User login
Face-to-Face Improvement
The American Medical Association recently released Current Procedural Terminology (CPT) 2009. New, deleted, and revised codes went into effect Jan. 1. The biggest change to hospitalist billing involves prolonged care codes (99354-99357). CPT 2009 descriptor revisions make it possible for physicians to contribute non-face-to-face time toward prolonged care services.
Inpatient Prolonged Care
Previous versions of CPT defined code 99356 as the first hour of prolonged physician [inpatient] services requiring direct (face-to-face) patient contact beyond the usual services (reportable after the initial 30 minutes); and 99357 for each additional 30 minutes of prolonged [inpatient] care beyond the first hour (reportable after the first 15 minutes of each additional segment). CPT 2009 has changed prolonged care guidelines to be more consistent with other time-based services: all unit/floor time spent by the physician is considered when reporting 99356 and 99357.1
As with most other evaluation and management services, a face-to-face encounter still must occur. In addition to the time associated with the face-to-face encounter, count the time associated with all other physician activities occurring on the unit/floor (e.g., reviewing images, obtaining information involving overnight events, discussing management options with the family) directed toward an individual patient. The cumulative time spent by the billing provider on a single calendar day is considered for billing. Time spent by someone other than the billing provider cannot be credited toward prolonged care.
As example, a physician cares for a 65-year-old male with uncontrolled diabetes, diabetic nephropathy, and congestive heart failure. Early in the day, the physician rounds, spending a total of 20 minutes reviewing the overnight course of events on the unit, re-confirming the patient history, and performing an exam with the patient. Anticipating the patient’s needs, the physician discusses post-discharge options and care with the patient and his family for 45 minutes. After the discussion, the physician spends an additional 30 minutes relaying information to the team and coordinating care. Merely reporting the highest-level subsequent hospital care service (99233), does not capture the physician’s cumulative effort. It only would account for 40 of the 95 minutes spent throughout the day. In order to capture the remaining 55 minutes, the physician reports 99356 on the same claim form as 99233.
Do not report prolonged care codes on a separate claim form. Prolonged care codes do not represent an independent service. These codes are reported along with a primary service. They must appear as a separate line item on the claim form, which includes a code representing the primary service. For prolonged care in the inpatient setting, the primary service must be initial hospital care (99221-99223), subsequent hospital care (99231-99233), inpatient consultations (99251-99255), or nursing facility services (99304-99318). Additional examples of billable prolonged care services are in Section 30.6.15.1I of the Medicare manual, available at www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf.
Threshold Time
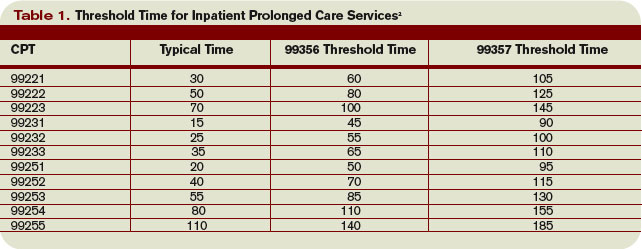
Prolonged care guidelines refer to “threshold” time. Threshold time requires the physician to exceed the time requirements associated with the “primary” codes before reporting prolonged care. Table 1 identifies the typical times associated with inpatient services qualifying for prolonged care. The physician must exceed the typical time by a minimum of 30 minutes. (For example, 99232 + 99356 = 25 minutes + 30 minutes = 55 total minutes). Additionally, the physician must document the total time spent during the face-to-face portion of the encounter, and the additional unit or floor time in one cumulative note or in separate notes representing the physician services provided to the patient throughout the day.
Prolonged Outpatient Services
Prolonged care (99354-99355) provided to outpatients remains unchanged. Physicians only report personally provided face-to-face time with the patient. Time spent by other staff members does not count toward prolonged care.
As with prolonged inpatient care, report 99354 and 99355 in addition to a primary service code. The companion outpatient codes are outpatient/office visits (99201-99205 or 99212–99215), outpatient consultation (99241–99245), domiciliary/custodial care (99324–99328 or 99334–99337), and home services (99341-99350). Hospitalists more often use outpatient prolonged care with office consultation codes for services provided in the emergency department, as appropriate.
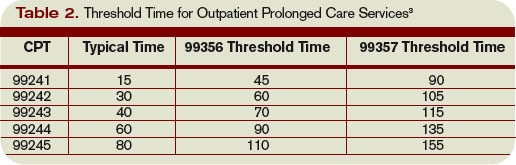
Do not report 99354 or 99355 with observation care (99217-99220) or emergency department visits (99281-99288), since these service categories typically require prolonged periods of physician monitoring, thereby prohibiting use of prolonged care codes. As with inpatient-prolonged care, the concept of threshold time exists. Refer to Table 2 (pg. 25) for the typical threshold times associated with office consultation codes.
Medicare Consideration
Although CPT has offered revisions to this code, Medicare guidelines remain unchanged. The Medicare Claims Processing Manual still states: “In the case of prolonged hospital services, time spent reviewing charts or discussion of a patient with house medical staff and not with direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities, cannot be billed as prolonged services.”4 It is yet to be determined if the Centers for Medicare and Medicaid Services (CMS) will issue a transmittal to revise the current description in the processing manual. Physicians and staff may access past and present transmittal information at www.cms.hhs.gov/ Transmittals/.
As always, be sure to query payers about prolonged care services, since some non-Medicare insurers may not recognize these codes.
Modifier 21
Modifier 21 has been deleted from the CPT. Modifier 21 was appended to an appropriate visit code (e.g., 99232-21) when the face-to-face or floor/unit service(s) provided is prolonged or otherwise greater than usually required for the highest level of evaluation and management service within a given category.5 Since the descriptors for codes 99354-99357 have been revised to more consistently reflect the description formerly associated with modifier 21, there is no need to maintain its existence. Additionally, Medicare and most other payers did not recognize this modifier.
Code This Case
Question: A newly diagnosed diabetic requires extensive counseling regarding lifestyle changes, medication regime, the disease process, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient (15 minutes), and performs an abbreviated service (problem-focused history and exam). The attending physician asks the resident to assist him with the remaining counseling efforts and coordination of care (30 minutes).
Each physician documents his or her portion of the service. What visit level can the hospitalist report?
Answer: When two billing providers (i.e., two attending physicians) from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service, since 99356 must be reported on the same invoice as the primary visit code (e.g., 99231).6
The example above involves the resident’s time as well as the attending physician’s time. Documentation must be very clear to demonstrate the attending physician actively participated in the entire 45-minute service. Otherwise, only the attending may report the amount of time he actually spent providing the service.
Billing options for this scenario can vary. When the physician performs and documents the key components of history, exam, and decision making for the primary encounter, report 99231 (0.76 physician work relative value units; $33.90) and 99356 (1.71 physician work relative value units; $76.46) for the cumulative service. Alternatively, in those evaluation and management services for which the [primary] code level is selected based on time alone (i.e., history and exam was not performed or required), prolonged services may only be reported with the highest code level in that family of codes as the companion code.7
Therefore, this 45-minute service may be reported as 99233 (2.0 physician work relative value units; $86.92) since more than half of the total visit time was dedicated to counseling/coordi-nation of care (see Section 30.6.1B-C available at www. cms.hhs.gov/manuals/ downloads/clm104c12.pdf for additional information on billing for counseling/coordination of care time).
If a payer does not recognize prolonged care codes, only the latter billing option is possible. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 25-26.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1G. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
3. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1F. www.cms.hhs.gov/manuals/dowloads/ clm104c12.pdf. Accessed November 19, 2008.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf. Accessed November 19, 2008.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 457.
6. Pohlig, C. Bill by time spent on case. The Hospitalist. Jul 2008;19.
7. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1H. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
The American Medical Association recently released Current Procedural Terminology (CPT) 2009. New, deleted, and revised codes went into effect Jan. 1. The biggest change to hospitalist billing involves prolonged care codes (99354-99357). CPT 2009 descriptor revisions make it possible for physicians to contribute non-face-to-face time toward prolonged care services.
Inpatient Prolonged Care
Previous versions of CPT defined code 99356 as the first hour of prolonged physician [inpatient] services requiring direct (face-to-face) patient contact beyond the usual services (reportable after the initial 30 minutes); and 99357 for each additional 30 minutes of prolonged [inpatient] care beyond the first hour (reportable after the first 15 minutes of each additional segment). CPT 2009 has changed prolonged care guidelines to be more consistent with other time-based services: all unit/floor time spent by the physician is considered when reporting 99356 and 99357.1
As with most other evaluation and management services, a face-to-face encounter still must occur. In addition to the time associated with the face-to-face encounter, count the time associated with all other physician activities occurring on the unit/floor (e.g., reviewing images, obtaining information involving overnight events, discussing management options with the family) directed toward an individual patient. The cumulative time spent by the billing provider on a single calendar day is considered for billing. Time spent by someone other than the billing provider cannot be credited toward prolonged care.
As example, a physician cares for a 65-year-old male with uncontrolled diabetes, diabetic nephropathy, and congestive heart failure. Early in the day, the physician rounds, spending a total of 20 minutes reviewing the overnight course of events on the unit, re-confirming the patient history, and performing an exam with the patient. Anticipating the patient’s needs, the physician discusses post-discharge options and care with the patient and his family for 45 minutes. After the discussion, the physician spends an additional 30 minutes relaying information to the team and coordinating care. Merely reporting the highest-level subsequent hospital care service (99233), does not capture the physician’s cumulative effort. It only would account for 40 of the 95 minutes spent throughout the day. In order to capture the remaining 55 minutes, the physician reports 99356 on the same claim form as 99233.
Do not report prolonged care codes on a separate claim form. Prolonged care codes do not represent an independent service. These codes are reported along with a primary service. They must appear as a separate line item on the claim form, which includes a code representing the primary service. For prolonged care in the inpatient setting, the primary service must be initial hospital care (99221-99223), subsequent hospital care (99231-99233), inpatient consultations (99251-99255), or nursing facility services (99304-99318). Additional examples of billable prolonged care services are in Section 30.6.15.1I of the Medicare manual, available at www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf.
Threshold Time
Prolonged care guidelines refer to “threshold” time. Threshold time requires the physician to exceed the time requirements associated with the “primary” codes before reporting prolonged care. Table 1 identifies the typical times associated with inpatient services qualifying for prolonged care. The physician must exceed the typical time by a minimum of 30 minutes. (For example, 99232 + 99356 = 25 minutes + 30 minutes = 55 total minutes). Additionally, the physician must document the total time spent during the face-to-face portion of the encounter, and the additional unit or floor time in one cumulative note or in separate notes representing the physician services provided to the patient throughout the day.
Prolonged Outpatient Services
Prolonged care (99354-99355) provided to outpatients remains unchanged. Physicians only report personally provided face-to-face time with the patient. Time spent by other staff members does not count toward prolonged care.
As with prolonged inpatient care, report 99354 and 99355 in addition to a primary service code. The companion outpatient codes are outpatient/office visits (99201-99205 or 99212–99215), outpatient consultation (99241–99245), domiciliary/custodial care (99324–99328 or 99334–99337), and home services (99341-99350). Hospitalists more often use outpatient prolonged care with office consultation codes for services provided in the emergency department, as appropriate.
Do not report 99354 or 99355 with observation care (99217-99220) or emergency department visits (99281-99288), since these service categories typically require prolonged periods of physician monitoring, thereby prohibiting use of prolonged care codes. As with inpatient-prolonged care, the concept of threshold time exists. Refer to Table 2 (pg. 25) for the typical threshold times associated with office consultation codes.
Medicare Consideration
Although CPT has offered revisions to this code, Medicare guidelines remain unchanged. The Medicare Claims Processing Manual still states: “In the case of prolonged hospital services, time spent reviewing charts or discussion of a patient with house medical staff and not with direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities, cannot be billed as prolonged services.”4 It is yet to be determined if the Centers for Medicare and Medicaid Services (CMS) will issue a transmittal to revise the current description in the processing manual. Physicians and staff may access past and present transmittal information at www.cms.hhs.gov/ Transmittals/.
As always, be sure to query payers about prolonged care services, since some non-Medicare insurers may not recognize these codes.
Modifier 21
Modifier 21 has been deleted from the CPT. Modifier 21 was appended to an appropriate visit code (e.g., 99232-21) when the face-to-face or floor/unit service(s) provided is prolonged or otherwise greater than usually required for the highest level of evaluation and management service within a given category.5 Since the descriptors for codes 99354-99357 have been revised to more consistently reflect the description formerly associated with modifier 21, there is no need to maintain its existence. Additionally, Medicare and most other payers did not recognize this modifier.
Code This Case
Question: A newly diagnosed diabetic requires extensive counseling regarding lifestyle changes, medication regime, the disease process, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient (15 minutes), and performs an abbreviated service (problem-focused history and exam). The attending physician asks the resident to assist him with the remaining counseling efforts and coordination of care (30 minutes).
Each physician documents his or her portion of the service. What visit level can the hospitalist report?
Answer: When two billing providers (i.e., two attending physicians) from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service, since 99356 must be reported on the same invoice as the primary visit code (e.g., 99231).6
The example above involves the resident’s time as well as the attending physician’s time. Documentation must be very clear to demonstrate the attending physician actively participated in the entire 45-minute service. Otherwise, only the attending may report the amount of time he actually spent providing the service.
Billing options for this scenario can vary. When the physician performs and documents the key components of history, exam, and decision making for the primary encounter, report 99231 (0.76 physician work relative value units; $33.90) and 99356 (1.71 physician work relative value units; $76.46) for the cumulative service. Alternatively, in those evaluation and management services for which the [primary] code level is selected based on time alone (i.e., history and exam was not performed or required), prolonged services may only be reported with the highest code level in that family of codes as the companion code.7
Therefore, this 45-minute service may be reported as 99233 (2.0 physician work relative value units; $86.92) since more than half of the total visit time was dedicated to counseling/coordi-nation of care (see Section 30.6.1B-C available at www. cms.hhs.gov/manuals/ downloads/clm104c12.pdf for additional information on billing for counseling/coordination of care time).
If a payer does not recognize prolonged care codes, only the latter billing option is possible. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 25-26.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1G. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
3. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1F. www.cms.hhs.gov/manuals/dowloads/ clm104c12.pdf. Accessed November 19, 2008.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf. Accessed November 19, 2008.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 457.
6. Pohlig, C. Bill by time spent on case. The Hospitalist. Jul 2008;19.
7. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1H. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
The American Medical Association recently released Current Procedural Terminology (CPT) 2009. New, deleted, and revised codes went into effect Jan. 1. The biggest change to hospitalist billing involves prolonged care codes (99354-99357). CPT 2009 descriptor revisions make it possible for physicians to contribute non-face-to-face time toward prolonged care services.
Inpatient Prolonged Care
Previous versions of CPT defined code 99356 as the first hour of prolonged physician [inpatient] services requiring direct (face-to-face) patient contact beyond the usual services (reportable after the initial 30 minutes); and 99357 for each additional 30 minutes of prolonged [inpatient] care beyond the first hour (reportable after the first 15 minutes of each additional segment). CPT 2009 has changed prolonged care guidelines to be more consistent with other time-based services: all unit/floor time spent by the physician is considered when reporting 99356 and 99357.1
As with most other evaluation and management services, a face-to-face encounter still must occur. In addition to the time associated with the face-to-face encounter, count the time associated with all other physician activities occurring on the unit/floor (e.g., reviewing images, obtaining information involving overnight events, discussing management options with the family) directed toward an individual patient. The cumulative time spent by the billing provider on a single calendar day is considered for billing. Time spent by someone other than the billing provider cannot be credited toward prolonged care.
As example, a physician cares for a 65-year-old male with uncontrolled diabetes, diabetic nephropathy, and congestive heart failure. Early in the day, the physician rounds, spending a total of 20 minutes reviewing the overnight course of events on the unit, re-confirming the patient history, and performing an exam with the patient. Anticipating the patient’s needs, the physician discusses post-discharge options and care with the patient and his family for 45 minutes. After the discussion, the physician spends an additional 30 minutes relaying information to the team and coordinating care. Merely reporting the highest-level subsequent hospital care service (99233), does not capture the physician’s cumulative effort. It only would account for 40 of the 95 minutes spent throughout the day. In order to capture the remaining 55 minutes, the physician reports 99356 on the same claim form as 99233.
Do not report prolonged care codes on a separate claim form. Prolonged care codes do not represent an independent service. These codes are reported along with a primary service. They must appear as a separate line item on the claim form, which includes a code representing the primary service. For prolonged care in the inpatient setting, the primary service must be initial hospital care (99221-99223), subsequent hospital care (99231-99233), inpatient consultations (99251-99255), or nursing facility services (99304-99318). Additional examples of billable prolonged care services are in Section 30.6.15.1I of the Medicare manual, available at www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf.
Threshold Time
Prolonged care guidelines refer to “threshold” time. Threshold time requires the physician to exceed the time requirements associated with the “primary” codes before reporting prolonged care. Table 1 identifies the typical times associated with inpatient services qualifying for prolonged care. The physician must exceed the typical time by a minimum of 30 minutes. (For example, 99232 + 99356 = 25 minutes + 30 minutes = 55 total minutes). Additionally, the physician must document the total time spent during the face-to-face portion of the encounter, and the additional unit or floor time in one cumulative note or in separate notes representing the physician services provided to the patient throughout the day.
Prolonged Outpatient Services
Prolonged care (99354-99355) provided to outpatients remains unchanged. Physicians only report personally provided face-to-face time with the patient. Time spent by other staff members does not count toward prolonged care.
As with prolonged inpatient care, report 99354 and 99355 in addition to a primary service code. The companion outpatient codes are outpatient/office visits (99201-99205 or 99212–99215), outpatient consultation (99241–99245), domiciliary/custodial care (99324–99328 or 99334–99337), and home services (99341-99350). Hospitalists more often use outpatient prolonged care with office consultation codes for services provided in the emergency department, as appropriate.
Do not report 99354 or 99355 with observation care (99217-99220) or emergency department visits (99281-99288), since these service categories typically require prolonged periods of physician monitoring, thereby prohibiting use of prolonged care codes. As with inpatient-prolonged care, the concept of threshold time exists. Refer to Table 2 (pg. 25) for the typical threshold times associated with office consultation codes.
Medicare Consideration
Although CPT has offered revisions to this code, Medicare guidelines remain unchanged. The Medicare Claims Processing Manual still states: “In the case of prolonged hospital services, time spent reviewing charts or discussion of a patient with house medical staff and not with direct face-to-face contact with the patient, or waiting for test results, for changes in the patient’s condition, for end of a therapy, or for use of facilities, cannot be billed as prolonged services.”4 It is yet to be determined if the Centers for Medicare and Medicaid Services (CMS) will issue a transmittal to revise the current description in the processing manual. Physicians and staff may access past and present transmittal information at www.cms.hhs.gov/ Transmittals/.
As always, be sure to query payers about prolonged care services, since some non-Medicare insurers may not recognize these codes.
Modifier 21
Modifier 21 has been deleted from the CPT. Modifier 21 was appended to an appropriate visit code (e.g., 99232-21) when the face-to-face or floor/unit service(s) provided is prolonged or otherwise greater than usually required for the highest level of evaluation and management service within a given category.5 Since the descriptors for codes 99354-99357 have been revised to more consistently reflect the description formerly associated with modifier 21, there is no need to maintain its existence. Additionally, Medicare and most other payers did not recognize this modifier.
Code This Case
Question: A newly diagnosed diabetic requires extensive counseling regarding lifestyle changes, medication regime, the disease process, as well as coordination of care for outpatient programs and services. The hospitalist reviews some of the pertinent information with the patient (15 minutes), and performs an abbreviated service (problem-focused history and exam). The attending physician asks the resident to assist him with the remaining counseling efforts and coordination of care (30 minutes).
Each physician documents his or her portion of the service. What visit level can the hospitalist report?
Answer: When two billing providers (i.e., two attending physicians) from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service, since 99356 must be reported on the same invoice as the primary visit code (e.g., 99231).6
The example above involves the resident’s time as well as the attending physician’s time. Documentation must be very clear to demonstrate the attending physician actively participated in the entire 45-minute service. Otherwise, only the attending may report the amount of time he actually spent providing the service.
Billing options for this scenario can vary. When the physician performs and documents the key components of history, exam, and decision making for the primary encounter, report 99231 (0.76 physician work relative value units; $33.90) and 99356 (1.71 physician work relative value units; $76.46) for the cumulative service. Alternatively, in those evaluation and management services for which the [primary] code level is selected based on time alone (i.e., history and exam was not performed or required), prolonged services may only be reported with the highest code level in that family of codes as the companion code.7
Therefore, this 45-minute service may be reported as 99233 (2.0 physician work relative value units; $86.92) since more than half of the total visit time was dedicated to counseling/coordi-nation of care (see Section 30.6.1B-C available at www. cms.hhs.gov/manuals/ downloads/clm104c12.pdf for additional information on billing for counseling/coordination of care time).
If a payer does not recognize prolonged care codes, only the latter billing option is possible. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References
1. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 25-26.
2. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1G. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
3. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1F. www.cms.hhs.gov/manuals/dowloads/ clm104c12.pdf. Accessed November 19, 2008.
4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1C. www.cms.hhs.gov/manuals/ downloads/clm104c12.pdf. Accessed November 19, 2008.
5. Beebe M, Dalton J, Espronceda M, Evans D, Glenn R. Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2008; 457.
6. Pohlig, C. Bill by time spent on case. The Hospitalist. Jul 2008;19.
7. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.15.1H. www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed November 19, 2008.
Keeping Your Money Safe: Cash Controls and Security for Physician Practices
Medical Verdicts
Sutures in sciatic nerve cause multiple problems
A GYNECOLOGIC ONCOLOGIST recommended and repaired a cystocele that was causing urinary incontinence in a patient. Immediately following the surgery, the patient experienced severe pain radiating from her right buttock to her right knee and developed numbness in her right toes. Two days later, after consultation with a neurologist, she underwent further surgery. After it was found that the first physician had placed sutures in the right sciatic nerve, they were removed. The nerve sustained permanent injury, and the patient continues to have chronic pain, paresthesia, weakness, fatigue, and an altered gait.
PATIENT’S CLAIM The physician was negligent for placing the sutures in the sciatic nerve.
PHYSICIAN’S DEFENSE The physician denied any negligence.
VERDICT $700,000 Indiana verdict, which included $25,000 for loss of consortium for the patient’s husband.
Was retained sponge from C-section—or later surgery?
A 16-YEAR-OLD PATIENT delivered a baby by C-section, which proceeded uneventfully. Eight months later, because of abdominal pain, the patient underwent an exploratory laparotomy performed by Dr. A, a surgeon. She continued to experience abdominal pain, the origin of which could not be found. After another 8 months, in exploratory surgery performed by Dr. B, a retained lap sponge was found and removed. At this time, the patient was 5 months pregnant. Two months later, the baby was delivered prematurely and lived for 12 days.
PATIENT’S CLAIM The retained lap sponge was left there during the laparotomy surgery performed by Dr. A, and it should have been found sooner.
PHYSICIAN’S DEFENSE The retained sponge was left during the C-section. Also, the death of the second child was unrelated to the retained sponge.
VERDICT Kentucky defense verdict. An appeal was pending.
$22 million award follows preeclamptic mother’s death
A 29-YEAR-OLD WOMAN who was 9 months pregnant presented at the hospital with a severe headache. She was admitted to labor and delivery, where she was examined by an experienced nurse and a 2nd year resident. A diagnosis of preeclampsia and HELLP syndrome, as indicated by lab tests, was given. The patient was administered three 10-mg doses of labetalol—despite hospital policy of administering the drug every 10 minutes in increasing doses until the blood pressure returns to a safe level. When labor was induced, her blood pressure rose dangerously and she became unresponsive. The baby was delivered successfully by emergency C-section. A CT scan indicated that the mother had suffered a massive brain hemorrhage. She was placed on a ventilator for 4 days, and died when it was disconnected.
PLAINTIFF’S CLAIM Labetalol was not administered properly and according to hospital policy.
PHYSICIAN’S DEFENSE The patient would likely not have survived because the preeclampsia and HELLP syndrome were so severe.
VERDICT $22 million Illinois verdict.
Woman conceives after undergoing tubal ligation
A 29-YEAR-OLD WOMAN underwent a tubal ligation. But 9 to 10 months later, she became pregnant. A subsequent ligation indicated a “normal appearing” right fallopian tube.
PATIENT’S CLAIM The physician failed to ligate the proper structure.
PHYSICIAN’S DEFENSE The right fallopian tube had recanalized and appeared normal. However, there was no negligence in performing the tubal ligation.
VERDICT District of Columbia defense verdict.
Placental fragment, aggressive D&C—failed pregnancy
A WEEK AFTER DELIVERING a healthy baby, a woman underwent an emergency dilation and curettage (D&C) because of severe, life-threatening bleeding. Two years later, she suffered a miscarriage, and 7 months after that an ectopic pregnancy.
PATIENT’S CLAIM The obstetrician negligent for failing to examine the placenta after the birth, leading to a retained placental fragment that caused the bleeding. An aggressively performed D&C resulted in Asherman’s syndrome, which caused the miscarriage and ectopic pregnancy.
PHYSICIAN’S DEFENSE At the time of delivery, the placenta was inspected properly. There was nothing to indicate a retained placental fragment, which is a recognized complication of delivery. The D&C was performed properly; uterine scarring is a recognized complication of the procedure.
VERDICT Illinois defense verdict.
Gallbladder disease during pregnancy is not properly treated
FOR A MONTH BEFORE DELIVERY of her child, a woman suffered severe abdominal pain and vomiting, for which she took over-the-counter calcium carbonate antacids. Two days before giving birth, she was admitted to the hospital dehydrated and with life-threatening elevated calcium in her blood. She was transferred to another hospital, where she gave birth to a child with cerebral palsy at 28 weeks’ gestation. She then underwent removal of her gallbladder.
PATIENT’S CLAIM The plaintiff child claimed the treating ObGyn failed to properly treat the mother’s gallbladder disease and pancreatitis.
PHYSICIAN’S DEFENSE The mother’s problems were mainly due to ingestion of an off-label dosage of over-the-counter calcium carbonate antacids.
VERDICT Nebraska defense verdict. The plaintiff appealed the case on the basis of exclusion of some expert testimony. The case was affirmed on appeal.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Sutures in sciatic nerve cause multiple problems
A GYNECOLOGIC ONCOLOGIST recommended and repaired a cystocele that was causing urinary incontinence in a patient. Immediately following the surgery, the patient experienced severe pain radiating from her right buttock to her right knee and developed numbness in her right toes. Two days later, after consultation with a neurologist, she underwent further surgery. After it was found that the first physician had placed sutures in the right sciatic nerve, they were removed. The nerve sustained permanent injury, and the patient continues to have chronic pain, paresthesia, weakness, fatigue, and an altered gait.
PATIENT’S CLAIM The physician was negligent for placing the sutures in the sciatic nerve.
PHYSICIAN’S DEFENSE The physician denied any negligence.
VERDICT $700,000 Indiana verdict, which included $25,000 for loss of consortium for the patient’s husband.
Was retained sponge from C-section—or later surgery?
A 16-YEAR-OLD PATIENT delivered a baby by C-section, which proceeded uneventfully. Eight months later, because of abdominal pain, the patient underwent an exploratory laparotomy performed by Dr. A, a surgeon. She continued to experience abdominal pain, the origin of which could not be found. After another 8 months, in exploratory surgery performed by Dr. B, a retained lap sponge was found and removed. At this time, the patient was 5 months pregnant. Two months later, the baby was delivered prematurely and lived for 12 days.
PATIENT’S CLAIM The retained lap sponge was left there during the laparotomy surgery performed by Dr. A, and it should have been found sooner.
PHYSICIAN’S DEFENSE The retained sponge was left during the C-section. Also, the death of the second child was unrelated to the retained sponge.
VERDICT Kentucky defense verdict. An appeal was pending.
$22 million award follows preeclamptic mother’s death
A 29-YEAR-OLD WOMAN who was 9 months pregnant presented at the hospital with a severe headache. She was admitted to labor and delivery, where she was examined by an experienced nurse and a 2nd year resident. A diagnosis of preeclampsia and HELLP syndrome, as indicated by lab tests, was given. The patient was administered three 10-mg doses of labetalol—despite hospital policy of administering the drug every 10 minutes in increasing doses until the blood pressure returns to a safe level. When labor was induced, her blood pressure rose dangerously and she became unresponsive. The baby was delivered successfully by emergency C-section. A CT scan indicated that the mother had suffered a massive brain hemorrhage. She was placed on a ventilator for 4 days, and died when it was disconnected.
PLAINTIFF’S CLAIM Labetalol was not administered properly and according to hospital policy.
PHYSICIAN’S DEFENSE The patient would likely not have survived because the preeclampsia and HELLP syndrome were so severe.
VERDICT $22 million Illinois verdict.
Woman conceives after undergoing tubal ligation
A 29-YEAR-OLD WOMAN underwent a tubal ligation. But 9 to 10 months later, she became pregnant. A subsequent ligation indicated a “normal appearing” right fallopian tube.
PATIENT’S CLAIM The physician failed to ligate the proper structure.
PHYSICIAN’S DEFENSE The right fallopian tube had recanalized and appeared normal. However, there was no negligence in performing the tubal ligation.
VERDICT District of Columbia defense verdict.
Placental fragment, aggressive D&C—failed pregnancy
A WEEK AFTER DELIVERING a healthy baby, a woman underwent an emergency dilation and curettage (D&C) because of severe, life-threatening bleeding. Two years later, she suffered a miscarriage, and 7 months after that an ectopic pregnancy.
PATIENT’S CLAIM The obstetrician negligent for failing to examine the placenta after the birth, leading to a retained placental fragment that caused the bleeding. An aggressively performed D&C resulted in Asherman’s syndrome, which caused the miscarriage and ectopic pregnancy.
PHYSICIAN’S DEFENSE At the time of delivery, the placenta was inspected properly. There was nothing to indicate a retained placental fragment, which is a recognized complication of delivery. The D&C was performed properly; uterine scarring is a recognized complication of the procedure.
VERDICT Illinois defense verdict.
Gallbladder disease during pregnancy is not properly treated
FOR A MONTH BEFORE DELIVERY of her child, a woman suffered severe abdominal pain and vomiting, for which she took over-the-counter calcium carbonate antacids. Two days before giving birth, she was admitted to the hospital dehydrated and with life-threatening elevated calcium in her blood. She was transferred to another hospital, where she gave birth to a child with cerebral palsy at 28 weeks’ gestation. She then underwent removal of her gallbladder.
PATIENT’S CLAIM The plaintiff child claimed the treating ObGyn failed to properly treat the mother’s gallbladder disease and pancreatitis.
PHYSICIAN’S DEFENSE The mother’s problems were mainly due to ingestion of an off-label dosage of over-the-counter calcium carbonate antacids.
VERDICT Nebraska defense verdict. The plaintiff appealed the case on the basis of exclusion of some expert testimony. The case was affirmed on appeal.
Sutures in sciatic nerve cause multiple problems
A GYNECOLOGIC ONCOLOGIST recommended and repaired a cystocele that was causing urinary incontinence in a patient. Immediately following the surgery, the patient experienced severe pain radiating from her right buttock to her right knee and developed numbness in her right toes. Two days later, after consultation with a neurologist, she underwent further surgery. After it was found that the first physician had placed sutures in the right sciatic nerve, they were removed. The nerve sustained permanent injury, and the patient continues to have chronic pain, paresthesia, weakness, fatigue, and an altered gait.
PATIENT’S CLAIM The physician was negligent for placing the sutures in the sciatic nerve.
PHYSICIAN’S DEFENSE The physician denied any negligence.
VERDICT $700,000 Indiana verdict, which included $25,000 for loss of consortium for the patient’s husband.
Was retained sponge from C-section—or later surgery?
A 16-YEAR-OLD PATIENT delivered a baby by C-section, which proceeded uneventfully. Eight months later, because of abdominal pain, the patient underwent an exploratory laparotomy performed by Dr. A, a surgeon. She continued to experience abdominal pain, the origin of which could not be found. After another 8 months, in exploratory surgery performed by Dr. B, a retained lap sponge was found and removed. At this time, the patient was 5 months pregnant. Two months later, the baby was delivered prematurely and lived for 12 days.
PATIENT’S CLAIM The retained lap sponge was left there during the laparotomy surgery performed by Dr. A, and it should have been found sooner.
PHYSICIAN’S DEFENSE The retained sponge was left during the C-section. Also, the death of the second child was unrelated to the retained sponge.
VERDICT Kentucky defense verdict. An appeal was pending.
$22 million award follows preeclamptic mother’s death
A 29-YEAR-OLD WOMAN who was 9 months pregnant presented at the hospital with a severe headache. She was admitted to labor and delivery, where she was examined by an experienced nurse and a 2nd year resident. A diagnosis of preeclampsia and HELLP syndrome, as indicated by lab tests, was given. The patient was administered three 10-mg doses of labetalol—despite hospital policy of administering the drug every 10 minutes in increasing doses until the blood pressure returns to a safe level. When labor was induced, her blood pressure rose dangerously and she became unresponsive. The baby was delivered successfully by emergency C-section. A CT scan indicated that the mother had suffered a massive brain hemorrhage. She was placed on a ventilator for 4 days, and died when it was disconnected.
PLAINTIFF’S CLAIM Labetalol was not administered properly and according to hospital policy.
PHYSICIAN’S DEFENSE The patient would likely not have survived because the preeclampsia and HELLP syndrome were so severe.
VERDICT $22 million Illinois verdict.
Woman conceives after undergoing tubal ligation
A 29-YEAR-OLD WOMAN underwent a tubal ligation. But 9 to 10 months later, she became pregnant. A subsequent ligation indicated a “normal appearing” right fallopian tube.
PATIENT’S CLAIM The physician failed to ligate the proper structure.
PHYSICIAN’S DEFENSE The right fallopian tube had recanalized and appeared normal. However, there was no negligence in performing the tubal ligation.
VERDICT District of Columbia defense verdict.
Placental fragment, aggressive D&C—failed pregnancy
A WEEK AFTER DELIVERING a healthy baby, a woman underwent an emergency dilation and curettage (D&C) because of severe, life-threatening bleeding. Two years later, she suffered a miscarriage, and 7 months after that an ectopic pregnancy.
PATIENT’S CLAIM The obstetrician negligent for failing to examine the placenta after the birth, leading to a retained placental fragment that caused the bleeding. An aggressively performed D&C resulted in Asherman’s syndrome, which caused the miscarriage and ectopic pregnancy.
PHYSICIAN’S DEFENSE At the time of delivery, the placenta was inspected properly. There was nothing to indicate a retained placental fragment, which is a recognized complication of delivery. The D&C was performed properly; uterine scarring is a recognized complication of the procedure.
VERDICT Illinois defense verdict.
Gallbladder disease during pregnancy is not properly treated
FOR A MONTH BEFORE DELIVERY of her child, a woman suffered severe abdominal pain and vomiting, for which she took over-the-counter calcium carbonate antacids. Two days before giving birth, she was admitted to the hospital dehydrated and with life-threatening elevated calcium in her blood. She was transferred to another hospital, where she gave birth to a child with cerebral palsy at 28 weeks’ gestation. She then underwent removal of her gallbladder.
PATIENT’S CLAIM The plaintiff child claimed the treating ObGyn failed to properly treat the mother’s gallbladder disease and pancreatitis.
PHYSICIAN’S DEFENSE The mother’s problems were mainly due to ingestion of an off-label dosage of over-the-counter calcium carbonate antacids.
VERDICT Nebraska defense verdict. The plaintiff appealed the case on the basis of exclusion of some expert testimony. The case was affirmed on appeal.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
A new year, a new CPT: Will these changes rattle your practice?
Take note, ObGyns: A number of changes in Current Procedural Terminology (CPT) 2009—those changes took effect January 1—are going to modify the way you bill and will have an impact on your reimbursement. Most of these changes are minor, although renumbering of infusion codes will require changes to the encounter form. And I have good and bad news for urogynecologists who perform vaginal paravaginal repairs and sling procedures for stress urinary incontinence. Read on for details!
Mesh for vaginal paravaginal defect repair—
code error corrected
Code 57267 is an add-on code that describes the insertion of mesh, or other prosthesis, through a vaginal approach when native tissues have been determined to be weak and inadequate for repair—especially in patients who have undergone a previous attempt at repair. As an add-on code, it can be billed only in addition to other, specific procedures.
Before January 1, code 57267 could only be reported with an anterior or posterior colporrhaphy, or both, or with a rectocele repair without colporrhaphy.
When performing a vaginal approach paravaginal defect repair, however, the same weakened tissues also require use of the mesh, yet code 57825 (paravaginal defect repair [including repair of cystocele, if performed]) was not included as one of the allowed codes. This error is rectified in 2009.
You must still be aware that reporting the 57267 add-on code requires that you establish medical necessity for its use. Documentation of weakened, attenuated, or incompetent pubocervical tissue in the case of a paravaginal repair (International Classification of Diseases Clinical Modification [ICD-9-CM] code 618.81) or rectovaginal tissue for rectocele/enterocele repair (618.82) continues to be important when reporting the add-on mesh code.
A reminder about anesthesia
Until January 1, codes 57400 (dilation of vagina), 57410 (pelvic examination), and 57415 (removal of impacted vaginal foreign body) read “under anesthesia.” In a move to standardize terminology, these codes will be revised to add the wording “other than local.” The revision clarifies that 1) all surgical codes include administration of a local anesthetic and 2) codes designated with “under anesthesia” refer to regional blocks and general anesthesia.
of 2 urogynecology procedures for UI!
Although not a CPT change, it’s worth noting that physicians who perform 1) sling operations for correcting stress urinary incontinence or 2) subsequent revisions because of problems with fascia or synthetic mesh need to be aware that the physician work relative value for these procedures has been decreased in 2009 by the Centers for Medicare and Medicaid Services (CMS). Why the drop? According to CMS, results of surveys by the American Urogynecologic Society and the American Urological Association indicate that the procedures are not as difficult to perform as once considered.
The two affected codes are:
| 57288 | Sling operation for stress incontinence (e.g., fascia or synthetic) |
| 57287 | Removal or revision of sling for stress urinary incontinence (e.g., fascia or synthetic) |
The change will result in a decline in payment for these procedures by Medicare and some non-Medicare payers, and will be felt harder with sling procedures than with revisions. Why? The work relative value units (RVUs) decreased for 57287, but that decrease was offset by an increase in practice expense relative value—which resulted in total RVUs increasing for this code in 2009, from 18.31 to 18.53.
Code 57288, on the other hand, has been tagged with a decrease in both the physician work and practice expense RVUs. Total RVUs for this code, therefore, have dropped from 21.59 to 19.62. In Medicare dollars, that equates to about $118 less for the same procedure when one applies the 2009 Medicare conversion factor of $36.07.
New human papillomavirus vaccine, new code
A new code, 90650, has been added to report the newer bivalent human papillomavirus (HPV) vaccine, which contains an adjuvant formulation and is intended to protect against infection by high-risk HPV types 16 and 18. The existing HPV vaccine code, 90649, targets those high-risk types of HPV and two low-risk types (6 and 11).
Coverage recommendations for the new vaccine match those of the existing, quadrivalent vaccine, but not all payers are covering the HPV vaccine based on those recommendations. The new vaccine offers a less costly alternative for patients whose health-care insurance does not cover the vaccine or who are uninsured.
Wholesale reorganization of injection and infusion codes
Codes 90760–90779 (covering therapeutic, prophylactic, and diagnostic injections and infusions) are deleted in 2009 and renumbered, with the same descriptors, to 96360–96379. This was done to organize all infusions and injections together. The biggest change for you and every other ObGyn? You must revise the practice’s encounter form to reflect the requirement that intramuscular and subcutaneous injections are now coded 96372 instead of 90772.
Modifier -21 and prolonged E/M services
Now deleted is Modifier -21 (prolonged evaluation and management [E/M] service). This modifier represented acknowledgment that a continuous face-to-face E/M service could exceed the maximum time allowed by the highest level of E/M service for the type being billed.
In other words, before January 1, 2009, if a patient’s condition was such that you documented an established or new patient visit (99215 or 99205) but in fact spent more time with her than the 45 or 60 minutes that typically accompanies these codes, you added modifier -21 in the hope of receiving higher reimbursement. Now the modifier is deleted because there is already a mechanism in place to report such prolonged service.
Add-on codes 99354–99357 are used to report face-to-face outpatient and inpatient prolonged E/M services. Guidelines for these codes mandate cumulative time rather than continuous time, and using the add-on codes is contingent on the additional time spent being 30 or more minutes above the typical time allotted for the basic E/M service that you are billing.
Here’s a case that exemplifies how coding works in these circumstances:
CASE
You evaluate a patient for severe uterine bleeding, and report a level-4 visit (99214), which has a typical time of 25 minutes. At the same visit, you determine that endometrial biopsy is required, and you perform it during the visit. But the patient faints during the procedure—and you spend an additional 35 minutes (cumulative time) with her before you send her home.
Because the typical time of 25 minutes was exceeded by at least 30 minutes, you should report 99354 (prolonged physician service in the office or other outpatient setting requiring direct [face-to-face] patient contact beyond the usual service; first hour [list separately in addition to code for office or other outpatient Evaluation and Management service]) in addition to 99214.
Guidelines for correct use of these codes are also being revised to emphasize that only outpatient prolonged services codes are intended to be used to report total duration of face-to-face time; on the other hand, inpatient codes are intended to report the total duration of the time spent (whether continuous or noncontinuous) by the physician on the unit actively involved in caring for the patient.
Take note, ObGyns: A number of changes in Current Procedural Terminology (CPT) 2009—those changes took effect January 1—are going to modify the way you bill and will have an impact on your reimbursement. Most of these changes are minor, although renumbering of infusion codes will require changes to the encounter form. And I have good and bad news for urogynecologists who perform vaginal paravaginal repairs and sling procedures for stress urinary incontinence. Read on for details!
Mesh for vaginal paravaginal defect repair—
code error corrected
Code 57267 is an add-on code that describes the insertion of mesh, or other prosthesis, through a vaginal approach when native tissues have been determined to be weak and inadequate for repair—especially in patients who have undergone a previous attempt at repair. As an add-on code, it can be billed only in addition to other, specific procedures.
Before January 1, code 57267 could only be reported with an anterior or posterior colporrhaphy, or both, or with a rectocele repair without colporrhaphy.
When performing a vaginal approach paravaginal defect repair, however, the same weakened tissues also require use of the mesh, yet code 57825 (paravaginal defect repair [including repair of cystocele, if performed]) was not included as one of the allowed codes. This error is rectified in 2009.
You must still be aware that reporting the 57267 add-on code requires that you establish medical necessity for its use. Documentation of weakened, attenuated, or incompetent pubocervical tissue in the case of a paravaginal repair (International Classification of Diseases Clinical Modification [ICD-9-CM] code 618.81) or rectovaginal tissue for rectocele/enterocele repair (618.82) continues to be important when reporting the add-on mesh code.
A reminder about anesthesia
Until January 1, codes 57400 (dilation of vagina), 57410 (pelvic examination), and 57415 (removal of impacted vaginal foreign body) read “under anesthesia.” In a move to standardize terminology, these codes will be revised to add the wording “other than local.” The revision clarifies that 1) all surgical codes include administration of a local anesthetic and 2) codes designated with “under anesthesia” refer to regional blocks and general anesthesia.
of 2 urogynecology procedures for UI!
Although not a CPT change, it’s worth noting that physicians who perform 1) sling operations for correcting stress urinary incontinence or 2) subsequent revisions because of problems with fascia or synthetic mesh need to be aware that the physician work relative value for these procedures has been decreased in 2009 by the Centers for Medicare and Medicaid Services (CMS). Why the drop? According to CMS, results of surveys by the American Urogynecologic Society and the American Urological Association indicate that the procedures are not as difficult to perform as once considered.
The two affected codes are:
| 57288 | Sling operation for stress incontinence (e.g., fascia or synthetic) |
| 57287 | Removal or revision of sling for stress urinary incontinence (e.g., fascia or synthetic) |
The change will result in a decline in payment for these procedures by Medicare and some non-Medicare payers, and will be felt harder with sling procedures than with revisions. Why? The work relative value units (RVUs) decreased for 57287, but that decrease was offset by an increase in practice expense relative value—which resulted in total RVUs increasing for this code in 2009, from 18.31 to 18.53.
Code 57288, on the other hand, has been tagged with a decrease in both the physician work and practice expense RVUs. Total RVUs for this code, therefore, have dropped from 21.59 to 19.62. In Medicare dollars, that equates to about $118 less for the same procedure when one applies the 2009 Medicare conversion factor of $36.07.
New human papillomavirus vaccine, new code
A new code, 90650, has been added to report the newer bivalent human papillomavirus (HPV) vaccine, which contains an adjuvant formulation and is intended to protect against infection by high-risk HPV types 16 and 18. The existing HPV vaccine code, 90649, targets those high-risk types of HPV and two low-risk types (6 and 11).
Coverage recommendations for the new vaccine match those of the existing, quadrivalent vaccine, but not all payers are covering the HPV vaccine based on those recommendations. The new vaccine offers a less costly alternative for patients whose health-care insurance does not cover the vaccine or who are uninsured.
Wholesale reorganization of injection and infusion codes
Codes 90760–90779 (covering therapeutic, prophylactic, and diagnostic injections and infusions) are deleted in 2009 and renumbered, with the same descriptors, to 96360–96379. This was done to organize all infusions and injections together. The biggest change for you and every other ObGyn? You must revise the practice’s encounter form to reflect the requirement that intramuscular and subcutaneous injections are now coded 96372 instead of 90772.
Modifier -21 and prolonged E/M services
Now deleted is Modifier -21 (prolonged evaluation and management [E/M] service). This modifier represented acknowledgment that a continuous face-to-face E/M service could exceed the maximum time allowed by the highest level of E/M service for the type being billed.
In other words, before January 1, 2009, if a patient’s condition was such that you documented an established or new patient visit (99215 or 99205) but in fact spent more time with her than the 45 or 60 minutes that typically accompanies these codes, you added modifier -21 in the hope of receiving higher reimbursement. Now the modifier is deleted because there is already a mechanism in place to report such prolonged service.
Add-on codes 99354–99357 are used to report face-to-face outpatient and inpatient prolonged E/M services. Guidelines for these codes mandate cumulative time rather than continuous time, and using the add-on codes is contingent on the additional time spent being 30 or more minutes above the typical time allotted for the basic E/M service that you are billing.
Here’s a case that exemplifies how coding works in these circumstances:
CASE
You evaluate a patient for severe uterine bleeding, and report a level-4 visit (99214), which has a typical time of 25 minutes. At the same visit, you determine that endometrial biopsy is required, and you perform it during the visit. But the patient faints during the procedure—and you spend an additional 35 minutes (cumulative time) with her before you send her home.
Because the typical time of 25 minutes was exceeded by at least 30 minutes, you should report 99354 (prolonged physician service in the office or other outpatient setting requiring direct [face-to-face] patient contact beyond the usual service; first hour [list separately in addition to code for office or other outpatient Evaluation and Management service]) in addition to 99214.
Guidelines for correct use of these codes are also being revised to emphasize that only outpatient prolonged services codes are intended to be used to report total duration of face-to-face time; on the other hand, inpatient codes are intended to report the total duration of the time spent (whether continuous or noncontinuous) by the physician on the unit actively involved in caring for the patient.
Take note, ObGyns: A number of changes in Current Procedural Terminology (CPT) 2009—those changes took effect January 1—are going to modify the way you bill and will have an impact on your reimbursement. Most of these changes are minor, although renumbering of infusion codes will require changes to the encounter form. And I have good and bad news for urogynecologists who perform vaginal paravaginal repairs and sling procedures for stress urinary incontinence. Read on for details!
Mesh for vaginal paravaginal defect repair—
code error corrected
Code 57267 is an add-on code that describes the insertion of mesh, or other prosthesis, through a vaginal approach when native tissues have been determined to be weak and inadequate for repair—especially in patients who have undergone a previous attempt at repair. As an add-on code, it can be billed only in addition to other, specific procedures.
Before January 1, code 57267 could only be reported with an anterior or posterior colporrhaphy, or both, or with a rectocele repair without colporrhaphy.
When performing a vaginal approach paravaginal defect repair, however, the same weakened tissues also require use of the mesh, yet code 57825 (paravaginal defect repair [including repair of cystocele, if performed]) was not included as one of the allowed codes. This error is rectified in 2009.
You must still be aware that reporting the 57267 add-on code requires that you establish medical necessity for its use. Documentation of weakened, attenuated, or incompetent pubocervical tissue in the case of a paravaginal repair (International Classification of Diseases Clinical Modification [ICD-9-CM] code 618.81) or rectovaginal tissue for rectocele/enterocele repair (618.82) continues to be important when reporting the add-on mesh code.
A reminder about anesthesia
Until January 1, codes 57400 (dilation of vagina), 57410 (pelvic examination), and 57415 (removal of impacted vaginal foreign body) read “under anesthesia.” In a move to standardize terminology, these codes will be revised to add the wording “other than local.” The revision clarifies that 1) all surgical codes include administration of a local anesthetic and 2) codes designated with “under anesthesia” refer to regional blocks and general anesthesia.
of 2 urogynecology procedures for UI!
Although not a CPT change, it’s worth noting that physicians who perform 1) sling operations for correcting stress urinary incontinence or 2) subsequent revisions because of problems with fascia or synthetic mesh need to be aware that the physician work relative value for these procedures has been decreased in 2009 by the Centers for Medicare and Medicaid Services (CMS). Why the drop? According to CMS, results of surveys by the American Urogynecologic Society and the American Urological Association indicate that the procedures are not as difficult to perform as once considered.
The two affected codes are:
| 57288 | Sling operation for stress incontinence (e.g., fascia or synthetic) |
| 57287 | Removal or revision of sling for stress urinary incontinence (e.g., fascia or synthetic) |
The change will result in a decline in payment for these procedures by Medicare and some non-Medicare payers, and will be felt harder with sling procedures than with revisions. Why? The work relative value units (RVUs) decreased for 57287, but that decrease was offset by an increase in practice expense relative value—which resulted in total RVUs increasing for this code in 2009, from 18.31 to 18.53.
Code 57288, on the other hand, has been tagged with a decrease in both the physician work and practice expense RVUs. Total RVUs for this code, therefore, have dropped from 21.59 to 19.62. In Medicare dollars, that equates to about $118 less for the same procedure when one applies the 2009 Medicare conversion factor of $36.07.
New human papillomavirus vaccine, new code
A new code, 90650, has been added to report the newer bivalent human papillomavirus (HPV) vaccine, which contains an adjuvant formulation and is intended to protect against infection by high-risk HPV types 16 and 18. The existing HPV vaccine code, 90649, targets those high-risk types of HPV and two low-risk types (6 and 11).
Coverage recommendations for the new vaccine match those of the existing, quadrivalent vaccine, but not all payers are covering the HPV vaccine based on those recommendations. The new vaccine offers a less costly alternative for patients whose health-care insurance does not cover the vaccine or who are uninsured.
Wholesale reorganization of injection and infusion codes
Codes 90760–90779 (covering therapeutic, prophylactic, and diagnostic injections and infusions) are deleted in 2009 and renumbered, with the same descriptors, to 96360–96379. This was done to organize all infusions and injections together. The biggest change for you and every other ObGyn? You must revise the practice’s encounter form to reflect the requirement that intramuscular and subcutaneous injections are now coded 96372 instead of 90772.
Modifier -21 and prolonged E/M services
Now deleted is Modifier -21 (prolonged evaluation and management [E/M] service). This modifier represented acknowledgment that a continuous face-to-face E/M service could exceed the maximum time allowed by the highest level of E/M service for the type being billed.
In other words, before January 1, 2009, if a patient’s condition was such that you documented an established or new patient visit (99215 or 99205) but in fact spent more time with her than the 45 or 60 minutes that typically accompanies these codes, you added modifier -21 in the hope of receiving higher reimbursement. Now the modifier is deleted because there is already a mechanism in place to report such prolonged service.
Add-on codes 99354–99357 are used to report face-to-face outpatient and inpatient prolonged E/M services. Guidelines for these codes mandate cumulative time rather than continuous time, and using the add-on codes is contingent on the additional time spent being 30 or more minutes above the typical time allotted for the basic E/M service that you are billing.
Here’s a case that exemplifies how coding works in these circumstances:
CASE
You evaluate a patient for severe uterine bleeding, and report a level-4 visit (99214), which has a typical time of 25 minutes. At the same visit, you determine that endometrial biopsy is required, and you perform it during the visit. But the patient faints during the procedure—and you spend an additional 35 minutes (cumulative time) with her before you send her home.
Because the typical time of 25 minutes was exceeded by at least 30 minutes, you should report 99354 (prolonged physician service in the office or other outpatient setting requiring direct [face-to-face] patient contact beyond the usual service; first hour [list separately in addition to code for office or other outpatient Evaluation and Management service]) in addition to 99214.
Guidelines for correct use of these codes are also being revised to emphasize that only outpatient prolonged services codes are intended to be used to report total duration of face-to-face time; on the other hand, inpatient codes are intended to report the total duration of the time spent (whether continuous or noncontinuous) by the physician on the unit actively involved in caring for the patient.
Winning the Insurance Claim Game
A dermatologist in the Midwest wrote to me for advice on dealing with everyone's worst nightmare, the burglary and arson of his office.
Filing an insurance claim was his first priority, of course. We all buy insurance hoping we will never need it, but when we do, it's important to get it right.
Prompt claim filing is key. All policies have a filing deadline, which varies for different policies and states, but just because you file promptly does not mean you have to settle on a payment just as fast.
Most insurers want a quick resolution as much as you do, but if you allow yourself to be rushed, you could end up with a smaller settlement than you deserve.
If you're a regular reader, you're quite familiar with my first rule of dealing with health insurers: Everything is negotiable. It's no different with casualty insurers. Regardless of what adjusters tell you, the initial amount offered is never engraved in stone. Adjusters are evaluated on the basis of how much money they “save” on claims, so their initial number will usually be low.
As with health insurance claims, casualty policies have gray areas. Those areas include reasonable expenses for repairing or replacing damaged medical equipment or the rental of alternative office space.
Other negotiable costs include moving expenses, storage of damaged and undamaged equipment, and depreciation on specific items. And as we all know from our health insurance experience, injuries are fertile areas for negotiation.
Another adjuster's trick, which you may have already encountered with a damaged car, is to steer people to certain repair shops and contractors that give the insurer better prices for their work but may offer inferior parts and service. Most policies do not require that you accept the insurer's choice of contractors. Insist on having work done by people you know and trust.
Do your own research on the value of lost and damaged items—the more documentation you have, the less likely an adjuster is to question your claim.
Document your losses very specifically. Adjusters often attempt to group material losses nonselectively, just as health insurers sometimes attempt to bundle your services. If a certain cabinet contained medical supplies, be very specific about the supplies it contained so you can assign value to the individual items.
Also remember that, after the trauma of a burglary or fire, you may overlook some losses. Your insurer may not tell you that you can file another claim for additional losses, even after you settle.
Don't be intimidated by the limits of your policy coverage. Depending on the policy, you may be able to recover more than the cited policy limit if you have “replacement cost” coverage. And don't assume you won't make your deductible in spite of initial estimates. Damage that is not immediately apparent can add up to a significant sum later.
It is usually not wise to rely solely on your insurance agent in such situations because an agent's loyalty resides primarily with the insurance company, not the insured. Retaining a lawyer is often a good idea, if only to review paperwork and help you value your losses. It will cost comparatively little and is usually money well spent.
A lawyer also can help negotiate any disputes with the insurer, but a public insurance adjuster may be a less expensive alternative. Public adjusters are professionals, employed by policyholders rather than insurers, who handle all aspects of a claim. You can find more information at the Web site of the National Association of Public Insurance Adjusters www.napia.com
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
A dermatologist in the Midwest wrote to me for advice on dealing with everyone's worst nightmare, the burglary and arson of his office.
Filing an insurance claim was his first priority, of course. We all buy insurance hoping we will never need it, but when we do, it's important to get it right.
Prompt claim filing is key. All policies have a filing deadline, which varies for different policies and states, but just because you file promptly does not mean you have to settle on a payment just as fast.
Most insurers want a quick resolution as much as you do, but if you allow yourself to be rushed, you could end up with a smaller settlement than you deserve.
If you're a regular reader, you're quite familiar with my first rule of dealing with health insurers: Everything is negotiable. It's no different with casualty insurers. Regardless of what adjusters tell you, the initial amount offered is never engraved in stone. Adjusters are evaluated on the basis of how much money they “save” on claims, so their initial number will usually be low.
As with health insurance claims, casualty policies have gray areas. Those areas include reasonable expenses for repairing or replacing damaged medical equipment or the rental of alternative office space.
Other negotiable costs include moving expenses, storage of damaged and undamaged equipment, and depreciation on specific items. And as we all know from our health insurance experience, injuries are fertile areas for negotiation.
Another adjuster's trick, which you may have already encountered with a damaged car, is to steer people to certain repair shops and contractors that give the insurer better prices for their work but may offer inferior parts and service. Most policies do not require that you accept the insurer's choice of contractors. Insist on having work done by people you know and trust.
Do your own research on the value of lost and damaged items—the more documentation you have, the less likely an adjuster is to question your claim.
Document your losses very specifically. Adjusters often attempt to group material losses nonselectively, just as health insurers sometimes attempt to bundle your services. If a certain cabinet contained medical supplies, be very specific about the supplies it contained so you can assign value to the individual items.
Also remember that, after the trauma of a burglary or fire, you may overlook some losses. Your insurer may not tell you that you can file another claim for additional losses, even after you settle.
Don't be intimidated by the limits of your policy coverage. Depending on the policy, you may be able to recover more than the cited policy limit if you have “replacement cost” coverage. And don't assume you won't make your deductible in spite of initial estimates. Damage that is not immediately apparent can add up to a significant sum later.
It is usually not wise to rely solely on your insurance agent in such situations because an agent's loyalty resides primarily with the insurance company, not the insured. Retaining a lawyer is often a good idea, if only to review paperwork and help you value your losses. It will cost comparatively little and is usually money well spent.
A lawyer also can help negotiate any disputes with the insurer, but a public insurance adjuster may be a less expensive alternative. Public adjusters are professionals, employed by policyholders rather than insurers, who handle all aspects of a claim. You can find more information at the Web site of the National Association of Public Insurance Adjusters www.napia.com
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
A dermatologist in the Midwest wrote to me for advice on dealing with everyone's worst nightmare, the burglary and arson of his office.
Filing an insurance claim was his first priority, of course. We all buy insurance hoping we will never need it, but when we do, it's important to get it right.
Prompt claim filing is key. All policies have a filing deadline, which varies for different policies and states, but just because you file promptly does not mean you have to settle on a payment just as fast.
Most insurers want a quick resolution as much as you do, but if you allow yourself to be rushed, you could end up with a smaller settlement than you deserve.
If you're a regular reader, you're quite familiar with my first rule of dealing with health insurers: Everything is negotiable. It's no different with casualty insurers. Regardless of what adjusters tell you, the initial amount offered is never engraved in stone. Adjusters are evaluated on the basis of how much money they “save” on claims, so their initial number will usually be low.
As with health insurance claims, casualty policies have gray areas. Those areas include reasonable expenses for repairing or replacing damaged medical equipment or the rental of alternative office space.
Other negotiable costs include moving expenses, storage of damaged and undamaged equipment, and depreciation on specific items. And as we all know from our health insurance experience, injuries are fertile areas for negotiation.
Another adjuster's trick, which you may have already encountered with a damaged car, is to steer people to certain repair shops and contractors that give the insurer better prices for their work but may offer inferior parts and service. Most policies do not require that you accept the insurer's choice of contractors. Insist on having work done by people you know and trust.
Do your own research on the value of lost and damaged items—the more documentation you have, the less likely an adjuster is to question your claim.
Document your losses very specifically. Adjusters often attempt to group material losses nonselectively, just as health insurers sometimes attempt to bundle your services. If a certain cabinet contained medical supplies, be very specific about the supplies it contained so you can assign value to the individual items.
Also remember that, after the trauma of a burglary or fire, you may overlook some losses. Your insurer may not tell you that you can file another claim for additional losses, even after you settle.
Don't be intimidated by the limits of your policy coverage. Depending on the policy, you may be able to recover more than the cited policy limit if you have “replacement cost” coverage. And don't assume you won't make your deductible in spite of initial estimates. Damage that is not immediately apparent can add up to a significant sum later.
It is usually not wise to rely solely on your insurance agent in such situations because an agent's loyalty resides primarily with the insurance company, not the insured. Retaining a lawyer is often a good idea, if only to review paperwork and help you value your losses. It will cost comparatively little and is usually money well spent.
A lawyer also can help negotiate any disputes with the insurer, but a public insurance adjuster may be a less expensive alternative. Public adjusters are professionals, employed by policyholders rather than insurers, who handle all aspects of a claim. You can find more information at the Web site of the National Association of Public Insurance Adjusters www.napia.com
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Don't Keep Your Patients Waiting
Consumer Reports surveyed its readers last year regarding their satisfaction with their medical care and found that the “overwhelming majority … were highly satisfied with their doctors.” Of course, they did have some complaints.
As you might expect, their top complaint was the time spent waiting to see their doctors—24% said they frequently waited 30 minutes or longer. Here are some suggestions to help keep you on track:
▸ Start on time. That seems obvious, but I'm always amazed at the number of doctors who admit to running late who also admit that they start late. If you're in the hole before you start, you can seldom dig yourself out. Sometimes an on-time start is the solution to the entire problem. Try it.
▸ Book realistically. Everyone works at a different pace. Determine the number of patients you can comfortably see in an hour, and book only that number. If you want to see more patients, the solution is working longer hours or hiring physicians or physician extenders (or both), not overloading your schedule.
▸ Time-stamp each chart. Every office should have a time clock, not only for employees, but for patients as well. As each patient arrives, have your receptionist time-stamp the “encounter form” that goes to the back with the chart. As you take each chart off the door and enter the room, a quick glance at the time stamp will tell you how long the patient has been waiting.
▸ Schedule all procedures. If you haven't scheduled the time necessary for a procedure, don't do it. It may be tempting to squeeze it in because you feel guilty that the patient has had to wait for you, but every unscheduled procedure puts you that much further behind. And hurrying increases the risk of mistakes. Tell the patient the procedure requires extra time and can't be rushed, so you will have to schedule.
▸ Work-ins come last, not first. Patients with urgent problems should be seen after scheduled patients. Receptionists often assume it's better to squeeze them in early, while you're still running on time, but doing that guarantees you will run late, and it isn't fair to patients who have appointments and expect to be seen promptly. Work-ins expect a wait because they have no appointment. We tell them our schedule is full, but if they come at the end of hours, they'll see a doctor though they may have a wait. Far from complaining, they invariably thank us for seeing them.
▸ Seize the list. You know which list I mean: “No. 16: My right big toe itches. No. 17: I think I feel something on my back…” When a list is produced, the best option is to read it yourself. Identify the most important two or three problems and address them. For the rest, I will say, “This group of problems deserves a visit of its own, and we will schedule that visit.” Ask if you can place the list (or a photocopy) in the patient's chart. It is, after all, important clinical information. All of these problems are important to the patient and should be addressed—but on your schedule, not the patient's.
▸ Avoid interruptions. Especially phone calls. Unless it's an emergency or an immediate family member, my receptionists say, “I'm sorry, the doctor is with patients. May I take a message?” Everyone—even other physicians—understands. Just be sure to return those calls promptly.
Pharmaceutical reps should not be allowed to interrupt you, either. Have them make an appointment. Don't stop to open the mail, do paperwork, or perform any other task that can be delegated.
There will be times, of course, when you run late, but they should be the exception rather than the rule.
Incidentally, the other leading patient complaints in the Consumer Reports survey were: couldn't schedule an appointment within a week (19%), spent too little time with me (9%), didn't provide test results promptly (7%), and didn't respond to my phone calls promptly (6%).
Now would be an excellent opportunity to identify and address any of those problems as well.
Consumer Reports surveyed its readers last year regarding their satisfaction with their medical care and found that the “overwhelming majority … were highly satisfied with their doctors.” Of course, they did have some complaints.
As you might expect, their top complaint was the time spent waiting to see their doctors—24% said they frequently waited 30 minutes or longer. Here are some suggestions to help keep you on track:
▸ Start on time. That seems obvious, but I'm always amazed at the number of doctors who admit to running late who also admit that they start late. If you're in the hole before you start, you can seldom dig yourself out. Sometimes an on-time start is the solution to the entire problem. Try it.
▸ Book realistically. Everyone works at a different pace. Determine the number of patients you can comfortably see in an hour, and book only that number. If you want to see more patients, the solution is working longer hours or hiring physicians or physician extenders (or both), not overloading your schedule.
▸ Time-stamp each chart. Every office should have a time clock, not only for employees, but for patients as well. As each patient arrives, have your receptionist time-stamp the “encounter form” that goes to the back with the chart. As you take each chart off the door and enter the room, a quick glance at the time stamp will tell you how long the patient has been waiting.
▸ Schedule all procedures. If you haven't scheduled the time necessary for a procedure, don't do it. It may be tempting to squeeze it in because you feel guilty that the patient has had to wait for you, but every unscheduled procedure puts you that much further behind. And hurrying increases the risk of mistakes. Tell the patient the procedure requires extra time and can't be rushed, so you will have to schedule.
▸ Work-ins come last, not first. Patients with urgent problems should be seen after scheduled patients. Receptionists often assume it's better to squeeze them in early, while you're still running on time, but doing that guarantees you will run late, and it isn't fair to patients who have appointments and expect to be seen promptly. Work-ins expect a wait because they have no appointment. We tell them our schedule is full, but if they come at the end of hours, they'll see a doctor though they may have a wait. Far from complaining, they invariably thank us for seeing them.
▸ Seize the list. You know which list I mean: “No. 16: My right big toe itches. No. 17: I think I feel something on my back…” When a list is produced, the best option is to read it yourself. Identify the most important two or three problems and address them. For the rest, I will say, “This group of problems deserves a visit of its own, and we will schedule that visit.” Ask if you can place the list (or a photocopy) in the patient's chart. It is, after all, important clinical information. All of these problems are important to the patient and should be addressed—but on your schedule, not the patient's.
▸ Avoid interruptions. Especially phone calls. Unless it's an emergency or an immediate family member, my receptionists say, “I'm sorry, the doctor is with patients. May I take a message?” Everyone—even other physicians—understands. Just be sure to return those calls promptly.
Pharmaceutical reps should not be allowed to interrupt you, either. Have them make an appointment. Don't stop to open the mail, do paperwork, or perform any other task that can be delegated.
There will be times, of course, when you run late, but they should be the exception rather than the rule.
Incidentally, the other leading patient complaints in the Consumer Reports survey were: couldn't schedule an appointment within a week (19%), spent too little time with me (9%), didn't provide test results promptly (7%), and didn't respond to my phone calls promptly (6%).
Now would be an excellent opportunity to identify and address any of those problems as well.
Consumer Reports surveyed its readers last year regarding their satisfaction with their medical care and found that the “overwhelming majority … were highly satisfied with their doctors.” Of course, they did have some complaints.
As you might expect, their top complaint was the time spent waiting to see their doctors—24% said they frequently waited 30 minutes or longer. Here are some suggestions to help keep you on track:
▸ Start on time. That seems obvious, but I'm always amazed at the number of doctors who admit to running late who also admit that they start late. If you're in the hole before you start, you can seldom dig yourself out. Sometimes an on-time start is the solution to the entire problem. Try it.
▸ Book realistically. Everyone works at a different pace. Determine the number of patients you can comfortably see in an hour, and book only that number. If you want to see more patients, the solution is working longer hours or hiring physicians or physician extenders (or both), not overloading your schedule.
▸ Time-stamp each chart. Every office should have a time clock, not only for employees, but for patients as well. As each patient arrives, have your receptionist time-stamp the “encounter form” that goes to the back with the chart. As you take each chart off the door and enter the room, a quick glance at the time stamp will tell you how long the patient has been waiting.
▸ Schedule all procedures. If you haven't scheduled the time necessary for a procedure, don't do it. It may be tempting to squeeze it in because you feel guilty that the patient has had to wait for you, but every unscheduled procedure puts you that much further behind. And hurrying increases the risk of mistakes. Tell the patient the procedure requires extra time and can't be rushed, so you will have to schedule.
▸ Work-ins come last, not first. Patients with urgent problems should be seen after scheduled patients. Receptionists often assume it's better to squeeze them in early, while you're still running on time, but doing that guarantees you will run late, and it isn't fair to patients who have appointments and expect to be seen promptly. Work-ins expect a wait because they have no appointment. We tell them our schedule is full, but if they come at the end of hours, they'll see a doctor though they may have a wait. Far from complaining, they invariably thank us for seeing them.
▸ Seize the list. You know which list I mean: “No. 16: My right big toe itches. No. 17: I think I feel something on my back…” When a list is produced, the best option is to read it yourself. Identify the most important two or three problems and address them. For the rest, I will say, “This group of problems deserves a visit of its own, and we will schedule that visit.” Ask if you can place the list (or a photocopy) in the patient's chart. It is, after all, important clinical information. All of these problems are important to the patient and should be addressed—but on your schedule, not the patient's.
▸ Avoid interruptions. Especially phone calls. Unless it's an emergency or an immediate family member, my receptionists say, “I'm sorry, the doctor is with patients. May I take a message?” Everyone—even other physicians—understands. Just be sure to return those calls promptly.
Pharmaceutical reps should not be allowed to interrupt you, either. Have them make an appointment. Don't stop to open the mail, do paperwork, or perform any other task that can be delegated.
There will be times, of course, when you run late, but they should be the exception rather than the rule.
Incidentally, the other leading patient complaints in the Consumer Reports survey were: couldn't schedule an appointment within a week (19%), spent too little time with me (9%), didn't provide test results promptly (7%), and didn't respond to my phone calls promptly (6%).
Now would be an excellent opportunity to identify and address any of those problems as well.
The Bare Necessities
Medicare reimburses for procedures and services deemed “reasonable and necessary.” By statute, Medicare only may pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury, or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g., colorectal cancer screening).1 Medical necessity is determined by evidence-based clinical standards of care, which guide the physician’s diagnostic and treatment process for certain patient populations, illnesses, or clinical circumstances.
National Coverage Determinations
The Centers for Medicare and Medicaid Services (CMS) develop national coverage determinations (NCDs) through an evidence-based process with opportunities for public participation. In some cases, CMS’ own research is supplemented by an outside technology assessment and/or consultation with the Medicare Evidence Development and Coverage Advisory Committee (MEDCAC).
All Medicare contractors must adhere to NCDs and cannot create additional limitations or guidelines. As an example, the NCD for pronouncement of death states an individual only is considered to have died as of the time he orshe is pronounced dead by a person who is legally authorized to make such a pronouncement, usually a physician; and medical services rendered up to and including pronouncement are considered reasonable and necessary.2 Further guidance authorizes physicians to report discharge day management codes (99238-99239) for the face-to-face pronouncement encounter.3 See the Medicare National Coverage Determination Manual (www.cms.hhs.gov/Manuals/ IOM/itemdetail.asp?filterType=none&filterByDID=-99&sortByDID=1&sort Order=ascending&itemID=CMS014961&intNumPerPage=10) for other applicable NCDs.
Local Coverage Determinations
In the absence of a national coverage policy, an item or service may be covered at the discretion of the Medicare contractors based on a local coverage determination (LCD).4
An LCD, as established by Section 522 of the Benefits Improvement and Protection Act (BIPA), is a decision made by a fiscal intermediary or carrier to cover a particular service on an intermediary-wide or carrier-wide basis, in accordance with Section 1862(a)(1)(A) of the Social Security Act (i.e., a determination as to whether the service is reasonable and necessary).5 LCDs may vary by state, causing an inconsistent approach to medical coverage. Non-Medicare payers do not have to follow federal guidelines, unless the member participates in a Medicare managed care plan. A list of Medicare contractor LCDs can be found at www.cms.hhs.gov/DeterminationProcess/04_LCDs.asp.
Certain payers develop coverage requirements for frequent or problematic procedures or services. Coverage requirements identify specific conditions (i.e., ICD-9-CM codes) for which the services or procedures are considered medically necessary. For example, echocardiography (99307) may not be considered medically necessary for a patient who presents with chest pain unless documentation also supports suspected acute myocardial ischemia and baseline electrocardiogram (ECG) is nondiagnostic; or in cases when the physician suspects aortic dissection.6
Medical Review Program
It is insufficient to develop billing compliance policies and standards without enforcement of these guidelines. In an effort to verify the appropriateness of claims and payment, CMS contracts with Medicare Administrative Contractors (MACs), Fiscal Intermediaries (FIs), and Program Safeguard Contractors (PSCs) to perform medical reviews. The goals of the Medical Review Program are reducing Medicare claims payment errors; decreased denials and increased timely payments; and increased educational opportunities.7
In order to determine which providers should be subject to medical review, contractors must analyze provider compliance with coverage and coding rules and take corrective action when necessary. The corrective action aims to modify behavior in need of change, collect overpayments, and deny improper payments.8 Several types of review exist:
- Prepayment review: The Medicare contractor requests medical records prior to payment;
- Postpayment review: The contractor requests medical records after payment has been received by the physician; this may result in upholding or reversing the initial payment determination;
- Probe review: The contractor requests medical records associated with 20 to 40 claims based upon provider-specific issues; and
- Comprehensive error rate testing (CERT) review: CMS measures the error rate and estimates improper claim payments by randomly selecting and reviewing a sample of claims for compliance.9
Prepayment reviews seem to be expanding as a response to the error rate for certain services. For example, high-level consultation services (99245 and 99255) have prompted review over the last several years to ensure documentation and medical necessity are appropriately supported and maintained. Hospitalists may have noticed a recent increase in prepayment record requests for subsequent hospital care (99232 or 99233) and discharge day management (99239) services. Responses to these and other record requests must be timely in order to prevent claim denial or repayment requests. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References:
1. Exclusions from coverage and Medicare as a secondary payer. Social Security Online. www.ssa.gov/ OP_Home/ssact/title18/1862.htm. Updated October 28, 2008. Accessed October 15, 2008.
2. Centers for Medicare and Medicaid Services. Medicare national coverage determination manual: chapter 1, part 1, section 70.4. www.cms.hhs.gov/manuals/ downloads/ncd103c1_Part1.pdf. Accessed October 14, 2008.
3. Centers for Medicare and Medicaid Services. Transmittal 1460: Subsequent hospital visits and hospital discharge day management services (Codes 99231-99239). www.cms.hhs.gov/transmittals/downloads/R1460CP.pdf. Accessed October 14, 2008.
4. Centers for Medicare and Medicaid Services. Medicare coverage determination process: overview. www. cms.hhs.gov/DeterminationProcess/01_Overview.asp#TopOfPage. Updated August 5, 2008. Accessed October 15, 2008.
5. Centers for Medicare and Medicaid Services. Medicare coverage determination process: local coverage determinations. www.cms.hhs.gov/DeterminationProcess/ 04_LCDs.asp. Updated October 7, 2008. Accessed October 15, 2008.
6. Highmark Medicare Services. LCD L27536: transthoracic echocardiography. www.highmarkmedicareservices. com/policy/mac-ab/l27536-r3.html. Updated Septem-ber 23, 2008. Accessed October 16, 2008.
7. Centers for Medicare and Medicaid Services. The Medicare medical review program. www.cms. hhs.gov/MedicalReviewProcess/Downloads/mrfactsheet.pdf. Published September 2004. Accessed October 15, 2008.
8. Rudolph P, Shuren A. Dealing with Medicare. In: coding for chest medicine 2008. Northbrook, IL: Am Coll of Chest Physicians. 2008;23-35.
9. Centers for Medicare and Medicaid Services. Comprehensive error rate testing: overview. www. cms.hhs.gov/CERT/. Updated December 14, 2005. Accessed October 16, 2008.
10. Centers for Medicare and Medicaid Services. Medicare claims processing manual: chapter 12, section 30.6.10G. www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Updated July 9, 2008. Accessed October 16, 2008.
Medicare reimburses for procedures and services deemed “reasonable and necessary.” By statute, Medicare only may pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury, or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g., colorectal cancer screening).1 Medical necessity is determined by evidence-based clinical standards of care, which guide the physician’s diagnostic and treatment process for certain patient populations, illnesses, or clinical circumstances.
National Coverage Determinations
The Centers for Medicare and Medicaid Services (CMS) develop national coverage determinations (NCDs) through an evidence-based process with opportunities for public participation. In some cases, CMS’ own research is supplemented by an outside technology assessment and/or consultation with the Medicare Evidence Development and Coverage Advisory Committee (MEDCAC).
All Medicare contractors must adhere to NCDs and cannot create additional limitations or guidelines. As an example, the NCD for pronouncement of death states an individual only is considered to have died as of the time he orshe is pronounced dead by a person who is legally authorized to make such a pronouncement, usually a physician; and medical services rendered up to and including pronouncement are considered reasonable and necessary.2 Further guidance authorizes physicians to report discharge day management codes (99238-99239) for the face-to-face pronouncement encounter.3 See the Medicare National Coverage Determination Manual (www.cms.hhs.gov/Manuals/ IOM/itemdetail.asp?filterType=none&filterByDID=-99&sortByDID=1&sort Order=ascending&itemID=CMS014961&intNumPerPage=10) for other applicable NCDs.
Local Coverage Determinations
In the absence of a national coverage policy, an item or service may be covered at the discretion of the Medicare contractors based on a local coverage determination (LCD).4
An LCD, as established by Section 522 of the Benefits Improvement and Protection Act (BIPA), is a decision made by a fiscal intermediary or carrier to cover a particular service on an intermediary-wide or carrier-wide basis, in accordance with Section 1862(a)(1)(A) of the Social Security Act (i.e., a determination as to whether the service is reasonable and necessary).5 LCDs may vary by state, causing an inconsistent approach to medical coverage. Non-Medicare payers do not have to follow federal guidelines, unless the member participates in a Medicare managed care plan. A list of Medicare contractor LCDs can be found at www.cms.hhs.gov/DeterminationProcess/04_LCDs.asp.
Certain payers develop coverage requirements for frequent or problematic procedures or services. Coverage requirements identify specific conditions (i.e., ICD-9-CM codes) for which the services or procedures are considered medically necessary. For example, echocardiography (99307) may not be considered medically necessary for a patient who presents with chest pain unless documentation also supports suspected acute myocardial ischemia and baseline electrocardiogram (ECG) is nondiagnostic; or in cases when the physician suspects aortic dissection.6
Medical Review Program
It is insufficient to develop billing compliance policies and standards without enforcement of these guidelines. In an effort to verify the appropriateness of claims and payment, CMS contracts with Medicare Administrative Contractors (MACs), Fiscal Intermediaries (FIs), and Program Safeguard Contractors (PSCs) to perform medical reviews. The goals of the Medical Review Program are reducing Medicare claims payment errors; decreased denials and increased timely payments; and increased educational opportunities.7
In order to determine which providers should be subject to medical review, contractors must analyze provider compliance with coverage and coding rules and take corrective action when necessary. The corrective action aims to modify behavior in need of change, collect overpayments, and deny improper payments.8 Several types of review exist:
- Prepayment review: The Medicare contractor requests medical records prior to payment;
- Postpayment review: The contractor requests medical records after payment has been received by the physician; this may result in upholding or reversing the initial payment determination;
- Probe review: The contractor requests medical records associated with 20 to 40 claims based upon provider-specific issues; and
- Comprehensive error rate testing (CERT) review: CMS measures the error rate and estimates improper claim payments by randomly selecting and reviewing a sample of claims for compliance.9
Prepayment reviews seem to be expanding as a response to the error rate for certain services. For example, high-level consultation services (99245 and 99255) have prompted review over the last several years to ensure documentation and medical necessity are appropriately supported and maintained. Hospitalists may have noticed a recent increase in prepayment record requests for subsequent hospital care (99232 or 99233) and discharge day management (99239) services. Responses to these and other record requests must be timely in order to prevent claim denial or repayment requests. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References:
1. Exclusions from coverage and Medicare as a secondary payer. Social Security Online. www.ssa.gov/ OP_Home/ssact/title18/1862.htm. Updated October 28, 2008. Accessed October 15, 2008.
2. Centers for Medicare and Medicaid Services. Medicare national coverage determination manual: chapter 1, part 1, section 70.4. www.cms.hhs.gov/manuals/ downloads/ncd103c1_Part1.pdf. Accessed October 14, 2008.
3. Centers for Medicare and Medicaid Services. Transmittal 1460: Subsequent hospital visits and hospital discharge day management services (Codes 99231-99239). www.cms.hhs.gov/transmittals/downloads/R1460CP.pdf. Accessed October 14, 2008.
4. Centers for Medicare and Medicaid Services. Medicare coverage determination process: overview. www. cms.hhs.gov/DeterminationProcess/01_Overview.asp#TopOfPage. Updated August 5, 2008. Accessed October 15, 2008.
5. Centers for Medicare and Medicaid Services. Medicare coverage determination process: local coverage determinations. www.cms.hhs.gov/DeterminationProcess/ 04_LCDs.asp. Updated October 7, 2008. Accessed October 15, 2008.
6. Highmark Medicare Services. LCD L27536: transthoracic echocardiography. www.highmarkmedicareservices. com/policy/mac-ab/l27536-r3.html. Updated Septem-ber 23, 2008. Accessed October 16, 2008.
7. Centers for Medicare and Medicaid Services. The Medicare medical review program. www.cms. hhs.gov/MedicalReviewProcess/Downloads/mrfactsheet.pdf. Published September 2004. Accessed October 15, 2008.
8. Rudolph P, Shuren A. Dealing with Medicare. In: coding for chest medicine 2008. Northbrook, IL: Am Coll of Chest Physicians. 2008;23-35.
9. Centers for Medicare and Medicaid Services. Comprehensive error rate testing: overview. www. cms.hhs.gov/CERT/. Updated December 14, 2005. Accessed October 16, 2008.
10. Centers for Medicare and Medicaid Services. Medicare claims processing manual: chapter 12, section 30.6.10G. www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Updated July 9, 2008. Accessed October 16, 2008.
Medicare reimburses for procedures and services deemed “reasonable and necessary.” By statute, Medicare only may pay for items and services that are “reasonable and necessary for the diagnosis or treatment of illness or injury, or to improve the functioning of a malformed body member,” unless there is another statutory authorization for payment (e.g., colorectal cancer screening).1 Medical necessity is determined by evidence-based clinical standards of care, which guide the physician’s diagnostic and treatment process for certain patient populations, illnesses, or clinical circumstances.
National Coverage Determinations
The Centers for Medicare and Medicaid Services (CMS) develop national coverage determinations (NCDs) through an evidence-based process with opportunities for public participation. In some cases, CMS’ own research is supplemented by an outside technology assessment and/or consultation with the Medicare Evidence Development and Coverage Advisory Committee (MEDCAC).
All Medicare contractors must adhere to NCDs and cannot create additional limitations or guidelines. As an example, the NCD for pronouncement of death states an individual only is considered to have died as of the time he orshe is pronounced dead by a person who is legally authorized to make such a pronouncement, usually a physician; and medical services rendered up to and including pronouncement are considered reasonable and necessary.2 Further guidance authorizes physicians to report discharge day management codes (99238-99239) for the face-to-face pronouncement encounter.3 See the Medicare National Coverage Determination Manual (www.cms.hhs.gov/Manuals/ IOM/itemdetail.asp?filterType=none&filterByDID=-99&sortByDID=1&sort Order=ascending&itemID=CMS014961&intNumPerPage=10) for other applicable NCDs.
Local Coverage Determinations
In the absence of a national coverage policy, an item or service may be covered at the discretion of the Medicare contractors based on a local coverage determination (LCD).4
An LCD, as established by Section 522 of the Benefits Improvement and Protection Act (BIPA), is a decision made by a fiscal intermediary or carrier to cover a particular service on an intermediary-wide or carrier-wide basis, in accordance with Section 1862(a)(1)(A) of the Social Security Act (i.e., a determination as to whether the service is reasonable and necessary).5 LCDs may vary by state, causing an inconsistent approach to medical coverage. Non-Medicare payers do not have to follow federal guidelines, unless the member participates in a Medicare managed care plan. A list of Medicare contractor LCDs can be found at www.cms.hhs.gov/DeterminationProcess/04_LCDs.asp.
Certain payers develop coverage requirements for frequent or problematic procedures or services. Coverage requirements identify specific conditions (i.e., ICD-9-CM codes) for which the services or procedures are considered medically necessary. For example, echocardiography (99307) may not be considered medically necessary for a patient who presents with chest pain unless documentation also supports suspected acute myocardial ischemia and baseline electrocardiogram (ECG) is nondiagnostic; or in cases when the physician suspects aortic dissection.6
Medical Review Program
It is insufficient to develop billing compliance policies and standards without enforcement of these guidelines. In an effort to verify the appropriateness of claims and payment, CMS contracts with Medicare Administrative Contractors (MACs), Fiscal Intermediaries (FIs), and Program Safeguard Contractors (PSCs) to perform medical reviews. The goals of the Medical Review Program are reducing Medicare claims payment errors; decreased denials and increased timely payments; and increased educational opportunities.7
In order to determine which providers should be subject to medical review, contractors must analyze provider compliance with coverage and coding rules and take corrective action when necessary. The corrective action aims to modify behavior in need of change, collect overpayments, and deny improper payments.8 Several types of review exist:
- Prepayment review: The Medicare contractor requests medical records prior to payment;
- Postpayment review: The contractor requests medical records after payment has been received by the physician; this may result in upholding or reversing the initial payment determination;
- Probe review: The contractor requests medical records associated with 20 to 40 claims based upon provider-specific issues; and
- Comprehensive error rate testing (CERT) review: CMS measures the error rate and estimates improper claim payments by randomly selecting and reviewing a sample of claims for compliance.9
Prepayment reviews seem to be expanding as a response to the error rate for certain services. For example, high-level consultation services (99245 and 99255) have prompted review over the last several years to ensure documentation and medical necessity are appropriately supported and maintained. Hospitalists may have noticed a recent increase in prepayment record requests for subsequent hospital care (99232 or 99233) and discharge day management (99239) services. Responses to these and other record requests must be timely in order to prevent claim denial or repayment requests. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is on the faculty of SHM’s inpatient coding course.
References:
1. Exclusions from coverage and Medicare as a secondary payer. Social Security Online. www.ssa.gov/ OP_Home/ssact/title18/1862.htm. Updated October 28, 2008. Accessed October 15, 2008.
2. Centers for Medicare and Medicaid Services. Medicare national coverage determination manual: chapter 1, part 1, section 70.4. www.cms.hhs.gov/manuals/ downloads/ncd103c1_Part1.pdf. Accessed October 14, 2008.
3. Centers for Medicare and Medicaid Services. Transmittal 1460: Subsequent hospital visits and hospital discharge day management services (Codes 99231-99239). www.cms.hhs.gov/transmittals/downloads/R1460CP.pdf. Accessed October 14, 2008.
4. Centers for Medicare and Medicaid Services. Medicare coverage determination process: overview. www. cms.hhs.gov/DeterminationProcess/01_Overview.asp#TopOfPage. Updated August 5, 2008. Accessed October 15, 2008.
5. Centers for Medicare and Medicaid Services. Medicare coverage determination process: local coverage determinations. www.cms.hhs.gov/DeterminationProcess/ 04_LCDs.asp. Updated October 7, 2008. Accessed October 15, 2008.
6. Highmark Medicare Services. LCD L27536: transthoracic echocardiography. www.highmarkmedicareservices. com/policy/mac-ab/l27536-r3.html. Updated Septem-ber 23, 2008. Accessed October 16, 2008.
7. Centers for Medicare and Medicaid Services. The Medicare medical review program. www.cms. hhs.gov/MedicalReviewProcess/Downloads/mrfactsheet.pdf. Published September 2004. Accessed October 15, 2008.
8. Rudolph P, Shuren A. Dealing with Medicare. In: coding for chest medicine 2008. Northbrook, IL: Am Coll of Chest Physicians. 2008;23-35.
9. Centers for Medicare and Medicaid Services. Comprehensive error rate testing: overview. www. cms.hhs.gov/CERT/. Updated December 14, 2005. Accessed October 16, 2008.
10. Centers for Medicare and Medicaid Services. Medicare claims processing manual: chapter 12, section 30.6.10G. www.cms.hhs.gov/manuals/downloads/clm104c12.pdf. Updated July 9, 2008. Accessed October 16, 2008.
Disaster Preparedness—Don't Get Caught Without a Plan
Medical Verdicts: Only on the Web
Parents claim fetal body was mistreated
A WOMAN presented at the hospital with excessive vaginal bleeding at 18 to 20 weeks’ gestation. A sonogram indicated the absence of amniotic fluid and a fetal heart rate of 86 to 102 bpm. The patient was admitted to labor and delivery. A nurse found no fetal heart tones, and the attending OB, Dr. A, used ultrasonography to confirm fetal death. Labor induction to deliver the fetus was begun. When a breech position was found, Dr. A, who was now unavailable, had the nurse contact Dr. B. The fetal body was delivered without the head—but Dr. B completed no delivery note and the medical records did not mention decapitation. After the body was placed in a sterile basin, the head was delivered using a ring forceps. Nurses removed the body parts and swaddled them in a baby blanket. The parents, who had not seen the decapitation, refused to hold the wrapped fetus, fearing the head would fall off. The remains were put in a closed casket for the viewing and funeral.
- PLAINTIFFS’ CLAIM The plaintiff mother claimed medical malpractice. Both parents said the fetus should have been left to deliver spontaneously without intervention. There was negligence in the mistreatment of the fetal body and also in the application of excessive force or traction to the body, which caused the decapitation.
- PHYSICIAN’S DEFENSE The delivery was carried out correctly. Delivery of a stillborn fetus requires guidance, as the cervix cannot fully dilate. Also, an 18- to 20-week fetus is friable and delicate; thus, contractions created a sheering force on the fetal body and caused the decapitation. The latter was not caused by traction.
- VERDICT Missouri defense verdict. A posttrial motion was pending.
Myomectomy causes uterine and bowel injuries
A 47-YEAR-OLD WOMAN suffered from heavy menstrual bleeding caused by submucosal uterine fibroids. Her gynecologist tried to resect the largest fibroid using a resectoscope, but the fibroid did not free itself from the uterine wall when he applied electrical current. He continued the procedure until it was apparent he had perforated the uterus. He stopped and sent the patient home with pain medications and antibiotics. Because of a bowel injury, she developed peritonitis and sepsis and eventually required surgical repair of the bowel. Her recovery was good, but it required her to miss work for 1 month and aggravated an existing anxiety disorder.
- PATIENT’S CLAIM Because of the high risk of uterine and bowel injury, the procedure should have been terminated when the application of electrical current did not free the fibroid from the uterine wall.
- PHYSICIAN’S DEFENSE Not reported.
- VERDICT $500,000 Minnesota settlement.
Patient attempts suicide after Lupron injection
A 27-YEAR-OLD WOMAN suffering from depression was given a diagnosis of endometriosis. Her ObGyn injected her with leuprolide (Lupron), which can decrease the production of some hormones and influence moods, and has an effect that lasts for about 3 months. Five days later the patient reported depression, and then returned to the facility the next day. Eleven days after that, she attempted suicide. A diagnosis of bipolar disorder was made following 3 days of inpatient psychiatric evaluation. She was treated for 1 month as an outpatient.
- PATIENT’S CLAIM Lupron should not have been administered. The ObGyn was negligent for treating her with the drug and for not disclosing that it can cause depression. She was unable to handle the presence of other people, and thus did not return to work.
- PHYSICIAN’S DEFENSE First, because depression is a rare side effect of Lupron, it was unnecessary to disclose the risk. Second, given that the depression did not subside until 3 years after leuprolide injection, the drug had not caused the depression.
- VERDICT New York defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Parents claim fetal body was mistreated
A WOMAN presented at the hospital with excessive vaginal bleeding at 18 to 20 weeks’ gestation. A sonogram indicated the absence of amniotic fluid and a fetal heart rate of 86 to 102 bpm. The patient was admitted to labor and delivery. A nurse found no fetal heart tones, and the attending OB, Dr. A, used ultrasonography to confirm fetal death. Labor induction to deliver the fetus was begun. When a breech position was found, Dr. A, who was now unavailable, had the nurse contact Dr. B. The fetal body was delivered without the head—but Dr. B completed no delivery note and the medical records did not mention decapitation. After the body was placed in a sterile basin, the head was delivered using a ring forceps. Nurses removed the body parts and swaddled them in a baby blanket. The parents, who had not seen the decapitation, refused to hold the wrapped fetus, fearing the head would fall off. The remains were put in a closed casket for the viewing and funeral.
- PLAINTIFFS’ CLAIM The plaintiff mother claimed medical malpractice. Both parents said the fetus should have been left to deliver spontaneously without intervention. There was negligence in the mistreatment of the fetal body and also in the application of excessive force or traction to the body, which caused the decapitation.
- PHYSICIAN’S DEFENSE The delivery was carried out correctly. Delivery of a stillborn fetus requires guidance, as the cervix cannot fully dilate. Also, an 18- to 20-week fetus is friable and delicate; thus, contractions created a sheering force on the fetal body and caused the decapitation. The latter was not caused by traction.
- VERDICT Missouri defense verdict. A posttrial motion was pending.
Myomectomy causes uterine and bowel injuries
A 47-YEAR-OLD WOMAN suffered from heavy menstrual bleeding caused by submucosal uterine fibroids. Her gynecologist tried to resect the largest fibroid using a resectoscope, but the fibroid did not free itself from the uterine wall when he applied electrical current. He continued the procedure until it was apparent he had perforated the uterus. He stopped and sent the patient home with pain medications and antibiotics. Because of a bowel injury, she developed peritonitis and sepsis and eventually required surgical repair of the bowel. Her recovery was good, but it required her to miss work for 1 month and aggravated an existing anxiety disorder.
- PATIENT’S CLAIM Because of the high risk of uterine and bowel injury, the procedure should have been terminated when the application of electrical current did not free the fibroid from the uterine wall.
- PHYSICIAN’S DEFENSE Not reported.
- VERDICT $500,000 Minnesota settlement.
Patient attempts suicide after Lupron injection
A 27-YEAR-OLD WOMAN suffering from depression was given a diagnosis of endometriosis. Her ObGyn injected her with leuprolide (Lupron), which can decrease the production of some hormones and influence moods, and has an effect that lasts for about 3 months. Five days later the patient reported depression, and then returned to the facility the next day. Eleven days after that, she attempted suicide. A diagnosis of bipolar disorder was made following 3 days of inpatient psychiatric evaluation. She was treated for 1 month as an outpatient.
- PATIENT’S CLAIM Lupron should not have been administered. The ObGyn was negligent for treating her with the drug and for not disclosing that it can cause depression. She was unable to handle the presence of other people, and thus did not return to work.
- PHYSICIAN’S DEFENSE First, because depression is a rare side effect of Lupron, it was unnecessary to disclose the risk. Second, given that the depression did not subside until 3 years after leuprolide injection, the drug had not caused the depression.
- VERDICT New York defense verdict.
Parents claim fetal body was mistreated
A WOMAN presented at the hospital with excessive vaginal bleeding at 18 to 20 weeks’ gestation. A sonogram indicated the absence of amniotic fluid and a fetal heart rate of 86 to 102 bpm. The patient was admitted to labor and delivery. A nurse found no fetal heart tones, and the attending OB, Dr. A, used ultrasonography to confirm fetal death. Labor induction to deliver the fetus was begun. When a breech position was found, Dr. A, who was now unavailable, had the nurse contact Dr. B. The fetal body was delivered without the head—but Dr. B completed no delivery note and the medical records did not mention decapitation. After the body was placed in a sterile basin, the head was delivered using a ring forceps. Nurses removed the body parts and swaddled them in a baby blanket. The parents, who had not seen the decapitation, refused to hold the wrapped fetus, fearing the head would fall off. The remains were put in a closed casket for the viewing and funeral.
- PLAINTIFFS’ CLAIM The plaintiff mother claimed medical malpractice. Both parents said the fetus should have been left to deliver spontaneously without intervention. There was negligence in the mistreatment of the fetal body and also in the application of excessive force or traction to the body, which caused the decapitation.
- PHYSICIAN’S DEFENSE The delivery was carried out correctly. Delivery of a stillborn fetus requires guidance, as the cervix cannot fully dilate. Also, an 18- to 20-week fetus is friable and delicate; thus, contractions created a sheering force on the fetal body and caused the decapitation. The latter was not caused by traction.
- VERDICT Missouri defense verdict. A posttrial motion was pending.
Myomectomy causes uterine and bowel injuries
A 47-YEAR-OLD WOMAN suffered from heavy menstrual bleeding caused by submucosal uterine fibroids. Her gynecologist tried to resect the largest fibroid using a resectoscope, but the fibroid did not free itself from the uterine wall when he applied electrical current. He continued the procedure until it was apparent he had perforated the uterus. He stopped and sent the patient home with pain medications and antibiotics. Because of a bowel injury, she developed peritonitis and sepsis and eventually required surgical repair of the bowel. Her recovery was good, but it required her to miss work for 1 month and aggravated an existing anxiety disorder.
- PATIENT’S CLAIM Because of the high risk of uterine and bowel injury, the procedure should have been terminated when the application of electrical current did not free the fibroid from the uterine wall.
- PHYSICIAN’S DEFENSE Not reported.
- VERDICT $500,000 Minnesota settlement.
Patient attempts suicide after Lupron injection
A 27-YEAR-OLD WOMAN suffering from depression was given a diagnosis of endometriosis. Her ObGyn injected her with leuprolide (Lupron), which can decrease the production of some hormones and influence moods, and has an effect that lasts for about 3 months. Five days later the patient reported depression, and then returned to the facility the next day. Eleven days after that, she attempted suicide. A diagnosis of bipolar disorder was made following 3 days of inpatient psychiatric evaluation. She was treated for 1 month as an outpatient.
- PATIENT’S CLAIM Lupron should not have been administered. The ObGyn was negligent for treating her with the drug and for not disclosing that it can cause depression. She was unable to handle the presence of other people, and thus did not return to work.
- PHYSICIAN’S DEFENSE First, because depression is a rare side effect of Lupron, it was unnecessary to disclose the risk. Second, given that the depression did not subside until 3 years after leuprolide injection, the drug had not caused the depression.
- VERDICT New York defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Medical Verdicts
$28 million award against government for failure to test
A WOMAN delivered her first child a month early, due to fetal distress, at Balboa Naval Medical Center, where he was determined to have brain damage and given a diagnosis of cerebral palsy. She was told that his problems were due to premature separation of the placenta. When discussing the risks of a second pregnancy with physicians at Bethesda Medical Center 2.5 years later, she told them she had lupus, migraine, and supraventricular tachycardia, which caused palpitations—and that she was taking a ß-blocker and another medication. These physicians told her that the risk of brain hemorrhage—which had caused her child’s injuries—could be reduced with regular ultrasonography (US) growth studies and tests to track fetal movement and heart rate. When the physicians asked her the results of such studies—routine in a woman with her history—during her pregnancy, she said there had been no such studies. She later learned that a specialist had been consulted during that pregnancy, and that testing had been recommended. This was never discussed with her, nor the testing performed. The child, now age 9, has an IQ of 48 and functions at the level of a 3-year-old.
PATIENT’S CLAIM Intrauterine growth restriction occurred during her pregnancy because of the ß-blocker she was taking. Additional monitoring should have been conducted when this was recognized.
PHYSICIAN’S DEFENSE Not reported.
VERDICT $28 million award in Virginia, resulting from a claim brought under the Federal Torts Claim Act.
Patient says lymph node sampling was unnecessary
A 53-YEAR-OLD WOMAN went to Dr. A, her ObGyn, complaining of heavy discharge since menopause. A workup indicated an enlarged uterus with well-differentiated adenocarcinoma. Dr. A consulted with gynecologic oncologist Dr. B, and they decided on a two-phase surgical plan. Dr. A was the primary surgeon in the first phase, which involved a hysterectomy with removal of the fallopian tubes and ovaries. Surgical specimens showed that the uterine cancer was noninvasive. In the second phase, Dr. B removed the pelvic, periaortic, and renal lymph nodes. Frozen section analysis of the specimens indicated no invasive or metastatic disease. The permanent section, available 48 hours after surgery, revealed moderately differentiated adenocarcinoma with a 2-cm tumor mass, but no evidence of metastatic disease. The patient reported to the emergency room with abdominal pain 9 days after the surgery. A ureteral injury was found. A ureteral stent was placed, and stricture developed, requiring further procedures.
PATIENT’S CLAIM A hemoclip placed on the ureter during the periaortic lymph node dissection caused injury to the ureter. This phase of the surgery was unnecessary and inappropriate because preoperative evidence and specimen analysis indicated that the cancer was noninvasive—so there was no need for lymph node sampling.
PHYSICIAN’S DEFENSE Dr. A said he was entitled to rely on Dr. B’s recommendations for the treatment, as Dr. B was an expert in the field. Dr. B indicated that results from frozen samples can be unreliable, and that the risk of injury to the ureter was low.
VERDICT California defense verdict.
Lump is cancer—not sebaceous cyst as diagnosed
A WOMAN had a growing breast lump that was diagnosed as a sebaceous cyst by her gynecologist. She was advised to have it drained if it became painful, but was given no formal referral. Eleven months later, the patient was given a diagnosis of stage IV cancer.
PATIENT’S CLAIM A biopsy should have been performed when she first presented with the lump. Following the cancer diagnosis, the gynecologist altered the medical records when he added a note. Because of the note, the jury might believe that he had referred the patient to the diagnosing physician at that initial visit.
PHYSICIAN’S DEFENSE The patient did not have regular mammograms or US and, instead of following traditional protocols, underwent alternative treatment. When he learned of the cancer diagnosis, he added a note in the chart and said he had spoken with the diagnosing physician. The note was circled and in a different pen, and it did not alter information in the chart.
VERDICT $3.9 million Pennsylvania verdict, which was reduced to $2.5 million because the patient was found to be 35% at fault.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
$28 million award against government for failure to test
A WOMAN delivered her first child a month early, due to fetal distress, at Balboa Naval Medical Center, where he was determined to have brain damage and given a diagnosis of cerebral palsy. She was told that his problems were due to premature separation of the placenta. When discussing the risks of a second pregnancy with physicians at Bethesda Medical Center 2.5 years later, she told them she had lupus, migraine, and supraventricular tachycardia, which caused palpitations—and that she was taking a ß-blocker and another medication. These physicians told her that the risk of brain hemorrhage—which had caused her child’s injuries—could be reduced with regular ultrasonography (US) growth studies and tests to track fetal movement and heart rate. When the physicians asked her the results of such studies—routine in a woman with her history—during her pregnancy, she said there had been no such studies. She later learned that a specialist had been consulted during that pregnancy, and that testing had been recommended. This was never discussed with her, nor the testing performed. The child, now age 9, has an IQ of 48 and functions at the level of a 3-year-old.
PATIENT’S CLAIM Intrauterine growth restriction occurred during her pregnancy because of the ß-blocker she was taking. Additional monitoring should have been conducted when this was recognized.
PHYSICIAN’S DEFENSE Not reported.
VERDICT $28 million award in Virginia, resulting from a claim brought under the Federal Torts Claim Act.
Patient says lymph node sampling was unnecessary
A 53-YEAR-OLD WOMAN went to Dr. A, her ObGyn, complaining of heavy discharge since menopause. A workup indicated an enlarged uterus with well-differentiated adenocarcinoma. Dr. A consulted with gynecologic oncologist Dr. B, and they decided on a two-phase surgical plan. Dr. A was the primary surgeon in the first phase, which involved a hysterectomy with removal of the fallopian tubes and ovaries. Surgical specimens showed that the uterine cancer was noninvasive. In the second phase, Dr. B removed the pelvic, periaortic, and renal lymph nodes. Frozen section analysis of the specimens indicated no invasive or metastatic disease. The permanent section, available 48 hours after surgery, revealed moderately differentiated adenocarcinoma with a 2-cm tumor mass, but no evidence of metastatic disease. The patient reported to the emergency room with abdominal pain 9 days after the surgery. A ureteral injury was found. A ureteral stent was placed, and stricture developed, requiring further procedures.
PATIENT’S CLAIM A hemoclip placed on the ureter during the periaortic lymph node dissection caused injury to the ureter. This phase of the surgery was unnecessary and inappropriate because preoperative evidence and specimen analysis indicated that the cancer was noninvasive—so there was no need for lymph node sampling.
PHYSICIAN’S DEFENSE Dr. A said he was entitled to rely on Dr. B’s recommendations for the treatment, as Dr. B was an expert in the field. Dr. B indicated that results from frozen samples can be unreliable, and that the risk of injury to the ureter was low.
VERDICT California defense verdict.
Lump is cancer—not sebaceous cyst as diagnosed
A WOMAN had a growing breast lump that was diagnosed as a sebaceous cyst by her gynecologist. She was advised to have it drained if it became painful, but was given no formal referral. Eleven months later, the patient was given a diagnosis of stage IV cancer.
PATIENT’S CLAIM A biopsy should have been performed when she first presented with the lump. Following the cancer diagnosis, the gynecologist altered the medical records when he added a note. Because of the note, the jury might believe that he had referred the patient to the diagnosing physician at that initial visit.
PHYSICIAN’S DEFENSE The patient did not have regular mammograms or US and, instead of following traditional protocols, underwent alternative treatment. When he learned of the cancer diagnosis, he added a note in the chart and said he had spoken with the diagnosing physician. The note was circled and in a different pen, and it did not alter information in the chart.
VERDICT $3.9 million Pennsylvania verdict, which was reduced to $2.5 million because the patient was found to be 35% at fault.
$28 million award against government for failure to test
A WOMAN delivered her first child a month early, due to fetal distress, at Balboa Naval Medical Center, where he was determined to have brain damage and given a diagnosis of cerebral palsy. She was told that his problems were due to premature separation of the placenta. When discussing the risks of a second pregnancy with physicians at Bethesda Medical Center 2.5 years later, she told them she had lupus, migraine, and supraventricular tachycardia, which caused palpitations—and that she was taking a ß-blocker and another medication. These physicians told her that the risk of brain hemorrhage—which had caused her child’s injuries—could be reduced with regular ultrasonography (US) growth studies and tests to track fetal movement and heart rate. When the physicians asked her the results of such studies—routine in a woman with her history—during her pregnancy, she said there had been no such studies. She later learned that a specialist had been consulted during that pregnancy, and that testing had been recommended. This was never discussed with her, nor the testing performed. The child, now age 9, has an IQ of 48 and functions at the level of a 3-year-old.
PATIENT’S CLAIM Intrauterine growth restriction occurred during her pregnancy because of the ß-blocker she was taking. Additional monitoring should have been conducted when this was recognized.
PHYSICIAN’S DEFENSE Not reported.
VERDICT $28 million award in Virginia, resulting from a claim brought under the Federal Torts Claim Act.
Patient says lymph node sampling was unnecessary
A 53-YEAR-OLD WOMAN went to Dr. A, her ObGyn, complaining of heavy discharge since menopause. A workup indicated an enlarged uterus with well-differentiated adenocarcinoma. Dr. A consulted with gynecologic oncologist Dr. B, and they decided on a two-phase surgical plan. Dr. A was the primary surgeon in the first phase, which involved a hysterectomy with removal of the fallopian tubes and ovaries. Surgical specimens showed that the uterine cancer was noninvasive. In the second phase, Dr. B removed the pelvic, periaortic, and renal lymph nodes. Frozen section analysis of the specimens indicated no invasive or metastatic disease. The permanent section, available 48 hours after surgery, revealed moderately differentiated adenocarcinoma with a 2-cm tumor mass, but no evidence of metastatic disease. The patient reported to the emergency room with abdominal pain 9 days after the surgery. A ureteral injury was found. A ureteral stent was placed, and stricture developed, requiring further procedures.
PATIENT’S CLAIM A hemoclip placed on the ureter during the periaortic lymph node dissection caused injury to the ureter. This phase of the surgery was unnecessary and inappropriate because preoperative evidence and specimen analysis indicated that the cancer was noninvasive—so there was no need for lymph node sampling.
PHYSICIAN’S DEFENSE Dr. A said he was entitled to rely on Dr. B’s recommendations for the treatment, as Dr. B was an expert in the field. Dr. B indicated that results from frozen samples can be unreliable, and that the risk of injury to the ureter was low.
VERDICT California defense verdict.
Lump is cancer—not sebaceous cyst as diagnosed
A WOMAN had a growing breast lump that was diagnosed as a sebaceous cyst by her gynecologist. She was advised to have it drained if it became painful, but was given no formal referral. Eleven months later, the patient was given a diagnosis of stage IV cancer.
PATIENT’S CLAIM A biopsy should have been performed when she first presented with the lump. Following the cancer diagnosis, the gynecologist altered the medical records when he added a note. Because of the note, the jury might believe that he had referred the patient to the diagnosing physician at that initial visit.
PHYSICIAN’S DEFENSE The patient did not have regular mammograms or US and, instead of following traditional protocols, underwent alternative treatment. When he learned of the cancer diagnosis, he added a note in the chart and said he had spoken with the diagnosing physician. The note was circled and in a different pen, and it did not alter information in the chart.
VERDICT $3.9 million Pennsylvania verdict, which was reduced to $2.5 million because the patient was found to be 35% at fault.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.