User login
MD-IQ only
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Metabolic modulation may represent a viable therapeutic strategy in pulmonary hypertension (PH), report researchers from the Veterans Affairs Atlanta Healthcare System. Metformin and thiazolidinedione (TZD) were associated with significantly improved survival in their recent retrospective study of 41,670 veterans with PH and diabetes mellitus (DM). Insulin, on the other hand, was associated with increased mortality.
PH is a complex condition that may combine pulmonary vascular disease, heart disease, lung disease, and chronic thromboembolism. More than one-third of veterans with PH also have DM. Veterans are more likely than nonveterans to have chronic cardiopulmonary disease, which may make them particularly susceptible to PH. Moreover, those who served in Iraq and Afghanistan may have respiratory issues that predispose them to PH.
Another study from the same researchers assessed the influence of DM and weight, both potentially modifiable risk factors, on PH outcomes in 110,495 veterans. Veterans with PH survived an average of 3.9 years after PH diagnosis. Roughly one-third had DM, which increased risk of death by 31%. The analysis showed that lower weight and DM were strong risk factors for mortality in PH.
The most striking finding in the current study, according to the researchers, was a consistent reduction of about 20% in mortality risk associated with metformin and a similar association of 18% lower risk with TZD. The contrast with the 28% higher mortality with insulin “likely reflects fundamental differences” in how these medications influence cellular energy metabolism, they reported.
Interactions were observed between drug effects and both renal function and PH comorbidities, with metformin's protective effect enhanced in patients with lower estimated glomerular filtration rate but attenuated in those with lung disease. The associations remained “robust across multiple analytical approaches,” the researchers note.
Hemoglobin A1c was not associated with outcome, suggesting that these therapies' association with outcome may be irrespective of their glycemic effects. The researchers say this emphasizes the complex interplay between DM and PH pathobiology, known differences in mechanisms of action of antidiabetic medications, and potentially off target impacts of these metabolically active therapies.
Metabolic modulation may represent a viable therapeutic strategy in pulmonary hypertension (PH), report researchers from the Veterans Affairs Atlanta Healthcare System. Metformin and thiazolidinedione (TZD) were associated with significantly improved survival in their recent retrospective study of 41,670 veterans with PH and diabetes mellitus (DM). Insulin, on the other hand, was associated with increased mortality.
PH is a complex condition that may combine pulmonary vascular disease, heart disease, lung disease, and chronic thromboembolism. More than one-third of veterans with PH also have DM. Veterans are more likely than nonveterans to have chronic cardiopulmonary disease, which may make them particularly susceptible to PH. Moreover, those who served in Iraq and Afghanistan may have respiratory issues that predispose them to PH.
Another study from the same researchers assessed the influence of DM and weight, both potentially modifiable risk factors, on PH outcomes in 110,495 veterans. Veterans with PH survived an average of 3.9 years after PH diagnosis. Roughly one-third had DM, which increased risk of death by 31%. The analysis showed that lower weight and DM were strong risk factors for mortality in PH.
The most striking finding in the current study, according to the researchers, was a consistent reduction of about 20% in mortality risk associated with metformin and a similar association of 18% lower risk with TZD. The contrast with the 28% higher mortality with insulin “likely reflects fundamental differences” in how these medications influence cellular energy metabolism, they reported.
Interactions were observed between drug effects and both renal function and PH comorbidities, with metformin's protective effect enhanced in patients with lower estimated glomerular filtration rate but attenuated in those with lung disease. The associations remained “robust across multiple analytical approaches,” the researchers note.
Hemoglobin A1c was not associated with outcome, suggesting that these therapies' association with outcome may be irrespective of their glycemic effects. The researchers say this emphasizes the complex interplay between DM and PH pathobiology, known differences in mechanisms of action of antidiabetic medications, and potentially off target impacts of these metabolically active therapies.
Metabolic modulation may represent a viable therapeutic strategy in pulmonary hypertension (PH), report researchers from the Veterans Affairs Atlanta Healthcare System. Metformin and thiazolidinedione (TZD) were associated with significantly improved survival in their recent retrospective study of 41,670 veterans with PH and diabetes mellitus (DM). Insulin, on the other hand, was associated with increased mortality.
PH is a complex condition that may combine pulmonary vascular disease, heart disease, lung disease, and chronic thromboembolism. More than one-third of veterans with PH also have DM. Veterans are more likely than nonveterans to have chronic cardiopulmonary disease, which may make them particularly susceptible to PH. Moreover, those who served in Iraq and Afghanistan may have respiratory issues that predispose them to PH.
Another study from the same researchers assessed the influence of DM and weight, both potentially modifiable risk factors, on PH outcomes in 110,495 veterans. Veterans with PH survived an average of 3.9 years after PH diagnosis. Roughly one-third had DM, which increased risk of death by 31%. The analysis showed that lower weight and DM were strong risk factors for mortality in PH.
The most striking finding in the current study, according to the researchers, was a consistent reduction of about 20% in mortality risk associated with metformin and a similar association of 18% lower risk with TZD. The contrast with the 28% higher mortality with insulin “likely reflects fundamental differences” in how these medications influence cellular energy metabolism, they reported.
Interactions were observed between drug effects and both renal function and PH comorbidities, with metformin's protective effect enhanced in patients with lower estimated glomerular filtration rate but attenuated in those with lung disease. The associations remained “robust across multiple analytical approaches,” the researchers note.
Hemoglobin A1c was not associated with outcome, suggesting that these therapies' association with outcome may be irrespective of their glycemic effects. The researchers say this emphasizes the complex interplay between DM and PH pathobiology, known differences in mechanisms of action of antidiabetic medications, and potentially off target impacts of these metabolically active therapies.
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Antidiabetic Therapies May Help Comorbid Pulmonary Hypertension in Veterans
Ralinepag Offers Once Daily Oral Option for PAH
Ralinepag Offers Once Daily Oral Option for PAH
Treatment with ralinepag, an investigational prostacyclin receptor agonist, reduced the risk for clinical disease worsening by 55% compared to placebo in patients with pulmonary arterial hypertension (PAH), based on new data from the ADVANCE Outcomes study presented at the American Thoracic Society (ATS) 2026 International Conference.
Ralinepag works by restoring prostacyclin signaling and activating prostacyclin receptors to affect pathways that play a role in the progression of PAH. The drug was originally formulated as an immediate-release capsule but modified to the extended-release tablet used in the current study as a way to optimize once daily dosing.
“The prostacyclin pathway is foundational in the management of PAH, and advancing prostacyclin science has benefited patients over the years,” said lead author Vallerie V. McLaughlin, MD, professor of cardiovascular medicine and director of the Pulmonary Hypertension Program at the University of Michigan, Ann Arbor, Michigan, who presented the findings at the meeting. Although other oral prostacyclin pathway agents available, ralinepag has the advantages of high potency and longer half-life that could be effective and well-tolerated in a more patient-friendly once daily formulation, McLaughlin said.
The international study population included 687 adults with PAH from 30 countries across five continents. Participants were randomized to ralinepag or placebo in addition to their standard PAH background therapies. Ralinepag was orally dosed once daily and titrated for tolerability and response. The mean age of the participants was 52 years, 80% were White, and the median time since PAH diagnosis was 2.3 years. A majority of 62% had idiopathic or heritable PAH, 28.2% had PAH as a result of connective tissue disease, 4.1% had a congenital heart defect, 3.1% had drug- or toxin-induced PAH, and 2.6% had PAH as a result of HIV infection. More than two thirds were considered low risk (characterized as Functional Class II).
The primary endpoint was the time to first indication of clinical worsening, which was defined as death, hospital admission for worsening PAH, initiation of a parenteral or inhaled prostacyclin pathway agent for worsening PAH, or unsatisfactory long-term clinical response.
Overall, patients treated with ralinepag were significantly less likely to experience a clinical worsening event than placebo patients (hazard ratio [HR], 0.45; 95% CI, 0.33-0.62; P < .0001), and 47% more likely to achieve the secondary endpoint of clinical improvement (P = .015).
Patients treated with ralinepag also showed significant improvements over placebo patients in the secondary endpoints of pro-B-type natriuretic peptide levels (24.3% reduction from baseline to week 28 over placebo; P = .0013), and in the 6-minute walk test (a placebo-corrected difference of 20.4 m from baseline to week 28; P = .0033).
Although more than 90% of participants treated with ralinepag reported an adverse event related to the drug, approximately 5% experienced drug-related serious adverse events, and the overall safety profile reflected previous ralinepag studies, with a positive risk-benefit ratio, the investigators noted.
Support for Early Introduction
The researchers expected the efficacy associated with prostacyclin therapy, said McLaughlin. “We were very pleased to see such a strong treatment effect in a relatively low-risk population, primarily Functional Class II with a mean 6-minute walk of nearly 440 meters, with the majority of patients on dual oral therapy,” she said.
If approved, ralinepag could help optimized risk status in PAH, said McLaughlin. “Many patients do not get to low risk with first-line therapy, and oral and inhaled prostacyclin pathway agents are often used in addition to dual therapy with phosphodiesterase type-5 inhibitors and endothelin receptor antagonists,” she said. “The impressive treatment effect of ralinepag in patients primarily treated with dual oral therapy reflects this real-world scenario,” she added. The significant event reduction makes a case for earlier introduction of ralinepag in relatively low-risk patients; a highly effective therapy that targets the prostacyclin pathway may reduce the need for more cumbersome and invasive prostacyclin therapies, McLaughlin added.
Ralinepag remains an investigational drug, but the company plans to seek a New Drug Application from the FDA for the treatment of PAH by the second half of 2026, according to a press release.
The research team would like to continue evaluating the ADVANCE Outcomes database to learn more about dose response, tolerability, and subgroup response, said McLaughlin. At that point, real-world data would be useful, and additional research areas in that setting would include combination therapy with other agents such as sotatercept, as well as the use of ralinepag to transition patients on more complicated and invasive therapy, she said.
Attention to Adverse Effects
Prostacyclin therapies are often offered in oral, inhaled, and the most invasive intravenous/subcutaneous routes, but a gap remains between the strong efficacy seen with parenteral therapy and what many patients are willing or able to use in real-world practice, said Parth M. Rali, MD, director of the Temple University Health System Pulmonary Embolism Response Team Program, Section Temple Lung Pulmonary Vascular Disease Program, Philadelphia, who was not involved in the study.
“Ralinepag provides sustained activation of IP receptors and has very long effective half-life, giving drug exposure comparable to parenteral therapy, and offers the first daily treatment option, which is important for the patients with PAH who are often on multiple drugs therapies,” Rali said.
Given the encouraging phase 2 findings demonstrating meaningful reductions in pulmonary vascular resistance and signals toward clinical benefit, we would like to see a favorable outcome in the phase 3 program. Primary outcome studied was time to clinical worsening in the large, randomized trial that involved global populations from the US, Europe, Latin-America, and Asia Pacific Region. Ralinepag arm had 55% reduction in risk for clinical worsening (HR, ~ 0.45) compared to placebo arm. “The positive results of the trial were primarily driven by disease progression, initiation of prostacyclin therapy, and unsatisfactory long-term clinical response at 28 weeks in ralinepag group compared to placebo group,” Rali said.
Although ralinepag offers a good option for once-a-day oral prostacyclin options for the patients, the significant number of patients in the new study who discontinued because of adverse effects is notable, said Rali. “Treating clinicians will have to watch very closely, as the real-world patient population seems to be more complex than clinical trial populations,” he said. “At the same time, clinicians will have an option to weigh against growing list of inhaled prostacyclin pathway therapies that may not have systemic side effects of the oral agents,” he added.
“Given the strong scientific data in the ADVANCE trials, ralinepag may become drug of choice for oral prostacyclin pathway agents,” Rali added. However, its place in the treatment sequence, whether it is best used early in the disease course, as an add-on for patients already receiving dual oral therapy, or potentially part of upfront combination strategies, will call for some clinician judgement, Rali said. “Patient education and gradual dose titration will likely play a major role in improving adherence and limiting prostacyclin-related adverse effects,” he added.
Questions for future research include what percentage of the patients were able to tolerate the maximum dose of the drug, and whether any changes in primary or secondary outcomes occurred depending on the dose, said Rali. Other areas of interest include whether certain patient populations derive greater benefit than others, including connective tissue disease-associated PAH, idiopathic PAH, and higher-risk patient populations. “Comparative effectiveness data against currently available oral prostacyclin pathway agents and studies evaluating transition strategies from parenteral or inhaled therapies would help clinicians better understand where ralinepag ultimately fits in the PAH treatment algorithm,” Rali said. “I also would be curious to see what the authors thought of the failure to achieve the primary endpoint in cohorts of patients from Latin America and Asia Pacific regions,” he added.
The study was funded by United Therapeutics, and McLaughlin disclosed serving as a consultant for the company. Rali had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Treatment with ralinepag, an investigational prostacyclin receptor agonist, reduced the risk for clinical disease worsening by 55% compared to placebo in patients with pulmonary arterial hypertension (PAH), based on new data from the ADVANCE Outcomes study presented at the American Thoracic Society (ATS) 2026 International Conference.
Ralinepag works by restoring prostacyclin signaling and activating prostacyclin receptors to affect pathways that play a role in the progression of PAH. The drug was originally formulated as an immediate-release capsule but modified to the extended-release tablet used in the current study as a way to optimize once daily dosing.
“The prostacyclin pathway is foundational in the management of PAH, and advancing prostacyclin science has benefited patients over the years,” said lead author Vallerie V. McLaughlin, MD, professor of cardiovascular medicine and director of the Pulmonary Hypertension Program at the University of Michigan, Ann Arbor, Michigan, who presented the findings at the meeting. Although other oral prostacyclin pathway agents available, ralinepag has the advantages of high potency and longer half-life that could be effective and well-tolerated in a more patient-friendly once daily formulation, McLaughlin said.
The international study population included 687 adults with PAH from 30 countries across five continents. Participants were randomized to ralinepag or placebo in addition to their standard PAH background therapies. Ralinepag was orally dosed once daily and titrated for tolerability and response. The mean age of the participants was 52 years, 80% were White, and the median time since PAH diagnosis was 2.3 years. A majority of 62% had idiopathic or heritable PAH, 28.2% had PAH as a result of connective tissue disease, 4.1% had a congenital heart defect, 3.1% had drug- or toxin-induced PAH, and 2.6% had PAH as a result of HIV infection. More than two thirds were considered low risk (characterized as Functional Class II).
The primary endpoint was the time to first indication of clinical worsening, which was defined as death, hospital admission for worsening PAH, initiation of a parenteral or inhaled prostacyclin pathway agent for worsening PAH, or unsatisfactory long-term clinical response.
Overall, patients treated with ralinepag were significantly less likely to experience a clinical worsening event than placebo patients (hazard ratio [HR], 0.45; 95% CI, 0.33-0.62; P < .0001), and 47% more likely to achieve the secondary endpoint of clinical improvement (P = .015).
Patients treated with ralinepag also showed significant improvements over placebo patients in the secondary endpoints of pro-B-type natriuretic peptide levels (24.3% reduction from baseline to week 28 over placebo; P = .0013), and in the 6-minute walk test (a placebo-corrected difference of 20.4 m from baseline to week 28; P = .0033).
Although more than 90% of participants treated with ralinepag reported an adverse event related to the drug, approximately 5% experienced drug-related serious adverse events, and the overall safety profile reflected previous ralinepag studies, with a positive risk-benefit ratio, the investigators noted.
Support for Early Introduction
The researchers expected the efficacy associated with prostacyclin therapy, said McLaughlin. “We were very pleased to see such a strong treatment effect in a relatively low-risk population, primarily Functional Class II with a mean 6-minute walk of nearly 440 meters, with the majority of patients on dual oral therapy,” she said.
If approved, ralinepag could help optimized risk status in PAH, said McLaughlin. “Many patients do not get to low risk with first-line therapy, and oral and inhaled prostacyclin pathway agents are often used in addition to dual therapy with phosphodiesterase type-5 inhibitors and endothelin receptor antagonists,” she said. “The impressive treatment effect of ralinepag in patients primarily treated with dual oral therapy reflects this real-world scenario,” she added. The significant event reduction makes a case for earlier introduction of ralinepag in relatively low-risk patients; a highly effective therapy that targets the prostacyclin pathway may reduce the need for more cumbersome and invasive prostacyclin therapies, McLaughlin added.
Ralinepag remains an investigational drug, but the company plans to seek a New Drug Application from the FDA for the treatment of PAH by the second half of 2026, according to a press release.
The research team would like to continue evaluating the ADVANCE Outcomes database to learn more about dose response, tolerability, and subgroup response, said McLaughlin. At that point, real-world data would be useful, and additional research areas in that setting would include combination therapy with other agents such as sotatercept, as well as the use of ralinepag to transition patients on more complicated and invasive therapy, she said.
Attention to Adverse Effects
Prostacyclin therapies are often offered in oral, inhaled, and the most invasive intravenous/subcutaneous routes, but a gap remains between the strong efficacy seen with parenteral therapy and what many patients are willing or able to use in real-world practice, said Parth M. Rali, MD, director of the Temple University Health System Pulmonary Embolism Response Team Program, Section Temple Lung Pulmonary Vascular Disease Program, Philadelphia, who was not involved in the study.
“Ralinepag provides sustained activation of IP receptors and has very long effective half-life, giving drug exposure comparable to parenteral therapy, and offers the first daily treatment option, which is important for the patients with PAH who are often on multiple drugs therapies,” Rali said.
Given the encouraging phase 2 findings demonstrating meaningful reductions in pulmonary vascular resistance and signals toward clinical benefit, we would like to see a favorable outcome in the phase 3 program. Primary outcome studied was time to clinical worsening in the large, randomized trial that involved global populations from the US, Europe, Latin-America, and Asia Pacific Region. Ralinepag arm had 55% reduction in risk for clinical worsening (HR, ~ 0.45) compared to placebo arm. “The positive results of the trial were primarily driven by disease progression, initiation of prostacyclin therapy, and unsatisfactory long-term clinical response at 28 weeks in ralinepag group compared to placebo group,” Rali said.
Although ralinepag offers a good option for once-a-day oral prostacyclin options for the patients, the significant number of patients in the new study who discontinued because of adverse effects is notable, said Rali. “Treating clinicians will have to watch very closely, as the real-world patient population seems to be more complex than clinical trial populations,” he said. “At the same time, clinicians will have an option to weigh against growing list of inhaled prostacyclin pathway therapies that may not have systemic side effects of the oral agents,” he added.
“Given the strong scientific data in the ADVANCE trials, ralinepag may become drug of choice for oral prostacyclin pathway agents,” Rali added. However, its place in the treatment sequence, whether it is best used early in the disease course, as an add-on for patients already receiving dual oral therapy, or potentially part of upfront combination strategies, will call for some clinician judgement, Rali said. “Patient education and gradual dose titration will likely play a major role in improving adherence and limiting prostacyclin-related adverse effects,” he added.
Questions for future research include what percentage of the patients were able to tolerate the maximum dose of the drug, and whether any changes in primary or secondary outcomes occurred depending on the dose, said Rali. Other areas of interest include whether certain patient populations derive greater benefit than others, including connective tissue disease-associated PAH, idiopathic PAH, and higher-risk patient populations. “Comparative effectiveness data against currently available oral prostacyclin pathway agents and studies evaluating transition strategies from parenteral or inhaled therapies would help clinicians better understand where ralinepag ultimately fits in the PAH treatment algorithm,” Rali said. “I also would be curious to see what the authors thought of the failure to achieve the primary endpoint in cohorts of patients from Latin America and Asia Pacific regions,” he added.
The study was funded by United Therapeutics, and McLaughlin disclosed serving as a consultant for the company. Rali had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Treatment with ralinepag, an investigational prostacyclin receptor agonist, reduced the risk for clinical disease worsening by 55% compared to placebo in patients with pulmonary arterial hypertension (PAH), based on new data from the ADVANCE Outcomes study presented at the American Thoracic Society (ATS) 2026 International Conference.
Ralinepag works by restoring prostacyclin signaling and activating prostacyclin receptors to affect pathways that play a role in the progression of PAH. The drug was originally formulated as an immediate-release capsule but modified to the extended-release tablet used in the current study as a way to optimize once daily dosing.
“The prostacyclin pathway is foundational in the management of PAH, and advancing prostacyclin science has benefited patients over the years,” said lead author Vallerie V. McLaughlin, MD, professor of cardiovascular medicine and director of the Pulmonary Hypertension Program at the University of Michigan, Ann Arbor, Michigan, who presented the findings at the meeting. Although other oral prostacyclin pathway agents available, ralinepag has the advantages of high potency and longer half-life that could be effective and well-tolerated in a more patient-friendly once daily formulation, McLaughlin said.
The international study population included 687 adults with PAH from 30 countries across five continents. Participants were randomized to ralinepag or placebo in addition to their standard PAH background therapies. Ralinepag was orally dosed once daily and titrated for tolerability and response. The mean age of the participants was 52 years, 80% were White, and the median time since PAH diagnosis was 2.3 years. A majority of 62% had idiopathic or heritable PAH, 28.2% had PAH as a result of connective tissue disease, 4.1% had a congenital heart defect, 3.1% had drug- or toxin-induced PAH, and 2.6% had PAH as a result of HIV infection. More than two thirds were considered low risk (characterized as Functional Class II).
The primary endpoint was the time to first indication of clinical worsening, which was defined as death, hospital admission for worsening PAH, initiation of a parenteral or inhaled prostacyclin pathway agent for worsening PAH, or unsatisfactory long-term clinical response.
Overall, patients treated with ralinepag were significantly less likely to experience a clinical worsening event than placebo patients (hazard ratio [HR], 0.45; 95% CI, 0.33-0.62; P < .0001), and 47% more likely to achieve the secondary endpoint of clinical improvement (P = .015).
Patients treated with ralinepag also showed significant improvements over placebo patients in the secondary endpoints of pro-B-type natriuretic peptide levels (24.3% reduction from baseline to week 28 over placebo; P = .0013), and in the 6-minute walk test (a placebo-corrected difference of 20.4 m from baseline to week 28; P = .0033).
Although more than 90% of participants treated with ralinepag reported an adverse event related to the drug, approximately 5% experienced drug-related serious adverse events, and the overall safety profile reflected previous ralinepag studies, with a positive risk-benefit ratio, the investigators noted.
Support for Early Introduction
The researchers expected the efficacy associated with prostacyclin therapy, said McLaughlin. “We were very pleased to see such a strong treatment effect in a relatively low-risk population, primarily Functional Class II with a mean 6-minute walk of nearly 440 meters, with the majority of patients on dual oral therapy,” she said.
If approved, ralinepag could help optimized risk status in PAH, said McLaughlin. “Many patients do not get to low risk with first-line therapy, and oral and inhaled prostacyclin pathway agents are often used in addition to dual therapy with phosphodiesterase type-5 inhibitors and endothelin receptor antagonists,” she said. “The impressive treatment effect of ralinepag in patients primarily treated with dual oral therapy reflects this real-world scenario,” she added. The significant event reduction makes a case for earlier introduction of ralinepag in relatively low-risk patients; a highly effective therapy that targets the prostacyclin pathway may reduce the need for more cumbersome and invasive prostacyclin therapies, McLaughlin added.
Ralinepag remains an investigational drug, but the company plans to seek a New Drug Application from the FDA for the treatment of PAH by the second half of 2026, according to a press release.
The research team would like to continue evaluating the ADVANCE Outcomes database to learn more about dose response, tolerability, and subgroup response, said McLaughlin. At that point, real-world data would be useful, and additional research areas in that setting would include combination therapy with other agents such as sotatercept, as well as the use of ralinepag to transition patients on more complicated and invasive therapy, she said.
Attention to Adverse Effects
Prostacyclin therapies are often offered in oral, inhaled, and the most invasive intravenous/subcutaneous routes, but a gap remains between the strong efficacy seen with parenteral therapy and what many patients are willing or able to use in real-world practice, said Parth M. Rali, MD, director of the Temple University Health System Pulmonary Embolism Response Team Program, Section Temple Lung Pulmonary Vascular Disease Program, Philadelphia, who was not involved in the study.
“Ralinepag provides sustained activation of IP receptors and has very long effective half-life, giving drug exposure comparable to parenteral therapy, and offers the first daily treatment option, which is important for the patients with PAH who are often on multiple drugs therapies,” Rali said.
Given the encouraging phase 2 findings demonstrating meaningful reductions in pulmonary vascular resistance and signals toward clinical benefit, we would like to see a favorable outcome in the phase 3 program. Primary outcome studied was time to clinical worsening in the large, randomized trial that involved global populations from the US, Europe, Latin-America, and Asia Pacific Region. Ralinepag arm had 55% reduction in risk for clinical worsening (HR, ~ 0.45) compared to placebo arm. “The positive results of the trial were primarily driven by disease progression, initiation of prostacyclin therapy, and unsatisfactory long-term clinical response at 28 weeks in ralinepag group compared to placebo group,” Rali said.
Although ralinepag offers a good option for once-a-day oral prostacyclin options for the patients, the significant number of patients in the new study who discontinued because of adverse effects is notable, said Rali. “Treating clinicians will have to watch very closely, as the real-world patient population seems to be more complex than clinical trial populations,” he said. “At the same time, clinicians will have an option to weigh against growing list of inhaled prostacyclin pathway therapies that may not have systemic side effects of the oral agents,” he added.
“Given the strong scientific data in the ADVANCE trials, ralinepag may become drug of choice for oral prostacyclin pathway agents,” Rali added. However, its place in the treatment sequence, whether it is best used early in the disease course, as an add-on for patients already receiving dual oral therapy, or potentially part of upfront combination strategies, will call for some clinician judgement, Rali said. “Patient education and gradual dose titration will likely play a major role in improving adherence and limiting prostacyclin-related adverse effects,” he added.
Questions for future research include what percentage of the patients were able to tolerate the maximum dose of the drug, and whether any changes in primary or secondary outcomes occurred depending on the dose, said Rali. Other areas of interest include whether certain patient populations derive greater benefit than others, including connective tissue disease-associated PAH, idiopathic PAH, and higher-risk patient populations. “Comparative effectiveness data against currently available oral prostacyclin pathway agents and studies evaluating transition strategies from parenteral or inhaled therapies would help clinicians better understand where ralinepag ultimately fits in the PAH treatment algorithm,” Rali said. “I also would be curious to see what the authors thought of the failure to achieve the primary endpoint in cohorts of patients from Latin America and Asia Pacific regions,” he added.
The study was funded by United Therapeutics, and McLaughlin disclosed serving as a consultant for the company. Rali had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Ralinepag Offers Once Daily Oral Option for PAH
Ralinepag Offers Once Daily Oral Option for PAH
Pulmonology Data Trends 2024
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:

Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:
Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Pulmonology Data Trends 2024 is a supplement to CHEST Physician highlighting the latest breakthroughs in pulmonology research and treatments through a series of infographics.
Read more:
Artificial Intelligence in Sleep Apnea
Ritwick Agrawal, MD, MS, FCCP
RSV Updates: Prophylaxis Approval and Hospitalization for Severe RSV
Riddhi Upadhyay, MD
Biologics in Asthma: Changing the Severe Asthma Paradigm
Shyam Subramanian, MD, FCCP
Updates in COPD Guidelines and Treatment
Dharani K. Narendra, MD, FCCP
Targeted Therapies and Surgical Resection for Lung Cancer: Evolving Treatment Options
Saadia A. Faiz, MD, FCCP
Closing the GAP in Idiopathic Pulmonary Fibrosis
Humayun Anjum, MD, FCCP
Severe Community-Acquired Pneumonia: Diagnostic Criteria, Treatment, and COVID-19
Sujith V. Cherian, MD, FCCP
Pulmonary Hypertension: Comorbidities and Novel Therapies
Mary Jo S. Farmer, MD, PhD, FCCP
The Genetic Side of Interstitial Lung Disease
Priya Balakrishnan, MD, MS, FCCP
Noninvasive Ventilation in Neuromuscular Disease
Sreelatha Naik, MD, FCCP, and Kelly Lobrutto, CRNP
Pulmonary Hypertension: Comorbidities and Novel Therapeutics
- Cullivan S, Gaine S, Sitbon O. New trends in pulmonary hypertension. Eur Respir Rev. 2023;32(167):220211. doi:10.1183/16000617.0211-2022
- Mocumbi A, Humbert M, Saxena A, et al. Pulmonary hypertension [published correction appears in Nat Rev Dis Primers. 2024;10(1):5]. Nat Rev Dis Primers. 2024;10(1):1. doi:10.1038/s41572-023-00486-7
- Lang IM, Palazzini M. The burden of comorbidities in pulmonary arterial hypertension. Eur Heart J Suppl. 2019;21(suppl K):K21-K28. doi:10.1093/ eurheartj/suz205
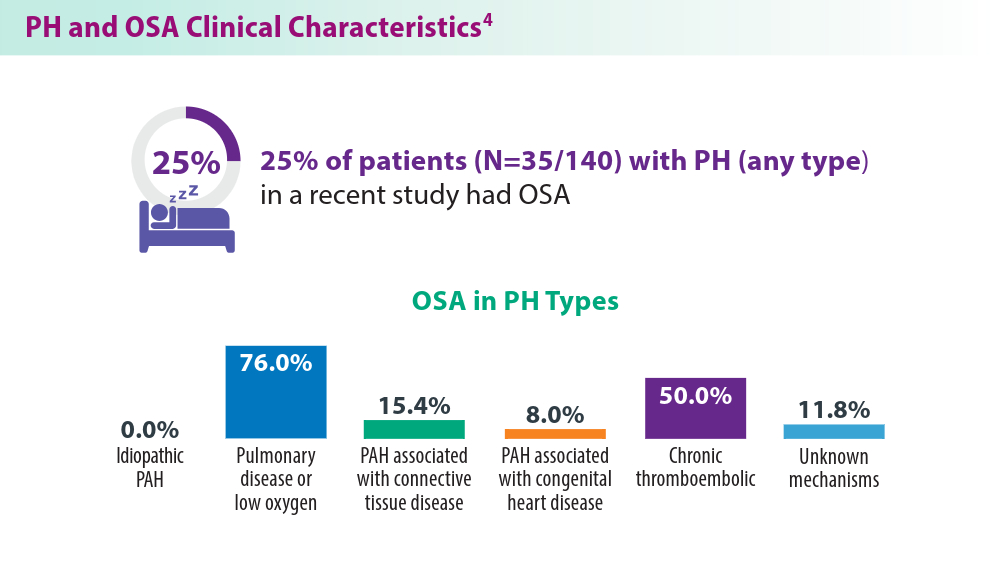
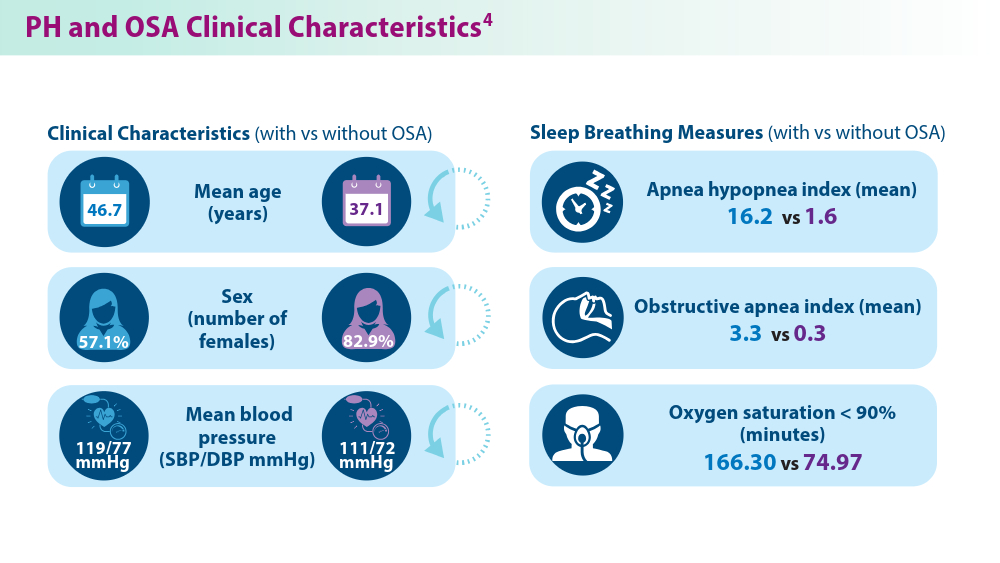
- Yan L, Zhao Z, Zhao Q, et al. The clinical characteristics of patients with pulmonary hypertension combined with obstructive sleep apnoea. BMC Pulm Med. 2021;21(1):378. doi:10.1186/s12890-021-01755-5
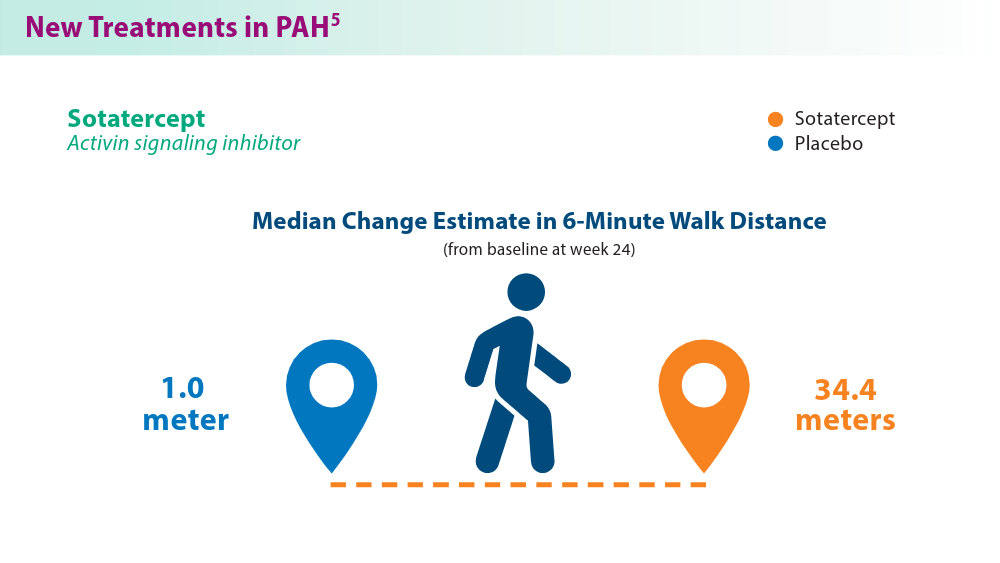
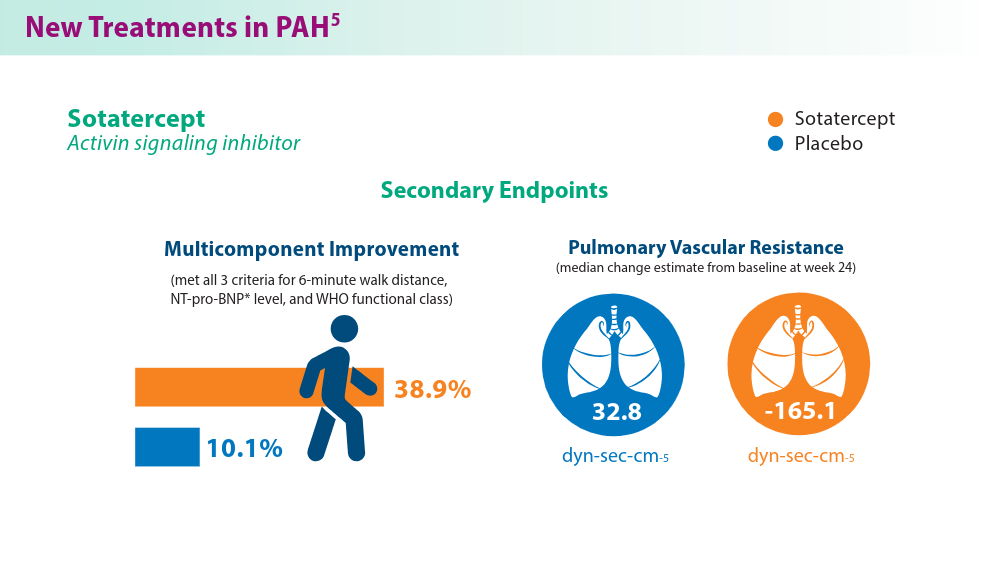
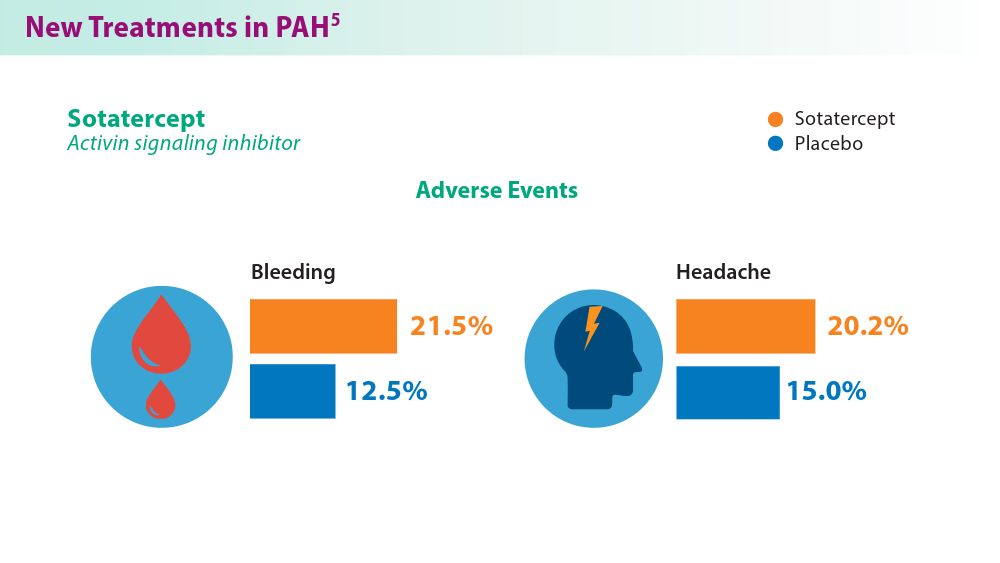
- Hoeper MM, Badesch DB, Ghofrani HA, et al; for the STELLAR Trial Investigators. Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. N Engl J Med. 2023;388(16):1478-1490. doi:10.1056/NEJMoa2213558
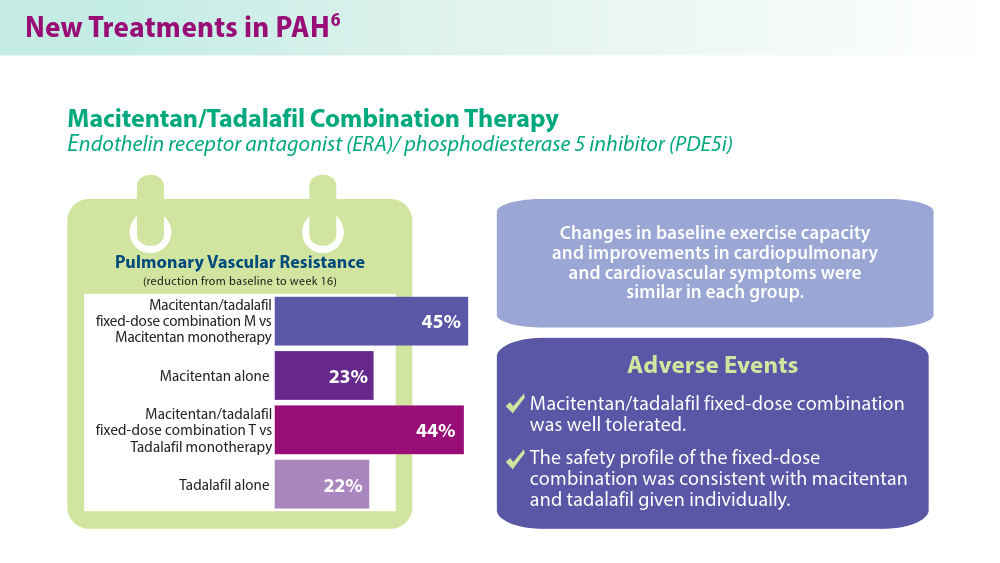
- Grünig E, Jansa P, Fan F, et al. Randomized trial of macitentan/tadalafil single-tablet combination therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2024;83(4):473-484. doi:10.1016/j.jacc.2023.10.045
- Higuchi S, Horinouchi H, Aoki T, et al. Balloon pulmonary angioplasty in the management of chronic thromboembolic pulmonary hypertension. Radiographics. 2022;42(6):1881-1896. doi:10.1148/rg.210102
- Cullivan S, Gaine S, Sitbon O. New trends in pulmonary hypertension. Eur Respir Rev. 2023;32(167):220211. doi:10.1183/16000617.0211-2022
- Mocumbi A, Humbert M, Saxena A, et al. Pulmonary hypertension [published correction appears in Nat Rev Dis Primers. 2024;10(1):5]. Nat Rev Dis Primers. 2024;10(1):1. doi:10.1038/s41572-023-00486-7
- Lang IM, Palazzini M. The burden of comorbidities in pulmonary arterial hypertension. Eur Heart J Suppl. 2019;21(suppl K):K21-K28. doi:10.1093/ eurheartj/suz205
- Yan L, Zhao Z, Zhao Q, et al. The clinical characteristics of patients with pulmonary hypertension combined with obstructive sleep apnoea. BMC Pulm Med. 2021;21(1):378. doi:10.1186/s12890-021-01755-5
- Hoeper MM, Badesch DB, Ghofrani HA, et al; for the STELLAR Trial Investigators. Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. N Engl J Med. 2023;388(16):1478-1490. doi:10.1056/NEJMoa2213558
- Grünig E, Jansa P, Fan F, et al. Randomized trial of macitentan/tadalafil single-tablet combination therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2024;83(4):473-484. doi:10.1016/j.jacc.2023.10.045
- Higuchi S, Horinouchi H, Aoki T, et al. Balloon pulmonary angioplasty in the management of chronic thromboembolic pulmonary hypertension. Radiographics. 2022;42(6):1881-1896. doi:10.1148/rg.210102
- Cullivan S, Gaine S, Sitbon O. New trends in pulmonary hypertension. Eur Respir Rev. 2023;32(167):220211. doi:10.1183/16000617.0211-2022
- Mocumbi A, Humbert M, Saxena A, et al. Pulmonary hypertension [published correction appears in Nat Rev Dis Primers. 2024;10(1):5]. Nat Rev Dis Primers. 2024;10(1):1. doi:10.1038/s41572-023-00486-7
- Lang IM, Palazzini M. The burden of comorbidities in pulmonary arterial hypertension. Eur Heart J Suppl. 2019;21(suppl K):K21-K28. doi:10.1093/ eurheartj/suz205
- Yan L, Zhao Z, Zhao Q, et al. The clinical characteristics of patients with pulmonary hypertension combined with obstructive sleep apnoea. BMC Pulm Med. 2021;21(1):378. doi:10.1186/s12890-021-01755-5
- Hoeper MM, Badesch DB, Ghofrani HA, et al; for the STELLAR Trial Investigators. Phase 3 trial of sotatercept for treatment of pulmonary arterial hypertension. N Engl J Med. 2023;388(16):1478-1490. doi:10.1056/NEJMoa2213558
- Grünig E, Jansa P, Fan F, et al. Randomized trial of macitentan/tadalafil single-tablet combination therapy for pulmonary arterial hypertension. J Am Coll Cardiol. 2024;83(4):473-484. doi:10.1016/j.jacc.2023.10.045
- Higuchi S, Horinouchi H, Aoki T, et al. Balloon pulmonary angioplasty in the management of chronic thromboembolic pulmonary hypertension. Radiographics. 2022;42(6):1881-1896. doi:10.1148/rg.210102
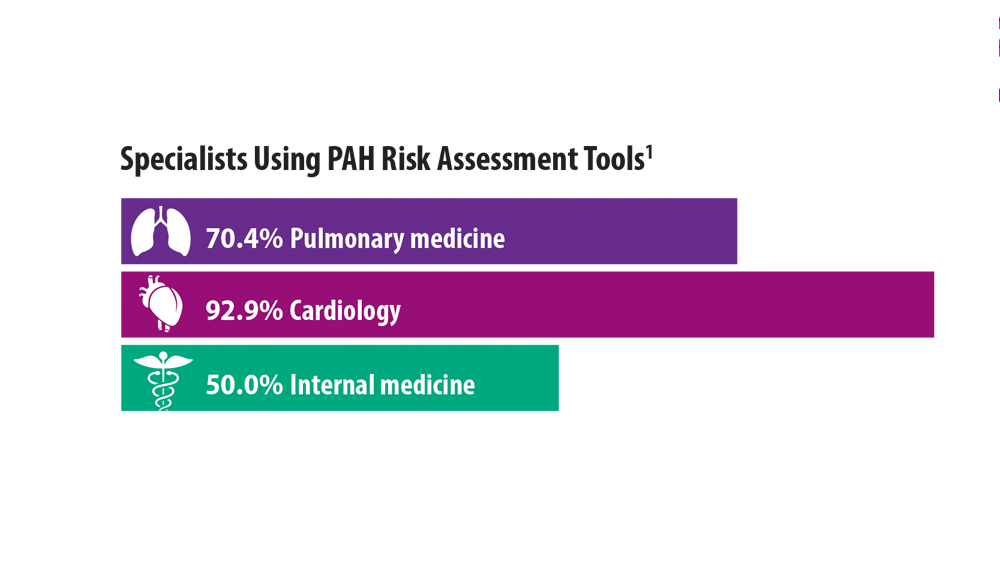
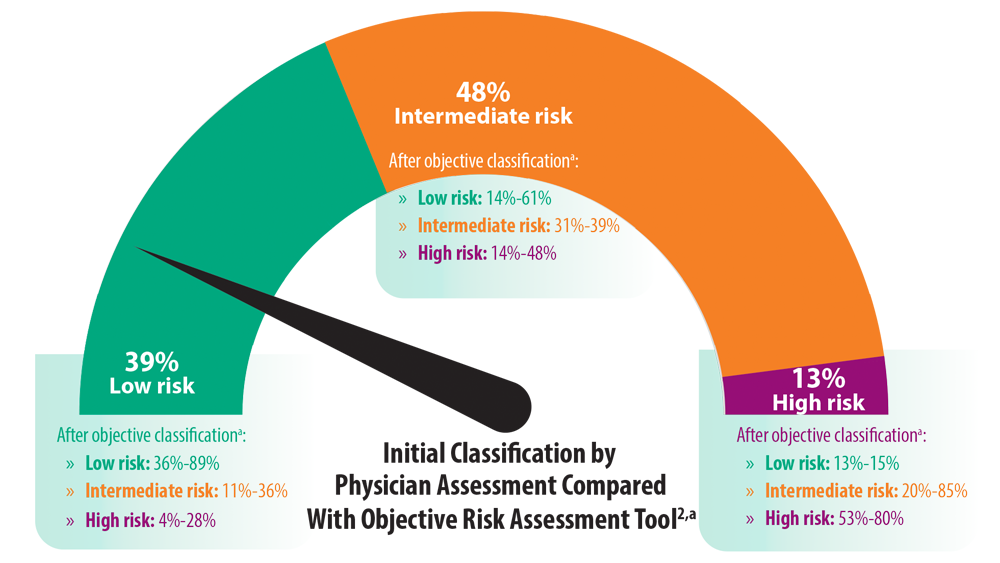
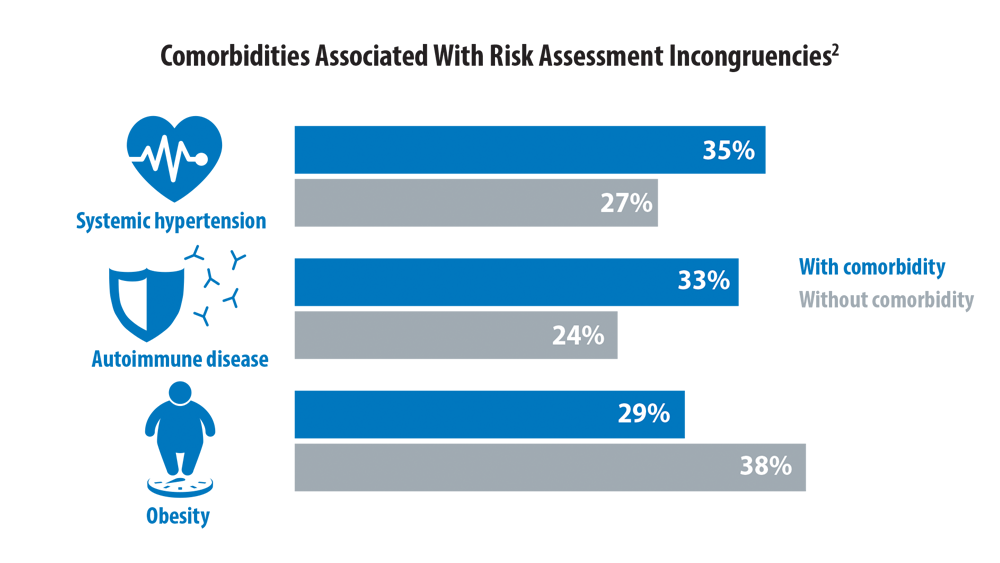
Risk Assessment in Pulmonary Arterial Hypertension
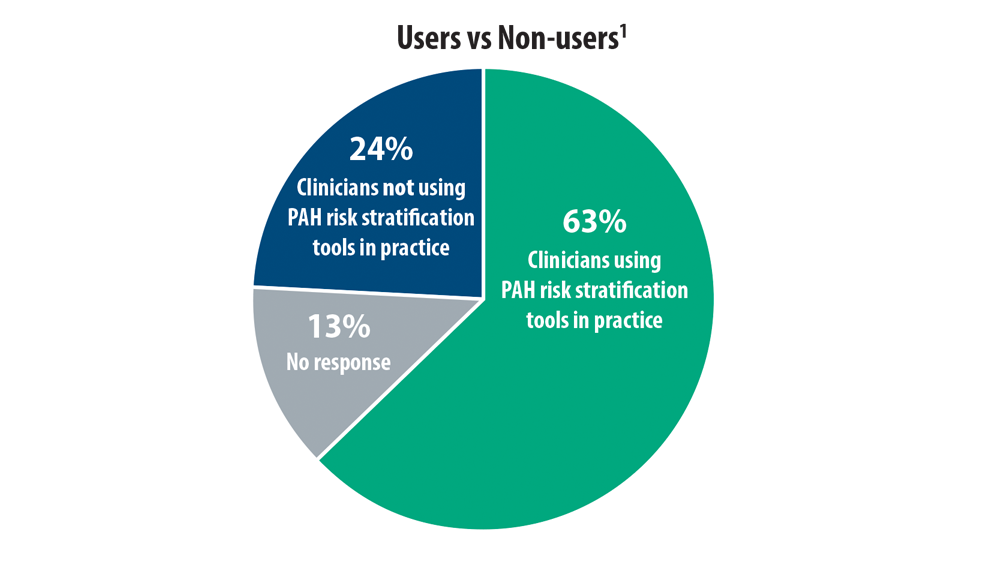
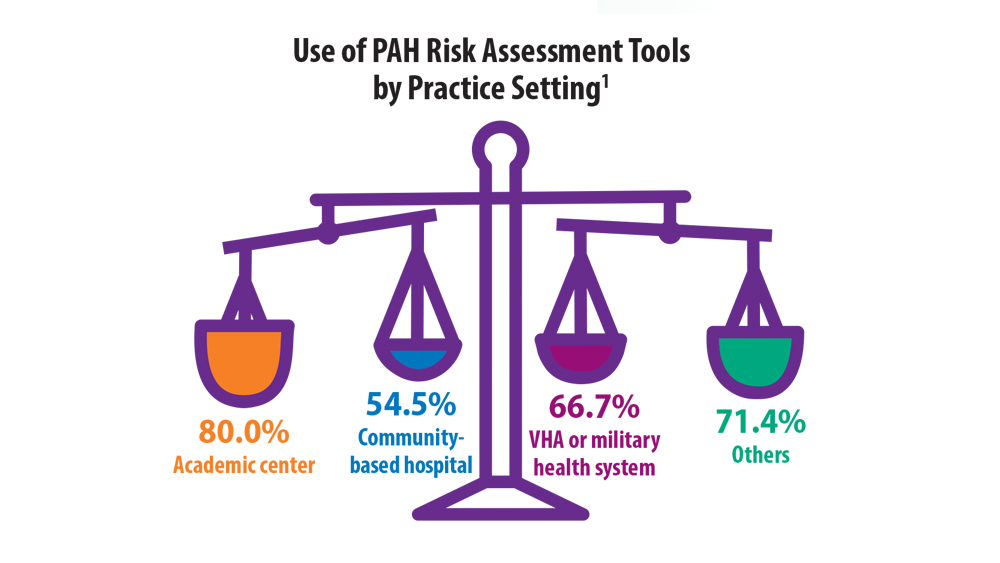
- Sahay S, Balasubramanian V, Memon H, et al. Utilization of risk assessment tools in management of PAH: a PAH provider survey. Pulm Circ. 2022;12(2):e12057. doi:10.1002/pul2.12057
- Sahay S, Tonelli AR, Selej M, Watson Z, Benza RL. Risk assessment in patients with functional class II pulmonary arterial hypertension: comparison of physician gestalt with ESC/ERS and the REVEAL 2.0 risk score. PLoS One. 2020;15(11):e0241504. doi:10.1371/journal.pone.0241504
- Galiè N, Channick RN, Frantz RP, et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur Respir J. 2019;53(1):1801889. doi:10.1183/13993003.01889-2018
- Boucly A, Weatherald J, Savale L, et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur Respir J. 2017;50(2):1700889. doi:10.1183/13993003.00889-2017
- Wilson M, Keeley J, Kingman M, Wang J, Rogers F. Current clinical utilization of risk assessment tools in pulmonary arterial hypertension: a descriptive survey of facilitation strategies, patterns, and barriers to use in the United States. Pulm Circ. 2020;10(3):2045894020950186. doi:10.1177/2045894020950186
- Sahay S, Balasubramanian V, Memon H, et al. Utilization of risk assessment tools in management of PAH: a PAH provider survey. Pulm Circ. 2022;12(2):e12057. doi:10.1002/pul2.12057
- Sahay S, Tonelli AR, Selej M, Watson Z, Benza RL. Risk assessment in patients with functional class II pulmonary arterial hypertension: comparison of physician gestalt with ESC/ERS and the REVEAL 2.0 risk score. PLoS One. 2020;15(11):e0241504. doi:10.1371/journal.pone.0241504
- Galiè N, Channick RN, Frantz RP, et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur Respir J. 2019;53(1):1801889. doi:10.1183/13993003.01889-2018
- Boucly A, Weatherald J, Savale L, et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur Respir J. 2017;50(2):1700889. doi:10.1183/13993003.00889-2017
- Wilson M, Keeley J, Kingman M, Wang J, Rogers F. Current clinical utilization of risk assessment tools in pulmonary arterial hypertension: a descriptive survey of facilitation strategies, patterns, and barriers to use in the United States. Pulm Circ. 2020;10(3):2045894020950186. doi:10.1177/2045894020950186
- Sahay S, Balasubramanian V, Memon H, et al. Utilization of risk assessment tools in management of PAH: a PAH provider survey. Pulm Circ. 2022;12(2):e12057. doi:10.1002/pul2.12057
- Sahay S, Tonelli AR, Selej M, Watson Z, Benza RL. Risk assessment in patients with functional class II pulmonary arterial hypertension: comparison of physician gestalt with ESC/ERS and the REVEAL 2.0 risk score. PLoS One. 2020;15(11):e0241504. doi:10.1371/journal.pone.0241504
- Galiè N, Channick RN, Frantz RP, et al. Risk stratification and medical therapy of pulmonary arterial hypertension. Eur Respir J. 2019;53(1):1801889. doi:10.1183/13993003.01889-2018
- Boucly A, Weatherald J, Savale L, et al. Risk assessment, prognosis and guideline implementation in pulmonary arterial hypertension. Eur Respir J. 2017;50(2):1700889. doi:10.1183/13993003.00889-2017
- Wilson M, Keeley J, Kingman M, Wang J, Rogers F. Current clinical utilization of risk assessment tools in pulmonary arterial hypertension: a descriptive survey of facilitation strategies, patterns, and barriers to use in the United States. Pulm Circ. 2020;10(3):2045894020950186. doi:10.1177/2045894020950186
In PAH trials, clinical worsening risk rose with time
Current clinical trials evaluating combination therapy for pulmonary artery hypertension (PAH) may be longer than what is needed to demonstrate treatment benefit, results of a recent meta-analysis suggest.
, according to results of the study published in the May issue of the journal Chest®.
The meta-analysis by Dr. Lajoie and her colleagues included 3,801 patients enrolled in one of 15 previously published randomized clinical trials. Of those trials, four were long-term, event driven studies, with a mean duration of 87 weeks, while the remainder were shorter studies with a mean duration of 15 weeks.
For the long-term, event-driven trials, the mean number needed to treat (NNT) was 17.4 at week 16, gradually decreasing to 8.8 at 52 weeks of follow-up, remaining stable after that, according to investigators.
Consistent with that finding, the mean relative risk of clinical worsening was 0.38 at 16 weeks, and similarly, 0.41 at 26 weeks, investigators reported. After that, the relative risk progressively increased to 0.54 at 52 weeks and 0.68 at 104 weeks.
Looking at all trials combined, Dr. Lajoie and her colleagues observed that longer trial duration had a positive correlation with relative risk of clinical worsening (P = .0002).
Pragmatically, these results raise the possibility that PAH combination therapy trials could be shorter in duration. Some recent event-driven studies have lasted up to 6 years, with patients on treatment for about 2 of those years, investigators noted.
“In the context of an orphan disease with limited and competing recruitment for trials and the rapidly changing treatment paradigm in PAH, the optimal duration of future trials should be revisited,” Dr. Lajoie and her colleagues wrote in a discussion of their findings.
They also cautioned that NNT, a measure of how many patient treatments are needed to prevent one additional adverse event, could be “misleading” despite its value as a simple measure of treatment impact.
Likewise, relative risk can be misleading; for example, a treatment reducing event risk from 30% to 20% represents a relative risk reduction of approximately 35%, but so does a treatment reducing event risk from 3% to 2%, the researchers noted.
“Multiple factors, in addition to the efficacy of the therapy and the comparator, may directly influence the NNT and relative risk and should be taken into account in their interpretation,” they said in their report.
Dr. Lajoie had no disclosures related to the study. Her coauthors had disclosures related to Actelion Pharmaceuticals, Bayer, and GlaxoSmithKline, among others.
SOURCE: Lajoie AC et al. Chest. 2017 May;153(5):1142-52.
Key clinical point: A meta-analysis calls into question the need to perform pulmonary arterial hypertension (PAH) trials beyond 6 to 12 months of treatment in the future.
Major finding: The mean number needed to treat was stable at 52 weeks of follow-up and thereafter, while the mean relative risk of clinical worsening progressively increased from approximately 0.38 at week 16 to 0.68 at week 104.
Study details: A systematic review of 3,801 patients enrolled in 15 randomized clinical trials.
Disclosures: The authors reported disclosures related to Actelion Pharmaceuticals, Bayer, and GlaxoSmithKline, among other entities.
Source: Lajoie AC et al. Chest. 2017 May;153(5):1142-52.
Key clinical point: A meta-analysis calls into question the need to perform pulmonary arterial hypertension (PAH) trials beyond 6 to 12 months of treatment in the future.
Major finding: The mean number needed to treat was stable at 52 weeks of follow-up and thereafter, while the mean relative risk of clinical worsening progressively increased from approximately 0.38 at week 16 to 0.68 at week 104.
Study details: A systematic review of 3,801 patients enrolled in 15 randomized clinical trials.
Disclosures: The authors reported disclosures related to Actelion Pharmaceuticals, Bayer, and GlaxoSmithKline, among other entities.
Source: Lajoie AC et al. Chest. 2017 May;153(5):1142-52.
Key clinical point: A meta-analysis calls into question the need to perform pulmonary arterial hypertension (PAH) trials beyond 6 to 12 months of treatment in the future.
Major finding: The mean number needed to treat was stable at 52 weeks of follow-up and thereafter, while the mean relative risk of clinical worsening progressively increased from approximately 0.38 at week 16 to 0.68 at week 104.
Study details: A systematic review of 3,801 patients enrolled in 15 randomized clinical trials.
Disclosures: The authors reported disclosures related to Actelion Pharmaceuticals, Bayer, and GlaxoSmithKline, among other entities.
Source: Lajoie AC et al. Chest. 2017 May;153(5):1142-52.
Current clinical trials evaluating combination therapy for pulmonary artery hypertension (PAH) may be longer than what is needed to demonstrate treatment benefit, results of a recent meta-analysis suggest.
, according to results of the study published in the May issue of the journal Chest®.
The meta-analysis by Dr. Lajoie and her colleagues included 3,801 patients enrolled in one of 15 previously published randomized clinical trials. Of those trials, four were long-term, event driven studies, with a mean duration of 87 weeks, while the remainder were shorter studies with a mean duration of 15 weeks.
For the long-term, event-driven trials, the mean number needed to treat (NNT) was 17.4 at week 16, gradually decreasing to 8.8 at 52 weeks of follow-up, remaining stable after that, according to investigators.
Consistent with that finding, the mean relative risk of clinical worsening was 0.38 at 16 weeks, and similarly, 0.41 at 26 weeks, investigators reported. After that, the relative risk progressively increased to 0.54 at 52 weeks and 0.68 at 104 weeks.
Looking at all trials combined, Dr. Lajoie and her colleagues observed that longer trial duration had a positive correlation with relative risk of clinical worsening (P = .0002).
Pragmatically, these results raise the possibility that PAH combination therapy trials could be shorter in duration. Some recent event-driven studies have lasted up to 6 years, with patients on treatment for about 2 of those years, investigators noted.
“In the context of an orphan disease with limited and competing recruitment for trials and the rapidly changing treatment paradigm in PAH, the optimal duration of future trials should be revisited,” Dr. Lajoie and her colleagues wrote in a discussion of their findings.
They also cautioned that NNT, a measure of how many patient treatments are needed to prevent one additional adverse event, could be “misleading” despite its value as a simple measure of treatment impact.
Likewise, relative risk can be misleading; for example, a treatment reducing event risk from 30% to 20% represents a relative risk reduction of approximately 35%, but so does a treatment reducing event risk from 3% to 2%, the researchers noted.
“Multiple factors, in addition to the efficacy of the therapy and the comparator, may directly influence the NNT and relative risk and should be taken into account in their interpretation,” they said in their report.
Dr. Lajoie had no disclosures related to the study. Her coauthors had disclosures related to Actelion Pharmaceuticals, Bayer, and GlaxoSmithKline, among others.
SOURCE: Lajoie AC et al. Chest. 2017 May;153(5):1142-52.
Current clinical trials evaluating combination therapy for pulmonary artery hypertension (PAH) may be longer than what is needed to demonstrate treatment benefit, results of a recent meta-analysis suggest.
, according to results of the study published in the May issue of the journal Chest®.
The meta-analysis by Dr. Lajoie and her colleagues included 3,801 patients enrolled in one of 15 previously published randomized clinical trials. Of those trials, four were long-term, event driven studies, with a mean duration of 87 weeks, while the remainder were shorter studies with a mean duration of 15 weeks.
For the long-term, event-driven trials, the mean number needed to treat (NNT) was 17.4 at week 16, gradually decreasing to 8.8 at 52 weeks of follow-up, remaining stable after that, according to investigators.
Consistent with that finding, the mean relative risk of clinical worsening was 0.38 at 16 weeks, and similarly, 0.41 at 26 weeks, investigators reported. After that, the relative risk progressively increased to 0.54 at 52 weeks and 0.68 at 104 weeks.
Looking at all trials combined, Dr. Lajoie and her colleagues observed that longer trial duration had a positive correlation with relative risk of clinical worsening (P = .0002).
Pragmatically, these results raise the possibility that PAH combination therapy trials could be shorter in duration. Some recent event-driven studies have lasted up to 6 years, with patients on treatment for about 2 of those years, investigators noted.
“In the context of an orphan disease with limited and competing recruitment for trials and the rapidly changing treatment paradigm in PAH, the optimal duration of future trials should be revisited,” Dr. Lajoie and her colleagues wrote in a discussion of their findings.
They also cautioned that NNT, a measure of how many patient treatments are needed to prevent one additional adverse event, could be “misleading” despite its value as a simple measure of treatment impact.
Likewise, relative risk can be misleading; for example, a treatment reducing event risk from 30% to 20% represents a relative risk reduction of approximately 35%, but so does a treatment reducing event risk from 3% to 2%, the researchers noted.
“Multiple factors, in addition to the efficacy of the therapy and the comparator, may directly influence the NNT and relative risk and should be taken into account in their interpretation,” they said in their report.
Dr. Lajoie had no disclosures related to the study. Her coauthors had disclosures related to Actelion Pharmaceuticals, Bayer, and GlaxoSmithKline, among others.
SOURCE: Lajoie AC et al. Chest. 2017 May;153(5):1142-52.
FROM CHEST®