User login
FDA approves pembrolizumab for cervical cancer
with disease progression on or after chemotherapy whose tumors express programmed cell death ligand 1, as determined by an FDA approved test.
“This indication is approved under accelerated approval based on tumor response rate and durability of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in the confirmatory trials,” the FDA said in updated labeling.
Two patients (2.6%) had a complete response, and nine (11.7%) had a partial response. Of these 11 patients, 10 had response durations of 6 months or longer. Patients were treated with 200 mg every 3 weeks until unacceptable toxicity or documented disease progression. Over a third had serious adverse reactions, most frequently anemia, fistula, hemorrhage, and infection.
“Keytruda is now the first anti-PD-1 [anti–programmed cell death 1] therapy approved for the treatment of advanced cervical cancer, providing an important new second-line option for certain patients with this disease,” Roy Baynes, MD, a Merck executive, said in a company press release.
with disease progression on or after chemotherapy whose tumors express programmed cell death ligand 1, as determined by an FDA approved test.
“This indication is approved under accelerated approval based on tumor response rate and durability of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in the confirmatory trials,” the FDA said in updated labeling.
Two patients (2.6%) had a complete response, and nine (11.7%) had a partial response. Of these 11 patients, 10 had response durations of 6 months or longer. Patients were treated with 200 mg every 3 weeks until unacceptable toxicity or documented disease progression. Over a third had serious adverse reactions, most frequently anemia, fistula, hemorrhage, and infection.
“Keytruda is now the first anti-PD-1 [anti–programmed cell death 1] therapy approved for the treatment of advanced cervical cancer, providing an important new second-line option for certain patients with this disease,” Roy Baynes, MD, a Merck executive, said in a company press release.
with disease progression on or after chemotherapy whose tumors express programmed cell death ligand 1, as determined by an FDA approved test.
“This indication is approved under accelerated approval based on tumor response rate and durability of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in the confirmatory trials,” the FDA said in updated labeling.
Two patients (2.6%) had a complete response, and nine (11.7%) had a partial response. Of these 11 patients, 10 had response durations of 6 months or longer. Patients were treated with 200 mg every 3 weeks until unacceptable toxicity or documented disease progression. Over a third had serious adverse reactions, most frequently anemia, fistula, hemorrhage, and infection.
“Keytruda is now the first anti-PD-1 [anti–programmed cell death 1] therapy approved for the treatment of advanced cervical cancer, providing an important new second-line option for certain patients with this disease,” Roy Baynes, MD, a Merck executive, said in a company press release.
A new way to classify endometrial cancer
We classify endometrial cancer so that we can communicate and define each patient’s disease status, the potential for harm, and the likelihood that adjuvant therapies might provide help. Traditional forms of classification have clearly fallen short in achieving this aim, as we all know of patients with apparent low-risk disease (such as stage IA grade 1 endometrioid carcinoma) who have had recurrences and died from their disease, and we know that many patients have been subjected to overtreatment for their cancer and have acquired lifelong toxicities of therapy. This column will explore the newer, more sophisticated molecular-based classifications that are being validated for endometrial cancer, and the ways in which this promises to personalize the treatment of endometrial cancer.

Breast cancer and melanoma are examples of the inclusion of molecular data such as hormone receptor status, HER2/neu status, or BRAF positivity resulting in advancements in personalizing therapeutics. We are now moving toward this for endometrial cancer.
What is the Cancer Genome Atlas?
In 2006 the National Institutes of Health announced an initiative to coordinate work between the National Cancer Institute and the National Human Genome Research Institute taking information about the human genome and analyzing it for key genomic alterations found in 33 common cancers. These data were combined with clinical information (such as survival) to classify the behaviors of those cancers with respect to their individual genomic alternations, in order to look for patterns in mutations and behaviors. The goal of this analysis was to shift the paradigm of cancer classification from being centered around primary organ site toward tumors’ shared genomic patterns.
In 2013 the Cancer Genome Atlas published their results of complete gene sequencing in endometrial cancer.3 The authors identified four discrete subgroups of endometrial cancer with distinct molecular mutational profiles and distinct clinical outcomes: polymerase epsilon (POLE, pronounced “pole-ee”) ultramutated, microsatellite instability (MSI) high, copy number high, and copy number low.
POLE ultramutated
An important subgroup identified in the Cancer Genome Atlas was a group of patients with a POLE ultramutated state. POLE encodes for a subunit of DNA polymerase, the enzyme responsible for replicating the leading DNA strand. Nonfunctioning POLE results in proofreading errors and a subsequent ultramutated cellular state with a predominance of single nucleotide variants. POLE proofreading domain mutations in endometrial cancer and colon cancer are associated with excellent prognosis, likely secondary to the immune response that is elicited by this ultramutated state from creation of “antigenic neoepitopes” that stimulate T-cell response. Effectively, the very mutated cell is seen as “more foreign” to the body’s immune system.
Approximately 10% of patients with endometrial cancer have a POLE ultramutated state, and, as stated above, prognosis is excellent, even if coexisting with a histologic cell type (such as serous) that is normally associated with adverse outcomes. These women tend to be younger, with a lower body mass index, higher-grade endometrioid cell type, the presence of lymphovascular space invasion, and low stage.
MSI high
MSI (microsatellite instability) is a result of epigenetic/hypermethylations or loss of expression in mismatch repair genes (such as MLH1, MSH2, MSH6, PMS2). These genes code for proteins critical in the repair of mismatches in short repeated sequences of DNA. Loss of their function results in an accumulation of errors in these sequences: MSI. It is a feature of the Lynch syndrome inherited state, but is also found sporadically in endometrial tumors. These tumors accumulate a number of mutations during cell replication that, as in POLE hypermutated tumors, are associated with eliciting an immune response.
These tumors tend to be associated with a higher-grade endometrioid cell type, the presence of lymphovascular space invasion, and an advanced stage. Patients with tumors that have been described as MSI high are candidates for “immune therapy” with the PDL1 inhibitor pembrolizumab because of their proinflammatory state and observed favorable responses in clinical trials.4
Copy number high/low
Copy number (CN) high and low refers to the results of microarrays in which hierarchical clustering was applied to identify reoccurring amplification or deletion regions. The CN-high group was associated with the poorest outcomes (recurrence and survival). There is significant overlap with mutations in TP53. Most serous carcinomas were CN high; however, 25% of patients with high-grade endometrioid cell type shared the CN-high classification. These tumors shared great molecular similarity to high-grade serous ovarian cancers and basal-like breast cancer.
Those patients who did not possess mutations that classified them as POLE hypermutated, MSI high, or CN high were classified as CN low. This group included predominantly grades 1 and 2 endometrioid adenocarcinomas of an early stage and had a favorable prognostic profile, though less favorable than those with a POLE ultramutated state, which appears to be somewhat protective.
Molecular/metabolic interactions
While molecular data are clearly important in driving a cancer cell’s behavior, other clinical and metabolic factors influence cancer behavior. For example, body mass index, adiposity, glucose, and lipid metabolism have been shown to be important drivers of cellular behavior and responsiveness to targeted therapies.5,6 Additionally age, race, and other metabolic states contribute to oncologic behavior. Future classifications of endometrial cancer are unlikely to use molecular profiles in isolation but will need to incorporate these additional patient-specific data to better predict and prognosticate outcomes.
Clinical applications
If researchers can better define and describe a patient’s endometrial cancer from the time of their biopsy, important clinical decisions might be able to be tackled. For example, in a premenopausal patient with an endometrial cancer who is considering fertility-sparing treatments, preoperative knowledge of a POLE ultramutated state (and therefore an anticipated good prognosis) might favor fertility preservation or avoid comprehensive staging which may be of limited value. Similarly, if an MSI-high profile is identified leading to a Lynch syndrome diagnosis, she may be more inclined to undergo a hysterectomy with bilateral salpingo-oophorectomy and staging as she is at known increased risk for a more advanced endometrial cancer, as well as the potential for ovarian cancer.
Postoperative incorporation of molecular data promises to be particularly helpful in guiding adjuvant therapies and sparing some women from unnecessary treatments. For example, women with high-grade endometrioid tumors who are CN high were historically treated with radiotherapy but might do better treated with systemic adjuvant therapies traditionally reserved for nonendometrioid carcinomas. Costly therapies such as immunotherapy can be directed toward those with MSI-high tumors, and the rare patient with a POLE ultramutated state who has a recurrence or advanced disease. Clinical trials will be able to cluster enrollment of patients with CN-high, serouslike cancers with those with serous cancers, rather than combining them with patients whose cancers predictably behave much differently.
Much work is still needed to validate this molecular profiling in endometrial cancer and define the algorithms associated with treatment decisions; however, it is likely that the way we describe endometrial cancer in the near future will be quite different.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures.
References
1. Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983;15(1):10-7.
2. Clarke BA et al. Endometrial carcinoma: controversies in histopathological assessment of grade and tumour cell type. J Clin Pathol. 2010;63(5):410-5.
3. Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67-73.
4. Ott PA et al. Pembrolizumab in advanced endometrial cancer: Preliminary results from the phase Ib KEYNOTE-028 study. J Clin Oncol. 2016;34(suppl):Abstract 5581.
5. Roque DR et al. Association between differential gene expression and body mass index among endometrial cancers from the Cancer Genome Atlas Project. Gynecol Oncol. 2016;142(2):317-22.
6. Talhouk A et al. New classification of endometrial cancers: The development and potential applications of genomic-based classification in research and clinical care. Gynecol Oncol Res Pract. 2016 Dec;3:14.
We classify endometrial cancer so that we can communicate and define each patient’s disease status, the potential for harm, and the likelihood that adjuvant therapies might provide help. Traditional forms of classification have clearly fallen short in achieving this aim, as we all know of patients with apparent low-risk disease (such as stage IA grade 1 endometrioid carcinoma) who have had recurrences and died from their disease, and we know that many patients have been subjected to overtreatment for their cancer and have acquired lifelong toxicities of therapy. This column will explore the newer, more sophisticated molecular-based classifications that are being validated for endometrial cancer, and the ways in which this promises to personalize the treatment of endometrial cancer.
Breast cancer and melanoma are examples of the inclusion of molecular data such as hormone receptor status, HER2/neu status, or BRAF positivity resulting in advancements in personalizing therapeutics. We are now moving toward this for endometrial cancer.
What is the Cancer Genome Atlas?
In 2006 the National Institutes of Health announced an initiative to coordinate work between the National Cancer Institute and the National Human Genome Research Institute taking information about the human genome and analyzing it for key genomic alterations found in 33 common cancers. These data were combined with clinical information (such as survival) to classify the behaviors of those cancers with respect to their individual genomic alternations, in order to look for patterns in mutations and behaviors. The goal of this analysis was to shift the paradigm of cancer classification from being centered around primary organ site toward tumors’ shared genomic patterns.
In 2013 the Cancer Genome Atlas published their results of complete gene sequencing in endometrial cancer.3 The authors identified four discrete subgroups of endometrial cancer with distinct molecular mutational profiles and distinct clinical outcomes: polymerase epsilon (POLE, pronounced “pole-ee”) ultramutated, microsatellite instability (MSI) high, copy number high, and copy number low.
POLE ultramutated
An important subgroup identified in the Cancer Genome Atlas was a group of patients with a POLE ultramutated state. POLE encodes for a subunit of DNA polymerase, the enzyme responsible for replicating the leading DNA strand. Nonfunctioning POLE results in proofreading errors and a subsequent ultramutated cellular state with a predominance of single nucleotide variants. POLE proofreading domain mutations in endometrial cancer and colon cancer are associated with excellent prognosis, likely secondary to the immune response that is elicited by this ultramutated state from creation of “antigenic neoepitopes” that stimulate T-cell response. Effectively, the very mutated cell is seen as “more foreign” to the body’s immune system.
Approximately 10% of patients with endometrial cancer have a POLE ultramutated state, and, as stated above, prognosis is excellent, even if coexisting with a histologic cell type (such as serous) that is normally associated with adverse outcomes. These women tend to be younger, with a lower body mass index, higher-grade endometrioid cell type, the presence of lymphovascular space invasion, and low stage.
MSI high
MSI (microsatellite instability) is a result of epigenetic/hypermethylations or loss of expression in mismatch repair genes (such as MLH1, MSH2, MSH6, PMS2). These genes code for proteins critical in the repair of mismatches in short repeated sequences of DNA. Loss of their function results in an accumulation of errors in these sequences: MSI. It is a feature of the Lynch syndrome inherited state, but is also found sporadically in endometrial tumors. These tumors accumulate a number of mutations during cell replication that, as in POLE hypermutated tumors, are associated with eliciting an immune response.
These tumors tend to be associated with a higher-grade endometrioid cell type, the presence of lymphovascular space invasion, and an advanced stage. Patients with tumors that have been described as MSI high are candidates for “immune therapy” with the PDL1 inhibitor pembrolizumab because of their proinflammatory state and observed favorable responses in clinical trials.4
Copy number high/low
Copy number (CN) high and low refers to the results of microarrays in which hierarchical clustering was applied to identify reoccurring amplification or deletion regions. The CN-high group was associated with the poorest outcomes (recurrence and survival). There is significant overlap with mutations in TP53. Most serous carcinomas were CN high; however, 25% of patients with high-grade endometrioid cell type shared the CN-high classification. These tumors shared great molecular similarity to high-grade serous ovarian cancers and basal-like breast cancer.
Those patients who did not possess mutations that classified them as POLE hypermutated, MSI high, or CN high were classified as CN low. This group included predominantly grades 1 and 2 endometrioid adenocarcinomas of an early stage and had a favorable prognostic profile, though less favorable than those with a POLE ultramutated state, which appears to be somewhat protective.
Molecular/metabolic interactions
While molecular data are clearly important in driving a cancer cell’s behavior, other clinical and metabolic factors influence cancer behavior. For example, body mass index, adiposity, glucose, and lipid metabolism have been shown to be important drivers of cellular behavior and responsiveness to targeted therapies.5,6 Additionally age, race, and other metabolic states contribute to oncologic behavior. Future classifications of endometrial cancer are unlikely to use molecular profiles in isolation but will need to incorporate these additional patient-specific data to better predict and prognosticate outcomes.
Clinical applications
If researchers can better define and describe a patient’s endometrial cancer from the time of their biopsy, important clinical decisions might be able to be tackled. For example, in a premenopausal patient with an endometrial cancer who is considering fertility-sparing treatments, preoperative knowledge of a POLE ultramutated state (and therefore an anticipated good prognosis) might favor fertility preservation or avoid comprehensive staging which may be of limited value. Similarly, if an MSI-high profile is identified leading to a Lynch syndrome diagnosis, she may be more inclined to undergo a hysterectomy with bilateral salpingo-oophorectomy and staging as she is at known increased risk for a more advanced endometrial cancer, as well as the potential for ovarian cancer.
Postoperative incorporation of molecular data promises to be particularly helpful in guiding adjuvant therapies and sparing some women from unnecessary treatments. For example, women with high-grade endometrioid tumors who are CN high were historically treated with radiotherapy but might do better treated with systemic adjuvant therapies traditionally reserved for nonendometrioid carcinomas. Costly therapies such as immunotherapy can be directed toward those with MSI-high tumors, and the rare patient with a POLE ultramutated state who has a recurrence or advanced disease. Clinical trials will be able to cluster enrollment of patients with CN-high, serouslike cancers with those with serous cancers, rather than combining them with patients whose cancers predictably behave much differently.
Much work is still needed to validate this molecular profiling in endometrial cancer and define the algorithms associated with treatment decisions; however, it is likely that the way we describe endometrial cancer in the near future will be quite different.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures.
References
1. Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983;15(1):10-7.
2. Clarke BA et al. Endometrial carcinoma: controversies in histopathological assessment of grade and tumour cell type. J Clin Pathol. 2010;63(5):410-5.
3. Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67-73.
4. Ott PA et al. Pembrolizumab in advanced endometrial cancer: Preliminary results from the phase Ib KEYNOTE-028 study. J Clin Oncol. 2016;34(suppl):Abstract 5581.
5. Roque DR et al. Association between differential gene expression and body mass index among endometrial cancers from the Cancer Genome Atlas Project. Gynecol Oncol. 2016;142(2):317-22.
6. Talhouk A et al. New classification of endometrial cancers: The development and potential applications of genomic-based classification in research and clinical care. Gynecol Oncol Res Pract. 2016 Dec;3:14.
We classify endometrial cancer so that we can communicate and define each patient’s disease status, the potential for harm, and the likelihood that adjuvant therapies might provide help. Traditional forms of classification have clearly fallen short in achieving this aim, as we all know of patients with apparent low-risk disease (such as stage IA grade 1 endometrioid carcinoma) who have had recurrences and died from their disease, and we know that many patients have been subjected to overtreatment for their cancer and have acquired lifelong toxicities of therapy. This column will explore the newer, more sophisticated molecular-based classifications that are being validated for endometrial cancer, and the ways in which this promises to personalize the treatment of endometrial cancer.
Breast cancer and melanoma are examples of the inclusion of molecular data such as hormone receptor status, HER2/neu status, or BRAF positivity resulting in advancements in personalizing therapeutics. We are now moving toward this for endometrial cancer.
What is the Cancer Genome Atlas?
In 2006 the National Institutes of Health announced an initiative to coordinate work between the National Cancer Institute and the National Human Genome Research Institute taking information about the human genome and analyzing it for key genomic alterations found in 33 common cancers. These data were combined with clinical information (such as survival) to classify the behaviors of those cancers with respect to their individual genomic alternations, in order to look for patterns in mutations and behaviors. The goal of this analysis was to shift the paradigm of cancer classification from being centered around primary organ site toward tumors’ shared genomic patterns.
In 2013 the Cancer Genome Atlas published their results of complete gene sequencing in endometrial cancer.3 The authors identified four discrete subgroups of endometrial cancer with distinct molecular mutational profiles and distinct clinical outcomes: polymerase epsilon (POLE, pronounced “pole-ee”) ultramutated, microsatellite instability (MSI) high, copy number high, and copy number low.
POLE ultramutated
An important subgroup identified in the Cancer Genome Atlas was a group of patients with a POLE ultramutated state. POLE encodes for a subunit of DNA polymerase, the enzyme responsible for replicating the leading DNA strand. Nonfunctioning POLE results in proofreading errors and a subsequent ultramutated cellular state with a predominance of single nucleotide variants. POLE proofreading domain mutations in endometrial cancer and colon cancer are associated with excellent prognosis, likely secondary to the immune response that is elicited by this ultramutated state from creation of “antigenic neoepitopes” that stimulate T-cell response. Effectively, the very mutated cell is seen as “more foreign” to the body’s immune system.
Approximately 10% of patients with endometrial cancer have a POLE ultramutated state, and, as stated above, prognosis is excellent, even if coexisting with a histologic cell type (such as serous) that is normally associated with adverse outcomes. These women tend to be younger, with a lower body mass index, higher-grade endometrioid cell type, the presence of lymphovascular space invasion, and low stage.
MSI high
MSI (microsatellite instability) is a result of epigenetic/hypermethylations or loss of expression in mismatch repair genes (such as MLH1, MSH2, MSH6, PMS2). These genes code for proteins critical in the repair of mismatches in short repeated sequences of DNA. Loss of their function results in an accumulation of errors in these sequences: MSI. It is a feature of the Lynch syndrome inherited state, but is also found sporadically in endometrial tumors. These tumors accumulate a number of mutations during cell replication that, as in POLE hypermutated tumors, are associated with eliciting an immune response.
These tumors tend to be associated with a higher-grade endometrioid cell type, the presence of lymphovascular space invasion, and an advanced stage. Patients with tumors that have been described as MSI high are candidates for “immune therapy” with the PDL1 inhibitor pembrolizumab because of their proinflammatory state and observed favorable responses in clinical trials.4
Copy number high/low
Copy number (CN) high and low refers to the results of microarrays in which hierarchical clustering was applied to identify reoccurring amplification or deletion regions. The CN-high group was associated with the poorest outcomes (recurrence and survival). There is significant overlap with mutations in TP53. Most serous carcinomas were CN high; however, 25% of patients with high-grade endometrioid cell type shared the CN-high classification. These tumors shared great molecular similarity to high-grade serous ovarian cancers and basal-like breast cancer.
Those patients who did not possess mutations that classified them as POLE hypermutated, MSI high, or CN high were classified as CN low. This group included predominantly grades 1 and 2 endometrioid adenocarcinomas of an early stage and had a favorable prognostic profile, though less favorable than those with a POLE ultramutated state, which appears to be somewhat protective.
Molecular/metabolic interactions
While molecular data are clearly important in driving a cancer cell’s behavior, other clinical and metabolic factors influence cancer behavior. For example, body mass index, adiposity, glucose, and lipid metabolism have been shown to be important drivers of cellular behavior and responsiveness to targeted therapies.5,6 Additionally age, race, and other metabolic states contribute to oncologic behavior. Future classifications of endometrial cancer are unlikely to use molecular profiles in isolation but will need to incorporate these additional patient-specific data to better predict and prognosticate outcomes.
Clinical applications
If researchers can better define and describe a patient’s endometrial cancer from the time of their biopsy, important clinical decisions might be able to be tackled. For example, in a premenopausal patient with an endometrial cancer who is considering fertility-sparing treatments, preoperative knowledge of a POLE ultramutated state (and therefore an anticipated good prognosis) might favor fertility preservation or avoid comprehensive staging which may be of limited value. Similarly, if an MSI-high profile is identified leading to a Lynch syndrome diagnosis, she may be more inclined to undergo a hysterectomy with bilateral salpingo-oophorectomy and staging as she is at known increased risk for a more advanced endometrial cancer, as well as the potential for ovarian cancer.
Postoperative incorporation of molecular data promises to be particularly helpful in guiding adjuvant therapies and sparing some women from unnecessary treatments. For example, women with high-grade endometrioid tumors who are CN high were historically treated with radiotherapy but might do better treated with systemic adjuvant therapies traditionally reserved for nonendometrioid carcinomas. Costly therapies such as immunotherapy can be directed toward those with MSI-high tumors, and the rare patient with a POLE ultramutated state who has a recurrence or advanced disease. Clinical trials will be able to cluster enrollment of patients with CN-high, serouslike cancers with those with serous cancers, rather than combining them with patients whose cancers predictably behave much differently.
Much work is still needed to validate this molecular profiling in endometrial cancer and define the algorithms associated with treatment decisions; however, it is likely that the way we describe endometrial cancer in the near future will be quite different.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no disclosures.
References
1. Bokhman JV. Two pathogenetic types of endometrial carcinoma. Gynecol Oncol. 1983;15(1):10-7.
2. Clarke BA et al. Endometrial carcinoma: controversies in histopathological assessment of grade and tumour cell type. J Clin Pathol. 2010;63(5):410-5.
3. Cancer Genome Atlas Research Network. Integrated genomic characterization of endometrial carcinoma. Nature. 2013;497(7447):67-73.
4. Ott PA et al. Pembrolizumab in advanced endometrial cancer: Preliminary results from the phase Ib KEYNOTE-028 study. J Clin Oncol. 2016;34(suppl):Abstract 5581.
5. Roque DR et al. Association between differential gene expression and body mass index among endometrial cancers from the Cancer Genome Atlas Project. Gynecol Oncol. 2016;142(2):317-22.
6. Talhouk A et al. New classification of endometrial cancers: The development and potential applications of genomic-based classification in research and clinical care. Gynecol Oncol Res Pract. 2016 Dec;3:14.
Trachelectomy rate for early-stage cervical cancer rises to 17% in younger women
based on a recent analysis of the National Cancer Database.
Of 15,150 patients analyzed, the vast majority (97.1%) underwent hysterectomy, but trachelectomy performance increased from 1.5% (95% confidence interval, 0.8%-2.2%; P less than .001) in 2004 to 3.8% (95% CI, 2.7%-4.8%; P less than .001) by 2014. The increase was mostly seen among women younger than 30 years old. In that group, trachelectomy increased from 4.6% (95% CI, 1.0%-8.2%; P less than .001) in 2004 to 17% (95% CI, 10.2%-23.7%; P less than .001) in 2014. Rates among women aged 30-49 years were relatively stable over the same period.
“A possible explanation for this rise in trachelectomy is the trend in delayed childbearing in women in the United States,” wrote Rosa R. Cui, MD, a resident at Columbia University, New York, and her coauthors.
In the analysis, mortality risk and 5-year survival rates were similar between the two procedures. Overall cohort 5-year survival was nearly identical with hysterectomy and trachelectomy at 92.4% and 92.3%, respectively. For stages IA2, IB1, and IB not specified, tumor stage was not associated with differences in 5-year survival for the two procedures. As few patients with stage IB2 tumors received trachelectomy, that data was excluded from the analysis.
Though increasing tumor size made trachelectomy less likely, 30% of patients in the study who underwent trachelectomy had a tumor greater than 2 cm in diameter, and 4% had a tumor greater than 4 cm in diameter. The researchers noted studies published in the past few years suggest abdominal radical trachelectomy may be a safe option for larger tumors, compared with vaginal trachelectomy. In the current analysis, they did not find a statistically significant decrease in survival for trachelectomy patients with tumors greater than 2 cm in diameter, but the sample size was small.
“The trachelectomy procedure has evolved significantly since it was initially described and now encompasses several approaches,” and can be performed more or less conservatively depending on the diagnosis “without compromising outcomes,” wrote Dr. Cui and her coauthors.
The researchers noted that the National Cancer Database does not have data on fertility outcomes, a possible focus of future studies of trachelectomy.
Two coauthors disclosed grants and a fellowship from the National Cancer Institute, and others disclosed consulting for several pharmaceutical companies including Pfizer, Teva, and Eisai.
SOURCE: Cui RR et al. Obstet Gynecol. 2018 Jun;131(6):1085-94.
based on a recent analysis of the National Cancer Database.
Of 15,150 patients analyzed, the vast majority (97.1%) underwent hysterectomy, but trachelectomy performance increased from 1.5% (95% confidence interval, 0.8%-2.2%; P less than .001) in 2004 to 3.8% (95% CI, 2.7%-4.8%; P less than .001) by 2014. The increase was mostly seen among women younger than 30 years old. In that group, trachelectomy increased from 4.6% (95% CI, 1.0%-8.2%; P less than .001) in 2004 to 17% (95% CI, 10.2%-23.7%; P less than .001) in 2014. Rates among women aged 30-49 years were relatively stable over the same period.
“A possible explanation for this rise in trachelectomy is the trend in delayed childbearing in women in the United States,” wrote Rosa R. Cui, MD, a resident at Columbia University, New York, and her coauthors.
In the analysis, mortality risk and 5-year survival rates were similar between the two procedures. Overall cohort 5-year survival was nearly identical with hysterectomy and trachelectomy at 92.4% and 92.3%, respectively. For stages IA2, IB1, and IB not specified, tumor stage was not associated with differences in 5-year survival for the two procedures. As few patients with stage IB2 tumors received trachelectomy, that data was excluded from the analysis.
Though increasing tumor size made trachelectomy less likely, 30% of patients in the study who underwent trachelectomy had a tumor greater than 2 cm in diameter, and 4% had a tumor greater than 4 cm in diameter. The researchers noted studies published in the past few years suggest abdominal radical trachelectomy may be a safe option for larger tumors, compared with vaginal trachelectomy. In the current analysis, they did not find a statistically significant decrease in survival for trachelectomy patients with tumors greater than 2 cm in diameter, but the sample size was small.
“The trachelectomy procedure has evolved significantly since it was initially described and now encompasses several approaches,” and can be performed more or less conservatively depending on the diagnosis “without compromising outcomes,” wrote Dr. Cui and her coauthors.
The researchers noted that the National Cancer Database does not have data on fertility outcomes, a possible focus of future studies of trachelectomy.
Two coauthors disclosed grants and a fellowship from the National Cancer Institute, and others disclosed consulting for several pharmaceutical companies including Pfizer, Teva, and Eisai.
SOURCE: Cui RR et al. Obstet Gynecol. 2018 Jun;131(6):1085-94.
based on a recent analysis of the National Cancer Database.
Of 15,150 patients analyzed, the vast majority (97.1%) underwent hysterectomy, but trachelectomy performance increased from 1.5% (95% confidence interval, 0.8%-2.2%; P less than .001) in 2004 to 3.8% (95% CI, 2.7%-4.8%; P less than .001) by 2014. The increase was mostly seen among women younger than 30 years old. In that group, trachelectomy increased from 4.6% (95% CI, 1.0%-8.2%; P less than .001) in 2004 to 17% (95% CI, 10.2%-23.7%; P less than .001) in 2014. Rates among women aged 30-49 years were relatively stable over the same period.
“A possible explanation for this rise in trachelectomy is the trend in delayed childbearing in women in the United States,” wrote Rosa R. Cui, MD, a resident at Columbia University, New York, and her coauthors.
In the analysis, mortality risk and 5-year survival rates were similar between the two procedures. Overall cohort 5-year survival was nearly identical with hysterectomy and trachelectomy at 92.4% and 92.3%, respectively. For stages IA2, IB1, and IB not specified, tumor stage was not associated with differences in 5-year survival for the two procedures. As few patients with stage IB2 tumors received trachelectomy, that data was excluded from the analysis.
Though increasing tumor size made trachelectomy less likely, 30% of patients in the study who underwent trachelectomy had a tumor greater than 2 cm in diameter, and 4% had a tumor greater than 4 cm in diameter. The researchers noted studies published in the past few years suggest abdominal radical trachelectomy may be a safe option for larger tumors, compared with vaginal trachelectomy. In the current analysis, they did not find a statistically significant decrease in survival for trachelectomy patients with tumors greater than 2 cm in diameter, but the sample size was small.
“The trachelectomy procedure has evolved significantly since it was initially described and now encompasses several approaches,” and can be performed more or less conservatively depending on the diagnosis “without compromising outcomes,” wrote Dr. Cui and her coauthors.
The researchers noted that the National Cancer Database does not have data on fertility outcomes, a possible focus of future studies of trachelectomy.
Two coauthors disclosed grants and a fellowship from the National Cancer Institute, and others disclosed consulting for several pharmaceutical companies including Pfizer, Teva, and Eisai.
SOURCE: Cui RR et al. Obstet Gynecol. 2018 Jun;131(6):1085-94.
FROM OBSTETRICS & GYNECOLOGY
Pembrolizumab monotherapy shows activity in advanced recurrent ovarian cancer
CHICAGO – Pembrolizumab monotherapy is associated with antitumor activity in patients with advanced recurrent ovarian cancer, interim results from the phase 2 KEYNOTE-100 study suggest.
Notably, objective response rates among study subjects increased in tandem with increased programmed death-ligand 1 (PD-L1) expression, which helps define the population most likely to benefit from single agent pembrolizumab (Keytruda), Ursula A. Matulonis reported during an oral abstract session at the annual meeting of the American Society of Clinical Oncology.
Further, no new safety signals were identified, said Dr. Matulonis, medical director and program leader of the Medical Gynecologic Oncology Program at of Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, both in Boston.
All patients received intravenous pembrolizumab at 200 mg every 3 weeks for 2 years or until progression, death, unacceptable toxicity, or consent withdrawal, and tumor imaging was performed every 9 weeks for a year, then every 12 weeks thereafter until progressive disease, death, or study completion.
The overall response rate (ORR) among 285 patients in Cohort A, who had one to three prior chemotherapy lines for recurrent advanced ovarian cancer and a platinum-free or treatment-free interval of 3-12 months, was 7.4%, with mean duration of response of 8.2 months. The ORR among 91 patients in Cohort B, who had four to six prior chemotherapy lines and a platinum-free or treatment-free interval of at least 3 months, was 9.9%; the mean duration of response was not reached in Cohort B.
Among all-comers, the ORR was 8.0%, including 7 complete responses and 23 partial responses. Mean duration of response was 8.2 months, and 65.5% of responses lasted at least 6 months. Further, responses were observed across all subgroups, Dr. Matulonis said, noting that responses were seen regardless of age, prior lines of treatment, progression-free/treatment-free interval duration, platinum sensitivity, and histology.
“The one factor that did predict response was a [combined positive score] of 10 or higher, where there were more responses,” she said.
The ORRs among those with PD-L1 expression as measured using the combined positive score (CPS), which is defined as the number of PD-L1–positive cells out of the total number of tumor cells x 100, was 5.0% in those with CPS less than 1, 10.2% in those with CPS of 1 or greater, and 17.1% in those with CPS of 10 or greater (vs. the 8.0% ORR in the study), she explained, noting that all complete responses occurred in those with CPS of 10 or higher.
Grade 3-4 treatment-related adverse events occurred in 19.7% of patients, and included fatigue in 2.7%, and anemia, colitis, increased amylase, increased blood alkaline phosphatase, ascites, and diarrhea in 0.8-1.3%. One treatment-related death occurred in a patient with Stevens-Johnson syndrome, and another occurred in a patient with hypoaldosteronism. Immune-mediated adverse events and infusion reactions were most commonly hyperthyroidism and hypothyroidism, and most cases were grade 1-2, she said.
KEYNOTE-100 is an ongoing study that followed KEYNOTE-028, which demonstrated the clinical activity of pembrolizumab in patients with advanced ovarian cancer. To date, KEYNOTE-100 has enrolled 376 patients with epithelial ovarian, fallopian tube, or primary peritoneal cancer and confirmed recurrence after frontline platinum-based therapy. All had a tumor sample available for biomarker analysis.
The patients had a mean age of 61 years, 64% and 35% had performance status scores of 0 and 1, respectively, and 75% had high-grade serous disease.
Median follow-up in Cohort A at the time of the current analysis was 16.7 months, and in Cohort B, the median follow-up was 17.3 months. Treatment was ongoing in 15 and 6 patients in the cohorts, respectively. Reasons for discontinuation included radiographic progression (204 and 62 patients), clinical progression (24 and 17 patients), adverse events (22 and 3 patients), and patient withdrawal (9 and 3 patients). Complete responses occurred in 1 and 0 patients in the groups, respectively.
Median progression-free survival in both cohorts was 2.1 months, and overall survival was not reached in Cohort A, while it was 17.6 months in the more heavily pretreated Cohort B.
“Recurrent ovarian cancer is the leading cause of death from gynecologic cancer. The majority of our patients relapse after first-line platinum and taxane-based chemotherapy, and the degree of platinum sensitivity will predict the tumor response rates with platinum, as well as survival time,” she said, noting that subsequent recurrences become increasingly platinum and treatment resistant.
Current treatment options in these patients include chemotherapy with or without bevacizumab; the ORRs with single-agent immune checkpoint blockade are about 10%, but in KEYNOTE-028, patients with PD-L1–positive advanced recurrent ovarian cancer had an ORR of 11.5% with pembrolizumab treatment, she said.
“With 16.9 months median follow-up, the results confirm that pembrolizumab monotherapy in recurrent ovarian cancer elicits modest antitumor efficacy,” Dr. Matulonis concluded, noting that further analysis for biomarkers predictive of pembrolizumab response are ongoing.
Invited discussant Janos Laszlo Tanyi, MD, of the University of Pennsylvania, Philadelphia, said the findings underscore the overall modest ORRs of 5.9%-15% seen with anti-PD-1 or PD-L1 monotherapy in patients with advanced recurrent ovarian cancer, but noted the importance of the finding that the subpopulation of patients with increased PD-L1 expression may experience greater benefit.
Dr. Matulonis reported consulting or advisory roles with 2X Oncology, Clovis Oncology, Fujifilm, Geneos Therapeutics, Lilly, Merck, and Myriad Genetics, and research funding from Merck and Novartis. Dr .Tanyi reported having no disclosures.
SOURCE: Matulonis UA et al. ASCO 2018, Abstract 5511.
CHICAGO – Pembrolizumab monotherapy is associated with antitumor activity in patients with advanced recurrent ovarian cancer, interim results from the phase 2 KEYNOTE-100 study suggest.
Notably, objective response rates among study subjects increased in tandem with increased programmed death-ligand 1 (PD-L1) expression, which helps define the population most likely to benefit from single agent pembrolizumab (Keytruda), Ursula A. Matulonis reported during an oral abstract session at the annual meeting of the American Society of Clinical Oncology.
Further, no new safety signals were identified, said Dr. Matulonis, medical director and program leader of the Medical Gynecologic Oncology Program at of Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, both in Boston.
All patients received intravenous pembrolizumab at 200 mg every 3 weeks for 2 years or until progression, death, unacceptable toxicity, or consent withdrawal, and tumor imaging was performed every 9 weeks for a year, then every 12 weeks thereafter until progressive disease, death, or study completion.
The overall response rate (ORR) among 285 patients in Cohort A, who had one to three prior chemotherapy lines for recurrent advanced ovarian cancer and a platinum-free or treatment-free interval of 3-12 months, was 7.4%, with mean duration of response of 8.2 months. The ORR among 91 patients in Cohort B, who had four to six prior chemotherapy lines and a platinum-free or treatment-free interval of at least 3 months, was 9.9%; the mean duration of response was not reached in Cohort B.
Among all-comers, the ORR was 8.0%, including 7 complete responses and 23 partial responses. Mean duration of response was 8.2 months, and 65.5% of responses lasted at least 6 months. Further, responses were observed across all subgroups, Dr. Matulonis said, noting that responses were seen regardless of age, prior lines of treatment, progression-free/treatment-free interval duration, platinum sensitivity, and histology.
“The one factor that did predict response was a [combined positive score] of 10 or higher, where there were more responses,” she said.
The ORRs among those with PD-L1 expression as measured using the combined positive score (CPS), which is defined as the number of PD-L1–positive cells out of the total number of tumor cells x 100, was 5.0% in those with CPS less than 1, 10.2% in those with CPS of 1 or greater, and 17.1% in those with CPS of 10 or greater (vs. the 8.0% ORR in the study), she explained, noting that all complete responses occurred in those with CPS of 10 or higher.
Grade 3-4 treatment-related adverse events occurred in 19.7% of patients, and included fatigue in 2.7%, and anemia, colitis, increased amylase, increased blood alkaline phosphatase, ascites, and diarrhea in 0.8-1.3%. One treatment-related death occurred in a patient with Stevens-Johnson syndrome, and another occurred in a patient with hypoaldosteronism. Immune-mediated adverse events and infusion reactions were most commonly hyperthyroidism and hypothyroidism, and most cases were grade 1-2, she said.
KEYNOTE-100 is an ongoing study that followed KEYNOTE-028, which demonstrated the clinical activity of pembrolizumab in patients with advanced ovarian cancer. To date, KEYNOTE-100 has enrolled 376 patients with epithelial ovarian, fallopian tube, or primary peritoneal cancer and confirmed recurrence after frontline platinum-based therapy. All had a tumor sample available for biomarker analysis.
The patients had a mean age of 61 years, 64% and 35% had performance status scores of 0 and 1, respectively, and 75% had high-grade serous disease.
Median follow-up in Cohort A at the time of the current analysis was 16.7 months, and in Cohort B, the median follow-up was 17.3 months. Treatment was ongoing in 15 and 6 patients in the cohorts, respectively. Reasons for discontinuation included radiographic progression (204 and 62 patients), clinical progression (24 and 17 patients), adverse events (22 and 3 patients), and patient withdrawal (9 and 3 patients). Complete responses occurred in 1 and 0 patients in the groups, respectively.
Median progression-free survival in both cohorts was 2.1 months, and overall survival was not reached in Cohort A, while it was 17.6 months in the more heavily pretreated Cohort B.
“Recurrent ovarian cancer is the leading cause of death from gynecologic cancer. The majority of our patients relapse after first-line platinum and taxane-based chemotherapy, and the degree of platinum sensitivity will predict the tumor response rates with platinum, as well as survival time,” she said, noting that subsequent recurrences become increasingly platinum and treatment resistant.
Current treatment options in these patients include chemotherapy with or without bevacizumab; the ORRs with single-agent immune checkpoint blockade are about 10%, but in KEYNOTE-028, patients with PD-L1–positive advanced recurrent ovarian cancer had an ORR of 11.5% with pembrolizumab treatment, she said.
“With 16.9 months median follow-up, the results confirm that pembrolizumab monotherapy in recurrent ovarian cancer elicits modest antitumor efficacy,” Dr. Matulonis concluded, noting that further analysis for biomarkers predictive of pembrolizumab response are ongoing.
Invited discussant Janos Laszlo Tanyi, MD, of the University of Pennsylvania, Philadelphia, said the findings underscore the overall modest ORRs of 5.9%-15% seen with anti-PD-1 or PD-L1 monotherapy in patients with advanced recurrent ovarian cancer, but noted the importance of the finding that the subpopulation of patients with increased PD-L1 expression may experience greater benefit.
Dr. Matulonis reported consulting or advisory roles with 2X Oncology, Clovis Oncology, Fujifilm, Geneos Therapeutics, Lilly, Merck, and Myriad Genetics, and research funding from Merck and Novartis. Dr .Tanyi reported having no disclosures.
SOURCE: Matulonis UA et al. ASCO 2018, Abstract 5511.
CHICAGO – Pembrolizumab monotherapy is associated with antitumor activity in patients with advanced recurrent ovarian cancer, interim results from the phase 2 KEYNOTE-100 study suggest.
Notably, objective response rates among study subjects increased in tandem with increased programmed death-ligand 1 (PD-L1) expression, which helps define the population most likely to benefit from single agent pembrolizumab (Keytruda), Ursula A. Matulonis reported during an oral abstract session at the annual meeting of the American Society of Clinical Oncology.
Further, no new safety signals were identified, said Dr. Matulonis, medical director and program leader of the Medical Gynecologic Oncology Program at of Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, both in Boston.
All patients received intravenous pembrolizumab at 200 mg every 3 weeks for 2 years or until progression, death, unacceptable toxicity, or consent withdrawal, and tumor imaging was performed every 9 weeks for a year, then every 12 weeks thereafter until progressive disease, death, or study completion.
The overall response rate (ORR) among 285 patients in Cohort A, who had one to three prior chemotherapy lines for recurrent advanced ovarian cancer and a platinum-free or treatment-free interval of 3-12 months, was 7.4%, with mean duration of response of 8.2 months. The ORR among 91 patients in Cohort B, who had four to six prior chemotherapy lines and a platinum-free or treatment-free interval of at least 3 months, was 9.9%; the mean duration of response was not reached in Cohort B.
Among all-comers, the ORR was 8.0%, including 7 complete responses and 23 partial responses. Mean duration of response was 8.2 months, and 65.5% of responses lasted at least 6 months. Further, responses were observed across all subgroups, Dr. Matulonis said, noting that responses were seen regardless of age, prior lines of treatment, progression-free/treatment-free interval duration, platinum sensitivity, and histology.
“The one factor that did predict response was a [combined positive score] of 10 or higher, where there were more responses,” she said.
The ORRs among those with PD-L1 expression as measured using the combined positive score (CPS), which is defined as the number of PD-L1–positive cells out of the total number of tumor cells x 100, was 5.0% in those with CPS less than 1, 10.2% in those with CPS of 1 or greater, and 17.1% in those with CPS of 10 or greater (vs. the 8.0% ORR in the study), she explained, noting that all complete responses occurred in those with CPS of 10 or higher.
Grade 3-4 treatment-related adverse events occurred in 19.7% of patients, and included fatigue in 2.7%, and anemia, colitis, increased amylase, increased blood alkaline phosphatase, ascites, and diarrhea in 0.8-1.3%. One treatment-related death occurred in a patient with Stevens-Johnson syndrome, and another occurred in a patient with hypoaldosteronism. Immune-mediated adverse events and infusion reactions were most commonly hyperthyroidism and hypothyroidism, and most cases were grade 1-2, she said.
KEYNOTE-100 is an ongoing study that followed KEYNOTE-028, which demonstrated the clinical activity of pembrolizumab in patients with advanced ovarian cancer. To date, KEYNOTE-100 has enrolled 376 patients with epithelial ovarian, fallopian tube, or primary peritoneal cancer and confirmed recurrence after frontline platinum-based therapy. All had a tumor sample available for biomarker analysis.
The patients had a mean age of 61 years, 64% and 35% had performance status scores of 0 and 1, respectively, and 75% had high-grade serous disease.
Median follow-up in Cohort A at the time of the current analysis was 16.7 months, and in Cohort B, the median follow-up was 17.3 months. Treatment was ongoing in 15 and 6 patients in the cohorts, respectively. Reasons for discontinuation included radiographic progression (204 and 62 patients), clinical progression (24 and 17 patients), adverse events (22 and 3 patients), and patient withdrawal (9 and 3 patients). Complete responses occurred in 1 and 0 patients in the groups, respectively.
Median progression-free survival in both cohorts was 2.1 months, and overall survival was not reached in Cohort A, while it was 17.6 months in the more heavily pretreated Cohort B.
“Recurrent ovarian cancer is the leading cause of death from gynecologic cancer. The majority of our patients relapse after first-line platinum and taxane-based chemotherapy, and the degree of platinum sensitivity will predict the tumor response rates with platinum, as well as survival time,” she said, noting that subsequent recurrences become increasingly platinum and treatment resistant.
Current treatment options in these patients include chemotherapy with or without bevacizumab; the ORRs with single-agent immune checkpoint blockade are about 10%, but in KEYNOTE-028, patients with PD-L1–positive advanced recurrent ovarian cancer had an ORR of 11.5% with pembrolizumab treatment, she said.
“With 16.9 months median follow-up, the results confirm that pembrolizumab monotherapy in recurrent ovarian cancer elicits modest antitumor efficacy,” Dr. Matulonis concluded, noting that further analysis for biomarkers predictive of pembrolizumab response are ongoing.
Invited discussant Janos Laszlo Tanyi, MD, of the University of Pennsylvania, Philadelphia, said the findings underscore the overall modest ORRs of 5.9%-15% seen with anti-PD-1 or PD-L1 monotherapy in patients with advanced recurrent ovarian cancer, but noted the importance of the finding that the subpopulation of patients with increased PD-L1 expression may experience greater benefit.
Dr. Matulonis reported consulting or advisory roles with 2X Oncology, Clovis Oncology, Fujifilm, Geneos Therapeutics, Lilly, Merck, and Myriad Genetics, and research funding from Merck and Novartis. Dr .Tanyi reported having no disclosures.
SOURCE: Matulonis UA et al. ASCO 2018, Abstract 5511.
REPORTING FROM ASCO 2018
Key clinical point: Pembrolizumab monotherapy shows antitumor activity in advanced recurrent OC, particularly in those with higher PD-L1 expression.
Major finding: Overall response rates: 8.0% overall, 5.0% with CPS up to 1, 10.2% with CPS of 1+, and 17.1% with CPS of 10+.
Study details: Interim findings from the 376-patient phase 2 KEYNOTE-100 study.
Disclosures: Dr. Matulonis reported consulting or advisory roles with 2X Oncology, Clovis Oncology, Fujifilm, Geneos Therapeutics, Lilly, Merck, and Myriad Genetics, and research funding from Merck and Novartis. Dr. Tanyi reported having no disclosures.
Source: Matulonis UA et al. ASCO 2018, Abstract 5511.
Tumor analysis: Test all MSI-high patients for Lynch Syndrome
CHICAGO – , according to “absolutely practice changing” findings from a prospective analysis of more than 15,000 tumor samples.

“The impact of these findings cannot be understated,” ASCO expert Shannon N. Westin, MD, said during a discussion of the findings presented by Zsofia K. Stadler, MD, at a press briefing at the annual meeting of the American Society of Clinical Oncology.
Lynch Syndrome (LS), an autosomal dominant inherited cancer predisposition syndrome caused by germline mutation in the DNA mismatch repair genes, is responsible for about 3% of colorectal and endometrial cancers; universal testing for tumor markers of LS is recommended in all patients with these types of cancers, said Dr. Stadler, director of the Clinical Genetics Service at Memorial Sloan Kettering Cancer Center, New York.
“This is usually done either via MSI analysis or immunohistochemical staining for the DNA mismatch repair proteins,” she said, noting that genetic testing and counseling is recommended in patients with tumors suggestive of LS, and increased surveillance and/or risk-reducing surgery is recommended in those recognized as having LS.
MSI-high is a hallmark of LS-associated cancers and has recently been implicated as a marker for response to immunotherapy. This has led to increased MSI testing in metastatic cancer regardless of cancer type.
However, the prevalence of germline mutations in the DNA mismatch repair genes diagnostic of LS across all MSI-high tumors is unknown, she said.
In 15,045 tumor samples across more than 50 cancer types, germline mutations were analyzed across tumor types and according to MSI status.
As expected, the highest level of MSI-high was seen in small bowel cancer (25%), followed by endometrial, colorectal, and gastric cancer (16%, 14%, and 6%, respectively), Dr. Stadler said.
“High frequency MSI was also seen in a number of other tumors as suggested by other papers previously,” she noted.
LS was present in 16.3% of MSI-high tumors vs. 1.9% of MSI-indeterminate (moderate MSI level) tumors, and 0.3% of microsatellite stable (MSS) tumors, she added.
Additional tumor evaluations, including immunohistochemical staining for the mismatch repair genes, were also performed.
“Our analysis corroborated the finding that in these Lynch patients, the MSI-high and MSI-indeterminate tumors were caused by Lynch Syndrome. This is in contrast to our Lynch Syndrome patients with microsatellite stable tumors; their tumor signature suggested that the Lynch Syndrome did not cause these cancers,” she said. “In fact, the prevalence of Lynch Syndrome in the MSS cohort of 0.3% is equivalent to the presence of Lynch Syndrome in the general at-large population.”
Of note, 50% of LS patients with MSI-high and indeterminate tumors had cancers other than colorectal or endometrial cancer, including prostate, sarcoma, mesothelioma, adrenocortical carcinoma, and ovarian germ cell carcinoma, which have been rarely or not previously associated with LS, and 45% of those patients did not meet clinical testing criteria for LS and would not have undergone LS testing.
This finding underscores the previously unknown heterogeneity of the phenotype.
“Our study supports that MSI-high is predictive of LS across tumor types...and also supports that the spectrum of cancers associated with Lynch Syndrome seems to be much broader that previously thought, she said, concluding that “MSI-high tumor signature, regardless of cancer subtype and irrespective of the family cancer history, should prompt germline genetic assessment for the evaluation of Lynch [Syndrome].
“This will result in an increased ability to recognize Lynch Syndrome not only in cancer patients, but also in at-risk family members who will benefit from genetic testing for Lynch [Syndrome] and subsequent enhanced cancer surveillance and risk reduction measures.”
In emphasizing the practice-changing nature of these findings, Dr. Westin, a gynecologic oncologist at MD Anderson Cancer Center, Houston, said that with the rise of precision medicine, increasing numbers of patients are undergoing testing for microsatellite instability, mainly to determine if their tumor can be affected by an-approved therapy.
“What we’ve learned is that MSI not only has therapeutic implications, it also has cancer prevention implications,” she said. “We’ve only been testing the tip of the iceberg of patients who are affected by Lynch Syndrome, and what we now know is that under the surface there is a larger number of patients with specific cancer types that should be tested for Lynch Syndrome.”
She added that this is “a straightforward testing strategy which can be immediately implemented to impact not only the patients themselves and their risk of cancer, but also their family members and their risk of cancer.”
This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
SOURCE: Schwark A et al., ASCO 2018 LBA1509.
CHICAGO – , according to “absolutely practice changing” findings from a prospective analysis of more than 15,000 tumor samples.
“The impact of these findings cannot be understated,” ASCO expert Shannon N. Westin, MD, said during a discussion of the findings presented by Zsofia K. Stadler, MD, at a press briefing at the annual meeting of the American Society of Clinical Oncology.
Lynch Syndrome (LS), an autosomal dominant inherited cancer predisposition syndrome caused by germline mutation in the DNA mismatch repair genes, is responsible for about 3% of colorectal and endometrial cancers; universal testing for tumor markers of LS is recommended in all patients with these types of cancers, said Dr. Stadler, director of the Clinical Genetics Service at Memorial Sloan Kettering Cancer Center, New York.
“This is usually done either via MSI analysis or immunohistochemical staining for the DNA mismatch repair proteins,” she said, noting that genetic testing and counseling is recommended in patients with tumors suggestive of LS, and increased surveillance and/or risk-reducing surgery is recommended in those recognized as having LS.
MSI-high is a hallmark of LS-associated cancers and has recently been implicated as a marker for response to immunotherapy. This has led to increased MSI testing in metastatic cancer regardless of cancer type.
However, the prevalence of germline mutations in the DNA mismatch repair genes diagnostic of LS across all MSI-high tumors is unknown, she said.
In 15,045 tumor samples across more than 50 cancer types, germline mutations were analyzed across tumor types and according to MSI status.
As expected, the highest level of MSI-high was seen in small bowel cancer (25%), followed by endometrial, colorectal, and gastric cancer (16%, 14%, and 6%, respectively), Dr. Stadler said.
“High frequency MSI was also seen in a number of other tumors as suggested by other papers previously,” she noted.
LS was present in 16.3% of MSI-high tumors vs. 1.9% of MSI-indeterminate (moderate MSI level) tumors, and 0.3% of microsatellite stable (MSS) tumors, she added.
Additional tumor evaluations, including immunohistochemical staining for the mismatch repair genes, were also performed.
“Our analysis corroborated the finding that in these Lynch patients, the MSI-high and MSI-indeterminate tumors were caused by Lynch Syndrome. This is in contrast to our Lynch Syndrome patients with microsatellite stable tumors; their tumor signature suggested that the Lynch Syndrome did not cause these cancers,” she said. “In fact, the prevalence of Lynch Syndrome in the MSS cohort of 0.3% is equivalent to the presence of Lynch Syndrome in the general at-large population.”
Of note, 50% of LS patients with MSI-high and indeterminate tumors had cancers other than colorectal or endometrial cancer, including prostate, sarcoma, mesothelioma, adrenocortical carcinoma, and ovarian germ cell carcinoma, which have been rarely or not previously associated with LS, and 45% of those patients did not meet clinical testing criteria for LS and would not have undergone LS testing.
This finding underscores the previously unknown heterogeneity of the phenotype.
“Our study supports that MSI-high is predictive of LS across tumor types...and also supports that the spectrum of cancers associated with Lynch Syndrome seems to be much broader that previously thought, she said, concluding that “MSI-high tumor signature, regardless of cancer subtype and irrespective of the family cancer history, should prompt germline genetic assessment for the evaluation of Lynch [Syndrome].
“This will result in an increased ability to recognize Lynch Syndrome not only in cancer patients, but also in at-risk family members who will benefit from genetic testing for Lynch [Syndrome] and subsequent enhanced cancer surveillance and risk reduction measures.”
In emphasizing the practice-changing nature of these findings, Dr. Westin, a gynecologic oncologist at MD Anderson Cancer Center, Houston, said that with the rise of precision medicine, increasing numbers of patients are undergoing testing for microsatellite instability, mainly to determine if their tumor can be affected by an-approved therapy.
“What we’ve learned is that MSI not only has therapeutic implications, it also has cancer prevention implications,” she said. “We’ve only been testing the tip of the iceberg of patients who are affected by Lynch Syndrome, and what we now know is that under the surface there is a larger number of patients with specific cancer types that should be tested for Lynch Syndrome.”
She added that this is “a straightforward testing strategy which can be immediately implemented to impact not only the patients themselves and their risk of cancer, but also their family members and their risk of cancer.”
This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
SOURCE: Schwark A et al., ASCO 2018 LBA1509.
CHICAGO – , according to “absolutely practice changing” findings from a prospective analysis of more than 15,000 tumor samples.
“The impact of these findings cannot be understated,” ASCO expert Shannon N. Westin, MD, said during a discussion of the findings presented by Zsofia K. Stadler, MD, at a press briefing at the annual meeting of the American Society of Clinical Oncology.
Lynch Syndrome (LS), an autosomal dominant inherited cancer predisposition syndrome caused by germline mutation in the DNA mismatch repair genes, is responsible for about 3% of colorectal and endometrial cancers; universal testing for tumor markers of LS is recommended in all patients with these types of cancers, said Dr. Stadler, director of the Clinical Genetics Service at Memorial Sloan Kettering Cancer Center, New York.
“This is usually done either via MSI analysis or immunohistochemical staining for the DNA mismatch repair proteins,” she said, noting that genetic testing and counseling is recommended in patients with tumors suggestive of LS, and increased surveillance and/or risk-reducing surgery is recommended in those recognized as having LS.
MSI-high is a hallmark of LS-associated cancers and has recently been implicated as a marker for response to immunotherapy. This has led to increased MSI testing in metastatic cancer regardless of cancer type.
However, the prevalence of germline mutations in the DNA mismatch repair genes diagnostic of LS across all MSI-high tumors is unknown, she said.
In 15,045 tumor samples across more than 50 cancer types, germline mutations were analyzed across tumor types and according to MSI status.
As expected, the highest level of MSI-high was seen in small bowel cancer (25%), followed by endometrial, colorectal, and gastric cancer (16%, 14%, and 6%, respectively), Dr. Stadler said.
“High frequency MSI was also seen in a number of other tumors as suggested by other papers previously,” she noted.
LS was present in 16.3% of MSI-high tumors vs. 1.9% of MSI-indeterminate (moderate MSI level) tumors, and 0.3% of microsatellite stable (MSS) tumors, she added.
Additional tumor evaluations, including immunohistochemical staining for the mismatch repair genes, were also performed.
“Our analysis corroborated the finding that in these Lynch patients, the MSI-high and MSI-indeterminate tumors were caused by Lynch Syndrome. This is in contrast to our Lynch Syndrome patients with microsatellite stable tumors; their tumor signature suggested that the Lynch Syndrome did not cause these cancers,” she said. “In fact, the prevalence of Lynch Syndrome in the MSS cohort of 0.3% is equivalent to the presence of Lynch Syndrome in the general at-large population.”
Of note, 50% of LS patients with MSI-high and indeterminate tumors had cancers other than colorectal or endometrial cancer, including prostate, sarcoma, mesothelioma, adrenocortical carcinoma, and ovarian germ cell carcinoma, which have been rarely or not previously associated with LS, and 45% of those patients did not meet clinical testing criteria for LS and would not have undergone LS testing.
This finding underscores the previously unknown heterogeneity of the phenotype.
“Our study supports that MSI-high is predictive of LS across tumor types...and also supports that the spectrum of cancers associated with Lynch Syndrome seems to be much broader that previously thought, she said, concluding that “MSI-high tumor signature, regardless of cancer subtype and irrespective of the family cancer history, should prompt germline genetic assessment for the evaluation of Lynch [Syndrome].
“This will result in an increased ability to recognize Lynch Syndrome not only in cancer patients, but also in at-risk family members who will benefit from genetic testing for Lynch [Syndrome] and subsequent enhanced cancer surveillance and risk reduction measures.”
In emphasizing the practice-changing nature of these findings, Dr. Westin, a gynecologic oncologist at MD Anderson Cancer Center, Houston, said that with the rise of precision medicine, increasing numbers of patients are undergoing testing for microsatellite instability, mainly to determine if their tumor can be affected by an-approved therapy.
“What we’ve learned is that MSI not only has therapeutic implications, it also has cancer prevention implications,” she said. “We’ve only been testing the tip of the iceberg of patients who are affected by Lynch Syndrome, and what we now know is that under the surface there is a larger number of patients with specific cancer types that should be tested for Lynch Syndrome.”
She added that this is “a straightforward testing strategy which can be immediately implemented to impact not only the patients themselves and their risk of cancer, but also their family members and their risk of cancer.”
This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
SOURCE: Schwark A et al., ASCO 2018 LBA1509.
REPORTING FROM ASCO 2018
Key clinical point: All MSI-high patients should be tested for LS regardless of cancer type or family history.
Major finding: LS was present in 16.3% of MSI-high tumors vs. 1.9% and 0.3% of MSI-indeterminate and stable tumors, respectively.
Study details: An analysis of 15,045 tumor samples.
Disclosures: This study was funded by Romeo Milio Lynch Syndrome Foundation, the Marie-Josee and Henry R. Kravis Center for Molecular Oncology, the Robert and Kate Niehaus Center for Inherited Cancer Genomics, the Fieldstone Family Fund, Stand Up to Cancer Colorectal Cancer Dream Team Translational Research Grant, and the NIH/NCI Cancer Center Support Grant. Dr. Stadler reported consulting or advisory roles on the part of an immediate family member for Allergan, Genentech/Roche, Regeneron, Optos, and Adverum.
Source: Schwark A et al. ASCO 2018 LBA 1509.
Who needs breast cancer genetics testing?
Advances in cancer genetics are rapidly changing how clinicians assess an individual’s risk for breast cancer. ObGyns counsel many women with a personal or family history of the disease, many of whom can benefit from genetics counseling and testing. As patients with a hereditary predisposition to breast cancer are at higher risk and are younger at diagnosis, it is imperative to identify them early so they can benefit from enhanced surveillance, chemoprevention, and discussions regarding risk-reducing surgeries. ObGyns are uniquely poised to identify young women at risk for hereditary cancer syndromes, and they play a crucial role in screening and prevention over the life span.
CASE Patient with breast cancer history asks about screening for her daughters
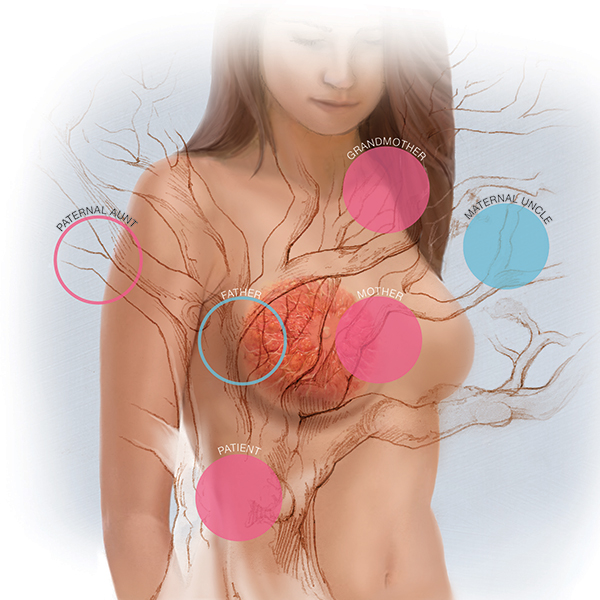
A 52-year-old woman presents for her annual examination. She underwent breast cancer treatment 10 years earlier and has done well since then. When asked about family history of breast cancer and ethnicity, she reports her mother had breast cancer later in life, and her mother’s father was of Ashkenazi Jewish ancestry.In addition, a maternal uncle had metastatic prostate cancer. You recall that breast cancer diagnosed before age 50 years and Ashkenazi ancestry are “red flags” for a hereditary cancer syndrome. The patient wonders how her daughters should be screened. What do you do next?
Having a risk assessment plan is crucial
Given increasing demands, limited time, and the abundance of information to be discussed with patients, primary care physicians may find it challenging to assess breast cancer risk, consider genetics testing for appropriate individuals, and counsel patients about risk management options. The process has become even more complex since the expansion in genetics knowledge and the advent of multigene panel testing. Not only is risk assessment crucial for this woman and her daughters, and for other patients, but a delay in diagnosing and treating breast cancer in patients with hereditary and familial cancer risks may represent a worrisome new trend in medical litigation.1,2 Clinicians must have a process in place for assessing risk in all patients and treating them appropriately.
The American Cancer Society (ACS) estimated that 252,710 cases of breast cancer would be diagnosed in 2017, leading to 40,610 deaths.3 Twelve percent to 14% of breast cancers are thought to be related to hereditary cancer predisposition syndromes.4–8 This means that, every year, almost 35,000 cases of breast cancer are attributable to hereditary risk. These cases can be detected early with enhanced surveillance, which carries the highest chance for cure, or prevented with risk-reducing surgery in identified genetic mutation carriers. Each child of a person with a genetic mutation predisposing to breast cancer has a 50% chance of inheriting the mutation and having a very high risk of cancer.
In this patient’s case, basic information is collected about her cancer-related personal and family history.
Asking a few key questions can help in stratifying risk:
- Have you or anyone in your family had cancer? What type, and at what age?
- If breast cancer, did it involve both breasts, or was it triple-negative?
- Is there a family history of ovarian cancer?
- Is there a family history of male breast cancer?
- Is there a family history of metastatic prostate cancer?
- Are you of Ashkenazi Jewish ethnicity?
- Have you or anyone in your family ever had genetics testing for cancer?
The hallmarks of hereditary cancer are multiple cancers in an individual or family; young age at diagnosis; and ovarian, pancreatic, or another rare cancer. Metastatic prostate cancer was added as a red flag for hereditary risk after a recent large series found that 11.8% of men with metastatic prostate cancer harbor germline mutations.9
CASE Continued
On further questioning, the patient reports she had triple-negative (estrogen receptor–, progesterone receptor–, and human epidermal growth factor receptor 2 [HER2]–negative) breast cancer, a feature of patients with germline BRCA1 (breast cancer susceptibility gene 1) mutations.10 In addition, her Ashkenazi ancestry is concerning, as there is a 1-in-40 chance of carrying 1 of the 3 Ashkenazi founder BRCA mutations.11 Is a genetics consultation needed?
Read about guidelines for referral and testing.
Guidelines for genetics referral and testing
According to the TABLE, which summarizes national guidelines for genetics referral, maternal and paternal family histories are equally important. Our patient was under age 50 at diagnosis, has a history of triple-negative breast cancer, is of Ashkenazi ancestry, and has a family history of metastatic prostate cancer. She meets the criteria for genetics testing, and screening for her daughters most certainly will depend on the findings of that testing. If she carries a BRCA1 mutation, as might be anticipated, each daughter would have a 50% chance of having inherited the mutation. If they carry the mutation as well, they would begin breast magnetic resonance imaging (MRI) screening at age 25.12 If they decide against genetics testing, they could still undergo MRI screening as untested first-degree relatives of a BRCA carrier, per ACS recommendations.13
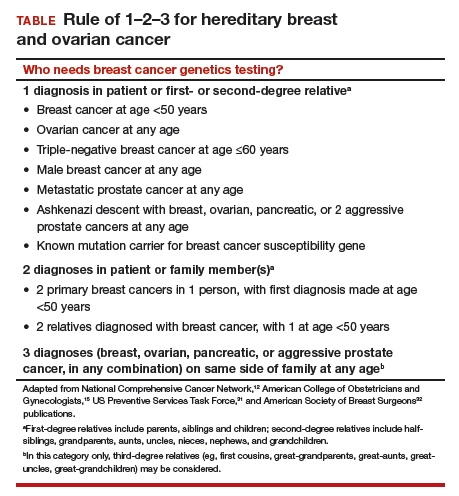
Integrating evidence and experience
Over the past 10 to 20 years, other breast cancer susceptibility genes (eg, BRCA2, PALB2, CHEK2) have been identified. More recently, next-generation sequencing has become commercially available. Laboratories can use this newer method to sequence multiple genes rapidly and in parallel, and its cost is similar to that of single-syndrome testing.14 When more than 1 gene can explain an inherited cancer syndrome, multigene panel testing may be more efficient and cost-effective. Use of multigene panel testing is supported in guidelines issued by the National Comprehensive Cancer Network,12 the American College of Obstetricians and Gynecologists,15 and other medical societies.
For our patient, the most logical strategy would be to test for the 3 mutations most common in the Ashkenazi population and then, if no mutation is found, perform multigene panel testing.
Formal genetics counseling can be very helpful for a patient, particularly in the era of multigene panel testing.16,17 A detailed pedigree (family tree) is elicited, and a genetics specialist determines whether testing is indicated and which test is best for the patient. Possible test findings are explained. The patient may be found to have a pathogenic variant with associated increased cancer risk, a negative test result (informative or uninformative), or a variant of uncertain significance (VUS). VUS is a gene mutation identified with an unknown effect on protein function and an unclear association with cancer risk. A finding of VUS may make the patient anxious,18 create uncertainty in the treating physician,19 and lead to harmful overtreatment, excessive surveillance, or unnecessary use of a preventive measure.19–21 Genetics counseling allows the patient, even the patient with VUS, to make appropriate decisions.22 Counseling may also help a patient or family process emotional responses, such as fear and guilt. In addition, counselors are familiar with relevant laws and regulations, such as the Genetic Information Nondiscrimination Act of 2008 (GINA), which protects patients from insurance and employment discrimination. Many professional guidelines recommend providing genetics counseling in conjunction with genetics testing,12,23 and some insurance companies and some states require counseling for coverage of testing.
Cost of genetics counseling. If patients are concerned about the cost of genetics testing, they can be reassured with the following information24–26:
- The Patient Protection and Affordable Care Act (ACA) identifies BRCA testing as a preventive service
- Medicare provides coverage for affected patients with a qualifying personal history
- 97% of commercial insurers and most state Medicaid programs provide coverage for hereditary cancer testing
- Most commercial laboratories have affordability programs that may provide additional support.
If a BRCA mutation is found: Many patients question the value of knowing whether they have a BRCA mutation. What our patient, her daughters, and others may not realize is that, if a BRCA mutation is found, breast MRI screening can begin at age 25. Although contrast-enhanced MRI screening is highly sensitive in detecting breast cancer,27–29 it lacks specificity and commonly yields false positives.
Some patients also worry about overdiagnosis with this highly sensitive test. Many do not realize that preventively prescribed oral contraceptives can reduce the risk of ovarian cancer by 50%, and cosmetically acceptable risk-reducing breast surgeries can reduce the risk by 90%.
Many are unaware of the associated risks with ovarian, prostate, pancreatic, and other cancers; of risk management options; and of assisted reproduction options, such as preimplantation genetics diagnosis, which can prevent the passing of a genetic mutation to future generations. The guidelines on risk management options are increasingly clear and helpful,12,30–32 and women often turn to their ObGyns for advice about health and prevention.
ObGyns are often the first-line providers for women with a personal or family history of breast cancer. Identification of at-risk patients begins with taking a careful family history and becoming familiar with the rapidly evolving guidelines in this important field. Identification of appropriate candidates for breast cancer genetics testing is a key step toward prevention, value-based care, and avoidance of legal liability.
CASE Resolved
In this case, testing for the 3 common Ashkenazi BRCA founder mutations was negative, and multigene panel testing was also negative. Her husband is not of Ashkenazi Jewish descent and there is no significant family history of cancer on his side. The daughters are advised to begin high-risk screening at the age of 32, 10 years earlier than their mother was diagnosed, but no genetic testing is indicated for them.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Phillips RL Jr, Bartholomew LA, Dovey SM, Fryer GE Jr, Miyoshi TJ, Green LA. Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care. 2004;13(2):121–126.
- Saber Tehrani AS, Lee H, Mathews SC, et al. 25-year summary of US malpractice claims for diagnostic errors 1986–2010: an analysis from the National Practitioner Data Bank. BMJ Qual Saf. 2013;22(8):672–680.
- American Cancer Society. Breast Cancer Facts & Figures 2017-2018. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-factsand-figures/breast-cancer-facts-and-figures-2017-2018.pdf. Published 2017. Accessed December 28, 2017.
- Tung N, Battelli C, Allen B, et al. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer. 2015;121(1):25–33.
- Tung N, Lin NU, Kidd J, et al. Frequency of germline mutations in 25 cancer susceptibility genes in a sequential series of patients with breast cancer. J Clin Oncol. 2016;34(13):1460–1468.
- Kurian AW, Hare EE, Mills MA, et al. Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J Clin Oncol. 2014;32(19):2001–2009.
- Easton DF, Pharoah PD, Antoniou AC, et al. Gene-panel sequencing and the prediction of breast-cancer risk. N Engl J Med. 2015;372(23):2243–2257.
- Yurgelun MB, Allen B, Kaldate RR, et al. Identification of a variety of mutations in cancer predisposition genes in patients with suspected Lynch syndrome. Gastroenterology. 2015;149(3):604–613.e20.
- Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443–453.
- Mavaddat N, Barrowdale D, Andrulis IL, et al; Consortium of Investigators of Modifiers of BRCA1/2. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol Biomarkers Prev. 2012;21(1):134–147.
- Struewing JP, Hartge P, Wacholder S, et al. The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med. 1997;336(20):1401–1408.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 1.2018. https://www.nccn.org. Accessed December 28, 2017.
- Saslow D, Boetes C, Burke W, et al; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57(2):75–89.
- Heather JM, Chain B. The sequence of sequencers: the history of sequencing DNA. Genomics. 2016;107(1):1–8.
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin No. 182: Hereditary breast and ovarian cancer syndrome. Obstet Gynecol. 2017;130(3):e110–e126.
- Mester JL, Schreiber AH, Moran RT. Genetic counselors: your partners in clinical practice. Cleve Clin J Med. 2012;79(8):560–568.
- Smith M, Mester J, Eng C. How to spot heritable breast cancer: a primary care physician’s guide. Cleve Clin J Med. 2014;81(1):31–40.
- Welsh JL, Hoskin TL, Day CN, et al. Clinical decision-making in patients with variant of uncertain significance in BRCA1 or BRCA2 genes. Ann Surg Oncol. 2017;24(10):3067–3072.
- Kurian AW, Li Y, Hamilton AS, et al. Gaps in incorporating germline genetic testing into treatment decision-making for early-stage breast cancer. J Clin Oncol. 2017;35(20):2232–2239.
- Tung N, Domchek SM, Stadler Z, et al. Counselling framework for moderate-penetrance cancer-susceptibility mutations. Nat Rev Clin Oncol. 2016;13(9):581–588.
- Yu PP, Vose JM, Hayes DF. Genetic cancer susceptibility testing: increased technology, increased complexity. J Clin Oncol. 2015;33(31):3533–3534.
- Pederson HJ, Gopalakrishnan D, Noss R, Yanda C, Eng C, Grobmyer SR. Impact of multigene panel testing on surgical decision making in breast cancer patients. J Am Coll Surg. 2018;226(4):560–565.
- Robson ME, Bradbury AR, Arun B, et al. American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. 2015;33(31):3660–3667.
- Preventive care benefits for women: What Marketplace health insurance plans cover. HealthCare.gov. https://www.healthcare.gov/coverage/what-marketplace-plans-cover/. Accessed May 15, 2018.
- Centers for Medicare & Medicaid Services. The Center for Consumer Information & Insurance Oversight: Affordable Care Act Implementation FAQs – Set 12. https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/aca_implementation_faqs12.html. Accessed May 15, 2018.
- US Preventive Services Task Force. Final Recommendation Statement: BRCA-Related Cancer: Risk Assessment, Genetic Counseling, and Genetic Testing. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/brca-related-cancer-risk-assessment-genetic-counseling-and-genetic-testing. Published December 2013. Accessed May 15, 2018.
- Kuhl CK, Schrading S, Leutner CC, et al. Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol. 2005;23(33):8469–8476.
- Lehman CD, Blume JD, Weatherall P, et al; International Breast MRI Consortium Working Group. Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer. 2005;103(9):1898–1905.
- Kriege M, Brekelmans CT, Boetes C, et al; Magnetic Resonance Imaging Screening Study Group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004;351(5):427–437.
- Pederson HJ, Padia SA, May M, Grobmyer S. Managing patients at genetic risk of breast cancer. Cleve Clin J Med. 2016;83(3):199–206.
- Moyer VA; US Preventive Services Task Force. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(4):271–281.
- American Society of Breast Surgeons. Consensus Guideline on Hereditary Genetic Testing for Patients With and Without Breast Cancer. Columbia, MD: American Society of Breast Surgeons. https://www.breastsurgeons.org/new_layout/about/statements/PDF_Statements/BRCA_Testing.pdf. Published March 14, 2017. Accessed December 28, 2017.

Dr. Pederson is Director of Medical Breast Services at the Cleveland Clinic, Cleveland, Ohio.
The author reports she is a consultant to Myriad Genetics.
Dr. Pederson is Director of Medical Breast Services at the Cleveland Clinic, Cleveland, Ohio.
The author reports she is a consultant to Myriad Genetics.
Dr. Pederson is Director of Medical Breast Services at the Cleveland Clinic, Cleveland, Ohio.
The author reports she is a consultant to Myriad Genetics.
Advances in cancer genetics are rapidly changing how clinicians assess an individual’s risk for breast cancer. ObGyns counsel many women with a personal or family history of the disease, many of whom can benefit from genetics counseling and testing. As patients with a hereditary predisposition to breast cancer are at higher risk and are younger at diagnosis, it is imperative to identify them early so they can benefit from enhanced surveillance, chemoprevention, and discussions regarding risk-reducing surgeries. ObGyns are uniquely poised to identify young women at risk for hereditary cancer syndromes, and they play a crucial role in screening and prevention over the life span.
CASE Patient with breast cancer history asks about screening for her daughters
A 52-year-old woman presents for her annual examination. She underwent breast cancer treatment 10 years earlier and has done well since then. When asked about family history of breast cancer and ethnicity, she reports her mother had breast cancer later in life, and her mother’s father was of Ashkenazi Jewish ancestry.In addition, a maternal uncle had metastatic prostate cancer. You recall that breast cancer diagnosed before age 50 years and Ashkenazi ancestry are “red flags” for a hereditary cancer syndrome. The patient wonders how her daughters should be screened. What do you do next?
Having a risk assessment plan is crucial
Given increasing demands, limited time, and the abundance of information to be discussed with patients, primary care physicians may find it challenging to assess breast cancer risk, consider genetics testing for appropriate individuals, and counsel patients about risk management options. The process has become even more complex since the expansion in genetics knowledge and the advent of multigene panel testing. Not only is risk assessment crucial for this woman and her daughters, and for other patients, but a delay in diagnosing and treating breast cancer in patients with hereditary and familial cancer risks may represent a worrisome new trend in medical litigation.1,2 Clinicians must have a process in place for assessing risk in all patients and treating them appropriately.
The American Cancer Society (ACS) estimated that 252,710 cases of breast cancer would be diagnosed in 2017, leading to 40,610 deaths.3 Twelve percent to 14% of breast cancers are thought to be related to hereditary cancer predisposition syndromes.4–8 This means that, every year, almost 35,000 cases of breast cancer are attributable to hereditary risk. These cases can be detected early with enhanced surveillance, which carries the highest chance for cure, or prevented with risk-reducing surgery in identified genetic mutation carriers. Each child of a person with a genetic mutation predisposing to breast cancer has a 50% chance of inheriting the mutation and having a very high risk of cancer.
In this patient’s case, basic information is collected about her cancer-related personal and family history.
Asking a few key questions can help in stratifying risk:
- Have you or anyone in your family had cancer? What type, and at what age?
- If breast cancer, did it involve both breasts, or was it triple-negative?
- Is there a family history of ovarian cancer?
- Is there a family history of male breast cancer?
- Is there a family history of metastatic prostate cancer?
- Are you of Ashkenazi Jewish ethnicity?
- Have you or anyone in your family ever had genetics testing for cancer?
The hallmarks of hereditary cancer are multiple cancers in an individual or family; young age at diagnosis; and ovarian, pancreatic, or another rare cancer. Metastatic prostate cancer was added as a red flag for hereditary risk after a recent large series found that 11.8% of men with metastatic prostate cancer harbor germline mutations.9
CASE Continued
On further questioning, the patient reports she had triple-negative (estrogen receptor–, progesterone receptor–, and human epidermal growth factor receptor 2 [HER2]–negative) breast cancer, a feature of patients with germline BRCA1 (breast cancer susceptibility gene 1) mutations.10 In addition, her Ashkenazi ancestry is concerning, as there is a 1-in-40 chance of carrying 1 of the 3 Ashkenazi founder BRCA mutations.11 Is a genetics consultation needed?
Read about guidelines for referral and testing.
Guidelines for genetics referral and testing
According to the TABLE, which summarizes national guidelines for genetics referral, maternal and paternal family histories are equally important. Our patient was under age 50 at diagnosis, has a history of triple-negative breast cancer, is of Ashkenazi ancestry, and has a family history of metastatic prostate cancer. She meets the criteria for genetics testing, and screening for her daughters most certainly will depend on the findings of that testing. If she carries a BRCA1 mutation, as might be anticipated, each daughter would have a 50% chance of having inherited the mutation. If they carry the mutation as well, they would begin breast magnetic resonance imaging (MRI) screening at age 25.12 If they decide against genetics testing, they could still undergo MRI screening as untested first-degree relatives of a BRCA carrier, per ACS recommendations.13
Integrating evidence and experience
Over the past 10 to 20 years, other breast cancer susceptibility genes (eg, BRCA2, PALB2, CHEK2) have been identified. More recently, next-generation sequencing has become commercially available. Laboratories can use this newer method to sequence multiple genes rapidly and in parallel, and its cost is similar to that of single-syndrome testing.14 When more than 1 gene can explain an inherited cancer syndrome, multigene panel testing may be more efficient and cost-effective. Use of multigene panel testing is supported in guidelines issued by the National Comprehensive Cancer Network,12 the American College of Obstetricians and Gynecologists,15 and other medical societies.
For our patient, the most logical strategy would be to test for the 3 mutations most common in the Ashkenazi population and then, if no mutation is found, perform multigene panel testing.
Formal genetics counseling can be very helpful for a patient, particularly in the era of multigene panel testing.16,17 A detailed pedigree (family tree) is elicited, and a genetics specialist determines whether testing is indicated and which test is best for the patient. Possible test findings are explained. The patient may be found to have a pathogenic variant with associated increased cancer risk, a negative test result (informative or uninformative), or a variant of uncertain significance (VUS). VUS is a gene mutation identified with an unknown effect on protein function and an unclear association with cancer risk. A finding of VUS may make the patient anxious,18 create uncertainty in the treating physician,19 and lead to harmful overtreatment, excessive surveillance, or unnecessary use of a preventive measure.19–21 Genetics counseling allows the patient, even the patient with VUS, to make appropriate decisions.22 Counseling may also help a patient or family process emotional responses, such as fear and guilt. In addition, counselors are familiar with relevant laws and regulations, such as the Genetic Information Nondiscrimination Act of 2008 (GINA), which protects patients from insurance and employment discrimination. Many professional guidelines recommend providing genetics counseling in conjunction with genetics testing,12,23 and some insurance companies and some states require counseling for coverage of testing.
Cost of genetics counseling. If patients are concerned about the cost of genetics testing, they can be reassured with the following information24–26:
- The Patient Protection and Affordable Care Act (ACA) identifies BRCA testing as a preventive service
- Medicare provides coverage for affected patients with a qualifying personal history
- 97% of commercial insurers and most state Medicaid programs provide coverage for hereditary cancer testing
- Most commercial laboratories have affordability programs that may provide additional support.
If a BRCA mutation is found: Many patients question the value of knowing whether they have a BRCA mutation. What our patient, her daughters, and others may not realize is that, if a BRCA mutation is found, breast MRI screening can begin at age 25. Although contrast-enhanced MRI screening is highly sensitive in detecting breast cancer,27–29 it lacks specificity and commonly yields false positives.
Some patients also worry about overdiagnosis with this highly sensitive test. Many do not realize that preventively prescribed oral contraceptives can reduce the risk of ovarian cancer by 50%, and cosmetically acceptable risk-reducing breast surgeries can reduce the risk by 90%.
Many are unaware of the associated risks with ovarian, prostate, pancreatic, and other cancers; of risk management options; and of assisted reproduction options, such as preimplantation genetics diagnosis, which can prevent the passing of a genetic mutation to future generations. The guidelines on risk management options are increasingly clear and helpful,12,30–32 and women often turn to their ObGyns for advice about health and prevention.
ObGyns are often the first-line providers for women with a personal or family history of breast cancer. Identification of at-risk patients begins with taking a careful family history and becoming familiar with the rapidly evolving guidelines in this important field. Identification of appropriate candidates for breast cancer genetics testing is a key step toward prevention, value-based care, and avoidance of legal liability.
CASE Resolved
In this case, testing for the 3 common Ashkenazi BRCA founder mutations was negative, and multigene panel testing was also negative. Her husband is not of Ashkenazi Jewish descent and there is no significant family history of cancer on his side. The daughters are advised to begin high-risk screening at the age of 32, 10 years earlier than their mother was diagnosed, but no genetic testing is indicated for them.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
Advances in cancer genetics are rapidly changing how clinicians assess an individual’s risk for breast cancer. ObGyns counsel many women with a personal or family history of the disease, many of whom can benefit from genetics counseling and testing. As patients with a hereditary predisposition to breast cancer are at higher risk and are younger at diagnosis, it is imperative to identify them early so they can benefit from enhanced surveillance, chemoprevention, and discussions regarding risk-reducing surgeries. ObGyns are uniquely poised to identify young women at risk for hereditary cancer syndromes, and they play a crucial role in screening and prevention over the life span.
CASE Patient with breast cancer history asks about screening for her daughters
A 52-year-old woman presents for her annual examination. She underwent breast cancer treatment 10 years earlier and has done well since then. When asked about family history of breast cancer and ethnicity, she reports her mother had breast cancer later in life, and her mother’s father was of Ashkenazi Jewish ancestry.In addition, a maternal uncle had metastatic prostate cancer. You recall that breast cancer diagnosed before age 50 years and Ashkenazi ancestry are “red flags” for a hereditary cancer syndrome. The patient wonders how her daughters should be screened. What do you do next?
Having a risk assessment plan is crucial
Given increasing demands, limited time, and the abundance of information to be discussed with patients, primary care physicians may find it challenging to assess breast cancer risk, consider genetics testing for appropriate individuals, and counsel patients about risk management options. The process has become even more complex since the expansion in genetics knowledge and the advent of multigene panel testing. Not only is risk assessment crucial for this woman and her daughters, and for other patients, but a delay in diagnosing and treating breast cancer in patients with hereditary and familial cancer risks may represent a worrisome new trend in medical litigation.1,2 Clinicians must have a process in place for assessing risk in all patients and treating them appropriately.
The American Cancer Society (ACS) estimated that 252,710 cases of breast cancer would be diagnosed in 2017, leading to 40,610 deaths.3 Twelve percent to 14% of breast cancers are thought to be related to hereditary cancer predisposition syndromes.4–8 This means that, every year, almost 35,000 cases of breast cancer are attributable to hereditary risk. These cases can be detected early with enhanced surveillance, which carries the highest chance for cure, or prevented with risk-reducing surgery in identified genetic mutation carriers. Each child of a person with a genetic mutation predisposing to breast cancer has a 50% chance of inheriting the mutation and having a very high risk of cancer.
In this patient’s case, basic information is collected about her cancer-related personal and family history.
Asking a few key questions can help in stratifying risk:
- Have you or anyone in your family had cancer? What type, and at what age?
- If breast cancer, did it involve both breasts, or was it triple-negative?
- Is there a family history of ovarian cancer?
- Is there a family history of male breast cancer?
- Is there a family history of metastatic prostate cancer?
- Are you of Ashkenazi Jewish ethnicity?
- Have you or anyone in your family ever had genetics testing for cancer?
The hallmarks of hereditary cancer are multiple cancers in an individual or family; young age at diagnosis; and ovarian, pancreatic, or another rare cancer. Metastatic prostate cancer was added as a red flag for hereditary risk after a recent large series found that 11.8% of men with metastatic prostate cancer harbor germline mutations.9
CASE Continued
On further questioning, the patient reports she had triple-negative (estrogen receptor–, progesterone receptor–, and human epidermal growth factor receptor 2 [HER2]–negative) breast cancer, a feature of patients with germline BRCA1 (breast cancer susceptibility gene 1) mutations.10 In addition, her Ashkenazi ancestry is concerning, as there is a 1-in-40 chance of carrying 1 of the 3 Ashkenazi founder BRCA mutations.11 Is a genetics consultation needed?
Read about guidelines for referral and testing.
Guidelines for genetics referral and testing
According to the TABLE, which summarizes national guidelines for genetics referral, maternal and paternal family histories are equally important. Our patient was under age 50 at diagnosis, has a history of triple-negative breast cancer, is of Ashkenazi ancestry, and has a family history of metastatic prostate cancer. She meets the criteria for genetics testing, and screening for her daughters most certainly will depend on the findings of that testing. If she carries a BRCA1 mutation, as might be anticipated, each daughter would have a 50% chance of having inherited the mutation. If they carry the mutation as well, they would begin breast magnetic resonance imaging (MRI) screening at age 25.12 If they decide against genetics testing, they could still undergo MRI screening as untested first-degree relatives of a BRCA carrier, per ACS recommendations.13
Integrating evidence and experience
Over the past 10 to 20 years, other breast cancer susceptibility genes (eg, BRCA2, PALB2, CHEK2) have been identified. More recently, next-generation sequencing has become commercially available. Laboratories can use this newer method to sequence multiple genes rapidly and in parallel, and its cost is similar to that of single-syndrome testing.14 When more than 1 gene can explain an inherited cancer syndrome, multigene panel testing may be more efficient and cost-effective. Use of multigene panel testing is supported in guidelines issued by the National Comprehensive Cancer Network,12 the American College of Obstetricians and Gynecologists,15 and other medical societies.
For our patient, the most logical strategy would be to test for the 3 mutations most common in the Ashkenazi population and then, if no mutation is found, perform multigene panel testing.
Formal genetics counseling can be very helpful for a patient, particularly in the era of multigene panel testing.16,17 A detailed pedigree (family tree) is elicited, and a genetics specialist determines whether testing is indicated and which test is best for the patient. Possible test findings are explained. The patient may be found to have a pathogenic variant with associated increased cancer risk, a negative test result (informative or uninformative), or a variant of uncertain significance (VUS). VUS is a gene mutation identified with an unknown effect on protein function and an unclear association with cancer risk. A finding of VUS may make the patient anxious,18 create uncertainty in the treating physician,19 and lead to harmful overtreatment, excessive surveillance, or unnecessary use of a preventive measure.19–21 Genetics counseling allows the patient, even the patient with VUS, to make appropriate decisions.22 Counseling may also help a patient or family process emotional responses, such as fear and guilt. In addition, counselors are familiar with relevant laws and regulations, such as the Genetic Information Nondiscrimination Act of 2008 (GINA), which protects patients from insurance and employment discrimination. Many professional guidelines recommend providing genetics counseling in conjunction with genetics testing,12,23 and some insurance companies and some states require counseling for coverage of testing.
Cost of genetics counseling. If patients are concerned about the cost of genetics testing, they can be reassured with the following information24–26:
- The Patient Protection and Affordable Care Act (ACA) identifies BRCA testing as a preventive service
- Medicare provides coverage for affected patients with a qualifying personal history
- 97% of commercial insurers and most state Medicaid programs provide coverage for hereditary cancer testing
- Most commercial laboratories have affordability programs that may provide additional support.
If a BRCA mutation is found: Many patients question the value of knowing whether they have a BRCA mutation. What our patient, her daughters, and others may not realize is that, if a BRCA mutation is found, breast MRI screening can begin at age 25. Although contrast-enhanced MRI screening is highly sensitive in detecting breast cancer,27–29 it lacks specificity and commonly yields false positives.
Some patients also worry about overdiagnosis with this highly sensitive test. Many do not realize that preventively prescribed oral contraceptives can reduce the risk of ovarian cancer by 50%, and cosmetically acceptable risk-reducing breast surgeries can reduce the risk by 90%.
Many are unaware of the associated risks with ovarian, prostate, pancreatic, and other cancers; of risk management options; and of assisted reproduction options, such as preimplantation genetics diagnosis, which can prevent the passing of a genetic mutation to future generations. The guidelines on risk management options are increasingly clear and helpful,12,30–32 and women often turn to their ObGyns for advice about health and prevention.
ObGyns are often the first-line providers for women with a personal or family history of breast cancer. Identification of at-risk patients begins with taking a careful family history and becoming familiar with the rapidly evolving guidelines in this important field. Identification of appropriate candidates for breast cancer genetics testing is a key step toward prevention, value-based care, and avoidance of legal liability.
CASE Resolved
In this case, testing for the 3 common Ashkenazi BRCA founder mutations was negative, and multigene panel testing was also negative. Her husband is not of Ashkenazi Jewish descent and there is no significant family history of cancer on his side. The daughters are advised to begin high-risk screening at the age of 32, 10 years earlier than their mother was diagnosed, but no genetic testing is indicated for them.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Phillips RL Jr, Bartholomew LA, Dovey SM, Fryer GE Jr, Miyoshi TJ, Green LA. Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care. 2004;13(2):121–126.
- Saber Tehrani AS, Lee H, Mathews SC, et al. 25-year summary of US malpractice claims for diagnostic errors 1986–2010: an analysis from the National Practitioner Data Bank. BMJ Qual Saf. 2013;22(8):672–680.
- American Cancer Society. Breast Cancer Facts & Figures 2017-2018. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-factsand-figures/breast-cancer-facts-and-figures-2017-2018.pdf. Published 2017. Accessed December 28, 2017.
- Tung N, Battelli C, Allen B, et al. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer. 2015;121(1):25–33.
- Tung N, Lin NU, Kidd J, et al. Frequency of germline mutations in 25 cancer susceptibility genes in a sequential series of patients with breast cancer. J Clin Oncol. 2016;34(13):1460–1468.
- Kurian AW, Hare EE, Mills MA, et al. Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J Clin Oncol. 2014;32(19):2001–2009.
- Easton DF, Pharoah PD, Antoniou AC, et al. Gene-panel sequencing and the prediction of breast-cancer risk. N Engl J Med. 2015;372(23):2243–2257.
- Yurgelun MB, Allen B, Kaldate RR, et al. Identification of a variety of mutations in cancer predisposition genes in patients with suspected Lynch syndrome. Gastroenterology. 2015;149(3):604–613.e20.
- Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443–453.
- Mavaddat N, Barrowdale D, Andrulis IL, et al; Consortium of Investigators of Modifiers of BRCA1/2. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol Biomarkers Prev. 2012;21(1):134–147.
- Struewing JP, Hartge P, Wacholder S, et al. The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med. 1997;336(20):1401–1408.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 1.2018. https://www.nccn.org. Accessed December 28, 2017.
- Saslow D, Boetes C, Burke W, et al; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57(2):75–89.
- Heather JM, Chain B. The sequence of sequencers: the history of sequencing DNA. Genomics. 2016;107(1):1–8.
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin No. 182: Hereditary breast and ovarian cancer syndrome. Obstet Gynecol. 2017;130(3):e110–e126.
- Mester JL, Schreiber AH, Moran RT. Genetic counselors: your partners in clinical practice. Cleve Clin J Med. 2012;79(8):560–568.
- Smith M, Mester J, Eng C. How to spot heritable breast cancer: a primary care physician’s guide. Cleve Clin J Med. 2014;81(1):31–40.
- Welsh JL, Hoskin TL, Day CN, et al. Clinical decision-making in patients with variant of uncertain significance in BRCA1 or BRCA2 genes. Ann Surg Oncol. 2017;24(10):3067–3072.
- Kurian AW, Li Y, Hamilton AS, et al. Gaps in incorporating germline genetic testing into treatment decision-making for early-stage breast cancer. J Clin Oncol. 2017;35(20):2232–2239.
- Tung N, Domchek SM, Stadler Z, et al. Counselling framework for moderate-penetrance cancer-susceptibility mutations. Nat Rev Clin Oncol. 2016;13(9):581–588.
- Yu PP, Vose JM, Hayes DF. Genetic cancer susceptibility testing: increased technology, increased complexity. J Clin Oncol. 2015;33(31):3533–3534.
- Pederson HJ, Gopalakrishnan D, Noss R, Yanda C, Eng C, Grobmyer SR. Impact of multigene panel testing on surgical decision making in breast cancer patients. J Am Coll Surg. 2018;226(4):560–565.
- Robson ME, Bradbury AR, Arun B, et al. American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. 2015;33(31):3660–3667.
- Preventive care benefits for women: What Marketplace health insurance plans cover. HealthCare.gov. https://www.healthcare.gov/coverage/what-marketplace-plans-cover/. Accessed May 15, 2018.
- Centers for Medicare & Medicaid Services. The Center for Consumer Information & Insurance Oversight: Affordable Care Act Implementation FAQs – Set 12. https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/aca_implementation_faqs12.html. Accessed May 15, 2018.
- US Preventive Services Task Force. Final Recommendation Statement: BRCA-Related Cancer: Risk Assessment, Genetic Counseling, and Genetic Testing. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/brca-related-cancer-risk-assessment-genetic-counseling-and-genetic-testing. Published December 2013. Accessed May 15, 2018.
- Kuhl CK, Schrading S, Leutner CC, et al. Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol. 2005;23(33):8469–8476.
- Lehman CD, Blume JD, Weatherall P, et al; International Breast MRI Consortium Working Group. Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer. 2005;103(9):1898–1905.
- Kriege M, Brekelmans CT, Boetes C, et al; Magnetic Resonance Imaging Screening Study Group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004;351(5):427–437.
- Pederson HJ, Padia SA, May M, Grobmyer S. Managing patients at genetic risk of breast cancer. Cleve Clin J Med. 2016;83(3):199–206.
- Moyer VA; US Preventive Services Task Force. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(4):271–281.
- American Society of Breast Surgeons. Consensus Guideline on Hereditary Genetic Testing for Patients With and Without Breast Cancer. Columbia, MD: American Society of Breast Surgeons. https://www.breastsurgeons.org/new_layout/about/statements/PDF_Statements/BRCA_Testing.pdf. Published March 14, 2017. Accessed December 28, 2017.
- Phillips RL Jr, Bartholomew LA, Dovey SM, Fryer GE Jr, Miyoshi TJ, Green LA. Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care. 2004;13(2):121–126.
- Saber Tehrani AS, Lee H, Mathews SC, et al. 25-year summary of US malpractice claims for diagnostic errors 1986–2010: an analysis from the National Practitioner Data Bank. BMJ Qual Saf. 2013;22(8):672–680.
- American Cancer Society. Breast Cancer Facts & Figures 2017-2018. https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/breast-cancer-factsand-figures/breast-cancer-facts-and-figures-2017-2018.pdf. Published 2017. Accessed December 28, 2017.
- Tung N, Battelli C, Allen B, et al. Frequency of mutations in individuals with breast cancer referred for BRCA1 and BRCA2 testing using next-generation sequencing with a 25-gene panel. Cancer. 2015;121(1):25–33.
- Tung N, Lin NU, Kidd J, et al. Frequency of germline mutations in 25 cancer susceptibility genes in a sequential series of patients with breast cancer. J Clin Oncol. 2016;34(13):1460–1468.
- Kurian AW, Hare EE, Mills MA, et al. Clinical evaluation of a multiple-gene sequencing panel for hereditary cancer risk assessment. J Clin Oncol. 2014;32(19):2001–2009.
- Easton DF, Pharoah PD, Antoniou AC, et al. Gene-panel sequencing and the prediction of breast-cancer risk. N Engl J Med. 2015;372(23):2243–2257.
- Yurgelun MB, Allen B, Kaldate RR, et al. Identification of a variety of mutations in cancer predisposition genes in patients with suspected Lynch syndrome. Gastroenterology. 2015;149(3):604–613.e20.
- Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443–453.
- Mavaddat N, Barrowdale D, Andrulis IL, et al; Consortium of Investigators of Modifiers of BRCA1/2. Pathology of breast and ovarian cancers among BRCA1 and BRCA2 mutation carriers: results from the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA). Cancer Epidemiol Biomarkers Prev. 2012;21(1):134–147.
- Struewing JP, Hartge P, Wacholder S, et al. The risk of cancer associated with specific mutations of BRCA1 and BRCA2 among Ashkenazi Jews. N Engl J Med. 1997;336(20):1401–1408.
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 1.2018. https://www.nccn.org. Accessed December 28, 2017.
- Saslow D, Boetes C, Burke W, et al; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007;57(2):75–89.
- Heather JM, Chain B. The sequence of sequencers: the history of sequencing DNA. Genomics. 2016;107(1):1–8.
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins-Gynecology. ACOG Practice Bulletin No. 182: Hereditary breast and ovarian cancer syndrome. Obstet Gynecol. 2017;130(3):e110–e126.
- Mester JL, Schreiber AH, Moran RT. Genetic counselors: your partners in clinical practice. Cleve Clin J Med. 2012;79(8):560–568.
- Smith M, Mester J, Eng C. How to spot heritable breast cancer: a primary care physician’s guide. Cleve Clin J Med. 2014;81(1):31–40.
- Welsh JL, Hoskin TL, Day CN, et al. Clinical decision-making in patients with variant of uncertain significance in BRCA1 or BRCA2 genes. Ann Surg Oncol. 2017;24(10):3067–3072.
- Kurian AW, Li Y, Hamilton AS, et al. Gaps in incorporating germline genetic testing into treatment decision-making for early-stage breast cancer. J Clin Oncol. 2017;35(20):2232–2239.
- Tung N, Domchek SM, Stadler Z, et al. Counselling framework for moderate-penetrance cancer-susceptibility mutations. Nat Rev Clin Oncol. 2016;13(9):581–588.
- Yu PP, Vose JM, Hayes DF. Genetic cancer susceptibility testing: increased technology, increased complexity. J Clin Oncol. 2015;33(31):3533–3534.
- Pederson HJ, Gopalakrishnan D, Noss R, Yanda C, Eng C, Grobmyer SR. Impact of multigene panel testing on surgical decision making in breast cancer patients. J Am Coll Surg. 2018;226(4):560–565.
- Robson ME, Bradbury AR, Arun B, et al. American Society of Clinical Oncology policy statement update: genetic and genomic testing for cancer susceptibility. J Clin Oncol. 2015;33(31):3660–3667.
- Preventive care benefits for women: What Marketplace health insurance plans cover. HealthCare.gov. https://www.healthcare.gov/coverage/what-marketplace-plans-cover/. Accessed May 15, 2018.
- Centers for Medicare & Medicaid Services. The Center for Consumer Information & Insurance Oversight: Affordable Care Act Implementation FAQs – Set 12. https://www.cms.gov/CCIIO/Resources/Fact-Sheets-and-FAQs/aca_implementation_faqs12.html. Accessed May 15, 2018.
- US Preventive Services Task Force. Final Recommendation Statement: BRCA-Related Cancer: Risk Assessment, Genetic Counseling, and Genetic Testing. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/brca-related-cancer-risk-assessment-genetic-counseling-and-genetic-testing. Published December 2013. Accessed May 15, 2018.
- Kuhl CK, Schrading S, Leutner CC, et al. Mammography, breast ultrasound, and magnetic resonance imaging for surveillance of women at high familial risk for breast cancer. J Clin Oncol. 2005;23(33):8469–8476.
- Lehman CD, Blume JD, Weatherall P, et al; International Breast MRI Consortium Working Group. Screening women at high risk for breast cancer with mammography and magnetic resonance imaging. Cancer. 2005;103(9):1898–1905.
- Kriege M, Brekelmans CT, Boetes C, et al; Magnetic Resonance Imaging Screening Study Group. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. N Engl J Med. 2004;351(5):427–437.
- Pederson HJ, Padia SA, May M, Grobmyer S. Managing patients at genetic risk of breast cancer. Cleve Clin J Med. 2016;83(3):199–206.
- Moyer VA; US Preventive Services Task Force. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(4):271–281.
- American Society of Breast Surgeons. Consensus Guideline on Hereditary Genetic Testing for Patients With and Without Breast Cancer. Columbia, MD: American Society of Breast Surgeons. https://www.breastsurgeons.org/new_layout/about/statements/PDF_Statements/BRCA_Testing.pdf. Published March 14, 2017. Accessed December 28, 2017.
Take-home points
- The best genetics test is a good family history, updated annually
- Each year, 35,000 breast cancers are attributable to hereditary risk
- It is crucial to identify families at risk for hereditary breast cancer early, as cancers may begin in a woman's 30s; screening begins at age 25
- Multigene panel testing is efficient and cost-effective
- For patients who have highly penetrant pathogenic variants and are of childbearing age, preimplantation genetics diagnosis is an option

Ovarian masses: Surgery or surveillance?
A meaningful evolution has occurred over the past 30 years in the evaluation of ovarian tumors. In the 1980s, any palpable ovarian tumor was recommended for surgical removal.1 In the early 2000s, studies showed that unilocular cysts were at very low risk for malignancy, and surveillance was recommended.2 In the following decade, septate cysts were added to the list of ovarian tumors unlikely to be malignant, and nonsurgical therapy was suggested.3 It is estimated that 10% of women will undergo surgery for an adnexal mass in their lifetime, despite the fact that only 1 in 6 (13%–21%) of these masses is found to be malignant.4,5
A comprehensive, morphology-based pelvic ultrasonography is the first and most important step in evaluating an ovarian tumor’s risk of malignancy to determine whether surgery or surveillance is required.
Ovarian cancer continues to be the leading cause of gynecologic cancer death. Despite achieving superior surgical and cancer outcomes, a gynecologic oncologist performs only 40% of the initial ovarian cancer surgeries.6 Premenopausal and menopausal ovarian tumors are different in cause and consequence. Only 15% of premenopausal tumors are malignant, most commonly germ cell tumors, borderline ovarian tumors, and epithelial ovarian cancers. Tumors in menopausal women are less common but are more likely to be malignant. In actuality, up to 50% of tumors in this population are malignant. The most common of these malignancies are epithelial ovarian cancers, cancers metastatic to the ovary, and malignant stromal tumors.
Effective and evidence-based preoperative evaluations are available to help the clinician estimate a tumor’s risk of malignancy and determine which tumors are appropriate for referral to a specialist for surgery.
The actual incidence and prevalence of ovarian tumors are not known. From a review of almost 40,000 ultrasonography scans performed in the University of Kentucky Ovarian Cancer Screening Program, the estimated incidence and prevalence of ovarian abnormalities are 8.2 per 100 women annuallyand 17%, respectively.7 Seventy percent of these abnormalities have a unilocular or simple septate morphology and are at low risk for malignancy.7 The remaining 30% of abnormalities are high risk, although this represents only 9% of the total population evaluated. Since the vast majority of these abnormalities are expected to be asymptomatic, most will go unrecognized in the general population. For women who have an ovarian abnormality on ultrasonography, the majority will be at low risk for malignancy and will not require surgery.
Ovarian ultrasonography plus morphologic scoring comprise a comprehensive approach
The recently published recommendations of the First International Consensus Conference report on adnexal masses are summarized in TABLE 1.8 The expert panel reviewed the evidence and concluded that effective ultrasonography strategies exist and are well validated, and that low-risk asymptomatic ovarian cysts do not require surgical removal.

While no single ultrasonographic findingcan differentiate a benign from a malignant mass, morphologic scoring systems improve our ability to estimate a tumor’s malignant potential. In the United States, most practitioners in women’s health have ready access to gynecologic ultrasonography, but individual training and proficiency vary. Since not everyone is an expert sonographer, it is useful to employ an objective strategy when evaluating an ovarian tumor. The focus of a comprehensive ovarian ultrasonography is to recognize morphologic patterns that reflect a tumor’s malignant potential. While tumor volume is useful, tumor morphology is the most prognostic feature.
International Ovarian Tumor Analysis group
The International Ovarian Tumor Analysis (IOTA) group has published extensively on sonographic definitions and patterns that categorize tumors based on appearance.9 Simple rules and the ADNEX risk model are 2 of the group’s approaches (FIGURE 1).10,11 Both methods have been validated as effective for differentiating benign from malignant ovarian tumors, but neither has been used to study serial changes in ovarian morphology.
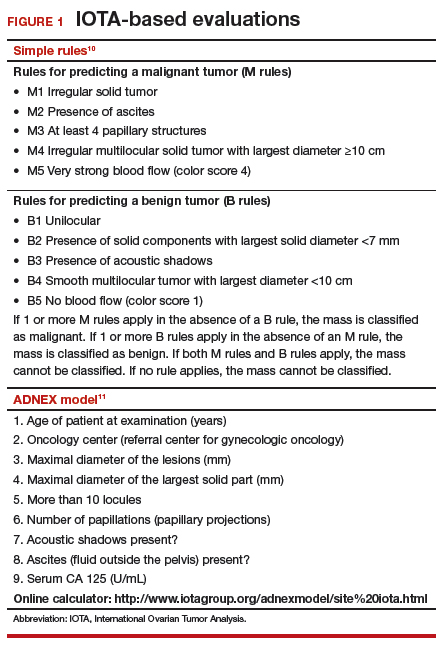
Regardless of the strategy employed, 25% of ovarian ultrasonography evaluations will be interpreted as “indeterminate” or “risk unknown.”10 The IOTA strategies have been successfully used in Europe for years, but they have not yet been studied or adopted in the United States.
Kentucky morphology index
The morphology index (MI) from the University of Kentucky is an ultrasonography-based scoring system that combines tumor volume and tumor structure into a simple and effective index with a score ranging from 0 to 10 (FIGURE 2).12 A rising Kentucky MI score has a linear and predictable increase in the risk of ovarian malignancy. In a review of almost 40,000 sonograms, 85% of the malignancies had an MI score of 5 or greater (TABLE 2).12 Using this as a cutoff, the sensitivity and specificity for predicting malignancy was 86% and 98%, respectively.12
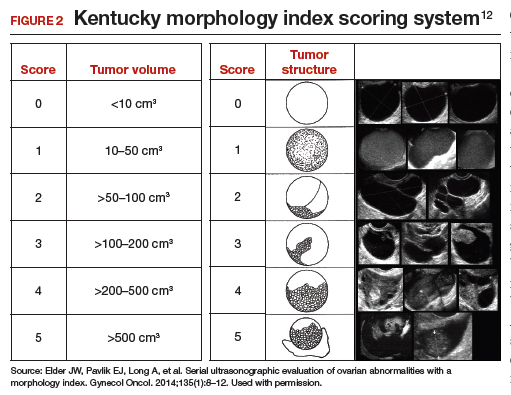
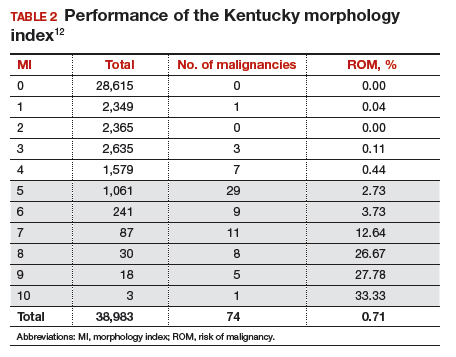
When comparing the ADNEX risk model with the Kentucky MI, investigators reviewed 45,000 ultrasound results and found that the majority of cancers were categorized by the ADNEX model in the lowest 4 of the 10 risk-of-malignancy groups, compared with only 15% for the MI.13 This clustering or skew is potentially problematic, since we expect higher scores to be more predictive of cancer than lower scores. It also infers that the ADNEX model may not be useful in serial surveillance strategies. Moreover, the ADNEX model identified only 30% of early stage cancers compared with identification of 80% with use of the MI.13
Serial ultrasonography
Serial ultrasonography is a concept similar to any longitudinal biomarker evaluation. In the United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS) program, the Risk of Ovarian Cancer Algorithm (ROCA) employs serial measurements of cancer antigen 125 (CA 125) to improve cancer detection. Serial ultrasonography similarly can be applied to better characterize a tumor’s physiology as well as its morphology. Over time, malignant ovarian tumors grow naturally in volume and complexity, and they do so at a rate faster than nonmalignant tumors. If this physical change can be measured objectively with ultrasonography, then serial sonography becomes a valuable diagnostic aid.
In comparing serial MI scores with clinical outcomes, studies have shown that malignant tumors exhibit a rapid increase, nonmalignant tumors have a stable or gradual rise, and resolving cysts show a decrease in MI score over time (FIGURE 3).12 An increase in the MI score of 1 or more per month (≥1 per month) is concerning for malignancy, and surgical removal should be considered. If the MI score of an asymptomatic ovarian tumor does not increase by 1 per month, it can be surveilled with intermittent ultrasonography.
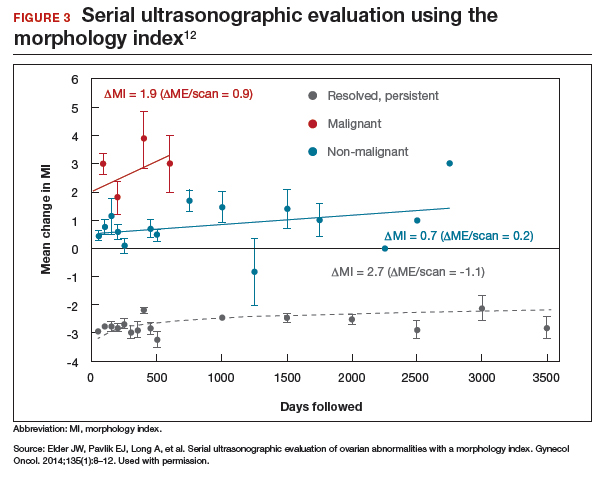
Read about evaluating with serum biomarkers and sonography.
Serum biomarkers useful for determining risk, need for referral
Serum biomarkers can be used to complement an ultrasonographic evaluation. They are particularly useful when surgery is recommended but the sonographic evaluation is indeterminate for malignancy risk. Many serum biomarkers are commonly used for the preoperative evaluation of an ovarian tumor or for surveillance of a malignancy following diagnosis (TABLE 3).
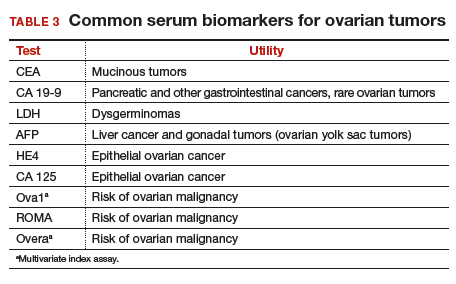
CA 125 is the most commonly ordered serum biomarker test for ovarian cancer. It is estimated that three‐quarters of CA 125 tests are ordered for preoperative use, which is not the US Food and Drug Administration (FDA) approved indication. Despite our clinical reliance on CA 125 as a diagnostic test prior to surgery, its utility is limited because of a low sensitivity for predicting cancer in premenopausal women and early stage disease.14,15 CA 125 specificity also varies widely, depending on patient age and other clinical factors, ranging from as low as 26% in premenopausal women to as high as 100% in postmenopausal women.16 Because CA 125 often is negative when early stage cancer is present, or positive when cancer is not, it is not recommended for preoperative use for determining whether an ovarian tumor is malignant or whether surgery is indicated. CA 125 should be used to monitor patients with a known ovarian malignancy.
The new triage serum biomarkers, Overa, Ova1, and ROMA (Risk of Ovarian Malignancy Algorithm), are FDA cleared for preoperative use to help determine whether a woman needing surgery for an ovarian mass should be referred to a gynecologic oncologist.17–20 These tests should not be used to decide if surgery is indicated, but rather should be considered when the decision for surgery has already been made but the malignancy risk is unknown. A woman with a “high risk” result should be referred to a gynecologic oncologist, while one with a “low risk” score is very unlikely to have a malignancy and referral to a specialist is not necessary. TABLE 4 lists a comparison of the relative performance of these serum biomarkers.14,15,17–20 There are no published data on the use of serial triage biomarkers.
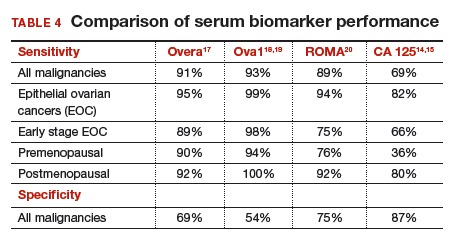
How to evaluate an ovarian tumor
Approximately 65% of the time, ovarian cystic tumors can be identified accurately as low risk based on the initial sonographic evaluation (TABLE 5). In this scenario, the risk of malignancy is very low (<1%), no secondary testing is needed, and no surgery is recommended.1,3,21
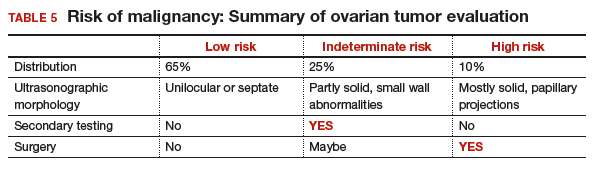
About 10% of tumors are expected to have a high-risk morphology on ultrasonography, where the risk of malignancy exceeds 25% and referral to a gynecologic oncologist is required.
The remaining 25% of tumors cannot be accurately classified with a single ultrasonographic evaluation and are considered indeterminate.22 Indeterminate tumors require secondary testing to ascertain whether surgery is indicated. Secondary testing may consist of serial ultrasonography, magnetic resonance imaging (MRI), or serum triage biomarker testing if the decision for surgery has been made.
A 2-step process is recommended for evaluating an ovarian tumor.
Step 1. Perform a detailed ultrasonography study using a morphology-based system. Classify the tumor as:
- low risk (65%): unilocular, simple septate, no flow on color Doppler
- simple rules: benign
- MI score 0–3
- no secondary testing; no referral is recommended
- high risk (10%): irregular, mostly solid, papillary projections, very strong flow on color Doppler
- simple rules: malignant
- MI score ≥5
- no secondary testing; refer to a gynecologic oncologist
- indeterminate (25%): partly solid, small wall abnormalities, minimal or moderate flow on color Doppler
- simple rules: both M and B rules apply or no rule applies
- MI score usually 4–6
- perform secondary testing (step 2).
Step 2. Perform secondary testing as follows:
- serum triage biomarkers if surgery is planned (Ova1, ROMA, Overa), or
- MRI, or
- serial sonography.
The 3 case scenarios that follow illustrate how the ovarian tumor evaluation process may be applied in clinical practice, with referral to a gynecologic oncologist as appropriate.
CASE 1 Postmenopausal woman with urinary symptoms and pelvic pressure
A 61-year-old woman is referred with a newly identified ovarian tumor. She has had 1 month of urinary urgency, frequency, and pelvic pressure, but she denies vaginal bleeding or fever. She has no family history of cancer. The referring physician included results of a serum CA 125 (48 U/mL; normal, ≤35 U/mL). A pelvic examination reveals a palpable, irregular mass in the anterior pelvis with limited mobility.
What would be your next step in the evaluation of this patient?
Start with ultrasonography
Step 1. Perform pelvic ultrasonography. In this patient, transvaginal sonography revealed a 6-cm (volume, 89 mL) mostly solid tumor (FIGURE 4). The maximum solid diameter of the tumor was 4.0 cm. There was a 20-mL pocket of pelvic ascites.
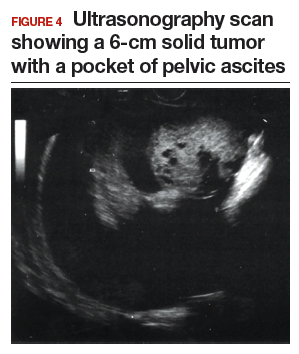
Results of morphology-based classification were as follows:
- simple rules: M1 and M5 positive; B rules: negative (malignant; high risk)
- ADNEX: 51.6% risk of malignancy (high risk)
- MI: 7 (high risk).
Step 2. Consider secondary testing. In this case, no secondary testing was recommended. Treatment plan. The patient was referred to a gynecologic oncologist for surgery and was found to have a stage IIA serous ovarian carcinoma.
CASE 2 Woman with history of pelvic symptoms and worsening pain
A 46-year-old woman presents with worsening pelvic pain over the last month. She has a long-standing history of pelvic pain, dysmenorrhea, and dyspareunia from suspected endometriosis. She has no family history of cancer. The referring physician included the following serum biomarker results: CA 125, 48 U/mL (normal, ≤35 U/mL), and HE4, 60 pM (normal, ≤150 pM). On pelvic examination, there is a palpable mass with limited mobility in the posterior cul-de-sac.
Based on the patient’s available history, physical examination, and biomarker information, how would you proceed?
Follow the 2-step process
Step 1. Perform pelvic ultrasonography. Transvaginal sonography revealed a 6-cm (volume, 89 mL) partly solid tumor with regular internal borders (FIGURE 5). The maximum solid diameter of the tumor was 4.5 cm. There was no pelvic ascites.
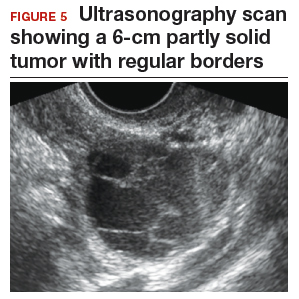
Morphology classification was as follows:
- simple rules: M5 equivocal; B4 positive (indeterminate risk)
- ADNEX: 42.7% risk of malignancy (high risk)
- MI: 6 (indeterminate risk).
Step 2. Secondary testing was recommended for this patient. Test results were:
- repeat ultrasonography in 4 weeks with MI of 7 (volume score increase from 2 to 3, structure score unchanged at 4). Change in MI score +1 per month (high risk)
- Overa: 5.2 (high risk)
- ROMA: 11.8% (low risk).
Treatment plan. The patient was referred to a gynecologic oncologist because of an increasing MI score on serial sonography. Surgery revealed a stage IA grade 2 endometrioid adenocarcinoma of the ovary with surrounding endometriosis.
Read about treating a woman with postmenstrual bleeding.
CASE 3 Woman with postmenopausal bleeding seeks medical care
A 62-year-old woman is referred with new-onset postmenopausal spotting for 1 month. She was recently prescribed antibiotics for diverticulitis. She has no family history of cancer. The referring physician included the results of a serum CA 125, which was 48 U/mL (normal, ≤35 U/mL). On pelvic examination, a mobile cystic mass is noted in the posterior cul-de-sac.
Use the stepwise protocol to sort out findings
Step 1. Pelvic ultrasonography. Transvaginal sonography suggested the presence of an endometrial polyp and revealed a 6-cm (volume, 89 mL) septate ovarian cyst (FIGURE 6).
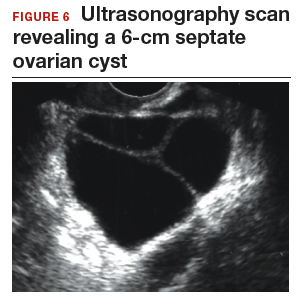
Based on morphology classification, risk was categorized as:
- simple rules: M rules negative; B2, B4, B5 positive (benign; low risk)
- ADNEX: 2.9% risk of malignancy (low risk)
- MI: 2 (low risk).
Step 2. No secondary testing was recommended in this case.
Treatment plan. The patient’s gynecologist performed a hysteroscopic polypectomy that revealed no cancer. Serial monitoring was recommended for the low-risk ovarian cyst. The next ultrasonography scan, at 6 months, was unchanged; a subsequent scan was ordered for 12 months later, and at that time the cyst had resolved.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Barber HR, Graber EA. The PMPO syndrome (postmenopausal palpable ovary syndrome). Obstet Gynecol. 1971;38(6):921–923.
- Modesitt SC, Pavlik EJ, Ueland FR, DePriest PD, Kryscio RJ, van Nagell JR Jr. Risk of malignancy in unilocular ovarian cystic tumors less than 10 centimeters in diameter. Obstet Gynecol. 2003;102(3):594–599.
- Saunders BA, Podzielinski I, Ware RA, et al. Risk of malignancy in sonographically confirmed septated cystic ovarian tumors. Gynecol Oncol. 2010;118(3):278–282.
- Moore RG, McMeekin DS, Brown AK, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol. 2009;112(1):40–46.
- Jordan SM, Bristow RE. Ovarian cancer biomarkers as diagnostic triage tests. Current Biomarker Findings. 2013;3:35–42.
- Giede KC, Kieser K, Dodge J, Rosen B. Who should operate on patients with ovarian cancer? An evidence-based review. Gynecol Oncol. 2005;99(2):447–461.
- Pavlik EJ, Ueland FR, Miller RW, et al. Frequency and disposition of ovarian abnormalities followed with serial transvaginal ultrasonography. Obstet Gynecol. 2013;122(2 pt 1):210–217.
- Glanc P, Benacerraf B, Bourne T, et al. First International Consensus Report on adnexal masses: management recommendations. J Ultrasound Med. 2017;36(5):849–863.
- Timmerman D, Valentin L, Bourne TGH, Collins WP, Verrelst H, Vergote I; International Ovarian Tumor Analysis (IOTA) Group. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) group. Ultrasound Obstet Gynecol. 2000;6(5):500–505.
- Timmerman D, Testa AC, Bourne T, et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet Gynecol. 2008;31(6):681–690.
- Van Calser B, Van Hoorde K, Valentin L, et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study. BMJ. 2014;349:g5920.
- Elder JW, Pavlik EJ, Long A, et al. Serial ultrasonographic evaluation of ovarian abnormalities with a morphology index. Gynecol Oncol. 2014;135(1):8–12.
- Lefringhouse J, Ueland F, Ore R, et al. Comparing 2 sonographic scoring systems for distinguishing benign from malignant ovarian tumors [abstract]. Gynecol Oncol. 2016;141(suppl 1):57.
- Bast RC Jr, Klug TL, St John E, et al. A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Engl J Med. 1983;309(15):883–887.
- Jacobs I, Bast RC Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989;4(1):1–12.
- Myers ER, Bastian LA, Havrilesky LJ, et al. Management of adnexal mass. Agency for Healthcare Research and Quality. https://archive.ahrq.gov/downloads/pub/evidence/pdf/adnexal/adnexal.pdf. Published February 2006. Accessed May 15, 2018.
- Coleman RL, Herzog TJ, Chan DW, et al. Validation of a second-generation multivariate index assay for malignancy risk of adnexal masses. Am J Obstet Gynecol. 2016;215(1):82.e1–e11.
- Ueland FR, Desimone CP, Seamon LG, et al. Effectiveness of a multivariate index assay in the preoperative assessment of ovarian tumors. Obstet Gynecol. 2011;117(6):1289–1297.
- Bristow RE, Smith A, Zhang Z, et al. Ovarian malignancy risk stratification of the adnexal mass using a multivariate index assay. Gynecol Oncol. 2013;128(2):252–259.
- Moore RG, McMeekin DS, Brown AK, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol. 2009;112(1):40–46.
- Valentin L, Ameye L, Franchi D, et al. Risk of malignancy in unilocular cysts: a study of 1148 adnexal masses classified as unilocular cysts on transvaginal ultrasound and review of the literature. Ultrasound Obstet Gynecol. 2013;41(1):80–89.
- Timmerman D, Ameye L, Fischerova D, et al. Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: prospective validation by IOTA group. BMJ. 2010;341:c6839.

Dr. Ueland is Professor and Director of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Kentucky, Lexington.

Dr. Fredericks is Fellow, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Kentucky, Lexington.
The authors report no financial relationships relevant to this article.
Dr. Ueland is Professor and Director of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Kentucky, Lexington.
Dr. Fredericks is Fellow, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Kentucky, Lexington.
The authors report no financial relationships relevant to this article.
Dr. Ueland is Professor and Director of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Kentucky, Lexington.
Dr. Fredericks is Fellow, Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, University of Kentucky, Lexington.
The authors report no financial relationships relevant to this article.
A meaningful evolution has occurred over the past 30 years in the evaluation of ovarian tumors. In the 1980s, any palpable ovarian tumor was recommended for surgical removal.1 In the early 2000s, studies showed that unilocular cysts were at very low risk for malignancy, and surveillance was recommended.2 In the following decade, septate cysts were added to the list of ovarian tumors unlikely to be malignant, and nonsurgical therapy was suggested.3 It is estimated that 10% of women will undergo surgery for an adnexal mass in their lifetime, despite the fact that only 1 in 6 (13%–21%) of these masses is found to be malignant.4,5
A comprehensive, morphology-based pelvic ultrasonography is the first and most important step in evaluating an ovarian tumor’s risk of malignancy to determine whether surgery or surveillance is required.
Ovarian cancer continues to be the leading cause of gynecologic cancer death. Despite achieving superior surgical and cancer outcomes, a gynecologic oncologist performs only 40% of the initial ovarian cancer surgeries.6 Premenopausal and menopausal ovarian tumors are different in cause and consequence. Only 15% of premenopausal tumors are malignant, most commonly germ cell tumors, borderline ovarian tumors, and epithelial ovarian cancers. Tumors in menopausal women are less common but are more likely to be malignant. In actuality, up to 50% of tumors in this population are malignant. The most common of these malignancies are epithelial ovarian cancers, cancers metastatic to the ovary, and malignant stromal tumors.
Effective and evidence-based preoperative evaluations are available to help the clinician estimate a tumor’s risk of malignancy and determine which tumors are appropriate for referral to a specialist for surgery.
The actual incidence and prevalence of ovarian tumors are not known. From a review of almost 40,000 ultrasonography scans performed in the University of Kentucky Ovarian Cancer Screening Program, the estimated incidence and prevalence of ovarian abnormalities are 8.2 per 100 women annuallyand 17%, respectively.7 Seventy percent of these abnormalities have a unilocular or simple septate morphology and are at low risk for malignancy.7 The remaining 30% of abnormalities are high risk, although this represents only 9% of the total population evaluated. Since the vast majority of these abnormalities are expected to be asymptomatic, most will go unrecognized in the general population. For women who have an ovarian abnormality on ultrasonography, the majority will be at low risk for malignancy and will not require surgery.
Ovarian ultrasonography plus morphologic scoring comprise a comprehensive approach
The recently published recommendations of the First International Consensus Conference report on adnexal masses are summarized in TABLE 1.8 The expert panel reviewed the evidence and concluded that effective ultrasonography strategies exist and are well validated, and that low-risk asymptomatic ovarian cysts do not require surgical removal.
While no single ultrasonographic findingcan differentiate a benign from a malignant mass, morphologic scoring systems improve our ability to estimate a tumor’s malignant potential. In the United States, most practitioners in women’s health have ready access to gynecologic ultrasonography, but individual training and proficiency vary. Since not everyone is an expert sonographer, it is useful to employ an objective strategy when evaluating an ovarian tumor. The focus of a comprehensive ovarian ultrasonography is to recognize morphologic patterns that reflect a tumor’s malignant potential. While tumor volume is useful, tumor morphology is the most prognostic feature.
International Ovarian Tumor Analysis group
The International Ovarian Tumor Analysis (IOTA) group has published extensively on sonographic definitions and patterns that categorize tumors based on appearance.9 Simple rules and the ADNEX risk model are 2 of the group’s approaches (FIGURE 1).10,11 Both methods have been validated as effective for differentiating benign from malignant ovarian tumors, but neither has been used to study serial changes in ovarian morphology.
Regardless of the strategy employed, 25% of ovarian ultrasonography evaluations will be interpreted as “indeterminate” or “risk unknown.”10 The IOTA strategies have been successfully used in Europe for years, but they have not yet been studied or adopted in the United States.
Kentucky morphology index
The morphology index (MI) from the University of Kentucky is an ultrasonography-based scoring system that combines tumor volume and tumor structure into a simple and effective index with a score ranging from 0 to 10 (FIGURE 2).12 A rising Kentucky MI score has a linear and predictable increase in the risk of ovarian malignancy. In a review of almost 40,000 sonograms, 85% of the malignancies had an MI score of 5 or greater (TABLE 2).12 Using this as a cutoff, the sensitivity and specificity for predicting malignancy was 86% and 98%, respectively.12
When comparing the ADNEX risk model with the Kentucky MI, investigators reviewed 45,000 ultrasound results and found that the majority of cancers were categorized by the ADNEX model in the lowest 4 of the 10 risk-of-malignancy groups, compared with only 15% for the MI.13 This clustering or skew is potentially problematic, since we expect higher scores to be more predictive of cancer than lower scores. It also infers that the ADNEX model may not be useful in serial surveillance strategies. Moreover, the ADNEX model identified only 30% of early stage cancers compared with identification of 80% with use of the MI.13
Serial ultrasonography
Serial ultrasonography is a concept similar to any longitudinal biomarker evaluation. In the United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS) program, the Risk of Ovarian Cancer Algorithm (ROCA) employs serial measurements of cancer antigen 125 (CA 125) to improve cancer detection. Serial ultrasonography similarly can be applied to better characterize a tumor’s physiology as well as its morphology. Over time, malignant ovarian tumors grow naturally in volume and complexity, and they do so at a rate faster than nonmalignant tumors. If this physical change can be measured objectively with ultrasonography, then serial sonography becomes a valuable diagnostic aid.
In comparing serial MI scores with clinical outcomes, studies have shown that malignant tumors exhibit a rapid increase, nonmalignant tumors have a stable or gradual rise, and resolving cysts show a decrease in MI score over time (FIGURE 3).12 An increase in the MI score of 1 or more per month (≥1 per month) is concerning for malignancy, and surgical removal should be considered. If the MI score of an asymptomatic ovarian tumor does not increase by 1 per month, it can be surveilled with intermittent ultrasonography.
Read about evaluating with serum biomarkers and sonography.
Serum biomarkers useful for determining risk, need for referral
Serum biomarkers can be used to complement an ultrasonographic evaluation. They are particularly useful when surgery is recommended but the sonographic evaluation is indeterminate for malignancy risk. Many serum biomarkers are commonly used for the preoperative evaluation of an ovarian tumor or for surveillance of a malignancy following diagnosis (TABLE 3).
CA 125 is the most commonly ordered serum biomarker test for ovarian cancer. It is estimated that three‐quarters of CA 125 tests are ordered for preoperative use, which is not the US Food and Drug Administration (FDA) approved indication. Despite our clinical reliance on CA 125 as a diagnostic test prior to surgery, its utility is limited because of a low sensitivity for predicting cancer in premenopausal women and early stage disease.14,15 CA 125 specificity also varies widely, depending on patient age and other clinical factors, ranging from as low as 26% in premenopausal women to as high as 100% in postmenopausal women.16 Because CA 125 often is negative when early stage cancer is present, or positive when cancer is not, it is not recommended for preoperative use for determining whether an ovarian tumor is malignant or whether surgery is indicated. CA 125 should be used to monitor patients with a known ovarian malignancy.
The new triage serum biomarkers, Overa, Ova1, and ROMA (Risk of Ovarian Malignancy Algorithm), are FDA cleared for preoperative use to help determine whether a woman needing surgery for an ovarian mass should be referred to a gynecologic oncologist.17–20 These tests should not be used to decide if surgery is indicated, but rather should be considered when the decision for surgery has already been made but the malignancy risk is unknown. A woman with a “high risk” result should be referred to a gynecologic oncologist, while one with a “low risk” score is very unlikely to have a malignancy and referral to a specialist is not necessary. TABLE 4 lists a comparison of the relative performance of these serum biomarkers.14,15,17–20 There are no published data on the use of serial triage biomarkers.
How to evaluate an ovarian tumor
Approximately 65% of the time, ovarian cystic tumors can be identified accurately as low risk based on the initial sonographic evaluation (TABLE 5). In this scenario, the risk of malignancy is very low (<1%), no secondary testing is needed, and no surgery is recommended.1,3,21
About 10% of tumors are expected to have a high-risk morphology on ultrasonography, where the risk of malignancy exceeds 25% and referral to a gynecologic oncologist is required.
The remaining 25% of tumors cannot be accurately classified with a single ultrasonographic evaluation and are considered indeterminate.22 Indeterminate tumors require secondary testing to ascertain whether surgery is indicated. Secondary testing may consist of serial ultrasonography, magnetic resonance imaging (MRI), or serum triage biomarker testing if the decision for surgery has been made.
A 2-step process is recommended for evaluating an ovarian tumor.
Step 1. Perform a detailed ultrasonography study using a morphology-based system. Classify the tumor as:
- low risk (65%): unilocular, simple septate, no flow on color Doppler
- simple rules: benign
- MI score 0–3
- no secondary testing; no referral is recommended
- high risk (10%): irregular, mostly solid, papillary projections, very strong flow on color Doppler
- simple rules: malignant
- MI score ≥5
- no secondary testing; refer to a gynecologic oncologist
- indeterminate (25%): partly solid, small wall abnormalities, minimal or moderate flow on color Doppler
- simple rules: both M and B rules apply or no rule applies
- MI score usually 4–6
- perform secondary testing (step 2).
Step 2. Perform secondary testing as follows:
- serum triage biomarkers if surgery is planned (Ova1, ROMA, Overa), or
- MRI, or
- serial sonography.
The 3 case scenarios that follow illustrate how the ovarian tumor evaluation process may be applied in clinical practice, with referral to a gynecologic oncologist as appropriate.
CASE 1 Postmenopausal woman with urinary symptoms and pelvic pressure
A 61-year-old woman is referred with a newly identified ovarian tumor. She has had 1 month of urinary urgency, frequency, and pelvic pressure, but she denies vaginal bleeding or fever. She has no family history of cancer. The referring physician included results of a serum CA 125 (48 U/mL; normal, ≤35 U/mL). A pelvic examination reveals a palpable, irregular mass in the anterior pelvis with limited mobility.
What would be your next step in the evaluation of this patient?
Start with ultrasonography
Step 1. Perform pelvic ultrasonography. In this patient, transvaginal sonography revealed a 6-cm (volume, 89 mL) mostly solid tumor (FIGURE 4). The maximum solid diameter of the tumor was 4.0 cm. There was a 20-mL pocket of pelvic ascites.
Results of morphology-based classification were as follows:
- simple rules: M1 and M5 positive; B rules: negative (malignant; high risk)
- ADNEX: 51.6% risk of malignancy (high risk)
- MI: 7 (high risk).
Step 2. Consider secondary testing. In this case, no secondary testing was recommended. Treatment plan. The patient was referred to a gynecologic oncologist for surgery and was found to have a stage IIA serous ovarian carcinoma.
CASE 2 Woman with history of pelvic symptoms and worsening pain
A 46-year-old woman presents with worsening pelvic pain over the last month. She has a long-standing history of pelvic pain, dysmenorrhea, and dyspareunia from suspected endometriosis. She has no family history of cancer. The referring physician included the following serum biomarker results: CA 125, 48 U/mL (normal, ≤35 U/mL), and HE4, 60 pM (normal, ≤150 pM). On pelvic examination, there is a palpable mass with limited mobility in the posterior cul-de-sac.
Based on the patient’s available history, physical examination, and biomarker information, how would you proceed?
Follow the 2-step process
Step 1. Perform pelvic ultrasonography. Transvaginal sonography revealed a 6-cm (volume, 89 mL) partly solid tumor with regular internal borders (FIGURE 5). The maximum solid diameter of the tumor was 4.5 cm. There was no pelvic ascites.
Morphology classification was as follows:
- simple rules: M5 equivocal; B4 positive (indeterminate risk)
- ADNEX: 42.7% risk of malignancy (high risk)
- MI: 6 (indeterminate risk).
Step 2. Secondary testing was recommended for this patient. Test results were:
- repeat ultrasonography in 4 weeks with MI of 7 (volume score increase from 2 to 3, structure score unchanged at 4). Change in MI score +1 per month (high risk)
- Overa: 5.2 (high risk)
- ROMA: 11.8% (low risk).
Treatment plan. The patient was referred to a gynecologic oncologist because of an increasing MI score on serial sonography. Surgery revealed a stage IA grade 2 endometrioid adenocarcinoma of the ovary with surrounding endometriosis.
Read about treating a woman with postmenstrual bleeding.
CASE 3 Woman with postmenopausal bleeding seeks medical care
A 62-year-old woman is referred with new-onset postmenopausal spotting for 1 month. She was recently prescribed antibiotics for diverticulitis. She has no family history of cancer. The referring physician included the results of a serum CA 125, which was 48 U/mL (normal, ≤35 U/mL). On pelvic examination, a mobile cystic mass is noted in the posterior cul-de-sac.
Use the stepwise protocol to sort out findings
Step 1. Pelvic ultrasonography. Transvaginal sonography suggested the presence of an endometrial polyp and revealed a 6-cm (volume, 89 mL) septate ovarian cyst (FIGURE 6).
Based on morphology classification, risk was categorized as:
- simple rules: M rules negative; B2, B4, B5 positive (benign; low risk)
- ADNEX: 2.9% risk of malignancy (low risk)
- MI: 2 (low risk).
Step 2. No secondary testing was recommended in this case.
Treatment plan. The patient’s gynecologist performed a hysteroscopic polypectomy that revealed no cancer. Serial monitoring was recommended for the low-risk ovarian cyst. The next ultrasonography scan, at 6 months, was unchanged; a subsequent scan was ordered for 12 months later, and at that time the cyst had resolved.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
A meaningful evolution has occurred over the past 30 years in the evaluation of ovarian tumors. In the 1980s, any palpable ovarian tumor was recommended for surgical removal.1 In the early 2000s, studies showed that unilocular cysts were at very low risk for malignancy, and surveillance was recommended.2 In the following decade, septate cysts were added to the list of ovarian tumors unlikely to be malignant, and nonsurgical therapy was suggested.3 It is estimated that 10% of women will undergo surgery for an adnexal mass in their lifetime, despite the fact that only 1 in 6 (13%–21%) of these masses is found to be malignant.4,5
A comprehensive, morphology-based pelvic ultrasonography is the first and most important step in evaluating an ovarian tumor’s risk of malignancy to determine whether surgery or surveillance is required.
Ovarian cancer continues to be the leading cause of gynecologic cancer death. Despite achieving superior surgical and cancer outcomes, a gynecologic oncologist performs only 40% of the initial ovarian cancer surgeries.6 Premenopausal and menopausal ovarian tumors are different in cause and consequence. Only 15% of premenopausal tumors are malignant, most commonly germ cell tumors, borderline ovarian tumors, and epithelial ovarian cancers. Tumors in menopausal women are less common but are more likely to be malignant. In actuality, up to 50% of tumors in this population are malignant. The most common of these malignancies are epithelial ovarian cancers, cancers metastatic to the ovary, and malignant stromal tumors.
Effective and evidence-based preoperative evaluations are available to help the clinician estimate a tumor’s risk of malignancy and determine which tumors are appropriate for referral to a specialist for surgery.
The actual incidence and prevalence of ovarian tumors are not known. From a review of almost 40,000 ultrasonography scans performed in the University of Kentucky Ovarian Cancer Screening Program, the estimated incidence and prevalence of ovarian abnormalities are 8.2 per 100 women annuallyand 17%, respectively.7 Seventy percent of these abnormalities have a unilocular or simple septate morphology and are at low risk for malignancy.7 The remaining 30% of abnormalities are high risk, although this represents only 9% of the total population evaluated. Since the vast majority of these abnormalities are expected to be asymptomatic, most will go unrecognized in the general population. For women who have an ovarian abnormality on ultrasonography, the majority will be at low risk for malignancy and will not require surgery.
Ovarian ultrasonography plus morphologic scoring comprise a comprehensive approach
The recently published recommendations of the First International Consensus Conference report on adnexal masses are summarized in TABLE 1.8 The expert panel reviewed the evidence and concluded that effective ultrasonography strategies exist and are well validated, and that low-risk asymptomatic ovarian cysts do not require surgical removal.
While no single ultrasonographic findingcan differentiate a benign from a malignant mass, morphologic scoring systems improve our ability to estimate a tumor’s malignant potential. In the United States, most practitioners in women’s health have ready access to gynecologic ultrasonography, but individual training and proficiency vary. Since not everyone is an expert sonographer, it is useful to employ an objective strategy when evaluating an ovarian tumor. The focus of a comprehensive ovarian ultrasonography is to recognize morphologic patterns that reflect a tumor’s malignant potential. While tumor volume is useful, tumor morphology is the most prognostic feature.
International Ovarian Tumor Analysis group
The International Ovarian Tumor Analysis (IOTA) group has published extensively on sonographic definitions and patterns that categorize tumors based on appearance.9 Simple rules and the ADNEX risk model are 2 of the group’s approaches (FIGURE 1).10,11 Both methods have been validated as effective for differentiating benign from malignant ovarian tumors, but neither has been used to study serial changes in ovarian morphology.
Regardless of the strategy employed, 25% of ovarian ultrasonography evaluations will be interpreted as “indeterminate” or “risk unknown.”10 The IOTA strategies have been successfully used in Europe for years, but they have not yet been studied or adopted in the United States.
Kentucky morphology index
The morphology index (MI) from the University of Kentucky is an ultrasonography-based scoring system that combines tumor volume and tumor structure into a simple and effective index with a score ranging from 0 to 10 (FIGURE 2).12 A rising Kentucky MI score has a linear and predictable increase in the risk of ovarian malignancy. In a review of almost 40,000 sonograms, 85% of the malignancies had an MI score of 5 or greater (TABLE 2).12 Using this as a cutoff, the sensitivity and specificity for predicting malignancy was 86% and 98%, respectively.12
When comparing the ADNEX risk model with the Kentucky MI, investigators reviewed 45,000 ultrasound results and found that the majority of cancers were categorized by the ADNEX model in the lowest 4 of the 10 risk-of-malignancy groups, compared with only 15% for the MI.13 This clustering or skew is potentially problematic, since we expect higher scores to be more predictive of cancer than lower scores. It also infers that the ADNEX model may not be useful in serial surveillance strategies. Moreover, the ADNEX model identified only 30% of early stage cancers compared with identification of 80% with use of the MI.13
Serial ultrasonography
Serial ultrasonography is a concept similar to any longitudinal biomarker evaluation. In the United Kingdom Collaborative Trial of Ovarian Cancer Screening (UKCTOCS) program, the Risk of Ovarian Cancer Algorithm (ROCA) employs serial measurements of cancer antigen 125 (CA 125) to improve cancer detection. Serial ultrasonography similarly can be applied to better characterize a tumor’s physiology as well as its morphology. Over time, malignant ovarian tumors grow naturally in volume and complexity, and they do so at a rate faster than nonmalignant tumors. If this physical change can be measured objectively with ultrasonography, then serial sonography becomes a valuable diagnostic aid.
In comparing serial MI scores with clinical outcomes, studies have shown that malignant tumors exhibit a rapid increase, nonmalignant tumors have a stable or gradual rise, and resolving cysts show a decrease in MI score over time (FIGURE 3).12 An increase in the MI score of 1 or more per month (≥1 per month) is concerning for malignancy, and surgical removal should be considered. If the MI score of an asymptomatic ovarian tumor does not increase by 1 per month, it can be surveilled with intermittent ultrasonography.
Read about evaluating with serum biomarkers and sonography.
Serum biomarkers useful for determining risk, need for referral
Serum biomarkers can be used to complement an ultrasonographic evaluation. They are particularly useful when surgery is recommended but the sonographic evaluation is indeterminate for malignancy risk. Many serum biomarkers are commonly used for the preoperative evaluation of an ovarian tumor or for surveillance of a malignancy following diagnosis (TABLE 3).
CA 125 is the most commonly ordered serum biomarker test for ovarian cancer. It is estimated that three‐quarters of CA 125 tests are ordered for preoperative use, which is not the US Food and Drug Administration (FDA) approved indication. Despite our clinical reliance on CA 125 as a diagnostic test prior to surgery, its utility is limited because of a low sensitivity for predicting cancer in premenopausal women and early stage disease.14,15 CA 125 specificity also varies widely, depending on patient age and other clinical factors, ranging from as low as 26% in premenopausal women to as high as 100% in postmenopausal women.16 Because CA 125 often is negative when early stage cancer is present, or positive when cancer is not, it is not recommended for preoperative use for determining whether an ovarian tumor is malignant or whether surgery is indicated. CA 125 should be used to monitor patients with a known ovarian malignancy.
The new triage serum biomarkers, Overa, Ova1, and ROMA (Risk of Ovarian Malignancy Algorithm), are FDA cleared for preoperative use to help determine whether a woman needing surgery for an ovarian mass should be referred to a gynecologic oncologist.17–20 These tests should not be used to decide if surgery is indicated, but rather should be considered when the decision for surgery has already been made but the malignancy risk is unknown. A woman with a “high risk” result should be referred to a gynecologic oncologist, while one with a “low risk” score is very unlikely to have a malignancy and referral to a specialist is not necessary. TABLE 4 lists a comparison of the relative performance of these serum biomarkers.14,15,17–20 There are no published data on the use of serial triage biomarkers.
How to evaluate an ovarian tumor
Approximately 65% of the time, ovarian cystic tumors can be identified accurately as low risk based on the initial sonographic evaluation (TABLE 5). In this scenario, the risk of malignancy is very low (<1%), no secondary testing is needed, and no surgery is recommended.1,3,21
About 10% of tumors are expected to have a high-risk morphology on ultrasonography, where the risk of malignancy exceeds 25% and referral to a gynecologic oncologist is required.
The remaining 25% of tumors cannot be accurately classified with a single ultrasonographic evaluation and are considered indeterminate.22 Indeterminate tumors require secondary testing to ascertain whether surgery is indicated. Secondary testing may consist of serial ultrasonography, magnetic resonance imaging (MRI), or serum triage biomarker testing if the decision for surgery has been made.
A 2-step process is recommended for evaluating an ovarian tumor.
Step 1. Perform a detailed ultrasonography study using a morphology-based system. Classify the tumor as:
- low risk (65%): unilocular, simple septate, no flow on color Doppler
- simple rules: benign
- MI score 0–3
- no secondary testing; no referral is recommended
- high risk (10%): irregular, mostly solid, papillary projections, very strong flow on color Doppler
- simple rules: malignant
- MI score ≥5
- no secondary testing; refer to a gynecologic oncologist
- indeterminate (25%): partly solid, small wall abnormalities, minimal or moderate flow on color Doppler
- simple rules: both M and B rules apply or no rule applies
- MI score usually 4–6
- perform secondary testing (step 2).
Step 2. Perform secondary testing as follows:
- serum triage biomarkers if surgery is planned (Ova1, ROMA, Overa), or
- MRI, or
- serial sonography.
The 3 case scenarios that follow illustrate how the ovarian tumor evaluation process may be applied in clinical practice, with referral to a gynecologic oncologist as appropriate.
CASE 1 Postmenopausal woman with urinary symptoms and pelvic pressure
A 61-year-old woman is referred with a newly identified ovarian tumor. She has had 1 month of urinary urgency, frequency, and pelvic pressure, but she denies vaginal bleeding or fever. She has no family history of cancer. The referring physician included results of a serum CA 125 (48 U/mL; normal, ≤35 U/mL). A pelvic examination reveals a palpable, irregular mass in the anterior pelvis with limited mobility.
What would be your next step in the evaluation of this patient?
Start with ultrasonography
Step 1. Perform pelvic ultrasonography. In this patient, transvaginal sonography revealed a 6-cm (volume, 89 mL) mostly solid tumor (FIGURE 4). The maximum solid diameter of the tumor was 4.0 cm. There was a 20-mL pocket of pelvic ascites.
Results of morphology-based classification were as follows:
- simple rules: M1 and M5 positive; B rules: negative (malignant; high risk)
- ADNEX: 51.6% risk of malignancy (high risk)
- MI: 7 (high risk).
Step 2. Consider secondary testing. In this case, no secondary testing was recommended. Treatment plan. The patient was referred to a gynecologic oncologist for surgery and was found to have a stage IIA serous ovarian carcinoma.
CASE 2 Woman with history of pelvic symptoms and worsening pain
A 46-year-old woman presents with worsening pelvic pain over the last month. She has a long-standing history of pelvic pain, dysmenorrhea, and dyspareunia from suspected endometriosis. She has no family history of cancer. The referring physician included the following serum biomarker results: CA 125, 48 U/mL (normal, ≤35 U/mL), and HE4, 60 pM (normal, ≤150 pM). On pelvic examination, there is a palpable mass with limited mobility in the posterior cul-de-sac.
Based on the patient’s available history, physical examination, and biomarker information, how would you proceed?
Follow the 2-step process
Step 1. Perform pelvic ultrasonography. Transvaginal sonography revealed a 6-cm (volume, 89 mL) partly solid tumor with regular internal borders (FIGURE 5). The maximum solid diameter of the tumor was 4.5 cm. There was no pelvic ascites.
Morphology classification was as follows:
- simple rules: M5 equivocal; B4 positive (indeterminate risk)
- ADNEX: 42.7% risk of malignancy (high risk)
- MI: 6 (indeterminate risk).
Step 2. Secondary testing was recommended for this patient. Test results were:
- repeat ultrasonography in 4 weeks with MI of 7 (volume score increase from 2 to 3, structure score unchanged at 4). Change in MI score +1 per month (high risk)
- Overa: 5.2 (high risk)
- ROMA: 11.8% (low risk).
Treatment plan. The patient was referred to a gynecologic oncologist because of an increasing MI score on serial sonography. Surgery revealed a stage IA grade 2 endometrioid adenocarcinoma of the ovary with surrounding endometriosis.
Read about treating a woman with postmenstrual bleeding.
CASE 3 Woman with postmenopausal bleeding seeks medical care
A 62-year-old woman is referred with new-onset postmenopausal spotting for 1 month. She was recently prescribed antibiotics for diverticulitis. She has no family history of cancer. The referring physician included the results of a serum CA 125, which was 48 U/mL (normal, ≤35 U/mL). On pelvic examination, a mobile cystic mass is noted in the posterior cul-de-sac.
Use the stepwise protocol to sort out findings
Step 1. Pelvic ultrasonography. Transvaginal sonography suggested the presence of an endometrial polyp and revealed a 6-cm (volume, 89 mL) septate ovarian cyst (FIGURE 6).
Based on morphology classification, risk was categorized as:
- simple rules: M rules negative; B2, B4, B5 positive (benign; low risk)
- ADNEX: 2.9% risk of malignancy (low risk)
- MI: 2 (low risk).
Step 2. No secondary testing was recommended in this case.
Treatment plan. The patient’s gynecologist performed a hysteroscopic polypectomy that revealed no cancer. Serial monitoring was recommended for the low-risk ovarian cyst. The next ultrasonography scan, at 6 months, was unchanged; a subsequent scan was ordered for 12 months later, and at that time the cyst had resolved.
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Barber HR, Graber EA. The PMPO syndrome (postmenopausal palpable ovary syndrome). Obstet Gynecol. 1971;38(6):921–923.
- Modesitt SC, Pavlik EJ, Ueland FR, DePriest PD, Kryscio RJ, van Nagell JR Jr. Risk of malignancy in unilocular ovarian cystic tumors less than 10 centimeters in diameter. Obstet Gynecol. 2003;102(3):594–599.
- Saunders BA, Podzielinski I, Ware RA, et al. Risk of malignancy in sonographically confirmed septated cystic ovarian tumors. Gynecol Oncol. 2010;118(3):278–282.
- Moore RG, McMeekin DS, Brown AK, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol. 2009;112(1):40–46.
- Jordan SM, Bristow RE. Ovarian cancer biomarkers as diagnostic triage tests. Current Biomarker Findings. 2013;3:35–42.
- Giede KC, Kieser K, Dodge J, Rosen B. Who should operate on patients with ovarian cancer? An evidence-based review. Gynecol Oncol. 2005;99(2):447–461.
- Pavlik EJ, Ueland FR, Miller RW, et al. Frequency and disposition of ovarian abnormalities followed with serial transvaginal ultrasonography. Obstet Gynecol. 2013;122(2 pt 1):210–217.
- Glanc P, Benacerraf B, Bourne T, et al. First International Consensus Report on adnexal masses: management recommendations. J Ultrasound Med. 2017;36(5):849–863.
- Timmerman D, Valentin L, Bourne TGH, Collins WP, Verrelst H, Vergote I; International Ovarian Tumor Analysis (IOTA) Group. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) group. Ultrasound Obstet Gynecol. 2000;6(5):500–505.
- Timmerman D, Testa AC, Bourne T, et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet Gynecol. 2008;31(6):681–690.
- Van Calser B, Van Hoorde K, Valentin L, et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study. BMJ. 2014;349:g5920.
- Elder JW, Pavlik EJ, Long A, et al. Serial ultrasonographic evaluation of ovarian abnormalities with a morphology index. Gynecol Oncol. 2014;135(1):8–12.
- Lefringhouse J, Ueland F, Ore R, et al. Comparing 2 sonographic scoring systems for distinguishing benign from malignant ovarian tumors [abstract]. Gynecol Oncol. 2016;141(suppl 1):57.
- Bast RC Jr, Klug TL, St John E, et al. A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Engl J Med. 1983;309(15):883–887.
- Jacobs I, Bast RC Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989;4(1):1–12.
- Myers ER, Bastian LA, Havrilesky LJ, et al. Management of adnexal mass. Agency for Healthcare Research and Quality. https://archive.ahrq.gov/downloads/pub/evidence/pdf/adnexal/adnexal.pdf. Published February 2006. Accessed May 15, 2018.
- Coleman RL, Herzog TJ, Chan DW, et al. Validation of a second-generation multivariate index assay for malignancy risk of adnexal masses. Am J Obstet Gynecol. 2016;215(1):82.e1–e11.
- Ueland FR, Desimone CP, Seamon LG, et al. Effectiveness of a multivariate index assay in the preoperative assessment of ovarian tumors. Obstet Gynecol. 2011;117(6):1289–1297.
- Bristow RE, Smith A, Zhang Z, et al. Ovarian malignancy risk stratification of the adnexal mass using a multivariate index assay. Gynecol Oncol. 2013;128(2):252–259.
- Moore RG, McMeekin DS, Brown AK, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol. 2009;112(1):40–46.
- Valentin L, Ameye L, Franchi D, et al. Risk of malignancy in unilocular cysts: a study of 1148 adnexal masses classified as unilocular cysts on transvaginal ultrasound and review of the literature. Ultrasound Obstet Gynecol. 2013;41(1):80–89.
- Timmerman D, Ameye L, Fischerova D, et al. Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: prospective validation by IOTA group. BMJ. 2010;341:c6839.
- Barber HR, Graber EA. The PMPO syndrome (postmenopausal palpable ovary syndrome). Obstet Gynecol. 1971;38(6):921–923.
- Modesitt SC, Pavlik EJ, Ueland FR, DePriest PD, Kryscio RJ, van Nagell JR Jr. Risk of malignancy in unilocular ovarian cystic tumors less than 10 centimeters in diameter. Obstet Gynecol. 2003;102(3):594–599.
- Saunders BA, Podzielinski I, Ware RA, et al. Risk of malignancy in sonographically confirmed septated cystic ovarian tumors. Gynecol Oncol. 2010;118(3):278–282.
- Moore RG, McMeekin DS, Brown AK, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol. 2009;112(1):40–46.
- Jordan SM, Bristow RE. Ovarian cancer biomarkers as diagnostic triage tests. Current Biomarker Findings. 2013;3:35–42.
- Giede KC, Kieser K, Dodge J, Rosen B. Who should operate on patients with ovarian cancer? An evidence-based review. Gynecol Oncol. 2005;99(2):447–461.
- Pavlik EJ, Ueland FR, Miller RW, et al. Frequency and disposition of ovarian abnormalities followed with serial transvaginal ultrasonography. Obstet Gynecol. 2013;122(2 pt 1):210–217.
- Glanc P, Benacerraf B, Bourne T, et al. First International Consensus Report on adnexal masses: management recommendations. J Ultrasound Med. 2017;36(5):849–863.
- Timmerman D, Valentin L, Bourne TGH, Collins WP, Verrelst H, Vergote I; International Ovarian Tumor Analysis (IOTA) Group. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) group. Ultrasound Obstet Gynecol. 2000;6(5):500–505.
- Timmerman D, Testa AC, Bourne T, et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer. Ultrasound Obstet Gynecol. 2008;31(6):681–690.
- Van Calser B, Van Hoorde K, Valentin L, et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study. BMJ. 2014;349:g5920.
- Elder JW, Pavlik EJ, Long A, et al. Serial ultrasonographic evaluation of ovarian abnormalities with a morphology index. Gynecol Oncol. 2014;135(1):8–12.
- Lefringhouse J, Ueland F, Ore R, et al. Comparing 2 sonographic scoring systems for distinguishing benign from malignant ovarian tumors [abstract]. Gynecol Oncol. 2016;141(suppl 1):57.
- Bast RC Jr, Klug TL, St John E, et al. A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Engl J Med. 1983;309(15):883–887.
- Jacobs I, Bast RC Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod. 1989;4(1):1–12.
- Myers ER, Bastian LA, Havrilesky LJ, et al. Management of adnexal mass. Agency for Healthcare Research and Quality. https://archive.ahrq.gov/downloads/pub/evidence/pdf/adnexal/adnexal.pdf. Published February 2006. Accessed May 15, 2018.
- Coleman RL, Herzog TJ, Chan DW, et al. Validation of a second-generation multivariate index assay for malignancy risk of adnexal masses. Am J Obstet Gynecol. 2016;215(1):82.e1–e11.
- Ueland FR, Desimone CP, Seamon LG, et al. Effectiveness of a multivariate index assay in the preoperative assessment of ovarian tumors. Obstet Gynecol. 2011;117(6):1289–1297.
- Bristow RE, Smith A, Zhang Z, et al. Ovarian malignancy risk stratification of the adnexal mass using a multivariate index assay. Gynecol Oncol. 2013;128(2):252–259.
- Moore RG, McMeekin DS, Brown AK, et al. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol. 2009;112(1):40–46.
- Valentin L, Ameye L, Franchi D, et al. Risk of malignancy in unilocular cysts: a study of 1148 adnexal masses classified as unilocular cysts on transvaginal ultrasound and review of the literature. Ultrasound Obstet Gynecol. 2013;41(1):80–89.
- Timmerman D, Ameye L, Fischerova D, et al. Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: prospective validation by IOTA group. BMJ. 2010;341:c6839.

Should breast cancer screening guidelines be tailored to a patient’s race and ethnicity?
EXPERT COMMENTARY
Breast cancer screening is an important aspect of women’s preventative health care, with proven mortality benefits.1,2 Different recommendations have been made for the age at initiation and the frequency of breast cancer screening in an effort to maximize benefit while minimizing unnecessary health care costs and harms of screening.
The American College of Obstetricians and Gynecologists (ACOG) and the National Comprehensive Cancer Network (NCCN) recommend initiating mammography screening at age 40, with annual screening (although ACOG offers deferral of screening to age 50 and biennial screening through shared decision making).3,4 The American Cancer Society (ACS) recommends offering annual mammography at ages 40 to 44 and recommends routinely starting annual mammography from 45 to 54, followed by either annual or biennial screening for women 55 and older.1 Finally, the US Preventive Services Task Force (USPSTF) recommends biennial mammography screening starting at age 50.5 No organization alters screening recommendations based on a woman’s race/ethnicity.
Details of the study
Stapleton and colleagues recently performed a retrospective population-based cohort study using the Surveillance, Epidemiology, and End Results (SEER) Program database to evaluate the age and stage at breast cancer diagnosis across different racial groups in the United States.6 The study (timeframe, January 1, 1973 to December 31, 2010) included 747,763 women, with a racial/ethnic distribution of 77.0% white, 9.3% black, 7.0% Hispanic, and 6.2% Asian.
The investigators found 2 distinct age distributions of breast cancer based on race. Among nonwhite women, the highest peak of breast cancer diagnoses occurred between 45 and 50 years (FIGURE). By contrast, breast cancer diagnoses peaked at 60 to 65 years in white women.
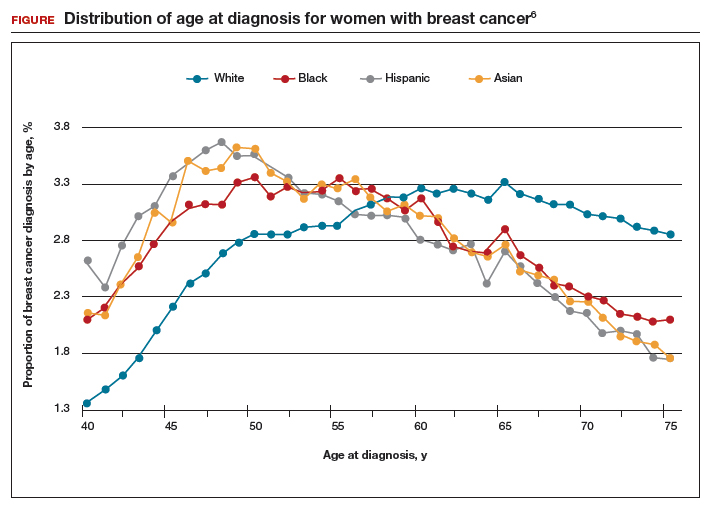
Similarly, a higher proportion of nonwhite women were diagnosed with their breast cancer prior to age 50 compared with white women. While one-quarter of white women with breast cancer develop disease prior to age 50, approximately one-third of black, Asian, and Hispanic women with breast cancer will be diagnosed before age 50 (TABLE).
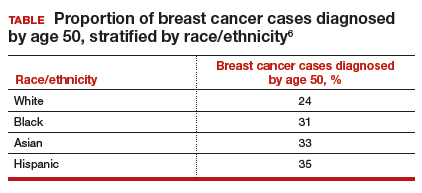
These data suggest that the peak proportion of breast cancer diagnoses in nonwhite women occurs prior to the age of initiation of screening recommended by the USPSTF. Based on these results, Stapleton and colleagues recommend reconsideration of the current USPSTF guidelines to incorporate race/ethnicity–based differences. To diagnose the same proportion of breast cancer cases among nonwhite women as is currently possible among white women at age 50, initiation of breast cancer screening would need to be adjusted to age 47 for black women, age 46 for Hispanic women, and age 47 for Asian women.
Study strengths and weaknesses
This is a unique study that uses the SEER database to capture a large cross section of the American population. The SEER database is a valuable tool because it gathers data from numerous major US metropolitan areas, creating a diverse representative population that minimizes confounding from geographical trends. Nevertheless, any study utilizing a large database is limited by the accuracy and completeness of the data collected at the level of the individual cancer registry. Furthermore, information regarding medical comorbidities and access and adherence to breast cancer screening is lacking in the SEER database; this provides an opportunity for confounding.
Approximately one-third of breast cancer cases in nonwhite women, and one-quarter of cases in white women, occur prior to the age of initiation of screening (50 years) recommended by the USPSTF.
While some screening organizations do recommend that breast cancer screening be initiated prior to age 50, no organizations alter the recommendations for screening based on a woman's race/ethnicity.
Health care providers should be aware that initiation of breast cancer screening at age 50 in nonwhite women misses a disproportionate number of breast cancer cases compared with white women.
Providers should counsel nonwhite women about these differences in age of diagnosis and include that in their consideration of initiating breast cancer screening prior to the age of 50, more in accordance with recommendations of ACOG, NCCN, and ACS.
-- Dana M. Scott, MD, and Mark D. Pearlman, MD
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599–1614.
- Arleo EK, Hendrick RE, Helvie MA, Sickles EA. Comparison of recommendations for screening mammography using CISNET models. Cancer. 2017;123(19):3673–3680.
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Gynecology. Practice Bulletin No. 179: Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1–e16.
- Bevers TB, Anderson BO, Bonaccio E, et al; National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009;7(10):1060–1096.
- US Preventive Services Task Force. Screening for breast cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(10):716–726.
- Stapleton SM, Oseni TO, Bababekov YJ, Hung Y-C, Chang DC. Race/ethnicity and age distribution of breast cancer diagnosis in the United States. JAMA Surg. Published online March 7, 2018. doi:10.1001/jamasurg.2018.0035.
EXPERT COMMENTARY
Breast cancer screening is an important aspect of women’s preventative health care, with proven mortality benefits.1,2 Different recommendations have been made for the age at initiation and the frequency of breast cancer screening in an effort to maximize benefit while minimizing unnecessary health care costs and harms of screening.
The American College of Obstetricians and Gynecologists (ACOG) and the National Comprehensive Cancer Network (NCCN) recommend initiating mammography screening at age 40, with annual screening (although ACOG offers deferral of screening to age 50 and biennial screening through shared decision making).3,4 The American Cancer Society (ACS) recommends offering annual mammography at ages 40 to 44 and recommends routinely starting annual mammography from 45 to 54, followed by either annual or biennial screening for women 55 and older.1 Finally, the US Preventive Services Task Force (USPSTF) recommends biennial mammography screening starting at age 50.5 No organization alters screening recommendations based on a woman’s race/ethnicity.
Details of the study
Stapleton and colleagues recently performed a retrospective population-based cohort study using the Surveillance, Epidemiology, and End Results (SEER) Program database to evaluate the age and stage at breast cancer diagnosis across different racial groups in the United States.6 The study (timeframe, January 1, 1973 to December 31, 2010) included 747,763 women, with a racial/ethnic distribution of 77.0% white, 9.3% black, 7.0% Hispanic, and 6.2% Asian.
The investigators found 2 distinct age distributions of breast cancer based on race. Among nonwhite women, the highest peak of breast cancer diagnoses occurred between 45 and 50 years (FIGURE). By contrast, breast cancer diagnoses peaked at 60 to 65 years in white women.
Similarly, a higher proportion of nonwhite women were diagnosed with their breast cancer prior to age 50 compared with white women. While one-quarter of white women with breast cancer develop disease prior to age 50, approximately one-third of black, Asian, and Hispanic women with breast cancer will be diagnosed before age 50 (TABLE).
These data suggest that the peak proportion of breast cancer diagnoses in nonwhite women occurs prior to the age of initiation of screening recommended by the USPSTF. Based on these results, Stapleton and colleagues recommend reconsideration of the current USPSTF guidelines to incorporate race/ethnicity–based differences. To diagnose the same proportion of breast cancer cases among nonwhite women as is currently possible among white women at age 50, initiation of breast cancer screening would need to be adjusted to age 47 for black women, age 46 for Hispanic women, and age 47 for Asian women.
Study strengths and weaknesses
This is a unique study that uses the SEER database to capture a large cross section of the American population. The SEER database is a valuable tool because it gathers data from numerous major US metropolitan areas, creating a diverse representative population that minimizes confounding from geographical trends. Nevertheless, any study utilizing a large database is limited by the accuracy and completeness of the data collected at the level of the individual cancer registry. Furthermore, information regarding medical comorbidities and access and adherence to breast cancer screening is lacking in the SEER database; this provides an opportunity for confounding.
Approximately one-third of breast cancer cases in nonwhite women, and one-quarter of cases in white women, occur prior to the age of initiation of screening (50 years) recommended by the USPSTF.
While some screening organizations do recommend that breast cancer screening be initiated prior to age 50, no organizations alter the recommendations for screening based on a woman's race/ethnicity.
Health care providers should be aware that initiation of breast cancer screening at age 50 in nonwhite women misses a disproportionate number of breast cancer cases compared with white women.
Providers should counsel nonwhite women about these differences in age of diagnosis and include that in their consideration of initiating breast cancer screening prior to the age of 50, more in accordance with recommendations of ACOG, NCCN, and ACS.
-- Dana M. Scott, MD, and Mark D. Pearlman, MD
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
EXPERT COMMENTARY
Breast cancer screening is an important aspect of women’s preventative health care, with proven mortality benefits.1,2 Different recommendations have been made for the age at initiation and the frequency of breast cancer screening in an effort to maximize benefit while minimizing unnecessary health care costs and harms of screening.
The American College of Obstetricians and Gynecologists (ACOG) and the National Comprehensive Cancer Network (NCCN) recommend initiating mammography screening at age 40, with annual screening (although ACOG offers deferral of screening to age 50 and biennial screening through shared decision making).3,4 The American Cancer Society (ACS) recommends offering annual mammography at ages 40 to 44 and recommends routinely starting annual mammography from 45 to 54, followed by either annual or biennial screening for women 55 and older.1 Finally, the US Preventive Services Task Force (USPSTF) recommends biennial mammography screening starting at age 50.5 No organization alters screening recommendations based on a woman’s race/ethnicity.
Details of the study
Stapleton and colleagues recently performed a retrospective population-based cohort study using the Surveillance, Epidemiology, and End Results (SEER) Program database to evaluate the age and stage at breast cancer diagnosis across different racial groups in the United States.6 The study (timeframe, January 1, 1973 to December 31, 2010) included 747,763 women, with a racial/ethnic distribution of 77.0% white, 9.3% black, 7.0% Hispanic, and 6.2% Asian.
The investigators found 2 distinct age distributions of breast cancer based on race. Among nonwhite women, the highest peak of breast cancer diagnoses occurred between 45 and 50 years (FIGURE). By contrast, breast cancer diagnoses peaked at 60 to 65 years in white women.
Similarly, a higher proportion of nonwhite women were diagnosed with their breast cancer prior to age 50 compared with white women. While one-quarter of white women with breast cancer develop disease prior to age 50, approximately one-third of black, Asian, and Hispanic women with breast cancer will be diagnosed before age 50 (TABLE).
These data suggest that the peak proportion of breast cancer diagnoses in nonwhite women occurs prior to the age of initiation of screening recommended by the USPSTF. Based on these results, Stapleton and colleagues recommend reconsideration of the current USPSTF guidelines to incorporate race/ethnicity–based differences. To diagnose the same proportion of breast cancer cases among nonwhite women as is currently possible among white women at age 50, initiation of breast cancer screening would need to be adjusted to age 47 for black women, age 46 for Hispanic women, and age 47 for Asian women.
Study strengths and weaknesses
This is a unique study that uses the SEER database to capture a large cross section of the American population. The SEER database is a valuable tool because it gathers data from numerous major US metropolitan areas, creating a diverse representative population that minimizes confounding from geographical trends. Nevertheless, any study utilizing a large database is limited by the accuracy and completeness of the data collected at the level of the individual cancer registry. Furthermore, information regarding medical comorbidities and access and adherence to breast cancer screening is lacking in the SEER database; this provides an opportunity for confounding.
Approximately one-third of breast cancer cases in nonwhite women, and one-quarter of cases in white women, occur prior to the age of initiation of screening (50 years) recommended by the USPSTF.
While some screening organizations do recommend that breast cancer screening be initiated prior to age 50, no organizations alter the recommendations for screening based on a woman's race/ethnicity.
Health care providers should be aware that initiation of breast cancer screening at age 50 in nonwhite women misses a disproportionate number of breast cancer cases compared with white women.
Providers should counsel nonwhite women about these differences in age of diagnosis and include that in their consideration of initiating breast cancer screening prior to the age of 50, more in accordance with recommendations of ACOG, NCCN, and ACS.
-- Dana M. Scott, MD, and Mark D. Pearlman, MD
Share your thoughts! Send your Letter to the Editor to rbarbieri@mdedge.com. Please include your name and the city and state in which you practice.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599–1614.
- Arleo EK, Hendrick RE, Helvie MA, Sickles EA. Comparison of recommendations for screening mammography using CISNET models. Cancer. 2017;123(19):3673–3680.
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Gynecology. Practice Bulletin No. 179: Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1–e16.
- Bevers TB, Anderson BO, Bonaccio E, et al; National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009;7(10):1060–1096.
- US Preventive Services Task Force. Screening for breast cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(10):716–726.
- Stapleton SM, Oseni TO, Bababekov YJ, Hung Y-C, Chang DC. Race/ethnicity and age distribution of breast cancer diagnosis in the United States. JAMA Surg. Published online March 7, 2018. doi:10.1001/jamasurg.2018.0035.
- Oeffinger KC, Fontham ET, Etzioni R, et al; American Cancer Society. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015;314(15):1599–1614.
- Arleo EK, Hendrick RE, Helvie MA, Sickles EA. Comparison of recommendations for screening mammography using CISNET models. Cancer. 2017;123(19):3673–3680.
- American College of Obstetricians and Gynecologists Committee on Practice Bulletins–Gynecology. Practice Bulletin No. 179: Breast cancer risk assessment and screening in average-risk women. Obstet Gynecol. 2017;130:e1–e16.
- Bevers TB, Anderson BO, Bonaccio E, et al; National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer screening and diagnosis. J Natl Compr Canc Netw. 2009;7(10):1060–1096.
- US Preventive Services Task Force. Screening for breast cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2009;151(10):716–726.
- Stapleton SM, Oseni TO, Bababekov YJ, Hung Y-C, Chang DC. Race/ethnicity and age distribution of breast cancer diagnosis in the United States. JAMA Surg. Published online March 7, 2018. doi:10.1001/jamasurg.2018.0035.
Endometrial cancer survivors may need long-term cardiovascular monitoring
Endometrial cancer survivors are at increased long-term risk for a number of adverse cardiovascular outcomes, results of a large, population-based study suggest.
Even after adjustment for potentially confounding factors, the cohort of 2,648 endometrial cancer survivors in this retrospective study had a “high burden” of cardiovascular events compared with 10,503 age-matched women, according to the investigators.
That finding highlights a need for increased monitoring and risk management for cardiovascular disease in endometrial cancer survivors, potentially for up to 10 years, according to Sean Soisson, a PhD student in the division of public health at the University of Utah, Salt Lake City, and his coinvestigators.
The study, published in the Journal of the National Cancer Institute, is not the first to find associations between endometrial cancer and long-term cardiovascular outcomes. However, many of the previous studies had small sample sizes, relied on patient-reported outcomes, or lacked a comparison group, according to investigators.
The study was based on data from the Surveillance, Epidemiology, and End Results (SEER) Utah Cancer Registry for women diagnosed between 1997 and 2012 with an invasive first primary endometrial cancer. The investigators identified cardiovascular disease diagnoses in those patients based on review of electronic medical records and ambulatory surgery and inpatient data.
Endometrial cancer survivors had elevated risks for hypertension, heart disease, and blood vessel diseases at 1-5 years after diagnosis, and for some diseases, the risk persisted at 5-10 years after diagnosis, the investigators found.
Survivors were about 50% more likely to be diagnosed with cardiac dysrhythmias compared with the general population both at 1-5 years (hazard ratio, 1.55; 99% confidence interval, 1.23-1.97) and 5-10 years (HR, 1.41; 99% CI, 1.06-1.88) after diagnosis, according to reported data.
There was a twofold increase in risk of phlebitis, thrombophlebitis, and thromboembolism for survivors (HR, 2.07, 99% CI, 1.57-2.72), and risk remained elevated in the 5- to 10-year time frame (HR, 1.53; 99% CI, 1.08-2.17), data show.
Similar increases in risk were reported for other cardiovascular diseases at 1-5 years, and in some cases also at 5-10 years. Cerebrovascular disease was the only major category where no increased risk was found among endometrial cancer survivors, the investigators said.
Type of cancer treatment also may have influenced risk. Among patients who had endometrial cancer, radiation therapy and chemotherapy both increased risk for cardiovascular disorders versus surgery. Advanced age and obesity may have increased risk, the investigators added.
“Studies that examine risk for long-term cardiovascular outcomes among endometrial cancer survivors are becoming increasingly more critical because of the high overall survival rate among individuals diagnosed with endometrial cancer, the large number of endometrial cancer survivors, the projected increase in the number of endometrial cancer diagnoses, the introduction of more complex therapies, and the high mortality due to cardiovascular disease among endometrial cancer survivors,” the authors wrote.
The National Cancer Institute and other organizations supported the study. The authors had no conflicts of interest to disclose.
SOURCE: Soisson S, et al. J Natl Cancer Inst. 2018 May 8. doi: 10.1093/jnci/djy070.
Endometrial cancer survivors are at increased long-term risk for a number of adverse cardiovascular outcomes, results of a large, population-based study suggest.
Even after adjustment for potentially confounding factors, the cohort of 2,648 endometrial cancer survivors in this retrospective study had a “high burden” of cardiovascular events compared with 10,503 age-matched women, according to the investigators.
That finding highlights a need for increased monitoring and risk management for cardiovascular disease in endometrial cancer survivors, potentially for up to 10 years, according to Sean Soisson, a PhD student in the division of public health at the University of Utah, Salt Lake City, and his coinvestigators.
The study, published in the Journal of the National Cancer Institute, is not the first to find associations between endometrial cancer and long-term cardiovascular outcomes. However, many of the previous studies had small sample sizes, relied on patient-reported outcomes, or lacked a comparison group, according to investigators.
The study was based on data from the Surveillance, Epidemiology, and End Results (SEER) Utah Cancer Registry for women diagnosed between 1997 and 2012 with an invasive first primary endometrial cancer. The investigators identified cardiovascular disease diagnoses in those patients based on review of electronic medical records and ambulatory surgery and inpatient data.
Endometrial cancer survivors had elevated risks for hypertension, heart disease, and blood vessel diseases at 1-5 years after diagnosis, and for some diseases, the risk persisted at 5-10 years after diagnosis, the investigators found.
Survivors were about 50% more likely to be diagnosed with cardiac dysrhythmias compared with the general population both at 1-5 years (hazard ratio, 1.55; 99% confidence interval, 1.23-1.97) and 5-10 years (HR, 1.41; 99% CI, 1.06-1.88) after diagnosis, according to reported data.
There was a twofold increase in risk of phlebitis, thrombophlebitis, and thromboembolism for survivors (HR, 2.07, 99% CI, 1.57-2.72), and risk remained elevated in the 5- to 10-year time frame (HR, 1.53; 99% CI, 1.08-2.17), data show.
Similar increases in risk were reported for other cardiovascular diseases at 1-5 years, and in some cases also at 5-10 years. Cerebrovascular disease was the only major category where no increased risk was found among endometrial cancer survivors, the investigators said.
Type of cancer treatment also may have influenced risk. Among patients who had endometrial cancer, radiation therapy and chemotherapy both increased risk for cardiovascular disorders versus surgery. Advanced age and obesity may have increased risk, the investigators added.
“Studies that examine risk for long-term cardiovascular outcomes among endometrial cancer survivors are becoming increasingly more critical because of the high overall survival rate among individuals diagnosed with endometrial cancer, the large number of endometrial cancer survivors, the projected increase in the number of endometrial cancer diagnoses, the introduction of more complex therapies, and the high mortality due to cardiovascular disease among endometrial cancer survivors,” the authors wrote.
The National Cancer Institute and other organizations supported the study. The authors had no conflicts of interest to disclose.
SOURCE: Soisson S, et al. J Natl Cancer Inst. 2018 May 8. doi: 10.1093/jnci/djy070.
Endometrial cancer survivors are at increased long-term risk for a number of adverse cardiovascular outcomes, results of a large, population-based study suggest.
Even after adjustment for potentially confounding factors, the cohort of 2,648 endometrial cancer survivors in this retrospective study had a “high burden” of cardiovascular events compared with 10,503 age-matched women, according to the investigators.
That finding highlights a need for increased monitoring and risk management for cardiovascular disease in endometrial cancer survivors, potentially for up to 10 years, according to Sean Soisson, a PhD student in the division of public health at the University of Utah, Salt Lake City, and his coinvestigators.
The study, published in the Journal of the National Cancer Institute, is not the first to find associations between endometrial cancer and long-term cardiovascular outcomes. However, many of the previous studies had small sample sizes, relied on patient-reported outcomes, or lacked a comparison group, according to investigators.
The study was based on data from the Surveillance, Epidemiology, and End Results (SEER) Utah Cancer Registry for women diagnosed between 1997 and 2012 with an invasive first primary endometrial cancer. The investigators identified cardiovascular disease diagnoses in those patients based on review of electronic medical records and ambulatory surgery and inpatient data.
Endometrial cancer survivors had elevated risks for hypertension, heart disease, and blood vessel diseases at 1-5 years after diagnosis, and for some diseases, the risk persisted at 5-10 years after diagnosis, the investigators found.
Survivors were about 50% more likely to be diagnosed with cardiac dysrhythmias compared with the general population both at 1-5 years (hazard ratio, 1.55; 99% confidence interval, 1.23-1.97) and 5-10 years (HR, 1.41; 99% CI, 1.06-1.88) after diagnosis, according to reported data.
There was a twofold increase in risk of phlebitis, thrombophlebitis, and thromboembolism for survivors (HR, 2.07, 99% CI, 1.57-2.72), and risk remained elevated in the 5- to 10-year time frame (HR, 1.53; 99% CI, 1.08-2.17), data show.
Similar increases in risk were reported for other cardiovascular diseases at 1-5 years, and in some cases also at 5-10 years. Cerebrovascular disease was the only major category where no increased risk was found among endometrial cancer survivors, the investigators said.
Type of cancer treatment also may have influenced risk. Among patients who had endometrial cancer, radiation therapy and chemotherapy both increased risk for cardiovascular disorders versus surgery. Advanced age and obesity may have increased risk, the investigators added.
“Studies that examine risk for long-term cardiovascular outcomes among endometrial cancer survivors are becoming increasingly more critical because of the high overall survival rate among individuals diagnosed with endometrial cancer, the large number of endometrial cancer survivors, the projected increase in the number of endometrial cancer diagnoses, the introduction of more complex therapies, and the high mortality due to cardiovascular disease among endometrial cancer survivors,” the authors wrote.
The National Cancer Institute and other organizations supported the study. The authors had no conflicts of interest to disclose.
SOURCE: Soisson S, et al. J Natl Cancer Inst. 2018 May 8. doi: 10.1093/jnci/djy070.
FROM THE JOURNAL OF THE NATIONAL CANCER INSTITUTE
Key clinical point: Endometrial cancer survivors may require increased monitoring for cardiovascular disease up to 10 years after diagnosis.
Major finding: Survivors were at increased risk of phlebitis, thrombophlebitis, and thromboembolism (HR, 2.07), cardiac dysrhythmias (HR, 1.55), and other cardiovascular diseases at 1-5 years after diagnosis, with some risks persisting in the 5- to 10-year evaluation time frame.
Study details: A retrospective, population-based cohort study of 2,648 endometrial cancer survivors diagnosed between 1997 and 2012 and 10,503 age-matched controls.
Disclosures: The National Cancer Institute and other organizations supported the study. The authors had no conflicts of interest to disclose.
Source: Soisson S et al. J Natl Cancer Inst. 2018 May 8. doi: 10.1093/jnci/djy070.
Female cancer researchers receive less funding than male counterparts
Female cancer researchers receive significantly less funding than their male counterparts in terms of total investment, number of awards, and mean and median funding, according to an analysis of data on public and philanthropic cancer research funding awarded to U.K. institutions between 2000 and 2013.
In an analysis of 4,186 awards totaling 2.33 billion pounds, 2,890 grants (69%) with a total value of 1.82 billion pounds (78%) were awarded to male primary investigators (PIs), compared with just 1,296 grants (31%) with a total value of 512 million pounds(22%) for female PIs, investigators reported in BMJ Open.
Investigators studied openly accessible information on funding awards from public and philanthropic sources including the Medical Research Council, Department of Health, Biotechnology and Biological Sciences Research Council, Engineering and Physical Science Research Council, Wellcome Trust, European Commission, and nine members of the Association of Medical Research Charities. Awards were excluded if they were not relevant to oncology, led by a non-U.K. institution, and/or not considered a research and development activity, wrote Charlie D. Zhou, MD, of the Royal Free NHS Foundation Trust Department of Nuclear Medicine in London, and coauthors.
Median grant value was greater for men (252,647 pounds; interquartile range, 127,343-553,560 pounds) than for women (198,485 pounds; IQR, 99,317-382,650 pounds) (P less than .001). Mean grant value was also greater for men (630,324 pounds; standard deviation, 1,662,559 pounds) than for women (394,730 pounds; SD, 666,574 pounds), Dr. Zhou and colleagues reported.
Large funding discrepancies were seen for sex-specific cancer research. For instance, males received 13.8, 3.5, and 2.0 times the investment of their female counterparts in total, mean, and median prostate cancer funding, respectively. Likewise, men received 9.9, 6.6, and 2.9 times the funding of women PIs in total, mean, and median funding, respectively, for cervical cancer research. This pattern was true for ovarian cancer and breast cancer research, as well.
Men also received significantly greater median funding at all points of the research and development pipeline. For preclinical, phase 1, 2, or 3 clinical trials; and public health, men received 20%, 90%, and 50% more, respectively (P less than .001); for product development and cross-disciplinary research, the difference was 50% and 20%, respectively (P less than .01).
The results of the analysis demonstrate that “female PIs clearly and consistently receive less funding than their male counterparts,” the authors wrote. Although the study results are descriptive in nature and do not identify the underlying mechanisms for these discrepancies, they “demonstrate substantial gender imbalances in cancer research investment.
“We would strongly urge policy makers, funders and the academic and scientific community to investigate the factors leading to our observed differences and seek to ensure that women are appropriately supported in scientific endeavor,” they concluded.
No disclosures or conflicts of interest were reported.
SOURCE: Zhou CD et al. BMJ Open. 2018 Apr 30. doi: 10.1136/bmjopen-2017-018625.
Female cancer researchers receive significantly less funding than their male counterparts in terms of total investment, number of awards, and mean and median funding, according to an analysis of data on public and philanthropic cancer research funding awarded to U.K. institutions between 2000 and 2013.
In an analysis of 4,186 awards totaling 2.33 billion pounds, 2,890 grants (69%) with a total value of 1.82 billion pounds (78%) were awarded to male primary investigators (PIs), compared with just 1,296 grants (31%) with a total value of 512 million pounds(22%) for female PIs, investigators reported in BMJ Open.
Investigators studied openly accessible information on funding awards from public and philanthropic sources including the Medical Research Council, Department of Health, Biotechnology and Biological Sciences Research Council, Engineering and Physical Science Research Council, Wellcome Trust, European Commission, and nine members of the Association of Medical Research Charities. Awards were excluded if they were not relevant to oncology, led by a non-U.K. institution, and/or not considered a research and development activity, wrote Charlie D. Zhou, MD, of the Royal Free NHS Foundation Trust Department of Nuclear Medicine in London, and coauthors.
Median grant value was greater for men (252,647 pounds; interquartile range, 127,343-553,560 pounds) than for women (198,485 pounds; IQR, 99,317-382,650 pounds) (P less than .001). Mean grant value was also greater for men (630,324 pounds; standard deviation, 1,662,559 pounds) than for women (394,730 pounds; SD, 666,574 pounds), Dr. Zhou and colleagues reported.
Large funding discrepancies were seen for sex-specific cancer research. For instance, males received 13.8, 3.5, and 2.0 times the investment of their female counterparts in total, mean, and median prostate cancer funding, respectively. Likewise, men received 9.9, 6.6, and 2.9 times the funding of women PIs in total, mean, and median funding, respectively, for cervical cancer research. This pattern was true for ovarian cancer and breast cancer research, as well.
Men also received significantly greater median funding at all points of the research and development pipeline. For preclinical, phase 1, 2, or 3 clinical trials; and public health, men received 20%, 90%, and 50% more, respectively (P less than .001); for product development and cross-disciplinary research, the difference was 50% and 20%, respectively (P less than .01).
The results of the analysis demonstrate that “female PIs clearly and consistently receive less funding than their male counterparts,” the authors wrote. Although the study results are descriptive in nature and do not identify the underlying mechanisms for these discrepancies, they “demonstrate substantial gender imbalances in cancer research investment.
“We would strongly urge policy makers, funders and the academic and scientific community to investigate the factors leading to our observed differences and seek to ensure that women are appropriately supported in scientific endeavor,” they concluded.
No disclosures or conflicts of interest were reported.
SOURCE: Zhou CD et al. BMJ Open. 2018 Apr 30. doi: 10.1136/bmjopen-2017-018625.
Female cancer researchers receive significantly less funding than their male counterparts in terms of total investment, number of awards, and mean and median funding, according to an analysis of data on public and philanthropic cancer research funding awarded to U.K. institutions between 2000 and 2013.
In an analysis of 4,186 awards totaling 2.33 billion pounds, 2,890 grants (69%) with a total value of 1.82 billion pounds (78%) were awarded to male primary investigators (PIs), compared with just 1,296 grants (31%) with a total value of 512 million pounds(22%) for female PIs, investigators reported in BMJ Open.
Investigators studied openly accessible information on funding awards from public and philanthropic sources including the Medical Research Council, Department of Health, Biotechnology and Biological Sciences Research Council, Engineering and Physical Science Research Council, Wellcome Trust, European Commission, and nine members of the Association of Medical Research Charities. Awards were excluded if they were not relevant to oncology, led by a non-U.K. institution, and/or not considered a research and development activity, wrote Charlie D. Zhou, MD, of the Royal Free NHS Foundation Trust Department of Nuclear Medicine in London, and coauthors.
Median grant value was greater for men (252,647 pounds; interquartile range, 127,343-553,560 pounds) than for women (198,485 pounds; IQR, 99,317-382,650 pounds) (P less than .001). Mean grant value was also greater for men (630,324 pounds; standard deviation, 1,662,559 pounds) than for women (394,730 pounds; SD, 666,574 pounds), Dr. Zhou and colleagues reported.
Large funding discrepancies were seen for sex-specific cancer research. For instance, males received 13.8, 3.5, and 2.0 times the investment of their female counterparts in total, mean, and median prostate cancer funding, respectively. Likewise, men received 9.9, 6.6, and 2.9 times the funding of women PIs in total, mean, and median funding, respectively, for cervical cancer research. This pattern was true for ovarian cancer and breast cancer research, as well.
Men also received significantly greater median funding at all points of the research and development pipeline. For preclinical, phase 1, 2, or 3 clinical trials; and public health, men received 20%, 90%, and 50% more, respectively (P less than .001); for product development and cross-disciplinary research, the difference was 50% and 20%, respectively (P less than .01).
The results of the analysis demonstrate that “female PIs clearly and consistently receive less funding than their male counterparts,” the authors wrote. Although the study results are descriptive in nature and do not identify the underlying mechanisms for these discrepancies, they “demonstrate substantial gender imbalances in cancer research investment.
“We would strongly urge policy makers, funders and the academic and scientific community to investigate the factors leading to our observed differences and seek to ensure that women are appropriately supported in scientific endeavor,” they concluded.
No disclosures or conflicts of interest were reported.
SOURCE: Zhou CD et al. BMJ Open. 2018 Apr 30. doi: 10.1136/bmjopen-2017-018625.
FROM BMJ OPEN
Key clinical point: Female cancer researchers receive significantly less funding than their male counterparts.
Major finding: Of 4,186 awards, 2,890 grants (69%) were awarded to male primary investigators (PIs), compared with 1,296 grants (31%) for female PIs.
Study details: An analysis of data on public and philanthropic cancer research funding awarded to U.K. institutions between 2000 and 2013.
Disclosures: No disclosures or conflicts of interest were reported.
Source: Zhou CD et al. BMJ Open. 2018 Apr 30. doi: 10.1136/bmjopen-2017-018625.