User login
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
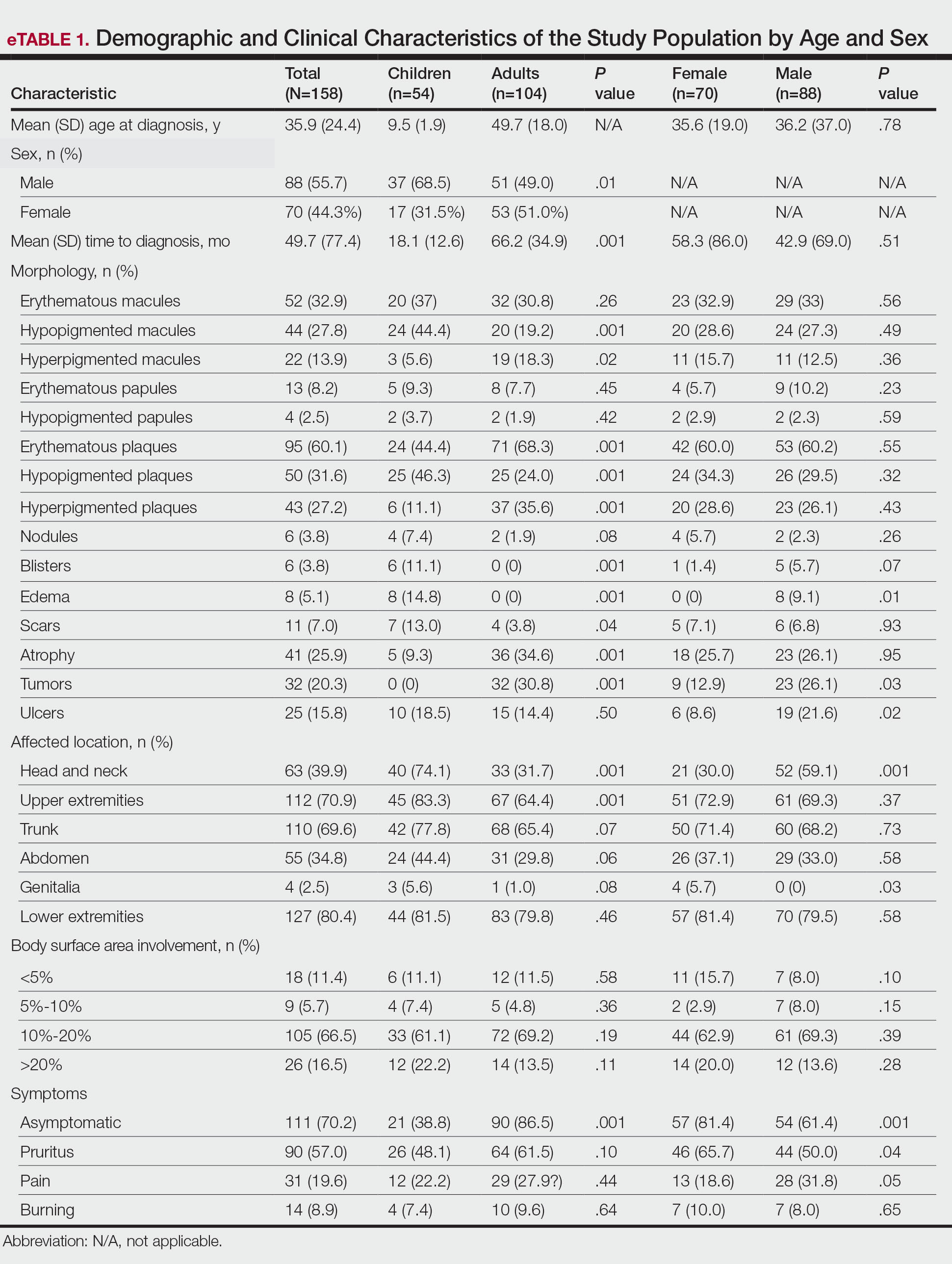
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
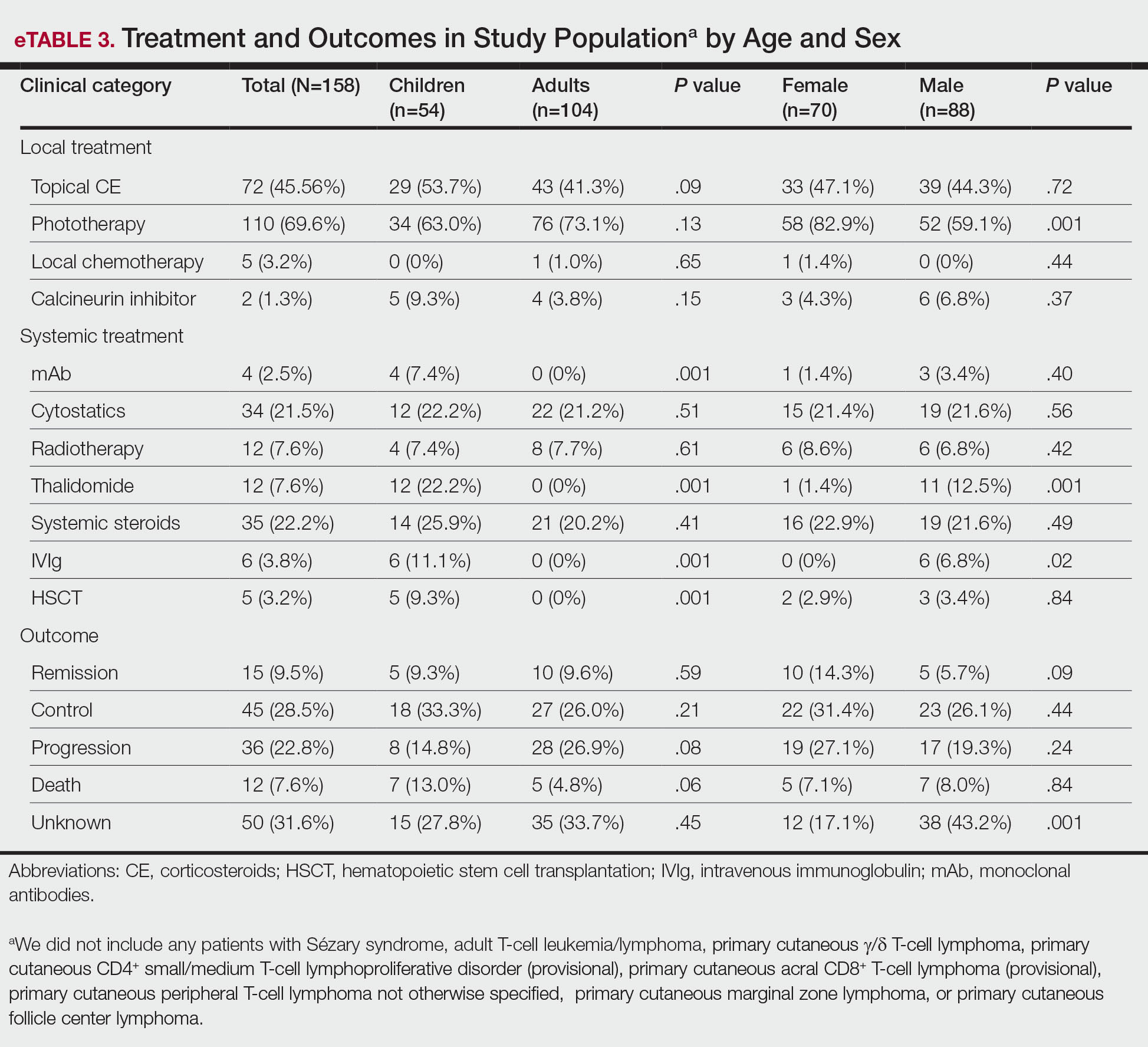
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
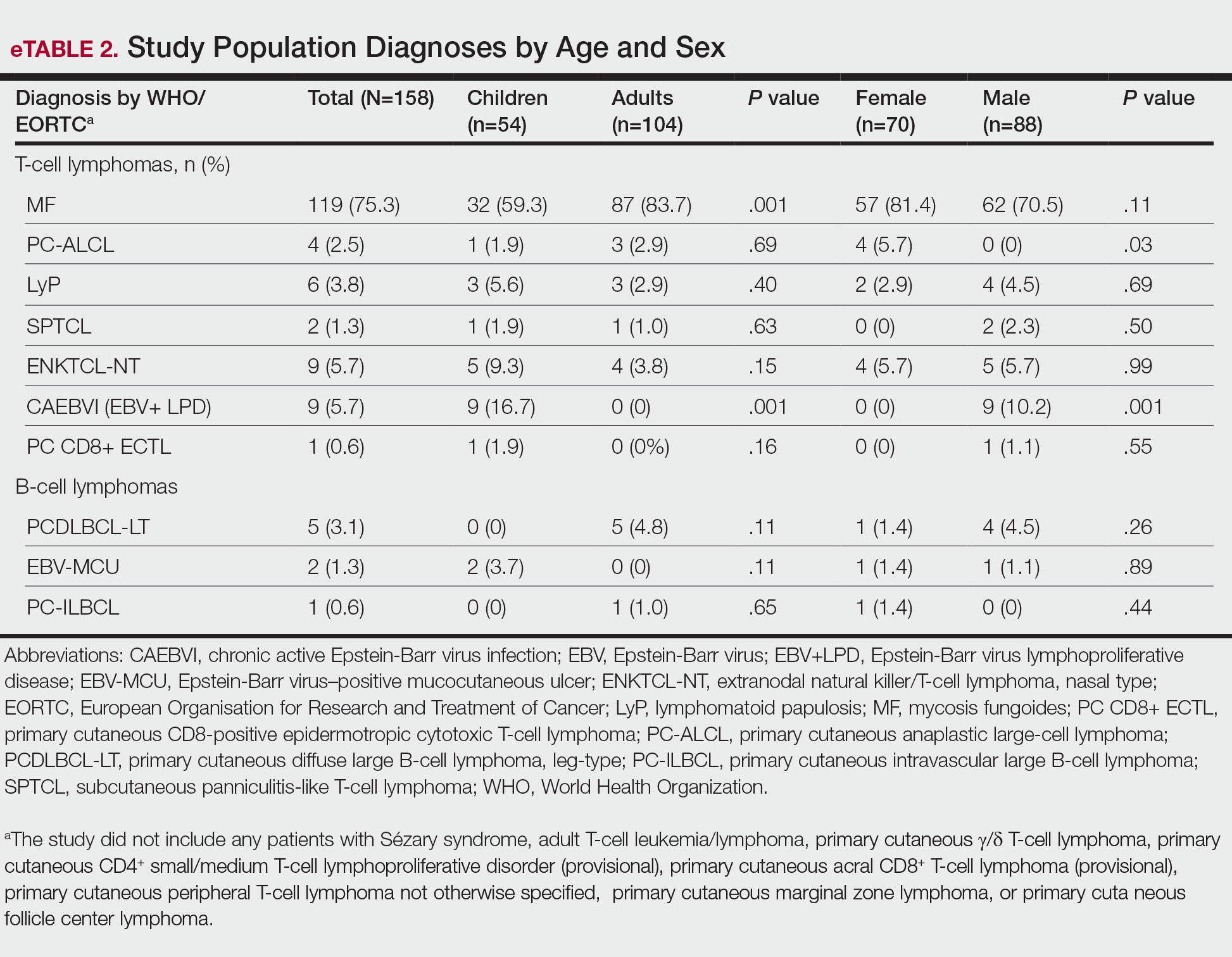
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
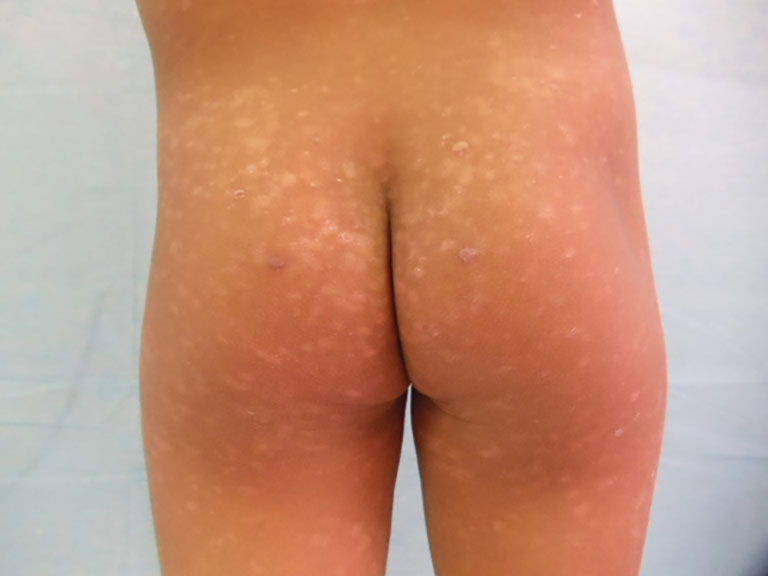
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).

Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).

Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).
Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).
Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
Non-Hodgkin lymphomas (NHLs) are a heterogeneous group of lymphoproliferative malignancies originating from T, B, or natural killer (NK) lymphocytes.1 Compared to Hodgkin lymphomas, NHLs exhibit a broader clinical spectrum and have a poorer prognosis and frequent extranodal involvement, with the skin being the second most frequent extranodal site.2 Primary cutaneous lymphomas (PCLs) are NHLs that are first evident on the skin without evidence of extracutaneous disease at diagnosis. They include a heterogeneous group of cutaneous T-cell lymphomas (CTCLs) and cutaneous B-cell lymphomas. Among CTCLs, mycosis fungoides (MF) is the most prevalent subtype, generally following an indolent course. Cutaneous B-cell lymphomas primarily include follicle center lymphoma and diffuse large B-cell lymphoma.3,4
The clinical behavior and incidence of PCLs vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.5,6 However, there is a notable lack of comparative studies in the literature addressing these variations, limiting a comprehensive understanding of PCLs and hindering the development of tailored therapeutic strategies. The main objective of this study was to evaluate the different clinical characteristics, subtypes, treatment options, and prognosis in PCLs between pediatric and adult populations.7,8
Methods
This retrospective observational study included pediatric (aged ≤18 years at diagnosis) and adult (aged >18 years at diagnosis) patients with a clinical and histopathologic diagnosis of PCL who were diagnosed and treated at either of 2 tertiary institutions (Dr. Manuel Gea Gonzalez General Hospital or the National Institute of Pediatrics, both in Mexico City, Mexico) between January 1, 1999, and December 31, 2019. The data analysis included demographic and clinical characteristics, type of PCL (according to World Health Organization [WHO]/European Organisation for Research and Treatment of Cancer [EORTC]) classification,3,4 treatment administered, and outcome. Disease remission was defined as remittance of clinical PCL manifestations for 3 months or more. Disease control was defined as stable clinical manifestations with no change in PCL stage following treatment initiation. Disease progression was defined as worsening clinical manifestations with an increase in PCL stage and/or development of systemic lymphoma. Beyond similarities and differences across age groups, we also analyzed differences by sex. χ² and Mann-Whitney U tests were used to assess differences between groups. Statistical significance was set at P≤.05. Institutional approval was obtained from both tertiary centers.
Results
Our analysis included a total of 158 patients: 54 (34.2%) were children and 104 (65.8%) were adults. Eighty-eight (55.7%) patients were male (eTable 1). The mean (SD) age at diagnosis was 9.5 (1.9) years in children and 49.7 (18) years in adults. Regarding differences between age groups, adult patients had a similar sex distribution, while in children, the majority of patients were male (37/54 [68.5%]; P=.01).
Overall, the most frequent diagnosis was MF, which occurred in 119 (75.3%) patients, and the most common lesions were erythematous plaques, noted in 95 (60.1%) patients. The lower extremities were the most affected body sites, impacting 127 (80.4%) patients, and the most common treatment was phototherapy, used to treat 110 (69.6%) patients. Reported outcomes included disease control in 45 (28.5%) patients and progression in 36 (22.8%) patients; 50 (31.6%) patients were lost to follow-up. Only 15 (9.5%) patients experienced disease remission, and 12 (7.6%) died.
The mean (SD) time between the onset of symptoms and diagnosis was shorter in children than in adults (18.1 [12.6] months vs 66.2 [34.9] months; P<.001). Regarding involved body sites, the head and neck more frequently affected children than adults (40 [74.1%] vs 33 [31.7%]; P<.001), while the upper extremities were more frequently involved in adults than in children (67 [64.4%] vs 45 [83.3%]; P<.001).
There were significant differences in the morphology of lesions and diagnoses. Children most frequently had hypopigmented plaques (25 [46.3%]) and macules (24 [44.4%])(P<.001) associated with MF, and scars (7 [13.0%]), blisters (6 [11.1%]), and edema (8 [14.8%])(P<.001) associated with positive Epstein-Barr virus (EBV) infection. Adults presented more frequently with hyperpigmented macules (19 [18.3%]) and plaques (37 [35.6%]), erythematous plaques (71 [68.3%]), atrophy (36 [34.6%]), and tumors (32 [30.8%])(P<.001). Adults were more often asymptomatic (86.5% vs 38.8%; P<.001).
Subtypes of PCL differed by age group (eTable 2), with MF being more frequent in adults (87 [83.6%] vs 32 [59.2%]; P<.001), while chronic active positive EBV infection (CAEBVI) manifesting as lymphoproliferative disease (LPD) was exclusive to male children (9 [16.6%])(P<.001). Accordingly, we found variations in systemic treatments used: monoclonal antibodies (mAb), thalidomide, intravenous immunoglobulin (IVIg), and hematopoietic stem cell transplantation (HSCT) were used exclusively for treating children (all P<.001). Outcomes were distributed similarly by age group.
The type of PCL, clinical manifestations, and treatment also varied by sex (eTables 2 and 3). Only males had CAEBVI and presented with edema (8 [9.1%] vs 0%; P<.01). Males also had tumors (23 [26.1%] vs 9 [12.9%]; P=.03) and lesions affecting the head and neck (52 [59.1%] vs 21 [30.0%]; P<.001) more frequently than females. Males were more likely than females to report pain (28 [31.8%] vs 13 [18.6%]; P=.05) and receive systemic treatment with thalidomide (11 [12.5%] vs 1 [1.4%]; P<.001) and IVIg (6 [6.8%] vs 0%; P=.02). Only females were diagnosed with primary cutaneous anaplastic large cell lymphoma (PC-ALCL)(4 [5.7%] vs 0%; P=.03) and had genital involvement (4 [5.7%] vs 0%; P=.03). Females were more likely to be asymptomatic (57 [81.4%] vs 54 [61.4%]; P<.001) or report pruritus (46 [65.7%] vs 44 [50%]; P<.001) and receive local treatment with phototherapy (58 [82.9%] vs 52 [59.1%]; P<.001) compared to males. Although distribution of outcomes was similar by sex, we found males were more frequently lost to follow-up (38 [43.2%] vs 12 [17.1%]; P<.001).
We further searched for differences in clinical manifestations according to the PCL subtype in each age group. The most frequent lesions in 32 children with MF were hypopigmented macules (21 [65.6%]; P<.001)(Figure 1). Three of 5 (60%) children with extranodal NK/T-cell lymphoma, nasal type (ENKTCL), had nodules (P=.002). Of 9 children with CAEBVI, 8 (88.9%) had edema (P<.001), ulcers (P<.001), erythematous plaques (P=.007), and hypopigmented plaques (P=.008); 5 (55.6%) children presented with scars (P<.001) and atrophy (P<.001); and 4 (44.4%) children had blisters (P=.005)(Figure 2). The 2 children with EBV-positive mucocutaneous ulcer (EBV-MCU) had crusts (P=.002) and blisters (P=.01).
Of 87 adults with MF, 54 (62%) had scaly lesions (P=.006)(Figure 3). Of 3 adult patients with PC-ALCL, 2 (66.7%) had crusts (P=.04) and ulcers (P=.05). Two of 3 (66.7%) adults with lymphomatoid papulosis (LyP) had erythematous papules (P<.001). All 4 adult patients with ENKTCL (P=.008) and all 5 patients with primary cutaneous diffuse large B-cell lymphoma, leg-type, had tumors (P<.001).
Finally, we found no differences in outcomes according to types of PCL overall or by age group; however, when categorized by sex, we found males with EBV-MCU more frequently had disease progression than females with EBV-MCU (P=.04).
Comment
Primary cutaneous lymphomas were similarly distributed among males and females (55.6% vs 44.3%, respectively). This slight male predominance was similar to other reports in the literature: one US study reported a male-to-female incidence rate ratio of 1.72, indicating a significantly higher incidence in males (P<.001).6 Similar trends have been observed in other geographic regions, with reported male-to-female ratios of 1.56 in Greece and 1.35 in Argentina.9,10 These findings suggest that PCLs are slightly more prevalent in males across different populations; however, when we stratified by age, pediatric cases of PCL were significantly more frequent in males than in females (68.5% vs. 31.4%; P=.01).
Our analysis revealed that the time to diagnosis was significantly longer in adults than in children (66.2 months vs 18.1 months) for all PCLs (P<.001). The most common type of PCL in both age groups was MF, with a notably higher prevalence in adults than in children (87 [83.7%] vs 32 [59.2%]). The prolonged course of MF in adults, often taking years to progress from early to advanced stages (47.0-52.7 months) may contribute to delayed diagnosis.8,11,12 Additionally, classic lesions of MF (erythematous scaly plaques) may resemble other common dermatologic conditions, further complicating early recognition and treatment in adults more than in children.11,12 Conversely, more aggressive and rapidly progressing PCL subtypes, including CAEBVI and ENKTCL-NT, were more frequent in children and would likely be diagnosed more promptly because of the acute onset and fast evolution of signs and symptoms.13
Mycosis fungoides is the most common CTCL, followed by CD30+ T-cell disorders such as LyP and PC-ALCL.14 While MF was the predominant subtype in both age groups, similar to previous reports,6,7 pediatric patients in our study exhibited distinctive features, such as hypopigmented macules and plaques. Hypopigmented lesions may suggest an underlying immunologic mechanism unique to younger patients, specifically children, in contrast to the hyperpigmented or violaceous lesions predominating in adults.7 The hypopigmented variant of MF has been reported to be more prevalent in children, similar to our data, accounting for 54.5% of all pediatric MF cases. These hypopigmented lesions typically manifest at an early stage and follow an indolent course.15,16 Jung et al8 conducted a systematic review of children with MF and reported a mean age at diagnosis of 12.2 years, whereas in our cohort, the mean age was 9.5 years. These findings highlight the different clinical manifestations of MF in children, which may aid in early recognition and diagnosis.
In adults, MF most commonly manifested as hyperpigmented macules and plaques, erythematous plaques, atrophic lesions, and tumors. In this population, MF remained the most frequently diagnosed PCL subtype, followed by PC-ALCL.
There were notable differences in symptom presentation between age groups and sexes. Adults were more often asymptomatic, and males reported pain more frequently.
When analyzing PCL subtypes in our study, we found that CAEBVI was exclusive to children, specifically males. The updated WHO/EORTC classification contains a new section on EBV-positive LPD in childhood, including hydroa vacciniforme–like LPD and hypersensitivity reactions to mosquito bites.4 Both are cutaneous manifestations of CAEBVI with a risk for progression to systemic EBV-positive T-cell or NK-cell lymphoma. These disorders mainly affect children and adolescents from Asia or Indigenous populations from Mexico and Central and South America.3,4,17 Cases in both female and male patients have been reported, without a clear sex predominance; however, mutations in the Src homology 2 domain containing 1A (SH2D1A) gene recently have been shown to cause X-linked lymphoproliferative disease, which is associated with predilection for EBV infection and subsequent EBV-positive LPD, including CAEBVI.18,19 Thus, it is possible some of the children with CAEBVI in our study may have an underlying X-linked lymphoproliferative disease, accounting for the male predominance.
Similarly, ENKTCL-NT tended to occur more in children than in adults in our study. Both CAEBVI-LPD and ENKTCL-NT are aggressive lymphomas with a suboptimal prognosis. Although treatment with immunomodulatory agents may lead to temporary remission in most cases, disease progression has been reported in larger cohorts, emphasizing the need for long-term follow-up and more aggressive treatments in severe cases of CAEBVI.13,17 Treatment options for EBV-positive LPD include mAb such as rituximab, IVIg, HSCT, antiviral agents, interferons α and γ, and corticosteroids.20
Treatment approaches were notably different between children and adults (P<.0001). Monoclonal antibodies, immunomodulatory agents such as thalidomide, IVIg, and HSCT were exclusively used in pediatric patients, reflecting the presence of CAEBVI and ENKTCL-NT (P<.0001). Additionally, edema, blisters, and scars were observed more frequently in children, likely due to the clinical manifestations of these EBV-related disorders.
A recent review of systemic NHL highlighted various age-related differences in clinical presentation, biology, and outcomes.13 In general, children tend to present with more aggressive subtypes and achieve better outcomes compared to adults.13 These differences may be attributed to variations in tumor biology, immune responses, and/or the benefits of early and intensive interventions in pediatric populations. These findings resonate with our results, as pediatric PCL patients received more aggressive treatments—including mAb, thalidomide, IVIg, and HSCT—likely due to the higher frequency of CAEBVI/ENKTCL-NT; however, we were unable to properly assess treatment outcomes, as many patients, both adults and children, were lost to follow-up.
Overall, our findings and comparisons with existing studies highlight the need for age-specific research and management approaches for PCL. The distinct clinical and biological profiles across age groups highlight opportunities for personalized therapies and further investigation into the molecular drivers of these differences to optimize outcomes for pediatric and adult patients.
When analyzing differences by sex, we found that CAEBVI was diagnosed exclusively in male children, who correspondingly exhibited clinical features such as edema and tumors, with lesions predominantly located on the head and neck. This also influenced treatment approach, as these patients were more likely to receive thalidomide and IVIg. In contrast, PC-ALCL was observed only in female patients, a finding that deviates from previously reported epidemiology.14 Females with PC-ALCL were more likely to have genital involvement and be asymptomatic, which could suggest a sex-related bias in disease recognition and seeking health care.
Recognizing distinctive clinical manifestations across different diagnoses and age groups can aid health care providers in early identification and accurate diagnosis of PCL. Our findings revealed several notable differences: adults with MF more frequently had scaly lesions, those with PC-ALCL had crusts and ulcers, and those with LyP had erythematous papules. All adults with ENKTCL and primary cutaneous diffuse large B-cell lymphoma, leg-type, presented with tumors. While children with MF had an increased frequency of hypopigmented macules, those with ENKTCL more frequently developed nodules, and children with EBV-MCU often had crusts and ulcers. As has already been mentioned, children with CAEBVI displayed a broad range of lesions, including edema, ulcers, erythematous and hypopigmented plaques, atrophy, blisters, and scars.
Our study was limited by the retrospective design and missing data from one-third of patients, which prevented outcome comparison. We also lacked molecular profiling of patients, which could help refine therapeutic strategies for PCL.13 Finally, as both centers included are reference institutions, results may be biased and overestimated and could differ from the rest of the population.
Conclusion
This comparative study of PCL highlighted age-related differences in clinical presentation, diagnostic distribution, and treatment patterns, including a higher prevalence among male children than female children. Adult patients with PCL had a notably longer time to diagnosis than children. The most common type of PCL identified in both age groups and sex categories was MF, but hypopigmented lesions predominated in children with this condition. Epstein-Barr virus–associated PCL occurred almost exclusively in children and manifested with nodules, edema, blisters, and scars. In terms of treatment, children received more aggressive and advanced therapies, including mAb, thalidomide, IVIg, and HSCT. Further prospective research is needed to establish variations in clinical manifestations, diagnoses, treatments, and outcomes.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
- Singh R, Shaik S, Negi BS, et al. Non-Hodgkin’s lymphoma: a review.J Family Med Prim Care. 2020;9:1834-1840.
- Armitage JO, Gascoyne RD, Lunning MA, et al. Non-Hodgkin lymphoma. Lancet. 2017;390:298-310.
- Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127:2375-2390.
- Willemze R, Cerroni L, Kempf W, et al. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood. 2019;133:1703-1714.
- Willemze R, Hodak E, Zinzani PL, et al; ESMO Guidelines Committee. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29:iv30-iv40.
- Bradford PT, Devesa SS, Anderson WF, et al. Cutaneous lymphoma incidence patterns in the United States: a population-based study of 3884 cases. Blood. 2009;113:5064-5073.
- Moon IJ, Won CH, Chang SE, et al. Prevalence, clinical features, and survival outcome trends of 627 patients with primary cutaneous lymphoma over 29 years: a retrospective review from a single tertiary center in Korea. Sci Rep. 2024;14:20118.
- Jung JM, Lim DJ, Won CH, et al. Mycosis fungoides in children and adolescents: a systematic review. JAMA Dermatol. 2021;157:431-438.
- Kaliampou S, Nikolaou V, Niforou A, et al. Epidemiological trends in cutaneous lymphomas in Greece. Eur J Dermatol. 2023;33:664-673.
- Abeldaño A, Enz P, Maskin M, et al. Primary cutaneous lymphoma in Argentina: a report of a nationwide study of 416 patients. Int J Dermatol. 2019;58:449-455.
- Cervini AB, Torres-Huamani AN, Sanchez-La-Rosa C, et al. Mycosis fungoides: experience in a pediatric hospital. Actas Dermosifiliogr. 2017;108:564-570.
- Welfringer-Morin A, Barroil M, Fraitag S, et al. Clinical features, histological characteristics, and disease outcomes of mycosis fungoides in children and adolescents: a nationwide multicentre cohort of 46 patients. Dermatology. 2023;239:132-139.
- Sandlund JT, Martin MG. Non-Hodgkin lymphoma across the pediatric and adolescent and young adult age spectrum. Hematology Am Soc Hematol Educ Program. 2016;2016:589-597.
- Ortiz-Hidalgo C, Pina-Oviedo S. Primary cutaneous anaplastic large cell lymphoma-a review of clinical, morphological, immunohistochemical, and molecular features. Cancers (Basel). 2023;15:4098.
- Nielsen PR, Eriksen JO, Wehkamp U, et al. Clinical and histological characteristics of mycosis fungoides and Sézary syndrome: a retrospective, single-centre study of 43 patients from eastern Denmark. Acta Derm Venereol. 2019;99:1231-1236.
- Suh KS, Jang MS, Jung JH, et al. Clinical characteristics and long-term outcome of 223 patients with mycosis fungoides at a single tertiary center in Korea: a 29-year review. J Am Acad Dermatol. 2022;86:1275-1284.
- Quintanilla-Martinez L, Ridaura C, Nagl F, et al. Hydroa vacciniforme-like lymphoma: a chronic EBV+ lymphoproliferative disorder with risk to develop a systemic lymphoma. Blood. 2013;122:3101-3110.
- Fujiwara S, Nakamura H. Chronic active Epstein-Barr virus infection: is it immunodeficiency, malignancy, or both? Cancers (Basel). 2020;12:3202.
- Sumazaki R, Kanegane H, Osaki M, et al. SH2D1A mutations in Japanese males with severe Epstein-Barr virus–associated illnesses. Blood. 2001;98:1268-1270.
- Kimura H. Pathogenesis of chronic active Epstein-Barr virus infection: is this an infectious disease, lymphoproliferative disorder, or immunodeficiency? Rev Med Virol. 2006;16:251-261.
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Age- and Sex-Related Differences in Primary Cutaneous Lymphoma
Practice Points
- The clinical behavior and incidence of primary cutaneous lymphomas vary dramatically between children and adults, suggesting underlying biologic, immunologic, and genetic differences.
- Primary cutaneous lymphoma is more common among males, particularly in children.
- Adults experience longer diagnostic delays due to slower symptom progression and overlap with benign skin conditions, whereas children often present with rapidly progressive, severe variants requiring more aggressive therapies.
