User login
Biomarker correlates with pancreatic cancer severity
HOUSTON – A circulating biomarker has the potential to identify metastatic pancreatic cancer and may be able to predict prognosis, investigators said.
Levels of a gene encoding for the gap-junction beta 3 (GJB3) protein were highly elevated in both pancreatic cancer cell lines and in blood samples from patients with pancreatic ductal adenocarcinoma (PDAC), but the gene was undetectable in blood samples from patients without cancer, reported Dr. Raoud Marayati from the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.

An analysis of gene expression in tumors from patients with PDAC also showed that patients with tumors expressing higher levels of GJB3 had significantly worse overall survival rates.
“GJB3 is highly expressed in blood samples from patients with metastatic versus local pancreatic cancer. GJB3 is a potential circulating biomarker for metastatic pancreatic cancer,” Dr. Marayati said at the annual Society of Surgical Oncology Cancer Symposium.
Markers lacking
PDAC is a highly aggressive cancer with a propensity for early invasion and metastasis. More than half of all patients (53%) have metastatic disease at the time of diagnosis, and 5-year survival for these patients is only 2.3%, according to the Surveillance, Epidemiology, and End Results (SEER) cancer statistics review for 2014, she noted.
The only currently available clinical biomarker for PDAC, carbohydrate antigen 19-9 (CA 19-9), generally correlates with treatment response and disease recurrence but has low sensitivity and specificity, Dr. Marayati said.
Circulating tumor cells (CTCs) – cells shed from the primary tumor into circulation – hold promise for better detection of cancer, but CTCs from pancreatic tumors have proven to be extremely difficult to isolate and count, she added.
To see whether they could identify circulating biomarkers of metastatic PDAC, Dr. Marayati and colleagues working in the laboratory of Dr. Jen Jen Yeh at the university first identified 76 genes that are differentially overexpressed in metastatic PDAC tumors, compared with localized primary tumors and with normal tissues.
The investigators looked for expression of the genes in 11 pancreatic cancer cell lines and in blood samples from 20 patients with pancreatic cancer and four without cancer. As noted, one gene, GJB3, was highly expressed in all of the cell-line samples but could not be detected in white blood cells from patients without PDAC.
To validate GJB3 as a potential cancer marker, the authors looked at expression levels in circulating tumor cells and found that, among the patients with cancer, expression levels of GBJ3 were significantly higher in those with metastatic disease, compared with localized disease (P = .016).
“That would suggest that GJB3 is a potential circulating biomarker specifically for metastatic pancreatic cancer patients,” Dr. Marayati said.
The investigators hypothesized that GJB3 may play a role in the biology of pancreatic cancer metastasis. To test this idea, they looked at resected tumors from 131 patients with primary pancreatic cancer and found that high tumor expression of GJB3 was associated with worse survival. Median overall survival among 32 patients with low levels of gene expression in their tumors was 24 months, compared with 15 months for 99 patients with high levels of GJB3 expression (P = .031).
The investigators plan to further validate the marker by testing it with larger samples from both patients with pancreatic cancer and controls.
The study funding source was not disclosed. Dr. Marayati reported having no disclosures.
HOUSTON – A circulating biomarker has the potential to identify metastatic pancreatic cancer and may be able to predict prognosis, investigators said.
Levels of a gene encoding for the gap-junction beta 3 (GJB3) protein were highly elevated in both pancreatic cancer cell lines and in blood samples from patients with pancreatic ductal adenocarcinoma (PDAC), but the gene was undetectable in blood samples from patients without cancer, reported Dr. Raoud Marayati from the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
An analysis of gene expression in tumors from patients with PDAC also showed that patients with tumors expressing higher levels of GJB3 had significantly worse overall survival rates.
“GJB3 is highly expressed in blood samples from patients with metastatic versus local pancreatic cancer. GJB3 is a potential circulating biomarker for metastatic pancreatic cancer,” Dr. Marayati said at the annual Society of Surgical Oncology Cancer Symposium.
Markers lacking
PDAC is a highly aggressive cancer with a propensity for early invasion and metastasis. More than half of all patients (53%) have metastatic disease at the time of diagnosis, and 5-year survival for these patients is only 2.3%, according to the Surveillance, Epidemiology, and End Results (SEER) cancer statistics review for 2014, she noted.
The only currently available clinical biomarker for PDAC, carbohydrate antigen 19-9 (CA 19-9), generally correlates with treatment response and disease recurrence but has low sensitivity and specificity, Dr. Marayati said.
Circulating tumor cells (CTCs) – cells shed from the primary tumor into circulation – hold promise for better detection of cancer, but CTCs from pancreatic tumors have proven to be extremely difficult to isolate and count, she added.
To see whether they could identify circulating biomarkers of metastatic PDAC, Dr. Marayati and colleagues working in the laboratory of Dr. Jen Jen Yeh at the university first identified 76 genes that are differentially overexpressed in metastatic PDAC tumors, compared with localized primary tumors and with normal tissues.
The investigators looked for expression of the genes in 11 pancreatic cancer cell lines and in blood samples from 20 patients with pancreatic cancer and four without cancer. As noted, one gene, GJB3, was highly expressed in all of the cell-line samples but could not be detected in white blood cells from patients without PDAC.
To validate GJB3 as a potential cancer marker, the authors looked at expression levels in circulating tumor cells and found that, among the patients with cancer, expression levels of GBJ3 were significantly higher in those with metastatic disease, compared with localized disease (P = .016).
“That would suggest that GJB3 is a potential circulating biomarker specifically for metastatic pancreatic cancer patients,” Dr. Marayati said.
The investigators hypothesized that GJB3 may play a role in the biology of pancreatic cancer metastasis. To test this idea, they looked at resected tumors from 131 patients with primary pancreatic cancer and found that high tumor expression of GJB3 was associated with worse survival. Median overall survival among 32 patients with low levels of gene expression in their tumors was 24 months, compared with 15 months for 99 patients with high levels of GJB3 expression (P = .031).
The investigators plan to further validate the marker by testing it with larger samples from both patients with pancreatic cancer and controls.
The study funding source was not disclosed. Dr. Marayati reported having no disclosures.
HOUSTON – A circulating biomarker has the potential to identify metastatic pancreatic cancer and may be able to predict prognosis, investigators said.
Levels of a gene encoding for the gap-junction beta 3 (GJB3) protein were highly elevated in both pancreatic cancer cell lines and in blood samples from patients with pancreatic ductal adenocarcinoma (PDAC), but the gene was undetectable in blood samples from patients without cancer, reported Dr. Raoud Marayati from the Lineberger Comprehensive Cancer Center at the University of North Carolina, Chapel Hill.
An analysis of gene expression in tumors from patients with PDAC also showed that patients with tumors expressing higher levels of GJB3 had significantly worse overall survival rates.
“GJB3 is highly expressed in blood samples from patients with metastatic versus local pancreatic cancer. GJB3 is a potential circulating biomarker for metastatic pancreatic cancer,” Dr. Marayati said at the annual Society of Surgical Oncology Cancer Symposium.
Markers lacking
PDAC is a highly aggressive cancer with a propensity for early invasion and metastasis. More than half of all patients (53%) have metastatic disease at the time of diagnosis, and 5-year survival for these patients is only 2.3%, according to the Surveillance, Epidemiology, and End Results (SEER) cancer statistics review for 2014, she noted.
The only currently available clinical biomarker for PDAC, carbohydrate antigen 19-9 (CA 19-9), generally correlates with treatment response and disease recurrence but has low sensitivity and specificity, Dr. Marayati said.
Circulating tumor cells (CTCs) – cells shed from the primary tumor into circulation – hold promise for better detection of cancer, but CTCs from pancreatic tumors have proven to be extremely difficult to isolate and count, she added.
To see whether they could identify circulating biomarkers of metastatic PDAC, Dr. Marayati and colleagues working in the laboratory of Dr. Jen Jen Yeh at the university first identified 76 genes that are differentially overexpressed in metastatic PDAC tumors, compared with localized primary tumors and with normal tissues.
The investigators looked for expression of the genes in 11 pancreatic cancer cell lines and in blood samples from 20 patients with pancreatic cancer and four without cancer. As noted, one gene, GJB3, was highly expressed in all of the cell-line samples but could not be detected in white blood cells from patients without PDAC.
To validate GJB3 as a potential cancer marker, the authors looked at expression levels in circulating tumor cells and found that, among the patients with cancer, expression levels of GBJ3 were significantly higher in those with metastatic disease, compared with localized disease (P = .016).
“That would suggest that GJB3 is a potential circulating biomarker specifically for metastatic pancreatic cancer patients,” Dr. Marayati said.
The investigators hypothesized that GJB3 may play a role in the biology of pancreatic cancer metastasis. To test this idea, they looked at resected tumors from 131 patients with primary pancreatic cancer and found that high tumor expression of GJB3 was associated with worse survival. Median overall survival among 32 patients with low levels of gene expression in their tumors was 24 months, compared with 15 months for 99 patients with high levels of GJB3 expression (P = .031).
The investigators plan to further validate the marker by testing it with larger samples from both patients with pancreatic cancer and controls.
The study funding source was not disclosed. Dr. Marayati reported having no disclosures.
AT SSO 2015
Key clinical point: GJB3 may be a serum marker for metastatic pancreatic ductal adenocarcinoma.
Major finding: GJB3 was expressed at significantly higher levels in patients with metastatic vs. localized PDAC.
Data source: Gene expression analyses involving patient tumor samples and 11 pancreatic cancer cell lines.
Disclosures: The study funding source was not disclosed. Dr. Marayati reported having no disclosures.

SSIs a factor in postop colon cancer survival
HOUSTON – Surgical-site infections occurring in patients who underwent curative resection for localized colon cancer were associated with worse overall survival in a large retrospective study.
Among nearly 10,000 patients with nonmetastatic colon cancer who underwent surgery with curative intent, surgical-site infections (SSIs) were associated with both worse overall survival and a reduced likelihood of receiving adjuvant chemotherapy, reported Dr. Gala Markia Barden, a surgical resident at Baylor College of Medicine, Houston.

Both SSIs and failure to receive adjuvant chemotherapy are independently associated with worse overall survival, she said at the annual Society of Surgical Oncology Cancer Symposium.
“Future studies and practice guidelines should focus on target areas for improving these potentially preventable problems, including active surveillance for and early recognition of surgical-site infections, as well as vigilant follow-up to ensure treatment completion and to improve the transition between the surgical and medical oncology teams to mitigate losses to follow-up,” she said.
Tapping into the merged Veterans Affairs Surgical Quality Improvement Program and VA Central Cancer Registry (VASQIP-VA) databases, the authors identified 9,946 patients aged 18 years and older who underwent radical resection for colon cancer from 1999 through 2009. Patients with rectal cancers or early postoperative deaths (within 90 days of surgery) were excluded.
The investigators examined the relationships between SSIs and both 5-year overall survival and receipt of adjuvant chemotherapy, which has been documented to improve survival in patients with stage III colon cancer. Delivery of adjuvant chemotherapy in these patients is considered to be a measure of the quality of cancer care, Dr. Barden noted.
Of the 9,946 patients included in the study, 1,340 (13.5%) developed SSIs. These patients were slightly but significantly younger (P < .001), had worse functional status (P = .002), and had higher American Society of Anesthesiologists (ASA) physical status scores (P < .001).
In univariate analysis, the investigators found that, in the entire cohort, SSIs were associated with worse overall survival (OS); in multivariate analysis controlling for sex, nutrition, functional status, ASA score, and number of lymph nodes resected, they saw that SSI was associated with a hazard ratio (HR) for worse overall survival of 1.35 (P < .0001).
When they looked at the association of SSI and OS stratified by cancer stage, however, they found that it was significant only for stage III disease. Patients with stage III who developed an SSI had a median OS of 29 months, compared with 33 months for those with no site infections (P< .001).
Dr. Barden and her associates also found that 42% of patients with infections did not receive adjuvant chemotherapy, compared with 34% of patients without SSIs (P = .002).
To see whether the worse survival among patients with SSI was primarily driven by the failure to deliver chemotherapy, they created a model adjusted for cancer risk factors, which showed that patients with stage III disease who developed an SSI and did not undergo adjuvant chemotherapy had an HR of worse overall survival of 1.59 (P < .0001).
They then added into the model those patients with SSIs who did receive adjuvant therapy but, contrary to their expectations, saw that the HR was only slightly reduced (1.56) and remained significant (P < .0001). The model also confirmed that failure to deliver chemotherapy was associated with worse survival (HR 1.52, P <.0001)
Dr. Barden acknowledged that the study was limited by the retrospective design, predominantly male VA cohort, and the lack of information in the databases about why patients did not receive adjuvant therapy.
The study was internally supported. Dr. Barden reported having no conflicts of interest.
HOUSTON – Surgical-site infections occurring in patients who underwent curative resection for localized colon cancer were associated with worse overall survival in a large retrospective study.
Among nearly 10,000 patients with nonmetastatic colon cancer who underwent surgery with curative intent, surgical-site infections (SSIs) were associated with both worse overall survival and a reduced likelihood of receiving adjuvant chemotherapy, reported Dr. Gala Markia Barden, a surgical resident at Baylor College of Medicine, Houston.
Both SSIs and failure to receive adjuvant chemotherapy are independently associated with worse overall survival, she said at the annual Society of Surgical Oncology Cancer Symposium.
“Future studies and practice guidelines should focus on target areas for improving these potentially preventable problems, including active surveillance for and early recognition of surgical-site infections, as well as vigilant follow-up to ensure treatment completion and to improve the transition between the surgical and medical oncology teams to mitigate losses to follow-up,” she said.
Tapping into the merged Veterans Affairs Surgical Quality Improvement Program and VA Central Cancer Registry (VASQIP-VA) databases, the authors identified 9,946 patients aged 18 years and older who underwent radical resection for colon cancer from 1999 through 2009. Patients with rectal cancers or early postoperative deaths (within 90 days of surgery) were excluded.
The investigators examined the relationships between SSIs and both 5-year overall survival and receipt of adjuvant chemotherapy, which has been documented to improve survival in patients with stage III colon cancer. Delivery of adjuvant chemotherapy in these patients is considered to be a measure of the quality of cancer care, Dr. Barden noted.
Of the 9,946 patients included in the study, 1,340 (13.5%) developed SSIs. These patients were slightly but significantly younger (P < .001), had worse functional status (P = .002), and had higher American Society of Anesthesiologists (ASA) physical status scores (P < .001).
In univariate analysis, the investigators found that, in the entire cohort, SSIs were associated with worse overall survival (OS); in multivariate analysis controlling for sex, nutrition, functional status, ASA score, and number of lymph nodes resected, they saw that SSI was associated with a hazard ratio (HR) for worse overall survival of 1.35 (P < .0001).
When they looked at the association of SSI and OS stratified by cancer stage, however, they found that it was significant only for stage III disease. Patients with stage III who developed an SSI had a median OS of 29 months, compared with 33 months for those with no site infections (P< .001).
Dr. Barden and her associates also found that 42% of patients with infections did not receive adjuvant chemotherapy, compared with 34% of patients without SSIs (P = .002).
To see whether the worse survival among patients with SSI was primarily driven by the failure to deliver chemotherapy, they created a model adjusted for cancer risk factors, which showed that patients with stage III disease who developed an SSI and did not undergo adjuvant chemotherapy had an HR of worse overall survival of 1.59 (P < .0001).
They then added into the model those patients with SSIs who did receive adjuvant therapy but, contrary to their expectations, saw that the HR was only slightly reduced (1.56) and remained significant (P < .0001). The model also confirmed that failure to deliver chemotherapy was associated with worse survival (HR 1.52, P <.0001)
Dr. Barden acknowledged that the study was limited by the retrospective design, predominantly male VA cohort, and the lack of information in the databases about why patients did not receive adjuvant therapy.
The study was internally supported. Dr. Barden reported having no conflicts of interest.
HOUSTON – Surgical-site infections occurring in patients who underwent curative resection for localized colon cancer were associated with worse overall survival in a large retrospective study.
Among nearly 10,000 patients with nonmetastatic colon cancer who underwent surgery with curative intent, surgical-site infections (SSIs) were associated with both worse overall survival and a reduced likelihood of receiving adjuvant chemotherapy, reported Dr. Gala Markia Barden, a surgical resident at Baylor College of Medicine, Houston.
Both SSIs and failure to receive adjuvant chemotherapy are independently associated with worse overall survival, she said at the annual Society of Surgical Oncology Cancer Symposium.
“Future studies and practice guidelines should focus on target areas for improving these potentially preventable problems, including active surveillance for and early recognition of surgical-site infections, as well as vigilant follow-up to ensure treatment completion and to improve the transition between the surgical and medical oncology teams to mitigate losses to follow-up,” she said.
Tapping into the merged Veterans Affairs Surgical Quality Improvement Program and VA Central Cancer Registry (VASQIP-VA) databases, the authors identified 9,946 patients aged 18 years and older who underwent radical resection for colon cancer from 1999 through 2009. Patients with rectal cancers or early postoperative deaths (within 90 days of surgery) were excluded.
The investigators examined the relationships between SSIs and both 5-year overall survival and receipt of adjuvant chemotherapy, which has been documented to improve survival in patients with stage III colon cancer. Delivery of adjuvant chemotherapy in these patients is considered to be a measure of the quality of cancer care, Dr. Barden noted.
Of the 9,946 patients included in the study, 1,340 (13.5%) developed SSIs. These patients were slightly but significantly younger (P < .001), had worse functional status (P = .002), and had higher American Society of Anesthesiologists (ASA) physical status scores (P < .001).
In univariate analysis, the investigators found that, in the entire cohort, SSIs were associated with worse overall survival (OS); in multivariate analysis controlling for sex, nutrition, functional status, ASA score, and number of lymph nodes resected, they saw that SSI was associated with a hazard ratio (HR) for worse overall survival of 1.35 (P < .0001).
When they looked at the association of SSI and OS stratified by cancer stage, however, they found that it was significant only for stage III disease. Patients with stage III who developed an SSI had a median OS of 29 months, compared with 33 months for those with no site infections (P< .001).
Dr. Barden and her associates also found that 42% of patients with infections did not receive adjuvant chemotherapy, compared with 34% of patients without SSIs (P = .002).
To see whether the worse survival among patients with SSI was primarily driven by the failure to deliver chemotherapy, they created a model adjusted for cancer risk factors, which showed that patients with stage III disease who developed an SSI and did not undergo adjuvant chemotherapy had an HR of worse overall survival of 1.59 (P < .0001).
They then added into the model those patients with SSIs who did receive adjuvant therapy but, contrary to their expectations, saw that the HR was only slightly reduced (1.56) and remained significant (P < .0001). The model also confirmed that failure to deliver chemotherapy was associated with worse survival (HR 1.52, P <.0001)
Dr. Barden acknowledged that the study was limited by the retrospective design, predominantly male VA cohort, and the lack of information in the databases about why patients did not receive adjuvant therapy.
The study was internally supported. Dr. Barden reported having no conflicts of interest.
AT SSO 2015
Key clinical point: Surgical site infections in patients with colon cancer are associated with both worse overall survival and lower chance of receiving adjuvant chemotherapy.
Major finding: Median overall survival for stage III patients with SSIs was 29 months, vs. 33 for no SSIs.
Data source: Retrospective cohort study of 9,946 patients who underwent radical colon cancer resection with curative intent.
Disclosures: The study was internally supported. Dr. Barden reported having no conflicts of interest.

Rectal preservation feasible after cancer clinical remission
HOUSTON – Patients who achieve complete clinical responses after neoadjuvant therapy for locally advanced rectal cancer may, in many cases, be safely spared the trauma and morbidity of total mesorectal excision.
That’s the opinion of investigators at Memorial Sloan Kettering Cancer Center, New York, who found that nearly two-thirds of patients followed with nonoperative management (NOM) had durable complete clinical remissions (cCR) for at least 4 years.
Disease-specific survival and overall survival rates among patients who had nonoperative management were similar to those seen in patients with pathologic complete responses (pCR), defined as no viable tumor cells in the resected specimen.

“We know that there is a very good overall and disease-free survival associated with a [pCR]. Clinical complete response is also associated with pathologic complete response. In that regard, this brings up the question: Is an operation always necessary in these patients?” Dr. Jesse Joshua Smith of the cancer center said at the annual Society of Surgical Oncology Cancer Symposium.
Dr. Smith and colleagues conducted a review of their center’s experience to date with NOM for patients with locally advanced rectal cancer, asking whether the data support the approach as oncologically safe and effective for organ preservation.
They identified 442 patients with rectal cancer treated with neoadjuvant chemotherapy from 2006 through 2014 and compared results for 73 who achieved a cCR and were followed with nonoperative management with those of 72 patients who had a pCR following total mesorectal excision.
Demographic and clinical characteristics between the groups were generally similar, although patients in the pCR group were significantly younger (58 years vs. 65 years, P = .01), had a greater tumor distance from the anal verge (median of 6 cm vs. 5.25 cm, P = .02), and higher proportions of clinical stage II (32% vs. 24%) and III (66% vs. 62%, P = .02).
Among the 73 patients managed with NOM, 54 had durable cCR at 4 years. Of the remaining 19 with local tumor regrowth, 2 had local excisions with no further recurrence and 17 went on to have rectal resections. The total number of patients with rectal preservation in this group was 56 (77%).
Of the 19 patients in the conservatively managed group who had local regrowths, all but three of the recurrences were detected within 13 months.
As noted before, neither disease-specific survival nor overall survival were significantly different between patients managed with NOM or with total mesorectal excision.
There were numerically more distant recurrences at both 1 and 4 years among patients treated with NOM compared with total mesorectal excision (7% vs. 2%, and 17% vs. 9%, respectively), but the differences were not statistically significant, the authors found.
Dr. Smith noted that patients who are offered the option of NOM have a discussion with the surgeon emphasizing that the practice is nonstandard management, carries about a 25% risk of local regrowth, and requires increased endoscopic and radiographic surveillance. Patients also are informed about the risks of salvage abdominoperineal resection or extended resections, and about the potential risk of compromising cure.
The study was supported in part by the Berezuk Colorectal Cancer Fund. Dr. Smith reported having no disclosures.
HOUSTON – Patients who achieve complete clinical responses after neoadjuvant therapy for locally advanced rectal cancer may, in many cases, be safely spared the trauma and morbidity of total mesorectal excision.
That’s the opinion of investigators at Memorial Sloan Kettering Cancer Center, New York, who found that nearly two-thirds of patients followed with nonoperative management (NOM) had durable complete clinical remissions (cCR) for at least 4 years.
Disease-specific survival and overall survival rates among patients who had nonoperative management were similar to those seen in patients with pathologic complete responses (pCR), defined as no viable tumor cells in the resected specimen.
“We know that there is a very good overall and disease-free survival associated with a [pCR]. Clinical complete response is also associated with pathologic complete response. In that regard, this brings up the question: Is an operation always necessary in these patients?” Dr. Jesse Joshua Smith of the cancer center said at the annual Society of Surgical Oncology Cancer Symposium.
Dr. Smith and colleagues conducted a review of their center’s experience to date with NOM for patients with locally advanced rectal cancer, asking whether the data support the approach as oncologically safe and effective for organ preservation.
They identified 442 patients with rectal cancer treated with neoadjuvant chemotherapy from 2006 through 2014 and compared results for 73 who achieved a cCR and were followed with nonoperative management with those of 72 patients who had a pCR following total mesorectal excision.
Demographic and clinical characteristics between the groups were generally similar, although patients in the pCR group were significantly younger (58 years vs. 65 years, P = .01), had a greater tumor distance from the anal verge (median of 6 cm vs. 5.25 cm, P = .02), and higher proportions of clinical stage II (32% vs. 24%) and III (66% vs. 62%, P = .02).
Among the 73 patients managed with NOM, 54 had durable cCR at 4 years. Of the remaining 19 with local tumor regrowth, 2 had local excisions with no further recurrence and 17 went on to have rectal resections. The total number of patients with rectal preservation in this group was 56 (77%).
Of the 19 patients in the conservatively managed group who had local regrowths, all but three of the recurrences were detected within 13 months.
As noted before, neither disease-specific survival nor overall survival were significantly different between patients managed with NOM or with total mesorectal excision.
There were numerically more distant recurrences at both 1 and 4 years among patients treated with NOM compared with total mesorectal excision (7% vs. 2%, and 17% vs. 9%, respectively), but the differences were not statistically significant, the authors found.
Dr. Smith noted that patients who are offered the option of NOM have a discussion with the surgeon emphasizing that the practice is nonstandard management, carries about a 25% risk of local regrowth, and requires increased endoscopic and radiographic surveillance. Patients also are informed about the risks of salvage abdominoperineal resection or extended resections, and about the potential risk of compromising cure.
The study was supported in part by the Berezuk Colorectal Cancer Fund. Dr. Smith reported having no disclosures.
HOUSTON – Patients who achieve complete clinical responses after neoadjuvant therapy for locally advanced rectal cancer may, in many cases, be safely spared the trauma and morbidity of total mesorectal excision.
That’s the opinion of investigators at Memorial Sloan Kettering Cancer Center, New York, who found that nearly two-thirds of patients followed with nonoperative management (NOM) had durable complete clinical remissions (cCR) for at least 4 years.
Disease-specific survival and overall survival rates among patients who had nonoperative management were similar to those seen in patients with pathologic complete responses (pCR), defined as no viable tumor cells in the resected specimen.
“We know that there is a very good overall and disease-free survival associated with a [pCR]. Clinical complete response is also associated with pathologic complete response. In that regard, this brings up the question: Is an operation always necessary in these patients?” Dr. Jesse Joshua Smith of the cancer center said at the annual Society of Surgical Oncology Cancer Symposium.
Dr. Smith and colleagues conducted a review of their center’s experience to date with NOM for patients with locally advanced rectal cancer, asking whether the data support the approach as oncologically safe and effective for organ preservation.
They identified 442 patients with rectal cancer treated with neoadjuvant chemotherapy from 2006 through 2014 and compared results for 73 who achieved a cCR and were followed with nonoperative management with those of 72 patients who had a pCR following total mesorectal excision.
Demographic and clinical characteristics between the groups were generally similar, although patients in the pCR group were significantly younger (58 years vs. 65 years, P = .01), had a greater tumor distance from the anal verge (median of 6 cm vs. 5.25 cm, P = .02), and higher proportions of clinical stage II (32% vs. 24%) and III (66% vs. 62%, P = .02).
Among the 73 patients managed with NOM, 54 had durable cCR at 4 years. Of the remaining 19 with local tumor regrowth, 2 had local excisions with no further recurrence and 17 went on to have rectal resections. The total number of patients with rectal preservation in this group was 56 (77%).
Of the 19 patients in the conservatively managed group who had local regrowths, all but three of the recurrences were detected within 13 months.
As noted before, neither disease-specific survival nor overall survival were significantly different between patients managed with NOM or with total mesorectal excision.
There were numerically more distant recurrences at both 1 and 4 years among patients treated with NOM compared with total mesorectal excision (7% vs. 2%, and 17% vs. 9%, respectively), but the differences were not statistically significant, the authors found.
Dr. Smith noted that patients who are offered the option of NOM have a discussion with the surgeon emphasizing that the practice is nonstandard management, carries about a 25% risk of local regrowth, and requires increased endoscopic and radiographic surveillance. Patients also are informed about the risks of salvage abdominoperineal resection or extended resections, and about the potential risk of compromising cure.
The study was supported in part by the Berezuk Colorectal Cancer Fund. Dr. Smith reported having no disclosures.
Key clinical point: Patients with complete clinical response after neoadjuvant chemotherapy for rectal cancer may be able to be safely followed with nonoperative management.
Major finding: There were no significant differences at 4 years in either disease-specific or overall survival among patients with rectal cancer managed conservatively or with total mesorectal excision.
Data source: Review of prospectively collected data on 145 patients with locally advanced rectal cancer.
Disclosures: The study was supported in part by the Berezuk Colorectal Cancer Fund. Dr. Smith reported having no disclosures.

Neoadjuvant therapy facilitates breast conservation
HOUSTON – For some women with breast cancer, neoadjuvant therapy can increase the likelihood of breast-conserving treatment and may limit the extent of axillary dissection, a breast cancer researcher says.
“Neoadjuvant chemotherapy has long been used in the management of inflammatory breast cancer, in patients with locally advanced, or inoperable disease, and it’s increasingly being used in patients who have operable breast cancer,” said Dr. Elizabeth A. Mittendorf of the University of Texas MD Anderson Cancer Center, Houston.

A meta-analysis published in 2007 suggested that neoadjuvant therapy in patients with operable breast cancer reduced the mastectomy rate by 17%, a figure that Dr. Mittendorf said likely underestimates the benefit, because many of the trials included in the analysis did not require patients to be considered for breast conservation at presentation.
The meta-analysis also showed that local recurrence rates did not differ from those seen with mastectomy when patients treated with neoadjuvant therapy were downstaged to breast-conserving therapy, and that there were no differences in local recurrence rates for neoadjuvant vs. adjuvant chemotherapy stratified by type of surgery, Dr. Mittendorf said at the annual Society of Surgical Oncology Cancer Symposium.
Key clinical trials, including the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-18 and B-27 trials, showed that neoadjuvant chemotherapy did not have an effect on either disease-free or overall survival compared with adjuvant chemotherapy, Dr. Mittendorf noted.
Response to neoadjuvant chemotherapy is also a good predictor of prognosis, she said, pointing to a pooled analysis of 12 studies published in 2014 in The Lancet. The authors of the analysis reported that patients with a pathologic complete response (pCR; no invasive disease in either the breast or axilla) after neoadjuvant chemotherapy had significantly improved survival, with the greatest prognostic values seen in patients with aggressive tumor subtypes.
Factors to consider when selecting neoadjuvant chemotherapy include:
• Tumor size.
• Lymph node status.
• Estrogen, progesterone, and/or HER2 status.
• Treatment sensitivity (as measured by Ki-67 or other markers).
• Pathologic complete response rates.
Chemo for HR-positive?
“With respect to hormone receptor–positive breast cancer, I think the most important question for these patients is do they even need chemotherapy?” Dr. Mittendorf said.
Hormone receptor–positive (HR-positive) breast cancers have been shown to be less responsive to neoadjuvant chemotherapy, and pCR is less prognostic of outcome in this tumor subtype. Older patients with HR-positive cancers who are borderline candidates for breast-conserving therapy might benefit from neoadjuvant therapy with an aromatase inhibitor, she noted.
HER2-positive disease
For patients with HER2-positive breast cancers, it may be possible to tailor neoadjuvant therapy, so that patients who achieve a pCR with neoadjuvant trastuzumab (Herceptin) might be spared an additional 6 months of adjuvant therapy. Dr. Mittendorf’s group published a recent study
Combination anti-HER2 therapies (trastuzumab and pertuzumab [Perjeta] as used in the NeoSphere Trial may help to improve pCR rates and outcomes in patients with HER2-positive tumors, Dr. Mittendorf said.
Triple negative disease
Among patients with triple-negative breast cancer (tumors lacking hormonal receptors and HER2), those who have residual cancer after neoadjuvant chemotherapy have a poor prognosis. At MD Anderson, patients with localized triple-negative breast cancer who are scheduled to receive neoadjuvant chemotherapy first have a biopsy with molecular profiling, and are immediately started on an anthracycline-based regimen.
Patients who have a response to the chemotherapy proceed to receive a taxane, while nonresponders will be triaged onto phase II studies based on the subtype of triple-negative breast cancer. Patients who are positive for BRCA mutations will be started on a carboplatin/paclitaxel regimen, while those with mesenchymal tumor subtypes will be started on a phosphoinositide 3-kinase (PI3K) inhibitor, and those with basal-like tumors will be started on an immunotherapy protocol.Better understanding of the biology of different tumor subtypes may also help to reduce the extent of axillary surgery, by helping clinicians to identify those patients who are likely to have a nodal pCR, Dr. Mittendorf said.
HOUSTON – For some women with breast cancer, neoadjuvant therapy can increase the likelihood of breast-conserving treatment and may limit the extent of axillary dissection, a breast cancer researcher says.
“Neoadjuvant chemotherapy has long been used in the management of inflammatory breast cancer, in patients with locally advanced, or inoperable disease, and it’s increasingly being used in patients who have operable breast cancer,” said Dr. Elizabeth A. Mittendorf of the University of Texas MD Anderson Cancer Center, Houston.
A meta-analysis published in 2007 suggested that neoadjuvant therapy in patients with operable breast cancer reduced the mastectomy rate by 17%, a figure that Dr. Mittendorf said likely underestimates the benefit, because many of the trials included in the analysis did not require patients to be considered for breast conservation at presentation.
The meta-analysis also showed that local recurrence rates did not differ from those seen with mastectomy when patients treated with neoadjuvant therapy were downstaged to breast-conserving therapy, and that there were no differences in local recurrence rates for neoadjuvant vs. adjuvant chemotherapy stratified by type of surgery, Dr. Mittendorf said at the annual Society of Surgical Oncology Cancer Symposium.
Key clinical trials, including the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-18 and B-27 trials, showed that neoadjuvant chemotherapy did not have an effect on either disease-free or overall survival compared with adjuvant chemotherapy, Dr. Mittendorf noted.
Response to neoadjuvant chemotherapy is also a good predictor of prognosis, she said, pointing to a pooled analysis of 12 studies published in 2014 in The Lancet. The authors of the analysis reported that patients with a pathologic complete response (pCR; no invasive disease in either the breast or axilla) after neoadjuvant chemotherapy had significantly improved survival, with the greatest prognostic values seen in patients with aggressive tumor subtypes.
Factors to consider when selecting neoadjuvant chemotherapy include:
• Tumor size.
• Lymph node status.
• Estrogen, progesterone, and/or HER2 status.
• Treatment sensitivity (as measured by Ki-67 or other markers).
• Pathologic complete response rates.
Chemo for HR-positive?
“With respect to hormone receptor–positive breast cancer, I think the most important question for these patients is do they even need chemotherapy?” Dr. Mittendorf said.
Hormone receptor–positive (HR-positive) breast cancers have been shown to be less responsive to neoadjuvant chemotherapy, and pCR is less prognostic of outcome in this tumor subtype. Older patients with HR-positive cancers who are borderline candidates for breast-conserving therapy might benefit from neoadjuvant therapy with an aromatase inhibitor, she noted.
HER2-positive disease
For patients with HER2-positive breast cancers, it may be possible to tailor neoadjuvant therapy, so that patients who achieve a pCR with neoadjuvant trastuzumab (Herceptin) might be spared an additional 6 months of adjuvant therapy. Dr. Mittendorf’s group published a recent study
Combination anti-HER2 therapies (trastuzumab and pertuzumab [Perjeta] as used in the NeoSphere Trial may help to improve pCR rates and outcomes in patients with HER2-positive tumors, Dr. Mittendorf said.
Triple negative disease
Among patients with triple-negative breast cancer (tumors lacking hormonal receptors and HER2), those who have residual cancer after neoadjuvant chemotherapy have a poor prognosis. At MD Anderson, patients with localized triple-negative breast cancer who are scheduled to receive neoadjuvant chemotherapy first have a biopsy with molecular profiling, and are immediately started on an anthracycline-based regimen.
Patients who have a response to the chemotherapy proceed to receive a taxane, while nonresponders will be triaged onto phase II studies based on the subtype of triple-negative breast cancer. Patients who are positive for BRCA mutations will be started on a carboplatin/paclitaxel regimen, while those with mesenchymal tumor subtypes will be started on a phosphoinositide 3-kinase (PI3K) inhibitor, and those with basal-like tumors will be started on an immunotherapy protocol.Better understanding of the biology of different tumor subtypes may also help to reduce the extent of axillary surgery, by helping clinicians to identify those patients who are likely to have a nodal pCR, Dr. Mittendorf said.
HOUSTON – For some women with breast cancer, neoadjuvant therapy can increase the likelihood of breast-conserving treatment and may limit the extent of axillary dissection, a breast cancer researcher says.
“Neoadjuvant chemotherapy has long been used in the management of inflammatory breast cancer, in patients with locally advanced, or inoperable disease, and it’s increasingly being used in patients who have operable breast cancer,” said Dr. Elizabeth A. Mittendorf of the University of Texas MD Anderson Cancer Center, Houston.
A meta-analysis published in 2007 suggested that neoadjuvant therapy in patients with operable breast cancer reduced the mastectomy rate by 17%, a figure that Dr. Mittendorf said likely underestimates the benefit, because many of the trials included in the analysis did not require patients to be considered for breast conservation at presentation.
The meta-analysis also showed that local recurrence rates did not differ from those seen with mastectomy when patients treated with neoadjuvant therapy were downstaged to breast-conserving therapy, and that there were no differences in local recurrence rates for neoadjuvant vs. adjuvant chemotherapy stratified by type of surgery, Dr. Mittendorf said at the annual Society of Surgical Oncology Cancer Symposium.
Key clinical trials, including the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-18 and B-27 trials, showed that neoadjuvant chemotherapy did not have an effect on either disease-free or overall survival compared with adjuvant chemotherapy, Dr. Mittendorf noted.
Response to neoadjuvant chemotherapy is also a good predictor of prognosis, she said, pointing to a pooled analysis of 12 studies published in 2014 in The Lancet. The authors of the analysis reported that patients with a pathologic complete response (pCR; no invasive disease in either the breast or axilla) after neoadjuvant chemotherapy had significantly improved survival, with the greatest prognostic values seen in patients with aggressive tumor subtypes.
Factors to consider when selecting neoadjuvant chemotherapy include:
• Tumor size.
• Lymph node status.
• Estrogen, progesterone, and/or HER2 status.
• Treatment sensitivity (as measured by Ki-67 or other markers).
• Pathologic complete response rates.
Chemo for HR-positive?
“With respect to hormone receptor–positive breast cancer, I think the most important question for these patients is do they even need chemotherapy?” Dr. Mittendorf said.
Hormone receptor–positive (HR-positive) breast cancers have been shown to be less responsive to neoadjuvant chemotherapy, and pCR is less prognostic of outcome in this tumor subtype. Older patients with HR-positive cancers who are borderline candidates for breast-conserving therapy might benefit from neoadjuvant therapy with an aromatase inhibitor, she noted.
HER2-positive disease
For patients with HER2-positive breast cancers, it may be possible to tailor neoadjuvant therapy, so that patients who achieve a pCR with neoadjuvant trastuzumab (Herceptin) might be spared an additional 6 months of adjuvant therapy. Dr. Mittendorf’s group published a recent study
Combination anti-HER2 therapies (trastuzumab and pertuzumab [Perjeta] as used in the NeoSphere Trial may help to improve pCR rates and outcomes in patients with HER2-positive tumors, Dr. Mittendorf said.
Triple negative disease
Among patients with triple-negative breast cancer (tumors lacking hormonal receptors and HER2), those who have residual cancer after neoadjuvant chemotherapy have a poor prognosis. At MD Anderson, patients with localized triple-negative breast cancer who are scheduled to receive neoadjuvant chemotherapy first have a biopsy with molecular profiling, and are immediately started on an anthracycline-based regimen.
Patients who have a response to the chemotherapy proceed to receive a taxane, while nonresponders will be triaged onto phase II studies based on the subtype of triple-negative breast cancer. Patients who are positive for BRCA mutations will be started on a carboplatin/paclitaxel regimen, while those with mesenchymal tumor subtypes will be started on a phosphoinositide 3-kinase (PI3K) inhibitor, and those with basal-like tumors will be started on an immunotherapy protocol.Better understanding of the biology of different tumor subtypes may also help to reduce the extent of axillary surgery, by helping clinicians to identify those patients who are likely to have a nodal pCR, Dr. Mittendorf said.

New melanoma therapies may break the bank
HOUSTON – Newer systemic therapies for metastatic malignant melanoma have resulted in significant gains in survival, but at a cost that may be unsustainable in the near future, according to Dr. Jeffrey E. Gershenwald.
Up to one-half of all expenses related to the treatment of malignant melanoma are accounted for by the care of patients with advanced disease, yet patients with distant metastases (stage IV disease) account for only about 2% of all patients, said Dr. Gershenwald, professor of surgical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.

“How best can we achieve the right therapy for the right patient at the right time, and as we learn more and more about some of the therapies, particularly in melanoma, for the right length of time? We can’t really afford to give treatments in perpetuity, so we need to know how long they actually need to be delivered in order to have optimal value for the patient,” he said at the annual Society of Surgical Oncology Cancer Symposium.
Over the last 3 decades, and particularly over the last 5 years, there have been tremendous forward strides in therapy. In 1975, when dacarbazine became the standard of care for metastatic melanoma, it was associated with response rates of only about 6%-15%, durable responses in only 5%-15% of patients, and a median overall survival of about 6-9 months, Dr. Gershenwald reported.
Treatment toxicities, but not response rates, increased with the introduction of interleukin-2 in 1998, which for want of a better drug became the new preferred treatment.
But with the introduction of new systemic therapies, such as immune checkpoint inhibitors (ipilimumab [Yervoy], nivolumab [Opdivo], and pembrolizumab [Keytruda]) and targeted agents (vemurafenib [Zelboraf], dabrafenib [Tafinlar], and trametinib [Mekinist]), response rates have soared, resulting in an improvement in 1-year survival rates from about 30% to 35% in 1970 to as high as 80% in clinical trials in 2014.
Increased survival, higher costs
Dr. Gershenwald pointed to a recently published cost-effectiveness analysis of treatment strategies for BRAF-mutated metastatic melanoma. In it, the authors noted that vemurafenib costs $13,000 per month, translating into $207,000 for a patient with median survival. Patients for whom vemurafenib fails are often put on ipilimumab, at $150,000 per course.
The authors calculated that the incremental cost-effectiveness ratio (ICER) for vemurafenib compared with dacarbazine was nearly $354,993 per quality-adjusted life-year (QALY) gained, a figure that is more than threefold higher than widely accepted thresholds for cost-effective treatment ($50,000-$100,000 per QALY gained).
The ICER for firstline vemurafenib followed by ipilimumab was $158,139, still well above the accepted limits.
The authors of the cost analysis noted that the treatments could become cost effective if drug prices were to drop significantly, or if clinical trials could establish whether it was possible to achieve a durable response without continued therapy.
Going forward, clinicians will need to consider disease burden, including both the extent and growth rate of the disease, as well as the risk of recurrence, in deciding whether to use adjuvant therapies, Dr. Gershenwald said.
In addition, clinical choices will be based on disease biology, predictors of response (although few such predictors currently exist), the likelihood of resistance, and drug toxicities, quality of life, and ease of administration, he said.
Dr. Gershenwald disclosed serving on a Merck advisory board.
HOUSTON – Newer systemic therapies for metastatic malignant melanoma have resulted in significant gains in survival, but at a cost that may be unsustainable in the near future, according to Dr. Jeffrey E. Gershenwald.
Up to one-half of all expenses related to the treatment of malignant melanoma are accounted for by the care of patients with advanced disease, yet patients with distant metastases (stage IV disease) account for only about 2% of all patients, said Dr. Gershenwald, professor of surgical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.
“How best can we achieve the right therapy for the right patient at the right time, and as we learn more and more about some of the therapies, particularly in melanoma, for the right length of time? We can’t really afford to give treatments in perpetuity, so we need to know how long they actually need to be delivered in order to have optimal value for the patient,” he said at the annual Society of Surgical Oncology Cancer Symposium.
Over the last 3 decades, and particularly over the last 5 years, there have been tremendous forward strides in therapy. In 1975, when dacarbazine became the standard of care for metastatic melanoma, it was associated with response rates of only about 6%-15%, durable responses in only 5%-15% of patients, and a median overall survival of about 6-9 months, Dr. Gershenwald reported.
Treatment toxicities, but not response rates, increased with the introduction of interleukin-2 in 1998, which for want of a better drug became the new preferred treatment.
But with the introduction of new systemic therapies, such as immune checkpoint inhibitors (ipilimumab [Yervoy], nivolumab [Opdivo], and pembrolizumab [Keytruda]) and targeted agents (vemurafenib [Zelboraf], dabrafenib [Tafinlar], and trametinib [Mekinist]), response rates have soared, resulting in an improvement in 1-year survival rates from about 30% to 35% in 1970 to as high as 80% in clinical trials in 2014.
Increased survival, higher costs
Dr. Gershenwald pointed to a recently published cost-effectiveness analysis of treatment strategies for BRAF-mutated metastatic melanoma. In it, the authors noted that vemurafenib costs $13,000 per month, translating into $207,000 for a patient with median survival. Patients for whom vemurafenib fails are often put on ipilimumab, at $150,000 per course.
The authors calculated that the incremental cost-effectiveness ratio (ICER) for vemurafenib compared with dacarbazine was nearly $354,993 per quality-adjusted life-year (QALY) gained, a figure that is more than threefold higher than widely accepted thresholds for cost-effective treatment ($50,000-$100,000 per QALY gained).
The ICER for firstline vemurafenib followed by ipilimumab was $158,139, still well above the accepted limits.
The authors of the cost analysis noted that the treatments could become cost effective if drug prices were to drop significantly, or if clinical trials could establish whether it was possible to achieve a durable response without continued therapy.
Going forward, clinicians will need to consider disease burden, including both the extent and growth rate of the disease, as well as the risk of recurrence, in deciding whether to use adjuvant therapies, Dr. Gershenwald said.
In addition, clinical choices will be based on disease biology, predictors of response (although few such predictors currently exist), the likelihood of resistance, and drug toxicities, quality of life, and ease of administration, he said.
Dr. Gershenwald disclosed serving on a Merck advisory board.
HOUSTON – Newer systemic therapies for metastatic malignant melanoma have resulted in significant gains in survival, but at a cost that may be unsustainable in the near future, according to Dr. Jeffrey E. Gershenwald.
Up to one-half of all expenses related to the treatment of malignant melanoma are accounted for by the care of patients with advanced disease, yet patients with distant metastases (stage IV disease) account for only about 2% of all patients, said Dr. Gershenwald, professor of surgical oncology at the University of Texas M.D. Anderson Cancer Center, Houston.
“How best can we achieve the right therapy for the right patient at the right time, and as we learn more and more about some of the therapies, particularly in melanoma, for the right length of time? We can’t really afford to give treatments in perpetuity, so we need to know how long they actually need to be delivered in order to have optimal value for the patient,” he said at the annual Society of Surgical Oncology Cancer Symposium.
Over the last 3 decades, and particularly over the last 5 years, there have been tremendous forward strides in therapy. In 1975, when dacarbazine became the standard of care for metastatic melanoma, it was associated with response rates of only about 6%-15%, durable responses in only 5%-15% of patients, and a median overall survival of about 6-9 months, Dr. Gershenwald reported.
Treatment toxicities, but not response rates, increased with the introduction of interleukin-2 in 1998, which for want of a better drug became the new preferred treatment.
But with the introduction of new systemic therapies, such as immune checkpoint inhibitors (ipilimumab [Yervoy], nivolumab [Opdivo], and pembrolizumab [Keytruda]) and targeted agents (vemurafenib [Zelboraf], dabrafenib [Tafinlar], and trametinib [Mekinist]), response rates have soared, resulting in an improvement in 1-year survival rates from about 30% to 35% in 1970 to as high as 80% in clinical trials in 2014.
Increased survival, higher costs
Dr. Gershenwald pointed to a recently published cost-effectiveness analysis of treatment strategies for BRAF-mutated metastatic melanoma. In it, the authors noted that vemurafenib costs $13,000 per month, translating into $207,000 for a patient with median survival. Patients for whom vemurafenib fails are often put on ipilimumab, at $150,000 per course.
The authors calculated that the incremental cost-effectiveness ratio (ICER) for vemurafenib compared with dacarbazine was nearly $354,993 per quality-adjusted life-year (QALY) gained, a figure that is more than threefold higher than widely accepted thresholds for cost-effective treatment ($50,000-$100,000 per QALY gained).
The ICER for firstline vemurafenib followed by ipilimumab was $158,139, still well above the accepted limits.
The authors of the cost analysis noted that the treatments could become cost effective if drug prices were to drop significantly, or if clinical trials could establish whether it was possible to achieve a durable response without continued therapy.
Going forward, clinicians will need to consider disease burden, including both the extent and growth rate of the disease, as well as the risk of recurrence, in deciding whether to use adjuvant therapies, Dr. Gershenwald said.
In addition, clinical choices will be based on disease biology, predictors of response (although few such predictors currently exist), the likelihood of resistance, and drug toxicities, quality of life, and ease of administration, he said.
Dr. Gershenwald disclosed serving on a Merck advisory board.
AT SSO 2015
Key clinical point: Immunotherapies and targeted agents for metastatic melanoma are effective but very costly.
Major finding: The incremental cost-effectiveness ratio for vemurafenib, compared with dacarbazine, was nearly $354,993 per quality-adjusted life-year gained.
Data source: A review of data on the efficacy and costs of therapy for metastatic malignant melanoma.
Disclosures: Dr. Gershenwald disclosed serving on a Merck advisory board.

Clinical doc improvement ups income, quality
HOUSTON – Results of a pilot program suggest that a surgeon-led Clinical Documentation Improvement (CDI) program can improve the accuracy of diagnostic coding, validate the quality of care delivered, and help ensure that hospitals are fairly compensated for the complexity of care they provide.
A comparison of outcomes of cases from four surgical oncologists from the periods before and after implementation of a CDI suggested that the actual case mix index (CMI) was 9% higher than the original charts indicated, a change that would translate into a more than $700,000 increase in reimbursement, said Dr. Keith Gray from the University of Tennessee Medical Center in Knoxville.

“CDI is low-hanging fruit in the era of pay for quality and dwindling hospital margins. Physicians and hospitals can benefit, and surgical oncologists are the natural physicians in the hospital to lead this process, “ Dr. Gray said at the Society of Surgical Oncology 2015 Cancer Symposium.
CDI programs are collaborative efforts between clinicians and health information management professionals, designed to document the quality of care the institution delivers through improved diagnostic coding, he explained.
The benefits of CDI include more accurate reflection of the severity of illness of patients, better sharing of data among caregivers, optimizing of claims processing, and a stronger bottom line.
“We all think we have the sickest patients in the country, and that’s why our results don’t match up. Clinical documentation is an opportunity for you to prove that,” he said.
In the study, a physician extender trained in CDI audited and update all inpatient diagnoses made by four surgical oncologists in a hospital-based practice from November 2012 through May 2013. The diagnoses were listed as being present on admission or recorded during the inpatient stay.
The investigators looked at data on the CMI, average mortality risk, and average severity of illness for 489 patients treated during the study period. These data were compared with a control set from 482 patients treated from March 2011 through October 2012, the period immediately prior to the implementation of the CDI.
The authors found that with the clinical documentation program in place, the CMI, risk of mortality estimates, and severity of illness index all increased.
The practice’s mean CMI, for example, increased from 2.38 to 2.59 (P < .001), a 9% relative increase. Dr. Gray noted that every 0.1 change in CMI represents a $700/patient difference in reimbursement. Therefore, the change would translate into a $718,830 relative increase in reimbursement.
Similarly, the severity of illness index, based on patient comorbidities, age, procedures, and principal diagnosis also increased, from a mean of 2.32 for controls to 2.54 during the study period, translating into a 9.5% increase (P < .001).
Risk of mortality estimates – the likelihood of in-hospital death based on comorbidities, age, procedures, and principal diagnosis – also increased, from a mean 1.88 to 2.07, a 10% increase (P < .001).
Although the CMI, risk of mortality, and severity of illness all increased during the study period, compared with the control period, the percentage of cases above the average length of stay, a measure of quality care, declined significantly, from 45.6% pre-CDI to 31.1% after CDI was implemented (P = .0001). Other measures of quality such as the observed to expected mortality ratio, length of stay ratio, and percentage of cases above the average cost also improved, but the changes were not statistically significant.
“CDI is relatively easy to implement with the resources that we have in place, and there’s minimal additional training to become efficient in this process,” Dr. Gray said.
The study was internally funded. Dr. Gray did not report potential conflicts of interest.
HOUSTON – Results of a pilot program suggest that a surgeon-led Clinical Documentation Improvement (CDI) program can improve the accuracy of diagnostic coding, validate the quality of care delivered, and help ensure that hospitals are fairly compensated for the complexity of care they provide.
A comparison of outcomes of cases from four surgical oncologists from the periods before and after implementation of a CDI suggested that the actual case mix index (CMI) was 9% higher than the original charts indicated, a change that would translate into a more than $700,000 increase in reimbursement, said Dr. Keith Gray from the University of Tennessee Medical Center in Knoxville.
“CDI is low-hanging fruit in the era of pay for quality and dwindling hospital margins. Physicians and hospitals can benefit, and surgical oncologists are the natural physicians in the hospital to lead this process, “ Dr. Gray said at the Society of Surgical Oncology 2015 Cancer Symposium.
CDI programs are collaborative efforts between clinicians and health information management professionals, designed to document the quality of care the institution delivers through improved diagnostic coding, he explained.
The benefits of CDI include more accurate reflection of the severity of illness of patients, better sharing of data among caregivers, optimizing of claims processing, and a stronger bottom line.
“We all think we have the sickest patients in the country, and that’s why our results don’t match up. Clinical documentation is an opportunity for you to prove that,” he said.
In the study, a physician extender trained in CDI audited and update all inpatient diagnoses made by four surgical oncologists in a hospital-based practice from November 2012 through May 2013. The diagnoses were listed as being present on admission or recorded during the inpatient stay.
The investigators looked at data on the CMI, average mortality risk, and average severity of illness for 489 patients treated during the study period. These data were compared with a control set from 482 patients treated from March 2011 through October 2012, the period immediately prior to the implementation of the CDI.
The authors found that with the clinical documentation program in place, the CMI, risk of mortality estimates, and severity of illness index all increased.
The practice’s mean CMI, for example, increased from 2.38 to 2.59 (P < .001), a 9% relative increase. Dr. Gray noted that every 0.1 change in CMI represents a $700/patient difference in reimbursement. Therefore, the change would translate into a $718,830 relative increase in reimbursement.
Similarly, the severity of illness index, based on patient comorbidities, age, procedures, and principal diagnosis also increased, from a mean of 2.32 for controls to 2.54 during the study period, translating into a 9.5% increase (P < .001).
Risk of mortality estimates – the likelihood of in-hospital death based on comorbidities, age, procedures, and principal diagnosis – also increased, from a mean 1.88 to 2.07, a 10% increase (P < .001).
Although the CMI, risk of mortality, and severity of illness all increased during the study period, compared with the control period, the percentage of cases above the average length of stay, a measure of quality care, declined significantly, from 45.6% pre-CDI to 31.1% after CDI was implemented (P = .0001). Other measures of quality such as the observed to expected mortality ratio, length of stay ratio, and percentage of cases above the average cost also improved, but the changes were not statistically significant.
“CDI is relatively easy to implement with the resources that we have in place, and there’s minimal additional training to become efficient in this process,” Dr. Gray said.
The study was internally funded. Dr. Gray did not report potential conflicts of interest.
HOUSTON – Results of a pilot program suggest that a surgeon-led Clinical Documentation Improvement (CDI) program can improve the accuracy of diagnostic coding, validate the quality of care delivered, and help ensure that hospitals are fairly compensated for the complexity of care they provide.
A comparison of outcomes of cases from four surgical oncologists from the periods before and after implementation of a CDI suggested that the actual case mix index (CMI) was 9% higher than the original charts indicated, a change that would translate into a more than $700,000 increase in reimbursement, said Dr. Keith Gray from the University of Tennessee Medical Center in Knoxville.
“CDI is low-hanging fruit in the era of pay for quality and dwindling hospital margins. Physicians and hospitals can benefit, and surgical oncologists are the natural physicians in the hospital to lead this process, “ Dr. Gray said at the Society of Surgical Oncology 2015 Cancer Symposium.
CDI programs are collaborative efforts between clinicians and health information management professionals, designed to document the quality of care the institution delivers through improved diagnostic coding, he explained.
The benefits of CDI include more accurate reflection of the severity of illness of patients, better sharing of data among caregivers, optimizing of claims processing, and a stronger bottom line.
“We all think we have the sickest patients in the country, and that’s why our results don’t match up. Clinical documentation is an opportunity for you to prove that,” he said.
In the study, a physician extender trained in CDI audited and update all inpatient diagnoses made by four surgical oncologists in a hospital-based practice from November 2012 through May 2013. The diagnoses were listed as being present on admission or recorded during the inpatient stay.
The investigators looked at data on the CMI, average mortality risk, and average severity of illness for 489 patients treated during the study period. These data were compared with a control set from 482 patients treated from March 2011 through October 2012, the period immediately prior to the implementation of the CDI.
The authors found that with the clinical documentation program in place, the CMI, risk of mortality estimates, and severity of illness index all increased.
The practice’s mean CMI, for example, increased from 2.38 to 2.59 (P < .001), a 9% relative increase. Dr. Gray noted that every 0.1 change in CMI represents a $700/patient difference in reimbursement. Therefore, the change would translate into a $718,830 relative increase in reimbursement.
Similarly, the severity of illness index, based on patient comorbidities, age, procedures, and principal diagnosis also increased, from a mean of 2.32 for controls to 2.54 during the study period, translating into a 9.5% increase (P < .001).
Risk of mortality estimates – the likelihood of in-hospital death based on comorbidities, age, procedures, and principal diagnosis – also increased, from a mean 1.88 to 2.07, a 10% increase (P < .001).
Although the CMI, risk of mortality, and severity of illness all increased during the study period, compared with the control period, the percentage of cases above the average length of stay, a measure of quality care, declined significantly, from 45.6% pre-CDI to 31.1% after CDI was implemented (P = .0001). Other measures of quality such as the observed to expected mortality ratio, length of stay ratio, and percentage of cases above the average cost also improved, but the changes were not statistically significant.
“CDI is relatively easy to implement with the resources that we have in place, and there’s minimal additional training to become efficient in this process,” Dr. Gray said.
The study was internally funded. Dr. Gray did not report potential conflicts of interest.
AT SSO 2015
Key clinical point: A surgeon-led clinical documentation program can increase revenue by demonstrating case-mix severity.
Major finding: An audit of previous cases showed that proper documentation would yield $718,830 in additional reimbursements.
Data source: Pilot program and retrospective case audit involving cases of 489 patients and 482 controls.
Disclosures: The study was internally funded. Dr. Gray did not report potential conflicts of interest.

Risk scale predicts mortality after gastric cancer surgery
HOUSTON – A simple preoperative scale can accurately predict a patient’s risk for near-term death following surgery for gastric cancer, investigators say.
The scale accounts for both patient and hospital factors, and is useful as a clinical tool for preoperative counseling of patients, reported Dr. Cristina Harnsberger of the University of California San Diego.

“Male gender, increasing age, and comorbid disease increase risk of in-hospital mortality for patients who undergo gastric resection for malignancy. Additionally, low hospital volume was an independent risk factor,” she said at the annual Society of Surgical Oncology Cancer Symposium.
The scale was able to accurately classify patients as being at low or high risk, and the observed and expected mortality rates for each risk score were well correlated, she said.
Weighing risks
Perioperative mortality rates following resection for gastric malignancies range from 0.6% to 15%. Risk scales and nomograms are intended to help clinicians predict risks for individual patients, but most incorporate postoperative data rather than preoperative or hospital data, Dr. Harnsberger said.
She and her colleagues conducted a study to determine whether a simple preoperative scale based on patient and hospital factors could accurately predict risk for death following gastric resection for malignancy.
They drew on data from the Nationwide Inpatient Sample database to identify adult patients with a diagnosis of gastric cancer who underwent potentially curative partial or total gastrectomy from 1998 through 2011.
They identified a total 24,538 patients, based on International Classification of Diseases, Revision 9 (ICD-9) diagnosis and procedure codes.
They then created multivariate logistic regression models to identify independent predictors of mortality, create a predictive model, and construct a risk scale. The models controlled for sex, age, race, comorbidities, insurance status, hospital volume (less than 25 vs. 25 or more gastric resections for malignancy per year), laparoscopic vs. open approach, poverty level, alcohol abuse, tobacco use, diabetes mellitus, and year of procedure.
The mean length of stay for the patient sample was 11 days. The overall in-hospital mortality was 5.5%.
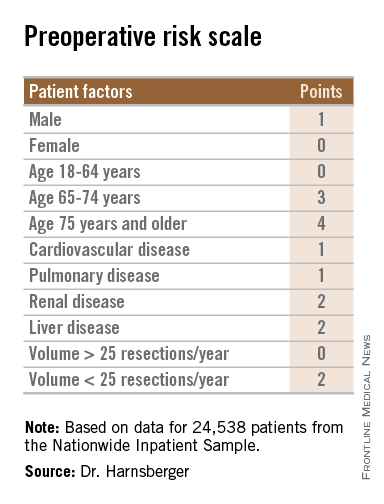
The models identified three patient-related factors and one hospital-related factor that were predictive of mortality and when combined in a risk scale proved to be accurate.
The patient factors were male sex, age 65 and older, and comorbid disease, specifically cardiovascular, pulmonary, renal, and/or hepatic.
The hospital factor, expressed as protective, was 25 or more gastric resections for cancer per year.
The maximum possible score is 13. Patients with scores lower than 6 are at low risk for perioperative mortality, while those with scores 6 and higher are at high risk. Among patients with a score of 0-5, the perioperative death rate ranged from 1.3% to 4.5%. In contrast, patients with higher scores had death rates ranging from 6.0% to 23.1%.
Clinical applications for the bedside risk scale include perioperative patient counseling, aiding in informed consent discussions, and as an adjunct to postoperative risk calculators, Dr. Harnsberger said.The study funding source was not disclosed. Dr. Harnsberger reported having no disclosures.
HOUSTON – A simple preoperative scale can accurately predict a patient’s risk for near-term death following surgery for gastric cancer, investigators say.
The scale accounts for both patient and hospital factors, and is useful as a clinical tool for preoperative counseling of patients, reported Dr. Cristina Harnsberger of the University of California San Diego.
“Male gender, increasing age, and comorbid disease increase risk of in-hospital mortality for patients who undergo gastric resection for malignancy. Additionally, low hospital volume was an independent risk factor,” she said at the annual Society of Surgical Oncology Cancer Symposium.
The scale was able to accurately classify patients as being at low or high risk, and the observed and expected mortality rates for each risk score were well correlated, she said.
Weighing risks
Perioperative mortality rates following resection for gastric malignancies range from 0.6% to 15%. Risk scales and nomograms are intended to help clinicians predict risks for individual patients, but most incorporate postoperative data rather than preoperative or hospital data, Dr. Harnsberger said.
She and her colleagues conducted a study to determine whether a simple preoperative scale based on patient and hospital factors could accurately predict risk for death following gastric resection for malignancy.
They drew on data from the Nationwide Inpatient Sample database to identify adult patients with a diagnosis of gastric cancer who underwent potentially curative partial or total gastrectomy from 1998 through 2011.
They identified a total 24,538 patients, based on International Classification of Diseases, Revision 9 (ICD-9) diagnosis and procedure codes.
They then created multivariate logistic regression models to identify independent predictors of mortality, create a predictive model, and construct a risk scale. The models controlled for sex, age, race, comorbidities, insurance status, hospital volume (less than 25 vs. 25 or more gastric resections for malignancy per year), laparoscopic vs. open approach, poverty level, alcohol abuse, tobacco use, diabetes mellitus, and year of procedure.
The mean length of stay for the patient sample was 11 days. The overall in-hospital mortality was 5.5%.
The models identified three patient-related factors and one hospital-related factor that were predictive of mortality and when combined in a risk scale proved to be accurate.
The patient factors were male sex, age 65 and older, and comorbid disease, specifically cardiovascular, pulmonary, renal, and/or hepatic.
The hospital factor, expressed as protective, was 25 or more gastric resections for cancer per year.
The maximum possible score is 13. Patients with scores lower than 6 are at low risk for perioperative mortality, while those with scores 6 and higher are at high risk. Among patients with a score of 0-5, the perioperative death rate ranged from 1.3% to 4.5%. In contrast, patients with higher scores had death rates ranging from 6.0% to 23.1%.
Clinical applications for the bedside risk scale include perioperative patient counseling, aiding in informed consent discussions, and as an adjunct to postoperative risk calculators, Dr. Harnsberger said.The study funding source was not disclosed. Dr. Harnsberger reported having no disclosures.
HOUSTON – A simple preoperative scale can accurately predict a patient’s risk for near-term death following surgery for gastric cancer, investigators say.
The scale accounts for both patient and hospital factors, and is useful as a clinical tool for preoperative counseling of patients, reported Dr. Cristina Harnsberger of the University of California San Diego.
“Male gender, increasing age, and comorbid disease increase risk of in-hospital mortality for patients who undergo gastric resection for malignancy. Additionally, low hospital volume was an independent risk factor,” she said at the annual Society of Surgical Oncology Cancer Symposium.
The scale was able to accurately classify patients as being at low or high risk, and the observed and expected mortality rates for each risk score were well correlated, she said.
Weighing risks
Perioperative mortality rates following resection for gastric malignancies range from 0.6% to 15%. Risk scales and nomograms are intended to help clinicians predict risks for individual patients, but most incorporate postoperative data rather than preoperative or hospital data, Dr. Harnsberger said.
She and her colleagues conducted a study to determine whether a simple preoperative scale based on patient and hospital factors could accurately predict risk for death following gastric resection for malignancy.
They drew on data from the Nationwide Inpatient Sample database to identify adult patients with a diagnosis of gastric cancer who underwent potentially curative partial or total gastrectomy from 1998 through 2011.
They identified a total 24,538 patients, based on International Classification of Diseases, Revision 9 (ICD-9) diagnosis and procedure codes.
They then created multivariate logistic regression models to identify independent predictors of mortality, create a predictive model, and construct a risk scale. The models controlled for sex, age, race, comorbidities, insurance status, hospital volume (less than 25 vs. 25 or more gastric resections for malignancy per year), laparoscopic vs. open approach, poverty level, alcohol abuse, tobacco use, diabetes mellitus, and year of procedure.
The mean length of stay for the patient sample was 11 days. The overall in-hospital mortality was 5.5%.
The models identified three patient-related factors and one hospital-related factor that were predictive of mortality and when combined in a risk scale proved to be accurate.
The patient factors were male sex, age 65 and older, and comorbid disease, specifically cardiovascular, pulmonary, renal, and/or hepatic.
The hospital factor, expressed as protective, was 25 or more gastric resections for cancer per year.
The maximum possible score is 13. Patients with scores lower than 6 are at low risk for perioperative mortality, while those with scores 6 and higher are at high risk. Among patients with a score of 0-5, the perioperative death rate ranged from 1.3% to 4.5%. In contrast, patients with higher scores had death rates ranging from 6.0% to 23.1%.
Clinical applications for the bedside risk scale include perioperative patient counseling, aiding in informed consent discussions, and as an adjunct to postoperative risk calculators, Dr. Harnsberger said.The study funding source was not disclosed. Dr. Harnsberger reported having no disclosures.
AT SSO 2015
Key clinical point: The bedside risk scale can be used in patient counseling prior to surgery for gastric malignancies.
Major finding: Patients with scores of 0-5 had perioperative death rates of 1.3%-4.5%. Patients with higher scores had death rates ranging from 6.0% to 23.1%.
Data source: Review of retrospective data on 24,538 adults who underwent partial or total gastric resection for malignancies.
Disclosures: The study funding source was not disclosed. Dr. Harnsberger reported having no disclosures.

Palliative surgery eases pain at end of life
HOUSTON – Palliative surgery can alleviate pain and improve the quality of life for patients dying from advanced cancers, without compromising performance status, a study showed.
Among 202 patients with stage III or IV cancers who underwent surgery with palliation as the goal, pain scores were significantly improved after surgery, while Karnofsky Performance Status (KPS) scores remained unchanged, said Dr. Anne Falor, a surgical oncology fellow at City of Hope in Duarte, Calif.

“Surgical oncology has not been historically involved in palliative care. If a patient is deemed unresectable, his or her treatment is often the purview of medical or radiation oncology,” she said at the annual Society of Surgical Oncology Cancer Symposium.
But for patients who are likely to have prolonged disease-free intervals, palliative surgery can be performed with low morbidity, she said.
Dr. Falor and her colleagues reviewed their center’s experience with palliative surgery in 2011, during which time 202 patients with a predicted 5-year survival of less than 5% underwent a total of 247 palliative procedures.
The patients had malignancies at various sites, including the large intestine, lung, stomach, breast, prostate, lymph nodes, esophagus, pancreas, and ovaries.
The primary indications for the procedure included dysphagia, pain/wound problems, dyspnea, nausea and vomiting, and dysuria.
Most of the patients (83%) had a single procedure, but 13% had two operations, 4% had three operations, 1% had four procedures, and 0.4% had five or more interventions.
The majority of procedures performed were endoscopic interventions characterized as minor in nature, followed by minor genitourinary and thoracic interventions, although a nearly equal proportion of thoracic interventions (about 28%) were major procedures such as diverting ostomy.
When the investigators looked at 30-day outcomes following palliative surgery, they found that only 13% of patients needed an urgent care visit, 2% required a triage call, 22% were readmitted, and 60% had an institutional supportive care referral.
Total 30-day morbidity of any kind was seen in 37% of patients; 15% of patients died within 30 days of surgery.
Looking at quality of life outcomes, the investigators found no differences in the percentage of patients with KPS scores from 80 to 100 between the presurgery and postsurgery periods (78% and 70%, respectively, P = ns).
There were significant improvements, however, in pain scores, which dropped by a mean of 1.2 points from the preoperative period to discharge (P < .0001), and decreased by 0.6 points before surgery to the first follow-up visit (P = .0037).
Dr. Falor said that it’s important for patients and their care team to have a discussion regarding expectations for surgery and the goals of care.
The study was internally funded. Dr. Falor reported having no conflicts of interest.
Over the past decade palliative surgery has been increasingly discussed and scrutinized, as the concept of palliative care has gained greater traction with medical professionals and the public. Not too long ago the designation “palliative” when applied to a surgical procedure had an apologetic connotation because the operation would fail to heal. In some cases the term was even used to describe positive tumor margins at the conclusion of a resection – something totally irrelevant when assessing the direct impact of the operation upon a patient’s self-designated symptoms.
Only recently has a more positive perspective emerged, helped by data such as these researchers have presented. Palliative surgery now is not failing to cure, but succeeding to comfort.
New perspectives, however, will raise new and necessary questions to better define the role of surgery in the greater context of relief of suffering in all its manifestations. In our wish to respond surgically to pain and other symptoms we must be vigilant against the temptation to “do something” when surgery for cure or palliation is unlikely to help in order to assuage our feelings of hopelessness. Hopelessness is not an indication for surgery – pain, obstruction, and saving life are. Indications for surgery must be more specific, as this article points out, and it is more likely to help with localized and pressing symptoms. A rule of thumb passed down to me from my surgeon grandfather who practiced in an era when the vast majority of operations were palliative, the more pressing and clear the indication for surgery, the better the result.
Dr. Geoffrey Dunn, an ACS Fellow based in Erie, Pa.
Over the past decade palliative surgery has been increasingly discussed and scrutinized, as the concept of palliative care has gained greater traction with medical professionals and the public. Not too long ago the designation “palliative” when applied to a surgical procedure had an apologetic connotation because the operation would fail to heal. In some cases the term was even used to describe positive tumor margins at the conclusion of a resection – something totally irrelevant when assessing the direct impact of the operation upon a patient’s self-designated symptoms.
Only recently has a more positive perspective emerged, helped by data such as these researchers have presented. Palliative surgery now is not failing to cure, but succeeding to comfort.
New perspectives, however, will raise new and necessary questions to better define the role of surgery in the greater context of relief of suffering in all its manifestations. In our wish to respond surgically to pain and other symptoms we must be vigilant against the temptation to “do something” when surgery for cure or palliation is unlikely to help in order to assuage our feelings of hopelessness. Hopelessness is not an indication for surgery – pain, obstruction, and saving life are. Indications for surgery must be more specific, as this article points out, and it is more likely to help with localized and pressing symptoms. A rule of thumb passed down to me from my surgeon grandfather who practiced in an era when the vast majority of operations were palliative, the more pressing and clear the indication for surgery, the better the result.
Dr. Geoffrey Dunn, an ACS Fellow based in Erie, Pa.
Over the past decade palliative surgery has been increasingly discussed and scrutinized, as the concept of palliative care has gained greater traction with medical professionals and the public. Not too long ago the designation “palliative” when applied to a surgical procedure had an apologetic connotation because the operation would fail to heal. In some cases the term was even used to describe positive tumor margins at the conclusion of a resection – something totally irrelevant when assessing the direct impact of the operation upon a patient’s self-designated symptoms.
Only recently has a more positive perspective emerged, helped by data such as these researchers have presented. Palliative surgery now is not failing to cure, but succeeding to comfort.
New perspectives, however, will raise new and necessary questions to better define the role of surgery in the greater context of relief of suffering in all its manifestations. In our wish to respond surgically to pain and other symptoms we must be vigilant against the temptation to “do something” when surgery for cure or palliation is unlikely to help in order to assuage our feelings of hopelessness. Hopelessness is not an indication for surgery – pain, obstruction, and saving life are. Indications for surgery must be more specific, as this article points out, and it is more likely to help with localized and pressing symptoms. A rule of thumb passed down to me from my surgeon grandfather who practiced in an era when the vast majority of operations were palliative, the more pressing and clear the indication for surgery, the better the result.
Dr. Geoffrey Dunn, an ACS Fellow based in Erie, Pa.
HOUSTON – Palliative surgery can alleviate pain and improve the quality of life for patients dying from advanced cancers, without compromising performance status, a study showed.
Among 202 patients with stage III or IV cancers who underwent surgery with palliation as the goal, pain scores were significantly improved after surgery, while Karnofsky Performance Status (KPS) scores remained unchanged, said Dr. Anne Falor, a surgical oncology fellow at City of Hope in Duarte, Calif.
“Surgical oncology has not been historically involved in palliative care. If a patient is deemed unresectable, his or her treatment is often the purview of medical or radiation oncology,” she said at the annual Society of Surgical Oncology Cancer Symposium.
But for patients who are likely to have prolonged disease-free intervals, palliative surgery can be performed with low morbidity, she said.
Dr. Falor and her colleagues reviewed their center’s experience with palliative surgery in 2011, during which time 202 patients with a predicted 5-year survival of less than 5% underwent a total of 247 palliative procedures.
The patients had malignancies at various sites, including the large intestine, lung, stomach, breast, prostate, lymph nodes, esophagus, pancreas, and ovaries.
The primary indications for the procedure included dysphagia, pain/wound problems, dyspnea, nausea and vomiting, and dysuria.
Most of the patients (83%) had a single procedure, but 13% had two operations, 4% had three operations, 1% had four procedures, and 0.4% had five or more interventions.
The majority of procedures performed were endoscopic interventions characterized as minor in nature, followed by minor genitourinary and thoracic interventions, although a nearly equal proportion of thoracic interventions (about 28%) were major procedures such as diverting ostomy.
When the investigators looked at 30-day outcomes following palliative surgery, they found that only 13% of patients needed an urgent care visit, 2% required a triage call, 22% were readmitted, and 60% had an institutional supportive care referral.
Total 30-day morbidity of any kind was seen in 37% of patients; 15% of patients died within 30 days of surgery.
Looking at quality of life outcomes, the investigators found no differences in the percentage of patients with KPS scores from 80 to 100 between the presurgery and postsurgery periods (78% and 70%, respectively, P = ns).
There were significant improvements, however, in pain scores, which dropped by a mean of 1.2 points from the preoperative period to discharge (P < .0001), and decreased by 0.6 points before surgery to the first follow-up visit (P = .0037).
Dr. Falor said that it’s important for patients and their care team to have a discussion regarding expectations for surgery and the goals of care.
The study was internally funded. Dr. Falor reported having no conflicts of interest.
HOUSTON – Palliative surgery can alleviate pain and improve the quality of life for patients dying from advanced cancers, without compromising performance status, a study showed.
Among 202 patients with stage III or IV cancers who underwent surgery with palliation as the goal, pain scores were significantly improved after surgery, while Karnofsky Performance Status (KPS) scores remained unchanged, said Dr. Anne Falor, a surgical oncology fellow at City of Hope in Duarte, Calif.
“Surgical oncology has not been historically involved in palliative care. If a patient is deemed unresectable, his or her treatment is often the purview of medical or radiation oncology,” she said at the annual Society of Surgical Oncology Cancer Symposium.
But for patients who are likely to have prolonged disease-free intervals, palliative surgery can be performed with low morbidity, she said.
Dr. Falor and her colleagues reviewed their center’s experience with palliative surgery in 2011, during which time 202 patients with a predicted 5-year survival of less than 5% underwent a total of 247 palliative procedures.
The patients had malignancies at various sites, including the large intestine, lung, stomach, breast, prostate, lymph nodes, esophagus, pancreas, and ovaries.
The primary indications for the procedure included dysphagia, pain/wound problems, dyspnea, nausea and vomiting, and dysuria.
Most of the patients (83%) had a single procedure, but 13% had two operations, 4% had three operations, 1% had four procedures, and 0.4% had five or more interventions.
The majority of procedures performed were endoscopic interventions characterized as minor in nature, followed by minor genitourinary and thoracic interventions, although a nearly equal proportion of thoracic interventions (about 28%) were major procedures such as diverting ostomy.
When the investigators looked at 30-day outcomes following palliative surgery, they found that only 13% of patients needed an urgent care visit, 2% required a triage call, 22% were readmitted, and 60% had an institutional supportive care referral.
Total 30-day morbidity of any kind was seen in 37% of patients; 15% of patients died within 30 days of surgery.
Looking at quality of life outcomes, the investigators found no differences in the percentage of patients with KPS scores from 80 to 100 between the presurgery and postsurgery periods (78% and 70%, respectively, P = ns).
There were significant improvements, however, in pain scores, which dropped by a mean of 1.2 points from the preoperative period to discharge (P < .0001), and decreased by 0.6 points before surgery to the first follow-up visit (P = .0037).
Dr. Falor said that it’s important for patients and their care team to have a discussion regarding expectations for surgery and the goals of care.
The study was internally funded. Dr. Falor reported having no conflicts of interest.
Key clinical point: Palliative surgery in patients with advanced cancers can relieve pain with minimal morbidity.
Major finding: Pain scores improved significantly from the pre- to postoperative periods, without a significant decline in performance status scores.
Data source: Case series of 202 patients with stage III or IV malignancies who underwent 247 palliative procedures.
Disclosures: The study was internally funded. Dr. Falor reported having no conflicts of interest.

Higher BMI linked to better metastatic RCC outcomes
ORLANDO – Talk about a paradox: high body mass index is a known risk factor for renal cell carcinoma, but previous studies have shown that patients with high BMI who develop localized RCC generally present with lower grade disease and have better outcomes than normal-weight patients.
Now, investigators confirm that overweight or obese patients with metastatic renal cell carcinoma (mRCC) also tend to have a better prognosis than their leaner counterparts when treated with targeted therapies.

“We externally validate that BMI impacts the outcome of patients with metastatic kidney cancer treated with targeted therapy in terms of overall survival (OS), progression-free survival, and overall response rates,” said Dr. Laurence Albiges, a visiting scientist in the Kidney Cancer Center at the Dana-Farber/Brigham and Women’s Cancer Center, Boston.
Although the mechanism for a protective effect of excess weight is not clear, there is some evidence to suggest that fatty acid metabolism in mRCC may play a role, she said at the 2015 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology.
In tissues samples from The Cancer Genome Atlas (TCGA, a joint repository of the National Cancer Institute and National Human Genome Research Institute), expression of FASN, a gene that encodes for fatty acid synthase, was associated with overall survival (OS), but in other samples FASN expression was not an independent prognostic factor for OS, she said.
Investigate and verify
To clarify the role of BMI in mRCC, Dr. Albiges and colleagues looked at data from clinical trials, specimens from the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC), and biologic data from the TCGA.
As the group reported at the 2014 ASCO annual meeting (Abstract 4576), they first looked at the effect of low BMI (< 25 kg/m2) vs. high BMI (≥ 25) in 1,975 patients with mRCC in clinical trials, and found that after adjustment for IMDC prognosis groups, higher BMI was associated with better OS (median 25.6 months vs. 17.1 months; hazard ratio, 0.84; P = .0079) and longer time to treatment failure (median 8.1 vs. 5.7 months; HR, 0.86; P = .0067).
They then, in collaboration with Pfizer Oncology, conducted an external validation study using data on 4,657 patients with mRCC treated in phase II-III clinical trials from 2003 through 2013.
After adjustment for various risk factors, they found again that BMI of 25 or greater was associated with better outcomes in terms of overall survival (23.4 vs. 14.5 months; HR, 0.830; P = .0008), progression free survival (8.2 vs. 5.5 months; HR, 0.821; P < .0001), and overall response rate (25.3% vs. 17.6; adjusted odds ratio, 1.527; P < .0001).
Dr. Albiges noted that when patients were stratified by histologic subtype, “the favorable outcome associated with high BMI was only observed in clear cell RCC.”
The investigators next looked at information from the TCGA dataset on patients with metastatic clear cell RCC to see whether there was correlation between BMI and survival and between BMI and FASN expression. Although they did not detect a significant survival advantage for higher BMI in this cohort, they did find that higher BMI was significantly associated with lower FASN expression levels (P = .034), and that FASN expression below the median level was associated with better overall survival (P = .002).

Finally, they examined biospecimens from the IMDC dataset with information about outcomes under targeted therapy. Here, they found that FASN staining was associated with prognosis groups, but was not an independent prognostic factor for OS in multivariable analysis.
“BMI, however, is associated with overall survival independently of FASN,” Dr. Albiges said.
Although the mechanisms for the effect of BMI on survival are not clear, the study supports observations that many oncologists have made in clinic, said Dr. Ulka Vaishampayan, chair of genitourinary oncology at the Karmanos Cancer Institute at Wayne State University in Detroit.
“There is obviously, I think, a clinical gestalt that we all have, that people who are not losing a lot of weight are in general doing better across a number of malignancies,” she said. Dr. Vaishampayan was the invited discussant.
ORLANDO – Talk about a paradox: high body mass index is a known risk factor for renal cell carcinoma, but previous studies have shown that patients with high BMI who develop localized RCC generally present with lower grade disease and have better outcomes than normal-weight patients.
Now, investigators confirm that overweight or obese patients with metastatic renal cell carcinoma (mRCC) also tend to have a better prognosis than their leaner counterparts when treated with targeted therapies.
“We externally validate that BMI impacts the outcome of patients with metastatic kidney cancer treated with targeted therapy in terms of overall survival (OS), progression-free survival, and overall response rates,” said Dr. Laurence Albiges, a visiting scientist in the Kidney Cancer Center at the Dana-Farber/Brigham and Women’s Cancer Center, Boston.
Although the mechanism for a protective effect of excess weight is not clear, there is some evidence to suggest that fatty acid metabolism in mRCC may play a role, she said at the 2015 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology.
In tissues samples from The Cancer Genome Atlas (TCGA, a joint repository of the National Cancer Institute and National Human Genome Research Institute), expression of FASN, a gene that encodes for fatty acid synthase, was associated with overall survival (OS), but in other samples FASN expression was not an independent prognostic factor for OS, she said.
Investigate and verify
To clarify the role of BMI in mRCC, Dr. Albiges and colleagues looked at data from clinical trials, specimens from the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC), and biologic data from the TCGA.
As the group reported at the 2014 ASCO annual meeting (Abstract 4576), they first looked at the effect of low BMI (< 25 kg/m2) vs. high BMI (≥ 25) in 1,975 patients with mRCC in clinical trials, and found that after adjustment for IMDC prognosis groups, higher BMI was associated with better OS (median 25.6 months vs. 17.1 months; hazard ratio, 0.84; P = .0079) and longer time to treatment failure (median 8.1 vs. 5.7 months; HR, 0.86; P = .0067).
They then, in collaboration with Pfizer Oncology, conducted an external validation study using data on 4,657 patients with mRCC treated in phase II-III clinical trials from 2003 through 2013.
After adjustment for various risk factors, they found again that BMI of 25 or greater was associated with better outcomes in terms of overall survival (23.4 vs. 14.5 months; HR, 0.830; P = .0008), progression free survival (8.2 vs. 5.5 months; HR, 0.821; P < .0001), and overall response rate (25.3% vs. 17.6; adjusted odds ratio, 1.527; P < .0001).
Dr. Albiges noted that when patients were stratified by histologic subtype, “the favorable outcome associated with high BMI was only observed in clear cell RCC.”
The investigators next looked at information from the TCGA dataset on patients with metastatic clear cell RCC to see whether there was correlation between BMI and survival and between BMI and FASN expression. Although they did not detect a significant survival advantage for higher BMI in this cohort, they did find that higher BMI was significantly associated with lower FASN expression levels (P = .034), and that FASN expression below the median level was associated with better overall survival (P = .002).
Finally, they examined biospecimens from the IMDC dataset with information about outcomes under targeted therapy. Here, they found that FASN staining was associated with prognosis groups, but was not an independent prognostic factor for OS in multivariable analysis.
“BMI, however, is associated with overall survival independently of FASN,” Dr. Albiges said.
Although the mechanisms for the effect of BMI on survival are not clear, the study supports observations that many oncologists have made in clinic, said Dr. Ulka Vaishampayan, chair of genitourinary oncology at the Karmanos Cancer Institute at Wayne State University in Detroit.
“There is obviously, I think, a clinical gestalt that we all have, that people who are not losing a lot of weight are in general doing better across a number of malignancies,” she said. Dr. Vaishampayan was the invited discussant.
ORLANDO – Talk about a paradox: high body mass index is a known risk factor for renal cell carcinoma, but previous studies have shown that patients with high BMI who develop localized RCC generally present with lower grade disease and have better outcomes than normal-weight patients.
Now, investigators confirm that overweight or obese patients with metastatic renal cell carcinoma (mRCC) also tend to have a better prognosis than their leaner counterparts when treated with targeted therapies.
“We externally validate that BMI impacts the outcome of patients with metastatic kidney cancer treated with targeted therapy in terms of overall survival (OS), progression-free survival, and overall response rates,” said Dr. Laurence Albiges, a visiting scientist in the Kidney Cancer Center at the Dana-Farber/Brigham and Women’s Cancer Center, Boston.
Although the mechanism for a protective effect of excess weight is not clear, there is some evidence to suggest that fatty acid metabolism in mRCC may play a role, she said at the 2015 Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology.
In tissues samples from The Cancer Genome Atlas (TCGA, a joint repository of the National Cancer Institute and National Human Genome Research Institute), expression of FASN, a gene that encodes for fatty acid synthase, was associated with overall survival (OS), but in other samples FASN expression was not an independent prognostic factor for OS, she said.
Investigate and verify
To clarify the role of BMI in mRCC, Dr. Albiges and colleagues looked at data from clinical trials, specimens from the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC), and biologic data from the TCGA.
As the group reported at the 2014 ASCO annual meeting (Abstract 4576), they first looked at the effect of low BMI (< 25 kg/m2) vs. high BMI (≥ 25) in 1,975 patients with mRCC in clinical trials, and found that after adjustment for IMDC prognosis groups, higher BMI was associated with better OS (median 25.6 months vs. 17.1 months; hazard ratio, 0.84; P = .0079) and longer time to treatment failure (median 8.1 vs. 5.7 months; HR, 0.86; P = .0067).
They then, in collaboration with Pfizer Oncology, conducted an external validation study using data on 4,657 patients with mRCC treated in phase II-III clinical trials from 2003 through 2013.
After adjustment for various risk factors, they found again that BMI of 25 or greater was associated with better outcomes in terms of overall survival (23.4 vs. 14.5 months; HR, 0.830; P = .0008), progression free survival (8.2 vs. 5.5 months; HR, 0.821; P < .0001), and overall response rate (25.3% vs. 17.6; adjusted odds ratio, 1.527; P < .0001).
Dr. Albiges noted that when patients were stratified by histologic subtype, “the favorable outcome associated with high BMI was only observed in clear cell RCC.”
The investigators next looked at information from the TCGA dataset on patients with metastatic clear cell RCC to see whether there was correlation between BMI and survival and between BMI and FASN expression. Although they did not detect a significant survival advantage for higher BMI in this cohort, they did find that higher BMI was significantly associated with lower FASN expression levels (P = .034), and that FASN expression below the median level was associated with better overall survival (P = .002).
Finally, they examined biospecimens from the IMDC dataset with information about outcomes under targeted therapy. Here, they found that FASN staining was associated with prognosis groups, but was not an independent prognostic factor for OS in multivariable analysis.
“BMI, however, is associated with overall survival independently of FASN,” Dr. Albiges said.
Although the mechanisms for the effect of BMI on survival are not clear, the study supports observations that many oncologists have made in clinic, said Dr. Ulka Vaishampayan, chair of genitourinary oncology at the Karmanos Cancer Institute at Wayne State University in Detroit.
“There is obviously, I think, a clinical gestalt that we all have, that people who are not losing a lot of weight are in general doing better across a number of malignancies,” she said. Dr. Vaishampayan was the invited discussant.
Key clinical point: Patients with metastatic renal cell carcinoma and high BMI have better outcomes than patients with low or normal BMI.
Major finding: Median OS of patients with BMI ≥ 25 was 25.6 months vs. 17.1 months for patients with BMI < 25.
Data source: Retrospective data review with external validation cohorts.
Disclosures: The study was supported by grants to investigators and to the Dana-Farber/Harvard Kidney Cancer Center. Dr. Albiges disclosed serving in an advisory or consulting role to Novartis, Pfizer, Sanofi, and Amgen, and receiving research funding from Novartis and Pfizer. Dr. Vaishampayan disclosed honoraria, speaking, consulting and/or research funding from Astellas, Pfizer, Jannsen, Novarity, Bayer, and Exellxis.

Dual angiogenesis inhibition shows promise in advanced RCC
ORLANDO – A combination of a multitarget tyrosine kinase inhibitor (TKI) with an experimental angiogenesis inhibitor showed “clinically meaningful” activity in the treatment of patients with advanced renal cell cancers.
Early results from a phase II study showed an overall response rate of 25% and median progression-free survival of 8.3 months with a combination of the TKI axitinib (Inlyta) and the investigational drug dalantercept, reported Dr. Martin H. Voss from the Memorial Sloan Kettering Cancer Center, New York.

Dalantercept is an angiogenesis inhibitor with a mechanism of action distinct from that of currently marketed TKIs that target vascular endothelial growth-factor receptors (VEGFR). Dalantercept works within the activin receptor-like kinase 1 (ALK1) pathway. This pathway is distinct from the anaplastic lymphoma kinase (a.k.a. “ALK”) pathway targeted by drugs such as crizotinib (Xalkori) and ceritinib (Zykadia).
ALK1 is selectively expressed on activated endothelial cells, and is activated by its ligands, bone morphogenetic proteins (BMP) 9 and 10. It promotes vascular maturation and stabilization. The processes with which ALK1 is involved occur later in angiogenesis than do the processes targeted by VEGF inhibitors.
Dalantercept “is designed as a soluble decoy receptor that has high affinity for BMP 9 and 10 and thus acts as an ALK1 ligand trap,” Dr. Voss explained at the Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology.
In preclinical studies, dalantercept was shown to inhibit the maturation of vascular cells and impair angiogenesis stimulated by both VEGF-A and basic fibroblast growth factor.
Modest single-agent activity
In a phase I study of dalantercept monotherapy in 37 patients with a variety of solid tumors that were refractory to standard therapies, there was modest activity of the drug with acceptable toxicities (primarily edema that was noncardiogenic and could be treated with diuretics).
Dr. Voss presented results of the first part of the phase II DART trial, a randomized, double-blind study of dalantercept and axitinib, compared with placebo and axitinib in patients with advanced renal cell cancers (RCC).
Patients with advanced RCC and at least one prior VEFGR-targeted TKI but no more than three prior lines of therapy were randomized to one of three open-label dose-escalation cohorts, consisting of axitinib 5 mg twice daily plus dalantercept in doses of either 0.6, 0.9. or 1.2 mg/kg subcutaneously every 3 weeks. There were also two dose escalation cohorts added later, one at the 0.9 mg/kg dalantercept level, and one at the 1.2 mg/kg dose. A total of 29 patients were enrolled in all cohorts.
Originally, nine patients were enrolled in the 1.2 mg/kg expansion cohort, but when these patients developed more fluid retention than was seen in the lower dose groups, the safety review team recommended expansion of the 0.9 mg/kg cohort, with an additional five patients. The patients appeared to tolerate this dose level well, and the 0.9 mg/kg dose was chose for part 2 of the study, results of which will be presented at a later date.
“Overall, the toxicity profile of the combination was in keeping with the single-agent experience of both of the medications,” Dr. Voss said.
Among the 28 patients available for an efficacy analysis, there were seven partial responses, 17 cases of stable disease, and four cases of progressive disease. The overall disease control rate after at least eight cycles of therapy (approximately 6 months) was 57.1% (16 patients); more than 20% of the population maintained disease control for 1 year, The median PFS, as noted before, was 8.3 months, with the upper limit of the 95% confidence interval not being reached yet.
“Along the same lines, I would say that the recommended phase II dose level has not reached its median progression-free survival in this analysis,” Dr. Voss noted.
Among the 17 patients with two or more prior lines of therapy, the response rate was 29%.
“Part 2 of the study is justified by these very encouraging results and is actively accruing patients.
The investigators plan to enroll 130 patients in the second phase, which will have a primary endpoint of PFS, with secondary endpoints of overall response rate, overall survival, safety, pharmacokinetics, and exploratory biomarkers for disease progression.

Dr. Ulka Vaishampayan, the invited discussant, commented that ALK1 “is an interesting and intriguing target, especially in combination with VEGF. This target does seem to be relevant in kidney cancer, at least in the preclinical testing that has been conducted.”
She noted that although the study has a small sample size, “preliminary results appear to be promising. The rationale is interesting and appears to be robust: of overcoming the mechanism of resistance to VEGF inhibition. However, so far we have no preselection based on target, and I worry will that be a problem moving forward, as the study moves into the randomized setting,”
She said that the investigators should attempt, even in retrospect, to identify a target for selecting patients who might benefit from the combination.
Dr. Vaishampayan is chair of genitourinary oncology at the Karmanos Cancer Institute at Wayne State University in Detroit.
ORLANDO – A combination of a multitarget tyrosine kinase inhibitor (TKI) with an experimental angiogenesis inhibitor showed “clinically meaningful” activity in the treatment of patients with advanced renal cell cancers.
Early results from a phase II study showed an overall response rate of 25% and median progression-free survival of 8.3 months with a combination of the TKI axitinib (Inlyta) and the investigational drug dalantercept, reported Dr. Martin H. Voss from the Memorial Sloan Kettering Cancer Center, New York.
Dalantercept is an angiogenesis inhibitor with a mechanism of action distinct from that of currently marketed TKIs that target vascular endothelial growth-factor receptors (VEGFR). Dalantercept works within the activin receptor-like kinase 1 (ALK1) pathway. This pathway is distinct from the anaplastic lymphoma kinase (a.k.a. “ALK”) pathway targeted by drugs such as crizotinib (Xalkori) and ceritinib (Zykadia).
ALK1 is selectively expressed on activated endothelial cells, and is activated by its ligands, bone morphogenetic proteins (BMP) 9 and 10. It promotes vascular maturation and stabilization. The processes with which ALK1 is involved occur later in angiogenesis than do the processes targeted by VEGF inhibitors.
Dalantercept “is designed as a soluble decoy receptor that has high affinity for BMP 9 and 10 and thus acts as an ALK1 ligand trap,” Dr. Voss explained at the Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology.
In preclinical studies, dalantercept was shown to inhibit the maturation of vascular cells and impair angiogenesis stimulated by both VEGF-A and basic fibroblast growth factor.
Modest single-agent activity
In a phase I study of dalantercept monotherapy in 37 patients with a variety of solid tumors that were refractory to standard therapies, there was modest activity of the drug with acceptable toxicities (primarily edema that was noncardiogenic and could be treated with diuretics).
Dr. Voss presented results of the first part of the phase II DART trial, a randomized, double-blind study of dalantercept and axitinib, compared with placebo and axitinib in patients with advanced renal cell cancers (RCC).
Patients with advanced RCC and at least one prior VEFGR-targeted TKI but no more than three prior lines of therapy were randomized to one of three open-label dose-escalation cohorts, consisting of axitinib 5 mg twice daily plus dalantercept in doses of either 0.6, 0.9. or 1.2 mg/kg subcutaneously every 3 weeks. There were also two dose escalation cohorts added later, one at the 0.9 mg/kg dalantercept level, and one at the 1.2 mg/kg dose. A total of 29 patients were enrolled in all cohorts.
Originally, nine patients were enrolled in the 1.2 mg/kg expansion cohort, but when these patients developed more fluid retention than was seen in the lower dose groups, the safety review team recommended expansion of the 0.9 mg/kg cohort, with an additional five patients. The patients appeared to tolerate this dose level well, and the 0.9 mg/kg dose was chose for part 2 of the study, results of which will be presented at a later date.
“Overall, the toxicity profile of the combination was in keeping with the single-agent experience of both of the medications,” Dr. Voss said.
Among the 28 patients available for an efficacy analysis, there were seven partial responses, 17 cases of stable disease, and four cases of progressive disease. The overall disease control rate after at least eight cycles of therapy (approximately 6 months) was 57.1% (16 patients); more than 20% of the population maintained disease control for 1 year, The median PFS, as noted before, was 8.3 months, with the upper limit of the 95% confidence interval not being reached yet.
“Along the same lines, I would say that the recommended phase II dose level has not reached its median progression-free survival in this analysis,” Dr. Voss noted.
Among the 17 patients with two or more prior lines of therapy, the response rate was 29%.
“Part 2 of the study is justified by these very encouraging results and is actively accruing patients.
The investigators plan to enroll 130 patients in the second phase, which will have a primary endpoint of PFS, with secondary endpoints of overall response rate, overall survival, safety, pharmacokinetics, and exploratory biomarkers for disease progression.
Dr. Ulka Vaishampayan, the invited discussant, commented that ALK1 “is an interesting and intriguing target, especially in combination with VEGF. This target does seem to be relevant in kidney cancer, at least in the preclinical testing that has been conducted.”
She noted that although the study has a small sample size, “preliminary results appear to be promising. The rationale is interesting and appears to be robust: of overcoming the mechanism of resistance to VEGF inhibition. However, so far we have no preselection based on target, and I worry will that be a problem moving forward, as the study moves into the randomized setting,”
She said that the investigators should attempt, even in retrospect, to identify a target for selecting patients who might benefit from the combination.
Dr. Vaishampayan is chair of genitourinary oncology at the Karmanos Cancer Institute at Wayne State University in Detroit.
ORLANDO – A combination of a multitarget tyrosine kinase inhibitor (TKI) with an experimental angiogenesis inhibitor showed “clinically meaningful” activity in the treatment of patients with advanced renal cell cancers.
Early results from a phase II study showed an overall response rate of 25% and median progression-free survival of 8.3 months with a combination of the TKI axitinib (Inlyta) and the investigational drug dalantercept, reported Dr. Martin H. Voss from the Memorial Sloan Kettering Cancer Center, New York.
Dalantercept is an angiogenesis inhibitor with a mechanism of action distinct from that of currently marketed TKIs that target vascular endothelial growth-factor receptors (VEGFR). Dalantercept works within the activin receptor-like kinase 1 (ALK1) pathway. This pathway is distinct from the anaplastic lymphoma kinase (a.k.a. “ALK”) pathway targeted by drugs such as crizotinib (Xalkori) and ceritinib (Zykadia).
ALK1 is selectively expressed on activated endothelial cells, and is activated by its ligands, bone morphogenetic proteins (BMP) 9 and 10. It promotes vascular maturation and stabilization. The processes with which ALK1 is involved occur later in angiogenesis than do the processes targeted by VEGF inhibitors.
Dalantercept “is designed as a soluble decoy receptor that has high affinity for BMP 9 and 10 and thus acts as an ALK1 ligand trap,” Dr. Voss explained at the Genitourinary Cancers Symposium sponsored by the American Society of Clinical Oncology.
In preclinical studies, dalantercept was shown to inhibit the maturation of vascular cells and impair angiogenesis stimulated by both VEGF-A and basic fibroblast growth factor.
Modest single-agent activity
In a phase I study of dalantercept monotherapy in 37 patients with a variety of solid tumors that were refractory to standard therapies, there was modest activity of the drug with acceptable toxicities (primarily edema that was noncardiogenic and could be treated with diuretics).
Dr. Voss presented results of the first part of the phase II DART trial, a randomized, double-blind study of dalantercept and axitinib, compared with placebo and axitinib in patients with advanced renal cell cancers (RCC).
Patients with advanced RCC and at least one prior VEFGR-targeted TKI but no more than three prior lines of therapy were randomized to one of three open-label dose-escalation cohorts, consisting of axitinib 5 mg twice daily plus dalantercept in doses of either 0.6, 0.9. or 1.2 mg/kg subcutaneously every 3 weeks. There were also two dose escalation cohorts added later, one at the 0.9 mg/kg dalantercept level, and one at the 1.2 mg/kg dose. A total of 29 patients were enrolled in all cohorts.
Originally, nine patients were enrolled in the 1.2 mg/kg expansion cohort, but when these patients developed more fluid retention than was seen in the lower dose groups, the safety review team recommended expansion of the 0.9 mg/kg cohort, with an additional five patients. The patients appeared to tolerate this dose level well, and the 0.9 mg/kg dose was chose for part 2 of the study, results of which will be presented at a later date.
“Overall, the toxicity profile of the combination was in keeping with the single-agent experience of both of the medications,” Dr. Voss said.
Among the 28 patients available for an efficacy analysis, there were seven partial responses, 17 cases of stable disease, and four cases of progressive disease. The overall disease control rate after at least eight cycles of therapy (approximately 6 months) was 57.1% (16 patients); more than 20% of the population maintained disease control for 1 year, The median PFS, as noted before, was 8.3 months, with the upper limit of the 95% confidence interval not being reached yet.
“Along the same lines, I would say that the recommended phase II dose level has not reached its median progression-free survival in this analysis,” Dr. Voss noted.
Among the 17 patients with two or more prior lines of therapy, the response rate was 29%.
“Part 2 of the study is justified by these very encouraging results and is actively accruing patients.
The investigators plan to enroll 130 patients in the second phase, which will have a primary endpoint of PFS, with secondary endpoints of overall response rate, overall survival, safety, pharmacokinetics, and exploratory biomarkers for disease progression.
Dr. Ulka Vaishampayan, the invited discussant, commented that ALK1 “is an interesting and intriguing target, especially in combination with VEGF. This target does seem to be relevant in kidney cancer, at least in the preclinical testing that has been conducted.”
She noted that although the study has a small sample size, “preliminary results appear to be promising. The rationale is interesting and appears to be robust: of overcoming the mechanism of resistance to VEGF inhibition. However, so far we have no preselection based on target, and I worry will that be a problem moving forward, as the study moves into the randomized setting,”
She said that the investigators should attempt, even in retrospect, to identify a target for selecting patients who might benefit from the combination.
Dr. Vaishampayan is chair of genitourinary oncology at the Karmanos Cancer Institute at Wayne State University in Detroit.
AT THE GENITOURINARY CANCERS SYMPOSIUM
Key clinical point: A combination antiangiogenesis regimen appears to have good activity in heavily pretreated patients with advanced metastatic renal cell cancers.
Major finding: The overall response rate was 25% and median progression-free survival was 8.3 months with a combination of dalantercept and axitinib.
Data source: Part 1 (safety) phase of a phase II randomized trial in patients with advanced RCC.
Disclosures: The study was sponsored by Acceleron Pharma. Dr. Voss disclosed honoraria and travel expenses from Novartis, consulting with Bayer and Novartis, and research funds form Bristol-Myers Squibb and Pfizer. Dr. Vaishampayan disclosed honoraria, speaking, consulting, and/or research funding from Astellas, Pfizer, Janssen, Novartis, Bayer, and Exelixis.
