User login
Education sessions upped COPD patients’ knowledge of their disease
A brief patient-directed education program delivered at the time of hospitalization for an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) improved disease-specific knowledge, according to results of a pilot randomized trial.
Patients who participated in education sessions had a significant improvement in their scores on the Bristol COPD Knowledge Questionnaire (BCKQ), compared with control patients who received no education, study investigators reported in the journal Chest.
“Early education may be a bridge to more active approaches and could provide an important contribution to self-management interventions post-AECOPD,” wrote first author Tania Janaudis-Ferreira, PhD, of the School of Physical and Occupational Therapy, McGill University, Montreal, and her co-authors.
In the study, patients admitted to a community hospital with an AECOPD were randomized to standard care plus brief education or standard care alone. The education consisted of two 30-minute sessions delivered by a physiotherapist, either in the hospital or at home up to 2 weeks after the admission.
Before and after the intervention period, participant knowledge was measured using both the BCKQ and the Lung Information Needs Questionnaire (LINQ).
A total of 31 patients participated, including 15 in the intervention group and 16 in the control group, although 3 patients in the control group did not complete the follow-up testing, investigators said in their report.
The mean change in BCKQ was 8 points for the educational intervention group, and 3.4 for the control group (P = 0.02). That result was in keeping with findings of a previous randomized study noting an 8.3-point change in BCKQ scores for COPD patients who received education in the primary care setting, Dr. Janaudis-Ferreira and co-authors said.
“The change itself is relatively modest, suggesting more frequent sessions might result in greater improvements,” they wrote. For example, they said, an 8-week educational intervention delivered in the context of pulmonary rehabilitation program in one study yielded a mean change of 18.3 points on the BCKQ in the intervention group.
By contrast, the investigators found no significant difference in LINQ score changes between the intervention and control groups (P = .8).
That may indicate that two 30-minute sessions were not sufficient to attend to patients’ learning needs, authors said, though it could also have been an issue with the instrument itself in the setting of this study.
“The majority of the questions in the LINQ ask whether or not a doctor or nurse has explained a specific question to the patient,” authors explained. “Since a physiotherapist delivered the program, had the wording been altered to include physiotherapists or a more general term for healthcare professionals, we may have seen a change in these results.”
Dr. Janaudis-Ferreira and co-authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
SOURCE: Janaudis-Ferreira T, et al. Chest
A brief patient-directed education program delivered at the time of hospitalization for an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) improved disease-specific knowledge, according to results of a pilot randomized trial.
Patients who participated in education sessions had a significant improvement in their scores on the Bristol COPD Knowledge Questionnaire (BCKQ), compared with control patients who received no education, study investigators reported in the journal Chest.
“Early education may be a bridge to more active approaches and could provide an important contribution to self-management interventions post-AECOPD,” wrote first author Tania Janaudis-Ferreira, PhD, of the School of Physical and Occupational Therapy, McGill University, Montreal, and her co-authors.
In the study, patients admitted to a community hospital with an AECOPD were randomized to standard care plus brief education or standard care alone. The education consisted of two 30-minute sessions delivered by a physiotherapist, either in the hospital or at home up to 2 weeks after the admission.
Before and after the intervention period, participant knowledge was measured using both the BCKQ and the Lung Information Needs Questionnaire (LINQ).
A total of 31 patients participated, including 15 in the intervention group and 16 in the control group, although 3 patients in the control group did not complete the follow-up testing, investigators said in their report.
The mean change in BCKQ was 8 points for the educational intervention group, and 3.4 for the control group (P = 0.02). That result was in keeping with findings of a previous randomized study noting an 8.3-point change in BCKQ scores for COPD patients who received education in the primary care setting, Dr. Janaudis-Ferreira and co-authors said.
“The change itself is relatively modest, suggesting more frequent sessions might result in greater improvements,” they wrote. For example, they said, an 8-week educational intervention delivered in the context of pulmonary rehabilitation program in one study yielded a mean change of 18.3 points on the BCKQ in the intervention group.
By contrast, the investigators found no significant difference in LINQ score changes between the intervention and control groups (P = .8).
That may indicate that two 30-minute sessions were not sufficient to attend to patients’ learning needs, authors said, though it could also have been an issue with the instrument itself in the setting of this study.
“The majority of the questions in the LINQ ask whether or not a doctor or nurse has explained a specific question to the patient,” authors explained. “Since a physiotherapist delivered the program, had the wording been altered to include physiotherapists or a more general term for healthcare professionals, we may have seen a change in these results.”
Dr. Janaudis-Ferreira and co-authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
SOURCE: Janaudis-Ferreira T, et al. Chest
A brief patient-directed education program delivered at the time of hospitalization for an acute exacerbation of chronic obstructive pulmonary disease (AECOPD) improved disease-specific knowledge, according to results of a pilot randomized trial.
Patients who participated in education sessions had a significant improvement in their scores on the Bristol COPD Knowledge Questionnaire (BCKQ), compared with control patients who received no education, study investigators reported in the journal Chest.
“Early education may be a bridge to more active approaches and could provide an important contribution to self-management interventions post-AECOPD,” wrote first author Tania Janaudis-Ferreira, PhD, of the School of Physical and Occupational Therapy, McGill University, Montreal, and her co-authors.
In the study, patients admitted to a community hospital with an AECOPD were randomized to standard care plus brief education or standard care alone. The education consisted of two 30-minute sessions delivered by a physiotherapist, either in the hospital or at home up to 2 weeks after the admission.
Before and after the intervention period, participant knowledge was measured using both the BCKQ and the Lung Information Needs Questionnaire (LINQ).
A total of 31 patients participated, including 15 in the intervention group and 16 in the control group, although 3 patients in the control group did not complete the follow-up testing, investigators said in their report.
The mean change in BCKQ was 8 points for the educational intervention group, and 3.4 for the control group (P = 0.02). That result was in keeping with findings of a previous randomized study noting an 8.3-point change in BCKQ scores for COPD patients who received education in the primary care setting, Dr. Janaudis-Ferreira and co-authors said.
“The change itself is relatively modest, suggesting more frequent sessions might result in greater improvements,” they wrote. For example, they said, an 8-week educational intervention delivered in the context of pulmonary rehabilitation program in one study yielded a mean change of 18.3 points on the BCKQ in the intervention group.
By contrast, the investigators found no significant difference in LINQ score changes between the intervention and control groups (P = .8).
That may indicate that two 30-minute sessions were not sufficient to attend to patients’ learning needs, authors said, though it could also have been an issue with the instrument itself in the setting of this study.
“The majority of the questions in the LINQ ask whether or not a doctor or nurse has explained a specific question to the patient,” authors explained. “Since a physiotherapist delivered the program, had the wording been altered to include physiotherapists or a more general term for healthcare professionals, we may have seen a change in these results.”
Dr. Janaudis-Ferreira and co-authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
SOURCE: Janaudis-Ferreira T, et al. Chest
FROM CHEST
Key clinical point: Two 30-minute education sessions improved patients’ disease-specific knowledge for an acute exacerbation of COPD.
Major finding: Mean change on the Bristol COPD Knowledge Questionnaire (BCKQ) was 8 points for the educational intervention, and 3.4 for controls.
Study details: A pilot randomized controlled trial of 31 patients admitted to a community hospital.
Disclosures: Authors had no conflicts of interest to disclose. The study was funded by a grant from the Canadian Respiratory Health Professionals, which did not have input in research or manuscript development.
Source: Janaudis-Ferreira T, et al. Chest 2018 Jun 4.
AZD8871 delivered significant bronchodilation in two-week study
SAN DIEGO – , results from a phase 2a trial showed.
AZD8871 is a long-acting, bifunctional bronchodilator that combines a muscarinic antagonist and a beta-2 adrenoceptor agonist. “There are some interesting avenues that you can explore with such a molecule,” one of the study authors, Dave Singh, MD, said at an international conference of the American Thoracic Society. “First, theoretically, as a single molecule you will be able to deposit both the active ingredients to the same site in the lung. On a more practical note, if you want to add something else to a dual bronchodilator, which is essentially what AZD8871 is, this provides a platform. Perhaps that’s the most interesting use of this type of approach.”
Single doses of AZD8871 (400 mcg and 1,800 mcg) administered in COPD patients demonstrated sustained bronchodilation over 36 hours. In a study presented at the 2017 meeting of the European Respiratory Society, Dr. Singh and his associates found that AZD8871 1,800 mcg showed greater bronchodilation than both indacaterol and tiotropium for peak and trough FEV1.
For the current study, researchers at one site in the United Kingdom and one site in Germany conducted a phase 2 randomized, double-blind, placebo-controlled trial of AZD8871 in 42 patients aged 40-80 years with moderate to severe reversible COPD. Patients were randomized to receive repeated once-daily doses of AZD8871 100 mcg, 600 mcg, or placebo via a dry powder inhaler device for 14 days. Between-treatment washout periods were 28-35 days. “We keep the patients in-house on day one and day 14 of each treatment period, and we measure lung function over 24 hours,” said Dr. Singh, professor of clinical pharmacology and respiratory medicine at the University of Manchester, United Kingdom. “Patients were allowed to continue any pre-existing steroid therapy, but at the end of screening they had to withdraw any long-acting bronchodilator therapy.”
The primary efficacy endpoint was change from baseline trough FEV1 on day 15. Secondary endpoints included change from baseline in peak FEV1, total score of breathlessness, cough, sputum scale questionnaire, and rescue medication use.
At baseline, the mean age of the 42 patients was 64 years, and 67% were male. Their mean FEV1 was about 58% predicted, and their FEV1 absolute reversibility was a mean of 379 mL, “which is rather high,” he said.
Of the 42 randomized patients, 31 completed all three treatments. Both doses of AZD8871 had a positive, dose-dependent effect on FEV1, compared with placebo, and both doses demonstrated an onset of action within 15 minutes. On day 15, least square mean change from baseline differences in trough FEV1 for AZD8871 100 mcg and 600 mcg versus placebo were 161 mL and 260 mL, respectively.
A similar association was observed with peak FEV1, which between baseline and day 14 increased by 380 mL at the 100 mcg dose and by 420 mL at the 600 mcg dose, compared with placebo. Sustained bronchodilation was observed over 24 hours on both day 1 and day 14.
Statistically significant COPD symptom improvements, measured by breathlessness, cough and sputum scale (BCSS), were observed for AZD8871 600 mcg on day 8 (P=0.002) and day 14 (P less than 0.001), compared with placebo.
In addition, substantial symptomatic improvements were observed for AZD8871 600 mcg on D14 versus placebo (least square mean of -1.16). Similar results were observed for individual domains of the BCSS. “When you separate out the different components of the scale, most of this is driven by the change in breathlessness,” he said. “We were surprised that we could capture this in such a small number of patients.”
On days 1-8 and days 9-14, the researchers observed a statistically significant improvement in change from baseline rescue medication use for AZD8871 600 mcg (P less than 0.001) and 100 mcg (P=0.029 and P=0.012, respectively), compared with placebo.
The most common adverse events for patients in all three treatment groups were headache (21.4%) and worsening of COPD-related symptoms (14.3%). No dose-dependence was observed with any adverse event, including serious adverse events and/or those leading to discontinuation.
AstraZeneca, the developer of AZD8871, sponsored the study. Dr. Singh reported being a consultant to and receiving research support from AstraZeneca and numerous other pharmaceutical companies.
SOURCE: Singh, D., et al, Abstract 7708, ATS 2018.
SAN DIEGO – , results from a phase 2a trial showed.
AZD8871 is a long-acting, bifunctional bronchodilator that combines a muscarinic antagonist and a beta-2 adrenoceptor agonist. “There are some interesting avenues that you can explore with such a molecule,” one of the study authors, Dave Singh, MD, said at an international conference of the American Thoracic Society. “First, theoretically, as a single molecule you will be able to deposit both the active ingredients to the same site in the lung. On a more practical note, if you want to add something else to a dual bronchodilator, which is essentially what AZD8871 is, this provides a platform. Perhaps that’s the most interesting use of this type of approach.”
Single doses of AZD8871 (400 mcg and 1,800 mcg) administered in COPD patients demonstrated sustained bronchodilation over 36 hours. In a study presented at the 2017 meeting of the European Respiratory Society, Dr. Singh and his associates found that AZD8871 1,800 mcg showed greater bronchodilation than both indacaterol and tiotropium for peak and trough FEV1.
For the current study, researchers at one site in the United Kingdom and one site in Germany conducted a phase 2 randomized, double-blind, placebo-controlled trial of AZD8871 in 42 patients aged 40-80 years with moderate to severe reversible COPD. Patients were randomized to receive repeated once-daily doses of AZD8871 100 mcg, 600 mcg, or placebo via a dry powder inhaler device for 14 days. Between-treatment washout periods were 28-35 days. “We keep the patients in-house on day one and day 14 of each treatment period, and we measure lung function over 24 hours,” said Dr. Singh, professor of clinical pharmacology and respiratory medicine at the University of Manchester, United Kingdom. “Patients were allowed to continue any pre-existing steroid therapy, but at the end of screening they had to withdraw any long-acting bronchodilator therapy.”
The primary efficacy endpoint was change from baseline trough FEV1 on day 15. Secondary endpoints included change from baseline in peak FEV1, total score of breathlessness, cough, sputum scale questionnaire, and rescue medication use.
At baseline, the mean age of the 42 patients was 64 years, and 67% were male. Their mean FEV1 was about 58% predicted, and their FEV1 absolute reversibility was a mean of 379 mL, “which is rather high,” he said.
Of the 42 randomized patients, 31 completed all three treatments. Both doses of AZD8871 had a positive, dose-dependent effect on FEV1, compared with placebo, and both doses demonstrated an onset of action within 15 minutes. On day 15, least square mean change from baseline differences in trough FEV1 for AZD8871 100 mcg and 600 mcg versus placebo were 161 mL and 260 mL, respectively.
A similar association was observed with peak FEV1, which between baseline and day 14 increased by 380 mL at the 100 mcg dose and by 420 mL at the 600 mcg dose, compared with placebo. Sustained bronchodilation was observed over 24 hours on both day 1 and day 14.
Statistically significant COPD symptom improvements, measured by breathlessness, cough and sputum scale (BCSS), were observed for AZD8871 600 mcg on day 8 (P=0.002) and day 14 (P less than 0.001), compared with placebo.
In addition, substantial symptomatic improvements were observed for AZD8871 600 mcg on D14 versus placebo (least square mean of -1.16). Similar results were observed for individual domains of the BCSS. “When you separate out the different components of the scale, most of this is driven by the change in breathlessness,” he said. “We were surprised that we could capture this in such a small number of patients.”
On days 1-8 and days 9-14, the researchers observed a statistically significant improvement in change from baseline rescue medication use for AZD8871 600 mcg (P less than 0.001) and 100 mcg (P=0.029 and P=0.012, respectively), compared with placebo.
The most common adverse events for patients in all three treatment groups were headache (21.4%) and worsening of COPD-related symptoms (14.3%). No dose-dependence was observed with any adverse event, including serious adverse events and/or those leading to discontinuation.
AstraZeneca, the developer of AZD8871, sponsored the study. Dr. Singh reported being a consultant to and receiving research support from AstraZeneca and numerous other pharmaceutical companies.
SOURCE: Singh, D., et al, Abstract 7708, ATS 2018.
SAN DIEGO – , results from a phase 2a trial showed.
AZD8871 is a long-acting, bifunctional bronchodilator that combines a muscarinic antagonist and a beta-2 adrenoceptor agonist. “There are some interesting avenues that you can explore with such a molecule,” one of the study authors, Dave Singh, MD, said at an international conference of the American Thoracic Society. “First, theoretically, as a single molecule you will be able to deposit both the active ingredients to the same site in the lung. On a more practical note, if you want to add something else to a dual bronchodilator, which is essentially what AZD8871 is, this provides a platform. Perhaps that’s the most interesting use of this type of approach.”
Single doses of AZD8871 (400 mcg and 1,800 mcg) administered in COPD patients demonstrated sustained bronchodilation over 36 hours. In a study presented at the 2017 meeting of the European Respiratory Society, Dr. Singh and his associates found that AZD8871 1,800 mcg showed greater bronchodilation than both indacaterol and tiotropium for peak and trough FEV1.
For the current study, researchers at one site in the United Kingdom and one site in Germany conducted a phase 2 randomized, double-blind, placebo-controlled trial of AZD8871 in 42 patients aged 40-80 years with moderate to severe reversible COPD. Patients were randomized to receive repeated once-daily doses of AZD8871 100 mcg, 600 mcg, or placebo via a dry powder inhaler device for 14 days. Between-treatment washout periods were 28-35 days. “We keep the patients in-house on day one and day 14 of each treatment period, and we measure lung function over 24 hours,” said Dr. Singh, professor of clinical pharmacology and respiratory medicine at the University of Manchester, United Kingdom. “Patients were allowed to continue any pre-existing steroid therapy, but at the end of screening they had to withdraw any long-acting bronchodilator therapy.”
The primary efficacy endpoint was change from baseline trough FEV1 on day 15. Secondary endpoints included change from baseline in peak FEV1, total score of breathlessness, cough, sputum scale questionnaire, and rescue medication use.
At baseline, the mean age of the 42 patients was 64 years, and 67% were male. Their mean FEV1 was about 58% predicted, and their FEV1 absolute reversibility was a mean of 379 mL, “which is rather high,” he said.
Of the 42 randomized patients, 31 completed all three treatments. Both doses of AZD8871 had a positive, dose-dependent effect on FEV1, compared with placebo, and both doses demonstrated an onset of action within 15 minutes. On day 15, least square mean change from baseline differences in trough FEV1 for AZD8871 100 mcg and 600 mcg versus placebo were 161 mL and 260 mL, respectively.
A similar association was observed with peak FEV1, which between baseline and day 14 increased by 380 mL at the 100 mcg dose and by 420 mL at the 600 mcg dose, compared with placebo. Sustained bronchodilation was observed over 24 hours on both day 1 and day 14.
Statistically significant COPD symptom improvements, measured by breathlessness, cough and sputum scale (BCSS), were observed for AZD8871 600 mcg on day 8 (P=0.002) and day 14 (P less than 0.001), compared with placebo.
In addition, substantial symptomatic improvements were observed for AZD8871 600 mcg on D14 versus placebo (least square mean of -1.16). Similar results were observed for individual domains of the BCSS. “When you separate out the different components of the scale, most of this is driven by the change in breathlessness,” he said. “We were surprised that we could capture this in such a small number of patients.”
On days 1-8 and days 9-14, the researchers observed a statistically significant improvement in change from baseline rescue medication use for AZD8871 600 mcg (P less than 0.001) and 100 mcg (P=0.029 and P=0.012, respectively), compared with placebo.
The most common adverse events for patients in all three treatment groups were headache (21.4%) and worsening of COPD-related symptoms (14.3%). No dose-dependence was observed with any adverse event, including serious adverse events and/or those leading to discontinuation.
AstraZeneca, the developer of AZD8871, sponsored the study. Dr. Singh reported being a consultant to and receiving research support from AstraZeneca and numerous other pharmaceutical companies.
SOURCE: Singh, D., et al, Abstract 7708, ATS 2018.
REPORTING FROM ATS 2018
Key clinical point: Once daily doses of AZD8871 100 mcg and 600 mcg elicited significant and clinically relevant differences in trough FEV1, compared with placebo.
Major finding: On day 15, least square mean change from baseline differences in trough FEV1 for AZD8871 100 mcg and 600 mcg versus placebo were 161 mL and 260 mL, respectively.
Study details: A phase 2a trial of 42 patients aged 40-80 years with moderate to severe reversible COPD.
Disclosures: AstraZeneca sponsored the study. Dr. Singh reported financial affiliations with AstraZeneca and numerous other pharmaceutical companies.Source: Singh, D., et al. Abstract 7708, ATS 2018.
COPD patient subset gains no benefit from low-dose theophylline
, results from a large trial funded by the United Kingdom found.
“Globally, theophylline was used for decades as a bronchodilator,” one of the study authors, David B. Price, MB BChir, said at an international conference of the American Thoracic Society. “The problem is theophylline has a narrow therapeutic index, it requires some blood monitoring, and it has been replaced by more effective inhaled bronchodilators. However, there has been a lot of discussion about whether low-dose theophylline has anti-inflammatory effects on its own and whether it increases sensitivity to inhaled steroids in COPD.”
According to the 2018 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, there is “limited and contradictory evidence regarding the effect of low-dose theophylline on exacerbation rates,” and its clinical relevance has “not yet been fully established.” Dr. Price, a professor of primary care respiratory medicine at the University of Aberdeen, United Kingdom, and his associates hypothesized that the addition of low-dose theophylline to inhaled steroid therapy in COPD would reduce the risk of moderate to severe COPD exacerbations after one year of treatment. “If it worked, it would be wonderful; it would save the National Health Service a fortune,” he said.
In a government-funded trial known as Theophylline With Inhaled Corticosteroids (TWICS), people aged 40 years and older with COPD on a drug regimen including inhaled corticosteroids with a history of at least two exacerbations treated with antibiotics and/or oral corticosteroids in the previous year were recruited in 121 U.K. primary and secondary care sites from January 2014 through August 2016. They were randomized to receive low-dose theophylline or placebo for one year. Theophylline dose (200 mg once/twice a day) was determined by ideal body weight and smoking status. Primary outcome was the number of participant-reported exacerbations in the one year treatment period treated with antibiotics and/or oral corticosteroids. Participants were assessed six and 12 months after randomization. The study was powered to detect a 15% reduction in exacerbations and aimed to recruit 1,424 participants.
In all, 1,578 people were randomized: 791 to theophylline and 787 to placebo. Of these, primary outcome data were available for 98% of participants: 772 in the theophylline group and 764 in the placebo group, which amounted to 1,489 person-years of follow-up data. The mean age of patients was 68 years, 54% were male, 32% currently smoked, 80% were using inhaled corticosteroids/long-acting beta 2-agonists/long-acting muscarinic agents, and their mean FEV1 was 51.7% predicted.
Slightly more than one-quarter of study participants (26%) ceased study medication. Dr. Price said that this was balanced between the theophylline and placebo groups and mitigated by over-recruitment and a high rate of follow-up.
He reported that there were 3,430 moderate to severe exacerbations: 1,727 in the theophylline group and 1,703 in the placebo group. The mean number of exacerbations in participants allocated to theophylline and placebo groups were essentially the same: 2.24 vs. 2.23. However, there were a fewer number of exacerbations that required hospitalization in the theophylline group, compared with the placebo groups (0.17 vs. 0.24, for an adjusted rate ratio of 0.72). Dr. Price was quick to point out that this finding applied to a relatively small number of study participants, about 3% overall.
“How you interpret this, I don’t know,” he said. “Our conclusion is that in the broad population there is no benefit [of low-dose theophylline], but maybe someone might want to study its use in frequent exacerbation patients who are getting hospitalized.”
The study was funded by the National Institute for Health Research (NIHR), United Kingdom. Dr. Price reported having no financial disclosures.
SOURCE: Price, D., et al, Abstract 7709, ATS 2018.
, results from a large trial funded by the United Kingdom found.
“Globally, theophylline was used for decades as a bronchodilator,” one of the study authors, David B. Price, MB BChir, said at an international conference of the American Thoracic Society. “The problem is theophylline has a narrow therapeutic index, it requires some blood monitoring, and it has been replaced by more effective inhaled bronchodilators. However, there has been a lot of discussion about whether low-dose theophylline has anti-inflammatory effects on its own and whether it increases sensitivity to inhaled steroids in COPD.”
According to the 2018 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, there is “limited and contradictory evidence regarding the effect of low-dose theophylline on exacerbation rates,” and its clinical relevance has “not yet been fully established.” Dr. Price, a professor of primary care respiratory medicine at the University of Aberdeen, United Kingdom, and his associates hypothesized that the addition of low-dose theophylline to inhaled steroid therapy in COPD would reduce the risk of moderate to severe COPD exacerbations after one year of treatment. “If it worked, it would be wonderful; it would save the National Health Service a fortune,” he said.
In a government-funded trial known as Theophylline With Inhaled Corticosteroids (TWICS), people aged 40 years and older with COPD on a drug regimen including inhaled corticosteroids with a history of at least two exacerbations treated with antibiotics and/or oral corticosteroids in the previous year were recruited in 121 U.K. primary and secondary care sites from January 2014 through August 2016. They were randomized to receive low-dose theophylline or placebo for one year. Theophylline dose (200 mg once/twice a day) was determined by ideal body weight and smoking status. Primary outcome was the number of participant-reported exacerbations in the one year treatment period treated with antibiotics and/or oral corticosteroids. Participants were assessed six and 12 months after randomization. The study was powered to detect a 15% reduction in exacerbations and aimed to recruit 1,424 participants.
In all, 1,578 people were randomized: 791 to theophylline and 787 to placebo. Of these, primary outcome data were available for 98% of participants: 772 in the theophylline group and 764 in the placebo group, which amounted to 1,489 person-years of follow-up data. The mean age of patients was 68 years, 54% were male, 32% currently smoked, 80% were using inhaled corticosteroids/long-acting beta 2-agonists/long-acting muscarinic agents, and their mean FEV1 was 51.7% predicted.
Slightly more than one-quarter of study participants (26%) ceased study medication. Dr. Price said that this was balanced between the theophylline and placebo groups and mitigated by over-recruitment and a high rate of follow-up.
He reported that there were 3,430 moderate to severe exacerbations: 1,727 in the theophylline group and 1,703 in the placebo group. The mean number of exacerbations in participants allocated to theophylline and placebo groups were essentially the same: 2.24 vs. 2.23. However, there were a fewer number of exacerbations that required hospitalization in the theophylline group, compared with the placebo groups (0.17 vs. 0.24, for an adjusted rate ratio of 0.72). Dr. Price was quick to point out that this finding applied to a relatively small number of study participants, about 3% overall.
“How you interpret this, I don’t know,” he said. “Our conclusion is that in the broad population there is no benefit [of low-dose theophylline], but maybe someone might want to study its use in frequent exacerbation patients who are getting hospitalized.”
The study was funded by the National Institute for Health Research (NIHR), United Kingdom. Dr. Price reported having no financial disclosures.
SOURCE: Price, D., et al, Abstract 7709, ATS 2018.
, results from a large trial funded by the United Kingdom found.
“Globally, theophylline was used for decades as a bronchodilator,” one of the study authors, David B. Price, MB BChir, said at an international conference of the American Thoracic Society. “The problem is theophylline has a narrow therapeutic index, it requires some blood monitoring, and it has been replaced by more effective inhaled bronchodilators. However, there has been a lot of discussion about whether low-dose theophylline has anti-inflammatory effects on its own and whether it increases sensitivity to inhaled steroids in COPD.”
According to the 2018 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, there is “limited and contradictory evidence regarding the effect of low-dose theophylline on exacerbation rates,” and its clinical relevance has “not yet been fully established.” Dr. Price, a professor of primary care respiratory medicine at the University of Aberdeen, United Kingdom, and his associates hypothesized that the addition of low-dose theophylline to inhaled steroid therapy in COPD would reduce the risk of moderate to severe COPD exacerbations after one year of treatment. “If it worked, it would be wonderful; it would save the National Health Service a fortune,” he said.
In a government-funded trial known as Theophylline With Inhaled Corticosteroids (TWICS), people aged 40 years and older with COPD on a drug regimen including inhaled corticosteroids with a history of at least two exacerbations treated with antibiotics and/or oral corticosteroids in the previous year were recruited in 121 U.K. primary and secondary care sites from January 2014 through August 2016. They were randomized to receive low-dose theophylline or placebo for one year. Theophylline dose (200 mg once/twice a day) was determined by ideal body weight and smoking status. Primary outcome was the number of participant-reported exacerbations in the one year treatment period treated with antibiotics and/or oral corticosteroids. Participants were assessed six and 12 months after randomization. The study was powered to detect a 15% reduction in exacerbations and aimed to recruit 1,424 participants.
In all, 1,578 people were randomized: 791 to theophylline and 787 to placebo. Of these, primary outcome data were available for 98% of participants: 772 in the theophylline group and 764 in the placebo group, which amounted to 1,489 person-years of follow-up data. The mean age of patients was 68 years, 54% were male, 32% currently smoked, 80% were using inhaled corticosteroids/long-acting beta 2-agonists/long-acting muscarinic agents, and their mean FEV1 was 51.7% predicted.
Slightly more than one-quarter of study participants (26%) ceased study medication. Dr. Price said that this was balanced between the theophylline and placebo groups and mitigated by over-recruitment and a high rate of follow-up.
He reported that there were 3,430 moderate to severe exacerbations: 1,727 in the theophylline group and 1,703 in the placebo group. The mean number of exacerbations in participants allocated to theophylline and placebo groups were essentially the same: 2.24 vs. 2.23. However, there were a fewer number of exacerbations that required hospitalization in the theophylline group, compared with the placebo groups (0.17 vs. 0.24, for an adjusted rate ratio of 0.72). Dr. Price was quick to point out that this finding applied to a relatively small number of study participants, about 3% overall.
“How you interpret this, I don’t know,” he said. “Our conclusion is that in the broad population there is no benefit [of low-dose theophylline], but maybe someone might want to study its use in frequent exacerbation patients who are getting hospitalized.”
The study was funded by the National Institute for Health Research (NIHR), United Kingdom. Dr. Price reported having no financial disclosures.
SOURCE: Price, D., et al, Abstract 7709, ATS 2018.
AT ATS 2018
Key clinical point: Among COPD patients at high risk of exacerbation, adding low-dose oral theophylline to a drug regimen that includes an inhaled corticosteroid provides no overall clinical benefit.
Major finding: The number of exacerbations was 2.24 in participants allocated to theophylline and 2.23 for participants allocated to placebo.
Study details: A trial of 1,578 people with COPD and a history of at least two exacerbations in the previous year who were randomized to receive low-dose theophylline or placebo for one year.
Disclosures: The study was funded by National Institute for Health Research (NIHR), United Kingdom. Dr. Price reported having no financial disclosures.
Source: Price, D., et al. Abstract 7709, ATS 2018.
Most COPD patients on triple therapy can withdraw steroids
SAN DIEGO – In patients on long-term triple therapy and up to one exacerbation in the previous year, the withdrawal of inhaled corticosteroids (ICS) led to a small decrease in lung function that was not clinically important, with no associated difference in the rates of chronic obstructive pulmonary disease (COPD) exacerbations, dyspnea or as-needed bronchodilator use.
Those are key findings from the SUNSET trial, a 26-week, randomized, double-blind, parallel-group multicenter study to assess the efficacy and safety of the switch from long-term triple therapy to indacaterol/glycopyrronium (IND/GLY, 110/50 mcg once daily) or continuation of triple therapy with tiotropium 18 mcg once daily and salmeterol/fluticasone propionate fixed-dose combination 50/500 mcg b.i.d.
Dr. Chapman, director of the asthma and airways clinic at University Health Network, Toronto, noted that relatively few patients with COPD benefit from inhaled steroids. “Given the risk of adverse events (pneumonia, osteoporosis, etc.), we’d rather not give them when they’re not needed,” he said. “Inhaled steroids seem to play only one role in COPD: They tend to reduce exacerbations in the exacerbation-prone COPD patient. That’s about 20% of the COPD population. Despite this, a great many patients end up on triple therapy [long-acting bronchodilators/long-acting muscarinic antagonist (LABA/LAMA) and ICS] needlessly.”
For the study, Dr. Chapman and his associates enrolled 1,053 patients with moderate to severe COPD who’d had no more than one exacerbation in the previous year who had used triple therapy for at least 6 months prior to study inclusion. The primary endpoint of the study was noninferiority on change from baseline in postdose trough forced expiratory volume in 1 second (FEV1) (with a noninferiority margin of –50 mL) after 26 weeks. Exacerbations, health-related quality of life as measured by the St. George’s Respiratory Questionnaire (SGRQ-C), and breathlessness as measures by the Transition Dyspnea Index also were evaluated. Of the 1,053 patients, 527 were randomized to IND/GLY and 526 to triple therapy. Their mean age was 65 years and their mean postbronchodilator FEV1 was 1.6 L.
The researchers found that ICS withdrawal led to a mean reduction in trough FEV1 of –26 mL, which exceeded the noninferiority margin. This difference between treatments on trough FEV1 was driven by the subset of patients with high blood eosinophil counts at baseline (a mean of –68 mL for patients with at least 300 cells/mcL and a mean of –13 mL for patients with fewer than 300 cells/mcL). The two treatments showed similar annualized rates of moderate/severe COPD exacerbations (rate ratio, 1.08) and all (mild/moderate/severe) exacerbations (RR, 1.07). ICS withdrawal led to a small difference in SGRQ-C (1.4 U on week 26), but no differences in Transition Dyspnea Index or use of rescue medication over 26 weeks. Safety and tolerability were balanced across the two treatment groups.
“Although we found no overall increase in exacerbations with ‘de-escalation,’ there were, of course, exacerbations that occurred during the trial,” Dr. Chapman said. “We found that they tended to occur in the minority of patients who had elevated blood eosinophil counts, especially if the counts were elevated persistently (at screening and randomization). The relevant cut-point was blood eosinophil counts above 300/UL. If exacerbations did occur in this easily identifiable subpopulation, they tended to occur early, in the first month after de-escalation. This gives physicians a simply way to identify a population they might exercise caution and a period when careful monitoring is useful.”
He acknowledged certain limitations of the study, including its 6-month duration, which is shorter than most exacerbation studies. “But by recruiting at multiple sites in multiple countries and across seasons, we don’t think this was an importation limitation,” he said. “Of course, like most investigators, I can always think of things I wish I had tracked. My personal hunch is that FeNO [exhaled nitric oxide levels] might offer some useful information but that will be a hunch to explore in another study.”
SUNSET was sponsored by Novartis. Dr. Chapman disclosed that he has received fees for research, consulting and lectures from Novartis, as well as from several other pharmaceutical companies.
dbrunk@mdedge.com
SOURCE: Chapman K et al. ATS 2018 Abstract A1009.
SAN DIEGO – In patients on long-term triple therapy and up to one exacerbation in the previous year, the withdrawal of inhaled corticosteroids (ICS) led to a small decrease in lung function that was not clinically important, with no associated difference in the rates of chronic obstructive pulmonary disease (COPD) exacerbations, dyspnea or as-needed bronchodilator use.
Those are key findings from the SUNSET trial, a 26-week, randomized, double-blind, parallel-group multicenter study to assess the efficacy and safety of the switch from long-term triple therapy to indacaterol/glycopyrronium (IND/GLY, 110/50 mcg once daily) or continuation of triple therapy with tiotropium 18 mcg once daily and salmeterol/fluticasone propionate fixed-dose combination 50/500 mcg b.i.d.
Dr. Chapman, director of the asthma and airways clinic at University Health Network, Toronto, noted that relatively few patients with COPD benefit from inhaled steroids. “Given the risk of adverse events (pneumonia, osteoporosis, etc.), we’d rather not give them when they’re not needed,” he said. “Inhaled steroids seem to play only one role in COPD: They tend to reduce exacerbations in the exacerbation-prone COPD patient. That’s about 20% of the COPD population. Despite this, a great many patients end up on triple therapy [long-acting bronchodilators/long-acting muscarinic antagonist (LABA/LAMA) and ICS] needlessly.”
For the study, Dr. Chapman and his associates enrolled 1,053 patients with moderate to severe COPD who’d had no more than one exacerbation in the previous year who had used triple therapy for at least 6 months prior to study inclusion. The primary endpoint of the study was noninferiority on change from baseline in postdose trough forced expiratory volume in 1 second (FEV1) (with a noninferiority margin of –50 mL) after 26 weeks. Exacerbations, health-related quality of life as measured by the St. George’s Respiratory Questionnaire (SGRQ-C), and breathlessness as measures by the Transition Dyspnea Index also were evaluated. Of the 1,053 patients, 527 were randomized to IND/GLY and 526 to triple therapy. Their mean age was 65 years and their mean postbronchodilator FEV1 was 1.6 L.
The researchers found that ICS withdrawal led to a mean reduction in trough FEV1 of –26 mL, which exceeded the noninferiority margin. This difference between treatments on trough FEV1 was driven by the subset of patients with high blood eosinophil counts at baseline (a mean of –68 mL for patients with at least 300 cells/mcL and a mean of –13 mL for patients with fewer than 300 cells/mcL). The two treatments showed similar annualized rates of moderate/severe COPD exacerbations (rate ratio, 1.08) and all (mild/moderate/severe) exacerbations (RR, 1.07). ICS withdrawal led to a small difference in SGRQ-C (1.4 U on week 26), but no differences in Transition Dyspnea Index or use of rescue medication over 26 weeks. Safety and tolerability were balanced across the two treatment groups.
“Although we found no overall increase in exacerbations with ‘de-escalation,’ there were, of course, exacerbations that occurred during the trial,” Dr. Chapman said. “We found that they tended to occur in the minority of patients who had elevated blood eosinophil counts, especially if the counts were elevated persistently (at screening and randomization). The relevant cut-point was blood eosinophil counts above 300/UL. If exacerbations did occur in this easily identifiable subpopulation, they tended to occur early, in the first month after de-escalation. This gives physicians a simply way to identify a population they might exercise caution and a period when careful monitoring is useful.”
He acknowledged certain limitations of the study, including its 6-month duration, which is shorter than most exacerbation studies. “But by recruiting at multiple sites in multiple countries and across seasons, we don’t think this was an importation limitation,” he said. “Of course, like most investigators, I can always think of things I wish I had tracked. My personal hunch is that FeNO [exhaled nitric oxide levels] might offer some useful information but that will be a hunch to explore in another study.”
SUNSET was sponsored by Novartis. Dr. Chapman disclosed that he has received fees for research, consulting and lectures from Novartis, as well as from several other pharmaceutical companies.
dbrunk@mdedge.com
SOURCE: Chapman K et al. ATS 2018 Abstract A1009.
SAN DIEGO – In patients on long-term triple therapy and up to one exacerbation in the previous year, the withdrawal of inhaled corticosteroids (ICS) led to a small decrease in lung function that was not clinically important, with no associated difference in the rates of chronic obstructive pulmonary disease (COPD) exacerbations, dyspnea or as-needed bronchodilator use.
Those are key findings from the SUNSET trial, a 26-week, randomized, double-blind, parallel-group multicenter study to assess the efficacy and safety of the switch from long-term triple therapy to indacaterol/glycopyrronium (IND/GLY, 110/50 mcg once daily) or continuation of triple therapy with tiotropium 18 mcg once daily and salmeterol/fluticasone propionate fixed-dose combination 50/500 mcg b.i.d.
Dr. Chapman, director of the asthma and airways clinic at University Health Network, Toronto, noted that relatively few patients with COPD benefit from inhaled steroids. “Given the risk of adverse events (pneumonia, osteoporosis, etc.), we’d rather not give them when they’re not needed,” he said. “Inhaled steroids seem to play only one role in COPD: They tend to reduce exacerbations in the exacerbation-prone COPD patient. That’s about 20% of the COPD population. Despite this, a great many patients end up on triple therapy [long-acting bronchodilators/long-acting muscarinic antagonist (LABA/LAMA) and ICS] needlessly.”
For the study, Dr. Chapman and his associates enrolled 1,053 patients with moderate to severe COPD who’d had no more than one exacerbation in the previous year who had used triple therapy for at least 6 months prior to study inclusion. The primary endpoint of the study was noninferiority on change from baseline in postdose trough forced expiratory volume in 1 second (FEV1) (with a noninferiority margin of –50 mL) after 26 weeks. Exacerbations, health-related quality of life as measured by the St. George’s Respiratory Questionnaire (SGRQ-C), and breathlessness as measures by the Transition Dyspnea Index also were evaluated. Of the 1,053 patients, 527 were randomized to IND/GLY and 526 to triple therapy. Their mean age was 65 years and their mean postbronchodilator FEV1 was 1.6 L.
The researchers found that ICS withdrawal led to a mean reduction in trough FEV1 of –26 mL, which exceeded the noninferiority margin. This difference between treatments on trough FEV1 was driven by the subset of patients with high blood eosinophil counts at baseline (a mean of –68 mL for patients with at least 300 cells/mcL and a mean of –13 mL for patients with fewer than 300 cells/mcL). The two treatments showed similar annualized rates of moderate/severe COPD exacerbations (rate ratio, 1.08) and all (mild/moderate/severe) exacerbations (RR, 1.07). ICS withdrawal led to a small difference in SGRQ-C (1.4 U on week 26), but no differences in Transition Dyspnea Index or use of rescue medication over 26 weeks. Safety and tolerability were balanced across the two treatment groups.
“Although we found no overall increase in exacerbations with ‘de-escalation,’ there were, of course, exacerbations that occurred during the trial,” Dr. Chapman said. “We found that they tended to occur in the minority of patients who had elevated blood eosinophil counts, especially if the counts were elevated persistently (at screening and randomization). The relevant cut-point was blood eosinophil counts above 300/UL. If exacerbations did occur in this easily identifiable subpopulation, they tended to occur early, in the first month after de-escalation. This gives physicians a simply way to identify a population they might exercise caution and a period when careful monitoring is useful.”
He acknowledged certain limitations of the study, including its 6-month duration, which is shorter than most exacerbation studies. “But by recruiting at multiple sites in multiple countries and across seasons, we don’t think this was an importation limitation,” he said. “Of course, like most investigators, I can always think of things I wish I had tracked. My personal hunch is that FeNO [exhaled nitric oxide levels] might offer some useful information but that will be a hunch to explore in another study.”
SUNSET was sponsored by Novartis. Dr. Chapman disclosed that he has received fees for research, consulting and lectures from Novartis, as well as from several other pharmaceutical companies.
dbrunk@mdedge.com
SOURCE: Chapman K et al. ATS 2018 Abstract A1009.
REPORTING FROM ATS 2018
Key clinical point: Switching from triple therapy to indacaterol/glycopyrronium (IND/GLY) is effective in COPD patients and avoids long-term exposure to inhaled corticosteroids.
Major finding: ICS withdrawal led to a mean reduction in trough FEV1 of –26 mL, which exceeded the noninferiority margin.
Study details: A randomized trial of COPD patients in which 527 were randomized to IND/GLY and 526 to triple therapy.
Disclosures: SUNSET was sponsored by Novartis. Dr. Chapman disclosed that he has received fees for research, consulting, and lectures from Novartis, as well as from several other pharmaceutical companies.
Source: Chapman K et al. ATS 2018. Abstract A1009.
CHEST® Physician’s preview of ATS 2018
Here is a glimpse of some of the important research that will be presented at this meeting.

The findings of several chronic obstructive pulmonary disease (COPD) drug trials will be discussed during a session entitled “ICS [Inhaled corticosteroids] in COPD: The Pendulum Keeps Swinging,” which is scheduled to occur at 9:15 a.m. in Room 14 A-B (Mezzanine Level). Among the research to be presented are the latest findings of the phase 3 IMPACT study of 10,355 symptomatic COPD patients with a history of moderate to severe exacerbations. This study compared the use of an inhaled therapy that comprised a corticosteroid, a long-acting muscarinic antagonist (LAMA), and a long-acting beta2-agonist (LABA) with the use of two other therapy combinations – a corticosteroid and a LABA, or a LABA and a LAMA. (Lipson DA et al. N Engl J Med. 2018 Apr 18;378:1671-80). Patients were randomized to receive either a once-daily combination of 100 mcg fluticasone furoate (a corticosteroid); 62.5 mcg of the LAMA, umeclidinium; and 25 mcg of the LABA, vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol for 52 weeks.
One of the updates on this trial is that using the triple therapy significantly reduced on-treatment all-cause mortality over using the LAMA (62.5 mcg of umeclidinium) plus LABA (25 mcg of the vilanterol) dual therapy. Fifty of the patients who received triple therapy died (1.20%), versus 49 patients in the corticosteroid plus LABA group (1.19%) and 30 patients (1.88%) in the LAMA plus LABA group. A 42.1% reduction in risk of all-cause mortality occurred for patients who took the triple therapy, when compared with patients who took the LAMA/LABA combo (95% confidence interval, 11.9%-61.9%; P = .011), according to an abstract on the ATS International Conference’s website.
At the same time on Sunday, researchers will be presenting their research in a session entitled “Sleep Disordered Breathing, Cardiovascular Disease, and Mortality,” in Room 3 (Upper Level) of the convention center. One of the abstracts that will be discussed compared the long-term effectiveness of noninvasive ventilation (NIV) with continuous positive airway pressure (CPAP) in patients with obesity hypoventilation syndrome with severe obstructive sleep apnea. In this multicenter open-label, randomized, controlled trial, Sanchez Quiroga M et al. analyzed the results for 202 patients who used one of the two treatments for at least 3 years. Among this study’s findings were that the mortality rates and the number of cardiovascular events that occurred were similar in the two treatment groups. The mortality rate for patients who used CPAP was 14.7%, compared with 11.3% for the patients who received NIV (adjusted hazard ratio, 0.73; P = .439), and the cardiovascular events per 100 person-years were 5.1 for CPAP and 7.46 for NIV (P = .315). The researchers concluded that both treatments are equally effective for the long term, but that CPAP should be “the preferred treatment modality,” because it’s cheaper and easier to implement.
On Monday morning, researchers will present their findings of the short-term cardiovascular effects of 30 pulmonary arterial hypertension patients’ use of the beta blocker carvedilol, in 3.125 mg doses taken twice a day. Right ventricular systolic pressure (RVSP) decreased by an average of 11 mmHg (P = .003) in this double-blinded, randomized, controlled open-label trial with a 1-week run-in period. Cardiac output decreased by an average of –1.8 L/min (P less than .0001), but RVSP was inversely associated with cardiac output. “Short-term carvedilol could potentially identify a subgroup for long-term therapy based on initial drop in RVSP and heart rate response,” noted Farha SY et al. in their abstract. None of the patients experienced any side effects from taking the drug. More details on this research and other studies on pulmonary hypertension will be presented at 9:15 am in Area B (Hall A-B2, Ground level) of the convention center, in the session entitled “Surf’s Up: Riding the Wave of Clinical Research in Pulmonary Hypertension.”
Look for all of our on-site coverage of the conference at mdedge.com/chestphysician next week.
Here is a glimpse of some of the important research that will be presented at this meeting.
The findings of several chronic obstructive pulmonary disease (COPD) drug trials will be discussed during a session entitled “ICS [Inhaled corticosteroids] in COPD: The Pendulum Keeps Swinging,” which is scheduled to occur at 9:15 a.m. in Room 14 A-B (Mezzanine Level). Among the research to be presented are the latest findings of the phase 3 IMPACT study of 10,355 symptomatic COPD patients with a history of moderate to severe exacerbations. This study compared the use of an inhaled therapy that comprised a corticosteroid, a long-acting muscarinic antagonist (LAMA), and a long-acting beta2-agonist (LABA) with the use of two other therapy combinations – a corticosteroid and a LABA, or a LABA and a LAMA. (Lipson DA et al. N Engl J Med. 2018 Apr 18;378:1671-80). Patients were randomized to receive either a once-daily combination of 100 mcg fluticasone furoate (a corticosteroid); 62.5 mcg of the LAMA, umeclidinium; and 25 mcg of the LABA, vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol for 52 weeks.
One of the updates on this trial is that using the triple therapy significantly reduced on-treatment all-cause mortality over using the LAMA (62.5 mcg of umeclidinium) plus LABA (25 mcg of the vilanterol) dual therapy. Fifty of the patients who received triple therapy died (1.20%), versus 49 patients in the corticosteroid plus LABA group (1.19%) and 30 patients (1.88%) in the LAMA plus LABA group. A 42.1% reduction in risk of all-cause mortality occurred for patients who took the triple therapy, when compared with patients who took the LAMA/LABA combo (95% confidence interval, 11.9%-61.9%; P = .011), according to an abstract on the ATS International Conference’s website.
At the same time on Sunday, researchers will be presenting their research in a session entitled “Sleep Disordered Breathing, Cardiovascular Disease, and Mortality,” in Room 3 (Upper Level) of the convention center. One of the abstracts that will be discussed compared the long-term effectiveness of noninvasive ventilation (NIV) with continuous positive airway pressure (CPAP) in patients with obesity hypoventilation syndrome with severe obstructive sleep apnea. In this multicenter open-label, randomized, controlled trial, Sanchez Quiroga M et al. analyzed the results for 202 patients who used one of the two treatments for at least 3 years. Among this study’s findings were that the mortality rates and the number of cardiovascular events that occurred were similar in the two treatment groups. The mortality rate for patients who used CPAP was 14.7%, compared with 11.3% for the patients who received NIV (adjusted hazard ratio, 0.73; P = .439), and the cardiovascular events per 100 person-years were 5.1 for CPAP and 7.46 for NIV (P = .315). The researchers concluded that both treatments are equally effective for the long term, but that CPAP should be “the preferred treatment modality,” because it’s cheaper and easier to implement.
On Monday morning, researchers will present their findings of the short-term cardiovascular effects of 30 pulmonary arterial hypertension patients’ use of the beta blocker carvedilol, in 3.125 mg doses taken twice a day. Right ventricular systolic pressure (RVSP) decreased by an average of 11 mmHg (P = .003) in this double-blinded, randomized, controlled open-label trial with a 1-week run-in period. Cardiac output decreased by an average of –1.8 L/min (P less than .0001), but RVSP was inversely associated with cardiac output. “Short-term carvedilol could potentially identify a subgroup for long-term therapy based on initial drop in RVSP and heart rate response,” noted Farha SY et al. in their abstract. None of the patients experienced any side effects from taking the drug. More details on this research and other studies on pulmonary hypertension will be presented at 9:15 am in Area B (Hall A-B2, Ground level) of the convention center, in the session entitled “Surf’s Up: Riding the Wave of Clinical Research in Pulmonary Hypertension.”
Look for all of our on-site coverage of the conference at mdedge.com/chestphysician next week.
Here is a glimpse of some of the important research that will be presented at this meeting.
The findings of several chronic obstructive pulmonary disease (COPD) drug trials will be discussed during a session entitled “ICS [Inhaled corticosteroids] in COPD: The Pendulum Keeps Swinging,” which is scheduled to occur at 9:15 a.m. in Room 14 A-B (Mezzanine Level). Among the research to be presented are the latest findings of the phase 3 IMPACT study of 10,355 symptomatic COPD patients with a history of moderate to severe exacerbations. This study compared the use of an inhaled therapy that comprised a corticosteroid, a long-acting muscarinic antagonist (LAMA), and a long-acting beta2-agonist (LABA) with the use of two other therapy combinations – a corticosteroid and a LABA, or a LABA and a LAMA. (Lipson DA et al. N Engl J Med. 2018 Apr 18;378:1671-80). Patients were randomized to receive either a once-daily combination of 100 mcg fluticasone furoate (a corticosteroid); 62.5 mcg of the LAMA, umeclidinium; and 25 mcg of the LABA, vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol for 52 weeks.
One of the updates on this trial is that using the triple therapy significantly reduced on-treatment all-cause mortality over using the LAMA (62.5 mcg of umeclidinium) plus LABA (25 mcg of the vilanterol) dual therapy. Fifty of the patients who received triple therapy died (1.20%), versus 49 patients in the corticosteroid plus LABA group (1.19%) and 30 patients (1.88%) in the LAMA plus LABA group. A 42.1% reduction in risk of all-cause mortality occurred for patients who took the triple therapy, when compared with patients who took the LAMA/LABA combo (95% confidence interval, 11.9%-61.9%; P = .011), according to an abstract on the ATS International Conference’s website.
At the same time on Sunday, researchers will be presenting their research in a session entitled “Sleep Disordered Breathing, Cardiovascular Disease, and Mortality,” in Room 3 (Upper Level) of the convention center. One of the abstracts that will be discussed compared the long-term effectiveness of noninvasive ventilation (NIV) with continuous positive airway pressure (CPAP) in patients with obesity hypoventilation syndrome with severe obstructive sleep apnea. In this multicenter open-label, randomized, controlled trial, Sanchez Quiroga M et al. analyzed the results for 202 patients who used one of the two treatments for at least 3 years. Among this study’s findings were that the mortality rates and the number of cardiovascular events that occurred were similar in the two treatment groups. The mortality rate for patients who used CPAP was 14.7%, compared with 11.3% for the patients who received NIV (adjusted hazard ratio, 0.73; P = .439), and the cardiovascular events per 100 person-years were 5.1 for CPAP and 7.46 for NIV (P = .315). The researchers concluded that both treatments are equally effective for the long term, but that CPAP should be “the preferred treatment modality,” because it’s cheaper and easier to implement.
On Monday morning, researchers will present their findings of the short-term cardiovascular effects of 30 pulmonary arterial hypertension patients’ use of the beta blocker carvedilol, in 3.125 mg doses taken twice a day. Right ventricular systolic pressure (RVSP) decreased by an average of 11 mmHg (P = .003) in this double-blinded, randomized, controlled open-label trial with a 1-week run-in period. Cardiac output decreased by an average of –1.8 L/min (P less than .0001), but RVSP was inversely associated with cardiac output. “Short-term carvedilol could potentially identify a subgroup for long-term therapy based on initial drop in RVSP and heart rate response,” noted Farha SY et al. in their abstract. None of the patients experienced any side effects from taking the drug. More details on this research and other studies on pulmonary hypertension will be presented at 9:15 am in Area B (Hall A-B2, Ground level) of the convention center, in the session entitled “Surf’s Up: Riding the Wave of Clinical Research in Pulmonary Hypertension.”
Look for all of our on-site coverage of the conference at mdedge.com/chestphysician next week.
FROM ATS 2018
COPD-OSA overlap syndrome
Chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA) each affect at least 10% of the general adult population and, thus, both disorders together, commonly referred to as the overlap syndrome, could be expected in at least 1% of adults by chance alone. However, there is evidence of important interactions between the disorders that influence the prevalence of the overlap, which have implications for the development of comorbidities,and also for management (McNicholas WT. Chest. 2017; 152[6]:1318). Furthermore, sleep quality is typically poor in COPD, which has been linked to worse pulmonary function and lung hyperinflation and may contribute to daytime fatigue.
Interactions between COPD and OSA that may influence the prevalence of overlap
Previous reports have presented conflicting results regarding the likely association between COPD and OSA, which may partly reflect different definitions of OSA, patient populations, and methodologies of investigation. However, COPD represents a spectrum of clinical phenotypes ranging from the hyperinflated patient with low BMI (predominant emphysema phenotype) to the patient with higher BMI and tendency to right-sided heart failure (predominant chronic bronchitis phenotype). The predominant emphysema phenotype may predispose to a lower likelihood of OSA, and there is recent evidence that lung hyperinflation is protective against the development of OSA by lowering the critical closing pressure of the upper airway during sleep. Furthermore, the degree of emphysema and gas trapping on CT scan of the thorax correlates inversely with apnea-hypopnia index in patients with severe COPD (Krachman SL et al. Ann Am Thorac Soc. 2016;13[7]:1129).

In contrast, the predominant chronic bronchitis phenotype predisposes to a higher likelihood of OSA because of higher BMI and likelihood of right-sided heart failure. Peripheral fluid retention in such patients predisposes to OSA because of the rostral fluid shift that occurs during sleep in the supine position, predisposing to upper airway obstruction by airway narrowing. The COPDGene study reports that the chronic bronchitis phenotype has a higher prevalence of OSA even in the absence of differences in BMI and lung function (Kim V et al. Chest. 2011;140[3]:626). Upper airway inflammation associated with cigarette smoking may also contribute to the development of OSA, and corticosteroid therapy may adversely affect upper airway muscle function. OSA also appears to exacerbate lower airway inflammation in COPD. In practice, most patients with COPD have a mixture of emphysema and chronic bronchitis, and the probability of OSA will represent the balance of these protective and promoting factors in individual patients (Fig 1).
While there is evidence of increased mortality in patients with COPD and OSA alone, a recent report based on the Sleep Heart Health Study somewhat surprisingly found that the incremental contribution of declining lung function to mortality diminished with increasing severity of SDB measured by AHI (Putcha N et al. Am J Respir Crit Care Med. 2016;194[8]:1007). Thus, the epidemiologic relationship of COPD and OSA and related clinical outcomes remains an important research topic comparing different clinical phenotypes.
Mechanisms of interaction in the overlap syndrome and implications for comorbidity
COPD and OSA are associated with several overlapping physiological and biological disturbances, including hypoxia and inflammation, which may contribute to cardiovascular and other comorbidities. Thus, the probability should be high that the overlap syndrome will be associated with a greater risk of comorbidity than with either disease alone. Patients with the overlap syndrome demonstrate greater degrees of oxygen desaturation predisposing to pulmonary hypertension, which is especially common in these patients.
COPD and OSA are each associated with systemic inflammation and oxidative stress, and C-reactive protein (CRP) has been identified as a measure of systemic inflammation that is commonly elevated in both disorders, although in OSA, concurrent obesity is an important confounding factor. Systemic inflammation contributes to the development of cardiovascular disease, which is a common complication of both COPD and OSA. Thus, one could expect that cardiovascular disease is particularly prevalent in patients with overlap syndrome, but there are limited data on this relationship, which represents an important research topic.
Clinical assessment
Patients with the overlap syndrome present with typical clinical features of each disorder and additional features that reflect the higher prevalence of hypoxemia, hypercapnia, and pulmonary hypertension. Thus, morning headaches reflecting hypercapnia and peripheral edema reflecting right-sided heart failure may be especially common. Screening questionnaires may be helpful in the initial evaluation of likely OSA in patients with COPD, and objective clinical data, including anthropometrics such as age, sex, and BMI, and medical history such as cardiovascular comorbidity, are especially useful in clinical prediction (McNicholas WT. Lancet Respir Med. 2016;4[9]:683). Thus, screening for OSA in patients with COPD should not be complicated, and the widespread failure to do so may reflect a lack of awareness of the possible association by the clinician involved.
The specific diagnosis of OSA in COPD requires some form of overnight sleep study, and there is a growing move toward ambulatory studies that focus on cardiorespiratory variables. Overnight monitoring of oxygen saturation is especially useful, particularly if linked to special analysis software, and may be sufficient in many cases. Full polysomnography can be reserved for select cases where the diagnosis remains in doubt.
Management and outcomes
Nocturnal hypoxemia in patients with COPD benefits from inhaled, long-acting beta-agonist and anticholinergic therapy, and mean nocturnal oxygen saturation is 2% to 3% higher on each medication compared with placebo. Supplemental oxygen may be indicated when nocturnal oxygen desaturation persists despite optimum pharmacotherapy and does not appear to be associated with significant additional risk of hypercapnia.
However, in patients with COPD-OSA overlap, nonnvasive pressure support is the most appropriate management option. In patients with predominant OSA, continuous positive airway pressure therapy (CPAP) is the preferred option, but where COPD is the dominant component, noninvasive ventilation (NIV) in the form of bi-level positive airway pressure (BIPAP) may be more appropriate. Recent reports in severe COPD indicate that NIV targeted to markedly reduce hypercapnia is associated with improved quality of life and prolonged survival (Köhnlein T et al. Lancet Respir Med. 2014;2[9]:698), and patients with COPD with persistent hypercapnia following hospitalization with an acute exacerbation show improved clinical outcomes and survival with continuing home NIV (Murphy PB et al. JAMA. 2017;317[21]:2177).
The recognition of co-existing OSA in patients with COPD has important clinical relevance as the management of patients with overlap syndrome is different from COPD alone, and the long-term survival of patients with overlap syndrome not treated with nocturnal positive airway pressure is significantly inferior to those patients with overlap syndrome appropriately treated (Marin JM et al. Am J Respir Crit Care Med. 2010;182[3]:325).
Dr. McNicholas is with the Department of Respiratory and Sleep Medicine, St. Vincent’s University Hospital, Dublin School of Medicine, University College Dublin, Ireland.
Chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA) each affect at least 10% of the general adult population and, thus, both disorders together, commonly referred to as the overlap syndrome, could be expected in at least 1% of adults by chance alone. However, there is evidence of important interactions between the disorders that influence the prevalence of the overlap, which have implications for the development of comorbidities,and also for management (McNicholas WT. Chest. 2017; 152[6]:1318). Furthermore, sleep quality is typically poor in COPD, which has been linked to worse pulmonary function and lung hyperinflation and may contribute to daytime fatigue.
Interactions between COPD and OSA that may influence the prevalence of overlap
Previous reports have presented conflicting results regarding the likely association between COPD and OSA, which may partly reflect different definitions of OSA, patient populations, and methodologies of investigation. However, COPD represents a spectrum of clinical phenotypes ranging from the hyperinflated patient with low BMI (predominant emphysema phenotype) to the patient with higher BMI and tendency to right-sided heart failure (predominant chronic bronchitis phenotype). The predominant emphysema phenotype may predispose to a lower likelihood of OSA, and there is recent evidence that lung hyperinflation is protective against the development of OSA by lowering the critical closing pressure of the upper airway during sleep. Furthermore, the degree of emphysema and gas trapping on CT scan of the thorax correlates inversely with apnea-hypopnia index in patients with severe COPD (Krachman SL et al. Ann Am Thorac Soc. 2016;13[7]:1129).
In contrast, the predominant chronic bronchitis phenotype predisposes to a higher likelihood of OSA because of higher BMI and likelihood of right-sided heart failure. Peripheral fluid retention in such patients predisposes to OSA because of the rostral fluid shift that occurs during sleep in the supine position, predisposing to upper airway obstruction by airway narrowing. The COPDGene study reports that the chronic bronchitis phenotype has a higher prevalence of OSA even in the absence of differences in BMI and lung function (Kim V et al. Chest. 2011;140[3]:626). Upper airway inflammation associated with cigarette smoking may also contribute to the development of OSA, and corticosteroid therapy may adversely affect upper airway muscle function. OSA also appears to exacerbate lower airway inflammation in COPD. In practice, most patients with COPD have a mixture of emphysema and chronic bronchitis, and the probability of OSA will represent the balance of these protective and promoting factors in individual patients (Fig 1).
While there is evidence of increased mortality in patients with COPD and OSA alone, a recent report based on the Sleep Heart Health Study somewhat surprisingly found that the incremental contribution of declining lung function to mortality diminished with increasing severity of SDB measured by AHI (Putcha N et al. Am J Respir Crit Care Med. 2016;194[8]:1007). Thus, the epidemiologic relationship of COPD and OSA and related clinical outcomes remains an important research topic comparing different clinical phenotypes.
Mechanisms of interaction in the overlap syndrome and implications for comorbidity
COPD and OSA are associated with several overlapping physiological and biological disturbances, including hypoxia and inflammation, which may contribute to cardiovascular and other comorbidities. Thus, the probability should be high that the overlap syndrome will be associated with a greater risk of comorbidity than with either disease alone. Patients with the overlap syndrome demonstrate greater degrees of oxygen desaturation predisposing to pulmonary hypertension, which is especially common in these patients.
COPD and OSA are each associated with systemic inflammation and oxidative stress, and C-reactive protein (CRP) has been identified as a measure of systemic inflammation that is commonly elevated in both disorders, although in OSA, concurrent obesity is an important confounding factor. Systemic inflammation contributes to the development of cardiovascular disease, which is a common complication of both COPD and OSA. Thus, one could expect that cardiovascular disease is particularly prevalent in patients with overlap syndrome, but there are limited data on this relationship, which represents an important research topic.
Clinical assessment
Patients with the overlap syndrome present with typical clinical features of each disorder and additional features that reflect the higher prevalence of hypoxemia, hypercapnia, and pulmonary hypertension. Thus, morning headaches reflecting hypercapnia and peripheral edema reflecting right-sided heart failure may be especially common. Screening questionnaires may be helpful in the initial evaluation of likely OSA in patients with COPD, and objective clinical data, including anthropometrics such as age, sex, and BMI, and medical history such as cardiovascular comorbidity, are especially useful in clinical prediction (McNicholas WT. Lancet Respir Med. 2016;4[9]:683). Thus, screening for OSA in patients with COPD should not be complicated, and the widespread failure to do so may reflect a lack of awareness of the possible association by the clinician involved.
The specific diagnosis of OSA in COPD requires some form of overnight sleep study, and there is a growing move toward ambulatory studies that focus on cardiorespiratory variables. Overnight monitoring of oxygen saturation is especially useful, particularly if linked to special analysis software, and may be sufficient in many cases. Full polysomnography can be reserved for select cases where the diagnosis remains in doubt.
Management and outcomes
Nocturnal hypoxemia in patients with COPD benefits from inhaled, long-acting beta-agonist and anticholinergic therapy, and mean nocturnal oxygen saturation is 2% to 3% higher on each medication compared with placebo. Supplemental oxygen may be indicated when nocturnal oxygen desaturation persists despite optimum pharmacotherapy and does not appear to be associated with significant additional risk of hypercapnia.
However, in patients with COPD-OSA overlap, nonnvasive pressure support is the most appropriate management option. In patients with predominant OSA, continuous positive airway pressure therapy (CPAP) is the preferred option, but where COPD is the dominant component, noninvasive ventilation (NIV) in the form of bi-level positive airway pressure (BIPAP) may be more appropriate. Recent reports in severe COPD indicate that NIV targeted to markedly reduce hypercapnia is associated with improved quality of life and prolonged survival (Köhnlein T et al. Lancet Respir Med. 2014;2[9]:698), and patients with COPD with persistent hypercapnia following hospitalization with an acute exacerbation show improved clinical outcomes and survival with continuing home NIV (Murphy PB et al. JAMA. 2017;317[21]:2177).
The recognition of co-existing OSA in patients with COPD has important clinical relevance as the management of patients with overlap syndrome is different from COPD alone, and the long-term survival of patients with overlap syndrome not treated with nocturnal positive airway pressure is significantly inferior to those patients with overlap syndrome appropriately treated (Marin JM et al. Am J Respir Crit Care Med. 2010;182[3]:325).
Dr. McNicholas is with the Department of Respiratory and Sleep Medicine, St. Vincent’s University Hospital, Dublin School of Medicine, University College Dublin, Ireland.
Chronic obstructive pulmonary disease (COPD) and obstructive sleep apnea (OSA) each affect at least 10% of the general adult population and, thus, both disorders together, commonly referred to as the overlap syndrome, could be expected in at least 1% of adults by chance alone. However, there is evidence of important interactions between the disorders that influence the prevalence of the overlap, which have implications for the development of comorbidities,and also for management (McNicholas WT. Chest. 2017; 152[6]:1318). Furthermore, sleep quality is typically poor in COPD, which has been linked to worse pulmonary function and lung hyperinflation and may contribute to daytime fatigue.
Interactions between COPD and OSA that may influence the prevalence of overlap
Previous reports have presented conflicting results regarding the likely association between COPD and OSA, which may partly reflect different definitions of OSA, patient populations, and methodologies of investigation. However, COPD represents a spectrum of clinical phenotypes ranging from the hyperinflated patient with low BMI (predominant emphysema phenotype) to the patient with higher BMI and tendency to right-sided heart failure (predominant chronic bronchitis phenotype). The predominant emphysema phenotype may predispose to a lower likelihood of OSA, and there is recent evidence that lung hyperinflation is protective against the development of OSA by lowering the critical closing pressure of the upper airway during sleep. Furthermore, the degree of emphysema and gas trapping on CT scan of the thorax correlates inversely with apnea-hypopnia index in patients with severe COPD (Krachman SL et al. Ann Am Thorac Soc. 2016;13[7]:1129).
In contrast, the predominant chronic bronchitis phenotype predisposes to a higher likelihood of OSA because of higher BMI and likelihood of right-sided heart failure. Peripheral fluid retention in such patients predisposes to OSA because of the rostral fluid shift that occurs during sleep in the supine position, predisposing to upper airway obstruction by airway narrowing. The COPDGene study reports that the chronic bronchitis phenotype has a higher prevalence of OSA even in the absence of differences in BMI and lung function (Kim V et al. Chest. 2011;140[3]:626). Upper airway inflammation associated with cigarette smoking may also contribute to the development of OSA, and corticosteroid therapy may adversely affect upper airway muscle function. OSA also appears to exacerbate lower airway inflammation in COPD. In practice, most patients with COPD have a mixture of emphysema and chronic bronchitis, and the probability of OSA will represent the balance of these protective and promoting factors in individual patients (Fig 1).
While there is evidence of increased mortality in patients with COPD and OSA alone, a recent report based on the Sleep Heart Health Study somewhat surprisingly found that the incremental contribution of declining lung function to mortality diminished with increasing severity of SDB measured by AHI (Putcha N et al. Am J Respir Crit Care Med. 2016;194[8]:1007). Thus, the epidemiologic relationship of COPD and OSA and related clinical outcomes remains an important research topic comparing different clinical phenotypes.
Mechanisms of interaction in the overlap syndrome and implications for comorbidity
COPD and OSA are associated with several overlapping physiological and biological disturbances, including hypoxia and inflammation, which may contribute to cardiovascular and other comorbidities. Thus, the probability should be high that the overlap syndrome will be associated with a greater risk of comorbidity than with either disease alone. Patients with the overlap syndrome demonstrate greater degrees of oxygen desaturation predisposing to pulmonary hypertension, which is especially common in these patients.
COPD and OSA are each associated with systemic inflammation and oxidative stress, and C-reactive protein (CRP) has been identified as a measure of systemic inflammation that is commonly elevated in both disorders, although in OSA, concurrent obesity is an important confounding factor. Systemic inflammation contributes to the development of cardiovascular disease, which is a common complication of both COPD and OSA. Thus, one could expect that cardiovascular disease is particularly prevalent in patients with overlap syndrome, but there are limited data on this relationship, which represents an important research topic.
Clinical assessment
Patients with the overlap syndrome present with typical clinical features of each disorder and additional features that reflect the higher prevalence of hypoxemia, hypercapnia, and pulmonary hypertension. Thus, morning headaches reflecting hypercapnia and peripheral edema reflecting right-sided heart failure may be especially common. Screening questionnaires may be helpful in the initial evaluation of likely OSA in patients with COPD, and objective clinical data, including anthropometrics such as age, sex, and BMI, and medical history such as cardiovascular comorbidity, are especially useful in clinical prediction (McNicholas WT. Lancet Respir Med. 2016;4[9]:683). Thus, screening for OSA in patients with COPD should not be complicated, and the widespread failure to do so may reflect a lack of awareness of the possible association by the clinician involved.
The specific diagnosis of OSA in COPD requires some form of overnight sleep study, and there is a growing move toward ambulatory studies that focus on cardiorespiratory variables. Overnight monitoring of oxygen saturation is especially useful, particularly if linked to special analysis software, and may be sufficient in many cases. Full polysomnography can be reserved for select cases where the diagnosis remains in doubt.
Management and outcomes
Nocturnal hypoxemia in patients with COPD benefits from inhaled, long-acting beta-agonist and anticholinergic therapy, and mean nocturnal oxygen saturation is 2% to 3% higher on each medication compared with placebo. Supplemental oxygen may be indicated when nocturnal oxygen desaturation persists despite optimum pharmacotherapy and does not appear to be associated with significant additional risk of hypercapnia.
However, in patients with COPD-OSA overlap, nonnvasive pressure support is the most appropriate management option. In patients with predominant OSA, continuous positive airway pressure therapy (CPAP) is the preferred option, but where COPD is the dominant component, noninvasive ventilation (NIV) in the form of bi-level positive airway pressure (BIPAP) may be more appropriate. Recent reports in severe COPD indicate that NIV targeted to markedly reduce hypercapnia is associated with improved quality of life and prolonged survival (Köhnlein T et al. Lancet Respir Med. 2014;2[9]:698), and patients with COPD with persistent hypercapnia following hospitalization with an acute exacerbation show improved clinical outcomes and survival with continuing home NIV (Murphy PB et al. JAMA. 2017;317[21]:2177).
The recognition of co-existing OSA in patients with COPD has important clinical relevance as the management of patients with overlap syndrome is different from COPD alone, and the long-term survival of patients with overlap syndrome not treated with nocturnal positive airway pressure is significantly inferior to those patients with overlap syndrome appropriately treated (Marin JM et al. Am J Respir Crit Care Med. 2010;182[3]:325).
Dr. McNicholas is with the Department of Respiratory and Sleep Medicine, St. Vincent’s University Hospital, Dublin School of Medicine, University College Dublin, Ireland.
In COPD, tai chi confers long-term benefit
and seems to confer better long-term improvement, suggests a study published online in the journal CHEST®.

Following 12 weeks of participation in tai chi or pulmonary rehabilitation, patients improved in most of the measurements taken, although no significant between-group differences were observed at that time. However, further improvements were observed in the tai chi group 12 weeks after the intervention had ended. These improvements manifested as a statistically significant 4.5 between-group difference in St. George’s Respiratory Questionnaire points in favor of tai chi (P less than .001)
“This observation, supported also by improvements in dyspnea and exercise performance, suggests that tai chi could be substituted for PR [pulmonary rehabilitation] in the treatment of COPD with greater convenience for patients,” the researchers concluded.
SOURCE: Polkey MI et al. CHEST. 2018 May;153[5]:1116-24.
and seems to confer better long-term improvement, suggests a study published online in the journal CHEST®.
Following 12 weeks of participation in tai chi or pulmonary rehabilitation, patients improved in most of the measurements taken, although no significant between-group differences were observed at that time. However, further improvements were observed in the tai chi group 12 weeks after the intervention had ended. These improvements manifested as a statistically significant 4.5 between-group difference in St. George’s Respiratory Questionnaire points in favor of tai chi (P less than .001)
“This observation, supported also by improvements in dyspnea and exercise performance, suggests that tai chi could be substituted for PR [pulmonary rehabilitation] in the treatment of COPD with greater convenience for patients,” the researchers concluded.
SOURCE: Polkey MI et al. CHEST. 2018 May;153[5]:1116-24.
and seems to confer better long-term improvement, suggests a study published online in the journal CHEST®.
Following 12 weeks of participation in tai chi or pulmonary rehabilitation, patients improved in most of the measurements taken, although no significant between-group differences were observed at that time. However, further improvements were observed in the tai chi group 12 weeks after the intervention had ended. These improvements manifested as a statistically significant 4.5 between-group difference in St. George’s Respiratory Questionnaire points in favor of tai chi (P less than .001)
“This observation, supported also by improvements in dyspnea and exercise performance, suggests that tai chi could be substituted for PR [pulmonary rehabilitation] in the treatment of COPD with greater convenience for patients,” the researchers concluded.
SOURCE: Polkey MI et al. CHEST. 2018 May;153[5]:1116-24.
FROM THE JOURNAL CHEST®
FDA: More COPD patients can use triple therapy
The Food and Drug Administration has approved a new indication for the chronic obstructive pulmonary disease (COPD) therapy fluticasone furoate/umeclidinium/vilanterol (Trelegy Ellipta), which allows physicians to prescribe the drug to a broader class of COPD patients, according to a statement from two pharmaceutical companies.

“Following the initial approval of Trelegy Ellipta in September, we have analysed the data from the IMPACT study and identified additional benefits that this important medicine offers patients with [COPD],” said Hal Barron, MD, chief scientific officer and president of research and development at GlaxoSmithKline, in the statement. “We are pleased that the robust data from the IMPACT study has enabled the expanded indication announced today and the FDA action has been taken so swiftly.”
The results of the IMPACT trial, which was the first study to compare a single-inhaler triple therapy with two dual therapies, were published on April 18 (N Engl J Med 2018. doi: 10.1056/NEJMoa1713901).
This study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate, 62.5 mcg of umeclidinium, and 25 mcg of vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction, compared with vilanterol-umeclidinium (P less than .001 for both).
The Food and Drug Administration has approved a new indication for the chronic obstructive pulmonary disease (COPD) therapy fluticasone furoate/umeclidinium/vilanterol (Trelegy Ellipta), which allows physicians to prescribe the drug to a broader class of COPD patients, according to a statement from two pharmaceutical companies.
“Following the initial approval of Trelegy Ellipta in September, we have analysed the data from the IMPACT study and identified additional benefits that this important medicine offers patients with [COPD],” said Hal Barron, MD, chief scientific officer and president of research and development at GlaxoSmithKline, in the statement. “We are pleased that the robust data from the IMPACT study has enabled the expanded indication announced today and the FDA action has been taken so swiftly.”
The results of the IMPACT trial, which was the first study to compare a single-inhaler triple therapy with two dual therapies, were published on April 18 (N Engl J Med 2018. doi: 10.1056/NEJMoa1713901).
This study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate, 62.5 mcg of umeclidinium, and 25 mcg of vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction, compared with vilanterol-umeclidinium (P less than .001 for both).
The Food and Drug Administration has approved a new indication for the chronic obstructive pulmonary disease (COPD) therapy fluticasone furoate/umeclidinium/vilanterol (Trelegy Ellipta), which allows physicians to prescribe the drug to a broader class of COPD patients, according to a statement from two pharmaceutical companies.
“Following the initial approval of Trelegy Ellipta in September, we have analysed the data from the IMPACT study and identified additional benefits that this important medicine offers patients with [COPD],” said Hal Barron, MD, chief scientific officer and president of research and development at GlaxoSmithKline, in the statement. “We are pleased that the robust data from the IMPACT study has enabled the expanded indication announced today and the FDA action has been taken so swiftly.”
The results of the IMPACT trial, which was the first study to compare a single-inhaler triple therapy with two dual therapies, were published on April 18 (N Engl J Med 2018. doi: 10.1056/NEJMoa1713901).
This study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate, 62.5 mcg of umeclidinium, and 25 mcg of vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction, compared with vilanterol-umeclidinium (P less than .001 for both).
Triple-therapy cuts COPD exacerbations
Triple therapy for chronic obstructive pulmonary disease (COPD) achieved reductions in moderate to severe exacerbations when compared with two kinds of dual therapy, in a study published online in the New England Journal of Medicine.
The trial compared the outcomes of COPD patients using an inhaled therapy comprising a corticosteroid, a long-acting muscarinic antagonist (LAMA), and a long-acting beta2-agonist (LABA) with the outcomes of similar patients taking one of two other therapy combinations – a corticosteroid and a LABA, or a LABA and a LAMA. This trial – Informing the Pathway of COPD Treatment (IMPACT) – included 10,355 patients with symptomatic COPD in 37 countries, according to David A. Lipson, MD, and his colleagues (N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMoa1713901).
The study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate (a corticosteroid), 62.5 mcg of the LAMA umeclidinium and 25 mcg of the LABA vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction compared with vilanterol-umeclidinium (P less than .001 for both).
When the analysis was limited to severe exacerbations alone, the difference was significant only between the triple therapy, which GSK is marketing as Trelegy Ellipta, and the vilanterol-umeclidinium dual therapy.
Dr. Lipson, of GSK and the University of Pennsylvania, and his coauthors noted that their finding of a greater benefit with the glucocorticoid-containing dual-therapy compared with the LABA-LAMA vilanterol-umeclidinium combination contradicted the findings of the earlier FLAME trial. This was likely due to differences in patient populations and design, as all patients in the FLAME trial had a 1-month run-in treatment with the bronchodilator tiotropium, the researchers explained.
“Therefore any patients who would require an inhaled glucocorticoid may have had an increase in exacerbations and a decrease in lung function during the run-in period and would have been forced to leave the trial,” they wrote.
Patients with higher eosinophil levels seemed to do even better with triple therapy. In those with eosinophil levels of 150 cells per microliter or above, the annual rate of moderate to severe exacerbations was 0.95 with triple therapy, 1.08 with fluticasone furoate–vilanterol, and 1.39 with vilanterol-umeclidinium.
Triple therapy also was associated with a significantly longer time to first event and greater improvements in quality of life, compared with the dual therapies.
Overall, the adverse event profile of triple therapy was similar to that of dual therapy. Contrasting that finding were differences in the incidences of physician-diagnosed pneumonia between the treatment groups. Physician-diagnosed pneumonia was 53% higher among patients who received fluticasone furoate – either in dual or triple therapy combinations. Eight percent of patients in the triple therapy group experienced pneumonia, compared with 7% of patients in the fluticasone furoate–vilanterol group and 5% in the vilanterol-umeclidinium group.
All-cause mortality was significantly lower in patients who received the inhaled glucocorticoid, although the authors said this finding was “fragile” and needed further investigation.
The rate of discontinuation or withdrawal from the trial was 6% for the triple therapy group, 8% for the fluticasone furoate–vilanterol group, and 9% for the vilanterol-umeclidinium group. The rates of serious adverse events in each group were 22%, 21%, and 23%, respectively.
At trial entry, 38% of patients were already receiving triple therapy and 29% were taking an inhaled glucocorticoid. The authors noted that any patients taking an inhaled glucocorticoid who were randomized to the vilanterol-umeclidinium group would have had to abruptly stop taking their inhaled glucocorticoids.
“It is unknown whether the abrupt discontinuation of inhaled glucocorticoids would have contributed to our finding of a lower rate of exacerbations in the inhaled glucocorticoid groups than in the LAMA-LABA group,” they wrote.
Fernando Martinez, MD, chief of the division of pulmonary and critical care medicine at New York–Presbyterian Hospital/Weill Cornell Medical Center, said the study advanced the understanding of COPD management by addressing some key evidence gaps, in a statement issued by GSK.
“By comparing various combinations of effective medications in the same device the study clarifies which type of patient gains greatest benefit from each class of medicine,” Dr Martinez said in the statement. “As many patients experience frequent exacerbations or ‘flare ups,’ which can often result in hospitalization, these data will be highly relevant to patients and clinicians as they consider the optimal treatment.”
The study was funded by GSK, which manufactures Trelegy Ellipta triple therapy for COPD. Eight authors were employees of GSK and two were on advisory boards for the company. Seven authors declared funding from a range of pharmaceutical companies including GSK. One author had no conflicts of interest to declare.
SOURCE: Lipson D et al. N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMoa1713901.
The data from the IMPACT study fills a gap in the evidence supporting a step-up from dual to triple inhaled therapy for COPD, which so far has been recommended only for patients with severe loss of lung function and those with frequent exacerbations despite maximum bronchodilator treatment. The study has the strengths of comparing the step-up to triple therapy with the GOLD guideline–recommended dual therapies and using the same dosages in the triple therapy as in the dual therapy
However, it is important to note that nearly 40% of patients enrolled in the trial were already being treated with triple therapy, 70% were receiving a glucocorticoid, and patients with a history of asthma were not excluded. This means patients assigned to the dual therapy without glucocorticoids would have had an abrupt cessation of their glucocorticoid therapy, which may explain a rapid surge in exacerbations in the first month and the lower rate of exacerbations in the dual-therapy group that did include glucocorticoids. The choice of patients for the study could potentially have artificially inflated the observed effectiveness of triple therapy over dual bronchodilator treatment.
As such, we suggest clinicians stick with the GOLD 2017 recommendations that escalation to triple therapy only occur after maximization of bronchodilator treatment.
Dr. Samy Suissa (PhD) is with the Center for Clinical Epidemiology at Lady Davis Institute–Jewish General Hospital, and the departments of epidemiology and biostatistics and medicine at McGill University, Montreal. Dr. Jeffrey M. Drazen is editor-in-chief of the New England Journal of Medicine. These comments are taken from an editorial (N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMe1716802 ). Dr. Suissa declared personal fees and grants from the pharmaceutical industry outside the submitted work.
The data from the IMPACT study fills a gap in the evidence supporting a step-up from dual to triple inhaled therapy for COPD, which so far has been recommended only for patients with severe loss of lung function and those with frequent exacerbations despite maximum bronchodilator treatment. The study has the strengths of comparing the step-up to triple therapy with the GOLD guideline–recommended dual therapies and using the same dosages in the triple therapy as in the dual therapy
However, it is important to note that nearly 40% of patients enrolled in the trial were already being treated with triple therapy, 70% were receiving a glucocorticoid, and patients with a history of asthma were not excluded. This means patients assigned to the dual therapy without glucocorticoids would have had an abrupt cessation of their glucocorticoid therapy, which may explain a rapid surge in exacerbations in the first month and the lower rate of exacerbations in the dual-therapy group that did include glucocorticoids. The choice of patients for the study could potentially have artificially inflated the observed effectiveness of triple therapy over dual bronchodilator treatment.
As such, we suggest clinicians stick with the GOLD 2017 recommendations that escalation to triple therapy only occur after maximization of bronchodilator treatment.
Dr. Samy Suissa (PhD) is with the Center for Clinical Epidemiology at Lady Davis Institute–Jewish General Hospital, and the departments of epidemiology and biostatistics and medicine at McGill University, Montreal. Dr. Jeffrey M. Drazen is editor-in-chief of the New England Journal of Medicine. These comments are taken from an editorial (N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMe1716802 ). Dr. Suissa declared personal fees and grants from the pharmaceutical industry outside the submitted work.
The data from the IMPACT study fills a gap in the evidence supporting a step-up from dual to triple inhaled therapy for COPD, which so far has been recommended only for patients with severe loss of lung function and those with frequent exacerbations despite maximum bronchodilator treatment. The study has the strengths of comparing the step-up to triple therapy with the GOLD guideline–recommended dual therapies and using the same dosages in the triple therapy as in the dual therapy
However, it is important to note that nearly 40% of patients enrolled in the trial were already being treated with triple therapy, 70% were receiving a glucocorticoid, and patients with a history of asthma were not excluded. This means patients assigned to the dual therapy without glucocorticoids would have had an abrupt cessation of their glucocorticoid therapy, which may explain a rapid surge in exacerbations in the first month and the lower rate of exacerbations in the dual-therapy group that did include glucocorticoids. The choice of patients for the study could potentially have artificially inflated the observed effectiveness of triple therapy over dual bronchodilator treatment.
As such, we suggest clinicians stick with the GOLD 2017 recommendations that escalation to triple therapy only occur after maximization of bronchodilator treatment.
Dr. Samy Suissa (PhD) is with the Center for Clinical Epidemiology at Lady Davis Institute–Jewish General Hospital, and the departments of epidemiology and biostatistics and medicine at McGill University, Montreal. Dr. Jeffrey M. Drazen is editor-in-chief of the New England Journal of Medicine. These comments are taken from an editorial (N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMe1716802 ). Dr. Suissa declared personal fees and grants from the pharmaceutical industry outside the submitted work.
Triple therapy for chronic obstructive pulmonary disease (COPD) achieved reductions in moderate to severe exacerbations when compared with two kinds of dual therapy, in a study published online in the New England Journal of Medicine.
The trial compared the outcomes of COPD patients using an inhaled therapy comprising a corticosteroid, a long-acting muscarinic antagonist (LAMA), and a long-acting beta2-agonist (LABA) with the outcomes of similar patients taking one of two other therapy combinations – a corticosteroid and a LABA, or a LABA and a LAMA. This trial – Informing the Pathway of COPD Treatment (IMPACT) – included 10,355 patients with symptomatic COPD in 37 countries, according to David A. Lipson, MD, and his colleagues (N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMoa1713901).
The study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate (a corticosteroid), 62.5 mcg of the LAMA umeclidinium and 25 mcg of the LABA vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction compared with vilanterol-umeclidinium (P less than .001 for both).
When the analysis was limited to severe exacerbations alone, the difference was significant only between the triple therapy, which GSK is marketing as Trelegy Ellipta, and the vilanterol-umeclidinium dual therapy.
Dr. Lipson, of GSK and the University of Pennsylvania, and his coauthors noted that their finding of a greater benefit with the glucocorticoid-containing dual-therapy compared with the LABA-LAMA vilanterol-umeclidinium combination contradicted the findings of the earlier FLAME trial. This was likely due to differences in patient populations and design, as all patients in the FLAME trial had a 1-month run-in treatment with the bronchodilator tiotropium, the researchers explained.
“Therefore any patients who would require an inhaled glucocorticoid may have had an increase in exacerbations and a decrease in lung function during the run-in period and would have been forced to leave the trial,” they wrote.
Patients with higher eosinophil levels seemed to do even better with triple therapy. In those with eosinophil levels of 150 cells per microliter or above, the annual rate of moderate to severe exacerbations was 0.95 with triple therapy, 1.08 with fluticasone furoate–vilanterol, and 1.39 with vilanterol-umeclidinium.
Triple therapy also was associated with a significantly longer time to first event and greater improvements in quality of life, compared with the dual therapies.
Overall, the adverse event profile of triple therapy was similar to that of dual therapy. Contrasting that finding were differences in the incidences of physician-diagnosed pneumonia between the treatment groups. Physician-diagnosed pneumonia was 53% higher among patients who received fluticasone furoate – either in dual or triple therapy combinations. Eight percent of patients in the triple therapy group experienced pneumonia, compared with 7% of patients in the fluticasone furoate–vilanterol group and 5% in the vilanterol-umeclidinium group.
All-cause mortality was significantly lower in patients who received the inhaled glucocorticoid, although the authors said this finding was “fragile” and needed further investigation.
The rate of discontinuation or withdrawal from the trial was 6% for the triple therapy group, 8% for the fluticasone furoate–vilanterol group, and 9% for the vilanterol-umeclidinium group. The rates of serious adverse events in each group were 22%, 21%, and 23%, respectively.
At trial entry, 38% of patients were already receiving triple therapy and 29% were taking an inhaled glucocorticoid. The authors noted that any patients taking an inhaled glucocorticoid who were randomized to the vilanterol-umeclidinium group would have had to abruptly stop taking their inhaled glucocorticoids.
“It is unknown whether the abrupt discontinuation of inhaled glucocorticoids would have contributed to our finding of a lower rate of exacerbations in the inhaled glucocorticoid groups than in the LAMA-LABA group,” they wrote.
Fernando Martinez, MD, chief of the division of pulmonary and critical care medicine at New York–Presbyterian Hospital/Weill Cornell Medical Center, said the study advanced the understanding of COPD management by addressing some key evidence gaps, in a statement issued by GSK.
“By comparing various combinations of effective medications in the same device the study clarifies which type of patient gains greatest benefit from each class of medicine,” Dr Martinez said in the statement. “As many patients experience frequent exacerbations or ‘flare ups,’ which can often result in hospitalization, these data will be highly relevant to patients and clinicians as they consider the optimal treatment.”
The study was funded by GSK, which manufactures Trelegy Ellipta triple therapy for COPD. Eight authors were employees of GSK and two were on advisory boards for the company. Seven authors declared funding from a range of pharmaceutical companies including GSK. One author had no conflicts of interest to declare.
SOURCE: Lipson D et al. N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMoa1713901.
Triple therapy for chronic obstructive pulmonary disease (COPD) achieved reductions in moderate to severe exacerbations when compared with two kinds of dual therapy, in a study published online in the New England Journal of Medicine.
The trial compared the outcomes of COPD patients using an inhaled therapy comprising a corticosteroid, a long-acting muscarinic antagonist (LAMA), and a long-acting beta2-agonist (LABA) with the outcomes of similar patients taking one of two other therapy combinations – a corticosteroid and a LABA, or a LABA and a LAMA. This trial – Informing the Pathway of COPD Treatment (IMPACT) – included 10,355 patients with symptomatic COPD in 37 countries, according to David A. Lipson, MD, and his colleagues (N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMoa1713901).
The study randomized patients to 52 weeks of either triple inhaled therapy involving a once-daily combination of 100 mcg fluticasone furoate (a corticosteroid), 62.5 mcg of the LAMA umeclidinium and 25 mcg of the LABA vilanterol; or dual inhaled therapy involving either 100 mcg fluticasone furoate plus 25 mcg of vilanterol, or 62.5 mcg of umeclidinium plus 25 mcg of vilanterol.
After 1 year, the rate of moderate to severe COPD exacerbations in the triple-therapy group was 0.91 per year, compared with 1.07 in the fluticasone furoate–vilanterol group and 1.21 in the vilanterol-umeclidinium group. This translated to a 15% reduction with triple therapy compared with fluticasone furoate–vilanterol and a 25% reduction compared with vilanterol-umeclidinium (P less than .001 for both).
When the analysis was limited to severe exacerbations alone, the difference was significant only between the triple therapy, which GSK is marketing as Trelegy Ellipta, and the vilanterol-umeclidinium dual therapy.
Dr. Lipson, of GSK and the University of Pennsylvania, and his coauthors noted that their finding of a greater benefit with the glucocorticoid-containing dual-therapy compared with the LABA-LAMA vilanterol-umeclidinium combination contradicted the findings of the earlier FLAME trial. This was likely due to differences in patient populations and design, as all patients in the FLAME trial had a 1-month run-in treatment with the bronchodilator tiotropium, the researchers explained.
“Therefore any patients who would require an inhaled glucocorticoid may have had an increase in exacerbations and a decrease in lung function during the run-in period and would have been forced to leave the trial,” they wrote.
Patients with higher eosinophil levels seemed to do even better with triple therapy. In those with eosinophil levels of 150 cells per microliter or above, the annual rate of moderate to severe exacerbations was 0.95 with triple therapy, 1.08 with fluticasone furoate–vilanterol, and 1.39 with vilanterol-umeclidinium.
Triple therapy also was associated with a significantly longer time to first event and greater improvements in quality of life, compared with the dual therapies.
Overall, the adverse event profile of triple therapy was similar to that of dual therapy. Contrasting that finding were differences in the incidences of physician-diagnosed pneumonia between the treatment groups. Physician-diagnosed pneumonia was 53% higher among patients who received fluticasone furoate – either in dual or triple therapy combinations. Eight percent of patients in the triple therapy group experienced pneumonia, compared with 7% of patients in the fluticasone furoate–vilanterol group and 5% in the vilanterol-umeclidinium group.
All-cause mortality was significantly lower in patients who received the inhaled glucocorticoid, although the authors said this finding was “fragile” and needed further investigation.
The rate of discontinuation or withdrawal from the trial was 6% for the triple therapy group, 8% for the fluticasone furoate–vilanterol group, and 9% for the vilanterol-umeclidinium group. The rates of serious adverse events in each group were 22%, 21%, and 23%, respectively.
At trial entry, 38% of patients were already receiving triple therapy and 29% were taking an inhaled glucocorticoid. The authors noted that any patients taking an inhaled glucocorticoid who were randomized to the vilanterol-umeclidinium group would have had to abruptly stop taking their inhaled glucocorticoids.
“It is unknown whether the abrupt discontinuation of inhaled glucocorticoids would have contributed to our finding of a lower rate of exacerbations in the inhaled glucocorticoid groups than in the LAMA-LABA group,” they wrote.
Fernando Martinez, MD, chief of the division of pulmonary and critical care medicine at New York–Presbyterian Hospital/Weill Cornell Medical Center, said the study advanced the understanding of COPD management by addressing some key evidence gaps, in a statement issued by GSK.
“By comparing various combinations of effective medications in the same device the study clarifies which type of patient gains greatest benefit from each class of medicine,” Dr Martinez said in the statement. “As many patients experience frequent exacerbations or ‘flare ups,’ which can often result in hospitalization, these data will be highly relevant to patients and clinicians as they consider the optimal treatment.”
The study was funded by GSK, which manufactures Trelegy Ellipta triple therapy for COPD. Eight authors were employees of GSK and two were on advisory boards for the company. Seven authors declared funding from a range of pharmaceutical companies including GSK. One author had no conflicts of interest to declare.
SOURCE: Lipson D et al. N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMoa1713901.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Triple COPD therapy shows fewer exacerbations than does dual therapy.
Major finding: Triple COPD therapy achieves a 15%-25% greater reduction in exacerbations compared with dual therapy.
Study details: Randomized controlled trial of 10,355 patients with symptomatic COPD.
Disclosures: The study was funded by GlaxoSmithKline, which manufactures Trelegy Ellipta triple therapy for COPD. Eight authors were employees of GlaxoSmithKline and two were on advisory boards for the company. Seven authors declared funding from a range of pharmaceutical companies including GlaxoSmithKline. One author had no conflicts of interest to declare.
Source: Lipson D et al. N Engl J Med. 2018 Apr 18. doi: 10.1056/NEJMoa1713901.
Life and health are not even across the U.S.
While U.S. death rates have declined overall, marked geographic disparities exist at the state level in burden of disease, injuries, and risk factors, according to a comprehensive analysis.
Life expectancy varies substantially, for example, ranging from a high of 81.3 years in Hawaii to a low of 74.7 years in Mississippi, according to results from the analysis of data from the Global Burden of Disease (GBD) study (JAMA. 2018;319[14]:1444-72).
Previously decreasing death rates for adults have reversed in 19 states, according to the analysis, which covers the years 1990 to 2016.
Hardest hit were Kentucky, New Mexico, Oklahoma, West Virginia, and Wyoming, which had mortality increases of more than 10% among adults aged 20-55 years. Those increases were largely due to causes such as substance use disorders, self-harm, and cirrhosis, according to the US Burden of Disease Collaborators, who authored the report.
“These findings should be used to examine the causes of health variations and to plan, develop, and implement programs and policies to improve health overall and eliminate disparities in the United States,” the authors wrote.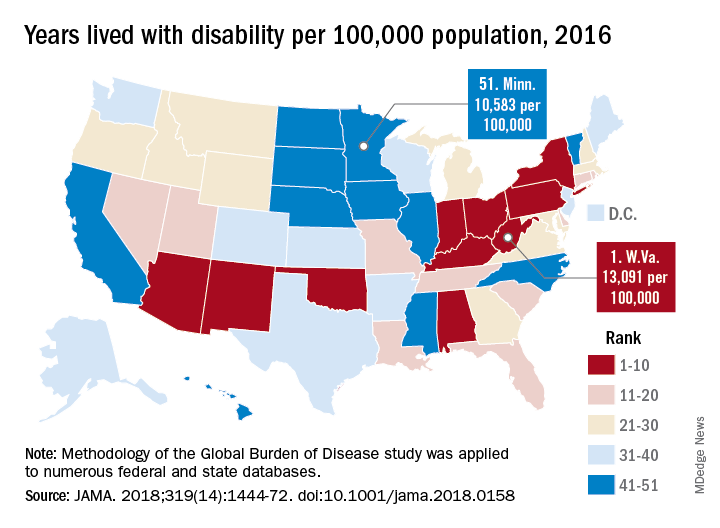
Overall, U.S. death rates have declined from 745.2 per 100,000 persons in 1990 to 578.0 per 100,000 persons in 2016, according to the report.
Likewise, health outcomes throughout the United States have improved over time for some conditions, such as ischemic heart disease, lung cancer, and neonatal preterm complications, the report says.
However, those gains are offset by rising death rates due to drug-use disorders, chronic kidney disease, cirrhosis, chronic obstructive pulmonary disease, hypertension, and self-harm.
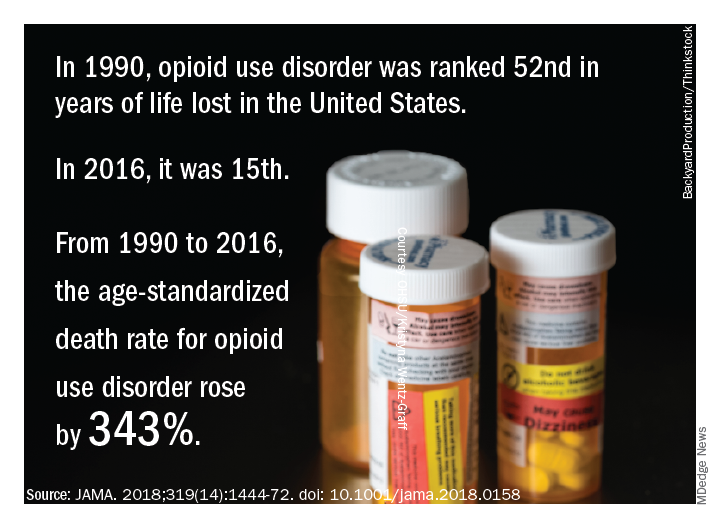
The three most important risk factors in the United States are high body mass index, smoking, and high fasting plasma glucose, the analysis showed. Of those risk factors, only smoking is decreasing, authors noted.
Many risk factors contributing to disparities in burden among states are amenable to medical treatment that emphasizes supportive behavioral and lifestyle changes, according to the authors.
“Expanding health coverage for certain conditions and medications should be considered and adopted to reduce burden,” they said.
Substance abuse disorders, cirrhosis, and self-harm, the causes of the mortality reversal in Kentucky, New Mexico, and other states, could be addressed via a wide range of interventions, according to the investigators.
Prevention programs could address the root causes of substance use and causes of relapse, while physicians can play a “major role” in addiction control through counseling of patients on pain control medication, they said.
Interventions to treat hepatitis C and decrease excessive alcohol consumption could help address cirrhosis, while for self-harm, the most promising approaches focus on restricting access to lethal means, they said, noting that a large proportion of U.S. suicides are due to firearms.
“While multiple strategies are available for dealing with these problems, they have not until very recently garnered attention,” investigators wrote.
The study was supported in part by the National Institute of Environmental Health Sciences and the Bill and Melinda Gates Foundation. Some individual study collaborators reported disclosures related to Savient, Takeda, Crealta/Horizon, Regeneron, Allergan, and others.
SOURCE: The US Burden of Disease Collaborators. JAMA 2018;319(14):1444-72.
This report on Global Burden of Disease (GBD) study data profoundly and powerfully illuminates U.S. health trends over time and by geography. There is much unfinished business for us, nationally and at the state level.
Clinicians and policy makers can use the rankings to evaluate why many individuals are still experiencing injury, disease, and deaths that are preventable; in doing so, the entire nation could move closely resemble a United States of health.
Clinicians could use the results to help guide patients through evidence-based disease prevention and early intervention, a strategy that has led to decreases in death due to cancer and cardiovascular disease over the past few decades.
At the same time, policy makers could use GBD 2016 results to reevaluate current national attitudes toward disease prevention.
Howard K. Koh, MD, MPH, is with the Harvard T.H. Chan School of Public Health, Boston. Anand K. Parekh, MD, MPH, is with the Bipartisan Policy Center in Washington. The comments above are derived from an editorial accompanying the report from the US Burden of Disease Collaborators ( JAMA. 2018;319[14]:1438-40 ). Dr. Koh and Dr. Parekh reported no conflicts of interest related to the editorial.
This report on Global Burden of Disease (GBD) study data profoundly and powerfully illuminates U.S. health trends over time and by geography. There is much unfinished business for us, nationally and at the state level.
Clinicians and policy makers can use the rankings to evaluate why many individuals are still experiencing injury, disease, and deaths that are preventable; in doing so, the entire nation could move closely resemble a United States of health.
Clinicians could use the results to help guide patients through evidence-based disease prevention and early intervention, a strategy that has led to decreases in death due to cancer and cardiovascular disease over the past few decades.
At the same time, policy makers could use GBD 2016 results to reevaluate current national attitudes toward disease prevention.
Howard K. Koh, MD, MPH, is with the Harvard T.H. Chan School of Public Health, Boston. Anand K. Parekh, MD, MPH, is with the Bipartisan Policy Center in Washington. The comments above are derived from an editorial accompanying the report from the US Burden of Disease Collaborators ( JAMA. 2018;319[14]:1438-40 ). Dr. Koh and Dr. Parekh reported no conflicts of interest related to the editorial.
This report on Global Burden of Disease (GBD) study data profoundly and powerfully illuminates U.S. health trends over time and by geography. There is much unfinished business for us, nationally and at the state level.
Clinicians and policy makers can use the rankings to evaluate why many individuals are still experiencing injury, disease, and deaths that are preventable; in doing so, the entire nation could move closely resemble a United States of health.
Clinicians could use the results to help guide patients through evidence-based disease prevention and early intervention, a strategy that has led to decreases in death due to cancer and cardiovascular disease over the past few decades.
At the same time, policy makers could use GBD 2016 results to reevaluate current national attitudes toward disease prevention.
Howard K. Koh, MD, MPH, is with the Harvard T.H. Chan School of Public Health, Boston. Anand K. Parekh, MD, MPH, is with the Bipartisan Policy Center in Washington. The comments above are derived from an editorial accompanying the report from the US Burden of Disease Collaborators ( JAMA. 2018;319[14]:1438-40 ). Dr. Koh and Dr. Parekh reported no conflicts of interest related to the editorial.
While U.S. death rates have declined overall, marked geographic disparities exist at the state level in burden of disease, injuries, and risk factors, according to a comprehensive analysis.
Life expectancy varies substantially, for example, ranging from a high of 81.3 years in Hawaii to a low of 74.7 years in Mississippi, according to results from the analysis of data from the Global Burden of Disease (GBD) study (JAMA. 2018;319[14]:1444-72).
Previously decreasing death rates for adults have reversed in 19 states, according to the analysis, which covers the years 1990 to 2016.
Hardest hit were Kentucky, New Mexico, Oklahoma, West Virginia, and Wyoming, which had mortality increases of more than 10% among adults aged 20-55 years. Those increases were largely due to causes such as substance use disorders, self-harm, and cirrhosis, according to the US Burden of Disease Collaborators, who authored the report.
“These findings should be used to examine the causes of health variations and to plan, develop, and implement programs and policies to improve health overall and eliminate disparities in the United States,” the authors wrote.
Overall, U.S. death rates have declined from 745.2 per 100,000 persons in 1990 to 578.0 per 100,000 persons in 2016, according to the report.
Likewise, health outcomes throughout the United States have improved over time for some conditions, such as ischemic heart disease, lung cancer, and neonatal preterm complications, the report says.
However, those gains are offset by rising death rates due to drug-use disorders, chronic kidney disease, cirrhosis, chronic obstructive pulmonary disease, hypertension, and self-harm.
The three most important risk factors in the United States are high body mass index, smoking, and high fasting plasma glucose, the analysis showed. Of those risk factors, only smoking is decreasing, authors noted.
Many risk factors contributing to disparities in burden among states are amenable to medical treatment that emphasizes supportive behavioral and lifestyle changes, according to the authors.
“Expanding health coverage for certain conditions and medications should be considered and adopted to reduce burden,” they said.
Substance abuse disorders, cirrhosis, and self-harm, the causes of the mortality reversal in Kentucky, New Mexico, and other states, could be addressed via a wide range of interventions, according to the investigators.
Prevention programs could address the root causes of substance use and causes of relapse, while physicians can play a “major role” in addiction control through counseling of patients on pain control medication, they said.
Interventions to treat hepatitis C and decrease excessive alcohol consumption could help address cirrhosis, while for self-harm, the most promising approaches focus on restricting access to lethal means, they said, noting that a large proportion of U.S. suicides are due to firearms.
“While multiple strategies are available for dealing with these problems, they have not until very recently garnered attention,” investigators wrote.
The study was supported in part by the National Institute of Environmental Health Sciences and the Bill and Melinda Gates Foundation. Some individual study collaborators reported disclosures related to Savient, Takeda, Crealta/Horizon, Regeneron, Allergan, and others.
SOURCE: The US Burden of Disease Collaborators. JAMA 2018;319(14):1444-72.
While U.S. death rates have declined overall, marked geographic disparities exist at the state level in burden of disease, injuries, and risk factors, according to a comprehensive analysis.
Life expectancy varies substantially, for example, ranging from a high of 81.3 years in Hawaii to a low of 74.7 years in Mississippi, according to results from the analysis of data from the Global Burden of Disease (GBD) study (JAMA. 2018;319[14]:1444-72).
Previously decreasing death rates for adults have reversed in 19 states, according to the analysis, which covers the years 1990 to 2016.
Hardest hit were Kentucky, New Mexico, Oklahoma, West Virginia, and Wyoming, which had mortality increases of more than 10% among adults aged 20-55 years. Those increases were largely due to causes such as substance use disorders, self-harm, and cirrhosis, according to the US Burden of Disease Collaborators, who authored the report.
“These findings should be used to examine the causes of health variations and to plan, develop, and implement programs and policies to improve health overall and eliminate disparities in the United States,” the authors wrote.
Overall, U.S. death rates have declined from 745.2 per 100,000 persons in 1990 to 578.0 per 100,000 persons in 2016, according to the report.
Likewise, health outcomes throughout the United States have improved over time for some conditions, such as ischemic heart disease, lung cancer, and neonatal preterm complications, the report says.
However, those gains are offset by rising death rates due to drug-use disorders, chronic kidney disease, cirrhosis, chronic obstructive pulmonary disease, hypertension, and self-harm.
The three most important risk factors in the United States are high body mass index, smoking, and high fasting plasma glucose, the analysis showed. Of those risk factors, only smoking is decreasing, authors noted.
Many risk factors contributing to disparities in burden among states are amenable to medical treatment that emphasizes supportive behavioral and lifestyle changes, according to the authors.
“Expanding health coverage for certain conditions and medications should be considered and adopted to reduce burden,” they said.
Substance abuse disorders, cirrhosis, and self-harm, the causes of the mortality reversal in Kentucky, New Mexico, and other states, could be addressed via a wide range of interventions, according to the investigators.
Prevention programs could address the root causes of substance use and causes of relapse, while physicians can play a “major role” in addiction control through counseling of patients on pain control medication, they said.
Interventions to treat hepatitis C and decrease excessive alcohol consumption could help address cirrhosis, while for self-harm, the most promising approaches focus on restricting access to lethal means, they said, noting that a large proportion of U.S. suicides are due to firearms.
“While multiple strategies are available for dealing with these problems, they have not until very recently garnered attention,” investigators wrote.
The study was supported in part by the National Institute of Environmental Health Sciences and the Bill and Melinda Gates Foundation. Some individual study collaborators reported disclosures related to Savient, Takeda, Crealta/Horizon, Regeneron, Allergan, and others.
SOURCE: The US Burden of Disease Collaborators. JAMA 2018;319(14):1444-72.
FROM JAMA
Key clinical point: While U.S. death rates have declined overall, marked geographic disparities exist at the state level in burden of disease, injuries, and risk factors.
Major finding: Life expectancy ranged from a high of 81.3 years in Hawaii to a low of 74.7 years in Mississippi, and previously decreasing death rates for adults have reversed in 19 states.
Study details: A U.S. state-level analysis of results from the Global Burden of Disease (GBD) study illustrating trends in diseases, injuries, risk factors, and deaths from 1990 to 2016.
Disclosures: The study was supported in part by the National Institute of Environmental Health Sciences and the Bill and Melinda Gates Foundation. Study authors reported disclosures related to Savient, Takeda, Crealta/Horizon, Regeneron, Allergan, and others.
Source: The US Burden of Disease Collaborators. JAMA 2018;319(14):1444-1472.