User login
Managing eczema in children—a treatment update
• Emollients should be used during acute flares as well as regularly for maintenance therapy in children with atopic dermatitis (AD). A
• Topical corticosteroids are the first-line therapy for acute AD flares. A
• There is no evidence to support the use of antihistamines for treatment of AD. A
• Exclusion of cow’s milk and eggs is not recommended except in proven cases of milk or egg allergy with sensitivity testing and food challenge. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Dylan, an 8-month-old boy whom you had seen for a routine check-up a little over a month ago, is in your office today because of a rash on his face and elbows. The rash began about 2 weeks ago, his mother reports—shortly after she had weaned him from the breast milk to formula. Certain that Dylan has a milk allergy, his mother tells you she plans to switch to a soy-based formula—and wants you to give her something to put on the rash to help clear it up.
CASE 2 Eighteen-month-old Angela had a mild case of atopic dermatitis when you saw her about 3 months ago. The reason for today’s visit is that “her eczema is getting worse,” according to her mother, and the moisturizing cream that you recommended at her last visit “stopped working.” The rash, which had been confined to the patient’s forearms and knees (FIGURE 1), now covers much of her face, forearms, knees, and trunk. Angela’s mother says that the rash appears to be very itchy and that her daughter has been crying and scratching at night.
If Dylan and Angela were your patients, what would you advise their parents to do, and how would you treat them?
FIGURE 1
An 18-month-old girl with an acute flare
This child has moderate atopic dermatitis, with erythema and localized thickened skin at the medial knee—a typical site for atopic dermatitis.
Atopic dermatitis (AD), or eczema, is a chronic inflammatory skin condition that affects up to 20% of children.1 The incidence of pediatric AD has increased 2- to 3-fold in the last 30 years (it’s not clear why), and the condition is a common reason for pediatric visits to family physicians.1,2
AD is marked by phases of pruritus and rash and, depending on the severity, can significantly affect the quality of life of young patients and their families.1-4 The pathophysiology involves structural abnormalities of the epidermis—leading to dry and sensitive skin—combined with immune dysregulation.

Topical corticosteroids to decrease the inflammation and emollients to repair and hydrate the skin are the mainstay of treatment.3,5,6 But numerous considerations, including what triggers patients should avoid; how potent a steroid to prescribe; how long to continue treatment; and when, or whether, to initiate systemic treatment, remain. The evidence-based review of traditional and alternative treatments (TABLE)1-3,7-19 and practical step-wise approach (FIGURE 2)1-3,5,6,9,19-22 that follow can help ensure that you give children with AD the best possible care.
FIGURE 2
A stepped approach to atopic dermatitis1-3,5,6,9,19-22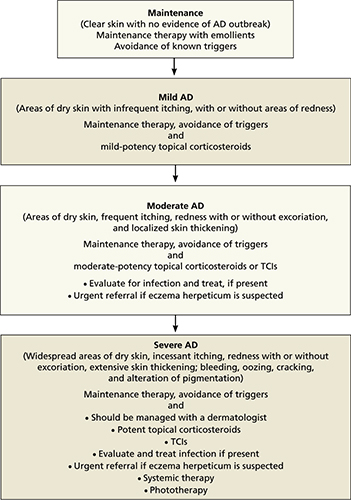
AD, atopic dermatitis; TCIs, topical calcineurin inhibitors.
TABLE
Treating atopic dermatitis: What the evidence shows
| Intervention (SOR) | Comments |
|---|---|
| Maintenance | |
| Emollients (A)1,2,7,8 | Mainstay of maintenance therapy |
| Treatment | |
| Corticosteroids9-15 – Topical (A) – Oral (B) | First-line treatment No proven benefit |
| TCIs:3,16,17 – Pimecrolimus (A) – Tacrolimus (A) | Second-line treatment |
| Symptom relief | |
| Antihistamines (A)11,14 | No proven benefit in the treatment of AD; sedating antihistamines may improve sleep |
| Tar (C)14 | |
| Wet wrap dressings (C )18 | |
| Infection1,11 | |
| Antibiotics – Topical (A) – Oral (A) | |
| Antifungals – Topical (A) – Oral (A) | |
| Alternative/preventive measures11,19 | |
| Breastfeeding (B) | May reduce risk of developing AD (poor quality study) |
| Essential fatty acids* | No proven benefit |
| Exclusion of eggs or cow’s milk (B) | Only in proven cases of allergy |
| Multivitamins, B6, zinc supplements (C) | No proven benefit |
| Probiotics (B) | No proven benefit |
| Vitamin D supplementation (C) | More studies needed |
| *Black currant seed oil, evening primrose oil, fish oil. AD, atopic dermatitis; TCIs, topical calcineurin inhibitors. | |
The patient has a rash, but what’s the trigger?
Epidemiologic studies have identified numerous AD triggers, including sweating, stress, dust, hard water, food allergies, and seasonality.23 Environmental or situational triggers should be avoided whenever possible,20 of course, but first, they must be identified—an often-difficult task. Establishing the role of any exacerbating factor in AD involves documentation of a temporal relationship between exposure and the development or worsening of symptoms; a dose-response effect; and remission after withdrawal of the trigger.
What’s more, avoidance does not always have the desired result. There is a well-demonstrated correlation between house dust mite sensitization and AD, especially in children of preschool age and older.7,21 Studies performed to determine whether decreasing house dust mite antigen would have a positive effect on disease severity, however, have had conflicting results.23
Food allergies are more likely in the youngest patients
For about a third (35%) of children with AD, the trigger is a food allergy.22 This is most common in infants, with one study showing a peak at 18 months.20,24 The most common food allergens are milk and egg, but wheat, soy, and peanuts are potential allergens, as well.22,25 Food allergies, which are difficult to identify, should be suspected in patients with a poor response to first-line treatment. Sensitivity testing with food challenge may be worthwhile only in severe cases that are refractory to routine care.20
We caution parents not to attempt to withhold a suspected food allergen on their own. To avoid the risk of malnutrition, young children should be placed on elimination diet trials only if the allergen has first been identified by sensitivity testing and food challenge tests, because the allergen may not be clinically significant.21,22 Neither skin prick tests nor serum tests for allergies have been found to be accurate, and parents themselves are often mistaken. Several studies have found a discrepancy between the foods parents think their child is allergic to and the substances that are later found to be clinically significant allergens.21
CASE 1 You advise Dylan’s mother not to switch formulas because answers to further questions about other symptoms were unremarkable (eg, diarrhea). Dylan is treated with a low-potency (class VII) topical steroid (1% hydrocortisone cream) with instructions for the parents to maintain hydration and call you in 5 to 7 days.
Topical corticosteroids are first-line treatment
Two major classes of pharmacologic agents are used for the treatment of AD: topical corticosteroids and topical calcineurin inhibitors (TCIs). Corticosteroids are first-line treatment, as their clinical effectiveness has been well established; TCIs are indicated only as second-line therapy.26,27
Which dosing regimen is best?
The potency of corticosteroids is expressed by a numerical scale, ranging from class I (the most potent) to class VII (the least potent). Class I steroids are about 1800 times more potent than class VII preparations.8
A decision about which strength to use is based on several factors, including the severity of the child’s AD, his or her age, and the affected body site. For infants ≤12 months old, the lowest potency preparations (such as 1% hydrocortisone) are preferable, but should be used in the diaper area for no more than 3 to 7 days at a time.8 In general, potent topical corticosteroids should not be used for children <12 months of age without a dermatology consult.8,9
For children ages 1 through 5 years, intermittent (1- to 2-week) bursts of mild to moderate potency corticosteroids (class VI and VII) are suitable; for older children, a 7- to 10-day course of more potent preparations (class II-V) can be used for nonflexural and nonfacial skin.
While clinical trials have addressed the issues of quantity, duration, potency, and frequency (one large systematic review found twice-daily application of topical corticosteroids to be no more effective than once-daily applications10), an optimal approach to their use in the long-term management of pediatric AD is largely undefined. Various approaches include:
- starting with a more potent preparation to induce remission, followed by a less potent corticosteroid as the AD improves
- using short bursts (5-7 days) of a potent topical corticosteroid, followed by emollient use until a flare-up occurs
- relying on prolonged, or continuous, treatment with less potent preparations.11,23
Long-term use of topical corticosteroids of any potency should be avoided in areas of high risk for cutaneous side effects, such as the face and intertriginous areas.
Emollients are also an important part of therapy for all pediatric patients. Emollients help restore the integrity of the skin barrier and inhibit water loss,1,2,12,20 and should be used not only during an acute flare, but also for maintenance therapy. Tell parents to look for emollients that are unscented and contain fewer additives, and to apply the emollient at least twice daily, and after bathing or swimming.5,20
CASE 2 You prescribe a class V steroid (triamcinolone ointment 0.025%) for Angela, to be applied once a day for 5 to 7 days. You instruct her mother in basic skin care and stress the importance of using an emollient regularly, not just during a flare-up.
What to tell parents about side effects
Discuss the benefits and potential harms of topical corticosteroids with parents (and youngsters who are old enough to understand), emphasizing that when used correctly, the benefits outweigh the risks.
Potential side effects include skin atrophy, striae, telangiectasia, hypopigmentation, rosacea, glaucoma, and cataracts, with studies suggesting that local adverse effects are related to the potency.13 Because there are few prospective controlled trials of sufficient duration, however, the incidence of local reactions to topical corticosteroids in patients with AD is uncertain.
The potential for topical corticosteroids to suppress the hypothalamic-pituitary-adrenal (HPA) axis has been investigated in a small number of studies, with inconclusive results. Effects on the HPA axis appear to be associated with percutaneous absorption in patients who either have a more severe case of AD or are <2 years old.14 A recent systematic review confirmed that the degree of systemic absorption is based on the severity and extent of the disease as well as the formulation and potency of the topical agent.14,15
When to consider TCIs
Pimecrolimus and tacrolimus, the 2 TCIs on the market, are second-line agents for AD. Both have US Food and Drug Administration (FDA) approval for short-term treatment of moderate to severe AD in immunocompetent patients who have failed to respond to topical corticosteroids and children >2 years.26,27 Both TCIs provide targeted anti-inflammatory activity without the local and systemic side effects of topical corticosteroids.
Pimecrolimus cream 1% is approved for treatment in children >2 years.27 Tacrolimus ointment 0.03% is approved for children ages 2 to 15 years with moderate to severe AD, and tacrolimus ointment 0.1% is approved for children older than 16 years with moderate to severe AD.26 Data from clinical trials have shown that pimecrolimus reduces the number and severity of flares, extends the time between flares, and decreases pruritus and other cutaneous signs associated with AD.3 Common side effects, which are usually mild and resolve within days, include pruritus, burning, and stinging at the application site.
In 2006 the FDA added a black-box warning stating that their long-term safety has not been established—a response to widespread off-label use of TCIs in children <2 years and concerns about a theoretical cancer risk based on their mechanism of action—and concluded in 2010 that the labeling adequately warns providers of the potential safety risks.28 Recent reviews have concluded that systemic exposure to topical TCIs is minimal and that there is no evidence linking TCIs to an increased risk of lymphoproliferative disease.16,17,29
Combining corticosteroids and TCIs
In clinical practice, both topical corticosteroids and TCIs are often used for long-term management of moderate to severe AD. TCIs are valuable alternatives to continuous use of corticosteroids for patients with persistent AD and recurrent flares. They’re also beneficial for patients with outbreaks in sensitive areas, such as the face and genitals.
Adjunctive therapies—what’s best for pruritus?
Pruritus is a major feature of AD, and a source of considerable distress. Here are some treatment options that often come up, and what we know about their usefulness.
Antihistamines. There is no evidence to support the use of nonsedating antihistamines in the treatment of AD. Sedating systemic antihistamines such as hydroxyzine and diphenhydramine don’t have a direct effect on the pruritus either, but they can be used to help patients with acute flare-ups improve their sleep.9,14
CASE 2 Antihistamines would not be recommended for Angela at this time; instead, you wait to see whether the topical corticosteroid you have just prescribed is effective. If the patient is still having trouble sleeping after she completes the corticosteroid trial, you can recommend the use of a sedating antihistamine at night as a sleeping aid.
Wet wraps. Wet wrap treatments using occlusive dressings were first recommended as a safe and effective treatment more than 20 years ago.18 Their application may be indicated for children with severe or refractory AD, provided there are no signs or symptoms of infection.
No large prospective studies have evaluated the safety and efficacy of wet wrap treatment or compared it with more conventional modalities. In a recent review, temporary systemic bioactivity of the corticosteroid was the only reported adverse effect.18
There are numerous wet wrap techniques. One effective short-term intervention is to use cream or ointment and a double layer of cotton bandages, with a moist first layer and a dry second layer. Wet wrap dressings with once-daily diluted topical corticosteroids can be used for up to 14 days.18
Coal tar. Although coal tar and coal tar derivatives have been used for many years in the treatment of AD, a lack of data on the clinical efficacy of their application, along with the cosmetic disadvantage, makes compliance with this treatment challenging.
Alternative treatments. A number of alternative measures purport to reduce a child’s risk of developing AD and/or reduce its severity (TABLE), but in most cases, evidence is lacking.
Consider systemic treatment for refractory AD
In a subgroup of patients with moderate to severe AD, the condition is refractory to standard topical therapy and systemic treatment is required. Systemic treatments—including oral corticosteroids, cyclosporine, mycophenolate mofetil, azathioprine, methotrexate, and interferon—should be undertaken only under supervision of a dermatologist.
Oral corticosteroids (typically, prednisone) are sometimes used for short-term treatment of severe AD, although rarely for young children. Evidence of their efficacy is insufficient, and their use is controversial. Patients may have severe symptom flares when an oral corticosteroid is tapered or discontinued. And no randomized controlled trials of prednisone therapy for AD were found in the peer-reviewed medical literature, despite the drug’s long-standing use in AD treatment.30
Systemic immunomodulatory therapies such as cyclosporine, azathioprine, interferon gamma, intravenous immune globulin, mycophenolate, and infliximab have been used for recalcitrant AD. Cyclosporine, an immunosuppressant that acts directly on the cells of the immune system and has an inhibitory effect on T cells, decreases AD severity in the short term. Cyclosporine has been found to be safe, effective, and well tolerated in children with AD, but the potential for hypertension and renal toxicity limits its usefulness for long-term therapy.30
Other systemic immunomodulatory therapies, including those listed above, should be considered when cyclosporine is contraindicated or does not produce a suitable response. Prospective controlled trials in a pediatric population are needed to evaluate the long-term effectiveness and safety of other agents.
Phototherapy is another option
Phototherapy has evolved as a treatment for recalcitrant AD, based on the observation that the condition often improves during the summer months with increased exposure to natural light. Adverse effects of phototherapy can include erythema, pruritus, and pigment changes. Ultraviolet light is also known to cause premature aging of the skin, as well as cutaneous malignancies.4,10,14 Therefore, phototherapy, like systemic treatment, should be undertaken only with the supervision of a dermatologist.
When infection complicates care
Colonization with Staphylococcus aureus is common in patients with AD. In addition to contributing to pruritus and chronic inflammation, S aureus is a risk factor for infection.
Treatment with topical or systemic antibiotics has no clear benefit for patients with AD, except when skin infection is present, When there is evidence of infection, however, methicillin-resistant S aureus must be considered, and any abscess incised and drained.1
Herpes simplex virus infection, another possibility in patients with AD, should be treated immediately with antiviral therapy. If the lesions are widely distributed or the patient has a toxic appearance, hospitalization and IV therapy is warranted—as is an ophthalmology consult when eye or periocular involvement is suspected.1,9
Dermatophyte infections are also more common in patients with AD and can be treated with standard regimens of topical or oral antifungals. Fungi may play a role in chronic inflammation; if there is no infection, however, patients respond better to anti-inflammatory agents than to antifungals.1
Time for a referral
As already noted, a dermatology consult is indicated for refractory AD and when systemic treatment and/or phototherapy is being considered. The suspicion of eczema herpeticum indicates a need for an immediate dermatology referral. An urgent referral is needed for patients with severe AD that has not responded to a week of optimum topical therapy—or whose treatment of bacterial infection has failed. Consider a dermatology consult, as well, when the diagnosis is uncertain or the patient’s symptoms have been poorly controlled. If you (or the child’s parents) suspect that a food allergy is the cause of a severe case of AD, a referral to an allergist is recommended.6,19,21,22
CASE 1 Dylan’s mother calls to tell you that, to her surprise, his eczema has completely cleared up, even though she did not change his formula. You advise her to continue to use the emollient at least twice a day and to bring him in if he develops another flare.
CASE 2 Two weeks after Angela’s office visit, her mother calls to report that her daughter has responded well to triamcinolone ointment 0.025%, the topical steroid you prescribed. When Angela comes in for a well-child visit at age 2, however, she has a mild flare. You prescribe a brief course of triamcinolone ointment and remind her mother to be diligent about skin care.
CORRESPONDENCE Joanne Dempster, MD, New York Presbyterian Hospital, Family & Community Medicine, 610 West 158th Street, New York, NY 10032; jd2745@columbia.edu
1. Boguniewicz M, Leung D. Recent insights into atopic dermatitis and implications for management of infectious complications. J Allergy Clin Immunol. 2010;125:4-13.
2. Lucinda BM. Treatment options for atopic dermatitis. Am Fam Physician. 2007;75:523-530.
3. Levy ML. Atopic dermatitis: understanding the disease and its management. Curr Med Res Opin. 2007;23:3091-3103.
4. Brown S, Reynolds NJ. Atopic and non-atopic eczema. BMJ. 2006;332:584-588.
5. Carbone A, Siu A, Patel R, et al. Pediatric atopic dermatitis: a review of the medical management. Ann Pharmacother. 2010;44:1448-1458.
6. Akadis CA, Akadis M, Beiber T, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergy and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL consensus report. Allergy. 2006;61:969-987.
7. Schafer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol. 2008;8:418-422.
8. Charman C, Williams H. The use of corticosteroids and corticosteroid phobia in atopic dermatitis. Clin Dermatol. 2003;21:193-200.
9. National Collaborating Centre for Women’s and Children’s Health. Atopic eczema in children. Management of atopic eczema in children from birth up to age of 12 years. Clinical guideline no. 57. London, UK: National Institute for Health and Clinical Excellence (NICE); 2007.
10. Hoare C, Li Wan Po A, Williams H. Systematic review of treatments of atopic eczema. Health Technol Assess. 2000;4:1-191.
11. Simpson E, Hanifin J. Atopic dermatitis. J Am Acad Dermatol. 2005;53:115-128.
12. Grimalt R, Mengeaud V, Cambazard F, et al. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214:61-67.
13. Callen J, Chamlin S, Eichenfield LF, et al. A systematic review of the safety of topical therapies for atopic dermatitis. Br J Dermatol. 2007;156:203-221.
14. Hanifin JM, Cooper KD, Ho VC, et al. Guidelines for the care of atopic dermatitis developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association. “Administrative regulations for evidence-based clinical practice guidelines”. J Am Acad Dermatol. 2004;50:391-404.
15. Simpson E. Atopic dermatitis: a review of topical treatment options. Curr Med Res Opin. 2010;26:633-640.
16. Munzenberger PJ, Monejo JM. Safety of topical calcineurin inhibitors for the treatment of atopic dermatitis. Pharmacotherapy. 2007;27:1020-1028.
17. Kang S, Lucky AW, Pariser D, et al. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol. 2001;44(suppl):S58-S64.
18. Devillers ACA, Oranje AP. Efficacy and safety of ‘wet wrap’ dressings as an intervention treatment in children with severe and/or refractory atopic dermatitis: a critical review of the literature. Br J Dermatol. 2006;154:579-585.
19. Boyl RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.-
20. Ellis C, Luger T. International Consensus Conference of Atopic Dermatitis (ICCAD II*): clinical update and current treatment strategies. Br J Dermatol. 2003;148(suppl 63):S3-S10.
21. Han KL, Leung TF, Ching G, et al. Patterns of food and aeroallergen sensitization in childhood eczema. Acta Pediatrica. 2008;97:1734-1737.
22. Greenhawt M. The role of food allergy in atopic dermatitis. Allergy Asthma Proc. 2010;31:392-397.
23. Langan SM, Williams HC. What causes worsening of eczema? A systemic review. Br J Dermatol. 2006;155:505-514.
24. Eller E, Kjaer HF, et al. Food allergy and food sensitization in early childhood: results from the DARC cohort. Allergy. 2009;63:1023-1029.
25. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361:151-160.
26. Protopic [prescribing information]. Deerfield, IL: Astellas Pharma US, Inc; 2006.
27. Elidel [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.
28. US Food and Drug Administration. Topical calcineurin inhibitors. Pediatric safety update: regulatory background. FDA Pediatric Advisory Committee Meeting; March 22, 2010; Bethesda, Md.
29. Kalavala M, Dohil MA. Calcineurin inhibitors in pediatric atopic dermatitis: a review of current evidence. Am J Clin Dermatol. 2011;12:15-24.
30. Ricci G, Dondi A, Patrizi A, et al. Systemic therapy of atopic dermatitis in children. Drugs. 2009;69:297-306.
• Emollients should be used during acute flares as well as regularly for maintenance therapy in children with atopic dermatitis (AD). A
• Topical corticosteroids are the first-line therapy for acute AD flares. A
• There is no evidence to support the use of antihistamines for treatment of AD. A
• Exclusion of cow’s milk and eggs is not recommended except in proven cases of milk or egg allergy with sensitivity testing and food challenge. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Dylan, an 8-month-old boy whom you had seen for a routine check-up a little over a month ago, is in your office today because of a rash on his face and elbows. The rash began about 2 weeks ago, his mother reports—shortly after she had weaned him from the breast milk to formula. Certain that Dylan has a milk allergy, his mother tells you she plans to switch to a soy-based formula—and wants you to give her something to put on the rash to help clear it up.
CASE 2 Eighteen-month-old Angela had a mild case of atopic dermatitis when you saw her about 3 months ago. The reason for today’s visit is that “her eczema is getting worse,” according to her mother, and the moisturizing cream that you recommended at her last visit “stopped working.” The rash, which had been confined to the patient’s forearms and knees (FIGURE 1), now covers much of her face, forearms, knees, and trunk. Angela’s mother says that the rash appears to be very itchy and that her daughter has been crying and scratching at night.
If Dylan and Angela were your patients, what would you advise their parents to do, and how would you treat them?
FIGURE 1
An 18-month-old girl with an acute flare
This child has moderate atopic dermatitis, with erythema and localized thickened skin at the medial knee—a typical site for atopic dermatitis.
Atopic dermatitis (AD), or eczema, is a chronic inflammatory skin condition that affects up to 20% of children.1 The incidence of pediatric AD has increased 2- to 3-fold in the last 30 years (it’s not clear why), and the condition is a common reason for pediatric visits to family physicians.1,2
AD is marked by phases of pruritus and rash and, depending on the severity, can significantly affect the quality of life of young patients and their families.1-4 The pathophysiology involves structural abnormalities of the epidermis—leading to dry and sensitive skin—combined with immune dysregulation.
Topical corticosteroids to decrease the inflammation and emollients to repair and hydrate the skin are the mainstay of treatment.3,5,6 But numerous considerations, including what triggers patients should avoid; how potent a steroid to prescribe; how long to continue treatment; and when, or whether, to initiate systemic treatment, remain. The evidence-based review of traditional and alternative treatments (TABLE)1-3,7-19 and practical step-wise approach (FIGURE 2)1-3,5,6,9,19-22 that follow can help ensure that you give children with AD the best possible care.
FIGURE 2
A stepped approach to atopic dermatitis1-3,5,6,9,19-22
AD, atopic dermatitis; TCIs, topical calcineurin inhibitors.
TABLE
Treating atopic dermatitis: What the evidence shows
| Intervention (SOR) | Comments |
|---|---|
| Maintenance | |
| Emollients (A)1,2,7,8 | Mainstay of maintenance therapy |
| Treatment | |
| Corticosteroids9-15 – Topical (A) – Oral (B) | First-line treatment No proven benefit |
| TCIs:3,16,17 – Pimecrolimus (A) – Tacrolimus (A) | Second-line treatment |
| Symptom relief | |
| Antihistamines (A)11,14 | No proven benefit in the treatment of AD; sedating antihistamines may improve sleep |
| Tar (C)14 | |
| Wet wrap dressings (C )18 | |
| Infection1,11 | |
| Antibiotics – Topical (A) – Oral (A) | |
| Antifungals – Topical (A) – Oral (A) | |
| Alternative/preventive measures11,19 | |
| Breastfeeding (B) | May reduce risk of developing AD (poor quality study) |
| Essential fatty acids* | No proven benefit |
| Exclusion of eggs or cow’s milk (B) | Only in proven cases of allergy |
| Multivitamins, B6, zinc supplements (C) | No proven benefit |
| Probiotics (B) | No proven benefit |
| Vitamin D supplementation (C) | More studies needed |
| *Black currant seed oil, evening primrose oil, fish oil. AD, atopic dermatitis; TCIs, topical calcineurin inhibitors. | |
The patient has a rash, but what’s the trigger?
Epidemiologic studies have identified numerous AD triggers, including sweating, stress, dust, hard water, food allergies, and seasonality.23 Environmental or situational triggers should be avoided whenever possible,20 of course, but first, they must be identified—an often-difficult task. Establishing the role of any exacerbating factor in AD involves documentation of a temporal relationship between exposure and the development or worsening of symptoms; a dose-response effect; and remission after withdrawal of the trigger.
What’s more, avoidance does not always have the desired result. There is a well-demonstrated correlation between house dust mite sensitization and AD, especially in children of preschool age and older.7,21 Studies performed to determine whether decreasing house dust mite antigen would have a positive effect on disease severity, however, have had conflicting results.23
Food allergies are more likely in the youngest patients
For about a third (35%) of children with AD, the trigger is a food allergy.22 This is most common in infants, with one study showing a peak at 18 months.20,24 The most common food allergens are milk and egg, but wheat, soy, and peanuts are potential allergens, as well.22,25 Food allergies, which are difficult to identify, should be suspected in patients with a poor response to first-line treatment. Sensitivity testing with food challenge may be worthwhile only in severe cases that are refractory to routine care.20
We caution parents not to attempt to withhold a suspected food allergen on their own. To avoid the risk of malnutrition, young children should be placed on elimination diet trials only if the allergen has first been identified by sensitivity testing and food challenge tests, because the allergen may not be clinically significant.21,22 Neither skin prick tests nor serum tests for allergies have been found to be accurate, and parents themselves are often mistaken. Several studies have found a discrepancy between the foods parents think their child is allergic to and the substances that are later found to be clinically significant allergens.21
CASE 1 You advise Dylan’s mother not to switch formulas because answers to further questions about other symptoms were unremarkable (eg, diarrhea). Dylan is treated with a low-potency (class VII) topical steroid (1% hydrocortisone cream) with instructions for the parents to maintain hydration and call you in 5 to 7 days.
Topical corticosteroids are first-line treatment
Two major classes of pharmacologic agents are used for the treatment of AD: topical corticosteroids and topical calcineurin inhibitors (TCIs). Corticosteroids are first-line treatment, as their clinical effectiveness has been well established; TCIs are indicated only as second-line therapy.26,27
Which dosing regimen is best?
The potency of corticosteroids is expressed by a numerical scale, ranging from class I (the most potent) to class VII (the least potent). Class I steroids are about 1800 times more potent than class VII preparations.8
A decision about which strength to use is based on several factors, including the severity of the child’s AD, his or her age, and the affected body site. For infants ≤12 months old, the lowest potency preparations (such as 1% hydrocortisone) are preferable, but should be used in the diaper area for no more than 3 to 7 days at a time.8 In general, potent topical corticosteroids should not be used for children <12 months of age without a dermatology consult.8,9
For children ages 1 through 5 years, intermittent (1- to 2-week) bursts of mild to moderate potency corticosteroids (class VI and VII) are suitable; for older children, a 7- to 10-day course of more potent preparations (class II-V) can be used for nonflexural and nonfacial skin.
While clinical trials have addressed the issues of quantity, duration, potency, and frequency (one large systematic review found twice-daily application of topical corticosteroids to be no more effective than once-daily applications10), an optimal approach to their use in the long-term management of pediatric AD is largely undefined. Various approaches include:
- starting with a more potent preparation to induce remission, followed by a less potent corticosteroid as the AD improves
- using short bursts (5-7 days) of a potent topical corticosteroid, followed by emollient use until a flare-up occurs
- relying on prolonged, or continuous, treatment with less potent preparations.11,23
Long-term use of topical corticosteroids of any potency should be avoided in areas of high risk for cutaneous side effects, such as the face and intertriginous areas.
Emollients are also an important part of therapy for all pediatric patients. Emollients help restore the integrity of the skin barrier and inhibit water loss,1,2,12,20 and should be used not only during an acute flare, but also for maintenance therapy. Tell parents to look for emollients that are unscented and contain fewer additives, and to apply the emollient at least twice daily, and after bathing or swimming.5,20
CASE 2 You prescribe a class V steroid (triamcinolone ointment 0.025%) for Angela, to be applied once a day for 5 to 7 days. You instruct her mother in basic skin care and stress the importance of using an emollient regularly, not just during a flare-up.
What to tell parents about side effects
Discuss the benefits and potential harms of topical corticosteroids with parents (and youngsters who are old enough to understand), emphasizing that when used correctly, the benefits outweigh the risks.
Potential side effects include skin atrophy, striae, telangiectasia, hypopigmentation, rosacea, glaucoma, and cataracts, with studies suggesting that local adverse effects are related to the potency.13 Because there are few prospective controlled trials of sufficient duration, however, the incidence of local reactions to topical corticosteroids in patients with AD is uncertain.
The potential for topical corticosteroids to suppress the hypothalamic-pituitary-adrenal (HPA) axis has been investigated in a small number of studies, with inconclusive results. Effects on the HPA axis appear to be associated with percutaneous absorption in patients who either have a more severe case of AD or are <2 years old.14 A recent systematic review confirmed that the degree of systemic absorption is based on the severity and extent of the disease as well as the formulation and potency of the topical agent.14,15
When to consider TCIs
Pimecrolimus and tacrolimus, the 2 TCIs on the market, are second-line agents for AD. Both have US Food and Drug Administration (FDA) approval for short-term treatment of moderate to severe AD in immunocompetent patients who have failed to respond to topical corticosteroids and children >2 years.26,27 Both TCIs provide targeted anti-inflammatory activity without the local and systemic side effects of topical corticosteroids.
Pimecrolimus cream 1% is approved for treatment in children >2 years.27 Tacrolimus ointment 0.03% is approved for children ages 2 to 15 years with moderate to severe AD, and tacrolimus ointment 0.1% is approved for children older than 16 years with moderate to severe AD.26 Data from clinical trials have shown that pimecrolimus reduces the number and severity of flares, extends the time between flares, and decreases pruritus and other cutaneous signs associated with AD.3 Common side effects, which are usually mild and resolve within days, include pruritus, burning, and stinging at the application site.
In 2006 the FDA added a black-box warning stating that their long-term safety has not been established—a response to widespread off-label use of TCIs in children <2 years and concerns about a theoretical cancer risk based on their mechanism of action—and concluded in 2010 that the labeling adequately warns providers of the potential safety risks.28 Recent reviews have concluded that systemic exposure to topical TCIs is minimal and that there is no evidence linking TCIs to an increased risk of lymphoproliferative disease.16,17,29
Combining corticosteroids and TCIs
In clinical practice, both topical corticosteroids and TCIs are often used for long-term management of moderate to severe AD. TCIs are valuable alternatives to continuous use of corticosteroids for patients with persistent AD and recurrent flares. They’re also beneficial for patients with outbreaks in sensitive areas, such as the face and genitals.
Adjunctive therapies—what’s best for pruritus?
Pruritus is a major feature of AD, and a source of considerable distress. Here are some treatment options that often come up, and what we know about their usefulness.
Antihistamines. There is no evidence to support the use of nonsedating antihistamines in the treatment of AD. Sedating systemic antihistamines such as hydroxyzine and diphenhydramine don’t have a direct effect on the pruritus either, but they can be used to help patients with acute flare-ups improve their sleep.9,14
CASE 2 Antihistamines would not be recommended for Angela at this time; instead, you wait to see whether the topical corticosteroid you have just prescribed is effective. If the patient is still having trouble sleeping after she completes the corticosteroid trial, you can recommend the use of a sedating antihistamine at night as a sleeping aid.
Wet wraps. Wet wrap treatments using occlusive dressings were first recommended as a safe and effective treatment more than 20 years ago.18 Their application may be indicated for children with severe or refractory AD, provided there are no signs or symptoms of infection.
No large prospective studies have evaluated the safety and efficacy of wet wrap treatment or compared it with more conventional modalities. In a recent review, temporary systemic bioactivity of the corticosteroid was the only reported adverse effect.18
There are numerous wet wrap techniques. One effective short-term intervention is to use cream or ointment and a double layer of cotton bandages, with a moist first layer and a dry second layer. Wet wrap dressings with once-daily diluted topical corticosteroids can be used for up to 14 days.18
Coal tar. Although coal tar and coal tar derivatives have been used for many years in the treatment of AD, a lack of data on the clinical efficacy of their application, along with the cosmetic disadvantage, makes compliance with this treatment challenging.
Alternative treatments. A number of alternative measures purport to reduce a child’s risk of developing AD and/or reduce its severity (TABLE), but in most cases, evidence is lacking.
Consider systemic treatment for refractory AD
In a subgroup of patients with moderate to severe AD, the condition is refractory to standard topical therapy and systemic treatment is required. Systemic treatments—including oral corticosteroids, cyclosporine, mycophenolate mofetil, azathioprine, methotrexate, and interferon—should be undertaken only under supervision of a dermatologist.
Oral corticosteroids (typically, prednisone) are sometimes used for short-term treatment of severe AD, although rarely for young children. Evidence of their efficacy is insufficient, and their use is controversial. Patients may have severe symptom flares when an oral corticosteroid is tapered or discontinued. And no randomized controlled trials of prednisone therapy for AD were found in the peer-reviewed medical literature, despite the drug’s long-standing use in AD treatment.30
Systemic immunomodulatory therapies such as cyclosporine, azathioprine, interferon gamma, intravenous immune globulin, mycophenolate, and infliximab have been used for recalcitrant AD. Cyclosporine, an immunosuppressant that acts directly on the cells of the immune system and has an inhibitory effect on T cells, decreases AD severity in the short term. Cyclosporine has been found to be safe, effective, and well tolerated in children with AD, but the potential for hypertension and renal toxicity limits its usefulness for long-term therapy.30
Other systemic immunomodulatory therapies, including those listed above, should be considered when cyclosporine is contraindicated or does not produce a suitable response. Prospective controlled trials in a pediatric population are needed to evaluate the long-term effectiveness and safety of other agents.
Phototherapy is another option
Phototherapy has evolved as a treatment for recalcitrant AD, based on the observation that the condition often improves during the summer months with increased exposure to natural light. Adverse effects of phototherapy can include erythema, pruritus, and pigment changes. Ultraviolet light is also known to cause premature aging of the skin, as well as cutaneous malignancies.4,10,14 Therefore, phototherapy, like systemic treatment, should be undertaken only with the supervision of a dermatologist.
When infection complicates care
Colonization with Staphylococcus aureus is common in patients with AD. In addition to contributing to pruritus and chronic inflammation, S aureus is a risk factor for infection.
Treatment with topical or systemic antibiotics has no clear benefit for patients with AD, except when skin infection is present, When there is evidence of infection, however, methicillin-resistant S aureus must be considered, and any abscess incised and drained.1
Herpes simplex virus infection, another possibility in patients with AD, should be treated immediately with antiviral therapy. If the lesions are widely distributed or the patient has a toxic appearance, hospitalization and IV therapy is warranted—as is an ophthalmology consult when eye or periocular involvement is suspected.1,9
Dermatophyte infections are also more common in patients with AD and can be treated with standard regimens of topical or oral antifungals. Fungi may play a role in chronic inflammation; if there is no infection, however, patients respond better to anti-inflammatory agents than to antifungals.1
Time for a referral
As already noted, a dermatology consult is indicated for refractory AD and when systemic treatment and/or phototherapy is being considered. The suspicion of eczema herpeticum indicates a need for an immediate dermatology referral. An urgent referral is needed for patients with severe AD that has not responded to a week of optimum topical therapy—or whose treatment of bacterial infection has failed. Consider a dermatology consult, as well, when the diagnosis is uncertain or the patient’s symptoms have been poorly controlled. If you (or the child’s parents) suspect that a food allergy is the cause of a severe case of AD, a referral to an allergist is recommended.6,19,21,22
CASE 1 Dylan’s mother calls to tell you that, to her surprise, his eczema has completely cleared up, even though she did not change his formula. You advise her to continue to use the emollient at least twice a day and to bring him in if he develops another flare.
CASE 2 Two weeks after Angela’s office visit, her mother calls to report that her daughter has responded well to triamcinolone ointment 0.025%, the topical steroid you prescribed. When Angela comes in for a well-child visit at age 2, however, she has a mild flare. You prescribe a brief course of triamcinolone ointment and remind her mother to be diligent about skin care.
CORRESPONDENCE Joanne Dempster, MD, New York Presbyterian Hospital, Family & Community Medicine, 610 West 158th Street, New York, NY 10032; jd2745@columbia.edu
• Emollients should be used during acute flares as well as regularly for maintenance therapy in children with atopic dermatitis (AD). A
• Topical corticosteroids are the first-line therapy for acute AD flares. A
• There is no evidence to support the use of antihistamines for treatment of AD. A
• Exclusion of cow’s milk and eggs is not recommended except in proven cases of milk or egg allergy with sensitivity testing and food challenge. B
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE 1 Dylan, an 8-month-old boy whom you had seen for a routine check-up a little over a month ago, is in your office today because of a rash on his face and elbows. The rash began about 2 weeks ago, his mother reports—shortly after she had weaned him from the breast milk to formula. Certain that Dylan has a milk allergy, his mother tells you she plans to switch to a soy-based formula—and wants you to give her something to put on the rash to help clear it up.
CASE 2 Eighteen-month-old Angela had a mild case of atopic dermatitis when you saw her about 3 months ago. The reason for today’s visit is that “her eczema is getting worse,” according to her mother, and the moisturizing cream that you recommended at her last visit “stopped working.” The rash, which had been confined to the patient’s forearms and knees (FIGURE 1), now covers much of her face, forearms, knees, and trunk. Angela’s mother says that the rash appears to be very itchy and that her daughter has been crying and scratching at night.
If Dylan and Angela were your patients, what would you advise their parents to do, and how would you treat them?
FIGURE 1
An 18-month-old girl with an acute flare
This child has moderate atopic dermatitis, with erythema and localized thickened skin at the medial knee—a typical site for atopic dermatitis.
Atopic dermatitis (AD), or eczema, is a chronic inflammatory skin condition that affects up to 20% of children.1 The incidence of pediatric AD has increased 2- to 3-fold in the last 30 years (it’s not clear why), and the condition is a common reason for pediatric visits to family physicians.1,2
AD is marked by phases of pruritus and rash and, depending on the severity, can significantly affect the quality of life of young patients and their families.1-4 The pathophysiology involves structural abnormalities of the epidermis—leading to dry and sensitive skin—combined with immune dysregulation.
Topical corticosteroids to decrease the inflammation and emollients to repair and hydrate the skin are the mainstay of treatment.3,5,6 But numerous considerations, including what triggers patients should avoid; how potent a steroid to prescribe; how long to continue treatment; and when, or whether, to initiate systemic treatment, remain. The evidence-based review of traditional and alternative treatments (TABLE)1-3,7-19 and practical step-wise approach (FIGURE 2)1-3,5,6,9,19-22 that follow can help ensure that you give children with AD the best possible care.
FIGURE 2
A stepped approach to atopic dermatitis1-3,5,6,9,19-22
AD, atopic dermatitis; TCIs, topical calcineurin inhibitors.
TABLE
Treating atopic dermatitis: What the evidence shows
| Intervention (SOR) | Comments |
|---|---|
| Maintenance | |
| Emollients (A)1,2,7,8 | Mainstay of maintenance therapy |
| Treatment | |
| Corticosteroids9-15 – Topical (A) – Oral (B) | First-line treatment No proven benefit |
| TCIs:3,16,17 – Pimecrolimus (A) – Tacrolimus (A) | Second-line treatment |
| Symptom relief | |
| Antihistamines (A)11,14 | No proven benefit in the treatment of AD; sedating antihistamines may improve sleep |
| Tar (C)14 | |
| Wet wrap dressings (C )18 | |
| Infection1,11 | |
| Antibiotics – Topical (A) – Oral (A) | |
| Antifungals – Topical (A) – Oral (A) | |
| Alternative/preventive measures11,19 | |
| Breastfeeding (B) | May reduce risk of developing AD (poor quality study) |
| Essential fatty acids* | No proven benefit |
| Exclusion of eggs or cow’s milk (B) | Only in proven cases of allergy |
| Multivitamins, B6, zinc supplements (C) | No proven benefit |
| Probiotics (B) | No proven benefit |
| Vitamin D supplementation (C) | More studies needed |
| *Black currant seed oil, evening primrose oil, fish oil. AD, atopic dermatitis; TCIs, topical calcineurin inhibitors. | |
The patient has a rash, but what’s the trigger?
Epidemiologic studies have identified numerous AD triggers, including sweating, stress, dust, hard water, food allergies, and seasonality.23 Environmental or situational triggers should be avoided whenever possible,20 of course, but first, they must be identified—an often-difficult task. Establishing the role of any exacerbating factor in AD involves documentation of a temporal relationship between exposure and the development or worsening of symptoms; a dose-response effect; and remission after withdrawal of the trigger.
What’s more, avoidance does not always have the desired result. There is a well-demonstrated correlation between house dust mite sensitization and AD, especially in children of preschool age and older.7,21 Studies performed to determine whether decreasing house dust mite antigen would have a positive effect on disease severity, however, have had conflicting results.23
Food allergies are more likely in the youngest patients
For about a third (35%) of children with AD, the trigger is a food allergy.22 This is most common in infants, with one study showing a peak at 18 months.20,24 The most common food allergens are milk and egg, but wheat, soy, and peanuts are potential allergens, as well.22,25 Food allergies, which are difficult to identify, should be suspected in patients with a poor response to first-line treatment. Sensitivity testing with food challenge may be worthwhile only in severe cases that are refractory to routine care.20
We caution parents not to attempt to withhold a suspected food allergen on their own. To avoid the risk of malnutrition, young children should be placed on elimination diet trials only if the allergen has first been identified by sensitivity testing and food challenge tests, because the allergen may not be clinically significant.21,22 Neither skin prick tests nor serum tests for allergies have been found to be accurate, and parents themselves are often mistaken. Several studies have found a discrepancy between the foods parents think their child is allergic to and the substances that are later found to be clinically significant allergens.21
CASE 1 You advise Dylan’s mother not to switch formulas because answers to further questions about other symptoms were unremarkable (eg, diarrhea). Dylan is treated with a low-potency (class VII) topical steroid (1% hydrocortisone cream) with instructions for the parents to maintain hydration and call you in 5 to 7 days.
Topical corticosteroids are first-line treatment
Two major classes of pharmacologic agents are used for the treatment of AD: topical corticosteroids and topical calcineurin inhibitors (TCIs). Corticosteroids are first-line treatment, as their clinical effectiveness has been well established; TCIs are indicated only as second-line therapy.26,27
Which dosing regimen is best?
The potency of corticosteroids is expressed by a numerical scale, ranging from class I (the most potent) to class VII (the least potent). Class I steroids are about 1800 times more potent than class VII preparations.8
A decision about which strength to use is based on several factors, including the severity of the child’s AD, his or her age, and the affected body site. For infants ≤12 months old, the lowest potency preparations (such as 1% hydrocortisone) are preferable, but should be used in the diaper area for no more than 3 to 7 days at a time.8 In general, potent topical corticosteroids should not be used for children <12 months of age without a dermatology consult.8,9
For children ages 1 through 5 years, intermittent (1- to 2-week) bursts of mild to moderate potency corticosteroids (class VI and VII) are suitable; for older children, a 7- to 10-day course of more potent preparations (class II-V) can be used for nonflexural and nonfacial skin.
While clinical trials have addressed the issues of quantity, duration, potency, and frequency (one large systematic review found twice-daily application of topical corticosteroids to be no more effective than once-daily applications10), an optimal approach to their use in the long-term management of pediatric AD is largely undefined. Various approaches include:
- starting with a more potent preparation to induce remission, followed by a less potent corticosteroid as the AD improves
- using short bursts (5-7 days) of a potent topical corticosteroid, followed by emollient use until a flare-up occurs
- relying on prolonged, or continuous, treatment with less potent preparations.11,23
Long-term use of topical corticosteroids of any potency should be avoided in areas of high risk for cutaneous side effects, such as the face and intertriginous areas.
Emollients are also an important part of therapy for all pediatric patients. Emollients help restore the integrity of the skin barrier and inhibit water loss,1,2,12,20 and should be used not only during an acute flare, but also for maintenance therapy. Tell parents to look for emollients that are unscented and contain fewer additives, and to apply the emollient at least twice daily, and after bathing or swimming.5,20
CASE 2 You prescribe a class V steroid (triamcinolone ointment 0.025%) for Angela, to be applied once a day for 5 to 7 days. You instruct her mother in basic skin care and stress the importance of using an emollient regularly, not just during a flare-up.
What to tell parents about side effects
Discuss the benefits and potential harms of topical corticosteroids with parents (and youngsters who are old enough to understand), emphasizing that when used correctly, the benefits outweigh the risks.
Potential side effects include skin atrophy, striae, telangiectasia, hypopigmentation, rosacea, glaucoma, and cataracts, with studies suggesting that local adverse effects are related to the potency.13 Because there are few prospective controlled trials of sufficient duration, however, the incidence of local reactions to topical corticosteroids in patients with AD is uncertain.
The potential for topical corticosteroids to suppress the hypothalamic-pituitary-adrenal (HPA) axis has been investigated in a small number of studies, with inconclusive results. Effects on the HPA axis appear to be associated with percutaneous absorption in patients who either have a more severe case of AD or are <2 years old.14 A recent systematic review confirmed that the degree of systemic absorption is based on the severity and extent of the disease as well as the formulation and potency of the topical agent.14,15
When to consider TCIs
Pimecrolimus and tacrolimus, the 2 TCIs on the market, are second-line agents for AD. Both have US Food and Drug Administration (FDA) approval for short-term treatment of moderate to severe AD in immunocompetent patients who have failed to respond to topical corticosteroids and children >2 years.26,27 Both TCIs provide targeted anti-inflammatory activity without the local and systemic side effects of topical corticosteroids.
Pimecrolimus cream 1% is approved for treatment in children >2 years.27 Tacrolimus ointment 0.03% is approved for children ages 2 to 15 years with moderate to severe AD, and tacrolimus ointment 0.1% is approved for children older than 16 years with moderate to severe AD.26 Data from clinical trials have shown that pimecrolimus reduces the number and severity of flares, extends the time between flares, and decreases pruritus and other cutaneous signs associated with AD.3 Common side effects, which are usually mild and resolve within days, include pruritus, burning, and stinging at the application site.
In 2006 the FDA added a black-box warning stating that their long-term safety has not been established—a response to widespread off-label use of TCIs in children <2 years and concerns about a theoretical cancer risk based on their mechanism of action—and concluded in 2010 that the labeling adequately warns providers of the potential safety risks.28 Recent reviews have concluded that systemic exposure to topical TCIs is minimal and that there is no evidence linking TCIs to an increased risk of lymphoproliferative disease.16,17,29
Combining corticosteroids and TCIs
In clinical practice, both topical corticosteroids and TCIs are often used for long-term management of moderate to severe AD. TCIs are valuable alternatives to continuous use of corticosteroids for patients with persistent AD and recurrent flares. They’re also beneficial for patients with outbreaks in sensitive areas, such as the face and genitals.
Adjunctive therapies—what’s best for pruritus?
Pruritus is a major feature of AD, and a source of considerable distress. Here are some treatment options that often come up, and what we know about their usefulness.
Antihistamines. There is no evidence to support the use of nonsedating antihistamines in the treatment of AD. Sedating systemic antihistamines such as hydroxyzine and diphenhydramine don’t have a direct effect on the pruritus either, but they can be used to help patients with acute flare-ups improve their sleep.9,14
CASE 2 Antihistamines would not be recommended for Angela at this time; instead, you wait to see whether the topical corticosteroid you have just prescribed is effective. If the patient is still having trouble sleeping after she completes the corticosteroid trial, you can recommend the use of a sedating antihistamine at night as a sleeping aid.
Wet wraps. Wet wrap treatments using occlusive dressings were first recommended as a safe and effective treatment more than 20 years ago.18 Their application may be indicated for children with severe or refractory AD, provided there are no signs or symptoms of infection.
No large prospective studies have evaluated the safety and efficacy of wet wrap treatment or compared it with more conventional modalities. In a recent review, temporary systemic bioactivity of the corticosteroid was the only reported adverse effect.18
There are numerous wet wrap techniques. One effective short-term intervention is to use cream or ointment and a double layer of cotton bandages, with a moist first layer and a dry second layer. Wet wrap dressings with once-daily diluted topical corticosteroids can be used for up to 14 days.18
Coal tar. Although coal tar and coal tar derivatives have been used for many years in the treatment of AD, a lack of data on the clinical efficacy of their application, along with the cosmetic disadvantage, makes compliance with this treatment challenging.
Alternative treatments. A number of alternative measures purport to reduce a child’s risk of developing AD and/or reduce its severity (TABLE), but in most cases, evidence is lacking.
Consider systemic treatment for refractory AD
In a subgroup of patients with moderate to severe AD, the condition is refractory to standard topical therapy and systemic treatment is required. Systemic treatments—including oral corticosteroids, cyclosporine, mycophenolate mofetil, azathioprine, methotrexate, and interferon—should be undertaken only under supervision of a dermatologist.
Oral corticosteroids (typically, prednisone) are sometimes used for short-term treatment of severe AD, although rarely for young children. Evidence of their efficacy is insufficient, and their use is controversial. Patients may have severe symptom flares when an oral corticosteroid is tapered or discontinued. And no randomized controlled trials of prednisone therapy for AD were found in the peer-reviewed medical literature, despite the drug’s long-standing use in AD treatment.30
Systemic immunomodulatory therapies such as cyclosporine, azathioprine, interferon gamma, intravenous immune globulin, mycophenolate, and infliximab have been used for recalcitrant AD. Cyclosporine, an immunosuppressant that acts directly on the cells of the immune system and has an inhibitory effect on T cells, decreases AD severity in the short term. Cyclosporine has been found to be safe, effective, and well tolerated in children with AD, but the potential for hypertension and renal toxicity limits its usefulness for long-term therapy.30
Other systemic immunomodulatory therapies, including those listed above, should be considered when cyclosporine is contraindicated or does not produce a suitable response. Prospective controlled trials in a pediatric population are needed to evaluate the long-term effectiveness and safety of other agents.
Phototherapy is another option
Phototherapy has evolved as a treatment for recalcitrant AD, based on the observation that the condition often improves during the summer months with increased exposure to natural light. Adverse effects of phototherapy can include erythema, pruritus, and pigment changes. Ultraviolet light is also known to cause premature aging of the skin, as well as cutaneous malignancies.4,10,14 Therefore, phototherapy, like systemic treatment, should be undertaken only with the supervision of a dermatologist.
When infection complicates care
Colonization with Staphylococcus aureus is common in patients with AD. In addition to contributing to pruritus and chronic inflammation, S aureus is a risk factor for infection.
Treatment with topical or systemic antibiotics has no clear benefit for patients with AD, except when skin infection is present, When there is evidence of infection, however, methicillin-resistant S aureus must be considered, and any abscess incised and drained.1
Herpes simplex virus infection, another possibility in patients with AD, should be treated immediately with antiviral therapy. If the lesions are widely distributed or the patient has a toxic appearance, hospitalization and IV therapy is warranted—as is an ophthalmology consult when eye or periocular involvement is suspected.1,9
Dermatophyte infections are also more common in patients with AD and can be treated with standard regimens of topical or oral antifungals. Fungi may play a role in chronic inflammation; if there is no infection, however, patients respond better to anti-inflammatory agents than to antifungals.1
Time for a referral
As already noted, a dermatology consult is indicated for refractory AD and when systemic treatment and/or phototherapy is being considered. The suspicion of eczema herpeticum indicates a need for an immediate dermatology referral. An urgent referral is needed for patients with severe AD that has not responded to a week of optimum topical therapy—or whose treatment of bacterial infection has failed. Consider a dermatology consult, as well, when the diagnosis is uncertain or the patient’s symptoms have been poorly controlled. If you (or the child’s parents) suspect that a food allergy is the cause of a severe case of AD, a referral to an allergist is recommended.6,19,21,22
CASE 1 Dylan’s mother calls to tell you that, to her surprise, his eczema has completely cleared up, even though she did not change his formula. You advise her to continue to use the emollient at least twice a day and to bring him in if he develops another flare.
CASE 2 Two weeks after Angela’s office visit, her mother calls to report that her daughter has responded well to triamcinolone ointment 0.025%, the topical steroid you prescribed. When Angela comes in for a well-child visit at age 2, however, she has a mild flare. You prescribe a brief course of triamcinolone ointment and remind her mother to be diligent about skin care.
CORRESPONDENCE Joanne Dempster, MD, New York Presbyterian Hospital, Family & Community Medicine, 610 West 158th Street, New York, NY 10032; jd2745@columbia.edu
1. Boguniewicz M, Leung D. Recent insights into atopic dermatitis and implications for management of infectious complications. J Allergy Clin Immunol. 2010;125:4-13.
2. Lucinda BM. Treatment options for atopic dermatitis. Am Fam Physician. 2007;75:523-530.
3. Levy ML. Atopic dermatitis: understanding the disease and its management. Curr Med Res Opin. 2007;23:3091-3103.
4. Brown S, Reynolds NJ. Atopic and non-atopic eczema. BMJ. 2006;332:584-588.
5. Carbone A, Siu A, Patel R, et al. Pediatric atopic dermatitis: a review of the medical management. Ann Pharmacother. 2010;44:1448-1458.
6. Akadis CA, Akadis M, Beiber T, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergy and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL consensus report. Allergy. 2006;61:969-987.
7. Schafer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol. 2008;8:418-422.
8. Charman C, Williams H. The use of corticosteroids and corticosteroid phobia in atopic dermatitis. Clin Dermatol. 2003;21:193-200.
9. National Collaborating Centre for Women’s and Children’s Health. Atopic eczema in children. Management of atopic eczema in children from birth up to age of 12 years. Clinical guideline no. 57. London, UK: National Institute for Health and Clinical Excellence (NICE); 2007.
10. Hoare C, Li Wan Po A, Williams H. Systematic review of treatments of atopic eczema. Health Technol Assess. 2000;4:1-191.
11. Simpson E, Hanifin J. Atopic dermatitis. J Am Acad Dermatol. 2005;53:115-128.
12. Grimalt R, Mengeaud V, Cambazard F, et al. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214:61-67.
13. Callen J, Chamlin S, Eichenfield LF, et al. A systematic review of the safety of topical therapies for atopic dermatitis. Br J Dermatol. 2007;156:203-221.
14. Hanifin JM, Cooper KD, Ho VC, et al. Guidelines for the care of atopic dermatitis developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association. “Administrative regulations for evidence-based clinical practice guidelines”. J Am Acad Dermatol. 2004;50:391-404.
15. Simpson E. Atopic dermatitis: a review of topical treatment options. Curr Med Res Opin. 2010;26:633-640.
16. Munzenberger PJ, Monejo JM. Safety of topical calcineurin inhibitors for the treatment of atopic dermatitis. Pharmacotherapy. 2007;27:1020-1028.
17. Kang S, Lucky AW, Pariser D, et al. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol. 2001;44(suppl):S58-S64.
18. Devillers ACA, Oranje AP. Efficacy and safety of ‘wet wrap’ dressings as an intervention treatment in children with severe and/or refractory atopic dermatitis: a critical review of the literature. Br J Dermatol. 2006;154:579-585.
19. Boyl RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.-
20. Ellis C, Luger T. International Consensus Conference of Atopic Dermatitis (ICCAD II*): clinical update and current treatment strategies. Br J Dermatol. 2003;148(suppl 63):S3-S10.
21. Han KL, Leung TF, Ching G, et al. Patterns of food and aeroallergen sensitization in childhood eczema. Acta Pediatrica. 2008;97:1734-1737.
22. Greenhawt M. The role of food allergy in atopic dermatitis. Allergy Asthma Proc. 2010;31:392-397.
23. Langan SM, Williams HC. What causes worsening of eczema? A systemic review. Br J Dermatol. 2006;155:505-514.
24. Eller E, Kjaer HF, et al. Food allergy and food sensitization in early childhood: results from the DARC cohort. Allergy. 2009;63:1023-1029.
25. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361:151-160.
26. Protopic [prescribing information]. Deerfield, IL: Astellas Pharma US, Inc; 2006.
27. Elidel [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.
28. US Food and Drug Administration. Topical calcineurin inhibitors. Pediatric safety update: regulatory background. FDA Pediatric Advisory Committee Meeting; March 22, 2010; Bethesda, Md.
29. Kalavala M, Dohil MA. Calcineurin inhibitors in pediatric atopic dermatitis: a review of current evidence. Am J Clin Dermatol. 2011;12:15-24.
30. Ricci G, Dondi A, Patrizi A, et al. Systemic therapy of atopic dermatitis in children. Drugs. 2009;69:297-306.
1. Boguniewicz M, Leung D. Recent insights into atopic dermatitis and implications for management of infectious complications. J Allergy Clin Immunol. 2010;125:4-13.
2. Lucinda BM. Treatment options for atopic dermatitis. Am Fam Physician. 2007;75:523-530.
3. Levy ML. Atopic dermatitis: understanding the disease and its management. Curr Med Res Opin. 2007;23:3091-3103.
4. Brown S, Reynolds NJ. Atopic and non-atopic eczema. BMJ. 2006;332:584-588.
5. Carbone A, Siu A, Patel R, et al. Pediatric atopic dermatitis: a review of the medical management. Ann Pharmacother. 2010;44:1448-1458.
6. Akadis CA, Akadis M, Beiber T, et al. Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergy and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL consensus report. Allergy. 2006;61:969-987.
7. Schafer T. The impact of allergy on atopic eczema from data from epidemiological studies. Curr Opin Allergy Clin Immunol. 2008;8:418-422.
8. Charman C, Williams H. The use of corticosteroids and corticosteroid phobia in atopic dermatitis. Clin Dermatol. 2003;21:193-200.
9. National Collaborating Centre for Women’s and Children’s Health. Atopic eczema in children. Management of atopic eczema in children from birth up to age of 12 years. Clinical guideline no. 57. London, UK: National Institute for Health and Clinical Excellence (NICE); 2007.
10. Hoare C, Li Wan Po A, Williams H. Systematic review of treatments of atopic eczema. Health Technol Assess. 2000;4:1-191.
11. Simpson E, Hanifin J. Atopic dermatitis. J Am Acad Dermatol. 2005;53:115-128.
12. Grimalt R, Mengeaud V, Cambazard F, et al. The steroid-sparing effect of an emollient therapy in infants with atopic dermatitis: a randomized controlled study. Dermatology. 2007;214:61-67.
13. Callen J, Chamlin S, Eichenfield LF, et al. A systematic review of the safety of topical therapies for atopic dermatitis. Br J Dermatol. 2007;156:203-221.
14. Hanifin JM, Cooper KD, Ho VC, et al. Guidelines for the care of atopic dermatitis developed in accordance with the American Academy of Dermatology (AAD)/American Academy of Dermatology Association. “Administrative regulations for evidence-based clinical practice guidelines”. J Am Acad Dermatol. 2004;50:391-404.
15. Simpson E. Atopic dermatitis: a review of topical treatment options. Curr Med Res Opin. 2010;26:633-640.
16. Munzenberger PJ, Monejo JM. Safety of topical calcineurin inhibitors for the treatment of atopic dermatitis. Pharmacotherapy. 2007;27:1020-1028.
17. Kang S, Lucky AW, Pariser D, et al. Long-term safety and efficacy of tacrolimus ointment for the treatment of atopic dermatitis in children. J Am Acad Dermatol. 2001;44(suppl):S58-S64.
18. Devillers ACA, Oranje AP. Efficacy and safety of ‘wet wrap’ dressings as an intervention treatment in children with severe and/or refractory atopic dermatitis: a critical review of the literature. Br J Dermatol. 2006;154:579-585.
19. Boyl RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.-
20. Ellis C, Luger T. International Consensus Conference of Atopic Dermatitis (ICCAD II*): clinical update and current treatment strategies. Br J Dermatol. 2003;148(suppl 63):S3-S10.
21. Han KL, Leung TF, Ching G, et al. Patterns of food and aeroallergen sensitization in childhood eczema. Acta Pediatrica. 2008;97:1734-1737.
22. Greenhawt M. The role of food allergy in atopic dermatitis. Allergy Asthma Proc. 2010;31:392-397.
23. Langan SM, Williams HC. What causes worsening of eczema? A systemic review. Br J Dermatol. 2006;155:505-514.
24. Eller E, Kjaer HF, et al. Food allergy and food sensitization in early childhood: results from the DARC cohort. Allergy. 2009;63:1023-1029.
25. Leung DY, Bieber T. Atopic dermatitis. Lancet. 2003;361:151-160.
26. Protopic [prescribing information]. Deerfield, IL: Astellas Pharma US, Inc; 2006.
27. Elidel [prescribing information]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2006.
28. US Food and Drug Administration. Topical calcineurin inhibitors. Pediatric safety update: regulatory background. FDA Pediatric Advisory Committee Meeting; March 22, 2010; Bethesda, Md.
29. Kalavala M, Dohil MA. Calcineurin inhibitors in pediatric atopic dermatitis: a review of current evidence. Am J Clin Dermatol. 2011;12:15-24.
30. Ricci G, Dondi A, Patrizi A, et al. Systemic therapy of atopic dermatitis in children. Drugs. 2009;69:297-306.