User login
Managing Office Supply Scams
It doesn’t occur to most physicians that a supplier might be ripping them off; but if adequate purchase controls are not in place, then it’s possible, and even likely. You should be aware of the common scams, how to avoid them, and the options if you’re victimized.
Con artists take advantage of unsuspecting employees (and physicians) and lax purchasing procedures. Typically, the scam begins with a phone call from a “representative” who asks questions about the office and the supplies commonly ordered in bulk, such as paper, disposable gloves, printer cartridges, gauze pads, and cleaning supplies. (They may claim to be conducting a survey.)
The scammer might pretend to be a regular supplier who is “overstocked” on printer ink or toner. (Toner scams are so common that perpetrators are nicknamed “toner phoners.”)
Here is how this scenario might play out: You receive a shipment of poor quality merchandise you didn’t order. Later, you receive an invoice for 5 to 10 times the amount you would pay a legitimate supplier for better quality supplies.
You can’t be sure you didn’t place the order, because you have no system in place for checking such things; your employees may have already opened the boxes; and you’re under the mistaken impression that you have to return unordered merchandise or pay for it if you’ve started using it. (More on this later.)
A variation can occur when the caller offers your receptionist or office manager a free “promotional item” with “no further obligation.” Your employee figures why not, and accepts the gift. You receive overpriced unordered merchandise, followed by an invoice with the employee’s name prominently displayed. The crooks are betting you will blame the employee, who you assume placed the order to get the gift (despite his or her denials), and now you have to pay.
Regardless of the method, the goal is the same: to get an invoice into your hands. Once that is accomplished, the scammers get very aggressive; they will dun you with letters and phone calls, send you to real or fake collection agents, and even threaten legal action.
You’re at a disadvantage because you’re not positive, and certainly can’t prove, that you didn’t order the supplies. And, if you pay the bill, you think maybe they will get off your back; however, you will only be targeted for additional scams. The scammer may even sell your “account” to other con artists.
Prevention, fortunately, is mostly a matter of good organization and training. Put one person in charge of ordering supplies, and instruct everyone (including physicians) to tell all solicitors, “I’m not authorized to order anything or answer surveys. You’ll need to speak to our purchaser.”
Instruct your purchaser to be suspicious of all cold calls and unfamiliar salespeople, and to never yield to pressure to make an immediate decision. Even if an offer appears legitimate, ask to see a catalog or printed price list before ordering anything.
Standardize your ordering procedure. Acquire a supply of purchase orders – either electronic or written –and make sure one is filled out for every order, and every order is assigned an order number. The employee who pays bills, ideally someone different than the one who does the ordering, should receive a copy of every purchase order. Keep blank order forms locked up or password protected.
When shipments arrive, verify they match the shipper’s invoice and the purchase order. If everything reconciles, send a copy of the shipping invoice to your accounts payable employee. Bills for services should be reconciled the same way.
If a scammer still gets through your defenses, you have rights, and you should exercise them. According to the Federal Trade Commission, you are not required to pay for supplies or services you didn’t order, nor are you required to return them. You may treat unordered merchandise as a gift. But of course, you have to be able to prove you didn’t order it – which should be easy if you always use purchase orders.
The FTC has a good template of instructions for avoiding scams at www.ftc.gov/bcp/edu/pubs/business/alerts/alt065.shtm that can be printed and used to train employees. Don’t forget to put a copy in your employee manual, as well.
It doesn’t occur to most physicians that a supplier might be ripping them off; but if adequate purchase controls are not in place, then it’s possible, and even likely. You should be aware of the common scams, how to avoid them, and the options if you’re victimized.
Con artists take advantage of unsuspecting employees (and physicians) and lax purchasing procedures. Typically, the scam begins with a phone call from a “representative” who asks questions about the office and the supplies commonly ordered in bulk, such as paper, disposable gloves, printer cartridges, gauze pads, and cleaning supplies. (They may claim to be conducting a survey.)
The scammer might pretend to be a regular supplier who is “overstocked” on printer ink or toner. (Toner scams are so common that perpetrators are nicknamed “toner phoners.”)
Here is how this scenario might play out: You receive a shipment of poor quality merchandise you didn’t order. Later, you receive an invoice for 5 to 10 times the amount you would pay a legitimate supplier for better quality supplies.
You can’t be sure you didn’t place the order, because you have no system in place for checking such things; your employees may have already opened the boxes; and you’re under the mistaken impression that you have to return unordered merchandise or pay for it if you’ve started using it. (More on this later.)
A variation can occur when the caller offers your receptionist or office manager a free “promotional item” with “no further obligation.” Your employee figures why not, and accepts the gift. You receive overpriced unordered merchandise, followed by an invoice with the employee’s name prominently displayed. The crooks are betting you will blame the employee, who you assume placed the order to get the gift (despite his or her denials), and now you have to pay.
Regardless of the method, the goal is the same: to get an invoice into your hands. Once that is accomplished, the scammers get very aggressive; they will dun you with letters and phone calls, send you to real or fake collection agents, and even threaten legal action.
You’re at a disadvantage because you’re not positive, and certainly can’t prove, that you didn’t order the supplies. And, if you pay the bill, you think maybe they will get off your back; however, you will only be targeted for additional scams. The scammer may even sell your “account” to other con artists.
Prevention, fortunately, is mostly a matter of good organization and training. Put one person in charge of ordering supplies, and instruct everyone (including physicians) to tell all solicitors, “I’m not authorized to order anything or answer surveys. You’ll need to speak to our purchaser.”
Instruct your purchaser to be suspicious of all cold calls and unfamiliar salespeople, and to never yield to pressure to make an immediate decision. Even if an offer appears legitimate, ask to see a catalog or printed price list before ordering anything.
Standardize your ordering procedure. Acquire a supply of purchase orders – either electronic or written –and make sure one is filled out for every order, and every order is assigned an order number. The employee who pays bills, ideally someone different than the one who does the ordering, should receive a copy of every purchase order. Keep blank order forms locked up or password protected.
When shipments arrive, verify they match the shipper’s invoice and the purchase order. If everything reconciles, send a copy of the shipping invoice to your accounts payable employee. Bills for services should be reconciled the same way.
If a scammer still gets through your defenses, you have rights, and you should exercise them. According to the Federal Trade Commission, you are not required to pay for supplies or services you didn’t order, nor are you required to return them. You may treat unordered merchandise as a gift. But of course, you have to be able to prove you didn’t order it – which should be easy if you always use purchase orders.
The FTC has a good template of instructions for avoiding scams at www.ftc.gov/bcp/edu/pubs/business/alerts/alt065.shtm that can be printed and used to train employees. Don’t forget to put a copy in your employee manual, as well.
It doesn’t occur to most physicians that a supplier might be ripping them off; but if adequate purchase controls are not in place, then it’s possible, and even likely. You should be aware of the common scams, how to avoid them, and the options if you’re victimized.
Con artists take advantage of unsuspecting employees (and physicians) and lax purchasing procedures. Typically, the scam begins with a phone call from a “representative” who asks questions about the office and the supplies commonly ordered in bulk, such as paper, disposable gloves, printer cartridges, gauze pads, and cleaning supplies. (They may claim to be conducting a survey.)
The scammer might pretend to be a regular supplier who is “overstocked” on printer ink or toner. (Toner scams are so common that perpetrators are nicknamed “toner phoners.”)
Here is how this scenario might play out: You receive a shipment of poor quality merchandise you didn’t order. Later, you receive an invoice for 5 to 10 times the amount you would pay a legitimate supplier for better quality supplies.
You can’t be sure you didn’t place the order, because you have no system in place for checking such things; your employees may have already opened the boxes; and you’re under the mistaken impression that you have to return unordered merchandise or pay for it if you’ve started using it. (More on this later.)
A variation can occur when the caller offers your receptionist or office manager a free “promotional item” with “no further obligation.” Your employee figures why not, and accepts the gift. You receive overpriced unordered merchandise, followed by an invoice with the employee’s name prominently displayed. The crooks are betting you will blame the employee, who you assume placed the order to get the gift (despite his or her denials), and now you have to pay.
Regardless of the method, the goal is the same: to get an invoice into your hands. Once that is accomplished, the scammers get very aggressive; they will dun you with letters and phone calls, send you to real or fake collection agents, and even threaten legal action.
You’re at a disadvantage because you’re not positive, and certainly can’t prove, that you didn’t order the supplies. And, if you pay the bill, you think maybe they will get off your back; however, you will only be targeted for additional scams. The scammer may even sell your “account” to other con artists.
Prevention, fortunately, is mostly a matter of good organization and training. Put one person in charge of ordering supplies, and instruct everyone (including physicians) to tell all solicitors, “I’m not authorized to order anything or answer surveys. You’ll need to speak to our purchaser.”
Instruct your purchaser to be suspicious of all cold calls and unfamiliar salespeople, and to never yield to pressure to make an immediate decision. Even if an offer appears legitimate, ask to see a catalog or printed price list before ordering anything.
Standardize your ordering procedure. Acquire a supply of purchase orders – either electronic or written –and make sure one is filled out for every order, and every order is assigned an order number. The employee who pays bills, ideally someone different than the one who does the ordering, should receive a copy of every purchase order. Keep blank order forms locked up or password protected.
When shipments arrive, verify they match the shipper’s invoice and the purchase order. If everything reconciles, send a copy of the shipping invoice to your accounts payable employee. Bills for services should be reconciled the same way.
If a scammer still gets through your defenses, you have rights, and you should exercise them. According to the Federal Trade Commission, you are not required to pay for supplies or services you didn’t order, nor are you required to return them. You may treat unordered merchandise as a gift. But of course, you have to be able to prove you didn’t order it – which should be easy if you always use purchase orders.
The FTC has a good template of instructions for avoiding scams at www.ftc.gov/bcp/edu/pubs/business/alerts/alt065.shtm that can be printed and used to train employees. Don’t forget to put a copy in your employee manual, as well.
To Discount or Not to Discount?
As the “Great Recession” continues, there is much discussion on medical forums about how to increase cash flow, decrease administrative expenses, and deal with ever-increasing numbers of unemployed and uninsured patients.
Extending discounts to patients who pay at the time of service or pay out of pocket is one effective way of addressing all three of these issues. Caution is necessary, though, because discounts can run afoul of federal and state laws. These include state antikickback statutes, the anti-inducement provision of the Health Insurance Portability and Accountability Act (HIPAA), the Medicare exclusion provision, and state insurance antidiscrimination provisions.
From a legal standpoint, any discount is a kickback of sorts—you are returning part of your fee to the patient—and many laws designed to thwart real kickbacks can apply in such situations.
Take the relatively straightforward case of time-of-service discounts for cosmetic procedures and other services not covered by insurance. You would think such transactions are strictly between you and your patients, but you need to avoid the appearance of using these discounts as marketing incentives; that is, as inducements to attract patients.
There is also the possibility that a shrewd third-party payer could try to pull a fast one on you. Many provider agreements contain what are often called “most favored nation” clauses, which require you to automatically give that provider the lowest price you offer to anyone else, regardless of what they would otherwise pay. In other words, they could demand that you give them the same discount.
My response, should that situation ever arise, would be that a time-of-service discount is exactly that: It is offered only when payment is made immediately. Third parties, which never pay at the time of service, are not entitled to it.
Things get more complicated if you also want to extend discounts for covered services. You must be sure that the discounted fee you charge the patient is also reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud. And you must avoid discounting so regularly that the discounted fee becomes your new usual and customary rate.
Waiving coinsurance and deductibles can be trouble too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare and Medicaid Services may see it as an inducement or kickback, especially if you do it routinely. CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need” (according to the Office of Inspector General), but thorough documentation is in order in such cases.
Waiving copays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable copays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and there has been litigation against providers who flout this requirement. As with CMS, accommodating patients with individually documented financial limitations is acceptable, but when there is a pattern of routine waivers and no documentation, you will have difficulty defending it.
In addition to antikickback laws, some states also have antidiscrimination laws that forbid either lower charges to any subset of insurance payers or any noninsurance payer than to any insurance payer. Some states make specific exceptions for legitimate discounts—as in cases of financial hardship, or when you are just trying to pass along your lower billing and collections costs—but other states do not. So you need to check your state’s laws and, as always, run everything past your attorney.
As for how much of a discount you can give, I cannot suggest an amount, but if it is completely out of proportion to the administrative costs of submitting paperwork and the hassles associated with waiting for your money, you could, once again, be accused of offering a discount that is a de facto increase to insurance carriers, and that could result in charges of fraud.
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies and all hospitals have a written policy for this, often based on federal poverty guidelines. Do a little homework: Contact local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient’s indigence. Once again, consistency of administration, objectivity in policies, and documentation of individual eligibility are essential.
As the “Great Recession” continues, there is much discussion on medical forums about how to increase cash flow, decrease administrative expenses, and deal with ever-increasing numbers of unemployed and uninsured patients.
Extending discounts to patients who pay at the time of service or pay out of pocket is one effective way of addressing all three of these issues. Caution is necessary, though, because discounts can run afoul of federal and state laws. These include state antikickback statutes, the anti-inducement provision of the Health Insurance Portability and Accountability Act (HIPAA), the Medicare exclusion provision, and state insurance antidiscrimination provisions.
From a legal standpoint, any discount is a kickback of sorts—you are returning part of your fee to the patient—and many laws designed to thwart real kickbacks can apply in such situations.
Take the relatively straightforward case of time-of-service discounts for cosmetic procedures and other services not covered by insurance. You would think such transactions are strictly between you and your patients, but you need to avoid the appearance of using these discounts as marketing incentives; that is, as inducements to attract patients.
There is also the possibility that a shrewd third-party payer could try to pull a fast one on you. Many provider agreements contain what are often called “most favored nation” clauses, which require you to automatically give that provider the lowest price you offer to anyone else, regardless of what they would otherwise pay. In other words, they could demand that you give them the same discount.
My response, should that situation ever arise, would be that a time-of-service discount is exactly that: It is offered only when payment is made immediately. Third parties, which never pay at the time of service, are not entitled to it.
Things get more complicated if you also want to extend discounts for covered services. You must be sure that the discounted fee you charge the patient is also reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud. And you must avoid discounting so regularly that the discounted fee becomes your new usual and customary rate.
Waiving coinsurance and deductibles can be trouble too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare and Medicaid Services may see it as an inducement or kickback, especially if you do it routinely. CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need” (according to the Office of Inspector General), but thorough documentation is in order in such cases.
Waiving copays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable copays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and there has been litigation against providers who flout this requirement. As with CMS, accommodating patients with individually documented financial limitations is acceptable, but when there is a pattern of routine waivers and no documentation, you will have difficulty defending it.
In addition to antikickback laws, some states also have antidiscrimination laws that forbid either lower charges to any subset of insurance payers or any noninsurance payer than to any insurance payer. Some states make specific exceptions for legitimate discounts—as in cases of financial hardship, or when you are just trying to pass along your lower billing and collections costs—but other states do not. So you need to check your state’s laws and, as always, run everything past your attorney.
As for how much of a discount you can give, I cannot suggest an amount, but if it is completely out of proportion to the administrative costs of submitting paperwork and the hassles associated with waiting for your money, you could, once again, be accused of offering a discount that is a de facto increase to insurance carriers, and that could result in charges of fraud.
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies and all hospitals have a written policy for this, often based on federal poverty guidelines. Do a little homework: Contact local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient’s indigence. Once again, consistency of administration, objectivity in policies, and documentation of individual eligibility are essential.
As the “Great Recession” continues, there is much discussion on medical forums about how to increase cash flow, decrease administrative expenses, and deal with ever-increasing numbers of unemployed and uninsured patients.
Extending discounts to patients who pay at the time of service or pay out of pocket is one effective way of addressing all three of these issues. Caution is necessary, though, because discounts can run afoul of federal and state laws. These include state antikickback statutes, the anti-inducement provision of the Health Insurance Portability and Accountability Act (HIPAA), the Medicare exclusion provision, and state insurance antidiscrimination provisions.
From a legal standpoint, any discount is a kickback of sorts—you are returning part of your fee to the patient—and many laws designed to thwart real kickbacks can apply in such situations.
Take the relatively straightforward case of time-of-service discounts for cosmetic procedures and other services not covered by insurance. You would think such transactions are strictly between you and your patients, but you need to avoid the appearance of using these discounts as marketing incentives; that is, as inducements to attract patients.
There is also the possibility that a shrewd third-party payer could try to pull a fast one on you. Many provider agreements contain what are often called “most favored nation” clauses, which require you to automatically give that provider the lowest price you offer to anyone else, regardless of what they would otherwise pay. In other words, they could demand that you give them the same discount.
My response, should that situation ever arise, would be that a time-of-service discount is exactly that: It is offered only when payment is made immediately. Third parties, which never pay at the time of service, are not entitled to it.
Things get more complicated if you also want to extend discounts for covered services. You must be sure that the discounted fee you charge the patient is also reflected on the claim submitted to the insurer. Billing the insurer more than you charged the patient invites a charge of fraud. And you must avoid discounting so regularly that the discounted fee becomes your new usual and customary rate.
Waiving coinsurance and deductibles can be trouble too, particularly with Medicare and Medicaid. You might intend it as a good deed, but the Centers for Medicare and Medicaid Services may see it as an inducement or kickback, especially if you do it routinely. CMS has no problem with an occasional waiver, especially “after determining in good faith that the individual is in financial need” (according to the Office of Inspector General), but thorough documentation is in order in such cases.
Waiving copays for privately insured patients can be equally problematic. Nearly all insurers impose a contractual duty on providers to make a reasonable effort to collect applicable copays and/or deductibles. They view the routine waiver of patient payments as a breach of contract, and there has been litigation against providers who flout this requirement. As with CMS, accommodating patients with individually documented financial limitations is acceptable, but when there is a pattern of routine waivers and no documentation, you will have difficulty defending it.
In addition to antikickback laws, some states also have antidiscrimination laws that forbid either lower charges to any subset of insurance payers or any noninsurance payer than to any insurance payer. Some states make specific exceptions for legitimate discounts—as in cases of financial hardship, or when you are just trying to pass along your lower billing and collections costs—but other states do not. So you need to check your state’s laws and, as always, run everything past your attorney.
As for how much of a discount you can give, I cannot suggest an amount, but if it is completely out of proportion to the administrative costs of submitting paperwork and the hassles associated with waiting for your money, you could, once again, be accused of offering a discount that is a de facto increase to insurance carriers, and that could result in charges of fraud.
In cases of legitimate financial hardship, the most effective and least problematic strategy may be to offer a sliding scale. Many large clinics and community agencies and all hospitals have a written policy for this, often based on federal poverty guidelines. Do a little homework: Contact local social service agencies and welfare clinics, learn the community standard in your area, and formulate a written policy with guidelines for determining a patient’s indigence. Once again, consistency of administration, objectivity in policies, and documentation of individual eligibility are essential.
Now Is the Time to Hire
If you have plans to enlarge your office staff anytime soon, consider doing it sooner, rather than later.
In March, President Obama signed the Hiring Incentives to Restore Employment (HIRE) Act into law. Known popularly as the “Jobs Bill,” its intended purpose is to get the unemployed back to work by encouraging the hiring of employees now.
The new law exempts private-sector employers from their 6.2% share of the Social Security payroll tax for the remainder of 2010 on all new hires who had been unemployed for the previous 60 days or more.
This is a hiring incentive that, for once, works to your advantage, as well as that of your new employees. For one thing, the tax benefit is immediate; it helps your cash flow instantly, because there are no refunds—the tax is simply not collected in the first place. For another, if you keep your new employees on payroll for at least 52 weeks, you, as the employer, can take an additional tax credit of up to $1,000 for each new employee, on your own 2011 tax return.
(More precisely, the credit is the lesser of either $1,000 or 6.2% of the wages paid to the worker during the 52 consecutive-week period; that means it will be $1,000 for any employee paid more than about $16,130 over that period.)
There is no limit to the number of employees you can hire, no maximum or minimum salary you need to pay, and no cap on the total dollar amount of tax that may be forgiven; your office saves 6.2% whether your new employee is a $30,000 medical assistant, a $100,000 physician assistant, or a $250,000 physician.
Part-time employees also are eligible; there is no minimum number of hours that new employees must work. However, the salary you pay a part-time employee in the second 26 weeks of that first year must total at least 80% of his or her pay over the first 26 weeks.
The objective of the new law is to create new jobs, not to hire the unemployed at the expense of those who have jobs already. So if you are thinking about laying off your entire staff and hiring a completely new crew solely for the purpose of taking the payroll exemption, forget about it. A new hire who replaces another employee who performed the same job is not eligible for the benefit, unless the prior employee left voluntarily or was fired for cause.
Congress anticipated and proactively plugged some other obvious loopholes; you cannot get the exemption by firing employees for 60 days and then hiring them back, for example. And you cannot claim the new tax breaks by hiring family members or by employing domestic workers in your home.
The law also forbids double dipping: If you have employees who are eligible for the Work Opportunity Tax Credit (WOTC), you must select one benefit or the other for 2010, not both.
The law requires each eligible worker to certify by signed affidavit that he or she has not been employed for more than 40 hours during the preceding 60-day period, that no one was fired without cause to create the job being taken, and that the employer is not a relative or family member.
You should explain to these new hires that they will not be paying into Social Security in 2010, but their eventual Social Security benefits will not be decreased because of it.
Remember, the incentive only applies to wages paid to eligible new employees for the remainder of this year; the idea is to decrease unemployment now. So the sooner you hire, the longer your payroll tax holiday will last.
The IRS will be watching, so be sure to check with your lawyer and accountant, and get all your documentation straight.
If you have plans to enlarge your office staff anytime soon, consider doing it sooner, rather than later.
In March, President Obama signed the Hiring Incentives to Restore Employment (HIRE) Act into law. Known popularly as the “Jobs Bill,” its intended purpose is to get the unemployed back to work by encouraging the hiring of employees now.
The new law exempts private-sector employers from their 6.2% share of the Social Security payroll tax for the remainder of 2010 on all new hires who had been unemployed for the previous 60 days or more.
This is a hiring incentive that, for once, works to your advantage, as well as that of your new employees. For one thing, the tax benefit is immediate; it helps your cash flow instantly, because there are no refunds—the tax is simply not collected in the first place. For another, if you keep your new employees on payroll for at least 52 weeks, you, as the employer, can take an additional tax credit of up to $1,000 for each new employee, on your own 2011 tax return.
(More precisely, the credit is the lesser of either $1,000 or 6.2% of the wages paid to the worker during the 52 consecutive-week period; that means it will be $1,000 for any employee paid more than about $16,130 over that period.)
There is no limit to the number of employees you can hire, no maximum or minimum salary you need to pay, and no cap on the total dollar amount of tax that may be forgiven; your office saves 6.2% whether your new employee is a $30,000 medical assistant, a $100,000 physician assistant, or a $250,000 physician.
Part-time employees also are eligible; there is no minimum number of hours that new employees must work. However, the salary you pay a part-time employee in the second 26 weeks of that first year must total at least 80% of his or her pay over the first 26 weeks.
The objective of the new law is to create new jobs, not to hire the unemployed at the expense of those who have jobs already. So if you are thinking about laying off your entire staff and hiring a completely new crew solely for the purpose of taking the payroll exemption, forget about it. A new hire who replaces another employee who performed the same job is not eligible for the benefit, unless the prior employee left voluntarily or was fired for cause.
Congress anticipated and proactively plugged some other obvious loopholes; you cannot get the exemption by firing employees for 60 days and then hiring them back, for example. And you cannot claim the new tax breaks by hiring family members or by employing domestic workers in your home.
The law also forbids double dipping: If you have employees who are eligible for the Work Opportunity Tax Credit (WOTC), you must select one benefit or the other for 2010, not both.
The law requires each eligible worker to certify by signed affidavit that he or she has not been employed for more than 40 hours during the preceding 60-day period, that no one was fired without cause to create the job being taken, and that the employer is not a relative or family member.
You should explain to these new hires that they will not be paying into Social Security in 2010, but their eventual Social Security benefits will not be decreased because of it.
Remember, the incentive only applies to wages paid to eligible new employees for the remainder of this year; the idea is to decrease unemployment now. So the sooner you hire, the longer your payroll tax holiday will last.
The IRS will be watching, so be sure to check with your lawyer and accountant, and get all your documentation straight.
If you have plans to enlarge your office staff anytime soon, consider doing it sooner, rather than later.
In March, President Obama signed the Hiring Incentives to Restore Employment (HIRE) Act into law. Known popularly as the “Jobs Bill,” its intended purpose is to get the unemployed back to work by encouraging the hiring of employees now.
The new law exempts private-sector employers from their 6.2% share of the Social Security payroll tax for the remainder of 2010 on all new hires who had been unemployed for the previous 60 days or more.
This is a hiring incentive that, for once, works to your advantage, as well as that of your new employees. For one thing, the tax benefit is immediate; it helps your cash flow instantly, because there are no refunds—the tax is simply not collected in the first place. For another, if you keep your new employees on payroll for at least 52 weeks, you, as the employer, can take an additional tax credit of up to $1,000 for each new employee, on your own 2011 tax return.
(More precisely, the credit is the lesser of either $1,000 or 6.2% of the wages paid to the worker during the 52 consecutive-week period; that means it will be $1,000 for any employee paid more than about $16,130 over that period.)
There is no limit to the number of employees you can hire, no maximum or minimum salary you need to pay, and no cap on the total dollar amount of tax that may be forgiven; your office saves 6.2% whether your new employee is a $30,000 medical assistant, a $100,000 physician assistant, or a $250,000 physician.
Part-time employees also are eligible; there is no minimum number of hours that new employees must work. However, the salary you pay a part-time employee in the second 26 weeks of that first year must total at least 80% of his or her pay over the first 26 weeks.
The objective of the new law is to create new jobs, not to hire the unemployed at the expense of those who have jobs already. So if you are thinking about laying off your entire staff and hiring a completely new crew solely for the purpose of taking the payroll exemption, forget about it. A new hire who replaces another employee who performed the same job is not eligible for the benefit, unless the prior employee left voluntarily or was fired for cause.
Congress anticipated and proactively plugged some other obvious loopholes; you cannot get the exemption by firing employees for 60 days and then hiring them back, for example. And you cannot claim the new tax breaks by hiring family members or by employing domestic workers in your home.
The law also forbids double dipping: If you have employees who are eligible for the Work Opportunity Tax Credit (WOTC), you must select one benefit or the other for 2010, not both.
The law requires each eligible worker to certify by signed affidavit that he or she has not been employed for more than 40 hours during the preceding 60-day period, that no one was fired without cause to create the job being taken, and that the employer is not a relative or family member.
You should explain to these new hires that they will not be paying into Social Security in 2010, but their eventual Social Security benefits will not be decreased because of it.
Remember, the incentive only applies to wages paid to eligible new employees for the remainder of this year; the idea is to decrease unemployment now. So the sooner you hire, the longer your payroll tax holiday will last.
The IRS will be watching, so be sure to check with your lawyer and accountant, and get all your documentation straight.
Square Peg, Square Hole

I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
I encounter a lot of hospitalists who complain that the other doctors at their hospital think of hospitalists as second-class citizens, as sort of like career residents. HM program directors need to make sure that is not the case for the hospitalists in their practice.
SHM has worked with the AMA’s Organized Medical Staff Section to assess the perception of hospitalists by primary-care physicians (PCPs) and hospitalists themselves. When asked in a 2009 survey, “Do you agree or disagree that hospitalists are respected members of the medical staff at a hospital?” only 3 out of 4 respondents agreed or highly agreed. That percentage is up slightly from the same survey conducted in 2007, and we don’t have data regarding how the responses would have been different if the question had been asked about other specialties. But I still find it concerning that about 25% of PCPs and hospitalists don’t see hospitalists as respected members of a medical staff. (If you are wondering, there wasn’t much of a difference between how hospitalists and PCPs answered the question.)
Use First Names
In the 1980s, I left residency and entered private practice as a hospitalist in a nonteaching, suburban hospital. I had a really hard time calling other doctors by their first names, especially the highly regarded senior internist who was my former roommate’s dad. He had always been Dr. McCollough to me, and I insisted calling him “Doctor” until we had been peers on the same medical staff for about a year.
Finally, in a somewhat annoyed voice, he told me I had to start calling him “Bob,” and that I should call all the doctors by their first names. It took a while, but using first names began to feel normal. Looking back on it, I think Dr. McCollough Bob taught me an important lesson about fitting in.
So make sure the hospitalists in your group call other doctors by their first names, too.
Dress the Part
I’ve come to believe that there are a number of things some hospitalists do to sabotage their own interest in being respected by the medical staff at their hospital. To my surprise, I’ve worked with a number of hospitalist groups in which most dress and act like residents, then complain that other doctors at their hospital treat them like residents. I think the way we dress, especially early in our careers, is a pretty big deal. If you’re similar in age to residents, then you’ll sure look like a resident if you dress like them. So don’t wear scrubs and Skechers unless all of the doctors in your hospital wear scrubs and Skechers.
The best advice is to dress the way the respected doctors dress. Follow the lead on things like neckties, dresses, and the white coat (the latter is almost unheard of at my hospital unless it is used to cover up scrubs). Fortunately, few doctors dress formally anymore (e.g., suit, and tie or sport coat for men). Emerging research might push all of us toward shedding ties, long sleeves, and the white coat before long.
Of course, you should keep in mind the way patients would like to see you dress. You can find information about patient expectations through a simple Internet search or by asking the person in charge of patient satisfaction at your hospital.
Seek Social Connections
Just like the issue of dress, I’ve encountered a number of hospitalist groups that have a habit of sneaking into the physician lunchroom, grabbing food in a “to go” container, and heading back to their office to eat together. These hospitalists are missing a valuable opportunity to enjoy social conversation with physicians of all specialties. If your hospital has a physician lunch room that is crowded with doctors, take advantage of the opportunity to build social networks.
You don’t need to eat there every day. (For a number of years, I enjoyed having lunch with the social workers in our main cafeteria.) But you should eat there more frequently than sneaking back to your office to eat only with other hospitalists. (If you don’t have time for lunch, then we need to talk about workload and efficiency issues.)
Look for other opportunities to make connections with other doctors through service on hospital committees, participation in social events at the hospital, or speaking at grand rounds. Although any single activity might not have significant impact, if you do these things regularly, you will form better relationships and be less likely to be or feel “dumped on,” and if it does happen, you’re in a much better position to address it if the dumping doctor is a friend.
Leadership Positions
Work to ensure a member of your group always sits on the medical staff executive committee, and seek out leadership positions like chief of medicine or chief of staff. Don’t simply assume you are too young or too inexperienced. Your hospital really needs the leadership of doctors who have a broad view of hospital operations and medical staff affairs. Few doctors have a broader view than hospitalists.
And if you have an interest in medical staff leadership, think about whether you’d like to serve as your hospital’s chief medical officer (aka vice president of medical affairs). All of these activities are important ways to influence what happens at your hospital, but aside from that, they are an excellent way to build relationships and gain respect from throughout the medical staff.
Worthwhile Effort
Ensuring that the hospitalists in your group feel respected and valued by other doctors and everyone they work with is important. Don’t make the mistake of thinking that working on this is just about stroking hospitalists’ egos.
I coauthored a 2001 research study on hospitalist burnout that failed to show a correlation between workload and burnout, but the study found that things like poor occupational solidarity are associated with burnout.1
Feeling like you fit in and are a respected member of your peer group (medical staff) is important and worth working on diligently. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is cofounder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is course co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Reference
- Hoff T, Whitcomb WF, Nelson JR. Thriving and surviving in a new medical career: the case of hospitalist physicians. Jrl Health Social Behavior. 2001;43:72-91.
Transitions Telethon

The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The headline was as biting as it was inciting. “Frustrations with hospitalist care: Need to improve transitions and communication,” it screamed from the cover of a recent issue of the Annals of Internal Medicine.1 Reading on the run, I thumbed to page 469 and glanced at the first few paragraphs, my mind spinning with the implications.
The article was an editorial following a recent thought piece by a primary-care physician (PCP) frustrated with his interactions with the HM model—mainly around the lack of communication from hospitalists about his patients, his marginalized role with his patients’ hospital care, and the lack of information transfer around transitions.2
Frustrations and Slapstick Comedy
Frustration with hospitalist care? Is this how PCPs see us? Are we really “frustrating” our outpatient colleagues? To an outsider, this presented a one-sided view of the issue—the side that sounds simplistically negative. What if someone important to our group should read this article, someone like my hospital CEO? I didn’t have to wonder for long as I looked up from my elevator reading to note my hospital CEO entering.
What followed eerily resembled one of those scenes from a slapstick comedy, as the boob, played perfectly by me, obviously fumbles something he intends to hide from his boss behind his back to escape the knowing eye of said boss. And, like a pornographic-magazine-sniffing parent, my CEO knowingly diagnosed the situation.
“Whatcha reading?” he sagely queried.
“Nothing,” I replied unconvincingly.
“Nothing? It sure looks like you hastily stuffed a magazine or something down the back of your pants as I walked in.”
“Oh, this?” I responded, unearthing a large medical journal from my pants, leaving an untucked shirt in its wake. “This is just a medical journal. You know, lots of medical stuff. It’s pretty complex. Probably hard for nonmedical types to understand,” I replied, employing a bit of professorial condescension to throw him off track.
“Annals of Internal Medicine,” he replied. “What a coincidence. I just received an e-mail from a friend with an Annals article about the issues of transitions of care with the hospitalist model. Sounds like a real problem. Maybe our new electronic health records will fix that. If not, you should fix it. Let’s chat about it soon.”
“Right,” I said as the elevator doors swished behind him, leaving me disheveled in both appearance and thoughts.
Testimonials?
The more recent Annals editorial summarized—and then printed—a few of the many online responses to the original thought piece.3 The responses ranged from outrage with the HM model of care to more measured discussions of the limitations of the “old” model it replaced. However, the tone and implications were clear: At least some, if not many, PCPs are displeased with the HM model.
One writer related a recent example in which his elderly patient was admitted unbeknownst to him. After receiving a query from a family member, he called the hospitalist on duty, who was uninformed about the patient details, had made questionable therapeutic changes, and was “unapologetic” about her team’s lack of communication, arguing that the ED physician “should have called.” That led this PCP to conclude that the system is “disjointed and isolating,” leaving “patients feeling abandoned.” Another writer commented that the current system of communication results in “potentially detrimental and demoralizing degrees of separation.” A response by a hospitalist detailed how they were able to put a system in place to contact PCPs with whom they are contracted 80% of the time.
The Annals editors concluded that the letters they received in response to the first article “reflect a schism that exists in internal medicine about the positive and negative effects of hospitalist care,” noting that “the evidence is still deficient about how to deliver care optimally when complex, seriously-ill patients must transition between multiple providers in diverse health care settings.” The authors go on to call for “intensive research and productive debates” about the HM model of care.
A Challenge to You
“Disjointed and isolating”? … “Detrimental and demoralizing”? … Lauding 80% PCP contact rates? … “Intensive research and debate”?
I get that this is a complex issue and that healthcare in the U.S. is fragmented to the point of fracture. To wit, it can be agonizingly time-consuming to track down PCPs and wade through their automated phone systems. And this assumes that your patient has a PCP, can identify that PCP, and has their phone number. If they don’t, you’re left to sift through online phone books, clinic websites, or Google searches with the hopes that you can summon the right Dr. Davis, Davies, or Daves—the patient’s not quite sure of the spelling but knows “she’s a nice lady doctor.” I know firsthand the tension between taking the time to make that PCP call and getting home in time for dinner with my family—I’m often guilty of choosing dinner.
However, I’m not sure “intensive research” is the answer. Nor is this a problem that can wait for technological solutions. I don’t want to diminish the great strides that have been made or understate the need to continue to innovate around transitions—this needs to be an area of ongoing study. But this is a problem that has at least one relatively simple, short-term solution: Just pick up the phone. As one Annals writer rightly questions: “How has inter-physician communication come to be regarded as an unexpected courtesy rather than an obligation?”
Good question.
So, I have a simple challenge for you: For one week, join me in committing to calling 100% of the available PCPs on patient discharge. I can guarantee you this will prove to be a hard, time-consuming, and, at times, migraine-inducing process. But it is an intervention that will make a difference, can be launched tomorrow, and does not require “intensive research and debate.”
We’ll no doubt gain some insight into our patients’ current therapeutic regimens, enlist PCPs’ help with the treatment decisions, and ensure that our patients’ transitions are as safe as possible. My guess is that we’ll also find it valuable to the point it becomes habit.
Start by committing with me to just one week.
Then go home and have dinner. TH
Dr. Glasheen is associate professor of medicine at the University of Colorado Denver, where he serves as director of the Hospital Medicine Program and the Hospitalist Training Program, and as associate program director of the Internal Medicine Residency Program.
References
- Frustrations with hospitalist care: need to improve transitions and communication. Ann Intern Med. 2010;152(7):469.
- Beckman H. Three degrees of separation. Ann Intern Med. 2009;151(12):890-891.
- The relationship between hospitalists and primary care physicians. Ann Intern Med. 2010;152(7):474-6.
The Cost of Regulation
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?

The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
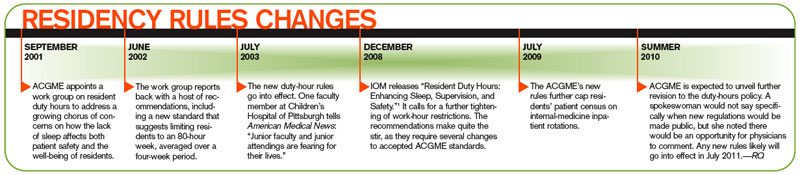
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.

At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
The impact of last summer’s new restrictions from the Accreditation Council for Graduate Medical Education (ACGME) on how many hospitalized patients a first-year resident can treat on an internal-medicine (IM) rotation was as immediate as it was evident at Monmouth Medical Center, a 527-bed teaching hospital in Long Branch, N.J. The institution had a class of eight rookie residents whose caseloads were cut from 12 to the new threshold of 10.
Physicians “had to find some other way of getting attention . . . for 16 patients,” says Sarah Wallach, MD, FACP, director of Monmouth’s IM residency program and vice chair of the department of medicine at the hospital. At Monmouth, the solution came in the form of a new hire—a nurse practitioner (NP)—to handle the overflow. The NP service is used predominantly for referral patients from primary-care physicians (PCPs), as opposed to independent hospital admissions.
But because the NP service does not provide 24-hour coverage, the hospital can get away with only one person in the position. To extend coverage all day long, Dr. Wallach estimates she would need to hire two or three additional NPs, plus another one or two administrative positions to provide relief on holidays and vacations. “You would need five people,” she says. “I can’t afford that.”
Few hospitals or HM groups can afford new hires in today’s world of Medicare reimbursement cuts, shrinking budgets, and—courtesy of the newest rules—restricting patient caps for residents. The latest rules took hold about a year ago, but hospitalists in both academic and community settings say the impact already is noticeable.
Many hospitals have had to craft solutions, which have included burdening academic hospitals with more clinical responsibilities, turning to private HM groups (HMGs) to assume the patients residents can no longer care for, or hiring nonphysician providers (NPPs) to pick up the slack. As Dr. Wallach pointedly notes, the latter two solutions cost money at a time when hospitals have less to go around.
Already, teaching hospitals have begun discussions about how the newest rules—and the future changes they presage—will change the playing field. Will a wave of academics flee their classroom (the teaching hospital), as nonteaching duties become an intrusion? Will teaching hospitals face financial pressure as they struggle to replace the low-cost labor force that residents represent?
Perhaps most importantly from a medical perspective, will graduate trainees be as prepared as their predecessors when they enter practice?
The answers will have a direct correlation to private HMGs, which are poised to see more patients in the wake of residency restrictions, particularly on overnight services. The cost of hospital care will increase for hospitals, putting more pressure on hospitalist groups that tout themselves to C-suites as engines for cost savings. Long-term implications, unfortunately, remain murky, as the newest rules have been in place for a relatively short time. Plus, ACGME is expected—at the end of this month, according to a recent memo to program directors—to announce more changes to residency guidelines.
“Hospitalists will always be involved in teaching—it will never go away,” says Julia Wright, MD, FHM, clinical professor of medicine and director of hospital medicine at the University of Wisconsin School of Medicine and Public Health in Madison and a member of Team Hospitalist. “But it will be a very different balance, a different kind of feel.”
The Past to the Future
To understand the concerns moving forward, it’s important to first look back. In July 2003, new ACGME rules went into place capping the workweeks of residents at 80 hours. Rules were put into place that regulated the number of patients that residents could be assigned, and those thresholds were further tightened on July 1, 2009. The most notable 2009 change: A first-year resident’s patient census must not exceed 10 patients. ACGME CEO Thomas J. Nasca, MD, MACP, sent a letter to program directors in early May announcing more changes to resident work hours. The letter indicates proposals will be announced by the end of this month, and public comment will follow. At the earliest, new rules changes would go into effect in 2011. “The board may adopt a modification to the duty-hours standard,” says Julie Jacob, a spokeswoman for Chicago-based ACGME. “Any proposed standards would get a public comment.”
Jacob declined further comment, but various hospitalists and academics say they wouldn’t be surprised if new rules reflect 2008 Institute of Medicine (IOM) recommendations.1 The IOM report called for a maximum resident shift length of 30 hours, with admission of patients for up to 16 hours, plus a five-hour uninterrupted sleep period between 10 p.m. and 8 a.m. It also suggested the remaining workweek hours be used for transitional and educational activities.
However those IOM recommendations are incorporated, one thing is clear: Any adoption of those standards will have a financial impact. In fact, a study published last year reported that annual labor costs from implementing the IOM standards was estimated to be $1.6 billion in 2006 dollars (see “The Cost of Progress,” p. 25).2
“Any replacement of a resident costs more than a resident, whether it’s an NP, a PA (physician assistant), an MD, or a DO,” says Kevin O’Leary, MD, MS, associate program director of the IM residency program at Northwestern University’s Feinberg School of Medicine in Chicago. “Everybody costs more.”
The Fate of Teachers
Some of the largest academic centers, including the Feinberg School, the University of Michigan, and the teaching service at St. Luke’s-Roosevelt Hospital in New York City, reduced patient caseloads ahead of the 2009 round of residency rule changes. Hospitalists and educators at those institutions say the proactive approach helped them adjust to the newest rules, which by some estimates reduce resident productivity by 20%.
But the changes shift the workload to academic hospitalists, many of whom forego higher-paying positions to pursue teaching and research. According to the latest SHM survey data, academic hospitalists make about $50,000 less per year than the average community hospitalist. But as clinical work intrudes further, as residents are unable to assume the patient care they once did, educators are put into positions of having to balance the educational portion of their job with patient care, says John Del Valle, MD, professor and residency program director in the department of internal medicine at the University of Michigan Health System in Ann Arbor.
“This is where difficult decisions have to be made,” Dr. Del Valle says. “This is not the blend of activities that traditional academics signed up for.”
Solutions to relieve current and impending pressure on teaching hospitalists have presented themselves in different ways. In Dr. Del Valle’s hospital, there is a split between the hospitalist service and the house staff, which is aimed at keeping up with the growth in IM admissions. That tally has climbed an average of 4% per year for the past five years, reaching some 18,000 admissions last year. To handle that workload, the nonresident service last year added three clinical full-time equivalents (FTEs) to bring its total to nearly 30 FTEs.
Dr. Del Valle notes his institution has been fortunate to be able to afford growth, thanks in large part to a payor mix with a relatively low percentage of charity care and high level of activity.
At Brigham and Women’s Hospital in Boston, the answer is a freestanding PA service that has been in place since 2005. Last summer, the program went to a 24-hour rotation to increase continuity for overnight services and to provide coverage on night shifts, an area most in the industry agree will be hit hardest by the resident caps. Physicians at Brigham’s, a teaching affiliate of Harvard Medical School, are now discussing an expansion of the PA service, or perhaps even an overhaul to a more cost-efficient solution, says Danielle Scheurer, MD, MSc, FHM, assistant professor of medicine at Harvard and director of Brigham’s general medicine service.
At Medical Center Hospital (MCH) in Odessa, Texas, the hospitalists were added to the ED call schedule once every five nights. The plan was under discussion before the new residency rules went into place; however, it was implemented to keep the IM residency program within the new limits, says Bruce Becker, MD, MCH’s chief medical officer.
And at St. Luke’s-Roosevelt Hospital, discussions are under way on how to best extend the nonteaching staff, says Ethan Fried, MD, MS, FACP, assistant professor of clinical medicine at Columbia University, vice chair for education in the department of medicine and director of graduate medical education at St. Luke’s-Roosevelt. “The adjustment has to come from the nonteaching side because the house staff at this point is saturated,” says Dr. Fried, president-elect of the Association of Program Directors in Internal Medicine (APDIM). “You can’t be cheap about acquiring your nonteaching staff.”
The Fate of Students
Perhaps paramount to the fears of how teaching hospitalists will react to current or future restrictions is the effect those limits have on the residents they safeguard. Some physicians think the new rules will produce crops of ill-prepared residents because they have been coddled with limited patient censuses. Other physicians argue that the new thresholds will actually better prepare physicians when HM groups are hiring residents for full-time positions.
Dr. Del Valle acknowledges there is as yet no rigorous data to show the impact of the current restrictions, but he agrees it’s a simple equation of patient-care mathematics. “You can’t [easily] replace 100-110 hours [of care per week],” he says.
Others say patient caps and rules to limit how much work residents do are in line with the purpose of medical training programs. “I’ve bought into the fact that these programs exist to train residents, not to provide clinical care,” Dr. O’Leary says. “I’ve drunk that Kool-Aid. … I think there’s more variation, person to person, than ‘my era vs. the current era.’ Like any new hospitalist that you hire, you need to give an orientation and give enough support to them so when they begin to see patients that they are not overwhelmed.”
Shaun Frost, MD, FACP, FHM, might be best described as halfway between those two extremes. A regional director for the eastern U.S. for Cogent Healthcare, he says duty-hour restrictions have had deleterious impacts but also create learning opportunities.
“The residency work-hour restrictions have inhibited our ability to train people to work as efficiently as trainees who were taught in the past,” says Dr. Frost, an SHM board member. “That doesn’t necessarily mean you can’t teach people to work more efficiently . . . but in the future, my hope is that residency training programs will recognize the deficit that exists in personal work efficiencies between their completion and their responsibilities as a hospitalist.”
To that end, Dr. Frost works with others to develop both structured curriculum and classroom didactics that help new hospitalists make up for gaps in preparation that weren’t addressed in residency. In some cases, that can be practice management and billing issues, but often, according to Dr. Frost, it is addressing personal workflow and bridging the “unnatural discontinuity” in patient care from residency to the real world.
“There is a cost to this investment for the future,” Dr. Frost adds. “If people don’t recognize the potential return on investment as being critical to the development of an educated workforce—an efficient and competent workforce—and thus critical to the retention of high-performing hospitalists, they are selling themselves, unfortunately, significantly short.”
Caught in the Middle
One man’s trash is another man’s treasure, the axiom tells us. Well, in healthcare circles, that could just as easily read: The woes of academic hospitalists are the wealth of community hospitalists.
The new rules “may result in more opportunities for hospitalists to provide needed clinical services,” Dr. Wright says.
The long-term implications, though, remain to be seen. While academic hospitalists say they have seen preliminary increases in care-delivery costs because of the latest rules changes, many say it’s too soon to tell just how high those costs might climb and what ripple effect might follow.
Some physicians, including Dr. Del Valle, note that while the 2009 changes and the expectation of more changes in 2011 are cause for attention, that doesn’t translate to cause for concern. In 2003, months before the 80-hour workweek rules were first put in place by ACGME, many of the same debates were already under way: How will the faculty of IM residency programs cope? How will institutions pay the bills while putting money aside for other physicians picking up the slack?
“This is a pendulum,” Dr. Del Valle says. “I think it will come back to a balanced place.”
Dr. Fried, who is more optimistic that the residency rules can have a positive, long-term effect, agrees. He says residency caps and limits should not be viewed as “things that limit education. We [should] look at them as things that ensure education continues while patient care continues.” TH
Richard Quinn is a freelance writer based in New Jersey.
References
- Institute of Medicine. Resident Duty Hours: Enhancing Sleep, Supervision, and Safety. Ulmer C, Wolman DM, Johns MM, eds. Washington, D.C.: The National Academies Press; 2008.
- Nuckols TK, Bhattacharya J, Wolman DM, Ulmer C, Escarce JJ. Cost implications of reduced work hours and workloads for resident physicians. N Engl J Med. 2009:360(21):2202-2215.
From Entrepreneur to Employee: Part 1. Ambiguity in Attitudes About Hospital Employment
“HT caused my breast cancer” … and more
Patient sues drug companies: “HT caused my breast cancer”
A WOMAN IN HER LATE 50S took a combination of Premarin and Provera for 6 years to treat menopausal symptoms. She was then switched to Prempro for 4 years until she detected a lump in her breast. Her physician diagnosed invasive ductal breast cancer and the patient underwent a left mastectomy. Cancer spread to her lymph nodes; she underwent chemotherapy and radiation treatments. She sued the drug manufacturers.
PATIENT’S CLAIM Years of combination hormone therapy (HT) caused her breast cancer. The pharmaceutical companies failed to adequately test the drugs despite knowledge of their cancer-causing potential. If the defendants had begun cancer studies in the early 1980s when they first learned about the cancer risk, the risk would have been discovered before she began taking HT in 1991. She provided letters dated as early as 1976 from the FDA, independent researchers, and internal drug company scientists urging that cancer risk research be conducted. She claimed the defendants intentionally restricted the publication of medical data outlining the cancerous effects of combination HT to physicians and patients.
DEFENDANTS’ DEFENSE The FDA has reviewed the benefits and risks of HT for decades, always finding that the benefits outweighed the risks. Defendants cited 19 studies examining HT and breast cancer risk, the first published in 1959. The Women’s Health Initiative reaffirmed the increased risk of breast cancer, available in the labeling for Prempro in 1995. Labeling for Premarin and Provera included FDA-approved warnings of the breast cancer risk. The physician and patient were adequately warned of risks before use.
VERDICT $34.3 million verdict was returned, including $28 million in total punitive damages against the drug companies.
Was hypertension properly treated in this stroke victim?
AFTER HEAVY VAGINAL BLEEDING was diagnosed in a 49-year-old woman, her gynecologist prescribed medroxyprogesterone acetate. Several months later, she underwent a dilation and curettage for continued bleeding. A year later, her blood pressure (BP) was 140/94 mm Hg, which the physician believed was “white coat” hypertension. The woman returned 10 months later, still complaining of abnormal uterine bleeding, but she refused surgical options; the physician prescribed birth control pills. She returned for a routine exam a year later, when her BP was again elevated. The physician continued the patient’s oral contraceptive prescription and initiated treatment for high BP with triamterene. When the patient called to complain of excessive bleeding the next month, a nurse told her to take ibuprofen and call back if symptoms persisted. Shortly thereafter, the patient suffered a stroke. After rehabilitation, she regained use of her arms and legs, but suffered from foot drop and decreased fine motor skills.
PATIENT’S CLAIM The stroke was caused by uncontrolled hypertension and/or birth control pills. The physician should have initiated treatment the first time her BP was elevated, and it should have been checked more frequently. Birth control pills should have been discontinued when high BP was diagnosed because they are contraindicated in women older than 35 years whose BP is elevated.
PHYSICIAN’S DEFENSE The use of birth control pills was proper; the physician prescribed a low-dose combination medication commonly given to perimenopausal women to control abnormal bleeding. When high BP was first suspected, the physician commenced treatment.
VERDICT A defense verdict was returned.
Painful intercourse reported following incontinence surgery
EIGHT SURGERIES WERE PERFORMED to correct a 54-year-old woman’s cystocele, enterocele, and retrocele. The patient’s bladder, colon, and intestines had been pressing on her vaginal canal causing abdominal pain, painful intercourse, and urinary and fecal incontinence.
PATIENT’S CLAIM The procedures reduced the size of her vaginal opening and the length of her vaginal canal, causing constant pain as well as severe pain with intercourse. She was not informed that this was a risk of surgery.
PHYSICIAN’S DEFENSE The patient’s vaginal opening did shrink due to the release of pressure placed on the vaginal canal by the other organs, but it is still within normal range of vaginal size. The procedures resolved the patient’s incontinence issues.
VERDICT A defense verdict was returned.
Radiotherapy wrong for sarcoma; caused short bowel syndrome
FIBROIDS WERE MORCELLATED during a vaginal hysterectomy in a 56-year-old woman. The patient’s pathology report indicated endometrial stromal sarcoma (ESS). She underwent open surgery for staging and to remove any residual cancer cells that could be identified. The gynecologist referred her to a radiation oncologist. After receiving radiotherapy for 4 months, the patient complained of bowel-related symptoms. Three months later, she sought treatment closer to home for diarrhea and gastrointestinal problems. A surgeon diagnosed radiation-induced short bowel syndrome causing inadequate nutritional absorption. The patient underwent two operations, during which large sections of her bowel were removed, a permanent colostomy was placed. She then required total parenteral nutrition tube feedings.
PLAINTIFF’S CLAIM The radiation oncologist was negligent for recommending and administering radiotherapy because of its limited value in ESS. Hormonal therapy should have been used instead.
PHYSICIAN’S DEFENSE Radiotherapy was necessary because of the patient’s history and disease type. Morcellation during vaginal hysterectomy increased the risk of microscopic cancer cells remaining in the pelvis, supported by the finding of residual cancer cells during the second procedure. Radiotherapy was necessary to treat the residual cancer cells.
VERDICT A defense verdict was returned.
No response to alarm when fetal heart tones are lost
A WOMAN ATTEMPTED VAGINAL BIRTH after having one vaginal birth and one cesarean delivery in the past. Labor progressed slowly with inadequate contractions and lack of descent. After the mother pushed five or six times without progress, the OB left to deliver another baby. Because of lack of progression, the mother requested cesarean delivery, and the husband conveyed their concerns to the nursing staff. The nurses assured them that all was well but did not discuss the parents’ concerns with the OB or other hospital personnel. One hour later, the mother’s uterus ruptured, fetal heart tones were lost from the external fetal monitor, and an alarm sounded.
PLAINTIFF’S CLAIM The nursing staff failed to respond to the alarm immediately; when a response did come, a nurse allegedly stated with excitement that she was amazed that no one had responded. This statement was confirmed by the OB. After 9 minutes of signal loss, a fetal heartbeat of 60 was found, but it was severely bradycardic. The mother was rushed to the OR and the baby was delivered expeditiously. The child was born limp and without respiratory effort, and sustained hypoxic ischemic encephalopathy. At age 5, he had no purposeful movement of his extremities, could not communicate, and was wheelchair-bound, although he was not cognitively impaired.
DEFENDANTS’ DEFENSE The OB offered full policy limits before trial. The hospital claimed that the 9-minute delay in detecting the loss of fetal heart tone and seeking the OB’s intervention was not the proximate cause of the child’s handicaps.
VERDICT A $4.9 million Michigan verdict was reached.
Untreated postpartum infection necessitated hysterectomy
AN 18-YEAR-OLD WOMAN was discharged from the hospital two days after the vaginal birth of her healthy child, although she claimed to not feel well. When a hospital-employed nurse visited her the next day, the patient reported abdominal pain and cramping. Five days later, she returned to the hospital in extreme pain. She was diagnosed with severe Streptococcus A infection, air-lifted to another hospital, and treated with antibiotics for 5 days. A hysterectomy was later performed.
PLAINTIFF’S CLAIM The physician, visiting nurse, and hospital failed to diagnose and treat the infection in a timely manner, resulting in a hysterectomy. Laboratory tests taken before the patient’s hospital discharge showed an elevated white blood cell (WBC) count; the patient should have been prescribed antibiotics before leaving the hospital. The visiting nurse did not react appropriately when the patient reported pain. The hospital was responsible because the results of the WBC test were not entered into the patient’s chart.
DEFENDANTS’ DEFENSE The physician claimed that the elevated WBC count was not recorded in the patient’s medical chart with other lab values. The hospital claimed that a high WBC count is common after childbirth; the test is rarely performed at that time. The only reason it was performed was that the technology automatically recorded WBC when it evaluated hemoglobin and hemocrit. Abdominal cramping reported to the visiting nurse is normal 3 days after childbirth. The patient did not have an infection at discharge or at the time of the nurse’s visit.
VERDICT Suit against the physician was dismissed prior to jury deliberations. A $2.3 million verdict was returned against the hospital.
Did retained sponges lead to PID and gallbladder disease?
A 6-INCH VAGINAL LACERATION was discovered after a woman delivered a healthy baby. The ObGyn, who was covering for the patient’s regular ObGyn because of a snowstorm, could not repair the laceration in the delivery room. He packed the patient’s vagina with gauze sponges, and took her to the OR where he repaired the laceration. The next day, he removed sponges placed after surgery. The patient was discharged with instructions to follow-up with her regular ObGyn. Eight days after delivery, the patient complained to her ObGyn of severe abdominal pain and a foul odor. Antibiotics were prescribed, but she refused a vaginal examination because of the pain. Six weeks after delivery, four gauze sponges were removed from the patient’s vagina.
PLAINTIFF’S CLAIM The physician was negligent in leaving the sponges in her vagina. He should have conducted the follow-up himself because he delivered her child. The infection caused chronic pain from pelvic inflammatory disease (PID), and necessitated the removal of her gallbladder.
PHYSICIAN’S DEFENSE Retained sponges can occur in the absence of negligence. It was proper for the patient to return to her own physician for postoperative follow-up treatment. The patient’s PID and gallbladder problems were unrelated to the retained sponges.
VERDICT A defense verdict was returned. The defendant was granted costs and attorney fees exceeding $27,000.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Patient sues drug companies: “HT caused my breast cancer”
A WOMAN IN HER LATE 50S took a combination of Premarin and Provera for 6 years to treat menopausal symptoms. She was then switched to Prempro for 4 years until she detected a lump in her breast. Her physician diagnosed invasive ductal breast cancer and the patient underwent a left mastectomy. Cancer spread to her lymph nodes; she underwent chemotherapy and radiation treatments. She sued the drug manufacturers.
PATIENT’S CLAIM Years of combination hormone therapy (HT) caused her breast cancer. The pharmaceutical companies failed to adequately test the drugs despite knowledge of their cancer-causing potential. If the defendants had begun cancer studies in the early 1980s when they first learned about the cancer risk, the risk would have been discovered before she began taking HT in 1991. She provided letters dated as early as 1976 from the FDA, independent researchers, and internal drug company scientists urging that cancer risk research be conducted. She claimed the defendants intentionally restricted the publication of medical data outlining the cancerous effects of combination HT to physicians and patients.
DEFENDANTS’ DEFENSE The FDA has reviewed the benefits and risks of HT for decades, always finding that the benefits outweighed the risks. Defendants cited 19 studies examining HT and breast cancer risk, the first published in 1959. The Women’s Health Initiative reaffirmed the increased risk of breast cancer, available in the labeling for Prempro in 1995. Labeling for Premarin and Provera included FDA-approved warnings of the breast cancer risk. The physician and patient were adequately warned of risks before use.
VERDICT $34.3 million verdict was returned, including $28 million in total punitive damages against the drug companies.
Was hypertension properly treated in this stroke victim?
AFTER HEAVY VAGINAL BLEEDING was diagnosed in a 49-year-old woman, her gynecologist prescribed medroxyprogesterone acetate. Several months later, she underwent a dilation and curettage for continued bleeding. A year later, her blood pressure (BP) was 140/94 mm Hg, which the physician believed was “white coat” hypertension. The woman returned 10 months later, still complaining of abnormal uterine bleeding, but she refused surgical options; the physician prescribed birth control pills. She returned for a routine exam a year later, when her BP was again elevated. The physician continued the patient’s oral contraceptive prescription and initiated treatment for high BP with triamterene. When the patient called to complain of excessive bleeding the next month, a nurse told her to take ibuprofen and call back if symptoms persisted. Shortly thereafter, the patient suffered a stroke. After rehabilitation, she regained use of her arms and legs, but suffered from foot drop and decreased fine motor skills.
PATIENT’S CLAIM The stroke was caused by uncontrolled hypertension and/or birth control pills. The physician should have initiated treatment the first time her BP was elevated, and it should have been checked more frequently. Birth control pills should have been discontinued when high BP was diagnosed because they are contraindicated in women older than 35 years whose BP is elevated.
PHYSICIAN’S DEFENSE The use of birth control pills was proper; the physician prescribed a low-dose combination medication commonly given to perimenopausal women to control abnormal bleeding. When high BP was first suspected, the physician commenced treatment.
VERDICT A defense verdict was returned.
Painful intercourse reported following incontinence surgery
EIGHT SURGERIES WERE PERFORMED to correct a 54-year-old woman’s cystocele, enterocele, and retrocele. The patient’s bladder, colon, and intestines had been pressing on her vaginal canal causing abdominal pain, painful intercourse, and urinary and fecal incontinence.
PATIENT’S CLAIM The procedures reduced the size of her vaginal opening and the length of her vaginal canal, causing constant pain as well as severe pain with intercourse. She was not informed that this was a risk of surgery.
PHYSICIAN’S DEFENSE The patient’s vaginal opening did shrink due to the release of pressure placed on the vaginal canal by the other organs, but it is still within normal range of vaginal size. The procedures resolved the patient’s incontinence issues.
VERDICT A defense verdict was returned.
Radiotherapy wrong for sarcoma; caused short bowel syndrome
FIBROIDS WERE MORCELLATED during a vaginal hysterectomy in a 56-year-old woman. The patient’s pathology report indicated endometrial stromal sarcoma (ESS). She underwent open surgery for staging and to remove any residual cancer cells that could be identified. The gynecologist referred her to a radiation oncologist. After receiving radiotherapy for 4 months, the patient complained of bowel-related symptoms. Three months later, she sought treatment closer to home for diarrhea and gastrointestinal problems. A surgeon diagnosed radiation-induced short bowel syndrome causing inadequate nutritional absorption. The patient underwent two operations, during which large sections of her bowel were removed, a permanent colostomy was placed. She then required total parenteral nutrition tube feedings.
PLAINTIFF’S CLAIM The radiation oncologist was negligent for recommending and administering radiotherapy because of its limited value in ESS. Hormonal therapy should have been used instead.
PHYSICIAN’S DEFENSE Radiotherapy was necessary because of the patient’s history and disease type. Morcellation during vaginal hysterectomy increased the risk of microscopic cancer cells remaining in the pelvis, supported by the finding of residual cancer cells during the second procedure. Radiotherapy was necessary to treat the residual cancer cells.
VERDICT A defense verdict was returned.
No response to alarm when fetal heart tones are lost
A WOMAN ATTEMPTED VAGINAL BIRTH after having one vaginal birth and one cesarean delivery in the past. Labor progressed slowly with inadequate contractions and lack of descent. After the mother pushed five or six times without progress, the OB left to deliver another baby. Because of lack of progression, the mother requested cesarean delivery, and the husband conveyed their concerns to the nursing staff. The nurses assured them that all was well but did not discuss the parents’ concerns with the OB or other hospital personnel. One hour later, the mother’s uterus ruptured, fetal heart tones were lost from the external fetal monitor, and an alarm sounded.
PLAINTIFF’S CLAIM The nursing staff failed to respond to the alarm immediately; when a response did come, a nurse allegedly stated with excitement that she was amazed that no one had responded. This statement was confirmed by the OB. After 9 minutes of signal loss, a fetal heartbeat of 60 was found, but it was severely bradycardic. The mother was rushed to the OR and the baby was delivered expeditiously. The child was born limp and without respiratory effort, and sustained hypoxic ischemic encephalopathy. At age 5, he had no purposeful movement of his extremities, could not communicate, and was wheelchair-bound, although he was not cognitively impaired.
DEFENDANTS’ DEFENSE The OB offered full policy limits before trial. The hospital claimed that the 9-minute delay in detecting the loss of fetal heart tone and seeking the OB’s intervention was not the proximate cause of the child’s handicaps.
VERDICT A $4.9 million Michigan verdict was reached.
Untreated postpartum infection necessitated hysterectomy
AN 18-YEAR-OLD WOMAN was discharged from the hospital two days after the vaginal birth of her healthy child, although she claimed to not feel well. When a hospital-employed nurse visited her the next day, the patient reported abdominal pain and cramping. Five days later, she returned to the hospital in extreme pain. She was diagnosed with severe Streptococcus A infection, air-lifted to another hospital, and treated with antibiotics for 5 days. A hysterectomy was later performed.
PLAINTIFF’S CLAIM The physician, visiting nurse, and hospital failed to diagnose and treat the infection in a timely manner, resulting in a hysterectomy. Laboratory tests taken before the patient’s hospital discharge showed an elevated white blood cell (WBC) count; the patient should have been prescribed antibiotics before leaving the hospital. The visiting nurse did not react appropriately when the patient reported pain. The hospital was responsible because the results of the WBC test were not entered into the patient’s chart.
DEFENDANTS’ DEFENSE The physician claimed that the elevated WBC count was not recorded in the patient’s medical chart with other lab values. The hospital claimed that a high WBC count is common after childbirth; the test is rarely performed at that time. The only reason it was performed was that the technology automatically recorded WBC when it evaluated hemoglobin and hemocrit. Abdominal cramping reported to the visiting nurse is normal 3 days after childbirth. The patient did not have an infection at discharge or at the time of the nurse’s visit.
VERDICT Suit against the physician was dismissed prior to jury deliberations. A $2.3 million verdict was returned against the hospital.
Did retained sponges lead to PID and gallbladder disease?
A 6-INCH VAGINAL LACERATION was discovered after a woman delivered a healthy baby. The ObGyn, who was covering for the patient’s regular ObGyn because of a snowstorm, could not repair the laceration in the delivery room. He packed the patient’s vagina with gauze sponges, and took her to the OR where he repaired the laceration. The next day, he removed sponges placed after surgery. The patient was discharged with instructions to follow-up with her regular ObGyn. Eight days after delivery, the patient complained to her ObGyn of severe abdominal pain and a foul odor. Antibiotics were prescribed, but she refused a vaginal examination because of the pain. Six weeks after delivery, four gauze sponges were removed from the patient’s vagina.
PLAINTIFF’S CLAIM The physician was negligent in leaving the sponges in her vagina. He should have conducted the follow-up himself because he delivered her child. The infection caused chronic pain from pelvic inflammatory disease (PID), and necessitated the removal of her gallbladder.
PHYSICIAN’S DEFENSE Retained sponges can occur in the absence of negligence. It was proper for the patient to return to her own physician for postoperative follow-up treatment. The patient’s PID and gallbladder problems were unrelated to the retained sponges.
VERDICT A defense verdict was returned. The defendant was granted costs and attorney fees exceeding $27,000.
Patient sues drug companies: “HT caused my breast cancer”
A WOMAN IN HER LATE 50S took a combination of Premarin and Provera for 6 years to treat menopausal symptoms. She was then switched to Prempro for 4 years until she detected a lump in her breast. Her physician diagnosed invasive ductal breast cancer and the patient underwent a left mastectomy. Cancer spread to her lymph nodes; she underwent chemotherapy and radiation treatments. She sued the drug manufacturers.
PATIENT’S CLAIM Years of combination hormone therapy (HT) caused her breast cancer. The pharmaceutical companies failed to adequately test the drugs despite knowledge of their cancer-causing potential. If the defendants had begun cancer studies in the early 1980s when they first learned about the cancer risk, the risk would have been discovered before she began taking HT in 1991. She provided letters dated as early as 1976 from the FDA, independent researchers, and internal drug company scientists urging that cancer risk research be conducted. She claimed the defendants intentionally restricted the publication of medical data outlining the cancerous effects of combination HT to physicians and patients.
DEFENDANTS’ DEFENSE The FDA has reviewed the benefits and risks of HT for decades, always finding that the benefits outweighed the risks. Defendants cited 19 studies examining HT and breast cancer risk, the first published in 1959. The Women’s Health Initiative reaffirmed the increased risk of breast cancer, available in the labeling for Prempro in 1995. Labeling for Premarin and Provera included FDA-approved warnings of the breast cancer risk. The physician and patient were adequately warned of risks before use.
VERDICT $34.3 million verdict was returned, including $28 million in total punitive damages against the drug companies.
Was hypertension properly treated in this stroke victim?
AFTER HEAVY VAGINAL BLEEDING was diagnosed in a 49-year-old woman, her gynecologist prescribed medroxyprogesterone acetate. Several months later, she underwent a dilation and curettage for continued bleeding. A year later, her blood pressure (BP) was 140/94 mm Hg, which the physician believed was “white coat” hypertension. The woman returned 10 months later, still complaining of abnormal uterine bleeding, but she refused surgical options; the physician prescribed birth control pills. She returned for a routine exam a year later, when her BP was again elevated. The physician continued the patient’s oral contraceptive prescription and initiated treatment for high BP with triamterene. When the patient called to complain of excessive bleeding the next month, a nurse told her to take ibuprofen and call back if symptoms persisted. Shortly thereafter, the patient suffered a stroke. After rehabilitation, she regained use of her arms and legs, but suffered from foot drop and decreased fine motor skills.
PATIENT’S CLAIM The stroke was caused by uncontrolled hypertension and/or birth control pills. The physician should have initiated treatment the first time her BP was elevated, and it should have been checked more frequently. Birth control pills should have been discontinued when high BP was diagnosed because they are contraindicated in women older than 35 years whose BP is elevated.
PHYSICIAN’S DEFENSE The use of birth control pills was proper; the physician prescribed a low-dose combination medication commonly given to perimenopausal women to control abnormal bleeding. When high BP was first suspected, the physician commenced treatment.
VERDICT A defense verdict was returned.
Painful intercourse reported following incontinence surgery
EIGHT SURGERIES WERE PERFORMED to correct a 54-year-old woman’s cystocele, enterocele, and retrocele. The patient’s bladder, colon, and intestines had been pressing on her vaginal canal causing abdominal pain, painful intercourse, and urinary and fecal incontinence.
PATIENT’S CLAIM The procedures reduced the size of her vaginal opening and the length of her vaginal canal, causing constant pain as well as severe pain with intercourse. She was not informed that this was a risk of surgery.
PHYSICIAN’S DEFENSE The patient’s vaginal opening did shrink due to the release of pressure placed on the vaginal canal by the other organs, but it is still within normal range of vaginal size. The procedures resolved the patient’s incontinence issues.
VERDICT A defense verdict was returned.
Radiotherapy wrong for sarcoma; caused short bowel syndrome
FIBROIDS WERE MORCELLATED during a vaginal hysterectomy in a 56-year-old woman. The patient’s pathology report indicated endometrial stromal sarcoma (ESS). She underwent open surgery for staging and to remove any residual cancer cells that could be identified. The gynecologist referred her to a radiation oncologist. After receiving radiotherapy for 4 months, the patient complained of bowel-related symptoms. Three months later, she sought treatment closer to home for diarrhea and gastrointestinal problems. A surgeon diagnosed radiation-induced short bowel syndrome causing inadequate nutritional absorption. The patient underwent two operations, during which large sections of her bowel were removed, a permanent colostomy was placed. She then required total parenteral nutrition tube feedings.
PLAINTIFF’S CLAIM The radiation oncologist was negligent for recommending and administering radiotherapy because of its limited value in ESS. Hormonal therapy should have been used instead.
PHYSICIAN’S DEFENSE Radiotherapy was necessary because of the patient’s history and disease type. Morcellation during vaginal hysterectomy increased the risk of microscopic cancer cells remaining in the pelvis, supported by the finding of residual cancer cells during the second procedure. Radiotherapy was necessary to treat the residual cancer cells.
VERDICT A defense verdict was returned.
No response to alarm when fetal heart tones are lost
A WOMAN ATTEMPTED VAGINAL BIRTH after having one vaginal birth and one cesarean delivery in the past. Labor progressed slowly with inadequate contractions and lack of descent. After the mother pushed five or six times without progress, the OB left to deliver another baby. Because of lack of progression, the mother requested cesarean delivery, and the husband conveyed their concerns to the nursing staff. The nurses assured them that all was well but did not discuss the parents’ concerns with the OB or other hospital personnel. One hour later, the mother’s uterus ruptured, fetal heart tones were lost from the external fetal monitor, and an alarm sounded.
PLAINTIFF’S CLAIM The nursing staff failed to respond to the alarm immediately; when a response did come, a nurse allegedly stated with excitement that she was amazed that no one had responded. This statement was confirmed by the OB. After 9 minutes of signal loss, a fetal heartbeat of 60 was found, but it was severely bradycardic. The mother was rushed to the OR and the baby was delivered expeditiously. The child was born limp and without respiratory effort, and sustained hypoxic ischemic encephalopathy. At age 5, he had no purposeful movement of his extremities, could not communicate, and was wheelchair-bound, although he was not cognitively impaired.
DEFENDANTS’ DEFENSE The OB offered full policy limits before trial. The hospital claimed that the 9-minute delay in detecting the loss of fetal heart tone and seeking the OB’s intervention was not the proximate cause of the child’s handicaps.
VERDICT A $4.9 million Michigan verdict was reached.
Untreated postpartum infection necessitated hysterectomy
AN 18-YEAR-OLD WOMAN was discharged from the hospital two days after the vaginal birth of her healthy child, although she claimed to not feel well. When a hospital-employed nurse visited her the next day, the patient reported abdominal pain and cramping. Five days later, she returned to the hospital in extreme pain. She was diagnosed with severe Streptococcus A infection, air-lifted to another hospital, and treated with antibiotics for 5 days. A hysterectomy was later performed.
PLAINTIFF’S CLAIM The physician, visiting nurse, and hospital failed to diagnose and treat the infection in a timely manner, resulting in a hysterectomy. Laboratory tests taken before the patient’s hospital discharge showed an elevated white blood cell (WBC) count; the patient should have been prescribed antibiotics before leaving the hospital. The visiting nurse did not react appropriately when the patient reported pain. The hospital was responsible because the results of the WBC test were not entered into the patient’s chart.
DEFENDANTS’ DEFENSE The physician claimed that the elevated WBC count was not recorded in the patient’s medical chart with other lab values. The hospital claimed that a high WBC count is common after childbirth; the test is rarely performed at that time. The only reason it was performed was that the technology automatically recorded WBC when it evaluated hemoglobin and hemocrit. Abdominal cramping reported to the visiting nurse is normal 3 days after childbirth. The patient did not have an infection at discharge or at the time of the nurse’s visit.
VERDICT Suit against the physician was dismissed prior to jury deliberations. A $2.3 million verdict was returned against the hospital.
Did retained sponges lead to PID and gallbladder disease?
A 6-INCH VAGINAL LACERATION was discovered after a woman delivered a healthy baby. The ObGyn, who was covering for the patient’s regular ObGyn because of a snowstorm, could not repair the laceration in the delivery room. He packed the patient’s vagina with gauze sponges, and took her to the OR where he repaired the laceration. The next day, he removed sponges placed after surgery. The patient was discharged with instructions to follow-up with her regular ObGyn. Eight days after delivery, the patient complained to her ObGyn of severe abdominal pain and a foul odor. Antibiotics were prescribed, but she refused a vaginal examination because of the pain. Six weeks after delivery, four gauze sponges were removed from the patient’s vagina.
PLAINTIFF’S CLAIM The physician was negligent in leaving the sponges in her vagina. He should have conducted the follow-up himself because he delivered her child. The infection caused chronic pain from pelvic inflammatory disease (PID), and necessitated the removal of her gallbladder.
PHYSICIAN’S DEFENSE Retained sponges can occur in the absence of negligence. It was proper for the patient to return to her own physician for postoperative follow-up treatment. The patient’s PID and gallbladder problems were unrelated to the retained sponges.
VERDICT A defense verdict was returned. The defendant was granted costs and attorney fees exceeding $27,000.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Business Lessons I Didn't Learn in Residency
Do you ever wish that your residency years had prepared you better for managing the business side of your practice?
It's critical to learn how to get paid for what we do, yet my experience in residency provided little preparation for doing just that. Here are a few tips I wish I had learned back in residency and that I think are important to pass along to the residents who I teach:
1. Always read your mail. Delegating this task to an office manager means you're out of the loop when it comes to knowing the trends occurring with your explanations of benefits and denials for payment. It's important to know what you are—and are not—getting paid for. Don't assume that if you bill for a service, you'll get paid for it. And don't assume that the amount you bill always covers your own costs. Manufacturers of vaccines and devices can change their charges on a dime, and that can eat into your margin if you're not paying attention. If you can't find the time to read your mail, train someone on your staff to push the information to you.
2. Develop solid relationships with patients. Medicare patients are constantly receiving reminders in the mail to report cases of fraud. Although absolutely no one should ever take advantage of these patients, sometimes they feel they are being taken advantage of due to miscommunication. A Medicare patient of mine recently called to question why I had billed for tobacco cessation, since she believed our discussion about her plans to quit smoking was just part of being a good doctor. I was relieved to be given the opportunity to explain to her that it was a legitimate claim, given that Medicare now reimburses physicians for providing such counseling. Not all your patients are going to like you. The aim is to develop an open relationship so they feel that they can come to you first if they have a question about their bill.
3. Be complete on review of systems. In cases of audit, inadequate review of systems (ROS) is the leading reason for physicians to write checks back to insurance companies. If you're doing the work of a ROS for a higher level of visit, make sure that you're documenting that fact. With any code, you need to at least spell out the pertinent ROS to justify payment.
4. Understand the difference between 99213 and 99214. Over the course of a year, the cumulative difference between billing for a level-3 visit versus a level-4 visit can be huge. Unfortunately, because residents are not allowed to bill above a 99213, they never really become used to doing the expanded documentation required for a 99214. And that's what they stick to once they are in practice, even when they are doing the work of a 99214.5
5. Learn how to code based on time in situations that warrant it. Family physicians in particular manage patients who may not always involve a high level of complexity but who do require a lot of time. The patient who has just been diagnosed with diabetes or the patient with depression, for example, both require considerable counseling time. To get paid for that time, you need to document that you spent at least 50% of the visit counseling and educating these patients on issues related to their diagnosis.
6. Remember consultation codes are a thing of the past. Learn how to add AI modifiers if you are the principal provider or consultant for a Medicare patient. These AI modifiers help explain to Medicare how there can be two codes for the same patient on the same day. They explain who is the principal provider and who is the consultant on the case, and if you don't use them your claim may be denied.
7. Use tobacco cessation counseling codes when appropriate. Codes 99406 and 99407 have been around since 2005, but a lot of physicians still aren't using them. In a patient with a disease or condition affected by tobacco use, these codes allow reimbursement for smoking cessation counseling for two quit attempts per patient during the year, and coverage is for four counseling interactions for each quit attempt. For 99406, the physician must document 3-10 minutes of counseling per interaction; for 99407, more than 10 minutes of counseling must be documented.
8. Use all the codes for diabetic foot exams and care. Physicians can bill for an initial foot exam for loss of protective sensation, or LOPS (G0245), as well as a follow-up exam code for LOPS at subsequent visits. In addition to the LOPS code, the code for routine foot care (G0247) can be used if you address the causes of LOPS, by shaving calluses, for example.
9. Keep au courant. Even if you think you know all there is to know about coding, take a coding class every now and then because things change. I pay very close attention to coding and I still have to look up the rules and coding changes.
10. Count your time for home health or hospice care plan certification and recertification. If you spend 30 minutes every month reviewing the care plan for a patient in home health or hospice you can bill for that. A lot of home heath care companies have cheat sheets to help you keep track of your time. Reviewing a new care plan can be coded as G0180. Recertification of the care plan after 60 days can be coded as G0179.
Do you ever wish that your residency years had prepared you better for managing the business side of your practice?
It's critical to learn how to get paid for what we do, yet my experience in residency provided little preparation for doing just that. Here are a few tips I wish I had learned back in residency and that I think are important to pass along to the residents who I teach:
1. Always read your mail. Delegating this task to an office manager means you're out of the loop when it comes to knowing the trends occurring with your explanations of benefits and denials for payment. It's important to know what you are—and are not—getting paid for. Don't assume that if you bill for a service, you'll get paid for it. And don't assume that the amount you bill always covers your own costs. Manufacturers of vaccines and devices can change their charges on a dime, and that can eat into your margin if you're not paying attention. If you can't find the time to read your mail, train someone on your staff to push the information to you.
2. Develop solid relationships with patients. Medicare patients are constantly receiving reminders in the mail to report cases of fraud. Although absolutely no one should ever take advantage of these patients, sometimes they feel they are being taken advantage of due to miscommunication. A Medicare patient of mine recently called to question why I had billed for tobacco cessation, since she believed our discussion about her plans to quit smoking was just part of being a good doctor. I was relieved to be given the opportunity to explain to her that it was a legitimate claim, given that Medicare now reimburses physicians for providing such counseling. Not all your patients are going to like you. The aim is to develop an open relationship so they feel that they can come to you first if they have a question about their bill.
3. Be complete on review of systems. In cases of audit, inadequate review of systems (ROS) is the leading reason for physicians to write checks back to insurance companies. If you're doing the work of a ROS for a higher level of visit, make sure that you're documenting that fact. With any code, you need to at least spell out the pertinent ROS to justify payment.
4. Understand the difference between 99213 and 99214. Over the course of a year, the cumulative difference between billing for a level-3 visit versus a level-4 visit can be huge. Unfortunately, because residents are not allowed to bill above a 99213, they never really become used to doing the expanded documentation required for a 99214. And that's what they stick to once they are in practice, even when they are doing the work of a 99214.5
5. Learn how to code based on time in situations that warrant it. Family physicians in particular manage patients who may not always involve a high level of complexity but who do require a lot of time. The patient who has just been diagnosed with diabetes or the patient with depression, for example, both require considerable counseling time. To get paid for that time, you need to document that you spent at least 50% of the visit counseling and educating these patients on issues related to their diagnosis.
6. Remember consultation codes are a thing of the past. Learn how to add AI modifiers if you are the principal provider or consultant for a Medicare patient. These AI modifiers help explain to Medicare how there can be two codes for the same patient on the same day. They explain who is the principal provider and who is the consultant on the case, and if you don't use them your claim may be denied.
7. Use tobacco cessation counseling codes when appropriate. Codes 99406 and 99407 have been around since 2005, but a lot of physicians still aren't using them. In a patient with a disease or condition affected by tobacco use, these codes allow reimbursement for smoking cessation counseling for two quit attempts per patient during the year, and coverage is for four counseling interactions for each quit attempt. For 99406, the physician must document 3-10 minutes of counseling per interaction; for 99407, more than 10 minutes of counseling must be documented.
8. Use all the codes for diabetic foot exams and care. Physicians can bill for an initial foot exam for loss of protective sensation, or LOPS (G0245), as well as a follow-up exam code for LOPS at subsequent visits. In addition to the LOPS code, the code for routine foot care (G0247) can be used if you address the causes of LOPS, by shaving calluses, for example.
9. Keep au courant. Even if you think you know all there is to know about coding, take a coding class every now and then because things change. I pay very close attention to coding and I still have to look up the rules and coding changes.
10. Count your time for home health or hospice care plan certification and recertification. If you spend 30 minutes every month reviewing the care plan for a patient in home health or hospice you can bill for that. A lot of home heath care companies have cheat sheets to help you keep track of your time. Reviewing a new care plan can be coded as G0180. Recertification of the care plan after 60 days can be coded as G0179.
Do you ever wish that your residency years had prepared you better for managing the business side of your practice?
It's critical to learn how to get paid for what we do, yet my experience in residency provided little preparation for doing just that. Here are a few tips I wish I had learned back in residency and that I think are important to pass along to the residents who I teach:
1. Always read your mail. Delegating this task to an office manager means you're out of the loop when it comes to knowing the trends occurring with your explanations of benefits and denials for payment. It's important to know what you are—and are not—getting paid for. Don't assume that if you bill for a service, you'll get paid for it. And don't assume that the amount you bill always covers your own costs. Manufacturers of vaccines and devices can change their charges on a dime, and that can eat into your margin if you're not paying attention. If you can't find the time to read your mail, train someone on your staff to push the information to you.
2. Develop solid relationships with patients. Medicare patients are constantly receiving reminders in the mail to report cases of fraud. Although absolutely no one should ever take advantage of these patients, sometimes they feel they are being taken advantage of due to miscommunication. A Medicare patient of mine recently called to question why I had billed for tobacco cessation, since she believed our discussion about her plans to quit smoking was just part of being a good doctor. I was relieved to be given the opportunity to explain to her that it was a legitimate claim, given that Medicare now reimburses physicians for providing such counseling. Not all your patients are going to like you. The aim is to develop an open relationship so they feel that they can come to you first if they have a question about their bill.
3. Be complete on review of systems. In cases of audit, inadequate review of systems (ROS) is the leading reason for physicians to write checks back to insurance companies. If you're doing the work of a ROS for a higher level of visit, make sure that you're documenting that fact. With any code, you need to at least spell out the pertinent ROS to justify payment.
4. Understand the difference between 99213 and 99214. Over the course of a year, the cumulative difference between billing for a level-3 visit versus a level-4 visit can be huge. Unfortunately, because residents are not allowed to bill above a 99213, they never really become used to doing the expanded documentation required for a 99214. And that's what they stick to once they are in practice, even when they are doing the work of a 99214.5
5. Learn how to code based on time in situations that warrant it. Family physicians in particular manage patients who may not always involve a high level of complexity but who do require a lot of time. The patient who has just been diagnosed with diabetes or the patient with depression, for example, both require considerable counseling time. To get paid for that time, you need to document that you spent at least 50% of the visit counseling and educating these patients on issues related to their diagnosis.
6. Remember consultation codes are a thing of the past. Learn how to add AI modifiers if you are the principal provider or consultant for a Medicare patient. These AI modifiers help explain to Medicare how there can be two codes for the same patient on the same day. They explain who is the principal provider and who is the consultant on the case, and if you don't use them your claim may be denied.
7. Use tobacco cessation counseling codes when appropriate. Codes 99406 and 99407 have been around since 2005, but a lot of physicians still aren't using them. In a patient with a disease or condition affected by tobacco use, these codes allow reimbursement for smoking cessation counseling for two quit attempts per patient during the year, and coverage is for four counseling interactions for each quit attempt. For 99406, the physician must document 3-10 minutes of counseling per interaction; for 99407, more than 10 minutes of counseling must be documented.
8. Use all the codes for diabetic foot exams and care. Physicians can bill for an initial foot exam for loss of protective sensation, or LOPS (G0245), as well as a follow-up exam code for LOPS at subsequent visits. In addition to the LOPS code, the code for routine foot care (G0247) can be used if you address the causes of LOPS, by shaving calluses, for example.
9. Keep au courant. Even if you think you know all there is to know about coding, take a coding class every now and then because things change. I pay very close attention to coding and I still have to look up the rules and coding changes.
10. Count your time for home health or hospice care plan certification and recertification. If you spend 30 minutes every month reviewing the care plan for a patient in home health or hospice you can bill for that. A lot of home heath care companies have cheat sheets to help you keep track of your time. Reviewing a new care plan can be coded as G0180. Recertification of the care plan after 60 days can be coded as G0179.
Spousal Consent
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.
When recruiting a hospitalist for his company, Jason Stuckey makes it a point to call the candidate’s home. His goal isn’t to speak with the hospitalist the company is interested in hiring—it’s to talk with the candidate’s spouse.
“One of the top five mistakes recruiters make is to not involve the spouse in the [recruitment] process,” says Stuckey, who directs HM recruiting for TeamHealth, a Knoxville, Tenn.-based company that provides healthcare staffing and administrative services to hospitals in 14 states.
Hospitalists are generally so busy with work that the spouse is often the person in the family who takes the lead in the job search, says Tim Lary, vice president of profession staffing for IPC: The Hospitalist Co., a national physician group practice based in North Hollywood, Calif.
The spouse often gives final approval on a decision to accept a job offer, adds Peggy Fricke, director of physician staffing for Eagle Hospital Physicians, an Atlanta-based company that manages hospitalist practices for hospitals in the Southeast and Mid-Atlantic regions.
“The physician could be making the most money, but if their spouse and family are not happy, then they won’t stay in the position long,” Stuckey explains. “I’ve also found that if the spouse is not on board with moving and uprooting the family to a new location, then it’s not going to happen.”
As a result, recruiters and prospective employers often spend just as much time engaging the spouse as they do the actual job candidate, the recruiters say. For this reason, hospitalists who are searching for a new job would be wise to include their husband or wife as early as possible in the job hunt in order to get the most out of the recruiting process.
For example, while the hospitalist focuses on determining if the work is the right fit professionally and financially, the spouse can appraise the community to see if it meets the family’s needs in such areas as schools, neighborhoods, religious services, community groups, and entertainment/cultural outlets. If the hospitalist is invited for an on-site interview, it’s important that their spouse makes the trip as well.
“We always do a community tour, and we will do school tours when asked,” Fricke says of Eagle’s recruiting efforts. “We can introduce the families of the other hospitalists in the practice so a spouse can meet and get to know them.”
—Jason Stuckey, director, HM recruitment, TeamHealth, Knoxville, Tenn.
Upfront Inclusion
When the spouse is involved in the process, they usually are more receptive to receiving information about what opportunities exist in other communities and more open to the idea of moving to a new place, Stuckey says.
For instances in which children are involved, the spouse is most often interested in learning about the location’s school districts and private schools, and determining if the community has a good quality of life for families, Fricke says. For situations in which there are no children or the children are grown, the spouse often focuses on job prospects in their own profession.
Hospitalists with a husband or wife who works and whose career is important to them should see if the HM recruiter can help put their spouse in touch with potential employers in the community, because many times they will, says Fricke, who has connected spouses in IT and engineering fields with people who could assist them in their job search.
“It goes back to making sure everyone is happy. If the spouse can’t find work, that is going to affect their happiness,” says Darren Swenson, MD, medical affairs director for IPC of Nevada and regional chair of IPC’s national advisory board.
Aside from schools, quality of life, and their own job opportunities, spouses also ask about what their hospitalist husband or wife’s work schedule would be and how much vacation and holiday time they would have in the prospective job, Dr. Swenson says.
“It’s extremely important that we look at our hospitalists and their spouses being happy in their home life, because if they’re not, that is going to spill over into in their work life,” IPC’s Lary says.
Good Partnership, Bad Partnership
Times arise when the spouse takes a proactive role in evaluating the actual HM job offer, the recruiters say. “In all couples, there is someone who is dominant and someone who is not,” says Fricke, who has seen spouses participate in job interviews with hospital administrators. “If the spouse is dominant, we try to understand them and listen to what is important to them.”
Sometimes the spouse is an attorney or other type of professional who wants to review the hospitalist contract and has the most questions about it, Dr. Swenson says. When that happens, recruiters will often have group members sit in to answer their questions, he says.
“Absolutely, without question, the spouse has to be involved. But if the spouse is too demanding and everything has to be run through them, to an employer, that can be a big turnoff,” Stuckey says.
When it comes to business matters, the physician—not the spouse—has to take the lead, he says. If the physician doesn’t, it could make the prospective employer wonder what challenges could be ahead should the candidate be hired, Stuckey says.
Two-Physician Families
One time when it is acceptable for a spouse to get intimately involved in the contract and negotiations is when he or she is a hospitalist who also is being recruited by the same prospective employer.
“It’s a unique situation. It’s great to have two for the price of one, so to speak,” Stuckey says. “But there are challenges from the employer’s perspective—for example, scheduling—that have to be resolved on the front end rather than when they get there.”
While still relatively rare, husband-wife hospitalist couples are becoming more prevalent because there are more hospitalists, Fricke says. They tend to meet each other in medical school or residency, she says.
“Even though they are a couple, we treat them as individuals during the recruiting process,” Fricke says. “I think the most important thing is we try to do anything we can—within reason, of course—to help the hospitalist and their spouse make the best decision for themselves and their family.” TH
Lisa Ryan is a freelance writer based in New Jersey.