User login
1.02 Common Clinical Diagnoses and Conditions: Acute Gastroenteritis
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
Introduction
Acute gastroenteritis (AGE) is one of the most common diseases of childhood. Admission to the hospital can be prevented in many cases with appropriate use of oral rehydration. Despite this, annual hospitalization rates in the United States have been reported to be as high 3 to 5 per 1000 US children, and the financial burden of emergency department care and hospitalization accounts for up to $350 million in costs annually. Although uncommon in developed countries, morbidity can be profound, and mortality can occur. Among hospitalized patients, complications including electrolyte abnormalities, sepsis, and malnutrition have been noted. Misdiagnosis of AGE may occur, particularly when vomiting is the predominant symptom, which can lead to inappropriate treatment for potentially life-threatening conditions. Pediatric hospitalists routinely encounter patients with AGE and should provide immediate medical care in an efficient and effective manner.
Knowledge
Pediatric hospitalists should be able to:
- Describe the signs, symptoms, and common or concerning complications of AGE, including electrolyte disturbances, dehydration, ileus, and hemolytic uremic syndrome.
- List the common pathogens and related epidemiologic factors for AGE depending upon age, immunization status, geographic location, and exposure and travel history.
- Discuss the pathophysiology of electrolyte disturbances in AGE.
- Discuss the indications for hospital admission, including the need for intravenous fluids, correction of fluid, electrolyte and acid base disturbances, close clinical monitoring, and/or further diagnostic evaluation.
- Discuss essential elements of the history for patients with AGE, including immunization status, water and food sources, method of food preparation, daycare attendance, and recent travel.
- Describe the elements of the physical examination that aid in the diagnosis of AGE and associated complications.
- Compare and contrast clinical findings associated with viral, bacterial, and parasitic AGE.
- Compare and contrast conditions with presentations like that of AGE or its complications, including critical medical and surgical diagnoses such as diabetic ketoacidosis, inborn errors of metabolism, malrotation with midgut volvulus, and bowel obstruction.
- Compare and contrast the differential diagnoses of isolated emesis, bilious emesis, and emesis with diarrhea.
- Describe the differences in approach toward diagnosis and treatment for patients with co-morbid conditions or immunosuppression.
- Discuss the role of infection control in the hospital, as well as public health reporting mandates.
- Describe the indications for diagnostic laboratory tests, including stool, blood, and urine studies, attending to age groups, predictive value of tests, and cost-effectiveness.
- Describe the indications and contraindications of the interventions used to manage the symptoms of AGE, including the role of oral rehydration solutions in the treatment of related dehydration.
- Discuss indications for specialty consultation, such as gastroenterology, nutrition, surgery, and others.
- Describe criteria for hospital discharge, including specific measures of clinical stability for safe care transition.
Skills
Pediatric hospitalists should be able to:
- Diagnose gastroenteritis by efficiently performing an accurate history and physical examination, determining if key features of the disease are present.
- Identify and correctly manage fluid, electrolyte, and acid base derangements.
- Assess patients efficiently and effectively for complications of gastroenteritis such as sepsis, ileus, and hemolytic uremic syndrome.
- Identify and appropriately treat patients at risk for AGE secondary to unusual pathogens.
- Direct a cost-effective and evidence-based evaluation and treatment plan, especially regarding laboratory studies, antibiotics, and oral or intravenous fluid resuscitation.
- Adhere consistently to infection control practices.
- Perform careful reassessments daily and as needed, note changes in clinical status, and respond with appropriate actions, taking care to consider alternative conditions as appropriate.
- Engage consultants efficiently when indicated.
- Communicate effectively with the family/caregivers and healthcare providers regarding findings and plans.
- Ensure coordination of care for diagnostic tests and treatment between subspecialists.
- Create a comprehensive discharge plan that can be expediently activated when appropriate.
Attitudes
Pediatric hospitalists should be able to:
- Realize responsibility for educating the family/caregivers on the natural course of the disease, identification and management of common complications, and infection control practices to manage expectations and decrease pathogen transmission.
- Ensure coordination of care for diagnostic tests and treatments between subspecialists.
- Exemplify and advocate for strict adherence to infection control practices.
- Exemplify effective communication with patients, the family/caregivers, and healthcare providers regarding findings, care plans, and anticipated health needs after discharge.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in the development and implementation of cost-effective, safe, evidence-based care pathways to standardize the evaluation and management for hospitalized children with AGE.
- Collaborate with hospital administration to create and sustain a process to follow up on laboratory tests pending at discharge.
- Collaborate with institutional infection control practitioners to improve processes to prevent nosocomial infection related to gastroenteritis.
- Lead, coordinate, or participate in efforts to assure consistent public health reporting of appropriate infections and response to trends.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
1. Chow CM, Leung AKC, Hon KL. Acute gastroenteritis: from guidelines to real life. Cli Exp Gastro. 2010; 3:97-112. https://doi.org/10.2147/ceg.s6554.
2. Freedman SB, Gouin S, Bhatt M, et al. Prospective assessment of practice pattern variations in the treatment of pediatric gastroenteritis. Pediatrics.2011;127(2) e287-e295. https://pediatrics.aappublications.org/content/127/2/e287. Accessed August 28, 2019.
1.01 Common Clinical Diagnoses and Conditions: Acute Abdominal Pain and Acute Abdomen
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
Introduction
Acute abdominal pain is a common presenting symptom of children and adolescents and prompts the consideration of an extensive differential diagnosis. Pediatric hospitalists frequently encounter children with acute abdominal pain. Acute abdominal pain may be due to common and self-limited medical conditions such as gastroenteritis or constipation, but it may also herald life threatening surgical conditions or systemic illness. The differential diagnosis of acute abdominal pain is broad, making a careful, skilled, and thorough history and physical examination essential in the evaluation of children presenting with this symptom. Identifying children with a true medical or surgical emergency is critical. Early diagnosis and treatment reduce morbidity, mortality, and length of hospital stay.
Knowledge
Pediatric hospitalists should be able to:
- Describe features of the medical history and physical examination that prompt specific and expedient diagnostic evaluation.
- Compare and contrast the differential diagnoses of acute abdominal pain and acute abdomen for children of varying ages.
- Describe and differentiate the clinical presentation consistent with intestinal obstruction from other causes of acute abdominal pain such as appendicitis, acute cholecystitis, and others.
- Differentiate etiologies of acute abdominal pain related to biological sex, such as testicular torsion, ovarian cyst rupture, ectopic pregnancy, and others.
- Discuss the presenting symptoms associated with abdominal emergencies (such as mid-gut volvulus and intussusception), including bilious emesis, bloody diarrhea, and severe pain.
- List the appropriate radiological studies for evaluation of various abdominal emergencies.
- Identify how the presentation of abdominal emergencies may differ in neonates and infants by including nonspecific symptoms, such as vomiting or lethargy.
- List conditions that may mimic the acute abdomen, including lower lobe pneumonia, diabetic ketoacidosis, and others.
- Discuss the benefits, risks, and limitations of commonly performed diagnostic studies, including abdominal radiography, ultrasonography, computed tomography, magnetic resonance imaging, and nuclear medicine scans, noting the benefits of and barriers to use of contrast enhancement for these studies.
- Describe the laboratory tests indicated to evaluate acute abdominal pain and acute abdomen.
- Discuss the importance of and indications for early surgical consultation in the child with an acute abdomen.
- Describe the principles of stabilization of the child with an acute abdomen, including volume resuscitation, antibiotics, and bowel decompression.
- Discuss the approach toward pain management in patients presenting with acute abdominal pain, including the impact of medication on serial exams.
- Describe indications for patient placement in various locations in the hospital system, such as an observation unit, surgical or medical ward, step-down, or intensive care unit.
- Discuss indications for patient transfer to a referral center, such as need for pediatric-specific services not available at the local facility.
Skills
Pediatric hospitalists should be able to:
- Obtain an accurate and thorough history to identify symptoms, triggers, and clinical course of acute abdominal pain and acute abdomen.
- Perform a physical exam to elicit signs of abdominal pain, differentiate findings of acute abdomen, and assess illness severity.
- Formulate a targeted differential diagnosis based on elements from the history and physical examination.
- Identify the child with an acute abdomen who requires emergent surgical consultation.
- Identify and manage the child with concomitant hypovolemia or sepsis requiring immediate medical stabilization.
- Direct an appropriate and cost-effective evaluation for acute abdominal pain and acute abdomen.
- Create and implement a treatment plan for non-surgical causes of abdominal pain.
- Order and correctly interpret basic diagnostic imaging and laboratory studies.
- Consult surgeons and other subspecialists effectively and efficiently when indicated.
- Provide pre- and post-operative general pediatric care for the child requiring surgery, including pain management, according to local practice parameters.
- Coordinate care with the primary care provider and subspecialists to arrange an appropriate transition plan for hospital discharge.
Attitudes
Pediatric hospitalists should be able to:
- Exemplify collaborative practice with subspecialists, including surgical teams and primary care providers, to ensure efficient care within the hospital setting and coordinated longitudinal care.
- Realize responsibility for promoting effective communication with patients, family/caregivers, and healthcare providers regarding findings and care plans.
Systems Organization and Improvement
In order to improve efficiency and quality within their organizations, pediatric hospitalists should:
- Lead, coordinate, or participate in education of healthcare providers, trainees, the family/caregivers regarding the signs and symptoms of the acute abdomen to encourage early detection and prompt evaluation.
- Lead, coordinate, or participate in a multidisciplinary team to provide optimal care for children with acute abdominal pain with and without acute abdomen.
- Lead, coordinate, or participate in institutional efforts to improve the expediency of diagnostic laboratory and radiographic studies, availability of specialty care, and other resources for children with acute abdominal pain and acute abdomen.
- Lead, coordinate, or participate in institutional efforts to develop surgical consultation or co-management models, clearly defining roles to ensure timely, high quality, and comprehensive care for pediatric patients requiring surgical care.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
1. Baker RD. Acute Abdominal Pain. Peds Rev. 2018;39(3):130-139.
2. Tsao K. and Anderson K.T. Evaluation of abdominal pain in children. BMJ Best Practice. https://bestpractice.bmj.com/topics/en-us/787/diagnosis-approach. Accessed August 27, 2019.
Pediatric Hospital Medicine Core Competencies: 2020 Revision. Table of Contents
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
Authors and Editors.............................................................3
External Reviewers.............................................................11
ORIGINAL RESEARCH
The Pediatric Hospital Medicine Core Competencies:
2020 Revision—Introduction and Methodology.............................................................12
Jennifer Maniscalco, MD, MPH, MAcM, FAAP; Sandra Gage, MD, PhD, SFHM, FAAP; Sofia Teferi, MD, SFHM, FAAP; Erin Stucky Fisher, MD, MHM, FAAP
SECTION 1: COMMON CLINICAL DIAGNOSES AND CONDITIONS
1.01 Acute Abdominal Pain and Acute Abdomen.............................................................18
1.02 Acute Gastroenteritis.............................................................20
1.03 Acute Respiratory Failure.............................................................22
1.04 Altered Mental Status.............................................................24
1.05 Asthma.............................................................26
1.06 Bone and Joint Infections.............................................................28
1.07 Brief Resolved Unexplained Event.............................................................30
1.08 Bronchiolitis.............................................................32
1.09 Central Nervous System Infections.............................................................34
1.10 Constipation.............................................................36
1.11 Diabetes Mellitus.............................................................37
1.12 Failure to Thrive.............................................................39
1.13 Fever of Unknown Origin.............................................................41
1.14 Fluid and Electrolyte Management.............................................................43
1.15 Gastrointestinal and Digestive Disorders.............................................................45
1.16 Head and Neck Disorders.............................................................47
1.17 Kawasaki Disease.............................................................49
1.18 Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome.............................................................50
1.19 Neonatal Fever.............................................................52
1.20 Neonatal Jaundice.............................................................54
1.21 Pneumonia.............................................................56
1.22 Seizures.............................................................57
1.23 Sepsis and Shock.............................................................59
1.24 Sickle Cell Disease.............................................................61
1.25 Skin and Soft Tissue Infections.............................................................63
1.26 Toxin Ingestion and Exposure.............................................................65
1.27 Urinary Tract Infections.............................................................67
SECTION 2: CORE SKILLS
2.01 Bladder Catheterization and Interpretation
of Urinalysis.............................................................68
2.02 Communication.............................................................70
2.03 Diagnostic Imaging.............................................................72
2.04 Electrocardiogram Interpretation.............................................................74
2.05 Feeding Tubes.............................................................75
2.06 Intravenous Access and Phlebotomy.............................................................77
2.07 Lumbar Puncture.............................................................79
2.08 Non-invasive Monitoring.............................................................81
2.09 Nutrition.............................................................82
2.10 Oxygen Delivery and Airway Management.............................................................84
2.11 Pain Management.............................................................86
2.12 Pediatric Advanced Life Support.............................................................88
2.13 Peri-procedural Care.............................................................90
2.14 Preventive Care Services.............................................................92
2.15 Procedural Sedation.............................................................94
SECTION 3: SPECIALIZED SERVICES
3.01 Acute Behavioral and Psychiatric Conditions.............................................................96
3.02 Adolescent and Young Adult Medicine.............................................................98
3.03 Child Abuse and Neglect.............................................................100
3.04 Child with Medical Complexity.............................................................102
3.05 Chronic Behavioral and Psychiatric Conditions.............................................................104
3.06 Newborn Care and Delivery Room Management.............................................................106
3.07 Palliative Care and Hospice.............................................................108
3.08 Pediatric Interfacility Transport.............................................................110
SECTION 4: HEALTHCARE SYSTEMS: SUPPORTING AND ADVANCING CHILD HEALTH
4.01 Advocacy.............................................................112
4.02 Business Practices.............................................................114
4.03 Consultation and Co-management.............................................................116
4.04 Education.............................................................118
4.05 Ethics.............................................................120
4.06 Evidence-based Medicine.............................................................122
4.07 Family Centered Care.............................................................123
4.08 Handoffs and Transitions of Care.............................................................125
4.09 Health Information Technology.............................................................127
4.10 High Value Care.............................................................129
4.11 Infection Control and Antimicrobial Stewardship.............................................................131
4.12 Leadership in Healthcare.............................................................133
4.13 Legal Issues and Risk Management.............................................................134
4.14 Patient Safety.............................................................136
4.15 Quality Improvement.............................................................138
4.16 Research.............................................................140
APPENDIX
Chapter Links.............................................................142
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
Figure: Needs Assessment Survey.............................................................145
Dedication.............................................................153
To Michael Burke, our friend and colleague
The Pediatric Hospital Medicine Core Competencies: 2020 Revision Dedication

Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
Thank you, Michael, for making us a stronger and more compassionate PHM Community.
The Editors and Associate Editors of The Pediatric Hospital Medicine Core Competencies: 2020 Revision:
Francisco Alvarez; Weijen Chang; Erin Fisher; Sandra Gage; Jennifer Maniscalco; Vineeta Mittal; Anand Sekaran; Amit Singh; Sofia Teferi
APPENDIX
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
NEEDS ASSESSMENT SURVEY
The editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council,and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
CHAPTER LINKS
These chapter links are guides to assist the reader in identifying chapters where some key relationships across knowledge, skills, attitudes, and systems organization and improvement may overlap. Chapter links are limited to 5 per chapter, are not comprehensive, and are intended as a general guide for the reader.
The Pediatric Hospital Medicine Core Competencies: 2020 Revision. Authors, Editors, and Reviewers
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
AUTHORS
Francisco Alvarez, MD
Associate Chief, Regional Pediatric Hospitalist Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Brian Alverson, MD
Director, Division of Pediatric Hospital Medicine
Hasbro Children’s Hospital
Professor of Pediatrics
Alpert School of Medicine, Bro
Providence, RI
Pneumonia
Eric Balighian, MD
Director, Pediatric Emergency Department
St. Agnes Hospital
Asistant Professor, Department of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Acute Abdominal Pain and Acute Abdomen
Julia Beauchamp-Walters, MD
Medical Director, Helen Bernardy Center for Medically Fragile Children
Medical Director, Home Care
Co-Medical Director, Emergency Transport Program
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Feeding Tubes
Pediatric Interfacility Transport
Eric Biondi, MD, MS
Director, Pediatric Hospital Medicine Division
Johns Hopkins Children’s Center
Associate Professor of Pediatrics
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Neonatal Fever
Rebecca Blankenberg, MD, MPH
Associate Chair of Education
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics and Emergency Medicine
Stanford University School of Medicine
Stanford, CA
Education
Colin Bridgeman, MD
Penn State Children’s Hospital
Assistant Professor of Pediatrics
Division of General Inpatient Pediatrics
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Jeffrey Brown, MD, MPH, CAP, FAAP
Texas Newborn Services/Pediatrix Medical Group
Clinical Professor of Pediatrics
University of Colorado School of Medicine
Fort Worth, TX
Business Practices
April O. Buchanan, MD
Associate Dean for Curriculum
Prisma Health Children’s Hospital at Greenville
Associate Professor of Clinical Pediatrics
University of South Carolina School of Medicine
Greenville, SC
Sepsis and Shock
Douglas Carlson, MD
Medical Director
HSHS St. John’s Children’s Hospital
Professor and Chair of Pediatrics
Southern Illinois University School of Medicine
Springfield, MO
Procedural Sedation
Pearl Chang, MD
Seattle Children’s Hospital
Assistant Professor
Department of Pediatrics, University of Washington
Seattle, WA
Neonatal Jaundice
Eric Coon, MD, MS
Co-Director, Pediatric Hospital Medicine Fellowship
Primary Children’s Medical Center
Assistant Professor of Pediatrics
University of Utah Health Science
Salt Lake City, UT
Research
Yasmeen N. Daud, MD
St. Louis Children’s Hospital
Associate Professor of Pediatrics
Washington University School of Medicine
St. Louise, MO
Oxygen Delivery and Airway Management
Sarah Denniston, MD, FAAP
Fellowship Director, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center
Assistant Professor of Pediatrics
Tufts University School of Medicine
Associate DIO for Quality and Safety
Tufts Medical Center
Boston, MA
Peri-procedural Care
Craig C. DeWolfe, MD, MEd, FAAP
Children’s National Health System
Director of Medical Student Education in Pediatrics
Associate Professor of Pediatrics,
George Washington University School of Medicine
Washington, DC
Brief Resolved Unexplained Event
Stephanie Anne Deutsch, MD, MS, FAAP
Section Chief, Child Abuse Pediatrics
Nemours/Alfred I. duPont Hospital for Children
Co-medical Director, CARE (Children at Risk Evaluation) Program
Assistant Clinical Professor of Pediatrics
Sidney Kimmel Medical College at Thomas Jefferson University
Wilmington, Delaware
Child Abuse and Neglect
Ami Doshi, MD
Medical Director, Inpatient Palliative Care Program
Rady Children’s Hospital San Diego
Clinical Associate Professor of Pediatrics
University of California San Diego School of Medicine
San Diego, CA
Palliative Care and Hospice
Erin Fisher, MD, FAAP, MHM
Medical Director, Quality Improvement
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Director, Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
San Diego, CA
Quality Improvement
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Mary Pat Gallagher, MD
Director, Pediatric Diabetes Center
Division of Pediatric Endocrinology, Hassenfeld Children’s Hospital
Assistant Professor
Department of Pediatrics
NYU Langone
New York, NY
Diabetes Mellitus
Amrit Gill, MD
Cleveland Clinic Children’s Hospital
Clinical Assistant Professor of Pediatrics
Case Western Reserve University School of Medicine
Cleveland, OH
Patient Safety
Veena Goel Jones, MD, FAAP
Medical Director, Digital Patient Experience, Sutter Health
Sutter Palo Alto Medical Foundation
Palo Alto, CA
Health Information Technology
Jeffrey Grill, MD
Vice Chair, Community Relations and Outreach
Chief, Division of Pediatric Hospital Medicine
Director, Just for Kids Hospitalist Service
Norton Children’s Hospital
Professor, Department of Pediatrics
University of Louisville School of Medicine
Louisville, KY
Constipation
Arun Gupta, MD
Director, Neonatal Hospitalist Program
Lucile Packard Children’s Hospital Stanford
Clinical Associate Professor, Pediatrics
Stanford University School of Medicine
Stanford, CA
Newborn Care and Delivery Room Management
Brian F Herbst Jr, MD
Medical Director, Hospital Medicine Adult Care
Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Internal Medicine and Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Daniel Hershey, MD, SFHM
Rady Children’s Hospital
Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Non-invasive Monitoring
Kim Hoang, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Education
Alison Volpe Holmes, MD, MPH
Children’s Hospital at Dartmouth-Hitchcock
Associate Dean for Student Affairs, Career Advising
Vice-Chair for Education, Department of Pediatrics
Associate Professor of Pediatrics and of The Dartmouth Institute
Geisel School of Medicine at Dartmouth
Hanover, NH
Neonatal Abstinence Syndrome/Neonatal Opioid Withdrawal Syndrome
Akshata Hopkins, MD, FAAP, FHM
Director, Pediatric Residency Program
Johns Hopkins All Children’s Hospital
Assistant Professor of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
High Value Care
Yemisi Jones, MD, FAAP, FHM
Co-Medical Director, Continuing Medical Education
Co-Director Liberty Simulation Education
Cincinnati Children’s Hospital Medical Center
Assistant Professor of Clinical Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Intravenous Access and Phlebotomy
Alisa Khan, MD, MPH
Health Services Researcher
Division of General Pediatrics, Boston Children’s Hospital
Clinical Instructor in Pediatrics
Harvard Medical School
Boston, MA
Family Centered Care
Vivian Lee, MD
Children’s Hospital Los Angeles
Clinical Assistant Professor of Pediatrics
University of Southern California Keck School of Medicine
Los Angeles, CA
Altered Mental Status
Su-Ting T. Li, MD, MPH
Associate Vice Chair of Education
Pediatric Residency Program Director
University of California Davis Children’s Hospital
Professor of Pediatrics
University of California, Davis
Sacramento, CA
Skin and Soft Tissue Infections
Patricia S. Lye, MD, MEd, FAAP
Children’s Hospital of Wisconsin
Professor of Pediatrics, Retired
Medical College of Wisconsin
Milwaukee, WI
Handoffs and Transitions of Care
Tamara Maginot, PhD
Pediatric Psychologist
Program Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Assistant Professor, Department of Psychiatry
UC San Diego Eating Disorders Center for Treatment and Research Behavioral Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Christopher Maloney, MD, PhD, FAAP
Chief Medical Officer and Senior Vice President
Children’s Hospital & Medical Center
Professor of Pediatrics and Pediatric Critical Care
Department of Pediatrics
University of Nebraska Medical Center College of Medicine
Omaha, NE
Pediatric Advanced Life Support
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Failure to Thrive
Elizabeth Mannino Avila, MD
Rady Children’s Hospital
Assistant Clinical Professor of Pediatrics
University of California, San Diego
San Diego, CA
Kawasaki Disease
Alison Markowsky, MD, MSHS, FAAP
Medical Director
Children’s National Pediatric Hospitalist Program at Mary Washington Healthcare
Children’s National Health System
Assistant Professor of Pediatrics
The George Washington University School of Medicine & Health Sciences
Washington, DC
Newborn Care and Delivery Room Management
Michelle Marks, DO, FAAP, SFHM
Chair, Pediatric Hospital Medicine
Cleveland Clinic Children’s Hospital
Clinical Associate Professor
Cleveland Clinic Lerner College of Medicine, Case Western Reserve University
Cleveland, OH
Nutrition
Armand H. Matheny Antommaria, MD, PhD, FAAP
Lee Ault Carter Chair Pediatric Ethics and Pediatric Hospitalist
Cincinnati Children’s Hospital
Associate Professor of Clinical-Affiliated
University of Cincinnati School of Medicine
Cincinnati, OH
Ethics
Erich Maul, MD
Division Chief, Hospital Medicine
Medical Director, Acute Care and Progressive Care
Kentucky Children’s Hospital
Professor of Pediatrics
University of Kentucky School of Medicine
Lexington, KY
Electrocardiogram Interpretation
Rusty McCulloh, MD
Chief, Division of Hospital Medicine
Children’s Hospital & Medical Center
Associate Professor, Division of Hospital Medicine
University of Nebraska College of Medicine
Omaha, NE
Infection Control and Antimicrobial Stewardship
Anjna Melwani, MD
Director, Preoperative Care Clinic
Children’s National Medical Center
Associate Professor of Pediatrics
George Washington University School of Medicine and Health Sciences
Washington, DC
Consultation and Co-management
Christopher Miller, MD
Pediatric Allergist
Children’s Mercy Hospitals and Clinics
Assistant Professor of Pediatrics
Section of Allergy and Immunology
University of Missouri-Kansas City School of Medicine
Kansas City, MO
Asthma
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System Dallas
Dallas, TX
Acute Respiratory Failure
Beth Natt, MD, MPH, FAAP, SFHM
Director, Pediatric Hospital Medicine, Regional Programs
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Farmington, CT
Bladder Catheterization and Interpretation of Urinalysis
Jennifer O’Toole, MD, MEd, FAAP, SFHM
Program Director, Internal Medicine – Pediatrics Residency
Director of Education, Division of Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Associate Professor of Pediatrics and Internal Medicine
University of Cincinnati College of Medicine
Cincinnati, OH
Adolescent and Young Adult Medicine
Mary Ottolini, MD, MPH, MEd, FAAP
George W. Hallett Chair of Pediatrics
Barbara Bush Children’s Hospital at Maine Medical Center
Professor of Pediatrics
Tufts University School of Medicine
Portland, ME
Fluid and Electrolyte Management
Jack Percelay, MD, MPH, FAAP, MHM
Stanford Lucile Packard Children’s Hospital
Clinical Associate Professor of Pediatrics
Stanford University School of Medicine
Stanford, CA
Advocacy
Seizures
Shannon Phillips, MD, MPH
Chief Patient Safety and Experience Officer
Primary Children’s Medical Center
Intermountain Healthcare, Inc.
Adjunct Associate Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Patient Safety
David Pressel, MD, PhD, FAAP, FHM
Medical Director, Pediatric Hospitalist Program
Capital Health Medical Center- Hopewell
Pennington, NJ
Acute Behavioral and Psychiatric Conditions
Child Abuse and Neglect
Ricardo Quinonez, MD, FAAP
Chief, Pediatric Hospital Medicine
Texas Children’s Hospital
Associate Professor of Pediatrics
Baylor College of Medicine
Houston, TX
High Value Care
Shawn Ralston, MA, MD, MS
Johns Hopkins Children’s Center
Editor, Hospital Pediatrics, American Academy of Pediatrics
Associate Professor of Pediatrics
Division of Pediatric Quality and Safety
The Johns Hopkins Hospital University School of Medicine
Baltimore, MD
Evidence Based Medicine
David I. Rappaport, MD, FAAP, FHM
Associate Residency Program Director
Division of General Pediatrics
Nemours/AI duPont Hospital for Children
Wilmington, DE
Associate Professor of Pediatrics
Sidney Kimmel Medical College at Jefferson
Philadelphia, PA
Consultation and Co-management
Daniel Rauch, MD, FAAP, SFHM
Chief, Pediatric Hospital Medicine
The Floating Hospital for Children at Tufts Medical Center.
Professor of Pediatrics
Tufts University School of Medicine
Boston, MA
Preventive Care Services
Kyung (Kay) Rhee, MD, MSc, MA
Director of Research, Division of Pediatric Hospital Medicine
Medical Director, Medical Behavioral Unit
Rady Children’s Hospital San Diego
Professor of Clinical Pediatrics
Department of Pediatrics, Division of General Academic Pediatrics, Developmental Pediatrics, and Center for Community Health
University of San Diego School of Medicine
San Diego, CA
Chronic Behavioral and Psychiatric Conditions
Jeffrey Riese, MD
Associate Pediatric Residency Program Director
Hasbro Children’s Hospital
Associate Professor of Pediatrics
Warren Alpert School of Medicine at Brown University
Providence, RI
Neonatal Fever
Ken Roberts, MD, FAAP
Professor Emeritus of Pediatrics
University of North Carolina School of Medicine
Chapel Hill, NC
Urinary Tract Infections
Amanda Rogers, MD
Associate Pediatric Residency Program Director
Children’s Hospital of Wisconsin
Assistant Professor, Section of Hospital Medicine
Medical College of Wisconsin
Milwaukee, WI
Lumbar Puncture
Rebecca E. Rosenberg, MD, MPH
Chief, Section of Hospital Medicine, Division of General Pediatrics
Hassenfeld Children’s Hospital at NYU Langone Health
Associate Professor of Pediatrics
NYU School of Medicine
New York, NY
Peri-procedural Care
Michael Ruhlen, MD, MHCM, FHM, FACHE
Vice President, Division of Medical Education
Vice Chair, RRC ACGME
Atrium Health System
Charlotte, NC
Legal Issues and Risk Management
Christopher J. Russell, MD, MS, FAAP
Research Director, Division of Hospital Medicine
Children’s Hospital Los Angeles
Assistant Professor of Clinical Pediatrics
Keck School of Medicine, University of Southern California
Los Angeles, CA
Child with Medical Complexity
Christopher Russo, MD
Director of Pediatrics
Central Lynchburg General Hospital
Assistant Professor of Pediatrics
Liberty University College of Osteopathic Medicine
Lynchburg, VA
Advocacy
Klint M. Schwenk, MD, MBA, FAAP, FHM
Associate Division Chief, Pediatric Hospital Medicine
Norton Children’s Hospital
Associate Professor of Pediatrics
University of Louisville
Louisville, KY
Acute Gastroenteritis
Gastrointestinal and Digestive Disorders
Anand Sekaran, MD, FAAP
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Diagnostic Imaging
Kristin A. Shadman, MD, FAAP
American Family Children’s Hospital
Associate Professor of Pediatrics
Division of Hospital Medicine
University of Wisconsin School of Medicine and Public Health
Madison, WI
Oxygen Delivery and Airway Management
Samir S. Shah, MD, MSCE
Director, Division of Hospital Medicine
James M. Ewell Endowed Chair
Attending Physician in Hospital Medicine & Infectious Diseases
Chief Metrics Officer
Cincinnati Children’s Hospital Medical Center
Professor, Department of Pediatrics
University of Cincinnati College of Medicine
Cincinnati, OH
Bone and Joint Infections
Mark Shen, MD, MBA, FAAP, SFHM
Associate Professor of Pediatrics
Dell Medical School at the University of Texas at Austin
Austin, TX
Leadership in Healthcare
Tamara Simon, MD, MSPH, FAAP
Principal Investigator, Center for Clinical and Translational Research
Seattle Children’s Research Institute
Associate Professor of Pediatrics
Divisions of Hospital Medicine and General Pediatrics, Department of Pediatrics
University of Washington
Seattle, WA
Child with Medical Complexity
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine, Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
Communication
Karen Smith, MD, MEd, SFHM, FAAP
Chief, Division of Pediatric Hospital Medicine
Children’s National Medical Center
Associate Professor of Pediatrics
The George Washington School of Medicine and Health Sciences
Washington, DC
Business Practices
Nita Srinivas, MD
Pediatric Hospitalist and Infectious Disease Specialist
Fellowship Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Fever of Unknown Origin
Rajendu Srivastava, MD, FRCP(C), MPH
Primary Children’s Medical Center
Assistant Vice President of Research and Medical Director of the Office of Research
Intermountain Healthcare Inc.
Professor of Pediatrics
University of Utah Health Sciences
Salt Lake City, UT
Research
Lynne Sterni, MD
Pediatric Anesthesiology and Pain Medicine
Naval Medical Center San Diego
Assistant Professor
Uniformed Services University School of Health Sciences
San Diego, CA
Pain Management
E. Douglas Thompson Jr, MD, FAAP
Chief, Section of Hospital Medicine
Associate Chair, Access and Partnerships
St. Christopher’s Hospital for Children
Associate Professor of Pediatrics
Drexel University School of Medicine and Health Sciences
Philadelphia, PA
Sickle Cell Disease
Joanna Thomson, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Cincinnati Children’s Hospital Medical Center
Assistant Professor, Department of Pediatrics
University of Cincinnati School of Medicine
Cincinnati, OH
Acute Respiratory Failure
Joel Tieder, MD, MPH
Seattle Children’s Hospital
Associate Professor of Pediatrics, Division of Hospital Medicine
University of Washington School of Medicine
Seattle, WA
Brief Resolved Unexplained Event
Adriana Tremoulet, MD, MAS
Associate Director, Kawasaki Disease Research Center
Division of Host-Microbe Systems and Therapeutics
Pediatric Infectious Diseases and Kawasaki Disease
Associate Professor of Pediatrics, University of California San Diego
San Diego, CA
Kawasaki Disease
Marie E. Wang, MD, MPH, FAAP
Associate Fellowship Program Director, Pediatric Hospital Medicine
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Stanford University School of Medicine
Stanford, CA
Central Nervous System Infections
Ronald Williams, MD, FAAP, FACP
Director, Combined Internal Medicine/Pediatrics Residency Program
Penn State Hershey Children’s Hospital
Professor of Pediatrics and Medicine
Penn State College of Medicine
Hershey, PA
Head and Neck Disorders
Susan Wu, MD, FAAP
Children’s Hospital Los Angeles
Associate Professor of Clinical Pediatrics
Division of Hospital Medicine, Department of Pediatrics
USC Keck School of Medicine
Los Angeles, CA
Bronchiolitis
EDITORS
Sandra Gage, MD, PhD, FAAP, SFHM
Associate Division Chief and Associate Fellowship Director
Division of Hospital Medicine
Phoenix Children’s Hospital
Clinical Associate Professor
University of Arizona College of Medicine – Phoenix
Department of Child Health
Phoenix, AZ
Jennifer Maniscalco, MD, MPH, MAcM, FAAP
Designated Institutional Official
Johns Hopkins All Children’s Hospital
Assistant Professor
Department of Pediatrics
Johns Hopkins University School of Medicine
St. Petersburg, FL
Erin Fisher, MD, MHM, FAAP
Medical Director Quality Improvement
Rady Children’s Hospital
Professor of Clinical Pediatrics
Director of Pediatric Quality and Safety Graduate Medical Education
Fellowship Director and Division Director, Pediatric Hospital Medicine
University of California San Diego School of Medicine
Department of Pediatrics
San Diego, CA
CONTRIBUTING EDITOR, COMMUNITY PERSPECTIVE EXPERTISE
Sofia Teferi, MD, FAAP, SFHM
Physician Executive
Richmond, VA
ASSOCIATE EDITORS
Francisco Alvarez, MD, FAAP
Associate Chief, Regional Pediatric Hospital Medicine Programs
Lucile Packard Children’s Hospital
Clinical Associate Professor
Stanford School of Medicine
Stanford, CA
Michael Burke, MD (1957 – 2019)
In memory: Chairman of Pediatrics
Saint Agnes Hospital
Associate Professor of Pediatrics
Johns Hopkins University School of Medicine
Baltimore, MD
Weijen Chang, MD
Division Chief, Pediatric Hospital Medicine
Vice Chair for Clinical Affairs, Department of Pediatrics
Baystate Children’s Hospital
Associate Professor of Pediatrics
University of Massachusetts Medical School-Baystate
Springfield, MA
Vineeta Mittal, MD, MBA
Imm. Past President of the Medical/Dental Staff
Children’s Medical Center
Associate Professor of Pediatrics
Director of Pediatric Hospital Medicine
Department of Pediatrics
UT Southwestern Medical Center & Children’s Health System, Dallas
Dallas, TX
Anand Sekaran, MD
Associate Chair of Pediatrics, Clinical Affairs
Division Chief, Hospital Medicine
Connecticut Children’s Medical Center
Associate Professor of Pediatrics
University of Connecticut School of Medicine
Hartford, CT
Amit Singh, MD, FAAP
Lucile Packard Children’s Hospital
Clinical Assistant Professor
Division of Pediatric Hospital Medicine
Department of Pediatrics
Stanford University School of Medicine
Stanford, CA
EXTERNAL REVIEWERS
Academic Pediatric Association Hospital Medicine Special Interest Group
American Academy of Pediatrics
- Committee on Psychological Aspects of Child and Family Health
- Council on Children with Disabilities
- Council on Community Pediatrics
- Disaster Preparedness Advisory Council
- Family Partnerships Network
- Section on Anesthesiology and Pain Medicine
- Section on Breastfeeding
- Section on Cardiology and Cardiac Surgery
- Section on Critical Care
- Section on Hematology/Oncology
- Section on Hospice and Palliative Medicine
- Section on Hospital Medicine
- Section on LGBT Health and Wellness
- Section on Medicine-Pediatrics
- Section on Nephrology
- Section on Neurology
- Section on Pediatric Trainees
- Section on Surgery
- Section on Transport Medicine
- Section on Urology
Association of Pediatric Program Directors Curriculum Committee
Society of Hospital Medicine Pediatrics Special Interest Group
Society of Hospital Medicine Medicine-Pediatrics Special Interest Group
The Pediatric Hospital Medicine Core Competencies: 2020 Revision. Introduction and Methodology
The Pediatric Hospital Medicine Core Competencies were first published in 2010 to help define a specific body of knowledge and measurable skills needed to practice high quality care for hospitalized pediatric patients across all practice settings.1 Since then, the number of practicing pediatric hospitalists has grown to a conservative estimate of 3,000 physicians and the scope of practice among pediatric hospitalists has matured.2 Pediatric hospitalists are increasingly leading or participating in organizational and national efforts that emphasize interprofessional collaboration and the delivery of high value care to hospitalized children and their caregivers—including innovative and family-centered care models, patient safety and quality improvement initiatives, and research and educational enterprises.3-8 In response to these changes, the American Board of Medical Specialties designated Pediatric Hospital Medicine (PHM) as a pediatric subspecialty in 2016.
The field of PHM in the United States continues to be supported by three core societies—Society of Hospital Medicine (SHM), American Academy of Pediatrics (AAP), and Academic Pediatric Association (APA). Together, these societies serve as tri-sponsors of the annual Pediatric Hospital Medicine national conference, which now welcomes over 1,200 attendees from the United States and abroad.9 Each society also individually sponsors a variety of professional development and continuing medical education activities specific to PHM.
In addition, pediatric hospitalists often serve a pivotal role in teaching learners (medical students, residents, and other health profession students), physician colleagues, and other healthcare professionals on the hospital wards and via institutional educational programs. Nearly 50 institutions in the United States offer graduate medical education training in PHM.10 The PHM Fellowship Directors Council has developed a standardized curricular framework and entrustable professional activities, which reflect the tenets of competency-based medical education, for use in PHM training programs.11-13
These changes in the practice environment of pediatric hospitalists, as well as the changing landscape of graduate and continuing medical education in PHM, have informed this revision of The PHM Core Competencies. The purpose of this article is to describe the methodology of the review and revision process.
OVERVIEW OF THE PHM CORECOMPETENCIES: 2020
Revision
The PHM Core Competencies: 2020 Revision provide a framework for graduate and continuing medical education that reflects the current roles and expectations for all pediatric hospitalists in the United States. The acuity and complexity of hospitalized children, the availability of pediatric subspecialty care and other resources, and the institutional orientation towards pediatric populations vary across community, tertiary, and children’s hospital settings. In order to unify the practice of PHM across these environments, The PHM Core Competencies: 2020 Revision address the fundamental and most common components of PHM which are encountered by the majority of practicing pediatric hospitalists, as opposed to an extensive review of all aspects of the field.
The compendium includes 66 chapters on both clinical and nonclinical topics, divided into four sections—Common Clinical Diagnoses and Conditions, Core Skills, Specialized Services, and Healthcare Systems: Supporting and Advancing Child Health (Table 1). Within each chapter is an introductory paragraph and learning objectives in three domains of educational outcomes—cognitive (knowledge), psychomotor (skills), and affective (attitudes)—as well as systems organization and improvement, to reflect the emphasis of PHM practice on improving healthcare systems. The objectives encompass a range of observable behaviors and other attributes, from foundational skills such as taking a history and performing a physical exam to more advanced actions such as participating in the development of care models to support the health of complex patient populations. Implicit in these objectives is the expectation that pediatric hospitalists build on experiences in medical school and residency training to attain a level of competency at the advanced levels of a developmental continuum, such as proficient, expert, or master.14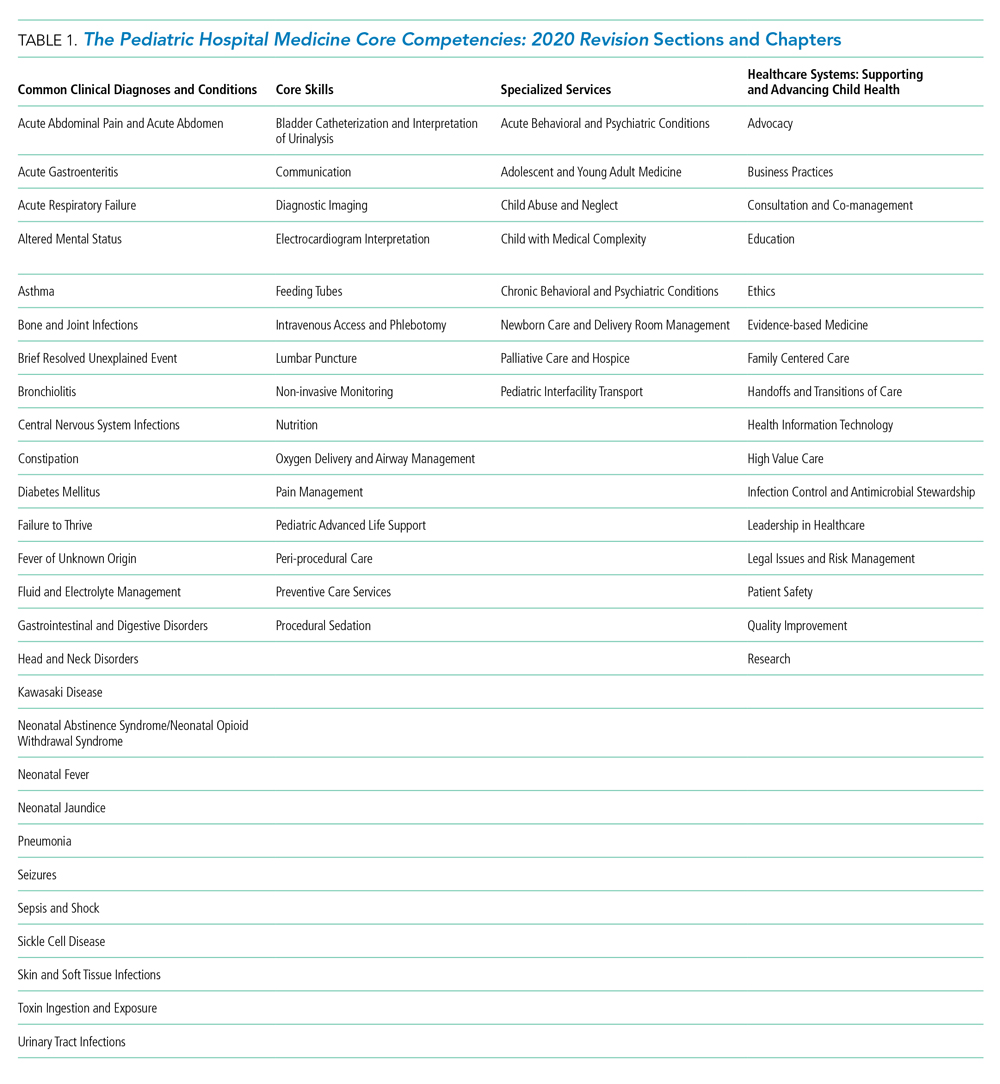
The objectives also balance specificity to the topic with a timeless quality, allowing for flexibility both as new information emerges and when applied to various educational activities and learner groups. Each chapter can stand alone, and thus themes recur if one reads the compendium in its entirety. However, in order to reflect related content among the chapters, the appendix contains a list of associated chapters (Chapter Links) for further exploration. In addition, a short reference list is provided in each chapter to reflect the literature and best practices at the time of publication.
Finally, The PHM Core Competencies: 2020 Revision reflect the status of children as a vulnerable population. Care for hospitalized children requires attention to many elements unique to the pediatric population. These include age-based differences in development, behavior, physiology, and prevalence of clinical conditions, the impact of acute and chronic disease states on child development, the use of medications and other medical interventions with limited investigative guidance, and the role of caregivers in decision-making and care delivery. Heightened awareness of these factors is required in the hospital setting, where diagnoses and interventions often include the use of high-risk modalities and require coordination of care across multiple providers.
METHODS
Project Initiation
Revision of The PHM Core Competencies: 2020 Revision began in early 2017 following SHM’s work on The Core Competencies in Hospital Medicine 2017 Revision.15 The Executive Committee of the SHM Pediatrics Special Interest Group (SIG) supported the initiation of the revision. The 3 editors from the original compendium created an initial plan for the project that included a proposed timeline, processes for engagement of previously involved experts and new talent, and performance of a needs assessment to guide content selection. The Figure highlights these and other important steps in the revision process.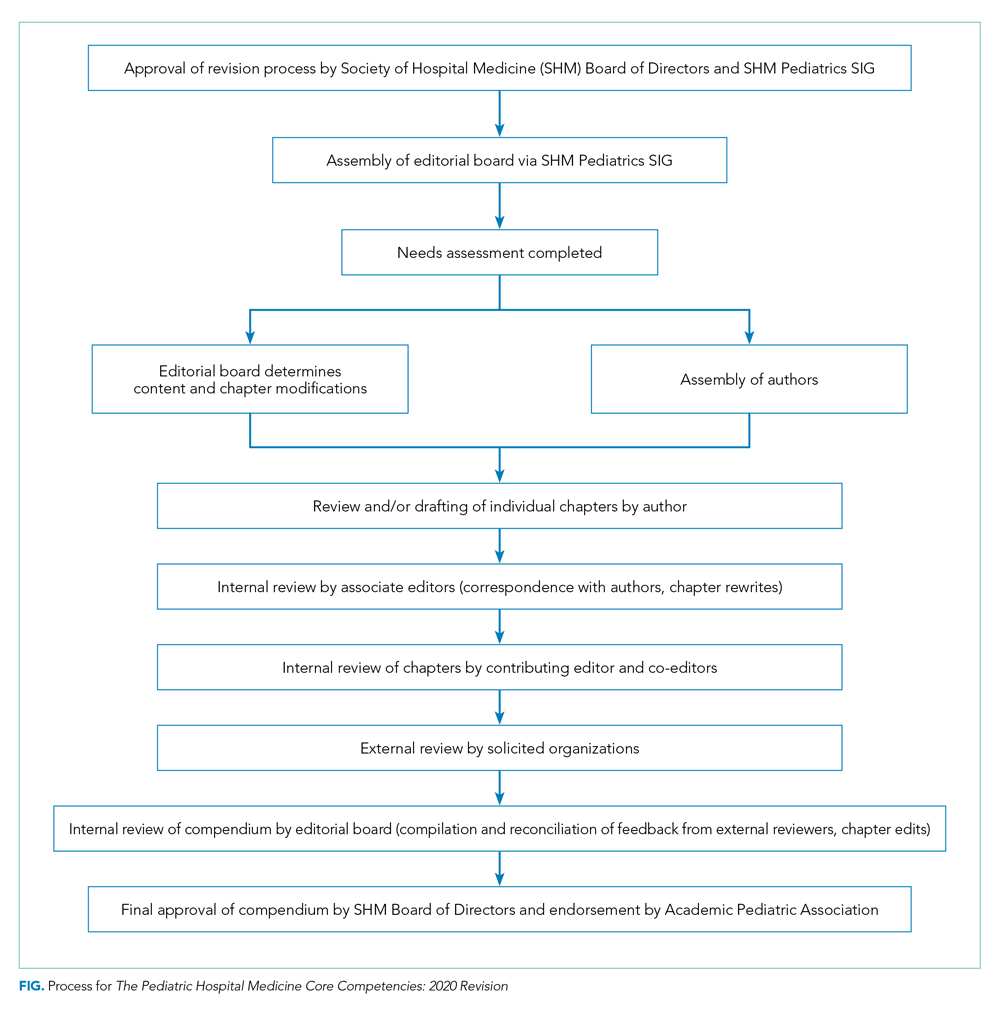
Editor and Associate Editor Selection
The above editors reviewed best practice examples of roles and responsibilities for editor and associate editor positions from relevant, leading societies and journals. From this review, the editors created an editorial structure specifically for The PHM Core Competencies: 2020 Revision. A new position of Contributing Editor was created to address the need for dedicated attention to the community site perspective and ensure review of all content, within and across chapters, by a pediatric hospitalist who is dedicated to this environment. Solicitation for additional editors and associate editors occurred via the SHM Pediatrics SIG to the wider SHM membership. The criteria for selection included active engagement in regional or national activities related to the growth and operations of PHM, strong organizational and leadership skills, including the ability to manage tasks and foster creativity, among others. In addition, a deliberate effort was made to recruit a diverse editorial cohort, considering geographic location, primary work environment, organizational affiliations, content expertise, time in practice, gender, and other factors.
Chapter Topic Selection
The editors conducted a two-pronged needs assessment related to optimal content for inclusion in The PHM Core Competencies: 2020 Revision. First, the editors reviewed content from conferences, textbooks, and handbooks specific to the field of PHM, including the conference programs for the most recent 5 years of both the annual PHM national conference and annual meetings of PHM’s 3 core societies in the United States—SHM, AAP, and APA. Second, the editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council, and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
The entire editorial board then reviewed all of the needs assessment data and considered potential changes (additions or deletions) based on emerging trends in pediatric healthcare, the frequency, relevance, and value of the item across all environments in which pediatric hospitalists function, and the value to or impact on hospitalized children and caregivers. Almost all survey ratings and comments were either incorporated into an existing chapter or used to create a new chapter. There was a paucity of comments related to the deletion of chapters, and thus no chapters were entirely excluded. However, there were several comments supporting the exclusion of the suprapubic bladder tap procedure, and thus related content was eliminated from the relevant section in Core Skills. Of the 66 chapters in this revision, the needs assessment data directly informed the creation of 12 new chapters, as well as adjustments and/or additions to the titles of 7 chapters and the content of 29 chapters. In addition, the title of the Specialized Clinical Services section was changed to Specialized Services to represent that both clinical and nonclinical competencies reside in this section devoted to comprehensive management of these unique patient populations commonly encountered by pediatric hospitalists. Many of these changes are highlighted in Table 2.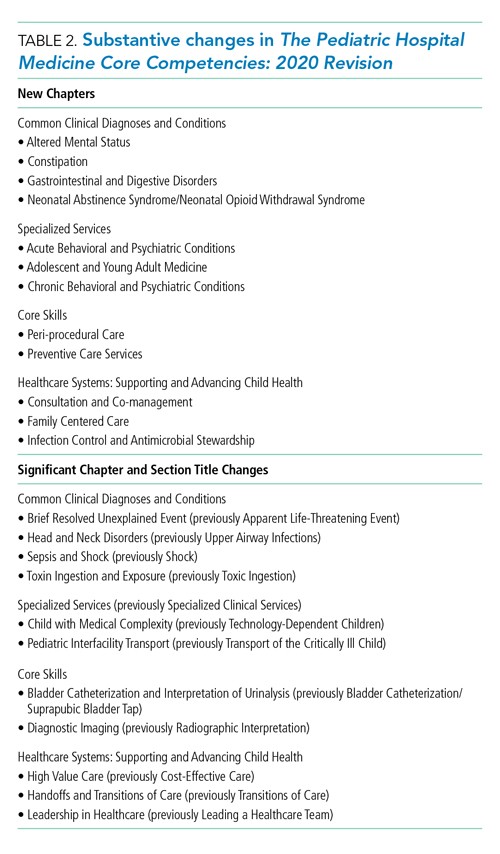
Author selection
Authors from the initial work were invited to participate again as author of their given chapter. Subsequently, authors were identified for new chapters and chapters for which previous authors were no longer able to be engaged. Authors with content expertise were found by reviewing content from conferences, textbooks, and handbooks specific to the field of PHM. Any content expert who was not identified as a pediatric hospitalist was paired with a pediatric hospitalist as coauthor. In addition, as with the editorial board, a deliberate effort was made to recruit a diverse author cohort, considering geographic location, primary work environment, time in practice, gender, and other factors.
The editorial board held numerous conference calls to review potential authors, and the SHM Pediatrics SIG was directly engaged to ensure authorship opportunities were extended broadly. This vetting process resulted in a robust author list and included members of all three of PHM’s sponsoring societies in the United States. Once participation was confirmed, authors received an “author packet” detailing the process with the proposed timeline, resources related to writing learning objectives, the past chapter (if applicable), assigned associate editor, and other helpful resources.
Internal and External Review Process
After all chapters were drafted, the editorial board conducted a rigorous, internal review process. Each chapter was reviewed by at least one associate editor and two editors, with a focus on content, scope, and a standard approach to phrasing and formatting. In addition, the contributing editor reviewed all the chapters to ensure the community hospitalist perspective was adequately represented.
Thirty-two agencies and societies were solicited for external review, including both those involved in review of the previous edition and new stakeholder groups. External reviewers were first contacted to ascertain their interest in participating in the review process, and if interested, were provided with information on the review process. Robust feedback was received from the APA Hospital Medicine SIG, SHM Pediatrics and Medicine-Pediatrics SIGs, Association of Pediatric Program Directors Curriculum Committee, and 20 AAP committees, councils, and sections.
The feedback from the external reviewers and subsequent edits for each chapter were reviewed by at least one associate editor, two editors, and the contributing editor. Authors were engaged to address any salient changes recommended. As the final steps in the review process, the SHM Board of Directors approved the compendium and the APA provided their endorsement.
SUMMARY AND FUTURE DIRECTIONS
This second edition of The PHM Core Competencies: 2020 Revision addresses the knowledge, skills, attitudes, and systems organization and improvement objectives that define the field of pediatric hospital medicine and the leadership roles of pediatric hospitalists. This compendium reflects the recent changes in the practice and educational environments of pediatric hospitalists and can inform education, training, and career development for pediatric hospitalists across all environments in which comprehensive care is rendered for the hospitalized child. Future work at the local and national level can lead to development of associated curricula, conference content, and other training materials.
Acknowledgments
We wish to humbly and respectfully acknowledge the work of the authors, editors, and reviewers involved in the creation of the first edition, as well as this revision, of The PHM Core Competencies. In addition, we are grateful for the input of all pediatric hospitalists and other stakeholders who informed this compendium via contributions to the needs assessment survey, conference proceedings, publications, and other works. Finally, we acknowledge the support and work of SHM project coordinator, Nyla Nicholson, the SHM Pediatrics SIG, and the SHM Board of Directors.
Disclosures
SHM provided administrative support for project coordination (N. Nicholson). No author, editor, or other involved member received any compensation for efforts related to this work. There are no reported conflicts of interest.
1. Pediatric hospital medicine core competencies. Stucky ER, Ottolini MC, Maniscalco J, editors. J Hosp Med April 2010; Vol 5 No 2 (Supplement), 86 pages. Available at: https://www.journalofhospitalmedicine.com/jhospmed/issue/128018/journal-hospital-medicine-52. Accessed August 7, 2019.
2. Association of American Medical Colleges: Analysis in Brief. Estimating the Number and Characteristics of Hospitalist Physicians in the United States and Their Possible Workforce Implications. August 2012 Edition. https://www.aamc.org/download/300620/data/aibvol12_no3-hospitalist.pdf. Accessed August 19, 2019.
3. White CM, Thomson JE, Statile AM, et al. Development of a new care model for hospitalized children with medical complexity. Hosp Pediatr. 2017;7(7):410-414. https://doi.org/10.1542/hpeds.2016-0149.
4. Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatr. 2012;129(2):394-404. https://doi.org/10.1542/peds.2011-3084.
5. Pediatric Research in Inpatient Setting. https://www.prisnetwork.org/. Accessed August 27, 2019.
6. American Academy of Pediatrics. Value in Inpatient Pediatric Network. 2019 Edition. https://www.aap.org/en-us/professional-resources/quality-improvement/Pages/Value-in-Inpatient-Pediatrics.aspx. Accessed August 27, 2019.
7. American Academy of Pediatrics. Advancing Pediatric Educator Excellence Teaching Program. 2019 Edition. https://www.aap.org/en-us/continuing-medical-education/APEX/Pages/APEX.aspx. Accessed August 27, 2019.
8. O’Toole JK, Starmer AJ, Calaman S, et al. I-PASS mentored implementation handoff curriculum: Champion training materials. MedEdPORTAL. 2019;15:10794. https://doi.org/10.15766/mep_2374-8265.10794.
9. Academic Pediatric Association. Pediatric Hospital Medicine 2018 Recap. 2018 Edition. http://2018.phmmeeting.org/. Accessed July 20, 2019.
10. PHM Fellowship Programs. 2019 Edition. http://phmfellows.org/phm-programs/. Accessed July 20, 2019.
11. Shah NH, Rhim HJH, Maniscalco J, et al. The current state of pediatric hospital medicine fellowships: A survey of program directors. J Hosp Med. 2016;11:324–328.21. https://doi.org/10.1002/jhm.2571.
12. Jerardi K, Fisher E, Rassbach C, et al. Development of a curricular framework for pediatric hospital medicine fellowships. Pediatr. 2017;140(1): e20170698.22. https://doi.org/10.1542/peds.2017-0698.
13. Blankenburg R, Chase L, Maniscalco J, Ottolini M. Hospital Medicine Entrustable Professional Activities, American Board of Pediatrics, 2018. https://www.abp.org/subspecialty-epas#Hospitalist%20Medicine. Accessed July 20, 2019.
14. Carraccio CL, Benson BJ, Nixon LJ, Derstine PL. From the educational bench to the clinical bedside: translating the Dreyfus Developmental Model to the learning of clinical skills. Accad Med. 2008;83(8):761-767. https://doi.org/10.1097/ACM.0b013e31817eb632.
15. Nichani S, Crocker J, Fetterman N, Lukela M. Updating the core competencies in hospital medicine—2017 revision: Introduction and methodology. J Hosp Med. 2017;4;283-287. https://doi.org/10.12788/jhm.2715.
The Pediatric Hospital Medicine Core Competencies were first published in 2010 to help define a specific body of knowledge and measurable skills needed to practice high quality care for hospitalized pediatric patients across all practice settings.1 Since then, the number of practicing pediatric hospitalists has grown to a conservative estimate of 3,000 physicians and the scope of practice among pediatric hospitalists has matured.2 Pediatric hospitalists are increasingly leading or participating in organizational and national efforts that emphasize interprofessional collaboration and the delivery of high value care to hospitalized children and their caregivers—including innovative and family-centered care models, patient safety and quality improvement initiatives, and research and educational enterprises.3-8 In response to these changes, the American Board of Medical Specialties designated Pediatric Hospital Medicine (PHM) as a pediatric subspecialty in 2016.
The field of PHM in the United States continues to be supported by three core societies—Society of Hospital Medicine (SHM), American Academy of Pediatrics (AAP), and Academic Pediatric Association (APA). Together, these societies serve as tri-sponsors of the annual Pediatric Hospital Medicine national conference, which now welcomes over 1,200 attendees from the United States and abroad.9 Each society also individually sponsors a variety of professional development and continuing medical education activities specific to PHM.
In addition, pediatric hospitalists often serve a pivotal role in teaching learners (medical students, residents, and other health profession students), physician colleagues, and other healthcare professionals on the hospital wards and via institutional educational programs. Nearly 50 institutions in the United States offer graduate medical education training in PHM.10 The PHM Fellowship Directors Council has developed a standardized curricular framework and entrustable professional activities, which reflect the tenets of competency-based medical education, for use in PHM training programs.11-13
These changes in the practice environment of pediatric hospitalists, as well as the changing landscape of graduate and continuing medical education in PHM, have informed this revision of The PHM Core Competencies. The purpose of this article is to describe the methodology of the review and revision process.
OVERVIEW OF THE PHM CORECOMPETENCIES: 2020
Revision
The PHM Core Competencies: 2020 Revision provide a framework for graduate and continuing medical education that reflects the current roles and expectations for all pediatric hospitalists in the United States. The acuity and complexity of hospitalized children, the availability of pediatric subspecialty care and other resources, and the institutional orientation towards pediatric populations vary across community, tertiary, and children’s hospital settings. In order to unify the practice of PHM across these environments, The PHM Core Competencies: 2020 Revision address the fundamental and most common components of PHM which are encountered by the majority of practicing pediatric hospitalists, as opposed to an extensive review of all aspects of the field.
The compendium includes 66 chapters on both clinical and nonclinical topics, divided into four sections—Common Clinical Diagnoses and Conditions, Core Skills, Specialized Services, and Healthcare Systems: Supporting and Advancing Child Health (Table 1). Within each chapter is an introductory paragraph and learning objectives in three domains of educational outcomes—cognitive (knowledge), psychomotor (skills), and affective (attitudes)—as well as systems organization and improvement, to reflect the emphasis of PHM practice on improving healthcare systems. The objectives encompass a range of observable behaviors and other attributes, from foundational skills such as taking a history and performing a physical exam to more advanced actions such as participating in the development of care models to support the health of complex patient populations. Implicit in these objectives is the expectation that pediatric hospitalists build on experiences in medical school and residency training to attain a level of competency at the advanced levels of a developmental continuum, such as proficient, expert, or master.14
The objectives also balance specificity to the topic with a timeless quality, allowing for flexibility both as new information emerges and when applied to various educational activities and learner groups. Each chapter can stand alone, and thus themes recur if one reads the compendium in its entirety. However, in order to reflect related content among the chapters, the appendix contains a list of associated chapters (Chapter Links) for further exploration. In addition, a short reference list is provided in each chapter to reflect the literature and best practices at the time of publication.
Finally, The PHM Core Competencies: 2020 Revision reflect the status of children as a vulnerable population. Care for hospitalized children requires attention to many elements unique to the pediatric population. These include age-based differences in development, behavior, physiology, and prevalence of clinical conditions, the impact of acute and chronic disease states on child development, the use of medications and other medical interventions with limited investigative guidance, and the role of caregivers in decision-making and care delivery. Heightened awareness of these factors is required in the hospital setting, where diagnoses and interventions often include the use of high-risk modalities and require coordination of care across multiple providers.
METHODS
Project Initiation
Revision of The PHM Core Competencies: 2020 Revision began in early 2017 following SHM’s work on The Core Competencies in Hospital Medicine 2017 Revision.15 The Executive Committee of the SHM Pediatrics Special Interest Group (SIG) supported the initiation of the revision. The 3 editors from the original compendium created an initial plan for the project that included a proposed timeline, processes for engagement of previously involved experts and new talent, and performance of a needs assessment to guide content selection. The Figure highlights these and other important steps in the revision process.
Editor and Associate Editor Selection
The above editors reviewed best practice examples of roles and responsibilities for editor and associate editor positions from relevant, leading societies and journals. From this review, the editors created an editorial structure specifically for The PHM Core Competencies: 2020 Revision. A new position of Contributing Editor was created to address the need for dedicated attention to the community site perspective and ensure review of all content, within and across chapters, by a pediatric hospitalist who is dedicated to this environment. Solicitation for additional editors and associate editors occurred via the SHM Pediatrics SIG to the wider SHM membership. The criteria for selection included active engagement in regional or national activities related to the growth and operations of PHM, strong organizational and leadership skills, including the ability to manage tasks and foster creativity, among others. In addition, a deliberate effort was made to recruit a diverse editorial cohort, considering geographic location, primary work environment, organizational affiliations, content expertise, time in practice, gender, and other factors.
Chapter Topic Selection
The editors conducted a two-pronged needs assessment related to optimal content for inclusion in The PHM Core Competencies: 2020 Revision. First, the editors reviewed content from conferences, textbooks, and handbooks specific to the field of PHM, including the conference programs for the most recent 5 years of both the annual PHM national conference and annual meetings of PHM’s 3 core societies in the United States—SHM, AAP, and APA. Second, the editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council, and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
The entire editorial board then reviewed all of the needs assessment data and considered potential changes (additions or deletions) based on emerging trends in pediatric healthcare, the frequency, relevance, and value of the item across all environments in which pediatric hospitalists function, and the value to or impact on hospitalized children and caregivers. Almost all survey ratings and comments were either incorporated into an existing chapter or used to create a new chapter. There was a paucity of comments related to the deletion of chapters, and thus no chapters were entirely excluded. However, there were several comments supporting the exclusion of the suprapubic bladder tap procedure, and thus related content was eliminated from the relevant section in Core Skills. Of the 66 chapters in this revision, the needs assessment data directly informed the creation of 12 new chapters, as well as adjustments and/or additions to the titles of 7 chapters and the content of 29 chapters. In addition, the title of the Specialized Clinical Services section was changed to Specialized Services to represent that both clinical and nonclinical competencies reside in this section devoted to comprehensive management of these unique patient populations commonly encountered by pediatric hospitalists. Many of these changes are highlighted in Table 2.
Author selection
Authors from the initial work were invited to participate again as author of their given chapter. Subsequently, authors were identified for new chapters and chapters for which previous authors were no longer able to be engaged. Authors with content expertise were found by reviewing content from conferences, textbooks, and handbooks specific to the field of PHM. Any content expert who was not identified as a pediatric hospitalist was paired with a pediatric hospitalist as coauthor. In addition, as with the editorial board, a deliberate effort was made to recruit a diverse author cohort, considering geographic location, primary work environment, time in practice, gender, and other factors.
The editorial board held numerous conference calls to review potential authors, and the SHM Pediatrics SIG was directly engaged to ensure authorship opportunities were extended broadly. This vetting process resulted in a robust author list and included members of all three of PHM’s sponsoring societies in the United States. Once participation was confirmed, authors received an “author packet” detailing the process with the proposed timeline, resources related to writing learning objectives, the past chapter (if applicable), assigned associate editor, and other helpful resources.
Internal and External Review Process
After all chapters were drafted, the editorial board conducted a rigorous, internal review process. Each chapter was reviewed by at least one associate editor and two editors, with a focus on content, scope, and a standard approach to phrasing and formatting. In addition, the contributing editor reviewed all the chapters to ensure the community hospitalist perspective was adequately represented.
Thirty-two agencies and societies were solicited for external review, including both those involved in review of the previous edition and new stakeholder groups. External reviewers were first contacted to ascertain their interest in participating in the review process, and if interested, were provided with information on the review process. Robust feedback was received from the APA Hospital Medicine SIG, SHM Pediatrics and Medicine-Pediatrics SIGs, Association of Pediatric Program Directors Curriculum Committee, and 20 AAP committees, councils, and sections.
The feedback from the external reviewers and subsequent edits for each chapter were reviewed by at least one associate editor, two editors, and the contributing editor. Authors were engaged to address any salient changes recommended. As the final steps in the review process, the SHM Board of Directors approved the compendium and the APA provided their endorsement.
SUMMARY AND FUTURE DIRECTIONS
This second edition of The PHM Core Competencies: 2020 Revision addresses the knowledge, skills, attitudes, and systems organization and improvement objectives that define the field of pediatric hospital medicine and the leadership roles of pediatric hospitalists. This compendium reflects the recent changes in the practice and educational environments of pediatric hospitalists and can inform education, training, and career development for pediatric hospitalists across all environments in which comprehensive care is rendered for the hospitalized child. Future work at the local and national level can lead to development of associated curricula, conference content, and other training materials.
Acknowledgments
We wish to humbly and respectfully acknowledge the work of the authors, editors, and reviewers involved in the creation of the first edition, as well as this revision, of The PHM Core Competencies. In addition, we are grateful for the input of all pediatric hospitalists and other stakeholders who informed this compendium via contributions to the needs assessment survey, conference proceedings, publications, and other works. Finally, we acknowledge the support and work of SHM project coordinator, Nyla Nicholson, the SHM Pediatrics SIG, and the SHM Board of Directors.
Disclosures
SHM provided administrative support for project coordination (N. Nicholson). No author, editor, or other involved member received any compensation for efforts related to this work. There are no reported conflicts of interest.
The Pediatric Hospital Medicine Core Competencies were first published in 2010 to help define a specific body of knowledge and measurable skills needed to practice high quality care for hospitalized pediatric patients across all practice settings.1 Since then, the number of practicing pediatric hospitalists has grown to a conservative estimate of 3,000 physicians and the scope of practice among pediatric hospitalists has matured.2 Pediatric hospitalists are increasingly leading or participating in organizational and national efforts that emphasize interprofessional collaboration and the delivery of high value care to hospitalized children and their caregivers—including innovative and family-centered care models, patient safety and quality improvement initiatives, and research and educational enterprises.3-8 In response to these changes, the American Board of Medical Specialties designated Pediatric Hospital Medicine (PHM) as a pediatric subspecialty in 2016.
The field of PHM in the United States continues to be supported by three core societies—Society of Hospital Medicine (SHM), American Academy of Pediatrics (AAP), and Academic Pediatric Association (APA). Together, these societies serve as tri-sponsors of the annual Pediatric Hospital Medicine national conference, which now welcomes over 1,200 attendees from the United States and abroad.9 Each society also individually sponsors a variety of professional development and continuing medical education activities specific to PHM.
In addition, pediatric hospitalists often serve a pivotal role in teaching learners (medical students, residents, and other health profession students), physician colleagues, and other healthcare professionals on the hospital wards and via institutional educational programs. Nearly 50 institutions in the United States offer graduate medical education training in PHM.10 The PHM Fellowship Directors Council has developed a standardized curricular framework and entrustable professional activities, which reflect the tenets of competency-based medical education, for use in PHM training programs.11-13
These changes in the practice environment of pediatric hospitalists, as well as the changing landscape of graduate and continuing medical education in PHM, have informed this revision of The PHM Core Competencies. The purpose of this article is to describe the methodology of the review and revision process.
OVERVIEW OF THE PHM CORECOMPETENCIES: 2020
Revision
The PHM Core Competencies: 2020 Revision provide a framework for graduate and continuing medical education that reflects the current roles and expectations for all pediatric hospitalists in the United States. The acuity and complexity of hospitalized children, the availability of pediatric subspecialty care and other resources, and the institutional orientation towards pediatric populations vary across community, tertiary, and children’s hospital settings. In order to unify the practice of PHM across these environments, The PHM Core Competencies: 2020 Revision address the fundamental and most common components of PHM which are encountered by the majority of practicing pediatric hospitalists, as opposed to an extensive review of all aspects of the field.
The compendium includes 66 chapters on both clinical and nonclinical topics, divided into four sections—Common Clinical Diagnoses and Conditions, Core Skills, Specialized Services, and Healthcare Systems: Supporting and Advancing Child Health (Table 1). Within each chapter is an introductory paragraph and learning objectives in three domains of educational outcomes—cognitive (knowledge), psychomotor (skills), and affective (attitudes)—as well as systems organization and improvement, to reflect the emphasis of PHM practice on improving healthcare systems. The objectives encompass a range of observable behaviors and other attributes, from foundational skills such as taking a history and performing a physical exam to more advanced actions such as participating in the development of care models to support the health of complex patient populations. Implicit in these objectives is the expectation that pediatric hospitalists build on experiences in medical school and residency training to attain a level of competency at the advanced levels of a developmental continuum, such as proficient, expert, or master.14
The objectives also balance specificity to the topic with a timeless quality, allowing for flexibility both as new information emerges and when applied to various educational activities and learner groups. Each chapter can stand alone, and thus themes recur if one reads the compendium in its entirety. However, in order to reflect related content among the chapters, the appendix contains a list of associated chapters (Chapter Links) for further exploration. In addition, a short reference list is provided in each chapter to reflect the literature and best practices at the time of publication.
Finally, The PHM Core Competencies: 2020 Revision reflect the status of children as a vulnerable population. Care for hospitalized children requires attention to many elements unique to the pediatric population. These include age-based differences in development, behavior, physiology, and prevalence of clinical conditions, the impact of acute and chronic disease states on child development, the use of medications and other medical interventions with limited investigative guidance, and the role of caregivers in decision-making and care delivery. Heightened awareness of these factors is required in the hospital setting, where diagnoses and interventions often include the use of high-risk modalities and require coordination of care across multiple providers.
METHODS
Project Initiation
Revision of The PHM Core Competencies: 2020 Revision began in early 2017 following SHM’s work on The Core Competencies in Hospital Medicine 2017 Revision.15 The Executive Committee of the SHM Pediatrics Special Interest Group (SIG) supported the initiation of the revision. The 3 editors from the original compendium created an initial plan for the project that included a proposed timeline, processes for engagement of previously involved experts and new talent, and performance of a needs assessment to guide content selection. The Figure highlights these and other important steps in the revision process.
Editor and Associate Editor Selection
The above editors reviewed best practice examples of roles and responsibilities for editor and associate editor positions from relevant, leading societies and journals. From this review, the editors created an editorial structure specifically for The PHM Core Competencies: 2020 Revision. A new position of Contributing Editor was created to address the need for dedicated attention to the community site perspective and ensure review of all content, within and across chapters, by a pediatric hospitalist who is dedicated to this environment. Solicitation for additional editors and associate editors occurred via the SHM Pediatrics SIG to the wider SHM membership. The criteria for selection included active engagement in regional or national activities related to the growth and operations of PHM, strong organizational and leadership skills, including the ability to manage tasks and foster creativity, among others. In addition, a deliberate effort was made to recruit a diverse editorial cohort, considering geographic location, primary work environment, organizational affiliations, content expertise, time in practice, gender, and other factors.
Chapter Topic Selection
The editors conducted a two-pronged needs assessment related to optimal content for inclusion in The PHM Core Competencies: 2020 Revision. First, the editors reviewed content from conferences, textbooks, and handbooks specific to the field of PHM, including the conference programs for the most recent 5 years of both the annual PHM national conference and annual meetings of PHM’s 3 core societies in the United States—SHM, AAP, and APA. Second, the editors conducted a needs assessment survey with several stakeholder groups, including SHM’s Pediatrics and Medicine-Pediatrics SIGs, AAP Section on Hospital Medicine and its subcommittees, APA Hospital Medicine SIG, PHM Fellowship Directors Council, and PHM Division Directors, with encouragement to pass the survey link to others in the PHM community interested in providing input (Appendix Figure). The solicitation asked for comment on existing chapters and suggestions for new chapters. For any new chapter, respondents were asked to note the intended purpose of the chapter and the anticipated value that chapter would bring to our profession and the children and the caregivers served by pediatric hospitalists.
The entire editorial board then reviewed all of the needs assessment data and considered potential changes (additions or deletions) based on emerging trends in pediatric healthcare, the frequency, relevance, and value of the item across all environments in which pediatric hospitalists function, and the value to or impact on hospitalized children and caregivers. Almost all survey ratings and comments were either incorporated into an existing chapter or used to create a new chapter. There was a paucity of comments related to the deletion of chapters, and thus no chapters were entirely excluded. However, there were several comments supporting the exclusion of the suprapubic bladder tap procedure, and thus related content was eliminated from the relevant section in Core Skills. Of the 66 chapters in this revision, the needs assessment data directly informed the creation of 12 new chapters, as well as adjustments and/or additions to the titles of 7 chapters and the content of 29 chapters. In addition, the title of the Specialized Clinical Services section was changed to Specialized Services to represent that both clinical and nonclinical competencies reside in this section devoted to comprehensive management of these unique patient populations commonly encountered by pediatric hospitalists. Many of these changes are highlighted in Table 2.
Author selection
Authors from the initial work were invited to participate again as author of their given chapter. Subsequently, authors were identified for new chapters and chapters for which previous authors were no longer able to be engaged. Authors with content expertise were found by reviewing content from conferences, textbooks, and handbooks specific to the field of PHM. Any content expert who was not identified as a pediatric hospitalist was paired with a pediatric hospitalist as coauthor. In addition, as with the editorial board, a deliberate effort was made to recruit a diverse author cohort, considering geographic location, primary work environment, time in practice, gender, and other factors.
The editorial board held numerous conference calls to review potential authors, and the SHM Pediatrics SIG was directly engaged to ensure authorship opportunities were extended broadly. This vetting process resulted in a robust author list and included members of all three of PHM’s sponsoring societies in the United States. Once participation was confirmed, authors received an “author packet” detailing the process with the proposed timeline, resources related to writing learning objectives, the past chapter (if applicable), assigned associate editor, and other helpful resources.
Internal and External Review Process
After all chapters were drafted, the editorial board conducted a rigorous, internal review process. Each chapter was reviewed by at least one associate editor and two editors, with a focus on content, scope, and a standard approach to phrasing and formatting. In addition, the contributing editor reviewed all the chapters to ensure the community hospitalist perspective was adequately represented.
Thirty-two agencies and societies were solicited for external review, including both those involved in review of the previous edition and new stakeholder groups. External reviewers were first contacted to ascertain their interest in participating in the review process, and if interested, were provided with information on the review process. Robust feedback was received from the APA Hospital Medicine SIG, SHM Pediatrics and Medicine-Pediatrics SIGs, Association of Pediatric Program Directors Curriculum Committee, and 20 AAP committees, councils, and sections.
The feedback from the external reviewers and subsequent edits for each chapter were reviewed by at least one associate editor, two editors, and the contributing editor. Authors were engaged to address any salient changes recommended. As the final steps in the review process, the SHM Board of Directors approved the compendium and the APA provided their endorsement.
SUMMARY AND FUTURE DIRECTIONS
This second edition of The PHM Core Competencies: 2020 Revision addresses the knowledge, skills, attitudes, and systems organization and improvement objectives that define the field of pediatric hospital medicine and the leadership roles of pediatric hospitalists. This compendium reflects the recent changes in the practice and educational environments of pediatric hospitalists and can inform education, training, and career development for pediatric hospitalists across all environments in which comprehensive care is rendered for the hospitalized child. Future work at the local and national level can lead to development of associated curricula, conference content, and other training materials.
Acknowledgments
We wish to humbly and respectfully acknowledge the work of the authors, editors, and reviewers involved in the creation of the first edition, as well as this revision, of The PHM Core Competencies. In addition, we are grateful for the input of all pediatric hospitalists and other stakeholders who informed this compendium via contributions to the needs assessment survey, conference proceedings, publications, and other works. Finally, we acknowledge the support and work of SHM project coordinator, Nyla Nicholson, the SHM Pediatrics SIG, and the SHM Board of Directors.
Disclosures
SHM provided administrative support for project coordination (N. Nicholson). No author, editor, or other involved member received any compensation for efforts related to this work. There are no reported conflicts of interest.
1. Pediatric hospital medicine core competencies. Stucky ER, Ottolini MC, Maniscalco J, editors. J Hosp Med April 2010; Vol 5 No 2 (Supplement), 86 pages. Available at: https://www.journalofhospitalmedicine.com/jhospmed/issue/128018/journal-hospital-medicine-52. Accessed August 7, 2019.
2. Association of American Medical Colleges: Analysis in Brief. Estimating the Number and Characteristics of Hospitalist Physicians in the United States and Their Possible Workforce Implications. August 2012 Edition. https://www.aamc.org/download/300620/data/aibvol12_no3-hospitalist.pdf. Accessed August 19, 2019.
3. White CM, Thomson JE, Statile AM, et al. Development of a new care model for hospitalized children with medical complexity. Hosp Pediatr. 2017;7(7):410-414. https://doi.org/10.1542/hpeds.2016-0149.
4. Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatr. 2012;129(2):394-404. https://doi.org/10.1542/peds.2011-3084.
5. Pediatric Research in Inpatient Setting. https://www.prisnetwork.org/. Accessed August 27, 2019.
6. American Academy of Pediatrics. Value in Inpatient Pediatric Network. 2019 Edition. https://www.aap.org/en-us/professional-resources/quality-improvement/Pages/Value-in-Inpatient-Pediatrics.aspx. Accessed August 27, 2019.
7. American Academy of Pediatrics. Advancing Pediatric Educator Excellence Teaching Program. 2019 Edition. https://www.aap.org/en-us/continuing-medical-education/APEX/Pages/APEX.aspx. Accessed August 27, 2019.
8. O’Toole JK, Starmer AJ, Calaman S, et al. I-PASS mentored implementation handoff curriculum: Champion training materials. MedEdPORTAL. 2019;15:10794. https://doi.org/10.15766/mep_2374-8265.10794.
9. Academic Pediatric Association. Pediatric Hospital Medicine 2018 Recap. 2018 Edition. http://2018.phmmeeting.org/. Accessed July 20, 2019.
10. PHM Fellowship Programs. 2019 Edition. http://phmfellows.org/phm-programs/. Accessed July 20, 2019.
11. Shah NH, Rhim HJH, Maniscalco J, et al. The current state of pediatric hospital medicine fellowships: A survey of program directors. J Hosp Med. 2016;11:324–328.21. https://doi.org/10.1002/jhm.2571.
12. Jerardi K, Fisher E, Rassbach C, et al. Development of a curricular framework for pediatric hospital medicine fellowships. Pediatr. 2017;140(1): e20170698.22. https://doi.org/10.1542/peds.2017-0698.
13. Blankenburg R, Chase L, Maniscalco J, Ottolini M. Hospital Medicine Entrustable Professional Activities, American Board of Pediatrics, 2018. https://www.abp.org/subspecialty-epas#Hospitalist%20Medicine. Accessed July 20, 2019.
14. Carraccio CL, Benson BJ, Nixon LJ, Derstine PL. From the educational bench to the clinical bedside: translating the Dreyfus Developmental Model to the learning of clinical skills. Accad Med. 2008;83(8):761-767. https://doi.org/10.1097/ACM.0b013e31817eb632.
15. Nichani S, Crocker J, Fetterman N, Lukela M. Updating the core competencies in hospital medicine—2017 revision: Introduction and methodology. J Hosp Med. 2017;4;283-287. https://doi.org/10.12788/jhm.2715.
1. Pediatric hospital medicine core competencies. Stucky ER, Ottolini MC, Maniscalco J, editors. J Hosp Med April 2010; Vol 5 No 2 (Supplement), 86 pages. Available at: https://www.journalofhospitalmedicine.com/jhospmed/issue/128018/journal-hospital-medicine-52. Accessed August 7, 2019.
2. Association of American Medical Colleges: Analysis in Brief. Estimating the Number and Characteristics of Hospitalist Physicians in the United States and Their Possible Workforce Implications. August 2012 Edition. https://www.aamc.org/download/300620/data/aibvol12_no3-hospitalist.pdf. Accessed August 19, 2019.
3. White CM, Thomson JE, Statile AM, et al. Development of a new care model for hospitalized children with medical complexity. Hosp Pediatr. 2017;7(7):410-414. https://doi.org/10.1542/hpeds.2016-0149.
4. Committee on Hospital Care and Institute for Patient- and Family-Centered Care. Patient- and family-centered care and the pediatrician’s role. Pediatr. 2012;129(2):394-404. https://doi.org/10.1542/peds.2011-3084.
5. Pediatric Research in Inpatient Setting. https://www.prisnetwork.org/. Accessed August 27, 2019.
6. American Academy of Pediatrics. Value in Inpatient Pediatric Network. 2019 Edition. https://www.aap.org/en-us/professional-resources/quality-improvement/Pages/Value-in-Inpatient-Pediatrics.aspx. Accessed August 27, 2019.
7. American Academy of Pediatrics. Advancing Pediatric Educator Excellence Teaching Program. 2019 Edition. https://www.aap.org/en-us/continuing-medical-education/APEX/Pages/APEX.aspx. Accessed August 27, 2019.
8. O’Toole JK, Starmer AJ, Calaman S, et al. I-PASS mentored implementation handoff curriculum: Champion training materials. MedEdPORTAL. 2019;15:10794. https://doi.org/10.15766/mep_2374-8265.10794.
9. Academic Pediatric Association. Pediatric Hospital Medicine 2018 Recap. 2018 Edition. http://2018.phmmeeting.org/. Accessed July 20, 2019.
10. PHM Fellowship Programs. 2019 Edition. http://phmfellows.org/phm-programs/. Accessed July 20, 2019.
11. Shah NH, Rhim HJH, Maniscalco J, et al. The current state of pediatric hospital medicine fellowships: A survey of program directors. J Hosp Med. 2016;11:324–328.21. https://doi.org/10.1002/jhm.2571.
12. Jerardi K, Fisher E, Rassbach C, et al. Development of a curricular framework for pediatric hospital medicine fellowships. Pediatr. 2017;140(1): e20170698.22. https://doi.org/10.1542/peds.2017-0698.
13. Blankenburg R, Chase L, Maniscalco J, Ottolini M. Hospital Medicine Entrustable Professional Activities, American Board of Pediatrics, 2018. https://www.abp.org/subspecialty-epas#Hospitalist%20Medicine. Accessed July 20, 2019.
14. Carraccio CL, Benson BJ, Nixon LJ, Derstine PL. From the educational bench to the clinical bedside: translating the Dreyfus Developmental Model to the learning of clinical skills. Accad Med. 2008;83(8):761-767. https://doi.org/10.1097/ACM.0b013e31817eb632.
15. Nichani S, Crocker J, Fetterman N, Lukela M. Updating the core competencies in hospital medicine—2017 revision: Introduction and methodology. J Hosp Med. 2017;4;283-287. https://doi.org/10.12788/jhm.2715.
© 2020 Society of Hospital Medicine
Robotic and manual total knee arthroplasty found at least comparable
When results in a series of robotic-assisted total knee arthroplasties (TKA) were compared with a series of arthroplasties performed manually by the same surgeon, results were comparable even though the robotic procedures included a learning phase. The results of the study were reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled because of COVID-19.
“Robotics appears to level the playing field for those who are less experienced, so that robotic total knee arthroplasty might be particularly well suited to low-volume surgeons,” reported Sridhar R. Rachala, MD, assistant professor of orthopaedic surgery, University of Buffalo (N.Y.).
In this retrospective cohort study, radiographic and clinical outcomes were evaluated in 164 total knee arthroplasties performed manually over an 8-month period and compared with 300 procedures performed robotically by the same experienced surgeon over the subsequent 15-month period.
There were no significant differences between patient groups for mean age or body mass index. Dr. Rachala, who performed both sets of procedures, reported inherent differences in technique. Specifically, the mechanical alignment was planned for a traditional neutral mechanical axis, while the robotic procedures were planned in kinematic alignment.
When evaluated at 1 year, the mean KOOS JR (Knee Injury and Osteoarthritis Outcome for Joint Replacement) scores were not significantly different for the robotic and manually performed procedures (76.0 vs. 73.9; P = .54). There were also no differences in the final extension (P = .64) or flexion (P = .59).
However, the difference in mean length of stay (2.0 vs. 2.4 days; P = .0002) favored the robotic approach, and the higher proportion of patients discharged to home after robotic surgery (73% vs. 66%; P = .11) suggested a favorable trend. Planned and postoperative alignment was within two degrees for both groups and not significantly different.
“The robotic series were at a disadvantage because it included cases that I performed when first switching to this approach,” reported Dr. Rachala in an interview.
Although a growing number of total hip arthroplasties are performed robotically, there have not so far been many comparisons of clinical outcomes among surgeons experienced with both approaches, according to Dr. Rachala. Acknowledging that a single-surgeon experience could be considered a limitation of this series, Dr. Rachala also considers it a potential strength. Dr. Rachala was highly experienced with manually instrumented total knee arthroplasty when he switched.
“Positioning and alignment are not just more accurate but easier to perform with robotic assistance,” he said, explaining why this approach is likely to offer a particular advantage to surgeons who perform these types of arthroplasties at low volume. He noted that robotic programming helps prevent errors and adopt alternative more personalized alignments.
Although Dr. Rachala acknowledged that long-term and controlled studies are needed, his experience suggests that robotic-assisted procedures are emerging as a viable alternative with advantages for the surgeon as well as the patient.
The principle that robotic assistance can add consistency to total joint arthroplasty is valid, according to Gwo-Chin Lee, MD, an associate professor of orthopaedic surgery, University of Pennsylvania, Philadelphia. “Robotic-assisted arthroplasty improves the accuracy and consistency of the procedure, which can potentially reduce the likelihood of failure. In knees, it is proven to be valuable in unicompartmental replacements in which results are correlated to a surgeon’s surgical volume. It has an equalizing effect relative to a surgeon with more extensive experience,” Dr. Lee said.
The senior author of a recent systematic review and meta-analysis of robotic-assisted unicompartmental knee arthroplasty (J Knee Surg. 2020 Jan 30; doi: 10.1055/s-0040-1701455), Dr. Lee said, “While the impact of robotics on other metrics including patient satisfaction and early recovery continues to be debated among surgeons who specialize in total knee arthroplasties, the technology can aid surgeons in component position, sizing, and ligament balance, particularly for the lower-volume surgeons and ultimately lead to more predictable outcomes.”
Dr. Rachala reports a financial relationship with Avanos and Stryker.
SOURCE: Rachala S et al. AAOS 2020. Abstract P0091.
When results in a series of robotic-assisted total knee arthroplasties (TKA) were compared with a series of arthroplasties performed manually by the same surgeon, results were comparable even though the robotic procedures included a learning phase. The results of the study were reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled because of COVID-19.
“Robotics appears to level the playing field for those who are less experienced, so that robotic total knee arthroplasty might be particularly well suited to low-volume surgeons,” reported Sridhar R. Rachala, MD, assistant professor of orthopaedic surgery, University of Buffalo (N.Y.).
In this retrospective cohort study, radiographic and clinical outcomes were evaluated in 164 total knee arthroplasties performed manually over an 8-month period and compared with 300 procedures performed robotically by the same experienced surgeon over the subsequent 15-month period.
There were no significant differences between patient groups for mean age or body mass index. Dr. Rachala, who performed both sets of procedures, reported inherent differences in technique. Specifically, the mechanical alignment was planned for a traditional neutral mechanical axis, while the robotic procedures were planned in kinematic alignment.
When evaluated at 1 year, the mean KOOS JR (Knee Injury and Osteoarthritis Outcome for Joint Replacement) scores were not significantly different for the robotic and manually performed procedures (76.0 vs. 73.9; P = .54). There were also no differences in the final extension (P = .64) or flexion (P = .59).
However, the difference in mean length of stay (2.0 vs. 2.4 days; P = .0002) favored the robotic approach, and the higher proportion of patients discharged to home after robotic surgery (73% vs. 66%; P = .11) suggested a favorable trend. Planned and postoperative alignment was within two degrees for both groups and not significantly different.
“The robotic series were at a disadvantage because it included cases that I performed when first switching to this approach,” reported Dr. Rachala in an interview.
Although a growing number of total hip arthroplasties are performed robotically, there have not so far been many comparisons of clinical outcomes among surgeons experienced with both approaches, according to Dr. Rachala. Acknowledging that a single-surgeon experience could be considered a limitation of this series, Dr. Rachala also considers it a potential strength. Dr. Rachala was highly experienced with manually instrumented total knee arthroplasty when he switched.
“Positioning and alignment are not just more accurate but easier to perform with robotic assistance,” he said, explaining why this approach is likely to offer a particular advantage to surgeons who perform these types of arthroplasties at low volume. He noted that robotic programming helps prevent errors and adopt alternative more personalized alignments.
Although Dr. Rachala acknowledged that long-term and controlled studies are needed, his experience suggests that robotic-assisted procedures are emerging as a viable alternative with advantages for the surgeon as well as the patient.
The principle that robotic assistance can add consistency to total joint arthroplasty is valid, according to Gwo-Chin Lee, MD, an associate professor of orthopaedic surgery, University of Pennsylvania, Philadelphia. “Robotic-assisted arthroplasty improves the accuracy and consistency of the procedure, which can potentially reduce the likelihood of failure. In knees, it is proven to be valuable in unicompartmental replacements in which results are correlated to a surgeon’s surgical volume. It has an equalizing effect relative to a surgeon with more extensive experience,” Dr. Lee said.
The senior author of a recent systematic review and meta-analysis of robotic-assisted unicompartmental knee arthroplasty (J Knee Surg. 2020 Jan 30; doi: 10.1055/s-0040-1701455), Dr. Lee said, “While the impact of robotics on other metrics including patient satisfaction and early recovery continues to be debated among surgeons who specialize in total knee arthroplasties, the technology can aid surgeons in component position, sizing, and ligament balance, particularly for the lower-volume surgeons and ultimately lead to more predictable outcomes.”
Dr. Rachala reports a financial relationship with Avanos and Stryker.
SOURCE: Rachala S et al. AAOS 2020. Abstract P0091.
When results in a series of robotic-assisted total knee arthroplasties (TKA) were compared with a series of arthroplasties performed manually by the same surgeon, results were comparable even though the robotic procedures included a learning phase. The results of the study were reported in an abstract scheduled for release at the annual meeting of the American Academy of Orthopaedic Surgeons. The meeting was canceled because of COVID-19.
“Robotics appears to level the playing field for those who are less experienced, so that robotic total knee arthroplasty might be particularly well suited to low-volume surgeons,” reported Sridhar R. Rachala, MD, assistant professor of orthopaedic surgery, University of Buffalo (N.Y.).
In this retrospective cohort study, radiographic and clinical outcomes were evaluated in 164 total knee arthroplasties performed manually over an 8-month period and compared with 300 procedures performed robotically by the same experienced surgeon over the subsequent 15-month period.
There were no significant differences between patient groups for mean age or body mass index. Dr. Rachala, who performed both sets of procedures, reported inherent differences in technique. Specifically, the mechanical alignment was planned for a traditional neutral mechanical axis, while the robotic procedures were planned in kinematic alignment.
When evaluated at 1 year, the mean KOOS JR (Knee Injury and Osteoarthritis Outcome for Joint Replacement) scores were not significantly different for the robotic and manually performed procedures (76.0 vs. 73.9; P = .54). There were also no differences in the final extension (P = .64) or flexion (P = .59).
However, the difference in mean length of stay (2.0 vs. 2.4 days; P = .0002) favored the robotic approach, and the higher proportion of patients discharged to home after robotic surgery (73% vs. 66%; P = .11) suggested a favorable trend. Planned and postoperative alignment was within two degrees for both groups and not significantly different.
“The robotic series were at a disadvantage because it included cases that I performed when first switching to this approach,” reported Dr. Rachala in an interview.
Although a growing number of total hip arthroplasties are performed robotically, there have not so far been many comparisons of clinical outcomes among surgeons experienced with both approaches, according to Dr. Rachala. Acknowledging that a single-surgeon experience could be considered a limitation of this series, Dr. Rachala also considers it a potential strength. Dr. Rachala was highly experienced with manually instrumented total knee arthroplasty when he switched.
“Positioning and alignment are not just more accurate but easier to perform with robotic assistance,” he said, explaining why this approach is likely to offer a particular advantage to surgeons who perform these types of arthroplasties at low volume. He noted that robotic programming helps prevent errors and adopt alternative more personalized alignments.
Although Dr. Rachala acknowledged that long-term and controlled studies are needed, his experience suggests that robotic-assisted procedures are emerging as a viable alternative with advantages for the surgeon as well as the patient.
The principle that robotic assistance can add consistency to total joint arthroplasty is valid, according to Gwo-Chin Lee, MD, an associate professor of orthopaedic surgery, University of Pennsylvania, Philadelphia. “Robotic-assisted arthroplasty improves the accuracy and consistency of the procedure, which can potentially reduce the likelihood of failure. In knees, it is proven to be valuable in unicompartmental replacements in which results are correlated to a surgeon’s surgical volume. It has an equalizing effect relative to a surgeon with more extensive experience,” Dr. Lee said.
The senior author of a recent systematic review and meta-analysis of robotic-assisted unicompartmental knee arthroplasty (J Knee Surg. 2020 Jan 30; doi: 10.1055/s-0040-1701455), Dr. Lee said, “While the impact of robotics on other metrics including patient satisfaction and early recovery continues to be debated among surgeons who specialize in total knee arthroplasties, the technology can aid surgeons in component position, sizing, and ligament balance, particularly for the lower-volume surgeons and ultimately lead to more predictable outcomes.”
Dr. Rachala reports a financial relationship with Avanos and Stryker.
SOURCE: Rachala S et al. AAOS 2020. Abstract P0091.
FROM aaos 2020
Implementation of a Patient Blood Management Program in a Large, Diverse Multi-Hospital System
From BJC HealthCare, St. Louis, MO.
Abstract
Background: There is limited literature relating to patient blood management (PBM) programs in large multi-hospital systems or addressing challenges of implementation across diverse systems comprised of community and academic hospitals.
Objective: To establish a PBM program to improve utilization of blood transfusion units at a multi-hospital system in the Midwest (BJC HealthCare).
Methods: High-impact strategies in establishing the PBM program included formation of Clinical Expert Councils (CECs) of providers, establishment of consensus utilization guidelines, and development of a robust reporting tool. CECs enabled collaboration and facilitated standardization across a complex system of academic, private practice, and tertiary facilities with a diverse community of medical providers. Consensus guidelines and the PBM reporting tool were key to creating meaningful reports to drive provider practice change.
Results: Over the 5 years following implementation of the PBM program, there has been a steady decrease in red blood cell (RBC) utilization. Noticeable changes have taken place at individual hospitals in the system, including reductions in transfusions falling outside guideline parameters from 300 per quarter to less than 8 per quarter at 1 of our community hospitals. No negative impact on patient care has been identified.
Conclusion: In response to current transfusion guidelines and the need for optimizing stewardship of blood product resources, this hospital system successfully implemented a robust PBM program that engaged academic and non-academic community providers and decreased utilization of blood transfusion resources in line with consensus guidelines.
Keywords: quality improvement; RBC transfusion; transfusion practices; provider practice change; utilization trends.
Evidence from clinical trials and published clinical guidelines support the adoption of a restrictive blood transfusion approach in hospitalized, stable patients as best practice.1-5 As such, the development and implementation of patient blood management (PBM) programs has become an increasingly important process improvement for reducing variability in transfusion practices and clinical outcomes.
As recently as 2013, BJC HealthCare, a multi-hospital system in the Midwest, had no standardized, system-wide blood management program, and transfusion practices varied widely across providers and between individual hospitals based on size, patient population, and resources. The system consisted of 13 hospitals, ranging from large tertiary to smaller community and academic hospitals. Although adults constituted the vast majority of the patient population, the hospital system also included a pediatric specialty hospital, St. Louis Children’s Hospital. In addition, some sites were staffed by private practice providers and others by university-based providers, including blood bank medical directors. Due to the diversity of settings and populations, efforts to align transfusion and other practices often faced multiple challenges. However, improving the management of blood transfusions was identified as a key resource stewardship priority in 2013, and implementation of a system-wide program began after extensive discussions and consensus approval by senior hospital system and medical leadership. The primary aim of the program was to optimize overall blood product resource stewardship. Specifically, we sought to control or reduce costs per patient-care episode using strategies that would not negatively impact patient care and could potentially even improve patient outcomes (eg, by avoiding unnecessary transfusions and their attendant risks).
There is a plethora of literature related to the implemention of PBM programs in individual hospitals,6-18 but few reports specifically relate to large multi-hospital health systems,19-21 or directly address the unique challenges of implementation across a diverse system of community and academic hospitals and providers.19 Here, we discuss our experience with establishing a PBM program in a large, diverse, multi-hospital health system, provide examples of innovative strategies, and address challenges faced and lessons learned. Future endeavors of the PBM program at BJC HealthCare are also described.
Setting
BJC HealthCare is one of the largest nonprofit health care organizations in the United States, delivering services to the greater St. Louis, southern Illinois, and mid-Missouri regions, and addressing the health care needs of urban, suburban, and rural communities. As of 2018, the system included 15 hospitals and multiple community health locations comprising more than 3400 staffed beds, 31,500 employees, and 4300 physicians with privileges. The system annually has more than 151,000 hospital admissions, 81,000 outpatient surgery visits, and 537,000 emergency department visits. In addition to inpatient and outpatient care, services include primary care, community health and wellness, workplace health, home health, community mental health, rehabilitation, long-term care, and hospice. As a nonprofit system, BJC is the largest provider of charity care, unreimbursed care, and community benefit in Missouri, highlighting the fact that resource stewardship is a critical issue across the entire system and the communities served.22
PBM Project
Preparation for large-scale change across several hospitals began with creating a framework for the initiative, which consisted of a “burning platform,” a guiding vision, and a coalition. The burning platform identifies the importance and urgency of a change and helps to establish commitment. Between 2012 and 2014, the American Association of Blood Banks (AABB) released new evidence-based guidelines and recommendations calling for more restrictive transfusion practices pertaining to red blood cells (RBCs; ie, a hemoglobin threshold of 7 to 8 g/dL) in both inpatient and outpatient care.2 In addition, use of single-unit transfusions was recognized as best practice by the AABB in the Choosing Wisely campaign.23 Historically, adult patients requiring transfusions were given 2 units in succession. The new recommendations provided a strong basis for changing transfusion practices at BJC. It was believed that aligning transfusion practices with the new guidelines was consistent with the mission and vision of the work: that these changes could lead to optimization of resources, cost control, reductions in unnecessary blood transfusions, and potentially improved care (eg, fewer transfusion-related complications). We used the national guidelines to initiate discussions and to identify clinical conditions and associated laboratory parameters for transfusion therapy.
Once this burning platform was established, a team comprised of physicians, blood bank experts, quality consultants, data analysts, and supply managers, referred to as the Outcomes Team, was formed to lead the change efforts across the system. Initial projects for the team included developing system-wide consensus-based transfusion guidelines, providing education to providers on the new evidence in transfusion practice, and sharing BJC-specific historical utilization data. The guiding principle for the group was that “blood is a valuable resource, but not without risk, and less is more.” In order to disseminate the vision of the initiative across the system, campaign signs with the slogans “7 is the new 10” (referring to the g/dL transfusion threshold) and “1 is the new 2” (referring to the new practice of the preferential transfusion of single units rather than 2 at a time) were displayed in system hospitals.
Last, a guiding coalition of system leaders was needed to help push the initiative forward and sustain the program once fully implemented. Thus, a multidisciplinary PBM Clinical Expert Counciel (CEC) was formed to assist with implementation and maintenance of the program.
Role of PBM Clinical Expert Council
The PBM CEC was designed to improve overall physician and expert engagement and provide a forum where stakeholders from across the system could participate to voice their expert opinion. CECs (which BJC formed in other clinical areas as well) are multidisciplinary teams consisting of clinical, administrative, and technical staff. The open, multidisciplinary structure of the councils allows for collaboration that promotes change across a complex multi-hospital system. Each hospital is represented by key physicians and technical leaders, opening opportunity for both horizontal and vertical partnership.
As part of the overall physician engagement strategy, the PBM CEC was launched across BJC in November 2013 as a decision-making body for gaining system consensus on matters relating to blood management. The initial goals for the PBM CEC were to share information and educate providers and others on the latest evidence, to subsequently debate and develop consensus for guidelines to be applied across BJC, and to identify and adopt gold standard practices to drive and sustain compliance across the system. More specifically, we wanted to focus on how to avoid unnecessary blood transfusions known to be associated with increased risk for adverse reactions, other morbidity, mortality, and longer length of stay. Council members met quarterly to address 6 key drivers: patient safety, informatics and data, quality improvement, efficiencies and workflows, education and competency, and communication and engagement. Members then voted to approve guidelines, policies, and procedures. The group continues to assist in updating and standardizing guidelines and providing input on improving the functionality of the PBM reporting tool.
Development of the PBM Reporting Tool
Providing and sharing data on blood utilization and practices with the CEC and hospital leaders was imperative to driving change. The Outcomes Team deliberated on how best to generate and provide such information, conducting comparisons between selected vendor-based tools and potential internal BJC solutions. After investigation, BJC leadership approved the development of an in-house PBM dashboard tool using Tableau Desktop (Tableau Software, Inc.). The tool consists of an executive page with 5 additional tabs for navigating to the appropriate information (Figure 1 and Figure 2); data within the tool are organized by facility, service, provider, ICD diagnosis, transfusion indication, and the Clinical Classifications Software category, as defined by the Agency for Healthcare Research and Quality.
")
The PBM reporting tool was launched on December 31, 2014. The next priority after the launch was to validate the tool’s blood utilization data and implement enhancements to make the tool more effective for users. A super-user group consisting of blood bank supervisors and managers was established. The goals of the user group were to preview any enhancements before presenting the tool to the larger CEC, test and validate data once new information was added, and share and prioritize future enhancements. User group meetings were held monthly to share best practices and discuss individual facilities’ blood utilization data. In addition, each facility’s representative(s) shared how they were driving changes in provider practice and discussed challenges specific to their facility. Enhancements suggested through the user group included: incorporation of additional lab values into the tool to correspond with other blood products (eg, fibrinogen, hematocrit, international normalized ratio, and platelet count), addition of the specific location where the blood product was administered, and standard naming conventions of locations to allow comparisons across facilities (eg, Emergency Department instead of ED, ER, or EU).

All hospital users were given access to a test version of the reporting tool where they could review enhancements, identify what worked well and what could be done better, and suggest corrections. As changes were made to the hospital lab systems, a sample of data was reviewed and validated with affected facilities to confirm the continued accuracy of the data. To ensure its practicality to users, the tool continues to be improved upon with input from council stakeholders and subject-matter experts.
Measurements
To monitor blood utilization across the health system, we tracked the total RBC units administered by hospital, service, and provider and also tracked pre- and post-transfusion hemoglobin values.
Results
Overall, the system has seen a steady decrease in RBC utilization over the 5 years since the PBM program was implemented (Table

In addition to system-wide improvement, noticeable changes have taken place at individual hospitals in the BJC system. For example, Boone Hospital Center in Columbia, Missouri, began critically reviewing all RBC transfusions starting in 2015 and, to raise awareness, communicating with any provider who transfused a patient outside of transfusion guidelines. Since then, Boone Hospital has seen a dramatic reduction in transfusions considered noncompliant (ie, falling outside guideline parameters), from 300 transfusions per quarter, down to less than 8 per quarter. St. Louis Children’s Hospital also began reviewing blood products utilized by providers that fell outside of the standardized guidelines. At this hospital, physician champions discuss any outliers with the providers involved and use multiple methods for disseminating information to providers, including grand rounds, faculty meetings, and new resident orientations.
Another success has been the partnership between Barnes Jewish St. Peters and Progress West Hospitals in providing PBM education. Their joint effort resulted in implementation of education modules in BJC’s internal learning system, and has provided PBM-related education to more than 367 nurses, blood bank staff, and physicians.
Challenges and Lessons Learned
Implementation of the PBM program was generally successful, but it was not without challenges. One of the biggest challenges was addressing the variation in care and practices across the hospital enterprise. Due to the varying sizes and service goals of individual hospitals, lack of standardization was a significant barrier to change. Gaining trust and buy-in was imperative to increasing compliance with new transfusion policies. The primary concern was finding a balance between respecting physician autonomy and emphasizing and aligning practices with new evidence in the literature. Thus, understanding and applying principles of thoughtful change management was imperative to advancing the framework of the PBM program. The CEC venue enabled collaboration among hospitals and staff and was ultimately used to facilitate the necessary standardization process. To gain the trust of hospital and medical staff, the Outcomes Team conducted several site visits, enabling face-to-face interaction with frontline staff and operational leaders. Moreover, the team’s emphasis on the use of the latest evidence-based guidelines in discussions with hospital and medical staff underscored the need for change.
Frank et al19 describes using an approach similar to our Outcomes Team at the Johns Hopkins Health System. A designated multidisciplinary quality improvement team, referred to as the “clinical community,” worked on implementing best practices for blood management across a system of 5 hospitals. The authors reported similar results, with an overall decrease in number of units transfused, as well as substantial cost savings.19 Our project, along with the project implemented by Frank et al, shows how a “consensus-community” approach, involving stakeholders and various experts across the system, can be be used to align practices among multiple hospitals.
Development of a robust PBM reporting tool was key to creating meaningful monthly reports and driving provider practice change. However, this did require several training sessions, site visits, and computer-based training. Members of the Outcomes Team engaged in one-on-one sessions with tool users as a way of addressing specific areas of concern raised by staff at individual blood banks, and also took part in system-wide initiatives. The team also attended blood bank staff meetings and hospital transfusion committee meetings to educate staff on the evidence and initiative, provide demos of the reporting tool, and allow for a more robust discussion of how the data could be used and shared with other departments. These sessions provided opportunities to identify and prioritize future enhancements, as well as opportunities for continued education and discussion at hospitals, which were critical to ongoing improvement of the reporting tool.
Conclusion and Future Directions
Blood products remain extremely valuable and scarce resources, and all health care professionals must work to prevent unnecessary transfusions and improve clinical outcomes by adhering to the latest evidence-based guidelines. In response to current transfusion guidelines and the need to optimize blood product resources, our system successfully implemented a robust PBM program that engaged both academic and non-academic providers and communities. Several elements of the program helped us overcome the challenges relating to standardization of transfusion practices: consensus-based development of guidelines using the latest scientific evidence; formation and utilization of the CEC venue to gain system-wide consensus around both guidelines and approaches to change; development of a trustworthy and accessible PBM reporting tool (as well as continuing education sessions to improve adoption and utilization of the tool); and ongoing multidisciplinary discussions and support of thoughtful change and sustaining activities. We have seen a system-wide decrease in the number of RBC units transfused (absolute and per case mix-adjusted patient day) since implementing the PBM program, and in the following years have noted a trending decrease in transfusion-related safety events. Although there was a slight increase in reported safety events from 2018 to 2019, this was likely due to the systematic implementation of a new electronic medical record system and improved reporting infrastructure.
Upcoming phases of our system-wide PBM program will include looking at opportunities to improve blood utilization in other specific clinical areas. For example, we have begun discussions with hematology and oncology experts across the system to expand their patient population data within the PBM reporting tool, and to identify areas of opportunity for provider practice change within their specialty. We are also reviewing cardiothoracic surgery transfusion data to identify opportunities for reducing blood utilization in specific clinical scenarios. In addition, we are working to incorporate our 2 newest hospital system members (Memorial Hospital East and Memorial Hospital Belleville) into the PBM program. In collaboration with perioperative leaders across the system, the surgical blood ordering process is being reviewed. The goal of this effort is to reduce blood products ordered in preparation for surgical procedures. We are also currently investigating whether an impact on safety events (ie, reduction in transfusion reactions) can yet be detected. Last, our health care system recently launched a system-wide electronic medical record, and we are eager to see how this will provide us with new methods to monitor and analyze blood administration and utilization data. We look forward to reporting on the expansion of our program and on any clinical outcome improvements gained through avoidance of unnecessary transfusions.
Acknowledgment: The authors thank the leadership within the Center for Clinical Excellence and Supply Chain at BJC HealthCare for their support of this manuscript, as well as all system participants who have contributed to these efforts, especially Mohammad Agha, MD, MHA, current physician leader of the PBM CEC, for his thoughtful edits of this manuscript.
Corresponding author: Audrey A. Gronemeyer, MPH, Center for Clinical Excellence, BJC HealthCare, 8300 Eager Road, Suite 400A, St. Louis, MO 63144; audrey.gronemeyer@bjc.org.
Financial disclosures: None.
1. Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: A clinical practice guideline from the AABB*. Ann Intern Med. 2012;157:49-58.
2. Goodnough LT, Levy JH, Murphy MF. Concepts of blood transfusion in adults. Lancet. 2013;381:1845-1854.
3. Hébert PC, Carson JL. Transfusion threshold of 7 g per deciliter—The new normal. N Engl J Med. 2014;371:1459-1461.
4. Gani F, Cerullo M, Ejaz A, et al. Implementation of a blood management program at a tertiary care hospital: Effect on transfusion practices and clinical outcomes among patients undergoing surgery. Ann Surg. 2019;269:1073-1079.
5. Podlasek SJ, Thakkar RN, Rotello LC, et al. Implementing a “why give 2 when 1 will do?” Choosing Wisely campaign. Transfusion. 2016;56:2164.
6. Boral LI, Bernard A, Hjorth T, et al. How do I implement a more restrictive transfusion trigger of hemoglobin level of 7 g/dL at my hospital? Transfusion. 2015;55:937-945.
7. Geissler RG, Kosters C, Franz D, et al. Utilization of blood components in trauma surgery: A single-center, retrospective analysis before and after the implementation of an educative PBM initiative. Transfuse Med Hemother. 2015;42:83-89.
8. Goel R, Cushing MM, Tobian AA. Pediatric patient blood management programs: Not just transfusing little adults. Transfus Med Rev. 2016;30:235-241.
9. Gupta PB, DeMario VM, Amin RM, et al. Patient blood management program improves blood use and clinical outcomes in orthopedic surgery. Anesthesiology. 2018;129;1082-1091.
10. Leahy MF, Roberts H, Mukhtar SA, et al. A pragmatic approach to embedding patient blood management in a tertiary hospital. Transfusion. 2014;54:1133-1145.
11. Leahy MF, Hofmann A, Towler S, et al. Improved outcomes and reduced costs associated with a health-system-wide patient blood management program: A retrospective observational study in four major adult tertiary-care hospitals. Transfusion. 2017;57:1347-1358.
12. Meybohm P, Herrmann E, Steinbicker AU, et al. Patient blood management is associated with a substantial reduction of red blood cell utilization and safe for patient’s outcome: A prospective, multicenter cohort study with a noninferiority design. Ann Surg. 2016;264:203-211.
13. Morgan PN, Coleman PL, Martinez-Garduno CM, et al. Implementation of a patient blood management program in an Australian private hospital orthopedic unit. J Blood Med. 2018;9;83-90.
14. Norgaard A, Stensballe J, de Lichtenberg TH, et al. Three-year follow-up of implementation of evidence-based transfusion practice in a tertiary hospital. Vox Sang. 2017;112:229-239.
15. Meuller MM, Van Remoortel H, Meybohm P, et al. Patient blood management: Recommendations from the 2018 Frankfurt Consensus Conference. JAMA. 2019;321:983-997.
16. Oliver JC, Griffin RL, Hannon T, Marques MB. The success of our patient blood management program depended on an institution-wide change in transfusion practices. Transfusion. 2014;54:2617-2624.
17. Thakkar RN, Lee KH, Ness PM, et al. Relative impact of a patient blood management program on utilization of all three major blood components. Transfusion. 2016;56:2212-2220.
18. Yang WW, Thakkar RN, Gehrie EA, et al. Single-unit transfusions and hemoglobin trigger: relative impact on red cell utilization. Transfusion. 2017;57:1163-1170.
19. Frank SM, Thakkar RN, Podlasek SJ, et al. Implementing a health system-wide patient blood management program with a clinical community approach. Anesthesiology. 2017;127;754-764.
20. Verdecchia NM, Wisniewski MK, Waters JH, et al. Changes in blood product utilization in a seven-hospital system after the implementation of a patient blood management program: A 9-year follow-up. Hematology. 2016;21:490-499.
21. Yazer MH, Waters JH. How do I implement a hospital-based blood management program? Transfusion. 2012;52:1640-1645.
22. BJC HealthCare. Facts and Figures.. BJC HealthCare website. www.bjc.org/About-Us/Facts-Figures. Accessed November 18, 2019.
23. Callum JL, Waters JH, Shaz BH, et al. The AABB recommendations for the Choosing Wisely campaign of the American Board of Internal Medicine. Transfusion. 2014;54:2344-2352.
From BJC HealthCare, St. Louis, MO.
Abstract
Background: There is limited literature relating to patient blood management (PBM) programs in large multi-hospital systems or addressing challenges of implementation across diverse systems comprised of community and academic hospitals.
Objective: To establish a PBM program to improve utilization of blood transfusion units at a multi-hospital system in the Midwest (BJC HealthCare).
Methods: High-impact strategies in establishing the PBM program included formation of Clinical Expert Councils (CECs) of providers, establishment of consensus utilization guidelines, and development of a robust reporting tool. CECs enabled collaboration and facilitated standardization across a complex system of academic, private practice, and tertiary facilities with a diverse community of medical providers. Consensus guidelines and the PBM reporting tool were key to creating meaningful reports to drive provider practice change.
Results: Over the 5 years following implementation of the PBM program, there has been a steady decrease in red blood cell (RBC) utilization. Noticeable changes have taken place at individual hospitals in the system, including reductions in transfusions falling outside guideline parameters from 300 per quarter to less than 8 per quarter at 1 of our community hospitals. No negative impact on patient care has been identified.
Conclusion: In response to current transfusion guidelines and the need for optimizing stewardship of blood product resources, this hospital system successfully implemented a robust PBM program that engaged academic and non-academic community providers and decreased utilization of blood transfusion resources in line with consensus guidelines.
Keywords: quality improvement; RBC transfusion; transfusion practices; provider practice change; utilization trends.
Evidence from clinical trials and published clinical guidelines support the adoption of a restrictive blood transfusion approach in hospitalized, stable patients as best practice.1-5 As such, the development and implementation of patient blood management (PBM) programs has become an increasingly important process improvement for reducing variability in transfusion practices and clinical outcomes.
As recently as 2013, BJC HealthCare, a multi-hospital system in the Midwest, had no standardized, system-wide blood management program, and transfusion practices varied widely across providers and between individual hospitals based on size, patient population, and resources. The system consisted of 13 hospitals, ranging from large tertiary to smaller community and academic hospitals. Although adults constituted the vast majority of the patient population, the hospital system also included a pediatric specialty hospital, St. Louis Children’s Hospital. In addition, some sites were staffed by private practice providers and others by university-based providers, including blood bank medical directors. Due to the diversity of settings and populations, efforts to align transfusion and other practices often faced multiple challenges. However, improving the management of blood transfusions was identified as a key resource stewardship priority in 2013, and implementation of a system-wide program began after extensive discussions and consensus approval by senior hospital system and medical leadership. The primary aim of the program was to optimize overall blood product resource stewardship. Specifically, we sought to control or reduce costs per patient-care episode using strategies that would not negatively impact patient care and could potentially even improve patient outcomes (eg, by avoiding unnecessary transfusions and their attendant risks).
There is a plethora of literature related to the implemention of PBM programs in individual hospitals,6-18 but few reports specifically relate to large multi-hospital health systems,19-21 or directly address the unique challenges of implementation across a diverse system of community and academic hospitals and providers.19 Here, we discuss our experience with establishing a PBM program in a large, diverse, multi-hospital health system, provide examples of innovative strategies, and address challenges faced and lessons learned. Future endeavors of the PBM program at BJC HealthCare are also described.
Setting
BJC HealthCare is one of the largest nonprofit health care organizations in the United States, delivering services to the greater St. Louis, southern Illinois, and mid-Missouri regions, and addressing the health care needs of urban, suburban, and rural communities. As of 2018, the system included 15 hospitals and multiple community health locations comprising more than 3400 staffed beds, 31,500 employees, and 4300 physicians with privileges. The system annually has more than 151,000 hospital admissions, 81,000 outpatient surgery visits, and 537,000 emergency department visits. In addition to inpatient and outpatient care, services include primary care, community health and wellness, workplace health, home health, community mental health, rehabilitation, long-term care, and hospice. As a nonprofit system, BJC is the largest provider of charity care, unreimbursed care, and community benefit in Missouri, highlighting the fact that resource stewardship is a critical issue across the entire system and the communities served.22
PBM Project
Preparation for large-scale change across several hospitals began with creating a framework for the initiative, which consisted of a “burning platform,” a guiding vision, and a coalition. The burning platform identifies the importance and urgency of a change and helps to establish commitment. Between 2012 and 2014, the American Association of Blood Banks (AABB) released new evidence-based guidelines and recommendations calling for more restrictive transfusion practices pertaining to red blood cells (RBCs; ie, a hemoglobin threshold of 7 to 8 g/dL) in both inpatient and outpatient care.2 In addition, use of single-unit transfusions was recognized as best practice by the AABB in the Choosing Wisely campaign.23 Historically, adult patients requiring transfusions were given 2 units in succession. The new recommendations provided a strong basis for changing transfusion practices at BJC. It was believed that aligning transfusion practices with the new guidelines was consistent with the mission and vision of the work: that these changes could lead to optimization of resources, cost control, reductions in unnecessary blood transfusions, and potentially improved care (eg, fewer transfusion-related complications). We used the national guidelines to initiate discussions and to identify clinical conditions and associated laboratory parameters for transfusion therapy.
Once this burning platform was established, a team comprised of physicians, blood bank experts, quality consultants, data analysts, and supply managers, referred to as the Outcomes Team, was formed to lead the change efforts across the system. Initial projects for the team included developing system-wide consensus-based transfusion guidelines, providing education to providers on the new evidence in transfusion practice, and sharing BJC-specific historical utilization data. The guiding principle for the group was that “blood is a valuable resource, but not without risk, and less is more.” In order to disseminate the vision of the initiative across the system, campaign signs with the slogans “7 is the new 10” (referring to the g/dL transfusion threshold) and “1 is the new 2” (referring to the new practice of the preferential transfusion of single units rather than 2 at a time) were displayed in system hospitals.
Last, a guiding coalition of system leaders was needed to help push the initiative forward and sustain the program once fully implemented. Thus, a multidisciplinary PBM Clinical Expert Counciel (CEC) was formed to assist with implementation and maintenance of the program.
Role of PBM Clinical Expert Council
The PBM CEC was designed to improve overall physician and expert engagement and provide a forum where stakeholders from across the system could participate to voice their expert opinion. CECs (which BJC formed in other clinical areas as well) are multidisciplinary teams consisting of clinical, administrative, and technical staff. The open, multidisciplinary structure of the councils allows for collaboration that promotes change across a complex multi-hospital system. Each hospital is represented by key physicians and technical leaders, opening opportunity for both horizontal and vertical partnership.
As part of the overall physician engagement strategy, the PBM CEC was launched across BJC in November 2013 as a decision-making body for gaining system consensus on matters relating to blood management. The initial goals for the PBM CEC were to share information and educate providers and others on the latest evidence, to subsequently debate and develop consensus for guidelines to be applied across BJC, and to identify and adopt gold standard practices to drive and sustain compliance across the system. More specifically, we wanted to focus on how to avoid unnecessary blood transfusions known to be associated with increased risk for adverse reactions, other morbidity, mortality, and longer length of stay. Council members met quarterly to address 6 key drivers: patient safety, informatics and data, quality improvement, efficiencies and workflows, education and competency, and communication and engagement. Members then voted to approve guidelines, policies, and procedures. The group continues to assist in updating and standardizing guidelines and providing input on improving the functionality of the PBM reporting tool.
Development of the PBM Reporting Tool
Providing and sharing data on blood utilization and practices with the CEC and hospital leaders was imperative to driving change. The Outcomes Team deliberated on how best to generate and provide such information, conducting comparisons between selected vendor-based tools and potential internal BJC solutions. After investigation, BJC leadership approved the development of an in-house PBM dashboard tool using Tableau Desktop (Tableau Software, Inc.). The tool consists of an executive page with 5 additional tabs for navigating to the appropriate information (Figure 1 and Figure 2); data within the tool are organized by facility, service, provider, ICD diagnosis, transfusion indication, and the Clinical Classifications Software category, as defined by the Agency for Healthcare Research and Quality.
The PBM reporting tool was launched on December 31, 2014. The next priority after the launch was to validate the tool’s blood utilization data and implement enhancements to make the tool more effective for users. A super-user group consisting of blood bank supervisors and managers was established. The goals of the user group were to preview any enhancements before presenting the tool to the larger CEC, test and validate data once new information was added, and share and prioritize future enhancements. User group meetings were held monthly to share best practices and discuss individual facilities’ blood utilization data. In addition, each facility’s representative(s) shared how they were driving changes in provider practice and discussed challenges specific to their facility. Enhancements suggested through the user group included: incorporation of additional lab values into the tool to correspond with other blood products (eg, fibrinogen, hematocrit, international normalized ratio, and platelet count), addition of the specific location where the blood product was administered, and standard naming conventions of locations to allow comparisons across facilities (eg, Emergency Department instead of ED, ER, or EU).
All hospital users were given access to a test version of the reporting tool where they could review enhancements, identify what worked well and what could be done better, and suggest corrections. As changes were made to the hospital lab systems, a sample of data was reviewed and validated with affected facilities to confirm the continued accuracy of the data. To ensure its practicality to users, the tool continues to be improved upon with input from council stakeholders and subject-matter experts.
Measurements
To monitor blood utilization across the health system, we tracked the total RBC units administered by hospital, service, and provider and also tracked pre- and post-transfusion hemoglobin values.
Results
Overall, the system has seen a steady decrease in RBC utilization over the 5 years since the PBM program was implemented (Table
In addition to system-wide improvement, noticeable changes have taken place at individual hospitals in the BJC system. For example, Boone Hospital Center in Columbia, Missouri, began critically reviewing all RBC transfusions starting in 2015 and, to raise awareness, communicating with any provider who transfused a patient outside of transfusion guidelines. Since then, Boone Hospital has seen a dramatic reduction in transfusions considered noncompliant (ie, falling outside guideline parameters), from 300 transfusions per quarter, down to less than 8 per quarter. St. Louis Children’s Hospital also began reviewing blood products utilized by providers that fell outside of the standardized guidelines. At this hospital, physician champions discuss any outliers with the providers involved and use multiple methods for disseminating information to providers, including grand rounds, faculty meetings, and new resident orientations.
Another success has been the partnership between Barnes Jewish St. Peters and Progress West Hospitals in providing PBM education. Their joint effort resulted in implementation of education modules in BJC’s internal learning system, and has provided PBM-related education to more than 367 nurses, blood bank staff, and physicians.
Challenges and Lessons Learned
Implementation of the PBM program was generally successful, but it was not without challenges. One of the biggest challenges was addressing the variation in care and practices across the hospital enterprise. Due to the varying sizes and service goals of individual hospitals, lack of standardization was a significant barrier to change. Gaining trust and buy-in was imperative to increasing compliance with new transfusion policies. The primary concern was finding a balance between respecting physician autonomy and emphasizing and aligning practices with new evidence in the literature. Thus, understanding and applying principles of thoughtful change management was imperative to advancing the framework of the PBM program. The CEC venue enabled collaboration among hospitals and staff and was ultimately used to facilitate the necessary standardization process. To gain the trust of hospital and medical staff, the Outcomes Team conducted several site visits, enabling face-to-face interaction with frontline staff and operational leaders. Moreover, the team’s emphasis on the use of the latest evidence-based guidelines in discussions with hospital and medical staff underscored the need for change.
Frank et al19 describes using an approach similar to our Outcomes Team at the Johns Hopkins Health System. A designated multidisciplinary quality improvement team, referred to as the “clinical community,” worked on implementing best practices for blood management across a system of 5 hospitals. The authors reported similar results, with an overall decrease in number of units transfused, as well as substantial cost savings.19 Our project, along with the project implemented by Frank et al, shows how a “consensus-community” approach, involving stakeholders and various experts across the system, can be be used to align practices among multiple hospitals.
Development of a robust PBM reporting tool was key to creating meaningful monthly reports and driving provider practice change. However, this did require several training sessions, site visits, and computer-based training. Members of the Outcomes Team engaged in one-on-one sessions with tool users as a way of addressing specific areas of concern raised by staff at individual blood banks, and also took part in system-wide initiatives. The team also attended blood bank staff meetings and hospital transfusion committee meetings to educate staff on the evidence and initiative, provide demos of the reporting tool, and allow for a more robust discussion of how the data could be used and shared with other departments. These sessions provided opportunities to identify and prioritize future enhancements, as well as opportunities for continued education and discussion at hospitals, which were critical to ongoing improvement of the reporting tool.
Conclusion and Future Directions
Blood products remain extremely valuable and scarce resources, and all health care professionals must work to prevent unnecessary transfusions and improve clinical outcomes by adhering to the latest evidence-based guidelines. In response to current transfusion guidelines and the need to optimize blood product resources, our system successfully implemented a robust PBM program that engaged both academic and non-academic providers and communities. Several elements of the program helped us overcome the challenges relating to standardization of transfusion practices: consensus-based development of guidelines using the latest scientific evidence; formation and utilization of the CEC venue to gain system-wide consensus around both guidelines and approaches to change; development of a trustworthy and accessible PBM reporting tool (as well as continuing education sessions to improve adoption and utilization of the tool); and ongoing multidisciplinary discussions and support of thoughtful change and sustaining activities. We have seen a system-wide decrease in the number of RBC units transfused (absolute and per case mix-adjusted patient day) since implementing the PBM program, and in the following years have noted a trending decrease in transfusion-related safety events. Although there was a slight increase in reported safety events from 2018 to 2019, this was likely due to the systematic implementation of a new electronic medical record system and improved reporting infrastructure.
Upcoming phases of our system-wide PBM program will include looking at opportunities to improve blood utilization in other specific clinical areas. For example, we have begun discussions with hematology and oncology experts across the system to expand their patient population data within the PBM reporting tool, and to identify areas of opportunity for provider practice change within their specialty. We are also reviewing cardiothoracic surgery transfusion data to identify opportunities for reducing blood utilization in specific clinical scenarios. In addition, we are working to incorporate our 2 newest hospital system members (Memorial Hospital East and Memorial Hospital Belleville) into the PBM program. In collaboration with perioperative leaders across the system, the surgical blood ordering process is being reviewed. The goal of this effort is to reduce blood products ordered in preparation for surgical procedures. We are also currently investigating whether an impact on safety events (ie, reduction in transfusion reactions) can yet be detected. Last, our health care system recently launched a system-wide electronic medical record, and we are eager to see how this will provide us with new methods to monitor and analyze blood administration and utilization data. We look forward to reporting on the expansion of our program and on any clinical outcome improvements gained through avoidance of unnecessary transfusions.
Acknowledgment: The authors thank the leadership within the Center for Clinical Excellence and Supply Chain at BJC HealthCare for their support of this manuscript, as well as all system participants who have contributed to these efforts, especially Mohammad Agha, MD, MHA, current physician leader of the PBM CEC, for his thoughtful edits of this manuscript.
Corresponding author: Audrey A. Gronemeyer, MPH, Center for Clinical Excellence, BJC HealthCare, 8300 Eager Road, Suite 400A, St. Louis, MO 63144; audrey.gronemeyer@bjc.org.
Financial disclosures: None.
From BJC HealthCare, St. Louis, MO.
Abstract
Background: There is limited literature relating to patient blood management (PBM) programs in large multi-hospital systems or addressing challenges of implementation across diverse systems comprised of community and academic hospitals.
Objective: To establish a PBM program to improve utilization of blood transfusion units at a multi-hospital system in the Midwest (BJC HealthCare).
Methods: High-impact strategies in establishing the PBM program included formation of Clinical Expert Councils (CECs) of providers, establishment of consensus utilization guidelines, and development of a robust reporting tool. CECs enabled collaboration and facilitated standardization across a complex system of academic, private practice, and tertiary facilities with a diverse community of medical providers. Consensus guidelines and the PBM reporting tool were key to creating meaningful reports to drive provider practice change.
Results: Over the 5 years following implementation of the PBM program, there has been a steady decrease in red blood cell (RBC) utilization. Noticeable changes have taken place at individual hospitals in the system, including reductions in transfusions falling outside guideline parameters from 300 per quarter to less than 8 per quarter at 1 of our community hospitals. No negative impact on patient care has been identified.
Conclusion: In response to current transfusion guidelines and the need for optimizing stewardship of blood product resources, this hospital system successfully implemented a robust PBM program that engaged academic and non-academic community providers and decreased utilization of blood transfusion resources in line with consensus guidelines.
Keywords: quality improvement; RBC transfusion; transfusion practices; provider practice change; utilization trends.
Evidence from clinical trials and published clinical guidelines support the adoption of a restrictive blood transfusion approach in hospitalized, stable patients as best practice.1-5 As such, the development and implementation of patient blood management (PBM) programs has become an increasingly important process improvement for reducing variability in transfusion practices and clinical outcomes.
As recently as 2013, BJC HealthCare, a multi-hospital system in the Midwest, had no standardized, system-wide blood management program, and transfusion practices varied widely across providers and between individual hospitals based on size, patient population, and resources. The system consisted of 13 hospitals, ranging from large tertiary to smaller community and academic hospitals. Although adults constituted the vast majority of the patient population, the hospital system also included a pediatric specialty hospital, St. Louis Children’s Hospital. In addition, some sites were staffed by private practice providers and others by university-based providers, including blood bank medical directors. Due to the diversity of settings and populations, efforts to align transfusion and other practices often faced multiple challenges. However, improving the management of blood transfusions was identified as a key resource stewardship priority in 2013, and implementation of a system-wide program began after extensive discussions and consensus approval by senior hospital system and medical leadership. The primary aim of the program was to optimize overall blood product resource stewardship. Specifically, we sought to control or reduce costs per patient-care episode using strategies that would not negatively impact patient care and could potentially even improve patient outcomes (eg, by avoiding unnecessary transfusions and their attendant risks).
There is a plethora of literature related to the implemention of PBM programs in individual hospitals,6-18 but few reports specifically relate to large multi-hospital health systems,19-21 or directly address the unique challenges of implementation across a diverse system of community and academic hospitals and providers.19 Here, we discuss our experience with establishing a PBM program in a large, diverse, multi-hospital health system, provide examples of innovative strategies, and address challenges faced and lessons learned. Future endeavors of the PBM program at BJC HealthCare are also described.
Setting
BJC HealthCare is one of the largest nonprofit health care organizations in the United States, delivering services to the greater St. Louis, southern Illinois, and mid-Missouri regions, and addressing the health care needs of urban, suburban, and rural communities. As of 2018, the system included 15 hospitals and multiple community health locations comprising more than 3400 staffed beds, 31,500 employees, and 4300 physicians with privileges. The system annually has more than 151,000 hospital admissions, 81,000 outpatient surgery visits, and 537,000 emergency department visits. In addition to inpatient and outpatient care, services include primary care, community health and wellness, workplace health, home health, community mental health, rehabilitation, long-term care, and hospice. As a nonprofit system, BJC is the largest provider of charity care, unreimbursed care, and community benefit in Missouri, highlighting the fact that resource stewardship is a critical issue across the entire system and the communities served.22
PBM Project
Preparation for large-scale change across several hospitals began with creating a framework for the initiative, which consisted of a “burning platform,” a guiding vision, and a coalition. The burning platform identifies the importance and urgency of a change and helps to establish commitment. Between 2012 and 2014, the American Association of Blood Banks (AABB) released new evidence-based guidelines and recommendations calling for more restrictive transfusion practices pertaining to red blood cells (RBCs; ie, a hemoglobin threshold of 7 to 8 g/dL) in both inpatient and outpatient care.2 In addition, use of single-unit transfusions was recognized as best practice by the AABB in the Choosing Wisely campaign.23 Historically, adult patients requiring transfusions were given 2 units in succession. The new recommendations provided a strong basis for changing transfusion practices at BJC. It was believed that aligning transfusion practices with the new guidelines was consistent with the mission and vision of the work: that these changes could lead to optimization of resources, cost control, reductions in unnecessary blood transfusions, and potentially improved care (eg, fewer transfusion-related complications). We used the national guidelines to initiate discussions and to identify clinical conditions and associated laboratory parameters for transfusion therapy.
Once this burning platform was established, a team comprised of physicians, blood bank experts, quality consultants, data analysts, and supply managers, referred to as the Outcomes Team, was formed to lead the change efforts across the system. Initial projects for the team included developing system-wide consensus-based transfusion guidelines, providing education to providers on the new evidence in transfusion practice, and sharing BJC-specific historical utilization data. The guiding principle for the group was that “blood is a valuable resource, but not without risk, and less is more.” In order to disseminate the vision of the initiative across the system, campaign signs with the slogans “7 is the new 10” (referring to the g/dL transfusion threshold) and “1 is the new 2” (referring to the new practice of the preferential transfusion of single units rather than 2 at a time) were displayed in system hospitals.
Last, a guiding coalition of system leaders was needed to help push the initiative forward and sustain the program once fully implemented. Thus, a multidisciplinary PBM Clinical Expert Counciel (CEC) was formed to assist with implementation and maintenance of the program.
Role of PBM Clinical Expert Council
The PBM CEC was designed to improve overall physician and expert engagement and provide a forum where stakeholders from across the system could participate to voice their expert opinion. CECs (which BJC formed in other clinical areas as well) are multidisciplinary teams consisting of clinical, administrative, and technical staff. The open, multidisciplinary structure of the councils allows for collaboration that promotes change across a complex multi-hospital system. Each hospital is represented by key physicians and technical leaders, opening opportunity for both horizontal and vertical partnership.
As part of the overall physician engagement strategy, the PBM CEC was launched across BJC in November 2013 as a decision-making body for gaining system consensus on matters relating to blood management. The initial goals for the PBM CEC were to share information and educate providers and others on the latest evidence, to subsequently debate and develop consensus for guidelines to be applied across BJC, and to identify and adopt gold standard practices to drive and sustain compliance across the system. More specifically, we wanted to focus on how to avoid unnecessary blood transfusions known to be associated with increased risk for adverse reactions, other morbidity, mortality, and longer length of stay. Council members met quarterly to address 6 key drivers: patient safety, informatics and data, quality improvement, efficiencies and workflows, education and competency, and communication and engagement. Members then voted to approve guidelines, policies, and procedures. The group continues to assist in updating and standardizing guidelines and providing input on improving the functionality of the PBM reporting tool.
Development of the PBM Reporting Tool
Providing and sharing data on blood utilization and practices with the CEC and hospital leaders was imperative to driving change. The Outcomes Team deliberated on how best to generate and provide such information, conducting comparisons between selected vendor-based tools and potential internal BJC solutions. After investigation, BJC leadership approved the development of an in-house PBM dashboard tool using Tableau Desktop (Tableau Software, Inc.). The tool consists of an executive page with 5 additional tabs for navigating to the appropriate information (Figure 1 and Figure 2); data within the tool are organized by facility, service, provider, ICD diagnosis, transfusion indication, and the Clinical Classifications Software category, as defined by the Agency for Healthcare Research and Quality.
The PBM reporting tool was launched on December 31, 2014. The next priority after the launch was to validate the tool’s blood utilization data and implement enhancements to make the tool more effective for users. A super-user group consisting of blood bank supervisors and managers was established. The goals of the user group were to preview any enhancements before presenting the tool to the larger CEC, test and validate data once new information was added, and share and prioritize future enhancements. User group meetings were held monthly to share best practices and discuss individual facilities’ blood utilization data. In addition, each facility’s representative(s) shared how they were driving changes in provider practice and discussed challenges specific to their facility. Enhancements suggested through the user group included: incorporation of additional lab values into the tool to correspond with other blood products (eg, fibrinogen, hematocrit, international normalized ratio, and platelet count), addition of the specific location where the blood product was administered, and standard naming conventions of locations to allow comparisons across facilities (eg, Emergency Department instead of ED, ER, or EU).
All hospital users were given access to a test version of the reporting tool where they could review enhancements, identify what worked well and what could be done better, and suggest corrections. As changes were made to the hospital lab systems, a sample of data was reviewed and validated with affected facilities to confirm the continued accuracy of the data. To ensure its practicality to users, the tool continues to be improved upon with input from council stakeholders and subject-matter experts.
Measurements
To monitor blood utilization across the health system, we tracked the total RBC units administered by hospital, service, and provider and also tracked pre- and post-transfusion hemoglobin values.
Results
Overall, the system has seen a steady decrease in RBC utilization over the 5 years since the PBM program was implemented (Table
In addition to system-wide improvement, noticeable changes have taken place at individual hospitals in the BJC system. For example, Boone Hospital Center in Columbia, Missouri, began critically reviewing all RBC transfusions starting in 2015 and, to raise awareness, communicating with any provider who transfused a patient outside of transfusion guidelines. Since then, Boone Hospital has seen a dramatic reduction in transfusions considered noncompliant (ie, falling outside guideline parameters), from 300 transfusions per quarter, down to less than 8 per quarter. St. Louis Children’s Hospital also began reviewing blood products utilized by providers that fell outside of the standardized guidelines. At this hospital, physician champions discuss any outliers with the providers involved and use multiple methods for disseminating information to providers, including grand rounds, faculty meetings, and new resident orientations.
Another success has been the partnership between Barnes Jewish St. Peters and Progress West Hospitals in providing PBM education. Their joint effort resulted in implementation of education modules in BJC’s internal learning system, and has provided PBM-related education to more than 367 nurses, blood bank staff, and physicians.
Challenges and Lessons Learned
Implementation of the PBM program was generally successful, but it was not without challenges. One of the biggest challenges was addressing the variation in care and practices across the hospital enterprise. Due to the varying sizes and service goals of individual hospitals, lack of standardization was a significant barrier to change. Gaining trust and buy-in was imperative to increasing compliance with new transfusion policies. The primary concern was finding a balance between respecting physician autonomy and emphasizing and aligning practices with new evidence in the literature. Thus, understanding and applying principles of thoughtful change management was imperative to advancing the framework of the PBM program. The CEC venue enabled collaboration among hospitals and staff and was ultimately used to facilitate the necessary standardization process. To gain the trust of hospital and medical staff, the Outcomes Team conducted several site visits, enabling face-to-face interaction with frontline staff and operational leaders. Moreover, the team’s emphasis on the use of the latest evidence-based guidelines in discussions with hospital and medical staff underscored the need for change.
Frank et al19 describes using an approach similar to our Outcomes Team at the Johns Hopkins Health System. A designated multidisciplinary quality improvement team, referred to as the “clinical community,” worked on implementing best practices for blood management across a system of 5 hospitals. The authors reported similar results, with an overall decrease in number of units transfused, as well as substantial cost savings.19 Our project, along with the project implemented by Frank et al, shows how a “consensus-community” approach, involving stakeholders and various experts across the system, can be be used to align practices among multiple hospitals.
Development of a robust PBM reporting tool was key to creating meaningful monthly reports and driving provider practice change. However, this did require several training sessions, site visits, and computer-based training. Members of the Outcomes Team engaged in one-on-one sessions with tool users as a way of addressing specific areas of concern raised by staff at individual blood banks, and also took part in system-wide initiatives. The team also attended blood bank staff meetings and hospital transfusion committee meetings to educate staff on the evidence and initiative, provide demos of the reporting tool, and allow for a more robust discussion of how the data could be used and shared with other departments. These sessions provided opportunities to identify and prioritize future enhancements, as well as opportunities for continued education and discussion at hospitals, which were critical to ongoing improvement of the reporting tool.
Conclusion and Future Directions
Blood products remain extremely valuable and scarce resources, and all health care professionals must work to prevent unnecessary transfusions and improve clinical outcomes by adhering to the latest evidence-based guidelines. In response to current transfusion guidelines and the need to optimize blood product resources, our system successfully implemented a robust PBM program that engaged both academic and non-academic providers and communities. Several elements of the program helped us overcome the challenges relating to standardization of transfusion practices: consensus-based development of guidelines using the latest scientific evidence; formation and utilization of the CEC venue to gain system-wide consensus around both guidelines and approaches to change; development of a trustworthy and accessible PBM reporting tool (as well as continuing education sessions to improve adoption and utilization of the tool); and ongoing multidisciplinary discussions and support of thoughtful change and sustaining activities. We have seen a system-wide decrease in the number of RBC units transfused (absolute and per case mix-adjusted patient day) since implementing the PBM program, and in the following years have noted a trending decrease in transfusion-related safety events. Although there was a slight increase in reported safety events from 2018 to 2019, this was likely due to the systematic implementation of a new electronic medical record system and improved reporting infrastructure.
Upcoming phases of our system-wide PBM program will include looking at opportunities to improve blood utilization in other specific clinical areas. For example, we have begun discussions with hematology and oncology experts across the system to expand their patient population data within the PBM reporting tool, and to identify areas of opportunity for provider practice change within their specialty. We are also reviewing cardiothoracic surgery transfusion data to identify opportunities for reducing blood utilization in specific clinical scenarios. In addition, we are working to incorporate our 2 newest hospital system members (Memorial Hospital East and Memorial Hospital Belleville) into the PBM program. In collaboration with perioperative leaders across the system, the surgical blood ordering process is being reviewed. The goal of this effort is to reduce blood products ordered in preparation for surgical procedures. We are also currently investigating whether an impact on safety events (ie, reduction in transfusion reactions) can yet be detected. Last, our health care system recently launched a system-wide electronic medical record, and we are eager to see how this will provide us with new methods to monitor and analyze blood administration and utilization data. We look forward to reporting on the expansion of our program and on any clinical outcome improvements gained through avoidance of unnecessary transfusions.
Acknowledgment: The authors thank the leadership within the Center for Clinical Excellence and Supply Chain at BJC HealthCare for their support of this manuscript, as well as all system participants who have contributed to these efforts, especially Mohammad Agha, MD, MHA, current physician leader of the PBM CEC, for his thoughtful edits of this manuscript.
Corresponding author: Audrey A. Gronemeyer, MPH, Center for Clinical Excellence, BJC HealthCare, 8300 Eager Road, Suite 400A, St. Louis, MO 63144; audrey.gronemeyer@bjc.org.
Financial disclosures: None.
1. Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: A clinical practice guideline from the AABB*. Ann Intern Med. 2012;157:49-58.
2. Goodnough LT, Levy JH, Murphy MF. Concepts of blood transfusion in adults. Lancet. 2013;381:1845-1854.
3. Hébert PC, Carson JL. Transfusion threshold of 7 g per deciliter—The new normal. N Engl J Med. 2014;371:1459-1461.
4. Gani F, Cerullo M, Ejaz A, et al. Implementation of a blood management program at a tertiary care hospital: Effect on transfusion practices and clinical outcomes among patients undergoing surgery. Ann Surg. 2019;269:1073-1079.
5. Podlasek SJ, Thakkar RN, Rotello LC, et al. Implementing a “why give 2 when 1 will do?” Choosing Wisely campaign. Transfusion. 2016;56:2164.
6. Boral LI, Bernard A, Hjorth T, et al. How do I implement a more restrictive transfusion trigger of hemoglobin level of 7 g/dL at my hospital? Transfusion. 2015;55:937-945.
7. Geissler RG, Kosters C, Franz D, et al. Utilization of blood components in trauma surgery: A single-center, retrospective analysis before and after the implementation of an educative PBM initiative. Transfuse Med Hemother. 2015;42:83-89.
8. Goel R, Cushing MM, Tobian AA. Pediatric patient blood management programs: Not just transfusing little adults. Transfus Med Rev. 2016;30:235-241.
9. Gupta PB, DeMario VM, Amin RM, et al. Patient blood management program improves blood use and clinical outcomes in orthopedic surgery. Anesthesiology. 2018;129;1082-1091.
10. Leahy MF, Roberts H, Mukhtar SA, et al. A pragmatic approach to embedding patient blood management in a tertiary hospital. Transfusion. 2014;54:1133-1145.
11. Leahy MF, Hofmann A, Towler S, et al. Improved outcomes and reduced costs associated with a health-system-wide patient blood management program: A retrospective observational study in four major adult tertiary-care hospitals. Transfusion. 2017;57:1347-1358.
12. Meybohm P, Herrmann E, Steinbicker AU, et al. Patient blood management is associated with a substantial reduction of red blood cell utilization and safe for patient’s outcome: A prospective, multicenter cohort study with a noninferiority design. Ann Surg. 2016;264:203-211.
13. Morgan PN, Coleman PL, Martinez-Garduno CM, et al. Implementation of a patient blood management program in an Australian private hospital orthopedic unit. J Blood Med. 2018;9;83-90.
14. Norgaard A, Stensballe J, de Lichtenberg TH, et al. Three-year follow-up of implementation of evidence-based transfusion practice in a tertiary hospital. Vox Sang. 2017;112:229-239.
15. Meuller MM, Van Remoortel H, Meybohm P, et al. Patient blood management: Recommendations from the 2018 Frankfurt Consensus Conference. JAMA. 2019;321:983-997.
16. Oliver JC, Griffin RL, Hannon T, Marques MB. The success of our patient blood management program depended on an institution-wide change in transfusion practices. Transfusion. 2014;54:2617-2624.
17. Thakkar RN, Lee KH, Ness PM, et al. Relative impact of a patient blood management program on utilization of all three major blood components. Transfusion. 2016;56:2212-2220.
18. Yang WW, Thakkar RN, Gehrie EA, et al. Single-unit transfusions and hemoglobin trigger: relative impact on red cell utilization. Transfusion. 2017;57:1163-1170.
19. Frank SM, Thakkar RN, Podlasek SJ, et al. Implementing a health system-wide patient blood management program with a clinical community approach. Anesthesiology. 2017;127;754-764.
20. Verdecchia NM, Wisniewski MK, Waters JH, et al. Changes in blood product utilization in a seven-hospital system after the implementation of a patient blood management program: A 9-year follow-up. Hematology. 2016;21:490-499.
21. Yazer MH, Waters JH. How do I implement a hospital-based blood management program? Transfusion. 2012;52:1640-1645.
22. BJC HealthCare. Facts and Figures.. BJC HealthCare website. www.bjc.org/About-Us/Facts-Figures. Accessed November 18, 2019.
23. Callum JL, Waters JH, Shaz BH, et al. The AABB recommendations for the Choosing Wisely campaign of the American Board of Internal Medicine. Transfusion. 2014;54:2344-2352.
1. Carson JL, Grossman BJ, Kleinman S, et al. Red blood cell transfusion: A clinical practice guideline from the AABB*. Ann Intern Med. 2012;157:49-58.
2. Goodnough LT, Levy JH, Murphy MF. Concepts of blood transfusion in adults. Lancet. 2013;381:1845-1854.
3. Hébert PC, Carson JL. Transfusion threshold of 7 g per deciliter—The new normal. N Engl J Med. 2014;371:1459-1461.
4. Gani F, Cerullo M, Ejaz A, et al. Implementation of a blood management program at a tertiary care hospital: Effect on transfusion practices and clinical outcomes among patients undergoing surgery. Ann Surg. 2019;269:1073-1079.
5. Podlasek SJ, Thakkar RN, Rotello LC, et al. Implementing a “why give 2 when 1 will do?” Choosing Wisely campaign. Transfusion. 2016;56:2164.
6. Boral LI, Bernard A, Hjorth T, et al. How do I implement a more restrictive transfusion trigger of hemoglobin level of 7 g/dL at my hospital? Transfusion. 2015;55:937-945.
7. Geissler RG, Kosters C, Franz D, et al. Utilization of blood components in trauma surgery: A single-center, retrospective analysis before and after the implementation of an educative PBM initiative. Transfuse Med Hemother. 2015;42:83-89.
8. Goel R, Cushing MM, Tobian AA. Pediatric patient blood management programs: Not just transfusing little adults. Transfus Med Rev. 2016;30:235-241.
9. Gupta PB, DeMario VM, Amin RM, et al. Patient blood management program improves blood use and clinical outcomes in orthopedic surgery. Anesthesiology. 2018;129;1082-1091.
10. Leahy MF, Roberts H, Mukhtar SA, et al. A pragmatic approach to embedding patient blood management in a tertiary hospital. Transfusion. 2014;54:1133-1145.
11. Leahy MF, Hofmann A, Towler S, et al. Improved outcomes and reduced costs associated with a health-system-wide patient blood management program: A retrospective observational study in four major adult tertiary-care hospitals. Transfusion. 2017;57:1347-1358.
12. Meybohm P, Herrmann E, Steinbicker AU, et al. Patient blood management is associated with a substantial reduction of red blood cell utilization and safe for patient’s outcome: A prospective, multicenter cohort study with a noninferiority design. Ann Surg. 2016;264:203-211.
13. Morgan PN, Coleman PL, Martinez-Garduno CM, et al. Implementation of a patient blood management program in an Australian private hospital orthopedic unit. J Blood Med. 2018;9;83-90.
14. Norgaard A, Stensballe J, de Lichtenberg TH, et al. Three-year follow-up of implementation of evidence-based transfusion practice in a tertiary hospital. Vox Sang. 2017;112:229-239.
15. Meuller MM, Van Remoortel H, Meybohm P, et al. Patient blood management: Recommendations from the 2018 Frankfurt Consensus Conference. JAMA. 2019;321:983-997.
16. Oliver JC, Griffin RL, Hannon T, Marques MB. The success of our patient blood management program depended on an institution-wide change in transfusion practices. Transfusion. 2014;54:2617-2624.
17. Thakkar RN, Lee KH, Ness PM, et al. Relative impact of a patient blood management program on utilization of all three major blood components. Transfusion. 2016;56:2212-2220.
18. Yang WW, Thakkar RN, Gehrie EA, et al. Single-unit transfusions and hemoglobin trigger: relative impact on red cell utilization. Transfusion. 2017;57:1163-1170.
19. Frank SM, Thakkar RN, Podlasek SJ, et al. Implementing a health system-wide patient blood management program with a clinical community approach. Anesthesiology. 2017;127;754-764.
20. Verdecchia NM, Wisniewski MK, Waters JH, et al. Changes in blood product utilization in a seven-hospital system after the implementation of a patient blood management program: A 9-year follow-up. Hematology. 2016;21:490-499.
21. Yazer MH, Waters JH. How do I implement a hospital-based blood management program? Transfusion. 2012;52:1640-1645.
22. BJC HealthCare. Facts and Figures.. BJC HealthCare website. www.bjc.org/About-Us/Facts-Figures. Accessed November 18, 2019.
23. Callum JL, Waters JH, Shaz BH, et al. The AABB recommendations for the Choosing Wisely campaign of the American Board of Internal Medicine. Transfusion. 2014;54:2344-2352.

An eConsults Program to Improve Patient Access to Specialty Care in an Academic Health System
From the Department of Medicine, University of California, Irvine, Orange, CA.
Abstract
Background: Orange County’s residents have difficulty accessing timely, quality, affordable specialty care services. As the county’s only academic health system, the University of California, Irvine (UCI) aimed to improve specialty care access for the communities it serves by implementing an electronic consultations (eConsults) program that allows primary care providers (PCPs) to efficiently receive specialist recommendations on referral problems that do not require an in-person evaluation.
Objective: To implement an eConsults program at the UCI that enhances access to and the delivery of coordinated specialty care for lower-complexity referral problems.
Methods: We developed custom solutions to integrate eConsults into UCI’s 2 electronic health record platforms. The impact of the eConsults program was assessed by continuously evaluating usage and outcomes. Measures used to track usage included the number of submitted eConsult requests per PCP, the number of completed responses per specialty, and the response time for eConsult requests. Outcome measures included the specialist recommendation (eg, in-office visit, consultation avoided) and physician feedback.
Results: Over 4.5 years, more than 1400 successful eConsults have been completed, and the program has expanded to 17 specialties. The average turnaround time for an eConsult response across all specialties was 1 business day. Moreover, more than 50% of the eConsults received specialty responses within the same day of the eConsult request. Most important, about 80% of eConsult requests were addressed without the need for an in-office visit with a specialist.
Conclusion: The enhanced access to and the delivery of coordinated specialty care provided by eConsults resulted in improved efficiency and specialty access, while likely reducing costs and improving patient satisfaction. The improved communication and collaboration among providers with eConsults has also led to overwhelmingly positive feedback from both PCPs and specialists.
Keywords: electronic consultation; access to care; primary care; specialty referral; telehealth.
Orange County’s growing, aging, and diverse population is driving an increased demand for health care.1 But with the county’s high cost of living and worsening shortage of physicians,1-3 many of its residents are struggling to access timely, quality, affordable care. Access to specialty care services is especially frustrating for many patients and their providers, both primary care providers (PCPs) and specialists, due to problems with the referral process. Many patients experience increased wait times for a visit with a specialist due to poor communication between providers, insufficient guidance on the information or diagnostic results needed by specialists, and lack of care coordination.4-6 One promising approach to overcome these challenges is the use of an electronic consultation, or eConsult, in place of a standard in-person referral. An eConsult is an asynchronous, non-face-to-face, provider-to-provider exchange using a secure electronic communication platform. For appropriate referral problems, the patient is able to receive timely access to specialist expertise through electronic referral by their PCP,7-9 and avoid the time and costs associated with a visit to the specialist,10,11 such as travel, missed work, co-pays, and child-care expenses. Clinical questions addressed using an eConsult system subsequently free up office visit appointment slots, improving access for patients requiring in-office evaluation.8,12
Orange County’s only academic health system, the University of California, Irvine (UCI), serves a population of 3.5 million, and its principal priority is providing the communities in the county (which is the sixth largest in United States) and the surrounding region with the highest quality health care possible. Thus, UCI aimed to improve its referral processes and provide timely access to specialty care for its patients by implementing an eConsults program that allows PCPs to efficiently receive specialist recommendations on referral problems that do not require the specialist to evaluate the patient in person. This report describes our experiences with developing and implementing a custom-built eConsults workflow in UCI’s prior electronic health record (EHR) platform, Allscripts, and subsequently transitioning our mature eConsults program to a new EHR system when UCI adopted Epic. UCI is likely the only academic medical center to have experience in successfully implementing eConsults into 2 different EHR systems.
Setting
UCI’s medical center is a 417-bed acute care hospital providing tertiary and quaternary care, ambulatory and specialty medical clinics, behavioral health care, and rehabilitation services. It is located in Orange, CA, and serves a diverse population of 3.5 million persons with broad health care needs. With more than 400 specialty and primary care physicians, UCI offers a full scope of acute and general care services. It is also the primary teaching location for UCI medical and nursing students, medical residents, and fellows, and is home to Orange County’s only adult Level I and pediatric Level II trauma centers and the regional burn center.
eConsults Program
We designed the initial eConsults program within UCI’s Allscripts EHR platform. Our information technology (IT) build team developed unique “documents-based” eConsults workflows that simplified the process of initiating requests directly from the EHR and facilitated rapid responses from participating specialties. The requesting provider’s eConsults interface was user-friendly, and referring providers were able to initiate an eConsult easily by selecting the customized eConsult icon from the Allscripts main toolbar. To ensure that all relevant information is provided to the specialists, condition-specific templates are embedded in the requesting provider’s eConsults workflow that allow PCPs to enter a focused, patient-specific clinical question and provide guidance on recommended patient information (eg, health history, laboratory results, and digital images) that may help the specialist provide an informed response. The eConsult templates were adapted from standardized forms developed by partner University of California Health Systems in an initiative funded by the University of California Center for Health Quality and Innovation.
To facilitate timely responses from specialists, an innovative notification system was created in the responding provider’s eConsults workflow to automatically send an email to participating specialists when a new eConsult is requested. The responding provider’s workflow also includes an option for the specialist to decline the eConsult if the case is deemed too complex to be addressed electronically. For every completed eConsult that does not result in an in-person patient evaluation, the requesting provider and responding specialist each receives a modest reimbursement, which was initially paid by UCI Health System funds.
Implementation
The design and implementation of the eConsults program began in November 2014, and was guided by a steering committee that included the chair of the department of medicine, chief medical information officer, primary care and specialty physician leads, IT build team, and a project manager. Early on, members of this committee engaged UCI leadership to affirm support for the program and obtain the IT resources needed to build the eConsults workflow. Regular steering committee meetings were established to discuss the design of the workflow, adapt the clinical content of the referral templates, and develop a provider reimbursement plan. After completion of the workflow build, the eConsults system was tested to identify failure points and obtain feedback from users. Prior to going live, the eConsults program was publicized by members of the steering committee through meetings with primary care groups and email communications. Committee members also hosted in-person training and orientation sessions with PCPs and participating specialists, and distributed tip sheets summarizing the steps to complete the PCP and specialist eConsult workflows.
The eConsults workflow build, testing, and launch were completed within 5 months (April 2015; Figure 1). eConsults went live in the 3 initial specialties (endocrinology, cardiology, and rheumatology) that were interested in participating in the first wave of the program. UCI’s eConsults service has subsequently expanded to 17 total specialties (allergy, cardiology, dermatology, endocrinology, gastroenterology, geriatrics, gynecology, hematology, hepatology, infectious disease, nephrology, neurology, palliative care, psychiatry, pulmonary, rheumatology, and sports medicine).

Two and half years after the eConsults program was implemented in Allscripts, UCI adopted a new EHR platform, Epic. By this time, the eConsults service had grown into a mature program with greater numbers of PCP users and submitted eConsults (Figure 2). Using our experience with the Allscripts build, our IT team was able to efficiently transition the eConsults service to the new EHR system. In contrast to the “documents-based” eConsult workflows on Allscripts, our IT team utilized an “orders-based” strategy on Epic, which followed a more traditional approach to requesting a consultation. We re-launched the service in Epic within 3 months (February 2018). However, both platforms utilized user-friendly workflows to achieve similar goals, and the program has continued to grow with respect to the number of users and eConsults.

Measurement/Analysis
The impact of the program was assessed by continuously evaluating usage and outcomes. Measures used to track usage included the number of PCP users, the number of submitted eConsult requests per PCP, and the number of requests per specialty. The response time for eConsult requests and the self-reported amount of time spent by specialists on the response were also tracked. Outcome measures included the specialist recommendation (eg, in-office visit, consultation avoided) and physician feedback. Provider satisfaction was primarily obtained by soliciting feedback from individual eConsult users.
Implementation of this eConsults program constituted a quality improvement activity and did not require Institutional Review Board review.
Results
Since the program was launched in April 2015, more than 1400 eConsults have been completed across 17 specialties (Figure 3). There were 654 completed eConsults on the Allscripts platform, and 808 eConsults have been completed using the Epic platform to date. The busiest eConsult specialties were endocrinology (receiving 276, or 19%, of the eConsults requests), hematology (receiving 249 requests, or 17%), infectious disease (receiving 244 requests, or 17% ), and cardiology (receiving 148 requests, or 10%).

The self-reported amount of time specialists spent on the response was different between the 2 EHR systems (Figure 4). On Allscripts, specialists reported that 23% of eConsults took 10 minutes or less to complete, 47% took 11 to 20 minutes, 23% took 21 to 30 minutes, and 7% took more than 30 minutes. On Epic, specialists reported that 42% of eConsults took 10 minutes or less to complete, 44% took 11 to 20 minutes, 12% took 21 to 30 minutes, and 2% took more than 30 minutes. This difference in time spent fielding eConsults likely represents the subtle nuances between Allscripts’ “documents-based” and Epic’s “orders-based” workflows.
 and Epic (inner ring)")
As a result of the automated notification system that was introduced early in the eConsults implementation process on Allscripts, the specialty response times were much faster than the expected 3 business days’ turnaround goal instituted by the Center for Health Quality and Innovation initiative, regardless of the EHR platform used. In fact, the average turnaround time for an eConsult response across all specialties was 1 business day, which was similar for both EHR systems (Figure 5). Furthermore, more than 50% of the eConsults on both EHR systems received specialist responses within the same day of the eConsult request (63% on Allscripts, 54% on Epic). There was a small decrease in the percentage of same-day responses when we transitioned to Epic, likely because the functionality of an automated notification email could not be restored in Epic. Regardless, the specialty response times on Epic remained expeditious, likely because the automated notifications on Allscripts instilled good practices for the specialists, and regularly checking for new eConsult requests became an ingrained behavior.
 and Epic (inner ring)")
Our most important finding was that approximately 80% of eConsult requests were addressed without the need for an in-office visit with a specialist. This measure was similar for both EHR platforms (83% on Allscripts and 78% on Epic).
Provider feedback has been overwhelmingly positive. PCPs are impressed with the robust educational content of the eConsult responses, since the goal for specialists is to justify their recommendations. Specialists appreciate the convenience and efficiency that eConsults offer, as well as the improved communication and collaboration among physicians. eConsults have been especially beneficial to PCPs at UCI’s Family Health Centers, who are now able to receive subspecialty consultations from UCI specialists despite insurance barriers.
Discussion
Our eConsults program uniquely contrasts with other programs because UCI is likely the only academic medical center to have experience in successfully incorporating eConsults into 2 different EHR systems: initial development of the eConsults workflow in UCI’s existing Allscripts EHR platform, and subsequently transitioning a mature eConsults program to a new EHR system when the institution adopted Epic.
We measured the impact of the eConsults program on access to care by the response time for eConsult requests and the percentage of eConsults that averted an in-office visit with a specialist. We found that the eConsults program at UCI provided our PCPs access to specialist consultations in a timely manner, with much shorter response times than standard in-person referrals. The average turnaround time for an eConsult response we reported is consistent with findings from other studies.12-15 Additionally, our program was able to address about 80% of its eConsults electronically, helping to reduce unnecessary in-person specialist referrals. In the literature, the percentage of eConsults that avoided an in-person specialist visit varies widely.8,12-16
We reported very positive feedback from both PCPs and specialists on UCI’s eConsults service. Similarly, other studies described PCP satisfaction with their respective eConsults programs to be uniformly high,8,9,13,14,17-19 though some reported that the level of satisfaction among specialists was more varied.18-21
Lessons Learned
The successful design and implementation of our eConsults program began with assembling the right clinical champions and technology partners for our steering committee. Establishing regular steering committee meetings helped maintain an appropriate timeline for completion of different aspects of the project. Engaging support from UCI’s leadership also provided us with a dedicated IT team that helped us with the build, training resources, troubleshooting issues, and reporting for the project.
Our experience with implementing the eConsults program on 2 different EHR systems highlighted the importance of creating efficient, user-friendly workflows to foster provider adoption and achieve sustainability. Allscripts’ open platform gave our IT team the ability to create a homegrown solution to implementing an eConsult model that was simple and easy to use. The Epic platform’s interoperability allowed us to leverage our learnings from the Allscripts build to efficiently implement eConsults in Epic.
We also found that providing modest incentive payments or reimbursements to both PCPs and specialists for each completed eConsult helps with both adoption and program sustainability. Initially, credit for the eConsult work was paid by internal UCI Health System funds. Two payers, UC Care (a preferred provider organization plan created just for the University of California) and more recently, the Centers for Medicare & Medicaid Services, have agreed to reimburse for outpatient eConsults. Securing additional payers for reimbursement of the eConsult service will not only ensure the program’s long-term sustainability, but also represents an acknowledgment of the value of eConsults in supporting access to care.
Applicability
Other health care settings that are experiencing issues with specialty care access can successfully implement their own eConsults program by employing strategies similar to those described in this report—assembling the right team, creating user-friendly workflows, and providing incentives. Our advice for successful implementation is to clearly communicate your goals to all involved, including primary care, specialists, leadership, and IT partners, and establish with these stakeholders the appropriate support and resources needed to facilitate the development of the program and overcome any barriers to adoption.
Current Status and Future Directions
Our future plans include continuing to optimize the Epic eConsult backend build and workflows using our experience in Allscripts. We have implemented eConsult workflows for use by graduate medical education trainees and advanced practice providers, with attending supervision. Further work is in progress to optimize these workflows, which will allow for appropriate education and supervision without delaying care. Furthermore, we plan to expand the program to include inpatient-to-inpatient and emergency department-to-inpatient eConsults. We will continue to expand the eConsults program by offering additional specialties, engage providers to encourage ongoing participation, and maximize PCP use by continuing to market the program through regular newsletters and email communications. Finally, the eConsults has served as an effective, important resource in the current era of COVID-19 in several ways: it allows for optimization of specialty input in patient care delivery without subjecting more health care workers to unnecessary exposure; saves on utilization of precious personal protective equipment; and enhances our ability to deal with a potential surge by providing access to specialists remotely and electronically all hours of the day, thus expanding care to the evening and weekend hours.
Acknowledgment: The authors thank our steering committee members (Dr. Ralph Cygan, Dr. Andrew Reikes, Dr. Byron Allen, Dr. George Lawry) and IT build team (Lori Bocchicchio, Meghan van Witsen, Jaymee Zillgitt, Tanya Sickles, Dennis Hoang, Jeanette Lisak-Phillips) for their contributions in the design and implementation of our eConsults program. We also thank additional team members Kurt McArthur and Neaktisia Lee for their assistance with generating reports, and Kathy LaPierre, Jennifer Rios, and Debra Webb Torres for their guidance with compliance and billing issues.
Corresponding author: Alpesh N. Amin, MD, MBA, University of California, Irvine, 101 The City Drive South, Building 26, Room 1000, ZC-4076H, Orange, CA 92868; anamin@uci.edu.
Financial disclosures: None.
1. County of Orange, Health Care Agency, Public Health Services. Orange County Health Profile 2013.
2. Coffman JM, Fix M Ko, M. California physician supply and distribution: headed for a drought? California Health Care Foundation, June 2018.
3. Spetz J, Coffman J, Geyn I. California’s primary care workforce: forecasted supply, demand, and pipeline of trainees, 2016-2030. Healthforce Center at the University of California, San Francisco, August 2017.
4. Gandhi TK, Sittig DF, Franklin M, et al. Communication breakdown in the outpatient referral process. J Gen Intern Med. 2000;15:626-631.
5. McPhee SJ, Lo B, Saika GY, Meltzer R. How good is communication between primary care physicians and subspecialty consultants? Arch Intern Med. 1984;144:1265-1268.
6. Mehrotra A, Forrest CB, Lin CY. Dropping the baton: specialty referrals in the United States. Milbank Q. 2011;89:39-68.
7. Wrenn K, Catschegn S, Cruz M, et al. Analysis of an electronic consultation program at an academic medical centre: Primary care provider questions, specialist responses, and primary care provider actions. J Telemed Telecare. 2017;23: 217-224.
8. Gleason N, Prasad PA, Ackerman S, et al. Adoption and impact of an eConsult system in a fee-for-service setting. Healthc (Amst). 2017;5(1-2):40-45.
9. Stoves J, Connolly J, Cheung CK, et al. Electronic consultation as an alternative to hospital referral for patients with chronic kidney disease: a novel application for networked electronic health records to improve the accessibility and efficiency of healthcare. Qual Saf Health Care. 2010;19: e54.
10. Datta SK, Warshaw EM, Edison KE, et al. Cost and utility analysis of a store-and-forward teledermatology referral system: a randomized clinical trial. JAMA Dermatol. 2015;151:1323-1329.
11. Liddy C, Drosinis P, Deri Armstrong C, et al. What are the cost savings associated with providing access to specialist care through the Champlain BASE eConsult service? A costing evaluation. BMJ Open. 2016;6:e010920.
12. Barnett ML, Yee HF Jr, Mehrotra A, Giboney P. Los Angeles safety-net program eConsult system was rapidly adopted and decreased wait times to see specialists. Health Aff. 2017;36:492-499.
13. Malagrino GD, Chaudhry R, Gardner M, et al. A study of 6,000 electronic specialty consultations for person-centered care at The Mayo Clinic. Int J Person Centered Med. 2012;2:458-466.
14. Keely E, Liddy C, Afkham A. Utilization, benefits, and impact of an e-consultation service across diverse specialties and primary care providers. Telemed J E Health. 2013;19:733-738.
15. Scherpbier-de Haan ND, van Gelder VA, Van Weel C, et al. Initial implementation of a web-based consultation process for patients with chronic kidney disease. Ann Fam Med. 2013;11:151-156.
16. Palen TE, Price D, Shetterly S, Wallace KB. Comparing virtual consults to traditional consults using an electronic health record: an observational case-control study. BMC Med Inform Decis Mak. 2012;12:65.
17. Liddy C, Afkham A, Drosinis P, et al. Impact of and satisfaction with a new eConsult service: a mixed methods study of primary care providers. J Am Board Fam Med. 2015;28:394-403.
18. Angstman KB, Adamson SC, Furst JW, et al. Provider satisfaction with virtual specialist consultations in a family medicine department. Health Care Manag (Frederick). 2009;28:14-18.
19. McAdams M, Cannavo L, Orlander JD. A medical specialty e-consult program in a VA health care system. Fed Pract. 2014; 31:26–31.
20. Keely E, Williams R, Epstein G, et al. Specialist perspectives on Ontario Provincial electronic consultation services. Telemed J E Health. 2019;25:3-10.
21. Kim-Hwang JE, Chen AH, Bell DS, et al. Evaluating electronic referrals for specialty care at a public hospital. J Gen Intern Med. 2010;25:1123-1128.
From the Department of Medicine, University of California, Irvine, Orange, CA.
Abstract
Background: Orange County’s residents have difficulty accessing timely, quality, affordable specialty care services. As the county’s only academic health system, the University of California, Irvine (UCI) aimed to improve specialty care access for the communities it serves by implementing an electronic consultations (eConsults) program that allows primary care providers (PCPs) to efficiently receive specialist recommendations on referral problems that do not require an in-person evaluation.
Objective: To implement an eConsults program at the UCI that enhances access to and the delivery of coordinated specialty care for lower-complexity referral problems.
Methods: We developed custom solutions to integrate eConsults into UCI’s 2 electronic health record platforms. The impact of the eConsults program was assessed by continuously evaluating usage and outcomes. Measures used to track usage included the number of submitted eConsult requests per PCP, the number of completed responses per specialty, and the response time for eConsult requests. Outcome measures included the specialist recommendation (eg, in-office visit, consultation avoided) and physician feedback.
Results: Over 4.5 years, more than 1400 successful eConsults have been completed, and the program has expanded to 17 specialties. The average turnaround time for an eConsult response across all specialties was 1 business day. Moreover, more than 50% of the eConsults received specialty responses within the same day of the eConsult request. Most important, about 80% of eConsult requests were addressed without the need for an in-office visit with a specialist.
Conclusion: The enhanced access to and the delivery of coordinated specialty care provided by eConsults resulted in improved efficiency and specialty access, while likely reducing costs and improving patient satisfaction. The improved communication and collaboration among providers with eConsults has also led to overwhelmingly positive feedback from both PCPs and specialists.
Keywords: electronic consultation; access to care; primary care; specialty referral; telehealth.
Orange County’s growing, aging, and diverse population is driving an increased demand for health care.1 But with the county’s high cost of living and worsening shortage of physicians,1-3 many of its residents are struggling to access timely, quality, affordable care. Access to specialty care services is especially frustrating for many patients and their providers, both primary care providers (PCPs) and specialists, due to problems with the referral process. Many patients experience increased wait times for a visit with a specialist due to poor communication between providers, insufficient guidance on the information or diagnostic results needed by specialists, and lack of care coordination.4-6 One promising approach to overcome these challenges is the use of an electronic consultation, or eConsult, in place of a standard in-person referral. An eConsult is an asynchronous, non-face-to-face, provider-to-provider exchange using a secure electronic communication platform. For appropriate referral problems, the patient is able to receive timely access to specialist expertise through electronic referral by their PCP,7-9 and avoid the time and costs associated with a visit to the specialist,10,11 such as travel, missed work, co-pays, and child-care expenses. Clinical questions addressed using an eConsult system subsequently free up office visit appointment slots, improving access for patients requiring in-office evaluation.8,12
Orange County’s only academic health system, the University of California, Irvine (UCI), serves a population of 3.5 million, and its principal priority is providing the communities in the county (which is the sixth largest in United States) and the surrounding region with the highest quality health care possible. Thus, UCI aimed to improve its referral processes and provide timely access to specialty care for its patients by implementing an eConsults program that allows PCPs to efficiently receive specialist recommendations on referral problems that do not require the specialist to evaluate the patient in person. This report describes our experiences with developing and implementing a custom-built eConsults workflow in UCI’s prior electronic health record (EHR) platform, Allscripts, and subsequently transitioning our mature eConsults program to a new EHR system when UCI adopted Epic. UCI is likely the only academic medical center to have experience in successfully implementing eConsults into 2 different EHR systems.
Setting
UCI’s medical center is a 417-bed acute care hospital providing tertiary and quaternary care, ambulatory and specialty medical clinics, behavioral health care, and rehabilitation services. It is located in Orange, CA, and serves a diverse population of 3.5 million persons with broad health care needs. With more than 400 specialty and primary care physicians, UCI offers a full scope of acute and general care services. It is also the primary teaching location for UCI medical and nursing students, medical residents, and fellows, and is home to Orange County’s only adult Level I and pediatric Level II trauma centers and the regional burn center.
eConsults Program
We designed the initial eConsults program within UCI’s Allscripts EHR platform. Our information technology (IT) build team developed unique “documents-based” eConsults workflows that simplified the process of initiating requests directly from the EHR and facilitated rapid responses from participating specialties. The requesting provider’s eConsults interface was user-friendly, and referring providers were able to initiate an eConsult easily by selecting the customized eConsult icon from the Allscripts main toolbar. To ensure that all relevant information is provided to the specialists, condition-specific templates are embedded in the requesting provider’s eConsults workflow that allow PCPs to enter a focused, patient-specific clinical question and provide guidance on recommended patient information (eg, health history, laboratory results, and digital images) that may help the specialist provide an informed response. The eConsult templates were adapted from standardized forms developed by partner University of California Health Systems in an initiative funded by the University of California Center for Health Quality and Innovation.
To facilitate timely responses from specialists, an innovative notification system was created in the responding provider’s eConsults workflow to automatically send an email to participating specialists when a new eConsult is requested. The responding provider’s workflow also includes an option for the specialist to decline the eConsult if the case is deemed too complex to be addressed electronically. For every completed eConsult that does not result in an in-person patient evaluation, the requesting provider and responding specialist each receives a modest reimbursement, which was initially paid by UCI Health System funds.
Implementation
The design and implementation of the eConsults program began in November 2014, and was guided by a steering committee that included the chair of the department of medicine, chief medical information officer, primary care and specialty physician leads, IT build team, and a project manager. Early on, members of this committee engaged UCI leadership to affirm support for the program and obtain the IT resources needed to build the eConsults workflow. Regular steering committee meetings were established to discuss the design of the workflow, adapt the clinical content of the referral templates, and develop a provider reimbursement plan. After completion of the workflow build, the eConsults system was tested to identify failure points and obtain feedback from users. Prior to going live, the eConsults program was publicized by members of the steering committee through meetings with primary care groups and email communications. Committee members also hosted in-person training and orientation sessions with PCPs and participating specialists, and distributed tip sheets summarizing the steps to complete the PCP and specialist eConsult workflows.
The eConsults workflow build, testing, and launch were completed within 5 months (April 2015; Figure 1). eConsults went live in the 3 initial specialties (endocrinology, cardiology, and rheumatology) that were interested in participating in the first wave of the program. UCI’s eConsults service has subsequently expanded to 17 total specialties (allergy, cardiology, dermatology, endocrinology, gastroenterology, geriatrics, gynecology, hematology, hepatology, infectious disease, nephrology, neurology, palliative care, psychiatry, pulmonary, rheumatology, and sports medicine).
Two and half years after the eConsults program was implemented in Allscripts, UCI adopted a new EHR platform, Epic. By this time, the eConsults service had grown into a mature program with greater numbers of PCP users and submitted eConsults (Figure 2). Using our experience with the Allscripts build, our IT team was able to efficiently transition the eConsults service to the new EHR system. In contrast to the “documents-based” eConsult workflows on Allscripts, our IT team utilized an “orders-based” strategy on Epic, which followed a more traditional approach to requesting a consultation. We re-launched the service in Epic within 3 months (February 2018). However, both platforms utilized user-friendly workflows to achieve similar goals, and the program has continued to grow with respect to the number of users and eConsults.
Measurement/Analysis
The impact of the program was assessed by continuously evaluating usage and outcomes. Measures used to track usage included the number of PCP users, the number of submitted eConsult requests per PCP, and the number of requests per specialty. The response time for eConsult requests and the self-reported amount of time spent by specialists on the response were also tracked. Outcome measures included the specialist recommendation (eg, in-office visit, consultation avoided) and physician feedback. Provider satisfaction was primarily obtained by soliciting feedback from individual eConsult users.
Implementation of this eConsults program constituted a quality improvement activity and did not require Institutional Review Board review.
Results
Since the program was launched in April 2015, more than 1400 eConsults have been completed across 17 specialties (Figure 3). There were 654 completed eConsults on the Allscripts platform, and 808 eConsults have been completed using the Epic platform to date. The busiest eConsult specialties were endocrinology (receiving 276, or 19%, of the eConsults requests), hematology (receiving 249 requests, or 17%), infectious disease (receiving 244 requests, or 17% ), and cardiology (receiving 148 requests, or 10%).
The self-reported amount of time specialists spent on the response was different between the 2 EHR systems (Figure 4). On Allscripts, specialists reported that 23% of eConsults took 10 minutes or less to complete, 47% took 11 to 20 minutes, 23% took 21 to 30 minutes, and 7% took more than 30 minutes. On Epic, specialists reported that 42% of eConsults took 10 minutes or less to complete, 44% took 11 to 20 minutes, 12% took 21 to 30 minutes, and 2% took more than 30 minutes. This difference in time spent fielding eConsults likely represents the subtle nuances between Allscripts’ “documents-based” and Epic’s “orders-based” workflows.
As a result of the automated notification system that was introduced early in the eConsults implementation process on Allscripts, the specialty response times were much faster than the expected 3 business days’ turnaround goal instituted by the Center for Health Quality and Innovation initiative, regardless of the EHR platform used. In fact, the average turnaround time for an eConsult response across all specialties was 1 business day, which was similar for both EHR systems (Figure 5). Furthermore, more than 50% of the eConsults on both EHR systems received specialist responses within the same day of the eConsult request (63% on Allscripts, 54% on Epic). There was a small decrease in the percentage of same-day responses when we transitioned to Epic, likely because the functionality of an automated notification email could not be restored in Epic. Regardless, the specialty response times on Epic remained expeditious, likely because the automated notifications on Allscripts instilled good practices for the specialists, and regularly checking for new eConsult requests became an ingrained behavior.
Our most important finding was that approximately 80% of eConsult requests were addressed without the need for an in-office visit with a specialist. This measure was similar for both EHR platforms (83% on Allscripts and 78% on Epic).
Provider feedback has been overwhelmingly positive. PCPs are impressed with the robust educational content of the eConsult responses, since the goal for specialists is to justify their recommendations. Specialists appreciate the convenience and efficiency that eConsults offer, as well as the improved communication and collaboration among physicians. eConsults have been especially beneficial to PCPs at UCI’s Family Health Centers, who are now able to receive subspecialty consultations from UCI specialists despite insurance barriers.
Discussion
Our eConsults program uniquely contrasts with other programs because UCI is likely the only academic medical center to have experience in successfully incorporating eConsults into 2 different EHR systems: initial development of the eConsults workflow in UCI’s existing Allscripts EHR platform, and subsequently transitioning a mature eConsults program to a new EHR system when the institution adopted Epic.
We measured the impact of the eConsults program on access to care by the response time for eConsult requests and the percentage of eConsults that averted an in-office visit with a specialist. We found that the eConsults program at UCI provided our PCPs access to specialist consultations in a timely manner, with much shorter response times than standard in-person referrals. The average turnaround time for an eConsult response we reported is consistent with findings from other studies.12-15 Additionally, our program was able to address about 80% of its eConsults electronically, helping to reduce unnecessary in-person specialist referrals. In the literature, the percentage of eConsults that avoided an in-person specialist visit varies widely.8,12-16
We reported very positive feedback from both PCPs and specialists on UCI’s eConsults service. Similarly, other studies described PCP satisfaction with their respective eConsults programs to be uniformly high,8,9,13,14,17-19 though some reported that the level of satisfaction among specialists was more varied.18-21
Lessons Learned
The successful design and implementation of our eConsults program began with assembling the right clinical champions and technology partners for our steering committee. Establishing regular steering committee meetings helped maintain an appropriate timeline for completion of different aspects of the project. Engaging support from UCI’s leadership also provided us with a dedicated IT team that helped us with the build, training resources, troubleshooting issues, and reporting for the project.
Our experience with implementing the eConsults program on 2 different EHR systems highlighted the importance of creating efficient, user-friendly workflows to foster provider adoption and achieve sustainability. Allscripts’ open platform gave our IT team the ability to create a homegrown solution to implementing an eConsult model that was simple and easy to use. The Epic platform’s interoperability allowed us to leverage our learnings from the Allscripts build to efficiently implement eConsults in Epic.
We also found that providing modest incentive payments or reimbursements to both PCPs and specialists for each completed eConsult helps with both adoption and program sustainability. Initially, credit for the eConsult work was paid by internal UCI Health System funds. Two payers, UC Care (a preferred provider organization plan created just for the University of California) and more recently, the Centers for Medicare & Medicaid Services, have agreed to reimburse for outpatient eConsults. Securing additional payers for reimbursement of the eConsult service will not only ensure the program’s long-term sustainability, but also represents an acknowledgment of the value of eConsults in supporting access to care.
Applicability
Other health care settings that are experiencing issues with specialty care access can successfully implement their own eConsults program by employing strategies similar to those described in this report—assembling the right team, creating user-friendly workflows, and providing incentives. Our advice for successful implementation is to clearly communicate your goals to all involved, including primary care, specialists, leadership, and IT partners, and establish with these stakeholders the appropriate support and resources needed to facilitate the development of the program and overcome any barriers to adoption.
Current Status and Future Directions
Our future plans include continuing to optimize the Epic eConsult backend build and workflows using our experience in Allscripts. We have implemented eConsult workflows for use by graduate medical education trainees and advanced practice providers, with attending supervision. Further work is in progress to optimize these workflows, which will allow for appropriate education and supervision without delaying care. Furthermore, we plan to expand the program to include inpatient-to-inpatient and emergency department-to-inpatient eConsults. We will continue to expand the eConsults program by offering additional specialties, engage providers to encourage ongoing participation, and maximize PCP use by continuing to market the program through regular newsletters and email communications. Finally, the eConsults has served as an effective, important resource in the current era of COVID-19 in several ways: it allows for optimization of specialty input in patient care delivery without subjecting more health care workers to unnecessary exposure; saves on utilization of precious personal protective equipment; and enhances our ability to deal with a potential surge by providing access to specialists remotely and electronically all hours of the day, thus expanding care to the evening and weekend hours.
Acknowledgment: The authors thank our steering committee members (Dr. Ralph Cygan, Dr. Andrew Reikes, Dr. Byron Allen, Dr. George Lawry) and IT build team (Lori Bocchicchio, Meghan van Witsen, Jaymee Zillgitt, Tanya Sickles, Dennis Hoang, Jeanette Lisak-Phillips) for their contributions in the design and implementation of our eConsults program. We also thank additional team members Kurt McArthur and Neaktisia Lee for their assistance with generating reports, and Kathy LaPierre, Jennifer Rios, and Debra Webb Torres for their guidance with compliance and billing issues.
Corresponding author: Alpesh N. Amin, MD, MBA, University of California, Irvine, 101 The City Drive South, Building 26, Room 1000, ZC-4076H, Orange, CA 92868; anamin@uci.edu.
Financial disclosures: None.
From the Department of Medicine, University of California, Irvine, Orange, CA.
Abstract
Background: Orange County’s residents have difficulty accessing timely, quality, affordable specialty care services. As the county’s only academic health system, the University of California, Irvine (UCI) aimed to improve specialty care access for the communities it serves by implementing an electronic consultations (eConsults) program that allows primary care providers (PCPs) to efficiently receive specialist recommendations on referral problems that do not require an in-person evaluation.
Objective: To implement an eConsults program at the UCI that enhances access to and the delivery of coordinated specialty care for lower-complexity referral problems.
Methods: We developed custom solutions to integrate eConsults into UCI’s 2 electronic health record platforms. The impact of the eConsults program was assessed by continuously evaluating usage and outcomes. Measures used to track usage included the number of submitted eConsult requests per PCP, the number of completed responses per specialty, and the response time for eConsult requests. Outcome measures included the specialist recommendation (eg, in-office visit, consultation avoided) and physician feedback.
Results: Over 4.5 years, more than 1400 successful eConsults have been completed, and the program has expanded to 17 specialties. The average turnaround time for an eConsult response across all specialties was 1 business day. Moreover, more than 50% of the eConsults received specialty responses within the same day of the eConsult request. Most important, about 80% of eConsult requests were addressed without the need for an in-office visit with a specialist.
Conclusion: The enhanced access to and the delivery of coordinated specialty care provided by eConsults resulted in improved efficiency and specialty access, while likely reducing costs and improving patient satisfaction. The improved communication and collaboration among providers with eConsults has also led to overwhelmingly positive feedback from both PCPs and specialists.
Keywords: electronic consultation; access to care; primary care; specialty referral; telehealth.
Orange County’s growing, aging, and diverse population is driving an increased demand for health care.1 But with the county’s high cost of living and worsening shortage of physicians,1-3 many of its residents are struggling to access timely, quality, affordable care. Access to specialty care services is especially frustrating for many patients and their providers, both primary care providers (PCPs) and specialists, due to problems with the referral process. Many patients experience increased wait times for a visit with a specialist due to poor communication between providers, insufficient guidance on the information or diagnostic results needed by specialists, and lack of care coordination.4-6 One promising approach to overcome these challenges is the use of an electronic consultation, or eConsult, in place of a standard in-person referral. An eConsult is an asynchronous, non-face-to-face, provider-to-provider exchange using a secure electronic communication platform. For appropriate referral problems, the patient is able to receive timely access to specialist expertise through electronic referral by their PCP,7-9 and avoid the time and costs associated with a visit to the specialist,10,11 such as travel, missed work, co-pays, and child-care expenses. Clinical questions addressed using an eConsult system subsequently free up office visit appointment slots, improving access for patients requiring in-office evaluation.8,12
Orange County’s only academic health system, the University of California, Irvine (UCI), serves a population of 3.5 million, and its principal priority is providing the communities in the county (which is the sixth largest in United States) and the surrounding region with the highest quality health care possible. Thus, UCI aimed to improve its referral processes and provide timely access to specialty care for its patients by implementing an eConsults program that allows PCPs to efficiently receive specialist recommendations on referral problems that do not require the specialist to evaluate the patient in person. This report describes our experiences with developing and implementing a custom-built eConsults workflow in UCI’s prior electronic health record (EHR) platform, Allscripts, and subsequently transitioning our mature eConsults program to a new EHR system when UCI adopted Epic. UCI is likely the only academic medical center to have experience in successfully implementing eConsults into 2 different EHR systems.
Setting
UCI’s medical center is a 417-bed acute care hospital providing tertiary and quaternary care, ambulatory and specialty medical clinics, behavioral health care, and rehabilitation services. It is located in Orange, CA, and serves a diverse population of 3.5 million persons with broad health care needs. With more than 400 specialty and primary care physicians, UCI offers a full scope of acute and general care services. It is also the primary teaching location for UCI medical and nursing students, medical residents, and fellows, and is home to Orange County’s only adult Level I and pediatric Level II trauma centers and the regional burn center.
eConsults Program
We designed the initial eConsults program within UCI’s Allscripts EHR platform. Our information technology (IT) build team developed unique “documents-based” eConsults workflows that simplified the process of initiating requests directly from the EHR and facilitated rapid responses from participating specialties. The requesting provider’s eConsults interface was user-friendly, and referring providers were able to initiate an eConsult easily by selecting the customized eConsult icon from the Allscripts main toolbar. To ensure that all relevant information is provided to the specialists, condition-specific templates are embedded in the requesting provider’s eConsults workflow that allow PCPs to enter a focused, patient-specific clinical question and provide guidance on recommended patient information (eg, health history, laboratory results, and digital images) that may help the specialist provide an informed response. The eConsult templates were adapted from standardized forms developed by partner University of California Health Systems in an initiative funded by the University of California Center for Health Quality and Innovation.
To facilitate timely responses from specialists, an innovative notification system was created in the responding provider’s eConsults workflow to automatically send an email to participating specialists when a new eConsult is requested. The responding provider’s workflow also includes an option for the specialist to decline the eConsult if the case is deemed too complex to be addressed electronically. For every completed eConsult that does not result in an in-person patient evaluation, the requesting provider and responding specialist each receives a modest reimbursement, which was initially paid by UCI Health System funds.
Implementation
The design and implementation of the eConsults program began in November 2014, and was guided by a steering committee that included the chair of the department of medicine, chief medical information officer, primary care and specialty physician leads, IT build team, and a project manager. Early on, members of this committee engaged UCI leadership to affirm support for the program and obtain the IT resources needed to build the eConsults workflow. Regular steering committee meetings were established to discuss the design of the workflow, adapt the clinical content of the referral templates, and develop a provider reimbursement plan. After completion of the workflow build, the eConsults system was tested to identify failure points and obtain feedback from users. Prior to going live, the eConsults program was publicized by members of the steering committee through meetings with primary care groups and email communications. Committee members also hosted in-person training and orientation sessions with PCPs and participating specialists, and distributed tip sheets summarizing the steps to complete the PCP and specialist eConsult workflows.
The eConsults workflow build, testing, and launch were completed within 5 months (April 2015; Figure 1). eConsults went live in the 3 initial specialties (endocrinology, cardiology, and rheumatology) that were interested in participating in the first wave of the program. UCI’s eConsults service has subsequently expanded to 17 total specialties (allergy, cardiology, dermatology, endocrinology, gastroenterology, geriatrics, gynecology, hematology, hepatology, infectious disease, nephrology, neurology, palliative care, psychiatry, pulmonary, rheumatology, and sports medicine).
Two and half years after the eConsults program was implemented in Allscripts, UCI adopted a new EHR platform, Epic. By this time, the eConsults service had grown into a mature program with greater numbers of PCP users and submitted eConsults (Figure 2). Using our experience with the Allscripts build, our IT team was able to efficiently transition the eConsults service to the new EHR system. In contrast to the “documents-based” eConsult workflows on Allscripts, our IT team utilized an “orders-based” strategy on Epic, which followed a more traditional approach to requesting a consultation. We re-launched the service in Epic within 3 months (February 2018). However, both platforms utilized user-friendly workflows to achieve similar goals, and the program has continued to grow with respect to the number of users and eConsults.
Measurement/Analysis
The impact of the program was assessed by continuously evaluating usage and outcomes. Measures used to track usage included the number of PCP users, the number of submitted eConsult requests per PCP, and the number of requests per specialty. The response time for eConsult requests and the self-reported amount of time spent by specialists on the response were also tracked. Outcome measures included the specialist recommendation (eg, in-office visit, consultation avoided) and physician feedback. Provider satisfaction was primarily obtained by soliciting feedback from individual eConsult users.
Implementation of this eConsults program constituted a quality improvement activity and did not require Institutional Review Board review.
Results
Since the program was launched in April 2015, more than 1400 eConsults have been completed across 17 specialties (Figure 3). There were 654 completed eConsults on the Allscripts platform, and 808 eConsults have been completed using the Epic platform to date. The busiest eConsult specialties were endocrinology (receiving 276, or 19%, of the eConsults requests), hematology (receiving 249 requests, or 17%), infectious disease (receiving 244 requests, or 17% ), and cardiology (receiving 148 requests, or 10%).
The self-reported amount of time specialists spent on the response was different between the 2 EHR systems (Figure 4). On Allscripts, specialists reported that 23% of eConsults took 10 minutes or less to complete, 47% took 11 to 20 minutes, 23% took 21 to 30 minutes, and 7% took more than 30 minutes. On Epic, specialists reported that 42% of eConsults took 10 minutes or less to complete, 44% took 11 to 20 minutes, 12% took 21 to 30 minutes, and 2% took more than 30 minutes. This difference in time spent fielding eConsults likely represents the subtle nuances between Allscripts’ “documents-based” and Epic’s “orders-based” workflows.
As a result of the automated notification system that was introduced early in the eConsults implementation process on Allscripts, the specialty response times were much faster than the expected 3 business days’ turnaround goal instituted by the Center for Health Quality and Innovation initiative, regardless of the EHR platform used. In fact, the average turnaround time for an eConsult response across all specialties was 1 business day, which was similar for both EHR systems (Figure 5). Furthermore, more than 50% of the eConsults on both EHR systems received specialist responses within the same day of the eConsult request (63% on Allscripts, 54% on Epic). There was a small decrease in the percentage of same-day responses when we transitioned to Epic, likely because the functionality of an automated notification email could not be restored in Epic. Regardless, the specialty response times on Epic remained expeditious, likely because the automated notifications on Allscripts instilled good practices for the specialists, and regularly checking for new eConsult requests became an ingrained behavior.
Our most important finding was that approximately 80% of eConsult requests were addressed without the need for an in-office visit with a specialist. This measure was similar for both EHR platforms (83% on Allscripts and 78% on Epic).
Provider feedback has been overwhelmingly positive. PCPs are impressed with the robust educational content of the eConsult responses, since the goal for specialists is to justify their recommendations. Specialists appreciate the convenience and efficiency that eConsults offer, as well as the improved communication and collaboration among physicians. eConsults have been especially beneficial to PCPs at UCI’s Family Health Centers, who are now able to receive subspecialty consultations from UCI specialists despite insurance barriers.
Discussion
Our eConsults program uniquely contrasts with other programs because UCI is likely the only academic medical center to have experience in successfully incorporating eConsults into 2 different EHR systems: initial development of the eConsults workflow in UCI’s existing Allscripts EHR platform, and subsequently transitioning a mature eConsults program to a new EHR system when the institution adopted Epic.
We measured the impact of the eConsults program on access to care by the response time for eConsult requests and the percentage of eConsults that averted an in-office visit with a specialist. We found that the eConsults program at UCI provided our PCPs access to specialist consultations in a timely manner, with much shorter response times than standard in-person referrals. The average turnaround time for an eConsult response we reported is consistent with findings from other studies.12-15 Additionally, our program was able to address about 80% of its eConsults electronically, helping to reduce unnecessary in-person specialist referrals. In the literature, the percentage of eConsults that avoided an in-person specialist visit varies widely.8,12-16
We reported very positive feedback from both PCPs and specialists on UCI’s eConsults service. Similarly, other studies described PCP satisfaction with their respective eConsults programs to be uniformly high,8,9,13,14,17-19 though some reported that the level of satisfaction among specialists was more varied.18-21
Lessons Learned
The successful design and implementation of our eConsults program began with assembling the right clinical champions and technology partners for our steering committee. Establishing regular steering committee meetings helped maintain an appropriate timeline for completion of different aspects of the project. Engaging support from UCI’s leadership also provided us with a dedicated IT team that helped us with the build, training resources, troubleshooting issues, and reporting for the project.
Our experience with implementing the eConsults program on 2 different EHR systems highlighted the importance of creating efficient, user-friendly workflows to foster provider adoption and achieve sustainability. Allscripts’ open platform gave our IT team the ability to create a homegrown solution to implementing an eConsult model that was simple and easy to use. The Epic platform’s interoperability allowed us to leverage our learnings from the Allscripts build to efficiently implement eConsults in Epic.
We also found that providing modest incentive payments or reimbursements to both PCPs and specialists for each completed eConsult helps with both adoption and program sustainability. Initially, credit for the eConsult work was paid by internal UCI Health System funds. Two payers, UC Care (a preferred provider organization plan created just for the University of California) and more recently, the Centers for Medicare & Medicaid Services, have agreed to reimburse for outpatient eConsults. Securing additional payers for reimbursement of the eConsult service will not only ensure the program’s long-term sustainability, but also represents an acknowledgment of the value of eConsults in supporting access to care.
Applicability
Other health care settings that are experiencing issues with specialty care access can successfully implement their own eConsults program by employing strategies similar to those described in this report—assembling the right team, creating user-friendly workflows, and providing incentives. Our advice for successful implementation is to clearly communicate your goals to all involved, including primary care, specialists, leadership, and IT partners, and establish with these stakeholders the appropriate support and resources needed to facilitate the development of the program and overcome any barriers to adoption.
Current Status and Future Directions
Our future plans include continuing to optimize the Epic eConsult backend build and workflows using our experience in Allscripts. We have implemented eConsult workflows for use by graduate medical education trainees and advanced practice providers, with attending supervision. Further work is in progress to optimize these workflows, which will allow for appropriate education and supervision without delaying care. Furthermore, we plan to expand the program to include inpatient-to-inpatient and emergency department-to-inpatient eConsults. We will continue to expand the eConsults program by offering additional specialties, engage providers to encourage ongoing participation, and maximize PCP use by continuing to market the program through regular newsletters and email communications. Finally, the eConsults has served as an effective, important resource in the current era of COVID-19 in several ways: it allows for optimization of specialty input in patient care delivery without subjecting more health care workers to unnecessary exposure; saves on utilization of precious personal protective equipment; and enhances our ability to deal with a potential surge by providing access to specialists remotely and electronically all hours of the day, thus expanding care to the evening and weekend hours.
Acknowledgment: The authors thank our steering committee members (Dr. Ralph Cygan, Dr. Andrew Reikes, Dr. Byron Allen, Dr. George Lawry) and IT build team (Lori Bocchicchio, Meghan van Witsen, Jaymee Zillgitt, Tanya Sickles, Dennis Hoang, Jeanette Lisak-Phillips) for their contributions in the design and implementation of our eConsults program. We also thank additional team members Kurt McArthur and Neaktisia Lee for their assistance with generating reports, and Kathy LaPierre, Jennifer Rios, and Debra Webb Torres for their guidance with compliance and billing issues.
Corresponding author: Alpesh N. Amin, MD, MBA, University of California, Irvine, 101 The City Drive South, Building 26, Room 1000, ZC-4076H, Orange, CA 92868; anamin@uci.edu.
Financial disclosures: None.
1. County of Orange, Health Care Agency, Public Health Services. Orange County Health Profile 2013.
2. Coffman JM, Fix M Ko, M. California physician supply and distribution: headed for a drought? California Health Care Foundation, June 2018.
3. Spetz J, Coffman J, Geyn I. California’s primary care workforce: forecasted supply, demand, and pipeline of trainees, 2016-2030. Healthforce Center at the University of California, San Francisco, August 2017.
4. Gandhi TK, Sittig DF, Franklin M, et al. Communication breakdown in the outpatient referral process. J Gen Intern Med. 2000;15:626-631.
5. McPhee SJ, Lo B, Saika GY, Meltzer R. How good is communication between primary care physicians and subspecialty consultants? Arch Intern Med. 1984;144:1265-1268.
6. Mehrotra A, Forrest CB, Lin CY. Dropping the baton: specialty referrals in the United States. Milbank Q. 2011;89:39-68.
7. Wrenn K, Catschegn S, Cruz M, et al. Analysis of an electronic consultation program at an academic medical centre: Primary care provider questions, specialist responses, and primary care provider actions. J Telemed Telecare. 2017;23: 217-224.
8. Gleason N, Prasad PA, Ackerman S, et al. Adoption and impact of an eConsult system in a fee-for-service setting. Healthc (Amst). 2017;5(1-2):40-45.
9. Stoves J, Connolly J, Cheung CK, et al. Electronic consultation as an alternative to hospital referral for patients with chronic kidney disease: a novel application for networked electronic health records to improve the accessibility and efficiency of healthcare. Qual Saf Health Care. 2010;19: e54.
10. Datta SK, Warshaw EM, Edison KE, et al. Cost and utility analysis of a store-and-forward teledermatology referral system: a randomized clinical trial. JAMA Dermatol. 2015;151:1323-1329.
11. Liddy C, Drosinis P, Deri Armstrong C, et al. What are the cost savings associated with providing access to specialist care through the Champlain BASE eConsult service? A costing evaluation. BMJ Open. 2016;6:e010920.
12. Barnett ML, Yee HF Jr, Mehrotra A, Giboney P. Los Angeles safety-net program eConsult system was rapidly adopted and decreased wait times to see specialists. Health Aff. 2017;36:492-499.
13. Malagrino GD, Chaudhry R, Gardner M, et al. A study of 6,000 electronic specialty consultations for person-centered care at The Mayo Clinic. Int J Person Centered Med. 2012;2:458-466.
14. Keely E, Liddy C, Afkham A. Utilization, benefits, and impact of an e-consultation service across diverse specialties and primary care providers. Telemed J E Health. 2013;19:733-738.
15. Scherpbier-de Haan ND, van Gelder VA, Van Weel C, et al. Initial implementation of a web-based consultation process for patients with chronic kidney disease. Ann Fam Med. 2013;11:151-156.
16. Palen TE, Price D, Shetterly S, Wallace KB. Comparing virtual consults to traditional consults using an electronic health record: an observational case-control study. BMC Med Inform Decis Mak. 2012;12:65.
17. Liddy C, Afkham A, Drosinis P, et al. Impact of and satisfaction with a new eConsult service: a mixed methods study of primary care providers. J Am Board Fam Med. 2015;28:394-403.
18. Angstman KB, Adamson SC, Furst JW, et al. Provider satisfaction with virtual specialist consultations in a family medicine department. Health Care Manag (Frederick). 2009;28:14-18.
19. McAdams M, Cannavo L, Orlander JD. A medical specialty e-consult program in a VA health care system. Fed Pract. 2014; 31:26–31.
20. Keely E, Williams R, Epstein G, et al. Specialist perspectives on Ontario Provincial electronic consultation services. Telemed J E Health. 2019;25:3-10.
21. Kim-Hwang JE, Chen AH, Bell DS, et al. Evaluating electronic referrals for specialty care at a public hospital. J Gen Intern Med. 2010;25:1123-1128.
1. County of Orange, Health Care Agency, Public Health Services. Orange County Health Profile 2013.
2. Coffman JM, Fix M Ko, M. California physician supply and distribution: headed for a drought? California Health Care Foundation, June 2018.
3. Spetz J, Coffman J, Geyn I. California’s primary care workforce: forecasted supply, demand, and pipeline of trainees, 2016-2030. Healthforce Center at the University of California, San Francisco, August 2017.
4. Gandhi TK, Sittig DF, Franklin M, et al. Communication breakdown in the outpatient referral process. J Gen Intern Med. 2000;15:626-631.
5. McPhee SJ, Lo B, Saika GY, Meltzer R. How good is communication between primary care physicians and subspecialty consultants? Arch Intern Med. 1984;144:1265-1268.
6. Mehrotra A, Forrest CB, Lin CY. Dropping the baton: specialty referrals in the United States. Milbank Q. 2011;89:39-68.
7. Wrenn K, Catschegn S, Cruz M, et al. Analysis of an electronic consultation program at an academic medical centre: Primary care provider questions, specialist responses, and primary care provider actions. J Telemed Telecare. 2017;23: 217-224.
8. Gleason N, Prasad PA, Ackerman S, et al. Adoption and impact of an eConsult system in a fee-for-service setting. Healthc (Amst). 2017;5(1-2):40-45.
9. Stoves J, Connolly J, Cheung CK, et al. Electronic consultation as an alternative to hospital referral for patients with chronic kidney disease: a novel application for networked electronic health records to improve the accessibility and efficiency of healthcare. Qual Saf Health Care. 2010;19: e54.
10. Datta SK, Warshaw EM, Edison KE, et al. Cost and utility analysis of a store-and-forward teledermatology referral system: a randomized clinical trial. JAMA Dermatol. 2015;151:1323-1329.
11. Liddy C, Drosinis P, Deri Armstrong C, et al. What are the cost savings associated with providing access to specialist care through the Champlain BASE eConsult service? A costing evaluation. BMJ Open. 2016;6:e010920.
12. Barnett ML, Yee HF Jr, Mehrotra A, Giboney P. Los Angeles safety-net program eConsult system was rapidly adopted and decreased wait times to see specialists. Health Aff. 2017;36:492-499.
13. Malagrino GD, Chaudhry R, Gardner M, et al. A study of 6,000 electronic specialty consultations for person-centered care at The Mayo Clinic. Int J Person Centered Med. 2012;2:458-466.
14. Keely E, Liddy C, Afkham A. Utilization, benefits, and impact of an e-consultation service across diverse specialties and primary care providers. Telemed J E Health. 2013;19:733-738.
15. Scherpbier-de Haan ND, van Gelder VA, Van Weel C, et al. Initial implementation of a web-based consultation process for patients with chronic kidney disease. Ann Fam Med. 2013;11:151-156.
16. Palen TE, Price D, Shetterly S, Wallace KB. Comparing virtual consults to traditional consults using an electronic health record: an observational case-control study. BMC Med Inform Decis Mak. 2012;12:65.
17. Liddy C, Afkham A, Drosinis P, et al. Impact of and satisfaction with a new eConsult service: a mixed methods study of primary care providers. J Am Board Fam Med. 2015;28:394-403.
18. Angstman KB, Adamson SC, Furst JW, et al. Provider satisfaction with virtual specialist consultations in a family medicine department. Health Care Manag (Frederick). 2009;28:14-18.
19. McAdams M, Cannavo L, Orlander JD. A medical specialty e-consult program in a VA health care system. Fed Pract. 2014; 31:26–31.
20. Keely E, Williams R, Epstein G, et al. Specialist perspectives on Ontario Provincial electronic consultation services. Telemed J E Health. 2019;25:3-10.
21. Kim-Hwang JE, Chen AH, Bell DS, et al. Evaluating electronic referrals for specialty care at a public hospital. J Gen Intern Med. 2010;25:1123-1128.