User login
Bariatric surgery for obesity: Does it decrease mortality?
Principal Source: Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch Surg 2007; 142(10):923-8.
Discussant: Glen L. Xiong, MD
Dr. Xiong is assistant clinical professor, departments of internal medicine and psychiatry and behavioral sciences, University of California, Davis.
- keep current with important developments in internal medicine
- knowledgeably discuss these developments with medical colleagues
- determine when to refer patients to a primary care physician or specialist
- manage psychiatric issues while your patients undergo evaluation or treatment for a medical condition.
Many obese patients suffer from depression, bipolar disorder, panic disorder, personality disorders, or other psychiatric conditions.1 Morbidly obese patients searching for a lasting solution to their weight problems might seek a psychiatric evaluation for bariatric surgery. However, before giving the green light for the procedure, consider that a recent study questions if bariatric surgery decreases mortality in obese patients.
Most bariatric surgery practice guidelines require evaluation and treatment of comorbid psychiatric conditions such as eating disorders, depression, and substance use disorder, which can worsen postoperative outcomes. Indications for bariatric surgery include a body mass index (BMI) ≥40 kg/m2 or ≥35 kg/m2 with significant obesity-related comorbid medical conditions, such as diabetes ( Table 3 ).
A large-scale epidemiologic study found that bariatric surgery patients had a higher long-term risk of dying from coronary artery disease and suicide than the general population ( Table 4 ).2 Bariatric surgery patients also have a higher mortality rate than the general population, although they may have an absolute 1% survival advantage over closely matched obese patients who do not have the surgery.3 This advantage might disappear when selection bias is controlled, however, because patients who undergo surgery are more motivated to improve their health than patients who remain obese.
Table 3
Body mass index (BMI) values
| Obesity class | BMI |
|---|---|
| Underweight | 2 |
| Normal | 18.5 to 24.9 kg/m2 |
| Overweight | 25 to 29.9 kg/m2 |
| Mild obesity | 30 to 34.9 kg/m2 |
| Moderate obesity | 35 to 39.9 kg/m2 |
| Morbid obesity | ≥40 kg/m2 |
Of 16,683 bariatric operations performed in Pennsylvania over 10 years, 440 (2.6%) patients died. Nearly 1% of these deaths occurred within 30 days. The total death rate was approximately 1% per year and almost 6% at 5 years. In addition to the medical causes, 45 bariatric patients died from traumatic causes:
- 16 suicides (4%)
- 14 drug overdoses (3%)
- 10 motor vehicle accidents (2%)
- 3 homicides (0.7%)
- 2 falls (0.5%).
Women accounted for 10 of the 16 suicides (62.5%) and 12 of the 14 (85.7%) drug overdoses.
Treatment options. When treating obese patients, choose medications with a low risk for weight gain, which may include switching to a medication in the same class that is less likely to cause weight gain. Also, give patients educational handouts and resources about dietary and exercise regimens that focus on behavioral reinforcement. Although important, lifestyle modification and medication management produce nonsustained and modest results for most obese patients. Benefits are even more limited in morbidly obese patients with BMI ≥40 kg/m2.
Bariatric surgery is an emerging treatment option for obese patients, although its use has been limited by safety concerns, availability, and lack of coverage by many insurance companies. Among obesity treatments, only bariatric surgery has demonstrated enduring weight loss and reduced medical comorbidities such as diabetes.4
Table 4
Leading medical causes of death after bariatric surgery
| 30-day mortality n = 150 | Overall mortality* n = 395 | |
|---|---|---|
| Surgical complication | 28 (25.3%) | 45 (11.4%) |
| Pulmonary embolism | 31 (20.7%) | 47 (11.9%) |
| Coronary artery disease | 26 (17.3%) | 76 (19.2%) |
| Sepsis | 17 (11.3%) | 55 (13.9%) |
| * Up to 9 years of follow-up | ||
| Source: Reference 2 | ||
A new epidemic. The prevalence of obesity—nearly 1 in 3 Americans—has increased dramatically over the last few decades for reasons that include dietary indiscretion and sedentary lifestyle.5 Obesity is associated with decreased life expectancy,6 reduced quality of life, and higher incidence of diabetes, hypertension, arthritis, cardiovascular disease, sleep apnea, gastroesophageal reflux disease, and other chronic medical conditions. In addition, metabolic side effects of some psychotropic medications—especially antipsychotics—can exacerbate weight gain.
- Do not recommend bariatric surgery for patients with unstable psychiatric symptoms and psychosocial conditions or those who cannot follow up with postoperative care and required lifestyle modifications.
- Evaluate obese patients for psychiatric symptoms and suicidal thoughts because bariatric surgery patients may have an elevated risk of suicide.
- Consider referring patients with a BMI≥40 kg/m2 or a ≥35 kg/m2 with significant obesity-related comorbid medical conditions for bariatric surgery.
- Bariatric surgery patients have an increased risk of coronary disease-related adverse events, so refer bariatric surgery patients to primary care providers for follow-up.
Related resources
- American Society for Bariatric Surgery. Pre-surgical psychological assessment of bariatric surgery candidates. www.asbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
- National Heart Lung and Blood Institute. Body mass index calculator. www.nhlbisupport.com/bmi/bmicalc.htm.
- Torpy JM, Burke A, Glass RM. JAMA patient page. Bariatric surgery. JAMA 2005;294;(15):1986. Available at: http://jama.ama-assn.org/cgi/reprint/294/15/1986.pdf.
Disclosure
Dr. Xiong reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Pickering RP, Grant BF, Chou SP, Compton WM. Are overweight, obesity, and extreme obesity associated with psychopathology? Results from the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry 2007;68(7):998-1009.
2. Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch Surg 2007;142(10):923-8.
3. Livingston EH. Obesity, mortality, and bariatric surgery death rates. JAMA 2007;298(20):2406-8.
4. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004;351(26):2683-93.
5. Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 2006;295:1549-55.
6. Grundy SM. Obesity, metabolic syndrome, and coronary atherosclerosis. Circulation 2002;105(23):2696-8.
Principal Source: Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch Surg 2007; 142(10):923-8.
Discussant: Glen L. Xiong, MD
Dr. Xiong is assistant clinical professor, departments of internal medicine and psychiatry and behavioral sciences, University of California, Davis.
- keep current with important developments in internal medicine
- knowledgeably discuss these developments with medical colleagues
- determine when to refer patients to a primary care physician or specialist
- manage psychiatric issues while your patients undergo evaluation or treatment for a medical condition.
Many obese patients suffer from depression, bipolar disorder, panic disorder, personality disorders, or other psychiatric conditions.1 Morbidly obese patients searching for a lasting solution to their weight problems might seek a psychiatric evaluation for bariatric surgery. However, before giving the green light for the procedure, consider that a recent study questions if bariatric surgery decreases mortality in obese patients.
Most bariatric surgery practice guidelines require evaluation and treatment of comorbid psychiatric conditions such as eating disorders, depression, and substance use disorder, which can worsen postoperative outcomes. Indications for bariatric surgery include a body mass index (BMI) ≥40 kg/m2 or ≥35 kg/m2 with significant obesity-related comorbid medical conditions, such as diabetes ( Table 3 ).
A large-scale epidemiologic study found that bariatric surgery patients had a higher long-term risk of dying from coronary artery disease and suicide than the general population ( Table 4 ).2 Bariatric surgery patients also have a higher mortality rate than the general population, although they may have an absolute 1% survival advantage over closely matched obese patients who do not have the surgery.3 This advantage might disappear when selection bias is controlled, however, because patients who undergo surgery are more motivated to improve their health than patients who remain obese.
Table 3
Body mass index (BMI) values
| Obesity class | BMI |
|---|---|
| Underweight | 2 |
| Normal | 18.5 to 24.9 kg/m2 |
| Overweight | 25 to 29.9 kg/m2 |
| Mild obesity | 30 to 34.9 kg/m2 |
| Moderate obesity | 35 to 39.9 kg/m2 |
| Morbid obesity | ≥40 kg/m2 |
Of 16,683 bariatric operations performed in Pennsylvania over 10 years, 440 (2.6%) patients died. Nearly 1% of these deaths occurred within 30 days. The total death rate was approximately 1% per year and almost 6% at 5 years. In addition to the medical causes, 45 bariatric patients died from traumatic causes:
- 16 suicides (4%)
- 14 drug overdoses (3%)
- 10 motor vehicle accidents (2%)
- 3 homicides (0.7%)
- 2 falls (0.5%).
Women accounted for 10 of the 16 suicides (62.5%) and 12 of the 14 (85.7%) drug overdoses.
Treatment options. When treating obese patients, choose medications with a low risk for weight gain, which may include switching to a medication in the same class that is less likely to cause weight gain. Also, give patients educational handouts and resources about dietary and exercise regimens that focus on behavioral reinforcement. Although important, lifestyle modification and medication management produce nonsustained and modest results for most obese patients. Benefits are even more limited in morbidly obese patients with BMI ≥40 kg/m2.
Bariatric surgery is an emerging treatment option for obese patients, although its use has been limited by safety concerns, availability, and lack of coverage by many insurance companies. Among obesity treatments, only bariatric surgery has demonstrated enduring weight loss and reduced medical comorbidities such as diabetes.4
Table 4
Leading medical causes of death after bariatric surgery
| 30-day mortality n = 150 | Overall mortality* n = 395 | |
|---|---|---|
| Surgical complication | 28 (25.3%) | 45 (11.4%) |
| Pulmonary embolism | 31 (20.7%) | 47 (11.9%) |
| Coronary artery disease | 26 (17.3%) | 76 (19.2%) |
| Sepsis | 17 (11.3%) | 55 (13.9%) |
| * Up to 9 years of follow-up | ||
| Source: Reference 2 | ||
A new epidemic. The prevalence of obesity—nearly 1 in 3 Americans—has increased dramatically over the last few decades for reasons that include dietary indiscretion and sedentary lifestyle.5 Obesity is associated with decreased life expectancy,6 reduced quality of life, and higher incidence of diabetes, hypertension, arthritis, cardiovascular disease, sleep apnea, gastroesophageal reflux disease, and other chronic medical conditions. In addition, metabolic side effects of some psychotropic medications—especially antipsychotics—can exacerbate weight gain.
- Do not recommend bariatric surgery for patients with unstable psychiatric symptoms and psychosocial conditions or those who cannot follow up with postoperative care and required lifestyle modifications.
- Evaluate obese patients for psychiatric symptoms and suicidal thoughts because bariatric surgery patients may have an elevated risk of suicide.
- Consider referring patients with a BMI≥40 kg/m2 or a ≥35 kg/m2 with significant obesity-related comorbid medical conditions for bariatric surgery.
- Bariatric surgery patients have an increased risk of coronary disease-related adverse events, so refer bariatric surgery patients to primary care providers for follow-up.
Related resources
- American Society for Bariatric Surgery. Pre-surgical psychological assessment of bariatric surgery candidates. www.asbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
- National Heart Lung and Blood Institute. Body mass index calculator. www.nhlbisupport.com/bmi/bmicalc.htm.
- Torpy JM, Burke A, Glass RM. JAMA patient page. Bariatric surgery. JAMA 2005;294;(15):1986. Available at: http://jama.ama-assn.org/cgi/reprint/294/15/1986.pdf.
Disclosure
Dr. Xiong reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Principal Source: Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch Surg 2007; 142(10):923-8.
Discussant: Glen L. Xiong, MD
Dr. Xiong is assistant clinical professor, departments of internal medicine and psychiatry and behavioral sciences, University of California, Davis.
- keep current with important developments in internal medicine
- knowledgeably discuss these developments with medical colleagues
- determine when to refer patients to a primary care physician or specialist
- manage psychiatric issues while your patients undergo evaluation or treatment for a medical condition.
Many obese patients suffer from depression, bipolar disorder, panic disorder, personality disorders, or other psychiatric conditions.1 Morbidly obese patients searching for a lasting solution to their weight problems might seek a psychiatric evaluation for bariatric surgery. However, before giving the green light for the procedure, consider that a recent study questions if bariatric surgery decreases mortality in obese patients.
Most bariatric surgery practice guidelines require evaluation and treatment of comorbid psychiatric conditions such as eating disorders, depression, and substance use disorder, which can worsen postoperative outcomes. Indications for bariatric surgery include a body mass index (BMI) ≥40 kg/m2 or ≥35 kg/m2 with significant obesity-related comorbid medical conditions, such as diabetes ( Table 3 ).
A large-scale epidemiologic study found that bariatric surgery patients had a higher long-term risk of dying from coronary artery disease and suicide than the general population ( Table 4 ).2 Bariatric surgery patients also have a higher mortality rate than the general population, although they may have an absolute 1% survival advantage over closely matched obese patients who do not have the surgery.3 This advantage might disappear when selection bias is controlled, however, because patients who undergo surgery are more motivated to improve their health than patients who remain obese.
Table 3
Body mass index (BMI) values
| Obesity class | BMI |
|---|---|
| Underweight | 2 |
| Normal | 18.5 to 24.9 kg/m2 |
| Overweight | 25 to 29.9 kg/m2 |
| Mild obesity | 30 to 34.9 kg/m2 |
| Moderate obesity | 35 to 39.9 kg/m2 |
| Morbid obesity | ≥40 kg/m2 |
Of 16,683 bariatric operations performed in Pennsylvania over 10 years, 440 (2.6%) patients died. Nearly 1% of these deaths occurred within 30 days. The total death rate was approximately 1% per year and almost 6% at 5 years. In addition to the medical causes, 45 bariatric patients died from traumatic causes:
- 16 suicides (4%)
- 14 drug overdoses (3%)
- 10 motor vehicle accidents (2%)
- 3 homicides (0.7%)
- 2 falls (0.5%).
Women accounted for 10 of the 16 suicides (62.5%) and 12 of the 14 (85.7%) drug overdoses.
Treatment options. When treating obese patients, choose medications with a low risk for weight gain, which may include switching to a medication in the same class that is less likely to cause weight gain. Also, give patients educational handouts and resources about dietary and exercise regimens that focus on behavioral reinforcement. Although important, lifestyle modification and medication management produce nonsustained and modest results for most obese patients. Benefits are even more limited in morbidly obese patients with BMI ≥40 kg/m2.
Bariatric surgery is an emerging treatment option for obese patients, although its use has been limited by safety concerns, availability, and lack of coverage by many insurance companies. Among obesity treatments, only bariatric surgery has demonstrated enduring weight loss and reduced medical comorbidities such as diabetes.4
Table 4
Leading medical causes of death after bariatric surgery
| 30-day mortality n = 150 | Overall mortality* n = 395 | |
|---|---|---|
| Surgical complication | 28 (25.3%) | 45 (11.4%) |
| Pulmonary embolism | 31 (20.7%) | 47 (11.9%) |
| Coronary artery disease | 26 (17.3%) | 76 (19.2%) |
| Sepsis | 17 (11.3%) | 55 (13.9%) |
| * Up to 9 years of follow-up | ||
| Source: Reference 2 | ||
A new epidemic. The prevalence of obesity—nearly 1 in 3 Americans—has increased dramatically over the last few decades for reasons that include dietary indiscretion and sedentary lifestyle.5 Obesity is associated with decreased life expectancy,6 reduced quality of life, and higher incidence of diabetes, hypertension, arthritis, cardiovascular disease, sleep apnea, gastroesophageal reflux disease, and other chronic medical conditions. In addition, metabolic side effects of some psychotropic medications—especially antipsychotics—can exacerbate weight gain.
- Do not recommend bariatric surgery for patients with unstable psychiatric symptoms and psychosocial conditions or those who cannot follow up with postoperative care and required lifestyle modifications.
- Evaluate obese patients for psychiatric symptoms and suicidal thoughts because bariatric surgery patients may have an elevated risk of suicide.
- Consider referring patients with a BMI≥40 kg/m2 or a ≥35 kg/m2 with significant obesity-related comorbid medical conditions for bariatric surgery.
- Bariatric surgery patients have an increased risk of coronary disease-related adverse events, so refer bariatric surgery patients to primary care providers for follow-up.
Related resources
- American Society for Bariatric Surgery. Pre-surgical psychological assessment of bariatric surgery candidates. www.asbs.org/html/pdf/PsychPreSurgicalAssessment.pdf.
- National Heart Lung and Blood Institute. Body mass index calculator. www.nhlbisupport.com/bmi/bmicalc.htm.
- Torpy JM, Burke A, Glass RM. JAMA patient page. Bariatric surgery. JAMA 2005;294;(15):1986. Available at: http://jama.ama-assn.org/cgi/reprint/294/15/1986.pdf.
Disclosure
Dr. Xiong reports no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Pickering RP, Grant BF, Chou SP, Compton WM. Are overweight, obesity, and extreme obesity associated with psychopathology? Results from the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry 2007;68(7):998-1009.
2. Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch Surg 2007;142(10):923-8.
3. Livingston EH. Obesity, mortality, and bariatric surgery death rates. JAMA 2007;298(20):2406-8.
4. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004;351(26):2683-93.
5. Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 2006;295:1549-55.
6. Grundy SM. Obesity, metabolic syndrome, and coronary atherosclerosis. Circulation 2002;105(23):2696-8.
1. Pickering RP, Grant BF, Chou SP, Compton WM. Are overweight, obesity, and extreme obesity associated with psychopathology? Results from the national epidemiologic survey on alcohol and related conditions. J Clin Psychiatry 2007;68(7):998-1009.
2. Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for Pennsylvania residents, 1995 to 2004. Arch Surg 2007;142(10):923-8.
3. Livingston EH. Obesity, mortality, and bariatric surgery death rates. JAMA 2007;298(20):2406-8.
4. Sjöström L, Lindroos AK, Peltonen M, et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med 2004;351(26):2683-93.
5. Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 2006;295:1549-55.
6. Grundy SM. Obesity, metabolic syndrome, and coronary atherosclerosis. Circulation 2002;105(23):2696-8.
Is multiple sclerosis patient depressed, stressed, or both?
Mrs. S, age 50, has had relapsing-remitting multiple sclerosis (MS) for approximately 10 years. She describes her mood as “up and down” and is referred by her neurologist for psychiatric assessment of mood swings and possible depression. Fatigue limits her ability to work full-time, perform household duties, socialize with friends and family, and enjoy mental or physical exercise. In addition, her 18-year-old daughter—an important source of psychological support—is planning to leave home.
Mrs. S experienced depression 5 years ago during her divorce. She was prescribed paroxetine, 20 mg/d, and had a positive response. She took the medication for 6 months, then discontinued.
One-half of MS patients experience major depression in their lifetimes,1 and the suicide rate is approximately doubled in MS patients compared with the general population.2 Depression in MS patients often has an atypical presentation, with irritability and anger being as prominent as sadness.3 Not all emotional changes experienced by MS patients represent depressive disorders, however.
When evaluating MS patients who are struggling with depression, you can help them by diagnosing comorbid mood disorders, determining suicide risk, and providing psychological support as they cope with the impact of their illness.
MS disease course
MS is a disease of the brain and spinal cord, characterized by:
- inflammatory demyelination and gliosis
- neuronal and axonal loss
- a variety of presenting symptoms as different CNS regions are affected.
Focal areas of demyelination followed by a reactive gliosis cause white matter lesions in the brain, spinal cord, and optic nerve. Neurologic dysfunction can manifest as visual changes, spastic paresis, hypoesthesia and paresthesia, ataxia, and bowel and bladder dysfunction. MS presentation also can include optic neuritis and transverse myelitis. MS symptoms often are intensified by heat exposure.
After the initial episode, months or years may pass before additional neurologic symptoms appear. Based on its course, MS can be classified as:
- relapsing-remitting, when the disease does not progress between attacks
- secondary progressive, characterized by a gradually progressive course after an initial relapsing-remitting pattern
- primary progressive, when patients experience gradual progressive disability from symptom onset (Table 1).
Table 1
Clinical classification of multiple sclerosis (MS)
| Type | Characteristics |
|---|---|
| Relapsing-remitting* | Symptoms appear during relapses, resolve during remissions, and do not progress between relapses |
| Secondary progressive | MS symptoms that previously followed a relapsing-remitting pattern steadily become more severe and progress without relapse |
| Primary progressive | Gradual progression from symptom onset, without relapses or remission |
| Clinically isolated syndrome | A single attack that may indicate MS has occurred—such as optic neuritis or transverse myelitis—but clinical requirements for the diagnosis have not been met |
| * Patients often progress from relapsing-remitting to secondary progressive MS | |
CASE CONTINUED: Progressing symptoms
Mrs. S has had multiple MS presentations, including optic neuritis, lower extremity weakness, balance problems, and urinary incontinence. Recently, her MS symptoms have gradually progressed even in the absence of attacks, and her diagnosis has been revised to secondary progressive MS.
During psychiatric evaluation, Mrs. S denies persistent changes in sleep or appetite. She describes fatigue that starts after physical exertion and increases as the day progresses. She denies feelings of worthlessness, helplessness, excessive guilt, and suicidal ideation and does not have a history of inappropriate anger or irritability.
Diagnosing depression in MS
Normal emotional adjustment to MS can include reactions to loss of function or changes in social or occupational roles. Further, MS patients—similar to non-MS patients—experience life changes and transitions not related to the illness, such as divorce or a grown child moving away. Emotional responses to life stressors often are self-limited but may warrant an adjustment disorder diagnosis if they are associated with excessive distress or substantial impairment in social, occupational, or academic functioning (Table 2).4
Table 2
Questions to consider when assessing MS patients for depression
| Ask yourself | Reason |
|---|---|
| Are symptoms part of normal emotional changes? | Not all mood changes are pathologic or meet criteria for major depression |
| Is this an adjustment disorder? | Mood symptoms can be caused by a major stressor such as a recent diagnosis or personal loss |
| Is fatigue secondary to MS or depression? | MS typically causes fatigue after physical activity and heat exposure; fatigue early in the day points to depression |
| Are cognitive deficits related to MS or depression? | Negative thoughts point to depression whereas cognitive deficits may be caused by depression, MS, or both |
| Is this an atypical presentation? | MS patients may present with anger or irritability |
| Is this a pseudobulbar problem? | Patients with IEED might describe more concern about affect dysregulation than mood swings |
| MS: multiple sclerosis; IEED: involuntary emotional expression disorder | |
Female MS patients and those who report high stress or a family history of affective disorder may be more likely to develop clinical depression.5 Several studies have reported correlations between structural brain abnormalities and depression in MS. Feinstein et al
6 reported that extensive hyper intense lesion volume in the left medial inferior prefrontal region with atrophy affecting the dominant anterior temporal lobe was associated with major depression. However, a depression diagnosis in MS patients remains a clinical one that does not require brain imaging studies.
Lack of interest or enjoyment as a symptom of depression can be difficult to identify because MS can diminish enjoyment of some activities. Although patients with MS may need to change their activity patterns to accommodate their illness, the lack of enjoyment in all—or almost all—activities remains a valid indicator of depressive disorder.
MS treatment includes the use of disease-modifying medications such as interferon beta-1b and interferon beta-1a. Several years ago researchers were concerned that interferon beta might cause depression in MS patients based on reports of a suicide and attempted suicide during an early trial of interferon beta-1b in relapsing-remitting MS.7 Subsequent studies did not substantiate this concern, however (Box 1).8,9
Overlapping symptoms such as fatigue and cognitive deterioration could complicate the diagnosis. Look for changing patterns of these symptoms and other signs of depression. Rating scales that do not emphasize fatigue and cognitive impairment—such as the Beck Depression Inventory10 and the Center for Epidemiologic Studies Depression Rating Scale11—can help identify depression in MS patients.
Fatigue is one of MS’ most common and troublesome symptoms.12,13 It typically mounts gradually during the day and after activity or heat exposure. Thus, fatigue early in the morning or manifesting as diminished motivation may point to a depressive disorder.
Cognitive deterioration. Clinically significant cognitive dysfunction occurs in 45% to 65% of MS patients.14 The disease can cause losses in short-term memory, attention, information processing, problem solving, multitasking, and language function.
Bedside cognitive function tests such as the Mini-Mental State Examination15 often are not sensitive enough to detect MS-related cognitive dysfunction. Be alert for changes in cognitive style when assessing for depressive disorders in these patients. Feelings of worthlessness and guilt or suicidal ideation are not normal MS symptoms and point to depression.
MS patients may experience pathological laughing and crying—also known as involuntary emotional expression disorder (IEED)—a neurologic phenomenon that causes uncontrollable laughing, crying, or anger in the absence of subjective emotional distress. IEED has been reported in approximately 10% of patients with MS (Box 2).16-22
CASE CONTINUED: Learning to adjust
Since discontinuing paroxetine 5 years ago, Mrs. S has not experienced another depressive episode. However, she describes a history of mood changes associated with pressured speech, increased activity, irritability, and insomnia during cortisone treatment for idiopathic thrombocytopenic purpura 4 years earlier. These episodes were mild, and she did not seek psychiatric treatment.
Mrs. S’ mood episode does not seem to be a recurrence of major depressive disorder because she lacks persistent depressed mood and major depressive symptoms. Her diagnosis is best understood as an adjustment disorder to the progression of her illness and her daughter leaving home. Fatigue is her most debilitating MS symptom.
Medication options
Use a cautious approach to pharmacotherapy. MS patients may have diminished cognitive reserves and might be at increased risk of medication-related delirium.
Depression. Two randomized, controlled trials have confirmed antidepressants’ efficacy for treating depression in MS patients. The studies investigated the tricyclic antidepressant desipramine23 and the selective serotonin reuptake inhibitor (SSRI) sertraline.24
In a double-blind clinical trial, 28 patients were randomly assigned to a 5-week trial of desipramine and individual psychotherapy or placebo and psychotherapy. Patients receiving desipramine showed significantly greater improvement than the placebo group, as measured by clinical judgment.
A 16-week study compared the efficacy of cognitive-behavioral therapy (CBT), supportive-expressive group therapy (SEG), and sertraline in 63 MS patients with major depressive disorder. Results showed that CBT and sertraline were more effective in reducing depression than SEG.24
SSRIs are a common first choice because of their ease of use and general tolerability among MS patients.25 Recommended dosages include:
- citalopram, 20 to 40 mg/d
- fluoxetine, 20 to 40 mg/d
- fluvoxamine, 50 to 300 mg/d
- paroxetine, 20 to 50 mg/d
- sertraline, 50 to 200 mg/d.
There is no consensus that any one antidepressant is best for all MS patients, however. When selecting an antidepressant, consider side-effect profiles, potential for drug-drug interactions, and a history of response to a particular antidepressant. Highly sedating antidepressants such as mirtazapine could aggravate fatigue. Highly anticholinergic agents such as amitriptyline may impair cognitive function.
Fatigue. Amantadine is the mainstay pharmacologic treatment for fatigue in MS, but evidence for its efficacy is weak.26 Clinical trials of psychostimulants generally have reported disappointing results. One randomized, double-blind trial found no significant differences in fatigue levels between patients receiving pemoline or placebo.27
Some studies have reported reduced MS-related fatigue with modafinil,28-30 but the only double-blind, placebo-controlled trial showed no significant difference between modafinil and placebo in patient fatigue levels.31 In this study, modafinil reduced physical fatigue only in patients with daytime somnolence.
Do interferon beta-1a and 1b—agents used to treat relapsing-remitting MS—cause or aggravate depression?
Two large-scale clinical trials of interferon beta-1a included a validated measure of depressive symptoms—the Center for Epidemiologic Studies Depression Rating Scale.8,9 This scale allowed researchers to conduct a detailed analysis that compared changes in depression symptoms over time in study participants treated with interferon or placebo. Evidence did not indicate increased depressive symptoms in association with interferon treatment.
Conclusion. Depression symptoms that emerge during treatment with one of these agents are not likely caused by the treatment and usually can be managed without discontinuing the drug.
Other psychiatric disorders
Bipolar disorder occurs more frequently in MS patients than in the general population.32 Additionally, some patients with advanced MS might experience benign feelings of euphoria.33 Euphoria can be differentiated from mania by assessing for mania’s other symptoms, such as erratic and disinhibited behavior, rapid speech, increased libido, decreased need for sleep, and excessive energy.
Antidepressants and corticosteroids could aggravate the course of bipolar disorder, and drug-illness interactions with lithium could make side effects such as tremor, diarrhea, and polyuria more difficult to tolerate. Mood stabilizing anticonvulsants such as valproate and carbamazepine are a useful alternative for treating the bipolar patient with comorbid MS. To avoid sedation, start with a low dose and increase gradually.
Approximately 10% of multiple sclerosis (MS) patients develop inappropriate affective expression—anger, laughing, or crying—in the absence of prominent mood changes.16 Involuntary emotional expression disorder (IEED)—or pathologic laughing or crying—is a form of pseudobulbar affect. IEED occurs when affective motor control becomes disinhibited as a result of brain damage from neurologic disease or injury. Conditions associated with IEED include amyotrophic lateral sclerosis, MS, traumatic brain injury, stroke, and dementia.17
IEED can prompt a psychiatric evaluation because uncontrolled crying can seem like intense depression. Symptoms range in severity and include exaggerated and inappropriate affective responses and perceived lack of control over responses. IEED episodes are paroxysmal, occurring in a brief and stereotyped manner, whereas crying in depression is more sustained, less stereotyped, and relates to the underlying mood.17,18 In addition, patients with depressive disorders often suffer difficulties with sleep and appetite as well as thoughts of guilt, hopelessness, and worthlessness not present in IEED.17,19
Studies have shown successful treatment of IEED with antidepressants including tricyclic antidepressants and serotonin reuptake inhibitors.20 A recent randomized, controlled trial suggested that dextromethorphan and quinidine may be beneficial in treating potentially disabling pseudobulbar affect in MS.21 Rating scales such as the 7-item Center for Neurologic Study Lability Scale may help establish a baseline against which to monitor treatment response.22
Insomnia. Sedative hypnotics such as zopiclone can be used for short-term treatment of sleep disturbances. Carefully consider hypnotics’ possible negative effects on balance, coordination, and memory, however.
Psychotic disturbances are rare in MS but occur more frequently in MS patients than in the general population.34 Use low doses of antipsychotics such as olanzapine, quetiapine, or risperidone in MS patients with psychosis. These atypical agents are associated with a lower risk of parkinsonian side effects than typical antipsychotics.
CASE CONTINUED: Coping mechanisms
Mrs. S has difficulty coping with her increasing symptom burden and functional limitations, but she says it is hard for her to ask for help. Her treatment plan includes recruiting support to help her deal with feelings of loss over her daughter’s move. We encourage her to reconnect with friends and family and use community supports for MS patients.
We discuss her treatment options, including biological treatments for fatigue, CBT, and behavioral activation therapy for her mood symptoms. She chooses a course of modafinil, 50 mg/d, and weekly CBT incorporating behavioral activation therapy to increase her activity level and target depressive symptoms and fatigue.
Psychosocial interventions
CBT is an effective treatment for depression in MS patients24 and is preferred for most patients with mild depression. CBT focuses on improving coping through behavioral activation and cognitive restructuring.35 CBT can incorporate teaching patients skills for managing MS-related problems such as fatigue, mild cognitive impairment, pain, stress, communication, sexual dysfunction, intimacy, and social difficulties secondary to MS.
Behavioral activation strategies focus on the relationship between activity and mood. They target a common pattern of avoidance and withdrawal from social, occupational, and physical demands that relieves MS patients’ anxiety in the short term but leads to problems associated with inactivity.35 Behavioral activation strategies—including exercise—have a strong evidence base supporting their use alone to manage depression and as a component of CBT.36
Active coping strategies. In early MS, patients often use avoidance and denial to cope with their disease. As symptoms become more intrusive, however, patients usually need to learn active coping strategies. These often begin with symptom management and evolve to include individually meaningful tasks such as reevaluating personal goals, values, and priorities.
Other psychotherapy modalities. In one study, patients randomized to an insight-oriented treatment group improved more than those in a placebo intervention based on discussing current events.37 Although not formally assessed in the literature, psychoeducation can help the patient maintain a sense of control over his or her treatment. Interpersonal therapy can help patients deal with role transitions caused by their illness and subsequent disabilities, although its use in this population has not been studied.
Although the literature does not favor supportive psychotherapy for treating depression in MS patients,24 this modality can help alleviate feelings of grief and loss that can emerge when MS symptoms worsen. Patients often appreciate having an opportunity to articulate their feelings and fears in a professional therapeutic relationship. MS patients often value validation and normalization of their emotional responses, and many therapists choose to integrate supportive strategies with CBT’s more “action oriented” elements.
Exercise is an effective treatment for fatigue in MS38 and also helps combat loss of physical fitness. MS patients who use energy conservation strategies to manage fatigue can participate in suitably paced physical exercise. Aquatic exercise is a popular option because it often does not cause overheating.
CASE CONTINUED: Energy surge
At the second follow-up appointment, Mrs. S notes that her energy level is better early in the day but decreases by late afternoon. An additional dose of modafinil, 50 mg, is added at noon, which increases her overall energy level.
CBT helps Mrs. S to develop reasonable expectations of herself and others and addresses the possibility that she could try part-time work. Including exercise as behavioral activation also lessens her fatigue. Reconnecting with family and friends helps relieve feelings of isolation resulting from her daughter moving away.
Related resources
- National Multiple Sclerosis Society. www.nationalmssociety.org.
- The Goldman Consensus Group. The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 2005;11:328-37.
- Feinstein A. The clinical neuropsychiatry of multiple sclerosis. Cambridge, UK: Cambridge University Press; 2007.
Drug brand names
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Interferon beta-1a • Avonex, Rebif
- Interferon beta-1b • Betaseron
- Lithium • Eskalith, Lithobid
- Mirtazapine • Remeron
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pemoline • Cylert
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Valproate • Depacon
- Zopiclone • Imovane, Zimovane
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Patten SB, Beck CA, Williams JVA, et al. Major depression in multiple sclerosis: a population-based perspective. Neurology 2003;61:1524-7.
2. Stenager EN, Stenager E, Koch-Henriksen N, et al. Suicide and multiple sclerosis: an epidemiological investigation. J Neurol Neurosurg Psychiatry 1992;55:542-5.
3. Minden SL, Orav J, Reich P. Depression in multiple sclerosis. Gen Hosp Psychiatry 1987;9:426-34.
4. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
5. Patten SB, Metz LM, Reimer MA. Biopsychosocial correlates of major depression in a multiple sclerosis population. Mult Scler 2000;6:115-20.
6. Feinstein A, Roy P, Lobaugh N, et al. Structural brain abnormalities in multiple sclerosis patients with major depression. Neurology 2004;62:586-90.
7. Klapper JA. Interferon beta treatment of multiple sclerosis. Neurology 1994;44:188.-
8. Patten SB, Metz LM. Interferon β-1a and depression in secondary progressive MS: data from the SPECTRIMS trial. Neurology 2002;59(744):746.-
9. Patten SB, Metz LM. Interferon b-1a and depression in relapsing-remitting multiple sclerosis: an analysis of depression data from the PRISMS clinical trial. Mult Scler 2001;7:243-8.
10. Beck AT, Ward CH, Mendelson M, et al. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:53-63.
11. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Applied Psychol Measurement 1977;1:385-401.
12. Fisk JD, Pontefract A, Ritvo PG, et al. The impact of fatigue on patients with multiple sclerosis. Can J Neurol Sci 1995;21:9-14.
13. Freal JE, Kraft GH, Coryell JK. Symptomatic fatigue in multiple sclerosis. Arch Phys Med Rehabil 1984;65:135-8.
14. Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis. Natural history, pathophysiology and management. CNS Drugs 2002;16:445-55.
15. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State Examination. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-98.
16. Feinstein A, Feinstein K, Gray T, O’Connor P. The prevalence and neurobehavioural correlates of pathological laughter and crying in multiple sclerosis. Arch Neurol 1997;54:1116-21.
17. Cummings JL. Involuntary emotional expression disorder: definition, diagnosis, and measurement scales. CNS Spectr 2007;12(4 suppl 5):11-6.
18. Paradiso S, Chemerinski E, Yazici KM, et al. Frontal lobe syndrome reassessed: comparison of patients with lateral or medial frontal brain damage. J Neurol Neurosurg Psychiatry 1999;67(5):664-7.
19. Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63(1):89-93.
20. Schiffer RB, Herndon RM, Rudick RA. Treatment of pathological laughing and weeping with amitriptyline. N Eng J Med 1985;312:1480-2.
21. Panitch HS, Thisted RA, Smith RA, et al. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann Neurol 2006;59:780-7.
22. Smith RA, Berg JE, Pope LE, Thisted RA. Measuring pseudobulbar affect in ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2004;5(suppl 1):99-102.
23. Schiffer RB, Wineman NM. Antidepressant pharmacotherapy of depression associated with multiple sclerosis. Am J Psychiatry 1990;147(11):1493-7.
24. Mohr DC, Boudewyn AC, Goodkin DE, et al. Comparative outcomes for individual cognitive-behavior therapy, supportive-expressive group psychotherapy, and sertraline for the treatment of depression in multiple sclerosis. J Cons Clin Psychol 2001;69:942-9.
25. The Goldman Consensus Group. The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 2005;11:328-37.
26. Taus C, Giulani G, Pucci E, et al. Amantadine for fatigue in multiple sclerosis. Cochrane Database Syst Rev 2003;(2):CD002818.-
27. Krupp LB, Coyle PK, Doscher C, et al. Fatigue therapy in multiple sclerosis: results of a double-bind, randomized, parallel trial of amantadine, pemoline and placebo. Neurology 1995;45:1956-61.
28. Zifko UA, Rupp M, Schwarz S, et al. Modafinil in treatment of fatigue in multiple sclerosis. Results of an open-label study. J Neurol 2002;249:983-7.
29. Zifko UA. Management of fatigue in patients with multiple sclerosis. Drugs 2004;64:1295-304.
30. Rammohan KW, Rosenberg JH, Lynn DJ, et al. Efficacy and safety of modafinil (Provigil) for the treatment of fatigue in multiple sclerosis: a two centre phase 2 study. J Neurol Neurosurg Psychiatry 2002;72:179-83.
31. Stankoff B, Waubant E, Confavreux C, et al. Modafinil for fatigue in MS: a randomized placebo-controlled double-blind study. Neurology 2005;64:1139-43.
32. Joffe RT, Lippert GP, Gray TA, et al. Mood disorders and multiple sclerosis. Arch Neurol 1987;44:376-8.
33. Finger S. A happy state of mind. A history of mild elation, denial of disability, optimism, and laughing in multiple sclerosis. Arch Neurol 1998;55:241-50.
34. Patten SB, Svenson LW, Metz LM. Psychotic disorders in MS: population-based evidence of an association. Neurology 2005;1123-5.
35. Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive therapy of depression. New York, NY: Guilford; 1979.
36. Jacobson NS, Dobson KS, Truax PA, et al. A component analysis of cognitive-behavioral treatment for depression. J Cons Clin Psychol 1996;64:295-304.
37. Crawford JD, McIvor GP. Group psychotherapy: benefits in multiple sclerosis. Arch Phys Med Rehabil 1985;66:810-3.
38. Comi G, Leocani L. Assessment, pathophysiology and treatment of fatigue in multiple sclerosis. Expert Rev Neurother 2002;2(6):867-76.
Mrs. S, age 50, has had relapsing-remitting multiple sclerosis (MS) for approximately 10 years. She describes her mood as “up and down” and is referred by her neurologist for psychiatric assessment of mood swings and possible depression. Fatigue limits her ability to work full-time, perform household duties, socialize with friends and family, and enjoy mental or physical exercise. In addition, her 18-year-old daughter—an important source of psychological support—is planning to leave home.
Mrs. S experienced depression 5 years ago during her divorce. She was prescribed paroxetine, 20 mg/d, and had a positive response. She took the medication for 6 months, then discontinued.
One-half of MS patients experience major depression in their lifetimes,1 and the suicide rate is approximately doubled in MS patients compared with the general population.2 Depression in MS patients often has an atypical presentation, with irritability and anger being as prominent as sadness.3 Not all emotional changes experienced by MS patients represent depressive disorders, however.
When evaluating MS patients who are struggling with depression, you can help them by diagnosing comorbid mood disorders, determining suicide risk, and providing psychological support as they cope with the impact of their illness.
MS disease course
MS is a disease of the brain and spinal cord, characterized by:
- inflammatory demyelination and gliosis
- neuronal and axonal loss
- a variety of presenting symptoms as different CNS regions are affected.
Focal areas of demyelination followed by a reactive gliosis cause white matter lesions in the brain, spinal cord, and optic nerve. Neurologic dysfunction can manifest as visual changes, spastic paresis, hypoesthesia and paresthesia, ataxia, and bowel and bladder dysfunction. MS presentation also can include optic neuritis and transverse myelitis. MS symptoms often are intensified by heat exposure.
After the initial episode, months or years may pass before additional neurologic symptoms appear. Based on its course, MS can be classified as:
- relapsing-remitting, when the disease does not progress between attacks
- secondary progressive, characterized by a gradually progressive course after an initial relapsing-remitting pattern
- primary progressive, when patients experience gradual progressive disability from symptom onset (Table 1).
Table 1
Clinical classification of multiple sclerosis (MS)
| Type | Characteristics |
|---|---|
| Relapsing-remitting* | Symptoms appear during relapses, resolve during remissions, and do not progress between relapses |
| Secondary progressive | MS symptoms that previously followed a relapsing-remitting pattern steadily become more severe and progress without relapse |
| Primary progressive | Gradual progression from symptom onset, without relapses or remission |
| Clinically isolated syndrome | A single attack that may indicate MS has occurred—such as optic neuritis or transverse myelitis—but clinical requirements for the diagnosis have not been met |
| * Patients often progress from relapsing-remitting to secondary progressive MS | |
CASE CONTINUED: Progressing symptoms
Mrs. S has had multiple MS presentations, including optic neuritis, lower extremity weakness, balance problems, and urinary incontinence. Recently, her MS symptoms have gradually progressed even in the absence of attacks, and her diagnosis has been revised to secondary progressive MS.
During psychiatric evaluation, Mrs. S denies persistent changes in sleep or appetite. She describes fatigue that starts after physical exertion and increases as the day progresses. She denies feelings of worthlessness, helplessness, excessive guilt, and suicidal ideation and does not have a history of inappropriate anger or irritability.
Diagnosing depression in MS
Normal emotional adjustment to MS can include reactions to loss of function or changes in social or occupational roles. Further, MS patients—similar to non-MS patients—experience life changes and transitions not related to the illness, such as divorce or a grown child moving away. Emotional responses to life stressors often are self-limited but may warrant an adjustment disorder diagnosis if they are associated with excessive distress or substantial impairment in social, occupational, or academic functioning (Table 2).4
Table 2
Questions to consider when assessing MS patients for depression
| Ask yourself | Reason |
|---|---|
| Are symptoms part of normal emotional changes? | Not all mood changes are pathologic or meet criteria for major depression |
| Is this an adjustment disorder? | Mood symptoms can be caused by a major stressor such as a recent diagnosis or personal loss |
| Is fatigue secondary to MS or depression? | MS typically causes fatigue after physical activity and heat exposure; fatigue early in the day points to depression |
| Are cognitive deficits related to MS or depression? | Negative thoughts point to depression whereas cognitive deficits may be caused by depression, MS, or both |
| Is this an atypical presentation? | MS patients may present with anger or irritability |
| Is this a pseudobulbar problem? | Patients with IEED might describe more concern about affect dysregulation than mood swings |
| MS: multiple sclerosis; IEED: involuntary emotional expression disorder | |
Female MS patients and those who report high stress or a family history of affective disorder may be more likely to develop clinical depression.5 Several studies have reported correlations between structural brain abnormalities and depression in MS. Feinstein et al
6 reported that extensive hyper intense lesion volume in the left medial inferior prefrontal region with atrophy affecting the dominant anterior temporal lobe was associated with major depression. However, a depression diagnosis in MS patients remains a clinical one that does not require brain imaging studies.
Lack of interest or enjoyment as a symptom of depression can be difficult to identify because MS can diminish enjoyment of some activities. Although patients with MS may need to change their activity patterns to accommodate their illness, the lack of enjoyment in all—or almost all—activities remains a valid indicator of depressive disorder.
MS treatment includes the use of disease-modifying medications such as interferon beta-1b and interferon beta-1a. Several years ago researchers were concerned that interferon beta might cause depression in MS patients based on reports of a suicide and attempted suicide during an early trial of interferon beta-1b in relapsing-remitting MS.7 Subsequent studies did not substantiate this concern, however (Box 1).8,9
Overlapping symptoms such as fatigue and cognitive deterioration could complicate the diagnosis. Look for changing patterns of these symptoms and other signs of depression. Rating scales that do not emphasize fatigue and cognitive impairment—such as the Beck Depression Inventory10 and the Center for Epidemiologic Studies Depression Rating Scale11—can help identify depression in MS patients.
Fatigue is one of MS’ most common and troublesome symptoms.12,13 It typically mounts gradually during the day and after activity or heat exposure. Thus, fatigue early in the morning or manifesting as diminished motivation may point to a depressive disorder.
Cognitive deterioration. Clinically significant cognitive dysfunction occurs in 45% to 65% of MS patients.14 The disease can cause losses in short-term memory, attention, information processing, problem solving, multitasking, and language function.
Bedside cognitive function tests such as the Mini-Mental State Examination15 often are not sensitive enough to detect MS-related cognitive dysfunction. Be alert for changes in cognitive style when assessing for depressive disorders in these patients. Feelings of worthlessness and guilt or suicidal ideation are not normal MS symptoms and point to depression.
MS patients may experience pathological laughing and crying—also known as involuntary emotional expression disorder (IEED)—a neurologic phenomenon that causes uncontrollable laughing, crying, or anger in the absence of subjective emotional distress. IEED has been reported in approximately 10% of patients with MS (Box 2).16-22
CASE CONTINUED: Learning to adjust
Since discontinuing paroxetine 5 years ago, Mrs. S has not experienced another depressive episode. However, she describes a history of mood changes associated with pressured speech, increased activity, irritability, and insomnia during cortisone treatment for idiopathic thrombocytopenic purpura 4 years earlier. These episodes were mild, and she did not seek psychiatric treatment.
Mrs. S’ mood episode does not seem to be a recurrence of major depressive disorder because she lacks persistent depressed mood and major depressive symptoms. Her diagnosis is best understood as an adjustment disorder to the progression of her illness and her daughter leaving home. Fatigue is her most debilitating MS symptom.
Medication options
Use a cautious approach to pharmacotherapy. MS patients may have diminished cognitive reserves and might be at increased risk of medication-related delirium.
Depression. Two randomized, controlled trials have confirmed antidepressants’ efficacy for treating depression in MS patients. The studies investigated the tricyclic antidepressant desipramine23 and the selective serotonin reuptake inhibitor (SSRI) sertraline.24
In a double-blind clinical trial, 28 patients were randomly assigned to a 5-week trial of desipramine and individual psychotherapy or placebo and psychotherapy. Patients receiving desipramine showed significantly greater improvement than the placebo group, as measured by clinical judgment.
A 16-week study compared the efficacy of cognitive-behavioral therapy (CBT), supportive-expressive group therapy (SEG), and sertraline in 63 MS patients with major depressive disorder. Results showed that CBT and sertraline were more effective in reducing depression than SEG.24
SSRIs are a common first choice because of their ease of use and general tolerability among MS patients.25 Recommended dosages include:
- citalopram, 20 to 40 mg/d
- fluoxetine, 20 to 40 mg/d
- fluvoxamine, 50 to 300 mg/d
- paroxetine, 20 to 50 mg/d
- sertraline, 50 to 200 mg/d.
There is no consensus that any one antidepressant is best for all MS patients, however. When selecting an antidepressant, consider side-effect profiles, potential for drug-drug interactions, and a history of response to a particular antidepressant. Highly sedating antidepressants such as mirtazapine could aggravate fatigue. Highly anticholinergic agents such as amitriptyline may impair cognitive function.
Fatigue. Amantadine is the mainstay pharmacologic treatment for fatigue in MS, but evidence for its efficacy is weak.26 Clinical trials of psychostimulants generally have reported disappointing results. One randomized, double-blind trial found no significant differences in fatigue levels between patients receiving pemoline or placebo.27
Some studies have reported reduced MS-related fatigue with modafinil,28-30 but the only double-blind, placebo-controlled trial showed no significant difference between modafinil and placebo in patient fatigue levels.31 In this study, modafinil reduced physical fatigue only in patients with daytime somnolence.
Do interferon beta-1a and 1b—agents used to treat relapsing-remitting MS—cause or aggravate depression?
Two large-scale clinical trials of interferon beta-1a included a validated measure of depressive symptoms—the Center for Epidemiologic Studies Depression Rating Scale.8,9 This scale allowed researchers to conduct a detailed analysis that compared changes in depression symptoms over time in study participants treated with interferon or placebo. Evidence did not indicate increased depressive symptoms in association with interferon treatment.
Conclusion. Depression symptoms that emerge during treatment with one of these agents are not likely caused by the treatment and usually can be managed without discontinuing the drug.
Other psychiatric disorders
Bipolar disorder occurs more frequently in MS patients than in the general population.32 Additionally, some patients with advanced MS might experience benign feelings of euphoria.33 Euphoria can be differentiated from mania by assessing for mania’s other symptoms, such as erratic and disinhibited behavior, rapid speech, increased libido, decreased need for sleep, and excessive energy.
Antidepressants and corticosteroids could aggravate the course of bipolar disorder, and drug-illness interactions with lithium could make side effects such as tremor, diarrhea, and polyuria more difficult to tolerate. Mood stabilizing anticonvulsants such as valproate and carbamazepine are a useful alternative for treating the bipolar patient with comorbid MS. To avoid sedation, start with a low dose and increase gradually.
Approximately 10% of multiple sclerosis (MS) patients develop inappropriate affective expression—anger, laughing, or crying—in the absence of prominent mood changes.16 Involuntary emotional expression disorder (IEED)—or pathologic laughing or crying—is a form of pseudobulbar affect. IEED occurs when affective motor control becomes disinhibited as a result of brain damage from neurologic disease or injury. Conditions associated with IEED include amyotrophic lateral sclerosis, MS, traumatic brain injury, stroke, and dementia.17
IEED can prompt a psychiatric evaluation because uncontrolled crying can seem like intense depression. Symptoms range in severity and include exaggerated and inappropriate affective responses and perceived lack of control over responses. IEED episodes are paroxysmal, occurring in a brief and stereotyped manner, whereas crying in depression is more sustained, less stereotyped, and relates to the underlying mood.17,18 In addition, patients with depressive disorders often suffer difficulties with sleep and appetite as well as thoughts of guilt, hopelessness, and worthlessness not present in IEED.17,19
Studies have shown successful treatment of IEED with antidepressants including tricyclic antidepressants and serotonin reuptake inhibitors.20 A recent randomized, controlled trial suggested that dextromethorphan and quinidine may be beneficial in treating potentially disabling pseudobulbar affect in MS.21 Rating scales such as the 7-item Center for Neurologic Study Lability Scale may help establish a baseline against which to monitor treatment response.22
Insomnia. Sedative hypnotics such as zopiclone can be used for short-term treatment of sleep disturbances. Carefully consider hypnotics’ possible negative effects on balance, coordination, and memory, however.
Psychotic disturbances are rare in MS but occur more frequently in MS patients than in the general population.34 Use low doses of antipsychotics such as olanzapine, quetiapine, or risperidone in MS patients with psychosis. These atypical agents are associated with a lower risk of parkinsonian side effects than typical antipsychotics.
CASE CONTINUED: Coping mechanisms
Mrs. S has difficulty coping with her increasing symptom burden and functional limitations, but she says it is hard for her to ask for help. Her treatment plan includes recruiting support to help her deal with feelings of loss over her daughter’s move. We encourage her to reconnect with friends and family and use community supports for MS patients.
We discuss her treatment options, including biological treatments for fatigue, CBT, and behavioral activation therapy for her mood symptoms. She chooses a course of modafinil, 50 mg/d, and weekly CBT incorporating behavioral activation therapy to increase her activity level and target depressive symptoms and fatigue.
Psychosocial interventions
CBT is an effective treatment for depression in MS patients24 and is preferred for most patients with mild depression. CBT focuses on improving coping through behavioral activation and cognitive restructuring.35 CBT can incorporate teaching patients skills for managing MS-related problems such as fatigue, mild cognitive impairment, pain, stress, communication, sexual dysfunction, intimacy, and social difficulties secondary to MS.
Behavioral activation strategies focus on the relationship between activity and mood. They target a common pattern of avoidance and withdrawal from social, occupational, and physical demands that relieves MS patients’ anxiety in the short term but leads to problems associated with inactivity.35 Behavioral activation strategies—including exercise—have a strong evidence base supporting their use alone to manage depression and as a component of CBT.36
Active coping strategies. In early MS, patients often use avoidance and denial to cope with their disease. As symptoms become more intrusive, however, patients usually need to learn active coping strategies. These often begin with symptom management and evolve to include individually meaningful tasks such as reevaluating personal goals, values, and priorities.
Other psychotherapy modalities. In one study, patients randomized to an insight-oriented treatment group improved more than those in a placebo intervention based on discussing current events.37 Although not formally assessed in the literature, psychoeducation can help the patient maintain a sense of control over his or her treatment. Interpersonal therapy can help patients deal with role transitions caused by their illness and subsequent disabilities, although its use in this population has not been studied.
Although the literature does not favor supportive psychotherapy for treating depression in MS patients,24 this modality can help alleviate feelings of grief and loss that can emerge when MS symptoms worsen. Patients often appreciate having an opportunity to articulate their feelings and fears in a professional therapeutic relationship. MS patients often value validation and normalization of their emotional responses, and many therapists choose to integrate supportive strategies with CBT’s more “action oriented” elements.
Exercise is an effective treatment for fatigue in MS38 and also helps combat loss of physical fitness. MS patients who use energy conservation strategies to manage fatigue can participate in suitably paced physical exercise. Aquatic exercise is a popular option because it often does not cause overheating.
CASE CONTINUED: Energy surge
At the second follow-up appointment, Mrs. S notes that her energy level is better early in the day but decreases by late afternoon. An additional dose of modafinil, 50 mg, is added at noon, which increases her overall energy level.
CBT helps Mrs. S to develop reasonable expectations of herself and others and addresses the possibility that she could try part-time work. Including exercise as behavioral activation also lessens her fatigue. Reconnecting with family and friends helps relieve feelings of isolation resulting from her daughter moving away.
Related resources
- National Multiple Sclerosis Society. www.nationalmssociety.org.
- The Goldman Consensus Group. The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 2005;11:328-37.
- Feinstein A. The clinical neuropsychiatry of multiple sclerosis. Cambridge, UK: Cambridge University Press; 2007.
Drug brand names
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Interferon beta-1a • Avonex, Rebif
- Interferon beta-1b • Betaseron
- Lithium • Eskalith, Lithobid
- Mirtazapine • Remeron
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pemoline • Cylert
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Valproate • Depacon
- Zopiclone • Imovane, Zimovane
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. S, age 50, has had relapsing-remitting multiple sclerosis (MS) for approximately 10 years. She describes her mood as “up and down” and is referred by her neurologist for psychiatric assessment of mood swings and possible depression. Fatigue limits her ability to work full-time, perform household duties, socialize with friends and family, and enjoy mental or physical exercise. In addition, her 18-year-old daughter—an important source of psychological support—is planning to leave home.
Mrs. S experienced depression 5 years ago during her divorce. She was prescribed paroxetine, 20 mg/d, and had a positive response. She took the medication for 6 months, then discontinued.
One-half of MS patients experience major depression in their lifetimes,1 and the suicide rate is approximately doubled in MS patients compared with the general population.2 Depression in MS patients often has an atypical presentation, with irritability and anger being as prominent as sadness.3 Not all emotional changes experienced by MS patients represent depressive disorders, however.
When evaluating MS patients who are struggling with depression, you can help them by diagnosing comorbid mood disorders, determining suicide risk, and providing psychological support as they cope with the impact of their illness.
MS disease course
MS is a disease of the brain and spinal cord, characterized by:
- inflammatory demyelination and gliosis
- neuronal and axonal loss
- a variety of presenting symptoms as different CNS regions are affected.
Focal areas of demyelination followed by a reactive gliosis cause white matter lesions in the brain, spinal cord, and optic nerve. Neurologic dysfunction can manifest as visual changes, spastic paresis, hypoesthesia and paresthesia, ataxia, and bowel and bladder dysfunction. MS presentation also can include optic neuritis and transverse myelitis. MS symptoms often are intensified by heat exposure.
After the initial episode, months or years may pass before additional neurologic symptoms appear. Based on its course, MS can be classified as:
- relapsing-remitting, when the disease does not progress between attacks
- secondary progressive, characterized by a gradually progressive course after an initial relapsing-remitting pattern
- primary progressive, when patients experience gradual progressive disability from symptom onset (Table 1).
Table 1
Clinical classification of multiple sclerosis (MS)
| Type | Characteristics |
|---|---|
| Relapsing-remitting* | Symptoms appear during relapses, resolve during remissions, and do not progress between relapses |
| Secondary progressive | MS symptoms that previously followed a relapsing-remitting pattern steadily become more severe and progress without relapse |
| Primary progressive | Gradual progression from symptom onset, without relapses or remission |
| Clinically isolated syndrome | A single attack that may indicate MS has occurred—such as optic neuritis or transverse myelitis—but clinical requirements for the diagnosis have not been met |
| * Patients often progress from relapsing-remitting to secondary progressive MS | |
CASE CONTINUED: Progressing symptoms
Mrs. S has had multiple MS presentations, including optic neuritis, lower extremity weakness, balance problems, and urinary incontinence. Recently, her MS symptoms have gradually progressed even in the absence of attacks, and her diagnosis has been revised to secondary progressive MS.
During psychiatric evaluation, Mrs. S denies persistent changes in sleep or appetite. She describes fatigue that starts after physical exertion and increases as the day progresses. She denies feelings of worthlessness, helplessness, excessive guilt, and suicidal ideation and does not have a history of inappropriate anger or irritability.
Diagnosing depression in MS
Normal emotional adjustment to MS can include reactions to loss of function or changes in social or occupational roles. Further, MS patients—similar to non-MS patients—experience life changes and transitions not related to the illness, such as divorce or a grown child moving away. Emotional responses to life stressors often are self-limited but may warrant an adjustment disorder diagnosis if they are associated with excessive distress or substantial impairment in social, occupational, or academic functioning (Table 2).4
Table 2
Questions to consider when assessing MS patients for depression
| Ask yourself | Reason |
|---|---|
| Are symptoms part of normal emotional changes? | Not all mood changes are pathologic or meet criteria for major depression |
| Is this an adjustment disorder? | Mood symptoms can be caused by a major stressor such as a recent diagnosis or personal loss |
| Is fatigue secondary to MS or depression? | MS typically causes fatigue after physical activity and heat exposure; fatigue early in the day points to depression |
| Are cognitive deficits related to MS or depression? | Negative thoughts point to depression whereas cognitive deficits may be caused by depression, MS, or both |
| Is this an atypical presentation? | MS patients may present with anger or irritability |
| Is this a pseudobulbar problem? | Patients with IEED might describe more concern about affect dysregulation than mood swings |
| MS: multiple sclerosis; IEED: involuntary emotional expression disorder | |
Female MS patients and those who report high stress or a family history of affective disorder may be more likely to develop clinical depression.5 Several studies have reported correlations between structural brain abnormalities and depression in MS. Feinstein et al
6 reported that extensive hyper intense lesion volume in the left medial inferior prefrontal region with atrophy affecting the dominant anterior temporal lobe was associated with major depression. However, a depression diagnosis in MS patients remains a clinical one that does not require brain imaging studies.
Lack of interest or enjoyment as a symptom of depression can be difficult to identify because MS can diminish enjoyment of some activities. Although patients with MS may need to change their activity patterns to accommodate their illness, the lack of enjoyment in all—or almost all—activities remains a valid indicator of depressive disorder.
MS treatment includes the use of disease-modifying medications such as interferon beta-1b and interferon beta-1a. Several years ago researchers were concerned that interferon beta might cause depression in MS patients based on reports of a suicide and attempted suicide during an early trial of interferon beta-1b in relapsing-remitting MS.7 Subsequent studies did not substantiate this concern, however (Box 1).8,9
Overlapping symptoms such as fatigue and cognitive deterioration could complicate the diagnosis. Look for changing patterns of these symptoms and other signs of depression. Rating scales that do not emphasize fatigue and cognitive impairment—such as the Beck Depression Inventory10 and the Center for Epidemiologic Studies Depression Rating Scale11—can help identify depression in MS patients.
Fatigue is one of MS’ most common and troublesome symptoms.12,13 It typically mounts gradually during the day and after activity or heat exposure. Thus, fatigue early in the morning or manifesting as diminished motivation may point to a depressive disorder.
Cognitive deterioration. Clinically significant cognitive dysfunction occurs in 45% to 65% of MS patients.14 The disease can cause losses in short-term memory, attention, information processing, problem solving, multitasking, and language function.
Bedside cognitive function tests such as the Mini-Mental State Examination15 often are not sensitive enough to detect MS-related cognitive dysfunction. Be alert for changes in cognitive style when assessing for depressive disorders in these patients. Feelings of worthlessness and guilt or suicidal ideation are not normal MS symptoms and point to depression.
MS patients may experience pathological laughing and crying—also known as involuntary emotional expression disorder (IEED)—a neurologic phenomenon that causes uncontrollable laughing, crying, or anger in the absence of subjective emotional distress. IEED has been reported in approximately 10% of patients with MS (Box 2).16-22
CASE CONTINUED: Learning to adjust
Since discontinuing paroxetine 5 years ago, Mrs. S has not experienced another depressive episode. However, she describes a history of mood changes associated with pressured speech, increased activity, irritability, and insomnia during cortisone treatment for idiopathic thrombocytopenic purpura 4 years earlier. These episodes were mild, and she did not seek psychiatric treatment.
Mrs. S’ mood episode does not seem to be a recurrence of major depressive disorder because she lacks persistent depressed mood and major depressive symptoms. Her diagnosis is best understood as an adjustment disorder to the progression of her illness and her daughter leaving home. Fatigue is her most debilitating MS symptom.
Medication options
Use a cautious approach to pharmacotherapy. MS patients may have diminished cognitive reserves and might be at increased risk of medication-related delirium.
Depression. Two randomized, controlled trials have confirmed antidepressants’ efficacy for treating depression in MS patients. The studies investigated the tricyclic antidepressant desipramine23 and the selective serotonin reuptake inhibitor (SSRI) sertraline.24
In a double-blind clinical trial, 28 patients were randomly assigned to a 5-week trial of desipramine and individual psychotherapy or placebo and psychotherapy. Patients receiving desipramine showed significantly greater improvement than the placebo group, as measured by clinical judgment.
A 16-week study compared the efficacy of cognitive-behavioral therapy (CBT), supportive-expressive group therapy (SEG), and sertraline in 63 MS patients with major depressive disorder. Results showed that CBT and sertraline were more effective in reducing depression than SEG.24
SSRIs are a common first choice because of their ease of use and general tolerability among MS patients.25 Recommended dosages include:
- citalopram, 20 to 40 mg/d
- fluoxetine, 20 to 40 mg/d
- fluvoxamine, 50 to 300 mg/d
- paroxetine, 20 to 50 mg/d
- sertraline, 50 to 200 mg/d.
There is no consensus that any one antidepressant is best for all MS patients, however. When selecting an antidepressant, consider side-effect profiles, potential for drug-drug interactions, and a history of response to a particular antidepressant. Highly sedating antidepressants such as mirtazapine could aggravate fatigue. Highly anticholinergic agents such as amitriptyline may impair cognitive function.
Fatigue. Amantadine is the mainstay pharmacologic treatment for fatigue in MS, but evidence for its efficacy is weak.26 Clinical trials of psychostimulants generally have reported disappointing results. One randomized, double-blind trial found no significant differences in fatigue levels between patients receiving pemoline or placebo.27
Some studies have reported reduced MS-related fatigue with modafinil,28-30 but the only double-blind, placebo-controlled trial showed no significant difference between modafinil and placebo in patient fatigue levels.31 In this study, modafinil reduced physical fatigue only in patients with daytime somnolence.
Do interferon beta-1a and 1b—agents used to treat relapsing-remitting MS—cause or aggravate depression?
Two large-scale clinical trials of interferon beta-1a included a validated measure of depressive symptoms—the Center for Epidemiologic Studies Depression Rating Scale.8,9 This scale allowed researchers to conduct a detailed analysis that compared changes in depression symptoms over time in study participants treated with interferon or placebo. Evidence did not indicate increased depressive symptoms in association with interferon treatment.
Conclusion. Depression symptoms that emerge during treatment with one of these agents are not likely caused by the treatment and usually can be managed without discontinuing the drug.
Other psychiatric disorders
Bipolar disorder occurs more frequently in MS patients than in the general population.32 Additionally, some patients with advanced MS might experience benign feelings of euphoria.33 Euphoria can be differentiated from mania by assessing for mania’s other symptoms, such as erratic and disinhibited behavior, rapid speech, increased libido, decreased need for sleep, and excessive energy.
Antidepressants and corticosteroids could aggravate the course of bipolar disorder, and drug-illness interactions with lithium could make side effects such as tremor, diarrhea, and polyuria more difficult to tolerate. Mood stabilizing anticonvulsants such as valproate and carbamazepine are a useful alternative for treating the bipolar patient with comorbid MS. To avoid sedation, start with a low dose and increase gradually.
Approximately 10% of multiple sclerosis (MS) patients develop inappropriate affective expression—anger, laughing, or crying—in the absence of prominent mood changes.16 Involuntary emotional expression disorder (IEED)—or pathologic laughing or crying—is a form of pseudobulbar affect. IEED occurs when affective motor control becomes disinhibited as a result of brain damage from neurologic disease or injury. Conditions associated with IEED include amyotrophic lateral sclerosis, MS, traumatic brain injury, stroke, and dementia.17
IEED can prompt a psychiatric evaluation because uncontrolled crying can seem like intense depression. Symptoms range in severity and include exaggerated and inappropriate affective responses and perceived lack of control over responses. IEED episodes are paroxysmal, occurring in a brief and stereotyped manner, whereas crying in depression is more sustained, less stereotyped, and relates to the underlying mood.17,18 In addition, patients with depressive disorders often suffer difficulties with sleep and appetite as well as thoughts of guilt, hopelessness, and worthlessness not present in IEED.17,19
Studies have shown successful treatment of IEED with antidepressants including tricyclic antidepressants and serotonin reuptake inhibitors.20 A recent randomized, controlled trial suggested that dextromethorphan and quinidine may be beneficial in treating potentially disabling pseudobulbar affect in MS.21 Rating scales such as the 7-item Center for Neurologic Study Lability Scale may help establish a baseline against which to monitor treatment response.22
Insomnia. Sedative hypnotics such as zopiclone can be used for short-term treatment of sleep disturbances. Carefully consider hypnotics’ possible negative effects on balance, coordination, and memory, however.
Psychotic disturbances are rare in MS but occur more frequently in MS patients than in the general population.34 Use low doses of antipsychotics such as olanzapine, quetiapine, or risperidone in MS patients with psychosis. These atypical agents are associated with a lower risk of parkinsonian side effects than typical antipsychotics.
CASE CONTINUED: Coping mechanisms
Mrs. S has difficulty coping with her increasing symptom burden and functional limitations, but she says it is hard for her to ask for help. Her treatment plan includes recruiting support to help her deal with feelings of loss over her daughter’s move. We encourage her to reconnect with friends and family and use community supports for MS patients.
We discuss her treatment options, including biological treatments for fatigue, CBT, and behavioral activation therapy for her mood symptoms. She chooses a course of modafinil, 50 mg/d, and weekly CBT incorporating behavioral activation therapy to increase her activity level and target depressive symptoms and fatigue.
Psychosocial interventions
CBT is an effective treatment for depression in MS patients24 and is preferred for most patients with mild depression. CBT focuses on improving coping through behavioral activation and cognitive restructuring.35 CBT can incorporate teaching patients skills for managing MS-related problems such as fatigue, mild cognitive impairment, pain, stress, communication, sexual dysfunction, intimacy, and social difficulties secondary to MS.
Behavioral activation strategies focus on the relationship between activity and mood. They target a common pattern of avoidance and withdrawal from social, occupational, and physical demands that relieves MS patients’ anxiety in the short term but leads to problems associated with inactivity.35 Behavioral activation strategies—including exercise—have a strong evidence base supporting their use alone to manage depression and as a component of CBT.36
Active coping strategies. In early MS, patients often use avoidance and denial to cope with their disease. As symptoms become more intrusive, however, patients usually need to learn active coping strategies. These often begin with symptom management and evolve to include individually meaningful tasks such as reevaluating personal goals, values, and priorities.
Other psychotherapy modalities. In one study, patients randomized to an insight-oriented treatment group improved more than those in a placebo intervention based on discussing current events.37 Although not formally assessed in the literature, psychoeducation can help the patient maintain a sense of control over his or her treatment. Interpersonal therapy can help patients deal with role transitions caused by their illness and subsequent disabilities, although its use in this population has not been studied.
Although the literature does not favor supportive psychotherapy for treating depression in MS patients,24 this modality can help alleviate feelings of grief and loss that can emerge when MS symptoms worsen. Patients often appreciate having an opportunity to articulate their feelings and fears in a professional therapeutic relationship. MS patients often value validation and normalization of their emotional responses, and many therapists choose to integrate supportive strategies with CBT’s more “action oriented” elements.
Exercise is an effective treatment for fatigue in MS38 and also helps combat loss of physical fitness. MS patients who use energy conservation strategies to manage fatigue can participate in suitably paced physical exercise. Aquatic exercise is a popular option because it often does not cause overheating.
CASE CONTINUED: Energy surge
At the second follow-up appointment, Mrs. S notes that her energy level is better early in the day but decreases by late afternoon. An additional dose of modafinil, 50 mg, is added at noon, which increases her overall energy level.
CBT helps Mrs. S to develop reasonable expectations of herself and others and addresses the possibility that she could try part-time work. Including exercise as behavioral activation also lessens her fatigue. Reconnecting with family and friends helps relieve feelings of isolation resulting from her daughter moving away.
Related resources
- National Multiple Sclerosis Society. www.nationalmssociety.org.
- The Goldman Consensus Group. The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 2005;11:328-37.
- Feinstein A. The clinical neuropsychiatry of multiple sclerosis. Cambridge, UK: Cambridge University Press; 2007.
Drug brand names
- Amantadine • Symmetrel
- Amitriptyline • Elavil
- Carbamazepine • Tegretol
- Citalopram • Celexa
- Desipramine • Norpramin
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Interferon beta-1a • Avonex, Rebif
- Interferon beta-1b • Betaseron
- Lithium • Eskalith, Lithobid
- Mirtazapine • Remeron
- Modafinil • Provigil
- Olanzapine • Zyprexa
- Paroxetine • Paxil
- Pemoline • Cylert
- Quetiapine • Seroquel
- Risperidone • Risperdal
- Sertraline • Zoloft
- Valproate • Depacon
- Zopiclone • Imovane, Zimovane
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Patten SB, Beck CA, Williams JVA, et al. Major depression in multiple sclerosis: a population-based perspective. Neurology 2003;61:1524-7.
2. Stenager EN, Stenager E, Koch-Henriksen N, et al. Suicide and multiple sclerosis: an epidemiological investigation. J Neurol Neurosurg Psychiatry 1992;55:542-5.
3. Minden SL, Orav J, Reich P. Depression in multiple sclerosis. Gen Hosp Psychiatry 1987;9:426-34.
4. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
5. Patten SB, Metz LM, Reimer MA. Biopsychosocial correlates of major depression in a multiple sclerosis population. Mult Scler 2000;6:115-20.
6. Feinstein A, Roy P, Lobaugh N, et al. Structural brain abnormalities in multiple sclerosis patients with major depression. Neurology 2004;62:586-90.
7. Klapper JA. Interferon beta treatment of multiple sclerosis. Neurology 1994;44:188.-
8. Patten SB, Metz LM. Interferon β-1a and depression in secondary progressive MS: data from the SPECTRIMS trial. Neurology 2002;59(744):746.-
9. Patten SB, Metz LM. Interferon b-1a and depression in relapsing-remitting multiple sclerosis: an analysis of depression data from the PRISMS clinical trial. Mult Scler 2001;7:243-8.
10. Beck AT, Ward CH, Mendelson M, et al. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:53-63.
11. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Applied Psychol Measurement 1977;1:385-401.
12. Fisk JD, Pontefract A, Ritvo PG, et al. The impact of fatigue on patients with multiple sclerosis. Can J Neurol Sci 1995;21:9-14.
13. Freal JE, Kraft GH, Coryell JK. Symptomatic fatigue in multiple sclerosis. Arch Phys Med Rehabil 1984;65:135-8.
14. Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis. Natural history, pathophysiology and management. CNS Drugs 2002;16:445-55.
15. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State Examination. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-98.
16. Feinstein A, Feinstein K, Gray T, O’Connor P. The prevalence and neurobehavioural correlates of pathological laughter and crying in multiple sclerosis. Arch Neurol 1997;54:1116-21.
17. Cummings JL. Involuntary emotional expression disorder: definition, diagnosis, and measurement scales. CNS Spectr 2007;12(4 suppl 5):11-6.
18. Paradiso S, Chemerinski E, Yazici KM, et al. Frontal lobe syndrome reassessed: comparison of patients with lateral or medial frontal brain damage. J Neurol Neurosurg Psychiatry 1999;67(5):664-7.
19. Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63(1):89-93.
20. Schiffer RB, Herndon RM, Rudick RA. Treatment of pathological laughing and weeping with amitriptyline. N Eng J Med 1985;312:1480-2.
21. Panitch HS, Thisted RA, Smith RA, et al. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann Neurol 2006;59:780-7.
22. Smith RA, Berg JE, Pope LE, Thisted RA. Measuring pseudobulbar affect in ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2004;5(suppl 1):99-102.
23. Schiffer RB, Wineman NM. Antidepressant pharmacotherapy of depression associated with multiple sclerosis. Am J Psychiatry 1990;147(11):1493-7.
24. Mohr DC, Boudewyn AC, Goodkin DE, et al. Comparative outcomes for individual cognitive-behavior therapy, supportive-expressive group psychotherapy, and sertraline for the treatment of depression in multiple sclerosis. J Cons Clin Psychol 2001;69:942-9.
25. The Goldman Consensus Group. The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 2005;11:328-37.
26. Taus C, Giulani G, Pucci E, et al. Amantadine for fatigue in multiple sclerosis. Cochrane Database Syst Rev 2003;(2):CD002818.-
27. Krupp LB, Coyle PK, Doscher C, et al. Fatigue therapy in multiple sclerosis: results of a double-bind, randomized, parallel trial of amantadine, pemoline and placebo. Neurology 1995;45:1956-61.
28. Zifko UA, Rupp M, Schwarz S, et al. Modafinil in treatment of fatigue in multiple sclerosis. Results of an open-label study. J Neurol 2002;249:983-7.
29. Zifko UA. Management of fatigue in patients with multiple sclerosis. Drugs 2004;64:1295-304.
30. Rammohan KW, Rosenberg JH, Lynn DJ, et al. Efficacy and safety of modafinil (Provigil) for the treatment of fatigue in multiple sclerosis: a two centre phase 2 study. J Neurol Neurosurg Psychiatry 2002;72:179-83.
31. Stankoff B, Waubant E, Confavreux C, et al. Modafinil for fatigue in MS: a randomized placebo-controlled double-blind study. Neurology 2005;64:1139-43.
32. Joffe RT, Lippert GP, Gray TA, et al. Mood disorders and multiple sclerosis. Arch Neurol 1987;44:376-8.
33. Finger S. A happy state of mind. A history of mild elation, denial of disability, optimism, and laughing in multiple sclerosis. Arch Neurol 1998;55:241-50.
34. Patten SB, Svenson LW, Metz LM. Psychotic disorders in MS: population-based evidence of an association. Neurology 2005;1123-5.
35. Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive therapy of depression. New York, NY: Guilford; 1979.
36. Jacobson NS, Dobson KS, Truax PA, et al. A component analysis of cognitive-behavioral treatment for depression. J Cons Clin Psychol 1996;64:295-304.
37. Crawford JD, McIvor GP. Group psychotherapy: benefits in multiple sclerosis. Arch Phys Med Rehabil 1985;66:810-3.
38. Comi G, Leocani L. Assessment, pathophysiology and treatment of fatigue in multiple sclerosis. Expert Rev Neurother 2002;2(6):867-76.
1. Patten SB, Beck CA, Williams JVA, et al. Major depression in multiple sclerosis: a population-based perspective. Neurology 2003;61:1524-7.
2. Stenager EN, Stenager E, Koch-Henriksen N, et al. Suicide and multiple sclerosis: an epidemiological investigation. J Neurol Neurosurg Psychiatry 1992;55:542-5.
3. Minden SL, Orav J, Reich P. Depression in multiple sclerosis. Gen Hosp Psychiatry 1987;9:426-34.
4. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed, text rev. Washington, DC: American Psychiatric Association; 2000.
5. Patten SB, Metz LM, Reimer MA. Biopsychosocial correlates of major depression in a multiple sclerosis population. Mult Scler 2000;6:115-20.
6. Feinstein A, Roy P, Lobaugh N, et al. Structural brain abnormalities in multiple sclerosis patients with major depression. Neurology 2004;62:586-90.
7. Klapper JA. Interferon beta treatment of multiple sclerosis. Neurology 1994;44:188.-
8. Patten SB, Metz LM. Interferon β-1a and depression in secondary progressive MS: data from the SPECTRIMS trial. Neurology 2002;59(744):746.-
9. Patten SB, Metz LM. Interferon b-1a and depression in relapsing-remitting multiple sclerosis: an analysis of depression data from the PRISMS clinical trial. Mult Scler 2001;7:243-8.
10. Beck AT, Ward CH, Mendelson M, et al. An inventory for measuring depression. Arch Gen Psychiatry 1961;4:53-63.
11. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Applied Psychol Measurement 1977;1:385-401.
12. Fisk JD, Pontefract A, Ritvo PG, et al. The impact of fatigue on patients with multiple sclerosis. Can J Neurol Sci 1995;21:9-14.
13. Freal JE, Kraft GH, Coryell JK. Symptomatic fatigue in multiple sclerosis. Arch Phys Med Rehabil 1984;65:135-8.
14. Bagert B, Camplair P, Bourdette D. Cognitive dysfunction in multiple sclerosis. Natural history, pathophysiology and management. CNS Drugs 2002;16:445-55.
15. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State Examination. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 1975;12:189-98.
16. Feinstein A, Feinstein K, Gray T, O’Connor P. The prevalence and neurobehavioural correlates of pathological laughter and crying in multiple sclerosis. Arch Neurol 1997;54:1116-21.
17. Cummings JL. Involuntary emotional expression disorder: definition, diagnosis, and measurement scales. CNS Spectr 2007;12(4 suppl 5):11-6.
18. Paradiso S, Chemerinski E, Yazici KM, et al. Frontal lobe syndrome reassessed: comparison of patients with lateral or medial frontal brain damage. J Neurol Neurosurg Psychiatry 1999;67(5):664-7.
19. Moore SR, Gresham LS, Bromberg MB, et al. A self report measure of affective lability. J Neurol Neurosurg Psychiatry 1997;63(1):89-93.
20. Schiffer RB, Herndon RM, Rudick RA. Treatment of pathological laughing and weeping with amitriptyline. N Eng J Med 1985;312:1480-2.
21. Panitch HS, Thisted RA, Smith RA, et al. Randomized, controlled trial of dextromethorphan/quinidine for pseudobulbar affect in multiple sclerosis. Ann Neurol 2006;59:780-7.
22. Smith RA, Berg JE, Pope LE, Thisted RA. Measuring pseudobulbar affect in ALS. Amyotroph Lateral Scler Other Motor Neuron Disord 2004;5(suppl 1):99-102.
23. Schiffer RB, Wineman NM. Antidepressant pharmacotherapy of depression associated with multiple sclerosis. Am J Psychiatry 1990;147(11):1493-7.
24. Mohr DC, Boudewyn AC, Goodkin DE, et al. Comparative outcomes for individual cognitive-behavior therapy, supportive-expressive group psychotherapy, and sertraline for the treatment of depression in multiple sclerosis. J Cons Clin Psychol 2001;69:942-9.
25. The Goldman Consensus Group. The Goldman Consensus statement on depression in multiple sclerosis. Mult Scler 2005;11:328-37.
26. Taus C, Giulani G, Pucci E, et al. Amantadine for fatigue in multiple sclerosis. Cochrane Database Syst Rev 2003;(2):CD002818.-
27. Krupp LB, Coyle PK, Doscher C, et al. Fatigue therapy in multiple sclerosis: results of a double-bind, randomized, parallel trial of amantadine, pemoline and placebo. Neurology 1995;45:1956-61.
28. Zifko UA, Rupp M, Schwarz S, et al. Modafinil in treatment of fatigue in multiple sclerosis. Results of an open-label study. J Neurol 2002;249:983-7.
29. Zifko UA. Management of fatigue in patients with multiple sclerosis. Drugs 2004;64:1295-304.
30. Rammohan KW, Rosenberg JH, Lynn DJ, et al. Efficacy and safety of modafinil (Provigil) for the treatment of fatigue in multiple sclerosis: a two centre phase 2 study. J Neurol Neurosurg Psychiatry 2002;72:179-83.
31. Stankoff B, Waubant E, Confavreux C, et al. Modafinil for fatigue in MS: a randomized placebo-controlled double-blind study. Neurology 2005;64:1139-43.
32. Joffe RT, Lippert GP, Gray TA, et al. Mood disorders and multiple sclerosis. Arch Neurol 1987;44:376-8.
33. Finger S. A happy state of mind. A history of mild elation, denial of disability, optimism, and laughing in multiple sclerosis. Arch Neurol 1998;55:241-50.
34. Patten SB, Svenson LW, Metz LM. Psychotic disorders in MS: population-based evidence of an association. Neurology 2005;1123-5.
35. Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive therapy of depression. New York, NY: Guilford; 1979.
36. Jacobson NS, Dobson KS, Truax PA, et al. A component analysis of cognitive-behavioral treatment for depression. J Cons Clin Psychol 1996;64:295-304.
37. Crawford JD, McIvor GP. Group psychotherapy: benefits in multiple sclerosis. Arch Phys Med Rehabil 1985;66:810-3.
38. Comi G, Leocani L. Assessment, pathophysiology and treatment of fatigue in multiple sclerosis. Expert Rev Neurother 2002;2(6):867-76.
Tools, techniques to assess organ transplant candidates
With nearly 30,000 organ transplants being performed in the United States each year (Box 1),1 demand is growing for psychiatrists to provide presurgical and ongoing care.
How you might collaborate with a transplant team depends on each medical center’s protocols and individual patients’ mental health needs. A transplant candidate with depressive or anxiety symptoms may be referred to you for presurgical stabilization, for example, particularly if the patient lives far from a highly specialized transplant center.
Transplant assessments differ from usual psychiatric evaluations. Your findings will be used to help the transplant team evaluate the patient’s demographics, disease severity, and resources to give the patient the best chance for medical recovery. Inform patients at the beginning of the pretransplant evaluation that the results:
- will be shared with the transplant team
- may be used to help make decisions about transplant
- will not be the only factor determining if a transplant center will place a patient on an organ wait list.2
Pretransplant evaluation
Presurgical assessment helps determine the patient’s understanding of the transplant process and ability to provide consent (Table 1).3 Patients do not need a high level of medical sophistication to discuss transplantation, but they must understand the basics of the procedure and be able to rationally discuss their options. If a patient has severe cognitive impairment, dementia, or hepatic encephalopathy and cannot participate in the consent process, a surrogate is necessary.
Explore the patient’s attitudes and beliefs about transplant. If other team members have educated the patient about the procedure, your assessment can help determine how much the patient understood and if the patient has the capacity to make treatment decisions. Some patients believe the operation will “cure” them, despite education about the rigorous posttransplant routine. Alert the transplant team to these views, and begin aligning the patient’s views with reality.
In 2006, U.S. surgeons performed 28,931 organ transplants, bringing the total number of transplants since 1988 to >400,000. Each year, more kidney transplants are performed (17,091 in 2006) than all other organ transplants combined, according to the nonprofit United Network of Organ Sharing.1
Other organs being transplanted include liver, pancreas, heart, lung, and intestine. Some patients receive multiple organs, such as kidney/pancreas or heart/lung. As this article went to press, >96,000 candidates were on wait lists for organ donations.
Survival after transplantation has improved because of better immunosuppressant therapies introduced in the early 1980s and evolving physician and institutional experience. One-year survival rates for single-organ transplants range from 85% for lung to 98% for living donor kidney. Five-year survival rates range from 47% for lung to 86% for living donor kidney.
Source: Reference 1
Table 1
Psychiatric assessment of the pretransplant patient
| Assess understanding of his or her illness |
| Assess understanding of transplant process and ability to provide informed consent |
| Assess history of compliance with medical and psychiatric treatments |
| Identify substance abuse and other psychiatric comorbidities |
| Assess mental status |
| Evaluate social support system and possible interventions to bolster supports |
| Provide transplant team with information about patient’s need for education and support |
| Recommend treatment plan to address substance abuse and other psychiatric comorbidities |
| Source: Adapted from reference 3 |
Assessing psychiatric comorbidity. Like other patients with life-threatening medical illnesses, many transplant patients present with major depression and anxiety. Screen for symptoms of mood and anxiety disorders and past episodes of depression or mania. Explore the patient’s response to psychiatric treatment, current therapies, and history of treatment adherence.
Depression. Patients listed for transplant are seriously ill and coping with the difficulties of the sick role. Organ failure symptoms and resultant disability—such as insomnia, anorexia, fatigue, and impaired concentration—overlap with depression’s neurovegetative signs. Suspect depression if a patient presents with anhedonia, tearfulness, apathy, or guilt.
Among heart, lung, and liver transplant candidates, the reported lifetime prevalence of depression averages approximately 20%.4-6
Anxiety disorders. An estimated 40% of transplant patients have anxiety disorders,7 which may be caused by:
- stress of chronic illness
- uncertainty of the transplant process
- medical conditions such as hypothyroidism or pulmonary embolism.
Chronic mental illness. Patients with major mental illnesses such as schizophrenia might be appropriate candidates for organ transplant if they have adequate social support and history of treatment compliance.
Pharmacotherapy. Because of the variety of medical problems seen in transplant candidates, carefully consider medication side effects and drug-drug interactions when prescribing psychotropics.
Antidepressants. Among the selective serotonin reuptake inhibitors (SSRIs), citalopram, escitalopram, and sertraline are least likely to affect hepatic metabolism of other medications (Table 2).8 If a patient presents with liver failure, reduce the dosages of medications with hepatic metabolism.
Benzodiazepines. Use caution when treating anxiety with benzodiazepines because of the risk of tolerance, withdrawal, and dependence. Avoid benzodiazepines when treating transplant candidates with a substance abuse history. Also, these drugs might worsen hepatic encephalopathy and increase confusion.
Patients awaiting lung transplantation, especially those with high levels of CO2 retention, require special care because benzodiazepines might decrease respiratory drive. Try other agents such as buspirone, gabapentin, SSRIs, or second-generation antipsychotics to treat their anxiety.
Psychotherapy. Supportive psychotherapy can help patients navigate the often-lengthy process of waiting for a donor organ. Support groups for organ transplant candidates may help ease patients’ depressive symptoms.
Table 2
Antidepressants’ half-life and effect on hepatic metabolism
| Hepatic enzyme alterations | Half-life (hours) | |
|---|---|---|
| SSRIs | ||
| Fluoxetine | 2D6, 2C9, 2C19, 3A4 inhibition | 72 |
| Citalopram | None | 35 |
| Escitalopram | 2D6 inhibition (weak) | 32 |
| Sertraline | 2D6 inhibition (weak) | 30 |
| Paroxetine | 2D6 inhibition (strong) | 18 |
| Fluvoxamine | 1A2, 2C19, 2C9, 3A4 inhibition | 18 |
| Others | ||
| Mirtazapine | None | 30 |
| Bupropion SR | 2D6 inhibition | 21 |
| Venlafaxine XR | 2D6 inhibition | 5 |
| Trazodone | None | 5 |
| SSRIs: selective serotonin reuptake inhibitors | ||
| Source: Reference 8 | ||
Assessing substance abuse
Up to 50% of liver transplant candidates have a history of alcohol and/or drug abuse,9 the highest rate among transplant populations. Alcohol-induced cirrhosis and hepatitis C contracted from IV drug use are common indications for liver transplant. Effective treatment of substance abuse is essential because 30% to 50% of these patients relapse after the procedure.10 Assess:
- each substance abused, including onset, peak, and current use
- family history of substance abuse disorders
- past efforts at rehabilitation
- tobacco use (smoking before and after transplant is related to an increased incidence of new cancer diagnoses).11
Some transplant centers require patients with substance
use disorders to participate in 12-step programs or
rehabilitation. Regardless of the institutions’
requirements, encourage patients to participate in
rehabilitation to prevent relapse and mitigate the
negative impact of substance abuse on physical
and mental well-being.
Mental status examination includes the usual elements such as appearance, behavior, speech, affect, and thought process. Assess for suicidal thinking or hopelessness, which have been linked to serious medical illness.12 Question patients about hallucinations and give special attention to visual aberrations, which may occur in medically ill patients.
Cognitive testing. Use tools such as the Mini-Mental State Examination, clock drawing test, and Trail Making A and B tests to assess cognitive ability. If patients show signs of cognitive impairment, arrange for follow-up examinations and refer for neuropsychological testing.
Some cognitive impairment—such as that caused by hepatic encephalopathy—will likely improve after transplant, but other types—such as that caused by vascular disease—will not. If confusion is caused by hepatic encephalopathy, treatment with lactulose might rapidly improve symptoms. Remember that patients with hepatic encephalopathy might not exhibit elevated ammonia levels. Underlying causes of worsening hepatic encephalopathy—such as infections or bleeding—might require treatment.
Assessing adherence. Medication adherence after transplant is essential to prevent organ rejection and other complications. Posttransplant regimens are complex, and the frequency of follow-up assessments can be intense—particularly in the first year after transplant.
Your pretransplant assessment can identify where patients have struggled with adherence in the past. Before the transplant, your team can work to correct barriers such as inability to pay for medications, child care problems, or transportation needs.
Personality disorders have been identified as predictors of posttransplant nonadherence, and 50% to 60% of transplant programs consider personality disorders a relative contraindication to organ transplant.13 Address other contributors to poor adherence—such as substance abuse or depression—with ongoing psychiatric care.
When assessing a patient’s social support, look for evidence of:
- stable living situations
- long-term relationships with spouses, parents, children, or close friends
- adequate financial resources, including health insurance.
These factors help the patient manage the posttransplant process and numerous follow-up physician visits. Religious organizations or other social institutions also appear to provide the emotional support patients need to cope with an organ transplant.
Social support is essential to help with the normal difficulties such as frequent clinic visits and initial physical disability patients face after successful transplant (Box 2). Ask about the candidate’s family, friends, spirituality, and finances during your pretransplant assessment. Poor social support is related to the development of posttransplant psychiatric disorders14 and adherence difficulties.15
Assessment instruments—such as the Psychosocial Assessment of Candidates for Transplantation and the Transplant Evaluation Rating Scale3—include social support items and can be useful in identifying weak areas.
Data collected by other team members can be invaluable. A nurse or social worker, for example, may observe that a patient is unwilling to take medications, contrary to the patient’s report. Other sources of information include the patient’s family and friends, a primary care physician, or other mental health providers such as a therapist or case manager.
Posttransplant psychiatric care
Depression. The incidence of depression is higher in the year following transplant than before transplant or in the immediate posttransplant period.5 Predictors of posttransplant depression include:
- history of depression
- poor social support
- passive coping strategies
- poor physical status after transplantation.16,17
Carefully monitor patients who present with these factors after transplant. Treat depression with supportive measures designed to improve the patient’s social network and coping skills and pharmacotherapy. Select antidepressant medications based on side effect profiles and impact on the patient’s transplanted organs.
Substance abuse. Patients with a pretransplant history of substance abuse often relapse. Among transplant recipients with a history of alcoholic liver disease, drinking rates of 30% to 40% have been reported 5 years after transplant. Most of these data represent occasional use, not heavy or regular drinking.18 Relapse can occur despite careful assessment and follow-up.
Some evidence suggests that transplant patients who resume drinking have worse outcomes than those who abstain. Alcoholism relapse has other negative consequences, such as relationship problems and employment difficulties.
Predictors of relapse include:
- pretransplant history of alcohol dependence
- family history of alcoholism
- rehabilitation history, which could indicate a severe substance abuse disorder.3
Medications for alcoholism treatment have not been studied systematically in transplant patients, but low doses of acamprosate, ≤2 g/d, and naltrexone, ≤200 mg/d, are options for patients interested in pharmacotherapy. Support from 12-step programs also helps treat substance-abusing patients.
Altered mental status. Immunosuppressive medications—including cyclosporine, tacrolimus, and prednisone—can have neuropsychiatric effects and could cause a change in mental status (Table 3).19 Check cyclosporine and tacrolimus serum levels against reference ranges when delirium is present. If levels are toxic the dosage often can be lowered, which might lead to clinical improvement.
Quality of life. In general, patients’ quality of life improves after their transplant. After the first year—which patients might find difficult because of changes in physical and social status—quality of life typically improves.5
Table 3
Neuropsychiatric side effects of medications
commonly used in transplant patients
| Medication | Side effects |
|---|---|
| Cyclosporine | Tremor, headache, seizures, hallucinations, delirium |
| Tacrolimus | Tremor, headache, vivid dreams, anxiety, anorexia, seizures, delirium |
| Prednisone | Depression, mania, psychosis, delirium |
| Source: Adapted from references 3,7 | |
Psychiatric disorders such as depression can worsen quality of life. However, quality of life can improve after depression is diagnosed and treated. Other predictors of improved quality of life include older age, marriage, and the absence of a personality disorder.4
Other posttransplant concerns of patients include changes in employment, finances, and relationships. Patients often have been away from work before transplant, and returning after a long absence can be stressful. Patients may find that they cannot work as well as before becoming ill, which may lead to frustration, depression, and/or anxiety symptoms. Transplant surgery requires a large financial investment, and money concerns usually persist long after the transplant.
The transplant recipient’s role within the family may shift after surgery. Families might expect the patient to “return to normal” and resume old activities. Alternatively, family members might continue to treat the patient as a person with chronic illness despite physical improvement. If patients are struggling with these changes, supportive psychotherapy is indicated.
Related resource
- United Network for Organ Sharing. www.unos.org.
- Transplant living. www.transplantliving.org.
- Trzepacz PT, DiMartini AF, eds. The transplant patient. Cambridge, UK: Cambridge University Press; 2000.
- Klapheke MM. The role of the psychiatrist in organ transplantation. Bull Menninger Clin 1999;63(1):13-39.
Drug brand names
- Acamprosate • Campral
- Buspirone • BuSpar
- Bupropion SR • Wellbutrin SR
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lactulose • Cephulac, Chronulac
- Mirtazapine • Remeron
- Naltrexone • ReVia
- Paroxetine • Paxil
- Prednisone • Deltasone
- Sertraline • Zoloft
- Tacrolimus • Prograf
- Trazodone • Desyrel
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. United Network for Organ Sharing. Transplants by donor type. U.S. transplants performed: January 1, 1988 – April 30, 2007. Organ Procurement and Transplantation Network. Available at: http://www.unos.org. Accessed July 26, 2007.
2. Crone CC, Wise TN. Psychiatric aspects of transplantation, I: evaluation and selection of candidates. Crit Care Nurs 1999;19:79-87.
3. DiMartini AF, Dew MA, Trzepacz PT. Organ transplantation. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington DC: American Psychiatric Publishing, Inc, 2005:675-700.
4. Cupples S, Dew MA, Grady KL, et al. Report of the psychosocial outcomes workgroup of the nursing and social sciences council of the international society for heart and lung transplantation: present status of research on psychosocial outcomes in cardiothoracic transplantation: review and recommendations for the field. J Heart Lung Transplant 2006;25:716-25.
5. Dew MA, DiMartini AF. Psychological disorders and distress after adult cardiothoracic transplantation. J Cardiovasc Nurs 2005;20:S51-S66.
6. Barbour KA, Blumenthal JA, Palmer SM. Psychosocial issues in the assessment and management of patients undergoing lung transplantation. Chest 2006;129:1367-74.
7. Trzepacz PT, Levenson JL, Tringali RA. Psychopharmacology and neuropsychiatric syndromes in organ transplantation. Gen Hosp Psychiatry 1991;13:233-45.
8. Crone CC, Gabriel GM. Treatment of anxiety and depression in transplant patients. Clin Pharmacokinet 2004;43:361-94.
9. DiMartini A, Weinrieb R, Mireman M. Liver transplantation in patients with alcohol and other substance use disorders. Psychiatr Clin North Am 2002;25:195-209.
10. Weinrieb RM, Van Horn DHA, McLellan AT, et al. Alcoholism treatment after liver transplantation: lessons learned from a clinical trial that failed. Psychosomatics 2001;42:110-6.
11. Jimenez C, Manrique A, Marques E, et al. Incidence and risk factors for the development of lung tumors after liver transplantation. Transpl Int 2007;20:57-63.
12. Juurlink DN, Herrmann N, Szalai JP, et al. Medical illness and the risk of suicide in the elderly. Arch Intern Med 2004;14:1179-84.
13. Levenson JL, Olbrisch ME. Psychosocial screening and selection of candidates for organ transplantation. In: Trzepacz PT, DiMartini AF, eds. The transplant patient. Cambridge, UK: Cambridge University Press, 2000:21-41.
14. Dew MA, Kormos RL, DiMartini AF, et al. Prevalence and risk of depression and anxiety-related disorders during the first three years after heart transplantation. Psychosomatics 2001;42:300-13.
15. Dew MA, Roth LH, Thompson ME, et al. Medical compliance and its predictors in the first year after cardiac transplantation. J Heart Lung Transplant 1996;15:631-45.
16. Dew MA, Myaskovsky L, Switzer GE, et al. Profiles and predictors of the course of psychological distress across four years after heart transplantation. Psychol Med 2005;35:1215-27.
17. Goetzmann L, Klaghofer R, Wagner-Huber R, et al. Psychosocial vulnerability predicts psychosocial outcome after an organ transplant: results of a prospective study with lung, liver, and bone-marrow patients. J Psychosom Res 2007;62:93-100.
18. Lucey M. Liver transplantation for alcoholic liver disease: a progress report. Graft 1999;2:S73-9.
19. Beresford TP. Neuropsychiatric complications of liver and other solid organ transplantation. Liver Transpl 2001;7(11 suppl 1):S36-S45.
With nearly 30,000 organ transplants being performed in the United States each year (Box 1),1 demand is growing for psychiatrists to provide presurgical and ongoing care.
How you might collaborate with a transplant team depends on each medical center’s protocols and individual patients’ mental health needs. A transplant candidate with depressive or anxiety symptoms may be referred to you for presurgical stabilization, for example, particularly if the patient lives far from a highly specialized transplant center.
Transplant assessments differ from usual psychiatric evaluations. Your findings will be used to help the transplant team evaluate the patient’s demographics, disease severity, and resources to give the patient the best chance for medical recovery. Inform patients at the beginning of the pretransplant evaluation that the results:
- will be shared with the transplant team
- may be used to help make decisions about transplant
- will not be the only factor determining if a transplant center will place a patient on an organ wait list.2
Pretransplant evaluation
Presurgical assessment helps determine the patient’s understanding of the transplant process and ability to provide consent (Table 1).3 Patients do not need a high level of medical sophistication to discuss transplantation, but they must understand the basics of the procedure and be able to rationally discuss their options. If a patient has severe cognitive impairment, dementia, or hepatic encephalopathy and cannot participate in the consent process, a surrogate is necessary.
Explore the patient’s attitudes and beliefs about transplant. If other team members have educated the patient about the procedure, your assessment can help determine how much the patient understood and if the patient has the capacity to make treatment decisions. Some patients believe the operation will “cure” them, despite education about the rigorous posttransplant routine. Alert the transplant team to these views, and begin aligning the patient’s views with reality.
In 2006, U.S. surgeons performed 28,931 organ transplants, bringing the total number of transplants since 1988 to >400,000. Each year, more kidney transplants are performed (17,091 in 2006) than all other organ transplants combined, according to the nonprofit United Network of Organ Sharing.1
Other organs being transplanted include liver, pancreas, heart, lung, and intestine. Some patients receive multiple organs, such as kidney/pancreas or heart/lung. As this article went to press, >96,000 candidates were on wait lists for organ donations.
Survival after transplantation has improved because of better immunosuppressant therapies introduced in the early 1980s and evolving physician and institutional experience. One-year survival rates for single-organ transplants range from 85% for lung to 98% for living donor kidney. Five-year survival rates range from 47% for lung to 86% for living donor kidney.
Source: Reference 1
Table 1
Psychiatric assessment of the pretransplant patient
| Assess understanding of his or her illness |
| Assess understanding of transplant process and ability to provide informed consent |
| Assess history of compliance with medical and psychiatric treatments |
| Identify substance abuse and other psychiatric comorbidities |
| Assess mental status |
| Evaluate social support system and possible interventions to bolster supports |
| Provide transplant team with information about patient’s need for education and support |
| Recommend treatment plan to address substance abuse and other psychiatric comorbidities |
| Source: Adapted from reference 3 |
Assessing psychiatric comorbidity. Like other patients with life-threatening medical illnesses, many transplant patients present with major depression and anxiety. Screen for symptoms of mood and anxiety disorders and past episodes of depression or mania. Explore the patient’s response to psychiatric treatment, current therapies, and history of treatment adherence.
Depression. Patients listed for transplant are seriously ill and coping with the difficulties of the sick role. Organ failure symptoms and resultant disability—such as insomnia, anorexia, fatigue, and impaired concentration—overlap with depression’s neurovegetative signs. Suspect depression if a patient presents with anhedonia, tearfulness, apathy, or guilt.
Among heart, lung, and liver transplant candidates, the reported lifetime prevalence of depression averages approximately 20%.4-6
Anxiety disorders. An estimated 40% of transplant patients have anxiety disorders,7 which may be caused by:
- stress of chronic illness
- uncertainty of the transplant process
- medical conditions such as hypothyroidism or pulmonary embolism.
Chronic mental illness. Patients with major mental illnesses such as schizophrenia might be appropriate candidates for organ transplant if they have adequate social support and history of treatment compliance.
Pharmacotherapy. Because of the variety of medical problems seen in transplant candidates, carefully consider medication side effects and drug-drug interactions when prescribing psychotropics.
Antidepressants. Among the selective serotonin reuptake inhibitors (SSRIs), citalopram, escitalopram, and sertraline are least likely to affect hepatic metabolism of other medications (Table 2).8 If a patient presents with liver failure, reduce the dosages of medications with hepatic metabolism.
Benzodiazepines. Use caution when treating anxiety with benzodiazepines because of the risk of tolerance, withdrawal, and dependence. Avoid benzodiazepines when treating transplant candidates with a substance abuse history. Also, these drugs might worsen hepatic encephalopathy and increase confusion.
Patients awaiting lung transplantation, especially those with high levels of CO2 retention, require special care because benzodiazepines might decrease respiratory drive. Try other agents such as buspirone, gabapentin, SSRIs, or second-generation antipsychotics to treat their anxiety.
Psychotherapy. Supportive psychotherapy can help patients navigate the often-lengthy process of waiting for a donor organ. Support groups for organ transplant candidates may help ease patients’ depressive symptoms.
Table 2
Antidepressants’ half-life and effect on hepatic metabolism
| Hepatic enzyme alterations | Half-life (hours) | |
|---|---|---|
| SSRIs | ||
| Fluoxetine | 2D6, 2C9, 2C19, 3A4 inhibition | 72 |
| Citalopram | None | 35 |
| Escitalopram | 2D6 inhibition (weak) | 32 |
| Sertraline | 2D6 inhibition (weak) | 30 |
| Paroxetine | 2D6 inhibition (strong) | 18 |
| Fluvoxamine | 1A2, 2C19, 2C9, 3A4 inhibition | 18 |
| Others | ||
| Mirtazapine | None | 30 |
| Bupropion SR | 2D6 inhibition | 21 |
| Venlafaxine XR | 2D6 inhibition | 5 |
| Trazodone | None | 5 |
| SSRIs: selective serotonin reuptake inhibitors | ||
| Source: Reference 8 | ||
Assessing substance abuse
Up to 50% of liver transplant candidates have a history of alcohol and/or drug abuse,9 the highest rate among transplant populations. Alcohol-induced cirrhosis and hepatitis C contracted from IV drug use are common indications for liver transplant. Effective treatment of substance abuse is essential because 30% to 50% of these patients relapse after the procedure.10 Assess:
- each substance abused, including onset, peak, and current use
- family history of substance abuse disorders
- past efforts at rehabilitation
- tobacco use (smoking before and after transplant is related to an increased incidence of new cancer diagnoses).11
Some transplant centers require patients with substance
use disorders to participate in 12-step programs or
rehabilitation. Regardless of the institutions’
requirements, encourage patients to participate in
rehabilitation to prevent relapse and mitigate the
negative impact of substance abuse on physical
and mental well-being.
Mental status examination includes the usual elements such as appearance, behavior, speech, affect, and thought process. Assess for suicidal thinking or hopelessness, which have been linked to serious medical illness.12 Question patients about hallucinations and give special attention to visual aberrations, which may occur in medically ill patients.
Cognitive testing. Use tools such as the Mini-Mental State Examination, clock drawing test, and Trail Making A and B tests to assess cognitive ability. If patients show signs of cognitive impairment, arrange for follow-up examinations and refer for neuropsychological testing.
Some cognitive impairment—such as that caused by hepatic encephalopathy—will likely improve after transplant, but other types—such as that caused by vascular disease—will not. If confusion is caused by hepatic encephalopathy, treatment with lactulose might rapidly improve symptoms. Remember that patients with hepatic encephalopathy might not exhibit elevated ammonia levels. Underlying causes of worsening hepatic encephalopathy—such as infections or bleeding—might require treatment.
Assessing adherence. Medication adherence after transplant is essential to prevent organ rejection and other complications. Posttransplant regimens are complex, and the frequency of follow-up assessments can be intense—particularly in the first year after transplant.
Your pretransplant assessment can identify where patients have struggled with adherence in the past. Before the transplant, your team can work to correct barriers such as inability to pay for medications, child care problems, or transportation needs.
Personality disorders have been identified as predictors of posttransplant nonadherence, and 50% to 60% of transplant programs consider personality disorders a relative contraindication to organ transplant.13 Address other contributors to poor adherence—such as substance abuse or depression—with ongoing psychiatric care.
When assessing a patient’s social support, look for evidence of:
- stable living situations
- long-term relationships with spouses, parents, children, or close friends
- adequate financial resources, including health insurance.
These factors help the patient manage the posttransplant process and numerous follow-up physician visits. Religious organizations or other social institutions also appear to provide the emotional support patients need to cope with an organ transplant.
Social support is essential to help with the normal difficulties such as frequent clinic visits and initial physical disability patients face after successful transplant (Box 2). Ask about the candidate’s family, friends, spirituality, and finances during your pretransplant assessment. Poor social support is related to the development of posttransplant psychiatric disorders14 and adherence difficulties.15
Assessment instruments—such as the Psychosocial Assessment of Candidates for Transplantation and the Transplant Evaluation Rating Scale3—include social support items and can be useful in identifying weak areas.
Data collected by other team members can be invaluable. A nurse or social worker, for example, may observe that a patient is unwilling to take medications, contrary to the patient’s report. Other sources of information include the patient’s family and friends, a primary care physician, or other mental health providers such as a therapist or case manager.
Posttransplant psychiatric care
Depression. The incidence of depression is higher in the year following transplant than before transplant or in the immediate posttransplant period.5 Predictors of posttransplant depression include:
- history of depression
- poor social support
- passive coping strategies
- poor physical status after transplantation.16,17
Carefully monitor patients who present with these factors after transplant. Treat depression with supportive measures designed to improve the patient’s social network and coping skills and pharmacotherapy. Select antidepressant medications based on side effect profiles and impact on the patient’s transplanted organs.
Substance abuse. Patients with a pretransplant history of substance abuse often relapse. Among transplant recipients with a history of alcoholic liver disease, drinking rates of 30% to 40% have been reported 5 years after transplant. Most of these data represent occasional use, not heavy or regular drinking.18 Relapse can occur despite careful assessment and follow-up.
Some evidence suggests that transplant patients who resume drinking have worse outcomes than those who abstain. Alcoholism relapse has other negative consequences, such as relationship problems and employment difficulties.
Predictors of relapse include:
- pretransplant history of alcohol dependence
- family history of alcoholism
- rehabilitation history, which could indicate a severe substance abuse disorder.3
Medications for alcoholism treatment have not been studied systematically in transplant patients, but low doses of acamprosate, ≤2 g/d, and naltrexone, ≤200 mg/d, are options for patients interested in pharmacotherapy. Support from 12-step programs also helps treat substance-abusing patients.
Altered mental status. Immunosuppressive medications—including cyclosporine, tacrolimus, and prednisone—can have neuropsychiatric effects and could cause a change in mental status (Table 3).19 Check cyclosporine and tacrolimus serum levels against reference ranges when delirium is present. If levels are toxic the dosage often can be lowered, which might lead to clinical improvement.
Quality of life. In general, patients’ quality of life improves after their transplant. After the first year—which patients might find difficult because of changes in physical and social status—quality of life typically improves.5
Table 3
Neuropsychiatric side effects of medications
commonly used in transplant patients
| Medication | Side effects |
|---|---|
| Cyclosporine | Tremor, headache, seizures, hallucinations, delirium |
| Tacrolimus | Tremor, headache, vivid dreams, anxiety, anorexia, seizures, delirium |
| Prednisone | Depression, mania, psychosis, delirium |
| Source: Adapted from references 3,7 | |
Psychiatric disorders such as depression can worsen quality of life. However, quality of life can improve after depression is diagnosed and treated. Other predictors of improved quality of life include older age, marriage, and the absence of a personality disorder.4
Other posttransplant concerns of patients include changes in employment, finances, and relationships. Patients often have been away from work before transplant, and returning after a long absence can be stressful. Patients may find that they cannot work as well as before becoming ill, which may lead to frustration, depression, and/or anxiety symptoms. Transplant surgery requires a large financial investment, and money concerns usually persist long after the transplant.
The transplant recipient’s role within the family may shift after surgery. Families might expect the patient to “return to normal” and resume old activities. Alternatively, family members might continue to treat the patient as a person with chronic illness despite physical improvement. If patients are struggling with these changes, supportive psychotherapy is indicated.
Related resource
- United Network for Organ Sharing. www.unos.org.
- Transplant living. www.transplantliving.org.
- Trzepacz PT, DiMartini AF, eds. The transplant patient. Cambridge, UK: Cambridge University Press; 2000.
- Klapheke MM. The role of the psychiatrist in organ transplantation. Bull Menninger Clin 1999;63(1):13-39.
Drug brand names
- Acamprosate • Campral
- Buspirone • BuSpar
- Bupropion SR • Wellbutrin SR
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lactulose • Cephulac, Chronulac
- Mirtazapine • Remeron
- Naltrexone • ReVia
- Paroxetine • Paxil
- Prednisone • Deltasone
- Sertraline • Zoloft
- Tacrolimus • Prograf
- Trazodone • Desyrel
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
With nearly 30,000 organ transplants being performed in the United States each year (Box 1),1 demand is growing for psychiatrists to provide presurgical and ongoing care.
How you might collaborate with a transplant team depends on each medical center’s protocols and individual patients’ mental health needs. A transplant candidate with depressive or anxiety symptoms may be referred to you for presurgical stabilization, for example, particularly if the patient lives far from a highly specialized transplant center.
Transplant assessments differ from usual psychiatric evaluations. Your findings will be used to help the transplant team evaluate the patient’s demographics, disease severity, and resources to give the patient the best chance for medical recovery. Inform patients at the beginning of the pretransplant evaluation that the results:
- will be shared with the transplant team
- may be used to help make decisions about transplant
- will not be the only factor determining if a transplant center will place a patient on an organ wait list.2
Pretransplant evaluation
Presurgical assessment helps determine the patient’s understanding of the transplant process and ability to provide consent (Table 1).3 Patients do not need a high level of medical sophistication to discuss transplantation, but they must understand the basics of the procedure and be able to rationally discuss their options. If a patient has severe cognitive impairment, dementia, or hepatic encephalopathy and cannot participate in the consent process, a surrogate is necessary.
Explore the patient’s attitudes and beliefs about transplant. If other team members have educated the patient about the procedure, your assessment can help determine how much the patient understood and if the patient has the capacity to make treatment decisions. Some patients believe the operation will “cure” them, despite education about the rigorous posttransplant routine. Alert the transplant team to these views, and begin aligning the patient’s views with reality.
In 2006, U.S. surgeons performed 28,931 organ transplants, bringing the total number of transplants since 1988 to >400,000. Each year, more kidney transplants are performed (17,091 in 2006) than all other organ transplants combined, according to the nonprofit United Network of Organ Sharing.1
Other organs being transplanted include liver, pancreas, heart, lung, and intestine. Some patients receive multiple organs, such as kidney/pancreas or heart/lung. As this article went to press, >96,000 candidates were on wait lists for organ donations.
Survival after transplantation has improved because of better immunosuppressant therapies introduced in the early 1980s and evolving physician and institutional experience. One-year survival rates for single-organ transplants range from 85% for lung to 98% for living donor kidney. Five-year survival rates range from 47% for lung to 86% for living donor kidney.
Source: Reference 1
Table 1
Psychiatric assessment of the pretransplant patient
| Assess understanding of his or her illness |
| Assess understanding of transplant process and ability to provide informed consent |
| Assess history of compliance with medical and psychiatric treatments |
| Identify substance abuse and other psychiatric comorbidities |
| Assess mental status |
| Evaluate social support system and possible interventions to bolster supports |
| Provide transplant team with information about patient’s need for education and support |
| Recommend treatment plan to address substance abuse and other psychiatric comorbidities |
| Source: Adapted from reference 3 |
Assessing psychiatric comorbidity. Like other patients with life-threatening medical illnesses, many transplant patients present with major depression and anxiety. Screen for symptoms of mood and anxiety disorders and past episodes of depression or mania. Explore the patient’s response to psychiatric treatment, current therapies, and history of treatment adherence.
Depression. Patients listed for transplant are seriously ill and coping with the difficulties of the sick role. Organ failure symptoms and resultant disability—such as insomnia, anorexia, fatigue, and impaired concentration—overlap with depression’s neurovegetative signs. Suspect depression if a patient presents with anhedonia, tearfulness, apathy, or guilt.
Among heart, lung, and liver transplant candidates, the reported lifetime prevalence of depression averages approximately 20%.4-6
Anxiety disorders. An estimated 40% of transplant patients have anxiety disorders,7 which may be caused by:
- stress of chronic illness
- uncertainty of the transplant process
- medical conditions such as hypothyroidism or pulmonary embolism.
Chronic mental illness. Patients with major mental illnesses such as schizophrenia might be appropriate candidates for organ transplant if they have adequate social support and history of treatment compliance.
Pharmacotherapy. Because of the variety of medical problems seen in transplant candidates, carefully consider medication side effects and drug-drug interactions when prescribing psychotropics.
Antidepressants. Among the selective serotonin reuptake inhibitors (SSRIs), citalopram, escitalopram, and sertraline are least likely to affect hepatic metabolism of other medications (Table 2).8 If a patient presents with liver failure, reduce the dosages of medications with hepatic metabolism.
Benzodiazepines. Use caution when treating anxiety with benzodiazepines because of the risk of tolerance, withdrawal, and dependence. Avoid benzodiazepines when treating transplant candidates with a substance abuse history. Also, these drugs might worsen hepatic encephalopathy and increase confusion.
Patients awaiting lung transplantation, especially those with high levels of CO2 retention, require special care because benzodiazepines might decrease respiratory drive. Try other agents such as buspirone, gabapentin, SSRIs, or second-generation antipsychotics to treat their anxiety.
Psychotherapy. Supportive psychotherapy can help patients navigate the often-lengthy process of waiting for a donor organ. Support groups for organ transplant candidates may help ease patients’ depressive symptoms.
Table 2
Antidepressants’ half-life and effect on hepatic metabolism
| Hepatic enzyme alterations | Half-life (hours) | |
|---|---|---|
| SSRIs | ||
| Fluoxetine | 2D6, 2C9, 2C19, 3A4 inhibition | 72 |
| Citalopram | None | 35 |
| Escitalopram | 2D6 inhibition (weak) | 32 |
| Sertraline | 2D6 inhibition (weak) | 30 |
| Paroxetine | 2D6 inhibition (strong) | 18 |
| Fluvoxamine | 1A2, 2C19, 2C9, 3A4 inhibition | 18 |
| Others | ||
| Mirtazapine | None | 30 |
| Bupropion SR | 2D6 inhibition | 21 |
| Venlafaxine XR | 2D6 inhibition | 5 |
| Trazodone | None | 5 |
| SSRIs: selective serotonin reuptake inhibitors | ||
| Source: Reference 8 | ||
Assessing substance abuse
Up to 50% of liver transplant candidates have a history of alcohol and/or drug abuse,9 the highest rate among transplant populations. Alcohol-induced cirrhosis and hepatitis C contracted from IV drug use are common indications for liver transplant. Effective treatment of substance abuse is essential because 30% to 50% of these patients relapse after the procedure.10 Assess:
- each substance abused, including onset, peak, and current use
- family history of substance abuse disorders
- past efforts at rehabilitation
- tobacco use (smoking before and after transplant is related to an increased incidence of new cancer diagnoses).11
Some transplant centers require patients with substance
use disorders to participate in 12-step programs or
rehabilitation. Regardless of the institutions’
requirements, encourage patients to participate in
rehabilitation to prevent relapse and mitigate the
negative impact of substance abuse on physical
and mental well-being.
Mental status examination includes the usual elements such as appearance, behavior, speech, affect, and thought process. Assess for suicidal thinking or hopelessness, which have been linked to serious medical illness.12 Question patients about hallucinations and give special attention to visual aberrations, which may occur in medically ill patients.
Cognitive testing. Use tools such as the Mini-Mental State Examination, clock drawing test, and Trail Making A and B tests to assess cognitive ability. If patients show signs of cognitive impairment, arrange for follow-up examinations and refer for neuropsychological testing.
Some cognitive impairment—such as that caused by hepatic encephalopathy—will likely improve after transplant, but other types—such as that caused by vascular disease—will not. If confusion is caused by hepatic encephalopathy, treatment with lactulose might rapidly improve symptoms. Remember that patients with hepatic encephalopathy might not exhibit elevated ammonia levels. Underlying causes of worsening hepatic encephalopathy—such as infections or bleeding—might require treatment.
Assessing adherence. Medication adherence after transplant is essential to prevent organ rejection and other complications. Posttransplant regimens are complex, and the frequency of follow-up assessments can be intense—particularly in the first year after transplant.
Your pretransplant assessment can identify where patients have struggled with adherence in the past. Before the transplant, your team can work to correct barriers such as inability to pay for medications, child care problems, or transportation needs.
Personality disorders have been identified as predictors of posttransplant nonadherence, and 50% to 60% of transplant programs consider personality disorders a relative contraindication to organ transplant.13 Address other contributors to poor adherence—such as substance abuse or depression—with ongoing psychiatric care.
When assessing a patient’s social support, look for evidence of:
- stable living situations
- long-term relationships with spouses, parents, children, or close friends
- adequate financial resources, including health insurance.
These factors help the patient manage the posttransplant process and numerous follow-up physician visits. Religious organizations or other social institutions also appear to provide the emotional support patients need to cope with an organ transplant.
Social support is essential to help with the normal difficulties such as frequent clinic visits and initial physical disability patients face after successful transplant (Box 2). Ask about the candidate’s family, friends, spirituality, and finances during your pretransplant assessment. Poor social support is related to the development of posttransplant psychiatric disorders14 and adherence difficulties.15
Assessment instruments—such as the Psychosocial Assessment of Candidates for Transplantation and the Transplant Evaluation Rating Scale3—include social support items and can be useful in identifying weak areas.
Data collected by other team members can be invaluable. A nurse or social worker, for example, may observe that a patient is unwilling to take medications, contrary to the patient’s report. Other sources of information include the patient’s family and friends, a primary care physician, or other mental health providers such as a therapist or case manager.
Posttransplant psychiatric care
Depression. The incidence of depression is higher in the year following transplant than before transplant or in the immediate posttransplant period.5 Predictors of posttransplant depression include:
- history of depression
- poor social support
- passive coping strategies
- poor physical status after transplantation.16,17
Carefully monitor patients who present with these factors after transplant. Treat depression with supportive measures designed to improve the patient’s social network and coping skills and pharmacotherapy. Select antidepressant medications based on side effect profiles and impact on the patient’s transplanted organs.
Substance abuse. Patients with a pretransplant history of substance abuse often relapse. Among transplant recipients with a history of alcoholic liver disease, drinking rates of 30% to 40% have been reported 5 years after transplant. Most of these data represent occasional use, not heavy or regular drinking.18 Relapse can occur despite careful assessment and follow-up.
Some evidence suggests that transplant patients who resume drinking have worse outcomes than those who abstain. Alcoholism relapse has other negative consequences, such as relationship problems and employment difficulties.
Predictors of relapse include:
- pretransplant history of alcohol dependence
- family history of alcoholism
- rehabilitation history, which could indicate a severe substance abuse disorder.3
Medications for alcoholism treatment have not been studied systematically in transplant patients, but low doses of acamprosate, ≤2 g/d, and naltrexone, ≤200 mg/d, are options for patients interested in pharmacotherapy. Support from 12-step programs also helps treat substance-abusing patients.
Altered mental status. Immunosuppressive medications—including cyclosporine, tacrolimus, and prednisone—can have neuropsychiatric effects and could cause a change in mental status (Table 3).19 Check cyclosporine and tacrolimus serum levels against reference ranges when delirium is present. If levels are toxic the dosage often can be lowered, which might lead to clinical improvement.
Quality of life. In general, patients’ quality of life improves after their transplant. After the first year—which patients might find difficult because of changes in physical and social status—quality of life typically improves.5
Table 3
Neuropsychiatric side effects of medications
commonly used in transplant patients
| Medication | Side effects |
|---|---|
| Cyclosporine | Tremor, headache, seizures, hallucinations, delirium |
| Tacrolimus | Tremor, headache, vivid dreams, anxiety, anorexia, seizures, delirium |
| Prednisone | Depression, mania, psychosis, delirium |
| Source: Adapted from references 3,7 | |
Psychiatric disorders such as depression can worsen quality of life. However, quality of life can improve after depression is diagnosed and treated. Other predictors of improved quality of life include older age, marriage, and the absence of a personality disorder.4
Other posttransplant concerns of patients include changes in employment, finances, and relationships. Patients often have been away from work before transplant, and returning after a long absence can be stressful. Patients may find that they cannot work as well as before becoming ill, which may lead to frustration, depression, and/or anxiety symptoms. Transplant surgery requires a large financial investment, and money concerns usually persist long after the transplant.
The transplant recipient’s role within the family may shift after surgery. Families might expect the patient to “return to normal” and resume old activities. Alternatively, family members might continue to treat the patient as a person with chronic illness despite physical improvement. If patients are struggling with these changes, supportive psychotherapy is indicated.
Related resource
- United Network for Organ Sharing. www.unos.org.
- Transplant living. www.transplantliving.org.
- Trzepacz PT, DiMartini AF, eds. The transplant patient. Cambridge, UK: Cambridge University Press; 2000.
- Klapheke MM. The role of the psychiatrist in organ transplantation. Bull Menninger Clin 1999;63(1):13-39.
Drug brand names
- Acamprosate • Campral
- Buspirone • BuSpar
- Bupropion SR • Wellbutrin SR
- Citalopram • Celexa
- Cyclosporine • Sandimmune
- Escitalopram • Lexapro
- Fluoxetine • Prozac
- Fluvoxamine • Luvox
- Gabapentin • Neurontin
- Lactulose • Cephulac, Chronulac
- Mirtazapine • Remeron
- Naltrexone • ReVia
- Paroxetine • Paxil
- Prednisone • Deltasone
- Sertraline • Zoloft
- Tacrolimus • Prograf
- Trazodone • Desyrel
Disclosure
The authors report no financial relationship with any company whose products are mentioned in this article or with manufacturers of competing products.
1. United Network for Organ Sharing. Transplants by donor type. U.S. transplants performed: January 1, 1988 – April 30, 2007. Organ Procurement and Transplantation Network. Available at: http://www.unos.org. Accessed July 26, 2007.
2. Crone CC, Wise TN. Psychiatric aspects of transplantation, I: evaluation and selection of candidates. Crit Care Nurs 1999;19:79-87.
3. DiMartini AF, Dew MA, Trzepacz PT. Organ transplantation. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington DC: American Psychiatric Publishing, Inc, 2005:675-700.
4. Cupples S, Dew MA, Grady KL, et al. Report of the psychosocial outcomes workgroup of the nursing and social sciences council of the international society for heart and lung transplantation: present status of research on psychosocial outcomes in cardiothoracic transplantation: review and recommendations for the field. J Heart Lung Transplant 2006;25:716-25.
5. Dew MA, DiMartini AF. Psychological disorders and distress after adult cardiothoracic transplantation. J Cardiovasc Nurs 2005;20:S51-S66.
6. Barbour KA, Blumenthal JA, Palmer SM. Psychosocial issues in the assessment and management of patients undergoing lung transplantation. Chest 2006;129:1367-74.
7. Trzepacz PT, Levenson JL, Tringali RA. Psychopharmacology and neuropsychiatric syndromes in organ transplantation. Gen Hosp Psychiatry 1991;13:233-45.
8. Crone CC, Gabriel GM. Treatment of anxiety and depression in transplant patients. Clin Pharmacokinet 2004;43:361-94.
9. DiMartini A, Weinrieb R, Mireman M. Liver transplantation in patients with alcohol and other substance use disorders. Psychiatr Clin North Am 2002;25:195-209.
10. Weinrieb RM, Van Horn DHA, McLellan AT, et al. Alcoholism treatment after liver transplantation: lessons learned from a clinical trial that failed. Psychosomatics 2001;42:110-6.
11. Jimenez C, Manrique A, Marques E, et al. Incidence and risk factors for the development of lung tumors after liver transplantation. Transpl Int 2007;20:57-63.
12. Juurlink DN, Herrmann N, Szalai JP, et al. Medical illness and the risk of suicide in the elderly. Arch Intern Med 2004;14:1179-84.
13. Levenson JL, Olbrisch ME. Psychosocial screening and selection of candidates for organ transplantation. In: Trzepacz PT, DiMartini AF, eds. The transplant patient. Cambridge, UK: Cambridge University Press, 2000:21-41.
14. Dew MA, Kormos RL, DiMartini AF, et al. Prevalence and risk of depression and anxiety-related disorders during the first three years after heart transplantation. Psychosomatics 2001;42:300-13.
15. Dew MA, Roth LH, Thompson ME, et al. Medical compliance and its predictors in the first year after cardiac transplantation. J Heart Lung Transplant 1996;15:631-45.
16. Dew MA, Myaskovsky L, Switzer GE, et al. Profiles and predictors of the course of psychological distress across four years after heart transplantation. Psychol Med 2005;35:1215-27.
17. Goetzmann L, Klaghofer R, Wagner-Huber R, et al. Psychosocial vulnerability predicts psychosocial outcome after an organ transplant: results of a prospective study with lung, liver, and bone-marrow patients. J Psychosom Res 2007;62:93-100.
18. Lucey M. Liver transplantation for alcoholic liver disease: a progress report. Graft 1999;2:S73-9.
19. Beresford TP. Neuropsychiatric complications of liver and other solid organ transplantation. Liver Transpl 2001;7(11 suppl 1):S36-S45.
1. United Network for Organ Sharing. Transplants by donor type. U.S. transplants performed: January 1, 1988 – April 30, 2007. Organ Procurement and Transplantation Network. Available at: http://www.unos.org. Accessed July 26, 2007.
2. Crone CC, Wise TN. Psychiatric aspects of transplantation, I: evaluation and selection of candidates. Crit Care Nurs 1999;19:79-87.
3. DiMartini AF, Dew MA, Trzepacz PT. Organ transplantation. In: Levenson JL, ed. The American Psychiatric Publishing textbook of psychosomatic medicine. Washington DC: American Psychiatric Publishing, Inc, 2005:675-700.
4. Cupples S, Dew MA, Grady KL, et al. Report of the psychosocial outcomes workgroup of the nursing and social sciences council of the international society for heart and lung transplantation: present status of research on psychosocial outcomes in cardiothoracic transplantation: review and recommendations for the field. J Heart Lung Transplant 2006;25:716-25.
5. Dew MA, DiMartini AF. Psychological disorders and distress after adult cardiothoracic transplantation. J Cardiovasc Nurs 2005;20:S51-S66.
6. Barbour KA, Blumenthal JA, Palmer SM. Psychosocial issues in the assessment and management of patients undergoing lung transplantation. Chest 2006;129:1367-74.
7. Trzepacz PT, Levenson JL, Tringali RA. Psychopharmacology and neuropsychiatric syndromes in organ transplantation. Gen Hosp Psychiatry 1991;13:233-45.
8. Crone CC, Gabriel GM. Treatment of anxiety and depression in transplant patients. Clin Pharmacokinet 2004;43:361-94.
9. DiMartini A, Weinrieb R, Mireman M. Liver transplantation in patients with alcohol and other substance use disorders. Psychiatr Clin North Am 2002;25:195-209.
10. Weinrieb RM, Van Horn DHA, McLellan AT, et al. Alcoholism treatment after liver transplantation: lessons learned from a clinical trial that failed. Psychosomatics 2001;42:110-6.
11. Jimenez C, Manrique A, Marques E, et al. Incidence and risk factors for the development of lung tumors after liver transplantation. Transpl Int 2007;20:57-63.
12. Juurlink DN, Herrmann N, Szalai JP, et al. Medical illness and the risk of suicide in the elderly. Arch Intern Med 2004;14:1179-84.
13. Levenson JL, Olbrisch ME. Psychosocial screening and selection of candidates for organ transplantation. In: Trzepacz PT, DiMartini AF, eds. The transplant patient. Cambridge, UK: Cambridge University Press, 2000:21-41.
14. Dew MA, Kormos RL, DiMartini AF, et al. Prevalence and risk of depression and anxiety-related disorders during the first three years after heart transplantation. Psychosomatics 2001;42:300-13.
15. Dew MA, Roth LH, Thompson ME, et al. Medical compliance and its predictors in the first year after cardiac transplantation. J Heart Lung Transplant 1996;15:631-45.
16. Dew MA, Myaskovsky L, Switzer GE, et al. Profiles and predictors of the course of psychological distress across four years after heart transplantation. Psychol Med 2005;35:1215-27.
17. Goetzmann L, Klaghofer R, Wagner-Huber R, et al. Psychosocial vulnerability predicts psychosocial outcome after an organ transplant: results of a prospective study with lung, liver, and bone-marrow patients. J Psychosom Res 2007;62:93-100.
18. Lucey M. Liver transplantation for alcoholic liver disease: a progress report. Graft 1999;2:S73-9.
19. Beresford TP. Neuropsychiatric complications of liver and other solid organ transplantation. Liver Transpl 2001;7(11 suppl 1):S36-S45.
Interpreting liver function tests
Mrs. W, age 53, is referred by her primary provider for consultation on depressive symptoms, including worsening depressed mood, anhedonia, anxiety, and suicidal thoughts for 2 months. She reports at least 2 similar episodes in the past 15 years. Mrs. W has a remote history of IV drug use and history of alcohol abuse, but she attends Alcoholics Anonymous and has 10 years of sobriety. She has no history of hospitalizations for medical illness and denies any medical problems.
Mrs. W is taking amitriptyline, 50 mg, for insomnia. She has no history of manic or psychotic symptoms, and the mental status examination is consistent with major depression. Her past depressive episodes were treated successfully with a medication that she does not recall.
The psychiatrist diagnoses recurrent and severe major depression and prescribes cognitive-behavioral therapy and sertraline, 25 mg/d, titrated to 50 mg/d over the next 2 weeks. Amitriptyline is discontinued.
When the psychiatrist receives Mrs. W’s medical records, electrolytes, complete blood count, thyroid stimulating hormone level, and fasting glucose are within normal limits, but alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are greatly elevated at 250 U/L and 150 U/L, respectively. Progress notes contain no references to liver disease.
Interpreting psychiatric patients’ liver function tests (LFTs) can be challenging, especially in those with polypharmacy, co-occurring substance abuse, or risk factors for viral hepatitis. You can improve collaboration with primary care providers by understanding:
- what an LFT measures
- how to interpret abnormal results
- which conditions to suspect, based on the results.
A standard LFT usually measures several enzymes and proteins, typically ALT, AST, alkaline phosphatase (ALP), total bilirubin (TBIL), albumin (ALB), and total protein (TP). Measures of gamma-glutamyl transpeptidase (GGT) and prothrombin time (PT) are often requested with an LFT. Table 1 provides normal ranges and ranges that indicate liver damage for several of these parameters.1,2
“Liver function test” is a misnomer because LFTs do not directly measure liver function. Rather, they reflect hepatocyte injury or cholestasis (blockage or damage in the biliary system). ALB and PT measure liver synthetic function, but are nonspecific. ALB levels can be altered by nutritional status, protein-losing enteropathies, or nephropathies, whereas PT may be modified by warfarin, vitamin K deficiency, or consumptive coagulopathy.
Table 1
Test results: what’s normal, what suggests liver damage
| Parameter | Description | Normal range | Range indicating liver damage |
|---|---|---|---|
| Alanine aminotransferase (ALT) | Enzyme highly concentrated in the liver | 3 to 30 U/L | >3 times upper limit of normal |
| Alkaline phosphatase (ALP) | Enzyme highly concentrated in the liver, bile ducts, placenta, and bone | 35 to 150 U/L | >2 times upper limit of normal |
| Aspartate aminotransferase (AST) | Enzyme highly concentrated in heart muscle, liver cells, skeletal muscle cells, and (to a lesser degree) other tissues | 11 to 32 U/L | Used to evaluate elevations in other serum enzyme level |
| Gamma-glutamyl transpeptidase (GGT) | Enzyme highly concentrated in the liver, bile ducts, and kidneys | 5 to 40 U/L | Used to evaluate elevations in other serum enzyme levels |
| Total bilirubin (TBIL) | Yellow bile pigment produced when liver processes waste products | 0.3 to 1.1 mg/dL | >2 times upper limit of normal if associated with elevation in ALT or ALP |
| Sources: References 1,2 | |||
CASE CONTINUED: Spotting a pattern of injury
Mrs. W’s elevated ALT and AST levels are of unknown duration. Her AST:ALT ratio is approximately 2:1, suggesting hepatocellular injury.
Interpreting abnormal LFT results
To properly interpret LFTs, consider the patient’s symptoms, physical exam findings, medical history, medical illnesses, potential substance use, risk factors for HIV and viral hepatitis, and medication list. Collaborate with the patient’s primary care provider or facilitate primary care (Figure 1).
ALT and AST are highly concentrated in the liver, but ALT is a more specific indicator of liver injury. For both, levels may vary according to age, sex, and ethnicity but in general, levels <30 U/L are considered normal.1,2
ALP originates predominately from the liver and from bone. Persistently elevated ALP levels in the liver may indicate chronic cholestasis or infiltrative liver disease.
GGT is best used to evaluate the meaning of elevations in other serum enzymes.3 Elevated GGT can help confirm hepatic origin of elevated ALP or support a suspicion of alcohol use in patients with an AST: ALT ratio >2:1.
If an asymptomatic patient has elevated LFT results, first repeat the test. If repeat results are normal, perform the test again in 3-6 months. Keep in mind, however, that normal LFT results do not always indicate the absence of disease. For example, up to 16% of patients with hepatitis C and 13% of patients with nonalcoholic steatohepatitis (NASH) have normal LFT results despite histologic abnormalities.4
If repeat results are abnormal, obtain the patient’s consent to inform the primary care provider. Then take a thorough history and perform a focused physical exam. In the history, focus on use of prescription and nonprescription medications, including over-the-counter and herbal therapies, alcohol, and drugs of abuse, such as MDMA (“ecstasy”), phencyclidine (“angel dust”), and glues or solvents. Also assess for risk factors for infectious hepatitis, such as IV drug use, work-related blood exposure, and tattoos. Ask about a family history of liver disease. Focus your physical exam on visible stigmata of chronic liver disease, such as jaundice, temporal wasting, ascites, and palmar erythema.
Next, analyze the severity and pattern of the LFT abnormality. Liver injury is defined as:
- ALT >3 times the upper limit of normal
- ALP >2 times the upper limit of normal
- or total bilirubin >2 times the upper limit of normal if associated with any elevation of ALT or ALP.5
If ALT elevations predominate, consider hepatocellular injury. If ALP elevations predominate, suspect cholestatic injury. Elevations of both ALT and ALP suggest a mixed pattern of hepatocellular and cholestatic injury.
Figure 1 Interpreting liver function test results
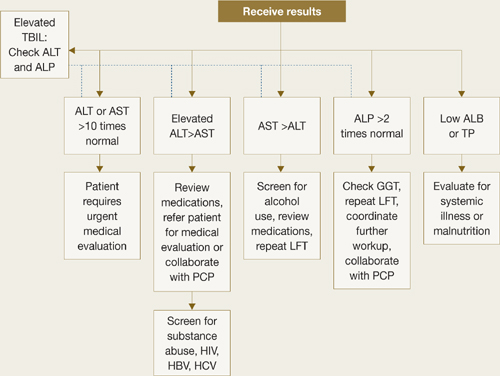
ALB: albumin; ALP: alkaline phosphatase; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyl transpeptidase; HBV: hepatitis B virus; HCV: hepatitis C virus; HIV: human immunodeficiency virus; LFT: liver function test; PCP: primary care provider; TBIL: total bilirubin; TP: total protein
CASE CONTINUED: Pinpointing a diagnosis
Mrs. W undergoes repeat LFTs with GGT testing, screening tests for hepatitis B and C, and a comprehensive physical exam. The psychiatrist screens for alcohol use, asks the patient about her use of herbal therapies and substance abuse relapse, and evaluates cognitive mental status for symptoms of encephalopathy. Results reveal that Mrs. W’s ALT and AST are elevated because of chronic active hepatitis C.
Causes of hepatocellular injury
Further evaluation of your patient’s test results can help narrow down potential causes of liver damage. If your patient’s ALT is disproportionately elevated, estimate the:
- severity of aminotransferase elevation
- ratio of AST:ALT
- rate of change over multiple LFTs.
If AST or ALT is >10 times normal, consider toxin-induced or ischemic injury.6 An AST:ALT ratio of 2:1 or 3:1, especially when associated with elevated GGT, strongly suggests alcohol-induced injury. With acute mild transaminase elevations—ALT>AST, 2 to 3 times normal—suspect medication-related injury.
A variety of factors and conditions can result in hepatocellular damage:
Common causes
Medications. Many drugs, including common psychotropics, can cause elevated liver enzymes (Table 2).5 As little as 4 grams per day of acetaminophen can cause mild transaminitis.4 Antidepressants, second-generation antipsychotics (SGAs), and anticonvulsants can cause increases in AST and ALT.7 If liver enzymes rise after a patient starts a new medication, drug-related liver toxicity is likely. Remember to consider a patient’s use of drugs of abuse and herbal therapies.
Discontinuing the suspect agent usually produces steady (although sometimes slow) improvement in LFTs. Use serial LFT testing and focused history and physical examinations to confirm improvement.
Alcohol. Screen for alcohol abuse using the CAGE questionnaire, the Alcohol Use Disorders Identification Test, or a similar tool. More than 90% of patients with an AST:ALT ratio of 2:1 have alcoholic liver disease; this percentage increases to >96% when the ratio is 3:1.1 A 2-fold increase in GGT in a patient with an AST:ALT ratio >2:1 further supports the diagnosis. In patients with alcohol abuse, AST rarely exceeds 10 times normal.5
Hepatitis C. The prevalence of hepatitis C is increasing among patients with severe mental illness, especially a dual diagnosis.8 Hepatitis C rarely causes acute symptoms.
Offer a hepatitis C antibody screening to test patients with even a remote history of IV drug use or comorbid substance abuse. Patients with a positive hepatitis C antibody test or a negative hepatitis C antibody test but a high risk for the disease should receive further testing.9
Hepatitis B. Risk factors include exposure to blood, sexual transmission, and emigration from endemic areas in Southeast Asia and sub-Saharan Africa. Initial screening panels include tests for hepatitis B surface antigen, hepatitis B surface antibody, and hepatitis B core antibody. Positive B surface antigen and core antibody tests indicate infection.
NASH. Nonalcoholic steatohepatitis (NASH) is the most common cause of mild transaminitis in the Western world (Box).4,10,11
Nonalcoholic steatohepatitis (NASH) is inflammatory liver disease of uncertain pathogenesis that commonly occurs with metabolic syndrome. It affects up to 5% of Americans, most often those who are middle-aged and overweight or obese, hyperlipidemic, or diabetic. NASH resembles alcoholic liver disease but occurs in people who drink little or no alcohol. In addition to inflammation, it is characterized by accumulation of fat and fibrous tissue in the liver. Typically patients are asymptomatic, but NASH can lead to cirrhosis.
NASH is a common cause of mild transaminitis. Aminotransferase levels are usually <4 times the normal value.10 Thirteen percent of patients with NASH have normal LFT results despite histologic abnormalities.4 NASH is a diagnosis of exclusion that is confirmed by liver biopsy.
NASH has no specific therapies or cure. Treatment focuses on controlling associated conditions such as diabetes, obesity, and hyperlipidemia. In obese patients, weight loss is the cornerstone of treatment. If you prescribe a second-generation antipsychotic (SGA) for a patient who has NASH, be aware that SGAs increase the risk of hyperglycemia and dyslipidemia, which can exacerbate NASH.11
Table 2
Medications that affect liver function test (LFT) results
| Medication class | Hepatocellular injury (↑ALT) | Cholestatic injury (↑ALP and ↑ALT) | Mixed injury (↑ALP and ↑TBIL) |
|---|---|---|---|
| Psychotropic | Bupropion, fluoxetine, paroxetine, risperidone, sertraline, trazodone, valproic acid | Chlorpromazine, mirtazapine, tricyclic antidepressants | Amitriptyline, Amitriptyline, phenobarbital, phenytoin, trazodone |
| Cardiovascular | Amiodarone, lisinopril, losartan, statins | Clopidogrel, irbesartan | Captopril, enalapril, verapamil |
| Endocrine | Acarbose, allopurinol | – | – |
| Gastrointestinal | Omeprazole | – | – |
| Herbal remedies | Germander, kava | – | – |
| Anti-infectives | HAART drugs, isoniazid, ketoconazole, pyrazinamide, rifampin, tetracycline, trovafloxacin | Amoxicillin/clavulanic acid, erythromycins, terbinafine | Clindamycin, nitrofurantoin, trimethoprim-sulfamethoxazole |
| Rheumatologic | Acetaminophen, baclofen, methotrexate, NSAIDs | Anabolic steroids | Azathioprine, sulfonamides |
| Others | – | Oral contraceptives, estrogens, phenothiazines | Cyproheptadine, flutamide |
| ALP: alkaline phosphatase; ALT: alanine aminotransferase; HAART: highly active antiretroviral therapy; NSAID: nonsteroidal anti-inflammatory drug; TBIL: total bilirubin | |||
| Source: Reference 5 | |||
Less common causes
Hemochromatosis is an autosomal recessive disease that causes pathologic deposition of iron in the liver, pancreas, and heart and leads to cirrhosis, diabetes, and heart disease. Suspect it in patients with a clinical syndrome and transferrin saturation index >45%.12 A hemochromatosis gene mutation analysis confirms the diagnosis.
Autoimmune hepatitis occurs primarily in women ages 20 to 50 years.13 Because >80% of patients with autoimmune hepatitis have hypergammaglobulinemia, serum protein electrophores is a useful screening test.5
Wilson’s disease is a genetic disorder of biliary copper excretion classically diagnosed in young people with concomitant neurologic or psychiatric conditions. Those affected have low serum ceruloplasmin. Neuropsychiatric symptoms include parkinsonian-like tremor, rigidity, clumsiness of gait, slurred speech, drooling, and inappropriate and uncontrollable grinning (risus sardonicus).8 Psychosis and suicidality also are common in patients with Wilson’s disease.
Alpha-1 antitrypsin deficiency. Alpha-1 antitrypsin is a protein produced primarily in the liver that protects the lungs from neutrophil elastase. Suspect alpha-1 antitrypsin deficiency in patients with abnormal LFTs and emphysema. Low serum alpha-1 antitrypsin confirms the diagnosis.
Celiac disease. Consider celiac disease in patients with chronic diarrhea or abdominal distension and abnormal LFTs. Small bowel biopsy and elevated tissue transglutaminase antibodies and anti-endomysial antibodies confirm the diagnosis.
Causes of cholestatic injury
If your patient has a disproportionate ALP elevation, identify the source of the ALP by testing GGT. GGT levels are elevated in liver disease but not in bone disease. Partial bile duct obstruction is a common cause of ALP elevation. For initial testing, include ultrasonography of the right upper quadrant.
Medications. Many medications can cause biliary stasis and cholestatic LFTs, including mirtazapine, tricyclic antidepressants, anabolic steroids, phenytoin, and estrogens.
Primary sclerosing cholangitis is inflammatory disease of the bile ducts that can lead to cholestasis (blockage of bile transport blockage). Consider it in patients with inflammatory bowel disease. Endoscopic retrograde cholangiopancreatography and magnetic resonance cholangiopancreatography aid diagnosis.
Primary biliary cirrhosis generally presents in middle-aged women with other autoimmune processes, cholestasis, and pruritus. Consider testing serum antimitochondrial antibodies.
Infiltrative liver diseases such as sarcoidosis, metastatic disease, or lymphoma can also present with cholestasis. Liver imaging is required for these diagnoses.
Causes of mixed injury
If LFT results suggest a mixed injury pattern, focus on the predominant pattern and evaluate the causes listed above. Certain medications typically result in a mixed injury pattern.
Related resources
- American Gastroenterological Association medical position statement: evaluation of liver chemistry tests. www.guideline.gov/summary/summary.aspx?ss=15&doc_id=3492&nbr=002718.
- Johnston DE. Special considerations in interpreting liver function tests. Am Fam Physician 1999;59(8):2223-30.
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Carbatrol, Equetro, Tegretol
- Chlorpromazine • Thorazine
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel
- Valproic acid • Depakene
- Warfarin • Coumadin
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137(1):1-10.
2. Gopal DV, Rosen HR. Abnormal findings on liver function tests. Interpreting results to narrow the diagnosis and establish a prognosis. Postgrad Med 2000;107(2):100-14.
3. Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med 2000;342(17):1266-71.
4. Ioannou GN, Boyko EJ, Lee SP. The prevalence and predictors of elevated serum aminotransferase activity in the United States in 1999-2002. Am J Gastroenterol 2006;101(1):76-82.
5. Navarro VJ, Senior JR. Drug-related hepatotoxicity. N Engl J Med 2006;354(7):731-9.
6. Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. CMAJ 2005;172(3):367-79.
7. Bezchilibny-Butler KZ, Jeffries JJ, eds. Clinical handbook of psychotropic drugs, 15th ed. Cambridge Hogrefe & Huber; 2005.
8. Crone CC, Gabriel GM, Dimartini A. An overview of psychiatric issues in liver disease for the consultation-liaison psychiatrist. Psychosomatics 2006;47(3):188-205.
9. Kaplan MA. Approach to the patient with abnormal liver function tests. Available at: http://www.uptodate.com. Accessed December 12, 2006.
10. Bacon BR, Farahvash MJ, Janney CG, Neuschwander-Tetri BA. Nonalcoholic steatohepatitis: an expanded clinical entity. Gastroenterology 1994;107(4):1103-9.
11. Lieberman JA, Stroup SS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353(12):1209-23.
12. Yen AW, Fancher TL, Bowlus CL. Revisiting hereditary hemochromatosis: current concepts and progress. Am J Med 2006;119(5):391-9.
13. Krawitt EL. Autoimmune hepatitis. N Engl J Med 1996;334(14):897-903.
Mrs. W, age 53, is referred by her primary provider for consultation on depressive symptoms, including worsening depressed mood, anhedonia, anxiety, and suicidal thoughts for 2 months. She reports at least 2 similar episodes in the past 15 years. Mrs. W has a remote history of IV drug use and history of alcohol abuse, but she attends Alcoholics Anonymous and has 10 years of sobriety. She has no history of hospitalizations for medical illness and denies any medical problems.
Mrs. W is taking amitriptyline, 50 mg, for insomnia. She has no history of manic or psychotic symptoms, and the mental status examination is consistent with major depression. Her past depressive episodes were treated successfully with a medication that she does not recall.
The psychiatrist diagnoses recurrent and severe major depression and prescribes cognitive-behavioral therapy and sertraline, 25 mg/d, titrated to 50 mg/d over the next 2 weeks. Amitriptyline is discontinued.
When the psychiatrist receives Mrs. W’s medical records, electrolytes, complete blood count, thyroid stimulating hormone level, and fasting glucose are within normal limits, but alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are greatly elevated at 250 U/L and 150 U/L, respectively. Progress notes contain no references to liver disease.
Interpreting psychiatric patients’ liver function tests (LFTs) can be challenging, especially in those with polypharmacy, co-occurring substance abuse, or risk factors for viral hepatitis. You can improve collaboration with primary care providers by understanding:
- what an LFT measures
- how to interpret abnormal results
- which conditions to suspect, based on the results.
A standard LFT usually measures several enzymes and proteins, typically ALT, AST, alkaline phosphatase (ALP), total bilirubin (TBIL), albumin (ALB), and total protein (TP). Measures of gamma-glutamyl transpeptidase (GGT) and prothrombin time (PT) are often requested with an LFT. Table 1 provides normal ranges and ranges that indicate liver damage for several of these parameters.1,2
“Liver function test” is a misnomer because LFTs do not directly measure liver function. Rather, they reflect hepatocyte injury or cholestasis (blockage or damage in the biliary system). ALB and PT measure liver synthetic function, but are nonspecific. ALB levels can be altered by nutritional status, protein-losing enteropathies, or nephropathies, whereas PT may be modified by warfarin, vitamin K deficiency, or consumptive coagulopathy.
Table 1
Test results: what’s normal, what suggests liver damage
| Parameter | Description | Normal range | Range indicating liver damage |
|---|---|---|---|
| Alanine aminotransferase (ALT) | Enzyme highly concentrated in the liver | 3 to 30 U/L | >3 times upper limit of normal |
| Alkaline phosphatase (ALP) | Enzyme highly concentrated in the liver, bile ducts, placenta, and bone | 35 to 150 U/L | >2 times upper limit of normal |
| Aspartate aminotransferase (AST) | Enzyme highly concentrated in heart muscle, liver cells, skeletal muscle cells, and (to a lesser degree) other tissues | 11 to 32 U/L | Used to evaluate elevations in other serum enzyme level |
| Gamma-glutamyl transpeptidase (GGT) | Enzyme highly concentrated in the liver, bile ducts, and kidneys | 5 to 40 U/L | Used to evaluate elevations in other serum enzyme levels |
| Total bilirubin (TBIL) | Yellow bile pigment produced when liver processes waste products | 0.3 to 1.1 mg/dL | >2 times upper limit of normal if associated with elevation in ALT or ALP |
| Sources: References 1,2 | |||
CASE CONTINUED: Spotting a pattern of injury
Mrs. W’s elevated ALT and AST levels are of unknown duration. Her AST:ALT ratio is approximately 2:1, suggesting hepatocellular injury.
Interpreting abnormal LFT results
To properly interpret LFTs, consider the patient’s symptoms, physical exam findings, medical history, medical illnesses, potential substance use, risk factors for HIV and viral hepatitis, and medication list. Collaborate with the patient’s primary care provider or facilitate primary care (Figure 1).
ALT and AST are highly concentrated in the liver, but ALT is a more specific indicator of liver injury. For both, levels may vary according to age, sex, and ethnicity but in general, levels <30 U/L are considered normal.1,2
ALP originates predominately from the liver and from bone. Persistently elevated ALP levels in the liver may indicate chronic cholestasis or infiltrative liver disease.
GGT is best used to evaluate the meaning of elevations in other serum enzymes.3 Elevated GGT can help confirm hepatic origin of elevated ALP or support a suspicion of alcohol use in patients with an AST: ALT ratio >2:1.
If an asymptomatic patient has elevated LFT results, first repeat the test. If repeat results are normal, perform the test again in 3-6 months. Keep in mind, however, that normal LFT results do not always indicate the absence of disease. For example, up to 16% of patients with hepatitis C and 13% of patients with nonalcoholic steatohepatitis (NASH) have normal LFT results despite histologic abnormalities.4
If repeat results are abnormal, obtain the patient’s consent to inform the primary care provider. Then take a thorough history and perform a focused physical exam. In the history, focus on use of prescription and nonprescription medications, including over-the-counter and herbal therapies, alcohol, and drugs of abuse, such as MDMA (“ecstasy”), phencyclidine (“angel dust”), and glues or solvents. Also assess for risk factors for infectious hepatitis, such as IV drug use, work-related blood exposure, and tattoos. Ask about a family history of liver disease. Focus your physical exam on visible stigmata of chronic liver disease, such as jaundice, temporal wasting, ascites, and palmar erythema.
Next, analyze the severity and pattern of the LFT abnormality. Liver injury is defined as:
- ALT >3 times the upper limit of normal
- ALP >2 times the upper limit of normal
- or total bilirubin >2 times the upper limit of normal if associated with any elevation of ALT or ALP.5
If ALT elevations predominate, consider hepatocellular injury. If ALP elevations predominate, suspect cholestatic injury. Elevations of both ALT and ALP suggest a mixed pattern of hepatocellular and cholestatic injury.
Figure 1 Interpreting liver function test results
ALB: albumin; ALP: alkaline phosphatase; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyl transpeptidase; HBV: hepatitis B virus; HCV: hepatitis C virus; HIV: human immunodeficiency virus; LFT: liver function test; PCP: primary care provider; TBIL: total bilirubin; TP: total protein
CASE CONTINUED: Pinpointing a diagnosis
Mrs. W undergoes repeat LFTs with GGT testing, screening tests for hepatitis B and C, and a comprehensive physical exam. The psychiatrist screens for alcohol use, asks the patient about her use of herbal therapies and substance abuse relapse, and evaluates cognitive mental status for symptoms of encephalopathy. Results reveal that Mrs. W’s ALT and AST are elevated because of chronic active hepatitis C.
Causes of hepatocellular injury
Further evaluation of your patient’s test results can help narrow down potential causes of liver damage. If your patient’s ALT is disproportionately elevated, estimate the:
- severity of aminotransferase elevation
- ratio of AST:ALT
- rate of change over multiple LFTs.
If AST or ALT is >10 times normal, consider toxin-induced or ischemic injury.6 An AST:ALT ratio of 2:1 or 3:1, especially when associated with elevated GGT, strongly suggests alcohol-induced injury. With acute mild transaminase elevations—ALT>AST, 2 to 3 times normal—suspect medication-related injury.
A variety of factors and conditions can result in hepatocellular damage:
Common causes
Medications. Many drugs, including common psychotropics, can cause elevated liver enzymes (Table 2).5 As little as 4 grams per day of acetaminophen can cause mild transaminitis.4 Antidepressants, second-generation antipsychotics (SGAs), and anticonvulsants can cause increases in AST and ALT.7 If liver enzymes rise after a patient starts a new medication, drug-related liver toxicity is likely. Remember to consider a patient’s use of drugs of abuse and herbal therapies.
Discontinuing the suspect agent usually produces steady (although sometimes slow) improvement in LFTs. Use serial LFT testing and focused history and physical examinations to confirm improvement.
Alcohol. Screen for alcohol abuse using the CAGE questionnaire, the Alcohol Use Disorders Identification Test, or a similar tool. More than 90% of patients with an AST:ALT ratio of 2:1 have alcoholic liver disease; this percentage increases to >96% when the ratio is 3:1.1 A 2-fold increase in GGT in a patient with an AST:ALT ratio >2:1 further supports the diagnosis. In patients with alcohol abuse, AST rarely exceeds 10 times normal.5
Hepatitis C. The prevalence of hepatitis C is increasing among patients with severe mental illness, especially a dual diagnosis.8 Hepatitis C rarely causes acute symptoms.
Offer a hepatitis C antibody screening to test patients with even a remote history of IV drug use or comorbid substance abuse. Patients with a positive hepatitis C antibody test or a negative hepatitis C antibody test but a high risk for the disease should receive further testing.9
Hepatitis B. Risk factors include exposure to blood, sexual transmission, and emigration from endemic areas in Southeast Asia and sub-Saharan Africa. Initial screening panels include tests for hepatitis B surface antigen, hepatitis B surface antibody, and hepatitis B core antibody. Positive B surface antigen and core antibody tests indicate infection.
NASH. Nonalcoholic steatohepatitis (NASH) is the most common cause of mild transaminitis in the Western world (Box).4,10,11
Nonalcoholic steatohepatitis (NASH) is inflammatory liver disease of uncertain pathogenesis that commonly occurs with metabolic syndrome. It affects up to 5% of Americans, most often those who are middle-aged and overweight or obese, hyperlipidemic, or diabetic. NASH resembles alcoholic liver disease but occurs in people who drink little or no alcohol. In addition to inflammation, it is characterized by accumulation of fat and fibrous tissue in the liver. Typically patients are asymptomatic, but NASH can lead to cirrhosis.
NASH is a common cause of mild transaminitis. Aminotransferase levels are usually <4 times the normal value.10 Thirteen percent of patients with NASH have normal LFT results despite histologic abnormalities.4 NASH is a diagnosis of exclusion that is confirmed by liver biopsy.
NASH has no specific therapies or cure. Treatment focuses on controlling associated conditions such as diabetes, obesity, and hyperlipidemia. In obese patients, weight loss is the cornerstone of treatment. If you prescribe a second-generation antipsychotic (SGA) for a patient who has NASH, be aware that SGAs increase the risk of hyperglycemia and dyslipidemia, which can exacerbate NASH.11
Table 2
Medications that affect liver function test (LFT) results
| Medication class | Hepatocellular injury (↑ALT) | Cholestatic injury (↑ALP and ↑ALT) | Mixed injury (↑ALP and ↑TBIL) |
|---|---|---|---|
| Psychotropic | Bupropion, fluoxetine, paroxetine, risperidone, sertraline, trazodone, valproic acid | Chlorpromazine, mirtazapine, tricyclic antidepressants | Amitriptyline, Amitriptyline, phenobarbital, phenytoin, trazodone |
| Cardiovascular | Amiodarone, lisinopril, losartan, statins | Clopidogrel, irbesartan | Captopril, enalapril, verapamil |
| Endocrine | Acarbose, allopurinol | – | – |
| Gastrointestinal | Omeprazole | – | – |
| Herbal remedies | Germander, kava | – | – |
| Anti-infectives | HAART drugs, isoniazid, ketoconazole, pyrazinamide, rifampin, tetracycline, trovafloxacin | Amoxicillin/clavulanic acid, erythromycins, terbinafine | Clindamycin, nitrofurantoin, trimethoprim-sulfamethoxazole |
| Rheumatologic | Acetaminophen, baclofen, methotrexate, NSAIDs | Anabolic steroids | Azathioprine, sulfonamides |
| Others | – | Oral contraceptives, estrogens, phenothiazines | Cyproheptadine, flutamide |
| ALP: alkaline phosphatase; ALT: alanine aminotransferase; HAART: highly active antiretroviral therapy; NSAID: nonsteroidal anti-inflammatory drug; TBIL: total bilirubin | |||
| Source: Reference 5 | |||
Less common causes
Hemochromatosis is an autosomal recessive disease that causes pathologic deposition of iron in the liver, pancreas, and heart and leads to cirrhosis, diabetes, and heart disease. Suspect it in patients with a clinical syndrome and transferrin saturation index >45%.12 A hemochromatosis gene mutation analysis confirms the diagnosis.
Autoimmune hepatitis occurs primarily in women ages 20 to 50 years.13 Because >80% of patients with autoimmune hepatitis have hypergammaglobulinemia, serum protein electrophores is a useful screening test.5
Wilson’s disease is a genetic disorder of biliary copper excretion classically diagnosed in young people with concomitant neurologic or psychiatric conditions. Those affected have low serum ceruloplasmin. Neuropsychiatric symptoms include parkinsonian-like tremor, rigidity, clumsiness of gait, slurred speech, drooling, and inappropriate and uncontrollable grinning (risus sardonicus).8 Psychosis and suicidality also are common in patients with Wilson’s disease.
Alpha-1 antitrypsin deficiency. Alpha-1 antitrypsin is a protein produced primarily in the liver that protects the lungs from neutrophil elastase. Suspect alpha-1 antitrypsin deficiency in patients with abnormal LFTs and emphysema. Low serum alpha-1 antitrypsin confirms the diagnosis.
Celiac disease. Consider celiac disease in patients with chronic diarrhea or abdominal distension and abnormal LFTs. Small bowel biopsy and elevated tissue transglutaminase antibodies and anti-endomysial antibodies confirm the diagnosis.
Causes of cholestatic injury
If your patient has a disproportionate ALP elevation, identify the source of the ALP by testing GGT. GGT levels are elevated in liver disease but not in bone disease. Partial bile duct obstruction is a common cause of ALP elevation. For initial testing, include ultrasonography of the right upper quadrant.
Medications. Many medications can cause biliary stasis and cholestatic LFTs, including mirtazapine, tricyclic antidepressants, anabolic steroids, phenytoin, and estrogens.
Primary sclerosing cholangitis is inflammatory disease of the bile ducts that can lead to cholestasis (blockage of bile transport blockage). Consider it in patients with inflammatory bowel disease. Endoscopic retrograde cholangiopancreatography and magnetic resonance cholangiopancreatography aid diagnosis.
Primary biliary cirrhosis generally presents in middle-aged women with other autoimmune processes, cholestasis, and pruritus. Consider testing serum antimitochondrial antibodies.
Infiltrative liver diseases such as sarcoidosis, metastatic disease, or lymphoma can also present with cholestasis. Liver imaging is required for these diagnoses.
Causes of mixed injury
If LFT results suggest a mixed injury pattern, focus on the predominant pattern and evaluate the causes listed above. Certain medications typically result in a mixed injury pattern.
Related resources
- American Gastroenterological Association medical position statement: evaluation of liver chemistry tests. www.guideline.gov/summary/summary.aspx?ss=15&doc_id=3492&nbr=002718.
- Johnston DE. Special considerations in interpreting liver function tests. Am Fam Physician 1999;59(8):2223-30.
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Carbatrol, Equetro, Tegretol
- Chlorpromazine • Thorazine
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel
- Valproic acid • Depakene
- Warfarin • Coumadin
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
Mrs. W, age 53, is referred by her primary provider for consultation on depressive symptoms, including worsening depressed mood, anhedonia, anxiety, and suicidal thoughts for 2 months. She reports at least 2 similar episodes in the past 15 years. Mrs. W has a remote history of IV drug use and history of alcohol abuse, but she attends Alcoholics Anonymous and has 10 years of sobriety. She has no history of hospitalizations for medical illness and denies any medical problems.
Mrs. W is taking amitriptyline, 50 mg, for insomnia. She has no history of manic or psychotic symptoms, and the mental status examination is consistent with major depression. Her past depressive episodes were treated successfully with a medication that she does not recall.
The psychiatrist diagnoses recurrent and severe major depression and prescribes cognitive-behavioral therapy and sertraline, 25 mg/d, titrated to 50 mg/d over the next 2 weeks. Amitriptyline is discontinued.
When the psychiatrist receives Mrs. W’s medical records, electrolytes, complete blood count, thyroid stimulating hormone level, and fasting glucose are within normal limits, but alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are greatly elevated at 250 U/L and 150 U/L, respectively. Progress notes contain no references to liver disease.
Interpreting psychiatric patients’ liver function tests (LFTs) can be challenging, especially in those with polypharmacy, co-occurring substance abuse, or risk factors for viral hepatitis. You can improve collaboration with primary care providers by understanding:
- what an LFT measures
- how to interpret abnormal results
- which conditions to suspect, based on the results.
A standard LFT usually measures several enzymes and proteins, typically ALT, AST, alkaline phosphatase (ALP), total bilirubin (TBIL), albumin (ALB), and total protein (TP). Measures of gamma-glutamyl transpeptidase (GGT) and prothrombin time (PT) are often requested with an LFT. Table 1 provides normal ranges and ranges that indicate liver damage for several of these parameters.1,2
“Liver function test” is a misnomer because LFTs do not directly measure liver function. Rather, they reflect hepatocyte injury or cholestasis (blockage or damage in the biliary system). ALB and PT measure liver synthetic function, but are nonspecific. ALB levels can be altered by nutritional status, protein-losing enteropathies, or nephropathies, whereas PT may be modified by warfarin, vitamin K deficiency, or consumptive coagulopathy.
Table 1
Test results: what’s normal, what suggests liver damage
| Parameter | Description | Normal range | Range indicating liver damage |
|---|---|---|---|
| Alanine aminotransferase (ALT) | Enzyme highly concentrated in the liver | 3 to 30 U/L | >3 times upper limit of normal |
| Alkaline phosphatase (ALP) | Enzyme highly concentrated in the liver, bile ducts, placenta, and bone | 35 to 150 U/L | >2 times upper limit of normal |
| Aspartate aminotransferase (AST) | Enzyme highly concentrated in heart muscle, liver cells, skeletal muscle cells, and (to a lesser degree) other tissues | 11 to 32 U/L | Used to evaluate elevations in other serum enzyme level |
| Gamma-glutamyl transpeptidase (GGT) | Enzyme highly concentrated in the liver, bile ducts, and kidneys | 5 to 40 U/L | Used to evaluate elevations in other serum enzyme levels |
| Total bilirubin (TBIL) | Yellow bile pigment produced when liver processes waste products | 0.3 to 1.1 mg/dL | >2 times upper limit of normal if associated with elevation in ALT or ALP |
| Sources: References 1,2 | |||
CASE CONTINUED: Spotting a pattern of injury
Mrs. W’s elevated ALT and AST levels are of unknown duration. Her AST:ALT ratio is approximately 2:1, suggesting hepatocellular injury.
Interpreting abnormal LFT results
To properly interpret LFTs, consider the patient’s symptoms, physical exam findings, medical history, medical illnesses, potential substance use, risk factors for HIV and viral hepatitis, and medication list. Collaborate with the patient’s primary care provider or facilitate primary care (Figure 1).
ALT and AST are highly concentrated in the liver, but ALT is a more specific indicator of liver injury. For both, levels may vary according to age, sex, and ethnicity but in general, levels <30 U/L are considered normal.1,2
ALP originates predominately from the liver and from bone. Persistently elevated ALP levels in the liver may indicate chronic cholestasis or infiltrative liver disease.
GGT is best used to evaluate the meaning of elevations in other serum enzymes.3 Elevated GGT can help confirm hepatic origin of elevated ALP or support a suspicion of alcohol use in patients with an AST: ALT ratio >2:1.
If an asymptomatic patient has elevated LFT results, first repeat the test. If repeat results are normal, perform the test again in 3-6 months. Keep in mind, however, that normal LFT results do not always indicate the absence of disease. For example, up to 16% of patients with hepatitis C and 13% of patients with nonalcoholic steatohepatitis (NASH) have normal LFT results despite histologic abnormalities.4
If repeat results are abnormal, obtain the patient’s consent to inform the primary care provider. Then take a thorough history and perform a focused physical exam. In the history, focus on use of prescription and nonprescription medications, including over-the-counter and herbal therapies, alcohol, and drugs of abuse, such as MDMA (“ecstasy”), phencyclidine (“angel dust”), and glues or solvents. Also assess for risk factors for infectious hepatitis, such as IV drug use, work-related blood exposure, and tattoos. Ask about a family history of liver disease. Focus your physical exam on visible stigmata of chronic liver disease, such as jaundice, temporal wasting, ascites, and palmar erythema.
Next, analyze the severity and pattern of the LFT abnormality. Liver injury is defined as:
- ALT >3 times the upper limit of normal
- ALP >2 times the upper limit of normal
- or total bilirubin >2 times the upper limit of normal if associated with any elevation of ALT or ALP.5
If ALT elevations predominate, consider hepatocellular injury. If ALP elevations predominate, suspect cholestatic injury. Elevations of both ALT and ALP suggest a mixed pattern of hepatocellular and cholestatic injury.
Figure 1 Interpreting liver function test results
ALB: albumin; ALP: alkaline phosphatase; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyl transpeptidase; HBV: hepatitis B virus; HCV: hepatitis C virus; HIV: human immunodeficiency virus; LFT: liver function test; PCP: primary care provider; TBIL: total bilirubin; TP: total protein
CASE CONTINUED: Pinpointing a diagnosis
Mrs. W undergoes repeat LFTs with GGT testing, screening tests for hepatitis B and C, and a comprehensive physical exam. The psychiatrist screens for alcohol use, asks the patient about her use of herbal therapies and substance abuse relapse, and evaluates cognitive mental status for symptoms of encephalopathy. Results reveal that Mrs. W’s ALT and AST are elevated because of chronic active hepatitis C.
Causes of hepatocellular injury
Further evaluation of your patient’s test results can help narrow down potential causes of liver damage. If your patient’s ALT is disproportionately elevated, estimate the:
- severity of aminotransferase elevation
- ratio of AST:ALT
- rate of change over multiple LFTs.
If AST or ALT is >10 times normal, consider toxin-induced or ischemic injury.6 An AST:ALT ratio of 2:1 or 3:1, especially when associated with elevated GGT, strongly suggests alcohol-induced injury. With acute mild transaminase elevations—ALT>AST, 2 to 3 times normal—suspect medication-related injury.
A variety of factors and conditions can result in hepatocellular damage:
Common causes
Medications. Many drugs, including common psychotropics, can cause elevated liver enzymes (Table 2).5 As little as 4 grams per day of acetaminophen can cause mild transaminitis.4 Antidepressants, second-generation antipsychotics (SGAs), and anticonvulsants can cause increases in AST and ALT.7 If liver enzymes rise after a patient starts a new medication, drug-related liver toxicity is likely. Remember to consider a patient’s use of drugs of abuse and herbal therapies.
Discontinuing the suspect agent usually produces steady (although sometimes slow) improvement in LFTs. Use serial LFT testing and focused history and physical examinations to confirm improvement.
Alcohol. Screen for alcohol abuse using the CAGE questionnaire, the Alcohol Use Disorders Identification Test, or a similar tool. More than 90% of patients with an AST:ALT ratio of 2:1 have alcoholic liver disease; this percentage increases to >96% when the ratio is 3:1.1 A 2-fold increase in GGT in a patient with an AST:ALT ratio >2:1 further supports the diagnosis. In patients with alcohol abuse, AST rarely exceeds 10 times normal.5
Hepatitis C. The prevalence of hepatitis C is increasing among patients with severe mental illness, especially a dual diagnosis.8 Hepatitis C rarely causes acute symptoms.
Offer a hepatitis C antibody screening to test patients with even a remote history of IV drug use or comorbid substance abuse. Patients with a positive hepatitis C antibody test or a negative hepatitis C antibody test but a high risk for the disease should receive further testing.9
Hepatitis B. Risk factors include exposure to blood, sexual transmission, and emigration from endemic areas in Southeast Asia and sub-Saharan Africa. Initial screening panels include tests for hepatitis B surface antigen, hepatitis B surface antibody, and hepatitis B core antibody. Positive B surface antigen and core antibody tests indicate infection.
NASH. Nonalcoholic steatohepatitis (NASH) is the most common cause of mild transaminitis in the Western world (Box).4,10,11
Nonalcoholic steatohepatitis (NASH) is inflammatory liver disease of uncertain pathogenesis that commonly occurs with metabolic syndrome. It affects up to 5% of Americans, most often those who are middle-aged and overweight or obese, hyperlipidemic, or diabetic. NASH resembles alcoholic liver disease but occurs in people who drink little or no alcohol. In addition to inflammation, it is characterized by accumulation of fat and fibrous tissue in the liver. Typically patients are asymptomatic, but NASH can lead to cirrhosis.
NASH is a common cause of mild transaminitis. Aminotransferase levels are usually <4 times the normal value.10 Thirteen percent of patients with NASH have normal LFT results despite histologic abnormalities.4 NASH is a diagnosis of exclusion that is confirmed by liver biopsy.
NASH has no specific therapies or cure. Treatment focuses on controlling associated conditions such as diabetes, obesity, and hyperlipidemia. In obese patients, weight loss is the cornerstone of treatment. If you prescribe a second-generation antipsychotic (SGA) for a patient who has NASH, be aware that SGAs increase the risk of hyperglycemia and dyslipidemia, which can exacerbate NASH.11
Table 2
Medications that affect liver function test (LFT) results
| Medication class | Hepatocellular injury (↑ALT) | Cholestatic injury (↑ALP and ↑ALT) | Mixed injury (↑ALP and ↑TBIL) |
|---|---|---|---|
| Psychotropic | Bupropion, fluoxetine, paroxetine, risperidone, sertraline, trazodone, valproic acid | Chlorpromazine, mirtazapine, tricyclic antidepressants | Amitriptyline, Amitriptyline, phenobarbital, phenytoin, trazodone |
| Cardiovascular | Amiodarone, lisinopril, losartan, statins | Clopidogrel, irbesartan | Captopril, enalapril, verapamil |
| Endocrine | Acarbose, allopurinol | – | – |
| Gastrointestinal | Omeprazole | – | – |
| Herbal remedies | Germander, kava | – | – |
| Anti-infectives | HAART drugs, isoniazid, ketoconazole, pyrazinamide, rifampin, tetracycline, trovafloxacin | Amoxicillin/clavulanic acid, erythromycins, terbinafine | Clindamycin, nitrofurantoin, trimethoprim-sulfamethoxazole |
| Rheumatologic | Acetaminophen, baclofen, methotrexate, NSAIDs | Anabolic steroids | Azathioprine, sulfonamides |
| Others | – | Oral contraceptives, estrogens, phenothiazines | Cyproheptadine, flutamide |
| ALP: alkaline phosphatase; ALT: alanine aminotransferase; HAART: highly active antiretroviral therapy; NSAID: nonsteroidal anti-inflammatory drug; TBIL: total bilirubin | |||
| Source: Reference 5 | |||
Less common causes
Hemochromatosis is an autosomal recessive disease that causes pathologic deposition of iron in the liver, pancreas, and heart and leads to cirrhosis, diabetes, and heart disease. Suspect it in patients with a clinical syndrome and transferrin saturation index >45%.12 A hemochromatosis gene mutation analysis confirms the diagnosis.
Autoimmune hepatitis occurs primarily in women ages 20 to 50 years.13 Because >80% of patients with autoimmune hepatitis have hypergammaglobulinemia, serum protein electrophores is a useful screening test.5
Wilson’s disease is a genetic disorder of biliary copper excretion classically diagnosed in young people with concomitant neurologic or psychiatric conditions. Those affected have low serum ceruloplasmin. Neuropsychiatric symptoms include parkinsonian-like tremor, rigidity, clumsiness of gait, slurred speech, drooling, and inappropriate and uncontrollable grinning (risus sardonicus).8 Psychosis and suicidality also are common in patients with Wilson’s disease.
Alpha-1 antitrypsin deficiency. Alpha-1 antitrypsin is a protein produced primarily in the liver that protects the lungs from neutrophil elastase. Suspect alpha-1 antitrypsin deficiency in patients with abnormal LFTs and emphysema. Low serum alpha-1 antitrypsin confirms the diagnosis.
Celiac disease. Consider celiac disease in patients with chronic diarrhea or abdominal distension and abnormal LFTs. Small bowel biopsy and elevated tissue transglutaminase antibodies and anti-endomysial antibodies confirm the diagnosis.
Causes of cholestatic injury
If your patient has a disproportionate ALP elevation, identify the source of the ALP by testing GGT. GGT levels are elevated in liver disease but not in bone disease. Partial bile duct obstruction is a common cause of ALP elevation. For initial testing, include ultrasonography of the right upper quadrant.
Medications. Many medications can cause biliary stasis and cholestatic LFTs, including mirtazapine, tricyclic antidepressants, anabolic steroids, phenytoin, and estrogens.
Primary sclerosing cholangitis is inflammatory disease of the bile ducts that can lead to cholestasis (blockage of bile transport blockage). Consider it in patients with inflammatory bowel disease. Endoscopic retrograde cholangiopancreatography and magnetic resonance cholangiopancreatography aid diagnosis.
Primary biliary cirrhosis generally presents in middle-aged women with other autoimmune processes, cholestasis, and pruritus. Consider testing serum antimitochondrial antibodies.
Infiltrative liver diseases such as sarcoidosis, metastatic disease, or lymphoma can also present with cholestasis. Liver imaging is required for these diagnoses.
Causes of mixed injury
If LFT results suggest a mixed injury pattern, focus on the predominant pattern and evaluate the causes listed above. Certain medications typically result in a mixed injury pattern.
Related resources
- American Gastroenterological Association medical position statement: evaluation of liver chemistry tests. www.guideline.gov/summary/summary.aspx?ss=15&doc_id=3492&nbr=002718.
- Johnston DE. Special considerations in interpreting liver function tests. Am Fam Physician 1999;59(8):2223-30.
Drug brand names
- Amitriptyline • Elavil
- Bupropion • Wellbutrin
- Carbamazepine • Carbatrol, Equetro, Tegretol
- Chlorpromazine • Thorazine
- Fluoxetine • Prozac
- Mirtazapine • Remeron
- Paroxetine • Paxil
- Phenobarbital • Luminal
- Phenytoin • Dilantin
- Risperidone • Risperdal
- Sertraline • Zoloft
- Trazodone • Desyrel
- Valproic acid • Depakene
- Warfarin • Coumadin
Disclosure
The authors report no financial relationships with any company whose products are mentioned in this article or with manufacturers of competing products.
1. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137(1):1-10.
2. Gopal DV, Rosen HR. Abnormal findings on liver function tests. Interpreting results to narrow the diagnosis and establish a prognosis. Postgrad Med 2000;107(2):100-14.
3. Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med 2000;342(17):1266-71.
4. Ioannou GN, Boyko EJ, Lee SP. The prevalence and predictors of elevated serum aminotransferase activity in the United States in 1999-2002. Am J Gastroenterol 2006;101(1):76-82.
5. Navarro VJ, Senior JR. Drug-related hepatotoxicity. N Engl J Med 2006;354(7):731-9.
6. Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. CMAJ 2005;172(3):367-79.
7. Bezchilibny-Butler KZ, Jeffries JJ, eds. Clinical handbook of psychotropic drugs, 15th ed. Cambridge Hogrefe & Huber; 2005.
8. Crone CC, Gabriel GM, Dimartini A. An overview of psychiatric issues in liver disease for the consultation-liaison psychiatrist. Psychosomatics 2006;47(3):188-205.
9. Kaplan MA. Approach to the patient with abnormal liver function tests. Available at: http://www.uptodate.com. Accessed December 12, 2006.
10. Bacon BR, Farahvash MJ, Janney CG, Neuschwander-Tetri BA. Nonalcoholic steatohepatitis: an expanded clinical entity. Gastroenterology 1994;107(4):1103-9.
11. Lieberman JA, Stroup SS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353(12):1209-23.
12. Yen AW, Fancher TL, Bowlus CL. Revisiting hereditary hemochromatosis: current concepts and progress. Am J Med 2006;119(5):391-9.
13. Krawitt EL. Autoimmune hepatitis. N Engl J Med 1996;334(14):897-903.
1. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137(1):1-10.
2. Gopal DV, Rosen HR. Abnormal findings on liver function tests. Interpreting results to narrow the diagnosis and establish a prognosis. Postgrad Med 2000;107(2):100-14.
3. Pratt DS, Kaplan MM. Evaluation of abnormal liver-enzyme results in asymptomatic patients. N Engl J Med 2000;342(17):1266-71.
4. Ioannou GN, Boyko EJ, Lee SP. The prevalence and predictors of elevated serum aminotransferase activity in the United States in 1999-2002. Am J Gastroenterol 2006;101(1):76-82.
5. Navarro VJ, Senior JR. Drug-related hepatotoxicity. N Engl J Med 2006;354(7):731-9.
6. Giannini EG, Testa R, Savarino V. Liver enzyme alteration: a guide for clinicians. CMAJ 2005;172(3):367-79.
7. Bezchilibny-Butler KZ, Jeffries JJ, eds. Clinical handbook of psychotropic drugs, 15th ed. Cambridge Hogrefe & Huber; 2005.
8. Crone CC, Gabriel GM, Dimartini A. An overview of psychiatric issues in liver disease for the consultation-liaison psychiatrist. Psychosomatics 2006;47(3):188-205.
9. Kaplan MA. Approach to the patient with abnormal liver function tests. Available at: http://www.uptodate.com. Accessed December 12, 2006.
10. Bacon BR, Farahvash MJ, Janney CG, Neuschwander-Tetri BA. Nonalcoholic steatohepatitis: an expanded clinical entity. Gastroenterology 1994;107(4):1103-9.
11. Lieberman JA, Stroup SS, McEvoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med 2005;353(12):1209-23.
12. Yen AW, Fancher TL, Bowlus CL. Revisiting hereditary hemochromatosis: current concepts and progress. Am J Med 2006;119(5):391-9.
13. Krawitt EL. Autoimmune hepatitis. N Engl J Med 1996;334(14):897-903.