User login
The Hospitalist only
LISTEN NOW: Hospitalist Lisa Shieh on Choosing Wisely
Excerpt of our interviews with Choosing Wisely, Lisa Shieh, MD, PhD, of Stanford University School of Medicine, discusses an example of a Choosing Wisely program.
Excerpt of our interviews with Choosing Wisely, Lisa Shieh, MD, PhD, of Stanford University School of Medicine, discusses an example of a Choosing Wisely program.
Excerpt of our interviews with Choosing Wisely, Lisa Shieh, MD, PhD, of Stanford University School of Medicine, discusses an example of a Choosing Wisely program.
LISTEN NOW: Gregory Seymann, MD, on Choosing Wisely
Gregory Seymann, MD, discusses a Choosing Wisely program.
Gregory Seymann, MD, discusses a Choosing Wisely program.
Gregory Seymann, MD, discusses a Choosing Wisely program.
Standard Text Messaging for Smartphones Not HIPAA Compliant

Doctors were the first to begin using pagers and, along with drug dealers, appear to be the last to give them up. But we really need to get rid of them.
Sadly, for the foreseeable future, we will need a pager replacement, but, in the longer term, I’m hopeful that we can:
- Reduce the frequency of electronic interruptions—all forms of interruptions—and the adverse effects that reliably accompany them, and
- Ensure that each interruption has value—that is, reduce or eliminate the many low value and non-urgent messages we all get (e.g. the ones informing you of a lab result you’ve already seen).
Death to the Pager
I can’t imagine anyone who will be more pleased than I will if pagers go the way of now rare hospital-wide PA announcements. Some hospitals have eliminated these announcements entirely, and even critical messages like “code blue” announcements are sent directly to each responder via a pager or other personal device.
Around the time the first iPhone was born, hospital signs banning cell phones began coming down. It seems the fear that they would disrupt hospital electronics, such as telemetry and other monitoring devices, has proven largely unfounded (though, along with things like computer keyboards and stethoscopes, pagers and cell phones can serve as dangerous repositories of bacteria).
Now nearly everyone, from staff to patients, keeps a cell phone with them while in the hospital. I think that is the most important step toward getting rid of pagers. Many doctors already are using the standard text messaging apps that come with the phone to communicate with one another efficiently.
“Regular” Texting Won’t Cut It
Unfortunately, the standard text messaging that comes with every smartphone is not HIPAA compliant. Though I certainly don’t know how anyone would do it, it is apparently too easy for another person to intercept the message. So, if you’re texting information related to your clinical work, you need to make sure it doesn’t include anything that could be considered protected health information. It isn’t enough just to leave the patient’s name off the message. If you’re in the habit of regularly texting doctors, nurses, and other healthcare personnel about patient care, you are at high risk of violating HIPAA, even if you try hard to avoid it.
Another big drawback is that there isn’t a good way to turn off work-related texting when you’re off duty, while leaving your texting app open for communication with your friends and family. Hospital staff will sometimes fail to check whether you’re on duty before texting, and that will lead to your personal time being interrupted by work reminders.
I think these shortcomings mean that none of us should rely on the standard text messaging apps that come with our phones.
But in order for a different app or service to be of any value, we will need to ensure that most providers associated with our hospital are on the same messaging system. That is a tall order, but fortunately there are a lot of companies trying to produce an attractive product that makes it as easy as possible to attract a critical mass of users at your institution.
HIPAA-Compliant Texting Vendors
Many healthcare tech companies provide secure messaging, usually at no additional cost, as an add-on to their main products, such as charge capture software (e.g. IngeniousMed), or physician social networking (e.g. Doximity). Something like 30 companies now offer a dedicated HIPAA-compliant texting option, including IM Your Doc, Voalte, Telmediq, PerfectServe, Vocera, and TigerText. There are so many that it is awfully tough to understand all of their strengths and shortcomings in detail, but I’m having fun trying to do just that. And I anticipate there will be significant consolidation in vendors within the next two to three years.
The dedicated HIPAA-compliant texting services range in price from free for basic features to a monthly fee per user that varies depending on the features you choose to enable. Some offer integration with the hospital’s EHR, which can let a message sender who only knows the patient’s name to see which doctor, nurse, or other caregiver is currently responsible for the patient. Some offer integration with a call schedule and answering service, or even replace an answering service.
No pager replacement will be viable if there are sites in the hospital or elsewhere where it is out of contact; a solution that works on both cellular networks and Wi-Fi is essential. Some vendors offer the ability for messages not delivered to or acknowledged by the recipient to escalate to other forms of delivery after a specified period of time.
I would love to see a feature that I don’t think any vendor offers yet. It would be great if all messages the sender hasn’t marked “stat” or “urgent” first went to a queue in the EHR rather than immediately interrupting the recipient. That way a doctor or other caregiver could see messages while already working in the EHR, rather than glancing at each new message as it arrives, something that all too often needlessly interrupts another important task such as talking with a patient.
And, since most work in EHRs is done in front of a larger device with a full keyboard, it would be easier to type a quick reply message than it would be to rely on a smartphone keyboard for return messaging. Protocols could be established such that messages waiting in the EHR without a reply or dismissal after a specified time would then be sent to the recipient’s personal device.
A Texting Ecosystem
In nearly every case, the hospital will select the text messaging vendor, though hospitalists and nurses, who will typically be among the highest-volume users, should participate in the decision. But the real value of the system hinges on ensuring its wide adoption by most, or nearly all, hospital caregivers and affiliated ambulatory providers.
I would enjoy hearing from those who are already using a HIPAA-secure texting and pager replacement service now, as well as those still researching their options. This has the potential to meaningfully change the way hospitalists and others do their work.

Doctors were the first to begin using pagers and, along with drug dealers, appear to be the last to give them up. But we really need to get rid of them.
Sadly, for the foreseeable future, we will need a pager replacement, but, in the longer term, I’m hopeful that we can:
- Reduce the frequency of electronic interruptions—all forms of interruptions—and the adverse effects that reliably accompany them, and
- Ensure that each interruption has value—that is, reduce or eliminate the many low value and non-urgent messages we all get (e.g. the ones informing you of a lab result you’ve already seen).
Death to the Pager
I can’t imagine anyone who will be more pleased than I will if pagers go the way of now rare hospital-wide PA announcements. Some hospitals have eliminated these announcements entirely, and even critical messages like “code blue” announcements are sent directly to each responder via a pager or other personal device.
Around the time the first iPhone was born, hospital signs banning cell phones began coming down. It seems the fear that they would disrupt hospital electronics, such as telemetry and other monitoring devices, has proven largely unfounded (though, along with things like computer keyboards and stethoscopes, pagers and cell phones can serve as dangerous repositories of bacteria).
Now nearly everyone, from staff to patients, keeps a cell phone with them while in the hospital. I think that is the most important step toward getting rid of pagers. Many doctors already are using the standard text messaging apps that come with the phone to communicate with one another efficiently.
“Regular” Texting Won’t Cut It
Unfortunately, the standard text messaging that comes with every smartphone is not HIPAA compliant. Though I certainly don’t know how anyone would do it, it is apparently too easy for another person to intercept the message. So, if you’re texting information related to your clinical work, you need to make sure it doesn’t include anything that could be considered protected health information. It isn’t enough just to leave the patient’s name off the message. If you’re in the habit of regularly texting doctors, nurses, and other healthcare personnel about patient care, you are at high risk of violating HIPAA, even if you try hard to avoid it.
Another big drawback is that there isn’t a good way to turn off work-related texting when you’re off duty, while leaving your texting app open for communication with your friends and family. Hospital staff will sometimes fail to check whether you’re on duty before texting, and that will lead to your personal time being interrupted by work reminders.
I think these shortcomings mean that none of us should rely on the standard text messaging apps that come with our phones.
But in order for a different app or service to be of any value, we will need to ensure that most providers associated with our hospital are on the same messaging system. That is a tall order, but fortunately there are a lot of companies trying to produce an attractive product that makes it as easy as possible to attract a critical mass of users at your institution.
HIPAA-Compliant Texting Vendors
Many healthcare tech companies provide secure messaging, usually at no additional cost, as an add-on to their main products, such as charge capture software (e.g. IngeniousMed), or physician social networking (e.g. Doximity). Something like 30 companies now offer a dedicated HIPAA-compliant texting option, including IM Your Doc, Voalte, Telmediq, PerfectServe, Vocera, and TigerText. There are so many that it is awfully tough to understand all of their strengths and shortcomings in detail, but I’m having fun trying to do just that. And I anticipate there will be significant consolidation in vendors within the next two to three years.
The dedicated HIPAA-compliant texting services range in price from free for basic features to a monthly fee per user that varies depending on the features you choose to enable. Some offer integration with the hospital’s EHR, which can let a message sender who only knows the patient’s name to see which doctor, nurse, or other caregiver is currently responsible for the patient. Some offer integration with a call schedule and answering service, or even replace an answering service.
No pager replacement will be viable if there are sites in the hospital or elsewhere where it is out of contact; a solution that works on both cellular networks and Wi-Fi is essential. Some vendors offer the ability for messages not delivered to or acknowledged by the recipient to escalate to other forms of delivery after a specified period of time.
I would love to see a feature that I don’t think any vendor offers yet. It would be great if all messages the sender hasn’t marked “stat” or “urgent” first went to a queue in the EHR rather than immediately interrupting the recipient. That way a doctor or other caregiver could see messages while already working in the EHR, rather than glancing at each new message as it arrives, something that all too often needlessly interrupts another important task such as talking with a patient.
And, since most work in EHRs is done in front of a larger device with a full keyboard, it would be easier to type a quick reply message than it would be to rely on a smartphone keyboard for return messaging. Protocols could be established such that messages waiting in the EHR without a reply or dismissal after a specified time would then be sent to the recipient’s personal device.
A Texting Ecosystem
In nearly every case, the hospital will select the text messaging vendor, though hospitalists and nurses, who will typically be among the highest-volume users, should participate in the decision. But the real value of the system hinges on ensuring its wide adoption by most, or nearly all, hospital caregivers and affiliated ambulatory providers.
I would enjoy hearing from those who are already using a HIPAA-secure texting and pager replacement service now, as well as those still researching their options. This has the potential to meaningfully change the way hospitalists and others do their work.
Doctors were the first to begin using pagers and, along with drug dealers, appear to be the last to give them up. But we really need to get rid of them.
Sadly, for the foreseeable future, we will need a pager replacement, but, in the longer term, I’m hopeful that we can:
- Reduce the frequency of electronic interruptions—all forms of interruptions—and the adverse effects that reliably accompany them, and
- Ensure that each interruption has value—that is, reduce or eliminate the many low value and non-urgent messages we all get (e.g. the ones informing you of a lab result you’ve already seen).
Death to the Pager
I can’t imagine anyone who will be more pleased than I will if pagers go the way of now rare hospital-wide PA announcements. Some hospitals have eliminated these announcements entirely, and even critical messages like “code blue” announcements are sent directly to each responder via a pager or other personal device.
Around the time the first iPhone was born, hospital signs banning cell phones began coming down. It seems the fear that they would disrupt hospital electronics, such as telemetry and other monitoring devices, has proven largely unfounded (though, along with things like computer keyboards and stethoscopes, pagers and cell phones can serve as dangerous repositories of bacteria).
Now nearly everyone, from staff to patients, keeps a cell phone with them while in the hospital. I think that is the most important step toward getting rid of pagers. Many doctors already are using the standard text messaging apps that come with the phone to communicate with one another efficiently.
“Regular” Texting Won’t Cut It
Unfortunately, the standard text messaging that comes with every smartphone is not HIPAA compliant. Though I certainly don’t know how anyone would do it, it is apparently too easy for another person to intercept the message. So, if you’re texting information related to your clinical work, you need to make sure it doesn’t include anything that could be considered protected health information. It isn’t enough just to leave the patient’s name off the message. If you’re in the habit of regularly texting doctors, nurses, and other healthcare personnel about patient care, you are at high risk of violating HIPAA, even if you try hard to avoid it.
Another big drawback is that there isn’t a good way to turn off work-related texting when you’re off duty, while leaving your texting app open for communication with your friends and family. Hospital staff will sometimes fail to check whether you’re on duty before texting, and that will lead to your personal time being interrupted by work reminders.
I think these shortcomings mean that none of us should rely on the standard text messaging apps that come with our phones.
But in order for a different app or service to be of any value, we will need to ensure that most providers associated with our hospital are on the same messaging system. That is a tall order, but fortunately there are a lot of companies trying to produce an attractive product that makes it as easy as possible to attract a critical mass of users at your institution.
HIPAA-Compliant Texting Vendors
Many healthcare tech companies provide secure messaging, usually at no additional cost, as an add-on to their main products, such as charge capture software (e.g. IngeniousMed), or physician social networking (e.g. Doximity). Something like 30 companies now offer a dedicated HIPAA-compliant texting option, including IM Your Doc, Voalte, Telmediq, PerfectServe, Vocera, and TigerText. There are so many that it is awfully tough to understand all of their strengths and shortcomings in detail, but I’m having fun trying to do just that. And I anticipate there will be significant consolidation in vendors within the next two to three years.
The dedicated HIPAA-compliant texting services range in price from free for basic features to a monthly fee per user that varies depending on the features you choose to enable. Some offer integration with the hospital’s EHR, which can let a message sender who only knows the patient’s name to see which doctor, nurse, or other caregiver is currently responsible for the patient. Some offer integration with a call schedule and answering service, or even replace an answering service.
No pager replacement will be viable if there are sites in the hospital or elsewhere where it is out of contact; a solution that works on both cellular networks and Wi-Fi is essential. Some vendors offer the ability for messages not delivered to or acknowledged by the recipient to escalate to other forms of delivery after a specified period of time.
I would love to see a feature that I don’t think any vendor offers yet. It would be great if all messages the sender hasn’t marked “stat” or “urgent” first went to a queue in the EHR rather than immediately interrupting the recipient. That way a doctor or other caregiver could see messages while already working in the EHR, rather than glancing at each new message as it arrives, something that all too often needlessly interrupts another important task such as talking with a patient.
And, since most work in EHRs is done in front of a larger device with a full keyboard, it would be easier to type a quick reply message than it would be to rely on a smartphone keyboard for return messaging. Protocols could be established such that messages waiting in the EHR without a reply or dismissal after a specified time would then be sent to the recipient’s personal device.
A Texting Ecosystem
In nearly every case, the hospital will select the text messaging vendor, though hospitalists and nurses, who will typically be among the highest-volume users, should participate in the decision. But the real value of the system hinges on ensuring its wide adoption by most, or nearly all, hospital caregivers and affiliated ambulatory providers.
I would enjoy hearing from those who are already using a HIPAA-secure texting and pager replacement service now, as well as those still researching their options. This has the potential to meaningfully change the way hospitalists and others do their work.
Hospitals with Hotel-Like Amenities Don’t Improve Satisfaction Scores
Hospital design may not contribute to patients’ satisfaction with the care given by their hospital professionals, according to new research from Johns Hopkins Hospital in Baltimore, published in the Journal of Hospital Medicine. Newly built hospitals often emphasize patient-centered features like reduced noise, natural light, visitor-friendly facilities, well-designed rooms, and hotel-like amenities, note the authors, led by Zishan Siddiqui, MD, attending physician and assistant professor of medicine at Johns Hopkins.
When Hopkins moved a number of its hospital units to the sleek new Sheikh Zayed Tower in 2012, researchers used a pre-post design experiment to compare patient satisfaction in the newer, more pleasing surroundings via Press Ganey and HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) survey scores. Patients responded positively to the new environment, with significant improvement in facility-related satisfaction, but were able to distinguish that satisfaction from their ratings of their doctors and nurses, which were not impacted by the new environment.
“It is more likely that provider-level interventions will have a greater impact on provider level and overall satisfaction,” the authors conclude. “Hospital administrators should not use outdated facilities as an excuse for suboptimal provider satisfaction scores.”
Hospital design may not contribute to patients’ satisfaction with the care given by their hospital professionals, according to new research from Johns Hopkins Hospital in Baltimore, published in the Journal of Hospital Medicine. Newly built hospitals often emphasize patient-centered features like reduced noise, natural light, visitor-friendly facilities, well-designed rooms, and hotel-like amenities, note the authors, led by Zishan Siddiqui, MD, attending physician and assistant professor of medicine at Johns Hopkins.
When Hopkins moved a number of its hospital units to the sleek new Sheikh Zayed Tower in 2012, researchers used a pre-post design experiment to compare patient satisfaction in the newer, more pleasing surroundings via Press Ganey and HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) survey scores. Patients responded positively to the new environment, with significant improvement in facility-related satisfaction, but were able to distinguish that satisfaction from their ratings of their doctors and nurses, which were not impacted by the new environment.
“It is more likely that provider-level interventions will have a greater impact on provider level and overall satisfaction,” the authors conclude. “Hospital administrators should not use outdated facilities as an excuse for suboptimal provider satisfaction scores.”
Hospital design may not contribute to patients’ satisfaction with the care given by their hospital professionals, according to new research from Johns Hopkins Hospital in Baltimore, published in the Journal of Hospital Medicine. Newly built hospitals often emphasize patient-centered features like reduced noise, natural light, visitor-friendly facilities, well-designed rooms, and hotel-like amenities, note the authors, led by Zishan Siddiqui, MD, attending physician and assistant professor of medicine at Johns Hopkins.
When Hopkins moved a number of its hospital units to the sleek new Sheikh Zayed Tower in 2012, researchers used a pre-post design experiment to compare patient satisfaction in the newer, more pleasing surroundings via Press Ganey and HCAHPS (Hospital Consumer Assessment of Healthcare Providers and Systems) survey scores. Patients responded positively to the new environment, with significant improvement in facility-related satisfaction, but were able to distinguish that satisfaction from their ratings of their doctors and nurses, which were not impacted by the new environment.
“It is more likely that provider-level interventions will have a greater impact on provider level and overall satisfaction,” the authors conclude. “Hospital administrators should not use outdated facilities as an excuse for suboptimal provider satisfaction scores.”
Hospitalists Should Make Commitment to Improve Healthcare Safety

Peter Pronovost, MD, PhD, FCCM, knows how to deliver a great talk. It is no wonder he is highly sought after and was asked to speak at the plenary for SHM’s annual meeting. Dr. Pronovost, also known as the “Checklist Doctor,” knows how to combine just the right amount of sadness, inspiration, and humor to make his audience feel motivated and compelled to DO something. And, in fact, he implores you—DO something.
Most of us feel excited and inspired during the annual meeting. But those feelings serve little purpose unless we translate them into actions that will make the medical industry a better place for clinicians to work and for patients to receive care. As Dr. Pronovost said, “We are the only hope that the healthcare system has of improving quality and safety.”
He was inspired years ago by the watershed event that will forever be imprinted upon Johns Hopkins Hospital in Baltimore, the preventable death of 18-month-old Josie King on Feb. 22, 2001. Years after the event, her mother, Sorrel King, a passionate patient safety advocate, wanted to know if hospitals are any safer than they were the day that Josie died. She wanted to know what patient safety experts at Hopkins had done to ensure there would not be another Josie King story.
Patients and their families consistently voice similar desires after they have suffered preventable harm. They want to know what happened, why it happened, what it means for them, and what will be done to prevent it from happening again.1 The latter question is one I am frequently asked by patients and their families at my hospital. “What are you going to do to make sure this does not happen again?”
I would venture to guess most hospitalists have been responsible for some type of preventable patient harm during their careers. We work in complex, high-volume, unpredictable, and continuously changing environments. Many of the patients and families in our care are new to us and are with us for only short periods of time. Those of us who have been responsible for preventable patient harm know that it is an unforgettable moment in time that can weigh upon your conscious. And, of course, we all want to do something to make sure it does not happen again.
That is exactly what patients and their families expect of all of us—to DO something—and they should.
But this can be an overwhelming responsibility, especially when the root causes of harm are difficult either to identify or to fix—such as a miscommunication, a diagnostic error, or an inadequate handoff.
Which gets me back to Dr. Pronovost giving a great talk. His appeal to our audience of about 3,000 hospitalists was to DO something. To make the healthcare system improve quality and safety for future patients. To not wait until we or our colleagues are involved in a preventable harm event. To do something, anything, now, that contributes to safer care, today and every day going forward.
He ended his talk with “I will….” Dr. Pronovost (and I would venture to guess patients and their families) wants each of us to fill in the blank with a statement of personal accountability for action. Unfortunately, many of us still believe that we are personally unable to make complex systems safer for patients. Many of us still believe that patients and the systems they traverse are too complex, unpredictable, unreliable, or noncompliant.
The truth is, patients and systems are indeed complex, unpredictable, unreliable, and noncompliant. The further truth is, the only way to make care safer is for each of us to start with a collective shared mental model that we can make it better—and for each of us to commit to personal accountability for action.
My “I Will”
So, while I really enjoyed Dr. Pronovost’s talk, what I enjoyed even more was reading the section in last month’s edition of The Hospitalist in which about a half dozen hospitalists interviewed after the plenary accepted the challenge of filling in the blank “I will….” A few excerpts:
- “I will let them know that everything is possible…”
- “I will improve healthcare…”
- “[I will] make sure the patient is heard…”
By a simple proclamation of personal accountability, a mere thousand hospitalists attending an annual meeting can collectively and progressively change the safety of healthcare in thousands of hospitals around the country. It starts with thinking we can do it and publicly committing to the journey. Although we are still a relatively new specialty, we have permeated almost every hospital in the country, and we have outpaced the growth of any specialty in the history of modern medicine. We are perfectly poised to be the safety change agents for every hospital system. As Margaret Meade famously said, “Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it’s the only thing that ever has….”
So don’t delay. Whether or not you had the good fortune of being inspired at the SHM annual meeting, each of us owes it to our patients to commit to improving the safety of healthcare and paving the future of hospital care. Get out your pen, craft a commitment now, follow through with it, and make hospitals safer tomorrow than they were yesterday.
I will…

Reference
- Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA. 2003;289(8):1001-1007.
Peter Pronovost, MD, PhD, FCCM, knows how to deliver a great talk. It is no wonder he is highly sought after and was asked to speak at the plenary for SHM’s annual meeting. Dr. Pronovost, also known as the “Checklist Doctor,” knows how to combine just the right amount of sadness, inspiration, and humor to make his audience feel motivated and compelled to DO something. And, in fact, he implores you—DO something.
Most of us feel excited and inspired during the annual meeting. But those feelings serve little purpose unless we translate them into actions that will make the medical industry a better place for clinicians to work and for patients to receive care. As Dr. Pronovost said, “We are the only hope that the healthcare system has of improving quality and safety.”
He was inspired years ago by the watershed event that will forever be imprinted upon Johns Hopkins Hospital in Baltimore, the preventable death of 18-month-old Josie King on Feb. 22, 2001. Years after the event, her mother, Sorrel King, a passionate patient safety advocate, wanted to know if hospitals are any safer than they were the day that Josie died. She wanted to know what patient safety experts at Hopkins had done to ensure there would not be another Josie King story.
Patients and their families consistently voice similar desires after they have suffered preventable harm. They want to know what happened, why it happened, what it means for them, and what will be done to prevent it from happening again.1 The latter question is one I am frequently asked by patients and their families at my hospital. “What are you going to do to make sure this does not happen again?”
I would venture to guess most hospitalists have been responsible for some type of preventable patient harm during their careers. We work in complex, high-volume, unpredictable, and continuously changing environments. Many of the patients and families in our care are new to us and are with us for only short periods of time. Those of us who have been responsible for preventable patient harm know that it is an unforgettable moment in time that can weigh upon your conscious. And, of course, we all want to do something to make sure it does not happen again.
That is exactly what patients and their families expect of all of us—to DO something—and they should.
But this can be an overwhelming responsibility, especially when the root causes of harm are difficult either to identify or to fix—such as a miscommunication, a diagnostic error, or an inadequate handoff.
Which gets me back to Dr. Pronovost giving a great talk. His appeal to our audience of about 3,000 hospitalists was to DO something. To make the healthcare system improve quality and safety for future patients. To not wait until we or our colleagues are involved in a preventable harm event. To do something, anything, now, that contributes to safer care, today and every day going forward.
He ended his talk with “I will….” Dr. Pronovost (and I would venture to guess patients and their families) wants each of us to fill in the blank with a statement of personal accountability for action. Unfortunately, many of us still believe that we are personally unable to make complex systems safer for patients. Many of us still believe that patients and the systems they traverse are too complex, unpredictable, unreliable, or noncompliant.
The truth is, patients and systems are indeed complex, unpredictable, unreliable, and noncompliant. The further truth is, the only way to make care safer is for each of us to start with a collective shared mental model that we can make it better—and for each of us to commit to personal accountability for action.
My “I Will”
So, while I really enjoyed Dr. Pronovost’s talk, what I enjoyed even more was reading the section in last month’s edition of The Hospitalist in which about a half dozen hospitalists interviewed after the plenary accepted the challenge of filling in the blank “I will….” A few excerpts:
- “I will let them know that everything is possible…”
- “I will improve healthcare…”
- “[I will] make sure the patient is heard…”
By a simple proclamation of personal accountability, a mere thousand hospitalists attending an annual meeting can collectively and progressively change the safety of healthcare in thousands of hospitals around the country. It starts with thinking we can do it and publicly committing to the journey. Although we are still a relatively new specialty, we have permeated almost every hospital in the country, and we have outpaced the growth of any specialty in the history of modern medicine. We are perfectly poised to be the safety change agents for every hospital system. As Margaret Meade famously said, “Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it’s the only thing that ever has….”
So don’t delay. Whether or not you had the good fortune of being inspired at the SHM annual meeting, each of us owes it to our patients to commit to improving the safety of healthcare and paving the future of hospital care. Get out your pen, craft a commitment now, follow through with it, and make hospitals safer tomorrow than they were yesterday.
I will…
Reference
- Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA. 2003;289(8):1001-1007.
Peter Pronovost, MD, PhD, FCCM, knows how to deliver a great talk. It is no wonder he is highly sought after and was asked to speak at the plenary for SHM’s annual meeting. Dr. Pronovost, also known as the “Checklist Doctor,” knows how to combine just the right amount of sadness, inspiration, and humor to make his audience feel motivated and compelled to DO something. And, in fact, he implores you—DO something.
Most of us feel excited and inspired during the annual meeting. But those feelings serve little purpose unless we translate them into actions that will make the medical industry a better place for clinicians to work and for patients to receive care. As Dr. Pronovost said, “We are the only hope that the healthcare system has of improving quality and safety.”
He was inspired years ago by the watershed event that will forever be imprinted upon Johns Hopkins Hospital in Baltimore, the preventable death of 18-month-old Josie King on Feb. 22, 2001. Years after the event, her mother, Sorrel King, a passionate patient safety advocate, wanted to know if hospitals are any safer than they were the day that Josie died. She wanted to know what patient safety experts at Hopkins had done to ensure there would not be another Josie King story.
Patients and their families consistently voice similar desires after they have suffered preventable harm. They want to know what happened, why it happened, what it means for them, and what will be done to prevent it from happening again.1 The latter question is one I am frequently asked by patients and their families at my hospital. “What are you going to do to make sure this does not happen again?”
I would venture to guess most hospitalists have been responsible for some type of preventable patient harm during their careers. We work in complex, high-volume, unpredictable, and continuously changing environments. Many of the patients and families in our care are new to us and are with us for only short periods of time. Those of us who have been responsible for preventable patient harm know that it is an unforgettable moment in time that can weigh upon your conscious. And, of course, we all want to do something to make sure it does not happen again.
That is exactly what patients and their families expect of all of us—to DO something—and they should.
But this can be an overwhelming responsibility, especially when the root causes of harm are difficult either to identify or to fix—such as a miscommunication, a diagnostic error, or an inadequate handoff.
Which gets me back to Dr. Pronovost giving a great talk. His appeal to our audience of about 3,000 hospitalists was to DO something. To make the healthcare system improve quality and safety for future patients. To not wait until we or our colleagues are involved in a preventable harm event. To do something, anything, now, that contributes to safer care, today and every day going forward.
He ended his talk with “I will….” Dr. Pronovost (and I would venture to guess patients and their families) wants each of us to fill in the blank with a statement of personal accountability for action. Unfortunately, many of us still believe that we are personally unable to make complex systems safer for patients. Many of us still believe that patients and the systems they traverse are too complex, unpredictable, unreliable, or noncompliant.
The truth is, patients and systems are indeed complex, unpredictable, unreliable, and noncompliant. The further truth is, the only way to make care safer is for each of us to start with a collective shared mental model that we can make it better—and for each of us to commit to personal accountability for action.
My “I Will”
So, while I really enjoyed Dr. Pronovost’s talk, what I enjoyed even more was reading the section in last month’s edition of The Hospitalist in which about a half dozen hospitalists interviewed after the plenary accepted the challenge of filling in the blank “I will….” A few excerpts:
- “I will let them know that everything is possible…”
- “I will improve healthcare…”
- “[I will] make sure the patient is heard…”
By a simple proclamation of personal accountability, a mere thousand hospitalists attending an annual meeting can collectively and progressively change the safety of healthcare in thousands of hospitals around the country. It starts with thinking we can do it and publicly committing to the journey. Although we are still a relatively new specialty, we have permeated almost every hospital in the country, and we have outpaced the growth of any specialty in the history of modern medicine. We are perfectly poised to be the safety change agents for every hospital system. As Margaret Meade famously said, “Never doubt that a small group of thoughtful, committed citizens can change the world; indeed, it’s the only thing that ever has….”
So don’t delay. Whether or not you had the good fortune of being inspired at the SHM annual meeting, each of us owes it to our patients to commit to improving the safety of healthcare and paving the future of hospital care. Get out your pen, craft a commitment now, follow through with it, and make hospitals safer tomorrow than they were yesterday.
I will…
Reference
- Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and physicians’ attitudes regarding the disclosure of medical errors. JAMA. 2003;289(8):1001-1007.
To Battle Burnout, Jerome C. Siy, MD, CHIE, SFHM, Instructs Hospitalist Leaders to Engage, Communicate, and Create a “Culture”
Studies show nearly one in three hospitalists will experience long-term exhaustion or diminished interest in their work.1 Burned out physicians have low empathy, don’t communicate well, and provide poor quality of care. Not only does burnout lower quality of care, it is also costly and affects physicians’ personal lives. Unfortunately, despite more than a decade of research and effort to improve burnout, there seems to be no secret formula.
“We see burnout in our quality metrics. We see it in increased medical errors. Patient compliance can be tied to burnout and poor patient satisfaction, as well,” said Jerome C. Siy, MD, CHIE, SFHM, during his HM15 session last month at the Gaylord National Resort and Conference Center in National Harbor, Md. “What is really important to understand is that burnout results in high turnover and early retirement. Conservative estimates tell us a burned out physician can cost the hospital system $250,000.”
Dr. Siy’s talk, “Preventing Hospitalist Burnout through Engagement,” went beyond the basics of burnout (higher rates of substance abuse, depression, suicidal ideation, and family conflicts) and explored the systematic reasons for its occurrence in hospital medicine. The 2009 winner of SHM’s Award for Clinical Excellence also outlined a handful of ways HM groups can engage and combat burnout.
“What is interesting is that the rate that our profession has burnout is inversely proportional to the rate of the U.S. general population,” said Dr. Siy, assistant professor of medicine at the University of Minnesota Medical School and department head of hospital medicine at HealthPartners Medical Group in Minneapolis. “In the general U.S. population, the higher your level of education, the lower the rates of burnout. And yet we, physicians, have a remarkably high rate of burnout compared with those at our education level.
“And when they broke it out by specialty, it was front-line physicians that have the highest rates of burnout.”
Dr. Siy says burnout is partly the fault of the “system,” in terms of workload and performance pressures. His hospitalist group has implemented mindfulness training with a guru and empathy training with age simulators. They employ geographic-based teams and bedside rounds with nursing. They’ve even hired scribes on the observation unit.
“Not only are we trying to address burnout from the individual physician perspective, but we’re trying to address the causes of burnout,” he says.
Dr. Siy also showed attendees a video on engagement by best-selling author Daniel Pink. The three factors Pink believes lead to better performance and personal satisfaction are autonomy, mastery, purpose. And Pink encourages business leaders to “take compensation off the table.”
“He talks about how compensation is important and drives things, but actually, if you are fair with your compensation, it no longer incents your workforce,” Dr. Siy reiterates. “So if compensation is a big issue for you, you should know that.”
Most important, he says, “It’s about creating a culture.” He provided this list of ways to engage hospitalists:
- Add a measure of physician engagement to your scorecard;
- Translate engagement data by having presence in the workspace, even when off service;
- Employ individualized and group time to provide feedback and mentoring, develop relationships, learn new skills, and grow;
- Have physicians lead and partner in quality improvement efforts;
- Have regular, formal meetings with opportunities for open discussion;
- Incorporate professional development into your culture;
- Develop a common sense of purpose inside and outside of the hospital; and
- Structure compensation to reflect your values.
“Everyone in your group has to have an opportunity to grow,” he says. “They need to know that you, the group leaders … and the system care about them.” TH
Reference
1. Hinami K, Whelan CT, Miller JA, Wolosin RJ, Wetterneck TB, Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402-410.
Studies show nearly one in three hospitalists will experience long-term exhaustion or diminished interest in their work.1 Burned out physicians have low empathy, don’t communicate well, and provide poor quality of care. Not only does burnout lower quality of care, it is also costly and affects physicians’ personal lives. Unfortunately, despite more than a decade of research and effort to improve burnout, there seems to be no secret formula.
“We see burnout in our quality metrics. We see it in increased medical errors. Patient compliance can be tied to burnout and poor patient satisfaction, as well,” said Jerome C. Siy, MD, CHIE, SFHM, during his HM15 session last month at the Gaylord National Resort and Conference Center in National Harbor, Md. “What is really important to understand is that burnout results in high turnover and early retirement. Conservative estimates tell us a burned out physician can cost the hospital system $250,000.”
Dr. Siy’s talk, “Preventing Hospitalist Burnout through Engagement,” went beyond the basics of burnout (higher rates of substance abuse, depression, suicidal ideation, and family conflicts) and explored the systematic reasons for its occurrence in hospital medicine. The 2009 winner of SHM’s Award for Clinical Excellence also outlined a handful of ways HM groups can engage and combat burnout.
“What is interesting is that the rate that our profession has burnout is inversely proportional to the rate of the U.S. general population,” said Dr. Siy, assistant professor of medicine at the University of Minnesota Medical School and department head of hospital medicine at HealthPartners Medical Group in Minneapolis. “In the general U.S. population, the higher your level of education, the lower the rates of burnout. And yet we, physicians, have a remarkably high rate of burnout compared with those at our education level.
“And when they broke it out by specialty, it was front-line physicians that have the highest rates of burnout.”
Dr. Siy says burnout is partly the fault of the “system,” in terms of workload and performance pressures. His hospitalist group has implemented mindfulness training with a guru and empathy training with age simulators. They employ geographic-based teams and bedside rounds with nursing. They’ve even hired scribes on the observation unit.
“Not only are we trying to address burnout from the individual physician perspective, but we’re trying to address the causes of burnout,” he says.
Dr. Siy also showed attendees a video on engagement by best-selling author Daniel Pink. The three factors Pink believes lead to better performance and personal satisfaction are autonomy, mastery, purpose. And Pink encourages business leaders to “take compensation off the table.”
“He talks about how compensation is important and drives things, but actually, if you are fair with your compensation, it no longer incents your workforce,” Dr. Siy reiterates. “So if compensation is a big issue for you, you should know that.”
Most important, he says, “It’s about creating a culture.” He provided this list of ways to engage hospitalists:
- Add a measure of physician engagement to your scorecard;
- Translate engagement data by having presence in the workspace, even when off service;
- Employ individualized and group time to provide feedback and mentoring, develop relationships, learn new skills, and grow;
- Have physicians lead and partner in quality improvement efforts;
- Have regular, formal meetings with opportunities for open discussion;
- Incorporate professional development into your culture;
- Develop a common sense of purpose inside and outside of the hospital; and
- Structure compensation to reflect your values.
“Everyone in your group has to have an opportunity to grow,” he says. “They need to know that you, the group leaders … and the system care about them.” TH
Reference
1. Hinami K, Whelan CT, Miller JA, Wolosin RJ, Wetterneck TB, Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402-410.
Studies show nearly one in three hospitalists will experience long-term exhaustion or diminished interest in their work.1 Burned out physicians have low empathy, don’t communicate well, and provide poor quality of care. Not only does burnout lower quality of care, it is also costly and affects physicians’ personal lives. Unfortunately, despite more than a decade of research and effort to improve burnout, there seems to be no secret formula.
“We see burnout in our quality metrics. We see it in increased medical errors. Patient compliance can be tied to burnout and poor patient satisfaction, as well,” said Jerome C. Siy, MD, CHIE, SFHM, during his HM15 session last month at the Gaylord National Resort and Conference Center in National Harbor, Md. “What is really important to understand is that burnout results in high turnover and early retirement. Conservative estimates tell us a burned out physician can cost the hospital system $250,000.”
Dr. Siy’s talk, “Preventing Hospitalist Burnout through Engagement,” went beyond the basics of burnout (higher rates of substance abuse, depression, suicidal ideation, and family conflicts) and explored the systematic reasons for its occurrence in hospital medicine. The 2009 winner of SHM’s Award for Clinical Excellence also outlined a handful of ways HM groups can engage and combat burnout.
“What is interesting is that the rate that our profession has burnout is inversely proportional to the rate of the U.S. general population,” said Dr. Siy, assistant professor of medicine at the University of Minnesota Medical School and department head of hospital medicine at HealthPartners Medical Group in Minneapolis. “In the general U.S. population, the higher your level of education, the lower the rates of burnout. And yet we, physicians, have a remarkably high rate of burnout compared with those at our education level.
“And when they broke it out by specialty, it was front-line physicians that have the highest rates of burnout.”
Dr. Siy says burnout is partly the fault of the “system,” in terms of workload and performance pressures. His hospitalist group has implemented mindfulness training with a guru and empathy training with age simulators. They employ geographic-based teams and bedside rounds with nursing. They’ve even hired scribes on the observation unit.
“Not only are we trying to address burnout from the individual physician perspective, but we’re trying to address the causes of burnout,” he says.
Dr. Siy also showed attendees a video on engagement by best-selling author Daniel Pink. The three factors Pink believes lead to better performance and personal satisfaction are autonomy, mastery, purpose. And Pink encourages business leaders to “take compensation off the table.”
“He talks about how compensation is important and drives things, but actually, if you are fair with your compensation, it no longer incents your workforce,” Dr. Siy reiterates. “So if compensation is a big issue for you, you should know that.”
Most important, he says, “It’s about creating a culture.” He provided this list of ways to engage hospitalists:
- Add a measure of physician engagement to your scorecard;
- Translate engagement data by having presence in the workspace, even when off service;
- Employ individualized and group time to provide feedback and mentoring, develop relationships, learn new skills, and grow;
- Have physicians lead and partner in quality improvement efforts;
- Have regular, formal meetings with opportunities for open discussion;
- Incorporate professional development into your culture;
- Develop a common sense of purpose inside and outside of the hospital; and
- Structure compensation to reflect your values.
“Everyone in your group has to have an opportunity to grow,” he says. “They need to know that you, the group leaders … and the system care about them.” TH
Reference
1. Hinami K, Whelan CT, Miller JA, Wolosin RJ, Wetterneck TB, Society of Hospital Medicine Career Satisfaction Task Force. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402-410.
HM15 Offers Hospitalist Leaders Training, Encouragement
NATIONAL HARBOR, Md.—Patient satisfaction, physician engagement, and administrator buy-in, oh my.
So went the thoughts of Jaidev Bhoopal, MD, last month at HM15. He’d been a hospitalist for about eight years, but he was named section chair about a month before he arrived at the annual meeting. His calculated first stop was the daylong practice management pre-course titled “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform.”
The timing couldn’t have been better.

“I’m starting a new role and I wanted to get input and ideas,” said Dr. Bhoopal, section chair of the hospitalist department at St. Mary’s Medical Center in Duluth, Minn. “This gives you a playbook of where you want to be and where you want to go.”
A playbook for where to go could just as well be the slogan for practice management’s role at SHM’s annual meeting. An educational track, a dedicated—and ever-popular—pre-course, and a chance to ask the field’s founding fathers their best practices were among the highlights of this spring’s four-day confab.
The need for practice management and leadership training is greater in the past few years as hospitalists have been more confounded than ever with how to best run their practices under a myriad of new rules and regulations tied to the Affordable Care Act and the digitization of healthcare. At their core, the changes are shifting hospital-based care from fee-for-service to value-based payments.
“The tipping point is really here for us,” said Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners of Darien, Conn.

Dr. Whitcomb, a founder of SHM and regular columnist for The Hospitalist, said that HM group (HMG) leaders have to be well versed in how to navigate a landscape of alternative payment models to excel in the new paradigm. Particularly after the announcement earlier this year that the federal government has set a goal of tying 85% of Medicare hospital fee-for-service payments to quality or value by 2016, and that percentage could increase to 90% by 2018. The January announcement was the first time in Medicare’s history that explicit goals for alternative payment models and value-based payments were set, according to an announcement from the U.S. Department of Health and Human Services.
“Strategically, these things are essential to work into the plan of what the hospital medicine group is doing in the coming three to five years,” Dr. Whitcomb said. “Hospitalists can’t do this alone. They have to do it with teams. It’s not only teams of other professionals in the hospital and around the hospital, but it’s other physicians.”
Dr. Whitcomb said key to the new paradigm is shared financial and clinical responsibilities. He says hospitalists have to “change our thinking…to a mindset where we’re in this together.”
Part of that shared responsibility extends to the post-acute care setting, where SHM senior vice president for practice management Joseph Miller said that some 30% of HMGs are practicing. To help those practitioners, SHM and IPC Healthcare of North Hollywood, Calif., debuted the “Primer for Hospitalists on Skilled Nursing Facilities” at HM15.
The educational program, housed at SHM’s Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post-acute care facilities. It is grouped in five sections and two modules, with a focus on skilled-nursing facilities (SNFs), which are the most common post-acute care settings.
“The types of resources that are available are different, and that’s not only in terms of staff, but the availability of specialists, the availability of testing capabilities,” Miller said. “If you need to work with a cardiologist for a particular patient...how do you engage them? You’re not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?”
Another communication hassle involves the growing number of HMGs spread over multiple sites. For Sara Shraibman, MD, an assistant program director at Syosset Hospital in Syosset, N.Y., those sites are two hospitals covered by the North Shore LIJ Medical Group.
“It’s actually a new program, so we are trying to look at our compensation, models comparing them across two hospitals…and how we manage,” she said. “Not every hospitalist will go back and forth. Some will, some won’t. Some will work nights to help cover, some won’t. It’s very interesting trying to come up with a schedule.”
The best way to address conflict at multi-site groups is communicating and focusing on shared goals, said David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., and a new member of Team Hospitalist.
“Make sure that no matter what conflict might be up front, that everybody is looking at the goals downstream and saying, ‘Yes, that is a goal we want to achieve. We want to have better patient safety metrics. We want to have decreased readmissions. We want to have better transitions of care,’” Dr. Weidig said. “The common goal all the way from hospital administrators all the way down to hospital physicians is going to be the key.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—Patient satisfaction, physician engagement, and administrator buy-in, oh my.
So went the thoughts of Jaidev Bhoopal, MD, last month at HM15. He’d been a hospitalist for about eight years, but he was named section chair about a month before he arrived at the annual meeting. His calculated first stop was the daylong practice management pre-course titled “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform.”
The timing couldn’t have been better.
“I’m starting a new role and I wanted to get input and ideas,” said Dr. Bhoopal, section chair of the hospitalist department at St. Mary’s Medical Center in Duluth, Minn. “This gives you a playbook of where you want to be and where you want to go.”
A playbook for where to go could just as well be the slogan for practice management’s role at SHM’s annual meeting. An educational track, a dedicated—and ever-popular—pre-course, and a chance to ask the field’s founding fathers their best practices were among the highlights of this spring’s four-day confab.
The need for practice management and leadership training is greater in the past few years as hospitalists have been more confounded than ever with how to best run their practices under a myriad of new rules and regulations tied to the Affordable Care Act and the digitization of healthcare. At their core, the changes are shifting hospital-based care from fee-for-service to value-based payments.
“The tipping point is really here for us,” said Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners of Darien, Conn.
Dr. Whitcomb, a founder of SHM and regular columnist for The Hospitalist, said that HM group (HMG) leaders have to be well versed in how to navigate a landscape of alternative payment models to excel in the new paradigm. Particularly after the announcement earlier this year that the federal government has set a goal of tying 85% of Medicare hospital fee-for-service payments to quality or value by 2016, and that percentage could increase to 90% by 2018. The January announcement was the first time in Medicare’s history that explicit goals for alternative payment models and value-based payments were set, according to an announcement from the U.S. Department of Health and Human Services.
“Strategically, these things are essential to work into the plan of what the hospital medicine group is doing in the coming three to five years,” Dr. Whitcomb said. “Hospitalists can’t do this alone. They have to do it with teams. It’s not only teams of other professionals in the hospital and around the hospital, but it’s other physicians.”
Dr. Whitcomb said key to the new paradigm is shared financial and clinical responsibilities. He says hospitalists have to “change our thinking…to a mindset where we’re in this together.”
Part of that shared responsibility extends to the post-acute care setting, where SHM senior vice president for practice management Joseph Miller said that some 30% of HMGs are practicing. To help those practitioners, SHM and IPC Healthcare of North Hollywood, Calif., debuted the “Primer for Hospitalists on Skilled Nursing Facilities” at HM15.
The educational program, housed at SHM’s Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post-acute care facilities. It is grouped in five sections and two modules, with a focus on skilled-nursing facilities (SNFs), which are the most common post-acute care settings.
“The types of resources that are available are different, and that’s not only in terms of staff, but the availability of specialists, the availability of testing capabilities,” Miller said. “If you need to work with a cardiologist for a particular patient...how do you engage them? You’re not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?”
Another communication hassle involves the growing number of HMGs spread over multiple sites. For Sara Shraibman, MD, an assistant program director at Syosset Hospital in Syosset, N.Y., those sites are two hospitals covered by the North Shore LIJ Medical Group.
“It’s actually a new program, so we are trying to look at our compensation, models comparing them across two hospitals…and how we manage,” she said. “Not every hospitalist will go back and forth. Some will, some won’t. Some will work nights to help cover, some won’t. It’s very interesting trying to come up with a schedule.”
The best way to address conflict at multi-site groups is communicating and focusing on shared goals, said David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., and a new member of Team Hospitalist.
“Make sure that no matter what conflict might be up front, that everybody is looking at the goals downstream and saying, ‘Yes, that is a goal we want to achieve. We want to have better patient safety metrics. We want to have decreased readmissions. We want to have better transitions of care,’” Dr. Weidig said. “The common goal all the way from hospital administrators all the way down to hospital physicians is going to be the key.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—Patient satisfaction, physician engagement, and administrator buy-in, oh my.
So went the thoughts of Jaidev Bhoopal, MD, last month at HM15. He’d been a hospitalist for about eight years, but he was named section chair about a month before he arrived at the annual meeting. His calculated first stop was the daylong practice management pre-course titled “Where the Rubber Meets the Road: Managing in the Era of Healthcare Reform.”
The timing couldn’t have been better.
“I’m starting a new role and I wanted to get input and ideas,” said Dr. Bhoopal, section chair of the hospitalist department at St. Mary’s Medical Center in Duluth, Minn. “This gives you a playbook of where you want to be and where you want to go.”
A playbook for where to go could just as well be the slogan for practice management’s role at SHM’s annual meeting. An educational track, a dedicated—and ever-popular—pre-course, and a chance to ask the field’s founding fathers their best practices were among the highlights of this spring’s four-day confab.
The need for practice management and leadership training is greater in the past few years as hospitalists have been more confounded than ever with how to best run their practices under a myriad of new rules and regulations tied to the Affordable Care Act and the digitization of healthcare. At their core, the changes are shifting hospital-based care from fee-for-service to value-based payments.
“The tipping point is really here for us,” said Win Whitcomb, MD, MHM, chief medical officer of Remedy Partners of Darien, Conn.
Dr. Whitcomb, a founder of SHM and regular columnist for The Hospitalist, said that HM group (HMG) leaders have to be well versed in how to navigate a landscape of alternative payment models to excel in the new paradigm. Particularly after the announcement earlier this year that the federal government has set a goal of tying 85% of Medicare hospital fee-for-service payments to quality or value by 2016, and that percentage could increase to 90% by 2018. The January announcement was the first time in Medicare’s history that explicit goals for alternative payment models and value-based payments were set, according to an announcement from the U.S. Department of Health and Human Services.
“Strategically, these things are essential to work into the plan of what the hospital medicine group is doing in the coming three to five years,” Dr. Whitcomb said. “Hospitalists can’t do this alone. They have to do it with teams. It’s not only teams of other professionals in the hospital and around the hospital, but it’s other physicians.”
Dr. Whitcomb said key to the new paradigm is shared financial and clinical responsibilities. He says hospitalists have to “change our thinking…to a mindset where we’re in this together.”
Part of that shared responsibility extends to the post-acute care setting, where SHM senior vice president for practice management Joseph Miller said that some 30% of HMGs are practicing. To help those practitioners, SHM and IPC Healthcare of North Hollywood, Calif., debuted the “Primer for Hospitalists on Skilled Nursing Facilities” at HM15.
The educational program, housed at SHM’s Learning Portal, has 32 lessons meant to differentiate the traditional acute-care hospital from post-acute care facilities. It is grouped in five sections and two modules, with a focus on skilled-nursing facilities (SNFs), which are the most common post-acute care settings.
“The types of resources that are available are different, and that’s not only in terms of staff, but the availability of specialists, the availability of testing capabilities,” Miller said. “If you need to work with a cardiologist for a particular patient...how do you engage them? You’re not going to be able to have them come and see that patient frequently. How do you communicate with them to get the feedback you need as the attending physician?”
Another communication hassle involves the growing number of HMGs spread over multiple sites. For Sara Shraibman, MD, an assistant program director at Syosset Hospital in Syosset, N.Y., those sites are two hospitals covered by the North Shore LIJ Medical Group.
“It’s actually a new program, so we are trying to look at our compensation, models comparing them across two hospitals…and how we manage,” she said. “Not every hospitalist will go back and forth. Some will, some won’t. Some will work nights to help cover, some won’t. It’s very interesting trying to come up with a schedule.”
The best way to address conflict at multi-site groups is communicating and focusing on shared goals, said David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., and a new member of Team Hospitalist.
“Make sure that no matter what conflict might be up front, that everybody is looking at the goals downstream and saying, ‘Yes, that is a goal we want to achieve. We want to have better patient safety metrics. We want to have decreased readmissions. We want to have better transitions of care,’” Dr. Weidig said. “The common goal all the way from hospital administrators all the way down to hospital physicians is going to be the key.”
Richard Quinn is a freelance writer in New Jersey.
HM15 Speakers Urge Hospitalists to Use Technology, Teamwork, Talent

NATIONAL HARBOR, Md.—In the convention business, some say an annual meeting is only as good as its keynote addresses. Those people would call HM15 a home run, because the thousands of hospitalists who made their way to just outside the nation’s capital last month were treated to a trinity of talented talkers.
First up was patient safety guru Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore. Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement (IHI), echoed his patient-centered focus in her address. The four-day confab ended with hospitalist dean Bob Wachter, MD, MHM, reading from his new book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age.”
The three came from different perspectives but ended up in the same place: Hospitalists can use technology, teamwork, and talent to be the people who make healthcare in this country safer. In fact, HM has the responsibility to do so.
“We are the only hope that the healthcare system has of improving quality and safety,” Dr. Pronovost said.
Famous for creating a five-step checklist designed to reduce the incidence of central line-associated infections, he talked about healthcare in terms of physicians telling “depressing” stories that hold change back.
“The first is that we still tell a story that harm is inevitable,” he said. “‘You’re sick, you’re old, you’re young, stuff happens.’ Second, we still tell stories that [show that] safety and quality are based on the heroism of our clinicians rather than design of safe systems. And, third, we still tell a story that ‘I am powerless to do anything about it.’
“We need some new stories.”
Reframing the discussion of healthcare into a story of preventing all harm is ambitious but doable, he added. Hospitalists need to team with others, though, because an overhauled healthcare system needs buy-in from all physicians.
“The trick of this is to have enough details that people want to join you, but don’t completely tell the story, because others have to co-create it with you,” Dr. Pronovost said. “You tell the why and the what, but the how is co-created by all of your colleagues who are working with you.”
Bisognano says hospitalists can help hospitalists achieve IHI’s Triple Aim, an initiative to simultaneously improve the patient experience and the health of populations, reducing the per capita cost of healthcare. But, like Dr. Pronovost, her argument is based on a new view of the healthcare system.
“We need not a system that says, ‘What’s the matter?’ but a system that understands deeply what matters to each patient,” Bisognano said.
That prism requires speaking a new “language,” one that uses quality of care delivered and defines it more broadly than simply mortality rates and adverse events.
“You can look at health and care, but you also can drive out unnecessary cost,” she said. “And being a former hospital CEO, I can say it was magic when a clinician could walk in and be able to talk in both languages.”
Dr. Wachter spoke of the past, present, and future of the digital age of medicine. He is as frustrated by poor electronic health record (EHR) rollouts as front-line hospitalists but notes that healthcare in the past five years has seen a digital revolution in a much shorter time period than most industries, thanks to federal incentives.
“Most fields that go digital do so over the course of 10 or 20 years, in a very organic way, with the early adopters, the rank and file, and then the laggards,” he said. “And in that kind of organic adoption curve, you see problems arise, and people begin to deal with them and understand them and mitigate them.
“What the federal intervention did was essentially turbocharge the digitization of healthcare. We’ve seen this in a very telescoped way. … It’s like we got started on a huge dose of chemo, stat.”
Moving forward, Dr. Wachter said the focus has to be on improving the use and integration of healthcare to ensure that it translates to better patient care. For example, going to digital radiology has in many ways ended the daily meetings that once were commonplace in hospital “film rooms.” In essence, the move from “analog to digital” meant people communicated less. Now, multidisciplinary rounds and other unit-based approaches are trying to recreate teamwork.
“Places are doing some pretty impressive things to try to bring teams back together in a digital environment,” Dr. Wachter said. “But, the point is, I didn’t give this any thought. I don’t know whether you did. What didn’t cross my own cognitive radar screen was that when we go digital, we will screw up the relationships, because people can now be wherever they want to be to do their work.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—In the convention business, some say an annual meeting is only as good as its keynote addresses. Those people would call HM15 a home run, because the thousands of hospitalists who made their way to just outside the nation’s capital last month were treated to a trinity of talented talkers.
First up was patient safety guru Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore. Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement (IHI), echoed his patient-centered focus in her address. The four-day confab ended with hospitalist dean Bob Wachter, MD, MHM, reading from his new book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age.”
The three came from different perspectives but ended up in the same place: Hospitalists can use technology, teamwork, and talent to be the people who make healthcare in this country safer. In fact, HM has the responsibility to do so.
“We are the only hope that the healthcare system has of improving quality and safety,” Dr. Pronovost said.
Famous for creating a five-step checklist designed to reduce the incidence of central line-associated infections, he talked about healthcare in terms of physicians telling “depressing” stories that hold change back.
“The first is that we still tell a story that harm is inevitable,” he said. “‘You’re sick, you’re old, you’re young, stuff happens.’ Second, we still tell stories that [show that] safety and quality are based on the heroism of our clinicians rather than design of safe systems. And, third, we still tell a story that ‘I am powerless to do anything about it.’
“We need some new stories.”
Reframing the discussion of healthcare into a story of preventing all harm is ambitious but doable, he added. Hospitalists need to team with others, though, because an overhauled healthcare system needs buy-in from all physicians.
“The trick of this is to have enough details that people want to join you, but don’t completely tell the story, because others have to co-create it with you,” Dr. Pronovost said. “You tell the why and the what, but the how is co-created by all of your colleagues who are working with you.”
Bisognano says hospitalists can help hospitalists achieve IHI’s Triple Aim, an initiative to simultaneously improve the patient experience and the health of populations, reducing the per capita cost of healthcare. But, like Dr. Pronovost, her argument is based on a new view of the healthcare system.
“We need not a system that says, ‘What’s the matter?’ but a system that understands deeply what matters to each patient,” Bisognano said.
That prism requires speaking a new “language,” one that uses quality of care delivered and defines it more broadly than simply mortality rates and adverse events.
“You can look at health and care, but you also can drive out unnecessary cost,” she said. “And being a former hospital CEO, I can say it was magic when a clinician could walk in and be able to talk in both languages.”
Dr. Wachter spoke of the past, present, and future of the digital age of medicine. He is as frustrated by poor electronic health record (EHR) rollouts as front-line hospitalists but notes that healthcare in the past five years has seen a digital revolution in a much shorter time period than most industries, thanks to federal incentives.
“Most fields that go digital do so over the course of 10 or 20 years, in a very organic way, with the early adopters, the rank and file, and then the laggards,” he said. “And in that kind of organic adoption curve, you see problems arise, and people begin to deal with them and understand them and mitigate them.
“What the federal intervention did was essentially turbocharge the digitization of healthcare. We’ve seen this in a very telescoped way. … It’s like we got started on a huge dose of chemo, stat.”
Moving forward, Dr. Wachter said the focus has to be on improving the use and integration of healthcare to ensure that it translates to better patient care. For example, going to digital radiology has in many ways ended the daily meetings that once were commonplace in hospital “film rooms.” In essence, the move from “analog to digital” meant people communicated less. Now, multidisciplinary rounds and other unit-based approaches are trying to recreate teamwork.
“Places are doing some pretty impressive things to try to bring teams back together in a digital environment,” Dr. Wachter said. “But, the point is, I didn’t give this any thought. I don’t know whether you did. What didn’t cross my own cognitive radar screen was that when we go digital, we will screw up the relationships, because people can now be wherever they want to be to do their work.”
Richard Quinn is a freelance writer in New Jersey.
NATIONAL HARBOR, Md.—In the convention business, some say an annual meeting is only as good as its keynote addresses. Those people would call HM15 a home run, because the thousands of hospitalists who made their way to just outside the nation’s capital last month were treated to a trinity of talented talkers.
First up was patient safety guru Peter Pronovost, MD, PhD, FCCM, senior vice president for patient safety and quality at Johns Hopkins Medicine in Baltimore. Maureen Bisognano, president and CEO of the Institute for Healthcare Improvement (IHI), echoed his patient-centered focus in her address. The four-day confab ended with hospitalist dean Bob Wachter, MD, MHM, reading from his new book, “The Digital Doctor: Hope, Hype, and Harm at the Dawn of Medicine’s Computer Age.”
The three came from different perspectives but ended up in the same place: Hospitalists can use technology, teamwork, and talent to be the people who make healthcare in this country safer. In fact, HM has the responsibility to do so.
“We are the only hope that the healthcare system has of improving quality and safety,” Dr. Pronovost said.
Famous for creating a five-step checklist designed to reduce the incidence of central line-associated infections, he talked about healthcare in terms of physicians telling “depressing” stories that hold change back.
“The first is that we still tell a story that harm is inevitable,” he said. “‘You’re sick, you’re old, you’re young, stuff happens.’ Second, we still tell stories that [show that] safety and quality are based on the heroism of our clinicians rather than design of safe systems. And, third, we still tell a story that ‘I am powerless to do anything about it.’
“We need some new stories.”
Reframing the discussion of healthcare into a story of preventing all harm is ambitious but doable, he added. Hospitalists need to team with others, though, because an overhauled healthcare system needs buy-in from all physicians.
“The trick of this is to have enough details that people want to join you, but don’t completely tell the story, because others have to co-create it with you,” Dr. Pronovost said. “You tell the why and the what, but the how is co-created by all of your colleagues who are working with you.”
Bisognano says hospitalists can help hospitalists achieve IHI’s Triple Aim, an initiative to simultaneously improve the patient experience and the health of populations, reducing the per capita cost of healthcare. But, like Dr. Pronovost, her argument is based on a new view of the healthcare system.
“We need not a system that says, ‘What’s the matter?’ but a system that understands deeply what matters to each patient,” Bisognano said.
That prism requires speaking a new “language,” one that uses quality of care delivered and defines it more broadly than simply mortality rates and adverse events.
“You can look at health and care, but you also can drive out unnecessary cost,” she said. “And being a former hospital CEO, I can say it was magic when a clinician could walk in and be able to talk in both languages.”
Dr. Wachter spoke of the past, present, and future of the digital age of medicine. He is as frustrated by poor electronic health record (EHR) rollouts as front-line hospitalists but notes that healthcare in the past five years has seen a digital revolution in a much shorter time period than most industries, thanks to federal incentives.
“Most fields that go digital do so over the course of 10 or 20 years, in a very organic way, with the early adopters, the rank and file, and then the laggards,” he said. “And in that kind of organic adoption curve, you see problems arise, and people begin to deal with them and understand them and mitigate them.
“What the federal intervention did was essentially turbocharge the digitization of healthcare. We’ve seen this in a very telescoped way. … It’s like we got started on a huge dose of chemo, stat.”
Moving forward, Dr. Wachter said the focus has to be on improving the use and integration of healthcare to ensure that it translates to better patient care. For example, going to digital radiology has in many ways ended the daily meetings that once were commonplace in hospital “film rooms.” In essence, the move from “analog to digital” meant people communicated less. Now, multidisciplinary rounds and other unit-based approaches are trying to recreate teamwork.
“Places are doing some pretty impressive things to try to bring teams back together in a digital environment,” Dr. Wachter said. “But, the point is, I didn’t give this any thought. I don’t know whether you did. What didn’t cross my own cognitive radar screen was that when we go digital, we will screw up the relationships, because people can now be wherever they want to be to do their work.”
Richard Quinn is a freelance writer in New Jersey.
Family Medicine’s Increasing Presence in Hospital Medicine
Years ago, I struggled with a difficult decision. Given the fact that the military disallowed dual training tracks, such as internal medicine/pediatrics (med/peds), I had to choose from internal medicine (IM), pediatrics (Peds), or family practice (FP) residencies. My personal history and experiential data remained incomplete and the view ahead blurry; still, the choice remained.
Over time, I’ve embraced the uncertainty inherent in most analyses. Such is the case with the current composition of specialties that make up hospital medicine nationwide. Available data remains in flux, yet I see apparent trends.
A new question in the 2014 State of Hospital Medicine (SOHM) report asked, “Did your hospital medicine group employ hospitalist physicians trained and certified in the following specialties…?” Strikingly, a full 59% of groups serving adult patients only reported having at least one family medicine-trained provider in their midst! And in these adult-only practices, 98% of groups utilized at least one internal medicine physician, 24% reported a med/peds doc, and none reported pediatricians.

Meanwhile, of 40 groups caring for children only, 95% reported using pediatrics, 2.5% internal medicine (huh?), 22.5% med/peds, and zero FPs. The 19 groups serving both adults and children revealed participation from all four nonsurgical hospitalist specialties (IM, peds, FP, med/peds).
So what is the specialty distribution of medical hospitalists overall? There’s no good data about this.
The 2014 Medical Group Management Association (MGMA) sample, licensed for use in SOHM, reported data for roughly 4,200 community hospital medicine providers: 82% were internal medicine, 10% family medicine, 7% pediatrics, and <1% med/peds. MGMA, however, cautions against assuming that this represents the entire population of hospitalists and their training. Although representative of the groups who participated in the survey, it may not be representative of groups that didn’t participate, and thus it would be misleading to suggest that this distribution holds true nationally.
In an effort to corroborate the MGMA distribution, I reviewed other compensation and productivity surveys; one such survey, conducted by the American Medical Group Association, reported hospitalists by training program. It contained over 3,700 community hospital providers—89% internal medicine, 6% family medicine, 5% pediatrics—but did not inquire about medicine/pediatrics.
Finally, if one combines the academic and community provider samples from MGMA (n=4,867), the distribution is 80% IM, 8.5% FP, 10% peds, and <1% med/peds.
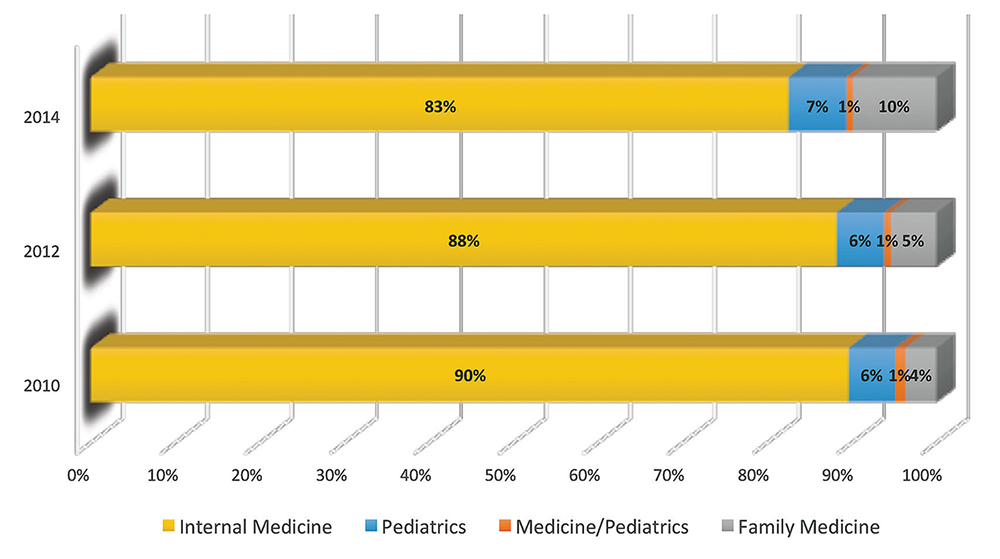
Which of these, if any, is the actual distribution of nonprocedural hospitalists? Although we cannot know exactly, I believe something close to the following to be current state: internal medicine 80%, family medicine 10%, pediatrics 10%, and medicine/pediatrics <1%.
It is clear from survey trends that the proportion of family medicine providers is growing, while the internal medicine super-majority is shrinking somewhat. Pediatrics appears to remain stable as a proportion of the total, as does med/peds, with the latter unable to grow in numbers proportionally given the small number of providers nationally compared to the other three fields.
The growth of family medicine-trained hospitalists relates to the continued high demand for the profession, with such residents comprising the largest pool of available providers, second only to internal medicine.
Based on the SHM survey, family medicine hospitalists seem to practice similarly to IM; they generally see adults only. It appears that they are accepted into traditional adult hospitalist practices, readily contrasting with groups serving children, which report no FP participation. Meanwhile, med/peds hospitalists provide care across the spectrum of hospitalist groups, though they often report splitting their duties between adults-only services and pediatric services.
As for me, a generation removed from my election of a family practice internship and subsequent transition to internal medicine residency, I should not have worried so. Both paths can lead to hospital medicine.
Dr. Ahlstrom is a hospitalist at Indigo Health Partners in Traverse City, Mich., and a member of SHM’s Practice Analysis Committee.
Years ago, I struggled with a difficult decision. Given the fact that the military disallowed dual training tracks, such as internal medicine/pediatrics (med/peds), I had to choose from internal medicine (IM), pediatrics (Peds), or family practice (FP) residencies. My personal history and experiential data remained incomplete and the view ahead blurry; still, the choice remained.
Over time, I’ve embraced the uncertainty inherent in most analyses. Such is the case with the current composition of specialties that make up hospital medicine nationwide. Available data remains in flux, yet I see apparent trends.
A new question in the 2014 State of Hospital Medicine (SOHM) report asked, “Did your hospital medicine group employ hospitalist physicians trained and certified in the following specialties…?” Strikingly, a full 59% of groups serving adult patients only reported having at least one family medicine-trained provider in their midst! And in these adult-only practices, 98% of groups utilized at least one internal medicine physician, 24% reported a med/peds doc, and none reported pediatricians.
Meanwhile, of 40 groups caring for children only, 95% reported using pediatrics, 2.5% internal medicine (huh?), 22.5% med/peds, and zero FPs. The 19 groups serving both adults and children revealed participation from all four nonsurgical hospitalist specialties (IM, peds, FP, med/peds).
So what is the specialty distribution of medical hospitalists overall? There’s no good data about this.
The 2014 Medical Group Management Association (MGMA) sample, licensed for use in SOHM, reported data for roughly 4,200 community hospital medicine providers: 82% were internal medicine, 10% family medicine, 7% pediatrics, and <1% med/peds. MGMA, however, cautions against assuming that this represents the entire population of hospitalists and their training. Although representative of the groups who participated in the survey, it may not be representative of groups that didn’t participate, and thus it would be misleading to suggest that this distribution holds true nationally.
In an effort to corroborate the MGMA distribution, I reviewed other compensation and productivity surveys; one such survey, conducted by the American Medical Group Association, reported hospitalists by training program. It contained over 3,700 community hospital providers—89% internal medicine, 6% family medicine, 5% pediatrics—but did not inquire about medicine/pediatrics.
Finally, if one combines the academic and community provider samples from MGMA (n=4,867), the distribution is 80% IM, 8.5% FP, 10% peds, and <1% med/peds.
Which of these, if any, is the actual distribution of nonprocedural hospitalists? Although we cannot know exactly, I believe something close to the following to be current state: internal medicine 80%, family medicine 10%, pediatrics 10%, and medicine/pediatrics <1%.
It is clear from survey trends that the proportion of family medicine providers is growing, while the internal medicine super-majority is shrinking somewhat. Pediatrics appears to remain stable as a proportion of the total, as does med/peds, with the latter unable to grow in numbers proportionally given the small number of providers nationally compared to the other three fields.
The growth of family medicine-trained hospitalists relates to the continued high demand for the profession, with such residents comprising the largest pool of available providers, second only to internal medicine.
Based on the SHM survey, family medicine hospitalists seem to practice similarly to IM; they generally see adults only. It appears that they are accepted into traditional adult hospitalist practices, readily contrasting with groups serving children, which report no FP participation. Meanwhile, med/peds hospitalists provide care across the spectrum of hospitalist groups, though they often report splitting their duties between adults-only services and pediatric services.
As for me, a generation removed from my election of a family practice internship and subsequent transition to internal medicine residency, I should not have worried so. Both paths can lead to hospital medicine.
Dr. Ahlstrom is a hospitalist at Indigo Health Partners in Traverse City, Mich., and a member of SHM’s Practice Analysis Committee.
Years ago, I struggled with a difficult decision. Given the fact that the military disallowed dual training tracks, such as internal medicine/pediatrics (med/peds), I had to choose from internal medicine (IM), pediatrics (Peds), or family practice (FP) residencies. My personal history and experiential data remained incomplete and the view ahead blurry; still, the choice remained.
Over time, I’ve embraced the uncertainty inherent in most analyses. Such is the case with the current composition of specialties that make up hospital medicine nationwide. Available data remains in flux, yet I see apparent trends.
A new question in the 2014 State of Hospital Medicine (SOHM) report asked, “Did your hospital medicine group employ hospitalist physicians trained and certified in the following specialties…?” Strikingly, a full 59% of groups serving adult patients only reported having at least one family medicine-trained provider in their midst! And in these adult-only practices, 98% of groups utilized at least one internal medicine physician, 24% reported a med/peds doc, and none reported pediatricians.
Meanwhile, of 40 groups caring for children only, 95% reported using pediatrics, 2.5% internal medicine (huh?), 22.5% med/peds, and zero FPs. The 19 groups serving both adults and children revealed participation from all four nonsurgical hospitalist specialties (IM, peds, FP, med/peds).
So what is the specialty distribution of medical hospitalists overall? There’s no good data about this.
The 2014 Medical Group Management Association (MGMA) sample, licensed for use in SOHM, reported data for roughly 4,200 community hospital medicine providers: 82% were internal medicine, 10% family medicine, 7% pediatrics, and <1% med/peds. MGMA, however, cautions against assuming that this represents the entire population of hospitalists and their training. Although representative of the groups who participated in the survey, it may not be representative of groups that didn’t participate, and thus it would be misleading to suggest that this distribution holds true nationally.
In an effort to corroborate the MGMA distribution, I reviewed other compensation and productivity surveys; one such survey, conducted by the American Medical Group Association, reported hospitalists by training program. It contained over 3,700 community hospital providers—89% internal medicine, 6% family medicine, 5% pediatrics—but did not inquire about medicine/pediatrics.
Finally, if one combines the academic and community provider samples from MGMA (n=4,867), the distribution is 80% IM, 8.5% FP, 10% peds, and <1% med/peds.
Which of these, if any, is the actual distribution of nonprocedural hospitalists? Although we cannot know exactly, I believe something close to the following to be current state: internal medicine 80%, family medicine 10%, pediatrics 10%, and medicine/pediatrics <1%.
It is clear from survey trends that the proportion of family medicine providers is growing, while the internal medicine super-majority is shrinking somewhat. Pediatrics appears to remain stable as a proportion of the total, as does med/peds, with the latter unable to grow in numbers proportionally given the small number of providers nationally compared to the other three fields.
The growth of family medicine-trained hospitalists relates to the continued high demand for the profession, with such residents comprising the largest pool of available providers, second only to internal medicine.
Based on the SHM survey, family medicine hospitalists seem to practice similarly to IM; they generally see adults only. It appears that they are accepted into traditional adult hospitalist practices, readily contrasting with groups serving children, which report no FP participation. Meanwhile, med/peds hospitalists provide care across the spectrum of hospitalist groups, though they often report splitting their duties between adults-only services and pediatric services.
As for me, a generation removed from my election of a family practice internship and subsequent transition to internal medicine residency, I should not have worried so. Both paths can lead to hospital medicine.
Dr. Ahlstrom is a hospitalist at Indigo Health Partners in Traverse City, Mich., and a member of SHM’s Practice Analysis Committee.
LISTEN NOW: David Weidig, MD, talks about best practices for multi-site hospital medicine
Excerpts from our interview with Team Hospitalist member David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., about best practices for multi-site hospital medicine.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/05/David-Weidig_HM15_FINAL_050215.mp3"][/audio]
Excerpts from our interview with Team Hospitalist member David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., about best practices for multi-site hospital medicine.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/05/David-Weidig_HM15_FINAL_050215.mp3"][/audio]
Excerpts from our interview with Team Hospitalist member David Weidig, MD, director of hospital medicine for Aurora Medical Group in West Allis, Wis., about best practices for multi-site hospital medicine.
[audio mp3="http://www.the-hospitalist.org/wp-content/uploads/2015/05/David-Weidig_HM15_FINAL_050215.mp3"][/audio]