User login
Listen Up
A recent claim against a New Jersey physician attracted considerable attention in the medical community, not because it resulted in a substantial jury award, but because the award was not covered by the doctor's malpractice insurance.
It is a good reminder for the rest of us: Your malpractice policy covers allegations of malpractice only, which is generally defined as negligence or deviation from the standard of care. This case involved a charge of discrimination against a hearing-impaired patient—which meant the physician not only had to fund his own defense, but he was personally responsible for the $400,000 award against him. (The case is now on appeal.)
The Americans With Disabilities Act (ADA) was designed to protect individuals with various disabilities against discrimination in various public situations—including, specifically, “the professional office of a health care professional.”
When the disability is impaired hearing, the law requires physicians to provide any “auxiliary aids and services” that might be necessary to ensure clear communication between doctor and patient. In the vast majority of such situations, a pad and pencil will satisfy that requirement. But occasionally, it does not, particularly when complex medical concepts are involved, and in such cases, as the New Jersey trial demonstrated, failure to make the necessary extra effort can be very expensive.
The claim involved a hearing-impaired patient with lupus erythematosus who was being treated by a rheumatologist. For almost 2 years, the patient's partner and her daughter provided translation, but that arrangement was inadequate, the patient testified, because her partner and daughter were unfamiliar with medical terminology, and the patient was “unable to understand and participate in her care,” which left her “unaware of risks and available alternatives.”
So she repeatedly requested that the rheumatologist provide an American Sign Language interpreter for her office visits. He refused on grounds that the cost of an interpreter would exceed the payment he would receive for the visits, which made it an “undue financial burden,” and, therefore, exempt from ADA requirements.
But the “undue burden” exemption is not automatic; it must be demonstrated in court. And the jury decided the rheumatologist's annual income of $425,000 rendered the cost of an interpreter quite affordable.
The lessons are clear: Physicians must take antidiscrimination laws seriously, particularly when uninsurable issues are involved, and we must be constantly aware of the needs of disabled patients, to be sure their care is not substantially different from that of any other patient.
In the case of hearing-impaired or deaf patients, it is important to remember that forms of communication that are quite adequate for most are not appropriate for some. Lip reading, written notes, and the use of family members as interpreters may be perfectly acceptable to one patient and unsuitable for another.
If the patient agrees to written notes and lip reading, as most do, you need to remember to speak slowly, and to write down critical information to avoid any miscommunication. And as always, it is crucial to document all communication and the methods used for that communication—specifically the fact that the patient agreed to those forms of communication.
As I so often say, documentation is like garlic: There is no such thing as too much.
Should a patient not agree that written notes are sufficient, other alternatives can be offered: computer transcription, assisted listening devices, videotext displays (often available in hospitals), and telecommunication devices such as TTY and TDD. But if the patient rejects all of those options and continues to insist on a professional interpreter, the precedent set by the New Jersey case (if upheld on appeal) suggests that you need to acquiesce, even if the interpreter's fee exceeds the visit reimbursement; the ADA prohibits you from passing your cost along to the patient. But any such cost will be far less than a noninsured judgment against you.
If you must go that route, make sure the interpreter you hire is familiar with medical terminology, and is not acquainted with or related to the patient (for confidentiality reasons). Your state may have an online registry of available interpreters, as, for example, New Jersey does at www.njrid.org
The good news is several states have responded to this issue by introducing legislation that would require health insurance carriers to pay for the cost of interpreters.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
A recent claim against a New Jersey physician attracted considerable attention in the medical community, not because it resulted in a substantial jury award, but because the award was not covered by the doctor's malpractice insurance.
It is a good reminder for the rest of us: Your malpractice policy covers allegations of malpractice only, which is generally defined as negligence or deviation from the standard of care. This case involved a charge of discrimination against a hearing-impaired patient—which meant the physician not only had to fund his own defense, but he was personally responsible for the $400,000 award against him. (The case is now on appeal.)
The Americans With Disabilities Act (ADA) was designed to protect individuals with various disabilities against discrimination in various public situations—including, specifically, “the professional office of a health care professional.”
When the disability is impaired hearing, the law requires physicians to provide any “auxiliary aids and services” that might be necessary to ensure clear communication between doctor and patient. In the vast majority of such situations, a pad and pencil will satisfy that requirement. But occasionally, it does not, particularly when complex medical concepts are involved, and in such cases, as the New Jersey trial demonstrated, failure to make the necessary extra effort can be very expensive.
The claim involved a hearing-impaired patient with lupus erythematosus who was being treated by a rheumatologist. For almost 2 years, the patient's partner and her daughter provided translation, but that arrangement was inadequate, the patient testified, because her partner and daughter were unfamiliar with medical terminology, and the patient was “unable to understand and participate in her care,” which left her “unaware of risks and available alternatives.”
So she repeatedly requested that the rheumatologist provide an American Sign Language interpreter for her office visits. He refused on grounds that the cost of an interpreter would exceed the payment he would receive for the visits, which made it an “undue financial burden,” and, therefore, exempt from ADA requirements.
But the “undue burden” exemption is not automatic; it must be demonstrated in court. And the jury decided the rheumatologist's annual income of $425,000 rendered the cost of an interpreter quite affordable.
The lessons are clear: Physicians must take antidiscrimination laws seriously, particularly when uninsurable issues are involved, and we must be constantly aware of the needs of disabled patients, to be sure their care is not substantially different from that of any other patient.
In the case of hearing-impaired or deaf patients, it is important to remember that forms of communication that are quite adequate for most are not appropriate for some. Lip reading, written notes, and the use of family members as interpreters may be perfectly acceptable to one patient and unsuitable for another.
If the patient agrees to written notes and lip reading, as most do, you need to remember to speak slowly, and to write down critical information to avoid any miscommunication. And as always, it is crucial to document all communication and the methods used for that communication—specifically the fact that the patient agreed to those forms of communication.
As I so often say, documentation is like garlic: There is no such thing as too much.
Should a patient not agree that written notes are sufficient, other alternatives can be offered: computer transcription, assisted listening devices, videotext displays (often available in hospitals), and telecommunication devices such as TTY and TDD. But if the patient rejects all of those options and continues to insist on a professional interpreter, the precedent set by the New Jersey case (if upheld on appeal) suggests that you need to acquiesce, even if the interpreter's fee exceeds the visit reimbursement; the ADA prohibits you from passing your cost along to the patient. But any such cost will be far less than a noninsured judgment against you.
If you must go that route, make sure the interpreter you hire is familiar with medical terminology, and is not acquainted with or related to the patient (for confidentiality reasons). Your state may have an online registry of available interpreters, as, for example, New Jersey does at www.njrid.org
The good news is several states have responded to this issue by introducing legislation that would require health insurance carriers to pay for the cost of interpreters.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
A recent claim against a New Jersey physician attracted considerable attention in the medical community, not because it resulted in a substantial jury award, but because the award was not covered by the doctor's malpractice insurance.
It is a good reminder for the rest of us: Your malpractice policy covers allegations of malpractice only, which is generally defined as negligence or deviation from the standard of care. This case involved a charge of discrimination against a hearing-impaired patient—which meant the physician not only had to fund his own defense, but he was personally responsible for the $400,000 award against him. (The case is now on appeal.)
The Americans With Disabilities Act (ADA) was designed to protect individuals with various disabilities against discrimination in various public situations—including, specifically, “the professional office of a health care professional.”
When the disability is impaired hearing, the law requires physicians to provide any “auxiliary aids and services” that might be necessary to ensure clear communication between doctor and patient. In the vast majority of such situations, a pad and pencil will satisfy that requirement. But occasionally, it does not, particularly when complex medical concepts are involved, and in such cases, as the New Jersey trial demonstrated, failure to make the necessary extra effort can be very expensive.
The claim involved a hearing-impaired patient with lupus erythematosus who was being treated by a rheumatologist. For almost 2 years, the patient's partner and her daughter provided translation, but that arrangement was inadequate, the patient testified, because her partner and daughter were unfamiliar with medical terminology, and the patient was “unable to understand and participate in her care,” which left her “unaware of risks and available alternatives.”
So she repeatedly requested that the rheumatologist provide an American Sign Language interpreter for her office visits. He refused on grounds that the cost of an interpreter would exceed the payment he would receive for the visits, which made it an “undue financial burden,” and, therefore, exempt from ADA requirements.
But the “undue burden” exemption is not automatic; it must be demonstrated in court. And the jury decided the rheumatologist's annual income of $425,000 rendered the cost of an interpreter quite affordable.
The lessons are clear: Physicians must take antidiscrimination laws seriously, particularly when uninsurable issues are involved, and we must be constantly aware of the needs of disabled patients, to be sure their care is not substantially different from that of any other patient.
In the case of hearing-impaired or deaf patients, it is important to remember that forms of communication that are quite adequate for most are not appropriate for some. Lip reading, written notes, and the use of family members as interpreters may be perfectly acceptable to one patient and unsuitable for another.
If the patient agrees to written notes and lip reading, as most do, you need to remember to speak slowly, and to write down critical information to avoid any miscommunication. And as always, it is crucial to document all communication and the methods used for that communication—specifically the fact that the patient agreed to those forms of communication.
As I so often say, documentation is like garlic: There is no such thing as too much.
Should a patient not agree that written notes are sufficient, other alternatives can be offered: computer transcription, assisted listening devices, videotext displays (often available in hospitals), and telecommunication devices such as TTY and TDD. But if the patient rejects all of those options and continues to insist on a professional interpreter, the precedent set by the New Jersey case (if upheld on appeal) suggests that you need to acquiesce, even if the interpreter's fee exceeds the visit reimbursement; the ADA prohibits you from passing your cost along to the patient. But any such cost will be far less than a noninsured judgment against you.
If you must go that route, make sure the interpreter you hire is familiar with medical terminology, and is not acquainted with or related to the patient (for confidentiality reasons). Your state may have an online registry of available interpreters, as, for example, New Jersey does at www.njrid.org
The good news is several states have responded to this issue by introducing legislation that would require health insurance carriers to pay for the cost of interpreters.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Listen Up
A recent claim against a physician in New Jersey attracted considerable attention, not because it resulted in a substantial jury award, but because the award was not covered by the doctor's malpractice insurance.
It is a good reminder for the rest of us: Your malpractice policy covers allegations of malpractice only, which is generally defined as negligence or deviation from the standard of care. This case involved a charge of discrimination against a hearing-impaired patient—which meant the physician not only had to fund his own defense, but he was personally responsible for the $400,000 award against him. (The case is now on appeal.)
The Americans With Disabilities Act (ADA) was designed to protect individuals with various disabilities against discrimination in various public situations—including, specifically, “the professional office of a health care professional.”
When the disability is impaired hearing, the law requires physicians to provide any “auxiliary aids and services” that might be necessary to ensure clear communication between doctor and patient. In the vast majority of such situations, a pad and pencil will satisfy that requirement. But occasionally, it does not, particularly when complex medical concepts are involved, and in such cases, as the New Jersey trial demonstrated, failure to make the necessary extra effort can be very expensive.
The claim involved a hearing-impaired patient with lupus erythematosus who was being treated by a rheumatologist. For almost 2 years, the patient's partner and her daughter provided translation, but that arrangement was inadequate, the patient testified, because her partner and daughter were unfamiliar with medical terminology, and the patient was “unable to understand and participate in her care,” which left her “unaware of risks and available alternatives.”
So she repeatedly requested that the rheumatologist provide an American Sign Language interpreter for her office visits. He refused on grounds that the cost of an interpreter would exceed the payment he would receive for the visits, which made it an “undue financial burden,” and, therefore, exempt from ADA requirements.
But the “undue burden” exemption is not automatic; it must be demonstrated in court. And the jury decided the rheumatologist's annual income of $425,000 rendered the cost of an interpreter affordable.
The lessons are clear: Physicians must take antidiscrimination laws seriously, particularly when uninsurable issues are involved, and we must be constantly aware of the needs of disabled patients, to be sure their care is not substantially different from that of any other patient.
In the case of hearing-impaired or deaf patients, it is important to remember that forms of communication that are quite adequate for most are not appropriate for some. Lip reading, written notes, and the use of family members as interpreters may be acceptable to one patient and unsuitable for another.
If the patient agrees to written notes and lip reading, you need to remember to speak slowly, and to write down critical information to avoid any miscommunication. And it is crucial to document all communication and the methods.
Should a patient insist on a professional interpreter, the precedent set by the New Jersey case (if upheld on appeal) suggests that you need to acquiesce, even if the interpreter's fee exceeds the visit reimbursement; the ADA prohibits you from passing your cost along to the patient. But any such cost will be far less than a noninsured judgment against you.
If you must go that route, make sure the interpreter you hire is familiar with medical terminology, and is not acquainted with or related to the patient (for confidentiality reasons). Your state may have an online registry of available interpreters.
A recent claim against a physician in New Jersey attracted considerable attention, not because it resulted in a substantial jury award, but because the award was not covered by the doctor's malpractice insurance.
It is a good reminder for the rest of us: Your malpractice policy covers allegations of malpractice only, which is generally defined as negligence or deviation from the standard of care. This case involved a charge of discrimination against a hearing-impaired patient—which meant the physician not only had to fund his own defense, but he was personally responsible for the $400,000 award against him. (The case is now on appeal.)
The Americans With Disabilities Act (ADA) was designed to protect individuals with various disabilities against discrimination in various public situations—including, specifically, “the professional office of a health care professional.”
When the disability is impaired hearing, the law requires physicians to provide any “auxiliary aids and services” that might be necessary to ensure clear communication between doctor and patient. In the vast majority of such situations, a pad and pencil will satisfy that requirement. But occasionally, it does not, particularly when complex medical concepts are involved, and in such cases, as the New Jersey trial demonstrated, failure to make the necessary extra effort can be very expensive.
The claim involved a hearing-impaired patient with lupus erythematosus who was being treated by a rheumatologist. For almost 2 years, the patient's partner and her daughter provided translation, but that arrangement was inadequate, the patient testified, because her partner and daughter were unfamiliar with medical terminology, and the patient was “unable to understand and participate in her care,” which left her “unaware of risks and available alternatives.”
So she repeatedly requested that the rheumatologist provide an American Sign Language interpreter for her office visits. He refused on grounds that the cost of an interpreter would exceed the payment he would receive for the visits, which made it an “undue financial burden,” and, therefore, exempt from ADA requirements.
But the “undue burden” exemption is not automatic; it must be demonstrated in court. And the jury decided the rheumatologist's annual income of $425,000 rendered the cost of an interpreter affordable.
The lessons are clear: Physicians must take antidiscrimination laws seriously, particularly when uninsurable issues are involved, and we must be constantly aware of the needs of disabled patients, to be sure their care is not substantially different from that of any other patient.
In the case of hearing-impaired or deaf patients, it is important to remember that forms of communication that are quite adequate for most are not appropriate for some. Lip reading, written notes, and the use of family members as interpreters may be acceptable to one patient and unsuitable for another.
If the patient agrees to written notes and lip reading, you need to remember to speak slowly, and to write down critical information to avoid any miscommunication. And it is crucial to document all communication and the methods.
Should a patient insist on a professional interpreter, the precedent set by the New Jersey case (if upheld on appeal) suggests that you need to acquiesce, even if the interpreter's fee exceeds the visit reimbursement; the ADA prohibits you from passing your cost along to the patient. But any such cost will be far less than a noninsured judgment against you.
If you must go that route, make sure the interpreter you hire is familiar with medical terminology, and is not acquainted with or related to the patient (for confidentiality reasons). Your state may have an online registry of available interpreters.
A recent claim against a physician in New Jersey attracted considerable attention, not because it resulted in a substantial jury award, but because the award was not covered by the doctor's malpractice insurance.
It is a good reminder for the rest of us: Your malpractice policy covers allegations of malpractice only, which is generally defined as negligence or deviation from the standard of care. This case involved a charge of discrimination against a hearing-impaired patient—which meant the physician not only had to fund his own defense, but he was personally responsible for the $400,000 award against him. (The case is now on appeal.)
The Americans With Disabilities Act (ADA) was designed to protect individuals with various disabilities against discrimination in various public situations—including, specifically, “the professional office of a health care professional.”
When the disability is impaired hearing, the law requires physicians to provide any “auxiliary aids and services” that might be necessary to ensure clear communication between doctor and patient. In the vast majority of such situations, a pad and pencil will satisfy that requirement. But occasionally, it does not, particularly when complex medical concepts are involved, and in such cases, as the New Jersey trial demonstrated, failure to make the necessary extra effort can be very expensive.
The claim involved a hearing-impaired patient with lupus erythematosus who was being treated by a rheumatologist. For almost 2 years, the patient's partner and her daughter provided translation, but that arrangement was inadequate, the patient testified, because her partner and daughter were unfamiliar with medical terminology, and the patient was “unable to understand and participate in her care,” which left her “unaware of risks and available alternatives.”
So she repeatedly requested that the rheumatologist provide an American Sign Language interpreter for her office visits. He refused on grounds that the cost of an interpreter would exceed the payment he would receive for the visits, which made it an “undue financial burden,” and, therefore, exempt from ADA requirements.
But the “undue burden” exemption is not automatic; it must be demonstrated in court. And the jury decided the rheumatologist's annual income of $425,000 rendered the cost of an interpreter affordable.
The lessons are clear: Physicians must take antidiscrimination laws seriously, particularly when uninsurable issues are involved, and we must be constantly aware of the needs of disabled patients, to be sure their care is not substantially different from that of any other patient.
In the case of hearing-impaired or deaf patients, it is important to remember that forms of communication that are quite adequate for most are not appropriate for some. Lip reading, written notes, and the use of family members as interpreters may be acceptable to one patient and unsuitable for another.
If the patient agrees to written notes and lip reading, you need to remember to speak slowly, and to write down critical information to avoid any miscommunication. And it is crucial to document all communication and the methods.
Should a patient insist on a professional interpreter, the precedent set by the New Jersey case (if upheld on appeal) suggests that you need to acquiesce, even if the interpreter's fee exceeds the visit reimbursement; the ADA prohibits you from passing your cost along to the patient. But any such cost will be far less than a noninsured judgment against you.
If you must go that route, make sure the interpreter you hire is familiar with medical terminology, and is not acquainted with or related to the patient (for confidentiality reasons). Your state may have an online registry of available interpreters.
E-Prescribing and the Physician Quality Reporting Initiative: Get in While the Getting is Good!
Medical Verdicts
Would you recognize appendicitis here?
A 20-YEAR-OLD WOMAN in the third trimester of pregnancy went to Dr. A, her ObGyn, complaining of abdominal pain. On each of the next 3 days, she presented at the emergency room with the same complaint. She was discharged twice, but was admitted on the third day. Dr. B provided care that day, and Dr. A took over on the following day. The patient was prescribed antibiotics after an infection was diagnosed. Then, after giving birth on that same day, her condition worsened. A ruptured appendix was discovered during exploratory laparotomy. The patient continued to decline and then died 3 weeks later.
PLAINTIFF’S CLAIM Failing to diagnose the appendicitis was negligent. On the 4 days the patient complained of pain, there was neither hands-on examination of her abdomen nor CT scans ordered. The nurses failed to recognize her condition and to see that she was properly evaluated.
PHYSICIANS’ DEFENSE Dr. A claimed his evaluation was performed properly. Dr. B claimed that, on the day the patient was admitted, he made a proper evaluation based on phone triage. The hospital claimed that the nurses performed proper triage and monitored her properly. And all claimed that a laparotomy required waiting until after delivery to be performed.
VERDICT Kentucky defense verdict. Posttrial motions were pending.
When findings are benign, should you refer, just to be safe?
A 36-YEAR-OLD PATIENT with presumptive fibroid tumors underwent a hysterectomy in which the ovaries and fallopian tubes were not removed. The pathologist initially reported that one tumor was benign, but that he was performing further tests. His second report confirmed the benign diagnosis and included mitotic count and spindle cells in the description of the microscopic exam. A year later, the patient developed abdominal pain, and the physician removed the fallopian tubes and ovaries. This time the same pathologist reported malignant uterine sarcoma in the ovaries. Upon reexamination of the previous year’s tissue, he believed the first tumor to be similar. A diagnosis of metastasis was given almost 2 years later.
PATIENT’S CLAIM She should have been referred to a gynecologic oncologist when the tumors were removed. This would have allowed her to be treated earlier and more effectively.
PHYSICIAN’S DEFENSE The initial diagnosis was benign and thus did not require a referral. Also, no adjuvant therapy would have improved the patient’s prognosis with this rare cancer.
VERDICT $2 million Illinois verdict.
Dystocia case is heard in bench trial
SHOULDER DYSTOCIA was encountered during delivery of the plaintiff child at a federally funded clinic. The OB used traction to complete the delivery, and the child suffered right brachial plexus injury, resulting in Erb’s palsy. No surgery was performed. The clinic was covered by the Federal Tort Claims Act, and the case was tried in a bench trial.
PATIENT’S CLAIM The treating OB used excessive traction, causing injury to the right brachial plexus.
PHYSICIAN’S DEFENSE Only moderate traction was used.
VERDICT $2,525,584 Illinois bench verdict. The court found the following: (1) negligence by the physician for repeatedly applying moderate traction to the point of excessive traction and rotating the infant’s head while the shoulder was trapped; (2) inappropriate grasping of the head while applying excessive traction; (3) failure to cut a generous episiotomy after shoulder dystocia was recognized; (4) failure to try other noninvasive measures before using excessive force; and (5) failure to recognize the likelihood of a macrosomic fetus.
No OB is available; complications ensue
SHORTLY AFTER a woman was admitted to the hospital for the birth of her child, complications occurred. The infant was delivered but suffered hypoxia and brain damage.
PATIENT’S CLAIM No OB was readily available to assist with the delivery. The nurses acted to delay the birth despite evidence that a hypoxic event was in progress and immediate delivery—even by a nurse—was essential. Fetal bradycardia continued for 5 to 6 minutes, resulting in hypoxia and brain damage in the infant.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Utah settlement with the hospital. The physicians had been dismissed in summary judgment rulings.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Would you recognize appendicitis here?
A 20-YEAR-OLD WOMAN in the third trimester of pregnancy went to Dr. A, her ObGyn, complaining of abdominal pain. On each of the next 3 days, she presented at the emergency room with the same complaint. She was discharged twice, but was admitted on the third day. Dr. B provided care that day, and Dr. A took over on the following day. The patient was prescribed antibiotics after an infection was diagnosed. Then, after giving birth on that same day, her condition worsened. A ruptured appendix was discovered during exploratory laparotomy. The patient continued to decline and then died 3 weeks later.
PLAINTIFF’S CLAIM Failing to diagnose the appendicitis was negligent. On the 4 days the patient complained of pain, there was neither hands-on examination of her abdomen nor CT scans ordered. The nurses failed to recognize her condition and to see that she was properly evaluated.
PHYSICIANS’ DEFENSE Dr. A claimed his evaluation was performed properly. Dr. B claimed that, on the day the patient was admitted, he made a proper evaluation based on phone triage. The hospital claimed that the nurses performed proper triage and monitored her properly. And all claimed that a laparotomy required waiting until after delivery to be performed.
VERDICT Kentucky defense verdict. Posttrial motions were pending.
When findings are benign, should you refer, just to be safe?
A 36-YEAR-OLD PATIENT with presumptive fibroid tumors underwent a hysterectomy in which the ovaries and fallopian tubes were not removed. The pathologist initially reported that one tumor was benign, but that he was performing further tests. His second report confirmed the benign diagnosis and included mitotic count and spindle cells in the description of the microscopic exam. A year later, the patient developed abdominal pain, and the physician removed the fallopian tubes and ovaries. This time the same pathologist reported malignant uterine sarcoma in the ovaries. Upon reexamination of the previous year’s tissue, he believed the first tumor to be similar. A diagnosis of metastasis was given almost 2 years later.
PATIENT’S CLAIM She should have been referred to a gynecologic oncologist when the tumors were removed. This would have allowed her to be treated earlier and more effectively.
PHYSICIAN’S DEFENSE The initial diagnosis was benign and thus did not require a referral. Also, no adjuvant therapy would have improved the patient’s prognosis with this rare cancer.
VERDICT $2 million Illinois verdict.
Dystocia case is heard in bench trial
SHOULDER DYSTOCIA was encountered during delivery of the plaintiff child at a federally funded clinic. The OB used traction to complete the delivery, and the child suffered right brachial plexus injury, resulting in Erb’s palsy. No surgery was performed. The clinic was covered by the Federal Tort Claims Act, and the case was tried in a bench trial.
PATIENT’S CLAIM The treating OB used excessive traction, causing injury to the right brachial plexus.
PHYSICIAN’S DEFENSE Only moderate traction was used.
VERDICT $2,525,584 Illinois bench verdict. The court found the following: (1) negligence by the physician for repeatedly applying moderate traction to the point of excessive traction and rotating the infant’s head while the shoulder was trapped; (2) inappropriate grasping of the head while applying excessive traction; (3) failure to cut a generous episiotomy after shoulder dystocia was recognized; (4) failure to try other noninvasive measures before using excessive force; and (5) failure to recognize the likelihood of a macrosomic fetus.
No OB is available; complications ensue
SHORTLY AFTER a woman was admitted to the hospital for the birth of her child, complications occurred. The infant was delivered but suffered hypoxia and brain damage.
PATIENT’S CLAIM No OB was readily available to assist with the delivery. The nurses acted to delay the birth despite evidence that a hypoxic event was in progress and immediate delivery—even by a nurse—was essential. Fetal bradycardia continued for 5 to 6 minutes, resulting in hypoxia and brain damage in the infant.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Utah settlement with the hospital. The physicians had been dismissed in summary judgment rulings.
Would you recognize appendicitis here?
A 20-YEAR-OLD WOMAN in the third trimester of pregnancy went to Dr. A, her ObGyn, complaining of abdominal pain. On each of the next 3 days, she presented at the emergency room with the same complaint. She was discharged twice, but was admitted on the third day. Dr. B provided care that day, and Dr. A took over on the following day. The patient was prescribed antibiotics after an infection was diagnosed. Then, after giving birth on that same day, her condition worsened. A ruptured appendix was discovered during exploratory laparotomy. The patient continued to decline and then died 3 weeks later.
PLAINTIFF’S CLAIM Failing to diagnose the appendicitis was negligent. On the 4 days the patient complained of pain, there was neither hands-on examination of her abdomen nor CT scans ordered. The nurses failed to recognize her condition and to see that she was properly evaluated.
PHYSICIANS’ DEFENSE Dr. A claimed his evaluation was performed properly. Dr. B claimed that, on the day the patient was admitted, he made a proper evaluation based on phone triage. The hospital claimed that the nurses performed proper triage and monitored her properly. And all claimed that a laparotomy required waiting until after delivery to be performed.
VERDICT Kentucky defense verdict. Posttrial motions were pending.
When findings are benign, should you refer, just to be safe?
A 36-YEAR-OLD PATIENT with presumptive fibroid tumors underwent a hysterectomy in which the ovaries and fallopian tubes were not removed. The pathologist initially reported that one tumor was benign, but that he was performing further tests. His second report confirmed the benign diagnosis and included mitotic count and spindle cells in the description of the microscopic exam. A year later, the patient developed abdominal pain, and the physician removed the fallopian tubes and ovaries. This time the same pathologist reported malignant uterine sarcoma in the ovaries. Upon reexamination of the previous year’s tissue, he believed the first tumor to be similar. A diagnosis of metastasis was given almost 2 years later.
PATIENT’S CLAIM She should have been referred to a gynecologic oncologist when the tumors were removed. This would have allowed her to be treated earlier and more effectively.
PHYSICIAN’S DEFENSE The initial diagnosis was benign and thus did not require a referral. Also, no adjuvant therapy would have improved the patient’s prognosis with this rare cancer.
VERDICT $2 million Illinois verdict.
Dystocia case is heard in bench trial
SHOULDER DYSTOCIA was encountered during delivery of the plaintiff child at a federally funded clinic. The OB used traction to complete the delivery, and the child suffered right brachial plexus injury, resulting in Erb’s palsy. No surgery was performed. The clinic was covered by the Federal Tort Claims Act, and the case was tried in a bench trial.
PATIENT’S CLAIM The treating OB used excessive traction, causing injury to the right brachial plexus.
PHYSICIAN’S DEFENSE Only moderate traction was used.
VERDICT $2,525,584 Illinois bench verdict. The court found the following: (1) negligence by the physician for repeatedly applying moderate traction to the point of excessive traction and rotating the infant’s head while the shoulder was trapped; (2) inappropriate grasping of the head while applying excessive traction; (3) failure to cut a generous episiotomy after shoulder dystocia was recognized; (4) failure to try other noninvasive measures before using excessive force; and (5) failure to recognize the likelihood of a macrosomic fetus.
No OB is available; complications ensue
SHORTLY AFTER a woman was admitted to the hospital for the birth of her child, complications occurred. The infant was delivered but suffered hypoxia and brain damage.
PATIENT’S CLAIM No OB was readily available to assist with the delivery. The nurses acted to delay the birth despite evidence that a hypoxic event was in progress and immediate delivery—even by a nurse—was essential. Fetal bradycardia continued for 5 to 6 minutes, resulting in hypoxia and brain damage in the infant.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Confidential Utah settlement with the hospital. The physicians had been dismissed in summary judgment rulings.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Ready for the Red Flags Rule?
By now, you are probably aware of the Fair and Accurate Credit Transactions (FACT) Act of 2003 and its “Identity Theft Red Flags Rule,” which require creditors to establish a program to prevent identity theft. The law will be enforced beginning this month, so if you haven't taken any action yet you'd better get cracking.
The law was originally aimed only at financial institutions, but the Federal Trade Commission, which is charged with enforcing it, subsequently decided it could apply to any group that would be considered a creditor, which the law defines as “any entity that regularly extends, renews, continues credit or arranges for the extension of credit.”
The FTC has specifically said that it will include medical providers in this definition “if [the provider] does not regularly demand payment in full for services or supplies at the time of service.”
In other words, if you routinely bill patients for any portion of your fees, including the portions not paid by insurance carriers, you are considered a creditor under this law.
To comply with the law, the FTC says that you must develop a program that allows you to do four things: identify relevant red flags (more on that below), detect red flags, prevent and mitigate identity theft, and update your program periodically.
So what is a red flag? Basically, it is a warning sign that should alert your practice to suspicious activity that may indicate identity theft. The FTC guidelines list five categories of warning signs that should be identified and addressed:
▸ Alerts, notifications, or warnings from a consumer reporting agency or any entity that performs services on your “covered accounts.”
▸ Suspicious documents.
▸ Suspicious identification documents.
▸ Suspicious activity relating to a “covered account.”
▸ Notices from customers, victims of identity theft, law enforcement authorities, or other entities about possible identity theft in connection with “covered accounts.”
Okay, so what is a “covered account?” It is any financial account used mostly for personal purposes that involves multiple payments or transactions, for which there is a foreseeable risk of identity theft.
The FTC says it is particularly worried about medical billing accounts because the theft of a patient's information to fraudulently obtain medical care can cause a variety of serious problems over and above those usually associated with identity theft, including exhaustion of the victim's health benefits and a potentially life-threatening corruption of medical records.
The law requires you to develop a written program appropriate to the size and complexity of your practice that spells out your responses to red flags and the preventive actions you plan to take if there is a breach or attempted breach of your database. The program should include appropriate staff training, as well as a plan for monitoring staff to ensure that they are all following the program.
You must update your program “periodically” (the law is no more specific than that) to reflect changes in risks to patients, ensuring that the program remains current and relevant as methods of identity theft change.
In other words, designing a program and putting it on a shelf to collect dust will not satisfy the law's requirements, nor adequately protect your patients.
If you employ a billing service and/or collection agency, or any other outside entity that has access to your covered accounts, you also must take steps to ensure that their activities are conducted using a reasonable identity theft program. This could be done through a written contract with the service provider, or by amending your existing HIPAA Business Associate Agreements.
Some states have their own additional rules that may need to be incorporated into your identity theft prevention program. Check with relevant agencies in your state regarding that possibility.
Violations of the Red Flags Rule can subject your practice to significant penalties—particularly if a patient suffers an identity theft that could have been prevented by your program, had it been properly implemented.
The exercise is not as onerous or time consuming as many assume. The American Academy of Dermatology points out that the law permits great flexibility, so if you determine that your practice has a low risk of identity theft, developing a program should be simple and straightforward, with only a few red flags to identify and deal with.
Medical practices and other businesses can find help online for developing their own programs. One good example, with a template that should be modifiable to fit most dermatology offices, is online at the California Society of Municipal Finance Officers' Web site www.csmfo.org/index.cfm?fuseaction=DetailGroup&CID=2478&NavID=181
The AAD also has more information at its site www.aad.org/pm/_doc/FTCRedFlagsRulesFactSheet.pdf
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
By now, you are probably aware of the Fair and Accurate Credit Transactions (FACT) Act of 2003 and its “Identity Theft Red Flags Rule,” which require creditors to establish a program to prevent identity theft. The law will be enforced beginning this month, so if you haven't taken any action yet you'd better get cracking.
The law was originally aimed only at financial institutions, but the Federal Trade Commission, which is charged with enforcing it, subsequently decided it could apply to any group that would be considered a creditor, which the law defines as “any entity that regularly extends, renews, continues credit or arranges for the extension of credit.”
The FTC has specifically said that it will include medical providers in this definition “if [the provider] does not regularly demand payment in full for services or supplies at the time of service.”
In other words, if you routinely bill patients for any portion of your fees, including the portions not paid by insurance carriers, you are considered a creditor under this law.
To comply with the law, the FTC says that you must develop a program that allows you to do four things: identify relevant red flags (more on that below), detect red flags, prevent and mitigate identity theft, and update your program periodically.
So what is a red flag? Basically, it is a warning sign that should alert your practice to suspicious activity that may indicate identity theft. The FTC guidelines list five categories of warning signs that should be identified and addressed:
▸ Alerts, notifications, or warnings from a consumer reporting agency or any entity that performs services on your “covered accounts.”
▸ Suspicious documents.
▸ Suspicious identification documents.
▸ Suspicious activity relating to a “covered account.”
▸ Notices from customers, victims of identity theft, law enforcement authorities, or other entities about possible identity theft in connection with “covered accounts.”
Okay, so what is a “covered account?” It is any financial account used mostly for personal purposes that involves multiple payments or transactions, for which there is a foreseeable risk of identity theft.
The FTC says it is particularly worried about medical billing accounts because the theft of a patient's information to fraudulently obtain medical care can cause a variety of serious problems over and above those usually associated with identity theft, including exhaustion of the victim's health benefits and a potentially life-threatening corruption of medical records.
The law requires you to develop a written program appropriate to the size and complexity of your practice that spells out your responses to red flags and the preventive actions you plan to take if there is a breach or attempted breach of your database. The program should include appropriate staff training, as well as a plan for monitoring staff to ensure that they are all following the program.
You must update your program “periodically” (the law is no more specific than that) to reflect changes in risks to patients, ensuring that the program remains current and relevant as methods of identity theft change.
In other words, designing a program and putting it on a shelf to collect dust will not satisfy the law's requirements, nor adequately protect your patients.
If you employ a billing service and/or collection agency, or any other outside entity that has access to your covered accounts, you also must take steps to ensure that their activities are conducted using a reasonable identity theft program. This could be done through a written contract with the service provider, or by amending your existing HIPAA Business Associate Agreements.
Some states have their own additional rules that may need to be incorporated into your identity theft prevention program. Check with relevant agencies in your state regarding that possibility.
Violations of the Red Flags Rule can subject your practice to significant penalties—particularly if a patient suffers an identity theft that could have been prevented by your program, had it been properly implemented.
The exercise is not as onerous or time consuming as many assume. The American Academy of Dermatology points out that the law permits great flexibility, so if you determine that your practice has a low risk of identity theft, developing a program should be simple and straightforward, with only a few red flags to identify and deal with.
Medical practices and other businesses can find help online for developing their own programs. One good example, with a template that should be modifiable to fit most dermatology offices, is online at the California Society of Municipal Finance Officers' Web site www.csmfo.org/index.cfm?fuseaction=DetailGroup&CID=2478&NavID=181
The AAD also has more information at its site www.aad.org/pm/_doc/FTCRedFlagsRulesFactSheet.pdf
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
By now, you are probably aware of the Fair and Accurate Credit Transactions (FACT) Act of 2003 and its “Identity Theft Red Flags Rule,” which require creditors to establish a program to prevent identity theft. The law will be enforced beginning this month, so if you haven't taken any action yet you'd better get cracking.
The law was originally aimed only at financial institutions, but the Federal Trade Commission, which is charged with enforcing it, subsequently decided it could apply to any group that would be considered a creditor, which the law defines as “any entity that regularly extends, renews, continues credit or arranges for the extension of credit.”
The FTC has specifically said that it will include medical providers in this definition “if [the provider] does not regularly demand payment in full for services or supplies at the time of service.”
In other words, if you routinely bill patients for any portion of your fees, including the portions not paid by insurance carriers, you are considered a creditor under this law.
To comply with the law, the FTC says that you must develop a program that allows you to do four things: identify relevant red flags (more on that below), detect red flags, prevent and mitigate identity theft, and update your program periodically.
So what is a red flag? Basically, it is a warning sign that should alert your practice to suspicious activity that may indicate identity theft. The FTC guidelines list five categories of warning signs that should be identified and addressed:
▸ Alerts, notifications, or warnings from a consumer reporting agency or any entity that performs services on your “covered accounts.”
▸ Suspicious documents.
▸ Suspicious identification documents.
▸ Suspicious activity relating to a “covered account.”
▸ Notices from customers, victims of identity theft, law enforcement authorities, or other entities about possible identity theft in connection with “covered accounts.”
Okay, so what is a “covered account?” It is any financial account used mostly for personal purposes that involves multiple payments or transactions, for which there is a foreseeable risk of identity theft.
The FTC says it is particularly worried about medical billing accounts because the theft of a patient's information to fraudulently obtain medical care can cause a variety of serious problems over and above those usually associated with identity theft, including exhaustion of the victim's health benefits and a potentially life-threatening corruption of medical records.
The law requires you to develop a written program appropriate to the size and complexity of your practice that spells out your responses to red flags and the preventive actions you plan to take if there is a breach or attempted breach of your database. The program should include appropriate staff training, as well as a plan for monitoring staff to ensure that they are all following the program.
You must update your program “periodically” (the law is no more specific than that) to reflect changes in risks to patients, ensuring that the program remains current and relevant as methods of identity theft change.
In other words, designing a program and putting it on a shelf to collect dust will not satisfy the law's requirements, nor adequately protect your patients.
If you employ a billing service and/or collection agency, or any other outside entity that has access to your covered accounts, you also must take steps to ensure that their activities are conducted using a reasonable identity theft program. This could be done through a written contract with the service provider, or by amending your existing HIPAA Business Associate Agreements.
Some states have their own additional rules that may need to be incorporated into your identity theft prevention program. Check with relevant agencies in your state regarding that possibility.
Violations of the Red Flags Rule can subject your practice to significant penalties—particularly if a patient suffers an identity theft that could have been prevented by your program, had it been properly implemented.
The exercise is not as onerous or time consuming as many assume. The American Academy of Dermatology points out that the law permits great flexibility, so if you determine that your practice has a low risk of identity theft, developing a program should be simple and straightforward, with only a few red flags to identify and deal with.
Medical practices and other businesses can find help online for developing their own programs. One good example, with a template that should be modifiable to fit most dermatology offices, is online at the California Society of Municipal Finance Officers' Web site www.csmfo.org/index.cfm?fuseaction=DetailGroup&CID=2478&NavID=181
The AAD also has more information at its site www.aad.org/pm/_doc/FTCRedFlagsRulesFactSheet.pdf
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Palliative-Care Payment
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
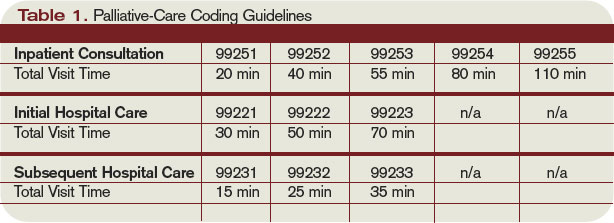
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Many hospitalists provide palliative-care services to patients at the request of physicians within their own groups or from other specialists. Varying factors affect how hospitalists report these services—namely, the nature of the request and the type of service provided. Palliative-care programs can be quite costly as they involve several team members and a substantial amount of time delivering these services. Capturing services appropriately and obtaining reimbursement to help continue program initiatives is pertinent.
Nature of the Request
Members of a palliative-care team often are called on to provide management options to assist in reducing pain and suffering associated with both terminal and nonterminal disease, thereby improving a patient’s quality of life. When a palliative-care specialist is asked to provide an opinion or advice, the initial service could qualify as a consultation. However, all requirements must be met in order to report the service as an inpatient consultation (codes 99251-99255).
There must be a written request from a qualified healthcare provider involved in the patient’s care (e.g., a physician, resident, or nurse practitioner). In the inpatient setting, this request can be documented as a physician order or in the assessment of the requesting provider’s progress note. Standing orders for consultation are not permitted. Ideally, the requesting provider should identify the reason for a consult to support the medical necessity of the service.
Additionally, the palliative-care physician renders and documents the service, then reports findings to the requesting physician. The consultant’s required written report does not have to be sent separately to the requesting physician. Because the requesting physician and the consultant share a common medical record in an inpatient setting, the consultant’s inpatient progress note suffices the “written report” requirement.
One concern about billing consultations involves the nature of the request. If the requesting physician documents the need for an opinion or advice from the palliative-care specialist, the service can be reported as a consultation. If, however, the request states consult for “medical management” or “palliative management,” it’s less likely that payors will consider the service a consultation. In the latter situation, it appears as if the requesting physician is not seeking an opinion or advice from the consultant to incorporate into his own plan of care for the patient and would rather the consultant take over that portion of patient care.
Recently revised billing policies prevent the consultant from billing consults under these circumstances. Without a sufficient request for consultation, the palliative-care specialist can only report “subsequent” hospital care services.1 Language that better supports the consultative nature of the request is:
- Consult for an opinion or advice on palliative measures;
- Consult for evaluation of palliative options; and
- Consult palliative care for treatment options.
Proper Documentation
The requesting physician can be in the same or different provider group as the consultant. The consultant must possess expertise in an area beyond that of the requesting provider. Because the specialty designation for most hospitalists is internal medicine, palliative-care claims could be scrutinized more closely. This does not necessarily occur when the requesting provider has a different two-digit specialty designation (e.g., internal medicine and gastroenterology).2 Scrutiny is more likely to occur when the requesting provider has the same internal-medicine designation as the palliative-care consultant, even if they are in different provider groups.
Payor concern escalates when physicians of the same designated specialty submit claims for the same patient on the same date. Having different primary diagnosis codes attached to each visit level does not necessarily help. The payor is likely to deny the second claim received, pending a review of documentation. If this happens, the provider who received the denial should submit a copy of both progress notes for the date in question. Hopefully, the distinction between the services is demonstrated in the documentation.
Service Type
Palliative services might involve obtaining and documenting the standard key components for visit-level selection: history, exam, and medical decision-making.3 However, the palliative-care specialist might spend more time providing counseling or coordination of care for a patient and family. When this occurs, the palliative-care specialist should not forget about the guidelines for reporting time-based services.4 Inpatient services may be reported on the basis of time, as long as a face-to-face service between the provider and the patient occurs. Consider the total time spent face to face with the patient, and the time spent obtaining, discussing, and coordinating patient care, while you are in the patient’s unit or floor.
As a reminder, document the total time, the amount of time spent counseling, and the details of discussion and coordination. The physician may count the time spent counseling the patient’s family regarding the treatment and care, as long as the focus is not emotional support for the family, the meeting takes place in the patient’s unit or floor, and the patient is present, unless there is medically supported reason for which the patient is unable to participate (e.g., cognitive impairment). The palliative-care specialist can then select the visit level based on time.5 (See Table 1, above.) TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.10. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 26, Section 10.8. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c26.pdf. Accessed Jan. 30, 2009.
3. Centers for Medicare and Medicaid Services. Documentation Guidelines for Evaluation and Management Services. CMS Web site. Available at: www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp. Accessed Jan. 30, 2009.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.1B. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Jan. 30, 2009.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association Press; 2008.
Boost Your Bargaining Power
Earlier this month, United Healthcare implemented a new fee schedule that essentially freezes physician reimbursement fees at Medicare's 2008 resource-based relative value unit scale. The move affects 12% of physicians in the UHC network, or about 70,000 providers.
According to United Healthcare, the transition was made to simplify fee schedule administration and increase the reliability and predictability of physician payments.
The new method for calculating reimbursement replaces the “progressive fee schedule,” which used a fixed conversion factor and RVU values that changed on an annual basis. The new “stated year fee schedule” bases physician reimbursement on their existing conversion factors and 2008 Medicare RVUs and non-RVU based fees.
This solution is not ideal because 2009 Medicare rates are higher than 2008 rates, but it does offer physicians a predictable rate of reimbursement. Under the progressive fee schedule, physicians experienced drops in their reimbursement for certain CPT codes, some by as much as 9.5%.
With that said, physicians may choose to renegotiate their contracts with United Healthcare. But what would be the first step?
First, I would call United Healthcare to get some details and clarification from them. Besides the fee schedule, for example, what other aspects of the contract are changing?
Second, ask the health plan to map out what the steps are for renegotiating the contract. What information do they require from the physician to justify an increase in the fees? How long would it take for that increase to take place? Check on your rights to appeal the change and find out what their expectations are. The process may seem like an uphill fight, but getting all the information you can is key.
Third, if it seems daunting to renegotiate on your own, consider creating an independent network of practices to raise your bargaining power.
Such networks are emerging all over the country. They must adhere to strict federal antitrust guidelines. So, for example, it's illegal for such networks to collectively boycott a health plan, but if they are set up correctly they can be the most effective way for small players to renegotiate contracts with health plans.
Large, nationally organized provider networks exist, but they tend to be so large that they deeply discount their reimbursement rates in order to compete with other large practice networks.
An alternative to joining a large network is to identify a cluster of 15-20 small group or solo physician practices that can be more nimble in their decision making and that can leverage their bargaining power at a local level when negotiating contracts or buying medical supplies.
This so-called group practice without walls concept gives a solo practice the bargaining strength of a large group practice without having to give up a solo practice.
Earlier this month, United Healthcare implemented a new fee schedule that essentially freezes physician reimbursement fees at Medicare's 2008 resource-based relative value unit scale. The move affects 12% of physicians in the UHC network, or about 70,000 providers.
According to United Healthcare, the transition was made to simplify fee schedule administration and increase the reliability and predictability of physician payments.
The new method for calculating reimbursement replaces the “progressive fee schedule,” which used a fixed conversion factor and RVU values that changed on an annual basis. The new “stated year fee schedule” bases physician reimbursement on their existing conversion factors and 2008 Medicare RVUs and non-RVU based fees.
This solution is not ideal because 2009 Medicare rates are higher than 2008 rates, but it does offer physicians a predictable rate of reimbursement. Under the progressive fee schedule, physicians experienced drops in their reimbursement for certain CPT codes, some by as much as 9.5%.
With that said, physicians may choose to renegotiate their contracts with United Healthcare. But what would be the first step?
First, I would call United Healthcare to get some details and clarification from them. Besides the fee schedule, for example, what other aspects of the contract are changing?
Second, ask the health plan to map out what the steps are for renegotiating the contract. What information do they require from the physician to justify an increase in the fees? How long would it take for that increase to take place? Check on your rights to appeal the change and find out what their expectations are. The process may seem like an uphill fight, but getting all the information you can is key.
Third, if it seems daunting to renegotiate on your own, consider creating an independent network of practices to raise your bargaining power.
Such networks are emerging all over the country. They must adhere to strict federal antitrust guidelines. So, for example, it's illegal for such networks to collectively boycott a health plan, but if they are set up correctly they can be the most effective way for small players to renegotiate contracts with health plans.
Large, nationally organized provider networks exist, but they tend to be so large that they deeply discount their reimbursement rates in order to compete with other large practice networks.
An alternative to joining a large network is to identify a cluster of 15-20 small group or solo physician practices that can be more nimble in their decision making and that can leverage their bargaining power at a local level when negotiating contracts or buying medical supplies.
This so-called group practice without walls concept gives a solo practice the bargaining strength of a large group practice without having to give up a solo practice.
Earlier this month, United Healthcare implemented a new fee schedule that essentially freezes physician reimbursement fees at Medicare's 2008 resource-based relative value unit scale. The move affects 12% of physicians in the UHC network, or about 70,000 providers.
According to United Healthcare, the transition was made to simplify fee schedule administration and increase the reliability and predictability of physician payments.
The new method for calculating reimbursement replaces the “progressive fee schedule,” which used a fixed conversion factor and RVU values that changed on an annual basis. The new “stated year fee schedule” bases physician reimbursement on their existing conversion factors and 2008 Medicare RVUs and non-RVU based fees.
This solution is not ideal because 2009 Medicare rates are higher than 2008 rates, but it does offer physicians a predictable rate of reimbursement. Under the progressive fee schedule, physicians experienced drops in their reimbursement for certain CPT codes, some by as much as 9.5%.
With that said, physicians may choose to renegotiate their contracts with United Healthcare. But what would be the first step?
First, I would call United Healthcare to get some details and clarification from them. Besides the fee schedule, for example, what other aspects of the contract are changing?
Second, ask the health plan to map out what the steps are for renegotiating the contract. What information do they require from the physician to justify an increase in the fees? How long would it take for that increase to take place? Check on your rights to appeal the change and find out what their expectations are. The process may seem like an uphill fight, but getting all the information you can is key.
Third, if it seems daunting to renegotiate on your own, consider creating an independent network of practices to raise your bargaining power.
Such networks are emerging all over the country. They must adhere to strict federal antitrust guidelines. So, for example, it's illegal for such networks to collectively boycott a health plan, but if they are set up correctly they can be the most effective way for small players to renegotiate contracts with health plans.
Large, nationally organized provider networks exist, but they tend to be so large that they deeply discount their reimbursement rates in order to compete with other large practice networks.
An alternative to joining a large network is to identify a cluster of 15-20 small group or solo physician practices that can be more nimble in their decision making and that can leverage their bargaining power at a local level when negotiating contracts or buying medical supplies.
This so-called group practice without walls concept gives a solo practice the bargaining strength of a large group practice without having to give up a solo practice.
Misunderstood Modifiers
Modifiers are two-digit representations used in conjunction with a service or procedure code (e.g., 99233-25) during claim submission to alert payors that the service or procedure was performed under a special circumstance. Modifiers can:
- Identify body areas;
- Distinguish multiple, separately identifiable services;
- Identify reduced or multiple services of the same or a different nature; or
- Categorize unusual events surrounding a particular service.1
Many questions arise over appropriate modifier use. Hospitalist misconceptions typically involve surgical comanagement or multiple services on the same day. Understanding when to use modifiers is imperative for proper claim submission and reimbursement.
Multiple Visits
Most hospitalists know payors allow reimbursement for only one visit per specialty, per patient, per day; however, some payors further limit coverage to a single service (i.e., a visit or a procedure) unless physician documentation demonstrates a medical necessity for each billed service. When two visits are performed on the same date by the same physician, or by two physicians of the same specialty within the same group, only one cumulative service should be reported.2
Consideration of two notes during visit-level selection does not authorize physicians to report a higher visit level (e.g., 99233 for two notes instead of 99232 for one note). If the cumulative documentation does not include the necessary elements of history, exam, or medical decision-making that are associated with 99233, the physician must report the lower visit level that accurately reflects the content of the progress note (for more information on documentation guidelines, visit www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp).
One exception to this “single cumulative service” rule occurs when a physician provides a typical inpatient service (e.g., admission or subsequent hospital care) for chronic obstructive bronchitis with acute exacerbation (diagnosis code 491.21) early in the day, and later the patient requires a second, more intense encounter for acute respiratory distress (diagnosis code 518.82) that meets the definition of critical care (99291). In this scenario, the physician is allowed to report both services on the same date, appending modifier 25 to the initial service (i.e., 99233-25) because each service was performed for distinct reasons.
If different physicians in the same provider group and specialty provided the initial and follow-up services, each physician reports the corresponding service in their own name with modifier 25 appended to the subsequent hospital care service (as above). Please note that physicians may not report both services if critical care is the initial service of the day. In this latter scenario, the physician reports critical-care codes (99291, 99292) for all of his or other group members’ encounters provided in one calendar day.3
Visits and Procedures
When a physician bills for a procedure and a visit (inpatient or outpatient) on the same day, most payors “bundle” the visit payment into that of the procedure. Some payors do provide separate payment for the visit, if the service is separately identifiable from the procedure (i.e., performed for a separate reason). To electronically demonstrate this on the claim form, the physician appends modifier 25 to the visit. Although not required, it is strongly suggested that, when possible, the primary diagnosis for the visit differs from the one used with the procedure. This will further distinguish the services. However, different diagnoses may not be possible when the physician evaluates the patient and decides, during the course of the evaluation, that a procedure is warranted. In this case, the physician may only have a single diagnosis to list with the procedure and the visit.
Payors may request documentation prior to payment to ensure that the visit is not associated with the required preprocedure history and physical. Modifier 57 is not to be confused with modifier 25. Modifier 57 indicates that the physician made the decision for “surgery” during the visit, but this modifier is used with preprocedural visits involving major surgical procedures (i.e., procedures associated with 90-day global periods). Since hospitalists do not perform major surgical procedures, they would not use this modifier with preprocedural visits.
Keep in mind that this “bundling” concept only applies when same-day visits and procedures are performed by the same physician or members of the same provider group with the same specialty designation. In other words, hospitalist visits are typically considered separate from procedures performed by a surgeon, and there is no need to append a modifier to visits on the same day as the surgeon’s procedure. The surgeon’s packaged payment includes preoperative visits after the decision for surgery is made beginning one day prior to surgery, and postoperative visits by the surgeon related to recovery from surgery, postoperative pain management, and discharge care.4 The surgeon is entitled to the full global payment if he provides the preoperative, intraoperative, and postoperative management.
If the surgeon relinquishes care and formally transfers the preoperative or postoperative management to another physician not associated with the surgical group, the other physician may bill for his portion of the perioperative management by appending modifier 56 (preop) or 55 (postop) to the procedure code. Unfortunately, the hospitalist is subject to the surgeon’s claim reporting. If the surgeon fails to solely report his intraoperative management (modifier 54 appended to the procedure code), the surgeon receives the full packaged payment. The payor will deny the hospitalist’s claim.
The payor is unlikely to retrieve money from one provider to pay another provider, unless a pattern of inappropriate claim submission is detected. Surgical intraoperative responsibilities are not typically reassigned to other provider groups unless special circumstances occur (e.g., geographical restrictions). Therefore, if the surgeon does not relinquish care but merely wants the hospitalist to assist in medical management, the hospitalist reports his medically necessary services with the appropriate inpatient visit code (subsequent hospital care, 99231-99233). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Holmes A. Appropriate Use of Modifiers In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians; 2008:273-282.
2. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
3. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
4. Pohlig, C. Sort out surgical cases. The Hospitalist. 2008;12(8):19.
Modifiers are two-digit representations used in conjunction with a service or procedure code (e.g., 99233-25) during claim submission to alert payors that the service or procedure was performed under a special circumstance. Modifiers can:
- Identify body areas;
- Distinguish multiple, separately identifiable services;
- Identify reduced or multiple services of the same or a different nature; or
- Categorize unusual events surrounding a particular service.1
Many questions arise over appropriate modifier use. Hospitalist misconceptions typically involve surgical comanagement or multiple services on the same day. Understanding when to use modifiers is imperative for proper claim submission and reimbursement.
Multiple Visits
Most hospitalists know payors allow reimbursement for only one visit per specialty, per patient, per day; however, some payors further limit coverage to a single service (i.e., a visit or a procedure) unless physician documentation demonstrates a medical necessity for each billed service. When two visits are performed on the same date by the same physician, or by two physicians of the same specialty within the same group, only one cumulative service should be reported.2
Consideration of two notes during visit-level selection does not authorize physicians to report a higher visit level (e.g., 99233 for two notes instead of 99232 for one note). If the cumulative documentation does not include the necessary elements of history, exam, or medical decision-making that are associated with 99233, the physician must report the lower visit level that accurately reflects the content of the progress note (for more information on documentation guidelines, visit www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp).
One exception to this “single cumulative service” rule occurs when a physician provides a typical inpatient service (e.g., admission or subsequent hospital care) for chronic obstructive bronchitis with acute exacerbation (diagnosis code 491.21) early in the day, and later the patient requires a second, more intense encounter for acute respiratory distress (diagnosis code 518.82) that meets the definition of critical care (99291). In this scenario, the physician is allowed to report both services on the same date, appending modifier 25 to the initial service (i.e., 99233-25) because each service was performed for distinct reasons.
If different physicians in the same provider group and specialty provided the initial and follow-up services, each physician reports the corresponding service in their own name with modifier 25 appended to the subsequent hospital care service (as above). Please note that physicians may not report both services if critical care is the initial service of the day. In this latter scenario, the physician reports critical-care codes (99291, 99292) for all of his or other group members’ encounters provided in one calendar day.3
Visits and Procedures
When a physician bills for a procedure and a visit (inpatient or outpatient) on the same day, most payors “bundle” the visit payment into that of the procedure. Some payors do provide separate payment for the visit, if the service is separately identifiable from the procedure (i.e., performed for a separate reason). To electronically demonstrate this on the claim form, the physician appends modifier 25 to the visit. Although not required, it is strongly suggested that, when possible, the primary diagnosis for the visit differs from the one used with the procedure. This will further distinguish the services. However, different diagnoses may not be possible when the physician evaluates the patient and decides, during the course of the evaluation, that a procedure is warranted. In this case, the physician may only have a single diagnosis to list with the procedure and the visit.
Payors may request documentation prior to payment to ensure that the visit is not associated with the required preprocedure history and physical. Modifier 57 is not to be confused with modifier 25. Modifier 57 indicates that the physician made the decision for “surgery” during the visit, but this modifier is used with preprocedural visits involving major surgical procedures (i.e., procedures associated with 90-day global periods). Since hospitalists do not perform major surgical procedures, they would not use this modifier with preprocedural visits.
Keep in mind that this “bundling” concept only applies when same-day visits and procedures are performed by the same physician or members of the same provider group with the same specialty designation. In other words, hospitalist visits are typically considered separate from procedures performed by a surgeon, and there is no need to append a modifier to visits on the same day as the surgeon’s procedure. The surgeon’s packaged payment includes preoperative visits after the decision for surgery is made beginning one day prior to surgery, and postoperative visits by the surgeon related to recovery from surgery, postoperative pain management, and discharge care.4 The surgeon is entitled to the full global payment if he provides the preoperative, intraoperative, and postoperative management.
If the surgeon relinquishes care and formally transfers the preoperative or postoperative management to another physician not associated with the surgical group, the other physician may bill for his portion of the perioperative management by appending modifier 56 (preop) or 55 (postop) to the procedure code. Unfortunately, the hospitalist is subject to the surgeon’s claim reporting. If the surgeon fails to solely report his intraoperative management (modifier 54 appended to the procedure code), the surgeon receives the full packaged payment. The payor will deny the hospitalist’s claim.
The payor is unlikely to retrieve money from one provider to pay another provider, unless a pattern of inappropriate claim submission is detected. Surgical intraoperative responsibilities are not typically reassigned to other provider groups unless special circumstances occur (e.g., geographical restrictions). Therefore, if the surgeon does not relinquish care but merely wants the hospitalist to assist in medical management, the hospitalist reports his medically necessary services with the appropriate inpatient visit code (subsequent hospital care, 99231-99233). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Holmes A. Appropriate Use of Modifiers In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians; 2008:273-282.
2. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
3. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
4. Pohlig, C. Sort out surgical cases. The Hospitalist. 2008;12(8):19.
Modifiers are two-digit representations used in conjunction with a service or procedure code (e.g., 99233-25) during claim submission to alert payors that the service or procedure was performed under a special circumstance. Modifiers can:
- Identify body areas;
- Distinguish multiple, separately identifiable services;
- Identify reduced or multiple services of the same or a different nature; or
- Categorize unusual events surrounding a particular service.1
Many questions arise over appropriate modifier use. Hospitalist misconceptions typically involve surgical comanagement or multiple services on the same day. Understanding when to use modifiers is imperative for proper claim submission and reimbursement.
Multiple Visits
Most hospitalists know payors allow reimbursement for only one visit per specialty, per patient, per day; however, some payors further limit coverage to a single service (i.e., a visit or a procedure) unless physician documentation demonstrates a medical necessity for each billed service. When two visits are performed on the same date by the same physician, or by two physicians of the same specialty within the same group, only one cumulative service should be reported.2
Consideration of two notes during visit-level selection does not authorize physicians to report a higher visit level (e.g., 99233 for two notes instead of 99232 for one note). If the cumulative documentation does not include the necessary elements of history, exam, or medical decision-making that are associated with 99233, the physician must report the lower visit level that accurately reflects the content of the progress note (for more information on documentation guidelines, visit www.cms.hhs.gov/MLNEdWebGuide/25_EMDOC.asp).
One exception to this “single cumulative service” rule occurs when a physician provides a typical inpatient service (e.g., admission or subsequent hospital care) for chronic obstructive bronchitis with acute exacerbation (diagnosis code 491.21) early in the day, and later the patient requires a second, more intense encounter for acute respiratory distress (diagnosis code 518.82) that meets the definition of critical care (99291). In this scenario, the physician is allowed to report both services on the same date, appending modifier 25 to the initial service (i.e., 99233-25) because each service was performed for distinct reasons.
If different physicians in the same provider group and specialty provided the initial and follow-up services, each physician reports the corresponding service in their own name with modifier 25 appended to the subsequent hospital care service (as above). Please note that physicians may not report both services if critical care is the initial service of the day. In this latter scenario, the physician reports critical-care codes (99291, 99292) for all of his or other group members’ encounters provided in one calendar day.3
Visits and Procedures
When a physician bills for a procedure and a visit (inpatient or outpatient) on the same day, most payors “bundle” the visit payment into that of the procedure. Some payors do provide separate payment for the visit, if the service is separately identifiable from the procedure (i.e., performed for a separate reason). To electronically demonstrate this on the claim form, the physician appends modifier 25 to the visit. Although not required, it is strongly suggested that, when possible, the primary diagnosis for the visit differs from the one used with the procedure. This will further distinguish the services. However, different diagnoses may not be possible when the physician evaluates the patient and decides, during the course of the evaluation, that a procedure is warranted. In this case, the physician may only have a single diagnosis to list with the procedure and the visit.
Payors may request documentation prior to payment to ensure that the visit is not associated with the required preprocedure history and physical. Modifier 57 is not to be confused with modifier 25. Modifier 57 indicates that the physician made the decision for “surgery” during the visit, but this modifier is used with preprocedural visits involving major surgical procedures (i.e., procedures associated with 90-day global periods). Since hospitalists do not perform major surgical procedures, they would not use this modifier with preprocedural visits.
Keep in mind that this “bundling” concept only applies when same-day visits and procedures are performed by the same physician or members of the same provider group with the same specialty designation. In other words, hospitalist visits are typically considered separate from procedures performed by a surgeon, and there is no need to append a modifier to visits on the same day as the surgeon’s procedure. The surgeon’s packaged payment includes preoperative visits after the decision for surgery is made beginning one day prior to surgery, and postoperative visits by the surgeon related to recovery from surgery, postoperative pain management, and discharge care.4 The surgeon is entitled to the full global payment if he provides the preoperative, intraoperative, and postoperative management.
If the surgeon relinquishes care and formally transfers the preoperative or postoperative management to another physician not associated with the surgical group, the other physician may bill for his portion of the perioperative management by appending modifier 56 (preop) or 55 (postop) to the procedure code. Unfortunately, the hospitalist is subject to the surgeon’s claim reporting. If the surgeon fails to solely report his intraoperative management (modifier 54 appended to the procedure code), the surgeon receives the full packaged payment. The payor will deny the hospitalist’s claim.
The payor is unlikely to retrieve money from one provider to pay another provider, unless a pattern of inappropriate claim submission is detected. Surgical intraoperative responsibilities are not typically reassigned to other provider groups unless special circumstances occur (e.g., geographical restrictions). Therefore, if the surgeon does not relinquish care but merely wants the hospitalist to assist in medical management, the hospitalist reports his medically necessary services with the appropriate inpatient visit code (subsequent hospital care, 99231-99233). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Holmes A. Appropriate Use of Modifiers In: Coding for Chest Medicine 2009. Northbrook, Ill.: American College of Chest Physicians; 2008:273-282.
2. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
3. Centers for Medicare and Medicaid Services. Medicare claims processing manual. CMS Web site. Available at: www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Accessed Feb. 10, 2009.
4. Pohlig, C. Sort out surgical cases. The Hospitalist. 2008;12(8):19.
Medical Verdicts
Long after surgery, clips continue to migrate to bladder
A 34-YEAR-OLD WOMAN underwent a total vaginal hysterectomy with a laparoscopic Burch procedure. Following surgery, she developed a fever and tenderness in her lower left quadrant. Cystoscopy indicated multiple areas of petechial hemorrhages when her bladder was filled. A week after the surgery, she was discharged but continued treatment for ongoing pelvic pain. Two years later, exploratory surgery showed that two clips from the hysterectomy procedure had migrated into her bladder. These were removed. A third clip was removed a year later. Eight years after the original surgery, Prolene mesh and more clips were discovered embedded in her bladder. The following year, to correct the migrating clips and help with pain, she underwent a vaginal sling procedure, bilateral ureteral catheterization, and right inguinal hernia repair.
PATIENT’S CLAIM The physician was negligent in placing the mesh and clips during the hysterectomy, and as a result additional procedures were required.
PHYSICIAN’S DEFENSE There was no negligence. Also, erosion of a tack is a known complication of the surgery.
VERDICT Massachusetts defense verdict.
Defense reneges on settlement, so patient fights back
FOLLOWING SURGERY to excise a Bartholin’s cyst from her labium, a patient developed first one hematoma and then a second, each of which was excised in turn. Then tissue became necrotic and was also excised.
PATIENT’S CLAIM The procedures caused disfigurement and subsequent embarrassment. One labium was removed entirely, and nerve damage resulted in loss of sensation and painful intercourse. She also claimed lack of consent because she was advised of neither the risks of nor alternatives to surgery. Although married at the time of the procedures, she is now divorced.
PHYSICIAN’S DEFENSE Many of the patient’s problems resulted from her mental health issues.
VERDICT Confidential Utah settlement. The patient had originally accepted the defense attorney’s offer of an $85,000 settlement. This was never paid, as the adjustor would allow only up to $72,500. When the patient filed a motion to enforce the $85,000 settlement, the matter was settled for an undisclosed amount.
Removed ovaries weren’t diseased, but defense wins at trial
A 31-YEAR-OLD WOMAN with persistent abdominal pain and heavy, painful periods underwent a hysterectomy as recommended by her ObGyn. Believing the ovaries were diseased, he removed them during the procedure—but a pathology report indicated no disease. He also branded the patient’s uterus with a “UK” symbol. Although this branding received attention from the national media, the trial dealt with removal of the ovaries.
PATIENT’S CLAIM (1) She had told her ObGyn that she wanted to keep her ovaries, so she was unhappy they had been removed. (2) She experienced insomnia, depression, and decreased libido. (3) The surgery was not necessary; she should have been treated conservatively at first. (4) She did not give informed consent. (5) And the ObGyn performed 120 hysterectomies in the year of her surgery, eight times the national average of only 15.
PHYSICIAN’S DEFENSE The frequency of the procedures he performed was based on his expertise in laparoscopic hysterectomy. Removal of the ovaries was necessary and within the patient’s consent.
VERDICT Kentucky defense verdict.
MD claims cervix was removed, but it was there 3 years later
A 48-YEAR-OLD WOMAN underwent a total abdominal hysterectomy because of bleeding and cancer concerns. Three years later, she underwent further gynecologic surgery to remove her cervix.
PATIENT’S CLAIM The defendant had not removed her cervix during the hysterectomy, as she learned 3 years after the procedure. She suffered abdominal pain and the fear of cancer, and she required additional surgery to remove the cervix.
PHYSICIAN’S DEFENSE The cervix was removed during the hysterectomy, but if a small portion had been left, it was not negligent to leave it behind.
VERDICT Illinois defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Long after surgery, clips continue to migrate to bladder
A 34-YEAR-OLD WOMAN underwent a total vaginal hysterectomy with a laparoscopic Burch procedure. Following surgery, she developed a fever and tenderness in her lower left quadrant. Cystoscopy indicated multiple areas of petechial hemorrhages when her bladder was filled. A week after the surgery, she was discharged but continued treatment for ongoing pelvic pain. Two years later, exploratory surgery showed that two clips from the hysterectomy procedure had migrated into her bladder. These were removed. A third clip was removed a year later. Eight years after the original surgery, Prolene mesh and more clips were discovered embedded in her bladder. The following year, to correct the migrating clips and help with pain, she underwent a vaginal sling procedure, bilateral ureteral catheterization, and right inguinal hernia repair.
PATIENT’S CLAIM The physician was negligent in placing the mesh and clips during the hysterectomy, and as a result additional procedures were required.
PHYSICIAN’S DEFENSE There was no negligence. Also, erosion of a tack is a known complication of the surgery.
VERDICT Massachusetts defense verdict.
Defense reneges on settlement, so patient fights back
FOLLOWING SURGERY to excise a Bartholin’s cyst from her labium, a patient developed first one hematoma and then a second, each of which was excised in turn. Then tissue became necrotic and was also excised.
PATIENT’S CLAIM The procedures caused disfigurement and subsequent embarrassment. One labium was removed entirely, and nerve damage resulted in loss of sensation and painful intercourse. She also claimed lack of consent because she was advised of neither the risks of nor alternatives to surgery. Although married at the time of the procedures, she is now divorced.
PHYSICIAN’S DEFENSE Many of the patient’s problems resulted from her mental health issues.
VERDICT Confidential Utah settlement. The patient had originally accepted the defense attorney’s offer of an $85,000 settlement. This was never paid, as the adjustor would allow only up to $72,500. When the patient filed a motion to enforce the $85,000 settlement, the matter was settled for an undisclosed amount.
Removed ovaries weren’t diseased, but defense wins at trial
A 31-YEAR-OLD WOMAN with persistent abdominal pain and heavy, painful periods underwent a hysterectomy as recommended by her ObGyn. Believing the ovaries were diseased, he removed them during the procedure—but a pathology report indicated no disease. He also branded the patient’s uterus with a “UK” symbol. Although this branding received attention from the national media, the trial dealt with removal of the ovaries.
PATIENT’S CLAIM (1) She had told her ObGyn that she wanted to keep her ovaries, so she was unhappy they had been removed. (2) She experienced insomnia, depression, and decreased libido. (3) The surgery was not necessary; she should have been treated conservatively at first. (4) She did not give informed consent. (5) And the ObGyn performed 120 hysterectomies in the year of her surgery, eight times the national average of only 15.
PHYSICIAN’S DEFENSE The frequency of the procedures he performed was based on his expertise in laparoscopic hysterectomy. Removal of the ovaries was necessary and within the patient’s consent.
VERDICT Kentucky defense verdict.
MD claims cervix was removed, but it was there 3 years later
A 48-YEAR-OLD WOMAN underwent a total abdominal hysterectomy because of bleeding and cancer concerns. Three years later, she underwent further gynecologic surgery to remove her cervix.
PATIENT’S CLAIM The defendant had not removed her cervix during the hysterectomy, as she learned 3 years after the procedure. She suffered abdominal pain and the fear of cancer, and she required additional surgery to remove the cervix.
PHYSICIAN’S DEFENSE The cervix was removed during the hysterectomy, but if a small portion had been left, it was not negligent to leave it behind.
VERDICT Illinois defense verdict.
Long after surgery, clips continue to migrate to bladder
A 34-YEAR-OLD WOMAN underwent a total vaginal hysterectomy with a laparoscopic Burch procedure. Following surgery, she developed a fever and tenderness in her lower left quadrant. Cystoscopy indicated multiple areas of petechial hemorrhages when her bladder was filled. A week after the surgery, she was discharged but continued treatment for ongoing pelvic pain. Two years later, exploratory surgery showed that two clips from the hysterectomy procedure had migrated into her bladder. These were removed. A third clip was removed a year later. Eight years after the original surgery, Prolene mesh and more clips were discovered embedded in her bladder. The following year, to correct the migrating clips and help with pain, she underwent a vaginal sling procedure, bilateral ureteral catheterization, and right inguinal hernia repair.
PATIENT’S CLAIM The physician was negligent in placing the mesh and clips during the hysterectomy, and as a result additional procedures were required.
PHYSICIAN’S DEFENSE There was no negligence. Also, erosion of a tack is a known complication of the surgery.
VERDICT Massachusetts defense verdict.
Defense reneges on settlement, so patient fights back
FOLLOWING SURGERY to excise a Bartholin’s cyst from her labium, a patient developed first one hematoma and then a second, each of which was excised in turn. Then tissue became necrotic and was also excised.
PATIENT’S CLAIM The procedures caused disfigurement and subsequent embarrassment. One labium was removed entirely, and nerve damage resulted in loss of sensation and painful intercourse. She also claimed lack of consent because she was advised of neither the risks of nor alternatives to surgery. Although married at the time of the procedures, she is now divorced.
PHYSICIAN’S DEFENSE Many of the patient’s problems resulted from her mental health issues.
VERDICT Confidential Utah settlement. The patient had originally accepted the defense attorney’s offer of an $85,000 settlement. This was never paid, as the adjustor would allow only up to $72,500. When the patient filed a motion to enforce the $85,000 settlement, the matter was settled for an undisclosed amount.
Removed ovaries weren’t diseased, but defense wins at trial
A 31-YEAR-OLD WOMAN with persistent abdominal pain and heavy, painful periods underwent a hysterectomy as recommended by her ObGyn. Believing the ovaries were diseased, he removed them during the procedure—but a pathology report indicated no disease. He also branded the patient’s uterus with a “UK” symbol. Although this branding received attention from the national media, the trial dealt with removal of the ovaries.
PATIENT’S CLAIM (1) She had told her ObGyn that she wanted to keep her ovaries, so she was unhappy they had been removed. (2) She experienced insomnia, depression, and decreased libido. (3) The surgery was not necessary; she should have been treated conservatively at first. (4) She did not give informed consent. (5) And the ObGyn performed 120 hysterectomies in the year of her surgery, eight times the national average of only 15.
PHYSICIAN’S DEFENSE The frequency of the procedures he performed was based on his expertise in laparoscopic hysterectomy. Removal of the ovaries was necessary and within the patient’s consent.
VERDICT Kentucky defense verdict.
MD claims cervix was removed, but it was there 3 years later
A 48-YEAR-OLD WOMAN underwent a total abdominal hysterectomy because of bleeding and cancer concerns. Three years later, she underwent further gynecologic surgery to remove her cervix.
PATIENT’S CLAIM The defendant had not removed her cervix during the hysterectomy, as she learned 3 years after the procedure. She suffered abdominal pain and the fear of cancer, and she required additional surgery to remove the cervix.
PHYSICIAN’S DEFENSE The cervix was removed during the hysterectomy, but if a small portion had been left, it was not negligent to leave it behind.
VERDICT Illinois defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Safeguarding Against Embezzlers
As the economy continues to founder, fraud and economic crime are on the rise, according to many law enforcement officials around the country.
Tight money increases embezzlement temptations, so this is an excellent time to review your bookkeeping procedures and remove any obvious opportunities for theft by your employees.
People who investigate embezzlement crimes for a living say that most cases are uncovered by accident. Finding it is usually relatively easy, because most embezzlers are not particularly skillful nor very good at covering their tracks, but many cases go undetected, sometimes for years, because no one is looking.
The experience of a friend of mine was all too typical: His bookkeeper wrote sizable checks to herself, entering them in the ledger as payments to vendors commonly used by his practice. Since she also balanced the checkbook, she got away with it for many months.
Detecting fraud is an inexact science. There is no textbook approach that one can follow, but a few simple measures will uncover or prevent a large percentage of dishonest behavior:
Hire honest employees. It is amazing how few doctors check applicants' references. Find out if the applicants are really as good as they look on paper. For a few dollars, you can screen prospective employees on public information Web sites to see if they have criminal records or if they have been sued or are suing others.
Minimize opportunities for dishonesty. Theft and embezzlement are the products of motivation and opportunity. It is hard to control motivation, but there ways to minimize opportunities for dishonesty. No one person should be in charge of the entire bookkeeping process. The person who enters charges should be different from the one who enters payments. The employee who writes the checks should not balance the checkbook, and so on. Internal audits should be done on a regular basis, and all employees should know that.
Reconcile receipts and cash daily. The most common form of embezzlement is simply taking cash out of the till. In a typical scenario, a patient pays a $15 copay in cash but the receptionist records the payment as $5 and pockets the rest. Make sure a receipt is generated, and that someone other than the person accepting cash reconciles the receipts and the cash daily.
Insist on separate accounting duties. Another common scam is false invoices: You think you are paying for supplies and services, but the money is going to an employee. One employee should enter invoices into the system, another should issue the check, and a third should match invoices to goods and services received.
Verify expense reports. False expense reports are another common form of fraud. When an employee asks for reimbursement of expenses, make sure they are real.
Safeguard your computer. Computers have made embezzlement easier and more tempting. Data are usually concentrated in one place, accounts can be accessed from remote workstations or off-premises servers, and a paper trail is often eliminated. Your computer vendor should be aware of this, and should have safeguards built into your system.
Look for red flags. Do you have an employee who refuses to take vacations, because someone else will have to look at the books? Does someone insist on approving or entering expenses that are another employee's responsibility?
Consider bonding your employees. The mere knowledge that your staff is bonded will scare away most applicants with a history of dishonesty, and you will be assured of some measure of recovery should the above safeguards fail.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
As the economy continues to founder, fraud and economic crime are on the rise, according to many law enforcement officials around the country.
Tight money increases embezzlement temptations, so this is an excellent time to review your bookkeeping procedures and remove any obvious opportunities for theft by your employees.
People who investigate embezzlement crimes for a living say that most cases are uncovered by accident. Finding it is usually relatively easy, because most embezzlers are not particularly skillful nor very good at covering their tracks, but many cases go undetected, sometimes for years, because no one is looking.
The experience of a friend of mine was all too typical: His bookkeeper wrote sizable checks to herself, entering them in the ledger as payments to vendors commonly used by his practice. Since she also balanced the checkbook, she got away with it for many months.
Detecting fraud is an inexact science. There is no textbook approach that one can follow, but a few simple measures will uncover or prevent a large percentage of dishonest behavior:
Hire honest employees. It is amazing how few doctors check applicants' references. Find out if the applicants are really as good as they look on paper. For a few dollars, you can screen prospective employees on public information Web sites to see if they have criminal records or if they have been sued or are suing others.
Minimize opportunities for dishonesty. Theft and embezzlement are the products of motivation and opportunity. It is hard to control motivation, but there ways to minimize opportunities for dishonesty. No one person should be in charge of the entire bookkeeping process. The person who enters charges should be different from the one who enters payments. The employee who writes the checks should not balance the checkbook, and so on. Internal audits should be done on a regular basis, and all employees should know that.
Reconcile receipts and cash daily. The most common form of embezzlement is simply taking cash out of the till. In a typical scenario, a patient pays a $15 copay in cash but the receptionist records the payment as $5 and pockets the rest. Make sure a receipt is generated, and that someone other than the person accepting cash reconciles the receipts and the cash daily.
Insist on separate accounting duties. Another common scam is false invoices: You think you are paying for supplies and services, but the money is going to an employee. One employee should enter invoices into the system, another should issue the check, and a third should match invoices to goods and services received.
Verify expense reports. False expense reports are another common form of fraud. When an employee asks for reimbursement of expenses, make sure they are real.
Safeguard your computer. Computers have made embezzlement easier and more tempting. Data are usually concentrated in one place, accounts can be accessed from remote workstations or off-premises servers, and a paper trail is often eliminated. Your computer vendor should be aware of this, and should have safeguards built into your system.
Look for red flags. Do you have an employee who refuses to take vacations, because someone else will have to look at the books? Does someone insist on approving or entering expenses that are another employee's responsibility?
Consider bonding your employees. The mere knowledge that your staff is bonded will scare away most applicants with a history of dishonesty, and you will be assured of some measure of recovery should the above safeguards fail.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
As the economy continues to founder, fraud and economic crime are on the rise, according to many law enforcement officials around the country.
Tight money increases embezzlement temptations, so this is an excellent time to review your bookkeeping procedures and remove any obvious opportunities for theft by your employees.
People who investigate embezzlement crimes for a living say that most cases are uncovered by accident. Finding it is usually relatively easy, because most embezzlers are not particularly skillful nor very good at covering their tracks, but many cases go undetected, sometimes for years, because no one is looking.
The experience of a friend of mine was all too typical: His bookkeeper wrote sizable checks to herself, entering them in the ledger as payments to vendors commonly used by his practice. Since she also balanced the checkbook, she got away with it for many months.
Detecting fraud is an inexact science. There is no textbook approach that one can follow, but a few simple measures will uncover or prevent a large percentage of dishonest behavior:
Hire honest employees. It is amazing how few doctors check applicants' references. Find out if the applicants are really as good as they look on paper. For a few dollars, you can screen prospective employees on public information Web sites to see if they have criminal records or if they have been sued or are suing others.
Minimize opportunities for dishonesty. Theft and embezzlement are the products of motivation and opportunity. It is hard to control motivation, but there ways to minimize opportunities for dishonesty. No one person should be in charge of the entire bookkeeping process. The person who enters charges should be different from the one who enters payments. The employee who writes the checks should not balance the checkbook, and so on. Internal audits should be done on a regular basis, and all employees should know that.
Reconcile receipts and cash daily. The most common form of embezzlement is simply taking cash out of the till. In a typical scenario, a patient pays a $15 copay in cash but the receptionist records the payment as $5 and pockets the rest. Make sure a receipt is generated, and that someone other than the person accepting cash reconciles the receipts and the cash daily.
Insist on separate accounting duties. Another common scam is false invoices: You think you are paying for supplies and services, but the money is going to an employee. One employee should enter invoices into the system, another should issue the check, and a third should match invoices to goods and services received.
Verify expense reports. False expense reports are another common form of fraud. When an employee asks for reimbursement of expenses, make sure they are real.
Safeguard your computer. Computers have made embezzlement easier and more tempting. Data are usually concentrated in one place, accounts can be accessed from remote workstations or off-premises servers, and a paper trail is often eliminated. Your computer vendor should be aware of this, and should have safeguards built into your system.
Look for red flags. Do you have an employee who refuses to take vacations, because someone else will have to look at the books? Does someone insist on approving or entering expenses that are another employee's responsibility?
Consider bonding your employees. The mere knowledge that your staff is bonded will scare away most applicants with a history of dishonesty, and you will be assured of some measure of recovery should the above safeguards fail.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com