User login
Computer program refines postsurgical insulin treatment
PALM BEACH, FLA. – A commercially available computer program designed to calculate optimal insulin dosages for postsurgical ICU patients halved the rate of hyperglycemic episodes that patients experienced while dropping the rate of hypoglycemic events by 95% in a single-center, U.S. experience with a total of more than 2,000 patients.
The computer program also resulted in a dramatic reduction in the number of blood glucose measures the nursing staff performed, cutting testing down from 7,495 blood glucose measures/month before the system began to 4,072 blood measures/month once it was in place, Dr. Christopher C. Baker, FACS, said at the annual meeting of the Southern Surgical Association.
An additional associated benefit was a substantial reduction in hospital-acquired infections in the postsurgery patients once computer-guided insulin dosing came online, but this was only a temporal association that may have also been driven by other improvements in patient management that happened at about the same time, said Dr. Baker, chairman of surgery at the Carilion Clinic in Roanoke, Va.
"People have shied away from glucose controls systems [like the one introduced at the Carilion Clinic] because the results from the NICE-SUGAR [Normoglycemia in Intensive Care Evaluation–Survival Using Glucose Algorithm Regulation] trial (N. Engl. J. Med. 2009;360:1283-97) showed that hypoglycemia episodes increase when you do this," commented Dr. David Herndon, FACS, professor of surgery at the University of Texas Medical branch in Galveston. "What is important in the Carilion results is that the computerized support system reduced hypoglycemia. If that can be done across the board, they might have a winner. We need to better control sugar in the ICU."
The next step is to prove the efficacy of this computer program in a prospective, randomized controlled trial, said Dr. Herndon, a suggestion that Dr. Baker also endorsed.
"The reduced incidence of hypoglycemia was incredibly impressive," commented Dr. Michael Rotondo, FACS, professor and chairman of surgery at East Carolina University in Greenville, N.C., who also called for results from a prospective, controlled study.
Surgeons at Carilion introduced the computerized support program for insulin dosing in early 2010 into five surgical intensive care departments: surgical ICU, trauma ICU, neurotrauma ICU, cardiac surgery ICU, and the cardiac surgery progressive care unit. Dr. Baker and his associates compared data collected on patients from all five units with the computerized system in place during July 2010-December 2011, a total of 1,682 patients treated using the computer program, with 449 patients treated in the five units during July 2009-December 2009, before use of the computer program started.
When using the program, nurses take an initial blood specimen from a patient newly arrived at the unit and enter the blood glucose level into the program along with the patient’s weight and blood creatinine level. The program then immediately calculates the appropriate bolus insulin dose, the insulin infusion rate, and the time to the next blood draw, said Dr. Sandy L. Fogel, FACS, a surgeon at Carilion who collaborated on the study. At first, the next blood draw is specified for about 15-30 minutes following the first, but subsequently the blood draws are directed to occur at longer and longer intervals as the patient’s blood glucose comes under control, within the target range of 70-150 mg/dL. Eventually, draws occur at 6-8 hour intervals, Dr. Fogel said.
During the 6-month historical control, nurses drew 44,972 blood specimens for glucose measurement, an average of 7,495/month, compared with 73,290 blood draws during the 18-month period with the program in place, an average of 4,072 blood specimens drawn/month.
During the 18 months with the program in use, hyperglycemic episodes, defined as a blood glucose level greater than 150 mg/dL, dropped by 45%-57% across the five units using the system compared with each unit’s historical control. Overall, hyperglycemic events fell by 50%, a statistically significant difference.
The incidence of hypoglycemic episodes, defined as a blood glucose level below 40 mg/dL, fell from a 1% rate during the historical control period, to rates that ranged from zero to 0.12% with the program in place, with an overall rate across all five units of 0.05%, a 95% relative decrease that was statistically significant.
The substantial decline in hypoglycemic episodes "was a surprise for us," Dr. Fogel said. In addition, out of all the blood measures performed using the computer program 17% had glucose levels of 60-69 mg/dL, and 3% were below 60 mg/dL. In short, the computer program "did not increase hypoglycemic episodes by any way you measure it," Dr. Fogel said.
The insulin-dosing program used at Carilion is the EndoTool, marketed by Hospira, Inc.
Dr. Baker, Dr. Herndon, Dr. Rotondo, and Dr. Fogel had no disclosures.
On Twitter @mitchelzoler
PALM BEACH, FLA. – A commercially available computer program designed to calculate optimal insulin dosages for postsurgical ICU patients halved the rate of hyperglycemic episodes that patients experienced while dropping the rate of hypoglycemic events by 95% in a single-center, U.S. experience with a total of more than 2,000 patients.
The computer program also resulted in a dramatic reduction in the number of blood glucose measures the nursing staff performed, cutting testing down from 7,495 blood glucose measures/month before the system began to 4,072 blood measures/month once it was in place, Dr. Christopher C. Baker, FACS, said at the annual meeting of the Southern Surgical Association.
An additional associated benefit was a substantial reduction in hospital-acquired infections in the postsurgery patients once computer-guided insulin dosing came online, but this was only a temporal association that may have also been driven by other improvements in patient management that happened at about the same time, said Dr. Baker, chairman of surgery at the Carilion Clinic in Roanoke, Va.
"People have shied away from glucose controls systems [like the one introduced at the Carilion Clinic] because the results from the NICE-SUGAR [Normoglycemia in Intensive Care Evaluation–Survival Using Glucose Algorithm Regulation] trial (N. Engl. J. Med. 2009;360:1283-97) showed that hypoglycemia episodes increase when you do this," commented Dr. David Herndon, FACS, professor of surgery at the University of Texas Medical branch in Galveston. "What is important in the Carilion results is that the computerized support system reduced hypoglycemia. If that can be done across the board, they might have a winner. We need to better control sugar in the ICU."
The next step is to prove the efficacy of this computer program in a prospective, randomized controlled trial, said Dr. Herndon, a suggestion that Dr. Baker also endorsed.
"The reduced incidence of hypoglycemia was incredibly impressive," commented Dr. Michael Rotondo, FACS, professor and chairman of surgery at East Carolina University in Greenville, N.C., who also called for results from a prospective, controlled study.
Surgeons at Carilion introduced the computerized support program for insulin dosing in early 2010 into five surgical intensive care departments: surgical ICU, trauma ICU, neurotrauma ICU, cardiac surgery ICU, and the cardiac surgery progressive care unit. Dr. Baker and his associates compared data collected on patients from all five units with the computerized system in place during July 2010-December 2011, a total of 1,682 patients treated using the computer program, with 449 patients treated in the five units during July 2009-December 2009, before use of the computer program started.
When using the program, nurses take an initial blood specimen from a patient newly arrived at the unit and enter the blood glucose level into the program along with the patient’s weight and blood creatinine level. The program then immediately calculates the appropriate bolus insulin dose, the insulin infusion rate, and the time to the next blood draw, said Dr. Sandy L. Fogel, FACS, a surgeon at Carilion who collaborated on the study. At first, the next blood draw is specified for about 15-30 minutes following the first, but subsequently the blood draws are directed to occur at longer and longer intervals as the patient’s blood glucose comes under control, within the target range of 70-150 mg/dL. Eventually, draws occur at 6-8 hour intervals, Dr. Fogel said.
During the 6-month historical control, nurses drew 44,972 blood specimens for glucose measurement, an average of 7,495/month, compared with 73,290 blood draws during the 18-month period with the program in place, an average of 4,072 blood specimens drawn/month.
During the 18 months with the program in use, hyperglycemic episodes, defined as a blood glucose level greater than 150 mg/dL, dropped by 45%-57% across the five units using the system compared with each unit’s historical control. Overall, hyperglycemic events fell by 50%, a statistically significant difference.
The incidence of hypoglycemic episodes, defined as a blood glucose level below 40 mg/dL, fell from a 1% rate during the historical control period, to rates that ranged from zero to 0.12% with the program in place, with an overall rate across all five units of 0.05%, a 95% relative decrease that was statistically significant.
The substantial decline in hypoglycemic episodes "was a surprise for us," Dr. Fogel said. In addition, out of all the blood measures performed using the computer program 17% had glucose levels of 60-69 mg/dL, and 3% were below 60 mg/dL. In short, the computer program "did not increase hypoglycemic episodes by any way you measure it," Dr. Fogel said.
The insulin-dosing program used at Carilion is the EndoTool, marketed by Hospira, Inc.
Dr. Baker, Dr. Herndon, Dr. Rotondo, and Dr. Fogel had no disclosures.
On Twitter @mitchelzoler
PALM BEACH, FLA. – A commercially available computer program designed to calculate optimal insulin dosages for postsurgical ICU patients halved the rate of hyperglycemic episodes that patients experienced while dropping the rate of hypoglycemic events by 95% in a single-center, U.S. experience with a total of more than 2,000 patients.
The computer program also resulted in a dramatic reduction in the number of blood glucose measures the nursing staff performed, cutting testing down from 7,495 blood glucose measures/month before the system began to 4,072 blood measures/month once it was in place, Dr. Christopher C. Baker, FACS, said at the annual meeting of the Southern Surgical Association.
An additional associated benefit was a substantial reduction in hospital-acquired infections in the postsurgery patients once computer-guided insulin dosing came online, but this was only a temporal association that may have also been driven by other improvements in patient management that happened at about the same time, said Dr. Baker, chairman of surgery at the Carilion Clinic in Roanoke, Va.
"People have shied away from glucose controls systems [like the one introduced at the Carilion Clinic] because the results from the NICE-SUGAR [Normoglycemia in Intensive Care Evaluation–Survival Using Glucose Algorithm Regulation] trial (N. Engl. J. Med. 2009;360:1283-97) showed that hypoglycemia episodes increase when you do this," commented Dr. David Herndon, FACS, professor of surgery at the University of Texas Medical branch in Galveston. "What is important in the Carilion results is that the computerized support system reduced hypoglycemia. If that can be done across the board, they might have a winner. We need to better control sugar in the ICU."
The next step is to prove the efficacy of this computer program in a prospective, randomized controlled trial, said Dr. Herndon, a suggestion that Dr. Baker also endorsed.
"The reduced incidence of hypoglycemia was incredibly impressive," commented Dr. Michael Rotondo, FACS, professor and chairman of surgery at East Carolina University in Greenville, N.C., who also called for results from a prospective, controlled study.
Surgeons at Carilion introduced the computerized support program for insulin dosing in early 2010 into five surgical intensive care departments: surgical ICU, trauma ICU, neurotrauma ICU, cardiac surgery ICU, and the cardiac surgery progressive care unit. Dr. Baker and his associates compared data collected on patients from all five units with the computerized system in place during July 2010-December 2011, a total of 1,682 patients treated using the computer program, with 449 patients treated in the five units during July 2009-December 2009, before use of the computer program started.
When using the program, nurses take an initial blood specimen from a patient newly arrived at the unit and enter the blood glucose level into the program along with the patient’s weight and blood creatinine level. The program then immediately calculates the appropriate bolus insulin dose, the insulin infusion rate, and the time to the next blood draw, said Dr. Sandy L. Fogel, FACS, a surgeon at Carilion who collaborated on the study. At first, the next blood draw is specified for about 15-30 minutes following the first, but subsequently the blood draws are directed to occur at longer and longer intervals as the patient’s blood glucose comes under control, within the target range of 70-150 mg/dL. Eventually, draws occur at 6-8 hour intervals, Dr. Fogel said.
During the 6-month historical control, nurses drew 44,972 blood specimens for glucose measurement, an average of 7,495/month, compared with 73,290 blood draws during the 18-month period with the program in place, an average of 4,072 blood specimens drawn/month.
During the 18 months with the program in use, hyperglycemic episodes, defined as a blood glucose level greater than 150 mg/dL, dropped by 45%-57% across the five units using the system compared with each unit’s historical control. Overall, hyperglycemic events fell by 50%, a statistically significant difference.
The incidence of hypoglycemic episodes, defined as a blood glucose level below 40 mg/dL, fell from a 1% rate during the historical control period, to rates that ranged from zero to 0.12% with the program in place, with an overall rate across all five units of 0.05%, a 95% relative decrease that was statistically significant.
The substantial decline in hypoglycemic episodes "was a surprise for us," Dr. Fogel said. In addition, out of all the blood measures performed using the computer program 17% had glucose levels of 60-69 mg/dL, and 3% were below 60 mg/dL. In short, the computer program "did not increase hypoglycemic episodes by any way you measure it," Dr. Fogel said.
The insulin-dosing program used at Carilion is the EndoTool, marketed by Hospira, Inc.
Dr. Baker, Dr. Herndon, Dr. Rotondo, and Dr. Fogel had no disclosures.
On Twitter @mitchelzoler
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: A computer program for calculating insulin doses for postsurgical patients cut hyperglycemic episodes by 50%, and hypoglycemic episodes by 95%, compared with historic controls.
Data Source: A study of 1,682 postsurgical patients treated in five intensive care units at one U.S. center and 449 historical controls from the same units.
Disclosures: Dr. Baker, Dr. Herndon, Dr. Rotondo, and Dr. Fogel had no disclosures.
Minority of surgical ICU patients drive costs
PALM BEACH, FLA. – Only a small percent of all trauma and acute care surgery patients require more than 10 days in the ICU, but the ones who do rack up an enormous chunk of ICU costs, a single-center study with more than 6,000 U.S. patients has shown.
A more detailed look at what contributes to these very prolonged ICU stays and their costs may provide new opportunities for hospital cost controls, Dr. Samir M. Fakhry, FACS, said at the annual meeting of the Southern Surgical Association.
"I think we need a paradigm shift in how these patients are managed," such as a step-down protocol that allows them to exit the ICU and wean off their ventilator, said Dr. Fakhry, professor and chief of general surgery at the Medical University of South Carolina in Charleston.
But trauma and acute care surgery patients who need less than a day in the ICU can’t be ignored either. Although their per-patient cost is relatively small, their aggregate cost is high, because many patients fall into this group.
"You need two approaches" for trying to save on surgical ICU costs, one for patients who need prolonged intensive care and a second approach for patients who require only a day, he said. "For patients with short lengths of stay and lower costs, small things like one or two fewer doses of an antibiotic or fewer tests would make a difference" when multiplied by thousands of patients, Dr. Fahkry said. Further insight into ICU costs and cost-saving approaches could come from expanding his analysis to a larger number of U.S. surgical ICUs, he added.
His analysis of data collected by the surgical ICU at the Medical University of South Carolina, a level 1 trauma center, during 2007-2011 also highlighted that the number of patients admitted to the unit jumped by 26%, rising from 1,084 patients in fiscal year 2007 to 1,364 in FY 2011. The rise was especially pronounced among nontrauma patients, increasing from 319 in 2007 to 502 in 2011, a 57% rise.
Dr. Fahkry and his associates analyzed data from a total of 6,008 patients admitted to his hospital’s surgical ICU during the 5-year period studied. Costs for this care rose from $17,243 per patient in 2007 to $26,468 in 2011, a 53% increase.
A total of 423 of these patients, 7%, stayed in the ICU for more than 10 days. This group consisted primarily of trauma patients, 320 (76%) of the 423 patients. The average length of stay among the prolonged-stay patients was about 17 days, with an overall duration of hospitalization of 31 days. About three-quarters of these patients had at least three comorbidities. Mortality was also high in this subgroup, especially in the nontrauma patients, who had a 40% death rate; in-hospital mortality among the trauma patients with prolonged ICU stays was 10%.
Although accounting for just 7% of all surgical ICU patients, this subgroup racked up 41% of total ICU costs during the 5 years studied. In contrast, 4,236 surgical ICU patients who remained in the unit for less than a full day, 71% of all patients in the analysis, were responsible for 30% of total surgical ICU costs.
The analysis also identified another marker of substantially increased ICU costs: patients who ultimately died during their index hospitalization. Among nontrauma patients who died while hospitalized, the average costs were nearly $60,000 per patient, almost eightfold higher than for the nontrauma patients who survived hospitalization. Among the trauma patients, those who died ran up more than $31,000 in costs, nearly threefold higher than the trauma patients who survived.
Dr. Fahkry said he had no relevant financial disclosures.
On Twitter @mitchelzoler
PALM BEACH, FLA. – Only a small percent of all trauma and acute care surgery patients require more than 10 days in the ICU, but the ones who do rack up an enormous chunk of ICU costs, a single-center study with more than 6,000 U.S. patients has shown.
A more detailed look at what contributes to these very prolonged ICU stays and their costs may provide new opportunities for hospital cost controls, Dr. Samir M. Fakhry, FACS, said at the annual meeting of the Southern Surgical Association.
"I think we need a paradigm shift in how these patients are managed," such as a step-down protocol that allows them to exit the ICU and wean off their ventilator, said Dr. Fakhry, professor and chief of general surgery at the Medical University of South Carolina in Charleston.
But trauma and acute care surgery patients who need less than a day in the ICU can’t be ignored either. Although their per-patient cost is relatively small, their aggregate cost is high, because many patients fall into this group.
"You need two approaches" for trying to save on surgical ICU costs, one for patients who need prolonged intensive care and a second approach for patients who require only a day, he said. "For patients with short lengths of stay and lower costs, small things like one or two fewer doses of an antibiotic or fewer tests would make a difference" when multiplied by thousands of patients, Dr. Fahkry said. Further insight into ICU costs and cost-saving approaches could come from expanding his analysis to a larger number of U.S. surgical ICUs, he added.
His analysis of data collected by the surgical ICU at the Medical University of South Carolina, a level 1 trauma center, during 2007-2011 also highlighted that the number of patients admitted to the unit jumped by 26%, rising from 1,084 patients in fiscal year 2007 to 1,364 in FY 2011. The rise was especially pronounced among nontrauma patients, increasing from 319 in 2007 to 502 in 2011, a 57% rise.
Dr. Fahkry and his associates analyzed data from a total of 6,008 patients admitted to his hospital’s surgical ICU during the 5-year period studied. Costs for this care rose from $17,243 per patient in 2007 to $26,468 in 2011, a 53% increase.
A total of 423 of these patients, 7%, stayed in the ICU for more than 10 days. This group consisted primarily of trauma patients, 320 (76%) of the 423 patients. The average length of stay among the prolonged-stay patients was about 17 days, with an overall duration of hospitalization of 31 days. About three-quarters of these patients had at least three comorbidities. Mortality was also high in this subgroup, especially in the nontrauma patients, who had a 40% death rate; in-hospital mortality among the trauma patients with prolonged ICU stays was 10%.
Although accounting for just 7% of all surgical ICU patients, this subgroup racked up 41% of total ICU costs during the 5 years studied. In contrast, 4,236 surgical ICU patients who remained in the unit for less than a full day, 71% of all patients in the analysis, were responsible for 30% of total surgical ICU costs.
The analysis also identified another marker of substantially increased ICU costs: patients who ultimately died during their index hospitalization. Among nontrauma patients who died while hospitalized, the average costs were nearly $60,000 per patient, almost eightfold higher than for the nontrauma patients who survived hospitalization. Among the trauma patients, those who died ran up more than $31,000 in costs, nearly threefold higher than the trauma patients who survived.
Dr. Fahkry said he had no relevant financial disclosures.
On Twitter @mitchelzoler
PALM BEACH, FLA. – Only a small percent of all trauma and acute care surgery patients require more than 10 days in the ICU, but the ones who do rack up an enormous chunk of ICU costs, a single-center study with more than 6,000 U.S. patients has shown.
A more detailed look at what contributes to these very prolonged ICU stays and their costs may provide new opportunities for hospital cost controls, Dr. Samir M. Fakhry, FACS, said at the annual meeting of the Southern Surgical Association.
"I think we need a paradigm shift in how these patients are managed," such as a step-down protocol that allows them to exit the ICU and wean off their ventilator, said Dr. Fakhry, professor and chief of general surgery at the Medical University of South Carolina in Charleston.
But trauma and acute care surgery patients who need less than a day in the ICU can’t be ignored either. Although their per-patient cost is relatively small, their aggregate cost is high, because many patients fall into this group.
"You need two approaches" for trying to save on surgical ICU costs, one for patients who need prolonged intensive care and a second approach for patients who require only a day, he said. "For patients with short lengths of stay and lower costs, small things like one or two fewer doses of an antibiotic or fewer tests would make a difference" when multiplied by thousands of patients, Dr. Fahkry said. Further insight into ICU costs and cost-saving approaches could come from expanding his analysis to a larger number of U.S. surgical ICUs, he added.
His analysis of data collected by the surgical ICU at the Medical University of South Carolina, a level 1 trauma center, during 2007-2011 also highlighted that the number of patients admitted to the unit jumped by 26%, rising from 1,084 patients in fiscal year 2007 to 1,364 in FY 2011. The rise was especially pronounced among nontrauma patients, increasing from 319 in 2007 to 502 in 2011, a 57% rise.
Dr. Fahkry and his associates analyzed data from a total of 6,008 patients admitted to his hospital’s surgical ICU during the 5-year period studied. Costs for this care rose from $17,243 per patient in 2007 to $26,468 in 2011, a 53% increase.
A total of 423 of these patients, 7%, stayed in the ICU for more than 10 days. This group consisted primarily of trauma patients, 320 (76%) of the 423 patients. The average length of stay among the prolonged-stay patients was about 17 days, with an overall duration of hospitalization of 31 days. About three-quarters of these patients had at least three comorbidities. Mortality was also high in this subgroup, especially in the nontrauma patients, who had a 40% death rate; in-hospital mortality among the trauma patients with prolonged ICU stays was 10%.
Although accounting for just 7% of all surgical ICU patients, this subgroup racked up 41% of total ICU costs during the 5 years studied. In contrast, 4,236 surgical ICU patients who remained in the unit for less than a full day, 71% of all patients in the analysis, were responsible for 30% of total surgical ICU costs.
The analysis also identified another marker of substantially increased ICU costs: patients who ultimately died during their index hospitalization. Among nontrauma patients who died while hospitalized, the average costs were nearly $60,000 per patient, almost eightfold higher than for the nontrauma patients who survived hospitalization. Among the trauma patients, those who died ran up more than $31,000 in costs, nearly threefold higher than the trauma patients who survived.
Dr. Fahkry said he had no relevant financial disclosures.
On Twitter @mitchelzoler
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Seven percent of surgical ICU patients stayed for more than 10 days but accounted for 41% of the costs.
Data Source: A review of 6,008 postsurgery patients admitted to the ICU of a single U.S. center during 2007-2011.
Disclosures: Dr. Fahkry said he had no relevant financial disclosures.
Adhesiolysis: An underestimated morbidity risk
Adhesiolysis, or the removal of adhesions immediately after abdominal surgery, is a risk factor for postoperative surgical complications, longer hospital stays, readmissions, and increased costs, according to findings from a large prospective cohort study.
And yet, to date, "adhesiolysis at repeat surgery has received less attention than bowel obstruction and infertility in reports assessing the clinical and socioeconomic burden of postoperative adhesions," wrote Dr. Richard P. G. ten Broek of Radboud University Nijmegen (the Netherlands) Medical Center and his associates.
He and his colleagues evaluated 755 consecutive elective abdominal procedures at the medical center between June 2008 and June 2010, of which adhesiolysis was deemed necessary and performed in 475. In both groups, most procedures were open rather than laparoscopic. Detailed data on adhesiolysis were gathered with direct observation of the procedures by an unaffiliated observer (Ann. Surg. 2012 Sept. 25 [doi: 10.1097/SLA.0b013e31826f4969]).
Primary outcomes were the incidence of adhesions; adhesiolysis time; and the incidence of bowel defects, seromuscular injury, injuries to other organs and structures, and major surgery-related complications.
In the adhesiolysis group, 111 (23.4%) of procedures had one or more major complications, compared with 50 (17.6%) in the nonadhesiolysis group (P = .047).
Adhesiolysis was associated with a significantly higher risk of sepsis (odds ratio, 5.12; 95% confidence interval, 1.06-24.71), intra-abdominal complications (OR, 3.46; 95% CI, 1.49-8.05), and wound infections (OR, 2.45; 95% CI, 1.01-5.94).
Operative time was a mean 20 minutes longer for the adhesiolysis group, and mean inpatient costs were $18,579 per operation, compared with $14,063 in the nonadhesiolysis group (P less than .001). Readmission within 30 days of discharge was also higher in the adhesiolysis group.
Full-thickness bowel defects, either in the form of inadvertent enterotomy or delayed diagnosed perforation, were seen in 10.5% of procedures with adhesiolysis (and in 40% of operations in which adhesiolysis lasted more than 1 hour). By contrast, no bowel defects were reported for the 280 procedures in which adhesiolysis was not performed.
Bowel defects were associated with an increase in in-hospital mortality, from 1.6% among patients without defects to 8%, along with significantly more surgical interventions and longer hospital stays. Patients with bowel defects incurred mean inpatient costs of $43,784.
The study demonstrated the substantial clinical and socioeconomic burden of adhesiolysis, "particularly when a bowel defect occurs. All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis," Dr. ten Broek and his colleagues wrote.
To date, they said, few clinicians appear to be taking the risks of adhesiolysis seriously. "Underestimation of the related morbidity and the passiveness of many physicians, who consider adhesiolysis an annoying but unavoidable part of redo surgery, account for the paucity of reports on the consequences of adhesiolysis," they wrote.
The investigators noted as weaknesses of their study the need for adhesiolysis in 60% of procedures in the cohort and the low number of laparoscopies – which, they said, could limit the generalizability of the study results.
The study was sponsored by Radboud University Nijmegen Medical Center. Dr. ten Broek and his associates stated that they had no conflicts of interest.
Adhesiolysis, or the removal of adhesions immediately after abdominal surgery, is a risk factor for postoperative surgical complications, longer hospital stays, readmissions, and increased costs, according to findings from a large prospective cohort study.
And yet, to date, "adhesiolysis at repeat surgery has received less attention than bowel obstruction and infertility in reports assessing the clinical and socioeconomic burden of postoperative adhesions," wrote Dr. Richard P. G. ten Broek of Radboud University Nijmegen (the Netherlands) Medical Center and his associates.
He and his colleagues evaluated 755 consecutive elective abdominal procedures at the medical center between June 2008 and June 2010, of which adhesiolysis was deemed necessary and performed in 475. In both groups, most procedures were open rather than laparoscopic. Detailed data on adhesiolysis were gathered with direct observation of the procedures by an unaffiliated observer (Ann. Surg. 2012 Sept. 25 [doi: 10.1097/SLA.0b013e31826f4969]).
Primary outcomes were the incidence of adhesions; adhesiolysis time; and the incidence of bowel defects, seromuscular injury, injuries to other organs and structures, and major surgery-related complications.
In the adhesiolysis group, 111 (23.4%) of procedures had one or more major complications, compared with 50 (17.6%) in the nonadhesiolysis group (P = .047).
Adhesiolysis was associated with a significantly higher risk of sepsis (odds ratio, 5.12; 95% confidence interval, 1.06-24.71), intra-abdominal complications (OR, 3.46; 95% CI, 1.49-8.05), and wound infections (OR, 2.45; 95% CI, 1.01-5.94).
Operative time was a mean 20 minutes longer for the adhesiolysis group, and mean inpatient costs were $18,579 per operation, compared with $14,063 in the nonadhesiolysis group (P less than .001). Readmission within 30 days of discharge was also higher in the adhesiolysis group.
Full-thickness bowel defects, either in the form of inadvertent enterotomy or delayed diagnosed perforation, were seen in 10.5% of procedures with adhesiolysis (and in 40% of operations in which adhesiolysis lasted more than 1 hour). By contrast, no bowel defects were reported for the 280 procedures in which adhesiolysis was not performed.
Bowel defects were associated with an increase in in-hospital mortality, from 1.6% among patients without defects to 8%, along with significantly more surgical interventions and longer hospital stays. Patients with bowel defects incurred mean inpatient costs of $43,784.
The study demonstrated the substantial clinical and socioeconomic burden of adhesiolysis, "particularly when a bowel defect occurs. All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis," Dr. ten Broek and his colleagues wrote.
To date, they said, few clinicians appear to be taking the risks of adhesiolysis seriously. "Underestimation of the related morbidity and the passiveness of many physicians, who consider adhesiolysis an annoying but unavoidable part of redo surgery, account for the paucity of reports on the consequences of adhesiolysis," they wrote.
The investigators noted as weaknesses of their study the need for adhesiolysis in 60% of procedures in the cohort and the low number of laparoscopies – which, they said, could limit the generalizability of the study results.
The study was sponsored by Radboud University Nijmegen Medical Center. Dr. ten Broek and his associates stated that they had no conflicts of interest.
Adhesiolysis, or the removal of adhesions immediately after abdominal surgery, is a risk factor for postoperative surgical complications, longer hospital stays, readmissions, and increased costs, according to findings from a large prospective cohort study.
And yet, to date, "adhesiolysis at repeat surgery has received less attention than bowel obstruction and infertility in reports assessing the clinical and socioeconomic burden of postoperative adhesions," wrote Dr. Richard P. G. ten Broek of Radboud University Nijmegen (the Netherlands) Medical Center and his associates.
He and his colleagues evaluated 755 consecutive elective abdominal procedures at the medical center between June 2008 and June 2010, of which adhesiolysis was deemed necessary and performed in 475. In both groups, most procedures were open rather than laparoscopic. Detailed data on adhesiolysis were gathered with direct observation of the procedures by an unaffiliated observer (Ann. Surg. 2012 Sept. 25 [doi: 10.1097/SLA.0b013e31826f4969]).
Primary outcomes were the incidence of adhesions; adhesiolysis time; and the incidence of bowel defects, seromuscular injury, injuries to other organs and structures, and major surgery-related complications.
In the adhesiolysis group, 111 (23.4%) of procedures had one or more major complications, compared with 50 (17.6%) in the nonadhesiolysis group (P = .047).
Adhesiolysis was associated with a significantly higher risk of sepsis (odds ratio, 5.12; 95% confidence interval, 1.06-24.71), intra-abdominal complications (OR, 3.46; 95% CI, 1.49-8.05), and wound infections (OR, 2.45; 95% CI, 1.01-5.94).
Operative time was a mean 20 minutes longer for the adhesiolysis group, and mean inpatient costs were $18,579 per operation, compared with $14,063 in the nonadhesiolysis group (P less than .001). Readmission within 30 days of discharge was also higher in the adhesiolysis group.
Full-thickness bowel defects, either in the form of inadvertent enterotomy or delayed diagnosed perforation, were seen in 10.5% of procedures with adhesiolysis (and in 40% of operations in which adhesiolysis lasted more than 1 hour). By contrast, no bowel defects were reported for the 280 procedures in which adhesiolysis was not performed.
Bowel defects were associated with an increase in in-hospital mortality, from 1.6% among patients without defects to 8%, along with significantly more surgical interventions and longer hospital stays. Patients with bowel defects incurred mean inpatient costs of $43,784.
The study demonstrated the substantial clinical and socioeconomic burden of adhesiolysis, "particularly when a bowel defect occurs. All physicians treating patients with disorders of the abdominal cavity that might require surgery should be aware of the adverse effects of adhesiolysis," Dr. ten Broek and his colleagues wrote.
To date, they said, few clinicians appear to be taking the risks of adhesiolysis seriously. "Underestimation of the related morbidity and the passiveness of many physicians, who consider adhesiolysis an annoying but unavoidable part of redo surgery, account for the paucity of reports on the consequences of adhesiolysis," they wrote.
The investigators noted as weaknesses of their study the need for adhesiolysis in 60% of procedures in the cohort and the low number of laparoscopies – which, they said, could limit the generalizability of the study results.
The study was sponsored by Radboud University Nijmegen Medical Center. Dr. ten Broek and his associates stated that they had no conflicts of interest.
FROM ANNALS OF SURGERY
Major finding: Adhesiolysis was required in 62.9% of patients undergoing elective abdominal operations, and bowel defects were incurred in 10.5% of the adhesiolysis patients.
Data source: A prospective cohort study of 755 directly observed procedures in 715 patients at a surgical center in the Netherlands.
Disclosures: The study was sponsored by Radboud University Nijmegen Medical Center. Dr ten Broek and his colleagues stated that they had no conflicts of interest.
U.S. surgeon supply projected to drop 18% by 2028
The supply of surgeons in the United States will decrease by nearly one-fifth by 2028, likely resulting in shortages in all but a handful of specialties, a study has shown.
Currently proposed changes to increase surgeon training will not be enough to offset the number of surgeons who will retire, predicted Erin P. Fraher, Ph.D., of the department of surgery at the University of North Carolina at Chapel Hill, and colleagues. If this trend continues, the overall supply of full-time-equivalent surgeons will have decreased 18% between 2009 and 2028, with declines in all specialties except colorectal, pediatric, neurologic, and vascular surgery.
Such a drop could result in a workforce insufficient to meet the needs of the U.S. population – particularly in light of the expanded access to and increased usage of health care services projected for the future. It could also exacerbate problems related to the geographic distribution of surgeons, the investigators cautioned, "leading to delayed or lost access to time-sensitive surgical procedures, particularly in rural areas" (Ann. Surg. 2012 [doi:10.1097/SLA.0b013e31826fccfa]).
These projections are lower than those forecast in a 2008 report by the U.S. Health Resources and Services Administration for general, cardiothoracic, orthopedic, urologic, plastic, ophthalmologic, and obstetrics/gynecologic surgeons. However, they are brighter than previously published projections for vascular and pediatric surgeons (J. Vasc. Surg. 2009;50:946-52; J. Pediatr. Surg. 2009;44:1677-82). Predictions of a decline in cardiothoracic surgeons are consistent with some earlier findings (Circulation 2009;120:488-94).
For the current research, the investigators used a stock-and-flow model, which calculates current numbers of physicians, projected numbers of physicians graduating from medical school, and physicians reentering the workforce, and subtracts from these anticipated deaths, retirements, and career breaks. They then adjusted the resulting head count to full-time-equivalent work participation rates of surgeons by age, sex, and specialty.
Data were drawn from databases maintained by the American Medical Association, the American Board of Medical Specialties, the National Resident Match Program, the San Francisco match for plastic surgery and ophthalmology, the American Urological Association, the Health Resources and Services Administration, and the North Carolina Health Professions Data System.
Unlike static projection models, this model allows for real-time updating to take into account changes in data and policy decisions, which enhances the accuracy of its workforce projections, according to the investigators.
Surgeons’ participation in patient care declines somewhat after age 60, they noted, making age a key factor in determining full-time equivalents for each specialty. Another factor considered in modeling was the "feminization" of various specialties. By 2019, Dr. Fraher and colleagues predicted, half of general surgery residents will be female, compared with 95% of obstetrics and gynecology residents and 28% of orthopedic surgery residents.
Furthermore, an estimated 25% of general surgery cases that have traditionally been performed by surgical specialists will, in the future, need to be made up by general surgeons, the investigators said.
The most important driver of future supply estimates, they said, "is whether anticipated declines in full-time equivalent rates will occur as expected and whether these full-time equivalent decreases will be offset, at least partially, by productivity gains."
Dr. Fraher and colleagues called their findings "a snapshot of trends that may or may not develop depending on whether there are changes in graduate medical education training pathways, in the length of training, and in attrition from residency programs."
Current proposals to either cut or increase graduate medical education funding under Medicare focus largely on increasing the supply of primary care physicians, but results from this model suggest that it is equally important to ensure an adequate supply of surgeons in the future, the authors said. They emphasized that current published recommendations to boost graduate medical education by the Council of Graduate Medical Education, Congress, and others, if implemented, would not avert declines in surgical workforce supply during the period forecasted.
Dr. Fraher and colleagues’ study was sponsored by the American College of Surgeons. None of its authors declared conflicts of interest.
The supply of surgeons in the United States will decrease by nearly one-fifth by 2028, likely resulting in shortages in all but a handful of specialties, a study has shown.
Currently proposed changes to increase surgeon training will not be enough to offset the number of surgeons who will retire, predicted Erin P. Fraher, Ph.D., of the department of surgery at the University of North Carolina at Chapel Hill, and colleagues. If this trend continues, the overall supply of full-time-equivalent surgeons will have decreased 18% between 2009 and 2028, with declines in all specialties except colorectal, pediatric, neurologic, and vascular surgery.
Such a drop could result in a workforce insufficient to meet the needs of the U.S. population – particularly in light of the expanded access to and increased usage of health care services projected for the future. It could also exacerbate problems related to the geographic distribution of surgeons, the investigators cautioned, "leading to delayed or lost access to time-sensitive surgical procedures, particularly in rural areas" (Ann. Surg. 2012 [doi:10.1097/SLA.0b013e31826fccfa]).
These projections are lower than those forecast in a 2008 report by the U.S. Health Resources and Services Administration for general, cardiothoracic, orthopedic, urologic, plastic, ophthalmologic, and obstetrics/gynecologic surgeons. However, they are brighter than previously published projections for vascular and pediatric surgeons (J. Vasc. Surg. 2009;50:946-52; J. Pediatr. Surg. 2009;44:1677-82). Predictions of a decline in cardiothoracic surgeons are consistent with some earlier findings (Circulation 2009;120:488-94).
For the current research, the investigators used a stock-and-flow model, which calculates current numbers of physicians, projected numbers of physicians graduating from medical school, and physicians reentering the workforce, and subtracts from these anticipated deaths, retirements, and career breaks. They then adjusted the resulting head count to full-time-equivalent work participation rates of surgeons by age, sex, and specialty.
Data were drawn from databases maintained by the American Medical Association, the American Board of Medical Specialties, the National Resident Match Program, the San Francisco match for plastic surgery and ophthalmology, the American Urological Association, the Health Resources and Services Administration, and the North Carolina Health Professions Data System.
Unlike static projection models, this model allows for real-time updating to take into account changes in data and policy decisions, which enhances the accuracy of its workforce projections, according to the investigators.
Surgeons’ participation in patient care declines somewhat after age 60, they noted, making age a key factor in determining full-time equivalents for each specialty. Another factor considered in modeling was the "feminization" of various specialties. By 2019, Dr. Fraher and colleagues predicted, half of general surgery residents will be female, compared with 95% of obstetrics and gynecology residents and 28% of orthopedic surgery residents.
Furthermore, an estimated 25% of general surgery cases that have traditionally been performed by surgical specialists will, in the future, need to be made up by general surgeons, the investigators said.
The most important driver of future supply estimates, they said, "is whether anticipated declines in full-time equivalent rates will occur as expected and whether these full-time equivalent decreases will be offset, at least partially, by productivity gains."
Dr. Fraher and colleagues called their findings "a snapshot of trends that may or may not develop depending on whether there are changes in graduate medical education training pathways, in the length of training, and in attrition from residency programs."
Current proposals to either cut or increase graduate medical education funding under Medicare focus largely on increasing the supply of primary care physicians, but results from this model suggest that it is equally important to ensure an adequate supply of surgeons in the future, the authors said. They emphasized that current published recommendations to boost graduate medical education by the Council of Graduate Medical Education, Congress, and others, if implemented, would not avert declines in surgical workforce supply during the period forecasted.
Dr. Fraher and colleagues’ study was sponsored by the American College of Surgeons. None of its authors declared conflicts of interest.
The supply of surgeons in the United States will decrease by nearly one-fifth by 2028, likely resulting in shortages in all but a handful of specialties, a study has shown.
Currently proposed changes to increase surgeon training will not be enough to offset the number of surgeons who will retire, predicted Erin P. Fraher, Ph.D., of the department of surgery at the University of North Carolina at Chapel Hill, and colleagues. If this trend continues, the overall supply of full-time-equivalent surgeons will have decreased 18% between 2009 and 2028, with declines in all specialties except colorectal, pediatric, neurologic, and vascular surgery.
Such a drop could result in a workforce insufficient to meet the needs of the U.S. population – particularly in light of the expanded access to and increased usage of health care services projected for the future. It could also exacerbate problems related to the geographic distribution of surgeons, the investigators cautioned, "leading to delayed or lost access to time-sensitive surgical procedures, particularly in rural areas" (Ann. Surg. 2012 [doi:10.1097/SLA.0b013e31826fccfa]).
These projections are lower than those forecast in a 2008 report by the U.S. Health Resources and Services Administration for general, cardiothoracic, orthopedic, urologic, plastic, ophthalmologic, and obstetrics/gynecologic surgeons. However, they are brighter than previously published projections for vascular and pediatric surgeons (J. Vasc. Surg. 2009;50:946-52; J. Pediatr. Surg. 2009;44:1677-82). Predictions of a decline in cardiothoracic surgeons are consistent with some earlier findings (Circulation 2009;120:488-94).
For the current research, the investigators used a stock-and-flow model, which calculates current numbers of physicians, projected numbers of physicians graduating from medical school, and physicians reentering the workforce, and subtracts from these anticipated deaths, retirements, and career breaks. They then adjusted the resulting head count to full-time-equivalent work participation rates of surgeons by age, sex, and specialty.
Data were drawn from databases maintained by the American Medical Association, the American Board of Medical Specialties, the National Resident Match Program, the San Francisco match for plastic surgery and ophthalmology, the American Urological Association, the Health Resources and Services Administration, and the North Carolina Health Professions Data System.
Unlike static projection models, this model allows for real-time updating to take into account changes in data and policy decisions, which enhances the accuracy of its workforce projections, according to the investigators.
Surgeons’ participation in patient care declines somewhat after age 60, they noted, making age a key factor in determining full-time equivalents for each specialty. Another factor considered in modeling was the "feminization" of various specialties. By 2019, Dr. Fraher and colleagues predicted, half of general surgery residents will be female, compared with 95% of obstetrics and gynecology residents and 28% of orthopedic surgery residents.
Furthermore, an estimated 25% of general surgery cases that have traditionally been performed by surgical specialists will, in the future, need to be made up by general surgeons, the investigators said.
The most important driver of future supply estimates, they said, "is whether anticipated declines in full-time equivalent rates will occur as expected and whether these full-time equivalent decreases will be offset, at least partially, by productivity gains."
Dr. Fraher and colleagues called their findings "a snapshot of trends that may or may not develop depending on whether there are changes in graduate medical education training pathways, in the length of training, and in attrition from residency programs."
Current proposals to either cut or increase graduate medical education funding under Medicare focus largely on increasing the supply of primary care physicians, but results from this model suggest that it is equally important to ensure an adequate supply of surgeons in the future, the authors said. They emphasized that current published recommendations to boost graduate medical education by the Council of Graduate Medical Education, Congress, and others, if implemented, would not avert declines in surgical workforce supply during the period forecasted.
Dr. Fraher and colleagues’ study was sponsored by the American College of Surgeons. None of its authors declared conflicts of interest.
FROM ANNALS OF SURGERY
Major Finding: The overall availability of surgeons in the United States will have decreased 18% by 2028 if current trends continue, with exceptions for some specialties.
Data Source: Databases maintained by the American Medical Association and several other organizations.
Disclosures: The study was sponsored by the American College of Surgeons. None of the authors declared conflicts of interest.
Lower esophageal electrical stimulation therapy targets GERD
Electrical stimulation of the lower esophageal sphincter using an implanted device shows promise for the treatment of gastroesophageal reflux, according to findings from three recent studies.
In one open-label pilot extension study, 77% of 23 patients treated with EndoStim’s Lower Esophageal Sphincter (LES) stimulation system reported normalization of (or at least a 50% reduction in) distal esophageal acid exposure at 12 months’ follow-up, Dr. Edy Soffer reported in October at the annual meeting of the American College of Gastroenterology.

The patients also experienced significant improvement in their median GERD-Health Related Quality of Life (GERD-HRQL) score while implanted with the LES stimulation system (LES-EST), compared with their score while on proton pump inhibitor (PPI) therapy (increase of 9 vs. 2 points) and while off PPI therapy (increase of 23.5 vs. 2), said Dr. Soffer, professor of clinical medicine and director of the GI motility program at the University of Southern California, Los Angeles.
All but one patient reported cessation of regular PPI use, and no implantation- or stimulation-related unanticipated adverse events or "untoward sensation" due to stimulation occurred during follow-up; nor was swallowing function as assessed by manometry affected.
Patients included in the study were GERD patients with a mean age of 53 years who were at least partially responsive to PPI therapy, and who had off-PPI GERD-HRQL scores of at least 20, as well as hiatal hernia.
The findings indicate that LES-EST, which uses low-energy electrical pulses to strengthen a weak or dysfunctional lower esophageal sphincter, is safe and effective for long-term use, he said.
In an interview, Dr. Soffer said that the findings have held up at 18 months of follow-up.
"The results are comparable to those observed at 12 months with regard to control of symptoms, and with near elimination of the use of PPIs," he said, noting that the safety profile remains excellent, with no new adverse event reported beyond those seen at 12 months’ follow-up.
Physiological studies such as esophageal pH will be conducted at 24 months, he said.
In a related study presented in a poster at the meeting, Michael Crowell, Ph.D., looked more closely at the effects of LES-EST on both distal and proximal esophageal acid exposure in a post hoc analysis.
In 19 patients with a median age of 54 years, LES-EST was associated with normalization of total and upright proximal esophageal acid exposure, which improved from 0.4% and 0.6%, respectively, at baseline to 0% at 12 months’ follow-up. Supine esophageal acid exposure was unchanged from 0% at baseline, said Dr. Crowell of the Mayo Clinic, Scottsdale, Ariz.
This was true even among seven patients with abnormal proximal esophageal pH, whose total, upright, and supine proximal esophageal acid exposure values at baseline were 1.7%, 2.9%, and 0.3%, respectively. Distal esophageal pH improved from 10.2% to 3.6% for the entire cohort, and from 9.3% to 3.4% in those seven patients.
Patients in this study had GERD that was at least partially responsive to PPIs, a hiatal hernia of less than 3 cm, and esophagitis of less than Los Angeles Classification grade D. Electrical stimulation was administered for 220 microseconds at 20 Hz and 5-8 mA in 6-12 30-minute sessions starting on day 1 after implantation.
No gastrointestinal side effects occurred in the patients, nor were there any device- or procedure-related adverse events.
LES-EST may be effective in treating proximal GERD, Dr. Crowell concluded.
In an interview, he added that the findings are important, particularly for the one-third of patients who remain symptomatic on PPIs.
"LES dysfunction is the root cause of GERD. Medications such as PPIs block stomach acid production, but do not address the pathophysiology of GERD. Hence, more than a third of patients continue to suffer from symptoms despite maximal medical therapy," he said.
Additionally, there are significant safety concerns with long-term acid suppression, he noted.
LES-EST, on the other hand, addresses the root cause of GERD by improving LES pressure and function, thereby restoring the LES physiology and its barrier function, preventing reflux of gastric acid into the esophagus.
"LES stimulation does not affect normal LES relaxation, allowing for the patient to swallow normally, and has no side effects," he said.
In a third, unrelated study also reported in a poster at the meeting, LES-EST was similarly effective.
Of 11 patients treated with EndoStim’s LES stimulation system as part of an international multicenter study, 10 were able to discontinue PPI therapy at 3-6 months of follow-up, according to Dr. Arjan J. Bredenoord of Academic Medical Center Utrecht, Rotterdam.
Those 10 patients experienced significant improvements in median GERD-HRQL scores from 32 (off PPIs) and 22 (on PPIs) to 9 (on LES-EST) at 3 months, and the scores remained stable at 9 points in 3 patients who were followed for 6 months.
Median esophageal acid exposure improved from 11.8% at baseline to 7.8% at 3 months and 7.3% at 6 months, Dr. Bredenoord said.
The remaining patient suffered a small bowl trocar perforation during implantation of the device and underwent successful repair. An additional 13 adverse events, including 1 serious adverse event, were reported in 4 patients. Nine of these were related to the device or procedure, including seven complaints of pain at the implant site and one case of postoperative nausea.
The treatment was safe, with no GI or cardiac side effects, Dr. Bredenoord concluded, noting that long-term safety and efficacy results in a larger group of patients are currently being analyzed.
In an interview, Dr. Bredenoord noted that the findings are among the first in patients outside South America, where the earliest trials of the EndoStim LES stimulation system were conducted.
"The data confirm the favorable outcome of the patients in Chile, and show that both symptoms and reflux are reduced in European patients as well," he said.
However, the experience remains limited, and additional study comparing the device with other treatments and/or with placebo is needed, as are longer-term outcomes data.
"I think that although these results suggest this is a promising treatment, it would be best to treat patients only in trials" at this point, he said. Because trial participants have been carefully selected, it remains unclear whether this treatment is suitable for the entire GERD population, he added.
Dr. Soffer agreed, and said that if the results are reproduced in additional studies with a larger number of patients, the intervention will provide an alternative therapy for GERD patients who are not satisfied with PPIs or who have concerns about side effects and the chronic use of treatment, and who also have concerns about the established surgical treatment for GERD.
"The importance of this intervention is in providing a bridge between the currently established drug therapy for GERD [PPIs] and the established surgical therapy [fundoplication]. While PPIs are effective in a substantial number of GERD patients, they do not correct the underlying pathophysiology of GERD, resulting in a substantial number of patients who remain symptomatic in spite of therapy," he said.
These patients can be offered fundoplication, which is effective in expert hands, but the surgery has side effects and is performed less and less often, he added.
"Consequently, there is a search for a bridge intervention, endoscopic or surgical, for the treatment of GERD," he said.
LES-EST appears to have the potential to be such a bridge intervention.
"The procedure is simple and nondisruptive, and addresses pathophysiology. The safety profile thus far is excellent, and the effect on esophageal acid exposure, symptoms, and PPI use is sustained over a period of 12-18 moths. Furthermore, the treatment can be optimized to individual needs by adjusting delivery of stimulation to coincide with periods when symptoms and acid reflux are detected," he said.
All three of these studies presented at the meeting were supported by EndoStim BV. Dr. Soffer disclosed that he has stockholder/ownership interest in the company. Dr. Crowell disclosed that he has served as a consultant to the company. Dr. Bredenoord reported receiving grant and/or research support from the company.
Gastroesophageal reflux disease is one of the most common chronic gastrointestinal disorders. The mainstay of medical therapy is to suppress gastric acid secretion with medications such as PPIs. An alternative approach to acid suppression is modulation of the antireflux barrier, composed of the lower esophageal sphincter (LES) and the crural diaphragm. Surgical fundoplication is a well-established method to augment the function of the antireflux barrier. Fundoplication has proven effective in high-quality trials, but it also has well-documented side effects such as dysphagia, bloating, and diarrhea in a subset of patients.
Additional means of enhancing the function of the antireflux barrier include pharmacological inhibition of transient LES relaxations (TLESR) with various agents and several endoscopic antireflux procedures. Unfortunately, the use of TLESR inhibitors and endoscopic procedures for GERD is very limited due to side effects and adverse events, along with insufficient efficacy.
Electrical stimulation of the LES has been previously shown to increase LES resting tone in an animal model (Am. J. Physiol. Gastrointest. Liver Physiol. 2008;295:G389-94). More recently, in a 6-month, open-label trial, electrical stimulation of the LES was found to reduce or eliminate PPI use and to improve symptoms and 24-hour esophageal pH parameters in GERD patients who were at least partially responsive to PPIs (Surg. Endosc. 2012 Oct. 17 [doi: 10.1007/s00464-012-2561-4]).
During the recent American College of Gastroenterology meeting, 1-year data for the open-label trial mentioned above was presented by Dr. Soffer, Dr. Crowell, and their collaborators, showing that improvement in symptoms, PPI use, and distal esophageal acid exposure persisted at 12 months with minimal side effects or adverse events.
Preliminary results of an international multicenter trial of LES electrical stimulation for refractory GERD were also presented at the meeting by Dr. Bredenoord and his colleagues. They found that LES electrical stimulation improved symptoms, PPI use, and esophageal acid exposure in this group of patients, but the preliminary number of patients was small and follow-up was mostly limited to 3 months. Importantly, they did report some adverse events.
These studies provide additional information to suggest that electrical stimulation of the LES may be an effective treatment for GERD. While the available data is compelling, more work will be required to evaluate the durability of the procedure, assess long-term safety and side effects, study the effects of stimulation on esophageal sensation, and define which GERD patients are best suited for this treatment. This will be ideally accomplished by randomized controlled trials that will compare electrical stimulation of the LES to the well-established pharmacological and surgical approaches currently used to treat GERD.
Marcelo F. Vela, M.D., is an associate professor of medicine and director of gastrointestinal motility at Baylor College of Medicine and the Michael E. DeBakey VA Medical Center, both in Houston. He is a member of an advisory panel for Given Imaging.
Gastroesophageal reflux disease is one of the most common chronic gastrointestinal disorders. The mainstay of medical therapy is to suppress gastric acid secretion with medications such as PPIs. An alternative approach to acid suppression is modulation of the antireflux barrier, composed of the lower esophageal sphincter (LES) and the crural diaphragm. Surgical fundoplication is a well-established method to augment the function of the antireflux barrier. Fundoplication has proven effective in high-quality trials, but it also has well-documented side effects such as dysphagia, bloating, and diarrhea in a subset of patients.
Additional means of enhancing the function of the antireflux barrier include pharmacological inhibition of transient LES relaxations (TLESR) with various agents and several endoscopic antireflux procedures. Unfortunately, the use of TLESR inhibitors and endoscopic procedures for GERD is very limited due to side effects and adverse events, along with insufficient efficacy.
Electrical stimulation of the LES has been previously shown to increase LES resting tone in an animal model (Am. J. Physiol. Gastrointest. Liver Physiol. 2008;295:G389-94). More recently, in a 6-month, open-label trial, electrical stimulation of the LES was found to reduce or eliminate PPI use and to improve symptoms and 24-hour esophageal pH parameters in GERD patients who were at least partially responsive to PPIs (Surg. Endosc. 2012 Oct. 17 [doi: 10.1007/s00464-012-2561-4]).
During the recent American College of Gastroenterology meeting, 1-year data for the open-label trial mentioned above was presented by Dr. Soffer, Dr. Crowell, and their collaborators, showing that improvement in symptoms, PPI use, and distal esophageal acid exposure persisted at 12 months with minimal side effects or adverse events.
Preliminary results of an international multicenter trial of LES electrical stimulation for refractory GERD were also presented at the meeting by Dr. Bredenoord and his colleagues. They found that LES electrical stimulation improved symptoms, PPI use, and esophageal acid exposure in this group of patients, but the preliminary number of patients was small and follow-up was mostly limited to 3 months. Importantly, they did report some adverse events.
These studies provide additional information to suggest that electrical stimulation of the LES may be an effective treatment for GERD. While the available data is compelling, more work will be required to evaluate the durability of the procedure, assess long-term safety and side effects, study the effects of stimulation on esophageal sensation, and define which GERD patients are best suited for this treatment. This will be ideally accomplished by randomized controlled trials that will compare electrical stimulation of the LES to the well-established pharmacological and surgical approaches currently used to treat GERD.
Marcelo F. Vela, M.D., is an associate professor of medicine and director of gastrointestinal motility at Baylor College of Medicine and the Michael E. DeBakey VA Medical Center, both in Houston. He is a member of an advisory panel for Given Imaging.
Gastroesophageal reflux disease is one of the most common chronic gastrointestinal disorders. The mainstay of medical therapy is to suppress gastric acid secretion with medications such as PPIs. An alternative approach to acid suppression is modulation of the antireflux barrier, composed of the lower esophageal sphincter (LES) and the crural diaphragm. Surgical fundoplication is a well-established method to augment the function of the antireflux barrier. Fundoplication has proven effective in high-quality trials, but it also has well-documented side effects such as dysphagia, bloating, and diarrhea in a subset of patients.
Additional means of enhancing the function of the antireflux barrier include pharmacological inhibition of transient LES relaxations (TLESR) with various agents and several endoscopic antireflux procedures. Unfortunately, the use of TLESR inhibitors and endoscopic procedures for GERD is very limited due to side effects and adverse events, along with insufficient efficacy.
Electrical stimulation of the LES has been previously shown to increase LES resting tone in an animal model (Am. J. Physiol. Gastrointest. Liver Physiol. 2008;295:G389-94). More recently, in a 6-month, open-label trial, electrical stimulation of the LES was found to reduce or eliminate PPI use and to improve symptoms and 24-hour esophageal pH parameters in GERD patients who were at least partially responsive to PPIs (Surg. Endosc. 2012 Oct. 17 [doi: 10.1007/s00464-012-2561-4]).
During the recent American College of Gastroenterology meeting, 1-year data for the open-label trial mentioned above was presented by Dr. Soffer, Dr. Crowell, and their collaborators, showing that improvement in symptoms, PPI use, and distal esophageal acid exposure persisted at 12 months with minimal side effects or adverse events.
Preliminary results of an international multicenter trial of LES electrical stimulation for refractory GERD were also presented at the meeting by Dr. Bredenoord and his colleagues. They found that LES electrical stimulation improved symptoms, PPI use, and esophageal acid exposure in this group of patients, but the preliminary number of patients was small and follow-up was mostly limited to 3 months. Importantly, they did report some adverse events.
These studies provide additional information to suggest that electrical stimulation of the LES may be an effective treatment for GERD. While the available data is compelling, more work will be required to evaluate the durability of the procedure, assess long-term safety and side effects, study the effects of stimulation on esophageal sensation, and define which GERD patients are best suited for this treatment. This will be ideally accomplished by randomized controlled trials that will compare electrical stimulation of the LES to the well-established pharmacological and surgical approaches currently used to treat GERD.
Marcelo F. Vela, M.D., is an associate professor of medicine and director of gastrointestinal motility at Baylor College of Medicine and the Michael E. DeBakey VA Medical Center, both in Houston. He is a member of an advisory panel for Given Imaging.
Electrical stimulation of the lower esophageal sphincter using an implanted device shows promise for the treatment of gastroesophageal reflux, according to findings from three recent studies.
In one open-label pilot extension study, 77% of 23 patients treated with EndoStim’s Lower Esophageal Sphincter (LES) stimulation system reported normalization of (or at least a 50% reduction in) distal esophageal acid exposure at 12 months’ follow-up, Dr. Edy Soffer reported in October at the annual meeting of the American College of Gastroenterology.
The patients also experienced significant improvement in their median GERD-Health Related Quality of Life (GERD-HRQL) score while implanted with the LES stimulation system (LES-EST), compared with their score while on proton pump inhibitor (PPI) therapy (increase of 9 vs. 2 points) and while off PPI therapy (increase of 23.5 vs. 2), said Dr. Soffer, professor of clinical medicine and director of the GI motility program at the University of Southern California, Los Angeles.
All but one patient reported cessation of regular PPI use, and no implantation- or stimulation-related unanticipated adverse events or "untoward sensation" due to stimulation occurred during follow-up; nor was swallowing function as assessed by manometry affected.
Patients included in the study were GERD patients with a mean age of 53 years who were at least partially responsive to PPI therapy, and who had off-PPI GERD-HRQL scores of at least 20, as well as hiatal hernia.
The findings indicate that LES-EST, which uses low-energy electrical pulses to strengthen a weak or dysfunctional lower esophageal sphincter, is safe and effective for long-term use, he said.
In an interview, Dr. Soffer said that the findings have held up at 18 months of follow-up.
"The results are comparable to those observed at 12 months with regard to control of symptoms, and with near elimination of the use of PPIs," he said, noting that the safety profile remains excellent, with no new adverse event reported beyond those seen at 12 months’ follow-up.
Physiological studies such as esophageal pH will be conducted at 24 months, he said.
In a related study presented in a poster at the meeting, Michael Crowell, Ph.D., looked more closely at the effects of LES-EST on both distal and proximal esophageal acid exposure in a post hoc analysis.
In 19 patients with a median age of 54 years, LES-EST was associated with normalization of total and upright proximal esophageal acid exposure, which improved from 0.4% and 0.6%, respectively, at baseline to 0% at 12 months’ follow-up. Supine esophageal acid exposure was unchanged from 0% at baseline, said Dr. Crowell of the Mayo Clinic, Scottsdale, Ariz.
This was true even among seven patients with abnormal proximal esophageal pH, whose total, upright, and supine proximal esophageal acid exposure values at baseline were 1.7%, 2.9%, and 0.3%, respectively. Distal esophageal pH improved from 10.2% to 3.6% for the entire cohort, and from 9.3% to 3.4% in those seven patients.
Patients in this study had GERD that was at least partially responsive to PPIs, a hiatal hernia of less than 3 cm, and esophagitis of less than Los Angeles Classification grade D. Electrical stimulation was administered for 220 microseconds at 20 Hz and 5-8 mA in 6-12 30-minute sessions starting on day 1 after implantation.
No gastrointestinal side effects occurred in the patients, nor were there any device- or procedure-related adverse events.
LES-EST may be effective in treating proximal GERD, Dr. Crowell concluded.
In an interview, he added that the findings are important, particularly for the one-third of patients who remain symptomatic on PPIs.
"LES dysfunction is the root cause of GERD. Medications such as PPIs block stomach acid production, but do not address the pathophysiology of GERD. Hence, more than a third of patients continue to suffer from symptoms despite maximal medical therapy," he said.
Additionally, there are significant safety concerns with long-term acid suppression, he noted.
LES-EST, on the other hand, addresses the root cause of GERD by improving LES pressure and function, thereby restoring the LES physiology and its barrier function, preventing reflux of gastric acid into the esophagus.
"LES stimulation does not affect normal LES relaxation, allowing for the patient to swallow normally, and has no side effects," he said.
In a third, unrelated study also reported in a poster at the meeting, LES-EST was similarly effective.
Of 11 patients treated with EndoStim’s LES stimulation system as part of an international multicenter study, 10 were able to discontinue PPI therapy at 3-6 months of follow-up, according to Dr. Arjan J. Bredenoord of Academic Medical Center Utrecht, Rotterdam.
Those 10 patients experienced significant improvements in median GERD-HRQL scores from 32 (off PPIs) and 22 (on PPIs) to 9 (on LES-EST) at 3 months, and the scores remained stable at 9 points in 3 patients who were followed for 6 months.
Median esophageal acid exposure improved from 11.8% at baseline to 7.8% at 3 months and 7.3% at 6 months, Dr. Bredenoord said.
The remaining patient suffered a small bowl trocar perforation during implantation of the device and underwent successful repair. An additional 13 adverse events, including 1 serious adverse event, were reported in 4 patients. Nine of these were related to the device or procedure, including seven complaints of pain at the implant site and one case of postoperative nausea.
The treatment was safe, with no GI or cardiac side effects, Dr. Bredenoord concluded, noting that long-term safety and efficacy results in a larger group of patients are currently being analyzed.
In an interview, Dr. Bredenoord noted that the findings are among the first in patients outside South America, where the earliest trials of the EndoStim LES stimulation system were conducted.
"The data confirm the favorable outcome of the patients in Chile, and show that both symptoms and reflux are reduced in European patients as well," he said.
However, the experience remains limited, and additional study comparing the device with other treatments and/or with placebo is needed, as are longer-term outcomes data.
"I think that although these results suggest this is a promising treatment, it would be best to treat patients only in trials" at this point, he said. Because trial participants have been carefully selected, it remains unclear whether this treatment is suitable for the entire GERD population, he added.
Dr. Soffer agreed, and said that if the results are reproduced in additional studies with a larger number of patients, the intervention will provide an alternative therapy for GERD patients who are not satisfied with PPIs or who have concerns about side effects and the chronic use of treatment, and who also have concerns about the established surgical treatment for GERD.
"The importance of this intervention is in providing a bridge between the currently established drug therapy for GERD [PPIs] and the established surgical therapy [fundoplication]. While PPIs are effective in a substantial number of GERD patients, they do not correct the underlying pathophysiology of GERD, resulting in a substantial number of patients who remain symptomatic in spite of therapy," he said.
These patients can be offered fundoplication, which is effective in expert hands, but the surgery has side effects and is performed less and less often, he added.
"Consequently, there is a search for a bridge intervention, endoscopic or surgical, for the treatment of GERD," he said.
LES-EST appears to have the potential to be such a bridge intervention.
"The procedure is simple and nondisruptive, and addresses pathophysiology. The safety profile thus far is excellent, and the effect on esophageal acid exposure, symptoms, and PPI use is sustained over a period of 12-18 moths. Furthermore, the treatment can be optimized to individual needs by adjusting delivery of stimulation to coincide with periods when symptoms and acid reflux are detected," he said.
All three of these studies presented at the meeting were supported by EndoStim BV. Dr. Soffer disclosed that he has stockholder/ownership interest in the company. Dr. Crowell disclosed that he has served as a consultant to the company. Dr. Bredenoord reported receiving grant and/or research support from the company.
Electrical stimulation of the lower esophageal sphincter using an implanted device shows promise for the treatment of gastroesophageal reflux, according to findings from three recent studies.
In one open-label pilot extension study, 77% of 23 patients treated with EndoStim’s Lower Esophageal Sphincter (LES) stimulation system reported normalization of (or at least a 50% reduction in) distal esophageal acid exposure at 12 months’ follow-up, Dr. Edy Soffer reported in October at the annual meeting of the American College of Gastroenterology.
The patients also experienced significant improvement in their median GERD-Health Related Quality of Life (GERD-HRQL) score while implanted with the LES stimulation system (LES-EST), compared with their score while on proton pump inhibitor (PPI) therapy (increase of 9 vs. 2 points) and while off PPI therapy (increase of 23.5 vs. 2), said Dr. Soffer, professor of clinical medicine and director of the GI motility program at the University of Southern California, Los Angeles.
All but one patient reported cessation of regular PPI use, and no implantation- or stimulation-related unanticipated adverse events or "untoward sensation" due to stimulation occurred during follow-up; nor was swallowing function as assessed by manometry affected.
Patients included in the study were GERD patients with a mean age of 53 years who were at least partially responsive to PPI therapy, and who had off-PPI GERD-HRQL scores of at least 20, as well as hiatal hernia.
The findings indicate that LES-EST, which uses low-energy electrical pulses to strengthen a weak or dysfunctional lower esophageal sphincter, is safe and effective for long-term use, he said.
In an interview, Dr. Soffer said that the findings have held up at 18 months of follow-up.
"The results are comparable to those observed at 12 months with regard to control of symptoms, and with near elimination of the use of PPIs," he said, noting that the safety profile remains excellent, with no new adverse event reported beyond those seen at 12 months’ follow-up.
Physiological studies such as esophageal pH will be conducted at 24 months, he said.
In a related study presented in a poster at the meeting, Michael Crowell, Ph.D., looked more closely at the effects of LES-EST on both distal and proximal esophageal acid exposure in a post hoc analysis.
In 19 patients with a median age of 54 years, LES-EST was associated with normalization of total and upright proximal esophageal acid exposure, which improved from 0.4% and 0.6%, respectively, at baseline to 0% at 12 months’ follow-up. Supine esophageal acid exposure was unchanged from 0% at baseline, said Dr. Crowell of the Mayo Clinic, Scottsdale, Ariz.
This was true even among seven patients with abnormal proximal esophageal pH, whose total, upright, and supine proximal esophageal acid exposure values at baseline were 1.7%, 2.9%, and 0.3%, respectively. Distal esophageal pH improved from 10.2% to 3.6% for the entire cohort, and from 9.3% to 3.4% in those seven patients.
Patients in this study had GERD that was at least partially responsive to PPIs, a hiatal hernia of less than 3 cm, and esophagitis of less than Los Angeles Classification grade D. Electrical stimulation was administered for 220 microseconds at 20 Hz and 5-8 mA in 6-12 30-minute sessions starting on day 1 after implantation.
No gastrointestinal side effects occurred in the patients, nor were there any device- or procedure-related adverse events.
LES-EST may be effective in treating proximal GERD, Dr. Crowell concluded.
In an interview, he added that the findings are important, particularly for the one-third of patients who remain symptomatic on PPIs.
"LES dysfunction is the root cause of GERD. Medications such as PPIs block stomach acid production, but do not address the pathophysiology of GERD. Hence, more than a third of patients continue to suffer from symptoms despite maximal medical therapy," he said.
Additionally, there are significant safety concerns with long-term acid suppression, he noted.
LES-EST, on the other hand, addresses the root cause of GERD by improving LES pressure and function, thereby restoring the LES physiology and its barrier function, preventing reflux of gastric acid into the esophagus.
"LES stimulation does not affect normal LES relaxation, allowing for the patient to swallow normally, and has no side effects," he said.
In a third, unrelated study also reported in a poster at the meeting, LES-EST was similarly effective.
Of 11 patients treated with EndoStim’s LES stimulation system as part of an international multicenter study, 10 were able to discontinue PPI therapy at 3-6 months of follow-up, according to Dr. Arjan J. Bredenoord of Academic Medical Center Utrecht, Rotterdam.
Those 10 patients experienced significant improvements in median GERD-HRQL scores from 32 (off PPIs) and 22 (on PPIs) to 9 (on LES-EST) at 3 months, and the scores remained stable at 9 points in 3 patients who were followed for 6 months.
Median esophageal acid exposure improved from 11.8% at baseline to 7.8% at 3 months and 7.3% at 6 months, Dr. Bredenoord said.
The remaining patient suffered a small bowl trocar perforation during implantation of the device and underwent successful repair. An additional 13 adverse events, including 1 serious adverse event, were reported in 4 patients. Nine of these were related to the device or procedure, including seven complaints of pain at the implant site and one case of postoperative nausea.
The treatment was safe, with no GI or cardiac side effects, Dr. Bredenoord concluded, noting that long-term safety and efficacy results in a larger group of patients are currently being analyzed.
In an interview, Dr. Bredenoord noted that the findings are among the first in patients outside South America, where the earliest trials of the EndoStim LES stimulation system were conducted.
"The data confirm the favorable outcome of the patients in Chile, and show that both symptoms and reflux are reduced in European patients as well," he said.
However, the experience remains limited, and additional study comparing the device with other treatments and/or with placebo is needed, as are longer-term outcomes data.
"I think that although these results suggest this is a promising treatment, it would be best to treat patients only in trials" at this point, he said. Because trial participants have been carefully selected, it remains unclear whether this treatment is suitable for the entire GERD population, he added.
Dr. Soffer agreed, and said that if the results are reproduced in additional studies with a larger number of patients, the intervention will provide an alternative therapy for GERD patients who are not satisfied with PPIs or who have concerns about side effects and the chronic use of treatment, and who also have concerns about the established surgical treatment for GERD.
"The importance of this intervention is in providing a bridge between the currently established drug therapy for GERD [PPIs] and the established surgical therapy [fundoplication]. While PPIs are effective in a substantial number of GERD patients, they do not correct the underlying pathophysiology of GERD, resulting in a substantial number of patients who remain symptomatic in spite of therapy," he said.
These patients can be offered fundoplication, which is effective in expert hands, but the surgery has side effects and is performed less and less often, he added.
"Consequently, there is a search for a bridge intervention, endoscopic or surgical, for the treatment of GERD," he said.
LES-EST appears to have the potential to be such a bridge intervention.
"The procedure is simple and nondisruptive, and addresses pathophysiology. The safety profile thus far is excellent, and the effect on esophageal acid exposure, symptoms, and PPI use is sustained over a period of 12-18 moths. Furthermore, the treatment can be optimized to individual needs by adjusting delivery of stimulation to coincide with periods when symptoms and acid reflux are detected," he said.
All three of these studies presented at the meeting were supported by EndoStim BV. Dr. Soffer disclosed that he has stockholder/ownership interest in the company. Dr. Crowell disclosed that he has served as a consultant to the company. Dr. Bredenoord reported receiving grant and/or research support from the company.
FROM THE ANNUAL MEETING OF THE AMERICAN COLLEGE OF GASTROENTEROLOGY
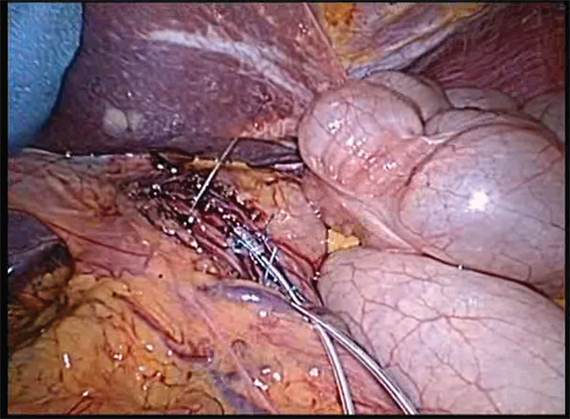
Contact precautions linked to fewer and shorter patient visits
Health care workers spent less time with patients who were on contact precautions, based on results from a prospective study in the January 2013 issue of Infection Control and Hospital Epidemiology.
Patients on contact precautions for drug-resistant infections had almost 40% fewer visits from health care workers. Further, when they did visit, health care workers spent significantly less time in the rooms of patients on precautions, reported Dr. Daniel Morgan and his associates.

On a positive note, handwashing hygiene improved when health care workers saw patient on contact precautions (Infect. Control Hosp. Epidemiol. 2013;34:69-73).
"Contact precautions modify health care workers’ behavior. This has positive and negative consequences," Dr. Morgan, the lead author, said in an interview.
"Health care workers should be aware of the tendency to visit patients less often and question their own behavior when caring for these patients," said Dr. Morgan of the University of Maryland and the Veterans Affairs (VA) Maryland Health Care System, Baltimore. "Do they visit them less often? Are they at risk of missing anything because a patient is on precautions? Are they creating workarounds for the inconvenience that may impact the patient?"
Research is underway looking at outcomes of patients on isolation and ways to improve these outcomes, "but for a start, it is important that health care workers consider how their behavior may be shaped by contact precautions," he added.
In the prospective cohort study, the activity of health care workers at four acute hospitals was observed for 1-hour periods over 19 months. The trained observers – so-called "secret shoppers" – observed a total of 7,743 visits over 1,989 hours in seven intensive care units and six medical surgical wards at three VA Hospitals and at one medical center, the University of Maryland Medical Center in Baltimore.
Patients on contact precautions had 2.78 visits per hour from health care workers, compared with 4.37 visits per hour among those not on precautions, a statistically significant difference.
Health care workers also spent significantly less time – nearly 18% less – with patients on contact precautions. Time spent per hour was 14 minutes for patients on precautions and 17 minutes for other patients. The time spent with patients in ICUs, however, was similar irrespective of contact precautions.
Health care workers were almost 16% more likely to comply with proper hand hygiene techniques when exiting the rooms of patients on contact precautions. Proper hand washing was observed 63% of the time when leaving the room of a patient on precautions and 47% of the time when exiting the room of a patient not on precautions. This statistically significant difference was "more pronounced" in the ICU setting, the authors wrote.
Contact precautions did not appear to affect compliance with hand hygiene when entering a patient’s room. Overall, the compliance rate with gowns and gloves was 66% for patients on contact precautions.
The compliance rates for hand hygiene and use of gown and gloves recorded in the study were lower than the rates hospitals often report to hospital regulators, but they are in the range of what is routinely reported in more rigorous research, Dr. Morgan said in an interview.
The reduced contact between patients on contact precautions and health care workers was "likely" caused by the "inconvenience of donning gowns and gloves," the authors wrote. The lack of a difference in contact in the ICU could be the "higher acuity of care" or the higher nurse-to-patient ratio, whereby gloves and gowns do not need to be changed as frequently.
The "unintended consequences" of contact precautions are a particular concern now that contact precautions have become more common with programs like the Department of Veterans Affairs MRSA Prevention Initiative, Dr. Morgan and his associates said. The decrease in contact with health care workers "may lead to increased adverse events and a lower quality of patient care due to less consistent patient monitoring and poorer adherence to standard adverse event prevention methods" such as protocols to prevent pressure ulcers, they suggested.
The only non-ICU units observed in the study were in VA hospitals, which was one of the limitations of the study cited by the authors. The strengths of the study included the nearly 2,000 hours of observations at hospitals in different parts of the country.
"We don’t know whether less frequent visits to the patient room necessarily means more adverse events," Dr. Anthony Harris, professor of epidemiology and public health at the University of Maryland, said in an interview. Previous research indicating that contact precautions led to adverse events had some serious methodological flaws.
Dr. Harris, acting medical director of infection control at the University of Maryland Medical Center, is involved in a randomized study evaluating whether universal glove and gown precautions lead to improved or worse outcomes. The study, funded by the Agency for Healthcare Research and Quality (AHRQ), also is examining the frequency of health care worker visits and adverse events and should "provide more definitive answers to the important question of whether contact precautions lead to more adverse events," he said.
Financial support for Dr. Morgan’s study was provided by the VA Health Affairs Services Research and Development Investigator Initiated Research, Association of American Medical Colleges/Centers for Disease Control and Prevention, and AHRQ. Dr. Morgan disclosed having received an unrestricted research grant from Merck; the other authors had no relevant conflicts of interest to disclose. Dr. Harris is on the board of the Society for Healthcare Epidemiology of America, which publishes Infection Control and Hospital Epidemiology.
E.Mechcatie@elsevier.com
Health care workers spent less time with patients who were on contact precautions, based on results from a prospective study in the January 2013 issue of Infection Control and Hospital Epidemiology.
Patients on contact precautions for drug-resistant infections had almost 40% fewer visits from health care workers. Further, when they did visit, health care workers spent significantly less time in the rooms of patients on precautions, reported Dr. Daniel Morgan and his associates.
On a positive note, handwashing hygiene improved when health care workers saw patient on contact precautions (Infect. Control Hosp. Epidemiol. 2013;34:69-73).
"Contact precautions modify health care workers’ behavior. This has positive and negative consequences," Dr. Morgan, the lead author, said in an interview.
"Health care workers should be aware of the tendency to visit patients less often and question their own behavior when caring for these patients," said Dr. Morgan of the University of Maryland and the Veterans Affairs (VA) Maryland Health Care System, Baltimore. "Do they visit them less often? Are they at risk of missing anything because a patient is on precautions? Are they creating workarounds for the inconvenience that may impact the patient?"
Research is underway looking at outcomes of patients on isolation and ways to improve these outcomes, "but for a start, it is important that health care workers consider how their behavior may be shaped by contact precautions," he added.
In the prospective cohort study, the activity of health care workers at four acute hospitals was observed for 1-hour periods over 19 months. The trained observers – so-called "secret shoppers" – observed a total of 7,743 visits over 1,989 hours in seven intensive care units and six medical surgical wards at three VA Hospitals and at one medical center, the University of Maryland Medical Center in Baltimore.
Patients on contact precautions had 2.78 visits per hour from health care workers, compared with 4.37 visits per hour among those not on precautions, a statistically significant difference.
Health care workers also spent significantly less time – nearly 18% less – with patients on contact precautions. Time spent per hour was 14 minutes for patients on precautions and 17 minutes for other patients. The time spent with patients in ICUs, however, was similar irrespective of contact precautions.
Health care workers were almost 16% more likely to comply with proper hand hygiene techniques when exiting the rooms of patients on contact precautions. Proper hand washing was observed 63% of the time when leaving the room of a patient on precautions and 47% of the time when exiting the room of a patient not on precautions. This statistically significant difference was "more pronounced" in the ICU setting, the authors wrote.
Contact precautions did not appear to affect compliance with hand hygiene when entering a patient’s room. Overall, the compliance rate with gowns and gloves was 66% for patients on contact precautions.
The compliance rates for hand hygiene and use of gown and gloves recorded in the study were lower than the rates hospitals often report to hospital regulators, but they are in the range of what is routinely reported in more rigorous research, Dr. Morgan said in an interview.
The reduced contact between patients on contact precautions and health care workers was "likely" caused by the "inconvenience of donning gowns and gloves," the authors wrote. The lack of a difference in contact in the ICU could be the "higher acuity of care" or the higher nurse-to-patient ratio, whereby gloves and gowns do not need to be changed as frequently.
The "unintended consequences" of contact precautions are a particular concern now that contact precautions have become more common with programs like the Department of Veterans Affairs MRSA Prevention Initiative, Dr. Morgan and his associates said. The decrease in contact with health care workers "may lead to increased adverse events and a lower quality of patient care due to less consistent patient monitoring and poorer adherence to standard adverse event prevention methods" such as protocols to prevent pressure ulcers, they suggested.
The only non-ICU units observed in the study were in VA hospitals, which was one of the limitations of the study cited by the authors. The strengths of the study included the nearly 2,000 hours of observations at hospitals in different parts of the country.
"We don’t know whether less frequent visits to the patient room necessarily means more adverse events," Dr. Anthony Harris, professor of epidemiology and public health at the University of Maryland, said in an interview. Previous research indicating that contact precautions led to adverse events had some serious methodological flaws.
Dr. Harris, acting medical director of infection control at the University of Maryland Medical Center, is involved in a randomized study evaluating whether universal glove and gown precautions lead to improved or worse outcomes. The study, funded by the Agency for Healthcare Research and Quality (AHRQ), also is examining the frequency of health care worker visits and adverse events and should "provide more definitive answers to the important question of whether contact precautions lead to more adverse events," he said.
Financial support for Dr. Morgan’s study was provided by the VA Health Affairs Services Research and Development Investigator Initiated Research, Association of American Medical Colleges/Centers for Disease Control and Prevention, and AHRQ. Dr. Morgan disclosed having received an unrestricted research grant from Merck; the other authors had no relevant conflicts of interest to disclose. Dr. Harris is on the board of the Society for Healthcare Epidemiology of America, which publishes Infection Control and Hospital Epidemiology.
E.Mechcatie@elsevier.com
Health care workers spent less time with patients who were on contact precautions, based on results from a prospective study in the January 2013 issue of Infection Control and Hospital Epidemiology.
Patients on contact precautions for drug-resistant infections had almost 40% fewer visits from health care workers. Further, when they did visit, health care workers spent significantly less time in the rooms of patients on precautions, reported Dr. Daniel Morgan and his associates.
On a positive note, handwashing hygiene improved when health care workers saw patient on contact precautions (Infect. Control Hosp. Epidemiol. 2013;34:69-73).
"Contact precautions modify health care workers’ behavior. This has positive and negative consequences," Dr. Morgan, the lead author, said in an interview.
"Health care workers should be aware of the tendency to visit patients less often and question their own behavior when caring for these patients," said Dr. Morgan of the University of Maryland and the Veterans Affairs (VA) Maryland Health Care System, Baltimore. "Do they visit them less often? Are they at risk of missing anything because a patient is on precautions? Are they creating workarounds for the inconvenience that may impact the patient?"
Research is underway looking at outcomes of patients on isolation and ways to improve these outcomes, "but for a start, it is important that health care workers consider how their behavior may be shaped by contact precautions," he added.
In the prospective cohort study, the activity of health care workers at four acute hospitals was observed for 1-hour periods over 19 months. The trained observers – so-called "secret shoppers" – observed a total of 7,743 visits over 1,989 hours in seven intensive care units and six medical surgical wards at three VA Hospitals and at one medical center, the University of Maryland Medical Center in Baltimore.
Patients on contact precautions had 2.78 visits per hour from health care workers, compared with 4.37 visits per hour among those not on precautions, a statistically significant difference.
Health care workers also spent significantly less time – nearly 18% less – with patients on contact precautions. Time spent per hour was 14 minutes for patients on precautions and 17 minutes for other patients. The time spent with patients in ICUs, however, was similar irrespective of contact precautions.
Health care workers were almost 16% more likely to comply with proper hand hygiene techniques when exiting the rooms of patients on contact precautions. Proper hand washing was observed 63% of the time when leaving the room of a patient on precautions and 47% of the time when exiting the room of a patient not on precautions. This statistically significant difference was "more pronounced" in the ICU setting, the authors wrote.
Contact precautions did not appear to affect compliance with hand hygiene when entering a patient’s room. Overall, the compliance rate with gowns and gloves was 66% for patients on contact precautions.
The compliance rates for hand hygiene and use of gown and gloves recorded in the study were lower than the rates hospitals often report to hospital regulators, but they are in the range of what is routinely reported in more rigorous research, Dr. Morgan said in an interview.
The reduced contact between patients on contact precautions and health care workers was "likely" caused by the "inconvenience of donning gowns and gloves," the authors wrote. The lack of a difference in contact in the ICU could be the "higher acuity of care" or the higher nurse-to-patient ratio, whereby gloves and gowns do not need to be changed as frequently.
The "unintended consequences" of contact precautions are a particular concern now that contact precautions have become more common with programs like the Department of Veterans Affairs MRSA Prevention Initiative, Dr. Morgan and his associates said. The decrease in contact with health care workers "may lead to increased adverse events and a lower quality of patient care due to less consistent patient monitoring and poorer adherence to standard adverse event prevention methods" such as protocols to prevent pressure ulcers, they suggested.
The only non-ICU units observed in the study were in VA hospitals, which was one of the limitations of the study cited by the authors. The strengths of the study included the nearly 2,000 hours of observations at hospitals in different parts of the country.
"We don’t know whether less frequent visits to the patient room necessarily means more adverse events," Dr. Anthony Harris, professor of epidemiology and public health at the University of Maryland, said in an interview. Previous research indicating that contact precautions led to adverse events had some serious methodological flaws.
Dr. Harris, acting medical director of infection control at the University of Maryland Medical Center, is involved in a randomized study evaluating whether universal glove and gown precautions lead to improved or worse outcomes. The study, funded by the Agency for Healthcare Research and Quality (AHRQ), also is examining the frequency of health care worker visits and adverse events and should "provide more definitive answers to the important question of whether contact precautions lead to more adverse events," he said.
Financial support for Dr. Morgan’s study was provided by the VA Health Affairs Services Research and Development Investigator Initiated Research, Association of American Medical Colleges/Centers for Disease Control and Prevention, and AHRQ. Dr. Morgan disclosed having received an unrestricted research grant from Merck; the other authors had no relevant conflicts of interest to disclose. Dr. Harris is on the board of the Society for Healthcare Epidemiology of America, which publishes Infection Control and Hospital Epidemiology.
E.Mechcatie@elsevier.com
FROM INFECTION CONTROL AND HOSPITAL EPIDEMIOLOGY
Major Finding: Patients on contact precautions had 2.78 visits per hour from health care workers, compared with 4.37 visits per hour among those not on precautions.
Data Source: In the prospective cohort study, trained observers secretly monitored the activity of health care workers at four acute care hospitals for a total of 7,743 visits.
Disclosures: Financial support for the study was provided by the VA Health Affairs Services Research and Development Investigator Initiated Research, Association of American Medical Colleges/Centers for Disease Control and Prevention, and the Agency for Healthcare Research and Quality. Dr. Morgan disclosed having received an unrestricted research grant from Merck; the other authors had no relevant conflicts.

Laparoscopic diverticulitis surgery linked to fewer complications
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.

"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
This work falls somewhat short of actually comparing the efficacy of the laparoscopic approach and open surgery in patients with complicated diverticulitis. Without an adequate standardized description of the disease process itself, the patients’ comorbidities, and their physiologic perturbation at the time of presentation, it is exceedingly difficult to measure outcomes and the efficacy of therapeutic interventions.
I’m afraid the authors have not satisfactorily controlled for or analyzed the confounding factors so that plausible conclusions can be reached. The results are striking that mortality and complications were higher for patients treated with open surgery. I have watched the evolution of laparoscopic surgery over the past 25 years, and I am convinced that patients greatly benefit from this technology.
While the laparoscopic approach for treating diverticulitis resonates with my sensibility, the data do not support a clear recommendation. I urge surgeons to focus on this emergency, general-surgery population so that we can do important comparative effectiveness research and address some of these questions.
Dr. Michael F. Rotondo is professor and chairman of surgery at East Carolina University in Greenville, N.C. He had no disclosures. He made these comments as a designated discussant of the report.
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.
"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
PALM BEACH, FLA.– Using laparoscopic surgery for colectomy with primary anastomosis in patients with complicated diverticulitis linked with significantly fewer major complications compared with open surgical management in a review of more than 10,000 patients from a nationwide database.
However, the inherent biases at play when surgeons decide whether to manage a diverticulitis patient by a laparoscopic or open approach make it difficult to draw definitive conclusions from the findings, Dr. Edward E. Cornwell III said at the annual meeting of the Southern Surgical Association.
"If a surgeon did an operation laparoscopically, that by itself is an indicator of how sick the patient was. The surgeon selects an open operation for sicker patients, and laparoscopy for the less sick patients," he said in an interview. "Have we accounted for that difference [in the analysis]? That’s an open question," said Dr. Cornwell, professor and chairman of surgery at Howard University in Washington.
"Patients whom the surgeon deem well enough physiologically to sustain colectomy with primary anastomosis deserve strong consideration for the laparoscopic approach because those patients had the greatest difference in complications" compared with open surgery, he said.
The data Dr. Cornwell and his associates reviewed also showed a marked skewing in how surgeons used laparoscopy. Among the 10,085 patients included in the analysis, 7,562 (75%) underwent colectomy with primary anastomosis, and in this subgroup, 5,105 patients (68%) had their surgery done laparoscopically, while the remaining 2,457 (32%) were done with open surgery. In contrast, the 2,523 other patients in the series underwent a colectomy with colostomy, and within this subgroup, 2,286 patients (91%) had open surgery, with only 237 (9%) having laparoscopic surgery.
The overwhelming use of open surgery for the colostomy patients makes sense as it is a more complex operation, Dr. Cornwell said.
He and his associates used data collected during 2005-2009 at 237 U.S. hospitals by the National Surgical Quality Improvement Program of the American College of Surgeons on patients who underwent surgical management of complicated diverticulitis. The average age of the patients was 58 years, and overall 30-day mortality was 2%, while the overall postoperative complication rate during the 30 days following surgery was 23%.
Among the patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients, a statistically significant difference. Major complications included surgical site infections, dehiscence, transfusion, respiratory failure, sepsis, myocardial infarction, pulmonary embolism, stroke, renal failure or need for rehospitalization.
In a multivariate analysis that controlled for demographic parameters, body mass index, comorbidities, and functional status, patients who underwent laparoscopy had about half the number of total complications and major complications compared with patients who underwent open surgery – statistically significant differences. The laparoscopically-treated patients also had roughly half the rate of several individual major complications – wound infections, respiratory complications, and sepsis – compared with the open surgery patients, all statistically significant differences.
Thirty-day mortality was about 50% lower with laparoscopy compared with open surgery among patients who underwent a primary anastomosis, but this difference fell short of statistical significance.
The advantage of laparoscopy over open surgery was not nearly so clear among patients who underwent colectomy with colostomy. The data showed no significant difference between laparoscopy and open surgery in the rate of all major complications, although the number of major complications with laparoscopy was about 20% lower. The only individual complications significantly reduced in the laparoscopy group were wound infections, reduced by about 40% in the adjusted analysis, and respiratory complications, cut by about 50% by laparoscopy. The two surgical subgroups showed virtually no difference in 30-day mortality among patients who underwent a colectomy.
The results suggest that because of the broad reduction of major complications with laparoscopy, this approach "should be considered when primary anastomosis is deemed appropriate," Dr. Cornwell concluded.
Dr. Cornwell said that he had no disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Among patients who underwent a primary anastomosis, the incidence of major complications during 30 days of follow-up was 13% in the open surgery patients and 6% in the laparoscopy patients.
Data Source: From 10,085 U.S. patients who had surgery for acute management of complicated diverticulitis during 2005-2009.
Disclosures: Dr. Cornwell said he had no disclosures.
Antibiotic prophylaxis reduces colorectal surgery readmissions
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
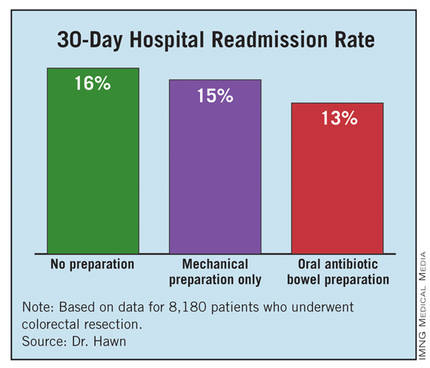
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
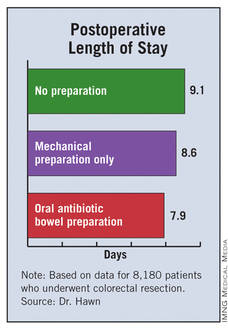
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.

Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |

At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |
At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
Surgical site infections (SSIs) remain a vexing problem despite the significant efforts by hospitals to increase compliance with measures of the Surgical Care Improvement Project. These efforts have so far failed to translate into improved outcomes. We need to identify additional processes that can be changed to improve surgical outcomes.
Elizabeth C. Wick |
At Johns Hopkins, we addressed SSIs by implementing the Comprehensive Unit-Based Safety Program for patients undergoing colorectal surgery. Interventions included standardization of skin preparation, administration of preoperative chlorhexidine showers, selective elimination of mechanical bowel preparation, warming of patients in the preanesthesia area, adoption of enhanced sterile techniques for skin and fascial closure, and addressing previously unrecognized lapses in antibiotic prophylaxis. The program was modeled on ICU processes designed to prevent central line bloodstream infections.
Our program improved the operating room culture by engaging and empowering front-line staff to address deficits and improve processes. A recent review of the rate of SSIs during the 12 months prior to and the 12 months after implementation of this program found that infection rates fell from 27% before implementation to 18% afterward – a 33% relative decrease (J. Am. Coll. Surg. 2012;215:193-200).
We are expanding this program to colon surgery programs at more than 100 U.S. hospitals. Hospitals want to institute new processes proven to improve patient outcomes. The report by Dr. Hawn and her associates is an important step toward identifying a new approach that might further reduce SSIs.
Dr. Elizabeth C. Wick is a colorectal surgeon at Johns Hopkins Hospital in Baltimore. She had no disclosures. She made these comments as a designated discussant for Dr. Hawn’s report.
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.
Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
PALM BEACH, FLA. – Administering a brief oral antibiotic regimen preoperatively to colorectal surgery patients cut the average postoperative hospitalization by more than a day and reduced 30-day readmissions by about 3% compared with no presurgical bowel preparation, a review of more than 8,000 patients found.
The primary driver of these beneficial effects was a reduced rate of surgical site infections, Dr. Mary T. Hawn said at the annual meeting of the Southern Surgical Association.
"Efforts to improve adherence with the use of oral antibiotic preparation may improve the efficiency of care for colorectal surgery," said Dr. Hawn, chief of gastrointestinal surgery at the University of Alabama, Birmingham. "Further research is needed to determine the best protocol for bowel prep prior to colorectal surgery, and to prospectively monitor the rate of Clostridium difficile infection."
The findings by Dr. Hawn’s group also showed that oral antibiotic bowel preparation (OABP) led to a small but statistically significant increase in the rate of hospital readmissions among patients with a principal diagnostic code of colitis caused by C. difficile infection. The OABP patients had a 0.5% readmission rate, compared with a 0.1% rate among patients who received no presurgical bowel preparation.
The value of OABP as shown in this study is particularly important because the use of OABP before colorectal surgery has declined in the United States over the past 20 years, Dr. Hawn added.
Using data collected as part of the VA Surgical Quality Improvement Program, Dr. Hawn and her colleagues analyzed results for 8,180 patients who underwent elective colorectal resection at any of 112 participating VA hospitals during 2005-2009. Patients who had a partial or total colectomy, a rectal resection, or an ostomy were included. Patients were excluded if they had a preoperative stay of more than 2 days, a postoperative stay of more than 30 days, or an American Surgical Association 5 classification, or if they died before hospital discharge.
Most of the patients (83%) underwent surgery for neoplasms; the next most common reason for surgery was diverticulitis, in 6%. OABP was the most common form of presurgical preparation, used on 44% of patients; mechanical preparation only was used on 39%, and no preparation was done in 17%. Ninety percent of the OABP patients also underwent mechanical preparation, while the other 10% had OABP only.
The average postoperative length of stay was 9.1 days among those who received no preparation, 8.6 days for those who got mechanical preparation only, and 7.9 days for those who had OABP – a statistically significant advantage for OABP. In a multivariate regression analysis that controlled for indication, age, and wound class, OABP cut length of stay by an average of 12% compared with no preparation, a statistically significant reduction. In the same analysis, mechanical preparation cut length of stay by only 4% compared with no preparation, also a significant effect.
The hospital readmission rate was 16% with no preparation, 15% with mechanical preparation only, and 13% with OABP. In the multivariate regression analysis with adjustment for procedure, age, and wound class, OABP cut the readmission rate by 19% compared with no preparation, a statistically significant reduction. Mechanical preparation only did not have a statistically significant effect.
Further analyses showed that the most common reason for readmission among all patients studied was postoperative infection, in 18%, followed by digestive-system complications, in 10%. C. difficile infection caused 3% of readmissions.
In addition, infections were responsible for readmissions among 6% of patients who underwent no presurgical preparation and in 4% of those who underwent OABP, a statistically significant difference. In contrast, use of OABP produced no statistically significant decline in noninfectious causes of readmission. This rate ran 10% among patients with no preparation, and 9% in patients who underwent OABP.
Dr. Hawn said that she had no disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Oral antibiotic preparation before colorectal surgery cut hospital readmissions by 19% compared with no preparation.
Data Source: A review of 8,180 U.S. patients who underwent colorectal surgery during 2005-2009 at 112 VA hospitals.
Disclosures: Dr. Hawn said that she had no disclosures.

Avatrombopag reduces preprocedure platelet needs in chronic liver disease
BOSTON – Avatrombopag, an investigational thrombopoietin receptor agonist, may reduce procedure-related bleeding risk in patients with chronic liver disease and thrombocytopenia, results of a phase II trial suggest.
Patients randomized to receive avatrambopag (E5501) before invasive surgical or diagnostic procedures had significantly more platelet count responses and required significantly fewer platelet transfusions than did patients randomized to placebo, Dr. Norah Terrault said at the annual meeting of the American Association for the Study of Liver Diseases.
"It was a well-tolerated drug with no dose-limiting adverse events," Dr. Terrault said, although she noted that one patient had a nonfatal episode of portal-vein thrombosis that may have been related to the drug.
Avatrombopag has been shown to mimic the effects of thrombopoietin both in vitro and in vivo, and in a phase II study it was shown to increase platelet counts in patients with chronic immune thrombocytopenia.
Dr. Terrault, associate professor of medicine in the division of gastroenterology at the University of California, San Francisco, and her colleagues tested the efficacy of short-course avatrombopag in 130 patients with chronic liver disease and thrombocytopenia prior to a planned invasive procedure. The patients were all adults with cirrhosis from viral hepatitis, nonalcoholic steatohepatitis, or alcoholic liver disease.
The trial, labeled E5501-G000-202, enrolled patients into two cohorts. In cohort A, 67 patients were randomly assigned to receive either placebo or a loading dose of a first-generation formulation of avatrombopag 100 mg on day 1, followed by a maintenance dose on days 2-7 of either 20, 40, or 80 mg daily.
In cohort B, 63 patients were randomized either to placebo or to a second-generation formulation of avatrombopag at 80 mg on day 1, followed by either 10 mg daily for days 2-7 or 20 mg/day for days 2-4 and placebo on days 5, 6, and 7.
Patients in both cohorts were scheduled for procedures 1-4 days after the end of drug dosing.
The primary end point was a platelet count response – defined as a platelet count increase from baseline of at least 20 × 109/L and at least one count of greater than 50 × 109/L during days 4-8 from the start of treatment. In an intention-to-treat analysis, the proportion of patients achieving the primary end point was significantly higher in each cohort compared with controls.
In cohort A, the respective responses in the 20- and 80-mg groups were seen in 7 of 18 patients on the 20-mg dose (38.9%) and in 13 of 17 on the 80-mg dose (76.5%), compared with 1 of 16 (6.3%) controls (P less than .05 for both comparisons). There was no significant difference between patients given a placebo vs. a 40-mg dose, however.
In cohort B, 9 of 21 patients on the 10-mg dose (42.9%) had a platelet count response, as did 11 of 21 (52.4%) in the 20-mg group, compared with 2 of 21 on placebo (9.5%; P less than .05 for both comparisons).
The investigators also performed an exploratory analysis looking at platelet transfusion requirements for 58 of the patients in cohort B and found that 7 of 20 (35%) controls needed preprocedure platelets, compared with 1 of 19 (5.3%) each in the 10- and 20-mg avatrombopag groups (P less than .05).
In the combined cohorts, 78 of 93 (83.9%) patients assigned to the drug had treatment-emergent adverse events, compared with 28 of 37 (75.7%) assigned to placebo. There were 15 grade-3 or -4 adverse events among avatrombopag patients (16.1%), compared with 5 among controls (13.5%).
There were three severe treatment-related events, all in patients who received the active drug, and 16 serious treatment-related events among those taking avatrombopag, compared with four on placebo (17.2% vs. 10.8%).
One patient – a 55-year-old with a history of cardiovascular disease, Child-Pugh class C cirrhosis, and a MELD (Model for End-Stage Liver Disease) score of 19 – died. The death was attributed to acute respiratory failure, cardiopulmonary arrest, and metabolic acidosis.
A 61-year-old man with Child-Pugh class C disease and a MELD score of 19 but no hepatocellular carcinoma had weight gain on study day 34, which was shown on Doppler ultrasound to be portal-vein thrombus. His peak platelet count was 199 × 109/L on day 17. He was successfully treated with embolization and anticoagulation therapy.
Investigators are currently planning phase III trials with avatrombopag, Dr. Terrault said.
The study was funded by Eisai, maker of avatrombopag. Dr. Terrault receives grant and research support from the company and serves in an advisory capacity.
BOSTON – Avatrombopag, an investigational thrombopoietin receptor agonist, may reduce procedure-related bleeding risk in patients with chronic liver disease and thrombocytopenia, results of a phase II trial suggest.
Patients randomized to receive avatrambopag (E5501) before invasive surgical or diagnostic procedures had significantly more platelet count responses and required significantly fewer platelet transfusions than did patients randomized to placebo, Dr. Norah Terrault said at the annual meeting of the American Association for the Study of Liver Diseases.
"It was a well-tolerated drug with no dose-limiting adverse events," Dr. Terrault said, although she noted that one patient had a nonfatal episode of portal-vein thrombosis that may have been related to the drug.
Avatrombopag has been shown to mimic the effects of thrombopoietin both in vitro and in vivo, and in a phase II study it was shown to increase platelet counts in patients with chronic immune thrombocytopenia.
Dr. Terrault, associate professor of medicine in the division of gastroenterology at the University of California, San Francisco, and her colleagues tested the efficacy of short-course avatrombopag in 130 patients with chronic liver disease and thrombocytopenia prior to a planned invasive procedure. The patients were all adults with cirrhosis from viral hepatitis, nonalcoholic steatohepatitis, or alcoholic liver disease.
The trial, labeled E5501-G000-202, enrolled patients into two cohorts. In cohort A, 67 patients were randomly assigned to receive either placebo or a loading dose of a first-generation formulation of avatrombopag 100 mg on day 1, followed by a maintenance dose on days 2-7 of either 20, 40, or 80 mg daily.
In cohort B, 63 patients were randomized either to placebo or to a second-generation formulation of avatrombopag at 80 mg on day 1, followed by either 10 mg daily for days 2-7 or 20 mg/day for days 2-4 and placebo on days 5, 6, and 7.
Patients in both cohorts were scheduled for procedures 1-4 days after the end of drug dosing.
The primary end point was a platelet count response – defined as a platelet count increase from baseline of at least 20 × 109/L and at least one count of greater than 50 × 109/L during days 4-8 from the start of treatment. In an intention-to-treat analysis, the proportion of patients achieving the primary end point was significantly higher in each cohort compared with controls.
In cohort A, the respective responses in the 20- and 80-mg groups were seen in 7 of 18 patients on the 20-mg dose (38.9%) and in 13 of 17 on the 80-mg dose (76.5%), compared with 1 of 16 (6.3%) controls (P less than .05 for both comparisons). There was no significant difference between patients given a placebo vs. a 40-mg dose, however.
In cohort B, 9 of 21 patients on the 10-mg dose (42.9%) had a platelet count response, as did 11 of 21 (52.4%) in the 20-mg group, compared with 2 of 21 on placebo (9.5%; P less than .05 for both comparisons).
The investigators also performed an exploratory analysis looking at platelet transfusion requirements for 58 of the patients in cohort B and found that 7 of 20 (35%) controls needed preprocedure platelets, compared with 1 of 19 (5.3%) each in the 10- and 20-mg avatrombopag groups (P less than .05).
In the combined cohorts, 78 of 93 (83.9%) patients assigned to the drug had treatment-emergent adverse events, compared with 28 of 37 (75.7%) assigned to placebo. There were 15 grade-3 or -4 adverse events among avatrombopag patients (16.1%), compared with 5 among controls (13.5%).
There were three severe treatment-related events, all in patients who received the active drug, and 16 serious treatment-related events among those taking avatrombopag, compared with four on placebo (17.2% vs. 10.8%).
One patient – a 55-year-old with a history of cardiovascular disease, Child-Pugh class C cirrhosis, and a MELD (Model for End-Stage Liver Disease) score of 19 – died. The death was attributed to acute respiratory failure, cardiopulmonary arrest, and metabolic acidosis.
A 61-year-old man with Child-Pugh class C disease and a MELD score of 19 but no hepatocellular carcinoma had weight gain on study day 34, which was shown on Doppler ultrasound to be portal-vein thrombus. His peak platelet count was 199 × 109/L on day 17. He was successfully treated with embolization and anticoagulation therapy.
Investigators are currently planning phase III trials with avatrombopag, Dr. Terrault said.
The study was funded by Eisai, maker of avatrombopag. Dr. Terrault receives grant and research support from the company and serves in an advisory capacity.
BOSTON – Avatrombopag, an investigational thrombopoietin receptor agonist, may reduce procedure-related bleeding risk in patients with chronic liver disease and thrombocytopenia, results of a phase II trial suggest.
Patients randomized to receive avatrambopag (E5501) before invasive surgical or diagnostic procedures had significantly more platelet count responses and required significantly fewer platelet transfusions than did patients randomized to placebo, Dr. Norah Terrault said at the annual meeting of the American Association for the Study of Liver Diseases.
"It was a well-tolerated drug with no dose-limiting adverse events," Dr. Terrault said, although she noted that one patient had a nonfatal episode of portal-vein thrombosis that may have been related to the drug.
Avatrombopag has been shown to mimic the effects of thrombopoietin both in vitro and in vivo, and in a phase II study it was shown to increase platelet counts in patients with chronic immune thrombocytopenia.
Dr. Terrault, associate professor of medicine in the division of gastroenterology at the University of California, San Francisco, and her colleagues tested the efficacy of short-course avatrombopag in 130 patients with chronic liver disease and thrombocytopenia prior to a planned invasive procedure. The patients were all adults with cirrhosis from viral hepatitis, nonalcoholic steatohepatitis, or alcoholic liver disease.
The trial, labeled E5501-G000-202, enrolled patients into two cohorts. In cohort A, 67 patients were randomly assigned to receive either placebo or a loading dose of a first-generation formulation of avatrombopag 100 mg on day 1, followed by a maintenance dose on days 2-7 of either 20, 40, or 80 mg daily.
In cohort B, 63 patients were randomized either to placebo or to a second-generation formulation of avatrombopag at 80 mg on day 1, followed by either 10 mg daily for days 2-7 or 20 mg/day for days 2-4 and placebo on days 5, 6, and 7.
Patients in both cohorts were scheduled for procedures 1-4 days after the end of drug dosing.
The primary end point was a platelet count response – defined as a platelet count increase from baseline of at least 20 × 109/L and at least one count of greater than 50 × 109/L during days 4-8 from the start of treatment. In an intention-to-treat analysis, the proportion of patients achieving the primary end point was significantly higher in each cohort compared with controls.
In cohort A, the respective responses in the 20- and 80-mg groups were seen in 7 of 18 patients on the 20-mg dose (38.9%) and in 13 of 17 on the 80-mg dose (76.5%), compared with 1 of 16 (6.3%) controls (P less than .05 for both comparisons). There was no significant difference between patients given a placebo vs. a 40-mg dose, however.
In cohort B, 9 of 21 patients on the 10-mg dose (42.9%) had a platelet count response, as did 11 of 21 (52.4%) in the 20-mg group, compared with 2 of 21 on placebo (9.5%; P less than .05 for both comparisons).
The investigators also performed an exploratory analysis looking at platelet transfusion requirements for 58 of the patients in cohort B and found that 7 of 20 (35%) controls needed preprocedure platelets, compared with 1 of 19 (5.3%) each in the 10- and 20-mg avatrombopag groups (P less than .05).
In the combined cohorts, 78 of 93 (83.9%) patients assigned to the drug had treatment-emergent adverse events, compared with 28 of 37 (75.7%) assigned to placebo. There were 15 grade-3 or -4 adverse events among avatrombopag patients (16.1%), compared with 5 among controls (13.5%).
There were three severe treatment-related events, all in patients who received the active drug, and 16 serious treatment-related events among those taking avatrombopag, compared with four on placebo (17.2% vs. 10.8%).
One patient – a 55-year-old with a history of cardiovascular disease, Child-Pugh class C cirrhosis, and a MELD (Model for End-Stage Liver Disease) score of 19 – died. The death was attributed to acute respiratory failure, cardiopulmonary arrest, and metabolic acidosis.
A 61-year-old man with Child-Pugh class C disease and a MELD score of 19 but no hepatocellular carcinoma had weight gain on study day 34, which was shown on Doppler ultrasound to be portal-vein thrombus. His peak platelet count was 199 × 109/L on day 17. He was successfully treated with embolization and anticoagulation therapy.
Investigators are currently planning phase III trials with avatrombopag, Dr. Terrault said.
The study was funded by Eisai, maker of avatrombopag. Dr. Terrault receives grant and research support from the company and serves in an advisory capacity.
AT THE ANNUAL MEETING OF THE AMERICAN ASSOCIATION FOR THE STUDY OF LIVER DISEASES
Major Finding: In a study cohort with a second-generation formulation of avatrombopag, 9 of 21 patients on a 10-mg daily dose (42.9%) had a platelet count response, as did 11 of 21 (52.4%) in the 20-mg group, compared with 2 of 21 on placebo (9.5%; P less than .05 for both comparisons).
Data Source: Randomized, double-blind, placebo-controlled phase II trial.
Disclosures: The study was funded by Eisai, maker of avatrombopag. Dr. Terrault receives grant and research support from the company and serves in an advisory capacity.
Bariatric surgery cut vascular events in diabetes
PALM BEACH, FLA. – Add another notch to the evidence base for bariatric surgery as effective treatment for type 2 diabetes in obese patients.
Patients with type 2 diabetes who underwent any type of bariatric surgery had a 61%-78% relative risk reduction in their rate of macrovascular, microvascular, or vascular events during an average 20-month follow-up in a review of more than 15,000 cases in South Carolina.

"We are trying to get primary care physicians to spread the word [to patients] that bariatric surgery has come a long way over the past 30 or 40 years; the risk-to-reward ratio is much more beneficial to patients," Dr. John D. Scott said at the annual meeting of the Southern Surgical Association.
The new finding "adds to the extensive list of papers that show bariatric surgery mitigates the long-term effects of type 2 diabetes," Dr. Scott added in an interview. "Some front-line medical providers still see bariatric surgery as a procedure of last resort, but findings like ours show that a discussion [with patients on whether they should consider bariatric surgery] should happen a lot sooner."
Dr. Scott, a surgeon at University Medical Center in Greenville, S.C., recommended that patients with a body mass index of at least 35 kg/m2 and two or more comorbidities be told that they have the option of undergoing bariatric surgery and reducing their risk.
"We have an epidemic [of obesity and type 2 diabetes], and for the first time since tuberculosis, this is an epidemic where surgery has a real opportunity to positively intervene," commented Dr. Josef E. Fischer, a professor of surgery at Harvard Medical School in Boston.
The study used hospital billing data collected by the South Carolina Office of Research and Statistics as well as state vital records data for 1995-2009. The analysis included 2,580 obese patients who underwent any type of bariatric surgery and 13,371 obese patients who did not have surgery. The researchers extracted the data from records of nearly 34,000 obese patients, but excluded patients with type 1 diabetes, patients with incomplete data, and patients with advanced cardiovascular or microvascular disease at the time of their surgery or entry into the state records during this period.
During a median follow-up of about 20 months, the rate of new-onset macro- or microvascular events was 2% in the bariatric surgery patients and 11% in the patients who did not undergo surgery. The rate of an incident vascular disease event was 2% in the patients who had surgery and 13% in those who did not. Macrovascular events included myocardial infarction, stroke, and all-cause death. Microvascular events included blindness in at least one eye, laser eye surgery, nontraumatic amputation, or placement of access for dialysis. Other vascular events included new-onset heart failure or angina, or revascularization of a coronary, carotid, or peripheral artery.
In a multivariate-adjusted analysis, patients who underwent bariatric surgery had a 61% reduction in macrovascular events, a 78% reduction in microvascular events, a 75% reduction in vascular events, and a 64% reduction in combined macro- and microvascular events, compared with patients who did not have this surgery – all statistically significant differences, reported Dr. Spence M. Taylor, a coinvestigator with Dr. Scott on the study. A propensity-score matched analysis that compared the bariatric surgery patients and matched nonsurgical patients showed very similar reductions in all three event categories.
"Bariatric surgery has a substantial and lasting mitigating association on major complications associated with type 2 diabetes in the obese population," concluded Dr. Taylor, chairman of surgery at the University Medical Center in Greenville.
Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.
PALM BEACH, FLA. – Add another notch to the evidence base for bariatric surgery as effective treatment for type 2 diabetes in obese patients.
Patients with type 2 diabetes who underwent any type of bariatric surgery had a 61%-78% relative risk reduction in their rate of macrovascular, microvascular, or vascular events during an average 20-month follow-up in a review of more than 15,000 cases in South Carolina.
"We are trying to get primary care physicians to spread the word [to patients] that bariatric surgery has come a long way over the past 30 or 40 years; the risk-to-reward ratio is much more beneficial to patients," Dr. John D. Scott said at the annual meeting of the Southern Surgical Association.
The new finding "adds to the extensive list of papers that show bariatric surgery mitigates the long-term effects of type 2 diabetes," Dr. Scott added in an interview. "Some front-line medical providers still see bariatric surgery as a procedure of last resort, but findings like ours show that a discussion [with patients on whether they should consider bariatric surgery] should happen a lot sooner."
Dr. Scott, a surgeon at University Medical Center in Greenville, S.C., recommended that patients with a body mass index of at least 35 kg/m2 and two or more comorbidities be told that they have the option of undergoing bariatric surgery and reducing their risk.
"We have an epidemic [of obesity and type 2 diabetes], and for the first time since tuberculosis, this is an epidemic where surgery has a real opportunity to positively intervene," commented Dr. Josef E. Fischer, a professor of surgery at Harvard Medical School in Boston.
The study used hospital billing data collected by the South Carolina Office of Research and Statistics as well as state vital records data for 1995-2009. The analysis included 2,580 obese patients who underwent any type of bariatric surgery and 13,371 obese patients who did not have surgery. The researchers extracted the data from records of nearly 34,000 obese patients, but excluded patients with type 1 diabetes, patients with incomplete data, and patients with advanced cardiovascular or microvascular disease at the time of their surgery or entry into the state records during this period.
During a median follow-up of about 20 months, the rate of new-onset macro- or microvascular events was 2% in the bariatric surgery patients and 11% in the patients who did not undergo surgery. The rate of an incident vascular disease event was 2% in the patients who had surgery and 13% in those who did not. Macrovascular events included myocardial infarction, stroke, and all-cause death. Microvascular events included blindness in at least one eye, laser eye surgery, nontraumatic amputation, or placement of access for dialysis. Other vascular events included new-onset heart failure or angina, or revascularization of a coronary, carotid, or peripheral artery.
In a multivariate-adjusted analysis, patients who underwent bariatric surgery had a 61% reduction in macrovascular events, a 78% reduction in microvascular events, a 75% reduction in vascular events, and a 64% reduction in combined macro- and microvascular events, compared with patients who did not have this surgery – all statistically significant differences, reported Dr. Spence M. Taylor, a coinvestigator with Dr. Scott on the study. A propensity-score matched analysis that compared the bariatric surgery patients and matched nonsurgical patients showed very similar reductions in all three event categories.
"Bariatric surgery has a substantial and lasting mitigating association on major complications associated with type 2 diabetes in the obese population," concluded Dr. Taylor, chairman of surgery at the University Medical Center in Greenville.
Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.
PALM BEACH, FLA. – Add another notch to the evidence base for bariatric surgery as effective treatment for type 2 diabetes in obese patients.
Patients with type 2 diabetes who underwent any type of bariatric surgery had a 61%-78% relative risk reduction in their rate of macrovascular, microvascular, or vascular events during an average 20-month follow-up in a review of more than 15,000 cases in South Carolina.
"We are trying to get primary care physicians to spread the word [to patients] that bariatric surgery has come a long way over the past 30 or 40 years; the risk-to-reward ratio is much more beneficial to patients," Dr. John D. Scott said at the annual meeting of the Southern Surgical Association.
The new finding "adds to the extensive list of papers that show bariatric surgery mitigates the long-term effects of type 2 diabetes," Dr. Scott added in an interview. "Some front-line medical providers still see bariatric surgery as a procedure of last resort, but findings like ours show that a discussion [with patients on whether they should consider bariatric surgery] should happen a lot sooner."
Dr. Scott, a surgeon at University Medical Center in Greenville, S.C., recommended that patients with a body mass index of at least 35 kg/m2 and two or more comorbidities be told that they have the option of undergoing bariatric surgery and reducing their risk.
"We have an epidemic [of obesity and type 2 diabetes], and for the first time since tuberculosis, this is an epidemic where surgery has a real opportunity to positively intervene," commented Dr. Josef E. Fischer, a professor of surgery at Harvard Medical School in Boston.
The study used hospital billing data collected by the South Carolina Office of Research and Statistics as well as state vital records data for 1995-2009. The analysis included 2,580 obese patients who underwent any type of bariatric surgery and 13,371 obese patients who did not have surgery. The researchers extracted the data from records of nearly 34,000 obese patients, but excluded patients with type 1 diabetes, patients with incomplete data, and patients with advanced cardiovascular or microvascular disease at the time of their surgery or entry into the state records during this period.
During a median follow-up of about 20 months, the rate of new-onset macro- or microvascular events was 2% in the bariatric surgery patients and 11% in the patients who did not undergo surgery. The rate of an incident vascular disease event was 2% in the patients who had surgery and 13% in those who did not. Macrovascular events included myocardial infarction, stroke, and all-cause death. Microvascular events included blindness in at least one eye, laser eye surgery, nontraumatic amputation, or placement of access for dialysis. Other vascular events included new-onset heart failure or angina, or revascularization of a coronary, carotid, or peripheral artery.
In a multivariate-adjusted analysis, patients who underwent bariatric surgery had a 61% reduction in macrovascular events, a 78% reduction in microvascular events, a 75% reduction in vascular events, and a 64% reduction in combined macro- and microvascular events, compared with patients who did not have this surgery – all statistically significant differences, reported Dr. Spence M. Taylor, a coinvestigator with Dr. Scott on the study. A propensity-score matched analysis that compared the bariatric surgery patients and matched nonsurgical patients showed very similar reductions in all three event categories.
"Bariatric surgery has a substantial and lasting mitigating association on major complications associated with type 2 diabetes in the obese population," concluded Dr. Taylor, chairman of surgery at the University Medical Center in Greenville.
Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.
AT THE ANNUAL MEETING OF THE SOUTHERN SURGICAL ASSOCIATION
Major Finding: Bariatric surgery was linked to a 64% decrease in macro- and microvascular events compared with no surgery in obese type 2 diabetes patients.
Data Source: Billing information collected on 15,951 obese patients in South Carolina during 1995-2009.
Disclosures: Dr. Scott, Dr. Fischer, and Dr. Taylor had no relevant disclosures.
