User login
Postmenopausal bleeding: First steps in the workup
• Screen all women with postmenopausal vaginal bleeding (PMB) for endometrial cancer. A
• Use transvaginal ultrasound for the initial study for patients at low risk for endometrial cancer, and endometrial biopsy for those at higher risk. B
• Use saline infusion sonography as a second step in the evaluation of PMB if the diagnosis remains unclear after a biopsy or the bleeding persists despite a normal initial workup. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Irene R, age 55, comes to see you because of vaginal bleeding, which started 7 days ago. The patient reports that she stopped menstruating about 4 years ago and is not on hormone replacement therapy or taking any medication. Irene, who is married and in a monogamous relationship with her husband of 20 years, denies any vaginal irritation, discharge, or dyspareunia. Her uterus is intact and she had a Pap smear about a year ago.
What will you include in a workup to determine the cause of her bleeding?
Endometrial cancer is the most common malignancy of the female reproductive organs, with more than 43,000 new cases detected in the United States in 2010 alone.1 More than half of all cases of endometrial cancer are diagnosed in women between the ages of 50 and 69 years.1,2
Vaginal bleeding, which more than 90% of women with endometrial cancer experience,3 is often the first sign of malignancy. Thus, all women who present with postmenopausal bleeding (PMB)—defined as any vaginal bleeding occurring ≥1 year after cessation of menses or any unscheduled bleeding in women on hormone replacement therapy (HRT)—require further evaluation.
Prognosis for endometrial cancer depends on the extent of the disease at the time of diagnosis. Most cases are diagnosed in the early stages and have a 5-year survival rate greater than 96%.1 Surgery alone can be curative if the malignancy is contained within the uterus.1,2
What are the essential elements of a workup for a woman with PMB? Which lab tests should be ordered and which procedures performed? You’ll find the answers in the at-a-glance ALGORITHM4-6 we created, and in the additional information provided in this evidence-based review.
ALGORITHM
Postmenopausal bleeding: An evidence-based workup4-6
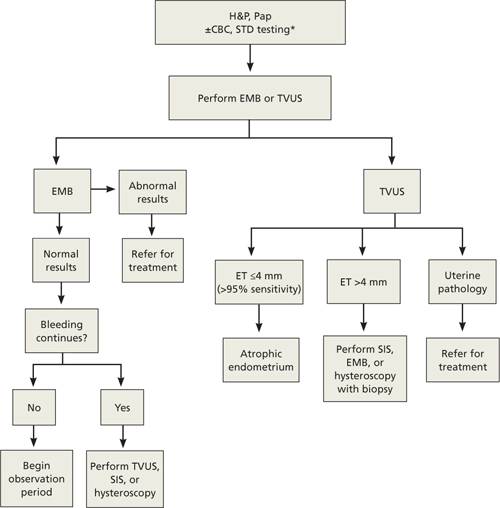
CBC, complete blood count; EMB, endometrial biopsy; ET, endometrial thickness; H&P, history and physical; Pap, Papanicolaou smear; SIS, saline infusion sonography; STD, sexually transmitted disease; TVUS, transvaginal ultrasonography.
*Laboratory tests are generally not helpful in evaluating postmenopausal bleeding, but a complete blood count is warranted if bleeding is prolonged or heavy and a test for sexually transmitted diseases may be appropriate based on patient history or physical exam.
Endometrial cancer is the key concern
While endometrial cancer is the most serious cause of PMB, it is not the most common. Atrophic endometrium is the culprit 60% to 80% of the time, while endometrial cancer accounts for up to 10% of cases. Endometrial polyps or hyperplasia, HRT, and cervical cancer are among the conditions included in the differential diagnosis (TABLE).7
A workup for PMB starts with a thorough medical history and a physical examination, including a Pap smear to screen for cervical cancer. Results from the Pap smear may suggest other pathology, such as benign endometrial cells, atypical endometrial cells, or atypical glandular cells.
Is lab work necessary? Laboratory tests are generally not helpful in evaluating PMB itself. A complete blood count is warranted if the bleeding is prolonged or heavy, however, and testing for sexually transmitted diseases may be appropriate, based on the patient’s history and/or physical exam.5,8
TABLE
Postmenopausal bleeding: The differential diagnosis7
| Cause | Incidence (%) |
|---|---|
| Atrophic endometrium | 60-80 |
| HRT | 15-25 |
| Endometrial cancer | 7-10 |
| Endometrial hyperplasia | 5-10 |
| Polyp(s) (endometrial or cervical) | 2-12 |
| Miscellaneous (uterine leiomyomas, cervicitis, atrophic vaginitis, tamoxifen therapy, trauma, anticoagulation) | <10 |
| HRT, hormone replacement therapy. | |
Endometrial biopsy or transvaginal ultrasound: Which test is better?
For many years, dilatation and curettage (D&C) of the endometrium was standard practice in the evaluation of patients with PMB. The Society of Radiologists in Ultrasound (SRU) and the American College of Obstetricians and Gynecologists (ACOG) now advise starting with either endometrial biopsy (EMB) or transvaginal ultrasound (TVUS).4,6 Both procedures are more advantageous than D&C for evaluating PMB because they can be done in an outpatient setting, are less expensive, provide faster results, and correlate with surgical findings more than 95% of the time.9
Although numerous studies have attempted to define the roles of EMB with Pipelle and TVUS, the literature is unclear as to which initial test is preferable.
Endometrial biopsy. Many physicians prefer to start with EMB, because it provides tissue samples for a histological diagnosis, is easily performed, and causes minimal cramping. The test does have limitations, such as difficulty in obtaining adequate tissue samples.
In a large cohort study (n=1535), EMB failed to provide an adequate tissue sample as much as 16% of the time.10 EMB’s sensitivity in detecting endometrial hyperplasia and cancer was 84%, the researchers reported, with a specificity of 99%; both the positive and negative predictive value were 94%. In a smaller study in which 97 women underwent TVUS and EMB was attempted, researchers reported that while no cases of endometrial cancer were missed when EMB sampling was successful, there was only a 27% probability of obtaining an adequate endometrial sample in women with an endometrial thickness (ET) <5 mm.11 EMB does a poorer job of detecting focal pathologies—with the potential to miss up to 18% of focal lesions, such as endometrial polyps, according to another study.12
Transvaginal ultrasound. TVUS is a safe, noninvasive, and cost-effective way to evaluate the endometrium, both to visualize focal lesions and assess ET. The technique, as defined by the SRU, involves scanning the uterus in a sagittal view and measuring the double-layer ET in the anteroposterior dimension from one basalis layer to the other.4
Reports of the sensitivity of TVUS in detecting endometrial cancer vary, depending on what cut point is used to rule it out. The SRU recommends an ET cutoff of ≤5 mm;4 ACOG recommends ≤4 mm.6 The consensus statements of both groups are based on a meta-analysis of 35 prospective studies that included data from nearly 6000 women with PMB. The sensitivity of TVUS in detecting endometrial cancer was 96%, whether the ≤4 or ≤5 mm cutoff was used, but specificity differed (53% for ≤4 mm vs 61% for ≤5 mm).13
In numerous studies with cut points of ≤4 or ≤5 mm, TVUS had a negative predictive value >99%.14-18 Because of this, ACOG states in an opinion issued in 2009 and reaffirmed in 2011, that TVUS is a “reasonable first approach.” The opinion further notes that in patients with an ET ≤4 mm, endometrial sampling is not required.6 In a meta-analysis of 3813 women, 3096 of whom were postmenopausal, researchers came to a different conclusion. An ET measurement on TVUS does not reduce the need for invasive diagnostic testing, the authors reported, because 4% of endometrial cancers would be missed even when a low threshold was used for reporting suspicious results.19
Type 2 endometrial cancer may be missed
A thin or indistinct endometrial lining on TVUS does not reliably exclude type 2 endometrial lesions20—which are not related to estrogen exposure or endometrial hyperplasia and typically present later in life, are diagnosed at a more advanced stage, and occur less frequently than type 1 endometrial cancer. A retrospective review of 52 patients with type 2 endometrial cancer found that 17% had an ET <4 mm, and another 17% had an indistinct endometrium.20
Factor risk level into decision-making
Researchers who conducted a decision analysis found that EMB is a more cost-effective initial diagnostic test for populations with a prevalence of endometrial cancer ≥15%.21 Overall, the prevalence among postmenopausal women in the United States is roughly 0.7%,22 but it is considerably higher among women with polycystic ovarian syndrome, obesity, diabetes, early menarche, late menopause, nulliparity, a history of tamoxifen use, or hereditary nonpolyposis colorectal cancer.5 For women with PMB and any of these risk factors, physicians should consider EMB as the first diagnostic test.
Because EMB is a substandard test for diagnosing benign endometrial abnormalities, such as polyps and submucosa leiomyomas, TVUS may be a better starting point for women at lower risk for endometrial cancer. In any case, an ET >4 mm requires further investigation using EMB, saline infusion sonography (SIS), or hysteroscopy with biopsy.9 Patients with uterine pathology noted with TVUS should be referred for treatment.
Next step? Consider saline infusion sonography
SIS is a procedure in which sterile saline is infused into the endometrial cavity, then TVUS is performed. The saline solution distends the uterus, promoting visualization and thus providing more detail than a conventional ultrasound.
Because SIS is expensive and uncomfortable, it is used mainly as a second step in the evaluation of PMB. It is useful when:
- a diagnosis remains unclear after biopsy
- TVUS finds evidence of a focal lesion
- bleeding persists despite a normal initial workup
- the patient has a relative contraindication for hysteroscopy with D&C.23,24
SIS is contraindicated in cases in which cancer cells were detected with either EMB or TVUS, as the procedure has been associated with a small but real risk of malignant cell dissemination.25
CASE Irene’s history did not reveal any significant risk factors for endometrial cancer. Physical exam revealed a cervical polyp. We obtained a Pap smear, which was normal, and removed the polyp, which was benign. Irene also underwent TVUS because of her low risk status. The test revealed an endometrial stripe of <4 mm and an endometrial polyp, prompting referral to a specialist.
The patient underwent a hysteroscopy and D&C. Her endometrial polyp was benign and the endometrial scrapings revealed atrophic squamous mucosa. Irene has had no further bleeding and is doing well at this time.
CORRESPONDENCE Danette B. Null, MD, 2411 Fox Hollow, Lake Charles, LA 70605; dnull@lcmh.com
1. American Cancer Society. Cancer facts and figures 2012. Atlanta: American Cancer Society; 2012.
2. Blair AR, Casas CM. Gynecologic cancers. Prim Care Clin Office Pract. 2009;36:115-130.
3. Doubilet PM. Society of Radiologists in Ultrasound consensus conference statement on postmenopausal bleeding. J Ultrasound Med. 2001;20:1037-1042.
4. Goldstein RB, Bree RL, Benson CB, et al. Evaluation of the woman with postmenopausal bleeding: Society of Radiologists in Ultrasound-Sponsored Consensus Conference statement. J Ultrasound Med. 2001;20:1025.-
5. Buchanan EM, Weinstein LC, Hillson C. Endometrial cancer. Am Fam Physician. 2009;80:1075-1080.
6. American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 440: the role of transvaginal ultrasonography in the evaluation of postmenopausal bleeding. Obstet Gynecol. 2009;114:409-411.Available at: http://journals.lww.com/greenjournal/Citation/2009/08000/ACOG_Committee_Opinion_No__440__The_Role_of.33.aspx. Accessed September 19, 2012.
7. Hsu C, Chen C, Wang K. Assessment of postmenopausal bleeding. Int J Gerontol. 2008;2:55-59.
8. Mounsey AL. Postmenopausal bleeding evaluation and management. Clinics Fam Pract. 2002;4:173-192.
9. O’Connell L, Fries M, Zeringue E, et al. Triage of abnormal postmenopausal bleeding: a comparison of endometrial biopsy and transvaginal sonohysterography versus factional curettage with hysteroscopy. Am J Obstet Gynecol. 1998;178:956-961
10. Machado F, Moreno J, Carazo M, et al. Accuracy of endometrial biopsy with the Cornier Pipelle for diagnosis of endometrial cancer and a typical hyperplasia. Eur J Gynaecol Oncol. 2003;23:279-281.
11. Elsandabesee D, Greenwood P. The performance of Pipelle endometrial sampling in a dedicated postmenopausal bleeding clinic. J Obstet Gynaecol. 2005;25:32-34.
12. Goldstein SR, Zeltser I, Horan CK, et al. Ultrasonography-based triage for perimenopausal patients with abnormal uterine bleeding. Am J Obstet Gynecol. 1997;177:102-108.
13. Smith-Bindman R, Kerlikowske K, Feldstein VA, et al. Endovaginal ultrasound to exclude endometrial cancer and other endometrial abnormalities. JAMA. 1998;280:1510-1517.
14. Karlsson B, Granberg S, Wikland M, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding—a Nordic multicenter study. Am J Obstet Gynecol. 1995;172:1488-1494.
15. Ferrazi E, Torri V, Trio D, et al. Sonographic endometrial thickness: a useful test to predict atrophy in patients with postmenopausal bleeding. An Italian multicenter study. Ultrasound Obstet Gynecol. 1996;7:315-321.
16. Gull B, Carlsson K, Karlsson B, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding; is it always necessary to perform an endometrial biopsy? Am J Obstet Gynecol. 2000;182:509-515.
17. Epstein E, Valentin L. Rebleeding and endometrial growth in women with postmenopausal bleeding and endometrial thickness <5 mm managed by dilatation and curettage or ultrasound follow-up: a randomized controlled study. Ultrasound Obstet Gynecol. 2001;18:499-504.
18. Gull B, Karlsson B, Milsom I, et al. Can ultrasound replace dilatation and curettage? A longitudinal evaluation of postmenopausal bleeding and transvaginal sonographic measurement of the endometrium as predictors of endometrial cancer. Am J Obstet Gynecol. 2003;18:401-408.
19. Tabor A, Watt HC, Wald NJ. Endometrial thickness as a test for endometrial cancer in women with postmenopausal vaginal bleeding. Obstet Gynecol. 2002;99:663-670.
20. Wang J, Wieslander C, Hansen G, et al. Thin endometrial echo complex on ultrasound does not reliably exclude type 2 endometrial cancers. Gynecol Oncol. 2006;101:120-125.
21. Dijkhuizen FP, Mol BW, Brolmann HA, et al. Cost-effectiveness of the use of transvaginal sonography in the evaluation of postmenopausal bleeding. Maturitas. 2003;45:275-282.
22. Howlader N, Noone AM, Krapcho M, et al (eds). SEER Cancer Statistics Review, 1975-2008. Bethesda, Md: National Cancer Institute. Available at: http://seer.cancer.gov/csr/1975_2008, based on November 2010 SEER data submission, posted to SEER web site, 2011.
23. Kamel HS, Darwish AM, Mohamed SA. Comparison of transvaginal ultrasonography and vaginal sonohysterography in the detection of endometrial polyps. Acta Obstet Gynecol Scand. 2000;79:60-64.
24. Krampl E, Bourne T, Hurlen-Solbakken H, et al. Transvaginal ultrasonography sonohysterography and operative hysteroscopy for the evaluation of abnormal uterine bleeding. Acta Obstet Gynecol Scand. 2001;80:616-622.
25. Alcazar JL, Errasti T, Zornoza A. Saline infusion sonohysterography in endometrial cancer: assessment of malignant cells dissemination risk. Acta Obstet Gynecol Scand. 2000;79:321-322.
• Screen all women with postmenopausal vaginal bleeding (PMB) for endometrial cancer. A
• Use transvaginal ultrasound for the initial study for patients at low risk for endometrial cancer, and endometrial biopsy for those at higher risk. B
• Use saline infusion sonography as a second step in the evaluation of PMB if the diagnosis remains unclear after a biopsy or the bleeding persists despite a normal initial workup. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Irene R, age 55, comes to see you because of vaginal bleeding, which started 7 days ago. The patient reports that she stopped menstruating about 4 years ago and is not on hormone replacement therapy or taking any medication. Irene, who is married and in a monogamous relationship with her husband of 20 years, denies any vaginal irritation, discharge, or dyspareunia. Her uterus is intact and she had a Pap smear about a year ago.
What will you include in a workup to determine the cause of her bleeding?
Endometrial cancer is the most common malignancy of the female reproductive organs, with more than 43,000 new cases detected in the United States in 2010 alone.1 More than half of all cases of endometrial cancer are diagnosed in women between the ages of 50 and 69 years.1,2
Vaginal bleeding, which more than 90% of women with endometrial cancer experience,3 is often the first sign of malignancy. Thus, all women who present with postmenopausal bleeding (PMB)—defined as any vaginal bleeding occurring ≥1 year after cessation of menses or any unscheduled bleeding in women on hormone replacement therapy (HRT)—require further evaluation.
Prognosis for endometrial cancer depends on the extent of the disease at the time of diagnosis. Most cases are diagnosed in the early stages and have a 5-year survival rate greater than 96%.1 Surgery alone can be curative if the malignancy is contained within the uterus.1,2
What are the essential elements of a workup for a woman with PMB? Which lab tests should be ordered and which procedures performed? You’ll find the answers in the at-a-glance ALGORITHM4-6 we created, and in the additional information provided in this evidence-based review.
ALGORITHM
Postmenopausal bleeding: An evidence-based workup4-6
CBC, complete blood count; EMB, endometrial biopsy; ET, endometrial thickness; H&P, history and physical; Pap, Papanicolaou smear; SIS, saline infusion sonography; STD, sexually transmitted disease; TVUS, transvaginal ultrasonography.
*Laboratory tests are generally not helpful in evaluating postmenopausal bleeding, but a complete blood count is warranted if bleeding is prolonged or heavy and a test for sexually transmitted diseases may be appropriate based on patient history or physical exam.
Endometrial cancer is the key concern
While endometrial cancer is the most serious cause of PMB, it is not the most common. Atrophic endometrium is the culprit 60% to 80% of the time, while endometrial cancer accounts for up to 10% of cases. Endometrial polyps or hyperplasia, HRT, and cervical cancer are among the conditions included in the differential diagnosis (TABLE).7
A workup for PMB starts with a thorough medical history and a physical examination, including a Pap smear to screen for cervical cancer. Results from the Pap smear may suggest other pathology, such as benign endometrial cells, atypical endometrial cells, or atypical glandular cells.
Is lab work necessary? Laboratory tests are generally not helpful in evaluating PMB itself. A complete blood count is warranted if the bleeding is prolonged or heavy, however, and testing for sexually transmitted diseases may be appropriate, based on the patient’s history and/or physical exam.5,8
TABLE
Postmenopausal bleeding: The differential diagnosis7
| Cause | Incidence (%) |
|---|---|
| Atrophic endometrium | 60-80 |
| HRT | 15-25 |
| Endometrial cancer | 7-10 |
| Endometrial hyperplasia | 5-10 |
| Polyp(s) (endometrial or cervical) | 2-12 |
| Miscellaneous (uterine leiomyomas, cervicitis, atrophic vaginitis, tamoxifen therapy, trauma, anticoagulation) | <10 |
| HRT, hormone replacement therapy. | |
Endometrial biopsy or transvaginal ultrasound: Which test is better?
For many years, dilatation and curettage (D&C) of the endometrium was standard practice in the evaluation of patients with PMB. The Society of Radiologists in Ultrasound (SRU) and the American College of Obstetricians and Gynecologists (ACOG) now advise starting with either endometrial biopsy (EMB) or transvaginal ultrasound (TVUS).4,6 Both procedures are more advantageous than D&C for evaluating PMB because they can be done in an outpatient setting, are less expensive, provide faster results, and correlate with surgical findings more than 95% of the time.9
Although numerous studies have attempted to define the roles of EMB with Pipelle and TVUS, the literature is unclear as to which initial test is preferable.
Endometrial biopsy. Many physicians prefer to start with EMB, because it provides tissue samples for a histological diagnosis, is easily performed, and causes minimal cramping. The test does have limitations, such as difficulty in obtaining adequate tissue samples.
In a large cohort study (n=1535), EMB failed to provide an adequate tissue sample as much as 16% of the time.10 EMB’s sensitivity in detecting endometrial hyperplasia and cancer was 84%, the researchers reported, with a specificity of 99%; both the positive and negative predictive value were 94%. In a smaller study in which 97 women underwent TVUS and EMB was attempted, researchers reported that while no cases of endometrial cancer were missed when EMB sampling was successful, there was only a 27% probability of obtaining an adequate endometrial sample in women with an endometrial thickness (ET) <5 mm.11 EMB does a poorer job of detecting focal pathologies—with the potential to miss up to 18% of focal lesions, such as endometrial polyps, according to another study.12
Transvaginal ultrasound. TVUS is a safe, noninvasive, and cost-effective way to evaluate the endometrium, both to visualize focal lesions and assess ET. The technique, as defined by the SRU, involves scanning the uterus in a sagittal view and measuring the double-layer ET in the anteroposterior dimension from one basalis layer to the other.4
Reports of the sensitivity of TVUS in detecting endometrial cancer vary, depending on what cut point is used to rule it out. The SRU recommends an ET cutoff of ≤5 mm;4 ACOG recommends ≤4 mm.6 The consensus statements of both groups are based on a meta-analysis of 35 prospective studies that included data from nearly 6000 women with PMB. The sensitivity of TVUS in detecting endometrial cancer was 96%, whether the ≤4 or ≤5 mm cutoff was used, but specificity differed (53% for ≤4 mm vs 61% for ≤5 mm).13
In numerous studies with cut points of ≤4 or ≤5 mm, TVUS had a negative predictive value >99%.14-18 Because of this, ACOG states in an opinion issued in 2009 and reaffirmed in 2011, that TVUS is a “reasonable first approach.” The opinion further notes that in patients with an ET ≤4 mm, endometrial sampling is not required.6 In a meta-analysis of 3813 women, 3096 of whom were postmenopausal, researchers came to a different conclusion. An ET measurement on TVUS does not reduce the need for invasive diagnostic testing, the authors reported, because 4% of endometrial cancers would be missed even when a low threshold was used for reporting suspicious results.19
Type 2 endometrial cancer may be missed
A thin or indistinct endometrial lining on TVUS does not reliably exclude type 2 endometrial lesions20—which are not related to estrogen exposure or endometrial hyperplasia and typically present later in life, are diagnosed at a more advanced stage, and occur less frequently than type 1 endometrial cancer. A retrospective review of 52 patients with type 2 endometrial cancer found that 17% had an ET <4 mm, and another 17% had an indistinct endometrium.20
Factor risk level into decision-making
Researchers who conducted a decision analysis found that EMB is a more cost-effective initial diagnostic test for populations with a prevalence of endometrial cancer ≥15%.21 Overall, the prevalence among postmenopausal women in the United States is roughly 0.7%,22 but it is considerably higher among women with polycystic ovarian syndrome, obesity, diabetes, early menarche, late menopause, nulliparity, a history of tamoxifen use, or hereditary nonpolyposis colorectal cancer.5 For women with PMB and any of these risk factors, physicians should consider EMB as the first diagnostic test.
Because EMB is a substandard test for diagnosing benign endometrial abnormalities, such as polyps and submucosa leiomyomas, TVUS may be a better starting point for women at lower risk for endometrial cancer. In any case, an ET >4 mm requires further investigation using EMB, saline infusion sonography (SIS), or hysteroscopy with biopsy.9 Patients with uterine pathology noted with TVUS should be referred for treatment.
Next step? Consider saline infusion sonography
SIS is a procedure in which sterile saline is infused into the endometrial cavity, then TVUS is performed. The saline solution distends the uterus, promoting visualization and thus providing more detail than a conventional ultrasound.
Because SIS is expensive and uncomfortable, it is used mainly as a second step in the evaluation of PMB. It is useful when:
- a diagnosis remains unclear after biopsy
- TVUS finds evidence of a focal lesion
- bleeding persists despite a normal initial workup
- the patient has a relative contraindication for hysteroscopy with D&C.23,24
SIS is contraindicated in cases in which cancer cells were detected with either EMB or TVUS, as the procedure has been associated with a small but real risk of malignant cell dissemination.25
CASE Irene’s history did not reveal any significant risk factors for endometrial cancer. Physical exam revealed a cervical polyp. We obtained a Pap smear, which was normal, and removed the polyp, which was benign. Irene also underwent TVUS because of her low risk status. The test revealed an endometrial stripe of <4 mm and an endometrial polyp, prompting referral to a specialist.
The patient underwent a hysteroscopy and D&C. Her endometrial polyp was benign and the endometrial scrapings revealed atrophic squamous mucosa. Irene has had no further bleeding and is doing well at this time.
CORRESPONDENCE Danette B. Null, MD, 2411 Fox Hollow, Lake Charles, LA 70605; dnull@lcmh.com
• Screen all women with postmenopausal vaginal bleeding (PMB) for endometrial cancer. A
• Use transvaginal ultrasound for the initial study for patients at low risk for endometrial cancer, and endometrial biopsy for those at higher risk. B
• Use saline infusion sonography as a second step in the evaluation of PMB if the diagnosis remains unclear after a biopsy or the bleeding persists despite a normal initial workup. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE Irene R, age 55, comes to see you because of vaginal bleeding, which started 7 days ago. The patient reports that she stopped menstruating about 4 years ago and is not on hormone replacement therapy or taking any medication. Irene, who is married and in a monogamous relationship with her husband of 20 years, denies any vaginal irritation, discharge, or dyspareunia. Her uterus is intact and she had a Pap smear about a year ago.
What will you include in a workup to determine the cause of her bleeding?
Endometrial cancer is the most common malignancy of the female reproductive organs, with more than 43,000 new cases detected in the United States in 2010 alone.1 More than half of all cases of endometrial cancer are diagnosed in women between the ages of 50 and 69 years.1,2
Vaginal bleeding, which more than 90% of women with endometrial cancer experience,3 is often the first sign of malignancy. Thus, all women who present with postmenopausal bleeding (PMB)—defined as any vaginal bleeding occurring ≥1 year after cessation of menses or any unscheduled bleeding in women on hormone replacement therapy (HRT)—require further evaluation.
Prognosis for endometrial cancer depends on the extent of the disease at the time of diagnosis. Most cases are diagnosed in the early stages and have a 5-year survival rate greater than 96%.1 Surgery alone can be curative if the malignancy is contained within the uterus.1,2
What are the essential elements of a workup for a woman with PMB? Which lab tests should be ordered and which procedures performed? You’ll find the answers in the at-a-glance ALGORITHM4-6 we created, and in the additional information provided in this evidence-based review.
ALGORITHM
Postmenopausal bleeding: An evidence-based workup4-6
CBC, complete blood count; EMB, endometrial biopsy; ET, endometrial thickness; H&P, history and physical; Pap, Papanicolaou smear; SIS, saline infusion sonography; STD, sexually transmitted disease; TVUS, transvaginal ultrasonography.
*Laboratory tests are generally not helpful in evaluating postmenopausal bleeding, but a complete blood count is warranted if bleeding is prolonged or heavy and a test for sexually transmitted diseases may be appropriate based on patient history or physical exam.
Endometrial cancer is the key concern
While endometrial cancer is the most serious cause of PMB, it is not the most common. Atrophic endometrium is the culprit 60% to 80% of the time, while endometrial cancer accounts for up to 10% of cases. Endometrial polyps or hyperplasia, HRT, and cervical cancer are among the conditions included in the differential diagnosis (TABLE).7
A workup for PMB starts with a thorough medical history and a physical examination, including a Pap smear to screen for cervical cancer. Results from the Pap smear may suggest other pathology, such as benign endometrial cells, atypical endometrial cells, or atypical glandular cells.
Is lab work necessary? Laboratory tests are generally not helpful in evaluating PMB itself. A complete blood count is warranted if the bleeding is prolonged or heavy, however, and testing for sexually transmitted diseases may be appropriate, based on the patient’s history and/or physical exam.5,8
TABLE
Postmenopausal bleeding: The differential diagnosis7
| Cause | Incidence (%) |
|---|---|
| Atrophic endometrium | 60-80 |
| HRT | 15-25 |
| Endometrial cancer | 7-10 |
| Endometrial hyperplasia | 5-10 |
| Polyp(s) (endometrial or cervical) | 2-12 |
| Miscellaneous (uterine leiomyomas, cervicitis, atrophic vaginitis, tamoxifen therapy, trauma, anticoagulation) | <10 |
| HRT, hormone replacement therapy. | |
Endometrial biopsy or transvaginal ultrasound: Which test is better?
For many years, dilatation and curettage (D&C) of the endometrium was standard practice in the evaluation of patients with PMB. The Society of Radiologists in Ultrasound (SRU) and the American College of Obstetricians and Gynecologists (ACOG) now advise starting with either endometrial biopsy (EMB) or transvaginal ultrasound (TVUS).4,6 Both procedures are more advantageous than D&C for evaluating PMB because they can be done in an outpatient setting, are less expensive, provide faster results, and correlate with surgical findings more than 95% of the time.9
Although numerous studies have attempted to define the roles of EMB with Pipelle and TVUS, the literature is unclear as to which initial test is preferable.
Endometrial biopsy. Many physicians prefer to start with EMB, because it provides tissue samples for a histological diagnosis, is easily performed, and causes minimal cramping. The test does have limitations, such as difficulty in obtaining adequate tissue samples.
In a large cohort study (n=1535), EMB failed to provide an adequate tissue sample as much as 16% of the time.10 EMB’s sensitivity in detecting endometrial hyperplasia and cancer was 84%, the researchers reported, with a specificity of 99%; both the positive and negative predictive value were 94%. In a smaller study in which 97 women underwent TVUS and EMB was attempted, researchers reported that while no cases of endometrial cancer were missed when EMB sampling was successful, there was only a 27% probability of obtaining an adequate endometrial sample in women with an endometrial thickness (ET) <5 mm.11 EMB does a poorer job of detecting focal pathologies—with the potential to miss up to 18% of focal lesions, such as endometrial polyps, according to another study.12
Transvaginal ultrasound. TVUS is a safe, noninvasive, and cost-effective way to evaluate the endometrium, both to visualize focal lesions and assess ET. The technique, as defined by the SRU, involves scanning the uterus in a sagittal view and measuring the double-layer ET in the anteroposterior dimension from one basalis layer to the other.4
Reports of the sensitivity of TVUS in detecting endometrial cancer vary, depending on what cut point is used to rule it out. The SRU recommends an ET cutoff of ≤5 mm;4 ACOG recommends ≤4 mm.6 The consensus statements of both groups are based on a meta-analysis of 35 prospective studies that included data from nearly 6000 women with PMB. The sensitivity of TVUS in detecting endometrial cancer was 96%, whether the ≤4 or ≤5 mm cutoff was used, but specificity differed (53% for ≤4 mm vs 61% for ≤5 mm).13
In numerous studies with cut points of ≤4 or ≤5 mm, TVUS had a negative predictive value >99%.14-18 Because of this, ACOG states in an opinion issued in 2009 and reaffirmed in 2011, that TVUS is a “reasonable first approach.” The opinion further notes that in patients with an ET ≤4 mm, endometrial sampling is not required.6 In a meta-analysis of 3813 women, 3096 of whom were postmenopausal, researchers came to a different conclusion. An ET measurement on TVUS does not reduce the need for invasive diagnostic testing, the authors reported, because 4% of endometrial cancers would be missed even when a low threshold was used for reporting suspicious results.19
Type 2 endometrial cancer may be missed
A thin or indistinct endometrial lining on TVUS does not reliably exclude type 2 endometrial lesions20—which are not related to estrogen exposure or endometrial hyperplasia and typically present later in life, are diagnosed at a more advanced stage, and occur less frequently than type 1 endometrial cancer. A retrospective review of 52 patients with type 2 endometrial cancer found that 17% had an ET <4 mm, and another 17% had an indistinct endometrium.20
Factor risk level into decision-making
Researchers who conducted a decision analysis found that EMB is a more cost-effective initial diagnostic test for populations with a prevalence of endometrial cancer ≥15%.21 Overall, the prevalence among postmenopausal women in the United States is roughly 0.7%,22 but it is considerably higher among women with polycystic ovarian syndrome, obesity, diabetes, early menarche, late menopause, nulliparity, a history of tamoxifen use, or hereditary nonpolyposis colorectal cancer.5 For women with PMB and any of these risk factors, physicians should consider EMB as the first diagnostic test.
Because EMB is a substandard test for diagnosing benign endometrial abnormalities, such as polyps and submucosa leiomyomas, TVUS may be a better starting point for women at lower risk for endometrial cancer. In any case, an ET >4 mm requires further investigation using EMB, saline infusion sonography (SIS), or hysteroscopy with biopsy.9 Patients with uterine pathology noted with TVUS should be referred for treatment.
Next step? Consider saline infusion sonography
SIS is a procedure in which sterile saline is infused into the endometrial cavity, then TVUS is performed. The saline solution distends the uterus, promoting visualization and thus providing more detail than a conventional ultrasound.
Because SIS is expensive and uncomfortable, it is used mainly as a second step in the evaluation of PMB. It is useful when:
- a diagnosis remains unclear after biopsy
- TVUS finds evidence of a focal lesion
- bleeding persists despite a normal initial workup
- the patient has a relative contraindication for hysteroscopy with D&C.23,24
SIS is contraindicated in cases in which cancer cells were detected with either EMB or TVUS, as the procedure has been associated with a small but real risk of malignant cell dissemination.25
CASE Irene’s history did not reveal any significant risk factors for endometrial cancer. Physical exam revealed a cervical polyp. We obtained a Pap smear, which was normal, and removed the polyp, which was benign. Irene also underwent TVUS because of her low risk status. The test revealed an endometrial stripe of <4 mm and an endometrial polyp, prompting referral to a specialist.
The patient underwent a hysteroscopy and D&C. Her endometrial polyp was benign and the endometrial scrapings revealed atrophic squamous mucosa. Irene has had no further bleeding and is doing well at this time.
CORRESPONDENCE Danette B. Null, MD, 2411 Fox Hollow, Lake Charles, LA 70605; dnull@lcmh.com
1. American Cancer Society. Cancer facts and figures 2012. Atlanta: American Cancer Society; 2012.
2. Blair AR, Casas CM. Gynecologic cancers. Prim Care Clin Office Pract. 2009;36:115-130.
3. Doubilet PM. Society of Radiologists in Ultrasound consensus conference statement on postmenopausal bleeding. J Ultrasound Med. 2001;20:1037-1042.
4. Goldstein RB, Bree RL, Benson CB, et al. Evaluation of the woman with postmenopausal bleeding: Society of Radiologists in Ultrasound-Sponsored Consensus Conference statement. J Ultrasound Med. 2001;20:1025.-
5. Buchanan EM, Weinstein LC, Hillson C. Endometrial cancer. Am Fam Physician. 2009;80:1075-1080.
6. American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 440: the role of transvaginal ultrasonography in the evaluation of postmenopausal bleeding. Obstet Gynecol. 2009;114:409-411.Available at: http://journals.lww.com/greenjournal/Citation/2009/08000/ACOG_Committee_Opinion_No__440__The_Role_of.33.aspx. Accessed September 19, 2012.
7. Hsu C, Chen C, Wang K. Assessment of postmenopausal bleeding. Int J Gerontol. 2008;2:55-59.
8. Mounsey AL. Postmenopausal bleeding evaluation and management. Clinics Fam Pract. 2002;4:173-192.
9. O’Connell L, Fries M, Zeringue E, et al. Triage of abnormal postmenopausal bleeding: a comparison of endometrial biopsy and transvaginal sonohysterography versus factional curettage with hysteroscopy. Am J Obstet Gynecol. 1998;178:956-961
10. Machado F, Moreno J, Carazo M, et al. Accuracy of endometrial biopsy with the Cornier Pipelle for diagnosis of endometrial cancer and a typical hyperplasia. Eur J Gynaecol Oncol. 2003;23:279-281.
11. Elsandabesee D, Greenwood P. The performance of Pipelle endometrial sampling in a dedicated postmenopausal bleeding clinic. J Obstet Gynaecol. 2005;25:32-34.
12. Goldstein SR, Zeltser I, Horan CK, et al. Ultrasonography-based triage for perimenopausal patients with abnormal uterine bleeding. Am J Obstet Gynecol. 1997;177:102-108.
13. Smith-Bindman R, Kerlikowske K, Feldstein VA, et al. Endovaginal ultrasound to exclude endometrial cancer and other endometrial abnormalities. JAMA. 1998;280:1510-1517.
14. Karlsson B, Granberg S, Wikland M, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding—a Nordic multicenter study. Am J Obstet Gynecol. 1995;172:1488-1494.
15. Ferrazi E, Torri V, Trio D, et al. Sonographic endometrial thickness: a useful test to predict atrophy in patients with postmenopausal bleeding. An Italian multicenter study. Ultrasound Obstet Gynecol. 1996;7:315-321.
16. Gull B, Carlsson K, Karlsson B, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding; is it always necessary to perform an endometrial biopsy? Am J Obstet Gynecol. 2000;182:509-515.
17. Epstein E, Valentin L. Rebleeding and endometrial growth in women with postmenopausal bleeding and endometrial thickness <5 mm managed by dilatation and curettage or ultrasound follow-up: a randomized controlled study. Ultrasound Obstet Gynecol. 2001;18:499-504.
18. Gull B, Karlsson B, Milsom I, et al. Can ultrasound replace dilatation and curettage? A longitudinal evaluation of postmenopausal bleeding and transvaginal sonographic measurement of the endometrium as predictors of endometrial cancer. Am J Obstet Gynecol. 2003;18:401-408.
19. Tabor A, Watt HC, Wald NJ. Endometrial thickness as a test for endometrial cancer in women with postmenopausal vaginal bleeding. Obstet Gynecol. 2002;99:663-670.
20. Wang J, Wieslander C, Hansen G, et al. Thin endometrial echo complex on ultrasound does not reliably exclude type 2 endometrial cancers. Gynecol Oncol. 2006;101:120-125.
21. Dijkhuizen FP, Mol BW, Brolmann HA, et al. Cost-effectiveness of the use of transvaginal sonography in the evaluation of postmenopausal bleeding. Maturitas. 2003;45:275-282.
22. Howlader N, Noone AM, Krapcho M, et al (eds). SEER Cancer Statistics Review, 1975-2008. Bethesda, Md: National Cancer Institute. Available at: http://seer.cancer.gov/csr/1975_2008, based on November 2010 SEER data submission, posted to SEER web site, 2011.
23. Kamel HS, Darwish AM, Mohamed SA. Comparison of transvaginal ultrasonography and vaginal sonohysterography in the detection of endometrial polyps. Acta Obstet Gynecol Scand. 2000;79:60-64.
24. Krampl E, Bourne T, Hurlen-Solbakken H, et al. Transvaginal ultrasonography sonohysterography and operative hysteroscopy for the evaluation of abnormal uterine bleeding. Acta Obstet Gynecol Scand. 2001;80:616-622.
25. Alcazar JL, Errasti T, Zornoza A. Saline infusion sonohysterography in endometrial cancer: assessment of malignant cells dissemination risk. Acta Obstet Gynecol Scand. 2000;79:321-322.
1. American Cancer Society. Cancer facts and figures 2012. Atlanta: American Cancer Society; 2012.
2. Blair AR, Casas CM. Gynecologic cancers. Prim Care Clin Office Pract. 2009;36:115-130.
3. Doubilet PM. Society of Radiologists in Ultrasound consensus conference statement on postmenopausal bleeding. J Ultrasound Med. 2001;20:1037-1042.
4. Goldstein RB, Bree RL, Benson CB, et al. Evaluation of the woman with postmenopausal bleeding: Society of Radiologists in Ultrasound-Sponsored Consensus Conference statement. J Ultrasound Med. 2001;20:1025.-
5. Buchanan EM, Weinstein LC, Hillson C. Endometrial cancer. Am Fam Physician. 2009;80:1075-1080.
6. American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 440: the role of transvaginal ultrasonography in the evaluation of postmenopausal bleeding. Obstet Gynecol. 2009;114:409-411.Available at: http://journals.lww.com/greenjournal/Citation/2009/08000/ACOG_Committee_Opinion_No__440__The_Role_of.33.aspx. Accessed September 19, 2012.
7. Hsu C, Chen C, Wang K. Assessment of postmenopausal bleeding. Int J Gerontol. 2008;2:55-59.
8. Mounsey AL. Postmenopausal bleeding evaluation and management. Clinics Fam Pract. 2002;4:173-192.
9. O’Connell L, Fries M, Zeringue E, et al. Triage of abnormal postmenopausal bleeding: a comparison of endometrial biopsy and transvaginal sonohysterography versus factional curettage with hysteroscopy. Am J Obstet Gynecol. 1998;178:956-961
10. Machado F, Moreno J, Carazo M, et al. Accuracy of endometrial biopsy with the Cornier Pipelle for diagnosis of endometrial cancer and a typical hyperplasia. Eur J Gynaecol Oncol. 2003;23:279-281.
11. Elsandabesee D, Greenwood P. The performance of Pipelle endometrial sampling in a dedicated postmenopausal bleeding clinic. J Obstet Gynaecol. 2005;25:32-34.
12. Goldstein SR, Zeltser I, Horan CK, et al. Ultrasonography-based triage for perimenopausal patients with abnormal uterine bleeding. Am J Obstet Gynecol. 1997;177:102-108.
13. Smith-Bindman R, Kerlikowske K, Feldstein VA, et al. Endovaginal ultrasound to exclude endometrial cancer and other endometrial abnormalities. JAMA. 1998;280:1510-1517.
14. Karlsson B, Granberg S, Wikland M, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding—a Nordic multicenter study. Am J Obstet Gynecol. 1995;172:1488-1494.
15. Ferrazi E, Torri V, Trio D, et al. Sonographic endometrial thickness: a useful test to predict atrophy in patients with postmenopausal bleeding. An Italian multicenter study. Ultrasound Obstet Gynecol. 1996;7:315-321.
16. Gull B, Carlsson K, Karlsson B, et al. Transvaginal ultrasonography of the endometrium in women with postmenopausal bleeding; is it always necessary to perform an endometrial biopsy? Am J Obstet Gynecol. 2000;182:509-515.
17. Epstein E, Valentin L. Rebleeding and endometrial growth in women with postmenopausal bleeding and endometrial thickness <5 mm managed by dilatation and curettage or ultrasound follow-up: a randomized controlled study. Ultrasound Obstet Gynecol. 2001;18:499-504.
18. Gull B, Karlsson B, Milsom I, et al. Can ultrasound replace dilatation and curettage? A longitudinal evaluation of postmenopausal bleeding and transvaginal sonographic measurement of the endometrium as predictors of endometrial cancer. Am J Obstet Gynecol. 2003;18:401-408.
19. Tabor A, Watt HC, Wald NJ. Endometrial thickness as a test for endometrial cancer in women with postmenopausal vaginal bleeding. Obstet Gynecol. 2002;99:663-670.
20. Wang J, Wieslander C, Hansen G, et al. Thin endometrial echo complex on ultrasound does not reliably exclude type 2 endometrial cancers. Gynecol Oncol. 2006;101:120-125.
21. Dijkhuizen FP, Mol BW, Brolmann HA, et al. Cost-effectiveness of the use of transvaginal sonography in the evaluation of postmenopausal bleeding. Maturitas. 2003;45:275-282.
22. Howlader N, Noone AM, Krapcho M, et al (eds). SEER Cancer Statistics Review, 1975-2008. Bethesda, Md: National Cancer Institute. Available at: http://seer.cancer.gov/csr/1975_2008, based on November 2010 SEER data submission, posted to SEER web site, 2011.
23. Kamel HS, Darwish AM, Mohamed SA. Comparison of transvaginal ultrasonography and vaginal sonohysterography in the detection of endometrial polyps. Acta Obstet Gynecol Scand. 2000;79:60-64.
24. Krampl E, Bourne T, Hurlen-Solbakken H, et al. Transvaginal ultrasonography sonohysterography and operative hysteroscopy for the evaluation of abnormal uterine bleeding. Acta Obstet Gynecol Scand. 2001;80:616-622.
25. Alcazar JL, Errasti T, Zornoza A. Saline infusion sonohysterography in endometrial cancer: assessment of malignant cells dissemination risk. Acta Obstet Gynecol Scand. 2000;79:321-322.