User login
Say What?
Research—not to mention common sense—shows that good communication between caregivers is essential for patient safety, particularly communication among doctors and nursing staff.
In the session “Nurse-Hospitalist Communication,” presenters Win Whitcomb, MD, Mercy Medical Center in Springfield, Mass., and Sally Szumlas, RN, MS, University of Chicago, each told their side of the story, outlining perceived problems and best practices for clear communications between MDs and RNs.
The RN Perspective
Szumlas began with an overview of the problem. “Nurses, through training, tend to be very descriptive, while MDs want to hear succinct information only,” she said. “This can lead to frustration, missed information, and poor communication.”
At the University of Chicago, a project focused on nurse-physician communications took the following steps to improve communication: The hospital instituted multidisciplinary rounding using the call light—indicating that when the physician reaches the patient’s bedside, he or she pushes the call light and the nurse will join if possible. The hospital also implemented the SBAR form—with sections for the nurse to fill in situation, background, assessment, and recommendations. This form ensures a standardized approach to critical communication, particularly when the nurse phones a physician with questions or patient information.
Szumlas concluded by listing common communication roadblocks, including a misunderstanding of roles, real and perceived power differentials, gender and ethnic differences, and differences in styles of communication.
The Hospitalist’s Viewpoint

Dr. Whitcomb presented the hospitalist’s view of nurse-MD communications, saying, “My sense is that collaborating with nurses is among the most satisfying thing we do.” However, he went on, there are common problems with communications between the two groups. “Interruptions are too frequent,” he pointed out. “We still practice telephone medicine too frequently, and nurses are not always available—they’re busy.”
And the addition of hospitalists has created communication problems that didn’t exist before. These include nurses not knowing which hospitalist to contact, or not being able to reach the hospitalist on duty. Nurses can be stuck bringing a hospitalist who’s starting a new shift up to speed on patients, or placating family members who want to see the unavailable hospitalist immediately.
Dr. Whitcomb offered an action plan hospital medicine programs can implement immediately: He suggested establishing a forum for improving nurse-physician communications, using dialogue, and creating action plans. In addition to this forum, the nurse leader and the hospital medicine director should meet regularly. You should also integrate nursing staff into daily rounds “any way that you can. Interdisciplinary rounds are very difficult,” Dr. Whitcomb admitted. “Everyone is busy.”
Additionally, hospital medicine programs should establish standards for team communication. “Seriously consider a daily goals sheet,” urged Dr. Whitcomb, “one for nurses and hospitalists to use to communicate their plan of care.” Adopt an SBAR tool for critical communications, and create an RN-MD communication log sheet on each patient’s chart. “This can replace the ‘stickies’ I find on the front the chart that aren’t dated or signed,” pointed out Dr. Whitcomb.
Hospitalists can also smooth communication problems by using a concise but detailed patient sign-out at shift changes; and nocturnists should add routine rounds to proactively address issues. Nurses, on the other hand, can help by pooling non-urgent calls during the night and, when appropriate, using text messaging when a quick return call is not critical.
Other basic best practices include distributing the hospitalists’ census to all nursing units by 8 a.m. (as well as to the receptionist), placing the hospitalist schedule at all nursing units, ensuring that day hospitalists leave their beepers on until designated times around the end of their shift, and dedicating a universal pager for rapid responses, codes, emergencies, and coverage questions. TH
Research—not to mention common sense—shows that good communication between caregivers is essential for patient safety, particularly communication among doctors and nursing staff.
In the session “Nurse-Hospitalist Communication,” presenters Win Whitcomb, MD, Mercy Medical Center in Springfield, Mass., and Sally Szumlas, RN, MS, University of Chicago, each told their side of the story, outlining perceived problems and best practices for clear communications between MDs and RNs.
The RN Perspective
Szumlas began with an overview of the problem. “Nurses, through training, tend to be very descriptive, while MDs want to hear succinct information only,” she said. “This can lead to frustration, missed information, and poor communication.”
At the University of Chicago, a project focused on nurse-physician communications took the following steps to improve communication: The hospital instituted multidisciplinary rounding using the call light—indicating that when the physician reaches the patient’s bedside, he or she pushes the call light and the nurse will join if possible. The hospital also implemented the SBAR form—with sections for the nurse to fill in situation, background, assessment, and recommendations. This form ensures a standardized approach to critical communication, particularly when the nurse phones a physician with questions or patient information.
Szumlas concluded by listing common communication roadblocks, including a misunderstanding of roles, real and perceived power differentials, gender and ethnic differences, and differences in styles of communication.
The Hospitalist’s Viewpoint
Dr. Whitcomb presented the hospitalist’s view of nurse-MD communications, saying, “My sense is that collaborating with nurses is among the most satisfying thing we do.” However, he went on, there are common problems with communications between the two groups. “Interruptions are too frequent,” he pointed out. “We still practice telephone medicine too frequently, and nurses are not always available—they’re busy.”
And the addition of hospitalists has created communication problems that didn’t exist before. These include nurses not knowing which hospitalist to contact, or not being able to reach the hospitalist on duty. Nurses can be stuck bringing a hospitalist who’s starting a new shift up to speed on patients, or placating family members who want to see the unavailable hospitalist immediately.
Dr. Whitcomb offered an action plan hospital medicine programs can implement immediately: He suggested establishing a forum for improving nurse-physician communications, using dialogue, and creating action plans. In addition to this forum, the nurse leader and the hospital medicine director should meet regularly. You should also integrate nursing staff into daily rounds “any way that you can. Interdisciplinary rounds are very difficult,” Dr. Whitcomb admitted. “Everyone is busy.”
Additionally, hospital medicine programs should establish standards for team communication. “Seriously consider a daily goals sheet,” urged Dr. Whitcomb, “one for nurses and hospitalists to use to communicate their plan of care.” Adopt an SBAR tool for critical communications, and create an RN-MD communication log sheet on each patient’s chart. “This can replace the ‘stickies’ I find on the front the chart that aren’t dated or signed,” pointed out Dr. Whitcomb.
Hospitalists can also smooth communication problems by using a concise but detailed patient sign-out at shift changes; and nocturnists should add routine rounds to proactively address issues. Nurses, on the other hand, can help by pooling non-urgent calls during the night and, when appropriate, using text messaging when a quick return call is not critical.
Other basic best practices include distributing the hospitalists’ census to all nursing units by 8 a.m. (as well as to the receptionist), placing the hospitalist schedule at all nursing units, ensuring that day hospitalists leave their beepers on until designated times around the end of their shift, and dedicating a universal pager for rapid responses, codes, emergencies, and coverage questions. TH
Research—not to mention common sense—shows that good communication between caregivers is essential for patient safety, particularly communication among doctors and nursing staff.
In the session “Nurse-Hospitalist Communication,” presenters Win Whitcomb, MD, Mercy Medical Center in Springfield, Mass., and Sally Szumlas, RN, MS, University of Chicago, each told their side of the story, outlining perceived problems and best practices for clear communications between MDs and RNs.
The RN Perspective
Szumlas began with an overview of the problem. “Nurses, through training, tend to be very descriptive, while MDs want to hear succinct information only,” she said. “This can lead to frustration, missed information, and poor communication.”
At the University of Chicago, a project focused on nurse-physician communications took the following steps to improve communication: The hospital instituted multidisciplinary rounding using the call light—indicating that when the physician reaches the patient’s bedside, he or she pushes the call light and the nurse will join if possible. The hospital also implemented the SBAR form—with sections for the nurse to fill in situation, background, assessment, and recommendations. This form ensures a standardized approach to critical communication, particularly when the nurse phones a physician with questions or patient information.
Szumlas concluded by listing common communication roadblocks, including a misunderstanding of roles, real and perceived power differentials, gender and ethnic differences, and differences in styles of communication.
The Hospitalist’s Viewpoint
Dr. Whitcomb presented the hospitalist’s view of nurse-MD communications, saying, “My sense is that collaborating with nurses is among the most satisfying thing we do.” However, he went on, there are common problems with communications between the two groups. “Interruptions are too frequent,” he pointed out. “We still practice telephone medicine too frequently, and nurses are not always available—they’re busy.”
And the addition of hospitalists has created communication problems that didn’t exist before. These include nurses not knowing which hospitalist to contact, or not being able to reach the hospitalist on duty. Nurses can be stuck bringing a hospitalist who’s starting a new shift up to speed on patients, or placating family members who want to see the unavailable hospitalist immediately.
Dr. Whitcomb offered an action plan hospital medicine programs can implement immediately: He suggested establishing a forum for improving nurse-physician communications, using dialogue, and creating action plans. In addition to this forum, the nurse leader and the hospital medicine director should meet regularly. You should also integrate nursing staff into daily rounds “any way that you can. Interdisciplinary rounds are very difficult,” Dr. Whitcomb admitted. “Everyone is busy.”
Additionally, hospital medicine programs should establish standards for team communication. “Seriously consider a daily goals sheet,” urged Dr. Whitcomb, “one for nurses and hospitalists to use to communicate their plan of care.” Adopt an SBAR tool for critical communications, and create an RN-MD communication log sheet on each patient’s chart. “This can replace the ‘stickies’ I find on the front the chart that aren’t dated or signed,” pointed out Dr. Whitcomb.
Hospitalists can also smooth communication problems by using a concise but detailed patient sign-out at shift changes; and nocturnists should add routine rounds to proactively address issues. Nurses, on the other hand, can help by pooling non-urgent calls during the night and, when appropriate, using text messaging when a quick return call is not critical.
Other basic best practices include distributing the hospitalists’ census to all nursing units by 8 a.m. (as well as to the receptionist), placing the hospitalist schedule at all nursing units, ensuring that day hospitalists leave their beepers on until designated times around the end of their shift, and dedicating a universal pager for rapid responses, codes, emergencies, and coverage questions. TH
Painful Truths
The session “Ethical and Legal Issues around Pain Management in Hospitalized Patients” shed light on issues that many hospitalists are aware of but perhaps not well versed in.
Speaker Vijay Rajput, MD, FACP, associate professor of medicine at the University of Medicine and Dentistry of New Jersey (UMDNJ), Robert Wood Johnson Medical School, and Cooper University Hospital, Camden, N.J., covered the many conflicts surrounding pain management, the law, and your conscience.
Hard Facts
Dr. Rajput shared what he called “hard facts” on pain medication, which include:
- 90% of cancer pain can be controlled with available options;
- 70% of the time chronic, nonmalignant pain is poorly managed, especially in nursing homes;
- 11% of admissions in the emergency department seek treatment for a chronic pain condition;
- 8.2% of, or 19.5 million, Americans use an illicit drug at least once a month; and
- 31.2 million reported non-medical use of pain relievers including hydrocodone (Vicodin), acetaminophen and hydrocodone (Lortab), oxycodone (Percocet), and others.
Dr. Rajput discussed barriers that lead to undertreatment of pain in hospitalized patients.
“There may be prioritization of diagnosis over pain relief by surgical colleagues on hospitalized patients,” he said. “There are also inadequacies in assessing pain, educational deficiencies, and cultural challenges. Some physicians are ruled by regulatory and ethical concerns in prescribing for pain.”
—Vijay Rajput, MD, FACP, associate professor of medicine at University of Medicine and Dentistry of New Jersey (UMDNJ), Robert Wood Johnson Medical School, and Cooper University Hospital, Camden, N.J.
Pain Management and the Law
There are several legal concerns regarding pain management that most physicians are aware of. In addition to liability for repercussions of undermedicating or overmedicating, the failure to refer a patient to a pain management specialist, the use of opioids when caring for end-of-life patients, and failure to get informed consent related to risk of treatment can all mean malpractice suits.
“The general rule for avoiding a malpractice charge is to follow national standards of care and any applicable clinical practice guidelines,” said Dr. Rajput. “There are Web-based databases that serve as national guidelines clearinghouses that you can refer to.”
The Ethical Side of Pain
“There are few common domains of ethical and legal issues in pain relief,” stated Dr. Rajput. These include the pain issues around end-of-life and palliative care of terminally ill patients, a subordination of pain relief to diagnosis, chronic pain issues and substance abuse, pain control in a patient’s transfer to a nursing home, and the risk of discontinuity of pain control after discharge.
“The ethical duty to relieve pain is well established,” Dr. Rajput said. Despite this, it is still common to subordinate pain relief to diagnosis. In 2003, the American Journal of Surgery stated, “Analgesia should be given prior to diagnosis only with the knowledge and consent of the surgeon who assumes the responsibility for decision-making.”
This “decision-making” can affect hospitalists because 86% of ED physicians follow this literature, and 89% of surgeons still prefer to hold the pain medication prior to surgical evaluation.
“Without ongoing education, senior physicians risk providing less, not more, pain control,” Dr. Rajput pointed out. “This will become more critical as we are co-managing more and more surgical patients in hospitals.”
What about End-of-Life Care?
The legal case of Estate of Henry James v. Hilhaven Corp. established that healthcare facilities have a duty to treat pain. However, Dr. Rajput stressed, patients, families, and physicians all remain confused about the role of opioids in caring for dying patients.
Dr. Rajput reviewed two cases where physicians were sued for undertreatment or negligent treatment of pain, and 11 cases where physicians were sued for administering medications that resulted in the deaths of terminally ill patients.
In a criminal prosecution involving the care of the dying, Dr. Rajput explained, the basic elements must be proved: There must be a criminal act, and that act must be intentional. Acts involving terminal pain are not investigated unless a nurse, supervisor, or ethics committee is informed. Nurses are the most common informants.
“Almost all cases are in hospital settings,” said Dr. Rajput. “And there are three major categories: withdrawal of life-sustaining support with accompanying pain meds, the use of opioids and sedations, and terminal care that includes the use of fatal agents such as insulin, potassium chloride, and chloroform.”
In 1997, the Supreme Court endorsed terminal sedation as an alternative to physician-assisted suicide, intensifying the legal debate in the so-called right-to-die controversy.
“Long before the Supreme Court intervention,” said Dr. Rajput, “terminal sedation was a palliative care option to relieve physical or non-physical pain, or to produce an unconscious state before the withdrawal of life support.”
There are clinical safeguards for terminal sedation. These include ensuring the effectiveness of palliative care, obtaining fully informed consent from the patient, maintaining diagnostic and prognostic clarity with respect to the patient’s disease and lifespan, obtaining an independent second opinion, and providing documentation and review.
Double Effect and Futility
In the “rule of double effect” in palliative care (or providing treatment to relieve suffering even though a foreseeable, unintended consequence of that treatment is to hasten death), the difference between permissible and prohibited action relies heavily on the clinician’s intent, Dr. Rajput pointed out.
He quoted the article “The Rule of Double Effect—A Critique of the Rule in End-of-Life Decision-Making,” saying, “A proportionately good effect (relief of suffering) may overcome a foreseeable bad effect (causing death) … as long as the actor does not intend to accomplish the bad effect.”
Another concept—medical futility—leads to three conceptual possibilities at end-of-life care:
- The treatment does not provide positive effects;
- The radical treatment has side effects that outweigh any positive effect; or
- It is futile to treat a disease when the patient is suffering from a more real-time, life-threatening disease.
In the event of physiological futility, a physician can withhold the treatment modality on the basis of having no effect on patient care, Dr. Rajput explained. But the decision needs to meet professional standards, and the physician must inform the patient and his or her family and give them an opportunity to seek a second opinion.
But what if there is no physiological futility?
“If it’s a matter of the appropriateness of sustaining a severely deteriorated life,” said Dr. Rajput, “then the scope of professional judgment is limited. This should not be a unilateral medical judgment.” You must include the patient and their family in decision-making, and you may want to consult with your hospital ethics committee.
“The bottom line is, futility is an elusive concept,” said Dr. Rajput. “The term is used more to make value-laden judgments,” He added, “Avoid the word ‘futility’ in communication and documentation. It can stop conversation.” Rather, communicate your
goals of care and treatments.
To determine those goals, your clinical ethical reasoning should follow these steps:
- State the problem plainly;
- Gather and organize the data;
- Consider the patient’s goals and preferences;
- Ask if this is an ethical problem;
- Ask if more information or dialogue is needed; and
- Determine the best course of action and support your position.
The complete PowerPoint presentation of “Ethical and Legal Issues around Pain Management in Hospitalized Patients” is available on the SHM Web site at www.hospitalmedicine.org/microsite/index.cfm. TH
The session “Ethical and Legal Issues around Pain Management in Hospitalized Patients” shed light on issues that many hospitalists are aware of but perhaps not well versed in.
Speaker Vijay Rajput, MD, FACP, associate professor of medicine at the University of Medicine and Dentistry of New Jersey (UMDNJ), Robert Wood Johnson Medical School, and Cooper University Hospital, Camden, N.J., covered the many conflicts surrounding pain management, the law, and your conscience.
Hard Facts
Dr. Rajput shared what he called “hard facts” on pain medication, which include:
- 90% of cancer pain can be controlled with available options;
- 70% of the time chronic, nonmalignant pain is poorly managed, especially in nursing homes;
- 11% of admissions in the emergency department seek treatment for a chronic pain condition;
- 8.2% of, or 19.5 million, Americans use an illicit drug at least once a month; and
- 31.2 million reported non-medical use of pain relievers including hydrocodone (Vicodin), acetaminophen and hydrocodone (Lortab), oxycodone (Percocet), and others.
Dr. Rajput discussed barriers that lead to undertreatment of pain in hospitalized patients.
“There may be prioritization of diagnosis over pain relief by surgical colleagues on hospitalized patients,” he said. “There are also inadequacies in assessing pain, educational deficiencies, and cultural challenges. Some physicians are ruled by regulatory and ethical concerns in prescribing for pain.”
—Vijay Rajput, MD, FACP, associate professor of medicine at University of Medicine and Dentistry of New Jersey (UMDNJ), Robert Wood Johnson Medical School, and Cooper University Hospital, Camden, N.J.
Pain Management and the Law
There are several legal concerns regarding pain management that most physicians are aware of. In addition to liability for repercussions of undermedicating or overmedicating, the failure to refer a patient to a pain management specialist, the use of opioids when caring for end-of-life patients, and failure to get informed consent related to risk of treatment can all mean malpractice suits.
“The general rule for avoiding a malpractice charge is to follow national standards of care and any applicable clinical practice guidelines,” said Dr. Rajput. “There are Web-based databases that serve as national guidelines clearinghouses that you can refer to.”
The Ethical Side of Pain
“There are few common domains of ethical and legal issues in pain relief,” stated Dr. Rajput. These include the pain issues around end-of-life and palliative care of terminally ill patients, a subordination of pain relief to diagnosis, chronic pain issues and substance abuse, pain control in a patient’s transfer to a nursing home, and the risk of discontinuity of pain control after discharge.
“The ethical duty to relieve pain is well established,” Dr. Rajput said. Despite this, it is still common to subordinate pain relief to diagnosis. In 2003, the American Journal of Surgery stated, “Analgesia should be given prior to diagnosis only with the knowledge and consent of the surgeon who assumes the responsibility for decision-making.”
This “decision-making” can affect hospitalists because 86% of ED physicians follow this literature, and 89% of surgeons still prefer to hold the pain medication prior to surgical evaluation.
“Without ongoing education, senior physicians risk providing less, not more, pain control,” Dr. Rajput pointed out. “This will become more critical as we are co-managing more and more surgical patients in hospitals.”
What about End-of-Life Care?
The legal case of Estate of Henry James v. Hilhaven Corp. established that healthcare facilities have a duty to treat pain. However, Dr. Rajput stressed, patients, families, and physicians all remain confused about the role of opioids in caring for dying patients.
Dr. Rajput reviewed two cases where physicians were sued for undertreatment or negligent treatment of pain, and 11 cases where physicians were sued for administering medications that resulted in the deaths of terminally ill patients.
In a criminal prosecution involving the care of the dying, Dr. Rajput explained, the basic elements must be proved: There must be a criminal act, and that act must be intentional. Acts involving terminal pain are not investigated unless a nurse, supervisor, or ethics committee is informed. Nurses are the most common informants.
“Almost all cases are in hospital settings,” said Dr. Rajput. “And there are three major categories: withdrawal of life-sustaining support with accompanying pain meds, the use of opioids and sedations, and terminal care that includes the use of fatal agents such as insulin, potassium chloride, and chloroform.”
In 1997, the Supreme Court endorsed terminal sedation as an alternative to physician-assisted suicide, intensifying the legal debate in the so-called right-to-die controversy.
“Long before the Supreme Court intervention,” said Dr. Rajput, “terminal sedation was a palliative care option to relieve physical or non-physical pain, or to produce an unconscious state before the withdrawal of life support.”
There are clinical safeguards for terminal sedation. These include ensuring the effectiveness of palliative care, obtaining fully informed consent from the patient, maintaining diagnostic and prognostic clarity with respect to the patient’s disease and lifespan, obtaining an independent second opinion, and providing documentation and review.
Double Effect and Futility
In the “rule of double effect” in palliative care (or providing treatment to relieve suffering even though a foreseeable, unintended consequence of that treatment is to hasten death), the difference between permissible and prohibited action relies heavily on the clinician’s intent, Dr. Rajput pointed out.
He quoted the article “The Rule of Double Effect—A Critique of the Rule in End-of-Life Decision-Making,” saying, “A proportionately good effect (relief of suffering) may overcome a foreseeable bad effect (causing death) … as long as the actor does not intend to accomplish the bad effect.”
Another concept—medical futility—leads to three conceptual possibilities at end-of-life care:
- The treatment does not provide positive effects;
- The radical treatment has side effects that outweigh any positive effect; or
- It is futile to treat a disease when the patient is suffering from a more real-time, life-threatening disease.
In the event of physiological futility, a physician can withhold the treatment modality on the basis of having no effect on patient care, Dr. Rajput explained. But the decision needs to meet professional standards, and the physician must inform the patient and his or her family and give them an opportunity to seek a second opinion.
But what if there is no physiological futility?
“If it’s a matter of the appropriateness of sustaining a severely deteriorated life,” said Dr. Rajput, “then the scope of professional judgment is limited. This should not be a unilateral medical judgment.” You must include the patient and their family in decision-making, and you may want to consult with your hospital ethics committee.
“The bottom line is, futility is an elusive concept,” said Dr. Rajput. “The term is used more to make value-laden judgments,” He added, “Avoid the word ‘futility’ in communication and documentation. It can stop conversation.” Rather, communicate your
goals of care and treatments.
To determine those goals, your clinical ethical reasoning should follow these steps:
- State the problem plainly;
- Gather and organize the data;
- Consider the patient’s goals and preferences;
- Ask if this is an ethical problem;
- Ask if more information or dialogue is needed; and
- Determine the best course of action and support your position.
The complete PowerPoint presentation of “Ethical and Legal Issues around Pain Management in Hospitalized Patients” is available on the SHM Web site at www.hospitalmedicine.org/microsite/index.cfm. TH
The session “Ethical and Legal Issues around Pain Management in Hospitalized Patients” shed light on issues that many hospitalists are aware of but perhaps not well versed in.
Speaker Vijay Rajput, MD, FACP, associate professor of medicine at the University of Medicine and Dentistry of New Jersey (UMDNJ), Robert Wood Johnson Medical School, and Cooper University Hospital, Camden, N.J., covered the many conflicts surrounding pain management, the law, and your conscience.
Hard Facts
Dr. Rajput shared what he called “hard facts” on pain medication, which include:
- 90% of cancer pain can be controlled with available options;
- 70% of the time chronic, nonmalignant pain is poorly managed, especially in nursing homes;
- 11% of admissions in the emergency department seek treatment for a chronic pain condition;
- 8.2% of, or 19.5 million, Americans use an illicit drug at least once a month; and
- 31.2 million reported non-medical use of pain relievers including hydrocodone (Vicodin), acetaminophen and hydrocodone (Lortab), oxycodone (Percocet), and others.
Dr. Rajput discussed barriers that lead to undertreatment of pain in hospitalized patients.
“There may be prioritization of diagnosis over pain relief by surgical colleagues on hospitalized patients,” he said. “There are also inadequacies in assessing pain, educational deficiencies, and cultural challenges. Some physicians are ruled by regulatory and ethical concerns in prescribing for pain.”
—Vijay Rajput, MD, FACP, associate professor of medicine at University of Medicine and Dentistry of New Jersey (UMDNJ), Robert Wood Johnson Medical School, and Cooper University Hospital, Camden, N.J.
Pain Management and the Law
There are several legal concerns regarding pain management that most physicians are aware of. In addition to liability for repercussions of undermedicating or overmedicating, the failure to refer a patient to a pain management specialist, the use of opioids when caring for end-of-life patients, and failure to get informed consent related to risk of treatment can all mean malpractice suits.
“The general rule for avoiding a malpractice charge is to follow national standards of care and any applicable clinical practice guidelines,” said Dr. Rajput. “There are Web-based databases that serve as national guidelines clearinghouses that you can refer to.”
The Ethical Side of Pain
“There are few common domains of ethical and legal issues in pain relief,” stated Dr. Rajput. These include the pain issues around end-of-life and palliative care of terminally ill patients, a subordination of pain relief to diagnosis, chronic pain issues and substance abuse, pain control in a patient’s transfer to a nursing home, and the risk of discontinuity of pain control after discharge.
“The ethical duty to relieve pain is well established,” Dr. Rajput said. Despite this, it is still common to subordinate pain relief to diagnosis. In 2003, the American Journal of Surgery stated, “Analgesia should be given prior to diagnosis only with the knowledge and consent of the surgeon who assumes the responsibility for decision-making.”
This “decision-making” can affect hospitalists because 86% of ED physicians follow this literature, and 89% of surgeons still prefer to hold the pain medication prior to surgical evaluation.
“Without ongoing education, senior physicians risk providing less, not more, pain control,” Dr. Rajput pointed out. “This will become more critical as we are co-managing more and more surgical patients in hospitals.”
What about End-of-Life Care?
The legal case of Estate of Henry James v. Hilhaven Corp. established that healthcare facilities have a duty to treat pain. However, Dr. Rajput stressed, patients, families, and physicians all remain confused about the role of opioids in caring for dying patients.
Dr. Rajput reviewed two cases where physicians were sued for undertreatment or negligent treatment of pain, and 11 cases where physicians were sued for administering medications that resulted in the deaths of terminally ill patients.
In a criminal prosecution involving the care of the dying, Dr. Rajput explained, the basic elements must be proved: There must be a criminal act, and that act must be intentional. Acts involving terminal pain are not investigated unless a nurse, supervisor, or ethics committee is informed. Nurses are the most common informants.
“Almost all cases are in hospital settings,” said Dr. Rajput. “And there are three major categories: withdrawal of life-sustaining support with accompanying pain meds, the use of opioids and sedations, and terminal care that includes the use of fatal agents such as insulin, potassium chloride, and chloroform.”
In 1997, the Supreme Court endorsed terminal sedation as an alternative to physician-assisted suicide, intensifying the legal debate in the so-called right-to-die controversy.
“Long before the Supreme Court intervention,” said Dr. Rajput, “terminal sedation was a palliative care option to relieve physical or non-physical pain, or to produce an unconscious state before the withdrawal of life support.”
There are clinical safeguards for terminal sedation. These include ensuring the effectiveness of palliative care, obtaining fully informed consent from the patient, maintaining diagnostic and prognostic clarity with respect to the patient’s disease and lifespan, obtaining an independent second opinion, and providing documentation and review.
Double Effect and Futility
In the “rule of double effect” in palliative care (or providing treatment to relieve suffering even though a foreseeable, unintended consequence of that treatment is to hasten death), the difference between permissible and prohibited action relies heavily on the clinician’s intent, Dr. Rajput pointed out.
He quoted the article “The Rule of Double Effect—A Critique of the Rule in End-of-Life Decision-Making,” saying, “A proportionately good effect (relief of suffering) may overcome a foreseeable bad effect (causing death) … as long as the actor does not intend to accomplish the bad effect.”
Another concept—medical futility—leads to three conceptual possibilities at end-of-life care:
- The treatment does not provide positive effects;
- The radical treatment has side effects that outweigh any positive effect; or
- It is futile to treat a disease when the patient is suffering from a more real-time, life-threatening disease.
In the event of physiological futility, a physician can withhold the treatment modality on the basis of having no effect on patient care, Dr. Rajput explained. But the decision needs to meet professional standards, and the physician must inform the patient and his or her family and give them an opportunity to seek a second opinion.
But what if there is no physiological futility?
“If it’s a matter of the appropriateness of sustaining a severely deteriorated life,” said Dr. Rajput, “then the scope of professional judgment is limited. This should not be a unilateral medical judgment.” You must include the patient and their family in decision-making, and you may want to consult with your hospital ethics committee.
“The bottom line is, futility is an elusive concept,” said Dr. Rajput. “The term is used more to make value-laden judgments,” He added, “Avoid the word ‘futility’ in communication and documentation. It can stop conversation.” Rather, communicate your
goals of care and treatments.
To determine those goals, your clinical ethical reasoning should follow these steps:
- State the problem plainly;
- Gather and organize the data;
- Consider the patient’s goals and preferences;
- Ask if this is an ethical problem;
- Ask if more information or dialogue is needed; and
- Determine the best course of action and support your position.
The complete PowerPoint presentation of “Ethical and Legal Issues around Pain Management in Hospitalized Patients” is available on the SHM Web site at www.hospitalmedicine.org/microsite/index.cfm. TH
Senior Syndromes

Attendees at the session “Managing Hospitalized Elders,” presented by Robert Palmer, MD, MPH, head of the section of Geriatric Medicine at Cleveland Clinic in Ohio, gained insights into the unique dangers hospitalization presents to their oldest patients.
“As every hospital-based physician knows, increasingly, hospital care is geriatric care,” said Dr. Palmer. “We’re seeing not only more people over 65, we’re seeing more people over age 85—the most complex and challenging cases. The question is, how do we work our way through the chronic diseases, the acute on top of chronic disease, deal with the psychosocial issues and family issues of the frail elderly person during hospitalization.”
The problem is that simply being hospitalized may trigger or exacerbate a functional decline in an elderly patient. Hospitalization itself can lead to delirium, undernutrition, immobility, pressure ulcers, incontinence, and ultimately placement in a nursing home.
“The process of care, a hostile environment, bed rest, starvation, medications—especially those that are inappropriate for use with older people—and depression all conspire to create a dysfunctional older person,” stressed Dr. Palmer. Common co-morbid conditions in the elderly include dehydration, chronic obstructive pulmonary disease (COPD), hypertension, chronic heart failure, diabetes, and anemia.
“We rarely treat these patients for just one condition,” Dr. Palmer pointed out.
Common Geriatric Syndromes
Common clinical presentations in elderly hospitalized patients include dysfunction, delirium, depression, and dementia.
“Some well-designed cohort studies show that 20% to 32% of these patients lose independent performance of one or more basic activities of daily living [ADL] at discharge,” said Dr. Palmer. Basic ADLs include bathing, dressing, moving from bed to chair, using the toilet, and eating. Why is this important? Patients admitted who were dependent in all six basic ADLs were at greater risk for in-hospital mortality or one-year mortality, 90-day nursing home use, and up to 50% higher DRG hospital costs.
“Not all older patients are at risk,” Dr. Palmer assured his audience. Risk factors for functional decline to watch for include patients over 75, those who are cognitively impaired, those dependent in two or more instrumental ADLs (shopping, housekeeping, taking medications), depression, and pressure ulcers.
—Robert Palmer, MD, MPH, head of the section of Geriatric Medicine at Cleveland Clinic in Ohio
Focus on Delirium
Dr. Palmer paid special attention to delirium.
“This is the most risky syndrome during hospitalization,” he warned. Delirium, or the acute decline of attention and cognition, can be called several things: acute confusional state, acute change in mental state, metabolic encephalopathy, toxic encephalopathy, acute brain syndrome, or acute toxic psychosis.
However it is categorized, delirium is found in 10% to 15% of hospitalized elders upon admission, and 10% to 15% of elderly patients develop it after admission. In ICUs, 70% to 84% of elderly patients suffer from delirium.
What causes delirium during hospitalization? Risk factors include severe illness, dementia, dehydration, sensory impairments (trouble hearing or seeing), and psychoactive medications. Identifiable precipitants of delirium are the use of physical restraints, malnutrition, the addition of three or more new medications, use of a bladder catheter, and any iatrogenic event.
“The major concern with delirium is the increased risk of mortality,” said Dr. Palmer. “But it also leads to prolonged length of stay, increased costs, and potential nursing home placement upon discharge.”
Diagnosing delirium versus dementia is based on four factors:
- The onset of confusion is abrupt with delirium and gradual for the early stages of dementia;
- Consciousness is fluctuating and clouded with delirium; with dementia it’s not affected;
- Attention span will be reduced with delirium but not with dementia; and
- A delirious patient will show hyperactive or hypoactive psychomotor changes, whereas this change will not show in early stages of dementia.
When evaluating for delirium, search for the cause and any possible precipitating factors, advised Dr. Palmer: “Consider multiple etiologies, and remember that fluctuation in the course is the rule.” Eliminating precipitating factors can help. Evaluation should include a targeted history and physical, and lab work to check things like drug levels and neuroimaging.
You may be able to manage delirium with nonpharmacologic changes in environment such as adding orienting stimuli of clocks, TV, and personal items; minimizing abrupt relocations; and sitting the patient in an upright position. You can also increase sensory input, said Dr. Palmer. You may also try a short course of meds: For severe agitation, haloperidol (0.5 to 1 mg every four hours as needed) or for anxiety symptoms use lorazepam (0.5 to 1 mg every four to six hours as needed).
Dr. Palmer offered a partial list of medications to avoid for elderly patients. “These patients are very vulnerable to bad outcomes,” he warned. His list included:
- Diphenhydramine;
- Hydroxyzine;
- Meperidine;
- Propoxyphene;
- Diazepam;
- Chlordiazepoxide;
- Amitriptyline;
- Imipramine;
- Doxepin;
- Promethazine;
- Prochlorperazine;
- Trimethobenzamide; and
- Famotidine (high dose).
Additionally, you should be aware that the following classes of drugs could cause delirium in the elderly:
- Antidepressants;
- Antianxiety medications;
- Antibiotics;
- Antihypertensives;
- Antihistamines;
- Antiarrhythmics;
- Antipsychotics; and
- Anti-inflammatory medications.
“Basically, any pharmacological class that begins with ‘anti’ should be avoided with elderly patients,” said Dr. Palmer.
Assess and Manage Undernutrition
An astonishing 40% to 60% of hospitalized, ill elderly patients suffer from malnutrition.
“This is often not diagnosed or adequately treated,” said Dr. Palmer. “It’s associated with terrible outcomes of hospital care, including length of stay, mortality, and affected ADL activities.”
There is no single blood test for malnutrition, Dr. Palmer continued, but indicators include a body mass index of less than 19, reduced muscle mass, reduced skin fold thickness, and biochemical measures including serum albumin of less than three and low hemoglobin and serum cholesterol.
To guard against dehydration and undernutrition in your elderly patients, Dr. Palmer advised assessing nutritional status at admission, prescribing and monitoring daily calorie and fluid intake for high-risk patients, giving priority to providing calories over restricted diet, and including consultation with a dietitian.
Take off the Restraints
“Why do we order bed rest for the weak and sick?” asked Dr. Palmer. He urged hospitalists to avoid bed-rest orders and instead encourage elderly patients to get out of bed and get physical activity or even physical therapy for transfer-dependent and gait-impaired patients.
Most of all, he said, “Avoid physical restraints.” These limit mobility, obviously, and can lead to pressure ulcers, deconditioning, falls, constipation, and incontinence.
Where to Send the Patient
Plan for discharging an independent elderly patient back home, not to a nursing home if you can, urged Dr. Palmer.
“Comprehensive discharge planning almost always requires an interdisciplinary team,” he said. “Goals of care and advanced directives should be discussed with the patient and family members, and post acute care needs should be considered.”
Following a “functional trajectory” from admission to discharge begins the first day. Dr. Palmer recommends the hospitalist, a nurse, and the case manager all interview the patient and family, establish a baseline and outline the expected hospital course including estimated length of stay and discharge site—nursing home, skilled nursing facility, or home.
“Work with physical or occupational therapy early to mobilize the patient and improve their functioning,” advised Dr. Palmer.
This type of comprehensive discharge planning, along with home follow-up, has reduced readmission rates. TH
Attendees at the session “Managing Hospitalized Elders,” presented by Robert Palmer, MD, MPH, head of the section of Geriatric Medicine at Cleveland Clinic in Ohio, gained insights into the unique dangers hospitalization presents to their oldest patients.
“As every hospital-based physician knows, increasingly, hospital care is geriatric care,” said Dr. Palmer. “We’re seeing not only more people over 65, we’re seeing more people over age 85—the most complex and challenging cases. The question is, how do we work our way through the chronic diseases, the acute on top of chronic disease, deal with the psychosocial issues and family issues of the frail elderly person during hospitalization.”
The problem is that simply being hospitalized may trigger or exacerbate a functional decline in an elderly patient. Hospitalization itself can lead to delirium, undernutrition, immobility, pressure ulcers, incontinence, and ultimately placement in a nursing home.
“The process of care, a hostile environment, bed rest, starvation, medications—especially those that are inappropriate for use with older people—and depression all conspire to create a dysfunctional older person,” stressed Dr. Palmer. Common co-morbid conditions in the elderly include dehydration, chronic obstructive pulmonary disease (COPD), hypertension, chronic heart failure, diabetes, and anemia.
“We rarely treat these patients for just one condition,” Dr. Palmer pointed out.
Common Geriatric Syndromes
Common clinical presentations in elderly hospitalized patients include dysfunction, delirium, depression, and dementia.
“Some well-designed cohort studies show that 20% to 32% of these patients lose independent performance of one or more basic activities of daily living [ADL] at discharge,” said Dr. Palmer. Basic ADLs include bathing, dressing, moving from bed to chair, using the toilet, and eating. Why is this important? Patients admitted who were dependent in all six basic ADLs were at greater risk for in-hospital mortality or one-year mortality, 90-day nursing home use, and up to 50% higher DRG hospital costs.
“Not all older patients are at risk,” Dr. Palmer assured his audience. Risk factors for functional decline to watch for include patients over 75, those who are cognitively impaired, those dependent in two or more instrumental ADLs (shopping, housekeeping, taking medications), depression, and pressure ulcers.
—Robert Palmer, MD, MPH, head of the section of Geriatric Medicine at Cleveland Clinic in Ohio
Focus on Delirium
Dr. Palmer paid special attention to delirium.
“This is the most risky syndrome during hospitalization,” he warned. Delirium, or the acute decline of attention and cognition, can be called several things: acute confusional state, acute change in mental state, metabolic encephalopathy, toxic encephalopathy, acute brain syndrome, or acute toxic psychosis.
However it is categorized, delirium is found in 10% to 15% of hospitalized elders upon admission, and 10% to 15% of elderly patients develop it after admission. In ICUs, 70% to 84% of elderly patients suffer from delirium.
What causes delirium during hospitalization? Risk factors include severe illness, dementia, dehydration, sensory impairments (trouble hearing or seeing), and psychoactive medications. Identifiable precipitants of delirium are the use of physical restraints, malnutrition, the addition of three or more new medications, use of a bladder catheter, and any iatrogenic event.
“The major concern with delirium is the increased risk of mortality,” said Dr. Palmer. “But it also leads to prolonged length of stay, increased costs, and potential nursing home placement upon discharge.”
Diagnosing delirium versus dementia is based on four factors:
- The onset of confusion is abrupt with delirium and gradual for the early stages of dementia;
- Consciousness is fluctuating and clouded with delirium; with dementia it’s not affected;
- Attention span will be reduced with delirium but not with dementia; and
- A delirious patient will show hyperactive or hypoactive psychomotor changes, whereas this change will not show in early stages of dementia.
When evaluating for delirium, search for the cause and any possible precipitating factors, advised Dr. Palmer: “Consider multiple etiologies, and remember that fluctuation in the course is the rule.” Eliminating precipitating factors can help. Evaluation should include a targeted history and physical, and lab work to check things like drug levels and neuroimaging.
You may be able to manage delirium with nonpharmacologic changes in environment such as adding orienting stimuli of clocks, TV, and personal items; minimizing abrupt relocations; and sitting the patient in an upright position. You can also increase sensory input, said Dr. Palmer. You may also try a short course of meds: For severe agitation, haloperidol (0.5 to 1 mg every four hours as needed) or for anxiety symptoms use lorazepam (0.5 to 1 mg every four to six hours as needed).
Dr. Palmer offered a partial list of medications to avoid for elderly patients. “These patients are very vulnerable to bad outcomes,” he warned. His list included:
- Diphenhydramine;
- Hydroxyzine;
- Meperidine;
- Propoxyphene;
- Diazepam;
- Chlordiazepoxide;
- Amitriptyline;
- Imipramine;
- Doxepin;
- Promethazine;
- Prochlorperazine;
- Trimethobenzamide; and
- Famotidine (high dose).
Additionally, you should be aware that the following classes of drugs could cause delirium in the elderly:
- Antidepressants;
- Antianxiety medications;
- Antibiotics;
- Antihypertensives;
- Antihistamines;
- Antiarrhythmics;
- Antipsychotics; and
- Anti-inflammatory medications.
“Basically, any pharmacological class that begins with ‘anti’ should be avoided with elderly patients,” said Dr. Palmer.
Assess and Manage Undernutrition
An astonishing 40% to 60% of hospitalized, ill elderly patients suffer from malnutrition.
“This is often not diagnosed or adequately treated,” said Dr. Palmer. “It’s associated with terrible outcomes of hospital care, including length of stay, mortality, and affected ADL activities.”
There is no single blood test for malnutrition, Dr. Palmer continued, but indicators include a body mass index of less than 19, reduced muscle mass, reduced skin fold thickness, and biochemical measures including serum albumin of less than three and low hemoglobin and serum cholesterol.
To guard against dehydration and undernutrition in your elderly patients, Dr. Palmer advised assessing nutritional status at admission, prescribing and monitoring daily calorie and fluid intake for high-risk patients, giving priority to providing calories over restricted diet, and including consultation with a dietitian.
Take off the Restraints
“Why do we order bed rest for the weak and sick?” asked Dr. Palmer. He urged hospitalists to avoid bed-rest orders and instead encourage elderly patients to get out of bed and get physical activity or even physical therapy for transfer-dependent and gait-impaired patients.
Most of all, he said, “Avoid physical restraints.” These limit mobility, obviously, and can lead to pressure ulcers, deconditioning, falls, constipation, and incontinence.
Where to Send the Patient
Plan for discharging an independent elderly patient back home, not to a nursing home if you can, urged Dr. Palmer.
“Comprehensive discharge planning almost always requires an interdisciplinary team,” he said. “Goals of care and advanced directives should be discussed with the patient and family members, and post acute care needs should be considered.”
Following a “functional trajectory” from admission to discharge begins the first day. Dr. Palmer recommends the hospitalist, a nurse, and the case manager all interview the patient and family, establish a baseline and outline the expected hospital course including estimated length of stay and discharge site—nursing home, skilled nursing facility, or home.
“Work with physical or occupational therapy early to mobilize the patient and improve their functioning,” advised Dr. Palmer.
This type of comprehensive discharge planning, along with home follow-up, has reduced readmission rates. TH
Attendees at the session “Managing Hospitalized Elders,” presented by Robert Palmer, MD, MPH, head of the section of Geriatric Medicine at Cleveland Clinic in Ohio, gained insights into the unique dangers hospitalization presents to their oldest patients.
“As every hospital-based physician knows, increasingly, hospital care is geriatric care,” said Dr. Palmer. “We’re seeing not only more people over 65, we’re seeing more people over age 85—the most complex and challenging cases. The question is, how do we work our way through the chronic diseases, the acute on top of chronic disease, deal with the psychosocial issues and family issues of the frail elderly person during hospitalization.”
The problem is that simply being hospitalized may trigger or exacerbate a functional decline in an elderly patient. Hospitalization itself can lead to delirium, undernutrition, immobility, pressure ulcers, incontinence, and ultimately placement in a nursing home.
“The process of care, a hostile environment, bed rest, starvation, medications—especially those that are inappropriate for use with older people—and depression all conspire to create a dysfunctional older person,” stressed Dr. Palmer. Common co-morbid conditions in the elderly include dehydration, chronic obstructive pulmonary disease (COPD), hypertension, chronic heart failure, diabetes, and anemia.
“We rarely treat these patients for just one condition,” Dr. Palmer pointed out.
Common Geriatric Syndromes
Common clinical presentations in elderly hospitalized patients include dysfunction, delirium, depression, and dementia.
“Some well-designed cohort studies show that 20% to 32% of these patients lose independent performance of one or more basic activities of daily living [ADL] at discharge,” said Dr. Palmer. Basic ADLs include bathing, dressing, moving from bed to chair, using the toilet, and eating. Why is this important? Patients admitted who were dependent in all six basic ADLs were at greater risk for in-hospital mortality or one-year mortality, 90-day nursing home use, and up to 50% higher DRG hospital costs.
“Not all older patients are at risk,” Dr. Palmer assured his audience. Risk factors for functional decline to watch for include patients over 75, those who are cognitively impaired, those dependent in two or more instrumental ADLs (shopping, housekeeping, taking medications), depression, and pressure ulcers.
—Robert Palmer, MD, MPH, head of the section of Geriatric Medicine at Cleveland Clinic in Ohio
Focus on Delirium
Dr. Palmer paid special attention to delirium.
“This is the most risky syndrome during hospitalization,” he warned. Delirium, or the acute decline of attention and cognition, can be called several things: acute confusional state, acute change in mental state, metabolic encephalopathy, toxic encephalopathy, acute brain syndrome, or acute toxic psychosis.
However it is categorized, delirium is found in 10% to 15% of hospitalized elders upon admission, and 10% to 15% of elderly patients develop it after admission. In ICUs, 70% to 84% of elderly patients suffer from delirium.
What causes delirium during hospitalization? Risk factors include severe illness, dementia, dehydration, sensory impairments (trouble hearing or seeing), and psychoactive medications. Identifiable precipitants of delirium are the use of physical restraints, malnutrition, the addition of three or more new medications, use of a bladder catheter, and any iatrogenic event.
“The major concern with delirium is the increased risk of mortality,” said Dr. Palmer. “But it also leads to prolonged length of stay, increased costs, and potential nursing home placement upon discharge.”
Diagnosing delirium versus dementia is based on four factors:
- The onset of confusion is abrupt with delirium and gradual for the early stages of dementia;
- Consciousness is fluctuating and clouded with delirium; with dementia it’s not affected;
- Attention span will be reduced with delirium but not with dementia; and
- A delirious patient will show hyperactive or hypoactive psychomotor changes, whereas this change will not show in early stages of dementia.
When evaluating for delirium, search for the cause and any possible precipitating factors, advised Dr. Palmer: “Consider multiple etiologies, and remember that fluctuation in the course is the rule.” Eliminating precipitating factors can help. Evaluation should include a targeted history and physical, and lab work to check things like drug levels and neuroimaging.
You may be able to manage delirium with nonpharmacologic changes in environment such as adding orienting stimuli of clocks, TV, and personal items; minimizing abrupt relocations; and sitting the patient in an upright position. You can also increase sensory input, said Dr. Palmer. You may also try a short course of meds: For severe agitation, haloperidol (0.5 to 1 mg every four hours as needed) or for anxiety symptoms use lorazepam (0.5 to 1 mg every four to six hours as needed).
Dr. Palmer offered a partial list of medications to avoid for elderly patients. “These patients are very vulnerable to bad outcomes,” he warned. His list included:
- Diphenhydramine;
- Hydroxyzine;
- Meperidine;
- Propoxyphene;
- Diazepam;
- Chlordiazepoxide;
- Amitriptyline;
- Imipramine;
- Doxepin;
- Promethazine;
- Prochlorperazine;
- Trimethobenzamide; and
- Famotidine (high dose).
Additionally, you should be aware that the following classes of drugs could cause delirium in the elderly:
- Antidepressants;
- Antianxiety medications;
- Antibiotics;
- Antihypertensives;
- Antihistamines;
- Antiarrhythmics;
- Antipsychotics; and
- Anti-inflammatory medications.
“Basically, any pharmacological class that begins with ‘anti’ should be avoided with elderly patients,” said Dr. Palmer.
Assess and Manage Undernutrition
An astonishing 40% to 60% of hospitalized, ill elderly patients suffer from malnutrition.
“This is often not diagnosed or adequately treated,” said Dr. Palmer. “It’s associated with terrible outcomes of hospital care, including length of stay, mortality, and affected ADL activities.”
There is no single blood test for malnutrition, Dr. Palmer continued, but indicators include a body mass index of less than 19, reduced muscle mass, reduced skin fold thickness, and biochemical measures including serum albumin of less than three and low hemoglobin and serum cholesterol.
To guard against dehydration and undernutrition in your elderly patients, Dr. Palmer advised assessing nutritional status at admission, prescribing and monitoring daily calorie and fluid intake for high-risk patients, giving priority to providing calories over restricted diet, and including consultation with a dietitian.
Take off the Restraints
“Why do we order bed rest for the weak and sick?” asked Dr. Palmer. He urged hospitalists to avoid bed-rest orders and instead encourage elderly patients to get out of bed and get physical activity or even physical therapy for transfer-dependent and gait-impaired patients.
Most of all, he said, “Avoid physical restraints.” These limit mobility, obviously, and can lead to pressure ulcers, deconditioning, falls, constipation, and incontinence.
Where to Send the Patient
Plan for discharging an independent elderly patient back home, not to a nursing home if you can, urged Dr. Palmer.
“Comprehensive discharge planning almost always requires an interdisciplinary team,” he said. “Goals of care and advanced directives should be discussed with the patient and family members, and post acute care needs should be considered.”
Following a “functional trajectory” from admission to discharge begins the first day. Dr. Palmer recommends the hospitalist, a nurse, and the case manager all interview the patient and family, establish a baseline and outline the expected hospital course including estimated length of stay and discharge site—nursing home, skilled nursing facility, or home.
“Work with physical or occupational therapy early to mobilize the patient and improve their functioning,” advised Dr. Palmer.
This type of comprehensive discharge planning, along with home follow-up, has reduced readmission rates. TH
A Hands-on Approach to Hand-offs

In “Developing Hand-off Standards for Hospitalists,” members of an SHM task force on hand-offs presented their findings from an extensive literature review and went on to propose basic standards for hospitalist hand-offs. The speakers included task force members Vineet Arora, MD, MA, assistant professor of medicine, University of Chicago; Lakshmi Halasyamani, MD, associate chairperson of the Department of Internal Medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich.; Sunil Kripalani, MD, MSc, an instructor at Emory University, Atlanta, Ga.; and Efren Manjarrez, MD, assistant clinical professor of medicine at the Miller School of Medicine, University of Miami.

Literature Review: Slim Pickings
Although the group hoped to determine best practices based on a literature review of hand-offs, shift changes and handovers (excluding transitions in and out of hospitals) they couldn’t find enough appropriate research to support this goal.
After a PubMed search, and a review of the Agency for Healthcare Research and Quality’s (AHRQ) Patient Safety Net—which is a categorized, reviewed collection of articles and references—the task force reported the following: Of the 334 promising articles they initially identified, only 107 were deemed relevant after a title review. And of those, a significant article review found only 10 met the criteria for inclusion. Three studies of hand-offs appeared in nursing publications and were the only provider-specific studies. The remaining seven were studies of technology solutions for hand-offs—although all articles revealed that any technology fixes were “homegrown,” as nothing specific to hand-offs is widely available commercially.

Those 10 studies included few interventions, with no studies of hospitalist-specific hand-offs. Studies of shift changes predominated, and there were few studies that included patient outcomes.
“A summary of the literature supports the use of supplementing verbal hand-offs with written documentation in some structured format,” said Dr. Manjarrez. “It also showed a technology solution provided added benefits such as reduced rounding time and prep time and increased time with patients.”
The literature summary also suggests involving the patient in the hand-off conversation. “Signing out in front of the patient does wonders for your patient satisfaction rate,” remarked Dr. Manjarrez.

As part of the literature review, the task force found and examined five major expert consensus and policy white papers deemed relevant to hand-offs. Dr. Arora cited these papers from the Australian Council for Safety and Quality in Healthcare, the British Medical Association Junior Doctors Committee, the University Health Consortium, the Department of Defense Patient Safety Program, and the Joint Commission’s (formerly JCAHO’s) National Patient Safety Goal 2006.
Dr. Arora reminded attendees that the Joint Commission’s National Patient Safety Goal states that, “hospitals should implement a standardized approach to hand-off communications. This applies to all staff, not just physicians.”
Common themes found in the five white papers include:
- Frontline providers must be educated about acceptable hand-off practices;
- Adequate time must be made by all parties for hand-offs, and interruptions should be reduced during hand-off communications;
- Information must be up to date;
- Interactive questioning should be facilitated;
- Ill patients must be made a priority; and
- Actions to be undertaken should be clearly delineated.
Recommended Standards for Hand-offs
Based on their literature review, the SHM task force has created basic standards for hospitalists to use for hand-offs.
“Our standards needed to be broad enough to work at all hospital medicine programs, so they’re pretty basic,” said Dr. Arora. “They’re actually minimal standards to be met—they’re fairly simplistic, and we do not consider them to be best practices by any means.”
The standards begin with what seems like an obvious statement, but a necessary one for some hospital medicine groups: “A formally recognized hand-off plan should be instituted at the end of a shift or a change in service.” The standards also state that, “Effective hand-offs will require not only a program policy, but standards for verbal exchange and content exchange,” said Dr. Arora.
To guide hospital medicine groups through this exchange, the speakers offered three mnemonic devices: The 3 T’s, the 4 I’s and the 3 A’s.
The 3 T’s: Your program should have a policy in place that stipulates:
- Time set aside for hand-offs. Ensure that busy hospitalists have adequate time blocked out.
- Template or technology solution. “You need a structured template to help people do their work,” said Dr. Arora. “The program needs to decide what kind of template to adopt—and a move to standardization meets that Joint Commission goal.”
- Train new staff on hand-off expectations. Keep everyone in your practice, including appropriate hospital staff, in the loop.
The 4 I’s of verbal, or face-to-face, exchange include:
- Interruptions are limited. There will always be interruptions, but you can take steps to limit them during hand-offs by designating a time and/or place as “interruption free,” or having someone cover the pagers of the involved hospitalists during hand-offs.
- Interactive process is used. “There should be some interactive dialogue” between the physicians, insisted Dr. Arora.
- Ill patients are given priority. Make sure that you give your sickest patients top priority during hand-offs.
- Insight given to receiver on what to expect or do. What would you do if you were staying on for the next shift? Give the receiver a list of “to-do” items.
The 3 A’s of content exchange standards are:
- All data are up to date. This can be a real problem in healthcare. Make sure all information you turn over, both written and oral, reflects your latest knowledge.
- Anticipated events are emphasized. “What do you anticipate will be a problem?” asked Dr. Arora. Think this through and let the receiver know.
- Action items are highlighted. Again, include a to-do list with the information.
What’s Next?
The task force didn’t stop with these new basic standards. They put together a research agenda, a “wish list” of what’s needed in hospital medicine research to improve hand-offs.
“We need to use research to evaluate these standards rigorously,” said Dr. Arora. “And we must emphasize controlled interventions because only 10 of the articles we found were controlled interventions. We have to urge the research community to do more in this area.”
The group would also like to encourage the development of patient-based outcomes that are sensitive to hand-off quality. “This is talked about a lot, but few people are doing anything about it,” Dr. Arora pointed out.
And finally, they’d like to enable additional funding for further research on hand-offs.
Attendees at the session were polled on their hand-off practices. By a show of hands, approximately 40% indicated they had a standardized hand-off procedure. However, virtually no one thought their procedure was ideal.
The task force encouraged attendees and other hospitalists to share their thoughts and input on hand-off standards. If you have ideas for the task force, you can e-mail them at handoffs@hospitalmedicine.org.
The task force plans to revise their recommendations, with attention to SHM member input. They’d also like to engage an expert panel for an external review of their work before they disseminate it. TH
In “Developing Hand-off Standards for Hospitalists,” members of an SHM task force on hand-offs presented their findings from an extensive literature review and went on to propose basic standards for hospitalist hand-offs. The speakers included task force members Vineet Arora, MD, MA, assistant professor of medicine, University of Chicago; Lakshmi Halasyamani, MD, associate chairperson of the Department of Internal Medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich.; Sunil Kripalani, MD, MSc, an instructor at Emory University, Atlanta, Ga.; and Efren Manjarrez, MD, assistant clinical professor of medicine at the Miller School of Medicine, University of Miami.
Literature Review: Slim Pickings
Although the group hoped to determine best practices based on a literature review of hand-offs, shift changes and handovers (excluding transitions in and out of hospitals) they couldn’t find enough appropriate research to support this goal.
After a PubMed search, and a review of the Agency for Healthcare Research and Quality’s (AHRQ) Patient Safety Net—which is a categorized, reviewed collection of articles and references—the task force reported the following: Of the 334 promising articles they initially identified, only 107 were deemed relevant after a title review. And of those, a significant article review found only 10 met the criteria for inclusion. Three studies of hand-offs appeared in nursing publications and were the only provider-specific studies. The remaining seven were studies of technology solutions for hand-offs—although all articles revealed that any technology fixes were “homegrown,” as nothing specific to hand-offs is widely available commercially.
Those 10 studies included few interventions, with no studies of hospitalist-specific hand-offs. Studies of shift changes predominated, and there were few studies that included patient outcomes.
“A summary of the literature supports the use of supplementing verbal hand-offs with written documentation in some structured format,” said Dr. Manjarrez. “It also showed a technology solution provided added benefits such as reduced rounding time and prep time and increased time with patients.”
The literature summary also suggests involving the patient in the hand-off conversation. “Signing out in front of the patient does wonders for your patient satisfaction rate,” remarked Dr. Manjarrez.
As part of the literature review, the task force found and examined five major expert consensus and policy white papers deemed relevant to hand-offs. Dr. Arora cited these papers from the Australian Council for Safety and Quality in Healthcare, the British Medical Association Junior Doctors Committee, the University Health Consortium, the Department of Defense Patient Safety Program, and the Joint Commission’s (formerly JCAHO’s) National Patient Safety Goal 2006.
Dr. Arora reminded attendees that the Joint Commission’s National Patient Safety Goal states that, “hospitals should implement a standardized approach to hand-off communications. This applies to all staff, not just physicians.”
Common themes found in the five white papers include:
- Frontline providers must be educated about acceptable hand-off practices;
- Adequate time must be made by all parties for hand-offs, and interruptions should be reduced during hand-off communications;
- Information must be up to date;
- Interactive questioning should be facilitated;
- Ill patients must be made a priority; and
- Actions to be undertaken should be clearly delineated.
Recommended Standards for Hand-offs
Based on their literature review, the SHM task force has created basic standards for hospitalists to use for hand-offs.
“Our standards needed to be broad enough to work at all hospital medicine programs, so they’re pretty basic,” said Dr. Arora. “They’re actually minimal standards to be met—they’re fairly simplistic, and we do not consider them to be best practices by any means.”
The standards begin with what seems like an obvious statement, but a necessary one for some hospital medicine groups: “A formally recognized hand-off plan should be instituted at the end of a shift or a change in service.” The standards also state that, “Effective hand-offs will require not only a program policy, but standards for verbal exchange and content exchange,” said Dr. Arora.
To guide hospital medicine groups through this exchange, the speakers offered three mnemonic devices: The 3 T’s, the 4 I’s and the 3 A’s.
The 3 T’s: Your program should have a policy in place that stipulates:
- Time set aside for hand-offs. Ensure that busy hospitalists have adequate time blocked out.
- Template or technology solution. “You need a structured template to help people do their work,” said Dr. Arora. “The program needs to decide what kind of template to adopt—and a move to standardization meets that Joint Commission goal.”
- Train new staff on hand-off expectations. Keep everyone in your practice, including appropriate hospital staff, in the loop.
The 4 I’s of verbal, or face-to-face, exchange include:
- Interruptions are limited. There will always be interruptions, but you can take steps to limit them during hand-offs by designating a time and/or place as “interruption free,” or having someone cover the pagers of the involved hospitalists during hand-offs.
- Interactive process is used. “There should be some interactive dialogue” between the physicians, insisted Dr. Arora.
- Ill patients are given priority. Make sure that you give your sickest patients top priority during hand-offs.
- Insight given to receiver on what to expect or do. What would you do if you were staying on for the next shift? Give the receiver a list of “to-do” items.
The 3 A’s of content exchange standards are:
- All data are up to date. This can be a real problem in healthcare. Make sure all information you turn over, both written and oral, reflects your latest knowledge.
- Anticipated events are emphasized. “What do you anticipate will be a problem?” asked Dr. Arora. Think this through and let the receiver know.
- Action items are highlighted. Again, include a to-do list with the information.
What’s Next?
The task force didn’t stop with these new basic standards. They put together a research agenda, a “wish list” of what’s needed in hospital medicine research to improve hand-offs.
“We need to use research to evaluate these standards rigorously,” said Dr. Arora. “And we must emphasize controlled interventions because only 10 of the articles we found were controlled interventions. We have to urge the research community to do more in this area.”
The group would also like to encourage the development of patient-based outcomes that are sensitive to hand-off quality. “This is talked about a lot, but few people are doing anything about it,” Dr. Arora pointed out.
And finally, they’d like to enable additional funding for further research on hand-offs.
Attendees at the session were polled on their hand-off practices. By a show of hands, approximately 40% indicated they had a standardized hand-off procedure. However, virtually no one thought their procedure was ideal.
The task force encouraged attendees and other hospitalists to share their thoughts and input on hand-off standards. If you have ideas for the task force, you can e-mail them at handoffs@hospitalmedicine.org.
The task force plans to revise their recommendations, with attention to SHM member input. They’d also like to engage an expert panel for an external review of their work before they disseminate it. TH
In “Developing Hand-off Standards for Hospitalists,” members of an SHM task force on hand-offs presented their findings from an extensive literature review and went on to propose basic standards for hospitalist hand-offs. The speakers included task force members Vineet Arora, MD, MA, assistant professor of medicine, University of Chicago; Lakshmi Halasyamani, MD, associate chairperson of the Department of Internal Medicine at St. Joseph Mercy Hospital in Ann Arbor, Mich.; Sunil Kripalani, MD, MSc, an instructor at Emory University, Atlanta, Ga.; and Efren Manjarrez, MD, assistant clinical professor of medicine at the Miller School of Medicine, University of Miami.
Literature Review: Slim Pickings
Although the group hoped to determine best practices based on a literature review of hand-offs, shift changes and handovers (excluding transitions in and out of hospitals) they couldn’t find enough appropriate research to support this goal.
After a PubMed search, and a review of the Agency for Healthcare Research and Quality’s (AHRQ) Patient Safety Net—which is a categorized, reviewed collection of articles and references—the task force reported the following: Of the 334 promising articles they initially identified, only 107 were deemed relevant after a title review. And of those, a significant article review found only 10 met the criteria for inclusion. Three studies of hand-offs appeared in nursing publications and were the only provider-specific studies. The remaining seven were studies of technology solutions for hand-offs—although all articles revealed that any technology fixes were “homegrown,” as nothing specific to hand-offs is widely available commercially.
Those 10 studies included few interventions, with no studies of hospitalist-specific hand-offs. Studies of shift changes predominated, and there were few studies that included patient outcomes.
“A summary of the literature supports the use of supplementing verbal hand-offs with written documentation in some structured format,” said Dr. Manjarrez. “It also showed a technology solution provided added benefits such as reduced rounding time and prep time and increased time with patients.”
The literature summary also suggests involving the patient in the hand-off conversation. “Signing out in front of the patient does wonders for your patient satisfaction rate,” remarked Dr. Manjarrez.
As part of the literature review, the task force found and examined five major expert consensus and policy white papers deemed relevant to hand-offs. Dr. Arora cited these papers from the Australian Council for Safety and Quality in Healthcare, the British Medical Association Junior Doctors Committee, the University Health Consortium, the Department of Defense Patient Safety Program, and the Joint Commission’s (formerly JCAHO’s) National Patient Safety Goal 2006.
Dr. Arora reminded attendees that the Joint Commission’s National Patient Safety Goal states that, “hospitals should implement a standardized approach to hand-off communications. This applies to all staff, not just physicians.”
Common themes found in the five white papers include:
- Frontline providers must be educated about acceptable hand-off practices;
- Adequate time must be made by all parties for hand-offs, and interruptions should be reduced during hand-off communications;
- Information must be up to date;
- Interactive questioning should be facilitated;
- Ill patients must be made a priority; and
- Actions to be undertaken should be clearly delineated.
Recommended Standards for Hand-offs
Based on their literature review, the SHM task force has created basic standards for hospitalists to use for hand-offs.
“Our standards needed to be broad enough to work at all hospital medicine programs, so they’re pretty basic,” said Dr. Arora. “They’re actually minimal standards to be met—they’re fairly simplistic, and we do not consider them to be best practices by any means.”
The standards begin with what seems like an obvious statement, but a necessary one for some hospital medicine groups: “A formally recognized hand-off plan should be instituted at the end of a shift or a change in service.” The standards also state that, “Effective hand-offs will require not only a program policy, but standards for verbal exchange and content exchange,” said Dr. Arora.
To guide hospital medicine groups through this exchange, the speakers offered three mnemonic devices: The 3 T’s, the 4 I’s and the 3 A’s.
The 3 T’s: Your program should have a policy in place that stipulates:
- Time set aside for hand-offs. Ensure that busy hospitalists have adequate time blocked out.
- Template or technology solution. “You need a structured template to help people do their work,” said Dr. Arora. “The program needs to decide what kind of template to adopt—and a move to standardization meets that Joint Commission goal.”
- Train new staff on hand-off expectations. Keep everyone in your practice, including appropriate hospital staff, in the loop.
The 4 I’s of verbal, or face-to-face, exchange include:
- Interruptions are limited. There will always be interruptions, but you can take steps to limit them during hand-offs by designating a time and/or place as “interruption free,” or having someone cover the pagers of the involved hospitalists during hand-offs.
- Interactive process is used. “There should be some interactive dialogue” between the physicians, insisted Dr. Arora.
- Ill patients are given priority. Make sure that you give your sickest patients top priority during hand-offs.
- Insight given to receiver on what to expect or do. What would you do if you were staying on for the next shift? Give the receiver a list of “to-do” items.
The 3 A’s of content exchange standards are:
- All data are up to date. This can be a real problem in healthcare. Make sure all information you turn over, both written and oral, reflects your latest knowledge.
- Anticipated events are emphasized. “What do you anticipate will be a problem?” asked Dr. Arora. Think this through and let the receiver know.
- Action items are highlighted. Again, include a to-do list with the information.
What’s Next?
The task force didn’t stop with these new basic standards. They put together a research agenda, a “wish list” of what’s needed in hospital medicine research to improve hand-offs.
“We need to use research to evaluate these standards rigorously,” said Dr. Arora. “And we must emphasize controlled interventions because only 10 of the articles we found were controlled interventions. We have to urge the research community to do more in this area.”
The group would also like to encourage the development of patient-based outcomes that are sensitive to hand-off quality. “This is talked about a lot, but few people are doing anything about it,” Dr. Arora pointed out.
And finally, they’d like to enable additional funding for further research on hand-offs.
Attendees at the session were polled on their hand-off practices. By a show of hands, approximately 40% indicated they had a standardized hand-off procedure. However, virtually no one thought their procedure was ideal.
The task force encouraged attendees and other hospitalists to share their thoughts and input on hand-off standards. If you have ideas for the task force, you can e-mail them at handoffs@hospitalmedicine.org.
The task force plans to revise their recommendations, with attention to SHM member input. They’d also like to engage an expert panel for an external review of their work before they disseminate it. TH
SHM Honors its Best
SHM recently presented its 2007 Awards of Excellence to four hospitalists whose work and research have contributed significantly to hospital medicine and to the betterment of patient care and quality improvement. The award winners were recognized at “Hospital Medicine 2007” held in Dallas in May:
- Award for Clinical Excellence: Adrienne Green, MD, hospitalist at the University of California, San Francisco (UCSF) Medical Center, associate chief medial officer, associate professor of medicine, and physician lead for the Department of Care Coordination at UCSF.
- Award for Excellence in Research: Vineet Arora, MD, MA, assistant professor for the University of Chicago’s Department of Medicine, associate program director for the Internal Medicine Residency Program and assistant dean for curricular innovation for the Pritzker School of Medicine.
- Award for Excellence in Teaching: Jeffrey Glasheen, MD, assistant professor of medicine, director of the hospital medicine unit and inpatient clinical services, associate program director of the Internal Medicine Residency Training Program and program director for the Hospitalist Training Program at the University of Colorado at Denver Health Sciences Center.
- Award for Outstanding Service in Hospital Medicine: Daniel Rauch, MD, director of the pediatric hospitalist program and assistant residency director of pediatrics for the New York University School of Medicine.

Dr. Green has been a clinically active hospitalist at UCSF Medical Center since 1998. She is engaged in improving systems at USCF, especially in the areas of patient safety, utilization management, compliance, and throughput.
She also enjoys the challenge of working to fix broken systems within the hospital and strives to engage providers across disciplines to work collaboratively to improve the care of hospitalized patients. For this work, she received the UCSF Exceptional Physician Award in 2005.
A graduate of Wesleyan University, Dr. Green received her bachelor’s in molecular biology and chemistry. She earned her medical degree from Hahnemann University School of Medicine and completed her residency at Stanford University (Calif.) in internal medicine.

Dr. Arora’s academic research work on medical education topics such as the effects of sleep deprivation on resident fatigue and patient care, as well as resident interaction with industry, and communication during the handoff process, earned her this year’s Award of Excellence in Research. Her research focuses on measuring and improving quality of care of hospitalized elderly patients. She is the recipient of the Hartford Geriatrics Health Outcomes Research Scholars Award and has also served as a content expert for the development of hospital care quality indicators as part of the ACOVE-3 (Assessing Care for the Vulnerable Elder) Project.
As an active member of SHM, Dr. Arora is the co-founder of the Young Physicians Committee, a member of the SHM Annual Meeting Planning Committee, chair of the Handoff Standards Task Force, and a reviewer for the Research Abstract Committee. She received her bachelor’s from Johns Hopkins University, completed her graduate studies at the University of Chicago Irving B. Harris School of Public Policy, and received her medical degree from Washington University. She completed her residency training in internal medicine and her fellowship in general medicine research at the University of Chicago.

Dr. Glasheen has received many awards recognizing his dedication to hospital medicine and teaching. He is a two-time winner of the Outstanding Clinical Teacher Award given by the students at the University of Colorado School of Medicine, as well as winner of the 7th Annual Elaine Cleary Faculty Teaching Award as the most outstanding educator in the University of Colorado’s Division of General Internal Medicine. As an active member of SHM, Dr. Glasheen participates in the Research, Annual Meeting, and Hospital Medicine Certification committees. He also serves as an SHM delegate to the American Board of Internal Medicine (ABIM) Task Force for Hospitalist Credentialing. Dr. Glasheen also has served as the assistant editor for the Journal of Hospital Medicine since its inception. Most recently, he has been named physician editor for The Hospitalist.
A graduate of Drake University in Des Moines, Iowa, Dr. Glasheen earned his bachelor’s in biology and earned his medical degree from the University of Wisconsin School of Medicine, where he also completed his residency training.

Dr. Rauch is a nationally recognized leader in pediatric hospital medicine. He has done extensive work with the SHRQ Pediatric Quality Indicators Project, resulting in an invitation to serve on the National Quality Forum Pediatric Technical Advisory Panel, as part of the National Voluntary Consensus Standards for Hospital Care: Additional Priorities, 2006-2007. He is an active member of SHM, serving on the Pediatrics and Benchmarks Committees. Additionally, he sits on the executive committee of the hospital medicine section and is a member of the National Committee on Residential Scholarships for the American Academy of Pediatrics.
Dr. Rauch is a graduate of Wesleyan University, where he received his bachelor’s in biology. He earned his medical degree from Wesleyan’s Albert Einstein College of Medicine, where he also completed his residency in pediatrics.
For additional information call (800) 843-3360 or visit www.hospitalmedicine.org. All Award of Excellence recipients receive an all expense-paid trip and complimentary registration to “Hospital Medicine 2008” in San Diego from April 3-5. TH
SHM recently presented its 2007 Awards of Excellence to four hospitalists whose work and research have contributed significantly to hospital medicine and to the betterment of patient care and quality improvement. The award winners were recognized at “Hospital Medicine 2007” held in Dallas in May:
- Award for Clinical Excellence: Adrienne Green, MD, hospitalist at the University of California, San Francisco (UCSF) Medical Center, associate chief medial officer, associate professor of medicine, and physician lead for the Department of Care Coordination at UCSF.
- Award for Excellence in Research: Vineet Arora, MD, MA, assistant professor for the University of Chicago’s Department of Medicine, associate program director for the Internal Medicine Residency Program and assistant dean for curricular innovation for the Pritzker School of Medicine.
- Award for Excellence in Teaching: Jeffrey Glasheen, MD, assistant professor of medicine, director of the hospital medicine unit and inpatient clinical services, associate program director of the Internal Medicine Residency Training Program and program director for the Hospitalist Training Program at the University of Colorado at Denver Health Sciences Center.
- Award for Outstanding Service in Hospital Medicine: Daniel Rauch, MD, director of the pediatric hospitalist program and assistant residency director of pediatrics for the New York University School of Medicine.
Dr. Green has been a clinically active hospitalist at UCSF Medical Center since 1998. She is engaged in improving systems at USCF, especially in the areas of patient safety, utilization management, compliance, and throughput.
She also enjoys the challenge of working to fix broken systems within the hospital and strives to engage providers across disciplines to work collaboratively to improve the care of hospitalized patients. For this work, she received the UCSF Exceptional Physician Award in 2005.
A graduate of Wesleyan University, Dr. Green received her bachelor’s in molecular biology and chemistry. She earned her medical degree from Hahnemann University School of Medicine and completed her residency at Stanford University (Calif.) in internal medicine.
Dr. Arora’s academic research work on medical education topics such as the effects of sleep deprivation on resident fatigue and patient care, as well as resident interaction with industry, and communication during the handoff process, earned her this year’s Award of Excellence in Research. Her research focuses on measuring and improving quality of care of hospitalized elderly patients. She is the recipient of the Hartford Geriatrics Health Outcomes Research Scholars Award and has also served as a content expert for the development of hospital care quality indicators as part of the ACOVE-3 (Assessing Care for the Vulnerable Elder) Project.
As an active member of SHM, Dr. Arora is the co-founder of the Young Physicians Committee, a member of the SHM Annual Meeting Planning Committee, chair of the Handoff Standards Task Force, and a reviewer for the Research Abstract Committee. She received her bachelor’s from Johns Hopkins University, completed her graduate studies at the University of Chicago Irving B. Harris School of Public Policy, and received her medical degree from Washington University. She completed her residency training in internal medicine and her fellowship in general medicine research at the University of Chicago.
Dr. Glasheen has received many awards recognizing his dedication to hospital medicine and teaching. He is a two-time winner of the Outstanding Clinical Teacher Award given by the students at the University of Colorado School of Medicine, as well as winner of the 7th Annual Elaine Cleary Faculty Teaching Award as the most outstanding educator in the University of Colorado’s Division of General Internal Medicine. As an active member of SHM, Dr. Glasheen participates in the Research, Annual Meeting, and Hospital Medicine Certification committees. He also serves as an SHM delegate to the American Board of Internal Medicine (ABIM) Task Force for Hospitalist Credentialing. Dr. Glasheen also has served as the assistant editor for the Journal of Hospital Medicine since its inception. Most recently, he has been named physician editor for The Hospitalist.
A graduate of Drake University in Des Moines, Iowa, Dr. Glasheen earned his bachelor’s in biology and earned his medical degree from the University of Wisconsin School of Medicine, where he also completed his residency training.
Dr. Rauch is a nationally recognized leader in pediatric hospital medicine. He has done extensive work with the SHRQ Pediatric Quality Indicators Project, resulting in an invitation to serve on the National Quality Forum Pediatric Technical Advisory Panel, as part of the National Voluntary Consensus Standards for Hospital Care: Additional Priorities, 2006-2007. He is an active member of SHM, serving on the Pediatrics and Benchmarks Committees. Additionally, he sits on the executive committee of the hospital medicine section and is a member of the National Committee on Residential Scholarships for the American Academy of Pediatrics.
Dr. Rauch is a graduate of Wesleyan University, where he received his bachelor’s in biology. He earned his medical degree from Wesleyan’s Albert Einstein College of Medicine, where he also completed his residency in pediatrics.
For additional information call (800) 843-3360 or visit www.hospitalmedicine.org. All Award of Excellence recipients receive an all expense-paid trip and complimentary registration to “Hospital Medicine 2008” in San Diego from April 3-5. TH
SHM recently presented its 2007 Awards of Excellence to four hospitalists whose work and research have contributed significantly to hospital medicine and to the betterment of patient care and quality improvement. The award winners were recognized at “Hospital Medicine 2007” held in Dallas in May:
- Award for Clinical Excellence: Adrienne Green, MD, hospitalist at the University of California, San Francisco (UCSF) Medical Center, associate chief medial officer, associate professor of medicine, and physician lead for the Department of Care Coordination at UCSF.
- Award for Excellence in Research: Vineet Arora, MD, MA, assistant professor for the University of Chicago’s Department of Medicine, associate program director for the Internal Medicine Residency Program and assistant dean for curricular innovation for the Pritzker School of Medicine.
- Award for Excellence in Teaching: Jeffrey Glasheen, MD, assistant professor of medicine, director of the hospital medicine unit and inpatient clinical services, associate program director of the Internal Medicine Residency Training Program and program director for the Hospitalist Training Program at the University of Colorado at Denver Health Sciences Center.
- Award for Outstanding Service in Hospital Medicine: Daniel Rauch, MD, director of the pediatric hospitalist program and assistant residency director of pediatrics for the New York University School of Medicine.
Dr. Green has been a clinically active hospitalist at UCSF Medical Center since 1998. She is engaged in improving systems at USCF, especially in the areas of patient safety, utilization management, compliance, and throughput.
She also enjoys the challenge of working to fix broken systems within the hospital and strives to engage providers across disciplines to work collaboratively to improve the care of hospitalized patients. For this work, she received the UCSF Exceptional Physician Award in 2005.
A graduate of Wesleyan University, Dr. Green received her bachelor’s in molecular biology and chemistry. She earned her medical degree from Hahnemann University School of Medicine and completed her residency at Stanford University (Calif.) in internal medicine.
Dr. Arora’s academic research work on medical education topics such as the effects of sleep deprivation on resident fatigue and patient care, as well as resident interaction with industry, and communication during the handoff process, earned her this year’s Award of Excellence in Research. Her research focuses on measuring and improving quality of care of hospitalized elderly patients. She is the recipient of the Hartford Geriatrics Health Outcomes Research Scholars Award and has also served as a content expert for the development of hospital care quality indicators as part of the ACOVE-3 (Assessing Care for the Vulnerable Elder) Project.
As an active member of SHM, Dr. Arora is the co-founder of the Young Physicians Committee, a member of the SHM Annual Meeting Planning Committee, chair of the Handoff Standards Task Force, and a reviewer for the Research Abstract Committee. She received her bachelor’s from Johns Hopkins University, completed her graduate studies at the University of Chicago Irving B. Harris School of Public Policy, and received her medical degree from Washington University. She completed her residency training in internal medicine and her fellowship in general medicine research at the University of Chicago.
Dr. Glasheen has received many awards recognizing his dedication to hospital medicine and teaching. He is a two-time winner of the Outstanding Clinical Teacher Award given by the students at the University of Colorado School of Medicine, as well as winner of the 7th Annual Elaine Cleary Faculty Teaching Award as the most outstanding educator in the University of Colorado’s Division of General Internal Medicine. As an active member of SHM, Dr. Glasheen participates in the Research, Annual Meeting, and Hospital Medicine Certification committees. He also serves as an SHM delegate to the American Board of Internal Medicine (ABIM) Task Force for Hospitalist Credentialing. Dr. Glasheen also has served as the assistant editor for the Journal of Hospital Medicine since its inception. Most recently, he has been named physician editor for The Hospitalist.
A graduate of Drake University in Des Moines, Iowa, Dr. Glasheen earned his bachelor’s in biology and earned his medical degree from the University of Wisconsin School of Medicine, where he also completed his residency training.
Dr. Rauch is a nationally recognized leader in pediatric hospital medicine. He has done extensive work with the SHRQ Pediatric Quality Indicators Project, resulting in an invitation to serve on the National Quality Forum Pediatric Technical Advisory Panel, as part of the National Voluntary Consensus Standards for Hospital Care: Additional Priorities, 2006-2007. He is an active member of SHM, serving on the Pediatrics and Benchmarks Committees. Additionally, he sits on the executive committee of the hospital medicine section and is a member of the National Committee on Residential Scholarships for the American Academy of Pediatrics.
Dr. Rauch is a graduate of Wesleyan University, where he received his bachelor’s in biology. He earned his medical degree from Wesleyan’s Albert Einstein College of Medicine, where he also completed his residency in pediatrics.
For additional information call (800) 843-3360 or visit www.hospitalmedicine.org. All Award of Excellence recipients receive an all expense-paid trip and complimentary registration to “Hospital Medicine 2008” in San Diego from April 3-5. TH
SHM Behind the Scenes
As I walked around our office during the week after this year’s SHM Annual Meeting, there was a simple question on the minds of many: What’s next?
After the 12-month planning of “Hospital Medicine 2007”—which culminated in a week away from family, getting out of bed before 5 a.m., and falling asleep after midnight—I guess “What’s next?” is a pretty reasonable question. It’s not at all a surprising question considering the “blood, sweat, and tears” so many volunteer leaders and staff gave to put on an event befitting the fastest-growing specialty in modern healthcare.

“What’s next?” is a fair question for our members to ask of us as well. After all, like so many other organizations, much of what SHM does is designed to come on line, or culminate, during the annual meeting.
I wanted to use this month’s column to give you a small glimpse inside our answer to this simple—yet powerful—question.
One of the surprise stories from “Hospital Medicine 2007” was the success of our Annual Meeting Blog. Over the course of three days, several hospital medicine leaders, including Bob Wachter, MD, shared their experiences—in real time—from Dallas. Augmenting the posts from these contributors were audio podcast interviews with notables that included keynote speaker David Brailer, MD, the first national coordinator for health information technology with the Department of Health and Human Services.

More than 1,000 people visited SHM’s first foray into the blogosphere. Even more exciting is that the blog had hits from hospitalists unable to join us in Dallas.
It used to be that we would say that the biggest meeting in hospital medicine took place each year at the site of the SHM Annual Meeting. With the introduction of the blog, we can now say that is no longer the case. The biggest meeting takes place in more than one city, in more than one hospital, with the geographic location of the SHM Annual Meeting just the hub.
The blog is just the beginning of the answer to the question “What’s next?”
During the coming year, we will use our blogging success as a building block to bringing what many call “new media” squarely into the framework of SHM. You are starting to see the first steps of that effort with the redesign of our homepage, www.hospitalmedicine.org.

To us, new media serves several purposes:
- Inform: The blog showed us a powerful way to deliver real-time news without the delay some publications require;
- Educate: We’re working on creating Webinars—audio conferences coupled with Internet presentations—that will bring education directly to you, at your institution, throughout the year;
- Connect: Through online discussions with thought leaders, including authors from The Hospitalist, we want to celebrate the fact that the most powerful connection we can facilitate is from physician to physician; and
- Differentiate: By bringing these elements together, from blogs and podcasts to Webinars and new online resources, we want to make the question “Why SHM?” one of the easiest you’ll ever have to answer.
What’s next? It’s an interesting question. To us, a major part of the answer is the same it’s always been: to continue innovating by building on our successes and being the group committed to blazing new trails that are focused squarely, and solely, on delivering benefit to our members and the hospital medicine movement.
As I walked around our office during the week after this year’s SHM Annual Meeting, there was a simple question on the minds of many: What’s next?
After the 12-month planning of “Hospital Medicine 2007”—which culminated in a week away from family, getting out of bed before 5 a.m., and falling asleep after midnight—I guess “What’s next?” is a pretty reasonable question. It’s not at all a surprising question considering the “blood, sweat, and tears” so many volunteer leaders and staff gave to put on an event befitting the fastest-growing specialty in modern healthcare.
“What’s next?” is a fair question for our members to ask of us as well. After all, like so many other organizations, much of what SHM does is designed to come on line, or culminate, during the annual meeting.
I wanted to use this month’s column to give you a small glimpse inside our answer to this simple—yet powerful—question.
One of the surprise stories from “Hospital Medicine 2007” was the success of our Annual Meeting Blog. Over the course of three days, several hospital medicine leaders, including Bob Wachter, MD, shared their experiences—in real time—from Dallas. Augmenting the posts from these contributors were audio podcast interviews with notables that included keynote speaker David Brailer, MD, the first national coordinator for health information technology with the Department of Health and Human Services.
More than 1,000 people visited SHM’s first foray into the blogosphere. Even more exciting is that the blog had hits from hospitalists unable to join us in Dallas.
It used to be that we would say that the biggest meeting in hospital medicine took place each year at the site of the SHM Annual Meeting. With the introduction of the blog, we can now say that is no longer the case. The biggest meeting takes place in more than one city, in more than one hospital, with the geographic location of the SHM Annual Meeting just the hub.
The blog is just the beginning of the answer to the question “What’s next?”
During the coming year, we will use our blogging success as a building block to bringing what many call “new media” squarely into the framework of SHM. You are starting to see the first steps of that effort with the redesign of our homepage, www.hospitalmedicine.org.
To us, new media serves several purposes:
- Inform: The blog showed us a powerful way to deliver real-time news without the delay some publications require;
- Educate: We’re working on creating Webinars—audio conferences coupled with Internet presentations—that will bring education directly to you, at your institution, throughout the year;
- Connect: Through online discussions with thought leaders, including authors from The Hospitalist, we want to celebrate the fact that the most powerful connection we can facilitate is from physician to physician; and
- Differentiate: By bringing these elements together, from blogs and podcasts to Webinars and new online resources, we want to make the question “Why SHM?” one of the easiest you’ll ever have to answer.
What’s next? It’s an interesting question. To us, a major part of the answer is the same it’s always been: to continue innovating by building on our successes and being the group committed to blazing new trails that are focused squarely, and solely, on delivering benefit to our members and the hospital medicine movement.
As I walked around our office during the week after this year’s SHM Annual Meeting, there was a simple question on the minds of many: What’s next?
After the 12-month planning of “Hospital Medicine 2007”—which culminated in a week away from family, getting out of bed before 5 a.m., and falling asleep after midnight—I guess “What’s next?” is a pretty reasonable question. It’s not at all a surprising question considering the “blood, sweat, and tears” so many volunteer leaders and staff gave to put on an event befitting the fastest-growing specialty in modern healthcare.
“What’s next?” is a fair question for our members to ask of us as well. After all, like so many other organizations, much of what SHM does is designed to come on line, or culminate, during the annual meeting.
I wanted to use this month’s column to give you a small glimpse inside our answer to this simple—yet powerful—question.
One of the surprise stories from “Hospital Medicine 2007” was the success of our Annual Meeting Blog. Over the course of three days, several hospital medicine leaders, including Bob Wachter, MD, shared their experiences—in real time—from Dallas. Augmenting the posts from these contributors were audio podcast interviews with notables that included keynote speaker David Brailer, MD, the first national coordinator for health information technology with the Department of Health and Human Services.
More than 1,000 people visited SHM’s first foray into the blogosphere. Even more exciting is that the blog had hits from hospitalists unable to join us in Dallas.
It used to be that we would say that the biggest meeting in hospital medicine took place each year at the site of the SHM Annual Meeting. With the introduction of the blog, we can now say that is no longer the case. The biggest meeting takes place in more than one city, in more than one hospital, with the geographic location of the SHM Annual Meeting just the hub.
The blog is just the beginning of the answer to the question “What’s next?”
During the coming year, we will use our blogging success as a building block to bringing what many call “new media” squarely into the framework of SHM. You are starting to see the first steps of that effort with the redesign of our homepage, www.hospitalmedicine.org.
To us, new media serves several purposes:
- Inform: The blog showed us a powerful way to deliver real-time news without the delay some publications require;
- Educate: We’re working on creating Webinars—audio conferences coupled with Internet presentations—that will bring education directly to you, at your institution, throughout the year;
- Connect: Through online discussions with thought leaders, including authors from The Hospitalist, we want to celebrate the fact that the most powerful connection we can facilitate is from physician to physician; and
- Differentiate: By bringing these elements together, from blogs and podcasts to Webinars and new online resources, we want to make the question “Why SHM?” one of the easiest you’ll ever have to answer.
What’s next? It’s an interesting question. To us, a major part of the answer is the same it’s always been: to continue innovating by building on our successes and being the group committed to blazing new trails that are focused squarely, and solely, on delivering benefit to our members and the hospital medicine movement.
Heinous Crimes
By the time a mortician in the northeast British town of Hyde, Greater Manchester, United Kingdom, noticed Dr. Harold Shipman’s patients were dying at an exorbitant rate, the doctor had probably killed close to 300 of them, according to Kenneth V. Iserson, MD, MBA, professor of emergency medicine at the University of Arizona College of Medicine and author of “Demon Doctors: Physicians as Serial Killers.”
Shipman, labeled ‘‘the most prolific serial killer in the history of the United Kingdom—and probably the world,’’ was officially convicted of killing 15 patients in 2000 and sentenced to 15 consecutive life sentences.1 In January 2004 he was found hanged in his prison cell.
Sometimes referred to as caregiver-associated serial killings, these incidents generate profound shock in the healthcare community. As repellent and relatively rare as this behavior is, and as controversial as the topic is, neither individuals nor institutions can afford to disassociate themselves from the subject. Hospitalists should not hide from this issue and should not feel they will be accused of “treason” if they educate themselves and bring suspicious behavior to the awareness of superiors, says Beatrice Crofts Yorker, JD, RN, MS, FAAN, dean of the College of Health and Human Services at California State University, Los Angeles. On the contrary, she says, “first, do no harm” also entails ensuring everyone else around you follows the same ethic.
Dr. Yorker, who has been studying this phenomenon since 1986, published the first examination of cases of serial murder by nurses in the American Journal of Nursing (AJN) in 1988. “It is a serious problem that has been under-recognized, and it is the right thing to blow the whistle when adverse patient incidents are associated with the presence of a specific healthcare provider,” says Dr. Yorker. “In fact, most of the cases came to the attention of authorities because a nurse blew the whistle. The sad thing is that some of the nurses were disciplined for their protective actions; however, they were ultimately vindicated.”
A veteran of the phenomenon urges continued vigilance. “As a general caveat, there needs to be a higher index of suspicion for these incidents,” says Kenneth W. Kizer, MD, MPH, the former head of the veterans healthcare system who had to deal with three incidents of serial murder at Veterans Affairs (VA) hospitals in the 1990s. “These incidents are grossly underreported.”
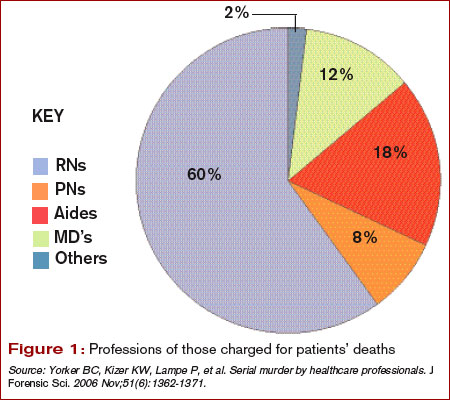
Incidence and Cause of Death
Drs. Kizer and Yorker were two of the investigators who reviewed epidemiologic studies, toxicology evidence, and court transcripts for data on healthcare professionals prosecuted between 1970 and 2006.
“Dr. Robert Forrest, who was a forensic toxicologist getting a law degree and wrote his dissertation on the topic of serial murder by healthcare providers, contacted me after the AJN article came out,” says Dr. Yorker. Dr. Forrest has been the testifying expert in most of the U.K. cases. “After the Charles Cullen case hit the news, The New York Times and Modern Healthcare contacted me regarding my study in AJN and the Journal of Nursing Law. That is how Ken Kizer and Paula Lampe found me.” (Cullen, a registered nurse, received 11 consecutive life sentences in 2006 after pleading guilty to administering lethal doses of medication to more than 40 patients in New Jersey and Pennsylvania.)
Lampe, an author, had been studying cases in Europe. “Because both Robert and Paula provided additional data on some cases, they were co-authors—as was Ken—who provided data on the VA cases and an important public policy perspective,” says Dr. Yorker.
The search showed 90 criminal prosecutions of healthcare providers who met the criteria of serial murder of patients. Of those, 54 have been convicted—45 for serial murder, four for attempted murder, and five on lesser charges. Since the publication of their study, one more of the accused has received a sentence of life in prison, another has been convicted and sentenced to 20 years, one committed suicide in prison, and two additional nurses in Germany and the Czech Republic have been arrested and confessed to serial murder of patients. In addition, Dr. Yorker is continuing to follow two large-scale murder-for-profit prosecutions. There are four defendants in each case. Further, three individuals have been found liable for wrongful death in the amounts of $27 million, $8 million, and $450,000 in damages.
Injection was the main method used by healthcare killers, followed by suffocation, poisoning, and tampering with equipment. Prosecutions were reported in 20 countries, with 40% of the incidents taking place in the United States. Nursing personnel were 86% of the healthcare providers prosecuted; 12% were physicians, and 2% were allied health professionals. The number of patient deaths that resulted in a murder conviction is 317, and the number of suspicious patient deaths attributed to the 54 convicted caregivers is 2,113.
“Physicians as serial killers are remarkably uncommon,” says Dr. Iserson, who is also director of the Arizona Bioethics Program at the University of Arizona College of Medicine in Tucson. “Nurses [who are serial killers] are much more common, but of course there are more nurses in the hospital, just as there are ancillary people.” (See Figure 1, left.) Dr. Iserson, who practices emergency medicine and consults nationally on bioethics, advises maintaining caution when examining data of charges or suspicions that were never proved.
Most of these crimes (70%) occur in hospital units. (See Figure 2, left.) Victims are almost always female, as are almost half (49%) of convicted serial killers and 55% of the total number of prosecuted healthcare providers. Males are disproportionately represented among prosecuted nurses.
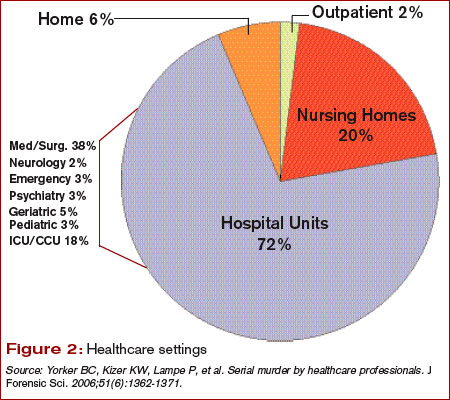
Motives: Who Is Always There?
Although the motives are complex, some common threads connect these crimes. “There are some classical signs, if you will,” says Dr. Kizer.
When the same person repeatedly calls a code and always seems to be in the thick of it, that is one prime indicator. These people are usually legitimately present in those settings and circumstances—for example, they are on call or working a shift—which makes it more difficult to discern when something is awry. Commonly, the perpetrators have easy access to high-alert drugs without sufficient accountability. Sometimes, once an investigation has been launched it is discovered the person has falsified his or her credentials.
In hospitals, experts say, the “rescuer” or “hero” personality is often on display in those who kill patients—the first person there to give the patient drugs or attempt to save the patient.
“What you are going to see as a pattern,” says Dr. Iserson, “is that they need to be near death.” Codes or calls for respiratory arrest are the most common; patients who have cardiac arrests are much harder to save. Being the hero is not always the motive; the converse can also apply.
Such is the case with nurse Orville Lynn Majors, LPN, convicted of six murders at the Vermillion county hospital in Clinton, Ind. The deaths were consistent with injections of potassium chloride and epinephrine according to prosecutors. Majors’ coworkers were concerned that patients were coding in alarming numbers while in his care. Although this information did not come out until after he was apprehended, his coworkers had a good idea which of his patients would not survive: Patients who were whiny, demanding, or required a lot of work. “The scuttlebutt or rumor among his coworkers,” says Dr. Kizer, “is that they could almost predict which patients would have a demise under his care.”
Although a typical profile of the serial healthcare murderer has been demonstrated in many cases, in many other cases the demographics and behaviors of these killers have deviated widely from generalized assumptions.2 Therefore, before looking at people, look at the numbers.
An unusual number of calls and codes may occur in a particular area of the hospital. “In ICUs you expect a lot of [codes and calls], but not on general post-op wards or the pediatrics MICU,” Dr. Kizer says. “When this happens in these settings it should raise a red flag.”
Unfortunately, most hospitals don’t track mortality on a monthly basis per unit or ward or ICU, so they may not recognize when something is out of line in a timely manner. Also, the hospital committee assigned to review deaths may be remiss in its duty to meet regularly or otherwise perform according to policy.
Another factor that should raise a red flag is a disproportionate number of codes or deaths on the same shift—most often the night shift. Often, someone says, “Gee, it seems like there’s an awful lot of codes lately,” explains Dr. Kizer. An unusually high rate of successful codes is another sign.
For example, in the 1995-1996 case of Kristen Gilbert, an RN convicted of four murders at the Veterans Affairs Medical Center in Northampton, Mass., she was having an extramarital affair with a hospital security guard who worked the evening shift. Protocol required that security be called to all cardiopulmonary arrests. Gilbert used stimulant epinephrine to make their hearts race out of control. The epidemiologic data later showed that suspicious codes occurred when both were on duty. “The patients always seemed to recover and she was the hero,” says Dr. Kizer. “She wanted to look good for her boyfriend.”
Similarly, Richard Angelo, a charge nurse at Good Samaritan Hospital in West Islip, Long Island, N.Y., admitted that between 1987 and 1989 he injected patients with paralyzing drugs Pavulon (pancuronium) and Anectine (succinylcholine). He wanted his colleagues to admire him for performing well in a code. During his confession, he likened himself to volunteer firefighters who set fires. In fact, Dr. Iserson makes this same parallel. “From what we can tell,” he says, “these people don’t really care whether the person dies or not. They would rather they not [die], so they can be seen as the hero. It’s all about them.” As with instances of arson, he says, the perpetrator is “the first one to show up at the fire watch, over and over again.”
Obstacles to Disclosure
Even when healthcare workers and related personnel come forward with their suspicions, law enforcement may be a barrier to prosecution.
In the United Kingdom, a Manchester mortician took her observations about the excessive deaths and cremations in Harold Shipman’s practice to her father and brother, who were also in the family business. She also obtained the support of a local female general practitioner. The two women went to the police, explaining that most patients who had died had not been critically ill and noted that the doctor had exhibited peculiar behavior when he was questioned.
But, says Dr. Iserson, the response again was typical: “‘Oh, foolish women. That can’t be happening.’ And it wasn’t until Shipman killed the wrong person [a former town mayor, mother of a prominent lawyer] that things started to unravel for him.” When police finally looked at other deaths Shipman had certified, a pattern emerged. He would overdose patients with diamorphine, sign their death certificates, then forge medical records to indicate they were in poor health.
A second common response by institutions is just as much of a barrier to bringing these crimes to light and ultimately, prosecution. “In essence,” says Dr. Iserson, “that response is, ‘Well, maybe it is happening but, boy, it sure is going to put our institution in a bad light. So let’s just not say anything.’ ”
This was the case with Michael Swango, a doctor who worked in several states and a number of countries. He was charged with five murders and may have been involved in 126 deaths. Swango confessed to the deaths that occurred in a Veterans Affairs hospital in Northport, N.Y., where he reportedly injected three veterans with a drug that stopped their hearts. He had forged “do not resuscitate” orders for the three. He was sentenced to two life sentences. It is possible that he killed as many as 35-60 people in the United States and Zimbabwe. But before it was all out in the open, “some very prominent people were involved in sweeping it under the rug,” says Dr. Iserson, “and they didn’t even get a slap on the wrist.”
Hiring Practices
One of the most shocking aspects of the Cullen case was that institutional coverup and employee privacy policies meant his prior employers never revealed the problems to prospective employers.
“Identifying potential serial killers is not at all the total problem,” says Dr. Iserson. “The problem is getting the powers that be to act. What they typically do is pass the problem on to somebody else, in effect, saying, ‘We don’t want you to work here anymore. We won’t necessarily write you a good letter of recommendation, but we will say that you worked here, and basically we just want you to go away.’ ”
An investigation revealed that Cullen had a history of reported incidents at hospitals in Pennsylvania and New Jersey, but there were no tracking or disclosure systems in place as he moved from one hospital to another. His employment history included termination from several hospitals because of misconduct, hospitalizations for mental illness, and a criminal investigation regarding improper medication administration.
In an open letter published in The New York Times on March 14, 2004, Somerset Medical Center (Somerville, N.J.) asserted: “Mr. Cullen worked at nine other healthcare facilities over a 16-year period. His former work history problems were not revealed to us. Nor were any state agencies or licensing boards able to provide us with accurate information about his employment history.”
Cullen had been investigated by three hospitals, a nursing home, and two prosecutors for suspicious patient deaths. He was fired by five hospitals and one nursing home for suspected wrongdoing. But Cullen continued to find employment and kill patients.
“Confidentiality is essential [as is] not leaking to the media, which can taint the investigation,” says Dr. Yorker. “The Charles Cullen case should motivate hospitalists to [participate in helping to stop the systemic mechanism that made possible] his killing over 40 patients in nine different hospitals and a nursing home before being stopped. This erodes the public trust in hospitals.”
The Health Care Quality Improvement Act provides some immunity for reporters of adverse information, but it applies only to physicians—not communications between employers.
The American Society for Healthcare Risk Management (ASHRM) and Dr. Kizer and his colleagues are in alignment in advocating for the provision of more comprehensive immunity to help healthcare employees and patients when they report these incidents.3
“If you have information that a worker is harming patients, the institution should be able to tell prospective employers and not worry about getting sued,” says Dr. Yorker. A number of states have passed varying forms of legislation so far, and ASHRM is recommending this be a federal matter. Dr. Kizer and his group recommend that reporting of suspected serial murderers should be considered for coverage under Good Samaritan laws.
Other Complicating Factors
Another problem in bringing legitimate cases to prosecution is when providers are accused on trumped-up charges, which in Dr. Iserson’s view amounts to prosecutorial malpractice. Examples are cases post-Hurricane Katrina, when physicians and nurses were charged with patient deaths.
Internationally, an example is the case in Libya where the main defendants—a Palestinian doctor and five Bulgarian nurses—were charged with injecting 426 children with HIV in 1998, causing an epidemic at El-Fath Children’s Hospital in Benghazi. According to World Politics Watch, dozens of foreign medical professionals were arrested, with six eventually charged and forced to confess by Libyan authorities. Subsequent research published in the journal Nature indicated that viral strains present in the infected children were present at the hospital before 1998.
“This was a case of political blackmail,” says Dr. Iserson. These cases may not be clear-cut and may be open to negative interpretations that “make people skittish. That is why institutions are prone to say, ‘Gee, maybe it’s just one of those kinds of cases. We don’t want to make that kind of mistake.’ ”
Also problematic is the variable rate at which hospitals perform autopsies.
“Autopsy rates are down in many communities to 1% or 2% or even lower,” says Dr. Kizer. “When the data point to the possibility of a crime on a particular unit, the site needs to be treated as a crime scene. In most hospitals, when someone dies, you get them off the floor and you clean up as quickly as possible. That shouldn’t be the case if it is a suspected crime scene. Ideally there should be standardized processes or protocols whenever there is suspicion. And those protocols may be different than when a patient ordinarily dies.”
Seeking Solutions
Hospitalists and other professionals—especially nurses and ancillary personnel—have an obligation to be informed and astute regarding individual characteristics and signs of suspicious patient deaths. Appropriate epidemiological, toxicological, and psychological data must be collected and analyzed routinely.
“Data about this phenomenon need to be disseminated to heighten awareness that serial murder of patients is a significant concern that extends beyond a few shocking, isolated incidents,” write Drs. Yorker and Kizer and their co-authors.
Institutional hiring practices must be changed so balance is achieved between preventing wrongful discharge or denial-of-employment lawsuits and protecting patient safety. Existing state legislation and future federal legislation for institutional immunity is an important element of patient advocacy that hospitalists can support.
Ultimately, hospitalists must be informed, aware, and alert. “Most [suspicions] will not be anything,” says Dr. Iserson. “Just pay attention to it.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Yorker BC, Kizer KW, Lampe P, et al. Serial murder by healthcare professionals. J Forensic Sci. 2006 Nov;51(6):1362-1371.
- Wolf BC, Lavezzi WA. Paths to destruction: the lives and crimes of two serial killers. J Forensic Sci. 2007 Jan;52(1):199-203.
- ASHRM. American Society for Healthcare Risk Management. A call for federal immunity to protect health care employers … and patients. Chicago: Monograph; April 1, 2005; www.ashrm.org/ashrm/resources/files/Monograph.Immunity.pdf.
By the time a mortician in the northeast British town of Hyde, Greater Manchester, United Kingdom, noticed Dr. Harold Shipman’s patients were dying at an exorbitant rate, the doctor had probably killed close to 300 of them, according to Kenneth V. Iserson, MD, MBA, professor of emergency medicine at the University of Arizona College of Medicine and author of “Demon Doctors: Physicians as Serial Killers.”
Shipman, labeled ‘‘the most prolific serial killer in the history of the United Kingdom—and probably the world,’’ was officially convicted of killing 15 patients in 2000 and sentenced to 15 consecutive life sentences.1 In January 2004 he was found hanged in his prison cell.
Sometimes referred to as caregiver-associated serial killings, these incidents generate profound shock in the healthcare community. As repellent and relatively rare as this behavior is, and as controversial as the topic is, neither individuals nor institutions can afford to disassociate themselves from the subject. Hospitalists should not hide from this issue and should not feel they will be accused of “treason” if they educate themselves and bring suspicious behavior to the awareness of superiors, says Beatrice Crofts Yorker, JD, RN, MS, FAAN, dean of the College of Health and Human Services at California State University, Los Angeles. On the contrary, she says, “first, do no harm” also entails ensuring everyone else around you follows the same ethic.
Dr. Yorker, who has been studying this phenomenon since 1986, published the first examination of cases of serial murder by nurses in the American Journal of Nursing (AJN) in 1988. “It is a serious problem that has been under-recognized, and it is the right thing to blow the whistle when adverse patient incidents are associated with the presence of a specific healthcare provider,” says Dr. Yorker. “In fact, most of the cases came to the attention of authorities because a nurse blew the whistle. The sad thing is that some of the nurses were disciplined for their protective actions; however, they were ultimately vindicated.”
A veteran of the phenomenon urges continued vigilance. “As a general caveat, there needs to be a higher index of suspicion for these incidents,” says Kenneth W. Kizer, MD, MPH, the former head of the veterans healthcare system who had to deal with three incidents of serial murder at Veterans Affairs (VA) hospitals in the 1990s. “These incidents are grossly underreported.”
Incidence and Cause of Death
Drs. Kizer and Yorker were two of the investigators who reviewed epidemiologic studies, toxicology evidence, and court transcripts for data on healthcare professionals prosecuted between 1970 and 2006.
“Dr. Robert Forrest, who was a forensic toxicologist getting a law degree and wrote his dissertation on the topic of serial murder by healthcare providers, contacted me after the AJN article came out,” says Dr. Yorker. Dr. Forrest has been the testifying expert in most of the U.K. cases. “After the Charles Cullen case hit the news, The New York Times and Modern Healthcare contacted me regarding my study in AJN and the Journal of Nursing Law. That is how Ken Kizer and Paula Lampe found me.” (Cullen, a registered nurse, received 11 consecutive life sentences in 2006 after pleading guilty to administering lethal doses of medication to more than 40 patients in New Jersey and Pennsylvania.)
Lampe, an author, had been studying cases in Europe. “Because both Robert and Paula provided additional data on some cases, they were co-authors—as was Ken—who provided data on the VA cases and an important public policy perspective,” says Dr. Yorker.
The search showed 90 criminal prosecutions of healthcare providers who met the criteria of serial murder of patients. Of those, 54 have been convicted—45 for serial murder, four for attempted murder, and five on lesser charges. Since the publication of their study, one more of the accused has received a sentence of life in prison, another has been convicted and sentenced to 20 years, one committed suicide in prison, and two additional nurses in Germany and the Czech Republic have been arrested and confessed to serial murder of patients. In addition, Dr. Yorker is continuing to follow two large-scale murder-for-profit prosecutions. There are four defendants in each case. Further, three individuals have been found liable for wrongful death in the amounts of $27 million, $8 million, and $450,000 in damages.
Injection was the main method used by healthcare killers, followed by suffocation, poisoning, and tampering with equipment. Prosecutions were reported in 20 countries, with 40% of the incidents taking place in the United States. Nursing personnel were 86% of the healthcare providers prosecuted; 12% were physicians, and 2% were allied health professionals. The number of patient deaths that resulted in a murder conviction is 317, and the number of suspicious patient deaths attributed to the 54 convicted caregivers is 2,113.
“Physicians as serial killers are remarkably uncommon,” says Dr. Iserson, who is also director of the Arizona Bioethics Program at the University of Arizona College of Medicine in Tucson. “Nurses [who are serial killers] are much more common, but of course there are more nurses in the hospital, just as there are ancillary people.” (See Figure 1, left.) Dr. Iserson, who practices emergency medicine and consults nationally on bioethics, advises maintaining caution when examining data of charges or suspicions that were never proved.
Most of these crimes (70%) occur in hospital units. (See Figure 2, left.) Victims are almost always female, as are almost half (49%) of convicted serial killers and 55% of the total number of prosecuted healthcare providers. Males are disproportionately represented among prosecuted nurses.
Motives: Who Is Always There?
Although the motives are complex, some common threads connect these crimes. “There are some classical signs, if you will,” says Dr. Kizer.
When the same person repeatedly calls a code and always seems to be in the thick of it, that is one prime indicator. These people are usually legitimately present in those settings and circumstances—for example, they are on call or working a shift—which makes it more difficult to discern when something is awry. Commonly, the perpetrators have easy access to high-alert drugs without sufficient accountability. Sometimes, once an investigation has been launched it is discovered the person has falsified his or her credentials.
In hospitals, experts say, the “rescuer” or “hero” personality is often on display in those who kill patients—the first person there to give the patient drugs or attempt to save the patient.
“What you are going to see as a pattern,” says Dr. Iserson, “is that they need to be near death.” Codes or calls for respiratory arrest are the most common; patients who have cardiac arrests are much harder to save. Being the hero is not always the motive; the converse can also apply.
Such is the case with nurse Orville Lynn Majors, LPN, convicted of six murders at the Vermillion county hospital in Clinton, Ind. The deaths were consistent with injections of potassium chloride and epinephrine according to prosecutors. Majors’ coworkers were concerned that patients were coding in alarming numbers while in his care. Although this information did not come out until after he was apprehended, his coworkers had a good idea which of his patients would not survive: Patients who were whiny, demanding, or required a lot of work. “The scuttlebutt or rumor among his coworkers,” says Dr. Kizer, “is that they could almost predict which patients would have a demise under his care.”
Although a typical profile of the serial healthcare murderer has been demonstrated in many cases, in many other cases the demographics and behaviors of these killers have deviated widely from generalized assumptions.2 Therefore, before looking at people, look at the numbers.
An unusual number of calls and codes may occur in a particular area of the hospital. “In ICUs you expect a lot of [codes and calls], but not on general post-op wards or the pediatrics MICU,” Dr. Kizer says. “When this happens in these settings it should raise a red flag.”
Unfortunately, most hospitals don’t track mortality on a monthly basis per unit or ward or ICU, so they may not recognize when something is out of line in a timely manner. Also, the hospital committee assigned to review deaths may be remiss in its duty to meet regularly or otherwise perform according to policy.
Another factor that should raise a red flag is a disproportionate number of codes or deaths on the same shift—most often the night shift. Often, someone says, “Gee, it seems like there’s an awful lot of codes lately,” explains Dr. Kizer. An unusually high rate of successful codes is another sign.
For example, in the 1995-1996 case of Kristen Gilbert, an RN convicted of four murders at the Veterans Affairs Medical Center in Northampton, Mass., she was having an extramarital affair with a hospital security guard who worked the evening shift. Protocol required that security be called to all cardiopulmonary arrests. Gilbert used stimulant epinephrine to make their hearts race out of control. The epidemiologic data later showed that suspicious codes occurred when both were on duty. “The patients always seemed to recover and she was the hero,” says Dr. Kizer. “She wanted to look good for her boyfriend.”
Similarly, Richard Angelo, a charge nurse at Good Samaritan Hospital in West Islip, Long Island, N.Y., admitted that between 1987 and 1989 he injected patients with paralyzing drugs Pavulon (pancuronium) and Anectine (succinylcholine). He wanted his colleagues to admire him for performing well in a code. During his confession, he likened himself to volunteer firefighters who set fires. In fact, Dr. Iserson makes this same parallel. “From what we can tell,” he says, “these people don’t really care whether the person dies or not. They would rather they not [die], so they can be seen as the hero. It’s all about them.” As with instances of arson, he says, the perpetrator is “the first one to show up at the fire watch, over and over again.”
Obstacles to Disclosure
Even when healthcare workers and related personnel come forward with their suspicions, law enforcement may be a barrier to prosecution.
In the United Kingdom, a Manchester mortician took her observations about the excessive deaths and cremations in Harold Shipman’s practice to her father and brother, who were also in the family business. She also obtained the support of a local female general practitioner. The two women went to the police, explaining that most patients who had died had not been critically ill and noted that the doctor had exhibited peculiar behavior when he was questioned.
But, says Dr. Iserson, the response again was typical: “‘Oh, foolish women. That can’t be happening.’ And it wasn’t until Shipman killed the wrong person [a former town mayor, mother of a prominent lawyer] that things started to unravel for him.” When police finally looked at other deaths Shipman had certified, a pattern emerged. He would overdose patients with diamorphine, sign their death certificates, then forge medical records to indicate they were in poor health.
A second common response by institutions is just as much of a barrier to bringing these crimes to light and ultimately, prosecution. “In essence,” says Dr. Iserson, “that response is, ‘Well, maybe it is happening but, boy, it sure is going to put our institution in a bad light. So let’s just not say anything.’ ”
This was the case with Michael Swango, a doctor who worked in several states and a number of countries. He was charged with five murders and may have been involved in 126 deaths. Swango confessed to the deaths that occurred in a Veterans Affairs hospital in Northport, N.Y., where he reportedly injected three veterans with a drug that stopped their hearts. He had forged “do not resuscitate” orders for the three. He was sentenced to two life sentences. It is possible that he killed as many as 35-60 people in the United States and Zimbabwe. But before it was all out in the open, “some very prominent people were involved in sweeping it under the rug,” says Dr. Iserson, “and they didn’t even get a slap on the wrist.”
Hiring Practices
One of the most shocking aspects of the Cullen case was that institutional coverup and employee privacy policies meant his prior employers never revealed the problems to prospective employers.
“Identifying potential serial killers is not at all the total problem,” says Dr. Iserson. “The problem is getting the powers that be to act. What they typically do is pass the problem on to somebody else, in effect, saying, ‘We don’t want you to work here anymore. We won’t necessarily write you a good letter of recommendation, but we will say that you worked here, and basically we just want you to go away.’ ”
An investigation revealed that Cullen had a history of reported incidents at hospitals in Pennsylvania and New Jersey, but there were no tracking or disclosure systems in place as he moved from one hospital to another. His employment history included termination from several hospitals because of misconduct, hospitalizations for mental illness, and a criminal investigation regarding improper medication administration.
In an open letter published in The New York Times on March 14, 2004, Somerset Medical Center (Somerville, N.J.) asserted: “Mr. Cullen worked at nine other healthcare facilities over a 16-year period. His former work history problems were not revealed to us. Nor were any state agencies or licensing boards able to provide us with accurate information about his employment history.”
Cullen had been investigated by three hospitals, a nursing home, and two prosecutors for suspicious patient deaths. He was fired by five hospitals and one nursing home for suspected wrongdoing. But Cullen continued to find employment and kill patients.
“Confidentiality is essential [as is] not leaking to the media, which can taint the investigation,” says Dr. Yorker. “The Charles Cullen case should motivate hospitalists to [participate in helping to stop the systemic mechanism that made possible] his killing over 40 patients in nine different hospitals and a nursing home before being stopped. This erodes the public trust in hospitals.”
The Health Care Quality Improvement Act provides some immunity for reporters of adverse information, but it applies only to physicians—not communications between employers.
The American Society for Healthcare Risk Management (ASHRM) and Dr. Kizer and his colleagues are in alignment in advocating for the provision of more comprehensive immunity to help healthcare employees and patients when they report these incidents.3
“If you have information that a worker is harming patients, the institution should be able to tell prospective employers and not worry about getting sued,” says Dr. Yorker. A number of states have passed varying forms of legislation so far, and ASHRM is recommending this be a federal matter. Dr. Kizer and his group recommend that reporting of suspected serial murderers should be considered for coverage under Good Samaritan laws.
Other Complicating Factors
Another problem in bringing legitimate cases to prosecution is when providers are accused on trumped-up charges, which in Dr. Iserson’s view amounts to prosecutorial malpractice. Examples are cases post-Hurricane Katrina, when physicians and nurses were charged with patient deaths.
Internationally, an example is the case in Libya where the main defendants—a Palestinian doctor and five Bulgarian nurses—were charged with injecting 426 children with HIV in 1998, causing an epidemic at El-Fath Children’s Hospital in Benghazi. According to World Politics Watch, dozens of foreign medical professionals were arrested, with six eventually charged and forced to confess by Libyan authorities. Subsequent research published in the journal Nature indicated that viral strains present in the infected children were present at the hospital before 1998.
“This was a case of political blackmail,” says Dr. Iserson. These cases may not be clear-cut and may be open to negative interpretations that “make people skittish. That is why institutions are prone to say, ‘Gee, maybe it’s just one of those kinds of cases. We don’t want to make that kind of mistake.’ ”
Also problematic is the variable rate at which hospitals perform autopsies.
“Autopsy rates are down in many communities to 1% or 2% or even lower,” says Dr. Kizer. “When the data point to the possibility of a crime on a particular unit, the site needs to be treated as a crime scene. In most hospitals, when someone dies, you get them off the floor and you clean up as quickly as possible. That shouldn’t be the case if it is a suspected crime scene. Ideally there should be standardized processes or protocols whenever there is suspicion. And those protocols may be different than when a patient ordinarily dies.”
Seeking Solutions
Hospitalists and other professionals—especially nurses and ancillary personnel—have an obligation to be informed and astute regarding individual characteristics and signs of suspicious patient deaths. Appropriate epidemiological, toxicological, and psychological data must be collected and analyzed routinely.
“Data about this phenomenon need to be disseminated to heighten awareness that serial murder of patients is a significant concern that extends beyond a few shocking, isolated incidents,” write Drs. Yorker and Kizer and their co-authors.
Institutional hiring practices must be changed so balance is achieved between preventing wrongful discharge or denial-of-employment lawsuits and protecting patient safety. Existing state legislation and future federal legislation for institutional immunity is an important element of patient advocacy that hospitalists can support.
Ultimately, hospitalists must be informed, aware, and alert. “Most [suspicions] will not be anything,” says Dr. Iserson. “Just pay attention to it.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Yorker BC, Kizer KW, Lampe P, et al. Serial murder by healthcare professionals. J Forensic Sci. 2006 Nov;51(6):1362-1371.
- Wolf BC, Lavezzi WA. Paths to destruction: the lives and crimes of two serial killers. J Forensic Sci. 2007 Jan;52(1):199-203.
- ASHRM. American Society for Healthcare Risk Management. A call for federal immunity to protect health care employers … and patients. Chicago: Monograph; April 1, 2005; www.ashrm.org/ashrm/resources/files/Monograph.Immunity.pdf.
By the time a mortician in the northeast British town of Hyde, Greater Manchester, United Kingdom, noticed Dr. Harold Shipman’s patients were dying at an exorbitant rate, the doctor had probably killed close to 300 of them, according to Kenneth V. Iserson, MD, MBA, professor of emergency medicine at the University of Arizona College of Medicine and author of “Demon Doctors: Physicians as Serial Killers.”
Shipman, labeled ‘‘the most prolific serial killer in the history of the United Kingdom—and probably the world,’’ was officially convicted of killing 15 patients in 2000 and sentenced to 15 consecutive life sentences.1 In January 2004 he was found hanged in his prison cell.
Sometimes referred to as caregiver-associated serial killings, these incidents generate profound shock in the healthcare community. As repellent and relatively rare as this behavior is, and as controversial as the topic is, neither individuals nor institutions can afford to disassociate themselves from the subject. Hospitalists should not hide from this issue and should not feel they will be accused of “treason” if they educate themselves and bring suspicious behavior to the awareness of superiors, says Beatrice Crofts Yorker, JD, RN, MS, FAAN, dean of the College of Health and Human Services at California State University, Los Angeles. On the contrary, she says, “first, do no harm” also entails ensuring everyone else around you follows the same ethic.
Dr. Yorker, who has been studying this phenomenon since 1986, published the first examination of cases of serial murder by nurses in the American Journal of Nursing (AJN) in 1988. “It is a serious problem that has been under-recognized, and it is the right thing to blow the whistle when adverse patient incidents are associated with the presence of a specific healthcare provider,” says Dr. Yorker. “In fact, most of the cases came to the attention of authorities because a nurse blew the whistle. The sad thing is that some of the nurses were disciplined for their protective actions; however, they were ultimately vindicated.”
A veteran of the phenomenon urges continued vigilance. “As a general caveat, there needs to be a higher index of suspicion for these incidents,” says Kenneth W. Kizer, MD, MPH, the former head of the veterans healthcare system who had to deal with three incidents of serial murder at Veterans Affairs (VA) hospitals in the 1990s. “These incidents are grossly underreported.”
Incidence and Cause of Death
Drs. Kizer and Yorker were two of the investigators who reviewed epidemiologic studies, toxicology evidence, and court transcripts for data on healthcare professionals prosecuted between 1970 and 2006.
“Dr. Robert Forrest, who was a forensic toxicologist getting a law degree and wrote his dissertation on the topic of serial murder by healthcare providers, contacted me after the AJN article came out,” says Dr. Yorker. Dr. Forrest has been the testifying expert in most of the U.K. cases. “After the Charles Cullen case hit the news, The New York Times and Modern Healthcare contacted me regarding my study in AJN and the Journal of Nursing Law. That is how Ken Kizer and Paula Lampe found me.” (Cullen, a registered nurse, received 11 consecutive life sentences in 2006 after pleading guilty to administering lethal doses of medication to more than 40 patients in New Jersey and Pennsylvania.)
Lampe, an author, had been studying cases in Europe. “Because both Robert and Paula provided additional data on some cases, they were co-authors—as was Ken—who provided data on the VA cases and an important public policy perspective,” says Dr. Yorker.
The search showed 90 criminal prosecutions of healthcare providers who met the criteria of serial murder of patients. Of those, 54 have been convicted—45 for serial murder, four for attempted murder, and five on lesser charges. Since the publication of their study, one more of the accused has received a sentence of life in prison, another has been convicted and sentenced to 20 years, one committed suicide in prison, and two additional nurses in Germany and the Czech Republic have been arrested and confessed to serial murder of patients. In addition, Dr. Yorker is continuing to follow two large-scale murder-for-profit prosecutions. There are four defendants in each case. Further, three individuals have been found liable for wrongful death in the amounts of $27 million, $8 million, and $450,000 in damages.
Injection was the main method used by healthcare killers, followed by suffocation, poisoning, and tampering with equipment. Prosecutions were reported in 20 countries, with 40% of the incidents taking place in the United States. Nursing personnel were 86% of the healthcare providers prosecuted; 12% were physicians, and 2% were allied health professionals. The number of patient deaths that resulted in a murder conviction is 317, and the number of suspicious patient deaths attributed to the 54 convicted caregivers is 2,113.
“Physicians as serial killers are remarkably uncommon,” says Dr. Iserson, who is also director of the Arizona Bioethics Program at the University of Arizona College of Medicine in Tucson. “Nurses [who are serial killers] are much more common, but of course there are more nurses in the hospital, just as there are ancillary people.” (See Figure 1, left.) Dr. Iserson, who practices emergency medicine and consults nationally on bioethics, advises maintaining caution when examining data of charges or suspicions that were never proved.
Most of these crimes (70%) occur in hospital units. (See Figure 2, left.) Victims are almost always female, as are almost half (49%) of convicted serial killers and 55% of the total number of prosecuted healthcare providers. Males are disproportionately represented among prosecuted nurses.
Motives: Who Is Always There?
Although the motives are complex, some common threads connect these crimes. “There are some classical signs, if you will,” says Dr. Kizer.
When the same person repeatedly calls a code and always seems to be in the thick of it, that is one prime indicator. These people are usually legitimately present in those settings and circumstances—for example, they are on call or working a shift—which makes it more difficult to discern when something is awry. Commonly, the perpetrators have easy access to high-alert drugs without sufficient accountability. Sometimes, once an investigation has been launched it is discovered the person has falsified his or her credentials.
In hospitals, experts say, the “rescuer” or “hero” personality is often on display in those who kill patients—the first person there to give the patient drugs or attempt to save the patient.
“What you are going to see as a pattern,” says Dr. Iserson, “is that they need to be near death.” Codes or calls for respiratory arrest are the most common; patients who have cardiac arrests are much harder to save. Being the hero is not always the motive; the converse can also apply.
Such is the case with nurse Orville Lynn Majors, LPN, convicted of six murders at the Vermillion county hospital in Clinton, Ind. The deaths were consistent with injections of potassium chloride and epinephrine according to prosecutors. Majors’ coworkers were concerned that patients were coding in alarming numbers while in his care. Although this information did not come out until after he was apprehended, his coworkers had a good idea which of his patients would not survive: Patients who were whiny, demanding, or required a lot of work. “The scuttlebutt or rumor among his coworkers,” says Dr. Kizer, “is that they could almost predict which patients would have a demise under his care.”
Although a typical profile of the serial healthcare murderer has been demonstrated in many cases, in many other cases the demographics and behaviors of these killers have deviated widely from generalized assumptions.2 Therefore, before looking at people, look at the numbers.
An unusual number of calls and codes may occur in a particular area of the hospital. “In ICUs you expect a lot of [codes and calls], but not on general post-op wards or the pediatrics MICU,” Dr. Kizer says. “When this happens in these settings it should raise a red flag.”
Unfortunately, most hospitals don’t track mortality on a monthly basis per unit or ward or ICU, so they may not recognize when something is out of line in a timely manner. Also, the hospital committee assigned to review deaths may be remiss in its duty to meet regularly or otherwise perform according to policy.
Another factor that should raise a red flag is a disproportionate number of codes or deaths on the same shift—most often the night shift. Often, someone says, “Gee, it seems like there’s an awful lot of codes lately,” explains Dr. Kizer. An unusually high rate of successful codes is another sign.
For example, in the 1995-1996 case of Kristen Gilbert, an RN convicted of four murders at the Veterans Affairs Medical Center in Northampton, Mass., she was having an extramarital affair with a hospital security guard who worked the evening shift. Protocol required that security be called to all cardiopulmonary arrests. Gilbert used stimulant epinephrine to make their hearts race out of control. The epidemiologic data later showed that suspicious codes occurred when both were on duty. “The patients always seemed to recover and she was the hero,” says Dr. Kizer. “She wanted to look good for her boyfriend.”
Similarly, Richard Angelo, a charge nurse at Good Samaritan Hospital in West Islip, Long Island, N.Y., admitted that between 1987 and 1989 he injected patients with paralyzing drugs Pavulon (pancuronium) and Anectine (succinylcholine). He wanted his colleagues to admire him for performing well in a code. During his confession, he likened himself to volunteer firefighters who set fires. In fact, Dr. Iserson makes this same parallel. “From what we can tell,” he says, “these people don’t really care whether the person dies or not. They would rather they not [die], so they can be seen as the hero. It’s all about them.” As with instances of arson, he says, the perpetrator is “the first one to show up at the fire watch, over and over again.”
Obstacles to Disclosure
Even when healthcare workers and related personnel come forward with their suspicions, law enforcement may be a barrier to prosecution.
In the United Kingdom, a Manchester mortician took her observations about the excessive deaths and cremations in Harold Shipman’s practice to her father and brother, who were also in the family business. She also obtained the support of a local female general practitioner. The two women went to the police, explaining that most patients who had died had not been critically ill and noted that the doctor had exhibited peculiar behavior when he was questioned.
But, says Dr. Iserson, the response again was typical: “‘Oh, foolish women. That can’t be happening.’ And it wasn’t until Shipman killed the wrong person [a former town mayor, mother of a prominent lawyer] that things started to unravel for him.” When police finally looked at other deaths Shipman had certified, a pattern emerged. He would overdose patients with diamorphine, sign their death certificates, then forge medical records to indicate they were in poor health.
A second common response by institutions is just as much of a barrier to bringing these crimes to light and ultimately, prosecution. “In essence,” says Dr. Iserson, “that response is, ‘Well, maybe it is happening but, boy, it sure is going to put our institution in a bad light. So let’s just not say anything.’ ”
This was the case with Michael Swango, a doctor who worked in several states and a number of countries. He was charged with five murders and may have been involved in 126 deaths. Swango confessed to the deaths that occurred in a Veterans Affairs hospital in Northport, N.Y., where he reportedly injected three veterans with a drug that stopped their hearts. He had forged “do not resuscitate” orders for the three. He was sentenced to two life sentences. It is possible that he killed as many as 35-60 people in the United States and Zimbabwe. But before it was all out in the open, “some very prominent people were involved in sweeping it under the rug,” says Dr. Iserson, “and they didn’t even get a slap on the wrist.”
Hiring Practices
One of the most shocking aspects of the Cullen case was that institutional coverup and employee privacy policies meant his prior employers never revealed the problems to prospective employers.
“Identifying potential serial killers is not at all the total problem,” says Dr. Iserson. “The problem is getting the powers that be to act. What they typically do is pass the problem on to somebody else, in effect, saying, ‘We don’t want you to work here anymore. We won’t necessarily write you a good letter of recommendation, but we will say that you worked here, and basically we just want you to go away.’ ”
An investigation revealed that Cullen had a history of reported incidents at hospitals in Pennsylvania and New Jersey, but there were no tracking or disclosure systems in place as he moved from one hospital to another. His employment history included termination from several hospitals because of misconduct, hospitalizations for mental illness, and a criminal investigation regarding improper medication administration.
In an open letter published in The New York Times on March 14, 2004, Somerset Medical Center (Somerville, N.J.) asserted: “Mr. Cullen worked at nine other healthcare facilities over a 16-year period. His former work history problems were not revealed to us. Nor were any state agencies or licensing boards able to provide us with accurate information about his employment history.”
Cullen had been investigated by three hospitals, a nursing home, and two prosecutors for suspicious patient deaths. He was fired by five hospitals and one nursing home for suspected wrongdoing. But Cullen continued to find employment and kill patients.
“Confidentiality is essential [as is] not leaking to the media, which can taint the investigation,” says Dr. Yorker. “The Charles Cullen case should motivate hospitalists to [participate in helping to stop the systemic mechanism that made possible] his killing over 40 patients in nine different hospitals and a nursing home before being stopped. This erodes the public trust in hospitals.”
The Health Care Quality Improvement Act provides some immunity for reporters of adverse information, but it applies only to physicians—not communications between employers.
The American Society for Healthcare Risk Management (ASHRM) and Dr. Kizer and his colleagues are in alignment in advocating for the provision of more comprehensive immunity to help healthcare employees and patients when they report these incidents.3
“If you have information that a worker is harming patients, the institution should be able to tell prospective employers and not worry about getting sued,” says Dr. Yorker. A number of states have passed varying forms of legislation so far, and ASHRM is recommending this be a federal matter. Dr. Kizer and his group recommend that reporting of suspected serial murderers should be considered for coverage under Good Samaritan laws.
Other Complicating Factors
Another problem in bringing legitimate cases to prosecution is when providers are accused on trumped-up charges, which in Dr. Iserson’s view amounts to prosecutorial malpractice. Examples are cases post-Hurricane Katrina, when physicians and nurses were charged with patient deaths.
Internationally, an example is the case in Libya where the main defendants—a Palestinian doctor and five Bulgarian nurses—were charged with injecting 426 children with HIV in 1998, causing an epidemic at El-Fath Children’s Hospital in Benghazi. According to World Politics Watch, dozens of foreign medical professionals were arrested, with six eventually charged and forced to confess by Libyan authorities. Subsequent research published in the journal Nature indicated that viral strains present in the infected children were present at the hospital before 1998.
“This was a case of political blackmail,” says Dr. Iserson. These cases may not be clear-cut and may be open to negative interpretations that “make people skittish. That is why institutions are prone to say, ‘Gee, maybe it’s just one of those kinds of cases. We don’t want to make that kind of mistake.’ ”
Also problematic is the variable rate at which hospitals perform autopsies.
“Autopsy rates are down in many communities to 1% or 2% or even lower,” says Dr. Kizer. “When the data point to the possibility of a crime on a particular unit, the site needs to be treated as a crime scene. In most hospitals, when someone dies, you get them off the floor and you clean up as quickly as possible. That shouldn’t be the case if it is a suspected crime scene. Ideally there should be standardized processes or protocols whenever there is suspicion. And those protocols may be different than when a patient ordinarily dies.”
Seeking Solutions
Hospitalists and other professionals—especially nurses and ancillary personnel—have an obligation to be informed and astute regarding individual characteristics and signs of suspicious patient deaths. Appropriate epidemiological, toxicological, and psychological data must be collected and analyzed routinely.
“Data about this phenomenon need to be disseminated to heighten awareness that serial murder of patients is a significant concern that extends beyond a few shocking, isolated incidents,” write Drs. Yorker and Kizer and their co-authors.
Institutional hiring practices must be changed so balance is achieved between preventing wrongful discharge or denial-of-employment lawsuits and protecting patient safety. Existing state legislation and future federal legislation for institutional immunity is an important element of patient advocacy that hospitalists can support.
Ultimately, hospitalists must be informed, aware, and alert. “Most [suspicions] will not be anything,” says Dr. Iserson. “Just pay attention to it.” TH
Andrea Sattinger is a frequent contributor to The Hospitalist.
References
- Yorker BC, Kizer KW, Lampe P, et al. Serial murder by healthcare professionals. J Forensic Sci. 2006 Nov;51(6):1362-1371.
- Wolf BC, Lavezzi WA. Paths to destruction: the lives and crimes of two serial killers. J Forensic Sci. 2007 Jan;52(1):199-203.
- ASHRM. American Society for Healthcare Risk Management. A call for federal immunity to protect health care employers … and patients. Chicago: Monograph; April 1, 2005; www.ashrm.org/ashrm/resources/files/Monograph.Immunity.pdf.
Rewards and Recognition

This is the third in a series of articles on the four pillars of career satisfaction in hospital medicine.
How much does your satisfaction with your job rely on your compensation level? What about your sense of being appreciated for what you do each day?
Many hospitalists would say the latter could be a key factor in their happiness with their career. This is confirmed in a new white paper from SHM, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). This document, created by SHM’s Career Satisfaction Task Force (CSTF), can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction. It outlines the four pillars of career satisfaction, the third of which is reward/recognition.
The Third Pillar
The reward/recognition pillar includes not just financial rewards but also social rewards (appreciation by your colleagues, leaders, patients, and family) and intrinsic rewards (healing patients or working efficiently and productively).
Achieving on-the-job recognition requires practicing high-quality medicine, communicating this to all the groups above, and participating in professional development and leadership. It also entails building relationships with peers and allied health professionals, hospital executives, patients, and the community.
“Reward and recognition ties in a lot with the other pillars—especially community,” says CSTF member Adrienne Bennett, MD, PhD, Ohio State University Medical Center, Columbus. “Part of what makes or breaks any hospitalist job is the group you work with and how you get along. This has to do with how you’re viewed and how you’re rewarded and supported.”
The classic dichotomy of values in hospital medicine is salary versus quality of life. Some groups offer higher salaries with heavy workloads and/or many shifts, and others value time over money. But there are additional values that affect reward and recognition. For example, let’s say you want to build a career or reputation in patient safety and quality of care but you work for a hospital medicine group focused mainly on high-volume patient care that is not engaged in quality improvement work. Your group may not value or reward your efforts. This can lead to job dissatisfaction.
“Make sure the group you join has a culture that shares or at least respects and supports your other career interests,” advises Dr. Bennett. “Working with a group where you’re a good fit and that supports your career aspirations is the most important aspect of career satisfaction.”
An Example of Reward Issues
To illustrate how reward/recognition works, here’s a fictional example of a hospitalist faced with a decision regarding her career:
“I’m ready to find my first job in hospital medicine, and my husband just accepted a pulmonary fellowship at a Midwestern university hospital. There are five hospital medicine groups in the area to choose from. I have to decide which I’d prefer to work for. My main priority is that I want to be ‘a name’ in hospital medicine—I want a chance to build a good reputation nationally.”
According to the white paper, a hospitalist in this position should take several steps to ensure career satisfaction:
Step 1: Assess your choices. Use the series of questions provided in the white paper to compare programs, including compensation and benefits.
“This hospitalist seems to want something more out of her work than just the rewards that come from taking excellent care of her patients,” observes Dr. Bennett. “When she’s interviewing, she needs to ask very carefully about opportunities for leadership development and for building her local reputation, which is the first step toward larger recognition. She needs to find out if the group supports and values work on hospital and/or medical association committees. Many community-based groups do support this.”
Step 2: Once you’re hired, set short- and long-term performance goals. Understand what you want to be recognized for, and outline what you want to accomplish—whether it’s a research project, a leadership role on a committee, or simply a standard of patient care you set for yourself.
Step 3: Participate in SHM chapter meetings. Network with physicians from other hospital medicine groups, get involved, and make a name for yourself.
How Your Rewards Stack up
Whether you’re questioning the compensation package at your long-term hospitalist position or weighing a decision on taking a new job, you’ll turn to available benchmark data on hospital medicine.
“There are a lot ways that benchmarks help and hurt,” warns Dr. Bennett. “Some of it isn’t very good because it’s based on very small numbers. If you’re dealing with an employer that relies on data [for compensation levels], it’s important to know what data they’re using. A reliable employer should share that information. Even the SHM benchmark data—which is probably the best we have, since it’s based on several thousand practicing hospitalists in a variety of settings—can’t always tell you how your job compares.”
Many variations within groups and individual jobs make it hard to compare positions side by side. Differentiating factors include salary and other compensation factors, patient load, shifts and schedule (including nights and weekends), and job responsibilities.
“Sometimes you can use the number of work [relative value units] RVUs to compare workloads,” Dr. Bennett suggests.
As with all the pillars of career satisfaction, the rewards and recognitions that come with your job must be measured against what other hospitalist positions offer—but more importantly against your values and priorities. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the third in a series of articles on the four pillars of career satisfaction in hospital medicine.
How much does your satisfaction with your job rely on your compensation level? What about your sense of being appreciated for what you do each day?
Many hospitalists would say the latter could be a key factor in their happiness with their career. This is confirmed in a new white paper from SHM, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). This document, created by SHM’s Career Satisfaction Task Force (CSTF), can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction. It outlines the four pillars of career satisfaction, the third of which is reward/recognition.
The Third Pillar
The reward/recognition pillar includes not just financial rewards but also social rewards (appreciation by your colleagues, leaders, patients, and family) and intrinsic rewards (healing patients or working efficiently and productively).
Achieving on-the-job recognition requires practicing high-quality medicine, communicating this to all the groups above, and participating in professional development and leadership. It also entails building relationships with peers and allied health professionals, hospital executives, patients, and the community.
“Reward and recognition ties in a lot with the other pillars—especially community,” says CSTF member Adrienne Bennett, MD, PhD, Ohio State University Medical Center, Columbus. “Part of what makes or breaks any hospitalist job is the group you work with and how you get along. This has to do with how you’re viewed and how you’re rewarded and supported.”
The classic dichotomy of values in hospital medicine is salary versus quality of life. Some groups offer higher salaries with heavy workloads and/or many shifts, and others value time over money. But there are additional values that affect reward and recognition. For example, let’s say you want to build a career or reputation in patient safety and quality of care but you work for a hospital medicine group focused mainly on high-volume patient care that is not engaged in quality improvement work. Your group may not value or reward your efforts. This can lead to job dissatisfaction.
“Make sure the group you join has a culture that shares or at least respects and supports your other career interests,” advises Dr. Bennett. “Working with a group where you’re a good fit and that supports your career aspirations is the most important aspect of career satisfaction.”
An Example of Reward Issues
To illustrate how reward/recognition works, here’s a fictional example of a hospitalist faced with a decision regarding her career:
“I’m ready to find my first job in hospital medicine, and my husband just accepted a pulmonary fellowship at a Midwestern university hospital. There are five hospital medicine groups in the area to choose from. I have to decide which I’d prefer to work for. My main priority is that I want to be ‘a name’ in hospital medicine—I want a chance to build a good reputation nationally.”
According to the white paper, a hospitalist in this position should take several steps to ensure career satisfaction:
Step 1: Assess your choices. Use the series of questions provided in the white paper to compare programs, including compensation and benefits.
“This hospitalist seems to want something more out of her work than just the rewards that come from taking excellent care of her patients,” observes Dr. Bennett. “When she’s interviewing, she needs to ask very carefully about opportunities for leadership development and for building her local reputation, which is the first step toward larger recognition. She needs to find out if the group supports and values work on hospital and/or medical association committees. Many community-based groups do support this.”
Step 2: Once you’re hired, set short- and long-term performance goals. Understand what you want to be recognized for, and outline what you want to accomplish—whether it’s a research project, a leadership role on a committee, or simply a standard of patient care you set for yourself.
Step 3: Participate in SHM chapter meetings. Network with physicians from other hospital medicine groups, get involved, and make a name for yourself.
How Your Rewards Stack up
Whether you’re questioning the compensation package at your long-term hospitalist position or weighing a decision on taking a new job, you’ll turn to available benchmark data on hospital medicine.
“There are a lot ways that benchmarks help and hurt,” warns Dr. Bennett. “Some of it isn’t very good because it’s based on very small numbers. If you’re dealing with an employer that relies on data [for compensation levels], it’s important to know what data they’re using. A reliable employer should share that information. Even the SHM benchmark data—which is probably the best we have, since it’s based on several thousand practicing hospitalists in a variety of settings—can’t always tell you how your job compares.”
Many variations within groups and individual jobs make it hard to compare positions side by side. Differentiating factors include salary and other compensation factors, patient load, shifts and schedule (including nights and weekends), and job responsibilities.
“Sometimes you can use the number of work [relative value units] RVUs to compare workloads,” Dr. Bennett suggests.
As with all the pillars of career satisfaction, the rewards and recognitions that come with your job must be measured against what other hospitalist positions offer—but more importantly against your values and priorities. TH
Jane Jerrard has written for The Hospitalist since 2005.
This is the third in a series of articles on the four pillars of career satisfaction in hospital medicine.
How much does your satisfaction with your job rely on your compensation level? What about your sense of being appreciated for what you do each day?
Many hospitalists would say the latter could be a key factor in their happiness with their career. This is confirmed in a new white paper from SHM, “A Challenge for a New Specialty: A White Paper on Hospitalist Career Satisfaction” (available online at www.hospitalmedicine.org). This document, created by SHM’s Career Satisfaction Task Force (CSTF), can be used by hospitalists and hospital medicine practices as a toolkit for improving or ensuring job satisfaction. It outlines the four pillars of career satisfaction, the third of which is reward/recognition.
The Third Pillar
The reward/recognition pillar includes not just financial rewards but also social rewards (appreciation by your colleagues, leaders, patients, and family) and intrinsic rewards (healing patients or working efficiently and productively).
Achieving on-the-job recognition requires practicing high-quality medicine, communicating this to all the groups above, and participating in professional development and leadership. It also entails building relationships with peers and allied health professionals, hospital executives, patients, and the community.
“Reward and recognition ties in a lot with the other pillars—especially community,” says CSTF member Adrienne Bennett, MD, PhD, Ohio State University Medical Center, Columbus. “Part of what makes or breaks any hospitalist job is the group you work with and how you get along. This has to do with how you’re viewed and how you’re rewarded and supported.”
The classic dichotomy of values in hospital medicine is salary versus quality of life. Some groups offer higher salaries with heavy workloads and/or many shifts, and others value time over money. But there are additional values that affect reward and recognition. For example, let’s say you want to build a career or reputation in patient safety and quality of care but you work for a hospital medicine group focused mainly on high-volume patient care that is not engaged in quality improvement work. Your group may not value or reward your efforts. This can lead to job dissatisfaction.
“Make sure the group you join has a culture that shares or at least respects and supports your other career interests,” advises Dr. Bennett. “Working with a group where you’re a good fit and that supports your career aspirations is the most important aspect of career satisfaction.”
An Example of Reward Issues
To illustrate how reward/recognition works, here’s a fictional example of a hospitalist faced with a decision regarding her career:
“I’m ready to find my first job in hospital medicine, and my husband just accepted a pulmonary fellowship at a Midwestern university hospital. There are five hospital medicine groups in the area to choose from. I have to decide which I’d prefer to work for. My main priority is that I want to be ‘a name’ in hospital medicine—I want a chance to build a good reputation nationally.”
According to the white paper, a hospitalist in this position should take several steps to ensure career satisfaction:
Step 1: Assess your choices. Use the series of questions provided in the white paper to compare programs, including compensation and benefits.
“This hospitalist seems to want something more out of her work than just the rewards that come from taking excellent care of her patients,” observes Dr. Bennett. “When she’s interviewing, she needs to ask very carefully about opportunities for leadership development and for building her local reputation, which is the first step toward larger recognition. She needs to find out if the group supports and values work on hospital and/or medical association committees. Many community-based groups do support this.”
Step 2: Once you’re hired, set short- and long-term performance goals. Understand what you want to be recognized for, and outline what you want to accomplish—whether it’s a research project, a leadership role on a committee, or simply a standard of patient care you set for yourself.
Step 3: Participate in SHM chapter meetings. Network with physicians from other hospital medicine groups, get involved, and make a name for yourself.
How Your Rewards Stack up
Whether you’re questioning the compensation package at your long-term hospitalist position or weighing a decision on taking a new job, you’ll turn to available benchmark data on hospital medicine.
“There are a lot ways that benchmarks help and hurt,” warns Dr. Bennett. “Some of it isn’t very good because it’s based on very small numbers. If you’re dealing with an employer that relies on data [for compensation levels], it’s important to know what data they’re using. A reliable employer should share that information. Even the SHM benchmark data—which is probably the best we have, since it’s based on several thousand practicing hospitalists in a variety of settings—can’t always tell you how your job compares.”
Many variations within groups and individual jobs make it hard to compare positions side by side. Differentiating factors include salary and other compensation factors, patient load, shifts and schedule (including nights and weekends), and job responsibilities.
“Sometimes you can use the number of work [relative value units] RVUs to compare workloads,” Dr. Bennett suggests.
As with all the pillars of career satisfaction, the rewards and recognitions that come with your job must be measured against what other hospitalist positions offer—but more importantly against your values and priorities. TH
Jane Jerrard has written for The Hospitalist since 2005.
Benefit Quest

The federal government is moving toward offering monetary rewards for reporting on specific performance indicators. When hospitals begin to seek those rewards, hospitalists will be integrally involved.
The Centers for Medicare and Medicaid Services (CMS) has been tasked with developing an approach to value-based purchasing (VBP) for Medicare hospital services beginning in fiscal year 2009. Once the proposal is complete and approved by Congress, hospitals will receive differential payments tied to their performance.
VBP is similar to pay for performance (P4P) in that it links a bonus payment to reporting on performance of specific procedures. But the payment in this case is awarded to a hospital rather than a physician. The goals for the CMS proposal include:
- Improve clinical quality;
- Address underuse, overuse, and misuse of services;
- Encourage patient-centered care;
- Reduce adverse events and improve patient safety;
- Avoid unnecessary costs;
- Stimulate investments in structural components and the re-engineering of care processes;
- Make performance results transparent to and usable by consumers; and
- Avoid creating additional disparities in healthcare and work to reduce existing disparities.
CMS has hosted two listening sessions on the VBP program, during which healthcare providers were able to directly offer suggestions and opinions. The latest information, including an options paper based on the first listening session, is available online at www.cms.hhs.gov/center/hospital.asp.
“I was impressed with their responsiveness to the feedback they received at two listening sessions,” says Gregory B. Seymann, MD, associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine, and a member of SHM’s Public Policy Committee. “I can see that the second options paper incorporates a lot of the comments from the first session.”
Aligning Measures
SHM has expressed support for CMS’ VBP proposal in a letter to the agency that also urged CMS to select candidate measures for hospitals that align with those for individual physicians under the Physician Quality Reporting Initiative (PQRI), which started July 1.
“These are very similar programs; one rewards hospitals for performing certain processes of care, and one rewards physicians for performing certain processes,” Dr. Seymann explains. “We’re simply asking CMS to make sure the measures [in VBP] match up with what physicians are asked to do. Many people voiced the same comment in the listening session.”
Although there are just 17 candidate measures proposed for the first year of the VBP program, the expectation is to add a considerable number as the program continues. Many candidate measures are similar or identical to those in the PQRI, such as giving aspirin on arrival and giving aspirin, beta-blockers, and ACE inhibitors on discharge for patients with acute myocardial infarction.
Additionally, the proposed measures are identical to those in the current P4P program most hospitals already participate in, known as Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU). The difference will be that instead of getting credit just for reporting the data as they do now, starting in 2009 hospitals must report publicly and perform at a certain level to get a payment update.
“Physicians, especially hospitalists, will need to watch this closely, as it is expected that the PQRI program, which is similar to RHQDAPU on the hospital level, will ultimately transition to a pay-for-performance program such as VBP,” says Dr. Seymann. “We can learn from the bumps in the road in the hospitals’ experience, and hopefully SHM can be active in ensuring that similar problems are anticipated prior to a physician-level pay-for-performance rollout. Furthermore, measures that will apply to hospitalists will likely mirror the hospital VBP measures.”
Rewards Program
Hospitals participating in the proposed VBP program can earn rewards based on two different criteria.
“This aspect is far and away the most important part of this program coming from CMS,” says Dr. Seymann. “They’ve learned from experience with the Premier [Hospital Quality Incentive Demonstration] project on hospital value-based purchasing that the hospitals that started out doing the best got the lion’s share of the reward because they were already doing well. Unfortunately, those that started at the bottom showed greater overall improvement but didn’t reach the top performance threshold, so they saw no financial recognition.”
So in the proposed VBP program, hospitals can demonstrate quality through overall performance on specific measures or through improvement over time in specific measures.
“Hospitals that reach the benchmark—the median of the top decile of performance—get the maximum number of points toward achieving the reward,” explains Dr. Seymann. “But hospitals can gain some points as long as they fall within the attainment range [between the 50th percentile and the mean of the top decile], proportional to how well they do. You get points for both the amount of improvement and the absolute attainment, and whichever score is higher comprises your score on that measure.”
Dr. Seymann calls this adjustment in the incentive structure “the most positive piece of this program,” explaining, “All hospitals have the opportunity to participate and to earn rewards.”
What It Means for Hospitalists
When VBP becomes a reality, how will that affect hospitalists?
“A lot of what hospitalists do for hospitals is improve quality,” says Dr. Seymann. “They’re likely to be asked to partner with their hospitals to put protocols in place for value-based purchasing. … Hospitals can’t make this work without physician participation, and a lot of hospital medicine groups are aligned with their hospitals on quality-improvement measures.”
It seems inevitable PQRI will morph into a CMS P4P or value-based purchasing program—or both. Whatever happens with these demonstration projects, hospitalists will be reporting on measures, and SHM wants to ensure those measures are appropriate.
“There are only 17 measures now; that’s a narrow sample to define quality at a hospital,” Dr. Seymann points out regarding VBP. “SHM will want to be involved in identifying gaps in care and recommending more measures in the future—like care coordination.” TH
Jane Jerrard also writes “Career Development” for The Hospitalist.
The federal government is moving toward offering monetary rewards for reporting on specific performance indicators. When hospitals begin to seek those rewards, hospitalists will be integrally involved.
The Centers for Medicare and Medicaid Services (CMS) has been tasked with developing an approach to value-based purchasing (VBP) for Medicare hospital services beginning in fiscal year 2009. Once the proposal is complete and approved by Congress, hospitals will receive differential payments tied to their performance.
VBP is similar to pay for performance (P4P) in that it links a bonus payment to reporting on performance of specific procedures. But the payment in this case is awarded to a hospital rather than a physician. The goals for the CMS proposal include:
- Improve clinical quality;
- Address underuse, overuse, and misuse of services;
- Encourage patient-centered care;
- Reduce adverse events and improve patient safety;
- Avoid unnecessary costs;
- Stimulate investments in structural components and the re-engineering of care processes;
- Make performance results transparent to and usable by consumers; and
- Avoid creating additional disparities in healthcare and work to reduce existing disparities.
CMS has hosted two listening sessions on the VBP program, during which healthcare providers were able to directly offer suggestions and opinions. The latest information, including an options paper based on the first listening session, is available online at www.cms.hhs.gov/center/hospital.asp.
“I was impressed with their responsiveness to the feedback they received at two listening sessions,” says Gregory B. Seymann, MD, associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine, and a member of SHM’s Public Policy Committee. “I can see that the second options paper incorporates a lot of the comments from the first session.”
Aligning Measures
SHM has expressed support for CMS’ VBP proposal in a letter to the agency that also urged CMS to select candidate measures for hospitals that align with those for individual physicians under the Physician Quality Reporting Initiative (PQRI), which started July 1.
“These are very similar programs; one rewards hospitals for performing certain processes of care, and one rewards physicians for performing certain processes,” Dr. Seymann explains. “We’re simply asking CMS to make sure the measures [in VBP] match up with what physicians are asked to do. Many people voiced the same comment in the listening session.”
Although there are just 17 candidate measures proposed for the first year of the VBP program, the expectation is to add a considerable number as the program continues. Many candidate measures are similar or identical to those in the PQRI, such as giving aspirin on arrival and giving aspirin, beta-blockers, and ACE inhibitors on discharge for patients with acute myocardial infarction.
Additionally, the proposed measures are identical to those in the current P4P program most hospitals already participate in, known as Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU). The difference will be that instead of getting credit just for reporting the data as they do now, starting in 2009 hospitals must report publicly and perform at a certain level to get a payment update.
“Physicians, especially hospitalists, will need to watch this closely, as it is expected that the PQRI program, which is similar to RHQDAPU on the hospital level, will ultimately transition to a pay-for-performance program such as VBP,” says Dr. Seymann. “We can learn from the bumps in the road in the hospitals’ experience, and hopefully SHM can be active in ensuring that similar problems are anticipated prior to a physician-level pay-for-performance rollout. Furthermore, measures that will apply to hospitalists will likely mirror the hospital VBP measures.”
Rewards Program
Hospitals participating in the proposed VBP program can earn rewards based on two different criteria.
“This aspect is far and away the most important part of this program coming from CMS,” says Dr. Seymann. “They’ve learned from experience with the Premier [Hospital Quality Incentive Demonstration] project on hospital value-based purchasing that the hospitals that started out doing the best got the lion’s share of the reward because they were already doing well. Unfortunately, those that started at the bottom showed greater overall improvement but didn’t reach the top performance threshold, so they saw no financial recognition.”
So in the proposed VBP program, hospitals can demonstrate quality through overall performance on specific measures or through improvement over time in specific measures.
“Hospitals that reach the benchmark—the median of the top decile of performance—get the maximum number of points toward achieving the reward,” explains Dr. Seymann. “But hospitals can gain some points as long as they fall within the attainment range [between the 50th percentile and the mean of the top decile], proportional to how well they do. You get points for both the amount of improvement and the absolute attainment, and whichever score is higher comprises your score on that measure.”
Dr. Seymann calls this adjustment in the incentive structure “the most positive piece of this program,” explaining, “All hospitals have the opportunity to participate and to earn rewards.”
What It Means for Hospitalists
When VBP becomes a reality, how will that affect hospitalists?
“A lot of what hospitalists do for hospitals is improve quality,” says Dr. Seymann. “They’re likely to be asked to partner with their hospitals to put protocols in place for value-based purchasing. … Hospitals can’t make this work without physician participation, and a lot of hospital medicine groups are aligned with their hospitals on quality-improvement measures.”
It seems inevitable PQRI will morph into a CMS P4P or value-based purchasing program—or both. Whatever happens with these demonstration projects, hospitalists will be reporting on measures, and SHM wants to ensure those measures are appropriate.
“There are only 17 measures now; that’s a narrow sample to define quality at a hospital,” Dr. Seymann points out regarding VBP. “SHM will want to be involved in identifying gaps in care and recommending more measures in the future—like care coordination.” TH
Jane Jerrard also writes “Career Development” for The Hospitalist.
The federal government is moving toward offering monetary rewards for reporting on specific performance indicators. When hospitals begin to seek those rewards, hospitalists will be integrally involved.
The Centers for Medicare and Medicaid Services (CMS) has been tasked with developing an approach to value-based purchasing (VBP) for Medicare hospital services beginning in fiscal year 2009. Once the proposal is complete and approved by Congress, hospitals will receive differential payments tied to their performance.
VBP is similar to pay for performance (P4P) in that it links a bonus payment to reporting on performance of specific procedures. But the payment in this case is awarded to a hospital rather than a physician. The goals for the CMS proposal include:
- Improve clinical quality;
- Address underuse, overuse, and misuse of services;
- Encourage patient-centered care;
- Reduce adverse events and improve patient safety;
- Avoid unnecessary costs;
- Stimulate investments in structural components and the re-engineering of care processes;
- Make performance results transparent to and usable by consumers; and
- Avoid creating additional disparities in healthcare and work to reduce existing disparities.
CMS has hosted two listening sessions on the VBP program, during which healthcare providers were able to directly offer suggestions and opinions. The latest information, including an options paper based on the first listening session, is available online at www.cms.hhs.gov/center/hospital.asp.
“I was impressed with their responsiveness to the feedback they received at two listening sessions,” says Gregory B. Seymann, MD, associate clinical professor, University of California, San Diego School of Medicine, Division of Hospital Medicine, and a member of SHM’s Public Policy Committee. “I can see that the second options paper incorporates a lot of the comments from the first session.”
Aligning Measures
SHM has expressed support for CMS’ VBP proposal in a letter to the agency that also urged CMS to select candidate measures for hospitals that align with those for individual physicians under the Physician Quality Reporting Initiative (PQRI), which started July 1.
“These are very similar programs; one rewards hospitals for performing certain processes of care, and one rewards physicians for performing certain processes,” Dr. Seymann explains. “We’re simply asking CMS to make sure the measures [in VBP] match up with what physicians are asked to do. Many people voiced the same comment in the listening session.”
Although there are just 17 candidate measures proposed for the first year of the VBP program, the expectation is to add a considerable number as the program continues. Many candidate measures are similar or identical to those in the PQRI, such as giving aspirin on arrival and giving aspirin, beta-blockers, and ACE inhibitors on discharge for patients with acute myocardial infarction.
Additionally, the proposed measures are identical to those in the current P4P program most hospitals already participate in, known as Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU). The difference will be that instead of getting credit just for reporting the data as they do now, starting in 2009 hospitals must report publicly and perform at a certain level to get a payment update.
“Physicians, especially hospitalists, will need to watch this closely, as it is expected that the PQRI program, which is similar to RHQDAPU on the hospital level, will ultimately transition to a pay-for-performance program such as VBP,” says Dr. Seymann. “We can learn from the bumps in the road in the hospitals’ experience, and hopefully SHM can be active in ensuring that similar problems are anticipated prior to a physician-level pay-for-performance rollout. Furthermore, measures that will apply to hospitalists will likely mirror the hospital VBP measures.”
Rewards Program
Hospitals participating in the proposed VBP program can earn rewards based on two different criteria.
“This aspect is far and away the most important part of this program coming from CMS,” says Dr. Seymann. “They’ve learned from experience with the Premier [Hospital Quality Incentive Demonstration] project on hospital value-based purchasing that the hospitals that started out doing the best got the lion’s share of the reward because they were already doing well. Unfortunately, those that started at the bottom showed greater overall improvement but didn’t reach the top performance threshold, so they saw no financial recognition.”
So in the proposed VBP program, hospitals can demonstrate quality through overall performance on specific measures or through improvement over time in specific measures.
“Hospitals that reach the benchmark—the median of the top decile of performance—get the maximum number of points toward achieving the reward,” explains Dr. Seymann. “But hospitals can gain some points as long as they fall within the attainment range [between the 50th percentile and the mean of the top decile], proportional to how well they do. You get points for both the amount of improvement and the absolute attainment, and whichever score is higher comprises your score on that measure.”
Dr. Seymann calls this adjustment in the incentive structure “the most positive piece of this program,” explaining, “All hospitals have the opportunity to participate and to earn rewards.”
What It Means for Hospitalists
When VBP becomes a reality, how will that affect hospitalists?
“A lot of what hospitalists do for hospitals is improve quality,” says Dr. Seymann. “They’re likely to be asked to partner with their hospitals to put protocols in place for value-based purchasing. … Hospitals can’t make this work without physician participation, and a lot of hospital medicine groups are aligned with their hospitals on quality-improvement measures.”
It seems inevitable PQRI will morph into a CMS P4P or value-based purchasing program—or both. Whatever happens with these demonstration projects, hospitalists will be reporting on measures, and SHM wants to ensure those measures are appropriate.
“There are only 17 measures now; that’s a narrow sample to define quality at a hospital,” Dr. Seymann points out regarding VBP. “SHM will want to be involved in identifying gaps in care and recommending more measures in the future—like care coordination.” TH
Jane Jerrard also writes “Career Development” for The Hospitalist.
For the Team

Many speakers at the recent SHM annual meeting in Dallas focused on the many ways hospitalists enhance quality of care. The teamwork necessary to effectively render inpatient services was an especially important topic.
Hospitalists have compiled a significant amount of descriptive material about their working environments and the composition and workloads of hospitalist teams. However, there is not much material available quantifying the ways that various disciplines impact the overall care-delivery metrics of multidisciplinary hospitalist teams.
The SHM Non-Physician Provider Committee is interested in collecting information on multidisciplinary programs, their component disciplines and individual providers to help identify and describe teams that have integrated nurse practitioners, physician assistants, clinical pharmacists and pharmacologists, nurse clinical care coordinators, and other related disciplines into their practices. Our goal is to develop descriptions of successful and unsuccessful implementation models.
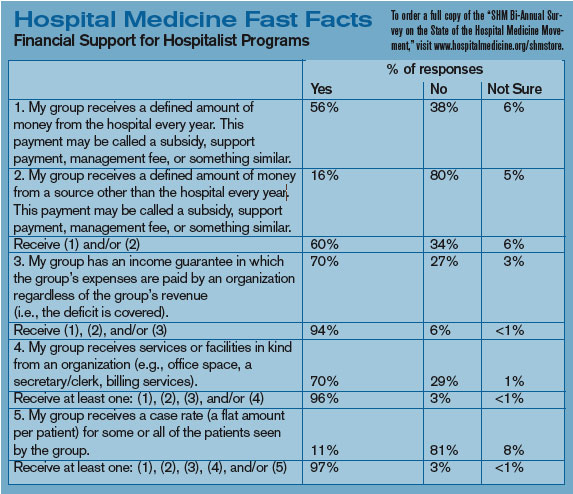
We would also like to collect information measuring additional domains of interest to major stakeholders. Such domains might include the clinical utilization of non-physician providers in relationship to both scope-of-practice and delegation of authority, the influence of multidisciplinary integration on patient-centered care and patient satisfaction, process and outcomes quality metrics, throughput and efficiency measures, documentation practices, hospital privileges for non-physicians, medical education in the multidisciplinary environment, risk management and, of course, reimbursement.
One might ask why the collection and analysis of such data should be of interest to hospitalists and to SHM. There are several immediate answers:
- The first reason involves manpower. Hospital medicine has become a growing discipline for physicians—one that did not exist on the radar screens of physician planners 10 years ago. However, given the growing demand for hospitalists there may be a significant shortage. To address this deficit, hospital medicine practices will need to attract new associates in the form of nurse practitioners and physician assistants. It is therefore imperative that hospitalists proactively identify barriers to the integration of non-physician providers into their practices and have successful implementation models to guide this effort.
- The second reason centers on the fact that hospitalists will continue to lead efforts to enhance quality of care. Incorporating a multidisciplinary approach—whether through the pre-rounding and follow-up of nurse clinical care coordinators, the counsel of clinical pharmacists, or the hands-on care of other disciplines—will facilitate throughput and improve quality as well as enhance patient satisfaction and communication. Identifying best practices in these particular domains will provide information crucial to success in these areas.
- The third reason is related to the cost of services. With declining reimbursements coupled with increasing costs, hospital medicine programs must identify and implement measures aimed at expense control and maximization of services. Used appropriately, non-physician providers provide a lower-cost alternative to a physician-only model. When one-to-one pairing occurs, physician/NPP team-care can be delivered in a parallel-versus-linear fashion, thus allowing for increased census as well as expedition of care.
The future of hospital medicine is one of continued growth with the demand for hospital medicine physicians far outstripping the available supply to meet the ever-increasing needs. SHM is committed to researching and sharing best practices, and views the use of multidisciplinary teams as an important model of care. Together, we can all achieve more.
If you are interested in being a part of this project or feel that this data would be of benefit to your practice, please contact the Non-Physician Provider Committee at nppcommittee@hospitalmedicine.org.
Chapter Reports
Nashville
Quite a bit of networking took place before the Medtronic-sponsored presentation at Ruth’s Chris in Nashville on April 26. The SHM Nashville Chapter has re-energized itself under the co-direction of Steven Embry, MD, and Kimberly Bell, MD. Eleven Nashville-area healthcare organizations were represented by more than 28 attendees. The attendees were a multidisciplinary mix of physicians, nurses, and administrators. Shashank Desai, MD, engaged the audience with his presentation “Simple to Complex: Advances in the Management of CHF.” Dr. Desai is the medical director of the Heart Failure and Transplant Program at Inova Fairfax Hospital.
Pacific Northwest
The latest Pacific Northwest Chapter meeting of SHM was held in Seattle on May 15. A change of venue and a new focus on speakers provided local hospitalists with information they won’t find elsewhere. Joseph Bennet, MD, former president of the local chapter, gave a presentation detailing his 15 months practicing hospitalist medicine in Dunedin, New Zealand. In addition to stunning photos of the terrain, Dr. Bennet delivered a thought-provoking presentation comparing New Zealand with the United States regarding culture, medical system financing, drug and care delivery, physician training, end-of-life issues, and many more aspects.
Pittsburgh
The Pittsburgh Chapter had a meeting May 10 at Morton’s Steakhouse. The speaker for the event was Rene Alvarez, MD, director of the Critical Care Unit at University of Pittsburgh Medical Center. Dr. Alvarez discussed “Strategies for Optimal Management of Patients with Heart Failure,” which generated an excellent discussion. Various hospital medicine topics including incentives, program structures, and 24/7 programs were also discussed. Attendees included hospitalists from six local hospitals. The next meeting will be held Oct. 30. For more information on the Pittsburgh Chapter, contact Michael Cratty, MD, PhD, at mcratty@wpahs.org.
Rocky Mountain
The Rocky Mountain Chapter held its spring meeting May 3 at the Denver Colorado Downtown Aquarium. Chapter President Eugene Chu, MD, welcomed attendees and was followed by an update from the Rocky Mountain Chapter Public Policy Committee presented by Bob Brockmann, MD, MSc. Guest speakers for the night were Edward Maa, MD, who spoke about “Seizure Management in Hospitalized Patients” and Daniel Mogyoros, MD, whose presentation was titled “Updates in Infectious Disease for Hospital Medicine.” Attendees received two AMA PRA [Physician’s Recognition Award] Category 1 credits.
San Diego
At its June 5 meeting, San Diego’s chapter discussed real-time, evidence-based practice as a means to improve patient care and share new clinical evidence with colleagues. Online access during the presentation allowed the group to review several evidence resources: PubMed, the Physician’s Information and Education Resource, the American College of Physicians Journal Club, and National Guideline Clearing House using real patient cases. Dinner was served by Blue Coral Seafood and Spirits, and Novartis sponsored the event.
Upstate South Carolina
The second meeting of the Upstate S.C. Chapter was held May 15, with close to 20 physicians representing five hospitals in upstate South Carolina. Kenneth Leeper, MD, pulmonologist, presented information on ventilator-associated pneumonia. Following the presentation, the business meeting was opened by outgoing President Raja Paladugu, MD.
The following officers were elected for 2007:
- President: Zafar Hossain, MD;
- Vice President: Imran Shaikh, MD; and
- Secretary: Shawn Morrow, MD.
The group decided to meet on a quarterly basis, with the next meeting to be held in September. TH
Many speakers at the recent SHM annual meeting in Dallas focused on the many ways hospitalists enhance quality of care. The teamwork necessary to effectively render inpatient services was an especially important topic.
Hospitalists have compiled a significant amount of descriptive material about their working environments and the composition and workloads of hospitalist teams. However, there is not much material available quantifying the ways that various disciplines impact the overall care-delivery metrics of multidisciplinary hospitalist teams.
The SHM Non-Physician Provider Committee is interested in collecting information on multidisciplinary programs, their component disciplines and individual providers to help identify and describe teams that have integrated nurse practitioners, physician assistants, clinical pharmacists and pharmacologists, nurse clinical care coordinators, and other related disciplines into their practices. Our goal is to develop descriptions of successful and unsuccessful implementation models.
We would also like to collect information measuring additional domains of interest to major stakeholders. Such domains might include the clinical utilization of non-physician providers in relationship to both scope-of-practice and delegation of authority, the influence of multidisciplinary integration on patient-centered care and patient satisfaction, process and outcomes quality metrics, throughput and efficiency measures, documentation practices, hospital privileges for non-physicians, medical education in the multidisciplinary environment, risk management and, of course, reimbursement.
One might ask why the collection and analysis of such data should be of interest to hospitalists and to SHM. There are several immediate answers:
- The first reason involves manpower. Hospital medicine has become a growing discipline for physicians—one that did not exist on the radar screens of physician planners 10 years ago. However, given the growing demand for hospitalists there may be a significant shortage. To address this deficit, hospital medicine practices will need to attract new associates in the form of nurse practitioners and physician assistants. It is therefore imperative that hospitalists proactively identify barriers to the integration of non-physician providers into their practices and have successful implementation models to guide this effort.
- The second reason centers on the fact that hospitalists will continue to lead efforts to enhance quality of care. Incorporating a multidisciplinary approach—whether through the pre-rounding and follow-up of nurse clinical care coordinators, the counsel of clinical pharmacists, or the hands-on care of other disciplines—will facilitate throughput and improve quality as well as enhance patient satisfaction and communication. Identifying best practices in these particular domains will provide information crucial to success in these areas.
- The third reason is related to the cost of services. With declining reimbursements coupled with increasing costs, hospital medicine programs must identify and implement measures aimed at expense control and maximization of services. Used appropriately, non-physician providers provide a lower-cost alternative to a physician-only model. When one-to-one pairing occurs, physician/NPP team-care can be delivered in a parallel-versus-linear fashion, thus allowing for increased census as well as expedition of care.
The future of hospital medicine is one of continued growth with the demand for hospital medicine physicians far outstripping the available supply to meet the ever-increasing needs. SHM is committed to researching and sharing best practices, and views the use of multidisciplinary teams as an important model of care. Together, we can all achieve more.
If you are interested in being a part of this project or feel that this data would be of benefit to your practice, please contact the Non-Physician Provider Committee at nppcommittee@hospitalmedicine.org.
Chapter Reports
Nashville
Quite a bit of networking took place before the Medtronic-sponsored presentation at Ruth’s Chris in Nashville on April 26. The SHM Nashville Chapter has re-energized itself under the co-direction of Steven Embry, MD, and Kimberly Bell, MD. Eleven Nashville-area healthcare organizations were represented by more than 28 attendees. The attendees were a multidisciplinary mix of physicians, nurses, and administrators. Shashank Desai, MD, engaged the audience with his presentation “Simple to Complex: Advances in the Management of CHF.” Dr. Desai is the medical director of the Heart Failure and Transplant Program at Inova Fairfax Hospital.
Pacific Northwest
The latest Pacific Northwest Chapter meeting of SHM was held in Seattle on May 15. A change of venue and a new focus on speakers provided local hospitalists with information they won’t find elsewhere. Joseph Bennet, MD, former president of the local chapter, gave a presentation detailing his 15 months practicing hospitalist medicine in Dunedin, New Zealand. In addition to stunning photos of the terrain, Dr. Bennet delivered a thought-provoking presentation comparing New Zealand with the United States regarding culture, medical system financing, drug and care delivery, physician training, end-of-life issues, and many more aspects.
Pittsburgh
The Pittsburgh Chapter had a meeting May 10 at Morton’s Steakhouse. The speaker for the event was Rene Alvarez, MD, director of the Critical Care Unit at University of Pittsburgh Medical Center. Dr. Alvarez discussed “Strategies for Optimal Management of Patients with Heart Failure,” which generated an excellent discussion. Various hospital medicine topics including incentives, program structures, and 24/7 programs were also discussed. Attendees included hospitalists from six local hospitals. The next meeting will be held Oct. 30. For more information on the Pittsburgh Chapter, contact Michael Cratty, MD, PhD, at mcratty@wpahs.org.
Rocky Mountain
The Rocky Mountain Chapter held its spring meeting May 3 at the Denver Colorado Downtown Aquarium. Chapter President Eugene Chu, MD, welcomed attendees and was followed by an update from the Rocky Mountain Chapter Public Policy Committee presented by Bob Brockmann, MD, MSc. Guest speakers for the night were Edward Maa, MD, who spoke about “Seizure Management in Hospitalized Patients” and Daniel Mogyoros, MD, whose presentation was titled “Updates in Infectious Disease for Hospital Medicine.” Attendees received two AMA PRA [Physician’s Recognition Award] Category 1 credits.
San Diego
At its June 5 meeting, San Diego’s chapter discussed real-time, evidence-based practice as a means to improve patient care and share new clinical evidence with colleagues. Online access during the presentation allowed the group to review several evidence resources: PubMed, the Physician’s Information and Education Resource, the American College of Physicians Journal Club, and National Guideline Clearing House using real patient cases. Dinner was served by Blue Coral Seafood and Spirits, and Novartis sponsored the event.
Upstate South Carolina
The second meeting of the Upstate S.C. Chapter was held May 15, with close to 20 physicians representing five hospitals in upstate South Carolina. Kenneth Leeper, MD, pulmonologist, presented information on ventilator-associated pneumonia. Following the presentation, the business meeting was opened by outgoing President Raja Paladugu, MD.
The following officers were elected for 2007:
- President: Zafar Hossain, MD;
- Vice President: Imran Shaikh, MD; and
- Secretary: Shawn Morrow, MD.
The group decided to meet on a quarterly basis, with the next meeting to be held in September. TH
Many speakers at the recent SHM annual meeting in Dallas focused on the many ways hospitalists enhance quality of care. The teamwork necessary to effectively render inpatient services was an especially important topic.
Hospitalists have compiled a significant amount of descriptive material about their working environments and the composition and workloads of hospitalist teams. However, there is not much material available quantifying the ways that various disciplines impact the overall care-delivery metrics of multidisciplinary hospitalist teams.
The SHM Non-Physician Provider Committee is interested in collecting information on multidisciplinary programs, their component disciplines and individual providers to help identify and describe teams that have integrated nurse practitioners, physician assistants, clinical pharmacists and pharmacologists, nurse clinical care coordinators, and other related disciplines into their practices. Our goal is to develop descriptions of successful and unsuccessful implementation models.
We would also like to collect information measuring additional domains of interest to major stakeholders. Such domains might include the clinical utilization of non-physician providers in relationship to both scope-of-practice and delegation of authority, the influence of multidisciplinary integration on patient-centered care and patient satisfaction, process and outcomes quality metrics, throughput and efficiency measures, documentation practices, hospital privileges for non-physicians, medical education in the multidisciplinary environment, risk management and, of course, reimbursement.
One might ask why the collection and analysis of such data should be of interest to hospitalists and to SHM. There are several immediate answers:
- The first reason involves manpower. Hospital medicine has become a growing discipline for physicians—one that did not exist on the radar screens of physician planners 10 years ago. However, given the growing demand for hospitalists there may be a significant shortage. To address this deficit, hospital medicine practices will need to attract new associates in the form of nurse practitioners and physician assistants. It is therefore imperative that hospitalists proactively identify barriers to the integration of non-physician providers into their practices and have successful implementation models to guide this effort.
- The second reason centers on the fact that hospitalists will continue to lead efforts to enhance quality of care. Incorporating a multidisciplinary approach—whether through the pre-rounding and follow-up of nurse clinical care coordinators, the counsel of clinical pharmacists, or the hands-on care of other disciplines—will facilitate throughput and improve quality as well as enhance patient satisfaction and communication. Identifying best practices in these particular domains will provide information crucial to success in these areas.
- The third reason is related to the cost of services. With declining reimbursements coupled with increasing costs, hospital medicine programs must identify and implement measures aimed at expense control and maximization of services. Used appropriately, non-physician providers provide a lower-cost alternative to a physician-only model. When one-to-one pairing occurs, physician/NPP team-care can be delivered in a parallel-versus-linear fashion, thus allowing for increased census as well as expedition of care.
The future of hospital medicine is one of continued growth with the demand for hospital medicine physicians far outstripping the available supply to meet the ever-increasing needs. SHM is committed to researching and sharing best practices, and views the use of multidisciplinary teams as an important model of care. Together, we can all achieve more.
If you are interested in being a part of this project or feel that this data would be of benefit to your practice, please contact the Non-Physician Provider Committee at nppcommittee@hospitalmedicine.org.
Chapter Reports
Nashville
Quite a bit of networking took place before the Medtronic-sponsored presentation at Ruth’s Chris in Nashville on April 26. The SHM Nashville Chapter has re-energized itself under the co-direction of Steven Embry, MD, and Kimberly Bell, MD. Eleven Nashville-area healthcare organizations were represented by more than 28 attendees. The attendees were a multidisciplinary mix of physicians, nurses, and administrators. Shashank Desai, MD, engaged the audience with his presentation “Simple to Complex: Advances in the Management of CHF.” Dr. Desai is the medical director of the Heart Failure and Transplant Program at Inova Fairfax Hospital.
Pacific Northwest
The latest Pacific Northwest Chapter meeting of SHM was held in Seattle on May 15. A change of venue and a new focus on speakers provided local hospitalists with information they won’t find elsewhere. Joseph Bennet, MD, former president of the local chapter, gave a presentation detailing his 15 months practicing hospitalist medicine in Dunedin, New Zealand. In addition to stunning photos of the terrain, Dr. Bennet delivered a thought-provoking presentation comparing New Zealand with the United States regarding culture, medical system financing, drug and care delivery, physician training, end-of-life issues, and many more aspects.
Pittsburgh
The Pittsburgh Chapter had a meeting May 10 at Morton’s Steakhouse. The speaker for the event was Rene Alvarez, MD, director of the Critical Care Unit at University of Pittsburgh Medical Center. Dr. Alvarez discussed “Strategies for Optimal Management of Patients with Heart Failure,” which generated an excellent discussion. Various hospital medicine topics including incentives, program structures, and 24/7 programs were also discussed. Attendees included hospitalists from six local hospitals. The next meeting will be held Oct. 30. For more information on the Pittsburgh Chapter, contact Michael Cratty, MD, PhD, at mcratty@wpahs.org.
Rocky Mountain
The Rocky Mountain Chapter held its spring meeting May 3 at the Denver Colorado Downtown Aquarium. Chapter President Eugene Chu, MD, welcomed attendees and was followed by an update from the Rocky Mountain Chapter Public Policy Committee presented by Bob Brockmann, MD, MSc. Guest speakers for the night were Edward Maa, MD, who spoke about “Seizure Management in Hospitalized Patients” and Daniel Mogyoros, MD, whose presentation was titled “Updates in Infectious Disease for Hospital Medicine.” Attendees received two AMA PRA [Physician’s Recognition Award] Category 1 credits.
San Diego
At its June 5 meeting, San Diego’s chapter discussed real-time, evidence-based practice as a means to improve patient care and share new clinical evidence with colleagues. Online access during the presentation allowed the group to review several evidence resources: PubMed, the Physician’s Information and Education Resource, the American College of Physicians Journal Club, and National Guideline Clearing House using real patient cases. Dinner was served by Blue Coral Seafood and Spirits, and Novartis sponsored the event.
Upstate South Carolina
The second meeting of the Upstate S.C. Chapter was held May 15, with close to 20 physicians representing five hospitals in upstate South Carolina. Kenneth Leeper, MD, pulmonologist, presented information on ventilator-associated pneumonia. Following the presentation, the business meeting was opened by outgoing President Raja Paladugu, MD.
The following officers were elected for 2007:
- President: Zafar Hossain, MD;
- Vice President: Imran Shaikh, MD; and
- Secretary: Shawn Morrow, MD.
The group decided to meet on a quarterly basis, with the next meeting to be held in September. TH