User login
Men Benefit Most From Combined Weight-Loss Procedure
SAN DIEGO – Significantly greater reductions in weight, body mass index, and adipose tissue were seen in men vs. women who underwent biliopancreatic diversion with duodenal switch surgery, a single-center study indicated.
The study, which was conducted at the Institute of Pneumology and Cardiology at Laval University in Quebec City, was designed to assess the impact of sex on weight loss along with changes in adiposity and skeletal muscle in 42 severely obese men and women who underwent biliopancreatic diversion with duodenal switch (BPD-DS) surgery. Audrey Auclair, a Ph.D. student in pharmacy at the university, presented the study results on behalf of her colleagues at the annual meeting of the American Society for Metabolic and Bariatric Surgery.

At baseline and 6 months, the 12 men and 30 women (mean age, 46 years) underwent anthropometric measurements and a midthigh CT scan. At baseline, the men and women were similar in terms of thickness of total, deep, and subcutaneous adipose tissue. However, the men weighed significantly more(mean, 156 vs. 118 kg, respectively), and had a higher body mass index (51.2 vs. 46.2 kg/m2) as well as greater midthigh composition in terms of total muscle (193 vs. 130 cm2), normal-density muscle (115 vs. 79 cm2), and low-density muscle (54 vs. 37 cm2), compared with the women (all P less than.001).
At 6 months, after adjustment for baseline weight, the researchers found that the men had a significantly greater reduction in weight (–30% vs. –26%, respectively), BMI (–30% vs. –26%), subcutaneous adipose tissue (–45% vs. –31%), and deep adipose tissue (–50% vs. –31%) than did the women (all P less than or equal to .05). There were no significant differences between the sexes in the percent decline at 6 months in total muscle, normal-density muscle, and low-density muscle.
"The BPD-DS has a major impact on weight and on both thigh muscle and fat mass in both sexes," Ms. Auclair concluded.
In a later interview, she speculated that the outcome differences between sexes may be attributable to greater physical activity among men compared with women, which would explain a similar loss in midthigh muscle between the sexes, despite a greater reduction in body weight and midthigh adipose tissue among men.
"In order to confirm this hypothesis, we plan to begin a new study to determine the effectiveness of a supervised exercise program on the maintenance of muscle mass in months after the BPD-DS," she said.
Ms. Auclair said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Significantly greater reductions in weight, body mass index, and adipose tissue were seen in men vs. women who underwent biliopancreatic diversion with duodenal switch surgery, a single-center study indicated.
The study, which was conducted at the Institute of Pneumology and Cardiology at Laval University in Quebec City, was designed to assess the impact of sex on weight loss along with changes in adiposity and skeletal muscle in 42 severely obese men and women who underwent biliopancreatic diversion with duodenal switch (BPD-DS) surgery. Audrey Auclair, a Ph.D. student in pharmacy at the university, presented the study results on behalf of her colleagues at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline and 6 months, the 12 men and 30 women (mean age, 46 years) underwent anthropometric measurements and a midthigh CT scan. At baseline, the men and women were similar in terms of thickness of total, deep, and subcutaneous adipose tissue. However, the men weighed significantly more(mean, 156 vs. 118 kg, respectively), and had a higher body mass index (51.2 vs. 46.2 kg/m2) as well as greater midthigh composition in terms of total muscle (193 vs. 130 cm2), normal-density muscle (115 vs. 79 cm2), and low-density muscle (54 vs. 37 cm2), compared with the women (all P less than.001).
At 6 months, after adjustment for baseline weight, the researchers found that the men had a significantly greater reduction in weight (–30% vs. –26%, respectively), BMI (–30% vs. –26%), subcutaneous adipose tissue (–45% vs. –31%), and deep adipose tissue (–50% vs. –31%) than did the women (all P less than or equal to .05). There were no significant differences between the sexes in the percent decline at 6 months in total muscle, normal-density muscle, and low-density muscle.
"The BPD-DS has a major impact on weight and on both thigh muscle and fat mass in both sexes," Ms. Auclair concluded.
In a later interview, she speculated that the outcome differences between sexes may be attributable to greater physical activity among men compared with women, which would explain a similar loss in midthigh muscle between the sexes, despite a greater reduction in body weight and midthigh adipose tissue among men.
"In order to confirm this hypothesis, we plan to begin a new study to determine the effectiveness of a supervised exercise program on the maintenance of muscle mass in months after the BPD-DS," she said.
Ms. Auclair said that she had no relevant financial conflicts to disclose.
SAN DIEGO – Significantly greater reductions in weight, body mass index, and adipose tissue were seen in men vs. women who underwent biliopancreatic diversion with duodenal switch surgery, a single-center study indicated.
The study, which was conducted at the Institute of Pneumology and Cardiology at Laval University in Quebec City, was designed to assess the impact of sex on weight loss along with changes in adiposity and skeletal muscle in 42 severely obese men and women who underwent biliopancreatic diversion with duodenal switch (BPD-DS) surgery. Audrey Auclair, a Ph.D. student in pharmacy at the university, presented the study results on behalf of her colleagues at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline and 6 months, the 12 men and 30 women (mean age, 46 years) underwent anthropometric measurements and a midthigh CT scan. At baseline, the men and women were similar in terms of thickness of total, deep, and subcutaneous adipose tissue. However, the men weighed significantly more(mean, 156 vs. 118 kg, respectively), and had a higher body mass index (51.2 vs. 46.2 kg/m2) as well as greater midthigh composition in terms of total muscle (193 vs. 130 cm2), normal-density muscle (115 vs. 79 cm2), and low-density muscle (54 vs. 37 cm2), compared with the women (all P less than.001).
At 6 months, after adjustment for baseline weight, the researchers found that the men had a significantly greater reduction in weight (–30% vs. –26%, respectively), BMI (–30% vs. –26%), subcutaneous adipose tissue (–45% vs. –31%), and deep adipose tissue (–50% vs. –31%) than did the women (all P less than or equal to .05). There were no significant differences between the sexes in the percent decline at 6 months in total muscle, normal-density muscle, and low-density muscle.
"The BPD-DS has a major impact on weight and on both thigh muscle and fat mass in both sexes," Ms. Auclair concluded.
In a later interview, she speculated that the outcome differences between sexes may be attributable to greater physical activity among men compared with women, which would explain a similar loss in midthigh muscle between the sexes, despite a greater reduction in body weight and midthigh adipose tissue among men.
"In order to confirm this hypothesis, we plan to begin a new study to determine the effectiveness of a supervised exercise program on the maintenance of muscle mass in months after the BPD-DS," she said.
Ms. Auclair said that she had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: At 6 months after undergoing BPD-DS surgery, men had a significantly greater reduction in weight (–-30% vs. –26%, respectively), body mass index (–30% vs. –26%), subcutaneous adipose tissue (–45% vs. –31%), and deep adipose tissue (–50% vs. –31%) than did women.
Data Source: The results are based on a single-center study of 42 severely obese patients who underwent BPD-DS.
Disclosures: Ms. Auclair said that she had no relevant financial conflicts to disclose.
Bariatric Surgery Yields Durable Results for Diabetic Nephropathy
SAN DIEGO – Bariatric surgery induced a significant and durable improvement in diabetic nephropathy after 5 years of follow-up, results from a single-center study showed.
"In addition to significant weight loss, [bariatric surgery] achieves profound metabolic effects, including improvements in glycemic control and insulin sensitivity, as well as a decrease in cardiovascular disease risk and mortality," lead author Dr. Helen M. Heneghan said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "We hypothesized that improving diabetic control with bariatric surgery may have positive effects on the end-organ complications of this disease, such as diabetic nephropathy. We also wanted to address one of the prevailing questions in this field: whether or not the effects of bariatric surgery on diabetes and its complications are durable."

Dr. Heneghan, a bariatric surgery fellow at the Cleveland Clinic Bariatric and Metabolic Institute, and her associates identified 52 patients who underwent bariatric surgery at the institute and had completed the 5-year follow-up. At baseline, the mean age of patients was 51 years, and 75% were women. Their preoperative mean body mass index was 49 kg/m2, 84% had hypertension, and 71% had hyperlipidemia. Preoperatively, the mean duration of diabetes was 8.6 years, and 29% were already taking insulin. Their mean hemoglobin A1c level was 7.7%, and 38% had diabetic nephropathy as indicated by microalbuminuria (30-299 mg of albumin per g of creatinine) or macroalbuminura (greater than 300 mg/g), and 22% of patients were prescribed an ACE inhibitor or angiotensin receptor blocker.
The majority of patients (69%) underwent gastric bypass; 25% had laparoscopic gastric banding and 6% had sleeve gastrectomy. Dr. Heneghan reported that 5 years after their surgery, 44% of patients had sustained remission of their type 2 diabetes, 33% had a significant improvement, and 23% had no change or worsening of their disease. This latter cohort "had the least amount of weight loss and were those who had the longest standing duration of diabetes preoperatively."
The rates of patients with remission, improvement, or change in hypertension were 16%, 50%, and 34%, respectively, whereas the rates for patients with dyslipidemia were 39%, 20%, and 41%.
Only 25% of patients who did not have diabetic nephropathy at the time of surgery went on to develop the condition. Among patients with preoperative microalbuminuria, 42% remained stable whereas 58% regressed and had no albuminuria 5 years after surgery. Similarly, among patients with preoperative macroalbuminuria, 50% remained stable and 50% regressed and had no albuminuria at 5 years.*
There were no preoperative differences in the mean urinary albumin to creatinine ratio (ACR) between patients who were and patients who were not prescribed a renoprotective agent. However, postoperatively, patients who were not on a renoprotective agent had a significantly lower urinary ACR, compared with those who remained on a renoprotective agent (P = .039). "This probably reflects the fact that patients who had improvement of their diabetes and regression or nonprogression of their nephropathy status also had a significant improvement in – or remission of – hypertension, and were no longer prescribed an antihypertensive medication," Dr. Heneghan explained.
She characterized the study’s overall findings as "remarkable, considering that diabetes is a chronic, progressive disease, and certainly warrant further investigation in the form of a prospective and larger study."
Dr. Heneghan said that she had no relevant financial conflicts to disclose.
*CORRECTION 8/28/12: The original sentence contained an error in describing the patients. The sentence should read" "Similarly, among patients with preoperative macroalbuminuria, 50% remained stable and 50% regressed and had no albuminuria at 5 years."
SAN DIEGO – Bariatric surgery induced a significant and durable improvement in diabetic nephropathy after 5 years of follow-up, results from a single-center study showed.
"In addition to significant weight loss, [bariatric surgery] achieves profound metabolic effects, including improvements in glycemic control and insulin sensitivity, as well as a decrease in cardiovascular disease risk and mortality," lead author Dr. Helen M. Heneghan said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "We hypothesized that improving diabetic control with bariatric surgery may have positive effects on the end-organ complications of this disease, such as diabetic nephropathy. We also wanted to address one of the prevailing questions in this field: whether or not the effects of bariatric surgery on diabetes and its complications are durable."
Dr. Heneghan, a bariatric surgery fellow at the Cleveland Clinic Bariatric and Metabolic Institute, and her associates identified 52 patients who underwent bariatric surgery at the institute and had completed the 5-year follow-up. At baseline, the mean age of patients was 51 years, and 75% were women. Their preoperative mean body mass index was 49 kg/m2, 84% had hypertension, and 71% had hyperlipidemia. Preoperatively, the mean duration of diabetes was 8.6 years, and 29% were already taking insulin. Their mean hemoglobin A1c level was 7.7%, and 38% had diabetic nephropathy as indicated by microalbuminuria (30-299 mg of albumin per g of creatinine) or macroalbuminura (greater than 300 mg/g), and 22% of patients were prescribed an ACE inhibitor or angiotensin receptor blocker.
The majority of patients (69%) underwent gastric bypass; 25% had laparoscopic gastric banding and 6% had sleeve gastrectomy. Dr. Heneghan reported that 5 years after their surgery, 44% of patients had sustained remission of their type 2 diabetes, 33% had a significant improvement, and 23% had no change or worsening of their disease. This latter cohort "had the least amount of weight loss and were those who had the longest standing duration of diabetes preoperatively."
The rates of patients with remission, improvement, or change in hypertension were 16%, 50%, and 34%, respectively, whereas the rates for patients with dyslipidemia were 39%, 20%, and 41%.
Only 25% of patients who did not have diabetic nephropathy at the time of surgery went on to develop the condition. Among patients with preoperative microalbuminuria, 42% remained stable whereas 58% regressed and had no albuminuria 5 years after surgery. Similarly, among patients with preoperative macroalbuminuria, 50% remained stable and 50% regressed and had no albuminuria at 5 years.*
There were no preoperative differences in the mean urinary albumin to creatinine ratio (ACR) between patients who were and patients who were not prescribed a renoprotective agent. However, postoperatively, patients who were not on a renoprotective agent had a significantly lower urinary ACR, compared with those who remained on a renoprotective agent (P = .039). "This probably reflects the fact that patients who had improvement of their diabetes and regression or nonprogression of their nephropathy status also had a significant improvement in – or remission of – hypertension, and were no longer prescribed an antihypertensive medication," Dr. Heneghan explained.
She characterized the study’s overall findings as "remarkable, considering that diabetes is a chronic, progressive disease, and certainly warrant further investigation in the form of a prospective and larger study."
Dr. Heneghan said that she had no relevant financial conflicts to disclose.
*CORRECTION 8/28/12: The original sentence contained an error in describing the patients. The sentence should read" "Similarly, among patients with preoperative macroalbuminuria, 50% remained stable and 50% regressed and had no albuminuria at 5 years."
SAN DIEGO – Bariatric surgery induced a significant and durable improvement in diabetic nephropathy after 5 years of follow-up, results from a single-center study showed.
"In addition to significant weight loss, [bariatric surgery] achieves profound metabolic effects, including improvements in glycemic control and insulin sensitivity, as well as a decrease in cardiovascular disease risk and mortality," lead author Dr. Helen M. Heneghan said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "We hypothesized that improving diabetic control with bariatric surgery may have positive effects on the end-organ complications of this disease, such as diabetic nephropathy. We also wanted to address one of the prevailing questions in this field: whether or not the effects of bariatric surgery on diabetes and its complications are durable."
Dr. Heneghan, a bariatric surgery fellow at the Cleveland Clinic Bariatric and Metabolic Institute, and her associates identified 52 patients who underwent bariatric surgery at the institute and had completed the 5-year follow-up. At baseline, the mean age of patients was 51 years, and 75% were women. Their preoperative mean body mass index was 49 kg/m2, 84% had hypertension, and 71% had hyperlipidemia. Preoperatively, the mean duration of diabetes was 8.6 years, and 29% were already taking insulin. Their mean hemoglobin A1c level was 7.7%, and 38% had diabetic nephropathy as indicated by microalbuminuria (30-299 mg of albumin per g of creatinine) or macroalbuminura (greater than 300 mg/g), and 22% of patients were prescribed an ACE inhibitor or angiotensin receptor blocker.
The majority of patients (69%) underwent gastric bypass; 25% had laparoscopic gastric banding and 6% had sleeve gastrectomy. Dr. Heneghan reported that 5 years after their surgery, 44% of patients had sustained remission of their type 2 diabetes, 33% had a significant improvement, and 23% had no change or worsening of their disease. This latter cohort "had the least amount of weight loss and were those who had the longest standing duration of diabetes preoperatively."
The rates of patients with remission, improvement, or change in hypertension were 16%, 50%, and 34%, respectively, whereas the rates for patients with dyslipidemia were 39%, 20%, and 41%.
Only 25% of patients who did not have diabetic nephropathy at the time of surgery went on to develop the condition. Among patients with preoperative microalbuminuria, 42% remained stable whereas 58% regressed and had no albuminuria 5 years after surgery. Similarly, among patients with preoperative macroalbuminuria, 50% remained stable and 50% regressed and had no albuminuria at 5 years.*
There were no preoperative differences in the mean urinary albumin to creatinine ratio (ACR) between patients who were and patients who were not prescribed a renoprotective agent. However, postoperatively, patients who were not on a renoprotective agent had a significantly lower urinary ACR, compared with those who remained on a renoprotective agent (P = .039). "This probably reflects the fact that patients who had improvement of their diabetes and regression or nonprogression of their nephropathy status also had a significant improvement in – or remission of – hypertension, and were no longer prescribed an antihypertensive medication," Dr. Heneghan explained.
She characterized the study’s overall findings as "remarkable, considering that diabetes is a chronic, progressive disease, and certainly warrant further investigation in the form of a prospective and larger study."
Dr. Heneghan said that she had no relevant financial conflicts to disclose.
*CORRECTION 8/28/12: The original sentence contained an error in describing the patients. The sentence should read" "Similarly, among patients with preoperative macroalbuminuria, 50% remained stable and 50% regressed and had no albuminuria at 5 years."
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: Among patients with preoperative microalbuminuria, 42% remained stable 5 years after their bariatric surgery, whereas 58% regressed and had no albuminuria. Similarly, among patients with preoperative macroalbuminuria, 50% remained stable, and 50% regressed and had no albuminuria at 5 years.
Data Source: The study included 52 patients who underwent bariatric surgery at the Cleveland Clinic and had completed the 5-year follow-up.
Disclosures: Dr. Heneghan said that she had no relevant financial conflicts to disclose.
BOLD Analysis Backs Safety of Sleeve Gastrectomy
SAN DIEGO – Laparoscopic sleeve gastrectomy is positioned between gastric banding and the laparoscopic gastric bypass for both safety and efficacy, results from the largest comparative study of its kind demonstrated.
The finding comes at a time when the Centers for Medicare and Medicaid Services is reviewing evidence to consider including sleeve gastrectomy as a covered benefit. Currently, gastric bypass, vertical banded gastroplasty, duodenal switch, and gastric banding are the only CMS-sanctioned bariatric procedures.

The study, which involved nearly 300,000 patients, "shows that across the board, regardless of the procedure, bariatric surgery is safe and effective," Dr. John M. Morton said in an interview at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "The emerging new procedure, the sleeve gastrectomy, is shown to be right between the bypass and the band. As a result, we have seen more interest from payers to cover it. In fact there are about 100 million lives that are covered. Our only outlier is CMS in deciding to cover. We hope that these data will help influence CMS in granting coverage for the sleeve gastrectomy."
Dr. Morton, associate professor of surgery and director of bariatric surgery at Stanford Hospitals and Clinics at Stanford (Calif.) University, and his associates examined BOLD (Bariatric Outcomes Longitudinal Database) to identify patients who had undergone laparoscopic Roux-en-Y gastric bypass (LRNYGB), gastric banding (LAGB), and sleeve gastrectomy (LSG) from June 2007 to December 2010. BOLD, the largest bariatric-specific database, is maintained by the ASMBS Bariatric Surgery Center of Excellence program, and includes more than 1,200 surgeons at 540 hospitals. Dr. Morton described the data as a "clinically rich" variable set that includes age, gender, race, insurance status, body mass index, excess body weight, and comorbidities.
"There is a definite need for more data around comparison of different procedures," Dr. Morton said at the meeting. "Our study hypothesis is very straightforward: Do demographics and outcomes for bariatric surgery vary by procedure?"
The primary outcomes were 30-day mortality, serious complications, and readmissions. The definitions of serious complications included death, anastomotic leakage, cardiac arrest, deep venous thrombosis, evisceration, heart failure and/or pulmonary edema, liver failure, and bleeding requiring transfusion.
Dr. Morton reported outcomes from 117,365 patients in the LAGB group, 138,222 in the LRNYGB group, and 16,139 in the LSG group. Patients in each group were generally the same age (a mean of 45, 46, and 45 years, respectively), mostly female (78%, 79%, and 74%), and mostly white (72%, 73%, and 72%). "The one area where there was a sizable difference was around self-pay," Dr. Morton said. About 21% of patients in the LSG group paid out-of-pocket, compared with 6% of those in the LAGB group and 2% of those in the LRNYGB group.
The proportion of preoperative comorbidities was similar among the three groups, with two exceptions. The prevalence of diabetes was highest in the LRNYGB group (37%, compared with 30% in the LSG group and 28% in the LAGB group; P less than .0001). A similar association was seen in the proportion of patients with five or more preoperative comorbidities (62%, 55%, and 52%, respectively; P less than .0001).
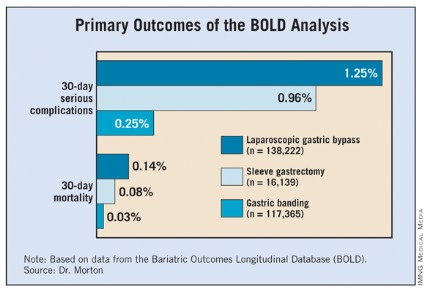
The mean length of stay was 0.7 days for the LAGB group, 1.9 days for the LSG group, and 2.3 days for the LRNYGB group. The percent change in BMI at 12 months was 7.6%, 13.4%, and 16.4%, respectively; the rate of 30-day serious complications was 0.25%, 0.96%, and 1.25%; and the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%. All differences between the groups were significant (P less than .0001).
"If you look at the remainder of the safety outcomes – everything from 30-day readmission to 30-day reoperation – it’s pretty much the same order, with the band group having the lowest [percentage], and the bypass having the highest, and the sleeve being right in between," Dr. Morton said. "When we looked at age greater than 65 in isolation, we found that the order of safety remains, with the banding having the least amount of mortality and the sleeve being right between the band procedure and the bypass."
Logistic regression analysis revealed several significant factors that predicted serious adverse events at 30 days: male gender (odds ratio, 1.67), having nonprivate insurance (OR, 1.15), stepwise progression with increasing age (for example, an OR of 1.27 for those aged 26-35 years and an OR of 4.42 for those above age 65), and stepwise progression with increasing BMI (for example, an OR of 1.37 for those with a BMI of 46-55 kg/m2 and an OR of 3.03 for those with a BMI greater than 65).
The invited discussant, Dr. Matthew M. Hutter, of Massachusetts General Hospital, Boston, described the size of the overall study cohort as remarkable. "What I find most interesting about this study is that it shows that sleeve gastrectomy – a brand-new, very complex procedure – can be introduced safely and effectively when performed under the standards of a bariatric accreditation program," Dr. Hutter said. "Other surgical procedures such as laparoscopic cholecystectomy or laparoscopic colectomy had very high morbidity and conversion rates when they were first implemented. However, this new complex procedure has been safe and effective from the get-go, and that is really quite impressive. The other remarkable finding is how consistent this is with all of the other major [bariatric surgery] data collection programs."
Dr. Morton acknowledged certain limitations of the study, including the fact that 1-year follow-up was available in only 60% of patients, while 30-day follow-up was available in 98% of the cohort. "Potentially, patients could have been admitted to other hospitals," he added. "These are research-consented patients, so about 70% consented. Some of this is surgeon-directed reporting."
Dr. Morton said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is positioned between gastric banding and the laparoscopic gastric bypass for both safety and efficacy, results from the largest comparative study of its kind demonstrated.
The finding comes at a time when the Centers for Medicare and Medicaid Services is reviewing evidence to consider including sleeve gastrectomy as a covered benefit. Currently, gastric bypass, vertical banded gastroplasty, duodenal switch, and gastric banding are the only CMS-sanctioned bariatric procedures.
The study, which involved nearly 300,000 patients, "shows that across the board, regardless of the procedure, bariatric surgery is safe and effective," Dr. John M. Morton said in an interview at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "The emerging new procedure, the sleeve gastrectomy, is shown to be right between the bypass and the band. As a result, we have seen more interest from payers to cover it. In fact there are about 100 million lives that are covered. Our only outlier is CMS in deciding to cover. We hope that these data will help influence CMS in granting coverage for the sleeve gastrectomy."
Dr. Morton, associate professor of surgery and director of bariatric surgery at Stanford Hospitals and Clinics at Stanford (Calif.) University, and his associates examined BOLD (Bariatric Outcomes Longitudinal Database) to identify patients who had undergone laparoscopic Roux-en-Y gastric bypass (LRNYGB), gastric banding (LAGB), and sleeve gastrectomy (LSG) from June 2007 to December 2010. BOLD, the largest bariatric-specific database, is maintained by the ASMBS Bariatric Surgery Center of Excellence program, and includes more than 1,200 surgeons at 540 hospitals. Dr. Morton described the data as a "clinically rich" variable set that includes age, gender, race, insurance status, body mass index, excess body weight, and comorbidities.
"There is a definite need for more data around comparison of different procedures," Dr. Morton said at the meeting. "Our study hypothesis is very straightforward: Do demographics and outcomes for bariatric surgery vary by procedure?"
The primary outcomes were 30-day mortality, serious complications, and readmissions. The definitions of serious complications included death, anastomotic leakage, cardiac arrest, deep venous thrombosis, evisceration, heart failure and/or pulmonary edema, liver failure, and bleeding requiring transfusion.
Dr. Morton reported outcomes from 117,365 patients in the LAGB group, 138,222 in the LRNYGB group, and 16,139 in the LSG group. Patients in each group were generally the same age (a mean of 45, 46, and 45 years, respectively), mostly female (78%, 79%, and 74%), and mostly white (72%, 73%, and 72%). "The one area where there was a sizable difference was around self-pay," Dr. Morton said. About 21% of patients in the LSG group paid out-of-pocket, compared with 6% of those in the LAGB group and 2% of those in the LRNYGB group.
The proportion of preoperative comorbidities was similar among the three groups, with two exceptions. The prevalence of diabetes was highest in the LRNYGB group (37%, compared with 30% in the LSG group and 28% in the LAGB group; P less than .0001). A similar association was seen in the proportion of patients with five or more preoperative comorbidities (62%, 55%, and 52%, respectively; P less than .0001).
The mean length of stay was 0.7 days for the LAGB group, 1.9 days for the LSG group, and 2.3 days for the LRNYGB group. The percent change in BMI at 12 months was 7.6%, 13.4%, and 16.4%, respectively; the rate of 30-day serious complications was 0.25%, 0.96%, and 1.25%; and the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%. All differences between the groups were significant (P less than .0001).
"If you look at the remainder of the safety outcomes – everything from 30-day readmission to 30-day reoperation – it’s pretty much the same order, with the band group having the lowest [percentage], and the bypass having the highest, and the sleeve being right in between," Dr. Morton said. "When we looked at age greater than 65 in isolation, we found that the order of safety remains, with the banding having the least amount of mortality and the sleeve being right between the band procedure and the bypass."
Logistic regression analysis revealed several significant factors that predicted serious adverse events at 30 days: male gender (odds ratio, 1.67), having nonprivate insurance (OR, 1.15), stepwise progression with increasing age (for example, an OR of 1.27 for those aged 26-35 years and an OR of 4.42 for those above age 65), and stepwise progression with increasing BMI (for example, an OR of 1.37 for those with a BMI of 46-55 kg/m2 and an OR of 3.03 for those with a BMI greater than 65).
The invited discussant, Dr. Matthew M. Hutter, of Massachusetts General Hospital, Boston, described the size of the overall study cohort as remarkable. "What I find most interesting about this study is that it shows that sleeve gastrectomy – a brand-new, very complex procedure – can be introduced safely and effectively when performed under the standards of a bariatric accreditation program," Dr. Hutter said. "Other surgical procedures such as laparoscopic cholecystectomy or laparoscopic colectomy had very high morbidity and conversion rates when they were first implemented. However, this new complex procedure has been safe and effective from the get-go, and that is really quite impressive. The other remarkable finding is how consistent this is with all of the other major [bariatric surgery] data collection programs."
Dr. Morton acknowledged certain limitations of the study, including the fact that 1-year follow-up was available in only 60% of patients, while 30-day follow-up was available in 98% of the cohort. "Potentially, patients could have been admitted to other hospitals," he added. "These are research-consented patients, so about 70% consented. Some of this is surgeon-directed reporting."
Dr. Morton said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is positioned between gastric banding and the laparoscopic gastric bypass for both safety and efficacy, results from the largest comparative study of its kind demonstrated.
The finding comes at a time when the Centers for Medicare and Medicaid Services is reviewing evidence to consider including sleeve gastrectomy as a covered benefit. Currently, gastric bypass, vertical banded gastroplasty, duodenal switch, and gastric banding are the only CMS-sanctioned bariatric procedures.
The study, which involved nearly 300,000 patients, "shows that across the board, regardless of the procedure, bariatric surgery is safe and effective," Dr. John M. Morton said in an interview at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "The emerging new procedure, the sleeve gastrectomy, is shown to be right between the bypass and the band. As a result, we have seen more interest from payers to cover it. In fact there are about 100 million lives that are covered. Our only outlier is CMS in deciding to cover. We hope that these data will help influence CMS in granting coverage for the sleeve gastrectomy."
Dr. Morton, associate professor of surgery and director of bariatric surgery at Stanford Hospitals and Clinics at Stanford (Calif.) University, and his associates examined BOLD (Bariatric Outcomes Longitudinal Database) to identify patients who had undergone laparoscopic Roux-en-Y gastric bypass (LRNYGB), gastric banding (LAGB), and sleeve gastrectomy (LSG) from June 2007 to December 2010. BOLD, the largest bariatric-specific database, is maintained by the ASMBS Bariatric Surgery Center of Excellence program, and includes more than 1,200 surgeons at 540 hospitals. Dr. Morton described the data as a "clinically rich" variable set that includes age, gender, race, insurance status, body mass index, excess body weight, and comorbidities.
"There is a definite need for more data around comparison of different procedures," Dr. Morton said at the meeting. "Our study hypothesis is very straightforward: Do demographics and outcomes for bariatric surgery vary by procedure?"
The primary outcomes were 30-day mortality, serious complications, and readmissions. The definitions of serious complications included death, anastomotic leakage, cardiac arrest, deep venous thrombosis, evisceration, heart failure and/or pulmonary edema, liver failure, and bleeding requiring transfusion.
Dr. Morton reported outcomes from 117,365 patients in the LAGB group, 138,222 in the LRNYGB group, and 16,139 in the LSG group. Patients in each group were generally the same age (a mean of 45, 46, and 45 years, respectively), mostly female (78%, 79%, and 74%), and mostly white (72%, 73%, and 72%). "The one area where there was a sizable difference was around self-pay," Dr. Morton said. About 21% of patients in the LSG group paid out-of-pocket, compared with 6% of those in the LAGB group and 2% of those in the LRNYGB group.
The proportion of preoperative comorbidities was similar among the three groups, with two exceptions. The prevalence of diabetes was highest in the LRNYGB group (37%, compared with 30% in the LSG group and 28% in the LAGB group; P less than .0001). A similar association was seen in the proportion of patients with five or more preoperative comorbidities (62%, 55%, and 52%, respectively; P less than .0001).
The mean length of stay was 0.7 days for the LAGB group, 1.9 days for the LSG group, and 2.3 days for the LRNYGB group. The percent change in BMI at 12 months was 7.6%, 13.4%, and 16.4%, respectively; the rate of 30-day serious complications was 0.25%, 0.96%, and 1.25%; and the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%. All differences between the groups were significant (P less than .0001).
"If you look at the remainder of the safety outcomes – everything from 30-day readmission to 30-day reoperation – it’s pretty much the same order, with the band group having the lowest [percentage], and the bypass having the highest, and the sleeve being right in between," Dr. Morton said. "When we looked at age greater than 65 in isolation, we found that the order of safety remains, with the banding having the least amount of mortality and the sleeve being right between the band procedure and the bypass."
Logistic regression analysis revealed several significant factors that predicted serious adverse events at 30 days: male gender (odds ratio, 1.67), having nonprivate insurance (OR, 1.15), stepwise progression with increasing age (for example, an OR of 1.27 for those aged 26-35 years and an OR of 4.42 for those above age 65), and stepwise progression with increasing BMI (for example, an OR of 1.37 for those with a BMI of 46-55 kg/m2 and an OR of 3.03 for those with a BMI greater than 65).
The invited discussant, Dr. Matthew M. Hutter, of Massachusetts General Hospital, Boston, described the size of the overall study cohort as remarkable. "What I find most interesting about this study is that it shows that sleeve gastrectomy – a brand-new, very complex procedure – can be introduced safely and effectively when performed under the standards of a bariatric accreditation program," Dr. Hutter said. "Other surgical procedures such as laparoscopic cholecystectomy or laparoscopic colectomy had very high morbidity and conversion rates when they were first implemented. However, this new complex procedure has been safe and effective from the get-go, and that is really quite impressive. The other remarkable finding is how consistent this is with all of the other major [bariatric surgery] data collection programs."
Dr. Morton acknowledged certain limitations of the study, including the fact that 1-year follow-up was available in only 60% of patients, while 30-day follow-up was available in 98% of the cohort. "Potentially, patients could have been admitted to other hospitals," he added. "These are research-consented patients, so about 70% consented. Some of this is surgeon-directed reporting."
Dr. Morton said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: The rate of 30-day serious complications was 0.25% among those who underwent laparoscopic gastric banding, 0.96% among those who underwent laparoscopic sleeve gastrectomy, and 1.25% among those who underwent laparoscopic Roux-en-Y gastric bypass, while the rate of 30-day mortality was 0.03%, 0.08%, and 0.14%, respectively.
Data Source: The data analysis was based on 271,726 patients from the Bariatric Outcomes Longitudinal Database who underwent bariatric surgery from June 2007 to December 2010.
Disclosures: Dr. Morton said that he had no relevant financial conflicts to disclose.
Race, Sex Factor Into Weight Loss After Gastric Bypass
SAN DIEGO – Being black, male, or older significantly raised the risk for weight-loss failure after gastric bypass in a single-center study of more than 1,200 patients.
"Long-term treatments of obesity are hampered by the fixed behaviors that induce obesity, the possibility of weight set points, and the ever-present exposure to high-calorie foods. The treatments of obesity all have great variability in outcome," Dr. Ramsey M. Dallal said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.

To determine predictors of weight-loss failure after gastric bypass surgery, Dr. Dallal and his associate at the department of surgery at Einstein Healthcare Network, Philadelphia, reviewed the medical records of 1,256 gastric bypass patients who had a least 1 year of follow-up. They separated patients into two groups: those who were above the 75th percentile in weight loss (success) and those who were below the 25th percentile in weight loss (failure). Multivariate logistic regression was performed to examine the impact of sex, race, age, initial weight, initial glycosylated hemoglobin (HbA1c) level, and insurance type (Medicare/Medicaid vs. private insurance).
The mean preoperative body mass index of the 1,256 patients was 48.3 kg/m2, their mean age was 42 years, and 82% were women. More than one-quarter of patients (27%) had diabetes, and the mean HbA1c level was 6.6% in blacks and 6.3% in whites. The majority of patients (75%) had private insurance, 19% were on Medicare, and 6% were on Medicaid.
Dr. Dallal reported that after a mean follow-up period of 665 days, the mean excess weight loss among all patients was 70%, and was significantly different between whites and blacks (72% vs. 63%, respectively), between those aged 65 years and older and those younger than age 40 (61% vs. 71%), and between men and women (62% vs. 71%). The calculated threshold estimated weight loss for the upper 75th and lower 25th percentiles was 82% vs. 57%, respectively.
Multivariate logistic regression analysis revealed the following independent predictors of weight-loss failure: being black (odds ratio, 3.1; P = .002), older (OR, 0.97; P = .001), or male (OR, 0.30; P less than .0005), and having a higher initial body weight (OR, 0.86; P less than .0005). Initial HbA1c and insurance type were not independent predictors of weight-loss failure.
Dr. Dallal acknowledged certain limitations of the study, including the fact that the ideal body weight calculations used "may not necessarily be valid for all ethnicities. Also, we did not distinguish between primary weight-loss failures (those who never reached adequate weight loss) and those [who had] a secondary weight-loss failure (regain of lost weight)."
Dr. Dallal said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Being black, male, or older significantly raised the risk for weight-loss failure after gastric bypass in a single-center study of more than 1,200 patients.
"Long-term treatments of obesity are hampered by the fixed behaviors that induce obesity, the possibility of weight set points, and the ever-present exposure to high-calorie foods. The treatments of obesity all have great variability in outcome," Dr. Ramsey M. Dallal said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
To determine predictors of weight-loss failure after gastric bypass surgery, Dr. Dallal and his associate at the department of surgery at Einstein Healthcare Network, Philadelphia, reviewed the medical records of 1,256 gastric bypass patients who had a least 1 year of follow-up. They separated patients into two groups: those who were above the 75th percentile in weight loss (success) and those who were below the 25th percentile in weight loss (failure). Multivariate logistic regression was performed to examine the impact of sex, race, age, initial weight, initial glycosylated hemoglobin (HbA1c) level, and insurance type (Medicare/Medicaid vs. private insurance).
The mean preoperative body mass index of the 1,256 patients was 48.3 kg/m2, their mean age was 42 years, and 82% were women. More than one-quarter of patients (27%) had diabetes, and the mean HbA1c level was 6.6% in blacks and 6.3% in whites. The majority of patients (75%) had private insurance, 19% were on Medicare, and 6% were on Medicaid.
Dr. Dallal reported that after a mean follow-up period of 665 days, the mean excess weight loss among all patients was 70%, and was significantly different between whites and blacks (72% vs. 63%, respectively), between those aged 65 years and older and those younger than age 40 (61% vs. 71%), and between men and women (62% vs. 71%). The calculated threshold estimated weight loss for the upper 75th and lower 25th percentiles was 82% vs. 57%, respectively.
Multivariate logistic regression analysis revealed the following independent predictors of weight-loss failure: being black (odds ratio, 3.1; P = .002), older (OR, 0.97; P = .001), or male (OR, 0.30; P less than .0005), and having a higher initial body weight (OR, 0.86; P less than .0005). Initial HbA1c and insurance type were not independent predictors of weight-loss failure.
Dr. Dallal acknowledged certain limitations of the study, including the fact that the ideal body weight calculations used "may not necessarily be valid for all ethnicities. Also, we did not distinguish between primary weight-loss failures (those who never reached adequate weight loss) and those [who had] a secondary weight-loss failure (regain of lost weight)."
Dr. Dallal said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Being black, male, or older significantly raised the risk for weight-loss failure after gastric bypass in a single-center study of more than 1,200 patients.
"Long-term treatments of obesity are hampered by the fixed behaviors that induce obesity, the possibility of weight set points, and the ever-present exposure to high-calorie foods. The treatments of obesity all have great variability in outcome," Dr. Ramsey M. Dallal said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
To determine predictors of weight-loss failure after gastric bypass surgery, Dr. Dallal and his associate at the department of surgery at Einstein Healthcare Network, Philadelphia, reviewed the medical records of 1,256 gastric bypass patients who had a least 1 year of follow-up. They separated patients into two groups: those who were above the 75th percentile in weight loss (success) and those who were below the 25th percentile in weight loss (failure). Multivariate logistic regression was performed to examine the impact of sex, race, age, initial weight, initial glycosylated hemoglobin (HbA1c) level, and insurance type (Medicare/Medicaid vs. private insurance).
The mean preoperative body mass index of the 1,256 patients was 48.3 kg/m2, their mean age was 42 years, and 82% were women. More than one-quarter of patients (27%) had diabetes, and the mean HbA1c level was 6.6% in blacks and 6.3% in whites. The majority of patients (75%) had private insurance, 19% were on Medicare, and 6% were on Medicaid.
Dr. Dallal reported that after a mean follow-up period of 665 days, the mean excess weight loss among all patients was 70%, and was significantly different between whites and blacks (72% vs. 63%, respectively), between those aged 65 years and older and those younger than age 40 (61% vs. 71%), and between men and women (62% vs. 71%). The calculated threshold estimated weight loss for the upper 75th and lower 25th percentiles was 82% vs. 57%, respectively.
Multivariate logistic regression analysis revealed the following independent predictors of weight-loss failure: being black (odds ratio, 3.1; P = .002), older (OR, 0.97; P = .001), or male (OR, 0.30; P less than .0005), and having a higher initial body weight (OR, 0.86; P less than .0005). Initial HbA1c and insurance type were not independent predictors of weight-loss failure.
Dr. Dallal acknowledged certain limitations of the study, including the fact that the ideal body weight calculations used "may not necessarily be valid for all ethnicities. Also, we did not distinguish between primary weight-loss failures (those who never reached adequate weight loss) and those [who had] a secondary weight-loss failure (regain of lost weight)."
Dr. Dallal said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: Following gastric bypass surgery, independent significant predictors of weight-loss failure were being black (OR, 3.1; P = .002), older (OR, 0.97; P = .001), or male (OR, 0.30; P less than .0005), and having higher initial body weight (OR, 0.86; P less than .0005).
Data Source: This single-center study comprised 1,256 gastric bypass patients who had a least 1 year of follow-up.
Disclosures: Dr. Dallal said that he had no relevant financial conflicts to disclose.
Tracking System Proposed for Medical Devices
Most medical devices distributed in the United States should carry an identification label to help identify and resolve problems associated with them, according to a statement issued the Food and Drug Administration on July 3.
The unique device identifier (UDI), an exclusive numeric or alphanumeric code, "has the potential to improve the quality of information in medical device adverse event reports, which will help the FDA identify product problems more quickly, better target recalls and improve patient safety," according to the statement.
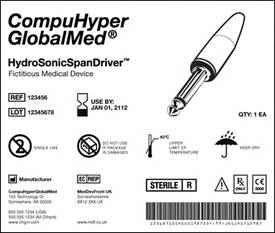
In the proposed rule, the label will include an illustration of the device, the product name, its expiration date, reference and lot numbers, manufacturer information, as well as a bar code.
The UDI system is required by legislation passed by Congress in 2007 directing the agency to develop regulations establishing such a system, and the agency worked closely with industry, clinical groups, as well as patient and consumer groups, and has conducted four pilot studies in developing the proposed rule, according to the statement.
Implementation will be phased in, with the highest-risk medical devices labeled first. Low-risk devices will be exempt from some or all of the requirements and over-the-counter devices will be exempt, since they usually have a universal product code.
In addition to improving the accuracy of device-related adverse event reporting, the system is expected to expedite the resolution of device-related problems. The system also will address counterfeit products and medical emergency preparation.
The FDA is accepting comments on the proposal for 120 days.
Most medical devices distributed in the United States should carry an identification label to help identify and resolve problems associated with them, according to a statement issued the Food and Drug Administration on July 3.
The unique device identifier (UDI), an exclusive numeric or alphanumeric code, "has the potential to improve the quality of information in medical device adverse event reports, which will help the FDA identify product problems more quickly, better target recalls and improve patient safety," according to the statement.
In the proposed rule, the label will include an illustration of the device, the product name, its expiration date, reference and lot numbers, manufacturer information, as well as a bar code.
The UDI system is required by legislation passed by Congress in 2007 directing the agency to develop regulations establishing such a system, and the agency worked closely with industry, clinical groups, as well as patient and consumer groups, and has conducted four pilot studies in developing the proposed rule, according to the statement.
Implementation will be phased in, with the highest-risk medical devices labeled first. Low-risk devices will be exempt from some or all of the requirements and over-the-counter devices will be exempt, since they usually have a universal product code.
In addition to improving the accuracy of device-related adverse event reporting, the system is expected to expedite the resolution of device-related problems. The system also will address counterfeit products and medical emergency preparation.
The FDA is accepting comments on the proposal for 120 days.
Most medical devices distributed in the United States should carry an identification label to help identify and resolve problems associated with them, according to a statement issued the Food and Drug Administration on July 3.
The unique device identifier (UDI), an exclusive numeric or alphanumeric code, "has the potential to improve the quality of information in medical device adverse event reports, which will help the FDA identify product problems more quickly, better target recalls and improve patient safety," according to the statement.
In the proposed rule, the label will include an illustration of the device, the product name, its expiration date, reference and lot numbers, manufacturer information, as well as a bar code.
The UDI system is required by legislation passed by Congress in 2007 directing the agency to develop regulations establishing such a system, and the agency worked closely with industry, clinical groups, as well as patient and consumer groups, and has conducted four pilot studies in developing the proposed rule, according to the statement.
Implementation will be phased in, with the highest-risk medical devices labeled first. Low-risk devices will be exempt from some or all of the requirements and over-the-counter devices will be exempt, since they usually have a universal product code.
In addition to improving the accuracy of device-related adverse event reporting, the system is expected to expedite the resolution of device-related problems. The system also will address counterfeit products and medical emergency preparation.
The FDA is accepting comments on the proposal for 120 days.
FDA Warns of Seizure Risk With Cefepime
The Food and Drug Administration has reported cases of a specific type of seizure called nonconvulsive status epilepticus that is associated with the use of the antibacterial drug cefepime in patients with renal impairment.
The seizures have been seen primarily in patients with renal impairment who did not receive appropriate dosage adjustments of cefepime, although in several cases patients received "dosage adjustment appropriate for their degree of renal impairment," according to the agency. The FDA is working to revise the "Warnings and Precautions" and "Adverse Reactions" sections of the cefepime label to highlight this risk.
The FDA advises health care professionals to adjust the dosage of cefepime in patients with a creatinine clearance of 60 mL/min or less in order to minimize the risk of seizures. If seizures associated with cefepime therapy occur, physicians should consider discontinuing cefepime or making appropriate dosage adjustments in patients with renal impairment.
Nonconvulsive status epilepticus associated with cefepime occurred in 59 patients from 1996 through February 2012. The cases were identified through the FDA’s Adverse Event Reporting System (AERS) database. The majority of seizures were reversible, and resolved after discontinuation of cefepime and/or after hemodialysis.
Cefepime is a cephalosporin antibacterial drug used to treat pneumonia, urinary tract, skin, and intra-abdominal infections.
*This article was updated on 7/3/2012*
The Food and Drug Administration has reported cases of a specific type of seizure called nonconvulsive status epilepticus that is associated with the use of the antibacterial drug cefepime in patients with renal impairment.
The seizures have been seen primarily in patients with renal impairment who did not receive appropriate dosage adjustments of cefepime, although in several cases patients received "dosage adjustment appropriate for their degree of renal impairment," according to the agency. The FDA is working to revise the "Warnings and Precautions" and "Adverse Reactions" sections of the cefepime label to highlight this risk.
The FDA advises health care professionals to adjust the dosage of cefepime in patients with a creatinine clearance of 60 mL/min or less in order to minimize the risk of seizures. If seizures associated with cefepime therapy occur, physicians should consider discontinuing cefepime or making appropriate dosage adjustments in patients with renal impairment.
Nonconvulsive status epilepticus associated with cefepime occurred in 59 patients from 1996 through February 2012. The cases were identified through the FDA’s Adverse Event Reporting System (AERS) database. The majority of seizures were reversible, and resolved after discontinuation of cefepime and/or after hemodialysis.
Cefepime is a cephalosporin antibacterial drug used to treat pneumonia, urinary tract, skin, and intra-abdominal infections.
*This article was updated on 7/3/2012*
The Food and Drug Administration has reported cases of a specific type of seizure called nonconvulsive status epilepticus that is associated with the use of the antibacterial drug cefepime in patients with renal impairment.
The seizures have been seen primarily in patients with renal impairment who did not receive appropriate dosage adjustments of cefepime, although in several cases patients received "dosage adjustment appropriate for their degree of renal impairment," according to the agency. The FDA is working to revise the "Warnings and Precautions" and "Adverse Reactions" sections of the cefepime label to highlight this risk.
The FDA advises health care professionals to adjust the dosage of cefepime in patients with a creatinine clearance of 60 mL/min or less in order to minimize the risk of seizures. If seizures associated with cefepime therapy occur, physicians should consider discontinuing cefepime or making appropriate dosage adjustments in patients with renal impairment.
Nonconvulsive status epilepticus associated with cefepime occurred in 59 patients from 1996 through February 2012. The cases were identified through the FDA’s Adverse Event Reporting System (AERS) database. The majority of seizures were reversible, and resolved after discontinuation of cefepime and/or after hemodialysis.
Cefepime is a cephalosporin antibacterial drug used to treat pneumonia, urinary tract, skin, and intra-abdominal infections.
*This article was updated on 7/3/2012*
Check Vitamin D in Adolescents Before Bariatric Surgery
HOUSTON – Fifty-four percent of 219 obese adolescents being evaluated for bariatric surgery were deficient in vitamin D, including 9% who were severely deficient, a retrospective analysis of preoperative laboratory measures found.
Eighty-two percent of the adolescents had insufficient levels of 25-hydroxyvitamin D (25OHD) in their blood, Dr. Marisa Censani and her associates reported at the annual meeting of the Endocrine Society.

The findings are so striking that all morbidly obese adolescents should be screened for vitamin D deficiency, and those who are deficient should be treated to replete vitamin D levels, suggested Dr. Censani of Columbia University, New York.
It’s particularly important to screen adolescents before bariatric surgery procedures, some of which have been associated with bone loss, which results from weight loss and decreased calcium and vitamin D absorption. Preoperative vitamin D deficiency could put adolescent patients at greater risk because they have not reached their peak bone mass, she said.
Previous studies have shown that obese adults undergoing bariatric surgery commonly are vitamin D deficient before surgery, but these are some of the first data in preoperative adolescent patients.
Of all adolescents undergoing bariatric surgery at her institution from March 2006 to June 2011, 219 had records on serum 25OHD and parathyroid hormone levels. The cohort was 65% female, 43% white, 35% Hispanic, and 15% African American, with the rest being other races/ethnicities. Patients had a mean age of 16 years (ranging from 13-18 years) and a mean body mass index of 48 kg/m2.
The mean serum 25OHD level was 21 ng/mL, which was considered insufficient. The study defined adequate levels of serum 25OHD as at least 30 ng/mL, insufficient levels as 20-29 ng/mL, deficient levels as less than 20 ng/mL, and severely deficient levels as less than 10 ng/mL.
Only 18% of patients had sufficient 25OHD levels. Twenty-nine percent had insufficient levels, 45% were vitamin D deficient, and 9% were severely deficient.
Patients with the highest BMIs were most likely to have deficient levels of 25OHD. Every kilogram increase in BMI correlated with a 0.2-ng decrease in 25OHD levels, Dr. Censani said.
Vitamin D deficiency was most common in African Americans, 82% of whom were deficient and none of whom had levels in the normal range. Fifty-nine percent of Hispanics and 37% of whites had vitamin D deficiency. Race was the strongest predictor of 25OHD levels.
Roughly 80% of African American patients were deficient in vitamin D and the rest had insufficient levels. In Hispanics, nearly 60% were deficient in vitamin D, close to 25% had insufficient levels, and about 25% had adequate levels. In whites, deficient or insufficient levels each were seen in nearly 40% of patients, with adequate levels in more than 20%.
Clear secondary hyperparathyroidism was seen in 5% of patients, though serum parathyroid levels varied inversely with 25OHD. African American race, BMI, and parathyroid levels explained 21% of the variance in 25OHD levels between patients.
To be eligible for bariatric surgery, adolescents had to have reached Tanner stage IV or V and had to have a BMI greater than 50, or above 35 kg/m2 if they had comorbidities.
A physician in the audience challenged Dr. Censani’s recommendation that all obese adolescents be screened and possibly treated for vitamin D deficiency, saying there is no evidence yet of clinical benefit from that approach. Dr. Censani agreed that more research is needed to support this strategy.
The current study was limited by the lack of a community-based, nonobese control group and lack of data on dietary calcium and vitamin D intake, sun exposure, or bone mineral density. The study’s large size and relatively good ethnic diversity are strengths, she said.
The U.S. adolescent obesity rate has more than tripled in the past 30 years, with 16% of children and adolescents now overweight, 4% obese, and 4% morbidly obese, studies suggest.
Dr. Censani reported having no financial disclosures. The National Institutes of Health funded the study.
25-hydroxyvitamin D, 25OHD, Dr. Marisa Censani, the Endocrine Society, vitamin D deficiency, parathyroid hormone levels,
HOUSTON – Fifty-four percent of 219 obese adolescents being evaluated for bariatric surgery were deficient in vitamin D, including 9% who were severely deficient, a retrospective analysis of preoperative laboratory measures found.
Eighty-two percent of the adolescents had insufficient levels of 25-hydroxyvitamin D (25OHD) in their blood, Dr. Marisa Censani and her associates reported at the annual meeting of the Endocrine Society.
The findings are so striking that all morbidly obese adolescents should be screened for vitamin D deficiency, and those who are deficient should be treated to replete vitamin D levels, suggested Dr. Censani of Columbia University, New York.
It’s particularly important to screen adolescents before bariatric surgery procedures, some of which have been associated with bone loss, which results from weight loss and decreased calcium and vitamin D absorption. Preoperative vitamin D deficiency could put adolescent patients at greater risk because they have not reached their peak bone mass, she said.
Previous studies have shown that obese adults undergoing bariatric surgery commonly are vitamin D deficient before surgery, but these are some of the first data in preoperative adolescent patients.
Of all adolescents undergoing bariatric surgery at her institution from March 2006 to June 2011, 219 had records on serum 25OHD and parathyroid hormone levels. The cohort was 65% female, 43% white, 35% Hispanic, and 15% African American, with the rest being other races/ethnicities. Patients had a mean age of 16 years (ranging from 13-18 years) and a mean body mass index of 48 kg/m2.
The mean serum 25OHD level was 21 ng/mL, which was considered insufficient. The study defined adequate levels of serum 25OHD as at least 30 ng/mL, insufficient levels as 20-29 ng/mL, deficient levels as less than 20 ng/mL, and severely deficient levels as less than 10 ng/mL.
Only 18% of patients had sufficient 25OHD levels. Twenty-nine percent had insufficient levels, 45% were vitamin D deficient, and 9% were severely deficient.
Patients with the highest BMIs were most likely to have deficient levels of 25OHD. Every kilogram increase in BMI correlated with a 0.2-ng decrease in 25OHD levels, Dr. Censani said.
Vitamin D deficiency was most common in African Americans, 82% of whom were deficient and none of whom had levels in the normal range. Fifty-nine percent of Hispanics and 37% of whites had vitamin D deficiency. Race was the strongest predictor of 25OHD levels.
Roughly 80% of African American patients were deficient in vitamin D and the rest had insufficient levels. In Hispanics, nearly 60% were deficient in vitamin D, close to 25% had insufficient levels, and about 25% had adequate levels. In whites, deficient or insufficient levels each were seen in nearly 40% of patients, with adequate levels in more than 20%.
Clear secondary hyperparathyroidism was seen in 5% of patients, though serum parathyroid levels varied inversely with 25OHD. African American race, BMI, and parathyroid levels explained 21% of the variance in 25OHD levels between patients.
To be eligible for bariatric surgery, adolescents had to have reached Tanner stage IV or V and had to have a BMI greater than 50, or above 35 kg/m2 if they had comorbidities.
A physician in the audience challenged Dr. Censani’s recommendation that all obese adolescents be screened and possibly treated for vitamin D deficiency, saying there is no evidence yet of clinical benefit from that approach. Dr. Censani agreed that more research is needed to support this strategy.
The current study was limited by the lack of a community-based, nonobese control group and lack of data on dietary calcium and vitamin D intake, sun exposure, or bone mineral density. The study’s large size and relatively good ethnic diversity are strengths, she said.
The U.S. adolescent obesity rate has more than tripled in the past 30 years, with 16% of children and adolescents now overweight, 4% obese, and 4% morbidly obese, studies suggest.
Dr. Censani reported having no financial disclosures. The National Institutes of Health funded the study.
HOUSTON – Fifty-four percent of 219 obese adolescents being evaluated for bariatric surgery were deficient in vitamin D, including 9% who were severely deficient, a retrospective analysis of preoperative laboratory measures found.
Eighty-two percent of the adolescents had insufficient levels of 25-hydroxyvitamin D (25OHD) in their blood, Dr. Marisa Censani and her associates reported at the annual meeting of the Endocrine Society.
The findings are so striking that all morbidly obese adolescents should be screened for vitamin D deficiency, and those who are deficient should be treated to replete vitamin D levels, suggested Dr. Censani of Columbia University, New York.
It’s particularly important to screen adolescents before bariatric surgery procedures, some of which have been associated with bone loss, which results from weight loss and decreased calcium and vitamin D absorption. Preoperative vitamin D deficiency could put adolescent patients at greater risk because they have not reached their peak bone mass, she said.
Previous studies have shown that obese adults undergoing bariatric surgery commonly are vitamin D deficient before surgery, but these are some of the first data in preoperative adolescent patients.
Of all adolescents undergoing bariatric surgery at her institution from March 2006 to June 2011, 219 had records on serum 25OHD and parathyroid hormone levels. The cohort was 65% female, 43% white, 35% Hispanic, and 15% African American, with the rest being other races/ethnicities. Patients had a mean age of 16 years (ranging from 13-18 years) and a mean body mass index of 48 kg/m2.
The mean serum 25OHD level was 21 ng/mL, which was considered insufficient. The study defined adequate levels of serum 25OHD as at least 30 ng/mL, insufficient levels as 20-29 ng/mL, deficient levels as less than 20 ng/mL, and severely deficient levels as less than 10 ng/mL.
Only 18% of patients had sufficient 25OHD levels. Twenty-nine percent had insufficient levels, 45% were vitamin D deficient, and 9% were severely deficient.
Patients with the highest BMIs were most likely to have deficient levels of 25OHD. Every kilogram increase in BMI correlated with a 0.2-ng decrease in 25OHD levels, Dr. Censani said.
Vitamin D deficiency was most common in African Americans, 82% of whom were deficient and none of whom had levels in the normal range. Fifty-nine percent of Hispanics and 37% of whites had vitamin D deficiency. Race was the strongest predictor of 25OHD levels.
Roughly 80% of African American patients were deficient in vitamin D and the rest had insufficient levels. In Hispanics, nearly 60% were deficient in vitamin D, close to 25% had insufficient levels, and about 25% had adequate levels. In whites, deficient or insufficient levels each were seen in nearly 40% of patients, with adequate levels in more than 20%.
Clear secondary hyperparathyroidism was seen in 5% of patients, though serum parathyroid levels varied inversely with 25OHD. African American race, BMI, and parathyroid levels explained 21% of the variance in 25OHD levels between patients.
To be eligible for bariatric surgery, adolescents had to have reached Tanner stage IV or V and had to have a BMI greater than 50, or above 35 kg/m2 if they had comorbidities.
A physician in the audience challenged Dr. Censani’s recommendation that all obese adolescents be screened and possibly treated for vitamin D deficiency, saying there is no evidence yet of clinical benefit from that approach. Dr. Censani agreed that more research is needed to support this strategy.
The current study was limited by the lack of a community-based, nonobese control group and lack of data on dietary calcium and vitamin D intake, sun exposure, or bone mineral density. The study’s large size and relatively good ethnic diversity are strengths, she said.
The U.S. adolescent obesity rate has more than tripled in the past 30 years, with 16% of children and adolescents now overweight, 4% obese, and 4% morbidly obese, studies suggest.
Dr. Censani reported having no financial disclosures. The National Institutes of Health funded the study.
25-hydroxyvitamin D, 25OHD, Dr. Marisa Censani, the Endocrine Society, vitamin D deficiency, parathyroid hormone levels,
25-hydroxyvitamin D, 25OHD, Dr. Marisa Censani, the Endocrine Society, vitamin D deficiency, parathyroid hormone levels,
AT THE ANNUAL MEETING OF THE ENDOCRINE SOCIETY
Major Finding: Fifty-four percent of obese adolescents being evaluated for bariatric surgery had vitamin D deficiency, including 8% with a severe deficiency.
Data Source: This was a retrospective analysis of preoperative laboratory measures from adolescents undergoing bariatric surgery at one institution from March 2006 to June 2011.
Disclosures: Dr. Censani reported having no financial disclosures. The National Institutes of Health funded the study.
AMA Delegates Slam PSA, Mammography Screening Recs
CHICAGO – Delegates to the American Medical Association’s legislative body are not happy with the U.S. Preventive Services Task Force.
They voted overwhelmingly (322 to 93) to express "concern" over the task force’s recommendations on screening mammography and prostate-specific antigen screening. Both recommendations attracted a firestorm of criticism when they were issued – the mammography recommendation in 2009 and those on PSA testing in May.
Many delegates also said they thought that the USPSTF, a quasi-governmental group operating under the auspices of the Agency for Healthcare Research and Quality, had reached its decisions without proper input from specialty societies or experts in each field.
In a second resolution, the delegates voted to encourage the USPSTF to "implement procedures that allow for meaningful input on recommendation development from specialists and stakeholders in the topic area under study."

Dr. Arl Van Moore Jr., a delegate from the American College of Radiology, said that neither the ACR nor any prominent breast imaging or surgical societies were contacted by the USPSTF in creating the screening mammography recommendations.
"None of the recognized experts in the field were contacted, to the best of our knowledge," said Dr. Moore, an interventional radiologist in Charlotte, N.C.
The American Urological Association delegate, Dr. William Gee, did not mince words when it came to the PSA screening guidelines.
"The [USPSTF] did not use an open process and ignored the public in reaching their conclusions," he said.
But Dr. Sally J. Trippel, a preventive medicine specialist at the Mayo Clinic and delegate from Minnesota, defended the USPSTF and its process. The task force is "about as politically independent as any national organization can get," and "about as free of conflict of interest as is possible in any organization developing guidelines for American clinicians," she said.
She quoted from task force documents showing that urologists provided peer review of the PSA evidence review. "So there were experts from urology involved in the development of that guideline," and also for the one on screening mammography.
To further show its consternation with the task force, AMA delegates also approved a report that stated that starting at age 40, women should be "eligible for screening mammography," and encouraging physicians "to regularly discuss with their individual patients the benefits and risks of screening mammography, and whether screening is appropriate for each clinical situation given that the balance of benefits and risks will be viewed differently by each patient."
Primary care delegates from the American Academy of Family Physicians and the American College of Physicians opposed the resolutions of concern against the USPSTF and the mammography report.
The AAFP supported the task force when it issued its mammography recommendations "because it was the most comprehensive pattern and set of preventive guidelines using current methodology with what was available in science at that time," said Dr. Roland Goertz, AAFP delegate.
The task force basically recommends what the AMA report urged: that physicians have discussions with their patients about risks and benefits, he said. The problem is not the USPSTF recommendations, but that they are being used to deny payment, he added.

Dr. Richard Reiling, a delegate from the American College of Surgeons, said that the task force had confused patients with its mammography recommendation, and called for the AMA to convene all interested parties to craft a single guideline. The USPSTF was "wrong in presenting this report without listening to the stakeholders in the past," he said, adding, "let’s get one guideline out there."
Dr. Goertz agreed that there needed to be a common guideline.
ACP Delegate Dr. William Golden expressed the ACP’s view that the House of Delegates was not the appropriate venue for voting on particular guidelines. "The House should not be in the position of voting on what guideline is best," he said.
CHICAGO – Delegates to the American Medical Association’s legislative body are not happy with the U.S. Preventive Services Task Force.
They voted overwhelmingly (322 to 93) to express "concern" over the task force’s recommendations on screening mammography and prostate-specific antigen screening. Both recommendations attracted a firestorm of criticism when they were issued – the mammography recommendation in 2009 and those on PSA testing in May.
Many delegates also said they thought that the USPSTF, a quasi-governmental group operating under the auspices of the Agency for Healthcare Research and Quality, had reached its decisions without proper input from specialty societies or experts in each field.
In a second resolution, the delegates voted to encourage the USPSTF to "implement procedures that allow for meaningful input on recommendation development from specialists and stakeholders in the topic area under study."
Dr. Arl Van Moore Jr., a delegate from the American College of Radiology, said that neither the ACR nor any prominent breast imaging or surgical societies were contacted by the USPSTF in creating the screening mammography recommendations.
"None of the recognized experts in the field were contacted, to the best of our knowledge," said Dr. Moore, an interventional radiologist in Charlotte, N.C.
The American Urological Association delegate, Dr. William Gee, did not mince words when it came to the PSA screening guidelines.
"The [USPSTF] did not use an open process and ignored the public in reaching their conclusions," he said.
But Dr. Sally J. Trippel, a preventive medicine specialist at the Mayo Clinic and delegate from Minnesota, defended the USPSTF and its process. The task force is "about as politically independent as any national organization can get," and "about as free of conflict of interest as is possible in any organization developing guidelines for American clinicians," she said.
She quoted from task force documents showing that urologists provided peer review of the PSA evidence review. "So there were experts from urology involved in the development of that guideline," and also for the one on screening mammography.
To further show its consternation with the task force, AMA delegates also approved a report that stated that starting at age 40, women should be "eligible for screening mammography," and encouraging physicians "to regularly discuss with their individual patients the benefits and risks of screening mammography, and whether screening is appropriate for each clinical situation given that the balance of benefits and risks will be viewed differently by each patient."
Primary care delegates from the American Academy of Family Physicians and the American College of Physicians opposed the resolutions of concern against the USPSTF and the mammography report.
The AAFP supported the task force when it issued its mammography recommendations "because it was the most comprehensive pattern and set of preventive guidelines using current methodology with what was available in science at that time," said Dr. Roland Goertz, AAFP delegate.
The task force basically recommends what the AMA report urged: that physicians have discussions with their patients about risks and benefits, he said. The problem is not the USPSTF recommendations, but that they are being used to deny payment, he added.
Dr. Richard Reiling, a delegate from the American College of Surgeons, said that the task force had confused patients with its mammography recommendation, and called for the AMA to convene all interested parties to craft a single guideline. The USPSTF was "wrong in presenting this report without listening to the stakeholders in the past," he said, adding, "let’s get one guideline out there."
Dr. Goertz agreed that there needed to be a common guideline.
ACP Delegate Dr. William Golden expressed the ACP’s view that the House of Delegates was not the appropriate venue for voting on particular guidelines. "The House should not be in the position of voting on what guideline is best," he said.
CHICAGO – Delegates to the American Medical Association’s legislative body are not happy with the U.S. Preventive Services Task Force.
They voted overwhelmingly (322 to 93) to express "concern" over the task force’s recommendations on screening mammography and prostate-specific antigen screening. Both recommendations attracted a firestorm of criticism when they were issued – the mammography recommendation in 2009 and those on PSA testing in May.
Many delegates also said they thought that the USPSTF, a quasi-governmental group operating under the auspices of the Agency for Healthcare Research and Quality, had reached its decisions without proper input from specialty societies or experts in each field.
In a second resolution, the delegates voted to encourage the USPSTF to "implement procedures that allow for meaningful input on recommendation development from specialists and stakeholders in the topic area under study."
Dr. Arl Van Moore Jr., a delegate from the American College of Radiology, said that neither the ACR nor any prominent breast imaging or surgical societies were contacted by the USPSTF in creating the screening mammography recommendations.
"None of the recognized experts in the field were contacted, to the best of our knowledge," said Dr. Moore, an interventional radiologist in Charlotte, N.C.
The American Urological Association delegate, Dr. William Gee, did not mince words when it came to the PSA screening guidelines.
"The [USPSTF] did not use an open process and ignored the public in reaching their conclusions," he said.
But Dr. Sally J. Trippel, a preventive medicine specialist at the Mayo Clinic and delegate from Minnesota, defended the USPSTF and its process. The task force is "about as politically independent as any national organization can get," and "about as free of conflict of interest as is possible in any organization developing guidelines for American clinicians," she said.
She quoted from task force documents showing that urologists provided peer review of the PSA evidence review. "So there were experts from urology involved in the development of that guideline," and also for the one on screening mammography.
To further show its consternation with the task force, AMA delegates also approved a report that stated that starting at age 40, women should be "eligible for screening mammography," and encouraging physicians "to regularly discuss with their individual patients the benefits and risks of screening mammography, and whether screening is appropriate for each clinical situation given that the balance of benefits and risks will be viewed differently by each patient."
Primary care delegates from the American Academy of Family Physicians and the American College of Physicians opposed the resolutions of concern against the USPSTF and the mammography report.
The AAFP supported the task force when it issued its mammography recommendations "because it was the most comprehensive pattern and set of preventive guidelines using current methodology with what was available in science at that time," said Dr. Roland Goertz, AAFP delegate.
The task force basically recommends what the AMA report urged: that physicians have discussions with their patients about risks and benefits, he said. The problem is not the USPSTF recommendations, but that they are being used to deny payment, he added.
Dr. Richard Reiling, a delegate from the American College of Surgeons, said that the task force had confused patients with its mammography recommendation, and called for the AMA to convene all interested parties to craft a single guideline. The USPSTF was "wrong in presenting this report without listening to the stakeholders in the past," he said, adding, "let’s get one guideline out there."
Dr. Goertz agreed that there needed to be a common guideline.
ACP Delegate Dr. William Golden expressed the ACP’s view that the House of Delegates was not the appropriate venue for voting on particular guidelines. "The House should not be in the position of voting on what guideline is best," he said.
AT THE ANNUAL MEETING OF THE AMERICAN MEDICAL ASSOCIATION'S HOUSE OF DELEGATES
Pancreatic Surgery Scorecard Aligns With IOM Quality Metrics
SAN DIEGO – A proposed quality measure for pancreatic surgery has the potential to assess performance more thoroughly than current volume and mortality measures, judging by surgeons’ responses to a recent survey.
The 12-item "Quality Scorecard," developed by Dr. Brian T. Kalish of Beth Israel Deaconess Medical Center, Boston, and a team of pancreatic surgeons from multiple academic medical centers, consists of actionable and meaningful measures. The scorecard is aligned with the Institute of Medicine’s health care quality domains: safety, timeliness, effectiveness, patient centeredness, efficiency, and equitability.
"Traditional quality metrics in high-acuity surgery on their own cannot measure or satisfy the [IOM] domains," Dr. Kalish explained in a plenary presentation at the annual Digestive Disease Week. "Our goal was to evaluate the need for broader quality metrics and whether such broader metrics would align to contemporary IOM domains."
"We expect the scorecard to reveal quality to an extent that volume and mortality alone cannot."
Toward this end, the development team worked with a professional market research firm to create a web-based survey and distribute it to expert pancreatic surgeons identified through specialty societies and verified by survey demographics, Dr. Kalish explained. "The survey asked respondents to rank [62] proposed quality metrics on level of importance, from essential to not important, and to align the metric to one or more of the [IOM] quality domains." Points were awarded for level of importance and multidomain alignment, and the two scores for a given quality metric were averaged to render a total quality score that was then normalized to a 100-point scale, he said.
The 21% survey response rate represented 106 surgeons primarily from academic medical centers in North America who perform an average of 43 pancreatic operations per year, said Dr. Kalish. The need for improved quality metrics was indicated by 90% of the respondents, while 81% believed that a "quality scorecard" in pancreatic surgery would probably or definitely be of value, he reported. More than one-third of the proposed metrics aligned to more than one IOM domain, and at least half of the respondents rated these as essential or very important, he said.
Of the 62 metrics, 12 emerged with the highest total quality score. In rank order, they are: multidisciplinary services for pancreatic diseases, major complication rate, perioperative mortality, overall complication rate, incidence of postoperative hemorrhage, venous thromboembolism prophylaxis, patients with malignancy who undergo adjuvant therapy, readmission rates (30 day, 90 day, total), incidence of postoperative pancreatic fistula, timely and appropriate perioperative antibiotics, survival rates (1 year and 5 year), and timing from diagnosis to surgical consultation.
"The metrics related to mortality, the rate and severity of complications, and access to multidisciplinary services for pancreatic disease had the highest total quality scores; technical and perioperative metrics had intermediate scores; and metrics related to patient satisfaction with care, costs of care, and patient demographics had the lowest total quality scores," Dr. Kalish observed. With respect to the IOM domains, "the least represented domains were equitability, efficiency, and patient-centeredness," he said.
Although the actual performance thresholds for each of the metrics require further definition and validation, "we expect the scorecard to reveal quality to an extent that volume and mortality alone cannot," Dr. Kalish stated, noting that the development process is ongoing.
Future efforts include the organization of patient focus groups and a formal survey of patients and family members to attain insight into which quality metrics are important to those receiving care, as well as a multicenter prospective validation.
Dr. Kalish reported having no relevant financial conflicts of interest.
SAN DIEGO – A proposed quality measure for pancreatic surgery has the potential to assess performance more thoroughly than current volume and mortality measures, judging by surgeons’ responses to a recent survey.
The 12-item "Quality Scorecard," developed by Dr. Brian T. Kalish of Beth Israel Deaconess Medical Center, Boston, and a team of pancreatic surgeons from multiple academic medical centers, consists of actionable and meaningful measures. The scorecard is aligned with the Institute of Medicine’s health care quality domains: safety, timeliness, effectiveness, patient centeredness, efficiency, and equitability.
"Traditional quality metrics in high-acuity surgery on their own cannot measure or satisfy the [IOM] domains," Dr. Kalish explained in a plenary presentation at the annual Digestive Disease Week. "Our goal was to evaluate the need for broader quality metrics and whether such broader metrics would align to contemporary IOM domains."
"We expect the scorecard to reveal quality to an extent that volume and mortality alone cannot."
Toward this end, the development team worked with a professional market research firm to create a web-based survey and distribute it to expert pancreatic surgeons identified through specialty societies and verified by survey demographics, Dr. Kalish explained. "The survey asked respondents to rank [62] proposed quality metrics on level of importance, from essential to not important, and to align the metric to one or more of the [IOM] quality domains." Points were awarded for level of importance and multidomain alignment, and the two scores for a given quality metric were averaged to render a total quality score that was then normalized to a 100-point scale, he said.
The 21% survey response rate represented 106 surgeons primarily from academic medical centers in North America who perform an average of 43 pancreatic operations per year, said Dr. Kalish. The need for improved quality metrics was indicated by 90% of the respondents, while 81% believed that a "quality scorecard" in pancreatic surgery would probably or definitely be of value, he reported. More than one-third of the proposed metrics aligned to more than one IOM domain, and at least half of the respondents rated these as essential or very important, he said.
Of the 62 metrics, 12 emerged with the highest total quality score. In rank order, they are: multidisciplinary services for pancreatic diseases, major complication rate, perioperative mortality, overall complication rate, incidence of postoperative hemorrhage, venous thromboembolism prophylaxis, patients with malignancy who undergo adjuvant therapy, readmission rates (30 day, 90 day, total), incidence of postoperative pancreatic fistula, timely and appropriate perioperative antibiotics, survival rates (1 year and 5 year), and timing from diagnosis to surgical consultation.
"The metrics related to mortality, the rate and severity of complications, and access to multidisciplinary services for pancreatic disease had the highest total quality scores; technical and perioperative metrics had intermediate scores; and metrics related to patient satisfaction with care, costs of care, and patient demographics had the lowest total quality scores," Dr. Kalish observed. With respect to the IOM domains, "the least represented domains were equitability, efficiency, and patient-centeredness," he said.
Although the actual performance thresholds for each of the metrics require further definition and validation, "we expect the scorecard to reveal quality to an extent that volume and mortality alone cannot," Dr. Kalish stated, noting that the development process is ongoing.
Future efforts include the organization of patient focus groups and a formal survey of patients and family members to attain insight into which quality metrics are important to those receiving care, as well as a multicenter prospective validation.
Dr. Kalish reported having no relevant financial conflicts of interest.
SAN DIEGO – A proposed quality measure for pancreatic surgery has the potential to assess performance more thoroughly than current volume and mortality measures, judging by surgeons’ responses to a recent survey.
The 12-item "Quality Scorecard," developed by Dr. Brian T. Kalish of Beth Israel Deaconess Medical Center, Boston, and a team of pancreatic surgeons from multiple academic medical centers, consists of actionable and meaningful measures. The scorecard is aligned with the Institute of Medicine’s health care quality domains: safety, timeliness, effectiveness, patient centeredness, efficiency, and equitability.
"Traditional quality metrics in high-acuity surgery on their own cannot measure or satisfy the [IOM] domains," Dr. Kalish explained in a plenary presentation at the annual Digestive Disease Week. "Our goal was to evaluate the need for broader quality metrics and whether such broader metrics would align to contemporary IOM domains."
"We expect the scorecard to reveal quality to an extent that volume and mortality alone cannot."
Toward this end, the development team worked with a professional market research firm to create a web-based survey and distribute it to expert pancreatic surgeons identified through specialty societies and verified by survey demographics, Dr. Kalish explained. "The survey asked respondents to rank [62] proposed quality metrics on level of importance, from essential to not important, and to align the metric to one or more of the [IOM] quality domains." Points were awarded for level of importance and multidomain alignment, and the two scores for a given quality metric were averaged to render a total quality score that was then normalized to a 100-point scale, he said.
The 21% survey response rate represented 106 surgeons primarily from academic medical centers in North America who perform an average of 43 pancreatic operations per year, said Dr. Kalish. The need for improved quality metrics was indicated by 90% of the respondents, while 81% believed that a "quality scorecard" in pancreatic surgery would probably or definitely be of value, he reported. More than one-third of the proposed metrics aligned to more than one IOM domain, and at least half of the respondents rated these as essential or very important, he said.
Of the 62 metrics, 12 emerged with the highest total quality score. In rank order, they are: multidisciplinary services for pancreatic diseases, major complication rate, perioperative mortality, overall complication rate, incidence of postoperative hemorrhage, venous thromboembolism prophylaxis, patients with malignancy who undergo adjuvant therapy, readmission rates (30 day, 90 day, total), incidence of postoperative pancreatic fistula, timely and appropriate perioperative antibiotics, survival rates (1 year and 5 year), and timing from diagnosis to surgical consultation.
"The metrics related to mortality, the rate and severity of complications, and access to multidisciplinary services for pancreatic disease had the highest total quality scores; technical and perioperative metrics had intermediate scores; and metrics related to patient satisfaction with care, costs of care, and patient demographics had the lowest total quality scores," Dr. Kalish observed. With respect to the IOM domains, "the least represented domains were equitability, efficiency, and patient-centeredness," he said.
Although the actual performance thresholds for each of the metrics require further definition and validation, "we expect the scorecard to reveal quality to an extent that volume and mortality alone cannot," Dr. Kalish stated, noting that the development process is ongoing.
Future efforts include the organization of patient focus groups and a formal survey of patients and family members to attain insight into which quality metrics are important to those receiving care, as well as a multicenter prospective validation.
Dr. Kalish reported having no relevant financial conflicts of interest.
AT THE ANNUAL DIGESTIVE DISEASE WEEK
Ventral Hernia Repair Incurs Overall Financial Losses
SAN DIEGO – Ventral hernia repair is associated with overall financial losses reaching the thousands of dollars in some cases, a single-center study demonstrated.
"These financial losses are just simply not sustainable," Dr. Drew Reynolds said in an interview prior to the annual Digestive Disease Week, where the study was presented.
In what is believed to be the first study of its kind, he and his associates set out to systematically evaluate hospital finances with respect to open ventral incisional hernia repair in the tertiary care environment.

"There is limited cost data currently available in the literature," he said. "These patients are complex and often require management in tertiary referral centers. Biologic meshes have a legitimate role in certain clinical scenarios, especially in those encountered in the tertiary care environment. Reimbursement strategies need to be reevaluated with more appropriate adjustment for preoperative risk factors and operative complexity."
Hospital costs associated with complex hernia repairs include direct costs (mesh materials, supplies, and non–surgeon labor), and indirect costs (facility fees, equipment depreciation, and unallocated labor), said Dr. Reynolds, a fellow in minimally invasive surgery at the University of Kentucky, Lexington. "Operative supplies including mesh represent a significant component of direct costs, especially in an era of proprietary synthetic meshes and biologic grafts," the researchers wrote in their abstract.
Dr. Reynolds and his associates evaluated cost data on 415 consecutive open ventral hernia repairs performed at the university’s hospital between July 1, 2008, and May 31, 2011, using CPT codes 49560, 49561, 49565, and 49566. They analyzed data based on hospital status (inpatient vs. outpatient) and whether the hernia repair was a primary or secondary procedure. The primary end points were hospital revenue and costs. Revenue calculations were adjusted for comorbid conditions/diagnosis-related groups, and readmission costs were not included.
Of the 415 patients, 353 were inpatients and 62 were outpatients. Among the 353 inpatients, ventral hernia repair was the primary procedure performed on 173 patients and was the secondary procedure for 180 patients. The median net revenue was significantly greater for those who underwent hernia repair as a secondary procedure compared with those who had hernia repair as a primary procedure ($17,310 vs. $10,360, P less than .01), as were net losses ($3,340 vs. $1,700, P less than .01).
Among the inpatient primary ventral hernia repairs, 46 were repaired without mesh, 79 were repaired with synthetic mesh, and 48 were repaired with biologic mesh, for median direct costs of $5,432, $7,590, and $16,970, respectively (P less than .01).
Dr. Reynolds also reported that among all inpatient ventral hernia repairs, the median net losses for repairs without mesh were $500, while synthetic mesh–based repairs yielded a median net profit of $60. The median contribution margin for cases involving biologic mesh was –$4,560, and the median net financial loss was $8,370.
Among patients who underwent outpatient ventral hernia repairs, median net losses among those performed with and without synthetic mesh reached $1,560 and $230, respectively.
"It was surprising to note that the vast majority of open ventral incisional hernia repairs are performed at an overall financial loss for the hospital," Dr. Reynolds said. "Further, it was surprising to note that inpatient biologic mesh–based ventral hernia repairs resulted in such a sizable negative median contribution margin ($4,560), and the striking median net financial loss of $8,370."
He acknowledged certain limitations of the study, including the fact that data used in the analysis were retrieved by CPT code search. "Hospital readmission costs were not included, which leads to underestimation of the costs," he added.
Dr. Reynolds said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Ventral hernia repair is associated with overall financial losses reaching the thousands of dollars in some cases, a single-center study demonstrated.
"These financial losses are just simply not sustainable," Dr. Drew Reynolds said in an interview prior to the annual Digestive Disease Week, where the study was presented.
In what is believed to be the first study of its kind, he and his associates set out to systematically evaluate hospital finances with respect to open ventral incisional hernia repair in the tertiary care environment.
"There is limited cost data currently available in the literature," he said. "These patients are complex and often require management in tertiary referral centers. Biologic meshes have a legitimate role in certain clinical scenarios, especially in those encountered in the tertiary care environment. Reimbursement strategies need to be reevaluated with more appropriate adjustment for preoperative risk factors and operative complexity."
Hospital costs associated with complex hernia repairs include direct costs (mesh materials, supplies, and non–surgeon labor), and indirect costs (facility fees, equipment depreciation, and unallocated labor), said Dr. Reynolds, a fellow in minimally invasive surgery at the University of Kentucky, Lexington. "Operative supplies including mesh represent a significant component of direct costs, especially in an era of proprietary synthetic meshes and biologic grafts," the researchers wrote in their abstract.
Dr. Reynolds and his associates evaluated cost data on 415 consecutive open ventral hernia repairs performed at the university’s hospital between July 1, 2008, and May 31, 2011, using CPT codes 49560, 49561, 49565, and 49566. They analyzed data based on hospital status (inpatient vs. outpatient) and whether the hernia repair was a primary or secondary procedure. The primary end points were hospital revenue and costs. Revenue calculations were adjusted for comorbid conditions/diagnosis-related groups, and readmission costs were not included.
Of the 415 patients, 353 were inpatients and 62 were outpatients. Among the 353 inpatients, ventral hernia repair was the primary procedure performed on 173 patients and was the secondary procedure for 180 patients. The median net revenue was significantly greater for those who underwent hernia repair as a secondary procedure compared with those who had hernia repair as a primary procedure ($17,310 vs. $10,360, P less than .01), as were net losses ($3,340 vs. $1,700, P less than .01).
Among the inpatient primary ventral hernia repairs, 46 were repaired without mesh, 79 were repaired with synthetic mesh, and 48 were repaired with biologic mesh, for median direct costs of $5,432, $7,590, and $16,970, respectively (P less than .01).
Dr. Reynolds also reported that among all inpatient ventral hernia repairs, the median net losses for repairs without mesh were $500, while synthetic mesh–based repairs yielded a median net profit of $60. The median contribution margin for cases involving biologic mesh was –$4,560, and the median net financial loss was $8,370.
Among patients who underwent outpatient ventral hernia repairs, median net losses among those performed with and without synthetic mesh reached $1,560 and $230, respectively.
"It was surprising to note that the vast majority of open ventral incisional hernia repairs are performed at an overall financial loss for the hospital," Dr. Reynolds said. "Further, it was surprising to note that inpatient biologic mesh–based ventral hernia repairs resulted in such a sizable negative median contribution margin ($4,560), and the striking median net financial loss of $8,370."
He acknowledged certain limitations of the study, including the fact that data used in the analysis were retrieved by CPT code search. "Hospital readmission costs were not included, which leads to underestimation of the costs," he added.
Dr. Reynolds said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Ventral hernia repair is associated with overall financial losses reaching the thousands of dollars in some cases, a single-center study demonstrated.
"These financial losses are just simply not sustainable," Dr. Drew Reynolds said in an interview prior to the annual Digestive Disease Week, where the study was presented.
In what is believed to be the first study of its kind, he and his associates set out to systematically evaluate hospital finances with respect to open ventral incisional hernia repair in the tertiary care environment.
"There is limited cost data currently available in the literature," he said. "These patients are complex and often require management in tertiary referral centers. Biologic meshes have a legitimate role in certain clinical scenarios, especially in those encountered in the tertiary care environment. Reimbursement strategies need to be reevaluated with more appropriate adjustment for preoperative risk factors and operative complexity."
Hospital costs associated with complex hernia repairs include direct costs (mesh materials, supplies, and non–surgeon labor), and indirect costs (facility fees, equipment depreciation, and unallocated labor), said Dr. Reynolds, a fellow in minimally invasive surgery at the University of Kentucky, Lexington. "Operative supplies including mesh represent a significant component of direct costs, especially in an era of proprietary synthetic meshes and biologic grafts," the researchers wrote in their abstract.
Dr. Reynolds and his associates evaluated cost data on 415 consecutive open ventral hernia repairs performed at the university’s hospital between July 1, 2008, and May 31, 2011, using CPT codes 49560, 49561, 49565, and 49566. They analyzed data based on hospital status (inpatient vs. outpatient) and whether the hernia repair was a primary or secondary procedure. The primary end points were hospital revenue and costs. Revenue calculations were adjusted for comorbid conditions/diagnosis-related groups, and readmission costs were not included.
Of the 415 patients, 353 were inpatients and 62 were outpatients. Among the 353 inpatients, ventral hernia repair was the primary procedure performed on 173 patients and was the secondary procedure for 180 patients. The median net revenue was significantly greater for those who underwent hernia repair as a secondary procedure compared with those who had hernia repair as a primary procedure ($17,310 vs. $10,360, P less than .01), as were net losses ($3,340 vs. $1,700, P less than .01).
Among the inpatient primary ventral hernia repairs, 46 were repaired without mesh, 79 were repaired with synthetic mesh, and 48 were repaired with biologic mesh, for median direct costs of $5,432, $7,590, and $16,970, respectively (P less than .01).
Dr. Reynolds also reported that among all inpatient ventral hernia repairs, the median net losses for repairs without mesh were $500, while synthetic mesh–based repairs yielded a median net profit of $60. The median contribution margin for cases involving biologic mesh was –$4,560, and the median net financial loss was $8,370.
Among patients who underwent outpatient ventral hernia repairs, median net losses among those performed with and without synthetic mesh reached $1,560 and $230, respectively.
"It was surprising to note that the vast majority of open ventral incisional hernia repairs are performed at an overall financial loss for the hospital," Dr. Reynolds said. "Further, it was surprising to note that inpatient biologic mesh–based ventral hernia repairs resulted in such a sizable negative median contribution margin ($4,560), and the striking median net financial loss of $8,370."
He acknowledged certain limitations of the study, including the fact that data used in the analysis were retrieved by CPT code search. "Hospital readmission costs were not included, which leads to underestimation of the costs," he added.
Dr. Reynolds said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL DIGESTIVE DISEASE WEEK