User login
Sterilized woman skips f/u HSG test, becomes pregnant…and more
Sterilized woman skips f/u HSG test, becomes pregnant
A 31-YEAR-OLD MOTHER OF THREE underwent a hysteroscopic tubal sterilization procedure because she wanted to avoid pregnancy. She neglected to return 3 months later for a hysterosalpingogram (HSG) to determine whether the procedure was effective. A few months after that, she discovered she was pregnant.
PATIENT’S CLAIM The physician was negligent for failing to inform her that postoperative testing was necessary, and importantly, to confirm her inability to become pregnant. He also failed to advise her to use alternative contraceptive methods.
PHYSICIAN’S DEFENSE The patient was told several times that the HSG test was needed and important, and that she should use alternative contraception. Also, five appointments were scheduled for her to have the HSG test, but each time she either canceled or failed to come for the test.
VERDICT Connecticut defense verdict.
Preeclampsia leads to infant’s death and 24/7 care for mother
A WOMAN AT 30 WEEKS’ GESTATION complained of headaches to her ObGyn during a routine examination. Her blood pressure, although within normal limits, was above her baseline level, and a dipstick urine demonstrated proteinuria. The next morning, she had a seizure and was taken to the hospital. Preeclampsia was diagnosed. An emergent cesarean delivery was performed. The infant, who suffered neurologic impairments, died at 18 months. The mother was hospitalized for 7 months due to hypoxia-induced neurologic injuries, sepsis, lung problems, a ministroke, and a second hypoxic episode. Wheelchair-bound, she is speech-impaired and requires 24-hour care.
PATIENT’S CLAIM The ObGyn’s failure to diagnose preeclampsia was negligent.
PHYSICIAN’S DEFENSE The patient showed no signs of preeclampsia. Despite protein in her urine and elevated blood pressure, the levels were not in a range indicating preeclampsia.
VERDICT South Carolina defense verdict.
Did emboli in utero from deceased twin cause other twin’s postnatal problems?
A WOMAN PREGNANT WITH TWINS was admitted to the hospital because of premature contractions. Tests performed 3 weeks later indicated the intrauterine demise of one twin. The other twin showed signs of distress 8 days later and was delivered by cesarean later that day. The infant experienced hypoxic-ischemic brain damage, which caused severe mental retardation, cerebral palsy, and spastic quadriparesis.
PATIENT’S CLAIM Prior to delivery, emboli of thromboplastin material from the deceased fetus traveled to the surviving fetus, contributing to that fetus’s injuries. The delivery should have been performed sooner.
PHYSICIAN’S DEFENSE The plaintiff’s proposed theory for the injuries was not supported scientifically.
VERDICT All defendants except the hospital settled for a total of $1.5 million prior to trial. A $4 million Florida verdict against the hospital for injuries to the surviving twin was reduced to $2.95 million.
Was excessive force applied in case of shoulder dystocia?
THE OBGYN WHO HAD PROVIDED ALL PRENATAL CARE encountered shoulder dystocia during the infant’s delivery. The problem was resolved with the McRoberts maneuver with suprapubic pressure, the Wood’s screw maneuver, and attempted delivery of the posterior arm. Born with a severe left brachial plexus injury, the child underwent surgery but still has limited use of his left arm and hand.
PATIENT’S CLAIM Among relatives present at the delivery were two nurses. They testified at the trial that the physician used excessive downward lateral traction and also allowed a nurse to apply fundal pressure.
PHYSICIAN’S DEFENSE Shoulder dystocia was unexpected, excessive traction was not used, and once dystocia was evident, fundal pressure was not used.
VERDICT $80,000 Illinois settlement with the hospital prior to trial. Although the jury delivered a defense verdict for the physician, a $1,000,000/$200,000 high/low agreement was in place.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Sterilized woman skips f/u HSG test, becomes pregnant
A 31-YEAR-OLD MOTHER OF THREE underwent a hysteroscopic tubal sterilization procedure because she wanted to avoid pregnancy. She neglected to return 3 months later for a hysterosalpingogram (HSG) to determine whether the procedure was effective. A few months after that, she discovered she was pregnant.
PATIENT’S CLAIM The physician was negligent for failing to inform her that postoperative testing was necessary, and importantly, to confirm her inability to become pregnant. He also failed to advise her to use alternative contraceptive methods.
PHYSICIAN’S DEFENSE The patient was told several times that the HSG test was needed and important, and that she should use alternative contraception. Also, five appointments were scheduled for her to have the HSG test, but each time she either canceled or failed to come for the test.
VERDICT Connecticut defense verdict.
Preeclampsia leads to infant’s death and 24/7 care for mother
A WOMAN AT 30 WEEKS’ GESTATION complained of headaches to her ObGyn during a routine examination. Her blood pressure, although within normal limits, was above her baseline level, and a dipstick urine demonstrated proteinuria. The next morning, she had a seizure and was taken to the hospital. Preeclampsia was diagnosed. An emergent cesarean delivery was performed. The infant, who suffered neurologic impairments, died at 18 months. The mother was hospitalized for 7 months due to hypoxia-induced neurologic injuries, sepsis, lung problems, a ministroke, and a second hypoxic episode. Wheelchair-bound, she is speech-impaired and requires 24-hour care.
PATIENT’S CLAIM The ObGyn’s failure to diagnose preeclampsia was negligent.
PHYSICIAN’S DEFENSE The patient showed no signs of preeclampsia. Despite protein in her urine and elevated blood pressure, the levels were not in a range indicating preeclampsia.
VERDICT South Carolina defense verdict.
Did emboli in utero from deceased twin cause other twin’s postnatal problems?
A WOMAN PREGNANT WITH TWINS was admitted to the hospital because of premature contractions. Tests performed 3 weeks later indicated the intrauterine demise of one twin. The other twin showed signs of distress 8 days later and was delivered by cesarean later that day. The infant experienced hypoxic-ischemic brain damage, which caused severe mental retardation, cerebral palsy, and spastic quadriparesis.
PATIENT’S CLAIM Prior to delivery, emboli of thromboplastin material from the deceased fetus traveled to the surviving fetus, contributing to that fetus’s injuries. The delivery should have been performed sooner.
PHYSICIAN’S DEFENSE The plaintiff’s proposed theory for the injuries was not supported scientifically.
VERDICT All defendants except the hospital settled for a total of $1.5 million prior to trial. A $4 million Florida verdict against the hospital for injuries to the surviving twin was reduced to $2.95 million.
Was excessive force applied in case of shoulder dystocia?
THE OBGYN WHO HAD PROVIDED ALL PRENATAL CARE encountered shoulder dystocia during the infant’s delivery. The problem was resolved with the McRoberts maneuver with suprapubic pressure, the Wood’s screw maneuver, and attempted delivery of the posterior arm. Born with a severe left brachial plexus injury, the child underwent surgery but still has limited use of his left arm and hand.
PATIENT’S CLAIM Among relatives present at the delivery were two nurses. They testified at the trial that the physician used excessive downward lateral traction and also allowed a nurse to apply fundal pressure.
PHYSICIAN’S DEFENSE Shoulder dystocia was unexpected, excessive traction was not used, and once dystocia was evident, fundal pressure was not used.
VERDICT $80,000 Illinois settlement with the hospital prior to trial. Although the jury delivered a defense verdict for the physician, a $1,000,000/$200,000 high/low agreement was in place.
Sterilized woman skips f/u HSG test, becomes pregnant
A 31-YEAR-OLD MOTHER OF THREE underwent a hysteroscopic tubal sterilization procedure because she wanted to avoid pregnancy. She neglected to return 3 months later for a hysterosalpingogram (HSG) to determine whether the procedure was effective. A few months after that, she discovered she was pregnant.
PATIENT’S CLAIM The physician was negligent for failing to inform her that postoperative testing was necessary, and importantly, to confirm her inability to become pregnant. He also failed to advise her to use alternative contraceptive methods.
PHYSICIAN’S DEFENSE The patient was told several times that the HSG test was needed and important, and that she should use alternative contraception. Also, five appointments were scheduled for her to have the HSG test, but each time she either canceled or failed to come for the test.
VERDICT Connecticut defense verdict.
Preeclampsia leads to infant’s death and 24/7 care for mother
A WOMAN AT 30 WEEKS’ GESTATION complained of headaches to her ObGyn during a routine examination. Her blood pressure, although within normal limits, was above her baseline level, and a dipstick urine demonstrated proteinuria. The next morning, she had a seizure and was taken to the hospital. Preeclampsia was diagnosed. An emergent cesarean delivery was performed. The infant, who suffered neurologic impairments, died at 18 months. The mother was hospitalized for 7 months due to hypoxia-induced neurologic injuries, sepsis, lung problems, a ministroke, and a second hypoxic episode. Wheelchair-bound, she is speech-impaired and requires 24-hour care.
PATIENT’S CLAIM The ObGyn’s failure to diagnose preeclampsia was negligent.
PHYSICIAN’S DEFENSE The patient showed no signs of preeclampsia. Despite protein in her urine and elevated blood pressure, the levels were not in a range indicating preeclampsia.
VERDICT South Carolina defense verdict.
Did emboli in utero from deceased twin cause other twin’s postnatal problems?
A WOMAN PREGNANT WITH TWINS was admitted to the hospital because of premature contractions. Tests performed 3 weeks later indicated the intrauterine demise of one twin. The other twin showed signs of distress 8 days later and was delivered by cesarean later that day. The infant experienced hypoxic-ischemic brain damage, which caused severe mental retardation, cerebral palsy, and spastic quadriparesis.
PATIENT’S CLAIM Prior to delivery, emboli of thromboplastin material from the deceased fetus traveled to the surviving fetus, contributing to that fetus’s injuries. The delivery should have been performed sooner.
PHYSICIAN’S DEFENSE The plaintiff’s proposed theory for the injuries was not supported scientifically.
VERDICT All defendants except the hospital settled for a total of $1.5 million prior to trial. A $4 million Florida verdict against the hospital for injuries to the surviving twin was reduced to $2.95 million.
Was excessive force applied in case of shoulder dystocia?
THE OBGYN WHO HAD PROVIDED ALL PRENATAL CARE encountered shoulder dystocia during the infant’s delivery. The problem was resolved with the McRoberts maneuver with suprapubic pressure, the Wood’s screw maneuver, and attempted delivery of the posterior arm. Born with a severe left brachial plexus injury, the child underwent surgery but still has limited use of his left arm and hand.
PATIENT’S CLAIM Among relatives present at the delivery were two nurses. They testified at the trial that the physician used excessive downward lateral traction and also allowed a nurse to apply fundal pressure.
PHYSICIAN’S DEFENSE Shoulder dystocia was unexpected, excessive traction was not used, and once dystocia was evident, fundal pressure was not used.
VERDICT $80,000 Illinois settlement with the hospital prior to trial. Although the jury delivered a defense verdict for the physician, a $1,000,000/$200,000 high/low agreement was in place.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Greening Your Practice
Physicians in private practice have a potentially large role to play in reducing medicine's impact on the environment. The opportunities to reduce your footprint are similar, whether you're running a large hospital or a small- to moderate-sized private practice.
There's no right or wrong way to approach this effort. Multiple points of intervention can make a difference, but the emphasis will vary depending on the practice's location, its size, and the urgency of the issues at hand. All practices, however, can start to make progress simply by looking at the flow of material coming in the front door and going out the back door.
Instituting a recycling program can go a long way toward reducing the volume of waste. So can converting from disposable to washable patient robes, to e-mail in lieu of paper-based communication, and to printing double-sided documents, when a paperless route isn't an option.
Energy efficient light bulbs are other simple way to reduce consumption.
Looking further upstream, consider the impact that your medical and office supply purchasing choices have on the environment. Practices that are able to band together in group purchasing organizations can have an enormous influence. When purchasers express an interest in environmental impacts of their choices, manufacturers listen. Even if you are not in a group purchasing arrangement, try voicing your concerns to manufacturers. Ask them for more clarity and transparency about what's in the products that you buy so that you can make more informed decisions. Ask them to reduce the amount of unnecessary packaging they use in shipping.
Big changes can occur when consumers let their wishes be known. For example, for years, highly toxic flame retardant chemicals were standard in all types of electronics such as computers. Such chemicals present a significant problem when it comes time to dispose of these technologies. In response to consumer pressure, several manufacturers have stepped up to phase out particularly toxic flame retardants.
Another hazardous material that's still common in smaller health care settings is mercury. Not too long ago, the health care sector was responsible for as much as 10% of the mercury levels emitted from waste incinerators. But pressure on suppliers led to increased use of mercury-free products.
Depending on the size of your practice, you also may be able to make considerable strides in energy efficiency. In many areas of the country, energy consumers can negotiate with competing suppliers to lock in a contracted price per kilowatt hour for the year. When energy companies compete with each other in a reverse auction to get your contract, prices drop. Consumers can also specify that a certain percentage of the energy come from renewable sources, such as solar, wind, or hydropower.
Encourage patients to avoid flushing unused prescription drugs down the toilet. Water treatment facilities are unable to eliminate most of these chemicals from the water system and trace amounts of pharmaceuticals have been found in streams and rivers across the country. Some pharmacies and municipalities have started take-back campaigns to safely dispose of unused medications. Another tactic is to avoid prescribing a large amount of a new drug, when a trial week might help determine if it's effective and well tolerated.
Don't know where to start? Try visiting the Web site of Health Care Without Harm
Physicians in private practice have a potentially large role to play in reducing medicine's impact on the environment. The opportunities to reduce your footprint are similar, whether you're running a large hospital or a small- to moderate-sized private practice.
There's no right or wrong way to approach this effort. Multiple points of intervention can make a difference, but the emphasis will vary depending on the practice's location, its size, and the urgency of the issues at hand. All practices, however, can start to make progress simply by looking at the flow of material coming in the front door and going out the back door.
Instituting a recycling program can go a long way toward reducing the volume of waste. So can converting from disposable to washable patient robes, to e-mail in lieu of paper-based communication, and to printing double-sided documents, when a paperless route isn't an option.
Energy efficient light bulbs are other simple way to reduce consumption.
Looking further upstream, consider the impact that your medical and office supply purchasing choices have on the environment. Practices that are able to band together in group purchasing organizations can have an enormous influence. When purchasers express an interest in environmental impacts of their choices, manufacturers listen. Even if you are not in a group purchasing arrangement, try voicing your concerns to manufacturers. Ask them for more clarity and transparency about what's in the products that you buy so that you can make more informed decisions. Ask them to reduce the amount of unnecessary packaging they use in shipping.
Big changes can occur when consumers let their wishes be known. For example, for years, highly toxic flame retardant chemicals were standard in all types of electronics such as computers. Such chemicals present a significant problem when it comes time to dispose of these technologies. In response to consumer pressure, several manufacturers have stepped up to phase out particularly toxic flame retardants.
Another hazardous material that's still common in smaller health care settings is mercury. Not too long ago, the health care sector was responsible for as much as 10% of the mercury levels emitted from waste incinerators. But pressure on suppliers led to increased use of mercury-free products.
Depending on the size of your practice, you also may be able to make considerable strides in energy efficiency. In many areas of the country, energy consumers can negotiate with competing suppliers to lock in a contracted price per kilowatt hour for the year. When energy companies compete with each other in a reverse auction to get your contract, prices drop. Consumers can also specify that a certain percentage of the energy come from renewable sources, such as solar, wind, or hydropower.
Encourage patients to avoid flushing unused prescription drugs down the toilet. Water treatment facilities are unable to eliminate most of these chemicals from the water system and trace amounts of pharmaceuticals have been found in streams and rivers across the country. Some pharmacies and municipalities have started take-back campaigns to safely dispose of unused medications. Another tactic is to avoid prescribing a large amount of a new drug, when a trial week might help determine if it's effective and well tolerated.
Don't know where to start? Try visiting the Web site of Health Care Without Harm
Physicians in private practice have a potentially large role to play in reducing medicine's impact on the environment. The opportunities to reduce your footprint are similar, whether you're running a large hospital or a small- to moderate-sized private practice.
There's no right or wrong way to approach this effort. Multiple points of intervention can make a difference, but the emphasis will vary depending on the practice's location, its size, and the urgency of the issues at hand. All practices, however, can start to make progress simply by looking at the flow of material coming in the front door and going out the back door.
Instituting a recycling program can go a long way toward reducing the volume of waste. So can converting from disposable to washable patient robes, to e-mail in lieu of paper-based communication, and to printing double-sided documents, when a paperless route isn't an option.
Energy efficient light bulbs are other simple way to reduce consumption.
Looking further upstream, consider the impact that your medical and office supply purchasing choices have on the environment. Practices that are able to band together in group purchasing organizations can have an enormous influence. When purchasers express an interest in environmental impacts of their choices, manufacturers listen. Even if you are not in a group purchasing arrangement, try voicing your concerns to manufacturers. Ask them for more clarity and transparency about what's in the products that you buy so that you can make more informed decisions. Ask them to reduce the amount of unnecessary packaging they use in shipping.
Big changes can occur when consumers let their wishes be known. For example, for years, highly toxic flame retardant chemicals were standard in all types of electronics such as computers. Such chemicals present a significant problem when it comes time to dispose of these technologies. In response to consumer pressure, several manufacturers have stepped up to phase out particularly toxic flame retardants.
Another hazardous material that's still common in smaller health care settings is mercury. Not too long ago, the health care sector was responsible for as much as 10% of the mercury levels emitted from waste incinerators. But pressure on suppliers led to increased use of mercury-free products.
Depending on the size of your practice, you also may be able to make considerable strides in energy efficiency. In many areas of the country, energy consumers can negotiate with competing suppliers to lock in a contracted price per kilowatt hour for the year. When energy companies compete with each other in a reverse auction to get your contract, prices drop. Consumers can also specify that a certain percentage of the energy come from renewable sources, such as solar, wind, or hydropower.
Encourage patients to avoid flushing unused prescription drugs down the toilet. Water treatment facilities are unable to eliminate most of these chemicals from the water system and trace amounts of pharmaceuticals have been found in streams and rivers across the country. Some pharmacies and municipalities have started take-back campaigns to safely dispose of unused medications. Another tactic is to avoid prescribing a large amount of a new drug, when a trial week might help determine if it's effective and well tolerated.
Don't know where to start? Try visiting the Web site of Health Care Without Harm
Practice Mergers
Tough economic times, coupled with the unpredictable consequences of health care reform, are prompting a growing number of small practices to consider protecting themselves by merging into larger entities.
While dermatology remains one of the last bastions of individual private medical practice, mergers offer significant advantages in stabilization of income and diversification of services. However, careful planning is essential.
It is certainly tempting for two honest and friendly parties to seal a merger with a simple handshake, but the bottom line is no one can ever be sure how things will work out. So, for peace of mind (if nothing else), a written agreement is in everyone's best interest, and the cost will be reasonable if lawyers are kept under control.
While every merger is unique, here are some general guidelines:
Management. An agreement will need to be reached on who will manage the new practice, and what percentage vote will be needed to approve group decisions. Typically the majority rules, but you may wish to specify important decisions that will require unanimous approval, such as purchasing expensive equipment, borrowing money, or adding new partners.
Retirement plans. Will you keep existing retirement plans or merge them? If the latter, you will have to agree on the terms of the new plan, which can be the same or different from any of the existing plans. You'll probably need some legal guidance to insure assets from each existing plan can be transferred into the new plan without tax issues.
Compensation. You will need to agree on a compensation formula. Will everyone be paid only for what they do individually or will revenue be shared equally? I favor a combination, so productivity is rewarded but your income doesn't drop to zero when you take time off.
Incorporation. If both practices are incorporated, there are two basic options for forming a single entity. The first option is to merge corporation A with corporation B. Corporation A ceases to exist, and its medical practice becomes a part of corporation B, the so-called "surviving entity."
Corporation B assumes all assets and liabilities of both old corporations, and the shareholders of corporation A exchange shares of its stock for shares of corporation B (with adjustments for inequalities in stock value).
The second option is to start a completely new corporation, which I'll call corporation C. Corporations A and B dissolve, and distribute their equipment and charts to their shareholders, who then transfer the assets to corporation C.
Option two is popular, but I am not a fan. It is billed as an opportunity to start fresh, shielding everyone from exposure to malpractice suits and other liabilities. However, the reality is, anyone looking to sue either old corporation will simply sue corporation C as the so-called "successor" corporation, on the grounds that it has assumed responsibility for its predecessors' liabilities.
You will also need new provider numbers, which may impede cash flow for months. Plus, the IRS treats corporate liquidations, even for merger purposes, as sales of assets, and taxes them.
I personally favor outright merger of the corporations; it is tax neutral, and while it may theoretically be less satisfactory liability-wise, you can minimize risk by examining financial and legal records, and by identifying any glaring flaws in charting or coding. Your lawyers can add verbiage known as "hold harmless" clauses to the merger agreement, indemnifying each party against the others' liabilities. This area, especially, is where you need experienced, competent legal advice.
Equalization of assets. Another common sticking point is known as "equalization." This happens when each party brings an equal amount of assets to the table, but that is hardly ever the case. One party may contribute more equipment, for example, and the others are often asked to make up the difference with something else, usually cash.
An alternative is to agree that any inequalities will be compensated at the other end, in the form of buy-out value; that is, physicians contributing more assets would receive larger buy-outs when they leave or retire than those contributing less.
Non-compete provisions. These are always a difficult issue, mostly because they are so hard (and expensive) to enforce. An increasingly popular alternative is, once again, to deal with it at the other end, with a buy-out penalty. An unhappy partner can leave and compete, but at the cost of a substantially reduced buy-out. This permits competition, but discourages it, and compensates the remaining partners.
These are only some of the pivotal business and legal issues that can never be settled with a handshake. A little planning and negotiation can prevent grief, regret, and legal expenses in the future.
Tough economic times, coupled with the unpredictable consequences of health care reform, are prompting a growing number of small practices to consider protecting themselves by merging into larger entities.
While dermatology remains one of the last bastions of individual private medical practice, mergers offer significant advantages in stabilization of income and diversification of services. However, careful planning is essential.
It is certainly tempting for two honest and friendly parties to seal a merger with a simple handshake, but the bottom line is no one can ever be sure how things will work out. So, for peace of mind (if nothing else), a written agreement is in everyone's best interest, and the cost will be reasonable if lawyers are kept under control.
While every merger is unique, here are some general guidelines:
Management. An agreement will need to be reached on who will manage the new practice, and what percentage vote will be needed to approve group decisions. Typically the majority rules, but you may wish to specify important decisions that will require unanimous approval, such as purchasing expensive equipment, borrowing money, or adding new partners.
Retirement plans. Will you keep existing retirement plans or merge them? If the latter, you will have to agree on the terms of the new plan, which can be the same or different from any of the existing plans. You'll probably need some legal guidance to insure assets from each existing plan can be transferred into the new plan without tax issues.
Compensation. You will need to agree on a compensation formula. Will everyone be paid only for what they do individually or will revenue be shared equally? I favor a combination, so productivity is rewarded but your income doesn't drop to zero when you take time off.
Incorporation. If both practices are incorporated, there are two basic options for forming a single entity. The first option is to merge corporation A with corporation B. Corporation A ceases to exist, and its medical practice becomes a part of corporation B, the so-called "surviving entity."
Corporation B assumes all assets and liabilities of both old corporations, and the shareholders of corporation A exchange shares of its stock for shares of corporation B (with adjustments for inequalities in stock value).
The second option is to start a completely new corporation, which I'll call corporation C. Corporations A and B dissolve, and distribute their equipment and charts to their shareholders, who then transfer the assets to corporation C.
Option two is popular, but I am not a fan. It is billed as an opportunity to start fresh, shielding everyone from exposure to malpractice suits and other liabilities. However, the reality is, anyone looking to sue either old corporation will simply sue corporation C as the so-called "successor" corporation, on the grounds that it has assumed responsibility for its predecessors' liabilities.
You will also need new provider numbers, which may impede cash flow for months. Plus, the IRS treats corporate liquidations, even for merger purposes, as sales of assets, and taxes them.
I personally favor outright merger of the corporations; it is tax neutral, and while it may theoretically be less satisfactory liability-wise, you can minimize risk by examining financial and legal records, and by identifying any glaring flaws in charting or coding. Your lawyers can add verbiage known as "hold harmless" clauses to the merger agreement, indemnifying each party against the others' liabilities. This area, especially, is where you need experienced, competent legal advice.
Equalization of assets. Another common sticking point is known as "equalization." This happens when each party brings an equal amount of assets to the table, but that is hardly ever the case. One party may contribute more equipment, for example, and the others are often asked to make up the difference with something else, usually cash.
An alternative is to agree that any inequalities will be compensated at the other end, in the form of buy-out value; that is, physicians contributing more assets would receive larger buy-outs when they leave or retire than those contributing less.
Non-compete provisions. These are always a difficult issue, mostly because they are so hard (and expensive) to enforce. An increasingly popular alternative is, once again, to deal with it at the other end, with a buy-out penalty. An unhappy partner can leave and compete, but at the cost of a substantially reduced buy-out. This permits competition, but discourages it, and compensates the remaining partners.
These are only some of the pivotal business and legal issues that can never be settled with a handshake. A little planning and negotiation can prevent grief, regret, and legal expenses in the future.
Tough economic times, coupled with the unpredictable consequences of health care reform, are prompting a growing number of small practices to consider protecting themselves by merging into larger entities.
While dermatology remains one of the last bastions of individual private medical practice, mergers offer significant advantages in stabilization of income and diversification of services. However, careful planning is essential.
It is certainly tempting for two honest and friendly parties to seal a merger with a simple handshake, but the bottom line is no one can ever be sure how things will work out. So, for peace of mind (if nothing else), a written agreement is in everyone's best interest, and the cost will be reasonable if lawyers are kept under control.
While every merger is unique, here are some general guidelines:
Management. An agreement will need to be reached on who will manage the new practice, and what percentage vote will be needed to approve group decisions. Typically the majority rules, but you may wish to specify important decisions that will require unanimous approval, such as purchasing expensive equipment, borrowing money, or adding new partners.
Retirement plans. Will you keep existing retirement plans or merge them? If the latter, you will have to agree on the terms of the new plan, which can be the same or different from any of the existing plans. You'll probably need some legal guidance to insure assets from each existing plan can be transferred into the new plan without tax issues.
Compensation. You will need to agree on a compensation formula. Will everyone be paid only for what they do individually or will revenue be shared equally? I favor a combination, so productivity is rewarded but your income doesn't drop to zero when you take time off.
Incorporation. If both practices are incorporated, there are two basic options for forming a single entity. The first option is to merge corporation A with corporation B. Corporation A ceases to exist, and its medical practice becomes a part of corporation B, the so-called "surviving entity."
Corporation B assumes all assets and liabilities of both old corporations, and the shareholders of corporation A exchange shares of its stock for shares of corporation B (with adjustments for inequalities in stock value).
The second option is to start a completely new corporation, which I'll call corporation C. Corporations A and B dissolve, and distribute their equipment and charts to their shareholders, who then transfer the assets to corporation C.
Option two is popular, but I am not a fan. It is billed as an opportunity to start fresh, shielding everyone from exposure to malpractice suits and other liabilities. However, the reality is, anyone looking to sue either old corporation will simply sue corporation C as the so-called "successor" corporation, on the grounds that it has assumed responsibility for its predecessors' liabilities.
You will also need new provider numbers, which may impede cash flow for months. Plus, the IRS treats corporate liquidations, even for merger purposes, as sales of assets, and taxes them.
I personally favor outright merger of the corporations; it is tax neutral, and while it may theoretically be less satisfactory liability-wise, you can minimize risk by examining financial and legal records, and by identifying any glaring flaws in charting or coding. Your lawyers can add verbiage known as "hold harmless" clauses to the merger agreement, indemnifying each party against the others' liabilities. This area, especially, is where you need experienced, competent legal advice.
Equalization of assets. Another common sticking point is known as "equalization." This happens when each party brings an equal amount of assets to the table, but that is hardly ever the case. One party may contribute more equipment, for example, and the others are often asked to make up the difference with something else, usually cash.
An alternative is to agree that any inequalities will be compensated at the other end, in the form of buy-out value; that is, physicians contributing more assets would receive larger buy-outs when they leave or retire than those contributing less.
Non-compete provisions. These are always a difficult issue, mostly because they are so hard (and expensive) to enforce. An increasingly popular alternative is, once again, to deal with it at the other end, with a buy-out penalty. An unhappy partner can leave and compete, but at the cost of a substantially reduced buy-out. This permits competition, but discourages it, and compensates the remaining partners.
These are only some of the pivotal business and legal issues that can never be settled with a handshake. A little planning and negotiation can prevent grief, regret, and legal expenses in the future.
Patient Distribution

Editor’s note: This is the first of a three-part series.
My experience is that some, maybe even most, hospitalists tend to assume there is a standard or “right” way to organize things like work schedules, compensation, or even the assignment of patients among the group’s providers. Some will say things like “SHM says the best hospitalist schedule is …” or “The best way to compensate hospitalists is …”
But there really isn’t a “best” way to manage any particular attribute of a practice. Don’t make the mistake of assuming your method is best, or that it’s the way “everybody else does it.” Although scheduling and compensation are marquee issues for hospitalists, approaches to distributing new patients is much less visible. Many groups tend to assume their method is the only reasonable approach. The best approach, however, varies from one practice to the next. You should be open to hearing approaches to scheduling that are different from your own.
Assign Patients by “Load Leveling”
I’ve come across a lot—and I mean a lot—of different approaches to distributing new patients in HM groups around the country, but it seems pretty clear that the most common method is to undertake “load leveling” on a daily or ongoing basis.
For example, groups that have a separate night shift (the night doctor performs no daytime work the day before or the day after a night shift) typically distribute the night’s new patients with the intent of having each daytime doctor start with the same number of patients. The group might more heavily weight some patients, such as those in the ICU (e.g., each ICU patient counts as 1.5 or two non-ICU patients), but most groups don’t. Over the course of the day shift, new referrals will be distributed evenly among the doctors one at a time, sort of like dealing a deck of cards.
This approach aims to avoid significant imbalances in patient loads and has the potential cultural benefit of everyone sharing equally in busy and slow days. Groups that use it tend to see it as the best option because it is the fairest way to divide up the workload.
Practices that use load-leveling almost always use a schedule built on shifts of a predetermined and fixed duration. For example, say the day shift always works from 7 a.m. to 7 p.m. This schedule usually has the majority of compensation paid via a fixed annual salary or fixed shift rate. One potential problem with this approach is that the doctor who is efficient and discharges a lot of patients today is “rewarded” with more new patients tomorrow. Hospitalists who are allergic to work might have an incentive to have a patient wait until tomorrow to discharge to avoid having to assume the care of yet another patient tomorrow morning. Hospital executives who are focused on length-of-stay management might be concerned if they knew this was a potential issue. Of course, the reverse is true as well. In a practice that doesn’t aggressively undertake load-leveling, a less-than-admirable hospitalist could push patients to discharge earlier than optimal just to have one less patient the next day.
Another cost of this approach is that the distribution of patients can be time-consuming each morning. It also offers the opportunity for some in the group to decide they’re treated unfairly. For instance, you might hear the occasional “just last Tuesday, I started with 16 patients, compared with 15 for everyone else. Now you want me to do it again? You’re being unfair to me; it’s someone else’s turn to take the extra patient.”
Assignment by Location
Groups that use “unit-based” hospitalists distribute patients according to the unit the patient is admitted to—and the hospitalist covering that unit. The pros and cons of unit-based hospitalists are many (see “A Unit-Based Approach,” September 2007), but there is an obvious tension between keeping patient loads even among hospitalists and ensuring that all of a hospitalist’s patients are on “their” unit. Practicality usually requires a compromise between pure unit-based assignment and load-leveling.
Uneven Assignments
Some groups assign patients according to a predetermined algorithm and employ load-leveling only when patient loads become extremely unbalanced. For example, Dr. Jones gets all the new referrals today, and Dr. James gets them tomorrow. The idea is that patient loads end up close to even over time, even if they’re unbalanced on any given day.
A system like this allows everyone, including the hospitalists themselves, ED staff, etc., to know who will take the next patient. It decreases the need to communicate the “who’s next” information time after time during the course of the day. In small- to medium-sized practices, it could mean no one needs to function as the triage doctor (i.e., the person who inefficiently answers the service calls, scribbles down clinical information, then calls the hospitalist who is due to take the next patient and relays all the pertinent patient info). This system allows the
hospitalists to know which days will be harder (e.g., taking on the care of new patients) and which days will be easier (e.g., rounding but not assuming care of new patients). Allowing uneven loads also eliminates the need to spend energy working to even the loads and risking that some in the group feel as if they aren’t being treated fairly.
Uncommon yet Intriguing Approaches
Pair referring primary-care physicians (PCPs) with specific hospitalists. I’ve encountered two groups that had hospitalists always admit patients from the same PCPs. In other words, hospitalist Dr. Hancock always serves as attending for patients referred by the same nine PCPs, and hospitalist Dr. Franklin always attends to patients from a different set of PCPs. It seems to me that there could be tremendous benefit in working closely with the same PCPs, most notably getting to know the PCPs’ office staff. But this system raises the risk of creating out-of-balance patient loads, among other problems. It is really attractive to me, but most groups will decide its costs outweigh its benefits.
Hospitalist and patient stay connected during admission. I’m not aware of any group that uses this method (let me know if you do!), but there could be benefits to having each patient see the same hospitalist during each hospital stay. Of course, that is assuming the hospitalist is on duty. Hospitalist and patient could be paired upon the patient’s first admission. The hospitalist could form an excellent relationship with the patient and family; the time spent by the hospitalist getting to know patients on admission would be reduced, and I suspect there might be some benefit in the quality of care.
This method, however, likely results in the most uneven patient loads, and load-leveling would be difficult, if not impossible. Even if hospitalist and patient did form a tight bond, there is a high probability that the hospitalist would be off for the duration of the patient’s next admission. So despite what I suspect are tremendous benefits, this approach may not be feasible for any group.
In next month’s column, I will discuss issues related to the way patients are distributed. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: This is the first of a three-part series.
My experience is that some, maybe even most, hospitalists tend to assume there is a standard or “right” way to organize things like work schedules, compensation, or even the assignment of patients among the group’s providers. Some will say things like “SHM says the best hospitalist schedule is …” or “The best way to compensate hospitalists is …”
But there really isn’t a “best” way to manage any particular attribute of a practice. Don’t make the mistake of assuming your method is best, or that it’s the way “everybody else does it.” Although scheduling and compensation are marquee issues for hospitalists, approaches to distributing new patients is much less visible. Many groups tend to assume their method is the only reasonable approach. The best approach, however, varies from one practice to the next. You should be open to hearing approaches to scheduling that are different from your own.
Assign Patients by “Load Leveling”
I’ve come across a lot—and I mean a lot—of different approaches to distributing new patients in HM groups around the country, but it seems pretty clear that the most common method is to undertake “load leveling” on a daily or ongoing basis.
For example, groups that have a separate night shift (the night doctor performs no daytime work the day before or the day after a night shift) typically distribute the night’s new patients with the intent of having each daytime doctor start with the same number of patients. The group might more heavily weight some patients, such as those in the ICU (e.g., each ICU patient counts as 1.5 or two non-ICU patients), but most groups don’t. Over the course of the day shift, new referrals will be distributed evenly among the doctors one at a time, sort of like dealing a deck of cards.
This approach aims to avoid significant imbalances in patient loads and has the potential cultural benefit of everyone sharing equally in busy and slow days. Groups that use it tend to see it as the best option because it is the fairest way to divide up the workload.
Practices that use load-leveling almost always use a schedule built on shifts of a predetermined and fixed duration. For example, say the day shift always works from 7 a.m. to 7 p.m. This schedule usually has the majority of compensation paid via a fixed annual salary or fixed shift rate. One potential problem with this approach is that the doctor who is efficient and discharges a lot of patients today is “rewarded” with more new patients tomorrow. Hospitalists who are allergic to work might have an incentive to have a patient wait until tomorrow to discharge to avoid having to assume the care of yet another patient tomorrow morning. Hospital executives who are focused on length-of-stay management might be concerned if they knew this was a potential issue. Of course, the reverse is true as well. In a practice that doesn’t aggressively undertake load-leveling, a less-than-admirable hospitalist could push patients to discharge earlier than optimal just to have one less patient the next day.
Another cost of this approach is that the distribution of patients can be time-consuming each morning. It also offers the opportunity for some in the group to decide they’re treated unfairly. For instance, you might hear the occasional “just last Tuesday, I started with 16 patients, compared with 15 for everyone else. Now you want me to do it again? You’re being unfair to me; it’s someone else’s turn to take the extra patient.”
Assignment by Location
Groups that use “unit-based” hospitalists distribute patients according to the unit the patient is admitted to—and the hospitalist covering that unit. The pros and cons of unit-based hospitalists are many (see “A Unit-Based Approach,” September 2007), but there is an obvious tension between keeping patient loads even among hospitalists and ensuring that all of a hospitalist’s patients are on “their” unit. Practicality usually requires a compromise between pure unit-based assignment and load-leveling.
Uneven Assignments
Some groups assign patients according to a predetermined algorithm and employ load-leveling only when patient loads become extremely unbalanced. For example, Dr. Jones gets all the new referrals today, and Dr. James gets them tomorrow. The idea is that patient loads end up close to even over time, even if they’re unbalanced on any given day.
A system like this allows everyone, including the hospitalists themselves, ED staff, etc., to know who will take the next patient. It decreases the need to communicate the “who’s next” information time after time during the course of the day. In small- to medium-sized practices, it could mean no one needs to function as the triage doctor (i.e., the person who inefficiently answers the service calls, scribbles down clinical information, then calls the hospitalist who is due to take the next patient and relays all the pertinent patient info). This system allows the
hospitalists to know which days will be harder (e.g., taking on the care of new patients) and which days will be easier (e.g., rounding but not assuming care of new patients). Allowing uneven loads also eliminates the need to spend energy working to even the loads and risking that some in the group feel as if they aren’t being treated fairly.
Uncommon yet Intriguing Approaches
Pair referring primary-care physicians (PCPs) with specific hospitalists. I’ve encountered two groups that had hospitalists always admit patients from the same PCPs. In other words, hospitalist Dr. Hancock always serves as attending for patients referred by the same nine PCPs, and hospitalist Dr. Franklin always attends to patients from a different set of PCPs. It seems to me that there could be tremendous benefit in working closely with the same PCPs, most notably getting to know the PCPs’ office staff. But this system raises the risk of creating out-of-balance patient loads, among other problems. It is really attractive to me, but most groups will decide its costs outweigh its benefits.
Hospitalist and patient stay connected during admission. I’m not aware of any group that uses this method (let me know if you do!), but there could be benefits to having each patient see the same hospitalist during each hospital stay. Of course, that is assuming the hospitalist is on duty. Hospitalist and patient could be paired upon the patient’s first admission. The hospitalist could form an excellent relationship with the patient and family; the time spent by the hospitalist getting to know patients on admission would be reduced, and I suspect there might be some benefit in the quality of care.
This method, however, likely results in the most uneven patient loads, and load-leveling would be difficult, if not impossible. Even if hospitalist and patient did form a tight bond, there is a high probability that the hospitalist would be off for the duration of the patient’s next admission. So despite what I suspect are tremendous benefits, this approach may not be feasible for any group.
In next month’s column, I will discuss issues related to the way patients are distributed. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Editor’s note: This is the first of a three-part series.
My experience is that some, maybe even most, hospitalists tend to assume there is a standard or “right” way to organize things like work schedules, compensation, or even the assignment of patients among the group’s providers. Some will say things like “SHM says the best hospitalist schedule is …” or “The best way to compensate hospitalists is …”
But there really isn’t a “best” way to manage any particular attribute of a practice. Don’t make the mistake of assuming your method is best, or that it’s the way “everybody else does it.” Although scheduling and compensation are marquee issues for hospitalists, approaches to distributing new patients is much less visible. Many groups tend to assume their method is the only reasonable approach. The best approach, however, varies from one practice to the next. You should be open to hearing approaches to scheduling that are different from your own.
Assign Patients by “Load Leveling”
I’ve come across a lot—and I mean a lot—of different approaches to distributing new patients in HM groups around the country, but it seems pretty clear that the most common method is to undertake “load leveling” on a daily or ongoing basis.
For example, groups that have a separate night shift (the night doctor performs no daytime work the day before or the day after a night shift) typically distribute the night’s new patients with the intent of having each daytime doctor start with the same number of patients. The group might more heavily weight some patients, such as those in the ICU (e.g., each ICU patient counts as 1.5 or two non-ICU patients), but most groups don’t. Over the course of the day shift, new referrals will be distributed evenly among the doctors one at a time, sort of like dealing a deck of cards.
This approach aims to avoid significant imbalances in patient loads and has the potential cultural benefit of everyone sharing equally in busy and slow days. Groups that use it tend to see it as the best option because it is the fairest way to divide up the workload.
Practices that use load-leveling almost always use a schedule built on shifts of a predetermined and fixed duration. For example, say the day shift always works from 7 a.m. to 7 p.m. This schedule usually has the majority of compensation paid via a fixed annual salary or fixed shift rate. One potential problem with this approach is that the doctor who is efficient and discharges a lot of patients today is “rewarded” with more new patients tomorrow. Hospitalists who are allergic to work might have an incentive to have a patient wait until tomorrow to discharge to avoid having to assume the care of yet another patient tomorrow morning. Hospital executives who are focused on length-of-stay management might be concerned if they knew this was a potential issue. Of course, the reverse is true as well. In a practice that doesn’t aggressively undertake load-leveling, a less-than-admirable hospitalist could push patients to discharge earlier than optimal just to have one less patient the next day.
Another cost of this approach is that the distribution of patients can be time-consuming each morning. It also offers the opportunity for some in the group to decide they’re treated unfairly. For instance, you might hear the occasional “just last Tuesday, I started with 16 patients, compared with 15 for everyone else. Now you want me to do it again? You’re being unfair to me; it’s someone else’s turn to take the extra patient.”
Assignment by Location
Groups that use “unit-based” hospitalists distribute patients according to the unit the patient is admitted to—and the hospitalist covering that unit. The pros and cons of unit-based hospitalists are many (see “A Unit-Based Approach,” September 2007), but there is an obvious tension between keeping patient loads even among hospitalists and ensuring that all of a hospitalist’s patients are on “their” unit. Practicality usually requires a compromise between pure unit-based assignment and load-leveling.
Uneven Assignments
Some groups assign patients according to a predetermined algorithm and employ load-leveling only when patient loads become extremely unbalanced. For example, Dr. Jones gets all the new referrals today, and Dr. James gets them tomorrow. The idea is that patient loads end up close to even over time, even if they’re unbalanced on any given day.
A system like this allows everyone, including the hospitalists themselves, ED staff, etc., to know who will take the next patient. It decreases the need to communicate the “who’s next” information time after time during the course of the day. In small- to medium-sized practices, it could mean no one needs to function as the triage doctor (i.e., the person who inefficiently answers the service calls, scribbles down clinical information, then calls the hospitalist who is due to take the next patient and relays all the pertinent patient info). This system allows the
hospitalists to know which days will be harder (e.g., taking on the care of new patients) and which days will be easier (e.g., rounding but not assuming care of new patients). Allowing uneven loads also eliminates the need to spend energy working to even the loads and risking that some in the group feel as if they aren’t being treated fairly.
Uncommon yet Intriguing Approaches
Pair referring primary-care physicians (PCPs) with specific hospitalists. I’ve encountered two groups that had hospitalists always admit patients from the same PCPs. In other words, hospitalist Dr. Hancock always serves as attending for patients referred by the same nine PCPs, and hospitalist Dr. Franklin always attends to patients from a different set of PCPs. It seems to me that there could be tremendous benefit in working closely with the same PCPs, most notably getting to know the PCPs’ office staff. But this system raises the risk of creating out-of-balance patient loads, among other problems. It is really attractive to me, but most groups will decide its costs outweigh its benefits.
Hospitalist and patient stay connected during admission. I’m not aware of any group that uses this method (let me know if you do!), but there could be benefits to having each patient see the same hospitalist during each hospital stay. Of course, that is assuming the hospitalist is on duty. Hospitalist and patient could be paired upon the patient’s first admission. The hospitalist could form an excellent relationship with the patient and family; the time spent by the hospitalist getting to know patients on admission would be reduced, and I suspect there might be some benefit in the quality of care.
This method, however, likely results in the most uneven patient loads, and load-leveling would be difficult, if not impossible. Even if hospitalist and patient did form a tight bond, there is a high probability that the hospitalist would be off for the duration of the patient’s next admission. So despite what I suspect are tremendous benefits, this approach may not be feasible for any group.
In next month’s column, I will discuss issues related to the way patients are distributed. TH
Dr. Nelson has been a practicing hospitalist since 1988 and is co-founder and past president of SHM. He is a principal in Nelson Flores Hospital Medicine Consultants, a national hospitalist practice management consulting firm (www.nelsonflores.com). He is co-director and faculty for SHM’s “Best Practices in Managing a Hospital Medicine Program” course. This column represents his views and is not intended to reflect an official position of SHM.
Because of migraines, severe preeclampsia diagnosis is delayed ...
Because of migraines, severe preeclampsia diagnosis is delayed
A WOMAN IN HER 35TH WEEK OF PREGNANCY awoke with what she thought was a migraine headache. When home remedies did not provide relief, she called her ObGyn. He sent her to the hospital for testing. The results suggested preeclampsia, and her blood pressure was at a level that would not cause bleeding in the brain, he believed. It was decided to admit the patient overnight, and then reassess her condition and consider a cesarean delivery on the following day. When the patient reported her headache was severe and the pain radiated to the back of her neck, she was administered Demerol. Her blood pressure and pain decreased. Two hours later, she was unresponsive and the fetal heart rate had dropped. An emergent cesarean delivery was performed, resulting in the birth of a healthy infant.
Following transfer of the mother to another hospital, a CT scan indicated acute intracranial bleeding at the left basal ganglia and frontal lobes. An emergency craniotomy left her semicomatose. During a 6-month stay at a rehabilitation hospital, a shunt placed in her head became infected and required several procedures to treat the infection and replace the shunt. At discharge, she required 24-hour care because of cognitive and physical impairments. She suffers severe memory lapses and poor vision and is unable to walk without a brace.
PATIENT’S CLAIM The ObGyn was negligent for failing to diagnose and treat severe preeclampsia in a timely manner.
PHYSICIAN’S DEFENSE Considering the patient’s history of migraines, the diagnosis and treatment were reasonable. The patient and her husband were informed of the benefits and risks of overnight observation at the hospital. They also wanted to delay the child’s delivery to avoid the complications of a premature birth.
VERDICT $6,420,000 Massachusetts verdict.
After removing right ovary, Gyn discovers no ovary on the left
BECAUSE OF A PAINFUL CYST, a gynecologist removed the right ovary of a 33-year-old patient. During the procedure, adhesions were found on the patient’s left side—but not the left ovary or fallopian tube. Postoperatively, the patient was found to be menopausal, suggesting the absence of a left ovary.
PATIENT’S CLAIM She did not give informed consent. The gynecologist was negligent for removing the right ovary before checking for the presence of the left ovary and for removing the right ovary rather than limiting surgery to removal of the cyst.
PHYSICIAN’S DEFENSE It was necessary to remove the right ovary, whether or not the patient had a left ovary.
VERDICT Texas defense verdict. Prior to trial, the radiologist settled for an undisclosed amount.
$11.5 million for waterbirth dystocia case; infant has CP
DURING A WATERBIRTH in a birthing tub, shoulder dystocia was encountered. The child has cerebral palsy as a result of oxygen deprivation and brain damage.
PATIENT’S CLAIM The birthing tub was not drained quickly enough to use the standard maneuvers for resolving shoulder dystocia.
PHYSICIAN’S DEFENSE The injuries resulted from an infection in the placenta. The maneuvers to resolve the dystocia were performed as quickly as if the mother had not been in a tub.
VERDICT $11.5 million Illinois settlement.
Patient needs vaginal sling, cystocele repair; suffers foot drop
A WOMAN WENT TO THE HOSPITAL for a vaginal sling procedure and repair of a cystocele. Two surgeons, Dr. A and Dr. B, performed the urology part of the surgery. Then an ObGyn, Dr. C, performed the sacrospinous vaginal vault suspension, which included placement of two sutures. Postoperatively, the patient suffered right foot drop. Four days later, Dr. C removed the sutures. The foot drop persisted. At first, she sued several parties. Only Dr. C and his group went to trial.
PATIENT’S CLAIM Not reported.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Alabama settlement. The first trial ended in a mistrial by the court. The second trial resulted in a $1 million verdict, but the court set it aside and ordered a new trial. Then the parties settled.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Because of migraines, severe preeclampsia diagnosis is delayed
A WOMAN IN HER 35TH WEEK OF PREGNANCY awoke with what she thought was a migraine headache. When home remedies did not provide relief, she called her ObGyn. He sent her to the hospital for testing. The results suggested preeclampsia, and her blood pressure was at a level that would not cause bleeding in the brain, he believed. It was decided to admit the patient overnight, and then reassess her condition and consider a cesarean delivery on the following day. When the patient reported her headache was severe and the pain radiated to the back of her neck, she was administered Demerol. Her blood pressure and pain decreased. Two hours later, she was unresponsive and the fetal heart rate had dropped. An emergent cesarean delivery was performed, resulting in the birth of a healthy infant.
Following transfer of the mother to another hospital, a CT scan indicated acute intracranial bleeding at the left basal ganglia and frontal lobes. An emergency craniotomy left her semicomatose. During a 6-month stay at a rehabilitation hospital, a shunt placed in her head became infected and required several procedures to treat the infection and replace the shunt. At discharge, she required 24-hour care because of cognitive and physical impairments. She suffers severe memory lapses and poor vision and is unable to walk without a brace.
PATIENT’S CLAIM The ObGyn was negligent for failing to diagnose and treat severe preeclampsia in a timely manner.
PHYSICIAN’S DEFENSE Considering the patient’s history of migraines, the diagnosis and treatment were reasonable. The patient and her husband were informed of the benefits and risks of overnight observation at the hospital. They also wanted to delay the child’s delivery to avoid the complications of a premature birth.
VERDICT $6,420,000 Massachusetts verdict.
After removing right ovary, Gyn discovers no ovary on the left
BECAUSE OF A PAINFUL CYST, a gynecologist removed the right ovary of a 33-year-old patient. During the procedure, adhesions were found on the patient’s left side—but not the left ovary or fallopian tube. Postoperatively, the patient was found to be menopausal, suggesting the absence of a left ovary.
PATIENT’S CLAIM She did not give informed consent. The gynecologist was negligent for removing the right ovary before checking for the presence of the left ovary and for removing the right ovary rather than limiting surgery to removal of the cyst.
PHYSICIAN’S DEFENSE It was necessary to remove the right ovary, whether or not the patient had a left ovary.
VERDICT Texas defense verdict. Prior to trial, the radiologist settled for an undisclosed amount.
$11.5 million for waterbirth dystocia case; infant has CP
DURING A WATERBIRTH in a birthing tub, shoulder dystocia was encountered. The child has cerebral palsy as a result of oxygen deprivation and brain damage.
PATIENT’S CLAIM The birthing tub was not drained quickly enough to use the standard maneuvers for resolving shoulder dystocia.
PHYSICIAN’S DEFENSE The injuries resulted from an infection in the placenta. The maneuvers to resolve the dystocia were performed as quickly as if the mother had not been in a tub.
VERDICT $11.5 million Illinois settlement.
Patient needs vaginal sling, cystocele repair; suffers foot drop
A WOMAN WENT TO THE HOSPITAL for a vaginal sling procedure and repair of a cystocele. Two surgeons, Dr. A and Dr. B, performed the urology part of the surgery. Then an ObGyn, Dr. C, performed the sacrospinous vaginal vault suspension, which included placement of two sutures. Postoperatively, the patient suffered right foot drop. Four days later, Dr. C removed the sutures. The foot drop persisted. At first, she sued several parties. Only Dr. C and his group went to trial.
PATIENT’S CLAIM Not reported.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Alabama settlement. The first trial ended in a mistrial by the court. The second trial resulted in a $1 million verdict, but the court set it aside and ordered a new trial. Then the parties settled.
Because of migraines, severe preeclampsia diagnosis is delayed
A WOMAN IN HER 35TH WEEK OF PREGNANCY awoke with what she thought was a migraine headache. When home remedies did not provide relief, she called her ObGyn. He sent her to the hospital for testing. The results suggested preeclampsia, and her blood pressure was at a level that would not cause bleeding in the brain, he believed. It was decided to admit the patient overnight, and then reassess her condition and consider a cesarean delivery on the following day. When the patient reported her headache was severe and the pain radiated to the back of her neck, she was administered Demerol. Her blood pressure and pain decreased. Two hours later, she was unresponsive and the fetal heart rate had dropped. An emergent cesarean delivery was performed, resulting in the birth of a healthy infant.
Following transfer of the mother to another hospital, a CT scan indicated acute intracranial bleeding at the left basal ganglia and frontal lobes. An emergency craniotomy left her semicomatose. During a 6-month stay at a rehabilitation hospital, a shunt placed in her head became infected and required several procedures to treat the infection and replace the shunt. At discharge, she required 24-hour care because of cognitive and physical impairments. She suffers severe memory lapses and poor vision and is unable to walk without a brace.
PATIENT’S CLAIM The ObGyn was negligent for failing to diagnose and treat severe preeclampsia in a timely manner.
PHYSICIAN’S DEFENSE Considering the patient’s history of migraines, the diagnosis and treatment were reasonable. The patient and her husband were informed of the benefits and risks of overnight observation at the hospital. They also wanted to delay the child’s delivery to avoid the complications of a premature birth.
VERDICT $6,420,000 Massachusetts verdict.
After removing right ovary, Gyn discovers no ovary on the left
BECAUSE OF A PAINFUL CYST, a gynecologist removed the right ovary of a 33-year-old patient. During the procedure, adhesions were found on the patient’s left side—but not the left ovary or fallopian tube. Postoperatively, the patient was found to be menopausal, suggesting the absence of a left ovary.
PATIENT’S CLAIM She did not give informed consent. The gynecologist was negligent for removing the right ovary before checking for the presence of the left ovary and for removing the right ovary rather than limiting surgery to removal of the cyst.
PHYSICIAN’S DEFENSE It was necessary to remove the right ovary, whether or not the patient had a left ovary.
VERDICT Texas defense verdict. Prior to trial, the radiologist settled for an undisclosed amount.
$11.5 million for waterbirth dystocia case; infant has CP
DURING A WATERBIRTH in a birthing tub, shoulder dystocia was encountered. The child has cerebral palsy as a result of oxygen deprivation and brain damage.
PATIENT’S CLAIM The birthing tub was not drained quickly enough to use the standard maneuvers for resolving shoulder dystocia.
PHYSICIAN’S DEFENSE The injuries resulted from an infection in the placenta. The maneuvers to resolve the dystocia were performed as quickly as if the mother had not been in a tub.
VERDICT $11.5 million Illinois settlement.
Patient needs vaginal sling, cystocele repair; suffers foot drop
A WOMAN WENT TO THE HOSPITAL for a vaginal sling procedure and repair of a cystocele. Two surgeons, Dr. A and Dr. B, performed the urology part of the surgery. Then an ObGyn, Dr. C, performed the sacrospinous vaginal vault suspension, which included placement of two sutures. Postoperatively, the patient suffered right foot drop. Four days later, Dr. C removed the sutures. The foot drop persisted. At first, she sued several parties. Only Dr. C and his group went to trial.
PATIENT’S CLAIM Not reported.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Alabama settlement. The first trial ended in a mistrial by the court. The second trial resulted in a $1 million verdict, but the court set it aside and ordered a new trial. Then the parties settled.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Effective Communication Ensures Patient Safety

Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Effective Communication Ensures Patient Safety
Can you explain to me what is meant by SBAR? I heard this acronym mentioned during a session at HM09, but I did not understand the term.
S. East, MD
Pullman, Wash.
Dr. Hospitalist responds: SBAR (pronounced “ess-bar”) is a standardized method of communication that originated in the Navy’s nuclear submarine program. It stands for:
- Situation: What is happening presently?
- Background: What circumstances led to this situation?
- Assessment: What do I think is the problem?
- Recommendation: What should we do to correct the problem?
The SBAR system was developed to prevent simple communication errors that could lead to global disaster.
Kaiser Permanente of Colorado was among the first to adopt this model of communication among its staff and has since popularized its use in healthcare. Numerous hospitals and healthcare organizations have implemented SBAR as an approach to minimize communication errors between healthcare providers. The idea is that eliminating communication errors between healthcare providers improves patient safety. SBAR encourages all providers (doctors, nurses, pharmacists, etc.) to communicate with a shared mental model for information transfer.
SBAR requires providers to organize their thoughts, understand what it is they want to convey, and make requests in an organized fashion. Adherence to SBAR allows providers to transmit factual information in a concise manner.
Highly effective communication is essential to any hospitalist program. The SBAR approach should not be limited to nurse-doctor communication. I encourage you to implement this tool at your institution.
For more information, an SBAR toolkit is available at www.azhha.org/patient_safety/sbar.aspx. TH
Consultation Elimination
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
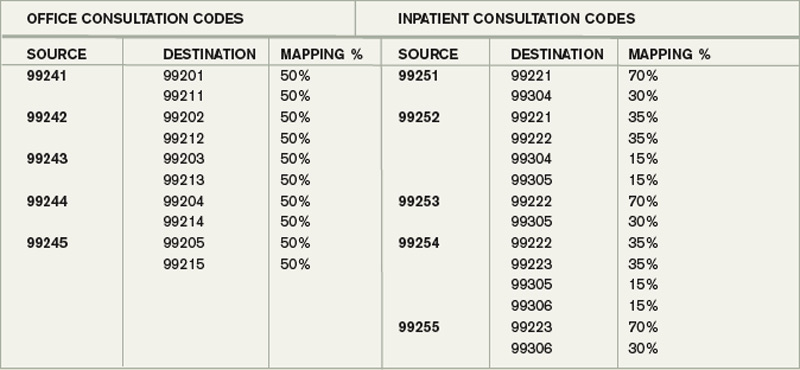
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
As of Jan. 1, the Centers for Medicare and Medicaid Services (CMS) ceased physician payment for consultations. The elimination of consult codes will affect physician group payments as well as relative-value-unit (RVU)-based incentive payments to individual physicians.
The Medicare-designated status of outpatient consultation (99241-99245) and inpatient consultation (99251-99255) codes has changed from “A” (separately payable under the physician fee schedule, when covered) to “I” (not valid for Medicare purposes; Medicare uses another code for the reporting of and the payment for these services). So if you submit consultation codes for Medicare beneficiaries, the result will be nonpayment.
While many physicians fear the negative impact of this ruling, hospitalists should consider its potential. Let’s take a look at a scenario hospitalists encounter on a routine basis.
Typical HM Scenario
A surgeon admits a 76-year-old man for aortic valve replacement. The patient’s history also includes well-controlled hypertension and chronic obstructive pulmonary disease (COPD). Postoperatively, the patient experiences an exacerbation of COPD related to anesthesia, elevated blood pressure, and hyperglycemia. The surgeon requests the hospitalist’s advice on appropriate medical interventions of these conditions. How should the hospitalist report the initial encounter with this Medicare beneficiary?
The hospitalist should select the CPT code that best fits the service and the payor. While most physicians regard this requested service as an inpatient consultation (99251-99255), Medicare no longer recognizes those codes. Instead, the hospitalist should report this encounter as an initial hospital care service (99221-99223).
Comanagement Issues
CMS and Medicare administrative contractors regularly uncover reporting errors for co-management requests. CMS decided the nature of these services were not consultative because the surgeon is not asking the physician or qualified nonphysician provider’s (NPP’s) opinion or advice for the surgeon’s use in treating the patient. Instead, these services constituted concurrent care and should have been billed using subsequent hospital care codes (99231-99233) in the hospital inpatient setting, subsequent NF care codes (99307-99310) in the SNF/NF setting, or office or other outpatient visit codes (99201-99215) in the office or outpatient settings.1
The new ruling simplifies coding and reduces reporting errors. The initial encounter with the patient is reported as such. Regardless of who is the attending of record or the consultant, the first physician from a particular provider group reports initial hospital care codes (i.e., 99221-99223) to represent the first patient encounter, even when this encounter does not occur on the admission date. Other physicians of the same specialty within the same provider group will not be permitted to report initial hospital care codes for their own initial encounter if someone from the group and specialty has already seen the patient during that hospitalization. In other words, the first hospitalist in the provider group reports 9922x, while the remaining hospitalists use subsequent hospital care codes (9923x).
In order to differentiate “consultant” services from “attending” services, CMS will be creating a modifier. The anticipated “AI” modifier must be appended to the attending physician’s initial encounter. Other initial hospital care codes reported throughout the hospital stay, as appropriate, are presumed to be that of “consultants” (i.e., physicians with a different specialty designation than the attending physician) participating in the case. Therefore, the hospitalist now can rightfully recover the increased work effort of the initial patient encounter (99223: 3.79 relative value units, ~$147 vs. 99233: 2.0 relative value units, ~$78, based on 2010 Medicare rates). Physicians will be required to meet the minimum documentation required for the selected visit code.
Other and Undefined Service Locations
Consultations in nursing facilities are handled much like inpatient hospital care. Physicians should report initial nursing facility services (99203-99306) for the first patient encounter, and subsequent nursing facility care codes (99307-99310) for each encounter thereafter. The attending physician of record appends the assigned modifier (presumed to be “AI”) when submitting their initial care service. All other initial care codes are presumed to be those of “consulting” physicians.
Initial information from CMS does not address observation services. Logically, these hospital-based services would follow the same methodology as inpatient care: report initial observation care (99218-99220) for the first “consulting” encounter. However, this might not be appropriate given Medicare’s existing rules for observation services, which guide physicians other than the admitting physician/group to “bill the office and other outpatient service codes or outpatient consultation codes as appropriate when they provide services to the patient.”2 With Medicare’s elimination of consultation codes, the consultant reports “office and other outpatient service codes” (i.e., new patient, 99201-99205, or established patient codes, 99212-99215) by default.
Without further clarification on observation services, hospitalists should report new or established patient service codes, depending on whether the patient has been seen by a group member within the last three years.
Medicare also has existing guidelines for the ED, which suggest that any physician not meeting the consultation criteria report ED service codes (99281-99285). Without further clarification, hospitalists should continue to follow this instruction for Medicare beneficiaries.
Nonphysician Providers
Medicare’s split/shared billing guidelines apply to most hospital inpatient, hospital outpatient, and ED evaluation and management (E/M) services, with consultations as one exception. Now, in accordance with the new ruling, hospitalists should select the appropriate initial service codes that correspond to patient’s location (e.g., 99223 for inpatients). NPPs can participate in the initial service provided to patients in these locations without the hospitalist having to replicate the entire service. The hospitalist can submit the claim in their name after selecting the visit level based upon the cumulative service personally provided on the same calendar day by both the NPP and the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center in Philadelphia. She also is faculty for SHM’s inpatient coding course.
References
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.10I. Centers for Medicare and Medicaid Services Web site. Available at: www.cms.hhs.gov/ manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- Medicare Claims Processing Manual: Chapter 12, Section 30.6.8A. CMS Web site. Available at: www. cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Nov. 14, 2009.
- PFS Federal Regulation Notices: Proposed Revisions to Payment Policies Under the Physician Fee Schedule and Part B for CY 2010. CMS Web site. Available at: www.cms.hhs.gov/PhysicianFeeSched/PFSFRN/itemdetail.asp?filterType=none&filterByDID=99&sortByDID=4&sortOrder=descending&itemID=CMS1223902&intNumPerPage=10. Accessed Nov. 12, 2009.
- Payment Policies Under the Physician Fee Schedule and Other Revisions to Part B (for CY 2010). CMS Web site. Available at: www.federalregister.gov/OFR Upload/OFRData/2009-26502_PI.pdf. Accessed Nov. 10, 2009.
The Bottom Line
The elimination of consults will affect physician group payments as well as RVU-based incentive payments to individual physicians. HM group leaders will want to refer to the CMS formula, also known as a crosswalk. The crosswalk outlines the utilization of consult codes and E/M codes for the sole purpose of establishing aggregate budget neutrality.3
The payment differential for consultations has been redistributed to increase payments for existing E/M services.
Here’s how it works: Use the “mapping percentage” column to project the distribution of consultative services between the “replacement” (i.e., “destination”) codes. For example, presumably 70% of 99251 will now be reported as initial hospital care (99221), whereas 30% will be reported as initial nursing facility care (99304). Please note that this table does not represent billing guidance or documentation equivalencies, but it does attempt to quantify sites of consultative service and their corresponding code categories for the basis of fiscal-year projections.
Physicians should select the visit code in the appropriate code category for the service location and in accordance with CMS documentation guidelines, which are available at www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp.
CPT changes for ObGyns are minor in 2010; the big news is Medicare’s toss of consult codes
Current Procedural Terminology (CPT) 2010, which took effect January 1, doesn’t bring many changes for ObGyn practice, but there’s been a major backpedaling in Medicare coverage of consultations that you must be aware of. In conjunction with this move by the Centers for Medicare & Medicaid Services (CMS), CPT has added a definition of “transfer of care” and established two possible reasons for providing a consultation. I’ll have more to report about these important developments later in this article.
Among the changes to billing codes for the work performed in ObGyn: rebundling of commonly performed urodynamics procedures and new codes for revision of a vaginal graft. There is also a new (and unpublished) code for administering the H1N1 influenza vaccine.
Last, CPT has revised the explanation of non–face-to-face prolonged services. Read on!
New codes bundle urodynamic studies—a product of joint CMS and CPT input
The biggest changes in coding for ObGyn procedures are urodynamics study codes. The American Medical Association (AMA) has 1) created three new codes that represent test bundles and, in the process, 2) deleted the stand-alone urodynamics codes 51772 (urethral pressure profile studies [UPP] [urethral closure pressure profile], any technique) and 51795 (voiding pressure studies; bladder voiding pressure, any technique).
These changes were made because the most commonly reported codes for a female patient were billed together 90% of the time (51726, 51772, 51795, and 51797); the AMA reasoned that the most frequent combinations were considered overvalued when billed separately—that is, there was no repeat of pre-test and post-test work when these combinations were performed and there was no duplication in the cost of supplies and staff time.
The new bundles were therefore considered to better reflect current medical practice, and the Relative Value Update Committee (RUC) recommended, and CMS accepted, the relative value units (RVU) for the combination codes to reflect the true physician work value and practice expense of the combined procedures.
New and revised codes are:
51726 Complex cystometrogram (i.e., calibrated electronic equipment)
51727 …with urethral pressure profile studies (i.e., urethral closure pressure profile), any technique
51728 …with voiding pressure studies (i.e., bladder voiding pressure), any technique
51729 …with voiding pressure studies (i.e., bladder voiding pressure) and urethral pressure profile studies (i.e., urethral closure pressure profile), any technique.
According to the clinical vignette submitted to the AMA for code 51727, this procedure will include a sustained Valsalva maneuver as part of the urethral closure pressure profile. CPT did, however, retain the add-on code +51797 (voiding pressure studies, intra-abdominal [i.e., rectal, gastric, intraperitoneal]) and has clarified that 51797 may be billed in addition to 51728 and 51729 if a rectal catheter is placed to determine if the patient is straining during the voiding event.
In other words, the add-on code may be reported only when the primary procedure includes a voiding pressure study.
RVU for these new procedures have also been revised (see the TABLE ). Notable is the seeming discrepancy in RVU between code 51726 (cystometrogram alone) and the bundled tests. This is the case because the practice expense for 51726 has not reached its final level (the practice expense RVU are being increased or decreased in increments over several years); for 2010 only, therefore, this code will have a higher total RVU value than the new codes (51727, 51728, 51729), despite having a lower physician work relative value.
The discrepancy will be corrected in 2011, when 51726 will have lower RVU than the other urodynamics combination test codes.
TABLE
Changes in 2010 to RVU for urodynamic studies
| 2009 | 2010 | |||
|---|---|---|---|---|
| CPT code | Work RVU | Total RVU | Work RVU | Total RVU |
| 51726 | 1.71 | 9.02 | 1.71 | 8.71 |
| 51727 | Not applicable (NA) | NA | 2.11 | 8.07 |
| 51728 | NA | NA | 2.11 | 8.06 |
| 51729 | NA | NA | 2.11 | 8.14 |
Laparoscopic revision of a vaginal graft
In 2006, the AMA added the code for a vaginal approach to revising a graft (57295, revision [including removal] of prosthetic vaginal graft; vaginal approach). Then, in 2007, it added a code for an abdominal approach (57296, revision [including removal] of prosthetic vaginal graft; open abdominal approach).
Now, you have a code for a laparoscopic approach, completing the code set for this procedure. As with 57295 and 57296, report the new code when the graft is either revised or removed entirely.
57426 Revision (including removal) of prosthetic vaginal graft, laparoscopic approach
Other, miscellaneous changes take effect
OBSTETRIC PANEL
Although code 80055 comprises a battery of tests that are performed routinely on obstetric patients, a new code, 86780, was created to report syphilis screening using a treponemal antibody method, in which IgM and IgG antibodies are measured. This test is not the same syphilis test that is now part of the 80055 panel. CPT has therefore cautioned that, when you use code 86780 instead of the standard syphilis test code 86592, you should not report the obstetrics panel but, instead, separately report each test performed.
REPRODUCTIVE MEDICINE
New code 89398 (unlisted reproductive medicine laboratory procedure) has been added, but CPT still directs billers to use the unlisted miscellaneous pathology test code 89240 to report cryopreservation of reproductive ovarian tissues.
BILLING FOR THE H1N1 INFLUENZA VACCINE
Because of the urgency of collecting data on the H1N1 influenza epidemic, CPT has revised code 90663 to include the H1N1 formulation of the flu vaccine product. In addition, CPT has created a new code, 90470, for administering the H1N1 flu vaccine, which became valid in September (but which isn’t included in the hard-copy version of CPT 2010). The new code is to be used for intramuscular injection or intranasal administration, and includes any time spent counseling.
In addition:
- Do not report established code 90471 (immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid]) when you administer the H1N1 flu vaccine
- Report the vaccine product code only when your practice has purchased the vaccine, or when the payer requires the code with a 0 charge to match the administration code.
- Medicare coding for administering the H1N1 flu vaccine is different than what I’ve just described. Do not use CPT codes for Medicare patients; instead, code H1N1 flu immunization as:
G9141 Influenza A (H1N1) immunization administration (includes the physician counseling the patient/family)
G9142 Influenza A (H1N1) vaccine, any route of administration
Medicare will not reimburse for the vaccine product because it is being given to its providers without cost. Some carriers may require that the new vaccine product code be listed with a 0 charge.
Prolonged inpatient E/M services
CPT has revised guidelines for prolonged services that do not involve direct face-to-face contact with a patient. Keep in mind, however, that, although these changes are welcome, many payers don’t reimburse separately for work that isn’t performed face to face.
These codes are no longer considered add-on codes; they can be reported on a different date than the related E/M service.
According to CPT, codes 99358 and 99359 are reported when the prolonged time:
- is greater than would be expected for normal pre-service and post-service work associated with the E/M service
- exceeds 30 minutes
- is related to an E/M service that has already occurred, or to one that will occur and represents ongoing patient management (for example, your review of extensive patient records that weren’t available at the time of the visit)
- is in addition to any telephone services codes (99441–99443)—but not with more specific codes, such as medical team conferences, online medical evaluation, or care plan oversight services, which have no upper limit to the time required to accomplish the service.
Consultation codes and clarifications
Two changes of note, from a CPT perspective, have been made in the area of consultations. CPT has:
- added a definition for a transfer of care
- defined two circumstances under which a consultation can be coded. These revisions come at the same time Medicare has made the decision to no longer pay for consultations other than tele-health consults (see following section).
For 2010, CPT defines transfer of care as
…the process whereby a physician who is providing management for some or all of a patient’s problems relinquishes this responsibility to another physician who agrees to accept this responsibility and who, from the initial encounter, is not providing consultative services.
The guidelines also explain that 1) a transferring physician is no longer responsible for caring for the problem for which the patient was referred and 2) the consultation codes should not be reported by the physician who accepts care.
Two alternative conditions must now apply for a consultation to be considered provided:
- A physician requested an opinion or advice for a specific condition or problem, or
- The consulting physician saw the patient first to determine whether to accept ongoing management of her entire care or of a specific condition or problem (i.e., transfer of care).
The second condition is new; it remains to be seen if payers will accept it as a valid reason to bill for consultation.
As with all billable services, you should ensure that the criteria required by the payer you are billing have been met. CPT also directs that the written request for consultation can be documented by either the requesting or the receiving physician—something that was unacceptable under Medicare guidelines.
Last, CPT has added instructions to clarify the type of consultation code to bill under certain circumstances:
- When the patient is admitted after an outpatient consultation but the physician does not see the patient on the unit on the date of admission, bill only for outpatient consultation
- When the patient is seen for an office visit, emergency room visit, or outpatient consult on the date of admission and the physician then sees the patient on the unit that day, bill only the inpatient consultation or initial hospital care code, whichever applies. All services that day are used to determine the final level of service.
Medicare tilts the playing field on consultations
Although CPT has retained all consultation codes, and although the hope is that commercial payers will continue to reimburse for such services in the near future, the big news is that Medicare has announced that it will no longer recognize (or reimburse for) codes for outpatient or inpatient consultations. (Note: This story is still unfolding, however. The changes announced by Medicare that I discuss below are still before Congress as this article goes to press. Although Medicare has, in fact, released the transmittal letter to all carriers instructing them about the changes, Senator Arlen Specter [D-Pa] has introduced an amendment to the Patient Protection and Affordable Care Act [H.R. 3590] to postpone the policy change for 1 year. If Congress has not passed this bill before the end of 2009, the changes go through as planned. Stay tuned for developments!)
Assuming the changes go through, here is what is expected of you in the circumstances of providing consultations and billing Medicare (Medicaid payers aren’t required to follow this policy change but may opt to do so).
Outpatients. Document, and report, the appropriate level of visit for a new or established Medicare patient using outpatient codes 99201–99215
Inpatients. If you are a non-admitting physician asked to see a patient for the first time, report the appropriate level of initial hospital care (codes 99221–99223). Note the following three points:
- Initial hospital care includes only three levels of service—not the five levels from which you choose for consultation codes
- The lowest level of history and exam for these initial visit codes is a detailed history and examination—no matter the level of medical decision-making. If the level of history or exam is documented lower than “detailed”—say, as “expanded problem-focused”—you are required to report the unlisted E/M code 99499.
- The admitting physician adds the new Healthcare Common Procedure Coding System (HCPCS) modifier –AI (that is, “‘A’ upper-case ‘i’”) to the initial visit code, so that Medicare can distinguish the admitting physician from others providing care for the patient.
- All subsequent visits with the inpatient continue to be billed with the subsequent care inpatient codes (99231–99233).
Fallout from this change? Medicare is studying the implications of its new policy on secondary payments—that is, when Medicare is the primary payer and there is a supplemental carrier, or when Medicare is the secondary payer. Note: Medicare strongly advises all providers to check with their primary payers, because 1) Medicare will not accept a consultation code when a primary insurer has paid on that code and 2) it’s doubtful that a commercial payer will accept a consultation code when Medicare has paid for a new or established patient service.
To add to the turmoil…
The CMS has announced that, as a result of the changes in Medicare policy on consultations, it is increasing the relative values for all new and established patient services and initial hospital care. CMS is doing this, however, by reducing the relative values of some consultation codes.
In addition, all surgical procedure codes that carry a 10- or 90-day global period will see an increase in work RVU because of the increase in E/M services that are a part of all global care. Keep in mind that payers who use the Resource-Based Relative Value Scale (RBRVS) to reimburse services will probably adopt the new values when contracts are up for renewal, although many will be unable to do so in the short term.
It also remains to be seen if any commercial payers adopt Medicare policy or continue to pay for consultations. This area might be a contract issue with payers.
Current Procedural Terminology (CPT) 2010, which took effect January 1, doesn’t bring many changes for ObGyn practice, but there’s been a major backpedaling in Medicare coverage of consultations that you must be aware of. In conjunction with this move by the Centers for Medicare & Medicaid Services (CMS), CPT has added a definition of “transfer of care” and established two possible reasons for providing a consultation. I’ll have more to report about these important developments later in this article.
Among the changes to billing codes for the work performed in ObGyn: rebundling of commonly performed urodynamics procedures and new codes for revision of a vaginal graft. There is also a new (and unpublished) code for administering the H1N1 influenza vaccine.
Last, CPT has revised the explanation of non–face-to-face prolonged services. Read on!
New codes bundle urodynamic studies—a product of joint CMS and CPT input
The biggest changes in coding for ObGyn procedures are urodynamics study codes. The American Medical Association (AMA) has 1) created three new codes that represent test bundles and, in the process, 2) deleted the stand-alone urodynamics codes 51772 (urethral pressure profile studies [UPP] [urethral closure pressure profile], any technique) and 51795 (voiding pressure studies; bladder voiding pressure, any technique).
These changes were made because the most commonly reported codes for a female patient were billed together 90% of the time (51726, 51772, 51795, and 51797); the AMA reasoned that the most frequent combinations were considered overvalued when billed separately—that is, there was no repeat of pre-test and post-test work when these combinations were performed and there was no duplication in the cost of supplies and staff time.
The new bundles were therefore considered to better reflect current medical practice, and the Relative Value Update Committee (RUC) recommended, and CMS accepted, the relative value units (RVU) for the combination codes to reflect the true physician work value and practice expense of the combined procedures.
New and revised codes are:
51726 Complex cystometrogram (i.e., calibrated electronic equipment)
51727 …with urethral pressure profile studies (i.e., urethral closure pressure profile), any technique
51728 …with voiding pressure studies (i.e., bladder voiding pressure), any technique
51729 …with voiding pressure studies (i.e., bladder voiding pressure) and urethral pressure profile studies (i.e., urethral closure pressure profile), any technique.
According to the clinical vignette submitted to the AMA for code 51727, this procedure will include a sustained Valsalva maneuver as part of the urethral closure pressure profile. CPT did, however, retain the add-on code +51797 (voiding pressure studies, intra-abdominal [i.e., rectal, gastric, intraperitoneal]) and has clarified that 51797 may be billed in addition to 51728 and 51729 if a rectal catheter is placed to determine if the patient is straining during the voiding event.
In other words, the add-on code may be reported only when the primary procedure includes a voiding pressure study.
RVU for these new procedures have also been revised (see the TABLE ). Notable is the seeming discrepancy in RVU between code 51726 (cystometrogram alone) and the bundled tests. This is the case because the practice expense for 51726 has not reached its final level (the practice expense RVU are being increased or decreased in increments over several years); for 2010 only, therefore, this code will have a higher total RVU value than the new codes (51727, 51728, 51729), despite having a lower physician work relative value.
The discrepancy will be corrected in 2011, when 51726 will have lower RVU than the other urodynamics combination test codes.
TABLE
Changes in 2010 to RVU for urodynamic studies
| 2009 | 2010 | |||
|---|---|---|---|---|
| CPT code | Work RVU | Total RVU | Work RVU | Total RVU |
| 51726 | 1.71 | 9.02 | 1.71 | 8.71 |
| 51727 | Not applicable (NA) | NA | 2.11 | 8.07 |
| 51728 | NA | NA | 2.11 | 8.06 |
| 51729 | NA | NA | 2.11 | 8.14 |
Laparoscopic revision of a vaginal graft
In 2006, the AMA added the code for a vaginal approach to revising a graft (57295, revision [including removal] of prosthetic vaginal graft; vaginal approach). Then, in 2007, it added a code for an abdominal approach (57296, revision [including removal] of prosthetic vaginal graft; open abdominal approach).
Now, you have a code for a laparoscopic approach, completing the code set for this procedure. As with 57295 and 57296, report the new code when the graft is either revised or removed entirely.
57426 Revision (including removal) of prosthetic vaginal graft, laparoscopic approach
Other, miscellaneous changes take effect
OBSTETRIC PANEL
Although code 80055 comprises a battery of tests that are performed routinely on obstetric patients, a new code, 86780, was created to report syphilis screening using a treponemal antibody method, in which IgM and IgG antibodies are measured. This test is not the same syphilis test that is now part of the 80055 panel. CPT has therefore cautioned that, when you use code 86780 instead of the standard syphilis test code 86592, you should not report the obstetrics panel but, instead, separately report each test performed.
REPRODUCTIVE MEDICINE
New code 89398 (unlisted reproductive medicine laboratory procedure) has been added, but CPT still directs billers to use the unlisted miscellaneous pathology test code 89240 to report cryopreservation of reproductive ovarian tissues.
BILLING FOR THE H1N1 INFLUENZA VACCINE
Because of the urgency of collecting data on the H1N1 influenza epidemic, CPT has revised code 90663 to include the H1N1 formulation of the flu vaccine product. In addition, CPT has created a new code, 90470, for administering the H1N1 flu vaccine, which became valid in September (but which isn’t included in the hard-copy version of CPT 2010). The new code is to be used for intramuscular injection or intranasal administration, and includes any time spent counseling.
In addition:
- Do not report established code 90471 (immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid]) when you administer the H1N1 flu vaccine
- Report the vaccine product code only when your practice has purchased the vaccine, or when the payer requires the code with a 0 charge to match the administration code.
- Medicare coding for administering the H1N1 flu vaccine is different than what I’ve just described. Do not use CPT codes for Medicare patients; instead, code H1N1 flu immunization as:
G9141 Influenza A (H1N1) immunization administration (includes the physician counseling the patient/family)
G9142 Influenza A (H1N1) vaccine, any route of administration
Medicare will not reimburse for the vaccine product because it is being given to its providers without cost. Some carriers may require that the new vaccine product code be listed with a 0 charge.
Prolonged inpatient E/M services
CPT has revised guidelines for prolonged services that do not involve direct face-to-face contact with a patient. Keep in mind, however, that, although these changes are welcome, many payers don’t reimburse separately for work that isn’t performed face to face.
These codes are no longer considered add-on codes; they can be reported on a different date than the related E/M service.
According to CPT, codes 99358 and 99359 are reported when the prolonged time:
- is greater than would be expected for normal pre-service and post-service work associated with the E/M service
- exceeds 30 minutes
- is related to an E/M service that has already occurred, or to one that will occur and represents ongoing patient management (for example, your review of extensive patient records that weren’t available at the time of the visit)
- is in addition to any telephone services codes (99441–99443)—but not with more specific codes, such as medical team conferences, online medical evaluation, or care plan oversight services, which have no upper limit to the time required to accomplish the service.
Consultation codes and clarifications
Two changes of note, from a CPT perspective, have been made in the area of consultations. CPT has:
- added a definition for a transfer of care
- defined two circumstances under which a consultation can be coded. These revisions come at the same time Medicare has made the decision to no longer pay for consultations other than tele-health consults (see following section).
For 2010, CPT defines transfer of care as
…the process whereby a physician who is providing management for some or all of a patient’s problems relinquishes this responsibility to another physician who agrees to accept this responsibility and who, from the initial encounter, is not providing consultative services.
The guidelines also explain that 1) a transferring physician is no longer responsible for caring for the problem for which the patient was referred and 2) the consultation codes should not be reported by the physician who accepts care.
Two alternative conditions must now apply for a consultation to be considered provided:
- A physician requested an opinion or advice for a specific condition or problem, or
- The consulting physician saw the patient first to determine whether to accept ongoing management of her entire care or of a specific condition or problem (i.e., transfer of care).
The second condition is new; it remains to be seen if payers will accept it as a valid reason to bill for consultation.
As with all billable services, you should ensure that the criteria required by the payer you are billing have been met. CPT also directs that the written request for consultation can be documented by either the requesting or the receiving physician—something that was unacceptable under Medicare guidelines.
Last, CPT has added instructions to clarify the type of consultation code to bill under certain circumstances:
- When the patient is admitted after an outpatient consultation but the physician does not see the patient on the unit on the date of admission, bill only for outpatient consultation
- When the patient is seen for an office visit, emergency room visit, or outpatient consult on the date of admission and the physician then sees the patient on the unit that day, bill only the inpatient consultation or initial hospital care code, whichever applies. All services that day are used to determine the final level of service.
Medicare tilts the playing field on consultations
Although CPT has retained all consultation codes, and although the hope is that commercial payers will continue to reimburse for such services in the near future, the big news is that Medicare has announced that it will no longer recognize (or reimburse for) codes for outpatient or inpatient consultations. (Note: This story is still unfolding, however. The changes announced by Medicare that I discuss below are still before Congress as this article goes to press. Although Medicare has, in fact, released the transmittal letter to all carriers instructing them about the changes, Senator Arlen Specter [D-Pa] has introduced an amendment to the Patient Protection and Affordable Care Act [H.R. 3590] to postpone the policy change for 1 year. If Congress has not passed this bill before the end of 2009, the changes go through as planned. Stay tuned for developments!)
Assuming the changes go through, here is what is expected of you in the circumstances of providing consultations and billing Medicare (Medicaid payers aren’t required to follow this policy change but may opt to do so).
Outpatients. Document, and report, the appropriate level of visit for a new or established Medicare patient using outpatient codes 99201–99215
Inpatients. If you are a non-admitting physician asked to see a patient for the first time, report the appropriate level of initial hospital care (codes 99221–99223). Note the following three points:
- Initial hospital care includes only three levels of service—not the five levels from which you choose for consultation codes
- The lowest level of history and exam for these initial visit codes is a detailed history and examination—no matter the level of medical decision-making. If the level of history or exam is documented lower than “detailed”—say, as “expanded problem-focused”—you are required to report the unlisted E/M code 99499.
- The admitting physician adds the new Healthcare Common Procedure Coding System (HCPCS) modifier –AI (that is, “‘A’ upper-case ‘i’”) to the initial visit code, so that Medicare can distinguish the admitting physician from others providing care for the patient.
- All subsequent visits with the inpatient continue to be billed with the subsequent care inpatient codes (99231–99233).
Fallout from this change? Medicare is studying the implications of its new policy on secondary payments—that is, when Medicare is the primary payer and there is a supplemental carrier, or when Medicare is the secondary payer. Note: Medicare strongly advises all providers to check with their primary payers, because 1) Medicare will not accept a consultation code when a primary insurer has paid on that code and 2) it’s doubtful that a commercial payer will accept a consultation code when Medicare has paid for a new or established patient service.
To add to the turmoil…
The CMS has announced that, as a result of the changes in Medicare policy on consultations, it is increasing the relative values for all new and established patient services and initial hospital care. CMS is doing this, however, by reducing the relative values of some consultation codes.
In addition, all surgical procedure codes that carry a 10- or 90-day global period will see an increase in work RVU because of the increase in E/M services that are a part of all global care. Keep in mind that payers who use the Resource-Based Relative Value Scale (RBRVS) to reimburse services will probably adopt the new values when contracts are up for renewal, although many will be unable to do so in the short term.
It also remains to be seen if any commercial payers adopt Medicare policy or continue to pay for consultations. This area might be a contract issue with payers.
Current Procedural Terminology (CPT) 2010, which took effect January 1, doesn’t bring many changes for ObGyn practice, but there’s been a major backpedaling in Medicare coverage of consultations that you must be aware of. In conjunction with this move by the Centers for Medicare & Medicaid Services (CMS), CPT has added a definition of “transfer of care” and established two possible reasons for providing a consultation. I’ll have more to report about these important developments later in this article.
Among the changes to billing codes for the work performed in ObGyn: rebundling of commonly performed urodynamics procedures and new codes for revision of a vaginal graft. There is also a new (and unpublished) code for administering the H1N1 influenza vaccine.
Last, CPT has revised the explanation of non–face-to-face prolonged services. Read on!
New codes bundle urodynamic studies—a product of joint CMS and CPT input
The biggest changes in coding for ObGyn procedures are urodynamics study codes. The American Medical Association (AMA) has 1) created three new codes that represent test bundles and, in the process, 2) deleted the stand-alone urodynamics codes 51772 (urethral pressure profile studies [UPP] [urethral closure pressure profile], any technique) and 51795 (voiding pressure studies; bladder voiding pressure, any technique).
These changes were made because the most commonly reported codes for a female patient were billed together 90% of the time (51726, 51772, 51795, and 51797); the AMA reasoned that the most frequent combinations were considered overvalued when billed separately—that is, there was no repeat of pre-test and post-test work when these combinations were performed and there was no duplication in the cost of supplies and staff time.
The new bundles were therefore considered to better reflect current medical practice, and the Relative Value Update Committee (RUC) recommended, and CMS accepted, the relative value units (RVU) for the combination codes to reflect the true physician work value and practice expense of the combined procedures.
New and revised codes are:
51726 Complex cystometrogram (i.e., calibrated electronic equipment)
51727 …with urethral pressure profile studies (i.e., urethral closure pressure profile), any technique
51728 …with voiding pressure studies (i.e., bladder voiding pressure), any technique
51729 …with voiding pressure studies (i.e., bladder voiding pressure) and urethral pressure profile studies (i.e., urethral closure pressure profile), any technique.
According to the clinical vignette submitted to the AMA for code 51727, this procedure will include a sustained Valsalva maneuver as part of the urethral closure pressure profile. CPT did, however, retain the add-on code +51797 (voiding pressure studies, intra-abdominal [i.e., rectal, gastric, intraperitoneal]) and has clarified that 51797 may be billed in addition to 51728 and 51729 if a rectal catheter is placed to determine if the patient is straining during the voiding event.
In other words, the add-on code may be reported only when the primary procedure includes a voiding pressure study.
RVU for these new procedures have also been revised (see the TABLE ). Notable is the seeming discrepancy in RVU between code 51726 (cystometrogram alone) and the bundled tests. This is the case because the practice expense for 51726 has not reached its final level (the practice expense RVU are being increased or decreased in increments over several years); for 2010 only, therefore, this code will have a higher total RVU value than the new codes (51727, 51728, 51729), despite having a lower physician work relative value.
The discrepancy will be corrected in 2011, when 51726 will have lower RVU than the other urodynamics combination test codes.
TABLE
Changes in 2010 to RVU for urodynamic studies
| 2009 | 2010 | |||
|---|---|---|---|---|
| CPT code | Work RVU | Total RVU | Work RVU | Total RVU |
| 51726 | 1.71 | 9.02 | 1.71 | 8.71 |
| 51727 | Not applicable (NA) | NA | 2.11 | 8.07 |
| 51728 | NA | NA | 2.11 | 8.06 |
| 51729 | NA | NA | 2.11 | 8.14 |
Laparoscopic revision of a vaginal graft
In 2006, the AMA added the code for a vaginal approach to revising a graft (57295, revision [including removal] of prosthetic vaginal graft; vaginal approach). Then, in 2007, it added a code for an abdominal approach (57296, revision [including removal] of prosthetic vaginal graft; open abdominal approach).
Now, you have a code for a laparoscopic approach, completing the code set for this procedure. As with 57295 and 57296, report the new code when the graft is either revised or removed entirely.
57426 Revision (including removal) of prosthetic vaginal graft, laparoscopic approach
Other, miscellaneous changes take effect
OBSTETRIC PANEL
Although code 80055 comprises a battery of tests that are performed routinely on obstetric patients, a new code, 86780, was created to report syphilis screening using a treponemal antibody method, in which IgM and IgG antibodies are measured. This test is not the same syphilis test that is now part of the 80055 panel. CPT has therefore cautioned that, when you use code 86780 instead of the standard syphilis test code 86592, you should not report the obstetrics panel but, instead, separately report each test performed.
REPRODUCTIVE MEDICINE
New code 89398 (unlisted reproductive medicine laboratory procedure) has been added, but CPT still directs billers to use the unlisted miscellaneous pathology test code 89240 to report cryopreservation of reproductive ovarian tissues.
BILLING FOR THE H1N1 INFLUENZA VACCINE
Because of the urgency of collecting data on the H1N1 influenza epidemic, CPT has revised code 90663 to include the H1N1 formulation of the flu vaccine product. In addition, CPT has created a new code, 90470, for administering the H1N1 flu vaccine, which became valid in September (but which isn’t included in the hard-copy version of CPT 2010). The new code is to be used for intramuscular injection or intranasal administration, and includes any time spent counseling.
In addition:
- Do not report established code 90471 (immunization administration [includes percutaneous, intradermal, subcutaneous, or intramuscular injections]; one vaccine [single or combination vaccine/toxoid]) when you administer the H1N1 flu vaccine
- Report the vaccine product code only when your practice has purchased the vaccine, or when the payer requires the code with a 0 charge to match the administration code.
- Medicare coding for administering the H1N1 flu vaccine is different than what I’ve just described. Do not use CPT codes for Medicare patients; instead, code H1N1 flu immunization as:
G9141 Influenza A (H1N1) immunization administration (includes the physician counseling the patient/family)
G9142 Influenza A (H1N1) vaccine, any route of administration
Medicare will not reimburse for the vaccine product because it is being given to its providers without cost. Some carriers may require that the new vaccine product code be listed with a 0 charge.
Prolonged inpatient E/M services
CPT has revised guidelines for prolonged services that do not involve direct face-to-face contact with a patient. Keep in mind, however, that, although these changes are welcome, many payers don’t reimburse separately for work that isn’t performed face to face.
These codes are no longer considered add-on codes; they can be reported on a different date than the related E/M service.
According to CPT, codes 99358 and 99359 are reported when the prolonged time:
- is greater than would be expected for normal pre-service and post-service work associated with the E/M service
- exceeds 30 minutes
- is related to an E/M service that has already occurred, or to one that will occur and represents ongoing patient management (for example, your review of extensive patient records that weren’t available at the time of the visit)
- is in addition to any telephone services codes (99441–99443)—but not with more specific codes, such as medical team conferences, online medical evaluation, or care plan oversight services, which have no upper limit to the time required to accomplish the service.
Consultation codes and clarifications
Two changes of note, from a CPT perspective, have been made in the area of consultations. CPT has:
- added a definition for a transfer of care
- defined two circumstances under which a consultation can be coded. These revisions come at the same time Medicare has made the decision to no longer pay for consultations other than tele-health consults (see following section).
For 2010, CPT defines transfer of care as
…the process whereby a physician who is providing management for some or all of a patient’s problems relinquishes this responsibility to another physician who agrees to accept this responsibility and who, from the initial encounter, is not providing consultative services.
The guidelines also explain that 1) a transferring physician is no longer responsible for caring for the problem for which the patient was referred and 2) the consultation codes should not be reported by the physician who accepts care.
Two alternative conditions must now apply for a consultation to be considered provided:
- A physician requested an opinion or advice for a specific condition or problem, or
- The consulting physician saw the patient first to determine whether to accept ongoing management of her entire care or of a specific condition or problem (i.e., transfer of care).
The second condition is new; it remains to be seen if payers will accept it as a valid reason to bill for consultation.
As with all billable services, you should ensure that the criteria required by the payer you are billing have been met. CPT also directs that the written request for consultation can be documented by either the requesting or the receiving physician—something that was unacceptable under Medicare guidelines.
Last, CPT has added instructions to clarify the type of consultation code to bill under certain circumstances:
- When the patient is admitted after an outpatient consultation but the physician does not see the patient on the unit on the date of admission, bill only for outpatient consultation
- When the patient is seen for an office visit, emergency room visit, or outpatient consult on the date of admission and the physician then sees the patient on the unit that day, bill only the inpatient consultation or initial hospital care code, whichever applies. All services that day are used to determine the final level of service.
Medicare tilts the playing field on consultations
Although CPT has retained all consultation codes, and although the hope is that commercial payers will continue to reimburse for such services in the near future, the big news is that Medicare has announced that it will no longer recognize (or reimburse for) codes for outpatient or inpatient consultations. (Note: This story is still unfolding, however. The changes announced by Medicare that I discuss below are still before Congress as this article goes to press. Although Medicare has, in fact, released the transmittal letter to all carriers instructing them about the changes, Senator Arlen Specter [D-Pa] has introduced an amendment to the Patient Protection and Affordable Care Act [H.R. 3590] to postpone the policy change for 1 year. If Congress has not passed this bill before the end of 2009, the changes go through as planned. Stay tuned for developments!)
Assuming the changes go through, here is what is expected of you in the circumstances of providing consultations and billing Medicare (Medicaid payers aren’t required to follow this policy change but may opt to do so).
Outpatients. Document, and report, the appropriate level of visit for a new or established Medicare patient using outpatient codes 99201–99215
Inpatients. If you are a non-admitting physician asked to see a patient for the first time, report the appropriate level of initial hospital care (codes 99221–99223). Note the following three points:
- Initial hospital care includes only three levels of service—not the five levels from which you choose for consultation codes
- The lowest level of history and exam for these initial visit codes is a detailed history and examination—no matter the level of medical decision-making. If the level of history or exam is documented lower than “detailed”—say, as “expanded problem-focused”—you are required to report the unlisted E/M code 99499.
- The admitting physician adds the new Healthcare Common Procedure Coding System (HCPCS) modifier –AI (that is, “‘A’ upper-case ‘i’”) to the initial visit code, so that Medicare can distinguish the admitting physician from others providing care for the patient.
- All subsequent visits with the inpatient continue to be billed with the subsequent care inpatient codes (99231–99233).
Fallout from this change? Medicare is studying the implications of its new policy on secondary payments—that is, when Medicare is the primary payer and there is a supplemental carrier, or when Medicare is the secondary payer. Note: Medicare strongly advises all providers to check with their primary payers, because 1) Medicare will not accept a consultation code when a primary insurer has paid on that code and 2) it’s doubtful that a commercial payer will accept a consultation code when Medicare has paid for a new or established patient service.
To add to the turmoil…
The CMS has announced that, as a result of the changes in Medicare policy on consultations, it is increasing the relative values for all new and established patient services and initial hospital care. CMS is doing this, however, by reducing the relative values of some consultation codes.
In addition, all surgical procedure codes that carry a 10- or 90-day global period will see an increase in work RVU because of the increase in E/M services that are a part of all global care. Keep in mind that payers who use the Resource-Based Relative Value Scale (RBRVS) to reimburse services will probably adopt the new values when contracts are up for renewal, although many will be unable to do so in the short term.
It also remains to be seen if any commercial payers adopt Medicare policy or continue to pay for consultations. This area might be a contract issue with payers.
Was gastroschisis of late onset—or visible on sonograms?... and more
Was gastroschisis of late onset—or visible on sonograms?
BECAUSE OF ADVANCED AGE and the presence of uterine fibroids, a woman underwent prenatal ultrasonography in the fifth, sixth, and seventh months of pregnancy. The sonograms were performed and interpreted by a specialist in maternal–fetal medicine. The baby was born with most of his intestines outside his abdomen and was transferred to another hospital, where surgery was performed nearly 4 hours after birth, revealing necrosis of a significant length of bowel. The child suffered short-gut syndrome and required intravenous catheter and tube feeding until the age of 5 years. His growth was stunted.
PATIENT’S CLAIM The sonograms showed gastroschisis. If this had been recognized at that time, the birth could have taken place in a hospital where surgical repair could be performed within 2 hours of birth. Because of the delay in surgery, necrosis of most of the small intestine occurred.
PHYSICIAN’S DEFENSE The child suffered late-onset gastroschisis, or ruptured umbilical hernia, which the sonograms did not show. No matter where the child was born, the outcome would have been the same.
VERDICT Illinois defense verdict for the specialist in maternal–fetal medicine. Prior to trial, the hospital and radiologist settled for $35,000 and $200,000, respectively.
Unsigned death certificate delays cremation of stillborn
FOLLOWING THE STILLBIRTH of their child, a couple waited 3 weeks for the death certificate to be signed. Only then were they given the body for cremation.
PLAINTIFFS’ CLAIM Dr. A, the attending physician, was negligent for not signing the baby’s death certificate in a timely manner, thus delaying the cremation and causing emotional distress. A death certificate should be signed within 1 day of determining the cause of death or knowing that there will be no further information about the cause.
PHYSICIAN’S DEFENSE According to Dr. A, his stated cause of death was rejected initially. While he was waiting for additional clinical information, Dr. B signed the certificate, giving only a general cause of death. Dr. A claimed his own actions caused no damages.
VERDICT $11,000 California verdict.
MDs find ovarian cyst, then, 7 months later, peritoneal cancer
A 49-YEAR-OLD WOMAN with an ovarian cyst underwent laparoscopy. Dr. C, the ObGyn who performed the surgery, found ovaries that were normal, but also the presence of endometriosis and adhesions. Dr. D and Dr. E provided follow-up care. When the patient visited Dr. E 5 months later complaining of bloating and gastrointestinal pain, ultrasonography was performed. She then followed up with her primary care physician and a gastroenterologist. Three months later, she underwent emergency surgery. Stage IIIC primary papillary serous carcinoma of the peritoneum was discovered in her pelvis and abdomen. Despite multiple surgeries and chemotherapy over the next year and a half, the patient died.
PLAINTIFF’S CLAIM Dr. C should have performed a biopsy during the original laparoscopy; this would have allowed an earlier diagnosis with a better prognosis.
PHYSICIAN’S DEFENSE A biopsy was not required initially; in fact, the cancer was probably either not present or microscopic at that time. Even with a diagnosis then, the odds of survival would have been much the same.
VERDICT Illinois defense verdict. The jury deadlocked, 11 to 1. The parties agreed to a less than unanimous verdict and a high/low agreement of $750,000/$100,000. Then the jury returned a defense verdict.
Still incontinent after undergoing retropubic urethropexy
A 43-YEAR-OLD WOMAN was experiencing urinary incontinence, gynecological pain, and bleeding. Her ObGyn diagnosed pelvic organ prolapse. A month later, the patient underwent a total abdominal hysterectomy with retropubic urethropexy. Following the surgery, the patient continued to be incontinent.
PATIENT’S CLAIM A sling procedure to correct the incontinence should have been performed.
PHYSICIAN’S DEFENSE The proper procedure and technique were used. As the patient was undergoing an abdominal hysterectomy, it was reasonable to perform a retropubic urethropexy at the same time.
VERDICT Texas defense verdict.
A $30.9 million verdict in the case of induced VBAC
ATTEMPTING A VAGINAL BIRTH after cesarean (VBAC), a woman arrived at the hospital for induced delivery of her child. During labor, the uterus ruptured and placental abruption occurred. For approximately 20 minutes, the fetus was deprived of oxygen. A cesarean delivery was performed, and the child was diagnosed with severe brain damage and cerebral palsy.
PATIENT’S CLAIM Uterine rupture was caused by hyperstimulation with oxytocin. After the loss of the fetal heart rate, the nurses delayed more than 15 minutes before notifying a physician.
PHYSICIAN’S DEFENSE The patient was informed of the increased risk of rupture when attempting VBAC. The nurses were following physician orders regarding use of oxytocin. Until the time of rupture and abruption, the uterus was not hyperstimulated and the heart rate was normal.
VERDICT $30,953,181 Ohio verdict against the hospital only. The case was settled under a confidential high/low agreement reached before the verdict.
While on HRT, patient with serious health concerns has stroke
DR. F PRESCRIBED oral hormone replacement therapy (HRT) to treat the menopausal symptoms of a 46-year-old patient. The following year he prescribed an estrogen patch and continued treating her for another 3 years until he died. Then Dr. G took over the patient’s care. She remained on some form of HRT until she suffered a stroke 2 years later. She suffered significant cognitive impairment and could no longer drive or work.
PATIENT’S CLAIM She should have been evaluated more thoroughly and weaned from artificial hormones. She had high blood pressure and high cholesterol, was overweight, and had a family history of cardiovascular problems.
PHYSICIAN’S DEFENSE The patient’s stroke was not necessarily related to HRT. In fact, it could have been caused by her cardiac condition.
VERDICT Missouri defense verdict.
Was laparoscopy to remove an ovary contraindicated?
A 39-YEAR-OLD WOMAN underwent multiple surgeries performed by her ObGyn: tubal ligation, dilation and curettage, hysteroscopy, and emergent hysterectomy. Following the hysterectomy, during which the ovaries were not removed, she had significant left upper quadrant pain. Ultrasonography revealed two cysts on the left ovary. During recommended surgery to remove the ovary, the physician continued laparoscopic dissection despite complications caused by extensive omental adhesions. The surgery lasted 5 hours, after which the patient required 2 days of hospitalization. Within 24 hours of leaving the hospital, she returned to the emergency room with fever, nausea, vomiting, and abdominal pain. A CT scan indicated a probable leak from the sigmoid colon. Follow-up surgery showed perforation of the sigmoid colon and a colostomy was placed. The patient developed acute respiratory distress syndrome and required intubation and mechanical ventilation during a 2-week hospitalization.
PATIENT’S CLAIM Because of her prior abdominal surgeries, laparoscopic surgery was contraindicated. Once begun, it should have been converted to an open procedure. Also, the physician should have recognized the injury to the sigmoid colon and treated it immediately.
PHYSICIAN’S DEFENSE Perforation is a known risk of laparoscopy, and the patient was informed of this.
VERDICT $437,438 Maryland verdict.
Nephrectomy is necessary after ureteral injury
A 52-YEAR-OLD WOMAN with a history of fibroids was told by her ObGyn, Dr. H, that the tumors had grown. After undergoing a recommended hysterectomy performed by Dr. H, the patient experienced ongoing pain. Three months after the surgery, she consulted Dr. J, who diagnosed ureteral obstruction. The patient then underwent surgical repair of the obstruction, but suffered permanent kidney damage. Nephrectomy was performed a month later.
PATIENT’S CLAIM Dr. H was negligent because he injured the ureter during the hysterectomy and was also negligent for failing to recognize the injury.
PHYSICIAN’S DEFENSE Ureteral injury is a known complication of the procedure. Also, the patient’s symptoms were inconsistent with such an injury.
VERDICT Tennessee defense verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Was gastroschisis of late onset—or visible on sonograms?
BECAUSE OF ADVANCED AGE and the presence of uterine fibroids, a woman underwent prenatal ultrasonography in the fifth, sixth, and seventh months of pregnancy. The sonograms were performed and interpreted by a specialist in maternal–fetal medicine. The baby was born with most of his intestines outside his abdomen and was transferred to another hospital, where surgery was performed nearly 4 hours after birth, revealing necrosis of a significant length of bowel. The child suffered short-gut syndrome and required intravenous catheter and tube feeding until the age of 5 years. His growth was stunted.
PATIENT’S CLAIM The sonograms showed gastroschisis. If this had been recognized at that time, the birth could have taken place in a hospital where surgical repair could be performed within 2 hours of birth. Because of the delay in surgery, necrosis of most of the small intestine occurred.
PHYSICIAN’S DEFENSE The child suffered late-onset gastroschisis, or ruptured umbilical hernia, which the sonograms did not show. No matter where the child was born, the outcome would have been the same.
VERDICT Illinois defense verdict for the specialist in maternal–fetal medicine. Prior to trial, the hospital and radiologist settled for $35,000 and $200,000, respectively.
Unsigned death certificate delays cremation of stillborn
FOLLOWING THE STILLBIRTH of their child, a couple waited 3 weeks for the death certificate to be signed. Only then were they given the body for cremation.
PLAINTIFFS’ CLAIM Dr. A, the attending physician, was negligent for not signing the baby’s death certificate in a timely manner, thus delaying the cremation and causing emotional distress. A death certificate should be signed within 1 day of determining the cause of death or knowing that there will be no further information about the cause.
PHYSICIAN’S DEFENSE According to Dr. A, his stated cause of death was rejected initially. While he was waiting for additional clinical information, Dr. B signed the certificate, giving only a general cause of death. Dr. A claimed his own actions caused no damages.
VERDICT $11,000 California verdict.
MDs find ovarian cyst, then, 7 months later, peritoneal cancer
A 49-YEAR-OLD WOMAN with an ovarian cyst underwent laparoscopy. Dr. C, the ObGyn who performed the surgery, found ovaries that were normal, but also the presence of endometriosis and adhesions. Dr. D and Dr. E provided follow-up care. When the patient visited Dr. E 5 months later complaining of bloating and gastrointestinal pain, ultrasonography was performed. She then followed up with her primary care physician and a gastroenterologist. Three months later, she underwent emergency surgery. Stage IIIC primary papillary serous carcinoma of the peritoneum was discovered in her pelvis and abdomen. Despite multiple surgeries and chemotherapy over the next year and a half, the patient died.
PLAINTIFF’S CLAIM Dr. C should have performed a biopsy during the original laparoscopy; this would have allowed an earlier diagnosis with a better prognosis.
PHYSICIAN’S DEFENSE A biopsy was not required initially; in fact, the cancer was probably either not present or microscopic at that time. Even with a diagnosis then, the odds of survival would have been much the same.
VERDICT Illinois defense verdict. The jury deadlocked, 11 to 1. The parties agreed to a less than unanimous verdict and a high/low agreement of $750,000/$100,000. Then the jury returned a defense verdict.
Still incontinent after undergoing retropubic urethropexy
A 43-YEAR-OLD WOMAN was experiencing urinary incontinence, gynecological pain, and bleeding. Her ObGyn diagnosed pelvic organ prolapse. A month later, the patient underwent a total abdominal hysterectomy with retropubic urethropexy. Following the surgery, the patient continued to be incontinent.
PATIENT’S CLAIM A sling procedure to correct the incontinence should have been performed.
PHYSICIAN’S DEFENSE The proper procedure and technique were used. As the patient was undergoing an abdominal hysterectomy, it was reasonable to perform a retropubic urethropexy at the same time.
VERDICT Texas defense verdict.
A $30.9 million verdict in the case of induced VBAC
ATTEMPTING A VAGINAL BIRTH after cesarean (VBAC), a woman arrived at the hospital for induced delivery of her child. During labor, the uterus ruptured and placental abruption occurred. For approximately 20 minutes, the fetus was deprived of oxygen. A cesarean delivery was performed, and the child was diagnosed with severe brain damage and cerebral palsy.
PATIENT’S CLAIM Uterine rupture was caused by hyperstimulation with oxytocin. After the loss of the fetal heart rate, the nurses delayed more than 15 minutes before notifying a physician.
PHYSICIAN’S DEFENSE The patient was informed of the increased risk of rupture when attempting VBAC. The nurses were following physician orders regarding use of oxytocin. Until the time of rupture and abruption, the uterus was not hyperstimulated and the heart rate was normal.
VERDICT $30,953,181 Ohio verdict against the hospital only. The case was settled under a confidential high/low agreement reached before the verdict.
While on HRT, patient with serious health concerns has stroke
DR. F PRESCRIBED oral hormone replacement therapy (HRT) to treat the menopausal symptoms of a 46-year-old patient. The following year he prescribed an estrogen patch and continued treating her for another 3 years until he died. Then Dr. G took over the patient’s care. She remained on some form of HRT until she suffered a stroke 2 years later. She suffered significant cognitive impairment and could no longer drive or work.
PATIENT’S CLAIM She should have been evaluated more thoroughly and weaned from artificial hormones. She had high blood pressure and high cholesterol, was overweight, and had a family history of cardiovascular problems.
PHYSICIAN’S DEFENSE The patient’s stroke was not necessarily related to HRT. In fact, it could have been caused by her cardiac condition.
VERDICT Missouri defense verdict.
Was laparoscopy to remove an ovary contraindicated?
A 39-YEAR-OLD WOMAN underwent multiple surgeries performed by her ObGyn: tubal ligation, dilation and curettage, hysteroscopy, and emergent hysterectomy. Following the hysterectomy, during which the ovaries were not removed, she had significant left upper quadrant pain. Ultrasonography revealed two cysts on the left ovary. During recommended surgery to remove the ovary, the physician continued laparoscopic dissection despite complications caused by extensive omental adhesions. The surgery lasted 5 hours, after which the patient required 2 days of hospitalization. Within 24 hours of leaving the hospital, she returned to the emergency room with fever, nausea, vomiting, and abdominal pain. A CT scan indicated a probable leak from the sigmoid colon. Follow-up surgery showed perforation of the sigmoid colon and a colostomy was placed. The patient developed acute respiratory distress syndrome and required intubation and mechanical ventilation during a 2-week hospitalization.
PATIENT’S CLAIM Because of her prior abdominal surgeries, laparoscopic surgery was contraindicated. Once begun, it should have been converted to an open procedure. Also, the physician should have recognized the injury to the sigmoid colon and treated it immediately.
PHYSICIAN’S DEFENSE Perforation is a known risk of laparoscopy, and the patient was informed of this.
VERDICT $437,438 Maryland verdict.
Nephrectomy is necessary after ureteral injury
A 52-YEAR-OLD WOMAN with a history of fibroids was told by her ObGyn, Dr. H, that the tumors had grown. After undergoing a recommended hysterectomy performed by Dr. H, the patient experienced ongoing pain. Three months after the surgery, she consulted Dr. J, who diagnosed ureteral obstruction. The patient then underwent surgical repair of the obstruction, but suffered permanent kidney damage. Nephrectomy was performed a month later.
PATIENT’S CLAIM Dr. H was negligent because he injured the ureter during the hysterectomy and was also negligent for failing to recognize the injury.
PHYSICIAN’S DEFENSE Ureteral injury is a known complication of the procedure. Also, the patient’s symptoms were inconsistent with such an injury.
VERDICT Tennessee defense verdict.
Was gastroschisis of late onset—or visible on sonograms?
BECAUSE OF ADVANCED AGE and the presence of uterine fibroids, a woman underwent prenatal ultrasonography in the fifth, sixth, and seventh months of pregnancy. The sonograms were performed and interpreted by a specialist in maternal–fetal medicine. The baby was born with most of his intestines outside his abdomen and was transferred to another hospital, where surgery was performed nearly 4 hours after birth, revealing necrosis of a significant length of bowel. The child suffered short-gut syndrome and required intravenous catheter and tube feeding until the age of 5 years. His growth was stunted.
PATIENT’S CLAIM The sonograms showed gastroschisis. If this had been recognized at that time, the birth could have taken place in a hospital where surgical repair could be performed within 2 hours of birth. Because of the delay in surgery, necrosis of most of the small intestine occurred.
PHYSICIAN’S DEFENSE The child suffered late-onset gastroschisis, or ruptured umbilical hernia, which the sonograms did not show. No matter where the child was born, the outcome would have been the same.
VERDICT Illinois defense verdict for the specialist in maternal–fetal medicine. Prior to trial, the hospital and radiologist settled for $35,000 and $200,000, respectively.
Unsigned death certificate delays cremation of stillborn
FOLLOWING THE STILLBIRTH of their child, a couple waited 3 weeks for the death certificate to be signed. Only then were they given the body for cremation.
PLAINTIFFS’ CLAIM Dr. A, the attending physician, was negligent for not signing the baby’s death certificate in a timely manner, thus delaying the cremation and causing emotional distress. A death certificate should be signed within 1 day of determining the cause of death or knowing that there will be no further information about the cause.
PHYSICIAN’S DEFENSE According to Dr. A, his stated cause of death was rejected initially. While he was waiting for additional clinical information, Dr. B signed the certificate, giving only a general cause of death. Dr. A claimed his own actions caused no damages.
VERDICT $11,000 California verdict.
MDs find ovarian cyst, then, 7 months later, peritoneal cancer
A 49-YEAR-OLD WOMAN with an ovarian cyst underwent laparoscopy. Dr. C, the ObGyn who performed the surgery, found ovaries that were normal, but also the presence of endometriosis and adhesions. Dr. D and Dr. E provided follow-up care. When the patient visited Dr. E 5 months later complaining of bloating and gastrointestinal pain, ultrasonography was performed. She then followed up with her primary care physician and a gastroenterologist. Three months later, she underwent emergency surgery. Stage IIIC primary papillary serous carcinoma of the peritoneum was discovered in her pelvis and abdomen. Despite multiple surgeries and chemotherapy over the next year and a half, the patient died.
PLAINTIFF’S CLAIM Dr. C should have performed a biopsy during the original laparoscopy; this would have allowed an earlier diagnosis with a better prognosis.
PHYSICIAN’S DEFENSE A biopsy was not required initially; in fact, the cancer was probably either not present or microscopic at that time. Even with a diagnosis then, the odds of survival would have been much the same.
VERDICT Illinois defense verdict. The jury deadlocked, 11 to 1. The parties agreed to a less than unanimous verdict and a high/low agreement of $750,000/$100,000. Then the jury returned a defense verdict.
Still incontinent after undergoing retropubic urethropexy
A 43-YEAR-OLD WOMAN was experiencing urinary incontinence, gynecological pain, and bleeding. Her ObGyn diagnosed pelvic organ prolapse. A month later, the patient underwent a total abdominal hysterectomy with retropubic urethropexy. Following the surgery, the patient continued to be incontinent.
PATIENT’S CLAIM A sling procedure to correct the incontinence should have been performed.
PHYSICIAN’S DEFENSE The proper procedure and technique were used. As the patient was undergoing an abdominal hysterectomy, it was reasonable to perform a retropubic urethropexy at the same time.
VERDICT Texas defense verdict.
A $30.9 million verdict in the case of induced VBAC
ATTEMPTING A VAGINAL BIRTH after cesarean (VBAC), a woman arrived at the hospital for induced delivery of her child. During labor, the uterus ruptured and placental abruption occurred. For approximately 20 minutes, the fetus was deprived of oxygen. A cesarean delivery was performed, and the child was diagnosed with severe brain damage and cerebral palsy.
PATIENT’S CLAIM Uterine rupture was caused by hyperstimulation with oxytocin. After the loss of the fetal heart rate, the nurses delayed more than 15 minutes before notifying a physician.
PHYSICIAN’S DEFENSE The patient was informed of the increased risk of rupture when attempting VBAC. The nurses were following physician orders regarding use of oxytocin. Until the time of rupture and abruption, the uterus was not hyperstimulated and the heart rate was normal.
VERDICT $30,953,181 Ohio verdict against the hospital only. The case was settled under a confidential high/low agreement reached before the verdict.
While on HRT, patient with serious health concerns has stroke
DR. F PRESCRIBED oral hormone replacement therapy (HRT) to treat the menopausal symptoms of a 46-year-old patient. The following year he prescribed an estrogen patch and continued treating her for another 3 years until he died. Then Dr. G took over the patient’s care. She remained on some form of HRT until she suffered a stroke 2 years later. She suffered significant cognitive impairment and could no longer drive or work.
PATIENT’S CLAIM She should have been evaluated more thoroughly and weaned from artificial hormones. She had high blood pressure and high cholesterol, was overweight, and had a family history of cardiovascular problems.
PHYSICIAN’S DEFENSE The patient’s stroke was not necessarily related to HRT. In fact, it could have been caused by her cardiac condition.
VERDICT Missouri defense verdict.
Was laparoscopy to remove an ovary contraindicated?
A 39-YEAR-OLD WOMAN underwent multiple surgeries performed by her ObGyn: tubal ligation, dilation and curettage, hysteroscopy, and emergent hysterectomy. Following the hysterectomy, during which the ovaries were not removed, she had significant left upper quadrant pain. Ultrasonography revealed two cysts on the left ovary. During recommended surgery to remove the ovary, the physician continued laparoscopic dissection despite complications caused by extensive omental adhesions. The surgery lasted 5 hours, after which the patient required 2 days of hospitalization. Within 24 hours of leaving the hospital, she returned to the emergency room with fever, nausea, vomiting, and abdominal pain. A CT scan indicated a probable leak from the sigmoid colon. Follow-up surgery showed perforation of the sigmoid colon and a colostomy was placed. The patient developed acute respiratory distress syndrome and required intubation and mechanical ventilation during a 2-week hospitalization.
PATIENT’S CLAIM Because of her prior abdominal surgeries, laparoscopic surgery was contraindicated. Once begun, it should have been converted to an open procedure. Also, the physician should have recognized the injury to the sigmoid colon and treated it immediately.
PHYSICIAN’S DEFENSE Perforation is a known risk of laparoscopy, and the patient was informed of this.
VERDICT $437,438 Maryland verdict.
Nephrectomy is necessary after ureteral injury
A 52-YEAR-OLD WOMAN with a history of fibroids was told by her ObGyn, Dr. H, that the tumors had grown. After undergoing a recommended hysterectomy performed by Dr. H, the patient experienced ongoing pain. Three months after the surgery, she consulted Dr. J, who diagnosed ureteral obstruction. The patient then underwent surgical repair of the obstruction, but suffered permanent kidney damage. Nephrectomy was performed a month later.
PATIENT’S CLAIM Dr. H was negligent because he injured the ureter during the hysterectomy and was also negligent for failing to recognize the injury.
PHYSICIAN’S DEFENSE Ureteral injury is a known complication of the procedure. Also, the patient’s symptoms were inconsistent with such an injury.
VERDICT Tennessee defense verdict.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
These cases were selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The information available to the editors about the cases presented here is sometimes incomplete. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Farewell Consultation Codes
A brand new year has begun, and that, as usual, means brand new surprises from our friends at the Centers for Medicare and Medicaid Services. This year's big surprise: The CMS has decided it will no longer pay for consultations in either outpatient (99241-99245) or inpatient (99251-99255) settings.
This decree has caused a great deal of protest, particularly from neurologists, rheumatologists, and other specialists who depend on consultations for a majority of their income. After all, specialists should be appropriately compensated for the special expertise they provide.
It is hard to envision how eliminating consultation payments could be anything but detrimental to patient care. At the least, consulting physicians may feel less inclined to provide reports to referring physicians, which will substantially hurt coordination of care at a time when policymakers claim to be looking for ways to improve it.
Further objections abound; nevertheless, the decision has been made, and adjustments must be taken to accommodate it.
For office visits, the CMS expects consultation codes to be replaced with new or established visit codes (99201-99205 or 99212-99215). They have increased relative value units for those visit codes by 6% to soften the blow, but the difference will be substantially noticeable if a lot of consultations were billed last year.
On the inpatient side, admission codes (99221-99223) are to be used in lieu of consultation codes. The “true” admitting physician will use a new modifier (not yet published at press time) along with the admit code, while all consulting physicians will use the admit code unmodified.
Physicians performing a lot of inpatient consultations should anticipate denials, appeals, and confusion as admitting physicians and consultants alike adjust to this change.
As usual, some commercial insurers will follow the CMS lead, while others will continue recognizing the consultation codes (which remain in the 2010 CPT book). This means a decision will need to be made about whether to continue billing consultations for non-Medicare patients whose insurers continue to pay for them. If this route is chosen, Medicare will provide secondary coverage, and will, of course, not pay its portion. So this situation needs to be recognized in advance.
It is probably worth reviewing some past explanation of benefits to determine how often Medicare is a secondary payer, and whether any extra revenue will be worth the extra vigilance and work involved.
Discussions on this issue have been widespread and heated, and opinions vary widely.
Some specialists claim they actually welcome the change because they will no longer need to worry about complying with the CMS's confusing and ever-changing consultation rules.
Others are understandably concerned about a potentially significant loss of income. Do not be tempted, however, to bill for more services, such as biopsies and surgical procedures, as compensation for lost revenue. The CMS is well aware of that tendency (they even have a name for it: “code creep”), and they will be watching.
If billing patterns change significantly, an audit can be expected; increased billings must be proved to be of medical necessity, not compensatory revenue generation. If increased billings cannot be proved to be medically necessary, abuse or fraud charges will come. In an audit, remember, everyone is guilty until proven innocent.
Billing patients directly for consults has been proposed as a way to recover lost revenue. If consults are no longer covered by the CMS, physicians have reasoned that they should be able to use a “noncovered service” code (such as 99199-GA) and have Medicare patients sign an Advance Beneficiary Notice (ABN). This signifies their understanding that Medicare will not pay for the service, the same procedure used for noncovered cosmetic services. It is not clear, however, if this is permissible by the CMS.
Another proposed counter strategy is to bill Medicare for a new patient visit and add a “surcharge” for consultative care, billed directly to the patient (again using a National Supplier Clearinghouse [NSC] code and an ABN). This would be considered a “priority service,” analogous to “concierge services” offered by some internists. No one knows if the CMS (or patients) would go along with this option either.
Even proponents of such strategies admit they are speculative and untested; I would not advise attempting them without a careful legal review with an experienced health care attorney.
No matter how individuals choose to deal with the loss of consultation codes, I believe physicians should continue sending reports to referring physicians even though they will not specifically be paid for them.
Doing what is best for patients should always be the top priority.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
A brand new year has begun, and that, as usual, means brand new surprises from our friends at the Centers for Medicare and Medicaid Services. This year's big surprise: The CMS has decided it will no longer pay for consultations in either outpatient (99241-99245) or inpatient (99251-99255) settings.
This decree has caused a great deal of protest, particularly from neurologists, rheumatologists, and other specialists who depend on consultations for a majority of their income. After all, specialists should be appropriately compensated for the special expertise they provide.
It is hard to envision how eliminating consultation payments could be anything but detrimental to patient care. At the least, consulting physicians may feel less inclined to provide reports to referring physicians, which will substantially hurt coordination of care at a time when policymakers claim to be looking for ways to improve it.
Further objections abound; nevertheless, the decision has been made, and adjustments must be taken to accommodate it.
For office visits, the CMS expects consultation codes to be replaced with new or established visit codes (99201-99205 or 99212-99215). They have increased relative value units for those visit codes by 6% to soften the blow, but the difference will be substantially noticeable if a lot of consultations were billed last year.
On the inpatient side, admission codes (99221-99223) are to be used in lieu of consultation codes. The “true” admitting physician will use a new modifier (not yet published at press time) along with the admit code, while all consulting physicians will use the admit code unmodified.
Physicians performing a lot of inpatient consultations should anticipate denials, appeals, and confusion as admitting physicians and consultants alike adjust to this change.
As usual, some commercial insurers will follow the CMS lead, while others will continue recognizing the consultation codes (which remain in the 2010 CPT book). This means a decision will need to be made about whether to continue billing consultations for non-Medicare patients whose insurers continue to pay for them. If this route is chosen, Medicare will provide secondary coverage, and will, of course, not pay its portion. So this situation needs to be recognized in advance.
It is probably worth reviewing some past explanation of benefits to determine how often Medicare is a secondary payer, and whether any extra revenue will be worth the extra vigilance and work involved.
Discussions on this issue have been widespread and heated, and opinions vary widely.
Some specialists claim they actually welcome the change because they will no longer need to worry about complying with the CMS's confusing and ever-changing consultation rules.
Others are understandably concerned about a potentially significant loss of income. Do not be tempted, however, to bill for more services, such as biopsies and surgical procedures, as compensation for lost revenue. The CMS is well aware of that tendency (they even have a name for it: “code creep”), and they will be watching.
If billing patterns change significantly, an audit can be expected; increased billings must be proved to be of medical necessity, not compensatory revenue generation. If increased billings cannot be proved to be medically necessary, abuse or fraud charges will come. In an audit, remember, everyone is guilty until proven innocent.
Billing patients directly for consults has been proposed as a way to recover lost revenue. If consults are no longer covered by the CMS, physicians have reasoned that they should be able to use a “noncovered service” code (such as 99199-GA) and have Medicare patients sign an Advance Beneficiary Notice (ABN). This signifies their understanding that Medicare will not pay for the service, the same procedure used for noncovered cosmetic services. It is not clear, however, if this is permissible by the CMS.
Another proposed counter strategy is to bill Medicare for a new patient visit and add a “surcharge” for consultative care, billed directly to the patient (again using a National Supplier Clearinghouse [NSC] code and an ABN). This would be considered a “priority service,” analogous to “concierge services” offered by some internists. No one knows if the CMS (or patients) would go along with this option either.
Even proponents of such strategies admit they are speculative and untested; I would not advise attempting them without a careful legal review with an experienced health care attorney.
No matter how individuals choose to deal with the loss of consultation codes, I believe physicians should continue sending reports to referring physicians even though they will not specifically be paid for them.
Doing what is best for patients should always be the top priority.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
A brand new year has begun, and that, as usual, means brand new surprises from our friends at the Centers for Medicare and Medicaid Services. This year's big surprise: The CMS has decided it will no longer pay for consultations in either outpatient (99241-99245) or inpatient (99251-99255) settings.
This decree has caused a great deal of protest, particularly from neurologists, rheumatologists, and other specialists who depend on consultations for a majority of their income. After all, specialists should be appropriately compensated for the special expertise they provide.
It is hard to envision how eliminating consultation payments could be anything but detrimental to patient care. At the least, consulting physicians may feel less inclined to provide reports to referring physicians, which will substantially hurt coordination of care at a time when policymakers claim to be looking for ways to improve it.
Further objections abound; nevertheless, the decision has been made, and adjustments must be taken to accommodate it.
For office visits, the CMS expects consultation codes to be replaced with new or established visit codes (99201-99205 or 99212-99215). They have increased relative value units for those visit codes by 6% to soften the blow, but the difference will be substantially noticeable if a lot of consultations were billed last year.
On the inpatient side, admission codes (99221-99223) are to be used in lieu of consultation codes. The “true” admitting physician will use a new modifier (not yet published at press time) along with the admit code, while all consulting physicians will use the admit code unmodified.
Physicians performing a lot of inpatient consultations should anticipate denials, appeals, and confusion as admitting physicians and consultants alike adjust to this change.
As usual, some commercial insurers will follow the CMS lead, while others will continue recognizing the consultation codes (which remain in the 2010 CPT book). This means a decision will need to be made about whether to continue billing consultations for non-Medicare patients whose insurers continue to pay for them. If this route is chosen, Medicare will provide secondary coverage, and will, of course, not pay its portion. So this situation needs to be recognized in advance.
It is probably worth reviewing some past explanation of benefits to determine how often Medicare is a secondary payer, and whether any extra revenue will be worth the extra vigilance and work involved.
Discussions on this issue have been widespread and heated, and opinions vary widely.
Some specialists claim they actually welcome the change because they will no longer need to worry about complying with the CMS's confusing and ever-changing consultation rules.
Others are understandably concerned about a potentially significant loss of income. Do not be tempted, however, to bill for more services, such as biopsies and surgical procedures, as compensation for lost revenue. The CMS is well aware of that tendency (they even have a name for it: “code creep”), and they will be watching.
If billing patterns change significantly, an audit can be expected; increased billings must be proved to be of medical necessity, not compensatory revenue generation. If increased billings cannot be proved to be medically necessary, abuse or fraud charges will come. In an audit, remember, everyone is guilty until proven innocent.
Billing patients directly for consults has been proposed as a way to recover lost revenue. If consults are no longer covered by the CMS, physicians have reasoned that they should be able to use a “noncovered service” code (such as 99199-GA) and have Medicare patients sign an Advance Beneficiary Notice (ABN). This signifies their understanding that Medicare will not pay for the service, the same procedure used for noncovered cosmetic services. It is not clear, however, if this is permissible by the CMS.
Another proposed counter strategy is to bill Medicare for a new patient visit and add a “surcharge” for consultative care, billed directly to the patient (again using a National Supplier Clearinghouse [NSC] code and an ABN). This would be considered a “priority service,” analogous to “concierge services” offered by some internists. No one knows if the CMS (or patients) would go along with this option either.
Even proponents of such strategies admit they are speculative and untested; I would not advise attempting them without a careful legal review with an experienced health care attorney.
No matter how individuals choose to deal with the loss of consultation codes, I believe physicians should continue sending reports to referring physicians even though they will not specifically be paid for them.
Doing what is best for patients should always be the top priority.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com