User login
The Hospitalist only
Contract Caveats
It happens at least once a year. One of the physicians we represent calls and says, “I want you to look at a contract I signed.” It’s the equivalent of a patient coming to the emergency department to show the doctor the job he did with his own stitches. Although you can try to clean up trouble spots, you can’t achieve the best result.
Nonetheless, because we know some hospitalists will continue to enter employment contracts without consulting an attorney, we want to provide some basics for evaluating contracts. These can be agreements signed with a hospital or hospitalist group, or with a group practice that covers a hospital or healthcare system.
Appropriate Mindset
Parties enter contracts expecting a mutually beneficial relationship. But our job is to assume the relationship will not only fail, it will go down in flames. By assuming worst-case scenarios we can assess the risks and benefits of each contract provision.
Identify the Parties
Although this may seem self-evident, it’s not. A physician may think he’s contracting with another physician, but the agreement is with a corporation. There are various options for structuring healthcare entities, each with advantages and disadvantages. All are designed to limit liability. There are also legal limits on physician arrangements with certain types of entities. It’s important to understand how the entity with which you’re contracting is organized and operated.
The status of the contracting physician is equally important. A hospitalist can contract individually as an employee, independent contractor, member (full or limited), or through his/her own professional corporation. These options have significant implications for compensation, tax, insurance, and liability.
Define the Purpose
Many contracts begin with recitals, or introductory paragraphs that explain the reasons for the contract. Most people zoom past the recitals—but that’s a mistake. A court asked to resolve a contract dispute attempts to construe the contract in a manner that effectuates the parties’ intent. Make sure recitals accurately state the parties’ intent.
Know the Benefits
All contracts include “consideration,” which is something of value exchanged for contractual obligations. What constitutes fair consideration varies by contract. Important considerations include:
- Compensation (salaries, bonuses, payment formulas, and profit distributions);
- Insurance (health, dental, vision, life, and disability);
- Paid time off (illness, vacation, and professional meetings);
- Retirement plans (401k and profit-sharing plans);
- Professional fees (hospital privileges, professional organizations, medical license, drug enforcement, administration registration, continuing medical education, subscriptions);
- Malpractice insurance and tail coverage;
- Indemnity; and
- Services and equipment (billing, support staff, equipment, and other resources).
All benefits must be adequately described in a contract to be enforceable because most contracts include “integration” clauses stating that the written agreement is the entire agreement between the parties and “no other agreements, written or oral, exist.” Courts will not let parties claim benefits not reflected in the written contract.
Know the Obligations
For a legally binding contract, each party must incur an obligation in exchange for consideration. For example, in a services agreement, a physician can readily agree to provide medical services in exchange for compensation and other benefits. Most contracts fail to provide enough detail about how obligations must be performed. When a physician agrees to “devote their full professional attention and best efforts” to a practice, what does that mean? Who determines whether one has devoted his “best efforts?”
Provisions that impose duties or obligations as described in other documents are also troublesome. Courts enforce obligations imposed by other documents incorporated into a contract, even if a party did not possess the other document at the time he signed the contract. Never agree to obligations contained in a document you haven’t read.
Reasonable Termination
Except for duties imposed by law or contract, parties generally don’t have continuing obligations to each other. For example, most states presume employment is at-will: Either party can terminate the employment at any time, without notice, for any lawful reason. Thus, the manager at McDonald’s can terminate a cashier in the middle of a shift because he thinks the cashier is rude. The cashier can quit his position in the middle of a shift because he doesn’t like his job.
Contract obligations limiting the circumstances under which employment can terminate comprise a major exception to employment at will. For example, a physician might agree to provide 90 days’ notice before leaving his employment. While the physician might agree to this provision, certain circumstances should allow for immediate termination. This includes when the practice has financial issues (fails to pay the physician or enters bankruptcy), allows insurance to lapse, fails to provide adequate staff, improperly bills, or sells to another owner. A healthcare entity can also have legitimate reasons for immediately terminating a physician, such as loss or suspension of his medical license, hospital privileges, or DEA registration.
Provisions that allow termination for vague reasons such as “conduct detrimental to the practice” or “failure to provide services in a professional manner” are problematic. It wouldn’t be hard to manufacture an instance where a physician engaged in conduct detrimental to the practice. Being late for an appointment is detrimental to the practice but probably unavoidable in some circumstances.
Be wary of contractual provisions that give one party unilateral or unlimited discretion over a term.
Evaluate Survival Terms
Some relationships simply end, with the parties going their separate ways. But contracts often include obligations that survive termination. A party to a contract should always make sure to understand the scope and effect of any contractual provision that continues after the parties’ relationship has otherwise ended.
In physician contracts, the most prevalent survival provisions are non-compete clauses. Non-compete clauses provide a good model to discuss post-termination obligations. A standard non-compete clause might read like this:
Dr. Jones will not, in the three years immediately following termination of this agreement, practice medicine in any location within a three-mile radius of any location where he has provided services for P.C.
If Dr. Jones has performed surgery at both area hospitals while under contract, this clause could require him to pack up his stethoscope and leave town. When coupled with a provision allowing an injunction or liquidated damages, non-compete clauses are a big deal and give rise to lots of lawsuits. Even in circumstances where a non-compete clause is unenforceable, a party is unlikely to receive a favorable determination without substantial litigation. Negotiate a non-compete clause or other survival terms everyone can live with.
Understand Remedies
Lawyers use the term “remedy” to describe the recourse available when a party breaches an agreement. Remedies come in three basic forms:
- Compensatory damages;
- Liquidated damages; and
- Equitable relief.
Compensatory damages are monetary awards designed to compensate an injured party for actual loss. The party seeking compensatory damages must prove the nature of the injury and the amount of compensation that should be awarded.
Liquidated damages are monetary awards to compensate a party for an agreed-upon loss. So long as the parties agree it would be difficult to calculate an actual award of damages, that the amount of liquidated damages is reasonable, and that the award of liquidated damages is not punitive, a court would likely enforce the liquidated damages provision.
Because liquidated damage provisions relieve a party of the burden of proving actual damages, they should be carefully considered.
Equitable relief consists of non-monetary remedies, such as an injunction. If a party agrees to injunctive relief to enforce a contract term, a judge could order the party discontinue certain conduct. If the party disobeys, he/she could be held in contempt of court and jailed. Injunctive relief alters a legal presumption that breaches of contract can be remedied through monetary awards. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
It happens at least once a year. One of the physicians we represent calls and says, “I want you to look at a contract I signed.” It’s the equivalent of a patient coming to the emergency department to show the doctor the job he did with his own stitches. Although you can try to clean up trouble spots, you can’t achieve the best result.
Nonetheless, because we know some hospitalists will continue to enter employment contracts without consulting an attorney, we want to provide some basics for evaluating contracts. These can be agreements signed with a hospital or hospitalist group, or with a group practice that covers a hospital or healthcare system.
Appropriate Mindset
Parties enter contracts expecting a mutually beneficial relationship. But our job is to assume the relationship will not only fail, it will go down in flames. By assuming worst-case scenarios we can assess the risks and benefits of each contract provision.
Identify the Parties
Although this may seem self-evident, it’s not. A physician may think he’s contracting with another physician, but the agreement is with a corporation. There are various options for structuring healthcare entities, each with advantages and disadvantages. All are designed to limit liability. There are also legal limits on physician arrangements with certain types of entities. It’s important to understand how the entity with which you’re contracting is organized and operated.
The status of the contracting physician is equally important. A hospitalist can contract individually as an employee, independent contractor, member (full or limited), or through his/her own professional corporation. These options have significant implications for compensation, tax, insurance, and liability.
Define the Purpose
Many contracts begin with recitals, or introductory paragraphs that explain the reasons for the contract. Most people zoom past the recitals—but that’s a mistake. A court asked to resolve a contract dispute attempts to construe the contract in a manner that effectuates the parties’ intent. Make sure recitals accurately state the parties’ intent.
Know the Benefits
All contracts include “consideration,” which is something of value exchanged for contractual obligations. What constitutes fair consideration varies by contract. Important considerations include:
- Compensation (salaries, bonuses, payment formulas, and profit distributions);
- Insurance (health, dental, vision, life, and disability);
- Paid time off (illness, vacation, and professional meetings);
- Retirement plans (401k and profit-sharing plans);
- Professional fees (hospital privileges, professional organizations, medical license, drug enforcement, administration registration, continuing medical education, subscriptions);
- Malpractice insurance and tail coverage;
- Indemnity; and
- Services and equipment (billing, support staff, equipment, and other resources).
All benefits must be adequately described in a contract to be enforceable because most contracts include “integration” clauses stating that the written agreement is the entire agreement between the parties and “no other agreements, written or oral, exist.” Courts will not let parties claim benefits not reflected in the written contract.
Know the Obligations
For a legally binding contract, each party must incur an obligation in exchange for consideration. For example, in a services agreement, a physician can readily agree to provide medical services in exchange for compensation and other benefits. Most contracts fail to provide enough detail about how obligations must be performed. When a physician agrees to “devote their full professional attention and best efforts” to a practice, what does that mean? Who determines whether one has devoted his “best efforts?”
Provisions that impose duties or obligations as described in other documents are also troublesome. Courts enforce obligations imposed by other documents incorporated into a contract, even if a party did not possess the other document at the time he signed the contract. Never agree to obligations contained in a document you haven’t read.
Reasonable Termination
Except for duties imposed by law or contract, parties generally don’t have continuing obligations to each other. For example, most states presume employment is at-will: Either party can terminate the employment at any time, without notice, for any lawful reason. Thus, the manager at McDonald’s can terminate a cashier in the middle of a shift because he thinks the cashier is rude. The cashier can quit his position in the middle of a shift because he doesn’t like his job.
Contract obligations limiting the circumstances under which employment can terminate comprise a major exception to employment at will. For example, a physician might agree to provide 90 days’ notice before leaving his employment. While the physician might agree to this provision, certain circumstances should allow for immediate termination. This includes when the practice has financial issues (fails to pay the physician or enters bankruptcy), allows insurance to lapse, fails to provide adequate staff, improperly bills, or sells to another owner. A healthcare entity can also have legitimate reasons for immediately terminating a physician, such as loss or suspension of his medical license, hospital privileges, or DEA registration.
Provisions that allow termination for vague reasons such as “conduct detrimental to the practice” or “failure to provide services in a professional manner” are problematic. It wouldn’t be hard to manufacture an instance where a physician engaged in conduct detrimental to the practice. Being late for an appointment is detrimental to the practice but probably unavoidable in some circumstances.
Be wary of contractual provisions that give one party unilateral or unlimited discretion over a term.
Evaluate Survival Terms
Some relationships simply end, with the parties going their separate ways. But contracts often include obligations that survive termination. A party to a contract should always make sure to understand the scope and effect of any contractual provision that continues after the parties’ relationship has otherwise ended.
In physician contracts, the most prevalent survival provisions are non-compete clauses. Non-compete clauses provide a good model to discuss post-termination obligations. A standard non-compete clause might read like this:
Dr. Jones will not, in the three years immediately following termination of this agreement, practice medicine in any location within a three-mile radius of any location where he has provided services for P.C.
If Dr. Jones has performed surgery at both area hospitals while under contract, this clause could require him to pack up his stethoscope and leave town. When coupled with a provision allowing an injunction or liquidated damages, non-compete clauses are a big deal and give rise to lots of lawsuits. Even in circumstances where a non-compete clause is unenforceable, a party is unlikely to receive a favorable determination without substantial litigation. Negotiate a non-compete clause or other survival terms everyone can live with.
Understand Remedies
Lawyers use the term “remedy” to describe the recourse available when a party breaches an agreement. Remedies come in three basic forms:
- Compensatory damages;
- Liquidated damages; and
- Equitable relief.
Compensatory damages are monetary awards designed to compensate an injured party for actual loss. The party seeking compensatory damages must prove the nature of the injury and the amount of compensation that should be awarded.
Liquidated damages are monetary awards to compensate a party for an agreed-upon loss. So long as the parties agree it would be difficult to calculate an actual award of damages, that the amount of liquidated damages is reasonable, and that the award of liquidated damages is not punitive, a court would likely enforce the liquidated damages provision.
Because liquidated damage provisions relieve a party of the burden of proving actual damages, they should be carefully considered.
Equitable relief consists of non-monetary remedies, such as an injunction. If a party agrees to injunctive relief to enforce a contract term, a judge could order the party discontinue certain conduct. If the party disobeys, he/she could be held in contempt of court and jailed. Injunctive relief alters a legal presumption that breaches of contract can be remedied through monetary awards. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
It happens at least once a year. One of the physicians we represent calls and says, “I want you to look at a contract I signed.” It’s the equivalent of a patient coming to the emergency department to show the doctor the job he did with his own stitches. Although you can try to clean up trouble spots, you can’t achieve the best result.
Nonetheless, because we know some hospitalists will continue to enter employment contracts without consulting an attorney, we want to provide some basics for evaluating contracts. These can be agreements signed with a hospital or hospitalist group, or with a group practice that covers a hospital or healthcare system.
Appropriate Mindset
Parties enter contracts expecting a mutually beneficial relationship. But our job is to assume the relationship will not only fail, it will go down in flames. By assuming worst-case scenarios we can assess the risks and benefits of each contract provision.
Identify the Parties
Although this may seem self-evident, it’s not. A physician may think he’s contracting with another physician, but the agreement is with a corporation. There are various options for structuring healthcare entities, each with advantages and disadvantages. All are designed to limit liability. There are also legal limits on physician arrangements with certain types of entities. It’s important to understand how the entity with which you’re contracting is organized and operated.
The status of the contracting physician is equally important. A hospitalist can contract individually as an employee, independent contractor, member (full or limited), or through his/her own professional corporation. These options have significant implications for compensation, tax, insurance, and liability.
Define the Purpose
Many contracts begin with recitals, or introductory paragraphs that explain the reasons for the contract. Most people zoom past the recitals—but that’s a mistake. A court asked to resolve a contract dispute attempts to construe the contract in a manner that effectuates the parties’ intent. Make sure recitals accurately state the parties’ intent.
Know the Benefits
All contracts include “consideration,” which is something of value exchanged for contractual obligations. What constitutes fair consideration varies by contract. Important considerations include:
- Compensation (salaries, bonuses, payment formulas, and profit distributions);
- Insurance (health, dental, vision, life, and disability);
- Paid time off (illness, vacation, and professional meetings);
- Retirement plans (401k and profit-sharing plans);
- Professional fees (hospital privileges, professional organizations, medical license, drug enforcement, administration registration, continuing medical education, subscriptions);
- Malpractice insurance and tail coverage;
- Indemnity; and
- Services and equipment (billing, support staff, equipment, and other resources).
All benefits must be adequately described in a contract to be enforceable because most contracts include “integration” clauses stating that the written agreement is the entire agreement between the parties and “no other agreements, written or oral, exist.” Courts will not let parties claim benefits not reflected in the written contract.
Know the Obligations
For a legally binding contract, each party must incur an obligation in exchange for consideration. For example, in a services agreement, a physician can readily agree to provide medical services in exchange for compensation and other benefits. Most contracts fail to provide enough detail about how obligations must be performed. When a physician agrees to “devote their full professional attention and best efforts” to a practice, what does that mean? Who determines whether one has devoted his “best efforts?”
Provisions that impose duties or obligations as described in other documents are also troublesome. Courts enforce obligations imposed by other documents incorporated into a contract, even if a party did not possess the other document at the time he signed the contract. Never agree to obligations contained in a document you haven’t read.
Reasonable Termination
Except for duties imposed by law or contract, parties generally don’t have continuing obligations to each other. For example, most states presume employment is at-will: Either party can terminate the employment at any time, without notice, for any lawful reason. Thus, the manager at McDonald’s can terminate a cashier in the middle of a shift because he thinks the cashier is rude. The cashier can quit his position in the middle of a shift because he doesn’t like his job.
Contract obligations limiting the circumstances under which employment can terminate comprise a major exception to employment at will. For example, a physician might agree to provide 90 days’ notice before leaving his employment. While the physician might agree to this provision, certain circumstances should allow for immediate termination. This includes when the practice has financial issues (fails to pay the physician or enters bankruptcy), allows insurance to lapse, fails to provide adequate staff, improperly bills, or sells to another owner. A healthcare entity can also have legitimate reasons for immediately terminating a physician, such as loss or suspension of his medical license, hospital privileges, or DEA registration.
Provisions that allow termination for vague reasons such as “conduct detrimental to the practice” or “failure to provide services in a professional manner” are problematic. It wouldn’t be hard to manufacture an instance where a physician engaged in conduct detrimental to the practice. Being late for an appointment is detrimental to the practice but probably unavoidable in some circumstances.
Be wary of contractual provisions that give one party unilateral or unlimited discretion over a term.
Evaluate Survival Terms
Some relationships simply end, with the parties going their separate ways. But contracts often include obligations that survive termination. A party to a contract should always make sure to understand the scope and effect of any contractual provision that continues after the parties’ relationship has otherwise ended.
In physician contracts, the most prevalent survival provisions are non-compete clauses. Non-compete clauses provide a good model to discuss post-termination obligations. A standard non-compete clause might read like this:
Dr. Jones will not, in the three years immediately following termination of this agreement, practice medicine in any location within a three-mile radius of any location where he has provided services for P.C.
If Dr. Jones has performed surgery at both area hospitals while under contract, this clause could require him to pack up his stethoscope and leave town. When coupled with a provision allowing an injunction or liquidated damages, non-compete clauses are a big deal and give rise to lots of lawsuits. Even in circumstances where a non-compete clause is unenforceable, a party is unlikely to receive a favorable determination without substantial litigation. Negotiate a non-compete clause or other survival terms everyone can live with.
Understand Remedies
Lawyers use the term “remedy” to describe the recourse available when a party breaches an agreement. Remedies come in three basic forms:
- Compensatory damages;
- Liquidated damages; and
- Equitable relief.
Compensatory damages are monetary awards designed to compensate an injured party for actual loss. The party seeking compensatory damages must prove the nature of the injury and the amount of compensation that should be awarded.
Liquidated damages are monetary awards to compensate a party for an agreed-upon loss. So long as the parties agree it would be difficult to calculate an actual award of damages, that the amount of liquidated damages is reasonable, and that the award of liquidated damages is not punitive, a court would likely enforce the liquidated damages provision.
Because liquidated damage provisions relieve a party of the burden of proving actual damages, they should be carefully considered.
Equitable relief consists of non-monetary remedies, such as an injunction. If a party agrees to injunctive relief to enforce a contract term, a judge could order the party discontinue certain conduct. If the party disobeys, he/she could be held in contempt of court and jailed. Injunctive relief alters a legal presumption that breaches of contract can be remedied through monetary awards. TH
Patrick O’Rourke works in the Office of University Counsel, Department of Litigation, University of Colorado, Denver.
The Admission Consult
When consultation services occur in inpatient and outpatient settings, physicians report the code category that best corresponds to the patient’s registered status at the time of service:
- Inpatient consultation (99251-99255) for services provided to an inpatient (acute care, inpatient rehabilitation, inpatient psychiatric, long-term acute care, or skilled nursing); or
- Outpatient consultation (99241-99245) for services provided to an outpatient (office, emergency department [ED], or observation care).
Regardless of location, consultants must meet each requirement before submitting a claim for these services. This article focuses on the coding and billing nuances of inpatient consultation services; outpatient consultations provided in the ED or during observation care will be addressed in a future issue.
The Three R’s
Reason and request: Consultants (physicians or qualified non-physician providers) are asked to give an opinion or recommendation, a suggestion, direction, or counsel in the treatment of a patient’s condition because the consultant has expertise in a specific medical area beyond the requesting professional’s knowledge.
The requesting professional must be a physician or other qualified healthcare provider (e.g., nurse practitioner, physician assistant, resident acting under guidance of a teaching physician) currently involved in the patient’s care. Do not report consultation codes when a patient, family member, or third party requests a second opinion. Instead, select the most appropriate subsequent hospital care code (99231-99233).
The request must be documented in the patient’s medical record. The initial request may be a verbal interaction between the requesting provider and the consulting physician; however, when this occurs, the verbal conversation must be documented by both the consultant (in the progress note) and the requesting provider (in the plan of care or as a written order). Standing orders for consultation are prohibited. Clearly document the reason for the service: the patient’s condition, sign, or symptoms that prompted the consult request, ensuring the medical necessity of the service.
Try to avoid terminology, such as “Consult hospitalist for perioperative management.” This leads to the payer’s confusion about co-management issues. The documentation should reflect the true intent of the service: “Consult hospitalist for perioperative risk assessment.” If necessary, ask the requesting provider to clarify the request. The consultant should further explain the request in his/her own note.
Report: After the patient’s assessment, the consultant documents the service and prepares a written report for the requesting provider, which includes the written request, consultation evaluation, findings, and recommendations.
It is appropriate for the consultant to initiate diagnostic services and treatment at the initial consultation service or at a subsequent visit, yet still qualify as a consult. In the inpatient setting, it is acceptable for the consultant’s report to appear as an entry in the shared medical record without need to forward a separate document to the requesting provider.
Code Use
Inpatient consultation codes are reported once per hospitalization. If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99251-99255 are denied. This happens even when the consultant signs off and is re-consulted for a different problem during the same hospitalization.
A physician who provides patient services after the initial consultation reports subsequent hospital care codes 99231-99233 for each date in which a face-to-face encounter occurs.
A physician or qualified nonphysician provider may request a consultation from a member of the same group practice as long as the consultant possesses a legitimate expertise in a specific medical area beyond the requesting professional’s knowledge (e.g., a hospitalist may consult a member of his group who specializes in infectious disease).
This situation is likely to produce a rejected consult claim. In appealing the claim, submit notes from each member of the group (i.e., the requesting provider and the consultant) to demonstrate medical necessity and distinguish the expertise involved in each service. Medicare and payers who follow Medicare guidelines should reimburse the consult after the documentation is reviewed.
Co-management
Preoperative consults: Preoperative consultations are permitted when performed by any physician or qualified nonphysician provider at the request of a surgeon—as long as all requirements for performing and reporting the consultation codes are met. The service must be medically necessary and not provided for routine screening (i.e., consults for healthy patients scheduled for elective surgery).
Postoperative management: If a physician or qualified nonphysician provider who has performed a preoperative consultation is subsequently consulted and/or assumes responsibility for the complete or partial management of the patient’s condition(s) during the postoperative period, the appropriate subsequent hospital care code 99231-99233 is used.
Additionally, do not report consultation codes when the surgeon asks the hospitalist to take responsibility for the management of an aspect of the patient’s condition during the postoperative period (i.e., consult for postoperative management). In this situation, the surgeon is not asking the consultant for an opinion or advice for the surgeon’s use in treating the patient, and the surgeon is not expected to continue on the case. This constitutes concurrent care and is billed with the appropriate subsequent hospital care codes.
Alternately, the surgeon may continue on the case, not transferring the care for the remaining portion of the hospitalization to the hospitalist, and incorporating the hospitalist’s recommendations into his/her own care plan, subsequently retaining the hospitalist’s services in assisting with care. Because the transfer did not occur prior to the consultation, this situation may constitute an inpatient consultation and be reported as such.
Unfortunately, some local Medicare contractors do not recognize this latter distinction and prohibit reporting post-surgical involvement with 99251-99255. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
When consultation services occur in inpatient and outpatient settings, physicians report the code category that best corresponds to the patient’s registered status at the time of service:
- Inpatient consultation (99251-99255) for services provided to an inpatient (acute care, inpatient rehabilitation, inpatient psychiatric, long-term acute care, or skilled nursing); or
- Outpatient consultation (99241-99245) for services provided to an outpatient (office, emergency department [ED], or observation care).
Regardless of location, consultants must meet each requirement before submitting a claim for these services. This article focuses on the coding and billing nuances of inpatient consultation services; outpatient consultations provided in the ED or during observation care will be addressed in a future issue.
The Three R’s
Reason and request: Consultants (physicians or qualified non-physician providers) are asked to give an opinion or recommendation, a suggestion, direction, or counsel in the treatment of a patient’s condition because the consultant has expertise in a specific medical area beyond the requesting professional’s knowledge.
The requesting professional must be a physician or other qualified healthcare provider (e.g., nurse practitioner, physician assistant, resident acting under guidance of a teaching physician) currently involved in the patient’s care. Do not report consultation codes when a patient, family member, or third party requests a second opinion. Instead, select the most appropriate subsequent hospital care code (99231-99233).
The request must be documented in the patient’s medical record. The initial request may be a verbal interaction between the requesting provider and the consulting physician; however, when this occurs, the verbal conversation must be documented by both the consultant (in the progress note) and the requesting provider (in the plan of care or as a written order). Standing orders for consultation are prohibited. Clearly document the reason for the service: the patient’s condition, sign, or symptoms that prompted the consult request, ensuring the medical necessity of the service.
Try to avoid terminology, such as “Consult hospitalist for perioperative management.” This leads to the payer’s confusion about co-management issues. The documentation should reflect the true intent of the service: “Consult hospitalist for perioperative risk assessment.” If necessary, ask the requesting provider to clarify the request. The consultant should further explain the request in his/her own note.
Report: After the patient’s assessment, the consultant documents the service and prepares a written report for the requesting provider, which includes the written request, consultation evaluation, findings, and recommendations.
It is appropriate for the consultant to initiate diagnostic services and treatment at the initial consultation service or at a subsequent visit, yet still qualify as a consult. In the inpatient setting, it is acceptable for the consultant’s report to appear as an entry in the shared medical record without need to forward a separate document to the requesting provider.
Code Use
Inpatient consultation codes are reported once per hospitalization. If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99251-99255 are denied. This happens even when the consultant signs off and is re-consulted for a different problem during the same hospitalization.
A physician who provides patient services after the initial consultation reports subsequent hospital care codes 99231-99233 for each date in which a face-to-face encounter occurs.
A physician or qualified nonphysician provider may request a consultation from a member of the same group practice as long as the consultant possesses a legitimate expertise in a specific medical area beyond the requesting professional’s knowledge (e.g., a hospitalist may consult a member of his group who specializes in infectious disease).
This situation is likely to produce a rejected consult claim. In appealing the claim, submit notes from each member of the group (i.e., the requesting provider and the consultant) to demonstrate medical necessity and distinguish the expertise involved in each service. Medicare and payers who follow Medicare guidelines should reimburse the consult after the documentation is reviewed.
Co-management
Preoperative consults: Preoperative consultations are permitted when performed by any physician or qualified nonphysician provider at the request of a surgeon—as long as all requirements for performing and reporting the consultation codes are met. The service must be medically necessary and not provided for routine screening (i.e., consults for healthy patients scheduled for elective surgery).
Postoperative management: If a physician or qualified nonphysician provider who has performed a preoperative consultation is subsequently consulted and/or assumes responsibility for the complete or partial management of the patient’s condition(s) during the postoperative period, the appropriate subsequent hospital care code 99231-99233 is used.
Additionally, do not report consultation codes when the surgeon asks the hospitalist to take responsibility for the management of an aspect of the patient’s condition during the postoperative period (i.e., consult for postoperative management). In this situation, the surgeon is not asking the consultant for an opinion or advice for the surgeon’s use in treating the patient, and the surgeon is not expected to continue on the case. This constitutes concurrent care and is billed with the appropriate subsequent hospital care codes.
Alternately, the surgeon may continue on the case, not transferring the care for the remaining portion of the hospitalization to the hospitalist, and incorporating the hospitalist’s recommendations into his/her own care plan, subsequently retaining the hospitalist’s services in assisting with care. Because the transfer did not occur prior to the consultation, this situation may constitute an inpatient consultation and be reported as such.
Unfortunately, some local Medicare contractors do not recognize this latter distinction and prohibit reporting post-surgical involvement with 99251-99255. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
When consultation services occur in inpatient and outpatient settings, physicians report the code category that best corresponds to the patient’s registered status at the time of service:
- Inpatient consultation (99251-99255) for services provided to an inpatient (acute care, inpatient rehabilitation, inpatient psychiatric, long-term acute care, or skilled nursing); or
- Outpatient consultation (99241-99245) for services provided to an outpatient (office, emergency department [ED], or observation care).
Regardless of location, consultants must meet each requirement before submitting a claim for these services. This article focuses on the coding and billing nuances of inpatient consultation services; outpatient consultations provided in the ED or during observation care will be addressed in a future issue.
The Three R’s
Reason and request: Consultants (physicians or qualified non-physician providers) are asked to give an opinion or recommendation, a suggestion, direction, or counsel in the treatment of a patient’s condition because the consultant has expertise in a specific medical area beyond the requesting professional’s knowledge.
The requesting professional must be a physician or other qualified healthcare provider (e.g., nurse practitioner, physician assistant, resident acting under guidance of a teaching physician) currently involved in the patient’s care. Do not report consultation codes when a patient, family member, or third party requests a second opinion. Instead, select the most appropriate subsequent hospital care code (99231-99233).
The request must be documented in the patient’s medical record. The initial request may be a verbal interaction between the requesting provider and the consulting physician; however, when this occurs, the verbal conversation must be documented by both the consultant (in the progress note) and the requesting provider (in the plan of care or as a written order). Standing orders for consultation are prohibited. Clearly document the reason for the service: the patient’s condition, sign, or symptoms that prompted the consult request, ensuring the medical necessity of the service.
Try to avoid terminology, such as “Consult hospitalist for perioperative management.” This leads to the payer’s confusion about co-management issues. The documentation should reflect the true intent of the service: “Consult hospitalist for perioperative risk assessment.” If necessary, ask the requesting provider to clarify the request. The consultant should further explain the request in his/her own note.
Report: After the patient’s assessment, the consultant documents the service and prepares a written report for the requesting provider, which includes the written request, consultation evaluation, findings, and recommendations.
It is appropriate for the consultant to initiate diagnostic services and treatment at the initial consultation service or at a subsequent visit, yet still qualify as a consult. In the inpatient setting, it is acceptable for the consultant’s report to appear as an entry in the shared medical record without need to forward a separate document to the requesting provider.
Code Use
Inpatient consultation codes are reported once per hospitalization. If reported more frequently, all claims within the same hospitalization subsequently reported with codes 99251-99255 are denied. This happens even when the consultant signs off and is re-consulted for a different problem during the same hospitalization.
A physician who provides patient services after the initial consultation reports subsequent hospital care codes 99231-99233 for each date in which a face-to-face encounter occurs.
A physician or qualified nonphysician provider may request a consultation from a member of the same group practice as long as the consultant possesses a legitimate expertise in a specific medical area beyond the requesting professional’s knowledge (e.g., a hospitalist may consult a member of his group who specializes in infectious disease).
This situation is likely to produce a rejected consult claim. In appealing the claim, submit notes from each member of the group (i.e., the requesting provider and the consultant) to demonstrate medical necessity and distinguish the expertise involved in each service. Medicare and payers who follow Medicare guidelines should reimburse the consult after the documentation is reviewed.
Co-management
Preoperative consults: Preoperative consultations are permitted when performed by any physician or qualified nonphysician provider at the request of a surgeon—as long as all requirements for performing and reporting the consultation codes are met. The service must be medically necessary and not provided for routine screening (i.e., consults for healthy patients scheduled for elective surgery).
Postoperative management: If a physician or qualified nonphysician provider who has performed a preoperative consultation is subsequently consulted and/or assumes responsibility for the complete or partial management of the patient’s condition(s) during the postoperative period, the appropriate subsequent hospital care code 99231-99233 is used.
Additionally, do not report consultation codes when the surgeon asks the hospitalist to take responsibility for the management of an aspect of the patient’s condition during the postoperative period (i.e., consult for postoperative management). In this situation, the surgeon is not asking the consultant for an opinion or advice for the surgeon’s use in treating the patient, and the surgeon is not expected to continue on the case. This constitutes concurrent care and is billed with the appropriate subsequent hospital care codes.
Alternately, the surgeon may continue on the case, not transferring the care for the remaining portion of the hospitalization to the hospitalist, and incorporating the hospitalist’s recommendations into his/her own care plan, subsequently retaining the hospitalist’s services in assisting with care. Because the transfer did not occur prior to the consultation, this situation may constitute an inpatient consultation and be reported as such.
Unfortunately, some local Medicare contractors do not recognize this latter distinction and prohibit reporting post-surgical involvement with 99251-99255. TH
Carol Pohlig is a billing and coding expert with the University of Pennsylvania Medical Center, Philadelphia. She is also on the faculty of SHM’s inpatient coding course.
Massachusetts Effect
With the first major statewide attempt at universal healthcare access under way in Massachusetts, everyone from presidential candidates to uninsured families on the other side of the U.S. is watching to see if the state’s plan will succeed. If so, it could become the basis of a national healthcare plan.
Massachusetts healthcare reform became law April 2006 as part of the Act Providing Access to Affordable, Quality, Accountable Health Care. It requires that virtually all state residents either purchase health insurance or get coverage through state-sponsored insurance for people with low incomes (May 2007 The Hospitalist, p. 1). The plan, based on insurance market reforms, merges the individual and small-group insurance market, allowing residents to get lower group insurance rates.
The law required coverage by July 1, and residents must show evidence of their coverage on their income tax return or face a substantial fine—up to 50% of the cost of a health insurance plan.
Many Massachusetts residents get healthcare coverage through their employers. The state plan requires companies with more than 10 employees to provide coverage or to pay a “Fair Share” contribution of up to $295 for each employee each year. Employers must also offer a “cafeteria plan” that allows workers to purchase healthcare with pre-tax income.
The bill created the Commonwealth Health Insurance Connector, which offers affordable, quality insurance to individuals and small businesses. The Connector board approved plans offered by seven insurers that include several options.
As for low-income residents, sliding-scale government-funded subsidies are provided by the Commonwealth Care Health Insurance Program (C-CHIP). As of June 1, nearly 80,000 low-income adults had enrolled in C-CHIP. In addition, the statute expanded MassHealth (Medicaid and SCHIP) coverage for children of low-income parents and restored MassHealth benefits such as dental and vision care.
The plan also includes a system for quality standards and for publicizing performance of providers.
The money for the plan comes from several sources. Gov. Deval Patrick has requested $1.725 billion to fund the program in the next fiscal year. This will supplement federal Medicaid payments, employer contributions, and general revenues.
What Hospitalists Face
How will universal healthcare coverage for state residents affect Massachusetts hospitalists and other physicians? Massachusetts resident Win Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, and co-founder of SHM, weighed the pros and cons.
“The first issue is the effect on primary care providers,” says Dr. Whitcomb. “A large number of patients will be steered into the system of primary care, which is already overwhelmed. A new [state] commission has been formed to address this shortage, but it’s too late—the system already lacks capacity.”
Soon-to-be-overwhelmed primary care physicians will take every step possible to share the workload: “I think [the plan] will be a new impetus for primary care providers to refer patients to hospitalists,” stresses Dr. Whitcomb. “Hospitalists may well see new demand from primary care providers.”
Will this trend mean more openings for hospitalists at Massachusetts institutions? “There are so many drivers behind [the growth of the hospital medicine]; this is just another driver,” says Dr. Whitcomb.
The second likely outcome of the plan will be a transformation of the types of patients treated by hospitalists. Hospitalists around the country are well aware of the problems of treating today’s uninsured patients. “The uninsured tend to show up in the ER in the middle of the night, with diseases in an advanced state” because they haven’t seen a doctor until the last minute, says Dr. Whitcomb. “That situation is not going to go away, but it might decrease” in Massachusetts under the new plan.
“The big question is, will the previously uninsured population, which hospitalists are all too familiar with, be a fundamentally different population?” muses Dr. Whitcomb. “In other words, if [patients] go through a primary care provider and have good management of their illness, will they become a different type of patient than hospitalists are seeing at present? This would be good for hospitalists; it will mean more control over chronic disease and illness.”
—Win Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, Mass., and co-founder of SHM
How Is It Working?
The plan is still in its infancy, but more than 150,000 of the state’s previously uninsured residents had coverage before the July deadline. However, the total estimated number of remaining uninsured is 250,000 to 375,000.
“The two roadblocks are the ability to enroll patients and finding primary care to handle everyone,” says Dr. Whitcomb. “It’s just one of those wait-and-see issues. I applaud the plan. It’s a sincere effort to deal with the uninsured. I think the primary care shortage is a major problem and will impact the success of the plan.”
Hospitalists around the country may want to keep an eye on developments in Massachusetts because the state’s healthcare system could affect their patient loads, daily work, and compensation. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
With the first major statewide attempt at universal healthcare access under way in Massachusetts, everyone from presidential candidates to uninsured families on the other side of the U.S. is watching to see if the state’s plan will succeed. If so, it could become the basis of a national healthcare plan.
Massachusetts healthcare reform became law April 2006 as part of the Act Providing Access to Affordable, Quality, Accountable Health Care. It requires that virtually all state residents either purchase health insurance or get coverage through state-sponsored insurance for people with low incomes (May 2007 The Hospitalist, p. 1). The plan, based on insurance market reforms, merges the individual and small-group insurance market, allowing residents to get lower group insurance rates.
The law required coverage by July 1, and residents must show evidence of their coverage on their income tax return or face a substantial fine—up to 50% of the cost of a health insurance plan.
Many Massachusetts residents get healthcare coverage through their employers. The state plan requires companies with more than 10 employees to provide coverage or to pay a “Fair Share” contribution of up to $295 for each employee each year. Employers must also offer a “cafeteria plan” that allows workers to purchase healthcare with pre-tax income.
The bill created the Commonwealth Health Insurance Connector, which offers affordable, quality insurance to individuals and small businesses. The Connector board approved plans offered by seven insurers that include several options.
As for low-income residents, sliding-scale government-funded subsidies are provided by the Commonwealth Care Health Insurance Program (C-CHIP). As of June 1, nearly 80,000 low-income adults had enrolled in C-CHIP. In addition, the statute expanded MassHealth (Medicaid and SCHIP) coverage for children of low-income parents and restored MassHealth benefits such as dental and vision care.
The plan also includes a system for quality standards and for publicizing performance of providers.
The money for the plan comes from several sources. Gov. Deval Patrick has requested $1.725 billion to fund the program in the next fiscal year. This will supplement federal Medicaid payments, employer contributions, and general revenues.
What Hospitalists Face
How will universal healthcare coverage for state residents affect Massachusetts hospitalists and other physicians? Massachusetts resident Win Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, and co-founder of SHM, weighed the pros and cons.
“The first issue is the effect on primary care providers,” says Dr. Whitcomb. “A large number of patients will be steered into the system of primary care, which is already overwhelmed. A new [state] commission has been formed to address this shortage, but it’s too late—the system already lacks capacity.”
Soon-to-be-overwhelmed primary care physicians will take every step possible to share the workload: “I think [the plan] will be a new impetus for primary care providers to refer patients to hospitalists,” stresses Dr. Whitcomb. “Hospitalists may well see new demand from primary care providers.”
Will this trend mean more openings for hospitalists at Massachusetts institutions? “There are so many drivers behind [the growth of the hospital medicine]; this is just another driver,” says Dr. Whitcomb.
The second likely outcome of the plan will be a transformation of the types of patients treated by hospitalists. Hospitalists around the country are well aware of the problems of treating today’s uninsured patients. “The uninsured tend to show up in the ER in the middle of the night, with diseases in an advanced state” because they haven’t seen a doctor until the last minute, says Dr. Whitcomb. “That situation is not going to go away, but it might decrease” in Massachusetts under the new plan.
“The big question is, will the previously uninsured population, which hospitalists are all too familiar with, be a fundamentally different population?” muses Dr. Whitcomb. “In other words, if [patients] go through a primary care provider and have good management of their illness, will they become a different type of patient than hospitalists are seeing at present? This would be good for hospitalists; it will mean more control over chronic disease and illness.”
—Win Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, Mass., and co-founder of SHM
How Is It Working?
The plan is still in its infancy, but more than 150,000 of the state’s previously uninsured residents had coverage before the July deadline. However, the total estimated number of remaining uninsured is 250,000 to 375,000.
“The two roadblocks are the ability to enroll patients and finding primary care to handle everyone,” says Dr. Whitcomb. “It’s just one of those wait-and-see issues. I applaud the plan. It’s a sincere effort to deal with the uninsured. I think the primary care shortage is a major problem and will impact the success of the plan.”
Hospitalists around the country may want to keep an eye on developments in Massachusetts because the state’s healthcare system could affect their patient loads, daily work, and compensation. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
With the first major statewide attempt at universal healthcare access under way in Massachusetts, everyone from presidential candidates to uninsured families on the other side of the U.S. is watching to see if the state’s plan will succeed. If so, it could become the basis of a national healthcare plan.
Massachusetts healthcare reform became law April 2006 as part of the Act Providing Access to Affordable, Quality, Accountable Health Care. It requires that virtually all state residents either purchase health insurance or get coverage through state-sponsored insurance for people with low incomes (May 2007 The Hospitalist, p. 1). The plan, based on insurance market reforms, merges the individual and small-group insurance market, allowing residents to get lower group insurance rates.
The law required coverage by July 1, and residents must show evidence of their coverage on their income tax return or face a substantial fine—up to 50% of the cost of a health insurance plan.
Many Massachusetts residents get healthcare coverage through their employers. The state plan requires companies with more than 10 employees to provide coverage or to pay a “Fair Share” contribution of up to $295 for each employee each year. Employers must also offer a “cafeteria plan” that allows workers to purchase healthcare with pre-tax income.
The bill created the Commonwealth Health Insurance Connector, which offers affordable, quality insurance to individuals and small businesses. The Connector board approved plans offered by seven insurers that include several options.
As for low-income residents, sliding-scale government-funded subsidies are provided by the Commonwealth Care Health Insurance Program (C-CHIP). As of June 1, nearly 80,000 low-income adults had enrolled in C-CHIP. In addition, the statute expanded MassHealth (Medicaid and SCHIP) coverage for children of low-income parents and restored MassHealth benefits such as dental and vision care.
The plan also includes a system for quality standards and for publicizing performance of providers.
The money for the plan comes from several sources. Gov. Deval Patrick has requested $1.725 billion to fund the program in the next fiscal year. This will supplement federal Medicaid payments, employer contributions, and general revenues.
What Hospitalists Face
How will universal healthcare coverage for state residents affect Massachusetts hospitalists and other physicians? Massachusetts resident Win Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, and co-founder of SHM, weighed the pros and cons.
“The first issue is the effect on primary care providers,” says Dr. Whitcomb. “A large number of patients will be steered into the system of primary care, which is already overwhelmed. A new [state] commission has been formed to address this shortage, but it’s too late—the system already lacks capacity.”
Soon-to-be-overwhelmed primary care physicians will take every step possible to share the workload: “I think [the plan] will be a new impetus for primary care providers to refer patients to hospitalists,” stresses Dr. Whitcomb. “Hospitalists may well see new demand from primary care providers.”
Will this trend mean more openings for hospitalists at Massachusetts institutions? “There are so many drivers behind [the growth of the hospital medicine]; this is just another driver,” says Dr. Whitcomb.
The second likely outcome of the plan will be a transformation of the types of patients treated by hospitalists. Hospitalists around the country are well aware of the problems of treating today’s uninsured patients. “The uninsured tend to show up in the ER in the middle of the night, with diseases in an advanced state” because they haven’t seen a doctor until the last minute, says Dr. Whitcomb. “That situation is not going to go away, but it might decrease” in Massachusetts under the new plan.
“The big question is, will the previously uninsured population, which hospitalists are all too familiar with, be a fundamentally different population?” muses Dr. Whitcomb. “In other words, if [patients] go through a primary care provider and have good management of their illness, will they become a different type of patient than hospitalists are seeing at present? This would be good for hospitalists; it will mean more control over chronic disease and illness.”
—Win Whitcomb, MD, director of clinical performance improvement at Mercy Medical Center in Springfield, Mass., and co-founder of SHM
How Is It Working?
The plan is still in its infancy, but more than 150,000 of the state’s previously uninsured residents had coverage before the July deadline. However, the total estimated number of remaining uninsured is 250,000 to 375,000.
“The two roadblocks are the ability to enroll patients and finding primary care to handle everyone,” says Dr. Whitcomb. “It’s just one of those wait-and-see issues. I applaud the plan. It’s a sincere effort to deal with the uninsured. I think the primary care shortage is a major problem and will impact the success of the plan.”
Hospitalists around the country may want to keep an eye on developments in Massachusetts because the state’s healthcare system could affect their patient loads, daily work, and compensation. TH
Jane Jerrard has been writing for The Hospitalist since 2005.
Succeed in Business
You may have an idea for a business you’d like to start, perhaps attracted by the prospect of controlling your time and work, chasing extra income, or fulfilling the dream of having an alternate career. Should you try turning your dream into reality—and if so, how?
Philippa Kennealy, MD, MPH, has guided hospitalists and other physicians along this path. She heads The Entrepreneurial MD, a Los Angeles-based coaching service for physicians who want to become more entrepreneurial with their practices or start a side business. She has a unique perspective on how physicians can add a satisfying second career to their practice of medicine. “I myself am a physician-entrepreneur,” says Dr. Kennealy.
Why Increase Workloads?
What makes busy hospitalists seek a side business? Why overload your schedule with the extra hours and responsibilities of running a business?
“It’s an opportunity to do something that feels creative, that gives you control,” explains Dr. Kennealy. “I feel that physicians don’t get to use creativity, and they don’t have much control. Their daily actions and decisions are quite regulated. Owning their own time is attractive to physicians. Hospitalists in particular are at it all day in the hospital.”
Is it really possible to continue to work as a hospitalist while shaping a second business? Yes—and others have done it.
“A lot of physicians dream of [entrepreneurship] but feel trapped by their existing time commitments,” says Dr. Kennealy. “But there are some who take the necessary steps, who carve out the time to do it. Many of them hook up with someone to form a partnership—often this is with a non-physician.”
Types of Endeavors
Some physicians are interested in a start-up business that goes hand in hand with their patient care; others may go in a completely different direction.
“There’s an enormous array of [physician-owned businesses] out there,” says Dr. Kennealy. “Many of my clients go into consulting, mostly within healthcare. Some have developed a software application that supports some aspect of healthcare.” Other physicians open health and wellness centers. One of Dr. Kennealy’s clients has developed a sculpting business and is ready to open her own gallery.
Lucia Ferreras-Cox, MD, works as an independent contractor in urgent care and hospital medicine while she runs her company, Ejerce Medecina USA, in Gilbert, Ariz. Ejerce offers Web-based training for Spanish-speaking physicians in other countries to help them pass the U.S. medical board review, then serves as a recruiting firm for those physicians once they get their U.S. licenses.
“I went back to business school for three months to refresh my skills,” says Dr. Ferreras-Cox, who previously had a pediatric practice. “I had to relearn—to learn that I was not a not-for-profit anymore.”
Marica Pook, MD, is a full-time hospitalist in Superior, Colo., and president of ExtraMD PC, a company that provides short-term physician staffing. Her start-up was quite simple. “I’ve been a hospitalist for seven years now, and of course part of my job is to call primary care physicians about patients,” Dr. Pook says. “I started thinking about what it’s like for those physicians and how they can get some help when they’re at their busiest.”
She decided to provide that help. In 2004 she used her contacts to start a kind of mini locum tenens job, working for different physician groups and hospitals. “Nine months into it, I started bringing in other physicians,” she says. Today, the business is thriving, with a growing number of local physicians involved, as well as some much-needed staff.
“I have an excellent bookkeeper, who does all the financials, invoicing, and budgeting—almost like a controller,” says Dr. Pook. “And I just hired a virtual assistant last week. I’ve found that it works best when I farm out the calling and scheduling and I just focus on the marketing. And I include talking to the physicians in that.”
Get Started
So how do you begin your transformation from hospitalist to hospitalist-entrepreneur?
“The basic steps begin with identifying whether this is an escapist fantasy or a deep, abiding interest,” stresses Dr. Kennealy. “It will take a deep interest to get you through the difficult times—it’s a real commitment.”
Once you determine you’re willing to invest time and expense in your own business, Dr. Kennealy advises you to assess your skills and acquire any new ones you’ll need. One way is to meet businesspeople, learn how they think, and understand the language of business. You can also study business and marketing books and journals or take business courses.
“I think physicians don’t know how to run a business,” says Dr. Pook. “We’re not trained to do this. What really helped me was a business coach. I’d advise others to either get a coach or get hooked up with someone who knows a lot about business.”
Before you make too deep a commitment, consider an important component. “You need some sense of the marketplace,” says Dr. Kennealy. Who will buy your product or service? Is there enough interest to support your efforts? What is the competition like in your area?
The next step, she says, is to develop a business plan. “There are free resources available at SCORE.org [the Web site of SCORE, Counselors to America’s Small Business],” she says. “As you start on your plan, you may see that you require further analysis. You need to close those knowledge gaps before you start the business.”
And finally, you have to have marketing savvy to make it work. “Wrap it all up in a sound marketing plan,” concludes Dr. Kennealy. “How will you reach your target audience, and how will you do it efficiently? You must learn the art of marketing, and most physicians don’t have a clue. You have to shift your thinking from a physician whose patients basically come flocking to someone who has to attract and keep customers.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
You may have an idea for a business you’d like to start, perhaps attracted by the prospect of controlling your time and work, chasing extra income, or fulfilling the dream of having an alternate career. Should you try turning your dream into reality—and if so, how?
Philippa Kennealy, MD, MPH, has guided hospitalists and other physicians along this path. She heads The Entrepreneurial MD, a Los Angeles-based coaching service for physicians who want to become more entrepreneurial with their practices or start a side business. She has a unique perspective on how physicians can add a satisfying second career to their practice of medicine. “I myself am a physician-entrepreneur,” says Dr. Kennealy.
Why Increase Workloads?
What makes busy hospitalists seek a side business? Why overload your schedule with the extra hours and responsibilities of running a business?
“It’s an opportunity to do something that feels creative, that gives you control,” explains Dr. Kennealy. “I feel that physicians don’t get to use creativity, and they don’t have much control. Their daily actions and decisions are quite regulated. Owning their own time is attractive to physicians. Hospitalists in particular are at it all day in the hospital.”
Is it really possible to continue to work as a hospitalist while shaping a second business? Yes—and others have done it.
“A lot of physicians dream of [entrepreneurship] but feel trapped by their existing time commitments,” says Dr. Kennealy. “But there are some who take the necessary steps, who carve out the time to do it. Many of them hook up with someone to form a partnership—often this is with a non-physician.”
Types of Endeavors
Some physicians are interested in a start-up business that goes hand in hand with their patient care; others may go in a completely different direction.
“There’s an enormous array of [physician-owned businesses] out there,” says Dr. Kennealy. “Many of my clients go into consulting, mostly within healthcare. Some have developed a software application that supports some aspect of healthcare.” Other physicians open health and wellness centers. One of Dr. Kennealy’s clients has developed a sculpting business and is ready to open her own gallery.
Lucia Ferreras-Cox, MD, works as an independent contractor in urgent care and hospital medicine while she runs her company, Ejerce Medecina USA, in Gilbert, Ariz. Ejerce offers Web-based training for Spanish-speaking physicians in other countries to help them pass the U.S. medical board review, then serves as a recruiting firm for those physicians once they get their U.S. licenses.
“I went back to business school for three months to refresh my skills,” says Dr. Ferreras-Cox, who previously had a pediatric practice. “I had to relearn—to learn that I was not a not-for-profit anymore.”
Marica Pook, MD, is a full-time hospitalist in Superior, Colo., and president of ExtraMD PC, a company that provides short-term physician staffing. Her start-up was quite simple. “I’ve been a hospitalist for seven years now, and of course part of my job is to call primary care physicians about patients,” Dr. Pook says. “I started thinking about what it’s like for those physicians and how they can get some help when they’re at their busiest.”
She decided to provide that help. In 2004 she used her contacts to start a kind of mini locum tenens job, working for different physician groups and hospitals. “Nine months into it, I started bringing in other physicians,” she says. Today, the business is thriving, with a growing number of local physicians involved, as well as some much-needed staff.
“I have an excellent bookkeeper, who does all the financials, invoicing, and budgeting—almost like a controller,” says Dr. Pook. “And I just hired a virtual assistant last week. I’ve found that it works best when I farm out the calling and scheduling and I just focus on the marketing. And I include talking to the physicians in that.”
Get Started
So how do you begin your transformation from hospitalist to hospitalist-entrepreneur?
“The basic steps begin with identifying whether this is an escapist fantasy or a deep, abiding interest,” stresses Dr. Kennealy. “It will take a deep interest to get you through the difficult times—it’s a real commitment.”
Once you determine you’re willing to invest time and expense in your own business, Dr. Kennealy advises you to assess your skills and acquire any new ones you’ll need. One way is to meet businesspeople, learn how they think, and understand the language of business. You can also study business and marketing books and journals or take business courses.
“I think physicians don’t know how to run a business,” says Dr. Pook. “We’re not trained to do this. What really helped me was a business coach. I’d advise others to either get a coach or get hooked up with someone who knows a lot about business.”
Before you make too deep a commitment, consider an important component. “You need some sense of the marketplace,” says Dr. Kennealy. Who will buy your product or service? Is there enough interest to support your efforts? What is the competition like in your area?
The next step, she says, is to develop a business plan. “There are free resources available at SCORE.org [the Web site of SCORE, Counselors to America’s Small Business],” she says. “As you start on your plan, you may see that you require further analysis. You need to close those knowledge gaps before you start the business.”
And finally, you have to have marketing savvy to make it work. “Wrap it all up in a sound marketing plan,” concludes Dr. Kennealy. “How will you reach your target audience, and how will you do it efficiently? You must learn the art of marketing, and most physicians don’t have a clue. You have to shift your thinking from a physician whose patients basically come flocking to someone who has to attract and keep customers.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
You may have an idea for a business you’d like to start, perhaps attracted by the prospect of controlling your time and work, chasing extra income, or fulfilling the dream of having an alternate career. Should you try turning your dream into reality—and if so, how?
Philippa Kennealy, MD, MPH, has guided hospitalists and other physicians along this path. She heads The Entrepreneurial MD, a Los Angeles-based coaching service for physicians who want to become more entrepreneurial with their practices or start a side business. She has a unique perspective on how physicians can add a satisfying second career to their practice of medicine. “I myself am a physician-entrepreneur,” says Dr. Kennealy.
Why Increase Workloads?
What makes busy hospitalists seek a side business? Why overload your schedule with the extra hours and responsibilities of running a business?
“It’s an opportunity to do something that feels creative, that gives you control,” explains Dr. Kennealy. “I feel that physicians don’t get to use creativity, and they don’t have much control. Their daily actions and decisions are quite regulated. Owning their own time is attractive to physicians. Hospitalists in particular are at it all day in the hospital.”
Is it really possible to continue to work as a hospitalist while shaping a second business? Yes—and others have done it.
“A lot of physicians dream of [entrepreneurship] but feel trapped by their existing time commitments,” says Dr. Kennealy. “But there are some who take the necessary steps, who carve out the time to do it. Many of them hook up with someone to form a partnership—often this is with a non-physician.”
Types of Endeavors
Some physicians are interested in a start-up business that goes hand in hand with their patient care; others may go in a completely different direction.
“There’s an enormous array of [physician-owned businesses] out there,” says Dr. Kennealy. “Many of my clients go into consulting, mostly within healthcare. Some have developed a software application that supports some aspect of healthcare.” Other physicians open health and wellness centers. One of Dr. Kennealy’s clients has developed a sculpting business and is ready to open her own gallery.
Lucia Ferreras-Cox, MD, works as an independent contractor in urgent care and hospital medicine while she runs her company, Ejerce Medecina USA, in Gilbert, Ariz. Ejerce offers Web-based training for Spanish-speaking physicians in other countries to help them pass the U.S. medical board review, then serves as a recruiting firm for those physicians once they get their U.S. licenses.
“I went back to business school for three months to refresh my skills,” says Dr. Ferreras-Cox, who previously had a pediatric practice. “I had to relearn—to learn that I was not a not-for-profit anymore.”
Marica Pook, MD, is a full-time hospitalist in Superior, Colo., and president of ExtraMD PC, a company that provides short-term physician staffing. Her start-up was quite simple. “I’ve been a hospitalist for seven years now, and of course part of my job is to call primary care physicians about patients,” Dr. Pook says. “I started thinking about what it’s like for those physicians and how they can get some help when they’re at their busiest.”
She decided to provide that help. In 2004 she used her contacts to start a kind of mini locum tenens job, working for different physician groups and hospitals. “Nine months into it, I started bringing in other physicians,” she says. Today, the business is thriving, with a growing number of local physicians involved, as well as some much-needed staff.
“I have an excellent bookkeeper, who does all the financials, invoicing, and budgeting—almost like a controller,” says Dr. Pook. “And I just hired a virtual assistant last week. I’ve found that it works best when I farm out the calling and scheduling and I just focus on the marketing. And I include talking to the physicians in that.”
Get Started
So how do you begin your transformation from hospitalist to hospitalist-entrepreneur?
“The basic steps begin with identifying whether this is an escapist fantasy or a deep, abiding interest,” stresses Dr. Kennealy. “It will take a deep interest to get you through the difficult times—it’s a real commitment.”
Once you determine you’re willing to invest time and expense in your own business, Dr. Kennealy advises you to assess your skills and acquire any new ones you’ll need. One way is to meet businesspeople, learn how they think, and understand the language of business. You can also study business and marketing books and journals or take business courses.
“I think physicians don’t know how to run a business,” says Dr. Pook. “We’re not trained to do this. What really helped me was a business coach. I’d advise others to either get a coach or get hooked up with someone who knows a lot about business.”
Before you make too deep a commitment, consider an important component. “You need some sense of the marketplace,” says Dr. Kennealy. Who will buy your product or service? Is there enough interest to support your efforts? What is the competition like in your area?
The next step, she says, is to develop a business plan. “There are free resources available at SCORE.org [the Web site of SCORE, Counselors to America’s Small Business],” she says. “As you start on your plan, you may see that you require further analysis. You need to close those knowledge gaps before you start the business.”
And finally, you have to have marketing savvy to make it work. “Wrap it all up in a sound marketing plan,” concludes Dr. Kennealy. “How will you reach your target audience, and how will you do it efficiently? You must learn the art of marketing, and most physicians don’t have a clue. You have to shift your thinking from a physician whose patients basically come flocking to someone who has to attract and keep customers.” TH
Jane Jerrard also writes “Public Policy” for The Hospitalist.
The DNR Dilemma

When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”

A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”
A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
When it comes to communicating do-not-resuscitate (DNR) orders, hospitals rely on a bewildering array of paper documentation, electronic records, and colored wristbands that can easily be misinterpreted.
These are the findings reported in the November-December issue of the Journal of Hospital Medicine by Niraj Sehgal, MD, and Robert Wachter, MD. Dr. Wachter is associate chair of the department of medicine at the University of California, San Francisco. Dr. Sehgal is an assistant clinical professor of medicine at the school.
In a survey of 69 nursing executives representing hospitals in a consortium of academic medical centers, “More than 70% of respondents recalled situations when confusion around a DNR order led to problems in patient care,” the authors say.
Everyone has a “near-miss” story, says Dr. Sehgal.
In one budget-minded hospital where materials were recycled, someone forgot to remove a DNR sticker from a previous patient’s folder before the folder was assigned to someone else. Several nurses told of instances in which patients were resuscitated inappropriately because hospital staff members did not see DNR stickers in the patient’s chart, the patient was off the unit for a procedure without a complete chart, or the DNR order was buried under other materials.
Much of the problem stems from the lack of a standardized method for making a patient’s DNR wishes known, Dr. Sehgal explains.
For example, in 2004 Dr. Sehgal saw a newspaper report that BayCare Health hospitals, in and around Tampa, Fla., were covering yellow “Livestrong” bracelets issued by the Lance Armstrong Foundation and worn by some patients to support those living with cancer. BayCare uses yellow bracelets for DNR patients. Nearly 20% of Americans wear “Livestrong” bracelets, posing a challenge for any hospital that also uses yellow bracelets to indicate DNR.
The newspaper story was the impetus for this study, Dr. Sehgal recalls. “I saw that article and thought, ‘What a great metaphor for the need for standardization.’”
He and Dr. Wachter designed a brief survey and distributed it via an e-mail listserve to senior nursing staff members of the University HealthSystem Consortium, an alliance of 97 academic medical centers and their affiliated hospitals. Those institutions represent 90% of the nation’s nonprofit academic medical centers.
Of the 127 nursing executives who received survey announcements, 69 (54%) returned completed questionnaires. Of those, 39 (56%) reported that their hospitals documented patients’ DNR preferences only in the charts, while 11 (16%) used only electronic health records (EHRs). Seventeen (25%) augmented the paper charts or EHRs with color-coded wristbands in eight colors.
“We expected variability, but even so we were struck by how much variability existed in our findings,” Dr. Sehgal says.
Hospitals use wristbands in a rainbow of colors to convey many messages. Of the hospitals represented in this survey, 55% used them to warn of allergies, fall risks, and even same last names. The authors found “12 different indications were depicted by various colors, with variations in both the color choice for a given indication (e.g., red and yellow used for allergy wristbands at different hospitals) and across indications (e.g., red for allergy at one hospital and red for bleeding risk at another).”
A national, standardized system for conveying patients’ DNR wishes would seem logical, but no system is in place, Dr. Sehgal says. Hospitals cannot even agree on which method to use. While some use wristbands, others use notices or stickers incorporated into the chart. Still others use EHRs.
A few states, including Arizona, Pennsylvania, and Colorado have established statewide standards for using wristbands—but each state chose a different color. “I suspect that many physicians don’t know the meaning of many of the wristbands used in their hospitals, especially if those doctors rotate among different hospitals or hospital systems,” Dr. Sehgal says.
Developing a system for making a patient’s wishes known to hospital staff is one of two challenges reflected in this study, he adds. The second is to use what might be perfunctory questions about advance directives as an opening for a deeper discussion about the patient’s thoughts on end-of-life care. Right now, those questions are just another process measure hospitals must document. “It becomes just another box to check instead of a tool for opening a conversation about what the patient’s wishes are,” he says.
Hospitalists should embrace the opportunity to involve the patient, the patient’s family members, and the primary care provider in an ongoing discussion about the patient’s desires over the course of the hospital stay. “This can give patients a mechanism for thinking about what they’d want under certain circumstances,” Dr. Sehgal explains.
From this study’s findings emerge two take-home messages for hospitalists, he maintains. The first is to remember that “we in inpatient settings spend a lot of time taking care of patients, and we must be aware of what those patients’ wishes are with respect to DNR.” The second is to step back and take an even broader view by remaining alert to processes other than DNR that might benefit from a standardized approach. “Maybe we should think about that, particularly when there is the potential to significantly harm patients,” he says. TH
Norra MacReady is a medical writer based in California.
Avoid Pancreatitis Risk
Drugs are an often-overlooked cause of pancreatitis in hospitalized patients.1,2 Knowing which drugs are associated with acute pancreatic inflammation can help the hospitalist consider specific drugs as the cause within their differential diagnosis.
The two most common causes of acute pancreatitis are biliary disease (30%-60%) and chronic alcohol use (15%-30%). Drug-induced pancreatitis (DIP) has occurred with more than 100 prescribed medications.3,4
Most cases of acute pancreatitis are reversible and resolve on their own within three to seven days after treatment begins. A small number of patients develop severe complications, and their mortality rate nears 30%. Symptoms may last a few days and can include mild to severe epigastric pain that can radiate to the back, chest, flank, or lower abdomen.
Other symptoms can include nausea, vomiting, fever, abdominal tenderness, jaundice, or hypotension. Serum amylase and lipase levels usually rise to three times the upper limit of normal. Use of computerized tomography (CT) or ultrasound can help the diagnosis.
The mechanism of DIP is not known, but is thought to be predominantly due to an idiosyncratic reaction, and for a few agents/classes, to intrinsic drug toxicity.5 The incidence of DIP is approximately 1.4%-5%. Not knowing the exact number of prescriptions for each medication and the cases of pancreatitis from each impedes the determination of incidence.
Most data on DIP are from case reports or reviews of compiled cases. The validity and severity of DIP is unknown mostly because cases are underreported to MedWatch. Reasons for underreporting include:
- Low index of suspicion for DIP compared with drug- induced hepatotoxicity;
- Milder cases due to missed lower enzyme levels (not routinely ascertained in a metabolic panel);
- Missed latency of exposure; and
- Erroneous classification as alcoholic or biliary disease by default.
Drug-induced pancreatitis is more common in patients who have inflammatory bowel disease, AIDS, cancer, or gastrointestinal disease. It is also common in those who are geriatric, HIV positive, or who are on immunomodulating agents.6
An early compilation of DIP reports was published by Lankisch, et al. This was a retrospective evaluation that excluded all other pancreatitis etiologies (e.g., post-endoscopic retrograde cholangiopancreatography (ERCP), post-traumatic, post-operative, viral), except drugs. Out of 1,613 patients with acute pancreatitis, there were 22 cases of DIP due to the following agents: azathioprine (n=6), mesalamine/sulfasalazine (n=5) didanosine (ddI, n=4), estrogens (n=3), furosemide (n=2), hydrochlorothiazide (HCTZ, n=1), and rifampicin (n=1). Rechallenge was not attempted for ethical reasons. The mean hospital stay was 25.5 days (range two to 78 days), with an incidence of 1.2%. Two patients died (from AIDS and tuberculosis). The authors noted that other studies show a high fatality rate from azathioprine, ddI, furosemide, and HCTZ.
New Drugs
![]()
Raltegravir (Isentress), an oral integrase inhibitor, is in a new class of antiretrovirals. This agent was FDA approved for use in combination with other antiretroviral therapy for treating HIV infection in patients with ongoing viral replication despite treatment.
New Indications
Levofloxacin 750 mg IV injection and oral tablets (Levaquin) have been FDA approved as a five-day, once-daily course for the treatment of complicated urinary tract infections and acute pyelonephritis.
Raloxifene 60 mg tablets (Evista) have been FDA approved to reduce the risk of invasive breast cancer in two populations of postmenopausal women: those with osteoporosis and those at high risk for invasive breast cancer.
Additionally, Triveldi, et al., evaluated cases reported in the literature or unpublished cases from 1966 through 2004. They then classified the drugs into one of three categories based on strength of evidence of DIP association.
Class I included medications causing more than 20 reported cases with at least one case following rechallenge. Class II were medications causing more than 10 but fewer than 20 reported cases with/without a positive rechallenge, and Class III were all medications in 10 or fewer cases or unpublished reports (FDA or pharmaceutical company records). Following are some of the most common reports from drugs available in the U.S.:
- Class I: ddI (n=883), asparaginase (n=177), azathioprine (n=86), valproic acid (n=80), pentavalent antimonials (parenterals to treat leishmaniasis, n=80), pentamidine (n=79), mercaptopurine (n=69), mesalamine (n=59), estrogens (n=42), opiates (n=42), tetracycline (n=34), cytarabine (n=26), steroids (n=25), sulfamethoxazole/trimethoprim (SMZ-TMP, n=24), sulfasalazine (n=23), furosemide (n=21), sulindac (n=21);
- Class II: rifampin, lamivudine, octreotide, carbamazepine, acetaminophen, interferon alfa-2b, enalapril, HCTZ, cisplatin, erythromycin; and
- Class III (numerous agents, including the following classes): quinolones, macrolides, angiotensin-converting enzyme inhibitors (ACEIs), statins, and others.
Most recently Badalov, et al., evaluated cases from Medline (through July 1, 2006) and classified them based on levels of evidence. These levels were:
- Definite (imaging study or autopsy confirmed diagnosis);
- Probable (typical symptoms present and threefold increase in amylase and/or lipase); or
- Possible (all others, not included in the final analysis).
Cases were further subclassified into four classes:
- Class Ia (1 or more cases with positive rechallenge, excluding all other causes): codeine, conjugated estrogens, enalapril, isoniazid, metronidazole, mesalamine, pravastatin (other statins), procainamide, simvastatin, sulindac, sulfa drugs, tetracycline, and valproic acid;
- Class Ib (1 or more cases with positive rechallenge, not excluding all other causes): amiodarone, azathioprine, clomiphene, cytosine arabinoside, dapsone, dexamethasone (other steroids), estrogens, furosemide, ifosfamide, lamivudine, losartan, 6-MP, methimazole, methyldopa, nelfinavir, omeprazole, pentamidine, SMZ-TMP, and trans-retinoic acid (not topical);
- Class II (four or more cases, consistent latency in 75% of cases): acetaminophen, clozapine, ddI, erythromycin, l-asparaginase/peg-asparaginase, pentamidine, propofol, and tamoxifen;
- Class III (two or more cases, no consistent latency, no rechallenge): alendronate, captopril, carbamazepine, ceftriaxone, HCTZ, interferon, lisinopril, metformin, mirtazapine, naproxen, and others; and
- Class IV (one case, no other class, without rechallenge): too numerous.
Additionally, the Australian Adverse Drug Reactions Advisory Committee reported on the top 12 DIP-associated medications (n=414 reports implicating 695 drugs). The most commonly reported drugs included azathioprine, ddI, valproate, stavudine, simvastatin, clozapine, lamivudine, ezetimibe, prednisolone, olanzapine, celecoxib and 6-MP, which are listed in each medication’s Australian product information.
The following drugs/classes have been implicated in causing DIP:
- AIDS therapies: ddI, pentamidine;
- Antimicrobials: metronidazole, sulfonamides, tetracyclines;
- Diuretics: furosemide, HCTZ;
- Anti-inflammatories: mesalamine, salicylates, sulindac, sulfasalazine;
- Immunosuppressives: asparaginase, azathioprine, mercaptopurine; and
- Neuropsychiatric agents: valproic acid.
The American Gastroenterologic Association Institute has developed a guide for managing acute pancreatitis. Additionally, they note that when assessing DIP, consider prescription, over-the-counter, and herbal products, too.7 Pancreatitis can occur with certain drugs or medication classes, some more often than others.
Consider DIP in the differential diagnosis of patients who present with or develop epigastric pain. Question all patients with acute pancreatitis about their medication use as a possible cause for the disease. Assessment of amylase/lipase will aid in the diagnosis. To prevent further compromise in cases where DIP is suspected, hold the offending agent (and substitute if possible) to decrease further episodes. TH
Michele B Kaufman is a freelance medical writer based in New York City.
References
- Lankisch PG, Dröge M, Gottesleben F. Drug-induced acute pancreatitis: incidence and severity. Gut. 1995 Oct;37(4):565-567.
- Eltookhy A, Pearson NL. Drug-induced pancreatitis. Can Pharm J. 2006;139(6):58-60.
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol. 2005 Sept;39(8):709-716.
- Badalov N, Baradarian R, Iswara K, et al. Drug-induced pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007 Jun;5(6):648-661.
- Vege SS, Chari ST. Etiology of acute pancreatitis. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass., 2007.
- Skirvin A. Drug-induced pancreatitis. Aust Adv Drug Reactions Bull. 2006 Dec;25(6):22.
- American Gastroenterological Association Institute Medical Position Statement on Acute Pancreatitis. Gastroenterology. 1998 Sep;115(3):763-764.
Drugs are an often-overlooked cause of pancreatitis in hospitalized patients.1,2 Knowing which drugs are associated with acute pancreatic inflammation can help the hospitalist consider specific drugs as the cause within their differential diagnosis.
The two most common causes of acute pancreatitis are biliary disease (30%-60%) and chronic alcohol use (15%-30%). Drug-induced pancreatitis (DIP) has occurred with more than 100 prescribed medications.3,4
Most cases of acute pancreatitis are reversible and resolve on their own within three to seven days after treatment begins. A small number of patients develop severe complications, and their mortality rate nears 30%. Symptoms may last a few days and can include mild to severe epigastric pain that can radiate to the back, chest, flank, or lower abdomen.
Other symptoms can include nausea, vomiting, fever, abdominal tenderness, jaundice, or hypotension. Serum amylase and lipase levels usually rise to three times the upper limit of normal. Use of computerized tomography (CT) or ultrasound can help the diagnosis.
The mechanism of DIP is not known, but is thought to be predominantly due to an idiosyncratic reaction, and for a few agents/classes, to intrinsic drug toxicity.5 The incidence of DIP is approximately 1.4%-5%. Not knowing the exact number of prescriptions for each medication and the cases of pancreatitis from each impedes the determination of incidence.
Most data on DIP are from case reports or reviews of compiled cases. The validity and severity of DIP is unknown mostly because cases are underreported to MedWatch. Reasons for underreporting include:
- Low index of suspicion for DIP compared with drug- induced hepatotoxicity;
- Milder cases due to missed lower enzyme levels (not routinely ascertained in a metabolic panel);
- Missed latency of exposure; and
- Erroneous classification as alcoholic or biliary disease by default.
Drug-induced pancreatitis is more common in patients who have inflammatory bowel disease, AIDS, cancer, or gastrointestinal disease. It is also common in those who are geriatric, HIV positive, or who are on immunomodulating agents.6
An early compilation of DIP reports was published by Lankisch, et al. This was a retrospective evaluation that excluded all other pancreatitis etiologies (e.g., post-endoscopic retrograde cholangiopancreatography (ERCP), post-traumatic, post-operative, viral), except drugs. Out of 1,613 patients with acute pancreatitis, there were 22 cases of DIP due to the following agents: azathioprine (n=6), mesalamine/sulfasalazine (n=5) didanosine (ddI, n=4), estrogens (n=3), furosemide (n=2), hydrochlorothiazide (HCTZ, n=1), and rifampicin (n=1). Rechallenge was not attempted for ethical reasons. The mean hospital stay was 25.5 days (range two to 78 days), with an incidence of 1.2%. Two patients died (from AIDS and tuberculosis). The authors noted that other studies show a high fatality rate from azathioprine, ddI, furosemide, and HCTZ.
New Drugs
![]()
Raltegravir (Isentress), an oral integrase inhibitor, is in a new class of antiretrovirals. This agent was FDA approved for use in combination with other antiretroviral therapy for treating HIV infection in patients with ongoing viral replication despite treatment.
New Indications
Levofloxacin 750 mg IV injection and oral tablets (Levaquin) have been FDA approved as a five-day, once-daily course for the treatment of complicated urinary tract infections and acute pyelonephritis.
Raloxifene 60 mg tablets (Evista) have been FDA approved to reduce the risk of invasive breast cancer in two populations of postmenopausal women: those with osteoporosis and those at high risk for invasive breast cancer.
Additionally, Triveldi, et al., evaluated cases reported in the literature or unpublished cases from 1966 through 2004. They then classified the drugs into one of three categories based on strength of evidence of DIP association.
Class I included medications causing more than 20 reported cases with at least one case following rechallenge. Class II were medications causing more than 10 but fewer than 20 reported cases with/without a positive rechallenge, and Class III were all medications in 10 or fewer cases or unpublished reports (FDA or pharmaceutical company records). Following are some of the most common reports from drugs available in the U.S.:
- Class I: ddI (n=883), asparaginase (n=177), azathioprine (n=86), valproic acid (n=80), pentavalent antimonials (parenterals to treat leishmaniasis, n=80), pentamidine (n=79), mercaptopurine (n=69), mesalamine (n=59), estrogens (n=42), opiates (n=42), tetracycline (n=34), cytarabine (n=26), steroids (n=25), sulfamethoxazole/trimethoprim (SMZ-TMP, n=24), sulfasalazine (n=23), furosemide (n=21), sulindac (n=21);
- Class II: rifampin, lamivudine, octreotide, carbamazepine, acetaminophen, interferon alfa-2b, enalapril, HCTZ, cisplatin, erythromycin; and
- Class III (numerous agents, including the following classes): quinolones, macrolides, angiotensin-converting enzyme inhibitors (ACEIs), statins, and others.
Most recently Badalov, et al., evaluated cases from Medline (through July 1, 2006) and classified them based on levels of evidence. These levels were:
- Definite (imaging study or autopsy confirmed diagnosis);
- Probable (typical symptoms present and threefold increase in amylase and/or lipase); or
- Possible (all others, not included in the final analysis).
Cases were further subclassified into four classes:
- Class Ia (1 or more cases with positive rechallenge, excluding all other causes): codeine, conjugated estrogens, enalapril, isoniazid, metronidazole, mesalamine, pravastatin (other statins), procainamide, simvastatin, sulindac, sulfa drugs, tetracycline, and valproic acid;
- Class Ib (1 or more cases with positive rechallenge, not excluding all other causes): amiodarone, azathioprine, clomiphene, cytosine arabinoside, dapsone, dexamethasone (other steroids), estrogens, furosemide, ifosfamide, lamivudine, losartan, 6-MP, methimazole, methyldopa, nelfinavir, omeprazole, pentamidine, SMZ-TMP, and trans-retinoic acid (not topical);
- Class II (four or more cases, consistent latency in 75% of cases): acetaminophen, clozapine, ddI, erythromycin, l-asparaginase/peg-asparaginase, pentamidine, propofol, and tamoxifen;
- Class III (two or more cases, no consistent latency, no rechallenge): alendronate, captopril, carbamazepine, ceftriaxone, HCTZ, interferon, lisinopril, metformin, mirtazapine, naproxen, and others; and
- Class IV (one case, no other class, without rechallenge): too numerous.
Additionally, the Australian Adverse Drug Reactions Advisory Committee reported on the top 12 DIP-associated medications (n=414 reports implicating 695 drugs). The most commonly reported drugs included azathioprine, ddI, valproate, stavudine, simvastatin, clozapine, lamivudine, ezetimibe, prednisolone, olanzapine, celecoxib and 6-MP, which are listed in each medication’s Australian product information.
The following drugs/classes have been implicated in causing DIP:
- AIDS therapies: ddI, pentamidine;
- Antimicrobials: metronidazole, sulfonamides, tetracyclines;
- Diuretics: furosemide, HCTZ;
- Anti-inflammatories: mesalamine, salicylates, sulindac, sulfasalazine;
- Immunosuppressives: asparaginase, azathioprine, mercaptopurine; and
- Neuropsychiatric agents: valproic acid.
The American Gastroenterologic Association Institute has developed a guide for managing acute pancreatitis. Additionally, they note that when assessing DIP, consider prescription, over-the-counter, and herbal products, too.7 Pancreatitis can occur with certain drugs or medication classes, some more often than others.
Consider DIP in the differential diagnosis of patients who present with or develop epigastric pain. Question all patients with acute pancreatitis about their medication use as a possible cause for the disease. Assessment of amylase/lipase will aid in the diagnosis. To prevent further compromise in cases where DIP is suspected, hold the offending agent (and substitute if possible) to decrease further episodes. TH
Michele B Kaufman is a freelance medical writer based in New York City.
References
- Lankisch PG, Dröge M, Gottesleben F. Drug-induced acute pancreatitis: incidence and severity. Gut. 1995 Oct;37(4):565-567.
- Eltookhy A, Pearson NL. Drug-induced pancreatitis. Can Pharm J. 2006;139(6):58-60.
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol. 2005 Sept;39(8):709-716.
- Badalov N, Baradarian R, Iswara K, et al. Drug-induced pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007 Jun;5(6):648-661.
- Vege SS, Chari ST. Etiology of acute pancreatitis. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass., 2007.
- Skirvin A. Drug-induced pancreatitis. Aust Adv Drug Reactions Bull. 2006 Dec;25(6):22.
- American Gastroenterological Association Institute Medical Position Statement on Acute Pancreatitis. Gastroenterology. 1998 Sep;115(3):763-764.
Drugs are an often-overlooked cause of pancreatitis in hospitalized patients.1,2 Knowing which drugs are associated with acute pancreatic inflammation can help the hospitalist consider specific drugs as the cause within their differential diagnosis.
The two most common causes of acute pancreatitis are biliary disease (30%-60%) and chronic alcohol use (15%-30%). Drug-induced pancreatitis (DIP) has occurred with more than 100 prescribed medications.3,4
Most cases of acute pancreatitis are reversible and resolve on their own within three to seven days after treatment begins. A small number of patients develop severe complications, and their mortality rate nears 30%. Symptoms may last a few days and can include mild to severe epigastric pain that can radiate to the back, chest, flank, or lower abdomen.
Other symptoms can include nausea, vomiting, fever, abdominal tenderness, jaundice, or hypotension. Serum amylase and lipase levels usually rise to three times the upper limit of normal. Use of computerized tomography (CT) or ultrasound can help the diagnosis.
The mechanism of DIP is not known, but is thought to be predominantly due to an idiosyncratic reaction, and for a few agents/classes, to intrinsic drug toxicity.5 The incidence of DIP is approximately 1.4%-5%. Not knowing the exact number of prescriptions for each medication and the cases of pancreatitis from each impedes the determination of incidence.
Most data on DIP are from case reports or reviews of compiled cases. The validity and severity of DIP is unknown mostly because cases are underreported to MedWatch. Reasons for underreporting include:
- Low index of suspicion for DIP compared with drug- induced hepatotoxicity;
- Milder cases due to missed lower enzyme levels (not routinely ascertained in a metabolic panel);
- Missed latency of exposure; and
- Erroneous classification as alcoholic or biliary disease by default.
Drug-induced pancreatitis is more common in patients who have inflammatory bowel disease, AIDS, cancer, or gastrointestinal disease. It is also common in those who are geriatric, HIV positive, or who are on immunomodulating agents.6
An early compilation of DIP reports was published by Lankisch, et al. This was a retrospective evaluation that excluded all other pancreatitis etiologies (e.g., post-endoscopic retrograde cholangiopancreatography (ERCP), post-traumatic, post-operative, viral), except drugs. Out of 1,613 patients with acute pancreatitis, there were 22 cases of DIP due to the following agents: azathioprine (n=6), mesalamine/sulfasalazine (n=5) didanosine (ddI, n=4), estrogens (n=3), furosemide (n=2), hydrochlorothiazide (HCTZ, n=1), and rifampicin (n=1). Rechallenge was not attempted for ethical reasons. The mean hospital stay was 25.5 days (range two to 78 days), with an incidence of 1.2%. Two patients died (from AIDS and tuberculosis). The authors noted that other studies show a high fatality rate from azathioprine, ddI, furosemide, and HCTZ.
New Drugs
![]()
Raltegravir (Isentress), an oral integrase inhibitor, is in a new class of antiretrovirals. This agent was FDA approved for use in combination with other antiretroviral therapy for treating HIV infection in patients with ongoing viral replication despite treatment.
New Indications
Levofloxacin 750 mg IV injection and oral tablets (Levaquin) have been FDA approved as a five-day, once-daily course for the treatment of complicated urinary tract infections and acute pyelonephritis.
Raloxifene 60 mg tablets (Evista) have been FDA approved to reduce the risk of invasive breast cancer in two populations of postmenopausal women: those with osteoporosis and those at high risk for invasive breast cancer.
Additionally, Triveldi, et al., evaluated cases reported in the literature or unpublished cases from 1966 through 2004. They then classified the drugs into one of three categories based on strength of evidence of DIP association.
Class I included medications causing more than 20 reported cases with at least one case following rechallenge. Class II were medications causing more than 10 but fewer than 20 reported cases with/without a positive rechallenge, and Class III were all medications in 10 or fewer cases or unpublished reports (FDA or pharmaceutical company records). Following are some of the most common reports from drugs available in the U.S.:
- Class I: ddI (n=883), asparaginase (n=177), azathioprine (n=86), valproic acid (n=80), pentavalent antimonials (parenterals to treat leishmaniasis, n=80), pentamidine (n=79), mercaptopurine (n=69), mesalamine (n=59), estrogens (n=42), opiates (n=42), tetracycline (n=34), cytarabine (n=26), steroids (n=25), sulfamethoxazole/trimethoprim (SMZ-TMP, n=24), sulfasalazine (n=23), furosemide (n=21), sulindac (n=21);
- Class II: rifampin, lamivudine, octreotide, carbamazepine, acetaminophen, interferon alfa-2b, enalapril, HCTZ, cisplatin, erythromycin; and
- Class III (numerous agents, including the following classes): quinolones, macrolides, angiotensin-converting enzyme inhibitors (ACEIs), statins, and others.
Most recently Badalov, et al., evaluated cases from Medline (through July 1, 2006) and classified them based on levels of evidence. These levels were:
- Definite (imaging study or autopsy confirmed diagnosis);
- Probable (typical symptoms present and threefold increase in amylase and/or lipase); or
- Possible (all others, not included in the final analysis).
Cases were further subclassified into four classes:
- Class Ia (1 or more cases with positive rechallenge, excluding all other causes): codeine, conjugated estrogens, enalapril, isoniazid, metronidazole, mesalamine, pravastatin (other statins), procainamide, simvastatin, sulindac, sulfa drugs, tetracycline, and valproic acid;
- Class Ib (1 or more cases with positive rechallenge, not excluding all other causes): amiodarone, azathioprine, clomiphene, cytosine arabinoside, dapsone, dexamethasone (other steroids), estrogens, furosemide, ifosfamide, lamivudine, losartan, 6-MP, methimazole, methyldopa, nelfinavir, omeprazole, pentamidine, SMZ-TMP, and trans-retinoic acid (not topical);
- Class II (four or more cases, consistent latency in 75% of cases): acetaminophen, clozapine, ddI, erythromycin, l-asparaginase/peg-asparaginase, pentamidine, propofol, and tamoxifen;
- Class III (two or more cases, no consistent latency, no rechallenge): alendronate, captopril, carbamazepine, ceftriaxone, HCTZ, interferon, lisinopril, metformin, mirtazapine, naproxen, and others; and
- Class IV (one case, no other class, without rechallenge): too numerous.
Additionally, the Australian Adverse Drug Reactions Advisory Committee reported on the top 12 DIP-associated medications (n=414 reports implicating 695 drugs). The most commonly reported drugs included azathioprine, ddI, valproate, stavudine, simvastatin, clozapine, lamivudine, ezetimibe, prednisolone, olanzapine, celecoxib and 6-MP, which are listed in each medication’s Australian product information.
The following drugs/classes have been implicated in causing DIP:
- AIDS therapies: ddI, pentamidine;
- Antimicrobials: metronidazole, sulfonamides, tetracyclines;
- Diuretics: furosemide, HCTZ;
- Anti-inflammatories: mesalamine, salicylates, sulindac, sulfasalazine;
- Immunosuppressives: asparaginase, azathioprine, mercaptopurine; and
- Neuropsychiatric agents: valproic acid.
The American Gastroenterologic Association Institute has developed a guide for managing acute pancreatitis. Additionally, they note that when assessing DIP, consider prescription, over-the-counter, and herbal products, too.7 Pancreatitis can occur with certain drugs or medication classes, some more often than others.
Consider DIP in the differential diagnosis of patients who present with or develop epigastric pain. Question all patients with acute pancreatitis about their medication use as a possible cause for the disease. Assessment of amylase/lipase will aid in the diagnosis. To prevent further compromise in cases where DIP is suspected, hold the offending agent (and substitute if possible) to decrease further episodes. TH
Michele B Kaufman is a freelance medical writer based in New York City.
References
- Lankisch PG, Dröge M, Gottesleben F. Drug-induced acute pancreatitis: incidence and severity. Gut. 1995 Oct;37(4):565-567.
- Eltookhy A, Pearson NL. Drug-induced pancreatitis. Can Pharm J. 2006;139(6):58-60.
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J Clin Gastroenterol. 2005 Sept;39(8):709-716.
- Badalov N, Baradarian R, Iswara K, et al. Drug-induced pancreatitis: an evidence-based review. Clin Gastroenterol Hepatol. 2007 Jun;5(6):648-661.
- Vege SS, Chari ST. Etiology of acute pancreatitis. In: UpToDate, Rose, BD (Ed), UpToDate, Waltham, Mass., 2007.
- Skirvin A. Drug-induced pancreatitis. Aust Adv Drug Reactions Bull. 2006 Dec;25(6):22.
- American Gastroenterological Association Institute Medical Position Statement on Acute Pancreatitis. Gastroenterology. 1998 Sep;115(3):763-764.
In the Literature
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
In This Edition
- C-reactive protein levels predict death from cardiac causes after MI.
- SSRIs reduce risk for recurrent cardiac events in acute coronary syndrome.
- Vancomycin is as effective as metronidazole in routine treatment of C. difficile and superior in severe infection.
- Prevalence and severity of C. difficile are increasing in hospitalized patients in the U.S.
- Deviations in recommended enoxaparin dosing in NSTEMI result in worse outcomes.
- Most outpatient VTE events occur in recently hospitalized patients.
- Poor health literacy predicts mortality in older adults.
- A validated model predicts the risk for delirium at hospital discharge.
Do C-reactive Protein Levels Predict Death from Heart Failure?
Background: Ultra-sensitive quantitative assessment of C-reactive protein (CRP), a surrogate marker of systemic inflammation, has previously been shown to predict plaque instability in acute coronary syndromes. Data are lacking as to whether this blood test can also predict subsequent risk of heart failure or death on presentation in patients admitted for acute myocardial infarction (MI).
Study design: Prospec-tive observational study.
Setting: Olmstead County, Minn.
Synopsis: Ultra-sensitive quantitative serum CRP levels were obtained a median of 6.1 hours following onset of symptoms in 329 patients admitted with acute MI. The patients were stratified into tertiles based levels of CRP less than 3 mg/L, 3-15 mg/L, and more than 15 mg/L.
Tertiles were similar in respect to age, male-predominance, most cardiac risk factors, body mass index, and electrocardiographic (EKG) changes. However, there were statistically significant differences between groups, particularly the frequency of diabetes (10.7%, 31.2%, and 38.0%), previous MI history (2.7%, 4.6%, and 9.3%), Killip class greater than one (15.2%, 31.2%, and 39.8%), peak cardiac enzyme levels (both were higher in the bottom tertile, and lowest in the top tertile), and likelihood of significant comorbidities (lower likelihood in the bottom tertile, higher likelihood in the top tertile).
One-year survival was highly correlated with CRP tertile (93%, 84%, and 62% respectively). Once corrected for age, gender, peak cardiac enzymes, Killip class, coronary history, and recurring ischemic events, there remained a robust hazard ratio for heart failure and death at one year based on CRP tertile (1.00, 1.73, and 3.96, respectively).
Bottom line: Ultra-sensitive quantitative CRP levels obtained on admission for acute MI predict one-year risk for heart failure or death. The ability to generalize these results into clinical practice may be limited due to heterogeneity of the studied groups with a higher frequency of diabetes, prior coronary disease, and higher comorbidities in the group that had the highest CRP levels and thus more mortality and heart failure.
Citation: Bursi F, Weston SA, Killian JM, et al. C-reactive protein and heart failure after myocardial infarction in the community. Am J Med. 2007;120(7):616-622.
Do Selective Serotonin Reuptake Inhibitors Confer Cardiac Benefit?
Background: Selective serotonin reuptake inhibitors (SSRIs) theoretically lead to qualitative platelet dysfunction due to inhibition of serotonin-induced platelet activation (and thus resultant inhibition of platelet aggregation and vasoconstriction).
Study design: Retrospective observational study.
Setting: Large teaching hospital in Baltimore.
Synopsis: Of 1,254 patients admitted during the three-year study, 158 patients were on an SSRI at the time of admission. Of the remaining 1,096 patients, a cohort of 158 propensity-matched patients was identified who were statistically similar to the study group in all comorbidities (except for depression, which was higher in the SSRI group).
There were no statistically significant differences between the SSRI group and the propensity-matched group in regards to treatment for acute coronary syndrome (ACS). Almost all received aspirin (98.7% versus 99.4%), clopidogrel (95.6% versus 93.7%), unfractionated heparin (96.8% versus 99.4%), and a glycoprotein IIb/IIIa inhibitor (100% in both).
Patients in the SSRI group had a statistically lower incidence of minor adverse cardiac events (7.0% versus 13.9%), but had increased bleeding events (37.3% versus 26.6%). Minor cardiac events were defined as recurrent EKG findings of ischemia without resultant cardiac enzyme increase, new heart failure, or asymptomatic cardiac enzyme elevation without EKG changes.
Bottom line: Patients taking SSRIs when admitted with an ACS (for an unknown duration) appear to be at lower risk for minor cardiac complications compared with patients not taking an SSRI on admission. These patients also appear to be at elevated risk for bleeding in the setting of maximum antiplatelet and heparin therapy typical in management of ACS.
Citation: Ziegelstein RC, Meuchel J, Kim TJ, et al. Selective serotonin reuptake inhibitor use by patients with acute coronary syndromes. Am J Med. 2007;120(6):525-530.
When Is Vancomycin Superior in Treating C. difficile-Associated Diarrhea?
Background: Epidemic strains of C. difficile raise issues about which antibiotic treatment for C. difficile-associated diarrhea (CDAD) may be superior, particularly due to the availability of more potent antibiotics that can wipe out the protective flora of the intestinal tract.
Study design: Prospec-tive, randomized, double-blind, placebo-controlled trial over 7.5 years.
Setting: A teaching hospital in Chicago.
Synopsis: One hundred seventy-two patients with diarrhea were stratified into mild (fewer than two risks) or severe (two or more risks) disease groups within 48 hours of randomization. These patients were older than 60, with temperature greater than 38.3°C, albumin level lower than 2.5 mg/dL, or peripheral white blood count greater than 15,000 cells/mm. Patients requiring intensive care unit treatment or those with colonscopic evidence of pseudomembranous colitis received an additional risk score of two.
One hundred fifty patients completed the study, 71 in the vancomycin group (125 mg orally, four times a day) and 79 in the metronidazole group (250 mg orally, four times a day). Both groups were similar in composition and numbers of patients with mild and severe CDAD. Patients received placebo plus either vancomycin or metronidazole.
Cure was defined as resolution of diarrhea by day six of therapy and negative C. difficile toxin A assays on days six and 10 of therapy. Results were statistically similar in both treatment groups with mild disease (98% vancomycin versus 90% metronidazole), but favored vancomycin in severe disease (97% versus 76%).
Relapse were not statistically different in either group (7% versus 14%). An albumin level less than 2.5 mg/dL or the presence of colonoscopy-confirmed pseudomembranous colitis showed statistically significant correlation with metronidazole treatment failure (relative risks of 12.70 and 6.67, respectively).
Bottom line: Oral vancomycin, with its commensurate potential for inducing vancomycin-resistant Enterococcus, proved to be equally effective as metronidazole in treating mild CDAD. It was statistically superior to metronidazole in severe disease with hypoalbuminemia and pseudomembranous colitis predicting failure of metronidazole therapy.
Citation: Zar FA, Bakkanagari SR, Moorthi KM, et al. A comparison of vancomycin and metronidazole for the treatment of C. difficile-associated diarrhea, stratified by disease severity. Clin Infect Dis. 2007;45(3):302-307.
What Risk Factors Affect VTE Development in Outpatients?
Background: Decreasing lengths of stay have raised concern that treatments that previously would have continued during the longer hospital stays in the past, such as deep vein thrombosis prophylaxis, may result in unintended adverse consequences after discharge.
Study design: Retrospective observational study
Setting: Worcester, Mass., in 1999, 2001, and 2003, comprising residents who had diagnosis of venous thromboembolism (VTE) at any one of the 12 hospitals in the region
Synopsis: VTE was diagnosed in 1,897 residents (71.1%, 15.0% had pulmonary embolism [PE], and 13.9% had both). Further, 73.7% of the patients presented as an outpatient or were diagnosed within one day of hospital admission.
Compared with inpatients with VTE, outpatients were younger (63.3 years versus 67.4), were less likely to have had a recent infection (18.6% versus 46.8%), central venous catheter (10.4% versus 41.0%), recent fracture (7.3% versus 18.7%), heart failure (4.2% versus 16.5%), cardiac procedures (2.9% versus 7.8%), or recent intensive care unit care stay (8.7% versus 38.2%), but were more likely to have had a prior episode of VTE (19.9% versus 10.2%) or to be taking hormonal therapy (8.0% versus 3.0%).
The prevalence of malignancy was similar in both groups (29.0% versus 32.3%). Most outpatients diagnosed with VTE (59.9%) had been hospitalized in the preceding three months with a majority of VTEs diagnosed within 30 days of discharge. Only 59.7% of those previously hospitalized had any DVT prophylaxis (42.8% received anticoagulants, 16.9% had mechanical prophylaxis).
Bottom line: In an era of decreasing lengths of stay, the possible high level of outpatient VTE attributable to recent hospitalization may be at least partially due to inadequate inpatient pharmacologic VTE prophylaxis in more than 50% of the patients.
Citation: Spencer FA, Lessard D, Emery C, et al. Venous thromboembolism in the outpatient setting. Arch Intern Med. 2007;167(14):1471-1475.
How Has C. difficile Colitis Changed in Severity and Prevalence?
Background: Recent epidemic strains of Clostridium difficile have been reported with several studies suggesting that C. difficile infection has become more serious with risks for sepsis, colectomy, and death.
Study design: Cohort analysis of nationwide inpatient sample (NIS) discharge data for 11 years.
Synopsis: Of the more than 78 million discharge abstracts available for analysis, 299,453 patients were discharged with either a principle or secondary diagnosis of Clostridium difficile colitis (CDC). Demographics trends comparing the early period (1993-1996) versus the middle period (1997-2000) versus the late period (2001-2003) showed CDC incidence:
- Increased in older groups (65.6 years, 66.9 years, 67.6 years);
- Decreased in females (59.8%, 59.1%, 58.9%); and
- Decreased in Caucasians (70.90%, 67.20%, 59.10%).
From 1993 to 2003, the prevalence of CDC discharge diagnoses increased from 261 to 546 cases per 100,000; the colectomy rate due to CDC increased from 1.2 up to 3.4 per 1000, and the case fatality rate statistically significantly increased from 7.84% to 9.26%.
Bottom line: Despite the limitations of using discharge coding abstracts, this study confirms the significantly increasing prevalence (particularly in older, non-Caucasian men) and severity of CDC over the previous decade. This has resulted in a higher incidence of colectomy and death.
Citation: Ricciardi R, Rothenberger DA, Madoff RD. Increasing prevalence and severity of Clostridium difficile colitis in hospitalized patients in the United States. Arch Surg. 2007;142(7):624-631.
How Often Do Clinicians Deviate from Recommended Enoxaparin Doses?
Background: Low molecular heparins have been increasingly utilized in the setting of non-ST-segment elevation myocardial infarctions (NSTEMI) in place of unfractionated heparin. They require careful dose adjustment to ensure appropriate therapeutic effect and prevent bleeding and thrombotic complications.
Study design: Retrospective observational cohort study.
Setting: Medical centers throughout the U.S. that participated in the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) initiative.
Synopsis: A total of 10,687 patients from 332 hospitals received enoxaparin for NSTEMI as part of CRUSADE. Patients were stratified by whether they received:
- The recommended dose of enoxaparin (1 mg/kg twice daily for glomerular filtration rate (GFR) more than 30 mL/min versus 0.5 mg/kg twice daily for estimated GFR of 30 mL/min or less; 52.1%);
- An excess dose (more than 10 mg/day over recommended dose; 18.7%); or
- A lower-than-recommended dose (more than 10 mg/day less than the recommended dose; 29.2%).
Those receiving an excess dose were more likely to be older, have lower body-mass indexes (BMI), weigh less, be female, have estimated GFRs less than 60 mL/min, and smoke. Those receiving less-than-recommended dosing were more likely to have a higher BMI, weigh more, and be male. Major bleeding episodes (14.2%) and deaths (5.6%) were more common statistically in the excess dose group compared with the recommended dose group (7.3% and 2.4%, respectively). Deaths, but not bleeding, also were higher in the lower-than-recommended dose group (3.3% versus 2.4%).
Bottom line: A little more than half of patients received the correct dose of enoxaparin in NSTEMIs. Those who received too high a dose had marked increases in risk of bleeding and death, and those receiving subtherapeutic doses suffered increased mortality.
Citation: LaPointe NMA, Chen AY, Alexander KP, et al. Enoxaparin dosing and associated risk of in-hospital bleeding and death in patients with non-ST-segment elevation acute coronary syndromes. Arch Intern Med. 2007;167(14):1539-1344.
Does Poor Health Literacy Predict Mortality?
Background: Prior studies have shown increased hospitalization rates in patients with poor health literacy (e.g., inability to comprehend prescriptions or educational materials). At least one study has shown an increase in mortality in 70-to-79-year-olds with impaired health literacy.
Study design: Prospective cohort study.
Setting: Four U.S. metropolitan areas.
Synopsis: Poor health literacy predicts patients’ inability to understand basic health information, such as prescription information, drug dosing intervals, or follow-up schedules. In 1997, 3,260 patients age 65 or older were included in the study, which used a face-to-face standardized test to quantify health literacy.
Patients were tracked via the National Death Index through 2003. Patients were stratified as having adequate, marginal, or inadequate health literacy (64.2%, 11.2%, and 24.5% of patients, respectively). Marginal and inadequate health literacy were strongly associated with increasing age, African American race, lower incomes, lower levels of education, worse physical and mental health, limitations in activities of daily living (ADLs), and lower BMIs. These patients were also less likely to perform vigorous exercise, and less likely to have smoked or used alcohol.
Health literacy (adequate, marginal, or inadequate) predicted unadjusted mortality rates (18.9%, 28.7%, and 39.4%, respectively). Adjusting for socioeconomic status, demographics, and baseline health, all-cause mortality hazard ratios of marginal and inadequate literacy (compared with adequate health literacy) were 1.13 (0.90-1.41 not statistically significant) and 1.52 (1.26-1.83, statistically significant).
Bottom line: Limited data exists regarding how to improve health literacy, and there is no easy bedside test to identify patients with varying levels of literacy. But there appears to be a strong, independent correlation to health literacy and mortality. Physicians need to remain vigilant in their patients’ understanding of their disease, treatment, and follow-up.
Citation: Baker DW, Wolf MS, Feinglass J, et al. Health literacy and mortality among elderly persons. Arch Intern Med. 2007;167(14):1503-1509.
Which Factors Predict Delirium at Discharge?
Background: Delirium at hospital discharge, which can persist for months following hospitalization, may be a contributing factor to dementia, results in increased medical errors during the traditionally high-risk period between discharge and follow-up. Further, it results in serious complications, and, if unrecognized, a high mortality rate.
Study design: Prospective validation model.
Synopsis: A model to predict delirium at hospital discharge was studied in a development cohort of 491 patients age 70 or older who had no evidence of delirium on admission. Of twenty-two different candidate factors, five factors correlated with high odds ratios of delirium at discharge in the 106 (21.6%) of those in the study group who developed delirium: dementia, vision impairment, inability to perform more than one ADL, multiple comorbidities (based on a Charlson score of four or more), and restraint use during delirium.
Patients were stratified into low-risk (zero-one factors), intermediate risk (two-three factors), or high risk (four or more factors) for delirium at hospital discharge. Relative risks (RR) for each group were 1, 4.4, and 15.3, respectively; RR for nursing home placement or death (NHPOD) at one year was 1, 2.4, and 3.4, respectively. A validation cohort of 461 statistically similar patients showed RR for development in the low-, intermediate-, and high-risk groups of 1, 5.4, 10.2, respectively; and RR at one year for NHPOD was 1, 2.7, and 4.4, respectively.
Bottom line: Dementia, vision impairment, inability to perform at least one ADL, multiple comorbidities, and use of restraints are risk factors that can stratify patients into low, intermediate, and high risk for delirium at hospital discharge. Commensurate risks exist for nursing home placement or death at one year.
Citation: Inouye SK, Zhang Y, Jones RN. Risk factors for delirium at discharge. Arch Intern Med. 2007;167(13):1406-1413.
Mission in D.C.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana

Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
SHM’s Public Policy Committee (PPC) has been monitoring federal legislation and regulations affecting hospital medicine and recommending appropriate action by the Society. Over the past several months, the PPC has been engaged in a variety of initiatives.
Physician Payment (Part B)
One of lawmakers’ top priorities in 2007 was addressing pending cuts in Medicare payments to physicians. Under the flawed sustainable growth rate (SGR) formula, Part B Medicare payments were to be reduced by 10% in 2008 and by an additional 5% in January 2009. SHM is working to influence the debate.
Chapter Summaries
Montana
Nashville
The Nashville chapter met Sept. 13 for a roundtable discussion on challenges in the management of hospitalist programs. Eleven hospitalist physicians attended, including five medical directors who represented five area hospitalist programs:
- Kimberly Bell, MD, HCA/Centennial Medical Center, Nashville;
- Rizwan Faisal, MD, Horizon Medical Center, Dickson;
- Randal Rampp, MD, River Park Hospital, McMinnville;
- James Snyder, MD, St. Thomas Hospital, Nashville; and
- James Tedesco, MD, Summit Medical Associates, Hermitage.
These medical directors de-scribed their programs and how they manage variation in daily patient volume, plan for staffing needs, and recruiting. They also discussed jeopardy plans, physician extenders, how to attract new applicants, and incentive plans.
As Congress began to consider legislation on physician payment reform, SHM quickly launched a comprehensive grassroots campaign to stop the cuts. In an e-mail to 7,745 hospitalists, PPC Chair Eric Siegal, MD, director of the hospital medicine program, Cogent Healthcare, Nashville, Tenn., urged members to contact their lawmakers using SHM’s online advocacy tool, Capwiz. Several issues of the e-newsletter also reminded members to write their representatives in support of two years of positive updates. As the congressional session came to a close, SHM members had sent a record 800 messages to their lawmakers urging them to block the pending reductions.
Then, in a letter to the chairs of the Ways and Means and Energy and Commerce committees, SHM commented on key provisions of draft Medicare legislation, expressing appreciation for the inclusion of language averting the scheduled cuts. SHM voiced concern about provisions of the bill that would reconfigure the Medicare payment formula into six service-specific categories with their own expenditure targets and conversion rates, in an effort to control volume of services. The letter also urged Congress to continue to provide funding for voluntary participation in the Physician Quality Reporting Initiative (PQRI) in 2008.
SHM also joined 130 state and national medical societies to urge Senate Majority Leader Harry Reid, D-Nev., to include two years of positive Medicare physician payment updates in pending legislation that would reauthorize the State Children’s Health Insurance Program. The letter underscored the importance of Congress acting sooner rather than later to reverse the cuts. “Temporary Congressional interventions to prevent past cuts, while necessary, have not kept up with increases in medical practice costs and have pushed the cost of fixing the problem to future years, making a meaningful long-term resolution more and more expensive,” the letter read. “Physician payment rates are about the same today as they were in 2001, while practice costs have increased nearly 20% and will increase another 20% over next nine years, according to the government’s conservative Medicare Economic Index (MEI).”
Last fall, two PPC members, Eric Howell, MD, from Maryland, and Greg Seymann, MD, from California, visited members of their congressional delegation on Capitol Hill. Dr. Howell is director of Collaborative Inpatient Medicine Service, Department of Medicine, Johns Hopkins Bayview Medical Center, Baltimore. Dr. Seymann is associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine. During their meetings, Drs. Howell and Seymann voiced support for legislation to avert the Medicare cuts and discussed other elements of SHM’s quality-centered legislative agenda, emphasizing the role of hospitalists in improving the quality of care provided in America’s hospitals.
Hospital Payment (Part A)
SHM joined the American Hospital Association in opposition to a provision in the fiscal year 2008 Medicare inpatient prospective payment system, a proposed rule that would have cut Medicare payment for hospital services in fiscal year 2008.
The Centers for Medicare and Medicaid Services (CMS) sought to reduce hospital payments by 2.4% in 2008 and 2009 based on the assumption that hospitals will adjust coding practices to receive higher payments as a result of proposed changes in the payment system designed to account more fully for patients’ severity of illness.
This proposed “behavioral offset” would have cut $24 billion over five years from payments to hospitals. Congress enacted legislation in September that significantly reduces the cuts hospitals face in the next two years.
Quality Reporting
Together with the Performance and Standards Task Force (PSTF), PPC and staff have posted educational material on our Web site and made other resources available to SHM members to help them determine whether or not they should participate in the PQRI, which began July 1.
For example, SHM sponsored a nationwide call with CMS on the “Nuts and Bolts of Applying the PQRI to Your Hospital Medicine Practice.” Staff have since surveyed the SHM members who participated in this members-only call to learn more about what led them to participate or not to participate in the program. Those participating were asked for information on their experiences to help inform our policy on the initiative.
PPC and the PSTF also collaborated on comments to CMS on the 2008 proposed physician payment rule that dealt with the PQRI and submitted comments to CMS staff on the draft feedback report that PQRI participating physicians and other health professionals will receive upon completion of the 2007 program.
In other action, at the PPC’s recommendation, SHM endorsed legislation that would authorize federal funding for the development and testing of inpatient pediatric quality measures. When it comes to measuring and reporting on healthcare quality, children’s measures lag far behind those for adult care. The Children’s Health Care Quality Act (S. 1226/H.R. 2723) would address this disparity.
FY 2008 Appropriations
SHM continues to call on Congress to increase funding for the Agency for Health Care Research and Quality (AHRQ) in view of the important role the agency plays in supporting quality improvement and patient safety initiatives.
Our efforts are paying off. Legislation approved by the House of Representatives and by the Senate Appropriations Committee would boost AHRQ funding in FY 2008 by $10 million to $329 million, the first increase for the agency in several years. SHM members sent 100 messages to Capitol Hill in support of increased spending for AHRQ. Research Committee Chair Andrew Auerbach, MD, visited with legislative staff Sept. 17 to advocate for greater funding for AHRQ and the creation of a new Center for Comparative Effectiveness Research within the agency. Dr. Auerbach is assistant professor of medicine in residence at the University of California, San Francisco.
At press time, Congress had not taken final action on FY 2008 appropriations for AHRQ.
The PPC keeps you informed about our legislative and regulatory activities through monthly updates posted via the SHM Web site, The Hospitalist, and our e-newsletter. SHM letters to Congress and CMS are on the SHM Web site as well. Depending on the issue, you might also get an e-mail urging you to visit our legislative action center at www.hospitalmedicine.org/beheard and contact your members of Congress. We depend on your involvement in the legislative process to be effective in Washington. We appreciate your feedback. You can reach me at lallendorf@hospitalmedicine.org.
SHM: BEHIND THE SCENES
Enter text here
Enter text here
Enter text here
What is the best surgical therapy for the secondary prevention of stroke?
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.


Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
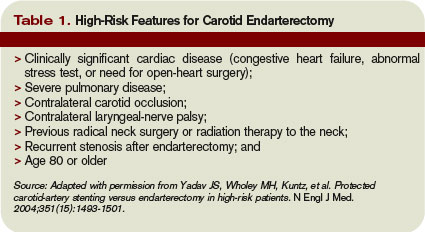
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.
Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.
Case
A 62-year-old obese woman with type 2 diabetes, hypertension, and a pack-a-day smoking habit presents to the emergency department for acute onset of left-side arm and leg weakness and sensory loss on awakening.
She reports taking a baby aspirin daily to “prevent heart attacks.” Her electrocardiogram demonstrates a left bundle branch block and frequent premature atrial contractions. She recovers partially but has residual mild hemiparesis. A duplex carotid ultrasound shows 80% stenosis of the right internal carotid artery.
Overview
In the United States each year approximately 700,000 cerebrovascular accidents (CVA) constitute the largest cause of age-adjusted morbidity of any illness.1 About 200,000 of these strokes are recurrent events.
CVA is the third-leading cause of death. Hospitalists increasingly are responsible for the inpatient care of patients with acute CVA. Atheroembolism from carotid atherosclerosis is the suspected cause for about one in five ischemic strokes.2
The link between carotid stenosis and stroke has been recognized for many years. The first carotid endarterectomy (CEA) was reported more than 50 years ago.3
This targeted review covers the natural history of symptomatic carotid stenosis, the key efficacy trials of CEA and carotid angioplasty and stenting (CAS) among symptomatic patients, and pitfalls for properly diagnosing the severity of carotid stenosis. The medical therapy of carotid stenosis and the secondary prevention of CVA were recently reviewed in The Hospitalist (October 2007, p. 34).
Natural History
The presence or absence of referable neurological symptoms is pivotal to understanding the near-term risk for recurrent CVA related to carotid stenosis. In the absence of symptoms, the risk for future CVA is essentially constant over years.
However, once symptoms occur, the risk for a second event accelerates substantially. Among patients with newly symptomatic carotid stenosis, the risk for another transient ischemic attack (TIA) or stroke within the following 24 months is 26%.4 This risk peaks within the first month or two following the index event, underscoring the time-dependent nature of carotid evaluation and intervention.
Guidelines from the American Heart Association and the American College of Cardiology on the management of ischemic stroke assign early carotid intervention, defined as within two weeks from the index event, a Class 2 indication.5 Hospitalists must rapidly identify the severity of carotid stenosis and make timely referrals to meet this recommended therapeutic window.
Carotid Endarterectomy
CEA is perhaps the best-studied surgical procedure, with multiple well-conducted prospective randomized trials demonstrating its efficacy. The procedure had been performed for hundreds of thousands of patients prior to this data being published in the early 1990s. The North American Symptomatic Carotid Endarterectomy Trial (NASCET) was the landmark study demonstrating the efficacy of intervention. The trial of patients with symptomatic carotid stenosis was stopped early for patients with severe stenosis, defined as 70% to 99% narrowing by conventional angiography. At two years, the rate of ipsilateral stroke or post-operative death in patients with severe stenosis decreased from 26% in the medical arm to 9% in the CEA arm [an absolute risk reduction of 17% and number needed to treat of six (p<0.001)].
Rarely has any medical or surgical procedure had such a robust effect over so short an interval for such an important outcome. Patients with less severe stenosis were followed out to five years, with the final results showing benefit among patients with moderate stenosis (50% to 69%).6 The Veterans Affairs Cooperative Trial 309 and the European Carotid Stenosis Trial (ECST) were combined with NASCET in a pooled analysis of more than 6,000 patients and about 35,000 patient-years of follow-up.7-9
Among patients with 70% or greater stenosis, CEA reduced the absolute five-year risk of ipsilateral ischemic stroke and any operative stroke or death by 16% (95% confidence interval 11.2% to 20.8%). The benefit was less pronounced among patients with 50% to 69% stenosis, in whom CEA conferred a 4.6% (95% confidence interval 0.6% to 8.6%) absolute five-year risk reduction.
The medical aspect of these trials required only the use of aspirin. Intensive lipid control and tight glycemic and blood pressure control would probably reduce the rate of events. The 30-day operative risk was consistently less than 6% across these trials, with the benefit seen by two years among patients with 70% to 99% stenosis and by five years among patients with 50% to 69% stenosis.
Referring hospitalists should know the operative event rates of the surgeons to whom they are referring. Hospitalists should also refer those patients whose anticipated life expectancy is at least two years for patients with 70% to 99% stenosis and at least five years for patients with 50% to 69% stenosis.
Carotid Angioplasty and Stenting
CAS is increasingly used as an alternative to CEA among selected patients. Two procedural developments have improved the safety of percutaneous carotid revascularization.
First, distal embolic protection filters deployed prior to angioplasty collect debris associated with the mechanical intervention and limit the risk of peri-procedural stroke. (See Figures 1 and 2, p. 36.)
Second, the use of self-expanding stents has improved long-term patency over balloon-expanding stents, which can be damaged by neck movement and external pressure.
The Stenting and Angioplasty with [distal embolic] Protection in Patients at High Risk for Endarterectomy trial demonstrated the noninferiority of CAS versus CEA among high-risk patients.10 Inclusion criteria were symptomatic carotid stenosis of greater than 50% or asymptomatic stenosis greater than 80%. Patients had to have one of several high-risk features to be included. (See Table 1, above)
The cumulative incidence of post-operative stroke, myocardial infarction, death, and ipsilateral stroke within one year after the procedure was 20.1% in the CEA arm and 12.2% in the CAS arm (p=0.004 for noninferiority and p=0.053 for superiority). The rate of post-procedural cranial nerve injury was substantially lower (zero) in the CEA arm.
However, among those patients with symptomatic carotid stenosis, the cumulative incidence of the primary endpoint was 16.8% in the CAS arm and 16.5% in the CEA arm. Based upon this trial, CAS has equivalent one-year outcomes versus CEA in a high-risk population.
The Carotid and Vertebral Artery Transluminal Angioplasty Study trial was the first large prospective trial comparing CEA and CAS among symptomatic patients with severe carotid stenosis (mean 86.4% stenosis).11 At 30 days, the rate of death or disabling stroke was 6.4% with CAS and 5.9% with CEA, which were not significantly different in this trial of about 500 patients.
The trial was begun in 1994, with a large portion of angioplasty performed without stents or distal embolic protection. There were fewer local complications but higher rates of restenosis in the CAS arm. The authors noted “no substantial difference in the rate of ipsilateral stroke … up to three years after randomization” but cautioned that the confidence intervals were wide.
Two recently published trials of CAS versus CEA in lower-risk populations do not support the overall safety of CAS among symptomatic patients. The Stent-Protected Angioplasty versus Carotid Endarterectomy trial randomized 1,200 average-risk patients with symptomatic carotid stenosis of 50% or greater by angiography or 70% of greater by ultrasound to either CAS or CEA.12
The trial design stipulated that both surgeons and percutaneous interventionalists perform at least 25 procedures prior to inclusion in the study and that independent quality committees review these procedures. The use of distal embolic protection devices was left to the discretion of the operators. The 30-day rate of death or ipsilateral ischemic stroke was 6.34% in the CEA arm and 6.84% in the CAS arm (p=0.09 for noninferiority).
The investigators concluded that CAS is not non-inferior to CEA (i.e., that CAS is inferior). The Endarterectomy versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial randomized 527 patients with symptomatic carotid stenosis of 70% or greater by angiography or magnetic resonance angiography (MRA) to either CAS or CEA within two weeks of the index event.13
This trial design also stipulated that surgeons had performed at least 25 CEAs in the prior year. Percutaneous interventionalists did not have similar numeric procedure requirements, although the investigators provided for tutoring of less experienced operators. The trial was stopped prematurely due to futility (in terms of noninferiority) and harm within the CAS arm.
The 30-day cumulative incidence of death or any stroke was 3.9% in the CEA arm and 9.6% in the CAS arm (p=0.01 for superiority of CEA). The trial was powered to detect only large differences among low- and high-volume operators. Nearly 10% of patients did not have distal embolic protection devices used during their CAS procedures. Ongoing trials will further define the role of CAS versus CEA in the interventional treatment of carotid stenosis.
Accurate Diagnosis
Different trials used different criteria for defining the percent stenosis of the diseased carotid arterial segment. These differences were based primarily on the mode of testing (i.e., conventional angiography versus ultrasound), and on what portion of the carotid artery was used as the reference or baseline segment to calculate the percent stenosis.
A meta-analysis of various non-invasive modes of testing for carotid stenosis concluded that duplex ultrasound had a pooled sensitivity and specificity of 86% and 87%, respectively, to distinguish 70% to 99% stenosis from less than 70% stenosis.14 MRA had a pooled sensitivity and specificity of 95% and 90%, respectively.
The authors selected trials comparing these non-invasive methods with the gold standard of digital subtraction angiography. Using ultrasonography to first identify patients with at least 50% stenosis, followed by MRA or conventional angiography to more accurately confirm the degree of stenosis has been shown to be cost-effective.15
Back to the Case
For the patient in the vignette, the positive ultrasonography should lead to an MRA or conventional angiography to more precisely determine the percent stenosis. Current guidelines would suggest referring the patient for CEA to be completed within the next two weeks to treat a 50% or greater stenosis. That’s provided the surgeons have an operative morbidity and mortality rate less than 6% and her life expectancy is at least five years. If the patient had high-risk features as listed in Table 1 (left), referral for CAS in the hands of an experienced operator would be an alternative. TH
Dr. Anderson is an assistant professor of medicine at the University of Colorado, Denver, and an associate program director of the internal medicine residency program.
References
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics-2007 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69-e171.
- White H, Boden-Albala B, Wang C, et al. Ischemic stroke subtype incidence among whites, blacks, and Hispanics: the Northern Manhattan Study. Circulation. 2005;111(10):1327-1331.
- Eastcott HH, Pickering GW, Rob CG. Reconstruction of internal carotid artery in a patient with intermittent attacks of hemiplegia. Lancet. 1954;267(6846):994-996.
- Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis: North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med. 1991; 325(7):445-453.
- Sacco RL, Adams R, Albers G, et al. American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention. Circulation. 2006;113:e409-e449.
- North American Symptomatic Carotid Endarterectomy Trialists’ Collaborative Group. The final results of the NASCET trial. N Engl J Med. 1998;339:1415-1425.
- Mayberg MR, Wilson E, Yatsu F, et al. Carotid endarterectomy and prevention of cerebral ischemia in symptomatic carotid stenosis. JAMA. 1991;266:3289-3294.
- European Carotid Surgery Trialists’ Investigators. Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet. 1998;351:1379-1387.
- Rothwell P, Eliasziw M, Gutnikov A, et al. Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361(9352):107-116.
- Yadav JS, Wholey MH, Kuntz, et al. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med. 2004;351(15):1493-1501.
- Endovascular versus surgical treatment in patients with carotid stenosis in the Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS): a randomised trial. Lancet. 2001;357:1729-1737.
- SPACE Collaborative Group. 30-day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised noninferiority trial. Lancet. 2006;368:1239-1247.
- Mas J, Chatellier G, Beyssen B, et al. EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med. 2006;355:1660-1671.
- Nederkoorn PJ, van der Graaf Y, Hunink MG. Duplex ultrasound and magnetic resonance angiography compared with digital subtraction angiography in carotid artery stenosis: a systematic review. Stroke. 2003;34:1324-1332.
- U-King-Im JM, Hollingworth W, Trivedi RA, et al. Cost-effectiveness of diagnostic strategies prior to carotid endarterectomy. Ann Neurol. 2005;58(4):506-515.