User login
Equity Evaluation: Analysis of the Prescribing Patterns of Isotretinoin Based on Reproductive Potential
Equity Evaluation: Analysis of the Prescribing Patterns of Isotretinoin Based on Reproductive Potential
To the Editor:
Isotretinoin is the most effective treatment option for acne vulgaris and is considered the first-line therapy for severe scarring acne.1-3 Isotretinoin therapy is indicated for moderate acne when other treatments have failed or when the condition causes distress.3 While there are treatment guidelines for moderate to severe acne, there is no gold standard, and most treatment options include a combination of topical and/or oral therapies.4 Isotretinoin is one of the few monotherapy options available, but its use often is limited by concerns for severe internal and external birth defects if taken during pregnancy.
To manage teratogenicity risks associated with isotretinoin, the US Food and Drug Administration implemented the iPLEDGE Risk Evaluation and Mitigation Strategy in 2006.5 The iPLEDGE compliance requirements differ vastly depending on the reproductive potential of the patient, and the process of obtaining an isotretinoin prescription is much more cumbersome for patients who can get pregnant. Previous studies have demonstrated that males are more likely to be prescribed isotretinoin compared to females, even though females attended more acne-related office visits than males.6,7 Additionally, the administrative burden of iPLEDGE may influence the prescribing patterns of isotretinoin. In a survey of 510 dermatologists, approximately 30% reported that they have at times chosen not to prescribe isotretinoin to patients with severe acne due to the administrative burden of iPLEDGE.8 In this study, we sought to further analyze the prescribing patterns of isotretinoin based on a patient’s reproductive potential.
In this single-center, retrospective cohort study, electronic medical records from 3292 patients diagnosed with acne vulgaris at the Department of Dermatology at Rush University Medical Center (Chicago, Illinois) between January 2013 and December 2019 were reviewed. A total of 188 patients who were prescribed isotretinoin for acne were identified, but only 171 met the study criteria. Eligible patients were aged 12 to 25 years and were prescribed oral isotretinoin for acne vulgaris during the study period. Patients younger than 12 or older than 25 years, those who were prescribed isotretinoin for indications other than acne vulgaris, and those who had previously received isotretinoin and either initiated an additional course or continued treatment at our institution were excluded. Eligible patients then were grouped by reproductive potential: patients who can get pregnant (positive reproductive potential [RP+]) and patients who cannot get pregnant (negative reproductive potential [RP–]). The number of months from initial acne visit, total number of office visits attended, and number of alternative medications that failed before isotretinoin therapy was discussed and initiated were compared between the 2 groups. To standardize between groups, the office visit at which patients were enrolled in iPLEDGE served as the date that isotretinoin therapy was initiated. Alternative medication type and sex of the prescriber were evaluated as secondary end points.
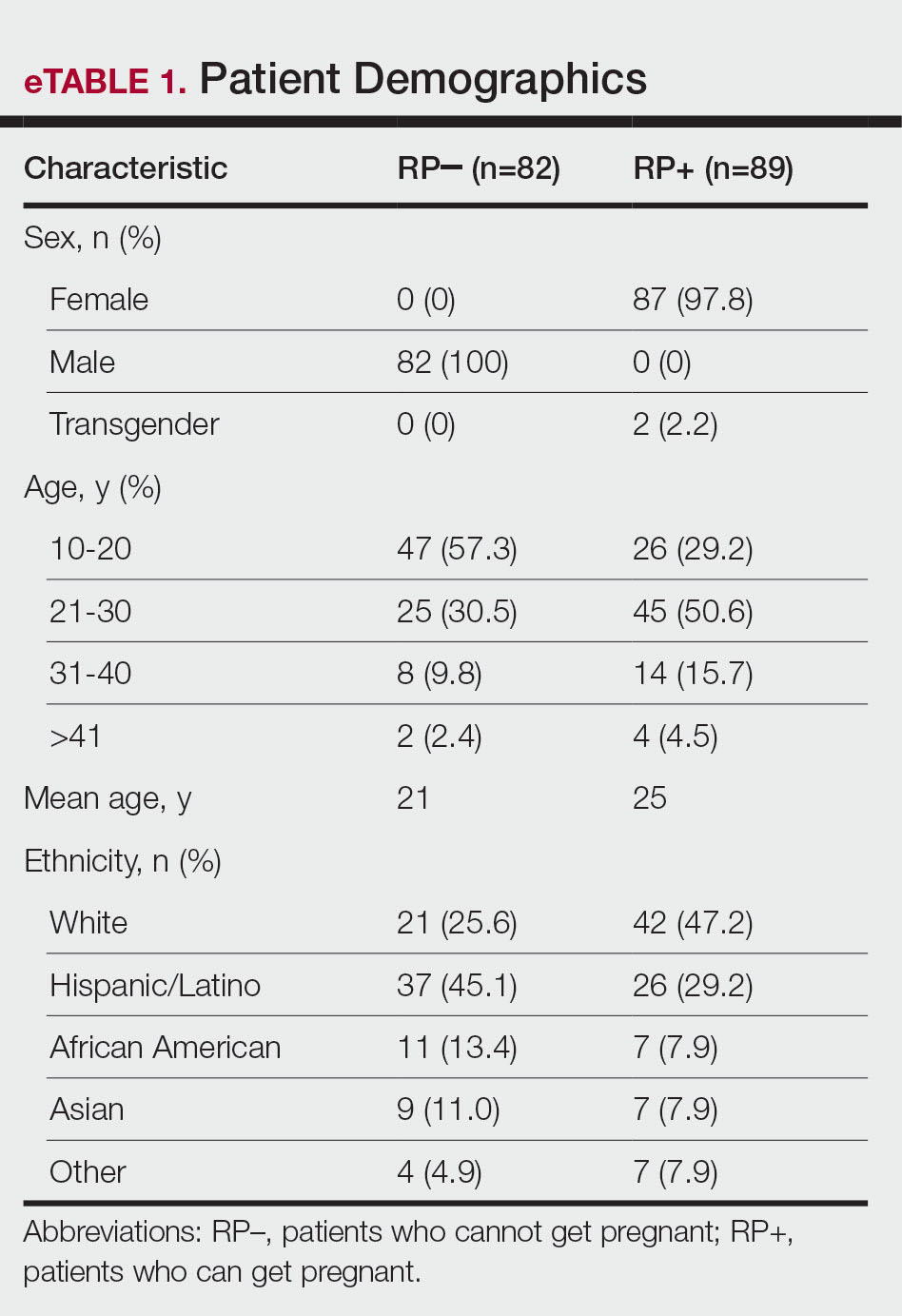
Eighty-nine RP+ patients and 82 RP– patients were prescribed isotretinoin for acne, including 85 females, 2 transgender males with female reproductive organs, 2 females with a history of tubal ligation, and 82 males. Of note, the iPLEDGE program considers tubal ligation as a primary form of contraception and classifies these patients as RP+. Patient demographics are summarized in eTable 1. There was a higher proportion of RP– patients aged 10 to 20 years compared to RP+ patients, for whom there was a higher number of patients aged 21 to 30 years. Most RP+ patients were White, while most RP– patients were Hispanic/Latino.
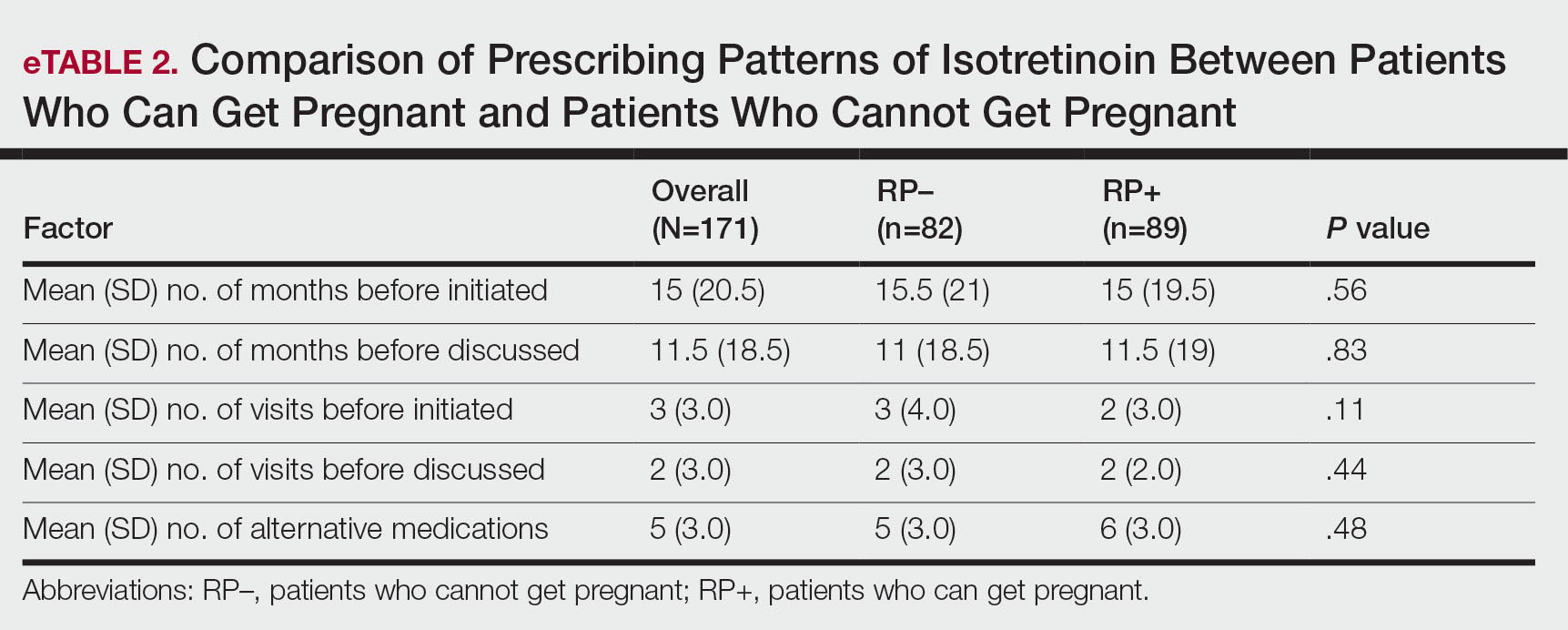
Overall isotretinoin prescribing patterns as well as prescribing patterns stratified by reproductive potential are presented in eTable 2. Overall, the average number of months before isotretinoin was discussed as a treatment option was 11.5 months and before isotretinoin therapy was initiated was 15 months. There was no significant difference between the number of months before isotretinoin was discussed (P=.83) or initiated (P=.56) between RP+ and RP– patients. On average, patients attended 2 office visits before isotretinoin was discussed as a treatment option and 3 office visits before isotretinoin therapy was initiated. The difference between the number of office visits patients attended before isotretinoin was discussed (P=.44) and before isotretinoin therapy was initiated (P=.11) was not significant between RP+ and RP– patients. The number of alternative medications that failed before initiation of isotretinoin therapy was comparable between groups. Patients in the RP– group experienced failure with an average of 5 alternative medications compared with 6 alternative medications in the RP+ group (P=.48).
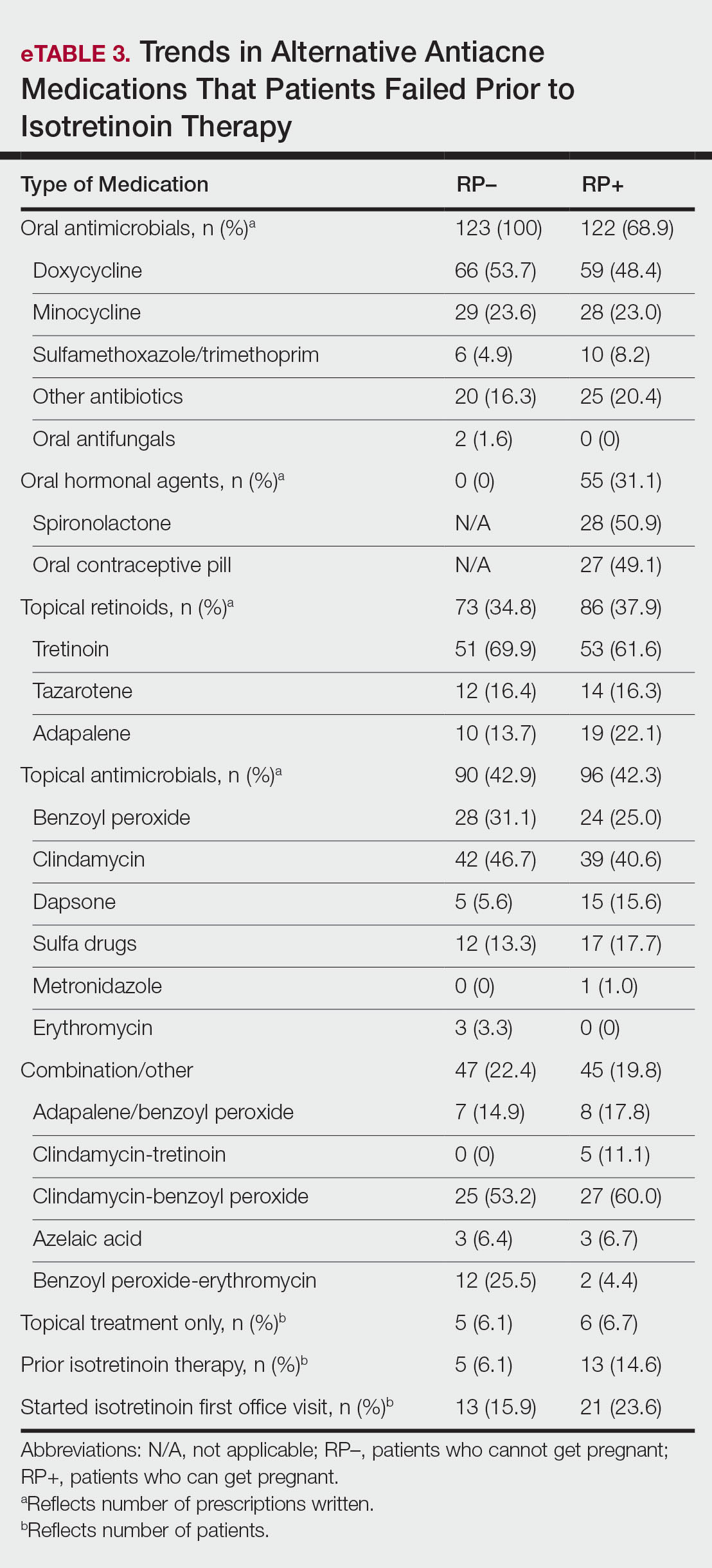
As shown in eTable 3, oral antibiotic therapy commonly was prescribed prior to isotretinoin in both groups, with doxycycline being prescribed most often. Hormonal therapy, including oral contraceptives and spironolactone, was trialed in 55 of 87 (63.2%) RP+ patients. Most patients experienced failure with other oral antiacne medications before isotretinoin therapy, with only 6 (6.7%) RP+ and 5 (6.1%) RP– patients trying topical therapy only. Prior isotretinoin therapy was documented in 13 (14.6%) RP+ patients compared with only 5 (6.1%) RP– patients. Interestingly, isotretinoin was initiated at the patient’s first office visit more often in the RP+ group.
At the time isotretinoin therapy was initiated, the sex of the prescribing provider was similar within the RP+ group, with 52% (46/89) of female and 48% (43/89) of male prescribers. In the RP– group, there was a slightly higher proportion of male prescribers, with 57% (47/82) male compared to 43% (35/82) female prescribers.
iPLEDGE (https://ipledgeprogram.com) is an online system mandated by the US Food and Drug Administration to be used by patients, physicians, and pharmacists for the duration of isotretinoin therapy to prevent and track isotretinoin-associated pregnancies.9 At its inception, the iPLEDGE program categorized patients as females of child-bearing potential, females not of child-bearing potential, or males. The program recently moved toward transgender-inclusive categorization of patients based on reproductive potential.10 Patients who can get pregnant include cisgender females and transgender males, and patients who cannot get pregnant include cisgender males, transgender females, and females and transgender males who have undergone a hysterectomy or bilateral oophorectomy or who are postmenopausal.9
The iPLEDGE compliance requirements for patients who can get pregnant are extensive. Patients with reproductive potential must obtain a negative baseline pregnancy test, enroll in iPLEDGE, undergo a 30-day waiting period, and obtain a second negative pregnancy test before they can start the medication. Each month thereafter, patients must obtain a negative pregnancy test, demonstrate risk comprehension, and report their methods of contraception on iPLEDGE before they can pick up their prescription. In addition, physicians and pharmacists must confirm patient counseling and obtain authorization codes from iPLEDGE to dispense the medication. If any of these steps are not completed by the patient, physician, or pharmacist within 7 days of the patient’s negative pregnancy test, all steps must be repeated by all parties.9,11
The efficacy and utility of iPLEDGE have been criticized and debated in the literature. Although there has been a general decrease in the number of fetal exposures to isotretinoin since the implementation of iPLEDGE in 2006, the average number of fetal exposures only decreased for 2 years until it plateaued in 2008.5 Some physicians have argued that the decrease in the number of fetal exposures is not attributed to the efficacy of iPLEDGE but rather because the program has made it difficult for patients who can get pregnant to obtain necessary isotretinoin prescriptions.12 Other physicians have reported that they have chosen not to prescribe isotretinoin due to the administrative burden of iPLEDGE.8 Although we expected to observe similar trends in our study, we ultimately had more eligible patients with reproductive potential than patients who could not get pregnant. Additionally, there was no difference in the number of months from initial acne visit, total number of office visits, and number of alternative medications that failed before isotretinoin initiation between patients who could and could not get pregnant. These findings suggest that iPLEDGE requirements did not dissuade prescribers from treating acne with isotretinoin in patients who could get pregnant and that the prescribing patterns of isotretinoin were similar regardless of reproductive potential.
Across all primary outcomes, the standard deviation was high in the overall dataset and in the RP– and RP+ subsets, indicating substantial variability in number of months from initial acne visit, total number of visits, and number of alternative medications that failed prior to initiation of isotretinoin. This implies that the prescribing patterns of isotretinoin may be patient and prescriber dependent, and other variables may influence these outcomes aside from the reproductive potential of the patient. Although there was a marginally higher percentage of male prescribers in the RP– group, the sex of the prescriber did not seem to have a major impact on the prescribing patterns of isotretinoin. Further research is indicated to investigate the impact of other factors that may influence the prescribing patterns of isotretinoin, including insurance coverage, access to contraception, and patient concerns about adverse effects.
The types of alternative medications that patients tried prior to isotretinoin were similar among patients who could get pregnant and patients who could not get pregnant. Hormonal therapy, including oral contraception pills and spironolactone, can be very effective in treating acne in patients with reproductive potential,13 as evidenced by the 55 (31.1%) prescriptions written for hormonal therapy in the RP+ group. Spironolactone for acne is contraindicated in male patients due to its antiandrogenic properties and risk for gynecomastia.14 As such, males have fewer alternative medication options for acne, and this may contribute to the higher prevalence of isotretinoin therapy in males that has been demonstrated in prior studies.6,7 Of note, patients obtained more than 100 prescriptions for oral antimicrobials in both groups. Although patients can see benefit with oral antimicrobials for acne, the volume of antimicrobial prescriptions seen in our cohort raises concerns about antibiotic stewardship.15 Whether isotretinoin is a safer therapeutic option compared to antibiotics is up for debate.2,16
Our study included a small sample size at a single institution, which may limit the external validity of our results. Additionally, our study focused on patients who were prescribed isotretinoin prior to 2020 to control for the influence of the COVID-19 pandemic on prescribing patterns. With this, our data may not reflect postpandemic prescribing trends. Further multi-institution studies that include postpandemic patient cohorts can be conducted to validate our findings.
There were no significant differences in the number of months from initial acne visit, total number of office visits, and number of alternative medications that failed prior to discussing isotretinoin as a treatment option or initiating isotretinoin therapy between patients who can get pregnant and those who cannot get pregnant. We observed substantial variability in these outcomes across datasets, indicating that the prescribing patterns of isotretinoin may be patient and prescriber dependent regardless of the reproductive potential of the patient. Follow-up studies are warranted to further investigate the specific influence of iPLEDGE on the utilization of isotretinoin.
- Aslam I, Fleischer A, Feldman S. Emerging drugs for the treatment of acne. Expert Opin Emerg Drugs. 2015;20:91-101. doi:10.1517/14728214.2015.990373
- Huang CY, Chang IJ, Bolick N, et al. Comparative efficacy of pharmacological treatments for acne vulgaris: a network meta-analysis of 221 randomized controlled trials. Ann Fam Med. 2023;21:358-369. doi:10.1370/afm.2995
- Hauk L. Acne vulgaris: treatment guidelines from the AAD. Am Fam Physician. 2017;95:740-741.
- Habeshian KA, Cohen BA. Current issues in the treatment of acne vulgaris. Pediatrics. 2020;145(suppl 2):S225-S230. doi:10.1542/peds.2019-2056L
- Tkachenko E, Singer S, Sharma P, et al. US Food and Drug Administration reports of pregnancy and pregnancy-related adverse events associated with isotretinoin. JAMA Dermatol. 2019;155:1175-1179. doi:10.1001/jamadermatol.2019.1388
- Fleischer AB Jr, Simpson JK, McMichael A, et al. Are there racial and sex differences in the use of oral isotretinoin for acne management in the United States? J Am Acad Dermatol. 2003;49:662-666. doi:10.1067/s0190-9622(03)01584-6
- Barbieri JS, Shin DB, Wang S, et al. Association of race/ethnicity and sex with differences in health care use and treatment for acne. JAMA Dermatol. 2020;156:312-319. doi:10.1001/jamadermatol.2019.4818
- Lee G, Wolf JR, Somers KE. Administrative burden of iPLEDGE deters isotretinoin prescriptions: results from a survey of dermatologists. Cutis. 2022;110:44-47. doi:10.12788/cutis.0558
- The iPLEDGE REMS Prescriber Guide. iPLEDGE. Updated March 2023. https://ipledgeprogram.com/ResourceDownloadRaw/GuideBestPractices
- Boos MD, Ginsberg BA, Peebles JK. Prescribing isotretinoin for transgender youth: a pledge for more inclusive care. Pediatr Dermatol. 2019;36:169-171. doi:10.1111/pde.13694
- iPLEDGE REMS Guide for Patients Who Can Get Pregnant: The Importance of Avoiding Pregnancy on Isotretinoin. iPLEDGE Program. Updated March 2023. https://ipledgeprogram.com/#Main/Resources
- Nagler AR. Early strides for necessary data-driven improvement in iPLEDGE. JAMA Dermatol. 2019;155:1111-1112. doi:10.1001/jamadermatol.2019.1247
- Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90:1006.E1-1006.E30. doi:10.1016/j.jaad.2023.12.017
- Sato K, Matsumoto D, Iizuka F, et al. Anti-androgenic therapy using oral spironolactone for acne vulgaris in Asians. Aesthetic Plast Surg. 2006;30:689-694. doi:10.1007/s00266-006-0081-0
- Issa NT, Kircik LH. Antibiotic stewardship in acne: 2023 update. J Drugs Dermatol. 2024;23:SF37896s4-SF378969s10. doi:10.36849/JDD.SF378969
- Vallerand IA, Lewinson RT, Farris MS, et al. Efficacy and adverse events of oral isotretinoin for acne: a systematic review. Br J Dermatol. 2018;178:76-85. doi:10.1111/bjd.15668
To the Editor:
Isotretinoin is the most effective treatment option for acne vulgaris and is considered the first-line therapy for severe scarring acne.1-3 Isotretinoin therapy is indicated for moderate acne when other treatments have failed or when the condition causes distress.3 While there are treatment guidelines for moderate to severe acne, there is no gold standard, and most treatment options include a combination of topical and/or oral therapies.4 Isotretinoin is one of the few monotherapy options available, but its use often is limited by concerns for severe internal and external birth defects if taken during pregnancy.
To manage teratogenicity risks associated with isotretinoin, the US Food and Drug Administration implemented the iPLEDGE Risk Evaluation and Mitigation Strategy in 2006.5 The iPLEDGE compliance requirements differ vastly depending on the reproductive potential of the patient, and the process of obtaining an isotretinoin prescription is much more cumbersome for patients who can get pregnant. Previous studies have demonstrated that males are more likely to be prescribed isotretinoin compared to females, even though females attended more acne-related office visits than males.6,7 Additionally, the administrative burden of iPLEDGE may influence the prescribing patterns of isotretinoin. In a survey of 510 dermatologists, approximately 30% reported that they have at times chosen not to prescribe isotretinoin to patients with severe acne due to the administrative burden of iPLEDGE.8 In this study, we sought to further analyze the prescribing patterns of isotretinoin based on a patient’s reproductive potential.
In this single-center, retrospective cohort study, electronic medical records from 3292 patients diagnosed with acne vulgaris at the Department of Dermatology at Rush University Medical Center (Chicago, Illinois) between January 2013 and December 2019 were reviewed. A total of 188 patients who were prescribed isotretinoin for acne were identified, but only 171 met the study criteria. Eligible patients were aged 12 to 25 years and were prescribed oral isotretinoin for acne vulgaris during the study period. Patients younger than 12 or older than 25 years, those who were prescribed isotretinoin for indications other than acne vulgaris, and those who had previously received isotretinoin and either initiated an additional course or continued treatment at our institution were excluded. Eligible patients then were grouped by reproductive potential: patients who can get pregnant (positive reproductive potential [RP+]) and patients who cannot get pregnant (negative reproductive potential [RP–]). The number of months from initial acne visit, total number of office visits attended, and number of alternative medications that failed before isotretinoin therapy was discussed and initiated were compared between the 2 groups. To standardize between groups, the office visit at which patients were enrolled in iPLEDGE served as the date that isotretinoin therapy was initiated. Alternative medication type and sex of the prescriber were evaluated as secondary end points.
Eighty-nine RP+ patients and 82 RP– patients were prescribed isotretinoin for acne, including 85 females, 2 transgender males with female reproductive organs, 2 females with a history of tubal ligation, and 82 males. Of note, the iPLEDGE program considers tubal ligation as a primary form of contraception and classifies these patients as RP+. Patient demographics are summarized in eTable 1. There was a higher proportion of RP– patients aged 10 to 20 years compared to RP+ patients, for whom there was a higher number of patients aged 21 to 30 years. Most RP+ patients were White, while most RP– patients were Hispanic/Latino.
Overall isotretinoin prescribing patterns as well as prescribing patterns stratified by reproductive potential are presented in eTable 2. Overall, the average number of months before isotretinoin was discussed as a treatment option was 11.5 months and before isotretinoin therapy was initiated was 15 months. There was no significant difference between the number of months before isotretinoin was discussed (P=.83) or initiated (P=.56) between RP+ and RP– patients. On average, patients attended 2 office visits before isotretinoin was discussed as a treatment option and 3 office visits before isotretinoin therapy was initiated. The difference between the number of office visits patients attended before isotretinoin was discussed (P=.44) and before isotretinoin therapy was initiated (P=.11) was not significant between RP+ and RP– patients. The number of alternative medications that failed before initiation of isotretinoin therapy was comparable between groups. Patients in the RP– group experienced failure with an average of 5 alternative medications compared with 6 alternative medications in the RP+ group (P=.48).
As shown in eTable 3, oral antibiotic therapy commonly was prescribed prior to isotretinoin in both groups, with doxycycline being prescribed most often. Hormonal therapy, including oral contraceptives and spironolactone, was trialed in 55 of 87 (63.2%) RP+ patients. Most patients experienced failure with other oral antiacne medications before isotretinoin therapy, with only 6 (6.7%) RP+ and 5 (6.1%) RP– patients trying topical therapy only. Prior isotretinoin therapy was documented in 13 (14.6%) RP+ patients compared with only 5 (6.1%) RP– patients. Interestingly, isotretinoin was initiated at the patient’s first office visit more often in the RP+ group.
At the time isotretinoin therapy was initiated, the sex of the prescribing provider was similar within the RP+ group, with 52% (46/89) of female and 48% (43/89) of male prescribers. In the RP– group, there was a slightly higher proportion of male prescribers, with 57% (47/82) male compared to 43% (35/82) female prescribers.
iPLEDGE (https://ipledgeprogram.com) is an online system mandated by the US Food and Drug Administration to be used by patients, physicians, and pharmacists for the duration of isotretinoin therapy to prevent and track isotretinoin-associated pregnancies.9 At its inception, the iPLEDGE program categorized patients as females of child-bearing potential, females not of child-bearing potential, or males. The program recently moved toward transgender-inclusive categorization of patients based on reproductive potential.10 Patients who can get pregnant include cisgender females and transgender males, and patients who cannot get pregnant include cisgender males, transgender females, and females and transgender males who have undergone a hysterectomy or bilateral oophorectomy or who are postmenopausal.9
The iPLEDGE compliance requirements for patients who can get pregnant are extensive. Patients with reproductive potential must obtain a negative baseline pregnancy test, enroll in iPLEDGE, undergo a 30-day waiting period, and obtain a second negative pregnancy test before they can start the medication. Each month thereafter, patients must obtain a negative pregnancy test, demonstrate risk comprehension, and report their methods of contraception on iPLEDGE before they can pick up their prescription. In addition, physicians and pharmacists must confirm patient counseling and obtain authorization codes from iPLEDGE to dispense the medication. If any of these steps are not completed by the patient, physician, or pharmacist within 7 days of the patient’s negative pregnancy test, all steps must be repeated by all parties.9,11
The efficacy and utility of iPLEDGE have been criticized and debated in the literature. Although there has been a general decrease in the number of fetal exposures to isotretinoin since the implementation of iPLEDGE in 2006, the average number of fetal exposures only decreased for 2 years until it plateaued in 2008.5 Some physicians have argued that the decrease in the number of fetal exposures is not attributed to the efficacy of iPLEDGE but rather because the program has made it difficult for patients who can get pregnant to obtain necessary isotretinoin prescriptions.12 Other physicians have reported that they have chosen not to prescribe isotretinoin due to the administrative burden of iPLEDGE.8 Although we expected to observe similar trends in our study, we ultimately had more eligible patients with reproductive potential than patients who could not get pregnant. Additionally, there was no difference in the number of months from initial acne visit, total number of office visits, and number of alternative medications that failed before isotretinoin initiation between patients who could and could not get pregnant. These findings suggest that iPLEDGE requirements did not dissuade prescribers from treating acne with isotretinoin in patients who could get pregnant and that the prescribing patterns of isotretinoin were similar regardless of reproductive potential.
Across all primary outcomes, the standard deviation was high in the overall dataset and in the RP– and RP+ subsets, indicating substantial variability in number of months from initial acne visit, total number of visits, and number of alternative medications that failed prior to initiation of isotretinoin. This implies that the prescribing patterns of isotretinoin may be patient and prescriber dependent, and other variables may influence these outcomes aside from the reproductive potential of the patient. Although there was a marginally higher percentage of male prescribers in the RP– group, the sex of the prescriber did not seem to have a major impact on the prescribing patterns of isotretinoin. Further research is indicated to investigate the impact of other factors that may influence the prescribing patterns of isotretinoin, including insurance coverage, access to contraception, and patient concerns about adverse effects.
The types of alternative medications that patients tried prior to isotretinoin were similar among patients who could get pregnant and patients who could not get pregnant. Hormonal therapy, including oral contraception pills and spironolactone, can be very effective in treating acne in patients with reproductive potential,13 as evidenced by the 55 (31.1%) prescriptions written for hormonal therapy in the RP+ group. Spironolactone for acne is contraindicated in male patients due to its antiandrogenic properties and risk for gynecomastia.14 As such, males have fewer alternative medication options for acne, and this may contribute to the higher prevalence of isotretinoin therapy in males that has been demonstrated in prior studies.6,7 Of note, patients obtained more than 100 prescriptions for oral antimicrobials in both groups. Although patients can see benefit with oral antimicrobials for acne, the volume of antimicrobial prescriptions seen in our cohort raises concerns about antibiotic stewardship.15 Whether isotretinoin is a safer therapeutic option compared to antibiotics is up for debate.2,16
Our study included a small sample size at a single institution, which may limit the external validity of our results. Additionally, our study focused on patients who were prescribed isotretinoin prior to 2020 to control for the influence of the COVID-19 pandemic on prescribing patterns. With this, our data may not reflect postpandemic prescribing trends. Further multi-institution studies that include postpandemic patient cohorts can be conducted to validate our findings.
There were no significant differences in the number of months from initial acne visit, total number of office visits, and number of alternative medications that failed prior to discussing isotretinoin as a treatment option or initiating isotretinoin therapy between patients who can get pregnant and those who cannot get pregnant. We observed substantial variability in these outcomes across datasets, indicating that the prescribing patterns of isotretinoin may be patient and prescriber dependent regardless of the reproductive potential of the patient. Follow-up studies are warranted to further investigate the specific influence of iPLEDGE on the utilization of isotretinoin.
To the Editor:
Isotretinoin is the most effective treatment option for acne vulgaris and is considered the first-line therapy for severe scarring acne.1-3 Isotretinoin therapy is indicated for moderate acne when other treatments have failed or when the condition causes distress.3 While there are treatment guidelines for moderate to severe acne, there is no gold standard, and most treatment options include a combination of topical and/or oral therapies.4 Isotretinoin is one of the few monotherapy options available, but its use often is limited by concerns for severe internal and external birth defects if taken during pregnancy.
To manage teratogenicity risks associated with isotretinoin, the US Food and Drug Administration implemented the iPLEDGE Risk Evaluation and Mitigation Strategy in 2006.5 The iPLEDGE compliance requirements differ vastly depending on the reproductive potential of the patient, and the process of obtaining an isotretinoin prescription is much more cumbersome for patients who can get pregnant. Previous studies have demonstrated that males are more likely to be prescribed isotretinoin compared to females, even though females attended more acne-related office visits than males.6,7 Additionally, the administrative burden of iPLEDGE may influence the prescribing patterns of isotretinoin. In a survey of 510 dermatologists, approximately 30% reported that they have at times chosen not to prescribe isotretinoin to patients with severe acne due to the administrative burden of iPLEDGE.8 In this study, we sought to further analyze the prescribing patterns of isotretinoin based on a patient’s reproductive potential.
In this single-center, retrospective cohort study, electronic medical records from 3292 patients diagnosed with acne vulgaris at the Department of Dermatology at Rush University Medical Center (Chicago, Illinois) between January 2013 and December 2019 were reviewed. A total of 188 patients who were prescribed isotretinoin for acne were identified, but only 171 met the study criteria. Eligible patients were aged 12 to 25 years and were prescribed oral isotretinoin for acne vulgaris during the study period. Patients younger than 12 or older than 25 years, those who were prescribed isotretinoin for indications other than acne vulgaris, and those who had previously received isotretinoin and either initiated an additional course or continued treatment at our institution were excluded. Eligible patients then were grouped by reproductive potential: patients who can get pregnant (positive reproductive potential [RP+]) and patients who cannot get pregnant (negative reproductive potential [RP–]). The number of months from initial acne visit, total number of office visits attended, and number of alternative medications that failed before isotretinoin therapy was discussed and initiated were compared between the 2 groups. To standardize between groups, the office visit at which patients were enrolled in iPLEDGE served as the date that isotretinoin therapy was initiated. Alternative medication type and sex of the prescriber were evaluated as secondary end points.
Eighty-nine RP+ patients and 82 RP– patients were prescribed isotretinoin for acne, including 85 females, 2 transgender males with female reproductive organs, 2 females with a history of tubal ligation, and 82 males. Of note, the iPLEDGE program considers tubal ligation as a primary form of contraception and classifies these patients as RP+. Patient demographics are summarized in eTable 1. There was a higher proportion of RP– patients aged 10 to 20 years compared to RP+ patients, for whom there was a higher number of patients aged 21 to 30 years. Most RP+ patients were White, while most RP– patients were Hispanic/Latino.
Overall isotretinoin prescribing patterns as well as prescribing patterns stratified by reproductive potential are presented in eTable 2. Overall, the average number of months before isotretinoin was discussed as a treatment option was 11.5 months and before isotretinoin therapy was initiated was 15 months. There was no significant difference between the number of months before isotretinoin was discussed (P=.83) or initiated (P=.56) between RP+ and RP– patients. On average, patients attended 2 office visits before isotretinoin was discussed as a treatment option and 3 office visits before isotretinoin therapy was initiated. The difference between the number of office visits patients attended before isotretinoin was discussed (P=.44) and before isotretinoin therapy was initiated (P=.11) was not significant between RP+ and RP– patients. The number of alternative medications that failed before initiation of isotretinoin therapy was comparable between groups. Patients in the RP– group experienced failure with an average of 5 alternative medications compared with 6 alternative medications in the RP+ group (P=.48).
As shown in eTable 3, oral antibiotic therapy commonly was prescribed prior to isotretinoin in both groups, with doxycycline being prescribed most often. Hormonal therapy, including oral contraceptives and spironolactone, was trialed in 55 of 87 (63.2%) RP+ patients. Most patients experienced failure with other oral antiacne medications before isotretinoin therapy, with only 6 (6.7%) RP+ and 5 (6.1%) RP– patients trying topical therapy only. Prior isotretinoin therapy was documented in 13 (14.6%) RP+ patients compared with only 5 (6.1%) RP– patients. Interestingly, isotretinoin was initiated at the patient’s first office visit more often in the RP+ group.
At the time isotretinoin therapy was initiated, the sex of the prescribing provider was similar within the RP+ group, with 52% (46/89) of female and 48% (43/89) of male prescribers. In the RP– group, there was a slightly higher proportion of male prescribers, with 57% (47/82) male compared to 43% (35/82) female prescribers.
iPLEDGE (https://ipledgeprogram.com) is an online system mandated by the US Food and Drug Administration to be used by patients, physicians, and pharmacists for the duration of isotretinoin therapy to prevent and track isotretinoin-associated pregnancies.9 At its inception, the iPLEDGE program categorized patients as females of child-bearing potential, females not of child-bearing potential, or males. The program recently moved toward transgender-inclusive categorization of patients based on reproductive potential.10 Patients who can get pregnant include cisgender females and transgender males, and patients who cannot get pregnant include cisgender males, transgender females, and females and transgender males who have undergone a hysterectomy or bilateral oophorectomy or who are postmenopausal.9
The iPLEDGE compliance requirements for patients who can get pregnant are extensive. Patients with reproductive potential must obtain a negative baseline pregnancy test, enroll in iPLEDGE, undergo a 30-day waiting period, and obtain a second negative pregnancy test before they can start the medication. Each month thereafter, patients must obtain a negative pregnancy test, demonstrate risk comprehension, and report their methods of contraception on iPLEDGE before they can pick up their prescription. In addition, physicians and pharmacists must confirm patient counseling and obtain authorization codes from iPLEDGE to dispense the medication. If any of these steps are not completed by the patient, physician, or pharmacist within 7 days of the patient’s negative pregnancy test, all steps must be repeated by all parties.9,11
The efficacy and utility of iPLEDGE have been criticized and debated in the literature. Although there has been a general decrease in the number of fetal exposures to isotretinoin since the implementation of iPLEDGE in 2006, the average number of fetal exposures only decreased for 2 years until it plateaued in 2008.5 Some physicians have argued that the decrease in the number of fetal exposures is not attributed to the efficacy of iPLEDGE but rather because the program has made it difficult for patients who can get pregnant to obtain necessary isotretinoin prescriptions.12 Other physicians have reported that they have chosen not to prescribe isotretinoin due to the administrative burden of iPLEDGE.8 Although we expected to observe similar trends in our study, we ultimately had more eligible patients with reproductive potential than patients who could not get pregnant. Additionally, there was no difference in the number of months from initial acne visit, total number of office visits, and number of alternative medications that failed before isotretinoin initiation between patients who could and could not get pregnant. These findings suggest that iPLEDGE requirements did not dissuade prescribers from treating acne with isotretinoin in patients who could get pregnant and that the prescribing patterns of isotretinoin were similar regardless of reproductive potential.
Across all primary outcomes, the standard deviation was high in the overall dataset and in the RP– and RP+ subsets, indicating substantial variability in number of months from initial acne visit, total number of visits, and number of alternative medications that failed prior to initiation of isotretinoin. This implies that the prescribing patterns of isotretinoin may be patient and prescriber dependent, and other variables may influence these outcomes aside from the reproductive potential of the patient. Although there was a marginally higher percentage of male prescribers in the RP– group, the sex of the prescriber did not seem to have a major impact on the prescribing patterns of isotretinoin. Further research is indicated to investigate the impact of other factors that may influence the prescribing patterns of isotretinoin, including insurance coverage, access to contraception, and patient concerns about adverse effects.
The types of alternative medications that patients tried prior to isotretinoin were similar among patients who could get pregnant and patients who could not get pregnant. Hormonal therapy, including oral contraception pills and spironolactone, can be very effective in treating acne in patients with reproductive potential,13 as evidenced by the 55 (31.1%) prescriptions written for hormonal therapy in the RP+ group. Spironolactone for acne is contraindicated in male patients due to its antiandrogenic properties and risk for gynecomastia.14 As such, males have fewer alternative medication options for acne, and this may contribute to the higher prevalence of isotretinoin therapy in males that has been demonstrated in prior studies.6,7 Of note, patients obtained more than 100 prescriptions for oral antimicrobials in both groups. Although patients can see benefit with oral antimicrobials for acne, the volume of antimicrobial prescriptions seen in our cohort raises concerns about antibiotic stewardship.15 Whether isotretinoin is a safer therapeutic option compared to antibiotics is up for debate.2,16
Our study included a small sample size at a single institution, which may limit the external validity of our results. Additionally, our study focused on patients who were prescribed isotretinoin prior to 2020 to control for the influence of the COVID-19 pandemic on prescribing patterns. With this, our data may not reflect postpandemic prescribing trends. Further multi-institution studies that include postpandemic patient cohorts can be conducted to validate our findings.
There were no significant differences in the number of months from initial acne visit, total number of office visits, and number of alternative medications that failed prior to discussing isotretinoin as a treatment option or initiating isotretinoin therapy between patients who can get pregnant and those who cannot get pregnant. We observed substantial variability in these outcomes across datasets, indicating that the prescribing patterns of isotretinoin may be patient and prescriber dependent regardless of the reproductive potential of the patient. Follow-up studies are warranted to further investigate the specific influence of iPLEDGE on the utilization of isotretinoin.
- Aslam I, Fleischer A, Feldman S. Emerging drugs for the treatment of acne. Expert Opin Emerg Drugs. 2015;20:91-101. doi:10.1517/14728214.2015.990373
- Huang CY, Chang IJ, Bolick N, et al. Comparative efficacy of pharmacological treatments for acne vulgaris: a network meta-analysis of 221 randomized controlled trials. Ann Fam Med. 2023;21:358-369. doi:10.1370/afm.2995
- Hauk L. Acne vulgaris: treatment guidelines from the AAD. Am Fam Physician. 2017;95:740-741.
- Habeshian KA, Cohen BA. Current issues in the treatment of acne vulgaris. Pediatrics. 2020;145(suppl 2):S225-S230. doi:10.1542/peds.2019-2056L
- Tkachenko E, Singer S, Sharma P, et al. US Food and Drug Administration reports of pregnancy and pregnancy-related adverse events associated with isotretinoin. JAMA Dermatol. 2019;155:1175-1179. doi:10.1001/jamadermatol.2019.1388
- Fleischer AB Jr, Simpson JK, McMichael A, et al. Are there racial and sex differences in the use of oral isotretinoin for acne management in the United States? J Am Acad Dermatol. 2003;49:662-666. doi:10.1067/s0190-9622(03)01584-6
- Barbieri JS, Shin DB, Wang S, et al. Association of race/ethnicity and sex with differences in health care use and treatment for acne. JAMA Dermatol. 2020;156:312-319. doi:10.1001/jamadermatol.2019.4818
- Lee G, Wolf JR, Somers KE. Administrative burden of iPLEDGE deters isotretinoin prescriptions: results from a survey of dermatologists. Cutis. 2022;110:44-47. doi:10.12788/cutis.0558
- The iPLEDGE REMS Prescriber Guide. iPLEDGE. Updated March 2023. https://ipledgeprogram.com/ResourceDownloadRaw/GuideBestPractices
- Boos MD, Ginsberg BA, Peebles JK. Prescribing isotretinoin for transgender youth: a pledge for more inclusive care. Pediatr Dermatol. 2019;36:169-171. doi:10.1111/pde.13694
- iPLEDGE REMS Guide for Patients Who Can Get Pregnant: The Importance of Avoiding Pregnancy on Isotretinoin. iPLEDGE Program. Updated March 2023. https://ipledgeprogram.com/#Main/Resources
- Nagler AR. Early strides for necessary data-driven improvement in iPLEDGE. JAMA Dermatol. 2019;155:1111-1112. doi:10.1001/jamadermatol.2019.1247
- Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90:1006.E1-1006.E30. doi:10.1016/j.jaad.2023.12.017
- Sato K, Matsumoto D, Iizuka F, et al. Anti-androgenic therapy using oral spironolactone for acne vulgaris in Asians. Aesthetic Plast Surg. 2006;30:689-694. doi:10.1007/s00266-006-0081-0
- Issa NT, Kircik LH. Antibiotic stewardship in acne: 2023 update. J Drugs Dermatol. 2024;23:SF37896s4-SF378969s10. doi:10.36849/JDD.SF378969
- Vallerand IA, Lewinson RT, Farris MS, et al. Efficacy and adverse events of oral isotretinoin for acne: a systematic review. Br J Dermatol. 2018;178:76-85. doi:10.1111/bjd.15668
- Aslam I, Fleischer A, Feldman S. Emerging drugs for the treatment of acne. Expert Opin Emerg Drugs. 2015;20:91-101. doi:10.1517/14728214.2015.990373
- Huang CY, Chang IJ, Bolick N, et al. Comparative efficacy of pharmacological treatments for acne vulgaris: a network meta-analysis of 221 randomized controlled trials. Ann Fam Med. 2023;21:358-369. doi:10.1370/afm.2995
- Hauk L. Acne vulgaris: treatment guidelines from the AAD. Am Fam Physician. 2017;95:740-741.
- Habeshian KA, Cohen BA. Current issues in the treatment of acne vulgaris. Pediatrics. 2020;145(suppl 2):S225-S230. doi:10.1542/peds.2019-2056L
- Tkachenko E, Singer S, Sharma P, et al. US Food and Drug Administration reports of pregnancy and pregnancy-related adverse events associated with isotretinoin. JAMA Dermatol. 2019;155:1175-1179. doi:10.1001/jamadermatol.2019.1388
- Fleischer AB Jr, Simpson JK, McMichael A, et al. Are there racial and sex differences in the use of oral isotretinoin for acne management in the United States? J Am Acad Dermatol. 2003;49:662-666. doi:10.1067/s0190-9622(03)01584-6
- Barbieri JS, Shin DB, Wang S, et al. Association of race/ethnicity and sex with differences in health care use and treatment for acne. JAMA Dermatol. 2020;156:312-319. doi:10.1001/jamadermatol.2019.4818
- Lee G, Wolf JR, Somers KE. Administrative burden of iPLEDGE deters isotretinoin prescriptions: results from a survey of dermatologists. Cutis. 2022;110:44-47. doi:10.12788/cutis.0558
- The iPLEDGE REMS Prescriber Guide. iPLEDGE. Updated March 2023. https://ipledgeprogram.com/ResourceDownloadRaw/GuideBestPractices
- Boos MD, Ginsberg BA, Peebles JK. Prescribing isotretinoin for transgender youth: a pledge for more inclusive care. Pediatr Dermatol. 2019;36:169-171. doi:10.1111/pde.13694
- iPLEDGE REMS Guide for Patients Who Can Get Pregnant: The Importance of Avoiding Pregnancy on Isotretinoin. iPLEDGE Program. Updated March 2023. https://ipledgeprogram.com/#Main/Resources
- Nagler AR. Early strides for necessary data-driven improvement in iPLEDGE. JAMA Dermatol. 2019;155:1111-1112. doi:10.1001/jamadermatol.2019.1247
- Reynolds RV, Yeung H, Cheng CE, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2024;90:1006.E1-1006.E30. doi:10.1016/j.jaad.2023.12.017
- Sato K, Matsumoto D, Iizuka F, et al. Anti-androgenic therapy using oral spironolactone for acne vulgaris in Asians. Aesthetic Plast Surg. 2006;30:689-694. doi:10.1007/s00266-006-0081-0
- Issa NT, Kircik LH. Antibiotic stewardship in acne: 2023 update. J Drugs Dermatol. 2024;23:SF37896s4-SF378969s10. doi:10.36849/JDD.SF378969
- Vallerand IA, Lewinson RT, Farris MS, et al. Efficacy and adverse events of oral isotretinoin for acne: a systematic review. Br J Dermatol. 2018;178:76-85. doi:10.1111/bjd.15668
Equity Evaluation: Analysis of the Prescribing Patterns of Isotretinoin Based on Reproductive Potential
Equity Evaluation: Analysis of the Prescribing Patterns of Isotretinoin Based on Reproductive Potential
Practice Points
- Isotretinoin is one of the few monotherapy options available for acne, but its use often is limited by concerns for severe internal and external birth defects if taken during pregnancy.
- The number of office visits attended, alternative acne medications used, and duration of acne treatment prior to isotretinoin therapy were similar between patients who can become pregnant and patients who cannot become pregnant.
- The reproductive potential of the patient did not appear to have a major impact on the prescribing patterns of isotretinoin; rather, the utilization of isotretinoin likely is dependent on individual prescriber preferences and other patient factors.
