User login
Bill by Time Spent on Case
In my recent columns, I addressed documentation guidelines with respect to the three key components: history, exam, and medical decision-making. However, time is considered the fourth key component.
Time-based billing places significant emphasis on the duration of the hospitalist-patient encounter more so than the detail or quality of the documentation. This month, I’ll focus on the guidelines for reporting inpatient hospital services based on time.
Counseling, Coordination
Hospitalists try to make their rounds as efficient as possible while still upholding a high standard of care. It is not unusual for a patient encounter to vary from the norm of updating the history, performing the necessary exam, and implementing the plan.
In fact, hospitalists often counsel patients with newly diagnosed conditions or when treatment options seem extensive and complicated. Based on these circumstances, physicians can document only a brief history and exam or none at all, since the bulk of the encounter focuses on medical decision-making, counseling, and coordination of care. Despite the minimal documentation compared with other physician services, it still is possible to report something more than the lowest service level (e.g., subsequent hospital care, 99231).
To use time as the determining factor for the visit level, more than 50% of the total visit time must involve counseling/coordination of care. The total visit time encompasses both the face-to-face time spent with the patient at the bedside and the additional time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers. Physicians providing care in academic settings cannot contribute teaching time toward the total visit time. Further, only the attending physician’s time counts.
Documentation
Hospitalists must document events during the patient encounter. There may be little or no history and an exam and counseling may dominate the entire visit.
Physicians must document both the counseling/coordination of care time and total visit time. The format may vary: “Total visit time = 25 minutes; more than 50% spent counseling/coordinating care,” or “20 of 25 minutes spent counseling/coordinating care.” Any given payer may prefer one documentation style over another. It always is best to query payers and review their documentation standards to determine the local preference.
In addition to the time, physicians must document the medical decision-making and details of the counseling/coordination of care. For example, patients with newly diagnosed diabetes need to be educated about their condition, lifestyle, and medication requirements. Physicians should include information regarding these factors in their progress notes as necessary.
Family Discussions
As noted in my previous article on critical care services (March 2008, p. 18), family discussions can contribute toward counseling/coordination of care time when:
- The patient is unable or clinically incompetent to participate in discussions;
- Time is spent on the unit/floor with family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; or
- The conversation bears directly on the management of the patient.
Prolonged Care
A physician makes his rounds in the morning. He cares for a 72-year-old female with diabetes, end-stage renal disease, and hypertension. In the afternoon, he returns to find the family waiting with questions. He spends an additional 30 minutes speaking at the bedside with the patient and family. The additional afternoon effort may be captured as prolonged care if both services are documented appropriately.
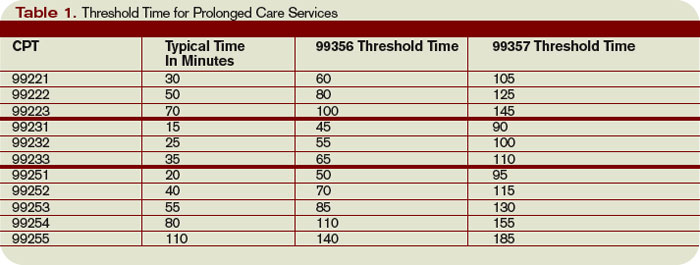
For inpatient services, CPT defines code 99356 as the first hour of prolonged physician services requiring face-to-face patient contact beyond the usual services (reportable after the initial 30 minutes). Code 99357 is used for each additional 30 minutes of prolonged care beyond the first hour (reportable after the first 15 minutes of each additional segment). Both codes are considered add-on codes and cannot be reported alone on a claim form; a primary code must be reported. Code 99357 must be used with 99356, and 99356 must be reported with one of the following inpatient service [primary] codes: 99221-99223, 99231-99233, or 99251-99255.
Prolonged care employs the concept of threshold time. This means total face-to-face physician visit time must exceed the time requirements associated with the primary codes by 30 minutes (e.g., 99232 plus 99356 = 25 minutes plus 30 minutes = 55 total face-to-face attending visit minutes). Accordingly, the physician must document the total face-to-face time spent during each portion of care in two separate notes or in one cumulative note. Be aware that this varies from the standard reporting of counseling and/or coordination of care time in that the physician must meet the threshold face-to-face-time requirements (see Table 1, left), making prolonged care services inefficient. When two providers from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service. To reiterate, 99356 must be reported on the same invoice as the primary visit code (e.g., 99232). Be sure once again to query payers, because most non-Medicare insurers do not recognize these codes. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
In my recent columns, I addressed documentation guidelines with respect to the three key components: history, exam, and medical decision-making. However, time is considered the fourth key component.
Time-based billing places significant emphasis on the duration of the hospitalist-patient encounter more so than the detail or quality of the documentation. This month, I’ll focus on the guidelines for reporting inpatient hospital services based on time.
Counseling, Coordination
Hospitalists try to make their rounds as efficient as possible while still upholding a high standard of care. It is not unusual for a patient encounter to vary from the norm of updating the history, performing the necessary exam, and implementing the plan.
In fact, hospitalists often counsel patients with newly diagnosed conditions or when treatment options seem extensive and complicated. Based on these circumstances, physicians can document only a brief history and exam or none at all, since the bulk of the encounter focuses on medical decision-making, counseling, and coordination of care. Despite the minimal documentation compared with other physician services, it still is possible to report something more than the lowest service level (e.g., subsequent hospital care, 99231).
To use time as the determining factor for the visit level, more than 50% of the total visit time must involve counseling/coordination of care. The total visit time encompasses both the face-to-face time spent with the patient at the bedside and the additional time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers. Physicians providing care in academic settings cannot contribute teaching time toward the total visit time. Further, only the attending physician’s time counts.
Documentation
Hospitalists must document events during the patient encounter. There may be little or no history and an exam and counseling may dominate the entire visit.
Physicians must document both the counseling/coordination of care time and total visit time. The format may vary: “Total visit time = 25 minutes; more than 50% spent counseling/coordinating care,” or “20 of 25 minutes spent counseling/coordinating care.” Any given payer may prefer one documentation style over another. It always is best to query payers and review their documentation standards to determine the local preference.
In addition to the time, physicians must document the medical decision-making and details of the counseling/coordination of care. For example, patients with newly diagnosed diabetes need to be educated about their condition, lifestyle, and medication requirements. Physicians should include information regarding these factors in their progress notes as necessary.
Family Discussions
As noted in my previous article on critical care services (March 2008, p. 18), family discussions can contribute toward counseling/coordination of care time when:
- The patient is unable or clinically incompetent to participate in discussions;
- Time is spent on the unit/floor with family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; or
- The conversation bears directly on the management of the patient.
Prolonged Care
A physician makes his rounds in the morning. He cares for a 72-year-old female with diabetes, end-stage renal disease, and hypertension. In the afternoon, he returns to find the family waiting with questions. He spends an additional 30 minutes speaking at the bedside with the patient and family. The additional afternoon effort may be captured as prolonged care if both services are documented appropriately.
For inpatient services, CPT defines code 99356 as the first hour of prolonged physician services requiring face-to-face patient contact beyond the usual services (reportable after the initial 30 minutes). Code 99357 is used for each additional 30 minutes of prolonged care beyond the first hour (reportable after the first 15 minutes of each additional segment). Both codes are considered add-on codes and cannot be reported alone on a claim form; a primary code must be reported. Code 99357 must be used with 99356, and 99356 must be reported with one of the following inpatient service [primary] codes: 99221-99223, 99231-99233, or 99251-99255.
Prolonged care employs the concept of threshold time. This means total face-to-face physician visit time must exceed the time requirements associated with the primary codes by 30 minutes (e.g., 99232 plus 99356 = 25 minutes plus 30 minutes = 55 total face-to-face attending visit minutes). Accordingly, the physician must document the total face-to-face time spent during each portion of care in two separate notes or in one cumulative note. Be aware that this varies from the standard reporting of counseling and/or coordination of care time in that the physician must meet the threshold face-to-face-time requirements (see Table 1, left), making prolonged care services inefficient. When two providers from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service. To reiterate, 99356 must be reported on the same invoice as the primary visit code (e.g., 99232). Be sure once again to query payers, because most non-Medicare insurers do not recognize these codes. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
In my recent columns, I addressed documentation guidelines with respect to the three key components: history, exam, and medical decision-making. However, time is considered the fourth key component.
Time-based billing places significant emphasis on the duration of the hospitalist-patient encounter more so than the detail or quality of the documentation. This month, I’ll focus on the guidelines for reporting inpatient hospital services based on time.
Counseling, Coordination
Hospitalists try to make their rounds as efficient as possible while still upholding a high standard of care. It is not unusual for a patient encounter to vary from the norm of updating the history, performing the necessary exam, and implementing the plan.
In fact, hospitalists often counsel patients with newly diagnosed conditions or when treatment options seem extensive and complicated. Based on these circumstances, physicians can document only a brief history and exam or none at all, since the bulk of the encounter focuses on medical decision-making, counseling, and coordination of care. Despite the minimal documentation compared with other physician services, it still is possible to report something more than the lowest service level (e.g., subsequent hospital care, 99231).
To use time as the determining factor for the visit level, more than 50% of the total visit time must involve counseling/coordination of care. The total visit time encompasses both the face-to-face time spent with the patient at the bedside and the additional time spent on the unit/floor reviewing data, obtaining relevant patient information, and discussing the case with other involved healthcare providers. Physicians providing care in academic settings cannot contribute teaching time toward the total visit time. Further, only the attending physician’s time counts.
Documentation
Hospitalists must document events during the patient encounter. There may be little or no history and an exam and counseling may dominate the entire visit.
Physicians must document both the counseling/coordination of care time and total visit time. The format may vary: “Total visit time = 25 minutes; more than 50% spent counseling/coordinating care,” or “20 of 25 minutes spent counseling/coordinating care.” Any given payer may prefer one documentation style over another. It always is best to query payers and review their documentation standards to determine the local preference.
In addition to the time, physicians must document the medical decision-making and details of the counseling/coordination of care. For example, patients with newly diagnosed diabetes need to be educated about their condition, lifestyle, and medication requirements. Physicians should include information regarding these factors in their progress notes as necessary.
Family Discussions
As noted in my previous article on critical care services (March 2008, p. 18), family discussions can contribute toward counseling/coordination of care time when:
- The patient is unable or clinically incompetent to participate in discussions;
- Time is spent on the unit/floor with family members or surrogate decision makers obtaining a medical history, reviewing the patient’s condition or prognosis, or discussing treatment or limitation(s) of treatment; or
- The conversation bears directly on the management of the patient.
Prolonged Care
A physician makes his rounds in the morning. He cares for a 72-year-old female with diabetes, end-stage renal disease, and hypertension. In the afternoon, he returns to find the family waiting with questions. He spends an additional 30 minutes speaking at the bedside with the patient and family. The additional afternoon effort may be captured as prolonged care if both services are documented appropriately.
For inpatient services, CPT defines code 99356 as the first hour of prolonged physician services requiring face-to-face patient contact beyond the usual services (reportable after the initial 30 minutes). Code 99357 is used for each additional 30 minutes of prolonged care beyond the first hour (reportable after the first 15 minutes of each additional segment). Both codes are considered add-on codes and cannot be reported alone on a claim form; a primary code must be reported. Code 99357 must be used with 99356, and 99356 must be reported with one of the following inpatient service [primary] codes: 99221-99223, 99231-99233, or 99251-99255.
Prolonged care employs the concept of threshold time. This means total face-to-face physician visit time must exceed the time requirements associated with the primary codes by 30 minutes (e.g., 99232 plus 99356 = 25 minutes plus 30 minutes = 55 total face-to-face attending visit minutes). Accordingly, the physician must document the total face-to-face time spent during each portion of care in two separate notes or in one cumulative note. Be aware that this varies from the standard reporting of counseling and/or coordination of care time in that the physician must meet the threshold face-to-face-time requirements (see Table 1, left), making prolonged care services inefficient. When two providers from the same group practice split the threshold time (e.g., physician A provided morning rounds, and physician B spoke with the family in the afternoon), only one physician can report the cumulative service. To reiterate, 99356 must be reported on the same invoice as the primary visit code (e.g., 99232). Be sure once again to query payers, because most non-Medicare insurers do not recognize these codes. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Use this quick gauge for retirement planning
If one issue dominates all others in financial planning, it’s retirement. Every client, at some point, asks two timeless questions of me: How much will I need in retirement? And how much do I need to save now to get there?
My answer is always the same: It depends.
The mobile home scenario
Depending on the client, I have proposed that he (or she) could retire today—if he’s willing to inhabit a mobile home and, probably, lose his spouse and custody of the kids. Sometimes clients smile at my proposal, sometimes they don’t.
Still, the mobile-home scenario is a good starting point for discussion because retirement, from a financial perspective, depends almost entirely on spending habits. Tell me how much you will spend in retirement and I can calculate, to some degree, what your portfolio should be and how much you have to save to get there. The trouble is, unless you are close to retirement, you can’t tell me how things will change between now and then.
A wish, and a plan
One of my oldest clients—dating back more than 20 years—was a senior executive with a major corporation until he retired last year. When we were talking about projections, at one point, he said that, in business, a 1-year projection may be accurate but a 5-year game plan is simply wishful thinking. So many things can change.
In personal financial planning, the same is true. If your retirement is years away, you could change jobs and spouse, and have children (or more of them) with varying college costs. Really, the only thing to do is to make some basic assumptions about the future based on your spending today, take into account likely future events, and, then, begin the process.
So, let’s start with the basics and work backward. This quick look at retirement planning focuses on three factors.
The 4% to 6% drawdown
First, how much can you draw off your portfolio without running out of money—or still have a relatively high probability that you will not run out of money? A multitude of studies on this topic have incorporated hundreds of economic and investment permutations (referred to as Monte Carlo simulations).
The clear consensus is that a balanced portfolio of stocks and bonds should yield an income stream of 4% to 6% annually, with a good chance the principal remains intact or grows. Pushing the withdrawal rate past 6% can be done, but you have to be willing to cut back during down markets.
My experience is that the high side of this range has worked well. But these clients have been in the position to cut back on expenses in down years.
Pay off that mortgage?
Second, paying off all debt before you retire is not an investment decision. Arguably, if your investments perform well and your mortgage is a low-interest one, paying it off may not be a good idea.
The reason planners, myself included, recommend paying off the mortgage is to reduce one’s fixed costs in retirement. Having low fixed costs but higher discretionary costs gives you the ability to cut back if necessary. Flexibility of spending can be as important as investment performance.
How much you’ll spend (really)
Third, you’ll need to make a realistic appraisal of your spending habits. My experience tells me that everyone, including me, lies about spending. When I began my practice, I asked clients to submit a detailed budget of their expenses over the past month. But one month did not cover all expenses.
So we tried three months, then a year—and still projections were off! I then tried the same on my own expenses and found that I could never capture all expenses. Or, more often, we considered such expenses as a new muffler for the car or a new roof to be onetime events. Wrong.
My personal and, I think, more accurate, preference is to simply determine how much you saved at the end of the year, subtract that from your income after taxes, and assume you spent the rest. This eliminates hours of trying to figure out where the money went. The only adjustment to this calculation would be to subtract those expenses that are eliminated at retirement—the mortgage and the costs of raising children, I would hope.
Running the numbers
Now you are armed with just about all you need. To take an example, suppose you have determined that you’re spending roughly $100,000 a year after taxes. If your portfolio will return 6% (net, 4% after taxes), then simply multiply by 25 (the inverse of 4%) to come up with the portfolio you’ll need: $2.5 million. If you want to be very conservative, assume a 4% return (3% net), and multiply by 33 to yield a needed retirement portfolio of $3.3 million.
- Take what you spend in a year
- Multiply that by the inverse of a 4% return on portfolio, or 25
Example:
You spend $100,000 a year
- $100,000 × 25
- You need $2.5 million
Many financial Web sites do allow you to calculate how much to save, however. A site that covers the gamut of calculations is www.dinkytown.com. One piece of information it asks for that is hard to define is the expected return on investments during preretirement years. With a portfolio tilted toward growth, using a pretax return of 7% to 9% is a safe assumption. Running the calculation at both 7% and 9% sets the parameters for how much you need to be saving now.
Hopefully, the number you come up with will not break the bank for you. But if it does, there is always that deluxe mobile home.
Go to www.dinkytown.com to evaluate your retirement savings, prepped with:
- Your age (now)
- Household income
- Rate of return before retirement
- Percentage of income to contribute
- Years of retirement income
- Expected rate of inflation
- Age at retirement
- Current retirement savings
- Rate of return during retirement
- Expected salary increases
- Percentage of income at retirement
If one issue dominates all others in financial planning, it’s retirement. Every client, at some point, asks two timeless questions of me: How much will I need in retirement? And how much do I need to save now to get there?
My answer is always the same: It depends.
The mobile home scenario
Depending on the client, I have proposed that he (or she) could retire today—if he’s willing to inhabit a mobile home and, probably, lose his spouse and custody of the kids. Sometimes clients smile at my proposal, sometimes they don’t.
Still, the mobile-home scenario is a good starting point for discussion because retirement, from a financial perspective, depends almost entirely on spending habits. Tell me how much you will spend in retirement and I can calculate, to some degree, what your portfolio should be and how much you have to save to get there. The trouble is, unless you are close to retirement, you can’t tell me how things will change between now and then.
A wish, and a plan
One of my oldest clients—dating back more than 20 years—was a senior executive with a major corporation until he retired last year. When we were talking about projections, at one point, he said that, in business, a 1-year projection may be accurate but a 5-year game plan is simply wishful thinking. So many things can change.
In personal financial planning, the same is true. If your retirement is years away, you could change jobs and spouse, and have children (or more of them) with varying college costs. Really, the only thing to do is to make some basic assumptions about the future based on your spending today, take into account likely future events, and, then, begin the process.
So, let’s start with the basics and work backward. This quick look at retirement planning focuses on three factors.
The 4% to 6% drawdown
First, how much can you draw off your portfolio without running out of money—or still have a relatively high probability that you will not run out of money? A multitude of studies on this topic have incorporated hundreds of economic and investment permutations (referred to as Monte Carlo simulations).
The clear consensus is that a balanced portfolio of stocks and bonds should yield an income stream of 4% to 6% annually, with a good chance the principal remains intact or grows. Pushing the withdrawal rate past 6% can be done, but you have to be willing to cut back during down markets.
My experience is that the high side of this range has worked well. But these clients have been in the position to cut back on expenses in down years.
Pay off that mortgage?
Second, paying off all debt before you retire is not an investment decision. Arguably, if your investments perform well and your mortgage is a low-interest one, paying it off may not be a good idea.
The reason planners, myself included, recommend paying off the mortgage is to reduce one’s fixed costs in retirement. Having low fixed costs but higher discretionary costs gives you the ability to cut back if necessary. Flexibility of spending can be as important as investment performance.
How much you’ll spend (really)
Third, you’ll need to make a realistic appraisal of your spending habits. My experience tells me that everyone, including me, lies about spending. When I began my practice, I asked clients to submit a detailed budget of their expenses over the past month. But one month did not cover all expenses.
So we tried three months, then a year—and still projections were off! I then tried the same on my own expenses and found that I could never capture all expenses. Or, more often, we considered such expenses as a new muffler for the car or a new roof to be onetime events. Wrong.
My personal and, I think, more accurate, preference is to simply determine how much you saved at the end of the year, subtract that from your income after taxes, and assume you spent the rest. This eliminates hours of trying to figure out where the money went. The only adjustment to this calculation would be to subtract those expenses that are eliminated at retirement—the mortgage and the costs of raising children, I would hope.
Running the numbers
Now you are armed with just about all you need. To take an example, suppose you have determined that you’re spending roughly $100,000 a year after taxes. If your portfolio will return 6% (net, 4% after taxes), then simply multiply by 25 (the inverse of 4%) to come up with the portfolio you’ll need: $2.5 million. If you want to be very conservative, assume a 4% return (3% net), and multiply by 33 to yield a needed retirement portfolio of $3.3 million.
- Take what you spend in a year
- Multiply that by the inverse of a 4% return on portfolio, or 25
Example:
You spend $100,000 a year
- $100,000 × 25
- You need $2.5 million
Many financial Web sites do allow you to calculate how much to save, however. A site that covers the gamut of calculations is www.dinkytown.com. One piece of information it asks for that is hard to define is the expected return on investments during preretirement years. With a portfolio tilted toward growth, using a pretax return of 7% to 9% is a safe assumption. Running the calculation at both 7% and 9% sets the parameters for how much you need to be saving now.
Hopefully, the number you come up with will not break the bank for you. But if it does, there is always that deluxe mobile home.
Go to www.dinkytown.com to evaluate your retirement savings, prepped with:
- Your age (now)
- Household income
- Rate of return before retirement
- Percentage of income to contribute
- Years of retirement income
- Expected rate of inflation
- Age at retirement
- Current retirement savings
- Rate of return during retirement
- Expected salary increases
- Percentage of income at retirement
If one issue dominates all others in financial planning, it’s retirement. Every client, at some point, asks two timeless questions of me: How much will I need in retirement? And how much do I need to save now to get there?
My answer is always the same: It depends.
The mobile home scenario
Depending on the client, I have proposed that he (or she) could retire today—if he’s willing to inhabit a mobile home and, probably, lose his spouse and custody of the kids. Sometimes clients smile at my proposal, sometimes they don’t.
Still, the mobile-home scenario is a good starting point for discussion because retirement, from a financial perspective, depends almost entirely on spending habits. Tell me how much you will spend in retirement and I can calculate, to some degree, what your portfolio should be and how much you have to save to get there. The trouble is, unless you are close to retirement, you can’t tell me how things will change between now and then.
A wish, and a plan
One of my oldest clients—dating back more than 20 years—was a senior executive with a major corporation until he retired last year. When we were talking about projections, at one point, he said that, in business, a 1-year projection may be accurate but a 5-year game plan is simply wishful thinking. So many things can change.
In personal financial planning, the same is true. If your retirement is years away, you could change jobs and spouse, and have children (or more of them) with varying college costs. Really, the only thing to do is to make some basic assumptions about the future based on your spending today, take into account likely future events, and, then, begin the process.
So, let’s start with the basics and work backward. This quick look at retirement planning focuses on three factors.
The 4% to 6% drawdown
First, how much can you draw off your portfolio without running out of money—or still have a relatively high probability that you will not run out of money? A multitude of studies on this topic have incorporated hundreds of economic and investment permutations (referred to as Monte Carlo simulations).
The clear consensus is that a balanced portfolio of stocks and bonds should yield an income stream of 4% to 6% annually, with a good chance the principal remains intact or grows. Pushing the withdrawal rate past 6% can be done, but you have to be willing to cut back during down markets.
My experience is that the high side of this range has worked well. But these clients have been in the position to cut back on expenses in down years.
Pay off that mortgage?
Second, paying off all debt before you retire is not an investment decision. Arguably, if your investments perform well and your mortgage is a low-interest one, paying it off may not be a good idea.
The reason planners, myself included, recommend paying off the mortgage is to reduce one’s fixed costs in retirement. Having low fixed costs but higher discretionary costs gives you the ability to cut back if necessary. Flexibility of spending can be as important as investment performance.
How much you’ll spend (really)
Third, you’ll need to make a realistic appraisal of your spending habits. My experience tells me that everyone, including me, lies about spending. When I began my practice, I asked clients to submit a detailed budget of their expenses over the past month. But one month did not cover all expenses.
So we tried three months, then a year—and still projections were off! I then tried the same on my own expenses and found that I could never capture all expenses. Or, more often, we considered such expenses as a new muffler for the car or a new roof to be onetime events. Wrong.
My personal and, I think, more accurate, preference is to simply determine how much you saved at the end of the year, subtract that from your income after taxes, and assume you spent the rest. This eliminates hours of trying to figure out where the money went. The only adjustment to this calculation would be to subtract those expenses that are eliminated at retirement—the mortgage and the costs of raising children, I would hope.
Running the numbers
Now you are armed with just about all you need. To take an example, suppose you have determined that you’re spending roughly $100,000 a year after taxes. If your portfolio will return 6% (net, 4% after taxes), then simply multiply by 25 (the inverse of 4%) to come up with the portfolio you’ll need: $2.5 million. If you want to be very conservative, assume a 4% return (3% net), and multiply by 33 to yield a needed retirement portfolio of $3.3 million.
- Take what you spend in a year
- Multiply that by the inverse of a 4% return on portfolio, or 25
Example:
You spend $100,000 a year
- $100,000 × 25
- You need $2.5 million
Many financial Web sites do allow you to calculate how much to save, however. A site that covers the gamut of calculations is www.dinkytown.com. One piece of information it asks for that is hard to define is the expected return on investments during preretirement years. With a portfolio tilted toward growth, using a pretax return of 7% to 9% is a safe assumption. Running the calculation at both 7% and 9% sets the parameters for how much you need to be saving now.
Hopefully, the number you come up with will not break the bank for you. But if it does, there is always that deluxe mobile home.
Go to www.dinkytown.com to evaluate your retirement savings, prepped with:
- Your age (now)
- Household income
- Rate of return before retirement
- Percentage of income to contribute
- Years of retirement income
- Expected rate of inflation
- Age at retirement
- Current retirement savings
- Rate of return during retirement
- Expected salary increases
- Percentage of income at retirement
Medical Verdicts
6 hours in lithotomy position leads to nerve damage
FOLLOWING A HYSTERECTOMY, a patient remained in the hospital for 18 days, during which time she developed agonizing pain in her legs. Also, her kidneys failed and she needed many rounds of dialysis.
- PATIENT’S CLAIM The physician was negligent for failing to reposition or lower her legs during the 6-hour surgery, for which she remained in a lithotomy position with her legs elevated. This caused compartment syndrome, as well as injury to motor and sensory femoral nerves and sciatic nerve involvement of the superficial perineal nerve.
- DOCTOR’S DEFENSE Although injury to the legs can occur if left in the lithotomy position for an extended time, the patient could not be repositioned because she was experiencing life-threatening hemorrhaging.
- VERDICT $700,000 California award, including $450,000 for economic losses and $250,000 for noneconomic losses.
Lost Pap smear delays diagnosis and treatment
A 36-YEAR-OLD WOMAN went to a new physician for gynecologic care. A Pap smear was not performed at her first visit, as her last one—only 6 months earlier—was normal. She was advised to return for another test in 6 months.
A Pap smear was performed at the patient’s next annual exam 10 months later. The physician said he would contact her if the results were abnormal. Three months later, the patient complained of vaginal discharge, and then continued to contact the physician’s office concerning urinary tract infections.
At her next annual exam the following year, a Pap smear was performed, during which the cervix bled easily. She learned that the results of the earlier Pap smear were not in the record. The current Pap test indicated low-grade intra-epithelial lesion and mild dysplasia with possible extension into the glands.
A few days after learning of the results, the patient underwent a colposcopy and biopsy. The pathology report revealed severe dysplasia with involvement of the endocervical glands. The physician noted at this time that the lab had never received the previous year’s specimen.
Two months later, the patient underwent a cone biopsy. Pathologic evaluation indicated moderate to severe dysplasia with extensive involvement in several areas. The patient had a vaginal hysterectomy for cervical carcinoma in situ 3 months later.
- PATIENT’S CLAIM If the physician had followed up on the results of the first Pap smear, he would have learned that the specimen never reached the laboratory, and he would have contacted the patient to have a repeat Pap test—instead of letting more than 2 years pass between two Pap smears. An earlier cancer diagnosis would have allowed her to undergo ablative therapy and avoid the hysterectomy.
- DOCTOR’S DEFENSE Nothing would have changed the patient’s outcome.
- VERDICT $500,000 Massachusetts settlement.
Sphincter laceration causes bowel and sexual problems
A 31-YEAR-OLD WOMAN gave birth by forceps delivery with the fetus at +2 station. The mother suffered a fourth degree laceration, which the OB tried to—but could not—repair. After discharge, the patient experienced constipation and difficulty controlling her bowel movements and could not have sexual intercourse. Nine months later, she underwent vaginal reconstruction, but impairment to her bowels and difficulties with intercourse are expected to continue.
- PATIENT’S CLAIM The physician was negligent during the delivery and repair of the laceration. The repair should have been performed by a physician with colorectal training and experience in such procedures. Also, forceps were used prematurely.
- DOCTOR’S DEFENSE Sphincter laceration is a recognized complication of delivery. Also, a colorectal surgeon was not needed.
- VERDICT $1,726,000 Pennsylvania verdict; recovery was limited by a confidential high–low agreement.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
6 hours in lithotomy position leads to nerve damage
FOLLOWING A HYSTERECTOMY, a patient remained in the hospital for 18 days, during which time she developed agonizing pain in her legs. Also, her kidneys failed and she needed many rounds of dialysis.
- PATIENT’S CLAIM The physician was negligent for failing to reposition or lower her legs during the 6-hour surgery, for which she remained in a lithotomy position with her legs elevated. This caused compartment syndrome, as well as injury to motor and sensory femoral nerves and sciatic nerve involvement of the superficial perineal nerve.
- DOCTOR’S DEFENSE Although injury to the legs can occur if left in the lithotomy position for an extended time, the patient could not be repositioned because she was experiencing life-threatening hemorrhaging.
- VERDICT $700,000 California award, including $450,000 for economic losses and $250,000 for noneconomic losses.
Lost Pap smear delays diagnosis and treatment
A 36-YEAR-OLD WOMAN went to a new physician for gynecologic care. A Pap smear was not performed at her first visit, as her last one—only 6 months earlier—was normal. She was advised to return for another test in 6 months.
A Pap smear was performed at the patient’s next annual exam 10 months later. The physician said he would contact her if the results were abnormal. Three months later, the patient complained of vaginal discharge, and then continued to contact the physician’s office concerning urinary tract infections.
At her next annual exam the following year, a Pap smear was performed, during which the cervix bled easily. She learned that the results of the earlier Pap smear were not in the record. The current Pap test indicated low-grade intra-epithelial lesion and mild dysplasia with possible extension into the glands.
A few days after learning of the results, the patient underwent a colposcopy and biopsy. The pathology report revealed severe dysplasia with involvement of the endocervical glands. The physician noted at this time that the lab had never received the previous year’s specimen.
Two months later, the patient underwent a cone biopsy. Pathologic evaluation indicated moderate to severe dysplasia with extensive involvement in several areas. The patient had a vaginal hysterectomy for cervical carcinoma in situ 3 months later.
- PATIENT’S CLAIM If the physician had followed up on the results of the first Pap smear, he would have learned that the specimen never reached the laboratory, and he would have contacted the patient to have a repeat Pap test—instead of letting more than 2 years pass between two Pap smears. An earlier cancer diagnosis would have allowed her to undergo ablative therapy and avoid the hysterectomy.
- DOCTOR’S DEFENSE Nothing would have changed the patient’s outcome.
- VERDICT $500,000 Massachusetts settlement.
Sphincter laceration causes bowel and sexual problems
A 31-YEAR-OLD WOMAN gave birth by forceps delivery with the fetus at +2 station. The mother suffered a fourth degree laceration, which the OB tried to—but could not—repair. After discharge, the patient experienced constipation and difficulty controlling her bowel movements and could not have sexual intercourse. Nine months later, she underwent vaginal reconstruction, but impairment to her bowels and difficulties with intercourse are expected to continue.
- PATIENT’S CLAIM The physician was negligent during the delivery and repair of the laceration. The repair should have been performed by a physician with colorectal training and experience in such procedures. Also, forceps were used prematurely.
- DOCTOR’S DEFENSE Sphincter laceration is a recognized complication of delivery. Also, a colorectal surgeon was not needed.
- VERDICT $1,726,000 Pennsylvania verdict; recovery was limited by a confidential high–low agreement.
6 hours in lithotomy position leads to nerve damage
FOLLOWING A HYSTERECTOMY, a patient remained in the hospital for 18 days, during which time she developed agonizing pain in her legs. Also, her kidneys failed and she needed many rounds of dialysis.
- PATIENT’S CLAIM The physician was negligent for failing to reposition or lower her legs during the 6-hour surgery, for which she remained in a lithotomy position with her legs elevated. This caused compartment syndrome, as well as injury to motor and sensory femoral nerves and sciatic nerve involvement of the superficial perineal nerve.
- DOCTOR’S DEFENSE Although injury to the legs can occur if left in the lithotomy position for an extended time, the patient could not be repositioned because she was experiencing life-threatening hemorrhaging.
- VERDICT $700,000 California award, including $450,000 for economic losses and $250,000 for noneconomic losses.
Lost Pap smear delays diagnosis and treatment
A 36-YEAR-OLD WOMAN went to a new physician for gynecologic care. A Pap smear was not performed at her first visit, as her last one—only 6 months earlier—was normal. She was advised to return for another test in 6 months.
A Pap smear was performed at the patient’s next annual exam 10 months later. The physician said he would contact her if the results were abnormal. Three months later, the patient complained of vaginal discharge, and then continued to contact the physician’s office concerning urinary tract infections.
At her next annual exam the following year, a Pap smear was performed, during which the cervix bled easily. She learned that the results of the earlier Pap smear were not in the record. The current Pap test indicated low-grade intra-epithelial lesion and mild dysplasia with possible extension into the glands.
A few days after learning of the results, the patient underwent a colposcopy and biopsy. The pathology report revealed severe dysplasia with involvement of the endocervical glands. The physician noted at this time that the lab had never received the previous year’s specimen.
Two months later, the patient underwent a cone biopsy. Pathologic evaluation indicated moderate to severe dysplasia with extensive involvement in several areas. The patient had a vaginal hysterectomy for cervical carcinoma in situ 3 months later.
- PATIENT’S CLAIM If the physician had followed up on the results of the first Pap smear, he would have learned that the specimen never reached the laboratory, and he would have contacted the patient to have a repeat Pap test—instead of letting more than 2 years pass between two Pap smears. An earlier cancer diagnosis would have allowed her to undergo ablative therapy and avoid the hysterectomy.
- DOCTOR’S DEFENSE Nothing would have changed the patient’s outcome.
- VERDICT $500,000 Massachusetts settlement.
Sphincter laceration causes bowel and sexual problems
A 31-YEAR-OLD WOMAN gave birth by forceps delivery with the fetus at +2 station. The mother suffered a fourth degree laceration, which the OB tried to—but could not—repair. After discharge, the patient experienced constipation and difficulty controlling her bowel movements and could not have sexual intercourse. Nine months later, she underwent vaginal reconstruction, but impairment to her bowels and difficulties with intercourse are expected to continue.
- PATIENT’S CLAIM The physician was negligent during the delivery and repair of the laceration. The repair should have been performed by a physician with colorectal training and experience in such procedures. Also, forceps were used prematurely.
- DOCTOR’S DEFENSE Sphincter laceration is a recognized complication of delivery. Also, a colorectal surgeon was not needed.
- VERDICT $1,726,000 Pennsylvania verdict; recovery was limited by a confidential high–low agreement.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Medical Verdicts: Only on the Web
Was bowel perforated during laparoscopy?
Patient, physician disagree
A 56-YEAR-OLD WOMAN underwent diagnostic laparoscopic surgery as an outpatient after she complained to her physician of abdominal pain. The evening after surgery, her husband called the physician to report that she was in pain. He was told that the pain was probably caused by gas and to have his wife telephone in the morning if pain persisted. The husband called 2 days later with the same complaint; 3 days after surgery, the woman was brought to an emergency room and admitted. Another physician performed further surgery and discovered two bowel perforations and an abdominal infection. The patient required colostomy for 5 months and underwent several more surgeries.
- PATIENT’S CLAIM The first physician was negligent for not diagnosing the bowel perforation in a timely manner. Also, the patient has ongoing bowel problems.
- DOCTOR’S DEFENSE Bowel perforation occurred after the patient left the hospital. No calls were made about the pain after surgery.
- VERDICT Missouri defense verdict.
Patient dies after surgery to repair second perforation
DURING A D&C PROCEDURE to remove a uterine mass, a gynecologist noted a small perforation in the patient’s uterine wall. During follow-up laparoscopic surgery, he repaired the uterine perforation and checked for other injuries, but failed to detect a small-bowel perforation. At discharge, he advised the patient to contact him if she suffered complications. At home, she began to deteriorate. Her husband took her back to her physician, who sent her to the hospital for emergency surgery to repair the bowel perforation. The patient suffered sepsis and necrosis, which led to septic shock and multiple-organ failure. She died the following week.
- PATIENT’S CLAIM The gynecologist failed to detect a small-bowel perforation during laparoscopic surgery to repair a prior small uterine perforation.
- DOCTOR’S DEFENSE Not reported.
- VERDICT Indiana defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Was bowel perforated during laparoscopy?
Patient, physician disagree
A 56-YEAR-OLD WOMAN underwent diagnostic laparoscopic surgery as an outpatient after she complained to her physician of abdominal pain. The evening after surgery, her husband called the physician to report that she was in pain. He was told that the pain was probably caused by gas and to have his wife telephone in the morning if pain persisted. The husband called 2 days later with the same complaint; 3 days after surgery, the woman was brought to an emergency room and admitted. Another physician performed further surgery and discovered two bowel perforations and an abdominal infection. The patient required colostomy for 5 months and underwent several more surgeries.
- PATIENT’S CLAIM The first physician was negligent for not diagnosing the bowel perforation in a timely manner. Also, the patient has ongoing bowel problems.
- DOCTOR’S DEFENSE Bowel perforation occurred after the patient left the hospital. No calls were made about the pain after surgery.
- VERDICT Missouri defense verdict.
Patient dies after surgery to repair second perforation
DURING A D&C PROCEDURE to remove a uterine mass, a gynecologist noted a small perforation in the patient’s uterine wall. During follow-up laparoscopic surgery, he repaired the uterine perforation and checked for other injuries, but failed to detect a small-bowel perforation. At discharge, he advised the patient to contact him if she suffered complications. At home, she began to deteriorate. Her husband took her back to her physician, who sent her to the hospital for emergency surgery to repair the bowel perforation. The patient suffered sepsis and necrosis, which led to septic shock and multiple-organ failure. She died the following week.
- PATIENT’S CLAIM The gynecologist failed to detect a small-bowel perforation during laparoscopic surgery to repair a prior small uterine perforation.
- DOCTOR’S DEFENSE Not reported.
- VERDICT Indiana defense verdict.
Was bowel perforated during laparoscopy?
Patient, physician disagree
A 56-YEAR-OLD WOMAN underwent diagnostic laparoscopic surgery as an outpatient after she complained to her physician of abdominal pain. The evening after surgery, her husband called the physician to report that she was in pain. He was told that the pain was probably caused by gas and to have his wife telephone in the morning if pain persisted. The husband called 2 days later with the same complaint; 3 days after surgery, the woman was brought to an emergency room and admitted. Another physician performed further surgery and discovered two bowel perforations and an abdominal infection. The patient required colostomy for 5 months and underwent several more surgeries.
- PATIENT’S CLAIM The first physician was negligent for not diagnosing the bowel perforation in a timely manner. Also, the patient has ongoing bowel problems.
- DOCTOR’S DEFENSE Bowel perforation occurred after the patient left the hospital. No calls were made about the pain after surgery.
- VERDICT Missouri defense verdict.
Patient dies after surgery to repair second perforation
DURING A D&C PROCEDURE to remove a uterine mass, a gynecologist noted a small perforation in the patient’s uterine wall. During follow-up laparoscopic surgery, he repaired the uterine perforation and checked for other injuries, but failed to detect a small-bowel perforation. At discharge, he advised the patient to contact him if she suffered complications. At home, she began to deteriorate. Her husband took her back to her physician, who sent her to the hospital for emergency surgery to repair the bowel perforation. The patient suffered sepsis and necrosis, which led to septic shock and multiple-organ failure. She died the following week.
- PATIENT’S CLAIM The gynecologist failed to detect a small-bowel perforation during laparoscopic surgery to repair a prior small uterine perforation.
- DOCTOR’S DEFENSE Not reported.
- VERDICT Indiana defense verdict.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Employee Lawsuit Coverage
Most physicians have a feeling that they carry too much insurance and that most of their policies are too expensive.
The policies you should have and how much they should cost will be covered in next month's column, but no matter what is in your insurance portfolio now, there is one relatively inexpensive policy—one you probably have never heard of—that you should definitely consider adding.
Recently, I corresponded with a dermatologist in California who experienced every employer's nightmare: He fired an incompetent employee, who promptly sued him for wrongful termination and accused him of sexual harassment to boot.
The charges were completely false, he told me, and the employee's transgressions were well documented, but defending the lawsuit would have been expensive, so his lawyer advised him to settle it for a significant sum of money.
Disasters like this are becoming more common. Plaintiffs' attorneys know all too well that most small businesses, including medical practices, are not protected against such legal actions and usually cannot afford to defend them in court.
Fortunately, there is a relatively inexpensive way to protect yourself: Employee practices liability insurance (EPLI) provides protection against many kinds of employee lawsuits that are not covered by conventional liability insurance. These include wrongful termination, sexual harassment, discrimination, breach of employment contract, negligent hiring or evaluation, failure to promote, wrongful discipline, mismanagement of benefits, and the ever-popular emotional distress.
EPLI would have defended the California dermatologist, had he carried it, against his employee's charges. In fact, there is a better than even chance that the plaintiff's attorney would have dropped the lawsuit entirely once informed that it would be aggressively defended.
As with all insurance, you should shop around for the best price and carefully read the policies on your short list.
All EPLI policies cover claims against your practice and its owners and employees, but some policies cover only claims against full-time employees.
Try to obtain the broadest coverage possible so that part-time, temporary, and seasonal employees, and, if possible, even applicants for employment and former employees also are covered.
You also should look for the most comprehensive policy in terms of coverage. Almost every EPLI policy covers the allegations mentioned above, but some offer a more comprehensive list of covered acts, such as invasion of privacy and defamation of character.
Also be aware of precisely what each policy does not cover. Most contain exclusions for punitive damages and court-imposed fines, as well as for criminal acts, fraud, and other clearly illegal conduct. For example, if it can be proved that you fired an employee because he or she refused to falsify insurance claims, any resulting civil suit against you will not be covered by EPLI, or any other type of insurance.
Depending on where you practice, it may be necessary to ask an employment lawyer to evaluate your individual EPLI needs.
An underwriter cannot anticipate every eventuality for you, particularly if he or she does not live in your area and is not familiar with employment conditions in your community.
Try to get a clause added that permits you to choose your own defense lawyer. Better still, pick a specific lawyer or firm that you trust and have that counsel named in an endorsement to the policy. Otherwise, the insurance carrier could select a lawyer who may not consider your interests to be a higher priority than those of the insurance company itself.
If you must accept the insurer's choice of counsel, you should find out whether that lawyer is experienced in employment law, which is a very specialized area. And just as with your malpractice policy, you will want to maintain as much control as possible over the settlement of claims. Ideally, no claim should be settled without your expressed permission.
As with any insurance policy you buy, be sure to choose an established carrier with ample EPLI experience and solid financial strength.
A low premium is no bargain if the carrier is new to EPLI, or goes belly up, or decides to cease covering employee practices liability. (As always, I have no financial interest in any company or product I discuss in this column.)
Above all, make sure that you can live with the claims definition and exclusions in the policy you choose and seek advice before you sign on the dotted line if you are unsure what your specific coverage needs are.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Most physicians have a feeling that they carry too much insurance and that most of their policies are too expensive.
The policies you should have and how much they should cost will be covered in next month's column, but no matter what is in your insurance portfolio now, there is one relatively inexpensive policy—one you probably have never heard of—that you should definitely consider adding.
Recently, I corresponded with a dermatologist in California who experienced every employer's nightmare: He fired an incompetent employee, who promptly sued him for wrongful termination and accused him of sexual harassment to boot.
The charges were completely false, he told me, and the employee's transgressions were well documented, but defending the lawsuit would have been expensive, so his lawyer advised him to settle it for a significant sum of money.
Disasters like this are becoming more common. Plaintiffs' attorneys know all too well that most small businesses, including medical practices, are not protected against such legal actions and usually cannot afford to defend them in court.
Fortunately, there is a relatively inexpensive way to protect yourself: Employee practices liability insurance (EPLI) provides protection against many kinds of employee lawsuits that are not covered by conventional liability insurance. These include wrongful termination, sexual harassment, discrimination, breach of employment contract, negligent hiring or evaluation, failure to promote, wrongful discipline, mismanagement of benefits, and the ever-popular emotional distress.
EPLI would have defended the California dermatologist, had he carried it, against his employee's charges. In fact, there is a better than even chance that the plaintiff's attorney would have dropped the lawsuit entirely once informed that it would be aggressively defended.
As with all insurance, you should shop around for the best price and carefully read the policies on your short list.
All EPLI policies cover claims against your practice and its owners and employees, but some policies cover only claims against full-time employees.
Try to obtain the broadest coverage possible so that part-time, temporary, and seasonal employees, and, if possible, even applicants for employment and former employees also are covered.
You also should look for the most comprehensive policy in terms of coverage. Almost every EPLI policy covers the allegations mentioned above, but some offer a more comprehensive list of covered acts, such as invasion of privacy and defamation of character.
Also be aware of precisely what each policy does not cover. Most contain exclusions for punitive damages and court-imposed fines, as well as for criminal acts, fraud, and other clearly illegal conduct. For example, if it can be proved that you fired an employee because he or she refused to falsify insurance claims, any resulting civil suit against you will not be covered by EPLI, or any other type of insurance.
Depending on where you practice, it may be necessary to ask an employment lawyer to evaluate your individual EPLI needs.
An underwriter cannot anticipate every eventuality for you, particularly if he or she does not live in your area and is not familiar with employment conditions in your community.
Try to get a clause added that permits you to choose your own defense lawyer. Better still, pick a specific lawyer or firm that you trust and have that counsel named in an endorsement to the policy. Otherwise, the insurance carrier could select a lawyer who may not consider your interests to be a higher priority than those of the insurance company itself.
If you must accept the insurer's choice of counsel, you should find out whether that lawyer is experienced in employment law, which is a very specialized area. And just as with your malpractice policy, you will want to maintain as much control as possible over the settlement of claims. Ideally, no claim should be settled without your expressed permission.
As with any insurance policy you buy, be sure to choose an established carrier with ample EPLI experience and solid financial strength.
A low premium is no bargain if the carrier is new to EPLI, or goes belly up, or decides to cease covering employee practices liability. (As always, I have no financial interest in any company or product I discuss in this column.)
Above all, make sure that you can live with the claims definition and exclusions in the policy you choose and seek advice before you sign on the dotted line if you are unsure what your specific coverage needs are.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Most physicians have a feeling that they carry too much insurance and that most of their policies are too expensive.
The policies you should have and how much they should cost will be covered in next month's column, but no matter what is in your insurance portfolio now, there is one relatively inexpensive policy—one you probably have never heard of—that you should definitely consider adding.
Recently, I corresponded with a dermatologist in California who experienced every employer's nightmare: He fired an incompetent employee, who promptly sued him for wrongful termination and accused him of sexual harassment to boot.
The charges were completely false, he told me, and the employee's transgressions were well documented, but defending the lawsuit would have been expensive, so his lawyer advised him to settle it for a significant sum of money.
Disasters like this are becoming more common. Plaintiffs' attorneys know all too well that most small businesses, including medical practices, are not protected against such legal actions and usually cannot afford to defend them in court.
Fortunately, there is a relatively inexpensive way to protect yourself: Employee practices liability insurance (EPLI) provides protection against many kinds of employee lawsuits that are not covered by conventional liability insurance. These include wrongful termination, sexual harassment, discrimination, breach of employment contract, negligent hiring or evaluation, failure to promote, wrongful discipline, mismanagement of benefits, and the ever-popular emotional distress.
EPLI would have defended the California dermatologist, had he carried it, against his employee's charges. In fact, there is a better than even chance that the plaintiff's attorney would have dropped the lawsuit entirely once informed that it would be aggressively defended.
As with all insurance, you should shop around for the best price and carefully read the policies on your short list.
All EPLI policies cover claims against your practice and its owners and employees, but some policies cover only claims against full-time employees.
Try to obtain the broadest coverage possible so that part-time, temporary, and seasonal employees, and, if possible, even applicants for employment and former employees also are covered.
You also should look for the most comprehensive policy in terms of coverage. Almost every EPLI policy covers the allegations mentioned above, but some offer a more comprehensive list of covered acts, such as invasion of privacy and defamation of character.
Also be aware of precisely what each policy does not cover. Most contain exclusions for punitive damages and court-imposed fines, as well as for criminal acts, fraud, and other clearly illegal conduct. For example, if it can be proved that you fired an employee because he or she refused to falsify insurance claims, any resulting civil suit against you will not be covered by EPLI, or any other type of insurance.
Depending on where you practice, it may be necessary to ask an employment lawyer to evaluate your individual EPLI needs.
An underwriter cannot anticipate every eventuality for you, particularly if he or she does not live in your area and is not familiar with employment conditions in your community.
Try to get a clause added that permits you to choose your own defense lawyer. Better still, pick a specific lawyer or firm that you trust and have that counsel named in an endorsement to the policy. Otherwise, the insurance carrier could select a lawyer who may not consider your interests to be a higher priority than those of the insurance company itself.
If you must accept the insurer's choice of counsel, you should find out whether that lawyer is experienced in employment law, which is a very specialized area. And just as with your malpractice policy, you will want to maintain as much control as possible over the settlement of claims. Ideally, no claim should be settled without your expressed permission.
As with any insurance policy you buy, be sure to choose an established carrier with ample EPLI experience and solid financial strength.
A low premium is no bargain if the carrier is new to EPLI, or goes belly up, or decides to cease covering employee practices liability. (As always, I have no financial interest in any company or product I discuss in this column.)
Above all, make sure that you can live with the claims definition and exclusions in the policy you choose and seek advice before you sign on the dotted line if you are unsure what your specific coverage needs are.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Three A's of Managed Care Contracting
The key to successful managed care contracting can be summed up in three words: attitude, analysis, and action. Adjust your attitude, analyze your practice, and take action to make sure you're getting paid for what you bring to the table.
To quote a renowned negotiation trainer, Chester L. Karrass, “In business, you don't get what you deserve; you get what you negotiate.” In the managed care arena, this translates to: “The payer will give you as little as you are willing to accept.” Unfortunately, many of us are accepting far too little.
With the demand for medical services at an all-time high and a diminishing supply of physicians to meet that demand, providers have a strong negotiating position. It is not your responsibility to ensure the profitability of private insurers by selling your services for less than their value. At the very least, you should expect payment that covers your overhead and allows you to take money home to feed and shelter your family; pay off your educational debt; educate your children; and save for your retirement.
Before undertaking a contract negotiation, a careful practice analysis should determine if you are being underpaid. It should help you to answer four fundamental questions:
Is the time you spend with patients who are covered by a given payer proportionate to the revenue you receive from that payer? If 25% of your visits come from a specific commercial payer, determine if that payer is providing a similar proportion of your income.
What is the effect on your revenue of ancillary carve-outs? If you normally provide laboratory services for your patients, but your contract with the payer prohibits you from doing them, determine the lost revenue from those carve-outs.
What are the hassle factors? Does the payer often downgrade your level 4 visits to level 3? Do they require a prepayment audit before paying higher levels of evaluation and management (E&M) services?
How long is your wait list? If you have a long wait list, consider this to be capital in the negotiation process.
A thorough business analysis also requires such considerations as the effect your practice's withdrawal would have on your competition, how dependent your practice is on a given payer, and how dependent that payer is on your practice.
When a business analysis reveals that a given managed care contract is more trouble than it's worth, be prepared to take action. A few years ago, an analysis of our practice revealed that our largest HMO was responsible for more than 13% of patient visits but only 4% of revenues. We realized that we had to see three of these HMO patients to earn what we received from one patient with an insurance company that carried its weight. We discontinued participation with that plan and saw a 20% increase in physician income the following year.
If a company is unwilling to negotiate, be prepared to pull out from that plan. Withdrawal—or a credible threat to withdraw—is the single most effective tool in improving reimbursement. But the primary purpose of withdrawal is to get out of a bad contract. If a company shows interest in negotiating once you have advised them of your withdrawal, they must offer you something that is substantially better.
The prospect of negotiating a managed care contract can seem daunting, but don't let it frighten you. You may be a stranger to managed care negotiations, but you negotiate all the time. You negotiate with your spouse, your children, your patients, vendors, and your staff. You can apply these same negotiating skills to this arena.
Remember that complex negotiations need to be paced, and they do take time. But don't lose momentum. One of the games negotiators play in the managed care business is to delay their responses. Time is money. The longer it takes them to get back to you to approve an increase, the more money they save.
The value of successful contract negotiations between physicians and managed care organizations extends beyond individuals to the profession as a whole. Medicine is at a crossroads right now. Our success can be measured by our ability to attract new physicians. Financial solvency and profitability are critical to this goal.
The key to successful managed care contracting can be summed up in three words: attitude, analysis, and action. Adjust your attitude, analyze your practice, and take action to make sure you're getting paid for what you bring to the table.
To quote a renowned negotiation trainer, Chester L. Karrass, “In business, you don't get what you deserve; you get what you negotiate.” In the managed care arena, this translates to: “The payer will give you as little as you are willing to accept.” Unfortunately, many of us are accepting far too little.
With the demand for medical services at an all-time high and a diminishing supply of physicians to meet that demand, providers have a strong negotiating position. It is not your responsibility to ensure the profitability of private insurers by selling your services for less than their value. At the very least, you should expect payment that covers your overhead and allows you to take money home to feed and shelter your family; pay off your educational debt; educate your children; and save for your retirement.
Before undertaking a contract negotiation, a careful practice analysis should determine if you are being underpaid. It should help you to answer four fundamental questions:
Is the time you spend with patients who are covered by a given payer proportionate to the revenue you receive from that payer? If 25% of your visits come from a specific commercial payer, determine if that payer is providing a similar proportion of your income.
What is the effect on your revenue of ancillary carve-outs? If you normally provide laboratory services for your patients, but your contract with the payer prohibits you from doing them, determine the lost revenue from those carve-outs.
What are the hassle factors? Does the payer often downgrade your level 4 visits to level 3? Do they require a prepayment audit before paying higher levels of evaluation and management (E&M) services?
How long is your wait list? If you have a long wait list, consider this to be capital in the negotiation process.
A thorough business analysis also requires such considerations as the effect your practice's withdrawal would have on your competition, how dependent your practice is on a given payer, and how dependent that payer is on your practice.
When a business analysis reveals that a given managed care contract is more trouble than it's worth, be prepared to take action. A few years ago, an analysis of our practice revealed that our largest HMO was responsible for more than 13% of patient visits but only 4% of revenues. We realized that we had to see three of these HMO patients to earn what we received from one patient with an insurance company that carried its weight. We discontinued participation with that plan and saw a 20% increase in physician income the following year.
If a company is unwilling to negotiate, be prepared to pull out from that plan. Withdrawal—or a credible threat to withdraw—is the single most effective tool in improving reimbursement. But the primary purpose of withdrawal is to get out of a bad contract. If a company shows interest in negotiating once you have advised them of your withdrawal, they must offer you something that is substantially better.
The prospect of negotiating a managed care contract can seem daunting, but don't let it frighten you. You may be a stranger to managed care negotiations, but you negotiate all the time. You negotiate with your spouse, your children, your patients, vendors, and your staff. You can apply these same negotiating skills to this arena.
Remember that complex negotiations need to be paced, and they do take time. But don't lose momentum. One of the games negotiators play in the managed care business is to delay their responses. Time is money. The longer it takes them to get back to you to approve an increase, the more money they save.
The value of successful contract negotiations between physicians and managed care organizations extends beyond individuals to the profession as a whole. Medicine is at a crossroads right now. Our success can be measured by our ability to attract new physicians. Financial solvency and profitability are critical to this goal.
The key to successful managed care contracting can be summed up in three words: attitude, analysis, and action. Adjust your attitude, analyze your practice, and take action to make sure you're getting paid for what you bring to the table.
To quote a renowned negotiation trainer, Chester L. Karrass, “In business, you don't get what you deserve; you get what you negotiate.” In the managed care arena, this translates to: “The payer will give you as little as you are willing to accept.” Unfortunately, many of us are accepting far too little.
With the demand for medical services at an all-time high and a diminishing supply of physicians to meet that demand, providers have a strong negotiating position. It is not your responsibility to ensure the profitability of private insurers by selling your services for less than their value. At the very least, you should expect payment that covers your overhead and allows you to take money home to feed and shelter your family; pay off your educational debt; educate your children; and save for your retirement.
Before undertaking a contract negotiation, a careful practice analysis should determine if you are being underpaid. It should help you to answer four fundamental questions:
Is the time you spend with patients who are covered by a given payer proportionate to the revenue you receive from that payer? If 25% of your visits come from a specific commercial payer, determine if that payer is providing a similar proportion of your income.
What is the effect on your revenue of ancillary carve-outs? If you normally provide laboratory services for your patients, but your contract with the payer prohibits you from doing them, determine the lost revenue from those carve-outs.
What are the hassle factors? Does the payer often downgrade your level 4 visits to level 3? Do they require a prepayment audit before paying higher levels of evaluation and management (E&M) services?
How long is your wait list? If you have a long wait list, consider this to be capital in the negotiation process.
A thorough business analysis also requires such considerations as the effect your practice's withdrawal would have on your competition, how dependent your practice is on a given payer, and how dependent that payer is on your practice.
When a business analysis reveals that a given managed care contract is more trouble than it's worth, be prepared to take action. A few years ago, an analysis of our practice revealed that our largest HMO was responsible for more than 13% of patient visits but only 4% of revenues. We realized that we had to see three of these HMO patients to earn what we received from one patient with an insurance company that carried its weight. We discontinued participation with that plan and saw a 20% increase in physician income the following year.
If a company is unwilling to negotiate, be prepared to pull out from that plan. Withdrawal—or a credible threat to withdraw—is the single most effective tool in improving reimbursement. But the primary purpose of withdrawal is to get out of a bad contract. If a company shows interest in negotiating once you have advised them of your withdrawal, they must offer you something that is substantially better.
The prospect of negotiating a managed care contract can seem daunting, but don't let it frighten you. You may be a stranger to managed care negotiations, but you negotiate all the time. You negotiate with your spouse, your children, your patients, vendors, and your staff. You can apply these same negotiating skills to this arena.
Remember that complex negotiations need to be paced, and they do take time. But don't lose momentum. One of the games negotiators play in the managed care business is to delay their responses. Time is money. The longer it takes them to get back to you to approve an increase, the more money they save.
The value of successful contract negotiations between physicians and managed care organizations extends beyond individuals to the profession as a whole. Medicine is at a crossroads right now. Our success can be measured by our ability to attract new physicians. Financial solvency and profitability are critical to this goal.
Document Your Decisions
For all the differences highlighted in my April and May columns studying the 1995 and 1997 documentation guidelines set forth by the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA), decision making remains consistent in both.
Physician documentation addresses the complexity of the patient’s condition in terms of the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality. The “diagnoses” and “data” categories follow a point system (see Table 1, below) determined by local Medicare contractors, whereas the “risk” category utilizes a universal table to define medical and/or procedural risks for the patient. The final result of complexity is classified as straightforward, low, moderate, or high.
A complete and accurate description of the patient’s condition should be conveyed through the plan of care. While acuity and severity may be inferred by a physician’s colleagues from particular pieces of information included in the record (e.g., critical lab values), the importance of this information may be lost on auditors and medical record reviewers. This article will assist in explaining the categories of medical decision making, as well as provide documentation tips to best represent patient complexity.
Diagnoses, Care Options
The plan of care outlines problems the physician personally manages and those that affect their management options, even if another physician directly oversees the problem. For example, the hospitalist may primarily manage a patient’s diabetes while the nephrologist manages renal insufficiency. Since the renal insufficiency may affect the hospitalist’s plan for diabetic management, the hospitalist receives credit for the documented renal insufficiency diagnosis and hospitalist-related care plan.
Physicians should address all problems in the documentation for each encounter regardless of any changes to the treatment plan. Credit is provided for each problem that has an associated plan, even if the plan states “continue same treatment.” Additional credit is provided when the treatment to be “continued” is referenced somewhere in the progress note (e.g., in the history).
The amount of credit varies depending upon the problem type. An established problem, defined as having a care plan established by the physician or someone from the same group practice during the current hospitalization, is considered less complex than an undiagnosed new problem for which a prognosis cannot be determined. Severity of the problem affects the weight of complexity. A stable, improving problem is not as complex as a progressing problem.
When documenting diagnoses/treatment options:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined; and
- Indicate the management/treatment option(s) for each problem.
When documentation indicates a continuation of current management options (e.g., “continue meds”), be sure the management options to be continued are noted somewhere in the progress note for that encounter (e.g., medication list).
Data Ordered/Reviewed
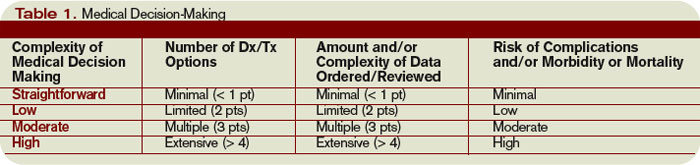
“Data” order/review comes in many forms: pathology/laboratory testing, radiology, and medicine-based diagnostics. Although an intuitive part of medical practice, the data section of the progress note is often underdocumented by physicians. Pertinent orders or results may be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note.
When documenting amount and/or complexity of data:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Test review may be documented by including a brief entry in the progress note (e.g., “decreased Hgb” or “CXR shows NAD”), or by dating and initialing the report;
- Physicians receive credit for reviewing old records or obtaining history from someone other than the patient, when necessary, as long as a summary of the review or discussion is documented in the medical record; and
- Indicate when images, tracings, or specimens are “personally reviewed” by the physician.
Discussion of unexpected or contradictory test results with the performing physician should be summarized in the medical record.
Risks of Complication
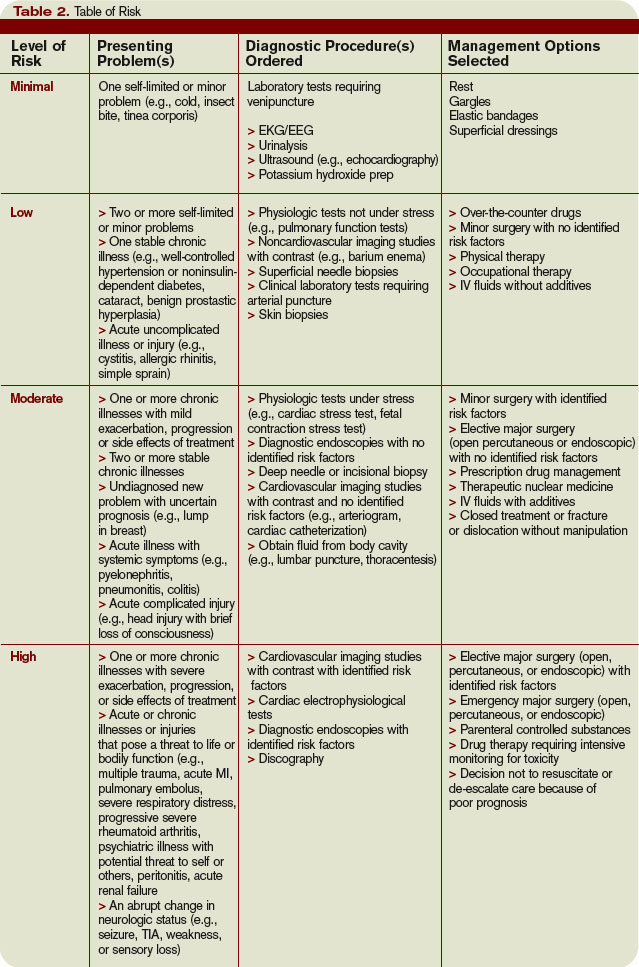
Risk is viewed in light of the patient’s presenting problem, diagnostic procedures ordered, and management options selected.
Risk is graded as minimal, low, moderate, and high with corresponding items that help to differentiate each level (see Table 2, right). The single highest item in any given risk category determines the risk level.
Chronic conditions and invasive procedures expose the patient to more risk than acute, uncomplicated illnesses or non-invasive procedures, respectively. As in the diagnoses/treatment options category, a stable or improving problem poses less risk than a progressing problem. Medication risk varies with the type and degree of potential adverse effects associated with each medication.
When documenting risk:
- Indicate status of all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), etc.;
- Document all diagnostic procedures being considered;
- Identify surgical risk factors involving co-morbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding. medication (e.g., “Continue coumadin, monitor PT/INR”). A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change.
Determine Complexity
To determine the final complexity of medical decision making, two of three categories must be met. For example, if a physician satisfies the requirements for “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician achieves moderate complexity decision-making.
Remember that decision-making is just one of three components of evaluation and management services, along with history and exam.
Determining the final visit level (e.g., 9922x) depends upon each of these three key components for initial hospital care and consultations, and two key components for subsequent hospital care. However, medical decision making always should drive visit level selection as it is the best representation of medical necessity for the service involved.
Contributory Factors
In addition to the three categories of medical decision making, a payer (e.g., TrailblazerHealth) may consider contributory factors when determining patient complexity and selecting visit levels.
For example, the nature of the presenting problem may play a role when reviewing claims for subsequent hospital care codes (99231-99233). Found in the code descriptors of the CPT manual, problems are identified as:
- 99231: Stable, recovering or improving;
- 99232: Responding inadequately to therapy or developed a minor complication; and
- 99233: Unstable or has developed a significant complication or a significant new problem.
Although this is not a general requirement, it represents a locally established standard for reviewing claims for medical necessity. It should not be used exclusively to determine the visit level.
Be sure to query your payer’s policy via written communication or Web site posting (e.g., www.trailblazerhealth.com/Publications/Job%20Aid/medical%20necessity.pdf) for guidance on how payers review documentation. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
For all the differences highlighted in my April and May columns studying the 1995 and 1997 documentation guidelines set forth by the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA), decision making remains consistent in both.
Physician documentation addresses the complexity of the patient’s condition in terms of the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality. The “diagnoses” and “data” categories follow a point system (see Table 1, below) determined by local Medicare contractors, whereas the “risk” category utilizes a universal table to define medical and/or procedural risks for the patient. The final result of complexity is classified as straightforward, low, moderate, or high.
A complete and accurate description of the patient’s condition should be conveyed through the plan of care. While acuity and severity may be inferred by a physician’s colleagues from particular pieces of information included in the record (e.g., critical lab values), the importance of this information may be lost on auditors and medical record reviewers. This article will assist in explaining the categories of medical decision making, as well as provide documentation tips to best represent patient complexity.
Diagnoses, Care Options
The plan of care outlines problems the physician personally manages and those that affect their management options, even if another physician directly oversees the problem. For example, the hospitalist may primarily manage a patient’s diabetes while the nephrologist manages renal insufficiency. Since the renal insufficiency may affect the hospitalist’s plan for diabetic management, the hospitalist receives credit for the documented renal insufficiency diagnosis and hospitalist-related care plan.
Physicians should address all problems in the documentation for each encounter regardless of any changes to the treatment plan. Credit is provided for each problem that has an associated plan, even if the plan states “continue same treatment.” Additional credit is provided when the treatment to be “continued” is referenced somewhere in the progress note (e.g., in the history).
The amount of credit varies depending upon the problem type. An established problem, defined as having a care plan established by the physician or someone from the same group practice during the current hospitalization, is considered less complex than an undiagnosed new problem for which a prognosis cannot be determined. Severity of the problem affects the weight of complexity. A stable, improving problem is not as complex as a progressing problem.
When documenting diagnoses/treatment options:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined; and
- Indicate the management/treatment option(s) for each problem.
When documentation indicates a continuation of current management options (e.g., “continue meds”), be sure the management options to be continued are noted somewhere in the progress note for that encounter (e.g., medication list).
Data Ordered/Reviewed
“Data” order/review comes in many forms: pathology/laboratory testing, radiology, and medicine-based diagnostics. Although an intuitive part of medical practice, the data section of the progress note is often underdocumented by physicians. Pertinent orders or results may be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note.
When documenting amount and/or complexity of data:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Test review may be documented by including a brief entry in the progress note (e.g., “decreased Hgb” or “CXR shows NAD”), or by dating and initialing the report;
- Physicians receive credit for reviewing old records or obtaining history from someone other than the patient, when necessary, as long as a summary of the review or discussion is documented in the medical record; and
- Indicate when images, tracings, or specimens are “personally reviewed” by the physician.
Discussion of unexpected or contradictory test results with the performing physician should be summarized in the medical record.
Risks of Complication
Risk is viewed in light of the patient’s presenting problem, diagnostic procedures ordered, and management options selected.
Risk is graded as minimal, low, moderate, and high with corresponding items that help to differentiate each level (see Table 2, right). The single highest item in any given risk category determines the risk level.
Chronic conditions and invasive procedures expose the patient to more risk than acute, uncomplicated illnesses or non-invasive procedures, respectively. As in the diagnoses/treatment options category, a stable or improving problem poses less risk than a progressing problem. Medication risk varies with the type and degree of potential adverse effects associated with each medication.
When documenting risk:
- Indicate status of all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), etc.;
- Document all diagnostic procedures being considered;
- Identify surgical risk factors involving co-morbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding. medication (e.g., “Continue coumadin, monitor PT/INR”). A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change.
Determine Complexity
To determine the final complexity of medical decision making, two of three categories must be met. For example, if a physician satisfies the requirements for “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician achieves moderate complexity decision-making.
Remember that decision-making is just one of three components of evaluation and management services, along with history and exam.
Determining the final visit level (e.g., 9922x) depends upon each of these three key components for initial hospital care and consultations, and two key components for subsequent hospital care. However, medical decision making always should drive visit level selection as it is the best representation of medical necessity for the service involved.
Contributory Factors
In addition to the three categories of medical decision making, a payer (e.g., TrailblazerHealth) may consider contributory factors when determining patient complexity and selecting visit levels.
For example, the nature of the presenting problem may play a role when reviewing claims for subsequent hospital care codes (99231-99233). Found in the code descriptors of the CPT manual, problems are identified as:
- 99231: Stable, recovering or improving;
- 99232: Responding inadequately to therapy or developed a minor complication; and
- 99233: Unstable or has developed a significant complication or a significant new problem.
Although this is not a general requirement, it represents a locally established standard for reviewing claims for medical necessity. It should not be used exclusively to determine the visit level.
Be sure to query your payer’s policy via written communication or Web site posting (e.g., www.trailblazerhealth.com/Publications/Job%20Aid/medical%20necessity.pdf) for guidance on how payers review documentation. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
For all the differences highlighted in my April and May columns studying the 1995 and 1997 documentation guidelines set forth by the Centers for Medicare and Medicaid Services (CMS) and the American Medical Association (AMA), decision making remains consistent in both.
Physician documentation addresses the complexity of the patient’s condition in terms of the number of diagnoses and/or treatment options, the amount and/or complexity of data ordered/reviewed, and the risk of complications/morbidity/mortality. The “diagnoses” and “data” categories follow a point system (see Table 1, below) determined by local Medicare contractors, whereas the “risk” category utilizes a universal table to define medical and/or procedural risks for the patient. The final result of complexity is classified as straightforward, low, moderate, or high.
A complete and accurate description of the patient’s condition should be conveyed through the plan of care. While acuity and severity may be inferred by a physician’s colleagues from particular pieces of information included in the record (e.g., critical lab values), the importance of this information may be lost on auditors and medical record reviewers. This article will assist in explaining the categories of medical decision making, as well as provide documentation tips to best represent patient complexity.
Diagnoses, Care Options
The plan of care outlines problems the physician personally manages and those that affect their management options, even if another physician directly oversees the problem. For example, the hospitalist may primarily manage a patient’s diabetes while the nephrologist manages renal insufficiency. Since the renal insufficiency may affect the hospitalist’s plan for diabetic management, the hospitalist receives credit for the documented renal insufficiency diagnosis and hospitalist-related care plan.
Physicians should address all problems in the documentation for each encounter regardless of any changes to the treatment plan. Credit is provided for each problem that has an associated plan, even if the plan states “continue same treatment.” Additional credit is provided when the treatment to be “continued” is referenced somewhere in the progress note (e.g., in the history).
The amount of credit varies depending upon the problem type. An established problem, defined as having a care plan established by the physician or someone from the same group practice during the current hospitalization, is considered less complex than an undiagnosed new problem for which a prognosis cannot be determined. Severity of the problem affects the weight of complexity. A stable, improving problem is not as complex as a progressing problem.
When documenting diagnoses/treatment options:
- Identify all problems managed or addressed during each encounter;
- Identify problems as stable or progressing, when appropriate;
- Indicate differential diagnoses when the problem remains undefined; and
- Indicate the management/treatment option(s) for each problem.
When documentation indicates a continuation of current management options (e.g., “continue meds”), be sure the management options to be continued are noted somewhere in the progress note for that encounter (e.g., medication list).
Data Ordered/Reviewed
“Data” order/review comes in many forms: pathology/laboratory testing, radiology, and medicine-based diagnostics. Although an intuitive part of medical practice, the data section of the progress note is often underdocumented by physicians. Pertinent orders or results may be noted in the visit record, but most of the background interactions and communications involving testing are undetected when reviewing the progress note.
When documenting amount and/or complexity of data:
- Specify tests ordered and rationale in the physician’s progress note or make an entry that refers to another auditor-accessible location for ordered tests and studies;
- Test review may be documented by including a brief entry in the progress note (e.g., “decreased Hgb” or “CXR shows NAD”), or by dating and initialing the report;
- Physicians receive credit for reviewing old records or obtaining history from someone other than the patient, when necessary, as long as a summary of the review or discussion is documented in the medical record; and
- Indicate when images, tracings, or specimens are “personally reviewed” by the physician.
Discussion of unexpected or contradictory test results with the performing physician should be summarized in the medical record.
Risks of Complication
Risk is viewed in light of the patient’s presenting problem, diagnostic procedures ordered, and management options selected.
Risk is graded as minimal, low, moderate, and high with corresponding items that help to differentiate each level (see Table 2, right). The single highest item in any given risk category determines the risk level.
Chronic conditions and invasive procedures expose the patient to more risk than acute, uncomplicated illnesses or non-invasive procedures, respectively. As in the diagnoses/treatment options category, a stable or improving problem poses less risk than a progressing problem. Medication risk varies with the type and degree of potential adverse effects associated with each medication.
When documenting risk:
- Indicate status of all problems in the plan of care; identify them as stable, worsening, exacerbating (mild or severe), etc.;
- Document all diagnostic procedures being considered;
- Identify surgical risk factors involving co-morbid conditions, when appropriate; and
- Associate the labs ordered to monitor for toxicity with the corresponding. medication (e.g., “Continue coumadin, monitor PT/INR”). A patient maintains the same level of risk for a given medication whether the dosage is increased, decreased, or continued without change.
Determine Complexity
To determine the final complexity of medical decision making, two of three categories must be met. For example, if a physician satisfies the requirements for “multiple” diagnoses/treatment options, “minimal” data, and “high” risk, the physician achieves moderate complexity decision-making.
Remember that decision-making is just one of three components of evaluation and management services, along with history and exam.
Determining the final visit level (e.g., 9922x) depends upon each of these three key components for initial hospital care and consultations, and two key components for subsequent hospital care. However, medical decision making always should drive visit level selection as it is the best representation of medical necessity for the service involved.
Contributory Factors
In addition to the three categories of medical decision making, a payer (e.g., TrailblazerHealth) may consider contributory factors when determining patient complexity and selecting visit levels.
For example, the nature of the presenting problem may play a role when reviewing claims for subsequent hospital care codes (99231-99233). Found in the code descriptors of the CPT manual, problems are identified as:
- 99231: Stable, recovering or improving;
- 99232: Responding inadequately to therapy or developed a minor complication; and
- 99233: Unstable or has developed a significant complication or a significant new problem.
Although this is not a general requirement, it represents a locally established standard for reviewing claims for medical necessity. It should not be used exclusively to determine the visit level.
Be sure to query your payer’s policy via written communication or Web site posting (e.g., www.trailblazerhealth.com/Publications/Job%20Aid/medical%20necessity.pdf) for guidance on how payers review documentation. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She also is on the faculty of SHM’s inpatient coding course.
Medical Verdicts
$24.5 million verdict after oxytocin, then uterine rupture
A 37-YEAR-OLD WOMAN in labor was administered oxytocin. Her uterus ruptured, and oxytocin was continued for another 3 minutes. In an emergency C-section, the baby was found to be half-extruded from the uterus into the abdominal cavity. He was born asphyxiated; his Apgar scores were low; and umbilical artery blood gas indicated hypoxia and metabolic acidosis. He was diagnosed with cerebral palsy and requires a feeding tube.
- PATIENT’S CLAIM The nurses were negligent for not contacting a physician and for continuing oxytocin.
- DOCTOR’S DEFENSE There was no negligence.
- VERDICT $24,554,880 Illinois bench verdict.
ObGyn follows fetal distress remotely—child born with CP
WHEN A PREGNANT WOMAN presented at the hospital, both she and her fetus were found to be healthy with no complications. About 4½ hours later, the fetal monitor indicated decelerations of the fetal heart rate, and the ObGyn was notified. After another 1½ hours, it had increased without returning to baseline, and the decelerations became more frequent, severe, and prolonged, with coupling of contractions. These changes were relayed to the ObGyn, who then reviewed the monitoring strips with the nurse and ordered oxytocin to be started. Increasing heart rate and decelerations continued over the next hour. The depressed heart rate then was slow to return to baseline, and the fetal tracings began to flatten. Again the strips were reviewed by the nurses and physician. After 3 more hours, the ObGyn was informed of the continuing signs of fetal distress—the patient was 8 cm dilated and labor had shown no progress in the previous 2 hours. The ObGyn ordered increased oxytocin. After 45 minutes, the mother was dilated 9 cm and was told to start pushing. When she pushed, fetal decelerations decreased to as low as 60 bpm during contractions. Again the ObGyn was informed of persistent ominous signs of fetal distress. Without assessing the patient, he asked to be told when the baby began to crown—and then went to take a nap. Nearly 2 hours later, informed of a lack of progress and continued decelerations, he reviewed the strips and ordered increased oxytocin. Within 2 hours, the baby was born. She was covered with meconium and had Apgar scores of 2, 3, and 4 at 1, 5, and 10 minutes. She was limp, gray, and not breathing, and cord gases indicated acute severe metabolic and respiratory acidosis. The infant was taken to the NICU with multiple problems, including no primary reflexes, seizure disorder, and cerebral edema. She was diagnosed with cerebral palsy with right hemiplegia, chronic head pain, memory deficits, motor dysfunction, and many other deficits.
- PATIENT’S CLAIM Not reported.
- DOCTOR’S DEFENSE Not reported.
- VERDICT $3.45 million California settlement: $1 million from the ObGyn; and $2.45 million from the hospital.
Midwife has turn, then MD finishes difficult delivery
DELIVERY OF AN INFANT at term was performed by a physician who used forceps to assist. The child suffered brain damage and died.
- PATIENT’S CLAIM The physician failed to deliver the child in a timely manner, which led to brain damage and death.
- DOCTOR’S DEFENSE Labor was managed primarily by a midwife. The physician responded immediately when called and used appropriate emergency measures to deliver the child as quickly as possible.
- VERDICT $1.5 million settlement with the hospital before trial; Illinois defense verdict for the physician.
Embolism after C-section causes death
A 38-YEAR-OLD WOMAN pregnant with her second child had a C-section and tubal ligation performed by her ObGyn. She developed a pulmonary embolism a few days later and died.
- PATIENT’S CLAIM The patient’s age and weight were risk factors for pulmonary embolism, and she was immobilized for over 72 hours following surgery, which also increased the risk. The defendants took no steps to prevent a pulmonary embolism.
- DOCTOR’S DEFENSE There was no negligence.
- VERDICT Ohio defense verdict.
Surgery for pelvic pain and cyst leads to … more surgery
A SONOGRAM REVEALED an ovarian cyst in a woman, in her mid-40s, who was experiencing pelvic pain. Her physician recommended and performed surgery to find the source of the pain, as well as to possibly remove the cyst and ovaries. Following surgery, the woman was diagnosed with a colon perforation. A colostomy and two further surgeries were necessary. In addition, the patient suffered a bowel obstruction, colovaginal fistula, and scarring.
- PATIENT’S CLAIM The original surgery was unnecessary, and the colon perforation was negligent.
- DOCTOR’S DEFENSE Surgery was necessary to determine and treat the cause of the pain. Perforation of the colon did not occur during surgery, but resulted from the patient’s diverticulitis.
- VERDICT A $3,497,000 Maryland verdict was returned; however, this was reduced to $702,000 pursuant to the state cap for noneconomic damages.
Femoral nerve palsy occurs after hysterectomy
A 39-YEAR-OLD WOMAN was diagnosed with a leiomyomata in her lower uterus. The tissue in the area became necrotic, and prolapse resulted. Surgery was performed. A week later, the patient returned to the hospital because of pain and bleeding. The ObGyn covering for the physician who had performed the surgery recommended—then performed—a hysterectomy. Following the surgery, the woman experienced numbness in the right anterior and lateral thigh. According to a neurological consultation, the femoral nerve was damaged. The patient suffers from persistent femoral nerve palsy, affecting her ability to walk. She has undergone physical therapy and rehabilitation, as well as nerve conduction studies.
- PATIENT’S CLAIM The ObGyn negligently placed the retractor or failed to reposition the retractor blades after they moved during the surgery.
- DOCTOR’S DEFENSE There was no negligence. Femoral nerve injury is a known risk of pelvic surgery. The patient suffered only minor sensory and motor palsy immediately following surgery, and her ongoing complaints had no physical basis.
- VERDICT California defense verdict.
Patient fails to report continued irregular bleeding
AT HER ANNUAL EXAM, a 49-year-old woman told her gynecologist, Dr. A, about cramping and bleeding on day 10 and sometimes day 17 of her menstrual cycle over the previous 6 months. Dr. A noted a normal pelvic exam. She told the patient that the bleeding was a normal perimenopausal symptom and suggested taking Advil for the pain. No further testing was recommended. The patient failed to report continued irregular vaginal bleeding. A year later, Dr. B conducted the next annual exam and found an enlarged uterus in the 7- to 8-week range. Endometrial biopsy showed the left ovary to be tender, slightly enlarged, with a possible mass present. A sonogram 2 days later showed an enlarged right ovary with multiple cystic areas and a large complex mass of the left ovary—findings suspicious for ovarian cancer. Pathology following a D&C 1 month later indicated adenocarcinoma consistent with primary endometrial cancer. The patient was diagnosed with endometrioid type adenocarcinoma involving both ovaries and the uterus, as well as metastatic disease to the omentum and diaphragm. She underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy, bilateral pelvic and periaortic lymph node dissection, omentectomy, and CUSA of the diaphragm. She is not expected to survive long-term.
- PATIENT’S CLAIM Dr. A was negligent for failing to timely diagnose and treat the cancer.
- DOCTOR’S DEFENSE As the patient reported irregular vaginal bleeding at one visit only, there was no indication for further testing of a woman her age and no reason to suspect any disease. Most likely, the irregular vaginal bleeding was unrelated to the ovarian cancer, and an endometrial biopsy after the first visit would not have changed the prognosis.
- VERDICT $750,000 Massachusetts settlement.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
$24.5 million verdict after oxytocin, then uterine rupture
A 37-YEAR-OLD WOMAN in labor was administered oxytocin. Her uterus ruptured, and oxytocin was continued for another 3 minutes. In an emergency C-section, the baby was found to be half-extruded from the uterus into the abdominal cavity. He was born asphyxiated; his Apgar scores were low; and umbilical artery blood gas indicated hypoxia and metabolic acidosis. He was diagnosed with cerebral palsy and requires a feeding tube.
- PATIENT’S CLAIM The nurses were negligent for not contacting a physician and for continuing oxytocin.
- DOCTOR’S DEFENSE There was no negligence.
- VERDICT $24,554,880 Illinois bench verdict.
ObGyn follows fetal distress remotely—child born with CP
WHEN A PREGNANT WOMAN presented at the hospital, both she and her fetus were found to be healthy with no complications. About 4½ hours later, the fetal monitor indicated decelerations of the fetal heart rate, and the ObGyn was notified. After another 1½ hours, it had increased without returning to baseline, and the decelerations became more frequent, severe, and prolonged, with coupling of contractions. These changes were relayed to the ObGyn, who then reviewed the monitoring strips with the nurse and ordered oxytocin to be started. Increasing heart rate and decelerations continued over the next hour. The depressed heart rate then was slow to return to baseline, and the fetal tracings began to flatten. Again the strips were reviewed by the nurses and physician. After 3 more hours, the ObGyn was informed of the continuing signs of fetal distress—the patient was 8 cm dilated and labor had shown no progress in the previous 2 hours. The ObGyn ordered increased oxytocin. After 45 minutes, the mother was dilated 9 cm and was told to start pushing. When she pushed, fetal decelerations decreased to as low as 60 bpm during contractions. Again the ObGyn was informed of persistent ominous signs of fetal distress. Without assessing the patient, he asked to be told when the baby began to crown—and then went to take a nap. Nearly 2 hours later, informed of a lack of progress and continued decelerations, he reviewed the strips and ordered increased oxytocin. Within 2 hours, the baby was born. She was covered with meconium and had Apgar scores of 2, 3, and 4 at 1, 5, and 10 minutes. She was limp, gray, and not breathing, and cord gases indicated acute severe metabolic and respiratory acidosis. The infant was taken to the NICU with multiple problems, including no primary reflexes, seizure disorder, and cerebral edema. She was diagnosed with cerebral palsy with right hemiplegia, chronic head pain, memory deficits, motor dysfunction, and many other deficits.
- PATIENT’S CLAIM Not reported.
- DOCTOR’S DEFENSE Not reported.
- VERDICT $3.45 million California settlement: $1 million from the ObGyn; and $2.45 million from the hospital.
Midwife has turn, then MD finishes difficult delivery
DELIVERY OF AN INFANT at term was performed by a physician who used forceps to assist. The child suffered brain damage and died.
- PATIENT’S CLAIM The physician failed to deliver the child in a timely manner, which led to brain damage and death.
- DOCTOR’S DEFENSE Labor was managed primarily by a midwife. The physician responded immediately when called and used appropriate emergency measures to deliver the child as quickly as possible.
- VERDICT $1.5 million settlement with the hospital before trial; Illinois defense verdict for the physician.
Embolism after C-section causes death
A 38-YEAR-OLD WOMAN pregnant with her second child had a C-section and tubal ligation performed by her ObGyn. She developed a pulmonary embolism a few days later and died.
- PATIENT’S CLAIM The patient’s age and weight were risk factors for pulmonary embolism, and she was immobilized for over 72 hours following surgery, which also increased the risk. The defendants took no steps to prevent a pulmonary embolism.
- DOCTOR’S DEFENSE There was no negligence.
- VERDICT Ohio defense verdict.
Surgery for pelvic pain and cyst leads to … more surgery
A SONOGRAM REVEALED an ovarian cyst in a woman, in her mid-40s, who was experiencing pelvic pain. Her physician recommended and performed surgery to find the source of the pain, as well as to possibly remove the cyst and ovaries. Following surgery, the woman was diagnosed with a colon perforation. A colostomy and two further surgeries were necessary. In addition, the patient suffered a bowel obstruction, colovaginal fistula, and scarring.
- PATIENT’S CLAIM The original surgery was unnecessary, and the colon perforation was negligent.
- DOCTOR’S DEFENSE Surgery was necessary to determine and treat the cause of the pain. Perforation of the colon did not occur during surgery, but resulted from the patient’s diverticulitis.
- VERDICT A $3,497,000 Maryland verdict was returned; however, this was reduced to $702,000 pursuant to the state cap for noneconomic damages.
Femoral nerve palsy occurs after hysterectomy
A 39-YEAR-OLD WOMAN was diagnosed with a leiomyomata in her lower uterus. The tissue in the area became necrotic, and prolapse resulted. Surgery was performed. A week later, the patient returned to the hospital because of pain and bleeding. The ObGyn covering for the physician who had performed the surgery recommended—then performed—a hysterectomy. Following the surgery, the woman experienced numbness in the right anterior and lateral thigh. According to a neurological consultation, the femoral nerve was damaged. The patient suffers from persistent femoral nerve palsy, affecting her ability to walk. She has undergone physical therapy and rehabilitation, as well as nerve conduction studies.
- PATIENT’S CLAIM The ObGyn negligently placed the retractor or failed to reposition the retractor blades after they moved during the surgery.
- DOCTOR’S DEFENSE There was no negligence. Femoral nerve injury is a known risk of pelvic surgery. The patient suffered only minor sensory and motor palsy immediately following surgery, and her ongoing complaints had no physical basis.
- VERDICT California defense verdict.
Patient fails to report continued irregular bleeding
AT HER ANNUAL EXAM, a 49-year-old woman told her gynecologist, Dr. A, about cramping and bleeding on day 10 and sometimes day 17 of her menstrual cycle over the previous 6 months. Dr. A noted a normal pelvic exam. She told the patient that the bleeding was a normal perimenopausal symptom and suggested taking Advil for the pain. No further testing was recommended. The patient failed to report continued irregular vaginal bleeding. A year later, Dr. B conducted the next annual exam and found an enlarged uterus in the 7- to 8-week range. Endometrial biopsy showed the left ovary to be tender, slightly enlarged, with a possible mass present. A sonogram 2 days later showed an enlarged right ovary with multiple cystic areas and a large complex mass of the left ovary—findings suspicious for ovarian cancer. Pathology following a D&C 1 month later indicated adenocarcinoma consistent with primary endometrial cancer. The patient was diagnosed with endometrioid type adenocarcinoma involving both ovaries and the uterus, as well as metastatic disease to the omentum and diaphragm. She underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy, bilateral pelvic and periaortic lymph node dissection, omentectomy, and CUSA of the diaphragm. She is not expected to survive long-term.
- PATIENT’S CLAIM Dr. A was negligent for failing to timely diagnose and treat the cancer.
- DOCTOR’S DEFENSE As the patient reported irregular vaginal bleeding at one visit only, there was no indication for further testing of a woman her age and no reason to suspect any disease. Most likely, the irregular vaginal bleeding was unrelated to the ovarian cancer, and an endometrial biopsy after the first visit would not have changed the prognosis.
- VERDICT $750,000 Massachusetts settlement.
$24.5 million verdict after oxytocin, then uterine rupture
A 37-YEAR-OLD WOMAN in labor was administered oxytocin. Her uterus ruptured, and oxytocin was continued for another 3 minutes. In an emergency C-section, the baby was found to be half-extruded from the uterus into the abdominal cavity. He was born asphyxiated; his Apgar scores were low; and umbilical artery blood gas indicated hypoxia and metabolic acidosis. He was diagnosed with cerebral palsy and requires a feeding tube.
- PATIENT’S CLAIM The nurses were negligent for not contacting a physician and for continuing oxytocin.
- DOCTOR’S DEFENSE There was no negligence.
- VERDICT $24,554,880 Illinois bench verdict.
ObGyn follows fetal distress remotely—child born with CP
WHEN A PREGNANT WOMAN presented at the hospital, both she and her fetus were found to be healthy with no complications. About 4½ hours later, the fetal monitor indicated decelerations of the fetal heart rate, and the ObGyn was notified. After another 1½ hours, it had increased without returning to baseline, and the decelerations became more frequent, severe, and prolonged, with coupling of contractions. These changes were relayed to the ObGyn, who then reviewed the monitoring strips with the nurse and ordered oxytocin to be started. Increasing heart rate and decelerations continued over the next hour. The depressed heart rate then was slow to return to baseline, and the fetal tracings began to flatten. Again the strips were reviewed by the nurses and physician. After 3 more hours, the ObGyn was informed of the continuing signs of fetal distress—the patient was 8 cm dilated and labor had shown no progress in the previous 2 hours. The ObGyn ordered increased oxytocin. After 45 minutes, the mother was dilated 9 cm and was told to start pushing. When she pushed, fetal decelerations decreased to as low as 60 bpm during contractions. Again the ObGyn was informed of persistent ominous signs of fetal distress. Without assessing the patient, he asked to be told when the baby began to crown—and then went to take a nap. Nearly 2 hours later, informed of a lack of progress and continued decelerations, he reviewed the strips and ordered increased oxytocin. Within 2 hours, the baby was born. She was covered with meconium and had Apgar scores of 2, 3, and 4 at 1, 5, and 10 minutes. She was limp, gray, and not breathing, and cord gases indicated acute severe metabolic and respiratory acidosis. The infant was taken to the NICU with multiple problems, including no primary reflexes, seizure disorder, and cerebral edema. She was diagnosed with cerebral palsy with right hemiplegia, chronic head pain, memory deficits, motor dysfunction, and many other deficits.
- PATIENT’S CLAIM Not reported.
- DOCTOR’S DEFENSE Not reported.
- VERDICT $3.45 million California settlement: $1 million from the ObGyn; and $2.45 million from the hospital.
Midwife has turn, then MD finishes difficult delivery
DELIVERY OF AN INFANT at term was performed by a physician who used forceps to assist. The child suffered brain damage and died.
- PATIENT’S CLAIM The physician failed to deliver the child in a timely manner, which led to brain damage and death.
- DOCTOR’S DEFENSE Labor was managed primarily by a midwife. The physician responded immediately when called and used appropriate emergency measures to deliver the child as quickly as possible.
- VERDICT $1.5 million settlement with the hospital before trial; Illinois defense verdict for the physician.
Embolism after C-section causes death
A 38-YEAR-OLD WOMAN pregnant with her second child had a C-section and tubal ligation performed by her ObGyn. She developed a pulmonary embolism a few days later and died.
- PATIENT’S CLAIM The patient’s age and weight were risk factors for pulmonary embolism, and she was immobilized for over 72 hours following surgery, which also increased the risk. The defendants took no steps to prevent a pulmonary embolism.
- DOCTOR’S DEFENSE There was no negligence.
- VERDICT Ohio defense verdict.
Surgery for pelvic pain and cyst leads to … more surgery
A SONOGRAM REVEALED an ovarian cyst in a woman, in her mid-40s, who was experiencing pelvic pain. Her physician recommended and performed surgery to find the source of the pain, as well as to possibly remove the cyst and ovaries. Following surgery, the woman was diagnosed with a colon perforation. A colostomy and two further surgeries were necessary. In addition, the patient suffered a bowel obstruction, colovaginal fistula, and scarring.
- PATIENT’S CLAIM The original surgery was unnecessary, and the colon perforation was negligent.
- DOCTOR’S DEFENSE Surgery was necessary to determine and treat the cause of the pain. Perforation of the colon did not occur during surgery, but resulted from the patient’s diverticulitis.
- VERDICT A $3,497,000 Maryland verdict was returned; however, this was reduced to $702,000 pursuant to the state cap for noneconomic damages.
Femoral nerve palsy occurs after hysterectomy
A 39-YEAR-OLD WOMAN was diagnosed with a leiomyomata in her lower uterus. The tissue in the area became necrotic, and prolapse resulted. Surgery was performed. A week later, the patient returned to the hospital because of pain and bleeding. The ObGyn covering for the physician who had performed the surgery recommended—then performed—a hysterectomy. Following the surgery, the woman experienced numbness in the right anterior and lateral thigh. According to a neurological consultation, the femoral nerve was damaged. The patient suffers from persistent femoral nerve palsy, affecting her ability to walk. She has undergone physical therapy and rehabilitation, as well as nerve conduction studies.
- PATIENT’S CLAIM The ObGyn negligently placed the retractor or failed to reposition the retractor blades after they moved during the surgery.
- DOCTOR’S DEFENSE There was no negligence. Femoral nerve injury is a known risk of pelvic surgery. The patient suffered only minor sensory and motor palsy immediately following surgery, and her ongoing complaints had no physical basis.
- VERDICT California defense verdict.
Patient fails to report continued irregular bleeding
AT HER ANNUAL EXAM, a 49-year-old woman told her gynecologist, Dr. A, about cramping and bleeding on day 10 and sometimes day 17 of her menstrual cycle over the previous 6 months. Dr. A noted a normal pelvic exam. She told the patient that the bleeding was a normal perimenopausal symptom and suggested taking Advil for the pain. No further testing was recommended. The patient failed to report continued irregular vaginal bleeding. A year later, Dr. B conducted the next annual exam and found an enlarged uterus in the 7- to 8-week range. Endometrial biopsy showed the left ovary to be tender, slightly enlarged, with a possible mass present. A sonogram 2 days later showed an enlarged right ovary with multiple cystic areas and a large complex mass of the left ovary—findings suspicious for ovarian cancer. Pathology following a D&C 1 month later indicated adenocarcinoma consistent with primary endometrial cancer. The patient was diagnosed with endometrioid type adenocarcinoma involving both ovaries and the uterus, as well as metastatic disease to the omentum and diaphragm. She underwent total abdominal hysterectomy, bilateral salpingo-oophorectomy, bilateral pelvic and periaortic lymph node dissection, omentectomy, and CUSA of the diaphragm. She is not expected to survive long-term.
- PATIENT’S CLAIM Dr. A was negligent for failing to timely diagnose and treat the cancer.
- DOCTOR’S DEFENSE As the patient reported irregular vaginal bleeding at one visit only, there was no indication for further testing of a woman her age and no reason to suspect any disease. Most likely, the irregular vaginal bleeding was unrelated to the ovarian cancer, and an endometrial biopsy after the first visit would not have changed the prognosis.
- VERDICT $750,000 Massachusetts settlement.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
The cases in this column are selected by the editors of OBG Management from Medical Malpractice Verdicts, Settlements & Experts, with permission of the editor, Lewis Laska (www.verdictslaska.com). The available information about the cases presented here is sometimes incomplete; pertinent details of a given situation therefore may be unavailable. Moreover, the cases may or may not have merit. Nevertheless, these cases represent the types of clinical situations that typically result in litigation and are meant to illustrate nationwide variation in jury verdicts and awards.
Paid Time Off
Many medical offices are following a popular trend in the business world—replacing employee sick leave, vacation, and any other miscellaneous time benefits with a combination of all of them, collectively referred to as “paid time off.”
There are several reasons why this is a good idea, but you should carefully consider all the pros and cons before you make such a change in your office. Contrary to what you may have read, a paid time off (PTO) policy is not without disadvantages.
Its advantages, however, are significant. Employees like the concept because most of them are generally healthy and never use all their sick leave. Allowing them to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate being treated more like adults who can make time-off decisions for themselves, and they like the increased flexibility that PTO provides.
Employers like it because there is less paperwork and less abuse of sick leave. They don't have to make any decisions about whether an employee is really sick or not since reasons for absence are now irrelevant, making feigned illnesses a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee's duties, you don't need to know or care about the reason for the request.
Critics of PTO say that employees are absent more frequently under a PTO system, which is sometimes true. Employees who never used their full allotment of sick leave will typically use all of their PTO every year, but most of these extra absences can be controlled by requiring prior approval for any PTO except emergencies.
Critics then point out that you are replacing decisions about what constitutes an illness with decisions about what constitutes an emergency, but as I will discuss below, most criteria for emergencies can be settled upon in advance.
You also have the option of allowing employees to take salary in exchange for unused PTO, which you can pay annually or when their employment ends. In general, though, I don't think that is a good idea. I believe vacations are necessary and important for good office morale, and they should be taken by all employees, as well as by all employers.
Remember Eastern's First Law: Your last words will not be, “I wish I had spent more time in the office.”
And as I've mentioned in several previous columns, you should be suspicious of any employee who refuses to take vacations. Such employees are often embezzlers who are afraid that someone will discover their illicit modus operandi during their absence.
If you're going to allow PTO to accrue and be paid later, it's probably best to allow only a portion (say, 25% maximum) to be taken that way.
The major disadvantage of PTO is the possibility that employees will resist staying home when they are ill. Some businesses converting to the PTO system have found that employees tend to view all paid time off as vacation time. So when they are sick, they don't want to “waste” any of their “vacation” days. The result is that many employees with upper respiratory infections and other communicable illnesses will come to work and transmit illness to fellow employees and patients alike. Productivity drops as more employees get sick, and patients, needless to say, are not happy about illnesses acquired (or suspected to be acquired) at the doctor's office.
So before switching to a paid time off system, it is important to weigh all the pros and cons and consider your options. Should you decide to proceed, anticipate the potential problems and put strategies in place to counter them.
First, define “advance notice”: Is it 24 hours, or is it a week? Then decide how you will define an emergency, and put these definitions in writing. Employees might regard waking up Monday morning with a bad hangover as an emergency, but you might not. Most would consider a sick child an emergency, but what about a malfunctioning car? Some circumstances will need to be decided on a case-by-case basis, but the more situations you can anticipate and settle in advance, the fewer hassles you will have.
Establish clear guidelines from the outset. Make sure everyone knows they will have to request PTO in advance except for emergencies.
Make it very clear that sick employees should stay home, and that if they come to work sick they will be sent home. You have an obligation to protect the rest of your employees, not to mention your patients (especially those who are elderly or immunocompromised), from a staff member with a potentially communicable illness.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Many medical offices are following a popular trend in the business world—replacing employee sick leave, vacation, and any other miscellaneous time benefits with a combination of all of them, collectively referred to as “paid time off.”
There are several reasons why this is a good idea, but you should carefully consider all the pros and cons before you make such a change in your office. Contrary to what you may have read, a paid time off (PTO) policy is not without disadvantages.
Its advantages, however, are significant. Employees like the concept because most of them are generally healthy and never use all their sick leave. Allowing them to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate being treated more like adults who can make time-off decisions for themselves, and they like the increased flexibility that PTO provides.
Employers like it because there is less paperwork and less abuse of sick leave. They don't have to make any decisions about whether an employee is really sick or not since reasons for absence are now irrelevant, making feigned illnesses a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee's duties, you don't need to know or care about the reason for the request.
Critics of PTO say that employees are absent more frequently under a PTO system, which is sometimes true. Employees who never used their full allotment of sick leave will typically use all of their PTO every year, but most of these extra absences can be controlled by requiring prior approval for any PTO except emergencies.
Critics then point out that you are replacing decisions about what constitutes an illness with decisions about what constitutes an emergency, but as I will discuss below, most criteria for emergencies can be settled upon in advance.
You also have the option of allowing employees to take salary in exchange for unused PTO, which you can pay annually or when their employment ends. In general, though, I don't think that is a good idea. I believe vacations are necessary and important for good office morale, and they should be taken by all employees, as well as by all employers.
Remember Eastern's First Law: Your last words will not be, “I wish I had spent more time in the office.”
And as I've mentioned in several previous columns, you should be suspicious of any employee who refuses to take vacations. Such employees are often embezzlers who are afraid that someone will discover their illicit modus operandi during their absence.
If you're going to allow PTO to accrue and be paid later, it's probably best to allow only a portion (say, 25% maximum) to be taken that way.
The major disadvantage of PTO is the possibility that employees will resist staying home when they are ill. Some businesses converting to the PTO system have found that employees tend to view all paid time off as vacation time. So when they are sick, they don't want to “waste” any of their “vacation” days. The result is that many employees with upper respiratory infections and other communicable illnesses will come to work and transmit illness to fellow employees and patients alike. Productivity drops as more employees get sick, and patients, needless to say, are not happy about illnesses acquired (or suspected to be acquired) at the doctor's office.
So before switching to a paid time off system, it is important to weigh all the pros and cons and consider your options. Should you decide to proceed, anticipate the potential problems and put strategies in place to counter them.
First, define “advance notice”: Is it 24 hours, or is it a week? Then decide how you will define an emergency, and put these definitions in writing. Employees might regard waking up Monday morning with a bad hangover as an emergency, but you might not. Most would consider a sick child an emergency, but what about a malfunctioning car? Some circumstances will need to be decided on a case-by-case basis, but the more situations you can anticipate and settle in advance, the fewer hassles you will have.
Establish clear guidelines from the outset. Make sure everyone knows they will have to request PTO in advance except for emergencies.
Make it very clear that sick employees should stay home, and that if they come to work sick they will be sent home. You have an obligation to protect the rest of your employees, not to mention your patients (especially those who are elderly or immunocompromised), from a staff member with a potentially communicable illness.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
Many medical offices are following a popular trend in the business world—replacing employee sick leave, vacation, and any other miscellaneous time benefits with a combination of all of them, collectively referred to as “paid time off.”
There are several reasons why this is a good idea, but you should carefully consider all the pros and cons before you make such a change in your office. Contrary to what you may have read, a paid time off (PTO) policy is not without disadvantages.
Its advantages, however, are significant. Employees like the concept because most of them are generally healthy and never use all their sick leave. Allowing them to take the difference as extra vacation time makes them happy and makes your office more attractive to excellent prospects. They also appreciate being treated more like adults who can make time-off decisions for themselves, and they like the increased flexibility that PTO provides.
Employers like it because there is less paperwork and less abuse of sick leave. They don't have to make any decisions about whether an employee is really sick or not since reasons for absence are now irrelevant, making feigned illnesses a thing of the past. If an employee requests a day off with adequate notice, and there is adequate coverage of that employee's duties, you don't need to know or care about the reason for the request.
Critics of PTO say that employees are absent more frequently under a PTO system, which is sometimes true. Employees who never used their full allotment of sick leave will typically use all of their PTO every year, but most of these extra absences can be controlled by requiring prior approval for any PTO except emergencies.
Critics then point out that you are replacing decisions about what constitutes an illness with decisions about what constitutes an emergency, but as I will discuss below, most criteria for emergencies can be settled upon in advance.
You also have the option of allowing employees to take salary in exchange for unused PTO, which you can pay annually or when their employment ends. In general, though, I don't think that is a good idea. I believe vacations are necessary and important for good office morale, and they should be taken by all employees, as well as by all employers.
Remember Eastern's First Law: Your last words will not be, “I wish I had spent more time in the office.”
And as I've mentioned in several previous columns, you should be suspicious of any employee who refuses to take vacations. Such employees are often embezzlers who are afraid that someone will discover their illicit modus operandi during their absence.
If you're going to allow PTO to accrue and be paid later, it's probably best to allow only a portion (say, 25% maximum) to be taken that way.
The major disadvantage of PTO is the possibility that employees will resist staying home when they are ill. Some businesses converting to the PTO system have found that employees tend to view all paid time off as vacation time. So when they are sick, they don't want to “waste” any of their “vacation” days. The result is that many employees with upper respiratory infections and other communicable illnesses will come to work and transmit illness to fellow employees and patients alike. Productivity drops as more employees get sick, and patients, needless to say, are not happy about illnesses acquired (or suspected to be acquired) at the doctor's office.
So before switching to a paid time off system, it is important to weigh all the pros and cons and consider your options. Should you decide to proceed, anticipate the potential problems and put strategies in place to counter them.
First, define “advance notice”: Is it 24 hours, or is it a week? Then decide how you will define an emergency, and put these definitions in writing. Employees might regard waking up Monday morning with a bad hangover as an emergency, but you might not. Most would consider a sick child an emergency, but what about a malfunctioning car? Some circumstances will need to be decided on a case-by-case basis, but the more situations you can anticipate and settle in advance, the fewer hassles you will have.
Establish clear guidelines from the outset. Make sure everyone knows they will have to request PTO in advance except for emergencies.
Make it very clear that sick employees should stay home, and that if they come to work sick they will be sent home. You have an obligation to protect the rest of your employees, not to mention your patients (especially those who are elderly or immunocompromised), from a staff member with a potentially communicable illness.
To respond to this column, e-mail Dr. Eastern at sknews@elsevier.com
The Value of Group Visits
As with so many things, I had heard about group medical visits long before I offered them. I had not remotely thought of offering them. Then that mother of invention, necessity, pushed her way into my office.
I had been struggling to help my most difficult patients. These were the patients with multiple problems. Many were obese with diabetes and chronic pain. In addition to their disease burden, many faced chaotic lives. They were living in poverty and lacked support at home.
Although they had frequent office visits, I was not succeeding in getting them to clinical goals. I felt like a nag when I tried to help them make changes. It wasn't good for them or me. And that was when I remembered I had a tool I was not using.
In October 2006, I began to offer group visits to patients with overlapping problems. We meet in my waiting room once a month from 5 p.m. to 6:30 p.m. The goal is to have the group work together on problem-solving skills and common problems.
Before each group meeting, I assess the patients' charts to see who needs refills or labs and what issues need to be addressed. I start each group off on a topic. Sometimes I give them a lighthearted quiz.
I am careful not to run the sessions as a class. The goal is for the patients to interact and solve problems with one another. I am there as a guide. I use an easel and markers to write down key words as they come up, to help define and reinforce take-home points. These are not group therapy sessions. The groups focus on medical issues such as accepting the need to take daily meds, affording care, and forming strategies for managing pain and achieving good nutrition despite the constraints of family and finances.
One of the most rewarding topics focuses on assertiveness skills. More than any other aspect, helping patients with this skill helps them feel more confident in managing their stress and their medical care. Another recurring topic is how to deal with setting goals and managing setbacks.
The ideal group size is from four to seven patients. This seems to be the magic number that allows everyone some airtime and prevents any one person from dominating the conversation.
During the group visits, I meet very briefly with each patient individually to check weight and vital signs and discuss any particular issues.
I bill the same way as with an individual visit. However, the evaluation and management (E/M) codes do tend to be less robust in this setting.
Privacy is important to address from the outset. From the beginning, I have made it clear that no one need reveal anything he or she does not wish to reveal. I wrote down a list of problems that many of my patients share and asked each person to think about which ones applied to him or her. Inevitably, the participants do reveal details about themselves as they become comfortable. In addition, when I communicate with participants via e-mail to remind them of group dates, I make sure that messages are sent individually to safeguard privacy.
Group visits are efficient. The work we all do with patients is repetitive, and it is more efficient to do it once for five people than five separate times. I run an individual medical practice, so my panel is small. Nevertheless, the group allows four to seven people to be seen in the duration of time I would have needed to see three patients during one-on-one office visits.
The bottom line is that my patients have benefited. The beauty is that when they solve problems with the support of their peers, they are more likely to set manageable goals. And when they achieve goals, there is a lovely positive feedback cycle that begins. This grows confidence.
Confidence is an undermeasured tool in our practices. Confident patients are more compliant and achieve better outcomes.
As a physician who is seeking to help motivate healthy behaviors, I find the synergistic value of group visits both humbling and rewarding.
As with so many things, I had heard about group medical visits long before I offered them. I had not remotely thought of offering them. Then that mother of invention, necessity, pushed her way into my office.
I had been struggling to help my most difficult patients. These were the patients with multiple problems. Many were obese with diabetes and chronic pain. In addition to their disease burden, many faced chaotic lives. They were living in poverty and lacked support at home.
Although they had frequent office visits, I was not succeeding in getting them to clinical goals. I felt like a nag when I tried to help them make changes. It wasn't good for them or me. And that was when I remembered I had a tool I was not using.
In October 2006, I began to offer group visits to patients with overlapping problems. We meet in my waiting room once a month from 5 p.m. to 6:30 p.m. The goal is to have the group work together on problem-solving skills and common problems.
Before each group meeting, I assess the patients' charts to see who needs refills or labs and what issues need to be addressed. I start each group off on a topic. Sometimes I give them a lighthearted quiz.
I am careful not to run the sessions as a class. The goal is for the patients to interact and solve problems with one another. I am there as a guide. I use an easel and markers to write down key words as they come up, to help define and reinforce take-home points. These are not group therapy sessions. The groups focus on medical issues such as accepting the need to take daily meds, affording care, and forming strategies for managing pain and achieving good nutrition despite the constraints of family and finances.
One of the most rewarding topics focuses on assertiveness skills. More than any other aspect, helping patients with this skill helps them feel more confident in managing their stress and their medical care. Another recurring topic is how to deal with setting goals and managing setbacks.
The ideal group size is from four to seven patients. This seems to be the magic number that allows everyone some airtime and prevents any one person from dominating the conversation.
During the group visits, I meet very briefly with each patient individually to check weight and vital signs and discuss any particular issues.
I bill the same way as with an individual visit. However, the evaluation and management (E/M) codes do tend to be less robust in this setting.
Privacy is important to address from the outset. From the beginning, I have made it clear that no one need reveal anything he or she does not wish to reveal. I wrote down a list of problems that many of my patients share and asked each person to think about which ones applied to him or her. Inevitably, the participants do reveal details about themselves as they become comfortable. In addition, when I communicate with participants via e-mail to remind them of group dates, I make sure that messages are sent individually to safeguard privacy.
Group visits are efficient. The work we all do with patients is repetitive, and it is more efficient to do it once for five people than five separate times. I run an individual medical practice, so my panel is small. Nevertheless, the group allows four to seven people to be seen in the duration of time I would have needed to see three patients during one-on-one office visits.
The bottom line is that my patients have benefited. The beauty is that when they solve problems with the support of their peers, they are more likely to set manageable goals. And when they achieve goals, there is a lovely positive feedback cycle that begins. This grows confidence.
Confidence is an undermeasured tool in our practices. Confident patients are more compliant and achieve better outcomes.
As a physician who is seeking to help motivate healthy behaviors, I find the synergistic value of group visits both humbling and rewarding.
As with so many things, I had heard about group medical visits long before I offered them. I had not remotely thought of offering them. Then that mother of invention, necessity, pushed her way into my office.
I had been struggling to help my most difficult patients. These were the patients with multiple problems. Many were obese with diabetes and chronic pain. In addition to their disease burden, many faced chaotic lives. They were living in poverty and lacked support at home.
Although they had frequent office visits, I was not succeeding in getting them to clinical goals. I felt like a nag when I tried to help them make changes. It wasn't good for them or me. And that was when I remembered I had a tool I was not using.
In October 2006, I began to offer group visits to patients with overlapping problems. We meet in my waiting room once a month from 5 p.m. to 6:30 p.m. The goal is to have the group work together on problem-solving skills and common problems.
Before each group meeting, I assess the patients' charts to see who needs refills or labs and what issues need to be addressed. I start each group off on a topic. Sometimes I give them a lighthearted quiz.
I am careful not to run the sessions as a class. The goal is for the patients to interact and solve problems with one another. I am there as a guide. I use an easel and markers to write down key words as they come up, to help define and reinforce take-home points. These are not group therapy sessions. The groups focus on medical issues such as accepting the need to take daily meds, affording care, and forming strategies for managing pain and achieving good nutrition despite the constraints of family and finances.
One of the most rewarding topics focuses on assertiveness skills. More than any other aspect, helping patients with this skill helps them feel more confident in managing their stress and their medical care. Another recurring topic is how to deal with setting goals and managing setbacks.
The ideal group size is from four to seven patients. This seems to be the magic number that allows everyone some airtime and prevents any one person from dominating the conversation.
During the group visits, I meet very briefly with each patient individually to check weight and vital signs and discuss any particular issues.
I bill the same way as with an individual visit. However, the evaluation and management (E/M) codes do tend to be less robust in this setting.
Privacy is important to address from the outset. From the beginning, I have made it clear that no one need reveal anything he or she does not wish to reveal. I wrote down a list of problems that many of my patients share and asked each person to think about which ones applied to him or her. Inevitably, the participants do reveal details about themselves as they become comfortable. In addition, when I communicate with participants via e-mail to remind them of group dates, I make sure that messages are sent individually to safeguard privacy.
Group visits are efficient. The work we all do with patients is repetitive, and it is more efficient to do it once for five people than five separate times. I run an individual medical practice, so my panel is small. Nevertheless, the group allows four to seven people to be seen in the duration of time I would have needed to see three patients during one-on-one office visits.
The bottom line is that my patients have benefited. The beauty is that when they solve problems with the support of their peers, they are more likely to set manageable goals. And when they achieve goals, there is a lovely positive feedback cycle that begins. This grows confidence.
Confidence is an undermeasured tool in our practices. Confident patients are more compliant and achieve better outcomes.
As a physician who is seeking to help motivate healthy behaviors, I find the synergistic value of group visits both humbling and rewarding.