User login
No EMR? Try the Bird in Hand
Even if you have yet to invest in an electronic medical records system, chances are that you already have some powerful tools at your disposal to make a difference in chronic disease management.
I'm referring to your practice management billing system. Most of these systems come with the option of having a scheduling component that is often built in for free. A few years ago, my family practice colleagues and I decided to make a concerted effort to institute a reminder system for patients with chronic conditions such as diabetes, asthma and chronic obstructive pulmonary disease, and hypertension. We wanted to make sure these patients came in for visits at regular recommended intervals instead of falling through the cracks.
Although we've had an electronic medical records (EMR) system since 1991, it didn't provide an efficient means to identify a list of target patients who missed visits or who were behind on disease management or prevention.
Many EMRs weren't and still are not set up to do disease management, although they desperately need to be. By comparison, our billing/scheduling system (www.athenahealth.com
Once that was in place, we started calling diabetes patients who hadn't been seen in 4 or more months to get them in for regular visits. During the visit, the EMR worked well to track patient details such as foot exams and fasting glucose checks, but the job of getting the patient to our office in the first place proved to be efficiently managed by our billing/scheduling system.
The return was impressive. Patients were called twice and then a letter was sent in the mail. For every dollar spent on this reminder system, five dollars were returned in the form of collected income for our practice.
In addition to using the system for patients with chronic conditions, we used it to remind healthy individuals to come in for their annual physical exams during the typically slow summer months. Parents were prompted to bring children in for well-child care and overdue immunizations. In the fall, others were reminded of their need to schedule an appointment for a flu shot.
If you cannot hire staff to help call patients, try paying your existing staff overtime to see how this works. If you can hire someone, it works well to bring aboard a part-time employee. Someone who is between college and medical school may be looking for research opportunities. Their remaining hours can be spent as a medical assistant.
Practices of at least five to eight physicians are ideal for this kind of effort because they have the infrastructure to support it, but a practice of any size can do this work, which improves quality as it generates income. Once a week, a physician leader needs to review the data to address any kinks in the process.
As primary care providers, we have more responsibility than ever in helping our patients manage their chronic diseases. We all have to institute ways to track these patients if we are going to decrease the prevalence of chronic diseases and the cost of care.
Even if you have yet to invest in an electronic medical records system, chances are that you already have some powerful tools at your disposal to make a difference in chronic disease management.
I'm referring to your practice management billing system. Most of these systems come with the option of having a scheduling component that is often built in for free. A few years ago, my family practice colleagues and I decided to make a concerted effort to institute a reminder system for patients with chronic conditions such as diabetes, asthma and chronic obstructive pulmonary disease, and hypertension. We wanted to make sure these patients came in for visits at regular recommended intervals instead of falling through the cracks.
Although we've had an electronic medical records (EMR) system since 1991, it didn't provide an efficient means to identify a list of target patients who missed visits or who were behind on disease management or prevention.
Many EMRs weren't and still are not set up to do disease management, although they desperately need to be. By comparison, our billing/scheduling system (www.athenahealth.com
Once that was in place, we started calling diabetes patients who hadn't been seen in 4 or more months to get them in for regular visits. During the visit, the EMR worked well to track patient details such as foot exams and fasting glucose checks, but the job of getting the patient to our office in the first place proved to be efficiently managed by our billing/scheduling system.
The return was impressive. Patients were called twice and then a letter was sent in the mail. For every dollar spent on this reminder system, five dollars were returned in the form of collected income for our practice.
In addition to using the system for patients with chronic conditions, we used it to remind healthy individuals to come in for their annual physical exams during the typically slow summer months. Parents were prompted to bring children in for well-child care and overdue immunizations. In the fall, others were reminded of their need to schedule an appointment for a flu shot.
If you cannot hire staff to help call patients, try paying your existing staff overtime to see how this works. If you can hire someone, it works well to bring aboard a part-time employee. Someone who is between college and medical school may be looking for research opportunities. Their remaining hours can be spent as a medical assistant.
Practices of at least five to eight physicians are ideal for this kind of effort because they have the infrastructure to support it, but a practice of any size can do this work, which improves quality as it generates income. Once a week, a physician leader needs to review the data to address any kinks in the process.
As primary care providers, we have more responsibility than ever in helping our patients manage their chronic diseases. We all have to institute ways to track these patients if we are going to decrease the prevalence of chronic diseases and the cost of care.
Even if you have yet to invest in an electronic medical records system, chances are that you already have some powerful tools at your disposal to make a difference in chronic disease management.
I'm referring to your practice management billing system. Most of these systems come with the option of having a scheduling component that is often built in for free. A few years ago, my family practice colleagues and I decided to make a concerted effort to institute a reminder system for patients with chronic conditions such as diabetes, asthma and chronic obstructive pulmonary disease, and hypertension. We wanted to make sure these patients came in for visits at regular recommended intervals instead of falling through the cracks.
Although we've had an electronic medical records (EMR) system since 1991, it didn't provide an efficient means to identify a list of target patients who missed visits or who were behind on disease management or prevention.
Many EMRs weren't and still are not set up to do disease management, although they desperately need to be. By comparison, our billing/scheduling system (www.athenahealth.com
Once that was in place, we started calling diabetes patients who hadn't been seen in 4 or more months to get them in for regular visits. During the visit, the EMR worked well to track patient details such as foot exams and fasting glucose checks, but the job of getting the patient to our office in the first place proved to be efficiently managed by our billing/scheduling system.
The return was impressive. Patients were called twice and then a letter was sent in the mail. For every dollar spent on this reminder system, five dollars were returned in the form of collected income for our practice.
In addition to using the system for patients with chronic conditions, we used it to remind healthy individuals to come in for their annual physical exams during the typically slow summer months. Parents were prompted to bring children in for well-child care and overdue immunizations. In the fall, others were reminded of their need to schedule an appointment for a flu shot.
If you cannot hire staff to help call patients, try paying your existing staff overtime to see how this works. If you can hire someone, it works well to bring aboard a part-time employee. Someone who is between college and medical school may be looking for research opportunities. Their remaining hours can be spent as a medical assistant.
Practices of at least five to eight physicians are ideal for this kind of effort because they have the infrastructure to support it, but a practice of any size can do this work, which improves quality as it generates income. Once a week, a physician leader needs to review the data to address any kinks in the process.
As primary care providers, we have more responsibility than ever in helping our patients manage their chronic diseases. We all have to institute ways to track these patients if we are going to decrease the prevalence of chronic diseases and the cost of care.
Eagle-Eye Your Payors
Protection of the Medicare program has reached new heights in recent years. One of the most important ways hospitalist groups can protect their Medicare funding is the discovery and recovery of improper contractor payments of Medicare claims.
The Centers for Medicare and Medicaid Services (CMS) reviews various types of contractors—Medicare administrative contractors (MACs), carriers, durable medical equipment regional carriers (DMERCs), fiscal intermediaries (FIs), and quality improvement organizations (QIOs)—through its protection efforts as part of the Comprehensive Error Rate Testing (CERT) program and Hospital Payment Monitoring Program (HPMP). The CERT program’s contractors review physician (i.e., professional) claims processed by MACs and carriers.
The primary goal of a contractor is to “pay it right”—that is, pay the correct amount to the right provider for covered and correctly coded services.1 During the 12-month reporting period ending Sept. 30, 2007, the CERT program sampled 129,875 claims from carriers, DMERCs, FIs, and MACs.
The CERT contractor randomly and electronically selects about 172 claims each month from each type of claims-processing contractor. Since some of these contractors were transitioning to MACs, the target Part B (i.e., professional) sample size for the May 2008 report was approximately 2,000 reviewable claims per MAC cluster. However, this might have varied if a MAC was not processing claims during the entire sampling period.
Document Requests
Physicians need to be mindful of CERT requests for documentation. When possible, every attempt is made to benefit the physician. Initial CERT requests are attempted by way of a letter. If the physician does not respond within 30 days, the CERT contractor attempts one to three more contacts with correspondence and phone calls. If documentation is received after 75 days, it is considered “late.” It then will be reviewed, unless the reporting period has expired.
However, this should not be considered a prudent approach, and timely responses are ideal. If the physician offers no response, and documentation is not received, it is counted as a “no documentation” error.
Physicians often worry about accusations of fraud. The purpose of the CERT program is not to assume or accuse physicians of fraud, although it may serve as a deterrent. It does not, and cannot, label a claim fraudulent.
One scenario of potential fraud the CERT program is able to identify occurs when a CERT documentation contractor is unable to locate a provider or supplier when requesting medical record documentation.2
Outcomes
Individual contractors are notified of improper payments. These include overpayments and underpayments. Unfortunately, contractors do not have to resolve CERT issues involving underpayments, although they are encouraged to do so by CMS.
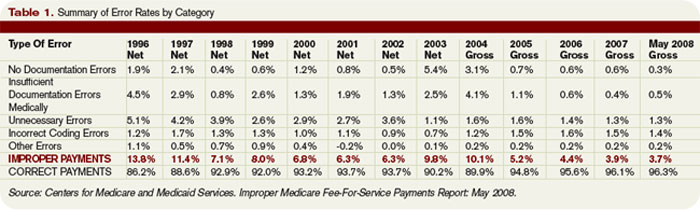
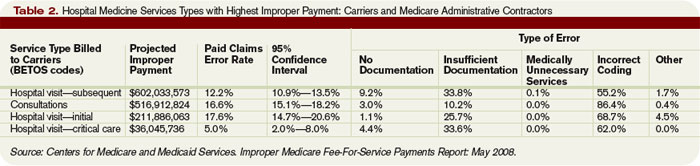
The CERT program identified overpayments totaling $875,005 during the 12-month reporting period, but collected only $650,418 in overpayments after consideration of appeals that overturned a CERT decision or the provider discontinued business operations. (See Table 1, p. 18, for error rates and Table 2, p. 18, for highest rates of improper payment)
To improve billing compliance and prevent repetitive errors, contractors must implement provider education regarding erroneously paid claims. A contractor may determine the best education method to distribute information about Medicare rules and effectively answer coverage and coding questions.
Some contractors have designed Web-based training modules, Web pages with frequently-asked-questions sections, or local coverage analyses to address contractor-specific errors. Detailed CERT contractor information can be found at www.cms.hhs.gov/ mcd/indexes.asp?from2=indexes.asp&
Due to its successful outcomes, future CMS goals include the continuation of the CERT program. MACs will look more closely at service types based on identified error rates.
Apart from CERT requests, prepayment contractor reviews already exist for most of the services included in Table 2 (p. 18). Timely response is crucial to justify and receive appropriate reimbursement. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Improper Medicare fee-for-service payments report: May 2008. CMS Web site. Available at: www.cms.hhs.gov/apps/er_report/preview_er_report.asp?from=public&which=long&reportID=9. Accessed Dec. 20, 2008.
2. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association; 2008.
Protection of the Medicare program has reached new heights in recent years. One of the most important ways hospitalist groups can protect their Medicare funding is the discovery and recovery of improper contractor payments of Medicare claims.
The Centers for Medicare and Medicaid Services (CMS) reviews various types of contractors—Medicare administrative contractors (MACs), carriers, durable medical equipment regional carriers (DMERCs), fiscal intermediaries (FIs), and quality improvement organizations (QIOs)—through its protection efforts as part of the Comprehensive Error Rate Testing (CERT) program and Hospital Payment Monitoring Program (HPMP). The CERT program’s contractors review physician (i.e., professional) claims processed by MACs and carriers.
The primary goal of a contractor is to “pay it right”—that is, pay the correct amount to the right provider for covered and correctly coded services.1 During the 12-month reporting period ending Sept. 30, 2007, the CERT program sampled 129,875 claims from carriers, DMERCs, FIs, and MACs.
The CERT contractor randomly and electronically selects about 172 claims each month from each type of claims-processing contractor. Since some of these contractors were transitioning to MACs, the target Part B (i.e., professional) sample size for the May 2008 report was approximately 2,000 reviewable claims per MAC cluster. However, this might have varied if a MAC was not processing claims during the entire sampling period.
Document Requests
Physicians need to be mindful of CERT requests for documentation. When possible, every attempt is made to benefit the physician. Initial CERT requests are attempted by way of a letter. If the physician does not respond within 30 days, the CERT contractor attempts one to three more contacts with correspondence and phone calls. If documentation is received after 75 days, it is considered “late.” It then will be reviewed, unless the reporting period has expired.
However, this should not be considered a prudent approach, and timely responses are ideal. If the physician offers no response, and documentation is not received, it is counted as a “no documentation” error.
Physicians often worry about accusations of fraud. The purpose of the CERT program is not to assume or accuse physicians of fraud, although it may serve as a deterrent. It does not, and cannot, label a claim fraudulent.
One scenario of potential fraud the CERT program is able to identify occurs when a CERT documentation contractor is unable to locate a provider or supplier when requesting medical record documentation.2
Outcomes
Individual contractors are notified of improper payments. These include overpayments and underpayments. Unfortunately, contractors do not have to resolve CERT issues involving underpayments, although they are encouraged to do so by CMS.
The CERT program identified overpayments totaling $875,005 during the 12-month reporting period, but collected only $650,418 in overpayments after consideration of appeals that overturned a CERT decision or the provider discontinued business operations. (See Table 1, p. 18, for error rates and Table 2, p. 18, for highest rates of improper payment)
To improve billing compliance and prevent repetitive errors, contractors must implement provider education regarding erroneously paid claims. A contractor may determine the best education method to distribute information about Medicare rules and effectively answer coverage and coding questions.
Some contractors have designed Web-based training modules, Web pages with frequently-asked-questions sections, or local coverage analyses to address contractor-specific errors. Detailed CERT contractor information can be found at www.cms.hhs.gov/ mcd/indexes.asp?from2=indexes.asp&
Due to its successful outcomes, future CMS goals include the continuation of the CERT program. MACs will look more closely at service types based on identified error rates.
Apart from CERT requests, prepayment contractor reviews already exist for most of the services included in Table 2 (p. 18). Timely response is crucial to justify and receive appropriate reimbursement. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Improper Medicare fee-for-service payments report: May 2008. CMS Web site. Available at: www.cms.hhs.gov/apps/er_report/preview_er_report.asp?from=public&which=long&reportID=9. Accessed Dec. 20, 2008.
2. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association; 2008.
Protection of the Medicare program has reached new heights in recent years. One of the most important ways hospitalist groups can protect their Medicare funding is the discovery and recovery of improper contractor payments of Medicare claims.
The Centers for Medicare and Medicaid Services (CMS) reviews various types of contractors—Medicare administrative contractors (MACs), carriers, durable medical equipment regional carriers (DMERCs), fiscal intermediaries (FIs), and quality improvement organizations (QIOs)—through its protection efforts as part of the Comprehensive Error Rate Testing (CERT) program and Hospital Payment Monitoring Program (HPMP). The CERT program’s contractors review physician (i.e., professional) claims processed by MACs and carriers.
The primary goal of a contractor is to “pay it right”—that is, pay the correct amount to the right provider for covered and correctly coded services.1 During the 12-month reporting period ending Sept. 30, 2007, the CERT program sampled 129,875 claims from carriers, DMERCs, FIs, and MACs.
The CERT contractor randomly and electronically selects about 172 claims each month from each type of claims-processing contractor. Since some of these contractors were transitioning to MACs, the target Part B (i.e., professional) sample size for the May 2008 report was approximately 2,000 reviewable claims per MAC cluster. However, this might have varied if a MAC was not processing claims during the entire sampling period.
Document Requests
Physicians need to be mindful of CERT requests for documentation. When possible, every attempt is made to benefit the physician. Initial CERT requests are attempted by way of a letter. If the physician does not respond within 30 days, the CERT contractor attempts one to three more contacts with correspondence and phone calls. If documentation is received after 75 days, it is considered “late.” It then will be reviewed, unless the reporting period has expired.
However, this should not be considered a prudent approach, and timely responses are ideal. If the physician offers no response, and documentation is not received, it is counted as a “no documentation” error.
Physicians often worry about accusations of fraud. The purpose of the CERT program is not to assume or accuse physicians of fraud, although it may serve as a deterrent. It does not, and cannot, label a claim fraudulent.
One scenario of potential fraud the CERT program is able to identify occurs when a CERT documentation contractor is unable to locate a provider or supplier when requesting medical record documentation.2
Outcomes
Individual contractors are notified of improper payments. These include overpayments and underpayments. Unfortunately, contractors do not have to resolve CERT issues involving underpayments, although they are encouraged to do so by CMS.
The CERT program identified overpayments totaling $875,005 during the 12-month reporting period, but collected only $650,418 in overpayments after consideration of appeals that overturned a CERT decision or the provider discontinued business operations. (See Table 1, p. 18, for error rates and Table 2, p. 18, for highest rates of improper payment)
To improve billing compliance and prevent repetitive errors, contractors must implement provider education regarding erroneously paid claims. A contractor may determine the best education method to distribute information about Medicare rules and effectively answer coverage and coding questions.
Some contractors have designed Web-based training modules, Web pages with frequently-asked-questions sections, or local coverage analyses to address contractor-specific errors. Detailed CERT contractor information can be found at www.cms.hhs.gov/ mcd/indexes.asp?from2=indexes.asp&
Due to its successful outcomes, future CMS goals include the continuation of the CERT program. MACs will look more closely at service types based on identified error rates.
Apart from CERT requests, prepayment contractor reviews already exist for most of the services included in Table 2 (p. 18). Timely response is crucial to justify and receive appropriate reimbursement. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Centers for Medicare and Medicaid Services. Improper Medicare fee-for-service payments report: May 2008. CMS Web site. Available at: www.cms.hhs.gov/apps/er_report/preview_er_report.asp?from=public&which=long&reportID=9. Accessed Dec. 20, 2008.
2. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago: American Medical Association; 2008.
Why off-label isn’t off base
This article is adapted from the February 2009 issue of Current Psychiatry, a Quadrant HealthCom Inc. publication.
The author reports no financial relationships relevant to this article.
CASE
A physician speaking with a colleague expressed his anxiety and uncertainty over off-label prescribing:
“When I was a resident, attending physicians occasionally cited journal articles in their consultation notes to substantiate their treatment choices. Since then, I’ve done this at times when I’ve prescribed a drug off label.
“Recently, I mentioned this practice to a physician who is trained as a lawyer. He thought citing articles in a patient’s chart was a bad idea, because by doing so I was automatically making the referred-to article the ‘expert witness.’ If a lawsuit occurred, I might be called upon to justify the article’s validity, statistical details, methodology, etc. My intent is to show that I have a detailed, well-thought-out justification for my treatment choice.
“Am I placing myself at greater risk of incurring liability should a lawsuit occur?”
This physician wants to know how he can minimize malpractice risk when prescribing a medication off label. He wonders if citing an article in a patient’s chart is a good—or bad—idea.
In law school, attorneys-in-training learn to answer very general legal questions with “It depends.” There’s little certainty about how to avoid successful malpractice litigation because few, if any, strategies have been tested systematically. However, this article will explain and, I hope, help you avoid the medicolegal pitfalls of off-label prescribing.
Limited testing for safety and effectiveness. Experiences such as the fen-phen (weight loss) controversy1 and estrogens for preventing vascular disease in postmenopausal women2 remind physicians that some untested treatments may do more harm than good.
Commercial influence. Pharmaceutical companies have used advisory boards, consultant meetings, and continuing medical education events to promote unproven off-label indications for drugs.3,4 Many studies that were, ostensibly, designed and proposed by researchers show evidence of so-called ghost authorship by commercial concerns.5
Study bias. Even peer-reviewed, double-blind studies that are published in the medical literature might not sufficiently support off-label prescribing practices because sponsors of such studies can structure them or use statistical analyses to make results look favorable. Former editors of the British Medical Journal and The Lancet have acknowledged that their publications unwittingly served as “an extension of the marketing arm” or “laundering operations” for drug manufacturers.6,7 Even for FDA-approved indications, a selective, positive-result publication bias and nonreporting of negative results may make drugs seem more effective than the full range of studies would justify.8
Legal use of labeling. Although off-label prescribing is accepted medical practice, doctors “may be found negligent if their decision to use a drug off label is sufficiently careless, imprudent, or unprofessional.”9 During a malpractice lawsuit, plaintiff’s counsel could try to use FDA-approved labeling or prescribing information to establish a presumptive standard of care. Such evidence usually is admissible if it is supported by expert testimony. The burden of proof is then placed on the defendant physician to show how an off-label use met the standard of care.10
References
1. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
2. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
3. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.-
4. Steinman MA, Bero L, Chren M, Landefeld CS. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
5. Gøtzsche PC, Hróbjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.-
6. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.-
7. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
8. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
9. Richardson v Miller. 44 SW3d 1 (Tenn Ct App 2000).
10. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
Off-label: Accepted and necessary
Off-label prescribing occurs when a physician prescribes a medication or uses a medical device outside the scope of FDA-approved labeling. Most commonly, off-label use involves prescribing a medication for something other than its FDA-approved indication. An example is sildenafil [Viagra] for women who have antidepressant-induced sexual dysfunction.1
Other examples are prescribing a drug:
- at an unapproved dose
- in an unapproved format (e.g., mixing capsule contents with applesauce)
- outside the approved age group
- for longer than the approved interval
- at a different dose schedule (e.g., qhs instead of bid or tid).
Typically, it takes years for a new drug to gain FDA approval and additional time for an already-approved drug to gain approval for a new indication. In the meantime, clinicians treat their patients with available drugs prescribed off label.
Off-label prescribing is legal. FDA approval means drugs may be sold and marketed in specific ways. But the FDA does not tell physicians how they can use approved drugs. As each edition of the Physicians’ Desk Reference explains, “Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling.”2 Federal statutes state that FDA approval does not “limit or interfere with the authority of a health care practitioner to prescribe” approved drugs or devices “for any condition or disease.”3
- Know why an article applies to your patient. If you are sued for malpractice, you can use an article to support your treatment choice by explaining how this information contributed to your decision-making.
- Tell your patient that the proposed treatment is an off-label use when you obtain consent, even though case law says you don’t have to do this. Telling your patient helps him understand your reasoning and prevents surprises that may give offense.
- Engage in ongoing informed consent. Uncertainty is part of medical practice and is heightened when physicians prescribe off label. Ongoing discussions help patients understand, accept, and share that uncertainty.
- Document informed consent. This will show—if it becomes necessary—that you and your patient made collaborative, conscientious decisions about treatment.1
Reference
1. Royal College of Psychiatrists. CR142. Use of unlicensed medicine for unlicensed applications in psychiatric practice. Available at: http://www.rcpsych.ac.uk/publications/collegereports/cr/cr142.aspx. Accessed March 4, 2009.
Does off-label constitute malpractice?
Off-label use is not only legal—it’s often wise medical practice. Many drug uses that now have FDA approval were off label just a few years ago. Examples include using selective serotonin reuptake inhibitors (SSRIs) to treat panic disorder and obsessive–compulsive disorder. Fluoxetine is the only FDA-approved drug for treating depression in adolescents, but other SSRIs may also have a favorable risk–benefit profile.6
The practice is common—we know that
Numerous studies have shown that off-label prescribing is common in, for example, psychiatry7 and other specialties.8,9 Because the practice is so common, the mere fact that a drug is not FDA-approved for a particular use does not imply that the drug was prescribed negligently.
Some commentators have suggested that off-label prescribing amounts to human experimentation.10 Without FDA approval, they say, physicians lack hard evidence, so to speak, that a product is safe and effective—making off-label prescribing a small-scale clinical trial based on the doctor’s educated guesses.
If this reasoning is correct, off-label prescribing would require the same human subject protections used in research, including institutional review board approval and special consent forms.
Although this argument sounds plausible, off-label prescribing is not experimentation or research (see “4 reasons why off-label prescribing can be controversial”).4,11-19 Researchers investigate hypotheses to obtain generalizable knowledge, whereas medical therapy aims to benefit individual patients. This experimentation–therapy distinction is not perfect because successful off-label treatment of one patient might imply beneficial effects for others.10 When courts have looked at this matter, though, they have found that “off-label use… by a physician seeking an optimal treatment for his or her patient is not necessarily…research or an investigational or experimental treatment when the use is customarily followed by physicians.”4
Courts also have said that off-label use does not require special informed consent. Just because a drug is prescribed off label doesn’t mean it’s risky. FDA approval “is not a material risk inherently involved in a proposed therapy which a physician should have disclosed to a patient prior to the therapy.”20 In other words, a physician is not required to discuss FDA regulatory status—such as off-label uses of a medication—to comply with standards of informed consent. FDA regulatory status has nothing to do with the risks or benefits of a medication and it does not provide information about treatment alternatives.21
What should you do?
For advice on protecting yourself when you prescribe off label, see the box above.
In addition, you should keep abreast of news and scientific evidence concerning drug uses, effects, interactions, and adverse effects, especially when prescribing for uses that are different from the manufacturer’s intended purposes.22
Last, collect articles on off-label uses, but keep them separate from your patients’ files. Good attorneys are highly skilled at using documents to score legal points, and opposing counsel will prepare questions to focus on the articles’ faults or limitations in isolation.
1. Nurnberg HG, Hensley PL, Heiman JR, et al. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300:395-404.
2. Physicians’ Desk Reference. 62nd ed. Montvale, NJ: Thomson Healthcare, Inc.; 2007.
3. Food, Drug and Cosmetic Act, 21USC §396
4. Richardson v Miller. 44 SW3d 1 (Tenn Ct App 2000).
5. Buckman Co. v Plaintiffs’ Legal Comm., 531 US 341 (2001).
6. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683-1696.
7. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Adv Psychiatr Treat. 2007;13:414-422.
8. Conroy S, Choonara I, Impicciatore P, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. European Network for Drug Investigation in Children. BMJ. 2000;320:79-82.
9. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166:1021-1026.
10. Mehlman MJ. Off-label prescribing. Available at: http://www.thedoctorwillseeyounow.com/articles/bioethics/offlabel_11. Accessed October 21, 2008.
11. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
12. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
13. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.-
14. Steinman MA, Bero L, Chren M, Landefeld CS. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
15. Gøtzsche PC, Hróbjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.-
16. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.-
17. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
18. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
19. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
20. Klein v Biscup. 673 NE2d 225 (Ohio App 1996).
21. Beck JM, Azari ED. FDA, off-label use, and informed consent: debunking myths and misconceptions. Food Drug Law J. 1998;53:71-104.
22. Shajnfeld A, Krueger RB. Reforming (purportedly) non-punitive responses to sexual offending. Dev Mental Health Law. 2006;25:81-99.
This article is adapted from the February 2009 issue of Current Psychiatry, a Quadrant HealthCom Inc. publication.
The author reports no financial relationships relevant to this article.
CASE
A physician speaking with a colleague expressed his anxiety and uncertainty over off-label prescribing:
“When I was a resident, attending physicians occasionally cited journal articles in their consultation notes to substantiate their treatment choices. Since then, I’ve done this at times when I’ve prescribed a drug off label.
“Recently, I mentioned this practice to a physician who is trained as a lawyer. He thought citing articles in a patient’s chart was a bad idea, because by doing so I was automatically making the referred-to article the ‘expert witness.’ If a lawsuit occurred, I might be called upon to justify the article’s validity, statistical details, methodology, etc. My intent is to show that I have a detailed, well-thought-out justification for my treatment choice.
“Am I placing myself at greater risk of incurring liability should a lawsuit occur?”
This physician wants to know how he can minimize malpractice risk when prescribing a medication off label. He wonders if citing an article in a patient’s chart is a good—or bad—idea.
In law school, attorneys-in-training learn to answer very general legal questions with “It depends.” There’s little certainty about how to avoid successful malpractice litigation because few, if any, strategies have been tested systematically. However, this article will explain and, I hope, help you avoid the medicolegal pitfalls of off-label prescribing.
Limited testing for safety and effectiveness. Experiences such as the fen-phen (weight loss) controversy1 and estrogens for preventing vascular disease in postmenopausal women2 remind physicians that some untested treatments may do more harm than good.
Commercial influence. Pharmaceutical companies have used advisory boards, consultant meetings, and continuing medical education events to promote unproven off-label indications for drugs.3,4 Many studies that were, ostensibly, designed and proposed by researchers show evidence of so-called ghost authorship by commercial concerns.5
Study bias. Even peer-reviewed, double-blind studies that are published in the medical literature might not sufficiently support off-label prescribing practices because sponsors of such studies can structure them or use statistical analyses to make results look favorable. Former editors of the British Medical Journal and The Lancet have acknowledged that their publications unwittingly served as “an extension of the marketing arm” or “laundering operations” for drug manufacturers.6,7 Even for FDA-approved indications, a selective, positive-result publication bias and nonreporting of negative results may make drugs seem more effective than the full range of studies would justify.8
Legal use of labeling. Although off-label prescribing is accepted medical practice, doctors “may be found negligent if their decision to use a drug off label is sufficiently careless, imprudent, or unprofessional.”9 During a malpractice lawsuit, plaintiff’s counsel could try to use FDA-approved labeling or prescribing information to establish a presumptive standard of care. Such evidence usually is admissible if it is supported by expert testimony. The burden of proof is then placed on the defendant physician to show how an off-label use met the standard of care.10
References
1. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
2. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
3. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.-
4. Steinman MA, Bero L, Chren M, Landefeld CS. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
5. Gøtzsche PC, Hróbjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.-
6. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.-
7. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
8. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
9. Richardson v Miller. 44 SW3d 1 (Tenn Ct App 2000).
10. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
Off-label: Accepted and necessary
Off-label prescribing occurs when a physician prescribes a medication or uses a medical device outside the scope of FDA-approved labeling. Most commonly, off-label use involves prescribing a medication for something other than its FDA-approved indication. An example is sildenafil [Viagra] for women who have antidepressant-induced sexual dysfunction.1
Other examples are prescribing a drug:
- at an unapproved dose
- in an unapproved format (e.g., mixing capsule contents with applesauce)
- outside the approved age group
- for longer than the approved interval
- at a different dose schedule (e.g., qhs instead of bid or tid).
Typically, it takes years for a new drug to gain FDA approval and additional time for an already-approved drug to gain approval for a new indication. In the meantime, clinicians treat their patients with available drugs prescribed off label.
Off-label prescribing is legal. FDA approval means drugs may be sold and marketed in specific ways. But the FDA does not tell physicians how they can use approved drugs. As each edition of the Physicians’ Desk Reference explains, “Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling.”2 Federal statutes state that FDA approval does not “limit or interfere with the authority of a health care practitioner to prescribe” approved drugs or devices “for any condition or disease.”3
- Know why an article applies to your patient. If you are sued for malpractice, you can use an article to support your treatment choice by explaining how this information contributed to your decision-making.
- Tell your patient that the proposed treatment is an off-label use when you obtain consent, even though case law says you don’t have to do this. Telling your patient helps him understand your reasoning and prevents surprises that may give offense.
- Engage in ongoing informed consent. Uncertainty is part of medical practice and is heightened when physicians prescribe off label. Ongoing discussions help patients understand, accept, and share that uncertainty.
- Document informed consent. This will show—if it becomes necessary—that you and your patient made collaborative, conscientious decisions about treatment.1
Reference
1. Royal College of Psychiatrists. CR142. Use of unlicensed medicine for unlicensed applications in psychiatric practice. Available at: http://www.rcpsych.ac.uk/publications/collegereports/cr/cr142.aspx. Accessed March 4, 2009.
Does off-label constitute malpractice?
Off-label use is not only legal—it’s often wise medical practice. Many drug uses that now have FDA approval were off label just a few years ago. Examples include using selective serotonin reuptake inhibitors (SSRIs) to treat panic disorder and obsessive–compulsive disorder. Fluoxetine is the only FDA-approved drug for treating depression in adolescents, but other SSRIs may also have a favorable risk–benefit profile.6
The practice is common—we know that
Numerous studies have shown that off-label prescribing is common in, for example, psychiatry7 and other specialties.8,9 Because the practice is so common, the mere fact that a drug is not FDA-approved for a particular use does not imply that the drug was prescribed negligently.
Some commentators have suggested that off-label prescribing amounts to human experimentation.10 Without FDA approval, they say, physicians lack hard evidence, so to speak, that a product is safe and effective—making off-label prescribing a small-scale clinical trial based on the doctor’s educated guesses.
If this reasoning is correct, off-label prescribing would require the same human subject protections used in research, including institutional review board approval and special consent forms.
Although this argument sounds plausible, off-label prescribing is not experimentation or research (see “4 reasons why off-label prescribing can be controversial”).4,11-19 Researchers investigate hypotheses to obtain generalizable knowledge, whereas medical therapy aims to benefit individual patients. This experimentation–therapy distinction is not perfect because successful off-label treatment of one patient might imply beneficial effects for others.10 When courts have looked at this matter, though, they have found that “off-label use… by a physician seeking an optimal treatment for his or her patient is not necessarily…research or an investigational or experimental treatment when the use is customarily followed by physicians.”4
Courts also have said that off-label use does not require special informed consent. Just because a drug is prescribed off label doesn’t mean it’s risky. FDA approval “is not a material risk inherently involved in a proposed therapy which a physician should have disclosed to a patient prior to the therapy.”20 In other words, a physician is not required to discuss FDA regulatory status—such as off-label uses of a medication—to comply with standards of informed consent. FDA regulatory status has nothing to do with the risks or benefits of a medication and it does not provide information about treatment alternatives.21
What should you do?
For advice on protecting yourself when you prescribe off label, see the box above.
In addition, you should keep abreast of news and scientific evidence concerning drug uses, effects, interactions, and adverse effects, especially when prescribing for uses that are different from the manufacturer’s intended purposes.22
Last, collect articles on off-label uses, but keep them separate from your patients’ files. Good attorneys are highly skilled at using documents to score legal points, and opposing counsel will prepare questions to focus on the articles’ faults or limitations in isolation.
This article is adapted from the February 2009 issue of Current Psychiatry, a Quadrant HealthCom Inc. publication.
The author reports no financial relationships relevant to this article.
CASE
A physician speaking with a colleague expressed his anxiety and uncertainty over off-label prescribing:
“When I was a resident, attending physicians occasionally cited journal articles in their consultation notes to substantiate their treatment choices. Since then, I’ve done this at times when I’ve prescribed a drug off label.
“Recently, I mentioned this practice to a physician who is trained as a lawyer. He thought citing articles in a patient’s chart was a bad idea, because by doing so I was automatically making the referred-to article the ‘expert witness.’ If a lawsuit occurred, I might be called upon to justify the article’s validity, statistical details, methodology, etc. My intent is to show that I have a detailed, well-thought-out justification for my treatment choice.
“Am I placing myself at greater risk of incurring liability should a lawsuit occur?”
This physician wants to know how he can minimize malpractice risk when prescribing a medication off label. He wonders if citing an article in a patient’s chart is a good—or bad—idea.
In law school, attorneys-in-training learn to answer very general legal questions with “It depends.” There’s little certainty about how to avoid successful malpractice litigation because few, if any, strategies have been tested systematically. However, this article will explain and, I hope, help you avoid the medicolegal pitfalls of off-label prescribing.
Limited testing for safety and effectiveness. Experiences such as the fen-phen (weight loss) controversy1 and estrogens for preventing vascular disease in postmenopausal women2 remind physicians that some untested treatments may do more harm than good.
Commercial influence. Pharmaceutical companies have used advisory boards, consultant meetings, and continuing medical education events to promote unproven off-label indications for drugs.3,4 Many studies that were, ostensibly, designed and proposed by researchers show evidence of so-called ghost authorship by commercial concerns.5
Study bias. Even peer-reviewed, double-blind studies that are published in the medical literature might not sufficiently support off-label prescribing practices because sponsors of such studies can structure them or use statistical analyses to make results look favorable. Former editors of the British Medical Journal and The Lancet have acknowledged that their publications unwittingly served as “an extension of the marketing arm” or “laundering operations” for drug manufacturers.6,7 Even for FDA-approved indications, a selective, positive-result publication bias and nonreporting of negative results may make drugs seem more effective than the full range of studies would justify.8
Legal use of labeling. Although off-label prescribing is accepted medical practice, doctors “may be found negligent if their decision to use a drug off label is sufficiently careless, imprudent, or unprofessional.”9 During a malpractice lawsuit, plaintiff’s counsel could try to use FDA-approved labeling or prescribing information to establish a presumptive standard of care. Such evidence usually is admissible if it is supported by expert testimony. The burden of proof is then placed on the defendant physician to show how an off-label use met the standard of care.10
References
1. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
2. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
3. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.-
4. Steinman MA, Bero L, Chren M, Landefeld CS. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
5. Gøtzsche PC, Hróbjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.-
6. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.-
7. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
8. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
9. Richardson v Miller. 44 SW3d 1 (Tenn Ct App 2000).
10. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
Off-label: Accepted and necessary
Off-label prescribing occurs when a physician prescribes a medication or uses a medical device outside the scope of FDA-approved labeling. Most commonly, off-label use involves prescribing a medication for something other than its FDA-approved indication. An example is sildenafil [Viagra] for women who have antidepressant-induced sexual dysfunction.1
Other examples are prescribing a drug:
- at an unapproved dose
- in an unapproved format (e.g., mixing capsule contents with applesauce)
- outside the approved age group
- for longer than the approved interval
- at a different dose schedule (e.g., qhs instead of bid or tid).
Typically, it takes years for a new drug to gain FDA approval and additional time for an already-approved drug to gain approval for a new indication. In the meantime, clinicians treat their patients with available drugs prescribed off label.
Off-label prescribing is legal. FDA approval means drugs may be sold and marketed in specific ways. But the FDA does not tell physicians how they can use approved drugs. As each edition of the Physicians’ Desk Reference explains, “Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling.”2 Federal statutes state that FDA approval does not “limit or interfere with the authority of a health care practitioner to prescribe” approved drugs or devices “for any condition or disease.”3
- Know why an article applies to your patient. If you are sued for malpractice, you can use an article to support your treatment choice by explaining how this information contributed to your decision-making.
- Tell your patient that the proposed treatment is an off-label use when you obtain consent, even though case law says you don’t have to do this. Telling your patient helps him understand your reasoning and prevents surprises that may give offense.
- Engage in ongoing informed consent. Uncertainty is part of medical practice and is heightened when physicians prescribe off label. Ongoing discussions help patients understand, accept, and share that uncertainty.
- Document informed consent. This will show—if it becomes necessary—that you and your patient made collaborative, conscientious decisions about treatment.1
Reference
1. Royal College of Psychiatrists. CR142. Use of unlicensed medicine for unlicensed applications in psychiatric practice. Available at: http://www.rcpsych.ac.uk/publications/collegereports/cr/cr142.aspx. Accessed March 4, 2009.
Does off-label constitute malpractice?
Off-label use is not only legal—it’s often wise medical practice. Many drug uses that now have FDA approval were off label just a few years ago. Examples include using selective serotonin reuptake inhibitors (SSRIs) to treat panic disorder and obsessive–compulsive disorder. Fluoxetine is the only FDA-approved drug for treating depression in adolescents, but other SSRIs may also have a favorable risk–benefit profile.6
The practice is common—we know that
Numerous studies have shown that off-label prescribing is common in, for example, psychiatry7 and other specialties.8,9 Because the practice is so common, the mere fact that a drug is not FDA-approved for a particular use does not imply that the drug was prescribed negligently.
Some commentators have suggested that off-label prescribing amounts to human experimentation.10 Without FDA approval, they say, physicians lack hard evidence, so to speak, that a product is safe and effective—making off-label prescribing a small-scale clinical trial based on the doctor’s educated guesses.
If this reasoning is correct, off-label prescribing would require the same human subject protections used in research, including institutional review board approval and special consent forms.
Although this argument sounds plausible, off-label prescribing is not experimentation or research (see “4 reasons why off-label prescribing can be controversial”).4,11-19 Researchers investigate hypotheses to obtain generalizable knowledge, whereas medical therapy aims to benefit individual patients. This experimentation–therapy distinction is not perfect because successful off-label treatment of one patient might imply beneficial effects for others.10 When courts have looked at this matter, though, they have found that “off-label use… by a physician seeking an optimal treatment for his or her patient is not necessarily…research or an investigational or experimental treatment when the use is customarily followed by physicians.”4
Courts also have said that off-label use does not require special informed consent. Just because a drug is prescribed off label doesn’t mean it’s risky. FDA approval “is not a material risk inherently involved in a proposed therapy which a physician should have disclosed to a patient prior to the therapy.”20 In other words, a physician is not required to discuss FDA regulatory status—such as off-label uses of a medication—to comply with standards of informed consent. FDA regulatory status has nothing to do with the risks or benefits of a medication and it does not provide information about treatment alternatives.21
What should you do?
For advice on protecting yourself when you prescribe off label, see the box above.
In addition, you should keep abreast of news and scientific evidence concerning drug uses, effects, interactions, and adverse effects, especially when prescribing for uses that are different from the manufacturer’s intended purposes.22
Last, collect articles on off-label uses, but keep them separate from your patients’ files. Good attorneys are highly skilled at using documents to score legal points, and opposing counsel will prepare questions to focus on the articles’ faults or limitations in isolation.
1. Nurnberg HG, Hensley PL, Heiman JR, et al. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300:395-404.
2. Physicians’ Desk Reference. 62nd ed. Montvale, NJ: Thomson Healthcare, Inc.; 2007.
3. Food, Drug and Cosmetic Act, 21USC §396
4. Richardson v Miller. 44 SW3d 1 (Tenn Ct App 2000).
5. Buckman Co. v Plaintiffs’ Legal Comm., 531 US 341 (2001).
6. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683-1696.
7. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Adv Psychiatr Treat. 2007;13:414-422.
8. Conroy S, Choonara I, Impicciatore P, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. European Network for Drug Investigation in Children. BMJ. 2000;320:79-82.
9. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166:1021-1026.
10. Mehlman MJ. Off-label prescribing. Available at: http://www.thedoctorwillseeyounow.com/articles/bioethics/offlabel_11. Accessed October 21, 2008.
11. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
12. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
13. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.-
14. Steinman MA, Bero L, Chren M, Landefeld CS. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
15. Gøtzsche PC, Hróbjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.-
16. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.-
17. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
18. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
19. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
20. Klein v Biscup. 673 NE2d 225 (Ohio App 1996).
21. Beck JM, Azari ED. FDA, off-label use, and informed consent: debunking myths and misconceptions. Food Drug Law J. 1998;53:71-104.
22. Shajnfeld A, Krueger RB. Reforming (purportedly) non-punitive responses to sexual offending. Dev Mental Health Law. 2006;25:81-99.
1. Nurnberg HG, Hensley PL, Heiman JR, et al. Sildenafil treatment of women with antidepressant-associated sexual dysfunction: a randomized controlled trial. JAMA. 2008;300:395-404.
2. Physicians’ Desk Reference. 62nd ed. Montvale, NJ: Thomson Healthcare, Inc.; 2007.
3. Food, Drug and Cosmetic Act, 21USC §396
4. Richardson v Miller. 44 SW3d 1 (Tenn Ct App 2000).
5. Buckman Co. v Plaintiffs’ Legal Comm., 531 US 341 (2001).
6. Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683-1696.
7. Baldwin DS, Kosky N. Off-label prescribing in psychiatric practice. Adv Psychiatr Treat. 2007;13:414-422.
8. Conroy S, Choonara I, Impicciatore P, et al. Survey of unlicensed and off label drug use in paediatric wards in European countries. European Network for Drug Investigation in Children. BMJ. 2000;320:79-82.
9. Radley DC, Finkelstein SN, Stafford RS. Off-label prescribing among office-based physicians. Arch Intern Med. 2006;166:1021-1026.
10. Mehlman MJ. Off-label prescribing. Available at: http://www.thedoctorwillseeyounow.com/articles/bioethics/offlabel_11. Accessed October 21, 2008.
11. Connolly H, Crary J, McGoon M, et al. Vascular heart disease associated with fenfluramine-phentermine. N Engl J Med. 1997;337:581-588.
12. Anderson GL, Limacher M, Assaf AR, et al. Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women’s Health Initiative randomized controlled trial. JAMA. 2004;291:1701-1712.
13. Sismondo S. Ghost management: how much of the medical literature is shaped behind the scenes by the pharmaceutical industry? PLoS Med. 2007;4(9):e286.-
14. Steinman MA, Bero L, Chren M, Landefeld CS. Narrative review: the promotion of gabapentin: an analysis of internal industry documents. Ann Intern Med. 2006;145:284-293.
15. Gøtzsche PC, Hróbjartsson A, Johansen H, et al. Ghost authorship in industry-initiated randomised trials. PLoS Med. 2007;4(1):e19.-
16. Smith R. Medical journals are an extension of the marketing arm of pharmaceutical companies. PLoS Med. 2005;2(5):e138.-
17. Horton R. The dawn of McScience. New York Rev Books. 2004;51(4):7-9.
18. Turner EH, Matthews A, Linardatos E, et al. Selective publication of antidepressant trials and its influence on apparent efficacy. N Engl J Med. 2008;358:252-260.
19. Henry V. Off-label prescribing. Legal implications. J Leg Med. 1999;20:365-383.
20. Klein v Biscup. 673 NE2d 225 (Ohio App 1996).
21. Beck JM, Azari ED. FDA, off-label use, and informed consent: debunking myths and misconceptions. Food Drug Law J. 1998;53:71-104.
22. Shajnfeld A, Krueger RB. Reforming (purportedly) non-punitive responses to sexual offending. Dev Mental Health Law. 2006;25:81-99.
Medical Verdicts: Only on the Web
Was surgery telecast without consent, as patient claims?
A 48-YEAR-OLD WOMAN underwent a minimally invasive hysteroscopic myomectomy. The surgery was telecast live for Ethicon, which paid the surgeon an honorarium of $500. The patient subsequently developed metastatic ovarian cancer. She sued her gynecologist for failing to detect her ovarian cancer in a timely manner. At the time of trial she was in hospice care. During discovery, she asked that a copy of the telecast be produced. The day before trial, her counsel found the video on the Internet and obtained a copy. It did not reveal any identifying information about the patient.
- PATIENT’S CLAIM The defendant was negligent for failure to: (1) send her for genetic testing/counseling based on her family history; (2) recommend/perform a hysterectomy, as her family history required aggressive treatment; (3) obtain informed consent for the surgery; (4) disclose that the surgery was to be telecast live for ethicon; and (5) disclose that he received an honorarium. The patient also claimed she was given a diagnosis of ovarian cancer 11 months after the surgery.
- PHYSICIAN’S DEFENSE At her first visit, the patient indicated she had already been counseled and didn’t need more counseling. She also refused a hysterectomy, choosing instead a minimally invasive procedure. The standard of care at the time did not require referral for genetic counseling/testing. The patient was informed about the telecast, but disclosing the honorarium to her was not required.
- VERDICT Illinois defense verdict. Ethicon was granted summary judgment, and the plaintiff voluntarily dismissed the physician from the misappropriation of identity claim.
One twin lives and other dies in delayed C-section
A WOMAN PREGNANT with twins presented at the hospital at 35.5 weeks’ gestation with spontaneous rupture of membranes. Dr. A, the ObGyn on call at the time, determined that both twins were in the breech position and the male twin had ruptured membranes. He ordered fetal heart monitoring. The following morning, Dr. B ordered an immediate cesarean delivery because of the possibility of a prolapsed cord. After a 2-hour delay, the twins were delivered—the female successfully, but the male twin was stillborn. The baby’s body was placed in the mother’s hospital room until it was removed for autopsy 2 days later.
- PATIENT’S CLAIM (1) Dr. A should have ordered an immediate cesarean delivery. (2) Dr. B should have made sure that the cesarean delivery he ordered was performed more timely. (3) Because of the patient’s large size, fetal heart rates could not be monitored properly. (4) The hospital should not have left the child’s body in the mother’s room for 2 days.
- PHYSICIAN’S DEFENSE Dr. A claimed an immediate cesarean delivery was not necessary.
- VERDICT Indiana defense verdict for Dr. A. Claims against Dr. B and the hospital were dismissed on summary judgment.
$19.6M for mother’s incontinence and child’s CP
A 37-YEAR-OLD WOMAN’S labor and delivery were managed by Dr. A, a resident, and Dr. B, an obstetrician. Following labor induction, the mother’s temperature rose and the heart rates of both mother and fetus increased. Believing the mother could have chorioamnionitis, Dr. A and Dr. B decided on a forceps delivery. During the delivery, the mother suffered a 4th degree laceration of the vagina. Dr. A repaired the laceration.
- PATIENT’S CLAIM Repair of the laceration was not effective, and she suffers permanent residual incontinence as a result. Also, the child suffered cerebral palsy resulting from injury during delivery.
- PHYSICIAN’S DEFENSE The mother made a good recovery. The child did not suffer a brain injury. Rather he has tibial torsion and is pigeon-toed—which caused problems with his gait.
- VERDICT $19.6 million New York verdict: $11,965,000 for the mother and $7,650,000 for the child.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Was surgery telecast without consent, as patient claims?
A 48-YEAR-OLD WOMAN underwent a minimally invasive hysteroscopic myomectomy. The surgery was telecast live for Ethicon, which paid the surgeon an honorarium of $500. The patient subsequently developed metastatic ovarian cancer. She sued her gynecologist for failing to detect her ovarian cancer in a timely manner. At the time of trial she was in hospice care. During discovery, she asked that a copy of the telecast be produced. The day before trial, her counsel found the video on the Internet and obtained a copy. It did not reveal any identifying information about the patient.
- PATIENT’S CLAIM The defendant was negligent for failure to: (1) send her for genetic testing/counseling based on her family history; (2) recommend/perform a hysterectomy, as her family history required aggressive treatment; (3) obtain informed consent for the surgery; (4) disclose that the surgery was to be telecast live for ethicon; and (5) disclose that he received an honorarium. The patient also claimed she was given a diagnosis of ovarian cancer 11 months after the surgery.
- PHYSICIAN’S DEFENSE At her first visit, the patient indicated she had already been counseled and didn’t need more counseling. She also refused a hysterectomy, choosing instead a minimally invasive procedure. The standard of care at the time did not require referral for genetic counseling/testing. The patient was informed about the telecast, but disclosing the honorarium to her was not required.
- VERDICT Illinois defense verdict. Ethicon was granted summary judgment, and the plaintiff voluntarily dismissed the physician from the misappropriation of identity claim.
One twin lives and other dies in delayed C-section
A WOMAN PREGNANT with twins presented at the hospital at 35.5 weeks’ gestation with spontaneous rupture of membranes. Dr. A, the ObGyn on call at the time, determined that both twins were in the breech position and the male twin had ruptured membranes. He ordered fetal heart monitoring. The following morning, Dr. B ordered an immediate cesarean delivery because of the possibility of a prolapsed cord. After a 2-hour delay, the twins were delivered—the female successfully, but the male twin was stillborn. The baby’s body was placed in the mother’s hospital room until it was removed for autopsy 2 days later.
- PATIENT’S CLAIM (1) Dr. A should have ordered an immediate cesarean delivery. (2) Dr. B should have made sure that the cesarean delivery he ordered was performed more timely. (3) Because of the patient’s large size, fetal heart rates could not be monitored properly. (4) The hospital should not have left the child’s body in the mother’s room for 2 days.
- PHYSICIAN’S DEFENSE Dr. A claimed an immediate cesarean delivery was not necessary.
- VERDICT Indiana defense verdict for Dr. A. Claims against Dr. B and the hospital were dismissed on summary judgment.
$19.6M for mother’s incontinence and child’s CP
A 37-YEAR-OLD WOMAN’S labor and delivery were managed by Dr. A, a resident, and Dr. B, an obstetrician. Following labor induction, the mother’s temperature rose and the heart rates of both mother and fetus increased. Believing the mother could have chorioamnionitis, Dr. A and Dr. B decided on a forceps delivery. During the delivery, the mother suffered a 4th degree laceration of the vagina. Dr. A repaired the laceration.
- PATIENT’S CLAIM Repair of the laceration was not effective, and she suffers permanent residual incontinence as a result. Also, the child suffered cerebral palsy resulting from injury during delivery.
- PHYSICIAN’S DEFENSE The mother made a good recovery. The child did not suffer a brain injury. Rather he has tibial torsion and is pigeon-toed—which caused problems with his gait.
- VERDICT $19.6 million New York verdict: $11,965,000 for the mother and $7,650,000 for the child.
Was surgery telecast without consent, as patient claims?
A 48-YEAR-OLD WOMAN underwent a minimally invasive hysteroscopic myomectomy. The surgery was telecast live for Ethicon, which paid the surgeon an honorarium of $500. The patient subsequently developed metastatic ovarian cancer. She sued her gynecologist for failing to detect her ovarian cancer in a timely manner. At the time of trial she was in hospice care. During discovery, she asked that a copy of the telecast be produced. The day before trial, her counsel found the video on the Internet and obtained a copy. It did not reveal any identifying information about the patient.
- PATIENT’S CLAIM The defendant was negligent for failure to: (1) send her for genetic testing/counseling based on her family history; (2) recommend/perform a hysterectomy, as her family history required aggressive treatment; (3) obtain informed consent for the surgery; (4) disclose that the surgery was to be telecast live for ethicon; and (5) disclose that he received an honorarium. The patient also claimed she was given a diagnosis of ovarian cancer 11 months after the surgery.
- PHYSICIAN’S DEFENSE At her first visit, the patient indicated she had already been counseled and didn’t need more counseling. She also refused a hysterectomy, choosing instead a minimally invasive procedure. The standard of care at the time did not require referral for genetic counseling/testing. The patient was informed about the telecast, but disclosing the honorarium to her was not required.
- VERDICT Illinois defense verdict. Ethicon was granted summary judgment, and the plaintiff voluntarily dismissed the physician from the misappropriation of identity claim.
One twin lives and other dies in delayed C-section
A WOMAN PREGNANT with twins presented at the hospital at 35.5 weeks’ gestation with spontaneous rupture of membranes. Dr. A, the ObGyn on call at the time, determined that both twins were in the breech position and the male twin had ruptured membranes. He ordered fetal heart monitoring. The following morning, Dr. B ordered an immediate cesarean delivery because of the possibility of a prolapsed cord. After a 2-hour delay, the twins were delivered—the female successfully, but the male twin was stillborn. The baby’s body was placed in the mother’s hospital room until it was removed for autopsy 2 days later.
- PATIENT’S CLAIM (1) Dr. A should have ordered an immediate cesarean delivery. (2) Dr. B should have made sure that the cesarean delivery he ordered was performed more timely. (3) Because of the patient’s large size, fetal heart rates could not be monitored properly. (4) The hospital should not have left the child’s body in the mother’s room for 2 days.
- PHYSICIAN’S DEFENSE Dr. A claimed an immediate cesarean delivery was not necessary.
- VERDICT Indiana defense verdict for Dr. A. Claims against Dr. B and the hospital were dismissed on summary judgment.
$19.6M for mother’s incontinence and child’s CP
A 37-YEAR-OLD WOMAN’S labor and delivery were managed by Dr. A, a resident, and Dr. B, an obstetrician. Following labor induction, the mother’s temperature rose and the heart rates of both mother and fetus increased. Believing the mother could have chorioamnionitis, Dr. A and Dr. B decided on a forceps delivery. During the delivery, the mother suffered a 4th degree laceration of the vagina. Dr. A repaired the laceration.
- PATIENT’S CLAIM Repair of the laceration was not effective, and she suffers permanent residual incontinence as a result. Also, the child suffered cerebral palsy resulting from injury during delivery.
- PHYSICIAN’S DEFENSE The mother made a good recovery. The child did not suffer a brain injury. Rather he has tibial torsion and is pigeon-toed—which caused problems with his gait.
- VERDICT $19.6 million New York verdict: $11,965,000 for the mother and $7,650,000 for the child.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Medical Verdicts
MD: “She had no complaints because I have no notes”
FOLLOWING HYSTERECTOMY, a 49-year-old woman complained of abdominal pain, fever, chills, and nausea. She continued to complain of the same symptoms on multiple visits to her physician. She also called him to report that her abdomen was painful to the touch. After one such call, the physician prescribed an antibiotic.
A routine x-ray of the patient’s prosthetic hip 5 months after the hysterectomy showed a surgical sponge in her abdomen. She reported this finding to the defendant, who then left a voicemail that (1) he was away, (2) she could live to 100 years old with that sponge inside her, and (3) she should return for a consultation in a few weeks.
Instead she sought the care of another physician.
A month later, she developed a bowel obstruction. In emergency surgery, the sponge was removed as it had created an abscess and bowel obstruction. After the surgery, the patient recovered and had no further abdominal complaints.
PATIENT’S CLAIM The physician was negligent for leaving the sponge in the abdomen and for failing to follow up on her consistent complaints of abdominal pain.
PHYSICIAN’S DEFENSE The nurses were responsible for a proper sponge count. Also, the patient did not complain of pain after surgery—because he had no notes stating that she did.
VERDICT $4,904,886 Maryland verdict, which was reduced by caps to $1,329,886.
Incontinence is worse after TVT and takedown
A WOMAN WHO WAS SUFFERING from stress urinary incontinence underwent a tension-free vaginal tape procedure (TVT). Following surgery, she developed urinary retention. To address this, her physician performed a TVT “takedown” procedure—and accidentally injured her bladder and urethra. The injuries were recognized and repaired. Because of worsening incontinence, the patient transferred her care to a urologist. Following a transvaginal sling procedure, her incontinence improved.
Eventually, she underwent a total abdominal hysterectomy as well as a procedure to address a prolapse involving her bladder. At this point, the patient became severely incontinent. A revision of the transvaginal sling repair was then performed.
PATIENT’S CLAIM Despite all the procedures, she remains incontinent. She also developed disabling chronic pelvic pain due to the procedures.
PHYSICIAN’S DEFENSE He denied negligence and insisted that the patient’s chronic pelvic pain was due to interstitial cystitis. He admitted causing the bladder and urethra injuries during the TVT takedown, but he recognized and repaired them immediately.
VERDICT Colorado defense verdict.
Colon is injured in D & E following fetal death
A 23-YEAR-OLD WOMAN suffered a fetal demise at 15 to 17 weeks’ gestation. Dr. A, an ObGyn, decided to perform a dilation and evacuation (D & E) involving removal of fetal parts in a blind procedure. On the preceding day, he inserted a laminaria to enlarge the cervix for the evacuation.
During the D & E, he inadvertently punctured the uterine wall with ring forceps and then grasped part of the sigmoid colon, believing he was removing a bone embedded in the wall. This caused vascular disruption and ischemia to the colon, but did not lacerate it. Aware that a complication had occurred, Dr. A switched to laparoscopy and consulted Dr. B, a general surgeon. When the scope indicated a 1.5- to 2-cm perforation in the fundus of the uterus, as well as bluish discoloration in the mesentery, Dr. B decided to resect the colon and perform a temporary colostomy.
The colostomy was reversed 3 months later. The patient has since given birth to a child by cesarean delivery.
PATIENT’S CLAIM Dr. A was negligent for pulling the colon into the uterus and clamping it to the uterine wall.
PHYSICIAN’S DEFENSE Dr. A claimed the uterus was penetrated accidently during the blind procedure. When he grasped the colon’s mesentery, he then released it in under 1 minute.
VERDICT Illinois defense verdict.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
MD: “She had no complaints because I have no notes”
FOLLOWING HYSTERECTOMY, a 49-year-old woman complained of abdominal pain, fever, chills, and nausea. She continued to complain of the same symptoms on multiple visits to her physician. She also called him to report that her abdomen was painful to the touch. After one such call, the physician prescribed an antibiotic.
A routine x-ray of the patient’s prosthetic hip 5 months after the hysterectomy showed a surgical sponge in her abdomen. She reported this finding to the defendant, who then left a voicemail that (1) he was away, (2) she could live to 100 years old with that sponge inside her, and (3) she should return for a consultation in a few weeks.
Instead she sought the care of another physician.
A month later, she developed a bowel obstruction. In emergency surgery, the sponge was removed as it had created an abscess and bowel obstruction. After the surgery, the patient recovered and had no further abdominal complaints.
PATIENT’S CLAIM The physician was negligent for leaving the sponge in the abdomen and for failing to follow up on her consistent complaints of abdominal pain.
PHYSICIAN’S DEFENSE The nurses were responsible for a proper sponge count. Also, the patient did not complain of pain after surgery—because he had no notes stating that she did.
VERDICT $4,904,886 Maryland verdict, which was reduced by caps to $1,329,886.
Incontinence is worse after TVT and takedown
A WOMAN WHO WAS SUFFERING from stress urinary incontinence underwent a tension-free vaginal tape procedure (TVT). Following surgery, she developed urinary retention. To address this, her physician performed a TVT “takedown” procedure—and accidentally injured her bladder and urethra. The injuries were recognized and repaired. Because of worsening incontinence, the patient transferred her care to a urologist. Following a transvaginal sling procedure, her incontinence improved.
Eventually, she underwent a total abdominal hysterectomy as well as a procedure to address a prolapse involving her bladder. At this point, the patient became severely incontinent. A revision of the transvaginal sling repair was then performed.
PATIENT’S CLAIM Despite all the procedures, she remains incontinent. She also developed disabling chronic pelvic pain due to the procedures.
PHYSICIAN’S DEFENSE He denied negligence and insisted that the patient’s chronic pelvic pain was due to interstitial cystitis. He admitted causing the bladder and urethra injuries during the TVT takedown, but he recognized and repaired them immediately.
VERDICT Colorado defense verdict.
Colon is injured in D & E following fetal death
A 23-YEAR-OLD WOMAN suffered a fetal demise at 15 to 17 weeks’ gestation. Dr. A, an ObGyn, decided to perform a dilation and evacuation (D & E) involving removal of fetal parts in a blind procedure. On the preceding day, he inserted a laminaria to enlarge the cervix for the evacuation.
During the D & E, he inadvertently punctured the uterine wall with ring forceps and then grasped part of the sigmoid colon, believing he was removing a bone embedded in the wall. This caused vascular disruption and ischemia to the colon, but did not lacerate it. Aware that a complication had occurred, Dr. A switched to laparoscopy and consulted Dr. B, a general surgeon. When the scope indicated a 1.5- to 2-cm perforation in the fundus of the uterus, as well as bluish discoloration in the mesentery, Dr. B decided to resect the colon and perform a temporary colostomy.
The colostomy was reversed 3 months later. The patient has since given birth to a child by cesarean delivery.
PATIENT’S CLAIM Dr. A was negligent for pulling the colon into the uterus and clamping it to the uterine wall.
PHYSICIAN’S DEFENSE Dr. A claimed the uterus was penetrated accidently during the blind procedure. When he grasped the colon’s mesentery, he then released it in under 1 minute.
VERDICT Illinois defense verdict.
MD: “She had no complaints because I have no notes”
FOLLOWING HYSTERECTOMY, a 49-year-old woman complained of abdominal pain, fever, chills, and nausea. She continued to complain of the same symptoms on multiple visits to her physician. She also called him to report that her abdomen was painful to the touch. After one such call, the physician prescribed an antibiotic.
A routine x-ray of the patient’s prosthetic hip 5 months after the hysterectomy showed a surgical sponge in her abdomen. She reported this finding to the defendant, who then left a voicemail that (1) he was away, (2) she could live to 100 years old with that sponge inside her, and (3) she should return for a consultation in a few weeks.
Instead she sought the care of another physician.
A month later, she developed a bowel obstruction. In emergency surgery, the sponge was removed as it had created an abscess and bowel obstruction. After the surgery, the patient recovered and had no further abdominal complaints.
PATIENT’S CLAIM The physician was negligent for leaving the sponge in the abdomen and for failing to follow up on her consistent complaints of abdominal pain.
PHYSICIAN’S DEFENSE The nurses were responsible for a proper sponge count. Also, the patient did not complain of pain after surgery—because he had no notes stating that she did.
VERDICT $4,904,886 Maryland verdict, which was reduced by caps to $1,329,886.
Incontinence is worse after TVT and takedown
A WOMAN WHO WAS SUFFERING from stress urinary incontinence underwent a tension-free vaginal tape procedure (TVT). Following surgery, she developed urinary retention. To address this, her physician performed a TVT “takedown” procedure—and accidentally injured her bladder and urethra. The injuries were recognized and repaired. Because of worsening incontinence, the patient transferred her care to a urologist. Following a transvaginal sling procedure, her incontinence improved.
Eventually, she underwent a total abdominal hysterectomy as well as a procedure to address a prolapse involving her bladder. At this point, the patient became severely incontinent. A revision of the transvaginal sling repair was then performed.
PATIENT’S CLAIM Despite all the procedures, she remains incontinent. She also developed disabling chronic pelvic pain due to the procedures.
PHYSICIAN’S DEFENSE He denied negligence and insisted that the patient’s chronic pelvic pain was due to interstitial cystitis. He admitted causing the bladder and urethra injuries during the TVT takedown, but he recognized and repaired them immediately.
VERDICT Colorado defense verdict.
Colon is injured in D & E following fetal death
A 23-YEAR-OLD WOMAN suffered a fetal demise at 15 to 17 weeks’ gestation. Dr. A, an ObGyn, decided to perform a dilation and evacuation (D & E) involving removal of fetal parts in a blind procedure. On the preceding day, he inserted a laminaria to enlarge the cervix for the evacuation.
During the D & E, he inadvertently punctured the uterine wall with ring forceps and then grasped part of the sigmoid colon, believing he was removing a bone embedded in the wall. This caused vascular disruption and ischemia to the colon, but did not lacerate it. Aware that a complication had occurred, Dr. A switched to laparoscopy and consulted Dr. B, a general surgeon. When the scope indicated a 1.5- to 2-cm perforation in the fundus of the uterus, as well as bluish discoloration in the mesentery, Dr. B decided to resect the colon and perform a temporary colostomy.
The colostomy was reversed 3 months later. The patient has since given birth to a child by cesarean delivery.
PATIENT’S CLAIM Dr. A was negligent for pulling the colon into the uterus and clamping it to the uterine wall.
PHYSICIAN’S DEFENSE Dr. A claimed the uterus was penetrated accidently during the blind procedure. When he grasped the colon’s mesentery, he then released it in under 1 minute.
VERDICT Illinois defense verdict.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Stepping Outside Your Comfort Zone
Each of us knows colleagues for whom medicine no longer holds the aura of excitement and fascination that we assume will last forever. Having faced their challenges and attained their goals, they are unwilling or unable to find new challenges and design new goals. In the modern vernacular, they are “burned out.”
These people are prisoners of the Comfort Zone.
The Comfort Zone is a product of a dangerous state of mind, complacency—the perception of doing okay, of having arrived, of believing it is okay to take it easy.
Complacency triggers the construction of a protective envelope of actions and situations that are familiar and comfortable and do not require any major risks or significant uncertainties. Unfortunately, the human psyche cannot function within the Comfort Zone for any length of time before it starts looking for distractions.
A patient of mine once owned one of the largest and most popular restaurants in northern New Jersey. He had all the wealth, power, and prestige he ever dreamed of. Now it's all gone. He gambled it all away.
I felt I knew him well enough to ask what had gone wrong. Why risk losing it all? Why did he allow such a catastrophe to happen? “Doc,” he replied, “if the game no longer challenges you, you will screw it up—just to have something to do!”
I found this lesson profound and enlightening, and it is a shame that this man had to learn it the hard way, as so many heretofore successful people do.
But if we cannot be happy within the Comfort Zone and have to constantly look for distractions, must the distractions necessarily be destructive? Why not look for constructive distractions? Why not push the other side of the envelope?
That is the solution to the Comfort Zone problem: Constantly expand the zone itself. You must continually incorporate new activities and situations into your envelope, so that you remain interested, focused, and enthused.
What do you look for? Anything that would make you uncomfortable. Such a situation, by definition, is outside your Comfort Zone. Of course, you must screen out detrimental things, considering only those additions to your zone that will improve you personally or professionally.
In your office, this can be as minor as trying a new appointment scheduling method or as major as adding a satellite office or purchasing a new, cutting edge piece of equipment and mastering its use. Rather than perpetuating the old, comfortable, risk-free, mind-numbing routine, conquer the fear and take some new risks. Once your Comfort Zone grows to encompass the new routine, you will be one step further away from burnout.
The concept of enlarging your Comfort Zone applies equally well to life outside the office. Find and seize opportunities to do things your zone tries to discourage but that you wish to learn to do comfortably. It doesn't have to be a life-changing project: Start small. If you tend to avoid talking on the phone, for example, make a conscious effort to initiate a phone call every day. When it becomes part of your zone, those important phone calls will be far easier and more comfortable to make.
“Do something every day that you don't want to do,” Mark Twain once wrote. “This is the golden rule for acquiring the habit of doing your duty without pain.”
So the solution to burnout is to recognize that your Comfort Zone exists and must be managed, rather than allowing it to manage you and restrict you. By molding your zone to activities and situations that will keep you enthused, you can keep complacency at bay. Rather than permitting distractions to take a destructive course, look for distractions that are constructive, educational, and pleasurable.
Next month, my wife and I will be leading a group of doctors on a trip to Uzbekistan in Central Asia on the old Silk Road. It will be a new experience in an unfamiliar part of the world, and the decision to take it on was not made lightly. It would have been easy to stay home or to plan a “safer” trip to a more familiar destination, but in settling for a comfortable option we would have missed a golden opportunity to push our envelope in an educational and exciting way.
So if you're burned out, find something uncomfortably new and constructive, and go for it. When you conquer the fear, you'll conquer complacency.
Each of us knows colleagues for whom medicine no longer holds the aura of excitement and fascination that we assume will last forever. Having faced their challenges and attained their goals, they are unwilling or unable to find new challenges and design new goals. In the modern vernacular, they are “burned out.”
These people are prisoners of the Comfort Zone.
The Comfort Zone is a product of a dangerous state of mind, complacency—the perception of doing okay, of having arrived, of believing it is okay to take it easy.
Complacency triggers the construction of a protective envelope of actions and situations that are familiar and comfortable and do not require any major risks or significant uncertainties. Unfortunately, the human psyche cannot function within the Comfort Zone for any length of time before it starts looking for distractions.
A patient of mine once owned one of the largest and most popular restaurants in northern New Jersey. He had all the wealth, power, and prestige he ever dreamed of. Now it's all gone. He gambled it all away.
I felt I knew him well enough to ask what had gone wrong. Why risk losing it all? Why did he allow such a catastrophe to happen? “Doc,” he replied, “if the game no longer challenges you, you will screw it up—just to have something to do!”
I found this lesson profound and enlightening, and it is a shame that this man had to learn it the hard way, as so many heretofore successful people do.
But if we cannot be happy within the Comfort Zone and have to constantly look for distractions, must the distractions necessarily be destructive? Why not look for constructive distractions? Why not push the other side of the envelope?
That is the solution to the Comfort Zone problem: Constantly expand the zone itself. You must continually incorporate new activities and situations into your envelope, so that you remain interested, focused, and enthused.
What do you look for? Anything that would make you uncomfortable. Such a situation, by definition, is outside your Comfort Zone. Of course, you must screen out detrimental things, considering only those additions to your zone that will improve you personally or professionally.
In your office, this can be as minor as trying a new appointment scheduling method or as major as adding a satellite office or purchasing a new, cutting edge piece of equipment and mastering its use. Rather than perpetuating the old, comfortable, risk-free, mind-numbing routine, conquer the fear and take some new risks. Once your Comfort Zone grows to encompass the new routine, you will be one step further away from burnout.
The concept of enlarging your Comfort Zone applies equally well to life outside the office. Find and seize opportunities to do things your zone tries to discourage but that you wish to learn to do comfortably. It doesn't have to be a life-changing project: Start small. If you tend to avoid talking on the phone, for example, make a conscious effort to initiate a phone call every day. When it becomes part of your zone, those important phone calls will be far easier and more comfortable to make.
“Do something every day that you don't want to do,” Mark Twain once wrote. “This is the golden rule for acquiring the habit of doing your duty without pain.”
So the solution to burnout is to recognize that your Comfort Zone exists and must be managed, rather than allowing it to manage you and restrict you. By molding your zone to activities and situations that will keep you enthused, you can keep complacency at bay. Rather than permitting distractions to take a destructive course, look for distractions that are constructive, educational, and pleasurable.
Next month, my wife and I will be leading a group of doctors on a trip to Uzbekistan in Central Asia on the old Silk Road. It will be a new experience in an unfamiliar part of the world, and the decision to take it on was not made lightly. It would have been easy to stay home or to plan a “safer” trip to a more familiar destination, but in settling for a comfortable option we would have missed a golden opportunity to push our envelope in an educational and exciting way.
So if you're burned out, find something uncomfortably new and constructive, and go for it. When you conquer the fear, you'll conquer complacency.
Each of us knows colleagues for whom medicine no longer holds the aura of excitement and fascination that we assume will last forever. Having faced their challenges and attained their goals, they are unwilling or unable to find new challenges and design new goals. In the modern vernacular, they are “burned out.”
These people are prisoners of the Comfort Zone.
The Comfort Zone is a product of a dangerous state of mind, complacency—the perception of doing okay, of having arrived, of believing it is okay to take it easy.
Complacency triggers the construction of a protective envelope of actions and situations that are familiar and comfortable and do not require any major risks or significant uncertainties. Unfortunately, the human psyche cannot function within the Comfort Zone for any length of time before it starts looking for distractions.
A patient of mine once owned one of the largest and most popular restaurants in northern New Jersey. He had all the wealth, power, and prestige he ever dreamed of. Now it's all gone. He gambled it all away.
I felt I knew him well enough to ask what had gone wrong. Why risk losing it all? Why did he allow such a catastrophe to happen? “Doc,” he replied, “if the game no longer challenges you, you will screw it up—just to have something to do!”
I found this lesson profound and enlightening, and it is a shame that this man had to learn it the hard way, as so many heretofore successful people do.
But if we cannot be happy within the Comfort Zone and have to constantly look for distractions, must the distractions necessarily be destructive? Why not look for constructive distractions? Why not push the other side of the envelope?
That is the solution to the Comfort Zone problem: Constantly expand the zone itself. You must continually incorporate new activities and situations into your envelope, so that you remain interested, focused, and enthused.
What do you look for? Anything that would make you uncomfortable. Such a situation, by definition, is outside your Comfort Zone. Of course, you must screen out detrimental things, considering only those additions to your zone that will improve you personally or professionally.
In your office, this can be as minor as trying a new appointment scheduling method or as major as adding a satellite office or purchasing a new, cutting edge piece of equipment and mastering its use. Rather than perpetuating the old, comfortable, risk-free, mind-numbing routine, conquer the fear and take some new risks. Once your Comfort Zone grows to encompass the new routine, you will be one step further away from burnout.
The concept of enlarging your Comfort Zone applies equally well to life outside the office. Find and seize opportunities to do things your zone tries to discourage but that you wish to learn to do comfortably. It doesn't have to be a life-changing project: Start small. If you tend to avoid talking on the phone, for example, make a conscious effort to initiate a phone call every day. When it becomes part of your zone, those important phone calls will be far easier and more comfortable to make.
“Do something every day that you don't want to do,” Mark Twain once wrote. “This is the golden rule for acquiring the habit of doing your duty without pain.”
So the solution to burnout is to recognize that your Comfort Zone exists and must be managed, rather than allowing it to manage you and restrict you. By molding your zone to activities and situations that will keep you enthused, you can keep complacency at bay. Rather than permitting distractions to take a destructive course, look for distractions that are constructive, educational, and pleasurable.
Next month, my wife and I will be leading a group of doctors on a trip to Uzbekistan in Central Asia on the old Silk Road. It will be a new experience in an unfamiliar part of the world, and the decision to take it on was not made lightly. It would have been easy to stay home or to plan a “safer” trip to a more familiar destination, but in settling for a comfortable option we would have missed a golden opportunity to push our envelope in an educational and exciting way.
So if you're burned out, find something uncomfortably new and constructive, and go for it. When you conquer the fear, you'll conquer complacency.
Protect Your Data!
All too often, our office computers are disasters waiting to happen. We store huge amounts of important information on them and risk losing it all by neglecting to back up the data. No amount of casualty insurance will recoup the loss of the data on stolen or destroyed computers.
Industry statistics show that fully 10% of hard drives fail in any given year and that 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, e-mail, documents, and other important information. Recovery of lost data, when it's possible at all, can be very expensive.
Yet a Harris Interactive study last year found that 35% of Americans admitted they never back up their computers. And amazingly, many people who have lost important data in a crash still refuse to do regular backups. Why do so many of us neglect such a basic precaution? Because it's inconvenient and time-consuming. Clearly, the only way to get many people to back up their data regularly is to make the process automatic.
Some computer companies have taken steps in that direction. Apple, for example, has a feature called Time Machine that backs up Macs to an external drive automatically. But that does you no good if, for example, a fire destroys the computers and also incinerates the backup drives.
So, the first rule is to store your backup drives in a different location from your computers. Unfortunately, that's a pain, too, and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup.
Several companies offer this service: two of the most popular are Mozy (www.mozy.comwww.carbonite.com
The cost is very reasonable for individual computers. In fact, Mozy lets you store up to two gigabytes of data for free. Its basic package, which includes unlimited storage, costs $4.95 a month per computer. Carbonite is a bit cheaper ($49.95 per year, also for unlimited capacity), but Mozy is a little more customizable, and you can specify the files you want regularly backed up and when it will be done. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it's still very reasonable and includes other services such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files to copy. Your first backup can take a long time, often days, depending on how much data you are sending and the speed of your Internet connection. After that, the program runs in the background, copying only files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service's data center, making them HIPAA compliant and, theoretically, accessible only to you.
To restore files, you open a sort of virtual representation of your backed-up files and click on what you want restored. You also can log into the Web site from any other computer and pick any file or folder to retrieve. If your computer is stolen or the hard drive is destroyed, you can go to a site to initiate a full restore to a new computer. Remote backups might even help you recover a lost or stolen machine: If the finder or thief opens new files, they will be backed up to your new machine, which could allow you (or the police) to trace the original computer's whereabouts.
If you ever decide to terminate the service or simply want a hard copy of your data, Mozy will send you a DVD of all your files, for a fee. (Carbonite does not mention this service on its site.)
Soon, though, you might be able to use these services for a lot more than simply storing and retrieving files. Mozy's parent company, EMC, has announced a new subsidiary called Decho (www.decho.com
All too often, our office computers are disasters waiting to happen. We store huge amounts of important information on them and risk losing it all by neglecting to back up the data. No amount of casualty insurance will recoup the loss of the data on stolen or destroyed computers.
Industry statistics show that fully 10% of hard drives fail in any given year and that 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, e-mail, documents, and other important information. Recovery of lost data, when it's possible at all, can be very expensive.
Yet a Harris Interactive study last year found that 35% of Americans admitted they never back up their computers. And amazingly, many people who have lost important data in a crash still refuse to do regular backups. Why do so many of us neglect such a basic precaution? Because it's inconvenient and time-consuming. Clearly, the only way to get many people to back up their data regularly is to make the process automatic.
Some computer companies have taken steps in that direction. Apple, for example, has a feature called Time Machine that backs up Macs to an external drive automatically. But that does you no good if, for example, a fire destroys the computers and also incinerates the backup drives.
So, the first rule is to store your backup drives in a different location from your computers. Unfortunately, that's a pain, too, and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup.
Several companies offer this service: two of the most popular are Mozy (www.mozy.comwww.carbonite.com
The cost is very reasonable for individual computers. In fact, Mozy lets you store up to two gigabytes of data for free. Its basic package, which includes unlimited storage, costs $4.95 a month per computer. Carbonite is a bit cheaper ($49.95 per year, also for unlimited capacity), but Mozy is a little more customizable, and you can specify the files you want regularly backed up and when it will be done. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it's still very reasonable and includes other services such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files to copy. Your first backup can take a long time, often days, depending on how much data you are sending and the speed of your Internet connection. After that, the program runs in the background, copying only files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service's data center, making them HIPAA compliant and, theoretically, accessible only to you.
To restore files, you open a sort of virtual representation of your backed-up files and click on what you want restored. You also can log into the Web site from any other computer and pick any file or folder to retrieve. If your computer is stolen or the hard drive is destroyed, you can go to a site to initiate a full restore to a new computer. Remote backups might even help you recover a lost or stolen machine: If the finder or thief opens new files, they will be backed up to your new machine, which could allow you (or the police) to trace the original computer's whereabouts.
If you ever decide to terminate the service or simply want a hard copy of your data, Mozy will send you a DVD of all your files, for a fee. (Carbonite does not mention this service on its site.)
Soon, though, you might be able to use these services for a lot more than simply storing and retrieving files. Mozy's parent company, EMC, has announced a new subsidiary called Decho (www.decho.com
All too often, our office computers are disasters waiting to happen. We store huge amounts of important information on them and risk losing it all by neglecting to back up the data. No amount of casualty insurance will recoup the loss of the data on stolen or destroyed computers.
Industry statistics show that fully 10% of hard drives fail in any given year and that 43% of computer users lose one or more files every year in the form of clinical data, financial records, photos, e-mail, documents, and other important information. Recovery of lost data, when it's possible at all, can be very expensive.
Yet a Harris Interactive study last year found that 35% of Americans admitted they never back up their computers. And amazingly, many people who have lost important data in a crash still refuse to do regular backups. Why do so many of us neglect such a basic precaution? Because it's inconvenient and time-consuming. Clearly, the only way to get many people to back up their data regularly is to make the process automatic.
Some computer companies have taken steps in that direction. Apple, for example, has a feature called Time Machine that backs up Macs to an external drive automatically. But that does you no good if, for example, a fire destroys the computers and also incinerates the backup drives.
So, the first rule is to store your backup drives in a different location from your computers. Unfortunately, that's a pain, too, and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup.
Several companies offer this service: two of the most popular are Mozy (www.mozy.comwww.carbonite.com
The cost is very reasonable for individual computers. In fact, Mozy lets you store up to two gigabytes of data for free. Its basic package, which includes unlimited storage, costs $4.95 a month per computer. Carbonite is a bit cheaper ($49.95 per year, also for unlimited capacity), but Mozy is a little more customizable, and you can specify the files you want regularly backed up and when it will be done. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it's still very reasonable and includes other services such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files to copy. Your first backup can take a long time, often days, depending on how much data you are sending and the speed of your Internet connection. After that, the program runs in the background, copying only files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service's data center, making them HIPAA compliant and, theoretically, accessible only to you.
To restore files, you open a sort of virtual representation of your backed-up files and click on what you want restored. You also can log into the Web site from any other computer and pick any file or folder to retrieve. If your computer is stolen or the hard drive is destroyed, you can go to a site to initiate a full restore to a new computer. Remote backups might even help you recover a lost or stolen machine: If the finder or thief opens new files, they will be backed up to your new machine, which could allow you (or the police) to trace the original computer's whereabouts.
If you ever decide to terminate the service or simply want a hard copy of your data, Mozy will send you a DVD of all your files, for a fee. (Carbonite does not mention this service on its site.)
Soon, though, you might be able to use these services for a lot more than simply storing and retrieving files. Mozy's parent company, EMC, has announced a new subsidiary called Decho (www.decho.com
Medical Verdicts
Emergent hysterectomy after abortion complications
A 40-YEAR-OLD WOMAN had a pregnancy termination at 8 weeks’ gestation. During the procedure, her uterus was perforated, resulting in excruciating pain. In a subsequent emergency hysterectomy, she lost 4 L of blood.
PATIENT’S CLAIM Even though she complained of pain during the abortion, the physician refused to stop, and clinic employees held her down until the procedure was completed.
PHYSICIAN’S DEFENSE The patient had been informed of the risks of the procedure, including a perforated uterus, and stopping in the middle was medically inappropriate. Also, the patient had been told it was important to remain still during the procedure, but she was unwilling or unable to do so.
VERDICT Confidential Nebraska settlement.
Extensive surgery precedes final report of “no ovarian Ca”
A 52-YEAR-OLD WOMAN underwent an exploratory laparotomy performed by Dr. A, a gynecologist. Tissues from her ovaries, peritoneal implant, and omentum were sent for testing. Preliminary findings indicated well-differentiated papillary serous cystadenocarcinoma, and were submitted for further consultation and definitive final diagnosis. The patient then met with Dr. B, a gynecological oncologist, who informed her that she had ovarian cancer with metastasis. She underwent extensive surgery: total abdominal hysterectomy, appendectomy, omentectomy, staging laparotomy, lymph-node dissection, and resection of pelvic implants. Following surgery, she was informed that she did not have ovarian cancer, and the final lab report indicated a borderline serous tumor.
PATIENT’S CLAIM The second surgery, 24 days following the initial surgery, was performed before a definitive diagnosis was received from the lab—and it was unnecessary.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Florida defense verdict. An appeal was pending.
Patient takes drug while pregnant; her infant dies
AFTER THE BIRTH of her first child, a woman developed symptoms of hypertension. Dr. A, an internist, prescribed valsartan (Diovan, an angiotensin II receptor blocker manufactured by Novartis). Seven years later, the patient went to Dr. B when Dr. A was out of town. Dr. B wrote a prescription for valsartan and instructed her to return in 1 month to check her blood pressure and again in 1 year. She did not return for that check. Eight months after that, she was pregnant. Dr. C, her ObGyn, knew she was taking valsartan, but did not tell her to discontinue its use. For the first 6 months of her pregnancy, she continued taking valsartan. She later returned to Dr. B, who told her she could double her daily dosage of valsartan. She gave birth to a baby who lived only a few days.
PATIENT’S CLAIM Valsartan’s packaging and the PDR indicate that it is inappropriate to take valsartan during pregnancy. As a result of its ingestion, the infant died. Initially, the lawsuit included a products-related claim against Novartis, as well as a claim against the pharmacy that filled the prescription.
PHYSICIAN’S DEFENSE Dr. B assumed that Dr. C was managing the patient’s pregnancy and hypertension concerns. Dr. C admitted he did not know of the risks of valsartan to a fetus.
VERDICT Alabama defense verdict for Dr. B; $700,000 settlement with Dr. C; and $60,000 settlement with the pharmacy. Novartis was granted a summary judgment.
$2.5 million award when child has lethal heritable disease
A PATIENT GAVE BIRTH to a child who had Canavan disease, a neurologic disorder characterized by spongy degeneration of the central nervous system, with death often occurring by 4 years. The disease is found especially in Eastern European Jews.
PATIENT’S CLAIM The intake nurse at the health center failed to ask proper questions that would have suggested the need for genetic testing. The nurse and three midwives should have performed genetic testing once they learned the patient was Jewish to determine if she was a carrier of Canavan disease.
PHYSICIAN’S DEFENSE The patient failed to fill out the intake form properly, because she neglected to indicate whether her parents had the Jewish background that could be a carrier for Canavan disease.
VERDICT $2.5 million New Jersey settlement.
Blood loss addressed too late, mother dies after childbirth
A 35-YEAR-OLD WOMAN went to her ObGyn for a routine prenatal visit. As she was 6 to 7 cm dilated, she was sent to the hospital for evaluation. Her baby was delivered by C-section very early the following morning, and the patient was moved to the recovery room. Her blood pressure was low and continued to drop. A second physician examined her 1.5 hours later and removed a 250-mL clot from her vagina—at which time her blood pressure was 71/32. She was administered crystalloid fluids, but no blood or blood products. Within half an hour, diastolic pressure could not be obtained. It was decided to perform an ileac artery embolization. However, the patient became bradycardic and went into ventricular fibrillation. She was resuscitated and taken for an emergency hysterectomy, during which blood and a clot were found in her abdominal cavity. Again she arrested and was resuscitated, and then continued to decline and died.
PLAINTIFF’S CLAIM The patient first showed signs of serious postsurgical bleeding while in the recovery room, but the blood loss was not addressed. The hysterectomy was not performed in a timely manner to address the uterine atony, which caused the bleeding.
PHYSICIAN’S DEFENSE Not reported.
VERDICT $1 million Maryland settlement.
Surgery, inadequate Paps—then stage IV endocervical Ca
FOLLOWING A DIAGNOSIS of cancer in her endocervix, a woman had the cancer removed surgically. Her physician scheduled her for semiannual Pap smears to monitor the endocervix for recurrence of the cancer, but he ordered no other testing. He performed the Pap smears; however, as the surgery had closed off the endocervix, the spatula could reach only the ectocervix and not the endocervix, which needed to be sampled. When the lab reported back that there were no endocervical cells on the smears, the patient was just told that the results were normal. She also was not informed that the endocervix could not be reached. Eventually, the patient received a diagnosis of stage IV endocervical cancer.
PLAINTIFF’S CLAIM Follow-up Pap smears to obtain adequate samples including endocervical cells were to have been performed. Her physician concealed the fact that he was unable to obtain an adequate sample from the previously cancerous area, and he failed to monitor her for recurrence of that cancer.
PHYSICIAN’S DEFENSE The claims for all but one of the Pap smears was time-barred, and the concealment argument did not apply.
VERDICT Confidential Florida settlement after a defense motion for summary judgment was denied.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Emergent hysterectomy after abortion complications
A 40-YEAR-OLD WOMAN had a pregnancy termination at 8 weeks’ gestation. During the procedure, her uterus was perforated, resulting in excruciating pain. In a subsequent emergency hysterectomy, she lost 4 L of blood.
PATIENT’S CLAIM Even though she complained of pain during the abortion, the physician refused to stop, and clinic employees held her down until the procedure was completed.
PHYSICIAN’S DEFENSE The patient had been informed of the risks of the procedure, including a perforated uterus, and stopping in the middle was medically inappropriate. Also, the patient had been told it was important to remain still during the procedure, but she was unwilling or unable to do so.
VERDICT Confidential Nebraska settlement.
Extensive surgery precedes final report of “no ovarian Ca”
A 52-YEAR-OLD WOMAN underwent an exploratory laparotomy performed by Dr. A, a gynecologist. Tissues from her ovaries, peritoneal implant, and omentum were sent for testing. Preliminary findings indicated well-differentiated papillary serous cystadenocarcinoma, and were submitted for further consultation and definitive final diagnosis. The patient then met with Dr. B, a gynecological oncologist, who informed her that she had ovarian cancer with metastasis. She underwent extensive surgery: total abdominal hysterectomy, appendectomy, omentectomy, staging laparotomy, lymph-node dissection, and resection of pelvic implants. Following surgery, she was informed that she did not have ovarian cancer, and the final lab report indicated a borderline serous tumor.
PATIENT’S CLAIM The second surgery, 24 days following the initial surgery, was performed before a definitive diagnosis was received from the lab—and it was unnecessary.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Florida defense verdict. An appeal was pending.
Patient takes drug while pregnant; her infant dies
AFTER THE BIRTH of her first child, a woman developed symptoms of hypertension. Dr. A, an internist, prescribed valsartan (Diovan, an angiotensin II receptor blocker manufactured by Novartis). Seven years later, the patient went to Dr. B when Dr. A was out of town. Dr. B wrote a prescription for valsartan and instructed her to return in 1 month to check her blood pressure and again in 1 year. She did not return for that check. Eight months after that, she was pregnant. Dr. C, her ObGyn, knew she was taking valsartan, but did not tell her to discontinue its use. For the first 6 months of her pregnancy, she continued taking valsartan. She later returned to Dr. B, who told her she could double her daily dosage of valsartan. She gave birth to a baby who lived only a few days.
PATIENT’S CLAIM Valsartan’s packaging and the PDR indicate that it is inappropriate to take valsartan during pregnancy. As a result of its ingestion, the infant died. Initially, the lawsuit included a products-related claim against Novartis, as well as a claim against the pharmacy that filled the prescription.
PHYSICIAN’S DEFENSE Dr. B assumed that Dr. C was managing the patient’s pregnancy and hypertension concerns. Dr. C admitted he did not know of the risks of valsartan to a fetus.
VERDICT Alabama defense verdict for Dr. B; $700,000 settlement with Dr. C; and $60,000 settlement with the pharmacy. Novartis was granted a summary judgment.
$2.5 million award when child has lethal heritable disease
A PATIENT GAVE BIRTH to a child who had Canavan disease, a neurologic disorder characterized by spongy degeneration of the central nervous system, with death often occurring by 4 years. The disease is found especially in Eastern European Jews.
PATIENT’S CLAIM The intake nurse at the health center failed to ask proper questions that would have suggested the need for genetic testing. The nurse and three midwives should have performed genetic testing once they learned the patient was Jewish to determine if she was a carrier of Canavan disease.
PHYSICIAN’S DEFENSE The patient failed to fill out the intake form properly, because she neglected to indicate whether her parents had the Jewish background that could be a carrier for Canavan disease.
VERDICT $2.5 million New Jersey settlement.
Blood loss addressed too late, mother dies after childbirth
A 35-YEAR-OLD WOMAN went to her ObGyn for a routine prenatal visit. As she was 6 to 7 cm dilated, she was sent to the hospital for evaluation. Her baby was delivered by C-section very early the following morning, and the patient was moved to the recovery room. Her blood pressure was low and continued to drop. A second physician examined her 1.5 hours later and removed a 250-mL clot from her vagina—at which time her blood pressure was 71/32. She was administered crystalloid fluids, but no blood or blood products. Within half an hour, diastolic pressure could not be obtained. It was decided to perform an ileac artery embolization. However, the patient became bradycardic and went into ventricular fibrillation. She was resuscitated and taken for an emergency hysterectomy, during which blood and a clot were found in her abdominal cavity. Again she arrested and was resuscitated, and then continued to decline and died.
PLAINTIFF’S CLAIM The patient first showed signs of serious postsurgical bleeding while in the recovery room, but the blood loss was not addressed. The hysterectomy was not performed in a timely manner to address the uterine atony, which caused the bleeding.
PHYSICIAN’S DEFENSE Not reported.
VERDICT $1 million Maryland settlement.
Surgery, inadequate Paps—then stage IV endocervical Ca
FOLLOWING A DIAGNOSIS of cancer in her endocervix, a woman had the cancer removed surgically. Her physician scheduled her for semiannual Pap smears to monitor the endocervix for recurrence of the cancer, but he ordered no other testing. He performed the Pap smears; however, as the surgery had closed off the endocervix, the spatula could reach only the ectocervix and not the endocervix, which needed to be sampled. When the lab reported back that there were no endocervical cells on the smears, the patient was just told that the results were normal. She also was not informed that the endocervix could not be reached. Eventually, the patient received a diagnosis of stage IV endocervical cancer.
PLAINTIFF’S CLAIM Follow-up Pap smears to obtain adequate samples including endocervical cells were to have been performed. Her physician concealed the fact that he was unable to obtain an adequate sample from the previously cancerous area, and he failed to monitor her for recurrence of that cancer.
PHYSICIAN’S DEFENSE The claims for all but one of the Pap smears was time-barred, and the concealment argument did not apply.
VERDICT Confidential Florida settlement after a defense motion for summary judgment was denied.
Emergent hysterectomy after abortion complications
A 40-YEAR-OLD WOMAN had a pregnancy termination at 8 weeks’ gestation. During the procedure, her uterus was perforated, resulting in excruciating pain. In a subsequent emergency hysterectomy, she lost 4 L of blood.
PATIENT’S CLAIM Even though she complained of pain during the abortion, the physician refused to stop, and clinic employees held her down until the procedure was completed.
PHYSICIAN’S DEFENSE The patient had been informed of the risks of the procedure, including a perforated uterus, and stopping in the middle was medically inappropriate. Also, the patient had been told it was important to remain still during the procedure, but she was unwilling or unable to do so.
VERDICT Confidential Nebraska settlement.
Extensive surgery precedes final report of “no ovarian Ca”
A 52-YEAR-OLD WOMAN underwent an exploratory laparotomy performed by Dr. A, a gynecologist. Tissues from her ovaries, peritoneal implant, and omentum were sent for testing. Preliminary findings indicated well-differentiated papillary serous cystadenocarcinoma, and were submitted for further consultation and definitive final diagnosis. The patient then met with Dr. B, a gynecological oncologist, who informed her that she had ovarian cancer with metastasis. She underwent extensive surgery: total abdominal hysterectomy, appendectomy, omentectomy, staging laparotomy, lymph-node dissection, and resection of pelvic implants. Following surgery, she was informed that she did not have ovarian cancer, and the final lab report indicated a borderline serous tumor.
PATIENT’S CLAIM The second surgery, 24 days following the initial surgery, was performed before a definitive diagnosis was received from the lab—and it was unnecessary.
PHYSICIAN’S DEFENSE Not reported.
VERDICT Florida defense verdict. An appeal was pending.
Patient takes drug while pregnant; her infant dies
AFTER THE BIRTH of her first child, a woman developed symptoms of hypertension. Dr. A, an internist, prescribed valsartan (Diovan, an angiotensin II receptor blocker manufactured by Novartis). Seven years later, the patient went to Dr. B when Dr. A was out of town. Dr. B wrote a prescription for valsartan and instructed her to return in 1 month to check her blood pressure and again in 1 year. She did not return for that check. Eight months after that, she was pregnant. Dr. C, her ObGyn, knew she was taking valsartan, but did not tell her to discontinue its use. For the first 6 months of her pregnancy, she continued taking valsartan. She later returned to Dr. B, who told her she could double her daily dosage of valsartan. She gave birth to a baby who lived only a few days.
PATIENT’S CLAIM Valsartan’s packaging and the PDR indicate that it is inappropriate to take valsartan during pregnancy. As a result of its ingestion, the infant died. Initially, the lawsuit included a products-related claim against Novartis, as well as a claim against the pharmacy that filled the prescription.
PHYSICIAN’S DEFENSE Dr. B assumed that Dr. C was managing the patient’s pregnancy and hypertension concerns. Dr. C admitted he did not know of the risks of valsartan to a fetus.
VERDICT Alabama defense verdict for Dr. B; $700,000 settlement with Dr. C; and $60,000 settlement with the pharmacy. Novartis was granted a summary judgment.
$2.5 million award when child has lethal heritable disease
A PATIENT GAVE BIRTH to a child who had Canavan disease, a neurologic disorder characterized by spongy degeneration of the central nervous system, with death often occurring by 4 years. The disease is found especially in Eastern European Jews.
PATIENT’S CLAIM The intake nurse at the health center failed to ask proper questions that would have suggested the need for genetic testing. The nurse and three midwives should have performed genetic testing once they learned the patient was Jewish to determine if she was a carrier of Canavan disease.
PHYSICIAN’S DEFENSE The patient failed to fill out the intake form properly, because she neglected to indicate whether her parents had the Jewish background that could be a carrier for Canavan disease.
VERDICT $2.5 million New Jersey settlement.
Blood loss addressed too late, mother dies after childbirth
A 35-YEAR-OLD WOMAN went to her ObGyn for a routine prenatal visit. As she was 6 to 7 cm dilated, she was sent to the hospital for evaluation. Her baby was delivered by C-section very early the following morning, and the patient was moved to the recovery room. Her blood pressure was low and continued to drop. A second physician examined her 1.5 hours later and removed a 250-mL clot from her vagina—at which time her blood pressure was 71/32. She was administered crystalloid fluids, but no blood or blood products. Within half an hour, diastolic pressure could not be obtained. It was decided to perform an ileac artery embolization. However, the patient became bradycardic and went into ventricular fibrillation. She was resuscitated and taken for an emergency hysterectomy, during which blood and a clot were found in her abdominal cavity. Again she arrested and was resuscitated, and then continued to decline and died.
PLAINTIFF’S CLAIM The patient first showed signs of serious postsurgical bleeding while in the recovery room, but the blood loss was not addressed. The hysterectomy was not performed in a timely manner to address the uterine atony, which caused the bleeding.
PHYSICIAN’S DEFENSE Not reported.
VERDICT $1 million Maryland settlement.
Surgery, inadequate Paps—then stage IV endocervical Ca
FOLLOWING A DIAGNOSIS of cancer in her endocervix, a woman had the cancer removed surgically. Her physician scheduled her for semiannual Pap smears to monitor the endocervix for recurrence of the cancer, but he ordered no other testing. He performed the Pap smears; however, as the surgery had closed off the endocervix, the spatula could reach only the ectocervix and not the endocervix, which needed to be sampled. When the lab reported back that there were no endocervical cells on the smears, the patient was just told that the results were normal. She also was not informed that the endocervix could not be reached. Eventually, the patient received a diagnosis of stage IV endocervical cancer.
PLAINTIFF’S CLAIM Follow-up Pap smears to obtain adequate samples including endocervical cells were to have been performed. Her physician concealed the fact that he was unable to obtain an adequate sample from the previously cancerous area, and he failed to monitor her for recurrence of that cancer.
PHYSICIAN’S DEFENSE The claims for all but one of the Pap smears was time-barred, and the concealment argument did not apply.
VERDICT Confidential Florida settlement after a defense motion for summary judgment was denied.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Protect Your Data!
Last month I wrote about a dermatologist from the Midwest whose office was ransacked and then set on fire. I covered the steps necessary to file a timely and accurate insurance claim.
No amount of insurance, however, will recoup one of his worst losses: the data on his destroyed computers.
Industry statistics show that fully 10% of hard drives fail in any given year and that 43% of computer users lose one or more files every year. Recovery of lost data, when it's possible at all, can be very expensive.
Despite that, a Harris Interactive study found that 35% of Americans admitted they never back up their computers. My guess is that the actual percentage is substantially higher. And amazingly, many people who have lost important, irretrievable data in a crash still refuse to do regular backups.
Why do so many of us neglect such a basic precaution? Because it's an annoyance and an inconvenience and takes too much time. Clearly, the only way to get many people to back up their data regularly is to make the process automatic.
Some computer companies have taken steps in that direction. Apple, for example, has a feature called Time Machine that backs up Macs to an external drive automatically. But that does you no good if, as happened to the Midwestern dermatologist, the fire that destroys the computers also incinerates the backup drives.
So, the first rule is to store your backup drives in a different location from your computers. Unfortunately, that's a pain, too, and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup.
There are several companies that offer this service: two of the most popular are Mozy (www.mozy.comwww.carbonite.com
(As always, I have no financial interest in any product or service discussed in this column.)
The cost is very reasonable. In fact, Mozy lets you store up to two gigabytes of data for free. Its basic package, which includes unlimited storage, costs $4.95 a month per computer. Carbonite is a bit cheaper ($49.95 per year, also for unlimited capacity), but Mozy is a little more customizable, and you can specify the files you want regularly backed up and when it will be done. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it's still very reasonable and includes other services such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and the speed of your Internet connection. After that, the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service's data center, making them HIPAA compliant and, theoretically, accessible only to you.
To restore files, you open a sort of virtual representation of your backed-up files and click on what you want restored. You also can log into the Web site from any other computer and pick any file or folder to retrieve. If your computer is stolen or the hard drive is destroyed, you can go to a site to initiate a full restore to a new computer.
If you ever decide to terminate the service or simply want a hard copy of your data, Mozy will send you a DVD of all your files, for a fee.
Mozy's parent company, EMC, has announced a new subsidiary called Decho www.decho.com
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Last month I wrote about a dermatologist from the Midwest whose office was ransacked and then set on fire. I covered the steps necessary to file a timely and accurate insurance claim.
No amount of insurance, however, will recoup one of his worst losses: the data on his destroyed computers.
Industry statistics show that fully 10% of hard drives fail in any given year and that 43% of computer users lose one or more files every year. Recovery of lost data, when it's possible at all, can be very expensive.
Despite that, a Harris Interactive study found that 35% of Americans admitted they never back up their computers. My guess is that the actual percentage is substantially higher. And amazingly, many people who have lost important, irretrievable data in a crash still refuse to do regular backups.
Why do so many of us neglect such a basic precaution? Because it's an annoyance and an inconvenience and takes too much time. Clearly, the only way to get many people to back up their data regularly is to make the process automatic.
Some computer companies have taken steps in that direction. Apple, for example, has a feature called Time Machine that backs up Macs to an external drive automatically. But that does you no good if, as happened to the Midwestern dermatologist, the fire that destroys the computers also incinerates the backup drives.
So, the first rule is to store your backup drives in a different location from your computers. Unfortunately, that's a pain, too, and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup.
There are several companies that offer this service: two of the most popular are Mozy (www.mozy.comwww.carbonite.com
(As always, I have no financial interest in any product or service discussed in this column.)
The cost is very reasonable. In fact, Mozy lets you store up to two gigabytes of data for free. Its basic package, which includes unlimited storage, costs $4.95 a month per computer. Carbonite is a bit cheaper ($49.95 per year, also for unlimited capacity), but Mozy is a little more customizable, and you can specify the files you want regularly backed up and when it will be done. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it's still very reasonable and includes other services such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and the speed of your Internet connection. After that, the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service's data center, making them HIPAA compliant and, theoretically, accessible only to you.
To restore files, you open a sort of virtual representation of your backed-up files and click on what you want restored. You also can log into the Web site from any other computer and pick any file or folder to retrieve. If your computer is stolen or the hard drive is destroyed, you can go to a site to initiate a full restore to a new computer.
If you ever decide to terminate the service or simply want a hard copy of your data, Mozy will send you a DVD of all your files, for a fee.
Mozy's parent company, EMC, has announced a new subsidiary called Decho www.decho.com
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Last month I wrote about a dermatologist from the Midwest whose office was ransacked and then set on fire. I covered the steps necessary to file a timely and accurate insurance claim.
No amount of insurance, however, will recoup one of his worst losses: the data on his destroyed computers.
Industry statistics show that fully 10% of hard drives fail in any given year and that 43% of computer users lose one or more files every year. Recovery of lost data, when it's possible at all, can be very expensive.
Despite that, a Harris Interactive study found that 35% of Americans admitted they never back up their computers. My guess is that the actual percentage is substantially higher. And amazingly, many people who have lost important, irretrievable data in a crash still refuse to do regular backups.
Why do so many of us neglect such a basic precaution? Because it's an annoyance and an inconvenience and takes too much time. Clearly, the only way to get many people to back up their data regularly is to make the process automatic.
Some computer companies have taken steps in that direction. Apple, for example, has a feature called Time Machine that backs up Macs to an external drive automatically. But that does you no good if, as happened to the Midwestern dermatologist, the fire that destroys the computers also incinerates the backup drives.
So, the first rule is to store your backup drives in a different location from your computers. Unfortunately, that's a pain, too, and external drives can be lost or stolen, creating a HIPAA nightmare. So an increasingly popular alternative is automatic remote backup.
There are several companies that offer this service: two of the most popular are Mozy (www.mozy.comwww.carbonite.com
(As always, I have no financial interest in any product or service discussed in this column.)
The cost is very reasonable. In fact, Mozy lets you store up to two gigabytes of data for free. Its basic package, which includes unlimited storage, costs $4.95 a month per computer. Carbonite is a bit cheaper ($49.95 per year, also for unlimited capacity), but Mozy is a little more customizable, and you can specify the files you want regularly backed up and when it will be done. Backing up an entire office costs more, depending on how many computers and/or servers you have, but it's still very reasonable and includes other services such as operating system and network share support.
The procedure is simple: You create an account and tell the service which files you want copied. Your first backup can take a long time, often days, depending on how much data you are sending and the speed of your Internet connection. After that, the program runs in the background, copying only those files that have changed since the previous backup. Files are encrypted before leaving your computer, and they remain encrypted at the service's data center, making them HIPAA compliant and, theoretically, accessible only to you.
To restore files, you open a sort of virtual representation of your backed-up files and click on what you want restored. You also can log into the Web site from any other computer and pick any file or folder to retrieve. If your computer is stolen or the hard drive is destroyed, you can go to a site to initiate a full restore to a new computer.
If you ever decide to terminate the service or simply want a hard copy of your data, Mozy will send you a DVD of all your files, for a fee.
Mozy's parent company, EMC, has announced a new subsidiary called Decho www.decho.com
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
CPR for EHRs
The truth about EHR systems is that their implementation is never easy. It's a lot of work. It takes time and money, and despite the best laid plans there will be trauma and frustration. So expecting problems to arise is key to keeping perspective.
When our office implemented an electronic health records system in 2000, our system crashed 25–75 times a day for 5 months, and we lost patient data each time. I repeat: We lost patient data each time. Extensive troubleshooting ensued. Ceiling tiles were ripped out to see if the fluorescent lights were interfering with the network cables, a consultant was brought in, and our server and network were reinstalled. Finally, the cause of the crashes was determined to be a bug in our Microsoft program. As nightmarish as this situation was, I would say that such technology challenges were nothing compared to challenges in managing processes and people.
From a process perspective, a common mistake involves attempting to make the EHR system conform to what is done with paper. The whole point is to imagine a process that can help your office save time and money instead of mirroring what you did for years with a paper-based system.
Staff challenges are by far the toughest ones to manage because they require changing the minds and habits of individuals who don't feel comfortable giving up paper-based processes. Persistent naysayers can sabotage EHR implementation by convincing others that the changes cannot be made. Over the years, four of five staff members have left. When new staff members were hired, we emphasized the fact that our office was computerized and those individuals have successfully adapted to a paperless system. Among the lessons we've learned over the years are these:
▸ Don't skimp on training. When you're spending thousands of dollars on an EHR system it's tempting to shave costs and training may appear to be part of the discretionary spending budget. But giving training short shrift can cost you a lot more than you saved in the long run.
Even if you're the most technologically savvy physician, avoid the “I can do it all” mentality. Your time is best spent seeing patients and making money. Make sure that others are well trained so you feel comfortable delegating EHR responsibilities.
▸ Train the Luddites last. Once you've worked out all the kinks in the training process with those who are most comfortable using computers, it'll go a lot more smoothly for those who are less tech-savvy. Don't let anyone opt out of training. That can cost tens of thousands of dollars in the long run.
▸ Include everyone in brainstorming sessions. While no one likes meetings, get everyone involved in implementation meetings, not just the doctors and the office manager, because you will get good ideas from everyone. In addition, if they are involved in the brainstorming sessions, they are far more likely to adopt new behaviors.
▸ It doesn't have to be perfect. During the transition phase to an EHR system, there's a temptation to try to make everything perfect. Soon after we went live with our system, I spent a lot of time checking electronic charts to make sure the staff had included consultation notes. It was really a wasted step, because 99% of the time they had done it. In the rare event that the notes don't get into the chart, it doesn't affect patient care. The key is knowing when to accept a process as good enough and move on.
▸ Get a leader. You need a leader with a vision to organize the troubleshooting, both to build support and to keep everyone on track. The most common cause of EHR failure is lack of a leader.
The truth about EHR systems is that their implementation is never easy. It's a lot of work. It takes time and money, and despite the best laid plans there will be trauma and frustration. So expecting problems to arise is key to keeping perspective.
When our office implemented an electronic health records system in 2000, our system crashed 25–75 times a day for 5 months, and we lost patient data each time. I repeat: We lost patient data each time. Extensive troubleshooting ensued. Ceiling tiles were ripped out to see if the fluorescent lights were interfering with the network cables, a consultant was brought in, and our server and network were reinstalled. Finally, the cause of the crashes was determined to be a bug in our Microsoft program. As nightmarish as this situation was, I would say that such technology challenges were nothing compared to challenges in managing processes and people.
From a process perspective, a common mistake involves attempting to make the EHR system conform to what is done with paper. The whole point is to imagine a process that can help your office save time and money instead of mirroring what you did for years with a paper-based system.
Staff challenges are by far the toughest ones to manage because they require changing the minds and habits of individuals who don't feel comfortable giving up paper-based processes. Persistent naysayers can sabotage EHR implementation by convincing others that the changes cannot be made. Over the years, four of five staff members have left. When new staff members were hired, we emphasized the fact that our office was computerized and those individuals have successfully adapted to a paperless system. Among the lessons we've learned over the years are these:
▸ Don't skimp on training. When you're spending thousands of dollars on an EHR system it's tempting to shave costs and training may appear to be part of the discretionary spending budget. But giving training short shrift can cost you a lot more than you saved in the long run.
Even if you're the most technologically savvy physician, avoid the “I can do it all” mentality. Your time is best spent seeing patients and making money. Make sure that others are well trained so you feel comfortable delegating EHR responsibilities.
▸ Train the Luddites last. Once you've worked out all the kinks in the training process with those who are most comfortable using computers, it'll go a lot more smoothly for those who are less tech-savvy. Don't let anyone opt out of training. That can cost tens of thousands of dollars in the long run.
▸ Include everyone in brainstorming sessions. While no one likes meetings, get everyone involved in implementation meetings, not just the doctors and the office manager, because you will get good ideas from everyone. In addition, if they are involved in the brainstorming sessions, they are far more likely to adopt new behaviors.
▸ It doesn't have to be perfect. During the transition phase to an EHR system, there's a temptation to try to make everything perfect. Soon after we went live with our system, I spent a lot of time checking electronic charts to make sure the staff had included consultation notes. It was really a wasted step, because 99% of the time they had done it. In the rare event that the notes don't get into the chart, it doesn't affect patient care. The key is knowing when to accept a process as good enough and move on.
▸ Get a leader. You need a leader with a vision to organize the troubleshooting, both to build support and to keep everyone on track. The most common cause of EHR failure is lack of a leader.
The truth about EHR systems is that their implementation is never easy. It's a lot of work. It takes time and money, and despite the best laid plans there will be trauma and frustration. So expecting problems to arise is key to keeping perspective.
When our office implemented an electronic health records system in 2000, our system crashed 25–75 times a day for 5 months, and we lost patient data each time. I repeat: We lost patient data each time. Extensive troubleshooting ensued. Ceiling tiles were ripped out to see if the fluorescent lights were interfering with the network cables, a consultant was brought in, and our server and network were reinstalled. Finally, the cause of the crashes was determined to be a bug in our Microsoft program. As nightmarish as this situation was, I would say that such technology challenges were nothing compared to challenges in managing processes and people.
From a process perspective, a common mistake involves attempting to make the EHR system conform to what is done with paper. The whole point is to imagine a process that can help your office save time and money instead of mirroring what you did for years with a paper-based system.
Staff challenges are by far the toughest ones to manage because they require changing the minds and habits of individuals who don't feel comfortable giving up paper-based processes. Persistent naysayers can sabotage EHR implementation by convincing others that the changes cannot be made. Over the years, four of five staff members have left. When new staff members were hired, we emphasized the fact that our office was computerized and those individuals have successfully adapted to a paperless system. Among the lessons we've learned over the years are these:
▸ Don't skimp on training. When you're spending thousands of dollars on an EHR system it's tempting to shave costs and training may appear to be part of the discretionary spending budget. But giving training short shrift can cost you a lot more than you saved in the long run.
Even if you're the most technologically savvy physician, avoid the “I can do it all” mentality. Your time is best spent seeing patients and making money. Make sure that others are well trained so you feel comfortable delegating EHR responsibilities.
▸ Train the Luddites last. Once you've worked out all the kinks in the training process with those who are most comfortable using computers, it'll go a lot more smoothly for those who are less tech-savvy. Don't let anyone opt out of training. That can cost tens of thousands of dollars in the long run.
▸ Include everyone in brainstorming sessions. While no one likes meetings, get everyone involved in implementation meetings, not just the doctors and the office manager, because you will get good ideas from everyone. In addition, if they are involved in the brainstorming sessions, they are far more likely to adopt new behaviors.
▸ It doesn't have to be perfect. During the transition phase to an EHR system, there's a temptation to try to make everything perfect. Soon after we went live with our system, I spent a lot of time checking electronic charts to make sure the staff had included consultation notes. It was really a wasted step, because 99% of the time they had done it. In the rare event that the notes don't get into the chart, it doesn't affect patient care. The key is knowing when to accept a process as good enough and move on.
▸ Get a leader. You need a leader with a vision to organize the troubleshooting, both to build support and to keep everyone on track. The most common cause of EHR failure is lack of a leader.