User login
Data Reveal Poor Outcomes With Delayed Cholecystectomy
ESTES PARK, COLO. – Patients hospitalized for prolonged biliary colic cholecystitis should be medically stabilized and then undergo cholecystectomy during the same admission, Dr. David Tanaka advised at a conference on internal medicine sponsored by the University of Colorado.
"I think that’s one of the big changes in the way we do things now. There’s really no benefit to cooling them off and sending them home and having them see the surgeon later. In fact, their outcomes are worse if you do that," according to Dr. Tanaka, a general internist at the university.

A major influence on this change in thinking was a meta-analysis involving five randomized clinical trials of early versus delayed laparoscopic cholecystectomy, with the delayed procedures being performed 6-12 weeks after symptoms settled. The analysis included 451 randomized patients with cholecystitis.
The incidence of bile duct injury was 36% lower and the conversion rate to open cholecystectomy was 12% lower in the early-surgery group, although neither of these differences achieved statistical significance.
However, the early-surgery group also averaged a mean 4.12-day shorter total hospital stay than did patients undergoing late cholecystectomy, and that difference was highly significant. Also, 17.5% of patients randomized to delayed laparoscopic surgery wound up undergoing emergency surgery as a consequence of incomplete resolution or recurrence of their cholecystitis during the waiting period. Fully 45% of these emergency laparoscopic cholecystectomies required conversion to open procedures (Br. J. Surg. 2010;97:141-50).
Ten to 15% of adults in Western countries have gallstones, and each year 1%-4% of these individuals become symptomatic. In the United States, historically only about 30% of patients with acute cholecystitis have undergone cholecystectomy during the acute episode.
It’s particularly important that patients admitted with gallstone pancreatitis undergo cholecystectomy prior to discharge. Otherwise they are at risk for frequent recurrences, Dr. Tanaka noted. Surgeons won’t want to operate on them when they have pancreatitis, though, so it’s necessary to treat that condition first. Preoperative endoscopic retrograde cholangiopancreatography is not indicated in all patients with gallstone pancreatitis, but it has been shown to be beneficial in those with persistent obstructive jaundice and/or biliary sepsis, he continued.
Most patients with gallbladder and common bile duct stones undergo preoperative endoscopic sphincterotomy followed by laparoscopic cholecystectomy. However, a recent meta-analysis demonstrated that intraoperative endoscopic sphincterotomy carried out during laparoscopic cholecystectomy is just as safe and effective as preoperative endoscopic sphincterotomy. And in this meta-analysis involving four randomized trials with 532 patients, intraoperative endoscopic sphincterotomy was associated with a mean 3-day shorter hospital stay (Br. J. Surg. 2011;98:908-16).
"So if you can get your gastroenterologist to coordinate with the surgeons to do it at the time of surgery, you’re probably going to save some hospital days," Dr. Tanaka said.
He reported having no financial conflicts.
ESTES PARK, COLO. – Patients hospitalized for prolonged biliary colic cholecystitis should be medically stabilized and then undergo cholecystectomy during the same admission, Dr. David Tanaka advised at a conference on internal medicine sponsored by the University of Colorado.
"I think that’s one of the big changes in the way we do things now. There’s really no benefit to cooling them off and sending them home and having them see the surgeon later. In fact, their outcomes are worse if you do that," according to Dr. Tanaka, a general internist at the university.
A major influence on this change in thinking was a meta-analysis involving five randomized clinical trials of early versus delayed laparoscopic cholecystectomy, with the delayed procedures being performed 6-12 weeks after symptoms settled. The analysis included 451 randomized patients with cholecystitis.
The incidence of bile duct injury was 36% lower and the conversion rate to open cholecystectomy was 12% lower in the early-surgery group, although neither of these differences achieved statistical significance.
However, the early-surgery group also averaged a mean 4.12-day shorter total hospital stay than did patients undergoing late cholecystectomy, and that difference was highly significant. Also, 17.5% of patients randomized to delayed laparoscopic surgery wound up undergoing emergency surgery as a consequence of incomplete resolution or recurrence of their cholecystitis during the waiting period. Fully 45% of these emergency laparoscopic cholecystectomies required conversion to open procedures (Br. J. Surg. 2010;97:141-50).
Ten to 15% of adults in Western countries have gallstones, and each year 1%-4% of these individuals become symptomatic. In the United States, historically only about 30% of patients with acute cholecystitis have undergone cholecystectomy during the acute episode.
It’s particularly important that patients admitted with gallstone pancreatitis undergo cholecystectomy prior to discharge. Otherwise they are at risk for frequent recurrences, Dr. Tanaka noted. Surgeons won’t want to operate on them when they have pancreatitis, though, so it’s necessary to treat that condition first. Preoperative endoscopic retrograde cholangiopancreatography is not indicated in all patients with gallstone pancreatitis, but it has been shown to be beneficial in those with persistent obstructive jaundice and/or biliary sepsis, he continued.
Most patients with gallbladder and common bile duct stones undergo preoperative endoscopic sphincterotomy followed by laparoscopic cholecystectomy. However, a recent meta-analysis demonstrated that intraoperative endoscopic sphincterotomy carried out during laparoscopic cholecystectomy is just as safe and effective as preoperative endoscopic sphincterotomy. And in this meta-analysis involving four randomized trials with 532 patients, intraoperative endoscopic sphincterotomy was associated with a mean 3-day shorter hospital stay (Br. J. Surg. 2011;98:908-16).
"So if you can get your gastroenterologist to coordinate with the surgeons to do it at the time of surgery, you’re probably going to save some hospital days," Dr. Tanaka said.
He reported having no financial conflicts.
ESTES PARK, COLO. – Patients hospitalized for prolonged biliary colic cholecystitis should be medically stabilized and then undergo cholecystectomy during the same admission, Dr. David Tanaka advised at a conference on internal medicine sponsored by the University of Colorado.
"I think that’s one of the big changes in the way we do things now. There’s really no benefit to cooling them off and sending them home and having them see the surgeon later. In fact, their outcomes are worse if you do that," according to Dr. Tanaka, a general internist at the university.
A major influence on this change in thinking was a meta-analysis involving five randomized clinical trials of early versus delayed laparoscopic cholecystectomy, with the delayed procedures being performed 6-12 weeks after symptoms settled. The analysis included 451 randomized patients with cholecystitis.
The incidence of bile duct injury was 36% lower and the conversion rate to open cholecystectomy was 12% lower in the early-surgery group, although neither of these differences achieved statistical significance.
However, the early-surgery group also averaged a mean 4.12-day shorter total hospital stay than did patients undergoing late cholecystectomy, and that difference was highly significant. Also, 17.5% of patients randomized to delayed laparoscopic surgery wound up undergoing emergency surgery as a consequence of incomplete resolution or recurrence of their cholecystitis during the waiting period. Fully 45% of these emergency laparoscopic cholecystectomies required conversion to open procedures (Br. J. Surg. 2010;97:141-50).
Ten to 15% of adults in Western countries have gallstones, and each year 1%-4% of these individuals become symptomatic. In the United States, historically only about 30% of patients with acute cholecystitis have undergone cholecystectomy during the acute episode.
It’s particularly important that patients admitted with gallstone pancreatitis undergo cholecystectomy prior to discharge. Otherwise they are at risk for frequent recurrences, Dr. Tanaka noted. Surgeons won’t want to operate on them when they have pancreatitis, though, so it’s necessary to treat that condition first. Preoperative endoscopic retrograde cholangiopancreatography is not indicated in all patients with gallstone pancreatitis, but it has been shown to be beneficial in those with persistent obstructive jaundice and/or biliary sepsis, he continued.
Most patients with gallbladder and common bile duct stones undergo preoperative endoscopic sphincterotomy followed by laparoscopic cholecystectomy. However, a recent meta-analysis demonstrated that intraoperative endoscopic sphincterotomy carried out during laparoscopic cholecystectomy is just as safe and effective as preoperative endoscopic sphincterotomy. And in this meta-analysis involving four randomized trials with 532 patients, intraoperative endoscopic sphincterotomy was associated with a mean 3-day shorter hospital stay (Br. J. Surg. 2011;98:908-16).
"So if you can get your gastroenterologist to coordinate with the surgeons to do it at the time of surgery, you’re probably going to save some hospital days," Dr. Tanaka said.
He reported having no financial conflicts.
EXPERT ANALYSIS FROM A CONFERENCE ON INTERNAL MEDICINE SPONSORED BY THE UNIVERSITY OF COLORADO

Bariatric Surgery Prevents Type 2 Diabetes
Bariatric surgery reduced the incidence of type 2 diabetes by 78% compared with usual care at 15 years in a prospective, case-matched study of more than 3,000 obese adults.
This significant risk reduction was seen with all types of bariatric surgery and regardless of baseline body mass index. And, it occurred despite the fact that the matching process unexpectedly resulted in the bariatric surgery group having a higher mean body weight and more severe risk factors at baseline than the controls.
The impact of bariatric surgery was even greater, with an 87% risk reduction, for those with impaired fasting glucose at baseline, said Dr. Lena M.S. Carlsson of the Sahlgrenska Academy at the University of Gothenburg, Sweden, and her associates (N. Engl. J. Med. 2012;367:695-704).

"Our data indicate that bariatric surgery has a preventive effect on incident type 2 diabetes, particularly in participants with impaired fasting glucose. In contrast, baseline BMI did not influence the preventive effect of bariatric surgery on type 2 diabetes, implying that anthropometric data are not useful in the selection of candidates for bariatric surgery, whereas data on impaired fasting glucose may be helpful," the authors wrote.
The finding comes from the Swedish Obese Subjects (SOS) trial, which included 1,658 patients who chose to undergo bariatric surgery and 1,771 matched controls. All patients in both groups entered the study with the intention of losing weight. None had diabetes at baseline.
In the bariatric surgery group, the types of procedures were banding in 311, vertical banded gastroplasty in 1,140, and gastric bypass in 207. Patients in the control group received the customary treatment for obesity at their primary health care centers, which in Sweden ranges from advanced lifestyle modification – including recommendations regarding eating behavior, food selection, energy intake, and physical activity – to no treatment. About half (54%) of the controls reported receiving professional guidance in attempts to lose weight.
There were several significant differences between groups at baseline. The bariatric surgery group weighed an average of 6 kg more than did the controls, and had a greater mean BMI (42.4 vs. 40.2 kg/m2). They also had higher mean blood pressures and total cholesterol and triglyceride levels, and were more likely to smoke and to be less active.
After adjustment for follow-up of less than 15 years and for death, the 15-year participation rate was 54%. At 15 years, the bariatric surgery group had lost 31 kg after 1 year, but then regained weight, so the average loss at 10 and 15 years was about 20 kg. The control group never lost or gained more than 3 kg over the entire study period, regardless of whether they had professional help.
During the follow-up, type 2 diabetes developed in 110 of the bariatric surgery patients and in 392 controls, corresponding to incidence rates of 6.8 and 28.4 cases per 1,000 person-years, respectively (P less than .001). The unadjusted hazard ratio was 0.22, which dropped to 0.17 following multivariate adjustments. Aside from treatment group, other strong univariate predictors of diabetes outcome were baseline blood glucose and the presence or absence of impaired fasting glucose, Dr. Carlsson and her associates reported.
In a sensitivity analysis performed to account for the low participation rate, the impact of treatment on the incidence of type 2 diabetes was at least as strong after 2 years and 10 years of follow-up as after 15 years. All types of bariatric surgery were associated with a reduced incidence of diabetes, with no significant differences among them. There were also no differences by receipt of professional weight-loss assistance, or by BMI at baseline, the investigators noted.
A total of 3 patients (0.2%) died within 90 days of surgery, and 245 patients in the surgery group (15%) reported at least one complication. Of those, 46 (2.8%) were serious enough to require a reoperation.
The risk reduction seen among those with impaired fasting glucose was at least twice as large as the risk reduction achieved with lifestyle interventions in large, long-term trials of moderately obese people with prediabetes (Lancet 2006;368:1673-9, Lancet 2009;374:1677-86, and Lancet 2008;371:1783-9), the investigators noted.
The ongoing SOS study is supported by grants from the Swedish Research Council, the Swedish Foundation for Strategic Research to the Sahlgrenska Center for Cardiovascular and Metabolic Research, the Swedish federal government, the VINNOVA-VINNMER program, and the Wenner-Gren Foundations. The SOS study has previously been supported by grants to one of the authors from Hoffmann-La Roche, AstraZeneca, and other companies. Dr. Carlsson reported receiving consulting fees from AstraZeneca and owning stock in Sahltech. Other coinvestigators also had financial disclosures.
The long-term findings of the SOS study are both provocative and exciting, especially the findings suggesting that bariatric surgery may prevent the conversion of abnormalities in glucose metabolism to frank diabetes.
The findings of previous studies, showing that bariatric surgery can have a prolonged, positive effect on blood sugar beyond that attainable with medication, have led to speculation about whether surgery might be considered earlier in the course of disease in patients with adult-onset diabetes.
However, it remains impractical and unjustified to contemplate the performance of bariatric surgery in the millions of eligible obese adults. And to be certain, the authors do not suggest such an approach. Rather, the current study should provide an impetus to develop a more complete understanding of the mechanisms by which the various bariatric procedures exert their beneficial effects. Such understanding will be important because it will enable the identification of individuals who are the most appropriate candidates for surgery.
The cause of type 2 diabetes is multifactorial, and this long-term study shows that surgery did not prevent the development of diabetes in all patients. Furthermore, it is possible that interventions that are even less invasive may accomplish the very desirable goal of decreasing the incidence of type 2 diabetes and its attendant complications.
Danny O. Jacobs, M.D., is chair of surgery at the Duke University School of Medicine, Durham, N.C. These remarks were taken from his editorial accompanying Dr. Carlson’s report (N. Engl. J. Med. 2012;367:764-5). Dr. Jacobs has consulting, research, and/or educational services working relationships with Ethicon, Surgisphere, and other companies.
The long-term findings of the SOS study are both provocative and exciting, especially the findings suggesting that bariatric surgery may prevent the conversion of abnormalities in glucose metabolism to frank diabetes.
The findings of previous studies, showing that bariatric surgery can have a prolonged, positive effect on blood sugar beyond that attainable with medication, have led to speculation about whether surgery might be considered earlier in the course of disease in patients with adult-onset diabetes.
However, it remains impractical and unjustified to contemplate the performance of bariatric surgery in the millions of eligible obese adults. And to be certain, the authors do not suggest such an approach. Rather, the current study should provide an impetus to develop a more complete understanding of the mechanisms by which the various bariatric procedures exert their beneficial effects. Such understanding will be important because it will enable the identification of individuals who are the most appropriate candidates for surgery.
The cause of type 2 diabetes is multifactorial, and this long-term study shows that surgery did not prevent the development of diabetes in all patients. Furthermore, it is possible that interventions that are even less invasive may accomplish the very desirable goal of decreasing the incidence of type 2 diabetes and its attendant complications.
Danny O. Jacobs, M.D., is chair of surgery at the Duke University School of Medicine, Durham, N.C. These remarks were taken from his editorial accompanying Dr. Carlson’s report (N. Engl. J. Med. 2012;367:764-5). Dr. Jacobs has consulting, research, and/or educational services working relationships with Ethicon, Surgisphere, and other companies.
The long-term findings of the SOS study are both provocative and exciting, especially the findings suggesting that bariatric surgery may prevent the conversion of abnormalities in glucose metabolism to frank diabetes.
The findings of previous studies, showing that bariatric surgery can have a prolonged, positive effect on blood sugar beyond that attainable with medication, have led to speculation about whether surgery might be considered earlier in the course of disease in patients with adult-onset diabetes.
However, it remains impractical and unjustified to contemplate the performance of bariatric surgery in the millions of eligible obese adults. And to be certain, the authors do not suggest such an approach. Rather, the current study should provide an impetus to develop a more complete understanding of the mechanisms by which the various bariatric procedures exert their beneficial effects. Such understanding will be important because it will enable the identification of individuals who are the most appropriate candidates for surgery.
The cause of type 2 diabetes is multifactorial, and this long-term study shows that surgery did not prevent the development of diabetes in all patients. Furthermore, it is possible that interventions that are even less invasive may accomplish the very desirable goal of decreasing the incidence of type 2 diabetes and its attendant complications.
Danny O. Jacobs, M.D., is chair of surgery at the Duke University School of Medicine, Durham, N.C. These remarks were taken from his editorial accompanying Dr. Carlson’s report (N. Engl. J. Med. 2012;367:764-5). Dr. Jacobs has consulting, research, and/or educational services working relationships with Ethicon, Surgisphere, and other companies.
Bariatric surgery reduced the incidence of type 2 diabetes by 78% compared with usual care at 15 years in a prospective, case-matched study of more than 3,000 obese adults.
This significant risk reduction was seen with all types of bariatric surgery and regardless of baseline body mass index. And, it occurred despite the fact that the matching process unexpectedly resulted in the bariatric surgery group having a higher mean body weight and more severe risk factors at baseline than the controls.
The impact of bariatric surgery was even greater, with an 87% risk reduction, for those with impaired fasting glucose at baseline, said Dr. Lena M.S. Carlsson of the Sahlgrenska Academy at the University of Gothenburg, Sweden, and her associates (N. Engl. J. Med. 2012;367:695-704).
"Our data indicate that bariatric surgery has a preventive effect on incident type 2 diabetes, particularly in participants with impaired fasting glucose. In contrast, baseline BMI did not influence the preventive effect of bariatric surgery on type 2 diabetes, implying that anthropometric data are not useful in the selection of candidates for bariatric surgery, whereas data on impaired fasting glucose may be helpful," the authors wrote.
The finding comes from the Swedish Obese Subjects (SOS) trial, which included 1,658 patients who chose to undergo bariatric surgery and 1,771 matched controls. All patients in both groups entered the study with the intention of losing weight. None had diabetes at baseline.
In the bariatric surgery group, the types of procedures were banding in 311, vertical banded gastroplasty in 1,140, and gastric bypass in 207. Patients in the control group received the customary treatment for obesity at their primary health care centers, which in Sweden ranges from advanced lifestyle modification – including recommendations regarding eating behavior, food selection, energy intake, and physical activity – to no treatment. About half (54%) of the controls reported receiving professional guidance in attempts to lose weight.
There were several significant differences between groups at baseline. The bariatric surgery group weighed an average of 6 kg more than did the controls, and had a greater mean BMI (42.4 vs. 40.2 kg/m2). They also had higher mean blood pressures and total cholesterol and triglyceride levels, and were more likely to smoke and to be less active.
After adjustment for follow-up of less than 15 years and for death, the 15-year participation rate was 54%. At 15 years, the bariatric surgery group had lost 31 kg after 1 year, but then regained weight, so the average loss at 10 and 15 years was about 20 kg. The control group never lost or gained more than 3 kg over the entire study period, regardless of whether they had professional help.
During the follow-up, type 2 diabetes developed in 110 of the bariatric surgery patients and in 392 controls, corresponding to incidence rates of 6.8 and 28.4 cases per 1,000 person-years, respectively (P less than .001). The unadjusted hazard ratio was 0.22, which dropped to 0.17 following multivariate adjustments. Aside from treatment group, other strong univariate predictors of diabetes outcome were baseline blood glucose and the presence or absence of impaired fasting glucose, Dr. Carlsson and her associates reported.
In a sensitivity analysis performed to account for the low participation rate, the impact of treatment on the incidence of type 2 diabetes was at least as strong after 2 years and 10 years of follow-up as after 15 years. All types of bariatric surgery were associated with a reduced incidence of diabetes, with no significant differences among them. There were also no differences by receipt of professional weight-loss assistance, or by BMI at baseline, the investigators noted.
A total of 3 patients (0.2%) died within 90 days of surgery, and 245 patients in the surgery group (15%) reported at least one complication. Of those, 46 (2.8%) were serious enough to require a reoperation.
The risk reduction seen among those with impaired fasting glucose was at least twice as large as the risk reduction achieved with lifestyle interventions in large, long-term trials of moderately obese people with prediabetes (Lancet 2006;368:1673-9, Lancet 2009;374:1677-86, and Lancet 2008;371:1783-9), the investigators noted.
The ongoing SOS study is supported by grants from the Swedish Research Council, the Swedish Foundation for Strategic Research to the Sahlgrenska Center for Cardiovascular and Metabolic Research, the Swedish federal government, the VINNOVA-VINNMER program, and the Wenner-Gren Foundations. The SOS study has previously been supported by grants to one of the authors from Hoffmann-La Roche, AstraZeneca, and other companies. Dr. Carlsson reported receiving consulting fees from AstraZeneca and owning stock in Sahltech. Other coinvestigators also had financial disclosures.
Bariatric surgery reduced the incidence of type 2 diabetes by 78% compared with usual care at 15 years in a prospective, case-matched study of more than 3,000 obese adults.
This significant risk reduction was seen with all types of bariatric surgery and regardless of baseline body mass index. And, it occurred despite the fact that the matching process unexpectedly resulted in the bariatric surgery group having a higher mean body weight and more severe risk factors at baseline than the controls.
The impact of bariatric surgery was even greater, with an 87% risk reduction, for those with impaired fasting glucose at baseline, said Dr. Lena M.S. Carlsson of the Sahlgrenska Academy at the University of Gothenburg, Sweden, and her associates (N. Engl. J. Med. 2012;367:695-704).
"Our data indicate that bariatric surgery has a preventive effect on incident type 2 diabetes, particularly in participants with impaired fasting glucose. In contrast, baseline BMI did not influence the preventive effect of bariatric surgery on type 2 diabetes, implying that anthropometric data are not useful in the selection of candidates for bariatric surgery, whereas data on impaired fasting glucose may be helpful," the authors wrote.
The finding comes from the Swedish Obese Subjects (SOS) trial, which included 1,658 patients who chose to undergo bariatric surgery and 1,771 matched controls. All patients in both groups entered the study with the intention of losing weight. None had diabetes at baseline.
In the bariatric surgery group, the types of procedures were banding in 311, vertical banded gastroplasty in 1,140, and gastric bypass in 207. Patients in the control group received the customary treatment for obesity at their primary health care centers, which in Sweden ranges from advanced lifestyle modification – including recommendations regarding eating behavior, food selection, energy intake, and physical activity – to no treatment. About half (54%) of the controls reported receiving professional guidance in attempts to lose weight.
There were several significant differences between groups at baseline. The bariatric surgery group weighed an average of 6 kg more than did the controls, and had a greater mean BMI (42.4 vs. 40.2 kg/m2). They also had higher mean blood pressures and total cholesterol and triglyceride levels, and were more likely to smoke and to be less active.
After adjustment for follow-up of less than 15 years and for death, the 15-year participation rate was 54%. At 15 years, the bariatric surgery group had lost 31 kg after 1 year, but then regained weight, so the average loss at 10 and 15 years was about 20 kg. The control group never lost or gained more than 3 kg over the entire study period, regardless of whether they had professional help.
During the follow-up, type 2 diabetes developed in 110 of the bariatric surgery patients and in 392 controls, corresponding to incidence rates of 6.8 and 28.4 cases per 1,000 person-years, respectively (P less than .001). The unadjusted hazard ratio was 0.22, which dropped to 0.17 following multivariate adjustments. Aside from treatment group, other strong univariate predictors of diabetes outcome were baseline blood glucose and the presence or absence of impaired fasting glucose, Dr. Carlsson and her associates reported.
In a sensitivity analysis performed to account for the low participation rate, the impact of treatment on the incidence of type 2 diabetes was at least as strong after 2 years and 10 years of follow-up as after 15 years. All types of bariatric surgery were associated with a reduced incidence of diabetes, with no significant differences among them. There were also no differences by receipt of professional weight-loss assistance, or by BMI at baseline, the investigators noted.
A total of 3 patients (0.2%) died within 90 days of surgery, and 245 patients in the surgery group (15%) reported at least one complication. Of those, 46 (2.8%) were serious enough to require a reoperation.
The risk reduction seen among those with impaired fasting glucose was at least twice as large as the risk reduction achieved with lifestyle interventions in large, long-term trials of moderately obese people with prediabetes (Lancet 2006;368:1673-9, Lancet 2009;374:1677-86, and Lancet 2008;371:1783-9), the investigators noted.
The ongoing SOS study is supported by grants from the Swedish Research Council, the Swedish Foundation for Strategic Research to the Sahlgrenska Center for Cardiovascular and Metabolic Research, the Swedish federal government, the VINNOVA-VINNMER program, and the Wenner-Gren Foundations. The SOS study has previously been supported by grants to one of the authors from Hoffmann-La Roche, AstraZeneca, and other companies. Dr. Carlsson reported receiving consulting fees from AstraZeneca and owning stock in Sahltech. Other coinvestigators also had financial disclosures.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: During follow-up, type 2 diabetes developed in 110 of the bariatric surgery patients and in 392 controls, corresponding to incidence rates of 6.8 versus 28.4 cases per 1,000 person-years, respectively (P less than .001).
Data Source: The Swedish Obese Subjects (SOS) study is a prospective, case-matched 15-year comparison of diabetes incidence between 1,658 obese nondiabetic individuals who chose to undergo bariatric surgery and 1,771 who received usual weight loss management.
Disclosures: The ongoing SOS study is supported by grants from the Swedish Research Council, the Swedish Foundation for Strategic Research to the Sahlgrenska Center for Cardiovascular and Metabolic Research, the Swedish federal government, the VINNOVA-VINNMER program, and the Wenner-Gren Foundations. The SOS study has previously been supported by grants to one of the authors from Hoffmann-La Roche, AstraZeneca, and other companies. Dr. Carlsson reported receiving consulting fees from AstraZeneca and owning stock in Sahltech. Other coinvestigators also had financial disclosures.

Transfusion Rates Vary Widely at Academic Hospitals
Wide variations in perioperative blood transfusion rates among patients undergoing major noncardiac procedures across U.S. hospitals highlight the need to further investigate evidence-based "transfusion triggers" in this population of surgical patients, according to a study published ahead of print in Annals of Surgery.
"In light of the increased risk of mortality and major complications associated with blood transfusion, the extensive variability in hospital transfusion practice in noncardiac surgery may represent an important opportunity to improve surgical outcomes," wrote Feng Qian, Ph.D., of the University of Rochester (N.Y.), and associates.
The researchers used the University HealthSystem Consortium hospital database to compare transfusion rates of allogeneic red blood cells, fresh frozen plasma, and platelets in patients undergoing elective primary total hip replacement (54,405 patients), colectomy (21,334), or pancreaticoduodenectomy (7,929) at 77 hospitals between June 2006 and September 2010. Most of the hospitals were teaching hospitals with at least 500 beds.
Transfusion rates varied widely before and after adjustment for comorbidities and other patient risk factors. Patients who were treated in hospitals with high rates of transfusions were about twice as likely to receive a blood transfusion as were patients at hospitals with average transfusion rates (Ann. Surg. 2012 July 13[doi:10.1097/SLA.0b013e31825ffc37]).
In hospitals where the transfusion rate for one procedure was high, transfusion rates also tended to be high for the other two procedures. There was some evidence indicating that a higher volume of surgical cases was associated with lower transfusion rates.
After adjusting for patient risk factors, the authors determined that transfusion rates for the different blood components among those undergoing a total hip replacement ranged from 1.3% to almost 75% (red blood cells), from 0.1% to 7.7% (fresh frozen plasma), and from 0.1% to 2% (platelets). Among colectomy patients, transfusion rates ranged from 1.9% to 47.8% (RBCs), from 1.4% to 17.7% (fresh frozen plasma), and from 1.3% to 6.2% (platelets). Among those undergoing a pancreaticoduodenectomy, the rates ranged from 3% to 78.6% (RBCs), from 1% to 47% (fresh frozen plasma), and from 1.4% to 12.6% (platelets).
The variability, the authors said, "reflects, in part, the complexity of the medical decision-making process underlying transfusion therapy." Because the data included patients from 90% of academic medical centers in the United States, the results provide "a broad and contemporary picture of transfusion practices in academic surgical centers" and "reflect transfusion practices that are being taught to the next generation of academic and private-practice clinicians during residency training," they noted.
To the best of their knowledge, the authors said, there are no large randomized studies that have compared liberal and restrictive transfusion strategies in noncardiac surgery patients, and they believe that such trials are "urgently needed to better define evidence-based transfusion triggers for patients undergoing noncardiac surgery."
The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester. No disclosures were reported by the authors.
Wide variations in perioperative blood transfusion rates among patients undergoing major noncardiac procedures across U.S. hospitals highlight the need to further investigate evidence-based "transfusion triggers" in this population of surgical patients, according to a study published ahead of print in Annals of Surgery.
"In light of the increased risk of mortality and major complications associated with blood transfusion, the extensive variability in hospital transfusion practice in noncardiac surgery may represent an important opportunity to improve surgical outcomes," wrote Feng Qian, Ph.D., of the University of Rochester (N.Y.), and associates.
The researchers used the University HealthSystem Consortium hospital database to compare transfusion rates of allogeneic red blood cells, fresh frozen plasma, and platelets in patients undergoing elective primary total hip replacement (54,405 patients), colectomy (21,334), or pancreaticoduodenectomy (7,929) at 77 hospitals between June 2006 and September 2010. Most of the hospitals were teaching hospitals with at least 500 beds.
Transfusion rates varied widely before and after adjustment for comorbidities and other patient risk factors. Patients who were treated in hospitals with high rates of transfusions were about twice as likely to receive a blood transfusion as were patients at hospitals with average transfusion rates (Ann. Surg. 2012 July 13[doi:10.1097/SLA.0b013e31825ffc37]).
In hospitals where the transfusion rate for one procedure was high, transfusion rates also tended to be high for the other two procedures. There was some evidence indicating that a higher volume of surgical cases was associated with lower transfusion rates.
After adjusting for patient risk factors, the authors determined that transfusion rates for the different blood components among those undergoing a total hip replacement ranged from 1.3% to almost 75% (red blood cells), from 0.1% to 7.7% (fresh frozen plasma), and from 0.1% to 2% (platelets). Among colectomy patients, transfusion rates ranged from 1.9% to 47.8% (RBCs), from 1.4% to 17.7% (fresh frozen plasma), and from 1.3% to 6.2% (platelets). Among those undergoing a pancreaticoduodenectomy, the rates ranged from 3% to 78.6% (RBCs), from 1% to 47% (fresh frozen plasma), and from 1.4% to 12.6% (platelets).
The variability, the authors said, "reflects, in part, the complexity of the medical decision-making process underlying transfusion therapy." Because the data included patients from 90% of academic medical centers in the United States, the results provide "a broad and contemporary picture of transfusion practices in academic surgical centers" and "reflect transfusion practices that are being taught to the next generation of academic and private-practice clinicians during residency training," they noted.
To the best of their knowledge, the authors said, there are no large randomized studies that have compared liberal and restrictive transfusion strategies in noncardiac surgery patients, and they believe that such trials are "urgently needed to better define evidence-based transfusion triggers for patients undergoing noncardiac surgery."
The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester. No disclosures were reported by the authors.
Wide variations in perioperative blood transfusion rates among patients undergoing major noncardiac procedures across U.S. hospitals highlight the need to further investigate evidence-based "transfusion triggers" in this population of surgical patients, according to a study published ahead of print in Annals of Surgery.
"In light of the increased risk of mortality and major complications associated with blood transfusion, the extensive variability in hospital transfusion practice in noncardiac surgery may represent an important opportunity to improve surgical outcomes," wrote Feng Qian, Ph.D., of the University of Rochester (N.Y.), and associates.
The researchers used the University HealthSystem Consortium hospital database to compare transfusion rates of allogeneic red blood cells, fresh frozen plasma, and platelets in patients undergoing elective primary total hip replacement (54,405 patients), colectomy (21,334), or pancreaticoduodenectomy (7,929) at 77 hospitals between June 2006 and September 2010. Most of the hospitals were teaching hospitals with at least 500 beds.
Transfusion rates varied widely before and after adjustment for comorbidities and other patient risk factors. Patients who were treated in hospitals with high rates of transfusions were about twice as likely to receive a blood transfusion as were patients at hospitals with average transfusion rates (Ann. Surg. 2012 July 13[doi:10.1097/SLA.0b013e31825ffc37]).
In hospitals where the transfusion rate for one procedure was high, transfusion rates also tended to be high for the other two procedures. There was some evidence indicating that a higher volume of surgical cases was associated with lower transfusion rates.
After adjusting for patient risk factors, the authors determined that transfusion rates for the different blood components among those undergoing a total hip replacement ranged from 1.3% to almost 75% (red blood cells), from 0.1% to 7.7% (fresh frozen plasma), and from 0.1% to 2% (platelets). Among colectomy patients, transfusion rates ranged from 1.9% to 47.8% (RBCs), from 1.4% to 17.7% (fresh frozen plasma), and from 1.3% to 6.2% (platelets). Among those undergoing a pancreaticoduodenectomy, the rates ranged from 3% to 78.6% (RBCs), from 1% to 47% (fresh frozen plasma), and from 1.4% to 12.6% (platelets).
The variability, the authors said, "reflects, in part, the complexity of the medical decision-making process underlying transfusion therapy." Because the data included patients from 90% of academic medical centers in the United States, the results provide "a broad and contemporary picture of transfusion practices in academic surgical centers" and "reflect transfusion practices that are being taught to the next generation of academic and private-practice clinicians during residency training," they noted.
To the best of their knowledge, the authors said, there are no large randomized studies that have compared liberal and restrictive transfusion strategies in noncardiac surgery patients, and they believe that such trials are "urgently needed to better define evidence-based transfusion triggers for patients undergoing noncardiac surgery."
The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester. No disclosures were reported by the authors.
FROM THE ANNALS OF SURGERY
Major Finding: Transfusion rates of red blood cells, fresh frozen plasma, and platelets among patients undergoing noncardiac procedures varied widely across different U.S. academic-affiliated hospitals.
Data Source: Data from a national database of academic medical centers were used to compare transfusions in patients undergoing one of three elective noncardiac surgical procedures at 77 academic hospitals between June 2006 and September 2010.
Disclosures: The study was supported by a grant from the Agency for Healthcare and Quality Research and funding from the department of anesthesiology at the University of Rochester (N.Y.). The authors reported no disclosures.
Gastric Bypass Tops Banding in Weight Loss
SAN DIEGO – Laparoscopic Roux-en-Y gastric bypass produced long-term weight loss results that were statistically superior to those of laparoscopic adjustable gastric banding, based on 10-years’ follow-up in a prospective randomized study.
Dr. Luigi Angrisani and his colleagues compared 10-year outcomes in 27 patients who underwent the Lap-Band via pars flaccida (group A) vs. those in 24 patients who underwent laparoscopic Roux-en-Y gastric bypass (group B) at San Giovanni Bosco Hospital, Naples, Italy, from January to November 2000.
Patients were included in the study if they had a body mass index (BMI) greater than 35 but less than 50 kg/m2, if they were older than age 19 years but younger than age 50, and if they lacked a hiatal hernia and had no previous abdominal surgery, Dr. Angrisani said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline, the mean age of patients was 34 years, their mean BMI was 44, their mean percentage of excess weight was 83%, and their mean weight was 118 kg.
Dr. Angrisani, who directs the general and laparoscopic surgery unit at San Giovanni Bosco Hospital, reported that the mean operative times were 60 minutes for group A and 220 minutes for group B (P greater than.001). There was no mortality, but five patients in group A and three in group B were lost to follow-up. The rate of reoperation was 41% in group A and 29% in group B.
After 10 years, the mean weight of patients in group A and B was 101 kg and 83 kg, respectively, their mean BMI was 37 vs. 30, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Reported compliance with the intake of multivitamins among patients in group B decreased over time. Compliance was 80% at 3 years, 66% at 5 years, 50% at 7 years, and just 33% at 10 years.
"Surgical complications in gastric bypass patients were life threatening, and long-term nutritional consequences remain to be defined, such as low compliance to vitamin supplementation," Dr. Angrisani said.
In his practice, potential candidates for gastric banding include "young and motivated" patients with a BMI of 40 or less; adolescents regardless of BMI; patients with BMI of 35 or less; high-risk patients, and those fearful of more-invasive procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass.
Dr. Angrisani said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic Roux-en-Y gastric bypass produced long-term weight loss results that were statistically superior to those of laparoscopic adjustable gastric banding, based on 10-years’ follow-up in a prospective randomized study.
Dr. Luigi Angrisani and his colleagues compared 10-year outcomes in 27 patients who underwent the Lap-Band via pars flaccida (group A) vs. those in 24 patients who underwent laparoscopic Roux-en-Y gastric bypass (group B) at San Giovanni Bosco Hospital, Naples, Italy, from January to November 2000.
Patients were included in the study if they had a body mass index (BMI) greater than 35 but less than 50 kg/m2, if they were older than age 19 years but younger than age 50, and if they lacked a hiatal hernia and had no previous abdominal surgery, Dr. Angrisani said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline, the mean age of patients was 34 years, their mean BMI was 44, their mean percentage of excess weight was 83%, and their mean weight was 118 kg.
Dr. Angrisani, who directs the general and laparoscopic surgery unit at San Giovanni Bosco Hospital, reported that the mean operative times were 60 minutes for group A and 220 minutes for group B (P greater than.001). There was no mortality, but five patients in group A and three in group B were lost to follow-up. The rate of reoperation was 41% in group A and 29% in group B.
After 10 years, the mean weight of patients in group A and B was 101 kg and 83 kg, respectively, their mean BMI was 37 vs. 30, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Reported compliance with the intake of multivitamins among patients in group B decreased over time. Compliance was 80% at 3 years, 66% at 5 years, 50% at 7 years, and just 33% at 10 years.
"Surgical complications in gastric bypass patients were life threatening, and long-term nutritional consequences remain to be defined, such as low compliance to vitamin supplementation," Dr. Angrisani said.
In his practice, potential candidates for gastric banding include "young and motivated" patients with a BMI of 40 or less; adolescents regardless of BMI; patients with BMI of 35 or less; high-risk patients, and those fearful of more-invasive procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass.
Dr. Angrisani said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic Roux-en-Y gastric bypass produced long-term weight loss results that were statistically superior to those of laparoscopic adjustable gastric banding, based on 10-years’ follow-up in a prospective randomized study.
Dr. Luigi Angrisani and his colleagues compared 10-year outcomes in 27 patients who underwent the Lap-Band via pars flaccida (group A) vs. those in 24 patients who underwent laparoscopic Roux-en-Y gastric bypass (group B) at San Giovanni Bosco Hospital, Naples, Italy, from January to November 2000.
Patients were included in the study if they had a body mass index (BMI) greater than 35 but less than 50 kg/m2, if they were older than age 19 years but younger than age 50, and if they lacked a hiatal hernia and had no previous abdominal surgery, Dr. Angrisani said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
At baseline, the mean age of patients was 34 years, their mean BMI was 44, their mean percentage of excess weight was 83%, and their mean weight was 118 kg.
Dr. Angrisani, who directs the general and laparoscopic surgery unit at San Giovanni Bosco Hospital, reported that the mean operative times were 60 minutes for group A and 220 minutes for group B (P greater than.001). There was no mortality, but five patients in group A and three in group B were lost to follow-up. The rate of reoperation was 41% in group A and 29% in group B.
After 10 years, the mean weight of patients in group A and B was 101 kg and 83 kg, respectively, their mean BMI was 37 vs. 30, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Reported compliance with the intake of multivitamins among patients in group B decreased over time. Compliance was 80% at 3 years, 66% at 5 years, 50% at 7 years, and just 33% at 10 years.
"Surgical complications in gastric bypass patients were life threatening, and long-term nutritional consequences remain to be defined, such as low compliance to vitamin supplementation," Dr. Angrisani said.
In his practice, potential candidates for gastric banding include "young and motivated" patients with a BMI of 40 or less; adolescents regardless of BMI; patients with BMI of 35 or less; high-risk patients, and those fearful of more-invasive procedures such as sleeve gastrectomy and Roux-en-Y gastric bypass.
Dr. Angrisani said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: At 10 years of follow-up, the mean weight among patients who underwent gastric banding was 101 kg, compared with 83 kg among those who underwent laparoscopic Roux-en-Y gastric bypass. In addition, their mean BMI was 37 vs. 30, respectively, and their mean loss of excess body weight was 46% vs. 69% (all P less than .05).
Data Source: This was a randomized, single-center study of 51 patients who underwent either procedure from January to November 2000.
Disclosures: Dr. Angrisani said that he had no relevant financial conflicts to disclose.
Modified Bariatric Surgery Tames Diabetes in Small Series
HOUSTON – Laparoscopic sleeve gastrectomy with ileal interposition sent diabetes into remission in 20 of 43 adults and reduced the need for diabetes medications in the other 23 patients during an average of 20 months of follow-up.
Among the 30 obese (defined as having a body mass index greater than 27 kg/m2) patients in the study, 26 showed remission of diabetes – an 86% success rate that’s similar to results reported for gastric bypass surgery, Dr. Kirtikumar D. Modi said in a press briefing at the annual meeting of the Endocrine Society.
Patients had an average disease duration of 10 years and an average BMI of 33. In laparoscopic sleeve gastrectomy with ileal interposition, stapling reduces the size of the stomach, and a segment of the ileum is shifted to the jejunal area closer to the stomach. The average BMI fell to 26 after surgery. Among 30 patients who had hypertension before surgery, 27 had no hypertension postoperatively.
The surgery seemed to have no significant effect on lipid levels, "maybe because [the patients] were already on lipid-lowering drugs," said Dr. Modi, chief endocrinologist at Medwin Hospital in Hyderabad, India.
There were few complications; approximately 25% of patients had nausea and loss of appetite during the first postoperative month. Difficulty with rapid swallowing in six patients subsided over 2 weeks.
In a second series, Dr. Modi and his associates performed a laparoscopic diverted sleeve gastrectomy with ileal interposition on 17 additional patients who were not obese and had had diabetes longer than 10 years – the characteristics of patients who responded less well to the sleeve gastrectomy with ileal interposition in the first series.
Laparoscopic diverted sleeve gastrectomy diverts food away from parts of the small intestine, including the duodenum, where the absorption of nutrients begins, and the ileal segment is shifted more proximally. Patients who underwent this procedure had had diabetes for 15 years on average, and they had an average BMI of 29 as well as stimulated C-peptide levels greater than 4 ng/mL.
As expected, the mean BMI decreased to 23 over 18 months, he said. Of the eight patients who had hypertension before surgery, seven (88%) had no hypertension afterward. This time, treatment produced significant decreases in glycemic, lipid, and microalbuminuria levels.
At 9 months after surgery, diabetes was in remission in 12 (70%) of the 17 patients, and the other 5 patients needed fewer oral hyperglycemic medications than did those in the first series.
All patients in both studies had poorly controlled diabetes. The investigators defined diabetes remission as a hemoglobin A1c level less than 6.5% and no further need for insulin or oral hypoglycemic agents.
The reduction in hemoglobin A1c was disproportionately greater than the decline in BMI, suggesting benefits that are "much more than the weight improvement," he said.
More complications were seen in the second series, including three patients with minor intraoperative complications. Another patient developed ileus with ileal perforation 2 weeks after surgery and underwent laparotomy for repair. Three patients experienced nausea and anorexia for 2 weeks. Two patients developed vitamin B12 deficiency at 12 months.
A previous study of 150 patients with uncontrolled type 2 diabetes reported better glycemic control in patients who were randomized to 12 months of medical therapy plus bariatric surgery (sleeve gastrectomy or Roux-en-Y gastric bypass), compared with those on medical treatment alone, Dr. Modi noted (N. Engl. J. Med. 2012;366:1567-76).
A separate retrospective study of 271,726 patients in the Bariatric Outcomes Longitudinal Database found that the efficacy and safety of laparoscopic sleeve gastrectomy fell between those of gastric banding and laparoscopic gastric bypass.
Dr. Modi reported having no financial disclosures.
HOUSTON – Laparoscopic sleeve gastrectomy with ileal interposition sent diabetes into remission in 20 of 43 adults and reduced the need for diabetes medications in the other 23 patients during an average of 20 months of follow-up.
Among the 30 obese (defined as having a body mass index greater than 27 kg/m2) patients in the study, 26 showed remission of diabetes – an 86% success rate that’s similar to results reported for gastric bypass surgery, Dr. Kirtikumar D. Modi said in a press briefing at the annual meeting of the Endocrine Society.
Patients had an average disease duration of 10 years and an average BMI of 33. In laparoscopic sleeve gastrectomy with ileal interposition, stapling reduces the size of the stomach, and a segment of the ileum is shifted to the jejunal area closer to the stomach. The average BMI fell to 26 after surgery. Among 30 patients who had hypertension before surgery, 27 had no hypertension postoperatively.
The surgery seemed to have no significant effect on lipid levels, "maybe because [the patients] were already on lipid-lowering drugs," said Dr. Modi, chief endocrinologist at Medwin Hospital in Hyderabad, India.
There were few complications; approximately 25% of patients had nausea and loss of appetite during the first postoperative month. Difficulty with rapid swallowing in six patients subsided over 2 weeks.
In a second series, Dr. Modi and his associates performed a laparoscopic diverted sleeve gastrectomy with ileal interposition on 17 additional patients who were not obese and had had diabetes longer than 10 years – the characteristics of patients who responded less well to the sleeve gastrectomy with ileal interposition in the first series.
Laparoscopic diverted sleeve gastrectomy diverts food away from parts of the small intestine, including the duodenum, where the absorption of nutrients begins, and the ileal segment is shifted more proximally. Patients who underwent this procedure had had diabetes for 15 years on average, and they had an average BMI of 29 as well as stimulated C-peptide levels greater than 4 ng/mL.
As expected, the mean BMI decreased to 23 over 18 months, he said. Of the eight patients who had hypertension before surgery, seven (88%) had no hypertension afterward. This time, treatment produced significant decreases in glycemic, lipid, and microalbuminuria levels.
At 9 months after surgery, diabetes was in remission in 12 (70%) of the 17 patients, and the other 5 patients needed fewer oral hyperglycemic medications than did those in the first series.
All patients in both studies had poorly controlled diabetes. The investigators defined diabetes remission as a hemoglobin A1c level less than 6.5% and no further need for insulin or oral hypoglycemic agents.
The reduction in hemoglobin A1c was disproportionately greater than the decline in BMI, suggesting benefits that are "much more than the weight improvement," he said.
More complications were seen in the second series, including three patients with minor intraoperative complications. Another patient developed ileus with ileal perforation 2 weeks after surgery and underwent laparotomy for repair. Three patients experienced nausea and anorexia for 2 weeks. Two patients developed vitamin B12 deficiency at 12 months.
A previous study of 150 patients with uncontrolled type 2 diabetes reported better glycemic control in patients who were randomized to 12 months of medical therapy plus bariatric surgery (sleeve gastrectomy or Roux-en-Y gastric bypass), compared with those on medical treatment alone, Dr. Modi noted (N. Engl. J. Med. 2012;366:1567-76).
A separate retrospective study of 271,726 patients in the Bariatric Outcomes Longitudinal Database found that the efficacy and safety of laparoscopic sleeve gastrectomy fell between those of gastric banding and laparoscopic gastric bypass.
Dr. Modi reported having no financial disclosures.
HOUSTON – Laparoscopic sleeve gastrectomy with ileal interposition sent diabetes into remission in 20 of 43 adults and reduced the need for diabetes medications in the other 23 patients during an average of 20 months of follow-up.
Among the 30 obese (defined as having a body mass index greater than 27 kg/m2) patients in the study, 26 showed remission of diabetes – an 86% success rate that’s similar to results reported for gastric bypass surgery, Dr. Kirtikumar D. Modi said in a press briefing at the annual meeting of the Endocrine Society.
Patients had an average disease duration of 10 years and an average BMI of 33. In laparoscopic sleeve gastrectomy with ileal interposition, stapling reduces the size of the stomach, and a segment of the ileum is shifted to the jejunal area closer to the stomach. The average BMI fell to 26 after surgery. Among 30 patients who had hypertension before surgery, 27 had no hypertension postoperatively.
The surgery seemed to have no significant effect on lipid levels, "maybe because [the patients] were already on lipid-lowering drugs," said Dr. Modi, chief endocrinologist at Medwin Hospital in Hyderabad, India.
There were few complications; approximately 25% of patients had nausea and loss of appetite during the first postoperative month. Difficulty with rapid swallowing in six patients subsided over 2 weeks.
In a second series, Dr. Modi and his associates performed a laparoscopic diverted sleeve gastrectomy with ileal interposition on 17 additional patients who were not obese and had had diabetes longer than 10 years – the characteristics of patients who responded less well to the sleeve gastrectomy with ileal interposition in the first series.
Laparoscopic diverted sleeve gastrectomy diverts food away from parts of the small intestine, including the duodenum, where the absorption of nutrients begins, and the ileal segment is shifted more proximally. Patients who underwent this procedure had had diabetes for 15 years on average, and they had an average BMI of 29 as well as stimulated C-peptide levels greater than 4 ng/mL.
As expected, the mean BMI decreased to 23 over 18 months, he said. Of the eight patients who had hypertension before surgery, seven (88%) had no hypertension afterward. This time, treatment produced significant decreases in glycemic, lipid, and microalbuminuria levels.
At 9 months after surgery, diabetes was in remission in 12 (70%) of the 17 patients, and the other 5 patients needed fewer oral hyperglycemic medications than did those in the first series.
All patients in both studies had poorly controlled diabetes. The investigators defined diabetes remission as a hemoglobin A1c level less than 6.5% and no further need for insulin or oral hypoglycemic agents.
The reduction in hemoglobin A1c was disproportionately greater than the decline in BMI, suggesting benefits that are "much more than the weight improvement," he said.
More complications were seen in the second series, including three patients with minor intraoperative complications. Another patient developed ileus with ileal perforation 2 weeks after surgery and underwent laparotomy for repair. Three patients experienced nausea and anorexia for 2 weeks. Two patients developed vitamin B12 deficiency at 12 months.
A previous study of 150 patients with uncontrolled type 2 diabetes reported better glycemic control in patients who were randomized to 12 months of medical therapy plus bariatric surgery (sleeve gastrectomy or Roux-en-Y gastric bypass), compared with those on medical treatment alone, Dr. Modi noted (N. Engl. J. Med. 2012;366:1567-76).
A separate retrospective study of 271,726 patients in the Bariatric Outcomes Longitudinal Database found that the efficacy and safety of laparoscopic sleeve gastrectomy fell between those of gastric banding and laparoscopic gastric bypass.
Dr. Modi reported having no financial disclosures.
AT THE ANNUAL MEETING OF THE ENDOCRINE SOCIETY
Major Finding: Diabetes went into remission in 20 of 43 adults after laparoscopic sleeve gastrectomy with ileal interposition; the procedure also reduced the need for medications in the other 23 patients.
Data Source: The study is based on a case series at one institution.
Disclosures: Dr. Modi reported having no financial disclosures.
Reversal of Lap-Band to Sleeve Gastrectomy Feasible
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
SAN DIEGO – Laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy is a safe and feasible operation, results from a two-center study showed.
"Since the Lap-Band was introduced in the United States in 2001, it has been a popular minimally invasive procedure for weight loss," Dr. Abdelkader A. Hawasli said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "However, recent reports have shown that there’s an increased rate of explantation (up to 49%)" because of complications or failure to lose weight. Options are removal, reversion, or reversal to a nonphysiological procedure, "such as Roux-en-Y gastric bypass or biliopancreatic diversion. However, recent reports have been showing that sleeve gastrectomy could be a possible physiologic alternative."
For the current study, Dr. Hawasli, a surgeon at St. John Hospital and Medical Center in Detroit and Beaumont Hospital in Grosse Pointe, Mich., and his associates set out to evaluate the safety of the laparoscopic reversal of the Lap-Band to sleeve gastrectomy, the feasibility of performing simultaneous laparoscopic removal of the Lap-Band and reversal to sleeve gastrectomy, and the results of the sleeve gastrectomy after reversal as the final bariatric procedure in continuing or maintaining weight loss.
Dr. Hawasli reported on 485 patients who had undergone Lap-Band placement at St. John Hospital and Medical Center and 4 who had undergone the procedure at another institution from January 2004 to October 2011.
Of the 489 patients, 34 (7%) had reversal of the Lap-Band to sleeve gastrectomy. Of these, 20 patients (group 1) underwent reversal because of slippage in 15 cases, erosion in 3 cases, and infection in 2 cases, whereas 14 patients (group 2) underwent reversal because they were dissatisfied with their weight loss. The mean time of the reversal to sleeve gastrectomy was more than 3 years from Lap-Band insertion among the slippage subset patients in group 1 and among all patients in group 2 (36.5 vs. 43.3 months, respectively).
The majority of patients (32) underwent simultaneous removal of the band with reversal to sleeve gastrectomy, whereas 2 underwent a staged sleeve gastrectomy.
Dr. Hawasli reported that there were just two complications in group 1: one leak, which occurred because of erosion, and one narrowing. Both cases were treated conservatively. There were no complications in group 2. There were no readmissions in group 1, whereas in group 2 one patient was readmitted for nausea and one for dehydration.
Patients in both groups lost weight after the reversal, but the loss was more pronounced in group 1, compared with group 2 (mean total body mass index loss, –15.8 kg/m2 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
To explain this difference in weight loss, Dr. Hawasli said that patients in group 1 lost most of their weight before the reversal (mean BMI loss, –11.7) and lost additional weight after the reversal (mean BMI loss, –3.8). However, group 2 patients struggled with weight loss before the reversal (mean BMI loss, –3.6) and they may have continued to struggle after the reversal, even though they lost more weight after the reversal than did group 1 patients (mean BMI loss, –7.2 vs. –3.8, respectively), which is expected.
"Another reason could be the short postreversal follow-up period (a mean of 9 months)," during which they did not get enough time to lose more weight, he explained.
In group 1, the mean operative time was 159 minutes for patients with Lap-Band slippage and 174 minutes for those with erosion or infection. The mean operative time in group 2 was 106 minutes.
Length of stay was about 2 days in both groups, but reached a mean of 3.6 days for the subset of group 1 patients who had reversal because of infection or erosion.
"The short-term results of weight loss after the reversal are better in patients who had the reversal secondary to complications," Dr. Hawasli concluded. "Concomitant removal of the band and reversal to sleeve gastrectomy did not increase the risk of complications except in patients with erosion. Thus, patients with erosion may benefit better from staged reversal."
Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: Weight loss was more pronounced among patients who underwent reversal of Lap-Band to sleeve gastrectomy because of band slippage, erosion, or infection than because of dissatisfaction with weight loss (mean total BMI loss, –15.8 vs. –10.8, respectively; mean percentage of excess BMI loss, –66.5% vs. –44.6%; all P less than .05).
Data Source: The study consisted of 34 patients who underwent reversal of Lap-Band to sleeve gastrectomy at two centers from January 2004 to October 2011.
Disclosures: Dr. Hawasli disclosed that he receives compensation from Covidien as a proctor.
Bariatric Surgery Most Common Elective Surgical Procedure
SAN DIEGO – Within the setting of academic medical centers, bariatric surgery is the most common elective general surgical operation and it has the highest use of laparoscopy.
In addition, the in-hospital mortality rate of laparoscopic bariatric surgery is now comparable to those of laparoscopic appendectomy and antireflux surgery, and is currently lower than that of laparoscopic cholecystectomy.
Those are main findings from an analysis of data from the University HealthSystem Consortium database, which contains data from 114 academic centers and 250 major teaching affiliates in the United States.
"Laparoscopy has revolutionized the performance of most intra-abdominal operations [and] is now widely utilized in many different types of general surgical operations," Brian Nguyen, a research student at the University of California, Irvine, said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
He and his associates searched the University HealthSystem database to determine the rate of laparoscopy use in seven common elective general surgical operations performed between Oct. 1, 2008, and March 31, 2012: antireflux surgery for gastroesophageal reflux disease (GERD) or hiatal hernia, cholecystectomy for chronic cholecystitis, bariatric surgery for morbid obesity, ventral hernia repair for incisional hernia, appendectomy for acute appendicitis, rectal resection for rectal cancer, and colectomy for colon cancer or diverticulitis. Secondary objectives were to determine the rate of conversion to open surgery, length of stay, overall complications, and in-hospital mortality.
The most common elective surgical procedure performed during the study period was bariatric surgery (53,958 cases), followed by colectomy (29,934 cases), ventral hernia repair (17,749 cases), antireflux surgery (13,918 cases), appendectomy (8,654 cases), cholecystectomy (8,512 cases), and rectal resection (4,729). Bariatric surgery also led the way with the highest rate of laparoscopy use (94%), followed by antireflux surgery (83%), appendectomy (79%), cholecystectomy (77%), colectomy (52%), ventral hernia repair (28%), and rectal resection (18%).
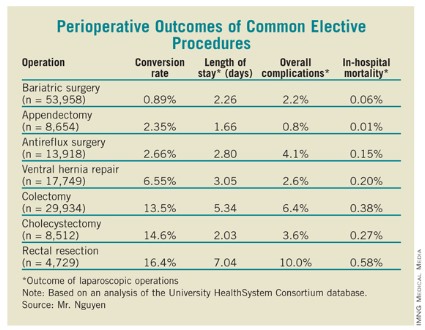
As for perioperative outcomes (see table), Mr. Nguyen reported that patients who underwent bariatric surgery had the lowest conversion rate to open procedures (0.89%). The overall complication rate of 2.2% and the in-hospital mortality rate of 0.06% associated with bariatric surgery were lower only in appendectomy, which had rates of 0.8% and 0.01%, respectively. The mean length of stay for bariatric surgery patients was 2.26 days, which was higher than that for appendectomy and cholecystectomy patients (a mean of 1.66 and 2.03 days, respectively), but lower than that for antireflux surgery (a mean of 2.80 days).
Mr. Nguyen acknowledged that the study was limited by the fact that it represented only inpatients at academic medical centers and affiliated hospitals.
He said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Within the setting of academic medical centers, bariatric surgery is the most common elective general surgical operation and it has the highest use of laparoscopy.
In addition, the in-hospital mortality rate of laparoscopic bariatric surgery is now comparable to those of laparoscopic appendectomy and antireflux surgery, and is currently lower than that of laparoscopic cholecystectomy.
Those are main findings from an analysis of data from the University HealthSystem Consortium database, which contains data from 114 academic centers and 250 major teaching affiliates in the United States.
"Laparoscopy has revolutionized the performance of most intra-abdominal operations [and] is now widely utilized in many different types of general surgical operations," Brian Nguyen, a research student at the University of California, Irvine, said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
He and his associates searched the University HealthSystem database to determine the rate of laparoscopy use in seven common elective general surgical operations performed between Oct. 1, 2008, and March 31, 2012: antireflux surgery for gastroesophageal reflux disease (GERD) or hiatal hernia, cholecystectomy for chronic cholecystitis, bariatric surgery for morbid obesity, ventral hernia repair for incisional hernia, appendectomy for acute appendicitis, rectal resection for rectal cancer, and colectomy for colon cancer or diverticulitis. Secondary objectives were to determine the rate of conversion to open surgery, length of stay, overall complications, and in-hospital mortality.
The most common elective surgical procedure performed during the study period was bariatric surgery (53,958 cases), followed by colectomy (29,934 cases), ventral hernia repair (17,749 cases), antireflux surgery (13,918 cases), appendectomy (8,654 cases), cholecystectomy (8,512 cases), and rectal resection (4,729). Bariatric surgery also led the way with the highest rate of laparoscopy use (94%), followed by antireflux surgery (83%), appendectomy (79%), cholecystectomy (77%), colectomy (52%), ventral hernia repair (28%), and rectal resection (18%).
As for perioperative outcomes (see table), Mr. Nguyen reported that patients who underwent bariatric surgery had the lowest conversion rate to open procedures (0.89%). The overall complication rate of 2.2% and the in-hospital mortality rate of 0.06% associated with bariatric surgery were lower only in appendectomy, which had rates of 0.8% and 0.01%, respectively. The mean length of stay for bariatric surgery patients was 2.26 days, which was higher than that for appendectomy and cholecystectomy patients (a mean of 1.66 and 2.03 days, respectively), but lower than that for antireflux surgery (a mean of 2.80 days).
Mr. Nguyen acknowledged that the study was limited by the fact that it represented only inpatients at academic medical centers and affiliated hospitals.
He said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Within the setting of academic medical centers, bariatric surgery is the most common elective general surgical operation and it has the highest use of laparoscopy.
In addition, the in-hospital mortality rate of laparoscopic bariatric surgery is now comparable to those of laparoscopic appendectomy and antireflux surgery, and is currently lower than that of laparoscopic cholecystectomy.
Those are main findings from an analysis of data from the University HealthSystem Consortium database, which contains data from 114 academic centers and 250 major teaching affiliates in the United States.
"Laparoscopy has revolutionized the performance of most intra-abdominal operations [and] is now widely utilized in many different types of general surgical operations," Brian Nguyen, a research student at the University of California, Irvine, said at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
He and his associates searched the University HealthSystem database to determine the rate of laparoscopy use in seven common elective general surgical operations performed between Oct. 1, 2008, and March 31, 2012: antireflux surgery for gastroesophageal reflux disease (GERD) or hiatal hernia, cholecystectomy for chronic cholecystitis, bariatric surgery for morbid obesity, ventral hernia repair for incisional hernia, appendectomy for acute appendicitis, rectal resection for rectal cancer, and colectomy for colon cancer or diverticulitis. Secondary objectives were to determine the rate of conversion to open surgery, length of stay, overall complications, and in-hospital mortality.
The most common elective surgical procedure performed during the study period was bariatric surgery (53,958 cases), followed by colectomy (29,934 cases), ventral hernia repair (17,749 cases), antireflux surgery (13,918 cases), appendectomy (8,654 cases), cholecystectomy (8,512 cases), and rectal resection (4,729). Bariatric surgery also led the way with the highest rate of laparoscopy use (94%), followed by antireflux surgery (83%), appendectomy (79%), cholecystectomy (77%), colectomy (52%), ventral hernia repair (28%), and rectal resection (18%).
As for perioperative outcomes (see table), Mr. Nguyen reported that patients who underwent bariatric surgery had the lowest conversion rate to open procedures (0.89%). The overall complication rate of 2.2% and the in-hospital mortality rate of 0.06% associated with bariatric surgery were lower only in appendectomy, which had rates of 0.8% and 0.01%, respectively. The mean length of stay for bariatric surgery patients was 2.26 days, which was higher than that for appendectomy and cholecystectomy patients (a mean of 1.66 and 2.03 days, respectively), but lower than that for antireflux surgery (a mean of 2.80 days).
Mr. Nguyen acknowledged that the study was limited by the fact that it represented only inpatients at academic medical centers and affiliated hospitals.
He said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: Between Oct. 1, 2008, and March 31, 2012, bariatric surgery ranked as the most common elective surgical procedure performed (53,958 cases), and led the way with use of laparoscopy (94% of cases).
Data Source: This study of seven common surgical elective procedures was based on a search of the University HealthSystem Consortium database, which is limited to 114 academic centers and 250 major teaching affiliates in the United States.
Disclosures: Mr. Nguyen said that he had no relevant financial conflicts to disclose.
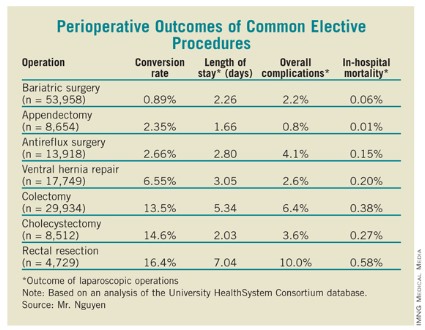
Sleeve Gastrectomy Feasible in Obese Transplant Candidates
SAN DIEGO – Laparoscopic sleeve gastrectomy is safe and effective in obese candidates for organ transplantation, results from a novel pilot study demonstrated.
Nationwide, 15%-20% of patients on the transplant waiting list are morbidly obese, with a body mass index of greater than 35 kg/m2, "but many cannot be transplanted unless they lose weight," said Dr. Matthew Y. Lin of the surgery department at the University of California, San Francisco (UCSF). "Morbid obesity can contribute to end-stage kidney or liver failure. For example, obesity-related nonalcoholic steatohepatitis is now the third most common indication for liver transplant in the United States and will likely become first in the future."

In what Dr. Lin said is the only reported case series of bariatric surgery in obese transplant candidates, he and his associates conducted a pilot study of 26 morbidly obese patients with liver or kidney failure who underwent laparoscopic sleeve gastrectomy at UCSF from 2006 to 2012. They chose sleeve gastrectomy over gastric banding "to avoid foreign body implantation, in anticipation of post-transplant immunosuppression," Dr. Lin explained at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
"We chose sleeve gastrectomy over gastric bypass to maintain endoscopic access to the biliary system, to reduce surgical complexity, and to avoid unpredictable immunosuppression absorption," he said.
Morbid obesity is a relative contraindication for solid organ transplantation at most centers because of poor post-transplant outcomes, according to Dr. Lin. "At UCSF, the selection criteria are a BMI of less than 40 for liver transplant, less than 38 for kidney transplant, and less than 34 for kidney transplant in patients with diabetes." The researchers hypothesized that laparoscopic sleeve gastrectomy could be safely performed in high-risk patients with liver or kidney failure and achieve enough weight loss to allow for transplantation.
The 26 patients had a mean age of 57 years, 17 were women, 20 were white, and their average preoperative BMI was 48. Twenty patients had liver insufficiency with a mean Model for End-Stage Liver Disease (MELD) score of 11, and 6 had kidney insufficiency with a mean glomerular filtration rate of 10 mL/min. Five of these patients were on hemodialysis.
All 26 patients had laparoscopic sleeve gastrectomy performed by the same surgeon. The mean operative time was 151 minutes, and the mean length of stay was 4.2 days. Complications that occurred within 30 days were two cases of superficial wound infection and one case each of worsened hepatic encephalopathy, acute renal insufficiency, need for blood transfusion, and staple line leak. There was no mortality within 30 days, but after that period two patients died awaiting transplant and one patient died from complications of the staple line leak and progressive liver failure 4 years after surgery.
After 2 years, the average BMI of study participants dropped from a mean of 48 to a mean of 29. "Between the 6- and 12-month marks, most patients were able to achieve a BMI that would make them acceptable for transplant," Dr. Lin said.
At 1, 3, 12, and 24 months, the percent of excess body weight lost was 17%, 26%, 50%, and 66%, respectively. "The weight-loss profile is similar to [those of] the general bariatric sleeve gastrectomy population," he noted.
Of the 13 patients who had diabetes preoperatively, 7 had complete resolution after the procedure and 1 had partial resolution. Mean postoperative albumin levels for all 26 patients after sleeve gastrectomy were 3.1 g/dL at 6 months and 3.3 g/dL at 12 months.
Eight patients went on to receive their organ transplant, Dr. Lin said. Their mean age was 56 years, and six were women. They waited a mean of 17 months for their procedures, which included six liver transplants, one liver and kidney transplant, and one kidney transplant. Their mean BMI before sleeve gastrectomy was 46, and their mean BMI prior to transplantation was 31. Immediately before transplant, their mean albumin level was 3.2 g/dL, and the most current measurement remained the same. "No increased acute rejection or difficulty maintaining immunosuppression was observed," he said.
Dr. Lin acknowledged certain limitations of the study, including its single-center design, lack of a control population, and the fact that "there is very little statistical power to estimate the true complication rate in this high-risk surgical group. Furthermore, we only have short-term follow-up."
Dr. Lin said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is safe and effective in obese candidates for organ transplantation, results from a novel pilot study demonstrated.
Nationwide, 15%-20% of patients on the transplant waiting list are morbidly obese, with a body mass index of greater than 35 kg/m2, "but many cannot be transplanted unless they lose weight," said Dr. Matthew Y. Lin of the surgery department at the University of California, San Francisco (UCSF). "Morbid obesity can contribute to end-stage kidney or liver failure. For example, obesity-related nonalcoholic steatohepatitis is now the third most common indication for liver transplant in the United States and will likely become first in the future."
In what Dr. Lin said is the only reported case series of bariatric surgery in obese transplant candidates, he and his associates conducted a pilot study of 26 morbidly obese patients with liver or kidney failure who underwent laparoscopic sleeve gastrectomy at UCSF from 2006 to 2012. They chose sleeve gastrectomy over gastric banding "to avoid foreign body implantation, in anticipation of post-transplant immunosuppression," Dr. Lin explained at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
"We chose sleeve gastrectomy over gastric bypass to maintain endoscopic access to the biliary system, to reduce surgical complexity, and to avoid unpredictable immunosuppression absorption," he said.
Morbid obesity is a relative contraindication for solid organ transplantation at most centers because of poor post-transplant outcomes, according to Dr. Lin. "At UCSF, the selection criteria are a BMI of less than 40 for liver transplant, less than 38 for kidney transplant, and less than 34 for kidney transplant in patients with diabetes." The researchers hypothesized that laparoscopic sleeve gastrectomy could be safely performed in high-risk patients with liver or kidney failure and achieve enough weight loss to allow for transplantation.
The 26 patients had a mean age of 57 years, 17 were women, 20 were white, and their average preoperative BMI was 48. Twenty patients had liver insufficiency with a mean Model for End-Stage Liver Disease (MELD) score of 11, and 6 had kidney insufficiency with a mean glomerular filtration rate of 10 mL/min. Five of these patients were on hemodialysis.
All 26 patients had laparoscopic sleeve gastrectomy performed by the same surgeon. The mean operative time was 151 minutes, and the mean length of stay was 4.2 days. Complications that occurred within 30 days were two cases of superficial wound infection and one case each of worsened hepatic encephalopathy, acute renal insufficiency, need for blood transfusion, and staple line leak. There was no mortality within 30 days, but after that period two patients died awaiting transplant and one patient died from complications of the staple line leak and progressive liver failure 4 years after surgery.
After 2 years, the average BMI of study participants dropped from a mean of 48 to a mean of 29. "Between the 6- and 12-month marks, most patients were able to achieve a BMI that would make them acceptable for transplant," Dr. Lin said.
At 1, 3, 12, and 24 months, the percent of excess body weight lost was 17%, 26%, 50%, and 66%, respectively. "The weight-loss profile is similar to [those of] the general bariatric sleeve gastrectomy population," he noted.
Of the 13 patients who had diabetes preoperatively, 7 had complete resolution after the procedure and 1 had partial resolution. Mean postoperative albumin levels for all 26 patients after sleeve gastrectomy were 3.1 g/dL at 6 months and 3.3 g/dL at 12 months.
Eight patients went on to receive their organ transplant, Dr. Lin said. Their mean age was 56 years, and six were women. They waited a mean of 17 months for their procedures, which included six liver transplants, one liver and kidney transplant, and one kidney transplant. Their mean BMI before sleeve gastrectomy was 46, and their mean BMI prior to transplantation was 31. Immediately before transplant, their mean albumin level was 3.2 g/dL, and the most current measurement remained the same. "No increased acute rejection or difficulty maintaining immunosuppression was observed," he said.
Dr. Lin acknowledged certain limitations of the study, including its single-center design, lack of a control population, and the fact that "there is very little statistical power to estimate the true complication rate in this high-risk surgical group. Furthermore, we only have short-term follow-up."
Dr. Lin said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Laparoscopic sleeve gastrectomy is safe and effective in obese candidates for organ transplantation, results from a novel pilot study demonstrated.
Nationwide, 15%-20% of patients on the transplant waiting list are morbidly obese, with a body mass index of greater than 35 kg/m2, "but many cannot be transplanted unless they lose weight," said Dr. Matthew Y. Lin of the surgery department at the University of California, San Francisco (UCSF). "Morbid obesity can contribute to end-stage kidney or liver failure. For example, obesity-related nonalcoholic steatohepatitis is now the third most common indication for liver transplant in the United States and will likely become first in the future."
In what Dr. Lin said is the only reported case series of bariatric surgery in obese transplant candidates, he and his associates conducted a pilot study of 26 morbidly obese patients with liver or kidney failure who underwent laparoscopic sleeve gastrectomy at UCSF from 2006 to 2012. They chose sleeve gastrectomy over gastric banding "to avoid foreign body implantation, in anticipation of post-transplant immunosuppression," Dr. Lin explained at the annual meeting of the American Society for Metabolic and Bariatric Surgery.
"We chose sleeve gastrectomy over gastric bypass to maintain endoscopic access to the biliary system, to reduce surgical complexity, and to avoid unpredictable immunosuppression absorption," he said.
Morbid obesity is a relative contraindication for solid organ transplantation at most centers because of poor post-transplant outcomes, according to Dr. Lin. "At UCSF, the selection criteria are a BMI of less than 40 for liver transplant, less than 38 for kidney transplant, and less than 34 for kidney transplant in patients with diabetes." The researchers hypothesized that laparoscopic sleeve gastrectomy could be safely performed in high-risk patients with liver or kidney failure and achieve enough weight loss to allow for transplantation.
The 26 patients had a mean age of 57 years, 17 were women, 20 were white, and their average preoperative BMI was 48. Twenty patients had liver insufficiency with a mean Model for End-Stage Liver Disease (MELD) score of 11, and 6 had kidney insufficiency with a mean glomerular filtration rate of 10 mL/min. Five of these patients were on hemodialysis.
All 26 patients had laparoscopic sleeve gastrectomy performed by the same surgeon. The mean operative time was 151 minutes, and the mean length of stay was 4.2 days. Complications that occurred within 30 days were two cases of superficial wound infection and one case each of worsened hepatic encephalopathy, acute renal insufficiency, need for blood transfusion, and staple line leak. There was no mortality within 30 days, but after that period two patients died awaiting transplant and one patient died from complications of the staple line leak and progressive liver failure 4 years after surgery.
After 2 years, the average BMI of study participants dropped from a mean of 48 to a mean of 29. "Between the 6- and 12-month marks, most patients were able to achieve a BMI that would make them acceptable for transplant," Dr. Lin said.
At 1, 3, 12, and 24 months, the percent of excess body weight lost was 17%, 26%, 50%, and 66%, respectively. "The weight-loss profile is similar to [those of] the general bariatric sleeve gastrectomy population," he noted.
Of the 13 patients who had diabetes preoperatively, 7 had complete resolution after the procedure and 1 had partial resolution. Mean postoperative albumin levels for all 26 patients after sleeve gastrectomy were 3.1 g/dL at 6 months and 3.3 g/dL at 12 months.
Eight patients went on to receive their organ transplant, Dr. Lin said. Their mean age was 56 years, and six were women. They waited a mean of 17 months for their procedures, which included six liver transplants, one liver and kidney transplant, and one kidney transplant. Their mean BMI before sleeve gastrectomy was 46, and their mean BMI prior to transplantation was 31. Immediately before transplant, their mean albumin level was 3.2 g/dL, and the most current measurement remained the same. "No increased acute rejection or difficulty maintaining immunosuppression was observed," he said.
Dr. Lin acknowledged certain limitations of the study, including its single-center design, lack of a control population, and the fact that "there is very little statistical power to estimate the true complication rate in this high-risk surgical group. Furthermore, we only have short-term follow-up."
Dr. Lin said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Survey: Long Surgical Career Raises Likelihood of Lawsuit
SAN DIEGO – The most experienced bariatric surgeons are those who are most likely to be sued, judging by responses to a survey from more than 300 members of the American Society for Metabolic and Bariatric Surgery.
"There are no resources, national registries, or easily accessible databases to analyze bariatric-specific medical malpractice claims in the United States," Dr. Ramsey M. Dallal said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "Without the ability to analyze aggregate data, surgeons cannot easily study common causes of medical malpractice litigation and develop patient safety improvements. Nor do there exist easily accessible measures of trends in bariatric surgery litigation."

In an effort to obtain a snapshot of the liability landscape in bariatric surgery, Dr. Dallal and other members of the ASMBS Patient Safety Committee e-mailed a survey to 1,672 surgeon members of the ASMBS in July 2011. A total of 330 surgeons in 46 states responded, for a response rate of 20%. Their mean number of years in practice was 15, which represented 5,042 years of bariatric surgery–specific liability exposure. Most respondents (38%) practiced in a hospital or academic group, 26% in a single specialty group, 20% in solo practice, 13% in a multispecialty group, and 3% in other settings.
Nine respondents chose not to have malpractice insurance. Those who were insured reported a mean yearly cost of malpractice insurance of $59,200.
Nearly half of respondents (48%) reported having no malpractice insurance cases since their careers began, but the average number of lifetime cases reported by their counterparts was 1.5.
Of the 464 lawsuits reported by 156 surgeons, 54% were dropped or dismissed, 27% were settled out of court, and 19% went to trial or arbitration.
Of those cases that went to trial, 72% were found in favor of the surgeon-defendant. The mean lifetime amount paid in lawsuits was $250,000, including one settlement for $7,000,000. The total amount paid by the respondents was $70,871,998.
Using multivariate logistic regression analysis, the researchers determined that the probability of reporting at least one lawsuit independently increased with the number of years in practice (odds ratio, 1.03; P = .03) and among those who have performed more than 1,000 cases (OR, 8.5%; P = .01). "In essence, our most experienced surgeons are the ones being sued the most," said Dr. Dallal, chief of bariatric/minimally invasive surgery at Einstein Healthcare Network, Philadelphia.
The odds of having lost a malpractice case that resulted in monetary compensation independently increased with the number of years in practice (OR, 1.09; P less than .0005), and the number of lawsuits experienced (OR, 1.42; P = .02). "The type of practice and the lack of a bariatric surgeon expert witness did not independently predict a payout," Dr. Dallal said.
Nearly 7% of survey respondents reported that the primary expert witness in determining the standard of bariatric surgery care was not a bariatric surgeon. In such cases, the surgeon-defendant had an 11-fold increased risk of having a lawsuit (P = .018). However, the use of an expert witness who was not a bariatric surgeon was not associated with the chance of settlement or the case’s going to trial.
Dr. Dallal noted that many lawsuits are filed about 2 years after the alleged injury, and another 1-2 years may pass before resolution of that lawsuit occurs. "So, there is a built-in bias against surgeons who have been in practice longer," he said.
He noted that successful lawsuits that are based on patient harm "do occur and are devastating to all involved. Improving the patient safety culture is the mainstay of reducing liability risk."
Dr. Dallal said that he had no relevant financial conflicts to disclose.
SAN DIEGO – The most experienced bariatric surgeons are those who are most likely to be sued, judging by responses to a survey from more than 300 members of the American Society for Metabolic and Bariatric Surgery.
"There are no resources, national registries, or easily accessible databases to analyze bariatric-specific medical malpractice claims in the United States," Dr. Ramsey M. Dallal said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "Without the ability to analyze aggregate data, surgeons cannot easily study common causes of medical malpractice litigation and develop patient safety improvements. Nor do there exist easily accessible measures of trends in bariatric surgery litigation."
In an effort to obtain a snapshot of the liability landscape in bariatric surgery, Dr. Dallal and other members of the ASMBS Patient Safety Committee e-mailed a survey to 1,672 surgeon members of the ASMBS in July 2011. A total of 330 surgeons in 46 states responded, for a response rate of 20%. Their mean number of years in practice was 15, which represented 5,042 years of bariatric surgery–specific liability exposure. Most respondents (38%) practiced in a hospital or academic group, 26% in a single specialty group, 20% in solo practice, 13% in a multispecialty group, and 3% in other settings.
Nine respondents chose not to have malpractice insurance. Those who were insured reported a mean yearly cost of malpractice insurance of $59,200.
Nearly half of respondents (48%) reported having no malpractice insurance cases since their careers began, but the average number of lifetime cases reported by their counterparts was 1.5.
Of the 464 lawsuits reported by 156 surgeons, 54% were dropped or dismissed, 27% were settled out of court, and 19% went to trial or arbitration.
Of those cases that went to trial, 72% were found in favor of the surgeon-defendant. The mean lifetime amount paid in lawsuits was $250,000, including one settlement for $7,000,000. The total amount paid by the respondents was $70,871,998.
Using multivariate logistic regression analysis, the researchers determined that the probability of reporting at least one lawsuit independently increased with the number of years in practice (odds ratio, 1.03; P = .03) and among those who have performed more than 1,000 cases (OR, 8.5%; P = .01). "In essence, our most experienced surgeons are the ones being sued the most," said Dr. Dallal, chief of bariatric/minimally invasive surgery at Einstein Healthcare Network, Philadelphia.
The odds of having lost a malpractice case that resulted in monetary compensation independently increased with the number of years in practice (OR, 1.09; P less than .0005), and the number of lawsuits experienced (OR, 1.42; P = .02). "The type of practice and the lack of a bariatric surgeon expert witness did not independently predict a payout," Dr. Dallal said.
Nearly 7% of survey respondents reported that the primary expert witness in determining the standard of bariatric surgery care was not a bariatric surgeon. In such cases, the surgeon-defendant had an 11-fold increased risk of having a lawsuit (P = .018). However, the use of an expert witness who was not a bariatric surgeon was not associated with the chance of settlement or the case’s going to trial.
Dr. Dallal noted that many lawsuits are filed about 2 years after the alleged injury, and another 1-2 years may pass before resolution of that lawsuit occurs. "So, there is a built-in bias against surgeons who have been in practice longer," he said.
He noted that successful lawsuits that are based on patient harm "do occur and are devastating to all involved. Improving the patient safety culture is the mainstay of reducing liability risk."
Dr. Dallal said that he had no relevant financial conflicts to disclose.
SAN DIEGO – The most experienced bariatric surgeons are those who are most likely to be sued, judging by responses to a survey from more than 300 members of the American Society for Metabolic and Bariatric Surgery.
"There are no resources, national registries, or easily accessible databases to analyze bariatric-specific medical malpractice claims in the United States," Dr. Ramsey M. Dallal said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "Without the ability to analyze aggregate data, surgeons cannot easily study common causes of medical malpractice litigation and develop patient safety improvements. Nor do there exist easily accessible measures of trends in bariatric surgery litigation."
In an effort to obtain a snapshot of the liability landscape in bariatric surgery, Dr. Dallal and other members of the ASMBS Patient Safety Committee e-mailed a survey to 1,672 surgeon members of the ASMBS in July 2011. A total of 330 surgeons in 46 states responded, for a response rate of 20%. Their mean number of years in practice was 15, which represented 5,042 years of bariatric surgery–specific liability exposure. Most respondents (38%) practiced in a hospital or academic group, 26% in a single specialty group, 20% in solo practice, 13% in a multispecialty group, and 3% in other settings.
Nine respondents chose not to have malpractice insurance. Those who were insured reported a mean yearly cost of malpractice insurance of $59,200.
Nearly half of respondents (48%) reported having no malpractice insurance cases since their careers began, but the average number of lifetime cases reported by their counterparts was 1.5.
Of the 464 lawsuits reported by 156 surgeons, 54% were dropped or dismissed, 27% were settled out of court, and 19% went to trial or arbitration.
Of those cases that went to trial, 72% were found in favor of the surgeon-defendant. The mean lifetime amount paid in lawsuits was $250,000, including one settlement for $7,000,000. The total amount paid by the respondents was $70,871,998.
Using multivariate logistic regression analysis, the researchers determined that the probability of reporting at least one lawsuit independently increased with the number of years in practice (odds ratio, 1.03; P = .03) and among those who have performed more than 1,000 cases (OR, 8.5%; P = .01). "In essence, our most experienced surgeons are the ones being sued the most," said Dr. Dallal, chief of bariatric/minimally invasive surgery at Einstein Healthcare Network, Philadelphia.
The odds of having lost a malpractice case that resulted in monetary compensation independently increased with the number of years in practice (OR, 1.09; P less than .0005), and the number of lawsuits experienced (OR, 1.42; P = .02). "The type of practice and the lack of a bariatric surgeon expert witness did not independently predict a payout," Dr. Dallal said.
Nearly 7% of survey respondents reported that the primary expert witness in determining the standard of bariatric surgery care was not a bariatric surgeon. In such cases, the surgeon-defendant had an 11-fold increased risk of having a lawsuit (P = .018). However, the use of an expert witness who was not a bariatric surgeon was not associated with the chance of settlement or the case’s going to trial.
Dr. Dallal noted that many lawsuits are filed about 2 years after the alleged injury, and another 1-2 years may pass before resolution of that lawsuit occurs. "So, there is a built-in bias against surgeons who have been in practice longer," he said.
He noted that successful lawsuits that are based on patient harm "do occur and are devastating to all involved. Improving the patient safety culture is the mainstay of reducing liability risk."
Dr. Dallal said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: The probability of reporting at least one lawsuit independently increased with the number of years in practice (OR, 1.03; P = .03) and among those who have performed more than 1,000 cases (OR, 8.5%; P = .01).
Data Source: The findings are based on responses to a survey from 330 members of the American Society of Metabolic and Bariatric Surgery.
Disclosures: Dr. Dallal said that he had no relevant financial conflicts to disclose.
Endoscopy Exposure Generally Low Among Surgical Trainees
SAN DIEGO – Exposure to endoscopy is generally low among surgical trainees, yet most bariatric surgeons continue to perform endoscopy and manage complications, responses to a survey indicate.
"There is a varying amount of endoscopic training during surgical residency and fellowship, and endoscopic practices are not standardized," Dr. Bipan Chand said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "Surgeons today perform varying degrees of endoscopy, pre- and postoperatively, as well as diagnostic and therapeutic procedures."
Dr. Chand and his associates sent a 19-question online survey to 1,670 active surgeon members of the ASMBS during a 1-month time frame in an effort to "obtain a better understanding on the current amount of exposure to endoscopy, to obtain information on the amount of diagnostic and therapeutic procedures being performed, by whom and [what the] the comfort level [is]."
Of the 1,670 members, 291 (17%) completed the survey, said Dr. Chand, director of metabolic surgery and bariatric care at Loyola University, Chicago. The largest proportion of respondents (30.9%) were more than 15 years removed from surgical training, whereas 18.9% were 11-15 years removed, 23.4% were 6-10 years removed, 23.4% were 1-5 years removed, and 3.4% were less than 1 year removed.
Nearly 60% of respondents completed a postresidency fellowship. Of these, 38% completed a fellowship in bariatric surgery with an emphasis in minimally invasive surgery (MIS), and 31% completed a fellowship in general MIS.
Dr. Chand, who chairs the ASMBS Emerging Technology and Procedures Committee, reported that during their combined residency and fellowship training, 25% of respondents performed fewer than 25 diagnostic procedures and 55% performed fewer than 5 therapeutic procedures such as dilation and treatment of bleeding.
After completing their training, 41% of respondents reported performing routine preoperative endoscopy for primary bariatric procedures, and 90% reported performing routine preoperative upper endoscopy for revisional bariatric procedures. More than 70% of these procedures were being done by the respondents or by their surgical partners.
Overall, 49% of respondents said they felt "very comfortable" with endoscopic management of bariatric complications, including bleeding, dilation of strictures, removal of foreign bodies, and stent placement.
More than three-quarters of respondents (78%) expressed interest in additional endoscopy training via postgraduate courses, particularly those related to advanced training techniques, whereas 53% and 56%, respectively, predicted that endoscopic procedures will play a role as primary and revisional endoluminal bariatric therapies.
More than two-thirds of surgeons (69%) said that they plan to increase the amount of endoscopy in their practice. "The ASMBS will continue to offer training labs to surgeons to help [them] acquire and refine these important skills," Dr. Chand said. "One such lab was offered at this year’s annual meeting."
Dr. Chand said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Exposure to endoscopy is generally low among surgical trainees, yet most bariatric surgeons continue to perform endoscopy and manage complications, responses to a survey indicate.
"There is a varying amount of endoscopic training during surgical residency and fellowship, and endoscopic practices are not standardized," Dr. Bipan Chand said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "Surgeons today perform varying degrees of endoscopy, pre- and postoperatively, as well as diagnostic and therapeutic procedures."
Dr. Chand and his associates sent a 19-question online survey to 1,670 active surgeon members of the ASMBS during a 1-month time frame in an effort to "obtain a better understanding on the current amount of exposure to endoscopy, to obtain information on the amount of diagnostic and therapeutic procedures being performed, by whom and [what the] the comfort level [is]."
Of the 1,670 members, 291 (17%) completed the survey, said Dr. Chand, director of metabolic surgery and bariatric care at Loyola University, Chicago. The largest proportion of respondents (30.9%) were more than 15 years removed from surgical training, whereas 18.9% were 11-15 years removed, 23.4% were 6-10 years removed, 23.4% were 1-5 years removed, and 3.4% were less than 1 year removed.
Nearly 60% of respondents completed a postresidency fellowship. Of these, 38% completed a fellowship in bariatric surgery with an emphasis in minimally invasive surgery (MIS), and 31% completed a fellowship in general MIS.
Dr. Chand, who chairs the ASMBS Emerging Technology and Procedures Committee, reported that during their combined residency and fellowship training, 25% of respondents performed fewer than 25 diagnostic procedures and 55% performed fewer than 5 therapeutic procedures such as dilation and treatment of bleeding.
After completing their training, 41% of respondents reported performing routine preoperative endoscopy for primary bariatric procedures, and 90% reported performing routine preoperative upper endoscopy for revisional bariatric procedures. More than 70% of these procedures were being done by the respondents or by their surgical partners.
Overall, 49% of respondents said they felt "very comfortable" with endoscopic management of bariatric complications, including bleeding, dilation of strictures, removal of foreign bodies, and stent placement.
More than three-quarters of respondents (78%) expressed interest in additional endoscopy training via postgraduate courses, particularly those related to advanced training techniques, whereas 53% and 56%, respectively, predicted that endoscopic procedures will play a role as primary and revisional endoluminal bariatric therapies.
More than two-thirds of surgeons (69%) said that they plan to increase the amount of endoscopy in their practice. "The ASMBS will continue to offer training labs to surgeons to help [them] acquire and refine these important skills," Dr. Chand said. "One such lab was offered at this year’s annual meeting."
Dr. Chand said that he had no relevant financial conflicts to disclose.
SAN DIEGO – Exposure to endoscopy is generally low among surgical trainees, yet most bariatric surgeons continue to perform endoscopy and manage complications, responses to a survey indicate.
"There is a varying amount of endoscopic training during surgical residency and fellowship, and endoscopic practices are not standardized," Dr. Bipan Chand said at the annual meeting of the American Society for Metabolic and Bariatric Surgery. "Surgeons today perform varying degrees of endoscopy, pre- and postoperatively, as well as diagnostic and therapeutic procedures."
Dr. Chand and his associates sent a 19-question online survey to 1,670 active surgeon members of the ASMBS during a 1-month time frame in an effort to "obtain a better understanding on the current amount of exposure to endoscopy, to obtain information on the amount of diagnostic and therapeutic procedures being performed, by whom and [what the] the comfort level [is]."
Of the 1,670 members, 291 (17%) completed the survey, said Dr. Chand, director of metabolic surgery and bariatric care at Loyola University, Chicago. The largest proportion of respondents (30.9%) were more than 15 years removed from surgical training, whereas 18.9% were 11-15 years removed, 23.4% were 6-10 years removed, 23.4% were 1-5 years removed, and 3.4% were less than 1 year removed.
Nearly 60% of respondents completed a postresidency fellowship. Of these, 38% completed a fellowship in bariatric surgery with an emphasis in minimally invasive surgery (MIS), and 31% completed a fellowship in general MIS.
Dr. Chand, who chairs the ASMBS Emerging Technology and Procedures Committee, reported that during their combined residency and fellowship training, 25% of respondents performed fewer than 25 diagnostic procedures and 55% performed fewer than 5 therapeutic procedures such as dilation and treatment of bleeding.
After completing their training, 41% of respondents reported performing routine preoperative endoscopy for primary bariatric procedures, and 90% reported performing routine preoperative upper endoscopy for revisional bariatric procedures. More than 70% of these procedures were being done by the respondents or by their surgical partners.
Overall, 49% of respondents said they felt "very comfortable" with endoscopic management of bariatric complications, including bleeding, dilation of strictures, removal of foreign bodies, and stent placement.
More than three-quarters of respondents (78%) expressed interest in additional endoscopy training via postgraduate courses, particularly those related to advanced training techniques, whereas 53% and 56%, respectively, predicted that endoscopic procedures will play a role as primary and revisional endoluminal bariatric therapies.
More than two-thirds of surgeons (69%) said that they plan to increase the amount of endoscopy in their practice. "The ASMBS will continue to offer training labs to surgeons to help [them] acquire and refine these important skills," Dr. Chand said. "One such lab was offered at this year’s annual meeting."
Dr. Chand said that he had no relevant financial conflicts to disclose.
AT THE ANNUAL MEETING OF THE AMERICAN SOCIETY FOR METABOLIC AND BARIATRIC SURGERY
Major Finding: During their combined residency and fellowship training, 25% of surgeons performed fewer than 25 diagnostic endoscopic procedures and 55% performed fewer than 5 endoscopic therapeutic procedures such as dilation and treatment of bleeding.
Data Source: The study was based on responses from 291 surgeons to an online survey sent to members of the American Society for Metabolic and Bariatric Surgery.
Disclosures: Dr. Chand said he had no relevant financial conflicts to disclose.