User login
The Observation Deck
Observation care provides a mechanism to evaluate and treat patients without the resource utilization and financial responsibility associated with an inpatient admission. Hospitalists may not understand the billing compliance risk and corresponding revenue implications when observation services (OBS) are not captured correctly.
Are OBS best reported with observation care codes (99218-99220, 99234-99236), office visit codes (99201-99215), or initial hospital care codes (99221-99223)? Code selection depends upon the patient’s registered status, the nature of the provided service, and the length of stay. Review the following information before reporting OBS to ensure an accurate claim submission.
Attending Physician Responsibilities
The physician-documented reason for observation substantiates the medical necessity for the OBS admission. Contractors often evaluate medical records to determine the consistency between the physician order (physician intent), the services actually provided (inpatient or outpatient), and the medical necessity of those services, including the medical appropriateness of the inpatient or observation stay.
Certain diagnoses and procedures generally do not support an inpatient admission and fall within the definitions of outpatient observation. Uncomplicated presentations of chest pain (rule out MI), mild asthma/COPD, mild CHF, syncope and decreased responsiveness, atrial arrhythmias, and renal colic all frequently are associated with the expectation of a brief (less than 24-hour) stay unless serious pathology is uncovered.2 Situations that do not meet the criteria for observation care are considered “not medically necessary” and separate payment is not permitted. Examples of circumstances that lack medical necessity include:
- Outpatient blood administration;
- Lack of/delay in patient transportation;
- Provision of a medical exam for patients who do not require skilled support;
- Routine preparation prior to and recovery after diagnostic testing;
- Routine recovery and post-operative care after ambulatory surgery;
- When used for the convenience of the physician, patient or patient’s family;
- While awaiting transfer to another facility;
- Duration of care exceeding 48 hours;
- When an overnight stay is planned prior to diagnostic testing;
- Standing orders following outpatient surgery;
- Services that would normally require inpatient stay;
- No physicians order to admit to observation;
- Observation following an uncomplicated treatment or procedure;
- Services that are not reasonable and necessary for care of the patient;
- Services provided concurrently with chemotherapy; and
- Inpatients discharged to outpatient observation status.3
The attending physician of record assumes responsibility for the patient’s admission to observation and is permitted to report observation care codes. In addition to the reason for admission, a medical record involving the observation stay must include dated and timed physician admitting orders outlining the care plan, physician progress notes, and discharge orders. This documentation must be added to any other record prepared as a result of an emergency department or outpatient clinic encounter. If physicians other than the admitting physician/group (i.e., physicians in different specialties) provide services to the patient during observation, they must use the appropriate outpatient visit (e.g., 99214) or consultation code (e.g., 99244).
Length of Stay4
In general, the duration of observation care services typically does not exceed 24 hours, although in some circumstances patients may require a second day. Observation care for greater than 48 hours without inpatient admission is not considered medically necessary but may be payable after medical review. When the stay spans two calendar days, physician billing is straightforward: Select an initial observation care code (99218-99220) for calendar day one and the observation discharge code (99217) for day two. Only the admitting physician/group may report the discharge service, when applicable. Documentation must demonstrate a face-to-face encounter by the physician for each date of service.
Should the stay only constitute one calendar day, the duration of care becomes a crucial factor in determining the code category. Standard OBS codes (99218-99220) are applicable if the patient stay is less than eight hours on any given date. The OBS discharge code (99217) is not reported in this instance, although the documentation should reflect the attending physician’s written order and appropriate discharge plan. Alternately, same day admit/discharge codes (99234-99236) apply to single-day stays lasting more than eight hours. The OBS discharge code (99217) also is not reported in this instance. Documentation must identify, at a minimum:
- Duration of the stay;
- Presence by the billing physician; and
- Physician performance of each service (i.e., both an admission and discharge note).
Inpatient Admission1,4-5
Sometimes the patient requires inpatient admission after initially being placed in observation. If the inpatient admission occurs on the same day as the OBS admission, only one service is reported (e.g., 99222). The physician need not redocument a complete history and physical (H&P) but merely write the new order for admission and update the OBS assessment with any relevant, new information.
Should the inpatient admission occur on the second calendar day of the OBS stay, the physician is able to report the initial observation care code (e.g., 99219) on day one, and the initial inpatient care code (e.g., 99223) on day two. However, the physician must meet the documentation guidelines for initial hospital care and redocument the H&P associated with the reported visit level. In the case of 99223, the physician must document a comprehensive history (only referring to the previous review of systems and histories, while rewriting the history of present illness) and high complexity decision making. If the physician chooses not to document to this extent, a subsequent hospital care code (99231-99233) is reasonable because the episode of care is a continuation from the observation phase.
Beware that some insurers may change the patient’s status for the entire episode of care. In other words, the conversion to inpatient status occurs on day two of the patient stay, but the insurer may convert the entire stay, including day one, to an inpatient status. Should this happen, the physician is responsible for reporting the visit category that corresponds with the patient’s status. Inpatient services codes are required for claim submission when the patient stay qualifies as an inpatient admission. Because these conversions occur with some frequency, it is advisable to hold claims intended for observation patients until the correct patient status can be confirmed by the utilization review team, and communicated to the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References
- 1. American Medical Association. cpt 2008, Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2007; 9-16 CPT codes, descriptions and other data only are copyright 2007 American Medical Association (AMA). All Rights Reserved (or such other date of publication of CPT). CPT is a trademark of the AMA.
- 2. Highmark Medicare Services. Local Coverage Determination L27548 Acute Care: Inpatient, Observation and Treatment Room Services. Available at www.highmarkmedicareservices.com/policy/mac-ab/127548.html. Accessed July 14, 2008.
- 3. Cigna. Healthcare Coverage Position: Observation Care. Available at www.cigna.com/customer_care/healthcare_ professional/coverage_positions/medical/mm_0411_coveragepositioncriteria_observation_care.pdf. Accessed July 12, 2008.
- 4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed July 13, 2008.
- 5. Pohlig C. Evaluation & Management Services: An Overview. Coding for Chest Medicine 2008. Northbrook, IL: American College of Chest Physicians, 2008; 57-69.
- 6. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 1, Section 50.3. Available at www.cms.hhs.gov/manuals/downloads/ clm104c01.pdf. Accessed July 13, 2008.
Observation care provides a mechanism to evaluate and treat patients without the resource utilization and financial responsibility associated with an inpatient admission. Hospitalists may not understand the billing compliance risk and corresponding revenue implications when observation services (OBS) are not captured correctly.
Are OBS best reported with observation care codes (99218-99220, 99234-99236), office visit codes (99201-99215), or initial hospital care codes (99221-99223)? Code selection depends upon the patient’s registered status, the nature of the provided service, and the length of stay. Review the following information before reporting OBS to ensure an accurate claim submission.
Attending Physician Responsibilities
The physician-documented reason for observation substantiates the medical necessity for the OBS admission. Contractors often evaluate medical records to determine the consistency between the physician order (physician intent), the services actually provided (inpatient or outpatient), and the medical necessity of those services, including the medical appropriateness of the inpatient or observation stay.
Certain diagnoses and procedures generally do not support an inpatient admission and fall within the definitions of outpatient observation. Uncomplicated presentations of chest pain (rule out MI), mild asthma/COPD, mild CHF, syncope and decreased responsiveness, atrial arrhythmias, and renal colic all frequently are associated with the expectation of a brief (less than 24-hour) stay unless serious pathology is uncovered.2 Situations that do not meet the criteria for observation care are considered “not medically necessary” and separate payment is not permitted. Examples of circumstances that lack medical necessity include:
- Outpatient blood administration;
- Lack of/delay in patient transportation;
- Provision of a medical exam for patients who do not require skilled support;
- Routine preparation prior to and recovery after diagnostic testing;
- Routine recovery and post-operative care after ambulatory surgery;
- When used for the convenience of the physician, patient or patient’s family;
- While awaiting transfer to another facility;
- Duration of care exceeding 48 hours;
- When an overnight stay is planned prior to diagnostic testing;
- Standing orders following outpatient surgery;
- Services that would normally require inpatient stay;
- No physicians order to admit to observation;
- Observation following an uncomplicated treatment or procedure;
- Services that are not reasonable and necessary for care of the patient;
- Services provided concurrently with chemotherapy; and
- Inpatients discharged to outpatient observation status.3
The attending physician of record assumes responsibility for the patient’s admission to observation and is permitted to report observation care codes. In addition to the reason for admission, a medical record involving the observation stay must include dated and timed physician admitting orders outlining the care plan, physician progress notes, and discharge orders. This documentation must be added to any other record prepared as a result of an emergency department or outpatient clinic encounter. If physicians other than the admitting physician/group (i.e., physicians in different specialties) provide services to the patient during observation, they must use the appropriate outpatient visit (e.g., 99214) or consultation code (e.g., 99244).
Length of Stay4
In general, the duration of observation care services typically does not exceed 24 hours, although in some circumstances patients may require a second day. Observation care for greater than 48 hours without inpatient admission is not considered medically necessary but may be payable after medical review. When the stay spans two calendar days, physician billing is straightforward: Select an initial observation care code (99218-99220) for calendar day one and the observation discharge code (99217) for day two. Only the admitting physician/group may report the discharge service, when applicable. Documentation must demonstrate a face-to-face encounter by the physician for each date of service.
Should the stay only constitute one calendar day, the duration of care becomes a crucial factor in determining the code category. Standard OBS codes (99218-99220) are applicable if the patient stay is less than eight hours on any given date. The OBS discharge code (99217) is not reported in this instance, although the documentation should reflect the attending physician’s written order and appropriate discharge plan. Alternately, same day admit/discharge codes (99234-99236) apply to single-day stays lasting more than eight hours. The OBS discharge code (99217) also is not reported in this instance. Documentation must identify, at a minimum:
- Duration of the stay;
- Presence by the billing physician; and
- Physician performance of each service (i.e., both an admission and discharge note).
Inpatient Admission1,4-5
Sometimes the patient requires inpatient admission after initially being placed in observation. If the inpatient admission occurs on the same day as the OBS admission, only one service is reported (e.g., 99222). The physician need not redocument a complete history and physical (H&P) but merely write the new order for admission and update the OBS assessment with any relevant, new information.
Should the inpatient admission occur on the second calendar day of the OBS stay, the physician is able to report the initial observation care code (e.g., 99219) on day one, and the initial inpatient care code (e.g., 99223) on day two. However, the physician must meet the documentation guidelines for initial hospital care and redocument the H&P associated with the reported visit level. In the case of 99223, the physician must document a comprehensive history (only referring to the previous review of systems and histories, while rewriting the history of present illness) and high complexity decision making. If the physician chooses not to document to this extent, a subsequent hospital care code (99231-99233) is reasonable because the episode of care is a continuation from the observation phase.
Beware that some insurers may change the patient’s status for the entire episode of care. In other words, the conversion to inpatient status occurs on day two of the patient stay, but the insurer may convert the entire stay, including day one, to an inpatient status. Should this happen, the physician is responsible for reporting the visit category that corresponds with the patient’s status. Inpatient services codes are required for claim submission when the patient stay qualifies as an inpatient admission. Because these conversions occur with some frequency, it is advisable to hold claims intended for observation patients until the correct patient status can be confirmed by the utilization review team, and communicated to the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References
- 1. American Medical Association. cpt 2008, Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2007; 9-16 CPT codes, descriptions and other data only are copyright 2007 American Medical Association (AMA). All Rights Reserved (or such other date of publication of CPT). CPT is a trademark of the AMA.
- 2. Highmark Medicare Services. Local Coverage Determination L27548 Acute Care: Inpatient, Observation and Treatment Room Services. Available at www.highmarkmedicareservices.com/policy/mac-ab/127548.html. Accessed July 14, 2008.
- 3. Cigna. Healthcare Coverage Position: Observation Care. Available at www.cigna.com/customer_care/healthcare_ professional/coverage_positions/medical/mm_0411_coveragepositioncriteria_observation_care.pdf. Accessed July 12, 2008.
- 4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed July 13, 2008.
- 5. Pohlig C. Evaluation & Management Services: An Overview. Coding for Chest Medicine 2008. Northbrook, IL: American College of Chest Physicians, 2008; 57-69.
- 6. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 1, Section 50.3. Available at www.cms.hhs.gov/manuals/downloads/ clm104c01.pdf. Accessed July 13, 2008.
Observation care provides a mechanism to evaluate and treat patients without the resource utilization and financial responsibility associated with an inpatient admission. Hospitalists may not understand the billing compliance risk and corresponding revenue implications when observation services (OBS) are not captured correctly.
Are OBS best reported with observation care codes (99218-99220, 99234-99236), office visit codes (99201-99215), or initial hospital care codes (99221-99223)? Code selection depends upon the patient’s registered status, the nature of the provided service, and the length of stay. Review the following information before reporting OBS to ensure an accurate claim submission.
Attending Physician Responsibilities
The physician-documented reason for observation substantiates the medical necessity for the OBS admission. Contractors often evaluate medical records to determine the consistency between the physician order (physician intent), the services actually provided (inpatient or outpatient), and the medical necessity of those services, including the medical appropriateness of the inpatient or observation stay.
Certain diagnoses and procedures generally do not support an inpatient admission and fall within the definitions of outpatient observation. Uncomplicated presentations of chest pain (rule out MI), mild asthma/COPD, mild CHF, syncope and decreased responsiveness, atrial arrhythmias, and renal colic all frequently are associated with the expectation of a brief (less than 24-hour) stay unless serious pathology is uncovered.2 Situations that do not meet the criteria for observation care are considered “not medically necessary” and separate payment is not permitted. Examples of circumstances that lack medical necessity include:
- Outpatient blood administration;
- Lack of/delay in patient transportation;
- Provision of a medical exam for patients who do not require skilled support;
- Routine preparation prior to and recovery after diagnostic testing;
- Routine recovery and post-operative care after ambulatory surgery;
- When used for the convenience of the physician, patient or patient’s family;
- While awaiting transfer to another facility;
- Duration of care exceeding 48 hours;
- When an overnight stay is planned prior to diagnostic testing;
- Standing orders following outpatient surgery;
- Services that would normally require inpatient stay;
- No physicians order to admit to observation;
- Observation following an uncomplicated treatment or procedure;
- Services that are not reasonable and necessary for care of the patient;
- Services provided concurrently with chemotherapy; and
- Inpatients discharged to outpatient observation status.3
The attending physician of record assumes responsibility for the patient’s admission to observation and is permitted to report observation care codes. In addition to the reason for admission, a medical record involving the observation stay must include dated and timed physician admitting orders outlining the care plan, physician progress notes, and discharge orders. This documentation must be added to any other record prepared as a result of an emergency department or outpatient clinic encounter. If physicians other than the admitting physician/group (i.e., physicians in different specialties) provide services to the patient during observation, they must use the appropriate outpatient visit (e.g., 99214) or consultation code (e.g., 99244).
Length of Stay4
In general, the duration of observation care services typically does not exceed 24 hours, although in some circumstances patients may require a second day. Observation care for greater than 48 hours without inpatient admission is not considered medically necessary but may be payable after medical review. When the stay spans two calendar days, physician billing is straightforward: Select an initial observation care code (99218-99220) for calendar day one and the observation discharge code (99217) for day two. Only the admitting physician/group may report the discharge service, when applicable. Documentation must demonstrate a face-to-face encounter by the physician for each date of service.
Should the stay only constitute one calendar day, the duration of care becomes a crucial factor in determining the code category. Standard OBS codes (99218-99220) are applicable if the patient stay is less than eight hours on any given date. The OBS discharge code (99217) is not reported in this instance, although the documentation should reflect the attending physician’s written order and appropriate discharge plan. Alternately, same day admit/discharge codes (99234-99236) apply to single-day stays lasting more than eight hours. The OBS discharge code (99217) also is not reported in this instance. Documentation must identify, at a minimum:
- Duration of the stay;
- Presence by the billing physician; and
- Physician performance of each service (i.e., both an admission and discharge note).
Inpatient Admission1,4-5
Sometimes the patient requires inpatient admission after initially being placed in observation. If the inpatient admission occurs on the same day as the OBS admission, only one service is reported (e.g., 99222). The physician need not redocument a complete history and physical (H&P) but merely write the new order for admission and update the OBS assessment with any relevant, new information.
Should the inpatient admission occur on the second calendar day of the OBS stay, the physician is able to report the initial observation care code (e.g., 99219) on day one, and the initial inpatient care code (e.g., 99223) on day two. However, the physician must meet the documentation guidelines for initial hospital care and redocument the H&P associated with the reported visit level. In the case of 99223, the physician must document a comprehensive history (only referring to the previous review of systems and histories, while rewriting the history of present illness) and high complexity decision making. If the physician chooses not to document to this extent, a subsequent hospital care code (99231-99233) is reasonable because the episode of care is a continuation from the observation phase.
Beware that some insurers may change the patient’s status for the entire episode of care. In other words, the conversion to inpatient status occurs on day two of the patient stay, but the insurer may convert the entire stay, including day one, to an inpatient status. Should this happen, the physician is responsible for reporting the visit category that corresponds with the patient’s status. Inpatient services codes are required for claim submission when the patient stay qualifies as an inpatient admission. Because these conversions occur with some frequency, it is advisable to hold claims intended for observation patients until the correct patient status can be confirmed by the utilization review team, and communicated to the physician. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
References
- 1. American Medical Association. cpt 2008, Current Procedural Terminology Professional Edition. Chicago, IL: American Medical Association, 2007; 9-16 CPT codes, descriptions and other data only are copyright 2007 American Medical Association (AMA). All Rights Reserved (or such other date of publication of CPT). CPT is a trademark of the AMA.
- 2. Highmark Medicare Services. Local Coverage Determination L27548 Acute Care: Inpatient, Observation and Treatment Room Services. Available at www.highmarkmedicareservices.com/policy/mac-ab/127548.html. Accessed July 14, 2008.
- 3. Cigna. Healthcare Coverage Position: Observation Care. Available at www.cigna.com/customer_care/healthcare_ professional/coverage_positions/medical/mm_0411_coveragepositioncriteria_observation_care.pdf. Accessed July 12, 2008.
- 4. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 12, Section 30.6.8. Available at www.cms.hhs.gov/manuals/downloads/ clm104c12.pdf. Accessed July 13, 2008.
- 5. Pohlig C. Evaluation & Management Services: An Overview. Coding for Chest Medicine 2008. Northbrook, IL: American College of Chest Physicians, 2008; 57-69.
- 6. Centers for Medicare and Medicaid Services. Medicare Claims Processing Manual: Chapter 1, Section 50.3. Available at www.cms.hhs.gov/manuals/downloads/ clm104c01.pdf. Accessed July 13, 2008.
Strategies for breaking bad news to patients
The author reports no financial relationships relevant to this article.
Editors’ note: This article appears under the “Focus on professional liability” series banner even though Dr. Bub’s discussion does not directly address matters of being sued. Our, and his, belief is that good communication brings a significant added benefit of lowering a physician’s litigation risk.
- It was tiring to try and think logically as the guy threw more and more facts at me.—An adolescent with cancer1
Consider the findings of two surveys of radiology residents and attending mammographers on breaking bad or troubling news to patients:
- 16% of residents and 4% of mammographers “didn’t feel confident communicating with patients who displayed strong emotional responses”
- 86% of residents and 81% of staff experienced “some or moderate stress communicating the need for biopsy”
- The majority of all respondents “hadn’t received feedback about their communication skills or communication training after medical school”
- 68% to 78% of respondents expressed interest in “improving their communication.”2
Breaking what you might perceive as “bad” news is never easy; even experienced practitioners may find the task stressful, as the results of these two surveys reveal. Physicians having been trained to do no harm, few find themselves at ease revealing information that has the potential to disappoint or upset, even devastate.
In this article, I offer an approach to breaking bad news in a manner that lessens the trauma to the patient and buffers you from the stress, and distress, of delivering it. The box near the end of this article gathers pearls for giving bad news based on my work and the experiences of others.
We are not unaffected by this task
Most of us find the act of breaking bad news a professional burden that we could just as soon do without. When we perceive an element of personal responsibility, our burden becomes greater: We may experience fear, guilt, or shame—and, for some, that leads to psychological stress disorders and burnout.
How do we cope, being occasional messengers of bad news?
We avoid. An obvious strategy. Consider Dr. D., a radiologist who heads a breast imaging center. He confides that many physicians ask him to inform their patients when he notes an abnormality on their mammogram. Still other physicians, Dr. D. points out, simply have their nurses call patients with troubling results.
Or we run. Another widely used strategy is to break the news and bolt. One cancer survivor lamented: “As soon as I started to cry, he ran off to fetch his nurse. Don’t you know doctors flee from suffering?”
Keeping matters in balance—that is the challenge
How do we maintain our sensitivity, humanity, and connection while, simultaneously, limiting our own vulnerability and pain? Many of us have wrestled with this issue from the earliest days of training:
- In the hospital’s predawn stillness, she confided fears about surgery to me, the medical student. I tried to reassure her. They operated. Finding extensive metastases, they closed immediately. That evening, aching for her, I cried.
- “Don’t worry,” another student reassured me. “It gets easier.”
- I hope not. If it does, I’ll have lost my humanity.3
Simultaneously, how do we handle our feelings of impotence, failure, and, perhaps, guilt—when every expression, gesture, word, and silence are potentially filled with meaning to those who are receiving the news?
David Lenz, an artist, in a commentary on his award-winning painting, “Sam and the Perfect World,” wrote:
- My wife Rosemarie had just given birth to our son Sam, and although he appeared perfectly healthy, something, nevertheless, didn’t seem right. There was an awkward silence in the room, no words of congratulation or comments about how cute he was—even though he was cute. Five minutes later the diagnosis was given: Sam has Down syndrome. “Are you going to keep him?” a nurse asked. Later that evening someone else came by to “console” us.
- “It’s every mother’s worst nightmare,” she said.
- Welcome to the world, Sam.4
5 and invest in deep and surface acting (of empathy).6 I disagree with this advice7 ; instead, I advocate that we notice, validate, and park our emotions. Later, we take time to integrate our emotions through self-care. Rather than relying on “the art of medicine” to communicate bad news, we should approach this task as a serious professional challenge and incorporate principles of trauma counseling, psychotherapy, and chaplaincy into the practice of medicine. Instead of distancing from our emotions and our patients, we draw closer.
Here is how one physician handles breaking bad news.
CASE
Dr. Bob, we’ll call him, typifies the overworked primary care physician. Yet, when a lab or imaging report that reveals an abnormal result lands on his desk, he, not a nurse, calls the patient. He waits a few days if the test or study was ordered by another physician; in that situation, he often reaches a frightened, confused person who had already been called by the specialist’s nurse.
When that happens, Dr. Bob invites the patient, and a close relative, to schedule an office visit with him. In the interim, he forms a liaison with the specialist so that they can function as a team.
At the office visit, Dr. Bob refuses to prognosticate. Instead, he recommends that they take matters “one step at a time.” His approach is positive and reassuring but not overly optimistic. His message is clear: “You are not alone. I will be a supportive presence throughout your journey.”
Two notable things about Dr. Bob: First, he does not suffer burnout or what some have called “compassion fatigue”; to the contrary, the relationship he forges with his patients and their loved ones, and the gratitude and loyalty he receives from them, sustain and reward him.
Second, Dr. Bob has never been sued.
The key to Dr. Bob’s success is that he does not shy from breaking bad news. Instead, he views the occasion as an opportunity for healing. His approach is to detach from the outcome but not from the patient. He relieves fear and isolation, and offers, as one patient said it, “candor with hope.”
Summon your personal strengths to succeed
But taking this approach requires a shift from the standard biomedical philosophy—a three-pronged cultivation of personal resources. Here is how you can make that shift.
First, cultivate equanimity—that evenness of mind
Consider that destruction is an inherent component of creation. There can’t be light without darkness, birth without death, joy without suffering, perfection without imperfection. The Sufi mystic, Rumi, said it succinctly: “A butterfly needs two wings to fly.”
Recognize that not all news is equally bad. The spectrum runs from merely inconvenient to utterly devastating; how the news is perceived and received is highly subjective. Avoid projecting your personal perspective onto the recipient:
- I was totally perplexed. I had just broken the news that Mrs. Smith had an incurable colon cancer, and they responded by nodding, then asking me whether I preferred a chocolate cake or an apple pie for their next visit because it was their custom to bring home-baked goodies for the staff.
- After her death, Mr. Smith faithfully continued this tradition. Then one day he arrived for his regular appointment unshaven, distressed and sans cake. He had lost weight and looked every bit of his 78 years. Something was very wrong.
- “She’s gone, she’s gone,” he lamented.
- At last he’s grieving flashed through my mind, so I responded: “Yes, it’s been about 9 months now, hasn’t it?”
- “No, just two weeks…she said she was my girlfriend…just 29 years old…moved in last month then left taking my money,” he cried.
- She assumed the mantle of a grieving widow. Only years later did she write that she had been secretly relieved that her husband was killed in an automobile accident. He had been abusive and she was planning to leave him anyway.
- It was my birthday, and we were about to celebrate with a dinner of leg of lamb and roast potatoes. My cell phone rang. It was my internist calling; my LDL cholesterol was mildly elevated and my dexa scan demonstrated slight osteopenia. The tone of his voice was matter-of-fact but I felt awful: I am getting old.
Realize that long-term well-being doesn’t depend on good vs. bad news:
- What do Chuck Close and Dan Gottlieb have in common? Each was a healthy young adult when suddenly becoming paraplegic—Chuck from a spinal artery thrombosis, Dan from a serious accident. Each adapted to his condition. Chuck developed a unique style of painting that established his fame as an artist. Dan, a psychotherapist, became an author, teacher, and highly regarded radio interviewer. Each has recently stated that he has never been happier.
Remind yourself of hidden opportunities. Bad news triggers a crisis—an unwelcome, unstable situation with obvious danger. Less apparent is the potential for positive personal transformation and gain:
- “It was the best thing that could have happened to me,” she said, lying with her right foot propped up, ankle heavily bandaged with pins and rods protruding. “Yes, it’s a horribly fractured ankle but I had been rushing, rushing, rushing, and when I fell down the steps, it was as if an angel was forcing me to slow down, be present to my family. I really think this fractured ankle was the best thing that could have happened—it may even have saved my marriage.”
Second, cultivate yourself as a healer
You may not always be able to cure but you can always facilitate healing. In addition to a treatment plan, remind yourself to create a parallel healing plan, listing the interventions that will help the recipient integrate losses and become as functionally whole as possible.
Your ability to heal depends as much on who you are as what you do:
- Work through your own trauma stories and you reduce the likelihood that you either attempt to rescue, or flee from engagement with, patients when their problems trigger painful memories for you
- Accept your imperfections as an inseparable aspect of your humanity
- Learn to accept life as a journey, with suffering and death being inevitable, and bad news ceases to be so exceptional
- Deepen your own joy, mindfulness, and faith and you find meaning in your work even when you cannot cure
- Have realistic expectations of your abilities and try to cultivate a realistic attitude in your patients:
- In Western culture there is a belief, conscious or not, that medicine can save us from the death that lies in wait for us… In a study conducted in 2006 among Israeli doctors, 68% of the participants reported that patients had unrealistic expectations of them. The study reflects unrealistic expectations of medicine in general.8
Third, cultivate skills to break really bad news
Sometimes news is so bad, so overwhelming, that it has the potential to trigger an acute stress reaction (ASR) and even posttraumatic stress disorder (PTSD) in the recipient. Typically, this is life-threatening news—a diagnosis of HIV infection or cancer; abortion or stillbirth; or the sudden, unexpected death of a loved one. The result is shock, horror, disorientation, and memory distortion.
So how can you approach a situation in which you must offer very bad news? To begin, the box, below “Pearls for breaking bad news…,” provides a set of skills and tools for delivering bad news.
In addition, as much as possible, break bad news in increments, so that the patient has time to cope and adjust. And there is more to keep in mind:
- Provide a safe, supportive environment
- Relieve the isolation that trauma inflicts by forging a relationship that is a partnership
- Relieve helplessness by empowering and assisting the patient to seek useful consultants, resources, and supports (One example: A patient who has breast or ovarian cancer can call the SHARE [Self-help for Women with Ovarian or Breast Cancer] hotline: [866] 891-2392)
- Over time, although not initially, help provide meaning to the experience for your patient and for you.
- Don’t have your assistant call with bad news unless she or he is trained to do this, humanely, and to handle the response. Don’t leave a message asking the patient to call back unless you are reasonably certain you will be able to take the call.
- Before you enter the room or place a call, pause, take a deep breath, acknowledge your feelings so you can set them aside, and be fully present. Remember: Empathy begins at home.
- Effective communication always begins and ends with listening. On entering a room, notice the people present, the atmosphere, and the interactions. Over the telephone, notice breath and tone of voice in addition to words spoken. Create space for the recipient to speak, even if silence is uncomfortably long.
- Begin the session by greeting everyone present by name and by shaking hands.
- Offer a general inquiry and listen. A simple “How are you?” allows the patient to express a feeling—“I’m OK but anxious,” for example. Respond with empathy early in the encounter: “Yes, it’s scary waiting for results.”
- Use simple, nontechnical language to describe the situation. Be brief, because a person in a high state of arousal has limited capacity to absorb details. Avoid harsh language (“aggressive,” “failure”) and use a calm, modulated tone.
- Listen and validate the responses you get, recognizing that you may be the recipient of an entire spectrum of emotional expression—from silence to an outburst of anger, from rage to grief. Keep in mind: Anything said in grief is acceptable.
- Remember: You are not responsible for your patients’ happiness. When a patient cries, it does not mean that you failed. An outpouring of grief is healing; your silent, supportive presence is invaluable.
- Don’t attempt to prematurely comfort; don’t try to “make it better,” because this stifles grief. Offering a box of tissues, on the other hand, is simply considerate.
- Don’t present the bleakest scenario. Later, as the patient adapts to her new reality, she will usually be able to tolerate more.
- Be forearmed with some basic treatment and referral options so that the patient isn’t left facing the dark unknown.
- Now, invite the patient’s perspective. Appreciate that she may be experiencing a sea of emotions, especially if the news is totally unexpected. It’s not sufficient to lay out options, then leave the final decision to her. Part of decision-making involves the processing of emotions. Gendlin’s technique of focusing is very useful at this point in the conversation.1
- If you are at the hospital, 1) consider having a chaplain present when the news is potentially devastating and 2) attend to privacy concerns when breaking bad news.
- Treat the person, not the pathology. Ask about her work, activities, and circle of support—all of which are relevant to her situation.
- Be clear that you will remain actively involved in her care even after you refer the patient to the best consultants available.
- Don’t limit yourself to the negative. Look for what is healthy about your patient’s situation, too, and support it.
- Give as much information as possible in writing at this time; amnesia is common. Offer to share the information with at least one family member over the telephone, or schedule a second visit at which a relative will be present.
- When you’re questioned directly, give yourself the benefit of a few moments to ground yourself before you respond.
- Ensure a safe exit for your patient. Does she have someone to drive her, keep her company, etc.?
- Consider calling her that evening to see how she is and to answer any additional questions.
- Invest in self-care. This might include debriefing, taking a break between patients for integration, and grounding and rituals that enable you to detoxify after a difficult day. Cultivate whatever spiritual and meditative practices are part of your life, even if it is simply a walk in the park.
- Empower yourself with relationship skills that enhance your ability to communicate and counsel.
- Have faith! The time that you invest in healthy practice and communication will save you much more over the course of your career.
Reference
1. Bub B. Communication skills that heal: a practical approach to a new professionalism in medicine. Abingdon, UK: Radcliffe Publishing; 2006.
Frankel E. Sacred Therapy. Boston: Shambhala; 2003.
Herman J. Trauma and Recovery. New York: Basic Books; 1992.
Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wis: Seasons Press; 1994.
1. Training workshop sponsored by Melissa’s Living Legacy Foundation, April 2004 (http://www.teenslivingwithcancer.org).
2. Sasson JP, Lown BA. Communicating practices in the diagnostic mammography suite. Med Encounter. 2006;20(4):66.-
3. Christianson AL. A piece of my mind. More stories. JAMA. 2002;288:931.-
4. Bub B. Medicine and the arts. Sam and the Perfect World by David Lenz. Commentary. Acad Med. 2007;82(2):200-201.
5. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA. 2001;286:3007-3014.
6. Larson EB, Yao X. Clinical empathy as emotional labor in the patient–physician relationship. JAMA. 2005;293:1100-1106.
7. Bub B. Focusing and the healing sequence: reclaiming authentic emotions as an aid to communication and well-being in medicine. Explore (NY). 2007;3:413-416.
8. Schwartzman O. White Doctor, Black Gods: White Psychiatric Medicine in the Jungles of Africa. Israel: Aryeh Nir Publishing House; 256 pages. http://www.haaretz.com/hasen/spages/834952.html.
The author reports no financial relationships relevant to this article.
Editors’ note: This article appears under the “Focus on professional liability” series banner even though Dr. Bub’s discussion does not directly address matters of being sued. Our, and his, belief is that good communication brings a significant added benefit of lowering a physician’s litigation risk.
- It was tiring to try and think logically as the guy threw more and more facts at me.—An adolescent with cancer1
Consider the findings of two surveys of radiology residents and attending mammographers on breaking bad or troubling news to patients:
- 16% of residents and 4% of mammographers “didn’t feel confident communicating with patients who displayed strong emotional responses”
- 86% of residents and 81% of staff experienced “some or moderate stress communicating the need for biopsy”
- The majority of all respondents “hadn’t received feedback about their communication skills or communication training after medical school”
- 68% to 78% of respondents expressed interest in “improving their communication.”2
Breaking what you might perceive as “bad” news is never easy; even experienced practitioners may find the task stressful, as the results of these two surveys reveal. Physicians having been trained to do no harm, few find themselves at ease revealing information that has the potential to disappoint or upset, even devastate.
In this article, I offer an approach to breaking bad news in a manner that lessens the trauma to the patient and buffers you from the stress, and distress, of delivering it. The box near the end of this article gathers pearls for giving bad news based on my work and the experiences of others.
We are not unaffected by this task
Most of us find the act of breaking bad news a professional burden that we could just as soon do without. When we perceive an element of personal responsibility, our burden becomes greater: We may experience fear, guilt, or shame—and, for some, that leads to psychological stress disorders and burnout.
How do we cope, being occasional messengers of bad news?
We avoid. An obvious strategy. Consider Dr. D., a radiologist who heads a breast imaging center. He confides that many physicians ask him to inform their patients when he notes an abnormality on their mammogram. Still other physicians, Dr. D. points out, simply have their nurses call patients with troubling results.
Or we run. Another widely used strategy is to break the news and bolt. One cancer survivor lamented: “As soon as I started to cry, he ran off to fetch his nurse. Don’t you know doctors flee from suffering?”
Keeping matters in balance—that is the challenge
How do we maintain our sensitivity, humanity, and connection while, simultaneously, limiting our own vulnerability and pain? Many of us have wrestled with this issue from the earliest days of training:
- In the hospital’s predawn stillness, she confided fears about surgery to me, the medical student. I tried to reassure her. They operated. Finding extensive metastases, they closed immediately. That evening, aching for her, I cried.
- “Don’t worry,” another student reassured me. “It gets easier.”
- I hope not. If it does, I’ll have lost my humanity.3
Simultaneously, how do we handle our feelings of impotence, failure, and, perhaps, guilt—when every expression, gesture, word, and silence are potentially filled with meaning to those who are receiving the news?
David Lenz, an artist, in a commentary on his award-winning painting, “Sam and the Perfect World,” wrote:
- My wife Rosemarie had just given birth to our son Sam, and although he appeared perfectly healthy, something, nevertheless, didn’t seem right. There was an awkward silence in the room, no words of congratulation or comments about how cute he was—even though he was cute. Five minutes later the diagnosis was given: Sam has Down syndrome. “Are you going to keep him?” a nurse asked. Later that evening someone else came by to “console” us.
- “It’s every mother’s worst nightmare,” she said.
- Welcome to the world, Sam.4
5 and invest in deep and surface acting (of empathy).6 I disagree with this advice7 ; instead, I advocate that we notice, validate, and park our emotions. Later, we take time to integrate our emotions through self-care. Rather than relying on “the art of medicine” to communicate bad news, we should approach this task as a serious professional challenge and incorporate principles of trauma counseling, psychotherapy, and chaplaincy into the practice of medicine. Instead of distancing from our emotions and our patients, we draw closer.
Here is how one physician handles breaking bad news.
CASE
Dr. Bob, we’ll call him, typifies the overworked primary care physician. Yet, when a lab or imaging report that reveals an abnormal result lands on his desk, he, not a nurse, calls the patient. He waits a few days if the test or study was ordered by another physician; in that situation, he often reaches a frightened, confused person who had already been called by the specialist’s nurse.
When that happens, Dr. Bob invites the patient, and a close relative, to schedule an office visit with him. In the interim, he forms a liaison with the specialist so that they can function as a team.
At the office visit, Dr. Bob refuses to prognosticate. Instead, he recommends that they take matters “one step at a time.” His approach is positive and reassuring but not overly optimistic. His message is clear: “You are not alone. I will be a supportive presence throughout your journey.”
Two notable things about Dr. Bob: First, he does not suffer burnout or what some have called “compassion fatigue”; to the contrary, the relationship he forges with his patients and their loved ones, and the gratitude and loyalty he receives from them, sustain and reward him.
Second, Dr. Bob has never been sued.
The key to Dr. Bob’s success is that he does not shy from breaking bad news. Instead, he views the occasion as an opportunity for healing. His approach is to detach from the outcome but not from the patient. He relieves fear and isolation, and offers, as one patient said it, “candor with hope.”
Summon your personal strengths to succeed
But taking this approach requires a shift from the standard biomedical philosophy—a three-pronged cultivation of personal resources. Here is how you can make that shift.
First, cultivate equanimity—that evenness of mind
Consider that destruction is an inherent component of creation. There can’t be light without darkness, birth without death, joy without suffering, perfection without imperfection. The Sufi mystic, Rumi, said it succinctly: “A butterfly needs two wings to fly.”
Recognize that not all news is equally bad. The spectrum runs from merely inconvenient to utterly devastating; how the news is perceived and received is highly subjective. Avoid projecting your personal perspective onto the recipient:
- I was totally perplexed. I had just broken the news that Mrs. Smith had an incurable colon cancer, and they responded by nodding, then asking me whether I preferred a chocolate cake or an apple pie for their next visit because it was their custom to bring home-baked goodies for the staff.
- After her death, Mr. Smith faithfully continued this tradition. Then one day he arrived for his regular appointment unshaven, distressed and sans cake. He had lost weight and looked every bit of his 78 years. Something was very wrong.
- “She’s gone, she’s gone,” he lamented.
- At last he’s grieving flashed through my mind, so I responded: “Yes, it’s been about 9 months now, hasn’t it?”
- “No, just two weeks…she said she was my girlfriend…just 29 years old…moved in last month then left taking my money,” he cried.
- She assumed the mantle of a grieving widow. Only years later did she write that she had been secretly relieved that her husband was killed in an automobile accident. He had been abusive and she was planning to leave him anyway.
- It was my birthday, and we were about to celebrate with a dinner of leg of lamb and roast potatoes. My cell phone rang. It was my internist calling; my LDL cholesterol was mildly elevated and my dexa scan demonstrated slight osteopenia. The tone of his voice was matter-of-fact but I felt awful: I am getting old.
Realize that long-term well-being doesn’t depend on good vs. bad news:
- What do Chuck Close and Dan Gottlieb have in common? Each was a healthy young adult when suddenly becoming paraplegic—Chuck from a spinal artery thrombosis, Dan from a serious accident. Each adapted to his condition. Chuck developed a unique style of painting that established his fame as an artist. Dan, a psychotherapist, became an author, teacher, and highly regarded radio interviewer. Each has recently stated that he has never been happier.
Remind yourself of hidden opportunities. Bad news triggers a crisis—an unwelcome, unstable situation with obvious danger. Less apparent is the potential for positive personal transformation and gain:
- “It was the best thing that could have happened to me,” she said, lying with her right foot propped up, ankle heavily bandaged with pins and rods protruding. “Yes, it’s a horribly fractured ankle but I had been rushing, rushing, rushing, and when I fell down the steps, it was as if an angel was forcing me to slow down, be present to my family. I really think this fractured ankle was the best thing that could have happened—it may even have saved my marriage.”
Second, cultivate yourself as a healer
You may not always be able to cure but you can always facilitate healing. In addition to a treatment plan, remind yourself to create a parallel healing plan, listing the interventions that will help the recipient integrate losses and become as functionally whole as possible.
Your ability to heal depends as much on who you are as what you do:
- Work through your own trauma stories and you reduce the likelihood that you either attempt to rescue, or flee from engagement with, patients when their problems trigger painful memories for you
- Accept your imperfections as an inseparable aspect of your humanity
- Learn to accept life as a journey, with suffering and death being inevitable, and bad news ceases to be so exceptional
- Deepen your own joy, mindfulness, and faith and you find meaning in your work even when you cannot cure
- Have realistic expectations of your abilities and try to cultivate a realistic attitude in your patients:
- In Western culture there is a belief, conscious or not, that medicine can save us from the death that lies in wait for us… In a study conducted in 2006 among Israeli doctors, 68% of the participants reported that patients had unrealistic expectations of them. The study reflects unrealistic expectations of medicine in general.8
Third, cultivate skills to break really bad news
Sometimes news is so bad, so overwhelming, that it has the potential to trigger an acute stress reaction (ASR) and even posttraumatic stress disorder (PTSD) in the recipient. Typically, this is life-threatening news—a diagnosis of HIV infection or cancer; abortion or stillbirth; or the sudden, unexpected death of a loved one. The result is shock, horror, disorientation, and memory distortion.
So how can you approach a situation in which you must offer very bad news? To begin, the box, below “Pearls for breaking bad news…,” provides a set of skills and tools for delivering bad news.
In addition, as much as possible, break bad news in increments, so that the patient has time to cope and adjust. And there is more to keep in mind:
- Provide a safe, supportive environment
- Relieve the isolation that trauma inflicts by forging a relationship that is a partnership
- Relieve helplessness by empowering and assisting the patient to seek useful consultants, resources, and supports (One example: A patient who has breast or ovarian cancer can call the SHARE [Self-help for Women with Ovarian or Breast Cancer] hotline: [866] 891-2392)
- Over time, although not initially, help provide meaning to the experience for your patient and for you.
- Don’t have your assistant call with bad news unless she or he is trained to do this, humanely, and to handle the response. Don’t leave a message asking the patient to call back unless you are reasonably certain you will be able to take the call.
- Before you enter the room or place a call, pause, take a deep breath, acknowledge your feelings so you can set them aside, and be fully present. Remember: Empathy begins at home.
- Effective communication always begins and ends with listening. On entering a room, notice the people present, the atmosphere, and the interactions. Over the telephone, notice breath and tone of voice in addition to words spoken. Create space for the recipient to speak, even if silence is uncomfortably long.
- Begin the session by greeting everyone present by name and by shaking hands.
- Offer a general inquiry and listen. A simple “How are you?” allows the patient to express a feeling—“I’m OK but anxious,” for example. Respond with empathy early in the encounter: “Yes, it’s scary waiting for results.”
- Use simple, nontechnical language to describe the situation. Be brief, because a person in a high state of arousal has limited capacity to absorb details. Avoid harsh language (“aggressive,” “failure”) and use a calm, modulated tone.
- Listen and validate the responses you get, recognizing that you may be the recipient of an entire spectrum of emotional expression—from silence to an outburst of anger, from rage to grief. Keep in mind: Anything said in grief is acceptable.
- Remember: You are not responsible for your patients’ happiness. When a patient cries, it does not mean that you failed. An outpouring of grief is healing; your silent, supportive presence is invaluable.
- Don’t attempt to prematurely comfort; don’t try to “make it better,” because this stifles grief. Offering a box of tissues, on the other hand, is simply considerate.
- Don’t present the bleakest scenario. Later, as the patient adapts to her new reality, she will usually be able to tolerate more.
- Be forearmed with some basic treatment and referral options so that the patient isn’t left facing the dark unknown.
- Now, invite the patient’s perspective. Appreciate that she may be experiencing a sea of emotions, especially if the news is totally unexpected. It’s not sufficient to lay out options, then leave the final decision to her. Part of decision-making involves the processing of emotions. Gendlin’s technique of focusing is very useful at this point in the conversation.1
- If you are at the hospital, 1) consider having a chaplain present when the news is potentially devastating and 2) attend to privacy concerns when breaking bad news.
- Treat the person, not the pathology. Ask about her work, activities, and circle of support—all of which are relevant to her situation.
- Be clear that you will remain actively involved in her care even after you refer the patient to the best consultants available.
- Don’t limit yourself to the negative. Look for what is healthy about your patient’s situation, too, and support it.
- Give as much information as possible in writing at this time; amnesia is common. Offer to share the information with at least one family member over the telephone, or schedule a second visit at which a relative will be present.
- When you’re questioned directly, give yourself the benefit of a few moments to ground yourself before you respond.
- Ensure a safe exit for your patient. Does she have someone to drive her, keep her company, etc.?
- Consider calling her that evening to see how she is and to answer any additional questions.
- Invest in self-care. This might include debriefing, taking a break between patients for integration, and grounding and rituals that enable you to detoxify after a difficult day. Cultivate whatever spiritual and meditative practices are part of your life, even if it is simply a walk in the park.
- Empower yourself with relationship skills that enhance your ability to communicate and counsel.
- Have faith! The time that you invest in healthy practice and communication will save you much more over the course of your career.
Reference
1. Bub B. Communication skills that heal: a practical approach to a new professionalism in medicine. Abingdon, UK: Radcliffe Publishing; 2006.
Frankel E. Sacred Therapy. Boston: Shambhala; 2003.
Herman J. Trauma and Recovery. New York: Basic Books; 1992.
Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wis: Seasons Press; 1994.
The author reports no financial relationships relevant to this article.
Editors’ note: This article appears under the “Focus on professional liability” series banner even though Dr. Bub’s discussion does not directly address matters of being sued. Our, and his, belief is that good communication brings a significant added benefit of lowering a physician’s litigation risk.
- It was tiring to try and think logically as the guy threw more and more facts at me.—An adolescent with cancer1
Consider the findings of two surveys of radiology residents and attending mammographers on breaking bad or troubling news to patients:
- 16% of residents and 4% of mammographers “didn’t feel confident communicating with patients who displayed strong emotional responses”
- 86% of residents and 81% of staff experienced “some or moderate stress communicating the need for biopsy”
- The majority of all respondents “hadn’t received feedback about their communication skills or communication training after medical school”
- 68% to 78% of respondents expressed interest in “improving their communication.”2
Breaking what you might perceive as “bad” news is never easy; even experienced practitioners may find the task stressful, as the results of these two surveys reveal. Physicians having been trained to do no harm, few find themselves at ease revealing information that has the potential to disappoint or upset, even devastate.
In this article, I offer an approach to breaking bad news in a manner that lessens the trauma to the patient and buffers you from the stress, and distress, of delivering it. The box near the end of this article gathers pearls for giving bad news based on my work and the experiences of others.
We are not unaffected by this task
Most of us find the act of breaking bad news a professional burden that we could just as soon do without. When we perceive an element of personal responsibility, our burden becomes greater: We may experience fear, guilt, or shame—and, for some, that leads to psychological stress disorders and burnout.
How do we cope, being occasional messengers of bad news?
We avoid. An obvious strategy. Consider Dr. D., a radiologist who heads a breast imaging center. He confides that many physicians ask him to inform their patients when he notes an abnormality on their mammogram. Still other physicians, Dr. D. points out, simply have their nurses call patients with troubling results.
Or we run. Another widely used strategy is to break the news and bolt. One cancer survivor lamented: “As soon as I started to cry, he ran off to fetch his nurse. Don’t you know doctors flee from suffering?”
Keeping matters in balance—that is the challenge
How do we maintain our sensitivity, humanity, and connection while, simultaneously, limiting our own vulnerability and pain? Many of us have wrestled with this issue from the earliest days of training:
- In the hospital’s predawn stillness, she confided fears about surgery to me, the medical student. I tried to reassure her. They operated. Finding extensive metastases, they closed immediately. That evening, aching for her, I cried.
- “Don’t worry,” another student reassured me. “It gets easier.”
- I hope not. If it does, I’ll have lost my humanity.3
Simultaneously, how do we handle our feelings of impotence, failure, and, perhaps, guilt—when every expression, gesture, word, and silence are potentially filled with meaning to those who are receiving the news?
David Lenz, an artist, in a commentary on his award-winning painting, “Sam and the Perfect World,” wrote:
- My wife Rosemarie had just given birth to our son Sam, and although he appeared perfectly healthy, something, nevertheless, didn’t seem right. There was an awkward silence in the room, no words of congratulation or comments about how cute he was—even though he was cute. Five minutes later the diagnosis was given: Sam has Down syndrome. “Are you going to keep him?” a nurse asked. Later that evening someone else came by to “console” us.
- “It’s every mother’s worst nightmare,” she said.
- Welcome to the world, Sam.4
5 and invest in deep and surface acting (of empathy).6 I disagree with this advice7 ; instead, I advocate that we notice, validate, and park our emotions. Later, we take time to integrate our emotions through self-care. Rather than relying on “the art of medicine” to communicate bad news, we should approach this task as a serious professional challenge and incorporate principles of trauma counseling, psychotherapy, and chaplaincy into the practice of medicine. Instead of distancing from our emotions and our patients, we draw closer.
Here is how one physician handles breaking bad news.
CASE
Dr. Bob, we’ll call him, typifies the overworked primary care physician. Yet, when a lab or imaging report that reveals an abnormal result lands on his desk, he, not a nurse, calls the patient. He waits a few days if the test or study was ordered by another physician; in that situation, he often reaches a frightened, confused person who had already been called by the specialist’s nurse.
When that happens, Dr. Bob invites the patient, and a close relative, to schedule an office visit with him. In the interim, he forms a liaison with the specialist so that they can function as a team.
At the office visit, Dr. Bob refuses to prognosticate. Instead, he recommends that they take matters “one step at a time.” His approach is positive and reassuring but not overly optimistic. His message is clear: “You are not alone. I will be a supportive presence throughout your journey.”
Two notable things about Dr. Bob: First, he does not suffer burnout or what some have called “compassion fatigue”; to the contrary, the relationship he forges with his patients and their loved ones, and the gratitude and loyalty he receives from them, sustain and reward him.
Second, Dr. Bob has never been sued.
The key to Dr. Bob’s success is that he does not shy from breaking bad news. Instead, he views the occasion as an opportunity for healing. His approach is to detach from the outcome but not from the patient. He relieves fear and isolation, and offers, as one patient said it, “candor with hope.”
Summon your personal strengths to succeed
But taking this approach requires a shift from the standard biomedical philosophy—a three-pronged cultivation of personal resources. Here is how you can make that shift.
First, cultivate equanimity—that evenness of mind
Consider that destruction is an inherent component of creation. There can’t be light without darkness, birth without death, joy without suffering, perfection without imperfection. The Sufi mystic, Rumi, said it succinctly: “A butterfly needs two wings to fly.”
Recognize that not all news is equally bad. The spectrum runs from merely inconvenient to utterly devastating; how the news is perceived and received is highly subjective. Avoid projecting your personal perspective onto the recipient:
- I was totally perplexed. I had just broken the news that Mrs. Smith had an incurable colon cancer, and they responded by nodding, then asking me whether I preferred a chocolate cake or an apple pie for their next visit because it was their custom to bring home-baked goodies for the staff.
- After her death, Mr. Smith faithfully continued this tradition. Then one day he arrived for his regular appointment unshaven, distressed and sans cake. He had lost weight and looked every bit of his 78 years. Something was very wrong.
- “She’s gone, she’s gone,” he lamented.
- At last he’s grieving flashed through my mind, so I responded: “Yes, it’s been about 9 months now, hasn’t it?”
- “No, just two weeks…she said she was my girlfriend…just 29 years old…moved in last month then left taking my money,” he cried.
- She assumed the mantle of a grieving widow. Only years later did she write that she had been secretly relieved that her husband was killed in an automobile accident. He had been abusive and she was planning to leave him anyway.
- It was my birthday, and we were about to celebrate with a dinner of leg of lamb and roast potatoes. My cell phone rang. It was my internist calling; my LDL cholesterol was mildly elevated and my dexa scan demonstrated slight osteopenia. The tone of his voice was matter-of-fact but I felt awful: I am getting old.
Realize that long-term well-being doesn’t depend on good vs. bad news:
- What do Chuck Close and Dan Gottlieb have in common? Each was a healthy young adult when suddenly becoming paraplegic—Chuck from a spinal artery thrombosis, Dan from a serious accident. Each adapted to his condition. Chuck developed a unique style of painting that established his fame as an artist. Dan, a psychotherapist, became an author, teacher, and highly regarded radio interviewer. Each has recently stated that he has never been happier.
Remind yourself of hidden opportunities. Bad news triggers a crisis—an unwelcome, unstable situation with obvious danger. Less apparent is the potential for positive personal transformation and gain:
- “It was the best thing that could have happened to me,” she said, lying with her right foot propped up, ankle heavily bandaged with pins and rods protruding. “Yes, it’s a horribly fractured ankle but I had been rushing, rushing, rushing, and when I fell down the steps, it was as if an angel was forcing me to slow down, be present to my family. I really think this fractured ankle was the best thing that could have happened—it may even have saved my marriage.”
Second, cultivate yourself as a healer
You may not always be able to cure but you can always facilitate healing. In addition to a treatment plan, remind yourself to create a parallel healing plan, listing the interventions that will help the recipient integrate losses and become as functionally whole as possible.
Your ability to heal depends as much on who you are as what you do:
- Work through your own trauma stories and you reduce the likelihood that you either attempt to rescue, or flee from engagement with, patients when their problems trigger painful memories for you
- Accept your imperfections as an inseparable aspect of your humanity
- Learn to accept life as a journey, with suffering and death being inevitable, and bad news ceases to be so exceptional
- Deepen your own joy, mindfulness, and faith and you find meaning in your work even when you cannot cure
- Have realistic expectations of your abilities and try to cultivate a realistic attitude in your patients:
- In Western culture there is a belief, conscious or not, that medicine can save us from the death that lies in wait for us… In a study conducted in 2006 among Israeli doctors, 68% of the participants reported that patients had unrealistic expectations of them. The study reflects unrealistic expectations of medicine in general.8
Third, cultivate skills to break really bad news
Sometimes news is so bad, so overwhelming, that it has the potential to trigger an acute stress reaction (ASR) and even posttraumatic stress disorder (PTSD) in the recipient. Typically, this is life-threatening news—a diagnosis of HIV infection or cancer; abortion or stillbirth; or the sudden, unexpected death of a loved one. The result is shock, horror, disorientation, and memory distortion.
So how can you approach a situation in which you must offer very bad news? To begin, the box, below “Pearls for breaking bad news…,” provides a set of skills and tools for delivering bad news.
In addition, as much as possible, break bad news in increments, so that the patient has time to cope and adjust. And there is more to keep in mind:
- Provide a safe, supportive environment
- Relieve the isolation that trauma inflicts by forging a relationship that is a partnership
- Relieve helplessness by empowering and assisting the patient to seek useful consultants, resources, and supports (One example: A patient who has breast or ovarian cancer can call the SHARE [Self-help for Women with Ovarian or Breast Cancer] hotline: [866] 891-2392)
- Over time, although not initially, help provide meaning to the experience for your patient and for you.
- Don’t have your assistant call with bad news unless she or he is trained to do this, humanely, and to handle the response. Don’t leave a message asking the patient to call back unless you are reasonably certain you will be able to take the call.
- Before you enter the room or place a call, pause, take a deep breath, acknowledge your feelings so you can set them aside, and be fully present. Remember: Empathy begins at home.
- Effective communication always begins and ends with listening. On entering a room, notice the people present, the atmosphere, and the interactions. Over the telephone, notice breath and tone of voice in addition to words spoken. Create space for the recipient to speak, even if silence is uncomfortably long.
- Begin the session by greeting everyone present by name and by shaking hands.
- Offer a general inquiry and listen. A simple “How are you?” allows the patient to express a feeling—“I’m OK but anxious,” for example. Respond with empathy early in the encounter: “Yes, it’s scary waiting for results.”
- Use simple, nontechnical language to describe the situation. Be brief, because a person in a high state of arousal has limited capacity to absorb details. Avoid harsh language (“aggressive,” “failure”) and use a calm, modulated tone.
- Listen and validate the responses you get, recognizing that you may be the recipient of an entire spectrum of emotional expression—from silence to an outburst of anger, from rage to grief. Keep in mind: Anything said in grief is acceptable.
- Remember: You are not responsible for your patients’ happiness. When a patient cries, it does not mean that you failed. An outpouring of grief is healing; your silent, supportive presence is invaluable.
- Don’t attempt to prematurely comfort; don’t try to “make it better,” because this stifles grief. Offering a box of tissues, on the other hand, is simply considerate.
- Don’t present the bleakest scenario. Later, as the patient adapts to her new reality, she will usually be able to tolerate more.
- Be forearmed with some basic treatment and referral options so that the patient isn’t left facing the dark unknown.
- Now, invite the patient’s perspective. Appreciate that she may be experiencing a sea of emotions, especially if the news is totally unexpected. It’s not sufficient to lay out options, then leave the final decision to her. Part of decision-making involves the processing of emotions. Gendlin’s technique of focusing is very useful at this point in the conversation.1
- If you are at the hospital, 1) consider having a chaplain present when the news is potentially devastating and 2) attend to privacy concerns when breaking bad news.
- Treat the person, not the pathology. Ask about her work, activities, and circle of support—all of which are relevant to her situation.
- Be clear that you will remain actively involved in her care even after you refer the patient to the best consultants available.
- Don’t limit yourself to the negative. Look for what is healthy about your patient’s situation, too, and support it.
- Give as much information as possible in writing at this time; amnesia is common. Offer to share the information with at least one family member over the telephone, or schedule a second visit at which a relative will be present.
- When you’re questioned directly, give yourself the benefit of a few moments to ground yourself before you respond.
- Ensure a safe exit for your patient. Does she have someone to drive her, keep her company, etc.?
- Consider calling her that evening to see how she is and to answer any additional questions.
- Invest in self-care. This might include debriefing, taking a break between patients for integration, and grounding and rituals that enable you to detoxify after a difficult day. Cultivate whatever spiritual and meditative practices are part of your life, even if it is simply a walk in the park.
- Empower yourself with relationship skills that enhance your ability to communicate and counsel.
- Have faith! The time that you invest in healthy practice and communication will save you much more over the course of your career.
Reference
1. Bub B. Communication skills that heal: a practical approach to a new professionalism in medicine. Abingdon, UK: Radcliffe Publishing; 2006.
Frankel E. Sacred Therapy. Boston: Shambhala; 2003.
Herman J. Trauma and Recovery. New York: Basic Books; 1992.
Schneider J. Finding My Way: Healing and Transformation Through Loss and Grief. Colfax, Wis: Seasons Press; 1994.
1. Training workshop sponsored by Melissa’s Living Legacy Foundation, April 2004 (http://www.teenslivingwithcancer.org).
2. Sasson JP, Lown BA. Communicating practices in the diagnostic mammography suite. Med Encounter. 2006;20(4):66.-
3. Christianson AL. A piece of my mind. More stories. JAMA. 2002;288:931.-
4. Bub B. Medicine and the arts. Sam and the Perfect World by David Lenz. Commentary. Acad Med. 2007;82(2):200-201.
5. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA. 2001;286:3007-3014.
6. Larson EB, Yao X. Clinical empathy as emotional labor in the patient–physician relationship. JAMA. 2005;293:1100-1106.
7. Bub B. Focusing and the healing sequence: reclaiming authentic emotions as an aid to communication and well-being in medicine. Explore (NY). 2007;3:413-416.
8. Schwartzman O. White Doctor, Black Gods: White Psychiatric Medicine in the Jungles of Africa. Israel: Aryeh Nir Publishing House; 256 pages. http://www.haaretz.com/hasen/spages/834952.html.
1. Training workshop sponsored by Melissa’s Living Legacy Foundation, April 2004 (http://www.teenslivingwithcancer.org).
2. Sasson JP, Lown BA. Communicating practices in the diagnostic mammography suite. Med Encounter. 2006;20(4):66.-
3. Christianson AL. A piece of my mind. More stories. JAMA. 2002;288:931.-
4. Bub B. Medicine and the arts. Sam and the Perfect World by David Lenz. Commentary. Acad Med. 2007;82(2):200-201.
5. Meier DE, Back AL, Morrison RS. The inner life of physicians and care of the seriously ill. JAMA. 2001;286:3007-3014.
6. Larson EB, Yao X. Clinical empathy as emotional labor in the patient–physician relationship. JAMA. 2005;293:1100-1106.
7. Bub B. Focusing and the healing sequence: reclaiming authentic emotions as an aid to communication and well-being in medicine. Explore (NY). 2007;3:413-416.
8. Schwartzman O. White Doctor, Black Gods: White Psychiatric Medicine in the Jungles of Africa. Israel: Aryeh Nir Publishing House; 256 pages. http://www.haaretz.com/hasen/spages/834952.html.
Come October 1, a multitude of ICD-9 code additions and revisions arrive
The author reports no financial relationships relevant to this article.
OBs get codes for unremarkable sonograms ordered on the basis of suspicion. For gyn practice, options expand for abnormal Pap smear results. Here are the details.
Revisions and additions to the International Classification of Diseases, Clinical Modification (ICD-9-CM) for 2009, which take effect on October 1, 2008, bring especially good news to obstetricians who are testing for “conditions not found,” evaluating or treating twin-to-twin transfusion syndrome, dealing with the aftermath of maternal surgery, and providing the correct diagnostic code match for screening tests.
Gyn practitioners, don’t feel slighted: Many new codes take effect on that October day, covering abnormal Pap smear results, prophylactic drug treatment, breast conditions, and taking a patient’s personal history.
Remember: 1) October 1 is the key date here—when all the new and revised codes described in this article (and others not reviewed here) are added to the national code set, and 2) as in past years, there will be no grace period!
New and revised OB codes
FOR “CONDITIONS NOT FOUND”
How many times have you ordered a sonogram for a suspected problem with a pregnancy, only to have the scan reveal that all is normal? You then had to use either 1) a screening code for the condition or 2) an unspecified code because you could not assign a code that gave a condition to the patient that she did not have.
With addition of a new category of codes (V89), this obstetrical problem will be solved.
V89.01 Suspected problem with amniotic cavity and membrane not found
V89.02 Suspected placenta not found
V89.03 Suspected fetal anomaly not found
V89.04 Suspected problem with fetal growth not found
V89.05 Suspected cervical shortening not found
V89.09 Other suspected maternal and fetal condition not found
CERVICAL SHORTENING
Women undergo cervical shortening normally as their body prepares for labor, of course, but, on occasion, cervical shortening can indicate impending premature birth. Until now, you might have reflected this condition with 654.5x (Cervical incompetence complicating pregnancy), 654.6x (Other congenital or acquired abnormality of cervix), or 644.1x (Other threatened labor). Starting October 1, however, you’ll have a more precise code available to report this condition: 649.7x (Cervical shortening).
HIGH-RISK PREGNANCY
The V23 category of codes, which represent supervision of high-risk pregnancy, becomes more specific with two additions: V23.85 (Pregnancy resulting from assisted reproductive technology) and V23.86 (Pregnancy with history of in utero procedure during previous pregnancy).
ANTENATAL SCREENING
How to select the right code to report a screening test has been less than clear. Were you performing it to screen for malformation of a fetus? Some other reason? Three new antenatal codes and revision of an existing code (V28.3) clarify the distinction.
V28.3 Encounter for routine screening for malformation using ultrasonics
V28.81 Encounter for fetal anatomic survey
V28.82 Encounter for screening for risk of preterm labor
V28.89 Other specified antenatal screening
ICD-9-CM now directs that the latter code, V28.89, be reported for screening as part of chorionic villus sampling, nuchal translucency testing, genomic screening, and proteomic screening.
COMPLICATIONS OF PREGNANCY AND IN UTERO PROCEDURES
At last, you have a specific code for fetal conjoined twins (678.1x) and one for such fetal hematologic conditions as fetal anemia, thrombocytopenia, and twin-to-twin transfusion syndrome (678.0x).
In addition, complications from an in utero procedure will have two new codes: 679.0x (Maternal complications from in utero procedure) and 679.1x (Fetal complications from in utero procedure).
Gynecologic code changes and additions
ABNORMAL RESULTS OF A PAP SMEAR
You already know to look at the 795 series for ICD-9 codes to support various abnormal Pap smear results; after October 1, you’ll have a lot of new options.
Key developments:
- The risk of dysplasia and carcinoma is the same for the anus as it is for the cervix, so physicians can take anal cytologic smears.
- The cervix and the anus both have transformation zones where mucosa turns from squamous to columnar, so parallel codes have been created for anal smears.
The new codes are listed below.
CERVIX
795.07 Satisfactory cervical smear but lacking transformation zone
VAGINA AND VULVA
795.10 Abnormal Papanicolaou smear of vagina
795.11 Papanicolaou smear of vagina with atypical squamous cells of undetermined significance (ASC-US)
795.12 Papanicolaou smear of vagina with atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H)
795.13 Papanicolaou smear of vagina with low grade squamous intraepithelial lesion (LGSIL)
795.14 Papanicolaou smear of vagina with high grade squamous intraepithelial lesion (HGSIL)
795.15 Vaginal high risk papillomavirus (HPV) DNA test positive
795.16 Papanicolaou smear of vagina with cytologic evidence of malignancy
795.18 Unsatisfactory cytology smear
795.19 Other abnormal smear of vagina and vaginal HPV
ANUS
796.70 Abnormal glandular Papanicolaou smear of anus
796.71 Papanicolaou smear of anus with atypical squamous cells of undetermined significance (ASC-US)
796.72 Papanicolaou smear of anus with atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H)
796.73 Papanicolaou smear of anus with low grade squamous intraepithelial lesion (LGSIL)
796.74 Papanicolaou smear of anus with high grade squamous intraepithelial lesion (HGSIL)
796.75 Anal high risk human papillomavirus (HPV) DNA test positive
796.76 Papanicolaou smear of anus with cytologic evidence of malignancy
796.77 Satisfactory anal smear but lacking transformation zone
796.78 Unsatisfactory anal cytology smear
796.79 Other abnormal Papanicolaou smear of anus and anal HPV
There is also a new code, 569.44 (Dysplasia of anus), to report anal dysplasia. In the past, this condition was reported using 569.49 (Other specified disorders of rectum and anus).
ACQUIRED ABSENCE CODES
Until now, only V45.77 (Acquired absence of genital organs) could be used to report this patient status. As of October 1, you’ll have to be more specific about what is absent, using any of the following three new codes. You might find these codes helpful in supporting the performance of screening Pap smears:
V88.01 Acquired absence of both cervix and uterus
V88.02 Acquired absence of uterus with remaining cervical stump
V88.03 Acquired absence of cervix with remaining uterus
These new codes can be reported in conjunction with V67.01 (Follow-up vaginal Pap smear) and V76.47 (Special screening for malignant neoplasm of vagina).
URINARY PROBLEMS
Use these three new codes to report various presentations of hematuria:
599.70 Hematuria, unspecified
599.71 Gross hematuria
599.72 Microscopic hematuria
Note: The old code for hematuria (599.7) did not require a fifth digit; after October 1, using that old code will trigger a denial of your claim.
In addition, you have two new codes with which to report urinary symptoms:
788.91 Functional urinary incontinence
788.99 Other symptoms involving urinary symptoms
VULVODYNIA AND VULVAR VESTIBULITIS
A single code (625.8) has been available to describe vulvodynia, and it was grouped into a general category that covered symptoms. This condition has been given three new codes.
625.70 Vulvodynia, unspecified
625.71 Vulvar vestibulitis
625.79 Other vulvodynia
BREAST DISORDERS
New codes for breast conditions are about to take effect. These include ptosis (611.81), hypoplasia (611.82), and other disorders of the breast, such as capsular contracture of a breast implant (611.89).
For surgeons who handle follow-up after breast surgery, two new codes describe problems with the reconstructed breast: 612.0 (Deformity of reconstructed breast) and 612.1 (Disproportion of reconstructed breast).
WOUND DISRUPTION
Under current ICD-9-CM guidelines, you must specify “external wound” or “internal wound” to code correctly for dehiscence. On October 1, you have the option to report an unspecified code, 998.30 (Disruption of wound, unspecified) if the record does not specify the type of wound.
PROPHYLACTIC USE OF AGENTS AFFECTING ESTROGEN RECEPTORS AND ESTROGEN LEVELS
ICD-9-CM created a V code to capture data on the many women who receive tamoxifen and raloxifene after treatment of breast cancer. This code has been expanded to include V codes for different classes of drugs used for this type of therapy:
V07.51 Prophylactic use of selective estrogen receptor modulators (SERMs)
V07.52 Prophylactic use of aromatase inhibitors
V07.59 Prophylactic use of agents affecting estrogen receptors and estrogen levels
From a guideline perspective, you can use the cancer code with one of these codes throughout the course of treatment, including during routine chemotherapy and radiation therapy. Long-term use of a drug that falls under the V07.5x category doesn’t require continued use of the cancer code, however.
You can provide additional information on your patient by reporting her estrogen receptor-positive status (V86.0), personal or family history of breast cancer (V10.3/V16.3), genetic susceptibility to cancer (V84.01–V84.09), and postmenopausal status (V49.81).
TAKING A PERSONAL HISTORY
This year, 11 codes make their debut to allow you to report a patient’s personal history. Use them for encounters in which the personal history has a direct impact on the patient’s complaints or status.
V13.51 Personal history of pathologic fracture
V13.52 Personal history of stress fracture
V13.59 Personal history of other musculoskeletal disorders
V15.51 Personal history of traumatic fracture
V15.59 Personal history of other injury
V15.21 Personal history of undergoing in utero procedure during pregnancy
V15.22 Personal history of undergoing in utero procedure while a fetus
V15.29 Personal history of surgery to other organs
V87.41 Personal history of antineoplastic chemotherapy
V87.42 Personal history of monoclonal drug therapy
V87.49 Personal history of other drug therapy
The author reports no financial relationships relevant to this article.
OBs get codes for unremarkable sonograms ordered on the basis of suspicion. For gyn practice, options expand for abnormal Pap smear results. Here are the details.
Revisions and additions to the International Classification of Diseases, Clinical Modification (ICD-9-CM) for 2009, which take effect on October 1, 2008, bring especially good news to obstetricians who are testing for “conditions not found,” evaluating or treating twin-to-twin transfusion syndrome, dealing with the aftermath of maternal surgery, and providing the correct diagnostic code match for screening tests.
Gyn practitioners, don’t feel slighted: Many new codes take effect on that October day, covering abnormal Pap smear results, prophylactic drug treatment, breast conditions, and taking a patient’s personal history.
Remember: 1) October 1 is the key date here—when all the new and revised codes described in this article (and others not reviewed here) are added to the national code set, and 2) as in past years, there will be no grace period!
New and revised OB codes
FOR “CONDITIONS NOT FOUND”
How many times have you ordered a sonogram for a suspected problem with a pregnancy, only to have the scan reveal that all is normal? You then had to use either 1) a screening code for the condition or 2) an unspecified code because you could not assign a code that gave a condition to the patient that she did not have.
With addition of a new category of codes (V89), this obstetrical problem will be solved.
V89.01 Suspected problem with amniotic cavity and membrane not found
V89.02 Suspected placenta not found
V89.03 Suspected fetal anomaly not found
V89.04 Suspected problem with fetal growth not found
V89.05 Suspected cervical shortening not found
V89.09 Other suspected maternal and fetal condition not found
CERVICAL SHORTENING
Women undergo cervical shortening normally as their body prepares for labor, of course, but, on occasion, cervical shortening can indicate impending premature birth. Until now, you might have reflected this condition with 654.5x (Cervical incompetence complicating pregnancy), 654.6x (Other congenital or acquired abnormality of cervix), or 644.1x (Other threatened labor). Starting October 1, however, you’ll have a more precise code available to report this condition: 649.7x (Cervical shortening).
HIGH-RISK PREGNANCY
The V23 category of codes, which represent supervision of high-risk pregnancy, becomes more specific with two additions: V23.85 (Pregnancy resulting from assisted reproductive technology) and V23.86 (Pregnancy with history of in utero procedure during previous pregnancy).
ANTENATAL SCREENING
How to select the right code to report a screening test has been less than clear. Were you performing it to screen for malformation of a fetus? Some other reason? Three new antenatal codes and revision of an existing code (V28.3) clarify the distinction.
V28.3 Encounter for routine screening for malformation using ultrasonics
V28.81 Encounter for fetal anatomic survey
V28.82 Encounter for screening for risk of preterm labor
V28.89 Other specified antenatal screening
ICD-9-CM now directs that the latter code, V28.89, be reported for screening as part of chorionic villus sampling, nuchal translucency testing, genomic screening, and proteomic screening.
COMPLICATIONS OF PREGNANCY AND IN UTERO PROCEDURES
At last, you have a specific code for fetal conjoined twins (678.1x) and one for such fetal hematologic conditions as fetal anemia, thrombocytopenia, and twin-to-twin transfusion syndrome (678.0x).
In addition, complications from an in utero procedure will have two new codes: 679.0x (Maternal complications from in utero procedure) and 679.1x (Fetal complications from in utero procedure).
Gynecologic code changes and additions
ABNORMAL RESULTS OF A PAP SMEAR
You already know to look at the 795 series for ICD-9 codes to support various abnormal Pap smear results; after October 1, you’ll have a lot of new options.
Key developments:
- The risk of dysplasia and carcinoma is the same for the anus as it is for the cervix, so physicians can take anal cytologic smears.
- The cervix and the anus both have transformation zones where mucosa turns from squamous to columnar, so parallel codes have been created for anal smears.
The new codes are listed below.
CERVIX
795.07 Satisfactory cervical smear but lacking transformation zone
VAGINA AND VULVA
795.10 Abnormal Papanicolaou smear of vagina
795.11 Papanicolaou smear of vagina with atypical squamous cells of undetermined significance (ASC-US)
795.12 Papanicolaou smear of vagina with atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H)
795.13 Papanicolaou smear of vagina with low grade squamous intraepithelial lesion (LGSIL)
795.14 Papanicolaou smear of vagina with high grade squamous intraepithelial lesion (HGSIL)
795.15 Vaginal high risk papillomavirus (HPV) DNA test positive
795.16 Papanicolaou smear of vagina with cytologic evidence of malignancy
795.18 Unsatisfactory cytology smear
795.19 Other abnormal smear of vagina and vaginal HPV
ANUS
796.70 Abnormal glandular Papanicolaou smear of anus
796.71 Papanicolaou smear of anus with atypical squamous cells of undetermined significance (ASC-US)
796.72 Papanicolaou smear of anus with atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H)
796.73 Papanicolaou smear of anus with low grade squamous intraepithelial lesion (LGSIL)
796.74 Papanicolaou smear of anus with high grade squamous intraepithelial lesion (HGSIL)
796.75 Anal high risk human papillomavirus (HPV) DNA test positive
796.76 Papanicolaou smear of anus with cytologic evidence of malignancy
796.77 Satisfactory anal smear but lacking transformation zone
796.78 Unsatisfactory anal cytology smear
796.79 Other abnormal Papanicolaou smear of anus and anal HPV
There is also a new code, 569.44 (Dysplasia of anus), to report anal dysplasia. In the past, this condition was reported using 569.49 (Other specified disorders of rectum and anus).
ACQUIRED ABSENCE CODES
Until now, only V45.77 (Acquired absence of genital organs) could be used to report this patient status. As of October 1, you’ll have to be more specific about what is absent, using any of the following three new codes. You might find these codes helpful in supporting the performance of screening Pap smears:
V88.01 Acquired absence of both cervix and uterus
V88.02 Acquired absence of uterus with remaining cervical stump
V88.03 Acquired absence of cervix with remaining uterus
These new codes can be reported in conjunction with V67.01 (Follow-up vaginal Pap smear) and V76.47 (Special screening for malignant neoplasm of vagina).
URINARY PROBLEMS
Use these three new codes to report various presentations of hematuria:
599.70 Hematuria, unspecified
599.71 Gross hematuria
599.72 Microscopic hematuria
Note: The old code for hematuria (599.7) did not require a fifth digit; after October 1, using that old code will trigger a denial of your claim.
In addition, you have two new codes with which to report urinary symptoms:
788.91 Functional urinary incontinence
788.99 Other symptoms involving urinary symptoms
VULVODYNIA AND VULVAR VESTIBULITIS
A single code (625.8) has been available to describe vulvodynia, and it was grouped into a general category that covered symptoms. This condition has been given three new codes.
625.70 Vulvodynia, unspecified
625.71 Vulvar vestibulitis
625.79 Other vulvodynia
BREAST DISORDERS
New codes for breast conditions are about to take effect. These include ptosis (611.81), hypoplasia (611.82), and other disorders of the breast, such as capsular contracture of a breast implant (611.89).
For surgeons who handle follow-up after breast surgery, two new codes describe problems with the reconstructed breast: 612.0 (Deformity of reconstructed breast) and 612.1 (Disproportion of reconstructed breast).
WOUND DISRUPTION
Under current ICD-9-CM guidelines, you must specify “external wound” or “internal wound” to code correctly for dehiscence. On October 1, you have the option to report an unspecified code, 998.30 (Disruption of wound, unspecified) if the record does not specify the type of wound.
PROPHYLACTIC USE OF AGENTS AFFECTING ESTROGEN RECEPTORS AND ESTROGEN LEVELS
ICD-9-CM created a V code to capture data on the many women who receive tamoxifen and raloxifene after treatment of breast cancer. This code has been expanded to include V codes for different classes of drugs used for this type of therapy:
V07.51 Prophylactic use of selective estrogen receptor modulators (SERMs)
V07.52 Prophylactic use of aromatase inhibitors
V07.59 Prophylactic use of agents affecting estrogen receptors and estrogen levels
From a guideline perspective, you can use the cancer code with one of these codes throughout the course of treatment, including during routine chemotherapy and radiation therapy. Long-term use of a drug that falls under the V07.5x category doesn’t require continued use of the cancer code, however.
You can provide additional information on your patient by reporting her estrogen receptor-positive status (V86.0), personal or family history of breast cancer (V10.3/V16.3), genetic susceptibility to cancer (V84.01–V84.09), and postmenopausal status (V49.81).
TAKING A PERSONAL HISTORY
This year, 11 codes make their debut to allow you to report a patient’s personal history. Use them for encounters in which the personal history has a direct impact on the patient’s complaints or status.
V13.51 Personal history of pathologic fracture
V13.52 Personal history of stress fracture
V13.59 Personal history of other musculoskeletal disorders
V15.51 Personal history of traumatic fracture
V15.59 Personal history of other injury
V15.21 Personal history of undergoing in utero procedure during pregnancy
V15.22 Personal history of undergoing in utero procedure while a fetus
V15.29 Personal history of surgery to other organs
V87.41 Personal history of antineoplastic chemotherapy
V87.42 Personal history of monoclonal drug therapy
V87.49 Personal history of other drug therapy
The author reports no financial relationships relevant to this article.
OBs get codes for unremarkable sonograms ordered on the basis of suspicion. For gyn practice, options expand for abnormal Pap smear results. Here are the details.
Revisions and additions to the International Classification of Diseases, Clinical Modification (ICD-9-CM) for 2009, which take effect on October 1, 2008, bring especially good news to obstetricians who are testing for “conditions not found,” evaluating or treating twin-to-twin transfusion syndrome, dealing with the aftermath of maternal surgery, and providing the correct diagnostic code match for screening tests.
Gyn practitioners, don’t feel slighted: Many new codes take effect on that October day, covering abnormal Pap smear results, prophylactic drug treatment, breast conditions, and taking a patient’s personal history.
Remember: 1) October 1 is the key date here—when all the new and revised codes described in this article (and others not reviewed here) are added to the national code set, and 2) as in past years, there will be no grace period!
New and revised OB codes
FOR “CONDITIONS NOT FOUND”
How many times have you ordered a sonogram for a suspected problem with a pregnancy, only to have the scan reveal that all is normal? You then had to use either 1) a screening code for the condition or 2) an unspecified code because you could not assign a code that gave a condition to the patient that she did not have.
With addition of a new category of codes (V89), this obstetrical problem will be solved.
V89.01 Suspected problem with amniotic cavity and membrane not found
V89.02 Suspected placenta not found
V89.03 Suspected fetal anomaly not found
V89.04 Suspected problem with fetal growth not found
V89.05 Suspected cervical shortening not found
V89.09 Other suspected maternal and fetal condition not found
CERVICAL SHORTENING
Women undergo cervical shortening normally as their body prepares for labor, of course, but, on occasion, cervical shortening can indicate impending premature birth. Until now, you might have reflected this condition with 654.5x (Cervical incompetence complicating pregnancy), 654.6x (Other congenital or acquired abnormality of cervix), or 644.1x (Other threatened labor). Starting October 1, however, you’ll have a more precise code available to report this condition: 649.7x (Cervical shortening).
HIGH-RISK PREGNANCY
The V23 category of codes, which represent supervision of high-risk pregnancy, becomes more specific with two additions: V23.85 (Pregnancy resulting from assisted reproductive technology) and V23.86 (Pregnancy with history of in utero procedure during previous pregnancy).
ANTENATAL SCREENING
How to select the right code to report a screening test has been less than clear. Were you performing it to screen for malformation of a fetus? Some other reason? Three new antenatal codes and revision of an existing code (V28.3) clarify the distinction.
V28.3 Encounter for routine screening for malformation using ultrasonics
V28.81 Encounter for fetal anatomic survey
V28.82 Encounter for screening for risk of preterm labor
V28.89 Other specified antenatal screening
ICD-9-CM now directs that the latter code, V28.89, be reported for screening as part of chorionic villus sampling, nuchal translucency testing, genomic screening, and proteomic screening.
COMPLICATIONS OF PREGNANCY AND IN UTERO PROCEDURES
At last, you have a specific code for fetal conjoined twins (678.1x) and one for such fetal hematologic conditions as fetal anemia, thrombocytopenia, and twin-to-twin transfusion syndrome (678.0x).
In addition, complications from an in utero procedure will have two new codes: 679.0x (Maternal complications from in utero procedure) and 679.1x (Fetal complications from in utero procedure).
Gynecologic code changes and additions
ABNORMAL RESULTS OF A PAP SMEAR
You already know to look at the 795 series for ICD-9 codes to support various abnormal Pap smear results; after October 1, you’ll have a lot of new options.
Key developments:
- The risk of dysplasia and carcinoma is the same for the anus as it is for the cervix, so physicians can take anal cytologic smears.
- The cervix and the anus both have transformation zones where mucosa turns from squamous to columnar, so parallel codes have been created for anal smears.
The new codes are listed below.
CERVIX
795.07 Satisfactory cervical smear but lacking transformation zone
VAGINA AND VULVA
795.10 Abnormal Papanicolaou smear of vagina
795.11 Papanicolaou smear of vagina with atypical squamous cells of undetermined significance (ASC-US)
795.12 Papanicolaou smear of vagina with atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H)
795.13 Papanicolaou smear of vagina with low grade squamous intraepithelial lesion (LGSIL)
795.14 Papanicolaou smear of vagina with high grade squamous intraepithelial lesion (HGSIL)
795.15 Vaginal high risk papillomavirus (HPV) DNA test positive
795.16 Papanicolaou smear of vagina with cytologic evidence of malignancy
795.18 Unsatisfactory cytology smear
795.19 Other abnormal smear of vagina and vaginal HPV
ANUS
796.70 Abnormal glandular Papanicolaou smear of anus
796.71 Papanicolaou smear of anus with atypical squamous cells of undetermined significance (ASC-US)
796.72 Papanicolaou smear of anus with atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H)
796.73 Papanicolaou smear of anus with low grade squamous intraepithelial lesion (LGSIL)
796.74 Papanicolaou smear of anus with high grade squamous intraepithelial lesion (HGSIL)
796.75 Anal high risk human papillomavirus (HPV) DNA test positive
796.76 Papanicolaou smear of anus with cytologic evidence of malignancy
796.77 Satisfactory anal smear but lacking transformation zone
796.78 Unsatisfactory anal cytology smear
796.79 Other abnormal Papanicolaou smear of anus and anal HPV
There is also a new code, 569.44 (Dysplasia of anus), to report anal dysplasia. In the past, this condition was reported using 569.49 (Other specified disorders of rectum and anus).
ACQUIRED ABSENCE CODES
Until now, only V45.77 (Acquired absence of genital organs) could be used to report this patient status. As of October 1, you’ll have to be more specific about what is absent, using any of the following three new codes. You might find these codes helpful in supporting the performance of screening Pap smears:
V88.01 Acquired absence of both cervix and uterus
V88.02 Acquired absence of uterus with remaining cervical stump
V88.03 Acquired absence of cervix with remaining uterus
These new codes can be reported in conjunction with V67.01 (Follow-up vaginal Pap smear) and V76.47 (Special screening for malignant neoplasm of vagina).
URINARY PROBLEMS
Use these three new codes to report various presentations of hematuria:
599.70 Hematuria, unspecified
599.71 Gross hematuria
599.72 Microscopic hematuria
Note: The old code for hematuria (599.7) did not require a fifth digit; after October 1, using that old code will trigger a denial of your claim.
In addition, you have two new codes with which to report urinary symptoms:
788.91 Functional urinary incontinence
788.99 Other symptoms involving urinary symptoms
VULVODYNIA AND VULVAR VESTIBULITIS
A single code (625.8) has been available to describe vulvodynia, and it was grouped into a general category that covered symptoms. This condition has been given three new codes.
625.70 Vulvodynia, unspecified
625.71 Vulvar vestibulitis
625.79 Other vulvodynia
BREAST DISORDERS
New codes for breast conditions are about to take effect. These include ptosis (611.81), hypoplasia (611.82), and other disorders of the breast, such as capsular contracture of a breast implant (611.89).
For surgeons who handle follow-up after breast surgery, two new codes describe problems with the reconstructed breast: 612.0 (Deformity of reconstructed breast) and 612.1 (Disproportion of reconstructed breast).
WOUND DISRUPTION
Under current ICD-9-CM guidelines, you must specify “external wound” or “internal wound” to code correctly for dehiscence. On October 1, you have the option to report an unspecified code, 998.30 (Disruption of wound, unspecified) if the record does not specify the type of wound.
PROPHYLACTIC USE OF AGENTS AFFECTING ESTROGEN RECEPTORS AND ESTROGEN LEVELS
ICD-9-CM created a V code to capture data on the many women who receive tamoxifen and raloxifene after treatment of breast cancer. This code has been expanded to include V codes for different classes of drugs used for this type of therapy:
V07.51 Prophylactic use of selective estrogen receptor modulators (SERMs)
V07.52 Prophylactic use of aromatase inhibitors
V07.59 Prophylactic use of agents affecting estrogen receptors and estrogen levels
From a guideline perspective, you can use the cancer code with one of these codes throughout the course of treatment, including during routine chemotherapy and radiation therapy. Long-term use of a drug that falls under the V07.5x category doesn’t require continued use of the cancer code, however.
You can provide additional information on your patient by reporting her estrogen receptor-positive status (V86.0), personal or family history of breast cancer (V10.3/V16.3), genetic susceptibility to cancer (V84.01–V84.09), and postmenopausal status (V49.81).
TAKING A PERSONAL HISTORY
This year, 11 codes make their debut to allow you to report a patient’s personal history. Use them for encounters in which the personal history has a direct impact on the patient’s complaints or status.
V13.51 Personal history of pathologic fracture
V13.52 Personal history of stress fracture
V13.59 Personal history of other musculoskeletal disorders
V15.51 Personal history of traumatic fracture
V15.59 Personal history of other injury
V15.21 Personal history of undergoing in utero procedure during pregnancy
V15.22 Personal history of undergoing in utero procedure while a fetus
V15.29 Personal history of surgery to other organs
V87.41 Personal history of antineoplastic chemotherapy
V87.42 Personal history of monoclonal drug therapy
V87.49 Personal history of other drug therapy
Adopt Guidelines for E-Mail Questions
I recently received a lengthy e-mail from a very worried woman. She claimed to be an established patient in my office, which I had no way of confirming because she did not sign her message. She asked many questions about sexually transmitted diseases and how they might affect her and a new boyfriend.
I was undecided on how to reply, or even whether to reply at all, so I posted my dilemma on the DermChat e-mail list to see how other dermatologists might handle such a situation.
Responses were all over the map—from “I never answer patient e-mails” to “What harm could it do, she's better off getting correct answers from you than incorrect answers from some 'advocacy' Web site”—and everything in between.
Clearly, this is a controversial issue that will only get more controversial in the future, so I decided to look at what has been published on the subject.
It turns out that, as early as 1998, two German investigators asked this same question and designed a study to address it (JAMA 1998;280:1333–5). Posing as a fictitious patient, they sent e-mails describing an acute dermatologic problem to random Web sites offering dermatologic information, tallied the responses they received, and followed up with a questionnaire to responders and nonresponders alike.
As with my informal survey, the authors found what they termed “a striking lack of consensus” on how to deal with this situation: Of the 50% who responded to the fictitious patient's e-mail, 31% refused to give advice without seeing the patient, but 59% offered a diagnosis, with a third of that group going on to provide specific advice about therapy.
In response to the questionnaire, 28% said that they tended not to answer any patient e-mails, 24% said they usually replied with a standard message, and 24% said they answered each request individually. The investigators concluded that “standards for physician response to unsolicited patient e-mail are needed.”
Unfortunately, my DermChat survey suggests that, 10 years later, there is still nothing like a consensus on this issue.
In the interim, several groups, including the American Medical Informatics Association http://134.174.100.34/AMIA%20E-mail%20Guidelines.pdfwww.medem.com/phy/phy_eriskguidelines.cfmwww.ama-assn.org/apps/pf_new/pf_oline?f_n=browse&doc=policyfiles/HnE/H-478.997.htm
Your guidelines may be very simple (if you decide never to answer any queries) or very complex, depending on your situation and personal philosophy, but all guidelines should cover such issues as authentication of patient correspondents, informed consent of those patients, licensing jurisdiction (if you receive e-mails from states in which you are not licensed), and above all, confidentiality.
Contrary to popular belief, ordinary unencrypted e-mail does not necessarily violate the Health Insurance Portability and Accountability Act (HIPAA). As I've noted many times, HIPAA allows you to handle medical information in just about any way you wish, as long as patients are informed of what you are doing and accept any associated risks of breach of privacy. As long as the Notice of Privacy Practices that you distribute to patients explains your e-mail policies, and each e-mail includes a standard confidentiality disclaimer, most experts say you will be HIPAA compliant.
If the lack of encryption and other privacy safeguards makes you or your patients uncomfortable, encryption software can be added to your practice's e-mail system. Rather than simply encrypting your e-mail, though, consider adopting Web-based messaging. Patients enter your Web site and send a message using an electronic template that you design. You (or a designated staffer) will be notified by regular e-mail when messages are received, and you can post a reply on a page that can only be accessed by the patient. Besides enhancing privacy and security, you can state your guidelines to preclude any misunderstanding of what you will and will not address online.
Web-based messaging services can be freestanding or incorporated into existing secure Web sites.
And the e-mail query that triggered all of this? I responded, but told the patient I could not provide specific answers to such personal questions over the Internet, particularly when they were asked anonymously. I said I would be happy to address her concerns in person, in my office.
And now, I'm writing my guidelines.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
I recently received a lengthy e-mail from a very worried woman. She claimed to be an established patient in my office, which I had no way of confirming because she did not sign her message. She asked many questions about sexually transmitted diseases and how they might affect her and a new boyfriend.
I was undecided on how to reply, or even whether to reply at all, so I posted my dilemma on the DermChat e-mail list to see how other dermatologists might handle such a situation.
Responses were all over the map—from “I never answer patient e-mails” to “What harm could it do, she's better off getting correct answers from you than incorrect answers from some 'advocacy' Web site”—and everything in between.
Clearly, this is a controversial issue that will only get more controversial in the future, so I decided to look at what has been published on the subject.
It turns out that, as early as 1998, two German investigators asked this same question and designed a study to address it (JAMA 1998;280:1333–5). Posing as a fictitious patient, they sent e-mails describing an acute dermatologic problem to random Web sites offering dermatologic information, tallied the responses they received, and followed up with a questionnaire to responders and nonresponders alike.
As with my informal survey, the authors found what they termed “a striking lack of consensus” on how to deal with this situation: Of the 50% who responded to the fictitious patient's e-mail, 31% refused to give advice without seeing the patient, but 59% offered a diagnosis, with a third of that group going on to provide specific advice about therapy.
In response to the questionnaire, 28% said that they tended not to answer any patient e-mails, 24% said they usually replied with a standard message, and 24% said they answered each request individually. The investigators concluded that “standards for physician response to unsolicited patient e-mail are needed.”
Unfortunately, my DermChat survey suggests that, 10 years later, there is still nothing like a consensus on this issue.
In the interim, several groups, including the American Medical Informatics Association http://134.174.100.34/AMIA%20E-mail%20Guidelines.pdfwww.medem.com/phy/phy_eriskguidelines.cfmwww.ama-assn.org/apps/pf_new/pf_oline?f_n=browse&doc=policyfiles/HnE/H-478.997.htm
Your guidelines may be very simple (if you decide never to answer any queries) or very complex, depending on your situation and personal philosophy, but all guidelines should cover such issues as authentication of patient correspondents, informed consent of those patients, licensing jurisdiction (if you receive e-mails from states in which you are not licensed), and above all, confidentiality.
Contrary to popular belief, ordinary unencrypted e-mail does not necessarily violate the Health Insurance Portability and Accountability Act (HIPAA). As I've noted many times, HIPAA allows you to handle medical information in just about any way you wish, as long as patients are informed of what you are doing and accept any associated risks of breach of privacy. As long as the Notice of Privacy Practices that you distribute to patients explains your e-mail policies, and each e-mail includes a standard confidentiality disclaimer, most experts say you will be HIPAA compliant.
If the lack of encryption and other privacy safeguards makes you or your patients uncomfortable, encryption software can be added to your practice's e-mail system. Rather than simply encrypting your e-mail, though, consider adopting Web-based messaging. Patients enter your Web site and send a message using an electronic template that you design. You (or a designated staffer) will be notified by regular e-mail when messages are received, and you can post a reply on a page that can only be accessed by the patient. Besides enhancing privacy and security, you can state your guidelines to preclude any misunderstanding of what you will and will not address online.
Web-based messaging services can be freestanding or incorporated into existing secure Web sites.
And the e-mail query that triggered all of this? I responded, but told the patient I could not provide specific answers to such personal questions over the Internet, particularly when they were asked anonymously. I said I would be happy to address her concerns in person, in my office.
And now, I'm writing my guidelines.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
I recently received a lengthy e-mail from a very worried woman. She claimed to be an established patient in my office, which I had no way of confirming because she did not sign her message. She asked many questions about sexually transmitted diseases and how they might affect her and a new boyfriend.
I was undecided on how to reply, or even whether to reply at all, so I posted my dilemma on the DermChat e-mail list to see how other dermatologists might handle such a situation.
Responses were all over the map—from “I never answer patient e-mails” to “What harm could it do, she's better off getting correct answers from you than incorrect answers from some 'advocacy' Web site”—and everything in between.
Clearly, this is a controversial issue that will only get more controversial in the future, so I decided to look at what has been published on the subject.
It turns out that, as early as 1998, two German investigators asked this same question and designed a study to address it (JAMA 1998;280:1333–5). Posing as a fictitious patient, they sent e-mails describing an acute dermatologic problem to random Web sites offering dermatologic information, tallied the responses they received, and followed up with a questionnaire to responders and nonresponders alike.
As with my informal survey, the authors found what they termed “a striking lack of consensus” on how to deal with this situation: Of the 50% who responded to the fictitious patient's e-mail, 31% refused to give advice without seeing the patient, but 59% offered a diagnosis, with a third of that group going on to provide specific advice about therapy.
In response to the questionnaire, 28% said that they tended not to answer any patient e-mails, 24% said they usually replied with a standard message, and 24% said they answered each request individually. The investigators concluded that “standards for physician response to unsolicited patient e-mail are needed.”
Unfortunately, my DermChat survey suggests that, 10 years later, there is still nothing like a consensus on this issue.
In the interim, several groups, including the American Medical Informatics Association http://134.174.100.34/AMIA%20E-mail%20Guidelines.pdfwww.medem.com/phy/phy_eriskguidelines.cfmwww.ama-assn.org/apps/pf_new/pf_oline?f_n=browse&doc=policyfiles/HnE/H-478.997.htm
Your guidelines may be very simple (if you decide never to answer any queries) or very complex, depending on your situation and personal philosophy, but all guidelines should cover such issues as authentication of patient correspondents, informed consent of those patients, licensing jurisdiction (if you receive e-mails from states in which you are not licensed), and above all, confidentiality.
Contrary to popular belief, ordinary unencrypted e-mail does not necessarily violate the Health Insurance Portability and Accountability Act (HIPAA). As I've noted many times, HIPAA allows you to handle medical information in just about any way you wish, as long as patients are informed of what you are doing and accept any associated risks of breach of privacy. As long as the Notice of Privacy Practices that you distribute to patients explains your e-mail policies, and each e-mail includes a standard confidentiality disclaimer, most experts say you will be HIPAA compliant.
If the lack of encryption and other privacy safeguards makes you or your patients uncomfortable, encryption software can be added to your practice's e-mail system. Rather than simply encrypting your e-mail, though, consider adopting Web-based messaging. Patients enter your Web site and send a message using an electronic template that you design. You (or a designated staffer) will be notified by regular e-mail when messages are received, and you can post a reply on a page that can only be accessed by the patient. Besides enhancing privacy and security, you can state your guidelines to preclude any misunderstanding of what you will and will not address online.
Web-based messaging services can be freestanding or incorporated into existing secure Web sites.
And the e-mail query that triggered all of this? I responded, but told the patient I could not provide specific answers to such personal questions over the Internet, particularly when they were asked anonymously. I said I would be happy to address her concerns in person, in my office.
And now, I'm writing my guidelines.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Making Paid Time Off Work
Many medical offices are following a popular trend in the business world by replacing employee sick leave, vacation, and any other miscellaneous time benefits with a combination of all of them, collectively referred to as “paid time off.”
There are several reasons why this is a good idea, but you should carefully consider all of the the pros and cons before you make such a change in your office. A paid time off (PTO) policy is not without disadvantages.
Nevertheless, the advantages are significant. Employees like the concept because most of them are generally healthy and never use all of their sick leave. They enjoy being able to take the difference as extra vacation time, making for a more contented staff and workplace in general. And they appreciate being able to make time-off decisions for themselves and the increased flexibility that comes with that.
Employers like the policy because there is less paperwork and less abuse of sick leave. They don't have to make decisions about whether an employee is really sick or not, because reasons for absence are now irrelevant. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee's duties, you don't need to know the reasons.
However, critics argue that under a PTO system, employees are absent more frequently, which is sometimes true. In addition, employees who never used their full allotment of sick leave will typically use all of their PTO every year. Most of these extra absences can be controlled by requiring preapproval for any PTO except emergencies, though some critics say that requirement effectively replaces decisions about what constitutes an illness with decisions about what constitutes an emergency.
Employees could take salary in exchange for unused PTO, to be paid annually or when employment ends. In general, though, I don't think that is a good idea. Vacations are necessary and important for good office morale, and they should be taken by all employees and employers.
If you are going to allow PTO to accrue and to be paid later, then it's probably best to allow only a portion—say, 25% maximum—to be taken that way.
A major disadvantage of PTO is the possibility that employees won't stay home when they are ill. Some businesses that have converted to the system have found that employees tend to view all paid time off as vacation time, so when they are sick, they don't want to “waste” any of their “vacation” days. The result is that many sick employees who should stay at home, come to the workplace where they risk infecting colleagues and patients and lowering their chances for quick recovery.
So before switching to a paid time off system, weigh all the pros and cons. Should you decide to proceed, try to anticipate potential problems and then establish clear guidelines to counter them.
Make sure everyone knows that, except for emergencies, they have to request PTO in advance. Define what is meant by “advance notice.” Is it 24 hours, or is it a week? Then define what constitutes an emergency, and put the definitions in writing. Some employees might regard waking up Monday morning with a bad hangover as an emergency, but you might not. Most would consider a sick child an emergency, but what about a malfunctioning car? Some circumstances will need to be decided on a case-by-case basis, but the more situations you can anticipate and settle in advance, the better.
Finally, make it clear that sick employees should stay home, and that if they come to work sick, then they will be sent home. You have an obligation to protect the rest of your employees, not to mention your patients (especially those who are elderly or immunocompromised), from a staff member with a potentially communicable illness.
Many medical offices are following a popular trend in the business world by replacing employee sick leave, vacation, and any other miscellaneous time benefits with a combination of all of them, collectively referred to as “paid time off.”
There are several reasons why this is a good idea, but you should carefully consider all of the the pros and cons before you make such a change in your office. A paid time off (PTO) policy is not without disadvantages.
Nevertheless, the advantages are significant. Employees like the concept because most of them are generally healthy and never use all of their sick leave. They enjoy being able to take the difference as extra vacation time, making for a more contented staff and workplace in general. And they appreciate being able to make time-off decisions for themselves and the increased flexibility that comes with that.
Employers like the policy because there is less paperwork and less abuse of sick leave. They don't have to make decisions about whether an employee is really sick or not, because reasons for absence are now irrelevant. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee's duties, you don't need to know the reasons.
However, critics argue that under a PTO system, employees are absent more frequently, which is sometimes true. In addition, employees who never used their full allotment of sick leave will typically use all of their PTO every year. Most of these extra absences can be controlled by requiring preapproval for any PTO except emergencies, though some critics say that requirement effectively replaces decisions about what constitutes an illness with decisions about what constitutes an emergency.
Employees could take salary in exchange for unused PTO, to be paid annually or when employment ends. In general, though, I don't think that is a good idea. Vacations are necessary and important for good office morale, and they should be taken by all employees and employers.
If you are going to allow PTO to accrue and to be paid later, then it's probably best to allow only a portion—say, 25% maximum—to be taken that way.
A major disadvantage of PTO is the possibility that employees won't stay home when they are ill. Some businesses that have converted to the system have found that employees tend to view all paid time off as vacation time, so when they are sick, they don't want to “waste” any of their “vacation” days. The result is that many sick employees who should stay at home, come to the workplace where they risk infecting colleagues and patients and lowering their chances for quick recovery.
So before switching to a paid time off system, weigh all the pros and cons. Should you decide to proceed, try to anticipate potential problems and then establish clear guidelines to counter them.
Make sure everyone knows that, except for emergencies, they have to request PTO in advance. Define what is meant by “advance notice.” Is it 24 hours, or is it a week? Then define what constitutes an emergency, and put the definitions in writing. Some employees might regard waking up Monday morning with a bad hangover as an emergency, but you might not. Most would consider a sick child an emergency, but what about a malfunctioning car? Some circumstances will need to be decided on a case-by-case basis, but the more situations you can anticipate and settle in advance, the better.
Finally, make it clear that sick employees should stay home, and that if they come to work sick, then they will be sent home. You have an obligation to protect the rest of your employees, not to mention your patients (especially those who are elderly or immunocompromised), from a staff member with a potentially communicable illness.
Many medical offices are following a popular trend in the business world by replacing employee sick leave, vacation, and any other miscellaneous time benefits with a combination of all of them, collectively referred to as “paid time off.”
There are several reasons why this is a good idea, but you should carefully consider all of the the pros and cons before you make such a change in your office. A paid time off (PTO) policy is not without disadvantages.
Nevertheless, the advantages are significant. Employees like the concept because most of them are generally healthy and never use all of their sick leave. They enjoy being able to take the difference as extra vacation time, making for a more contented staff and workplace in general. And they appreciate being able to make time-off decisions for themselves and the increased flexibility that comes with that.
Employers like the policy because there is less paperwork and less abuse of sick leave. They don't have to make decisions about whether an employee is really sick or not, because reasons for absence are now irrelevant. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee's duties, you don't need to know the reasons.
However, critics argue that under a PTO system, employees are absent more frequently, which is sometimes true. In addition, employees who never used their full allotment of sick leave will typically use all of their PTO every year. Most of these extra absences can be controlled by requiring preapproval for any PTO except emergencies, though some critics say that requirement effectively replaces decisions about what constitutes an illness with decisions about what constitutes an emergency.
Employees could take salary in exchange for unused PTO, to be paid annually or when employment ends. In general, though, I don't think that is a good idea. Vacations are necessary and important for good office morale, and they should be taken by all employees and employers.
If you are going to allow PTO to accrue and to be paid later, then it's probably best to allow only a portion—say, 25% maximum—to be taken that way.
A major disadvantage of PTO is the possibility that employees won't stay home when they are ill. Some businesses that have converted to the system have found that employees tend to view all paid time off as vacation time, so when they are sick, they don't want to “waste” any of their “vacation” days. The result is that many sick employees who should stay at home, come to the workplace where they risk infecting colleagues and patients and lowering their chances for quick recovery.
So before switching to a paid time off system, weigh all the pros and cons. Should you decide to proceed, try to anticipate potential problems and then establish clear guidelines to counter them.
Make sure everyone knows that, except for emergencies, they have to request PTO in advance. Define what is meant by “advance notice.” Is it 24 hours, or is it a week? Then define what constitutes an emergency, and put the definitions in writing. Some employees might regard waking up Monday morning with a bad hangover as an emergency, but you might not. Most would consider a sick child an emergency, but what about a malfunctioning car? Some circumstances will need to be decided on a case-by-case basis, but the more situations you can anticipate and settle in advance, the better.
Finally, make it clear that sick employees should stay home, and that if they come to work sick, then they will be sent home. You have an obligation to protect the rest of your employees, not to mention your patients (especially those who are elderly or immunocompromised), from a staff member with a potentially communicable illness.
Sort Out Surgical Cases
Hospitalists often are involved in the care of a surgical patient. Reimbursement for surgical procedures includes payment for pre-, intra-, and post-operative care.
Knowing the billing and coding responsibilities apart from those of the surgeon is imperative for the hospitalist’s accurate charge capture. There are several critical misconceptions in this regard:
- Hospitalists cannot bill for services when involved in a surgical case;
- Surgeons are not responsible for inpatient care if the patient is stable and does not require additional inpatient post-op visits; and
- Modifiers are not required for hospitalist claims unless the hospitalist reports under the same tax identification number as the surgeon.
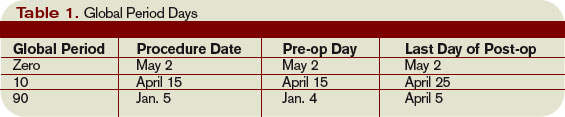
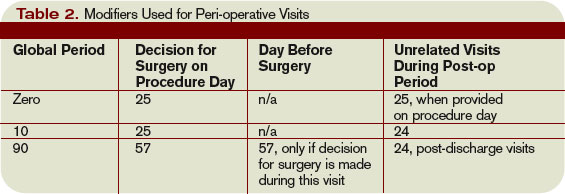
Determine Global Period
Procedures are categorized as major or minor surgery. A global period is assigned to each procedure code, designating post-operative periods of zero, 10, or 90 days. Physician services during this global period are considered part of the packaged payment and not separately reimbursed.
The global period for any given CPT code can be identified in the Medicare Physician Fee Schedule and accessed at www.cms.hhs.gov/PfsLookup. In addition to zero, 10, and 90 days, services can be noted with:
- XXX, indicating the global period concept does not apply; or
- ZZZ, indicating an “add-on” procedure that must always be reported with the relevant primary procedure code; “add-on” procedures assume the global period of the primary procedure.
Major surgery routinely is allotted 90-day global periods. Therefore, the surgeon is responsible for the patient and must provide all related care one day prior to the surgery forward thru 90 postoperative days at no additional charge. Minor surgery, including endoscopy, has zero or 10-day postoperative periods, bundling all services on the surgical day only, or the surgical day and the subsequent 10 days, respectively (see Table 1, p. above).
The Surgeon Defined
Any qualified physician able to perform “surgical” services within his scope of practice is considered a “surgeon” for billing purposes. For example, a pulmonologist, or primary care physician, must meet the surgical billing and documentation requirements when performing bronchoscopies or uncomplicated incision-and-drainage services, respectively.
Surgical services easily are identified as any code included in range 20000-69999. This code series includes major, minor, and endoscopic procedures. The “surgeon” and all physicians in the same group practice (i.e., reporting services under the same tax identification number) with the same specialty designation must adhere to the global period billing rules.
Alternately, physicians with different specialty designations in the same group practice (e.g., multispecialty group that reports services under the same tax identification number) or different group practices can perform and separately report medically necessary services during the surgeon’s global period, as long as a formal (mutually agreed upon) transfer of care did not occur. Information on physician specialty designations is available at www.highmarkmedicareservices.com/partb/refman/appendix-d.html.
Package Components
The following services are included in the surgeon’s packaged payment:
- Preoperative visits after the decision for surgery is made beginning one day prior to surgery;
- All additional post-operative medical or surgical services provided by the surgeon related to complications, but not require additional trips to the operating room;
- Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes; local incisional care; removal of cutaneous sutures and staples; line removals; changes and removal of tracheostomy tubes; and discharge services; and
- Post-operative pain management provided by the surgeon.
Services not included are:
- The initial consultation or evaluation of the problem by the surgeon to determine the need for surgery. Append modifier 57 to this visit if provided the day before or day of major surgery to alert the payer that the service resulted in the decision for surgery. Append modifier 25 to this visit if provided the day of minor surgery;
- Services of other physicians except where the other physicians are providing coverage for the surgeon or agree on a transfer of care. This agreement may be in the form of a letter or an annotation in the discharge summary, hospital record, or ASC record;
- Post-operative visits by the surgeon unrelated to the diagnosis for which the surgical procedure is performed, unless the visits occur due to complications of the surgery. These services only are payable after the patient has been discharged from the hospitalization in which the surgery occurred. Append modifier 24 to these unrelated post-op visits;
- Diagnostic tests and procedures, including diagnostic radiological procedures;
- Clearly distinct surgical procedures during the post-operative period that do not result in repeat operations or treatment for complications;
- Treatment for post-operative complications that require a return trip to the operating room, catheterization lab, or endoscopy suite;
- Immunosuppressive therapy for organ transplants; and
- Critical care services (CPT codes 99291 and 99292) unrelated to the surgery in which a seriously injured or burned patient is critically ill and requires constant attendance of the surgeon. Append modifier 24 to these unrelated critical care services (see Table 2, above).
Payer Variations
While Medicare does not require modifier usage by hospitalists providing medically necessary services on surgical cases, some private payers do. Their electronic claim systems may not differentiate services by non-surgical specialists, requiring all physicians to append the appropriate modifier depending on the reason and timing of the service (see “Key Modifiers” below). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Hospitalists often are involved in the care of a surgical patient. Reimbursement for surgical procedures includes payment for pre-, intra-, and post-operative care.
Knowing the billing and coding responsibilities apart from those of the surgeon is imperative for the hospitalist’s accurate charge capture. There are several critical misconceptions in this regard:
- Hospitalists cannot bill for services when involved in a surgical case;
- Surgeons are not responsible for inpatient care if the patient is stable and does not require additional inpatient post-op visits; and
- Modifiers are not required for hospitalist claims unless the hospitalist reports under the same tax identification number as the surgeon.
Determine Global Period
Procedures are categorized as major or minor surgery. A global period is assigned to each procedure code, designating post-operative periods of zero, 10, or 90 days. Physician services during this global period are considered part of the packaged payment and not separately reimbursed.
The global period for any given CPT code can be identified in the Medicare Physician Fee Schedule and accessed at www.cms.hhs.gov/PfsLookup. In addition to zero, 10, and 90 days, services can be noted with:
- XXX, indicating the global period concept does not apply; or
- ZZZ, indicating an “add-on” procedure that must always be reported with the relevant primary procedure code; “add-on” procedures assume the global period of the primary procedure.
Major surgery routinely is allotted 90-day global periods. Therefore, the surgeon is responsible for the patient and must provide all related care one day prior to the surgery forward thru 90 postoperative days at no additional charge. Minor surgery, including endoscopy, has zero or 10-day postoperative periods, bundling all services on the surgical day only, or the surgical day and the subsequent 10 days, respectively (see Table 1, p. above).
The Surgeon Defined
Any qualified physician able to perform “surgical” services within his scope of practice is considered a “surgeon” for billing purposes. For example, a pulmonologist, or primary care physician, must meet the surgical billing and documentation requirements when performing bronchoscopies or uncomplicated incision-and-drainage services, respectively.
Surgical services easily are identified as any code included in range 20000-69999. This code series includes major, minor, and endoscopic procedures. The “surgeon” and all physicians in the same group practice (i.e., reporting services under the same tax identification number) with the same specialty designation must adhere to the global period billing rules.
Alternately, physicians with different specialty designations in the same group practice (e.g., multispecialty group that reports services under the same tax identification number) or different group practices can perform and separately report medically necessary services during the surgeon’s global period, as long as a formal (mutually agreed upon) transfer of care did not occur. Information on physician specialty designations is available at www.highmarkmedicareservices.com/partb/refman/appendix-d.html.
Package Components
The following services are included in the surgeon’s packaged payment:
- Preoperative visits after the decision for surgery is made beginning one day prior to surgery;
- All additional post-operative medical or surgical services provided by the surgeon related to complications, but not require additional trips to the operating room;
- Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes; local incisional care; removal of cutaneous sutures and staples; line removals; changes and removal of tracheostomy tubes; and discharge services; and
- Post-operative pain management provided by the surgeon.
Services not included are:
- The initial consultation or evaluation of the problem by the surgeon to determine the need for surgery. Append modifier 57 to this visit if provided the day before or day of major surgery to alert the payer that the service resulted in the decision for surgery. Append modifier 25 to this visit if provided the day of minor surgery;
- Services of other physicians except where the other physicians are providing coverage for the surgeon or agree on a transfer of care. This agreement may be in the form of a letter or an annotation in the discharge summary, hospital record, or ASC record;
- Post-operative visits by the surgeon unrelated to the diagnosis for which the surgical procedure is performed, unless the visits occur due to complications of the surgery. These services only are payable after the patient has been discharged from the hospitalization in which the surgery occurred. Append modifier 24 to these unrelated post-op visits;
- Diagnostic tests and procedures, including diagnostic radiological procedures;
- Clearly distinct surgical procedures during the post-operative period that do not result in repeat operations or treatment for complications;
- Treatment for post-operative complications that require a return trip to the operating room, catheterization lab, or endoscopy suite;
- Immunosuppressive therapy for organ transplants; and
- Critical care services (CPT codes 99291 and 99292) unrelated to the surgery in which a seriously injured or burned patient is critically ill and requires constant attendance of the surgeon. Append modifier 24 to these unrelated critical care services (see Table 2, above).
Payer Variations
While Medicare does not require modifier usage by hospitalists providing medically necessary services on surgical cases, some private payers do. Their electronic claim systems may not differentiate services by non-surgical specialists, requiring all physicians to append the appropriate modifier depending on the reason and timing of the service (see “Key Modifiers” below). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Hospitalists often are involved in the care of a surgical patient. Reimbursement for surgical procedures includes payment for pre-, intra-, and post-operative care.
Knowing the billing and coding responsibilities apart from those of the surgeon is imperative for the hospitalist’s accurate charge capture. There are several critical misconceptions in this regard:
- Hospitalists cannot bill for services when involved in a surgical case;
- Surgeons are not responsible for inpatient care if the patient is stable and does not require additional inpatient post-op visits; and
- Modifiers are not required for hospitalist claims unless the hospitalist reports under the same tax identification number as the surgeon.
Determine Global Period
Procedures are categorized as major or minor surgery. A global period is assigned to each procedure code, designating post-operative periods of zero, 10, or 90 days. Physician services during this global period are considered part of the packaged payment and not separately reimbursed.
The global period for any given CPT code can be identified in the Medicare Physician Fee Schedule and accessed at www.cms.hhs.gov/PfsLookup. In addition to zero, 10, and 90 days, services can be noted with:
- XXX, indicating the global period concept does not apply; or
- ZZZ, indicating an “add-on” procedure that must always be reported with the relevant primary procedure code; “add-on” procedures assume the global period of the primary procedure.
Major surgery routinely is allotted 90-day global periods. Therefore, the surgeon is responsible for the patient and must provide all related care one day prior to the surgery forward thru 90 postoperative days at no additional charge. Minor surgery, including endoscopy, has zero or 10-day postoperative periods, bundling all services on the surgical day only, or the surgical day and the subsequent 10 days, respectively (see Table 1, p. above).
The Surgeon Defined
Any qualified physician able to perform “surgical” services within his scope of practice is considered a “surgeon” for billing purposes. For example, a pulmonologist, or primary care physician, must meet the surgical billing and documentation requirements when performing bronchoscopies or uncomplicated incision-and-drainage services, respectively.
Surgical services easily are identified as any code included in range 20000-69999. This code series includes major, minor, and endoscopic procedures. The “surgeon” and all physicians in the same group practice (i.e., reporting services under the same tax identification number) with the same specialty designation must adhere to the global period billing rules.
Alternately, physicians with different specialty designations in the same group practice (e.g., multispecialty group that reports services under the same tax identification number) or different group practices can perform and separately report medically necessary services during the surgeon’s global period, as long as a formal (mutually agreed upon) transfer of care did not occur. Information on physician specialty designations is available at www.highmarkmedicareservices.com/partb/refman/appendix-d.html.
Package Components
The following services are included in the surgeon’s packaged payment:
- Preoperative visits after the decision for surgery is made beginning one day prior to surgery;
- All additional post-operative medical or surgical services provided by the surgeon related to complications, but not require additional trips to the operating room;
- Post-operative visits by the surgeon related to recovery from surgery, including but not limited to dressing changes; local incisional care; removal of cutaneous sutures and staples; line removals; changes and removal of tracheostomy tubes; and discharge services; and
- Post-operative pain management provided by the surgeon.
Services not included are:
- The initial consultation or evaluation of the problem by the surgeon to determine the need for surgery. Append modifier 57 to this visit if provided the day before or day of major surgery to alert the payer that the service resulted in the decision for surgery. Append modifier 25 to this visit if provided the day of minor surgery;
- Services of other physicians except where the other physicians are providing coverage for the surgeon or agree on a transfer of care. This agreement may be in the form of a letter or an annotation in the discharge summary, hospital record, or ASC record;
- Post-operative visits by the surgeon unrelated to the diagnosis for which the surgical procedure is performed, unless the visits occur due to complications of the surgery. These services only are payable after the patient has been discharged from the hospitalization in which the surgery occurred. Append modifier 24 to these unrelated post-op visits;
- Diagnostic tests and procedures, including diagnostic radiological procedures;
- Clearly distinct surgical procedures during the post-operative period that do not result in repeat operations or treatment for complications;
- Treatment for post-operative complications that require a return trip to the operating room, catheterization lab, or endoscopy suite;
- Immunosuppressive therapy for organ transplants; and
- Critical care services (CPT codes 99291 and 99292) unrelated to the surgery in which a seriously injured or burned patient is critically ill and requires constant attendance of the surgeon. Append modifier 24 to these unrelated critical care services (see Table 2, above).
Payer Variations
While Medicare does not require modifier usage by hospitalists providing medically necessary services on surgical cases, some private payers do. Their electronic claim systems may not differentiate services by non-surgical specialists, requiring all physicians to append the appropriate modifier depending on the reason and timing of the service (see “Key Modifiers” below). TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Medical Verdicts
Vacuum extraction cause of child’s deep brain bleed?
A PREGNANT 24-YEAR-OLD WOMAN had regular prenatal care but smoked throughout her pregnancy. At 3 days past her due date, she was admitted to the hospital for induction of labor. Labor progressed normally but the fetal heart rate pattern was occasionally nonreassuring. A first-year resident performed a vacuum extraction under supervision and delivered the 8 lb 15 oz infant after one pull of the vacuum extractor. Apgar scores were 8 and 9, and blood gases were normal, but there was some molding of the head. The baby’s 25-hour stay in the hospital was normal. Three days later, a visiting nurse noted the child was not feeding well and was jaundiced. On a pediatrician’s advice, the child was taken to the hospital, where a cephalohematoma and jaundice were discovered. After suffering seizures, the child was transferred to another facility, where bleeding deep in the brain—believed to be due to the vacuum delivery—was diagnosed. The child has mild cerebral palsy and seizure disorder, as well as mild behavioral problems and learning deficits.
PATIENT’S CLAIM A C-section should have been performed.
DOCTOR’S DEFENSE There was no need for a C-section, as shown by the reassuring fetal strips, normal Apgar scores, and normal neonatal course in the hospital. There was no evidence of trauma, as vacuum succeeded with only one pull and was attached for only 1 or 2 minutes. Also, vacuum extraction cannot cause deep brain bleeds; the child must have suffered trauma after leaving the hospital. Surgery can correct the seizures.
VERDICT $1.125 million Michigan settlement.
Radiologist underestimates size of fetus—by 3.5 lb
ACCORDING TO THE RADIOLOGIST, a sonogram indicated the size of a woman’s fetus to be 8.5 lb at 39 weeks’ gestation. The attending physician thus planned a vaginal delivery, which was performed by a nurse-midwife. The infant, however, weighed 12 lb at birth. Shoulder dystocia occurred, and the baby was born with Erb’s palsy of the left arm.
PATIENT’S CLAIM The radiologist underestimated the fetus’s size, so that a vaginal delivery was planned instead of a C-section. Also, the nurse-midwife used excessive force when shoulder dystocia occurred, thus injuring the infant.
DOCTOR’S DEFENSE Not reported.
VERDICT $1.2 million New Jersey settlement; 60% to be paid on behalf of the nurse-midwife, and 40% on behalf of the radiologist.
New mother has uterine infection, sepsis; dies
SIX DAYS AFTER GIVING BIRTH TO TWINS, a 25-year-old woman was at a restaurant when she experienced a gush of bloody, smelly fluid from her vagina. The nurse who answered her call to her physician’s office advised her to wait and see. An ObGyn with the group reviewed the call card. When the patient was examined by a physician at the office 5 days later, she had obvious signs of an infection. Following exploratory surgery, the patient did not improve. She developed sepsis, adult respiratory distress syndrome, and further complications. Two months after her children’s birth, she died.
PATIENT’S CLAIM The nurse or ObGyn should have instructed the patient to go to the emergency room when she first called about the emitted fluid. She had a uterine infection and would have survived with earlier treatment.
DOCTOR’S DEFENSE The call was handled properly, and she was treated in a timely manner. Sepsis only began 3 days after her office visit, and it was pre-existing conditions—a pulmonary disorder and Crohn’s disease—that caused her death.
VERDICT Tennessee defense verdict.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Vacuum extraction cause of child’s deep brain bleed?
A PREGNANT 24-YEAR-OLD WOMAN had regular prenatal care but smoked throughout her pregnancy. At 3 days past her due date, she was admitted to the hospital for induction of labor. Labor progressed normally but the fetal heart rate pattern was occasionally nonreassuring. A first-year resident performed a vacuum extraction under supervision and delivered the 8 lb 15 oz infant after one pull of the vacuum extractor. Apgar scores were 8 and 9, and blood gases were normal, but there was some molding of the head. The baby’s 25-hour stay in the hospital was normal. Three days later, a visiting nurse noted the child was not feeding well and was jaundiced. On a pediatrician’s advice, the child was taken to the hospital, where a cephalohematoma and jaundice were discovered. After suffering seizures, the child was transferred to another facility, where bleeding deep in the brain—believed to be due to the vacuum delivery—was diagnosed. The child has mild cerebral palsy and seizure disorder, as well as mild behavioral problems and learning deficits.
PATIENT’S CLAIM A C-section should have been performed.
DOCTOR’S DEFENSE There was no need for a C-section, as shown by the reassuring fetal strips, normal Apgar scores, and normal neonatal course in the hospital. There was no evidence of trauma, as vacuum succeeded with only one pull and was attached for only 1 or 2 minutes. Also, vacuum extraction cannot cause deep brain bleeds; the child must have suffered trauma after leaving the hospital. Surgery can correct the seizures.
VERDICT $1.125 million Michigan settlement.
Radiologist underestimates size of fetus—by 3.5 lb
ACCORDING TO THE RADIOLOGIST, a sonogram indicated the size of a woman’s fetus to be 8.5 lb at 39 weeks’ gestation. The attending physician thus planned a vaginal delivery, which was performed by a nurse-midwife. The infant, however, weighed 12 lb at birth. Shoulder dystocia occurred, and the baby was born with Erb’s palsy of the left arm.
PATIENT’S CLAIM The radiologist underestimated the fetus’s size, so that a vaginal delivery was planned instead of a C-section. Also, the nurse-midwife used excessive force when shoulder dystocia occurred, thus injuring the infant.
DOCTOR’S DEFENSE Not reported.
VERDICT $1.2 million New Jersey settlement; 60% to be paid on behalf of the nurse-midwife, and 40% on behalf of the radiologist.
New mother has uterine infection, sepsis; dies
SIX DAYS AFTER GIVING BIRTH TO TWINS, a 25-year-old woman was at a restaurant when she experienced a gush of bloody, smelly fluid from her vagina. The nurse who answered her call to her physician’s office advised her to wait and see. An ObGyn with the group reviewed the call card. When the patient was examined by a physician at the office 5 days later, she had obvious signs of an infection. Following exploratory surgery, the patient did not improve. She developed sepsis, adult respiratory distress syndrome, and further complications. Two months after her children’s birth, she died.
PATIENT’S CLAIM The nurse or ObGyn should have instructed the patient to go to the emergency room when she first called about the emitted fluid. She had a uterine infection and would have survived with earlier treatment.
DOCTOR’S DEFENSE The call was handled properly, and she was treated in a timely manner. Sepsis only began 3 days after her office visit, and it was pre-existing conditions—a pulmonary disorder and Crohn’s disease—that caused her death.
VERDICT Tennessee defense verdict.
Vacuum extraction cause of child’s deep brain bleed?
A PREGNANT 24-YEAR-OLD WOMAN had regular prenatal care but smoked throughout her pregnancy. At 3 days past her due date, she was admitted to the hospital for induction of labor. Labor progressed normally but the fetal heart rate pattern was occasionally nonreassuring. A first-year resident performed a vacuum extraction under supervision and delivered the 8 lb 15 oz infant after one pull of the vacuum extractor. Apgar scores were 8 and 9, and blood gases were normal, but there was some molding of the head. The baby’s 25-hour stay in the hospital was normal. Three days later, a visiting nurse noted the child was not feeding well and was jaundiced. On a pediatrician’s advice, the child was taken to the hospital, where a cephalohematoma and jaundice were discovered. After suffering seizures, the child was transferred to another facility, where bleeding deep in the brain—believed to be due to the vacuum delivery—was diagnosed. The child has mild cerebral palsy and seizure disorder, as well as mild behavioral problems and learning deficits.
PATIENT’S CLAIM A C-section should have been performed.
DOCTOR’S DEFENSE There was no need for a C-section, as shown by the reassuring fetal strips, normal Apgar scores, and normal neonatal course in the hospital. There was no evidence of trauma, as vacuum succeeded with only one pull and was attached for only 1 or 2 minutes. Also, vacuum extraction cannot cause deep brain bleeds; the child must have suffered trauma after leaving the hospital. Surgery can correct the seizures.
VERDICT $1.125 million Michigan settlement.
Radiologist underestimates size of fetus—by 3.5 lb
ACCORDING TO THE RADIOLOGIST, a sonogram indicated the size of a woman’s fetus to be 8.5 lb at 39 weeks’ gestation. The attending physician thus planned a vaginal delivery, which was performed by a nurse-midwife. The infant, however, weighed 12 lb at birth. Shoulder dystocia occurred, and the baby was born with Erb’s palsy of the left arm.
PATIENT’S CLAIM The radiologist underestimated the fetus’s size, so that a vaginal delivery was planned instead of a C-section. Also, the nurse-midwife used excessive force when shoulder dystocia occurred, thus injuring the infant.
DOCTOR’S DEFENSE Not reported.
VERDICT $1.2 million New Jersey settlement; 60% to be paid on behalf of the nurse-midwife, and 40% on behalf of the radiologist.
New mother has uterine infection, sepsis; dies
SIX DAYS AFTER GIVING BIRTH TO TWINS, a 25-year-old woman was at a restaurant when she experienced a gush of bloody, smelly fluid from her vagina. The nurse who answered her call to her physician’s office advised her to wait and see. An ObGyn with the group reviewed the call card. When the patient was examined by a physician at the office 5 days later, she had obvious signs of an infection. Following exploratory surgery, the patient did not improve. She developed sepsis, adult respiratory distress syndrome, and further complications. Two months after her children’s birth, she died.
PATIENT’S CLAIM The nurse or ObGyn should have instructed the patient to go to the emergency room when she first called about the emitted fluid. She had a uterine infection and would have survived with earlier treatment.
DOCTOR’S DEFENSE The call was handled properly, and she was treated in a timely manner. Sepsis only began 3 days after her office visit, and it was pre-existing conditions—a pulmonary disorder and Crohn’s disease—that caused her death.
VERDICT Tennessee defense verdict.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG MANAGEMENT from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Stuff of nightmares: Criminal prosecution for malpractice
This overview is not intended as advice on any legal matter. Consult a medicolegal expert for advice.
Happily, criminal prosecutions for malpractice are rare in the United States—far, far less common than civil suits for malpractice. Nevertheless, criminal prosecutions do occur and seem to be increasingly frequent in recent years. Consider that, between 1809 and 1981, approximately 15 criminal cases involved the prosecution of a physician for medical malfeasance1; by contrast, between 1985 and 2004, another 15 cases were heard in US courts—every one involving the death of one or more patients.2
The two cases that I present in this article, both involving ObGyns, illustrate the distinguishing features of criminal and civil malpractice in the eyes of the law. My goal? To answer a question you may be considering: Am I safe from criminal prosecution for harm that comes to a patient at my hands?
Dr. Milos Klvana. The qualifications of Klvana to practice OB weren’t reassuring. After he received his medical education in Czechoslovakia, he was dismissed from an ObGyn residency in New York for poor academic performance, then forced to resign from an anesthesiology residency in California when a hospital held him responsible for a patient’s death. The California Medical Board put Klvana on license probation after he was convicted on 26 counts of inappropriately prescribing controlled substances and misrepresenting himself as “board-eligible” in ObGyn when he sought admitting privileges.
Klvana nevertheless continued practicing OB at his outpatient clinic after his convictions. There, over an 11-year period, nine babies whom he delivered died after grossly deficient management of labor.
Could Klvana have been prosecuted for causing these deaths?
- Depraved indifference to human life
- Lack of timely response
- Reckless endangerment
- Risky therapies
What crimes can a physician commit?
Any action that violates the law—insurance fraud, illicit sexual contact, theft, illegal distribution of narcotics, and tax evasion, to name several—is a criminal offense, whether perpetrated in the course of medical practice or under other circumstances.3 But a physician, by the nature of his (her) work, is in a unique position in regard to the law: When a patient in his care suffers severe or lethal injury, he may face a charge of criminal negligence, manslaughter, or second-degree murder2 (see the glossary of death-related charges).
- First-degree murder Many states require evidence of premeditation and intent to press this charge
- Second-degree murder Requires a reckless act and depraved indifference to human life
- Manslaughter Killing without malice aforethought
- Negligent homicide Killing because of carelessness, inattention, or indifference
CASE 1 CONTINUED
Klvana was charged with second-degree murder—as well as with insurance fraud, perjury, grand theft, and practicing medicine without a license.1-6 Expert witnesses testified that his conduct fell egregiously below the standard of proper obstetrical care. For example, Klvana repeatedly:
- failed to properly monitor oxytocin-stimulated labor
- disregarded signs of fetal and neonatal distress, including the presence of meconium
- was absent during delivery
- disregarded obvious signs of danger in newborns, including difficulty breathing
- failed to transfer high-risk patients to a hospital when labor became complicated.
A lengthy trial ensued. Klvana was convicted and sentenced to 53 years in prison.
Bad outcomes
The practice of medicine is full of uncertainties. There is never a guarantee that the out-come of a medical procedure or treatment will be curative or without risk.
When an outcome is bad, nothing the physician could have done would, in most instances, have averted the catastrophe. On rare occasions, however, a bad outcome is the result of physician negligence; when the patient (or her survivors) believes that a bad outcome was caused by the physician’s actions, they may institute a civil suit for malpractice. Very, very rarely does a prosecutor decide that the facts of a case warrant a charge of criminal malpractice.
What exactly puts a physician at risk of such a criminal charge?
The usual remedy is a civil suit
To understand why some medical actions constitute a crime, first let’s analyze the far more usual redress for a bad outcome—the malpractice suit. To be successful in such a suit, a plaintiff must prove four elements (see “Civil malpractice carries 4 elements”):
- duty
- breach
- damage
- causation.
A civil suit for malpractice is brought by the injured party or by his or her representatives. The compensation sought by the plaintiff is monetary.
- A relationship exists between physician and patient that establishes a duty on the physician’s part to perform a medical service
- A breach in the performance of that duty occurs, measured by applicable standards of care
- Monetary or physical damages to the patient result from that breach
- A proximate cause-and-effect relationship (causation) can be identified between the performance and the damage7
Dr. David Benjamin, repeat offender. Benjamin’s license had been revoked for gross incompetence after the fifth occasion on which he perforated a patient’s uterus during a gynecologic procedure. Unfortunately for his patients, Benjamin was given a window of opportunity to do more harm while he appealed the revocation of the license.
During that time, Benjamin performed an in-office abortion on a patient at 20 weeks’ gestation; state regulations at the time required that a second-trimester termination be performed in a hospital.
After the abortion, the patient bled excessively—the result of perforation of the uterus (a 1” × 4” wound) and cervical laceration. Benjamin was aware of the heavy bleeding but placed the patient in a clinic corridor while he performed an abortion on another patient. The first patient remained in the corridor for an hour, without adequate monitoring, until she went into shock and cardiac arrest. According to the testimony of witnesses, emergency medical services staff were misinformed about the patient’s condition, further delaying timely intervention.
Benjamin was indicted for second-degree murder after a grand jury found “depraved indifference to human life.” He was tried, convicted, and sentenced to imprisonment for 25 years to life.6-10
What made his conduct criminal?
What was he thinking?
Criminal malpractice is characterized by the same four elements as civil malpractice, and adds a fifth element: The physician’s state of mind (in legal terminology, mens rea). That state of mind can range from inattention to premeditation.
Here’s an example: One of Klvana’s residency faculty testified that the defendant-physician was “cavalier and casual in his approach and his duties.” Klvana’s training and experience should have been enough to alert him to the need for appropriate monitoring during augmented labor but, apparently, he chose to ignore these accepted standards of practice. He had, for example, used oxytocin stimulation by direct infusion and without fetal monitoring (and in his office, not the hospital) for a postdate gravida who had had two prior cesarean sections. Her newborn died of perinatal asphyxia.
Klvana repeatedly used this risky, life-endangering protocol, exhibiting what can be called a “wanton disregard for human life” and an indifference to his patients’ safety. His preference for more precarious, office-based delivery may have been the result of his difficulty obtaining admitting privileges.
Similarly, Benjamin may have been motivated by greed when he chose to perform an abortion on a second patient instead of attending to the patient who was bleeding to death in the corridor after an earlier procedure.
- Willful, reckless endangerment
- Wanton disregard of past negative outcomes
- Lack of timely response
- Improper motive
- Depraved indifference to human life
- Gross negligence
- Intoxication
- Deception
- Unjustifiable risk
The standard of care
In some prosecuted cases, the level of gross negligence is so high that proving that a departure from the standard of care has occurred is unnecessary. A case in point is the growing number of physicians who are under the influence of drugs or alcohol when they treat patients. As early as 1887, courts recognized as grossly negligent surgeons who operated while drunk.11 It is estimated that 10% to 15% of American doctors have had, or will have, a substance abuse problem sometime in their life. Many continue practicing while undergoing treatment for the illness.12
Note that chemical impairment is no longer accepted as an excuse for error. Just as a charge of driving while intoxicated that involves bodily injury may be tried as a felony, surgical damage done while intoxicated is now generally prosecuted as criminal negligence.3
In most criminal prosecutions for malpractice, however, expert testimony is required to 1) attest to the relevant standard of care and 2) characterize the defendant’s actions as a marked departure from such a standard. Deviating from accepted modes of treatment, or employing dubious approaches known to be highly risky, constitutes such a departure.
The applicable standard of care is defined locally and varies from jurisdiction to jurisdiction. Each societal unit determines and defines the limits of acceptable conduct by its professional members, beyond which certain actions become intolerable. (An example of this variability is that, in 1991, an ObGyn in the United States had, on average, been sued three times, but the typical ObGyn in the State of New York had been sued eight times.13)
Furthermore, those societal definitions of “acceptable conduct” may be influenced by prevailing social attitudes about such charged issues as abortion, sexual promiscuity, faith healing, or sedation at end of life.
Repeat performances
Physicians who have been found guilty of criminal malpractice don’t seem to learn from experience. They continue to produce similar adverse results when they treat particular medical problems. Consider Benjamin: Five times, he caused a life-endangering uterine perforation during gynecologic procedures before the fatal episode described earlier occurred. And Kvlana: nine stillborn and neonatal demises in 11 years as he persisted in his grossly deficient practice of managing labor. This sort of repetitive behavior, constituting a pattern of negligence, is another invitation to criminal prosecution.
Depraved indifference; reckless endangerment
The unwarranted delay in dealing with a postabortal hemorrhage led, in Benjamin’s case, directly to the patient’s death. Such a delay displays either a lack of understanding of basic physiology or a depraved indifference to human life. Benjamin’s behavior was not simply a matter of faulty medical judgment; it was a willful repetition of precarious substandard practices that constituted reckless endangerment. His criminally culpable error was twofold: the recurrence of uterine perforation (a risk he should have been aware of because it had happened in prior surgeries) and, more so, his willful neglect of a bleeding patient.
More recent criminal prosecutions may give “good-faith” physicians pause and make them wary of entering into particularly troubled areas of medical practice:
- Chronic pain Fear of prosecution by the US Drug Enforcement Administration (DEA) has had a chilling effect on the practice of physicians who prescribe opioids for chronic pain.
- Late-term abortions Federal legislation criminalizing so-called partial-birth abortions has, similarly, influenced the performance of all second-trimester abortion.
- End-of-life care Dispute over the legitimacy of terminal sedation has placed hospice physicians in legal jeopardy in some jurisdictions.
- Physician-assisted suicide Legal only in the state of Oregon, this practice has already sent its most prominent practitioner to jail. Legislation to legalize the highly controversial procedure has been introduced in other state legislatures.
- Prosecutors building support for re-election This appears to have been the impetus for Louisiana’s Attorney General charging Anna Pou, MD, with murder in the deaths of four elderly New Orleans nursing home patients stranded by Hurricane Katrina in 2005. Dr. Pou administered to her patients what she believed to be pain relief and comfort in the form of morphine and midazolam. The grand jury refused to return the indictment.1
Reference
1. Okie S. Dr. Pou and the hurricane—implications for patient care during disasters. N Engl J Med. 2008;358:1-5.
Is criminal prosecution necessary?
The legitimate desire of society 1) for its members to receive diligent treatment and 2) to prevent the repetition of inept or dangerous medical practices is central to the question posed atop this section. Consumers of health care are, increasingly, aware that the usual processes of professional discipline and state regulation do not always protect patients from harm: Dangerous physicians have eluded attempts to discipline them by moving from one jurisdiction to another, always a step ahead of attempts to control them. A civil malpractice suit, however large the settlement sometimes is, does not always deter a defendant from repeat performances of his or her negligent behavior.
It is reasonable to expect prosecutors to become more active in filing criminal charges as public frustration with inadequate self-policing grows.14 The Benjamin and Klvana cases are striking instances of the failure of government licensing agencies to take timely action to protect the public from harm. And, so, in the most egregious cases of physician misconduct, society resorts to criminal prosecution. Will such prosecutions become more frequent? The answer depends on how effectively quality assurance measures in health care are implemented.
Avoid prosecution with “quality medicine”
The best way to avoid criminal prosecution is, of course, to practice good medicine. Quality medicine rests on the principle that caregivers respond to patients’ needs in a timely, appropriate manner. Your patients will, of course, come to the end of their life sooner or later. But patients in the hands of a good physician will not have that end hastened by disregard for sound medical practices.
In 1980, the Massachusetts Supreme Judicial Court enunciated a standard for physicians that no honorable physician would have difficulty meeting: “A doctor will be protected,” the court said, “if he acts on a good faith judgment that is not grievously unreasonable by medical standards.”15
1. Monico E, Kulkarni R, Calise A, Calabro J. The criminal prosecution of medical negligence. Internet J Law Healthcare Ethics. 2007;5(1). www.ispub.com/journals/ijlhe.htm. Accessed July 5, 2008.
2. Filkins JA. Criminalization of medical negligence. In: Sanbar SS, Fiscina S, Firestone MH, eds. Legal Medicine. 7th ed. Philadelphia: Elsevier Health Sciences; 2007:507-512.
3. Twardy S. Crimes by health care providers. In: Sanbar SS, Fiscina S, Firestone MH, eds. Legal Medicine. 7th ed. Philadelphia: Elsevier Health Sciences; 2007:513-520.
4. People v Klvana, 11 Cal App 4th 1679, 15 Cal Rptr 2d 512 (1992)
5. Klvana v State of California, 911 F Supp 1228 (CD Cal 1995)
6. McCarthy KM. Doing time for clinical crime: the prosecution of incompetent physicians as an additional mechanism to assure quality health care. Seton Hall Law Rev. 1997;28:569-619.
7. Steinman GD. Doctor-to-Doctor: Avoiding Financial Suicide. New York: Baffin Books; 1998;53.
8. People v Benjamin, 270 AD 2d 428, 705 NYS 2d 386 (2d Dept 2000).
9. Sullivan R. Doctor faces murder count in abortion. New York Times. August 13, 1993.
10. Holloway L. 25 years to life for doctor in woman’s death after botched abortion. New York Times. September 13, 1995.
11. Holbrook J. The criminalisation of fatal medical mistakes. BMJ. 2003;327:1118-1119.
12. Addicted doctors still practice while in rehab www.msnbc.msn.com/id/22314486. Accessed July 5, 2008.
13. Glauser J. NPDB: malpractice, incompetency, and consent to settle. Emerg Med News. 2001;23(8):16-18.
14. Annas GJ. Medicine, death, and the criminal law. N Engl J Med. 1995;333:527-530.
15. In the matter of Spring, 380 Mass 629, 637 (1980)
This overview is not intended as advice on any legal matter. Consult a medicolegal expert for advice.
Happily, criminal prosecutions for malpractice are rare in the United States—far, far less common than civil suits for malpractice. Nevertheless, criminal prosecutions do occur and seem to be increasingly frequent in recent years. Consider that, between 1809 and 1981, approximately 15 criminal cases involved the prosecution of a physician for medical malfeasance1; by contrast, between 1985 and 2004, another 15 cases were heard in US courts—every one involving the death of one or more patients.2
The two cases that I present in this article, both involving ObGyns, illustrate the distinguishing features of criminal and civil malpractice in the eyes of the law. My goal? To answer a question you may be considering: Am I safe from criminal prosecution for harm that comes to a patient at my hands?
Dr. Milos Klvana. The qualifications of Klvana to practice OB weren’t reassuring. After he received his medical education in Czechoslovakia, he was dismissed from an ObGyn residency in New York for poor academic performance, then forced to resign from an anesthesiology residency in California when a hospital held him responsible for a patient’s death. The California Medical Board put Klvana on license probation after he was convicted on 26 counts of inappropriately prescribing controlled substances and misrepresenting himself as “board-eligible” in ObGyn when he sought admitting privileges.
Klvana nevertheless continued practicing OB at his outpatient clinic after his convictions. There, over an 11-year period, nine babies whom he delivered died after grossly deficient management of labor.
Could Klvana have been prosecuted for causing these deaths?
- Depraved indifference to human life
- Lack of timely response
- Reckless endangerment
- Risky therapies
What crimes can a physician commit?
Any action that violates the law—insurance fraud, illicit sexual contact, theft, illegal distribution of narcotics, and tax evasion, to name several—is a criminal offense, whether perpetrated in the course of medical practice or under other circumstances.3 But a physician, by the nature of his (her) work, is in a unique position in regard to the law: When a patient in his care suffers severe or lethal injury, he may face a charge of criminal negligence, manslaughter, or second-degree murder2 (see the glossary of death-related charges).
- First-degree murder Many states require evidence of premeditation and intent to press this charge
- Second-degree murder Requires a reckless act and depraved indifference to human life
- Manslaughter Killing without malice aforethought
- Negligent homicide Killing because of carelessness, inattention, or indifference
CASE 1 CONTINUED
Klvana was charged with second-degree murder—as well as with insurance fraud, perjury, grand theft, and practicing medicine without a license.1-6 Expert witnesses testified that his conduct fell egregiously below the standard of proper obstetrical care. For example, Klvana repeatedly:
- failed to properly monitor oxytocin-stimulated labor
- disregarded signs of fetal and neonatal distress, including the presence of meconium
- was absent during delivery
- disregarded obvious signs of danger in newborns, including difficulty breathing
- failed to transfer high-risk patients to a hospital when labor became complicated.
A lengthy trial ensued. Klvana was convicted and sentenced to 53 years in prison.
Bad outcomes
The practice of medicine is full of uncertainties. There is never a guarantee that the out-come of a medical procedure or treatment will be curative or without risk.
When an outcome is bad, nothing the physician could have done would, in most instances, have averted the catastrophe. On rare occasions, however, a bad outcome is the result of physician negligence; when the patient (or her survivors) believes that a bad outcome was caused by the physician’s actions, they may institute a civil suit for malpractice. Very, very rarely does a prosecutor decide that the facts of a case warrant a charge of criminal malpractice.
What exactly puts a physician at risk of such a criminal charge?
The usual remedy is a civil suit
To understand why some medical actions constitute a crime, first let’s analyze the far more usual redress for a bad outcome—the malpractice suit. To be successful in such a suit, a plaintiff must prove four elements (see “Civil malpractice carries 4 elements”):
- duty
- breach
- damage
- causation.
A civil suit for malpractice is brought by the injured party or by his or her representatives. The compensation sought by the plaintiff is monetary.
- A relationship exists between physician and patient that establishes a duty on the physician’s part to perform a medical service
- A breach in the performance of that duty occurs, measured by applicable standards of care
- Monetary or physical damages to the patient result from that breach
- A proximate cause-and-effect relationship (causation) can be identified between the performance and the damage7
Dr. David Benjamin, repeat offender. Benjamin’s license had been revoked for gross incompetence after the fifth occasion on which he perforated a patient’s uterus during a gynecologic procedure. Unfortunately for his patients, Benjamin was given a window of opportunity to do more harm while he appealed the revocation of the license.
During that time, Benjamin performed an in-office abortion on a patient at 20 weeks’ gestation; state regulations at the time required that a second-trimester termination be performed in a hospital.
After the abortion, the patient bled excessively—the result of perforation of the uterus (a 1” × 4” wound) and cervical laceration. Benjamin was aware of the heavy bleeding but placed the patient in a clinic corridor while he performed an abortion on another patient. The first patient remained in the corridor for an hour, without adequate monitoring, until she went into shock and cardiac arrest. According to the testimony of witnesses, emergency medical services staff were misinformed about the patient’s condition, further delaying timely intervention.
Benjamin was indicted for second-degree murder after a grand jury found “depraved indifference to human life.” He was tried, convicted, and sentenced to imprisonment for 25 years to life.6-10
What made his conduct criminal?
What was he thinking?
Criminal malpractice is characterized by the same four elements as civil malpractice, and adds a fifth element: The physician’s state of mind (in legal terminology, mens rea). That state of mind can range from inattention to premeditation.
Here’s an example: One of Klvana’s residency faculty testified that the defendant-physician was “cavalier and casual in his approach and his duties.” Klvana’s training and experience should have been enough to alert him to the need for appropriate monitoring during augmented labor but, apparently, he chose to ignore these accepted standards of practice. He had, for example, used oxytocin stimulation by direct infusion and without fetal monitoring (and in his office, not the hospital) for a postdate gravida who had had two prior cesarean sections. Her newborn died of perinatal asphyxia.
Klvana repeatedly used this risky, life-endangering protocol, exhibiting what can be called a “wanton disregard for human life” and an indifference to his patients’ safety. His preference for more precarious, office-based delivery may have been the result of his difficulty obtaining admitting privileges.
Similarly, Benjamin may have been motivated by greed when he chose to perform an abortion on a second patient instead of attending to the patient who was bleeding to death in the corridor after an earlier procedure.
- Willful, reckless endangerment
- Wanton disregard of past negative outcomes
- Lack of timely response
- Improper motive
- Depraved indifference to human life
- Gross negligence
- Intoxication
- Deception
- Unjustifiable risk
The standard of care
In some prosecuted cases, the level of gross negligence is so high that proving that a departure from the standard of care has occurred is unnecessary. A case in point is the growing number of physicians who are under the influence of drugs or alcohol when they treat patients. As early as 1887, courts recognized as grossly negligent surgeons who operated while drunk.11 It is estimated that 10% to 15% of American doctors have had, or will have, a substance abuse problem sometime in their life. Many continue practicing while undergoing treatment for the illness.12
Note that chemical impairment is no longer accepted as an excuse for error. Just as a charge of driving while intoxicated that involves bodily injury may be tried as a felony, surgical damage done while intoxicated is now generally prosecuted as criminal negligence.3
In most criminal prosecutions for malpractice, however, expert testimony is required to 1) attest to the relevant standard of care and 2) characterize the defendant’s actions as a marked departure from such a standard. Deviating from accepted modes of treatment, or employing dubious approaches known to be highly risky, constitutes such a departure.
The applicable standard of care is defined locally and varies from jurisdiction to jurisdiction. Each societal unit determines and defines the limits of acceptable conduct by its professional members, beyond which certain actions become intolerable. (An example of this variability is that, in 1991, an ObGyn in the United States had, on average, been sued three times, but the typical ObGyn in the State of New York had been sued eight times.13)
Furthermore, those societal definitions of “acceptable conduct” may be influenced by prevailing social attitudes about such charged issues as abortion, sexual promiscuity, faith healing, or sedation at end of life.
Repeat performances
Physicians who have been found guilty of criminal malpractice don’t seem to learn from experience. They continue to produce similar adverse results when they treat particular medical problems. Consider Benjamin: Five times, he caused a life-endangering uterine perforation during gynecologic procedures before the fatal episode described earlier occurred. And Kvlana: nine stillborn and neonatal demises in 11 years as he persisted in his grossly deficient practice of managing labor. This sort of repetitive behavior, constituting a pattern of negligence, is another invitation to criminal prosecution.
Depraved indifference; reckless endangerment
The unwarranted delay in dealing with a postabortal hemorrhage led, in Benjamin’s case, directly to the patient’s death. Such a delay displays either a lack of understanding of basic physiology or a depraved indifference to human life. Benjamin’s behavior was not simply a matter of faulty medical judgment; it was a willful repetition of precarious substandard practices that constituted reckless endangerment. His criminally culpable error was twofold: the recurrence of uterine perforation (a risk he should have been aware of because it had happened in prior surgeries) and, more so, his willful neglect of a bleeding patient.
More recent criminal prosecutions may give “good-faith” physicians pause and make them wary of entering into particularly troubled areas of medical practice:
- Chronic pain Fear of prosecution by the US Drug Enforcement Administration (DEA) has had a chilling effect on the practice of physicians who prescribe opioids for chronic pain.
- Late-term abortions Federal legislation criminalizing so-called partial-birth abortions has, similarly, influenced the performance of all second-trimester abortion.
- End-of-life care Dispute over the legitimacy of terminal sedation has placed hospice physicians in legal jeopardy in some jurisdictions.
- Physician-assisted suicide Legal only in the state of Oregon, this practice has already sent its most prominent practitioner to jail. Legislation to legalize the highly controversial procedure has been introduced in other state legislatures.
- Prosecutors building support for re-election This appears to have been the impetus for Louisiana’s Attorney General charging Anna Pou, MD, with murder in the deaths of four elderly New Orleans nursing home patients stranded by Hurricane Katrina in 2005. Dr. Pou administered to her patients what she believed to be pain relief and comfort in the form of morphine and midazolam. The grand jury refused to return the indictment.1
Reference
1. Okie S. Dr. Pou and the hurricane—implications for patient care during disasters. N Engl J Med. 2008;358:1-5.
Is criminal prosecution necessary?
The legitimate desire of society 1) for its members to receive diligent treatment and 2) to prevent the repetition of inept or dangerous medical practices is central to the question posed atop this section. Consumers of health care are, increasingly, aware that the usual processes of professional discipline and state regulation do not always protect patients from harm: Dangerous physicians have eluded attempts to discipline them by moving from one jurisdiction to another, always a step ahead of attempts to control them. A civil malpractice suit, however large the settlement sometimes is, does not always deter a defendant from repeat performances of his or her negligent behavior.
It is reasonable to expect prosecutors to become more active in filing criminal charges as public frustration with inadequate self-policing grows.14 The Benjamin and Klvana cases are striking instances of the failure of government licensing agencies to take timely action to protect the public from harm. And, so, in the most egregious cases of physician misconduct, society resorts to criminal prosecution. Will such prosecutions become more frequent? The answer depends on how effectively quality assurance measures in health care are implemented.
Avoid prosecution with “quality medicine”
The best way to avoid criminal prosecution is, of course, to practice good medicine. Quality medicine rests on the principle that caregivers respond to patients’ needs in a timely, appropriate manner. Your patients will, of course, come to the end of their life sooner or later. But patients in the hands of a good physician will not have that end hastened by disregard for sound medical practices.
In 1980, the Massachusetts Supreme Judicial Court enunciated a standard for physicians that no honorable physician would have difficulty meeting: “A doctor will be protected,” the court said, “if he acts on a good faith judgment that is not grievously unreasonable by medical standards.”15
This overview is not intended as advice on any legal matter. Consult a medicolegal expert for advice.
Happily, criminal prosecutions for malpractice are rare in the United States—far, far less common than civil suits for malpractice. Nevertheless, criminal prosecutions do occur and seem to be increasingly frequent in recent years. Consider that, between 1809 and 1981, approximately 15 criminal cases involved the prosecution of a physician for medical malfeasance1; by contrast, between 1985 and 2004, another 15 cases were heard in US courts—every one involving the death of one or more patients.2
The two cases that I present in this article, both involving ObGyns, illustrate the distinguishing features of criminal and civil malpractice in the eyes of the law. My goal? To answer a question you may be considering: Am I safe from criminal prosecution for harm that comes to a patient at my hands?
Dr. Milos Klvana. The qualifications of Klvana to practice OB weren’t reassuring. After he received his medical education in Czechoslovakia, he was dismissed from an ObGyn residency in New York for poor academic performance, then forced to resign from an anesthesiology residency in California when a hospital held him responsible for a patient’s death. The California Medical Board put Klvana on license probation after he was convicted on 26 counts of inappropriately prescribing controlled substances and misrepresenting himself as “board-eligible” in ObGyn when he sought admitting privileges.
Klvana nevertheless continued practicing OB at his outpatient clinic after his convictions. There, over an 11-year period, nine babies whom he delivered died after grossly deficient management of labor.
Could Klvana have been prosecuted for causing these deaths?
- Depraved indifference to human life
- Lack of timely response
- Reckless endangerment
- Risky therapies
What crimes can a physician commit?
Any action that violates the law—insurance fraud, illicit sexual contact, theft, illegal distribution of narcotics, and tax evasion, to name several—is a criminal offense, whether perpetrated in the course of medical practice or under other circumstances.3 But a physician, by the nature of his (her) work, is in a unique position in regard to the law: When a patient in his care suffers severe or lethal injury, he may face a charge of criminal negligence, manslaughter, or second-degree murder2 (see the glossary of death-related charges).
- First-degree murder Many states require evidence of premeditation and intent to press this charge
- Second-degree murder Requires a reckless act and depraved indifference to human life
- Manslaughter Killing without malice aforethought
- Negligent homicide Killing because of carelessness, inattention, or indifference
CASE 1 CONTINUED
Klvana was charged with second-degree murder—as well as with insurance fraud, perjury, grand theft, and practicing medicine without a license.1-6 Expert witnesses testified that his conduct fell egregiously below the standard of proper obstetrical care. For example, Klvana repeatedly:
- failed to properly monitor oxytocin-stimulated labor
- disregarded signs of fetal and neonatal distress, including the presence of meconium
- was absent during delivery
- disregarded obvious signs of danger in newborns, including difficulty breathing
- failed to transfer high-risk patients to a hospital when labor became complicated.
A lengthy trial ensued. Klvana was convicted and sentenced to 53 years in prison.
Bad outcomes
The practice of medicine is full of uncertainties. There is never a guarantee that the out-come of a medical procedure or treatment will be curative or without risk.
When an outcome is bad, nothing the physician could have done would, in most instances, have averted the catastrophe. On rare occasions, however, a bad outcome is the result of physician negligence; when the patient (or her survivors) believes that a bad outcome was caused by the physician’s actions, they may institute a civil suit for malpractice. Very, very rarely does a prosecutor decide that the facts of a case warrant a charge of criminal malpractice.
What exactly puts a physician at risk of such a criminal charge?
The usual remedy is a civil suit
To understand why some medical actions constitute a crime, first let’s analyze the far more usual redress for a bad outcome—the malpractice suit. To be successful in such a suit, a plaintiff must prove four elements (see “Civil malpractice carries 4 elements”):
- duty
- breach
- damage
- causation.
A civil suit for malpractice is brought by the injured party or by his or her representatives. The compensation sought by the plaintiff is monetary.
- A relationship exists between physician and patient that establishes a duty on the physician’s part to perform a medical service
- A breach in the performance of that duty occurs, measured by applicable standards of care
- Monetary or physical damages to the patient result from that breach
- A proximate cause-and-effect relationship (causation) can be identified between the performance and the damage7
Dr. David Benjamin, repeat offender. Benjamin’s license had been revoked for gross incompetence after the fifth occasion on which he perforated a patient’s uterus during a gynecologic procedure. Unfortunately for his patients, Benjamin was given a window of opportunity to do more harm while he appealed the revocation of the license.
During that time, Benjamin performed an in-office abortion on a patient at 20 weeks’ gestation; state regulations at the time required that a second-trimester termination be performed in a hospital.
After the abortion, the patient bled excessively—the result of perforation of the uterus (a 1” × 4” wound) and cervical laceration. Benjamin was aware of the heavy bleeding but placed the patient in a clinic corridor while he performed an abortion on another patient. The first patient remained in the corridor for an hour, without adequate monitoring, until she went into shock and cardiac arrest. According to the testimony of witnesses, emergency medical services staff were misinformed about the patient’s condition, further delaying timely intervention.
Benjamin was indicted for second-degree murder after a grand jury found “depraved indifference to human life.” He was tried, convicted, and sentenced to imprisonment for 25 years to life.6-10
What made his conduct criminal?
What was he thinking?
Criminal malpractice is characterized by the same four elements as civil malpractice, and adds a fifth element: The physician’s state of mind (in legal terminology, mens rea). That state of mind can range from inattention to premeditation.
Here’s an example: One of Klvana’s residency faculty testified that the defendant-physician was “cavalier and casual in his approach and his duties.” Klvana’s training and experience should have been enough to alert him to the need for appropriate monitoring during augmented labor but, apparently, he chose to ignore these accepted standards of practice. He had, for example, used oxytocin stimulation by direct infusion and without fetal monitoring (and in his office, not the hospital) for a postdate gravida who had had two prior cesarean sections. Her newborn died of perinatal asphyxia.
Klvana repeatedly used this risky, life-endangering protocol, exhibiting what can be called a “wanton disregard for human life” and an indifference to his patients’ safety. His preference for more precarious, office-based delivery may have been the result of his difficulty obtaining admitting privileges.
Similarly, Benjamin may have been motivated by greed when he chose to perform an abortion on a second patient instead of attending to the patient who was bleeding to death in the corridor after an earlier procedure.
- Willful, reckless endangerment
- Wanton disregard of past negative outcomes
- Lack of timely response
- Improper motive
- Depraved indifference to human life
- Gross negligence
- Intoxication
- Deception
- Unjustifiable risk
The standard of care
In some prosecuted cases, the level of gross negligence is so high that proving that a departure from the standard of care has occurred is unnecessary. A case in point is the growing number of physicians who are under the influence of drugs or alcohol when they treat patients. As early as 1887, courts recognized as grossly negligent surgeons who operated while drunk.11 It is estimated that 10% to 15% of American doctors have had, or will have, a substance abuse problem sometime in their life. Many continue practicing while undergoing treatment for the illness.12
Note that chemical impairment is no longer accepted as an excuse for error. Just as a charge of driving while intoxicated that involves bodily injury may be tried as a felony, surgical damage done while intoxicated is now generally prosecuted as criminal negligence.3
In most criminal prosecutions for malpractice, however, expert testimony is required to 1) attest to the relevant standard of care and 2) characterize the defendant’s actions as a marked departure from such a standard. Deviating from accepted modes of treatment, or employing dubious approaches known to be highly risky, constitutes such a departure.
The applicable standard of care is defined locally and varies from jurisdiction to jurisdiction. Each societal unit determines and defines the limits of acceptable conduct by its professional members, beyond which certain actions become intolerable. (An example of this variability is that, in 1991, an ObGyn in the United States had, on average, been sued three times, but the typical ObGyn in the State of New York had been sued eight times.13)
Furthermore, those societal definitions of “acceptable conduct” may be influenced by prevailing social attitudes about such charged issues as abortion, sexual promiscuity, faith healing, or sedation at end of life.
Repeat performances
Physicians who have been found guilty of criminal malpractice don’t seem to learn from experience. They continue to produce similar adverse results when they treat particular medical problems. Consider Benjamin: Five times, he caused a life-endangering uterine perforation during gynecologic procedures before the fatal episode described earlier occurred. And Kvlana: nine stillborn and neonatal demises in 11 years as he persisted in his grossly deficient practice of managing labor. This sort of repetitive behavior, constituting a pattern of negligence, is another invitation to criminal prosecution.
Depraved indifference; reckless endangerment
The unwarranted delay in dealing with a postabortal hemorrhage led, in Benjamin’s case, directly to the patient’s death. Such a delay displays either a lack of understanding of basic physiology or a depraved indifference to human life. Benjamin’s behavior was not simply a matter of faulty medical judgment; it was a willful repetition of precarious substandard practices that constituted reckless endangerment. His criminally culpable error was twofold: the recurrence of uterine perforation (a risk he should have been aware of because it had happened in prior surgeries) and, more so, his willful neglect of a bleeding patient.
More recent criminal prosecutions may give “good-faith” physicians pause and make them wary of entering into particularly troubled areas of medical practice:
- Chronic pain Fear of prosecution by the US Drug Enforcement Administration (DEA) has had a chilling effect on the practice of physicians who prescribe opioids for chronic pain.
- Late-term abortions Federal legislation criminalizing so-called partial-birth abortions has, similarly, influenced the performance of all second-trimester abortion.
- End-of-life care Dispute over the legitimacy of terminal sedation has placed hospice physicians in legal jeopardy in some jurisdictions.
- Physician-assisted suicide Legal only in the state of Oregon, this practice has already sent its most prominent practitioner to jail. Legislation to legalize the highly controversial procedure has been introduced in other state legislatures.
- Prosecutors building support for re-election This appears to have been the impetus for Louisiana’s Attorney General charging Anna Pou, MD, with murder in the deaths of four elderly New Orleans nursing home patients stranded by Hurricane Katrina in 2005. Dr. Pou administered to her patients what she believed to be pain relief and comfort in the form of morphine and midazolam. The grand jury refused to return the indictment.1
Reference
1. Okie S. Dr. Pou and the hurricane—implications for patient care during disasters. N Engl J Med. 2008;358:1-5.
Is criminal prosecution necessary?
The legitimate desire of society 1) for its members to receive diligent treatment and 2) to prevent the repetition of inept or dangerous medical practices is central to the question posed atop this section. Consumers of health care are, increasingly, aware that the usual processes of professional discipline and state regulation do not always protect patients from harm: Dangerous physicians have eluded attempts to discipline them by moving from one jurisdiction to another, always a step ahead of attempts to control them. A civil malpractice suit, however large the settlement sometimes is, does not always deter a defendant from repeat performances of his or her negligent behavior.
It is reasonable to expect prosecutors to become more active in filing criminal charges as public frustration with inadequate self-policing grows.14 The Benjamin and Klvana cases are striking instances of the failure of government licensing agencies to take timely action to protect the public from harm. And, so, in the most egregious cases of physician misconduct, society resorts to criminal prosecution. Will such prosecutions become more frequent? The answer depends on how effectively quality assurance measures in health care are implemented.
Avoid prosecution with “quality medicine”
The best way to avoid criminal prosecution is, of course, to practice good medicine. Quality medicine rests on the principle that caregivers respond to patients’ needs in a timely, appropriate manner. Your patients will, of course, come to the end of their life sooner or later. But patients in the hands of a good physician will not have that end hastened by disregard for sound medical practices.
In 1980, the Massachusetts Supreme Judicial Court enunciated a standard for physicians that no honorable physician would have difficulty meeting: “A doctor will be protected,” the court said, “if he acts on a good faith judgment that is not grievously unreasonable by medical standards.”15
1. Monico E, Kulkarni R, Calise A, Calabro J. The criminal prosecution of medical negligence. Internet J Law Healthcare Ethics. 2007;5(1). www.ispub.com/journals/ijlhe.htm. Accessed July 5, 2008.
2. Filkins JA. Criminalization of medical negligence. In: Sanbar SS, Fiscina S, Firestone MH, eds. Legal Medicine. 7th ed. Philadelphia: Elsevier Health Sciences; 2007:507-512.
3. Twardy S. Crimes by health care providers. In: Sanbar SS, Fiscina S, Firestone MH, eds. Legal Medicine. 7th ed. Philadelphia: Elsevier Health Sciences; 2007:513-520.
4. People v Klvana, 11 Cal App 4th 1679, 15 Cal Rptr 2d 512 (1992)
5. Klvana v State of California, 911 F Supp 1228 (CD Cal 1995)
6. McCarthy KM. Doing time for clinical crime: the prosecution of incompetent physicians as an additional mechanism to assure quality health care. Seton Hall Law Rev. 1997;28:569-619.
7. Steinman GD. Doctor-to-Doctor: Avoiding Financial Suicide. New York: Baffin Books; 1998;53.
8. People v Benjamin, 270 AD 2d 428, 705 NYS 2d 386 (2d Dept 2000).
9. Sullivan R. Doctor faces murder count in abortion. New York Times. August 13, 1993.
10. Holloway L. 25 years to life for doctor in woman’s death after botched abortion. New York Times. September 13, 1995.
11. Holbrook J. The criminalisation of fatal medical mistakes. BMJ. 2003;327:1118-1119.
12. Addicted doctors still practice while in rehab www.msnbc.msn.com/id/22314486. Accessed July 5, 2008.
13. Glauser J. NPDB: malpractice, incompetency, and consent to settle. Emerg Med News. 2001;23(8):16-18.
14. Annas GJ. Medicine, death, and the criminal law. N Engl J Med. 1995;333:527-530.
15. In the matter of Spring, 380 Mass 629, 637 (1980)
1. Monico E, Kulkarni R, Calise A, Calabro J. The criminal prosecution of medical negligence. Internet J Law Healthcare Ethics. 2007;5(1). www.ispub.com/journals/ijlhe.htm. Accessed July 5, 2008.
2. Filkins JA. Criminalization of medical negligence. In: Sanbar SS, Fiscina S, Firestone MH, eds. Legal Medicine. 7th ed. Philadelphia: Elsevier Health Sciences; 2007:507-512.
3. Twardy S. Crimes by health care providers. In: Sanbar SS, Fiscina S, Firestone MH, eds. Legal Medicine. 7th ed. Philadelphia: Elsevier Health Sciences; 2007:513-520.
4. People v Klvana, 11 Cal App 4th 1679, 15 Cal Rptr 2d 512 (1992)
5. Klvana v State of California, 911 F Supp 1228 (CD Cal 1995)
6. McCarthy KM. Doing time for clinical crime: the prosecution of incompetent physicians as an additional mechanism to assure quality health care. Seton Hall Law Rev. 1997;28:569-619.
7. Steinman GD. Doctor-to-Doctor: Avoiding Financial Suicide. New York: Baffin Books; 1998;53.
8. People v Benjamin, 270 AD 2d 428, 705 NYS 2d 386 (2d Dept 2000).
9. Sullivan R. Doctor faces murder count in abortion. New York Times. August 13, 1993.
10. Holloway L. 25 years to life for doctor in woman’s death after botched abortion. New York Times. September 13, 1995.
11. Holbrook J. The criminalisation of fatal medical mistakes. BMJ. 2003;327:1118-1119.
12. Addicted doctors still practice while in rehab www.msnbc.msn.com/id/22314486. Accessed July 5, 2008.
13. Glauser J. NPDB: malpractice, incompetency, and consent to settle. Emerg Med News. 2001;23(8):16-18.
14. Annas GJ. Medicine, death, and the criminal law. N Engl J Med. 1995;333:527-530.
15. In the matter of Spring, 380 Mass 629, 637 (1980)
Review Your Insurance Coverage
Insurance is one of the most necessary, and most hated, facts of life, particularly for physicians. We resent all the money we throw into a black hole every year, but in the event of an unforeseeable calamity it is indispensable.
Chances are that you're already insuring yourself against the worst calamities, but are you getting the most insurance for your premium money? To find out, it behooves you to meet with your insurance broker every couple of years and review all of your insurance coverage.
At first glance, malpractice insurance offers few opportunities to reduce costs, but more and more alternatives are becoming available as premiums on conventional policies continue to increase inexorably.
“Occurrence” policies remain the coverage of choice where they are available and affordable, but they are becoming an endangered species as fewer and fewer insurers remain willing to write them. “Claims made” policies are usually cheaper, and they provide the same coverage as long as you remain in practice. You will need “tail” coverage against belated claims after you retire, but some companies now provide free tail coverage once you've been insured for a minimum period (usually 5 years).
Other alternatives are gaining popularity as the demand for reasonably priced insurance increases. The most common, known as reciprocal exchanges, are very similar to traditional insurers but differ in certain aspects of start-up, funding, and operations. For example, most exchanges require policyholders to make capital contributions in addition to payment of premiums, at least in their early stages. You get your investment back, with interest, once the exchange becomes solvent.
Risk retention groups (RRGs) are similar to exchanges in that capital investments are usually required, but the owners are the insured parties themselves, who are ultimately responsible for all management and operational decisions, including the assurance of adequate funding. Most medical malpractice RRGs are licensed in Vermont or South Carolina because of favorable laws in those states, but they can be based in any state that allows them.
A third alternative is called a captive, which is generally defined as an insurance company formed by one or more noninsurance entities (such as medical practices) to write the insurance business of its owners. All participants are shareholders and all premiums (less administrative expenses) go toward enhancing the prosperity of the captive.
Reinsurance (usually not available to RRGs) protects the company against catastrophic losses. If all goes well, individual owners will be able to sell their shares at retirement for a nice profit—a profit that has grown tax free.
Exchanges, RRGs, and captives all carry risk: A few large claims can eat up all the profits and may even incur further financial obligations. But lack of profit is a certainty with traditional malpractice insurance.
If your current premiums are getting out of hand, ask your broker if any alternatives have become available in your area. While you are at it, you may want to review the rest of your insurance as well.
Worker's compensation insurance is mandatory in most states and heavily regulated, so there is little room for cutting expenses. Some states, however, do not require you, as the employer, to cover yourself, and eliminating that coverage could save you a substantial amount. This is only worth considering, of course, if you have adequate health and disability policies in place.
One additional policy to consider is employee practices liability insurance, which protects you from lawsuits brought by militant or disgruntled employees. I discussed this type of insurance in detail in last month's column, which can be found in the archives at www.skinandallergynews.com
If your financial situation has changed since your last insurance review, your life insurance needs have probably changed, too. As your retirement savings accumulate, less insurance is necessary. And if you own any expensive whole-life policies, you can probably convert them to much cheaper term insurance.
Disability insurance is not something to skimp on, but if you are approaching retirement age you may be able to decrease your coverage or even eliminate it if your retirement plan is far enough along.
Liability insurance is also no place to pinch pennies, but you might be able to add an umbrella policy providing comprehensive catastrophic coverage that may allow you to decrease your regular coverage or raise your deductible limits.
Health insurance offers numerous variables, with so many competing insurers and so many types of plans. If you still have expensive indemnity insurance, consider switching to an HMO, PPO, or any of the other plans in the alphabet soup available in today's market. Or consider raising your deductibles, which can lower premiums substantially.
If you're over 50 years of age, look into long-term care insurance. It's relatively inexpensive if you buy it while you're still healthy, and it could save you and your heirs a load of money on the other end.
Insurance is a necessary evil, but overinsurance is an unnecessary expense. Regular insurance reviews are the best way to be sure you have the right coverage, and only the right coverage.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Insurance is one of the most necessary, and most hated, facts of life, particularly for physicians. We resent all the money we throw into a black hole every year, but in the event of an unforeseeable calamity it is indispensable.
Chances are that you're already insuring yourself against the worst calamities, but are you getting the most insurance for your premium money? To find out, it behooves you to meet with your insurance broker every couple of years and review all of your insurance coverage.
At first glance, malpractice insurance offers few opportunities to reduce costs, but more and more alternatives are becoming available as premiums on conventional policies continue to increase inexorably.
“Occurrence” policies remain the coverage of choice where they are available and affordable, but they are becoming an endangered species as fewer and fewer insurers remain willing to write them. “Claims made” policies are usually cheaper, and they provide the same coverage as long as you remain in practice. You will need “tail” coverage against belated claims after you retire, but some companies now provide free tail coverage once you've been insured for a minimum period (usually 5 years).
Other alternatives are gaining popularity as the demand for reasonably priced insurance increases. The most common, known as reciprocal exchanges, are very similar to traditional insurers but differ in certain aspects of start-up, funding, and operations. For example, most exchanges require policyholders to make capital contributions in addition to payment of premiums, at least in their early stages. You get your investment back, with interest, once the exchange becomes solvent.
Risk retention groups (RRGs) are similar to exchanges in that capital investments are usually required, but the owners are the insured parties themselves, who are ultimately responsible for all management and operational decisions, including the assurance of adequate funding. Most medical malpractice RRGs are licensed in Vermont or South Carolina because of favorable laws in those states, but they can be based in any state that allows them.
A third alternative is called a captive, which is generally defined as an insurance company formed by one or more noninsurance entities (such as medical practices) to write the insurance business of its owners. All participants are shareholders and all premiums (less administrative expenses) go toward enhancing the prosperity of the captive.
Reinsurance (usually not available to RRGs) protects the company against catastrophic losses. If all goes well, individual owners will be able to sell their shares at retirement for a nice profit—a profit that has grown tax free.
Exchanges, RRGs, and captives all carry risk: A few large claims can eat up all the profits and may even incur further financial obligations. But lack of profit is a certainty with traditional malpractice insurance.
If your current premiums are getting out of hand, ask your broker if any alternatives have become available in your area. While you are at it, you may want to review the rest of your insurance as well.
Worker's compensation insurance is mandatory in most states and heavily regulated, so there is little room for cutting expenses. Some states, however, do not require you, as the employer, to cover yourself, and eliminating that coverage could save you a substantial amount. This is only worth considering, of course, if you have adequate health and disability policies in place.
One additional policy to consider is employee practices liability insurance, which protects you from lawsuits brought by militant or disgruntled employees. I discussed this type of insurance in detail in last month's column, which can be found in the archives at www.skinandallergynews.com
If your financial situation has changed since your last insurance review, your life insurance needs have probably changed, too. As your retirement savings accumulate, less insurance is necessary. And if you own any expensive whole-life policies, you can probably convert them to much cheaper term insurance.
Disability insurance is not something to skimp on, but if you are approaching retirement age you may be able to decrease your coverage or even eliminate it if your retirement plan is far enough along.
Liability insurance is also no place to pinch pennies, but you might be able to add an umbrella policy providing comprehensive catastrophic coverage that may allow you to decrease your regular coverage or raise your deductible limits.
Health insurance offers numerous variables, with so many competing insurers and so many types of plans. If you still have expensive indemnity insurance, consider switching to an HMO, PPO, or any of the other plans in the alphabet soup available in today's market. Or consider raising your deductibles, which can lower premiums substantially.
If you're over 50 years of age, look into long-term care insurance. It's relatively inexpensive if you buy it while you're still healthy, and it could save you and your heirs a load of money on the other end.
Insurance is a necessary evil, but overinsurance is an unnecessary expense. Regular insurance reviews are the best way to be sure you have the right coverage, and only the right coverage.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Insurance is one of the most necessary, and most hated, facts of life, particularly for physicians. We resent all the money we throw into a black hole every year, but in the event of an unforeseeable calamity it is indispensable.
Chances are that you're already insuring yourself against the worst calamities, but are you getting the most insurance for your premium money? To find out, it behooves you to meet with your insurance broker every couple of years and review all of your insurance coverage.
At first glance, malpractice insurance offers few opportunities to reduce costs, but more and more alternatives are becoming available as premiums on conventional policies continue to increase inexorably.
“Occurrence” policies remain the coverage of choice where they are available and affordable, but they are becoming an endangered species as fewer and fewer insurers remain willing to write them. “Claims made” policies are usually cheaper, and they provide the same coverage as long as you remain in practice. You will need “tail” coverage against belated claims after you retire, but some companies now provide free tail coverage once you've been insured for a minimum period (usually 5 years).
Other alternatives are gaining popularity as the demand for reasonably priced insurance increases. The most common, known as reciprocal exchanges, are very similar to traditional insurers but differ in certain aspects of start-up, funding, and operations. For example, most exchanges require policyholders to make capital contributions in addition to payment of premiums, at least in their early stages. You get your investment back, with interest, once the exchange becomes solvent.
Risk retention groups (RRGs) are similar to exchanges in that capital investments are usually required, but the owners are the insured parties themselves, who are ultimately responsible for all management and operational decisions, including the assurance of adequate funding. Most medical malpractice RRGs are licensed in Vermont or South Carolina because of favorable laws in those states, but they can be based in any state that allows them.
A third alternative is called a captive, which is generally defined as an insurance company formed by one or more noninsurance entities (such as medical practices) to write the insurance business of its owners. All participants are shareholders and all premiums (less administrative expenses) go toward enhancing the prosperity of the captive.
Reinsurance (usually not available to RRGs) protects the company against catastrophic losses. If all goes well, individual owners will be able to sell their shares at retirement for a nice profit—a profit that has grown tax free.
Exchanges, RRGs, and captives all carry risk: A few large claims can eat up all the profits and may even incur further financial obligations. But lack of profit is a certainty with traditional malpractice insurance.
If your current premiums are getting out of hand, ask your broker if any alternatives have become available in your area. While you are at it, you may want to review the rest of your insurance as well.
Worker's compensation insurance is mandatory in most states and heavily regulated, so there is little room for cutting expenses. Some states, however, do not require you, as the employer, to cover yourself, and eliminating that coverage could save you a substantial amount. This is only worth considering, of course, if you have adequate health and disability policies in place.
One additional policy to consider is employee practices liability insurance, which protects you from lawsuits brought by militant or disgruntled employees. I discussed this type of insurance in detail in last month's column, which can be found in the archives at www.skinandallergynews.com
If your financial situation has changed since your last insurance review, your life insurance needs have probably changed, too. As your retirement savings accumulate, less insurance is necessary. And if you own any expensive whole-life policies, you can probably convert them to much cheaper term insurance.
Disability insurance is not something to skimp on, but if you are approaching retirement age you may be able to decrease your coverage or even eliminate it if your retirement plan is far enough along.
Liability insurance is also no place to pinch pennies, but you might be able to add an umbrella policy providing comprehensive catastrophic coverage that may allow you to decrease your regular coverage or raise your deductible limits.
Health insurance offers numerous variables, with so many competing insurers and so many types of plans. If you still have expensive indemnity insurance, consider switching to an HMO, PPO, or any of the other plans in the alphabet soup available in today's market. Or consider raising your deductibles, which can lower premiums substantially.
If you're over 50 years of age, look into long-term care insurance. It's relatively inexpensive if you buy it while you're still healthy, and it could save you and your heirs a load of money on the other end.
Insurance is a necessary evil, but overinsurance is an unnecessary expense. Regular insurance reviews are the best way to be sure you have the right coverage, and only the right coverage.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
EHR Implementation … In Hindsight
DR. MICHAEL WOOLERY is a family physician and MS. ROBIN BROWN is the office manager at Family Physicians of Coshocton (Ohio) Inc.
If there's one thing we've learned about implementing an electronic health record system, it's that it doesn't make sense to train everyone about the big picture.
A brief overview makes sense. But learning all the details about how each employee uses the EHR isn't necessary and it's too much information. It overloads one's capacity to learn what's critical to know for one's job.
Before flipping the switch on our system about a year ago, we devoted 3 half days to training. Our preference had been to avoid closing the office for those days, so training was conducted on-site while the office was kept open for patient appointments. Half of the the staff participated in a morning session and the other half an afternoon session.
But all too often, people felt the tug of their work responsibilities and they couldn't focus on the training. In hindsight, it would have made more sense to close the office for those days and to conduct the training off site.
In our practice, we have seven full-time family physicians, 18 support staff members, seven nurses, one physician assistant, and two nurse practitioners. Attempting to train each of those employee groups together on how to use the EHR proved counterproductive. A better approach would have been to conduct shorter training sessions geared toward what individuals needed to know to get up and running. After 3–4 weeks of using the system, another session would then have been helpful to address problems and help maximize efficiencies.
Among the most helpful aspects of our EHR implementation was the fact that our vendor, iMedica, arranged to speak with us during weekly teleconferences for 10 months. These meetings started as we were gearing up for implementation and continued for several months afterward. Having this routine contact was very helpful and something that wewould encourage anyone considering investing in an EHR system to request.
We also took the opportunity to test-drive the tablet device that we would be using to enter patient information into the system and to request information from a database. Trying out this device for 60 days before we went live helped many of us develop a comfort level with the hardware.
Any practice that goes through the implementation of an EHR has to be prepared to take a temporary financial hit. Every physician in our practice had to cut their number of appointments back by half while they became used to using the EHR system. It took about 2 months for the practice's patient appointment schedule to return to normal.
To minimize the financial burden, we phased in the rollout by having a couple of physicians make the switch from paper to EHR each week, rather than converting everyone all at once. We wisely had our most computer-savvy physicians make the transition first. This most willing and able group went through the growing pains and passed along their tips to the self-described Luddites who watched for a while before having to switch from paper. That tactic worked well and helped the transition go smoothly.
One really nice feature of an EHR system is that it allows labs to automatically send their results to patient medical charts. But this feature is also enormously complicated to arrange.
No matter how many times your EHR vendor has worked with multiple interfaces, it always takes more time than expected to get multiple computer systems to speak to one another. So insist on starting this process early as soon as you select your EHR vendor.
DR. MICHAEL WOOLERY is a family physician and MS. ROBIN BROWN is the office manager at Family Physicians of Coshocton (Ohio) Inc.
If there's one thing we've learned about implementing an electronic health record system, it's that it doesn't make sense to train everyone about the big picture.
A brief overview makes sense. But learning all the details about how each employee uses the EHR isn't necessary and it's too much information. It overloads one's capacity to learn what's critical to know for one's job.
Before flipping the switch on our system about a year ago, we devoted 3 half days to training. Our preference had been to avoid closing the office for those days, so training was conducted on-site while the office was kept open for patient appointments. Half of the the staff participated in a morning session and the other half an afternoon session.
But all too often, people felt the tug of their work responsibilities and they couldn't focus on the training. In hindsight, it would have made more sense to close the office for those days and to conduct the training off site.
In our practice, we have seven full-time family physicians, 18 support staff members, seven nurses, one physician assistant, and two nurse practitioners. Attempting to train each of those employee groups together on how to use the EHR proved counterproductive. A better approach would have been to conduct shorter training sessions geared toward what individuals needed to know to get up and running. After 3–4 weeks of using the system, another session would then have been helpful to address problems and help maximize efficiencies.
Among the most helpful aspects of our EHR implementation was the fact that our vendor, iMedica, arranged to speak with us during weekly teleconferences for 10 months. These meetings started as we were gearing up for implementation and continued for several months afterward. Having this routine contact was very helpful and something that wewould encourage anyone considering investing in an EHR system to request.
We also took the opportunity to test-drive the tablet device that we would be using to enter patient information into the system and to request information from a database. Trying out this device for 60 days before we went live helped many of us develop a comfort level with the hardware.
Any practice that goes through the implementation of an EHR has to be prepared to take a temporary financial hit. Every physician in our practice had to cut their number of appointments back by half while they became used to using the EHR system. It took about 2 months for the practice's patient appointment schedule to return to normal.
To minimize the financial burden, we phased in the rollout by having a couple of physicians make the switch from paper to EHR each week, rather than converting everyone all at once. We wisely had our most computer-savvy physicians make the transition first. This most willing and able group went through the growing pains and passed along their tips to the self-described Luddites who watched for a while before having to switch from paper. That tactic worked well and helped the transition go smoothly.
One really nice feature of an EHR system is that it allows labs to automatically send their results to patient medical charts. But this feature is also enormously complicated to arrange.
No matter how many times your EHR vendor has worked with multiple interfaces, it always takes more time than expected to get multiple computer systems to speak to one another. So insist on starting this process early as soon as you select your EHR vendor.
DR. MICHAEL WOOLERY is a family physician and MS. ROBIN BROWN is the office manager at Family Physicians of Coshocton (Ohio) Inc.
If there's one thing we've learned about implementing an electronic health record system, it's that it doesn't make sense to train everyone about the big picture.
A brief overview makes sense. But learning all the details about how each employee uses the EHR isn't necessary and it's too much information. It overloads one's capacity to learn what's critical to know for one's job.
Before flipping the switch on our system about a year ago, we devoted 3 half days to training. Our preference had been to avoid closing the office for those days, so training was conducted on-site while the office was kept open for patient appointments. Half of the the staff participated in a morning session and the other half an afternoon session.
But all too often, people felt the tug of their work responsibilities and they couldn't focus on the training. In hindsight, it would have made more sense to close the office for those days and to conduct the training off site.
In our practice, we have seven full-time family physicians, 18 support staff members, seven nurses, one physician assistant, and two nurse practitioners. Attempting to train each of those employee groups together on how to use the EHR proved counterproductive. A better approach would have been to conduct shorter training sessions geared toward what individuals needed to know to get up and running. After 3–4 weeks of using the system, another session would then have been helpful to address problems and help maximize efficiencies.
Among the most helpful aspects of our EHR implementation was the fact that our vendor, iMedica, arranged to speak with us during weekly teleconferences for 10 months. These meetings started as we were gearing up for implementation and continued for several months afterward. Having this routine contact was very helpful and something that wewould encourage anyone considering investing in an EHR system to request.
We also took the opportunity to test-drive the tablet device that we would be using to enter patient information into the system and to request information from a database. Trying out this device for 60 days before we went live helped many of us develop a comfort level with the hardware.
Any practice that goes through the implementation of an EHR has to be prepared to take a temporary financial hit. Every physician in our practice had to cut their number of appointments back by half while they became used to using the EHR system. It took about 2 months for the practice's patient appointment schedule to return to normal.
To minimize the financial burden, we phased in the rollout by having a couple of physicians make the switch from paper to EHR each week, rather than converting everyone all at once. We wisely had our most computer-savvy physicians make the transition first. This most willing and able group went through the growing pains and passed along their tips to the self-described Luddites who watched for a while before having to switch from paper. That tactic worked well and helped the transition go smoothly.
One really nice feature of an EHR system is that it allows labs to automatically send their results to patient medical charts. But this feature is also enormously complicated to arrange.
No matter how many times your EHR vendor has worked with multiple interfaces, it always takes more time than expected to get multiple computer systems to speak to one another. So insist on starting this process early as soon as you select your EHR vendor.