User login
Which CAM modalities are worth considering?
› Consider referring your patients for guided imagery to reduce anxiety or pain. A
› Recommend a trial of glucosamine sulfate 1500 mg/d for 3 months for patients with osteoarthritis. B
› Consider acupuncture as a treatment option for patients with chronic pain. B
› Use probiotics to prevent antibiotic-associated diarrhea in pediatric patients, except for those who are immunocompromised or have an indwelling medical device. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Bob F, age 54, seeks care for chronic low back pain. The conservative treatments you have prescribed, including physical therapy, regular exercise, and an over-the-counter nonsteroidal anti-inflammatory drug, have provided minimal pain relief. Mr. F is reluctant to take a prescription pain medication and has expressed interest in trying a complementary and alternative medicine (CAM) therapy, such as acupuncture or yoga. What should you tell him?
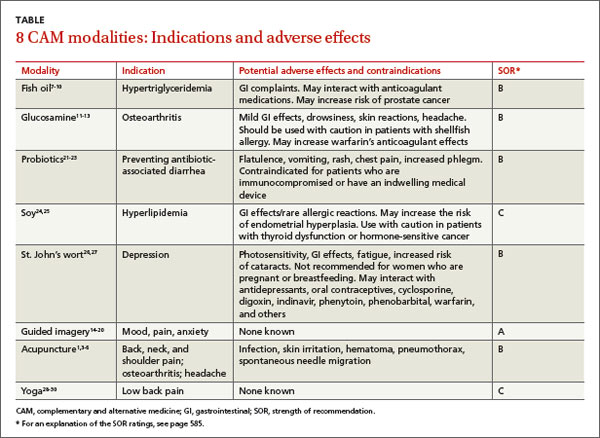
Almost 40% of Americans use CAM modalities to treat specific conditions or for overall well-being,1 and these practices are increasingly becoming a part of our approach to health care, as evidenced by the nearly 50 of facilities across the country that boast integrative health care programs, which combine CAM modalities with conventional medicine.2 Emerging evidence suggests several integrative practices may offer health benefits, and primary care physicians must become well-versed in these modalities to effectively communicate potential benefits and harms to patients. In this article, we present evidence from Cochrane reviews and other studies of 8 commonly used CAM therapies, including dietary interventions, a psychotherapeutic modality, and other treatments (TABLE).1,3-30 And while motivational interviewing technically is not a form of CAM, we also review this modality, which has proven useful in the treatment of patients for substance use. (See “Motivational interviewing for substance abuse.”)
Fish oil for hypertriglyceridemia
High triglyceride levels are a risk factor for cardiovascular disease and a component of metabolic syndrome.8 A 2008 review of 47 randomized controlled trials (RCTs) that included 16,511 participants found that omega-3 fatty acid (fish oil) supplements significantly reduced triglyceride levels compared to placebo.7 The American Heart Association recommends 2 to 4 g/d of eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA) to lower triglyceride levels.8
Most studies have found that fish oil supplements are associated with few adverse effects; gastrointestinal (GI) complaints are most common. However, these supplements should be discontinued following an acute bleeding event, such as hemorrhagic stroke, due to their anticoagulant properties.9 Some evidence suggests that the risk for prostate cancer is increased in men with high blood levels of omega-3 fatty acids.10
Glucosamine for osteoarthritis
Glucosamine is an amino sugar that is a building block of cartilage proteoglycans. Although it occurs naturally in the body, the glucosamine used in supplements is typically harvested from seashells. Glucosamine stimulates the metabolism of synovial cells and chondrocytes in articular cartilage and may delay joint degeneration.31,32
Glucosamine is widely used in the United States as a dietary supplement, most often as glucosamine sulfate but also as n-acetyl glucosamine and glucosamine hydrochloride, although there is limited evidence of effectiveness for the latter formulations.33
Most studies have examined the effects of oral glucosamine sulfate, 500 mg taken 3 times a day for 30 to 90 days. Once-a-day dosing as high as 1500 mg also has been used.
A Cochrane review of 25 studies with 4963 patients concluded that oral glucosamine sulfate may reduce osteoarthritis (OA) pain and improve functionality, without many adverse effects.11 A 2-year double-blind RCT compared the effects of glucosamine hydrochloride 500 mg tid, chondroitin sulfate 400 mg tid, glucosamine plus chondroitin, celecoxib 200 mg/d, or placebo in 662 patients with knee OA.12 While all groups experienced early and sustained symptomatic relief, the odds of achieving a 20% reduction in pain and improved functioning were highest with celecoxib and glucosamine.
Oral glucosamine sulfate can cause mild GI effects, but drowsiness, skin reactions, and headache also have been reported. Shellfish allergy also is a concern; however, shellfish allergies occur due to the proteins in the meat, and not from the shell from which glucosamine is derived. Glucosamine may increase glucose levels and the anticoagulant effects of warfarin.13
Probiotics to prevent antibiotic-associated diarrhea
Antibiotic-associated diarrhea (AAD) is a common problem.21 Probiotics—microorganisms found in oral supplements, yogurt, and other food—are commonly used to help maintain the balance of intestinal flora.34 A recent Cochrane review of 16 RCTs that included approximately 3400 patients found evidence that probiotics can prevent AAD.22 A 2012 systematic review and meta-analysis of 63 RCTs with more than 11,000 participants concluded that probiotics lowered the relative risk of developing diarrhea compared to control groups.35 The American Academy of Pediatrics supports the use of probiotics, citing results from a meta-analysis that found probiotics reduced the risk of developing diarrhea from 28.5% to 11.9% compared to placebo.36
Exact dosages for probiotics have not been established, and recommendations range from 5 billion to 40 billion colony-forming units/d.22 The most commonly used probiotics are from the Lactobacillus and Saccharomyces genera; relatively little evidence supports other genera.21,22,35,36
Probiotics are considered relatively safe, but are not recommended for patients who are immunocompromised or have an indwelling medical device.23 Adverse effects are rare, but may include flatulence, vomiting, rash, chest pain, and increased phlegm.21
For a review of the latest evidence on using probiotics to reduce crying in infants with colic, see "Probiotics for colic? A PURL update."
Soy for hyperlipidemia
Soybeans are a species of legume that contain significant amounts of protein, fiber, potassium, and iron. Although soy has been used to prevent or treat cancer, osteoporosis, and menopausal symptoms, current evidence is unfavorable or inconclusive for such conditions. Some RCTs have found soy has small, favorable effects on serum levels of low-density lipoprotein and total cholesterol,24 while others have shown modest improvements in triglyceride levels without significant improvements in other lipid levels.25
A 2011 meta-analysis of 10 RCTs that included 268 participants found that a diet high in non-soy legume products, such as alfalfa, lentils, and other beans, also improved lipid levels.37 A review of 136 studies that described 22 dietary interventions concluded that among other helpful dietary approaches to controlling hyperlipidemia, dietary soy—which contains fiber and polyunsaturated fats—is favored over supplementation of soy protein alone.38
Use caution when recommending soy for patients with thyroid dysfunction or hormone-sensitive cancers because some evidence suggests soy may interfere with absorption of levothyroxine and increase the risk of developing clinical symptoms of hypothyroidism.39
Soy also contains phytoestrogens, and prolonged use of soy supplements may increase the risk of endometrial hyperplasia.24 This risk has been documented only in the use of soy supplements, and not from dietary soy. GI disturbances and rare allergic reactions also have been reported.24
St. John’s wort for depression
Hypericum perforatum (St. John’s wort), a perennial herb, has been used to treat mood disorders and other ailments for more than 2000 years.40,41 Commercial preparations typically are alcohol extracts with an herb-to-extract ratio of 4:1 to 8:1.26 The normal dose ranges from 900 to 1500 mg/d in 2 to 3 divided doses of the alcohol extract standardized to 0.3% hypericin and/or 3% to 5% hyperforin.
St. John’s wort has been studied extensively as a treatment for depressive disorders. A 2001 double-blind RCT conducted in 11 US academic medical centers and community clinics between 1998 and 2000 that included 200 patients found that St. John’s wort was not effective for moderately severe major depression; a trend toward a positive effect was noted in both the placebo and St. John’s wort groups.26
However, a 2009 Cochrane review of 29 international studies (5489 patients) concluded that St. John’s wort may be better than placebo and as effective as antidepressants for mild to moderate major depression,27 and appeared to have fewer side effects than antidepressants. This review, conducted in German-speaking countries where medical professionals have long prescribed St. John’s wort, reported more positive results than those conducted in other countries.
St. John’s wort interacts with many medications, including antidepressants, oral contraceptives, cyclosporine, digoxin, indinavir, phenytoin, phenobarbital, warfarin, and others. It induces cytochrome P450 (CYP450) enzymes, and therefore can potentially reduce the efficacy of any medication that is metabolized by a CYP450 enzyme. When used in high doses in combination with antidepressants, St. John’s wort may cause serotonin syndrome. Other side effects include photosensitivity, GI complaints, fatigue, and increased risk of cataracts. Due to a lack of clinical data, St. John’s wort is contraindicated in women who are pregnant or breastfeeding.42
Motivational interviewing (MI) is an alternative approach to traditional provider-patient communication that entails using open-ended questions, reflective listening, affirmation, and assessing readiness to change.1 MI facilitators aim to elicit change and assist patients in forming a self-management plan with specific, measurable, achievable, realistic, and timely (SMART) goals.1-3
MI can be efficiently implemented in diverse settings and by a variety of trained facilitators.3-5 For example, the Brief Negotiation Interview requires only 7 minutes per emergency department patient and effectively improves long-term outcomes for substance abusers.4 A randomized controlled trial that included 135 patients admitted to a psychiatric emergency inpatient unit for substance abuse found that those who received 2 sessions of MI reported significantly less substance use than controls 2 years after the intervention.3
Training for providers to ensure proper implementation of MI techniques is essential because poor use of MI can be counter-therapeutic.5 Tools such as the Motivational Interviewing Treatment Integrity Scale and the Client Evaluation of Motivational Interviewing can be used to ensure providers are competent.4,6
References
1. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behavior. New York, NY: Guilford Press; 1991.
2. Levensky ER, Forcehimes A, O’Donohue WT, et al. Motivational interviewing: an evidence-based approach to counseling helps patients follow treatment recommendations. Am J Nurse. 2007;107:50-59.
3. Bagøien G, Bjørngaard JH, Østensen C, et al. The effects of motivational interviewing on patients with comorbid substance use admitted to a psychiatric emergency unit - a randomized controlled trial with two year follow-up. BMC Psychiatry. 2013;13:93.
4. D’Onofrio G, Fiellin DA, Pantalon MV, et al. A brief intervention reduces hazardous and harmful drinking in emergency department patients. Ann Emerg Med. 2012;60:181-192.
5. Tollison SJ, Mastroleo NR, Mallett KA, et al. The relationship between baseline drinking status, peer motivational interviewing microskills, and drinking outcomes in a brief alcohol intervention for matriculating college students: a replication. Behav Ther. 2013;44:137-151.
6. Madson MB, Mohn RS, Zuckoff A, et al. Measuring client perceptions of motivational interviewing: factor analysis of the Client Evaluation of Motivational Interviewing scale. J Subst Abuse Treat. 2013;44:330-335.
Guided imagery for anxiety and pain
Guided imagery is a relaxation technique that involves visualizing positive outcomes to reduce one’s reaction to anxiety-provoking or painful experiences.43 It can be practiced independently or under the direction of an instructor. One RCT of 96 women with newly diagnosed breast cancer found that adding relaxation and guided imagery to standard breast cancer treatment protocols positively affected mood and quality of life.14 While this study saw no change in pathologic responses to chemotherapy,14 a more recent RCT concluded that such biochemical advantages may be possible.44 Guided imagery has been linked to decreased anxiety in diverse studies of students, women in labor, individuals suffering from nightmares, and in occupational settings such as training for pilots and surgeons.15-18
A review of 9 RCTs of guided imagery for decreasing musculoskeletal pain involving 201 patients found 8 studies reported positive results, though the methodological quality of the studies was low.19 Of 6 high-quality studies included in a 2012 systematic review, 5 supported the use of guided imagery for postoperative, abdominal, and other nonmusculoskeletal pain.20 This initial evidence is promising, but additional research of high methodological quality is needed to validate the use of guided imagery for anxiety and pain.
Acupuncture for pain
From 2002 to 2007, the use of acupuncture significantly increased in the United States, primarily for the treatment of pain.1 A 2012 meta-analysis of 29 RCTs that included almost 18,000 participants evaluated the clinical usefulness of acupuncture for back, neck, and shoulder pain, OA, and headache.3 Compared to no treatment, both acupuncture and sham acupuncture significantly improved pain scores. The authors of this meta-analysis found that acupuncture offered a small but significant advantage over sham acupuncture, and concluded that the benefits of acupuncture were not due to a placebo effect.
In 2007, the American College of Physicians (ACP) and the American Pain Society (APS) issued a joint statement indicating that acupuncture should be considered for patients with chronic low back pain who do not respond to conventional therapies.4 The North American Spine Society also supports acupuncture, stating that it provides “...better short-term pain relief and functional improvement than no treatment and the addition of acupuncture to other treatment modalities provides a greater benefit than those treatments alone.”5 Additional evidence found acupuncture for chronic low back pain improves function and serves as an adjunct therapy.6
Reported adverse effects of acupuncture include—but may not be limited to—infection, skin irritation, hematoma, pneumothorax, and spontaneous needle migration.1,3-6
Yoga for low back pain
Back pain is the most common reason patients use CAM therapies.1 A systematic review of 10 RCTs that included 967 participants with chronic low back pain found strong evidence for the short-term effectiveness and moderate evidence for the long-term effectiveness of yoga.28 A review of 17 studies that included 1626 patients concluded that yoga improves both pain and functionality; this review did not recommend a specific type of yoga practice.29 In a recent study of 95 minority adults with moderate-to-severe chronic low back pain, once-weekly and twice-weekly yoga for 12 weeks were similarly effective for reducing pain and improving functionality.30
Guidelines from the ACP and the APS recommend yoga as part of an intensive interdisciplinary rehabilitation program for patients with chronic or subacute low back pain who do not improve using other self-care options.4 This recommendation is specifically for Viniyoga, a practice in which the instructor recommends modifications to body positioning for each individual based on past injuries and overall physical condition. (For more information on therapeutic uses of yoga, see “Yoga as therapy: When is it helpful?”)
CORRESPONDENCE
Roger Zoorob, MD, MPH, FAAFP; Department of Family and Community Medicine, Baylor College of Medicine, 3701 Kirby Drive, Suite 600, Houston, TX 77098; roger.zoorob@bcm.edu
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;10:1-23.
2. American Holistic Medicine Association. Integrative medicine centers. American Holistic Medicine Association Web site. Available at: http://www.holisticmedicine.org/content. asp?pl=30&sl=2&contentid=74. Accessed September 8, 2014.
3. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
4. Chou R, Qaseem A, Snow V, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians; American College of Physicians; American Pain Society Low Back Pain Guidelines Panel. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478-491.
5. Berman BM, Langevin HM, Witt CM, et al. Acupuncture for chronic low back pain. N Engl J Med. 2010;363:454-461.
6. Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009;79:1067-1074.
7. Eslik GD, Howe PR, Smith C, et al. Benefits of fish oil supplementation in hyperlipidemia: a systematic review and meta-analysis. Int J Cardiol. 2009;136:4-16.
8. Miller M, Stone NJ, Ballantyne C, et al; American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committeeof the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglyceride and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2292-2333.
9. Bays HE. Safety considerations with omega-3 fatty acid therapy. Am J Cardiol. 2007;99:35C-43C.
10. Brasky TM, Darke AK, Song X, et al. Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2013;105:1132-1141.
11. Towheed TE, Maxwell L, Anastassiades TP, et al. Glucosamine therapy for treating osteoarthritis. Cochrane Database Syst Rev. 2005;(2):CD002946.
12. Sawitzke AD, Shi H, Finco MF, et al. Clinical efficacy and safety of glucosamine, chondroitin sulphate, their combination, celecoxib or placebo taken to treat osteoarthritis of the knee: 2-year results from GAIT. Ann Rheum Dis. 2010;69:1459-1464.
13. Dostrovsky NR, Towheed TE, Hudson RW, et al. The effect of glucosamine on glucose metabolism in humans: a systematic review of the literature. Osteoarthritis Cartilage. 2011;19:375-380.
14. Walker LG, Walker MB, Ogston K, et al. Psychological, clinical and pathological effects of relaxation training and guided imagery during primary chemotherapy. Br J Cancer. 1999;80:262-268.
15. Thünker J, Pietrowsky R. Effectiveness of a manualized imagery rehearsal therapy for patients suffering from nightmare disorders with and without a comorbidity of depression or PTSD. Behav Res Ther. 2012;50:558-564.
16. Marc I, Toureche N, Ernst E, et al. Mind-body interventions during pregnancy for preventing or treating women’s anxiety. Cochrane Database Syst Rev. 2011;(7):CD007559.
17. Jing X, Wu P, Liu F, et al. Guided imagery, anxiety, heart rate, and heart rate variability during centrifuge training. Aviat Space Environ Med. 2011;82:92-96.
18. Arora S, Aggarwal R, Moran A, et al. Mental practice: effective stress management training for novice surgeons. J Am Coll Surg. 2011;212:225-233.
19. Posadzki P, Ernst E. Guided imagery for musculoskeletal pain: a systematic review. Clin J Pain. 2011;27:648-653.
20. Posadzki P, Lewandowski W, Terry R, et al. Guided imagery for non-musculoskeletal pain: a systematic review of randomized clinical trials. J Pain Symptom Manage. 2012;44:95-104.
21. Arvola T, Laiho K, Torkkeli S, et al. Prophylactic Lactobacillus GG reduces antibiotic-associated diarrhea in children with respiratory infections: a randomized study. Pediatrics. 1999;104:e64.
22. Johnston BC, Goldenberg JZ, Vandvik PO, et al. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database Syst Rev. 2011;(11):CD004827.
23. Williams NT. Probiotics. Am J Health-Syst Pharm. 2010;67:449-458.
24. Sacks FM, Lichtenstein A, Van Horn L, et al; American Heart Association Nutrition Committee. Soy protein, isoflavones, and cardiovascular health: an American Heart Association Science Advisory for professionals from the Nutrition Committee. Circulation. 2006;113:1034-1044.
25. Qin Y, Niu K, Zeng Y, et al. Isoflavones for hypercholesterolaemia in adults. Cochrane Database Syst Rev. 2013;6:CD009518.
26. Shelton RC, Keller MB, Gelenberg A, et al. Effectiveness of St John’s wort in major depression: a randomized controlled trial. JAMA. 2001;285:1978-1986.
27. Linde K, Berner MM, Kriston L. St John’s wort for major depression. Cochrane Database Syst Rev. 2008;(4):CD000448.
28. Cramer H, Lauche R, Haller H, et al. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29: 450-460.
29. Ward L, Stebbings S, Cherkin D, et al. Yoga for functional ability, pain and psychosocial outcomes in musculoskeletal conditions: a systematic review and meta-analysis. Musculoskeletal Care. 2013;11:203-217.
30. Saper RB, Boah AR, Keosaian J, et al. Comparing once- versus twice-weekly yoga classes for chronic low back pain in predominantly low income minorities: a randomized dosing trial. Evid Based Complement Alternat Med. 2013;2013:658030.
31. Uitterlinden EJ, Koevoet JLM, Verkoelen CF, et al. Glucosamine increases hyaluronic acid production in human osteoarthritic synovium explants. BMC Musculoskelet Disord. 2008;9:120.
32. Calamia V, Ruiz-Romero C, Rocha B, et al. Pharmacoproteomic study of the effects of chondroitin and glucosamine sulfate on human articular chondrocytes. Arthritis Res Ther. 2010;12:R138.
33. Rovati LC, Girolami F, Persiani S. Crystalline glucosamine sulfate in the management of knee osteoarthritis: efficacy, safety, and pharmacokinetic properties. Ther Adv Musculoskelet Dis. 2012;4:167-180.
34. National Center for Complementary and Alternative Medicine. Oral probiotics: An introduction. National Center for Complementary and Alternative Medicine Web site. Available at: http:// nccam.nih.gov/health/probiotics/introduction.htm. Updated December 2012. Accessed August 29, 2013.
35. Hempel S, Newberry SJ, Maher AR, et al. Probiotics for the prevention and treatment of antibiotic-associated diarrhea: a systematic review and meta-analysis. JAMA. 2012;307:1959-1969.
36. Thomas DW, Greer FR; American Academy of Pediatrics Committee on Nutrition; American Academy of Pediatrics Section on Gastroenterology, Hepatology, and Nutrition. Probiotics and prebiotics in pediatrics. Pediatrics. 2010;126:1217-1231.
37. Bazzano LA, Thompson AM, Tees MT, et al. Non-soy legume consumption lowers cholesterol levels: a meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2011;21:94-103.
38. Huang J, Frohlich J, Ignaszewski AP. The impact of dietary changes and dietary supplements on lipid profile. Can J Cardiol. 2011;27:488-505.
39. Messina M, Redmond G. Effects of soy protein and soybean isoflavones on thyroid function in healthy adults and hypothyroid patients: a review of the relevant literature. Thyroid. 2006;16: 249-258.
40. National Center for Complementary and Alternative Medicine. St. John’s Wort. National Center for Complementary and Alternative Medicine Web site. Available at: http://nccam.nih.gov/ health/stjohnswort. Accessed October 14, 2013.
41. Schulz V, Hänsel R, Tyler VE. Rational Phytotherapy: A Physicians’ Guide to Herbal Medicine. Berlin: Springer; 2001:62-81.
42. Mischoulon D. Update and critique of natural remedies as antidepressant treatments. Obstet Gynecol Clin North Am. 2009;36: 789-807.
43. Hanssen MM, Peters ML, Vlaeyen JW, et al. Optimism lowers pain: evidence of the causal status and underlying mechanisms. Pain. 2013;154:53-58.
44. Eremin O, Walker MB, Simpson E, et al. Immuno-modulatory effects of relaxation training and guided imagery in women with locally advanced breast cancer undergoing multimodality therapy: a randomised controlled trial. Breast. 2009;18:17-25.
› Consider referring your patients for guided imagery to reduce anxiety or pain. A
› Recommend a trial of glucosamine sulfate 1500 mg/d for 3 months for patients with osteoarthritis. B
› Consider acupuncture as a treatment option for patients with chronic pain. B
› Use probiotics to prevent antibiotic-associated diarrhea in pediatric patients, except for those who are immunocompromised or have an indwelling medical device. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Bob F, age 54, seeks care for chronic low back pain. The conservative treatments you have prescribed, including physical therapy, regular exercise, and an over-the-counter nonsteroidal anti-inflammatory drug, have provided minimal pain relief. Mr. F is reluctant to take a prescription pain medication and has expressed interest in trying a complementary and alternative medicine (CAM) therapy, such as acupuncture or yoga. What should you tell him?
Almost 40% of Americans use CAM modalities to treat specific conditions or for overall well-being,1 and these practices are increasingly becoming a part of our approach to health care, as evidenced by the nearly 50 of facilities across the country that boast integrative health care programs, which combine CAM modalities with conventional medicine.2 Emerging evidence suggests several integrative practices may offer health benefits, and primary care physicians must become well-versed in these modalities to effectively communicate potential benefits and harms to patients. In this article, we present evidence from Cochrane reviews and other studies of 8 commonly used CAM therapies, including dietary interventions, a psychotherapeutic modality, and other treatments (TABLE).1,3-30 And while motivational interviewing technically is not a form of CAM, we also review this modality, which has proven useful in the treatment of patients for substance use. (See “Motivational interviewing for substance abuse.”)
Fish oil for hypertriglyceridemia
High triglyceride levels are a risk factor for cardiovascular disease and a component of metabolic syndrome.8 A 2008 review of 47 randomized controlled trials (RCTs) that included 16,511 participants found that omega-3 fatty acid (fish oil) supplements significantly reduced triglyceride levels compared to placebo.7 The American Heart Association recommends 2 to 4 g/d of eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA) to lower triglyceride levels.8
Most studies have found that fish oil supplements are associated with few adverse effects; gastrointestinal (GI) complaints are most common. However, these supplements should be discontinued following an acute bleeding event, such as hemorrhagic stroke, due to their anticoagulant properties.9 Some evidence suggests that the risk for prostate cancer is increased in men with high blood levels of omega-3 fatty acids.10
Glucosamine for osteoarthritis
Glucosamine is an amino sugar that is a building block of cartilage proteoglycans. Although it occurs naturally in the body, the glucosamine used in supplements is typically harvested from seashells. Glucosamine stimulates the metabolism of synovial cells and chondrocytes in articular cartilage and may delay joint degeneration.31,32
Glucosamine is widely used in the United States as a dietary supplement, most often as glucosamine sulfate but also as n-acetyl glucosamine and glucosamine hydrochloride, although there is limited evidence of effectiveness for the latter formulations.33
Most studies have examined the effects of oral glucosamine sulfate, 500 mg taken 3 times a day for 30 to 90 days. Once-a-day dosing as high as 1500 mg also has been used.
A Cochrane review of 25 studies with 4963 patients concluded that oral glucosamine sulfate may reduce osteoarthritis (OA) pain and improve functionality, without many adverse effects.11 A 2-year double-blind RCT compared the effects of glucosamine hydrochloride 500 mg tid, chondroitin sulfate 400 mg tid, glucosamine plus chondroitin, celecoxib 200 mg/d, or placebo in 662 patients with knee OA.12 While all groups experienced early and sustained symptomatic relief, the odds of achieving a 20% reduction in pain and improved functioning were highest with celecoxib and glucosamine.
Oral glucosamine sulfate can cause mild GI effects, but drowsiness, skin reactions, and headache also have been reported. Shellfish allergy also is a concern; however, shellfish allergies occur due to the proteins in the meat, and not from the shell from which glucosamine is derived. Glucosamine may increase glucose levels and the anticoagulant effects of warfarin.13
Probiotics to prevent antibiotic-associated diarrhea
Antibiotic-associated diarrhea (AAD) is a common problem.21 Probiotics—microorganisms found in oral supplements, yogurt, and other food—are commonly used to help maintain the balance of intestinal flora.34 A recent Cochrane review of 16 RCTs that included approximately 3400 patients found evidence that probiotics can prevent AAD.22 A 2012 systematic review and meta-analysis of 63 RCTs with more than 11,000 participants concluded that probiotics lowered the relative risk of developing diarrhea compared to control groups.35 The American Academy of Pediatrics supports the use of probiotics, citing results from a meta-analysis that found probiotics reduced the risk of developing diarrhea from 28.5% to 11.9% compared to placebo.36
Exact dosages for probiotics have not been established, and recommendations range from 5 billion to 40 billion colony-forming units/d.22 The most commonly used probiotics are from the Lactobacillus and Saccharomyces genera; relatively little evidence supports other genera.21,22,35,36
Probiotics are considered relatively safe, but are not recommended for patients who are immunocompromised or have an indwelling medical device.23 Adverse effects are rare, but may include flatulence, vomiting, rash, chest pain, and increased phlegm.21
For a review of the latest evidence on using probiotics to reduce crying in infants with colic, see "Probiotics for colic? A PURL update."
Soy for hyperlipidemia
Soybeans are a species of legume that contain significant amounts of protein, fiber, potassium, and iron. Although soy has been used to prevent or treat cancer, osteoporosis, and menopausal symptoms, current evidence is unfavorable or inconclusive for such conditions. Some RCTs have found soy has small, favorable effects on serum levels of low-density lipoprotein and total cholesterol,24 while others have shown modest improvements in triglyceride levels without significant improvements in other lipid levels.25
A 2011 meta-analysis of 10 RCTs that included 268 participants found that a diet high in non-soy legume products, such as alfalfa, lentils, and other beans, also improved lipid levels.37 A review of 136 studies that described 22 dietary interventions concluded that among other helpful dietary approaches to controlling hyperlipidemia, dietary soy—which contains fiber and polyunsaturated fats—is favored over supplementation of soy protein alone.38
Use caution when recommending soy for patients with thyroid dysfunction or hormone-sensitive cancers because some evidence suggests soy may interfere with absorption of levothyroxine and increase the risk of developing clinical symptoms of hypothyroidism.39
Soy also contains phytoestrogens, and prolonged use of soy supplements may increase the risk of endometrial hyperplasia.24 This risk has been documented only in the use of soy supplements, and not from dietary soy. GI disturbances and rare allergic reactions also have been reported.24
St. John’s wort for depression
Hypericum perforatum (St. John’s wort), a perennial herb, has been used to treat mood disorders and other ailments for more than 2000 years.40,41 Commercial preparations typically are alcohol extracts with an herb-to-extract ratio of 4:1 to 8:1.26 The normal dose ranges from 900 to 1500 mg/d in 2 to 3 divided doses of the alcohol extract standardized to 0.3% hypericin and/or 3% to 5% hyperforin.
St. John’s wort has been studied extensively as a treatment for depressive disorders. A 2001 double-blind RCT conducted in 11 US academic medical centers and community clinics between 1998 and 2000 that included 200 patients found that St. John’s wort was not effective for moderately severe major depression; a trend toward a positive effect was noted in both the placebo and St. John’s wort groups.26
However, a 2009 Cochrane review of 29 international studies (5489 patients) concluded that St. John’s wort may be better than placebo and as effective as antidepressants for mild to moderate major depression,27 and appeared to have fewer side effects than antidepressants. This review, conducted in German-speaking countries where medical professionals have long prescribed St. John’s wort, reported more positive results than those conducted in other countries.
St. John’s wort interacts with many medications, including antidepressants, oral contraceptives, cyclosporine, digoxin, indinavir, phenytoin, phenobarbital, warfarin, and others. It induces cytochrome P450 (CYP450) enzymes, and therefore can potentially reduce the efficacy of any medication that is metabolized by a CYP450 enzyme. When used in high doses in combination with antidepressants, St. John’s wort may cause serotonin syndrome. Other side effects include photosensitivity, GI complaints, fatigue, and increased risk of cataracts. Due to a lack of clinical data, St. John’s wort is contraindicated in women who are pregnant or breastfeeding.42
Motivational interviewing (MI) is an alternative approach to traditional provider-patient communication that entails using open-ended questions, reflective listening, affirmation, and assessing readiness to change.1 MI facilitators aim to elicit change and assist patients in forming a self-management plan with specific, measurable, achievable, realistic, and timely (SMART) goals.1-3
MI can be efficiently implemented in diverse settings and by a variety of trained facilitators.3-5 For example, the Brief Negotiation Interview requires only 7 minutes per emergency department patient and effectively improves long-term outcomes for substance abusers.4 A randomized controlled trial that included 135 patients admitted to a psychiatric emergency inpatient unit for substance abuse found that those who received 2 sessions of MI reported significantly less substance use than controls 2 years after the intervention.3
Training for providers to ensure proper implementation of MI techniques is essential because poor use of MI can be counter-therapeutic.5 Tools such as the Motivational Interviewing Treatment Integrity Scale and the Client Evaluation of Motivational Interviewing can be used to ensure providers are competent.4,6
References
1. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behavior. New York, NY: Guilford Press; 1991.
2. Levensky ER, Forcehimes A, O’Donohue WT, et al. Motivational interviewing: an evidence-based approach to counseling helps patients follow treatment recommendations. Am J Nurse. 2007;107:50-59.
3. Bagøien G, Bjørngaard JH, Østensen C, et al. The effects of motivational interviewing on patients with comorbid substance use admitted to a psychiatric emergency unit - a randomized controlled trial with two year follow-up. BMC Psychiatry. 2013;13:93.
4. D’Onofrio G, Fiellin DA, Pantalon MV, et al. A brief intervention reduces hazardous and harmful drinking in emergency department patients. Ann Emerg Med. 2012;60:181-192.
5. Tollison SJ, Mastroleo NR, Mallett KA, et al. The relationship between baseline drinking status, peer motivational interviewing microskills, and drinking outcomes in a brief alcohol intervention for matriculating college students: a replication. Behav Ther. 2013;44:137-151.
6. Madson MB, Mohn RS, Zuckoff A, et al. Measuring client perceptions of motivational interviewing: factor analysis of the Client Evaluation of Motivational Interviewing scale. J Subst Abuse Treat. 2013;44:330-335.
Guided imagery for anxiety and pain
Guided imagery is a relaxation technique that involves visualizing positive outcomes to reduce one’s reaction to anxiety-provoking or painful experiences.43 It can be practiced independently or under the direction of an instructor. One RCT of 96 women with newly diagnosed breast cancer found that adding relaxation and guided imagery to standard breast cancer treatment protocols positively affected mood and quality of life.14 While this study saw no change in pathologic responses to chemotherapy,14 a more recent RCT concluded that such biochemical advantages may be possible.44 Guided imagery has been linked to decreased anxiety in diverse studies of students, women in labor, individuals suffering from nightmares, and in occupational settings such as training for pilots and surgeons.15-18
A review of 9 RCTs of guided imagery for decreasing musculoskeletal pain involving 201 patients found 8 studies reported positive results, though the methodological quality of the studies was low.19 Of 6 high-quality studies included in a 2012 systematic review, 5 supported the use of guided imagery for postoperative, abdominal, and other nonmusculoskeletal pain.20 This initial evidence is promising, but additional research of high methodological quality is needed to validate the use of guided imagery for anxiety and pain.
Acupuncture for pain
From 2002 to 2007, the use of acupuncture significantly increased in the United States, primarily for the treatment of pain.1 A 2012 meta-analysis of 29 RCTs that included almost 18,000 participants evaluated the clinical usefulness of acupuncture for back, neck, and shoulder pain, OA, and headache.3 Compared to no treatment, both acupuncture and sham acupuncture significantly improved pain scores. The authors of this meta-analysis found that acupuncture offered a small but significant advantage over sham acupuncture, and concluded that the benefits of acupuncture were not due to a placebo effect.
In 2007, the American College of Physicians (ACP) and the American Pain Society (APS) issued a joint statement indicating that acupuncture should be considered for patients with chronic low back pain who do not respond to conventional therapies.4 The North American Spine Society also supports acupuncture, stating that it provides “...better short-term pain relief and functional improvement than no treatment and the addition of acupuncture to other treatment modalities provides a greater benefit than those treatments alone.”5 Additional evidence found acupuncture for chronic low back pain improves function and serves as an adjunct therapy.6
Reported adverse effects of acupuncture include—but may not be limited to—infection, skin irritation, hematoma, pneumothorax, and spontaneous needle migration.1,3-6
Yoga for low back pain
Back pain is the most common reason patients use CAM therapies.1 A systematic review of 10 RCTs that included 967 participants with chronic low back pain found strong evidence for the short-term effectiveness and moderate evidence for the long-term effectiveness of yoga.28 A review of 17 studies that included 1626 patients concluded that yoga improves both pain and functionality; this review did not recommend a specific type of yoga practice.29 In a recent study of 95 minority adults with moderate-to-severe chronic low back pain, once-weekly and twice-weekly yoga for 12 weeks were similarly effective for reducing pain and improving functionality.30
Guidelines from the ACP and the APS recommend yoga as part of an intensive interdisciplinary rehabilitation program for patients with chronic or subacute low back pain who do not improve using other self-care options.4 This recommendation is specifically for Viniyoga, a practice in which the instructor recommends modifications to body positioning for each individual based on past injuries and overall physical condition. (For more information on therapeutic uses of yoga, see “Yoga as therapy: When is it helpful?”)
CORRESPONDENCE
Roger Zoorob, MD, MPH, FAAFP; Department of Family and Community Medicine, Baylor College of Medicine, 3701 Kirby Drive, Suite 600, Houston, TX 77098; roger.zoorob@bcm.edu
› Consider referring your patients for guided imagery to reduce anxiety or pain. A
› Recommend a trial of glucosamine sulfate 1500 mg/d for 3 months for patients with osteoarthritis. B
› Consider acupuncture as a treatment option for patients with chronic pain. B
› Use probiotics to prevent antibiotic-associated diarrhea in pediatric patients, except for those who are immunocompromised or have an indwelling medical device. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Bob F, age 54, seeks care for chronic low back pain. The conservative treatments you have prescribed, including physical therapy, regular exercise, and an over-the-counter nonsteroidal anti-inflammatory drug, have provided minimal pain relief. Mr. F is reluctant to take a prescription pain medication and has expressed interest in trying a complementary and alternative medicine (CAM) therapy, such as acupuncture or yoga. What should you tell him?
Almost 40% of Americans use CAM modalities to treat specific conditions or for overall well-being,1 and these practices are increasingly becoming a part of our approach to health care, as evidenced by the nearly 50 of facilities across the country that boast integrative health care programs, which combine CAM modalities with conventional medicine.2 Emerging evidence suggests several integrative practices may offer health benefits, and primary care physicians must become well-versed in these modalities to effectively communicate potential benefits and harms to patients. In this article, we present evidence from Cochrane reviews and other studies of 8 commonly used CAM therapies, including dietary interventions, a psychotherapeutic modality, and other treatments (TABLE).1,3-30 And while motivational interviewing technically is not a form of CAM, we also review this modality, which has proven useful in the treatment of patients for substance use. (See “Motivational interviewing for substance abuse.”)
Fish oil for hypertriglyceridemia
High triglyceride levels are a risk factor for cardiovascular disease and a component of metabolic syndrome.8 A 2008 review of 47 randomized controlled trials (RCTs) that included 16,511 participants found that omega-3 fatty acid (fish oil) supplements significantly reduced triglyceride levels compared to placebo.7 The American Heart Association recommends 2 to 4 g/d of eicosapentaenoic acid (EPA) plus docosahexaenoic acid (DHA) to lower triglyceride levels.8
Most studies have found that fish oil supplements are associated with few adverse effects; gastrointestinal (GI) complaints are most common. However, these supplements should be discontinued following an acute bleeding event, such as hemorrhagic stroke, due to their anticoagulant properties.9 Some evidence suggests that the risk for prostate cancer is increased in men with high blood levels of omega-3 fatty acids.10
Glucosamine for osteoarthritis
Glucosamine is an amino sugar that is a building block of cartilage proteoglycans. Although it occurs naturally in the body, the glucosamine used in supplements is typically harvested from seashells. Glucosamine stimulates the metabolism of synovial cells and chondrocytes in articular cartilage and may delay joint degeneration.31,32
Glucosamine is widely used in the United States as a dietary supplement, most often as glucosamine sulfate but also as n-acetyl glucosamine and glucosamine hydrochloride, although there is limited evidence of effectiveness for the latter formulations.33
Most studies have examined the effects of oral glucosamine sulfate, 500 mg taken 3 times a day for 30 to 90 days. Once-a-day dosing as high as 1500 mg also has been used.
A Cochrane review of 25 studies with 4963 patients concluded that oral glucosamine sulfate may reduce osteoarthritis (OA) pain and improve functionality, without many adverse effects.11 A 2-year double-blind RCT compared the effects of glucosamine hydrochloride 500 mg tid, chondroitin sulfate 400 mg tid, glucosamine plus chondroitin, celecoxib 200 mg/d, or placebo in 662 patients with knee OA.12 While all groups experienced early and sustained symptomatic relief, the odds of achieving a 20% reduction in pain and improved functioning were highest with celecoxib and glucosamine.
Oral glucosamine sulfate can cause mild GI effects, but drowsiness, skin reactions, and headache also have been reported. Shellfish allergy also is a concern; however, shellfish allergies occur due to the proteins in the meat, and not from the shell from which glucosamine is derived. Glucosamine may increase glucose levels and the anticoagulant effects of warfarin.13
Probiotics to prevent antibiotic-associated diarrhea
Antibiotic-associated diarrhea (AAD) is a common problem.21 Probiotics—microorganisms found in oral supplements, yogurt, and other food—are commonly used to help maintain the balance of intestinal flora.34 A recent Cochrane review of 16 RCTs that included approximately 3400 patients found evidence that probiotics can prevent AAD.22 A 2012 systematic review and meta-analysis of 63 RCTs with more than 11,000 participants concluded that probiotics lowered the relative risk of developing diarrhea compared to control groups.35 The American Academy of Pediatrics supports the use of probiotics, citing results from a meta-analysis that found probiotics reduced the risk of developing diarrhea from 28.5% to 11.9% compared to placebo.36
Exact dosages for probiotics have not been established, and recommendations range from 5 billion to 40 billion colony-forming units/d.22 The most commonly used probiotics are from the Lactobacillus and Saccharomyces genera; relatively little evidence supports other genera.21,22,35,36
Probiotics are considered relatively safe, but are not recommended for patients who are immunocompromised or have an indwelling medical device.23 Adverse effects are rare, but may include flatulence, vomiting, rash, chest pain, and increased phlegm.21
For a review of the latest evidence on using probiotics to reduce crying in infants with colic, see "Probiotics for colic? A PURL update."
Soy for hyperlipidemia
Soybeans are a species of legume that contain significant amounts of protein, fiber, potassium, and iron. Although soy has been used to prevent or treat cancer, osteoporosis, and menopausal symptoms, current evidence is unfavorable or inconclusive for such conditions. Some RCTs have found soy has small, favorable effects on serum levels of low-density lipoprotein and total cholesterol,24 while others have shown modest improvements in triglyceride levels without significant improvements in other lipid levels.25
A 2011 meta-analysis of 10 RCTs that included 268 participants found that a diet high in non-soy legume products, such as alfalfa, lentils, and other beans, also improved lipid levels.37 A review of 136 studies that described 22 dietary interventions concluded that among other helpful dietary approaches to controlling hyperlipidemia, dietary soy—which contains fiber and polyunsaturated fats—is favored over supplementation of soy protein alone.38
Use caution when recommending soy for patients with thyroid dysfunction or hormone-sensitive cancers because some evidence suggests soy may interfere with absorption of levothyroxine and increase the risk of developing clinical symptoms of hypothyroidism.39
Soy also contains phytoestrogens, and prolonged use of soy supplements may increase the risk of endometrial hyperplasia.24 This risk has been documented only in the use of soy supplements, and not from dietary soy. GI disturbances and rare allergic reactions also have been reported.24
St. John’s wort for depression
Hypericum perforatum (St. John’s wort), a perennial herb, has been used to treat mood disorders and other ailments for more than 2000 years.40,41 Commercial preparations typically are alcohol extracts with an herb-to-extract ratio of 4:1 to 8:1.26 The normal dose ranges from 900 to 1500 mg/d in 2 to 3 divided doses of the alcohol extract standardized to 0.3% hypericin and/or 3% to 5% hyperforin.
St. John’s wort has been studied extensively as a treatment for depressive disorders. A 2001 double-blind RCT conducted in 11 US academic medical centers and community clinics between 1998 and 2000 that included 200 patients found that St. John’s wort was not effective for moderately severe major depression; a trend toward a positive effect was noted in both the placebo and St. John’s wort groups.26
However, a 2009 Cochrane review of 29 international studies (5489 patients) concluded that St. John’s wort may be better than placebo and as effective as antidepressants for mild to moderate major depression,27 and appeared to have fewer side effects than antidepressants. This review, conducted in German-speaking countries where medical professionals have long prescribed St. John’s wort, reported more positive results than those conducted in other countries.
St. John’s wort interacts with many medications, including antidepressants, oral contraceptives, cyclosporine, digoxin, indinavir, phenytoin, phenobarbital, warfarin, and others. It induces cytochrome P450 (CYP450) enzymes, and therefore can potentially reduce the efficacy of any medication that is metabolized by a CYP450 enzyme. When used in high doses in combination with antidepressants, St. John’s wort may cause serotonin syndrome. Other side effects include photosensitivity, GI complaints, fatigue, and increased risk of cataracts. Due to a lack of clinical data, St. John’s wort is contraindicated in women who are pregnant or breastfeeding.42
Motivational interviewing (MI) is an alternative approach to traditional provider-patient communication that entails using open-ended questions, reflective listening, affirmation, and assessing readiness to change.1 MI facilitators aim to elicit change and assist patients in forming a self-management plan with specific, measurable, achievable, realistic, and timely (SMART) goals.1-3
MI can be efficiently implemented in diverse settings and by a variety of trained facilitators.3-5 For example, the Brief Negotiation Interview requires only 7 minutes per emergency department patient and effectively improves long-term outcomes for substance abusers.4 A randomized controlled trial that included 135 patients admitted to a psychiatric emergency inpatient unit for substance abuse found that those who received 2 sessions of MI reported significantly less substance use than controls 2 years after the intervention.3
Training for providers to ensure proper implementation of MI techniques is essential because poor use of MI can be counter-therapeutic.5 Tools such as the Motivational Interviewing Treatment Integrity Scale and the Client Evaluation of Motivational Interviewing can be used to ensure providers are competent.4,6
References
1. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behavior. New York, NY: Guilford Press; 1991.
2. Levensky ER, Forcehimes A, O’Donohue WT, et al. Motivational interviewing: an evidence-based approach to counseling helps patients follow treatment recommendations. Am J Nurse. 2007;107:50-59.
3. Bagøien G, Bjørngaard JH, Østensen C, et al. The effects of motivational interviewing on patients with comorbid substance use admitted to a psychiatric emergency unit - a randomized controlled trial with two year follow-up. BMC Psychiatry. 2013;13:93.
4. D’Onofrio G, Fiellin DA, Pantalon MV, et al. A brief intervention reduces hazardous and harmful drinking in emergency department patients. Ann Emerg Med. 2012;60:181-192.
5. Tollison SJ, Mastroleo NR, Mallett KA, et al. The relationship between baseline drinking status, peer motivational interviewing microskills, and drinking outcomes in a brief alcohol intervention for matriculating college students: a replication. Behav Ther. 2013;44:137-151.
6. Madson MB, Mohn RS, Zuckoff A, et al. Measuring client perceptions of motivational interviewing: factor analysis of the Client Evaluation of Motivational Interviewing scale. J Subst Abuse Treat. 2013;44:330-335.
Guided imagery for anxiety and pain
Guided imagery is a relaxation technique that involves visualizing positive outcomes to reduce one’s reaction to anxiety-provoking or painful experiences.43 It can be practiced independently or under the direction of an instructor. One RCT of 96 women with newly diagnosed breast cancer found that adding relaxation and guided imagery to standard breast cancer treatment protocols positively affected mood and quality of life.14 While this study saw no change in pathologic responses to chemotherapy,14 a more recent RCT concluded that such biochemical advantages may be possible.44 Guided imagery has been linked to decreased anxiety in diverse studies of students, women in labor, individuals suffering from nightmares, and in occupational settings such as training for pilots and surgeons.15-18
A review of 9 RCTs of guided imagery for decreasing musculoskeletal pain involving 201 patients found 8 studies reported positive results, though the methodological quality of the studies was low.19 Of 6 high-quality studies included in a 2012 systematic review, 5 supported the use of guided imagery for postoperative, abdominal, and other nonmusculoskeletal pain.20 This initial evidence is promising, but additional research of high methodological quality is needed to validate the use of guided imagery for anxiety and pain.
Acupuncture for pain
From 2002 to 2007, the use of acupuncture significantly increased in the United States, primarily for the treatment of pain.1 A 2012 meta-analysis of 29 RCTs that included almost 18,000 participants evaluated the clinical usefulness of acupuncture for back, neck, and shoulder pain, OA, and headache.3 Compared to no treatment, both acupuncture and sham acupuncture significantly improved pain scores. The authors of this meta-analysis found that acupuncture offered a small but significant advantage over sham acupuncture, and concluded that the benefits of acupuncture were not due to a placebo effect.
In 2007, the American College of Physicians (ACP) and the American Pain Society (APS) issued a joint statement indicating that acupuncture should be considered for patients with chronic low back pain who do not respond to conventional therapies.4 The North American Spine Society also supports acupuncture, stating that it provides “...better short-term pain relief and functional improvement than no treatment and the addition of acupuncture to other treatment modalities provides a greater benefit than those treatments alone.”5 Additional evidence found acupuncture for chronic low back pain improves function and serves as an adjunct therapy.6
Reported adverse effects of acupuncture include—but may not be limited to—infection, skin irritation, hematoma, pneumothorax, and spontaneous needle migration.1,3-6
Yoga for low back pain
Back pain is the most common reason patients use CAM therapies.1 A systematic review of 10 RCTs that included 967 participants with chronic low back pain found strong evidence for the short-term effectiveness and moderate evidence for the long-term effectiveness of yoga.28 A review of 17 studies that included 1626 patients concluded that yoga improves both pain and functionality; this review did not recommend a specific type of yoga practice.29 In a recent study of 95 minority adults with moderate-to-severe chronic low back pain, once-weekly and twice-weekly yoga for 12 weeks were similarly effective for reducing pain and improving functionality.30
Guidelines from the ACP and the APS recommend yoga as part of an intensive interdisciplinary rehabilitation program for patients with chronic or subacute low back pain who do not improve using other self-care options.4 This recommendation is specifically for Viniyoga, a practice in which the instructor recommends modifications to body positioning for each individual based on past injuries and overall physical condition. (For more information on therapeutic uses of yoga, see “Yoga as therapy: When is it helpful?”)
CORRESPONDENCE
Roger Zoorob, MD, MPH, FAAFP; Department of Family and Community Medicine, Baylor College of Medicine, 3701 Kirby Drive, Suite 600, Houston, TX 77098; roger.zoorob@bcm.edu
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;10:1-23.
2. American Holistic Medicine Association. Integrative medicine centers. American Holistic Medicine Association Web site. Available at: http://www.holisticmedicine.org/content. asp?pl=30&sl=2&contentid=74. Accessed September 8, 2014.
3. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
4. Chou R, Qaseem A, Snow V, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians; American College of Physicians; American Pain Society Low Back Pain Guidelines Panel. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478-491.
5. Berman BM, Langevin HM, Witt CM, et al. Acupuncture for chronic low back pain. N Engl J Med. 2010;363:454-461.
6. Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009;79:1067-1074.
7. Eslik GD, Howe PR, Smith C, et al. Benefits of fish oil supplementation in hyperlipidemia: a systematic review and meta-analysis. Int J Cardiol. 2009;136:4-16.
8. Miller M, Stone NJ, Ballantyne C, et al; American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committeeof the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglyceride and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2292-2333.
9. Bays HE. Safety considerations with omega-3 fatty acid therapy. Am J Cardiol. 2007;99:35C-43C.
10. Brasky TM, Darke AK, Song X, et al. Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2013;105:1132-1141.
11. Towheed TE, Maxwell L, Anastassiades TP, et al. Glucosamine therapy for treating osteoarthritis. Cochrane Database Syst Rev. 2005;(2):CD002946.
12. Sawitzke AD, Shi H, Finco MF, et al. Clinical efficacy and safety of glucosamine, chondroitin sulphate, their combination, celecoxib or placebo taken to treat osteoarthritis of the knee: 2-year results from GAIT. Ann Rheum Dis. 2010;69:1459-1464.
13. Dostrovsky NR, Towheed TE, Hudson RW, et al. The effect of glucosamine on glucose metabolism in humans: a systematic review of the literature. Osteoarthritis Cartilage. 2011;19:375-380.
14. Walker LG, Walker MB, Ogston K, et al. Psychological, clinical and pathological effects of relaxation training and guided imagery during primary chemotherapy. Br J Cancer. 1999;80:262-268.
15. Thünker J, Pietrowsky R. Effectiveness of a manualized imagery rehearsal therapy for patients suffering from nightmare disorders with and without a comorbidity of depression or PTSD. Behav Res Ther. 2012;50:558-564.
16. Marc I, Toureche N, Ernst E, et al. Mind-body interventions during pregnancy for preventing or treating women’s anxiety. Cochrane Database Syst Rev. 2011;(7):CD007559.
17. Jing X, Wu P, Liu F, et al. Guided imagery, anxiety, heart rate, and heart rate variability during centrifuge training. Aviat Space Environ Med. 2011;82:92-96.
18. Arora S, Aggarwal R, Moran A, et al. Mental practice: effective stress management training for novice surgeons. J Am Coll Surg. 2011;212:225-233.
19. Posadzki P, Ernst E. Guided imagery for musculoskeletal pain: a systematic review. Clin J Pain. 2011;27:648-653.
20. Posadzki P, Lewandowski W, Terry R, et al. Guided imagery for non-musculoskeletal pain: a systematic review of randomized clinical trials. J Pain Symptom Manage. 2012;44:95-104.
21. Arvola T, Laiho K, Torkkeli S, et al. Prophylactic Lactobacillus GG reduces antibiotic-associated diarrhea in children with respiratory infections: a randomized study. Pediatrics. 1999;104:e64.
22. Johnston BC, Goldenberg JZ, Vandvik PO, et al. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database Syst Rev. 2011;(11):CD004827.
23. Williams NT. Probiotics. Am J Health-Syst Pharm. 2010;67:449-458.
24. Sacks FM, Lichtenstein A, Van Horn L, et al; American Heart Association Nutrition Committee. Soy protein, isoflavones, and cardiovascular health: an American Heart Association Science Advisory for professionals from the Nutrition Committee. Circulation. 2006;113:1034-1044.
25. Qin Y, Niu K, Zeng Y, et al. Isoflavones for hypercholesterolaemia in adults. Cochrane Database Syst Rev. 2013;6:CD009518.
26. Shelton RC, Keller MB, Gelenberg A, et al. Effectiveness of St John’s wort in major depression: a randomized controlled trial. JAMA. 2001;285:1978-1986.
27. Linde K, Berner MM, Kriston L. St John’s wort for major depression. Cochrane Database Syst Rev. 2008;(4):CD000448.
28. Cramer H, Lauche R, Haller H, et al. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29: 450-460.
29. Ward L, Stebbings S, Cherkin D, et al. Yoga for functional ability, pain and psychosocial outcomes in musculoskeletal conditions: a systematic review and meta-analysis. Musculoskeletal Care. 2013;11:203-217.
30. Saper RB, Boah AR, Keosaian J, et al. Comparing once- versus twice-weekly yoga classes for chronic low back pain in predominantly low income minorities: a randomized dosing trial. Evid Based Complement Alternat Med. 2013;2013:658030.
31. Uitterlinden EJ, Koevoet JLM, Verkoelen CF, et al. Glucosamine increases hyaluronic acid production in human osteoarthritic synovium explants. BMC Musculoskelet Disord. 2008;9:120.
32. Calamia V, Ruiz-Romero C, Rocha B, et al. Pharmacoproteomic study of the effects of chondroitin and glucosamine sulfate on human articular chondrocytes. Arthritis Res Ther. 2010;12:R138.
33. Rovati LC, Girolami F, Persiani S. Crystalline glucosamine sulfate in the management of knee osteoarthritis: efficacy, safety, and pharmacokinetic properties. Ther Adv Musculoskelet Dis. 2012;4:167-180.
34. National Center for Complementary and Alternative Medicine. Oral probiotics: An introduction. National Center for Complementary and Alternative Medicine Web site. Available at: http:// nccam.nih.gov/health/probiotics/introduction.htm. Updated December 2012. Accessed August 29, 2013.
35. Hempel S, Newberry SJ, Maher AR, et al. Probiotics for the prevention and treatment of antibiotic-associated diarrhea: a systematic review and meta-analysis. JAMA. 2012;307:1959-1969.
36. Thomas DW, Greer FR; American Academy of Pediatrics Committee on Nutrition; American Academy of Pediatrics Section on Gastroenterology, Hepatology, and Nutrition. Probiotics and prebiotics in pediatrics. Pediatrics. 2010;126:1217-1231.
37. Bazzano LA, Thompson AM, Tees MT, et al. Non-soy legume consumption lowers cholesterol levels: a meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2011;21:94-103.
38. Huang J, Frohlich J, Ignaszewski AP. The impact of dietary changes and dietary supplements on lipid profile. Can J Cardiol. 2011;27:488-505.
39. Messina M, Redmond G. Effects of soy protein and soybean isoflavones on thyroid function in healthy adults and hypothyroid patients: a review of the relevant literature. Thyroid. 2006;16: 249-258.
40. National Center for Complementary and Alternative Medicine. St. John’s Wort. National Center for Complementary and Alternative Medicine Web site. Available at: http://nccam.nih.gov/ health/stjohnswort. Accessed October 14, 2013.
41. Schulz V, Hänsel R, Tyler VE. Rational Phytotherapy: A Physicians’ Guide to Herbal Medicine. Berlin: Springer; 2001:62-81.
42. Mischoulon D. Update and critique of natural remedies as antidepressant treatments. Obstet Gynecol Clin North Am. 2009;36: 789-807.
43. Hanssen MM, Peters ML, Vlaeyen JW, et al. Optimism lowers pain: evidence of the causal status and underlying mechanisms. Pain. 2013;154:53-58.
44. Eremin O, Walker MB, Simpson E, et al. Immuno-modulatory effects of relaxation training and guided imagery in women with locally advanced breast cancer undergoing multimodality therapy: a randomised controlled trial. Breast. 2009;18:17-25.
1. Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;10:1-23.
2. American Holistic Medicine Association. Integrative medicine centers. American Holistic Medicine Association Web site. Available at: http://www.holisticmedicine.org/content. asp?pl=30&sl=2&contentid=74. Accessed September 8, 2014.
3. Vickers AJ, Cronin AM, Maschino AC, et al; Acupuncture Trialists’ Collaboration. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172:1444-1453.
4. Chou R, Qaseem A, Snow V, et al; Clinical Efficacy Assessment Subcommittee of the American College of Physicians; American College of Physicians; American Pain Society Low Back Pain Guidelines Panel. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147:478-491.
5. Berman BM, Langevin HM, Witt CM, et al. Acupuncture for chronic low back pain. N Engl J Med. 2010;363:454-461.
6. Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009;79:1067-1074.
7. Eslik GD, Howe PR, Smith C, et al. Benefits of fish oil supplementation in hyperlipidemia: a systematic review and meta-analysis. Int J Cardiol. 2009;136:4-16.
8. Miller M, Stone NJ, Ballantyne C, et al; American Heart Association Clinical Lipidology, Thrombosis, and Prevention Committeeof the Council on Nutrition, Physical Activity, and Metabolism; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Nursing; Council on the Kidney in Cardiovascular Disease. Triglyceride and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2011;123:2292-2333.
9. Bays HE. Safety considerations with omega-3 fatty acid therapy. Am J Cardiol. 2007;99:35C-43C.
10. Brasky TM, Darke AK, Song X, et al. Plasma phospholipid fatty acids and prostate cancer risk in the SELECT trial. J Natl Cancer Inst. 2013;105:1132-1141.
11. Towheed TE, Maxwell L, Anastassiades TP, et al. Glucosamine therapy for treating osteoarthritis. Cochrane Database Syst Rev. 2005;(2):CD002946.
12. Sawitzke AD, Shi H, Finco MF, et al. Clinical efficacy and safety of glucosamine, chondroitin sulphate, their combination, celecoxib or placebo taken to treat osteoarthritis of the knee: 2-year results from GAIT. Ann Rheum Dis. 2010;69:1459-1464.
13. Dostrovsky NR, Towheed TE, Hudson RW, et al. The effect of glucosamine on glucose metabolism in humans: a systematic review of the literature. Osteoarthritis Cartilage. 2011;19:375-380.
14. Walker LG, Walker MB, Ogston K, et al. Psychological, clinical and pathological effects of relaxation training and guided imagery during primary chemotherapy. Br J Cancer. 1999;80:262-268.
15. Thünker J, Pietrowsky R. Effectiveness of a manualized imagery rehearsal therapy for patients suffering from nightmare disorders with and without a comorbidity of depression or PTSD. Behav Res Ther. 2012;50:558-564.
16. Marc I, Toureche N, Ernst E, et al. Mind-body interventions during pregnancy for preventing or treating women’s anxiety. Cochrane Database Syst Rev. 2011;(7):CD007559.
17. Jing X, Wu P, Liu F, et al. Guided imagery, anxiety, heart rate, and heart rate variability during centrifuge training. Aviat Space Environ Med. 2011;82:92-96.
18. Arora S, Aggarwal R, Moran A, et al. Mental practice: effective stress management training for novice surgeons. J Am Coll Surg. 2011;212:225-233.
19. Posadzki P, Ernst E. Guided imagery for musculoskeletal pain: a systematic review. Clin J Pain. 2011;27:648-653.
20. Posadzki P, Lewandowski W, Terry R, et al. Guided imagery for non-musculoskeletal pain: a systematic review of randomized clinical trials. J Pain Symptom Manage. 2012;44:95-104.
21. Arvola T, Laiho K, Torkkeli S, et al. Prophylactic Lactobacillus GG reduces antibiotic-associated diarrhea in children with respiratory infections: a randomized study. Pediatrics. 1999;104:e64.
22. Johnston BC, Goldenberg JZ, Vandvik PO, et al. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database Syst Rev. 2011;(11):CD004827.
23. Williams NT. Probiotics. Am J Health-Syst Pharm. 2010;67:449-458.
24. Sacks FM, Lichtenstein A, Van Horn L, et al; American Heart Association Nutrition Committee. Soy protein, isoflavones, and cardiovascular health: an American Heart Association Science Advisory for professionals from the Nutrition Committee. Circulation. 2006;113:1034-1044.
25. Qin Y, Niu K, Zeng Y, et al. Isoflavones for hypercholesterolaemia in adults. Cochrane Database Syst Rev. 2013;6:CD009518.
26. Shelton RC, Keller MB, Gelenberg A, et al. Effectiveness of St John’s wort in major depression: a randomized controlled trial. JAMA. 2001;285:1978-1986.
27. Linde K, Berner MM, Kriston L. St John’s wort for major depression. Cochrane Database Syst Rev. 2008;(4):CD000448.
28. Cramer H, Lauche R, Haller H, et al. A systematic review and meta-analysis of yoga for low back pain. Clin J Pain. 2013;29: 450-460.
29. Ward L, Stebbings S, Cherkin D, et al. Yoga for functional ability, pain and psychosocial outcomes in musculoskeletal conditions: a systematic review and meta-analysis. Musculoskeletal Care. 2013;11:203-217.
30. Saper RB, Boah AR, Keosaian J, et al. Comparing once- versus twice-weekly yoga classes for chronic low back pain in predominantly low income minorities: a randomized dosing trial. Evid Based Complement Alternat Med. 2013;2013:658030.
31. Uitterlinden EJ, Koevoet JLM, Verkoelen CF, et al. Glucosamine increases hyaluronic acid production in human osteoarthritic synovium explants. BMC Musculoskelet Disord. 2008;9:120.
32. Calamia V, Ruiz-Romero C, Rocha B, et al. Pharmacoproteomic study of the effects of chondroitin and glucosamine sulfate on human articular chondrocytes. Arthritis Res Ther. 2010;12:R138.
33. Rovati LC, Girolami F, Persiani S. Crystalline glucosamine sulfate in the management of knee osteoarthritis: efficacy, safety, and pharmacokinetic properties. Ther Adv Musculoskelet Dis. 2012;4:167-180.
34. National Center for Complementary and Alternative Medicine. Oral probiotics: An introduction. National Center for Complementary and Alternative Medicine Web site. Available at: http:// nccam.nih.gov/health/probiotics/introduction.htm. Updated December 2012. Accessed August 29, 2013.
35. Hempel S, Newberry SJ, Maher AR, et al. Probiotics for the prevention and treatment of antibiotic-associated diarrhea: a systematic review and meta-analysis. JAMA. 2012;307:1959-1969.
36. Thomas DW, Greer FR; American Academy of Pediatrics Committee on Nutrition; American Academy of Pediatrics Section on Gastroenterology, Hepatology, and Nutrition. Probiotics and prebiotics in pediatrics. Pediatrics. 2010;126:1217-1231.
37. Bazzano LA, Thompson AM, Tees MT, et al. Non-soy legume consumption lowers cholesterol levels: a meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2011;21:94-103.
38. Huang J, Frohlich J, Ignaszewski AP. The impact of dietary changes and dietary supplements on lipid profile. Can J Cardiol. 2011;27:488-505.
39. Messina M, Redmond G. Effects of soy protein and soybean isoflavones on thyroid function in healthy adults and hypothyroid patients: a review of the relevant literature. Thyroid. 2006;16: 249-258.
40. National Center for Complementary and Alternative Medicine. St. John’s Wort. National Center for Complementary and Alternative Medicine Web site. Available at: http://nccam.nih.gov/ health/stjohnswort. Accessed October 14, 2013.
41. Schulz V, Hänsel R, Tyler VE. Rational Phytotherapy: A Physicians’ Guide to Herbal Medicine. Berlin: Springer; 2001:62-81.
42. Mischoulon D. Update and critique of natural remedies as antidepressant treatments. Obstet Gynecol Clin North Am. 2009;36: 789-807.
43. Hanssen MM, Peters ML, Vlaeyen JW, et al. Optimism lowers pain: evidence of the causal status and underlying mechanisms. Pain. 2013;154:53-58.
44. Eremin O, Walker MB, Simpson E, et al. Immuno-modulatory effects of relaxation training and guided imagery in women with locally advanced breast cancer undergoing multimodality therapy: a randomised controlled trial. Breast. 2009;18:17-25.
