User login
Jeffrey Glasheen, New SHM Board Member, Committed to Raising Quality of Care
Although based in an academic hospital program at the University of Colorado Denver, new SHM board member Jeffrey Glasheen, MD, SFHM, does not view himself as representative of only academic hospitalist groups on the board.
"I'd like to say I represent the constituency that cares about the quality, safety, and efficiency of healthcare delivery—and that includes every hospitalist,” says Dr. Glasheen, who has played major roles in developing SHM's Academic Hospitalist Academy and Academic Hospital Medicine Leadership Summit, and now chairs its Academic Committee.
Dr. Glasheen, who recently resigned as physician editor of the The Hospitalist is a senior deputy editor of the Journal of Hospital Medicine and was course director of HM12 in San Diego earlier this month. He intends to "push the envelope" for quality issues in his service on the board. "Quality is the best conceivable care you can provide, and clearly, where we are today is not there yet," he says.
Dr. Glasheen, who is committed to giving hospitalists the skills they need to elevate the quality of hospital care, says that starts with redesigning residency programs and medical school curriculums to teach quality improvement (QI). He believes that payment and healthcare reform will put hospitalists in a great position to serve as their hospitals' quality leaders, "but it's also going to take inspired leadership," he says. Hospitalists and hospitals need to make quality a major priority, which he recognizes is hard to do when groups are understaffed. As such, he hopes to find solutions to HM's pipeline issues—how to fill the hospitalist positions that will be needed in the future.
"I've been blessed in my situation [at my institution] to have an administration that's really supportive of hospital medicine," he says. "Our administration really gets the value equation, and we as hospitalists do, too. But as I travel around the country, I don't always see that."
Although based in an academic hospital program at the University of Colorado Denver, new SHM board member Jeffrey Glasheen, MD, SFHM, does not view himself as representative of only academic hospitalist groups on the board.
"I'd like to say I represent the constituency that cares about the quality, safety, and efficiency of healthcare delivery—and that includes every hospitalist,” says Dr. Glasheen, who has played major roles in developing SHM's Academic Hospitalist Academy and Academic Hospital Medicine Leadership Summit, and now chairs its Academic Committee.
Dr. Glasheen, who recently resigned as physician editor of the The Hospitalist is a senior deputy editor of the Journal of Hospital Medicine and was course director of HM12 in San Diego earlier this month. He intends to "push the envelope" for quality issues in his service on the board. "Quality is the best conceivable care you can provide, and clearly, where we are today is not there yet," he says.
Dr. Glasheen, who is committed to giving hospitalists the skills they need to elevate the quality of hospital care, says that starts with redesigning residency programs and medical school curriculums to teach quality improvement (QI). He believes that payment and healthcare reform will put hospitalists in a great position to serve as their hospitals' quality leaders, "but it's also going to take inspired leadership," he says. Hospitalists and hospitals need to make quality a major priority, which he recognizes is hard to do when groups are understaffed. As such, he hopes to find solutions to HM's pipeline issues—how to fill the hospitalist positions that will be needed in the future.
"I've been blessed in my situation [at my institution] to have an administration that's really supportive of hospital medicine," he says. "Our administration really gets the value equation, and we as hospitalists do, too. But as I travel around the country, I don't always see that."
Although based in an academic hospital program at the University of Colorado Denver, new SHM board member Jeffrey Glasheen, MD, SFHM, does not view himself as representative of only academic hospitalist groups on the board.
"I'd like to say I represent the constituency that cares about the quality, safety, and efficiency of healthcare delivery—and that includes every hospitalist,” says Dr. Glasheen, who has played major roles in developing SHM's Academic Hospitalist Academy and Academic Hospital Medicine Leadership Summit, and now chairs its Academic Committee.
Dr. Glasheen, who recently resigned as physician editor of the The Hospitalist is a senior deputy editor of the Journal of Hospital Medicine and was course director of HM12 in San Diego earlier this month. He intends to "push the envelope" for quality issues in his service on the board. "Quality is the best conceivable care you can provide, and clearly, where we are today is not there yet," he says.
Dr. Glasheen, who is committed to giving hospitalists the skills they need to elevate the quality of hospital care, says that starts with redesigning residency programs and medical school curriculums to teach quality improvement (QI). He believes that payment and healthcare reform will put hospitalists in a great position to serve as their hospitals' quality leaders, "but it's also going to take inspired leadership," he says. Hospitalists and hospitals need to make quality a major priority, which he recognizes is hard to do when groups are understaffed. As such, he hopes to find solutions to HM's pipeline issues—how to fill the hospitalist positions that will be needed in the future.
"I've been blessed in my situation [at my institution] to have an administration that's really supportive of hospital medicine," he says. "Our administration really gets the value equation, and we as hospitalists do, too. But as I travel around the country, I don't always see that."
HM Tool Designed to Pinpoint Program Strengths, Weaknesses
The creators of the first measurement tool for hospitalist programs hope that it becomes a standardized gauge for HM practice performance.
The Greeno-Hawley Hospital Medicine Index, unveiled earlier this month by Cogent HMG, uses a 26-question survey to measure HM group performance in five categories: alignment, performance management, infrastructure, operational processes, and leadership and people. The score will offer HM leaders a perspective on where their group stands in comparison with other hospitalist programs.
"It's meant to be a snapshot in time," says Beth Hawley, MBA, FACHE, Cogent's chief customer experience officer, who helped develop the index with Ron Greeno, MD, MHM, the company's chief medical officer. It is intended to help programs pinpoint the areas on which they need to focus in order to improve their performance, she says.
The index will be formally demonstrated at the American College of Physician Executives meeting April 30 in San Francisco. It will be available online in May.
Hawley says that once programs begin using the index, Cogent can assimilate and review the data to determine whether the tool can serve as a predictive model. Until then, it can be a guidepost for practice improvement for HM leaders who have never before had comparative tools.
"People would sit there thinking they're doing a great job but they only know their little market or their hospital," she says, "and really don’t see the broad picture of where hospital medicine is going and what a hospital medicine program can do for a hospital."
The creators of the first measurement tool for hospitalist programs hope that it becomes a standardized gauge for HM practice performance.
The Greeno-Hawley Hospital Medicine Index, unveiled earlier this month by Cogent HMG, uses a 26-question survey to measure HM group performance in five categories: alignment, performance management, infrastructure, operational processes, and leadership and people. The score will offer HM leaders a perspective on where their group stands in comparison with other hospitalist programs.
"It's meant to be a snapshot in time," says Beth Hawley, MBA, FACHE, Cogent's chief customer experience officer, who helped develop the index with Ron Greeno, MD, MHM, the company's chief medical officer. It is intended to help programs pinpoint the areas on which they need to focus in order to improve their performance, she says.
The index will be formally demonstrated at the American College of Physician Executives meeting April 30 in San Francisco. It will be available online in May.
Hawley says that once programs begin using the index, Cogent can assimilate and review the data to determine whether the tool can serve as a predictive model. Until then, it can be a guidepost for practice improvement for HM leaders who have never before had comparative tools.
"People would sit there thinking they're doing a great job but they only know their little market or their hospital," she says, "and really don’t see the broad picture of where hospital medicine is going and what a hospital medicine program can do for a hospital."
The creators of the first measurement tool for hospitalist programs hope that it becomes a standardized gauge for HM practice performance.
The Greeno-Hawley Hospital Medicine Index, unveiled earlier this month by Cogent HMG, uses a 26-question survey to measure HM group performance in five categories: alignment, performance management, infrastructure, operational processes, and leadership and people. The score will offer HM leaders a perspective on where their group stands in comparison with other hospitalist programs.
"It's meant to be a snapshot in time," says Beth Hawley, MBA, FACHE, Cogent's chief customer experience officer, who helped develop the index with Ron Greeno, MD, MHM, the company's chief medical officer. It is intended to help programs pinpoint the areas on which they need to focus in order to improve their performance, she says.
The index will be formally demonstrated at the American College of Physician Executives meeting April 30 in San Francisco. It will be available online in May.
Hawley says that once programs begin using the index, Cogent can assimilate and review the data to determine whether the tool can serve as a predictive model. Until then, it can be a guidepost for practice improvement for HM leaders who have never before had comparative tools.
"People would sit there thinking they're doing a great job but they only know their little market or their hospital," she says, "and really don’t see the broad picture of where hospital medicine is going and what a hospital medicine program can do for a hospital."
Kids' Deadly Unintentional Injuries Drop 30%
Fewer children died from unintentional injuries between 2000 and 2009, but death rates from suffocation and poisoning increased, according to a report from the Centers for Disease Control and Prevention.
The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, according to an analysis of national mortality data. There were 9,143 childhood deaths from unintentional injuries in 2009, down from 12,441 in 2000. Yet, that’s about one child death per hour caused by unintentional injury, whether it’s a traffic crash, drowning, poisoning, or fire.

"One child’s death is still one too many," said Ileana Arias, Ph.D., principal deputy director at CDC, in a news conference. "We know most of these events are predictable and preventable."
Traffic crashes were the leading cause of death among children and adolescents (4,564 deaths), followed by suffocation (1,160), drowning (983), poisoning (824), fire/burn (391), and falls (151), according to the report.
Despite a drop in most of the mechanisms, the authors noted the increase in poisoning and suffocation death rates.
There was a 91% increase in poisoning death rate among adolescents aged 15-19 years over the 10-year period. The authors attributed the rise to prescription drug overdoses. Painkillers seem to be replacing marijuana as a gateway drug, said Dr. Arias.
"Strategies to reduce the misuse of prescription drugs include appropriate prescribing, proper storage and disposal, discouraging medication sharing, and state-based prescription drug monitoring programs," the report’s authors wrote (MMWR 2012;61:1-7).
Also, unintentional infant suffocation rates increased 54% between 2000 and 2009. The increase "underscores the importance of safe sleeping environments as recommended by the American Academy of Pediatrics, which includes supine positioning, a firm sleep surface, room-sharing without bed-sharing, and avoiding loose bedding," the investigators noted.
There was nearly a 41% decrease in deaths from traffic crashes during the 10-year-period, which could be due to several factors, including improvements in seat belt use, child safety seat and booster seat use, licensing requirements, and vehicle design, according to the report.
Drowning deaths decreased 28%; deaths from fire/burn decreased 45%, and deaths from accidental falls dropped 19%.
Despite the declines, injury remains the leading cause of death among children in the United States. The nation also ranks worst among all high-income countries when it comes to injury deaths among 0 to 14-year-olds, according to the CDC report, which is the first of its kind to describe trends among 0 to 19-year-olds by mechanism and by state.
Unintentional injury rates varied widely among states, suggesting that "environment, exposure to hazards, and difference in public policy might play a role," the authors wrote. The variation also "demonstrated that it is possible to prevent these injuries," said Dr. Arias. Massachusetts had the lowest unintentional injury death rate (4/100,000), and Mississippi had the highest (25.1/100,000).
The report is based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
The authors said the report has at least two limitations. First, the report is based on death certificate data, which are subject to misclassification errors. In addition, the report is limited to unintentional injury deaths and excludes nonfatal injuries. Thus, it underreports "the total burden from injury on the society and the medical care system."
CDC officials and their partners released the National Action Plan for Child Injury Prevention along with this report, hoping that the plan’s implementation "could result in significant reductions in needless deaths, injuries, and costs associated with injuries among children and adolescents in the United States."
Fewer children died from unintentional injuries between 2000 and 2009, but death rates from suffocation and poisoning increased, according to a report from the Centers for Disease Control and Prevention.
The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, according to an analysis of national mortality data. There were 9,143 childhood deaths from unintentional injuries in 2009, down from 12,441 in 2000. Yet, that’s about one child death per hour caused by unintentional injury, whether it’s a traffic crash, drowning, poisoning, or fire.
"One child’s death is still one too many," said Ileana Arias, Ph.D., principal deputy director at CDC, in a news conference. "We know most of these events are predictable and preventable."
Traffic crashes were the leading cause of death among children and adolescents (4,564 deaths), followed by suffocation (1,160), drowning (983), poisoning (824), fire/burn (391), and falls (151), according to the report.
Despite a drop in most of the mechanisms, the authors noted the increase in poisoning and suffocation death rates.
There was a 91% increase in poisoning death rate among adolescents aged 15-19 years over the 10-year period. The authors attributed the rise to prescription drug overdoses. Painkillers seem to be replacing marijuana as a gateway drug, said Dr. Arias.
"Strategies to reduce the misuse of prescription drugs include appropriate prescribing, proper storage and disposal, discouraging medication sharing, and state-based prescription drug monitoring programs," the report’s authors wrote (MMWR 2012;61:1-7).
Also, unintentional infant suffocation rates increased 54% between 2000 and 2009. The increase "underscores the importance of safe sleeping environments as recommended by the American Academy of Pediatrics, which includes supine positioning, a firm sleep surface, room-sharing without bed-sharing, and avoiding loose bedding," the investigators noted.
There was nearly a 41% decrease in deaths from traffic crashes during the 10-year-period, which could be due to several factors, including improvements in seat belt use, child safety seat and booster seat use, licensing requirements, and vehicle design, according to the report.
Drowning deaths decreased 28%; deaths from fire/burn decreased 45%, and deaths from accidental falls dropped 19%.
Despite the declines, injury remains the leading cause of death among children in the United States. The nation also ranks worst among all high-income countries when it comes to injury deaths among 0 to 14-year-olds, according to the CDC report, which is the first of its kind to describe trends among 0 to 19-year-olds by mechanism and by state.
Unintentional injury rates varied widely among states, suggesting that "environment, exposure to hazards, and difference in public policy might play a role," the authors wrote. The variation also "demonstrated that it is possible to prevent these injuries," said Dr. Arias. Massachusetts had the lowest unintentional injury death rate (4/100,000), and Mississippi had the highest (25.1/100,000).
The report is based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
The authors said the report has at least two limitations. First, the report is based on death certificate data, which are subject to misclassification errors. In addition, the report is limited to unintentional injury deaths and excludes nonfatal injuries. Thus, it underreports "the total burden from injury on the society and the medical care system."
CDC officials and their partners released the National Action Plan for Child Injury Prevention along with this report, hoping that the plan’s implementation "could result in significant reductions in needless deaths, injuries, and costs associated with injuries among children and adolescents in the United States."
Fewer children died from unintentional injuries between 2000 and 2009, but death rates from suffocation and poisoning increased, according to a report from the Centers for Disease Control and Prevention.
The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, according to an analysis of national mortality data. There were 9,143 childhood deaths from unintentional injuries in 2009, down from 12,441 in 2000. Yet, that’s about one child death per hour caused by unintentional injury, whether it’s a traffic crash, drowning, poisoning, or fire.
"One child’s death is still one too many," said Ileana Arias, Ph.D., principal deputy director at CDC, in a news conference. "We know most of these events are predictable and preventable."
Traffic crashes were the leading cause of death among children and adolescents (4,564 deaths), followed by suffocation (1,160), drowning (983), poisoning (824), fire/burn (391), and falls (151), according to the report.
Despite a drop in most of the mechanisms, the authors noted the increase in poisoning and suffocation death rates.
There was a 91% increase in poisoning death rate among adolescents aged 15-19 years over the 10-year period. The authors attributed the rise to prescription drug overdoses. Painkillers seem to be replacing marijuana as a gateway drug, said Dr. Arias.
"Strategies to reduce the misuse of prescription drugs include appropriate prescribing, proper storage and disposal, discouraging medication sharing, and state-based prescription drug monitoring programs," the report’s authors wrote (MMWR 2012;61:1-7).
Also, unintentional infant suffocation rates increased 54% between 2000 and 2009. The increase "underscores the importance of safe sleeping environments as recommended by the American Academy of Pediatrics, which includes supine positioning, a firm sleep surface, room-sharing without bed-sharing, and avoiding loose bedding," the investigators noted.
There was nearly a 41% decrease in deaths from traffic crashes during the 10-year-period, which could be due to several factors, including improvements in seat belt use, child safety seat and booster seat use, licensing requirements, and vehicle design, according to the report.
Drowning deaths decreased 28%; deaths from fire/burn decreased 45%, and deaths from accidental falls dropped 19%.
Despite the declines, injury remains the leading cause of death among children in the United States. The nation also ranks worst among all high-income countries when it comes to injury deaths among 0 to 14-year-olds, according to the CDC report, which is the first of its kind to describe trends among 0 to 19-year-olds by mechanism and by state.
Unintentional injury rates varied widely among states, suggesting that "environment, exposure to hazards, and difference in public policy might play a role," the authors wrote. The variation also "demonstrated that it is possible to prevent these injuries," said Dr. Arias. Massachusetts had the lowest unintentional injury death rate (4/100,000), and Mississippi had the highest (25.1/100,000).
The report is based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
The authors said the report has at least two limitations. First, the report is based on death certificate data, which are subject to misclassification errors. In addition, the report is limited to unintentional injury deaths and excludes nonfatal injuries. Thus, it underreports "the total burden from injury on the society and the medical care system."
CDC officials and their partners released the National Action Plan for Child Injury Prevention along with this report, hoping that the plan’s implementation "could result in significant reductions in needless deaths, injuries, and costs associated with injuries among children and adolescents in the United States."
FROM THE CENTERS FOR DISEASE CONTROL AND PREVENTION VITAL SIGNS REPORT
Major Finding: The overall death rate from unintentional injuries among children dropped by nearly 30% during the 10-year period, but death rate from poisoning and suffocation increased in subgroups.
Data Source: Based on analysis of national mortality data collected in the CDC’s National Vital Statistics Systems.
Disclosures: None.

Men, women, and migraine: The role of sex, hormones, obesity, and PTSD
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
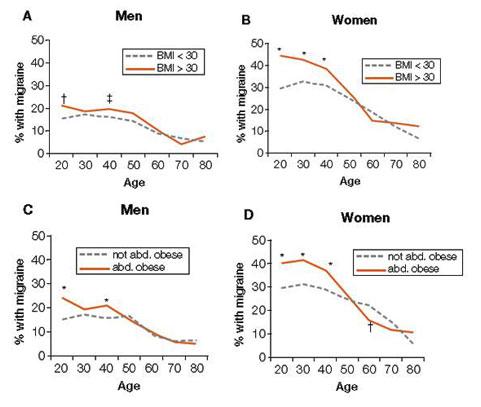
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
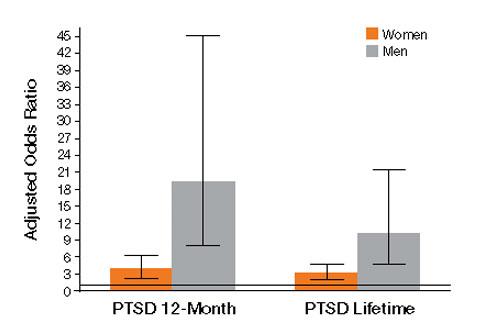
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
Migraine is a common neurologic disorder that occurs in approximately 3 times as many females as males in the United States. Among 30,000 respondents, the American Migraine Study II found that the prevalence of migraine was 18.2% among females and 6.5% among males, and was much higher in females from age 12 across the lifespan.1 In comparison, for tension-type headache the female to male ratio of occurrence is 5:4, occurring only slightly more in females.2 The reasons for this disparity in migraine prevalence are not well understood. The disproportionate number of women of reproductive age with migraine suggests that hormonal factors may play a role, but the complex pathophysiology of migraine indicates additional factors are involved.3
Recent research on menstrual-related migraine and two significant comorbidities of migraine—obesity and posttraumatic stress disorder (PTSD)—shed new light on the differences in how men and women present with and experience this often disabling disorder.
Epidemiologic differences
The incidence of migraine, defined here as age of first onset, is different in boys and girls. For migraine without aura, age of first onset is approximately 10 to 11 years in boys versus 14 to 17 years in girls. For migraine with aura, age of first onset is approximately 5 years in boys and 12 to 13 years in girls.4
The picture of migraine differs by sex before and after puberty. Before age 12, boys have a higher incidence and prevalence of migraine. After age 12, prevalence increases for both sexes, peaking between age 35 to 45, with an increase in the female-to-male ratio from 2:1 at age 20 to 3.3:1 at age 40.5,6
Disparities in migraine symptoms
Common symptoms associated with severe or unilateral migraine pain include photophobia, phonophobia, and nausea. In the American Migraine Study II, the most frequently reported symptoms were pulsatile pain (85%of migraineurs), light sensitivity (80%), sound sensitivity (76%), nausea (73%), unilateral pain (59%), blurred vision (44%), aura (36%), and vomiting (29%).1 Females were more likely than males to report light sensitivity, sound sensitivity, and nausea. More females experienced 1 to 2 days of migraine-associated activity restriction than males (30.5% vs 22.9%).1 Separate studies have shown neck pain to be second after menstruation in its predictive value for onset of migraine, and to be more prevalent than nausea at the time of treatment.7,8
Migraine comorbidities
Migraine is known to be comorbid with a variety of disorders including psychiatric conditions such as depression and anxiety,9,10 and medical comorbidities such as stroke, epilepsy, and hypothyroidism.11-13 In women, migraine is also comorbid with endometriosis.14
Hormonal factors: Menstrual-related migraine
With migraine disproportionately affecting women of reproductive age, as many as 70% of female migraineurs are aware of a menstrual association with their headaches.15 A menstrual migraine is defined as migraine without aura that occurs during the 5-day window that begins 2 days before the onset of bleeding and extends through the third day of active bleeding—and that occurs in at least two-thirds of menstrual cycles.16 Approximately 14% of women experience what is termed pure menstrual migraine, meaning the only time they experience migraine is during menstruation. For women who also have migraines triggered by other mechanisms, the menstrual migraine is typically their most severe migraine of the month.
For many women, menstrual migraines are more painful, longer lasting, and more resistant to acute therapy than migraines occurring at other times.17,18 It is specifically the reduction in estradiol in the late luteal phase that appears to be the greatest trigger for menstrual migraine.
About two-thirds of women with migraine improve in menopause, particularly those for whom migraine attacks were associated with menstruation.19,20 As disabling as menstrual related migraine can be, clinically it is often found to coexist with chronic migraine and medication overuse headache.21
In a study that looked at the impact of eliminating menstrual migraine, investigators treated women with hormonal preventives based on the hypothesis that, because these agents confer no known benefit for migraines that are not hormonally triggered, use of these agents might allow them to separate out menstrual-related migraine and its effect on the overall clinical picture.21 Among 229 consecutive women seen in follow-up, 81% of those patients who were taking the hormonal preventive as prescribed had a complete resolution of menstrual-related migraine. Among those in whom menstrual migraine was eliminated, 58.9% reverted back to episodic migraine, compared with only 11% of patients whose menstrual-migraine was not eliminated.21 Resolution of menstrual-related migraine also was associated with resolution of medication overuse. Patients in whom menstrual-related migraine resolved were >2 times as likely to stop medication overuse as those in whom the migraines were not eliminated. The results offer preliminary evidence that hormonal regimens may be of benefit in preventing menstrual-related migraine.
Migraine and obesity
Obesity, which results from excessive adipose tissue in relation to fat free mass, has been shown in clinical and population-based studies to be associated with migraine.22-25 Both migraine and the distribution of adipose tissue change substantially based on age and sex.25 Following puberty, girls have an increase in the subcutaneous to visceral adipose tissue ratio as compared with boys, a pattern that continues through the reproductive years for women. Postmenopausal women see an increase in visceral
adipose tissue volume and a decrease in the subcutaneous to visceral adipose tissue volume compared with premenopausal women. Similarly, migraine prevalence increases in women of reproductive age as compared with those of postreproductive age and it is greater in women of reproductive age as compared with men.25
To evaluate the prevalence of migraine and severe headaches in men and women with and without total body obesity (TBO), as measured by body mass index (BMI) and abdominal obesity (Abd-O), Peterlin and colleagues analyzed data from 21,783 participants in the National Health and Nutrition Examination Survey.26 The investigators found that the relationship between migraine and obesity varies by age, sex, and the distribution of adipose tissue. For men and women of reproductive age, migraine prevalence increased in those with either TBO or Abd-O compared with those without. For postreproductive aged men and women (>55 years), migraine prevalence was not increased in those with either Abd-O or TBO. [Figure 1]
FIGURE 1: Migraine prevalence in men and women in relation to TBO and Abd-O
Total body obesity (TBO) was estimated based on BMI. Abdominal obesity (Abd-O) was estimated
based on waist circumference.
*P ≤ .001; † P ≤ .01; ‡ P ≤ .05
Source: Adapted with permission from Peterlin BL, et al. Migraine and obesity: Epidemiology,
mechanisms, and implications. Headache. 2010;50:631-636.
Vo et al observed similar findings for women of reproductive age in analyses of data from the Omega study. In a cohort of 3,733 women during early pregnancy, researchers found that obesity was associated with increased odds for migraine and that the risk of migraine increased with increasing obesity.27 Specifically, while the overall odds of migraine in women with obesity of any level was 48% greater than in women without obesity (OR 1.48; 95%CI: 1.12-1.96), those women with severe or class II obesity (BMI 35 to 39.9) had a >200% increased risk (OR 2.07; 95%CI: 1.27-3.39), and those with morbid or class III obesity (BMI ≥40) had a 275% increased risk of migraine, (OR 2.75; 95%CI: 1.60-4.70).27 Furthermore, Vo et al demonstrated that women with a history of pediatric migraine had 67% increased odds of gaining ≥22 pounds above their weight at the age of 18 (OR 1.67; 95% CI:1.13-2.47).27
An association between obesity and migraine was also found in two small studies that assessed the effects of bariatric surgery on headache frequency in morbidly obese, episodic migraineurs.28,29 In these studies, at 6 months after surgery the monthly headache frequency declined from approximately 4 headache days per month at baseline to just 1 to 2 headache days per month. Researchers also noted that following bariatric surgery, the migraine-associated symptoms were reduced and headache related disability improved significantly. Larger, controlled studies will be needed to substantiate these findings and determine the true effect size before bariatric surgery could be considered as a component of migraine therapy.30 However, these results highlight the observation that clinicians should give consideration to obesity as a potentially modifiable risk factor for episodic migraine.
Migraine and PTSD
Posttraumatic stress disorder (PTSD), the result of traumatic life stressors, has a lifetime prevalence of approximately 7%—3.6% among men and 9.7% among women—according to the National Comorbidity Survey Replication (NCS-R), a cross-sectional, general population survey of mental disorders.31 Interpersonal trauma (such as physical or sexual abuse) is the most common cause of PTSD, but it can also result from life-threatening situations such as natural and man-made disasters or military combat.32,33 In a secondary analysis of a the NCS-R, Peterlin and colleagues and found that 21.5% of episodic migraineurs and 19.2% of chronic daily headache sufferers fulfilled PTSD criteria.34
Although both migraine and PTSD are up to 3 times more common in women than men, recent data suggest that the association between migraine and PTSD is stronger in men.34,35 Using the NCS-R data, Peterlin and colleagues found a more than 3-4 fold increase in the odds ratio of PTSD in men with migraine versus women with migraine—a result that renders PTSD, to the knowledge of the investigators, the first mental disorder to be reported as having a greater prevalence in men with migraine than women with migraine.34[Figure 2]
FIGURE 2: Sex-specific odds ratio of PTSD in episodic migraine
Source: Adapted with permission from Peterlin BL, et al. Post-traumatic distress disorder and migraine:
Epidemiology, sex differences, and potential mechanisms. Headache. 2011;51(6)860-868.
The neurobiological mechanism linking PTSD to migraine is not known. Although a variety of theories exist—including low serotonin levels, dysfunctions of the autonomic system and hypothalamic-pituitary-adrenal axis (HPA) in both migraine and PTSD, and elevated baseline cortisol levels in migraineurs—it remains unclear why the association is stronger in men than in women.34 Some studies suggest that sex-related differences of the HPA axis may play a role.36,37 Others consider fMRI findings of sex differences in cerebral blood flow to pain centers in response to psychological distress.37 Further research into the sex-related differences of migraineurs with PTSD will likely reveal insights into new therapeutic directions for men and women with these disorders.
Implications for clinicians
The preceding data add to the understanding that numerous comorbidities exist in individuals with migraine. If a patient is a migraineur, screen for PTSD as well as depression and anxiety. Treatment with cognitive behavioral therapy—alone or in combination with pharmacological therapy—should be considered, since treatment of PTSD alone has been shown to have a beneficial effect on both pain and disability in chronic pain patients.38
Given that obesity is a modifiable risk factor, educate all migraine patients about the association with obesity in general, the increasing risk of migraine associated with increasing obesity, and the potential effect of weight gain/loss on headache frequency.26,27 Also inform patients about the potential effects migraine medications may have on their weight, and encourage them to eat a healthy diet, exercise, and avoid gaining excessive weight. If other comorbidities are involved, tailor the therapeutic regimen based on that combination. If a migraine patient is obese and has high blood pressure, look for an antihypertensive agent that is relatively weight-neutral.
Eliminating menstrual migraine should be an important treatment goal for patients in whom it is the most disabling migraine of the month. Hormonal preventives may be the best approach for women whose menstrual attacks are resistant to acute treatment.21
Disclosures
B. Lee Peterlin, DO, has received grant/research support from GlaxoSmithKline, has served as a consultant to Nautilus, and has served on the speaker’s bureau of Zogenix. She holds a provisional patent for use of adiponectin-modulating drugs for migraine.
Anne H. Calhoun, MD, has no conflicts of interest to report.
Fred Balzac has no conflicts of interest to report.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
1. Lipton RB, Stewart WF, Diamond S, et al. Prevalence and burden of migraine in the United States: data from the American Migraine Study II. Headache. 2001;41:646-657.
2. Rasmussen BK, Jensen R, Schroll M, et al. Epidemiology of headache in a general population—a prevalence study. J Clin Epidemiol. 1991;44(11)1147-1157.
3. Peterlin BL, Katsnelson MJ, Calhoun AH. The associations between migraine, unipolar psychiatric comorbidities, and stress-related disorders and the role of estrogen. Curr Pain Headache Rep. 2009;13:404-412.
4. Stewart WF, Linet MS, Celentano DD, et al. Age- and sex-specific incidence rates of migraine with and without visual aura. Am J Epidemiol. 1991;134(10):1111-1120.
5. Stewart WF, Lipton RB, Celentano DD, et al. Prevalence of migraine headache in the United States: relation to age, income, race, and other sociodemographic factors. JAMA. 1992;267:64- 69.
6. Lipton RB, Stewart WF. Migraine in the United States: a review of epidemiology and health care use. Neurology. 1993;43(suppl 3):S6-10.
7. Wober C, Brannath W, Schmidt K, et al. Prospective analysis of factors related to migraine attacks: The PAMINA study. Cephalalgia. 2007;27:304-314.
8. Calhoun AH, Ford S, Millen C, et al. The prevalence of neck pain in migraine. Headache. 2010;50:1273-1277.
9. Breslau N, Lipton RB, Stewart WF, et al. Comorbidity of migraine and depression: Investigating potential etiology and prognosis. Neurology. 2003;60:1308-1312.
10. Stewart W, Breslau N, Keck PE Jr. Comorbidity of migraine and panic disorder. Neurology. 1994;44:S23-S27.
11. Scher AI, Terwindt GM, Picavet HS, et al. Cardiovascular risk factors and migraine: The GEM population based study. Neurology. 2005;64:614-620.
12. Ottman R, Lipton RB. Comorbidity of migraine and epilepsy. Neurology. 1994;44:2105-2110.
13. Moreau T, Manceau E, Giroud-Baleydier F, et al. Headache in hypothyroidism. Prevalence and outcome under thyroid hormone therapy. Cephalalgia. 1998;18:687-689.
14. Ferrero S, Pretta S, Bertoldi S, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. 2004;19:2927-2932.
15. MacGregor EA. “Menstrual” migraine: Towards a definition. Cephalalgia. 1996;16:11-21.
16. Calhoun AH, Hutchinson S. Hormonal therapies for menstrual migraine. Curr Pain Headache Rep.2009;13:381-385.
17. Granella F, Sances G, Allais G, et al. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia. 2004;24:707-716.
18. MacGregor EA, Hackshaw A. Prevalence of migraine on each day of the natural menstrual cycle. Neurology. 2004;63:351-353.
19. Neri I, Granella F, Nappi R, et al. Characteristics of headache at menopause: a clinico-epidemiologic study. Maturitas.1993;17:31-37.
20. Brandes JL. The influence of estrogen on migraine: a systematic review. JAMA. 2006;295(15):1824-1830.
21. Calhoun A, Ford S. Elimination of menstrual-related migraine beneficially impacts chronification and medication overuse. Headache. 2008;48:1186-1193.
22. Scher AI, Stewart WF, Ricci JA, et al. Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 2003;106:81-89.
23. Horev A, Wirguin I, Lantsberg L, et al. A high incidence of migraine with aura among morbidly obese women. Headache. 2005;45:936-938.
24. Ford ES, Li C, Pearson WS, et al. Body mass index and headaches: Findings from a national sample of US adults. Cephalalgia. 2008;28(12):1270-1276.
25. Peterlin BL, Rapoport AM, Kurth T. Migraine and obesity: Epidemiology, mechanisms, and implications. Headache. 2012;50:631-648.
26. Peterlin BL, Rosso AL, Rapoport AM, et al. Obesity and migraine: the effect of age, gender and adipose tissue distribution. Headache. 2010;50:52-62.
27. Vo M, Ainalem A, Qiu C, et al. Body mass index and adult weight gain among reproductive age women with migraine. Headache. 2011;51:559-569.
28. Novack V, Fuchs L, Lantsberg L, et al. Changes in headache frequency in premenopausal obese women with migraine after bariatric surgery: A case series. Cephalalgia. 2011;31(13):1336-1342.
29. Bond DS, Vithiananthan S, Nash JM, et al. Improvement of migraine headaches in severely obese patients after bariatric surgery. Neurology. 2011;76(13)1135-1138.
30. Peterlin BL. Bariatric surgery in obese migraineurs: Mounting evidence but important questions remain. Cephalalgia. 2011;31(13):1333-1335.
31. Kessler RC, Berglund P, Delmer O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
32. Butterfield MI, Becker M, Marx CE. Posttraumatic stress disorder in women: Current concepts and treatments. Curr Psychiatry Rep. 2002;4:474-486.
33. Breslau N. The epidemiology of trauma, PTSD, and other posttrauma disorders. Trauma Violence Abuse. 2009;10(3):198-210.
34. Peterlin BL, Rosso AL, Sheftell FD, et al. Post-traumatic stress disorder, drug abuse and migraine: new findings from the National Comorbidity Survey Replication (NCS-R). Cephalalgia. 2011;31:235-244.
35. Peterlin BL, Nijjar SS, Tietjen GE. Post-traumatic stress disorder and migraine: epidemiology, sex differences, and potential mechanisms. Headache. 2011;51:860-868.
36. Rainero I, Ferrero M, Rubino E, et al. Endocrine function is altered in chronic migraine patient with medication-overuse. Headache. 2006;46:597-603.
37. Wang J, Korczykowski, Rao H, et al. Gender difference in neural response to psychological stress. Soc Cog Affect Neurosci. 2007;2:227-239.
38. Peterlin BL, Tietjen GE, Brandes JL, et al. Posttraumatic stress disorder in migraine. Headache. 2009;49:541-551.
Found a Peanut: Dealing With Airway Obstructions in Kids
NATIONAL HARBOR, MD. – You may think that child’s cough is due to a respiratory infection. But it could be due to a peanut.
Peanuts, little plastic toys, apples, and especially pieces of hot dog: These are the things of which emergency department nightmares are made.
"Close to a million children visit emergency departments every year due to concerns over foreign bodies" in the airway or esophagus, Dr. Patrick C. Barth said at a meeting sponsored by the American College of Emergency Physicians. "And about 100 of those kids die from airway obstruction."
It’s not surprising that most of the choking incidents occur in young children – those between 3 and 4 years old. Learning how to chew, swallow, and breathe at the same time is a complicated physiologic task that takes a while to master, said Dr. Barth, an otolaryngologist at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Toddlers also explore all kinds of objects with their mouths as well as their hands, increasing the likelihood that they will swallow or inhale an object.
"If there is a history of a prior airway obstruction, you need to have a high level of suspicion."
"Seeds, popcorn, chunks of apple, or any foods with two different consistencies are hard for kids to manage. The slippery surface causes the food to quickly pass out of the mouth and they don’t have molars yet, so [they] can’t masticate well."
Peanuts, even though they are not large enough to block the trachea, can be really problematic, he added. "The oils set up a significant inflammatory reaction in the airways, so these kids can look really sick. And the inflammation makes endoscopy really difficult."
Children don’t always present in acute respiratory distress; they could just have a nagging wheeze or cough with no obvious illness. But if you think there might be a choking problem, look for one. "If there is a history of a prior airway obstruction, you need to have a high level of suspicion," he said.
A plain radiograph is usually the first diagnostic tool, although an x-ray won’t show radiolucent items, such as those made of plastic. But inspiratory and expiratory films might increase suspicion if there is asymmetric collapse when the child exhales.
CT may also be helpful, but the need should be balanced against the risks, since young children need to be sedated to acquire quality images.
The rigid bronchoscope is a good tool for both diagnosis and extraction of a foreign body, Dr. Barth said. The rigid type allows for simultaneous ventilation and the passage of instruments to remove the object. A flexible scope lacks this ability, and adequate ventilation is critically important in a child whose breathing may already be compromised. "If there’s a sharp object in the airway, the rigid bronchoscope also lets you sheathe it, so you don’t cause airway injury as you’re extracting it," he said.
In 30% of suspected cases, the bronchoscopy turns out to be negative. But in the case of airway obstruction, it’s better to be safe than sorry.
"This is a reasonable rate, because you really do not want to miss one of these. If you have a high level of suspicion, it’s not wrong to do a bronchoscopy."
Dr. Barth had no financial disclosures.
NATIONAL HARBOR, MD. – You may think that child’s cough is due to a respiratory infection. But it could be due to a peanut.
Peanuts, little plastic toys, apples, and especially pieces of hot dog: These are the things of which emergency department nightmares are made.
"Close to a million children visit emergency departments every year due to concerns over foreign bodies" in the airway or esophagus, Dr. Patrick C. Barth said at a meeting sponsored by the American College of Emergency Physicians. "And about 100 of those kids die from airway obstruction."
It’s not surprising that most of the choking incidents occur in young children – those between 3 and 4 years old. Learning how to chew, swallow, and breathe at the same time is a complicated physiologic task that takes a while to master, said Dr. Barth, an otolaryngologist at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Toddlers also explore all kinds of objects with their mouths as well as their hands, increasing the likelihood that they will swallow or inhale an object.
"If there is a history of a prior airway obstruction, you need to have a high level of suspicion."
"Seeds, popcorn, chunks of apple, or any foods with two different consistencies are hard for kids to manage. The slippery surface causes the food to quickly pass out of the mouth and they don’t have molars yet, so [they] can’t masticate well."
Peanuts, even though they are not large enough to block the trachea, can be really problematic, he added. "The oils set up a significant inflammatory reaction in the airways, so these kids can look really sick. And the inflammation makes endoscopy really difficult."
Children don’t always present in acute respiratory distress; they could just have a nagging wheeze or cough with no obvious illness. But if you think there might be a choking problem, look for one. "If there is a history of a prior airway obstruction, you need to have a high level of suspicion," he said.
A plain radiograph is usually the first diagnostic tool, although an x-ray won’t show radiolucent items, such as those made of plastic. But inspiratory and expiratory films might increase suspicion if there is asymmetric collapse when the child exhales.
CT may also be helpful, but the need should be balanced against the risks, since young children need to be sedated to acquire quality images.
The rigid bronchoscope is a good tool for both diagnosis and extraction of a foreign body, Dr. Barth said. The rigid type allows for simultaneous ventilation and the passage of instruments to remove the object. A flexible scope lacks this ability, and adequate ventilation is critically important in a child whose breathing may already be compromised. "If there’s a sharp object in the airway, the rigid bronchoscope also lets you sheathe it, so you don’t cause airway injury as you’re extracting it," he said.
In 30% of suspected cases, the bronchoscopy turns out to be negative. But in the case of airway obstruction, it’s better to be safe than sorry.
"This is a reasonable rate, because you really do not want to miss one of these. If you have a high level of suspicion, it’s not wrong to do a bronchoscopy."
Dr. Barth had no financial disclosures.
NATIONAL HARBOR, MD. – You may think that child’s cough is due to a respiratory infection. But it could be due to a peanut.
Peanuts, little plastic toys, apples, and especially pieces of hot dog: These are the things of which emergency department nightmares are made.
"Close to a million children visit emergency departments every year due to concerns over foreign bodies" in the airway or esophagus, Dr. Patrick C. Barth said at a meeting sponsored by the American College of Emergency Physicians. "And about 100 of those kids die from airway obstruction."
It’s not surprising that most of the choking incidents occur in young children – those between 3 and 4 years old. Learning how to chew, swallow, and breathe at the same time is a complicated physiologic task that takes a while to master, said Dr. Barth, an otolaryngologist at the Nemours/Alfred I. duPont Hospital for Children in Wilmington, Del.
Toddlers also explore all kinds of objects with their mouths as well as their hands, increasing the likelihood that they will swallow or inhale an object.
"If there is a history of a prior airway obstruction, you need to have a high level of suspicion."
"Seeds, popcorn, chunks of apple, or any foods with two different consistencies are hard for kids to manage. The slippery surface causes the food to quickly pass out of the mouth and they don’t have molars yet, so [they] can’t masticate well."
Peanuts, even though they are not large enough to block the trachea, can be really problematic, he added. "The oils set up a significant inflammatory reaction in the airways, so these kids can look really sick. And the inflammation makes endoscopy really difficult."
Children don’t always present in acute respiratory distress; they could just have a nagging wheeze or cough with no obvious illness. But if you think there might be a choking problem, look for one. "If there is a history of a prior airway obstruction, you need to have a high level of suspicion," he said.
A plain radiograph is usually the first diagnostic tool, although an x-ray won’t show radiolucent items, such as those made of plastic. But inspiratory and expiratory films might increase suspicion if there is asymmetric collapse when the child exhales.
CT may also be helpful, but the need should be balanced against the risks, since young children need to be sedated to acquire quality images.
The rigid bronchoscope is a good tool for both diagnosis and extraction of a foreign body, Dr. Barth said. The rigid type allows for simultaneous ventilation and the passage of instruments to remove the object. A flexible scope lacks this ability, and adequate ventilation is critically important in a child whose breathing may already be compromised. "If there’s a sharp object in the airway, the rigid bronchoscope also lets you sheathe it, so you don’t cause airway injury as you’re extracting it," he said.
In 30% of suspected cases, the bronchoscopy turns out to be negative. But in the case of airway obstruction, it’s better to be safe than sorry.
"This is a reasonable rate, because you really do not want to miss one of these. If you have a high level of suspicion, it’s not wrong to do a bronchoscopy."
Dr. Barth had no financial disclosures.
FROM A MEETING SPONSORED BY THE AMERICAN COLLEGE OF EMERGENCY PHYSICIANS
Evidence Suggests Pregnancies Can Survive Maternal Cancer Treatment
Emerging data on pregnancy and cancer can now help women and their doctors chart a safer course between effective treatment and protecting the developing fetus.
Two registries – one in the United States and another in Europe – agree: It’s not only possible to save a pregnancy in many situations, but children born to these women appear to be largely unaffected by in utero chemotherapy exposure. The combined studies followed more than 200 exposed children for up to 18 years; neither one found any elevated risk of congenital anomaly or any kind of cognitive or developmental delay.

"This is practice-changing information," Dr. Frédéric Amant, primary author on the European paper, said in an interview. "Until now, physicians were reluctant to administer chemotherapy and usually opted for termination, or at least for a delay in treatment or premature delivery in order to get treatment going," he said.
Dr. Amant’s study leads off a special section on cancer in pregnancy, published in the March issue of Lancet Oncology. The paper examined evidence that both supports and questions the clinical wisdom of treating a disease that threatens two very different patients – an adult woman and the fetus she carries.
Every case is different, depending on the type of cancer, its grade and potential aggressiveness, the stage of pregnancy, and the woman’s own desires, said Dr. Elyce Cardonick, an ob.gyn. at Cooper University Hospital in Camden, N.J., and the lead investigator of the Pregnancy and Cancer Registry.
"With solid tumors you usually have time to do the surgery, get the pathologic diagnosis, and let the patient recover. But if there is leukemia, for instance, you have to move faster. The first question should be ‘Could we delay treatment for this patient if she was not pregnant?’ I don’t want to limit their treatment, but at the same time, it’s true that they might not be getting the most up-to-date treatment – the newest agent on the block – because you would want to go with something there is at least some experience with. But this doesn’t necessarily mean they are going to do worse."
Cancer occurs in about 1 in 1,000 pregnancies, said Dr. Sarah Temkin, a gynecologic oncologist at the University of Maryland, Baltimore. Many of her patients are referred after a routine screening during early pregnancy finds something abnormal, or when a woman with an existing cancer is incidentally found to be pregnant. But signs that might raise a red flag in other situations don’t necessarily alert physicians to danger in pregnant women, she said in an interview. Pregnancy could obfuscate some symptoms, which might be further downplayed in light of a mother’s relatively young age. Breast cancer is a prime example.
"There are two problems, especially for breast cancers, which are the most common ones we see in pregnancy. First, a woman’s breasts are changing anyway during that time. Breast cancer is so rare in women of earlier childbearing age that both the patient and the doctor tend to disregard any new lumps and bumps."
But despite its rarity, cancer in all forms appears to be increasing among pregnant women, she said. This is probably a direct relation to age. "Cancer rates increase with increasing age, and women are becoming mothers at older and older ages."
When cancer coincides with pregnancy, Dr. Temkin views the mother’s health as paramount. "The mother is the person with cancer, and she deserves whatever the standard of care is for that particular cancer – the best care that would be offered to her if she was not pregnant."
Chemotherapy and Fetal Outcomes
To examine long-term neurodevelopmental risks associated with maternal cancer treatment, Dr. Amant, a gynecologic oncologist at the Leuven (Belgium) Cancer Institute, and his colleagues, are following 70 children from the age of 18 months until 18 years. In the newly published interim analysis, the mean follow-up time is 22 months. All the children had intrauterine exposure to chemotherapy, radiation, oncologic surgery, or combinations of these.
The analysis, which also appeared in Lancet Oncology’s special issue, includes data on all the children, including 18 who are now older than 9 years (Lancet Oncol. 2012;13:256-64).
The children – 68 singletons and one set of twins – were born from pregnancies exposed to a total of 236 chemotherapy cycles. Exposure varied by the mother’s cancer type and its stage at diagnosis. In all, 34 mothers were treated with only chemotherapy, 27 had chemotherapy and surgery, 1 received chemotherapy and radiation, and 6 women were treated with all three modalities. Most of the children also had in utero exposure to multiple imaging studies, including MRI, ultrasound, echocardiography, CT, and mammography. Chemotherapy regimens included doxorubicin, epirubicin, idarubicin and daunorubicin.

Fetuses also were exposed to a variety of other drugs, including antibiotics, antiemetics, pain medications, colony stimulating factors, and anxiolytics.
Breast cancer was the most common disease type (35). There were 18 cases of hematologic cancers, 6 ovarian cancers, 4 cervical cancers, and 1 each of basal cell carcinoma, brain tumor, Ewing’s sarcoma, colorectal cancer, and nasopharyngeal cancer.
The mean gestational age at cancer diagnosis was 18 weeks, although fetuses ranged in age from 2 to 33 weeks when their mothers were diagnosed. About a third of the babies (23) were born at term.
Seven were born at 28-32 weeks, nine at 32-34 weeks, and 31 at 34-37 weeks. Weight for gestational age was below the 10th percentile in 14 children (21%).
Seven congenital anomalies were found in the group of 70 children (10%) – a rate not significantly different from that in the background population. There were only two major malformations, for a 2.9% rate. Malformations included the following:
• Hip subluxation, pectus excavatum and hemangioma, associated with chemotherapy only.
• Bilateral partial syndactyly, associated with chemotherapy plus radiotherapy.
• Bilateral small protuberance on one finger, and rectal atresia, associated with chemotherapy plus surgery.
• Bilateral double cartilage ring in a child exposed to chemotherapy, surgery and radiotherapy.
None of the children showed any congenital cardiac issues.
All of the children showed neurocognitive development that was within normal range, except for the set of twins, who were delivered by cesarean section at 32.5 weeks after a preterm premature rupture of membranes. These children were so delayed that they were not able to complete cognitive testing. Their mother developed an acute myeloid leukemia – one of the true "emergency" cancers diagnosed in pregnancy, Dr. Amant said. The babies had been exposed to idarubicin and cytosine arabinoside at 15.5, 21.5, 26.5, and 31.5 weeks’ gestation.
The boy, who weighed 1,640 g at birth, had a normal karyotype but, at 3 years, brain imaging showed a unilateral polymicrogyria in the left perisylvian area. He showed an early developmental delay; at age 9 years, he had the developmental capacity of a 12-month old.
The girl, who weighed 1,390 g at birth, also had an early developmental delay, but at age 9 years she attended school with support. Her parents refused brain imaging.
"The other 68 children did well," Dr. Amant said. "This doesn’t mean they were all normal in every way, but in any population you will see learning and developmental delay issues. We think the problem for the delayed children was not related to chemotherapy exposure, but more likely to their prematurity."
Dr. Amant saw a direct correlation between gestational age and intelligence quota. "When we controlled for age, gender, and country of birth, we found that the IQ score increased by almost 12 points for each additional month of gestation."
The U.S. Experience

Dr. Cardonick has found similar results. Her registry now contains information on 280 women who were enrolled over a 13-year period. The children born from these pregnancies have been assessed annually since birth. It also includes 70 controls – children whose mothers had cancer but who were not exposed to chemotherapy.
She published interim results of the registry in 2010 (Cancer J. 2010;16:76-82). At that point, it contained information on 231 women and 157 children. The most common malignancy was breast cancer (128); the mean gestational age at diagnosis was 13 weeks. About a third of the women (54) were advised to terminate their pregnancy; 12 did so.
Among those who continued both pregnancy and treatment, neonatal outcomes were generally good. There were nine premature deliveries related to preterm labor or premature rupture of membranes. The congenital anomaly rate born was 4%, which was in line with the normal background rate and slightly lower than that seen in Dr. Amant’s cohort.
The infants’ mean birth weight was 2,647 g, which was significantly less than the mean 2,873 g in the control group, but probably clinically irrelevant, Dr. Cardonick wrote in the paper.
She continues to follow these children annually. At this point, the children are a mean 5 years old; her oldest subject is 14 years. So far, the rate of neurocognitive issues in the group is no different than would be observed in any other group, and none of the children has developed any health problem that could be conclusively tied to intrauterine chemotherapy exposure.
Her experience stresses several key factors that must be considered in this situation. Her patients received chemotherapy at a mean of 20 weeks’ gestation – safely outside the critical early period. Only two women received chemotherapy before 10 weeks; both were treated before they knew they were pregnant. Both children born of these pregnancies were considered well. One with intrauterine exposure to cytarabine was developmentally normal at age 7 years. The other, who was exposed to oxaliplatin and capecitabine, was normal at age 2 years.
Treatment also was stopped a mean of 40 days before delivery, to allow the mother’s bone marrow to fully recover before giving birth.
A second U.S. study was reported at the 2011 meeting of the American Society of Clinical Oncology. A poster by Dr. Jennifer Litton and her colleagues examined physiological outcomes in 81 children exposed to chemotherapy for maternal breast cancer. The mothers had taken a standardized chemotherapy regimen of 5-fluorouracil, doxorubicin and cyclophosphamide (FAC) given during the second and third trimesters (J. Clin. Oncol. 2011;29[May 20 suppl.]:abstract 1099).
One child was born with Down syndrome, one with a club foot, and one with ureteral reflux. Three parents reported language delay in later follow-up surveys. Other reported health issues included 15 children with allergies and/or eczema, 2 with asthma, and 1 with absence seizures.
Dr. Litton, a breast oncologist at the University of Texas M.D. Anderson Cancer Center in Houston, also cowrote a 2010 review of breast cancer treatment in pregnancy, in which she discusses maternal and fetal outcomes from several cohorts, and the possible impact of intrauterine exposure to a variety of chemotherapy agents (Oncologist 2010;15:1238-47).
Risks Vary With Cancer Type
Breast cancer during pregnancy may be the simplest to treat. If the cancer is caught very early, it may be reasonable to delay treatment until the fetus has passed the critical first trimester, waiting until organs are formed and the risk of chemically induced damage is reduced, Dr. Temkin said. "It’s safe to do breast surgery during pregnancy and it’s safe to give chemotherapy after the first trimester."
But physicians can miss a new breast tumor during a prenatal exam, so some present at a more advanced stage, according to Dr. Amant, who is also the lead author of the Lancet’s breast cancer report (Lancet 2012;379:570-9).
Infiltrating ductal adenocarcinomas account for more than 70% of the breast cancers diagnosed during pregnancy. These can be aggressive, said Dr. Amant. Estrogen receptor status is probably no different in pregnant and nonpregnant women.
If the tumor is discovered early and is pathologically favorable, chemotherapy probably can be delayed until 14 weeks’ gestation, allowing nearly complete fetal organogenesis without worsening the mother’s outcome. Women also may elect an early termination if the pathology is unfavorable, or for other personal reasons, Dr. Temkin said. "I think a lot of it depends on when the cancer is diagnosed. Patients of mine who already have a diagnosis and then become pregnant almost always elect to terminate. But if the cancer is discovered when the pregnancy is farther along, most will continue, especially if the woman is highly emotionally invested," she noted.
Tougher Cancers, Tougher Choices
Treating gynecologic cancers during pregnancy often comes down to a choice between the mother’s health and maintenance of the pregnancy, Dr. Temkin said. "The standard of care for ovarian cancers is surgery or radiation to the pelvis, where the fetus is. Cervical cancer is treated with a hysterectomy or radiation, and neither treatment is compatible with keeping a pregnancy. Neoadjuvant therapy is not considered standard of care for these tumors. These are complex decisions for the patient: ‘Do I accept a different treatment [that might not be as effective] or maintain the pregnancy?’ "
In early cervical cancers without nodal spread, the most common tactic is close observation with periodic imaging to rule out spread; therapy is given after delivery, Dr. Phillippe Morice wrote in the Lancet section’s review on gynecologic malignancies (Lancet 2012;379:558-69).
"Delayed treatment until fetal maturation for patients with stage IA disease has an excellent prognosis and is now the standard of care," wrote Dr. Morice of the Institut de Cancérologie Gustave-Roussy in Villejuif, France.
Locally advanced disease is often not compatible with pregnancy. "The main treatment choice is either neoadjuvant chemotherapy or chemotherapy and radiotherapy. In pregnant patients, this approach means that the pregnancy must be ended before the initiation of therapy, but in exceptional cases in which surgery to end the pregnancy is not technically feasible ([that is], a bulky cervical tumor), radiation therapy can be delivered with the fetus in utero, resulting in a spontaneous abortion in about 3 weeks," he wrote.
Ovarian tumors can be surgically staged and – if it is of low malignant potential – can be laparoscopically removed, usually without endangering the pregnancy. Large tumors or those with aggressive pathology, like epithelial tumors, are much more difficult. Advanced or large tumors often have uterine and pelvic involvement, and treatment usually means a hysterectomy.
The literature contains reports of a very few women who have undergone chemotherapy to control peritoneal spread while keeping a pregnancy. However, despite giving birth to normally developed children, a number of these women died from recurrent disease, Dr. Morice noted.
Hematologic Cancers: True Emergency
Cancers of the blood are rare in pregnancy, occurring in only 1 of every 6,000. But when they do occur, they can be devastating, Dr. Benjamin Brenner wrote in the special series (Lancet 2012;379:580-7).
Pregnant patients with Hodgkin’s lymphoma generally do as well as their nonpregnant counterparts and can receive the same chemotherapy regimens, observing the first-trimester delay to favor the fetus.
Those who present with non-Hodgkin’s lymphoma are likely to have a very poor outlook. This disease is very rare in pregnant women, and symptoms can overlap with Hodgkin’s. Those factors, combined with a desire to avoid imaging, can delay diagnosis until the cancer is more advanced, said Dr. Brenner of the Rambam Health Care Campus, Haifa, Israel.
Acute leukemia is also rare, but demands urgent attention regardless of gestational stage, Dr. Brenner warned. "Patients diagnosed with acute leukemia during the first trimester are recommended to terminate the pregnancy, in view of the high risk of toxic effects on the fetus and mother, along with the expected need for further intensive treatment including stem-cell transplantation, which is absolutely contraindicated during gestation."
Talking It Out
Despite the emerging positive evidence, treating cancer during pregnancy can be a tough sell, Dr. Amant said. "Women have been told over and over to avoid taking so much as an aspirin. It’s very difficult to convince them that a fetus can not only survive a mother’s cancer treatment, but have a good chance of developing normally."
The stress of a cancer diagnosis during a desired pregnancy is very hard on patients, Dr. Temkin added. "Pregnancy is a time when many women come to grips with their own mortality as well as that of giving new life. Adding a diagnosis of cancer of top of that – especially in the face of a much-desired pregnancy – can be devastating."
These women are faced with two options: terminate the pregnancy and concentrate on their own treatment, or continue the pregnancy knowing that their unborn child will be exposed to the possible risks of radiation, chemotherapy, and surgery. Either option can "inflict terrible guilt on a pregnant woman. We can try to minimize that to some degree, but it’s important to know from the outset that what is the right solution for one patient is not right for the next."
Connecting with other women who have experienced the same situation can be of immense value, Dr. Cardonick said. She participates in an online support group called "Hope for Two."
The organization’s main goal is to link new patients with survivors who can help educate them as well as lend emotional support. Patients call in or fill out a secure online request for a personal match-up with a survivor, who is often a woman who has had the same type of cancer.
The website also contains links to news and medical articles, books, and financial assistance sources, and allows new patients to securely contact Dr. Cardonick’s pregnancy registry. "We keep in touch with the baby’s pediatrician and the mom every year, to see how things are going and [to] collect information," she said. "The best way to treat these women in the future depends on the information we continue to gather in the present."
None of the researchers interviewed for this article had any relevant financial disclosures. Dr. Litton noted that she had no financial disclosures for her 2011 ASCO poster.
Emerging data on pregnancy and cancer can now help women and their doctors chart a safer course between effective treatment and protecting the developing fetus.
Two registries – one in the United States and another in Europe – agree: It’s not only possible to save a pregnancy in many situations, but children born to these women appear to be largely unaffected by in utero chemotherapy exposure. The combined studies followed more than 200 exposed children for up to 18 years; neither one found any elevated risk of congenital anomaly or any kind of cognitive or developmental delay.
"This is practice-changing information," Dr. Frédéric Amant, primary author on the European paper, said in an interview. "Until now, physicians were reluctant to administer chemotherapy and usually opted for termination, or at least for a delay in treatment or premature delivery in order to get treatment going," he said.
Dr. Amant’s study leads off a special section on cancer in pregnancy, published in the March issue of Lancet Oncology. The paper examined evidence that both supports and questions the clinical wisdom of treating a disease that threatens two very different patients – an adult woman and the fetus she carries.
Every case is different, depending on the type of cancer, its grade and potential aggressiveness, the stage of pregnancy, and the woman’s own desires, said Dr. Elyce Cardonick, an ob.gyn. at Cooper University Hospital in Camden, N.J., and the lead investigator of the Pregnancy and Cancer Registry.
"With solid tumors you usually have time to do the surgery, get the pathologic diagnosis, and let the patient recover. But if there is leukemia, for instance, you have to move faster. The first question should be ‘Could we delay treatment for this patient if she was not pregnant?’ I don’t want to limit their treatment, but at the same time, it’s true that they might not be getting the most up-to-date treatment – the newest agent on the block – because you would want to go with something there is at least some experience with. But this doesn’t necessarily mean they are going to do worse."
Cancer occurs in about 1 in 1,000 pregnancies, said Dr. Sarah Temkin, a gynecologic oncologist at the University of Maryland, Baltimore. Many of her patients are referred after a routine screening during early pregnancy finds something abnormal, or when a woman with an existing cancer is incidentally found to be pregnant. But signs that might raise a red flag in other situations don’t necessarily alert physicians to danger in pregnant women, she said in an interview. Pregnancy could obfuscate some symptoms, which might be further downplayed in light of a mother’s relatively young age. Breast cancer is a prime example.
"There are two problems, especially for breast cancers, which are the most common ones we see in pregnancy. First, a woman’s breasts are changing anyway during that time. Breast cancer is so rare in women of earlier childbearing age that both the patient and the doctor tend to disregard any new lumps and bumps."
But despite its rarity, cancer in all forms appears to be increasing among pregnant women, she said. This is probably a direct relation to age. "Cancer rates increase with increasing age, and women are becoming mothers at older and older ages."
When cancer coincides with pregnancy, Dr. Temkin views the mother’s health as paramount. "The mother is the person with cancer, and she deserves whatever the standard of care is for that particular cancer – the best care that would be offered to her if she was not pregnant."
Chemotherapy and Fetal Outcomes
To examine long-term neurodevelopmental risks associated with maternal cancer treatment, Dr. Amant, a gynecologic oncologist at the Leuven (Belgium) Cancer Institute, and his colleagues, are following 70 children from the age of 18 months until 18 years. In the newly published interim analysis, the mean follow-up time is 22 months. All the children had intrauterine exposure to chemotherapy, radiation, oncologic surgery, or combinations of these.
The analysis, which also appeared in Lancet Oncology’s special issue, includes data on all the children, including 18 who are now older than 9 years (Lancet Oncol. 2012;13:256-64).
The children – 68 singletons and one set of twins – were born from pregnancies exposed to a total of 236 chemotherapy cycles. Exposure varied by the mother’s cancer type and its stage at diagnosis. In all, 34 mothers were treated with only chemotherapy, 27 had chemotherapy and surgery, 1 received chemotherapy and radiation, and 6 women were treated with all three modalities. Most of the children also had in utero exposure to multiple imaging studies, including MRI, ultrasound, echocardiography, CT, and mammography. Chemotherapy regimens included doxorubicin, epirubicin, idarubicin and daunorubicin.
Fetuses also were exposed to a variety of other drugs, including antibiotics, antiemetics, pain medications, colony stimulating factors, and anxiolytics.
Breast cancer was the most common disease type (35). There were 18 cases of hematologic cancers, 6 ovarian cancers, 4 cervical cancers, and 1 each of basal cell carcinoma, brain tumor, Ewing’s sarcoma, colorectal cancer, and nasopharyngeal cancer.
The mean gestational age at cancer diagnosis was 18 weeks, although fetuses ranged in age from 2 to 33 weeks when their mothers were diagnosed. About a third of the babies (23) were born at term.
Seven were born at 28-32 weeks, nine at 32-34 weeks, and 31 at 34-37 weeks. Weight for gestational age was below the 10th percentile in 14 children (21%).
Seven congenital anomalies were found in the group of 70 children (10%) – a rate not significantly different from that in the background population. There were only two major malformations, for a 2.9% rate. Malformations included the following:
• Hip subluxation, pectus excavatum and hemangioma, associated with chemotherapy only.
• Bilateral partial syndactyly, associated with chemotherapy plus radiotherapy.
• Bilateral small protuberance on one finger, and rectal atresia, associated with chemotherapy plus surgery.
• Bilateral double cartilage ring in a child exposed to chemotherapy, surgery and radiotherapy.
None of the children showed any congenital cardiac issues.
All of the children showed neurocognitive development that was within normal range, except for the set of twins, who were delivered by cesarean section at 32.5 weeks after a preterm premature rupture of membranes. These children were so delayed that they were not able to complete cognitive testing. Their mother developed an acute myeloid leukemia – one of the true "emergency" cancers diagnosed in pregnancy, Dr. Amant said. The babies had been exposed to idarubicin and cytosine arabinoside at 15.5, 21.5, 26.5, and 31.5 weeks’ gestation.
The boy, who weighed 1,640 g at birth, had a normal karyotype but, at 3 years, brain imaging showed a unilateral polymicrogyria in the left perisylvian area. He showed an early developmental delay; at age 9 years, he had the developmental capacity of a 12-month old.
The girl, who weighed 1,390 g at birth, also had an early developmental delay, but at age 9 years she attended school with support. Her parents refused brain imaging.
"The other 68 children did well," Dr. Amant said. "This doesn’t mean they were all normal in every way, but in any population you will see learning and developmental delay issues. We think the problem for the delayed children was not related to chemotherapy exposure, but more likely to their prematurity."
Dr. Amant saw a direct correlation between gestational age and intelligence quota. "When we controlled for age, gender, and country of birth, we found that the IQ score increased by almost 12 points for each additional month of gestation."
The U.S. Experience
Dr. Cardonick has found similar results. Her registry now contains information on 280 women who were enrolled over a 13-year period. The children born from these pregnancies have been assessed annually since birth. It also includes 70 controls – children whose mothers had cancer but who were not exposed to chemotherapy.
She published interim results of the registry in 2010 (Cancer J. 2010;16:76-82). At that point, it contained information on 231 women and 157 children. The most common malignancy was breast cancer (128); the mean gestational age at diagnosis was 13 weeks. About a third of the women (54) were advised to terminate their pregnancy; 12 did so.
Among those who continued both pregnancy and treatment, neonatal outcomes were generally good. There were nine premature deliveries related to preterm labor or premature rupture of membranes. The congenital anomaly rate born was 4%, which was in line with the normal background rate and slightly lower than that seen in Dr. Amant’s cohort.
The infants’ mean birth weight was 2,647 g, which was significantly less than the mean 2,873 g in the control group, but probably clinically irrelevant, Dr. Cardonick wrote in the paper.
She continues to follow these children annually. At this point, the children are a mean 5 years old; her oldest subject is 14 years. So far, the rate of neurocognitive issues in the group is no different than would be observed in any other group, and none of the children has developed any health problem that could be conclusively tied to intrauterine chemotherapy exposure.
Her experience stresses several key factors that must be considered in this situation. Her patients received chemotherapy at a mean of 20 weeks’ gestation – safely outside the critical early period. Only two women received chemotherapy before 10 weeks; both were treated before they knew they were pregnant. Both children born of these pregnancies were considered well. One with intrauterine exposure to cytarabine was developmentally normal at age 7 years. The other, who was exposed to oxaliplatin and capecitabine, was normal at age 2 years.
Treatment also was stopped a mean of 40 days before delivery, to allow the mother’s bone marrow to fully recover before giving birth.
A second U.S. study was reported at the 2011 meeting of the American Society of Clinical Oncology. A poster by Dr. Jennifer Litton and her colleagues examined physiological outcomes in 81 children exposed to chemotherapy for maternal breast cancer. The mothers had taken a standardized chemotherapy regimen of 5-fluorouracil, doxorubicin and cyclophosphamide (FAC) given during the second and third trimesters (J. Clin. Oncol. 2011;29[May 20 suppl.]:abstract 1099).
One child was born with Down syndrome, one with a club foot, and one with ureteral reflux. Three parents reported language delay in later follow-up surveys. Other reported health issues included 15 children with allergies and/or eczema, 2 with asthma, and 1 with absence seizures.
Dr. Litton, a breast oncologist at the University of Texas M.D. Anderson Cancer Center in Houston, also cowrote a 2010 review of breast cancer treatment in pregnancy, in which she discusses maternal and fetal outcomes from several cohorts, and the possible impact of intrauterine exposure to a variety of chemotherapy agents (Oncologist 2010;15:1238-47).
Risks Vary With Cancer Type
Breast cancer during pregnancy may be the simplest to treat. If the cancer is caught very early, it may be reasonable to delay treatment until the fetus has passed the critical first trimester, waiting until organs are formed and the risk of chemically induced damage is reduced, Dr. Temkin said. "It’s safe to do breast surgery during pregnancy and it’s safe to give chemotherapy after the first trimester."
But physicians can miss a new breast tumor during a prenatal exam, so some present at a more advanced stage, according to Dr. Amant, who is also the lead author of the Lancet’s breast cancer report (Lancet 2012;379:570-9).
Infiltrating ductal adenocarcinomas account for more than 70% of the breast cancers diagnosed during pregnancy. These can be aggressive, said Dr. Amant. Estrogen receptor status is probably no different in pregnant and nonpregnant women.
If the tumor is discovered early and is pathologically favorable, chemotherapy probably can be delayed until 14 weeks’ gestation, allowing nearly complete fetal organogenesis without worsening the mother’s outcome. Women also may elect an early termination if the pathology is unfavorable, or for other personal reasons, Dr. Temkin said. "I think a lot of it depends on when the cancer is diagnosed. Patients of mine who already have a diagnosis and then become pregnant almost always elect to terminate. But if the cancer is discovered when the pregnancy is farther along, most will continue, especially if the woman is highly emotionally invested," she noted.
Tougher Cancers, Tougher Choices
Treating gynecologic cancers during pregnancy often comes down to a choice between the mother’s health and maintenance of the pregnancy, Dr. Temkin said. "The standard of care for ovarian cancers is surgery or radiation to the pelvis, where the fetus is. Cervical cancer is treated with a hysterectomy or radiation, and neither treatment is compatible with keeping a pregnancy. Neoadjuvant therapy is not considered standard of care for these tumors. These are complex decisions for the patient: ‘Do I accept a different treatment [that might not be as effective] or maintain the pregnancy?’ "
In early cervical cancers without nodal spread, the most common tactic is close observation with periodic imaging to rule out spread; therapy is given after delivery, Dr. Phillippe Morice wrote in the Lancet section’s review on gynecologic malignancies (Lancet 2012;379:558-69).
"Delayed treatment until fetal maturation for patients with stage IA disease has an excellent prognosis and is now the standard of care," wrote Dr. Morice of the Institut de Cancérologie Gustave-Roussy in Villejuif, France.
Locally advanced disease is often not compatible with pregnancy. "The main treatment choice is either neoadjuvant chemotherapy or chemotherapy and radiotherapy. In pregnant patients, this approach means that the pregnancy must be ended before the initiation of therapy, but in exceptional cases in which surgery to end the pregnancy is not technically feasible ([that is], a bulky cervical tumor), radiation therapy can be delivered with the fetus in utero, resulting in a spontaneous abortion in about 3 weeks," he wrote.
Ovarian tumors can be surgically staged and – if it is of low malignant potential – can be laparoscopically removed, usually without endangering the pregnancy. Large tumors or those with aggressive pathology, like epithelial tumors, are much more difficult. Advanced or large tumors often have uterine and pelvic involvement, and treatment usually means a hysterectomy.
The literature contains reports of a very few women who have undergone chemotherapy to control peritoneal spread while keeping a pregnancy. However, despite giving birth to normally developed children, a number of these women died from recurrent disease, Dr. Morice noted.
Hematologic Cancers: True Emergency
Cancers of the blood are rare in pregnancy, occurring in only 1 of every 6,000. But when they do occur, they can be devastating, Dr. Benjamin Brenner wrote in the special series (Lancet 2012;379:580-7).
Pregnant patients with Hodgkin’s lymphoma generally do as well as their nonpregnant counterparts and can receive the same chemotherapy regimens, observing the first-trimester delay to favor the fetus.
Those who present with non-Hodgkin’s lymphoma are likely to have a very poor outlook. This disease is very rare in pregnant women, and symptoms can overlap with Hodgkin’s. Those factors, combined with a desire to avoid imaging, can delay diagnosis until the cancer is more advanced, said Dr. Brenner of the Rambam Health Care Campus, Haifa, Israel.
Acute leukemia is also rare, but demands urgent attention regardless of gestational stage, Dr. Brenner warned. "Patients diagnosed with acute leukemia during the first trimester are recommended to terminate the pregnancy, in view of the high risk of toxic effects on the fetus and mother, along with the expected need for further intensive treatment including stem-cell transplantation, which is absolutely contraindicated during gestation."
Talking It Out
Despite the emerging positive evidence, treating cancer during pregnancy can be a tough sell, Dr. Amant said. "Women have been told over and over to avoid taking so much as an aspirin. It’s very difficult to convince them that a fetus can not only survive a mother’s cancer treatment, but have a good chance of developing normally."
The stress of a cancer diagnosis during a desired pregnancy is very hard on patients, Dr. Temkin added. "Pregnancy is a time when many women come to grips with their own mortality as well as that of giving new life. Adding a diagnosis of cancer of top of that – especially in the face of a much-desired pregnancy – can be devastating."
These women are faced with two options: terminate the pregnancy and concentrate on their own treatment, or continue the pregnancy knowing that their unborn child will be exposed to the possible risks of radiation, chemotherapy, and surgery. Either option can "inflict terrible guilt on a pregnant woman. We can try to minimize that to some degree, but it’s important to know from the outset that what is the right solution for one patient is not right for the next."
Connecting with other women who have experienced the same situation can be of immense value, Dr. Cardonick said. She participates in an online support group called "Hope for Two."
The organization’s main goal is to link new patients with survivors who can help educate them as well as lend emotional support. Patients call in or fill out a secure online request for a personal match-up with a survivor, who is often a woman who has had the same type of cancer.
The website also contains links to news and medical articles, books, and financial assistance sources, and allows new patients to securely contact Dr. Cardonick’s pregnancy registry. "We keep in touch with the baby’s pediatrician and the mom every year, to see how things are going and [to] collect information," she said. "The best way to treat these women in the future depends on the information we continue to gather in the present."
None of the researchers interviewed for this article had any relevant financial disclosures. Dr. Litton noted that she had no financial disclosures for her 2011 ASCO poster.
Emerging data on pregnancy and cancer can now help women and their doctors chart a safer course between effective treatment and protecting the developing fetus.
Two registries – one in the United States and another in Europe – agree: It’s not only possible to save a pregnancy in many situations, but children born to these women appear to be largely unaffected by in utero chemotherapy exposure. The combined studies followed more than 200 exposed children for up to 18 years; neither one found any elevated risk of congenital anomaly or any kind of cognitive or developmental delay.
"This is practice-changing information," Dr. Frédéric Amant, primary author on the European paper, said in an interview. "Until now, physicians were reluctant to administer chemotherapy and usually opted for termination, or at least for a delay in treatment or premature delivery in order to get treatment going," he said.
Dr. Amant’s study leads off a special section on cancer in pregnancy, published in the March issue of Lancet Oncology. The paper examined evidence that both supports and questions the clinical wisdom of treating a disease that threatens two very different patients – an adult woman and the fetus she carries.
Every case is different, depending on the type of cancer, its grade and potential aggressiveness, the stage of pregnancy, and the woman’s own desires, said Dr. Elyce Cardonick, an ob.gyn. at Cooper University Hospital in Camden, N.J., and the lead investigator of the Pregnancy and Cancer Registry.
"With solid tumors you usually have time to do the surgery, get the pathologic diagnosis, and let the patient recover. But if there is leukemia, for instance, you have to move faster. The first question should be ‘Could we delay treatment for this patient if she was not pregnant?’ I don’t want to limit their treatment, but at the same time, it’s true that they might not be getting the most up-to-date treatment – the newest agent on the block – because you would want to go with something there is at least some experience with. But this doesn’t necessarily mean they are going to do worse."
Cancer occurs in about 1 in 1,000 pregnancies, said Dr. Sarah Temkin, a gynecologic oncologist at the University of Maryland, Baltimore. Many of her patients are referred after a routine screening during early pregnancy finds something abnormal, or when a woman with an existing cancer is incidentally found to be pregnant. But signs that might raise a red flag in other situations don’t necessarily alert physicians to danger in pregnant women, she said in an interview. Pregnancy could obfuscate some symptoms, which might be further downplayed in light of a mother’s relatively young age. Breast cancer is a prime example.
"There are two problems, especially for breast cancers, which are the most common ones we see in pregnancy. First, a woman’s breasts are changing anyway during that time. Breast cancer is so rare in women of earlier childbearing age that both the patient and the doctor tend to disregard any new lumps and bumps."
But despite its rarity, cancer in all forms appears to be increasing among pregnant women, she said. This is probably a direct relation to age. "Cancer rates increase with increasing age, and women are becoming mothers at older and older ages."
When cancer coincides with pregnancy, Dr. Temkin views the mother’s health as paramount. "The mother is the person with cancer, and she deserves whatever the standard of care is for that particular cancer – the best care that would be offered to her if she was not pregnant."
Chemotherapy and Fetal Outcomes
To examine long-term neurodevelopmental risks associated with maternal cancer treatment, Dr. Amant, a gynecologic oncologist at the Leuven (Belgium) Cancer Institute, and his colleagues, are following 70 children from the age of 18 months until 18 years. In the newly published interim analysis, the mean follow-up time is 22 months. All the children had intrauterine exposure to chemotherapy, radiation, oncologic surgery, or combinations of these.
The analysis, which also appeared in Lancet Oncology’s special issue, includes data on all the children, including 18 who are now older than 9 years (Lancet Oncol. 2012;13:256-64).
The children – 68 singletons and one set of twins – were born from pregnancies exposed to a total of 236 chemotherapy cycles. Exposure varied by the mother’s cancer type and its stage at diagnosis. In all, 34 mothers were treated with only chemotherapy, 27 had chemotherapy and surgery, 1 received chemotherapy and radiation, and 6 women were treated with all three modalities. Most of the children also had in utero exposure to multiple imaging studies, including MRI, ultrasound, echocardiography, CT, and mammography. Chemotherapy regimens included doxorubicin, epirubicin, idarubicin and daunorubicin.
Fetuses also were exposed to a variety of other drugs, including antibiotics, antiemetics, pain medications, colony stimulating factors, and anxiolytics.
Breast cancer was the most common disease type (35). There were 18 cases of hematologic cancers, 6 ovarian cancers, 4 cervical cancers, and 1 each of basal cell carcinoma, brain tumor, Ewing’s sarcoma, colorectal cancer, and nasopharyngeal cancer.
The mean gestational age at cancer diagnosis was 18 weeks, although fetuses ranged in age from 2 to 33 weeks when their mothers were diagnosed. About a third of the babies (23) were born at term.
Seven were born at 28-32 weeks, nine at 32-34 weeks, and 31 at 34-37 weeks. Weight for gestational age was below the 10th percentile in 14 children (21%).
Seven congenital anomalies were found in the group of 70 children (10%) – a rate not significantly different from that in the background population. There were only two major malformations, for a 2.9% rate. Malformations included the following:
• Hip subluxation, pectus excavatum and hemangioma, associated with chemotherapy only.
• Bilateral partial syndactyly, associated with chemotherapy plus radiotherapy.
• Bilateral small protuberance on one finger, and rectal atresia, associated with chemotherapy plus surgery.
• Bilateral double cartilage ring in a child exposed to chemotherapy, surgery and radiotherapy.
None of the children showed any congenital cardiac issues.
All of the children showed neurocognitive development that was within normal range, except for the set of twins, who were delivered by cesarean section at 32.5 weeks after a preterm premature rupture of membranes. These children were so delayed that they were not able to complete cognitive testing. Their mother developed an acute myeloid leukemia – one of the true "emergency" cancers diagnosed in pregnancy, Dr. Amant said. The babies had been exposed to idarubicin and cytosine arabinoside at 15.5, 21.5, 26.5, and 31.5 weeks’ gestation.
The boy, who weighed 1,640 g at birth, had a normal karyotype but, at 3 years, brain imaging showed a unilateral polymicrogyria in the left perisylvian area. He showed an early developmental delay; at age 9 years, he had the developmental capacity of a 12-month old.
The girl, who weighed 1,390 g at birth, also had an early developmental delay, but at age 9 years she attended school with support. Her parents refused brain imaging.
"The other 68 children did well," Dr. Amant said. "This doesn’t mean they were all normal in every way, but in any population you will see learning and developmental delay issues. We think the problem for the delayed children was not related to chemotherapy exposure, but more likely to their prematurity."
Dr. Amant saw a direct correlation between gestational age and intelligence quota. "When we controlled for age, gender, and country of birth, we found that the IQ score increased by almost 12 points for each additional month of gestation."
The U.S. Experience
Dr. Cardonick has found similar results. Her registry now contains information on 280 women who were enrolled over a 13-year period. The children born from these pregnancies have been assessed annually since birth. It also includes 70 controls – children whose mothers had cancer but who were not exposed to chemotherapy.
She published interim results of the registry in 2010 (Cancer J. 2010;16:76-82). At that point, it contained information on 231 women and 157 children. The most common malignancy was breast cancer (128); the mean gestational age at diagnosis was 13 weeks. About a third of the women (54) were advised to terminate their pregnancy; 12 did so.
Among those who continued both pregnancy and treatment, neonatal outcomes were generally good. There were nine premature deliveries related to preterm labor or premature rupture of membranes. The congenital anomaly rate born was 4%, which was in line with the normal background rate and slightly lower than that seen in Dr. Amant’s cohort.
The infants’ mean birth weight was 2,647 g, which was significantly less than the mean 2,873 g in the control group, but probably clinically irrelevant, Dr. Cardonick wrote in the paper.
She continues to follow these children annually. At this point, the children are a mean 5 years old; her oldest subject is 14 years. So far, the rate of neurocognitive issues in the group is no different than would be observed in any other group, and none of the children has developed any health problem that could be conclusively tied to intrauterine chemotherapy exposure.
Her experience stresses several key factors that must be considered in this situation. Her patients received chemotherapy at a mean of 20 weeks’ gestation – safely outside the critical early period. Only two women received chemotherapy before 10 weeks; both were treated before they knew they were pregnant. Both children born of these pregnancies were considered well. One with intrauterine exposure to cytarabine was developmentally normal at age 7 years. The other, who was exposed to oxaliplatin and capecitabine, was normal at age 2 years.
Treatment also was stopped a mean of 40 days before delivery, to allow the mother’s bone marrow to fully recover before giving birth.
A second U.S. study was reported at the 2011 meeting of the American Society of Clinical Oncology. A poster by Dr. Jennifer Litton and her colleagues examined physiological outcomes in 81 children exposed to chemotherapy for maternal breast cancer. The mothers had taken a standardized chemotherapy regimen of 5-fluorouracil, doxorubicin and cyclophosphamide (FAC) given during the second and third trimesters (J. Clin. Oncol. 2011;29[May 20 suppl.]:abstract 1099).
One child was born with Down syndrome, one with a club foot, and one with ureteral reflux. Three parents reported language delay in later follow-up surveys. Other reported health issues included 15 children with allergies and/or eczema, 2 with asthma, and 1 with absence seizures.
Dr. Litton, a breast oncologist at the University of Texas M.D. Anderson Cancer Center in Houston, also cowrote a 2010 review of breast cancer treatment in pregnancy, in which she discusses maternal and fetal outcomes from several cohorts, and the possible impact of intrauterine exposure to a variety of chemotherapy agents (Oncologist 2010;15:1238-47).
Risks Vary With Cancer Type
Breast cancer during pregnancy may be the simplest to treat. If the cancer is caught very early, it may be reasonable to delay treatment until the fetus has passed the critical first trimester, waiting until organs are formed and the risk of chemically induced damage is reduced, Dr. Temkin said. "It’s safe to do breast surgery during pregnancy and it’s safe to give chemotherapy after the first trimester."
But physicians can miss a new breast tumor during a prenatal exam, so some present at a more advanced stage, according to Dr. Amant, who is also the lead author of the Lancet’s breast cancer report (Lancet 2012;379:570-9).
Infiltrating ductal adenocarcinomas account for more than 70% of the breast cancers diagnosed during pregnancy. These can be aggressive, said Dr. Amant. Estrogen receptor status is probably no different in pregnant and nonpregnant women.
If the tumor is discovered early and is pathologically favorable, chemotherapy probably can be delayed until 14 weeks’ gestation, allowing nearly complete fetal organogenesis without worsening the mother’s outcome. Women also may elect an early termination if the pathology is unfavorable, or for other personal reasons, Dr. Temkin said. "I think a lot of it depends on when the cancer is diagnosed. Patients of mine who already have a diagnosis and then become pregnant almost always elect to terminate. But if the cancer is discovered when the pregnancy is farther along, most will continue, especially if the woman is highly emotionally invested," she noted.
Tougher Cancers, Tougher Choices
Treating gynecologic cancers during pregnancy often comes down to a choice between the mother’s health and maintenance of the pregnancy, Dr. Temkin said. "The standard of care for ovarian cancers is surgery or radiation to the pelvis, where the fetus is. Cervical cancer is treated with a hysterectomy or radiation, and neither treatment is compatible with keeping a pregnancy. Neoadjuvant therapy is not considered standard of care for these tumors. These are complex decisions for the patient: ‘Do I accept a different treatment [that might not be as effective] or maintain the pregnancy?’ "
In early cervical cancers without nodal spread, the most common tactic is close observation with periodic imaging to rule out spread; therapy is given after delivery, Dr. Phillippe Morice wrote in the Lancet section’s review on gynecologic malignancies (Lancet 2012;379:558-69).
"Delayed treatment until fetal maturation for patients with stage IA disease has an excellent prognosis and is now the standard of care," wrote Dr. Morice of the Institut de Cancérologie Gustave-Roussy in Villejuif, France.
Locally advanced disease is often not compatible with pregnancy. "The main treatment choice is either neoadjuvant chemotherapy or chemotherapy and radiotherapy. In pregnant patients, this approach means that the pregnancy must be ended before the initiation of therapy, but in exceptional cases in which surgery to end the pregnancy is not technically feasible ([that is], a bulky cervical tumor), radiation therapy can be delivered with the fetus in utero, resulting in a spontaneous abortion in about 3 weeks," he wrote.
Ovarian tumors can be surgically staged and – if it is of low malignant potential – can be laparoscopically removed, usually without endangering the pregnancy. Large tumors or those with aggressive pathology, like epithelial tumors, are much more difficult. Advanced or large tumors often have uterine and pelvic involvement, and treatment usually means a hysterectomy.
The literature contains reports of a very few women who have undergone chemotherapy to control peritoneal spread while keeping a pregnancy. However, despite giving birth to normally developed children, a number of these women died from recurrent disease, Dr. Morice noted.
Hematologic Cancers: True Emergency
Cancers of the blood are rare in pregnancy, occurring in only 1 of every 6,000. But when they do occur, they can be devastating, Dr. Benjamin Brenner wrote in the special series (Lancet 2012;379:580-7).
Pregnant patients with Hodgkin’s lymphoma generally do as well as their nonpregnant counterparts and can receive the same chemotherapy regimens, observing the first-trimester delay to favor the fetus.
Those who present with non-Hodgkin’s lymphoma are likely to have a very poor outlook. This disease is very rare in pregnant women, and symptoms can overlap with Hodgkin’s. Those factors, combined with a desire to avoid imaging, can delay diagnosis until the cancer is more advanced, said Dr. Brenner of the Rambam Health Care Campus, Haifa, Israel.
Acute leukemia is also rare, but demands urgent attention regardless of gestational stage, Dr. Brenner warned. "Patients diagnosed with acute leukemia during the first trimester are recommended to terminate the pregnancy, in view of the high risk of toxic effects on the fetus and mother, along with the expected need for further intensive treatment including stem-cell transplantation, which is absolutely contraindicated during gestation."
Talking It Out
Despite the emerging positive evidence, treating cancer during pregnancy can be a tough sell, Dr. Amant said. "Women have been told over and over to avoid taking so much as an aspirin. It’s very difficult to convince them that a fetus can not only survive a mother’s cancer treatment, but have a good chance of developing normally."
The stress of a cancer diagnosis during a desired pregnancy is very hard on patients, Dr. Temkin added. "Pregnancy is a time when many women come to grips with their own mortality as well as that of giving new life. Adding a diagnosis of cancer of top of that – especially in the face of a much-desired pregnancy – can be devastating."
These women are faced with two options: terminate the pregnancy and concentrate on their own treatment, or continue the pregnancy knowing that their unborn child will be exposed to the possible risks of radiation, chemotherapy, and surgery. Either option can "inflict terrible guilt on a pregnant woman. We can try to minimize that to some degree, but it’s important to know from the outset that what is the right solution for one patient is not right for the next."
Connecting with other women who have experienced the same situation can be of immense value, Dr. Cardonick said. She participates in an online support group called "Hope for Two."
The organization’s main goal is to link new patients with survivors who can help educate them as well as lend emotional support. Patients call in or fill out a secure online request for a personal match-up with a survivor, who is often a woman who has had the same type of cancer.
The website also contains links to news and medical articles, books, and financial assistance sources, and allows new patients to securely contact Dr. Cardonick’s pregnancy registry. "We keep in touch with the baby’s pediatrician and the mom every year, to see how things are going and [to] collect information," she said. "The best way to treat these women in the future depends on the information we continue to gather in the present."
None of the researchers interviewed for this article had any relevant financial disclosures. Dr. Litton noted that she had no financial disclosures for her 2011 ASCO poster.
Consider Chemotherapy after Induction Failure for Childhood Leukemia
Allogeneic stem-cell transplantation is not always the best option when pediatric acute lymphoblastic leukemia fails to respond adequately to induction therapy, according to a report in the April 12 issue of the New England Journal of Medicine.
Children who have the precursor B-cell subtype and no other adverse features do better when treated with chemotherapy, investigators report. Those with T-cell leukemia appear to have better outcomes with allogeneic stem-cell transplantation, a common treatment of choice after induction failure.
Eighty percent of children with pediatric acute lymphoblastic leukemia (ALL) can be cured with standard treatments. The small proportion of children in the very-high-risk group that does not respond to induction therapy is much more heterogeneous than clinicians may realize, according to Dr. Martin Schrappe of Schleswig-Holstein University Medical Center, Christian-Albrechts University, Kiel (Germany) and his associates.
The authors pooled the findings of multiple clinical trials performed by 14 cooperative study groups in North America, Europe, and Asia between 1985 and 2000. Based on this observational analysis, ALL with induction failure was found to be a highly varied entity, with different clinical and biologic traits and a wide range of prognoses.
The study assessed outcomes in 44,017 children and adolescents (aged 0-18 years) with newly diagnosed ALL who were enrolled in clinical trials during that interval and were followed for a median of 8.3 years (range, 1.5-22.1 years). A total of 1,041 (2.4%) failed induction therapy, showing persistent leukemic blasts in the bone marrow or at extramedullary sites.
Overall 10-year survival was 32% but varied greatly across the cohort, from 4% to 73%, depending on biological and clinical factors.
Patients with induction failure were much more likely than ALL patients as a whole to have conventional adverse prognostic factors such as a high leukocyte count, older age at disease onset, the BCR-ABL1 gene, and T-cell phenotypes – and these factors conferred an even worse prognosis in this already high-risk population.
"Indeed, the clinical and biologic characteristics of the patients in our study and the course of the disease were similar to those in patients with relapse during receipt of therapy, another group of patients with a highly unfavorable prognosis," the researchers said.
Among patients who eventually achieved a late remission, 10-year survival was significantly higher (48%) than among those who never achieved a remission (14%).
A total of 198 patients underwent hematopoietic stem-cell transplantation and 427 received chemotherapy only. The 10-year survival was 43% with transplantation and 41% without it.
Surprisingly, allogeneic transplantation was shown to be of no benefit in patients younger than 6 years who had precursor B-cell ALL with induction failure and no high-risk features, compared with chemotherapy alone. This finding has "considerable clinical implications, since transplantation is generally considered to be the standard of care for such patients," Dr. Schrappe and his colleagues said (N. Engl. J. Med. 2012;366:1371-81).
In patients aged 6 years and older who had precursor B-cell ALL, a transplant from a matched, related donor appeared to improve outcome, while other types of allogeneic transplants actually worsened outcomes. This was due in part to a high number of transplantation-related deaths in the latter group.
In contrast, allogeneic transplantation appeared to improve outcomes in the subgroup of patients who had T-cell ALL and failed induction therapy.
Patients with high hyperdiploidy (more than 50 chromosomes) showed an excellent outcome, with a 10-year survival rate of 71%. This favorable outcome "may be due to the increased sensitivity of the blast cells to methotrexate and mercaptopurine, drugs that are generally not used during remission induction but are used at high doses after remission," the investigators said.
Patients who carried the genetic aberration ETV6-RUNX1 also had a high 10-year survival of 73%, which is more than double the survival rate in the cohort as a whole.
Survival was lower among patients who had M3 marrow after induction therapy, compared with those who had M1 marrow and extramedullary disease or M2 marrow. Subgroups with the worst outcomes included patients aged 6 years or older who had M3 marrow (10-year survival, 22%) and those of any age who had T-cell ALL and M3 marrow (10-year survival, 19%).
Among infants who had precursor B-cell ALL and did not have a rearrangement of the MLL gene or fusion of the BCR-ABL1 gene, outcomes were similar to those in children aged 1-5 years (10-year survivals of 65% and 63%, respectively). In contrast, infants who had a rearrangement of the MLL gene fared very poorly (10-year survival, 4%) compared with older children who had the same genetic abnormality (10-year survival, 26%).
Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
The study by Dr. Schrappe and colleagues, a "remarkable collaborative effort," demonstrates that "induction failure is not a single entity with a uniform prognosis but rather exhibits biologic and prognostic heterogeneity," said Dr. Karen R. Rabin.
Moreover, the "striking" finding that chemotherapy is superior to stem-cell transplantation in certain subgroups of patients "may substantially affect current practice, since stem-cell transplantation has generally been accepted as the preferred treatment for all cases of induction failure," she said.
Dr. Rabin is with the division of pediatric hematology/oncology at Texas Children’s Cancer Center and Baylor College of Medicine, Houston. She reported no financial conflicts of interest. These remarks were taken from her editorial comment accompanying Dr. Schrappe’s report (N. Engl. J. Med. 2012;366:1445-6).
The study by Dr. Schrappe and colleagues, a "remarkable collaborative effort," demonstrates that "induction failure is not a single entity with a uniform prognosis but rather exhibits biologic and prognostic heterogeneity," said Dr. Karen R. Rabin.
Moreover, the "striking" finding that chemotherapy is superior to stem-cell transplantation in certain subgroups of patients "may substantially affect current practice, since stem-cell transplantation has generally been accepted as the preferred treatment for all cases of induction failure," she said.
Dr. Rabin is with the division of pediatric hematology/oncology at Texas Children’s Cancer Center and Baylor College of Medicine, Houston. She reported no financial conflicts of interest. These remarks were taken from her editorial comment accompanying Dr. Schrappe’s report (N. Engl. J. Med. 2012;366:1445-6).
The study by Dr. Schrappe and colleagues, a "remarkable collaborative effort," demonstrates that "induction failure is not a single entity with a uniform prognosis but rather exhibits biologic and prognostic heterogeneity," said Dr. Karen R. Rabin.
Moreover, the "striking" finding that chemotherapy is superior to stem-cell transplantation in certain subgroups of patients "may substantially affect current practice, since stem-cell transplantation has generally been accepted as the preferred treatment for all cases of induction failure," she said.
Dr. Rabin is with the division of pediatric hematology/oncology at Texas Children’s Cancer Center and Baylor College of Medicine, Houston. She reported no financial conflicts of interest. These remarks were taken from her editorial comment accompanying Dr. Schrappe’s report (N. Engl. J. Med. 2012;366:1445-6).
Allogeneic stem-cell transplantation is not always the best option when pediatric acute lymphoblastic leukemia fails to respond adequately to induction therapy, according to a report in the April 12 issue of the New England Journal of Medicine.
Children who have the precursor B-cell subtype and no other adverse features do better when treated with chemotherapy, investigators report. Those with T-cell leukemia appear to have better outcomes with allogeneic stem-cell transplantation, a common treatment of choice after induction failure.
Eighty percent of children with pediatric acute lymphoblastic leukemia (ALL) can be cured with standard treatments. The small proportion of children in the very-high-risk group that does not respond to induction therapy is much more heterogeneous than clinicians may realize, according to Dr. Martin Schrappe of Schleswig-Holstein University Medical Center, Christian-Albrechts University, Kiel (Germany) and his associates.
The authors pooled the findings of multiple clinical trials performed by 14 cooperative study groups in North America, Europe, and Asia between 1985 and 2000. Based on this observational analysis, ALL with induction failure was found to be a highly varied entity, with different clinical and biologic traits and a wide range of prognoses.
The study assessed outcomes in 44,017 children and adolescents (aged 0-18 years) with newly diagnosed ALL who were enrolled in clinical trials during that interval and were followed for a median of 8.3 years (range, 1.5-22.1 years). A total of 1,041 (2.4%) failed induction therapy, showing persistent leukemic blasts in the bone marrow or at extramedullary sites.
Overall 10-year survival was 32% but varied greatly across the cohort, from 4% to 73%, depending on biological and clinical factors.
Patients with induction failure were much more likely than ALL patients as a whole to have conventional adverse prognostic factors such as a high leukocyte count, older age at disease onset, the BCR-ABL1 gene, and T-cell phenotypes – and these factors conferred an even worse prognosis in this already high-risk population.
"Indeed, the clinical and biologic characteristics of the patients in our study and the course of the disease were similar to those in patients with relapse during receipt of therapy, another group of patients with a highly unfavorable prognosis," the researchers said.
Among patients who eventually achieved a late remission, 10-year survival was significantly higher (48%) than among those who never achieved a remission (14%).
A total of 198 patients underwent hematopoietic stem-cell transplantation and 427 received chemotherapy only. The 10-year survival was 43% with transplantation and 41% without it.
Surprisingly, allogeneic transplantation was shown to be of no benefit in patients younger than 6 years who had precursor B-cell ALL with induction failure and no high-risk features, compared with chemotherapy alone. This finding has "considerable clinical implications, since transplantation is generally considered to be the standard of care for such patients," Dr. Schrappe and his colleagues said (N. Engl. J. Med. 2012;366:1371-81).
In patients aged 6 years and older who had precursor B-cell ALL, a transplant from a matched, related donor appeared to improve outcome, while other types of allogeneic transplants actually worsened outcomes. This was due in part to a high number of transplantation-related deaths in the latter group.
In contrast, allogeneic transplantation appeared to improve outcomes in the subgroup of patients who had T-cell ALL and failed induction therapy.
Patients with high hyperdiploidy (more than 50 chromosomes) showed an excellent outcome, with a 10-year survival rate of 71%. This favorable outcome "may be due to the increased sensitivity of the blast cells to methotrexate and mercaptopurine, drugs that are generally not used during remission induction but are used at high doses after remission," the investigators said.
Patients who carried the genetic aberration ETV6-RUNX1 also had a high 10-year survival of 73%, which is more than double the survival rate in the cohort as a whole.
Survival was lower among patients who had M3 marrow after induction therapy, compared with those who had M1 marrow and extramedullary disease or M2 marrow. Subgroups with the worst outcomes included patients aged 6 years or older who had M3 marrow (10-year survival, 22%) and those of any age who had T-cell ALL and M3 marrow (10-year survival, 19%).
Among infants who had precursor B-cell ALL and did not have a rearrangement of the MLL gene or fusion of the BCR-ABL1 gene, outcomes were similar to those in children aged 1-5 years (10-year survivals of 65% and 63%, respectively). In contrast, infants who had a rearrangement of the MLL gene fared very poorly (10-year survival, 4%) compared with older children who had the same genetic abnormality (10-year survival, 26%).
Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
Allogeneic stem-cell transplantation is not always the best option when pediatric acute lymphoblastic leukemia fails to respond adequately to induction therapy, according to a report in the April 12 issue of the New England Journal of Medicine.
Children who have the precursor B-cell subtype and no other adverse features do better when treated with chemotherapy, investigators report. Those with T-cell leukemia appear to have better outcomes with allogeneic stem-cell transplantation, a common treatment of choice after induction failure.
Eighty percent of children with pediatric acute lymphoblastic leukemia (ALL) can be cured with standard treatments. The small proportion of children in the very-high-risk group that does not respond to induction therapy is much more heterogeneous than clinicians may realize, according to Dr. Martin Schrappe of Schleswig-Holstein University Medical Center, Christian-Albrechts University, Kiel (Germany) and his associates.
The authors pooled the findings of multiple clinical trials performed by 14 cooperative study groups in North America, Europe, and Asia between 1985 and 2000. Based on this observational analysis, ALL with induction failure was found to be a highly varied entity, with different clinical and biologic traits and a wide range of prognoses.
The study assessed outcomes in 44,017 children and adolescents (aged 0-18 years) with newly diagnosed ALL who were enrolled in clinical trials during that interval and were followed for a median of 8.3 years (range, 1.5-22.1 years). A total of 1,041 (2.4%) failed induction therapy, showing persistent leukemic blasts in the bone marrow or at extramedullary sites.
Overall 10-year survival was 32% but varied greatly across the cohort, from 4% to 73%, depending on biological and clinical factors.
Patients with induction failure were much more likely than ALL patients as a whole to have conventional adverse prognostic factors such as a high leukocyte count, older age at disease onset, the BCR-ABL1 gene, and T-cell phenotypes – and these factors conferred an even worse prognosis in this already high-risk population.
"Indeed, the clinical and biologic characteristics of the patients in our study and the course of the disease were similar to those in patients with relapse during receipt of therapy, another group of patients with a highly unfavorable prognosis," the researchers said.
Among patients who eventually achieved a late remission, 10-year survival was significantly higher (48%) than among those who never achieved a remission (14%).
A total of 198 patients underwent hematopoietic stem-cell transplantation and 427 received chemotherapy only. The 10-year survival was 43% with transplantation and 41% without it.
Surprisingly, allogeneic transplantation was shown to be of no benefit in patients younger than 6 years who had precursor B-cell ALL with induction failure and no high-risk features, compared with chemotherapy alone. This finding has "considerable clinical implications, since transplantation is generally considered to be the standard of care for such patients," Dr. Schrappe and his colleagues said (N. Engl. J. Med. 2012;366:1371-81).
In patients aged 6 years and older who had precursor B-cell ALL, a transplant from a matched, related donor appeared to improve outcome, while other types of allogeneic transplants actually worsened outcomes. This was due in part to a high number of transplantation-related deaths in the latter group.
In contrast, allogeneic transplantation appeared to improve outcomes in the subgroup of patients who had T-cell ALL and failed induction therapy.
Patients with high hyperdiploidy (more than 50 chromosomes) showed an excellent outcome, with a 10-year survival rate of 71%. This favorable outcome "may be due to the increased sensitivity of the blast cells to methotrexate and mercaptopurine, drugs that are generally not used during remission induction but are used at high doses after remission," the investigators said.
Patients who carried the genetic aberration ETV6-RUNX1 also had a high 10-year survival of 73%, which is more than double the survival rate in the cohort as a whole.
Survival was lower among patients who had M3 marrow after induction therapy, compared with those who had M1 marrow and extramedullary disease or M2 marrow. Subgroups with the worst outcomes included patients aged 6 years or older who had M3 marrow (10-year survival, 22%) and those of any age who had T-cell ALL and M3 marrow (10-year survival, 19%).
Among infants who had precursor B-cell ALL and did not have a rearrangement of the MLL gene or fusion of the BCR-ABL1 gene, outcomes were similar to those in children aged 1-5 years (10-year survivals of 65% and 63%, respectively). In contrast, infants who had a rearrangement of the MLL gene fared very poorly (10-year survival, 4%) compared with older children who had the same genetic abnormality (10-year survival, 26%).
Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major Finding: 10-year survival ranged from 4% to 73% in children and adolescents with ALL who failed remission-induction therapy, depending on a wide variety of biological and clinical characteristics.
Data Source: The retrospective observational analysis of data pooled from 14 cooperative study groups in Europe, North America, and Asia, comprised 44,017 children with newly diagnosed ALL enrolled in clinical trials from 1985 through 2000 and followed for a mean of 8 years.
Disclosures: Numerous hospitals, charities, and government agencies supported this study. Dr. Schrappe reported ties to Medoc and EUSA Pharm; his associates reported ties to numerous industry sources.
ONLINE EXCLUSIVE: SHM President, NQF CEO Discuss SHM's Earning National Quality Award
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
Click here to listen to Dr. Li
Click here to listen to Janet Corrigan
ONLINE EXCLUSIVE: Listen to new physician editor Danielle Scheurer's vision for The Hospitalist
Click here to listen to Dr. Scheurer
Click here to listen to Dr. Scheurer
Click here to listen to Dr. Scheurer
ONLINE EXCLUSIVE: How the School of Medicine at Stanford University Is Addressing Female Physicians and Leadership
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.

—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.
—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.
Whenever Hannah Valantine, MD, needs reassurance that female leadership interventions at Stanford University’s School of Medicine are working, she looks at the numbers.
—Janet Nagamine, RN, MD, SFHM, hospitalist, Kaiser Permanente Medical Center, Santa Clara, Calif., SHM board member
In the span of five to six years, the medical school has increased the percentage of women at each faculty rank so that it now surpasses national averages as calculated by the Association of American Medical Colleges. Indeed, the percentage of women at the full professor rank jumped to 22% from 14.5%.
“We really are making progress,” says Dr. Valantine, full professor of medicine and the medical school’s senior associate dean for diversity and leadership.
With structural elements, such as tenure clock extension, extended maternity and family leave, onsite childcare, early-stage research funding support, and mentoring in place, Dr. Valantine is turning her attention to the next round of interventions, which focus more on the psychological and social factors that impair women’s advancement. She will use a National Institutes of Health grant to develop interventions for the phenomenon of stereotype threat, which is the fear that one's behavior will confirm an existing stereotype about one’s social group. This fear may lead to an impairment of performance.
Over the next six months, Dr. Valantine and her team will also conduct several pilot programs involving map career customization, a model that encourages people to chart their careers over the next five to 10 to 20 years, taking into consideration their life outside of work. The intent is to help individuals identify their priorities and goals and how they change over time, and also help supervisors better match the ebbs and flows of a person’s life to the workplace and identify and develop aspiring leaders.
Stanford’s medical school is organized around teams of doctors that care for groups of patients. Each team must achieve excellence in four academic missions: clinical care, education, research, and administration. The map career customization pilot programs are aimed at helping doctors within the team plan their career paths around these four missions, then put the individual plans together in a team context in order to meet the team’s goals, says Dr. Valantine.
“This way, the work and the four missions are entirely covered,” she says. “We create a vibrant academic environment where we create new things and have time to think and integrate our life and work. … It’s a little countercultural, but I think people are crying out for that, and I think it stands a great chance of making the culture change.”
Stanford’s burgeoning efforts in map career customization have intrigued SHM board member Janet Nagamine, RN, MD, SFHM, a hospitalist at Kaiser Permanente Medical Center in Santa Clara, Calif., and Stanford alum. She hopes to collaborate with Dr. Valantine and incorporate into hospital medicine the interventions that Stanford is doing while conducting studies and developing workforce planning initiatives specific to hospitalists. The goal is to create a hospital medicine model that replicates Stanford’s success in cultivating female physician leaders.
“We make this false assumption that your career is going to look the same throughout your life,” Dr. Nagamine says. “That’s just not realistic.”
Lisa Ryan is a freelance writer in New Jersey.