User login
Where Leading GOP Presidential Candidates Stand on Health Policies
As the long 2016 presidential election season draws on, Republican hopefuls strive to stand out among their fellow party candidates; however, many in the running remain tacit about specific policies on issues ranging from immigration to gun control and healthcare.
“Many of these candidates … do not feel like getting involved in an extensive policy discussion will influence whether they win Iowa and New Hampshire,” says Robert Blendon, ScD, professor of health policy and political analysis at the Harvard School of Public Health and Harvard Kennedy School of Government in Cambridge, Mass. “They see it as a distraction, because the people voting are not asking them.”
For physicians and others passionate about healthcare, “it’s very frustrating,” Dr. Blendon says. “People who are on the Republican side want a replacement [for the Affordable Care Act], but they are not driven—I have seen the surveys—to want to really know the details of that replacement.”
GOP candidates share many common ideas about the U.S. health system. Most say they want to allow people under age 26 to remain on their parents’ health plans and believe people with preexisting conditions should have access to coverage, generally through the creation of state-based, high-risk insurance pools. They believe expanded health savings accounts will give patients more skin in the game, and, across the board, they have vowed to “repeal and replace Obamacare.”
Listen to more of our interview with Robert Blendon, ScD
However, “with more than 10 candidates, there is going to be variation,” Dr. Blendon adds.
For instance, former Florida Governor Jeb Bush has proposed the Conservative Plan for 21st Century Health, which aims to “lower costs,” “promote innovation,” and “return power to states.”
Neurosurgeon Ben Carson originally suggested he would “abolish” Medicare and instead provide seniors with a $2,000-a-year federal subsidy to purchase private insurance. He has backtracked that idea and, in December 2015, issued a report highlighting the pillars of his health plan, which include creating “health empowerment accounts” and raising the Medicare age to 70.
New Jersey Governor Chris Christie’s plan suggests a priority for veterans, including the formation of a federal Secretary of Veterans Affairs, while Carly Fiorina says that “every healthcare provider “ought to publish its costs, its prices, its outcomes” so patients know what they are buying.
“As the field on the Republican side narrows, I think we will start to see more pressure on them to flesh those principles out a little bit more,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami (Fla.) Jackson Memorial Hospital and a member of SHM’s Public Policy Committee.
Some GOP candidates, like Kentucky Senator and ophthalmologist Rand Paul, have proposed reforming medical malpractice. Some wish to make insurance portable from one job to the next, like former Arkansas Governor Mike Huckabee, or across state lines, as Ohio Governor John Kasich has proposed.
Some of these ideas, says hospitalist and SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, MHM, “have been adequately dismembered, and they’re not going to carry weight.
“Buying insurance across state lines, fixing malpractice—that is not going to fix the healthcare system,” says Dr. Flansbaum, clinical professor of medicine at NYU School of Medicine in New York City.
Overall, a Republican-sponsored healthcare system will not guarantee the same level of comprehensive benefits patients have now under the ACA, Dr. Blendon says, and, in general, subsidies and tax credits will be less generous than they are today, in turn reducing federal expenditures.
Most Republican candidates are in favor of some version of free market healthcare, but Dr. Flansbaum points out that “there are so many imperfections in the market, everything from people having asymmetric information—a physician knows a lot more than a patient does—to opaque pricing,” he says. “It’s not exchanging goods like we are used to.”
Republicans are generally committed to “less federal government, less expenditures, more choices, and less expensive benefits,” in healthcare, but Dr. Blendon says the system “would not go back to 2009.”
For hospitalists interested in election-year or other healthcare policy issues, Dr. Flansbaum suggests getting involved in the SHM committee, visiting the advocacy section of the SHM website, and reaching out to local representatives and others who write and vote on laws.
“How do you affect change?” he asks. “It’s not sitting in the breakfast lounge at the hospital bellyaching to your colleagues.” TH
Editor's note: update Jan. 4, 2016.
Kelly April Tyrrell is a freelance writer in Madison, Wis.
As the long 2016 presidential election season draws on, Republican hopefuls strive to stand out among their fellow party candidates; however, many in the running remain tacit about specific policies on issues ranging from immigration to gun control and healthcare.
“Many of these candidates … do not feel like getting involved in an extensive policy discussion will influence whether they win Iowa and New Hampshire,” says Robert Blendon, ScD, professor of health policy and political analysis at the Harvard School of Public Health and Harvard Kennedy School of Government in Cambridge, Mass. “They see it as a distraction, because the people voting are not asking them.”
For physicians and others passionate about healthcare, “it’s very frustrating,” Dr. Blendon says. “People who are on the Republican side want a replacement [for the Affordable Care Act], but they are not driven—I have seen the surveys—to want to really know the details of that replacement.”
GOP candidates share many common ideas about the U.S. health system. Most say they want to allow people under age 26 to remain on their parents’ health plans and believe people with preexisting conditions should have access to coverage, generally through the creation of state-based, high-risk insurance pools. They believe expanded health savings accounts will give patients more skin in the game, and, across the board, they have vowed to “repeal and replace Obamacare.”
Listen to more of our interview with Robert Blendon, ScD
However, “with more than 10 candidates, there is going to be variation,” Dr. Blendon adds.
For instance, former Florida Governor Jeb Bush has proposed the Conservative Plan for 21st Century Health, which aims to “lower costs,” “promote innovation,” and “return power to states.”
Neurosurgeon Ben Carson originally suggested he would “abolish” Medicare and instead provide seniors with a $2,000-a-year federal subsidy to purchase private insurance. He has backtracked that idea and, in December 2015, issued a report highlighting the pillars of his health plan, which include creating “health empowerment accounts” and raising the Medicare age to 70.
New Jersey Governor Chris Christie’s plan suggests a priority for veterans, including the formation of a federal Secretary of Veterans Affairs, while Carly Fiorina says that “every healthcare provider “ought to publish its costs, its prices, its outcomes” so patients know what they are buying.
“As the field on the Republican side narrows, I think we will start to see more pressure on them to flesh those principles out a little bit more,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami (Fla.) Jackson Memorial Hospital and a member of SHM’s Public Policy Committee.
Some GOP candidates, like Kentucky Senator and ophthalmologist Rand Paul, have proposed reforming medical malpractice. Some wish to make insurance portable from one job to the next, like former Arkansas Governor Mike Huckabee, or across state lines, as Ohio Governor John Kasich has proposed.
Some of these ideas, says hospitalist and SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, MHM, “have been adequately dismembered, and they’re not going to carry weight.
“Buying insurance across state lines, fixing malpractice—that is not going to fix the healthcare system,” says Dr. Flansbaum, clinical professor of medicine at NYU School of Medicine in New York City.
Overall, a Republican-sponsored healthcare system will not guarantee the same level of comprehensive benefits patients have now under the ACA, Dr. Blendon says, and, in general, subsidies and tax credits will be less generous than they are today, in turn reducing federal expenditures.
Most Republican candidates are in favor of some version of free market healthcare, but Dr. Flansbaum points out that “there are so many imperfections in the market, everything from people having asymmetric information—a physician knows a lot more than a patient does—to opaque pricing,” he says. “It’s not exchanging goods like we are used to.”
Republicans are generally committed to “less federal government, less expenditures, more choices, and less expensive benefits,” in healthcare, but Dr. Blendon says the system “would not go back to 2009.”
For hospitalists interested in election-year or other healthcare policy issues, Dr. Flansbaum suggests getting involved in the SHM committee, visiting the advocacy section of the SHM website, and reaching out to local representatives and others who write and vote on laws.
“How do you affect change?” he asks. “It’s not sitting in the breakfast lounge at the hospital bellyaching to your colleagues.” TH
Editor's note: update Jan. 4, 2016.
Kelly April Tyrrell is a freelance writer in Madison, Wis.
As the long 2016 presidential election season draws on, Republican hopefuls strive to stand out among their fellow party candidates; however, many in the running remain tacit about specific policies on issues ranging from immigration to gun control and healthcare.
“Many of these candidates … do not feel like getting involved in an extensive policy discussion will influence whether they win Iowa and New Hampshire,” says Robert Blendon, ScD, professor of health policy and political analysis at the Harvard School of Public Health and Harvard Kennedy School of Government in Cambridge, Mass. “They see it as a distraction, because the people voting are not asking them.”
For physicians and others passionate about healthcare, “it’s very frustrating,” Dr. Blendon says. “People who are on the Republican side want a replacement [for the Affordable Care Act], but they are not driven—I have seen the surveys—to want to really know the details of that replacement.”
GOP candidates share many common ideas about the U.S. health system. Most say they want to allow people under age 26 to remain on their parents’ health plans and believe people with preexisting conditions should have access to coverage, generally through the creation of state-based, high-risk insurance pools. They believe expanded health savings accounts will give patients more skin in the game, and, across the board, they have vowed to “repeal and replace Obamacare.”
Listen to more of our interview with Robert Blendon, ScD
However, “with more than 10 candidates, there is going to be variation,” Dr. Blendon adds.
For instance, former Florida Governor Jeb Bush has proposed the Conservative Plan for 21st Century Health, which aims to “lower costs,” “promote innovation,” and “return power to states.”
Neurosurgeon Ben Carson originally suggested he would “abolish” Medicare and instead provide seniors with a $2,000-a-year federal subsidy to purchase private insurance. He has backtracked that idea and, in December 2015, issued a report highlighting the pillars of his health plan, which include creating “health empowerment accounts” and raising the Medicare age to 70.
New Jersey Governor Chris Christie’s plan suggests a priority for veterans, including the formation of a federal Secretary of Veterans Affairs, while Carly Fiorina says that “every healthcare provider “ought to publish its costs, its prices, its outcomes” so patients know what they are buying.
“As the field on the Republican side narrows, I think we will start to see more pressure on them to flesh those principles out a little bit more,” says Joshua Lenchus, DO, RPh, FACP, SFHM, a hospitalist at the University of Miami (Fla.) Jackson Memorial Hospital and a member of SHM’s Public Policy Committee.
Some GOP candidates, like Kentucky Senator and ophthalmologist Rand Paul, have proposed reforming medical malpractice. Some wish to make insurance portable from one job to the next, like former Arkansas Governor Mike Huckabee, or across state lines, as Ohio Governor John Kasich has proposed.
Some of these ideas, says hospitalist and SHM Public Policy Committee member Bradley Flansbaum, DO, MPH, MHM, “have been adequately dismembered, and they’re not going to carry weight.
“Buying insurance across state lines, fixing malpractice—that is not going to fix the healthcare system,” says Dr. Flansbaum, clinical professor of medicine at NYU School of Medicine in New York City.
Overall, a Republican-sponsored healthcare system will not guarantee the same level of comprehensive benefits patients have now under the ACA, Dr. Blendon says, and, in general, subsidies and tax credits will be less generous than they are today, in turn reducing federal expenditures.
Most Republican candidates are in favor of some version of free market healthcare, but Dr. Flansbaum points out that “there are so many imperfections in the market, everything from people having asymmetric information—a physician knows a lot more than a patient does—to opaque pricing,” he says. “It’s not exchanging goods like we are used to.”
Republicans are generally committed to “less federal government, less expenditures, more choices, and less expensive benefits,” in healthcare, but Dr. Blendon says the system “would not go back to 2009.”
For hospitalists interested in election-year or other healthcare policy issues, Dr. Flansbaum suggests getting involved in the SHM committee, visiting the advocacy section of the SHM website, and reaching out to local representatives and others who write and vote on laws.
“How do you affect change?” he asks. “It’s not sitting in the breakfast lounge at the hospital bellyaching to your colleagues.” TH
Editor's note: update Jan. 4, 2016.
Kelly April Tyrrell is a freelance writer in Madison, Wis.
New Medicare Rule Will Reimburse Physicians for Advance Care Planning
Hospitalists care for patients with the most serious, chronic, and complex illnesses. As a result, they are often faced with the daunting task of counseling their patients to help them clearly define their end-of-life wishes. The mere subject of death is met with apprehension and avoidance, but its inevitability warrants an early discussion.
End-of-life care, also known as Advance Care Planning (ACP), enables patients to formulate advanced directives: a living will, the designation of a healthcare proxy, Medical Orders for Life-Sustaining Treatment (MOLST), and the preparation for hospice care, among others. Patients should start thinking about their healthcare options and share such important decisions with their physicians and family before the need for hospitalization.
On October 30, 2015, the Centers for Medicare and Medicaid Services (CMS) released the final payment rules for Medicare reimbursement of physicians who consult with their patients on advance care planning. This separate payment system under the 2016 Physician Fee Schedule will impact the almost 55 million Medicare beneficiaries and their healthcare providers.
Effective January 1, 2016, Medicare will pay $86 for 30 minutes of ACP in a physician’s office and will pay $80 for the same service in a hospital (CPT billing code 99497). In both settings, Medicare will pay up to $75 for 30 additional minutes of consultation (add-on CPT billing code 99498). Such counseling can take place during a senior’s annual wellness visit or during a routine office visit and at various stages of health, always “at the discretion of the beneficiary.”
Six years ago, proposed legislation on Medicare reimbursement for ACP under the Accountable Care Act (ACA) sparked political debate over fears that the implementation of so-called “death panels” could influence decisions to avoid medical care. The goal was to reduce healthcare costs, but these controversial provisions were dropped with the passage of the ACA. This time, there was less resistance.
Proponents of this new legislation, such as the American Medical Association and the American Academy of Palliative and Hospice Medicine, say that this rule will encourage physicians to make time for these lengthy discussions and facilitate patient choices while improving quality of care for seniors. Opponents, including the Association of American Physicians and Surgeons, contend that such payments will “create financial incentives to persuade patients to consent to the denial of care.”
Patrick Conway, MD, CMS' chief medical officer, told the New York Times, "We received overwhelmingly positive comments about the importance of these conversations between physicians and patients. We know that many patients and families want to have these discussions."
Future endeavors should focus on efforts to improve the quality of delivering end-of-life care that honors and upholds a patient’s wishes. Strengthening the clinical training of physicians in palliative care, developing quality metrics and standards, and educating the public should remain a top priority.
Will tying a financial incentive to these services have an impact on the cost and quality of care delivered? Hospitalists can begin billing for valuable services they are already providing on a daily basis, and can better coordinate inpatient medical care when more seniors have clear advanced directives. TH
Dr. Zeitoun is a member of Team Hospitalist.
Hospitalists care for patients with the most serious, chronic, and complex illnesses. As a result, they are often faced with the daunting task of counseling their patients to help them clearly define their end-of-life wishes. The mere subject of death is met with apprehension and avoidance, but its inevitability warrants an early discussion.
End-of-life care, also known as Advance Care Planning (ACP), enables patients to formulate advanced directives: a living will, the designation of a healthcare proxy, Medical Orders for Life-Sustaining Treatment (MOLST), and the preparation for hospice care, among others. Patients should start thinking about their healthcare options and share such important decisions with their physicians and family before the need for hospitalization.
On October 30, 2015, the Centers for Medicare and Medicaid Services (CMS) released the final payment rules for Medicare reimbursement of physicians who consult with their patients on advance care planning. This separate payment system under the 2016 Physician Fee Schedule will impact the almost 55 million Medicare beneficiaries and their healthcare providers.
Effective January 1, 2016, Medicare will pay $86 for 30 minutes of ACP in a physician’s office and will pay $80 for the same service in a hospital (CPT billing code 99497). In both settings, Medicare will pay up to $75 for 30 additional minutes of consultation (add-on CPT billing code 99498). Such counseling can take place during a senior’s annual wellness visit or during a routine office visit and at various stages of health, always “at the discretion of the beneficiary.”
Six years ago, proposed legislation on Medicare reimbursement for ACP under the Accountable Care Act (ACA) sparked political debate over fears that the implementation of so-called “death panels” could influence decisions to avoid medical care. The goal was to reduce healthcare costs, but these controversial provisions were dropped with the passage of the ACA. This time, there was less resistance.
Proponents of this new legislation, such as the American Medical Association and the American Academy of Palliative and Hospice Medicine, say that this rule will encourage physicians to make time for these lengthy discussions and facilitate patient choices while improving quality of care for seniors. Opponents, including the Association of American Physicians and Surgeons, contend that such payments will “create financial incentives to persuade patients to consent to the denial of care.”
Patrick Conway, MD, CMS' chief medical officer, told the New York Times, "We received overwhelmingly positive comments about the importance of these conversations between physicians and patients. We know that many patients and families want to have these discussions."
Future endeavors should focus on efforts to improve the quality of delivering end-of-life care that honors and upholds a patient’s wishes. Strengthening the clinical training of physicians in palliative care, developing quality metrics and standards, and educating the public should remain a top priority.
Will tying a financial incentive to these services have an impact on the cost and quality of care delivered? Hospitalists can begin billing for valuable services they are already providing on a daily basis, and can better coordinate inpatient medical care when more seniors have clear advanced directives. TH
Dr. Zeitoun is a member of Team Hospitalist.
Hospitalists care for patients with the most serious, chronic, and complex illnesses. As a result, they are often faced with the daunting task of counseling their patients to help them clearly define their end-of-life wishes. The mere subject of death is met with apprehension and avoidance, but its inevitability warrants an early discussion.
End-of-life care, also known as Advance Care Planning (ACP), enables patients to formulate advanced directives: a living will, the designation of a healthcare proxy, Medical Orders for Life-Sustaining Treatment (MOLST), and the preparation for hospice care, among others. Patients should start thinking about their healthcare options and share such important decisions with their physicians and family before the need for hospitalization.
On October 30, 2015, the Centers for Medicare and Medicaid Services (CMS) released the final payment rules for Medicare reimbursement of physicians who consult with their patients on advance care planning. This separate payment system under the 2016 Physician Fee Schedule will impact the almost 55 million Medicare beneficiaries and their healthcare providers.
Effective January 1, 2016, Medicare will pay $86 for 30 minutes of ACP in a physician’s office and will pay $80 for the same service in a hospital (CPT billing code 99497). In both settings, Medicare will pay up to $75 for 30 additional minutes of consultation (add-on CPT billing code 99498). Such counseling can take place during a senior’s annual wellness visit or during a routine office visit and at various stages of health, always “at the discretion of the beneficiary.”
Six years ago, proposed legislation on Medicare reimbursement for ACP under the Accountable Care Act (ACA) sparked political debate over fears that the implementation of so-called “death panels” could influence decisions to avoid medical care. The goal was to reduce healthcare costs, but these controversial provisions were dropped with the passage of the ACA. This time, there was less resistance.
Proponents of this new legislation, such as the American Medical Association and the American Academy of Palliative and Hospice Medicine, say that this rule will encourage physicians to make time for these lengthy discussions and facilitate patient choices while improving quality of care for seniors. Opponents, including the Association of American Physicians and Surgeons, contend that such payments will “create financial incentives to persuade patients to consent to the denial of care.”
Patrick Conway, MD, CMS' chief medical officer, told the New York Times, "We received overwhelmingly positive comments about the importance of these conversations between physicians and patients. We know that many patients and families want to have these discussions."
Future endeavors should focus on efforts to improve the quality of delivering end-of-life care that honors and upholds a patient’s wishes. Strengthening the clinical training of physicians in palliative care, developing quality metrics and standards, and educating the public should remain a top priority.
Will tying a financial incentive to these services have an impact on the cost and quality of care delivered? Hospitalists can begin billing for valuable services they are already providing on a daily basis, and can better coordinate inpatient medical care when more seniors have clear advanced directives. TH
Dr. Zeitoun is a member of Team Hospitalist.
Medicare’s Readmission Reduction Program Cuts $420M to U.S. Hospitals This Year
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
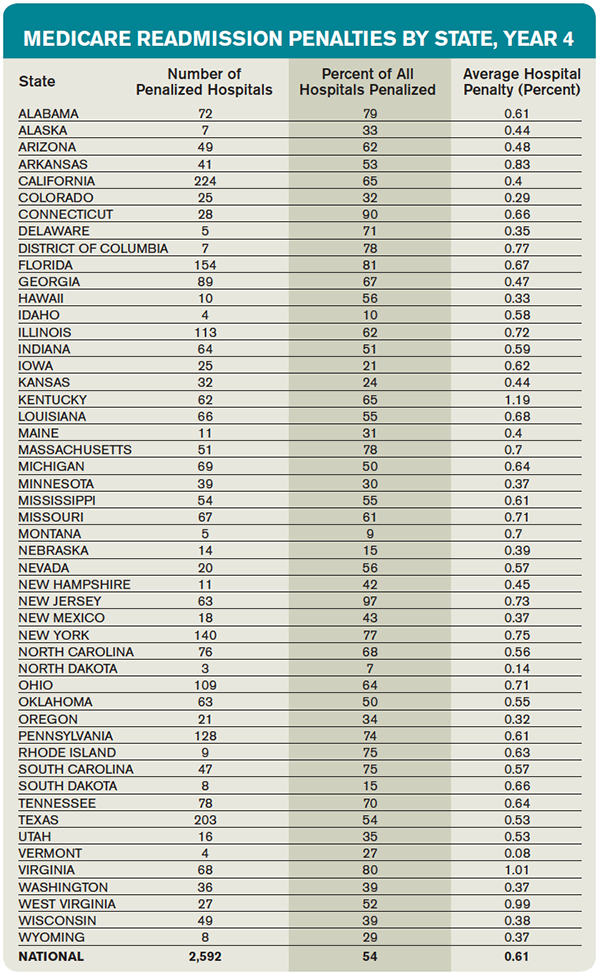
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.

References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.
References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
It’s that time of year again … the time when hospitals around the country are being notified of their 30-day readmission penalties from the Centers for Medicare and Medicaid Services (CMS). Now in the fourth year of the program, many hospitals have come to dread the announcement of how much they are being penalized each year.1
This year, the readmission reduction program will decrease Medicare payments within a total of 2,592 U.S. hospitals, for a combined total of $420 million. This year’s program included readmissions from July 2011 to June 2014; the program uses a three-year rolling average for its calculations.2
The readmission program, which initially was implemented through the Affordable Care Act in 2012, aimed to penalize hospitals with higher than expected 30-day readmission rates on select conditions (currently heart attack, heart failure, pneumonia, COPD, and hip/knee replacements). Medicare estimates that it spends $17 billion a year in avoidable readmissions, which prompted the initial support for the program. For each condition, CMS calculates expected readmission rates (based on risk adjustment models that include age, severity of illness, and comorbid conditions) and observed rates, and then calculates an “excess readmission ratio” for each hospital. Based on the overall ratio, the hospital is penalized up to 3% of its Medicare payments for all inpatient stays for that fiscal year. Each year, CMS reassesses the readmission rates for hospitals and readjusts the magnitude of the penalty. The purpose of the program is to incent hospitals to invest in discharge planning and care coordination efforts and do everything possible to avoid readmissions.1
Who Gets Penalized?
This year, most eligible hospitals were penalized to some extent, and all but 209 of the hospitals that were penalized last year were penalized again.
The average Medicare payment reduction will be 0.61% per patient stay.
A total of 506 hospitals will lose at least 1% of their Medicare payments, and 38 hospitals will receive the maximum 3% penalty.
Unfortunately, safety net hospitals were about 60% more likely than other hospitals to have been penalized in all three years of the program. In addition, hospitals with the lowest profit margins were 36% more likely to be penalized than those with higher margins.
Some states were disproportionately affected, with at least three-quarters of hospitals affected in Alabama, Connecticut, Florida, Massachusetts, New Jersey, New York, Rhode Island, South Carolina, Virginia, and the District of Columbia. States that fared the best were Idaho, Iowa, Kansas, Montana, Nebraska, North Dakota, and South Dakota.
Most of the 2,232 hospitals that avoided a penalty were spared because they were exempted from the program (Veterans Affairs hospitals, children’s hospitals, critical access hospitals, or those with too few Medicare patients), not because of exceptional performance.
Does the Program Work?
Despite criticism, there is no doubt that this program has forced hospitals to pay keen attention to transitions of care and avoidable readmissions. And it does appear to be an effective strategy for CMS to achieve its goals; there has been an overall decrease in 30-day readmission rates among Medicare recipients since the program began, in all types of hospitals.
Compared to 2012, there were 100,000 fewer readmissions among Medicare beneficiaries in the U.S. in 2013. As such, there is no evidence that the program will be discontinued, although it will hopefully be altered in some key aspects.3
What the Future Holds
The program has been criticized on many fronts. For one, it recalculates a three-year rolling average each year, which makes it incredibly difficult to “wash out” older (poor) performance and get off the penalty list.
In addition, critics have pointed out that the program fails to take into account the socioeconomic background of patients when assessing readmission penalties. Many argue that social determinants of readmissions that are beyond the immediate control of a hospital system can have a huge impact on readmission rates.
The National Quality Forum is examining the impact of these factors on readmissions, but this evaluation likely will take years.
In the meantime, the Hospital Readmissions Program Accuracy and Accountability Act of 2014 has been introduced as a bill that would require CMS to factor socioeconomic status into the equation when determining readmission penalties.
What All This Means for Hospitalists
All of us working within the confines of the current program can do a few things to improve our understanding and our hospitals’ performance:
- If your hospital is one that incurred a penalty, know that most “eligible” hospitals also incurred a penalty.
- Look at how your hospital fared within your state and find out if you are above or below average in the amount.3
- Continue to focus on exemplary care transition protocols, policies, and programs within your hospital system, because the penalties are unlikely to go away and are very likely to expand over time.
- Support any advocacy efforts toward improving risk adjustment methodologies for readmissions; all hospitals are likely to benefit from more accurate risk adjustments.
References
- Centers for Medicare and Medicaid Services. Readmissions reduction program. Accessed October 3, 2015.
- Rau J. Half of nation’s hospitals fail again to escape Medicare’s readmissions penalties. August 3, 2015. Accessed October 3, 2015.
- Medpac. The hospital readmission penalty: how well is it working?. Accessed October 3, 2015.
CMS Releases Updated Two-Midnight Rule for 2016
On November 13, the Centers for Medicare & Medicaid Services (CMS) is scheduled to publish its final OPPS rule for 2016. One of the biggest impacts for hospitalists is the update to the two-midnight rule. Here are six areas of interest to hospitalists:
1. The two-midnight rule became effective just over two years ago, on October 1, 2013. The purpose of the rule is to define which Medicare beneficiary hospital stays are appropriate for Medicare Part A payment.
2. The original rule stated that if the physician (or other practitioner) expects the patient to stay for fewer than two midnights, then the services should be billed as outpatient (Medicare Part B), and not inpatient.
3. In the first two years of this rule, the only exception was for those diagnoses that CMS designates as “inpatient only.”
4. The new rule modifies the exceptions to the two-midnight rule. Under the new rule, the exception can now be determined by the physician (or other practitioner) on a “case-by-case basis.” Every case can still be subjected to medical review.
5. Another change is that short stays will no longer be reviewed by Medicare administrative contractors or recovery audit contractors, which are usually funded on a contingency basis. Under the updated rule, the quality improvement organization contractors will review short inpatient stays. This went into effect on October 1, 2015.
6. Additionally, the new rule does state “we [CMS] continue to expect that stays under 24 hours would rarely qualify for an exception to the two-midnight benchmark.”
On November 13, the Centers for Medicare & Medicaid Services (CMS) is scheduled to publish its final OPPS rule for 2016. One of the biggest impacts for hospitalists is the update to the two-midnight rule. Here are six areas of interest to hospitalists:
1. The two-midnight rule became effective just over two years ago, on October 1, 2013. The purpose of the rule is to define which Medicare beneficiary hospital stays are appropriate for Medicare Part A payment.
2. The original rule stated that if the physician (or other practitioner) expects the patient to stay for fewer than two midnights, then the services should be billed as outpatient (Medicare Part B), and not inpatient.
3. In the first two years of this rule, the only exception was for those diagnoses that CMS designates as “inpatient only.”
4. The new rule modifies the exceptions to the two-midnight rule. Under the new rule, the exception can now be determined by the physician (or other practitioner) on a “case-by-case basis.” Every case can still be subjected to medical review.
5. Another change is that short stays will no longer be reviewed by Medicare administrative contractors or recovery audit contractors, which are usually funded on a contingency basis. Under the updated rule, the quality improvement organization contractors will review short inpatient stays. This went into effect on October 1, 2015.
6. Additionally, the new rule does state “we [CMS] continue to expect that stays under 24 hours would rarely qualify for an exception to the two-midnight benchmark.”
On November 13, the Centers for Medicare & Medicaid Services (CMS) is scheduled to publish its final OPPS rule for 2016. One of the biggest impacts for hospitalists is the update to the two-midnight rule. Here are six areas of interest to hospitalists:
1. The two-midnight rule became effective just over two years ago, on October 1, 2013. The purpose of the rule is to define which Medicare beneficiary hospital stays are appropriate for Medicare Part A payment.
2. The original rule stated that if the physician (or other practitioner) expects the patient to stay for fewer than two midnights, then the services should be billed as outpatient (Medicare Part B), and not inpatient.
3. In the first two years of this rule, the only exception was for those diagnoses that CMS designates as “inpatient only.”
4. The new rule modifies the exceptions to the two-midnight rule. Under the new rule, the exception can now be determined by the physician (or other practitioner) on a “case-by-case basis.” Every case can still be subjected to medical review.
5. Another change is that short stays will no longer be reviewed by Medicare administrative contractors or recovery audit contractors, which are usually funded on a contingency basis. Under the updated rule, the quality improvement organization contractors will review short inpatient stays. This went into effect on October 1, 2015.
6. Additionally, the new rule does state “we [CMS] continue to expect that stays under 24 hours would rarely qualify for an exception to the two-midnight benchmark.”
Hospitalists Support Medicare’s Plan to Reimburse Advance Care Planning

On July 8, following on the heels of the sustainable growth rate repeal, the Centers for Medicare and Medicaid Services released a proposed update to the 2016 Physician Fee Schedule that would reimburse physicians and other qualified providers for conversations with patients and patient families about end-of-life care.
It is yet another move toward higher quality patient-centered care, CMS said in a news release on its website the day the proposed rule change was published. The comment period, which spanned 90 days, closes Nov. 1. The final rule will take effect Jan. 1, 2016.
Although CMS specifically cites the recommendation made by the American Medical Association to make advance care planning a separate, payable service, many physician groups, including the Society of Hospital Medicine, have championed and continue to actively advocate for reimbursement for end-of-life conversations with patients and their families.
“We think that palliative care and hospice services are underutilized, so we support anything we can do to make sure there is more appropriate use of these services,” says Ronald A. Greeno, MD, FCCP, MHM, a founding member of SHM, a longtime SHM Public Policy Committee member, and a current member of its board of directors. “We think it’s important to encourage providers to take the time to have those discussions, and one way is getting reimbursement for that time.”
When CMS considered reimbursement for advance care planning last year but did not propose a rule, SHM wrote a letter in December 2014 to U.S. Department of Health and Human Services (HHS) acting administrator Marilynn Tavenner urging the agency to consider adopting the two codes for complex advance care planning developed by the AMA’s CPT Editorial Panel.1 In May 2015, SHM joined 65 other medical specialty and professional societies in signing a letter to HHS Secretary Sylvia Mathews Burwell asking for these codes to be formalized in CY 2016.2
In the more recent letter, the authors mention peer-reviewed research demonstrating that advance care planning leads to “better care, higher patient and family satisfaction, fewer unwanted hospitalizations and lower rates of caregiver distress, depression and lost productivity.” SHM also cites a 2014 Institute of Medicine report, Dying in America, in which advance care planning is listed as one of five key recommendations.3

—Dr. Greeno
Pending final rule adoption, the codes 99487 and 99498 will become payable starting in January 2016.
“We (hospitalists) are in this position pretty much every day, working with people in late life and at the end of life, cycling in and out of the hospital with end-stage chronic diseases,” says Howard Epstein, MD, FHM, CHIE, executive vice president and chief medical officer at PreferredOne Health Plans in Minnesota and a hospice and palliative medicine-certified hospitalist. “I’ll be quite honest: I don’t think reimbursement is going to pay for the time and expertise for these procedures; it’s more offsetting the costs of doing the right thing for patients and families.”
What reimbursement does is lend credibility to the goals of care and advance care planning discussions patients and providers are already having, Dr. Epstein says.
“Having a specific CPT code for this legitimizes it,” he says, “like the field of palliative medicine when it became a board-certified specialty; these kinds of things really matter. They say, ‘This is our procedure.’”
It also enables providers to take the time to have these conversations with patients and families. In a post on the SHM blog in July 2015, Dr. Epstein, also a member of the SHM board of directors, cites a New England Journal of Medicine study indicating that most of the 2.5 million deaths each year in the U.S. are due to progressive health conditions and another that found that a quarter of elderly Americans lack the ability to make critical decisions at the end of life.4,5 The proposed rule, he says, reflects a change in our culture.
“As our society ages, and more and more people go through the experience with loved ones, they are demanding this care,” Dr. Epstein says.
But simply providing reimbursement is not enough, nor should the onus fall squarely on physicians, Dr. Epstein says. Rather, he believes physicians should take advantage of resources provided by SHM, hospital systems, and other organizations that offer training in advance care planning, and all members of a patient care and support team should be well versed in how to have these conversations.
The rule comes just over five years after attempts to include advance care planning in health reform efforts failed, and SHM plans to continue to advocate for national consistency in applying the measure and to work to ensure there are no limits to the timing of advance care planning conversations or where they take place.
“It was just a matter of time. It was bound to happen,” Dr. Greeno says of the rule. “We held out during the discussions of death panels and things like that. There are always lots of political issues with misinformation on both sides. We’ve tried to really communicate how and why we are supportive, and the benefits for our patients and our healthcare system, which is always our goal.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Kealey BT. Re: Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule, Clinical Laboratory Fee Schedule, Access to Identifiable Data for the Center for Medicare and Medicaid Innovation Models and Other Revisions to Part B for CY 2015; Final Rule (CMS-1612-FC). Letter to Administrator Marilyn Tavenner, Centers for Medicare and Medicaid Services, Department of Health and Human Services. December 8, 2014. Accessed September 14, 2015.
- Letter to The Honorable Sylvia Mathews Burwell, Secretary of Health and Human Services. May 12, 2015. Accessed September 14, 2015.
- Institute of Medicine. Dying in America: improving quality and honoring individual preferences near the end of life. September 17, 2014. Accessed September 14, 2015.
- Wolf SM, Berlinger N, Jennings B. Forty years of work on end-of-life care - from patient’s rights to systemic reform. N Engl J Med. 2015;372(7):678-682. doi: 10.1056/NEJMms1410321.
- Silveira MJ, Kim SY, Langa KM. Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362(13):1211-1218. doi: 10.1056/NEJMsa0907901.
On July 8, following on the heels of the sustainable growth rate repeal, the Centers for Medicare and Medicaid Services released a proposed update to the 2016 Physician Fee Schedule that would reimburse physicians and other qualified providers for conversations with patients and patient families about end-of-life care.
It is yet another move toward higher quality patient-centered care, CMS said in a news release on its website the day the proposed rule change was published. The comment period, which spanned 90 days, closes Nov. 1. The final rule will take effect Jan. 1, 2016.
Although CMS specifically cites the recommendation made by the American Medical Association to make advance care planning a separate, payable service, many physician groups, including the Society of Hospital Medicine, have championed and continue to actively advocate for reimbursement for end-of-life conversations with patients and their families.
“We think that palliative care and hospice services are underutilized, so we support anything we can do to make sure there is more appropriate use of these services,” says Ronald A. Greeno, MD, FCCP, MHM, a founding member of SHM, a longtime SHM Public Policy Committee member, and a current member of its board of directors. “We think it’s important to encourage providers to take the time to have those discussions, and one way is getting reimbursement for that time.”
When CMS considered reimbursement for advance care planning last year but did not propose a rule, SHM wrote a letter in December 2014 to U.S. Department of Health and Human Services (HHS) acting administrator Marilynn Tavenner urging the agency to consider adopting the two codes for complex advance care planning developed by the AMA’s CPT Editorial Panel.1 In May 2015, SHM joined 65 other medical specialty and professional societies in signing a letter to HHS Secretary Sylvia Mathews Burwell asking for these codes to be formalized in CY 2016.2
In the more recent letter, the authors mention peer-reviewed research demonstrating that advance care planning leads to “better care, higher patient and family satisfaction, fewer unwanted hospitalizations and lower rates of caregiver distress, depression and lost productivity.” SHM also cites a 2014 Institute of Medicine report, Dying in America, in which advance care planning is listed as one of five key recommendations.3
—Dr. Greeno
Pending final rule adoption, the codes 99487 and 99498 will become payable starting in January 2016.
“We (hospitalists) are in this position pretty much every day, working with people in late life and at the end of life, cycling in and out of the hospital with end-stage chronic diseases,” says Howard Epstein, MD, FHM, CHIE, executive vice president and chief medical officer at PreferredOne Health Plans in Minnesota and a hospice and palliative medicine-certified hospitalist. “I’ll be quite honest: I don’t think reimbursement is going to pay for the time and expertise for these procedures; it’s more offsetting the costs of doing the right thing for patients and families.”
What reimbursement does is lend credibility to the goals of care and advance care planning discussions patients and providers are already having, Dr. Epstein says.
“Having a specific CPT code for this legitimizes it,” he says, “like the field of palliative medicine when it became a board-certified specialty; these kinds of things really matter. They say, ‘This is our procedure.’”
It also enables providers to take the time to have these conversations with patients and families. In a post on the SHM blog in July 2015, Dr. Epstein, also a member of the SHM board of directors, cites a New England Journal of Medicine study indicating that most of the 2.5 million deaths each year in the U.S. are due to progressive health conditions and another that found that a quarter of elderly Americans lack the ability to make critical decisions at the end of life.4,5 The proposed rule, he says, reflects a change in our culture.
“As our society ages, and more and more people go through the experience with loved ones, they are demanding this care,” Dr. Epstein says.
But simply providing reimbursement is not enough, nor should the onus fall squarely on physicians, Dr. Epstein says. Rather, he believes physicians should take advantage of resources provided by SHM, hospital systems, and other organizations that offer training in advance care planning, and all members of a patient care and support team should be well versed in how to have these conversations.
The rule comes just over five years after attempts to include advance care planning in health reform efforts failed, and SHM plans to continue to advocate for national consistency in applying the measure and to work to ensure there are no limits to the timing of advance care planning conversations or where they take place.
“It was just a matter of time. It was bound to happen,” Dr. Greeno says of the rule. “We held out during the discussions of death panels and things like that. There are always lots of political issues with misinformation on both sides. We’ve tried to really communicate how and why we are supportive, and the benefits for our patients and our healthcare system, which is always our goal.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Kealey BT. Re: Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule, Clinical Laboratory Fee Schedule, Access to Identifiable Data for the Center for Medicare and Medicaid Innovation Models and Other Revisions to Part B for CY 2015; Final Rule (CMS-1612-FC). Letter to Administrator Marilyn Tavenner, Centers for Medicare and Medicaid Services, Department of Health and Human Services. December 8, 2014. Accessed September 14, 2015.
- Letter to The Honorable Sylvia Mathews Burwell, Secretary of Health and Human Services. May 12, 2015. Accessed September 14, 2015.
- Institute of Medicine. Dying in America: improving quality and honoring individual preferences near the end of life. September 17, 2014. Accessed September 14, 2015.
- Wolf SM, Berlinger N, Jennings B. Forty years of work on end-of-life care - from patient’s rights to systemic reform. N Engl J Med. 2015;372(7):678-682. doi: 10.1056/NEJMms1410321.
- Silveira MJ, Kim SY, Langa KM. Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362(13):1211-1218. doi: 10.1056/NEJMsa0907901.
On July 8, following on the heels of the sustainable growth rate repeal, the Centers for Medicare and Medicaid Services released a proposed update to the 2016 Physician Fee Schedule that would reimburse physicians and other qualified providers for conversations with patients and patient families about end-of-life care.
It is yet another move toward higher quality patient-centered care, CMS said in a news release on its website the day the proposed rule change was published. The comment period, which spanned 90 days, closes Nov. 1. The final rule will take effect Jan. 1, 2016.
Although CMS specifically cites the recommendation made by the American Medical Association to make advance care planning a separate, payable service, many physician groups, including the Society of Hospital Medicine, have championed and continue to actively advocate for reimbursement for end-of-life conversations with patients and their families.
“We think that palliative care and hospice services are underutilized, so we support anything we can do to make sure there is more appropriate use of these services,” says Ronald A. Greeno, MD, FCCP, MHM, a founding member of SHM, a longtime SHM Public Policy Committee member, and a current member of its board of directors. “We think it’s important to encourage providers to take the time to have those discussions, and one way is getting reimbursement for that time.”
When CMS considered reimbursement for advance care planning last year but did not propose a rule, SHM wrote a letter in December 2014 to U.S. Department of Health and Human Services (HHS) acting administrator Marilynn Tavenner urging the agency to consider adopting the two codes for complex advance care planning developed by the AMA’s CPT Editorial Panel.1 In May 2015, SHM joined 65 other medical specialty and professional societies in signing a letter to HHS Secretary Sylvia Mathews Burwell asking for these codes to be formalized in CY 2016.2
In the more recent letter, the authors mention peer-reviewed research demonstrating that advance care planning leads to “better care, higher patient and family satisfaction, fewer unwanted hospitalizations and lower rates of caregiver distress, depression and lost productivity.” SHM also cites a 2014 Institute of Medicine report, Dying in America, in which advance care planning is listed as one of five key recommendations.3
—Dr. Greeno
Pending final rule adoption, the codes 99487 and 99498 will become payable starting in January 2016.
“We (hospitalists) are in this position pretty much every day, working with people in late life and at the end of life, cycling in and out of the hospital with end-stage chronic diseases,” says Howard Epstein, MD, FHM, CHIE, executive vice president and chief medical officer at PreferredOne Health Plans in Minnesota and a hospice and palliative medicine-certified hospitalist. “I’ll be quite honest: I don’t think reimbursement is going to pay for the time and expertise for these procedures; it’s more offsetting the costs of doing the right thing for patients and families.”
What reimbursement does is lend credibility to the goals of care and advance care planning discussions patients and providers are already having, Dr. Epstein says.
“Having a specific CPT code for this legitimizes it,” he says, “like the field of palliative medicine when it became a board-certified specialty; these kinds of things really matter. They say, ‘This is our procedure.’”
It also enables providers to take the time to have these conversations with patients and families. In a post on the SHM blog in July 2015, Dr. Epstein, also a member of the SHM board of directors, cites a New England Journal of Medicine study indicating that most of the 2.5 million deaths each year in the U.S. are due to progressive health conditions and another that found that a quarter of elderly Americans lack the ability to make critical decisions at the end of life.4,5 The proposed rule, he says, reflects a change in our culture.
“As our society ages, and more and more people go through the experience with loved ones, they are demanding this care,” Dr. Epstein says.
But simply providing reimbursement is not enough, nor should the onus fall squarely on physicians, Dr. Epstein says. Rather, he believes physicians should take advantage of resources provided by SHM, hospital systems, and other organizations that offer training in advance care planning, and all members of a patient care and support team should be well versed in how to have these conversations.
The rule comes just over five years after attempts to include advance care planning in health reform efforts failed, and SHM plans to continue to advocate for national consistency in applying the measure and to work to ensure there are no limits to the timing of advance care planning conversations or where they take place.
“It was just a matter of time. It was bound to happen,” Dr. Greeno says of the rule. “We held out during the discussions of death panels and things like that. There are always lots of political issues with misinformation on both sides. We’ve tried to really communicate how and why we are supportive, and the benefits for our patients and our healthcare system, which is always our goal.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Kealey BT. Re: Medicare Program; Revisions to Payment Policies under the Physician Fee Schedule, Clinical Laboratory Fee Schedule, Access to Identifiable Data for the Center for Medicare and Medicaid Innovation Models and Other Revisions to Part B for CY 2015; Final Rule (CMS-1612-FC). Letter to Administrator Marilyn Tavenner, Centers for Medicare and Medicaid Services, Department of Health and Human Services. December 8, 2014. Accessed September 14, 2015.
- Letter to The Honorable Sylvia Mathews Burwell, Secretary of Health and Human Services. May 12, 2015. Accessed September 14, 2015.
- Institute of Medicine. Dying in America: improving quality and honoring individual preferences near the end of life. September 17, 2014. Accessed September 14, 2015.
- Wolf SM, Berlinger N, Jennings B. Forty years of work on end-of-life care - from patient’s rights to systemic reform. N Engl J Med. 2015;372(7):678-682. doi: 10.1056/NEJMms1410321.
- Silveira MJ, Kim SY, Langa KM. Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362(13):1211-1218. doi: 10.1056/NEJMsa0907901.
Physicians Critical of Proposed Changes to Medicare's Two-Midnight Rule

In the wake of proposed changes to the Centers for Medicare and Medicaid Services’ two-midnight rule, physicians say new flexibilities and changes to the policy’s auditing mechanism add more uncertainty and ambiguity.
The 2016 Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System proposed rule was published on July 1, 2015, and included changes in response to concerns about portions of the original two-midnight rule.1 By classifying an inpatient stay as any hospitalization lasting more than two midnights, the rule, which attempted to clarify which services warranted billing under Part B and which qualified for Part A, initially was intended to limit the long observation stays negatively impacting Medicare beneficiaries. However, aggressive reviews by recovery auditors (RAs) and the notion that physician judgment was taking a backseat to arbitrary CMS policy caused a backlash.
In 2014, CMS solicited feedback on the two-midnight rule. SHM suggested a two-tiered approach to address immediate and long-term patient care needs.
“SHM suggests CMS pursue broader solutions to observation status instead of making minor adjustments to the two-midnight rule,” wrote then-SHM President Burke Kealey, MD, SFHM, in a public comment letter to CMS in June 2014. “However, SHM does recognize that in the interim, the two-midnight policy needs to be refined in order to reflect the realities of patient care. Some situations may not be appropriate for classification as outpatient, regardless of the length of stay.”
The proposed changes were supposed to be a solution, but some are saying that CMS has missed the mark. In trying to give physicians more flexibility to determine patient status at the time of admissions, the rule instead may leave physician judgment open to additional scrutiny. Also, the nature of short inpatient stay reviews by Quality Improvement Organizations (QIOs), rather than RAs, remains unclear, and an additional point of concern involves the question of how RAs will factor in.
“My personal opinion is that it will only muddy the waters, in terms of payment for [and] documentation and reviews of short stays for Medicare beneficiaries,” says Jeannine Engel, MD, FACP, in a statement she wrote and shared by email. Dr. Engel is an internist and physician advisor for billing compliance at University of Utah Health Care in Salt Lake City. “No matter who reviews medical documentation, when subjective criteria are used, there is room for interpretation.”
CMS has not defined what constitutes adequate documentation to justify short inpatient stays, nor has it indicated the threshold for “high rates of denials” that would kick reviews over to RAs.
“Details are lacking, and then what makes it even more confusing is what they’ve done with the tweak in policy is further muddied the definition of inpatient,” says Charles Locke, MD, internist and senior physician advisor at Johns Hopkins University School of Medicine in Baltimore. “Whether you agree or disagree with the two-midnight rule, it actually made more clear what inpatient should be.”
According to CMS, the two-midnight rule has reduced observation stays lasting longer than two midnights by 11%, and inpatient admissions are anticipated to increase. But, physicians say, it’s a billing distinction rather than one that impacts patient care.
“The reality is when you take someone in the hospital as outpatient, they can receive every service and care identical to inpatient,” Dr. Locke says. “CMS seems hung up on the idea that in the hospital there are two levels of care.”
In fact, with the changes, “CMS had all but abandoned the term ‘inpatient hospital care’ in favor of simply ‘hospital care.’ Now it is back,” says Dr. Engel, who is also a professor of medicine at Huntsman Cancer Institute. “The two-midnight rule was a payment policy, not a ‘care policy.’ Now we may be back to debating what constitutes ‘inpatient care’ versus what could have been ‘safely delivered in a different/lower status such as observation.’”
Dr. Engel and Dr. Locke recently published a study of RAs and the two-midnight rule in the Journal of Hospital Medicine, with University of Wisconsin-Madison School of Medicine and Public Health hospitalist Ann Sheehy, MD.2
The AHA-CMS Quarrel
In addition to SHM, other organizations are heartened by CMS’s responsiveness. Priya Bathija, senior associate director of policy at the American Hospital Association, called them a “step in the right direction,” but also highlighted some of the group’s lingering concerns.
“We think it’s a good thing they’re using QIOs as first-line medical review as opposed to RAs, but we still want to make sure RAs will not make inappropriate denials of claims,” Bathija says.
The AHA is fighting a legal battle against the U.S. Department of Health and Human Services over a 0.2% reduction in inpatient payments through the two-midnight rule, maintained in the proposed changes, which CMS says are warranted based on a projected increase in inpatient service claims.3 The AHA disputes these actuarial values, Bathija says.
The AHA is calling upon CMS to make changes to short stay payments and submitted a letter to CMS outlining six models.4 The agency accepted comment on the proposed changes through August 30.
The fundamental issue, however, is that the Medicare payment system is vastly out of date, Dr. Locke says. “What I have advocated is to get rid of Part A and Part B distinction, just like private insurance,” he says, “so when you’re hospitalized, you’re hospitalized, and there is no distinction except inpatient extended, recovery outpatient, or extended outpatient observation.”
If the proposed rule changes are finalized, hospitals are going to have to learn to live with them, despite ambiguous guidance, and adjust their workflow, Dr. Locke says.
“It costs a lot of money and time, and hospitals don’t want to do something thinking they’re doing it in good faith but then the Inspector General says you owe $10 million,” he says. “In general, I and others don’t see this fixing any fundamental problems.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- U.S. Department of Health and Human Services. Medicare program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center payment systems and quality reporting programs; short inpatient hospital stays; transition for certain Medicare-dependent, small rural hospitals under the Hospital Inpatient Prospective Payment System. July 1, 2015. Accessed July 29, 2015.
- Sheehy AM, Locke C, Engel JZ, et al. Recovery audit contractor audits and appeals at three academic medical centers. J Hosp Med. 2015;10(4):212-219. doi: 10.1002/jhm.2332.
- American Hospital Association. Associations, hospitals challenge two-midnight rule in federal court. April 14, 2014. Accessed July 29, 2015.
- Fishman LE. RE: Two-midnight policy and potential short stay payment solutions [letter]. American Hospital Association. February 13, 2015. Accessed July 29, 2015.
In the wake of proposed changes to the Centers for Medicare and Medicaid Services’ two-midnight rule, physicians say new flexibilities and changes to the policy’s auditing mechanism add more uncertainty and ambiguity.
The 2016 Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System proposed rule was published on July 1, 2015, and included changes in response to concerns about portions of the original two-midnight rule.1 By classifying an inpatient stay as any hospitalization lasting more than two midnights, the rule, which attempted to clarify which services warranted billing under Part B and which qualified for Part A, initially was intended to limit the long observation stays negatively impacting Medicare beneficiaries. However, aggressive reviews by recovery auditors (RAs) and the notion that physician judgment was taking a backseat to arbitrary CMS policy caused a backlash.
In 2014, CMS solicited feedback on the two-midnight rule. SHM suggested a two-tiered approach to address immediate and long-term patient care needs.
“SHM suggests CMS pursue broader solutions to observation status instead of making minor adjustments to the two-midnight rule,” wrote then-SHM President Burke Kealey, MD, SFHM, in a public comment letter to CMS in June 2014. “However, SHM does recognize that in the interim, the two-midnight policy needs to be refined in order to reflect the realities of patient care. Some situations may not be appropriate for classification as outpatient, regardless of the length of stay.”
The proposed changes were supposed to be a solution, but some are saying that CMS has missed the mark. In trying to give physicians more flexibility to determine patient status at the time of admissions, the rule instead may leave physician judgment open to additional scrutiny. Also, the nature of short inpatient stay reviews by Quality Improvement Organizations (QIOs), rather than RAs, remains unclear, and an additional point of concern involves the question of how RAs will factor in.
“My personal opinion is that it will only muddy the waters, in terms of payment for [and] documentation and reviews of short stays for Medicare beneficiaries,” says Jeannine Engel, MD, FACP, in a statement she wrote and shared by email. Dr. Engel is an internist and physician advisor for billing compliance at University of Utah Health Care in Salt Lake City. “No matter who reviews medical documentation, when subjective criteria are used, there is room for interpretation.”
CMS has not defined what constitutes adequate documentation to justify short inpatient stays, nor has it indicated the threshold for “high rates of denials” that would kick reviews over to RAs.
“Details are lacking, and then what makes it even more confusing is what they’ve done with the tweak in policy is further muddied the definition of inpatient,” says Charles Locke, MD, internist and senior physician advisor at Johns Hopkins University School of Medicine in Baltimore. “Whether you agree or disagree with the two-midnight rule, it actually made more clear what inpatient should be.”
According to CMS, the two-midnight rule has reduced observation stays lasting longer than two midnights by 11%, and inpatient admissions are anticipated to increase. But, physicians say, it’s a billing distinction rather than one that impacts patient care.
“The reality is when you take someone in the hospital as outpatient, they can receive every service and care identical to inpatient,” Dr. Locke says. “CMS seems hung up on the idea that in the hospital there are two levels of care.”
In fact, with the changes, “CMS had all but abandoned the term ‘inpatient hospital care’ in favor of simply ‘hospital care.’ Now it is back,” says Dr. Engel, who is also a professor of medicine at Huntsman Cancer Institute. “The two-midnight rule was a payment policy, not a ‘care policy.’ Now we may be back to debating what constitutes ‘inpatient care’ versus what could have been ‘safely delivered in a different/lower status such as observation.’”
Dr. Engel and Dr. Locke recently published a study of RAs and the two-midnight rule in the Journal of Hospital Medicine, with University of Wisconsin-Madison School of Medicine and Public Health hospitalist Ann Sheehy, MD.2
The AHA-CMS Quarrel
In addition to SHM, other organizations are heartened by CMS’s responsiveness. Priya Bathija, senior associate director of policy at the American Hospital Association, called them a “step in the right direction,” but also highlighted some of the group’s lingering concerns.
“We think it’s a good thing they’re using QIOs as first-line medical review as opposed to RAs, but we still want to make sure RAs will not make inappropriate denials of claims,” Bathija says.
The AHA is fighting a legal battle against the U.S. Department of Health and Human Services over a 0.2% reduction in inpatient payments through the two-midnight rule, maintained in the proposed changes, which CMS says are warranted based on a projected increase in inpatient service claims.3 The AHA disputes these actuarial values, Bathija says.
The AHA is calling upon CMS to make changes to short stay payments and submitted a letter to CMS outlining six models.4 The agency accepted comment on the proposed changes through August 30.
The fundamental issue, however, is that the Medicare payment system is vastly out of date, Dr. Locke says. “What I have advocated is to get rid of Part A and Part B distinction, just like private insurance,” he says, “so when you’re hospitalized, you’re hospitalized, and there is no distinction except inpatient extended, recovery outpatient, or extended outpatient observation.”
If the proposed rule changes are finalized, hospitals are going to have to learn to live with them, despite ambiguous guidance, and adjust their workflow, Dr. Locke says.
“It costs a lot of money and time, and hospitals don’t want to do something thinking they’re doing it in good faith but then the Inspector General says you owe $10 million,” he says. “In general, I and others don’t see this fixing any fundamental problems.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- U.S. Department of Health and Human Services. Medicare program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center payment systems and quality reporting programs; short inpatient hospital stays; transition for certain Medicare-dependent, small rural hospitals under the Hospital Inpatient Prospective Payment System. July 1, 2015. Accessed July 29, 2015.
- Sheehy AM, Locke C, Engel JZ, et al. Recovery audit contractor audits and appeals at three academic medical centers. J Hosp Med. 2015;10(4):212-219. doi: 10.1002/jhm.2332.
- American Hospital Association. Associations, hospitals challenge two-midnight rule in federal court. April 14, 2014. Accessed July 29, 2015.
- Fishman LE. RE: Two-midnight policy and potential short stay payment solutions [letter]. American Hospital Association. February 13, 2015. Accessed July 29, 2015.
In the wake of proposed changes to the Centers for Medicare and Medicaid Services’ two-midnight rule, physicians say new flexibilities and changes to the policy’s auditing mechanism add more uncertainty and ambiguity.
The 2016 Hospital Outpatient Prospective Payment System and Ambulatory Surgical Center Payment System proposed rule was published on July 1, 2015, and included changes in response to concerns about portions of the original two-midnight rule.1 By classifying an inpatient stay as any hospitalization lasting more than two midnights, the rule, which attempted to clarify which services warranted billing under Part B and which qualified for Part A, initially was intended to limit the long observation stays negatively impacting Medicare beneficiaries. However, aggressive reviews by recovery auditors (RAs) and the notion that physician judgment was taking a backseat to arbitrary CMS policy caused a backlash.
In 2014, CMS solicited feedback on the two-midnight rule. SHM suggested a two-tiered approach to address immediate and long-term patient care needs.
“SHM suggests CMS pursue broader solutions to observation status instead of making minor adjustments to the two-midnight rule,” wrote then-SHM President Burke Kealey, MD, SFHM, in a public comment letter to CMS in June 2014. “However, SHM does recognize that in the interim, the two-midnight policy needs to be refined in order to reflect the realities of patient care. Some situations may not be appropriate for classification as outpatient, regardless of the length of stay.”
The proposed changes were supposed to be a solution, but some are saying that CMS has missed the mark. In trying to give physicians more flexibility to determine patient status at the time of admissions, the rule instead may leave physician judgment open to additional scrutiny. Also, the nature of short inpatient stay reviews by Quality Improvement Organizations (QIOs), rather than RAs, remains unclear, and an additional point of concern involves the question of how RAs will factor in.
“My personal opinion is that it will only muddy the waters, in terms of payment for [and] documentation and reviews of short stays for Medicare beneficiaries,” says Jeannine Engel, MD, FACP, in a statement she wrote and shared by email. Dr. Engel is an internist and physician advisor for billing compliance at University of Utah Health Care in Salt Lake City. “No matter who reviews medical documentation, when subjective criteria are used, there is room for interpretation.”
CMS has not defined what constitutes adequate documentation to justify short inpatient stays, nor has it indicated the threshold for “high rates of denials” that would kick reviews over to RAs.
“Details are lacking, and then what makes it even more confusing is what they’ve done with the tweak in policy is further muddied the definition of inpatient,” says Charles Locke, MD, internist and senior physician advisor at Johns Hopkins University School of Medicine in Baltimore. “Whether you agree or disagree with the two-midnight rule, it actually made more clear what inpatient should be.”
According to CMS, the two-midnight rule has reduced observation stays lasting longer than two midnights by 11%, and inpatient admissions are anticipated to increase. But, physicians say, it’s a billing distinction rather than one that impacts patient care.
“The reality is when you take someone in the hospital as outpatient, they can receive every service and care identical to inpatient,” Dr. Locke says. “CMS seems hung up on the idea that in the hospital there are two levels of care.”
In fact, with the changes, “CMS had all but abandoned the term ‘inpatient hospital care’ in favor of simply ‘hospital care.’ Now it is back,” says Dr. Engel, who is also a professor of medicine at Huntsman Cancer Institute. “The two-midnight rule was a payment policy, not a ‘care policy.’ Now we may be back to debating what constitutes ‘inpatient care’ versus what could have been ‘safely delivered in a different/lower status such as observation.’”
Dr. Engel and Dr. Locke recently published a study of RAs and the two-midnight rule in the Journal of Hospital Medicine, with University of Wisconsin-Madison School of Medicine and Public Health hospitalist Ann Sheehy, MD.2
The AHA-CMS Quarrel
In addition to SHM, other organizations are heartened by CMS’s responsiveness. Priya Bathija, senior associate director of policy at the American Hospital Association, called them a “step in the right direction,” but also highlighted some of the group’s lingering concerns.
“We think it’s a good thing they’re using QIOs as first-line medical review as opposed to RAs, but we still want to make sure RAs will not make inappropriate denials of claims,” Bathija says.
The AHA is fighting a legal battle against the U.S. Department of Health and Human Services over a 0.2% reduction in inpatient payments through the two-midnight rule, maintained in the proposed changes, which CMS says are warranted based on a projected increase in inpatient service claims.3 The AHA disputes these actuarial values, Bathija says.
The AHA is calling upon CMS to make changes to short stay payments and submitted a letter to CMS outlining six models.4 The agency accepted comment on the proposed changes through August 30.
The fundamental issue, however, is that the Medicare payment system is vastly out of date, Dr. Locke says. “What I have advocated is to get rid of Part A and Part B distinction, just like private insurance,” he says, “so when you’re hospitalized, you’re hospitalized, and there is no distinction except inpatient extended, recovery outpatient, or extended outpatient observation.”
If the proposed rule changes are finalized, hospitals are going to have to learn to live with them, despite ambiguous guidance, and adjust their workflow, Dr. Locke says.
“It costs a lot of money and time, and hospitals don’t want to do something thinking they’re doing it in good faith but then the Inspector General says you owe $10 million,” he says. “In general, I and others don’t see this fixing any fundamental problems.”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- U.S. Department of Health and Human Services. Medicare program: Hospital Outpatient Prospective Payment and Ambulatory Surgical Center payment systems and quality reporting programs; short inpatient hospital stays; transition for certain Medicare-dependent, small rural hospitals under the Hospital Inpatient Prospective Payment System. July 1, 2015. Accessed July 29, 2015.
- Sheehy AM, Locke C, Engel JZ, et al. Recovery audit contractor audits and appeals at three academic medical centers. J Hosp Med. 2015;10(4):212-219. doi: 10.1002/jhm.2332.
- American Hospital Association. Associations, hospitals challenge two-midnight rule in federal court. April 14, 2014. Accessed July 29, 2015.
- Fishman LE. RE: Two-midnight policy and potential short stay payment solutions [letter]. American Hospital Association. February 13, 2015. Accessed July 29, 2015.
Medicare Rule May Needlessly Extend Hospital Stay
(Reuters Health) - A decades old Medicare rule requiring a three-day hospital stay before patients can transfer to skilled nursing facilities may needlessly prolong hospitalizations, a study suggests.
Researchers compared the average time patients were hospitalized between 2006 and 2010 in privately administered Medicare Advantage health plans that either stuck to this rule or allowed people to transfer to skilled nursing facilities sooner.
Lengths of hospital stays increased with the rule in place and declined when it was waived, the study found.
"The three-day stay rule may inappropriately lengthen the time spent in a hospital for patients who could be transferred to a skilled nursing facility earlier," senior author Dr. Amal Trivedi, a health policy researcher at Brown University in Providence, Rhode Island, said by email.
This minimum-stay rule dates back to the 1960s, when patients typically remained in the hospital for nearly two weeks, and three days was the minimum time needed to evaluate them and plan their post-hospital care, Trivedi and colleagues note in the journal Health Affairs for August.
Since then, typical stays have shortened, and skilled nursing facilities have become an increasingly common treatment setting for patients with complex medical problems who no longer require acute inpatient care.
To see how the three-day minimum stay requirement might impact hospitalization, researchers compared the typical number of hospital days for nearly 141,000 patients in 14 Medicare Advantage plans that upheld the rule and for nearly 117,000 people in 14 similar plans that waived it.
The people enrolled in plans that waived the rule were typically younger, poorer and less likely to be white.
For plans that waived the rule, 23.5% of hospitalized patients were admitted to skilled nursing facilities in the year before the rule was eliminated, compared with 25.7% in the year after it went away.
Plans that kept the rule saw a similar gain, from 22.8% to 26.3%.
But the average length of hospital stays for patients in plans that waived the three-day rule declined from 6.9 days to 6.7 days, compared with an increase from 6.1 days to 6.6 days in plans that kept the requirement in place.
Overall, the average reduction in hospital stays was 0.7 days with the rule elimination, translating into approximately $1,500 in savings for every admission that ended with a transfer to a skilled nursing facility, the researchers estimated.
One limitation of the study, however, is that it looked at hospital days over the entire year, rather then the number of days for each stay, the researchers acknowledge. It's also possible that the cost savings wouldn't be the same for people with traditional fee-for-service Medicare or other plans unlike the ones in the study.
Even so, as hospital stays become shorter and patients with complicated illnesses are treated in other settings, it makes sense to revisit whether the three days is the right cutoff to identify people who can appropriately transfer to a skilled nursing facility, said David Grabowski, a health policy researcher at Harvard Medical School in Boston.
Certain patients may also benefit from leaving the hospital sooner, because longer stays can increase their risk of infections and make it less likely that they get out of bed for physical activity that can aid recovery, Grabowski, who wasn't involved in the study, said by email.
"Some individuals with short hospital stays may be inappropriately excluded from skilled nursing facility care under the current system," he said. "Moreover, this rule has led to some unintended consequences like the growth in observational stays."
"There really aren't many benefits to staying beyond medical necessity," Grabowski added.
(Reuters Health) - A decades old Medicare rule requiring a three-day hospital stay before patients can transfer to skilled nursing facilities may needlessly prolong hospitalizations, a study suggests.
Researchers compared the average time patients were hospitalized between 2006 and 2010 in privately administered Medicare Advantage health plans that either stuck to this rule or allowed people to transfer to skilled nursing facilities sooner.
Lengths of hospital stays increased with the rule in place and declined when it was waived, the study found.
"The three-day stay rule may inappropriately lengthen the time spent in a hospital for patients who could be transferred to a skilled nursing facility earlier," senior author Dr. Amal Trivedi, a health policy researcher at Brown University in Providence, Rhode Island, said by email.
This minimum-stay rule dates back to the 1960s, when patients typically remained in the hospital for nearly two weeks, and three days was the minimum time needed to evaluate them and plan their post-hospital care, Trivedi and colleagues note in the journal Health Affairs for August.
Since then, typical stays have shortened, and skilled nursing facilities have become an increasingly common treatment setting for patients with complex medical problems who no longer require acute inpatient care.
To see how the three-day minimum stay requirement might impact hospitalization, researchers compared the typical number of hospital days for nearly 141,000 patients in 14 Medicare Advantage plans that upheld the rule and for nearly 117,000 people in 14 similar plans that waived it.
The people enrolled in plans that waived the rule were typically younger, poorer and less likely to be white.
For plans that waived the rule, 23.5% of hospitalized patients were admitted to skilled nursing facilities in the year before the rule was eliminated, compared with 25.7% in the year after it went away.
Plans that kept the rule saw a similar gain, from 22.8% to 26.3%.
But the average length of hospital stays for patients in plans that waived the three-day rule declined from 6.9 days to 6.7 days, compared with an increase from 6.1 days to 6.6 days in plans that kept the requirement in place.
Overall, the average reduction in hospital stays was 0.7 days with the rule elimination, translating into approximately $1,500 in savings for every admission that ended with a transfer to a skilled nursing facility, the researchers estimated.
One limitation of the study, however, is that it looked at hospital days over the entire year, rather then the number of days for each stay, the researchers acknowledge. It's also possible that the cost savings wouldn't be the same for people with traditional fee-for-service Medicare or other plans unlike the ones in the study.
Even so, as hospital stays become shorter and patients with complicated illnesses are treated in other settings, it makes sense to revisit whether the three days is the right cutoff to identify people who can appropriately transfer to a skilled nursing facility, said David Grabowski, a health policy researcher at Harvard Medical School in Boston.
Certain patients may also benefit from leaving the hospital sooner, because longer stays can increase their risk of infections and make it less likely that they get out of bed for physical activity that can aid recovery, Grabowski, who wasn't involved in the study, said by email.
"Some individuals with short hospital stays may be inappropriately excluded from skilled nursing facility care under the current system," he said. "Moreover, this rule has led to some unintended consequences like the growth in observational stays."
"There really aren't many benefits to staying beyond medical necessity," Grabowski added.
(Reuters Health) - A decades old Medicare rule requiring a three-day hospital stay before patients can transfer to skilled nursing facilities may needlessly prolong hospitalizations, a study suggests.
Researchers compared the average time patients were hospitalized between 2006 and 2010 in privately administered Medicare Advantage health plans that either stuck to this rule or allowed people to transfer to skilled nursing facilities sooner.
Lengths of hospital stays increased with the rule in place and declined when it was waived, the study found.
"The three-day stay rule may inappropriately lengthen the time spent in a hospital for patients who could be transferred to a skilled nursing facility earlier," senior author Dr. Amal Trivedi, a health policy researcher at Brown University in Providence, Rhode Island, said by email.
This minimum-stay rule dates back to the 1960s, when patients typically remained in the hospital for nearly two weeks, and three days was the minimum time needed to evaluate them and plan their post-hospital care, Trivedi and colleagues note in the journal Health Affairs for August.
Since then, typical stays have shortened, and skilled nursing facilities have become an increasingly common treatment setting for patients with complex medical problems who no longer require acute inpatient care.
To see how the three-day minimum stay requirement might impact hospitalization, researchers compared the typical number of hospital days for nearly 141,000 patients in 14 Medicare Advantage plans that upheld the rule and for nearly 117,000 people in 14 similar plans that waived it.
The people enrolled in plans that waived the rule were typically younger, poorer and less likely to be white.
For plans that waived the rule, 23.5% of hospitalized patients were admitted to skilled nursing facilities in the year before the rule was eliminated, compared with 25.7% in the year after it went away.
Plans that kept the rule saw a similar gain, from 22.8% to 26.3%.
But the average length of hospital stays for patients in plans that waived the three-day rule declined from 6.9 days to 6.7 days, compared with an increase from 6.1 days to 6.6 days in plans that kept the requirement in place.
Overall, the average reduction in hospital stays was 0.7 days with the rule elimination, translating into approximately $1,500 in savings for every admission that ended with a transfer to a skilled nursing facility, the researchers estimated.
One limitation of the study, however, is that it looked at hospital days over the entire year, rather then the number of days for each stay, the researchers acknowledge. It's also possible that the cost savings wouldn't be the same for people with traditional fee-for-service Medicare or other plans unlike the ones in the study.
Even so, as hospital stays become shorter and patients with complicated illnesses are treated in other settings, it makes sense to revisit whether the three days is the right cutoff to identify people who can appropriately transfer to a skilled nursing facility, said David Grabowski, a health policy researcher at Harvard Medical School in Boston.
Certain patients may also benefit from leaving the hospital sooner, because longer stays can increase their risk of infections and make it less likely that they get out of bed for physical activity that can aid recovery, Grabowski, who wasn't involved in the study, said by email.
"Some individuals with short hospital stays may be inappropriately excluded from skilled nursing facility care under the current system," he said. "Moreover, this rule has led to some unintended consequences like the growth in observational stays."
"There really aren't many benefits to staying beyond medical necessity," Grabowski added.
New Bill Hopes to Increase Residency Medicare Slots after Two Previous Bills Failed

Two federal bills introduced in 2013, the Resident Physician Shortage Reduction Act and the Training Tomorrow’s Doctors Today Act, would have increased the number of Medicare-funded residency slots by 15,000 over five years. The latter bill also would have required each teaching hospital to release annual reports on the costs of training residents and of running specialized services, and it would have tied 2% to 3% of IME funding to quality measures, such as how well an institution trains providers to work in teams and in different settings. (In 2010, the Medicare Payment Advisory Commission, also known as MedPAC, instead recommended redirecting more than half of Medicare’s IME funding to performance-based incentives.)
After both bills died in the House of Representatives, supporters resurrected some key features and incorporated them into the Resident Physician Shortage Reduction Act of 2015 (H.R. 2124), reintroduced this spring in both the House and the Senate. The new version again seeks to increase Medicare residency slots by 15,000 over five years, while attempting to identify physician shortage specialties and increase the workforce diversity.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and a member of the IOM committee that recommended a significant GME overhaul, says requirements to increase the transparency of actual training costs would be a step in the right direction if implemented appropriately. She is less enthusiastic about tying a small percentage of funding to quality measures without moving to a robust system that ties funding to residency education in a meaningful way. The IOM report concluded that overall reform of the system is needed, she says, “not tweaking at the edges.”
A bold overhaul may be a tough sell, however, and she acknowledges that the committee’s own recommendations have gained little traction so far.
Vikas Parekh, MD, FACP, SFHM, chair of the SHM Academic Hospitalist Committee, says putting 2% or 3% of a hospital’s total Medicare money at risk is more in line with what the agency is doing in other quality improvement programs.
“So far,” he says, “the indications are that that’s enough money for most big academic medical centers to pay attention to it.”
Two federal bills introduced in 2013, the Resident Physician Shortage Reduction Act and the Training Tomorrow’s Doctors Today Act, would have increased the number of Medicare-funded residency slots by 15,000 over five years. The latter bill also would have required each teaching hospital to release annual reports on the costs of training residents and of running specialized services, and it would have tied 2% to 3% of IME funding to quality measures, such as how well an institution trains providers to work in teams and in different settings. (In 2010, the Medicare Payment Advisory Commission, also known as MedPAC, instead recommended redirecting more than half of Medicare’s IME funding to performance-based incentives.)
After both bills died in the House of Representatives, supporters resurrected some key features and incorporated them into the Resident Physician Shortage Reduction Act of 2015 (H.R. 2124), reintroduced this spring in both the House and the Senate. The new version again seeks to increase Medicare residency slots by 15,000 over five years, while attempting to identify physician shortage specialties and increase the workforce diversity.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and a member of the IOM committee that recommended a significant GME overhaul, says requirements to increase the transparency of actual training costs would be a step in the right direction if implemented appropriately. She is less enthusiastic about tying a small percentage of funding to quality measures without moving to a robust system that ties funding to residency education in a meaningful way. The IOM report concluded that overall reform of the system is needed, she says, “not tweaking at the edges.”
A bold overhaul may be a tough sell, however, and she acknowledges that the committee’s own recommendations have gained little traction so far.
Vikas Parekh, MD, FACP, SFHM, chair of the SHM Academic Hospitalist Committee, says putting 2% or 3% of a hospital’s total Medicare money at risk is more in line with what the agency is doing in other quality improvement programs.
“So far,” he says, “the indications are that that’s enough money for most big academic medical centers to pay attention to it.”
Two federal bills introduced in 2013, the Resident Physician Shortage Reduction Act and the Training Tomorrow’s Doctors Today Act, would have increased the number of Medicare-funded residency slots by 15,000 over five years. The latter bill also would have required each teaching hospital to release annual reports on the costs of training residents and of running specialized services, and it would have tied 2% to 3% of IME funding to quality measures, such as how well an institution trains providers to work in teams and in different settings. (In 2010, the Medicare Payment Advisory Commission, also known as MedPAC, instead recommended redirecting more than half of Medicare’s IME funding to performance-based incentives.)
After both bills died in the House of Representatives, supporters resurrected some key features and incorporated them into the Resident Physician Shortage Reduction Act of 2015 (H.R. 2124), reintroduced this spring in both the House and the Senate. The new version again seeks to increase Medicare residency slots by 15,000 over five years, while attempting to identify physician shortage specialties and increase the workforce diversity.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and a member of the IOM committee that recommended a significant GME overhaul, says requirements to increase the transparency of actual training costs would be a step in the right direction if implemented appropriately. She is less enthusiastic about tying a small percentage of funding to quality measures without moving to a robust system that ties funding to residency education in a meaningful way. The IOM report concluded that overall reform of the system is needed, she says, “not tweaking at the edges.”
A bold overhaul may be a tough sell, however, and she acknowledges that the committee’s own recommendations have gained little traction so far.
Vikas Parekh, MD, FACP, SFHM, chair of the SHM Academic Hospitalist Committee, says putting 2% or 3% of a hospital’s total Medicare money at risk is more in line with what the agency is doing in other quality improvement programs.
“So far,” he says, “the indications are that that’s enough money for most big academic medical centers to pay attention to it.”
Institute of Medicine Report Prompts Debate Over Graduate Medical Education Funding, Oversight
Ever since 1997, when the federal Balanced Budget Act froze Medicare’s overall funding for graduate medical education, debates have flared regularly over whether and how the U.S. government should support medical resident training.
Discussions about the possible redistribution of billions of dollars are bound to make people nervous, but the controversy reached a fever pitch in 2014 when the Institute of Medicine released a report penned by a 21-member committee that recommended significant—and contentious—changes to the existing graduate medical education (GME) financing and governance structure to “address current deficiencies and better shape the physician workforce for the future.”
Should Medicare shake up the system to redistribute existing training slots to where they’re needed most, as the report recommends? Should it instead lift its funding cap to avert a potential bottleneck in the physician pipeline, as several medical associations have requested? One year later, the report has gained little traction amid a largely unchanged status quo that few experts believe is ultimately sustainable. The continuing debate, however, has prompted fresh questions about whether the current GME structure is adequately supporting the nation’s healthcare needs and has spurred widespread agreement on the need for greater transparency, accountability, and innovation.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and one of the report’s co-authors, says she has seen firsthand the challenges arising from a lack of physicians in multiple specialties, especially in rural areas. “We believed that simply adding new money to a system that is outdated would not solve the issues in physician education and physician workforce,” she says.
Some HM leaders and other physicians’ groups have cautiously welcomed the report’s focus on better equipping doctors for a rapidly changing reality.
“It wasn’t wrong for them to look at this,” says Darlene B. Tad-y, MD, FHM, chair of the SHM Physicians in Training Committee and assistant professor of medicine at the University of Colorado in Denver. “And it’s probably not wrong for them to propose new ways to think about how we fund GME.”
In fact, she says, efforts to align such funding with healthcare funding in general could be timely in the face of added pressures like ensuring that new insurance beneficiaries have access to primary care.
Scott Sears, MD, FACP, MBA, chief clinical officer of Tacoma, Wash.-based hospitalist management firm Sound Physicians, says healthcare is also moving rapidly toward managing populations as part of team-based care that increases quality while lowering costs. So why not better align GME with innovative Medicare initiatives like bundled payments, he asks, and then use the savings to reward those training programs that accept the risk and achieve results?
“Shifting some of our education to match what Medicare is trying to drive out in the real world, I think, is long overdue,” Dr. Sears says.
Other groups, such as the Association of American Medical Colleges, however, contend that the report’s prescriptions are far less helpful than its diagnoses. “Politically, there’s just stuff in there for everybody to hate,” says Atul Grover, MD, PhD, FACP, FCCP, the AAMC’s chief public policy officer. “I think [the IOM report] did a decent job of pointing out some of the things that we want to improve moving forward, but I’m not sure that the answers are quite right.”
An Uneven Funding Landscape
The strong opinions engendered by the topic underscore the high stakes involved in GME. Every year, the federal government doles out about $15 billion for residency training, including about $10 billion from Medicare coffers. Medicare’s share is divided into two main funding streams that flow primarily to academic medical centers: direct graduate medical education (DGME) and indirect medical education (IME) payments. The first covers training expenses, while the second reimburses teaching hospitals that care for Medicare patients while training residents.
Some skeptics have questioned whether the government should be funding medical education at all, noting that the arrangement is utterly unique to the field. Advocates have countered that the funding concept was embedded in the original Medicare legislation and that it correctly recognized the added cost of offering GME training while providing more complex Medicare beneficiaries with specialty services.
Nearly everyone acknowledges that there are still enough residency slots for all U.S. graduates, but Dr. Grover says residency programs aren’t growing nearly fast enough to keep pace with medical school enrollment, creating a growing mismatch and a looming bottleneck in the supply chain. Compared to medical school numbers in 2002, for example, the AAMC says enrollment is on track to expand 29% by 2019, while osteopathic schools are set to expand by 162% over the same timeframe.
It wasn’t wrong for the [Institute of Medicine] to look at this. And it’s probably not wrong for them to propose new ways to think about how we fund GME. 
—Darlene B. Tad-y, MD, FHM, assistant professor of medicine, University of Colorado, Denver, chair, SHM Physicians in Training Committee
Fundamentally, the idea is not a bad one, to say that programs that were more aligned with national needs and priorities in terms of how they train physicians would get more funding, and those that did not wouldn’t. I think the challenge is that the devil’s in the details of how you do that. 
—Vikas Parekh, MD, FACP, SFHM, associate director, hospitalist program, University of Michigan, Ann Arbor, chair, SHM Academic Hospitalist Committee
Despite the continued freeze in Medicare funding, many large medical institutions continue to add residency spots.
“We’ve been hundreds of residency positions over our cap for a very long time,” says Vikas Parekh, MD, FACP, SFHM, associate director of the hospitalist program at the University of Michigan in Ann Arbor. “The hospital funds them through hospital operating margin because in the net, they still view the investment as worthwhile.”
Alternatively, some non-university-based training programs have secured money from other sources to fund their residency positions, potentially creating new funding models for the future if the programs can demonstrate both quality and stability.
One key rationale for the IOM report’s proposed overhaul, however, is the longstanding and sizeable geographical disparity in Medicare’s per capita GME spending, which has skewed heavily toward the Northeast. A 2013 study, in fact, found that one-fifth of all DGME funding in 2010—an estimated $2 billion—went to New York State alone.1 Florida, which recently overtook New York as the third most populous state, received only one-eighth as much money. And Mississippi—the state with the lowest doctor-to-patient ratio—received only $22 million, or about one-ninetieth as much.
The IOM report also suggests that the long-standing GME payment plan has yielded little data on whether it actually accomplishes what it was designed to do: help establish a well-prepared medical workforce in a cost-effective way. In response, one major IOM recommendation is to maintain the overall level of Medicare support but tie some of the payments to performance to ensure oversight and accountability, and provide new incentives for innovation in the content and financing of training programs.
As with other CMS initiatives, however, getting everyone to agree on which quality metrics to use in evaluating GME training could take awhile. For example, should Medicare judge the performance of the trainees, the GME programs, or even the sponsoring institutions? Despite the proliferation of performance-based carrots and sticks elsewhere in healthcare, Dr. Tad-y says, such incentives may work less well for GME.
“One thing that’s inherent with trainees is that they’re trainees,” she says. “They’re not as efficient or as effective as someone who’s an expert, right? That’s why it’s training.”
Dr. Parekh, who also serves as chair of the SHM Academic Hospitalist Committee, agrees that finding the right outcome measures could be tough. “It gets very dicey, because how do you define who’s a good doctor?” he says. Currently, residents often are assessed via the reputation and history of the training program. “People say, ‘I know that the people coming out of that program are good because they’ve always been good, and it’s a reputable program and has a big name.’ But it’s not objective data,” he says.
Dr. Sears, of Sound Physicians, notes that it’s also often difficult to attribute patients to specific providers.
“Many times in graduate medical education, patients are going in and out of the program or in and out of the hospital, and how do you attribute?” he says. “I think it becomes very complex.”
A New Take on Transformation
Another IOM recommendation would create a single GME fund with two subsidiaries: an operational fund for ongoing support and a transformation fund. The latter fund would finance four new initiatives to:
- Develop and evaluate innovative GME programs;
- Determine and validate appropriate performance measures;
- Establish pilot projects to test out alternative payment methods; and
- Award new training positions based on priority disciplines—such as primary care—and underserved geographic areas.
A related recommendation seeks to modernize the GME payment methodology. For example, the committee urged Medicare to combine the indirect and direct funding streams into one payment based on a national per-resident amount and adjusted according to each location. In addition, the report endorsed performance-based payments based on the results of pilots launched under the transformation fund.
Dr. Sears says he appreciates the report’s effort to address shortfalls in primary care providers relative to specialists. “That’s not to say that specialty medicine isn’t incredibly important, because it is,” he says. “But I think incentivizing or reallocating spots to ensure that we have adequate primary care physician coverage throughout the country will have tremendous impact on the ability to care for an aging population in the United States, at least.”
I have had physicians tell me that they do not understand why our report said that there was not a physician shortage, and I try to point out that we did NOT say that. Rather, the report [and the committee] said that we could not find compelling evidence of an impending physician shortage and that physician workforce projections had been and are quite unreliable. —Deborah Powell, MD, dean emerita, University of Minnesota Medical School, IOM committee member 
Shifting some of our [medical] education to match what Medicare is trying to drive out in the real world, I think, is long overdue. —Scott Sears, MD, FACP, MBA, chief clinical officer, Sound Physicians, Tacoma, Wash. 
Dr. Parekh agrees, at least in part.
“Fundamentally, the idea is not a bad one, to say that programs that were more aligned with national needs and priorities in terms of how they train physicians would get more funding, and those that did not wouldn’t,” he says. “I think the challenge is that the devil’s in the details of how you do that.”
A priority-based GME system, he continues, could potentially influence what type of physicians are trained.
“In my mind, it’s not irrational to think that if GME funding was more targeted around expanding slots in certain specialties and not expanding slots in other specialties, that there would be some ability to influence the workforce,” Dr. Parekh says. Influencing where residents go may be more difficult, though a growing mismatch between medical graduates and available residency slots might add a new wrinkle to that debate, as well.
Currently, U.S. medical graduates fill only about 60% of residency slots for specialties like internal medicine—a main conduit for hospital medicine—while foreign graduates make up the remainder.
“So who’s the first that’s going to be squeezed out? It will be foreign medical graduates,” Dr. Parekh says. Many of those graduates come to the U.S. on J-1 visas, which carry a payback requirement: practicing in underserved areas. “One worry is, will rural and underserved areas suffer from a physician shortage because U.S. grads won’t want to work there after you start squeezing out all of the foreign medical grads?” he asks.
Clear Line of Sight?
Dr. Parekh also supports efforts to establish a clearer connection between the funding’s intent and where the money actually goes. The IOM report’s proposal to do so, however, raises yet another controversy around the true purpose of IME funding. Teaching hospitals argue that the money should continue to be used to reimburse them for the added costs of providing comprehensive and specialized care like level I trauma centers to their more complex Medicare patient populations.
Number one, [the IOM] came out and said, ‘We don’t know that there’s a shortage of physicians and we’re, if anything, going to remove money from the training system rather than putting in additional resources. We found that problematic, given all the evidence we have of the growing, aging population. —Atul Grover, MD, PhD, FACP, FCCP, chief public policy officer, Association of American Medical Colleges 
A big part of the problem here is that people are free agents. If you make more residency spots, but the economics are such that people decide to become cardiologists because cardiologists make twice or more what hospitalists make, then you may have increased residency spots but [added only] a very small increment in the number of hospitalists. —Daniel Brotman, MD, FACP, SFHM, chair, SHM Education Committee, director, hospitalist program, Johns Hopkins Hospital, Baltimore 
Accordingly, the AAMC panned the report’s recommendation to replace separate IME funding with a single fund directed toward the GME sponsoring institution and subdivided instead into the operational and transformation funds. Dr. Grover says setting up a transformation fund with new money would make sense, but not as a carve-out from existing support.
“You’re removing those resources from the system and not replacing them, which is a challenge,” he says.
Medical schools are more inclined to want the money directed toward training goals, especially if they are to be held accountable for GME outcomes. “Right now, the hospital gets it, and it’s basically somewhere in the bottom line,” Dr. Parekh says. “No one really knows where that money goes. There’s very little accountability or clarity of purpose for that dollar.”
Amid the ongoing debate, the call for more transparency and accountability in GME seems to be gaining the most ground. “I don’t see tons of downside from it,” Dr. Parekh says. “I think it sheds light on the current funding environment and makes people have to justify a little bit more what they’re doing with that money.”
Dr. Tad-y puts it this way: “If you made your own budget at home, the first thing you’d do is try to figure out where all your money goes and what you’re spending your money on.” If Medicare is concerned that its GME money isn’t being spent wisely, then, the first step would be to do some accounting. “And that means a little bit of transparency,” she says. “I don’t think that’s a bad thing, to know exactly what we’re paying for; that makes sense. I mean, we do that for everything else.”
SHM and most other medical associations also agree on the necessary goal of increasing the nation’s primary care capacity, even if they differ on the details of how best to do so. In the long run, however, some observers say growing the workforce—whether that of primary care providers or of hospitalists—may depend less on the total number of residency spots and more on the enthusiasm of program leadership and the attractiveness of job conditions such as salary and workload.
“A big part of the problem here is that people are free agents,” says Daniel Brotman, MD, FACP, SFHM, chair of the SHM Education Committee and director of the hospitalist program at the Johns Hopkins Hospital in Baltimore. “If you make more residency spots, but the economics are such that people decide to become cardiologists because cardiologists make twice or more what hospitalists make, then you may have increased residency spots but [added only] a very small increment in the number of hospitalists.”
Whatever happens, Dr. Parekh says hospitalists are well positioned to be integral parts of improving quality, accountability, and innovation in residency training programs.
“I think if more GME money is targeted toward the outcomes of the GME programs, hospitalists are going to be tapped to help with that work, in terms of training and broadening their skill sets,” he says. “So I think it’s a great opportunity.”
Bryn Nelson is a freelance medical writer in Seattle.
References
- Mullan F, Chen C, Steinmetz E. The geography of graduate medical education: imbalances signal need for new distribution policies. Health Aff. 2013;32(11):1914-1921.
Ever since 1997, when the federal Balanced Budget Act froze Medicare’s overall funding for graduate medical education, debates have flared regularly over whether and how the U.S. government should support medical resident training.
Discussions about the possible redistribution of billions of dollars are bound to make people nervous, but the controversy reached a fever pitch in 2014 when the Institute of Medicine released a report penned by a 21-member committee that recommended significant—and contentious—changes to the existing graduate medical education (GME) financing and governance structure to “address current deficiencies and better shape the physician workforce for the future.”
Should Medicare shake up the system to redistribute existing training slots to where they’re needed most, as the report recommends? Should it instead lift its funding cap to avert a potential bottleneck in the physician pipeline, as several medical associations have requested? One year later, the report has gained little traction amid a largely unchanged status quo that few experts believe is ultimately sustainable. The continuing debate, however, has prompted fresh questions about whether the current GME structure is adequately supporting the nation’s healthcare needs and has spurred widespread agreement on the need for greater transparency, accountability, and innovation.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and one of the report’s co-authors, says she has seen firsthand the challenges arising from a lack of physicians in multiple specialties, especially in rural areas. “We believed that simply adding new money to a system that is outdated would not solve the issues in physician education and physician workforce,” she says.
Some HM leaders and other physicians’ groups have cautiously welcomed the report’s focus on better equipping doctors for a rapidly changing reality.
“It wasn’t wrong for them to look at this,” says Darlene B. Tad-y, MD, FHM, chair of the SHM Physicians in Training Committee and assistant professor of medicine at the University of Colorado in Denver. “And it’s probably not wrong for them to propose new ways to think about how we fund GME.”
In fact, she says, efforts to align such funding with healthcare funding in general could be timely in the face of added pressures like ensuring that new insurance beneficiaries have access to primary care.
Scott Sears, MD, FACP, MBA, chief clinical officer of Tacoma, Wash.-based hospitalist management firm Sound Physicians, says healthcare is also moving rapidly toward managing populations as part of team-based care that increases quality while lowering costs. So why not better align GME with innovative Medicare initiatives like bundled payments, he asks, and then use the savings to reward those training programs that accept the risk and achieve results?
“Shifting some of our education to match what Medicare is trying to drive out in the real world, I think, is long overdue,” Dr. Sears says.
Other groups, such as the Association of American Medical Colleges, however, contend that the report’s prescriptions are far less helpful than its diagnoses. “Politically, there’s just stuff in there for everybody to hate,” says Atul Grover, MD, PhD, FACP, FCCP, the AAMC’s chief public policy officer. “I think [the IOM report] did a decent job of pointing out some of the things that we want to improve moving forward, but I’m not sure that the answers are quite right.”
An Uneven Funding Landscape
The strong opinions engendered by the topic underscore the high stakes involved in GME. Every year, the federal government doles out about $15 billion for residency training, including about $10 billion from Medicare coffers. Medicare’s share is divided into two main funding streams that flow primarily to academic medical centers: direct graduate medical education (DGME) and indirect medical education (IME) payments. The first covers training expenses, while the second reimburses teaching hospitals that care for Medicare patients while training residents.
Some skeptics have questioned whether the government should be funding medical education at all, noting that the arrangement is utterly unique to the field. Advocates have countered that the funding concept was embedded in the original Medicare legislation and that it correctly recognized the added cost of offering GME training while providing more complex Medicare beneficiaries with specialty services.
Nearly everyone acknowledges that there are still enough residency slots for all U.S. graduates, but Dr. Grover says residency programs aren’t growing nearly fast enough to keep pace with medical school enrollment, creating a growing mismatch and a looming bottleneck in the supply chain. Compared to medical school numbers in 2002, for example, the AAMC says enrollment is on track to expand 29% by 2019, while osteopathic schools are set to expand by 162% over the same timeframe.
It wasn’t wrong for the [Institute of Medicine] to look at this. And it’s probably not wrong for them to propose new ways to think about how we fund GME. —Darlene B. Tad-y, MD, FHM, assistant professor of medicine, University of Colorado, Denver, chair, SHM Physicians in Training Committee
Fundamentally, the idea is not a bad one, to say that programs that were more aligned with national needs and priorities in terms of how they train physicians would get more funding, and those that did not wouldn’t. I think the challenge is that the devil’s in the details of how you do that. —Vikas Parekh, MD, FACP, SFHM, associate director, hospitalist program, University of Michigan, Ann Arbor, chair, SHM Academic Hospitalist Committee
Despite the continued freeze in Medicare funding, many large medical institutions continue to add residency spots.
“We’ve been hundreds of residency positions over our cap for a very long time,” says Vikas Parekh, MD, FACP, SFHM, associate director of the hospitalist program at the University of Michigan in Ann Arbor. “The hospital funds them through hospital operating margin because in the net, they still view the investment as worthwhile.”
Alternatively, some non-university-based training programs have secured money from other sources to fund their residency positions, potentially creating new funding models for the future if the programs can demonstrate both quality and stability.
One key rationale for the IOM report’s proposed overhaul, however, is the longstanding and sizeable geographical disparity in Medicare’s per capita GME spending, which has skewed heavily toward the Northeast. A 2013 study, in fact, found that one-fifth of all DGME funding in 2010—an estimated $2 billion—went to New York State alone.1 Florida, which recently overtook New York as the third most populous state, received only one-eighth as much money. And Mississippi—the state with the lowest doctor-to-patient ratio—received only $22 million, or about one-ninetieth as much.
The IOM report also suggests that the long-standing GME payment plan has yielded little data on whether it actually accomplishes what it was designed to do: help establish a well-prepared medical workforce in a cost-effective way. In response, one major IOM recommendation is to maintain the overall level of Medicare support but tie some of the payments to performance to ensure oversight and accountability, and provide new incentives for innovation in the content and financing of training programs.
As with other CMS initiatives, however, getting everyone to agree on which quality metrics to use in evaluating GME training could take awhile. For example, should Medicare judge the performance of the trainees, the GME programs, or even the sponsoring institutions? Despite the proliferation of performance-based carrots and sticks elsewhere in healthcare, Dr. Tad-y says, such incentives may work less well for GME.
“One thing that’s inherent with trainees is that they’re trainees,” she says. “They’re not as efficient or as effective as someone who’s an expert, right? That’s why it’s training.”
Dr. Parekh, who also serves as chair of the SHM Academic Hospitalist Committee, agrees that finding the right outcome measures could be tough. “It gets very dicey, because how do you define who’s a good doctor?” he says. Currently, residents often are assessed via the reputation and history of the training program. “People say, ‘I know that the people coming out of that program are good because they’ve always been good, and it’s a reputable program and has a big name.’ But it’s not objective data,” he says.
Dr. Sears, of Sound Physicians, notes that it’s also often difficult to attribute patients to specific providers.
“Many times in graduate medical education, patients are going in and out of the program or in and out of the hospital, and how do you attribute?” he says. “I think it becomes very complex.”
A New Take on Transformation
Another IOM recommendation would create a single GME fund with two subsidiaries: an operational fund for ongoing support and a transformation fund. The latter fund would finance four new initiatives to:
- Develop and evaluate innovative GME programs;
- Determine and validate appropriate performance measures;
- Establish pilot projects to test out alternative payment methods; and
- Award new training positions based on priority disciplines—such as primary care—and underserved geographic areas.
A related recommendation seeks to modernize the GME payment methodology. For example, the committee urged Medicare to combine the indirect and direct funding streams into one payment based on a national per-resident amount and adjusted according to each location. In addition, the report endorsed performance-based payments based on the results of pilots launched under the transformation fund.
Dr. Sears says he appreciates the report’s effort to address shortfalls in primary care providers relative to specialists. “That’s not to say that specialty medicine isn’t incredibly important, because it is,” he says. “But I think incentivizing or reallocating spots to ensure that we have adequate primary care physician coverage throughout the country will have tremendous impact on the ability to care for an aging population in the United States, at least.”
I have had physicians tell me that they do not understand why our report said that there was not a physician shortage, and I try to point out that we did NOT say that. Rather, the report [and the committee] said that we could not find compelling evidence of an impending physician shortage and that physician workforce projections had been and are quite unreliable. —Deborah Powell, MD, dean emerita, University of Minnesota Medical School, IOM committee member
Shifting some of our [medical] education to match what Medicare is trying to drive out in the real world, I think, is long overdue. —Scott Sears, MD, FACP, MBA, chief clinical officer, Sound Physicians, Tacoma, Wash.
Dr. Parekh agrees, at least in part.
“Fundamentally, the idea is not a bad one, to say that programs that were more aligned with national needs and priorities in terms of how they train physicians would get more funding, and those that did not wouldn’t,” he says. “I think the challenge is that the devil’s in the details of how you do that.”
A priority-based GME system, he continues, could potentially influence what type of physicians are trained.
“In my mind, it’s not irrational to think that if GME funding was more targeted around expanding slots in certain specialties and not expanding slots in other specialties, that there would be some ability to influence the workforce,” Dr. Parekh says. Influencing where residents go may be more difficult, though a growing mismatch between medical graduates and available residency slots might add a new wrinkle to that debate, as well.
Currently, U.S. medical graduates fill only about 60% of residency slots for specialties like internal medicine—a main conduit for hospital medicine—while foreign graduates make up the remainder.
“So who’s the first that’s going to be squeezed out? It will be foreign medical graduates,” Dr. Parekh says. Many of those graduates come to the U.S. on J-1 visas, which carry a payback requirement: practicing in underserved areas. “One worry is, will rural and underserved areas suffer from a physician shortage because U.S. grads won’t want to work there after you start squeezing out all of the foreign medical grads?” he asks.
Clear Line of Sight?
Dr. Parekh also supports efforts to establish a clearer connection between the funding’s intent and where the money actually goes. The IOM report’s proposal to do so, however, raises yet another controversy around the true purpose of IME funding. Teaching hospitals argue that the money should continue to be used to reimburse them for the added costs of providing comprehensive and specialized care like level I trauma centers to their more complex Medicare patient populations.
Number one, [the IOM] came out and said, ‘We don’t know that there’s a shortage of physicians and we’re, if anything, going to remove money from the training system rather than putting in additional resources. We found that problematic, given all the evidence we have of the growing, aging population. —Atul Grover, MD, PhD, FACP, FCCP, chief public policy officer, Association of American Medical Colleges
A big part of the problem here is that people are free agents. If you make more residency spots, but the economics are such that people decide to become cardiologists because cardiologists make twice or more what hospitalists make, then you may have increased residency spots but [added only] a very small increment in the number of hospitalists. —Daniel Brotman, MD, FACP, SFHM, chair, SHM Education Committee, director, hospitalist program, Johns Hopkins Hospital, Baltimore
Accordingly, the AAMC panned the report’s recommendation to replace separate IME funding with a single fund directed toward the GME sponsoring institution and subdivided instead into the operational and transformation funds. Dr. Grover says setting up a transformation fund with new money would make sense, but not as a carve-out from existing support.
“You’re removing those resources from the system and not replacing them, which is a challenge,” he says.
Medical schools are more inclined to want the money directed toward training goals, especially if they are to be held accountable for GME outcomes. “Right now, the hospital gets it, and it’s basically somewhere in the bottom line,” Dr. Parekh says. “No one really knows where that money goes. There’s very little accountability or clarity of purpose for that dollar.”
Amid the ongoing debate, the call for more transparency and accountability in GME seems to be gaining the most ground. “I don’t see tons of downside from it,” Dr. Parekh says. “I think it sheds light on the current funding environment and makes people have to justify a little bit more what they’re doing with that money.”
Dr. Tad-y puts it this way: “If you made your own budget at home, the first thing you’d do is try to figure out where all your money goes and what you’re spending your money on.” If Medicare is concerned that its GME money isn’t being spent wisely, then, the first step would be to do some accounting. “And that means a little bit of transparency,” she says. “I don’t think that’s a bad thing, to know exactly what we’re paying for; that makes sense. I mean, we do that for everything else.”
SHM and most other medical associations also agree on the necessary goal of increasing the nation’s primary care capacity, even if they differ on the details of how best to do so. In the long run, however, some observers say growing the workforce—whether that of primary care providers or of hospitalists—may depend less on the total number of residency spots and more on the enthusiasm of program leadership and the attractiveness of job conditions such as salary and workload.
“A big part of the problem here is that people are free agents,” says Daniel Brotman, MD, FACP, SFHM, chair of the SHM Education Committee and director of the hospitalist program at the Johns Hopkins Hospital in Baltimore. “If you make more residency spots, but the economics are such that people decide to become cardiologists because cardiologists make twice or more what hospitalists make, then you may have increased residency spots but [added only] a very small increment in the number of hospitalists.”
Whatever happens, Dr. Parekh says hospitalists are well positioned to be integral parts of improving quality, accountability, and innovation in residency training programs.
“I think if more GME money is targeted toward the outcomes of the GME programs, hospitalists are going to be tapped to help with that work, in terms of training and broadening their skill sets,” he says. “So I think it’s a great opportunity.”
Bryn Nelson is a freelance medical writer in Seattle.
References
- Mullan F, Chen C, Steinmetz E. The geography of graduate medical education: imbalances signal need for new distribution policies. Health Aff. 2013;32(11):1914-1921.
Ever since 1997, when the federal Balanced Budget Act froze Medicare’s overall funding for graduate medical education, debates have flared regularly over whether and how the U.S. government should support medical resident training.
Discussions about the possible redistribution of billions of dollars are bound to make people nervous, but the controversy reached a fever pitch in 2014 when the Institute of Medicine released a report penned by a 21-member committee that recommended significant—and contentious—changes to the existing graduate medical education (GME) financing and governance structure to “address current deficiencies and better shape the physician workforce for the future.”
Should Medicare shake up the system to redistribute existing training slots to where they’re needed most, as the report recommends? Should it instead lift its funding cap to avert a potential bottleneck in the physician pipeline, as several medical associations have requested? One year later, the report has gained little traction amid a largely unchanged status quo that few experts believe is ultimately sustainable. The continuing debate, however, has prompted fresh questions about whether the current GME structure is adequately supporting the nation’s healthcare needs and has spurred widespread agreement on the need for greater transparency, accountability, and innovation.
Deborah Powell, MD, dean emerita of the University of Minnesota Medical School and one of the report’s co-authors, says she has seen firsthand the challenges arising from a lack of physicians in multiple specialties, especially in rural areas. “We believed that simply adding new money to a system that is outdated would not solve the issues in physician education and physician workforce,” she says.
Some HM leaders and other physicians’ groups have cautiously welcomed the report’s focus on better equipping doctors for a rapidly changing reality.
“It wasn’t wrong for them to look at this,” says Darlene B. Tad-y, MD, FHM, chair of the SHM Physicians in Training Committee and assistant professor of medicine at the University of Colorado in Denver. “And it’s probably not wrong for them to propose new ways to think about how we fund GME.”
In fact, she says, efforts to align such funding with healthcare funding in general could be timely in the face of added pressures like ensuring that new insurance beneficiaries have access to primary care.
Scott Sears, MD, FACP, MBA, chief clinical officer of Tacoma, Wash.-based hospitalist management firm Sound Physicians, says healthcare is also moving rapidly toward managing populations as part of team-based care that increases quality while lowering costs. So why not better align GME with innovative Medicare initiatives like bundled payments, he asks, and then use the savings to reward those training programs that accept the risk and achieve results?
“Shifting some of our education to match what Medicare is trying to drive out in the real world, I think, is long overdue,” Dr. Sears says.
Other groups, such as the Association of American Medical Colleges, however, contend that the report’s prescriptions are far less helpful than its diagnoses. “Politically, there’s just stuff in there for everybody to hate,” says Atul Grover, MD, PhD, FACP, FCCP, the AAMC’s chief public policy officer. “I think [the IOM report] did a decent job of pointing out some of the things that we want to improve moving forward, but I’m not sure that the answers are quite right.”
An Uneven Funding Landscape
The strong opinions engendered by the topic underscore the high stakes involved in GME. Every year, the federal government doles out about $15 billion for residency training, including about $10 billion from Medicare coffers. Medicare’s share is divided into two main funding streams that flow primarily to academic medical centers: direct graduate medical education (DGME) and indirect medical education (IME) payments. The first covers training expenses, while the second reimburses teaching hospitals that care for Medicare patients while training residents.
Some skeptics have questioned whether the government should be funding medical education at all, noting that the arrangement is utterly unique to the field. Advocates have countered that the funding concept was embedded in the original Medicare legislation and that it correctly recognized the added cost of offering GME training while providing more complex Medicare beneficiaries with specialty services.
Nearly everyone acknowledges that there are still enough residency slots for all U.S. graduates, but Dr. Grover says residency programs aren’t growing nearly fast enough to keep pace with medical school enrollment, creating a growing mismatch and a looming bottleneck in the supply chain. Compared to medical school numbers in 2002, for example, the AAMC says enrollment is on track to expand 29% by 2019, while osteopathic schools are set to expand by 162% over the same timeframe.
It wasn’t wrong for the [Institute of Medicine] to look at this. And it’s probably not wrong for them to propose new ways to think about how we fund GME. —Darlene B. Tad-y, MD, FHM, assistant professor of medicine, University of Colorado, Denver, chair, SHM Physicians in Training Committee
Fundamentally, the idea is not a bad one, to say that programs that were more aligned with national needs and priorities in terms of how they train physicians would get more funding, and those that did not wouldn’t. I think the challenge is that the devil’s in the details of how you do that. —Vikas Parekh, MD, FACP, SFHM, associate director, hospitalist program, University of Michigan, Ann Arbor, chair, SHM Academic Hospitalist Committee
Despite the continued freeze in Medicare funding, many large medical institutions continue to add residency spots.
“We’ve been hundreds of residency positions over our cap for a very long time,” says Vikas Parekh, MD, FACP, SFHM, associate director of the hospitalist program at the University of Michigan in Ann Arbor. “The hospital funds them through hospital operating margin because in the net, they still view the investment as worthwhile.”
Alternatively, some non-university-based training programs have secured money from other sources to fund their residency positions, potentially creating new funding models for the future if the programs can demonstrate both quality and stability.
One key rationale for the IOM report’s proposed overhaul, however, is the longstanding and sizeable geographical disparity in Medicare’s per capita GME spending, which has skewed heavily toward the Northeast. A 2013 study, in fact, found that one-fifth of all DGME funding in 2010—an estimated $2 billion—went to New York State alone.1 Florida, which recently overtook New York as the third most populous state, received only one-eighth as much money. And Mississippi—the state with the lowest doctor-to-patient ratio—received only $22 million, or about one-ninetieth as much.
The IOM report also suggests that the long-standing GME payment plan has yielded little data on whether it actually accomplishes what it was designed to do: help establish a well-prepared medical workforce in a cost-effective way. In response, one major IOM recommendation is to maintain the overall level of Medicare support but tie some of the payments to performance to ensure oversight and accountability, and provide new incentives for innovation in the content and financing of training programs.
As with other CMS initiatives, however, getting everyone to agree on which quality metrics to use in evaluating GME training could take awhile. For example, should Medicare judge the performance of the trainees, the GME programs, or even the sponsoring institutions? Despite the proliferation of performance-based carrots and sticks elsewhere in healthcare, Dr. Tad-y says, such incentives may work less well for GME.
“One thing that’s inherent with trainees is that they’re trainees,” she says. “They’re not as efficient or as effective as someone who’s an expert, right? That’s why it’s training.”
Dr. Parekh, who also serves as chair of the SHM Academic Hospitalist Committee, agrees that finding the right outcome measures could be tough. “It gets very dicey, because how do you define who’s a good doctor?” he says. Currently, residents often are assessed via the reputation and history of the training program. “People say, ‘I know that the people coming out of that program are good because they’ve always been good, and it’s a reputable program and has a big name.’ But it’s not objective data,” he says.
Dr. Sears, of Sound Physicians, notes that it’s also often difficult to attribute patients to specific providers.
“Many times in graduate medical education, patients are going in and out of the program or in and out of the hospital, and how do you attribute?” he says. “I think it becomes very complex.”
A New Take on Transformation
Another IOM recommendation would create a single GME fund with two subsidiaries: an operational fund for ongoing support and a transformation fund. The latter fund would finance four new initiatives to:
- Develop and evaluate innovative GME programs;
- Determine and validate appropriate performance measures;
- Establish pilot projects to test out alternative payment methods; and
- Award new training positions based on priority disciplines—such as primary care—and underserved geographic areas.
A related recommendation seeks to modernize the GME payment methodology. For example, the committee urged Medicare to combine the indirect and direct funding streams into one payment based on a national per-resident amount and adjusted according to each location. In addition, the report endorsed performance-based payments based on the results of pilots launched under the transformation fund.
Dr. Sears says he appreciates the report’s effort to address shortfalls in primary care providers relative to specialists. “That’s not to say that specialty medicine isn’t incredibly important, because it is,” he says. “But I think incentivizing or reallocating spots to ensure that we have adequate primary care physician coverage throughout the country will have tremendous impact on the ability to care for an aging population in the United States, at least.”
I have had physicians tell me that they do not understand why our report said that there was not a physician shortage, and I try to point out that we did NOT say that. Rather, the report [and the committee] said that we could not find compelling evidence of an impending physician shortage and that physician workforce projections had been and are quite unreliable. —Deborah Powell, MD, dean emerita, University of Minnesota Medical School, IOM committee member
Shifting some of our [medical] education to match what Medicare is trying to drive out in the real world, I think, is long overdue. —Scott Sears, MD, FACP, MBA, chief clinical officer, Sound Physicians, Tacoma, Wash.
Dr. Parekh agrees, at least in part.
“Fundamentally, the idea is not a bad one, to say that programs that were more aligned with national needs and priorities in terms of how they train physicians would get more funding, and those that did not wouldn’t,” he says. “I think the challenge is that the devil’s in the details of how you do that.”
A priority-based GME system, he continues, could potentially influence what type of physicians are trained.
“In my mind, it’s not irrational to think that if GME funding was more targeted around expanding slots in certain specialties and not expanding slots in other specialties, that there would be some ability to influence the workforce,” Dr. Parekh says. Influencing where residents go may be more difficult, though a growing mismatch between medical graduates and available residency slots might add a new wrinkle to that debate, as well.
Currently, U.S. medical graduates fill only about 60% of residency slots for specialties like internal medicine—a main conduit for hospital medicine—while foreign graduates make up the remainder.
“So who’s the first that’s going to be squeezed out? It will be foreign medical graduates,” Dr. Parekh says. Many of those graduates come to the U.S. on J-1 visas, which carry a payback requirement: practicing in underserved areas. “One worry is, will rural and underserved areas suffer from a physician shortage because U.S. grads won’t want to work there after you start squeezing out all of the foreign medical grads?” he asks.
Clear Line of Sight?
Dr. Parekh also supports efforts to establish a clearer connection between the funding’s intent and where the money actually goes. The IOM report’s proposal to do so, however, raises yet another controversy around the true purpose of IME funding. Teaching hospitals argue that the money should continue to be used to reimburse them for the added costs of providing comprehensive and specialized care like level I trauma centers to their more complex Medicare patient populations.
Number one, [the IOM] came out and said, ‘We don’t know that there’s a shortage of physicians and we’re, if anything, going to remove money from the training system rather than putting in additional resources. We found that problematic, given all the evidence we have of the growing, aging population. —Atul Grover, MD, PhD, FACP, FCCP, chief public policy officer, Association of American Medical Colleges
A big part of the problem here is that people are free agents. If you make more residency spots, but the economics are such that people decide to become cardiologists because cardiologists make twice or more what hospitalists make, then you may have increased residency spots but [added only] a very small increment in the number of hospitalists. —Daniel Brotman, MD, FACP, SFHM, chair, SHM Education Committee, director, hospitalist program, Johns Hopkins Hospital, Baltimore
Accordingly, the AAMC panned the report’s recommendation to replace separate IME funding with a single fund directed toward the GME sponsoring institution and subdivided instead into the operational and transformation funds. Dr. Grover says setting up a transformation fund with new money would make sense, but not as a carve-out from existing support.
“You’re removing those resources from the system and not replacing them, which is a challenge,” he says.
Medical schools are more inclined to want the money directed toward training goals, especially if they are to be held accountable for GME outcomes. “Right now, the hospital gets it, and it’s basically somewhere in the bottom line,” Dr. Parekh says. “No one really knows where that money goes. There’s very little accountability or clarity of purpose for that dollar.”
Amid the ongoing debate, the call for more transparency and accountability in GME seems to be gaining the most ground. “I don’t see tons of downside from it,” Dr. Parekh says. “I think it sheds light on the current funding environment and makes people have to justify a little bit more what they’re doing with that money.”
Dr. Tad-y puts it this way: “If you made your own budget at home, the first thing you’d do is try to figure out where all your money goes and what you’re spending your money on.” If Medicare is concerned that its GME money isn’t being spent wisely, then, the first step would be to do some accounting. “And that means a little bit of transparency,” she says. “I don’t think that’s a bad thing, to know exactly what we’re paying for; that makes sense. I mean, we do that for everything else.”
SHM and most other medical associations also agree on the necessary goal of increasing the nation’s primary care capacity, even if they differ on the details of how best to do so. In the long run, however, some observers say growing the workforce—whether that of primary care providers or of hospitalists—may depend less on the total number of residency spots and more on the enthusiasm of program leadership and the attractiveness of job conditions such as salary and workload.
“A big part of the problem here is that people are free agents,” says Daniel Brotman, MD, FACP, SFHM, chair of the SHM Education Committee and director of the hospitalist program at the Johns Hopkins Hospital in Baltimore. “If you make more residency spots, but the economics are such that people decide to become cardiologists because cardiologists make twice or more what hospitalists make, then you may have increased residency spots but [added only] a very small increment in the number of hospitalists.”
Whatever happens, Dr. Parekh says hospitalists are well positioned to be integral parts of improving quality, accountability, and innovation in residency training programs.
“I think if more GME money is targeted toward the outcomes of the GME programs, hospitalists are going to be tapped to help with that work, in terms of training and broadening their skill sets,” he says. “So I think it’s a great opportunity.”
Bryn Nelson is a freelance medical writer in Seattle.
References
- Mullan F, Chen C, Steinmetz E. The geography of graduate medical education: imbalances signal need for new distribution policies. Health Aff. 2013;32(11):1914-1921.
Experts Urge Extension to Medicaid's Parity Program
On the last day of 2014, a provision of the Affordable Care Act (ACA) that increased payments to some physicians providing primary care services to the country’s poorest patients expired. The Medicaid payment parity program, under section 1202 of the ACA, increased to Medicare levels Medicaid reimbursement for primary care services rendered by internists, pediatricians, family medicine physicians, some subspecialists, and hospitalists in all states in 2013 and 2014.
A bill introduced in 2015, the Ensuring Access to Primary Care for Women and Children Act—sponsored by Sherrod Brown (D-Ohio) and Patty Murray, (D-W. Va.) in the Senate and Kathy Castor (D-Fla.) in the House—seeks to extend the parity program another two years and expand it to other providers, like obstetricians and nurse practitioners.
The parity program was intended to improve access to healthcare for the millions of Americans newly eligible for Medicaid under the ACA. Currently, one in five Americans is on Medicaid.
Fewer physicians in the U.S. participate in Medicaid than in Medicare or private insurance, and low reimbursement rates are sometimes cited as a cause.1,2 In 2012, fee-for-service Medicaid reimbursement for primary care averaged just 59% of Medicare fee levels nationally, but during the years of increased payment, eligible physicians saw a 73% boost in reimbursement for Medicaid primary care services.1,2
The new bill is similar to one introduced unsuccessfully last year in the Senate, which sought to avoid a lapse in the program. Initially beset by delays, some experts say the program did not last long enough to gather sufficient data or to demonstrate its effectiveness. Others say the short duration of the program prevented new providers from accepting Medicaid patients.3
An extension “would give people the chance to get more data and show the payment increase resulted in a more cost-effective healthcare system,” says Ron Greeno, MD, FCCP, MHM, an SHM board member, chair of SHM’s Public Policy Committee, and chief strategy officer at IPC Healthcare. “Ideally, there would be permanent parity.”

–Dr. Greeno
In February, Dan Polsky, PhD, the Robert D. Eilers professor in healthcare management and economics at the University of Pennsylvania Perelman School of Medicine in Philadelphia, and colleagues published a study in the New England Journal of Medicine that showed an increase in primary care appointments for new Medicaid patients correlating with the temporary increase in reimbursement.4
“We saw a 10% increase in the number of providers willing to see new Medicaid patients,” Dr. Polsky says. “It was an economic behavior test to see how physicians respond to changes in payment rates, because in a lot of states, policy makers are being asked to extend parity, and the typical comment was: ‘We don’t know if it works; it’s not cheap.’”
Indeed, the Congressional Budget Office estimated that the two-year pay increase would cost between $11 and $12 billion.1
“We came up with evidence it works,” Dr. Polsky says.
However, further measures of the parity program’s success remain a challenge, according to the author of a Kaiser Family Foundation brief, because it’s difficult to separate it from other elements of the healthcare law. Studies have also conflicted with regard to the ability of payment boosts to improve access, and the reimbursement increase may not be compatible with a shift away from the fee-for-service model.1
Yet, experts like Dr. Polsky say that to encourage greater participation in Medicaid, some type of parity is needed. “If we’re going to maintain better provider availability, I think you would need something like this,” he says.
For hospitalists, the two-year boost meant the ability to provide better care for hospitalized patients, Dr. Greeno says. Anecdotally, hospitalists reported that it was easier to discharge Medicaid patients to primary care follow-up in the community, he says, and better pay meant better staffing ratios were possible.
As of Jan. 1, 2015, 16 states and the District of Columbia reported that they will continue to reimburse Medicaid primary care services at Medicare levels.2 Dr. Greeno says the disparity between states that reimburse at higher rates for Medicaid and those that won’t could start changing the macroeconomics of medical practice, similar to the situation that occurred when states differentially imposed caps on malpractice liability.
A May 2015 Health Affairs policy brief indicates that, despite the House and Senate bill, Congress is unlikely to act soon on increasing Medicaid reimbursement rates again. Dr. Greeno believes this a mistake.
“From a healthcare policy standpoint, it seems intellectually inconsistent, and from a public health standpoint, is it really justifiable?” he asks. “At the end of the day, the fundamental question is, do we really want to have two classes of access to American healthcare?”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Paradise J. Henry J. Kaiser Family Foundation. The Kaiser Commission on Medicaid and the Uninsured. Medicaid moving forward. March 9, 2015. Accessed July 7, 2015.
- Tollen L. Medicaid primary care parity. May 11, 2015. Health Affairs online. Accessed July 7, 2015.
- Medicaid and CHIP Payment and Access Commission (MACPAC). March 2015 report to Congress on Medicaid and CHIP, chapter 8: an update on the Medicaid primary care payment increase. Accessed July 7, 2015.
- Polsky D, Richards M, Basseyn S, et al. Appointment availability after increases in Medicaid payments for primary care. N Engl J Med. 2015;372:537-545. doi: 10.1056/NEJMsa1413299.
On the last day of 2014, a provision of the Affordable Care Act (ACA) that increased payments to some physicians providing primary care services to the country’s poorest patients expired. The Medicaid payment parity program, under section 1202 of the ACA, increased to Medicare levels Medicaid reimbursement for primary care services rendered by internists, pediatricians, family medicine physicians, some subspecialists, and hospitalists in all states in 2013 and 2014.
A bill introduced in 2015, the Ensuring Access to Primary Care for Women and Children Act—sponsored by Sherrod Brown (D-Ohio) and Patty Murray, (D-W. Va.) in the Senate and Kathy Castor (D-Fla.) in the House—seeks to extend the parity program another two years and expand it to other providers, like obstetricians and nurse practitioners.
The parity program was intended to improve access to healthcare for the millions of Americans newly eligible for Medicaid under the ACA. Currently, one in five Americans is on Medicaid.
Fewer physicians in the U.S. participate in Medicaid than in Medicare or private insurance, and low reimbursement rates are sometimes cited as a cause.1,2 In 2012, fee-for-service Medicaid reimbursement for primary care averaged just 59% of Medicare fee levels nationally, but during the years of increased payment, eligible physicians saw a 73% boost in reimbursement for Medicaid primary care services.1,2
The new bill is similar to one introduced unsuccessfully last year in the Senate, which sought to avoid a lapse in the program. Initially beset by delays, some experts say the program did not last long enough to gather sufficient data or to demonstrate its effectiveness. Others say the short duration of the program prevented new providers from accepting Medicaid patients.3
An extension “would give people the chance to get more data and show the payment increase resulted in a more cost-effective healthcare system,” says Ron Greeno, MD, FCCP, MHM, an SHM board member, chair of SHM’s Public Policy Committee, and chief strategy officer at IPC Healthcare. “Ideally, there would be permanent parity.”
–Dr. Greeno
In February, Dan Polsky, PhD, the Robert D. Eilers professor in healthcare management and economics at the University of Pennsylvania Perelman School of Medicine in Philadelphia, and colleagues published a study in the New England Journal of Medicine that showed an increase in primary care appointments for new Medicaid patients correlating with the temporary increase in reimbursement.4
“We saw a 10% increase in the number of providers willing to see new Medicaid patients,” Dr. Polsky says. “It was an economic behavior test to see how physicians respond to changes in payment rates, because in a lot of states, policy makers are being asked to extend parity, and the typical comment was: ‘We don’t know if it works; it’s not cheap.’”
Indeed, the Congressional Budget Office estimated that the two-year pay increase would cost between $11 and $12 billion.1
“We came up with evidence it works,” Dr. Polsky says.
However, further measures of the parity program’s success remain a challenge, according to the author of a Kaiser Family Foundation brief, because it’s difficult to separate it from other elements of the healthcare law. Studies have also conflicted with regard to the ability of payment boosts to improve access, and the reimbursement increase may not be compatible with a shift away from the fee-for-service model.1
Yet, experts like Dr. Polsky say that to encourage greater participation in Medicaid, some type of parity is needed. “If we’re going to maintain better provider availability, I think you would need something like this,” he says.
For hospitalists, the two-year boost meant the ability to provide better care for hospitalized patients, Dr. Greeno says. Anecdotally, hospitalists reported that it was easier to discharge Medicaid patients to primary care follow-up in the community, he says, and better pay meant better staffing ratios were possible.
As of Jan. 1, 2015, 16 states and the District of Columbia reported that they will continue to reimburse Medicaid primary care services at Medicare levels.2 Dr. Greeno says the disparity between states that reimburse at higher rates for Medicaid and those that won’t could start changing the macroeconomics of medical practice, similar to the situation that occurred when states differentially imposed caps on malpractice liability.
A May 2015 Health Affairs policy brief indicates that, despite the House and Senate bill, Congress is unlikely to act soon on increasing Medicaid reimbursement rates again. Dr. Greeno believes this a mistake.
“From a healthcare policy standpoint, it seems intellectually inconsistent, and from a public health standpoint, is it really justifiable?” he asks. “At the end of the day, the fundamental question is, do we really want to have two classes of access to American healthcare?”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Paradise J. Henry J. Kaiser Family Foundation. The Kaiser Commission on Medicaid and the Uninsured. Medicaid moving forward. March 9, 2015. Accessed July 7, 2015.
- Tollen L. Medicaid primary care parity. May 11, 2015. Health Affairs online. Accessed July 7, 2015.
- Medicaid and CHIP Payment and Access Commission (MACPAC). March 2015 report to Congress on Medicaid and CHIP, chapter 8: an update on the Medicaid primary care payment increase. Accessed July 7, 2015.
- Polsky D, Richards M, Basseyn S, et al. Appointment availability after increases in Medicaid payments for primary care. N Engl J Med. 2015;372:537-545. doi: 10.1056/NEJMsa1413299.
On the last day of 2014, a provision of the Affordable Care Act (ACA) that increased payments to some physicians providing primary care services to the country’s poorest patients expired. The Medicaid payment parity program, under section 1202 of the ACA, increased to Medicare levels Medicaid reimbursement for primary care services rendered by internists, pediatricians, family medicine physicians, some subspecialists, and hospitalists in all states in 2013 and 2014.
A bill introduced in 2015, the Ensuring Access to Primary Care for Women and Children Act—sponsored by Sherrod Brown (D-Ohio) and Patty Murray, (D-W. Va.) in the Senate and Kathy Castor (D-Fla.) in the House—seeks to extend the parity program another two years and expand it to other providers, like obstetricians and nurse practitioners.
The parity program was intended to improve access to healthcare for the millions of Americans newly eligible for Medicaid under the ACA. Currently, one in five Americans is on Medicaid.
Fewer physicians in the U.S. participate in Medicaid than in Medicare or private insurance, and low reimbursement rates are sometimes cited as a cause.1,2 In 2012, fee-for-service Medicaid reimbursement for primary care averaged just 59% of Medicare fee levels nationally, but during the years of increased payment, eligible physicians saw a 73% boost in reimbursement for Medicaid primary care services.1,2
The new bill is similar to one introduced unsuccessfully last year in the Senate, which sought to avoid a lapse in the program. Initially beset by delays, some experts say the program did not last long enough to gather sufficient data or to demonstrate its effectiveness. Others say the short duration of the program prevented new providers from accepting Medicaid patients.3
An extension “would give people the chance to get more data and show the payment increase resulted in a more cost-effective healthcare system,” says Ron Greeno, MD, FCCP, MHM, an SHM board member, chair of SHM’s Public Policy Committee, and chief strategy officer at IPC Healthcare. “Ideally, there would be permanent parity.”
–Dr. Greeno
In February, Dan Polsky, PhD, the Robert D. Eilers professor in healthcare management and economics at the University of Pennsylvania Perelman School of Medicine in Philadelphia, and colleagues published a study in the New England Journal of Medicine that showed an increase in primary care appointments for new Medicaid patients correlating with the temporary increase in reimbursement.4
“We saw a 10% increase in the number of providers willing to see new Medicaid patients,” Dr. Polsky says. “It was an economic behavior test to see how physicians respond to changes in payment rates, because in a lot of states, policy makers are being asked to extend parity, and the typical comment was: ‘We don’t know if it works; it’s not cheap.’”
Indeed, the Congressional Budget Office estimated that the two-year pay increase would cost between $11 and $12 billion.1
“We came up with evidence it works,” Dr. Polsky says.
However, further measures of the parity program’s success remain a challenge, according to the author of a Kaiser Family Foundation brief, because it’s difficult to separate it from other elements of the healthcare law. Studies have also conflicted with regard to the ability of payment boosts to improve access, and the reimbursement increase may not be compatible with a shift away from the fee-for-service model.1
Yet, experts like Dr. Polsky say that to encourage greater participation in Medicaid, some type of parity is needed. “If we’re going to maintain better provider availability, I think you would need something like this,” he says.
For hospitalists, the two-year boost meant the ability to provide better care for hospitalized patients, Dr. Greeno says. Anecdotally, hospitalists reported that it was easier to discharge Medicaid patients to primary care follow-up in the community, he says, and better pay meant better staffing ratios were possible.
As of Jan. 1, 2015, 16 states and the District of Columbia reported that they will continue to reimburse Medicaid primary care services at Medicare levels.2 Dr. Greeno says the disparity between states that reimburse at higher rates for Medicaid and those that won’t could start changing the macroeconomics of medical practice, similar to the situation that occurred when states differentially imposed caps on malpractice liability.
A May 2015 Health Affairs policy brief indicates that, despite the House and Senate bill, Congress is unlikely to act soon on increasing Medicaid reimbursement rates again. Dr. Greeno believes this a mistake.
“From a healthcare policy standpoint, it seems intellectually inconsistent, and from a public health standpoint, is it really justifiable?” he asks. “At the end of the day, the fundamental question is, do we really want to have two classes of access to American healthcare?”
Kelly April Tyrrell is a freelance writer in Madison, Wis.
References
- Paradise J. Henry J. Kaiser Family Foundation. The Kaiser Commission on Medicaid and the Uninsured. Medicaid moving forward. March 9, 2015. Accessed July 7, 2015.
- Tollen L. Medicaid primary care parity. May 11, 2015. Health Affairs online. Accessed July 7, 2015.
- Medicaid and CHIP Payment and Access Commission (MACPAC). March 2015 report to Congress on Medicaid and CHIP, chapter 8: an update on the Medicaid primary care payment increase. Accessed July 7, 2015.
- Polsky D, Richards M, Basseyn S, et al. Appointment availability after increases in Medicaid payments for primary care. N Engl J Med. 2015;372:537-545. doi: 10.1056/NEJMsa1413299.