User login
Single-port laparoscopy has few complications but BMI matters
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission. 
“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.
“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
NATIONAL HARBOR, MD. – Single-port laparoscopy is both safe and feasible, and has the potential to decrease surgical complications and increase efficiency, according to findings presented at the AAGL Global Congress.
Ahmed N. Al-Niaimi, MD, of the University of Wisconsin–Madison, and his colleagues, conducted a retrospective cohort study analyzing 587 consecutive patients who underwent single-port laparoscopy from March 2012 to December 2016. Of the 587 patients, there were 27 clinically-relevant complications among 18 patients (3%). The complications included intensive care unit admission, reoperation, end organ damage, organ space surgical site infection, and readmission.
“Those factors leading to those complications are similar to the factors that cause complications in any other surgery,” Dr. Al-Niaimi said in an interview before the meeting.
Body mass index was found to be a primary contributor to surgical complications. Patients with a BMI of more than 30 kg/m2 experienced a 1% increase in the risk of surgical complications per unit value increase of BMI. This is significant because the median BMI of the patient population in the study was 33.9 kg/m2 and 57% of the study participants were considered obese or morbidly obese.
“The heavier the patient, the higher the complication rate,” Dr. Al-Niaimi said.
Surgeons who are learning single-port laparoscopy should choose patients with lower BMIs to gain efficiency in using the new technique, Dr. Al-Niaimi suggested. This will allow patients to decrease their risk of surgical complications while allowing surgeons to hone their abilities in a new surgical technique, he said.
The other prime contributor to surgical complications is the length of surgical time. The average time of surgery during the study was 156 minutes. Dr. Al-Niaimi and his colleagues found that for each 10-minute increase in surgical time, the risk of complications increased by 2%.
While the results of the study demonstrate safety in the single-port approach, Dr. Al-Niaimi said a randomized controlled trial is needed to validate the findings and determine whether single-port laparoscopy is more effective than multi-port laparoscopy.
Dr. Al-Niaimi reported having no financial disclosures.
AT AAGL 2017
Key clinical point:
Major finding: Obese patients experienced a 1% increase in risk of surgical complications per unit value increase of BMI.
Data source: Retrospective cohort study of 587 consecutive patients undergoing single-port laparoscopy at a single academic institution.
Disclosures: Dr. Al-Niaimi reported having no financial disclosures.
Pain is a risk factor for endometrial ablation failure
NATIONAL HARBOR, MD. – Second-generation endometrial ablations performed for an indication related to pain were significantly more likely to fail, according to findings presented at the AAGL Global Congress.
“We know that endometrial ablation carries a reasonable risk of failure – meaning a second ablation or hysterectomy procedure – and that rate can vary institutionally,” Matthew Hoffman, MD, chair of obstetrics and gynecology at Christiana Care Health Center, Newark, Del., said in an interview prior to the meeting. “Part of our goal is to examine patients who had pain as an indication for their procedure and to better understand if that served as an independent risk factor for women who would ultimately require additional surgical intervention.”
In a retrospective study, researchers identified 5,818 women who had undergone an ablation between October 2003 and March 2016 at a community hospital affiliated with the Christina Care Health System. Patients had either a radiofrequency ablation (3,706), hydrothermablation (1,786), or uterine balloon ablation (326).
The majority of the patients were white. Pain indications included pelvic pain, dysmenorrhea, dyspareunia, lower abdominal pain, endometriosis, and adenomyosis.
Investigators found a hysterectomy rate of 19.2% among the 437 patients who had pain as an indication for ablation, compared with 13.5% of patients with different indications (P = .001).
Secondary outcomes showed older women who underwent ablation for pain were still less likely to fail than were younger patients (odds ratio, 0.96, 95% confidence interval, .95-.97). “Older age, especially age 50 years or older, with the indication of pain, was actually protective against hysterectomy,” Meagan Cramer, MD, a resident physician at Christina Care Health System and one of the study researchers, said in an interview. “So even though pain itself was a risk factor, if you were in pain and older than 50 you were less likely to need a hysterectomy.”
The data used were collected at a single center, potentially limiting the generalizability of the findings.
Dr. Hoffman and Dr. Cramer suggested using hormonal IUDs as an alternative treatment when counseling patients who may be at risk for a failed ablation.
“This is a call for folks to look at a diverse number of risk factors and to look at this data to better counsel patients in how they choose and select procedures to get to the endpoints that you want,” Dr. Hoffman said.
The researchers reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Second-generation endometrial ablations performed for an indication related to pain were significantly more likely to fail, according to findings presented at the AAGL Global Congress.
“We know that endometrial ablation carries a reasonable risk of failure – meaning a second ablation or hysterectomy procedure – and that rate can vary institutionally,” Matthew Hoffman, MD, chair of obstetrics and gynecology at Christiana Care Health Center, Newark, Del., said in an interview prior to the meeting. “Part of our goal is to examine patients who had pain as an indication for their procedure and to better understand if that served as an independent risk factor for women who would ultimately require additional surgical intervention.”
In a retrospective study, researchers identified 5,818 women who had undergone an ablation between October 2003 and March 2016 at a community hospital affiliated with the Christina Care Health System. Patients had either a radiofrequency ablation (3,706), hydrothermablation (1,786), or uterine balloon ablation (326).
The majority of the patients were white. Pain indications included pelvic pain, dysmenorrhea, dyspareunia, lower abdominal pain, endometriosis, and adenomyosis.
Investigators found a hysterectomy rate of 19.2% among the 437 patients who had pain as an indication for ablation, compared with 13.5% of patients with different indications (P = .001).
Secondary outcomes showed older women who underwent ablation for pain were still less likely to fail than were younger patients (odds ratio, 0.96, 95% confidence interval, .95-.97). “Older age, especially age 50 years or older, with the indication of pain, was actually protective against hysterectomy,” Meagan Cramer, MD, a resident physician at Christina Care Health System and one of the study researchers, said in an interview. “So even though pain itself was a risk factor, if you were in pain and older than 50 you were less likely to need a hysterectomy.”
The data used were collected at a single center, potentially limiting the generalizability of the findings.
Dr. Hoffman and Dr. Cramer suggested using hormonal IUDs as an alternative treatment when counseling patients who may be at risk for a failed ablation.
“This is a call for folks to look at a diverse number of risk factors and to look at this data to better counsel patients in how they choose and select procedures to get to the endpoints that you want,” Dr. Hoffman said.
The researchers reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
NATIONAL HARBOR, MD. – Second-generation endometrial ablations performed for an indication related to pain were significantly more likely to fail, according to findings presented at the AAGL Global Congress.
“We know that endometrial ablation carries a reasonable risk of failure – meaning a second ablation or hysterectomy procedure – and that rate can vary institutionally,” Matthew Hoffman, MD, chair of obstetrics and gynecology at Christiana Care Health Center, Newark, Del., said in an interview prior to the meeting. “Part of our goal is to examine patients who had pain as an indication for their procedure and to better understand if that served as an independent risk factor for women who would ultimately require additional surgical intervention.”
In a retrospective study, researchers identified 5,818 women who had undergone an ablation between October 2003 and March 2016 at a community hospital affiliated with the Christina Care Health System. Patients had either a radiofrequency ablation (3,706), hydrothermablation (1,786), or uterine balloon ablation (326).
The majority of the patients were white. Pain indications included pelvic pain, dysmenorrhea, dyspareunia, lower abdominal pain, endometriosis, and adenomyosis.
Investigators found a hysterectomy rate of 19.2% among the 437 patients who had pain as an indication for ablation, compared with 13.5% of patients with different indications (P = .001).
Secondary outcomes showed older women who underwent ablation for pain were still less likely to fail than were younger patients (odds ratio, 0.96, 95% confidence interval, .95-.97). “Older age, especially age 50 years or older, with the indication of pain, was actually protective against hysterectomy,” Meagan Cramer, MD, a resident physician at Christina Care Health System and one of the study researchers, said in an interview. “So even though pain itself was a risk factor, if you were in pain and older than 50 you were less likely to need a hysterectomy.”
The data used were collected at a single center, potentially limiting the generalizability of the findings.
Dr. Hoffman and Dr. Cramer suggested using hormonal IUDs as an alternative treatment when counseling patients who may be at risk for a failed ablation.
“This is a call for folks to look at a diverse number of risk factors and to look at this data to better counsel patients in how they choose and select procedures to get to the endpoints that you want,” Dr. Hoffman said.
The researchers reported no relevant financial disclosures.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
AT AAGL 2017
Key clinical point:
Major finding: Ablation had a hysterectomy rate of 19.2% when pain was an indication, compared with 13.5% for other indications.
Data source: Retrospective study of 5,818 endometrial ablations conducted between October 2003 and March 2016 at a single institution.
Disclosures: The researchers reported no relevant financial disclosures.
ACOG updates guidance on pelvic organ prolapse
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
(POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
(POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
Using polypropylene mesh to augment surgical repair of anterior vaginal wall prolapse improves anatomic and some subjective outcomes, compared with native tissue repair, but it also comes with increased morbidity, according to new guidance from the American College of Obstetricians and Gynecologists.
(POP) to incorporate recent systematic review evidence.
When using polypropylene mesh for anterior POP repair, 11% of patients develop mesh erosion, of which 7% require surgical correction, according to the updated practice bulletin (Obstet Gynecol. 2017;130:e234-50).
“Referral to an obstetrician-gynecologist with appropriate training and experience, such as a female pelvic medicine and reconstructive surgery specialist, is recommended for surgical treatment of prolapse mesh complications,” ACOG and AUGS wrote.
The practice bulletin updates the recommendations on mesh based on a recent systematic review and meta-analysis that concluded that biological graft repair and absorbable mesh offered minimal benefits compared with native tissue repair, and did not significantly reduce rates of prolapse awareness or repeat surgery (Cochrane Database Syst Rev. 2016 Nov 30;11:CD004014).
Porcine dermis graft, which was used in most of the studies, did not significantly reduce rates of anterior prolapse recurrence compared with native tissue repair. Use of polypropylene mesh also tends to prolong operating times and causes more blood loss than native tissue anterior repair, and is associated with an elevated combined risk of stress urinary incontinence, mesh erosion, and repeat surgery for prolapse, the review concluded.
“Uterosacral and sacrospinous ligament suspension for apical POP with native tissue are equally effective surgical treatments of POP, with comparable anatomic, functional, and adverse outcomes,” the authors wrote in the practice bulletin.
Neither synthetic mesh nor biologic grafts improve outcomes of transvaginal repair of posterior vaginal wall prolapse, they added. As an alternative to surgery, most women can be successfully fitted with a pessary and clinicians should offer them this option, the practice bulletin stated. In up to 9% of cases, pessaries cause local devascularization or erosion, in which case they should be removed for 2-4 weeks while the patient undergoes local estrogen therapy.
Although POP is common and benign, symptomatic cases undermine quality of life by causing vaginal bulge and pressure and problems voiding, defecating, and during sexual activity. Consequently, about 300,000 women in the United States undergo surgery for POP every year. By 2050, population aging in the United States will lead to about a 50% rise in the number of women with POP, according to the practice bulletin.
FROM OBSTETRICS & GYNECOLOGY
Chlamydia infection: Common, and consequential to women's health
Seven days of opioids adequate for most hernia and other general surgery procedures
A 7-day limit on the initial opioid prescription may be sufficient for many common general surgery procedures, including hernia surgery and gynecologic procedures, findings of a large retrospective study suggest.
Rebecca E. Scully, MD, of the Center for Surgery and Public Health at Brigham and Women’s Hospital in Boston, and her associates examined opioid pain medication prescriptions and refills from records of the Military Health System Data Repository and the TRICARE insurance program of 215,140 opioid-naive patients. These patients were aged 18-64 years who underwent either cholecystectomy, appendectomy, inguinal hernia repair, anterior cruciate ligament reconstruction, rotator cuff tear repair, discectomy, mastectomy, or hysterectomy (JAMA Surg. 2017. doi: 10.1001/jamasurg.2017.3132). Only 20% of the covered individuals are active members of the U.S. military. The mean age was 40 years; 50% were male, and 60% were white.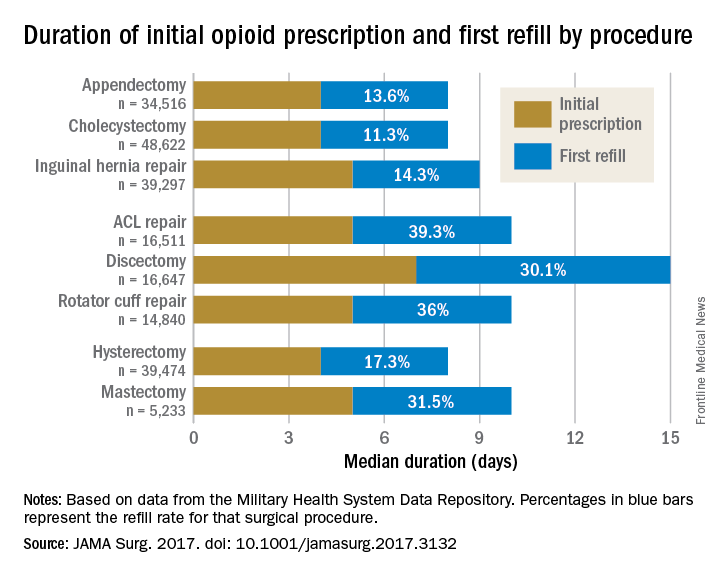
For appendectomy, cholecystectomy, and hysterectomy, the prescription was a median 4 days. For inguinal hernia repair, anterior cruciate ligament repair, rotator cuff repair, and mastectomy, the initial prescription was for 5 days. For discectomy, the median was 7 days.
Refill rates were the least at 11.3% for cholecystectomy and the most at 39.3% after anterior cruciate ligament repair. The time after the initial prescription until a refill was a median 6 days for appendectomy, cholecystectomy, and inguinal hernia repair, compared with a median 10 days for discectomy. The median duration of a refill prescription was 4 days for appendectomy, cholecystectomy, hernia repair, and hysterectomy versus 8 days for discectomy.
“Although 7 days appears to be more than adequate for many patients undergoing common general surgery and gynecologic procedures, prescription lengths likely should be extended to 10 days, particularly after common neurosurgical and musculoskeletal procedures, recognizing that as many as 40% of patients may still require one refill at a 7-day limit,” Dr. Scully and her associates said.
Although this study did not include rates of unused prescriptions or use of nonopioid pain relievers such as acetaminophen or NSAIDs, it did include a large population considered to be nationally representative “in many respects,” and it included a variety of procedures for which patients are commonly discharged to home, the researchers said.
The study was funded in part by the Department of Defense/Henry M. Jackson Foundation. The investigators had no conflict of interests. Adil H. Haider, MD, MPH, is deputy editor of JAMA Surgery, but he was not involved in any of the decisions regarding review of the manuscript or its acceptance.
A 7-day limit on the initial opioid prescription may be sufficient for many common general surgery procedures, including hernia surgery and gynecologic procedures, findings of a large retrospective study suggest.
Rebecca E. Scully, MD, of the Center for Surgery and Public Health at Brigham and Women’s Hospital in Boston, and her associates examined opioid pain medication prescriptions and refills from records of the Military Health System Data Repository and the TRICARE insurance program of 215,140 opioid-naive patients. These patients were aged 18-64 years who underwent either cholecystectomy, appendectomy, inguinal hernia repair, anterior cruciate ligament reconstruction, rotator cuff tear repair, discectomy, mastectomy, or hysterectomy (JAMA Surg. 2017. doi: 10.1001/jamasurg.2017.3132). Only 20% of the covered individuals are active members of the U.S. military. The mean age was 40 years; 50% were male, and 60% were white.
For appendectomy, cholecystectomy, and hysterectomy, the prescription was a median 4 days. For inguinal hernia repair, anterior cruciate ligament repair, rotator cuff repair, and mastectomy, the initial prescription was for 5 days. For discectomy, the median was 7 days.
Refill rates were the least at 11.3% for cholecystectomy and the most at 39.3% after anterior cruciate ligament repair. The time after the initial prescription until a refill was a median 6 days for appendectomy, cholecystectomy, and inguinal hernia repair, compared with a median 10 days for discectomy. The median duration of a refill prescription was 4 days for appendectomy, cholecystectomy, hernia repair, and hysterectomy versus 8 days for discectomy.
“Although 7 days appears to be more than adequate for many patients undergoing common general surgery and gynecologic procedures, prescription lengths likely should be extended to 10 days, particularly after common neurosurgical and musculoskeletal procedures, recognizing that as many as 40% of patients may still require one refill at a 7-day limit,” Dr. Scully and her associates said.
Although this study did not include rates of unused prescriptions or use of nonopioid pain relievers such as acetaminophen or NSAIDs, it did include a large population considered to be nationally representative “in many respects,” and it included a variety of procedures for which patients are commonly discharged to home, the researchers said.
The study was funded in part by the Department of Defense/Henry M. Jackson Foundation. The investigators had no conflict of interests. Adil H. Haider, MD, MPH, is deputy editor of JAMA Surgery, but he was not involved in any of the decisions regarding review of the manuscript or its acceptance.
A 7-day limit on the initial opioid prescription may be sufficient for many common general surgery procedures, including hernia surgery and gynecologic procedures, findings of a large retrospective study suggest.
Rebecca E. Scully, MD, of the Center for Surgery and Public Health at Brigham and Women’s Hospital in Boston, and her associates examined opioid pain medication prescriptions and refills from records of the Military Health System Data Repository and the TRICARE insurance program of 215,140 opioid-naive patients. These patients were aged 18-64 years who underwent either cholecystectomy, appendectomy, inguinal hernia repair, anterior cruciate ligament reconstruction, rotator cuff tear repair, discectomy, mastectomy, or hysterectomy (JAMA Surg. 2017. doi: 10.1001/jamasurg.2017.3132). Only 20% of the covered individuals are active members of the U.S. military. The mean age was 40 years; 50% were male, and 60% were white.
For appendectomy, cholecystectomy, and hysterectomy, the prescription was a median 4 days. For inguinal hernia repair, anterior cruciate ligament repair, rotator cuff repair, and mastectomy, the initial prescription was for 5 days. For discectomy, the median was 7 days.
Refill rates were the least at 11.3% for cholecystectomy and the most at 39.3% after anterior cruciate ligament repair. The time after the initial prescription until a refill was a median 6 days for appendectomy, cholecystectomy, and inguinal hernia repair, compared with a median 10 days for discectomy. The median duration of a refill prescription was 4 days for appendectomy, cholecystectomy, hernia repair, and hysterectomy versus 8 days for discectomy.
“Although 7 days appears to be more than adequate for many patients undergoing common general surgery and gynecologic procedures, prescription lengths likely should be extended to 10 days, particularly after common neurosurgical and musculoskeletal procedures, recognizing that as many as 40% of patients may still require one refill at a 7-day limit,” Dr. Scully and her associates said.
Although this study did not include rates of unused prescriptions or use of nonopioid pain relievers such as acetaminophen or NSAIDs, it did include a large population considered to be nationally representative “in many respects,” and it included a variety of procedures for which patients are commonly discharged to home, the researchers said.
The study was funded in part by the Department of Defense/Henry M. Jackson Foundation. The investigators had no conflict of interests. Adil H. Haider, MD, MPH, is deputy editor of JAMA Surgery, but he was not involved in any of the decisions regarding review of the manuscript or its acceptance.
FROM JAMA SURGERY
Key clinical point:
Major finding: The initial opioid prescription was a median 4 days for appendectomy and cholecystectomy, a median 5 days for inguinal hernia repair and anterior cruciate ligament and rotator cuff repair, and a median 7 days for discectomy.
Data source: A study of opioid prescriptions in 215,140 surgery patients aged 18-64 years.
Disclosures: The study was funded in part by the Department of Defense/Henry M. Jackson Foundation. The investigators had no conflict of interests. Adil H. Haider, MD, MPH, is deputy editor of JAMA Surgery, but he was not involved in any of the decisions regarding review of the manuscript or its acceptance.
Top research to be presented at AAGL
The 46th AAGL Global Congress on Minimally Invasive Gynecologic Surgery starts Nov. 12, 2017, in National Harbor, Md., and attendees will have a chance to hear presentations on more than 300 studies, plus numerous virtual posters.
Dr. Charles E. Miller, a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL, offered his top picks for not-to-be-missed research at this year’s meeting.
Cesarean-induced isthmoceles
On Wednesday, Nov. 15, at 12:17 p.m., researchers from West Virginia University in Morgantown and Universidad Autónoma de Nuevo León in Mexico will present data from a prospective study on the anatomy of cesarean-induced isthmoceles. The paper won the Golden Hysteroscope Award for best paper on hysteroscopy. It is being presented during the Open Communications 13 session on reproductive medicine.

“Isthmocele has become such a hot topic,” Dr. Miller said. “Besides the implications in terms of pelvic pain and abnormal bleeding, it can be a cause of infertility as fluid goes into the endometrial cavity and impacts implantation.”
Dr. Miller will be performing a telesurgery featuring robotic-assisted excision and repair of a cesarean section isthmocele on Thursday, Nov. 16, as part of General Session V from 8:30 a.m. to 12:30 p.m.
Rectosigmoid endometriosis
On Wednesday, Nov. 15, at 12:50 p.m., researchers from the University of Pittsburgh will show a surgical video on anterior discoid resection for rectosigmoid endometriosis. They use various laparoscopic instruments and techniques to assess and resect the nodule, including a “squeeze” technique, barbed suture, and a V-shaped closure. The video, which won the Golden Laparoscope Award for best surgical video, is being presented during the Plenary 6 session on endometriosis and adenomyosis.
“There is great debate in just how aggressively patients should be treated when a woman has deep infiltrative endometriosis involving the rectosigmoid area,” Dr. Miller said.
Most of the research in this area is from single-institution studies that do not always completely describe the procedure, leaving surgeons “unsure of which way to go,” Dr. Miller said. In addition, because many patients with endometriosis are young, surgeons need to consider how the procedure will impact them in 20 or even 50 years. While more aggressive than shaving, discoid resection is less aggressive than standard bowel resection.
Postsurgical pain control
On Tuesday, Nov. 14, at 3:46 p.m., researchers from the University of Pittsburgh, Oregon Health & Science University, Southern California Permanente Medical Group, and the University of Wisconsin, Madison, will present results from a prospective, double-blind, randomized study comparing intravenous acetaminophen with placebo for postsurgical pain control and patient satisfaction after laparoscopic hysterectomy. Their findings indicate no difference in either pain or satisfaction, casting doubt on routine use during hysterectomy. The study, which won the Jay M. Cooper Award for best paper on minimally invasive gynecology by a fellow, will be presented during the Open Communications 9 session on laparoscopy.
On Tuesday, Nov. 14, at 1:21 p.m., researchers from the University of Maryland, Baltimore; Mercy Medical Center, Baltimore; and Yoyodyne General Services, New York, will present a single-center, double-blind, randomized, placebo-controlled trial to assess the use of a single belladonna and opium suppository placed after laparoscopic or robotic hysterectomy to control postoperative pain. As with acetaminophen, they also found that the suppositories did not significantly lower pain or narcotic use. However, the belladonna/opium suppository reduced time to discharge from the postanesthesia care unit in phase I. The research, which won the Jerome J. Hoffman Award for best abstract by a resident or fellow, will be presented during Session 2 of the Virtual Posters.
“Here again are two treatments that really have minimal basis,” Dr. Miller said. “In the days of cost containment, is there really any reason for either?”
Cervical ripening
Dr. Miller also recommended that attendees take note of a randomized controlled trial evaluating whether misoprostol oral is as effective as vaginal tablets for cervical ripening. Researchers at Cairo University in Egypt considered this question among more than 350 women who were undergoing operative hysterectomy for various indications. They found no statistically significant difference in efficacy and similar adverse effects.
“There has been some concern raised about, is there a better way?” Dr. Miller said. “This is especially important as we move hysteroscopy to the office.”
The cervical priming study, which won the Robert B. Hunt Award for best paper published in the Journal of Minimally Invasive Gynecology between September 2016 and August 2017, will be presented on Tuesday, Nov. 14, at 7:10 a.m. during the journal’s editorial/advisory board breakfast. You can read the full article online (J Minim Invasive Gynecol. 2016 Nov - Dec;23[7]:1107-12).
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The 46th AAGL Global Congress on Minimally Invasive Gynecologic Surgery starts Nov. 12, 2017, in National Harbor, Md., and attendees will have a chance to hear presentations on more than 300 studies, plus numerous virtual posters.
Dr. Charles E. Miller, a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL, offered his top picks for not-to-be-missed research at this year’s meeting.
Cesarean-induced isthmoceles
On Wednesday, Nov. 15, at 12:17 p.m., researchers from West Virginia University in Morgantown and Universidad Autónoma de Nuevo León in Mexico will present data from a prospective study on the anatomy of cesarean-induced isthmoceles. The paper won the Golden Hysteroscope Award for best paper on hysteroscopy. It is being presented during the Open Communications 13 session on reproductive medicine.
“Isthmocele has become such a hot topic,” Dr. Miller said. “Besides the implications in terms of pelvic pain and abnormal bleeding, it can be a cause of infertility as fluid goes into the endometrial cavity and impacts implantation.”
Dr. Miller will be performing a telesurgery featuring robotic-assisted excision and repair of a cesarean section isthmocele on Thursday, Nov. 16, as part of General Session V from 8:30 a.m. to 12:30 p.m.
Rectosigmoid endometriosis
On Wednesday, Nov. 15, at 12:50 p.m., researchers from the University of Pittsburgh will show a surgical video on anterior discoid resection for rectosigmoid endometriosis. They use various laparoscopic instruments and techniques to assess and resect the nodule, including a “squeeze” technique, barbed suture, and a V-shaped closure. The video, which won the Golden Laparoscope Award for best surgical video, is being presented during the Plenary 6 session on endometriosis and adenomyosis.
“There is great debate in just how aggressively patients should be treated when a woman has deep infiltrative endometriosis involving the rectosigmoid area,” Dr. Miller said.
Most of the research in this area is from single-institution studies that do not always completely describe the procedure, leaving surgeons “unsure of which way to go,” Dr. Miller said. In addition, because many patients with endometriosis are young, surgeons need to consider how the procedure will impact them in 20 or even 50 years. While more aggressive than shaving, discoid resection is less aggressive than standard bowel resection.
Postsurgical pain control
On Tuesday, Nov. 14, at 3:46 p.m., researchers from the University of Pittsburgh, Oregon Health & Science University, Southern California Permanente Medical Group, and the University of Wisconsin, Madison, will present results from a prospective, double-blind, randomized study comparing intravenous acetaminophen with placebo for postsurgical pain control and patient satisfaction after laparoscopic hysterectomy. Their findings indicate no difference in either pain or satisfaction, casting doubt on routine use during hysterectomy. The study, which won the Jay M. Cooper Award for best paper on minimally invasive gynecology by a fellow, will be presented during the Open Communications 9 session on laparoscopy.
On Tuesday, Nov. 14, at 1:21 p.m., researchers from the University of Maryland, Baltimore; Mercy Medical Center, Baltimore; and Yoyodyne General Services, New York, will present a single-center, double-blind, randomized, placebo-controlled trial to assess the use of a single belladonna and opium suppository placed after laparoscopic or robotic hysterectomy to control postoperative pain. As with acetaminophen, they also found that the suppositories did not significantly lower pain or narcotic use. However, the belladonna/opium suppository reduced time to discharge from the postanesthesia care unit in phase I. The research, which won the Jerome J. Hoffman Award for best abstract by a resident or fellow, will be presented during Session 2 of the Virtual Posters.
“Here again are two treatments that really have minimal basis,” Dr. Miller said. “In the days of cost containment, is there really any reason for either?”
Cervical ripening
Dr. Miller also recommended that attendees take note of a randomized controlled trial evaluating whether misoprostol oral is as effective as vaginal tablets for cervical ripening. Researchers at Cairo University in Egypt considered this question among more than 350 women who were undergoing operative hysterectomy for various indications. They found no statistically significant difference in efficacy and similar adverse effects.
“There has been some concern raised about, is there a better way?” Dr. Miller said. “This is especially important as we move hysteroscopy to the office.”
The cervical priming study, which won the Robert B. Hunt Award for best paper published in the Journal of Minimally Invasive Gynecology between September 2016 and August 2017, will be presented on Tuesday, Nov. 14, at 7:10 a.m. during the journal’s editorial/advisory board breakfast. You can read the full article online (J Minim Invasive Gynecol. 2016 Nov - Dec;23[7]:1107-12).
mschneider@frontlinemedcom.com
On Twitter @maryellenny
The 46th AAGL Global Congress on Minimally Invasive Gynecologic Surgery starts Nov. 12, 2017, in National Harbor, Md., and attendees will have a chance to hear presentations on more than 300 studies, plus numerous virtual posters.
Dr. Charles E. Miller, a minimally invasive gynecologic surgeon in Naperville, Ill., and a past president of the AAGL, offered his top picks for not-to-be-missed research at this year’s meeting.
Cesarean-induced isthmoceles
On Wednesday, Nov. 15, at 12:17 p.m., researchers from West Virginia University in Morgantown and Universidad Autónoma de Nuevo León in Mexico will present data from a prospective study on the anatomy of cesarean-induced isthmoceles. The paper won the Golden Hysteroscope Award for best paper on hysteroscopy. It is being presented during the Open Communications 13 session on reproductive medicine.
“Isthmocele has become such a hot topic,” Dr. Miller said. “Besides the implications in terms of pelvic pain and abnormal bleeding, it can be a cause of infertility as fluid goes into the endometrial cavity and impacts implantation.”
Dr. Miller will be performing a telesurgery featuring robotic-assisted excision and repair of a cesarean section isthmocele on Thursday, Nov. 16, as part of General Session V from 8:30 a.m. to 12:30 p.m.
Rectosigmoid endometriosis
On Wednesday, Nov. 15, at 12:50 p.m., researchers from the University of Pittsburgh will show a surgical video on anterior discoid resection for rectosigmoid endometriosis. They use various laparoscopic instruments and techniques to assess and resect the nodule, including a “squeeze” technique, barbed suture, and a V-shaped closure. The video, which won the Golden Laparoscope Award for best surgical video, is being presented during the Plenary 6 session on endometriosis and adenomyosis.
“There is great debate in just how aggressively patients should be treated when a woman has deep infiltrative endometriosis involving the rectosigmoid area,” Dr. Miller said.
Most of the research in this area is from single-institution studies that do not always completely describe the procedure, leaving surgeons “unsure of which way to go,” Dr. Miller said. In addition, because many patients with endometriosis are young, surgeons need to consider how the procedure will impact them in 20 or even 50 years. While more aggressive than shaving, discoid resection is less aggressive than standard bowel resection.
Postsurgical pain control
On Tuesday, Nov. 14, at 3:46 p.m., researchers from the University of Pittsburgh, Oregon Health & Science University, Southern California Permanente Medical Group, and the University of Wisconsin, Madison, will present results from a prospective, double-blind, randomized study comparing intravenous acetaminophen with placebo for postsurgical pain control and patient satisfaction after laparoscopic hysterectomy. Their findings indicate no difference in either pain or satisfaction, casting doubt on routine use during hysterectomy. The study, which won the Jay M. Cooper Award for best paper on minimally invasive gynecology by a fellow, will be presented during the Open Communications 9 session on laparoscopy.
On Tuesday, Nov. 14, at 1:21 p.m., researchers from the University of Maryland, Baltimore; Mercy Medical Center, Baltimore; and Yoyodyne General Services, New York, will present a single-center, double-blind, randomized, placebo-controlled trial to assess the use of a single belladonna and opium suppository placed after laparoscopic or robotic hysterectomy to control postoperative pain. As with acetaminophen, they also found that the suppositories did not significantly lower pain or narcotic use. However, the belladonna/opium suppository reduced time to discharge from the postanesthesia care unit in phase I. The research, which won the Jerome J. Hoffman Award for best abstract by a resident or fellow, will be presented during Session 2 of the Virtual Posters.
“Here again are two treatments that really have minimal basis,” Dr. Miller said. “In the days of cost containment, is there really any reason for either?”
Cervical ripening
Dr. Miller also recommended that attendees take note of a randomized controlled trial evaluating whether misoprostol oral is as effective as vaginal tablets for cervical ripening. Researchers at Cairo University in Egypt considered this question among more than 350 women who were undergoing operative hysterectomy for various indications. They found no statistically significant difference in efficacy and similar adverse effects.
“There has been some concern raised about, is there a better way?” Dr. Miller said. “This is especially important as we move hysteroscopy to the office.”
The cervical priming study, which won the Robert B. Hunt Award for best paper published in the Journal of Minimally Invasive Gynecology between September 2016 and August 2017, will be presented on Tuesday, Nov. 14, at 7:10 a.m. during the journal’s editorial/advisory board breakfast. You can read the full article online (J Minim Invasive Gynecol. 2016 Nov - Dec;23[7]:1107-12).
mschneider@frontlinemedcom.com
On Twitter @maryellenny

Teach your adolescent patients about normal menses, so they know when it’s abnormal
CHICAGO – , according to S. Paige Hertweck, MD, chief of gynecology at Norton Children’s Hospital in Louisville, Ky.
“Remember to use the menstrual cycle as a vital sign,” Dr. Hertweck told attendees at the American Academy of Pediatrics annual meeting. “Even within the first year of menarche, most girls have a period at least every 90 days, so work up those who don’t.”
The median age of menarche is 12.4 years, typically beginning within 2-3 years of breast budding at Tanner Stage 4 breast development, she said. By 15 years of age, 98% of girls have begun menstruation.
Girls’ cycles typically last 21-45 days, an average of 32.2 days during their first year of menstruation, with flow for 7 days or less, requiring an average of 3-6 pads and/or tampons per day. Dr. Hertweck recommends you write down these features of normal menstruation so that your patients can tell you when their cycle is abnormal or menses doesn’t return.
“Cycle length is more variable for teens versus women 20-40 years old,” she said. However, “it’s not true that ‘anything goes’ for cycle length” in teens, she added. “Cycles that are consistently outside the range of 21-45 days are statistically uncommon.” Hence the need to evaluate causes of amenorrhea in girls whose cycles exceed 90 days.
Possible causes of amenorrhea include pregnancy, polycystic ovary syndrome, thyroid abnormalities, hyperprolactinemia, primary ovarian insufficiency, or hypogonadal amenorrhea, typically stimulated by the first instance of anorexia, Crohn’s disease, celiac disease, or a gluten intolerance.
Primary amenorrhea
Dr. Hertweck listed five benchmarks that indicate primary amenorrhea requiring evaluation. Those indicators include girls who have no menarche by age 15 years or within 3 years of breast budding, no breast development by age 13 years, or no menses by age 14 years with hirsutism or with a history of excessive exercise or of an eating disorder.
You can start by examining what normal menstruation relies on: an intact central nervous system with a functioning pituitary, an ovarian response, and a normal uterus, cervix, and vagina. You should check the patient’s follicle-stimulating hormone, thyroid-stimulating hormone, and prolactin levels to assess CNS functioning, and estradiol levels to assess ovarian response. A genital exam with a pelvic ultrasound can reveal any possible defects in the uterus, cervix, or vagina.
The presence of breasts without a uterus indicates normal estrogen production, so the missing uterus could be a congenital defect or result from androgen insensitivity, Dr. Hertweck explained. In those without breasts, gonadal dysgenesis or gonadal enzymatic deficiency may explain no estrogen production. If the patient has both breasts and a uterus, you should rule out pregnancy first and then track CNS changes via FSH, TSH, and prolactin levels.
Premature ovarian insufficiency
Approximately 1% of females experience premature ovarian insufficiency, which can be diagnosed as early as age 14 years and should be suspected in a patient with a uterus but without breasts who has low estradiol levels, CNS failure identified by a high FSH level, and gonadal failure.
Formal diagnosis requires two separate instances of FSH elevation, and chromosomal testing should be done to rule out gonadal dysgenesis. You also should test the serum anti-Müllerian hormone biomarker (readings above 8 are concerning) and look for two possible causes. The FMR1 (Fragile X) premutation carrier status could be a cause, or presence of 21-hydroxylase and/or adrenal antibodies indicate autoimmune polyglandular syndrome.
Catching premature ovarian insufficiency early enough may allow patients to preserve some fertility if they still have oocytes present. Aside from this, girls will need hormone replacement therapy to fulfill developmental emotional and physical needs, such as bone growth and overall health. Despite a history of treating teens with premature ovarian insufficiency like adults, you should follow the practice guidelines specific to adolescents by the American College of Obstetricians and Gynecologists committee opinion statement (Obstet Gynecol. 2014;123:193-7).
Menorrhagia: heavy menstrual bleeding
Even though average blood loss is estimated at 30 mL per period, that number means little in clinical practice because patients cannot measure the actual amount of menses. Better indicators of abnormally greater flow include flow lasting longer than 7 days, finding clots larger than a quarter, changing menstrual products every 1-2 hours, leaking onto clothing such that patients need to take extra clothes to school, and any heavy periods that occur with easy bruising or with a family history of bleeding disorders.
First-line treatment for heavy menstrual bleeding in teens is hormonal contraception, either combination oral contraceptive pills, the transdermal patch, or the intravaginal ring, which can be combined with other therapies.
An alternative for those under age 18 (per Food and Drug Administration labeling) is oral tranexamic acid, found in a crossover trial with an oral contraceptive pill to be just as effective at reducing average blood loss and improving quality of life, but with fewer side effects and better compliance. Before prescribing anything for heavy menstrual bleeding, however, you must consider possible causes and rule some out that require different management.
Aside from pregnancy, one potential cause of menorrhagia is infection such as chlamydia or gonorrhea, which should be considered even in those with a negative sexual history, Dr. Hertweck said. Other possible causes include an immature hypothalamic-pituitary-ovarian axis, polycystic ovary syndrome (even with low hemoglobin), malignancy with a hormone-producing tumor, hypothalamic dysfunction (often stimulated by eating disorders, obesity, rapid weight loss, or gluten intolerance), or coagulopathy.
“Teens with menorrhagia may need to be screened for a bleeding disorder,” Dr. Hertweck said. At a minimum, she recommends checking complete blood count, ferritin, and TSH. “The most common bleeding disorders associated with heavy menstrual bleeding include platelet function disorders and von Willebrand.”
Up to half of teen girls with menorrhagia who visit a hematologist or multidisciplinary clinic receive a diagnosis of a bleeding disorder, Dr. Hertweck said. And up to half of those with menorrhagia at menarche may have von Willebrand, as do one in six adolescents who go to the emergency department because of heavy menstrual bleeding.
Von Willebrand syndrome
Von Willebrand syndrome is a deficiency or dysfunction of von Willebrand factor (vWF), a protein with binding sites for platelets, collagen, and factor VIII that “serves as a bridge between platelets and injury sites in vessel walls” and “protects factor VIII from rapid proteolytic degradation,” Dr. Hertweck said. Von Willebrand syndrome is the most common inherited congenital bleeding disorder. Although acquired von Willebrand syndrome is rare, it has grown in incidence among those with complex cardiovascular, hematologic, or immunologic disorders.
“Correct diagnosis is complex and not always straightforward,” Dr. Hertweck said, but “a positive response to questions in four categories is highly sensitive.” They are as follows:
• Menses lasting at least 7 days and interfering with a person’s daily activities.
• “History of treatment for anemia.
• Family history of a diagnosed bleeding disorder.
• History of excessive bleeding after tooth extraction, delivery, miscarriage, or surgery.
Diagnostic assays include platelet concentration of vWF antigen, an activity test of vWF-platelet binding, and factor VIII activity. However, you often need to repeat diagnostic testing because vWF antigens vary according to race, blood type, age, acute phase response, and menstrual cycle timing, Dr. Hertweck said.
“Remember to draw von Willebrand testing only during the first 3 days of the menstrual cycle when estrogen levels are at the nadir,” she said.
Because estrogen increases vWF, treatment for von Willebrand syndrome should be progestin only, either oral pills, medroxyprogesterone acetate (MPA, or Depo-Provera injections), or an etonogestrel implant.
Dr. Hertweck presented several cases of abnormal menstruation and extreme conditions such as severe menorrhagia. Outside of von Willebrand in such patients, possible platelet disorders could include Glanzmann thrombasthenia (a platelet function disorder that is caused by an abnormality in the genes for glycoproteins IIb/IIIa) and platelet storage pool disorder, both of which should be diagnosed by a hematologist.
Dr. Hertweck reported having a research grant from Merck related to contraceptive implants in adolescents.
CHICAGO – , according to S. Paige Hertweck, MD, chief of gynecology at Norton Children’s Hospital in Louisville, Ky.
“Remember to use the menstrual cycle as a vital sign,” Dr. Hertweck told attendees at the American Academy of Pediatrics annual meeting. “Even within the first year of menarche, most girls have a period at least every 90 days, so work up those who don’t.”
The median age of menarche is 12.4 years, typically beginning within 2-3 years of breast budding at Tanner Stage 4 breast development, she said. By 15 years of age, 98% of girls have begun menstruation.
Girls’ cycles typically last 21-45 days, an average of 32.2 days during their first year of menstruation, with flow for 7 days or less, requiring an average of 3-6 pads and/or tampons per day. Dr. Hertweck recommends you write down these features of normal menstruation so that your patients can tell you when their cycle is abnormal or menses doesn’t return.
“Cycle length is more variable for teens versus women 20-40 years old,” she said. However, “it’s not true that ‘anything goes’ for cycle length” in teens, she added. “Cycles that are consistently outside the range of 21-45 days are statistically uncommon.” Hence the need to evaluate causes of amenorrhea in girls whose cycles exceed 90 days.
Possible causes of amenorrhea include pregnancy, polycystic ovary syndrome, thyroid abnormalities, hyperprolactinemia, primary ovarian insufficiency, or hypogonadal amenorrhea, typically stimulated by the first instance of anorexia, Crohn’s disease, celiac disease, or a gluten intolerance.
Primary amenorrhea
Dr. Hertweck listed five benchmarks that indicate primary amenorrhea requiring evaluation. Those indicators include girls who have no menarche by age 15 years or within 3 years of breast budding, no breast development by age 13 years, or no menses by age 14 years with hirsutism or with a history of excessive exercise or of an eating disorder.
You can start by examining what normal menstruation relies on: an intact central nervous system with a functioning pituitary, an ovarian response, and a normal uterus, cervix, and vagina. You should check the patient’s follicle-stimulating hormone, thyroid-stimulating hormone, and prolactin levels to assess CNS functioning, and estradiol levels to assess ovarian response. A genital exam with a pelvic ultrasound can reveal any possible defects in the uterus, cervix, or vagina.
The presence of breasts without a uterus indicates normal estrogen production, so the missing uterus could be a congenital defect or result from androgen insensitivity, Dr. Hertweck explained. In those without breasts, gonadal dysgenesis or gonadal enzymatic deficiency may explain no estrogen production. If the patient has both breasts and a uterus, you should rule out pregnancy first and then track CNS changes via FSH, TSH, and prolactin levels.
Premature ovarian insufficiency
Approximately 1% of females experience premature ovarian insufficiency, which can be diagnosed as early as age 14 years and should be suspected in a patient with a uterus but without breasts who has low estradiol levels, CNS failure identified by a high FSH level, and gonadal failure.
Formal diagnosis requires two separate instances of FSH elevation, and chromosomal testing should be done to rule out gonadal dysgenesis. You also should test the serum anti-Müllerian hormone biomarker (readings above 8 are concerning) and look for two possible causes. The FMR1 (Fragile X) premutation carrier status could be a cause, or presence of 21-hydroxylase and/or adrenal antibodies indicate autoimmune polyglandular syndrome.
Catching premature ovarian insufficiency early enough may allow patients to preserve some fertility if they still have oocytes present. Aside from this, girls will need hormone replacement therapy to fulfill developmental emotional and physical needs, such as bone growth and overall health. Despite a history of treating teens with premature ovarian insufficiency like adults, you should follow the practice guidelines specific to adolescents by the American College of Obstetricians and Gynecologists committee opinion statement (Obstet Gynecol. 2014;123:193-7).
Menorrhagia: heavy menstrual bleeding
Even though average blood loss is estimated at 30 mL per period, that number means little in clinical practice because patients cannot measure the actual amount of menses. Better indicators of abnormally greater flow include flow lasting longer than 7 days, finding clots larger than a quarter, changing menstrual products every 1-2 hours, leaking onto clothing such that patients need to take extra clothes to school, and any heavy periods that occur with easy bruising or with a family history of bleeding disorders.
First-line treatment for heavy menstrual bleeding in teens is hormonal contraception, either combination oral contraceptive pills, the transdermal patch, or the intravaginal ring, which can be combined with other therapies.
An alternative for those under age 18 (per Food and Drug Administration labeling) is oral tranexamic acid, found in a crossover trial with an oral contraceptive pill to be just as effective at reducing average blood loss and improving quality of life, but with fewer side effects and better compliance. Before prescribing anything for heavy menstrual bleeding, however, you must consider possible causes and rule some out that require different management.
Aside from pregnancy, one potential cause of menorrhagia is infection such as chlamydia or gonorrhea, which should be considered even in those with a negative sexual history, Dr. Hertweck said. Other possible causes include an immature hypothalamic-pituitary-ovarian axis, polycystic ovary syndrome (even with low hemoglobin), malignancy with a hormone-producing tumor, hypothalamic dysfunction (often stimulated by eating disorders, obesity, rapid weight loss, or gluten intolerance), or coagulopathy.
“Teens with menorrhagia may need to be screened for a bleeding disorder,” Dr. Hertweck said. At a minimum, she recommends checking complete blood count, ferritin, and TSH. “The most common bleeding disorders associated with heavy menstrual bleeding include platelet function disorders and von Willebrand.”
Up to half of teen girls with menorrhagia who visit a hematologist or multidisciplinary clinic receive a diagnosis of a bleeding disorder, Dr. Hertweck said. And up to half of those with menorrhagia at menarche may have von Willebrand, as do one in six adolescents who go to the emergency department because of heavy menstrual bleeding.
Von Willebrand syndrome
Von Willebrand syndrome is a deficiency or dysfunction of von Willebrand factor (vWF), a protein with binding sites for platelets, collagen, and factor VIII that “serves as a bridge between platelets and injury sites in vessel walls” and “protects factor VIII from rapid proteolytic degradation,” Dr. Hertweck said. Von Willebrand syndrome is the most common inherited congenital bleeding disorder. Although acquired von Willebrand syndrome is rare, it has grown in incidence among those with complex cardiovascular, hematologic, or immunologic disorders.
“Correct diagnosis is complex and not always straightforward,” Dr. Hertweck said, but “a positive response to questions in four categories is highly sensitive.” They are as follows:
• Menses lasting at least 7 days and interfering with a person’s daily activities.
• “History of treatment for anemia.
• Family history of a diagnosed bleeding disorder.
• History of excessive bleeding after tooth extraction, delivery, miscarriage, or surgery.
Diagnostic assays include platelet concentration of vWF antigen, an activity test of vWF-platelet binding, and factor VIII activity. However, you often need to repeat diagnostic testing because vWF antigens vary according to race, blood type, age, acute phase response, and menstrual cycle timing, Dr. Hertweck said.
“Remember to draw von Willebrand testing only during the first 3 days of the menstrual cycle when estrogen levels are at the nadir,” she said.
Because estrogen increases vWF, treatment for von Willebrand syndrome should be progestin only, either oral pills, medroxyprogesterone acetate (MPA, or Depo-Provera injections), or an etonogestrel implant.
Dr. Hertweck presented several cases of abnormal menstruation and extreme conditions such as severe menorrhagia. Outside of von Willebrand in such patients, possible platelet disorders could include Glanzmann thrombasthenia (a platelet function disorder that is caused by an abnormality in the genes for glycoproteins IIb/IIIa) and platelet storage pool disorder, both of which should be diagnosed by a hematologist.
Dr. Hertweck reported having a research grant from Merck related to contraceptive implants in adolescents.
CHICAGO – , according to S. Paige Hertweck, MD, chief of gynecology at Norton Children’s Hospital in Louisville, Ky.
“Remember to use the menstrual cycle as a vital sign,” Dr. Hertweck told attendees at the American Academy of Pediatrics annual meeting. “Even within the first year of menarche, most girls have a period at least every 90 days, so work up those who don’t.”
The median age of menarche is 12.4 years, typically beginning within 2-3 years of breast budding at Tanner Stage 4 breast development, she said. By 15 years of age, 98% of girls have begun menstruation.
Girls’ cycles typically last 21-45 days, an average of 32.2 days during their first year of menstruation, with flow for 7 days or less, requiring an average of 3-6 pads and/or tampons per day. Dr. Hertweck recommends you write down these features of normal menstruation so that your patients can tell you when their cycle is abnormal or menses doesn’t return.
“Cycle length is more variable for teens versus women 20-40 years old,” she said. However, “it’s not true that ‘anything goes’ for cycle length” in teens, she added. “Cycles that are consistently outside the range of 21-45 days are statistically uncommon.” Hence the need to evaluate causes of amenorrhea in girls whose cycles exceed 90 days.
Possible causes of amenorrhea include pregnancy, polycystic ovary syndrome, thyroid abnormalities, hyperprolactinemia, primary ovarian insufficiency, or hypogonadal amenorrhea, typically stimulated by the first instance of anorexia, Crohn’s disease, celiac disease, or a gluten intolerance.
Primary amenorrhea
Dr. Hertweck listed five benchmarks that indicate primary amenorrhea requiring evaluation. Those indicators include girls who have no menarche by age 15 years or within 3 years of breast budding, no breast development by age 13 years, or no menses by age 14 years with hirsutism or with a history of excessive exercise or of an eating disorder.
You can start by examining what normal menstruation relies on: an intact central nervous system with a functioning pituitary, an ovarian response, and a normal uterus, cervix, and vagina. You should check the patient’s follicle-stimulating hormone, thyroid-stimulating hormone, and prolactin levels to assess CNS functioning, and estradiol levels to assess ovarian response. A genital exam with a pelvic ultrasound can reveal any possible defects in the uterus, cervix, or vagina.
The presence of breasts without a uterus indicates normal estrogen production, so the missing uterus could be a congenital defect or result from androgen insensitivity, Dr. Hertweck explained. In those without breasts, gonadal dysgenesis or gonadal enzymatic deficiency may explain no estrogen production. If the patient has both breasts and a uterus, you should rule out pregnancy first and then track CNS changes via FSH, TSH, and prolactin levels.
Premature ovarian insufficiency
Approximately 1% of females experience premature ovarian insufficiency, which can be diagnosed as early as age 14 years and should be suspected in a patient with a uterus but without breasts who has low estradiol levels, CNS failure identified by a high FSH level, and gonadal failure.
Formal diagnosis requires two separate instances of FSH elevation, and chromosomal testing should be done to rule out gonadal dysgenesis. You also should test the serum anti-Müllerian hormone biomarker (readings above 8 are concerning) and look for two possible causes. The FMR1 (Fragile X) premutation carrier status could be a cause, or presence of 21-hydroxylase and/or adrenal antibodies indicate autoimmune polyglandular syndrome.
Catching premature ovarian insufficiency early enough may allow patients to preserve some fertility if they still have oocytes present. Aside from this, girls will need hormone replacement therapy to fulfill developmental emotional and physical needs, such as bone growth and overall health. Despite a history of treating teens with premature ovarian insufficiency like adults, you should follow the practice guidelines specific to adolescents by the American College of Obstetricians and Gynecologists committee opinion statement (Obstet Gynecol. 2014;123:193-7).
Menorrhagia: heavy menstrual bleeding
Even though average blood loss is estimated at 30 mL per period, that number means little in clinical practice because patients cannot measure the actual amount of menses. Better indicators of abnormally greater flow include flow lasting longer than 7 days, finding clots larger than a quarter, changing menstrual products every 1-2 hours, leaking onto clothing such that patients need to take extra clothes to school, and any heavy periods that occur with easy bruising or with a family history of bleeding disorders.
First-line treatment for heavy menstrual bleeding in teens is hormonal contraception, either combination oral contraceptive pills, the transdermal patch, or the intravaginal ring, which can be combined with other therapies.
An alternative for those under age 18 (per Food and Drug Administration labeling) is oral tranexamic acid, found in a crossover trial with an oral contraceptive pill to be just as effective at reducing average blood loss and improving quality of life, but with fewer side effects and better compliance. Before prescribing anything for heavy menstrual bleeding, however, you must consider possible causes and rule some out that require different management.
Aside from pregnancy, one potential cause of menorrhagia is infection such as chlamydia or gonorrhea, which should be considered even in those with a negative sexual history, Dr. Hertweck said. Other possible causes include an immature hypothalamic-pituitary-ovarian axis, polycystic ovary syndrome (even with low hemoglobin), malignancy with a hormone-producing tumor, hypothalamic dysfunction (often stimulated by eating disorders, obesity, rapid weight loss, or gluten intolerance), or coagulopathy.
“Teens with menorrhagia may need to be screened for a bleeding disorder,” Dr. Hertweck said. At a minimum, she recommends checking complete blood count, ferritin, and TSH. “The most common bleeding disorders associated with heavy menstrual bleeding include platelet function disorders and von Willebrand.”
Up to half of teen girls with menorrhagia who visit a hematologist or multidisciplinary clinic receive a diagnosis of a bleeding disorder, Dr. Hertweck said. And up to half of those with menorrhagia at menarche may have von Willebrand, as do one in six adolescents who go to the emergency department because of heavy menstrual bleeding.
Von Willebrand syndrome
Von Willebrand syndrome is a deficiency or dysfunction of von Willebrand factor (vWF), a protein with binding sites for platelets, collagen, and factor VIII that “serves as a bridge between platelets and injury sites in vessel walls” and “protects factor VIII from rapid proteolytic degradation,” Dr. Hertweck said. Von Willebrand syndrome is the most common inherited congenital bleeding disorder. Although acquired von Willebrand syndrome is rare, it has grown in incidence among those with complex cardiovascular, hematologic, or immunologic disorders.
“Correct diagnosis is complex and not always straightforward,” Dr. Hertweck said, but “a positive response to questions in four categories is highly sensitive.” They are as follows:
• Menses lasting at least 7 days and interfering with a person’s daily activities.
• “History of treatment for anemia.
• Family history of a diagnosed bleeding disorder.
• History of excessive bleeding after tooth extraction, delivery, miscarriage, or surgery.
Diagnostic assays include platelet concentration of vWF antigen, an activity test of vWF-platelet binding, and factor VIII activity. However, you often need to repeat diagnostic testing because vWF antigens vary according to race, blood type, age, acute phase response, and menstrual cycle timing, Dr. Hertweck said.
“Remember to draw von Willebrand testing only during the first 3 days of the menstrual cycle when estrogen levels are at the nadir,” she said.
Because estrogen increases vWF, treatment for von Willebrand syndrome should be progestin only, either oral pills, medroxyprogesterone acetate (MPA, or Depo-Provera injections), or an etonogestrel implant.
Dr. Hertweck presented several cases of abnormal menstruation and extreme conditions such as severe menorrhagia. Outside of von Willebrand in such patients, possible platelet disorders could include Glanzmann thrombasthenia (a platelet function disorder that is caused by an abnormality in the genes for glycoproteins IIb/IIIa) and platelet storage pool disorder, both of which should be diagnosed by a hematologist.
Dr. Hertweck reported having a research grant from Merck related to contraceptive implants in adolescents.
EXPERT ANALYSIS FROM AAP 2017
Are microRNAs the key to an endometriosis biomarker?
SAN ANTONIO – The results of a prospective study showed that, in patients without a surgical endometriosis diagnosis, a serum test of microRNA (miRNA) levels yielded a very high predictive value when endometriosis was later surgically confirmed.
“This is the first prospective study performed within a diverse population that identifies miRNAs can reliably be used to differentiate between endometriosis and other gynecologic pathologies,” Sarah Moustafa, MD, said at the annual meeting of the American Society for Reproductive Medicine. 
Dr. Moustafa and her collaborators found that the area under the receiver operating characteristic curve (AUC) for the combination of miRNAs 125, 451, and 3613 was 0.917. The AUC of another combination was even higher: the miRNAs let-7b, 150, 342, and 451 yielded an AUC of 0.977 for endometriosis. These figures support that the miRNA combinations give “an excellent diagnostic potential for endometriosis,” Dr. Moustafa said.
The study enrolled 86 women of reproductive age who were scheduled to have a laparotomy or laparoscopy for benign gynecologic reasons. Pregnant patients and those with malignancy were excluded. Patients had blood drawn before their surgeries to have blinded miRNA analysis via quantitative reverse transcriptase polymerase chain reaction.
Dr. Moustafa and her colleagues looked at the diagnostic value of individual miRNAs and also examined combinations of promising miRNAs by seeing which levels were elevated or depressed in patients who were later found to have surgically diagnosed endometriosis. The study built on previous retrospective work that had identified some candidate miRNAs.
In this prospective study, women with endometriosis had significantly lower serum levels of miRNAs 3613 and let-7b and significantly higher serum levels of miRNAs 150, 125b, 451, and 342. The investigators also analyzed the data to see if there were miRNA level differences between women who were on hormones and those who were not, and also to see if cycle timing affected results; neither of these factors affected miRNA levels, Dr. Moustafa reported.
When the enrolled patients had surgery, 36 were found to have endometriosis and 50 had a variety of other diagnoses, with uterine fibroids (48%) and no abnormal pathology (28%) predominating.
“A noninvasive diagnostic test does not currently exist” but is sorely needed, Dr. Moustafa said.
There’s a long gap from the onset of endometriosis symptoms to diagnosis, with one study showing that symptoms can be present for an average of 6.7-11 years before surgical diagnosis occurs. In one survey of more than 7,000 women, nearly half (46%) saw more than five physicians before they got the correct diagnosis, said Dr. Moustafa, a resident in the obstetrics, gynecology, and reproductive sciences department at Yale University, New Haven, Conn.
In a discussion following the presentation, attendee Steve Young, MD, PhD, professor of reproductive endocrinology and fertility at the University of North Carolina, Chapel Hill, said it would be useful to have a biomarker that could be a surrogate for disease burden. “You could look at miRNAs after surgery. Do you see changes back toward normal?” Dr. Young said.
Dr. Moustafa responded that the research team is in the process of collecting postoperative data to see whether levels change when the disease burden is diminished by surgery.
Next steps, she said, include looking for miRNAs in saliva to explore whether an even less invasive test might be possible. Also, there are suggestions that miRNA 125 might be a marker for more severe disease, so the team is investigating this association as well.
Whether the combination miRNA screen is ready for prime time is still an open question, she said. “Any time a new screening test is developed we have to have caution.” Current thinking, she said, points toward the utility of miRNA screening for patients with unexplained fertility, for example.
“At this point, the pendulum is so far on the side of underdiagnosis that we think patients would benefit from a screening test,” Dr. Moustafa added.
The study was supported by OvaScience. Dr. Moustafa reported having no relevant financial disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
SAN ANTONIO – The results of a prospective study showed that, in patients without a surgical endometriosis diagnosis, a serum test of microRNA (miRNA) levels yielded a very high predictive value when endometriosis was later surgically confirmed.
“This is the first prospective study performed within a diverse population that identifies miRNAs can reliably be used to differentiate between endometriosis and other gynecologic pathologies,” Sarah Moustafa, MD, said at the annual meeting of the American Society for Reproductive Medicine.
Dr. Moustafa and her collaborators found that the area under the receiver operating characteristic curve (AUC) for the combination of miRNAs 125, 451, and 3613 was 0.917. The AUC of another combination was even higher: the miRNAs let-7b, 150, 342, and 451 yielded an AUC of 0.977 for endometriosis. These figures support that the miRNA combinations give “an excellent diagnostic potential for endometriosis,” Dr. Moustafa said.
The study enrolled 86 women of reproductive age who were scheduled to have a laparotomy or laparoscopy for benign gynecologic reasons. Pregnant patients and those with malignancy were excluded. Patients had blood drawn before their surgeries to have blinded miRNA analysis via quantitative reverse transcriptase polymerase chain reaction.
Dr. Moustafa and her colleagues looked at the diagnostic value of individual miRNAs and also examined combinations of promising miRNAs by seeing which levels were elevated or depressed in patients who were later found to have surgically diagnosed endometriosis. The study built on previous retrospective work that had identified some candidate miRNAs.
In this prospective study, women with endometriosis had significantly lower serum levels of miRNAs 3613 and let-7b and significantly higher serum levels of miRNAs 150, 125b, 451, and 342. The investigators also analyzed the data to see if there were miRNA level differences between women who were on hormones and those who were not, and also to see if cycle timing affected results; neither of these factors affected miRNA levels, Dr. Moustafa reported.
When the enrolled patients had surgery, 36 were found to have endometriosis and 50 had a variety of other diagnoses, with uterine fibroids (48%) and no abnormal pathology (28%) predominating.
“A noninvasive diagnostic test does not currently exist” but is sorely needed, Dr. Moustafa said.
There’s a long gap from the onset of endometriosis symptoms to diagnosis, with one study showing that symptoms can be present for an average of 6.7-11 years before surgical diagnosis occurs. In one survey of more than 7,000 women, nearly half (46%) saw more than five physicians before they got the correct diagnosis, said Dr. Moustafa, a resident in the obstetrics, gynecology, and reproductive sciences department at Yale University, New Haven, Conn.
In a discussion following the presentation, attendee Steve Young, MD, PhD, professor of reproductive endocrinology and fertility at the University of North Carolina, Chapel Hill, said it would be useful to have a biomarker that could be a surrogate for disease burden. “You could look at miRNAs after surgery. Do you see changes back toward normal?” Dr. Young said.
Dr. Moustafa responded that the research team is in the process of collecting postoperative data to see whether levels change when the disease burden is diminished by surgery.
Next steps, she said, include looking for miRNAs in saliva to explore whether an even less invasive test might be possible. Also, there are suggestions that miRNA 125 might be a marker for more severe disease, so the team is investigating this association as well.
Whether the combination miRNA screen is ready for prime time is still an open question, she said. “Any time a new screening test is developed we have to have caution.” Current thinking, she said, points toward the utility of miRNA screening for patients with unexplained fertility, for example.
“At this point, the pendulum is so far on the side of underdiagnosis that we think patients would benefit from a screening test,” Dr. Moustafa added.
The study was supported by OvaScience. Dr. Moustafa reported having no relevant financial disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
SAN ANTONIO – The results of a prospective study showed that, in patients without a surgical endometriosis diagnosis, a serum test of microRNA (miRNA) levels yielded a very high predictive value when endometriosis was later surgically confirmed.
“This is the first prospective study performed within a diverse population that identifies miRNAs can reliably be used to differentiate between endometriosis and other gynecologic pathologies,” Sarah Moustafa, MD, said at the annual meeting of the American Society for Reproductive Medicine.
Dr. Moustafa and her collaborators found that the area under the receiver operating characteristic curve (AUC) for the combination of miRNAs 125, 451, and 3613 was 0.917. The AUC of another combination was even higher: the miRNAs let-7b, 150, 342, and 451 yielded an AUC of 0.977 for endometriosis. These figures support that the miRNA combinations give “an excellent diagnostic potential for endometriosis,” Dr. Moustafa said.
The study enrolled 86 women of reproductive age who were scheduled to have a laparotomy or laparoscopy for benign gynecologic reasons. Pregnant patients and those with malignancy were excluded. Patients had blood drawn before their surgeries to have blinded miRNA analysis via quantitative reverse transcriptase polymerase chain reaction.
Dr. Moustafa and her colleagues looked at the diagnostic value of individual miRNAs and also examined combinations of promising miRNAs by seeing which levels were elevated or depressed in patients who were later found to have surgically diagnosed endometriosis. The study built on previous retrospective work that had identified some candidate miRNAs.
In this prospective study, women with endometriosis had significantly lower serum levels of miRNAs 3613 and let-7b and significantly higher serum levels of miRNAs 150, 125b, 451, and 342. The investigators also analyzed the data to see if there were miRNA level differences between women who were on hormones and those who were not, and also to see if cycle timing affected results; neither of these factors affected miRNA levels, Dr. Moustafa reported.
When the enrolled patients had surgery, 36 were found to have endometriosis and 50 had a variety of other diagnoses, with uterine fibroids (48%) and no abnormal pathology (28%) predominating.
“A noninvasive diagnostic test does not currently exist” but is sorely needed, Dr. Moustafa said.
There’s a long gap from the onset of endometriosis symptoms to diagnosis, with one study showing that symptoms can be present for an average of 6.7-11 years before surgical diagnosis occurs. In one survey of more than 7,000 women, nearly half (46%) saw more than five physicians before they got the correct diagnosis, said Dr. Moustafa, a resident in the obstetrics, gynecology, and reproductive sciences department at Yale University, New Haven, Conn.
In a discussion following the presentation, attendee Steve Young, MD, PhD, professor of reproductive endocrinology and fertility at the University of North Carolina, Chapel Hill, said it would be useful to have a biomarker that could be a surrogate for disease burden. “You could look at miRNAs after surgery. Do you see changes back toward normal?” Dr. Young said.
Dr. Moustafa responded that the research team is in the process of collecting postoperative data to see whether levels change when the disease burden is diminished by surgery.
Next steps, she said, include looking for miRNAs in saliva to explore whether an even less invasive test might be possible. Also, there are suggestions that miRNA 125 might be a marker for more severe disease, so the team is investigating this association as well.
Whether the combination miRNA screen is ready for prime time is still an open question, she said. “Any time a new screening test is developed we have to have caution.” Current thinking, she said, points toward the utility of miRNA screening for patients with unexplained fertility, for example.
“At this point, the pendulum is so far on the side of underdiagnosis that we think patients would benefit from a screening test,” Dr. Moustafa added.
The study was supported by OvaScience. Dr. Moustafa reported having no relevant financial disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
AT ASRM 2017
Key clinical point:
Major finding: The areas under the receiver operating curve for the most promising miRNA combinations were 0.917 and 0.977.
Data source: Blinded, prospective study of 86 women slated to have diagnostic pelvic laparoscopy or laparotomy.
Disclosures: Dr. Moustafa reported no relevant disclosures. OvaScience supported the study.

FDA: Ultrasound surgical devices are contraindicated for uterine fibroid removal
, according to the Food and Drug Administration.
These devices have the potential to disseminate undetected tumor tissue, and there are no proven preoperative screening methods for detecting uterine sarcoma in uterine fibroids that otherwise appear to be benign, FDA officials wrote in a guidance document issued Oct. 30. The FDA is calling for new product labeling for these devices within 120 days.
The devices deliver ultrasonic energy through an oscillating tip, which leads to tissue fragmentation. This can lead to tissue dissemination that cannot be eliminated by suction/aspiration. In advanced cancers, the risk of dissemination may be outweighed by the benefits of the devices, including the debulking effect with no thermal collateral damage, as well as avoidance of the need for organ removal or resection.
The devices are currently labeled in a way that suggests they could be used in removing uterine fibroids, though the agency said that it is not aware that they are used for this purpose.
The agency recommended against their use in uterine fibroids, in part because there are alternative treatment options available. But the American College of Obstetricians and Gynecologists has challenged that assertion. When the FDA first issued a draft notice of the labeling guidance in November 2016, ACOG commented that abdominal hysterectomy is the alternative treatment option and is associated with significant morbidity and mortality beyond that seen with minimally invasive techniques. ACOG urged the FDA to prioritize informed consent and the weighing of risks and benefits.
Ultrasonic surgical aspirator devices are used for a wide range of surgical applications, but the recommendations apply specifically to laparoscopic surgery, open surgery, and gynecologic surgery.
, according to the Food and Drug Administration.
These devices have the potential to disseminate undetected tumor tissue, and there are no proven preoperative screening methods for detecting uterine sarcoma in uterine fibroids that otherwise appear to be benign, FDA officials wrote in a guidance document issued Oct. 30. The FDA is calling for new product labeling for these devices within 120 days.
The devices deliver ultrasonic energy through an oscillating tip, which leads to tissue fragmentation. This can lead to tissue dissemination that cannot be eliminated by suction/aspiration. In advanced cancers, the risk of dissemination may be outweighed by the benefits of the devices, including the debulking effect with no thermal collateral damage, as well as avoidance of the need for organ removal or resection.
The devices are currently labeled in a way that suggests they could be used in removing uterine fibroids, though the agency said that it is not aware that they are used for this purpose.
The agency recommended against their use in uterine fibroids, in part because there are alternative treatment options available. But the American College of Obstetricians and Gynecologists has challenged that assertion. When the FDA first issued a draft notice of the labeling guidance in November 2016, ACOG commented that abdominal hysterectomy is the alternative treatment option and is associated with significant morbidity and mortality beyond that seen with minimally invasive techniques. ACOG urged the FDA to prioritize informed consent and the weighing of risks and benefits.
Ultrasonic surgical aspirator devices are used for a wide range of surgical applications, but the recommendations apply specifically to laparoscopic surgery, open surgery, and gynecologic surgery.
, according to the Food and Drug Administration.
These devices have the potential to disseminate undetected tumor tissue, and there are no proven preoperative screening methods for detecting uterine sarcoma in uterine fibroids that otherwise appear to be benign, FDA officials wrote in a guidance document issued Oct. 30. The FDA is calling for new product labeling for these devices within 120 days.
The devices deliver ultrasonic energy through an oscillating tip, which leads to tissue fragmentation. This can lead to tissue dissemination that cannot be eliminated by suction/aspiration. In advanced cancers, the risk of dissemination may be outweighed by the benefits of the devices, including the debulking effect with no thermal collateral damage, as well as avoidance of the need for organ removal or resection.
The devices are currently labeled in a way that suggests they could be used in removing uterine fibroids, though the agency said that it is not aware that they are used for this purpose.
The agency recommended against their use in uterine fibroids, in part because there are alternative treatment options available. But the American College of Obstetricians and Gynecologists has challenged that assertion. When the FDA first issued a draft notice of the labeling guidance in November 2016, ACOG commented that abdominal hysterectomy is the alternative treatment option and is associated with significant morbidity and mortality beyond that seen with minimally invasive techniques. ACOG urged the FDA to prioritize informed consent and the weighing of risks and benefits.
Ultrasonic surgical aspirator devices are used for a wide range of surgical applications, but the recommendations apply specifically to laparoscopic surgery, open surgery, and gynecologic surgery.
Ulipristal acetate reduced bleeding for women with fibroids
SAN ANTONIO – About half of women with uterine fibroids became amenorrheic when taking the selective progesterone receptor modulator ulipristal acetate (UPA) during a 12-week study cycle, and women taking UPA experienced significant improvement of quality of life, compared with those taking placebo.
Of those women taking 5 mg of UPA, 40.5%-42% became amenorrheic; of those taking 10 mg, 54.8%-57.3% became amenorrheic, James Liu, MD, reported at the annual meeting of the American Society for Reproductive Medicine. These results compared to amenorrhea rates of 0%-8% for women on placebo (P less than .0001 for all values).
The primary aim of VENUS II was to evaluate UPA’s efficacy and safety as intermittent treatment of abnormal uterine bleeding associated with uterine fibroids. Patients received UPA at either 5 mg or 10 mg orally. Secondary efficacy measures included the maintenance effect of UPA at both doses when compared to placebo, by assessing the rate of amenorrhea and the time to amenorrhea. Another secondary measure assessed uterine fibroid–related quality of life.
Safety was assessed by tracking adverse events through both courses of treatment. The study was not powered to compare the two doses against each other, but rather compared each against placebo.
Altogether, 432 patients were randomized to one of the treatment arms, which was begun after an initial screening period of about 10-12 weeks. The first treatment course lasted 12 weeks, after which patients went off treatment for two menstrual cycles. They then began another treatment course for 12 weeks and were followed for an additional 12 weeks after treatment was stopped.
Patients were included if they were premenopausal, aged 18-50 years old, had prolonged bleeding in at least 4 of the last 6 menstrual periods, had menstrual blood loss of at least 80 mL by cycle by the alkaline hematin method, and had at least one discrete leiomyoma without a uterine size greater than 20 weeks. About two-thirds of patients were black, reflecting the higher prevalence of uterine fibroids in this population, said Dr. Liu, professor of medicine and reproductive biology at Case Western Reserve University, Cleveland.
Most patients (60%-80%) had their bleeding controlled on either dose of UPA, compared with fewer than 10% of women taking placebo.
Quality of life data, presented separately at ASRM by Lee Shulman, MD, examined the impact of treatment on patients’ physical and social activities, and also on the severity of symptoms and health-related quality of life.
“The majority of patients on UPA versus a minority of patients on placebo described their menstrual/vaginal bleeding at the end of treatment course 1 as ‘much better’ or ‘very much better,’ ” said Dr. Shulman, chief of clinical genetics in the department of ob.gyn. at Northwestern University in Evanston, Ill.
Of patients taking 5 mg UPA, 75% reported that degree of improvement, as did 87% of those on 10 mg UPA, compared with 17.9% of those taking placebo. .
Adverse events were rare, with hot flashes occurring in about 10% of women taking UPA, compared with less than 2% of those taking placebo. Headaches, fatigue, and nausea were also reported, but rates were not significantly different from rates for those taking placebo. One serious adverse event that was deemed treatment related was a uterine hemorrhage experienced by a woman taking UPA.
“Even in treatment course 1 we already had profound and statistically significant effects in symptoms across the board,” Dr. Shulman said. “How long will they last? We obviously need more data. But the study suggests that the benefits last significantly longer than that associated with leuprolide acetate.”
Ulipristal acetate is already approved by the Food and Drug Administration at a different dosage as emergency contraception. The VENUS II data support its use for women with uterine fibroids, the researchers said. “Our results provide reassurance,” Dr. Liu said. “We can conclude that UPA is effective and safe in the management of uterine fibroids in the U.S. population.”
Dr. Liu reported that he had no relevant disclosures. Dr. Shulman reported relationships with multiple pharmaceutical companies, including Allergan, which funded the VENUS II study.
koakes@frontlinemedcom.com
On Twitter @karioakes
SAN ANTONIO – About half of women with uterine fibroids became amenorrheic when taking the selective progesterone receptor modulator ulipristal acetate (UPA) during a 12-week study cycle, and women taking UPA experienced significant improvement of quality of life, compared with those taking placebo.
Of those women taking 5 mg of UPA, 40.5%-42% became amenorrheic; of those taking 10 mg, 54.8%-57.3% became amenorrheic, James Liu, MD, reported at the annual meeting of the American Society for Reproductive Medicine. These results compared to amenorrhea rates of 0%-8% for women on placebo (P less than .0001 for all values).
The primary aim of VENUS II was to evaluate UPA’s efficacy and safety as intermittent treatment of abnormal uterine bleeding associated with uterine fibroids. Patients received UPA at either 5 mg or 10 mg orally. Secondary efficacy measures included the maintenance effect of UPA at both doses when compared to placebo, by assessing the rate of amenorrhea and the time to amenorrhea. Another secondary measure assessed uterine fibroid–related quality of life.
Safety was assessed by tracking adverse events through both courses of treatment. The study was not powered to compare the two doses against each other, but rather compared each against placebo.
Altogether, 432 patients were randomized to one of the treatment arms, which was begun after an initial screening period of about 10-12 weeks. The first treatment course lasted 12 weeks, after which patients went off treatment for two menstrual cycles. They then began another treatment course for 12 weeks and were followed for an additional 12 weeks after treatment was stopped.
Patients were included if they were premenopausal, aged 18-50 years old, had prolonged bleeding in at least 4 of the last 6 menstrual periods, had menstrual blood loss of at least 80 mL by cycle by the alkaline hematin method, and had at least one discrete leiomyoma without a uterine size greater than 20 weeks. About two-thirds of patients were black, reflecting the higher prevalence of uterine fibroids in this population, said Dr. Liu, professor of medicine and reproductive biology at Case Western Reserve University, Cleveland.
Most patients (60%-80%) had their bleeding controlled on either dose of UPA, compared with fewer than 10% of women taking placebo.
Quality of life data, presented separately at ASRM by Lee Shulman, MD, examined the impact of treatment on patients’ physical and social activities, and also on the severity of symptoms and health-related quality of life.
“The majority of patients on UPA versus a minority of patients on placebo described their menstrual/vaginal bleeding at the end of treatment course 1 as ‘much better’ or ‘very much better,’ ” said Dr. Shulman, chief of clinical genetics in the department of ob.gyn. at Northwestern University in Evanston, Ill.
Of patients taking 5 mg UPA, 75% reported that degree of improvement, as did 87% of those on 10 mg UPA, compared with 17.9% of those taking placebo. .
Adverse events were rare, with hot flashes occurring in about 10% of women taking UPA, compared with less than 2% of those taking placebo. Headaches, fatigue, and nausea were also reported, but rates were not significantly different from rates for those taking placebo. One serious adverse event that was deemed treatment related was a uterine hemorrhage experienced by a woman taking UPA.
“Even in treatment course 1 we already had profound and statistically significant effects in symptoms across the board,” Dr. Shulman said. “How long will they last? We obviously need more data. But the study suggests that the benefits last significantly longer than that associated with leuprolide acetate.”
Ulipristal acetate is already approved by the Food and Drug Administration at a different dosage as emergency contraception. The VENUS II data support its use for women with uterine fibroids, the researchers said. “Our results provide reassurance,” Dr. Liu said. “We can conclude that UPA is effective and safe in the management of uterine fibroids in the U.S. population.”
Dr. Liu reported that he had no relevant disclosures. Dr. Shulman reported relationships with multiple pharmaceutical companies, including Allergan, which funded the VENUS II study.
koakes@frontlinemedcom.com
On Twitter @karioakes
SAN ANTONIO – About half of women with uterine fibroids became amenorrheic when taking the selective progesterone receptor modulator ulipristal acetate (UPA) during a 12-week study cycle, and women taking UPA experienced significant improvement of quality of life, compared with those taking placebo.
Of those women taking 5 mg of UPA, 40.5%-42% became amenorrheic; of those taking 10 mg, 54.8%-57.3% became amenorrheic, James Liu, MD, reported at the annual meeting of the American Society for Reproductive Medicine. These results compared to amenorrhea rates of 0%-8% for women on placebo (P less than .0001 for all values).
The primary aim of VENUS II was to evaluate UPA’s efficacy and safety as intermittent treatment of abnormal uterine bleeding associated with uterine fibroids. Patients received UPA at either 5 mg or 10 mg orally. Secondary efficacy measures included the maintenance effect of UPA at both doses when compared to placebo, by assessing the rate of amenorrhea and the time to amenorrhea. Another secondary measure assessed uterine fibroid–related quality of life.
Safety was assessed by tracking adverse events through both courses of treatment. The study was not powered to compare the two doses against each other, but rather compared each against placebo.
Altogether, 432 patients were randomized to one of the treatment arms, which was begun after an initial screening period of about 10-12 weeks. The first treatment course lasted 12 weeks, after which patients went off treatment for two menstrual cycles. They then began another treatment course for 12 weeks and were followed for an additional 12 weeks after treatment was stopped.
Patients were included if they were premenopausal, aged 18-50 years old, had prolonged bleeding in at least 4 of the last 6 menstrual periods, had menstrual blood loss of at least 80 mL by cycle by the alkaline hematin method, and had at least one discrete leiomyoma without a uterine size greater than 20 weeks. About two-thirds of patients were black, reflecting the higher prevalence of uterine fibroids in this population, said Dr. Liu, professor of medicine and reproductive biology at Case Western Reserve University, Cleveland.
Most patients (60%-80%) had their bleeding controlled on either dose of UPA, compared with fewer than 10% of women taking placebo.
Quality of life data, presented separately at ASRM by Lee Shulman, MD, examined the impact of treatment on patients’ physical and social activities, and also on the severity of symptoms and health-related quality of life.
“The majority of patients on UPA versus a minority of patients on placebo described their menstrual/vaginal bleeding at the end of treatment course 1 as ‘much better’ or ‘very much better,’ ” said Dr. Shulman, chief of clinical genetics in the department of ob.gyn. at Northwestern University in Evanston, Ill.
Of patients taking 5 mg UPA, 75% reported that degree of improvement, as did 87% of those on 10 mg UPA, compared with 17.9% of those taking placebo. .
Adverse events were rare, with hot flashes occurring in about 10% of women taking UPA, compared with less than 2% of those taking placebo. Headaches, fatigue, and nausea were also reported, but rates were not significantly different from rates for those taking placebo. One serious adverse event that was deemed treatment related was a uterine hemorrhage experienced by a woman taking UPA.
“Even in treatment course 1 we already had profound and statistically significant effects in symptoms across the board,” Dr. Shulman said. “How long will they last? We obviously need more data. But the study suggests that the benefits last significantly longer than that associated with leuprolide acetate.”
Ulipristal acetate is already approved by the Food and Drug Administration at a different dosage as emergency contraception. The VENUS II data support its use for women with uterine fibroids, the researchers said. “Our results provide reassurance,” Dr. Liu said. “We can conclude that UPA is effective and safe in the management of uterine fibroids in the U.S. population.”
Dr. Liu reported that he had no relevant disclosures. Dr. Shulman reported relationships with multiple pharmaceutical companies, including Allergan, which funded the VENUS II study.
koakes@frontlinemedcom.com
On Twitter @karioakes
AT ASRM 2017
Key clinical point:
Major finding: Between 40.5% and 57.3% of women taking ulipristal acetate (UPA) achieved amenorrhea, compared with 0%-8% of women on placebo (P less than .0001).
Data source: Venus II, a phase 3 prospective, randomized, double-blind, double-dummy, placebo-controlled study that was partially parallel and partially crossover, with 432 patients.
Disclosures: Dr. Liu reported no relevant disclosures; Dr. Shulman reported financial relationships with multiple pharmaceutical companies, including Allergan, which funded the trial.