User login
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
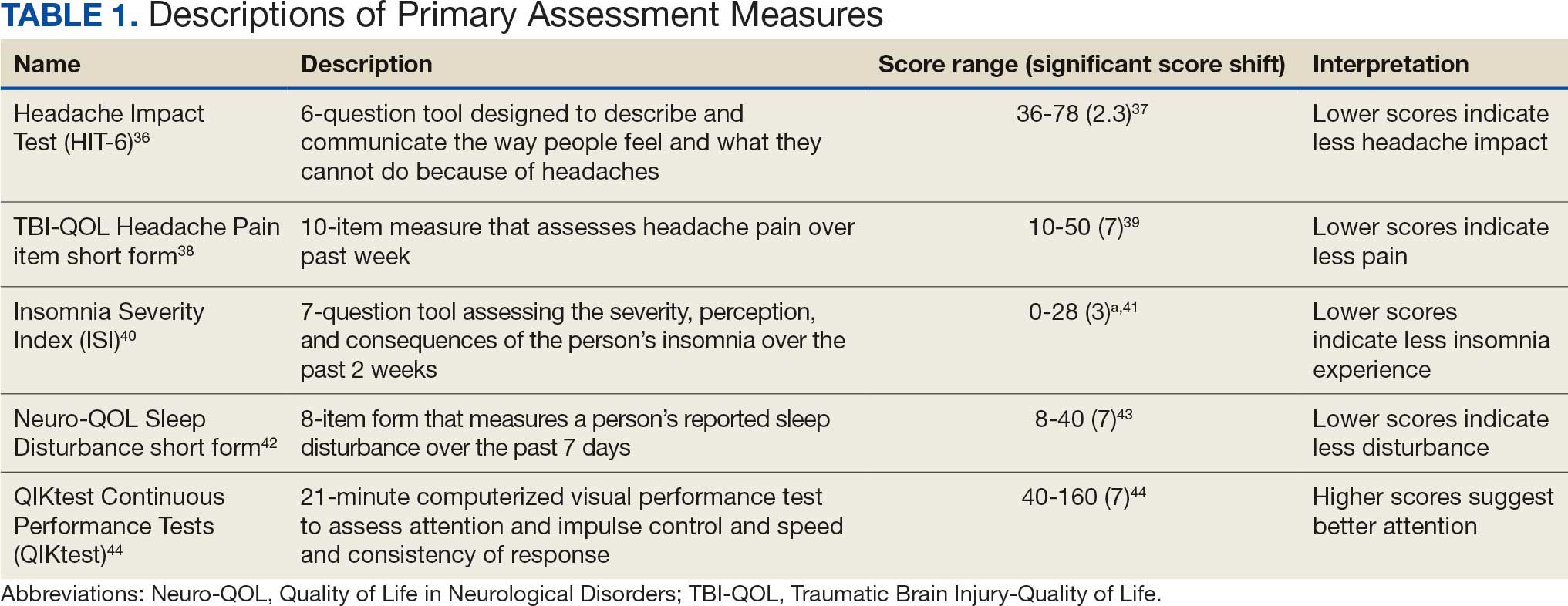
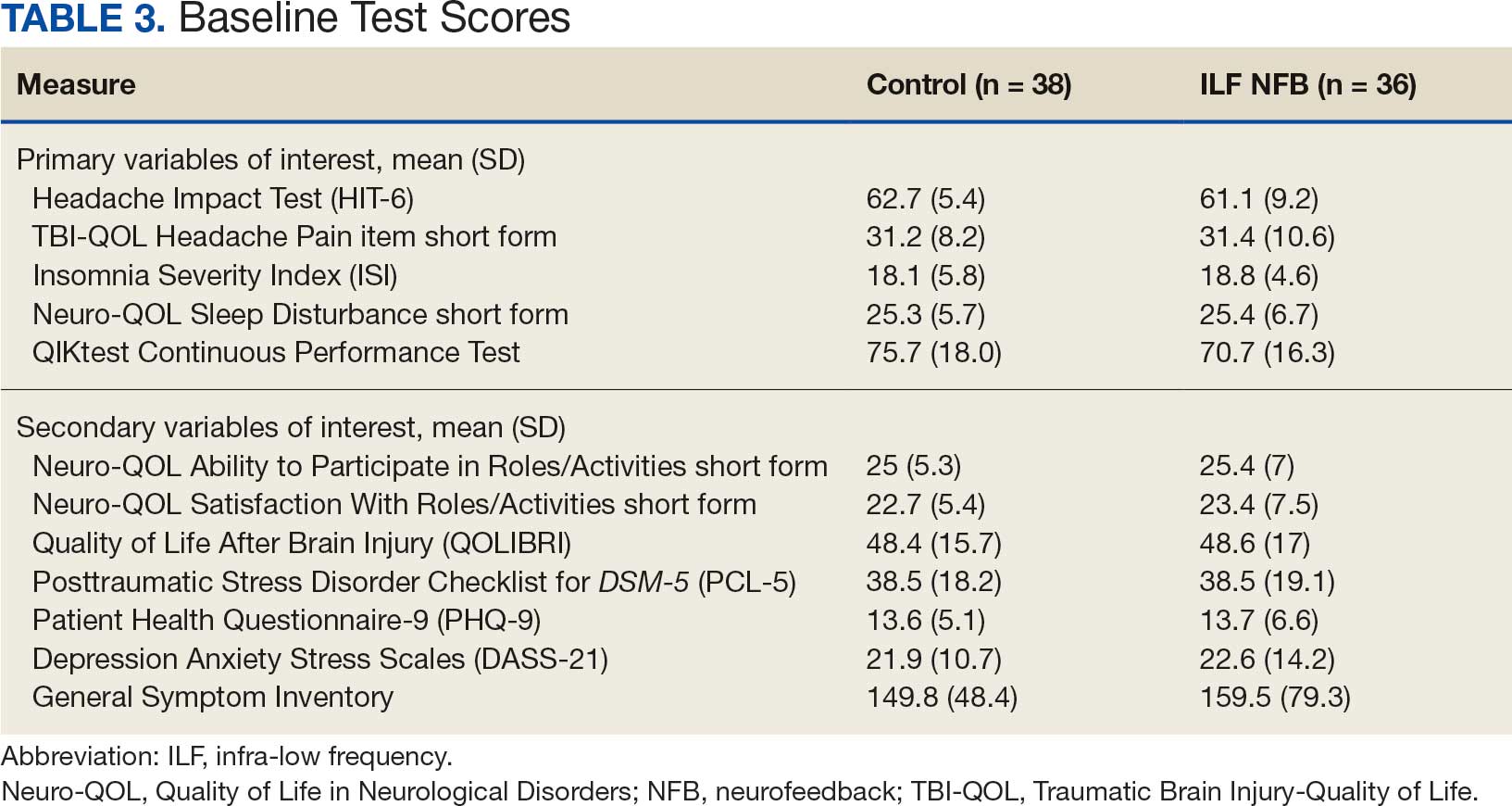
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
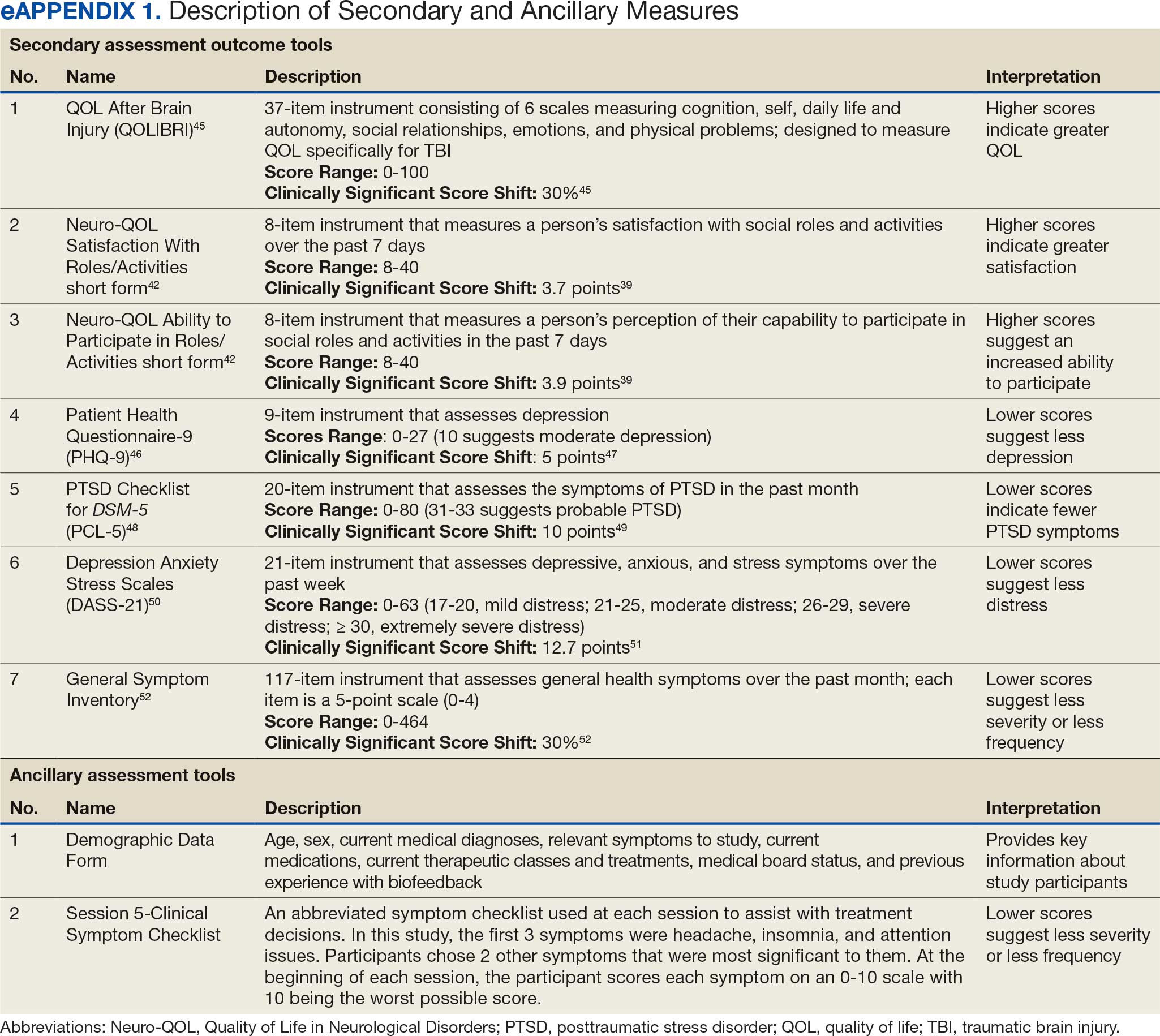
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
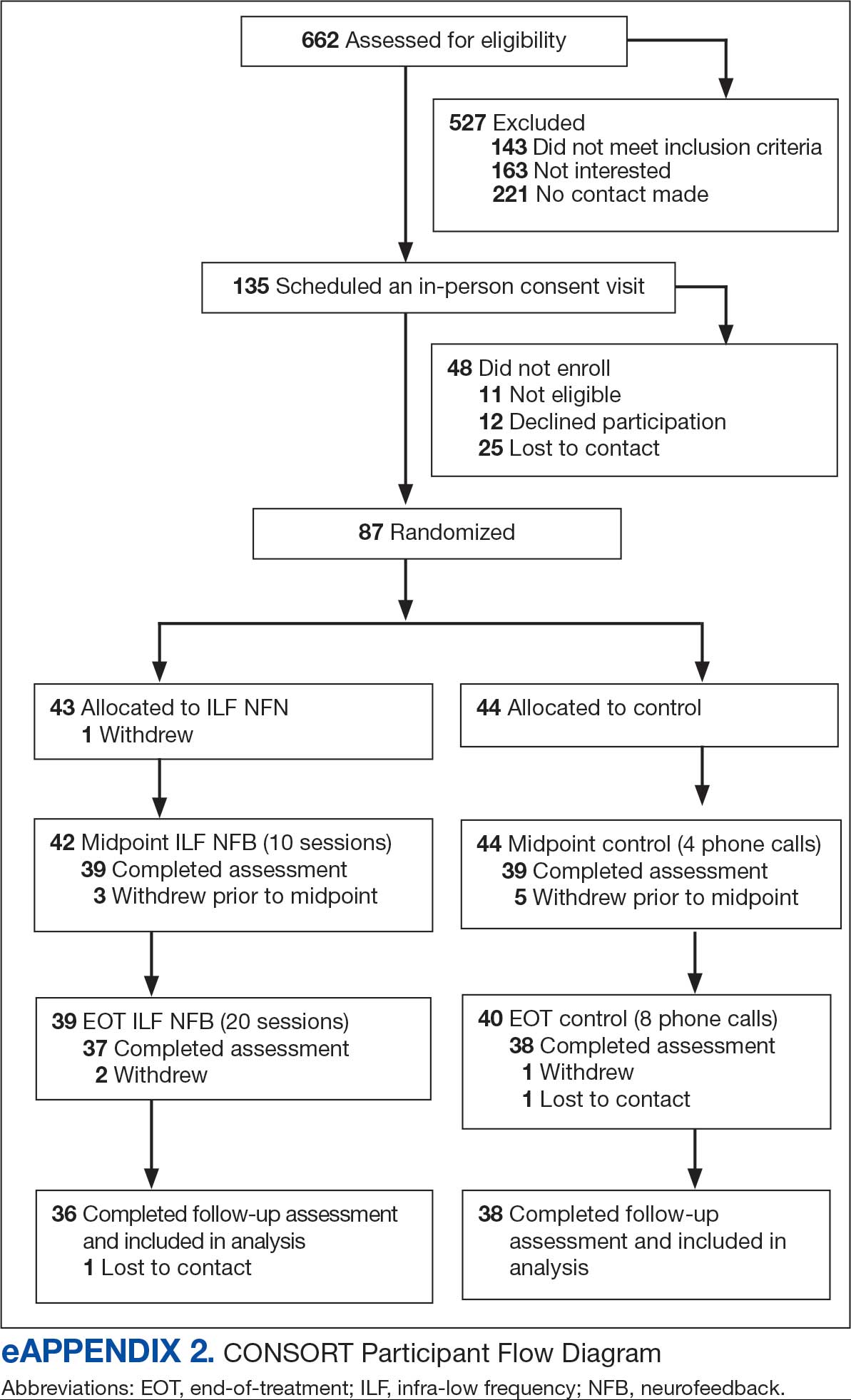
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
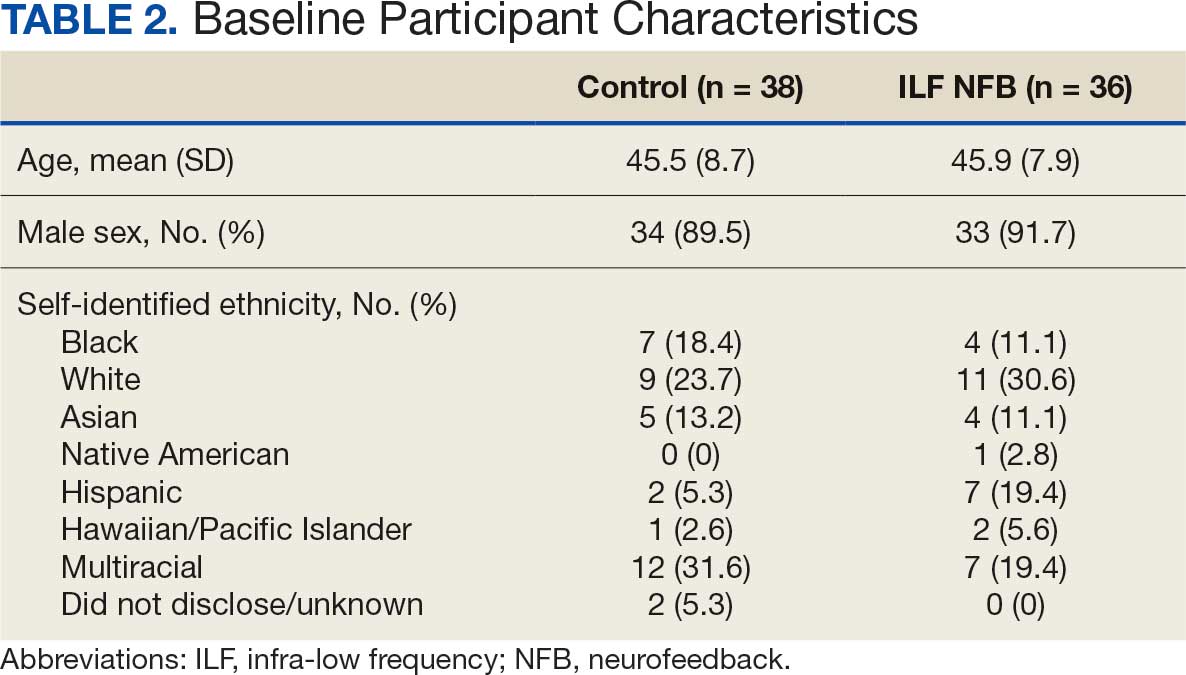
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
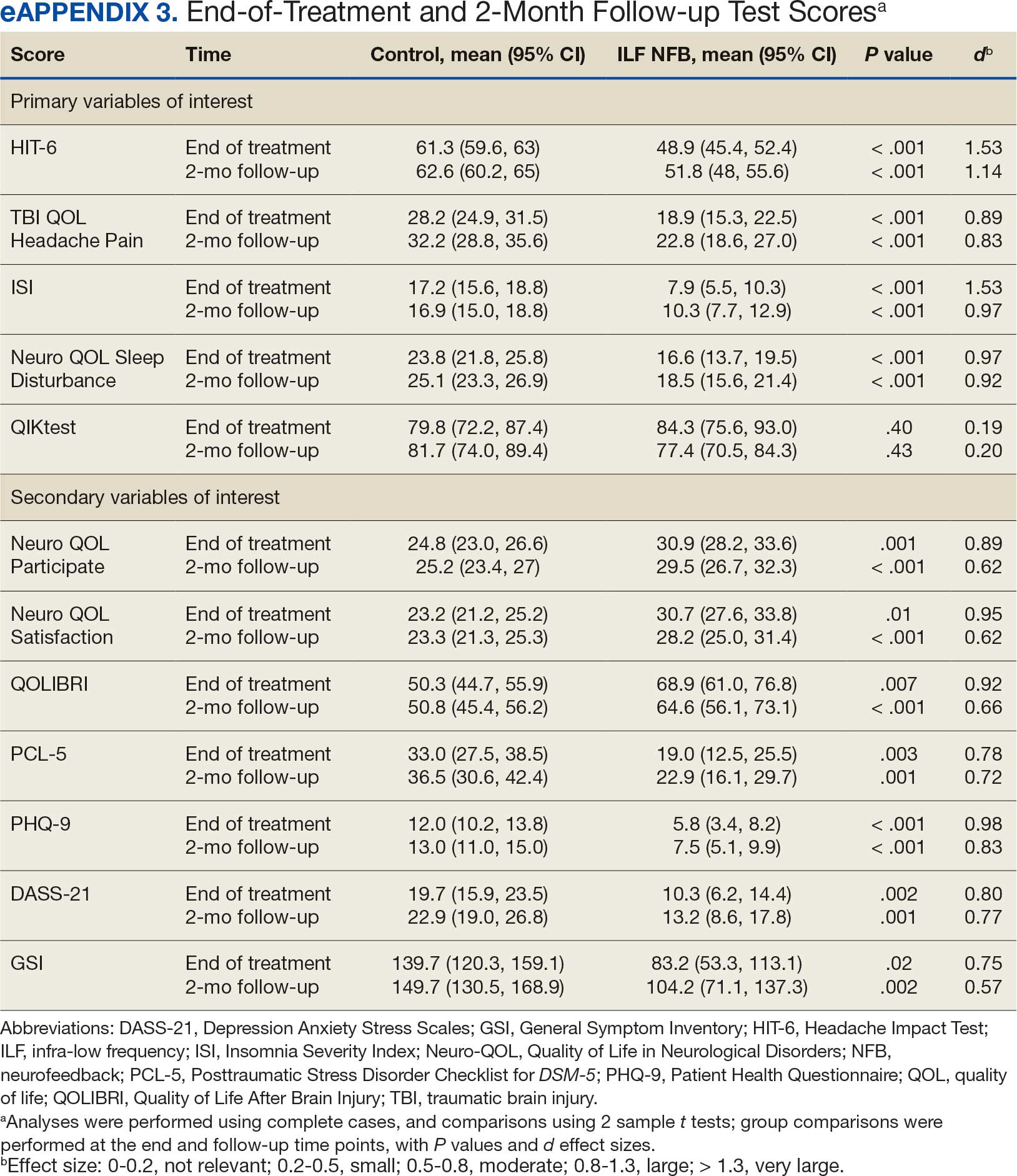
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
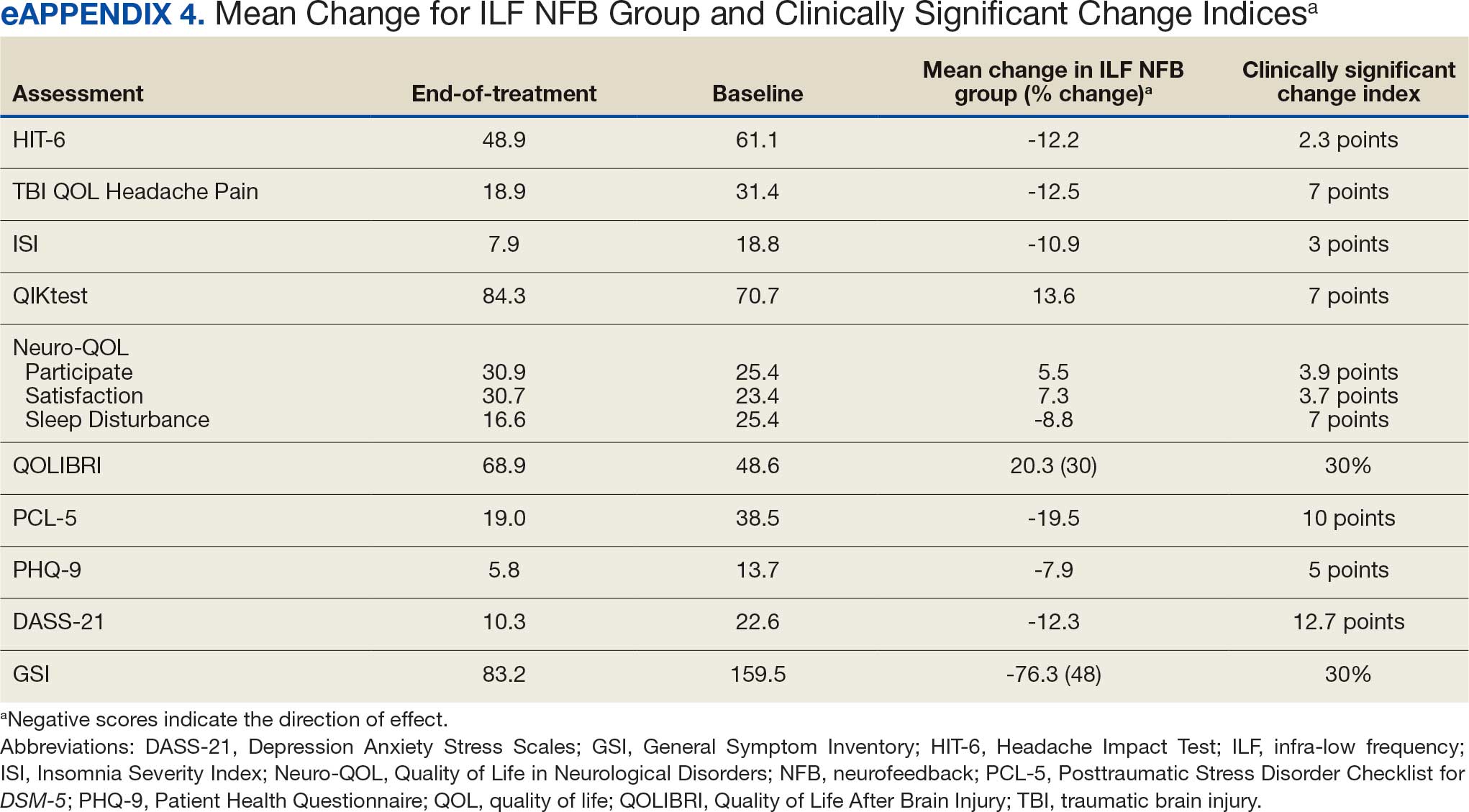
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
Traumatic brain injury (TBI) is the signature injury of post-9/11 military operations, impacting > 441,000 combat veterans from 2001 to 2021 and 87% diagnosed with mild TBI (mTBI).1,2 The most common cause of mTBI during these operations was blast exposures stemming from improvised explosive devices, rocket-propelled grenades, or land mines. mTBI was once thought to be self-limiting, lasting hours or days postinjury, but is now recognized as a complex focal and diffuse injury causing a cascade of molecular and biochemical responses with significant physiologic effects lasting for a longer duration. A significant number of combat veterans with mTBI (23%-48%) experience long-standing postconcussive symptoms (PCSs) for many years postinjury.3-5
Developing and implementing strategies to reduce persistent symptoms associated with mTBI is of critical importance. Veterans diagnosed with mTBI and experiencing PCSs present ongoing treatment challenges to the health care system due to limited or suboptimal treatment options.6,7 According to the 2021 US Department of Veterans Affairs (VA) and US Department of Defense (DoD) clinical guidelines for postacute mTBI, treatment for PCSs should be symptom focused. 8,9 For instance, veterans with migraine headaches associated with mTBIs are often treated with abortive agents (eg, triptans) and preventive medications (eg, anticonvulsants and tricyclics).10 Cognitive dysfunction and insomnia are treated with cognitive rehabilitation programs, cognitive behavioral therapy, occupational therapy, and medications (eg, hypnotics for insomnia).11,12 The 2021 VA/DoD guidelines note that veteran and military focus groups described greater success with nonpharmacologic treatments than with pharmacologic treatments.8 The VA launched an enterprise-wide Whole Health Service program with the requirement that complementary and integrative health approaches must be available to veterans.13 As a nonpharmacologic, integrative, and noninvasive modality, neurofeedback (NFB) supports the VA Whole Health initiative and veterans’ preferences for integrative treatments.14
Neurofeedback
Rather than a symptom management approach, Defina et al described the possibilities of brain repair in TBI by treatments to enhance neuroplasticity, thereby establishing a more normalized or stable brain environment and enabling the brain to reorganize itself and function more normally.15 NFB has been shown to influence neuroplasticity,16 as evident in microstructural changes in white and gray matter17 and its ability to contribute to functional rehabilitation by restoring connectivity in specific areas of the brain that may have been impaired.18 The benefits of neuroenhancement strategies include potentially reduced pain for patients with mTBI and improved quality of life (QOL).19
NFB assists individuals by helping them become more aware of and self-regulate their physiology.20,21 Because there are several types of NFB (eg, quantitative electroencephalography, Z-scored, α-θ) that differ in terms of equipment, mechanism of action, focus, and patient and clinician procedures, it is important to note that this study used a novel technologically advanced form of NFB, referred to as infra-low frequency (ILF) NFB. It works by reflecting a person’s brain wave activity via conventional electroencephalography back to the person through the visual cortex, thus providing relevant information to which the brain responds to improve core state regulation.22
In 2006, ILF NFB developers sought to extend NFB capability into the slow cortical potential domain (< 0.1 Hz) and then gradually extended to lower frequencies on the basis of favorable clinical responses.22,23 In 2017, the technology reached an ILF capacity that appeared to be helpful for several clinical issues. These developments depended on instrumentation capable of low noise signal detection down to the lowest frequency of interest. Instrumentation was developed for the purpose (eg, Bee Medic Cygnet NFB).
Although mTBI has been a clinical focus in NFB since the 1980s, there are few published studies demonstrating the efficacy of ILF NFB relating to the PCSs of interest in this study, and 2 suggested ILF NFB positively affected change in PCS severity.24,25 Other studies found that ILF NFB decreased incidence of migraines and tension type headaches.26,27 However, the findings of these studies had limited generalizability due to methodologic limitations, such as selection bias and small sample sizes.24-27 Of importance to this article, there are also several publications on the efficacy of ILF NFB in clinical settings.28-33
This article presents the second analysis of data from veterans who completed ILF NFB intervention and control group procedures during a 5-year randomized controlled trial (RCT). The RCT included veterans who experienced an mTBI while participating in post-9/11 military operations to evaluate the impact of ILF NFB on chronic PCSs, including headache, insomnia, and attention dysfunction. Initial results of this trial demonstrated significant differences between the intervention and control groups with strong effect sizes on all outcome measures at the end of treatment.34
Methods
Participants included male and nonpregnant female veterans with a diagnosed mTBI during post-9/11 military operations; aged 18 to 65 years; reports of persistent (ie, > 3 months in duration) headaches, insomnia, and attention difficulties; and able to read and write English, comprehend what is read, and follow directions. mTBI diagnosis was verified for each veteran via the electronic health record. Patients were excluded if they had a severe TBI diagnosis or impaired decision-making capacity; were unable to comply with study visit schedule; or endorsed active suicidal intent on the Columbia-Suicide Severity Rating Scale.35
Recruitment efforts included: (1) letters sent to eligible veterans with mTBI who were identified by clinical informatics data after waiver of Health Insurance Portability and Accountability Act was obtained; veterans could contact the research team directly or the research team would call the veteran 2 weeks after the letter was sent; (2) veterans could be referred by a clinician; and (3) veterans could self-refer based on flyers and other study marketing materials.
The study was conducted from 2019 to 2024 at Spark M. Matsunaga VA Medical Center, in Honolulu, Hawaii. Four private research spaces in compliance with human research standards were used for consent, treatment, and assessment.
Consenting Procedure and Randomization
The privacy rights of potential participants were observed, and interested veterans who met the eligibility criteria underwent an informed consent procedure and were administered the Columbia-Suicide Severity Rating Scale.35 Those veterans not indicating active suicidal intent were randomized into the intervention or control group. Once randomized, the participant was enrolled and scheduled for baseline assessment.
All procedures of this study were performed in adherence with relevant laws and institutional guidelines. The study was reviewed and approved by the VA Pacific Islands Health Care System Institutional Review Board (#2019-06-JC/Promise 0003).
Outcome Measures
The outcome measures were administered at baseline, midpoint (3-7 weeks), end of treatment (6-12 weeks), and at a 2-month follow-up appointment with the research assistant or project coordinator.
The primary outcome measures included the Headache Impact Test (HIT-6), TBIQOL Headache Pain item short form, Insomnia Severity Index (ISI), Quality of Life in Neurological Disorders (Neuro-QOL) Sleep Disturbance short form, and attention measure: QIKtest Continuous Performance Test (QIKtest) (Table 1).36-44
Secondary outcome measures included QOL After Brain Injury (QOLIBRI), Neuro- QOL Satisfaction With Roles/Activities short form (Neuro-QOL Satisfaction), Neuro-QOL Ability to Participate in Roles/Activities short form (Neuro-QOL Participate), Depression Anxiety Stress Scales (DASS-21), Patient Health Questionnaire-9 (PHQ-9), Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5), and the General Symptom Inventory (eAppendix 1).39,42,45-52
Sample
Seventy-two participants (36 in each group) were needed to have adequate statistical power for the analysis. Presuming attrition, the goal was to recruit 100 veterans. Literature on NFB studies of patients with mTBI have reported dropout rates ranging from 10% to 30%.53,54 Assuming a dropout rate of 28% and a moderate autocorrelation of 0.6 among repeated measures, this sample size ensured the detection of an average difference of at least 0.49 SDs with a power of 80% in the NFB intervention group compared with the control group using a 2-tailed significance level of 0.05.
Control Group
Following baseline assessment, control group participants received 8 phone calls (1 call/wk) from 1 of 4 clinical investigators over 8 to 10 weeks. During each 15-minute call, 1 of the following health topics was discussed: sleep hygiene, basic nutritional concepts, beverage choices, positive thinking, thought reframing, fitness, daily calming activity, and enhancement of focus strategies. A script for each topic was used to guide each call.
Intervention Group
Following baseline assessment, intervention group participants completed 20 half-hour ILF NFB sessions, typically receiving 3 sessions per week over an 8- to 10-week period. ILF NFB treatments were administered by 1 of 4 licensed health care employees who had received substantial ILF NFB training and achieved a skill reliability index score of 0.95, ensuring the skill level of the ILF NFB providers was equal. A script was used by the ILF NFB providers during the ILF NFB sessions to keep the interaction approach consistent with all participants.
All procedures were explained in advance to participants and voluntary participation affirmed. At the first session, participants filled out a clinical symptom checklist of 5 symptoms (eAppendix 1).39,42,45-49 The initial rating on the symptom checklist was reflective of their experience over the past month, while in each subsequent session, participants indicated their experience of those symptoms that day. ILF NFB providers were never privy to participants’ primary or secondary outcome measures data during the study, so these recurring clinical symptom checklist ratings, as well as other feedback provided by participants on their experience within and between sessions, were the clinical data used to make decisions about ILF NFB treatment protocol.
The Othmer Optimal Response Frequency (ORF) protocol was used for participants in this study.55 Through an iterative process, ORF protocol establishes the specific frequency point along the 0.000001 mHz to 0.1 Hz continuum, which is optimal to diminish symptoms experienced in real-time during the session (eg, tension or pain in shoulders; racing thoughts).
During each ILF NFB session, participants were seated comfortably and encouraged to look at the feedback screen. The moving images on the game screen provided almost instantaneous feedback (within 500 ms) to participants about their brain functioning, as ascertained by electrodes placed on the scalp as dictated by study protocol.56 A standardized protocol for site placement was used beginning with T3-T4, followed by the weekly addition of a site as tolerated in the following sequence: T4-P4, FP2-T4, and FP1-T4. More information about the ILF NFB procedures are outlined in the report of the pilot study and RCT initial results.22,34
Statistical Analysis
Eighty-seven participants were randomized, with 43 assigned to the intervention group and 44 to the control group to achieve the enrollment goal of ≥ 36 participants in each group. This report is the second analysis of data from this RCT that employed a per-protocol approach, analyzing a subset of participants who fully adhered to the study protocol and completed all study procedures. Outcome scores at baseline, midpoint, end of treatment, and 2-month follow-up were summarized as means with corresponding 95% CIs. Group comparisons at the end of treatment and 2-month follow-up time points were conducted using 2-sample t tests. All statistical tests were 2-sided with a significance level of .05 (Type I error rate). SAS software version 9.4 Maintenance 8 was used for statistical analysis. Cohen d analyses were used for effect sizes.
Results
Seventy-four participants fully adhered to the study protocol and were included in the present analyses, with 38 in the control group and 36 in the intervention group. eAppendix 2 depicts the flow of participants through this study. There were no adverse events related to treatment, and the 13 participants who withdrew typically reported difficulty with scheduling or transportation as the primary reason. This study also took place during the COVID-19 pandemic, which likely had some impact on enrollment; participants were differentially impacted by changes in employment and moves to the continental US.
Participants were aged 30 to 60 years (mean [SD], 45.4 [8.0]). Most participants (90.5%) were male, and multiracial and White were the most common racial identities (Table 2). Participant characteristics were largely balanced across randomized groups. Similarly, test scores on the primary variables of interest in this study and secondary clinical variables assessed were comparable across participants (Table 3).
Primary Variables of Interest Analyses
This study’s hypothesis was that those who completed ILF NFB treatment per protocol would demonstrate statistically significant improvement in symptoms related to headaches, sleep disturbance, and difficulty with attention when compared with veterans in the control group. This hypothesis was partially supported. A 2-sample t test showed that veterans in the intervention group demonstrated significant improvement in headache symptoms compared with veterans in the control group on the HIT-6 at the end-of-treatment (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 1.14). This pattern also was consistent with the TBI-QOL Headache Pain item short form, with veterans in the intervention group showing improvement beyond those in the control group at the end-of-treatment (P < .001, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.83). Two-sample t tests also demonstrated significant improvement in subjective reports of sleep; those in the intervention group had significantly lower scores on the ISI at the end-of-study (P < .001, d = 1.53) and 2-month follow-up assessment (P < .001, d = 0.97). This pattern also held true for the Neuro-QOL Sleep Disturbance short form subtest, which demonstrated significantly more improvement in the intervention group compared with the control group at the end-of-study (P < .001, d = 0.97) and 2-month follow- up assessment (P < .001, d = 0.92). improvement in attention was not supported by the present results. A 2-sample t test found no significant difference between performance on the QIKtest for veterans in the intervention group vs the control group at the end-of-study (P = .40, d = 0.19) or the 2-month follow-up (P = .43, d = 0.20) (eAppendix 3).
Secondary Variables of Interest Analysis
Secondary variables examined differences in QOL, PTSD, depressive symptoms, and general symptoms reported between veterans in the intervention and control groups. Results demonstrated that veterans in the intervention group showed improvement above and beyond those in the control group on all measures. In regard to QOL, veterans in the intervention group had significantly higher scores on the Neuro-QOL Participate subtest than those in the control group at the end-of-study (P = .01, d = 0.89) and 2-month follow-up assessment (P < .001, d = 0.62). A similar pattern was found for the Neuro-QOL Satisfaction subtest, with veterans in the intervention group showing significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.95) and 2-month follow-up assessment (P < .001, d = 0.62). This also held true on the QOLIBRI, with veterans in the intervention group demonstrating significantly higher scores than those in the control group at the end-of-study (P = .001, d = 0.92) and 2-month follow-up assessment (P < .001, d = 0.66).
Veterans in the intervention group had significantly lower scores on the PCL-5 than those in the control group at the end-of- study (P = .003, d = 0.78) and 2-month follow-up assessment (P = .001, d = 0.72). Veterans in the intervention group also had significantly lower scores on the PHQ-9 than those in the control group at the end-of-study (P < .001, d = 0.98) and 2-month follow-up assessment (P < .001, d = 0.83). Veterans in the intervention group had significantly lower scores on the DASS- 21 than those in the control group at the end-of-study (P = .002, d = 0.80) and 2-month follow-up assessment (P = .001, d = 0.77). They also had significantly lower scores on the General Symptom Inventory than those in the control group at the end-of-study (P = .02, d = 0.75) and 2-month follow-up assessment (P = .002, d = 0.57). A clinically significant shift of score occurred for each of the measures except DASS-21 (eAppendix 3). eAppendix 4 depicts the change in scores for the intervention group at the end of treatment and the clinically significant shift score of each measure.
Discussion
The results of this RCT revealed a promising impact of ILF NFB on the commonly experienced persistent PCSs of headaches and disrupted sleep. Veterans in the intervention group demonstrated statistically significant improvement in headache symptoms compared with veterans in the control group when assessed at the end of treatment and during a 2-month follow-up. The statistical significance of these improvements was also supported by large or very large effect sizes. In addition to these primary variables of interest, veterans in the intervention group notably demonstrated significant improvement compared with those in the control group in a number of secondary clinical measures, including QOL, traumatic stress-related symptoms, depressive symptoms, and general symptom report. The clinical impact was further supported by the clinically relevant shift in scores in the intervention group.
The data did not support the hypothesis that attention concerns would show significant improvement following ILF NFB. Performance on an attention measure did not differ significantly between groups at either the end-of-treatment or 2-month follow up assessment. The QIKtest, a continuous performance test used to measure attention, was a go/no-go task and calculated based on a combination of various types of errors and outlier responses. The stimulus for this task is a series of computerized, blinking lights, for which participants are tasked with discriminating targets and nontargets under time pressure. However, the order of the stimuli are consistent across administrations, rather than being randomized, introducing a potential confound of practice effects on this task since patients were administered the QIKtest 3 times in a 2-month period and again 2 months later. Veterans in the control group notably improved in their average performance of this task from baseline to the endpoint of their treatment participation and demonstrated further improvement at the 2-month follow-up assessment; this pattern would be consistent with potential practice effects and warrants caution in its interpretation for both groups.
Previously published ILF NFB clinical studies that used the QIKtest and found positive results were mostly conducted among children and teen populations across longer treatment periods. This research may indicate the QIKtest is not an appropriate measure to assess adults who have specialized training in responding to stimuli (ie, trained military personnel). This suggests the concept of attention dysfunction experienced by veterans and the best method to measure it may need to be explored further. This construct may not be related to the focus and skill in prolonged attention needed in selecting go/ no-go tasks, but rather related to a broader conceptual basis involving memory, recall, clarity of rational thought, and decision making impacted by the mTBI. For instance, a study among combat veterans with mTBI and PTSD found that performance on objective cognitive measures did not significantly correlate with their subjective reports of cognitive difficulties.57 This reflects the pattern of the present study, in which subjective reports of attention improved over time on the clinical symptom checklist filled out by participants at each session, but the objective measure did not. The mean attention dysfunction score was 6 at session 1 and 1 to 2 at session 20 (lower scores are better on a 10-point scale).
Strengths and Limitations
This study presents results stemming from the first RCT examining clinical effectiveness of ILF NFB in a VA setting for veterans with diagnoses of mTBI. The study design shows promising external validity. Veterans were able to participate in a treatment consisting of 20 sessions over a period of typically 8 to 10 weeks, entailing 2 to 3 sessions per week, with an attrition of only 18% over the course of the study. Notably, attrition rates may have been impacted by the time course of the study, which was recruiting and running participants throughout the COVID-19 pandemic (March 2020 to May 2023). No attrition was due to the intervention itself, and no adverse reactions to ILF NFB were reported during the course of the study. Other strengths of the study include the ethnically and racially diverse participants, representative of the population of veterans in Hawaii. Additionally, all ILF NFB providers underwent supervised ILF NFB training and achieved a skill reliability index score of 0.95 prior to providing ILF NFB to the intervention group.
This study was not blinded. Neither veterans nor ILF NFB clinicians were blinded and were therefore aware of the randomly assigned groups. Research assistants administering the periodic assessments were meant to be blinded to condition by design; however, as the study progressed, a research assistant became unintentionally aware of each study participant's condition based on required documentation in the veteran’s health records; more notes were present for those in the intervention group (20 specialist notes) than the control group (8 notes). While the presence of a control group represents a strength relative to much of the existing ILF NFB literature, the control group in this case did not account for the total time spent with the researchers. Participants in the intervention group met with researchers for 20 total sessions as opposed to 8 telephone calls. Therefore, the study design cannot fully rule out the differential impact of demand characteristics between the 2 groups, nor can it fully address or rule out the impact of differential motivation and expectations between groups. There is also evidence that technological innovation can influence the expectations of research participants, meaning that the intervention group may have been unduly influenced by the novelty of the ILF NFB technology, to which the control group did not have exposure.58
A second attention measure for this study would have been beneficial, perhaps in identifying true change in attention ability or providing more insight into finding better methods to assess attention among veterans with mTBI. ILF NFB demonstrated significant impact across multiple outcome measures of clinical relevance for veterans diagnosed with mTBI, including the primary outcome variables of headache and sleep. The strength of the improvements seen in these areas, supported by large practical effects as well as veterans’ subjective reports, indicates much promise. Follow-up studies may also focus on the potential effectiveness of ILF NFB as a treatment of the secondary concerns measured in this study, including traumatic stress-related and depressive symptoms, and may explore the added benefit, if any, of ILF NFB alongside other evidence-based treatments for traumatic stress-related and mood disorders (eg, cognitive behavioral therapy). Using functional magnetic resonance imaging before and after assessments to determine actual brain enhancement with ILF NFB for certain disorders in which a brain signature exists (ie, migraine) should be explored. Further examination of ILF NFB as an intervention for attention may also be warranted, using more effective measures of attention in the population of veterans with mTBI, given the concerns noted earlier. Future research on this topic will need to clearly define attention in relation to the veteran experience and use relevant measures.
Conclusions
This study supports ILF NFB as a safe, noninvasive, nonpharmacologic treatment that may be effective in addressing the complex clinical concerns of veterans diagnosed with mTBI, a population for whom effective treatments have been difficult to identify. This intervention can provide veterans with a desirable and effective nonpharmacologic alternative in their care.
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
- Hayward P. Traumatic brain injury: the signature of modern conflicts. Lancet Neurol. 2008;7:200-201. doi:10.1016/S1474-4422(08)70032-2
- Whiteneck G, Williams W, Almeida E, et al. Two decades of Department of Veterans Affairs traumatic brain injury care and benefits for veterans of post-9/11 conflicts. J Head Trauma Rehabil. 2024;39:E462-E469. doi:10.1097/HTR.0000000000000952
- Chapman JC, Diaz-Arrastia R. Military traumatic brain injury: a review. Alzheimers Dement. 2014;10(3 suppl):S97- S104. doi:10.1016/j.jalz.2014.04.012
- Dean PJA, O’Neill D, Sterr A. Post-concussion syndrome: prevalence after mild traumatic brain injury in comparison with a sample without head injury. Brain Inj. 2012;26:14-26. doi:10.3109/02699052.2011.635354
- Agimi Y, Hai T, Gano A, et al. Clinical trajectories of comorbidity associated with military-sustained mild traumatic brain injury: pre- and post-injury. J Head Trauma Rehabil. 2024;39:E564-E575. doi:10.1097/HTR.0000000000000934
- Hoge CW, McGurk D, Thomas JL, et al. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N Engl J Med. 2008;358:453-463. doi:10.1056/NEJMoa072972
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation. Neuropsychol Rev. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- Eapen BC, Bowles AO, Sall J, et al. The management and rehabilitation of post-acute mild traumatic brain injury. Brain Inj. 2022;36:693-702. doi:10.1080/02699052.2022.2033848
- Department of Veterans Affairs (VA) and Department of Defense (DoD). VA/DoD Clinical Practice Guideline for the management and Rehabilitation of Post-Acute Mild Traumatic Brain Injury, 2021, Version 3:1-128. https://www.healthquality.va.gov/HEALTHQUALITY/guidelines/Rehab/mtbi/index.asp
- Patil VK, St Andre JR, Crisan E, et al. Prevalence and treatment of headaches in veterans with mild traumatic brain injury. Headache. 2011;51:1112-1121. doi:10.1111/j.1526-4610.2011.01946.x
- Ayalon L, Borodkin K, Dishon L, Kanety H, Dagan Y. Circadian rhythm sleep disorders following mild traumatic brain injury. Neurology. 2007;68:1136-1140. doi:10.1212/01.wnl.0000258672.52836.30
- Bogdanova Y, Verfaellie M. Cognitive sequelae of blast-induced traumatic brain injury: recovery and rehabilitation, Neuropsychology Review. 2012;22:4-20. doi:10.1007/s11065-012-9192-3
- US Department of Veteran Affairs. VHA Directive 1137.December 13, 2022. https://www.va.gov/VHApublications/ViewPublication.asp?pub_ID=10072
- Taylor SL, Hoggatt KJ, Kligler B. Complementary and integrated health approaches: what do veterans use and want. J Gen Intern Med. 2019;34:1192-1199. doi:10.1007/s11606-019-04862-6
- DeFlna P, Fellus J, Polito MZ, et al. The new neuroscience frontier: promoting neuroplasticity and brain repair in traumatic brain injury. Clin Neuropsychol. 2009;23:1391-1399. doi:10.1080/13854040903058978
- Enriquez-Geppert S, Huster RJ, Herrmann CS. Boosting brain functions: improving executive functions with behavioral training, neurostimulation, and neurofeedback. Int J Psychophysiol. 2013;88:1-16. doi:10.1016/j.ijpsycho.2013.02.001
- Ghaziri J, Tucholka A, Larue V, et al. Neurofeedback training induces changes in white and gray matter. Clin EEG Neurosci. 2013;44:265-272. doi:10.1177/1550059413476031
- Ibric VL, Dragomirescu LG, Hudspeth WJ. Real-time changes in connectivities during neurofeedback. J Neurother. 2009;13:156-165. doi:10.1080/10874200903118378
- Clark VP, Parasuraman R. Neuroenhancement: enhancing brain and mind in health and in disease. Neuroimage. 2014;85:889-894. doi:10.1016/j.neuroimage.2013.08.071
- Larsen S, Sherlin L. Neurofeedback: an emerging technology for treating central nervous system dysregulation. Psychiatr Clin North Am. 2013;36:163-168. doi:10.1016/j.psc.2013.01.005
- Hammond DC. What is neurofeedback: an update. J Neurother. 2011; 15:305-336. doi:10.1080/10874208.2011.623090
- Othmer S. Endogenous neuromodulation at infra-low frequencies. In: Chartier DR, Dellinger MB, Evans JR, Budzynski HK, eds. Introduction to Quantitative EEG and Neurofeedback. 3rd ed. Academic Press; 2023:283-299. doi:10.1016/B978-0-323-89827-0.00001-2
- Othmer SF. History of the Othmer Method: an evolving clinical model and process. In: Evans JR, Dellinger MB, Russell HL, eds. Neurofeedback: The First Fifty Years. Academic Press; 2020:327-334. doi:10.1016/B978-0-12-817659-7.00043-9
- Legarda SB, Lahti CE, McDermott D, Michas-Martin A. Use of novel concussion protocol with infralow frequency neuromodulation demonstrates significant treatment response in patients with persistent postconcussion symptoms, a retrospective study. Front Hum Neurosci. 2022;16:894758. doi:10.3389/fnhum.2022.894758
- Carlson J, Ross GW. Neurofeedback impact on chronic headache, sleep, and attention disorders experienced by veterans with mild traumatic brain injury: a pilot study. Biofeedback. 2021;49:2-9. doi:10.5298/1081-5937-49.01.01
- Dobrushina O, Arina G, Osina E, Aziatskaya G. Clinical and psychological confirmation of stabilizing effect of neurofeedback in migraine. Eur Psychiatry. 2017;41:S253-S253. doi:10.1016/j.eurpsy.2017.02.045
- Arina GA, Dobrushina OR, Shvetsova ET, et al. Infra-low frequency neurofeedback in tension-type headache: a cross-over sham-controlled study. Front Hum Neurosci. 2022;16:891323. doi:10.3389/fnhum.2022.891323
- Kirk HW, Dahl MG. Infra low frequency neurofeedback training for trauma recovery: a case report. Front Hum Neurosci. 2022;16:905823. doi:10.3389/fnhum.2022.905823
- Benson A, LaDou T. The use of neurofeedback for combat veterans with post-traumatic stress. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. CRC Press; 2015.
- Legarda SB, McMahon D, Othmer S, Othmer S. Clinical neurofeedback: case studies, proposed mechanism, and implications for pediatric neurology practice. J Child Neurol. 2011;26:1045-1051. doi:10.1177/0883073811405052
- McMahon DE. Notes from clinical practice: an MD’s perspective on 9 years of neurofeedback practice. Semin Pediatr Neurol. 2013;20:258-260. doi:10.1016/j.spen.2013.10.007
- Othmer S, Othmer SF. Post traumatic stress disorder— the neurofeedback remedy. Biofeedback. 2009;37:24-31. doi:10.5298/1081-5937-37.1.24
- Shapero E, Prager J. ILF Neurofeedback and alpha-theta training in a multidisciplinary chronic pain program. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020:223-243.
- Carlson J, Ross G, Tyrrell C, et al. Infra-low frequency neurofeedback impact on post-concussive symptoms of headache, insomnia and attention disorder: results of a randomized control trial. Explore (NY). 2025;21:103137. doi:10.1016/j.explore.2025.103137
- Posner K, Brown GK, Stanley B, et al. The Columbia– Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168:1266- 1277. doi:10.1176/appi.ajp.2011.10111704
- Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: the HIT-6. Qual Life Res. 2003;12:963-974. doi:10.1023/a:1026119331193
- Coeytaux RR, Kaufman JS, Chao R, Mann JD, Devellis RF. Four methods of estimating the minimal important difference score were compared to establish a clinically significant change in Headache Impact Test. J Clin Epidemiol. 2006;59:374-380. doi:10.1016/j.jclinepi.2005.05.010
- Tulsky DS, Tyner CE, Boulton AJ, et al. Development of the TBI-QOL Headache Pain Item Bank and Short Form. J Head Trauma Rehabil. 2019;34:298-307. doi:10.1097/HTR.0000000000000532
- Poritz JMP, Sherer M, Kisala MA, et al. Responsiveness of the Traumatic Brain Injury-Quality of Life (TBI-QOL) measurement system. Arch Phys Med Rehabil. 2020;101:54- 61. doi:10.1016/j.apmr.2017.11.018
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2:297-307. doi:10.1016/s1389-9457(00)00065-4
- Yang M, Morin CM, Schaefer M, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25:2487-2494. doi:10.1185/03007990903167415
- Cella D, Lai J-S, Nowinski CJ, et al. Neuro-QOL Brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860-1867. doi:10.1212/WNL.0b013e318258f744
- Kozlowski AJ, Cella D, Nitsch KP, Heinemann AW. Evaluating individual change with the Quality of Life in Neurological Disorders (Neuro-QoL) short forms. Arch Phys Med Rehabil. 2016;97:650-654.e8. doi:10.1016/j.apmr.2015.12.010
- Versace M. QIKTest Report on EEG Expert: introduction and overview. 2014. Accessed February 24, 2026. https://media.voog.com/0000/0044/8343/files/EEGexpert_manual_newreport2014_EN.pdf
- Truelle J-L, Koskinen S, Hawthorne G, et al. Quality of life after traumatic brain injury: the clinical use of the QOLIBRI, a novel disease-specific instrument. Brain Inj. 2010;24:1272-1291. doi:10.3109/02699052.2010.506865
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606-613. doi:10.1046/j.1525-1497.2001.016009606.x
- Kroenke K. Enhancing the clinical utility of depression screening. CMAJ. 2012;184:281-282. doi:10.1503/cmaj.112004
- Weathers FW, Litz BT, Keane TM, et al. PTSD checklist for DSM-5 (PCL-5). National Center for PTSD. Updated September 10, 2025. Accessed February 24, 2026. https:// www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Henry JD, Crawford JR. The short]form version of the Depression Anxiety Stress Scales (DASS]21): construct validity and normative data in a large non]clinical sample. Br J Clin Psychol. 2005;44:227-239. doi:10.1348/014466505X29657
- Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995;33(3):335-343. doi:10.1016/0005-7967(94)00075-u
- Ronk FR, Korman JR, Hooke GR, Page AC. Assessing clinical significance of treatment outcomes using the DASS-21. Psychol Assess. 2013;25:1103-1110. doi:10.1037/a0033100
- Carlson J. General symptom inventory. Description published online 2021.
- Nelson DV, Esty ML. Neurotherapy of traumatic brain injury/ posttraumatic stress symptoms in OEF/OIF veterans. J Neuropsychiatry Clin Neurosci. 2012;24:237-240. doi:10.1176/appi.neuropsych.11020041
- Zoefel B, Huster RJ, Herrmann CS. Neurofeedback training of the upper alpha frequency band in EEG improves cognitive performance. Neuroimage. 2011;54:1427-1431. doi:10.1016/j.neuroimage.2010.08.078
- Othmer S, Othmer S. Toward a theory of infra-low frequency neurofeedback. In: Kirk HW, ed. Restoring the Brain: Neurofeedback as an Integrative Approach to Health. 2nd ed. Routledge; 2020.
- Huster RJ, Mokom ZN, Enriquez-Geppert S, Herrmann CS. Brain–computer interfaces for EEG neurofeedback: peculiarities and solutions. Int J Psychophysiol. 2014;91:36-45. doi:10.1016/j.ijpsycho.2013.08.011
- Ord AS, Martindale SL, Jenks ER, Rowland JA. Subjective cognitive complaints and objective cognitive functioning in combat veterans: effects of PTSD and deployment mild TBI. Appl Neuropsychol Adult. 2025;32:1400-1406. doi:10.1080/23279095.2023.2280807
- Lawton J, Blackburn M, Breckenridge J, Hallowell N, Farrington C, Rankin D. Ambassadors of hope, research pioneers and agents of change-individuals’ expectations and experiences of taking part in a randomised trial of an innovative health technology: longitudinal qualitative study. Trials. 2019;20:289. doi:10.1186/s13063-019-3373-9
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
Clinical Impact of Infra-Low Frequency Neurofeedback on Combat Veterans With Chronic Postconcussive Symptoms
