User login
Humira Pen topped per-person drug spending in 2016
Humira Pen (adalimumab) was the most expensive drug in 2016 when ranked by spending per person, according to pharmacy benefits manager Express Scripts.
Total spending per person with employer-sponsored insurance was $45.11 last year for Humira Pen, which is indicated for rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, and plaque psoriasis. Next in spending per person was Enbrel (etanercept) – another drug for arthritis, psoriatic arthritis, ankylosing spondylitis, and psoriasis – at $26.82, followed by the diabetes drug Lantus (insulin glargine) and two multiple sclerosis drugs: Tecfidera (dimethyl fumarate) and Copaxone (glatiramer), Express Scripts said in its “2016 Drug Trend Report.”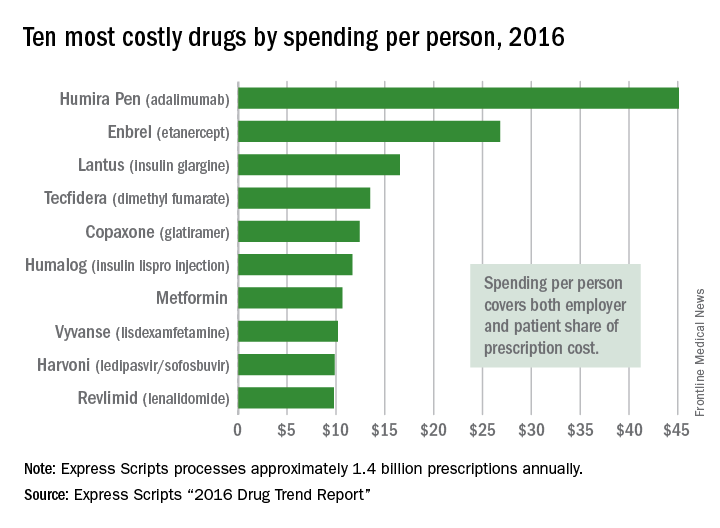
Humira Pen had the next-largest increase from 2015 – a mere 28% – while the hepatitis C drug Harvoni (ledipasvir/sofisbuvir) had the largest decrease in per-person spending among the top 10, dropping 54%, the report noted.
Express Scripts processes approximately 1.4 billion prescriptions annually for 85 million insured members from 3,000 client companies.
Humira Pen (adalimumab) was the most expensive drug in 2016 when ranked by spending per person, according to pharmacy benefits manager Express Scripts.
Total spending per person with employer-sponsored insurance was $45.11 last year for Humira Pen, which is indicated for rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, and plaque psoriasis. Next in spending per person was Enbrel (etanercept) – another drug for arthritis, psoriatic arthritis, ankylosing spondylitis, and psoriasis – at $26.82, followed by the diabetes drug Lantus (insulin glargine) and two multiple sclerosis drugs: Tecfidera (dimethyl fumarate) and Copaxone (glatiramer), Express Scripts said in its “2016 Drug Trend Report.”
Humira Pen had the next-largest increase from 2015 – a mere 28% – while the hepatitis C drug Harvoni (ledipasvir/sofisbuvir) had the largest decrease in per-person spending among the top 10, dropping 54%, the report noted.
Express Scripts processes approximately 1.4 billion prescriptions annually for 85 million insured members from 3,000 client companies.
Humira Pen (adalimumab) was the most expensive drug in 2016 when ranked by spending per person, according to pharmacy benefits manager Express Scripts.
Total spending per person with employer-sponsored insurance was $45.11 last year for Humira Pen, which is indicated for rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, Crohn’s disease, ulcerative colitis, and plaque psoriasis. Next in spending per person was Enbrel (etanercept) – another drug for arthritis, psoriatic arthritis, ankylosing spondylitis, and psoriasis – at $26.82, followed by the diabetes drug Lantus (insulin glargine) and two multiple sclerosis drugs: Tecfidera (dimethyl fumarate) and Copaxone (glatiramer), Express Scripts said in its “2016 Drug Trend Report.”
Humira Pen had the next-largest increase from 2015 – a mere 28% – while the hepatitis C drug Harvoni (ledipasvir/sofisbuvir) had the largest decrease in per-person spending among the top 10, dropping 54%, the report noted.
Express Scripts processes approximately 1.4 billion prescriptions annually for 85 million insured members from 3,000 client companies.
Ocrelizumab Reduces Disease Progression in MS
Ocrelizumab is associated with lower rates of disease activity and progression in patients with relapsing-remitting multiple sclerosis (MS), compared with interferon beta-1a, according to research published in the New England Journal of Medicine. A separate study published in the same journal indicates that ocrelizumab is associated with lower rates of clinical and MRI progression in patients with primary progressive MS, compared with placebo. Ocrelizumab selectively depletes CD20+ B cells, and both studies provide evidence that B cells contribute to the pathogenesis of MS.
“This is the first drug to show a significant effect in slowing disability progression in a phase III trial in primary progressive MS, and therefore the trial represents a landmark study in the field,” said Peter A. Calabresi, MD, Professor of Neurology at Johns Hopkins University School of Medicine in Baltimore, in an accompanying editorial. The articles and editorial were published online ahead of print December 21, 2016.
Ocrelizumab in Relapsing-Remitting MS
Stephen L. Hauser, MD, Chair of Neurology at the University of California, San Francisco School of Medicine, and colleagues conducted OPERA I and OPERA II, two phase III studies to investigate the safety and efficacy of ocrelizumab, compared with interferon beta-1a, in patients with relapsing-remitting MS. The trials had identical protocols, but were conducted at separate trial sites. Eligible participants were between ages 18 and 55, had an Expanded Disability Status Scale (EDSS) score no greater than 5.5 at screening, a history of relapses, and MRI abnormalities consistent with MS. Patients who previously had received a B-cell-targeted therapy or other immunosuppressive medication were excluded.
A total of 821 patients in OPERA I and 835 patients in OPERA II were randomized to 600 mg of IV ocrelizumab every 24 weeks or to 44 µg of subcutaneous interferon beta-1a three times weekly. The treatment period was 96 weeks. Each trial site had separate treating and examining investigators, all of whom were unaware of participants’ treatment assignments. The primary end point was the annualized relapse rate by 96 weeks. Secondary end points included the proportion of patients with disability progression confirmed at 12 weeks, the mean number of gadolinium-enhancing lesions identified on T1-weighted MRI, and the proportion of patients with disability improvement confirmed at 12 weeks.
The annualized relapse rate at 96 weeks in OPERA I was 0.16 in the ocrelizumab group, compared with 0.29 in the interferon beta-1a group. In OPERA II, the annualized relapse rate was 0.16 in the ocrelizumab group, compared with 0.29 in the interferon beta-1a group. These data suggest a 46% lower annualized relapse rate with ocrelizumab in OPERA I and a 47% lower rate with ocrelizumab in OPERA II.
The mean numbers of gadolinium-enhancing lesions in OPERA I were 0.02 with ocrelizumab versus 0.29 with interferon beta-1a. The numbers in OPERA II were 0.02 with ocrelizumab versus 0.42 with interferon beta-1a. The mean numbers of new or newly enlarged T2 hyperintense lesions in OPERA I were 0.32 with ocrelizumab and 1.41 with interferon beta-1a (ie, 77% fewer lesions with ocrelizumab). The values in OPERA II were 0.33 with ocrelizumab versus 1.90 with interferon beta-1a.
In a pooled analysis, 9.1% of patients in the ocrelizumab group had disability progression confirmed at 12 weeks, compared with 13.6% of patients in the interferon beta-1a group. The percentage of patients with disability improvement confirmed at 12 weeks was 20.7% in the ocrelizumab group, compared with 15.6% in the interferon beta-1a group (ie, a 33% higher rate of improvement with ocrelizumab). The effect of ocrelizumab on the rate of confirmed disability improvement was significant in OPERA I, but nonsignificant in OPERA II.
“Additional and extended studies will be required to determine whether the outcomes observed in these 96-week trials, including a near-complete cessation of new plaque formation, as assessed by MRI of the brain, translate into enhanced protection against accrual of disability over the long term,” said Dr. Hauser.
Ocrelizumab in Progressive MS
To examine the safety and efficacy of ocrelizumab in primary progressive MS, Xavier Montalban, MD, PhD, Chair of the Department of Neurology-Neuroimmunology and Director of the MS Centre of Catalonia at the Vall d’Hebron University Hospital in Barcelona, and colleagues conducted the phase III ORATORIO trial. Eligible patients were between ages 18 and 55 and had an EDSS score between 3.0 and 6.5 at screening. Patients with a history of relapsing-remitting MS, secondary progressive MS, or progressive relapsing MS were excluded, as were patients who had had previous treatment with B-cell-targeted therapies and other immunosuppressive medications.

Patients were randomized in a 2:1 ratio to receive 600 mg of IV ocrelizumab or matching placebo every 24 weeks. Double-blinded treatment was administered for at least 120 weeks. As in the OPERA trials, each trial site had separate treating and examining investigators. Patients who completed the blinded treatment phase were eligible to enter an open-label extension phase.
The primary end point was the percentage of patients with disability progression confirmed at 12 weeks in a time-to-event analysis. Secondary end points included the percentage of patients with disability progression confirmed at 24 weeks, change in performance on the timed 25-foot walk from baseline to week 120, change in the total volume of brain lesions on T2-weighted MRI from baseline to week 120, change in brain volume from week 24 to week 120, and change in the Physical Component Summary score of the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36), version 2, from baseline to week 120.
In all, 488 patients received ocrelizumab, and 244 received placebo. A total of 402 patients in the ocrelizumab arm and 174 controls completed the 120-week treatment period. The percentage of patients with 12-week confirmed disability progression was 32.9% with ocrelizumab versus 39.3% with placebo. The data suggest a 24% reduction in the risk of this outcome with ocrelizumab.
The percentage of patients with 24-week confirmed disability progression was 29.6% with ocrelizumab and 35.7% with placebo (ie, a relative risk reduction of 25% with ocrelizumab). The mean change from baseline to week 120 in performance on the timed 25-foot walk was 38.9% with ocrelizumab versus 55.1% with placebo (ie, a relative reduction of 29.3% with ocrelizumab). The researchers found no significant between-group difference in the change in the SF-36 Physical Component Summary score from baseline to week 120.
In addition, the total volume of hyperintense lesions on T2-weighted images from baseline to week 120 decreased with ocrelizumab and increased with placebo (mean percent change, −3.4% vs 7.4%). The adjusted mean percent change in brain volume from week 24 to week 120 was lower with ocrelizumab than with placebo (–0.90% vs –1.09%).
Infusion-related reactions were more common in the ocrelizumab group than among controls. Neoplasms were reported in 11 of 486 patients (2.3%) in the ocrelizumab group and in two of 239 patients (0.8%) in the placebo group. “Safety will continue to be assessed throughout the open-label extension phase,” said Dr. Montalban.
Unknown Mechanism of Action
The mechanism by which B-cell depletion slows disability progression is not fully understood. It “may be multifunctional, because B cells have important roles in antibody secretion, antigen presentation, and the release of effector cytokines,” said Dr. Calabresi. By virtue of their number, B cells may be more important than other antigen-presenting cells in MS.
One potential reason that ocrelizumab showed positive effects in ORATORIO is that the patient population was relatively young (mean age, 45) and had active MRI scans (more than 25% of the population had gadolinium-enhancing lesions). These factors enabled the demonstration of a measurable anti-inflammatory effect of ocrelizumab in patients with inflammation at an early, reversible stage of the disease. “Another possible explanation is that B cells may mediate pathologic processes by secretion of cytokines or by deposition of immunoglobulins after they enter the CNS,” said Dr. Calabresi. “B cells and plasma cells secrete antibodies that may target CNS antigens such as myelin, neurons, and glia, which could accelerate neurodegeneration or inhibit myelin repair. The continued separation of disability progression curves in the ORATORIO trial beyond 52 weeks, when anti-inflammatory effects have been maximized, and success in the relatively noninflammatory disorder of primary progressive MS suggest that additional mechanisms of action may be operational, and further study is warranted.”
Because ocrelizumab appears to entail a higher risk of herpes reactivation and of neoplasms, “clinicians are urged to carefully consider which patients might benefit the most from ocrelizumab and to stay vigilant with regard to monitoring for side effects that could be managed effectively if detected early,” Dr. Calabresi concluded.
—Erik Greb
Suggested Reading
Hauser SL, Bar-Or A, Comi G, et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Montalban X, Hauser SL, Kappos L, et al. Ocrelizumab versus placebo in primary progressive multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Calabresi PA. B-cell depletion - a frontier in monoclonal antibodies for multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Ocrelizumab is associated with lower rates of disease activity and progression in patients with relapsing-remitting multiple sclerosis (MS), compared with interferon beta-1a, according to research published in the New England Journal of Medicine. A separate study published in the same journal indicates that ocrelizumab is associated with lower rates of clinical and MRI progression in patients with primary progressive MS, compared with placebo. Ocrelizumab selectively depletes CD20+ B cells, and both studies provide evidence that B cells contribute to the pathogenesis of MS.
“This is the first drug to show a significant effect in slowing disability progression in a phase III trial in primary progressive MS, and therefore the trial represents a landmark study in the field,” said Peter A. Calabresi, MD, Professor of Neurology at Johns Hopkins University School of Medicine in Baltimore, in an accompanying editorial. The articles and editorial were published online ahead of print December 21, 2016.
Ocrelizumab in Relapsing-Remitting MS
Stephen L. Hauser, MD, Chair of Neurology at the University of California, San Francisco School of Medicine, and colleagues conducted OPERA I and OPERA II, two phase III studies to investigate the safety and efficacy of ocrelizumab, compared with interferon beta-1a, in patients with relapsing-remitting MS. The trials had identical protocols, but were conducted at separate trial sites. Eligible participants were between ages 18 and 55, had an Expanded Disability Status Scale (EDSS) score no greater than 5.5 at screening, a history of relapses, and MRI abnormalities consistent with MS. Patients who previously had received a B-cell-targeted therapy or other immunosuppressive medication were excluded.
A total of 821 patients in OPERA I and 835 patients in OPERA II were randomized to 600 mg of IV ocrelizumab every 24 weeks or to 44 µg of subcutaneous interferon beta-1a three times weekly. The treatment period was 96 weeks. Each trial site had separate treating and examining investigators, all of whom were unaware of participants’ treatment assignments. The primary end point was the annualized relapse rate by 96 weeks. Secondary end points included the proportion of patients with disability progression confirmed at 12 weeks, the mean number of gadolinium-enhancing lesions identified on T1-weighted MRI, and the proportion of patients with disability improvement confirmed at 12 weeks.
The annualized relapse rate at 96 weeks in OPERA I was 0.16 in the ocrelizumab group, compared with 0.29 in the interferon beta-1a group. In OPERA II, the annualized relapse rate was 0.16 in the ocrelizumab group, compared with 0.29 in the interferon beta-1a group. These data suggest a 46% lower annualized relapse rate with ocrelizumab in OPERA I and a 47% lower rate with ocrelizumab in OPERA II.
The mean numbers of gadolinium-enhancing lesions in OPERA I were 0.02 with ocrelizumab versus 0.29 with interferon beta-1a. The numbers in OPERA II were 0.02 with ocrelizumab versus 0.42 with interferon beta-1a. The mean numbers of new or newly enlarged T2 hyperintense lesions in OPERA I were 0.32 with ocrelizumab and 1.41 with interferon beta-1a (ie, 77% fewer lesions with ocrelizumab). The values in OPERA II were 0.33 with ocrelizumab versus 1.90 with interferon beta-1a.
In a pooled analysis, 9.1% of patients in the ocrelizumab group had disability progression confirmed at 12 weeks, compared with 13.6% of patients in the interferon beta-1a group. The percentage of patients with disability improvement confirmed at 12 weeks was 20.7% in the ocrelizumab group, compared with 15.6% in the interferon beta-1a group (ie, a 33% higher rate of improvement with ocrelizumab). The effect of ocrelizumab on the rate of confirmed disability improvement was significant in OPERA I, but nonsignificant in OPERA II.
“Additional and extended studies will be required to determine whether the outcomes observed in these 96-week trials, including a near-complete cessation of new plaque formation, as assessed by MRI of the brain, translate into enhanced protection against accrual of disability over the long term,” said Dr. Hauser.
Ocrelizumab in Progressive MS
To examine the safety and efficacy of ocrelizumab in primary progressive MS, Xavier Montalban, MD, PhD, Chair of the Department of Neurology-Neuroimmunology and Director of the MS Centre of Catalonia at the Vall d’Hebron University Hospital in Barcelona, and colleagues conducted the phase III ORATORIO trial. Eligible patients were between ages 18 and 55 and had an EDSS score between 3.0 and 6.5 at screening. Patients with a history of relapsing-remitting MS, secondary progressive MS, or progressive relapsing MS were excluded, as were patients who had had previous treatment with B-cell-targeted therapies and other immunosuppressive medications.
Patients were randomized in a 2:1 ratio to receive 600 mg of IV ocrelizumab or matching placebo every 24 weeks. Double-blinded treatment was administered for at least 120 weeks. As in the OPERA trials, each trial site had separate treating and examining investigators. Patients who completed the blinded treatment phase were eligible to enter an open-label extension phase.
The primary end point was the percentage of patients with disability progression confirmed at 12 weeks in a time-to-event analysis. Secondary end points included the percentage of patients with disability progression confirmed at 24 weeks, change in performance on the timed 25-foot walk from baseline to week 120, change in the total volume of brain lesions on T2-weighted MRI from baseline to week 120, change in brain volume from week 24 to week 120, and change in the Physical Component Summary score of the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36), version 2, from baseline to week 120.
In all, 488 patients received ocrelizumab, and 244 received placebo. A total of 402 patients in the ocrelizumab arm and 174 controls completed the 120-week treatment period. The percentage of patients with 12-week confirmed disability progression was 32.9% with ocrelizumab versus 39.3% with placebo. The data suggest a 24% reduction in the risk of this outcome with ocrelizumab.
The percentage of patients with 24-week confirmed disability progression was 29.6% with ocrelizumab and 35.7% with placebo (ie, a relative risk reduction of 25% with ocrelizumab). The mean change from baseline to week 120 in performance on the timed 25-foot walk was 38.9% with ocrelizumab versus 55.1% with placebo (ie, a relative reduction of 29.3% with ocrelizumab). The researchers found no significant between-group difference in the change in the SF-36 Physical Component Summary score from baseline to week 120.
In addition, the total volume of hyperintense lesions on T2-weighted images from baseline to week 120 decreased with ocrelizumab and increased with placebo (mean percent change, −3.4% vs 7.4%). The adjusted mean percent change in brain volume from week 24 to week 120 was lower with ocrelizumab than with placebo (–0.90% vs –1.09%).
Infusion-related reactions were more common in the ocrelizumab group than among controls. Neoplasms were reported in 11 of 486 patients (2.3%) in the ocrelizumab group and in two of 239 patients (0.8%) in the placebo group. “Safety will continue to be assessed throughout the open-label extension phase,” said Dr. Montalban.
Unknown Mechanism of Action
The mechanism by which B-cell depletion slows disability progression is not fully understood. It “may be multifunctional, because B cells have important roles in antibody secretion, antigen presentation, and the release of effector cytokines,” said Dr. Calabresi. By virtue of their number, B cells may be more important than other antigen-presenting cells in MS.
One potential reason that ocrelizumab showed positive effects in ORATORIO is that the patient population was relatively young (mean age, 45) and had active MRI scans (more than 25% of the population had gadolinium-enhancing lesions). These factors enabled the demonstration of a measurable anti-inflammatory effect of ocrelizumab in patients with inflammation at an early, reversible stage of the disease. “Another possible explanation is that B cells may mediate pathologic processes by secretion of cytokines or by deposition of immunoglobulins after they enter the CNS,” said Dr. Calabresi. “B cells and plasma cells secrete antibodies that may target CNS antigens such as myelin, neurons, and glia, which could accelerate neurodegeneration or inhibit myelin repair. The continued separation of disability progression curves in the ORATORIO trial beyond 52 weeks, when anti-inflammatory effects have been maximized, and success in the relatively noninflammatory disorder of primary progressive MS suggest that additional mechanisms of action may be operational, and further study is warranted.”
Because ocrelizumab appears to entail a higher risk of herpes reactivation and of neoplasms, “clinicians are urged to carefully consider which patients might benefit the most from ocrelizumab and to stay vigilant with regard to monitoring for side effects that could be managed effectively if detected early,” Dr. Calabresi concluded.
—Erik Greb
Suggested Reading
Hauser SL, Bar-Or A, Comi G, et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Montalban X, Hauser SL, Kappos L, et al. Ocrelizumab versus placebo in primary progressive multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Calabresi PA. B-cell depletion - a frontier in monoclonal antibodies for multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Ocrelizumab is associated with lower rates of disease activity and progression in patients with relapsing-remitting multiple sclerosis (MS), compared with interferon beta-1a, according to research published in the New England Journal of Medicine. A separate study published in the same journal indicates that ocrelizumab is associated with lower rates of clinical and MRI progression in patients with primary progressive MS, compared with placebo. Ocrelizumab selectively depletes CD20+ B cells, and both studies provide evidence that B cells contribute to the pathogenesis of MS.
“This is the first drug to show a significant effect in slowing disability progression in a phase III trial in primary progressive MS, and therefore the trial represents a landmark study in the field,” said Peter A. Calabresi, MD, Professor of Neurology at Johns Hopkins University School of Medicine in Baltimore, in an accompanying editorial. The articles and editorial were published online ahead of print December 21, 2016.
Ocrelizumab in Relapsing-Remitting MS
Stephen L. Hauser, MD, Chair of Neurology at the University of California, San Francisco School of Medicine, and colleagues conducted OPERA I and OPERA II, two phase III studies to investigate the safety and efficacy of ocrelizumab, compared with interferon beta-1a, in patients with relapsing-remitting MS. The trials had identical protocols, but were conducted at separate trial sites. Eligible participants were between ages 18 and 55, had an Expanded Disability Status Scale (EDSS) score no greater than 5.5 at screening, a history of relapses, and MRI abnormalities consistent with MS. Patients who previously had received a B-cell-targeted therapy or other immunosuppressive medication were excluded.
A total of 821 patients in OPERA I and 835 patients in OPERA II were randomized to 600 mg of IV ocrelizumab every 24 weeks or to 44 µg of subcutaneous interferon beta-1a three times weekly. The treatment period was 96 weeks. Each trial site had separate treating and examining investigators, all of whom were unaware of participants’ treatment assignments. The primary end point was the annualized relapse rate by 96 weeks. Secondary end points included the proportion of patients with disability progression confirmed at 12 weeks, the mean number of gadolinium-enhancing lesions identified on T1-weighted MRI, and the proportion of patients with disability improvement confirmed at 12 weeks.
The annualized relapse rate at 96 weeks in OPERA I was 0.16 in the ocrelizumab group, compared with 0.29 in the interferon beta-1a group. In OPERA II, the annualized relapse rate was 0.16 in the ocrelizumab group, compared with 0.29 in the interferon beta-1a group. These data suggest a 46% lower annualized relapse rate with ocrelizumab in OPERA I and a 47% lower rate with ocrelizumab in OPERA II.
The mean numbers of gadolinium-enhancing lesions in OPERA I were 0.02 with ocrelizumab versus 0.29 with interferon beta-1a. The numbers in OPERA II were 0.02 with ocrelizumab versus 0.42 with interferon beta-1a. The mean numbers of new or newly enlarged T2 hyperintense lesions in OPERA I were 0.32 with ocrelizumab and 1.41 with interferon beta-1a (ie, 77% fewer lesions with ocrelizumab). The values in OPERA II were 0.33 with ocrelizumab versus 1.90 with interferon beta-1a.
In a pooled analysis, 9.1% of patients in the ocrelizumab group had disability progression confirmed at 12 weeks, compared with 13.6% of patients in the interferon beta-1a group. The percentage of patients with disability improvement confirmed at 12 weeks was 20.7% in the ocrelizumab group, compared with 15.6% in the interferon beta-1a group (ie, a 33% higher rate of improvement with ocrelizumab). The effect of ocrelizumab on the rate of confirmed disability improvement was significant in OPERA I, but nonsignificant in OPERA II.
“Additional and extended studies will be required to determine whether the outcomes observed in these 96-week trials, including a near-complete cessation of new plaque formation, as assessed by MRI of the brain, translate into enhanced protection against accrual of disability over the long term,” said Dr. Hauser.
Ocrelizumab in Progressive MS
To examine the safety and efficacy of ocrelizumab in primary progressive MS, Xavier Montalban, MD, PhD, Chair of the Department of Neurology-Neuroimmunology and Director of the MS Centre of Catalonia at the Vall d’Hebron University Hospital in Barcelona, and colleagues conducted the phase III ORATORIO trial. Eligible patients were between ages 18 and 55 and had an EDSS score between 3.0 and 6.5 at screening. Patients with a history of relapsing-remitting MS, secondary progressive MS, or progressive relapsing MS were excluded, as were patients who had had previous treatment with B-cell-targeted therapies and other immunosuppressive medications.
Patients were randomized in a 2:1 ratio to receive 600 mg of IV ocrelizumab or matching placebo every 24 weeks. Double-blinded treatment was administered for at least 120 weeks. As in the OPERA trials, each trial site had separate treating and examining investigators. Patients who completed the blinded treatment phase were eligible to enter an open-label extension phase.
The primary end point was the percentage of patients with disability progression confirmed at 12 weeks in a time-to-event analysis. Secondary end points included the percentage of patients with disability progression confirmed at 24 weeks, change in performance on the timed 25-foot walk from baseline to week 120, change in the total volume of brain lesions on T2-weighted MRI from baseline to week 120, change in brain volume from week 24 to week 120, and change in the Physical Component Summary score of the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36), version 2, from baseline to week 120.
In all, 488 patients received ocrelizumab, and 244 received placebo. A total of 402 patients in the ocrelizumab arm and 174 controls completed the 120-week treatment period. The percentage of patients with 12-week confirmed disability progression was 32.9% with ocrelizumab versus 39.3% with placebo. The data suggest a 24% reduction in the risk of this outcome with ocrelizumab.
The percentage of patients with 24-week confirmed disability progression was 29.6% with ocrelizumab and 35.7% with placebo (ie, a relative risk reduction of 25% with ocrelizumab). The mean change from baseline to week 120 in performance on the timed 25-foot walk was 38.9% with ocrelizumab versus 55.1% with placebo (ie, a relative reduction of 29.3% with ocrelizumab). The researchers found no significant between-group difference in the change in the SF-36 Physical Component Summary score from baseline to week 120.
In addition, the total volume of hyperintense lesions on T2-weighted images from baseline to week 120 decreased with ocrelizumab and increased with placebo (mean percent change, −3.4% vs 7.4%). The adjusted mean percent change in brain volume from week 24 to week 120 was lower with ocrelizumab than with placebo (–0.90% vs –1.09%).
Infusion-related reactions were more common in the ocrelizumab group than among controls. Neoplasms were reported in 11 of 486 patients (2.3%) in the ocrelizumab group and in two of 239 patients (0.8%) in the placebo group. “Safety will continue to be assessed throughout the open-label extension phase,” said Dr. Montalban.
Unknown Mechanism of Action
The mechanism by which B-cell depletion slows disability progression is not fully understood. It “may be multifunctional, because B cells have important roles in antibody secretion, antigen presentation, and the release of effector cytokines,” said Dr. Calabresi. By virtue of their number, B cells may be more important than other antigen-presenting cells in MS.
One potential reason that ocrelizumab showed positive effects in ORATORIO is that the patient population was relatively young (mean age, 45) and had active MRI scans (more than 25% of the population had gadolinium-enhancing lesions). These factors enabled the demonstration of a measurable anti-inflammatory effect of ocrelizumab in patients with inflammation at an early, reversible stage of the disease. “Another possible explanation is that B cells may mediate pathologic processes by secretion of cytokines or by deposition of immunoglobulins after they enter the CNS,” said Dr. Calabresi. “B cells and plasma cells secrete antibodies that may target CNS antigens such as myelin, neurons, and glia, which could accelerate neurodegeneration or inhibit myelin repair. The continued separation of disability progression curves in the ORATORIO trial beyond 52 weeks, when anti-inflammatory effects have been maximized, and success in the relatively noninflammatory disorder of primary progressive MS suggest that additional mechanisms of action may be operational, and further study is warranted.”
Because ocrelizumab appears to entail a higher risk of herpes reactivation and of neoplasms, “clinicians are urged to carefully consider which patients might benefit the most from ocrelizumab and to stay vigilant with regard to monitoring for side effects that could be managed effectively if detected early,” Dr. Calabresi concluded.
—Erik Greb
Suggested Reading
Hauser SL, Bar-Or A, Comi G, et al. Ocrelizumab versus interferon beta-1a in relapsing multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Montalban X, Hauser SL, Kappos L, et al. Ocrelizumab versus placebo in primary progressive multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].
Calabresi PA. B-cell depletion - a frontier in monoclonal antibodies for multiple sclerosis. N Engl J Med. 2016 Dec 21 [Epub ahead of print].

Treatment Reduces Risk of Long-Term Disability in MS
Compared with the natural history of the disease, disease-modifying treatments for multiple sclerosis (MS) significantly reduce the risks of long-term disability worsening and evolution to secondary progressive MS (SPMS), according to research published in the October issue of Annals of Neurology. The data also suggest that patients who have no evidence of disease activity (NEDA) for two years are no more likely to have long-term stability than patients who do not reach this end point.
“These observations challenge the concept that NEDA represents remission. Although NEDA may be a useful measure for assessing relative therapeutic efficacy, many patients who meet NEDA criteria over two years go on to develop clinically significant disability,” said Bruce A. C. Cree, MD, PhD, Associate Professor of Neurology at the University of California, San Francisco School of Medicine. “Worsening in patients who meet the two-year NEDA end point could result from active spinal cord disease not captured with brain MRI, progressive axonal or neuronal degeneration, or an escape from a true but transient remission state.

Researchers had anticipated that between 36% and 50% of patients with relapsing MS (RMS) would develop SPMS, but 11.3% of the cohort transitioned to SPMS during the course of the study. Evolution of sustained disability was also slower than expected, said Dr. Cree.
Examining Long-Term Effects of Treatment
Natural history studies from the pretreatment era suggest that between one-third and one-half of patients with MS experience substantial worsening of neurologic disability approximately 15 years after disease onset. Disease-modifying therapies in MS have been studied during the past two decades and are associated with improvement in the short term. Their effect on long-term outcomes is unknown, however. Furthermore, little is known about the relationship between short-term MRI measurements and long-term disability in MS.
As a result, Dr. Cree and colleagues conducted a prospective study to characterize the accrual of long-term disability in a cohort of actively treated patients with MS. Additionally, they sought to assess whether clinical and MRI data used in clinical trials have long-term prognostic value.
Eligible participants had all clinical subtypes of MS and were first evaluated at the MS Center at the University of California, San Francisco between July 2004 and September 2005. Patients were excluded if they were unable to tolerate MRI scans, had poor venous access, or if they had other significant medical illnesses that might interfere with goals of the study. Investigators followed participants annually for five years. In addition, patients underwent re-evaluation at extended time points for as long as 10 years after baseline.
Researchers defined disability progression as a clinically significant worsening in the Expanded Disability Status Scale (EDSS), the timed 25-foot walk, the nine-hole peg test, and the paced serial auditory addition test.
Two Tiers of Therapy
The first tier of treatment, platform therapy, included interferon (IFN) beta, glatiramer acetate, and off-label therapies such as glucocorticoids, azathioprine, and mycophenolate mofetil. The second tier of treatment, high-potency therapy, included natalizumab, rituximab, mitoxantrone, and cyclophosphamide.
NEDA and Long-Term Disability
Of 517 actively managed patients with MS enrolled in the study, 366 had RMS, 48 had SPMS, 21 had primary progressive MS (PPMS), and 82 had clinically isolated syndrome (CIS). After 10 years of follow-up, neurologic disability was stable or improved, compared with baseline, in 41% of patients. Serum vitamin D levels were inversely associated with short-term MS disease activity, but were not associated with long-term disability. At a median time of 16.8 years after disease onset, 10.7% of patients reached an EDSS score of greater than or equal to 6, and 18.1% of patients evolved from RMS to SPMS.
The investigators concluded that evolution to SPMS in this study was significantly lower than expected, based on natural history studies. They also noted that short-term increases in EDSS did not necessarily predict future accumulation of long-term disability in patients with RMS. In addition, subjects with NEDA by clinical and MRI criteria during the first two years had long-term outcomes that were no different from those of the cohort as a whole.
“Treating to target with two-year NEDA as the goal may not result in protection against long-term disability,” said Dr. Cree. “Long-term studies are urgently needed to determine if high-intensity therapy, initiated at the time of diagnosis or used in patients with seemingly inactive disease, is superior to the escalation approach employed in this cohort.”
—Erica Tricarico
Suggested Reading
University of California, San Francisco MS-EPIC Team, Cree BA, Gourraud PA, et al. Long-term evolution of multiple sclerosis disability in the treatment era. Ann Neurol. 2016;80(4):499-510.
Compared with the natural history of the disease, disease-modifying treatments for multiple sclerosis (MS) significantly reduce the risks of long-term disability worsening and evolution to secondary progressive MS (SPMS), according to research published in the October issue of Annals of Neurology. The data also suggest that patients who have no evidence of disease activity (NEDA) for two years are no more likely to have long-term stability than patients who do not reach this end point.
“These observations challenge the concept that NEDA represents remission. Although NEDA may be a useful measure for assessing relative therapeutic efficacy, many patients who meet NEDA criteria over two years go on to develop clinically significant disability,” said Bruce A. C. Cree, MD, PhD, Associate Professor of Neurology at the University of California, San Francisco School of Medicine. “Worsening in patients who meet the two-year NEDA end point could result from active spinal cord disease not captured with brain MRI, progressive axonal or neuronal degeneration, or an escape from a true but transient remission state.
Researchers had anticipated that between 36% and 50% of patients with relapsing MS (RMS) would develop SPMS, but 11.3% of the cohort transitioned to SPMS during the course of the study. Evolution of sustained disability was also slower than expected, said Dr. Cree.
Examining Long-Term Effects of Treatment
Natural history studies from the pretreatment era suggest that between one-third and one-half of patients with MS experience substantial worsening of neurologic disability approximately 15 years after disease onset. Disease-modifying therapies in MS have been studied during the past two decades and are associated with improvement in the short term. Their effect on long-term outcomes is unknown, however. Furthermore, little is known about the relationship between short-term MRI measurements and long-term disability in MS.
As a result, Dr. Cree and colleagues conducted a prospective study to characterize the accrual of long-term disability in a cohort of actively treated patients with MS. Additionally, they sought to assess whether clinical and MRI data used in clinical trials have long-term prognostic value.
Eligible participants had all clinical subtypes of MS and were first evaluated at the MS Center at the University of California, San Francisco between July 2004 and September 2005. Patients were excluded if they were unable to tolerate MRI scans, had poor venous access, or if they had other significant medical illnesses that might interfere with goals of the study. Investigators followed participants annually for five years. In addition, patients underwent re-evaluation at extended time points for as long as 10 years after baseline.
Researchers defined disability progression as a clinically significant worsening in the Expanded Disability Status Scale (EDSS), the timed 25-foot walk, the nine-hole peg test, and the paced serial auditory addition test.
Two Tiers of Therapy
The first tier of treatment, platform therapy, included interferon (IFN) beta, glatiramer acetate, and off-label therapies such as glucocorticoids, azathioprine, and mycophenolate mofetil. The second tier of treatment, high-potency therapy, included natalizumab, rituximab, mitoxantrone, and cyclophosphamide.
NEDA and Long-Term Disability
Of 517 actively managed patients with MS enrolled in the study, 366 had RMS, 48 had SPMS, 21 had primary progressive MS (PPMS), and 82 had clinically isolated syndrome (CIS). After 10 years of follow-up, neurologic disability was stable or improved, compared with baseline, in 41% of patients. Serum vitamin D levels were inversely associated with short-term MS disease activity, but were not associated with long-term disability. At a median time of 16.8 years after disease onset, 10.7% of patients reached an EDSS score of greater than or equal to 6, and 18.1% of patients evolved from RMS to SPMS.
The investigators concluded that evolution to SPMS in this study was significantly lower than expected, based on natural history studies. They also noted that short-term increases in EDSS did not necessarily predict future accumulation of long-term disability in patients with RMS. In addition, subjects with NEDA by clinical and MRI criteria during the first two years had long-term outcomes that were no different from those of the cohort as a whole.
“Treating to target with two-year NEDA as the goal may not result in protection against long-term disability,” said Dr. Cree. “Long-term studies are urgently needed to determine if high-intensity therapy, initiated at the time of diagnosis or used in patients with seemingly inactive disease, is superior to the escalation approach employed in this cohort.”
—Erica Tricarico
Suggested Reading
University of California, San Francisco MS-EPIC Team, Cree BA, Gourraud PA, et al. Long-term evolution of multiple sclerosis disability in the treatment era. Ann Neurol. 2016;80(4):499-510.
Compared with the natural history of the disease, disease-modifying treatments for multiple sclerosis (MS) significantly reduce the risks of long-term disability worsening and evolution to secondary progressive MS (SPMS), according to research published in the October issue of Annals of Neurology. The data also suggest that patients who have no evidence of disease activity (NEDA) for two years are no more likely to have long-term stability than patients who do not reach this end point.
“These observations challenge the concept that NEDA represents remission. Although NEDA may be a useful measure for assessing relative therapeutic efficacy, many patients who meet NEDA criteria over two years go on to develop clinically significant disability,” said Bruce A. C. Cree, MD, PhD, Associate Professor of Neurology at the University of California, San Francisco School of Medicine. “Worsening in patients who meet the two-year NEDA end point could result from active spinal cord disease not captured with brain MRI, progressive axonal or neuronal degeneration, or an escape from a true but transient remission state.
Researchers had anticipated that between 36% and 50% of patients with relapsing MS (RMS) would develop SPMS, but 11.3% of the cohort transitioned to SPMS during the course of the study. Evolution of sustained disability was also slower than expected, said Dr. Cree.
Examining Long-Term Effects of Treatment
Natural history studies from the pretreatment era suggest that between one-third and one-half of patients with MS experience substantial worsening of neurologic disability approximately 15 years after disease onset. Disease-modifying therapies in MS have been studied during the past two decades and are associated with improvement in the short term. Their effect on long-term outcomes is unknown, however. Furthermore, little is known about the relationship between short-term MRI measurements and long-term disability in MS.
As a result, Dr. Cree and colleagues conducted a prospective study to characterize the accrual of long-term disability in a cohort of actively treated patients with MS. Additionally, they sought to assess whether clinical and MRI data used in clinical trials have long-term prognostic value.
Eligible participants had all clinical subtypes of MS and were first evaluated at the MS Center at the University of California, San Francisco between July 2004 and September 2005. Patients were excluded if they were unable to tolerate MRI scans, had poor venous access, or if they had other significant medical illnesses that might interfere with goals of the study. Investigators followed participants annually for five years. In addition, patients underwent re-evaluation at extended time points for as long as 10 years after baseline.
Researchers defined disability progression as a clinically significant worsening in the Expanded Disability Status Scale (EDSS), the timed 25-foot walk, the nine-hole peg test, and the paced serial auditory addition test.
Two Tiers of Therapy
The first tier of treatment, platform therapy, included interferon (IFN) beta, glatiramer acetate, and off-label therapies such as glucocorticoids, azathioprine, and mycophenolate mofetil. The second tier of treatment, high-potency therapy, included natalizumab, rituximab, mitoxantrone, and cyclophosphamide.
NEDA and Long-Term Disability
Of 517 actively managed patients with MS enrolled in the study, 366 had RMS, 48 had SPMS, 21 had primary progressive MS (PPMS), and 82 had clinically isolated syndrome (CIS). After 10 years of follow-up, neurologic disability was stable or improved, compared with baseline, in 41% of patients. Serum vitamin D levels were inversely associated with short-term MS disease activity, but were not associated with long-term disability. At a median time of 16.8 years after disease onset, 10.7% of patients reached an EDSS score of greater than or equal to 6, and 18.1% of patients evolved from RMS to SPMS.
The investigators concluded that evolution to SPMS in this study was significantly lower than expected, based on natural history studies. They also noted that short-term increases in EDSS did not necessarily predict future accumulation of long-term disability in patients with RMS. In addition, subjects with NEDA by clinical and MRI criteria during the first two years had long-term outcomes that were no different from those of the cohort as a whole.
“Treating to target with two-year NEDA as the goal may not result in protection against long-term disability,” said Dr. Cree. “Long-term studies are urgently needed to determine if high-intensity therapy, initiated at the time of diagnosis or used in patients with seemingly inactive disease, is superior to the escalation approach employed in this cohort.”
—Erica Tricarico
Suggested Reading
University of California, San Francisco MS-EPIC Team, Cree BA, Gourraud PA, et al. Long-term evolution of multiple sclerosis disability in the treatment era. Ann Neurol. 2016;80(4):499-510.

New report highlights gaps in knowledge on marijuana use
A new report by the National Academies of Sciences, Engineering and Medicine shines a light on what the existing literature says about the perceived health benefits and dangers of using cannabis and cannabinoids.
“What little we know for certain about the effects of marijuana on human health — and all that we have reason to suspect — justifies serious national concern,” wrote the authors of the report, the evidence and research review of which was chaired by Marie McCormick, MD, of Harvard University in Boston. “The committee’s major recommendation called for an intensification and more comprehensive research effort into the effects of marijuana on the health of the American people.”
The authors concluded current literature shows substantial evidence stating that cannabis is effective at managing chronic pain in adults, while oral cannabinoid use is effective in mitigating nausea or vomiting induced by chemotherapy and improving patient-reported spasticity in patients with multiple sclerosis. Additionally, cannabinoids – specifically, nabiximols – are moderately effective in the short term for improving sleep disturbances brought on by obstructive sleep apnea syndrome, fibromyalgia, chronic pain, and multiple sclerosis.
However, there is limited evidence to support cannabis or cannabinoid use for reducing weight loss or inducing appetite in HIV/AIDS patients, improving clinician-measured spasicity or Tourette syndrome symptoms, reducing anxiety, improving symptoms brought on by post-traumatic stress, and improving outcomes in patients who have suffered traumatic brain injury or intracranial hemorrhage.
Additionally, there is no evidence to support the use of cannabis or cannabinoids in treating cancers or cancer-related anorexia, irritable bowel syndrome symptoms, epilepsy, spinal cord-related spasticity, symptoms of amyotrophic lateral sclerosis, Huntington’s disease, Parkinson’s disease, schizophrenia, and dystonia.
“Present data on drug use progression neither support nor refute the suggestion that medical availability would increase drug abuse,” the authors noted. “However, this question is beyond the issues normally considered for medical uses of drugs and should not be a factor in evaluating the therapeutic potential of marijuana or cannabinoids.”
From a mental health standpoint, suicidal thoughts were found to be more likely in individuals who frequently used cannabis or cannabinoids. Symptoms like depression and anxiety are also more likely in those who smoke marijuana and have bipolar disorder. There is also “limited evidence of a statistical association between sustained abstinence from cannabis use [and] impairments in the cognitive domains of learning, memory, and attention.”
Among the other significant findings of the report, children who live in states where marijuana has been legalized are significantly more likely to ingest cannabis or cannabinoids; so far, marijuana use in some form – either recreational or medical – has been approved in 28 states and Washington, DC. Furthermore, adolescents who use marijuana are more likely to experience difficulties in social and educational development. And individuals of any age who smoke marijuana and drive are more likely to be involved in a car accident.
Also noteworthy is the lack of evidence pointing to marijuana use causing cancer. While chronic marijuana smoking was found to be linked to bronchitis, it was not found to cause cancers that are most commonly associated with chronic smoking of tobacco.
“This report highlights that there are critical gaps in our understanding of the health effects of cannabis,” explained John H. Krystal, MD, of Yale University in New Haven, Connecticut.
A reviewer of the report, Dr. Krystal elaborated on the gaps that exist in the current literature, saying “One reason for these gaps has been regulatory and practical challenges facing those who attempted to conduct this research. For example, what supply of cannabis should they use? Where, in the typical hospital settings where research is conducted, should patients participating in research be permitted to smoke cannabis? What standards should the institutional review committees employ when evaluating studies that involve the administration of cannabis or other cannabinoids?”
Ultimately, Dr. Krystal stated, “what should be evident from this summary is that only a few of the many publicized clinical applications for cannabis are adequately supported by acceptable research standards for determining safety or efficacy.” Specifically, states that have approved cannabis use for managing PTSD symptoms are doing so based off “meager” evidence, and in some cases, are circumventing FDA regulatory processes in a way. This could not only compromise patient care, but muddy the waters for physicians who want to treat their patients safely while also following legal avenues.
“Physicians may face a tension between their roles as physicians [and] their wish to provide a legal path for access to cannabinoids for their patients,” Dr. Krystal said, adding that “the endorsement of particular cannabis prescription practices by the states, even for clinical indications where cannabis has not been shown to be safe and effective, may create pressure for physicians to engage in ineffective or unsafe cannabis prescription practices.”
Ultimately, the report underlines areas of need in terms of understanding and effectively using cannabis and cannabinoid in treating patients. Calling the report a “call to arms” for those in the health care – and, specifically, the public health – arena, Dr. Krystal added that he hopes the findings of the report will be used for educating “legislators, physicians, and consumers [about the] potential benefits and risks of cannabis and thereby help to guide both legislation, clinical practice, and perhaps recreational use.”
A new report by the National Academies of Sciences, Engineering and Medicine shines a light on what the existing literature says about the perceived health benefits and dangers of using cannabis and cannabinoids.
“What little we know for certain about the effects of marijuana on human health — and all that we have reason to suspect — justifies serious national concern,” wrote the authors of the report, the evidence and research review of which was chaired by Marie McCormick, MD, of Harvard University in Boston. “The committee’s major recommendation called for an intensification and more comprehensive research effort into the effects of marijuana on the health of the American people.”
The authors concluded current literature shows substantial evidence stating that cannabis is effective at managing chronic pain in adults, while oral cannabinoid use is effective in mitigating nausea or vomiting induced by chemotherapy and improving patient-reported spasticity in patients with multiple sclerosis. Additionally, cannabinoids – specifically, nabiximols – are moderately effective in the short term for improving sleep disturbances brought on by obstructive sleep apnea syndrome, fibromyalgia, chronic pain, and multiple sclerosis.
However, there is limited evidence to support cannabis or cannabinoid use for reducing weight loss or inducing appetite in HIV/AIDS patients, improving clinician-measured spasicity or Tourette syndrome symptoms, reducing anxiety, improving symptoms brought on by post-traumatic stress, and improving outcomes in patients who have suffered traumatic brain injury or intracranial hemorrhage.
Additionally, there is no evidence to support the use of cannabis or cannabinoids in treating cancers or cancer-related anorexia, irritable bowel syndrome symptoms, epilepsy, spinal cord-related spasticity, symptoms of amyotrophic lateral sclerosis, Huntington’s disease, Parkinson’s disease, schizophrenia, and dystonia.
“Present data on drug use progression neither support nor refute the suggestion that medical availability would increase drug abuse,” the authors noted. “However, this question is beyond the issues normally considered for medical uses of drugs and should not be a factor in evaluating the therapeutic potential of marijuana or cannabinoids.”
From a mental health standpoint, suicidal thoughts were found to be more likely in individuals who frequently used cannabis or cannabinoids. Symptoms like depression and anxiety are also more likely in those who smoke marijuana and have bipolar disorder. There is also “limited evidence of a statistical association between sustained abstinence from cannabis use [and] impairments in the cognitive domains of learning, memory, and attention.”
Among the other significant findings of the report, children who live in states where marijuana has been legalized are significantly more likely to ingest cannabis or cannabinoids; so far, marijuana use in some form – either recreational or medical – has been approved in 28 states and Washington, DC. Furthermore, adolescents who use marijuana are more likely to experience difficulties in social and educational development. And individuals of any age who smoke marijuana and drive are more likely to be involved in a car accident.
Also noteworthy is the lack of evidence pointing to marijuana use causing cancer. While chronic marijuana smoking was found to be linked to bronchitis, it was not found to cause cancers that are most commonly associated with chronic smoking of tobacco.
“This report highlights that there are critical gaps in our understanding of the health effects of cannabis,” explained John H. Krystal, MD, of Yale University in New Haven, Connecticut.
A reviewer of the report, Dr. Krystal elaborated on the gaps that exist in the current literature, saying “One reason for these gaps has been regulatory and practical challenges facing those who attempted to conduct this research. For example, what supply of cannabis should they use? Where, in the typical hospital settings where research is conducted, should patients participating in research be permitted to smoke cannabis? What standards should the institutional review committees employ when evaluating studies that involve the administration of cannabis or other cannabinoids?”
Ultimately, Dr. Krystal stated, “what should be evident from this summary is that only a few of the many publicized clinical applications for cannabis are adequately supported by acceptable research standards for determining safety or efficacy.” Specifically, states that have approved cannabis use for managing PTSD symptoms are doing so based off “meager” evidence, and in some cases, are circumventing FDA regulatory processes in a way. This could not only compromise patient care, but muddy the waters for physicians who want to treat their patients safely while also following legal avenues.
“Physicians may face a tension between their roles as physicians [and] their wish to provide a legal path for access to cannabinoids for their patients,” Dr. Krystal said, adding that “the endorsement of particular cannabis prescription practices by the states, even for clinical indications where cannabis has not been shown to be safe and effective, may create pressure for physicians to engage in ineffective or unsafe cannabis prescription practices.”
Ultimately, the report underlines areas of need in terms of understanding and effectively using cannabis and cannabinoid in treating patients. Calling the report a “call to arms” for those in the health care – and, specifically, the public health – arena, Dr. Krystal added that he hopes the findings of the report will be used for educating “legislators, physicians, and consumers [about the] potential benefits and risks of cannabis and thereby help to guide both legislation, clinical practice, and perhaps recreational use.”
A new report by the National Academies of Sciences, Engineering and Medicine shines a light on what the existing literature says about the perceived health benefits and dangers of using cannabis and cannabinoids.
“What little we know for certain about the effects of marijuana on human health — and all that we have reason to suspect — justifies serious national concern,” wrote the authors of the report, the evidence and research review of which was chaired by Marie McCormick, MD, of Harvard University in Boston. “The committee’s major recommendation called for an intensification and more comprehensive research effort into the effects of marijuana on the health of the American people.”
The authors concluded current literature shows substantial evidence stating that cannabis is effective at managing chronic pain in adults, while oral cannabinoid use is effective in mitigating nausea or vomiting induced by chemotherapy and improving patient-reported spasticity in patients with multiple sclerosis. Additionally, cannabinoids – specifically, nabiximols – are moderately effective in the short term for improving sleep disturbances brought on by obstructive sleep apnea syndrome, fibromyalgia, chronic pain, and multiple sclerosis.
However, there is limited evidence to support cannabis or cannabinoid use for reducing weight loss or inducing appetite in HIV/AIDS patients, improving clinician-measured spasicity or Tourette syndrome symptoms, reducing anxiety, improving symptoms brought on by post-traumatic stress, and improving outcomes in patients who have suffered traumatic brain injury or intracranial hemorrhage.
Additionally, there is no evidence to support the use of cannabis or cannabinoids in treating cancers or cancer-related anorexia, irritable bowel syndrome symptoms, epilepsy, spinal cord-related spasticity, symptoms of amyotrophic lateral sclerosis, Huntington’s disease, Parkinson’s disease, schizophrenia, and dystonia.
“Present data on drug use progression neither support nor refute the suggestion that medical availability would increase drug abuse,” the authors noted. “However, this question is beyond the issues normally considered for medical uses of drugs and should not be a factor in evaluating the therapeutic potential of marijuana or cannabinoids.”
From a mental health standpoint, suicidal thoughts were found to be more likely in individuals who frequently used cannabis or cannabinoids. Symptoms like depression and anxiety are also more likely in those who smoke marijuana and have bipolar disorder. There is also “limited evidence of a statistical association between sustained abstinence from cannabis use [and] impairments in the cognitive domains of learning, memory, and attention.”
Among the other significant findings of the report, children who live in states where marijuana has been legalized are significantly more likely to ingest cannabis or cannabinoids; so far, marijuana use in some form – either recreational or medical – has been approved in 28 states and Washington, DC. Furthermore, adolescents who use marijuana are more likely to experience difficulties in social and educational development. And individuals of any age who smoke marijuana and drive are more likely to be involved in a car accident.
Also noteworthy is the lack of evidence pointing to marijuana use causing cancer. While chronic marijuana smoking was found to be linked to bronchitis, it was not found to cause cancers that are most commonly associated with chronic smoking of tobacco.
“This report highlights that there are critical gaps in our understanding of the health effects of cannabis,” explained John H. Krystal, MD, of Yale University in New Haven, Connecticut.
A reviewer of the report, Dr. Krystal elaborated on the gaps that exist in the current literature, saying “One reason for these gaps has been regulatory and practical challenges facing those who attempted to conduct this research. For example, what supply of cannabis should they use? Where, in the typical hospital settings where research is conducted, should patients participating in research be permitted to smoke cannabis? What standards should the institutional review committees employ when evaluating studies that involve the administration of cannabis or other cannabinoids?”
Ultimately, Dr. Krystal stated, “what should be evident from this summary is that only a few of the many publicized clinical applications for cannabis are adequately supported by acceptable research standards for determining safety or efficacy.” Specifically, states that have approved cannabis use for managing PTSD symptoms are doing so based off “meager” evidence, and in some cases, are circumventing FDA regulatory processes in a way. This could not only compromise patient care, but muddy the waters for physicians who want to treat their patients safely while also following legal avenues.
“Physicians may face a tension between their roles as physicians [and] their wish to provide a legal path for access to cannabinoids for their patients,” Dr. Krystal said, adding that “the endorsement of particular cannabis prescription practices by the states, even for clinical indications where cannabis has not been shown to be safe and effective, may create pressure for physicians to engage in ineffective or unsafe cannabis prescription practices.”
Ultimately, the report underlines areas of need in terms of understanding and effectively using cannabis and cannabinoid in treating patients. Calling the report a “call to arms” for those in the health care – and, specifically, the public health – arena, Dr. Krystal added that he hopes the findings of the report will be used for educating “legislators, physicians, and consumers [about the] potential benefits and risks of cannabis and thereby help to guide both legislation, clinical practice, and perhaps recreational use.”
FROM THE NATIONAL ACADEMIES OF SCIENCES, ENGINEERING AND MEDICINE
Switch from fingolimod to alemtuzumab might trigger MS relapse
Nine relapsing multiple sclerosis patients had significant and unexpected disease activity within 12 months of switching from fingolimod to alemtuzumab, according to a report from six European neuroscience centers.
The centers treated 174 patients with alemtuzumab (Lemtrada); 36 had been on fingolimod (Gilenya) beforehand. “Therefore, these nine patients ... represent 25% of the fingolimod-alemtuzumab cohort,” said investigators led by Mark Willis, MBBCh, a clinical research fellow at Cardiff University, Wales (Neurol Neuroimmunol Neuroinflamm. 2017 Jan 10. doi: 10.1212/NXI.0000000000000320).
“Careful consideration needs to be given to mode of action of individual therapies and sequential treatment effects,” the team concluded.
The nine patients were on fingolimod for 5-33 months, but it wasn’t working well so they were started on alemtuzumab following a median fingolimod washout period of 6 weeks. Eight patients had at least one clinical relapse within 12 months of the first alemtuzumab infusion cycle; the median time to relapse following alemtuzumab induction was 4.5 months. All nine patients had radiologic evidence of new disease activity.
Five patients had lymphocyte counts below normal when started on alemtuzumab.
Fingolimod has a half-life of 6-9 days, so “lymphocytes would be expected to normalize 2-4 weeks after discontinuation. However, there are case reports of prolonged lymphopenia following prolonged drug exposure, up to 37 months after discontinuation.” It has “been suggested that patients continue on an alternative [disease-modifying treatment] after fingolimod discontinuation, preferably until peripheral lymphocyte counts have normalized.” However, “there is currently no consensus as to which subsequent therapeutic agent is optimal,” the investigators said.
Despite the presence of disease activity in the first 12 months, all nine patients went on to the second planned infusion of alemtuzumab; eight were relapse free during a mean follow-up of 6 months after the second treatment cycle. Four of seven were radiologically stable, but three had new T2 lesions and one with a single new gadolinium-enhancing lesion.
Even so, the findings offers “some support to the hypothesis that, after a period, sequestrated lymphocytes eventually become available for depletion by alemtuzumab,” the researchers noted.
The mean age of the patients when diagnosed with MS was 21 years. The median disease duration to alemtuzumab treatment was 94 months.
There was no external funding. Dr. Willis had no disclosures. Other researchers reported ties to a number of companies, including Genzyme, maker of alemtuzumab, and Novartis, fingolimod’s maker.
Nine relapsing multiple sclerosis patients had significant and unexpected disease activity within 12 months of switching from fingolimod to alemtuzumab, according to a report from six European neuroscience centers.
The centers treated 174 patients with alemtuzumab (Lemtrada); 36 had been on fingolimod (Gilenya) beforehand. “Therefore, these nine patients ... represent 25% of the fingolimod-alemtuzumab cohort,” said investigators led by Mark Willis, MBBCh, a clinical research fellow at Cardiff University, Wales (Neurol Neuroimmunol Neuroinflamm. 2017 Jan 10. doi: 10.1212/NXI.0000000000000320).
“Careful consideration needs to be given to mode of action of individual therapies and sequential treatment effects,” the team concluded.
The nine patients were on fingolimod for 5-33 months, but it wasn’t working well so they were started on alemtuzumab following a median fingolimod washout period of 6 weeks. Eight patients had at least one clinical relapse within 12 months of the first alemtuzumab infusion cycle; the median time to relapse following alemtuzumab induction was 4.5 months. All nine patients had radiologic evidence of new disease activity.
Five patients had lymphocyte counts below normal when started on alemtuzumab.
Fingolimod has a half-life of 6-9 days, so “lymphocytes would be expected to normalize 2-4 weeks after discontinuation. However, there are case reports of prolonged lymphopenia following prolonged drug exposure, up to 37 months after discontinuation.” It has “been suggested that patients continue on an alternative [disease-modifying treatment] after fingolimod discontinuation, preferably until peripheral lymphocyte counts have normalized.” However, “there is currently no consensus as to which subsequent therapeutic agent is optimal,” the investigators said.
Despite the presence of disease activity in the first 12 months, all nine patients went on to the second planned infusion of alemtuzumab; eight were relapse free during a mean follow-up of 6 months after the second treatment cycle. Four of seven were radiologically stable, but three had new T2 lesions and one with a single new gadolinium-enhancing lesion.
Even so, the findings offers “some support to the hypothesis that, after a period, sequestrated lymphocytes eventually become available for depletion by alemtuzumab,” the researchers noted.
The mean age of the patients when diagnosed with MS was 21 years. The median disease duration to alemtuzumab treatment was 94 months.
There was no external funding. Dr. Willis had no disclosures. Other researchers reported ties to a number of companies, including Genzyme, maker of alemtuzumab, and Novartis, fingolimod’s maker.
Nine relapsing multiple sclerosis patients had significant and unexpected disease activity within 12 months of switching from fingolimod to alemtuzumab, according to a report from six European neuroscience centers.
The centers treated 174 patients with alemtuzumab (Lemtrada); 36 had been on fingolimod (Gilenya) beforehand. “Therefore, these nine patients ... represent 25% of the fingolimod-alemtuzumab cohort,” said investigators led by Mark Willis, MBBCh, a clinical research fellow at Cardiff University, Wales (Neurol Neuroimmunol Neuroinflamm. 2017 Jan 10. doi: 10.1212/NXI.0000000000000320).
“Careful consideration needs to be given to mode of action of individual therapies and sequential treatment effects,” the team concluded.
The nine patients were on fingolimod for 5-33 months, but it wasn’t working well so they were started on alemtuzumab following a median fingolimod washout period of 6 weeks. Eight patients had at least one clinical relapse within 12 months of the first alemtuzumab infusion cycle; the median time to relapse following alemtuzumab induction was 4.5 months. All nine patients had radiologic evidence of new disease activity.
Five patients had lymphocyte counts below normal when started on alemtuzumab.
Fingolimod has a half-life of 6-9 days, so “lymphocytes would be expected to normalize 2-4 weeks after discontinuation. However, there are case reports of prolonged lymphopenia following prolonged drug exposure, up to 37 months after discontinuation.” It has “been suggested that patients continue on an alternative [disease-modifying treatment] after fingolimod discontinuation, preferably until peripheral lymphocyte counts have normalized.” However, “there is currently no consensus as to which subsequent therapeutic agent is optimal,” the investigators said.
Despite the presence of disease activity in the first 12 months, all nine patients went on to the second planned infusion of alemtuzumab; eight were relapse free during a mean follow-up of 6 months after the second treatment cycle. Four of seven were radiologically stable, but three had new T2 lesions and one with a single new gadolinium-enhancing lesion.
Even so, the findings offers “some support to the hypothesis that, after a period, sequestrated lymphocytes eventually become available for depletion by alemtuzumab,” the researchers noted.
The mean age of the patients when diagnosed with MS was 21 years. The median disease duration to alemtuzumab treatment was 94 months.
There was no external funding. Dr. Willis had no disclosures. Other researchers reported ties to a number of companies, including Genzyme, maker of alemtuzumab, and Novartis, fingolimod’s maker.
FROM NEUROLOGY: NEUROIMMUNOLOGY AND NEUROINFLAMMATION
High-risk relatives of MS patients show early signs of disease
Asymptomatic first-degree relatives of multiple sclerosis patients at high risk for developing the disease were significantly more likely to show subclinical signs of MS than were family members at lower risk, in the Genes and Environment in Multiple Sclerosis prospective cohort study. The findings were published online on Jan. 17 in JAMA Neurology.
The Genes and Environment in Multiple Sclerosis (GEMS) project is the first prospective study of populations at risk for MS and is the first detailed cross-sectional examination of higher-risk and lower-risk family members to date, according to investigators led by Zongqi Xia, MD, PhD, of Brigham and Women’s Hospital, Boston. Although the totality of evidence put together through neuroimaging and numerous clinical tests in the study indicate that individuals with the highest risk for MS have higher risk for the disease than do those with the lowest risk, simple vibration threshold testing gave the best results, Dr. Xia and his colleagues reported.
The study involved 100 neurologically asymptomatic adults aged 18-50 years who were first-degree relatives of people with MS who participated in the GEMS project during August 2012 to July 2015. These 100 comprised 41 high-risk participants from the top 10% of a Genetic and Environmental Risk Score (GERS) and 59 low-risk participants from the bottom 10% on the GERS. The GERS included genetic risk factors (HLA alleles and several MS-associated non-HLA genetic variants) and environmental factors, such as smoking status, body mass index, history of infectious mononucleosis and migraine, and vitamin D levels.
However, because 40 of the 41 high-risk individuals were female and 25 of the 59 low-risk individuals were female, the investigators limited the study to the 65 female participants to avoid “attributing any potential difference primarily to the role of sex.”
To help in identifying early signs of MS, the researchers used brain MRI and optical coherence tomography and other measures of neurological function, including the Expanded Disability Status Scale, timed 25-foot walk, Nine-Hole Peg Test, Paced Auditory Serial Addition Test, Symbol Digit Modalities Test, Timed Up and Go, and high-contrast and low-contrast visual acuity (JAMA Neurol. 2017 Jan 17. doi: 10.1001/jamaneurol.2016.5056).
Overall, high-risk women showed more subclinical signs of MS than did low-risk women based on an omnibus test that globally assessed the burden of neurological dysfunction by comparing the overall differences between the two groups when considering all of the measured outcomes (P = .01). However, impaired vibration perception yielded a stronger result; of 47 women (27 high-risk and 20 low-risk) tested in this manner, high-risk women showed significantly reduced vibration perception in the distal lower extremities (P = .008).
One individual in the high-risk group converted to clinically definite MS during the study. Four of the high-risk women had T2-weighted hyperintense lesions that met the 2010 McDonald MRI criteria for dissemination in space, compared with one low-risk woman. The 2016 proposed consensus MRI criteria for MS diagnosis were met by two high-risk women and one low-risk woman. Radiological isolated syndrome occurred in one woman of each group, and there was a single foci of leptominengeal enhancement in three high-risk women and one low-risk woman.
The findings were limited by several factors including the small size, lack of male participants, cross-sectional nature of the study, and the fact that vibration sensitivity thresholds were in the normal range for high-risk and low-risk individuals. However, the researchers wrote that they “plan to confirm the finding of change in vibration sensitivity with a follow-up study,” and they noted that the “study highlights the important need to develop and test more sensitive measures, particularly with biometric devices, to detect subtle subclinical changes early in the disease process.”
The National Institutes of Health and the National Multiple Sclerosis Society supported the study. Some of the authors reported receiving awards from the National Multiple Sclerosis Society, the American Academy of Neurology, and the National Institute of Neurological Disorders and Stroke.
The GEMS study represents the most ambitious effort yet to identify presymptomatic individuals who are at increased risk for MS, and it is a valuable first step toward targeted screening. Even if we cannot yet intervene therapeutically using currently available disease-modifying treatments in presymptomatic stages of MS, the ability to better define high-risk individuals is likely to make active surveillance programs more cost effective. It also provides important information to counsel individuals about lifestyle changes, such as quitting smoking.
The GERS also can likely be further refined with more up-to-date data on the interaction between specific genetic and environmental factors.
Fredrik Piehl, MD, PhD, is a member of the department of neurology at the Karolinska Institutet and Karolinska University Hospital, Stockholm. His comments are derived from an editorial accompanying the report by Dr. Xia and colleagues (JAMA Neurol. 2017 Jan 17. doi: 10.1001/jamaneurol.2016.5126). He disclosed research support, travel grants, and other relationships with Biogen, Genzyme, Novartis, Merck, Roche, Serono, and Teva.
The GEMS study represents the most ambitious effort yet to identify presymptomatic individuals who are at increased risk for MS, and it is a valuable first step toward targeted screening. Even if we cannot yet intervene therapeutically using currently available disease-modifying treatments in presymptomatic stages of MS, the ability to better define high-risk individuals is likely to make active surveillance programs more cost effective. It also provides important information to counsel individuals about lifestyle changes, such as quitting smoking.
The GERS also can likely be further refined with more up-to-date data on the interaction between specific genetic and environmental factors.
Fredrik Piehl, MD, PhD, is a member of the department of neurology at the Karolinska Institutet and Karolinska University Hospital, Stockholm. His comments are derived from an editorial accompanying the report by Dr. Xia and colleagues (JAMA Neurol. 2017 Jan 17. doi: 10.1001/jamaneurol.2016.5126). He disclosed research support, travel grants, and other relationships with Biogen, Genzyme, Novartis, Merck, Roche, Serono, and Teva.
The GEMS study represents the most ambitious effort yet to identify presymptomatic individuals who are at increased risk for MS, and it is a valuable first step toward targeted screening. Even if we cannot yet intervene therapeutically using currently available disease-modifying treatments in presymptomatic stages of MS, the ability to better define high-risk individuals is likely to make active surveillance programs more cost effective. It also provides important information to counsel individuals about lifestyle changes, such as quitting smoking.
The GERS also can likely be further refined with more up-to-date data on the interaction between specific genetic and environmental factors.
Fredrik Piehl, MD, PhD, is a member of the department of neurology at the Karolinska Institutet and Karolinska University Hospital, Stockholm. His comments are derived from an editorial accompanying the report by Dr. Xia and colleagues (JAMA Neurol. 2017 Jan 17. doi: 10.1001/jamaneurol.2016.5126). He disclosed research support, travel grants, and other relationships with Biogen, Genzyme, Novartis, Merck, Roche, Serono, and Teva.
Asymptomatic first-degree relatives of multiple sclerosis patients at high risk for developing the disease were significantly more likely to show subclinical signs of MS than were family members at lower risk, in the Genes and Environment in Multiple Sclerosis prospective cohort study. The findings were published online on Jan. 17 in JAMA Neurology.
The Genes and Environment in Multiple Sclerosis (GEMS) project is the first prospective study of populations at risk for MS and is the first detailed cross-sectional examination of higher-risk and lower-risk family members to date, according to investigators led by Zongqi Xia, MD, PhD, of Brigham and Women’s Hospital, Boston. Although the totality of evidence put together through neuroimaging and numerous clinical tests in the study indicate that individuals with the highest risk for MS have higher risk for the disease than do those with the lowest risk, simple vibration threshold testing gave the best results, Dr. Xia and his colleagues reported.
The study involved 100 neurologically asymptomatic adults aged 18-50 years who were first-degree relatives of people with MS who participated in the GEMS project during August 2012 to July 2015. These 100 comprised 41 high-risk participants from the top 10% of a Genetic and Environmental Risk Score (GERS) and 59 low-risk participants from the bottom 10% on the GERS. The GERS included genetic risk factors (HLA alleles and several MS-associated non-HLA genetic variants) and environmental factors, such as smoking status, body mass index, history of infectious mononucleosis and migraine, and vitamin D levels.
However, because 40 of the 41 high-risk individuals were female and 25 of the 59 low-risk individuals were female, the investigators limited the study to the 65 female participants to avoid “attributing any potential difference primarily to the role of sex.”
To help in identifying early signs of MS, the researchers used brain MRI and optical coherence tomography and other measures of neurological function, including the Expanded Disability Status Scale, timed 25-foot walk, Nine-Hole Peg Test, Paced Auditory Serial Addition Test, Symbol Digit Modalities Test, Timed Up and Go, and high-contrast and low-contrast visual acuity (JAMA Neurol. 2017 Jan 17. doi: 10.1001/jamaneurol.2016.5056).
Overall, high-risk women showed more subclinical signs of MS than did low-risk women based on an omnibus test that globally assessed the burden of neurological dysfunction by comparing the overall differences between the two groups when considering all of the measured outcomes (P = .01). However, impaired vibration perception yielded a stronger result; of 47 women (27 high-risk and 20 low-risk) tested in this manner, high-risk women showed significantly reduced vibration perception in the distal lower extremities (P = .008).
One individual in the high-risk group converted to clinically definite MS during the study. Four of the high-risk women had T2-weighted hyperintense lesions that met the 2010 McDonald MRI criteria for dissemination in space, compared with one low-risk woman. The 2016 proposed consensus MRI criteria for MS diagnosis were met by two high-risk women and one low-risk woman. Radiological isolated syndrome occurred in one woman of each group, and there was a single foci of leptominengeal enhancement in three high-risk women and one low-risk woman.
The findings were limited by several factors including the small size, lack of male participants, cross-sectional nature of the study, and the fact that vibration sensitivity thresholds were in the normal range for high-risk and low-risk individuals. However, the researchers wrote that they “plan to confirm the finding of change in vibration sensitivity with a follow-up study,” and they noted that the “study highlights the important need to develop and test more sensitive measures, particularly with biometric devices, to detect subtle subclinical changes early in the disease process.”
The National Institutes of Health and the National Multiple Sclerosis Society supported the study. Some of the authors reported receiving awards from the National Multiple Sclerosis Society, the American Academy of Neurology, and the National Institute of Neurological Disorders and Stroke.
Asymptomatic first-degree relatives of multiple sclerosis patients at high risk for developing the disease were significantly more likely to show subclinical signs of MS than were family members at lower risk, in the Genes and Environment in Multiple Sclerosis prospective cohort study. The findings were published online on Jan. 17 in JAMA Neurology.
The Genes and Environment in Multiple Sclerosis (GEMS) project is the first prospective study of populations at risk for MS and is the first detailed cross-sectional examination of higher-risk and lower-risk family members to date, according to investigators led by Zongqi Xia, MD, PhD, of Brigham and Women’s Hospital, Boston. Although the totality of evidence put together through neuroimaging and numerous clinical tests in the study indicate that individuals with the highest risk for MS have higher risk for the disease than do those with the lowest risk, simple vibration threshold testing gave the best results, Dr. Xia and his colleagues reported.
The study involved 100 neurologically asymptomatic adults aged 18-50 years who were first-degree relatives of people with MS who participated in the GEMS project during August 2012 to July 2015. These 100 comprised 41 high-risk participants from the top 10% of a Genetic and Environmental Risk Score (GERS) and 59 low-risk participants from the bottom 10% on the GERS. The GERS included genetic risk factors (HLA alleles and several MS-associated non-HLA genetic variants) and environmental factors, such as smoking status, body mass index, history of infectious mononucleosis and migraine, and vitamin D levels.
However, because 40 of the 41 high-risk individuals were female and 25 of the 59 low-risk individuals were female, the investigators limited the study to the 65 female participants to avoid “attributing any potential difference primarily to the role of sex.”
To help in identifying early signs of MS, the researchers used brain MRI and optical coherence tomography and other measures of neurological function, including the Expanded Disability Status Scale, timed 25-foot walk, Nine-Hole Peg Test, Paced Auditory Serial Addition Test, Symbol Digit Modalities Test, Timed Up and Go, and high-contrast and low-contrast visual acuity (JAMA Neurol. 2017 Jan 17. doi: 10.1001/jamaneurol.2016.5056).
Overall, high-risk women showed more subclinical signs of MS than did low-risk women based on an omnibus test that globally assessed the burden of neurological dysfunction by comparing the overall differences between the two groups when considering all of the measured outcomes (P = .01). However, impaired vibration perception yielded a stronger result; of 47 women (27 high-risk and 20 low-risk) tested in this manner, high-risk women showed significantly reduced vibration perception in the distal lower extremities (P = .008).
One individual in the high-risk group converted to clinically definite MS during the study. Four of the high-risk women had T2-weighted hyperintense lesions that met the 2010 McDonald MRI criteria for dissemination in space, compared with one low-risk woman. The 2016 proposed consensus MRI criteria for MS diagnosis were met by two high-risk women and one low-risk woman. Radiological isolated syndrome occurred in one woman of each group, and there was a single foci of leptominengeal enhancement in three high-risk women and one low-risk woman.
The findings were limited by several factors including the small size, lack of male participants, cross-sectional nature of the study, and the fact that vibration sensitivity thresholds were in the normal range for high-risk and low-risk individuals. However, the researchers wrote that they “plan to confirm the finding of change in vibration sensitivity with a follow-up study,” and they noted that the “study highlights the important need to develop and test more sensitive measures, particularly with biometric devices, to detect subtle subclinical changes early in the disease process.”
The National Institutes of Health and the National Multiple Sclerosis Society supported the study. Some of the authors reported receiving awards from the National Multiple Sclerosis Society, the American Academy of Neurology, and the National Institute of Neurological Disorders and Stroke.
FROM JAMA NEUROLOGY
Key clinical point: Higher-risk asymptomatic female family relatives of patients with MS are more likely to have early subclinical manifestations of the disease and deserve further monitoring.
Major finding: Women at high risk for MS scored significantly higher on a composite of measured outcomes (P = .01) and on a vibration sensitivity test (P = .008), compared with lower-risk women.
Data source: A prospective, cross-sectional, cohort study of 65 adult women at risk for MS.
Disclosures: The National Institutes of Health and the National Multiple Sclerosis Society supported the study. Some of the authors reported receiving awards from the National Multiple Sclerosis Society, the American Academy of Neurology, and the National Institute of Neurological Disorders and Stroke.
Rituximab May Have Advantages Over Fingolimod and Natalizumab in MS
LONDON—As a first- or second-line agent for relapsing-remitting multiple sclerosis (MS), rituximab demonstrates superior drug survival (ie, the proportion of patients remaining on a
Rituximab Is Not Indicated for MS
Rituximab, a chimeric mouse–human anti-CD20 monoclonal antibody, is not approved as an MS treatment, but researchers have studied it for this indication. Naismith et al found that rituximab effectively treated breakthrough disease in patients with relapsing-remitting MS.
In a retrospective, observational study, Fredrik Piehl, MD, Professor of Neuroimmunology at Karolinska Institutet in Stockholm, and colleagues examined outcomes in patients with MS who switched from natalizumab to rituximab or fingolimod as part of a risk-management strategy. Compared with patients who switched to fingolimod, patients who switched to rituximab had lower risks of clinical relapses and adverse events.

These results prompted Dr. Piehl and colleagues to conduct a study to compare the baseline characteristics and outcomes of patients with relapsing-remitting MS starting rituximab, fingolimod, or natalizumab. The investigators used data from the Swedish Neuroregistry, which contains information on approximately 80% of all Swedish patients with MS. They included 4,244 patients in their final analysis and examined only the first period for each therapy and patient.
Rituximab Reduced Likelihood of Relapse
Approximately 14% of Swedish patients with relapsing-remitting MS received natalizumab, 10% received fingolimod, and 29% received rituximab. Patients who initiated therapy with natalizumab tended to be younger, have a higher Expanded Disability Status Scale (EDSS) score, and have more active disease at baseline, compared with the other participants.
Drug survival was greater among all patients who ever received rituximab, compared with all patients who ever received fingolimod or natalizumab. When the researchers examined the drugs as first-line agents, drug survival was greater with rituximab than with the other therapies. They found the same result when they analyzed the treatments as second-line agents. Among patients who switched from natalizumab, drug survival was greater in patients who initiated rituximab, compared with those who initiated fingolimod.
Relapse-free survival was most likely among patients receiving rituximab, compared with patients receiving fingolimod or natalizumab. When the researchers analyzed the drugs as first-line agents, they found that relapse-free survival was more likely with rituximab than with the other therapies, but the difference was small. The difference in relapse-free survival was greater, however, when the researchers analyzed the three drugs as second-line therapies.
“The strengths of this study are that it is nationwide and [that] it is a real-world population, including patients with various comorbidities,” said Dr. Piehl. The study results were susceptible to hidden confounding by indication, however. Another weakness of the study was its retrospective, observational design, said Dr. Piehl.
—Erik Greb
Suggested Reading
Naismith RT, Piccio L, Lyons JA, et al. Rituximab add-on therapy for breakthrough relapsing multiple sclerosis: a 52-week phase II trial. Neurology. 2010;74(23):1860-1867.
Salzer J, Svenningsson R, Alping P, et al. Rituximab in multiple sclerosis: A retrospective observational study on safety and efficacy. Neurology. 2016 Oct 19 [Epub ahead of print].
LONDON—As a first- or second-line agent for relapsing-remitting multiple sclerosis (MS), rituximab demonstrates superior drug survival (ie, the proportion of patients remaining on a
Rituximab Is Not Indicated for MS
Rituximab, a chimeric mouse–human anti-CD20 monoclonal antibody, is not approved as an MS treatment, but researchers have studied it for this indication. Naismith et al found that rituximab effectively treated breakthrough disease in patients with relapsing-remitting MS.
In a retrospective, observational study, Fredrik Piehl, MD, Professor of Neuroimmunology at Karolinska Institutet in Stockholm, and colleagues examined outcomes in patients with MS who switched from natalizumab to rituximab or fingolimod as part of a risk-management strategy. Compared with patients who switched to fingolimod, patients who switched to rituximab had lower risks of clinical relapses and adverse events.
These results prompted Dr. Piehl and colleagues to conduct a study to compare the baseline characteristics and outcomes of patients with relapsing-remitting MS starting rituximab, fingolimod, or natalizumab. The investigators used data from the Swedish Neuroregistry, which contains information on approximately 80% of all Swedish patients with MS. They included 4,244 patients in their final analysis and examined only the first period for each therapy and patient.
Rituximab Reduced Likelihood of Relapse
Approximately 14% of Swedish patients with relapsing-remitting MS received natalizumab, 10% received fingolimod, and 29% received rituximab. Patients who initiated therapy with natalizumab tended to be younger, have a higher Expanded Disability Status Scale (EDSS) score, and have more active disease at baseline, compared with the other participants.
Drug survival was greater among all patients who ever received rituximab, compared with all patients who ever received fingolimod or natalizumab. When the researchers examined the drugs as first-line agents, drug survival was greater with rituximab than with the other therapies. They found the same result when they analyzed the treatments as second-line agents. Among patients who switched from natalizumab, drug survival was greater in patients who initiated rituximab, compared with those who initiated fingolimod.
Relapse-free survival was most likely among patients receiving rituximab, compared with patients receiving fingolimod or natalizumab. When the researchers analyzed the drugs as first-line agents, they found that relapse-free survival was more likely with rituximab than with the other therapies, but the difference was small. The difference in relapse-free survival was greater, however, when the researchers analyzed the three drugs as second-line therapies.
“The strengths of this study are that it is nationwide and [that] it is a real-world population, including patients with various comorbidities,” said Dr. Piehl. The study results were susceptible to hidden confounding by indication, however. Another weakness of the study was its retrospective, observational design, said Dr. Piehl.
—Erik Greb
Suggested Reading
Naismith RT, Piccio L, Lyons JA, et al. Rituximab add-on therapy for breakthrough relapsing multiple sclerosis: a 52-week phase II trial. Neurology. 2010;74(23):1860-1867.
Salzer J, Svenningsson R, Alping P, et al. Rituximab in multiple sclerosis: A retrospective observational study on safety and efficacy. Neurology. 2016 Oct 19 [Epub ahead of print].
LONDON—As a first- or second-line agent for relapsing-remitting multiple sclerosis (MS), rituximab demonstrates superior drug survival (ie, the proportion of patients remaining on a
Rituximab Is Not Indicated for MS
Rituximab, a chimeric mouse–human anti-CD20 monoclonal antibody, is not approved as an MS treatment, but researchers have studied it for this indication. Naismith et al found that rituximab effectively treated breakthrough disease in patients with relapsing-remitting MS.
In a retrospective, observational study, Fredrik Piehl, MD, Professor of Neuroimmunology at Karolinska Institutet in Stockholm, and colleagues examined outcomes in patients with MS who switched from natalizumab to rituximab or fingolimod as part of a risk-management strategy. Compared with patients who switched to fingolimod, patients who switched to rituximab had lower risks of clinical relapses and adverse events.
These results prompted Dr. Piehl and colleagues to conduct a study to compare the baseline characteristics and outcomes of patients with relapsing-remitting MS starting rituximab, fingolimod, or natalizumab. The investigators used data from the Swedish Neuroregistry, which contains information on approximately 80% of all Swedish patients with MS. They included 4,244 patients in their final analysis and examined only the first period for each therapy and patient.
Rituximab Reduced Likelihood of Relapse
Approximately 14% of Swedish patients with relapsing-remitting MS received natalizumab, 10% received fingolimod, and 29% received rituximab. Patients who initiated therapy with natalizumab tended to be younger, have a higher Expanded Disability Status Scale (EDSS) score, and have more active disease at baseline, compared with the other participants.
Drug survival was greater among all patients who ever received rituximab, compared with all patients who ever received fingolimod or natalizumab. When the researchers examined the drugs as first-line agents, drug survival was greater with rituximab than with the other therapies. They found the same result when they analyzed the treatments as second-line agents. Among patients who switched from natalizumab, drug survival was greater in patients who initiated rituximab, compared with those who initiated fingolimod.
Relapse-free survival was most likely among patients receiving rituximab, compared with patients receiving fingolimod or natalizumab. When the researchers analyzed the drugs as first-line agents, they found that relapse-free survival was more likely with rituximab than with the other therapies, but the difference was small. The difference in relapse-free survival was greater, however, when the researchers analyzed the three drugs as second-line therapies.
“The strengths of this study are that it is nationwide and [that] it is a real-world population, including patients with various comorbidities,” said Dr. Piehl. The study results were susceptible to hidden confounding by indication, however. Another weakness of the study was its retrospective, observational design, said Dr. Piehl.
—Erik Greb
Suggested Reading
Naismith RT, Piccio L, Lyons JA, et al. Rituximab add-on therapy for breakthrough relapsing multiple sclerosis: a 52-week phase II trial. Neurology. 2010;74(23):1860-1867.
Salzer J, Svenningsson R, Alping P, et al. Rituximab in multiple sclerosis: A retrospective observational study on safety and efficacy. Neurology. 2016 Oct 19 [Epub ahead of print].

What Are the Best Treatments for Bladder Dysfunction in MS?
LONDON—Many patients with multiple sclerosis (MS) suffer from bladder dysfunction, however, few of these patients have their symptoms managed, according to an overview presented at the 32nd Congress of the European Committee for Treatment and Research in MS.
If a patient reports bladder symptoms, most often those bladder symptoms will persist and increase, said Jalesh Panicker, MD, DM, Consultant Neurologist and Clinical Lead in Uroneurology at the University College London Institute of Neurology in Queen Square, London. Symptoms of urinary frequency, urgency, incontinence, and nocturia, which are collectively called overactive bladder syndrome, increase with increased duration of MS and tend to correlate with the neurologic disability, especially lower limb parameter weakness.

In a large survey of 3,000 patients with MS, 90% rated bladder complications as one of the top five common symptomatic problems. Seventy percent of the group reported that bladder issues had a moderate or high impact on them. Only one-third of patients surveyed reported improvement after starting disease-modifying therapies.
Bladder symptoms in MS occur, on average, six years into the illness. Lower urinary tract symptoms are present in 10% of patients at first diagnosis. To help address this issue, the Actionable eight-item questionnaire was developed to help make it easier for doctors to assess bladder problems, said Dr. Panicker.
Lesion location plays a significant role in urinary tract dysfunction. Patients with suprapontine lesions present predominantly with overactive bladder, whereas patients with spinal lesions tend to report voiding symptoms such as hesitancy and poor stream. Plaques in the cerebral cord can also alter the pattern of lower urinary tract dysfunction.
Measuring post-void residue is critical for bladder dysfunction management. Unlike in urgency and incontinence, patients tend to have difficulties expressing voiding and voiding dysfunction symptoms. A high post-void residue can cause urinary tract infections and lead to devastating effects on patients, Dr. Panicker said. Using a bladder scanner to detect high post-void residuals may help reduce urinary tract infections.
Oral Agents
The three most commonly used treatments for bladder dysfunction in patients with MS are oral agents, botulinum toxin, and neuromodulation. Oral antimuscarinics work through the muscarinic receptors of the bladder, reducing bladder sensation and intrusive pressures, inhibiting detrusor overactivity, and improving bladder capacity. Oxybutynin, for example, can cause dry mouth and dry eyes, whereas newer antimuscarinics such as tolteradine, solifenancin, or fesoteradine are less likely to cause dry eyes, dry mouth, or constipation, Dr. Panicker noted.
Anticholinergic burden refers to the cumulative effect of multiple medications with anticholinergic properties. The higher the anticholinergic burden, the greater the risk of cognitive impairment, impaired functional performance, mortality, and brain atrophy. The Anticholinergic Burden Scale (ACB) grades medications according to their anticholinergic burden—mild (ACB1), moderate (ACB2), and severe (ACB3). Total ACB score is the sum of each medication the patient is on; any ACB score over 3 is considered clinically relevant.
Beta 3 agonists are another class of oral agents used to control bladder symptoms. Beta 3 agonists inhibit intrusive muscle contractions and increase relaxation by acting on the beta 3 receptors present on the wall of the bladder. Unlike antimuscarinics, beta 3 agonists are devoid of side effects like dry mouth, dry eyes, and constipation; however, these oral agents are associated with cardiovascular side effects. Currently, there are pivotal phase III studies on the efficacy of mirabegron in the UK, however, there is limited evidence from neurologic patients and there is a need for more long-term data, Dr. Panicker said.
Botulinum Toxin
Botulinum toxin is effective for bladder management. Evidence shows that patients with MS experienced significant improvement in urinary incontinence, frequency, and urgency as early as four weeks after injections, and this beneficial effect is not lost with repeated injections. Three pivotal phase III studies have demonstrated the efficacy of onabotulinumtoxinA for improving incontinence. Studies suggest that onabotulinumtoxinA significantly improved incontinence at week 12. The median duration of retreatment was 42 weeks.
Neuromodulation
Stimulating the tibial nerve is beneficial in managing overactive bladder symptoms such as urinary frequency and incontinence. Percutaneous tibial nerve stimulation is one of the few treatments that does not tend to worsen voiding dysfunction. It is also potentially a treatment for patients who are retaining urine or experiencing incomplete bladder emptying.
“With several disease-modifying therapies over the last few years, it is clear that the number of MS relapses in patients is coming down. There is evidence to suggest that the neurologic disability that accumulates is also either halted or possibly even reversed. Whether the nonmotor symptoms of MS, such as urinary tract dysfunction, also would get halted or reversed with these treatments is an area for further research,” said Dr. Panicker.
—Erica Tricarico
Suggested Reading
Ginsberg D, Gousse A, Keppenne V, et al. Phase 3 efficacy and tolerability study of onabotulinumtoxinA for urinary incontinence from neurogenic detrusor overactivity. J Urol. 2012;187(6):2131-2139.
Jongen PJ, Blok BF, Heesakkers JP, et al. Simplified scoring of the Actionable 8-item screening questionnaire for neurogenic bladder overactivity in multiple sclerosis: a comparative analysis of test performance at different cut-off points. BMC Urol. 2015;15:106.
Wintner A, Kim MM, Bechis SK, Kreydin El. Voiding dysfunction in multiple sclerosis. Semin Neurol. 2016;36(1):34-40.
LONDON—Many patients with multiple sclerosis (MS) suffer from bladder dysfunction, however, few of these patients have their symptoms managed, according to an overview presented at the 32nd Congress of the European Committee for Treatment and Research in MS.
If a patient reports bladder symptoms, most often those bladder symptoms will persist and increase, said Jalesh Panicker, MD, DM, Consultant Neurologist and Clinical Lead in Uroneurology at the University College London Institute of Neurology in Queen Square, London. Symptoms of urinary frequency, urgency, incontinence, and nocturia, which are collectively called overactive bladder syndrome, increase with increased duration of MS and tend to correlate with the neurologic disability, especially lower limb parameter weakness.
In a large survey of 3,000 patients with MS, 90% rated bladder complications as one of the top five common symptomatic problems. Seventy percent of the group reported that bladder issues had a moderate or high impact on them. Only one-third of patients surveyed reported improvement after starting disease-modifying therapies.
Bladder symptoms in MS occur, on average, six years into the illness. Lower urinary tract symptoms are present in 10% of patients at first diagnosis. To help address this issue, the Actionable eight-item questionnaire was developed to help make it easier for doctors to assess bladder problems, said Dr. Panicker.
Lesion location plays a significant role in urinary tract dysfunction. Patients with suprapontine lesions present predominantly with overactive bladder, whereas patients with spinal lesions tend to report voiding symptoms such as hesitancy and poor stream. Plaques in the cerebral cord can also alter the pattern of lower urinary tract dysfunction.
Measuring post-void residue is critical for bladder dysfunction management. Unlike in urgency and incontinence, patients tend to have difficulties expressing voiding and voiding dysfunction symptoms. A high post-void residue can cause urinary tract infections and lead to devastating effects on patients, Dr. Panicker said. Using a bladder scanner to detect high post-void residuals may help reduce urinary tract infections.
Oral Agents
The three most commonly used treatments for bladder dysfunction in patients with MS are oral agents, botulinum toxin, and neuromodulation. Oral antimuscarinics work through the muscarinic receptors of the bladder, reducing bladder sensation and intrusive pressures, inhibiting detrusor overactivity, and improving bladder capacity. Oxybutynin, for example, can cause dry mouth and dry eyes, whereas newer antimuscarinics such as tolteradine, solifenancin, or fesoteradine are less likely to cause dry eyes, dry mouth, or constipation, Dr. Panicker noted.
Anticholinergic burden refers to the cumulative effect of multiple medications with anticholinergic properties. The higher the anticholinergic burden, the greater the risk of cognitive impairment, impaired functional performance, mortality, and brain atrophy. The Anticholinergic Burden Scale (ACB) grades medications according to their anticholinergic burden—mild (ACB1), moderate (ACB2), and severe (ACB3). Total ACB score is the sum of each medication the patient is on; any ACB score over 3 is considered clinically relevant.
Beta 3 agonists are another class of oral agents used to control bladder symptoms. Beta 3 agonists inhibit intrusive muscle contractions and increase relaxation by acting on the beta 3 receptors present on the wall of the bladder. Unlike antimuscarinics, beta 3 agonists are devoid of side effects like dry mouth, dry eyes, and constipation; however, these oral agents are associated with cardiovascular side effects. Currently, there are pivotal phase III studies on the efficacy of mirabegron in the UK, however, there is limited evidence from neurologic patients and there is a need for more long-term data, Dr. Panicker said.
Botulinum Toxin
Botulinum toxin is effective for bladder management. Evidence shows that patients with MS experienced significant improvement in urinary incontinence, frequency, and urgency as early as four weeks after injections, and this beneficial effect is not lost with repeated injections. Three pivotal phase III studies have demonstrated the efficacy of onabotulinumtoxinA for improving incontinence. Studies suggest that onabotulinumtoxinA significantly improved incontinence at week 12. The median duration of retreatment was 42 weeks.
Neuromodulation
Stimulating the tibial nerve is beneficial in managing overactive bladder symptoms such as urinary frequency and incontinence. Percutaneous tibial nerve stimulation is one of the few treatments that does not tend to worsen voiding dysfunction. It is also potentially a treatment for patients who are retaining urine or experiencing incomplete bladder emptying.
“With several disease-modifying therapies over the last few years, it is clear that the number of MS relapses in patients is coming down. There is evidence to suggest that the neurologic disability that accumulates is also either halted or possibly even reversed. Whether the nonmotor symptoms of MS, such as urinary tract dysfunction, also would get halted or reversed with these treatments is an area for further research,” said Dr. Panicker.
—Erica Tricarico
Suggested Reading
Ginsberg D, Gousse A, Keppenne V, et al. Phase 3 efficacy and tolerability study of onabotulinumtoxinA for urinary incontinence from neurogenic detrusor overactivity. J Urol. 2012;187(6):2131-2139.
Jongen PJ, Blok BF, Heesakkers JP, et al. Simplified scoring of the Actionable 8-item screening questionnaire for neurogenic bladder overactivity in multiple sclerosis: a comparative analysis of test performance at different cut-off points. BMC Urol. 2015;15:106.
Wintner A, Kim MM, Bechis SK, Kreydin El. Voiding dysfunction in multiple sclerosis. Semin Neurol. 2016;36(1):34-40.
LONDON—Many patients with multiple sclerosis (MS) suffer from bladder dysfunction, however, few of these patients have their symptoms managed, according to an overview presented at the 32nd Congress of the European Committee for Treatment and Research in MS.
If a patient reports bladder symptoms, most often those bladder symptoms will persist and increase, said Jalesh Panicker, MD, DM, Consultant Neurologist and Clinical Lead in Uroneurology at the University College London Institute of Neurology in Queen Square, London. Symptoms of urinary frequency, urgency, incontinence, and nocturia, which are collectively called overactive bladder syndrome, increase with increased duration of MS and tend to correlate with the neurologic disability, especially lower limb parameter weakness.
In a large survey of 3,000 patients with MS, 90% rated bladder complications as one of the top five common symptomatic problems. Seventy percent of the group reported that bladder issues had a moderate or high impact on them. Only one-third of patients surveyed reported improvement after starting disease-modifying therapies.
Bladder symptoms in MS occur, on average, six years into the illness. Lower urinary tract symptoms are present in 10% of patients at first diagnosis. To help address this issue, the Actionable eight-item questionnaire was developed to help make it easier for doctors to assess bladder problems, said Dr. Panicker.
Lesion location plays a significant role in urinary tract dysfunction. Patients with suprapontine lesions present predominantly with overactive bladder, whereas patients with spinal lesions tend to report voiding symptoms such as hesitancy and poor stream. Plaques in the cerebral cord can also alter the pattern of lower urinary tract dysfunction.
Measuring post-void residue is critical for bladder dysfunction management. Unlike in urgency and incontinence, patients tend to have difficulties expressing voiding and voiding dysfunction symptoms. A high post-void residue can cause urinary tract infections and lead to devastating effects on patients, Dr. Panicker said. Using a bladder scanner to detect high post-void residuals may help reduce urinary tract infections.
Oral Agents
The three most commonly used treatments for bladder dysfunction in patients with MS are oral agents, botulinum toxin, and neuromodulation. Oral antimuscarinics work through the muscarinic receptors of the bladder, reducing bladder sensation and intrusive pressures, inhibiting detrusor overactivity, and improving bladder capacity. Oxybutynin, for example, can cause dry mouth and dry eyes, whereas newer antimuscarinics such as tolteradine, solifenancin, or fesoteradine are less likely to cause dry eyes, dry mouth, or constipation, Dr. Panicker noted.
Anticholinergic burden refers to the cumulative effect of multiple medications with anticholinergic properties. The higher the anticholinergic burden, the greater the risk of cognitive impairment, impaired functional performance, mortality, and brain atrophy. The Anticholinergic Burden Scale (ACB) grades medications according to their anticholinergic burden—mild (ACB1), moderate (ACB2), and severe (ACB3). Total ACB score is the sum of each medication the patient is on; any ACB score over 3 is considered clinically relevant.
Beta 3 agonists are another class of oral agents used to control bladder symptoms. Beta 3 agonists inhibit intrusive muscle contractions and increase relaxation by acting on the beta 3 receptors present on the wall of the bladder. Unlike antimuscarinics, beta 3 agonists are devoid of side effects like dry mouth, dry eyes, and constipation; however, these oral agents are associated with cardiovascular side effects. Currently, there are pivotal phase III studies on the efficacy of mirabegron in the UK, however, there is limited evidence from neurologic patients and there is a need for more long-term data, Dr. Panicker said.
Botulinum Toxin
Botulinum toxin is effective for bladder management. Evidence shows that patients with MS experienced significant improvement in urinary incontinence, frequency, and urgency as early as four weeks after injections, and this beneficial effect is not lost with repeated injections. Three pivotal phase III studies have demonstrated the efficacy of onabotulinumtoxinA for improving incontinence. Studies suggest that onabotulinumtoxinA significantly improved incontinence at week 12. The median duration of retreatment was 42 weeks.
Neuromodulation
Stimulating the tibial nerve is beneficial in managing overactive bladder symptoms such as urinary frequency and incontinence. Percutaneous tibial nerve stimulation is one of the few treatments that does not tend to worsen voiding dysfunction. It is also potentially a treatment for patients who are retaining urine or experiencing incomplete bladder emptying.
“With several disease-modifying therapies over the last few years, it is clear that the number of MS relapses in patients is coming down. There is evidence to suggest that the neurologic disability that accumulates is also either halted or possibly even reversed. Whether the nonmotor symptoms of MS, such as urinary tract dysfunction, also would get halted or reversed with these treatments is an area for further research,” said Dr. Panicker.
—Erica Tricarico
Suggested Reading
Ginsberg D, Gousse A, Keppenne V, et al. Phase 3 efficacy and tolerability study of onabotulinumtoxinA for urinary incontinence from neurogenic detrusor overactivity. J Urol. 2012;187(6):2131-2139.
Jongen PJ, Blok BF, Heesakkers JP, et al. Simplified scoring of the Actionable 8-item screening questionnaire for neurogenic bladder overactivity in multiple sclerosis: a comparative analysis of test performance at different cut-off points. BMC Urol. 2015;15:106.
Wintner A, Kim MM, Bechis SK, Kreydin El. Voiding dysfunction in multiple sclerosis. Semin Neurol. 2016;36(1):34-40.
Lack of natalizumab concentration increase before PML argues against extending dosing interval
Serum concentrations of natalizumab do not appear to rise before patients with relapsing-remitting multiple sclerosis are diagnosed with progressive multifocal leukoencephalopathy, contradicting the hypothesis that exposure to elevated concentrations of the drug is a risk factor for the disease, according to findings from a prospective, observational cohort study.
Zoé L.E. van Kempen, MD, and her colleagues at VU Medical Center Amsterdam noted that a small but increasing number of “neurologists are extending dose intervals of natalizumab [Tysabri] with the primary aim of reducing the risk of PML [progressive multifocal leukoencephalopathy] by lowering the natalizumab exposure per patient,” which also potentially has the benefit of decreasing drug costs, as well as clinic or hospital visits. However, there have been no prospective studies that confirm that extending natalizumab dose intervals does not affect efficacy.
Dr. van Kempen and her coinvestigators investigated this hypothesis by comparing serum concentrations of natalizumab in 5 patients with PML and 10 age- and sex-matched controls from a cohort of 219 relapsing-remitting multiple sclerosis patients taking natalizumab who had blood samples routinely drawn every 12 weeks before the infusion of natalizumab (Mult Scler. 2016 Dec 13. doi: 10.1177/1352458516684023). These 10 controls had a mean concentration of 23.8 mcg/mL, which was in the same range as the 18.9 mcg/mL level observed before the diagnosis of PML in the 5 cases from the cohort. The five cases also did not show a rise in concentration before the diagnosis of PML and did not have concentrations fluctuate more than 11 mcg/mL during treatment. The patients with PML received a mean of 43 infusions, whereas controls received an average of 106 infusions. A median number of 5 pre-PML samples underwent testing, compared with yearly concentration measurements in the 10 controls who had at least 7 years’ treatment duration.
The increased risk of PML that has been documented in other studies with more than 24 months of natalizumab treatment also was not explained in this study by a rise in serum concentration over long-term follow-up.
“Although this cohort is too small to draw definite conclusions, our results do not support the hypothesis of high serum concentrations as a risk factor for developing PML,” the investigators wrote.
“With our small cohort in mind and insufficient data on this subject so far, neurologists should be careful in extending dose intervals and not overstate a possible decrease in the risk of developing PML. Obviously, if neurologists choose to extend dosing intervals of natalizumab in [John Cunningham virus]–positive patients, these patients should still receive stringent PML monitoring according to current recommendations,” they advised.
The study received support from the Brain Foundation Netherlands. Five of the authors reported financial ties to various pharmaceutical companies that market MS drugs, including Biogen, which markets natalizumab.
Serum concentrations of natalizumab do not appear to rise before patients with relapsing-remitting multiple sclerosis are diagnosed with progressive multifocal leukoencephalopathy, contradicting the hypothesis that exposure to elevated concentrations of the drug is a risk factor for the disease, according to findings from a prospective, observational cohort study.
Zoé L.E. van Kempen, MD, and her colleagues at VU Medical Center Amsterdam noted that a small but increasing number of “neurologists are extending dose intervals of natalizumab [Tysabri] with the primary aim of reducing the risk of PML [progressive multifocal leukoencephalopathy] by lowering the natalizumab exposure per patient,” which also potentially has the benefit of decreasing drug costs, as well as clinic or hospital visits. However, there have been no prospective studies that confirm that extending natalizumab dose intervals does not affect efficacy.
Dr. van Kempen and her coinvestigators investigated this hypothesis by comparing serum concentrations of natalizumab in 5 patients with PML and 10 age- and sex-matched controls from a cohort of 219 relapsing-remitting multiple sclerosis patients taking natalizumab who had blood samples routinely drawn every 12 weeks before the infusion of natalizumab (Mult Scler. 2016 Dec 13. doi: 10.1177/1352458516684023). These 10 controls had a mean concentration of 23.8 mcg/mL, which was in the same range as the 18.9 mcg/mL level observed before the diagnosis of PML in the 5 cases from the cohort. The five cases also did not show a rise in concentration before the diagnosis of PML and did not have concentrations fluctuate more than 11 mcg/mL during treatment. The patients with PML received a mean of 43 infusions, whereas controls received an average of 106 infusions. A median number of 5 pre-PML samples underwent testing, compared with yearly concentration measurements in the 10 controls who had at least 7 years’ treatment duration.
The increased risk of PML that has been documented in other studies with more than 24 months of natalizumab treatment also was not explained in this study by a rise in serum concentration over long-term follow-up.
“Although this cohort is too small to draw definite conclusions, our results do not support the hypothesis of high serum concentrations as a risk factor for developing PML,” the investigators wrote.
“With our small cohort in mind and insufficient data on this subject so far, neurologists should be careful in extending dose intervals and not overstate a possible decrease in the risk of developing PML. Obviously, if neurologists choose to extend dosing intervals of natalizumab in [John Cunningham virus]–positive patients, these patients should still receive stringent PML monitoring according to current recommendations,” they advised.
The study received support from the Brain Foundation Netherlands. Five of the authors reported financial ties to various pharmaceutical companies that market MS drugs, including Biogen, which markets natalizumab.
Serum concentrations of natalizumab do not appear to rise before patients with relapsing-remitting multiple sclerosis are diagnosed with progressive multifocal leukoencephalopathy, contradicting the hypothesis that exposure to elevated concentrations of the drug is a risk factor for the disease, according to findings from a prospective, observational cohort study.
Zoé L.E. van Kempen, MD, and her colleagues at VU Medical Center Amsterdam noted that a small but increasing number of “neurologists are extending dose intervals of natalizumab [Tysabri] with the primary aim of reducing the risk of PML [progressive multifocal leukoencephalopathy] by lowering the natalizumab exposure per patient,” which also potentially has the benefit of decreasing drug costs, as well as clinic or hospital visits. However, there have been no prospective studies that confirm that extending natalizumab dose intervals does not affect efficacy.
Dr. van Kempen and her coinvestigators investigated this hypothesis by comparing serum concentrations of natalizumab in 5 patients with PML and 10 age- and sex-matched controls from a cohort of 219 relapsing-remitting multiple sclerosis patients taking natalizumab who had blood samples routinely drawn every 12 weeks before the infusion of natalizumab (Mult Scler. 2016 Dec 13. doi: 10.1177/1352458516684023). These 10 controls had a mean concentration of 23.8 mcg/mL, which was in the same range as the 18.9 mcg/mL level observed before the diagnosis of PML in the 5 cases from the cohort. The five cases also did not show a rise in concentration before the diagnosis of PML and did not have concentrations fluctuate more than 11 mcg/mL during treatment. The patients with PML received a mean of 43 infusions, whereas controls received an average of 106 infusions. A median number of 5 pre-PML samples underwent testing, compared with yearly concentration measurements in the 10 controls who had at least 7 years’ treatment duration.
The increased risk of PML that has been documented in other studies with more than 24 months of natalizumab treatment also was not explained in this study by a rise in serum concentration over long-term follow-up.
“Although this cohort is too small to draw definite conclusions, our results do not support the hypothesis of high serum concentrations as a risk factor for developing PML,” the investigators wrote.
“With our small cohort in mind and insufficient data on this subject so far, neurologists should be careful in extending dose intervals and not overstate a possible decrease in the risk of developing PML. Obviously, if neurologists choose to extend dosing intervals of natalizumab in [John Cunningham virus]–positive patients, these patients should still receive stringent PML monitoring according to current recommendations,” they advised.
The study received support from the Brain Foundation Netherlands. Five of the authors reported financial ties to various pharmaceutical companies that market MS drugs, including Biogen, which markets natalizumab.
FROM MULTIPLE SCLEROSIS JOURNAL
Key clinical point:
Major finding: A total of 10 control patients had a mean natalizumab serum concentration of 23.8 mcg/mL, which was in the same range as the 18.9 mcg/mL level observed in 5 patients before a diagnosis of PML.
Data source: A comparison of 5 patients with PML and 10 age- and sex-matched controls from a prospective cohort of 219 patients with relapsing-remitting MS who were treated with natalizumab at one center.
Disclosures: The study received support from the Brain Foundation Netherlands. Five of the authors reported financial ties to various pharmaceutical companies that market MS drugs, including Biogen, which markets natalizumab.
Nomogram predicts conversion of first demyelinating event to definite MS
Baseline and follow-up data from a prospective, multinational cohort of more than 3,000 patients with clinically isolated events allowed researchers to develop an accurate prognostic nomogram to calculate an individual’s risk for conversion to clinically definite multiple sclerosis at 12 months.
“Identification of patient, disease, and examination factors associated with higher probability of second attack in clinical practice may enable clinicians to flag patients that could benefit from more intensive follow-up and consideration of early DMD [disease-modifying drug] treatment intervention, facilitating more favorable patient outcomes,” wrote Tim Spelman, PhD, and his associates.
Risk of relapse was decreased when clinically isolated syndrome was diagnosed later, with an adjusted hazard ratio of 0.9 for every 5 additional years of age. Other risk factors for earlier relapse include higher Expanded Disability Status Scale score at the onset of the first demyelinating event, DMD exposure prior to the first attack, multiple brain and spinal MRI criteria, and oligoclonal bands.
“These results corroborate and extend prior, albeit smaller, studies observing similar sets of predictors of clinical conversion probability,” Dr. Spelman and his coauthors wrote.
The predictive nomogram had a concordance index of 0.81 between the 12-month estimated and observed conversion probabilities.
“While our own internal validation suggested good performance, both an additional training-validation approach and an external validation through the application of the nomogram to a separate MS data set or population are required to confirm the generalizability of the nomogram,” they wrote.
Read the full study in Multiple Sclerosis Journal (2016 Nov 24. doi: 10.1177/1352458516679893).
Baseline and follow-up data from a prospective, multinational cohort of more than 3,000 patients with clinically isolated events allowed researchers to develop an accurate prognostic nomogram to calculate an individual’s risk for conversion to clinically definite multiple sclerosis at 12 months.
“Identification of patient, disease, and examination factors associated with higher probability of second attack in clinical practice may enable clinicians to flag patients that could benefit from more intensive follow-up and consideration of early DMD [disease-modifying drug] treatment intervention, facilitating more favorable patient outcomes,” wrote Tim Spelman, PhD, and his associates.
Risk of relapse was decreased when clinically isolated syndrome was diagnosed later, with an adjusted hazard ratio of 0.9 for every 5 additional years of age. Other risk factors for earlier relapse include higher Expanded Disability Status Scale score at the onset of the first demyelinating event, DMD exposure prior to the first attack, multiple brain and spinal MRI criteria, and oligoclonal bands.
“These results corroborate and extend prior, albeit smaller, studies observing similar sets of predictors of clinical conversion probability,” Dr. Spelman and his coauthors wrote.
The predictive nomogram had a concordance index of 0.81 between the 12-month estimated and observed conversion probabilities.
“While our own internal validation suggested good performance, both an additional training-validation approach and an external validation through the application of the nomogram to a separate MS data set or population are required to confirm the generalizability of the nomogram,” they wrote.
Read the full study in Multiple Sclerosis Journal (2016 Nov 24. doi: 10.1177/1352458516679893).
Baseline and follow-up data from a prospective, multinational cohort of more than 3,000 patients with clinically isolated events allowed researchers to develop an accurate prognostic nomogram to calculate an individual’s risk for conversion to clinically definite multiple sclerosis at 12 months.
“Identification of patient, disease, and examination factors associated with higher probability of second attack in clinical practice may enable clinicians to flag patients that could benefit from more intensive follow-up and consideration of early DMD [disease-modifying drug] treatment intervention, facilitating more favorable patient outcomes,” wrote Tim Spelman, PhD, and his associates.
Risk of relapse was decreased when clinically isolated syndrome was diagnosed later, with an adjusted hazard ratio of 0.9 for every 5 additional years of age. Other risk factors for earlier relapse include higher Expanded Disability Status Scale score at the onset of the first demyelinating event, DMD exposure prior to the first attack, multiple brain and spinal MRI criteria, and oligoclonal bands.
“These results corroborate and extend prior, albeit smaller, studies observing similar sets of predictors of clinical conversion probability,” Dr. Spelman and his coauthors wrote.
The predictive nomogram had a concordance index of 0.81 between the 12-month estimated and observed conversion probabilities.
“While our own internal validation suggested good performance, both an additional training-validation approach and an external validation through the application of the nomogram to a separate MS data set or population are required to confirm the generalizability of the nomogram,” they wrote.
Read the full study in Multiple Sclerosis Journal (2016 Nov 24. doi: 10.1177/1352458516679893).
FROM MULTIPLE SCLEROSIS JOURNAL