User login
Defining Effective Clinician Roles in End-of-Life Care
OBJECTIVE: Our goal was to determine primary care clinician perceptions of what is important to the provision of quality end-of-life care.
STUDY DESIGN: We used ethnography, a qualitative research method involving the use of open-ended semistructured interviews.
POPULATION: We included 38 family practice residency faculty from 9 community residency programs of the Affiliated Family Practice Residency Network, Department of Family Medicine, University of Washington School of Medicine.
OUTCOMES MEASURED: The roles described by interviewees when discussing their best practices while delivering end-of-life care were compiled.
RESULTS: Primary care clinicians organize their delivery of quality end-of-life care predominantly through their relationships with patients and families. They play 3 roles when providing end-of-life care. As consultants, clinicians provide expert medical advice and treatment. As collaborators, they seek to understand the patient and family experience. Seasoned clinicians act as guides, using their personal intuitive knowledge of patient and family to facilitate everyone’s growth when providing end-of-life care.
CONCLUSIONS: Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve end-of-life care for patients, families, and clinicians.
- Exemplary end-of-life care is organized around relationships, meaning, and roles.
- Knowledge and skills are essential but are not how exemplary end-of-life care is organized.
- Clinicians providing end-of-life care play 3 roles: consultant, collaborator, and guide.
- Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve care.
Modern medicine has dramatically improved the length and quality of life for countless persons but has also created problems in integrating these advances with end-of-life care. Although 70% of Americans want to die in their own home supported by family, 74% of Americans currently die in institutions.1,2 Clearly, there is a disparity between patient preferences and the end-of-life services provided in America.
Most recommendations for the provision of quality end-of-life care are based on unresearched expert opinion that identifies problems and offers solutions.3-5 Studies have explored communication strategies,6 satisfaction levels with care,7 perceptions of management issues,8 and attitudes toward both death and dying patients.9 Yet little research addresses how practicing community clinicians develop the appropriate relationships and integrate the requisite knowledge, skills, and attitudes to provide quality end-of-life care.
The relationship between clinician, patient, and family and the personal meaning of events for each participant greatly influence end-of-life care.10 Although most commentary on physician roles and relationships in end-of-life care also reflects unresearched expert opinion,11-13 Steinmetz and Gabel14,15 theorized a model that was later validated against the experience of practicing family physicians. The role of the clinician in the successful provision of quality care has not been systematically researched and remains a major challenge to improving end-of-life care. We describe an exploratory qualitative study to determine the perceptions of practicing clinicians regarding quality end-of-life care.
Methods
With approval from the Human Subjects Committee of the University of Washington School of Medicine, faculty were recruited from 9 community programs in the Affiliated Family Practice Residency Network of the Department of Family Medicine. Twenty semistructured long interviews were conducted from a convenience sample at 3 residency sites.16 An additional 8 semistructured interviews and 2 focus groups (10 participants) further explored the data. Thus, a total of 38 clinicians participated in the study. Demographic characteristics of the study cohort have been published previously.10
We conducted the initial 20 interviews using open-ended questions designed to uncover faculty perceptions of quality end-of-life care. The questions explored may be found in the Table. Nonspecific prompts such as “tell me more” were used to enrich data and avoid interviewer bias. The interview was rehearsed with a medical school faculty expert in ethnographic research, field tested, and adjusted before final use. The interviews were audio-recorded and transcribed into qualitative research software.17
Throughout the interview process, the investigators met weekly to compare findings, discuss emerging categories, and jointly code the transcripts for model development using the process of grounded theory described by Glaser and Strauss.18 Common themes, communication and educational issues, and roles and relationships were identified. Data were constantly compared and winnowed to facilitate manageability; data collection and analysis occurred simultaneously.19,20 Common themes are published elsewhere.10 We report and discuss the analysis of the data pertaining to clinician roles and relationships.
We employed the following 3 strategies to assess the methodologic validity of the study and face validity of the themes and models emerging from the data analysis.
TABLE
INTERVIEW QUESTIONS
Remember a case in which you provided care for a patient and family facing a chronic, progressive, terminal illness:
|
Methodologic validation
The themes, models, and 2 interview transcripts were reviewed by 2 expert consultants with experience in qualitative research on end-of-life care and chronic debilitating disease. They assessed the validity of the research process and model development.21,22 These experts confirmed the methodologic approach, affirmed that the transcripts supported the coded model, and noted that the results were consistent with their own past research experience.
Face validity faculty interviews
Long interviews were conducted with a convenience sample of 8 faculty at 2 other residency sites. Researchers described the previous interview process and presented a written summary of the roles and relationship model coded from the data. Dialogue was encouraged with nonspecific prompts to enrich the data and avoid interviewer bias. Interviews were recorded, transcribed, and coded by the researchers to assess face validity and further develop the roles and relationship model using a grounded theory approach.
Face validity focus groups
Two focus groups were conducted with a total of 10 faculty at 2 additional sites. The entire model (themes, communication, roles, and relationships) was presented, and dialogue was encouraged. The researchers recorded, transcribed, and reviewed the focus groups to further assess face validity and refine the model.
Content validity
In a manner identical to that of the focus groups, the researchers presented the entire model at 2 of the 3 sites where faculty provided the initial 20 interviews. These sessions were audiotaped, transcribed, and reviewed by the researchers. The model presented was considered a valid, clinically plausible summary of the content of the initial interviews.
Results
Content analysis of the roles and relationships described by the study cohort revealed 3 distinct clinician roles in the provision of end-of-life care that we termed “consultant,” “collaborator,” and “guide.” All roles were viewed as important; none was more valuable than another; and the roles appeared to build on each other, often merging. Roles were implemented fluidly, with clinicians moving from one role to another as circumstances dictated. Although clinicians tended to describe successful cases, they freely discussed the challenges of end-of-life care, noting that less-than-ideal results were frequent. Thus, the models were described as “best practice” rather than routine care.
Consultant
The consultant provides expert medical information to the patient and family based on the biomedical model and the disease process. The power of the consultant role emanates from the clinician’s medical authority and special knowledge. The consultant presents information to help the patient and family understand the diagnosis, prognosis, and treatment. Once this knowledge is understood, the patient and family determine its meaning to them and decide on treatment. If the patient or family cannot decide or understand the medical implications of their particular situation, the consultant decides based on the medical facts.
A pediatrician illustrated the application of the consultant role in 2 situations involving newborns with severe heart anomalies. Here the physician describes the difficulty of using only medical facts to assist the family in deciding whether to discontinue the ventilator: “I remember saying: ‘The only thing that’s keeping the baby alive at this point is the ventilator. How do you feel about making the decision to turn that off?’ I remember it was a very cruel thing to have them make the decision.”
The physician continued: “Next time I said: ‘We have to sit down and talk about how your baby is doing because he died, and I’m going to turn off the machines now.’ I don’t think we should put them in the position of having to make this decision. We should make this decision and tell them what we’re going to do.” In this situation the clinician employed biomedical expertise to determine the appropriate medical care and outcome for the patient and family. In both cases the decision centered on continuing or discontinuing a medical intervention (respirator) and avoided discussion of the parents’ affective experience. Hallmarks of the consultant role include a biomedical focus, disease-centered decision-making processes, and the clinician’s assumption of authority based on biomedical expertise.
Collaborator
The collaborator exchanges information with the patient and family to promote a common understanding of the diagnosis and illness experience, working with them to choose a treatment path. The collaborator incorporates all components of the consultant role and additionally requires the clinician to understand the patient/family experience. The collaborator considers patient and family issues that need to be addressed to understand the medical facts, appreciates their past experiences with serious illness, determines what information would be difficult for them to accept but would benefit them if they were challenged to confront it, and recognizes that the patient and family hold ultimate responsibility for making treatment decisions.
The following quotes exemplify collaborative clinical care. In the first example, the physician steps outside his comfort zone to provide medical care based on the expressed wishes of a 30-year-old man dying of an advanced brain tumor: “The issue for me was letting go of control. He was going 4 hours away to a fishing cabin and going on a boat. I was really nervous…what if he all of a sudden crashed there? It took me a while to get used to the idea that he needs to be able to do what he enjoys doing, and everybody knows that there’s a risk.”
In a second example, the physician describes collaborating with the family of an 85-year-old woman suffering a massive stroke: “Having heard from the family that they understand that Grandma has had a big stroke and isn’t going to survive…then what wishes do Grandma and the family have? Have they ever discussed this sort of situation?”
In both these examples an understanding of the patient/family experience directs the clinician toward appropriate end-of-life care and is a major source of the collaborator’s power.
Guide
As a guide, the clinician actively and personally seeks solutions for the patient based not only on the medical facts (consultant) and the patient’s values and preferences (collaborator) but also on the guide’s greater understanding of the medical context. In essence, the guide not only knows why and where the patient and family prefer to go but also how to get there.
The following quote demonstrates a clinical application of the guide role. The physician first collaborates to understand the resistance of a terminally ill patient to hospice care:
“They had been very resistant to hospice for reasons that I wasn’t quite clear on. It wasn’t until I was in the home and listened to them talk that I realized they viewed hospice as ‘people are giving up on him.’ I think nobody really was talking to the patient about whether he was willing to give up or if he was ready to die.
“Once patient and family concerns were understood, the guide role was employed: I told the wife and family, ‘We’ve maxed out our medical therapies. There’s not much more we can do for him physically, but perhaps there’s something we can do for him spiritually and emotionally.’ When it was presented to them that way, they were much more understanding. We talked about hospice philosophy and looking at death as a part of life, saying: ‘That we’re not going to resuscitate does not mean do not treat.’ That’s where I came in more as the guide and said: ‘This is what I think is reasonable. What are your expectations? What do you want, Billy? And what do you want, as far as [his] wife and kids?”
The guide role requires that the clinician interpret the patient’s experience, integrate this interpretation with the clinician’s understanding of the clinical situation, and make a recommendation based on the guide’s personal and professional understanding of the situation. The power of the guide role emanates from the clinician’s understanding of how to use the medical system to see that the goals of patient and family are realized.
Discussion
The results of our study are consistent with reports over the past 3 decades by researchers, educators, and social critics who have explored how health professionals provide end-of-life care.23-29 Despite their varying perspectives, all reflect a common theme: the need to provide care based on the unique illness experience and values of the patient and family. The majority of clinicians in our study spoke of the importance of their relationships with patients and families. More than 50% of all interview commentary addressed clinician issues of relationship and personal meaning when providing end-of-life care.
The descriptions of consultant,30 collaborator,31,32 and guide33 confirm previous theoretical discussions regarding the nature of roles and relationships between patients and physicians. The guide is the most complex of the roles described by our study cohort and lends itself to ambivalence on the part of clinicians, in light of its potential to be misunderstood as paternalism. Yet, given the vulnerability and dependence of many patients who are terminally ill, the guide provides these patients with structure, safety, support, and care—based on the patients’ values and goals—reminiscent of the role of a nurturing parent.34
The personal nature of the decisions the guide facilitates reflects the reality of medicine as a moral enterprise.34,35 Having generally witnessed many more deaths than the patient, the guide has knowledge regarding the processes of dying and medical systems that is instrumental in assuring that the desires of the patient and family are realized. A knowledge of patient and family, an appreciation of the futility of the medical situation, and an insight into the process and systems of dying afford the clinician an opportunity to shape the death experience; as Nuland36 described: “Each of us needs a guide who knows us as well as he knows the pathways by which we can approach death.”
Facility with these roles may be a function of personal talent, introspection, and experience. The physicians studied reported that competence with these roles grew over time through delivering endof-life care and learning from patients, families, and other caregivers. Less experienced clinicians tended to describe the consultant and collaborator roles only. Clinicians describing the guide role had been in practice at least a decade and thus were at least 17 years into their training and practice in medicine. Apparently, expertise in all 3 roles requires not only excellent technical diagnostic and treatment skills but also the complex integrated skills of relational knowledge and caring gained through experience.
Our data indicate that relationship, meaning, and roles are primary moderators of the organization of exemplary end-of-life care. Yet, it appears to take nearly 2 decades for physicians to gain the confidence in their knowledge, skills, and attitudes necessary to comfortably guide patients and families through the nuances of end-of-life care. How to successfully educate clinicians to use such a model earlier is beyond our scope but appears crucial to improving training efforts. Current attempts to teach end-of-life care do not develop and explore the complex integrative domains of relational knowledge37-40 described in our study. Studies of educational interventions that stress the importance of the relational aspects of end-of-life care appear warranted.
To facilitate skill acquisition, the authors propose the steps diagrammed in the Figure to assist clinicians in providing quality end-of-life care. We believe the time spent determining patient-centered goals and the roles and relationships required by the clinician should at least equal the time spent determining which tests and treatments to provide. At the end of life, when tests and treatments result in fewer benefits and greater risks and burdens, determining patient and family needs and goals becomes increasingly important as management changes from cure to care.
FIGURE
FLOW DIAGRAM FOR CLINICIAN ROLES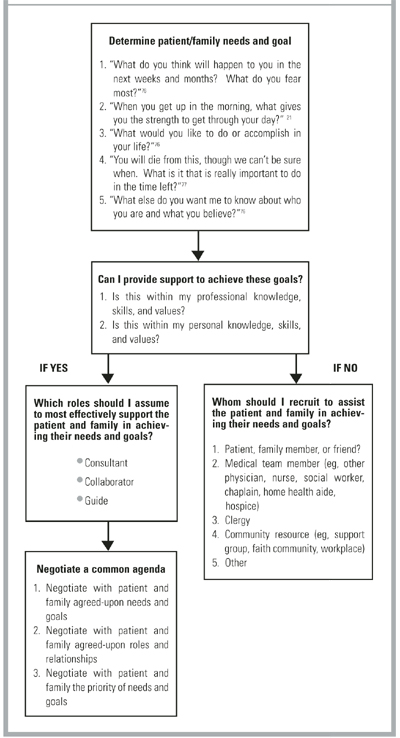
Limitations
This study is limited by a study sample of primary care, family practice faculty who geographically represent all practice in the Pacific Northwest and are predominantly Euro-American in ethnicity. The majority are family physicians, with the remainder pediatricians, internists, and a small number of nurse practitioners and physician assistants. Although no significant differences in terms of roles, relationships, and personal meanings between professional groups were noted, whether these findings are transferable to other primary care clinicians in community practice is unknown. Whether non–primary care specialists and clinicians of differing ethnicity or geographic region would respond differently is unknown. Generalizing these findings to non–primary care clinicians and clinicians of color requires further research.
Conclusions
Given the enormity of social and cultural values that make death a taboo topic, it is unclear how any single reform can easily overcome the multiple barriers to improved end-of-life care. Whether it is possible to teach attitudes and values, such as empathy and self-reflection, is uncertain, though promising curricula and research exist.41-42 If primary care physicians and other professionals improve their knowledge, skills, and attitudes in the delivery of such care, the ultimate effect on improving the experience of patients and families will require further study.
Acknowledgments
We wish to thank the Emily Davie and Joseph S. Kornfeld Foundation and The Nathan Cummings Foundation, New York, which provided generous grants that made our study and article possible. Additionally, we thank Phyllis Silverman, PhD, Harvard University, for her early counsel and advice; Tom Taylor, MD, PhD, University of Washington School of Medicine, for his thoughtful input into the study design, his sage guidance, and his review of the manuscript; Jeanne Quint Benoliel, DNS, Professor Emeritus, University of Washington School of Nursing, for her inspiration and review of the study design and results; and Greg Guldin, PhD, Pacific Lutheran University, for his thoughtful review of the manuscript.
1. The George Gallup International Institute. Spiritual beliefs and the dying process: a report on a national survey. Princeton, NJ: George Gallup International Institute;1997.
2. Field MJ, Cassel CK, eds. Approaching death: improving care at the end of life: Committee on Care at the End of Life, Division of Health Care Services, Institute of Medicine. Washington, DC: National Academy Press; 1997.
3. Schonwetter RS, Hawke W, Knight CF, eds. Hospice and palliative medicine core curriculum and review syllabus: American Academy of Hospice and Palliative Medicine. Dubuque, Iowa: Kendall/Hunt; 1999.
4. Emanuel LL, von Gunten CF, Ferris FD. The education for physicians on end-of-life care (EPEC) curriculum. Chicago, Ill: American Medical Association; 1999.
5. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744-49.
6. Todd C, Still A. General practitioners’ strategies and tactics of communication with the terminally ill. Fam Pract 1993;10:268-76.
7. Blyth AC. Audit of terminal care in a general practice. BMJ 1990;300:983-86.
8. Goodlin SJ, Jette AM, Lynn J, Wasson JH. Community physicians describe management issues for patients expected to live less than twelve months. J Palliat Care 1998;14:30-35.
9. Durand RP, Dickinson GE, Sumner DE, Lancaster CG. Family physicians’ attitudes toward death and the terminally-ill patient. Fam Pract Res J 1990;9:123-29.
10. Farber SJ, Egnew TR, Herman-Bertsch JL. Issues in end-of-life care: family practice faculty perceptions. J Fam Pract 1999;49:525-30.
11. Brewin TB. Not TLC but FPI. J R Soc Med 1990;83:172-75.
12. Mitchell G. The role of the general practitioner in palliative care. Aust Fam Physician 1994;23:1233-39.
13. Ogle KS, Plum JD. The role of the primary care physician in the care of the terminally ill. Clin Geriatr Med 1996;12:267-77.
14. Steinmetz D, Gabel LL. The family physician’s role in caring for the dying patient and family: a comprehensive theoretical model. Fam Pract 1992;9:433-36.
15. Steinmetz D, Walsh M, Gabel LL, Williams PT. Family physicians’ involvement with dying patients and their families. Arch Fam Med 1993;2:753-61.
16. Crabtree BF, Miller WL. A qualitative approach to primary care research: the long interview. Fam Med 1991;23:145-51.
17. Seidel J, Friese S, Leonard DC. The Ethnograph version 4.0 . Amherst, Mass: Qualis Research Associates; 1995.
18. Glaser B, Strauss A. The discovery of grounded theory. New York, NY: Aldine; 1967.
19. Strauss A, Corbin C. Basics of qualitative research. Newbury Park, Calif: Sage; 1990.
20. Wolcott HF. Writing up qualitative research. Newbury Park, Calif: Sage; 1990.
21. Benoliel JQ. Advancing nursing science: qualitative approaches. West J Nurs Res 1984;6:1-8.
22. Taylor TR, Gordon MJ, Ashworth CD. A systems perspective on clinical management. Behav Sci 1984;29:233-47.
23. Glaser BG, Strauss AL. Awareness of dying. Chicago, Ill: Aldine; 1965.
24. Kubler-Ross E. On death and dying. New York, NY: MacMillan; 1969.
25. Weisman A. On dying and denying: a psychiatric study on terminality. New York, NY: Behavioral Publications; 1972.
26. Saunders C, Baines M. Living with dying. New York, NY: Oxford University Press; 1983.
27. Corbin JM, Strauss AL. Unending work and care: managing chronic illness at home. San Francisco, Calif: Jossey-Bass; 1988.
28. Broyard A. Intoxicated by my illness. New York, NY: Potter; 1992.
29. Callahan D. Troubled dream of life. New York, NY: Simon & Schuster; 1993.
30. Balint J, Shelton W. Regaining the initiative: forging a new model of the patient-physician relationship. JAMA 1996;275:887-91.
31. Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med 1983;98:228-34.
32. Stewart M, Brown JB, Weston WW, McWhinney IR, Freeman TR. Patient centered medicine: transforming the clinical method. Thousand Oaks, Calif: Sage; 1995.
33. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA 1992;267:2221-26.
34. Cassell EJ. The nature of suffering and the goals of medicine. New York, NY: Oxford University Press; 1991.
35. Veatch RM. Contemporary bioethics and the demise of modern medicine. In Ormiston G, Sassower R, eds. Prescriptions: the dissemination of medical authority. New York, NY: Greenwood Press; 1990;23-39.
36. Nuland S. How we die. New York, NY: Knopf; 1994.
37. Rogers CR. Client-centered therapy: its current practice, implications, and theory. Boston, Mass: Houghton Mifflin; 1951.
38. Buber M. I and thou. New York, NY: MacMillan; 1974.
39. Mayeroff M. On caring. New York, NY: HarperPerennial; 1990.
40. Kleinman A, Kleinman J. Suffering and its professional transformation: toward an ethnography of interpersonal experience. Cult Med Psychiatry 1991;15:275-301.
41. Novack DH, Suchman AL, Clark W, Epstein RM, Najberg E, Kaplan C. Calibrating the physician: personal awareness and effective patient care. JAMA 1997;278:502-09.
42. Epstein RM. Mindful practice. JAMA 1999;282:833-39.
OBJECTIVE: Our goal was to determine primary care clinician perceptions of what is important to the provision of quality end-of-life care.
STUDY DESIGN: We used ethnography, a qualitative research method involving the use of open-ended semistructured interviews.
POPULATION: We included 38 family practice residency faculty from 9 community residency programs of the Affiliated Family Practice Residency Network, Department of Family Medicine, University of Washington School of Medicine.
OUTCOMES MEASURED: The roles described by interviewees when discussing their best practices while delivering end-of-life care were compiled.
RESULTS: Primary care clinicians organize their delivery of quality end-of-life care predominantly through their relationships with patients and families. They play 3 roles when providing end-of-life care. As consultants, clinicians provide expert medical advice and treatment. As collaborators, they seek to understand the patient and family experience. Seasoned clinicians act as guides, using their personal intuitive knowledge of patient and family to facilitate everyone’s growth when providing end-of-life care.
CONCLUSIONS: Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve end-of-life care for patients, families, and clinicians.
- Exemplary end-of-life care is organized around relationships, meaning, and roles.
- Knowledge and skills are essential but are not how exemplary end-of-life care is organized.
- Clinicians providing end-of-life care play 3 roles: consultant, collaborator, and guide.
- Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve care.
Modern medicine has dramatically improved the length and quality of life for countless persons but has also created problems in integrating these advances with end-of-life care. Although 70% of Americans want to die in their own home supported by family, 74% of Americans currently die in institutions.1,2 Clearly, there is a disparity between patient preferences and the end-of-life services provided in America.
Most recommendations for the provision of quality end-of-life care are based on unresearched expert opinion that identifies problems and offers solutions.3-5 Studies have explored communication strategies,6 satisfaction levels with care,7 perceptions of management issues,8 and attitudes toward both death and dying patients.9 Yet little research addresses how practicing community clinicians develop the appropriate relationships and integrate the requisite knowledge, skills, and attitudes to provide quality end-of-life care.
The relationship between clinician, patient, and family and the personal meaning of events for each participant greatly influence end-of-life care.10 Although most commentary on physician roles and relationships in end-of-life care also reflects unresearched expert opinion,11-13 Steinmetz and Gabel14,15 theorized a model that was later validated against the experience of practicing family physicians. The role of the clinician in the successful provision of quality care has not been systematically researched and remains a major challenge to improving end-of-life care. We describe an exploratory qualitative study to determine the perceptions of practicing clinicians regarding quality end-of-life care.
Methods
With approval from the Human Subjects Committee of the University of Washington School of Medicine, faculty were recruited from 9 community programs in the Affiliated Family Practice Residency Network of the Department of Family Medicine. Twenty semistructured long interviews were conducted from a convenience sample at 3 residency sites.16 An additional 8 semistructured interviews and 2 focus groups (10 participants) further explored the data. Thus, a total of 38 clinicians participated in the study. Demographic characteristics of the study cohort have been published previously.10
We conducted the initial 20 interviews using open-ended questions designed to uncover faculty perceptions of quality end-of-life care. The questions explored may be found in the Table. Nonspecific prompts such as “tell me more” were used to enrich data and avoid interviewer bias. The interview was rehearsed with a medical school faculty expert in ethnographic research, field tested, and adjusted before final use. The interviews were audio-recorded and transcribed into qualitative research software.17
Throughout the interview process, the investigators met weekly to compare findings, discuss emerging categories, and jointly code the transcripts for model development using the process of grounded theory described by Glaser and Strauss.18 Common themes, communication and educational issues, and roles and relationships were identified. Data were constantly compared and winnowed to facilitate manageability; data collection and analysis occurred simultaneously.19,20 Common themes are published elsewhere.10 We report and discuss the analysis of the data pertaining to clinician roles and relationships.
We employed the following 3 strategies to assess the methodologic validity of the study and face validity of the themes and models emerging from the data analysis.
TABLE
INTERVIEW QUESTIONS
Remember a case in which you provided care for a patient and family facing a chronic, progressive, terminal illness:
|
Methodologic validation
The themes, models, and 2 interview transcripts were reviewed by 2 expert consultants with experience in qualitative research on end-of-life care and chronic debilitating disease. They assessed the validity of the research process and model development.21,22 These experts confirmed the methodologic approach, affirmed that the transcripts supported the coded model, and noted that the results were consistent with their own past research experience.
Face validity faculty interviews
Long interviews were conducted with a convenience sample of 8 faculty at 2 other residency sites. Researchers described the previous interview process and presented a written summary of the roles and relationship model coded from the data. Dialogue was encouraged with nonspecific prompts to enrich the data and avoid interviewer bias. Interviews were recorded, transcribed, and coded by the researchers to assess face validity and further develop the roles and relationship model using a grounded theory approach.
Face validity focus groups
Two focus groups were conducted with a total of 10 faculty at 2 additional sites. The entire model (themes, communication, roles, and relationships) was presented, and dialogue was encouraged. The researchers recorded, transcribed, and reviewed the focus groups to further assess face validity and refine the model.
Content validity
In a manner identical to that of the focus groups, the researchers presented the entire model at 2 of the 3 sites where faculty provided the initial 20 interviews. These sessions were audiotaped, transcribed, and reviewed by the researchers. The model presented was considered a valid, clinically plausible summary of the content of the initial interviews.
Results
Content analysis of the roles and relationships described by the study cohort revealed 3 distinct clinician roles in the provision of end-of-life care that we termed “consultant,” “collaborator,” and “guide.” All roles were viewed as important; none was more valuable than another; and the roles appeared to build on each other, often merging. Roles were implemented fluidly, with clinicians moving from one role to another as circumstances dictated. Although clinicians tended to describe successful cases, they freely discussed the challenges of end-of-life care, noting that less-than-ideal results were frequent. Thus, the models were described as “best practice” rather than routine care.
Consultant
The consultant provides expert medical information to the patient and family based on the biomedical model and the disease process. The power of the consultant role emanates from the clinician’s medical authority and special knowledge. The consultant presents information to help the patient and family understand the diagnosis, prognosis, and treatment. Once this knowledge is understood, the patient and family determine its meaning to them and decide on treatment. If the patient or family cannot decide or understand the medical implications of their particular situation, the consultant decides based on the medical facts.
A pediatrician illustrated the application of the consultant role in 2 situations involving newborns with severe heart anomalies. Here the physician describes the difficulty of using only medical facts to assist the family in deciding whether to discontinue the ventilator: “I remember saying: ‘The only thing that’s keeping the baby alive at this point is the ventilator. How do you feel about making the decision to turn that off?’ I remember it was a very cruel thing to have them make the decision.”
The physician continued: “Next time I said: ‘We have to sit down and talk about how your baby is doing because he died, and I’m going to turn off the machines now.’ I don’t think we should put them in the position of having to make this decision. We should make this decision and tell them what we’re going to do.” In this situation the clinician employed biomedical expertise to determine the appropriate medical care and outcome for the patient and family. In both cases the decision centered on continuing or discontinuing a medical intervention (respirator) and avoided discussion of the parents’ affective experience. Hallmarks of the consultant role include a biomedical focus, disease-centered decision-making processes, and the clinician’s assumption of authority based on biomedical expertise.
Collaborator
The collaborator exchanges information with the patient and family to promote a common understanding of the diagnosis and illness experience, working with them to choose a treatment path. The collaborator incorporates all components of the consultant role and additionally requires the clinician to understand the patient/family experience. The collaborator considers patient and family issues that need to be addressed to understand the medical facts, appreciates their past experiences with serious illness, determines what information would be difficult for them to accept but would benefit them if they were challenged to confront it, and recognizes that the patient and family hold ultimate responsibility for making treatment decisions.
The following quotes exemplify collaborative clinical care. In the first example, the physician steps outside his comfort zone to provide medical care based on the expressed wishes of a 30-year-old man dying of an advanced brain tumor: “The issue for me was letting go of control. He was going 4 hours away to a fishing cabin and going on a boat. I was really nervous…what if he all of a sudden crashed there? It took me a while to get used to the idea that he needs to be able to do what he enjoys doing, and everybody knows that there’s a risk.”
In a second example, the physician describes collaborating with the family of an 85-year-old woman suffering a massive stroke: “Having heard from the family that they understand that Grandma has had a big stroke and isn’t going to survive…then what wishes do Grandma and the family have? Have they ever discussed this sort of situation?”
In both these examples an understanding of the patient/family experience directs the clinician toward appropriate end-of-life care and is a major source of the collaborator’s power.
Guide
As a guide, the clinician actively and personally seeks solutions for the patient based not only on the medical facts (consultant) and the patient’s values and preferences (collaborator) but also on the guide’s greater understanding of the medical context. In essence, the guide not only knows why and where the patient and family prefer to go but also how to get there.
The following quote demonstrates a clinical application of the guide role. The physician first collaborates to understand the resistance of a terminally ill patient to hospice care:
“They had been very resistant to hospice for reasons that I wasn’t quite clear on. It wasn’t until I was in the home and listened to them talk that I realized they viewed hospice as ‘people are giving up on him.’ I think nobody really was talking to the patient about whether he was willing to give up or if he was ready to die.
“Once patient and family concerns were understood, the guide role was employed: I told the wife and family, ‘We’ve maxed out our medical therapies. There’s not much more we can do for him physically, but perhaps there’s something we can do for him spiritually and emotionally.’ When it was presented to them that way, they were much more understanding. We talked about hospice philosophy and looking at death as a part of life, saying: ‘That we’re not going to resuscitate does not mean do not treat.’ That’s where I came in more as the guide and said: ‘This is what I think is reasonable. What are your expectations? What do you want, Billy? And what do you want, as far as [his] wife and kids?”
The guide role requires that the clinician interpret the patient’s experience, integrate this interpretation with the clinician’s understanding of the clinical situation, and make a recommendation based on the guide’s personal and professional understanding of the situation. The power of the guide role emanates from the clinician’s understanding of how to use the medical system to see that the goals of patient and family are realized.
Discussion
The results of our study are consistent with reports over the past 3 decades by researchers, educators, and social critics who have explored how health professionals provide end-of-life care.23-29 Despite their varying perspectives, all reflect a common theme: the need to provide care based on the unique illness experience and values of the patient and family. The majority of clinicians in our study spoke of the importance of their relationships with patients and families. More than 50% of all interview commentary addressed clinician issues of relationship and personal meaning when providing end-of-life care.
The descriptions of consultant,30 collaborator,31,32 and guide33 confirm previous theoretical discussions regarding the nature of roles and relationships between patients and physicians. The guide is the most complex of the roles described by our study cohort and lends itself to ambivalence on the part of clinicians, in light of its potential to be misunderstood as paternalism. Yet, given the vulnerability and dependence of many patients who are terminally ill, the guide provides these patients with structure, safety, support, and care—based on the patients’ values and goals—reminiscent of the role of a nurturing parent.34
The personal nature of the decisions the guide facilitates reflects the reality of medicine as a moral enterprise.34,35 Having generally witnessed many more deaths than the patient, the guide has knowledge regarding the processes of dying and medical systems that is instrumental in assuring that the desires of the patient and family are realized. A knowledge of patient and family, an appreciation of the futility of the medical situation, and an insight into the process and systems of dying afford the clinician an opportunity to shape the death experience; as Nuland36 described: “Each of us needs a guide who knows us as well as he knows the pathways by which we can approach death.”
Facility with these roles may be a function of personal talent, introspection, and experience. The physicians studied reported that competence with these roles grew over time through delivering endof-life care and learning from patients, families, and other caregivers. Less experienced clinicians tended to describe the consultant and collaborator roles only. Clinicians describing the guide role had been in practice at least a decade and thus were at least 17 years into their training and practice in medicine. Apparently, expertise in all 3 roles requires not only excellent technical diagnostic and treatment skills but also the complex integrated skills of relational knowledge and caring gained through experience.
Our data indicate that relationship, meaning, and roles are primary moderators of the organization of exemplary end-of-life care. Yet, it appears to take nearly 2 decades for physicians to gain the confidence in their knowledge, skills, and attitudes necessary to comfortably guide patients and families through the nuances of end-of-life care. How to successfully educate clinicians to use such a model earlier is beyond our scope but appears crucial to improving training efforts. Current attempts to teach end-of-life care do not develop and explore the complex integrative domains of relational knowledge37-40 described in our study. Studies of educational interventions that stress the importance of the relational aspects of end-of-life care appear warranted.
To facilitate skill acquisition, the authors propose the steps diagrammed in the Figure to assist clinicians in providing quality end-of-life care. We believe the time spent determining patient-centered goals and the roles and relationships required by the clinician should at least equal the time spent determining which tests and treatments to provide. At the end of life, when tests and treatments result in fewer benefits and greater risks and burdens, determining patient and family needs and goals becomes increasingly important as management changes from cure to care.
FIGURE
FLOW DIAGRAM FOR CLINICIAN ROLES
Limitations
This study is limited by a study sample of primary care, family practice faculty who geographically represent all practice in the Pacific Northwest and are predominantly Euro-American in ethnicity. The majority are family physicians, with the remainder pediatricians, internists, and a small number of nurse practitioners and physician assistants. Although no significant differences in terms of roles, relationships, and personal meanings between professional groups were noted, whether these findings are transferable to other primary care clinicians in community practice is unknown. Whether non–primary care specialists and clinicians of differing ethnicity or geographic region would respond differently is unknown. Generalizing these findings to non–primary care clinicians and clinicians of color requires further research.
Conclusions
Given the enormity of social and cultural values that make death a taboo topic, it is unclear how any single reform can easily overcome the multiple barriers to improved end-of-life care. Whether it is possible to teach attitudes and values, such as empathy and self-reflection, is uncertain, though promising curricula and research exist.41-42 If primary care physicians and other professionals improve their knowledge, skills, and attitudes in the delivery of such care, the ultimate effect on improving the experience of patients and families will require further study.
Acknowledgments
We wish to thank the Emily Davie and Joseph S. Kornfeld Foundation and The Nathan Cummings Foundation, New York, which provided generous grants that made our study and article possible. Additionally, we thank Phyllis Silverman, PhD, Harvard University, for her early counsel and advice; Tom Taylor, MD, PhD, University of Washington School of Medicine, for his thoughtful input into the study design, his sage guidance, and his review of the manuscript; Jeanne Quint Benoliel, DNS, Professor Emeritus, University of Washington School of Nursing, for her inspiration and review of the study design and results; and Greg Guldin, PhD, Pacific Lutheran University, for his thoughtful review of the manuscript.
OBJECTIVE: Our goal was to determine primary care clinician perceptions of what is important to the provision of quality end-of-life care.
STUDY DESIGN: We used ethnography, a qualitative research method involving the use of open-ended semistructured interviews.
POPULATION: We included 38 family practice residency faculty from 9 community residency programs of the Affiliated Family Practice Residency Network, Department of Family Medicine, University of Washington School of Medicine.
OUTCOMES MEASURED: The roles described by interviewees when discussing their best practices while delivering end-of-life care were compiled.
RESULTS: Primary care clinicians organize their delivery of quality end-of-life care predominantly through their relationships with patients and families. They play 3 roles when providing end-of-life care. As consultants, clinicians provide expert medical advice and treatment. As collaborators, they seek to understand the patient and family experience. Seasoned clinicians act as guides, using their personal intuitive knowledge of patient and family to facilitate everyone’s growth when providing end-of-life care.
CONCLUSIONS: Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve end-of-life care for patients, families, and clinicians.
- Exemplary end-of-life care is organized around relationships, meaning, and roles.
- Knowledge and skills are essential but are not how exemplary end-of-life care is organized.
- Clinicians providing end-of-life care play 3 roles: consultant, collaborator, and guide.
- Shifting clinician focus from skills and knowledge toward relationship, meaning, and roles provides new opportunities to improve care.
Modern medicine has dramatically improved the length and quality of life for countless persons but has also created problems in integrating these advances with end-of-life care. Although 70% of Americans want to die in their own home supported by family, 74% of Americans currently die in institutions.1,2 Clearly, there is a disparity between patient preferences and the end-of-life services provided in America.
Most recommendations for the provision of quality end-of-life care are based on unresearched expert opinion that identifies problems and offers solutions.3-5 Studies have explored communication strategies,6 satisfaction levels with care,7 perceptions of management issues,8 and attitudes toward both death and dying patients.9 Yet little research addresses how practicing community clinicians develop the appropriate relationships and integrate the requisite knowledge, skills, and attitudes to provide quality end-of-life care.
The relationship between clinician, patient, and family and the personal meaning of events for each participant greatly influence end-of-life care.10 Although most commentary on physician roles and relationships in end-of-life care also reflects unresearched expert opinion,11-13 Steinmetz and Gabel14,15 theorized a model that was later validated against the experience of practicing family physicians. The role of the clinician in the successful provision of quality care has not been systematically researched and remains a major challenge to improving end-of-life care. We describe an exploratory qualitative study to determine the perceptions of practicing clinicians regarding quality end-of-life care.
Methods
With approval from the Human Subjects Committee of the University of Washington School of Medicine, faculty were recruited from 9 community programs in the Affiliated Family Practice Residency Network of the Department of Family Medicine. Twenty semistructured long interviews were conducted from a convenience sample at 3 residency sites.16 An additional 8 semistructured interviews and 2 focus groups (10 participants) further explored the data. Thus, a total of 38 clinicians participated in the study. Demographic characteristics of the study cohort have been published previously.10
We conducted the initial 20 interviews using open-ended questions designed to uncover faculty perceptions of quality end-of-life care. The questions explored may be found in the Table. Nonspecific prompts such as “tell me more” were used to enrich data and avoid interviewer bias. The interview was rehearsed with a medical school faculty expert in ethnographic research, field tested, and adjusted before final use. The interviews were audio-recorded and transcribed into qualitative research software.17
Throughout the interview process, the investigators met weekly to compare findings, discuss emerging categories, and jointly code the transcripts for model development using the process of grounded theory described by Glaser and Strauss.18 Common themes, communication and educational issues, and roles and relationships were identified. Data were constantly compared and winnowed to facilitate manageability; data collection and analysis occurred simultaneously.19,20 Common themes are published elsewhere.10 We report and discuss the analysis of the data pertaining to clinician roles and relationships.
We employed the following 3 strategies to assess the methodologic validity of the study and face validity of the themes and models emerging from the data analysis.
TABLE
INTERVIEW QUESTIONS
Remember a case in which you provided care for a patient and family facing a chronic, progressive, terminal illness:
|
Methodologic validation
The themes, models, and 2 interview transcripts were reviewed by 2 expert consultants with experience in qualitative research on end-of-life care and chronic debilitating disease. They assessed the validity of the research process and model development.21,22 These experts confirmed the methodologic approach, affirmed that the transcripts supported the coded model, and noted that the results were consistent with their own past research experience.
Face validity faculty interviews
Long interviews were conducted with a convenience sample of 8 faculty at 2 other residency sites. Researchers described the previous interview process and presented a written summary of the roles and relationship model coded from the data. Dialogue was encouraged with nonspecific prompts to enrich the data and avoid interviewer bias. Interviews were recorded, transcribed, and coded by the researchers to assess face validity and further develop the roles and relationship model using a grounded theory approach.
Face validity focus groups
Two focus groups were conducted with a total of 10 faculty at 2 additional sites. The entire model (themes, communication, roles, and relationships) was presented, and dialogue was encouraged. The researchers recorded, transcribed, and reviewed the focus groups to further assess face validity and refine the model.
Content validity
In a manner identical to that of the focus groups, the researchers presented the entire model at 2 of the 3 sites where faculty provided the initial 20 interviews. These sessions were audiotaped, transcribed, and reviewed by the researchers. The model presented was considered a valid, clinically plausible summary of the content of the initial interviews.
Results
Content analysis of the roles and relationships described by the study cohort revealed 3 distinct clinician roles in the provision of end-of-life care that we termed “consultant,” “collaborator,” and “guide.” All roles were viewed as important; none was more valuable than another; and the roles appeared to build on each other, often merging. Roles were implemented fluidly, with clinicians moving from one role to another as circumstances dictated. Although clinicians tended to describe successful cases, they freely discussed the challenges of end-of-life care, noting that less-than-ideal results were frequent. Thus, the models were described as “best practice” rather than routine care.
Consultant
The consultant provides expert medical information to the patient and family based on the biomedical model and the disease process. The power of the consultant role emanates from the clinician’s medical authority and special knowledge. The consultant presents information to help the patient and family understand the diagnosis, prognosis, and treatment. Once this knowledge is understood, the patient and family determine its meaning to them and decide on treatment. If the patient or family cannot decide or understand the medical implications of their particular situation, the consultant decides based on the medical facts.
A pediatrician illustrated the application of the consultant role in 2 situations involving newborns with severe heart anomalies. Here the physician describes the difficulty of using only medical facts to assist the family in deciding whether to discontinue the ventilator: “I remember saying: ‘The only thing that’s keeping the baby alive at this point is the ventilator. How do you feel about making the decision to turn that off?’ I remember it was a very cruel thing to have them make the decision.”
The physician continued: “Next time I said: ‘We have to sit down and talk about how your baby is doing because he died, and I’m going to turn off the machines now.’ I don’t think we should put them in the position of having to make this decision. We should make this decision and tell them what we’re going to do.” In this situation the clinician employed biomedical expertise to determine the appropriate medical care and outcome for the patient and family. In both cases the decision centered on continuing or discontinuing a medical intervention (respirator) and avoided discussion of the parents’ affective experience. Hallmarks of the consultant role include a biomedical focus, disease-centered decision-making processes, and the clinician’s assumption of authority based on biomedical expertise.
Collaborator
The collaborator exchanges information with the patient and family to promote a common understanding of the diagnosis and illness experience, working with them to choose a treatment path. The collaborator incorporates all components of the consultant role and additionally requires the clinician to understand the patient/family experience. The collaborator considers patient and family issues that need to be addressed to understand the medical facts, appreciates their past experiences with serious illness, determines what information would be difficult for them to accept but would benefit them if they were challenged to confront it, and recognizes that the patient and family hold ultimate responsibility for making treatment decisions.
The following quotes exemplify collaborative clinical care. In the first example, the physician steps outside his comfort zone to provide medical care based on the expressed wishes of a 30-year-old man dying of an advanced brain tumor: “The issue for me was letting go of control. He was going 4 hours away to a fishing cabin and going on a boat. I was really nervous…what if he all of a sudden crashed there? It took me a while to get used to the idea that he needs to be able to do what he enjoys doing, and everybody knows that there’s a risk.”
In a second example, the physician describes collaborating with the family of an 85-year-old woman suffering a massive stroke: “Having heard from the family that they understand that Grandma has had a big stroke and isn’t going to survive…then what wishes do Grandma and the family have? Have they ever discussed this sort of situation?”
In both these examples an understanding of the patient/family experience directs the clinician toward appropriate end-of-life care and is a major source of the collaborator’s power.
Guide
As a guide, the clinician actively and personally seeks solutions for the patient based not only on the medical facts (consultant) and the patient’s values and preferences (collaborator) but also on the guide’s greater understanding of the medical context. In essence, the guide not only knows why and where the patient and family prefer to go but also how to get there.
The following quote demonstrates a clinical application of the guide role. The physician first collaborates to understand the resistance of a terminally ill patient to hospice care:
“They had been very resistant to hospice for reasons that I wasn’t quite clear on. It wasn’t until I was in the home and listened to them talk that I realized they viewed hospice as ‘people are giving up on him.’ I think nobody really was talking to the patient about whether he was willing to give up or if he was ready to die.
“Once patient and family concerns were understood, the guide role was employed: I told the wife and family, ‘We’ve maxed out our medical therapies. There’s not much more we can do for him physically, but perhaps there’s something we can do for him spiritually and emotionally.’ When it was presented to them that way, they were much more understanding. We talked about hospice philosophy and looking at death as a part of life, saying: ‘That we’re not going to resuscitate does not mean do not treat.’ That’s where I came in more as the guide and said: ‘This is what I think is reasonable. What are your expectations? What do you want, Billy? And what do you want, as far as [his] wife and kids?”
The guide role requires that the clinician interpret the patient’s experience, integrate this interpretation with the clinician’s understanding of the clinical situation, and make a recommendation based on the guide’s personal and professional understanding of the situation. The power of the guide role emanates from the clinician’s understanding of how to use the medical system to see that the goals of patient and family are realized.
Discussion
The results of our study are consistent with reports over the past 3 decades by researchers, educators, and social critics who have explored how health professionals provide end-of-life care.23-29 Despite their varying perspectives, all reflect a common theme: the need to provide care based on the unique illness experience and values of the patient and family. The majority of clinicians in our study spoke of the importance of their relationships with patients and families. More than 50% of all interview commentary addressed clinician issues of relationship and personal meaning when providing end-of-life care.
The descriptions of consultant,30 collaborator,31,32 and guide33 confirm previous theoretical discussions regarding the nature of roles and relationships between patients and physicians. The guide is the most complex of the roles described by our study cohort and lends itself to ambivalence on the part of clinicians, in light of its potential to be misunderstood as paternalism. Yet, given the vulnerability and dependence of many patients who are terminally ill, the guide provides these patients with structure, safety, support, and care—based on the patients’ values and goals—reminiscent of the role of a nurturing parent.34
The personal nature of the decisions the guide facilitates reflects the reality of medicine as a moral enterprise.34,35 Having generally witnessed many more deaths than the patient, the guide has knowledge regarding the processes of dying and medical systems that is instrumental in assuring that the desires of the patient and family are realized. A knowledge of patient and family, an appreciation of the futility of the medical situation, and an insight into the process and systems of dying afford the clinician an opportunity to shape the death experience; as Nuland36 described: “Each of us needs a guide who knows us as well as he knows the pathways by which we can approach death.”
Facility with these roles may be a function of personal talent, introspection, and experience. The physicians studied reported that competence with these roles grew over time through delivering endof-life care and learning from patients, families, and other caregivers. Less experienced clinicians tended to describe the consultant and collaborator roles only. Clinicians describing the guide role had been in practice at least a decade and thus were at least 17 years into their training and practice in medicine. Apparently, expertise in all 3 roles requires not only excellent technical diagnostic and treatment skills but also the complex integrated skills of relational knowledge and caring gained through experience.
Our data indicate that relationship, meaning, and roles are primary moderators of the organization of exemplary end-of-life care. Yet, it appears to take nearly 2 decades for physicians to gain the confidence in their knowledge, skills, and attitudes necessary to comfortably guide patients and families through the nuances of end-of-life care. How to successfully educate clinicians to use such a model earlier is beyond our scope but appears crucial to improving training efforts. Current attempts to teach end-of-life care do not develop and explore the complex integrative domains of relational knowledge37-40 described in our study. Studies of educational interventions that stress the importance of the relational aspects of end-of-life care appear warranted.
To facilitate skill acquisition, the authors propose the steps diagrammed in the Figure to assist clinicians in providing quality end-of-life care. We believe the time spent determining patient-centered goals and the roles and relationships required by the clinician should at least equal the time spent determining which tests and treatments to provide. At the end of life, when tests and treatments result in fewer benefits and greater risks and burdens, determining patient and family needs and goals becomes increasingly important as management changes from cure to care.
FIGURE
FLOW DIAGRAM FOR CLINICIAN ROLES
Limitations
This study is limited by a study sample of primary care, family practice faculty who geographically represent all practice in the Pacific Northwest and are predominantly Euro-American in ethnicity. The majority are family physicians, with the remainder pediatricians, internists, and a small number of nurse practitioners and physician assistants. Although no significant differences in terms of roles, relationships, and personal meanings between professional groups were noted, whether these findings are transferable to other primary care clinicians in community practice is unknown. Whether non–primary care specialists and clinicians of differing ethnicity or geographic region would respond differently is unknown. Generalizing these findings to non–primary care clinicians and clinicians of color requires further research.
Conclusions
Given the enormity of social and cultural values that make death a taboo topic, it is unclear how any single reform can easily overcome the multiple barriers to improved end-of-life care. Whether it is possible to teach attitudes and values, such as empathy and self-reflection, is uncertain, though promising curricula and research exist.41-42 If primary care physicians and other professionals improve their knowledge, skills, and attitudes in the delivery of such care, the ultimate effect on improving the experience of patients and families will require further study.
Acknowledgments
We wish to thank the Emily Davie and Joseph S. Kornfeld Foundation and The Nathan Cummings Foundation, New York, which provided generous grants that made our study and article possible. Additionally, we thank Phyllis Silverman, PhD, Harvard University, for her early counsel and advice; Tom Taylor, MD, PhD, University of Washington School of Medicine, for his thoughtful input into the study design, his sage guidance, and his review of the manuscript; Jeanne Quint Benoliel, DNS, Professor Emeritus, University of Washington School of Nursing, for her inspiration and review of the study design and results; and Greg Guldin, PhD, Pacific Lutheran University, for his thoughtful review of the manuscript.
1. The George Gallup International Institute. Spiritual beliefs and the dying process: a report on a national survey. Princeton, NJ: George Gallup International Institute;1997.
2. Field MJ, Cassel CK, eds. Approaching death: improving care at the end of life: Committee on Care at the End of Life, Division of Health Care Services, Institute of Medicine. Washington, DC: National Academy Press; 1997.
3. Schonwetter RS, Hawke W, Knight CF, eds. Hospice and palliative medicine core curriculum and review syllabus: American Academy of Hospice and Palliative Medicine. Dubuque, Iowa: Kendall/Hunt; 1999.
4. Emanuel LL, von Gunten CF, Ferris FD. The education for physicians on end-of-life care (EPEC) curriculum. Chicago, Ill: American Medical Association; 1999.
5. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744-49.
6. Todd C, Still A. General practitioners’ strategies and tactics of communication with the terminally ill. Fam Pract 1993;10:268-76.
7. Blyth AC. Audit of terminal care in a general practice. BMJ 1990;300:983-86.
8. Goodlin SJ, Jette AM, Lynn J, Wasson JH. Community physicians describe management issues for patients expected to live less than twelve months. J Palliat Care 1998;14:30-35.
9. Durand RP, Dickinson GE, Sumner DE, Lancaster CG. Family physicians’ attitudes toward death and the terminally-ill patient. Fam Pract Res J 1990;9:123-29.
10. Farber SJ, Egnew TR, Herman-Bertsch JL. Issues in end-of-life care: family practice faculty perceptions. J Fam Pract 1999;49:525-30.
11. Brewin TB. Not TLC but FPI. J R Soc Med 1990;83:172-75.
12. Mitchell G. The role of the general practitioner in palliative care. Aust Fam Physician 1994;23:1233-39.
13. Ogle KS, Plum JD. The role of the primary care physician in the care of the terminally ill. Clin Geriatr Med 1996;12:267-77.
14. Steinmetz D, Gabel LL. The family physician’s role in caring for the dying patient and family: a comprehensive theoretical model. Fam Pract 1992;9:433-36.
15. Steinmetz D, Walsh M, Gabel LL, Williams PT. Family physicians’ involvement with dying patients and their families. Arch Fam Med 1993;2:753-61.
16. Crabtree BF, Miller WL. A qualitative approach to primary care research: the long interview. Fam Med 1991;23:145-51.
17. Seidel J, Friese S, Leonard DC. The Ethnograph version 4.0 . Amherst, Mass: Qualis Research Associates; 1995.
18. Glaser B, Strauss A. The discovery of grounded theory. New York, NY: Aldine; 1967.
19. Strauss A, Corbin C. Basics of qualitative research. Newbury Park, Calif: Sage; 1990.
20. Wolcott HF. Writing up qualitative research. Newbury Park, Calif: Sage; 1990.
21. Benoliel JQ. Advancing nursing science: qualitative approaches. West J Nurs Res 1984;6:1-8.
22. Taylor TR, Gordon MJ, Ashworth CD. A systems perspective on clinical management. Behav Sci 1984;29:233-47.
23. Glaser BG, Strauss AL. Awareness of dying. Chicago, Ill: Aldine; 1965.
24. Kubler-Ross E. On death and dying. New York, NY: MacMillan; 1969.
25. Weisman A. On dying and denying: a psychiatric study on terminality. New York, NY: Behavioral Publications; 1972.
26. Saunders C, Baines M. Living with dying. New York, NY: Oxford University Press; 1983.
27. Corbin JM, Strauss AL. Unending work and care: managing chronic illness at home. San Francisco, Calif: Jossey-Bass; 1988.
28. Broyard A. Intoxicated by my illness. New York, NY: Potter; 1992.
29. Callahan D. Troubled dream of life. New York, NY: Simon & Schuster; 1993.
30. Balint J, Shelton W. Regaining the initiative: forging a new model of the patient-physician relationship. JAMA 1996;275:887-91.
31. Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med 1983;98:228-34.
32. Stewart M, Brown JB, Weston WW, McWhinney IR, Freeman TR. Patient centered medicine: transforming the clinical method. Thousand Oaks, Calif: Sage; 1995.
33. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA 1992;267:2221-26.
34. Cassell EJ. The nature of suffering and the goals of medicine. New York, NY: Oxford University Press; 1991.
35. Veatch RM. Contemporary bioethics and the demise of modern medicine. In Ormiston G, Sassower R, eds. Prescriptions: the dissemination of medical authority. New York, NY: Greenwood Press; 1990;23-39.
36. Nuland S. How we die. New York, NY: Knopf; 1994.
37. Rogers CR. Client-centered therapy: its current practice, implications, and theory. Boston, Mass: Houghton Mifflin; 1951.
38. Buber M. I and thou. New York, NY: MacMillan; 1974.
39. Mayeroff M. On caring. New York, NY: HarperPerennial; 1990.
40. Kleinman A, Kleinman J. Suffering and its professional transformation: toward an ethnography of interpersonal experience. Cult Med Psychiatry 1991;15:275-301.
41. Novack DH, Suchman AL, Clark W, Epstein RM, Najberg E, Kaplan C. Calibrating the physician: personal awareness and effective patient care. JAMA 1997;278:502-09.
42. Epstein RM. Mindful practice. JAMA 1999;282:833-39.
1. The George Gallup International Institute. Spiritual beliefs and the dying process: a report on a national survey. Princeton, NJ: George Gallup International Institute;1997.
2. Field MJ, Cassel CK, eds. Approaching death: improving care at the end of life: Committee on Care at the End of Life, Division of Health Care Services, Institute of Medicine. Washington, DC: National Academy Press; 1997.
3. Schonwetter RS, Hawke W, Knight CF, eds. Hospice and palliative medicine core curriculum and review syllabus: American Academy of Hospice and Palliative Medicine. Dubuque, Iowa: Kendall/Hunt; 1999.
4. Emanuel LL, von Gunten CF, Ferris FD. The education for physicians on end-of-life care (EPEC) curriculum. Chicago, Ill: American Medical Association; 1999.
5. Lo B, Quill T, Tulsky J. Discussing palliative care with patients. Ann Intern Med 1999;130:744-49.
6. Todd C, Still A. General practitioners’ strategies and tactics of communication with the terminally ill. Fam Pract 1993;10:268-76.
7. Blyth AC. Audit of terminal care in a general practice. BMJ 1990;300:983-86.
8. Goodlin SJ, Jette AM, Lynn J, Wasson JH. Community physicians describe management issues for patients expected to live less than twelve months. J Palliat Care 1998;14:30-35.
9. Durand RP, Dickinson GE, Sumner DE, Lancaster CG. Family physicians’ attitudes toward death and the terminally-ill patient. Fam Pract Res J 1990;9:123-29.
10. Farber SJ, Egnew TR, Herman-Bertsch JL. Issues in end-of-life care: family practice faculty perceptions. J Fam Pract 1999;49:525-30.
11. Brewin TB. Not TLC but FPI. J R Soc Med 1990;83:172-75.
12. Mitchell G. The role of the general practitioner in palliative care. Aust Fam Physician 1994;23:1233-39.
13. Ogle KS, Plum JD. The role of the primary care physician in the care of the terminally ill. Clin Geriatr Med 1996;12:267-77.
14. Steinmetz D, Gabel LL. The family physician’s role in caring for the dying patient and family: a comprehensive theoretical model. Fam Pract 1992;9:433-36.
15. Steinmetz D, Walsh M, Gabel LL, Williams PT. Family physicians’ involvement with dying patients and their families. Arch Fam Med 1993;2:753-61.
16. Crabtree BF, Miller WL. A qualitative approach to primary care research: the long interview. Fam Med 1991;23:145-51.
17. Seidel J, Friese S, Leonard DC. The Ethnograph version 4.0 . Amherst, Mass: Qualis Research Associates; 1995.
18. Glaser B, Strauss A. The discovery of grounded theory. New York, NY: Aldine; 1967.
19. Strauss A, Corbin C. Basics of qualitative research. Newbury Park, Calif: Sage; 1990.
20. Wolcott HF. Writing up qualitative research. Newbury Park, Calif: Sage; 1990.
21. Benoliel JQ. Advancing nursing science: qualitative approaches. West J Nurs Res 1984;6:1-8.
22. Taylor TR, Gordon MJ, Ashworth CD. A systems perspective on clinical management. Behav Sci 1984;29:233-47.
23. Glaser BG, Strauss AL. Awareness of dying. Chicago, Ill: Aldine; 1965.
24. Kubler-Ross E. On death and dying. New York, NY: MacMillan; 1969.
25. Weisman A. On dying and denying: a psychiatric study on terminality. New York, NY: Behavioral Publications; 1972.
26. Saunders C, Baines M. Living with dying. New York, NY: Oxford University Press; 1983.
27. Corbin JM, Strauss AL. Unending work and care: managing chronic illness at home. San Francisco, Calif: Jossey-Bass; 1988.
28. Broyard A. Intoxicated by my illness. New York, NY: Potter; 1992.
29. Callahan D. Troubled dream of life. New York, NY: Simon & Schuster; 1993.
30. Balint J, Shelton W. Regaining the initiative: forging a new model of the patient-physician relationship. JAMA 1996;275:887-91.
31. Quill TE. Partnerships in patient care: a contractual approach. Ann Intern Med 1983;98:228-34.
32. Stewart M, Brown JB, Weston WW, McWhinney IR, Freeman TR. Patient centered medicine: transforming the clinical method. Thousand Oaks, Calif: Sage; 1995.
33. Emanuel EJ, Emanuel LL. Four models of the physician-patient relationship. JAMA 1992;267:2221-26.
34. Cassell EJ. The nature of suffering and the goals of medicine. New York, NY: Oxford University Press; 1991.
35. Veatch RM. Contemporary bioethics and the demise of modern medicine. In Ormiston G, Sassower R, eds. Prescriptions: the dissemination of medical authority. New York, NY: Greenwood Press; 1990;23-39.
36. Nuland S. How we die. New York, NY: Knopf; 1994.
37. Rogers CR. Client-centered therapy: its current practice, implications, and theory. Boston, Mass: Houghton Mifflin; 1951.
38. Buber M. I and thou. New York, NY: MacMillan; 1974.
39. Mayeroff M. On caring. New York, NY: HarperPerennial; 1990.
40. Kleinman A, Kleinman J. Suffering and its professional transformation: toward an ethnography of interpersonal experience. Cult Med Psychiatry 1991;15:275-301.
41. Novack DH, Suchman AL, Clark W, Epstein RM, Najberg E, Kaplan C. Calibrating the physician: personal awareness and effective patient care. JAMA 1997;278:502-09.
42. Epstein RM. Mindful practice. JAMA 1999;282:833-39.