User login
Do new Alzheimer’s drugs get us closer to solving the Alzheimer’s disease riddle?
Two antiamyloid drugs were recently approved by the Food and Drug Administration for treating early-stage Alzheimer’s disease (AD). In trials of both lecanemab (Leqembi) and donanemab, a long-held neuropharmacologic dream was realized: Most amyloid plaques – the primary pathologic marker for AD – were eliminated from the brains of patients with late pre-AD or early AD.
Implications for the amyloid hypothesis
The reduction of amyloid plaques has been argued by many scientists and clinical authorities to be the likely pharmacologic solution for AD. These trials are appropriately viewed as a test of the hypothesis that amyloid bodies are a primary cause of the neurobehavioral symptoms we call AD.
In parallel with that striking reduction in amyloid bodies, drug-treated patients had an initially slower progression of neurobehavioral decline than did placebo-treated control patients. That slowing in symptom progression was accompanied by a modest but statistically significant difference in neurobehavioral ability. After several months in treatment, the rate of decline again paralleled that recorded in the control group. The sustained difference of about a half point on cognitive assessment scores separating treatment and control participants was well short of the 1.5-point difference typically considered clinically significant.
A small number of unexpected and unexplained deaths occurred in the treatment groups. Brain swelling and/or micro-hemorrhages were seen in 20%-30% of treated individuals. Significant brain shrinkage was recorded. These adverse findings are indicative of drug-induced trauma in the target organ for these drugs (i.e., the brain) and were the basis for a boxed warning label for drug usage. Antiamyloid drug treatment was not effective in patients who had higher initial numbers of amyloid plaques, indicating that these drugs would not measurably help the majority of AD patients, who are at more advanced disease stages.
These drugs do not appear to be an “answer” for AD. A modest delay in progression does not mean that we’re on a path to a “cure.” Treatment cost estimates are high – more than $80,000 per year. With requisite PET exams and high copays, patient accessibility issues will be daunting.
Of note, To the contrary, they add strong support for the counterargument that the emergence of amyloid plaques is an effect and not a fundamental cause of that progressive loss of neurologic function that we ultimately define as “Alzheimer’s disease.”
Time to switch gears
The more obvious path to winning the battle against this human scourge is prevention. A recent analysis published in The Lancet argued that about 40% of AD and other dementias are potentially preventable. I disagree. I believe that 80%-90% of prospective cases can be substantially delayed or prevented. Studies have shown that progression to AD or other dementias is driven primarily by the progressive deterioration of organic brain health, expressed by the loss of what psychologists have termed “cognitive reserve.” Cognitive reserve is resilience arising from active brain usage, akin to physical resilience attributable to a physically active life. Scientific studies have shown us that an individual’s cognitive resilience (reserve) is a greater predictor of risk for dementia than are amyloid plaques – indeed, greater than any combination of pathologic markers in dementia patients.
Building up cognitive reserve
It’s increasingly clear to this observer that cognitive reserve is synonymous with organic brain health. The primary factors that underlie cognitive reserve are processing speed in the brain, executive control, response withholding, memory acquisition, reasoning, and attention abilities. Faster, more accurate brains are necessarily more physically optimized. They necessarily sustain brain system connectivity. They are necessarily healthier. Such brains bear a relatively low risk of developing AD or other dementias, just as physically healthier bodies bear a lower risk of being prematurely banished to semi-permanent residence in an easy chair or a bed.
Brain health can be sustained by deploying inexpensive, self-administered, app-based assessments of neurologic performance limits, which inform patients and their medical teams about general brain health status. These assessments can help doctors guide their patients to adopt more intelligent brain-healthy lifestyles, or direct them to the “brain gym” to progressively exercise their brains in ways that contribute to rapid, potentially large-scale, rejuvenating improvements in physical and functional brain health.
Randomized controlled trials incorporating different combinations of physical exercise, diet, and cognitive training have recorded significant improvements in physical and functional neurologic status, indicating substantially advanced brain health. Consistent moderate-to-intense physical exercise, brain- and heart-healthy eating habits, and, particularly, computerized brain training have repeatedly been shown to improve cognitive function and physically rejuvenate the brain. With cognitive training in the right forms, improvements in processing speed and other measures manifest improving brain health and greater safety.
In the National Institutes of Health–funded ACTIVE study with more than 2,800 older adults, just 10-18 hours of a specific speed of processing training (now part of BrainHQ, a program that I was involved in developing) reduced the probability of a progression to dementia over the following 10 years by 29%, and by 48% in those who did the most training.
This approach is several orders of magnitude less expensive than the pricey new AD drugs. It presents less serious issues of accessibility and has no side effects. It delivers far more powerful therapeutic benefits in older normal and at-risk populations.
Sustained wellness supporting prevention is the far more sensible medical way forward to save people from AD and other dementias – at a far lower medical and societal cost.
Dr. Merzenich is professor emeritus, department of neuroscience, University of California, San Francisco. He reported conflicts of interest with Posit Science, Stronger Brains, and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Two antiamyloid drugs were recently approved by the Food and Drug Administration for treating early-stage Alzheimer’s disease (AD). In trials of both lecanemab (Leqembi) and donanemab, a long-held neuropharmacologic dream was realized: Most amyloid plaques – the primary pathologic marker for AD – were eliminated from the brains of patients with late pre-AD or early AD.
Implications for the amyloid hypothesis
The reduction of amyloid plaques has been argued by many scientists and clinical authorities to be the likely pharmacologic solution for AD. These trials are appropriately viewed as a test of the hypothesis that amyloid bodies are a primary cause of the neurobehavioral symptoms we call AD.
In parallel with that striking reduction in amyloid bodies, drug-treated patients had an initially slower progression of neurobehavioral decline than did placebo-treated control patients. That slowing in symptom progression was accompanied by a modest but statistically significant difference in neurobehavioral ability. After several months in treatment, the rate of decline again paralleled that recorded in the control group. The sustained difference of about a half point on cognitive assessment scores separating treatment and control participants was well short of the 1.5-point difference typically considered clinically significant.
A small number of unexpected and unexplained deaths occurred in the treatment groups. Brain swelling and/or micro-hemorrhages were seen in 20%-30% of treated individuals. Significant brain shrinkage was recorded. These adverse findings are indicative of drug-induced trauma in the target organ for these drugs (i.e., the brain) and were the basis for a boxed warning label for drug usage. Antiamyloid drug treatment was not effective in patients who had higher initial numbers of amyloid plaques, indicating that these drugs would not measurably help the majority of AD patients, who are at more advanced disease stages.
These drugs do not appear to be an “answer” for AD. A modest delay in progression does not mean that we’re on a path to a “cure.” Treatment cost estimates are high – more than $80,000 per year. With requisite PET exams and high copays, patient accessibility issues will be daunting.
Of note, To the contrary, they add strong support for the counterargument that the emergence of amyloid plaques is an effect and not a fundamental cause of that progressive loss of neurologic function that we ultimately define as “Alzheimer’s disease.”
Time to switch gears
The more obvious path to winning the battle against this human scourge is prevention. A recent analysis published in The Lancet argued that about 40% of AD and other dementias are potentially preventable. I disagree. I believe that 80%-90% of prospective cases can be substantially delayed or prevented. Studies have shown that progression to AD or other dementias is driven primarily by the progressive deterioration of organic brain health, expressed by the loss of what psychologists have termed “cognitive reserve.” Cognitive reserve is resilience arising from active brain usage, akin to physical resilience attributable to a physically active life. Scientific studies have shown us that an individual’s cognitive resilience (reserve) is a greater predictor of risk for dementia than are amyloid plaques – indeed, greater than any combination of pathologic markers in dementia patients.
Building up cognitive reserve
It’s increasingly clear to this observer that cognitive reserve is synonymous with organic brain health. The primary factors that underlie cognitive reserve are processing speed in the brain, executive control, response withholding, memory acquisition, reasoning, and attention abilities. Faster, more accurate brains are necessarily more physically optimized. They necessarily sustain brain system connectivity. They are necessarily healthier. Such brains bear a relatively low risk of developing AD or other dementias, just as physically healthier bodies bear a lower risk of being prematurely banished to semi-permanent residence in an easy chair or a bed.
Brain health can be sustained by deploying inexpensive, self-administered, app-based assessments of neurologic performance limits, which inform patients and their medical teams about general brain health status. These assessments can help doctors guide their patients to adopt more intelligent brain-healthy lifestyles, or direct them to the “brain gym” to progressively exercise their brains in ways that contribute to rapid, potentially large-scale, rejuvenating improvements in physical and functional brain health.
Randomized controlled trials incorporating different combinations of physical exercise, diet, and cognitive training have recorded significant improvements in physical and functional neurologic status, indicating substantially advanced brain health. Consistent moderate-to-intense physical exercise, brain- and heart-healthy eating habits, and, particularly, computerized brain training have repeatedly been shown to improve cognitive function and physically rejuvenate the brain. With cognitive training in the right forms, improvements in processing speed and other measures manifest improving brain health and greater safety.
In the National Institutes of Health–funded ACTIVE study with more than 2,800 older adults, just 10-18 hours of a specific speed of processing training (now part of BrainHQ, a program that I was involved in developing) reduced the probability of a progression to dementia over the following 10 years by 29%, and by 48% in those who did the most training.
This approach is several orders of magnitude less expensive than the pricey new AD drugs. It presents less serious issues of accessibility and has no side effects. It delivers far more powerful therapeutic benefits in older normal and at-risk populations.
Sustained wellness supporting prevention is the far more sensible medical way forward to save people from AD and other dementias – at a far lower medical and societal cost.
Dr. Merzenich is professor emeritus, department of neuroscience, University of California, San Francisco. He reported conflicts of interest with Posit Science, Stronger Brains, and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Two antiamyloid drugs were recently approved by the Food and Drug Administration for treating early-stage Alzheimer’s disease (AD). In trials of both lecanemab (Leqembi) and donanemab, a long-held neuropharmacologic dream was realized: Most amyloid plaques – the primary pathologic marker for AD – were eliminated from the brains of patients with late pre-AD or early AD.
Implications for the amyloid hypothesis
The reduction of amyloid plaques has been argued by many scientists and clinical authorities to be the likely pharmacologic solution for AD. These trials are appropriately viewed as a test of the hypothesis that amyloid bodies are a primary cause of the neurobehavioral symptoms we call AD.
In parallel with that striking reduction in amyloid bodies, drug-treated patients had an initially slower progression of neurobehavioral decline than did placebo-treated control patients. That slowing in symptom progression was accompanied by a modest but statistically significant difference in neurobehavioral ability. After several months in treatment, the rate of decline again paralleled that recorded in the control group. The sustained difference of about a half point on cognitive assessment scores separating treatment and control participants was well short of the 1.5-point difference typically considered clinically significant.
A small number of unexpected and unexplained deaths occurred in the treatment groups. Brain swelling and/or micro-hemorrhages were seen in 20%-30% of treated individuals. Significant brain shrinkage was recorded. These adverse findings are indicative of drug-induced trauma in the target organ for these drugs (i.e., the brain) and were the basis for a boxed warning label for drug usage. Antiamyloid drug treatment was not effective in patients who had higher initial numbers of amyloid plaques, indicating that these drugs would not measurably help the majority of AD patients, who are at more advanced disease stages.
These drugs do not appear to be an “answer” for AD. A modest delay in progression does not mean that we’re on a path to a “cure.” Treatment cost estimates are high – more than $80,000 per year. With requisite PET exams and high copays, patient accessibility issues will be daunting.
Of note, To the contrary, they add strong support for the counterargument that the emergence of amyloid plaques is an effect and not a fundamental cause of that progressive loss of neurologic function that we ultimately define as “Alzheimer’s disease.”
Time to switch gears
The more obvious path to winning the battle against this human scourge is prevention. A recent analysis published in The Lancet argued that about 40% of AD and other dementias are potentially preventable. I disagree. I believe that 80%-90% of prospective cases can be substantially delayed or prevented. Studies have shown that progression to AD or other dementias is driven primarily by the progressive deterioration of organic brain health, expressed by the loss of what psychologists have termed “cognitive reserve.” Cognitive reserve is resilience arising from active brain usage, akin to physical resilience attributable to a physically active life. Scientific studies have shown us that an individual’s cognitive resilience (reserve) is a greater predictor of risk for dementia than are amyloid plaques – indeed, greater than any combination of pathologic markers in dementia patients.
Building up cognitive reserve
It’s increasingly clear to this observer that cognitive reserve is synonymous with organic brain health. The primary factors that underlie cognitive reserve are processing speed in the brain, executive control, response withholding, memory acquisition, reasoning, and attention abilities. Faster, more accurate brains are necessarily more physically optimized. They necessarily sustain brain system connectivity. They are necessarily healthier. Such brains bear a relatively low risk of developing AD or other dementias, just as physically healthier bodies bear a lower risk of being prematurely banished to semi-permanent residence in an easy chair or a bed.
Brain health can be sustained by deploying inexpensive, self-administered, app-based assessments of neurologic performance limits, which inform patients and their medical teams about general brain health status. These assessments can help doctors guide their patients to adopt more intelligent brain-healthy lifestyles, or direct them to the “brain gym” to progressively exercise their brains in ways that contribute to rapid, potentially large-scale, rejuvenating improvements in physical and functional brain health.
Randomized controlled trials incorporating different combinations of physical exercise, diet, and cognitive training have recorded significant improvements in physical and functional neurologic status, indicating substantially advanced brain health. Consistent moderate-to-intense physical exercise, brain- and heart-healthy eating habits, and, particularly, computerized brain training have repeatedly been shown to improve cognitive function and physically rejuvenate the brain. With cognitive training in the right forms, improvements in processing speed and other measures manifest improving brain health and greater safety.
In the National Institutes of Health–funded ACTIVE study with more than 2,800 older adults, just 10-18 hours of a specific speed of processing training (now part of BrainHQ, a program that I was involved in developing) reduced the probability of a progression to dementia over the following 10 years by 29%, and by 48% in those who did the most training.
This approach is several orders of magnitude less expensive than the pricey new AD drugs. It presents less serious issues of accessibility and has no side effects. It delivers far more powerful therapeutic benefits in older normal and at-risk populations.
Sustained wellness supporting prevention is the far more sensible medical way forward to save people from AD and other dementias – at a far lower medical and societal cost.
Dr. Merzenich is professor emeritus, department of neuroscience, University of California, San Francisco. He reported conflicts of interest with Posit Science, Stronger Brains, and the National Institutes of Health.
A version of this article first appeared on Medscape.com.
Loneliness tied to increased risk for Parkinson’s disease
TOPLINE:
Loneliness is associated with a higher risk of developing Parkinson’s disease (PD) across demographic groups and independent of other risk factors, data from nearly 500,000 U.K. adults suggest.
METHODOLOGY:
- Loneliness is associated with illness and death, including higher risk of neurodegenerative diseases, but no study has examined whether the association between loneliness and detrimental outcomes extends to PD.
- The current analysis included 491,603 U.K. Biobank participants (mean age, 56; 54% women) without a diagnosis of PD at baseline.
- Loneliness was assessed by a single question at baseline and incident PD was ascertained via health records over 15 years.
- Researchers assessed whether the association between loneliness and PD was moderated by age, sex, or genetic risk and whether the association was accounted for by sociodemographic factors; behavioral, mental, physical, or social factors; or genetic risk.
TAKEAWAY:
- Roughly 19% of the cohort reported being lonely. Compared with those who were not lonely, those who did report being lonely were slightly younger and were more likely to be women. They also had fewer resources, more health risk behaviors (current smoker and physically inactive), and worse physical and mental health.
- Over 15+ years of follow-up, 2,822 participants developed PD (incidence rate: 47 per 100,000 person-years). Compared with those who did not develop PD, those who did were older and more likely to be male, former smokers, have higher BMI and PD polygenetic risk score, and to have diabetes, hypertension, myocardial infarction or stroke, anxiety, or depression.
- In the primary analysis, individuals who reported being lonely had a higher risk for PD (hazard ratio, 1.37) – an association that remained after accounting for demographic and socioeconomic status, social isolation, PD polygenetic risk score, smoking, physical activity, BMI, diabetes, hypertension, stroke, myocardial infarction, depression, and having ever seen a psychiatrist (fully adjusted HR, 1.25).
- The association between loneliness and incident PD was not moderated by sex, age, or polygenetic risk score.
- Contrary to expectations for a prodromal syndrome, loneliness was not associated with incident PD in the first 5 years after baseline but was associated with PD risk in the subsequent 10 years of follow-up (HR, 1.32).
IN PRACTICE:
“Our findings complement other evidence that loneliness is a psychosocial determinant of health associated with increased risk of morbidity and mortality [and] supports recent calls for the protective and healing effects of personally meaningful social connection,” the authors write.
SOURCE:
The study, with first author Antonio Terracciano, PhD, of Florida State University College of Medicine, Tallahassee, was published online in JAMA Neurology.
LIMITATIONS:
This observational study could not determine causality or whether reverse causality could explain the association. Loneliness was assessed by a single yes/no question. PD diagnosis relied on hospital admission and death records and may have missed early PD diagnoses.
DISCLOSURES:
Funding for the study was provided by the National Institutes of Health and National Institute on Aging. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
Loneliness is associated with a higher risk of developing Parkinson’s disease (PD) across demographic groups and independent of other risk factors, data from nearly 500,000 U.K. adults suggest.
METHODOLOGY:
- Loneliness is associated with illness and death, including higher risk of neurodegenerative diseases, but no study has examined whether the association between loneliness and detrimental outcomes extends to PD.
- The current analysis included 491,603 U.K. Biobank participants (mean age, 56; 54% women) without a diagnosis of PD at baseline.
- Loneliness was assessed by a single question at baseline and incident PD was ascertained via health records over 15 years.
- Researchers assessed whether the association between loneliness and PD was moderated by age, sex, or genetic risk and whether the association was accounted for by sociodemographic factors; behavioral, mental, physical, or social factors; or genetic risk.
TAKEAWAY:
- Roughly 19% of the cohort reported being lonely. Compared with those who were not lonely, those who did report being lonely were slightly younger and were more likely to be women. They also had fewer resources, more health risk behaviors (current smoker and physically inactive), and worse physical and mental health.
- Over 15+ years of follow-up, 2,822 participants developed PD (incidence rate: 47 per 100,000 person-years). Compared with those who did not develop PD, those who did were older and more likely to be male, former smokers, have higher BMI and PD polygenetic risk score, and to have diabetes, hypertension, myocardial infarction or stroke, anxiety, or depression.
- In the primary analysis, individuals who reported being lonely had a higher risk for PD (hazard ratio, 1.37) – an association that remained after accounting for demographic and socioeconomic status, social isolation, PD polygenetic risk score, smoking, physical activity, BMI, diabetes, hypertension, stroke, myocardial infarction, depression, and having ever seen a psychiatrist (fully adjusted HR, 1.25).
- The association between loneliness and incident PD was not moderated by sex, age, or polygenetic risk score.
- Contrary to expectations for a prodromal syndrome, loneliness was not associated with incident PD in the first 5 years after baseline but was associated with PD risk in the subsequent 10 years of follow-up (HR, 1.32).
IN PRACTICE:
“Our findings complement other evidence that loneliness is a psychosocial determinant of health associated with increased risk of morbidity and mortality [and] supports recent calls for the protective and healing effects of personally meaningful social connection,” the authors write.
SOURCE:
The study, with first author Antonio Terracciano, PhD, of Florida State University College of Medicine, Tallahassee, was published online in JAMA Neurology.
LIMITATIONS:
This observational study could not determine causality or whether reverse causality could explain the association. Loneliness was assessed by a single yes/no question. PD diagnosis relied on hospital admission and death records and may have missed early PD diagnoses.
DISCLOSURES:
Funding for the study was provided by the National Institutes of Health and National Institute on Aging. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
TOPLINE:
Loneliness is associated with a higher risk of developing Parkinson’s disease (PD) across demographic groups and independent of other risk factors, data from nearly 500,000 U.K. adults suggest.
METHODOLOGY:
- Loneliness is associated with illness and death, including higher risk of neurodegenerative diseases, but no study has examined whether the association between loneliness and detrimental outcomes extends to PD.
- The current analysis included 491,603 U.K. Biobank participants (mean age, 56; 54% women) without a diagnosis of PD at baseline.
- Loneliness was assessed by a single question at baseline and incident PD was ascertained via health records over 15 years.
- Researchers assessed whether the association between loneliness and PD was moderated by age, sex, or genetic risk and whether the association was accounted for by sociodemographic factors; behavioral, mental, physical, or social factors; or genetic risk.
TAKEAWAY:
- Roughly 19% of the cohort reported being lonely. Compared with those who were not lonely, those who did report being lonely were slightly younger and were more likely to be women. They also had fewer resources, more health risk behaviors (current smoker and physically inactive), and worse physical and mental health.
- Over 15+ years of follow-up, 2,822 participants developed PD (incidence rate: 47 per 100,000 person-years). Compared with those who did not develop PD, those who did were older and more likely to be male, former smokers, have higher BMI and PD polygenetic risk score, and to have diabetes, hypertension, myocardial infarction or stroke, anxiety, or depression.
- In the primary analysis, individuals who reported being lonely had a higher risk for PD (hazard ratio, 1.37) – an association that remained after accounting for demographic and socioeconomic status, social isolation, PD polygenetic risk score, smoking, physical activity, BMI, diabetes, hypertension, stroke, myocardial infarction, depression, and having ever seen a psychiatrist (fully adjusted HR, 1.25).
- The association between loneliness and incident PD was not moderated by sex, age, or polygenetic risk score.
- Contrary to expectations for a prodromal syndrome, loneliness was not associated with incident PD in the first 5 years after baseline but was associated with PD risk in the subsequent 10 years of follow-up (HR, 1.32).
IN PRACTICE:
“Our findings complement other evidence that loneliness is a psychosocial determinant of health associated with increased risk of morbidity and mortality [and] supports recent calls for the protective and healing effects of personally meaningful social connection,” the authors write.
SOURCE:
The study, with first author Antonio Terracciano, PhD, of Florida State University College of Medicine, Tallahassee, was published online in JAMA Neurology.
LIMITATIONS:
This observational study could not determine causality or whether reverse causality could explain the association. Loneliness was assessed by a single yes/no question. PD diagnosis relied on hospital admission and death records and may have missed early PD diagnoses.
DISCLOSURES:
Funding for the study was provided by the National Institutes of Health and National Institute on Aging. The authors report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Decoding AFib recurrence: PCPs’ role in personalized care
One in three patients who experience their first bout of atrial fibrillation (AFib) during hospitalization can expect to experience a recurrence of the arrhythmia within the year, new research shows.
The findings, reported in Annals of Internal Medicine, suggest these patients may be good candidates for oral anticoagulants to reduce their risk for stroke.
“Atrial fibrillation is very common in patients for the very first time in their life when they’re sick and in the hospital,” said William F. McIntyre, MD, PhD, a cardiologist at McMaster University, Hamilton, Ont., who led the study. These new insights into AFib management suggest there is a need for primary care physicians to be on the lookout for potential recurrence.
AFib is strongly linked to stroke, and patients at greater risk for stroke may be prescribed oral anticoagulants. Although the arrhythmia can be reversed before the patient is discharged from the hospital, risk for recurrence was unclear, Dr. McIntyre said.
“We wanted to know if the patient was in atrial fibrillation because of the physiologic stress that they were under, or if they just have the disease called atrial fibrillation, which should usually be followed lifelong by a specialist,” Dr. McIntyre said.
Dr. McIntyre and colleagues followed 139 patients (mean age, 71 years) at three medical centers in Ontario who experienced new-onset AFib during their hospital stay, along with an equal number of patients who had no history of AFib and who served as controls. The research team used a Holter monitor to record study participants’ heart rhythm for 14 days to detect incident AFib at 1 and 6 months after discharge. They also followed up with periodic phone calls for up to 12 months. Among the study participants, half were admitted for noncardiac surgeries, and the other half were admitted for medical illnesses, including infections and pneumonia. Participants with a prior history of AFib were excluded from the analysis.
The primary outcome of the study was an episode of AFib that lasted at least 30 seconds on the monitor or one detected during routine care at the 12-month mark.
Patients who experienced AFib for the first time in the hospital had roughly a 33% risk for recurrence within a year, nearly sevenfold higher than their age- and sex-matched counterparts who had not had an arrhythmia during their hospital stay (3%; confidence interval, 0%-6.4%).
“This study has important implications for management of patients who have a first presentation of AFib that is concurrent with a reversible physiologic stressor,” the authors wrote. “An AFib recurrence risk of 33.1% at 1 year is neither low enough to conclude that transient new-onset AFib in the setting of another illness is benign nor high enough that all such transient new-onset AFib can be assumed to be paroxysmal AFib. Instead, these results call for risk stratification and follow-up in these patients.”
The researchers reported that among people with recurrent AFib in the study, the median total time in arrhythmia was 9 hours. “This far exceeds the cutoff of 6 minutes that was established as being associated with stroke using simulated AFib screening in patients with implanted continuous monitors,” they wrote. “These results suggest that the patients in our study who had AFib detected in follow-up are similar to contemporary patients with AFib for whom evidence-based therapies, including oral anticoagulation, are warranted.”
Dr. McIntyre and colleagues were able to track outcomes and treatments for the patients in the study. In the group with recurrent AFib, 1 had a stroke, 2 experienced systemic embolism, 3 had a heart failure event, 6 experienced bleeding, and 11 died. In the other group, there was one case of stroke, one of heart failure, four cases involving bleeding, and seven deaths. “The proportion of participants with new-onset AFib during their initial hospitalization who were taking oral anticoagulants was 47.1% at 6 months and 49.2% at 12 months. This included 73% of participants with AFib detected during follow-up and 39% who did not have AFib detected during follow-up,” they wrote.
The uncertain nature of AFib recurrence complicates predictions about patients’ posthospitalization experiences within the following year. “We cannot just say: ‘Hey, this is just a reversible illness, and now we can forget about it,’ ” Dr. McIntyre said. “Nor is the risk of recurrence so strong in the other direction that you can give patients a lifelong diagnosis of atrial fibrillation.”
Role for primary care
Without that certainty, physicians cannot refer everyone who experiences new-onset AFib to a cardiologist for long-term care. The variability in recurrence rates necessitates a more nuanced and personalized approach. Here, primary care physicians step in, offering tailored care based on their established, long-term patient relationships, Dr. McIntyre said.
The study participants already have chronic health conditions that bring them into regular contact with their family physician. This gives primary care physicians a golden opportunity to be on lookout and to recommend care from a cardiologist at the appropriate time if it becomes necessary, he said.
“I have certainly seen cases of recurrent atrial fibrillation in patients who had an episode while hospitalized, and consistent with this study, this is a common clinical occurrence,” said Deepak L. Bhatt, MD, MPH, director of Mount Sinai Heart, New York. Primary care physicians must remain vigilant and avoid the temptation to attribute AFib solely to illness or surgery
“Ideally, we would have randomized clinical trial data to guide the decision about whether to use prophylactic anticoagulation,” said Dr. Bhatt, who added that a cardiology consultation may also be appropriate.
Dr. McIntyre reported no relevant financial relationships. Dr. Bhatt reported numerous relationships with industry.
A version of this article appeared on Medscape.com.
One in three patients who experience their first bout of atrial fibrillation (AFib) during hospitalization can expect to experience a recurrence of the arrhythmia within the year, new research shows.
The findings, reported in Annals of Internal Medicine, suggest these patients may be good candidates for oral anticoagulants to reduce their risk for stroke.
“Atrial fibrillation is very common in patients for the very first time in their life when they’re sick and in the hospital,” said William F. McIntyre, MD, PhD, a cardiologist at McMaster University, Hamilton, Ont., who led the study. These new insights into AFib management suggest there is a need for primary care physicians to be on the lookout for potential recurrence.
AFib is strongly linked to stroke, and patients at greater risk for stroke may be prescribed oral anticoagulants. Although the arrhythmia can be reversed before the patient is discharged from the hospital, risk for recurrence was unclear, Dr. McIntyre said.
“We wanted to know if the patient was in atrial fibrillation because of the physiologic stress that they were under, or if they just have the disease called atrial fibrillation, which should usually be followed lifelong by a specialist,” Dr. McIntyre said.
Dr. McIntyre and colleagues followed 139 patients (mean age, 71 years) at three medical centers in Ontario who experienced new-onset AFib during their hospital stay, along with an equal number of patients who had no history of AFib and who served as controls. The research team used a Holter monitor to record study participants’ heart rhythm for 14 days to detect incident AFib at 1 and 6 months after discharge. They also followed up with periodic phone calls for up to 12 months. Among the study participants, half were admitted for noncardiac surgeries, and the other half were admitted for medical illnesses, including infections and pneumonia. Participants with a prior history of AFib were excluded from the analysis.
The primary outcome of the study was an episode of AFib that lasted at least 30 seconds on the monitor or one detected during routine care at the 12-month mark.
Patients who experienced AFib for the first time in the hospital had roughly a 33% risk for recurrence within a year, nearly sevenfold higher than their age- and sex-matched counterparts who had not had an arrhythmia during their hospital stay (3%; confidence interval, 0%-6.4%).
“This study has important implications for management of patients who have a first presentation of AFib that is concurrent with a reversible physiologic stressor,” the authors wrote. “An AFib recurrence risk of 33.1% at 1 year is neither low enough to conclude that transient new-onset AFib in the setting of another illness is benign nor high enough that all such transient new-onset AFib can be assumed to be paroxysmal AFib. Instead, these results call for risk stratification and follow-up in these patients.”
The researchers reported that among people with recurrent AFib in the study, the median total time in arrhythmia was 9 hours. “This far exceeds the cutoff of 6 minutes that was established as being associated with stroke using simulated AFib screening in patients with implanted continuous monitors,” they wrote. “These results suggest that the patients in our study who had AFib detected in follow-up are similar to contemporary patients with AFib for whom evidence-based therapies, including oral anticoagulation, are warranted.”
Dr. McIntyre and colleagues were able to track outcomes and treatments for the patients in the study. In the group with recurrent AFib, 1 had a stroke, 2 experienced systemic embolism, 3 had a heart failure event, 6 experienced bleeding, and 11 died. In the other group, there was one case of stroke, one of heart failure, four cases involving bleeding, and seven deaths. “The proportion of participants with new-onset AFib during their initial hospitalization who were taking oral anticoagulants was 47.1% at 6 months and 49.2% at 12 months. This included 73% of participants with AFib detected during follow-up and 39% who did not have AFib detected during follow-up,” they wrote.
The uncertain nature of AFib recurrence complicates predictions about patients’ posthospitalization experiences within the following year. “We cannot just say: ‘Hey, this is just a reversible illness, and now we can forget about it,’ ” Dr. McIntyre said. “Nor is the risk of recurrence so strong in the other direction that you can give patients a lifelong diagnosis of atrial fibrillation.”
Role for primary care
Without that certainty, physicians cannot refer everyone who experiences new-onset AFib to a cardiologist for long-term care. The variability in recurrence rates necessitates a more nuanced and personalized approach. Here, primary care physicians step in, offering tailored care based on their established, long-term patient relationships, Dr. McIntyre said.
The study participants already have chronic health conditions that bring them into regular contact with their family physician. This gives primary care physicians a golden opportunity to be on lookout and to recommend care from a cardiologist at the appropriate time if it becomes necessary, he said.
“I have certainly seen cases of recurrent atrial fibrillation in patients who had an episode while hospitalized, and consistent with this study, this is a common clinical occurrence,” said Deepak L. Bhatt, MD, MPH, director of Mount Sinai Heart, New York. Primary care physicians must remain vigilant and avoid the temptation to attribute AFib solely to illness or surgery
“Ideally, we would have randomized clinical trial data to guide the decision about whether to use prophylactic anticoagulation,” said Dr. Bhatt, who added that a cardiology consultation may also be appropriate.
Dr. McIntyre reported no relevant financial relationships. Dr. Bhatt reported numerous relationships with industry.
A version of this article appeared on Medscape.com.
One in three patients who experience their first bout of atrial fibrillation (AFib) during hospitalization can expect to experience a recurrence of the arrhythmia within the year, new research shows.
The findings, reported in Annals of Internal Medicine, suggest these patients may be good candidates for oral anticoagulants to reduce their risk for stroke.
“Atrial fibrillation is very common in patients for the very first time in their life when they’re sick and in the hospital,” said William F. McIntyre, MD, PhD, a cardiologist at McMaster University, Hamilton, Ont., who led the study. These new insights into AFib management suggest there is a need for primary care physicians to be on the lookout for potential recurrence.
AFib is strongly linked to stroke, and patients at greater risk for stroke may be prescribed oral anticoagulants. Although the arrhythmia can be reversed before the patient is discharged from the hospital, risk for recurrence was unclear, Dr. McIntyre said.
“We wanted to know if the patient was in atrial fibrillation because of the physiologic stress that they were under, or if they just have the disease called atrial fibrillation, which should usually be followed lifelong by a specialist,” Dr. McIntyre said.
Dr. McIntyre and colleagues followed 139 patients (mean age, 71 years) at three medical centers in Ontario who experienced new-onset AFib during their hospital stay, along with an equal number of patients who had no history of AFib and who served as controls. The research team used a Holter monitor to record study participants’ heart rhythm for 14 days to detect incident AFib at 1 and 6 months after discharge. They also followed up with periodic phone calls for up to 12 months. Among the study participants, half were admitted for noncardiac surgeries, and the other half were admitted for medical illnesses, including infections and pneumonia. Participants with a prior history of AFib were excluded from the analysis.
The primary outcome of the study was an episode of AFib that lasted at least 30 seconds on the monitor or one detected during routine care at the 12-month mark.
Patients who experienced AFib for the first time in the hospital had roughly a 33% risk for recurrence within a year, nearly sevenfold higher than their age- and sex-matched counterparts who had not had an arrhythmia during their hospital stay (3%; confidence interval, 0%-6.4%).
“This study has important implications for management of patients who have a first presentation of AFib that is concurrent with a reversible physiologic stressor,” the authors wrote. “An AFib recurrence risk of 33.1% at 1 year is neither low enough to conclude that transient new-onset AFib in the setting of another illness is benign nor high enough that all such transient new-onset AFib can be assumed to be paroxysmal AFib. Instead, these results call for risk stratification and follow-up in these patients.”
The researchers reported that among people with recurrent AFib in the study, the median total time in arrhythmia was 9 hours. “This far exceeds the cutoff of 6 minutes that was established as being associated with stroke using simulated AFib screening in patients with implanted continuous monitors,” they wrote. “These results suggest that the patients in our study who had AFib detected in follow-up are similar to contemporary patients with AFib for whom evidence-based therapies, including oral anticoagulation, are warranted.”
Dr. McIntyre and colleagues were able to track outcomes and treatments for the patients in the study. In the group with recurrent AFib, 1 had a stroke, 2 experienced systemic embolism, 3 had a heart failure event, 6 experienced bleeding, and 11 died. In the other group, there was one case of stroke, one of heart failure, four cases involving bleeding, and seven deaths. “The proportion of participants with new-onset AFib during their initial hospitalization who were taking oral anticoagulants was 47.1% at 6 months and 49.2% at 12 months. This included 73% of participants with AFib detected during follow-up and 39% who did not have AFib detected during follow-up,” they wrote.
The uncertain nature of AFib recurrence complicates predictions about patients’ posthospitalization experiences within the following year. “We cannot just say: ‘Hey, this is just a reversible illness, and now we can forget about it,’ ” Dr. McIntyre said. “Nor is the risk of recurrence so strong in the other direction that you can give patients a lifelong diagnosis of atrial fibrillation.”
Role for primary care
Without that certainty, physicians cannot refer everyone who experiences new-onset AFib to a cardiologist for long-term care. The variability in recurrence rates necessitates a more nuanced and personalized approach. Here, primary care physicians step in, offering tailored care based on their established, long-term patient relationships, Dr. McIntyre said.
The study participants already have chronic health conditions that bring them into regular contact with their family physician. This gives primary care physicians a golden opportunity to be on lookout and to recommend care from a cardiologist at the appropriate time if it becomes necessary, he said.
“I have certainly seen cases of recurrent atrial fibrillation in patients who had an episode while hospitalized, and consistent with this study, this is a common clinical occurrence,” said Deepak L. Bhatt, MD, MPH, director of Mount Sinai Heart, New York. Primary care physicians must remain vigilant and avoid the temptation to attribute AFib solely to illness or surgery
“Ideally, we would have randomized clinical trial data to guide the decision about whether to use prophylactic anticoagulation,” said Dr. Bhatt, who added that a cardiology consultation may also be appropriate.
Dr. McIntyre reported no relevant financial relationships. Dr. Bhatt reported numerous relationships with industry.
A version of this article appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Support tool reduces hypoglycemia risk in type 2 diabetes
TOPLINE:
Use of a novel clinical-decision support tool and shared decision-making in elderly patients with type 2 diabetes managed in a primary care practice and at high risk for hypoglycemic episodes led to a 46% decrease in the number of at-risk patients and discontinuation of hypoglycemic agents in 20% in a prospective, 6-month, single-arm study with 94 patients.
METHODOLOGY:
- The HypoPrevent study enrolled 94 people from a Pennsylvania primary care practice who were at least 65 years old with type 2 diabetes and at risk for hypoglycemia because of treatment with insulin or sulfonylureas, and having a hemoglobin A1c of less than 7.0%.
- Clinicians and patients used a newly devised hypoglycemia reduction clinical-decision support tool developed by the Endocrine Society and a health care consulting company to help guide shared decision-making for a goal A1c level, potential changes to treatment, and other steps to reduce the risk of hypoglycemia.
- Primary outcomes during 6-month follow-up were impact of the intervention on A1c, changes in use of insulin or sulfonylureas, change in the number of study patients at risk for hypoglycemia, and impact on the incidence of nonsevere hypoglycemic events (NSHEs) measured with the Treatment-Related Impact Measure–Non-severe Hypoglycemic Events (TRIM-HYPO) survey.
TAKEAWAY:
- Patients averaged 74 years old, 57% were women, 95% were White, 61% had diabetes for more than 10 years, 48% had chronic kidney disease, 51% were on insulin, 47% on a sulfonylurea, and 80 of the 94 enrolled patients completed all three study visits.
- Nineteen patients (20%) reduced their dose of or discontinued insulin or sulfonylurea.
- In patients with both baseline and follow-up A1c measures, A1c rose from 6.29% at baseline to 6.82%.
- Fifty patients set an A1c goal and had a timely follow-up A1c measurement, and in this subgroup the number of patients at risk for hypoglycemia decreased by 46%, a significant change.
- Patients who reported at least one NSHE at baseline had a significant reduction between the baseline survey and follow-up visits in both the total score as well as each of the five scored domains.
IN PRACTICE:
The HypoPrevent study results with positive results,” concluded the researchers in their report.
SOURCE:
The HypoPrevent study was funded and organized by the Endocrine Society in collaboration with a multicenter team of researchers. The report appeared in the Journal of the American Geriatrics Society.
LIMITATIONS:
Lack of a control group makes it impossible to conclusively determine whether the intervention led to the observed increases in A1c levels, nor can the study exclude regression to the mean as the cause for lowered A1c levels.
DISCLOSURES:
The study received funding from Abbott, Lilly, Merck, Novo Nordisk, and Sanofi. Two coauthors had individual disclosures listed in the report; the other six coauthors had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
Use of a novel clinical-decision support tool and shared decision-making in elderly patients with type 2 diabetes managed in a primary care practice and at high risk for hypoglycemic episodes led to a 46% decrease in the number of at-risk patients and discontinuation of hypoglycemic agents in 20% in a prospective, 6-month, single-arm study with 94 patients.
METHODOLOGY:
- The HypoPrevent study enrolled 94 people from a Pennsylvania primary care practice who were at least 65 years old with type 2 diabetes and at risk for hypoglycemia because of treatment with insulin or sulfonylureas, and having a hemoglobin A1c of less than 7.0%.
- Clinicians and patients used a newly devised hypoglycemia reduction clinical-decision support tool developed by the Endocrine Society and a health care consulting company to help guide shared decision-making for a goal A1c level, potential changes to treatment, and other steps to reduce the risk of hypoglycemia.
- Primary outcomes during 6-month follow-up were impact of the intervention on A1c, changes in use of insulin or sulfonylureas, change in the number of study patients at risk for hypoglycemia, and impact on the incidence of nonsevere hypoglycemic events (NSHEs) measured with the Treatment-Related Impact Measure–Non-severe Hypoglycemic Events (TRIM-HYPO) survey.
TAKEAWAY:
- Patients averaged 74 years old, 57% were women, 95% were White, 61% had diabetes for more than 10 years, 48% had chronic kidney disease, 51% were on insulin, 47% on a sulfonylurea, and 80 of the 94 enrolled patients completed all three study visits.
- Nineteen patients (20%) reduced their dose of or discontinued insulin or sulfonylurea.
- In patients with both baseline and follow-up A1c measures, A1c rose from 6.29% at baseline to 6.82%.
- Fifty patients set an A1c goal and had a timely follow-up A1c measurement, and in this subgroup the number of patients at risk for hypoglycemia decreased by 46%, a significant change.
- Patients who reported at least one NSHE at baseline had a significant reduction between the baseline survey and follow-up visits in both the total score as well as each of the five scored domains.
IN PRACTICE:
The HypoPrevent study results with positive results,” concluded the researchers in their report.
SOURCE:
The HypoPrevent study was funded and organized by the Endocrine Society in collaboration with a multicenter team of researchers. The report appeared in the Journal of the American Geriatrics Society.
LIMITATIONS:
Lack of a control group makes it impossible to conclusively determine whether the intervention led to the observed increases in A1c levels, nor can the study exclude regression to the mean as the cause for lowered A1c levels.
DISCLOSURES:
The study received funding from Abbott, Lilly, Merck, Novo Nordisk, and Sanofi. Two coauthors had individual disclosures listed in the report; the other six coauthors had no disclosures.
A version of this article first appeared on Medscape.com.
TOPLINE:
Use of a novel clinical-decision support tool and shared decision-making in elderly patients with type 2 diabetes managed in a primary care practice and at high risk for hypoglycemic episodes led to a 46% decrease in the number of at-risk patients and discontinuation of hypoglycemic agents in 20% in a prospective, 6-month, single-arm study with 94 patients.
METHODOLOGY:
- The HypoPrevent study enrolled 94 people from a Pennsylvania primary care practice who were at least 65 years old with type 2 diabetes and at risk for hypoglycemia because of treatment with insulin or sulfonylureas, and having a hemoglobin A1c of less than 7.0%.
- Clinicians and patients used a newly devised hypoglycemia reduction clinical-decision support tool developed by the Endocrine Society and a health care consulting company to help guide shared decision-making for a goal A1c level, potential changes to treatment, and other steps to reduce the risk of hypoglycemia.
- Primary outcomes during 6-month follow-up were impact of the intervention on A1c, changes in use of insulin or sulfonylureas, change in the number of study patients at risk for hypoglycemia, and impact on the incidence of nonsevere hypoglycemic events (NSHEs) measured with the Treatment-Related Impact Measure–Non-severe Hypoglycemic Events (TRIM-HYPO) survey.
TAKEAWAY:
- Patients averaged 74 years old, 57% were women, 95% were White, 61% had diabetes for more than 10 years, 48% had chronic kidney disease, 51% were on insulin, 47% on a sulfonylurea, and 80 of the 94 enrolled patients completed all three study visits.
- Nineteen patients (20%) reduced their dose of or discontinued insulin or sulfonylurea.
- In patients with both baseline and follow-up A1c measures, A1c rose from 6.29% at baseline to 6.82%.
- Fifty patients set an A1c goal and had a timely follow-up A1c measurement, and in this subgroup the number of patients at risk for hypoglycemia decreased by 46%, a significant change.
- Patients who reported at least one NSHE at baseline had a significant reduction between the baseline survey and follow-up visits in both the total score as well as each of the five scored domains.
IN PRACTICE:
The HypoPrevent study results with positive results,” concluded the researchers in their report.
SOURCE:
The HypoPrevent study was funded and organized by the Endocrine Society in collaboration with a multicenter team of researchers. The report appeared in the Journal of the American Geriatrics Society.
LIMITATIONS:
Lack of a control group makes it impossible to conclusively determine whether the intervention led to the observed increases in A1c levels, nor can the study exclude regression to the mean as the cause for lowered A1c levels.
DISCLOSURES:
The study received funding from Abbott, Lilly, Merck, Novo Nordisk, and Sanofi. Two coauthors had individual disclosures listed in the report; the other six coauthors had no disclosures.
A version of this article first appeared on Medscape.com.
JOURNAL OF THE AMERICAN GERIATRICS SOCIETY
Are ketogenic supplements the key to healthy aging?
A century ago, pediatricians began prescribing for children with intractable seizures the “keto diet,” which they also used to treat diabetes in children and adults. The low-carbohydrate, high-fat meals were designed to induce a near hypoglycemic state, forcing the body to use ketones for fuel instead of glucose.
The strategy fell out of favor after the discovery of insulin in the 1920s and the development of better antiseizure medications. The global market for the ketogenic diet topped $11 billion in 2022.
Is it just a fad, or has the public – and science – caught up with the 100-year-old approach?
Although scientists still don’t know why the ketogenic diet was effective for controlling seizures, they have documented the effectiveness of ketogenic diets for the treatment of diabetes and metabolic syndrome. An extensive body of literature has documented their use in athletes, but less is known regarding conditions such as heart disease and dementia.
Although the data are promising, much of the research has been conducted with mice or has come from trials of short-term use in humans. But recently, the National Institutes of Health awarded a $3.5 million federal grant for a double-blind, randomized, placebo-controlled clinical trial to understand the effects of the long-term use of ketone ester supplementation on frailty. Developed 20 years ago, ketone esters are precursor molecules that the body quickly breaks down into ketone bodies when carbohydrates aren’t available.
“We’ve learned so much recently about how ketone bodies interact with aging biology,” John Newman, MD, PhD, of the Buck Institute for Research on Aging in Novato, Calif., and the study’s principal investigator, said in an interview. “And we’re only just starting to translate that out of the laboratory and into human studies to see how we can take advantage of ketone bodies to improve people’s health.”
Researchers from the Ohio State University and the University of Connecticut will also participate in the TAKEOFF (Targeting Aging With Ketone Ester in Older Adults for Function in Frailty) trial, which seeks to recruit a total of 180 people across the three sites.
Dr. Newman, assistant professor at the Buck Institute and associate professor in the division of geriatrics at the University of California, San Francisco, said
One of the common things that happen during aging is that tissues – such as of the heart, brain, and muscle – lose the ability to metabolize glucose effectively. Over time, resistance to insulin can develop.
Researchers can map out areas of the brain affected by Alzheimer’s disease, for example, by assessing where patients’ glucose uptake drops. In heart failure, the heart has difficulty obtaining enough energy from glucose and instead burns fats and ketone bodies.
How might ketones affect frailty in the elderly?
As a practicing geriatrician, Dr. Newman measures frailty by evaluating patients’ strength, endurance, and how they react to stresses. He and his colleagues believe certain molecular and cellular changes may make patients more likely to fall, to recover more slowly from surgery, or to lose mobility.
The main hypothesis of the TAKEOFF study is “that if you target these fundamental mechanisms of aging, you would be able to impact many different diseases of aging across different organ systems.”
Dr. Newman and Brianna Stubbs, DPhil, lead translational scientist at the Buck Institute, are still finishing up the BIKE (Buck Institute Ketone Ester) pilot study, which was the first double-blind, randomized, placebo-controlled study to evaluate the use of ketone ester supplements in adults older than 65 years. “The BIKE study is 12 weeks long. That’s actually the longest that anyone has studied ketone ester supplements in humans,” Dr. Stubbs said. The results will help them firm up the protocol for the TAKEOFF trial, which will likely treat patients for up to 24 weeks.
The primary outcome measure at all three study sites will be leg press strength. Researchers will also assess a variety of secondary outcomes that cover geriatric and cognitive function – measures such as gait speed and walking endurance, cognitive tests, and quality of life. And at the Buck, Dr. Newman and Dr. Stubbs will be evaluating the use of biomarkers that are often available in clinical labs – insulin, C-reactive protein, cystatin, and natriuretic peptide tests – for use as outcome measures that are responsive to treatment interventions and that can be used to track outcomes in future research on aging.
To achieve the goal of looking broadly at different organ systems likely to be affected by ketogenic supplements, they have assembled a team of coinvestigators with wide-ranging expertise in ketone and aging research.
Jeff Volek, PhD, professor in the department of human sciences at the Ohio State University, in Columbus, has contributed extensively to the literature on the use of ketogenic diets and supplements in a variety of populations, such as endurance athletes and patients with insulin resistance or diabetes.
Dr. Volek has demonstrated that ketones can have an anticatabolic effect on muscle tissue. “They could help offset some of the muscle loss with aging, which would in turn improve their physical functioning and ability to do daily activities,” he said.
The anti-inflammatory property of ketones may provide another benefit to older people. They can reduce oxidative stress, which is considered one of the chief pathologic mechanisms responsible for conditions such as heart disease, Alzheimer’s disease, asthma, and arthritis.
In addition to the main study outcomes, Dr. Volek’s lab will study muscle physiology by performing biopsies at baseline and after consumption of ketogenic supplements to assess metabolic changes in muscle cells as they consume energy. Study participants will also undergo MRIs to detect subtle changes in muscle size before and after treatment.
From elite athletes to everyday agers
As a graduate student in Dr. Volek’s lab, Jenna Bartley, PhD, studied the effects of a ketogenic diet on elite athletes. But her work has taken a turn. Now an assistant professor in the department of immunology and the center on aging at the University of Connecticut in Farmington, she focuses on how immune responses and physical function decline with age.
“Ketogenic diets and the main ketone bodies – mainly beta-hydroxybutyrate – have been shown to have really powerful influences on a lot of things that go wrong with aging,” Dr. Bartley said. The decline in immune function in the elderly is not isolated to one cell type or even one arm of the immune system. There is reason to believe ketone supplementation could improve immune function.
“T cells really love ketones for energy,” Dr. Bartley said. Some data show that production of ketone bodies is impaired in individuals with severe SARS-CoV-2 infection. Mouse models of SARS-CoV-2 infection have found that ketogenic diets led to improvement in the response to antiviral therapy.
In her lab, she’ll assess serum markers of inflammation in patients, as well as cytokine secretion following stimulation of T cells. T cells in culture from older people produce more inflammatory cytokines than those from younger people, leading to a dysfunctional immune response. Dr. Bartley is curious to see whether ketones can fix that. Additional work will include single-cell RNA sequencing of different classes of immune cells to investigate how ketones might change metabolic pathways.
Why use ketogenic supplements instead of having people consume ketogenic diets? “There are no cheat days in the keto diet,” Dr. Bartley said. Administering the diet requires intense supervision of research participants to enforce adherence. Use of supplements will improve compliance and likely make any findings translatable to more of the population, she said.
Drawbacks of the initial formulations of ketone esters, first developed 20 years ago, included high cost and terrible taste. Dr, Stubbs, a former world class rowing champion who competed in the Ironman World Championship last year, has firsthand experience with them as a research participant.
“It tasted like drinking nail polish,” she said. Recent advances in manufacturing have made them cheaper – roughly $5 per day – and more palatable, enabling research studies such as TAKEOFF.
For Dr. Newman, the studies are early building blocks in the emerging field of geroscience, which aims to translate fundamental mechanisms of aging into therapies to treat disease.
“We’re hoping that this will be an example of a proof-of-concept geroscience study that will really help to translate ketone body biology out of the laboratory and hopefully into a diversity of clinical applications,” he said. “There’s a lot we don’t understand still about the molecular mechanisms of frailty.”
Dr. Newman and Dr. Stubbs own stock in BHB Therapeutics Ltd, the company providing the product being studied, and are inventors on patents that relate to the product being studied. The Buck Institute has an ownership interest in BHB Therapeutics. Dr. Bartley and Dr. Volek report no relevant financial relationships.
A version of this article appeared on Medscape.com .
A century ago, pediatricians began prescribing for children with intractable seizures the “keto diet,” which they also used to treat diabetes in children and adults. The low-carbohydrate, high-fat meals were designed to induce a near hypoglycemic state, forcing the body to use ketones for fuel instead of glucose.
The strategy fell out of favor after the discovery of insulin in the 1920s and the development of better antiseizure medications. The global market for the ketogenic diet topped $11 billion in 2022.
Is it just a fad, or has the public – and science – caught up with the 100-year-old approach?
Although scientists still don’t know why the ketogenic diet was effective for controlling seizures, they have documented the effectiveness of ketogenic diets for the treatment of diabetes and metabolic syndrome. An extensive body of literature has documented their use in athletes, but less is known regarding conditions such as heart disease and dementia.
Although the data are promising, much of the research has been conducted with mice or has come from trials of short-term use in humans. But recently, the National Institutes of Health awarded a $3.5 million federal grant for a double-blind, randomized, placebo-controlled clinical trial to understand the effects of the long-term use of ketone ester supplementation on frailty. Developed 20 years ago, ketone esters are precursor molecules that the body quickly breaks down into ketone bodies when carbohydrates aren’t available.
“We’ve learned so much recently about how ketone bodies interact with aging biology,” John Newman, MD, PhD, of the Buck Institute for Research on Aging in Novato, Calif., and the study’s principal investigator, said in an interview. “And we’re only just starting to translate that out of the laboratory and into human studies to see how we can take advantage of ketone bodies to improve people’s health.”
Researchers from the Ohio State University and the University of Connecticut will also participate in the TAKEOFF (Targeting Aging With Ketone Ester in Older Adults for Function in Frailty) trial, which seeks to recruit a total of 180 people across the three sites.
Dr. Newman, assistant professor at the Buck Institute and associate professor in the division of geriatrics at the University of California, San Francisco, said
One of the common things that happen during aging is that tissues – such as of the heart, brain, and muscle – lose the ability to metabolize glucose effectively. Over time, resistance to insulin can develop.
Researchers can map out areas of the brain affected by Alzheimer’s disease, for example, by assessing where patients’ glucose uptake drops. In heart failure, the heart has difficulty obtaining enough energy from glucose and instead burns fats and ketone bodies.
How might ketones affect frailty in the elderly?
As a practicing geriatrician, Dr. Newman measures frailty by evaluating patients’ strength, endurance, and how they react to stresses. He and his colleagues believe certain molecular and cellular changes may make patients more likely to fall, to recover more slowly from surgery, or to lose mobility.
The main hypothesis of the TAKEOFF study is “that if you target these fundamental mechanisms of aging, you would be able to impact many different diseases of aging across different organ systems.”
Dr. Newman and Brianna Stubbs, DPhil, lead translational scientist at the Buck Institute, are still finishing up the BIKE (Buck Institute Ketone Ester) pilot study, which was the first double-blind, randomized, placebo-controlled study to evaluate the use of ketone ester supplements in adults older than 65 years. “The BIKE study is 12 weeks long. That’s actually the longest that anyone has studied ketone ester supplements in humans,” Dr. Stubbs said. The results will help them firm up the protocol for the TAKEOFF trial, which will likely treat patients for up to 24 weeks.
The primary outcome measure at all three study sites will be leg press strength. Researchers will also assess a variety of secondary outcomes that cover geriatric and cognitive function – measures such as gait speed and walking endurance, cognitive tests, and quality of life. And at the Buck, Dr. Newman and Dr. Stubbs will be evaluating the use of biomarkers that are often available in clinical labs – insulin, C-reactive protein, cystatin, and natriuretic peptide tests – for use as outcome measures that are responsive to treatment interventions and that can be used to track outcomes in future research on aging.
To achieve the goal of looking broadly at different organ systems likely to be affected by ketogenic supplements, they have assembled a team of coinvestigators with wide-ranging expertise in ketone and aging research.
Jeff Volek, PhD, professor in the department of human sciences at the Ohio State University, in Columbus, has contributed extensively to the literature on the use of ketogenic diets and supplements in a variety of populations, such as endurance athletes and patients with insulin resistance or diabetes.
Dr. Volek has demonstrated that ketones can have an anticatabolic effect on muscle tissue. “They could help offset some of the muscle loss with aging, which would in turn improve their physical functioning and ability to do daily activities,” he said.
The anti-inflammatory property of ketones may provide another benefit to older people. They can reduce oxidative stress, which is considered one of the chief pathologic mechanisms responsible for conditions such as heart disease, Alzheimer’s disease, asthma, and arthritis.
In addition to the main study outcomes, Dr. Volek’s lab will study muscle physiology by performing biopsies at baseline and after consumption of ketogenic supplements to assess metabolic changes in muscle cells as they consume energy. Study participants will also undergo MRIs to detect subtle changes in muscle size before and after treatment.
From elite athletes to everyday agers
As a graduate student in Dr. Volek’s lab, Jenna Bartley, PhD, studied the effects of a ketogenic diet on elite athletes. But her work has taken a turn. Now an assistant professor in the department of immunology and the center on aging at the University of Connecticut in Farmington, she focuses on how immune responses and physical function decline with age.
“Ketogenic diets and the main ketone bodies – mainly beta-hydroxybutyrate – have been shown to have really powerful influences on a lot of things that go wrong with aging,” Dr. Bartley said. The decline in immune function in the elderly is not isolated to one cell type or even one arm of the immune system. There is reason to believe ketone supplementation could improve immune function.
“T cells really love ketones for energy,” Dr. Bartley said. Some data show that production of ketone bodies is impaired in individuals with severe SARS-CoV-2 infection. Mouse models of SARS-CoV-2 infection have found that ketogenic diets led to improvement in the response to antiviral therapy.
In her lab, she’ll assess serum markers of inflammation in patients, as well as cytokine secretion following stimulation of T cells. T cells in culture from older people produce more inflammatory cytokines than those from younger people, leading to a dysfunctional immune response. Dr. Bartley is curious to see whether ketones can fix that. Additional work will include single-cell RNA sequencing of different classes of immune cells to investigate how ketones might change metabolic pathways.
Why use ketogenic supplements instead of having people consume ketogenic diets? “There are no cheat days in the keto diet,” Dr. Bartley said. Administering the diet requires intense supervision of research participants to enforce adherence. Use of supplements will improve compliance and likely make any findings translatable to more of the population, she said.
Drawbacks of the initial formulations of ketone esters, first developed 20 years ago, included high cost and terrible taste. Dr, Stubbs, a former world class rowing champion who competed in the Ironman World Championship last year, has firsthand experience with them as a research participant.
“It tasted like drinking nail polish,” she said. Recent advances in manufacturing have made them cheaper – roughly $5 per day – and more palatable, enabling research studies such as TAKEOFF.
For Dr. Newman, the studies are early building blocks in the emerging field of geroscience, which aims to translate fundamental mechanisms of aging into therapies to treat disease.
“We’re hoping that this will be an example of a proof-of-concept geroscience study that will really help to translate ketone body biology out of the laboratory and hopefully into a diversity of clinical applications,” he said. “There’s a lot we don’t understand still about the molecular mechanisms of frailty.”
Dr. Newman and Dr. Stubbs own stock in BHB Therapeutics Ltd, the company providing the product being studied, and are inventors on patents that relate to the product being studied. The Buck Institute has an ownership interest in BHB Therapeutics. Dr. Bartley and Dr. Volek report no relevant financial relationships.
A version of this article appeared on Medscape.com .
A century ago, pediatricians began prescribing for children with intractable seizures the “keto diet,” which they also used to treat diabetes in children and adults. The low-carbohydrate, high-fat meals were designed to induce a near hypoglycemic state, forcing the body to use ketones for fuel instead of glucose.
The strategy fell out of favor after the discovery of insulin in the 1920s and the development of better antiseizure medications. The global market for the ketogenic diet topped $11 billion in 2022.
Is it just a fad, or has the public – and science – caught up with the 100-year-old approach?
Although scientists still don’t know why the ketogenic diet was effective for controlling seizures, they have documented the effectiveness of ketogenic diets for the treatment of diabetes and metabolic syndrome. An extensive body of literature has documented their use in athletes, but less is known regarding conditions such as heart disease and dementia.
Although the data are promising, much of the research has been conducted with mice or has come from trials of short-term use in humans. But recently, the National Institutes of Health awarded a $3.5 million federal grant for a double-blind, randomized, placebo-controlled clinical trial to understand the effects of the long-term use of ketone ester supplementation on frailty. Developed 20 years ago, ketone esters are precursor molecules that the body quickly breaks down into ketone bodies when carbohydrates aren’t available.
“We’ve learned so much recently about how ketone bodies interact with aging biology,” John Newman, MD, PhD, of the Buck Institute for Research on Aging in Novato, Calif., and the study’s principal investigator, said in an interview. “And we’re only just starting to translate that out of the laboratory and into human studies to see how we can take advantage of ketone bodies to improve people’s health.”
Researchers from the Ohio State University and the University of Connecticut will also participate in the TAKEOFF (Targeting Aging With Ketone Ester in Older Adults for Function in Frailty) trial, which seeks to recruit a total of 180 people across the three sites.
Dr. Newman, assistant professor at the Buck Institute and associate professor in the division of geriatrics at the University of California, San Francisco, said
One of the common things that happen during aging is that tissues – such as of the heart, brain, and muscle – lose the ability to metabolize glucose effectively. Over time, resistance to insulin can develop.
Researchers can map out areas of the brain affected by Alzheimer’s disease, for example, by assessing where patients’ glucose uptake drops. In heart failure, the heart has difficulty obtaining enough energy from glucose and instead burns fats and ketone bodies.
How might ketones affect frailty in the elderly?
As a practicing geriatrician, Dr. Newman measures frailty by evaluating patients’ strength, endurance, and how they react to stresses. He and his colleagues believe certain molecular and cellular changes may make patients more likely to fall, to recover more slowly from surgery, or to lose mobility.
The main hypothesis of the TAKEOFF study is “that if you target these fundamental mechanisms of aging, you would be able to impact many different diseases of aging across different organ systems.”
Dr. Newman and Brianna Stubbs, DPhil, lead translational scientist at the Buck Institute, are still finishing up the BIKE (Buck Institute Ketone Ester) pilot study, which was the first double-blind, randomized, placebo-controlled study to evaluate the use of ketone ester supplements in adults older than 65 years. “The BIKE study is 12 weeks long. That’s actually the longest that anyone has studied ketone ester supplements in humans,” Dr. Stubbs said. The results will help them firm up the protocol for the TAKEOFF trial, which will likely treat patients for up to 24 weeks.
The primary outcome measure at all three study sites will be leg press strength. Researchers will also assess a variety of secondary outcomes that cover geriatric and cognitive function – measures such as gait speed and walking endurance, cognitive tests, and quality of life. And at the Buck, Dr. Newman and Dr. Stubbs will be evaluating the use of biomarkers that are often available in clinical labs – insulin, C-reactive protein, cystatin, and natriuretic peptide tests – for use as outcome measures that are responsive to treatment interventions and that can be used to track outcomes in future research on aging.
To achieve the goal of looking broadly at different organ systems likely to be affected by ketogenic supplements, they have assembled a team of coinvestigators with wide-ranging expertise in ketone and aging research.
Jeff Volek, PhD, professor in the department of human sciences at the Ohio State University, in Columbus, has contributed extensively to the literature on the use of ketogenic diets and supplements in a variety of populations, such as endurance athletes and patients with insulin resistance or diabetes.
Dr. Volek has demonstrated that ketones can have an anticatabolic effect on muscle tissue. “They could help offset some of the muscle loss with aging, which would in turn improve their physical functioning and ability to do daily activities,” he said.
The anti-inflammatory property of ketones may provide another benefit to older people. They can reduce oxidative stress, which is considered one of the chief pathologic mechanisms responsible for conditions such as heart disease, Alzheimer’s disease, asthma, and arthritis.
In addition to the main study outcomes, Dr. Volek’s lab will study muscle physiology by performing biopsies at baseline and after consumption of ketogenic supplements to assess metabolic changes in muscle cells as they consume energy. Study participants will also undergo MRIs to detect subtle changes in muscle size before and after treatment.
From elite athletes to everyday agers
As a graduate student in Dr. Volek’s lab, Jenna Bartley, PhD, studied the effects of a ketogenic diet on elite athletes. But her work has taken a turn. Now an assistant professor in the department of immunology and the center on aging at the University of Connecticut in Farmington, she focuses on how immune responses and physical function decline with age.
“Ketogenic diets and the main ketone bodies – mainly beta-hydroxybutyrate – have been shown to have really powerful influences on a lot of things that go wrong with aging,” Dr. Bartley said. The decline in immune function in the elderly is not isolated to one cell type or even one arm of the immune system. There is reason to believe ketone supplementation could improve immune function.
“T cells really love ketones for energy,” Dr. Bartley said. Some data show that production of ketone bodies is impaired in individuals with severe SARS-CoV-2 infection. Mouse models of SARS-CoV-2 infection have found that ketogenic diets led to improvement in the response to antiviral therapy.
In her lab, she’ll assess serum markers of inflammation in patients, as well as cytokine secretion following stimulation of T cells. T cells in culture from older people produce more inflammatory cytokines than those from younger people, leading to a dysfunctional immune response. Dr. Bartley is curious to see whether ketones can fix that. Additional work will include single-cell RNA sequencing of different classes of immune cells to investigate how ketones might change metabolic pathways.
Why use ketogenic supplements instead of having people consume ketogenic diets? “There are no cheat days in the keto diet,” Dr. Bartley said. Administering the diet requires intense supervision of research participants to enforce adherence. Use of supplements will improve compliance and likely make any findings translatable to more of the population, she said.
Drawbacks of the initial formulations of ketone esters, first developed 20 years ago, included high cost and terrible taste. Dr, Stubbs, a former world class rowing champion who competed in the Ironman World Championship last year, has firsthand experience with them as a research participant.
“It tasted like drinking nail polish,” she said. Recent advances in manufacturing have made them cheaper – roughly $5 per day – and more palatable, enabling research studies such as TAKEOFF.
For Dr. Newman, the studies are early building blocks in the emerging field of geroscience, which aims to translate fundamental mechanisms of aging into therapies to treat disease.
“We’re hoping that this will be an example of a proof-of-concept geroscience study that will really help to translate ketone body biology out of the laboratory and hopefully into a diversity of clinical applications,” he said. “There’s a lot we don’t understand still about the molecular mechanisms of frailty.”
Dr. Newman and Dr. Stubbs own stock in BHB Therapeutics Ltd, the company providing the product being studied, and are inventors on patents that relate to the product being studied. The Buck Institute has an ownership interest in BHB Therapeutics. Dr. Bartley and Dr. Volek report no relevant financial relationships.
A version of this article appeared on Medscape.com .
Older women who get mammograms risk overdiagnosis
TOPLINE:
Women who continue breast cancer screening after age 70 face a considerable risk for overdiagnosis.
METHODOLOGY:
- Overdiagnosis – the risk of detecting and treating cancers that would never have caused issues in a person’s lifetime – is increasingly recognized as a harm of breast cancer screening; however, the scope of the problem among older women remains uncertain.
- To get an idea, investigators linked Medicare claims data with Surveillance, Epidemiology, and End Results (SEER) data for 54,635 women 70 years or older to compare the incidence of breast cancer and breast cancer–specific death among women who continued screening mammography with those who did not.
- The women all had undergone recent screening mammograms and had no history of breast cancer at study entry. Those who had a subsequent mammogram within 3 years were classified as undergoing continued screening while those who did not were classified as not undergoing continued screening.
- Overdiagnosis was defined as the difference in cumulative incidence of breast cancer between screened and unscreened women divided by the cumulative incidence among screened women.
- Results were adjusted for potential confounders, including age, race, and ethnicity.
TAKEAWAY:
- Over 80% of women 70-84 years old and more than 60% of women 85 years or older continued screening.
- Among women 70-74 years old, the adjusted cumulative incidence of breast cancer was 6.1 cases per 100 screened women vs. 4.2 cases per 100 unscreened women; for women aged 75-84 years old, the cumulative incidence was 4.9 per 100 screened women vs. 2.6 per 100 unscreened women, and for women 85 years and older, the cumulative incidence was 2.8 vs. 1.3 per 100, respectively.
- Estimates of overdiagnosis ranged from 31% of breast cancer cases among screened women in the 70-74 age group to 54% of cases in the 85 and older group.
- The researchers found no statistically significant reduction in breast cancer–specific death associated with screening in any age or life-expectancy group. Overdiagnosis appeared to be driven by in situ and localized invasive breast cancer, not advanced breast cancer.
IN PRACTICE:
The proportion of older women who continue to receive screening mammograms and may experience breast cancer overdiagnosis is “considerable” and “increases with advancing age and with decreasing life expectancy,” the authors conclude. Given potential benefits and harms of screening in this population, “patient preferences, including risk tolerance, comfort with uncertainty, and willingness to undergo treatment, are important for informing screening decisions.”
SOURCE:
The study was led by Ilana Richman, MD, MHS, of the Yale School of Medicine, New Haven, Connecticut, and published in the Annals of Internal Medicine.
LIMITATIONS:
The definition of screening mammography in the study may have misclassified some diagnostic mammograms as screening. Using a more conservative definition of screening mammogram, which largely accounted for this misclassification, estimates for overdiagnosis were smaller, ranging from 15% of cases in the 70-74 age group to 44% of cases in the 85 and older group. Results could not be adjusted for breast density, family history, and other breast cancer risk factors not captured by the data.
DISCLOSURES:
The work was funded by the National Cancer Institute. One author reported funding from Genentech and Johnson & Johnson.
A version of this article first appeared on Medscape.com.
TOPLINE:
Women who continue breast cancer screening after age 70 face a considerable risk for overdiagnosis.
METHODOLOGY:
- Overdiagnosis – the risk of detecting and treating cancers that would never have caused issues in a person’s lifetime – is increasingly recognized as a harm of breast cancer screening; however, the scope of the problem among older women remains uncertain.
- To get an idea, investigators linked Medicare claims data with Surveillance, Epidemiology, and End Results (SEER) data for 54,635 women 70 years or older to compare the incidence of breast cancer and breast cancer–specific death among women who continued screening mammography with those who did not.
- The women all had undergone recent screening mammograms and had no history of breast cancer at study entry. Those who had a subsequent mammogram within 3 years were classified as undergoing continued screening while those who did not were classified as not undergoing continued screening.
- Overdiagnosis was defined as the difference in cumulative incidence of breast cancer between screened and unscreened women divided by the cumulative incidence among screened women.
- Results were adjusted for potential confounders, including age, race, and ethnicity.
TAKEAWAY:
- Over 80% of women 70-84 years old and more than 60% of women 85 years or older continued screening.
- Among women 70-74 years old, the adjusted cumulative incidence of breast cancer was 6.1 cases per 100 screened women vs. 4.2 cases per 100 unscreened women; for women aged 75-84 years old, the cumulative incidence was 4.9 per 100 screened women vs. 2.6 per 100 unscreened women, and for women 85 years and older, the cumulative incidence was 2.8 vs. 1.3 per 100, respectively.
- Estimates of overdiagnosis ranged from 31% of breast cancer cases among screened women in the 70-74 age group to 54% of cases in the 85 and older group.
- The researchers found no statistically significant reduction in breast cancer–specific death associated with screening in any age or life-expectancy group. Overdiagnosis appeared to be driven by in situ and localized invasive breast cancer, not advanced breast cancer.
IN PRACTICE:
The proportion of older women who continue to receive screening mammograms and may experience breast cancer overdiagnosis is “considerable” and “increases with advancing age and with decreasing life expectancy,” the authors conclude. Given potential benefits and harms of screening in this population, “patient preferences, including risk tolerance, comfort with uncertainty, and willingness to undergo treatment, are important for informing screening decisions.”
SOURCE:
The study was led by Ilana Richman, MD, MHS, of the Yale School of Medicine, New Haven, Connecticut, and published in the Annals of Internal Medicine.
LIMITATIONS:
The definition of screening mammography in the study may have misclassified some diagnostic mammograms as screening. Using a more conservative definition of screening mammogram, which largely accounted for this misclassification, estimates for overdiagnosis were smaller, ranging from 15% of cases in the 70-74 age group to 44% of cases in the 85 and older group. Results could not be adjusted for breast density, family history, and other breast cancer risk factors not captured by the data.
DISCLOSURES:
The work was funded by the National Cancer Institute. One author reported funding from Genentech and Johnson & Johnson.
A version of this article first appeared on Medscape.com.
TOPLINE:
Women who continue breast cancer screening after age 70 face a considerable risk for overdiagnosis.
METHODOLOGY:
- Overdiagnosis – the risk of detecting and treating cancers that would never have caused issues in a person’s lifetime – is increasingly recognized as a harm of breast cancer screening; however, the scope of the problem among older women remains uncertain.
- To get an idea, investigators linked Medicare claims data with Surveillance, Epidemiology, and End Results (SEER) data for 54,635 women 70 years or older to compare the incidence of breast cancer and breast cancer–specific death among women who continued screening mammography with those who did not.
- The women all had undergone recent screening mammograms and had no history of breast cancer at study entry. Those who had a subsequent mammogram within 3 years were classified as undergoing continued screening while those who did not were classified as not undergoing continued screening.
- Overdiagnosis was defined as the difference in cumulative incidence of breast cancer between screened and unscreened women divided by the cumulative incidence among screened women.
- Results were adjusted for potential confounders, including age, race, and ethnicity.
TAKEAWAY:
- Over 80% of women 70-84 years old and more than 60% of women 85 years or older continued screening.
- Among women 70-74 years old, the adjusted cumulative incidence of breast cancer was 6.1 cases per 100 screened women vs. 4.2 cases per 100 unscreened women; for women aged 75-84 years old, the cumulative incidence was 4.9 per 100 screened women vs. 2.6 per 100 unscreened women, and for women 85 years and older, the cumulative incidence was 2.8 vs. 1.3 per 100, respectively.
- Estimates of overdiagnosis ranged from 31% of breast cancer cases among screened women in the 70-74 age group to 54% of cases in the 85 and older group.
- The researchers found no statistically significant reduction in breast cancer–specific death associated with screening in any age or life-expectancy group. Overdiagnosis appeared to be driven by in situ and localized invasive breast cancer, not advanced breast cancer.
IN PRACTICE:
The proportion of older women who continue to receive screening mammograms and may experience breast cancer overdiagnosis is “considerable” and “increases with advancing age and with decreasing life expectancy,” the authors conclude. Given potential benefits and harms of screening in this population, “patient preferences, including risk tolerance, comfort with uncertainty, and willingness to undergo treatment, are important for informing screening decisions.”
SOURCE:
The study was led by Ilana Richman, MD, MHS, of the Yale School of Medicine, New Haven, Connecticut, and published in the Annals of Internal Medicine.
LIMITATIONS:
The definition of screening mammography in the study may have misclassified some diagnostic mammograms as screening. Using a more conservative definition of screening mammogram, which largely accounted for this misclassification, estimates for overdiagnosis were smaller, ranging from 15% of cases in the 70-74 age group to 44% of cases in the 85 and older group. Results could not be adjusted for breast density, family history, and other breast cancer risk factors not captured by the data.
DISCLOSURES:
The work was funded by the National Cancer Institute. One author reported funding from Genentech and Johnson & Johnson.
A version of this article first appeared on Medscape.com.
Atypical antipsychotics no safer than haloperidol for postoperative delirium: Study
Dae Hyun Kim, MD, ScD, associate professor of medicine at Harvard Medical School, in Boston, who is the lead author of the study, said the findings were especially relevant, as the use of atypical antipsychotics, such as quetiapine, olanzapine, and risperidone, has increased while use of haloperidol has fallen.
A separate but related study led by Dr. Kim, which was recently published in the Journal of the American Geriatrics Society, showed that between 2008 and 2018, use of haloperidol and benzodiazepines in community hospitals and academic medical centers decreased while use of atypical antipsychotics, antidepressants, antiepileptics, and dexmedetomidine rose (P < .01).
“Clinicians should not think atypical antipsychotics are the safer option to haloperidol,” Dr. Kim said. “We should focus on reducing prescriptions.”
Postoperative delirium
Postoperative delirium is the among the most common complications of surgery in older adults, affecting between 15% and 50% of those patients who undergo major operations. Postoperative delirium is associated with longer hospital stays, poor functional recovery, institutionalization, dementia, and death.
According to research from Harvard Medical School, postoperative delirium is linked to a 40% faster rate of cognitive decline among patients who develop the condition, compared with those who do not experience the complication.
While older patients often feel tired or a bit off after surgery, marked changes in mental function, such as confusion, disorientation, agitation, aggression, hallucinations, or persistent sleepiness, could indicate postoperative delirium.
“Antipsychotic medications are most commonly used off label for managing those symptoms of delirium,” Dr. Kim said. “What we’ve done is look at the comparative safety of two other drugs.”
Results
In the retrospective cohort study, researchers analyzed data from 17,115 patients aged 65 years and older who were without psychiatric disorders and who received oral antipsychotics after major surgery requiring general anesthesia.
“These results don’t apply to people in emergent situations where there is severe behavior that threatens their safety and others,” Dr. Kim noted.
There was no statistically significant difference in the risk for in-hospital death among patients treated with haloperidol (3.7%), olanzapine (2.8%; relative risk, 0.74; 95% confidence interval, 0.42-1.27), quetiapine (2.6%; RR, 0.70; 95% CI, 0.47-1.04), or risperidone (3.3%; RR, 0.90; CI, 0.53-1.41).
The study also found statistically insignificant differences in the risk for nonfatal clinical events. Those risks ranged from 2% to 2.6% for a cardiac arrhythmia, from 4.2% to 4.6% for pneumonia, and from 0.6% to 1.2% for strokes or transient ischemic attacks.
Esther Oh, MD, PhD, an associate professor at Johns Hopkins University, Baltimore, said that caring for patients who experience acute changes in mental status or behaviors during hospitalization can be difficult.
“Although there is a lot of evidence in the literature that nonpharmacological methods to address these problems are effective, staff shortages of recent years have made it even more difficult for the care team to institute these methods,” Dr. Oh said in an interview.
Prevention
Dr. Oh and Dr. Kim agreed that nonpharmacologic strategies, such as ensuring good nutrition and hydration, daily walking, cognitive-stimulating activities, and good sleep hygiene, are effective and safe in preventing postoperative delirium.
“These are common sense interventions, but they require a lot of staffing and training,” Dr. Kim said. “It’s a resource-intensive intervention that requires really changing the way hospital staff interacts with older patients in the hospital.”
Second-generation antipsychotic medications often are thought to be safer than haloperidol in terms of side effects, Dr. Oh said, but the new findings challenge that assumption.
“Based on the findings from this study and on prior studies of antipsychotic use for older adults, use of all antipsychotics, both first and second generation, should be reviewed carefully to ensure they are being administered at the lowest effective dose for the shortest duration possible,” she said.
The study was supported by the National Institute on Aging of the National Institutes of Health. Dr. Kim and Dr. Oh disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dae Hyun Kim, MD, ScD, associate professor of medicine at Harvard Medical School, in Boston, who is the lead author of the study, said the findings were especially relevant, as the use of atypical antipsychotics, such as quetiapine, olanzapine, and risperidone, has increased while use of haloperidol has fallen.
A separate but related study led by Dr. Kim, which was recently published in the Journal of the American Geriatrics Society, showed that between 2008 and 2018, use of haloperidol and benzodiazepines in community hospitals and academic medical centers decreased while use of atypical antipsychotics, antidepressants, antiepileptics, and dexmedetomidine rose (P < .01).
“Clinicians should not think atypical antipsychotics are the safer option to haloperidol,” Dr. Kim said. “We should focus on reducing prescriptions.”
Postoperative delirium
Postoperative delirium is the among the most common complications of surgery in older adults, affecting between 15% and 50% of those patients who undergo major operations. Postoperative delirium is associated with longer hospital stays, poor functional recovery, institutionalization, dementia, and death.
According to research from Harvard Medical School, postoperative delirium is linked to a 40% faster rate of cognitive decline among patients who develop the condition, compared with those who do not experience the complication.
While older patients often feel tired or a bit off after surgery, marked changes in mental function, such as confusion, disorientation, agitation, aggression, hallucinations, or persistent sleepiness, could indicate postoperative delirium.
“Antipsychotic medications are most commonly used off label for managing those symptoms of delirium,” Dr. Kim said. “What we’ve done is look at the comparative safety of two other drugs.”
Results
In the retrospective cohort study, researchers analyzed data from 17,115 patients aged 65 years and older who were without psychiatric disorders and who received oral antipsychotics after major surgery requiring general anesthesia.
“These results don’t apply to people in emergent situations where there is severe behavior that threatens their safety and others,” Dr. Kim noted.
There was no statistically significant difference in the risk for in-hospital death among patients treated with haloperidol (3.7%), olanzapine (2.8%; relative risk, 0.74; 95% confidence interval, 0.42-1.27), quetiapine (2.6%; RR, 0.70; 95% CI, 0.47-1.04), or risperidone (3.3%; RR, 0.90; CI, 0.53-1.41).
The study also found statistically insignificant differences in the risk for nonfatal clinical events. Those risks ranged from 2% to 2.6% for a cardiac arrhythmia, from 4.2% to 4.6% for pneumonia, and from 0.6% to 1.2% for strokes or transient ischemic attacks.
Esther Oh, MD, PhD, an associate professor at Johns Hopkins University, Baltimore, said that caring for patients who experience acute changes in mental status or behaviors during hospitalization can be difficult.
“Although there is a lot of evidence in the literature that nonpharmacological methods to address these problems are effective, staff shortages of recent years have made it even more difficult for the care team to institute these methods,” Dr. Oh said in an interview.
Prevention
Dr. Oh and Dr. Kim agreed that nonpharmacologic strategies, such as ensuring good nutrition and hydration, daily walking, cognitive-stimulating activities, and good sleep hygiene, are effective and safe in preventing postoperative delirium.
“These are common sense interventions, but they require a lot of staffing and training,” Dr. Kim said. “It’s a resource-intensive intervention that requires really changing the way hospital staff interacts with older patients in the hospital.”
Second-generation antipsychotic medications often are thought to be safer than haloperidol in terms of side effects, Dr. Oh said, but the new findings challenge that assumption.
“Based on the findings from this study and on prior studies of antipsychotic use for older adults, use of all antipsychotics, both first and second generation, should be reviewed carefully to ensure they are being administered at the lowest effective dose for the shortest duration possible,” she said.
The study was supported by the National Institute on Aging of the National Institutes of Health. Dr. Kim and Dr. Oh disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Dae Hyun Kim, MD, ScD, associate professor of medicine at Harvard Medical School, in Boston, who is the lead author of the study, said the findings were especially relevant, as the use of atypical antipsychotics, such as quetiapine, olanzapine, and risperidone, has increased while use of haloperidol has fallen.
A separate but related study led by Dr. Kim, which was recently published in the Journal of the American Geriatrics Society, showed that between 2008 and 2018, use of haloperidol and benzodiazepines in community hospitals and academic medical centers decreased while use of atypical antipsychotics, antidepressants, antiepileptics, and dexmedetomidine rose (P < .01).
“Clinicians should not think atypical antipsychotics are the safer option to haloperidol,” Dr. Kim said. “We should focus on reducing prescriptions.”
Postoperative delirium
Postoperative delirium is the among the most common complications of surgery in older adults, affecting between 15% and 50% of those patients who undergo major operations. Postoperative delirium is associated with longer hospital stays, poor functional recovery, institutionalization, dementia, and death.
According to research from Harvard Medical School, postoperative delirium is linked to a 40% faster rate of cognitive decline among patients who develop the condition, compared with those who do not experience the complication.
While older patients often feel tired or a bit off after surgery, marked changes in mental function, such as confusion, disorientation, agitation, aggression, hallucinations, or persistent sleepiness, could indicate postoperative delirium.
“Antipsychotic medications are most commonly used off label for managing those symptoms of delirium,” Dr. Kim said. “What we’ve done is look at the comparative safety of two other drugs.”
Results
In the retrospective cohort study, researchers analyzed data from 17,115 patients aged 65 years and older who were without psychiatric disorders and who received oral antipsychotics after major surgery requiring general anesthesia.
“These results don’t apply to people in emergent situations where there is severe behavior that threatens their safety and others,” Dr. Kim noted.
There was no statistically significant difference in the risk for in-hospital death among patients treated with haloperidol (3.7%), olanzapine (2.8%; relative risk, 0.74; 95% confidence interval, 0.42-1.27), quetiapine (2.6%; RR, 0.70; 95% CI, 0.47-1.04), or risperidone (3.3%; RR, 0.90; CI, 0.53-1.41).
The study also found statistically insignificant differences in the risk for nonfatal clinical events. Those risks ranged from 2% to 2.6% for a cardiac arrhythmia, from 4.2% to 4.6% for pneumonia, and from 0.6% to 1.2% for strokes or transient ischemic attacks.
Esther Oh, MD, PhD, an associate professor at Johns Hopkins University, Baltimore, said that caring for patients who experience acute changes in mental status or behaviors during hospitalization can be difficult.
“Although there is a lot of evidence in the literature that nonpharmacological methods to address these problems are effective, staff shortages of recent years have made it even more difficult for the care team to institute these methods,” Dr. Oh said in an interview.
Prevention
Dr. Oh and Dr. Kim agreed that nonpharmacologic strategies, such as ensuring good nutrition and hydration, daily walking, cognitive-stimulating activities, and good sleep hygiene, are effective and safe in preventing postoperative delirium.
“These are common sense interventions, but they require a lot of staffing and training,” Dr. Kim said. “It’s a resource-intensive intervention that requires really changing the way hospital staff interacts with older patients in the hospital.”
Second-generation antipsychotic medications often are thought to be safer than haloperidol in terms of side effects, Dr. Oh said, but the new findings challenge that assumption.
“Based on the findings from this study and on prior studies of antipsychotic use for older adults, use of all antipsychotics, both first and second generation, should be reviewed carefully to ensure they are being administered at the lowest effective dose for the shortest duration possible,” she said.
The study was supported by the National Institute on Aging of the National Institutes of Health. Dr. Kim and Dr. Oh disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Fighting disparities in palliative and end-of-life care
Palliative care has been shown to improve quality of life, receipt of goal-concordant care, end-of-life decision-making, and improvement in pain and symptoms in individuals with serious illness. However, palliative and end-of-life care remain underutilized in racial and ethnic minorities.1 Health disparities such as access, quality of care, and health outcomes among minority groups exist in delivery and receipt of care within the health care system, and this includes the care of individuals with serious illness and at the end of life.1
Racial and ethnic minorities are less likely to receive goal-concordant care, participate in advance care planning, and have access to palliative care or hospice.2-4 They are more likely to die in a hospital, have inadequate pain and symptom management, and experience poor provider-patient communication.5-7 Other contributing factors include lack of knowledge of hospice and palliative care services, mistrust of the health care system, spiritual and religious beliefs, provider bias, and cultural beliefs.1
Despite these disparities, interventions have had limited success,8 and there are gaps in content, methods, and inclusion of racial and ethnic groups within palliative care research.7
Efforts to improve health equity for people with serious illness have been identified as an “urgent call to action.”1
A few recommended actionable items include delivering culturally competent care by ensuring availability of culturally and linguistically appropriate materials and information, education, and training for providers, and practicing cultural humility; contributing to workforce diversity by hiring and training diverse staff; and partnering with community organizations to build trust and to facilitate dissemination of culturally and linguistically appropriate information to providers in caring for their diverse patient populations.1,9
One of the first steps identified is to recognize that there is a problem and prioritize efforts to understand its “multifaceted nature.”10 This should occur on multiple levels including the individual (patient and caregiver), interpersonal (health care team), organization, and policy levels,10 and be done through clinical, research, and educational platforms.
At the interpersonal level, we as the health care team can start by reflecting, acknowledging biases, seeking educational and training opportunities on cross-cultural interactions, learning about cultural and spiritual beliefs, and developing skills in culturally and linguistically appropriate communication regarding goals of care and advance care planning.1,10
For those seeking resources, organizations such as the Center to Advance Palliative Care’s Project Equity and the American Academy of Hospice and Palliative Medicine have ongoing efforts to educate and train physicians and health care professionals to improve and understand health equity in palliative care by providing resource portals, toolkits, training, and general information.
It is imperative to move forward in actionable ways to address not only racial and ethnic disparities, but advance equity in serious illness care for health care organizations, providers, and policymakers.1
Dr. Kang is in the division of gerontology and geriatric medicine at the University of Washington, Seattle.
References
1. Barrett NJ et al. N C Med J. 2020;81:254-6.
2. Johnson KS et al. J Am Geriatr Soc. 2011;59:732-7.
3. Sharma RK et al. J Clin Oncol. 2015;33:3802-8.
4. Muni S et al. Chest. 2011;139:1025-33.
5. Anderson KO et al. J Pain. 2009;10:1187-204.
6. Mack JW et al. Arch Intern Med. 2010;170:1533-40.
7. Johnson KS. J Palliat Med. 2013;16(11):1329-34.
8. Brown CE et al. J Pain Symptom Manage. 2021;63(5):e465-e71.
9. Chambers B. Center for Advancing Palliative Care. July 9, 2020.
10. Koffman J et al. BMC Palliat Care. 2023;22(64):1-3.
Palliative care has been shown to improve quality of life, receipt of goal-concordant care, end-of-life decision-making, and improvement in pain and symptoms in individuals with serious illness. However, palliative and end-of-life care remain underutilized in racial and ethnic minorities.1 Health disparities such as access, quality of care, and health outcomes among minority groups exist in delivery and receipt of care within the health care system, and this includes the care of individuals with serious illness and at the end of life.1
Racial and ethnic minorities are less likely to receive goal-concordant care, participate in advance care planning, and have access to palliative care or hospice.2-4 They are more likely to die in a hospital, have inadequate pain and symptom management, and experience poor provider-patient communication.5-7 Other contributing factors include lack of knowledge of hospice and palliative care services, mistrust of the health care system, spiritual and religious beliefs, provider bias, and cultural beliefs.1
Despite these disparities, interventions have had limited success,8 and there are gaps in content, methods, and inclusion of racial and ethnic groups within palliative care research.7
Efforts to improve health equity for people with serious illness have been identified as an “urgent call to action.”1
A few recommended actionable items include delivering culturally competent care by ensuring availability of culturally and linguistically appropriate materials and information, education, and training for providers, and practicing cultural humility; contributing to workforce diversity by hiring and training diverse staff; and partnering with community organizations to build trust and to facilitate dissemination of culturally and linguistically appropriate information to providers in caring for their diverse patient populations.1,9
One of the first steps identified is to recognize that there is a problem and prioritize efforts to understand its “multifaceted nature.”10 This should occur on multiple levels including the individual (patient and caregiver), interpersonal (health care team), organization, and policy levels,10 and be done through clinical, research, and educational platforms.
At the interpersonal level, we as the health care team can start by reflecting, acknowledging biases, seeking educational and training opportunities on cross-cultural interactions, learning about cultural and spiritual beliefs, and developing skills in culturally and linguistically appropriate communication regarding goals of care and advance care planning.1,10
For those seeking resources, organizations such as the Center to Advance Palliative Care’s Project Equity and the American Academy of Hospice and Palliative Medicine have ongoing efforts to educate and train physicians and health care professionals to improve and understand health equity in palliative care by providing resource portals, toolkits, training, and general information.
It is imperative to move forward in actionable ways to address not only racial and ethnic disparities, but advance equity in serious illness care for health care organizations, providers, and policymakers.1
Dr. Kang is in the division of gerontology and geriatric medicine at the University of Washington, Seattle.
References
1. Barrett NJ et al. N C Med J. 2020;81:254-6.
2. Johnson KS et al. J Am Geriatr Soc. 2011;59:732-7.
3. Sharma RK et al. J Clin Oncol. 2015;33:3802-8.
4. Muni S et al. Chest. 2011;139:1025-33.
5. Anderson KO et al. J Pain. 2009;10:1187-204.
6. Mack JW et al. Arch Intern Med. 2010;170:1533-40.
7. Johnson KS. J Palliat Med. 2013;16(11):1329-34.
8. Brown CE et al. J Pain Symptom Manage. 2021;63(5):e465-e71.
9. Chambers B. Center for Advancing Palliative Care. July 9, 2020.
10. Koffman J et al. BMC Palliat Care. 2023;22(64):1-3.
Palliative care has been shown to improve quality of life, receipt of goal-concordant care, end-of-life decision-making, and improvement in pain and symptoms in individuals with serious illness. However, palliative and end-of-life care remain underutilized in racial and ethnic minorities.1 Health disparities such as access, quality of care, and health outcomes among minority groups exist in delivery and receipt of care within the health care system, and this includes the care of individuals with serious illness and at the end of life.1
Racial and ethnic minorities are less likely to receive goal-concordant care, participate in advance care planning, and have access to palliative care or hospice.2-4 They are more likely to die in a hospital, have inadequate pain and symptom management, and experience poor provider-patient communication.5-7 Other contributing factors include lack of knowledge of hospice and palliative care services, mistrust of the health care system, spiritual and religious beliefs, provider bias, and cultural beliefs.1
Despite these disparities, interventions have had limited success,8 and there are gaps in content, methods, and inclusion of racial and ethnic groups within palliative care research.7
Efforts to improve health equity for people with serious illness have been identified as an “urgent call to action.”1
A few recommended actionable items include delivering culturally competent care by ensuring availability of culturally and linguistically appropriate materials and information, education, and training for providers, and practicing cultural humility; contributing to workforce diversity by hiring and training diverse staff; and partnering with community organizations to build trust and to facilitate dissemination of culturally and linguistically appropriate information to providers in caring for their diverse patient populations.1,9
One of the first steps identified is to recognize that there is a problem and prioritize efforts to understand its “multifaceted nature.”10 This should occur on multiple levels including the individual (patient and caregiver), interpersonal (health care team), organization, and policy levels,10 and be done through clinical, research, and educational platforms.
At the interpersonal level, we as the health care team can start by reflecting, acknowledging biases, seeking educational and training opportunities on cross-cultural interactions, learning about cultural and spiritual beliefs, and developing skills in culturally and linguistically appropriate communication regarding goals of care and advance care planning.1,10
For those seeking resources, organizations such as the Center to Advance Palliative Care’s Project Equity and the American Academy of Hospice and Palliative Medicine have ongoing efforts to educate and train physicians and health care professionals to improve and understand health equity in palliative care by providing resource portals, toolkits, training, and general information.
It is imperative to move forward in actionable ways to address not only racial and ethnic disparities, but advance equity in serious illness care for health care organizations, providers, and policymakers.1
Dr. Kang is in the division of gerontology and geriatric medicine at the University of Washington, Seattle.
References
1. Barrett NJ et al. N C Med J. 2020;81:254-6.
2. Johnson KS et al. J Am Geriatr Soc. 2011;59:732-7.
3. Sharma RK et al. J Clin Oncol. 2015;33:3802-8.
4. Muni S et al. Chest. 2011;139:1025-33.
5. Anderson KO et al. J Pain. 2009;10:1187-204.
6. Mack JW et al. Arch Intern Med. 2010;170:1533-40.
7. Johnson KS. J Palliat Med. 2013;16(11):1329-34.
8. Brown CE et al. J Pain Symptom Manage. 2021;63(5):e465-e71.
9. Chambers B. Center for Advancing Palliative Care. July 9, 2020.
10. Koffman J et al. BMC Palliat Care. 2023;22(64):1-3.
Steady VKA therapy beats switch to NOAC in frail AFib patients: FRAIL-AF
Switching frail patients with atrial fibrillation (AFib) from anticoagulation therapy with vitamin K antagonists (VKAs) to a novel oral anticoagulant (NOAC) resulted in more bleeding without any reduction in thromboembolic complications or all-cause mortality, randomized trial results show.
The study, FRAIL-AF, is the first randomized NOAC trial to exclusively include frail older patients, said lead author Linda P.T. Joosten, MD, Julius Center for Health Sciences and Primary Care in Utrecht, the Netherlands, and these unexpected findings provide evidence that goes beyond what is currently available.
“Data from the FRAIL-AF trial showed that switching from a VKA to a NOAC should not be considered without a clear indication in frail older patients with AF[ib], as switching to a NOAC leads to 69% more bleeding,” she concluded, without any benefit on secondary clinical endpoints, including thromboembolic events and all-cause mortality.
“The results turned out different than we expected,” Dr. Joosten said. “The hypothesis of this superiority trial was that switching from VKA therapy to a NOAC would result in less bleeding. However, we observed the opposite. After the interim analysis, the data and safety monitoring board advised to stop inclusion because switching from a VKA to a NOAC was clearly contraindicated with a hazard ratio of 1.69 and a highly significant P value of .001.”
Results of FRAIL-AF were presented at the annual congress of the European Society of Cardiology and published online in the journal Circulation.
Session moderator Renate B. Schnabel, MD, interventional cardiologist with University Heart & Vascular Center Hamburg (Germany), congratulated the researchers on these “astonishing” data.
“The thing I want to emphasize here is that, in the absence of randomized controlled trial data, we should be very cautious in extrapolating data from the landmark trials to populations not enrolled in those, and to rely on observational data only,” Dr. Schnabel told Dr. Joosten. “We need randomized controlled trials that sometimes give astonishing results.”
Frailty a clinical syndrome
Frailty is “a lot more than just aging, multiple comorbidities and polypharmacy,” Dr. Joosten explained. “It’s really a clinical syndrome, with people with a high biological vulnerability, dependency on significant others, and a reduced capacity to resist stressors, all leading to a reduced homeostatic reserve.”
Frailty is common in the community, with a prevalence of about 12%, she noted, “and even more important, AF[ib] in frail older people is very common, with a prevalence of 18%. And “without any doubt, we have to adequately anticoagulate frail AF[ib] patients, as they have a high stroke risk, with an incidence of 12.4% per year,” Dr. Joosten noted, compared with 3.9% per year among nonfrail AFib patients.
NOACs are preferred over VKAs in nonfrail AFib patients, after four major trials, RE-LY with dabigatran, ROCKET-AF with rivaroxaban, ARISTOTLE with apixaban, and ENGAGE-AF with edoxaban, showed that NOAC treatment resulted in less major bleeding while stroke risk was comparable with treatment with warfarin, she noted.
The 2023 European Heart Rhythm Association consensus document on management of arrhythmias in frailty syndrome concludes that the advantages of NOACs relative to VKAs are “likely consistent” in frail and nonfrail AFib patients, but the level of evidence is low.
So it’s unknown if NOACs are preferred over VKAs in frail AFib patients, “and it’s even more questionable whether patients on VKAs should switch to NOAC therapy,” Dr. Joosten said.
This new trial aimed to answer the question of whether switching frail AFib patients currently managed on a VKA to a NOAC would reduce bleeding. FRAIL-AF was a pragmatic, multicenter, open-label, randomized, controlled superiority trial.
Older AFib patients were deemed frail if they were aged 75 years or older and had a score of 3 or more on the validated Groningen Frailty Indicator (GFI). Patients with a glomerular filtration rate of less than 30 mL/min per 1.73 m2 or with valvular AFib were excluded.
Eligible patients were then assigned randomly to switch from their international normalized ratio (INR)–guided VKA treatment with either 1 mg acenocoumarol or 3 mg phenprocoumon, to a NOAC, or to continue VKA treatment. They were followed for 12 months for the primary outcome – major bleeding or clinically relevant nonmajor bleeding complication, whichever came first – accounting for death as a competing risk.
A total of 1,330 patients were randomly assigned between January 2018 and June 2022. Their mean age was 83 years, and they had a median GFI of 4. After randomization, 6 patients in the switch-to-NOAC arm, and 1 in the continue-VKA arm were found to have exclusion criteria, so in the end, 662 patients were switched from a VKA to NOAC, while 661 continued on VKA therapy. The choice of NOAC was made by the treating physician.
Major bleeding was defined as a fatal bleeding; bleeding in a critical area or organ; bleeding leading to transfusion; and/or bleeding leading to a fall in hemoglobin level of 2 g/dL (1.24 mmol/L) or more. Nonmajor bleeding was bleeding not considered major but requiring face-to-face consultation, hospitalization or increased level of care, or medical intervention.
After a prespecified futility analysis planned after 163 primary outcome events, the trial was halted when it was seen that there were 101 primary outcome events in the switch arm compared to 62 in the continue arm, Dr. Joosten said. The difference appeared to be driven by clinically relevant nonmajor bleeding.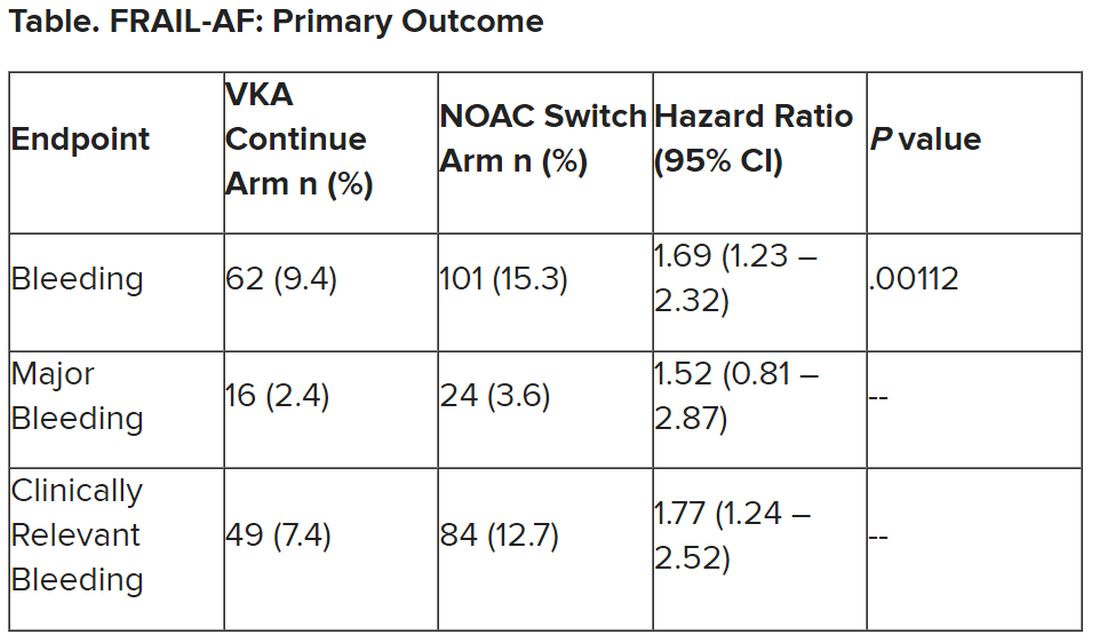
Secondary outcomes of thromboembolic events and all-cause mortality were similar between the groups.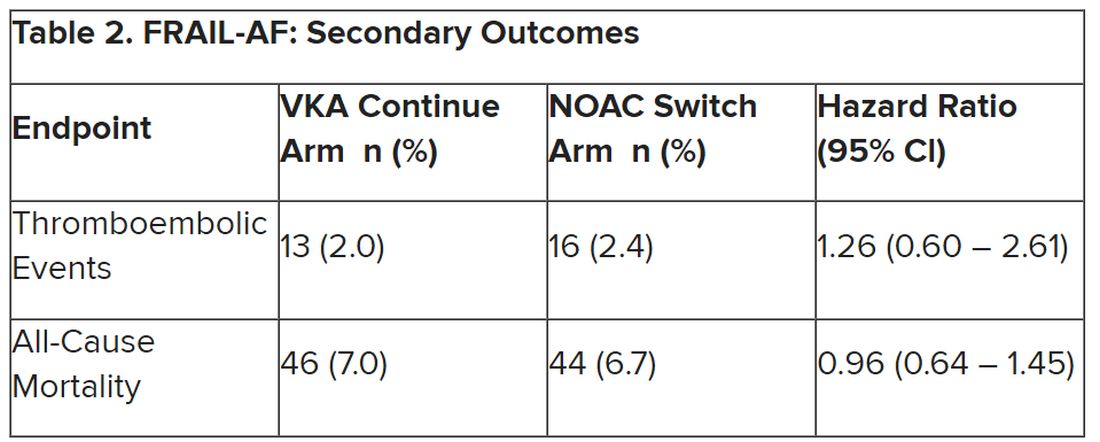
Completely different patients
Discussant at the meeting for the presentation was Isabelle C. Van Gelder, MD, University Medical Centre Groningen (the Netherlands). She said the results are important and relevant because it “provides data on an important gap of knowledge in our AF[ib] guidelines, and a note for all the cardiologists – this study was not done in the hospital. This trial was done in general practitioner practices, so that’s important to consider.”
Comparing FRAIL-AF patients with those of the four previous NOAC trials, “you see that enormous difference in age,” with an average age of 83 years versus 70-73 years in those trials. “These are completely different patients than have been included previously,” she said.
That GFI score of 4 or more includes patients on four or more different types of medication, as well as memory complaints, an inability to walk around the house, and problems with vision or hearing.
The finding of a 69% increase in bleeding with NOACs in FRAIL-AF was “completely unexpected, and I think that we as cardiologists and as NOAC believers did not expect it at all, but it is as clear as it is.” The curves don’t diverge immediately, but rather after 3 months or thereafter, “so it has nothing to do with the switching process. So why did it occur?”
The Netherlands has dedicated thrombosis services that might improve time in therapeutic range for VKA patients, but there is no real difference in TTRs in FRAIL-AF versus the other NOAC trials, Dr. Van Gelder noted.
The most likely suspect in her view is frailty itself, in particular the tendency for patients to be on a high number of medications. A previous study showed, for example, that polypharmacy could be used as a proxy for the effect of frailty on bleeding risk; patients on 10 or more medications had a higher risk for bleeding on treatment with rivaroxaban versus those on 4 or fewer medications.
“Therefore, in my view, why was there such a high risk of bleeding? It’s because these are other patients than we are normally used to treat, we as cardiologists,” although general practitioners see these patients all the time. “It’s all about frailty.”
NOACs are still relatively new drugs, with possible unknown interactions, she added. Because of their frailty and polypharmacy, these patients may benefit from INR control, Dr. Van Gelder speculated. “Therefore, I agree with them that we should be careful; if such old, frail patients survive on VKA, do not change medications and do not switch!”
The study was supported by the Dutch government with additional and unrestricted educational grants from Boehringer Ingelheim, BMS-Pfizer, Bayer, and Daiichi Sankyo. Dr. Joosten reported no relevant financial relationships. Dr. Van Gelder reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Switching frail patients with atrial fibrillation (AFib) from anticoagulation therapy with vitamin K antagonists (VKAs) to a novel oral anticoagulant (NOAC) resulted in more bleeding without any reduction in thromboembolic complications or all-cause mortality, randomized trial results show.
The study, FRAIL-AF, is the first randomized NOAC trial to exclusively include frail older patients, said lead author Linda P.T. Joosten, MD, Julius Center for Health Sciences and Primary Care in Utrecht, the Netherlands, and these unexpected findings provide evidence that goes beyond what is currently available.
“Data from the FRAIL-AF trial showed that switching from a VKA to a NOAC should not be considered without a clear indication in frail older patients with AF[ib], as switching to a NOAC leads to 69% more bleeding,” she concluded, without any benefit on secondary clinical endpoints, including thromboembolic events and all-cause mortality.
“The results turned out different than we expected,” Dr. Joosten said. “The hypothesis of this superiority trial was that switching from VKA therapy to a NOAC would result in less bleeding. However, we observed the opposite. After the interim analysis, the data and safety monitoring board advised to stop inclusion because switching from a VKA to a NOAC was clearly contraindicated with a hazard ratio of 1.69 and a highly significant P value of .001.”
Results of FRAIL-AF were presented at the annual congress of the European Society of Cardiology and published online in the journal Circulation.
Session moderator Renate B. Schnabel, MD, interventional cardiologist with University Heart & Vascular Center Hamburg (Germany), congratulated the researchers on these “astonishing” data.
“The thing I want to emphasize here is that, in the absence of randomized controlled trial data, we should be very cautious in extrapolating data from the landmark trials to populations not enrolled in those, and to rely on observational data only,” Dr. Schnabel told Dr. Joosten. “We need randomized controlled trials that sometimes give astonishing results.”
Frailty a clinical syndrome
Frailty is “a lot more than just aging, multiple comorbidities and polypharmacy,” Dr. Joosten explained. “It’s really a clinical syndrome, with people with a high biological vulnerability, dependency on significant others, and a reduced capacity to resist stressors, all leading to a reduced homeostatic reserve.”
Frailty is common in the community, with a prevalence of about 12%, she noted, “and even more important, AF[ib] in frail older people is very common, with a prevalence of 18%. And “without any doubt, we have to adequately anticoagulate frail AF[ib] patients, as they have a high stroke risk, with an incidence of 12.4% per year,” Dr. Joosten noted, compared with 3.9% per year among nonfrail AFib patients.
NOACs are preferred over VKAs in nonfrail AFib patients, after four major trials, RE-LY with dabigatran, ROCKET-AF with rivaroxaban, ARISTOTLE with apixaban, and ENGAGE-AF with edoxaban, showed that NOAC treatment resulted in less major bleeding while stroke risk was comparable with treatment with warfarin, she noted.
The 2023 European Heart Rhythm Association consensus document on management of arrhythmias in frailty syndrome concludes that the advantages of NOACs relative to VKAs are “likely consistent” in frail and nonfrail AFib patients, but the level of evidence is low.
So it’s unknown if NOACs are preferred over VKAs in frail AFib patients, “and it’s even more questionable whether patients on VKAs should switch to NOAC therapy,” Dr. Joosten said.
This new trial aimed to answer the question of whether switching frail AFib patients currently managed on a VKA to a NOAC would reduce bleeding. FRAIL-AF was a pragmatic, multicenter, open-label, randomized, controlled superiority trial.
Older AFib patients were deemed frail if they were aged 75 years or older and had a score of 3 or more on the validated Groningen Frailty Indicator (GFI). Patients with a glomerular filtration rate of less than 30 mL/min per 1.73 m2 or with valvular AFib were excluded.
Eligible patients were then assigned randomly to switch from their international normalized ratio (INR)–guided VKA treatment with either 1 mg acenocoumarol or 3 mg phenprocoumon, to a NOAC, or to continue VKA treatment. They were followed for 12 months for the primary outcome – major bleeding or clinically relevant nonmajor bleeding complication, whichever came first – accounting for death as a competing risk.
A total of 1,330 patients were randomly assigned between January 2018 and June 2022. Their mean age was 83 years, and they had a median GFI of 4. After randomization, 6 patients in the switch-to-NOAC arm, and 1 in the continue-VKA arm were found to have exclusion criteria, so in the end, 662 patients were switched from a VKA to NOAC, while 661 continued on VKA therapy. The choice of NOAC was made by the treating physician.
Major bleeding was defined as a fatal bleeding; bleeding in a critical area or organ; bleeding leading to transfusion; and/or bleeding leading to a fall in hemoglobin level of 2 g/dL (1.24 mmol/L) or more. Nonmajor bleeding was bleeding not considered major but requiring face-to-face consultation, hospitalization or increased level of care, or medical intervention.
After a prespecified futility analysis planned after 163 primary outcome events, the trial was halted when it was seen that there were 101 primary outcome events in the switch arm compared to 62 in the continue arm, Dr. Joosten said. The difference appeared to be driven by clinically relevant nonmajor bleeding.
Secondary outcomes of thromboembolic events and all-cause mortality were similar between the groups.
Completely different patients
Discussant at the meeting for the presentation was Isabelle C. Van Gelder, MD, University Medical Centre Groningen (the Netherlands). She said the results are important and relevant because it “provides data on an important gap of knowledge in our AF[ib] guidelines, and a note for all the cardiologists – this study was not done in the hospital. This trial was done in general practitioner practices, so that’s important to consider.”
Comparing FRAIL-AF patients with those of the four previous NOAC trials, “you see that enormous difference in age,” with an average age of 83 years versus 70-73 years in those trials. “These are completely different patients than have been included previously,” she said.
That GFI score of 4 or more includes patients on four or more different types of medication, as well as memory complaints, an inability to walk around the house, and problems with vision or hearing.
The finding of a 69% increase in bleeding with NOACs in FRAIL-AF was “completely unexpected, and I think that we as cardiologists and as NOAC believers did not expect it at all, but it is as clear as it is.” The curves don’t diverge immediately, but rather after 3 months or thereafter, “so it has nothing to do with the switching process. So why did it occur?”
The Netherlands has dedicated thrombosis services that might improve time in therapeutic range for VKA patients, but there is no real difference in TTRs in FRAIL-AF versus the other NOAC trials, Dr. Van Gelder noted.
The most likely suspect in her view is frailty itself, in particular the tendency for patients to be on a high number of medications. A previous study showed, for example, that polypharmacy could be used as a proxy for the effect of frailty on bleeding risk; patients on 10 or more medications had a higher risk for bleeding on treatment with rivaroxaban versus those on 4 or fewer medications.
“Therefore, in my view, why was there such a high risk of bleeding? It’s because these are other patients than we are normally used to treat, we as cardiologists,” although general practitioners see these patients all the time. “It’s all about frailty.”
NOACs are still relatively new drugs, with possible unknown interactions, she added. Because of their frailty and polypharmacy, these patients may benefit from INR control, Dr. Van Gelder speculated. “Therefore, I agree with them that we should be careful; if such old, frail patients survive on VKA, do not change medications and do not switch!”
The study was supported by the Dutch government with additional and unrestricted educational grants from Boehringer Ingelheim, BMS-Pfizer, Bayer, and Daiichi Sankyo. Dr. Joosten reported no relevant financial relationships. Dr. Van Gelder reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Switching frail patients with atrial fibrillation (AFib) from anticoagulation therapy with vitamin K antagonists (VKAs) to a novel oral anticoagulant (NOAC) resulted in more bleeding without any reduction in thromboembolic complications or all-cause mortality, randomized trial results show.
The study, FRAIL-AF, is the first randomized NOAC trial to exclusively include frail older patients, said lead author Linda P.T. Joosten, MD, Julius Center for Health Sciences and Primary Care in Utrecht, the Netherlands, and these unexpected findings provide evidence that goes beyond what is currently available.
“Data from the FRAIL-AF trial showed that switching from a VKA to a NOAC should not be considered without a clear indication in frail older patients with AF[ib], as switching to a NOAC leads to 69% more bleeding,” she concluded, without any benefit on secondary clinical endpoints, including thromboembolic events and all-cause mortality.
“The results turned out different than we expected,” Dr. Joosten said. “The hypothesis of this superiority trial was that switching from VKA therapy to a NOAC would result in less bleeding. However, we observed the opposite. After the interim analysis, the data and safety monitoring board advised to stop inclusion because switching from a VKA to a NOAC was clearly contraindicated with a hazard ratio of 1.69 and a highly significant P value of .001.”
Results of FRAIL-AF were presented at the annual congress of the European Society of Cardiology and published online in the journal Circulation.
Session moderator Renate B. Schnabel, MD, interventional cardiologist with University Heart & Vascular Center Hamburg (Germany), congratulated the researchers on these “astonishing” data.
“The thing I want to emphasize here is that, in the absence of randomized controlled trial data, we should be very cautious in extrapolating data from the landmark trials to populations not enrolled in those, and to rely on observational data only,” Dr. Schnabel told Dr. Joosten. “We need randomized controlled trials that sometimes give astonishing results.”
Frailty a clinical syndrome
Frailty is “a lot more than just aging, multiple comorbidities and polypharmacy,” Dr. Joosten explained. “It’s really a clinical syndrome, with people with a high biological vulnerability, dependency on significant others, and a reduced capacity to resist stressors, all leading to a reduced homeostatic reserve.”
Frailty is common in the community, with a prevalence of about 12%, she noted, “and even more important, AF[ib] in frail older people is very common, with a prevalence of 18%. And “without any doubt, we have to adequately anticoagulate frail AF[ib] patients, as they have a high stroke risk, with an incidence of 12.4% per year,” Dr. Joosten noted, compared with 3.9% per year among nonfrail AFib patients.
NOACs are preferred over VKAs in nonfrail AFib patients, after four major trials, RE-LY with dabigatran, ROCKET-AF with rivaroxaban, ARISTOTLE with apixaban, and ENGAGE-AF with edoxaban, showed that NOAC treatment resulted in less major bleeding while stroke risk was comparable with treatment with warfarin, she noted.
The 2023 European Heart Rhythm Association consensus document on management of arrhythmias in frailty syndrome concludes that the advantages of NOACs relative to VKAs are “likely consistent” in frail and nonfrail AFib patients, but the level of evidence is low.
So it’s unknown if NOACs are preferred over VKAs in frail AFib patients, “and it’s even more questionable whether patients on VKAs should switch to NOAC therapy,” Dr. Joosten said.
This new trial aimed to answer the question of whether switching frail AFib patients currently managed on a VKA to a NOAC would reduce bleeding. FRAIL-AF was a pragmatic, multicenter, open-label, randomized, controlled superiority trial.
Older AFib patients were deemed frail if they were aged 75 years or older and had a score of 3 or more on the validated Groningen Frailty Indicator (GFI). Patients with a glomerular filtration rate of less than 30 mL/min per 1.73 m2 or with valvular AFib were excluded.
Eligible patients were then assigned randomly to switch from their international normalized ratio (INR)–guided VKA treatment with either 1 mg acenocoumarol or 3 mg phenprocoumon, to a NOAC, or to continue VKA treatment. They were followed for 12 months for the primary outcome – major bleeding or clinically relevant nonmajor bleeding complication, whichever came first – accounting for death as a competing risk.
A total of 1,330 patients were randomly assigned between January 2018 and June 2022. Their mean age was 83 years, and they had a median GFI of 4. After randomization, 6 patients in the switch-to-NOAC arm, and 1 in the continue-VKA arm were found to have exclusion criteria, so in the end, 662 patients were switched from a VKA to NOAC, while 661 continued on VKA therapy. The choice of NOAC was made by the treating physician.
Major bleeding was defined as a fatal bleeding; bleeding in a critical area or organ; bleeding leading to transfusion; and/or bleeding leading to a fall in hemoglobin level of 2 g/dL (1.24 mmol/L) or more. Nonmajor bleeding was bleeding not considered major but requiring face-to-face consultation, hospitalization or increased level of care, or medical intervention.
After a prespecified futility analysis planned after 163 primary outcome events, the trial was halted when it was seen that there were 101 primary outcome events in the switch arm compared to 62 in the continue arm, Dr. Joosten said. The difference appeared to be driven by clinically relevant nonmajor bleeding.
Secondary outcomes of thromboembolic events and all-cause mortality were similar between the groups.
Completely different patients
Discussant at the meeting for the presentation was Isabelle C. Van Gelder, MD, University Medical Centre Groningen (the Netherlands). She said the results are important and relevant because it “provides data on an important gap of knowledge in our AF[ib] guidelines, and a note for all the cardiologists – this study was not done in the hospital. This trial was done in general practitioner practices, so that’s important to consider.”
Comparing FRAIL-AF patients with those of the four previous NOAC trials, “you see that enormous difference in age,” with an average age of 83 years versus 70-73 years in those trials. “These are completely different patients than have been included previously,” she said.
That GFI score of 4 or more includes patients on four or more different types of medication, as well as memory complaints, an inability to walk around the house, and problems with vision or hearing.
The finding of a 69% increase in bleeding with NOACs in FRAIL-AF was “completely unexpected, and I think that we as cardiologists and as NOAC believers did not expect it at all, but it is as clear as it is.” The curves don’t diverge immediately, but rather after 3 months or thereafter, “so it has nothing to do with the switching process. So why did it occur?”
The Netherlands has dedicated thrombosis services that might improve time in therapeutic range for VKA patients, but there is no real difference in TTRs in FRAIL-AF versus the other NOAC trials, Dr. Van Gelder noted.
The most likely suspect in her view is frailty itself, in particular the tendency for patients to be on a high number of medications. A previous study showed, for example, that polypharmacy could be used as a proxy for the effect of frailty on bleeding risk; patients on 10 or more medications had a higher risk for bleeding on treatment with rivaroxaban versus those on 4 or fewer medications.
“Therefore, in my view, why was there such a high risk of bleeding? It’s because these are other patients than we are normally used to treat, we as cardiologists,” although general practitioners see these patients all the time. “It’s all about frailty.”
NOACs are still relatively new drugs, with possible unknown interactions, she added. Because of their frailty and polypharmacy, these patients may benefit from INR control, Dr. Van Gelder speculated. “Therefore, I agree with them that we should be careful; if such old, frail patients survive on VKA, do not change medications and do not switch!”
The study was supported by the Dutch government with additional and unrestricted educational grants from Boehringer Ingelheim, BMS-Pfizer, Bayer, and Daiichi Sankyo. Dr. Joosten reported no relevant financial relationships. Dr. Van Gelder reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE ESC CONGRESS 2023
Should people who play sports pay higher medical insurance premiums?
This transcript has been edited for clarity.
If you’re anywhere near Seattle, anywhere near Florida, or anywhere where it might be not oppressively hot outside but encouraging some people who might want to go out and get a little exercise, you’ve undoubtedly seen or heard of pickleball.
This took off, I think, out of Bainbridge Island, Wash. It was meant as a gentlemanly game where people didn’t exert themselves too much. The joke is you could play it while holding a drink in one hand. It’s gotten more popular and more competitive. It’s kind of a miniature version of tennis, with a smaller court, a plastic ball, and a wooden paddle. The ball can go back and forth rapidly, but you’re always playing doubles and it doesn’t take as much energy, exertion, and, if you will, fitness as a game like singles tennis.
The upside is it’s gotten many people outdoors getting some exercise and socializing. That’s all to the good. But a recent study suggested that there are about $500 million worth of injuries coming into the health care system associated with pickleball. There have been leg sprains, broken bones, people getting hit in the eye, hamstring pulls, and many other problems. I’ve been told that many of the spectators who show up for pickleball matches are there with a cast or have some kind of a wrap on because they were injured.
Well, many people have argued in the past about what we are going to do about health care costs. Some suggest if you voluntarily incur health care damage, you ought to pay for that yourself and you ought to have a big copay.
If you decide you’re going to do cross-country skiing or downhill skiing and you injure yourself, you chose to do it, so you pay. If you’re not going to maintain your weight, you’re going to smoke, or you’re going to ride around without a helmet, that’s your choice. You ought to pay.
I think the pickleball example is really a good challenge to these views. You obviously want people to go out and get some exercise. Here, we’re talking about a population that’s a little older and oftentimes doesn’t get out there as much as doctors would like to get the exercise that’s still important that they need, and yet it does incur injuries and problems.
My suggestion would be to make the game a little safer. Let’s try to encourage people to warm up more before they get out there and jump out of the car and engage in their pickleball battles. Goggles might be important to prevent the eye injuries in a game that’s played up close. Maybe we want to make sure that people look out for one another out there. If they think they’re getting dehydrated or tired, they should say, “Let’s sit down.”
I’m not willing to put a tax or a copay on the pickleball players of America. I know they choose to do it. It’s got an upside and benefits, as many things like skiing and other behaviors that have some risk do, but I think we want to be encouraging, not discouraging, of it.
I don’t like a society where anybody who tries to do something that takes risk winds up bearing extra cost for doing that. I understand that that gets people irritated when it comes to dangerous, hyper-risky behavior like smoking and not wearing a motorcycle helmet. I think the way to engage is not to call out the sinner or to try and punish those who are trying to do things that bring them enjoyment, reward, or in some of these cases, physical fitness, but to try to make things safer and try to gradually improve and get rid of the risk side to capture the full benefit side.
I’m not sure I’ve come up with all the best ways to make pickleball safer, but I think that’s where our thinking in health care should go. My view is to get out there and play pickleball. If you do pull your hamstring, raise my insurance premium a little bit. I’ll help to pay for it. Better you get some enjoyment and some exercise.
I get the downside, but come on, folks, we ought to be, as a community, somewhat supportive of the fun and recreation that our fellow citizens engage in.
Dr. Caplan is director, division of medical ethics, New York University Langone Medical Center. He disclosed serving as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); and as a contributing author and adviser for Medscape.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
If you’re anywhere near Seattle, anywhere near Florida, or anywhere where it might be not oppressively hot outside but encouraging some people who might want to go out and get a little exercise, you’ve undoubtedly seen or heard of pickleball.
This took off, I think, out of Bainbridge Island, Wash. It was meant as a gentlemanly game where people didn’t exert themselves too much. The joke is you could play it while holding a drink in one hand. It’s gotten more popular and more competitive. It’s kind of a miniature version of tennis, with a smaller court, a plastic ball, and a wooden paddle. The ball can go back and forth rapidly, but you’re always playing doubles and it doesn’t take as much energy, exertion, and, if you will, fitness as a game like singles tennis.
The upside is it’s gotten many people outdoors getting some exercise and socializing. That’s all to the good. But a recent study suggested that there are about $500 million worth of injuries coming into the health care system associated with pickleball. There have been leg sprains, broken bones, people getting hit in the eye, hamstring pulls, and many other problems. I’ve been told that many of the spectators who show up for pickleball matches are there with a cast or have some kind of a wrap on because they were injured.
Well, many people have argued in the past about what we are going to do about health care costs. Some suggest if you voluntarily incur health care damage, you ought to pay for that yourself and you ought to have a big copay.
If you decide you’re going to do cross-country skiing or downhill skiing and you injure yourself, you chose to do it, so you pay. If you’re not going to maintain your weight, you’re going to smoke, or you’re going to ride around without a helmet, that’s your choice. You ought to pay.
I think the pickleball example is really a good challenge to these views. You obviously want people to go out and get some exercise. Here, we’re talking about a population that’s a little older and oftentimes doesn’t get out there as much as doctors would like to get the exercise that’s still important that they need, and yet it does incur injuries and problems.
My suggestion would be to make the game a little safer. Let’s try to encourage people to warm up more before they get out there and jump out of the car and engage in their pickleball battles. Goggles might be important to prevent the eye injuries in a game that’s played up close. Maybe we want to make sure that people look out for one another out there. If they think they’re getting dehydrated or tired, they should say, “Let’s sit down.”
I’m not willing to put a tax or a copay on the pickleball players of America. I know they choose to do it. It’s got an upside and benefits, as many things like skiing and other behaviors that have some risk do, but I think we want to be encouraging, not discouraging, of it.
I don’t like a society where anybody who tries to do something that takes risk winds up bearing extra cost for doing that. I understand that that gets people irritated when it comes to dangerous, hyper-risky behavior like smoking and not wearing a motorcycle helmet. I think the way to engage is not to call out the sinner or to try and punish those who are trying to do things that bring them enjoyment, reward, or in some of these cases, physical fitness, but to try to make things safer and try to gradually improve and get rid of the risk side to capture the full benefit side.
I’m not sure I’ve come up with all the best ways to make pickleball safer, but I think that’s where our thinking in health care should go. My view is to get out there and play pickleball. If you do pull your hamstring, raise my insurance premium a little bit. I’ll help to pay for it. Better you get some enjoyment and some exercise.
I get the downside, but come on, folks, we ought to be, as a community, somewhat supportive of the fun and recreation that our fellow citizens engage in.
Dr. Caplan is director, division of medical ethics, New York University Langone Medical Center. He disclosed serving as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); and as a contributing author and adviser for Medscape.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
If you’re anywhere near Seattle, anywhere near Florida, or anywhere where it might be not oppressively hot outside but encouraging some people who might want to go out and get a little exercise, you’ve undoubtedly seen or heard of pickleball.
This took off, I think, out of Bainbridge Island, Wash. It was meant as a gentlemanly game where people didn’t exert themselves too much. The joke is you could play it while holding a drink in one hand. It’s gotten more popular and more competitive. It’s kind of a miniature version of tennis, with a smaller court, a plastic ball, and a wooden paddle. The ball can go back and forth rapidly, but you’re always playing doubles and it doesn’t take as much energy, exertion, and, if you will, fitness as a game like singles tennis.
The upside is it’s gotten many people outdoors getting some exercise and socializing. That’s all to the good. But a recent study suggested that there are about $500 million worth of injuries coming into the health care system associated with pickleball. There have been leg sprains, broken bones, people getting hit in the eye, hamstring pulls, and many other problems. I’ve been told that many of the spectators who show up for pickleball matches are there with a cast or have some kind of a wrap on because they were injured.
Well, many people have argued in the past about what we are going to do about health care costs. Some suggest if you voluntarily incur health care damage, you ought to pay for that yourself and you ought to have a big copay.
If you decide you’re going to do cross-country skiing or downhill skiing and you injure yourself, you chose to do it, so you pay. If you’re not going to maintain your weight, you’re going to smoke, or you’re going to ride around without a helmet, that’s your choice. You ought to pay.
I think the pickleball example is really a good challenge to these views. You obviously want people to go out and get some exercise. Here, we’re talking about a population that’s a little older and oftentimes doesn’t get out there as much as doctors would like to get the exercise that’s still important that they need, and yet it does incur injuries and problems.
My suggestion would be to make the game a little safer. Let’s try to encourage people to warm up more before they get out there and jump out of the car and engage in their pickleball battles. Goggles might be important to prevent the eye injuries in a game that’s played up close. Maybe we want to make sure that people look out for one another out there. If they think they’re getting dehydrated or tired, they should say, “Let’s sit down.”
I’m not willing to put a tax or a copay on the pickleball players of America. I know they choose to do it. It’s got an upside and benefits, as many things like skiing and other behaviors that have some risk do, but I think we want to be encouraging, not discouraging, of it.
I don’t like a society where anybody who tries to do something that takes risk winds up bearing extra cost for doing that. I understand that that gets people irritated when it comes to dangerous, hyper-risky behavior like smoking and not wearing a motorcycle helmet. I think the way to engage is not to call out the sinner or to try and punish those who are trying to do things that bring them enjoyment, reward, or in some of these cases, physical fitness, but to try to make things safer and try to gradually improve and get rid of the risk side to capture the full benefit side.
I’m not sure I’ve come up with all the best ways to make pickleball safer, but I think that’s where our thinking in health care should go. My view is to get out there and play pickleball. If you do pull your hamstring, raise my insurance premium a little bit. I’ll help to pay for it. Better you get some enjoyment and some exercise.
I get the downside, but come on, folks, we ought to be, as a community, somewhat supportive of the fun and recreation that our fellow citizens engage in.
Dr. Caplan is director, division of medical ethics, New York University Langone Medical Center. He disclosed serving as a director, officer, partner, employee, adviser, consultant, or trustee for Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position); and as a contributing author and adviser for Medscape.
A version of this article appeared on Medscape.com.