User login
Black surgeons transcend artificial barriers
The emergence of African Americans as acclaimed leaders in the field of surgery over the last century is a triumph of personal struggle, brilliant minds, and sheer determination.
Disparities in educational and professional opportunities related to racial/ethnic identity persist, but LaSalle D. Leffall, Jr., MD, FACS, fondly recalls a favorite quote from pioneering African American surgeon Charles Drew: “Excellence of performance will transcend artificial barriers created by man.” The goals and abundant talent shared by the membership of the American College of Surgeons (ACS) and Society of Black Academic Surgeons (SBAS) are testimony to the ongoing dissolution of these artificial barriers.
Parallels are evident between the history of organized surgery in America and African American efforts to achieve health care equity. While the spectrum of surgical procedures mushroomed in the late 19th century, surgical training was characterized by inconsistency and instability. The ACS was established in 1913 with the mission of “improving the care of the surgical patient and to safeguarding standards of care in an optimal and ethical practice environment.”
Significant disparities in medical and surgical care existed for African Americans in this era. During the decades following the Civil War, black citizens were routinely denied care or they received substandard care delivered in segregated hospitals. Medical education opportunities for African Americans were nearly nonexistent.
Nonetheless, African Americans mobilized their talent and energy to address the same threats to quality medical care as those faced by the ACS founders, but having to overcome even greater obstacles in the form of systematic racism and exclusion.

Chicago’s Provident Hospital and Training School (the first African American-owned and -operated hospital) was established in 1891. Howard University College of Medicine in Washington, and Meharry Medical College in Nashville, Tenn., founded in 1868 and 1876, respectively, remained the predominent options for prospective African American medical students for several decades. Because African American medical professionals were denied membership in the American Medical Association, they formed their own professional society, the National Medical Association, in 1895.
In contrast, Dr. Daniel Hale Williams, founder of the Provident Hospital and founding member of the National Medical Association, was a charter member of ACS in 1913. However, more than 20 years passed before another African American surgeon (Louis Tompkins Wright, MD, FACS) became a Fellow of the College.

The number of African American surgeons in the College grew steadily after World War II, and in the past 3 years, approximately 6% of ACS inductees have been African Americans.
The value of race/ethnic diversity in optimizing quality of care is summarized by Dr. Otis Brawley, Chief Medical Officer for the American Cancer Society and past Director of the Office for Special Populations Research at the National Institutes of Health: “The practice of surgery is both a science and an art. Part of the art is understanding the patient’s needs and communicating well. Modern medicine has used the phrase ‘cultural competence’ to describe this. While a physician of one race certainly can and often does provide excellent service to a patient of another, diverse membership in the surgical community is essential for cultural competence of that community.”
Pioneering black surgeons
The following lists a few of the many African American surgical luminaries who fought incredible obstacles in order to improve health outcomes for all:
• Daniel Hale Williams, MD, FACS (1856-1931): Founder of Provident Hospital; performed one of the first successful open heart surgeries; charter member of the ACS.
• Louis Tompkins Wright, MD, FACS (1891-1952): Second African American admitted to ACS Fellowship (in 1934) amid much debate and controversy, despite graduating cum laude from Harvard Medical School and having an illustrious career as a decorated Army surgeon. Dr. Wright was the son of a slave (Ceah Ketcham Wright, MD) who pursued medical education at Meharry after obtaining his freedom.
• Charles Richard Drew, MD, FACS (1904-1950): Pioneer transfusion researcher; first American Red Cross Blood Bank director. Dr. Leffall, a Drew trainee, recalls, “After several applications for fellowship in ACS, Drew was approved for admission at the annual convocation October 1950. He was killed in an automobile accident April 1, 1950, en route to a medical meeting in Tuskegee, Ala. In a highly unusual action, the College’s Board of Regents approved him for posthumous fellowship October 1951.”

• Vivien Thomas (1910-1985): surgical technical assistant to Dr. Alfred Blalock at Vanderbilt, and supervisor of surgical laboratories at Johns Hopkins for 35 years; became pioneer in cardiac surgery despite having no formal education beyond high school and awarded honorary doctorate at Hopkins in 1976.
• Samuel Kountz, MD, FACS (1930-1981): Pioneer transplant surgeon; performed first successful human non-identical twin kidney transplant; developed Belzer kidney perfusion prototype.
• Claude Organ, MD, FACS (1926-2005): Professor of surgery at the University of California, Davis, and University of California, San Francisco East; editor of JAMA Archives of Surgery; founding member and President of SBAS (1995-1997) and second African American President of ACS (2003-2004).
• LaSalle D. Leffall, Jr., MD, FACS: Charles R. Drew Professor of Surgery and former chairman of surgery at Howard University; former chairman of the President’s Cancer Panel; SBAS president (1997-1998); first African American president of the American Cancer Society; first African American president of the ACS (1995-1996).
• Levi Watkins, MD: Professor of cardiac surgery, Johns Hopkins University; performed first human implantation of automatic implantable defibrillator; carried out landmark efforts to strengthen diversity among health care professionals. Dr. Watkins commented: “On the occasion of the national holiday of my former pastor, Dr. Martin Luther King, Jr., I am happy to say that given the opportunity the African American surgeon has shown very well that he or she is capable and worthy to serve and lead this nation in health equity and well-being. We must, however, not allow this progress and opportunity to slip from us using slogans to replace direct action on our part. I must compliment the ACS for its role in helping to bring about change in this area.”

• Harold P. Freeman, MD, FACS: Past president, American Cancer Society; past chairman, President’s Cancer Panel; pioneer architect of patient navigation programs; founder and president/CEO, Harold P. Freeman Patient Navigation Institute.
• Haile Debas, MD, FACS: Past chairman, University of California, San Francisco (UCSF) department of surgery; past dean, School of Medicine; founding executive director, UCSF Global Health Sciences; president, the American Surgical Association (2002-2003).
• Benjamin S. Carson, Sr., MD: Emeritus professor of neurosurgery, Johns Hopkins School of Medicine; president/CEO American Business Collaborative, LLC; awarded Presidential Medal of Freedom; renowned for historic 1987 surgical procedure separating craniopagus conjoined twins.
He recalled: “Twins joined at the back of the head had never before been separated with both surviving. The 22-hour operation which combined advanced neurosurgical techniques with hypothermic cardiac arrest proved successful. I intentionally remained in the background and did not reveal my role as the primary neurosurgeon until the press conference several hours after the completion of the operation. Historically, the accomplishments of Blacks in scientific endeavors have not been heavily covered by the news media. In order to inspire millions of Black youngsters who lacked scientific role models, I waited until the story was so big that the media could not back off. Thankfully our society has advanced to the point that this kind of thing is no longer necessary.”

• Alexa Canady, MD, FACS: First African American female neurosurgery resident (University of Minnesota); became chief of neurosurgery at the Children’s Hospital of Detroit at age 36.
• Henri R. Ford, MD, FACS: Past surgeon-in-chief, Children’s Hospital of Pittsburgh; past vice-president, chief of surgery, University of California, Los Angeles (UCLA); vice-dean for Medical Education, Keck School/UCLA; SBAS president (2010-2011).
• L.D. Britt, MD, MPH, D.Sc (Hon), FACS, FCCM, FRCSEng (Hon), FRCSEd (Hon), FWACS (Hon), FRCSI (Hon), FCS(SA) (Hon), FRCS(Glasg) (Hon):
Chairman, department of surgery at Eastern Virginia Medical School; past president of numerous academic societies (American College of Surgeons, 2010-2011; Southern Surgical Congress; American Association of Trauma; Halsted Society, SBAS 1999-2001; American Surgical Association; Society of Surgical Chairs); current SBAS executive director; Robert J. Glaser Distinguished Educator Award recipient (highest teaching award granted by Association of American Medical Colleges).
Professional and personal challenges

Many of these African American professionals tackle the same barriers to productive longevity as the African American general population – disparities in professional promotion opportunities, socioeconomic disadvantages, and reduced life expectancy (National Vital Statistics Reports; vol. 61 no. 4., National Center for Health Statistics 2013).
Black physicians are less likely to receive academic promotion in university programs and are underrepresented within the full professorship rank (JAMA 2000; 284:1085-92); African American researchers are less likely to receive NIH research funding (Science 2011;333:1015-19); and society has lost many academically accomplished African American surgeons to premature death from cancer and other illnesses as well as trauma. Icons Dr. Charles Drew and Dr. Sam Kountz both died in the prime of their professional careers. More recently, the surgical oncology community mourned the losses of Keith Amos, MD, FACS, assistant professor of surgery, University of North Carolina and Yvedt Matory, MD, FACS, assistant professor of surgery, Harvard Medical School. Both of these talented surgeons died before reaching age 50.
Socioeconomic disparities and downstream effects on the pipeline of African American students and trainees remain apparent in the pool of surgeons available to pursue academic careers. These inequities are poignantly described by Sha’shonda Revels, MD, chief resident in general surgery at the University of Michigan, Ann Arbor, with plans to pursue an academic career in cardiothoracic surgery: “I consider myself truly blessed to have the opportunity to learn a tangible skill that I can use to effect change in the lives of others. … I appreciate the struggles that others have made for me to have this opportunity. Those not so well known ‘others’ include my grandmother who cleaned houses, and took care of me so that my mother could finish high school and attend college. They also include my parents who were tenacious about academics and would not accept a B average.”

The SBAS is born
Despite post-WWII gains, opportunities remained limited for black surgeons to achieve prominence and recognition in academic surgical societies. The Society for Black Academic Surgeons was therefore established as a network that would promote the careers of African American surgeons in academia and accelerate their upward professional trajectory.
SBAS founding member and President (1993-1995) Eddie Hoover, MD, FACS, professor of surgery at the State University of New York Buffalo, and Editor-in-Chief for the Journal of the National Medical Association, provides this passionate account of its history and accomplishments: “SBAS was created in a hotel room at the Marriott in New Orleans in 1987 to address the paucity of academic African American surgeons; their poor retention, promotion, and research funding; and lack of a leadership role in American surgery. The hero of academic African American surgeons, Dr. Charles Drew, adorns the shield of SBAS as much for his defiance of ACS for refusing to accept other well-qualified African American surgeons in the 1940’s as for his scientific contributions …With strong ACS support, SBAS has been stunningly successful over the past 27 years with a dozen SBAS members serving as surgical chairs and four as deans of majority schools.”

Dr. Britt, first African American chair of the ACS Board of Regents and later SBAS president, emphasizes that these two organizations have shared goals. “The evolution of the American College of Surgeons, the world’s largest organization for surgeons, and its growing partnership with the Society of Black Academic Surgeons (demonstrated formally, informally, and sometimes tacitly) needs to be recognized, underscored, and continually enhanced. Many of the ideals of SBAS now mirror the ideals and achievements of the ACS, including an ever growing diverse membership, improved diversity at all levels of leadership, meaningful mentorships for underrepresented minorities, and the establishment of several initiatives to address severe health care disparities in the world’s wealthiest nation.”
The 25th Annual Scientific Meeting of the SBAS will be hosted by the University of North Carolina, Chapel Hill, April 9-11, 2015.
Frederick Cason, MD, FACS, professor of surgery and chief, Division of Surgical Education at Morehouse School of Medicine and the SBAS historian and archivist, stated, “With the strong academic activities of SBAS, the networking it fosters, and the partnerships with numerous academic institutions and members of the College… there developed some 10 academic chairmen and at least 4 deans leading our major medical centers in America.”

Andrea Hayes-Jordan, MD, SBAS 2015 Annual Meeting program chair and associate professor of surgery and Pediatrics and Director of Pediatric Surgical Oncology at the University of Texas M.D. Anderson Cancer Center, notes, “At the annual meeting we are not only able to see the results of excellent research efforts from minority surgeons from around the country, but one has the unique opportunity to interact with them on a personal level, at an intimate meeting. This personal interaction with successful chair persons of color is invaluable in receiving pearls of advice, and understanding the nuances of successful academic practice. We hope in the future to increase the membership of SBAS and continue to promote the timely advancement of our members.”

Robert Higgins, MD, FACS, Professor and Chairman of the Department of Surgery, Ohio State University and past SBAS president (2008-2009), commented, “As someone who has benefitted from the progress that the SBAS/ACS relationship has fostered, I think the critical strength of this effort in the future is based upon its ability to create foundations for the development of underrepresented men and women of diverse backgrounds to reach new heights in surgery.”
Gender diversity addressed
Health equity efforts must also address gender imbalance. Edward E. Cornwell III, MD, FACS, LaSalle D. Leffall, Jr. Professor and Chairman of Surgery, Howard University, and SBAS president (2003-2004), reminisced about the first national meeting photo (above) of SBAS leadership and notes the “most obvious sign of the times in April 1989 … no women surgeons in that photo (the woman in the top row wasn’t a physician). Today, at a time when 14 of my 25 categorical surgical residents are women … we stand on the precipice of the next 25 years of career milestones trumpeting gender diversity – that will surpass the explosion we saw over the last 25 years with male surgeons of color.”

Dr. Brawley also commented on the meteoric rise of African American women surgeons: “I take particular pride in the contribution today of black women who have come on strong in the past half-century. I appreciate and celebrate their achievement.”
Patricia Turner, MD, FACS, Director, ACS Division of Member Services, and Associate Professor of Surgery at the University of Chicago, summarized the African American female experience in surgery: “It is indeed a pleasure to note that in the years since the first SBAS photograph in 1989 … the number of women in medicine and surgery continues to surge. This recent growth is as much a reflection of an increased interest in surgery among women who may have been discouraged previously, as it is of a profession that has realized that previously accepted constraints around gender, race, and other factors limited access to colleagues exemplifying excellence in surgery. ACS and SBAS have consistently placed excellence, integrity, and outcomes at the forefront of their mission. Diversity brings quality, and the house of surgery is no different.”

Mentorship and Giving Back
Despite facing myriad obstacles, successful contemporary African American surgeons that are testimony to the mentorship and outreach efforts of SBAS as well as the ACS leadership have been acknowledged by an exhibit developed by the National Library of Medicine titled “Opening Doors: Contemporary African American Academic Surgeons,” and by a chapter contributed by Dr. Britt for the ACS Centennial textbook, “Setting the Course and Establishing Alliances: Fellows of the American College of Surgeons with African American Heritage.” The NLM exhibit specifically highlights the achievements of contemporary surgeons Drs. Alexa Canady; LaSalle Lefall; Claude Organ (1926-2005); Rosalyn Scott; L.D. Britt; Malcolm V. Brock; Karyn L.Butler; Benjamin Carson; Edward Cornwell; Kenneth Davis; Sharon Henry; Carla Pugh; Velma Scantlebury; Claudia Thomas; Errington Thompson; Levi Watkins; Patricia Bath; and Richard Scott. Dr. Britt (a legend in his own right as well as a contemporary icon) also acknowledges the accomplishments of the recent generations of academic surgeons (many of which overlap with the notables listed by the NLM), including Drs. Levi Watkins; Kenneth Forde; Alexa Canady; Clive Callender; Arthur Fleming; Lenworth Jacobs; Velma Scantlebury; Sharon Henry; Patricia Turner; Cato Laurencin; Butch Rossner; Kimberly Joseph; Debra Ford; Robert Higgins; Lisa Newman; Carla Pugh; Electron Kebenew; Terrence Fullum; David Jacobs; Andre Campbell; Kenneth Davis; Rhonda Henry-Tillman; Sherilyn Gordon-Burroughs; Hobart Harris; Michael Watkins; Raphael Lee; Karyn Butler; Edward Barksdale; Orlando Kirton; Jeffrey Upperman; Frederick Cason; Malcolm Brock; and Raymond Bynoe.

African Americans in medicine and surgery remain committed to improving the landscape of health care for underrepresented minority patients, students, and trainees today as in the past. This dedication was expressed by Dr. Daniel Hale Williams many decades ago: “My greatest reward is knowing that I can help my fellow man, especially those of my own race, who so deserve a better way of life.”
Today, trainee Dr. Revels echoes a similar allegiance to eradicating health care disparities by strengthening gender balance as well as racial/ethnic diversity in the health care profession: “I have a responsibility to stand for the next generation of young women of color who may be told that they didn’t need to take that algebra class or that AP classes would be too hard for them.”
Data continue to document that African American physicians are substantially more likely to establish practices that provide care to minority and impoverished patient populations (The Rationale for Diversity in the Health Professions: A Review of the Evidence. Washington, DC: U.S. Department of Health and Human Services Health Resources and Services Administration Bureau of Health Professions, October 2006).
Transcending artificial barriers
The ACS and the SBAS are in many ways bound together by their shared history, goals, and membership, and both have a critical role to play in the continuing struggle for equity and diversity in the surgical profession. Dr. Britt eloquently stated: “The month of February should not be the only time to highlight these milestones. On the contrary, there should be around-the-clock recognition, along with continual emphasis on even more advances. Let me be one of the first to toast this special partnership.”

Lisa Newman MD, MPH, FACS, FASCO, is Professor of Surgery and Director of the Breast Care Center at the University of Michigan in Ann Arbor.
Her research focus includes studies of high-risk/triple negative breast cancer and breast cancer disparities related to African ancestry. This research involves an international breast cancer registry. Dr. Newman also serves on the Program Committee for the Society of Black Academic Surgeons.
Several resources are available to those interested in learning more about the history of African Americans in medicine and surgery in particular:
“Opening Doors: Contemporary African American Academic Surgeons”; exhibit developed by the National Library of Medicine and the Reginald F. Lewis Museum of Maryland African American History and Culture” (http://www.nlm.nih.gov/exhibition/aframsurgeons/)
Organ, Claude, A Century of Black Surgeons: The USA Experience. Norman, OK: Transcript Press, 1987.
Leffall, LaSalle D., No Boundaries: A Cancer Surgeon’s Odyssey. Washington DC: Howard University Press, 2005.
O’Shea, JS., “Louis T. Wright and Henry W. Cave: How they paved the way for fellowships for black surgeons.” Bulletin of the American College of Surgeons 2005; 90(10):22-29.
Stain, SC, “Presidential Address: Dr. Organ, how are we doing”, American Journal of Surgery 2009; 197:137-41.
ACS Centennial textbook, pages 34-41, by Dr. L.D. Britt “Setting the Course and Establishing Alliances: Fellows of the American College of Surgeons with an African American Heritage”
Several resources are available to those interested in learning more about the history of African Americans in medicine and surgery in particular:
“Opening Doors: Contemporary African American Academic Surgeons”; exhibit developed by the National Library of Medicine and the Reginald F. Lewis Museum of Maryland African American History and Culture” (http://www.nlm.nih.gov/exhibition/aframsurgeons/)
Organ, Claude, A Century of Black Surgeons: The USA Experience. Norman, OK: Transcript Press, 1987.
Leffall, LaSalle D., No Boundaries: A Cancer Surgeon’s Odyssey. Washington DC: Howard University Press, 2005.
O’Shea, JS., “Louis T. Wright and Henry W. Cave: How they paved the way for fellowships for black surgeons.” Bulletin of the American College of Surgeons 2005; 90(10):22-29.
Stain, SC, “Presidential Address: Dr. Organ, how are we doing”, American Journal of Surgery 2009; 197:137-41.
ACS Centennial textbook, pages 34-41, by Dr. L.D. Britt “Setting the Course and Establishing Alliances: Fellows of the American College of Surgeons with an African American Heritage”
Several resources are available to those interested in learning more about the history of African Americans in medicine and surgery in particular:
“Opening Doors: Contemporary African American Academic Surgeons”; exhibit developed by the National Library of Medicine and the Reginald F. Lewis Museum of Maryland African American History and Culture” (http://www.nlm.nih.gov/exhibition/aframsurgeons/)
Organ, Claude, A Century of Black Surgeons: The USA Experience. Norman, OK: Transcript Press, 1987.
Leffall, LaSalle D., No Boundaries: A Cancer Surgeon’s Odyssey. Washington DC: Howard University Press, 2005.
O’Shea, JS., “Louis T. Wright and Henry W. Cave: How they paved the way for fellowships for black surgeons.” Bulletin of the American College of Surgeons 2005; 90(10):22-29.
Stain, SC, “Presidential Address: Dr. Organ, how are we doing”, American Journal of Surgery 2009; 197:137-41.
ACS Centennial textbook, pages 34-41, by Dr. L.D. Britt “Setting the Course and Establishing Alliances: Fellows of the American College of Surgeons with an African American Heritage”
The emergence of African Americans as acclaimed leaders in the field of surgery over the last century is a triumph of personal struggle, brilliant minds, and sheer determination.
Disparities in educational and professional opportunities related to racial/ethnic identity persist, but LaSalle D. Leffall, Jr., MD, FACS, fondly recalls a favorite quote from pioneering African American surgeon Charles Drew: “Excellence of performance will transcend artificial barriers created by man.” The goals and abundant talent shared by the membership of the American College of Surgeons (ACS) and Society of Black Academic Surgeons (SBAS) are testimony to the ongoing dissolution of these artificial barriers.
Parallels are evident between the history of organized surgery in America and African American efforts to achieve health care equity. While the spectrum of surgical procedures mushroomed in the late 19th century, surgical training was characterized by inconsistency and instability. The ACS was established in 1913 with the mission of “improving the care of the surgical patient and to safeguarding standards of care in an optimal and ethical practice environment.”
Significant disparities in medical and surgical care existed for African Americans in this era. During the decades following the Civil War, black citizens were routinely denied care or they received substandard care delivered in segregated hospitals. Medical education opportunities for African Americans were nearly nonexistent.
Nonetheless, African Americans mobilized their talent and energy to address the same threats to quality medical care as those faced by the ACS founders, but having to overcome even greater obstacles in the form of systematic racism and exclusion.
Chicago’s Provident Hospital and Training School (the first African American-owned and -operated hospital) was established in 1891. Howard University College of Medicine in Washington, and Meharry Medical College in Nashville, Tenn., founded in 1868 and 1876, respectively, remained the predominent options for prospective African American medical students for several decades. Because African American medical professionals were denied membership in the American Medical Association, they formed their own professional society, the National Medical Association, in 1895.
In contrast, Dr. Daniel Hale Williams, founder of the Provident Hospital and founding member of the National Medical Association, was a charter member of ACS in 1913. However, more than 20 years passed before another African American surgeon (Louis Tompkins Wright, MD, FACS) became a Fellow of the College.
The number of African American surgeons in the College grew steadily after World War II, and in the past 3 years, approximately 6% of ACS inductees have been African Americans.
The value of race/ethnic diversity in optimizing quality of care is summarized by Dr. Otis Brawley, Chief Medical Officer for the American Cancer Society and past Director of the Office for Special Populations Research at the National Institutes of Health: “The practice of surgery is both a science and an art. Part of the art is understanding the patient’s needs and communicating well. Modern medicine has used the phrase ‘cultural competence’ to describe this. While a physician of one race certainly can and often does provide excellent service to a patient of another, diverse membership in the surgical community is essential for cultural competence of that community.”
Pioneering black surgeons
The following lists a few of the many African American surgical luminaries who fought incredible obstacles in order to improve health outcomes for all:
• Daniel Hale Williams, MD, FACS (1856-1931): Founder of Provident Hospital; performed one of the first successful open heart surgeries; charter member of the ACS.
• Louis Tompkins Wright, MD, FACS (1891-1952): Second African American admitted to ACS Fellowship (in 1934) amid much debate and controversy, despite graduating cum laude from Harvard Medical School and having an illustrious career as a decorated Army surgeon. Dr. Wright was the son of a slave (Ceah Ketcham Wright, MD) who pursued medical education at Meharry after obtaining his freedom.
• Charles Richard Drew, MD, FACS (1904-1950): Pioneer transfusion researcher; first American Red Cross Blood Bank director. Dr. Leffall, a Drew trainee, recalls, “After several applications for fellowship in ACS, Drew was approved for admission at the annual convocation October 1950. He was killed in an automobile accident April 1, 1950, en route to a medical meeting in Tuskegee, Ala. In a highly unusual action, the College’s Board of Regents approved him for posthumous fellowship October 1951.”
• Vivien Thomas (1910-1985): surgical technical assistant to Dr. Alfred Blalock at Vanderbilt, and supervisor of surgical laboratories at Johns Hopkins for 35 years; became pioneer in cardiac surgery despite having no formal education beyond high school and awarded honorary doctorate at Hopkins in 1976.
• Samuel Kountz, MD, FACS (1930-1981): Pioneer transplant surgeon; performed first successful human non-identical twin kidney transplant; developed Belzer kidney perfusion prototype.
• Claude Organ, MD, FACS (1926-2005): Professor of surgery at the University of California, Davis, and University of California, San Francisco East; editor of JAMA Archives of Surgery; founding member and President of SBAS (1995-1997) and second African American President of ACS (2003-2004).
• LaSalle D. Leffall, Jr., MD, FACS: Charles R. Drew Professor of Surgery and former chairman of surgery at Howard University; former chairman of the President’s Cancer Panel; SBAS president (1997-1998); first African American president of the American Cancer Society; first African American president of the ACS (1995-1996).
• Levi Watkins, MD: Professor of cardiac surgery, Johns Hopkins University; performed first human implantation of automatic implantable defibrillator; carried out landmark efforts to strengthen diversity among health care professionals. Dr. Watkins commented: “On the occasion of the national holiday of my former pastor, Dr. Martin Luther King, Jr., I am happy to say that given the opportunity the African American surgeon has shown very well that he or she is capable and worthy to serve and lead this nation in health equity and well-being. We must, however, not allow this progress and opportunity to slip from us using slogans to replace direct action on our part. I must compliment the ACS for its role in helping to bring about change in this area.”
• Harold P. Freeman, MD, FACS: Past president, American Cancer Society; past chairman, President’s Cancer Panel; pioneer architect of patient navigation programs; founder and president/CEO, Harold P. Freeman Patient Navigation Institute.
• Haile Debas, MD, FACS: Past chairman, University of California, San Francisco (UCSF) department of surgery; past dean, School of Medicine; founding executive director, UCSF Global Health Sciences; president, the American Surgical Association (2002-2003).
• Benjamin S. Carson, Sr., MD: Emeritus professor of neurosurgery, Johns Hopkins School of Medicine; president/CEO American Business Collaborative, LLC; awarded Presidential Medal of Freedom; renowned for historic 1987 surgical procedure separating craniopagus conjoined twins.
He recalled: “Twins joined at the back of the head had never before been separated with both surviving. The 22-hour operation which combined advanced neurosurgical techniques with hypothermic cardiac arrest proved successful. I intentionally remained in the background and did not reveal my role as the primary neurosurgeon until the press conference several hours after the completion of the operation. Historically, the accomplishments of Blacks in scientific endeavors have not been heavily covered by the news media. In order to inspire millions of Black youngsters who lacked scientific role models, I waited until the story was so big that the media could not back off. Thankfully our society has advanced to the point that this kind of thing is no longer necessary.”
• Alexa Canady, MD, FACS: First African American female neurosurgery resident (University of Minnesota); became chief of neurosurgery at the Children’s Hospital of Detroit at age 36.
• Henri R. Ford, MD, FACS: Past surgeon-in-chief, Children’s Hospital of Pittsburgh; past vice-president, chief of surgery, University of California, Los Angeles (UCLA); vice-dean for Medical Education, Keck School/UCLA; SBAS president (2010-2011).
• L.D. Britt, MD, MPH, D.Sc (Hon), FACS, FCCM, FRCSEng (Hon), FRCSEd (Hon), FWACS (Hon), FRCSI (Hon), FCS(SA) (Hon), FRCS(Glasg) (Hon):
Chairman, department of surgery at Eastern Virginia Medical School; past president of numerous academic societies (American College of Surgeons, 2010-2011; Southern Surgical Congress; American Association of Trauma; Halsted Society, SBAS 1999-2001; American Surgical Association; Society of Surgical Chairs); current SBAS executive director; Robert J. Glaser Distinguished Educator Award recipient (highest teaching award granted by Association of American Medical Colleges).
Professional and personal challenges
Many of these African American professionals tackle the same barriers to productive longevity as the African American general population – disparities in professional promotion opportunities, socioeconomic disadvantages, and reduced life expectancy (National Vital Statistics Reports; vol. 61 no. 4., National Center for Health Statistics 2013).
Black physicians are less likely to receive academic promotion in university programs and are underrepresented within the full professorship rank (JAMA 2000; 284:1085-92); African American researchers are less likely to receive NIH research funding (Science 2011;333:1015-19); and society has lost many academically accomplished African American surgeons to premature death from cancer and other illnesses as well as trauma. Icons Dr. Charles Drew and Dr. Sam Kountz both died in the prime of their professional careers. More recently, the surgical oncology community mourned the losses of Keith Amos, MD, FACS, assistant professor of surgery, University of North Carolina and Yvedt Matory, MD, FACS, assistant professor of surgery, Harvard Medical School. Both of these talented surgeons died before reaching age 50.
Socioeconomic disparities and downstream effects on the pipeline of African American students and trainees remain apparent in the pool of surgeons available to pursue academic careers. These inequities are poignantly described by Sha’shonda Revels, MD, chief resident in general surgery at the University of Michigan, Ann Arbor, with plans to pursue an academic career in cardiothoracic surgery: “I consider myself truly blessed to have the opportunity to learn a tangible skill that I can use to effect change in the lives of others. … I appreciate the struggles that others have made for me to have this opportunity. Those not so well known ‘others’ include my grandmother who cleaned houses, and took care of me so that my mother could finish high school and attend college. They also include my parents who were tenacious about academics and would not accept a B average.”
The SBAS is born
Despite post-WWII gains, opportunities remained limited for black surgeons to achieve prominence and recognition in academic surgical societies. The Society for Black Academic Surgeons was therefore established as a network that would promote the careers of African American surgeons in academia and accelerate their upward professional trajectory.
SBAS founding member and President (1993-1995) Eddie Hoover, MD, FACS, professor of surgery at the State University of New York Buffalo, and Editor-in-Chief for the Journal of the National Medical Association, provides this passionate account of its history and accomplishments: “SBAS was created in a hotel room at the Marriott in New Orleans in 1987 to address the paucity of academic African American surgeons; their poor retention, promotion, and research funding; and lack of a leadership role in American surgery. The hero of academic African American surgeons, Dr. Charles Drew, adorns the shield of SBAS as much for his defiance of ACS for refusing to accept other well-qualified African American surgeons in the 1940’s as for his scientific contributions …With strong ACS support, SBAS has been stunningly successful over the past 27 years with a dozen SBAS members serving as surgical chairs and four as deans of majority schools.”
Dr. Britt, first African American chair of the ACS Board of Regents and later SBAS president, emphasizes that these two organizations have shared goals. “The evolution of the American College of Surgeons, the world’s largest organization for surgeons, and its growing partnership with the Society of Black Academic Surgeons (demonstrated formally, informally, and sometimes tacitly) needs to be recognized, underscored, and continually enhanced. Many of the ideals of SBAS now mirror the ideals and achievements of the ACS, including an ever growing diverse membership, improved diversity at all levels of leadership, meaningful mentorships for underrepresented minorities, and the establishment of several initiatives to address severe health care disparities in the world’s wealthiest nation.”
The 25th Annual Scientific Meeting of the SBAS will be hosted by the University of North Carolina, Chapel Hill, April 9-11, 2015.
Frederick Cason, MD, FACS, professor of surgery and chief, Division of Surgical Education at Morehouse School of Medicine and the SBAS historian and archivist, stated, “With the strong academic activities of SBAS, the networking it fosters, and the partnerships with numerous academic institutions and members of the College… there developed some 10 academic chairmen and at least 4 deans leading our major medical centers in America.”
Andrea Hayes-Jordan, MD, SBAS 2015 Annual Meeting program chair and associate professor of surgery and Pediatrics and Director of Pediatric Surgical Oncology at the University of Texas M.D. Anderson Cancer Center, notes, “At the annual meeting we are not only able to see the results of excellent research efforts from minority surgeons from around the country, but one has the unique opportunity to interact with them on a personal level, at an intimate meeting. This personal interaction with successful chair persons of color is invaluable in receiving pearls of advice, and understanding the nuances of successful academic practice. We hope in the future to increase the membership of SBAS and continue to promote the timely advancement of our members.”
Robert Higgins, MD, FACS, Professor and Chairman of the Department of Surgery, Ohio State University and past SBAS president (2008-2009), commented, “As someone who has benefitted from the progress that the SBAS/ACS relationship has fostered, I think the critical strength of this effort in the future is based upon its ability to create foundations for the development of underrepresented men and women of diverse backgrounds to reach new heights in surgery.”
Gender diversity addressed
Health equity efforts must also address gender imbalance. Edward E. Cornwell III, MD, FACS, LaSalle D. Leffall, Jr. Professor and Chairman of Surgery, Howard University, and SBAS president (2003-2004), reminisced about the first national meeting photo (above) of SBAS leadership and notes the “most obvious sign of the times in April 1989 … no women surgeons in that photo (the woman in the top row wasn’t a physician). Today, at a time when 14 of my 25 categorical surgical residents are women … we stand on the precipice of the next 25 years of career milestones trumpeting gender diversity – that will surpass the explosion we saw over the last 25 years with male surgeons of color.”
Dr. Brawley also commented on the meteoric rise of African American women surgeons: “I take particular pride in the contribution today of black women who have come on strong in the past half-century. I appreciate and celebrate their achievement.”
Patricia Turner, MD, FACS, Director, ACS Division of Member Services, and Associate Professor of Surgery at the University of Chicago, summarized the African American female experience in surgery: “It is indeed a pleasure to note that in the years since the first SBAS photograph in 1989 … the number of women in medicine and surgery continues to surge. This recent growth is as much a reflection of an increased interest in surgery among women who may have been discouraged previously, as it is of a profession that has realized that previously accepted constraints around gender, race, and other factors limited access to colleagues exemplifying excellence in surgery. ACS and SBAS have consistently placed excellence, integrity, and outcomes at the forefront of their mission. Diversity brings quality, and the house of surgery is no different.”
Mentorship and Giving Back
Despite facing myriad obstacles, successful contemporary African American surgeons that are testimony to the mentorship and outreach efforts of SBAS as well as the ACS leadership have been acknowledged by an exhibit developed by the National Library of Medicine titled “Opening Doors: Contemporary African American Academic Surgeons,” and by a chapter contributed by Dr. Britt for the ACS Centennial textbook, “Setting the Course and Establishing Alliances: Fellows of the American College of Surgeons with African American Heritage.” The NLM exhibit specifically highlights the achievements of contemporary surgeons Drs. Alexa Canady; LaSalle Lefall; Claude Organ (1926-2005); Rosalyn Scott; L.D. Britt; Malcolm V. Brock; Karyn L.Butler; Benjamin Carson; Edward Cornwell; Kenneth Davis; Sharon Henry; Carla Pugh; Velma Scantlebury; Claudia Thomas; Errington Thompson; Levi Watkins; Patricia Bath; and Richard Scott. Dr. Britt (a legend in his own right as well as a contemporary icon) also acknowledges the accomplishments of the recent generations of academic surgeons (many of which overlap with the notables listed by the NLM), including Drs. Levi Watkins; Kenneth Forde; Alexa Canady; Clive Callender; Arthur Fleming; Lenworth Jacobs; Velma Scantlebury; Sharon Henry; Patricia Turner; Cato Laurencin; Butch Rossner; Kimberly Joseph; Debra Ford; Robert Higgins; Lisa Newman; Carla Pugh; Electron Kebenew; Terrence Fullum; David Jacobs; Andre Campbell; Kenneth Davis; Rhonda Henry-Tillman; Sherilyn Gordon-Burroughs; Hobart Harris; Michael Watkins; Raphael Lee; Karyn Butler; Edward Barksdale; Orlando Kirton; Jeffrey Upperman; Frederick Cason; Malcolm Brock; and Raymond Bynoe.
African Americans in medicine and surgery remain committed to improving the landscape of health care for underrepresented minority patients, students, and trainees today as in the past. This dedication was expressed by Dr. Daniel Hale Williams many decades ago: “My greatest reward is knowing that I can help my fellow man, especially those of my own race, who so deserve a better way of life.”
Today, trainee Dr. Revels echoes a similar allegiance to eradicating health care disparities by strengthening gender balance as well as racial/ethnic diversity in the health care profession: “I have a responsibility to stand for the next generation of young women of color who may be told that they didn’t need to take that algebra class or that AP classes would be too hard for them.”
Data continue to document that African American physicians are substantially more likely to establish practices that provide care to minority and impoverished patient populations (The Rationale for Diversity in the Health Professions: A Review of the Evidence. Washington, DC: U.S. Department of Health and Human Services Health Resources and Services Administration Bureau of Health Professions, October 2006).
Transcending artificial barriers
The ACS and the SBAS are in many ways bound together by their shared history, goals, and membership, and both have a critical role to play in the continuing struggle for equity and diversity in the surgical profession. Dr. Britt eloquently stated: “The month of February should not be the only time to highlight these milestones. On the contrary, there should be around-the-clock recognition, along with continual emphasis on even more advances. Let me be one of the first to toast this special partnership.”
Lisa Newman MD, MPH, FACS, FASCO, is Professor of Surgery and Director of the Breast Care Center at the University of Michigan in Ann Arbor.
Her research focus includes studies of high-risk/triple negative breast cancer and breast cancer disparities related to African ancestry. This research involves an international breast cancer registry. Dr. Newman also serves on the Program Committee for the Society of Black Academic Surgeons.
The emergence of African Americans as acclaimed leaders in the field of surgery over the last century is a triumph of personal struggle, brilliant minds, and sheer determination.
Disparities in educational and professional opportunities related to racial/ethnic identity persist, but LaSalle D. Leffall, Jr., MD, FACS, fondly recalls a favorite quote from pioneering African American surgeon Charles Drew: “Excellence of performance will transcend artificial barriers created by man.” The goals and abundant talent shared by the membership of the American College of Surgeons (ACS) and Society of Black Academic Surgeons (SBAS) are testimony to the ongoing dissolution of these artificial barriers.
Parallels are evident between the history of organized surgery in America and African American efforts to achieve health care equity. While the spectrum of surgical procedures mushroomed in the late 19th century, surgical training was characterized by inconsistency and instability. The ACS was established in 1913 with the mission of “improving the care of the surgical patient and to safeguarding standards of care in an optimal and ethical practice environment.”
Significant disparities in medical and surgical care existed for African Americans in this era. During the decades following the Civil War, black citizens were routinely denied care or they received substandard care delivered in segregated hospitals. Medical education opportunities for African Americans were nearly nonexistent.
Nonetheless, African Americans mobilized their talent and energy to address the same threats to quality medical care as those faced by the ACS founders, but having to overcome even greater obstacles in the form of systematic racism and exclusion.
Chicago’s Provident Hospital and Training School (the first African American-owned and -operated hospital) was established in 1891. Howard University College of Medicine in Washington, and Meharry Medical College in Nashville, Tenn., founded in 1868 and 1876, respectively, remained the predominent options for prospective African American medical students for several decades. Because African American medical professionals were denied membership in the American Medical Association, they formed their own professional society, the National Medical Association, in 1895.
In contrast, Dr. Daniel Hale Williams, founder of the Provident Hospital and founding member of the National Medical Association, was a charter member of ACS in 1913. However, more than 20 years passed before another African American surgeon (Louis Tompkins Wright, MD, FACS) became a Fellow of the College.
The number of African American surgeons in the College grew steadily after World War II, and in the past 3 years, approximately 6% of ACS inductees have been African Americans.
The value of race/ethnic diversity in optimizing quality of care is summarized by Dr. Otis Brawley, Chief Medical Officer for the American Cancer Society and past Director of the Office for Special Populations Research at the National Institutes of Health: “The practice of surgery is both a science and an art. Part of the art is understanding the patient’s needs and communicating well. Modern medicine has used the phrase ‘cultural competence’ to describe this. While a physician of one race certainly can and often does provide excellent service to a patient of another, diverse membership in the surgical community is essential for cultural competence of that community.”
Pioneering black surgeons
The following lists a few of the many African American surgical luminaries who fought incredible obstacles in order to improve health outcomes for all:
• Daniel Hale Williams, MD, FACS (1856-1931): Founder of Provident Hospital; performed one of the first successful open heart surgeries; charter member of the ACS.
• Louis Tompkins Wright, MD, FACS (1891-1952): Second African American admitted to ACS Fellowship (in 1934) amid much debate and controversy, despite graduating cum laude from Harvard Medical School and having an illustrious career as a decorated Army surgeon. Dr. Wright was the son of a slave (Ceah Ketcham Wright, MD) who pursued medical education at Meharry after obtaining his freedom.
• Charles Richard Drew, MD, FACS (1904-1950): Pioneer transfusion researcher; first American Red Cross Blood Bank director. Dr. Leffall, a Drew trainee, recalls, “After several applications for fellowship in ACS, Drew was approved for admission at the annual convocation October 1950. He was killed in an automobile accident April 1, 1950, en route to a medical meeting in Tuskegee, Ala. In a highly unusual action, the College’s Board of Regents approved him for posthumous fellowship October 1951.”
• Vivien Thomas (1910-1985): surgical technical assistant to Dr. Alfred Blalock at Vanderbilt, and supervisor of surgical laboratories at Johns Hopkins for 35 years; became pioneer in cardiac surgery despite having no formal education beyond high school and awarded honorary doctorate at Hopkins in 1976.
• Samuel Kountz, MD, FACS (1930-1981): Pioneer transplant surgeon; performed first successful human non-identical twin kidney transplant; developed Belzer kidney perfusion prototype.
• Claude Organ, MD, FACS (1926-2005): Professor of surgery at the University of California, Davis, and University of California, San Francisco East; editor of JAMA Archives of Surgery; founding member and President of SBAS (1995-1997) and second African American President of ACS (2003-2004).
• LaSalle D. Leffall, Jr., MD, FACS: Charles R. Drew Professor of Surgery and former chairman of surgery at Howard University; former chairman of the President’s Cancer Panel; SBAS president (1997-1998); first African American president of the American Cancer Society; first African American president of the ACS (1995-1996).
• Levi Watkins, MD: Professor of cardiac surgery, Johns Hopkins University; performed first human implantation of automatic implantable defibrillator; carried out landmark efforts to strengthen diversity among health care professionals. Dr. Watkins commented: “On the occasion of the national holiday of my former pastor, Dr. Martin Luther King, Jr., I am happy to say that given the opportunity the African American surgeon has shown very well that he or she is capable and worthy to serve and lead this nation in health equity and well-being. We must, however, not allow this progress and opportunity to slip from us using slogans to replace direct action on our part. I must compliment the ACS for its role in helping to bring about change in this area.”
• Harold P. Freeman, MD, FACS: Past president, American Cancer Society; past chairman, President’s Cancer Panel; pioneer architect of patient navigation programs; founder and president/CEO, Harold P. Freeman Patient Navigation Institute.
• Haile Debas, MD, FACS: Past chairman, University of California, San Francisco (UCSF) department of surgery; past dean, School of Medicine; founding executive director, UCSF Global Health Sciences; president, the American Surgical Association (2002-2003).
• Benjamin S. Carson, Sr., MD: Emeritus professor of neurosurgery, Johns Hopkins School of Medicine; president/CEO American Business Collaborative, LLC; awarded Presidential Medal of Freedom; renowned for historic 1987 surgical procedure separating craniopagus conjoined twins.
He recalled: “Twins joined at the back of the head had never before been separated with both surviving. The 22-hour operation which combined advanced neurosurgical techniques with hypothermic cardiac arrest proved successful. I intentionally remained in the background and did not reveal my role as the primary neurosurgeon until the press conference several hours after the completion of the operation. Historically, the accomplishments of Blacks in scientific endeavors have not been heavily covered by the news media. In order to inspire millions of Black youngsters who lacked scientific role models, I waited until the story was so big that the media could not back off. Thankfully our society has advanced to the point that this kind of thing is no longer necessary.”
• Alexa Canady, MD, FACS: First African American female neurosurgery resident (University of Minnesota); became chief of neurosurgery at the Children’s Hospital of Detroit at age 36.
• Henri R. Ford, MD, FACS: Past surgeon-in-chief, Children’s Hospital of Pittsburgh; past vice-president, chief of surgery, University of California, Los Angeles (UCLA); vice-dean for Medical Education, Keck School/UCLA; SBAS president (2010-2011).
• L.D. Britt, MD, MPH, D.Sc (Hon), FACS, FCCM, FRCSEng (Hon), FRCSEd (Hon), FWACS (Hon), FRCSI (Hon), FCS(SA) (Hon), FRCS(Glasg) (Hon):
Chairman, department of surgery at Eastern Virginia Medical School; past president of numerous academic societies (American College of Surgeons, 2010-2011; Southern Surgical Congress; American Association of Trauma; Halsted Society, SBAS 1999-2001; American Surgical Association; Society of Surgical Chairs); current SBAS executive director; Robert J. Glaser Distinguished Educator Award recipient (highest teaching award granted by Association of American Medical Colleges).
Professional and personal challenges
Many of these African American professionals tackle the same barriers to productive longevity as the African American general population – disparities in professional promotion opportunities, socioeconomic disadvantages, and reduced life expectancy (National Vital Statistics Reports; vol. 61 no. 4., National Center for Health Statistics 2013).
Black physicians are less likely to receive academic promotion in university programs and are underrepresented within the full professorship rank (JAMA 2000; 284:1085-92); African American researchers are less likely to receive NIH research funding (Science 2011;333:1015-19); and society has lost many academically accomplished African American surgeons to premature death from cancer and other illnesses as well as trauma. Icons Dr. Charles Drew and Dr. Sam Kountz both died in the prime of their professional careers. More recently, the surgical oncology community mourned the losses of Keith Amos, MD, FACS, assistant professor of surgery, University of North Carolina and Yvedt Matory, MD, FACS, assistant professor of surgery, Harvard Medical School. Both of these talented surgeons died before reaching age 50.
Socioeconomic disparities and downstream effects on the pipeline of African American students and trainees remain apparent in the pool of surgeons available to pursue academic careers. These inequities are poignantly described by Sha’shonda Revels, MD, chief resident in general surgery at the University of Michigan, Ann Arbor, with plans to pursue an academic career in cardiothoracic surgery: “I consider myself truly blessed to have the opportunity to learn a tangible skill that I can use to effect change in the lives of others. … I appreciate the struggles that others have made for me to have this opportunity. Those not so well known ‘others’ include my grandmother who cleaned houses, and took care of me so that my mother could finish high school and attend college. They also include my parents who were tenacious about academics and would not accept a B average.”
The SBAS is born
Despite post-WWII gains, opportunities remained limited for black surgeons to achieve prominence and recognition in academic surgical societies. The Society for Black Academic Surgeons was therefore established as a network that would promote the careers of African American surgeons in academia and accelerate their upward professional trajectory.
SBAS founding member and President (1993-1995) Eddie Hoover, MD, FACS, professor of surgery at the State University of New York Buffalo, and Editor-in-Chief for the Journal of the National Medical Association, provides this passionate account of its history and accomplishments: “SBAS was created in a hotel room at the Marriott in New Orleans in 1987 to address the paucity of academic African American surgeons; their poor retention, promotion, and research funding; and lack of a leadership role in American surgery. The hero of academic African American surgeons, Dr. Charles Drew, adorns the shield of SBAS as much for his defiance of ACS for refusing to accept other well-qualified African American surgeons in the 1940’s as for his scientific contributions …With strong ACS support, SBAS has been stunningly successful over the past 27 years with a dozen SBAS members serving as surgical chairs and four as deans of majority schools.”
Dr. Britt, first African American chair of the ACS Board of Regents and later SBAS president, emphasizes that these two organizations have shared goals. “The evolution of the American College of Surgeons, the world’s largest organization for surgeons, and its growing partnership with the Society of Black Academic Surgeons (demonstrated formally, informally, and sometimes tacitly) needs to be recognized, underscored, and continually enhanced. Many of the ideals of SBAS now mirror the ideals and achievements of the ACS, including an ever growing diverse membership, improved diversity at all levels of leadership, meaningful mentorships for underrepresented minorities, and the establishment of several initiatives to address severe health care disparities in the world’s wealthiest nation.”
The 25th Annual Scientific Meeting of the SBAS will be hosted by the University of North Carolina, Chapel Hill, April 9-11, 2015.
Frederick Cason, MD, FACS, professor of surgery and chief, Division of Surgical Education at Morehouse School of Medicine and the SBAS historian and archivist, stated, “With the strong academic activities of SBAS, the networking it fosters, and the partnerships with numerous academic institutions and members of the College… there developed some 10 academic chairmen and at least 4 deans leading our major medical centers in America.”
Andrea Hayes-Jordan, MD, SBAS 2015 Annual Meeting program chair and associate professor of surgery and Pediatrics and Director of Pediatric Surgical Oncology at the University of Texas M.D. Anderson Cancer Center, notes, “At the annual meeting we are not only able to see the results of excellent research efforts from minority surgeons from around the country, but one has the unique opportunity to interact with them on a personal level, at an intimate meeting. This personal interaction with successful chair persons of color is invaluable in receiving pearls of advice, and understanding the nuances of successful academic practice. We hope in the future to increase the membership of SBAS and continue to promote the timely advancement of our members.”
Robert Higgins, MD, FACS, Professor and Chairman of the Department of Surgery, Ohio State University and past SBAS president (2008-2009), commented, “As someone who has benefitted from the progress that the SBAS/ACS relationship has fostered, I think the critical strength of this effort in the future is based upon its ability to create foundations for the development of underrepresented men and women of diverse backgrounds to reach new heights in surgery.”
Gender diversity addressed
Health equity efforts must also address gender imbalance. Edward E. Cornwell III, MD, FACS, LaSalle D. Leffall, Jr. Professor and Chairman of Surgery, Howard University, and SBAS president (2003-2004), reminisced about the first national meeting photo (above) of SBAS leadership and notes the “most obvious sign of the times in April 1989 … no women surgeons in that photo (the woman in the top row wasn’t a physician). Today, at a time when 14 of my 25 categorical surgical residents are women … we stand on the precipice of the next 25 years of career milestones trumpeting gender diversity – that will surpass the explosion we saw over the last 25 years with male surgeons of color.”
Dr. Brawley also commented on the meteoric rise of African American women surgeons: “I take particular pride in the contribution today of black women who have come on strong in the past half-century. I appreciate and celebrate their achievement.”
Patricia Turner, MD, FACS, Director, ACS Division of Member Services, and Associate Professor of Surgery at the University of Chicago, summarized the African American female experience in surgery: “It is indeed a pleasure to note that in the years since the first SBAS photograph in 1989 … the number of women in medicine and surgery continues to surge. This recent growth is as much a reflection of an increased interest in surgery among women who may have been discouraged previously, as it is of a profession that has realized that previously accepted constraints around gender, race, and other factors limited access to colleagues exemplifying excellence in surgery. ACS and SBAS have consistently placed excellence, integrity, and outcomes at the forefront of their mission. Diversity brings quality, and the house of surgery is no different.”
Mentorship and Giving Back
Despite facing myriad obstacles, successful contemporary African American surgeons that are testimony to the mentorship and outreach efforts of SBAS as well as the ACS leadership have been acknowledged by an exhibit developed by the National Library of Medicine titled “Opening Doors: Contemporary African American Academic Surgeons,” and by a chapter contributed by Dr. Britt for the ACS Centennial textbook, “Setting the Course and Establishing Alliances: Fellows of the American College of Surgeons with African American Heritage.” The NLM exhibit specifically highlights the achievements of contemporary surgeons Drs. Alexa Canady; LaSalle Lefall; Claude Organ (1926-2005); Rosalyn Scott; L.D. Britt; Malcolm V. Brock; Karyn L.Butler; Benjamin Carson; Edward Cornwell; Kenneth Davis; Sharon Henry; Carla Pugh; Velma Scantlebury; Claudia Thomas; Errington Thompson; Levi Watkins; Patricia Bath; and Richard Scott. Dr. Britt (a legend in his own right as well as a contemporary icon) also acknowledges the accomplishments of the recent generations of academic surgeons (many of which overlap with the notables listed by the NLM), including Drs. Levi Watkins; Kenneth Forde; Alexa Canady; Clive Callender; Arthur Fleming; Lenworth Jacobs; Velma Scantlebury; Sharon Henry; Patricia Turner; Cato Laurencin; Butch Rossner; Kimberly Joseph; Debra Ford; Robert Higgins; Lisa Newman; Carla Pugh; Electron Kebenew; Terrence Fullum; David Jacobs; Andre Campbell; Kenneth Davis; Rhonda Henry-Tillman; Sherilyn Gordon-Burroughs; Hobart Harris; Michael Watkins; Raphael Lee; Karyn Butler; Edward Barksdale; Orlando Kirton; Jeffrey Upperman; Frederick Cason; Malcolm Brock; and Raymond Bynoe.
African Americans in medicine and surgery remain committed to improving the landscape of health care for underrepresented minority patients, students, and trainees today as in the past. This dedication was expressed by Dr. Daniel Hale Williams many decades ago: “My greatest reward is knowing that I can help my fellow man, especially those of my own race, who so deserve a better way of life.”
Today, trainee Dr. Revels echoes a similar allegiance to eradicating health care disparities by strengthening gender balance as well as racial/ethnic diversity in the health care profession: “I have a responsibility to stand for the next generation of young women of color who may be told that they didn’t need to take that algebra class or that AP classes would be too hard for them.”
Data continue to document that African American physicians are substantially more likely to establish practices that provide care to minority and impoverished patient populations (The Rationale for Diversity in the Health Professions: A Review of the Evidence. Washington, DC: U.S. Department of Health and Human Services Health Resources and Services Administration Bureau of Health Professions, October 2006).
Transcending artificial barriers
The ACS and the SBAS are in many ways bound together by their shared history, goals, and membership, and both have a critical role to play in the continuing struggle for equity and diversity in the surgical profession. Dr. Britt eloquently stated: “The month of February should not be the only time to highlight these milestones. On the contrary, there should be around-the-clock recognition, along with continual emphasis on even more advances. Let me be one of the first to toast this special partnership.”
Lisa Newman MD, MPH, FACS, FASCO, is Professor of Surgery and Director of the Breast Care Center at the University of Michigan in Ann Arbor.
Her research focus includes studies of high-risk/triple negative breast cancer and breast cancer disparities related to African ancestry. This research involves an international breast cancer registry. Dr. Newman also serves on the Program Committee for the Society of Black Academic Surgeons.

VIDEO: Ask patients about metal-on-metal hip implants
MAUI, HAWAII – Rheumatologists and other providers need to ask patients if they’ve had metal-on-metal hip implants.
That goes for hip resurfacing – which by definition is metal on metal – as well as actual metal-on-metal hips. Signs of trouble can be as subtle as mental status changes, and they go well beyond the traditional issues with worn-out artificial joints.
During a video interview at the 2015 Rheumatology Winter Clinical Symposium, Dr. Bill Bugbee, an orthopedic surgeon and professor at the University of California, San Diego, explained the problems and the warning signs for which physicians should watch.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MAUI, HAWAII – Rheumatologists and other providers need to ask patients if they’ve had metal-on-metal hip implants.
That goes for hip resurfacing – which by definition is metal on metal – as well as actual metal-on-metal hips. Signs of trouble can be as subtle as mental status changes, and they go well beyond the traditional issues with worn-out artificial joints.
During a video interview at the 2015 Rheumatology Winter Clinical Symposium, Dr. Bill Bugbee, an orthopedic surgeon and professor at the University of California, San Diego, explained the problems and the warning signs for which physicians should watch.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
MAUI, HAWAII – Rheumatologists and other providers need to ask patients if they’ve had metal-on-metal hip implants.
That goes for hip resurfacing – which by definition is metal on metal – as well as actual metal-on-metal hips. Signs of trouble can be as subtle as mental status changes, and they go well beyond the traditional issues with worn-out artificial joints.
During a video interview at the 2015 Rheumatology Winter Clinical Symposium, Dr. Bill Bugbee, an orthopedic surgeon and professor at the University of California, San Diego, explained the problems and the warning signs for which physicians should watch.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT RWCS 2015

Early drain removal safe in 60% of pancreaticoduodenectomy patients
The majority of patients undergoing pancreaticoduodenectomy will not develop pancreatic fistula and may safely have drains removed on the first postoperative day, a prospective cohort study has found.
Less than 1% of patients with drain amylase levels below 600 U/L on postoperative day 1 will develop pancreatic fistula (PF). This means that in this group – which represents about 60% of PD patients – early drain removal may be a safe management option.
For their research, published online in Annals of Surgery (2015 Jan. 12 [doi:10.1097/SLA.0000000000001038), Dr. Zhi Ven Fong and colleagues at Massachusetts General Hospital and Harvard Medical School, Boston, sought to find the threshold value for drain amylase that predicts fistula, with the goal of helping guide surgeons’ decisions on drain management.
Most surgeons place intraperitoneal drains during PD to control leakage in the event that anastomoses fail. However, some surgeons have abandoned drain placement after PD out of concerns that drains can introduce infection and cause other complications, with risks increasing the longer drains are in place. Drain placement followed by amylase measurement and early removal in low-risk patients “represents a middle ground between the two practices,” Dr. Fong and colleagues wrote.
The investigators evaluated results from two cohorts of consecutive patients undergoing pancreaticoduodenectomy at their surgical center, an initial training cohort (n = 126) and a validation cohort (n = 369). Closed-suction drains were used in all patients, and drain output and amylase levels were prospectively measured daily until drain removal or patient discharge.
Results from the first cohort showed that a drain amylase level of 612 U/L or higher showed the best accuracy (86%), sensitivity (93%), and specificity (79%) in predicting fistula, compared with other established variables.
In the larger validation cohort, the 140 patients with drain amylase values of 600 or higher on postoperative day 1 saw a PF rate of 31.4% (odds ratio = 52, P < .0001). Of the 229 patients with values lower than 600, a group comprising 62.1% of the cohort, fistula developed in only two cases (0.9%). An amylase value below 600 proved a stronger predictor of the absence of PF (OR = 0.0192, P < .0001) than pancreatic gland texture (OR = 0.193, P = .002) and duct diameter (OR = 0.861, P = .835).
“We believe that the debate [over] current intraperitoneal drain management after PD should not be ‘to drain or not to drain’ but rather ‘who and when can we stop draining,’ ” Dr. Fong and colleagues wrote.
“Risk of PF is less than 1% if POD [postoperative day] 1 drain amylase level is lower than 600 U/L. We propose that in this group, which comprises more than 60% of patients, intraperitoneal drains should be removed on PODs 1 and 2, and are currently validating this strategy in our practice,” they wrote.
The investigators cautioned, however, that theirs was a one-site study at an institution whose fistula rates after PD are low, compared with historic rates. “Utilizing POD 1 drain amylase of less than 600 U/L as an early stratification of patients to guide drain removal should not be assumed to be a universally safe practice,” they wrote, until data from larger multisite studies become available.
Dr. Fong and colleagues disclosed no external funding or conflicts of interest.
The majority of patients undergoing pancreaticoduodenectomy will not develop pancreatic fistula and may safely have drains removed on the first postoperative day, a prospective cohort study has found.
Less than 1% of patients with drain amylase levels below 600 U/L on postoperative day 1 will develop pancreatic fistula (PF). This means that in this group – which represents about 60% of PD patients – early drain removal may be a safe management option.
For their research, published online in Annals of Surgery (2015 Jan. 12 [doi:10.1097/SLA.0000000000001038), Dr. Zhi Ven Fong and colleagues at Massachusetts General Hospital and Harvard Medical School, Boston, sought to find the threshold value for drain amylase that predicts fistula, with the goal of helping guide surgeons’ decisions on drain management.
Most surgeons place intraperitoneal drains during PD to control leakage in the event that anastomoses fail. However, some surgeons have abandoned drain placement after PD out of concerns that drains can introduce infection and cause other complications, with risks increasing the longer drains are in place. Drain placement followed by amylase measurement and early removal in low-risk patients “represents a middle ground between the two practices,” Dr. Fong and colleagues wrote.
The investigators evaluated results from two cohorts of consecutive patients undergoing pancreaticoduodenectomy at their surgical center, an initial training cohort (n = 126) and a validation cohort (n = 369). Closed-suction drains were used in all patients, and drain output and amylase levels were prospectively measured daily until drain removal or patient discharge.
Results from the first cohort showed that a drain amylase level of 612 U/L or higher showed the best accuracy (86%), sensitivity (93%), and specificity (79%) in predicting fistula, compared with other established variables.
In the larger validation cohort, the 140 patients with drain amylase values of 600 or higher on postoperative day 1 saw a PF rate of 31.4% (odds ratio = 52, P < .0001). Of the 229 patients with values lower than 600, a group comprising 62.1% of the cohort, fistula developed in only two cases (0.9%). An amylase value below 600 proved a stronger predictor of the absence of PF (OR = 0.0192, P < .0001) than pancreatic gland texture (OR = 0.193, P = .002) and duct diameter (OR = 0.861, P = .835).
“We believe that the debate [over] current intraperitoneal drain management after PD should not be ‘to drain or not to drain’ but rather ‘who and when can we stop draining,’ ” Dr. Fong and colleagues wrote.
“Risk of PF is less than 1% if POD [postoperative day] 1 drain amylase level is lower than 600 U/L. We propose that in this group, which comprises more than 60% of patients, intraperitoneal drains should be removed on PODs 1 and 2, and are currently validating this strategy in our practice,” they wrote.
The investigators cautioned, however, that theirs was a one-site study at an institution whose fistula rates after PD are low, compared with historic rates. “Utilizing POD 1 drain amylase of less than 600 U/L as an early stratification of patients to guide drain removal should not be assumed to be a universally safe practice,” they wrote, until data from larger multisite studies become available.
Dr. Fong and colleagues disclosed no external funding or conflicts of interest.
The majority of patients undergoing pancreaticoduodenectomy will not develop pancreatic fistula and may safely have drains removed on the first postoperative day, a prospective cohort study has found.
Less than 1% of patients with drain amylase levels below 600 U/L on postoperative day 1 will develop pancreatic fistula (PF). This means that in this group – which represents about 60% of PD patients – early drain removal may be a safe management option.
For their research, published online in Annals of Surgery (2015 Jan. 12 [doi:10.1097/SLA.0000000000001038), Dr. Zhi Ven Fong and colleagues at Massachusetts General Hospital and Harvard Medical School, Boston, sought to find the threshold value for drain amylase that predicts fistula, with the goal of helping guide surgeons’ decisions on drain management.
Most surgeons place intraperitoneal drains during PD to control leakage in the event that anastomoses fail. However, some surgeons have abandoned drain placement after PD out of concerns that drains can introduce infection and cause other complications, with risks increasing the longer drains are in place. Drain placement followed by amylase measurement and early removal in low-risk patients “represents a middle ground between the two practices,” Dr. Fong and colleagues wrote.
The investigators evaluated results from two cohorts of consecutive patients undergoing pancreaticoduodenectomy at their surgical center, an initial training cohort (n = 126) and a validation cohort (n = 369). Closed-suction drains were used in all patients, and drain output and amylase levels were prospectively measured daily until drain removal or patient discharge.
Results from the first cohort showed that a drain amylase level of 612 U/L or higher showed the best accuracy (86%), sensitivity (93%), and specificity (79%) in predicting fistula, compared with other established variables.
In the larger validation cohort, the 140 patients with drain amylase values of 600 or higher on postoperative day 1 saw a PF rate of 31.4% (odds ratio = 52, P < .0001). Of the 229 patients with values lower than 600, a group comprising 62.1% of the cohort, fistula developed in only two cases (0.9%). An amylase value below 600 proved a stronger predictor of the absence of PF (OR = 0.0192, P < .0001) than pancreatic gland texture (OR = 0.193, P = .002) and duct diameter (OR = 0.861, P = .835).
“We believe that the debate [over] current intraperitoneal drain management after PD should not be ‘to drain or not to drain’ but rather ‘who and when can we stop draining,’ ” Dr. Fong and colleagues wrote.
“Risk of PF is less than 1% if POD [postoperative day] 1 drain amylase level is lower than 600 U/L. We propose that in this group, which comprises more than 60% of patients, intraperitoneal drains should be removed on PODs 1 and 2, and are currently validating this strategy in our practice,” they wrote.
The investigators cautioned, however, that theirs was a one-site study at an institution whose fistula rates after PD are low, compared with historic rates. “Utilizing POD 1 drain amylase of less than 600 U/L as an early stratification of patients to guide drain removal should not be assumed to be a universally safe practice,” they wrote, until data from larger multisite studies become available.
Dr. Fong and colleagues disclosed no external funding or conflicts of interest.
FROM ANNALS OF SURGERY
Key clinical point: Most patients undergoing pancreaticoduodenectomy can safely have drains removed 1 or 2 days following the procedure, reducing complication risks associated with longer-term drain use.
Major finding: Drain amylase values below 600 U/L on postoperative day 1, seen in more than 60% of the cohort, correspond with a low risk of fistula development.
Data source: A prospective cohort study evaluating about 500 patients, all undergoing PD at a major surgical center.
Disclosures: Dr. Fong and colleagues disclosed no external funding or conflicts of interest.
Trio of risk factors predict gangrenous cholecystitis
LAKE BUENA VISTA, FL. – Older age, diabetes, and elevated bilirubin were significant risk factors for acute gangrenous cholecystitis in a retrospective study of 489 patients undergoing cholecystectomy.
Patients with acute gangrenous cholecystitis (AGC) were on average 15 years older than those with cholecystitis without necrosis (CN) were (55.8 vs. 40.8 years; P value ≤ .001), almost five times more likely to have comorbid diabetes (32% vs. 6.7%; P≤ .05), and had significantly higher bilirubin levels (1.96 mg/dL vs. 0.89 mg/dL; P≤ .001).
The findings are consistent with previous studies showing that all three risk factors are strongly associated with gangrenous cholecystitis, Seda Bourikian reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“Future studies may explore how the pathophysiology of diabetes, or the duration of illness in each patient, plays a role in the development of AGC,” the authors suggested in the poster presentation.
The chart review included 489 patients admitted to an emergency general surgery service who underwent cholecystectomy between January 2009 and April 2014. Retrospectively evaluated pathological specimen reports identified 464 patients with CN and 25 patients with AGC.
Male patients had a significantly higher incidence of AGC than CN (56% vs. 26%; P≤ .05), whereas women were less likely to have AGC (44% vs. 74%; NS), Ms. Bourikian and her colleagues at Virginia Commonwealth University in Richmond wrote.
Previous studies also have shown that acute cholecystitis is more common in men and patients over the age of 50 years.
Notably, lactate, obesity, and systolic blood pressure below 100 mm Hg were not different between groups.
As expected, patients with AGC were significantly more likely to die than their counterparts with cholecystitis without necrosis (16% vs. 0.86%; P≤ .05), the authors reported.
People with diabetes with AGC were almost five times more likely to die than were diabetics with CN (32% vs. 6.7%; P≤ .05). according to the authors.
Mortality, however, was nearly identical between AGC and CN patients with a systolic BP ≤ 100 mm Hg (0% vs. 0.02%; NS).
Logistic regression analysis showed that increased age (P≤ .001) and male gender (P≤ .05) were strongly associated with the development of AGC. The failure of more risk factors to pan out in logistic regression is likely because of the small number of patients with gangrenous cholecystitis, senior author and colleague Dr. Paula Ferrada of Virginia Commonwealth University suggested.
“This is not a common disease,” she said in an interview. “That’s why it’s so hard to diagnose and triage. Clinicians need to have a higher suspicion” of AGC.
LAKE BUENA VISTA, FL. – Older age, diabetes, and elevated bilirubin were significant risk factors for acute gangrenous cholecystitis in a retrospective study of 489 patients undergoing cholecystectomy.
Patients with acute gangrenous cholecystitis (AGC) were on average 15 years older than those with cholecystitis without necrosis (CN) were (55.8 vs. 40.8 years; P value ≤ .001), almost five times more likely to have comorbid diabetes (32% vs. 6.7%; P≤ .05), and had significantly higher bilirubin levels (1.96 mg/dL vs. 0.89 mg/dL; P≤ .001).
The findings are consistent with previous studies showing that all three risk factors are strongly associated with gangrenous cholecystitis, Seda Bourikian reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“Future studies may explore how the pathophysiology of diabetes, or the duration of illness in each patient, plays a role in the development of AGC,” the authors suggested in the poster presentation.
The chart review included 489 patients admitted to an emergency general surgery service who underwent cholecystectomy between January 2009 and April 2014. Retrospectively evaluated pathological specimen reports identified 464 patients with CN and 25 patients with AGC.
Male patients had a significantly higher incidence of AGC than CN (56% vs. 26%; P≤ .05), whereas women were less likely to have AGC (44% vs. 74%; NS), Ms. Bourikian and her colleagues at Virginia Commonwealth University in Richmond wrote.
Previous studies also have shown that acute cholecystitis is more common in men and patients over the age of 50 years.
Notably, lactate, obesity, and systolic blood pressure below 100 mm Hg were not different between groups.
As expected, patients with AGC were significantly more likely to die than their counterparts with cholecystitis without necrosis (16% vs. 0.86%; P≤ .05), the authors reported.
People with diabetes with AGC were almost five times more likely to die than were diabetics with CN (32% vs. 6.7%; P≤ .05). according to the authors.
Mortality, however, was nearly identical between AGC and CN patients with a systolic BP ≤ 100 mm Hg (0% vs. 0.02%; NS).
Logistic regression analysis showed that increased age (P≤ .001) and male gender (P≤ .05) were strongly associated with the development of AGC. The failure of more risk factors to pan out in logistic regression is likely because of the small number of patients with gangrenous cholecystitis, senior author and colleague Dr. Paula Ferrada of Virginia Commonwealth University suggested.
“This is not a common disease,” she said in an interview. “That’s why it’s so hard to diagnose and triage. Clinicians need to have a higher suspicion” of AGC.
LAKE BUENA VISTA, FL. – Older age, diabetes, and elevated bilirubin were significant risk factors for acute gangrenous cholecystitis in a retrospective study of 489 patients undergoing cholecystectomy.
Patients with acute gangrenous cholecystitis (AGC) were on average 15 years older than those with cholecystitis without necrosis (CN) were (55.8 vs. 40.8 years; P value ≤ .001), almost five times more likely to have comorbid diabetes (32% vs. 6.7%; P≤ .05), and had significantly higher bilirubin levels (1.96 mg/dL vs. 0.89 mg/dL; P≤ .001).
The findings are consistent with previous studies showing that all three risk factors are strongly associated with gangrenous cholecystitis, Seda Bourikian reported at the annual scientific assembly of the Eastern Association for the Surgery of Trauma (EAST).
“Future studies may explore how the pathophysiology of diabetes, or the duration of illness in each patient, plays a role in the development of AGC,” the authors suggested in the poster presentation.
The chart review included 489 patients admitted to an emergency general surgery service who underwent cholecystectomy between January 2009 and April 2014. Retrospectively evaluated pathological specimen reports identified 464 patients with CN and 25 patients with AGC.
Male patients had a significantly higher incidence of AGC than CN (56% vs. 26%; P≤ .05), whereas women were less likely to have AGC (44% vs. 74%; NS), Ms. Bourikian and her colleagues at Virginia Commonwealth University in Richmond wrote.
Previous studies also have shown that acute cholecystitis is more common in men and patients over the age of 50 years.
Notably, lactate, obesity, and systolic blood pressure below 100 mm Hg were not different between groups.
As expected, patients with AGC were significantly more likely to die than their counterparts with cholecystitis without necrosis (16% vs. 0.86%; P≤ .05), the authors reported.
People with diabetes with AGC were almost five times more likely to die than were diabetics with CN (32% vs. 6.7%; P≤ .05). according to the authors.
Mortality, however, was nearly identical between AGC and CN patients with a systolic BP ≤ 100 mm Hg (0% vs. 0.02%; NS).
Logistic regression analysis showed that increased age (P≤ .001) and male gender (P≤ .05) were strongly associated with the development of AGC. The failure of more risk factors to pan out in logistic regression is likely because of the small number of patients with gangrenous cholecystitis, senior author and colleague Dr. Paula Ferrada of Virginia Commonwealth University suggested.
“This is not a common disease,” she said in an interview. “That’s why it’s so hard to diagnose and triage. Clinicians need to have a higher suspicion” of AGC.
AT THE EAST SCIENTIFIC ASSEMBLY
Key clinical point: Older age, diabetes and elevated bilirubin were risk factors for acute gangrenous cholecystitis.
Major finding: Patients with acute gangrenous cholecystitis vs. cholecystitis without necrosis were older (55.8 vs. 40.8 years; P value ≤ .001), more likely to have diabetes (32% vs. 6.7%; P≤ .05) and an elevated bilirubin (1.96 mg/dL vs. 0.89 mg/dL; P≤ .001).
Data source: Retrospective analysis of 489 patients undergoing cholecystectomy.
Disclosures: The authors reported having no relevant financial disclosures.
FDA approves first internal tissue adhesive for use in abdominoplasty
The Food and Drug Administration has approved a urethane-based surgical adhesive for use during abdominoplasty, the first synthetic tissue adhesive approved for internal use, the FDA announced on Feb. 4.
The approved indication for the adhesive, called TissuGlu, is for “the approximation of tissue layers where subcutaneous dead space exists between the tissue planes in abdominoplasty.” The use of this product “will help some abdominoplasty patients get back to their daily routine after surgery more quickly than if surgical drains had been inserted,” Dr. William Maisel, deputy director for science at the FDA’s Center for Devices and Radiological Health, said in the statement announcing the approval.
To apply TissuGlu, the surgeon uses a hand-held applicator to apply drops of the adhesive to the tissue surface, then positions the abdominoplasty flap in place. “Water in the patient’s tissue starts a chemical reaction that bonds the flaps together. The surgeon then proceeds with standard closure of the skin using sutures,” according to the statement, which adds that use of an internal adhesive to connect the tissue flaps “may reduce or eliminate the need for postoperative surgical draining of fluid between the abdominoplasty tissue flaps.”
The data reviewed by the FDA included a study of 130 patients who were undergoing an elective abdominoplasty; surgical drains were used in half of the patients and half received TissuGlu only. Among those who received TissuGlu only, 73% required no postoperative interventions to drain fluid that had accumulated between the abdominoplasty tissue flaps, but those who needed interventions “were more likely to require another operation to insert surgical drains,” the statement said.
Patients treated with TissuGlu who did not require a surgical drain were “generally able to return to most daily activities such as showering, climbing stairs, and resuming their usual routines sooner than those who had surgical drains,” but the levels of surgery-related pain or discomfort reported by the patients were not different between the two groups.
Cohera Medical is the manufacturer of TissuGlu, which has been on the market in the European Union since 2011, according to the company.
TissuGlu was reviewed at a meeting of the FDA’s general and plastic surgery devices advisory panel in August 2014.
Information on the approval, as well as patient and physician labeling, is available on the FDA website.
The Food and Drug Administration has approved a urethane-based surgical adhesive for use during abdominoplasty, the first synthetic tissue adhesive approved for internal use, the FDA announced on Feb. 4.
The approved indication for the adhesive, called TissuGlu, is for “the approximation of tissue layers where subcutaneous dead space exists between the tissue planes in abdominoplasty.” The use of this product “will help some abdominoplasty patients get back to their daily routine after surgery more quickly than if surgical drains had been inserted,” Dr. William Maisel, deputy director for science at the FDA’s Center for Devices and Radiological Health, said in the statement announcing the approval.
To apply TissuGlu, the surgeon uses a hand-held applicator to apply drops of the adhesive to the tissue surface, then positions the abdominoplasty flap in place. “Water in the patient’s tissue starts a chemical reaction that bonds the flaps together. The surgeon then proceeds with standard closure of the skin using sutures,” according to the statement, which adds that use of an internal adhesive to connect the tissue flaps “may reduce or eliminate the need for postoperative surgical draining of fluid between the abdominoplasty tissue flaps.”
The data reviewed by the FDA included a study of 130 patients who were undergoing an elective abdominoplasty; surgical drains were used in half of the patients and half received TissuGlu only. Among those who received TissuGlu only, 73% required no postoperative interventions to drain fluid that had accumulated between the abdominoplasty tissue flaps, but those who needed interventions “were more likely to require another operation to insert surgical drains,” the statement said.
Patients treated with TissuGlu who did not require a surgical drain were “generally able to return to most daily activities such as showering, climbing stairs, and resuming their usual routines sooner than those who had surgical drains,” but the levels of surgery-related pain or discomfort reported by the patients were not different between the two groups.
Cohera Medical is the manufacturer of TissuGlu, which has been on the market in the European Union since 2011, according to the company.
TissuGlu was reviewed at a meeting of the FDA’s general and plastic surgery devices advisory panel in August 2014.
Information on the approval, as well as patient and physician labeling, is available on the FDA website.
The Food and Drug Administration has approved a urethane-based surgical adhesive for use during abdominoplasty, the first synthetic tissue adhesive approved for internal use, the FDA announced on Feb. 4.
The approved indication for the adhesive, called TissuGlu, is for “the approximation of tissue layers where subcutaneous dead space exists between the tissue planes in abdominoplasty.” The use of this product “will help some abdominoplasty patients get back to their daily routine after surgery more quickly than if surgical drains had been inserted,” Dr. William Maisel, deputy director for science at the FDA’s Center for Devices and Radiological Health, said in the statement announcing the approval.
To apply TissuGlu, the surgeon uses a hand-held applicator to apply drops of the adhesive to the tissue surface, then positions the abdominoplasty flap in place. “Water in the patient’s tissue starts a chemical reaction that bonds the flaps together. The surgeon then proceeds with standard closure of the skin using sutures,” according to the statement, which adds that use of an internal adhesive to connect the tissue flaps “may reduce or eliminate the need for postoperative surgical draining of fluid between the abdominoplasty tissue flaps.”
The data reviewed by the FDA included a study of 130 patients who were undergoing an elective abdominoplasty; surgical drains were used in half of the patients and half received TissuGlu only. Among those who received TissuGlu only, 73% required no postoperative interventions to drain fluid that had accumulated between the abdominoplasty tissue flaps, but those who needed interventions “were more likely to require another operation to insert surgical drains,” the statement said.
Patients treated with TissuGlu who did not require a surgical drain were “generally able to return to most daily activities such as showering, climbing stairs, and resuming their usual routines sooner than those who had surgical drains,” but the levels of surgery-related pain or discomfort reported by the patients were not different between the two groups.
Cohera Medical is the manufacturer of TissuGlu, which has been on the market in the European Union since 2011, according to the company.
TissuGlu was reviewed at a meeting of the FDA’s general and plastic surgery devices advisory panel in August 2014.
Information on the approval, as well as patient and physician labeling, is available on the FDA website.
Study: Surgical readmissions tied to new discharge complications, not prior conditions
Surgical site infection and ileus were the most frequent reason for hospital readmission within 30 days, according to an analysis of data from the National Surgical Quality Improvement Program.
The findings, published online in the Feb. 3 JAMA, suggest that policies that penalize hospitals for readmissions may be ineffective and potentially counterproductive.
Dr. Karl Y. Bilimoria of Northwestern University, Chicago, and his colleagues examined patient data from 346 hospitals participating in the American College of Surgeon’s National Surgical Quality Improvement Program (ACS NSQIP) between January 2012 and December 2012. Readmission rates and reasons were assessed for all surgical procedures and for six representative operations: bariatric surgery, colectomy or proctectomy, hysterectomy, total hip or knee arthroplasty, ventral hernia repair, and lower extremity vascular bypass (JAMA 2015;313;483-95 [doi:10.1001/jama.2014.18614]).
Of the 498, 875 patient sample, the overall readmission rate was 5.7%. For individual procedures, the readmission rate ranged from 3.8% for hysterectomy to 14.9% for lower extremity vascular bypass.

The most common reason for readmission was surgical site infection (SSI; 19.5%), ranging from 11.4% after bariatric surgery to 36.4% after lower extremity vascular bypass. Ileus was the most common reason for readmission after bariatric surgery (24.5%) and the second most common reason overall (10.3%). Other common causes for readmission included dehydration or nutritional deficiency, bleeding or anemia, venous thromboembolism, and prosthesis or graft issues (after arthroplasty and lower extremity vascular bypass procedures). Only 2% of patients were readmitted for the same complication they had experienced during their index hospitalization. Just 3% of patients readmitted for SSIs had experienced an SSI during their index hospitalization.
The results show readmissions after surgery may not be an appropriate measure for pay-for-performance and cost-containment programs, such as the Centers for Medicare & Medicaid Service’s Hospital Readmissions Reduction Program, Dr. Bilimoria said. Performance targets without accepted courses of intervention might be more prone to unintended or ineffective behaviors and consequences, he noted.
“Surgical readmissions mostly reflect postdischarge complications, and readmission rates may be difficult to reduce until effective strategies are put forth to reduce common complications such as SSI,” he said. “Efforts should focus on reducing complication rates overall than simply those that occur after discharge, and this will subsequently reduce readmission rates as well.”
On Twitter @legal_med
These findings provide an unprecedented opportunity to apply these lessons and make substantial reductions in surgical complications, Dr. Lucian L. Leape said in an editorial accompanying the study.
Changing systems is hard work and requires serious commitment. Changing hospital systems is especially difficult because of long-standing traditions and entrenched practices. Successful change requires leadership by those with the will, the determination, and the perseverance to overcome obstacles and motivate colleagues. It requires commitment, which comes from a sense of urgency and a sense of possibility.
One way to develop a sense of urgency is to translate rates into numbers – i.e., actual patients. For example, in this study, surgical site infections accounted for 19.5% of the unplanned readmissions. Even though this only represents 1% of the 498,875 ACS NSQIP patients undergoing surgery in 2012, that 1% equals 5,565 patients. Reducing that number by half would reduce pain and suffering for more than 2,700 patients. If similar success were achieved nationwide, the total would be many times that.
Dr. Lucian L. Leape is with the department of health policy and management at Harvard School of Public Health, Boston, and made these comments in an accompanying editorial (doi:10.1001/jama.2014.18666). He reported having no relevant financial disclosures.
These findings provide an unprecedented opportunity to apply these lessons and make substantial reductions in surgical complications, Dr. Lucian L. Leape said in an editorial accompanying the study.
Changing systems is hard work and requires serious commitment. Changing hospital systems is especially difficult because of long-standing traditions and entrenched practices. Successful change requires leadership by those with the will, the determination, and the perseverance to overcome obstacles and motivate colleagues. It requires commitment, which comes from a sense of urgency and a sense of possibility.
One way to develop a sense of urgency is to translate rates into numbers – i.e., actual patients. For example, in this study, surgical site infections accounted for 19.5% of the unplanned readmissions. Even though this only represents 1% of the 498,875 ACS NSQIP patients undergoing surgery in 2012, that 1% equals 5,565 patients. Reducing that number by half would reduce pain and suffering for more than 2,700 patients. If similar success were achieved nationwide, the total would be many times that.
Dr. Lucian L. Leape is with the department of health policy and management at Harvard School of Public Health, Boston, and made these comments in an accompanying editorial (doi:10.1001/jama.2014.18666). He reported having no relevant financial disclosures.
These findings provide an unprecedented opportunity to apply these lessons and make substantial reductions in surgical complications, Dr. Lucian L. Leape said in an editorial accompanying the study.
Changing systems is hard work and requires serious commitment. Changing hospital systems is especially difficult because of long-standing traditions and entrenched practices. Successful change requires leadership by those with the will, the determination, and the perseverance to overcome obstacles and motivate colleagues. It requires commitment, which comes from a sense of urgency and a sense of possibility.
One way to develop a sense of urgency is to translate rates into numbers – i.e., actual patients. For example, in this study, surgical site infections accounted for 19.5% of the unplanned readmissions. Even though this only represents 1% of the 498,875 ACS NSQIP patients undergoing surgery in 2012, that 1% equals 5,565 patients. Reducing that number by half would reduce pain and suffering for more than 2,700 patients. If similar success were achieved nationwide, the total would be many times that.
Dr. Lucian L. Leape is with the department of health policy and management at Harvard School of Public Health, Boston, and made these comments in an accompanying editorial (doi:10.1001/jama.2014.18666). He reported having no relevant financial disclosures.
Surgical site infection and ileus were the most frequent reason for hospital readmission within 30 days, according to an analysis of data from the National Surgical Quality Improvement Program.
The findings, published online in the Feb. 3 JAMA, suggest that policies that penalize hospitals for readmissions may be ineffective and potentially counterproductive.
Dr. Karl Y. Bilimoria of Northwestern University, Chicago, and his colleagues examined patient data from 346 hospitals participating in the American College of Surgeon’s National Surgical Quality Improvement Program (ACS NSQIP) between January 2012 and December 2012. Readmission rates and reasons were assessed for all surgical procedures and for six representative operations: bariatric surgery, colectomy or proctectomy, hysterectomy, total hip or knee arthroplasty, ventral hernia repair, and lower extremity vascular bypass (JAMA 2015;313;483-95 [doi:10.1001/jama.2014.18614]).
Of the 498, 875 patient sample, the overall readmission rate was 5.7%. For individual procedures, the readmission rate ranged from 3.8% for hysterectomy to 14.9% for lower extremity vascular bypass.
The most common reason for readmission was surgical site infection (SSI; 19.5%), ranging from 11.4% after bariatric surgery to 36.4% after lower extremity vascular bypass. Ileus was the most common reason for readmission after bariatric surgery (24.5%) and the second most common reason overall (10.3%). Other common causes for readmission included dehydration or nutritional deficiency, bleeding or anemia, venous thromboembolism, and prosthesis or graft issues (after arthroplasty and lower extremity vascular bypass procedures). Only 2% of patients were readmitted for the same complication they had experienced during their index hospitalization. Just 3% of patients readmitted for SSIs had experienced an SSI during their index hospitalization.
The results show readmissions after surgery may not be an appropriate measure for pay-for-performance and cost-containment programs, such as the Centers for Medicare & Medicaid Service’s Hospital Readmissions Reduction Program, Dr. Bilimoria said. Performance targets without accepted courses of intervention might be more prone to unintended or ineffective behaviors and consequences, he noted.
“Surgical readmissions mostly reflect postdischarge complications, and readmission rates may be difficult to reduce until effective strategies are put forth to reduce common complications such as SSI,” he said. “Efforts should focus on reducing complication rates overall than simply those that occur after discharge, and this will subsequently reduce readmission rates as well.”
On Twitter @legal_med
Surgical site infection and ileus were the most frequent reason for hospital readmission within 30 days, according to an analysis of data from the National Surgical Quality Improvement Program.
The findings, published online in the Feb. 3 JAMA, suggest that policies that penalize hospitals for readmissions may be ineffective and potentially counterproductive.
Dr. Karl Y. Bilimoria of Northwestern University, Chicago, and his colleagues examined patient data from 346 hospitals participating in the American College of Surgeon’s National Surgical Quality Improvement Program (ACS NSQIP) between January 2012 and December 2012. Readmission rates and reasons were assessed for all surgical procedures and for six representative operations: bariatric surgery, colectomy or proctectomy, hysterectomy, total hip or knee arthroplasty, ventral hernia repair, and lower extremity vascular bypass (JAMA 2015;313;483-95 [doi:10.1001/jama.2014.18614]).
Of the 498, 875 patient sample, the overall readmission rate was 5.7%. For individual procedures, the readmission rate ranged from 3.8% for hysterectomy to 14.9% for lower extremity vascular bypass.
The most common reason for readmission was surgical site infection (SSI; 19.5%), ranging from 11.4% after bariatric surgery to 36.4% after lower extremity vascular bypass. Ileus was the most common reason for readmission after bariatric surgery (24.5%) and the second most common reason overall (10.3%). Other common causes for readmission included dehydration or nutritional deficiency, bleeding or anemia, venous thromboembolism, and prosthesis or graft issues (after arthroplasty and lower extremity vascular bypass procedures). Only 2% of patients were readmitted for the same complication they had experienced during their index hospitalization. Just 3% of patients readmitted for SSIs had experienced an SSI during their index hospitalization.
The results show readmissions after surgery may not be an appropriate measure for pay-for-performance and cost-containment programs, such as the Centers for Medicare & Medicaid Service’s Hospital Readmissions Reduction Program, Dr. Bilimoria said. Performance targets without accepted courses of intervention might be more prone to unintended or ineffective behaviors and consequences, he noted.
“Surgical readmissions mostly reflect postdischarge complications, and readmission rates may be difficult to reduce until effective strategies are put forth to reduce common complications such as SSI,” he said. “Efforts should focus on reducing complication rates overall than simply those that occur after discharge, and this will subsequently reduce readmission rates as well.”
On Twitter @legal_med
Key clinical point: The majority of 30-day readmissions after surgery are associated with new postdischarge complications and not the worsening of medical conditions patients had when initially hospitalized.
Major finding: Of 498,875 patients, the overall unplanned readmission rate was 5.7%. Only 2% of patients were readmitted for the same complication they had experienced during their index hospitalization. The most common reason for readmission was surgical site infections (19.5%).
Data source: A study of 346 hospitals participating in the American College of Surgeon’s National Surgical Quality Improvement Program (ACS NSQIP) between January and December 2012.
Disclosures: The investigators reported no relevant conflicts of interest.

Abuse-deterrent formulation of extended-release hydrocodone approved
A new formulation of extended-release hydrocodone with abuse-deterrent properties has been approved by the Food and Drug Administration, the manufacturer, Zogenix, has announced.
The new formulation, marketed as Zohydro ER, contains extended-release hydrocodone with “pharmaceutical excipients that immediately form a viscous gel when crushed and dissolved in liquids or solvents,” according to the Jan. 30 statement released by the company. The technology is called “BeadTek.”
The company expects to start transitioning from the currently available Zohydro ER product to the newly formulated product in the second quarter of 2015 for all the prescribed strengths of Zohydro ER, to avoid disrupting patients who are being treated with the product, the statement said.
Zohydro ER is an opioid agonist approved for the management of pain “severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate,” according to the prescribing information.
In the second half of this year, the company plans to submit the results of ongoing Human Abuse Liability studies, “which will further characterize the abuse-deterrent properties of the new formulation” and will support the addition of abuse-deterrent claims to the prescribing information, the company statement said. The statement refers to the FDA’s draft guidance for the evaluation and labeling of abuse-deterrent opioids, which describes the abuse-deterrent claims.
Zohydro ER was approved by the FDA in 2013.
A new formulation of extended-release hydrocodone with abuse-deterrent properties has been approved by the Food and Drug Administration, the manufacturer, Zogenix, has announced.
The new formulation, marketed as Zohydro ER, contains extended-release hydrocodone with “pharmaceutical excipients that immediately form a viscous gel when crushed and dissolved in liquids or solvents,” according to the Jan. 30 statement released by the company. The technology is called “BeadTek.”
The company expects to start transitioning from the currently available Zohydro ER product to the newly formulated product in the second quarter of 2015 for all the prescribed strengths of Zohydro ER, to avoid disrupting patients who are being treated with the product, the statement said.
Zohydro ER is an opioid agonist approved for the management of pain “severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate,” according to the prescribing information.
In the second half of this year, the company plans to submit the results of ongoing Human Abuse Liability studies, “which will further characterize the abuse-deterrent properties of the new formulation” and will support the addition of abuse-deterrent claims to the prescribing information, the company statement said. The statement refers to the FDA’s draft guidance for the evaluation and labeling of abuse-deterrent opioids, which describes the abuse-deterrent claims.
Zohydro ER was approved by the FDA in 2013.
A new formulation of extended-release hydrocodone with abuse-deterrent properties has been approved by the Food and Drug Administration, the manufacturer, Zogenix, has announced.
The new formulation, marketed as Zohydro ER, contains extended-release hydrocodone with “pharmaceutical excipients that immediately form a viscous gel when crushed and dissolved in liquids or solvents,” according to the Jan. 30 statement released by the company. The technology is called “BeadTek.”
The company expects to start transitioning from the currently available Zohydro ER product to the newly formulated product in the second quarter of 2015 for all the prescribed strengths of Zohydro ER, to avoid disrupting patients who are being treated with the product, the statement said.
Zohydro ER is an opioid agonist approved for the management of pain “severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate,” according to the prescribing information.
In the second half of this year, the company plans to submit the results of ongoing Human Abuse Liability studies, “which will further characterize the abuse-deterrent properties of the new formulation” and will support the addition of abuse-deterrent claims to the prescribing information, the company statement said. The statement refers to the FDA’s draft guidance for the evaluation and labeling of abuse-deterrent opioids, which describes the abuse-deterrent claims.
Zohydro ER was approved by the FDA in 2013.
Transoral fundoplication can be effective against GERD symptoms
Transoral esophagogastric fundoplication can be an effective treatment for patients seeking to alleviate symptoms associated with gastroesophageal reflux disease, particularly in individuals with persistent regurgitation despite prior treatment with proton pump inhibitor therapy, according to the results of a new study published in the February issue of Gastroenterology (doi:10.1053/j.gastro.2014.10.009).
“Gastroesophageal reflux disease (GERD) remains one of the most common conditions for which Americans take daily medication, and PPI use has more than doubled in the last decade,” wrote lead authors Dr. John G. Hunter of Oregon Health & Science University in Portland, and Dr. Peter J. Kahrilas of Northwestern University in Chicago, and their associates. “Despite this, up to 40% of proton pump inhibitor (PPI)–dependent GERD patients have troublesome symptoms of GERD, despite PPI therapy.”
In the Randomized EsophyX vs Sham, Placebo-Controlled Transoral Fundoplication (RESPECT) trial, investigators screened 696 patients who were experiencing “troublesome regurgitation” despite daily PPI treatment. These subjects were evaluated via three validated GERD-specific symptom scales, and were either on or off PPI use at the time of trial commencement. Post trial, patients were blinded to therapy and were reassessed at intervals of 2, 12, and 26 weeks. All patients underwent 48-hour esophageal pH monitoring and esophagogastroduodenoscopy at 66 months after the trial ended.

Regurgitation severity was based on the Montreal definition, which was used to measure efficacy of treatments given as part of the study. The Montreal definition of reflux is described by the authors as “either mucosal damage or troublesome symptoms attributable to reflux.” Those with “least troublesome” regurgitation while on PPIs “underwent barium swallow, esophagogastroduodenoscopy, 48-hour esophageal pH monitoring (off PPIs), and high-resolution esophageal manometry analyses.”
Eighty-seven subjects with GERD and hiatal hernias of at least 2 centimeters were randomly assigned to groups that underwent transoral fundoplication (TF) followed by placebo treatment after 6 months, while 42 subjects, who made up the control group, underwent a “sham surgery” and began regimens of once- or twice-daily omeprazole medication for 6 months.
Results showed that 67% of patients who received TF treatment experienced elimination of adverse regurgitation vs. 45% of those treated with PPI (P = .023). Control of esophageal pH also improved noticeably in patients who received TF treatment versus those who did not (9.3% vs. 6.3% on average, respectively, P < .001), but not in patients who received the “sham surgery” (8.6% preop vs. 8.9% postop on average). Fewer patients who received TF treatment recorded having “no response” after 3 months compared with those in the control group (11% vs. 36%, respectively, P = .004).
“Transoral fundoplication may fill the ‘therapeutic gap’ that exists between PPI and laparoscopic fundoplication,” wrote the authors. “Considering the virtual absence of dysphagia and bloating after TF, which may be problematic with LINX [LINX Reflux Management System], it would appear that TF is an option for patients with troublesome regurgitation, as well as for patients with troublesome GERD symptoms who wish not to take PPI over a protracted period of time.”
Several coauthors disclosed ties with the study sponsor EndoGastric Solutions of Redmond, Wash., as well as individual potential conflicts of interest.
Transoral esophagogastric fundoplication can be an effective treatment for patients seeking to alleviate symptoms associated with gastroesophageal reflux disease, particularly in individuals with persistent regurgitation despite prior treatment with proton pump inhibitor therapy, according to the results of a new study published in the February issue of Gastroenterology (doi:10.1053/j.gastro.2014.10.009).
“Gastroesophageal reflux disease (GERD) remains one of the most common conditions for which Americans take daily medication, and PPI use has more than doubled in the last decade,” wrote lead authors Dr. John G. Hunter of Oregon Health & Science University in Portland, and Dr. Peter J. Kahrilas of Northwestern University in Chicago, and their associates. “Despite this, up to 40% of proton pump inhibitor (PPI)–dependent GERD patients have troublesome symptoms of GERD, despite PPI therapy.”
In the Randomized EsophyX vs Sham, Placebo-Controlled Transoral Fundoplication (RESPECT) trial, investigators screened 696 patients who were experiencing “troublesome regurgitation” despite daily PPI treatment. These subjects were evaluated via three validated GERD-specific symptom scales, and were either on or off PPI use at the time of trial commencement. Post trial, patients were blinded to therapy and were reassessed at intervals of 2, 12, and 26 weeks. All patients underwent 48-hour esophageal pH monitoring and esophagogastroduodenoscopy at 66 months after the trial ended.
Regurgitation severity was based on the Montreal definition, which was used to measure efficacy of treatments given as part of the study. The Montreal definition of reflux is described by the authors as “either mucosal damage or troublesome symptoms attributable to reflux.” Those with “least troublesome” regurgitation while on PPIs “underwent barium swallow, esophagogastroduodenoscopy, 48-hour esophageal pH monitoring (off PPIs), and high-resolution esophageal manometry analyses.”
Eighty-seven subjects with GERD and hiatal hernias of at least 2 centimeters were randomly assigned to groups that underwent transoral fundoplication (TF) followed by placebo treatment after 6 months, while 42 subjects, who made up the control group, underwent a “sham surgery” and began regimens of once- or twice-daily omeprazole medication for 6 months.
Results showed that 67% of patients who received TF treatment experienced elimination of adverse regurgitation vs. 45% of those treated with PPI (P = .023). Control of esophageal pH also improved noticeably in patients who received TF treatment versus those who did not (9.3% vs. 6.3% on average, respectively, P < .001), but not in patients who received the “sham surgery” (8.6% preop vs. 8.9% postop on average). Fewer patients who received TF treatment recorded having “no response” after 3 months compared with those in the control group (11% vs. 36%, respectively, P = .004).
“Transoral fundoplication may fill the ‘therapeutic gap’ that exists between PPI and laparoscopic fundoplication,” wrote the authors. “Considering the virtual absence of dysphagia and bloating after TF, which may be problematic with LINX [LINX Reflux Management System], it would appear that TF is an option for patients with troublesome regurgitation, as well as for patients with troublesome GERD symptoms who wish not to take PPI over a protracted period of time.”
Several coauthors disclosed ties with the study sponsor EndoGastric Solutions of Redmond, Wash., as well as individual potential conflicts of interest.
Transoral esophagogastric fundoplication can be an effective treatment for patients seeking to alleviate symptoms associated with gastroesophageal reflux disease, particularly in individuals with persistent regurgitation despite prior treatment with proton pump inhibitor therapy, according to the results of a new study published in the February issue of Gastroenterology (doi:10.1053/j.gastro.2014.10.009).
“Gastroesophageal reflux disease (GERD) remains one of the most common conditions for which Americans take daily medication, and PPI use has more than doubled in the last decade,” wrote lead authors Dr. John G. Hunter of Oregon Health & Science University in Portland, and Dr. Peter J. Kahrilas of Northwestern University in Chicago, and their associates. “Despite this, up to 40% of proton pump inhibitor (PPI)–dependent GERD patients have troublesome symptoms of GERD, despite PPI therapy.”
In the Randomized EsophyX vs Sham, Placebo-Controlled Transoral Fundoplication (RESPECT) trial, investigators screened 696 patients who were experiencing “troublesome regurgitation” despite daily PPI treatment. These subjects were evaluated via three validated GERD-specific symptom scales, and were either on or off PPI use at the time of trial commencement. Post trial, patients were blinded to therapy and were reassessed at intervals of 2, 12, and 26 weeks. All patients underwent 48-hour esophageal pH monitoring and esophagogastroduodenoscopy at 66 months after the trial ended.
Regurgitation severity was based on the Montreal definition, which was used to measure efficacy of treatments given as part of the study. The Montreal definition of reflux is described by the authors as “either mucosal damage or troublesome symptoms attributable to reflux.” Those with “least troublesome” regurgitation while on PPIs “underwent barium swallow, esophagogastroduodenoscopy, 48-hour esophageal pH monitoring (off PPIs), and high-resolution esophageal manometry analyses.”
Eighty-seven subjects with GERD and hiatal hernias of at least 2 centimeters were randomly assigned to groups that underwent transoral fundoplication (TF) followed by placebo treatment after 6 months, while 42 subjects, who made up the control group, underwent a “sham surgery” and began regimens of once- or twice-daily omeprazole medication for 6 months.
Results showed that 67% of patients who received TF treatment experienced elimination of adverse regurgitation vs. 45% of those treated with PPI (P = .023). Control of esophageal pH also improved noticeably in patients who received TF treatment versus those who did not (9.3% vs. 6.3% on average, respectively, P < .001), but not in patients who received the “sham surgery” (8.6% preop vs. 8.9% postop on average). Fewer patients who received TF treatment recorded having “no response” after 3 months compared with those in the control group (11% vs. 36%, respectively, P = .004).
“Transoral fundoplication may fill the ‘therapeutic gap’ that exists between PPI and laparoscopic fundoplication,” wrote the authors. “Considering the virtual absence of dysphagia and bloating after TF, which may be problematic with LINX [LINX Reflux Management System], it would appear that TF is an option for patients with troublesome regurgitation, as well as for patients with troublesome GERD symptoms who wish not to take PPI over a protracted period of time.”
Several coauthors disclosed ties with the study sponsor EndoGastric Solutions of Redmond, Wash., as well as individual potential conflicts of interest.
FROM GASTROENTEROLOGY
Key clinical point: Transoral esophagogastric fundoplication (TF) is an effective treatment for gastroesophageal reflux disease symptoms, particularly in patients with persistent regurgitation despite proton pump inhibitor therapy (PPI).
Major finding: Of patients who received TF, 67% experienced elimination of adverse regurgitation, compared with 45% of those treated with PPI (P = .023).
Data source: Randomized EsophyX vs Sham, Placebo-Controlled Transoral Fundoplication (RESPECT) trial.
Disclosures: Several coauthors disclosed ties with the study sponsor EndoGastric Solutions of Redmond, Wash., as well as individual potential conflicts of interest.

Postop pancreatectomy complications most deadly in elderly
Although rates of complications following pancreatectomy are relatively similar in patients both above and below the age of 80 years, significantly higher mortality rates occur in the older age group, according to the findings of a new study published online in the Annals of Surgery
“Previous studies have focused solely on mortality after pancreatectomy in older patients or failure to rescue for all patients undergoing pancreatectomy,” wrote lead author Dr. Nina P. Tamirisa of the University of Texas Medical Branch in Galveston, and her associates. “For older patients, it is not clear whether the observed increase in mortality rate is attributed to higher rates of postsurgical complications, higher failure to rescue from these postsurgical complications, or both” (Ann. Surg. 2015 [doi:10.1097/SLA.0000000000001093]).
In this study, “failure to rescue” was calculated as the number of patients who died from complications divided by total number of patients with complications and was understood to measure of a hospital’s ability to recognize and manage postoperative complications.
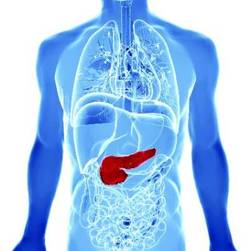
In a retrospective cohort study, Dr. Tamirisa and her coinvestigators looked at data on 2,805 patients in the American College of Surgeons’ National Surgical Quality Improvement Pancreatectomy Demonstration Project (ACS NSQIP) at 43 high-volume centers around the United States between November 2011 and December 2012. Institutions with fewer than 10 cases were excluded, leaving 2,694 subjects from 37 centers for the study.
Following this, patients were divided into cohorts of those younger than 80 years of age, and those aged 80 years or older, which contained 2,496 and 198 subjects, respectively. Overall and individual cohorts were split roughly evenly between males and females. Postoperative morbidity and in-hospital mortality rates were measured along with rate of “failure to rescue.”
Results indicated that there were no significant differences in the rates of complications between the cohorts: 41.4% in patients under 80 years and 39.4% in patients aged 80 years or older (P = .58). However, in-hospital mortality rates were significant higher in the 80 and older cohort (3.0%) than in the younger group (1.1%) (P = .01).
Overall, unadjusted complication rates in the 37 centers included in the study varied widely from 25.0% to as high as 72.2%, while failure to rescue rates at ranged from 0.0% to 25.0%.
Major complications were seen in 29.3% of patients aged 80 years or older and in 28.5% of patients under 80 years old (P = .79), with perioperative bleeding being the most prevalent. Among patients with postoperative complications, ascites, chronic obstructive pulmonary disease, and diabetes were the comorbidities most highly associated with failure to rescue, along with acute renal failure, septic shock, and postoperative pulmonary complications.
“It is always true that avoiding complications will decrease mortality for all patients undergoing pancreatectomy,” concluded the investigators, adding that it’s crucial for there to be more interventions to facilitate identification and aggressive treatment of complications to decrease mortality in vulnerable older patients.
“Several factors, such as individual surgeon volume, impact patient outcomes and failure to rescue rates are a significant but not the sole contributor to increased mortality rates in older patients undergoing pancreatectomy,” wrote Dr. Tamirisa and her coauthors.
This study was funded by grants from the Cancer Prevention Research Institute of Texas, UTMB Clinical and Translational Science Award, the National Institutes of Health, and the Agency for Healthcare Research & Quality. Coauthor Dr. Bruce L. Hall disclosed being a paid consulting director of the American College of Surgeons’ National Surgical Quality Improvement Program.
Although rates of complications following pancreatectomy are relatively similar in patients both above and below the age of 80 years, significantly higher mortality rates occur in the older age group, according to the findings of a new study published online in the Annals of Surgery
“Previous studies have focused solely on mortality after pancreatectomy in older patients or failure to rescue for all patients undergoing pancreatectomy,” wrote lead author Dr. Nina P. Tamirisa of the University of Texas Medical Branch in Galveston, and her associates. “For older patients, it is not clear whether the observed increase in mortality rate is attributed to higher rates of postsurgical complications, higher failure to rescue from these postsurgical complications, or both” (Ann. Surg. 2015 [doi:10.1097/SLA.0000000000001093]).
In this study, “failure to rescue” was calculated as the number of patients who died from complications divided by total number of patients with complications and was understood to measure of a hospital’s ability to recognize and manage postoperative complications.
In a retrospective cohort study, Dr. Tamirisa and her coinvestigators looked at data on 2,805 patients in the American College of Surgeons’ National Surgical Quality Improvement Pancreatectomy Demonstration Project (ACS NSQIP) at 43 high-volume centers around the United States between November 2011 and December 2012. Institutions with fewer than 10 cases were excluded, leaving 2,694 subjects from 37 centers for the study.
Following this, patients were divided into cohorts of those younger than 80 years of age, and those aged 80 years or older, which contained 2,496 and 198 subjects, respectively. Overall and individual cohorts were split roughly evenly between males and females. Postoperative morbidity and in-hospital mortality rates were measured along with rate of “failure to rescue.”
Results indicated that there were no significant differences in the rates of complications between the cohorts: 41.4% in patients under 80 years and 39.4% in patients aged 80 years or older (P = .58). However, in-hospital mortality rates were significant higher in the 80 and older cohort (3.0%) than in the younger group (1.1%) (P = .01).
Overall, unadjusted complication rates in the 37 centers included in the study varied widely from 25.0% to as high as 72.2%, while failure to rescue rates at ranged from 0.0% to 25.0%.
Major complications were seen in 29.3% of patients aged 80 years or older and in 28.5% of patients under 80 years old (P = .79), with perioperative bleeding being the most prevalent. Among patients with postoperative complications, ascites, chronic obstructive pulmonary disease, and diabetes were the comorbidities most highly associated with failure to rescue, along with acute renal failure, septic shock, and postoperative pulmonary complications.
“It is always true that avoiding complications will decrease mortality for all patients undergoing pancreatectomy,” concluded the investigators, adding that it’s crucial for there to be more interventions to facilitate identification and aggressive treatment of complications to decrease mortality in vulnerable older patients.
“Several factors, such as individual surgeon volume, impact patient outcomes and failure to rescue rates are a significant but not the sole contributor to increased mortality rates in older patients undergoing pancreatectomy,” wrote Dr. Tamirisa and her coauthors.
This study was funded by grants from the Cancer Prevention Research Institute of Texas, UTMB Clinical and Translational Science Award, the National Institutes of Health, and the Agency for Healthcare Research & Quality. Coauthor Dr. Bruce L. Hall disclosed being a paid consulting director of the American College of Surgeons’ National Surgical Quality Improvement Program.
Although rates of complications following pancreatectomy are relatively similar in patients both above and below the age of 80 years, significantly higher mortality rates occur in the older age group, according to the findings of a new study published online in the Annals of Surgery
“Previous studies have focused solely on mortality after pancreatectomy in older patients or failure to rescue for all patients undergoing pancreatectomy,” wrote lead author Dr. Nina P. Tamirisa of the University of Texas Medical Branch in Galveston, and her associates. “For older patients, it is not clear whether the observed increase in mortality rate is attributed to higher rates of postsurgical complications, higher failure to rescue from these postsurgical complications, or both” (Ann. Surg. 2015 [doi:10.1097/SLA.0000000000001093]).
In this study, “failure to rescue” was calculated as the number of patients who died from complications divided by total number of patients with complications and was understood to measure of a hospital’s ability to recognize and manage postoperative complications.
In a retrospective cohort study, Dr. Tamirisa and her coinvestigators looked at data on 2,805 patients in the American College of Surgeons’ National Surgical Quality Improvement Pancreatectomy Demonstration Project (ACS NSQIP) at 43 high-volume centers around the United States between November 2011 and December 2012. Institutions with fewer than 10 cases were excluded, leaving 2,694 subjects from 37 centers for the study.
Following this, patients were divided into cohorts of those younger than 80 years of age, and those aged 80 years or older, which contained 2,496 and 198 subjects, respectively. Overall and individual cohorts were split roughly evenly between males and females. Postoperative morbidity and in-hospital mortality rates were measured along with rate of “failure to rescue.”
Results indicated that there were no significant differences in the rates of complications between the cohorts: 41.4% in patients under 80 years and 39.4% in patients aged 80 years or older (P = .58). However, in-hospital mortality rates were significant higher in the 80 and older cohort (3.0%) than in the younger group (1.1%) (P = .01).
Overall, unadjusted complication rates in the 37 centers included in the study varied widely from 25.0% to as high as 72.2%, while failure to rescue rates at ranged from 0.0% to 25.0%.
Major complications were seen in 29.3% of patients aged 80 years or older and in 28.5% of patients under 80 years old (P = .79), with perioperative bleeding being the most prevalent. Among patients with postoperative complications, ascites, chronic obstructive pulmonary disease, and diabetes were the comorbidities most highly associated with failure to rescue, along with acute renal failure, septic shock, and postoperative pulmonary complications.
“It is always true that avoiding complications will decrease mortality for all patients undergoing pancreatectomy,” concluded the investigators, adding that it’s crucial for there to be more interventions to facilitate identification and aggressive treatment of complications to decrease mortality in vulnerable older patients.
“Several factors, such as individual surgeon volume, impact patient outcomes and failure to rescue rates are a significant but not the sole contributor to increased mortality rates in older patients undergoing pancreatectomy,” wrote Dr. Tamirisa and her coauthors.
This study was funded by grants from the Cancer Prevention Research Institute of Texas, UTMB Clinical and Translational Science Award, the National Institutes of Health, and the Agency for Healthcare Research & Quality. Coauthor Dr. Bruce L. Hall disclosed being a paid consulting director of the American College of Surgeons’ National Surgical Quality Improvement Program.
FROM THE ANNALS OF SURGERY
Key clinical point: Significantly higher rates of mortality are experienced in pancreatectomy patients aged 80 years or older, requiring urgent attention toward minimizing postoperative complications.
Major finding: In-hospital mortality rates were significant higher in the cohort aged 80 years and older (3.0%) than in the younger group (1.1%) (P = .01) even though rates of complications between the two groups were relatively similar.
Data source: Retrospective cohort study of 2,694 patients in the American College of Surgeons’ National Surgical Quality Improvement Pancreatectomy Demonstration Project at 37 high-volume U.S. centers.
Disclosures: Study was funded by grants from the Cancer Prevention Research Institute of Texas, UTMB Clinical and Translational Science Award, the National Institutes of Health, and the Agency for Healthcare Research & Quality. Coauthor Dr. Bruce L. Hall disclosed being a paid consulting director of the American College of Surgeons’ National Surgical Quality Improvement Program.
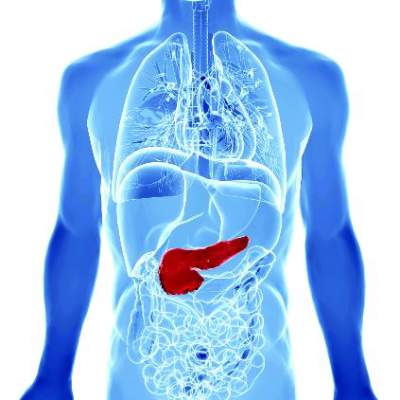
Bundled intervention tackles S. aureus SSIs
PHILADELPHIA – A bundled intervention including Staphylococcus aureus screening, decolonization, and targeted perioperative prophylaxis significantly decreased the rate of complex S. aureus surgical site infections in a multicenter quasi-experimental effectiveness study of patients undergoing cardiac operations or total joint arthroplasty.
The pooled rate of complex S. aureus surgical site infections (SSIs) decreased from 0.36% following 28,218 procedures performed during the preintervention period to 0.20% after 14,316 procedures performed during the intervention period (rate ratio, 0.58), Dr. Loreen A. Herwaldt of the University of Iowa, Iowa City, reported at an annual scientific meeting on infectious diseases.
Further, the number of months with no complex S. aureus SSIs increased from 2 of 39 months (5.1%) to 8 of 22 months (36.4%) Dr. Herwaldt said, noting that the median rate and range of complex SSIs became zero by intervention month 4.
The decrease in SSIs was greatest for joint arthroplasties, she said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Subgroup analyses also demonstrated significantly lower rates of complex SSIs for scheduled vs. nonscheduled or emergent operations (rate ratio, 0.55), fully adherent vs. partially or nonadherent operations (rate ratio, 0.26), and for operations in which the surgeon (in accordance with hospital participation) implemented at least some bundle elements vs. no bundle elements (rate ratio, 0.54), she said, explaining that surgeons could opt out of the study even if a hospital was participating.
The rate of complex SSIs caused by any pathogen also was reduced (rate ratio, 0.67).
“We were very pleased to note that gram negative SSIs did not increase. The rate ratio was 0.86, and the confidence interval did cross 1 and the P value was 0.67,” she said.
The study, known as STOP SSI, was conducted at 20 Hospital Corporation of America (HCA) hospitals in nine states from March 1, 2009, to March 31, 2014. Patients who tested positive for methicillin-resistant or methicillin-susceptible S. aureus on a preoperative nares screen within 30 days before surgery were asked to apply mupirocin intranasally twice daily for 5 days and to bathe with chlorhexidine gluconate once daily for 5 days prior to their operation, including on the night before and the morning of surgery. Those who tested negative for MRSA and MSSA bathed with chlorhexidine gluconate only on the night before surgery and the morning of surgery.
Those with MRSA were treated with vancomycin and cefazolin perioperatively, and those without MRSA received only cefazolin.
If the patient’s status was unknown at the time of the operation, the goal was to have the patient bathe in chlorhexidine and to give as many intranasal doses of mupirocin as possible before surgery. The patient was treated perioperatively with vancomycin and cefazolin, and if it was later determined that the patient was positive for MRSA, the mupirocin was continued after surgery until the patient had been treated for 5 days.
After a 3-month phase-in period, 48% of the hospitals were fully compliant with this protocol, and 20% were partially compliant.
The use of a bundled intervention similar to the one used in this study was shown in a recent meta-analysis (BMJ 2013;346:f2743) to be likely to reduce the rate of S. aureus SSIs, but the approach had not been studied in a multicenter trial, Dr. Herwaldt said.
“Implementation of this SSI bundle was associated with significantly lower rates of complex S. aureus SSIs in the total cohort and in the hip and knee arthroplasty group. It was not associated with an increase in gram-negative SSIs, and thus we feel that if people actually did implement this bundle, it could substantially reduce patient morbidity and the cost of care,” she concluded, noting that the effect was seen only with implementation of the full bundle.
The Agency for Healthcare Research and Quality funded the study. Dr. Herwaldt reported having no disclosures.
PHILADELPHIA – A bundled intervention including Staphylococcus aureus screening, decolonization, and targeted perioperative prophylaxis significantly decreased the rate of complex S. aureus surgical site infections in a multicenter quasi-experimental effectiveness study of patients undergoing cardiac operations or total joint arthroplasty.
The pooled rate of complex S. aureus surgical site infections (SSIs) decreased from 0.36% following 28,218 procedures performed during the preintervention period to 0.20% after 14,316 procedures performed during the intervention period (rate ratio, 0.58), Dr. Loreen A. Herwaldt of the University of Iowa, Iowa City, reported at an annual scientific meeting on infectious diseases.
Further, the number of months with no complex S. aureus SSIs increased from 2 of 39 months (5.1%) to 8 of 22 months (36.4%) Dr. Herwaldt said, noting that the median rate and range of complex SSIs became zero by intervention month 4.
The decrease in SSIs was greatest for joint arthroplasties, she said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Subgroup analyses also demonstrated significantly lower rates of complex SSIs for scheduled vs. nonscheduled or emergent operations (rate ratio, 0.55), fully adherent vs. partially or nonadherent operations (rate ratio, 0.26), and for operations in which the surgeon (in accordance with hospital participation) implemented at least some bundle elements vs. no bundle elements (rate ratio, 0.54), she said, explaining that surgeons could opt out of the study even if a hospital was participating.
The rate of complex SSIs caused by any pathogen also was reduced (rate ratio, 0.67).
“We were very pleased to note that gram negative SSIs did not increase. The rate ratio was 0.86, and the confidence interval did cross 1 and the P value was 0.67,” she said.
The study, known as STOP SSI, was conducted at 20 Hospital Corporation of America (HCA) hospitals in nine states from March 1, 2009, to March 31, 2014. Patients who tested positive for methicillin-resistant or methicillin-susceptible S. aureus on a preoperative nares screen within 30 days before surgery were asked to apply mupirocin intranasally twice daily for 5 days and to bathe with chlorhexidine gluconate once daily for 5 days prior to their operation, including on the night before and the morning of surgery. Those who tested negative for MRSA and MSSA bathed with chlorhexidine gluconate only on the night before surgery and the morning of surgery.
Those with MRSA were treated with vancomycin and cefazolin perioperatively, and those without MRSA received only cefazolin.
If the patient’s status was unknown at the time of the operation, the goal was to have the patient bathe in chlorhexidine and to give as many intranasal doses of mupirocin as possible before surgery. The patient was treated perioperatively with vancomycin and cefazolin, and if it was later determined that the patient was positive for MRSA, the mupirocin was continued after surgery until the patient had been treated for 5 days.
After a 3-month phase-in period, 48% of the hospitals were fully compliant with this protocol, and 20% were partially compliant.
The use of a bundled intervention similar to the one used in this study was shown in a recent meta-analysis (BMJ 2013;346:f2743) to be likely to reduce the rate of S. aureus SSIs, but the approach had not been studied in a multicenter trial, Dr. Herwaldt said.
“Implementation of this SSI bundle was associated with significantly lower rates of complex S. aureus SSIs in the total cohort and in the hip and knee arthroplasty group. It was not associated with an increase in gram-negative SSIs, and thus we feel that if people actually did implement this bundle, it could substantially reduce patient morbidity and the cost of care,” she concluded, noting that the effect was seen only with implementation of the full bundle.
The Agency for Healthcare Research and Quality funded the study. Dr. Herwaldt reported having no disclosures.
PHILADELPHIA – A bundled intervention including Staphylococcus aureus screening, decolonization, and targeted perioperative prophylaxis significantly decreased the rate of complex S. aureus surgical site infections in a multicenter quasi-experimental effectiveness study of patients undergoing cardiac operations or total joint arthroplasty.
The pooled rate of complex S. aureus surgical site infections (SSIs) decreased from 0.36% following 28,218 procedures performed during the preintervention period to 0.20% after 14,316 procedures performed during the intervention period (rate ratio, 0.58), Dr. Loreen A. Herwaldt of the University of Iowa, Iowa City, reported at an annual scientific meeting on infectious diseases.
Further, the number of months with no complex S. aureus SSIs increased from 2 of 39 months (5.1%) to 8 of 22 months (36.4%) Dr. Herwaldt said, noting that the median rate and range of complex SSIs became zero by intervention month 4.
The decrease in SSIs was greatest for joint arthroplasties, she said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
Subgroup analyses also demonstrated significantly lower rates of complex SSIs for scheduled vs. nonscheduled or emergent operations (rate ratio, 0.55), fully adherent vs. partially or nonadherent operations (rate ratio, 0.26), and for operations in which the surgeon (in accordance with hospital participation) implemented at least some bundle elements vs. no bundle elements (rate ratio, 0.54), she said, explaining that surgeons could opt out of the study even if a hospital was participating.
The rate of complex SSIs caused by any pathogen also was reduced (rate ratio, 0.67).
“We were very pleased to note that gram negative SSIs did not increase. The rate ratio was 0.86, and the confidence interval did cross 1 and the P value was 0.67,” she said.
The study, known as STOP SSI, was conducted at 20 Hospital Corporation of America (HCA) hospitals in nine states from March 1, 2009, to March 31, 2014. Patients who tested positive for methicillin-resistant or methicillin-susceptible S. aureus on a preoperative nares screen within 30 days before surgery were asked to apply mupirocin intranasally twice daily for 5 days and to bathe with chlorhexidine gluconate once daily for 5 days prior to their operation, including on the night before and the morning of surgery. Those who tested negative for MRSA and MSSA bathed with chlorhexidine gluconate only on the night before surgery and the morning of surgery.
Those with MRSA were treated with vancomycin and cefazolin perioperatively, and those without MRSA received only cefazolin.
If the patient’s status was unknown at the time of the operation, the goal was to have the patient bathe in chlorhexidine and to give as many intranasal doses of mupirocin as possible before surgery. The patient was treated perioperatively with vancomycin and cefazolin, and if it was later determined that the patient was positive for MRSA, the mupirocin was continued after surgery until the patient had been treated for 5 days.
After a 3-month phase-in period, 48% of the hospitals were fully compliant with this protocol, and 20% were partially compliant.
The use of a bundled intervention similar to the one used in this study was shown in a recent meta-analysis (BMJ 2013;346:f2743) to be likely to reduce the rate of S. aureus SSIs, but the approach had not been studied in a multicenter trial, Dr. Herwaldt said.
“Implementation of this SSI bundle was associated with significantly lower rates of complex S. aureus SSIs in the total cohort and in the hip and knee arthroplasty group. It was not associated with an increase in gram-negative SSIs, and thus we feel that if people actually did implement this bundle, it could substantially reduce patient morbidity and the cost of care,” she concluded, noting that the effect was seen only with implementation of the full bundle.
The Agency for Healthcare Research and Quality funded the study. Dr. Herwaldt reported having no disclosures.
AT IDWEEK 2014
Key clinical point: Implementing a bundled intervention reduced S. aureus SSIs and could reduce patient morbidity and costs.
Major finding: The pooled S. aureus SSI rate decreased from 0.36% to 0.20% (rate ratio, 0.58).
Data source: A multicenter quasi-experimental effectiveness study of 42,534 procedures.
Disclosures: The Agency for Healthcare Research and Quality funded the study. Dr. Herwaldt reported having no disclosures.