User login
Richard Quinn is an award-winning journalist with 15 years’ experience. He has worked at the Asbury Park Press in New Jersey and The Virginian-Pilot in Norfolk, Va., and currently is managing editor for a leading commercial real estate publication. His freelance work has appeared in The Jewish State, The Hospitalist, The Rheumatologist, ACEP Now, and ENT Today. He lives in New Jersey with his wife and three cats.
Hospitalist Salaries Show Steady Gains
The first wave of fiscal year 2010 (FY10) provider data from SHM-MGMA shows that hospitalist salaries and productivity appear to have to have crept up only slightly from the previous year.
The national median annual salary for internal-medicine hospitalists seeing adult patients is $220,144, up from $215,000 in FY09, a 2.4% increase. For pediatric hospitalists, the 2010 salary was $171,617, up from $160,038 in FY09, a 7% increase. Work RVUs for both categories saw even smaller increases: 4,174 for internal-medicine hospitalists (up 1.8%) and 1,976 for pediatric hospitalists (up 0.02%).
By comparison, the increase from SHM's 2007-2008 survey to 2009's salary data set from SHM-MGMA was 9%. SHM cautions against drawing too many conclusions from comparisons with older figures, as the population universes are different. However, Leslie Flores, MHA, SHM senior advisor for practice management, says that anecdotally, the data suggest the field is hitting a fiscal plateau.
"What I get out of this is both compensation and productivity appear to be leveling off somewhat," Flores says. "We're not seeing the big increases from year to year we have seen historically."
The data are publicly available as of today, even though snippets of the survey results were previewed at HM11 last month in Grapevine, Texas. The preview, however, only showed regional figures. Academic hospitalist data was removed from the study this year, as that provider universe now has its own survey.
Flores says it's hard to pin down exactly why increases in both salaries and productivity are slowing. It could be the natural evolution of the relatively young field, or it could be a narrowing of the supply-demand gap for hospitalists.
The data being released today serve as the foundation for the annual State of Hospital Medicine report, scheduled for release in September. That expanded data set will feature HM-centric data points including CPT code distribution, group leader compensation, and administrative time allocation and compensation and productivity for nocturnists. Until then, Flores says, hospitalists should consider data points like the ones currently available as key negotiating and practice-management guideposts. But national data only go so far.
"Even the regional numbers don't reflect what the individual numbers are in individual markets. You need to know what the hospitalist down the street is making," she says.
The first wave of fiscal year 2010 (FY10) provider data from SHM-MGMA shows that hospitalist salaries and productivity appear to have to have crept up only slightly from the previous year.
The national median annual salary for internal-medicine hospitalists seeing adult patients is $220,144, up from $215,000 in FY09, a 2.4% increase. For pediatric hospitalists, the 2010 salary was $171,617, up from $160,038 in FY09, a 7% increase. Work RVUs for both categories saw even smaller increases: 4,174 for internal-medicine hospitalists (up 1.8%) and 1,976 for pediatric hospitalists (up 0.02%).
By comparison, the increase from SHM's 2007-2008 survey to 2009's salary data set from SHM-MGMA was 9%. SHM cautions against drawing too many conclusions from comparisons with older figures, as the population universes are different. However, Leslie Flores, MHA, SHM senior advisor for practice management, says that anecdotally, the data suggest the field is hitting a fiscal plateau.
"What I get out of this is both compensation and productivity appear to be leveling off somewhat," Flores says. "We're not seeing the big increases from year to year we have seen historically."
The data are publicly available as of today, even though snippets of the survey results were previewed at HM11 last month in Grapevine, Texas. The preview, however, only showed regional figures. Academic hospitalist data was removed from the study this year, as that provider universe now has its own survey.
Flores says it's hard to pin down exactly why increases in both salaries and productivity are slowing. It could be the natural evolution of the relatively young field, or it could be a narrowing of the supply-demand gap for hospitalists.
The data being released today serve as the foundation for the annual State of Hospital Medicine report, scheduled for release in September. That expanded data set will feature HM-centric data points including CPT code distribution, group leader compensation, and administrative time allocation and compensation and productivity for nocturnists. Until then, Flores says, hospitalists should consider data points like the ones currently available as key negotiating and practice-management guideposts. But national data only go so far.
"Even the regional numbers don't reflect what the individual numbers are in individual markets. You need to know what the hospitalist down the street is making," she says.
The first wave of fiscal year 2010 (FY10) provider data from SHM-MGMA shows that hospitalist salaries and productivity appear to have to have crept up only slightly from the previous year.
The national median annual salary for internal-medicine hospitalists seeing adult patients is $220,144, up from $215,000 in FY09, a 2.4% increase. For pediatric hospitalists, the 2010 salary was $171,617, up from $160,038 in FY09, a 7% increase. Work RVUs for both categories saw even smaller increases: 4,174 for internal-medicine hospitalists (up 1.8%) and 1,976 for pediatric hospitalists (up 0.02%).
By comparison, the increase from SHM's 2007-2008 survey to 2009's salary data set from SHM-MGMA was 9%. SHM cautions against drawing too many conclusions from comparisons with older figures, as the population universes are different. However, Leslie Flores, MHA, SHM senior advisor for practice management, says that anecdotally, the data suggest the field is hitting a fiscal plateau.
"What I get out of this is both compensation and productivity appear to be leveling off somewhat," Flores says. "We're not seeing the big increases from year to year we have seen historically."
The data are publicly available as of today, even though snippets of the survey results were previewed at HM11 last month in Grapevine, Texas. The preview, however, only showed regional figures. Academic hospitalist data was removed from the study this year, as that provider universe now has its own survey.
Flores says it's hard to pin down exactly why increases in both salaries and productivity are slowing. It could be the natural evolution of the relatively young field, or it could be a narrowing of the supply-demand gap for hospitalists.
The data being released today serve as the foundation for the annual State of Hospital Medicine report, scheduled for release in September. That expanded data set will feature HM-centric data points including CPT code distribution, group leader compensation, and administrative time allocation and compensation and productivity for nocturnists. Until then, Flores says, hospitalists should consider data points like the ones currently available as key negotiating and practice-management guideposts. But national data only go so far.
"Even the regional numbers don't reflect what the individual numbers are in individual markets. You need to know what the hospitalist down the street is making," she says.
ONLINE EXCLUSIVE: Listen to experts discuss new anticoagulants
Click here to listen to Dr. Merli
Click here to listen to Dr. Merli
Click here to listen to Dr. Merli
A Numbers Game
New guidelines from the American College of Physicians (ACP) on the use of intensive insulin therapy (IIT) for glycemic control of hospitalized patients have prompted a backlash from physicians, including an SHM mentor, who think the rules could lead to needless confusion on best practices.
The guidelines, issued in February, recommend against using IIT to strictly control or normalize blood glucose in nonsurgical or medical ICU patients with or without diabetes. It also recommends a target blood-glucose level of 140 mg to 200 mg if insulin therapy is used in those patients.
Hospitalist Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego and a mentor with SHM’s Glycemic Control Mentored Implementation (GCMI) program, says the first two guidelines are in line with current practice, as laid out by a 2009 consensus statement from the American Association of Clinical Endocrinologists and the American Diabetes Association.
The guideline on glucose levels, however, has generated harsh feedback, with one cardiothoracic surgeon calling for ACP to pull the recommendations. Dr. Ramos doesn’t go that far, but he wonders whether that guideline was necessary, as he believes there is little strong evidence on outcomes from 180 mg to 200 mg.
The third guidelin "didn't really add much, other than confusion," Dr. Ramos says.
Dr. Ramos says it's too early to draw best practices from SHM's GCMI program, but the initiative is drawing attention to the issue. He hopes the ACP guidelines won't impede that growth.
"I want [hospitalists] not to focus on the numbers: 140 to 180, 140 to 200," Dr. Ramos explains. "What I want them to take from it is we need control ... we need safe targets and they need to be achievable."
New guidelines from the American College of Physicians (ACP) on the use of intensive insulin therapy (IIT) for glycemic control of hospitalized patients have prompted a backlash from physicians, including an SHM mentor, who think the rules could lead to needless confusion on best practices.
The guidelines, issued in February, recommend against using IIT to strictly control or normalize blood glucose in nonsurgical or medical ICU patients with or without diabetes. It also recommends a target blood-glucose level of 140 mg to 200 mg if insulin therapy is used in those patients.
Hospitalist Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego and a mentor with SHM’s Glycemic Control Mentored Implementation (GCMI) program, says the first two guidelines are in line with current practice, as laid out by a 2009 consensus statement from the American Association of Clinical Endocrinologists and the American Diabetes Association.
The guideline on glucose levels, however, has generated harsh feedback, with one cardiothoracic surgeon calling for ACP to pull the recommendations. Dr. Ramos doesn’t go that far, but he wonders whether that guideline was necessary, as he believes there is little strong evidence on outcomes from 180 mg to 200 mg.
The third guidelin "didn't really add much, other than confusion," Dr. Ramos says.
Dr. Ramos says it's too early to draw best practices from SHM's GCMI program, but the initiative is drawing attention to the issue. He hopes the ACP guidelines won't impede that growth.
"I want [hospitalists] not to focus on the numbers: 140 to 180, 140 to 200," Dr. Ramos explains. "What I want them to take from it is we need control ... we need safe targets and they need to be achievable."
New guidelines from the American College of Physicians (ACP) on the use of intensive insulin therapy (IIT) for glycemic control of hospitalized patients have prompted a backlash from physicians, including an SHM mentor, who think the rules could lead to needless confusion on best practices.
The guidelines, issued in February, recommend against using IIT to strictly control or normalize blood glucose in nonsurgical or medical ICU patients with or without diabetes. It also recommends a target blood-glucose level of 140 mg to 200 mg if insulin therapy is used in those patients.
Hospitalist Pedro Ramos, MD, assistant clinical professor of medicine at the University of California at San Diego and a mentor with SHM’s Glycemic Control Mentored Implementation (GCMI) program, says the first two guidelines are in line with current practice, as laid out by a 2009 consensus statement from the American Association of Clinical Endocrinologists and the American Diabetes Association.
The guideline on glucose levels, however, has generated harsh feedback, with one cardiothoracic surgeon calling for ACP to pull the recommendations. Dr. Ramos doesn’t go that far, but he wonders whether that guideline was necessary, as he believes there is little strong evidence on outcomes from 180 mg to 200 mg.
The third guidelin "didn't really add much, other than confusion," Dr. Ramos says.
Dr. Ramos says it's too early to draw best practices from SHM's GCMI program, but the initiative is drawing attention to the issue. He hopes the ACP guidelines won't impede that growth.
"I want [hospitalists] not to focus on the numbers: 140 to 180, 140 to 200," Dr. Ramos explains. "What I want them to take from it is we need control ... we need safe targets and they need to be achievable."
Patients Unaware of DVT Risk, Survey Shows
A new survey of patients showing that less than one-third reported receiving DVT prophylaxis, even though 2 out of every 5 had a family member who previously had an embolism clot in their leg or lung, is a sign physicians need to improve their communication skills, one hospitalist says.
The survey, conducted online by the National Blood Clot Alliance (NCBA) and presented at HM11, queried 500 patients with a length of stay of three days or higher. According to the survey, only 28% of patients had heard of DVT when the term was used, and just 15% knew pulmonary embolism when the term was used. In comparison, 83% knew what a blood clot was and 99% knew it could be life-threatening. Still, 46% said their doctor did not provide info about blood-clot-related risks.
Greg Maynard, MD, MSc, SFHM, chief of the Division of Hospital Medicine at the University of California at San Diego, says the results should serve as a wake-up call to hospitalists and other physicians. "They don't speak the language," says Dr. Maynard, a member of the NCBA's Medical and Scientific Advisory Board. "If we use that terminology with them, we fail. ... The first part of this puzzle is how we educate our patients."
Dr. Maynard says increased use of prophylaxis would help reduce care delivery costs and increase efficiency by eliminating preventable DVT or VTE incidences. Hospitalists are "well positioned" to lead the effort, but a few steps must happen first, he says. These changes require institutional commitment to do everything from adding prophylaxis checks to order sets to adopting new safety checklists to patient brochures explaining symptoms of blood clots. In addition, according to Dr. Maynard, baseline measurements must be set to determine what factors will classify patients as low-risk versus high-risk. Everyone above the low-risk line should receive prophylaxis, be it ambulation, compression stockings, or anticoagulant therapies, he says.
"It's all part of a bundle," Dr. Maynard says. "Any one of these things by themselves would not work as well."
A new survey of patients showing that less than one-third reported receiving DVT prophylaxis, even though 2 out of every 5 had a family member who previously had an embolism clot in their leg or lung, is a sign physicians need to improve their communication skills, one hospitalist says.
The survey, conducted online by the National Blood Clot Alliance (NCBA) and presented at HM11, queried 500 patients with a length of stay of three days or higher. According to the survey, only 28% of patients had heard of DVT when the term was used, and just 15% knew pulmonary embolism when the term was used. In comparison, 83% knew what a blood clot was and 99% knew it could be life-threatening. Still, 46% said their doctor did not provide info about blood-clot-related risks.
Greg Maynard, MD, MSc, SFHM, chief of the Division of Hospital Medicine at the University of California at San Diego, says the results should serve as a wake-up call to hospitalists and other physicians. "They don't speak the language," says Dr. Maynard, a member of the NCBA's Medical and Scientific Advisory Board. "If we use that terminology with them, we fail. ... The first part of this puzzle is how we educate our patients."
Dr. Maynard says increased use of prophylaxis would help reduce care delivery costs and increase efficiency by eliminating preventable DVT or VTE incidences. Hospitalists are "well positioned" to lead the effort, but a few steps must happen first, he says. These changes require institutional commitment to do everything from adding prophylaxis checks to order sets to adopting new safety checklists to patient brochures explaining symptoms of blood clots. In addition, according to Dr. Maynard, baseline measurements must be set to determine what factors will classify patients as low-risk versus high-risk. Everyone above the low-risk line should receive prophylaxis, be it ambulation, compression stockings, or anticoagulant therapies, he says.
"It's all part of a bundle," Dr. Maynard says. "Any one of these things by themselves would not work as well."
A new survey of patients showing that less than one-third reported receiving DVT prophylaxis, even though 2 out of every 5 had a family member who previously had an embolism clot in their leg or lung, is a sign physicians need to improve their communication skills, one hospitalist says.
The survey, conducted online by the National Blood Clot Alliance (NCBA) and presented at HM11, queried 500 patients with a length of stay of three days or higher. According to the survey, only 28% of patients had heard of DVT when the term was used, and just 15% knew pulmonary embolism when the term was used. In comparison, 83% knew what a blood clot was and 99% knew it could be life-threatening. Still, 46% said their doctor did not provide info about blood-clot-related risks.
Greg Maynard, MD, MSc, SFHM, chief of the Division of Hospital Medicine at the University of California at San Diego, says the results should serve as a wake-up call to hospitalists and other physicians. "They don't speak the language," says Dr. Maynard, a member of the NCBA's Medical and Scientific Advisory Board. "If we use that terminology with them, we fail. ... The first part of this puzzle is how we educate our patients."
Dr. Maynard says increased use of prophylaxis would help reduce care delivery costs and increase efficiency by eliminating preventable DVT or VTE incidences. Hospitalists are "well positioned" to lead the effort, but a few steps must happen first, he says. These changes require institutional commitment to do everything from adding prophylaxis checks to order sets to adopting new safety checklists to patient brochures explaining symptoms of blood clots. In addition, according to Dr. Maynard, baseline measurements must be set to determine what factors will classify patients as low-risk versus high-risk. Everyone above the low-risk line should receive prophylaxis, be it ambulation, compression stockings, or anticoagulant therapies, he says.
"It's all part of a bundle," Dr. Maynard says. "Any one of these things by themselves would not work as well."
Texas-Sized Excitement
SHM’s annual meeting was a Texas-sized birthday party for a teenager. Fifteen years after the term “hospitalist” was coined, more than 2,500 hospitalists, residents, nonphysician providers, and at least one pharmacist attended HM11 May 10-13 at the Gaylord Texan Resort and Convention Center in Grapevine, Texas.
The four-day celebration of all things HM drew arguably its most impressive batch of speakers, including AMA President Cecil Wilson, MD, and Robert
Kocher, MD, a former special assistant to President Obama. Robert Wachter, MD, MHM, who coauthored the term “hospitalist,” gave the penultimate address.
But attendees say the value of the meeting wasn’t the speeches, the more than 100 breakout sessions, or the endless networking opportunities. It was all of it.
“People talking about how excited they are about hospitalized medicine, you’re like, ‘Yeah, let’s do this,’ ” said first-time attendee Randa Perkins, MD, chief resident at Tallahassee Memorial’s Family Medicine Residency Program in Florida. “You feel like it is ‘Braveheart’!”
SHM’s annual meeting was a Texas-sized birthday party for a teenager. Fifteen years after the term “hospitalist” was coined, more than 2,500 hospitalists, residents, nonphysician providers, and at least one pharmacist attended HM11 May 10-13 at the Gaylord Texan Resort and Convention Center in Grapevine, Texas.
The four-day celebration of all things HM drew arguably its most impressive batch of speakers, including AMA President Cecil Wilson, MD, and Robert
Kocher, MD, a former special assistant to President Obama. Robert Wachter, MD, MHM, who coauthored the term “hospitalist,” gave the penultimate address.
But attendees say the value of the meeting wasn’t the speeches, the more than 100 breakout sessions, or the endless networking opportunities. It was all of it.
“People talking about how excited they are about hospitalized medicine, you’re like, ‘Yeah, let’s do this,’ ” said first-time attendee Randa Perkins, MD, chief resident at Tallahassee Memorial’s Family Medicine Residency Program in Florida. “You feel like it is ‘Braveheart’!”
SHM’s annual meeting was a Texas-sized birthday party for a teenager. Fifteen years after the term “hospitalist” was coined, more than 2,500 hospitalists, residents, nonphysician providers, and at least one pharmacist attended HM11 May 10-13 at the Gaylord Texan Resort and Convention Center in Grapevine, Texas.
The four-day celebration of all things HM drew arguably its most impressive batch of speakers, including AMA President Cecil Wilson, MD, and Robert
Kocher, MD, a former special assistant to President Obama. Robert Wachter, MD, MHM, who coauthored the term “hospitalist,” gave the penultimate address.
But attendees say the value of the meeting wasn’t the speeches, the more than 100 breakout sessions, or the endless networking opportunities. It was all of it.
“People talking about how excited they are about hospitalized medicine, you’re like, ‘Yeah, let’s do this,’ ” said first-time attendee Randa Perkins, MD, chief resident at Tallahassee Memorial’s Family Medicine Residency Program in Florida. “You feel like it is ‘Braveheart’!”
Med Students’ Simple Idea Has Serious Potential
The difficulties in routinely recalling each and every action to take with a patient has encouraged hospitalists to abide by checklists that remind them of just what to do. So why shouldn’t patients have the same systematic prodding? That’s exactly what two first-year students at the University of Michigan Medical School in Ann Arbor—Andrew Lin and Aaron Farberg—thought two years ago, prompting them to invent Dear Doctor.
With the help of senior physicians, including former SHM president Scott Flanders, MD, SFHM, FACP, Lin and Farberg conducted a three-month study that provided bedside notepads to patients. The patients were encouraged to jot down questions for their doctors whenever a question occurred to them, not just when the physician was in the room. The students produced 1,000 notepads, even shrink-wrapping them with companion pens.
The simple yet seemingly effective approach worked so well that “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication” earned the budding physicians the 2010 Innovation Poster award in the Research, Innovations, and Clinical Vignettes competition at HM10.
“This isn’t groundbreaking work here,” Lin says. “It’s a notepad, scraps of paper. Look around your desk and you’ve got sticky notes around. That’s what this is.”
Lin and Farberg both say they were surprised no one had crafted a similar communication tool as a potential quality-improvement (QI) measure. To wit, they are now working on publishing their research in the Journal of Hospital Medicine to further draw attention to the concept. They envision a day when the notes patients write down could be included in electronic medical records.
The ultimate goal is to give hospitalists and other physicians another way to communicate with their patients. “We want to institutionalize [Dear Doctor] to the point it’s a recognized necessity for the hospital system,” Lin says.—RQ
Toolkit Addresses Small-Business Security Concerns
The Healthcare Information and Management Systems Society (HIMSS) has had a privacy and security toolkit for physicians for a decade, but after its last annual security survey with the Medical Group Management Association (MGMA), it became clear that small- to medium-sized organizations were behind in implementation.
And so was born the HIMSS Privacy and Security Toolkit for Small Provider Organizations. The joint initiative is one that HM groups in rural or small settings should take advantage of, says Lisa Gallagher, HIMSS’ senior director of privacy and security.
Hospitalists “need to understand the reporting environment,” Gallagher says. “They are the subject of a lot of the policies and technology. We need them to be knowledgeable about it. They’re the ones who have access.”
HM’s role at the juncture of different departments and physicians, particularly at smaller hospitals that rely on hospitalists as traffic cops, makes it all the more important for hospitalists to understand the nuances of both privacy and security.
The interactive toolkit allows users to submit their own suggestions for improved processes and features introductions to the Centers for Medicare & Medicaid Services’ (CMS) “meaningful use” standard. Gallagher is hopeful that an engaged physician response to the toolkit will only bolster its efficacy in the coming months. “This is going to continue to evolve,” she says.—RQ
QUALITY RESEARCH
Care Transitions, Readmissions Concern Other Countries
International studies suggest that the recent torrent of attention toward improving care transitions and preventing hospital readmissions is not just an American trend. For example, a literature survey of physician “handovers” (aka handoffs) in international hospitals published in the British Medical Journal for Quality and Safety identified 32 papers on the subject.1 The authors conclude that the existing literature rarely examines pre- and post-handover phases or evaluates the quality of handover practices, and thus “does not fully identify where communication failures typically occur.” More systematic analysis of all stages of handoffs by physicians is warranted, the authors suggest.
In the same journal, a literature search of English-language publications from 1990 to 2010 found a dozen studies—eight from the U.S.—documenting failure to perform adequate follow-up for patients’ test results.2 The lack of follow-up ranged from 20% to 62% for hospitalized patients, and from 1% to 75% for patients treated in the ED. Two areas where problems were particularly evident were critical test results and results for patients moving across healthcare settings. “The existing evidence suggests that the problem of missed test results is considerable and reported negative impacts on patients warrant the exploration of solutions,” the authors conclude. They recommend further study of the effectiveness of such interventions as online endorsement of results, and integration of information technology into clinical work practices.
The World Alliance for Patient Safety, which was convened in 2004 by the World Health Organization, recently pointed to poor test result follow-up as one of the major processes contributing to unsafe patient care internationally.1 The organization has identified nine “patient-safety solutions,” one of which is ensuring medication accuracy at transitions of care.
For more information on the alliance and WHO’s interest in patient safety, visit http://www.who.int/topics/patient_safety/en/. —LB
References
- Raduma-Tomás MA, Flin R, Yule S, Williams D. Doctors’ handovers in hospi- tals: a literature review. BMJ Qual Saf. 2011;20:128-133.
- Callen J, Georgiou A, Li J, Westbrook JI. The safety implications of missed test results for hospitalised patients: a systematic review. BMJ Qual Saf. 2011;20:194-199.
The difficulties in routinely recalling each and every action to take with a patient has encouraged hospitalists to abide by checklists that remind them of just what to do. So why shouldn’t patients have the same systematic prodding? That’s exactly what two first-year students at the University of Michigan Medical School in Ann Arbor—Andrew Lin and Aaron Farberg—thought two years ago, prompting them to invent Dear Doctor.
With the help of senior physicians, including former SHM president Scott Flanders, MD, SFHM, FACP, Lin and Farberg conducted a three-month study that provided bedside notepads to patients. The patients were encouraged to jot down questions for their doctors whenever a question occurred to them, not just when the physician was in the room. The students produced 1,000 notepads, even shrink-wrapping them with companion pens.
The simple yet seemingly effective approach worked so well that “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication” earned the budding physicians the 2010 Innovation Poster award in the Research, Innovations, and Clinical Vignettes competition at HM10.
“This isn’t groundbreaking work here,” Lin says. “It’s a notepad, scraps of paper. Look around your desk and you’ve got sticky notes around. That’s what this is.”
Lin and Farberg both say they were surprised no one had crafted a similar communication tool as a potential quality-improvement (QI) measure. To wit, they are now working on publishing their research in the Journal of Hospital Medicine to further draw attention to the concept. They envision a day when the notes patients write down could be included in electronic medical records.
The ultimate goal is to give hospitalists and other physicians another way to communicate with their patients. “We want to institutionalize [Dear Doctor] to the point it’s a recognized necessity for the hospital system,” Lin says.—RQ
Toolkit Addresses Small-Business Security Concerns
The Healthcare Information and Management Systems Society (HIMSS) has had a privacy and security toolkit for physicians for a decade, but after its last annual security survey with the Medical Group Management Association (MGMA), it became clear that small- to medium-sized organizations were behind in implementation.
And so was born the HIMSS Privacy and Security Toolkit for Small Provider Organizations. The joint initiative is one that HM groups in rural or small settings should take advantage of, says Lisa Gallagher, HIMSS’ senior director of privacy and security.
Hospitalists “need to understand the reporting environment,” Gallagher says. “They are the subject of a lot of the policies and technology. We need them to be knowledgeable about it. They’re the ones who have access.”
HM’s role at the juncture of different departments and physicians, particularly at smaller hospitals that rely on hospitalists as traffic cops, makes it all the more important for hospitalists to understand the nuances of both privacy and security.
The interactive toolkit allows users to submit their own suggestions for improved processes and features introductions to the Centers for Medicare & Medicaid Services’ (CMS) “meaningful use” standard. Gallagher is hopeful that an engaged physician response to the toolkit will only bolster its efficacy in the coming months. “This is going to continue to evolve,” she says.—RQ
QUALITY RESEARCH
Care Transitions, Readmissions Concern Other Countries
International studies suggest that the recent torrent of attention toward improving care transitions and preventing hospital readmissions is not just an American trend. For example, a literature survey of physician “handovers” (aka handoffs) in international hospitals published in the British Medical Journal for Quality and Safety identified 32 papers on the subject.1 The authors conclude that the existing literature rarely examines pre- and post-handover phases or evaluates the quality of handover practices, and thus “does not fully identify where communication failures typically occur.” More systematic analysis of all stages of handoffs by physicians is warranted, the authors suggest.
In the same journal, a literature search of English-language publications from 1990 to 2010 found a dozen studies—eight from the U.S.—documenting failure to perform adequate follow-up for patients’ test results.2 The lack of follow-up ranged from 20% to 62% for hospitalized patients, and from 1% to 75% for patients treated in the ED. Two areas where problems were particularly evident were critical test results and results for patients moving across healthcare settings. “The existing evidence suggests that the problem of missed test results is considerable and reported negative impacts on patients warrant the exploration of solutions,” the authors conclude. They recommend further study of the effectiveness of such interventions as online endorsement of results, and integration of information technology into clinical work practices.
The World Alliance for Patient Safety, which was convened in 2004 by the World Health Organization, recently pointed to poor test result follow-up as one of the major processes contributing to unsafe patient care internationally.1 The organization has identified nine “patient-safety solutions,” one of which is ensuring medication accuracy at transitions of care.
For more information on the alliance and WHO’s interest in patient safety, visit http://www.who.int/topics/patient_safety/en/. —LB
References
- Raduma-Tomás MA, Flin R, Yule S, Williams D. Doctors’ handovers in hospi- tals: a literature review. BMJ Qual Saf. 2011;20:128-133.
- Callen J, Georgiou A, Li J, Westbrook JI. The safety implications of missed test results for hospitalised patients: a systematic review. BMJ Qual Saf. 2011;20:194-199.
The difficulties in routinely recalling each and every action to take with a patient has encouraged hospitalists to abide by checklists that remind them of just what to do. So why shouldn’t patients have the same systematic prodding? That’s exactly what two first-year students at the University of Michigan Medical School in Ann Arbor—Andrew Lin and Aaron Farberg—thought two years ago, prompting them to invent Dear Doctor.
With the help of senior physicians, including former SHM president Scott Flanders, MD, SFHM, FACP, Lin and Farberg conducted a three-month study that provided bedside notepads to patients. The patients were encouraged to jot down questions for their doctors whenever a question occurred to them, not just when the physician was in the room. The students produced 1,000 notepads, even shrink-wrapping them with companion pens.
The simple yet seemingly effective approach worked so well that “Dear Doctor: A Tool to Facilitate Patient-Centered Care and Enhance Communication” earned the budding physicians the 2010 Innovation Poster award in the Research, Innovations, and Clinical Vignettes competition at HM10.
“This isn’t groundbreaking work here,” Lin says. “It’s a notepad, scraps of paper. Look around your desk and you’ve got sticky notes around. That’s what this is.”
Lin and Farberg both say they were surprised no one had crafted a similar communication tool as a potential quality-improvement (QI) measure. To wit, they are now working on publishing their research in the Journal of Hospital Medicine to further draw attention to the concept. They envision a day when the notes patients write down could be included in electronic medical records.
The ultimate goal is to give hospitalists and other physicians another way to communicate with their patients. “We want to institutionalize [Dear Doctor] to the point it’s a recognized necessity for the hospital system,” Lin says.—RQ
Toolkit Addresses Small-Business Security Concerns
The Healthcare Information and Management Systems Society (HIMSS) has had a privacy and security toolkit for physicians for a decade, but after its last annual security survey with the Medical Group Management Association (MGMA), it became clear that small- to medium-sized organizations were behind in implementation.
And so was born the HIMSS Privacy and Security Toolkit for Small Provider Organizations. The joint initiative is one that HM groups in rural or small settings should take advantage of, says Lisa Gallagher, HIMSS’ senior director of privacy and security.
Hospitalists “need to understand the reporting environment,” Gallagher says. “They are the subject of a lot of the policies and technology. We need them to be knowledgeable about it. They’re the ones who have access.”
HM’s role at the juncture of different departments and physicians, particularly at smaller hospitals that rely on hospitalists as traffic cops, makes it all the more important for hospitalists to understand the nuances of both privacy and security.
The interactive toolkit allows users to submit their own suggestions for improved processes and features introductions to the Centers for Medicare & Medicaid Services’ (CMS) “meaningful use” standard. Gallagher is hopeful that an engaged physician response to the toolkit will only bolster its efficacy in the coming months. “This is going to continue to evolve,” she says.—RQ
QUALITY RESEARCH
Care Transitions, Readmissions Concern Other Countries
International studies suggest that the recent torrent of attention toward improving care transitions and preventing hospital readmissions is not just an American trend. For example, a literature survey of physician “handovers” (aka handoffs) in international hospitals published in the British Medical Journal for Quality and Safety identified 32 papers on the subject.1 The authors conclude that the existing literature rarely examines pre- and post-handover phases or evaluates the quality of handover practices, and thus “does not fully identify where communication failures typically occur.” More systematic analysis of all stages of handoffs by physicians is warranted, the authors suggest.
In the same journal, a literature search of English-language publications from 1990 to 2010 found a dozen studies—eight from the U.S.—documenting failure to perform adequate follow-up for patients’ test results.2 The lack of follow-up ranged from 20% to 62% for hospitalized patients, and from 1% to 75% for patients treated in the ED. Two areas where problems were particularly evident were critical test results and results for patients moving across healthcare settings. “The existing evidence suggests that the problem of missed test results is considerable and reported negative impacts on patients warrant the exploration of solutions,” the authors conclude. They recommend further study of the effectiveness of such interventions as online endorsement of results, and integration of information technology into clinical work practices.
The World Alliance for Patient Safety, which was convened in 2004 by the World Health Organization, recently pointed to poor test result follow-up as one of the major processes contributing to unsafe patient care internationally.1 The organization has identified nine “patient-safety solutions,” one of which is ensuring medication accuracy at transitions of care.
For more information on the alliance and WHO’s interest in patient safety, visit http://www.who.int/topics/patient_safety/en/. —LB
References
- Raduma-Tomás MA, Flin R, Yule S, Williams D. Doctors’ handovers in hospi- tals: a literature review. BMJ Qual Saf. 2011;20:128-133.
- Callen J, Georgiou A, Li J, Westbrook JI. The safety implications of missed test results for hospitalised patients: a systematic review. BMJ Qual Saf. 2011;20:194-199.
The Future Is Forward
GRAPEVINE, Texas—New SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, asked a question at HM11 that might be a first for the relatively nascent field. After explaining to the crowd in the ballroom at the Gaylord Texan Resort and Convention Center that the average hospitalist is 37 years old, Dr. Li asked: “What’s going to happen when the hospitalist gets older and their priorities change?”
A hopeful, if wary, eye on the future of the still-growing field was a common thread throughout HM11, as SHM leaders from the new president to CEO Larry Wellikson, MD, SFHM, laid out the pathway of growth for a 15-year-old specialty. Although each acknowledged uncertainties as they adjust to a domestic healthcare system in the throes of its largest reform in a generation, they agree on a few mainstays.
First, HM should continue to take ownership of quality-improvement (QI) and patient-safety initiatives that improve outcomes and reduce costs for hospitals, as the dual reward of better care for patients and lower costs for chief financial officers can serve as change agents for healthcare and leverage for the next contract.
Second, hospitalists should be careful to balance expansion of their duties—be it via such “hyphenated hospitalists” as laborists, say, or through comanagement of surgical and ED patients—with an appropriate amount of dedicated resources.
Finally, academic hospitalists, from residents to attendings, should continue to plan for this summer’s reduction in work hours and patient caps for residents, new rules from the Accreditation Council for Graduate Medical Education (ACGME) that some fear could create a future cast of ill-prepared internists.
“There’s a lot that’s bearing down on physicians and it’s been compressed in a short period of time,” said AMA President Cecil Wilson, MD. “We cannot go back to where we were and we cannot stay where we are. … We may not have a choice about change, but we do have a choice on how we respond to change and how we influence it.”
Dr. Li sees SHM sitting at the intersection of practical application and influence. He wants to continue with society-sponsored training academies and leadership programs that both impress upon hospitalists how important it is for them to take leadership roles in their hospitals and make sure they have the skills to do so. Dr. Li says the field needs to look no further than other fields adopting the in-hospital practice model as proof that the care model is vital to improving equality.

“We need to be laser-focused in terms of what we want to do. [We] want to improve the quality of care of patients both inside and outside the hospital,” he adds. “I say both inside and outside because, oftentimes, that transition is somewhere in between it. We have many hospitalists, like at my place, who provide care in the outpatient setting, in post-discharge clinics, and other places.”
Dr. Li also says that collaborations with fellow medical societies and organizations are key to SHM’s advocacy role. Society leaders are attending other specialty conferences to build and strengthen relationships that help extend HM’s reach into policy circles. In perhaps one of the strongest relationships, SHM leadership is meeting this summer with Donald Berwick, MD, administrator of the Centers for Medicare & Medicaid Services (CMS). The meeting is even more valuable in context of Dr. Berwick’s recent selection of Patrick Conway, MD, MSc, SFHM, a pediatric hospitalist and director of hospital medicine at Cincinnati Children’s Hospital Medical Center, as CMS’ chief medical officer. The government position is the highest-ranking policy role ever held by a hospitalist (see “Hospitalist Takes Charge” p. 28).
“We’re in a position going forward where we don’t talk alone,” says immediate past SHM president Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center in New Orleans. “It’s us and our partners talking together. That moves what is currently a loud voice to a stentorian voice. You can imagine where SHM and ACP [American College of Physicians] and the VA [Veterans Administration] and Society of Critical Care Medicine … if they’re all saying the same thing, that’s a very different message than if one organization is saying it alone.”
Adds SHM board member and former SHM Public Policy Committee chairman Eric Siegal, MD, SFHM, a critical-care fellow at the University of Wisconsin School of Medicine and Public Health in Madison, “We’re absolutely at the table in a way that’s, frankly, almost stunning how fast we have evolved [from] several years ago, when we first went to Washington, D.C., for our first advocacy day, and we had to explain to people that hospitalists were not in the hospitality industry. We punch well above our weight class right now.”
It’s a tall order for any specialty society to push the national healthcare discussion, but Dr. Li sees HM as perfectly perched “to train the trainers.” The field has grown to more than 30,000 hospitalists, well beyond the estimated ceiling of 20,000 hospitalists forecasted in the field’s earliest days. That rapid-fire growth–hospitalists are now present in the vast majority of hospitals that can either afford them or need them–means the field can now evolve past simply swelling numbers to creating better physicians. By encouraging more rank-and-file practitioners to become leaders, the logic goes, the number of groups will increase as practices sprout in those remaining hospitals without HM services: more practices, more hospitalists, more presence in future policy discussions.
To that end, Dr. Wellikson notes that SHM continues to introduce training courses and research repositories. Two recent additions are eQUIPS (Electronic Quality Improvement Programs), a series of QI and patient toolkits aimed at transitional care, glycemic control, and VTE prevention, and SQUINT, SHM’s new QI repository, which allows users to upload research projects to a searchable database that other physicians can then mine for data.
“We’re really only at the very beginning,” Dr. Li says. “All of hospital medicine only started 10, 15 years ago. For some folks, they believe that’s a long time. But this really is the very beginning of this movement.”
Richard Quinn is a freelance writer based in New Jersey.
GRAPEVINE, Texas—New SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, asked a question at HM11 that might be a first for the relatively nascent field. After explaining to the crowd in the ballroom at the Gaylord Texan Resort and Convention Center that the average hospitalist is 37 years old, Dr. Li asked: “What’s going to happen when the hospitalist gets older and their priorities change?”
A hopeful, if wary, eye on the future of the still-growing field was a common thread throughout HM11, as SHM leaders from the new president to CEO Larry Wellikson, MD, SFHM, laid out the pathway of growth for a 15-year-old specialty. Although each acknowledged uncertainties as they adjust to a domestic healthcare system in the throes of its largest reform in a generation, they agree on a few mainstays.
First, HM should continue to take ownership of quality-improvement (QI) and patient-safety initiatives that improve outcomes and reduce costs for hospitals, as the dual reward of better care for patients and lower costs for chief financial officers can serve as change agents for healthcare and leverage for the next contract.
Second, hospitalists should be careful to balance expansion of their duties—be it via such “hyphenated hospitalists” as laborists, say, or through comanagement of surgical and ED patients—with an appropriate amount of dedicated resources.
Finally, academic hospitalists, from residents to attendings, should continue to plan for this summer’s reduction in work hours and patient caps for residents, new rules from the Accreditation Council for Graduate Medical Education (ACGME) that some fear could create a future cast of ill-prepared internists.
“There’s a lot that’s bearing down on physicians and it’s been compressed in a short period of time,” said AMA President Cecil Wilson, MD. “We cannot go back to where we were and we cannot stay where we are. … We may not have a choice about change, but we do have a choice on how we respond to change and how we influence it.”
Dr. Li sees SHM sitting at the intersection of practical application and influence. He wants to continue with society-sponsored training academies and leadership programs that both impress upon hospitalists how important it is for them to take leadership roles in their hospitals and make sure they have the skills to do so. Dr. Li says the field needs to look no further than other fields adopting the in-hospital practice model as proof that the care model is vital to improving equality.
“We need to be laser-focused in terms of what we want to do. [We] want to improve the quality of care of patients both inside and outside the hospital,” he adds. “I say both inside and outside because, oftentimes, that transition is somewhere in between it. We have many hospitalists, like at my place, who provide care in the outpatient setting, in post-discharge clinics, and other places.”
Dr. Li also says that collaborations with fellow medical societies and organizations are key to SHM’s advocacy role. Society leaders are attending other specialty conferences to build and strengthen relationships that help extend HM’s reach into policy circles. In perhaps one of the strongest relationships, SHM leadership is meeting this summer with Donald Berwick, MD, administrator of the Centers for Medicare & Medicaid Services (CMS). The meeting is even more valuable in context of Dr. Berwick’s recent selection of Patrick Conway, MD, MSc, SFHM, a pediatric hospitalist and director of hospital medicine at Cincinnati Children’s Hospital Medical Center, as CMS’ chief medical officer. The government position is the highest-ranking policy role ever held by a hospitalist (see “Hospitalist Takes Charge” p. 28).
“We’re in a position going forward where we don’t talk alone,” says immediate past SHM president Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center in New Orleans. “It’s us and our partners talking together. That moves what is currently a loud voice to a stentorian voice. You can imagine where SHM and ACP [American College of Physicians] and the VA [Veterans Administration] and Society of Critical Care Medicine … if they’re all saying the same thing, that’s a very different message than if one organization is saying it alone.”
Adds SHM board member and former SHM Public Policy Committee chairman Eric Siegal, MD, SFHM, a critical-care fellow at the University of Wisconsin School of Medicine and Public Health in Madison, “We’re absolutely at the table in a way that’s, frankly, almost stunning how fast we have evolved [from] several years ago, when we first went to Washington, D.C., for our first advocacy day, and we had to explain to people that hospitalists were not in the hospitality industry. We punch well above our weight class right now.”
It’s a tall order for any specialty society to push the national healthcare discussion, but Dr. Li sees HM as perfectly perched “to train the trainers.” The field has grown to more than 30,000 hospitalists, well beyond the estimated ceiling of 20,000 hospitalists forecasted in the field’s earliest days. That rapid-fire growth–hospitalists are now present in the vast majority of hospitals that can either afford them or need them–means the field can now evolve past simply swelling numbers to creating better physicians. By encouraging more rank-and-file practitioners to become leaders, the logic goes, the number of groups will increase as practices sprout in those remaining hospitals without HM services: more practices, more hospitalists, more presence in future policy discussions.
To that end, Dr. Wellikson notes that SHM continues to introduce training courses and research repositories. Two recent additions are eQUIPS (Electronic Quality Improvement Programs), a series of QI and patient toolkits aimed at transitional care, glycemic control, and VTE prevention, and SQUINT, SHM’s new QI repository, which allows users to upload research projects to a searchable database that other physicians can then mine for data.
“We’re really only at the very beginning,” Dr. Li says. “All of hospital medicine only started 10, 15 years ago. For some folks, they believe that’s a long time. But this really is the very beginning of this movement.”
Richard Quinn is a freelance writer based in New Jersey.
GRAPEVINE, Texas—New SHM President Joseph Li, MD, SFHM, associate professor of medicine at Harvard Medical School and director of the hospital medicine division at Beth Israel Deaconess Medical Center in Boston, asked a question at HM11 that might be a first for the relatively nascent field. After explaining to the crowd in the ballroom at the Gaylord Texan Resort and Convention Center that the average hospitalist is 37 years old, Dr. Li asked: “What’s going to happen when the hospitalist gets older and their priorities change?”
A hopeful, if wary, eye on the future of the still-growing field was a common thread throughout HM11, as SHM leaders from the new president to CEO Larry Wellikson, MD, SFHM, laid out the pathway of growth for a 15-year-old specialty. Although each acknowledged uncertainties as they adjust to a domestic healthcare system in the throes of its largest reform in a generation, they agree on a few mainstays.
First, HM should continue to take ownership of quality-improvement (QI) and patient-safety initiatives that improve outcomes and reduce costs for hospitals, as the dual reward of better care for patients and lower costs for chief financial officers can serve as change agents for healthcare and leverage for the next contract.
Second, hospitalists should be careful to balance expansion of their duties—be it via such “hyphenated hospitalists” as laborists, say, or through comanagement of surgical and ED patients—with an appropriate amount of dedicated resources.
Finally, academic hospitalists, from residents to attendings, should continue to plan for this summer’s reduction in work hours and patient caps for residents, new rules from the Accreditation Council for Graduate Medical Education (ACGME) that some fear could create a future cast of ill-prepared internists.
“There’s a lot that’s bearing down on physicians and it’s been compressed in a short period of time,” said AMA President Cecil Wilson, MD. “We cannot go back to where we were and we cannot stay where we are. … We may not have a choice about change, but we do have a choice on how we respond to change and how we influence it.”
Dr. Li sees SHM sitting at the intersection of practical application and influence. He wants to continue with society-sponsored training academies and leadership programs that both impress upon hospitalists how important it is for them to take leadership roles in their hospitals and make sure they have the skills to do so. Dr. Li says the field needs to look no further than other fields adopting the in-hospital practice model as proof that the care model is vital to improving equality.
“We need to be laser-focused in terms of what we want to do. [We] want to improve the quality of care of patients both inside and outside the hospital,” he adds. “I say both inside and outside because, oftentimes, that transition is somewhere in between it. We have many hospitalists, like at my place, who provide care in the outpatient setting, in post-discharge clinics, and other places.”
Dr. Li also says that collaborations with fellow medical societies and organizations are key to SHM’s advocacy role. Society leaders are attending other specialty conferences to build and strengthen relationships that help extend HM’s reach into policy circles. In perhaps one of the strongest relationships, SHM leadership is meeting this summer with Donald Berwick, MD, administrator of the Centers for Medicare & Medicaid Services (CMS). The meeting is even more valuable in context of Dr. Berwick’s recent selection of Patrick Conway, MD, MSc, SFHM, a pediatric hospitalist and director of hospital medicine at Cincinnati Children’s Hospital Medical Center, as CMS’ chief medical officer. The government position is the highest-ranking policy role ever held by a hospitalist (see “Hospitalist Takes Charge” p. 28).
“We’re in a position going forward where we don’t talk alone,” says immediate past SHM president Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center in New Orleans. “It’s us and our partners talking together. That moves what is currently a loud voice to a stentorian voice. You can imagine where SHM and ACP [American College of Physicians] and the VA [Veterans Administration] and Society of Critical Care Medicine … if they’re all saying the same thing, that’s a very different message than if one organization is saying it alone.”
Adds SHM board member and former SHM Public Policy Committee chairman Eric Siegal, MD, SFHM, a critical-care fellow at the University of Wisconsin School of Medicine and Public Health in Madison, “We’re absolutely at the table in a way that’s, frankly, almost stunning how fast we have evolved [from] several years ago, when we first went to Washington, D.C., for our first advocacy day, and we had to explain to people that hospitalists were not in the hospitality industry. We punch well above our weight class right now.”
It’s a tall order for any specialty society to push the national healthcare discussion, but Dr. Li sees HM as perfectly perched “to train the trainers.” The field has grown to more than 30,000 hospitalists, well beyond the estimated ceiling of 20,000 hospitalists forecasted in the field’s earliest days. That rapid-fire growth–hospitalists are now present in the vast majority of hospitals that can either afford them or need them–means the field can now evolve past simply swelling numbers to creating better physicians. By encouraging more rank-and-file practitioners to become leaders, the logic goes, the number of groups will increase as practices sprout in those remaining hospitals without HM services: more practices, more hospitalists, more presence in future policy discussions.
To that end, Dr. Wellikson notes that SHM continues to introduce training courses and research repositories. Two recent additions are eQUIPS (Electronic Quality Improvement Programs), a series of QI and patient toolkits aimed at transitional care, glycemic control, and VTE prevention, and SQUINT, SHM’s new QI repository, which allows users to upload research projects to a searchable database that other physicians can then mine for data.
“We’re really only at the very beginning,” Dr. Li says. “All of hospital medicine only started 10, 15 years ago. For some folks, they believe that’s a long time. But this really is the very beginning of this movement.”
Richard Quinn is a freelance writer based in New Jersey.
The Future of Better Patient Care

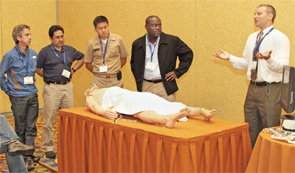
GRAPEVINE, Texas—Hospitalist Michael Monge, MD, of Cogent Healthcare in San Bernardino, Calif., watched an instructor squeeze the lubricating gel on the transponder and press it gently, but firmly, into the crook of a woman’s arm. Veins practically popped off an ultrasound monitor, serving as a literal road map for vascular access.
And he thought: Wouldn’t it be great if I had this technology all the time, just like I remember from my residency?
“A lot of my ER attendings were able to do a study at the bedside in a manner of minutes, not 30 or 45 minutes,” says Dr. Monge, who practices at Saint Bernardine Medical Center. “If they saw something abnormal, sure enough, they got the full study. But they were able to get that glimpse. Ultimately, it’s just better patient care.”
Dr. Monge’s ultrasound lesson was a first for the SHM annual meeting. In past years, training on ultrasounds was wrapped into the “Medical Procedures for the Hospitalist” pre-course. But at HM11, thanks to the growing prevalence and portability of the technology, the training was expanded into its own half-day pre-course, appropriately dubbed “Portable Ultrasound for the Hospitalist.”
“The ultrasound will be the stethoscope of the 21st century,” says Mark Ault, director of the Division of General Internal Medicine and assistant chairman for clinical affairs of the Department of Medicine at Cedars-Sinai Medical Center in Los Angeles. “And the goal will be to have an ultrasound in the hands of every internist.”
Only time will tell whether portable ultrasound becomes as commonplace as Dr. Ault envisions, but what is clear is that the evolution of the technology makes it widely applicable to hospitalists, says Bradley Rosen, MD, MBA, medical director of the Inpatient Specialty Program (ISP) at Cedars-Sinai Medical Center.
Pricing is one such example. In years past, ultrasound machines were bulky and costly, with price tags in the hundreds of thousands of dollars. Now, portable units, depending on the number of transducers and functionality, can come as low as $20,000, though more-advanced machines quickly jump into the $40,000 to $60,000 range.
Still, Dr. Rosen views the practical uses of the technology as almost endless, and could include vascular access, placing central and PICC lines, and insertion and removal of catheters. Most hospitalists, however, continue to have limited experience with portable ultrasound, meaning those interested in learning more likely have to seek out physicians in other departments to provide the training and mentorship required. Dr. Rosen suggests working with ED physicians, OB-GYNs, and radiologists, although he notes you should be careful to be clear that the HM community is not looking to supplant anyone, or take billing opportunities away.
Hospitalists “don’t know how to use it, and people don’t know where to go to learn how to use it,” he says. “This is a starting point that will allow people … to take these ideas back and, hopefully, generate enough of a critical mass that it becomes a louder and louder chorus asking for this technology.”
GRAPEVINE, Texas—Hospitalist Michael Monge, MD, of Cogent Healthcare in San Bernardino, Calif., watched an instructor squeeze the lubricating gel on the transponder and press it gently, but firmly, into the crook of a woman’s arm. Veins practically popped off an ultrasound monitor, serving as a literal road map for vascular access.
And he thought: Wouldn’t it be great if I had this technology all the time, just like I remember from my residency?
“A lot of my ER attendings were able to do a study at the bedside in a manner of minutes, not 30 or 45 minutes,” says Dr. Monge, who practices at Saint Bernardine Medical Center. “If they saw something abnormal, sure enough, they got the full study. But they were able to get that glimpse. Ultimately, it’s just better patient care.”
Dr. Monge’s ultrasound lesson was a first for the SHM annual meeting. In past years, training on ultrasounds was wrapped into the “Medical Procedures for the Hospitalist” pre-course. But at HM11, thanks to the growing prevalence and portability of the technology, the training was expanded into its own half-day pre-course, appropriately dubbed “Portable Ultrasound for the Hospitalist.”
“The ultrasound will be the stethoscope of the 21st century,” says Mark Ault, director of the Division of General Internal Medicine and assistant chairman for clinical affairs of the Department of Medicine at Cedars-Sinai Medical Center in Los Angeles. “And the goal will be to have an ultrasound in the hands of every internist.”
Only time will tell whether portable ultrasound becomes as commonplace as Dr. Ault envisions, but what is clear is that the evolution of the technology makes it widely applicable to hospitalists, says Bradley Rosen, MD, MBA, medical director of the Inpatient Specialty Program (ISP) at Cedars-Sinai Medical Center.
Pricing is one such example. In years past, ultrasound machines were bulky and costly, with price tags in the hundreds of thousands of dollars. Now, portable units, depending on the number of transducers and functionality, can come as low as $20,000, though more-advanced machines quickly jump into the $40,000 to $60,000 range.
Still, Dr. Rosen views the practical uses of the technology as almost endless, and could include vascular access, placing central and PICC lines, and insertion and removal of catheters. Most hospitalists, however, continue to have limited experience with portable ultrasound, meaning those interested in learning more likely have to seek out physicians in other departments to provide the training and mentorship required. Dr. Rosen suggests working with ED physicians, OB-GYNs, and radiologists, although he notes you should be careful to be clear that the HM community is not looking to supplant anyone, or take billing opportunities away.
Hospitalists “don’t know how to use it, and people don’t know where to go to learn how to use it,” he says. “This is a starting point that will allow people … to take these ideas back and, hopefully, generate enough of a critical mass that it becomes a louder and louder chorus asking for this technology.”
GRAPEVINE, Texas—Hospitalist Michael Monge, MD, of Cogent Healthcare in San Bernardino, Calif., watched an instructor squeeze the lubricating gel on the transponder and press it gently, but firmly, into the crook of a woman’s arm. Veins practically popped off an ultrasound monitor, serving as a literal road map for vascular access.
And he thought: Wouldn’t it be great if I had this technology all the time, just like I remember from my residency?
“A lot of my ER attendings were able to do a study at the bedside in a manner of minutes, not 30 or 45 minutes,” says Dr. Monge, who practices at Saint Bernardine Medical Center. “If they saw something abnormal, sure enough, they got the full study. But they were able to get that glimpse. Ultimately, it’s just better patient care.”
Dr. Monge’s ultrasound lesson was a first for the SHM annual meeting. In past years, training on ultrasounds was wrapped into the “Medical Procedures for the Hospitalist” pre-course. But at HM11, thanks to the growing prevalence and portability of the technology, the training was expanded into its own half-day pre-course, appropriately dubbed “Portable Ultrasound for the Hospitalist.”
“The ultrasound will be the stethoscope of the 21st century,” says Mark Ault, director of the Division of General Internal Medicine and assistant chairman for clinical affairs of the Department of Medicine at Cedars-Sinai Medical Center in Los Angeles. “And the goal will be to have an ultrasound in the hands of every internist.”
Only time will tell whether portable ultrasound becomes as commonplace as Dr. Ault envisions, but what is clear is that the evolution of the technology makes it widely applicable to hospitalists, says Bradley Rosen, MD, MBA, medical director of the Inpatient Specialty Program (ISP) at Cedars-Sinai Medical Center.
Pricing is one such example. In years past, ultrasound machines were bulky and costly, with price tags in the hundreds of thousands of dollars. Now, portable units, depending on the number of transducers and functionality, can come as low as $20,000, though more-advanced machines quickly jump into the $40,000 to $60,000 range.
Still, Dr. Rosen views the practical uses of the technology as almost endless, and could include vascular access, placing central and PICC lines, and insertion and removal of catheters. Most hospitalists, however, continue to have limited experience with portable ultrasound, meaning those interested in learning more likely have to seek out physicians in other departments to provide the training and mentorship required. Dr. Rosen suggests working with ED physicians, OB-GYNs, and radiologists, although he notes you should be careful to be clear that the HM community is not looking to supplant anyone, or take billing opportunities away.
Hospitalists “don’t know how to use it, and people don’t know where to go to learn how to use it,” he says. “This is a starting point that will allow people … to take these ideas back and, hopefully, generate enough of a critical mass that it becomes a louder and louder chorus asking for this technology.”
HM=Improved Patient Care

GRAPEVINE, Texas—The most successful companies tend to have superior branding. Starbucks owns coffee. Disney owns family fun. And hospitalists own patient-safety and quality-improvement (QI) initiatives within their hospitals.
“We were pretty confident that if we embraced this, we would have a clear running field to ourselves,” says Robert Wachter, MD, MHM, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president, and author of the Wachter’s World blog. “No other physician field would do the same thing, and by owning the patient-safety field, we would distinguish ourselves.”
Now comes the really hard part, though.
Three keynote speakers at HM11—Dr. Wachter, AMA President Cecil Wilson, MD, and Robert Kocher, MD, a healthcare policy advisor to President Obama—pointed to hospitalists as the physician cohort that can help shepherd the conceptual reform passed last year by Congress into daily practice in America’s hospitals. And all three also point to HM’s role at the vanguard of patient safety as a primary reason why.
Hurdles will arise, Dr. Wilson says. A solo practitioner most of his career, he says hospitalists can play a key role in the coming years as more patients receive insurance, but looming doctor shortages could stymie the cause. While many caution that the flood of newly insured patients will overburden primary-care physicians (PCPs), the expected shortage of physicians will plague HM as well.
“Hospitalists are primary-care physicians; the vast majority of them are general internists,” Dr. Wilson says. “… So when we say that the number of people who are going into primary care, particularly general internal medicine, is reducing, that reduces not only the pool of physicians in the community, but also the hospitalist pool. We’re in that boat together.”
Dr. Kocher, director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., says hospitalists are in the best position to push for on-the-ground reform as they are the doctors who bridge all hospital departments, floors, and wards. He sees four broad areas where HM can take a particularly leading role:

- Increasing labor productivity. HM’s role as a link between specialties from cardiology to the pharmacy makes HM a natural conduit to push institutional values from a unique vantage point.
- Driving decision-making. Whether it’s recommending less costly drugs with similar outcomes, questioning whether expensive test batteries are truly necessary or being done for fear of missing something, or pausing to ask whether a “90-year-old hip replacement patient should receive orthopedic implants that will last far longer than their grandkids will be alive,” hospitalists can use their data to be a common-sense lynchpin of daily operations.
- Using technology to lower delivery costs. Many insurance companies are willing to enter into risk-based contracts with hospitals, but some hospital executives worry whether they will be able to perform well enough to justify the risk. “Hospitalists can help say, ‘We can do this. We can hit the thresholds.’ ”
- Shifting compensation models from “selling work RVUs to selling years of health.”
“The biggest thing [hospitalists] should begin doing,” Dr. Kocher adds, “is stop thinking about units of work, or RVUs, and start thinking about how much better patients can be by virtue of the care they’re delivering, how many readmissions are they avoiding, how many core measures/outcomes are they hitting, how much better is the patient experience, and how much smoother is the handoff.”
The push to improve quality and show better outcomes, of course, is intrinsically tied to payment reform. Bundled payments that reimburse a set fee for a case from pre-admission to a preset post-discharge deadline worry some hospitalists, who fear how the payments will be divvied up and who will be in charge of said payment decisions. Dr. Kocher says that even when the initial rules are set, the system is likely to evolve.
However, the hospitalist’s role as a driver of QI positions the field well, all three speakers noted. By quarterbacking patient handoffs and continuing to be seen by hospital executives as quality and safety leaders, HM groups can make the argument that they are worth the financial support they ask for in negotiations. Dr. Wachter adds that while quality research has become a staple of academics and residents, hospitalists should look to now tie value to the equation, effectively linking better patient outcomes to HM’s bottom line.
“There’s no question that physicians that can care for patients more efficiently, in a higher-quality way, in hospitals at lower costs, are going to do better no matter how the system evolves,” Dr. Kocher says. “I’m positive, as long as hospitalists are confident—and I think they should be—that they can deliver, more consistently, better care than those who aren’t hospitalists practicing in hospitals … and they’re going to do better economically.”
GRAPEVINE, Texas—The most successful companies tend to have superior branding. Starbucks owns coffee. Disney owns family fun. And hospitalists own patient-safety and quality-improvement (QI) initiatives within their hospitals.
“We were pretty confident that if we embraced this, we would have a clear running field to ourselves,” says Robert Wachter, MD, MHM, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president, and author of the Wachter’s World blog. “No other physician field would do the same thing, and by owning the patient-safety field, we would distinguish ourselves.”
Now comes the really hard part, though.
Three keynote speakers at HM11—Dr. Wachter, AMA President Cecil Wilson, MD, and Robert Kocher, MD, a healthcare policy advisor to President Obama—pointed to hospitalists as the physician cohort that can help shepherd the conceptual reform passed last year by Congress into daily practice in America’s hospitals. And all three also point to HM’s role at the vanguard of patient safety as a primary reason why.
Hurdles will arise, Dr. Wilson says. A solo practitioner most of his career, he says hospitalists can play a key role in the coming years as more patients receive insurance, but looming doctor shortages could stymie the cause. While many caution that the flood of newly insured patients will overburden primary-care physicians (PCPs), the expected shortage of physicians will plague HM as well.
“Hospitalists are primary-care physicians; the vast majority of them are general internists,” Dr. Wilson says. “… So when we say that the number of people who are going into primary care, particularly general internal medicine, is reducing, that reduces not only the pool of physicians in the community, but also the hospitalist pool. We’re in that boat together.”
Dr. Kocher, director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., says hospitalists are in the best position to push for on-the-ground reform as they are the doctors who bridge all hospital departments, floors, and wards. He sees four broad areas where HM can take a particularly leading role:
- Increasing labor productivity. HM’s role as a link between specialties from cardiology to the pharmacy makes HM a natural conduit to push institutional values from a unique vantage point.
- Driving decision-making. Whether it’s recommending less costly drugs with similar outcomes, questioning whether expensive test batteries are truly necessary or being done for fear of missing something, or pausing to ask whether a “90-year-old hip replacement patient should receive orthopedic implants that will last far longer than their grandkids will be alive,” hospitalists can use their data to be a common-sense lynchpin of daily operations.
- Using technology to lower delivery costs. Many insurance companies are willing to enter into risk-based contracts with hospitals, but some hospital executives worry whether they will be able to perform well enough to justify the risk. “Hospitalists can help say, ‘We can do this. We can hit the thresholds.’ ”
- Shifting compensation models from “selling work RVUs to selling years of health.”
“The biggest thing [hospitalists] should begin doing,” Dr. Kocher adds, “is stop thinking about units of work, or RVUs, and start thinking about how much better patients can be by virtue of the care they’re delivering, how many readmissions are they avoiding, how many core measures/outcomes are they hitting, how much better is the patient experience, and how much smoother is the handoff.”
The push to improve quality and show better outcomes, of course, is intrinsically tied to payment reform. Bundled payments that reimburse a set fee for a case from pre-admission to a preset post-discharge deadline worry some hospitalists, who fear how the payments will be divvied up and who will be in charge of said payment decisions. Dr. Kocher says that even when the initial rules are set, the system is likely to evolve.
However, the hospitalist’s role as a driver of QI positions the field well, all three speakers noted. By quarterbacking patient handoffs and continuing to be seen by hospital executives as quality and safety leaders, HM groups can make the argument that they are worth the financial support they ask for in negotiations. Dr. Wachter adds that while quality research has become a staple of academics and residents, hospitalists should look to now tie value to the equation, effectively linking better patient outcomes to HM’s bottom line.
“There’s no question that physicians that can care for patients more efficiently, in a higher-quality way, in hospitals at lower costs, are going to do better no matter how the system evolves,” Dr. Kocher says. “I’m positive, as long as hospitalists are confident—and I think they should be—that they can deliver, more consistently, better care than those who aren’t hospitalists practicing in hospitals … and they’re going to do better economically.”
GRAPEVINE, Texas—The most successful companies tend to have superior branding. Starbucks owns coffee. Disney owns family fun. And hospitalists own patient-safety and quality-improvement (QI) initiatives within their hospitals.
“We were pretty confident that if we embraced this, we would have a clear running field to ourselves,” says Robert Wachter, MD, MHM, professor, chief of the Division of Hospital Medicine, and chief of the Medical Service at the University of California at San Francisco Medical Center, former SHM president, and author of the Wachter’s World blog. “No other physician field would do the same thing, and by owning the patient-safety field, we would distinguish ourselves.”
Now comes the really hard part, though.
Three keynote speakers at HM11—Dr. Wachter, AMA President Cecil Wilson, MD, and Robert Kocher, MD, a healthcare policy advisor to President Obama—pointed to hospitalists as the physician cohort that can help shepherd the conceptual reform passed last year by Congress into daily practice in America’s hospitals. And all three also point to HM’s role at the vanguard of patient safety as a primary reason why.
Hurdles will arise, Dr. Wilson says. A solo practitioner most of his career, he says hospitalists can play a key role in the coming years as more patients receive insurance, but looming doctor shortages could stymie the cause. While many caution that the flood of newly insured patients will overburden primary-care physicians (PCPs), the expected shortage of physicians will plague HM as well.
“Hospitalists are primary-care physicians; the vast majority of them are general internists,” Dr. Wilson says. “… So when we say that the number of people who are going into primary care, particularly general internal medicine, is reducing, that reduces not only the pool of physicians in the community, but also the hospitalist pool. We’re in that boat together.”
Dr. Kocher, director of the McKinsey Center for U.S. Health System Reform in Washington, D.C., says hospitalists are in the best position to push for on-the-ground reform as they are the doctors who bridge all hospital departments, floors, and wards. He sees four broad areas where HM can take a particularly leading role:
- Increasing labor productivity. HM’s role as a link between specialties from cardiology to the pharmacy makes HM a natural conduit to push institutional values from a unique vantage point.
- Driving decision-making. Whether it’s recommending less costly drugs with similar outcomes, questioning whether expensive test batteries are truly necessary or being done for fear of missing something, or pausing to ask whether a “90-year-old hip replacement patient should receive orthopedic implants that will last far longer than their grandkids will be alive,” hospitalists can use their data to be a common-sense lynchpin of daily operations.
- Using technology to lower delivery costs. Many insurance companies are willing to enter into risk-based contracts with hospitals, but some hospital executives worry whether they will be able to perform well enough to justify the risk. “Hospitalists can help say, ‘We can do this. We can hit the thresholds.’ ”
- Shifting compensation models from “selling work RVUs to selling years of health.”
“The biggest thing [hospitalists] should begin doing,” Dr. Kocher adds, “is stop thinking about units of work, or RVUs, and start thinking about how much better patients can be by virtue of the care they’re delivering, how many readmissions are they avoiding, how many core measures/outcomes are they hitting, how much better is the patient experience, and how much smoother is the handoff.”
The push to improve quality and show better outcomes, of course, is intrinsically tied to payment reform. Bundled payments that reimburse a set fee for a case from pre-admission to a preset post-discharge deadline worry some hospitalists, who fear how the payments will be divvied up and who will be in charge of said payment decisions. Dr. Kocher says that even when the initial rules are set, the system is likely to evolve.
However, the hospitalist’s role as a driver of QI positions the field well, all three speakers noted. By quarterbacking patient handoffs and continuing to be seen by hospital executives as quality and safety leaders, HM groups can make the argument that they are worth the financial support they ask for in negotiations. Dr. Wachter adds that while quality research has become a staple of academics and residents, hospitalists should look to now tie value to the equation, effectively linking better patient outcomes to HM’s bottom line.
“There’s no question that physicians that can care for patients more efficiently, in a higher-quality way, in hospitals at lower costs, are going to do better no matter how the system evolves,” Dr. Kocher says. “I’m positive, as long as hospitalists are confident—and I think they should be—that they can deliver, more consistently, better care than those who aren’t hospitalists practicing in hospitals … and they’re going to do better economically.”
HM11 BREAKOUT SESSIONS OVERVIEW





QUALITY
Utilizing Technology to Improve the Clinical and Operational Performance of Hospitalists
SPEAKERS: Jason Stein, MD, SFHM, associate vice chair for quality, Department of Medicine, Bryce Gartland, MD, FHM, associate director, section of hospital medicine, Emory University School of Medicine, Atlanta
In an age of increasing technology, just getting technology into a hospital isn’t the answer. It’s about integrating it into practice to improve care.
At Emory, the marriage of “low-tech solutions” and patented data displays has resulted in what Drs. Stein and Gartland call an accountable-care unit (ACU). The unit-based team features geographic ownership and structured interdisciplinary bedside rounds (SIBR). Perhaps more important, the unit generates real-time data captured on monitors, allowing teams of hospitalists, nonphysician providers (NPPs), residents, interns, and social workers to “visually digest immense amounts of information in a very short time period,” Dr. Gartland said.
Dr. Stein defined an ACU as a bounded geographic inpatient area responsible for the clinical, service, and cost outcomes it produces. To help manage beds, Emory instituted a system called “e-Bed,” a McKesson system that tracks room availability. The system shows whether rooms are occupied, being cleaned, or somewhere in between. It has icons to show whether patients are elsewhere in the hospital for treatment, as well as clinical data capacities. Unit teams round together and use a portable workstation or tablet computer to input clinical data, notes, or other comments into real-time dashboards that can then show everything from VTE prophylaxis to whether a patient is at high risk for falls.
The project has been in the works for several years, and Dr. Garltand noted that any hospitalists looking to push similar initiatives at their institution need to ensure that they have buy-in from providers and a commitment to seeing the project through.
“Timing is everything,” he said. “If we tried to force this … a few years ago, it would not have worked.”
PRACTICE MANAGEMENT
Recruiting and Retaining Hospitalists: Developing a Talent Facilitation Framework
SPEAKERS: Patrick Kneeland, MD, hospitalist, Providence Regional Medical Center, Everett, Wash.; Christine Kneeland, COO, Center Partners, Fort Collins, Colo.; Niraj Sehgal, associate professor of medicine, associate chair for quality and safety, Department of Medicine, University of California at San Francisco
Lincoln Godfrey, DO, a hospitalist at Baxter Regional Medical Center in Mountain Home, Ark., was sitting and listening to strategies to lure and keep hospitalists when his hospital CEO sent him a text asking how his recruiting efforts were going with a would-be hire.
“I said I’d get back to him,” Dr. Godfrey jokes.
The C-suite’s passion is understandable, though, as the fight to hire experienced staff outside of major markets continues to stymie many HM groups. Dr. Godfrey says he can’t hire anybody without first getting them to the Ozark Mountains to learn the hospital, its people, and its community.
“There’s going to be a limited talent pool of people who will come at all,” he says. “But I don’t get anybody who doesn’t work with us for a bit first.”
Christine Kneeland—Dr. Kneeland’s mother—said HM leaders tasked with their group’s personnel duties should focus on a few main concepts:
- Think outside the bank. Some physicians look only to earn as much as they can as quickly as they can, but many seek personal and professional satisfaction.
- Engagement is instrumental. A one-day orientation program for a lifetime job doesn’t sound like enough, does it?
In the coming years, hiring managers will have to focus on “millennials”—the generation of doctors born between 1977 and 1999—which Christine Kneeland described as tech-savvy doctors interested in a blended lifestyle of work and leisure. And while some might not agree with or understand their perspective, they’d better get used to it, she said. “The millennials are here, the workplace has changed, and they are leading that change,” she added. “Just embrace it.”
QUALITY
Patient Satisfaction: Tips for Improving Your HCAHPS Scores
MODERATORS: Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; Steven Deitelzweig, MD, MMM, SFHM, system chairman, Department of Hospital Medicine, regional vice president of medical affairs, Ochsner Health System, New Orleans
Patient satisfaction scores are a big deal right now, as many HM groups tie the scores to compensation and the federal government tethers the scores and a portion of hospital payment through the value-based purchasing (VBP) program.
So how does a hospitalist improve their HCAHPS score? Here’s what the experts said:
- Personalize things. Give a business card with a picture. Sit down. Smile. Ask the patient if they understand what you’ve said, and don’t get frustrated if they don’t.
- First and last. Make good impressions when introducing yourself to the patient and when it’s time to discharge or transition them to a different facility. “When the hospitalist hands a patient off,” Dr. Whitcomb said, “it doesn’t cut it to pull out your brochure of 40 practitioners when the patient asks, ‘Who am I going to see tomorrow?’”
- Be professional. Don’t vent about workplace issues in front of patients. Dr. Deitelzweig illustrated the point with the case of an elderly patient who got out of bed to help a practitioner they heard complaining about a heavy workload. The patient fell.
- Creative use of white space. Consider using in-room white boards to help keep patients informed of a day’s care plan.
David Jaworski, MD, director of the hospitalist service at Windham Hospital in Willimantic, Conn., says honesty was a key piece of advice he gleaned from the session.
“I think one of the things people appreciate the most when they’re in the hospital is being honest about our uncertainties,” he says. “I have had more people thank me for saying, ‘I don’t know, but we will find out by doing this, this, and this.’ ”
ACADEMIC
The Role of Hospital Medicine in Adapting to the New ACGME Requirements
SPEAKER: Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center, New Orleans
The new Accreditation Council for Graduate Medical Education (ACGME) work-hour rules that take effect July 1 have received a lot of attention since they were announced last summer. The guideline that has attracted the bulk of the attention limits intern shifts to 16 hours, with upper-level residents capped at 24 consecutive hours, with four hours of administrative follow-on allowed with the caveat that strategic napping is “strongly suggested.”
“I’m all for work hours,” said Dr. Wiese, immediate past president of SHM. “It’s the right thing to do; it’s safer. But I think we have to be careful we don’t super-fragment the system or double the intensity of the system. And on both of those plates, if you don’t do it right, what you end up with is people who will be ill-prepared.”
Dr. Wiese said an easy way to question the validity of one ACGME rule is to examine the guideline that limits a first-year resident’s census to 10 patients. He wondered which scenario offers more teaching opportunities: a roster of six chest-pain cases, two pneumonia cases, and two similarly familiar or relatively safe cases, or a resident with only four cases but each one having multiple comorbidities and complex decisions?
The new rules provide hospitals and HM groups an opportunity to change their way of thinking, adds Jeffrey Schnipper, MD, MPH, FHM, of Brigham and Women’s Hospital and Massachusetts General Hospital in Boston. “Every program has to change its entire way of doing business anyway, so let’s be at the table and say, ‘Well, while you’re redesigning your entire program, let’s inject patent safety and quality of care, and good pedagogy into the system,’” he says.
CLINICAL
Skin is In: Dermatological Images Every Hospitalist Should Recognize
MODERATOR: Paul Aronowitz, MD, FACP, internal medicine residency program director, California Pacific Medical Center, San Francisco
A patient comes into the ED with a blistering skin condition, but the diagnosis escapes the triage doctor on the case. The problem turns out to be bullosis diabeticorum, but the ED doc doesn’t know that yet and pushes to add a patient to the upstairs HM roster.
“The ED will usually try to admit because they’re worried [the patient has] some terrible drug eruption, but they can actually go home,” Dr. Aronowitz explained. “Hospitalists can help tell the difference.”
HM groups shouldn’t work to become amateur dermatologists, Dr. Aronowitz added. However, given that many hospitalists find themselves confronted by dermatologic cases several times a month, a rudimentary pedigree is a good idea to help sift out which cases require admission and which would take up bed space required for others.
He referred to it as knowing enough to know whether you know enough. “For sure, a hospitalist can diagnose a hypersensitivity reaction from a classic drug like Dilantin,” Dr. Aronowitz said, “and then stop the drug, because that would be one of the best things they could do.”
The session exposed hospitalists to dozens of images of skin conditions theymight come across in daily rounds, from snakebites to drug reactions to argyria.
“The idea is to help hospitalists recognize what’s serious and what’s not,” he said. “If you recognize those initial cutaneous clues, you can guide your antibiotic therapy, or whether you need antibiotics.”
CAREER
This Disease Is Easy; It’s the Patient Who’s Difficult
Speaker: Susan Block, chair, Department of Psychosocial Oncology and Palliative Care at Dana Farber Cancer Institute, Boston
Every physician will have their “button pushed” by a patient now and then, and hospitalists are in the unfortunate position of having little or no previous relationship with most patients, according to Dr. Block, a national expert in physician-patient conflict resolution who said “interpersonal challenges are an onerous part” of the job.
“We want to make sure we provide really good care to these patients, but it can be very challenging,” she said, noting that between 10% and 30% of patients in the healthcare setting present with difficult behaviors.
Whether it’s an empowered patient, a traumatized patient, an intrusive family member, or a patient with clear psychosocial issues, Dr. Block explained that “these patients can make physicians feel lousy. … Being aware of that and trying to stop that process is one of the key issues in professionalism and competence in working with difficult patients.”
She also warned hospitalists to recognize when they become a “magnet” for difficult patients, as many times the expert in the group will become the “go-to” doc. “I don’t think anyone can take care of a large panel of these patients; it’s just too much,” she said, noting you have to negotiate some limits or you will “burn out and lose perspective.”
Many doctors are very uncomfortable with scared or crying patients, Dr. Block said, explaining these are some of her most difficult patients. “Show me a patient in the hospital who isn’t scared,” she said. “Even it they aren’t, they are scared of dying.”
Other sources of workplace discomfort include the dependent or “needy” patient, the suspicious patient, and the extremely pushy patient. Dr. Block suggested setting clear boundaries with patients; she also noted physicians should be ready and willing to identify and reflect on your own emotions so that “you have the capacity to get perspective on the problem and keep yourself from being part of the problem.
“Limit-setting is one of the most therapeutic things you can do with difficult patients,” she said. “It feels to us as a form of sadism, as though we are punishing patients. But for many patients, the most dangerous, scary, and dysfunctional thing you can do for patients is not set limits.”
CLINICAL
The Art of Clinical Problem-Solving: Mystery Cases
SPEAKER: Gupreet Dhaliwal, MD, University of California at San Francisco
Humility, patience, and practice: Those are the keys to improving one’s clinical diagnostic skills, according to Dr. Dhaliwal, an acclaimed educator and clinician at UCSF who walked a packed room through two blind cases and encouraged hospitalists to work hard at their craft.
“If you want to reach your maximum potential, you have to view it the same way we do other things, the same way a great musician rehearses and a great soccer player scrimmages,” he said. “All of us are busy, but you either have to increase the number of cases you put your mind through, or you take the cases you have and you analyze them, you seek feedback, you try to improve the process around the diagnostic.
“The message isn’t always fun, because both of those things equal more work, but there is no way to hide it because there is no field in which people get better without more work.”
Dr. Dhaliwal says hospitalists should be “humble about diagnosis.” He explained that the more experienced people become, the more we shift from analytical reasoning, “thinking hard like we did when we were students and residents,” to intuitive reasoning, which “is basically saying, ‘I recognize a pattern, this is an old friend, I’ve seen gout before.’ I think any of us can be guilty of forgetting that it has pitfalls. And there is a whole list of cognitive biases that are associated with moving fast and building patterns.”
He also believes hospitalists who dedicate themselves to clinical greatness can parlay such improvement in the quality realm. “Every one of us has used diagnosis as a core part of our identity, but in terms of getting the community or other stakeholders behind improving diagnosis or improving judgment, I think the umbrella of quality and reducing diagnostic errors is the most appealing and most logical,” he says. “I think we start to take for granted we are good at it, but I think there are ways many of us, especially if we work at it, can become great at it.”
CLINICAL
The How, When, and Why of Noninvasive Ventilation
SPEAKER: Eric Siegal, MD, SFHM, critical care fellow, University of Wisconsin School of Medicine, Madison
Dr. Siegal’s review of literature in front of a packed crowd provided a road map to Noninvasive Positive Pressure Ventilation (NPPV) usage. In the end, NPPV should be a hospitalist’s first choice for patients with hypercarbic COPD exacerbations, and likely in patients with acute cardiogenic pulmonary edema, hypoxemic respiratory failure, immunocompromised patients, and pre-intubation patients.
Dr. Siegal stressed the use of NPPV in COPD, which has been studied thoroughly and “held up to repeated scrutiny.”
“If you put people on NPPV instead of intubating them … mortality is halved, intubation rate is less than half, treatment failure is much lower, you have a third of the complications, and huge reductions in length of stay,” Dr. Siegal said.
In the absence of contraindications, he stressed, NPPV should be the first line of therapy for patients with hypercarbic COPD exacerbations. “In fact, I would argue that you really should be asking yourself, ‘Why can’t I put these patients on NPPV?’ ” he asked, “because this has really shown to be life-saving.”
Dr. Siegal also explored recent findings on NPPV in acute cardiogenic pulmonary edema patients, which surprisingly showed “no better than supplemental oxygen.” He concluded that if your patient is not hypercarbic, “there is no advantage to adding pressure support.” He also said the benefit is more robust in ACPE patients who have acute coronary syndrome.
Dr. Siegal advised hospitalists to pick the right patients, start NPPV therapy early, and if the patient doesn’t improve within one or two hours, “it’s time to move on.”
QUALITY
Utilizing Technology to Improve the Clinical and Operational Performance of Hospitalists
SPEAKERS: Jason Stein, MD, SFHM, associate vice chair for quality, Department of Medicine, Bryce Gartland, MD, FHM, associate director, section of hospital medicine, Emory University School of Medicine, Atlanta
In an age of increasing technology, just getting technology into a hospital isn’t the answer. It’s about integrating it into practice to improve care.
At Emory, the marriage of “low-tech solutions” and patented data displays has resulted in what Drs. Stein and Gartland call an accountable-care unit (ACU). The unit-based team features geographic ownership and structured interdisciplinary bedside rounds (SIBR). Perhaps more important, the unit generates real-time data captured on monitors, allowing teams of hospitalists, nonphysician providers (NPPs), residents, interns, and social workers to “visually digest immense amounts of information in a very short time period,” Dr. Gartland said.
Dr. Stein defined an ACU as a bounded geographic inpatient area responsible for the clinical, service, and cost outcomes it produces. To help manage beds, Emory instituted a system called “e-Bed,” a McKesson system that tracks room availability. The system shows whether rooms are occupied, being cleaned, or somewhere in between. It has icons to show whether patients are elsewhere in the hospital for treatment, as well as clinical data capacities. Unit teams round together and use a portable workstation or tablet computer to input clinical data, notes, or other comments into real-time dashboards that can then show everything from VTE prophylaxis to whether a patient is at high risk for falls.
The project has been in the works for several years, and Dr. Garltand noted that any hospitalists looking to push similar initiatives at their institution need to ensure that they have buy-in from providers and a commitment to seeing the project through.
“Timing is everything,” he said. “If we tried to force this … a few years ago, it would not have worked.”
PRACTICE MANAGEMENT
Recruiting and Retaining Hospitalists: Developing a Talent Facilitation Framework
SPEAKERS: Patrick Kneeland, MD, hospitalist, Providence Regional Medical Center, Everett, Wash.; Christine Kneeland, COO, Center Partners, Fort Collins, Colo.; Niraj Sehgal, associate professor of medicine, associate chair for quality and safety, Department of Medicine, University of California at San Francisco
Lincoln Godfrey, DO, a hospitalist at Baxter Regional Medical Center in Mountain Home, Ark., was sitting and listening to strategies to lure and keep hospitalists when his hospital CEO sent him a text asking how his recruiting efforts were going with a would-be hire.
“I said I’d get back to him,” Dr. Godfrey jokes.
The C-suite’s passion is understandable, though, as the fight to hire experienced staff outside of major markets continues to stymie many HM groups. Dr. Godfrey says he can’t hire anybody without first getting them to the Ozark Mountains to learn the hospital, its people, and its community.
“There’s going to be a limited talent pool of people who will come at all,” he says. “But I don’t get anybody who doesn’t work with us for a bit first.”
Christine Kneeland—Dr. Kneeland’s mother—said HM leaders tasked with their group’s personnel duties should focus on a few main concepts:
- Think outside the bank. Some physicians look only to earn as much as they can as quickly as they can, but many seek personal and professional satisfaction.
- Engagement is instrumental. A one-day orientation program for a lifetime job doesn’t sound like enough, does it?
In the coming years, hiring managers will have to focus on “millennials”—the generation of doctors born between 1977 and 1999—which Christine Kneeland described as tech-savvy doctors interested in a blended lifestyle of work and leisure. And while some might not agree with or understand their perspective, they’d better get used to it, she said. “The millennials are here, the workplace has changed, and they are leading that change,” she added. “Just embrace it.”
QUALITY
Patient Satisfaction: Tips for Improving Your HCAHPS Scores
MODERATORS: Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; Steven Deitelzweig, MD, MMM, SFHM, system chairman, Department of Hospital Medicine, regional vice president of medical affairs, Ochsner Health System, New Orleans
Patient satisfaction scores are a big deal right now, as many HM groups tie the scores to compensation and the federal government tethers the scores and a portion of hospital payment through the value-based purchasing (VBP) program.
So how does a hospitalist improve their HCAHPS score? Here’s what the experts said:
- Personalize things. Give a business card with a picture. Sit down. Smile. Ask the patient if they understand what you’ve said, and don’t get frustrated if they don’t.
- First and last. Make good impressions when introducing yourself to the patient and when it’s time to discharge or transition them to a different facility. “When the hospitalist hands a patient off,” Dr. Whitcomb said, “it doesn’t cut it to pull out your brochure of 40 practitioners when the patient asks, ‘Who am I going to see tomorrow?’”
- Be professional. Don’t vent about workplace issues in front of patients. Dr. Deitelzweig illustrated the point with the case of an elderly patient who got out of bed to help a practitioner they heard complaining about a heavy workload. The patient fell.
- Creative use of white space. Consider using in-room white boards to help keep patients informed of a day’s care plan.
David Jaworski, MD, director of the hospitalist service at Windham Hospital in Willimantic, Conn., says honesty was a key piece of advice he gleaned from the session.
“I think one of the things people appreciate the most when they’re in the hospital is being honest about our uncertainties,” he says. “I have had more people thank me for saying, ‘I don’t know, but we will find out by doing this, this, and this.’ ”
ACADEMIC
The Role of Hospital Medicine in Adapting to the New ACGME Requirements
SPEAKER: Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center, New Orleans
The new Accreditation Council for Graduate Medical Education (ACGME) work-hour rules that take effect July 1 have received a lot of attention since they were announced last summer. The guideline that has attracted the bulk of the attention limits intern shifts to 16 hours, with upper-level residents capped at 24 consecutive hours, with four hours of administrative follow-on allowed with the caveat that strategic napping is “strongly suggested.”
“I’m all for work hours,” said Dr. Wiese, immediate past president of SHM. “It’s the right thing to do; it’s safer. But I think we have to be careful we don’t super-fragment the system or double the intensity of the system. And on both of those plates, if you don’t do it right, what you end up with is people who will be ill-prepared.”
Dr. Wiese said an easy way to question the validity of one ACGME rule is to examine the guideline that limits a first-year resident’s census to 10 patients. He wondered which scenario offers more teaching opportunities: a roster of six chest-pain cases, two pneumonia cases, and two similarly familiar or relatively safe cases, or a resident with only four cases but each one having multiple comorbidities and complex decisions?
The new rules provide hospitals and HM groups an opportunity to change their way of thinking, adds Jeffrey Schnipper, MD, MPH, FHM, of Brigham and Women’s Hospital and Massachusetts General Hospital in Boston. “Every program has to change its entire way of doing business anyway, so let’s be at the table and say, ‘Well, while you’re redesigning your entire program, let’s inject patent safety and quality of care, and good pedagogy into the system,’” he says.
CLINICAL
Skin is In: Dermatological Images Every Hospitalist Should Recognize
MODERATOR: Paul Aronowitz, MD, FACP, internal medicine residency program director, California Pacific Medical Center, San Francisco
A patient comes into the ED with a blistering skin condition, but the diagnosis escapes the triage doctor on the case. The problem turns out to be bullosis diabeticorum, but the ED doc doesn’t know that yet and pushes to add a patient to the upstairs HM roster.
“The ED will usually try to admit because they’re worried [the patient has] some terrible drug eruption, but they can actually go home,” Dr. Aronowitz explained. “Hospitalists can help tell the difference.”
HM groups shouldn’t work to become amateur dermatologists, Dr. Aronowitz added. However, given that many hospitalists find themselves confronted by dermatologic cases several times a month, a rudimentary pedigree is a good idea to help sift out which cases require admission and which would take up bed space required for others.
He referred to it as knowing enough to know whether you know enough. “For sure, a hospitalist can diagnose a hypersensitivity reaction from a classic drug like Dilantin,” Dr. Aronowitz said, “and then stop the drug, because that would be one of the best things they could do.”
The session exposed hospitalists to dozens of images of skin conditions theymight come across in daily rounds, from snakebites to drug reactions to argyria.
“The idea is to help hospitalists recognize what’s serious and what’s not,” he said. “If you recognize those initial cutaneous clues, you can guide your antibiotic therapy, or whether you need antibiotics.”
CAREER
This Disease Is Easy; It’s the Patient Who’s Difficult
Speaker: Susan Block, chair, Department of Psychosocial Oncology and Palliative Care at Dana Farber Cancer Institute, Boston
Every physician will have their “button pushed” by a patient now and then, and hospitalists are in the unfortunate position of having little or no previous relationship with most patients, according to Dr. Block, a national expert in physician-patient conflict resolution who said “interpersonal challenges are an onerous part” of the job.
“We want to make sure we provide really good care to these patients, but it can be very challenging,” she said, noting that between 10% and 30% of patients in the healthcare setting present with difficult behaviors.
Whether it’s an empowered patient, a traumatized patient, an intrusive family member, or a patient with clear psychosocial issues, Dr. Block explained that “these patients can make physicians feel lousy. … Being aware of that and trying to stop that process is one of the key issues in professionalism and competence in working with difficult patients.”
She also warned hospitalists to recognize when they become a “magnet” for difficult patients, as many times the expert in the group will become the “go-to” doc. “I don’t think anyone can take care of a large panel of these patients; it’s just too much,” she said, noting you have to negotiate some limits or you will “burn out and lose perspective.”
Many doctors are very uncomfortable with scared or crying patients, Dr. Block said, explaining these are some of her most difficult patients. “Show me a patient in the hospital who isn’t scared,” she said. “Even it they aren’t, they are scared of dying.”
Other sources of workplace discomfort include the dependent or “needy” patient, the suspicious patient, and the extremely pushy patient. Dr. Block suggested setting clear boundaries with patients; she also noted physicians should be ready and willing to identify and reflect on your own emotions so that “you have the capacity to get perspective on the problem and keep yourself from being part of the problem.
“Limit-setting is one of the most therapeutic things you can do with difficult patients,” she said. “It feels to us as a form of sadism, as though we are punishing patients. But for many patients, the most dangerous, scary, and dysfunctional thing you can do for patients is not set limits.”
CLINICAL
The Art of Clinical Problem-Solving: Mystery Cases
SPEAKER: Gupreet Dhaliwal, MD, University of California at San Francisco
Humility, patience, and practice: Those are the keys to improving one’s clinical diagnostic skills, according to Dr. Dhaliwal, an acclaimed educator and clinician at UCSF who walked a packed room through two blind cases and encouraged hospitalists to work hard at their craft.
“If you want to reach your maximum potential, you have to view it the same way we do other things, the same way a great musician rehearses and a great soccer player scrimmages,” he said. “All of us are busy, but you either have to increase the number of cases you put your mind through, or you take the cases you have and you analyze them, you seek feedback, you try to improve the process around the diagnostic.
“The message isn’t always fun, because both of those things equal more work, but there is no way to hide it because there is no field in which people get better without more work.”
Dr. Dhaliwal says hospitalists should be “humble about diagnosis.” He explained that the more experienced people become, the more we shift from analytical reasoning, “thinking hard like we did when we were students and residents,” to intuitive reasoning, which “is basically saying, ‘I recognize a pattern, this is an old friend, I’ve seen gout before.’ I think any of us can be guilty of forgetting that it has pitfalls. And there is a whole list of cognitive biases that are associated with moving fast and building patterns.”
He also believes hospitalists who dedicate themselves to clinical greatness can parlay such improvement in the quality realm. “Every one of us has used diagnosis as a core part of our identity, but in terms of getting the community or other stakeholders behind improving diagnosis or improving judgment, I think the umbrella of quality and reducing diagnostic errors is the most appealing and most logical,” he says. “I think we start to take for granted we are good at it, but I think there are ways many of us, especially if we work at it, can become great at it.”
CLINICAL
The How, When, and Why of Noninvasive Ventilation
SPEAKER: Eric Siegal, MD, SFHM, critical care fellow, University of Wisconsin School of Medicine, Madison
Dr. Siegal’s review of literature in front of a packed crowd provided a road map to Noninvasive Positive Pressure Ventilation (NPPV) usage. In the end, NPPV should be a hospitalist’s first choice for patients with hypercarbic COPD exacerbations, and likely in patients with acute cardiogenic pulmonary edema, hypoxemic respiratory failure, immunocompromised patients, and pre-intubation patients.
Dr. Siegal stressed the use of NPPV in COPD, which has been studied thoroughly and “held up to repeated scrutiny.”
“If you put people on NPPV instead of intubating them … mortality is halved, intubation rate is less than half, treatment failure is much lower, you have a third of the complications, and huge reductions in length of stay,” Dr. Siegal said.
In the absence of contraindications, he stressed, NPPV should be the first line of therapy for patients with hypercarbic COPD exacerbations. “In fact, I would argue that you really should be asking yourself, ‘Why can’t I put these patients on NPPV?’ ” he asked, “because this has really shown to be life-saving.”
Dr. Siegal also explored recent findings on NPPV in acute cardiogenic pulmonary edema patients, which surprisingly showed “no better than supplemental oxygen.” He concluded that if your patient is not hypercarbic, “there is no advantage to adding pressure support.” He also said the benefit is more robust in ACPE patients who have acute coronary syndrome.
Dr. Siegal advised hospitalists to pick the right patients, start NPPV therapy early, and if the patient doesn’t improve within one or two hours, “it’s time to move on.”
QUALITY
Utilizing Technology to Improve the Clinical and Operational Performance of Hospitalists
SPEAKERS: Jason Stein, MD, SFHM, associate vice chair for quality, Department of Medicine, Bryce Gartland, MD, FHM, associate director, section of hospital medicine, Emory University School of Medicine, Atlanta
In an age of increasing technology, just getting technology into a hospital isn’t the answer. It’s about integrating it into practice to improve care.
At Emory, the marriage of “low-tech solutions” and patented data displays has resulted in what Drs. Stein and Gartland call an accountable-care unit (ACU). The unit-based team features geographic ownership and structured interdisciplinary bedside rounds (SIBR). Perhaps more important, the unit generates real-time data captured on monitors, allowing teams of hospitalists, nonphysician providers (NPPs), residents, interns, and social workers to “visually digest immense amounts of information in a very short time period,” Dr. Gartland said.
Dr. Stein defined an ACU as a bounded geographic inpatient area responsible for the clinical, service, and cost outcomes it produces. To help manage beds, Emory instituted a system called “e-Bed,” a McKesson system that tracks room availability. The system shows whether rooms are occupied, being cleaned, or somewhere in between. It has icons to show whether patients are elsewhere in the hospital for treatment, as well as clinical data capacities. Unit teams round together and use a portable workstation or tablet computer to input clinical data, notes, or other comments into real-time dashboards that can then show everything from VTE prophylaxis to whether a patient is at high risk for falls.
The project has been in the works for several years, and Dr. Garltand noted that any hospitalists looking to push similar initiatives at their institution need to ensure that they have buy-in from providers and a commitment to seeing the project through.
“Timing is everything,” he said. “If we tried to force this … a few years ago, it would not have worked.”
PRACTICE MANAGEMENT
Recruiting and Retaining Hospitalists: Developing a Talent Facilitation Framework
SPEAKERS: Patrick Kneeland, MD, hospitalist, Providence Regional Medical Center, Everett, Wash.; Christine Kneeland, COO, Center Partners, Fort Collins, Colo.; Niraj Sehgal, associate professor of medicine, associate chair for quality and safety, Department of Medicine, University of California at San Francisco
Lincoln Godfrey, DO, a hospitalist at Baxter Regional Medical Center in Mountain Home, Ark., was sitting and listening to strategies to lure and keep hospitalists when his hospital CEO sent him a text asking how his recruiting efforts were going with a would-be hire.
“I said I’d get back to him,” Dr. Godfrey jokes.
The C-suite’s passion is understandable, though, as the fight to hire experienced staff outside of major markets continues to stymie many HM groups. Dr. Godfrey says he can’t hire anybody without first getting them to the Ozark Mountains to learn the hospital, its people, and its community.
“There’s going to be a limited talent pool of people who will come at all,” he says. “But I don’t get anybody who doesn’t work with us for a bit first.”
Christine Kneeland—Dr. Kneeland’s mother—said HM leaders tasked with their group’s personnel duties should focus on a few main concepts:
- Think outside the bank. Some physicians look only to earn as much as they can as quickly as they can, but many seek personal and professional satisfaction.
- Engagement is instrumental. A one-day orientation program for a lifetime job doesn’t sound like enough, does it?
In the coming years, hiring managers will have to focus on “millennials”—the generation of doctors born between 1977 and 1999—which Christine Kneeland described as tech-savvy doctors interested in a blended lifestyle of work and leisure. And while some might not agree with or understand their perspective, they’d better get used to it, she said. “The millennials are here, the workplace has changed, and they are leading that change,” she added. “Just embrace it.”
QUALITY
Patient Satisfaction: Tips for Improving Your HCAHPS Scores
MODERATORS: Win Whitcomb, MD, MHM, medical director of healthcare quality, Baystate Medical Center, Springfield, Mass.; Steven Deitelzweig, MD, MMM, SFHM, system chairman, Department of Hospital Medicine, regional vice president of medical affairs, Ochsner Health System, New Orleans
Patient satisfaction scores are a big deal right now, as many HM groups tie the scores to compensation and the federal government tethers the scores and a portion of hospital payment through the value-based purchasing (VBP) program.
So how does a hospitalist improve their HCAHPS score? Here’s what the experts said:
- Personalize things. Give a business card with a picture. Sit down. Smile. Ask the patient if they understand what you’ve said, and don’t get frustrated if they don’t.
- First and last. Make good impressions when introducing yourself to the patient and when it’s time to discharge or transition them to a different facility. “When the hospitalist hands a patient off,” Dr. Whitcomb said, “it doesn’t cut it to pull out your brochure of 40 practitioners when the patient asks, ‘Who am I going to see tomorrow?’”
- Be professional. Don’t vent about workplace issues in front of patients. Dr. Deitelzweig illustrated the point with the case of an elderly patient who got out of bed to help a practitioner they heard complaining about a heavy workload. The patient fell.
- Creative use of white space. Consider using in-room white boards to help keep patients informed of a day’s care plan.
David Jaworski, MD, director of the hospitalist service at Windham Hospital in Willimantic, Conn., says honesty was a key piece of advice he gleaned from the session.
“I think one of the things people appreciate the most when they’re in the hospital is being honest about our uncertainties,” he says. “I have had more people thank me for saying, ‘I don’t know, but we will find out by doing this, this, and this.’ ”
ACADEMIC
The Role of Hospital Medicine in Adapting to the New ACGME Requirements
SPEAKER: Jeff Wiese, MD, FACP, SFHM, associate professor of medicine at Tulane University Health Sciences Center, New Orleans
The new Accreditation Council for Graduate Medical Education (ACGME) work-hour rules that take effect July 1 have received a lot of attention since they were announced last summer. The guideline that has attracted the bulk of the attention limits intern shifts to 16 hours, with upper-level residents capped at 24 consecutive hours, with four hours of administrative follow-on allowed with the caveat that strategic napping is “strongly suggested.”
“I’m all for work hours,” said Dr. Wiese, immediate past president of SHM. “It’s the right thing to do; it’s safer. But I think we have to be careful we don’t super-fragment the system or double the intensity of the system. And on both of those plates, if you don’t do it right, what you end up with is people who will be ill-prepared.”
Dr. Wiese said an easy way to question the validity of one ACGME rule is to examine the guideline that limits a first-year resident’s census to 10 patients. He wondered which scenario offers more teaching opportunities: a roster of six chest-pain cases, two pneumonia cases, and two similarly familiar or relatively safe cases, or a resident with only four cases but each one having multiple comorbidities and complex decisions?
The new rules provide hospitals and HM groups an opportunity to change their way of thinking, adds Jeffrey Schnipper, MD, MPH, FHM, of Brigham and Women’s Hospital and Massachusetts General Hospital in Boston. “Every program has to change its entire way of doing business anyway, so let’s be at the table and say, ‘Well, while you’re redesigning your entire program, let’s inject patent safety and quality of care, and good pedagogy into the system,’” he says.
CLINICAL
Skin is In: Dermatological Images Every Hospitalist Should Recognize
MODERATOR: Paul Aronowitz, MD, FACP, internal medicine residency program director, California Pacific Medical Center, San Francisco
A patient comes into the ED with a blistering skin condition, but the diagnosis escapes the triage doctor on the case. The problem turns out to be bullosis diabeticorum, but the ED doc doesn’t know that yet and pushes to add a patient to the upstairs HM roster.
“The ED will usually try to admit because they’re worried [the patient has] some terrible drug eruption, but they can actually go home,” Dr. Aronowitz explained. “Hospitalists can help tell the difference.”
HM groups shouldn’t work to become amateur dermatologists, Dr. Aronowitz added. However, given that many hospitalists find themselves confronted by dermatologic cases several times a month, a rudimentary pedigree is a good idea to help sift out which cases require admission and which would take up bed space required for others.
He referred to it as knowing enough to know whether you know enough. “For sure, a hospitalist can diagnose a hypersensitivity reaction from a classic drug like Dilantin,” Dr. Aronowitz said, “and then stop the drug, because that would be one of the best things they could do.”
The session exposed hospitalists to dozens of images of skin conditions theymight come across in daily rounds, from snakebites to drug reactions to argyria.
“The idea is to help hospitalists recognize what’s serious and what’s not,” he said. “If you recognize those initial cutaneous clues, you can guide your antibiotic therapy, or whether you need antibiotics.”
CAREER
This Disease Is Easy; It’s the Patient Who’s Difficult
Speaker: Susan Block, chair, Department of Psychosocial Oncology and Palliative Care at Dana Farber Cancer Institute, Boston
Every physician will have their “button pushed” by a patient now and then, and hospitalists are in the unfortunate position of having little or no previous relationship with most patients, according to Dr. Block, a national expert in physician-patient conflict resolution who said “interpersonal challenges are an onerous part” of the job.
“We want to make sure we provide really good care to these patients, but it can be very challenging,” she said, noting that between 10% and 30% of patients in the healthcare setting present with difficult behaviors.
Whether it’s an empowered patient, a traumatized patient, an intrusive family member, or a patient with clear psychosocial issues, Dr. Block explained that “these patients can make physicians feel lousy. … Being aware of that and trying to stop that process is one of the key issues in professionalism and competence in working with difficult patients.”
She also warned hospitalists to recognize when they become a “magnet” for difficult patients, as many times the expert in the group will become the “go-to” doc. “I don’t think anyone can take care of a large panel of these patients; it’s just too much,” she said, noting you have to negotiate some limits or you will “burn out and lose perspective.”
Many doctors are very uncomfortable with scared or crying patients, Dr. Block said, explaining these are some of her most difficult patients. “Show me a patient in the hospital who isn’t scared,” she said. “Even it they aren’t, they are scared of dying.”
Other sources of workplace discomfort include the dependent or “needy” patient, the suspicious patient, and the extremely pushy patient. Dr. Block suggested setting clear boundaries with patients; she also noted physicians should be ready and willing to identify and reflect on your own emotions so that “you have the capacity to get perspective on the problem and keep yourself from being part of the problem.
“Limit-setting is one of the most therapeutic things you can do with difficult patients,” she said. “It feels to us as a form of sadism, as though we are punishing patients. But for many patients, the most dangerous, scary, and dysfunctional thing you can do for patients is not set limits.”
CLINICAL
The Art of Clinical Problem-Solving: Mystery Cases
SPEAKER: Gupreet Dhaliwal, MD, University of California at San Francisco
Humility, patience, and practice: Those are the keys to improving one’s clinical diagnostic skills, according to Dr. Dhaliwal, an acclaimed educator and clinician at UCSF who walked a packed room through two blind cases and encouraged hospitalists to work hard at their craft.
“If you want to reach your maximum potential, you have to view it the same way we do other things, the same way a great musician rehearses and a great soccer player scrimmages,” he said. “All of us are busy, but you either have to increase the number of cases you put your mind through, or you take the cases you have and you analyze them, you seek feedback, you try to improve the process around the diagnostic.
“The message isn’t always fun, because both of those things equal more work, but there is no way to hide it because there is no field in which people get better without more work.”
Dr. Dhaliwal says hospitalists should be “humble about diagnosis.” He explained that the more experienced people become, the more we shift from analytical reasoning, “thinking hard like we did when we were students and residents,” to intuitive reasoning, which “is basically saying, ‘I recognize a pattern, this is an old friend, I’ve seen gout before.’ I think any of us can be guilty of forgetting that it has pitfalls. And there is a whole list of cognitive biases that are associated with moving fast and building patterns.”
He also believes hospitalists who dedicate themselves to clinical greatness can parlay such improvement in the quality realm. “Every one of us has used diagnosis as a core part of our identity, but in terms of getting the community or other stakeholders behind improving diagnosis or improving judgment, I think the umbrella of quality and reducing diagnostic errors is the most appealing and most logical,” he says. “I think we start to take for granted we are good at it, but I think there are ways many of us, especially if we work at it, can become great at it.”
CLINICAL
The How, When, and Why of Noninvasive Ventilation
SPEAKER: Eric Siegal, MD, SFHM, critical care fellow, University of Wisconsin School of Medicine, Madison
Dr. Siegal’s review of literature in front of a packed crowd provided a road map to Noninvasive Positive Pressure Ventilation (NPPV) usage. In the end, NPPV should be a hospitalist’s first choice for patients with hypercarbic COPD exacerbations, and likely in patients with acute cardiogenic pulmonary edema, hypoxemic respiratory failure, immunocompromised patients, and pre-intubation patients.
Dr. Siegal stressed the use of NPPV in COPD, which has been studied thoroughly and “held up to repeated scrutiny.”
“If you put people on NPPV instead of intubating them … mortality is halved, intubation rate is less than half, treatment failure is much lower, you have a third of the complications, and huge reductions in length of stay,” Dr. Siegal said.
In the absence of contraindications, he stressed, NPPV should be the first line of therapy for patients with hypercarbic COPD exacerbations. “In fact, I would argue that you really should be asking yourself, ‘Why can’t I put these patients on NPPV?’ ” he asked, “because this has really shown to be life-saving.”
Dr. Siegal also explored recent findings on NPPV in acute cardiogenic pulmonary edema patients, which surprisingly showed “no better than supplemental oxygen.” He concluded that if your patient is not hypercarbic, “there is no advantage to adding pressure support.” He also said the benefit is more robust in ACPE patients who have acute coronary syndrome.
Dr. Siegal advised hospitalists to pick the right patients, start NPPV therapy early, and if the patient doesn’t improve within one or two hours, “it’s time to move on.”