User login
NICE recommends edoxaban for NVAF

Photo courtesy of the CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending the oral anticoagulant edoxaban tosylate (Lixiana) as an option for preventing stroke and systemic embolism in adults with non-valvular atrial fibrillation (NVAF).
The patients must have 1 or more risk factors for stroke, including congestive heart failure, hypertension, diabetes, prior stroke or transient ischemic attack, and age of 75 years or older.
Such patients are generally treated with warfarin or the newer oral anticoagulants dabigatran, rivaroxaban, and apixaban.
NICE said it wants to add edoxaban to that list because the drug is a clinically and cost-effective treatment option for these patients.
NICE’s draft guidance says the decision about whether to start treatment with edoxaban should be made after an informed discussion between the clinician and the patient about the risks and benefits of edoxaban compared with warfarin, apixaban, dabigatran, and rivaroxaban.
For patients considering switching from warfarin, edoxaban’s potential benefits should be weighed against its potential risks, taking into account the patient’s level of international normalized ratio control.
Clinical effectiveness
NICE’s conclusion that edoxaban is clinically effective was based primarily on results of the ENGAGE AF-TIMI 48 trial. In this trial, researchers compared edoxaban and warfarin as prophylaxis for stroke or systemic embolism in patients with NVAF.
Results suggested edoxaban was at least non-inferior to warfarin with regard to efficacy, and edoxaban was associated with a significantly lower rate of major and fatal bleeding.
A committee advising NICE also reviewed a meta-analysis prepared by Daiichi Sankyo Co., Ltd., the company developing edoxaban.
The goal of the meta-analysis was to compare edoxaban with rivaroxaban, apixaban, and dabigatran. The analysis included 4 trials: ENGAGE AF-TIMI 48, ARISTOTLE (apixaban), RE-LY (dabigatran), and ROCKET-AF (rivaroxaban). All 4 trials had a warfarin comparator arm.
The results of the meta-analysis indicated that, for the composite endpoint of stroke and systemic embolism, efficacy was similar for high-dose edoxaban and the other newer oral anticoagulants.
However, edoxaban significantly reduced major bleeding risk by 24% compared to rivaroxaban, 28% compared to dabigatran at 150 mg, and 17% compared to dabigatran at 110 mg. Major bleeding rates were similar for high-dose edoxaban and apixaban.
The committee advising NICE said these results should be interpreted with caution, but edoxaban is unlikely to be different from rivaroxaban, apixaban, and dabigatran in clinical practice.
Cost-effectiveness
Edoxaban costs £58.80 for a 28-tablet pack (60 mg or 30 mg), and the daily cost of treatment is £2.10 (excluding value-added tax). However, costs may vary in different settings because of negotiated procurement discounts.
The committee advising NICE analyzed cost information and concluded that edoxaban is cost-effective compared with warfarin, but there is insufficient evidence to distinguish between the clinical and cost-effectiveness of edoxaban and the newer oral anticoagulants.
Nevertheless, the committee recommended edoxaban as a cost-effective treatment for patients with NVAF who have 1 or more risk factors for stroke.
NICE’s draft guidance is now with consultees, who have the opportunity to appeal against it. Once NICE issues its final guidance on a technology, it replaces local recommendations. ![]()
Photo courtesy of the CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending the oral anticoagulant edoxaban tosylate (Lixiana) as an option for preventing stroke and systemic embolism in adults with non-valvular atrial fibrillation (NVAF).
The patients must have 1 or more risk factors for stroke, including congestive heart failure, hypertension, diabetes, prior stroke or transient ischemic attack, and age of 75 years or older.
Such patients are generally treated with warfarin or the newer oral anticoagulants dabigatran, rivaroxaban, and apixaban.
NICE said it wants to add edoxaban to that list because the drug is a clinically and cost-effective treatment option for these patients.
NICE’s draft guidance says the decision about whether to start treatment with edoxaban should be made after an informed discussion between the clinician and the patient about the risks and benefits of edoxaban compared with warfarin, apixaban, dabigatran, and rivaroxaban.
For patients considering switching from warfarin, edoxaban’s potential benefits should be weighed against its potential risks, taking into account the patient’s level of international normalized ratio control.
Clinical effectiveness
NICE’s conclusion that edoxaban is clinically effective was based primarily on results of the ENGAGE AF-TIMI 48 trial. In this trial, researchers compared edoxaban and warfarin as prophylaxis for stroke or systemic embolism in patients with NVAF.
Results suggested edoxaban was at least non-inferior to warfarin with regard to efficacy, and edoxaban was associated with a significantly lower rate of major and fatal bleeding.
A committee advising NICE also reviewed a meta-analysis prepared by Daiichi Sankyo Co., Ltd., the company developing edoxaban.
The goal of the meta-analysis was to compare edoxaban with rivaroxaban, apixaban, and dabigatran. The analysis included 4 trials: ENGAGE AF-TIMI 48, ARISTOTLE (apixaban), RE-LY (dabigatran), and ROCKET-AF (rivaroxaban). All 4 trials had a warfarin comparator arm.
The results of the meta-analysis indicated that, for the composite endpoint of stroke and systemic embolism, efficacy was similar for high-dose edoxaban and the other newer oral anticoagulants.
However, edoxaban significantly reduced major bleeding risk by 24% compared to rivaroxaban, 28% compared to dabigatran at 150 mg, and 17% compared to dabigatran at 110 mg. Major bleeding rates were similar for high-dose edoxaban and apixaban.
The committee advising NICE said these results should be interpreted with caution, but edoxaban is unlikely to be different from rivaroxaban, apixaban, and dabigatran in clinical practice.
Cost-effectiveness
Edoxaban costs £58.80 for a 28-tablet pack (60 mg or 30 mg), and the daily cost of treatment is £2.10 (excluding value-added tax). However, costs may vary in different settings because of negotiated procurement discounts.
The committee advising NICE analyzed cost information and concluded that edoxaban is cost-effective compared with warfarin, but there is insufficient evidence to distinguish between the clinical and cost-effectiveness of edoxaban and the newer oral anticoagulants.
Nevertheless, the committee recommended edoxaban as a cost-effective treatment for patients with NVAF who have 1 or more risk factors for stroke.
NICE’s draft guidance is now with consultees, who have the opportunity to appeal against it. Once NICE issues its final guidance on a technology, it replaces local recommendations. ![]()
Photo courtesy of the CDC
The UK’s National Institute for Health and Care Excellence (NICE) has issued a draft guidance recommending the oral anticoagulant edoxaban tosylate (Lixiana) as an option for preventing stroke and systemic embolism in adults with non-valvular atrial fibrillation (NVAF).
The patients must have 1 or more risk factors for stroke, including congestive heart failure, hypertension, diabetes, prior stroke or transient ischemic attack, and age of 75 years or older.
Such patients are generally treated with warfarin or the newer oral anticoagulants dabigatran, rivaroxaban, and apixaban.
NICE said it wants to add edoxaban to that list because the drug is a clinically and cost-effective treatment option for these patients.
NICE’s draft guidance says the decision about whether to start treatment with edoxaban should be made after an informed discussion between the clinician and the patient about the risks and benefits of edoxaban compared with warfarin, apixaban, dabigatran, and rivaroxaban.
For patients considering switching from warfarin, edoxaban’s potential benefits should be weighed against its potential risks, taking into account the patient’s level of international normalized ratio control.
Clinical effectiveness
NICE’s conclusion that edoxaban is clinically effective was based primarily on results of the ENGAGE AF-TIMI 48 trial. In this trial, researchers compared edoxaban and warfarin as prophylaxis for stroke or systemic embolism in patients with NVAF.
Results suggested edoxaban was at least non-inferior to warfarin with regard to efficacy, and edoxaban was associated with a significantly lower rate of major and fatal bleeding.
A committee advising NICE also reviewed a meta-analysis prepared by Daiichi Sankyo Co., Ltd., the company developing edoxaban.
The goal of the meta-analysis was to compare edoxaban with rivaroxaban, apixaban, and dabigatran. The analysis included 4 trials: ENGAGE AF-TIMI 48, ARISTOTLE (apixaban), RE-LY (dabigatran), and ROCKET-AF (rivaroxaban). All 4 trials had a warfarin comparator arm.
The results of the meta-analysis indicated that, for the composite endpoint of stroke and systemic embolism, efficacy was similar for high-dose edoxaban and the other newer oral anticoagulants.
However, edoxaban significantly reduced major bleeding risk by 24% compared to rivaroxaban, 28% compared to dabigatran at 150 mg, and 17% compared to dabigatran at 110 mg. Major bleeding rates were similar for high-dose edoxaban and apixaban.
The committee advising NICE said these results should be interpreted with caution, but edoxaban is unlikely to be different from rivaroxaban, apixaban, and dabigatran in clinical practice.
Cost-effectiveness
Edoxaban costs £58.80 for a 28-tablet pack (60 mg or 30 mg), and the daily cost of treatment is £2.10 (excluding value-added tax). However, costs may vary in different settings because of negotiated procurement discounts.
The committee advising NICE analyzed cost information and concluded that edoxaban is cost-effective compared with warfarin, but there is insufficient evidence to distinguish between the clinical and cost-effectiveness of edoxaban and the newer oral anticoagulants.
Nevertheless, the committee recommended edoxaban as a cost-effective treatment for patients with NVAF who have 1 or more risk factors for stroke.
NICE’s draft guidance is now with consultees, who have the opportunity to appeal against it. Once NICE issues its final guidance on a technology, it replaces local recommendations. ![]()
FDA approves IVIG product for kids

Photo by Bill Branson
The US Food and Drug Administration (FDA) has approved an intravenous human immune globulin (IVIG) product (Gammaplex) for pediatric patients age 2 years and older who have primary humoral immunodeficiencies.
This includes, but is not limited to, the humoral immune defect in common variable immunodeficiency, X-linked agammaglobulinemia, congenital agammaglobulinemia, Wiskott Aldrich syndrome, and severe combined immunodeficiencies.
The approval was based on data submitted to the FDA as part of a post-marketing commitment following approval of the product for replacement therapy in adults in 2009.
Data supporting the latest approval came from a study of 25 children and adolescents (ages 3 to 16) with primary immunodeficiencies who were treated with IVIG for 12 months.
The study’s primary efficacy endpoint was the incidence of serious, acute bacterial infections (SABIs) as defined by the FDA. Secondary endpoints were safety and tolerability.
Throughout the course of the study, there were 2 SABIs—both pneumonia—resulting in an annual SABI event rate of 0.09, well below the maximum SABI event rate of 0.5 per subject required for approval.
Fourteen subjects (56%) had an adverse event that was possibly related to IVIG. Two patients experienced events that were considered definitely related to the treatment—headache, fatigue, and myalgia.
The most common adverse events, occurring in ≥ 5% of subjects, were dyspnea (2/25, 8%), otitis media acute (2/25, 8%), and tonsillar disorder (2/25, 8%).
Two patients had a serious adverse event of lobar pneumonia. Neither of these was considered related to IVIG, and neither met FDA-defined SABI criteria. None of the subjects withdrew from the study due to adverse events.
IVIG is marketed as Gammaplex by Bio Products Laboratory Limited. For more details on the treatment, see the full prescribing information. ![]()
Photo by Bill Branson
The US Food and Drug Administration (FDA) has approved an intravenous human immune globulin (IVIG) product (Gammaplex) for pediatric patients age 2 years and older who have primary humoral immunodeficiencies.
This includes, but is not limited to, the humoral immune defect in common variable immunodeficiency, X-linked agammaglobulinemia, congenital agammaglobulinemia, Wiskott Aldrich syndrome, and severe combined immunodeficiencies.
The approval was based on data submitted to the FDA as part of a post-marketing commitment following approval of the product for replacement therapy in adults in 2009.
Data supporting the latest approval came from a study of 25 children and adolescents (ages 3 to 16) with primary immunodeficiencies who were treated with IVIG for 12 months.
The study’s primary efficacy endpoint was the incidence of serious, acute bacterial infections (SABIs) as defined by the FDA. Secondary endpoints were safety and tolerability.
Throughout the course of the study, there were 2 SABIs—both pneumonia—resulting in an annual SABI event rate of 0.09, well below the maximum SABI event rate of 0.5 per subject required for approval.
Fourteen subjects (56%) had an adverse event that was possibly related to IVIG. Two patients experienced events that were considered definitely related to the treatment—headache, fatigue, and myalgia.
The most common adverse events, occurring in ≥ 5% of subjects, were dyspnea (2/25, 8%), otitis media acute (2/25, 8%), and tonsillar disorder (2/25, 8%).
Two patients had a serious adverse event of lobar pneumonia. Neither of these was considered related to IVIG, and neither met FDA-defined SABI criteria. None of the subjects withdrew from the study due to adverse events.
IVIG is marketed as Gammaplex by Bio Products Laboratory Limited. For more details on the treatment, see the full prescribing information. ![]()
Photo by Bill Branson
The US Food and Drug Administration (FDA) has approved an intravenous human immune globulin (IVIG) product (Gammaplex) for pediatric patients age 2 years and older who have primary humoral immunodeficiencies.
This includes, but is not limited to, the humoral immune defect in common variable immunodeficiency, X-linked agammaglobulinemia, congenital agammaglobulinemia, Wiskott Aldrich syndrome, and severe combined immunodeficiencies.
The approval was based on data submitted to the FDA as part of a post-marketing commitment following approval of the product for replacement therapy in adults in 2009.
Data supporting the latest approval came from a study of 25 children and adolescents (ages 3 to 16) with primary immunodeficiencies who were treated with IVIG for 12 months.
The study’s primary efficacy endpoint was the incidence of serious, acute bacterial infections (SABIs) as defined by the FDA. Secondary endpoints were safety and tolerability.
Throughout the course of the study, there were 2 SABIs—both pneumonia—resulting in an annual SABI event rate of 0.09, well below the maximum SABI event rate of 0.5 per subject required for approval.
Fourteen subjects (56%) had an adverse event that was possibly related to IVIG. Two patients experienced events that were considered definitely related to the treatment—headache, fatigue, and myalgia.
The most common adverse events, occurring in ≥ 5% of subjects, were dyspnea (2/25, 8%), otitis media acute (2/25, 8%), and tonsillar disorder (2/25, 8%).
Two patients had a serious adverse event of lobar pneumonia. Neither of these was considered related to IVIG, and neither met FDA-defined SABI criteria. None of the subjects withdrew from the study due to adverse events.
IVIG is marketed as Gammaplex by Bio Products Laboratory Limited. For more details on the treatment, see the full prescribing information. ![]()
Drug on fast track to treat aHUS

Image by Kevin MacKenzie
The US Food and Drug Administration (FDA) has granted fast track designation to OMS721 for the treatment of atypical hemolytic uremic syndrome (aHUS).
OMS721 is a monoclonal antibody targeting mannan-binding lectin-associated serine protease-2 (MASP-2), a key regulator of the lectin pathway of the complement system.
The FDA previously granted OMS721 orphan designation for the prevention of thrombotic microangiopathies (TMAs).
Omeros Corporation, the company developing OMS721, has released results from a phase 1 trial of the drug in healthy subjects and an ongoing phase 2 trial in patients with TMAs, including aHUS.
Early positive responses in the phase 2 trial prompted the initiation of a compassionate use program for OMS721 to allow extended treatment of 2 patients who had completed 4 weeks of dosing.
Phase 1 results
In the phase 1 trial of healthy subjects, OMS721 was well tolerated and prompted a high degree of sustained lectin pathway inhibition, according to researchers.
Seven cohorts of subjects received OMS721 or placebo by either subcutaneous injection or intravenous infusion at increasing dose levels. The researchers observed no drug-related adverse events and no clinically significant abnormalities on laboratory tests or electrocardiograms.
At the highest dose evaluated, both routes of administration prompted inhibition of the lectin pathway and achieved the pharmacologic target of sustained inhibition for at least a week.
Phase 2 results and compassionate use
In the ongoing phase 2 study, all patients are receiving OMS721. The researchers said they have observed treatment-related, clinically meaningful improvements in disease markers among the patients treated thus far.
The first cohort in this trial consisted of 3 aHUS patients treated with the lowest dose of OMS721. All 3 patients had improvements in platelet counts after treatment. Serum haptoglobin improved in 2 patients, normalizing in 1.
Serum lactate dehydrogenase levels remained normal in 1 patient, substantially decreased to close to the normal range in another, and remained elevated in the third. Creatinine levels in the 1 patient with independent renal function improved.
One patient was taken off the trial because of a serious adverse event—a localized inflammatory response often related to certain types of infections, one of which the patient previously had for 3 years while on immunosuppressive therapy. All data to date indicate no active infection in this patient.
The patient relapsed after stopping OMS721 treatment. No other significant safety issues were observed in this trial or the phase 1 trial.
The other 2 aHUS patients in this cohort continue to receive OMS721 as part of a compassionate use program. Based on their improvements in disease markers, an investigator requested that Omeros continue to provide OMS721 to these patients.
Following European regulatory approval, Omeros released the shipment of OMS721 so these patients could continue treatment beyond the period that was initially planned for the phase 2 study.
About fast track and orphan designation
The FDA’s fast track program facilitates the development of drugs intended to treat serious or life-threatening conditions and that have the potential to address unmet medical needs. Fast track status affords the company developing a drug greater access to the FDA in order to expedite the drug’s development, review, and potential approval.
Many drugs that receive fast track designation also receive priority review, and their new drug applications may be accepted by the FDA as a rolling submission, in which portions of an application are reviewed before the complete application is submitted. Priority review and rolling submission can each provide further acceleration of the FDA’s approval process.
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US.
Orphan designation provides a drug’s developer with opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, 7 years of US marketing exclusivity if the drug is approved, and other benefits. ![]()
Image by Kevin MacKenzie
The US Food and Drug Administration (FDA) has granted fast track designation to OMS721 for the treatment of atypical hemolytic uremic syndrome (aHUS).
OMS721 is a monoclonal antibody targeting mannan-binding lectin-associated serine protease-2 (MASP-2), a key regulator of the lectin pathway of the complement system.
The FDA previously granted OMS721 orphan designation for the prevention of thrombotic microangiopathies (TMAs).
Omeros Corporation, the company developing OMS721, has released results from a phase 1 trial of the drug in healthy subjects and an ongoing phase 2 trial in patients with TMAs, including aHUS.
Early positive responses in the phase 2 trial prompted the initiation of a compassionate use program for OMS721 to allow extended treatment of 2 patients who had completed 4 weeks of dosing.
Phase 1 results
In the phase 1 trial of healthy subjects, OMS721 was well tolerated and prompted a high degree of sustained lectin pathway inhibition, according to researchers.
Seven cohorts of subjects received OMS721 or placebo by either subcutaneous injection or intravenous infusion at increasing dose levels. The researchers observed no drug-related adverse events and no clinically significant abnormalities on laboratory tests or electrocardiograms.
At the highest dose evaluated, both routes of administration prompted inhibition of the lectin pathway and achieved the pharmacologic target of sustained inhibition for at least a week.
Phase 2 results and compassionate use
In the ongoing phase 2 study, all patients are receiving OMS721. The researchers said they have observed treatment-related, clinically meaningful improvements in disease markers among the patients treated thus far.
The first cohort in this trial consisted of 3 aHUS patients treated with the lowest dose of OMS721. All 3 patients had improvements in platelet counts after treatment. Serum haptoglobin improved in 2 patients, normalizing in 1.
Serum lactate dehydrogenase levels remained normal in 1 patient, substantially decreased to close to the normal range in another, and remained elevated in the third. Creatinine levels in the 1 patient with independent renal function improved.
One patient was taken off the trial because of a serious adverse event—a localized inflammatory response often related to certain types of infections, one of which the patient previously had for 3 years while on immunosuppressive therapy. All data to date indicate no active infection in this patient.
The patient relapsed after stopping OMS721 treatment. No other significant safety issues were observed in this trial or the phase 1 trial.
The other 2 aHUS patients in this cohort continue to receive OMS721 as part of a compassionate use program. Based on their improvements in disease markers, an investigator requested that Omeros continue to provide OMS721 to these patients.
Following European regulatory approval, Omeros released the shipment of OMS721 so these patients could continue treatment beyond the period that was initially planned for the phase 2 study.
About fast track and orphan designation
The FDA’s fast track program facilitates the development of drugs intended to treat serious or life-threatening conditions and that have the potential to address unmet medical needs. Fast track status affords the company developing a drug greater access to the FDA in order to expedite the drug’s development, review, and potential approval.
Many drugs that receive fast track designation also receive priority review, and their new drug applications may be accepted by the FDA as a rolling submission, in which portions of an application are reviewed before the complete application is submitted. Priority review and rolling submission can each provide further acceleration of the FDA’s approval process.
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US.
Orphan designation provides a drug’s developer with opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, 7 years of US marketing exclusivity if the drug is approved, and other benefits. ![]()
Image by Kevin MacKenzie
The US Food and Drug Administration (FDA) has granted fast track designation to OMS721 for the treatment of atypical hemolytic uremic syndrome (aHUS).
OMS721 is a monoclonal antibody targeting mannan-binding lectin-associated serine protease-2 (MASP-2), a key regulator of the lectin pathway of the complement system.
The FDA previously granted OMS721 orphan designation for the prevention of thrombotic microangiopathies (TMAs).
Omeros Corporation, the company developing OMS721, has released results from a phase 1 trial of the drug in healthy subjects and an ongoing phase 2 trial in patients with TMAs, including aHUS.
Early positive responses in the phase 2 trial prompted the initiation of a compassionate use program for OMS721 to allow extended treatment of 2 patients who had completed 4 weeks of dosing.
Phase 1 results
In the phase 1 trial of healthy subjects, OMS721 was well tolerated and prompted a high degree of sustained lectin pathway inhibition, according to researchers.
Seven cohorts of subjects received OMS721 or placebo by either subcutaneous injection or intravenous infusion at increasing dose levels. The researchers observed no drug-related adverse events and no clinically significant abnormalities on laboratory tests or electrocardiograms.
At the highest dose evaluated, both routes of administration prompted inhibition of the lectin pathway and achieved the pharmacologic target of sustained inhibition for at least a week.
Phase 2 results and compassionate use
In the ongoing phase 2 study, all patients are receiving OMS721. The researchers said they have observed treatment-related, clinically meaningful improvements in disease markers among the patients treated thus far.
The first cohort in this trial consisted of 3 aHUS patients treated with the lowest dose of OMS721. All 3 patients had improvements in platelet counts after treatment. Serum haptoglobin improved in 2 patients, normalizing in 1.
Serum lactate dehydrogenase levels remained normal in 1 patient, substantially decreased to close to the normal range in another, and remained elevated in the third. Creatinine levels in the 1 patient with independent renal function improved.
One patient was taken off the trial because of a serious adverse event—a localized inflammatory response often related to certain types of infections, one of which the patient previously had for 3 years while on immunosuppressive therapy. All data to date indicate no active infection in this patient.
The patient relapsed after stopping OMS721 treatment. No other significant safety issues were observed in this trial or the phase 1 trial.
The other 2 aHUS patients in this cohort continue to receive OMS721 as part of a compassionate use program. Based on their improvements in disease markers, an investigator requested that Omeros continue to provide OMS721 to these patients.
Following European regulatory approval, Omeros released the shipment of OMS721 so these patients could continue treatment beyond the period that was initially planned for the phase 2 study.
About fast track and orphan designation
The FDA’s fast track program facilitates the development of drugs intended to treat serious or life-threatening conditions and that have the potential to address unmet medical needs. Fast track status affords the company developing a drug greater access to the FDA in order to expedite the drug’s development, review, and potential approval.
Many drugs that receive fast track designation also receive priority review, and their new drug applications may be accepted by the FDA as a rolling submission, in which portions of an application are reviewed before the complete application is submitted. Priority review and rolling submission can each provide further acceleration of the FDA’s approval process.
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US.
Orphan designation provides a drug’s developer with opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, 7 years of US marketing exclusivity if the drug is approved, and other benefits. ![]()
FDA grants drug orphan designation for ITP

Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted orphan designation to veltuzumab for the treatment of immune thrombocytopenia (ITP).
Veltuzumab is a 2nd-generation, humanized monoclonal antibody targeting CD20. The drug is being developed by Immunomedics as a treatment for ITP, other autoimmune diseases, and non-Hodgkin lymphoma.
Veltuzumab was considered active and well-tolerated in a phase 1 study of adults with ITP. The drug produced responses in about half of patients, with some responses lasting more than 4 years.
The study included 50 patients with primary ITP who had failed 1 or more types of standard therapy, had platelet levels of 30,000/μL or less, and did not have major bleeding. The patients’ median age was 54, and most were female (n=31). Eight patients had undergone splenectomy.
Patients were a median of 2 years from diagnosis. Fourteen had been diagnosed with ITP for a year or less and had received corticosteroids and/or immunoglobulins.
Thirty-six patients had chronic ITP and had received azathioprine or danazol (n=15), thrombopoietin-receptor agonists (n=10), rituximab (n=7), platelets (n=5), and/or chemotherapy (n=4).
The 34 patients assigned to cohort 1 received 2 doses of subcutaneous veltuzumab at 80 mg, 160 mg, or 320 mg, 2 weeks apart (total doses of 160 mg, 320 mg, and 640 mg, respectively). The 18 patients in cohort 2 (which included 2 rollovers) received once-weekly doses at 320 mg for 4 weeks (total dose of 1280 mg).
The researchers said veltuzumab was well tolerated. The only adverse events were grade 1-2, transient injection reactions.
Forty-seven patients were evaluable for response. Forty-seven percent (n=22) had objective responses (ORs), and 28% (n=13) had complete responses (CRs).
Responses did not differ much according to disease duration. Patients with chronic ITP had an OR rate of 42% and a CR rate of 27%. Patients who had ITP for a year or less had an OR rate of 51% and a CR rate of 29%.
The median time to relapse (TTR) did not differ much between patients with CRs and those with partial responses, but there was a sizable difference between patients with chronic ITP and those with newly diagnosed ITP.
The median TTR was 7.9 months for patients with a CR and 7.6 months for patients with a partial response. The median TTR was 6.9 months for patients with chronic ITP and 14.4 months for patients who had ITP for a year or less.
The phase 2 expansion trial of veltuzumab in ITP has completed accrual, and patients are being followed for up to 5 years.
About orphan designation
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US. Orphan designation provides the sponsor of a drug with various development incentives.
The orphan designation for veltuzumab provides Immunomedics with opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, 7 years of US marketing exclusivity if the drug is approved, and other benefits. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted orphan designation to veltuzumab for the treatment of immune thrombocytopenia (ITP).
Veltuzumab is a 2nd-generation, humanized monoclonal antibody targeting CD20. The drug is being developed by Immunomedics as a treatment for ITP, other autoimmune diseases, and non-Hodgkin lymphoma.
Veltuzumab was considered active and well-tolerated in a phase 1 study of adults with ITP. The drug produced responses in about half of patients, with some responses lasting more than 4 years.
The study included 50 patients with primary ITP who had failed 1 or more types of standard therapy, had platelet levels of 30,000/μL or less, and did not have major bleeding. The patients’ median age was 54, and most were female (n=31). Eight patients had undergone splenectomy.
Patients were a median of 2 years from diagnosis. Fourteen had been diagnosed with ITP for a year or less and had received corticosteroids and/or immunoglobulins.
Thirty-six patients had chronic ITP and had received azathioprine or danazol (n=15), thrombopoietin-receptor agonists (n=10), rituximab (n=7), platelets (n=5), and/or chemotherapy (n=4).
The 34 patients assigned to cohort 1 received 2 doses of subcutaneous veltuzumab at 80 mg, 160 mg, or 320 mg, 2 weeks apart (total doses of 160 mg, 320 mg, and 640 mg, respectively). The 18 patients in cohort 2 (which included 2 rollovers) received once-weekly doses at 320 mg for 4 weeks (total dose of 1280 mg).
The researchers said veltuzumab was well tolerated. The only adverse events were grade 1-2, transient injection reactions.
Forty-seven patients were evaluable for response. Forty-seven percent (n=22) had objective responses (ORs), and 28% (n=13) had complete responses (CRs).
Responses did not differ much according to disease duration. Patients with chronic ITP had an OR rate of 42% and a CR rate of 27%. Patients who had ITP for a year or less had an OR rate of 51% and a CR rate of 29%.
The median time to relapse (TTR) did not differ much between patients with CRs and those with partial responses, but there was a sizable difference between patients with chronic ITP and those with newly diagnosed ITP.
The median TTR was 7.9 months for patients with a CR and 7.6 months for patients with a partial response. The median TTR was 6.9 months for patients with chronic ITP and 14.4 months for patients who had ITP for a year or less.
The phase 2 expansion trial of veltuzumab in ITP has completed accrual, and patients are being followed for up to 5 years.
About orphan designation
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US. Orphan designation provides the sponsor of a drug with various development incentives.
The orphan designation for veltuzumab provides Immunomedics with opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, 7 years of US marketing exclusivity if the drug is approved, and other benefits. ![]()
Photo by Linda Bartlett
The US Food and Drug Administration (FDA) has granted orphan designation to veltuzumab for the treatment of immune thrombocytopenia (ITP).
Veltuzumab is a 2nd-generation, humanized monoclonal antibody targeting CD20. The drug is being developed by Immunomedics as a treatment for ITP, other autoimmune diseases, and non-Hodgkin lymphoma.
Veltuzumab was considered active and well-tolerated in a phase 1 study of adults with ITP. The drug produced responses in about half of patients, with some responses lasting more than 4 years.
The study included 50 patients with primary ITP who had failed 1 or more types of standard therapy, had platelet levels of 30,000/μL or less, and did not have major bleeding. The patients’ median age was 54, and most were female (n=31). Eight patients had undergone splenectomy.
Patients were a median of 2 years from diagnosis. Fourteen had been diagnosed with ITP for a year or less and had received corticosteroids and/or immunoglobulins.
Thirty-six patients had chronic ITP and had received azathioprine or danazol (n=15), thrombopoietin-receptor agonists (n=10), rituximab (n=7), platelets (n=5), and/or chemotherapy (n=4).
The 34 patients assigned to cohort 1 received 2 doses of subcutaneous veltuzumab at 80 mg, 160 mg, or 320 mg, 2 weeks apart (total doses of 160 mg, 320 mg, and 640 mg, respectively). The 18 patients in cohort 2 (which included 2 rollovers) received once-weekly doses at 320 mg for 4 weeks (total dose of 1280 mg).
The researchers said veltuzumab was well tolerated. The only adverse events were grade 1-2, transient injection reactions.
Forty-seven patients were evaluable for response. Forty-seven percent (n=22) had objective responses (ORs), and 28% (n=13) had complete responses (CRs).
Responses did not differ much according to disease duration. Patients with chronic ITP had an OR rate of 42% and a CR rate of 27%. Patients who had ITP for a year or less had an OR rate of 51% and a CR rate of 29%.
The median time to relapse (TTR) did not differ much between patients with CRs and those with partial responses, but there was a sizable difference between patients with chronic ITP and those with newly diagnosed ITP.
The median TTR was 7.9 months for patients with a CR and 7.6 months for patients with a partial response. The median TTR was 6.9 months for patients with chronic ITP and 14.4 months for patients who had ITP for a year or less.
The phase 2 expansion trial of veltuzumab in ITP has completed accrual, and patients are being followed for up to 5 years.
About orphan designation
The FDA grants orphan designation to drugs that are intended to treat diseases or conditions affecting fewer than 200,000 patients in the US. Orphan designation provides the sponsor of a drug with various development incentives.
The orphan designation for veltuzumab provides Immunomedics with opportunities to apply for research-related tax credits and grant funding, assistance in designing clinical trials, 7 years of US marketing exclusivity if the drug is approved, and other benefits. ![]()
Drug gets orphan designation for CTCL
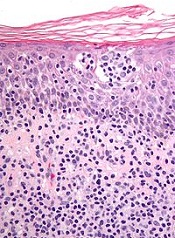
The European Commission has granted orphan drug designation to synthetic hypericin, the active pharmaceutical ingredient in SGX301, for the treatment of cutaneous T-cell lymphoma (CTCL).
SGX301 is a first-in-class, photodynamic therapy utilizing safe, visible light for activation. Synthetic hypericin is a potent photosensitizer that is topically applied to skin lesions and activated by visible fluorescent light 16 to 24 hours later.
This treatment approach is intended to prevent the secondary malignancies that may occur following chemotherapy or photodynamic therapies that are dependent on ultraviolet exposure.
Combined with photoactivation, hypericin has demonstrated significant antiproliferative effects on activated, normal human lymphoid cells and inhibited the growth of malignant T cells isolated from CTCL patients.
Topical hypericin has also proven safe in a phase 1 study of healthy volunteers.
In a phase 2 trial of patients with CTCL (mycosis fungoides only) or psoriasis, topical hypericin conferred a significant improvement over placebo. Among CTCL patients, the treatment prompted a response rate of 58.3%, compared to an 8.3% response rate for placebo (P≤0.04).
Topical hypericin was also well tolerated in this trial. There were no deaths or serious adverse events related to the treatment. However, there were reports of mild to moderate burning, itching, erythema, and pruritus at the application site.
Soligenix, Inc., the company developing SGX301, is currently working with CTCL centers, the National Organization for Rare Disorders, and the Cutaneous Lymphoma Foundation to begin a 120-subject phase 3 trial of SGX301.
About orphan designation
The European Commission grants orphan designation to medicines designed to treat a life-threatening or chronically debilitating condition that affects no more than 5 in 10,000 persons in the European Union and has no satisfactory treatment available.
In addition to a 10-year period of marketing exclusivity after product approval, orphan drug designation provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase, as well as direct access to the centralized authorization procedure.
SGX301 has both orphan designation and fast track designation from the US Food and Drug Administration for the first-line treatment of CTCL. ![]()
The European Commission has granted orphan drug designation to synthetic hypericin, the active pharmaceutical ingredient in SGX301, for the treatment of cutaneous T-cell lymphoma (CTCL).
SGX301 is a first-in-class, photodynamic therapy utilizing safe, visible light for activation. Synthetic hypericin is a potent photosensitizer that is topically applied to skin lesions and activated by visible fluorescent light 16 to 24 hours later.
This treatment approach is intended to prevent the secondary malignancies that may occur following chemotherapy or photodynamic therapies that are dependent on ultraviolet exposure.
Combined with photoactivation, hypericin has demonstrated significant antiproliferative effects on activated, normal human lymphoid cells and inhibited the growth of malignant T cells isolated from CTCL patients.
Topical hypericin has also proven safe in a phase 1 study of healthy volunteers.
In a phase 2 trial of patients with CTCL (mycosis fungoides only) or psoriasis, topical hypericin conferred a significant improvement over placebo. Among CTCL patients, the treatment prompted a response rate of 58.3%, compared to an 8.3% response rate for placebo (P≤0.04).
Topical hypericin was also well tolerated in this trial. There were no deaths or serious adverse events related to the treatment. However, there were reports of mild to moderate burning, itching, erythema, and pruritus at the application site.
Soligenix, Inc., the company developing SGX301, is currently working with CTCL centers, the National Organization for Rare Disorders, and the Cutaneous Lymphoma Foundation to begin a 120-subject phase 3 trial of SGX301.
About orphan designation
The European Commission grants orphan designation to medicines designed to treat a life-threatening or chronically debilitating condition that affects no more than 5 in 10,000 persons in the European Union and has no satisfactory treatment available.
In addition to a 10-year period of marketing exclusivity after product approval, orphan drug designation provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase, as well as direct access to the centralized authorization procedure.
SGX301 has both orphan designation and fast track designation from the US Food and Drug Administration for the first-line treatment of CTCL. ![]()
The European Commission has granted orphan drug designation to synthetic hypericin, the active pharmaceutical ingredient in SGX301, for the treatment of cutaneous T-cell lymphoma (CTCL).
SGX301 is a first-in-class, photodynamic therapy utilizing safe, visible light for activation. Synthetic hypericin is a potent photosensitizer that is topically applied to skin lesions and activated by visible fluorescent light 16 to 24 hours later.
This treatment approach is intended to prevent the secondary malignancies that may occur following chemotherapy or photodynamic therapies that are dependent on ultraviolet exposure.
Combined with photoactivation, hypericin has demonstrated significant antiproliferative effects on activated, normal human lymphoid cells and inhibited the growth of malignant T cells isolated from CTCL patients.
Topical hypericin has also proven safe in a phase 1 study of healthy volunteers.
In a phase 2 trial of patients with CTCL (mycosis fungoides only) or psoriasis, topical hypericin conferred a significant improvement over placebo. Among CTCL patients, the treatment prompted a response rate of 58.3%, compared to an 8.3% response rate for placebo (P≤0.04).
Topical hypericin was also well tolerated in this trial. There were no deaths or serious adverse events related to the treatment. However, there were reports of mild to moderate burning, itching, erythema, and pruritus at the application site.
Soligenix, Inc., the company developing SGX301, is currently working with CTCL centers, the National Organization for Rare Disorders, and the Cutaneous Lymphoma Foundation to begin a 120-subject phase 3 trial of SGX301.
About orphan designation
The European Commission grants orphan designation to medicines designed to treat a life-threatening or chronically debilitating condition that affects no more than 5 in 10,000 persons in the European Union and has no satisfactory treatment available.
In addition to a 10-year period of marketing exclusivity after product approval, orphan drug designation provides incentives for companies seeking protocol assistance from the European Medicines Agency during the product development phase, as well as direct access to the centralized authorization procedure.
SGX301 has both orphan designation and fast track designation from the US Food and Drug Administration for the first-line treatment of CTCL. ![]()
FDA warns of anticoagulant/antidepressant mix-up

Photo courtesy of AstraZeneca
The US Food and Drug Administration (FDA) has announced that confusion between the anticoagulant Brilinta (ticagrelor) and the antidepressant Brintellix (vortioxetine) is resulting in the wrong medication being prescribed or dispensed.
The FDA found the main reason for the confusion is the similarity of the drugs’ brand names.
None of the reports the FDA received indicate that a patient ingested the wrong medication. However, the FDA continues to receive reports of prescribing and dispensing errors.
As of June 2015, the agency has received 50 reports of name confusion between Brintellix and Brilinta. The FDA confirmed that the wrong medication was dispensed to a patient in 12 of the cases and may have been dispensed in 3 additional cases.
About the medications
Brilinta is a P2Y12 platelet inhibitor approved for use in patients with acute coronary syndrome to reduce the rate of thrombotic cardiovascular events. The drug comes in the form of a round, yellow tablet with a “90” above a “T” stamped on one side.
Brintellix is a selective serotonin reuptake inhibitor used to treat major depressive disorder in adults. The medication comes in the form of a tear-shaped tablet stamped with “TL” on one side of the tablet and a number that indicates the tablet strength on the other side. It varies in color depending upon the strength prescribed.
About the error reports
As of June 2015, the FDA has received 50 medication error reports describing brand name confusion with Brintellix (vortioxetine) and Brilinta (ticagrelor). In most cases, Brintellix was mistaken as Brilinta.
Some of the contributing factors to the name confusion included the following:
- Both brand names begin with the same 3 letters
- Both brand names are presented when selecting medications in a computerized physician order entry (CPOE) system
- The pharmacist was not familiar with the new medication Brintellix and so dispensed Brilinta
- The brand names look and sound similar.
Of these 50 reports, the wrong medication was actually dispensed in 12 cases and was possibly dispensed in 3 additional cases but could not be confirmed based on the case narrative information. None of the reports indicated a patient had ingested the wrong medication.
However, in one case, Brintellix was misinterpreted as Brilinta, and the pharmacist did not dispense any medication because the patient had a contraindication to antiplatelet therapy. As a result, the patient went untreated for the psychiatric indication for an unreported period.
In the 12 cases where a wrong medication was actually dispensed, the reports showed that, in 6 cases, the error occurred when prescribing the medication.
Five of these prescribing errors occurred during CPOE. Some CPOE systems auto-populate or present a drop-down menu after the first 3 letters are typed, at which point a prescriber can select the wrong medication.
In the other 6 cases, the error occurred during dispensing of the medication.
FDA recommendations
The FDA is recommending that healthcare professionals reduce the risk of name confusion when prescribing these medications by including the generic names, indications for use, correct dosage, and directions for use.
Healthcare professionals should also ensure that patients understand what their medication is used to treat and encourage patients and their caregivers to read the Medication Guides provided with their Brintellix and Brilinta prescriptions.
Healthcare professionals and patients can report name confusion and medication errors involving Brintellix and Brilinta to the FDA MedWatch Program. ![]()
Photo courtesy of AstraZeneca
The US Food and Drug Administration (FDA) has announced that confusion between the anticoagulant Brilinta (ticagrelor) and the antidepressant Brintellix (vortioxetine) is resulting in the wrong medication being prescribed or dispensed.
The FDA found the main reason for the confusion is the similarity of the drugs’ brand names.
None of the reports the FDA received indicate that a patient ingested the wrong medication. However, the FDA continues to receive reports of prescribing and dispensing errors.
As of June 2015, the agency has received 50 reports of name confusion between Brintellix and Brilinta. The FDA confirmed that the wrong medication was dispensed to a patient in 12 of the cases and may have been dispensed in 3 additional cases.
About the medications
Brilinta is a P2Y12 platelet inhibitor approved for use in patients with acute coronary syndrome to reduce the rate of thrombotic cardiovascular events. The drug comes in the form of a round, yellow tablet with a “90” above a “T” stamped on one side.
Brintellix is a selective serotonin reuptake inhibitor used to treat major depressive disorder in adults. The medication comes in the form of a tear-shaped tablet stamped with “TL” on one side of the tablet and a number that indicates the tablet strength on the other side. It varies in color depending upon the strength prescribed.
About the error reports
As of June 2015, the FDA has received 50 medication error reports describing brand name confusion with Brintellix (vortioxetine) and Brilinta (ticagrelor). In most cases, Brintellix was mistaken as Brilinta.
Some of the contributing factors to the name confusion included the following:
- Both brand names begin with the same 3 letters
- Both brand names are presented when selecting medications in a computerized physician order entry (CPOE) system
- The pharmacist was not familiar with the new medication Brintellix and so dispensed Brilinta
- The brand names look and sound similar.
Of these 50 reports, the wrong medication was actually dispensed in 12 cases and was possibly dispensed in 3 additional cases but could not be confirmed based on the case narrative information. None of the reports indicated a patient had ingested the wrong medication.
However, in one case, Brintellix was misinterpreted as Brilinta, and the pharmacist did not dispense any medication because the patient had a contraindication to antiplatelet therapy. As a result, the patient went untreated for the psychiatric indication for an unreported period.
In the 12 cases where a wrong medication was actually dispensed, the reports showed that, in 6 cases, the error occurred when prescribing the medication.
Five of these prescribing errors occurred during CPOE. Some CPOE systems auto-populate or present a drop-down menu after the first 3 letters are typed, at which point a prescriber can select the wrong medication.
In the other 6 cases, the error occurred during dispensing of the medication.
FDA recommendations
The FDA is recommending that healthcare professionals reduce the risk of name confusion when prescribing these medications by including the generic names, indications for use, correct dosage, and directions for use.
Healthcare professionals should also ensure that patients understand what their medication is used to treat and encourage patients and their caregivers to read the Medication Guides provided with their Brintellix and Brilinta prescriptions.
Healthcare professionals and patients can report name confusion and medication errors involving Brintellix and Brilinta to the FDA MedWatch Program. ![]()
Photo courtesy of AstraZeneca
The US Food and Drug Administration (FDA) has announced that confusion between the anticoagulant Brilinta (ticagrelor) and the antidepressant Brintellix (vortioxetine) is resulting in the wrong medication being prescribed or dispensed.
The FDA found the main reason for the confusion is the similarity of the drugs’ brand names.
None of the reports the FDA received indicate that a patient ingested the wrong medication. However, the FDA continues to receive reports of prescribing and dispensing errors.
As of June 2015, the agency has received 50 reports of name confusion between Brintellix and Brilinta. The FDA confirmed that the wrong medication was dispensed to a patient in 12 of the cases and may have been dispensed in 3 additional cases.
About the medications
Brilinta is a P2Y12 platelet inhibitor approved for use in patients with acute coronary syndrome to reduce the rate of thrombotic cardiovascular events. The drug comes in the form of a round, yellow tablet with a “90” above a “T” stamped on one side.
Brintellix is a selective serotonin reuptake inhibitor used to treat major depressive disorder in adults. The medication comes in the form of a tear-shaped tablet stamped with “TL” on one side of the tablet and a number that indicates the tablet strength on the other side. It varies in color depending upon the strength prescribed.
About the error reports
As of June 2015, the FDA has received 50 medication error reports describing brand name confusion with Brintellix (vortioxetine) and Brilinta (ticagrelor). In most cases, Brintellix was mistaken as Brilinta.
Some of the contributing factors to the name confusion included the following:
- Both brand names begin with the same 3 letters
- Both brand names are presented when selecting medications in a computerized physician order entry (CPOE) system
- The pharmacist was not familiar with the new medication Brintellix and so dispensed Brilinta
- The brand names look and sound similar.
Of these 50 reports, the wrong medication was actually dispensed in 12 cases and was possibly dispensed in 3 additional cases but could not be confirmed based on the case narrative information. None of the reports indicated a patient had ingested the wrong medication.
However, in one case, Brintellix was misinterpreted as Brilinta, and the pharmacist did not dispense any medication because the patient had a contraindication to antiplatelet therapy. As a result, the patient went untreated for the psychiatric indication for an unreported period.
In the 12 cases where a wrong medication was actually dispensed, the reports showed that, in 6 cases, the error occurred when prescribing the medication.
Five of these prescribing errors occurred during CPOE. Some CPOE systems auto-populate or present a drop-down menu after the first 3 letters are typed, at which point a prescriber can select the wrong medication.
In the other 6 cases, the error occurred during dispensing of the medication.
FDA recommendations
The FDA is recommending that healthcare professionals reduce the risk of name confusion when prescribing these medications by including the generic names, indications for use, correct dosage, and directions for use.
Healthcare professionals should also ensure that patients understand what their medication is used to treat and encourage patients and their caregivers to read the Medication Guides provided with their Brintellix and Brilinta prescriptions.
Healthcare professionals and patients can report name confusion and medication errors involving Brintellix and Brilinta to the FDA MedWatch Program. ![]()
Health Canada grants drug conditional approval for MCL

Photo courtesy of
Janssen Biotech, Inc.
Health Canada has granted conditional approval for the BTK inhibitor ibrutinib (Imbruvica) to treat patients with relapsed or refractory mantle cell lymphoma (MCL).
This approval was based on data from a phase 2 trial in which ibrutinib conferred an overall response rate of 68% in patients with relapsed/refractory MCL.
For ibrutinib to gain full approval, Health Canada must receive additional data confirming the drug provides a clinical benefit.
Ibrutinib was first approved in Canada in November 2014 for patients with chronic lymphocytic leukemia (CLL), including those with 17p deletion, who have received at least one prior therapy, or for the frontline treatment of patients with CLL with 17p deletion. For this use, ibrutinib was issued marketing authorization without conditions.
Now, Health Canada has issued ibrutinib conditional marketing authorization for the treatment of relapsed/refractory MCL. This decision was based on data from the phase 2 PCYC-1104 trial, which was presented at ASH 2012 and published in NEJM in August 2013.
The study included 111 MCL patients who had received at least one prior therapy. The primary endpoint of the study was overall response rate according to the revised International Working Group criteria for non-Hodgkin lymphoma.
The overall response rate was 68%, with a complete response rate of 21% and a partial response rate of 47%. With a median follow-up of 15.3 months, the median response duration was 17.5 months.
The estimated progression-free survival was 13.9 months, and the overall survival was not reached. The estimated rate of overall survival was 58% at 18 months.
Common nonhematologic adverse events included diarrhea (50%), fatigue (41%), nausea (31%), peripheral edema (28%), dyspnea (27%), constipation (25%), upper respiratory tract infection (23%), vomiting (23%), and decreased appetite (21%). The most common grade 3, 4, or 5 infection was pneumonia (6%).
Grade 3 and 4 hematologic adverse events included neutropenia (16%), thrombocytopenia (11%), and anemia (10%). Grade 3 bleeding events occurred in 5 patients.
Eight patients (7%) had an adverse event that led to treatment discontinuation.
Sixteen patients (14%) died during the trial, 12 due to disease progression and 4 due to an adverse event. Two patients died of pneumonia, 1 from sepsis, and 1 from a cardiac arrest that was not considered drug-related.
Ibrutinib is co-developed by Cilag GmbH International (a member of the Janssen Pharmaceutical Companies) and Pharmacyclics LLC, an AbbVie company. Janssen Inc. markets ibrutinib as Imbruvica in Canada. ![]()
Photo courtesy of
Janssen Biotech, Inc.
Health Canada has granted conditional approval for the BTK inhibitor ibrutinib (Imbruvica) to treat patients with relapsed or refractory mantle cell lymphoma (MCL).
This approval was based on data from a phase 2 trial in which ibrutinib conferred an overall response rate of 68% in patients with relapsed/refractory MCL.
For ibrutinib to gain full approval, Health Canada must receive additional data confirming the drug provides a clinical benefit.
Ibrutinib was first approved in Canada in November 2014 for patients with chronic lymphocytic leukemia (CLL), including those with 17p deletion, who have received at least one prior therapy, or for the frontline treatment of patients with CLL with 17p deletion. For this use, ibrutinib was issued marketing authorization without conditions.
Now, Health Canada has issued ibrutinib conditional marketing authorization for the treatment of relapsed/refractory MCL. This decision was based on data from the phase 2 PCYC-1104 trial, which was presented at ASH 2012 and published in NEJM in August 2013.
The study included 111 MCL patients who had received at least one prior therapy. The primary endpoint of the study was overall response rate according to the revised International Working Group criteria for non-Hodgkin lymphoma.
The overall response rate was 68%, with a complete response rate of 21% and a partial response rate of 47%. With a median follow-up of 15.3 months, the median response duration was 17.5 months.
The estimated progression-free survival was 13.9 months, and the overall survival was not reached. The estimated rate of overall survival was 58% at 18 months.
Common nonhematologic adverse events included diarrhea (50%), fatigue (41%), nausea (31%), peripheral edema (28%), dyspnea (27%), constipation (25%), upper respiratory tract infection (23%), vomiting (23%), and decreased appetite (21%). The most common grade 3, 4, or 5 infection was pneumonia (6%).
Grade 3 and 4 hematologic adverse events included neutropenia (16%), thrombocytopenia (11%), and anemia (10%). Grade 3 bleeding events occurred in 5 patients.
Eight patients (7%) had an adverse event that led to treatment discontinuation.
Sixteen patients (14%) died during the trial, 12 due to disease progression and 4 due to an adverse event. Two patients died of pneumonia, 1 from sepsis, and 1 from a cardiac arrest that was not considered drug-related.
Ibrutinib is co-developed by Cilag GmbH International (a member of the Janssen Pharmaceutical Companies) and Pharmacyclics LLC, an AbbVie company. Janssen Inc. markets ibrutinib as Imbruvica in Canada. ![]()
Photo courtesy of
Janssen Biotech, Inc.
Health Canada has granted conditional approval for the BTK inhibitor ibrutinib (Imbruvica) to treat patients with relapsed or refractory mantle cell lymphoma (MCL).
This approval was based on data from a phase 2 trial in which ibrutinib conferred an overall response rate of 68% in patients with relapsed/refractory MCL.
For ibrutinib to gain full approval, Health Canada must receive additional data confirming the drug provides a clinical benefit.
Ibrutinib was first approved in Canada in November 2014 for patients with chronic lymphocytic leukemia (CLL), including those with 17p deletion, who have received at least one prior therapy, or for the frontline treatment of patients with CLL with 17p deletion. For this use, ibrutinib was issued marketing authorization without conditions.
Now, Health Canada has issued ibrutinib conditional marketing authorization for the treatment of relapsed/refractory MCL. This decision was based on data from the phase 2 PCYC-1104 trial, which was presented at ASH 2012 and published in NEJM in August 2013.
The study included 111 MCL patients who had received at least one prior therapy. The primary endpoint of the study was overall response rate according to the revised International Working Group criteria for non-Hodgkin lymphoma.
The overall response rate was 68%, with a complete response rate of 21% and a partial response rate of 47%. With a median follow-up of 15.3 months, the median response duration was 17.5 months.
The estimated progression-free survival was 13.9 months, and the overall survival was not reached. The estimated rate of overall survival was 58% at 18 months.
Common nonhematologic adverse events included diarrhea (50%), fatigue (41%), nausea (31%), peripheral edema (28%), dyspnea (27%), constipation (25%), upper respiratory tract infection (23%), vomiting (23%), and decreased appetite (21%). The most common grade 3, 4, or 5 infection was pneumonia (6%).
Grade 3 and 4 hematologic adverse events included neutropenia (16%), thrombocytopenia (11%), and anemia (10%). Grade 3 bleeding events occurred in 5 patients.
Eight patients (7%) had an adverse event that led to treatment discontinuation.
Sixteen patients (14%) died during the trial, 12 due to disease progression and 4 due to an adverse event. Two patients died of pneumonia, 1 from sepsis, and 1 from a cardiac arrest that was not considered drug-related.
Ibrutinib is co-developed by Cilag GmbH International (a member of the Janssen Pharmaceutical Companies) and Pharmacyclics LLC, an AbbVie company. Janssen Inc. markets ibrutinib as Imbruvica in Canada.
Study suggests hemophilia therapies are too costly

Hemophilia therapies account for the largest portion of pharmacy expenditures among publicly insured children with serious chronic illnesses in California, according to a study published in JAMA.
Hemophilia therapies accounted for 41% of expenditures for these children, even though hemophilia patients made up only 0.4% of the group studied.
Researchers said this finding suggests a need to improve pricing for hemophilia therapies and other high-cost medications. However, they noted that pricing varies from state to state.
Sonja M. Swenson, of Stanford University in California, and her colleagues conducted this research, analyzing paid claims for children (ages 0-21 years) using the California Children’s Services (CCS) paid claims data set (2010-2012).
CCS provides insurance coverage, care coordination, and a regionalized system of pediatric specialty care facilities for approximately 180,000 publicly insured children with serious chronic illnesses.
The data set includes age, sex, race/ethnicity, county of residence, enrollment dates, primary and secondary eligible diagnoses, claim diagnoses, and procedures for every enrollee. This study included children enrolled through fee-for-service care for at least 6 continuous months.
The researchers examined the records of 34,330 children. Outpatient pharmacy expenditures totaled $475,718,130 (20% of total healthcare expenditures).
Per-child pharmacy expenditures ranged from $0.16 to $56,849,034. The average and median per-child expenditures were $13,857 and $791, respectively.
Expenditures for all products analyzed were as follows:
| Product Class | Expenditures | % of Total
Expenditures |
No. of Children | Expenditures/
Child |
|---|---|---|---|---|
| Blood formation, coagulation, and thrombosis agents | $199,498,843 | 41.9% | 3499 | $57,016 |
| Central nervous system agents | $43,633,418 | 9.2% | 23,351 | $1869 |
| Electrolytic, caloric, and water balance | $39,617,776 | 8.3% | 10,959 | $3615 |
| Anti-infective agents | $35,827,958 | 7.5% | 26,165 | $1369 |
| Respiratory agents | $29,614,645 | 6.2% | 16,706 | $1173 |
| Hormones and synthetic substitutes | $24,722,256 | 5.2% | 8542 | $2894 |
| Enzymes | $13,294,509 | 2.8% | 27 | $492,389 |
| Gastrointestinal drugs | $12,500,330 | 2.6% | 11,817 | $1058 |
| Heavy metal antagonists | $6,983,828 | 1.5% | 108 | $64,665 |
| Cardiovascular drugs | $6,173,792 | 1.3% | 4031 | $1532 |
Hemophilia expenditures
As seen in the above table, the product class of blood formation, coagulation, and thrombosis agents accounted for the greatest share of outpatient pharmacy expenditures (42%).
Antihemophilic factors represented 98% of this class’s expenditures, or 41% of total pharmacy expenditures. Children with an antihemophilic factor paid claim were 0.4% of the entire cohort (n=145). And the average per-child expenditure for antihemophilic factor was $1,343,262.
Among children with antihemophilic factor claims who were enrolled for all 3 years studied, the average and median per-child annualized expenditures were $634,054 and $152,280, respectively.
The researchers said these results suggest a need for better pricing for hemophilia therapies, but it’s important to note that expenditures vary from state to state.
For instance, CCS’s mean per-child antihemophilic factor annual expenditure ($634,054) significantly surpassed that of North Carolina’s Medicaid program ($233,968 in fiscal year 2012) and Medicaid programs in 10 other states ($148,215 in 2008).
Hemophilia therapies account for the largest portion of pharmacy expenditures among publicly insured children with serious chronic illnesses in California, according to a study published in JAMA.
Hemophilia therapies accounted for 41% of expenditures for these children, even though hemophilia patients made up only 0.4% of the group studied.
Researchers said this finding suggests a need to improve pricing for hemophilia therapies and other high-cost medications. However, they noted that pricing varies from state to state.
Sonja M. Swenson, of Stanford University in California, and her colleagues conducted this research, analyzing paid claims for children (ages 0-21 years) using the California Children’s Services (CCS) paid claims data set (2010-2012).
CCS provides insurance coverage, care coordination, and a regionalized system of pediatric specialty care facilities for approximately 180,000 publicly insured children with serious chronic illnesses.
The data set includes age, sex, race/ethnicity, county of residence, enrollment dates, primary and secondary eligible diagnoses, claim diagnoses, and procedures for every enrollee. This study included children enrolled through fee-for-service care for at least 6 continuous months.
The researchers examined the records of 34,330 children. Outpatient pharmacy expenditures totaled $475,718,130 (20% of total healthcare expenditures).
Per-child pharmacy expenditures ranged from $0.16 to $56,849,034. The average and median per-child expenditures were $13,857 and $791, respectively.
Expenditures for all products analyzed were as follows:
| Product Class | Expenditures | % of Total
Expenditures |
No. of Children | Expenditures/
Child |
|---|---|---|---|---|
| Blood formation, coagulation, and thrombosis agents | $199,498,843 | 41.9% | 3499 | $57,016 |
| Central nervous system agents | $43,633,418 | 9.2% | 23,351 | $1869 |
| Electrolytic, caloric, and water balance | $39,617,776 | 8.3% | 10,959 | $3615 |
| Anti-infective agents | $35,827,958 | 7.5% | 26,165 | $1369 |
| Respiratory agents | $29,614,645 | 6.2% | 16,706 | $1173 |
| Hormones and synthetic substitutes | $24,722,256 | 5.2% | 8542 | $2894 |
| Enzymes | $13,294,509 | 2.8% | 27 | $492,389 |
| Gastrointestinal drugs | $12,500,330 | 2.6% | 11,817 | $1058 |
| Heavy metal antagonists | $6,983,828 | 1.5% | 108 | $64,665 |
| Cardiovascular drugs | $6,173,792 | 1.3% | 4031 | $1532 |
Hemophilia expenditures
As seen in the above table, the product class of blood formation, coagulation, and thrombosis agents accounted for the greatest share of outpatient pharmacy expenditures (42%).
Antihemophilic factors represented 98% of this class’s expenditures, or 41% of total pharmacy expenditures. Children with an antihemophilic factor paid claim were 0.4% of the entire cohort (n=145). And the average per-child expenditure for antihemophilic factor was $1,343,262.
Among children with antihemophilic factor claims who were enrolled for all 3 years studied, the average and median per-child annualized expenditures were $634,054 and $152,280, respectively.
The researchers said these results suggest a need for better pricing for hemophilia therapies, but it’s important to note that expenditures vary from state to state.
For instance, CCS’s mean per-child antihemophilic factor annual expenditure ($634,054) significantly surpassed that of North Carolina’s Medicaid program ($233,968 in fiscal year 2012) and Medicaid programs in 10 other states ($148,215 in 2008).
Hemophilia therapies account for the largest portion of pharmacy expenditures among publicly insured children with serious chronic illnesses in California, according to a study published in JAMA.
Hemophilia therapies accounted for 41% of expenditures for these children, even though hemophilia patients made up only 0.4% of the group studied.
Researchers said this finding suggests a need to improve pricing for hemophilia therapies and other high-cost medications. However, they noted that pricing varies from state to state.
Sonja M. Swenson, of Stanford University in California, and her colleagues conducted this research, analyzing paid claims for children (ages 0-21 years) using the California Children’s Services (CCS) paid claims data set (2010-2012).
CCS provides insurance coverage, care coordination, and a regionalized system of pediatric specialty care facilities for approximately 180,000 publicly insured children with serious chronic illnesses.
The data set includes age, sex, race/ethnicity, county of residence, enrollment dates, primary and secondary eligible diagnoses, claim diagnoses, and procedures for every enrollee. This study included children enrolled through fee-for-service care for at least 6 continuous months.
The researchers examined the records of 34,330 children. Outpatient pharmacy expenditures totaled $475,718,130 (20% of total healthcare expenditures).
Per-child pharmacy expenditures ranged from $0.16 to $56,849,034. The average and median per-child expenditures were $13,857 and $791, respectively.
Expenditures for all products analyzed were as follows:
| Product Class | Expenditures | % of Total
Expenditures |
No. of Children | Expenditures/
Child |
|---|---|---|---|---|
| Blood formation, coagulation, and thrombosis agents | $199,498,843 | 41.9% | 3499 | $57,016 |
| Central nervous system agents | $43,633,418 | 9.2% | 23,351 | $1869 |
| Electrolytic, caloric, and water balance | $39,617,776 | 8.3% | 10,959 | $3615 |
| Anti-infective agents | $35,827,958 | 7.5% | 26,165 | $1369 |
| Respiratory agents | $29,614,645 | 6.2% | 16,706 | $1173 |
| Hormones and synthetic substitutes | $24,722,256 | 5.2% | 8542 | $2894 |
| Enzymes | $13,294,509 | 2.8% | 27 | $492,389 |
| Gastrointestinal drugs | $12,500,330 | 2.6% | 11,817 | $1058 |
| Heavy metal antagonists | $6,983,828 | 1.5% | 108 | $64,665 |
| Cardiovascular drugs | $6,173,792 | 1.3% | 4031 | $1532 |
Hemophilia expenditures
As seen in the above table, the product class of blood formation, coagulation, and thrombosis agents accounted for the greatest share of outpatient pharmacy expenditures (42%).
Antihemophilic factors represented 98% of this class’s expenditures, or 41% of total pharmacy expenditures. Children with an antihemophilic factor paid claim were 0.4% of the entire cohort (n=145). And the average per-child expenditure for antihemophilic factor was $1,343,262.
Among children with antihemophilic factor claims who were enrolled for all 3 years studied, the average and median per-child annualized expenditures were $634,054 and $152,280, respectively.
The researchers said these results suggest a need for better pricing for hemophilia therapies, but it’s important to note that expenditures vary from state to state.
For instance, CCS’s mean per-child antihemophilic factor annual expenditure ($634,054) significantly surpassed that of North Carolina’s Medicaid program ($233,968 in fiscal year 2012) and Medicaid programs in 10 other states ($148,215 in 2008).
CHMP recommends drug for acquired hemophilia A
Photo courtesy of
Baxter International Inc.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended approval for Obizur, a recombinant porcine
factor VIII (FVIII) product, to treat bleeding episodes in adults with acquired hemophilia A.
If the European Commission approves Obizur, it will be the first recombinant porcine FVIII treatment available in the European Union (EU) for this patient population. Obizur already has orphan designation in the EU.
The European Commission is expected to make a decision on Obizur later this year. The decision will be applicable to all 28 EU member states plus Iceland, Norway, and Liechtenstein.
About Obizur
Acquired hemophilia A is caused by the formation of antibodies directed against the body’s own FVIII. The underlying cause of this may be pregnancy, cancer, or the use of certain medications, but the cause is often unknown.
Obizur replaces inhibited human FVIII with a recombinant porcine sequence FVIII based on the rationale that porcine FVIII is less susceptible to inactivation by circulating human FVIII antibodies. Physicians can monitor patients’ response to Obizur by measuring FVIII activity levels.
The CHMP’s positive opinion of Obizur is based on a phase 2/3 trial in which patients with acquired hemophilia A received the drug as treatment for serious bleeding episodes.
Twenty-nine patients were enrolled and evaluated for safety. Researchers determined that one of the patients did not actually have acquired hemophilia A, so this patient could not be evaluated for efficacy.
At 24 hours after the initial infusion, all 28 patients in the efficacy analysis had a positive response to Obizur. This meant that bleeding stopped or decreased, the patients experienced clinical stabilization or improvement, and FVIII levels were 20% or higher.
Eighty-six percent of patients (24/28) had successful treatment of their initial bleeding episode. The overall treatment success was determined by the investigator based on the ability to discontinue or reduce the dose and/or dosing frequency of Obizur.
The adverse event most frequently reported in the 29 patients in the safety analysis was the development of inhibitors to porcine FVIII.
Nineteen patients were negative for anti-porcine FVIII antibodies at baseline, and 5 of these patients (26%) developed anti-porcine FVIII antibodies following exposure to Obizur.
Of the 10 patients with detectable anti-porcine FVIII antibodies at baseline, 2 (20%) experienced an increase in titer, and 8 (80%) decreased to a non-detectable titer.
Obizur is under development by Baxalta Incorporated. The product is already approved in the US and is under regulatory review in Canada, Switzerland, Australia, and Colombia.
Photo courtesy of
Baxter International Inc.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended approval for Obizur, a recombinant porcine
factor VIII (FVIII) product, to treat bleeding episodes in adults with acquired hemophilia A.
If the European Commission approves Obizur, it will be the first recombinant porcine FVIII treatment available in the European Union (EU) for this patient population. Obizur already has orphan designation in the EU.
The European Commission is expected to make a decision on Obizur later this year. The decision will be applicable to all 28 EU member states plus Iceland, Norway, and Liechtenstein.
About Obizur
Acquired hemophilia A is caused by the formation of antibodies directed against the body’s own FVIII. The underlying cause of this may be pregnancy, cancer, or the use of certain medications, but the cause is often unknown.
Obizur replaces inhibited human FVIII with a recombinant porcine sequence FVIII based on the rationale that porcine FVIII is less susceptible to inactivation by circulating human FVIII antibodies. Physicians can monitor patients’ response to Obizur by measuring FVIII activity levels.
The CHMP’s positive opinion of Obizur is based on a phase 2/3 trial in which patients with acquired hemophilia A received the drug as treatment for serious bleeding episodes.
Twenty-nine patients were enrolled and evaluated for safety. Researchers determined that one of the patients did not actually have acquired hemophilia A, so this patient could not be evaluated for efficacy.
At 24 hours after the initial infusion, all 28 patients in the efficacy analysis had a positive response to Obizur. This meant that bleeding stopped or decreased, the patients experienced clinical stabilization or improvement, and FVIII levels were 20% or higher.
Eighty-six percent of patients (24/28) had successful treatment of their initial bleeding episode. The overall treatment success was determined by the investigator based on the ability to discontinue or reduce the dose and/or dosing frequency of Obizur.
The adverse event most frequently reported in the 29 patients in the safety analysis was the development of inhibitors to porcine FVIII.
Nineteen patients were negative for anti-porcine FVIII antibodies at baseline, and 5 of these patients (26%) developed anti-porcine FVIII antibodies following exposure to Obizur.
Of the 10 patients with detectable anti-porcine FVIII antibodies at baseline, 2 (20%) experienced an increase in titer, and 8 (80%) decreased to a non-detectable titer.
Obizur is under development by Baxalta Incorporated. The product is already approved in the US and is under regulatory review in Canada, Switzerland, Australia, and Colombia.
Photo courtesy of
Baxter International Inc.
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended approval for Obizur, a recombinant porcine
factor VIII (FVIII) product, to treat bleeding episodes in adults with acquired hemophilia A.
If the European Commission approves Obizur, it will be the first recombinant porcine FVIII treatment available in the European Union (EU) for this patient population. Obizur already has orphan designation in the EU.
The European Commission is expected to make a decision on Obizur later this year. The decision will be applicable to all 28 EU member states plus Iceland, Norway, and Liechtenstein.
About Obizur
Acquired hemophilia A is caused by the formation of antibodies directed against the body’s own FVIII. The underlying cause of this may be pregnancy, cancer, or the use of certain medications, but the cause is often unknown.
Obizur replaces inhibited human FVIII with a recombinant porcine sequence FVIII based on the rationale that porcine FVIII is less susceptible to inactivation by circulating human FVIII antibodies. Physicians can monitor patients’ response to Obizur by measuring FVIII activity levels.
The CHMP’s positive opinion of Obizur is based on a phase 2/3 trial in which patients with acquired hemophilia A received the drug as treatment for serious bleeding episodes.
Twenty-nine patients were enrolled and evaluated for safety. Researchers determined that one of the patients did not actually have acquired hemophilia A, so this patient could not be evaluated for efficacy.
At 24 hours after the initial infusion, all 28 patients in the efficacy analysis had a positive response to Obizur. This meant that bleeding stopped or decreased, the patients experienced clinical stabilization or improvement, and FVIII levels were 20% or higher.
Eighty-six percent of patients (24/28) had successful treatment of their initial bleeding episode. The overall treatment success was determined by the investigator based on the ability to discontinue or reduce the dose and/or dosing frequency of Obizur.
The adverse event most frequently reported in the 29 patients in the safety analysis was the development of inhibitors to porcine FVIII.
Nineteen patients were negative for anti-porcine FVIII antibodies at baseline, and 5 of these patients (26%) developed anti-porcine FVIII antibodies following exposure to Obizur.
Of the 10 patients with detectable anti-porcine FVIII antibodies at baseline, 2 (20%) experienced an increase in titer, and 8 (80%) decreased to a non-detectable titer.
Obizur is under development by Baxalta Incorporated. The product is already approved in the US and is under regulatory review in Canada, Switzerland, Australia, and Colombia.
Some AEs not reported according to regulations

Photo courtesy of the FDA
A new study indicates that drug manufacturers fail to report about 10% of serious and unexpected adverse events (AEs) within the timeframe set out in federal regulations.
Manufacturers are required to report a serious AE (death, hospitalization, disability, etc.) or unexpected AE (anything not listed in the drug’s label) to the US Food and Drug Administration (FDA) within 15 calendar days of learning about the event.
But an analysis of more than 1.6 million AE reports showed that manufacturers failed to meet this requirement for nearly 10% of AEs.
Pinar Karaca-Mandic, PhD, of the University of Minnesota School of Public Health in Minneapolis, and her colleagues conducted the analysis and detailed the results in JAMA Internal Medicine.
The team examined data from the FDA Adverse Event Reporting System for AE reports made from January 2004 through June 2014. The final study sample included only reports that were subject to the regulation requiring submission within 15 days—a total of 1,613,079 reports.
The researchers found that 9.94% of reports were not received by the FDA within the 15-day timeframe. This was a total of 160,383 reports—40,464 cases in which patients died and 119,919 in which they did not.
So 90.06% of reports (n=1,452,696) were reported within 15 days, 5.28% (n=85,161) were reported within 16 to 90 days, 2.19% (n=35,392) were reported within 91 to 180 days, and 2.47% (n=39,830) were reported after 180 days.
Multivariate analysis revealed that patient death was positively associated with delayed AE reporting. About 91% (90.71%) of AEs that did not involve death were reported within 15 days, compared to 88.25% of AEs that did involve death.
The percentage of reports received within 16 to 90 days was 5.19% for AEs without death and 6.42% for AEs with death. The percentage of reports received within 91 to 180 days was 1.98% and 2.53%, respectively. And the percentage of reports received after 180 days was 2.12% and 2.80%, respectively.
The researchers said perhaps manufacturers spend additional time verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.
In a related Editor’s Note, Rita F. Redberg, MD, editor of JAMA Internal Medicine, wrote that delays in reporting AEs should never occur because they mean exposing patients to serious harm, including death, that could potentially be avoided.
“One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer . . . ,” she wrote. “Physicians and their patients must be knowledgeable of benefits, harms, and alternatives for a wide choice of treatments, especially those recently approved for which clinical experience is limited.”
Photo courtesy of the FDA
A new study indicates that drug manufacturers fail to report about 10% of serious and unexpected adverse events (AEs) within the timeframe set out in federal regulations.
Manufacturers are required to report a serious AE (death, hospitalization, disability, etc.) or unexpected AE (anything not listed in the drug’s label) to the US Food and Drug Administration (FDA) within 15 calendar days of learning about the event.
But an analysis of more than 1.6 million AE reports showed that manufacturers failed to meet this requirement for nearly 10% of AEs.
Pinar Karaca-Mandic, PhD, of the University of Minnesota School of Public Health in Minneapolis, and her colleagues conducted the analysis and detailed the results in JAMA Internal Medicine.
The team examined data from the FDA Adverse Event Reporting System for AE reports made from January 2004 through June 2014. The final study sample included only reports that were subject to the regulation requiring submission within 15 days—a total of 1,613,079 reports.
The researchers found that 9.94% of reports were not received by the FDA within the 15-day timeframe. This was a total of 160,383 reports—40,464 cases in which patients died and 119,919 in which they did not.
So 90.06% of reports (n=1,452,696) were reported within 15 days, 5.28% (n=85,161) were reported within 16 to 90 days, 2.19% (n=35,392) were reported within 91 to 180 days, and 2.47% (n=39,830) were reported after 180 days.
Multivariate analysis revealed that patient death was positively associated with delayed AE reporting. About 91% (90.71%) of AEs that did not involve death were reported within 15 days, compared to 88.25% of AEs that did involve death.
The percentage of reports received within 16 to 90 days was 5.19% for AEs without death and 6.42% for AEs with death. The percentage of reports received within 91 to 180 days was 1.98% and 2.53%, respectively. And the percentage of reports received after 180 days was 2.12% and 2.80%, respectively.
The researchers said perhaps manufacturers spend additional time verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.
In a related Editor’s Note, Rita F. Redberg, MD, editor of JAMA Internal Medicine, wrote that delays in reporting AEs should never occur because they mean exposing patients to serious harm, including death, that could potentially be avoided.
“One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer . . . ,” she wrote. “Physicians and their patients must be knowledgeable of benefits, harms, and alternatives for a wide choice of treatments, especially those recently approved for which clinical experience is limited.”
Photo courtesy of the FDA
A new study indicates that drug manufacturers fail to report about 10% of serious and unexpected adverse events (AEs) within the timeframe set out in federal regulations.
Manufacturers are required to report a serious AE (death, hospitalization, disability, etc.) or unexpected AE (anything not listed in the drug’s label) to the US Food and Drug Administration (FDA) within 15 calendar days of learning about the event.
But an analysis of more than 1.6 million AE reports showed that manufacturers failed to meet this requirement for nearly 10% of AEs.
Pinar Karaca-Mandic, PhD, of the University of Minnesota School of Public Health in Minneapolis, and her colleagues conducted the analysis and detailed the results in JAMA Internal Medicine.
The team examined data from the FDA Adverse Event Reporting System for AE reports made from January 2004 through June 2014. The final study sample included only reports that were subject to the regulation requiring submission within 15 days—a total of 1,613,079 reports.
The researchers found that 9.94% of reports were not received by the FDA within the 15-day timeframe. This was a total of 160,383 reports—40,464 cases in which patients died and 119,919 in which they did not.
So 90.06% of reports (n=1,452,696) were reported within 15 days, 5.28% (n=85,161) were reported within 16 to 90 days, 2.19% (n=35,392) were reported within 91 to 180 days, and 2.47% (n=39,830) were reported after 180 days.
Multivariate analysis revealed that patient death was positively associated with delayed AE reporting. About 91% (90.71%) of AEs that did not involve death were reported within 15 days, compared to 88.25% of AEs that did involve death.
The percentage of reports received within 16 to 90 days was 5.19% for AEs without death and 6.42% for AEs with death. The percentage of reports received within 91 to 180 days was 1.98% and 2.53%, respectively. And the percentage of reports received after 180 days was 2.12% and 2.80%, respectively.
The researchers said perhaps manufacturers spend additional time verifying reports concerning deaths, but this discretion is outside the scope of the current regulatory regime.
In a related Editor’s Note, Rita F. Redberg, MD, editor of JAMA Internal Medicine, wrote that delays in reporting AEs should never occur because they mean exposing patients to serious harm, including death, that could potentially be avoided.
“One improvement would be for AE reports to go directly to the FDA instead of via the manufacturer . . . ,” she wrote. “Physicians and their patients must be knowledgeable of benefits, harms, and alternatives for a wide choice of treatments, especially those recently approved for which clinical experience is limited.”