia classification systems or evidence-based treatment guidelines exist.
"This is a common yet inadequately studied condition that adds several billion dollars to our annual health care expenditures," said Dr. Harris, professor of surgery and chief of the division of general surgery at the University of California, San Francisco.
He offered some tough love for Dr. Mason and his coinvestigators: "Enthusiasm must not overshadow the evidence or lack thereof. Due to the limitations of the ACS NSQIP data, my respected colleagues are unable to comment on postoperative pain or recovery time, let alone operating room time or costs, or – perhaps most importantly – the recurrence rates for the two techniques," Dr. Harris pointed out.
Although the NSQIP analysis demonstrated statistically significant differences favoring laparoscopic repair, these differences are arguably too small to be clinically meaningful, in his view.
"In the absence of equivalent or superior long-term recurrence rate data, I fear that the jury is still out. And I am not alone in that view, given that only one in five of these hernias were repaired using laparoscopic techniques," Dr. Harris said.
Dr. John M. Kellum Jr. cautioned Dr. Mason against making sweeping declarations regarding the superiority of laparoscopic repair.
"I have a concern that the message from your study will be that if you don’t do a laparoscopic incisional hernia repair, you’re lacking in testosterone," said Dr. Kellum, professor of surgery at Virginia Commonwealth University, Richmond.
Dr. Kellum said that he likes doing laparoscopic hernia repairs, but if the CT scan of a large hernia shows significant adhesions of intestine to the abdominal wall, an open repair is probably the best way to go.
Dr. Mason declared having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN SURGICAL ASSOCIATION
Major Finding: The 0.18% mortality rate in the group having laparoscopic abdominal wall hernia repair was roughly half the 0.33% mortality rate in patients undergoing open repair. Complication and morbidity rates were also lower in the laparoscopic group.
Data Source: Database analysis of 71,026 patients.
Disclosures: Dr. Mason declared having no financial conflicts.
NSQIP Found Highly Cost Effective for Participating Hospitals
BOCA RATON, FLA. – Hospitals that embrace the National Surgical Quality Improvement Program can expect to face significant expenses initially, but within a couple of years, the program becomes highly cost effective.
That’s been the experience at Pennsylvania State University’s Milton S. Hershey Medical Center, in Hershey, Pa., where the general and vascular surgery postoperative complication rate has dropped steadily as a consequence of NSQIP participation.
Indeed, by the time NSQIP had been in place for 2 years, the cost of avoiding one postop adverse event through NSQIP participation was roughly $9,000 less than the average cost of actually dealing with such a complication, Dr. Peter W. Dillon said at the annual meeting of the American Surgical Association.
"What it means for our institution is that at the end of year 2, treating the complication cost a lot more than paying NSQIP to avoid the complication. By the time we got to year 2, the program had a potential cost savings to the institution," explained Dr. Dillon, professor and chairman of the department of surgery at Hershey Medical Center.

There’s an important lesson here for surgeons and hospital officials elsewhere around the country. Today, only about 5% of U.S. acute care hospitals are on board with NSQIP. A major barrier to implementation is the program’s hefty direct costs. Those costs averaged more than $138,800 annually during the first 2 years of Hershey Medical Center’s participation, including licensing fees, administrative costs, travel for training, and information technology expertise. But after implementation, reduced surgical/medical errors result in substantial cost savings.
At Hershey, the postop adverse event rate fell from 17.1% at baseline to 13.8% after 1 year and to 12.7% after 2 years.
NSQIP was a challenge at the start. During the first 6 months of NSQIP involvement, the hospital was paying $25,471 per complication avoided. That’s a prohibitive cost, especially considering that it was substantially more than the $16,371 average cost of managing a real postop event.
By 2 years, however, the cost of avoiding one postop adverse event had fallen to $7,319, or $9,072 less than the cost attributed to an actual adverse event.
Discussant Dr. Sean J. Mulvihill commented that the Hershey study is important because the nation faces unsustainable escalation in the cost of medical care, and it’s incumbent on surgeons to find ways to increase the value of their services. Along those lines, compelling evidence exists to show that NSQIP reduces surgical morbidity and improves outcomes.
Dr. Mulvihill said he believes the Hershey group’s calculations are too conservative. The actual savings accrued through NSQIP involvement may be substantially greater.
For example, NSQIP can replace previous less-effective surgical quality improvement efforts. That saves institutional costs. Plus, as hospital administrators and department heads know all too well, the time will soon be at hand when hospitals will be punished financially for certain postop complications that are deemed by payers to be preventable. Hospitals will simply no longer receive payment for such events. Thus, preventing those complications from happening will yield additional financial value, explained Dr. Mulvihill, professor and chair of the department of surgery at the University of Utah, Salt Lake City.
"I predict the Hershey group will find additional added value with further passage of time. Our hospitals at University of Utah have been participating in NSQIP since 2001. It took us several years of maturation of the program before we hit our stride with serious quality improvement efforts coming directly from the program," the surgeon said.
The NSQIP program is a project of the American College of Surgeons. Dr. Dillon declared having no financial conflicts of interest.
BOCA RATON, FLA. – Hospitals that embrace the National Surgical Quality Improvement Program can expect to face significant expenses initially, but within a couple of years, the program becomes highly cost effective.
That’s been the experience at Pennsylvania State University’s Milton S. Hershey Medical Center, in Hershey, Pa., where the general and vascular surgery postoperative complication rate has dropped steadily as a consequence of NSQIP participation.
Indeed, by the time NSQIP had been in place for 2 years, the cost of avoiding one postop adverse event through NSQIP participation was roughly $9,000 less than the average cost of actually dealing with such a complication, Dr. Peter W. Dillon said at the annual meeting of the American Surgical Association.
"What it means for our institution is that at the end of year 2, treating the complication cost a lot more than paying NSQIP to avoid the complication. By the time we got to year 2, the program had a potential cost savings to the institution," explained Dr. Dillon, professor and chairman of the department of surgery at Hershey Medical Center.
There’s an important lesson here for surgeons and hospital officials elsewhere around the country. Today, only about 5% of U.S. acute care hospitals are on board with NSQIP. A major barrier to implementation is the program’s hefty direct costs. Those costs averaged more than $138,800 annually during the first 2 years of Hershey Medical Center’s participation, including licensing fees, administrative costs, travel for training, and information technology expertise. But after implementation, reduced surgical/medical errors result in substantial cost savings.
At Hershey, the postop adverse event rate fell from 17.1% at baseline to 13.8% after 1 year and to 12.7% after 2 years.
NSQIP was a challenge at the start. During the first 6 months of NSQIP involvement, the hospital was paying $25,471 per complication avoided. That’s a prohibitive cost, especially considering that it was substantially more than the $16,371 average cost of managing a real postop event.
By 2 years, however, the cost of avoiding one postop adverse event had fallen to $7,319, or $9,072 less than the cost attributed to an actual adverse event.
Discussant Dr. Sean J. Mulvihill commented that the Hershey study is important because the nation faces unsustainable escalation in the cost of medical care, and it’s incumbent on surgeons to find ways to increase the value of their services. Along those lines, compelling evidence exists to show that NSQIP reduces surgical morbidity and improves outcomes.
Dr. Mulvihill said he believes the Hershey group’s calculations are too conservative. The actual savings accrued through NSQIP involvement may be substantially greater.
For example, NSQIP can replace previous less-effective surgical quality improvement efforts. That saves institutional costs. Plus, as hospital administrators and department heads know all too well, the time will soon be at hand when hospitals will be punished financially for certain postop complications that are deemed by payers to be preventable. Hospitals will simply no longer receive payment for such events. Thus, preventing those complications from happening will yield additional financial value, explained Dr. Mulvihill, professor and chair of the department of surgery at the University of Utah, Salt Lake City.
"I predict the Hershey group will find additional added value with further passage of time. Our hospitals at University of Utah have been participating in NSQIP since 2001. It took us several years of maturation of the program before we hit our stride with serious quality improvement efforts coming directly from the program," the surgeon said.
The NSQIP program is a project of the American College of Surgeons. Dr. Dillon declared having no financial conflicts of interest.
BOCA RATON, FLA. – Hospitals that embrace the National Surgical Quality Improvement Program can expect to face significant expenses initially, but within a couple of years, the program becomes highly cost effective.
That’s been the experience at Pennsylvania State University’s Milton S. Hershey Medical Center, in Hershey, Pa., where the general and vascular surgery postoperative complication rate has dropped steadily as a consequence of NSQIP participation.
Indeed, by the time NSQIP had been in place for 2 years, the cost of avoiding one postop adverse event through NSQIP participation was roughly $9,000 less than the average cost of actually dealing with such a complication, Dr. Peter W. Dillon said at the annual meeting of the American Surgical Association.
"What it means for our institution is that at the end of year 2, treating the complication cost a lot more than paying NSQIP to avoid the complication. By the time we got to year 2, the program had a potential cost savings to the institution," explained Dr. Dillon, professor and chairman of the department of surgery at Hershey Medical Center.
There’s an important lesson here for surgeons and hospital officials elsewhere around the country. Today, only about 5% of U.S. acute care hospitals are on board with NSQIP. A major barrier to implementation is the program’s hefty direct costs. Those costs averaged more than $138,800 annually during the first 2 years of Hershey Medical Center’s participation, including licensing fees, administrative costs, travel for training, and information technology expertise. But after implementation, reduced surgical/medical errors result in substantial cost savings.
At Hershey, the postop adverse event rate fell from 17.1% at baseline to 13.8% after 1 year and to 12.7% after 2 years.
NSQIP was a challenge at the start. During the first 6 months of NSQIP involvement, the hospital was paying $25,471 per complication avoided. That’s a prohibitive cost, especially considering that it was substantially more than the $16,371 average cost of managing a real postop event.
By 2 years, however, the cost of avoiding one postop adverse event had fallen to $7,319, or $9,072 less than the cost attributed to an actual adverse event.
Discussant Dr. Sean J. Mulvihill commented that the Hershey study is important because the nation faces unsustainable escalation in the cost of medical care, and it’s incumbent on surgeons to find ways to increase the value of their services. Along those lines, compelling evidence exists to show that NSQIP reduces surgical morbidity and improves outcomes.
Dr. Mulvihill said he believes the Hershey group’s calculations are too conservative. The actual savings accrued through NSQIP involvement may be substantially greater.
For example, NSQIP can replace previous less-effective surgical quality improvement efforts. That saves institutional costs. Plus, as hospital administrators and department heads know all too well, the time will soon be at hand when hospitals will be punished financially for certain postop complications that are deemed by payers to be preventable. Hospitals will simply no longer receive payment for such events. Thus, preventing those complications from happening will yield additional financial value, explained Dr. Mulvihill, professor and chair of the department of surgery at the University of Utah, Salt Lake City.
"I predict the Hershey group will find additional added value with further passage of time. Our hospitals at University of Utah have been participating in NSQIP since 2001. It took us several years of maturation of the program before we hit our stride with serious quality improvement efforts coming directly from the program," the surgeon said.
The NSQIP program is a project of the American College of Surgeons. Dr. Dillon declared having no financial conflicts of interest.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN SURGICAL ASSOCIATION
Simulator Tops Standard Training for Laparoscopic Hernia Repair
BOCA RATON, FLA. – A novel simulation-based training curriculum in laparoscopic totally extraperitoneal inguinal herniorrhaphy for general surgery residents led to shorter operating times, better trainee performance, and fewer patient complications in a randomized clinical trial.
The training program has two elements: a cognitive component featuring Web-based PowerPoint presentations and videos along with assigned readings, and psychomotor training on a totally extraperitoneal inguinal herniorrhaphy (TEP) simulator, Dr. Benjamin Zendejas said at the annual meeting of the American Surgical Association.

A key feature is that the skills training – with one instructor per resident – is performed until mastery is attained, however long that takes. Only then does the resident start performing TEPs in the operating room under supervision, explained Dr. Zendejas of the Mayo Clinic, Rochester, Minn.
He presented a study in which 50 general surgery residents performed a baseline TEP in the operating room, and then were randomized to the simulation-based training program or standard training.
The simulator was the Limbs & Things Ltd.’s TEP Guildford MATTU Hernia Trainer. Mastery was defined by the average 2 minutes required for five experienced instructors to perform a TEP on the simulator. An average of roughly eight attempts was required for fifth-year residents to achieve mastery on the simulator, compared with 26 for first-year residents.
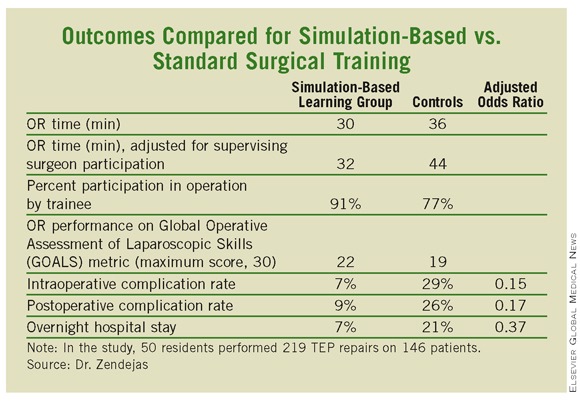
In the operating room, the 50 residents performed 219 TEP repairs on 146 patients. Each repair was evaluated immediately afterward by two independent raters. The simulation-based training group outperformed residents who were trained in the standard fashion in all outcome measures, including the key end point of operative time adjusted for the impact of supervising surgeon takeover for poorly performing trainees. (See box.)
Intraoperative complications, such as peritoneal tears and procedure conversions, occurred in 7% of procedures performed by simulation-trained residents, and in 29% of controls. Urinary retention, seroma, and other postoperative complications resulted from 9% of the simulation-trained residents’ operations, compared with 26% of those performed by residents trained in TEP in standard fashion. In all, 7% of procedures carried out by simulation-trained residents led to an overnight hospital stay, compared with 21% for controls.
"This will become a seminal paper in simulation-based training education," said discussant Dr. Gary L. Dunnington, who called the study "outstanding."
This work suggests that, on an hour-by-hour basis, training in a psychomotor skills laboratory may be more efficient for residents than time spent in the operating room. These data, "if further substantiated, will be of great value with the increasing constraints of decreasing duty hours," noted Dr. Dunnington, professor and chairman of the department of surgery at Southern Illinois University, Springfield.
He was impressed with the investigators’ documentation of improved clinically relevant patient outcomes in the operating room after simulation-based training – the first study to do so. He also liked the investigators’ use of video recordings rather than crude recall to facilitate the study of operative errors.
"This study sets a new bar for simulation researchers," he concluded.
Dr. Zendejas reported having no financial conflicts.
BOCA RATON, FLA. – A novel simulation-based training curriculum in laparoscopic totally extraperitoneal inguinal herniorrhaphy for general surgery residents led to shorter operating times, better trainee performance, and fewer patient complications in a randomized clinical trial.
The training program has two elements: a cognitive component featuring Web-based PowerPoint presentations and videos along with assigned readings, and psychomotor training on a totally extraperitoneal inguinal herniorrhaphy (TEP) simulator, Dr. Benjamin Zendejas said at the annual meeting of the American Surgical Association.
A key feature is that the skills training – with one instructor per resident – is performed until mastery is attained, however long that takes. Only then does the resident start performing TEPs in the operating room under supervision, explained Dr. Zendejas of the Mayo Clinic, Rochester, Minn.
He presented a study in which 50 general surgery residents performed a baseline TEP in the operating room, and then were randomized to the simulation-based training program or standard training.
The simulator was the Limbs & Things Ltd.’s TEP Guildford MATTU Hernia Trainer. Mastery was defined by the average 2 minutes required for five experienced instructors to perform a TEP on the simulator. An average of roughly eight attempts was required for fifth-year residents to achieve mastery on the simulator, compared with 26 for first-year residents.
In the operating room, the 50 residents performed 219 TEP repairs on 146 patients. Each repair was evaluated immediately afterward by two independent raters. The simulation-based training group outperformed residents who were trained in the standard fashion in all outcome measures, including the key end point of operative time adjusted for the impact of supervising surgeon takeover for poorly performing trainees. (See box.)
Intraoperative complications, such as peritoneal tears and procedure conversions, occurred in 7% of procedures performed by simulation-trained residents, and in 29% of controls. Urinary retention, seroma, and other postoperative complications resulted from 9% of the simulation-trained residents’ operations, compared with 26% of those performed by residents trained in TEP in standard fashion. In all, 7% of procedures carried out by simulation-trained residents led to an overnight hospital stay, compared with 21% for controls.
"This will become a seminal paper in simulation-based training education," said discussant Dr. Gary L. Dunnington, who called the study "outstanding."
This work suggests that, on an hour-by-hour basis, training in a psychomotor skills laboratory may be more efficient for residents than time spent in the operating room. These data, "if further substantiated, will be of great value with the increasing constraints of decreasing duty hours," noted Dr. Dunnington, professor and chairman of the department of surgery at Southern Illinois University, Springfield.
He was impressed with the investigators’ documentation of improved clinically relevant patient outcomes in the operating room after simulation-based training – the first study to do so. He also liked the investigators’ use of video recordings rather than crude recall to facilitate the study of operative errors.
"This study sets a new bar for simulation researchers," he concluded.
Dr. Zendejas reported having no financial conflicts.
BOCA RATON, FLA. – A novel simulation-based training curriculum in laparoscopic totally extraperitoneal inguinal herniorrhaphy for general surgery residents led to shorter operating times, better trainee performance, and fewer patient complications in a randomized clinical trial.
The training program has two elements: a cognitive component featuring Web-based PowerPoint presentations and videos along with assigned readings, and psychomotor training on a totally extraperitoneal inguinal herniorrhaphy (TEP) simulator, Dr. Benjamin Zendejas said at the annual meeting of the American Surgical Association.
A key feature is that the skills training – with one instructor per resident – is performed until mastery is attained, however long that takes. Only then does the resident start performing TEPs in the operating room under supervision, explained Dr. Zendejas of the Mayo Clinic, Rochester, Minn.
He presented a study in which 50 general surgery residents performed a baseline TEP in the operating room, and then were randomized to the simulation-based training program or standard training.
The simulator was the Limbs & Things Ltd.’s TEP Guildford MATTU Hernia Trainer. Mastery was defined by the average 2 minutes required for five experienced instructors to perform a TEP on the simulator. An average of roughly eight attempts was required for fifth-year residents to achieve mastery on the simulator, compared with 26 for first-year residents.
In the operating room, the 50 residents performed 219 TEP repairs on 146 patients. Each repair was evaluated immediately afterward by two independent raters. The simulation-based training group outperformed residents who were trained in the standard fashion in all outcome measures, including the key end point of operative time adjusted for the impact of supervising surgeon takeover for poorly performing trainees. (See box.)
Intraoperative complications, such as peritoneal tears and procedure conversions, occurred in 7% of procedures performed by simulation-trained residents, and in 29% of controls. Urinary retention, seroma, and other postoperative complications resulted from 9% of the simulation-trained residents’ operations, compared with 26% of those performed by residents trained in TEP in standard fashion. In all, 7% of procedures carried out by simulation-trained residents led to an overnight hospital stay, compared with 21% for controls.
"This will become a seminal paper in simulation-based training education," said discussant Dr. Gary L. Dunnington, who called the study "outstanding."
This work suggests that, on an hour-by-hour basis, training in a psychomotor skills laboratory may be more efficient for residents than time spent in the operating room. These data, "if further substantiated, will be of great value with the increasing constraints of decreasing duty hours," noted Dr. Dunnington, professor and chairman of the department of surgery at Southern Illinois University, Springfield.
He was impressed with the investigators’ documentation of improved clinically relevant patient outcomes in the operating room after simulation-based training – the first study to do so. He also liked the investigators’ use of video recordings rather than crude recall to facilitate the study of operative errors.
"This study sets a new bar for simulation researchers," he concluded.
Dr. Zendejas reported having no financial conflicts.
FROM THE ANNUAL MEETING OF THE AMERICAN SURGICAL ASSOCIATION
Major Finding: General surgery residents who learned laparoscopic totally extraperitoneal inguinal herniorrhaphy through a novel simulation-based training program significantly outperformed those trained in standard fashion.
Data Source: Randomized trial with 50 residents.
Disclosures: Dr. Zendejas reported having no financial conflicts.
Repair of Uncomplicated Diaphragmatic Hernia Can Avoid Worse Outcomes
PHILADELPHIA – Current clinical practice is to repair symptomatic diaphragmatic hernias to avoid complications such as obstruction or gangrene. However, practice patterns are based largely on limited data from institutional case series, according to Dr. Subroto Paul and his colleagues at Cornell University in New York.
Mortality was significantly higher in patients with uncomplicated hernia who went on to readmission with obstruction or gangrene, Dr. Paul said at the annual meeting of the American Association for Thoracic Surgery, where he presented an analysis of the National Inpatient Sample (NIS) database.
Over a 10-year-period, 193,554 patient admissions were identified for the primary diagnosis of diaphragmatic hernia of any type. An uncomplicated diaphragmatic hernia was the diagnosis in 161,777 (83.6%) admissions. Of these, 38,764 (24.0%) patients underwent an elective repair of their hernia as the principal procedure for their admission.
A diagnosis of diaphragmatic hernia with obstruction or gangrene was the reason for admission in 31,127 (16.1%) and 651 (0.3%) patients, respectively. Mortality was significantly higher in patients who were admitted with obstruction or gangrene (4.5% vs. 27.5%, respectively), compared with patients who were admitted for an elective hernia repair (1%).
Morbidity from pneumonia and sepsis was also significantly higher in patients who were admitted for obstruction or gangrene. Symptomatic admission was associated with more intensive hospitalization, as evidenced by significantly increasing length of stay – 6 days (uncomplicated) vs. 9 days (obstruction) vs. 17.5 days (gangrene) – and the need for mechanical ventilation (3.6% vs. 9.7 vs. 41.3%, respectively).
Based on their mortality data, the authors also performed a lifetime risk analysis that suggested that elective repair is associated with a favorable risk-benefit profile for patients in their 50s, 60s, and perhaps early 70s.
"In this large national database study, the prevalence of diaphragmatic hernia per hospital admission is 1:2,000. Admissions resulting from gangrene or obstruction are not uncommon and are associated with worse outcomes than [is repair] in uncomplicated hernias.
"This analysis suggests the practice of repair of uncomplicated diaphragmatic hernia may avoid the morbidity and mortality associated with either obstruction or gangrene," he concluded.
Dr. Paul reported that he had no relevant disclosures.
PHILADELPHIA – Current clinical practice is to repair symptomatic diaphragmatic hernias to avoid complications such as obstruction or gangrene. However, practice patterns are based largely on limited data from institutional case series, according to Dr. Subroto Paul and his colleagues at Cornell University in New York.
Mortality was significantly higher in patients with uncomplicated hernia who went on to readmission with obstruction or gangrene, Dr. Paul said at the annual meeting of the American Association for Thoracic Surgery, where he presented an analysis of the National Inpatient Sample (NIS) database.
Over a 10-year-period, 193,554 patient admissions were identified for the primary diagnosis of diaphragmatic hernia of any type. An uncomplicated diaphragmatic hernia was the diagnosis in 161,777 (83.6%) admissions. Of these, 38,764 (24.0%) patients underwent an elective repair of their hernia as the principal procedure for their admission.
A diagnosis of diaphragmatic hernia with obstruction or gangrene was the reason for admission in 31,127 (16.1%) and 651 (0.3%) patients, respectively. Mortality was significantly higher in patients who were admitted with obstruction or gangrene (4.5% vs. 27.5%, respectively), compared with patients who were admitted for an elective hernia repair (1%).
Morbidity from pneumonia and sepsis was also significantly higher in patients who were admitted for obstruction or gangrene. Symptomatic admission was associated with more intensive hospitalization, as evidenced by significantly increasing length of stay – 6 days (uncomplicated) vs. 9 days (obstruction) vs. 17.5 days (gangrene) – and the need for mechanical ventilation (3.6% vs. 9.7 vs. 41.3%, respectively).
Based on their mortality data, the authors also performed a lifetime risk analysis that suggested that elective repair is associated with a favorable risk-benefit profile for patients in their 50s, 60s, and perhaps early 70s.
"In this large national database study, the prevalence of diaphragmatic hernia per hospital admission is 1:2,000. Admissions resulting from gangrene or obstruction are not uncommon and are associated with worse outcomes than [is repair] in uncomplicated hernias.
"This analysis suggests the practice of repair of uncomplicated diaphragmatic hernia may avoid the morbidity and mortality associated with either obstruction or gangrene," he concluded.
Dr. Paul reported that he had no relevant disclosures.
PHILADELPHIA – Current clinical practice is to repair symptomatic diaphragmatic hernias to avoid complications such as obstruction or gangrene. However, practice patterns are based largely on limited data from institutional case series, according to Dr. Subroto Paul and his colleagues at Cornell University in New York.
Mortality was significantly higher in patients with uncomplicated hernia who went on to readmission with obstruction or gangrene, Dr. Paul said at the annual meeting of the American Association for Thoracic Surgery, where he presented an analysis of the National Inpatient Sample (NIS) database.
Over a 10-year-period, 193,554 patient admissions were identified for the primary diagnosis of diaphragmatic hernia of any type. An uncomplicated diaphragmatic hernia was the diagnosis in 161,777 (83.6%) admissions. Of these, 38,764 (24.0%) patients underwent an elective repair of their hernia as the principal procedure for their admission.
A diagnosis of diaphragmatic hernia with obstruction or gangrene was the reason for admission in 31,127 (16.1%) and 651 (0.3%) patients, respectively. Mortality was significantly higher in patients who were admitted with obstruction or gangrene (4.5% vs. 27.5%, respectively), compared with patients who were admitted for an elective hernia repair (1%).
Morbidity from pneumonia and sepsis was also significantly higher in patients who were admitted for obstruction or gangrene. Symptomatic admission was associated with more intensive hospitalization, as evidenced by significantly increasing length of stay – 6 days (uncomplicated) vs. 9 days (obstruction) vs. 17.5 days (gangrene) – and the need for mechanical ventilation (3.6% vs. 9.7 vs. 41.3%, respectively).
Based on their mortality data, the authors also performed a lifetime risk analysis that suggested that elective repair is associated with a favorable risk-benefit profile for patients in their 50s, 60s, and perhaps early 70s.
"In this large national database study, the prevalence of diaphragmatic hernia per hospital admission is 1:2,000. Admissions resulting from gangrene or obstruction are not uncommon and are associated with worse outcomes than [is repair] in uncomplicated hernias.
"This analysis suggests the practice of repair of uncomplicated diaphragmatic hernia may avoid the morbidity and mortality associated with either obstruction or gangrene," he concluded.
Dr. Paul reported that he had no relevant disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR THORACIC SURGERY
Major Finding: Compared with patients who were admitted for an elective repair of uncomplicated diaphragmatic hernia, mortality was significantly higher in patients who were admitted with obstruction or gangrene (1% vs. 4.5% vs. 27.5%, respectively).
Data Source: A National Inpatient Sample database analysis of 161,777 patients who were diagnosed with diaphragmatic hernia.
Disclosures: Dr. Paul reported that he had no relevant disclosures.