In treating hypertension, lower systolic pressure is better than higher—with caveats. This is the message of the Systolic Blood Pressure Intervention Trial (SPRINT),1 a large, federally funded study that was halted early when patients at high cardiovascular risk who were randomized to a goal systolic pressure of less than 120 mm Hg were found to have better outcomes, including lower rates of heart failure, death from cardiovascular causes, and death from any cause, than patients randomized to a goal of less than 140 mm Hg.
The caveats: the benefit came at a price of more adverse events. Also, the trial excluded patients who had diabetes mellitus or previous strokes, so it is uncertain if these subgroups would also benefit from intensive lowering of systolic pressure—and in earlier trials they did not.
This article reviews the trial design and protocol, summarizes the results, and briefly discusses the implications of these results.
BEFORE SPRINT
Hypertension is very common in adults in the United States, and is a risk factor for heart disease, stroke, heart failure, and kidney disease. The estimated prevalence of hypertension in the 2011–2014 National Health and Nutrition Examination Survey (NHANES) was 29%, and the prevalence increases with age (7.3% in those ages 18 to 39, 32.2% in those ages 40 to 59, and 64.9% in those ages 60 and older).2 Isolated systolic hypertension (ie, systolic blood pressure > 140 mm Hg with diastolic pressure < 90 mm Hg) is the most common form of hypertension after age 50.3
Clinical trials have provided substantial evidence that treating hypertension reduces the incidence of stroke, myocardial infarction, and heart failure.4,5 Although observational studies show a progressive and linear rise in cardiovascular risk as systolic blood pressure rises above 115 mm Hg,6 clinical trials in the general population have not documented benefits of lowering systolic pressure to this level.7–11 However, clinical trials that directly evaluated two different blood pressure goals in the general population showed benefit with achieving systolic blood pressure less than 150 mm Hg,7,9 with limited data on lower blood pressure targets.10–12
No benefit found in intensive systolic lowering in diabetes or after stroke
The Action to Control Cardiovascular Risk in Diabetes-Blood Pressure (ACCORD BP) trial13 in patients with type 2 diabetes found no benefit in lowering systolic pressure to less than 120 mm Hg compared with less than 140 mm Hg in terms of the trial’s primary composite cardiovascular outcome (ie, nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes). However, the intensively treated group in this trial did enjoy a benefit in terms of fewer stroke events.
The Secondary Prevention of Small Subcortical Strokes (SPS3) trial14 in patients with stroke found no significant benefit in lowering systolic pressure to less than 130 mm Hg compared with less than 150 mm Hg for overall risk of another stroke, but a significant benefit was noted in reduced risk of intracerebral hemorrhage.
Current guidelines, based on available evidence, advocate treatment to a systolic goal of less than 140 mm Hg in most patients, and recommend relaxing this goal to less than 150 mm Hg in the elderly.15,16
SPRINT was stopped early due to better outcomes in the intensive treatment group
Given the uncertainty surrounding optimal systolic targets, SPRINT was designed to test the hypothesis that a goal of less than 120 mm Hg would reduce the risk of cardiovascular events more than the generally accepted systolic goal of less than 140 mm Hg.17 Patients with diabetes and stroke were excluded because a similar hypothesis was tested in the ACCORD BP and SPS3 trials, which included patients with these conditions.
SPRINT DESIGN
SPRINT was a randomized, controlled, open-label trial sponsored by the National Institutes of Health and conducted at 102 US sites.
Inclusion criteria. Participants had to be at least 50 years old, with systolic pressure of 130 to 180 mm Hg, and had to have at least one cardiovascular risk factor, eg:
Clinical or subclinical cardiovascular disease (other than stroke)
Chronic kidney disease, defined as estimated glomerular filtration rate (eGFR), calculated by the Modification of Diet in Renal Disease (MDRD) study equation, of 20 to less than 60 mL/min/1.73 m2
Framingham risk score of 15% of more
Age 75 or older.
Major exclusion criteria included:
Diabetes
Stroke
Polycystic kidney disease
Chronic kidney disease with an eGFR less than 20 mL/min/1.73 m2
Proteinuria (excretion > 1 g/day).
Intensive vs standard treatment
Participants were randomized to receive intensive treatment (systolic goal < 120 mm Hg) or standard treatment (systolic goal < 140 mm Hg). Baseline antihypertensive medications were adjusted to achieve blood pressure goals based on randomization assignment.
Doses of medications were adjusted on the basis of an average of three seated office blood pressure measurements after a 5-minute period of rest, taken with an automated monitor (Omron Healthcare Model 907); the same monitor was used and the same protocol was followed at all participating sites. Blood pressure was also measured after standing for 1 minute to assess orthostatic change.
Intensive treatment required, on average, one more medication than standard treatment
Lifestyle modifications were encouraged in both groups. There was no restriction on using any antihypertensive medication, and this was at the discretion of individual investigators. Thiazide-type diuretics were encouraged as first-line agents (with chlorthalidone encouraged as the primary thiazide-type diuretic).
Outcomes measured
The primary outcome was a composite of myocardial infarction, acute coronary syndrome not resulting in myocardial infarction, stroke, acute decompensated heart failure, and cardiovascular mortality.
Secondary outcomes included individual components of the primary composite outcome, all-cause mortality, and the composite of primary outcome and all-cause mortality.
Renal outcomes were assessed as:
Incident albuminuria (doubling of the urinary albumin-to-creatinine ratio from less than 10 mg/g to more than 10 mg/g)
Composite of a 50% decrease in eGFR or development of end-stage renal disease requiring long-term dialysis or kidney transplantation (in those with baseline chronic kidney disease)
A 30% decrease in eGFR (in those without chronic kidney disease).1,17
SPRINT also recruited participants to two nested substudies: SPRINT MIND and SPRINT MIND MRI, to study differences in cognitive outcomes and small-vessel ischemic disease between intensive treatment and standard treatment.
STUDY RESULTS
Older patients at risk, but without diabetes
Of 14,692 participants screened, 9,361 were enrolled in the study between 2010 and 2013. Baseline characteristics were comparable in both groups.
Demographics. The mean age of the participants was 67.9, and about 28% were 75 or older. About 36% were women, 58% white, 30% black, and 11% Hispanic.
Cardiovascular risk. The mean Framingham risk score was 20% (ie, they had a 20% risk of having a cardiovascular event within 10 years), and 61% of the participants had a risk score of at least 15%. Twenty percent already had cardiovascular disease.
Blood pressure. The average baseline blood pressure was 139.7/78.2 mm Hg. One-third of the participants had baseline systolic pressures of 132 mm Hg or less, another third had pressures in the range of 132 to 145, and the rest had 145 mm Hg or higher.
Renal function. The mean serum creatinine level was about 1.1 mg/dL. The mean eGFR was about 71 mL/min/1.73 m2 as calculated by the MDRD equation, and about 28% had eGFRs less than 60. The mean ratio of urinary albumin to creatinine was 44.1 mg/g in the intensive treatment group and 41.1 in the standard treatment group.
Other. The mean total cholesterol level was 190 mg/dL, fasting plasma glucose 99 mg/dL, and body mass index nearly 30 kg/m2.
Blood pressure during treatment
People in the intensive treatment group were taking a mean of 2.8 antihypertensive medications, and those in the standard treatment group were taking 1.8. Patients in the intensive group required greater use of all classes of medications to achieve goal systolic pressure (Table 1).
Study halted early due to efficacy
Throughout the 3.26 years of follow-up, the average difference in systolic pressure between the two groups was 13.1 mm Hg, with a mean systolic pressure of 121.5 mm Hg in the intensive treatment group and 134.6 mm Hg in the standard treatment group. The mean diastolic blood pressure was 68.7 mm Hg in the intensive treatment group and 76.3 mm Hg in the standard treatment group.
Although the study was planned to run for an average follow-up of 5 years, the National Heart, Lung, and Blood Institute terminated it early at a median of 3.26 years in view of lower rates of the primary outcome and of heart failure and death in the intensive treatment group (Table 2).
The effects on the primary outcome and mortality were consistent across the prespecified subgroups of age (< 75 vs ≥ 75), sex (female vs male), race (black vs nonblack), cardiovascular disease (presence or absence at baseline), prior chronic kidney disease (presence or absence at baseline), and across blood pressure tertiles (≤ 132 mm Hg, > 132 to < 145 mm Hg, ≥ 145 mm Hg).
Follow-up for assessment of cognitive outcomes (SPRINT MIND) and small-vessel ischemic disease (SPRINT MIND MRI) is ongoing.
WHAT DOES THIS MEAN?
SPRINT is the first large, adequately powered, randomized trial to demonstrate cardiovascular and mortality benefit from lowering the systolic blood pressure (goal < 120 mm Hg) in older patients at cardiovascular risk but without a history of diabetes mellitus or stroke.1
Most SPRINT patients had reasonably controlled blood pressure at baseline (the mean systolic pressure was 139.7 mm Hg, and two-thirds of participants had systolic pressure < 145 mm Hg). Of note, however, this trial excluded patients with systolic pressure higher than 180 mm Hg. There was excellent separation of systolic pressure between the two groups beginning at 1 year, which was consistent through the course of the trial.
The cardiovascular benefit in the intensive treatment group was predominantly driven by lower rates of heart failure (a 38% reduction in the intensive treatment group, P = .0002) and cardiovascular mortality (a 43% reduction in the intensive treatment group, P = .005), while there was no significant difference between the two groups in myocardial infarction or stroke. The beneficial effect on heart failure events is consistent with results from other trials including the Systolic Hypertension in the Elderly Program,7 Systolic Hypertension in Europe,8 and Hypertension in the Very Elderly Trial,9 all of which showed greatest risk reduction for heart failure events with systolic pressure-lowering (although to higher systolic levels than SPRINT).7–9 It is unclear why there was no beneficial effect on stroke events. The reduction in all-cause mortality in the intensive treatment group in SPRINT was greater than the reduction in cardiovascular deaths, which is also unexplained.
Although the study was terminated early due to efficacy (which introduces the possible bias that the estimated effect size will be too high), the number of primary end points reached was large (562 in the two groups combined), providing reassurance that the findings are valid. There was no blinding in the study (both participants and study investigators were aware of treatment assignment and study medications), but there was a structured assessment of outcomes and adverse events, with adjudication done by blinded reviewers.
SPRINT used an automated device for blood pressure measurement, which is known to reduce the “white coat” effect and correlates tightly with average daytime blood pressure done by ambulatory blood pressure monitoring.18 However, in clinical practice automated devices may not be available and a strict protocol for correct measurement may not be followed, with the possible result that blood pressure may be overestimated and overtreated.
What about diastolic pressure?
The trial, by design, focused on lowering systolic pressure (given the greater prevalence of isolated systolic hypertension with age), and the implications of lowering diastolic pressure are unclear. The issue of a J-shaped relationship between diastolic pressure and cardiovascular risk is debated in the literature: patients with a diastolic pressure of 60 to 65 mm Hg, especially those with existing coronary artery disease, may not tolerate aggressive blood pressure-lowering.19,20 Further analysis of this association (if any) from SPRINT will be helpful.
What about patients with diabetes?
Patients were excluded from SPRINT if they were under age 50, were at low cardiovascular risk, or had diabetes, raising the question of whether the results apply to these groups as well.
The question is particularly relevant in diabetes, as the ACCORD BP study, which used the same blood pressure targets as SPRINT, did not show a significant difference in the primary cardiovascular outcome between the intensive and standard treatments in patients with diabetes (Table 3).13 In ACCORD BP, the rate of the primary outcome was 12% lower in the intensive treatment group than in the standard treatment group, but the 95% confidence interval was –27% to +6%, so the finding was not statistically significant. However, the wide confidence interval does not exclude the possibility of a benefit that was comparable to that observed in SPRINT.
It has been speculated that ACCORD BP was underpowered to detect significant differences in the primary outcome.21 An analysis combining data from both trials indicated that effects on individual outcomes were generally consistent in both trials (with no significant heterogeneity noted).22 Also, the primary composite outcome in ACCORD did not include heart failure, which is particularly sensitive to blood pressure reduction.
Additionally, ACCORD BP had a 2 × 2 factorial design involving a simultaneous comparison of intensive vs standard glycemic control, which may have influenced the effects due to blood pressure. Indeed, a post hoc analysis showed that there was a significant 26% lower risk of the primary outcome in ACCORD BP patients who received intensive systolic pressure control plus standard glycemic control than in those receiving standard systolic control plus standard glycemic control.23
Are more adverse events an acceptable trade-off?
Adverse events, including acute kidney injury, were more frequent in the intensive therapy group in SPRINT.
Acute kidney injury was coded as an adverse event on the basis of this diagnosis being included in the hospital discharge summary (as a primary or main secondary diagnosis) and if considered by the safety officer to be one of the top three reasons for admission or continued hospitalization. Further analysis of renal events should be forthcoming.
People in the intensive treatment group, on average, needed one more medication than those in the standard treatment group. Some of the adverse events may be related to the antihypertensive medications taken (eg, electrolyte abnormalities such as hyponatremia and hypokalemia due to diuretic use), and others may be related to blood pressure-lowering (eg, acute kidney injury due to renal hypoperfusion).
At this point, the long-term effects of these adverse events, especially on kidney function, are not known. Patients enrolled in clinical trials tend to be healthier than patients seen in clinical practice; thus, the rate of adverse events reported in the trial may be lower than one would see in the real world.
Does lower systolic pressure protect or harm the kidneys?
SPRINT included patients with stage 3 and 4 chronic kidney disease (ie, with eGFR 20–50 mL/min/1.73 m2), but it was designed to assess cardiovascular outcomes, not the progression of chronic kidney disease. The trial excluded patients with diabetic nephropathy or high degrees of proteinuria.
Only about half of hypertensive adults have their blood pressure under control, ie, < 140/90
Earlier randomized trials that focused on chronic kidney disease progression, including the MDRD24 and the African American Study of Kidney Disease and Hypertension,25 did not show benefit with more aggressive blood pressure-lowering (except in patients with higher degrees of proteinuria), and these trials were not powered to assess effects on cardiovascular outcomes.24,25
The Irbesartan Diabetic Nephropathy Trial,26,27 which was done in patients with overt diabetic nephropathy, showed that a progressively lower achieved systolic pressure down to 120 mm Hg predicted lower rates of heart failure, cardiovascular mortality, and renal events (although the trial target was ≤ 130/85 mm Hg and few participants achieved systolic pressure lower than 120 mm Hg).
IMPLICATIONS FOR MANAGEMENT
The recent estimates of hypertension prevalence and control from NHANES show that only about 53% of hypertensive adults have their blood pressure under control (defined as systolic pressure < 140 mm Hg and diastolic pressure < 90 mm Hg).2 Analysis of the NHANES 2007–2012 data showed that 16.7% or 8.2 million US adults with treated hypertension meet the eligibility criteria for SPRINT.28
Although the SPRINT results support the notion that “lower is better,” the risks and benefits of intensive control will need to be balanced in individual patients. Table 4 shows the number needed to treat and number needed to harm in the trial.
More aggressive management of hypertension is challenging. The median systolic pressure achieved in the intensive group in SPRINT was just over 120 mm Hg, which implies that at least half of the participants in the intensive group did not achieve the goal of less than 120 mm Hg. While it may be reasonable to aim for systolic pressure of less than 120 or 125 mm Hg in patients who fit the SPRINT criteria and can tolerate intensive blood pressure lowering, it would be prudent to aim for a more conservative goal in elderly patients who are frail and at risk for falls, considering the higher incidence of specified adverse events in the intensive group.
Results of cognitive outcomes, as well as data related to quality of life, are still awaited. Long-term renal outcomes are also unclear.
As noted above, the question of generalizability of SPRINT results to patients with diabetes is open to debate. In our opinion, with currently available evidence, it is difficult to conclusively answer the question of whether a lower systolic target provides cardiovascular benefit in diabetes. It is also unclear whether similar beneficial results would be seen with intensive treatment in a population at low cardiovascular risk. The American Heart Association and the American College of Cardiology are in the process of formulating new hypertension guidelines, and evidence from SPRINT will inform any new recommendations.
As more medications will likely be needed for intensive systolic blood pressure control, side effects and tolerability of medications with polypharmacy and potential nonadherence with increasing complexity of medication regimens should be kept in mind. Lifestyle modifications will need to be emphasized and reinforced, with greater use of combination antihypertensive therapy.
The data from SPRINT indicate that lower systolic pressure is better, as long as untoward clinical events can be monitored and avoided or easily managed. Careful monitoring will likely entail more frequent clinic visits and more frequent assessment of renal function and electrolyte levels (participants in the intensive group in the trial were seen every month until goal was achieved). A team approach that includes pharmacists and nurse practitioners, along with optimal use of best practice algorithms and remote monitoring technology, will need to be implemented for efficient and effective care.
References
SPRINT Research Group; Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373:2103–2116.
Yoon SS, Fryar CD, Carroll MD. Hypertension prevalence and control among adults: United States, 2011–2014. NCHS data brief, no. 220. Hyattsville, MD: National Center for Health Statistics. 2015.
Franklin SS, Jacobs MJ, Wong ND, L’Italien GJ, Lapuerta P. Predominance of isolated systolic hypertension among middle-aged and elderly US hypertensives: analysis based on National Health and Nutrition Examination Survey (NHANES) III. Hypertension 2001; 37:869–874.
Neal B, MacMahon S, Chapman N; Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet 2000; 356:1955–1964.
Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA 1997; 277:739–745.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360:1903–1913.
SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991; 265:3255–3264.
Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350:757–764.
Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358:1887–1898.
JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res 2008; 31:2115–2127.
Ogihara T, Saruta T, Rakugi H, et al; Valsartan in Elderly Isolated Systolic Hypertension Study Group. Target blood pressure for treatment of isolated systolic hypertension in the elderly: Valsartan in Elderly Isolated Systolic Hypertension study. Hypertension 2010; 56:196–202.
Liu L, Zhang Y, Liu G, Li W, Zhang X, Zanchetti A; FEVER Study Group. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens 2005; 23:2157–2172.
ACCORD Study Group; Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010; 362:1575–1585.
SPS3 Study Group; Benavente OR, Coffey CS, Conwit R, et al. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trial. Lancet 2013; 382:507–515.
James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311:507–520. Erratum in: JAMA. 2014; 311:1809.
Weber MA, Schiffrin EL, White WB, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich) 2014; 16:14–26.
Ambrosius WT, Sink KM, Foy CG, et al; SPRINT Study Research Group. The design and rationale of a multicenter clinical trial comparing two strategies for control of systolic blood pressure: the Systolic Blood Pressure Intervention Trial (SPRINT). Clin Trials 2014; 11:532–546.
Myers MG, Godwin M, Dawes M, Kiss A, Tobe SW, Kaczorowski J. Conventional versus automated measurement of blood pressure in the office (CAMBO) trial. Fam Pract 2012; 29:376–382.
Messerli FH, Mancia G, Conti CR, et al. Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann Intern Med 2006; 144:884–893.
Boutitie F, Gueyffier F, Pocock S, Fagard R, Boissel JP; INDANA Project Steering Committee; INdividual Data ANalysis of Antihypertensive intervention. J-shaped relationship between blood pressure and mortality in hypertensive patients: new insights from a meta-analysis of individual-patient data. Ann Intern Med 2002; 136:438–448.
Mancia G. Effects of intensive blood pressure control in the management of patients with type 2 diabetes mellitus in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Circulation 2010; 122:847–849.
Perkovic V, Rodgers A. Redefining blood-pressure targets—SPRINT starts the marathon. N Engl J Med 2015; 373:2175–2178.
Margolis KL, O’Connor PJ, Morgan TM, et al. Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial. Diabetes Care 2014; 37:1721–1728.
Peterson JC, Adler S, Burkart JM, et al. Blood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease study. Ann Intern Med 1995; 123:754–762.
Agodoa LY, Appel L, Bakris GL, et al; African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 2001; 285:2719–2728.
Berl T, Hunsicker LG, Lewis JB, et al; Collaborative Study Group. Impact of achieved blood pressure on cardiovascular outcomes in the Irbesartan Diabetic Nephropathy Trial. J Am Soc Nephrol 2005; 16:2170–2179.
Pohl MA, Blumenthal S, Cordonnier DJ, et al. Independent and additive impact of blood pressure control and angiotensin II receptor blockade on renal outcomes in the Irbesartan Diabetic Nephropathy Trial: clinical implications and limitations. J Am Soc Nephrol 2005; 16:3027–3037.
Bress AP, Tanner RM, Hess R, Colantonio LD, Shimbo D, Muntner P. Generalizability of results from the Systolic Blood Pressure Intervention Trial (SPRINT) to the US adult population. J Am Coll Cardiol 2015 Oct 31. doi: 10.1016/j.jacc.2015.10.037. Epub ahead of print.
George Thomas, MD, FACP, FASN Director, Center for Blood Pressure Disorders, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH; Cleveland Clinic Site Principal Investigator, Systolic Blood Pressure Intervention Trial (SPRINT)
Joseph V. Nally, MD Director, Center for Chronic Kidney Disease, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Clinical Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Marc A. Pohl, MD Ray W. Gifford Chair in Hypertension, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Chair, Clinical Management Committee, Irbesartan Diabetic Nephropathy Trial
Address: George Thomas, MD, Department of Nephrology and Hypertension, Q7, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: thomasg3@ccf.org
George Thomas, MD, FACP, FASN Director, Center for Blood Pressure Disorders, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH; Cleveland Clinic Site Principal Investigator, Systolic Blood Pressure Intervention Trial (SPRINT)
Joseph V. Nally, MD Director, Center for Chronic Kidney Disease, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Clinical Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Marc A. Pohl, MD Ray W. Gifford Chair in Hypertension, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Chair, Clinical Management Committee, Irbesartan Diabetic Nephropathy Trial
Address: George Thomas, MD, Department of Nephrology and Hypertension, Q7, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: thomasg3@ccf.org
Author and Disclosure Information
George Thomas, MD, FACP, FASN Director, Center for Blood Pressure Disorders, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH; Cleveland Clinic Site Principal Investigator, Systolic Blood Pressure Intervention Trial (SPRINT)
Joseph V. Nally, MD Director, Center for Chronic Kidney Disease, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Clinical Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Marc A. Pohl, MD Ray W. Gifford Chair in Hypertension, Department of Nephrology and Hypertension, Glickman Urological and Kidney Institute, Cleveland Clinic; Chair, Clinical Management Committee, Irbesartan Diabetic Nephropathy Trial
Address: George Thomas, MD, Department of Nephrology and Hypertension, Q7, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: thomasg3@ccf.org
In treating hypertension, lower systolic pressure is better than higher—with caveats. This is the message of the Systolic Blood Pressure Intervention Trial (SPRINT),1 a large, federally funded study that was halted early when patients at high cardiovascular risk who were randomized to a goal systolic pressure of less than 120 mm Hg were found to have better outcomes, including lower rates of heart failure, death from cardiovascular causes, and death from any cause, than patients randomized to a goal of less than 140 mm Hg.
The caveats: the benefit came at a price of more adverse events. Also, the trial excluded patients who had diabetes mellitus or previous strokes, so it is uncertain if these subgroups would also benefit from intensive lowering of systolic pressure—and in earlier trials they did not.
This article reviews the trial design and protocol, summarizes the results, and briefly discusses the implications of these results.
BEFORE SPRINT
Hypertension is very common in adults in the United States, and is a risk factor for heart disease, stroke, heart failure, and kidney disease. The estimated prevalence of hypertension in the 2011–2014 National Health and Nutrition Examination Survey (NHANES) was 29%, and the prevalence increases with age (7.3% in those ages 18 to 39, 32.2% in those ages 40 to 59, and 64.9% in those ages 60 and older).2 Isolated systolic hypertension (ie, systolic blood pressure > 140 mm Hg with diastolic pressure < 90 mm Hg) is the most common form of hypertension after age 50.3
Clinical trials have provided substantial evidence that treating hypertension reduces the incidence of stroke, myocardial infarction, and heart failure.4,5 Although observational studies show a progressive and linear rise in cardiovascular risk as systolic blood pressure rises above 115 mm Hg,6 clinical trials in the general population have not documented benefits of lowering systolic pressure to this level.7–11 However, clinical trials that directly evaluated two different blood pressure goals in the general population showed benefit with achieving systolic blood pressure less than 150 mm Hg,7,9 with limited data on lower blood pressure targets.10–12
No benefit found in intensive systolic lowering in diabetes or after stroke
The Action to Control Cardiovascular Risk in Diabetes-Blood Pressure (ACCORD BP) trial13 in patients with type 2 diabetes found no benefit in lowering systolic pressure to less than 120 mm Hg compared with less than 140 mm Hg in terms of the trial’s primary composite cardiovascular outcome (ie, nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes). However, the intensively treated group in this trial did enjoy a benefit in terms of fewer stroke events.
The Secondary Prevention of Small Subcortical Strokes (SPS3) trial14 in patients with stroke found no significant benefit in lowering systolic pressure to less than 130 mm Hg compared with less than 150 mm Hg for overall risk of another stroke, but a significant benefit was noted in reduced risk of intracerebral hemorrhage.
Current guidelines, based on available evidence, advocate treatment to a systolic goal of less than 140 mm Hg in most patients, and recommend relaxing this goal to less than 150 mm Hg in the elderly.15,16
SPRINT was stopped early due to better outcomes in the intensive treatment group
Given the uncertainty surrounding optimal systolic targets, SPRINT was designed to test the hypothesis that a goal of less than 120 mm Hg would reduce the risk of cardiovascular events more than the generally accepted systolic goal of less than 140 mm Hg.17 Patients with diabetes and stroke were excluded because a similar hypothesis was tested in the ACCORD BP and SPS3 trials, which included patients with these conditions.
SPRINT DESIGN
SPRINT was a randomized, controlled, open-label trial sponsored by the National Institutes of Health and conducted at 102 US sites.
Inclusion criteria. Participants had to be at least 50 years old, with systolic pressure of 130 to 180 mm Hg, and had to have at least one cardiovascular risk factor, eg:
Clinical or subclinical cardiovascular disease (other than stroke)
Chronic kidney disease, defined as estimated glomerular filtration rate (eGFR), calculated by the Modification of Diet in Renal Disease (MDRD) study equation, of 20 to less than 60 mL/min/1.73 m2
Framingham risk score of 15% of more
Age 75 or older.
Major exclusion criteria included:
Diabetes
Stroke
Polycystic kidney disease
Chronic kidney disease with an eGFR less than 20 mL/min/1.73 m2
Proteinuria (excretion > 1 g/day).
Intensive vs standard treatment
Participants were randomized to receive intensive treatment (systolic goal < 120 mm Hg) or standard treatment (systolic goal < 140 mm Hg). Baseline antihypertensive medications were adjusted to achieve blood pressure goals based on randomization assignment.
Doses of medications were adjusted on the basis of an average of three seated office blood pressure measurements after a 5-minute period of rest, taken with an automated monitor (Omron Healthcare Model 907); the same monitor was used and the same protocol was followed at all participating sites. Blood pressure was also measured after standing for 1 minute to assess orthostatic change.
Intensive treatment required, on average, one more medication than standard treatment
Lifestyle modifications were encouraged in both groups. There was no restriction on using any antihypertensive medication, and this was at the discretion of individual investigators. Thiazide-type diuretics were encouraged as first-line agents (with chlorthalidone encouraged as the primary thiazide-type diuretic).
Outcomes measured
The primary outcome was a composite of myocardial infarction, acute coronary syndrome not resulting in myocardial infarction, stroke, acute decompensated heart failure, and cardiovascular mortality.
Secondary outcomes included individual components of the primary composite outcome, all-cause mortality, and the composite of primary outcome and all-cause mortality.
Renal outcomes were assessed as:
Incident albuminuria (doubling of the urinary albumin-to-creatinine ratio from less than 10 mg/g to more than 10 mg/g)
Composite of a 50% decrease in eGFR or development of end-stage renal disease requiring long-term dialysis or kidney transplantation (in those with baseline chronic kidney disease)
A 30% decrease in eGFR (in those without chronic kidney disease).1,17
SPRINT also recruited participants to two nested substudies: SPRINT MIND and SPRINT MIND MRI, to study differences in cognitive outcomes and small-vessel ischemic disease between intensive treatment and standard treatment.
STUDY RESULTS
Older patients at risk, but without diabetes
Of 14,692 participants screened, 9,361 were enrolled in the study between 2010 and 2013. Baseline characteristics were comparable in both groups.
Demographics. The mean age of the participants was 67.9, and about 28% were 75 or older. About 36% were women, 58% white, 30% black, and 11% Hispanic.
Cardiovascular risk. The mean Framingham risk score was 20% (ie, they had a 20% risk of having a cardiovascular event within 10 years), and 61% of the participants had a risk score of at least 15%. Twenty percent already had cardiovascular disease.
Blood pressure. The average baseline blood pressure was 139.7/78.2 mm Hg. One-third of the participants had baseline systolic pressures of 132 mm Hg or less, another third had pressures in the range of 132 to 145, and the rest had 145 mm Hg or higher.
Renal function. The mean serum creatinine level was about 1.1 mg/dL. The mean eGFR was about 71 mL/min/1.73 m2 as calculated by the MDRD equation, and about 28% had eGFRs less than 60. The mean ratio of urinary albumin to creatinine was 44.1 mg/g in the intensive treatment group and 41.1 in the standard treatment group.
Other. The mean total cholesterol level was 190 mg/dL, fasting plasma glucose 99 mg/dL, and body mass index nearly 30 kg/m2.
Blood pressure during treatment
People in the intensive treatment group were taking a mean of 2.8 antihypertensive medications, and those in the standard treatment group were taking 1.8. Patients in the intensive group required greater use of all classes of medications to achieve goal systolic pressure (Table 1).
Study halted early due to efficacy
Throughout the 3.26 years of follow-up, the average difference in systolic pressure between the two groups was 13.1 mm Hg, with a mean systolic pressure of 121.5 mm Hg in the intensive treatment group and 134.6 mm Hg in the standard treatment group. The mean diastolic blood pressure was 68.7 mm Hg in the intensive treatment group and 76.3 mm Hg in the standard treatment group.
Although the study was planned to run for an average follow-up of 5 years, the National Heart, Lung, and Blood Institute terminated it early at a median of 3.26 years in view of lower rates of the primary outcome and of heart failure and death in the intensive treatment group (Table 2).
The effects on the primary outcome and mortality were consistent across the prespecified subgroups of age (< 75 vs ≥ 75), sex (female vs male), race (black vs nonblack), cardiovascular disease (presence or absence at baseline), prior chronic kidney disease (presence or absence at baseline), and across blood pressure tertiles (≤ 132 mm Hg, > 132 to < 145 mm Hg, ≥ 145 mm Hg).
Follow-up for assessment of cognitive outcomes (SPRINT MIND) and small-vessel ischemic disease (SPRINT MIND MRI) is ongoing.
WHAT DOES THIS MEAN?
SPRINT is the first large, adequately powered, randomized trial to demonstrate cardiovascular and mortality benefit from lowering the systolic blood pressure (goal < 120 mm Hg) in older patients at cardiovascular risk but without a history of diabetes mellitus or stroke.1
Most SPRINT patients had reasonably controlled blood pressure at baseline (the mean systolic pressure was 139.7 mm Hg, and two-thirds of participants had systolic pressure < 145 mm Hg). Of note, however, this trial excluded patients with systolic pressure higher than 180 mm Hg. There was excellent separation of systolic pressure between the two groups beginning at 1 year, which was consistent through the course of the trial.
The cardiovascular benefit in the intensive treatment group was predominantly driven by lower rates of heart failure (a 38% reduction in the intensive treatment group, P = .0002) and cardiovascular mortality (a 43% reduction in the intensive treatment group, P = .005), while there was no significant difference between the two groups in myocardial infarction or stroke. The beneficial effect on heart failure events is consistent with results from other trials including the Systolic Hypertension in the Elderly Program,7 Systolic Hypertension in Europe,8 and Hypertension in the Very Elderly Trial,9 all of which showed greatest risk reduction for heart failure events with systolic pressure-lowering (although to higher systolic levels than SPRINT).7–9 It is unclear why there was no beneficial effect on stroke events. The reduction in all-cause mortality in the intensive treatment group in SPRINT was greater than the reduction in cardiovascular deaths, which is also unexplained.
Although the study was terminated early due to efficacy (which introduces the possible bias that the estimated effect size will be too high), the number of primary end points reached was large (562 in the two groups combined), providing reassurance that the findings are valid. There was no blinding in the study (both participants and study investigators were aware of treatment assignment and study medications), but there was a structured assessment of outcomes and adverse events, with adjudication done by blinded reviewers.
SPRINT used an automated device for blood pressure measurement, which is known to reduce the “white coat” effect and correlates tightly with average daytime blood pressure done by ambulatory blood pressure monitoring.18 However, in clinical practice automated devices may not be available and a strict protocol for correct measurement may not be followed, with the possible result that blood pressure may be overestimated and overtreated.
What about diastolic pressure?
The trial, by design, focused on lowering systolic pressure (given the greater prevalence of isolated systolic hypertension with age), and the implications of lowering diastolic pressure are unclear. The issue of a J-shaped relationship between diastolic pressure and cardiovascular risk is debated in the literature: patients with a diastolic pressure of 60 to 65 mm Hg, especially those with existing coronary artery disease, may not tolerate aggressive blood pressure-lowering.19,20 Further analysis of this association (if any) from SPRINT will be helpful.
What about patients with diabetes?
Patients were excluded from SPRINT if they were under age 50, were at low cardiovascular risk, or had diabetes, raising the question of whether the results apply to these groups as well.
The question is particularly relevant in diabetes, as the ACCORD BP study, which used the same blood pressure targets as SPRINT, did not show a significant difference in the primary cardiovascular outcome between the intensive and standard treatments in patients with diabetes (Table 3).13 In ACCORD BP, the rate of the primary outcome was 12% lower in the intensive treatment group than in the standard treatment group, but the 95% confidence interval was –27% to +6%, so the finding was not statistically significant. However, the wide confidence interval does not exclude the possibility of a benefit that was comparable to that observed in SPRINT.
It has been speculated that ACCORD BP was underpowered to detect significant differences in the primary outcome.21 An analysis combining data from both trials indicated that effects on individual outcomes were generally consistent in both trials (with no significant heterogeneity noted).22 Also, the primary composite outcome in ACCORD did not include heart failure, which is particularly sensitive to blood pressure reduction.
Additionally, ACCORD BP had a 2 × 2 factorial design involving a simultaneous comparison of intensive vs standard glycemic control, which may have influenced the effects due to blood pressure. Indeed, a post hoc analysis showed that there was a significant 26% lower risk of the primary outcome in ACCORD BP patients who received intensive systolic pressure control plus standard glycemic control than in those receiving standard systolic control plus standard glycemic control.23
Are more adverse events an acceptable trade-off?
Adverse events, including acute kidney injury, were more frequent in the intensive therapy group in SPRINT.
Acute kidney injury was coded as an adverse event on the basis of this diagnosis being included in the hospital discharge summary (as a primary or main secondary diagnosis) and if considered by the safety officer to be one of the top three reasons for admission or continued hospitalization. Further analysis of renal events should be forthcoming.
People in the intensive treatment group, on average, needed one more medication than those in the standard treatment group. Some of the adverse events may be related to the antihypertensive medications taken (eg, electrolyte abnormalities such as hyponatremia and hypokalemia due to diuretic use), and others may be related to blood pressure-lowering (eg, acute kidney injury due to renal hypoperfusion).
At this point, the long-term effects of these adverse events, especially on kidney function, are not known. Patients enrolled in clinical trials tend to be healthier than patients seen in clinical practice; thus, the rate of adverse events reported in the trial may be lower than one would see in the real world.
Does lower systolic pressure protect or harm the kidneys?
SPRINT included patients with stage 3 and 4 chronic kidney disease (ie, with eGFR 20–50 mL/min/1.73 m2), but it was designed to assess cardiovascular outcomes, not the progression of chronic kidney disease. The trial excluded patients with diabetic nephropathy or high degrees of proteinuria.
Only about half of hypertensive adults have their blood pressure under control, ie, < 140/90
Earlier randomized trials that focused on chronic kidney disease progression, including the MDRD24 and the African American Study of Kidney Disease and Hypertension,25 did not show benefit with more aggressive blood pressure-lowering (except in patients with higher degrees of proteinuria), and these trials were not powered to assess effects on cardiovascular outcomes.24,25
The Irbesartan Diabetic Nephropathy Trial,26,27 which was done in patients with overt diabetic nephropathy, showed that a progressively lower achieved systolic pressure down to 120 mm Hg predicted lower rates of heart failure, cardiovascular mortality, and renal events (although the trial target was ≤ 130/85 mm Hg and few participants achieved systolic pressure lower than 120 mm Hg).
IMPLICATIONS FOR MANAGEMENT
The recent estimates of hypertension prevalence and control from NHANES show that only about 53% of hypertensive adults have their blood pressure under control (defined as systolic pressure < 140 mm Hg and diastolic pressure < 90 mm Hg).2 Analysis of the NHANES 2007–2012 data showed that 16.7% or 8.2 million US adults with treated hypertension meet the eligibility criteria for SPRINT.28
Although the SPRINT results support the notion that “lower is better,” the risks and benefits of intensive control will need to be balanced in individual patients. Table 4 shows the number needed to treat and number needed to harm in the trial.
More aggressive management of hypertension is challenging. The median systolic pressure achieved in the intensive group in SPRINT was just over 120 mm Hg, which implies that at least half of the participants in the intensive group did not achieve the goal of less than 120 mm Hg. While it may be reasonable to aim for systolic pressure of less than 120 or 125 mm Hg in patients who fit the SPRINT criteria and can tolerate intensive blood pressure lowering, it would be prudent to aim for a more conservative goal in elderly patients who are frail and at risk for falls, considering the higher incidence of specified adverse events in the intensive group.
Results of cognitive outcomes, as well as data related to quality of life, are still awaited. Long-term renal outcomes are also unclear.
As noted above, the question of generalizability of SPRINT results to patients with diabetes is open to debate. In our opinion, with currently available evidence, it is difficult to conclusively answer the question of whether a lower systolic target provides cardiovascular benefit in diabetes. It is also unclear whether similar beneficial results would be seen with intensive treatment in a population at low cardiovascular risk. The American Heart Association and the American College of Cardiology are in the process of formulating new hypertension guidelines, and evidence from SPRINT will inform any new recommendations.
As more medications will likely be needed for intensive systolic blood pressure control, side effects and tolerability of medications with polypharmacy and potential nonadherence with increasing complexity of medication regimens should be kept in mind. Lifestyle modifications will need to be emphasized and reinforced, with greater use of combination antihypertensive therapy.
The data from SPRINT indicate that lower systolic pressure is better, as long as untoward clinical events can be monitored and avoided or easily managed. Careful monitoring will likely entail more frequent clinic visits and more frequent assessment of renal function and electrolyte levels (participants in the intensive group in the trial were seen every month until goal was achieved). A team approach that includes pharmacists and nurse practitioners, along with optimal use of best practice algorithms and remote monitoring technology, will need to be implemented for efficient and effective care.
In treating hypertension, lower systolic pressure is better than higher—with caveats. This is the message of the Systolic Blood Pressure Intervention Trial (SPRINT),1 a large, federally funded study that was halted early when patients at high cardiovascular risk who were randomized to a goal systolic pressure of less than 120 mm Hg were found to have better outcomes, including lower rates of heart failure, death from cardiovascular causes, and death from any cause, than patients randomized to a goal of less than 140 mm Hg.
The caveats: the benefit came at a price of more adverse events. Also, the trial excluded patients who had diabetes mellitus or previous strokes, so it is uncertain if these subgroups would also benefit from intensive lowering of systolic pressure—and in earlier trials they did not.
This article reviews the trial design and protocol, summarizes the results, and briefly discusses the implications of these results.
BEFORE SPRINT
Hypertension is very common in adults in the United States, and is a risk factor for heart disease, stroke, heart failure, and kidney disease. The estimated prevalence of hypertension in the 2011–2014 National Health and Nutrition Examination Survey (NHANES) was 29%, and the prevalence increases with age (7.3% in those ages 18 to 39, 32.2% in those ages 40 to 59, and 64.9% in those ages 60 and older).2 Isolated systolic hypertension (ie, systolic blood pressure > 140 mm Hg with diastolic pressure < 90 mm Hg) is the most common form of hypertension after age 50.3
Clinical trials have provided substantial evidence that treating hypertension reduces the incidence of stroke, myocardial infarction, and heart failure.4,5 Although observational studies show a progressive and linear rise in cardiovascular risk as systolic blood pressure rises above 115 mm Hg,6 clinical trials in the general population have not documented benefits of lowering systolic pressure to this level.7–11 However, clinical trials that directly evaluated two different blood pressure goals in the general population showed benefit with achieving systolic blood pressure less than 150 mm Hg,7,9 with limited data on lower blood pressure targets.10–12
No benefit found in intensive systolic lowering in diabetes or after stroke
The Action to Control Cardiovascular Risk in Diabetes-Blood Pressure (ACCORD BP) trial13 in patients with type 2 diabetes found no benefit in lowering systolic pressure to less than 120 mm Hg compared with less than 140 mm Hg in terms of the trial’s primary composite cardiovascular outcome (ie, nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes). However, the intensively treated group in this trial did enjoy a benefit in terms of fewer stroke events.
The Secondary Prevention of Small Subcortical Strokes (SPS3) trial14 in patients with stroke found no significant benefit in lowering systolic pressure to less than 130 mm Hg compared with less than 150 mm Hg for overall risk of another stroke, but a significant benefit was noted in reduced risk of intracerebral hemorrhage.
Current guidelines, based on available evidence, advocate treatment to a systolic goal of less than 140 mm Hg in most patients, and recommend relaxing this goal to less than 150 mm Hg in the elderly.15,16
SPRINT was stopped early due to better outcomes in the intensive treatment group
Given the uncertainty surrounding optimal systolic targets, SPRINT was designed to test the hypothesis that a goal of less than 120 mm Hg would reduce the risk of cardiovascular events more than the generally accepted systolic goal of less than 140 mm Hg.17 Patients with diabetes and stroke were excluded because a similar hypothesis was tested in the ACCORD BP and SPS3 trials, which included patients with these conditions.
SPRINT DESIGN
SPRINT was a randomized, controlled, open-label trial sponsored by the National Institutes of Health and conducted at 102 US sites.
Inclusion criteria. Participants had to be at least 50 years old, with systolic pressure of 130 to 180 mm Hg, and had to have at least one cardiovascular risk factor, eg:
Clinical or subclinical cardiovascular disease (other than stroke)
Chronic kidney disease, defined as estimated glomerular filtration rate (eGFR), calculated by the Modification of Diet in Renal Disease (MDRD) study equation, of 20 to less than 60 mL/min/1.73 m2
Framingham risk score of 15% of more
Age 75 or older.
Major exclusion criteria included:
Diabetes
Stroke
Polycystic kidney disease
Chronic kidney disease with an eGFR less than 20 mL/min/1.73 m2
Proteinuria (excretion > 1 g/day).
Intensive vs standard treatment
Participants were randomized to receive intensive treatment (systolic goal < 120 mm Hg) or standard treatment (systolic goal < 140 mm Hg). Baseline antihypertensive medications were adjusted to achieve blood pressure goals based on randomization assignment.
Doses of medications were adjusted on the basis of an average of three seated office blood pressure measurements after a 5-minute period of rest, taken with an automated monitor (Omron Healthcare Model 907); the same monitor was used and the same protocol was followed at all participating sites. Blood pressure was also measured after standing for 1 minute to assess orthostatic change.
Intensive treatment required, on average, one more medication than standard treatment
Lifestyle modifications were encouraged in both groups. There was no restriction on using any antihypertensive medication, and this was at the discretion of individual investigators. Thiazide-type diuretics were encouraged as first-line agents (with chlorthalidone encouraged as the primary thiazide-type diuretic).
Outcomes measured
The primary outcome was a composite of myocardial infarction, acute coronary syndrome not resulting in myocardial infarction, stroke, acute decompensated heart failure, and cardiovascular mortality.
Secondary outcomes included individual components of the primary composite outcome, all-cause mortality, and the composite of primary outcome and all-cause mortality.
Renal outcomes were assessed as:
Incident albuminuria (doubling of the urinary albumin-to-creatinine ratio from less than 10 mg/g to more than 10 mg/g)
Composite of a 50% decrease in eGFR or development of end-stage renal disease requiring long-term dialysis or kidney transplantation (in those with baseline chronic kidney disease)
A 30% decrease in eGFR (in those without chronic kidney disease).1,17
SPRINT also recruited participants to two nested substudies: SPRINT MIND and SPRINT MIND MRI, to study differences in cognitive outcomes and small-vessel ischemic disease between intensive treatment and standard treatment.
STUDY RESULTS
Older patients at risk, but without diabetes
Of 14,692 participants screened, 9,361 were enrolled in the study between 2010 and 2013. Baseline characteristics were comparable in both groups.
Demographics. The mean age of the participants was 67.9, and about 28% were 75 or older. About 36% were women, 58% white, 30% black, and 11% Hispanic.
Cardiovascular risk. The mean Framingham risk score was 20% (ie, they had a 20% risk of having a cardiovascular event within 10 years), and 61% of the participants had a risk score of at least 15%. Twenty percent already had cardiovascular disease.
Blood pressure. The average baseline blood pressure was 139.7/78.2 mm Hg. One-third of the participants had baseline systolic pressures of 132 mm Hg or less, another third had pressures in the range of 132 to 145, and the rest had 145 mm Hg or higher.
Renal function. The mean serum creatinine level was about 1.1 mg/dL. The mean eGFR was about 71 mL/min/1.73 m2 as calculated by the MDRD equation, and about 28% had eGFRs less than 60. The mean ratio of urinary albumin to creatinine was 44.1 mg/g in the intensive treatment group and 41.1 in the standard treatment group.
Other. The mean total cholesterol level was 190 mg/dL, fasting plasma glucose 99 mg/dL, and body mass index nearly 30 kg/m2.
Blood pressure during treatment
People in the intensive treatment group were taking a mean of 2.8 antihypertensive medications, and those in the standard treatment group were taking 1.8. Patients in the intensive group required greater use of all classes of medications to achieve goal systolic pressure (Table 1).
Study halted early due to efficacy
Throughout the 3.26 years of follow-up, the average difference in systolic pressure between the two groups was 13.1 mm Hg, with a mean systolic pressure of 121.5 mm Hg in the intensive treatment group and 134.6 mm Hg in the standard treatment group. The mean diastolic blood pressure was 68.7 mm Hg in the intensive treatment group and 76.3 mm Hg in the standard treatment group.
Although the study was planned to run for an average follow-up of 5 years, the National Heart, Lung, and Blood Institute terminated it early at a median of 3.26 years in view of lower rates of the primary outcome and of heart failure and death in the intensive treatment group (Table 2).
The effects on the primary outcome and mortality were consistent across the prespecified subgroups of age (< 75 vs ≥ 75), sex (female vs male), race (black vs nonblack), cardiovascular disease (presence or absence at baseline), prior chronic kidney disease (presence or absence at baseline), and across blood pressure tertiles (≤ 132 mm Hg, > 132 to < 145 mm Hg, ≥ 145 mm Hg).
Follow-up for assessment of cognitive outcomes (SPRINT MIND) and small-vessel ischemic disease (SPRINT MIND MRI) is ongoing.
WHAT DOES THIS MEAN?
SPRINT is the first large, adequately powered, randomized trial to demonstrate cardiovascular and mortality benefit from lowering the systolic blood pressure (goal < 120 mm Hg) in older patients at cardiovascular risk but without a history of diabetes mellitus or stroke.1
Most SPRINT patients had reasonably controlled blood pressure at baseline (the mean systolic pressure was 139.7 mm Hg, and two-thirds of participants had systolic pressure < 145 mm Hg). Of note, however, this trial excluded patients with systolic pressure higher than 180 mm Hg. There was excellent separation of systolic pressure between the two groups beginning at 1 year, which was consistent through the course of the trial.
The cardiovascular benefit in the intensive treatment group was predominantly driven by lower rates of heart failure (a 38% reduction in the intensive treatment group, P = .0002) and cardiovascular mortality (a 43% reduction in the intensive treatment group, P = .005), while there was no significant difference between the two groups in myocardial infarction or stroke. The beneficial effect on heart failure events is consistent with results from other trials including the Systolic Hypertension in the Elderly Program,7 Systolic Hypertension in Europe,8 and Hypertension in the Very Elderly Trial,9 all of which showed greatest risk reduction for heart failure events with systolic pressure-lowering (although to higher systolic levels than SPRINT).7–9 It is unclear why there was no beneficial effect on stroke events. The reduction in all-cause mortality in the intensive treatment group in SPRINT was greater than the reduction in cardiovascular deaths, which is also unexplained.
Although the study was terminated early due to efficacy (which introduces the possible bias that the estimated effect size will be too high), the number of primary end points reached was large (562 in the two groups combined), providing reassurance that the findings are valid. There was no blinding in the study (both participants and study investigators were aware of treatment assignment and study medications), but there was a structured assessment of outcomes and adverse events, with adjudication done by blinded reviewers.
SPRINT used an automated device for blood pressure measurement, which is known to reduce the “white coat” effect and correlates tightly with average daytime blood pressure done by ambulatory blood pressure monitoring.18 However, in clinical practice automated devices may not be available and a strict protocol for correct measurement may not be followed, with the possible result that blood pressure may be overestimated and overtreated.
What about diastolic pressure?
The trial, by design, focused on lowering systolic pressure (given the greater prevalence of isolated systolic hypertension with age), and the implications of lowering diastolic pressure are unclear. The issue of a J-shaped relationship between diastolic pressure and cardiovascular risk is debated in the literature: patients with a diastolic pressure of 60 to 65 mm Hg, especially those with existing coronary artery disease, may not tolerate aggressive blood pressure-lowering.19,20 Further analysis of this association (if any) from SPRINT will be helpful.
What about patients with diabetes?
Patients were excluded from SPRINT if they were under age 50, were at low cardiovascular risk, or had diabetes, raising the question of whether the results apply to these groups as well.
The question is particularly relevant in diabetes, as the ACCORD BP study, which used the same blood pressure targets as SPRINT, did not show a significant difference in the primary cardiovascular outcome between the intensive and standard treatments in patients with diabetes (Table 3).13 In ACCORD BP, the rate of the primary outcome was 12% lower in the intensive treatment group than in the standard treatment group, but the 95% confidence interval was –27% to +6%, so the finding was not statistically significant. However, the wide confidence interval does not exclude the possibility of a benefit that was comparable to that observed in SPRINT.
It has been speculated that ACCORD BP was underpowered to detect significant differences in the primary outcome.21 An analysis combining data from both trials indicated that effects on individual outcomes were generally consistent in both trials (with no significant heterogeneity noted).22 Also, the primary composite outcome in ACCORD did not include heart failure, which is particularly sensitive to blood pressure reduction.
Additionally, ACCORD BP had a 2 × 2 factorial design involving a simultaneous comparison of intensive vs standard glycemic control, which may have influenced the effects due to blood pressure. Indeed, a post hoc analysis showed that there was a significant 26% lower risk of the primary outcome in ACCORD BP patients who received intensive systolic pressure control plus standard glycemic control than in those receiving standard systolic control plus standard glycemic control.23
Are more adverse events an acceptable trade-off?
Adverse events, including acute kidney injury, were more frequent in the intensive therapy group in SPRINT.
Acute kidney injury was coded as an adverse event on the basis of this diagnosis being included in the hospital discharge summary (as a primary or main secondary diagnosis) and if considered by the safety officer to be one of the top three reasons for admission or continued hospitalization. Further analysis of renal events should be forthcoming.
People in the intensive treatment group, on average, needed one more medication than those in the standard treatment group. Some of the adverse events may be related to the antihypertensive medications taken (eg, electrolyte abnormalities such as hyponatremia and hypokalemia due to diuretic use), and others may be related to blood pressure-lowering (eg, acute kidney injury due to renal hypoperfusion).
At this point, the long-term effects of these adverse events, especially on kidney function, are not known. Patients enrolled in clinical trials tend to be healthier than patients seen in clinical practice; thus, the rate of adverse events reported in the trial may be lower than one would see in the real world.
Does lower systolic pressure protect or harm the kidneys?
SPRINT included patients with stage 3 and 4 chronic kidney disease (ie, with eGFR 20–50 mL/min/1.73 m2), but it was designed to assess cardiovascular outcomes, not the progression of chronic kidney disease. The trial excluded patients with diabetic nephropathy or high degrees of proteinuria.
Only about half of hypertensive adults have their blood pressure under control, ie, < 140/90
Earlier randomized trials that focused on chronic kidney disease progression, including the MDRD24 and the African American Study of Kidney Disease and Hypertension,25 did not show benefit with more aggressive blood pressure-lowering (except in patients with higher degrees of proteinuria), and these trials were not powered to assess effects on cardiovascular outcomes.24,25
The Irbesartan Diabetic Nephropathy Trial,26,27 which was done in patients with overt diabetic nephropathy, showed that a progressively lower achieved systolic pressure down to 120 mm Hg predicted lower rates of heart failure, cardiovascular mortality, and renal events (although the trial target was ≤ 130/85 mm Hg and few participants achieved systolic pressure lower than 120 mm Hg).
IMPLICATIONS FOR MANAGEMENT
The recent estimates of hypertension prevalence and control from NHANES show that only about 53% of hypertensive adults have their blood pressure under control (defined as systolic pressure < 140 mm Hg and diastolic pressure < 90 mm Hg).2 Analysis of the NHANES 2007–2012 data showed that 16.7% or 8.2 million US adults with treated hypertension meet the eligibility criteria for SPRINT.28
Although the SPRINT results support the notion that “lower is better,” the risks and benefits of intensive control will need to be balanced in individual patients. Table 4 shows the number needed to treat and number needed to harm in the trial.
More aggressive management of hypertension is challenging. The median systolic pressure achieved in the intensive group in SPRINT was just over 120 mm Hg, which implies that at least half of the participants in the intensive group did not achieve the goal of less than 120 mm Hg. While it may be reasonable to aim for systolic pressure of less than 120 or 125 mm Hg in patients who fit the SPRINT criteria and can tolerate intensive blood pressure lowering, it would be prudent to aim for a more conservative goal in elderly patients who are frail and at risk for falls, considering the higher incidence of specified adverse events in the intensive group.
Results of cognitive outcomes, as well as data related to quality of life, are still awaited. Long-term renal outcomes are also unclear.
As noted above, the question of generalizability of SPRINT results to patients with diabetes is open to debate. In our opinion, with currently available evidence, it is difficult to conclusively answer the question of whether a lower systolic target provides cardiovascular benefit in diabetes. It is also unclear whether similar beneficial results would be seen with intensive treatment in a population at low cardiovascular risk. The American Heart Association and the American College of Cardiology are in the process of formulating new hypertension guidelines, and evidence from SPRINT will inform any new recommendations.
As more medications will likely be needed for intensive systolic blood pressure control, side effects and tolerability of medications with polypharmacy and potential nonadherence with increasing complexity of medication regimens should be kept in mind. Lifestyle modifications will need to be emphasized and reinforced, with greater use of combination antihypertensive therapy.
The data from SPRINT indicate that lower systolic pressure is better, as long as untoward clinical events can be monitored and avoided or easily managed. Careful monitoring will likely entail more frequent clinic visits and more frequent assessment of renal function and electrolyte levels (participants in the intensive group in the trial were seen every month until goal was achieved). A team approach that includes pharmacists and nurse practitioners, along with optimal use of best practice algorithms and remote monitoring technology, will need to be implemented for efficient and effective care.
References
SPRINT Research Group; Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373:2103–2116.
Yoon SS, Fryar CD, Carroll MD. Hypertension prevalence and control among adults: United States, 2011–2014. NCHS data brief, no. 220. Hyattsville, MD: National Center for Health Statistics. 2015.
Franklin SS, Jacobs MJ, Wong ND, L’Italien GJ, Lapuerta P. Predominance of isolated systolic hypertension among middle-aged and elderly US hypertensives: analysis based on National Health and Nutrition Examination Survey (NHANES) III. Hypertension 2001; 37:869–874.
Neal B, MacMahon S, Chapman N; Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet 2000; 356:1955–1964.
Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA 1997; 277:739–745.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360:1903–1913.
SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991; 265:3255–3264.
Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350:757–764.
Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358:1887–1898.
JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res 2008; 31:2115–2127.
Ogihara T, Saruta T, Rakugi H, et al; Valsartan in Elderly Isolated Systolic Hypertension Study Group. Target blood pressure for treatment of isolated systolic hypertension in the elderly: Valsartan in Elderly Isolated Systolic Hypertension study. Hypertension 2010; 56:196–202.
Liu L, Zhang Y, Liu G, Li W, Zhang X, Zanchetti A; FEVER Study Group. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens 2005; 23:2157–2172.
ACCORD Study Group; Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010; 362:1575–1585.
SPS3 Study Group; Benavente OR, Coffey CS, Conwit R, et al. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trial. Lancet 2013; 382:507–515.
James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311:507–520. Erratum in: JAMA. 2014; 311:1809.
Weber MA, Schiffrin EL, White WB, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich) 2014; 16:14–26.
Ambrosius WT, Sink KM, Foy CG, et al; SPRINT Study Research Group. The design and rationale of a multicenter clinical trial comparing two strategies for control of systolic blood pressure: the Systolic Blood Pressure Intervention Trial (SPRINT). Clin Trials 2014; 11:532–546.
Myers MG, Godwin M, Dawes M, Kiss A, Tobe SW, Kaczorowski J. Conventional versus automated measurement of blood pressure in the office (CAMBO) trial. Fam Pract 2012; 29:376–382.
Messerli FH, Mancia G, Conti CR, et al. Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann Intern Med 2006; 144:884–893.
Boutitie F, Gueyffier F, Pocock S, Fagard R, Boissel JP; INDANA Project Steering Committee; INdividual Data ANalysis of Antihypertensive intervention. J-shaped relationship between blood pressure and mortality in hypertensive patients: new insights from a meta-analysis of individual-patient data. Ann Intern Med 2002; 136:438–448.
Mancia G. Effects of intensive blood pressure control in the management of patients with type 2 diabetes mellitus in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Circulation 2010; 122:847–849.
Perkovic V, Rodgers A. Redefining blood-pressure targets—SPRINT starts the marathon. N Engl J Med 2015; 373:2175–2178.
Margolis KL, O’Connor PJ, Morgan TM, et al. Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial. Diabetes Care 2014; 37:1721–1728.
Peterson JC, Adler S, Burkart JM, et al. Blood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease study. Ann Intern Med 1995; 123:754–762.
Agodoa LY, Appel L, Bakris GL, et al; African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 2001; 285:2719–2728.
Berl T, Hunsicker LG, Lewis JB, et al; Collaborative Study Group. Impact of achieved blood pressure on cardiovascular outcomes in the Irbesartan Diabetic Nephropathy Trial. J Am Soc Nephrol 2005; 16:2170–2179.
Pohl MA, Blumenthal S, Cordonnier DJ, et al. Independent and additive impact of blood pressure control and angiotensin II receptor blockade on renal outcomes in the Irbesartan Diabetic Nephropathy Trial: clinical implications and limitations. J Am Soc Nephrol 2005; 16:3027–3037.
Bress AP, Tanner RM, Hess R, Colantonio LD, Shimbo D, Muntner P. Generalizability of results from the Systolic Blood Pressure Intervention Trial (SPRINT) to the US adult population. J Am Coll Cardiol 2015 Oct 31. doi: 10.1016/j.jacc.2015.10.037. Epub ahead of print.
References
SPRINT Research Group; Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373:2103–2116.
Yoon SS, Fryar CD, Carroll MD. Hypertension prevalence and control among adults: United States, 2011–2014. NCHS data brief, no. 220. Hyattsville, MD: National Center for Health Statistics. 2015.
Franklin SS, Jacobs MJ, Wong ND, L’Italien GJ, Lapuerta P. Predominance of isolated systolic hypertension among middle-aged and elderly US hypertensives: analysis based on National Health and Nutrition Examination Survey (NHANES) III. Hypertension 2001; 37:869–874.
Neal B, MacMahon S, Chapman N; Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of ACE inhibitors, calcium antagonists, and other blood-pressure-lowering drugs: results of prospectively designed overviews of randomised trials. Blood Pressure Lowering Treatment Trialists’ Collaboration. Lancet 2000; 356:1955–1964.
Psaty BM, Smith NL, Siscovick DS, et al. Health outcomes associated with antihypertensive therapies used as first-line agents. A systematic review and meta-analysis. JAMA 1997; 277:739–745.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360:1903–1913.
SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991; 265:3255–3264.
Staessen JA, Fagard R, Thijs L, et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The Systolic Hypertension in Europe (Syst-Eur) Trial Investigators. Lancet 1997; 350:757–764.
Beckett NS, Peters R, Fletcher AE, et al; HYVET Study Group. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008; 358:1887–1898.
JATOS Study Group. Principal results of the Japanese trial to assess optimal systolic blood pressure in elderly hypertensive patients (JATOS). Hypertens Res 2008; 31:2115–2127.
Ogihara T, Saruta T, Rakugi H, et al; Valsartan in Elderly Isolated Systolic Hypertension Study Group. Target blood pressure for treatment of isolated systolic hypertension in the elderly: Valsartan in Elderly Isolated Systolic Hypertension study. Hypertension 2010; 56:196–202.
Liu L, Zhang Y, Liu G, Li W, Zhang X, Zanchetti A; FEVER Study Group. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens 2005; 23:2157–2172.
ACCORD Study Group; Cushman WC, Evans GW, Byington RP, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010; 362:1575–1585.
SPS3 Study Group; Benavente OR, Coffey CS, Conwit R, et al. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trial. Lancet 2013; 382:507–515.
James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311:507–520. Erratum in: JAMA. 2014; 311:1809.
Weber MA, Schiffrin EL, White WB, et al. Clinical practice guidelines for the management of hypertension in the community: a statement by the American Society of Hypertension and the International Society of Hypertension. J Clin Hypertens (Greenwich) 2014; 16:14–26.
Ambrosius WT, Sink KM, Foy CG, et al; SPRINT Study Research Group. The design and rationale of a multicenter clinical trial comparing two strategies for control of systolic blood pressure: the Systolic Blood Pressure Intervention Trial (SPRINT). Clin Trials 2014; 11:532–546.
Myers MG, Godwin M, Dawes M, Kiss A, Tobe SW, Kaczorowski J. Conventional versus automated measurement of blood pressure in the office (CAMBO) trial. Fam Pract 2012; 29:376–382.
Messerli FH, Mancia G, Conti CR, et al. Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann Intern Med 2006; 144:884–893.
Boutitie F, Gueyffier F, Pocock S, Fagard R, Boissel JP; INDANA Project Steering Committee; INdividual Data ANalysis of Antihypertensive intervention. J-shaped relationship between blood pressure and mortality in hypertensive patients: new insights from a meta-analysis of individual-patient data. Ann Intern Med 2002; 136:438–448.
Mancia G. Effects of intensive blood pressure control in the management of patients with type 2 diabetes mellitus in the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Circulation 2010; 122:847–849.
Perkovic V, Rodgers A. Redefining blood-pressure targets—SPRINT starts the marathon. N Engl J Med 2015; 373:2175–2178.
Margolis KL, O’Connor PJ, Morgan TM, et al. Outcomes of combined cardiovascular risk factor management strategies in type 2 diabetes: the ACCORD randomized trial. Diabetes Care 2014; 37:1721–1728.
Peterson JC, Adler S, Burkart JM, et al. Blood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease study. Ann Intern Med 1995; 123:754–762.
Agodoa LY, Appel L, Bakris GL, et al; African American Study of Kidney Disease and Hypertension (AASK) Study Group. Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 2001; 285:2719–2728.
Berl T, Hunsicker LG, Lewis JB, et al; Collaborative Study Group. Impact of achieved blood pressure on cardiovascular outcomes in the Irbesartan Diabetic Nephropathy Trial. J Am Soc Nephrol 2005; 16:2170–2179.
Pohl MA, Blumenthal S, Cordonnier DJ, et al. Independent and additive impact of blood pressure control and angiotensin II receptor blockade on renal outcomes in the Irbesartan Diabetic Nephropathy Trial: clinical implications and limitations. J Am Soc Nephrol 2005; 16:3027–3037.
Bress AP, Tanner RM, Hess R, Colantonio LD, Shimbo D, Muntner P. Generalizability of results from the Systolic Blood Pressure Intervention Trial (SPRINT) to the US adult population. J Am Coll Cardiol 2015 Oct 31. doi: 10.1016/j.jacc.2015.10.037. Epub ahead of print.
SPRINT is the first large prospective randomized trial to show evidence of cardiovascular and mortality benefit for intensive lowering of systolic blood pressure (goal < 120 mm Hg) in older patients at cardiovascular risk, but without a history of diabetes mellitus or stroke.
A similar trial in patients with type 2 diabetes mellitus did not show significant benefit of intensive treatment.
Intensive treatment was associated with more adverse events, including hypotension, syncope, electrolyte abnormalities, and acute kidney injury.
It is unclear if these results can be extrapolated to patients with a history of diabetes or stroke, younger patients, or those with low cardiovascular risk.
Healthcare providers should engage patients in a shared decision-making process, with discussion of the benefits and risks associated with intensive lowering of blood pressure.
In a large phase trial, a combination drug that contains the angiotensin II receptor blocker (ARB) valsartan and the neprilysin inhibitor sacubitril was found to be superior to the angiotensin-converting enzyme (ACE) inhibitor enalapril in terms of important end points, including death and hospitalization for heart failure, in patients with heart failure with reduced ejection fraction.1
Recently approved by the US Food and Drug Administration, this combination drug, marketed under the brand name Entresto, represents a new drug class, angiotensin receptor-neprilysin inhibitors, or ARNIs.
This article is an overview of the Prospective Comparison of ARNI With ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial1 and the implications it may have on the care of patients with chronic heart failure.
NEED FOR NEW HEART FAILURE DRUGS
Heart failure is a major public health problem, and the care of patients with heart failure is challenging.
Almost 6 million US adults have heart failure, and the prevalence is projected to increase in the next few decades as the population continues to age.2 Furthermore, the total healthcare cost for heart failure patients was almost $31 billion in 2012 and is projected to rise to $70 billion by 2030.2
The care of patients with severely decompensated heart failure has changed dramatically in the last few decades with advances in heart transplantation and mechanical support devices. But day-to-day management of patients with chronic mildly to moderately symptomatic heart failure continues to pose a clinical challenge.
The drugs currently available for these patients include beta-blockers, ACE inhibitors, ARBs, aldosterone antagonists, digoxin, diuretics, and vasodilators. But even with these drugs, the death and readmission rates of patients with heart failure with reduced ejection fraction remain high. More than 50% of patients with heart failure die within 5 years of diagnosis,3 and 25% of patients hospitalized with heart failure are readmitted within 30 days of discharge.2 Furthermore, death rates are higher in those patients who have a history of heart failure hospitalization.4
Although heart failure with preserved ejection fraction encompasses an important group of heart failure patients with high morbidity, the focus of this article will be on patients with heart failure with reduced ejection fraction.
Available drugs to date
The cornerstone drugs that lower the odds of death in patients with heart failure with reduced ejection fraction are ACE inhibitors, ARBs, beta-blockers, and mineralocorticoid antagonists.
ACE inhibitors were the first class of drugs shown to reduce the death rate in patients with heart failure with reduced ejection fraction. The landmark CONSENSUS trial,5 published in 1987, found that the death rate in patients who received enalapril was 27% lower than in those receiving placebo, an effect driven entirely by a reduction in progressive heart failure. Similarly, the SOLVD trial,6 published in 1991, showed a 26% reduction in heart failure hospitalization and a 16% lower rate of death with enalapril compared with placebo, an effect driven predominantly by a decrease in the progression of heart failure.
ARBs have also been shown to decrease the rate of death, although not by as much as ACE inhibitors. In the CHARM trial,7 compared with placebo, candesartan significantly decreased the risk of death from any cause, of death from cardiovascular causes, and of hospitalization related to heart failure.7
Beta-blockers. The MERIT-HF trial,8 published in 1999, was stopped early because fewer patients were dying in the group receiving metoprolol succinate than in the group receiving placebo (relative risk 0.66). Similarly, in 2001, the COPERNICUS trial9 reported a 34% reduction in deaths in patients receiving carvedilol in addition to an ACE inhibitor compared with those receiving an ACE inhibitor alone.
Mineralocorticoid receptor antagonists were found to be beneficial when added to standard therapy for chronic symptomatic heart failure in the RALES10 and EMPHASIS-HF11 trials.
Vasodilators (specifically, the combination of isosorbide dinitrate and hydralazine) were found to have benefit in terms of mortality when added to standard therapy in African American patients in the A-HeEFT trial.12
WHY INHIBIT BOTH ANGIOTENSIN AND NEPRILYSIN?
The renin-angiotensin-aldosterone system is a major focus in treating heart failure, as overactivity of this system plays a key role in the pathophysiology of this disease. Therefore, essential drugs for heart failure patients include those that inhibit overactivity of this system such as ACE inhibitors, ARBs, and aldosterone antagonists.
The natriuretic peptide system is another important pathway that can be targeted in patients with heart failure. Natriuretic peptides are key molecules that counteract heart failure, as they contribute to diuresis and vasodilation and protect against vascular remodeling.13 An increased understanding of the importance of this system in slowing the progression of heart failure has motivated evaluation of drugs such as nesiritide in patients with symptomatic heart failure. However, these drugs can cause hypotension and have limited bioavailability.14
Neprilysin is an endopeptidase—an endogenous enzyme that degrades vasoactive peptides such as bradykinin and natriuretic peptides.14 Drugs that inhibit neprilysin increase the levels of these peptides and thus counteract neurohormonal stimuli that lead to cardiac remodeling, sodium retention, and vasoconstriction.15
However, neprilysin also hydrolyzes angiotensin I to angiotensin (1–7), an inhibitor of angiotensin II. Thus, inhibition of neprilysin alone could lead to increased activity of angiotensin II and so have an overall neutral effect. To be beneficial, neprilysin inhibition needs to be combined with renin-angiotensin system inhibition. Furthermore, the benefit of renin-angiotensin-aldosterone system blockade may be amplified by up-regulation of the endogenous natriuretic peptide system.15
Omapatrilat, the most studied combination neprilysin inhibitor and ACE inhibitor, improved cardiac function and decreased cardiac mass in animal experiments.15 In addition, this drug showed promise in terms of blood pressure, heart failure readmissions, death, and preservation of renal function when compared with ACE inhibitors in patients with heart failure.15–17 But in clinical trials this drug posed a greater risk of hypotension, dizziness, and, its major shortcoming, an unacceptably high incidence of angioedema compared with ACE inhibitors.15,16,18 This higher risk of angioedema is thought to be from inhibition of three enzymes that break down bradykinin: ACE, neprilysin, and aminopeptidase P.19
Figure 1. The final effect of sacubitril-valsartan is lower blood pressure, increased diuresis, and decreasedcardiac fibrosis and hypertrophy.ACE = angiotensin-converting enzyme; BNP = B-type natriuretic peptide; GC-A = guanylyl cyclase A
ARNIs contain an angiotensin receptor blocker rather than an ACE inhibitor, and thus in theory they may be associated with a lower risk of angioedema.19 Sacubitril-valsartan, the first drug of this class, contains its two constitutive drugs in a one-to-one molecular ratio (Figure 1).
PARADIGM-HF investigated the benefit of this drug in patients with systolic heart failure.1
STUDY DESIGN AND OBJECTIVES
PARADIGM-HF was a double-blind, randomized controlled trial comparing sacubitril-valsartan and enalapril in patients with chronic systolic heart failure. As such, it was the first trial in recent years to study a new drug in comparison with a well-established heart failure drug rather than as an add-on strategy.1
Inclusion criteria
To be included in the PARADIGM-HF trial, patients had to have:
A left ventricular ejection fraction of 40% or less (later changed to ≤ 35%)
New York Heart Association class II, III, or IV symptoms
A B-type natriuretic peptide (BNP) level of at least 150 pg/mL or an N-terminal proBNP (NT-proBNP) level of at least 600 pg/mL; for patients hospitalized for heart failure within the previous 12 months, the cut points were lower (BNP ≥ 100 pg/mL or NT-proBNP ≥ 400 pg/mL).
End points
The primary end point was the composite of cardiovascular death or first hospitalization for heart failure. Other outcomes assessed were time to death from any cause, the change from baseline in the Kansas City Cardiomyopathy Questionnaire (KCCQ) score at 8 months, time to new-onset atrial fibrillation, and the time to decline in renal function (defined as end-stage renal disease or a decrease in estimated glomerular filtration rate of at least 50% from randomization). All end points were blindly adjudicated by a clinical end points committee.
Two run-in periods
The study enrolled 10,521 patients from 1,043 centers in 47 countries, who entered the initial run-in period consisting of 2 weeks of treatment with enalapril at the study dosage (10 mg twice daily) in order to ensure no unacceptable side effects. At this point, 1,102 patients exited the study, leaving 9,419 who entered the second run-in period.
The second run-in period consisted of 4 weeks of treatment with sacubitril-valsartan, initially at half the study regimen (100 mg twice daily) and eventually at the full study dosage (200 mg twice daily). During the second run-in period, 977 participants left the study, leaving a total of 8,442 patients who underwent randomization. Forty-three patients were then excluded (6 because of invalid randomization and 37 because of four sites that closed because of major violations of good clinical practice).
Of those randomized, 4,187 patients were assigned to the sacubitril-valsartan treatment group and 4,212 were assigned to the enalapril group. The investigators used an intention-to-treat analysis for this study.
Most patients had NYHA class II symptoms
The randomized patients had a mean age of 64 years, 75% were men, 66% were white, and 58% were from Europe (only 7% were from North America). The mean left ventricular ejection fraction was about 30%, and 60% of the study participants had an ischemic cause for their cardiomyopathy. Although one of the inclusion criteria was New York Heart Association class II, III, or IV symptoms, about 5% of the patients had class I symptoms. Seventy percent had class II symptoms, 24% had class III, and less than 1% had class IV symptoms.
At the time of randomization, 78% of the patients were taking an ACE inhibitor and 93% were taking a beta-blocker, but only a little more than half were taking a mineralocorticoid antagonist and only about 15% had an implantable cardioverter-defibrillator.
STUDY OUTCOMES
This study was designed to detect a 15% lower risk of cardiovascular death in the sacubitril-valsartan group. It was projected to continue for at least 34 months but was stopped early because of an overwhelming benefit of the new drug at a median follow-up of 27 months.
Major findings
The primary composite outcome (cardiovascular death or first hospitalization for heart failure)1 occurred in 21.8% of the patients in the sacubitril-valsartan group vs 26.5% of patients in the enalapril group (hazard ratio [HR] 0.80, 95% confidence interval [CI] 0.73–0.87, P < .001). The number of patients who needed to be treated to prevent one occurrence of the primary composite outcome (100/absolute risk reduction) was only 21. The benefit was strong and consistent across both of the individual components of the composite outcome:
Cardiovascular death 13.3% vs 16.5%, HR 0.80 (95% CI 0.71–0.89), P < .001
First hospitalization for worsening heart failure 12.8% vs 15.6%, HR 0.79 (95% CI 0.71–0.89), P < .001.
Secondary outcomes. The sacubitril-valsartan group had a significantly lower rate of death from any cause (17.0% vs 19.8%, HR 0.84, 95% CI 0.76–0.93, P < .001) and a lower mean decrease in KCCQ clinical summary scores at 8 months (2.99 points vs 4.63 points, mean difference 1.64, 95% CI 0.63–2.65, P = .001). The KCCQ score measures subjective symptoms and physical limitations caused by heart failure; possible scores range from 0 to 100, with a higher score indicating better functional status. Notably, sacubitril-valsartan did not increase the KCCQ score in these patients; rather, sacubitril-valsartan recipients had a lower decrease in their scores than those in the enalapril group.
The incidence of new-onset atrial fibrillation was the same in both groups (3.1% and 3.1%).1 A decline in renal function (defined as end-stage renal disease, a decrease of 50% or more in estimated glomerular filtration rate from the value at randomization or a decrease in the estimated glomerular filtration rate of more than 30 mL/min/1.73 m2 to less than 60 mL/min/1.73 m2) occurred in 2.2% of the valsartan-sacubitril group and 2.6% of the enalapril group (P = .28).
The effects of the study drug on the primary composite outcome and on death from a cardiovascular cause were similar in all prespecified subgroups except for NYHA class: the reduction in the risk of the composite outcome was lower in sacubitril-valsartan recipients with NYHA I or II symptoms than in those with NYHA III or IV symptoms (P for interaction .03). However, there were no differences in the other prespecified subgroups, defined by age, sex, race, region, estimated glomerular filtration rate, diabetes, systolic blood pressure, ejection fraction, atrial fibrillation, NT-proBNP, hypertension, previous use of an ACE inhibitor, previous use of an aldosterone antagonist, previous heart failure hospitalization, and time since diagnosis of heart failure.
SAFETY: ANGIOEDEMA, HYPOTENSION, AND RENAL DYSFUNCTION
Angioedema
As noted above, the combination of neprilysin inhibitors and ACE inhibitors has been associated with an increased risk of angioedema. That was an important consideration before starting this study, which used a combination of a neprilysin inhibitor and an ARB in an attempt to avoid this serious side effect.
As it happened, there was no increased risk of significant angioedema with sacubitril-valsartan use compared with enalapril. Rates were similar to those in other studies, which showed a less than 1% risk of angioedema caused by ACE inhibitors.20,21 Only 19 patients (0.5%) in the sacubitril-valsartan group and 10 patients (0.2%) in the enalapril group experienced any angioedema. Of these, just three patients in the sacubitril-valsartan group and one patient in the enalapril group experienced angioedema that required hospitalization (P = .31). None of these patients had airway compromise due to angioedema.
Other safety issues that were assessed included hypotension, worsening renal function, increase in potassium levels, and cough. Patients in the sacubitril-valsartan group were more likely to have symptomatic hypotension than patients in the enalapril group (14.0% vs 9.2%, P < .001); however, the authors noted that this was a rare cause of drug discontinuation.
Patients in the sacubitril-valsartan group were less likely to develop cough (11.3% vs 14.3%, P < .001), a serum creatinine level of 2.5 mg/dL or more (3.3% vs 4.5%, P = .007), or a serum potassium level of more than 6.0 mmol/L (11.3% vs 14.3%, P = .007).1
During the two run-in periods combined, 12% of the patients in the study withdrew because of adverse events, including cough, renal dysfunction, hyperkalemia, and symptomatic hypotension. During the enalapril run-in period, 591 patients (5.6%) withdrew due to adverse events, and 547 patients (5.8%) withdrew due to these events during the sacubitril-valsartan run-in period. After adjusting for the shorter time on enalapril, there was a higher rate of withdrawal because of adverse events from enalapril than from sacubitril-valsartan.
LOWER RISK OF CLINICAL PROGRESSION
In a separate paper,22 the PARADIGM-HF investigators reported that, among the survivors in the study, those who received sacubitril-valsartan fared better in terms of a number of markers of progression of heart failure, with lower rates of:
Intensification of medical treatment for heart failure
Emergency department visits for worsening heart failure
Hospitalization for worsening heart failure
Need for intensive care
Need for intravenous inotropic agents
Need for cardiac devices or heart transplants
Worsening symptom scores
Elevation of biomarkers of myocardial injury.
QUESTIONS AND CONCERNS
Although this study, which was funded by the manufacturer, showed consistent benefit for sacubitril-valsartan over enalapril, questions remain.
Are the findings generalizable?
Despite the study’s rigorous run-in period, 12% of patients dropped out because of adverse events, and thus the patients who completed the study may not be representative of the general population of heart failure patients. The authors included this double-level wash-out to ensure patient tolerance of both drugs. But in everyday practice, a significant number of patients may be unable to tolerate one of these drugs.
Moreover, after adjusting for the difference in the run-in periods, patients actually withdrew more often during the enalapril run-in period than during the sacubitril-valsartan run-in period. However, there may be overlap in tolerability in these two drugs, which both affect the renin-angiotensin-aldosterone system. Thus, the enalapril run-in period may have contributed to the lower tolerability of this drug compared with sacubitril-valsartan.
Were patients receiving the best possible therapy?
Another important point when considering how we treat heart failure patients in the United States is how few patients in this study were using cardiac implantable electronic devices. Only 15% of the patients in this study had an implantable cardioverter-defibrillator despite a mean left ventricular ejection fraction less than 30%. This likely reflects differences in practice internationally; however, based on American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines, these patients would have a class I indication for an implantable cardioverter-defibrillator for primary prevention of sudden cardiac death.23
Therefore, based on these recommendations, the patients in this study were not necessarily on optimal medical and device therapy and furthermore may not be representative of heart failure patients in the United States.
Was enalapril 10 mg twice a day a fair comparison?
Another concern about the results of this study relates to the dosages used in the two treatment groups. The sacubitril-valsartan formulation included full-dose valsartan, whereas the ACE inhibitor group received enalapril at less than a full dose.
Although the authors explained that the dose of enalapril chosen for the study was based on the one used in previous studies that showed survival benefit, this raises the question of whether the significant difference in outcomes in this trial was due to a greater inhibition of the renin-angiotensin-aldosterone system related to a higher dose of drug in the sacubitril-valsartan group.
What about black patients taking hydralazine-isosorbide?
Only about 5% of patients in the PARADIGM-HF trial were black. Based on the A-HeFT study results, black patients can be prescribed an ACE inhibitor as well as hydralazine and isosorbide dinitrate as tolerated to decrease the risk of death. Does sacubitril-valsartan offer benefit to these patients compared with a regimen of an ACE inhibitor, hydralazine, and isosorbide dinitrate?
Another concern is that the incidence of angioedema observed with ACE inhibitors and omapatrilat is higher in black patients.15,21 Thus, it would be prudent to investigate whether the risk of angioedema with sacubitril-valsartan would be higher if more black patients are studied.
IMPLICATIONS AND CONSIDERATIONS
In this study, sacubitril-valsartan showed impressive and consistent results, with an almost 20% decrease in the composite end point of heart failure hospitalization or cardiovascular death and a similar decrease in the composite outcomes with a very low number needed to treat (21 patients). It did not show a decrease in the incidence of new-onset atrial fibrillation; however, only 80 cases of atrial fibrillation were reported, so there may have been a lack of statistical power to detect a difference.
To avoid angioedema, wait at least 36 hours after stopping an ACE inhibitor. Sacubitril-valsartan was not associated with an increased risk of severe angioedema, and no patients experienced life-threatening angioedema. In the trial, the sacubitril-valsartan run-in period was started at least 24 hours after enalapril was stopped, and thus the authors recommended at least a 1-day washout period after discontinuing an ACE inhibitor to avoid angioedema in patients starting sacubitril-valsartan.
Hypotension is a concern. Although there was actually a decreased risk of renal dysfunction, hyperkalemia, and cough compared with enalapril, there was a significantly increased rate of symptomatic hypotension in the sacubitril-valsartan group, which raises the question of patient tolerance and physician comfort when prescribing and titrating this drug in clinical practice. This side effect will be an important consideration when attempting to titrate the drug to target doses.
Start treatment early. This trial largely consisted of patients with NYHA class II or III symptoms, with about 70% of patients with class II symptoms. Since this drug showed benefit in patients with mildly to moderately symptomatic heart failure, clinicians who are considering prescribing this drug should not wait until the patient is closer to end-stage disease. Patients with mildly symptomatic heart failure may be followed by a general cardiologist, internist, or both, and thus it is important to emphasize to the entire medical community the need to start this medication early on.
How much will it cost? Cost is a concern that could heavily weigh on the decision to prescribe this drug. Generic ACE inhibitors are relatively inexpensive, and it may difficult to switch from an affordable generic drug to a new drug that is likely to be much more expensive. Arguably, this drug may be cost-effective in the long run owing to a large decrease in heart failure readmissions. We await further analyses to evaluate this issue.
Will patients take a twice-a-day drug as prescribed? Most patients who are prescribed an ACE inhibitor take it just once a day, and switching from a daily to a twice-daily drug may present a challenge for some.
What about other outcomes? Based on this study, it is unclear what effect sacubitril-valsartan has on the incidence of fatal arrhythmias, sudden cardiac death, and pump failure. Furthermore, the effect on quality of life is still uncertain. Quality of life is an integral component in the evaluation of heart failure patients, and in this study the changes in KCCQ scores were not impressive. We hope to see further evaluations of this drug’s impact on quality of life of patients with heart failure. Furthermore, it would be interesting to study if this drug has any long-term effects on the need for advanced therapies such as left ventricular assist devices and orthotopic heart transplant.
What about patients with heart failure with preserved ejection fraction? This study included only patients with heart failure with reduced ejection fraction. However PARAMOUNT, a phase 2 study that evaluated the benefit of sacubitril-valsartan in patients with heart failure with preserved ejection fraction, has shown encouraging results.24 We look forward to further investigation of this agent in patients with heart failure with preserved ejection fraction.
Sacubitril-valsartan, the first ARNI to be studied in humans, has a dual action in that it enhances the activity of the natriuretic peptide system and inhibits that of the renin-angiotensin-aldosterone system. It is the first drug in over a decade to show mortality benefit in patients with chronic systolic heart failure when compared with an already well-established heart failure medication. It appears to decrease rates of mortality and heart failure hospitalization without increasing the risk of severe angioedema in patients with mild or moderate chronic systolic heart failure. Symptomatic hypotension and high cost may pose the largest barriers to the use of this new drug. And we have yet to see how the clinical community and patients with heart failure will respond to it.
References
McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371:993–1004.
Dunlay SM, Pereira NL, Kushwaha SS. Contemporary strategies in the diagnosis and management of heart failure. Mayo Clin Proc 2014; 89:662–676.
Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation 2013; 127:e6–e245.
Bello NA, Claggett B, Desai AS, et al. Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction. Circ Heart Fail 2014; 7:590–595.
Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The CONSENSUS Trial Study Group. N Engl J Med 1987; 316:1429–1435.
Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The SOLVD Investigators. N Engl J Med 1991; 325:293–302.
Pfeffer MA, Swedberg K, Granger CB, et al; CHARM Investigators and Committees. Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programme. Lancet 2003; 362:759–766.
Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353:2001–2007.
Packer M, Coats AJ, Fowler MB, et al; Carvedilol Prospective Randomized Cumulative Survival Study Group. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 2001; 344:1651–1658.
Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999; 341:709–717.
Zannad F, McMurray JJ, Krum H, et al; EMPHASIS-HF Study Group. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 2011; 364:11–21.
Taylor AL, Ziesche S, Yancy C, et al; African-American Heart Failure Trial Investigators. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med 2004; 351:2049–2057.
Schreiner GF, Protter AA. B-type natriuretic peptide for the treatment of congestive heart failure. Curr Opin Pharmacol 2002; 2:142–147.
von Lueder TG, Sangaralingham SJ, Wang BH, et al. Renin-angiotensin blockade combined with natriuretic peptide system augmentation: novel therapeutic concepts to combat heart failure. Circ Heart Fail 2013; 6:594–605.
Abassi Z, Karram T, Ellaham S, Winaver J, Hoffman A. Implications of the natriuretic peptide system in the pathogenesis of heart failure: diagnostic and therapeutic importance. Pharmacol Ther 2004; 102:223–241.
Packer M, Califf RM, Konstam MA, et al. Comparison of omapatrilat and enalapril in patients with chronic heart failure: the Omapatrilat Versus Enalapril Randomized Trial of Utility in Reducing Events (OVERTURE). Circulation 2002; 106:920–926.
Rouleau JL, Pfeffer MA, Stewart DJ, et al. Comparison of vasopeptidase inhibitor, omapatrilat, and lisinopril on exercise tolerance and morbidity in patients with heart failure: IMPRESS randomised trial. Lancet 2000; 356:615–620.
Kostis JB, Packer M, Black HR, Schmieder R, Henry D, Levy E. Omapatrilat and enalapril in patients with hypertension: the Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am J Hypertens 2004; 17:103–111.
McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Committees and Investigators. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur J Heart Fail 2013; 15:1062–1073.
Toh S, Reichman ME, Houstoun M, et al. Comparative risk for angioedema associated with the use of drugs that target the renin-angiotensin-aldosterone system. Arch Intern Med 2012; 172:1582–1589.
Kostis JB, Kim HJ, Rusnak J, et al. Incidence and characteristics of angioedema associated with enalapril. Arch Intern Med 2005; 165:1637–1642.
Packer M, McMurray JJV, Desai AS, et al; on behalf of the PARADIGM-HF Investigators and Coordinators. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation 2015; 131:54–61.
Epstein AE, Dimarco JP, Ellenbogen KA, et al; American College of Cardiology/American Heart Association Task Force on Practice; American Association for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: executive summary. Heart Rhythm 2008; 5:934–955.
Solomon SD, Zile M, Pieske B, et al; Prospective comparison of ARNI with ARB on Management Of Heart Failure with Preserved Ejection Fraction (PARAMOUNT) Investigators. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet 2012; 380:1387–1395.
Address: David O. Taylor, MD, Department of Cardiovascular Medicine, J3-4, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: taylord2@ccf.org
Address: David O. Taylor, MD, Department of Cardiovascular Medicine, J3-4, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: taylord2@ccf.org
Author and Disclosure Information
Marwa A. Sabe, MD, MPH Department of Cardiovascular Medicine, Cleveland Clinic
Address: David O. Taylor, MD, Department of Cardiovascular Medicine, J3-4, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: taylord2@ccf.org
In a large phase trial, a combination drug that contains the angiotensin II receptor blocker (ARB) valsartan and the neprilysin inhibitor sacubitril was found to be superior to the angiotensin-converting enzyme (ACE) inhibitor enalapril in terms of important end points, including death and hospitalization for heart failure, in patients with heart failure with reduced ejection fraction.1
Recently approved by the US Food and Drug Administration, this combination drug, marketed under the brand name Entresto, represents a new drug class, angiotensin receptor-neprilysin inhibitors, or ARNIs.
This article is an overview of the Prospective Comparison of ARNI With ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial1 and the implications it may have on the care of patients with chronic heart failure.
NEED FOR NEW HEART FAILURE DRUGS
Heart failure is a major public health problem, and the care of patients with heart failure is challenging.
Almost 6 million US adults have heart failure, and the prevalence is projected to increase in the next few decades as the population continues to age.2 Furthermore, the total healthcare cost for heart failure patients was almost $31 billion in 2012 and is projected to rise to $70 billion by 2030.2
The care of patients with severely decompensated heart failure has changed dramatically in the last few decades with advances in heart transplantation and mechanical support devices. But day-to-day management of patients with chronic mildly to moderately symptomatic heart failure continues to pose a clinical challenge.
The drugs currently available for these patients include beta-blockers, ACE inhibitors, ARBs, aldosterone antagonists, digoxin, diuretics, and vasodilators. But even with these drugs, the death and readmission rates of patients with heart failure with reduced ejection fraction remain high. More than 50% of patients with heart failure die within 5 years of diagnosis,3 and 25% of patients hospitalized with heart failure are readmitted within 30 days of discharge.2 Furthermore, death rates are higher in those patients who have a history of heart failure hospitalization.4
Although heart failure with preserved ejection fraction encompasses an important group of heart failure patients with high morbidity, the focus of this article will be on patients with heart failure with reduced ejection fraction.
Available drugs to date
The cornerstone drugs that lower the odds of death in patients with heart failure with reduced ejection fraction are ACE inhibitors, ARBs, beta-blockers, and mineralocorticoid antagonists.
ACE inhibitors were the first class of drugs shown to reduce the death rate in patients with heart failure with reduced ejection fraction. The landmark CONSENSUS trial,5 published in 1987, found that the death rate in patients who received enalapril was 27% lower than in those receiving placebo, an effect driven entirely by a reduction in progressive heart failure. Similarly, the SOLVD trial,6 published in 1991, showed a 26% reduction in heart failure hospitalization and a 16% lower rate of death with enalapril compared with placebo, an effect driven predominantly by a decrease in the progression of heart failure.
ARBs have also been shown to decrease the rate of death, although not by as much as ACE inhibitors. In the CHARM trial,7 compared with placebo, candesartan significantly decreased the risk of death from any cause, of death from cardiovascular causes, and of hospitalization related to heart failure.7
Beta-blockers. The MERIT-HF trial,8 published in 1999, was stopped early because fewer patients were dying in the group receiving metoprolol succinate than in the group receiving placebo (relative risk 0.66). Similarly, in 2001, the COPERNICUS trial9 reported a 34% reduction in deaths in patients receiving carvedilol in addition to an ACE inhibitor compared with those receiving an ACE inhibitor alone.
Mineralocorticoid receptor antagonists were found to be beneficial when added to standard therapy for chronic symptomatic heart failure in the RALES10 and EMPHASIS-HF11 trials.
Vasodilators (specifically, the combination of isosorbide dinitrate and hydralazine) were found to have benefit in terms of mortality when added to standard therapy in African American patients in the A-HeEFT trial.12
WHY INHIBIT BOTH ANGIOTENSIN AND NEPRILYSIN?
The renin-angiotensin-aldosterone system is a major focus in treating heart failure, as overactivity of this system plays a key role in the pathophysiology of this disease. Therefore, essential drugs for heart failure patients include those that inhibit overactivity of this system such as ACE inhibitors, ARBs, and aldosterone antagonists.
The natriuretic peptide system is another important pathway that can be targeted in patients with heart failure. Natriuretic peptides are key molecules that counteract heart failure, as they contribute to diuresis and vasodilation and protect against vascular remodeling.13 An increased understanding of the importance of this system in slowing the progression of heart failure has motivated evaluation of drugs such as nesiritide in patients with symptomatic heart failure. However, these drugs can cause hypotension and have limited bioavailability.14
Neprilysin is an endopeptidase—an endogenous enzyme that degrades vasoactive peptides such as bradykinin and natriuretic peptides.14 Drugs that inhibit neprilysin increase the levels of these peptides and thus counteract neurohormonal stimuli that lead to cardiac remodeling, sodium retention, and vasoconstriction.15
However, neprilysin also hydrolyzes angiotensin I to angiotensin (1–7), an inhibitor of angiotensin II. Thus, inhibition of neprilysin alone could lead to increased activity of angiotensin II and so have an overall neutral effect. To be beneficial, neprilysin inhibition needs to be combined with renin-angiotensin system inhibition. Furthermore, the benefit of renin-angiotensin-aldosterone system blockade may be amplified by up-regulation of the endogenous natriuretic peptide system.15
Omapatrilat, the most studied combination neprilysin inhibitor and ACE inhibitor, improved cardiac function and decreased cardiac mass in animal experiments.15 In addition, this drug showed promise in terms of blood pressure, heart failure readmissions, death, and preservation of renal function when compared with ACE inhibitors in patients with heart failure.15–17 But in clinical trials this drug posed a greater risk of hypotension, dizziness, and, its major shortcoming, an unacceptably high incidence of angioedema compared with ACE inhibitors.15,16,18 This higher risk of angioedema is thought to be from inhibition of three enzymes that break down bradykinin: ACE, neprilysin, and aminopeptidase P.19
Figure 1. The final effect of sacubitril-valsartan is lower blood pressure, increased diuresis, and decreasedcardiac fibrosis and hypertrophy.ACE = angiotensin-converting enzyme; BNP = B-type natriuretic peptide; GC-A = guanylyl cyclase A
ARNIs contain an angiotensin receptor blocker rather than an ACE inhibitor, and thus in theory they may be associated with a lower risk of angioedema.19 Sacubitril-valsartan, the first drug of this class, contains its two constitutive drugs in a one-to-one molecular ratio (Figure 1).
PARADIGM-HF investigated the benefit of this drug in patients with systolic heart failure.1
STUDY DESIGN AND OBJECTIVES
PARADIGM-HF was a double-blind, randomized controlled trial comparing sacubitril-valsartan and enalapril in patients with chronic systolic heart failure. As such, it was the first trial in recent years to study a new drug in comparison with a well-established heart failure drug rather than as an add-on strategy.1
Inclusion criteria
To be included in the PARADIGM-HF trial, patients had to have:
A left ventricular ejection fraction of 40% or less (later changed to ≤ 35%)
New York Heart Association class II, III, or IV symptoms
A B-type natriuretic peptide (BNP) level of at least 150 pg/mL or an N-terminal proBNP (NT-proBNP) level of at least 600 pg/mL; for patients hospitalized for heart failure within the previous 12 months, the cut points were lower (BNP ≥ 100 pg/mL or NT-proBNP ≥ 400 pg/mL).
End points
The primary end point was the composite of cardiovascular death or first hospitalization for heart failure. Other outcomes assessed were time to death from any cause, the change from baseline in the Kansas City Cardiomyopathy Questionnaire (KCCQ) score at 8 months, time to new-onset atrial fibrillation, and the time to decline in renal function (defined as end-stage renal disease or a decrease in estimated glomerular filtration rate of at least 50% from randomization). All end points were blindly adjudicated by a clinical end points committee.
Two run-in periods
The study enrolled 10,521 patients from 1,043 centers in 47 countries, who entered the initial run-in period consisting of 2 weeks of treatment with enalapril at the study dosage (10 mg twice daily) in order to ensure no unacceptable side effects. At this point, 1,102 patients exited the study, leaving 9,419 who entered the second run-in period.
The second run-in period consisted of 4 weeks of treatment with sacubitril-valsartan, initially at half the study regimen (100 mg twice daily) and eventually at the full study dosage (200 mg twice daily). During the second run-in period, 977 participants left the study, leaving a total of 8,442 patients who underwent randomization. Forty-three patients were then excluded (6 because of invalid randomization and 37 because of four sites that closed because of major violations of good clinical practice).
Of those randomized, 4,187 patients were assigned to the sacubitril-valsartan treatment group and 4,212 were assigned to the enalapril group. The investigators used an intention-to-treat analysis for this study.
Most patients had NYHA class II symptoms
The randomized patients had a mean age of 64 years, 75% were men, 66% were white, and 58% were from Europe (only 7% were from North America). The mean left ventricular ejection fraction was about 30%, and 60% of the study participants had an ischemic cause for their cardiomyopathy. Although one of the inclusion criteria was New York Heart Association class II, III, or IV symptoms, about 5% of the patients had class I symptoms. Seventy percent had class II symptoms, 24% had class III, and less than 1% had class IV symptoms.
At the time of randomization, 78% of the patients were taking an ACE inhibitor and 93% were taking a beta-blocker, but only a little more than half were taking a mineralocorticoid antagonist and only about 15% had an implantable cardioverter-defibrillator.
STUDY OUTCOMES
This study was designed to detect a 15% lower risk of cardiovascular death in the sacubitril-valsartan group. It was projected to continue for at least 34 months but was stopped early because of an overwhelming benefit of the new drug at a median follow-up of 27 months.
Major findings
The primary composite outcome (cardiovascular death or first hospitalization for heart failure)1 occurred in 21.8% of the patients in the sacubitril-valsartan group vs 26.5% of patients in the enalapril group (hazard ratio [HR] 0.80, 95% confidence interval [CI] 0.73–0.87, P < .001). The number of patients who needed to be treated to prevent one occurrence of the primary composite outcome (100/absolute risk reduction) was only 21. The benefit was strong and consistent across both of the individual components of the composite outcome:
Cardiovascular death 13.3% vs 16.5%, HR 0.80 (95% CI 0.71–0.89), P < .001
First hospitalization for worsening heart failure 12.8% vs 15.6%, HR 0.79 (95% CI 0.71–0.89), P < .001.
Secondary outcomes. The sacubitril-valsartan group had a significantly lower rate of death from any cause (17.0% vs 19.8%, HR 0.84, 95% CI 0.76–0.93, P < .001) and a lower mean decrease in KCCQ clinical summary scores at 8 months (2.99 points vs 4.63 points, mean difference 1.64, 95% CI 0.63–2.65, P = .001). The KCCQ score measures subjective symptoms and physical limitations caused by heart failure; possible scores range from 0 to 100, with a higher score indicating better functional status. Notably, sacubitril-valsartan did not increase the KCCQ score in these patients; rather, sacubitril-valsartan recipients had a lower decrease in their scores than those in the enalapril group.
The incidence of new-onset atrial fibrillation was the same in both groups (3.1% and 3.1%).1 A decline in renal function (defined as end-stage renal disease, a decrease of 50% or more in estimated glomerular filtration rate from the value at randomization or a decrease in the estimated glomerular filtration rate of more than 30 mL/min/1.73 m2 to less than 60 mL/min/1.73 m2) occurred in 2.2% of the valsartan-sacubitril group and 2.6% of the enalapril group (P = .28).
The effects of the study drug on the primary composite outcome and on death from a cardiovascular cause were similar in all prespecified subgroups except for NYHA class: the reduction in the risk of the composite outcome was lower in sacubitril-valsartan recipients with NYHA I or II symptoms than in those with NYHA III or IV symptoms (P for interaction .03). However, there were no differences in the other prespecified subgroups, defined by age, sex, race, region, estimated glomerular filtration rate, diabetes, systolic blood pressure, ejection fraction, atrial fibrillation, NT-proBNP, hypertension, previous use of an ACE inhibitor, previous use of an aldosterone antagonist, previous heart failure hospitalization, and time since diagnosis of heart failure.
SAFETY: ANGIOEDEMA, HYPOTENSION, AND RENAL DYSFUNCTION
Angioedema
As noted above, the combination of neprilysin inhibitors and ACE inhibitors has been associated with an increased risk of angioedema. That was an important consideration before starting this study, which used a combination of a neprilysin inhibitor and an ARB in an attempt to avoid this serious side effect.
As it happened, there was no increased risk of significant angioedema with sacubitril-valsartan use compared with enalapril. Rates were similar to those in other studies, which showed a less than 1% risk of angioedema caused by ACE inhibitors.20,21 Only 19 patients (0.5%) in the sacubitril-valsartan group and 10 patients (0.2%) in the enalapril group experienced any angioedema. Of these, just three patients in the sacubitril-valsartan group and one patient in the enalapril group experienced angioedema that required hospitalization (P = .31). None of these patients had airway compromise due to angioedema.
Other safety issues that were assessed included hypotension, worsening renal function, increase in potassium levels, and cough. Patients in the sacubitril-valsartan group were more likely to have symptomatic hypotension than patients in the enalapril group (14.0% vs 9.2%, P < .001); however, the authors noted that this was a rare cause of drug discontinuation.
Patients in the sacubitril-valsartan group were less likely to develop cough (11.3% vs 14.3%, P < .001), a serum creatinine level of 2.5 mg/dL or more (3.3% vs 4.5%, P = .007), or a serum potassium level of more than 6.0 mmol/L (11.3% vs 14.3%, P = .007).1
During the two run-in periods combined, 12% of the patients in the study withdrew because of adverse events, including cough, renal dysfunction, hyperkalemia, and symptomatic hypotension. During the enalapril run-in period, 591 patients (5.6%) withdrew due to adverse events, and 547 patients (5.8%) withdrew due to these events during the sacubitril-valsartan run-in period. After adjusting for the shorter time on enalapril, there was a higher rate of withdrawal because of adverse events from enalapril than from sacubitril-valsartan.
LOWER RISK OF CLINICAL PROGRESSION
In a separate paper,22 the PARADIGM-HF investigators reported that, among the survivors in the study, those who received sacubitril-valsartan fared better in terms of a number of markers of progression of heart failure, with lower rates of:
Intensification of medical treatment for heart failure
Emergency department visits for worsening heart failure
Hospitalization for worsening heart failure
Need for intensive care
Need for intravenous inotropic agents
Need for cardiac devices or heart transplants
Worsening symptom scores
Elevation of biomarkers of myocardial injury.
QUESTIONS AND CONCERNS
Although this study, which was funded by the manufacturer, showed consistent benefit for sacubitril-valsartan over enalapril, questions remain.
Are the findings generalizable?
Despite the study’s rigorous run-in period, 12% of patients dropped out because of adverse events, and thus the patients who completed the study may not be representative of the general population of heart failure patients. The authors included this double-level wash-out to ensure patient tolerance of both drugs. But in everyday practice, a significant number of patients may be unable to tolerate one of these drugs.
Moreover, after adjusting for the difference in the run-in periods, patients actually withdrew more often during the enalapril run-in period than during the sacubitril-valsartan run-in period. However, there may be overlap in tolerability in these two drugs, which both affect the renin-angiotensin-aldosterone system. Thus, the enalapril run-in period may have contributed to the lower tolerability of this drug compared with sacubitril-valsartan.
Were patients receiving the best possible therapy?
Another important point when considering how we treat heart failure patients in the United States is how few patients in this study were using cardiac implantable electronic devices. Only 15% of the patients in this study had an implantable cardioverter-defibrillator despite a mean left ventricular ejection fraction less than 30%. This likely reflects differences in practice internationally; however, based on American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines, these patients would have a class I indication for an implantable cardioverter-defibrillator for primary prevention of sudden cardiac death.23
Therefore, based on these recommendations, the patients in this study were not necessarily on optimal medical and device therapy and furthermore may not be representative of heart failure patients in the United States.
Was enalapril 10 mg twice a day a fair comparison?
Another concern about the results of this study relates to the dosages used in the two treatment groups. The sacubitril-valsartan formulation included full-dose valsartan, whereas the ACE inhibitor group received enalapril at less than a full dose.
Although the authors explained that the dose of enalapril chosen for the study was based on the one used in previous studies that showed survival benefit, this raises the question of whether the significant difference in outcomes in this trial was due to a greater inhibition of the renin-angiotensin-aldosterone system related to a higher dose of drug in the sacubitril-valsartan group.
What about black patients taking hydralazine-isosorbide?
Only about 5% of patients in the PARADIGM-HF trial were black. Based on the A-HeFT study results, black patients can be prescribed an ACE inhibitor as well as hydralazine and isosorbide dinitrate as tolerated to decrease the risk of death. Does sacubitril-valsartan offer benefit to these patients compared with a regimen of an ACE inhibitor, hydralazine, and isosorbide dinitrate?
Another concern is that the incidence of angioedema observed with ACE inhibitors and omapatrilat is higher in black patients.15,21 Thus, it would be prudent to investigate whether the risk of angioedema with sacubitril-valsartan would be higher if more black patients are studied.
IMPLICATIONS AND CONSIDERATIONS
In this study, sacubitril-valsartan showed impressive and consistent results, with an almost 20% decrease in the composite end point of heart failure hospitalization or cardiovascular death and a similar decrease in the composite outcomes with a very low number needed to treat (21 patients). It did not show a decrease in the incidence of new-onset atrial fibrillation; however, only 80 cases of atrial fibrillation were reported, so there may have been a lack of statistical power to detect a difference.
To avoid angioedema, wait at least 36 hours after stopping an ACE inhibitor. Sacubitril-valsartan was not associated with an increased risk of severe angioedema, and no patients experienced life-threatening angioedema. In the trial, the sacubitril-valsartan run-in period was started at least 24 hours after enalapril was stopped, and thus the authors recommended at least a 1-day washout period after discontinuing an ACE inhibitor to avoid angioedema in patients starting sacubitril-valsartan.
Hypotension is a concern. Although there was actually a decreased risk of renal dysfunction, hyperkalemia, and cough compared with enalapril, there was a significantly increased rate of symptomatic hypotension in the sacubitril-valsartan group, which raises the question of patient tolerance and physician comfort when prescribing and titrating this drug in clinical practice. This side effect will be an important consideration when attempting to titrate the drug to target doses.
Start treatment early. This trial largely consisted of patients with NYHA class II or III symptoms, with about 70% of patients with class II symptoms. Since this drug showed benefit in patients with mildly to moderately symptomatic heart failure, clinicians who are considering prescribing this drug should not wait until the patient is closer to end-stage disease. Patients with mildly symptomatic heart failure may be followed by a general cardiologist, internist, or both, and thus it is important to emphasize to the entire medical community the need to start this medication early on.
How much will it cost? Cost is a concern that could heavily weigh on the decision to prescribe this drug. Generic ACE inhibitors are relatively inexpensive, and it may difficult to switch from an affordable generic drug to a new drug that is likely to be much more expensive. Arguably, this drug may be cost-effective in the long run owing to a large decrease in heart failure readmissions. We await further analyses to evaluate this issue.
Will patients take a twice-a-day drug as prescribed? Most patients who are prescribed an ACE inhibitor take it just once a day, and switching from a daily to a twice-daily drug may present a challenge for some.
What about other outcomes? Based on this study, it is unclear what effect sacubitril-valsartan has on the incidence of fatal arrhythmias, sudden cardiac death, and pump failure. Furthermore, the effect on quality of life is still uncertain. Quality of life is an integral component in the evaluation of heart failure patients, and in this study the changes in KCCQ scores were not impressive. We hope to see further evaluations of this drug’s impact on quality of life of patients with heart failure. Furthermore, it would be interesting to study if this drug has any long-term effects on the need for advanced therapies such as left ventricular assist devices and orthotopic heart transplant.
What about patients with heart failure with preserved ejection fraction? This study included only patients with heart failure with reduced ejection fraction. However PARAMOUNT, a phase 2 study that evaluated the benefit of sacubitril-valsartan in patients with heart failure with preserved ejection fraction, has shown encouraging results.24 We look forward to further investigation of this agent in patients with heart failure with preserved ejection fraction.
Sacubitril-valsartan, the first ARNI to be studied in humans, has a dual action in that it enhances the activity of the natriuretic peptide system and inhibits that of the renin-angiotensin-aldosterone system. It is the first drug in over a decade to show mortality benefit in patients with chronic systolic heart failure when compared with an already well-established heart failure medication. It appears to decrease rates of mortality and heart failure hospitalization without increasing the risk of severe angioedema in patients with mild or moderate chronic systolic heart failure. Symptomatic hypotension and high cost may pose the largest barriers to the use of this new drug. And we have yet to see how the clinical community and patients with heart failure will respond to it.
In a large phase trial, a combination drug that contains the angiotensin II receptor blocker (ARB) valsartan and the neprilysin inhibitor sacubitril was found to be superior to the angiotensin-converting enzyme (ACE) inhibitor enalapril in terms of important end points, including death and hospitalization for heart failure, in patients with heart failure with reduced ejection fraction.1
Recently approved by the US Food and Drug Administration, this combination drug, marketed under the brand name Entresto, represents a new drug class, angiotensin receptor-neprilysin inhibitors, or ARNIs.
This article is an overview of the Prospective Comparison of ARNI With ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) trial1 and the implications it may have on the care of patients with chronic heart failure.
NEED FOR NEW HEART FAILURE DRUGS
Heart failure is a major public health problem, and the care of patients with heart failure is challenging.
Almost 6 million US adults have heart failure, and the prevalence is projected to increase in the next few decades as the population continues to age.2 Furthermore, the total healthcare cost for heart failure patients was almost $31 billion in 2012 and is projected to rise to $70 billion by 2030.2
The care of patients with severely decompensated heart failure has changed dramatically in the last few decades with advances in heart transplantation and mechanical support devices. But day-to-day management of patients with chronic mildly to moderately symptomatic heart failure continues to pose a clinical challenge.
The drugs currently available for these patients include beta-blockers, ACE inhibitors, ARBs, aldosterone antagonists, digoxin, diuretics, and vasodilators. But even with these drugs, the death and readmission rates of patients with heart failure with reduced ejection fraction remain high. More than 50% of patients with heart failure die within 5 years of diagnosis,3 and 25% of patients hospitalized with heart failure are readmitted within 30 days of discharge.2 Furthermore, death rates are higher in those patients who have a history of heart failure hospitalization.4
Although heart failure with preserved ejection fraction encompasses an important group of heart failure patients with high morbidity, the focus of this article will be on patients with heart failure with reduced ejection fraction.
Available drugs to date
The cornerstone drugs that lower the odds of death in patients with heart failure with reduced ejection fraction are ACE inhibitors, ARBs, beta-blockers, and mineralocorticoid antagonists.
ACE inhibitors were the first class of drugs shown to reduce the death rate in patients with heart failure with reduced ejection fraction. The landmark CONSENSUS trial,5 published in 1987, found that the death rate in patients who received enalapril was 27% lower than in those receiving placebo, an effect driven entirely by a reduction in progressive heart failure. Similarly, the SOLVD trial,6 published in 1991, showed a 26% reduction in heart failure hospitalization and a 16% lower rate of death with enalapril compared with placebo, an effect driven predominantly by a decrease in the progression of heart failure.
ARBs have also been shown to decrease the rate of death, although not by as much as ACE inhibitors. In the CHARM trial,7 compared with placebo, candesartan significantly decreased the risk of death from any cause, of death from cardiovascular causes, and of hospitalization related to heart failure.7
Beta-blockers. The MERIT-HF trial,8 published in 1999, was stopped early because fewer patients were dying in the group receiving metoprolol succinate than in the group receiving placebo (relative risk 0.66). Similarly, in 2001, the COPERNICUS trial9 reported a 34% reduction in deaths in patients receiving carvedilol in addition to an ACE inhibitor compared with those receiving an ACE inhibitor alone.
Mineralocorticoid receptor antagonists were found to be beneficial when added to standard therapy for chronic symptomatic heart failure in the RALES10 and EMPHASIS-HF11 trials.
Vasodilators (specifically, the combination of isosorbide dinitrate and hydralazine) were found to have benefit in terms of mortality when added to standard therapy in African American patients in the A-HeEFT trial.12
WHY INHIBIT BOTH ANGIOTENSIN AND NEPRILYSIN?
The renin-angiotensin-aldosterone system is a major focus in treating heart failure, as overactivity of this system plays a key role in the pathophysiology of this disease. Therefore, essential drugs for heart failure patients include those that inhibit overactivity of this system such as ACE inhibitors, ARBs, and aldosterone antagonists.
The natriuretic peptide system is another important pathway that can be targeted in patients with heart failure. Natriuretic peptides are key molecules that counteract heart failure, as they contribute to diuresis and vasodilation and protect against vascular remodeling.13 An increased understanding of the importance of this system in slowing the progression of heart failure has motivated evaluation of drugs such as nesiritide in patients with symptomatic heart failure. However, these drugs can cause hypotension and have limited bioavailability.14
Neprilysin is an endopeptidase—an endogenous enzyme that degrades vasoactive peptides such as bradykinin and natriuretic peptides.14 Drugs that inhibit neprilysin increase the levels of these peptides and thus counteract neurohormonal stimuli that lead to cardiac remodeling, sodium retention, and vasoconstriction.15
However, neprilysin also hydrolyzes angiotensin I to angiotensin (1–7), an inhibitor of angiotensin II. Thus, inhibition of neprilysin alone could lead to increased activity of angiotensin II and so have an overall neutral effect. To be beneficial, neprilysin inhibition needs to be combined with renin-angiotensin system inhibition. Furthermore, the benefit of renin-angiotensin-aldosterone system blockade may be amplified by up-regulation of the endogenous natriuretic peptide system.15
Omapatrilat, the most studied combination neprilysin inhibitor and ACE inhibitor, improved cardiac function and decreased cardiac mass in animal experiments.15 In addition, this drug showed promise in terms of blood pressure, heart failure readmissions, death, and preservation of renal function when compared with ACE inhibitors in patients with heart failure.15–17 But in clinical trials this drug posed a greater risk of hypotension, dizziness, and, its major shortcoming, an unacceptably high incidence of angioedema compared with ACE inhibitors.15,16,18 This higher risk of angioedema is thought to be from inhibition of three enzymes that break down bradykinin: ACE, neprilysin, and aminopeptidase P.19
Figure 1. The final effect of sacubitril-valsartan is lower blood pressure, increased diuresis, and decreasedcardiac fibrosis and hypertrophy.ACE = angiotensin-converting enzyme; BNP = B-type natriuretic peptide; GC-A = guanylyl cyclase A
ARNIs contain an angiotensin receptor blocker rather than an ACE inhibitor, and thus in theory they may be associated with a lower risk of angioedema.19 Sacubitril-valsartan, the first drug of this class, contains its two constitutive drugs in a one-to-one molecular ratio (Figure 1).
PARADIGM-HF investigated the benefit of this drug in patients with systolic heart failure.1
STUDY DESIGN AND OBJECTIVES
PARADIGM-HF was a double-blind, randomized controlled trial comparing sacubitril-valsartan and enalapril in patients with chronic systolic heart failure. As such, it was the first trial in recent years to study a new drug in comparison with a well-established heart failure drug rather than as an add-on strategy.1
Inclusion criteria
To be included in the PARADIGM-HF trial, patients had to have:
A left ventricular ejection fraction of 40% or less (later changed to ≤ 35%)
New York Heart Association class II, III, or IV symptoms
A B-type natriuretic peptide (BNP) level of at least 150 pg/mL or an N-terminal proBNP (NT-proBNP) level of at least 600 pg/mL; for patients hospitalized for heart failure within the previous 12 months, the cut points were lower (BNP ≥ 100 pg/mL or NT-proBNP ≥ 400 pg/mL).
End points
The primary end point was the composite of cardiovascular death or first hospitalization for heart failure. Other outcomes assessed were time to death from any cause, the change from baseline in the Kansas City Cardiomyopathy Questionnaire (KCCQ) score at 8 months, time to new-onset atrial fibrillation, and the time to decline in renal function (defined as end-stage renal disease or a decrease in estimated glomerular filtration rate of at least 50% from randomization). All end points were blindly adjudicated by a clinical end points committee.
Two run-in periods
The study enrolled 10,521 patients from 1,043 centers in 47 countries, who entered the initial run-in period consisting of 2 weeks of treatment with enalapril at the study dosage (10 mg twice daily) in order to ensure no unacceptable side effects. At this point, 1,102 patients exited the study, leaving 9,419 who entered the second run-in period.
The second run-in period consisted of 4 weeks of treatment with sacubitril-valsartan, initially at half the study regimen (100 mg twice daily) and eventually at the full study dosage (200 mg twice daily). During the second run-in period, 977 participants left the study, leaving a total of 8,442 patients who underwent randomization. Forty-three patients were then excluded (6 because of invalid randomization and 37 because of four sites that closed because of major violations of good clinical practice).
Of those randomized, 4,187 patients were assigned to the sacubitril-valsartan treatment group and 4,212 were assigned to the enalapril group. The investigators used an intention-to-treat analysis for this study.
Most patients had NYHA class II symptoms
The randomized patients had a mean age of 64 years, 75% were men, 66% were white, and 58% were from Europe (only 7% were from North America). The mean left ventricular ejection fraction was about 30%, and 60% of the study participants had an ischemic cause for their cardiomyopathy. Although one of the inclusion criteria was New York Heart Association class II, III, or IV symptoms, about 5% of the patients had class I symptoms. Seventy percent had class II symptoms, 24% had class III, and less than 1% had class IV symptoms.
At the time of randomization, 78% of the patients were taking an ACE inhibitor and 93% were taking a beta-blocker, but only a little more than half were taking a mineralocorticoid antagonist and only about 15% had an implantable cardioverter-defibrillator.
STUDY OUTCOMES
This study was designed to detect a 15% lower risk of cardiovascular death in the sacubitril-valsartan group. It was projected to continue for at least 34 months but was stopped early because of an overwhelming benefit of the new drug at a median follow-up of 27 months.
Major findings
The primary composite outcome (cardiovascular death or first hospitalization for heart failure)1 occurred in 21.8% of the patients in the sacubitril-valsartan group vs 26.5% of patients in the enalapril group (hazard ratio [HR] 0.80, 95% confidence interval [CI] 0.73–0.87, P < .001). The number of patients who needed to be treated to prevent one occurrence of the primary composite outcome (100/absolute risk reduction) was only 21. The benefit was strong and consistent across both of the individual components of the composite outcome:
Cardiovascular death 13.3% vs 16.5%, HR 0.80 (95% CI 0.71–0.89), P < .001
First hospitalization for worsening heart failure 12.8% vs 15.6%, HR 0.79 (95% CI 0.71–0.89), P < .001.
Secondary outcomes. The sacubitril-valsartan group had a significantly lower rate of death from any cause (17.0% vs 19.8%, HR 0.84, 95% CI 0.76–0.93, P < .001) and a lower mean decrease in KCCQ clinical summary scores at 8 months (2.99 points vs 4.63 points, mean difference 1.64, 95% CI 0.63–2.65, P = .001). The KCCQ score measures subjective symptoms and physical limitations caused by heart failure; possible scores range from 0 to 100, with a higher score indicating better functional status. Notably, sacubitril-valsartan did not increase the KCCQ score in these patients; rather, sacubitril-valsartan recipients had a lower decrease in their scores than those in the enalapril group.
The incidence of new-onset atrial fibrillation was the same in both groups (3.1% and 3.1%).1 A decline in renal function (defined as end-stage renal disease, a decrease of 50% or more in estimated glomerular filtration rate from the value at randomization or a decrease in the estimated glomerular filtration rate of more than 30 mL/min/1.73 m2 to less than 60 mL/min/1.73 m2) occurred in 2.2% of the valsartan-sacubitril group and 2.6% of the enalapril group (P = .28).
The effects of the study drug on the primary composite outcome and on death from a cardiovascular cause were similar in all prespecified subgroups except for NYHA class: the reduction in the risk of the composite outcome was lower in sacubitril-valsartan recipients with NYHA I or II symptoms than in those with NYHA III or IV symptoms (P for interaction .03). However, there were no differences in the other prespecified subgroups, defined by age, sex, race, region, estimated glomerular filtration rate, diabetes, systolic blood pressure, ejection fraction, atrial fibrillation, NT-proBNP, hypertension, previous use of an ACE inhibitor, previous use of an aldosterone antagonist, previous heart failure hospitalization, and time since diagnosis of heart failure.
SAFETY: ANGIOEDEMA, HYPOTENSION, AND RENAL DYSFUNCTION
Angioedema
As noted above, the combination of neprilysin inhibitors and ACE inhibitors has been associated with an increased risk of angioedema. That was an important consideration before starting this study, which used a combination of a neprilysin inhibitor and an ARB in an attempt to avoid this serious side effect.
As it happened, there was no increased risk of significant angioedema with sacubitril-valsartan use compared with enalapril. Rates were similar to those in other studies, which showed a less than 1% risk of angioedema caused by ACE inhibitors.20,21 Only 19 patients (0.5%) in the sacubitril-valsartan group and 10 patients (0.2%) in the enalapril group experienced any angioedema. Of these, just three patients in the sacubitril-valsartan group and one patient in the enalapril group experienced angioedema that required hospitalization (P = .31). None of these patients had airway compromise due to angioedema.
Other safety issues that were assessed included hypotension, worsening renal function, increase in potassium levels, and cough. Patients in the sacubitril-valsartan group were more likely to have symptomatic hypotension than patients in the enalapril group (14.0% vs 9.2%, P < .001); however, the authors noted that this was a rare cause of drug discontinuation.
Patients in the sacubitril-valsartan group were less likely to develop cough (11.3% vs 14.3%, P < .001), a serum creatinine level of 2.5 mg/dL or more (3.3% vs 4.5%, P = .007), or a serum potassium level of more than 6.0 mmol/L (11.3% vs 14.3%, P = .007).1
During the two run-in periods combined, 12% of the patients in the study withdrew because of adverse events, including cough, renal dysfunction, hyperkalemia, and symptomatic hypotension. During the enalapril run-in period, 591 patients (5.6%) withdrew due to adverse events, and 547 patients (5.8%) withdrew due to these events during the sacubitril-valsartan run-in period. After adjusting for the shorter time on enalapril, there was a higher rate of withdrawal because of adverse events from enalapril than from sacubitril-valsartan.
LOWER RISK OF CLINICAL PROGRESSION
In a separate paper,22 the PARADIGM-HF investigators reported that, among the survivors in the study, those who received sacubitril-valsartan fared better in terms of a number of markers of progression of heart failure, with lower rates of:
Intensification of medical treatment for heart failure
Emergency department visits for worsening heart failure
Hospitalization for worsening heart failure
Need for intensive care
Need for intravenous inotropic agents
Need for cardiac devices or heart transplants
Worsening symptom scores
Elevation of biomarkers of myocardial injury.
QUESTIONS AND CONCERNS
Although this study, which was funded by the manufacturer, showed consistent benefit for sacubitril-valsartan over enalapril, questions remain.
Are the findings generalizable?
Despite the study’s rigorous run-in period, 12% of patients dropped out because of adverse events, and thus the patients who completed the study may not be representative of the general population of heart failure patients. The authors included this double-level wash-out to ensure patient tolerance of both drugs. But in everyday practice, a significant number of patients may be unable to tolerate one of these drugs.
Moreover, after adjusting for the difference in the run-in periods, patients actually withdrew more often during the enalapril run-in period than during the sacubitril-valsartan run-in period. However, there may be overlap in tolerability in these two drugs, which both affect the renin-angiotensin-aldosterone system. Thus, the enalapril run-in period may have contributed to the lower tolerability of this drug compared with sacubitril-valsartan.
Were patients receiving the best possible therapy?
Another important point when considering how we treat heart failure patients in the United States is how few patients in this study were using cardiac implantable electronic devices. Only 15% of the patients in this study had an implantable cardioverter-defibrillator despite a mean left ventricular ejection fraction less than 30%. This likely reflects differences in practice internationally; however, based on American College of Cardiology, American Heart Association, and Heart Rhythm Society guidelines, these patients would have a class I indication for an implantable cardioverter-defibrillator for primary prevention of sudden cardiac death.23
Therefore, based on these recommendations, the patients in this study were not necessarily on optimal medical and device therapy and furthermore may not be representative of heart failure patients in the United States.
Was enalapril 10 mg twice a day a fair comparison?
Another concern about the results of this study relates to the dosages used in the two treatment groups. The sacubitril-valsartan formulation included full-dose valsartan, whereas the ACE inhibitor group received enalapril at less than a full dose.
Although the authors explained that the dose of enalapril chosen for the study was based on the one used in previous studies that showed survival benefit, this raises the question of whether the significant difference in outcomes in this trial was due to a greater inhibition of the renin-angiotensin-aldosterone system related to a higher dose of drug in the sacubitril-valsartan group.
What about black patients taking hydralazine-isosorbide?
Only about 5% of patients in the PARADIGM-HF trial were black. Based on the A-HeFT study results, black patients can be prescribed an ACE inhibitor as well as hydralazine and isosorbide dinitrate as tolerated to decrease the risk of death. Does sacubitril-valsartan offer benefit to these patients compared with a regimen of an ACE inhibitor, hydralazine, and isosorbide dinitrate?
Another concern is that the incidence of angioedema observed with ACE inhibitors and omapatrilat is higher in black patients.15,21 Thus, it would be prudent to investigate whether the risk of angioedema with sacubitril-valsartan would be higher if more black patients are studied.
IMPLICATIONS AND CONSIDERATIONS
In this study, sacubitril-valsartan showed impressive and consistent results, with an almost 20% decrease in the composite end point of heart failure hospitalization or cardiovascular death and a similar decrease in the composite outcomes with a very low number needed to treat (21 patients). It did not show a decrease in the incidence of new-onset atrial fibrillation; however, only 80 cases of atrial fibrillation were reported, so there may have been a lack of statistical power to detect a difference.
To avoid angioedema, wait at least 36 hours after stopping an ACE inhibitor. Sacubitril-valsartan was not associated with an increased risk of severe angioedema, and no patients experienced life-threatening angioedema. In the trial, the sacubitril-valsartan run-in period was started at least 24 hours after enalapril was stopped, and thus the authors recommended at least a 1-day washout period after discontinuing an ACE inhibitor to avoid angioedema in patients starting sacubitril-valsartan.
Hypotension is a concern. Although there was actually a decreased risk of renal dysfunction, hyperkalemia, and cough compared with enalapril, there was a significantly increased rate of symptomatic hypotension in the sacubitril-valsartan group, which raises the question of patient tolerance and physician comfort when prescribing and titrating this drug in clinical practice. This side effect will be an important consideration when attempting to titrate the drug to target doses.
Start treatment early. This trial largely consisted of patients with NYHA class II or III symptoms, with about 70% of patients with class II symptoms. Since this drug showed benefit in patients with mildly to moderately symptomatic heart failure, clinicians who are considering prescribing this drug should not wait until the patient is closer to end-stage disease. Patients with mildly symptomatic heart failure may be followed by a general cardiologist, internist, or both, and thus it is important to emphasize to the entire medical community the need to start this medication early on.
How much will it cost? Cost is a concern that could heavily weigh on the decision to prescribe this drug. Generic ACE inhibitors are relatively inexpensive, and it may difficult to switch from an affordable generic drug to a new drug that is likely to be much more expensive. Arguably, this drug may be cost-effective in the long run owing to a large decrease in heart failure readmissions. We await further analyses to evaluate this issue.
Will patients take a twice-a-day drug as prescribed? Most patients who are prescribed an ACE inhibitor take it just once a day, and switching from a daily to a twice-daily drug may present a challenge for some.
What about other outcomes? Based on this study, it is unclear what effect sacubitril-valsartan has on the incidence of fatal arrhythmias, sudden cardiac death, and pump failure. Furthermore, the effect on quality of life is still uncertain. Quality of life is an integral component in the evaluation of heart failure patients, and in this study the changes in KCCQ scores were not impressive. We hope to see further evaluations of this drug’s impact on quality of life of patients with heart failure. Furthermore, it would be interesting to study if this drug has any long-term effects on the need for advanced therapies such as left ventricular assist devices and orthotopic heart transplant.
What about patients with heart failure with preserved ejection fraction? This study included only patients with heart failure with reduced ejection fraction. However PARAMOUNT, a phase 2 study that evaluated the benefit of sacubitril-valsartan in patients with heart failure with preserved ejection fraction, has shown encouraging results.24 We look forward to further investigation of this agent in patients with heart failure with preserved ejection fraction.
Sacubitril-valsartan, the first ARNI to be studied in humans, has a dual action in that it enhances the activity of the natriuretic peptide system and inhibits that of the renin-angiotensin-aldosterone system. It is the first drug in over a decade to show mortality benefit in patients with chronic systolic heart failure when compared with an already well-established heart failure medication. It appears to decrease rates of mortality and heart failure hospitalization without increasing the risk of severe angioedema in patients with mild or moderate chronic systolic heart failure. Symptomatic hypotension and high cost may pose the largest barriers to the use of this new drug. And we have yet to see how the clinical community and patients with heart failure will respond to it.
References
McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371:993–1004.
Dunlay SM, Pereira NL, Kushwaha SS. Contemporary strategies in the diagnosis and management of heart failure. Mayo Clin Proc 2014; 89:662–676.
Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation 2013; 127:e6–e245.
Bello NA, Claggett B, Desai AS, et al. Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction. Circ Heart Fail 2014; 7:590–595.
Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The CONSENSUS Trial Study Group. N Engl J Med 1987; 316:1429–1435.
Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The SOLVD Investigators. N Engl J Med 1991; 325:293–302.
Pfeffer MA, Swedberg K, Granger CB, et al; CHARM Investigators and Committees. Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programme. Lancet 2003; 362:759–766.
Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353:2001–2007.
Packer M, Coats AJ, Fowler MB, et al; Carvedilol Prospective Randomized Cumulative Survival Study Group. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 2001; 344:1651–1658.
Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999; 341:709–717.
Zannad F, McMurray JJ, Krum H, et al; EMPHASIS-HF Study Group. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 2011; 364:11–21.
Taylor AL, Ziesche S, Yancy C, et al; African-American Heart Failure Trial Investigators. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med 2004; 351:2049–2057.
Schreiner GF, Protter AA. B-type natriuretic peptide for the treatment of congestive heart failure. Curr Opin Pharmacol 2002; 2:142–147.
von Lueder TG, Sangaralingham SJ, Wang BH, et al. Renin-angiotensin blockade combined with natriuretic peptide system augmentation: novel therapeutic concepts to combat heart failure. Circ Heart Fail 2013; 6:594–605.
Abassi Z, Karram T, Ellaham S, Winaver J, Hoffman A. Implications of the natriuretic peptide system in the pathogenesis of heart failure: diagnostic and therapeutic importance. Pharmacol Ther 2004; 102:223–241.
Packer M, Califf RM, Konstam MA, et al. Comparison of omapatrilat and enalapril in patients with chronic heart failure: the Omapatrilat Versus Enalapril Randomized Trial of Utility in Reducing Events (OVERTURE). Circulation 2002; 106:920–926.
Rouleau JL, Pfeffer MA, Stewart DJ, et al. Comparison of vasopeptidase inhibitor, omapatrilat, and lisinopril on exercise tolerance and morbidity in patients with heart failure: IMPRESS randomised trial. Lancet 2000; 356:615–620.
Kostis JB, Packer M, Black HR, Schmieder R, Henry D, Levy E. Omapatrilat and enalapril in patients with hypertension: the Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am J Hypertens 2004; 17:103–111.
McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Committees and Investigators. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur J Heart Fail 2013; 15:1062–1073.
Toh S, Reichman ME, Houstoun M, et al. Comparative risk for angioedema associated with the use of drugs that target the renin-angiotensin-aldosterone system. Arch Intern Med 2012; 172:1582–1589.
Kostis JB, Kim HJ, Rusnak J, et al. Incidence and characteristics of angioedema associated with enalapril. Arch Intern Med 2005; 165:1637–1642.
Packer M, McMurray JJV, Desai AS, et al; on behalf of the PARADIGM-HF Investigators and Coordinators. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation 2015; 131:54–61.
Epstein AE, Dimarco JP, Ellenbogen KA, et al; American College of Cardiology/American Heart Association Task Force on Practice; American Association for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: executive summary. Heart Rhythm 2008; 5:934–955.
Solomon SD, Zile M, Pieske B, et al; Prospective comparison of ARNI with ARB on Management Of Heart Failure with Preserved Ejection Fraction (PARAMOUNT) Investigators. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet 2012; 380:1387–1395.
References
McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Investigators and Committees. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014; 371:993–1004.
Dunlay SM, Pereira NL, Kushwaha SS. Contemporary strategies in the diagnosis and management of heart failure. Mayo Clin Proc 2014; 89:662–676.
Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2013 update: a report from the American Heart Association. Circulation 2013; 127:e6–e245.
Bello NA, Claggett B, Desai AS, et al. Influence of previous heart failure hospitalization on cardiovascular events in patients with reduced and preserved ejection fraction. Circ Heart Fail 2014; 7:590–595.
Effects of enalapril on mortality in severe congestive heart failure. Results of the Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). The CONSENSUS Trial Study Group. N Engl J Med 1987; 316:1429–1435.
Effect of enalapril on survival in patients with reduced left ventricular ejection fractions and congestive heart failure. The SOLVD Investigators. N Engl J Med 1991; 325:293–302.
Pfeffer MA, Swedberg K, Granger CB, et al; CHARM Investigators and Committees. Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programme. Lancet 2003; 362:759–766.
Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL Randomised Intervention Trial in Congestive Heart Failure (MERIT-HF). Lancet 1999; 353:2001–2007.
Packer M, Coats AJ, Fowler MB, et al; Carvedilol Prospective Randomized Cumulative Survival Study Group. Effect of carvedilol on survival in severe chronic heart failure. N Engl J Med 2001; 344:1651–1658.
Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. Randomized Aldactone Evaluation Study Investigators. N Engl J Med 1999; 341:709–717.
Zannad F, McMurray JJ, Krum H, et al; EMPHASIS-HF Study Group. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med 2011; 364:11–21.
Taylor AL, Ziesche S, Yancy C, et al; African-American Heart Failure Trial Investigators. Combination of isosorbide dinitrate and hydralazine in blacks with heart failure. N Engl J Med 2004; 351:2049–2057.
Schreiner GF, Protter AA. B-type natriuretic peptide for the treatment of congestive heart failure. Curr Opin Pharmacol 2002; 2:142–147.
von Lueder TG, Sangaralingham SJ, Wang BH, et al. Renin-angiotensin blockade combined with natriuretic peptide system augmentation: novel therapeutic concepts to combat heart failure. Circ Heart Fail 2013; 6:594–605.
Abassi Z, Karram T, Ellaham S, Winaver J, Hoffman A. Implications of the natriuretic peptide system in the pathogenesis of heart failure: diagnostic and therapeutic importance. Pharmacol Ther 2004; 102:223–241.
Packer M, Califf RM, Konstam MA, et al. Comparison of omapatrilat and enalapril in patients with chronic heart failure: the Omapatrilat Versus Enalapril Randomized Trial of Utility in Reducing Events (OVERTURE). Circulation 2002; 106:920–926.
Rouleau JL, Pfeffer MA, Stewart DJ, et al. Comparison of vasopeptidase inhibitor, omapatrilat, and lisinopril on exercise tolerance and morbidity in patients with heart failure: IMPRESS randomised trial. Lancet 2000; 356:615–620.
Kostis JB, Packer M, Black HR, Schmieder R, Henry D, Levy E. Omapatrilat and enalapril in patients with hypertension: the Omapatrilat Cardiovascular Treatment vs. Enalapril (OCTAVE) trial. Am J Hypertens 2004; 17:103–111.
McMurray JJ, Packer M, Desai AS, et al; PARADIGM-HF Committees and Investigators. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-converting enzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparison of ARNI with ACEI to Determine Impact on Global Mortality and morbidity in Heart Failure trial (PARADIGM-HF). Eur J Heart Fail 2013; 15:1062–1073.
Toh S, Reichman ME, Houstoun M, et al. Comparative risk for angioedema associated with the use of drugs that target the renin-angiotensin-aldosterone system. Arch Intern Med 2012; 172:1582–1589.
Kostis JB, Kim HJ, Rusnak J, et al. Incidence and characteristics of angioedema associated with enalapril. Arch Intern Med 2005; 165:1637–1642.
Packer M, McMurray JJV, Desai AS, et al; on behalf of the PARADIGM-HF Investigators and Coordinators. Angiotensin receptor neprilysin inhibition compared with enalapril on the risk of clinical progression in surviving patients with heart failure. Circulation 2015; 131:54–61.
Epstein AE, Dimarco JP, Ellenbogen KA, et al; American College of Cardiology/American Heart Association Task Force on Practice; American Association for Thoracic Surgery; Society of Thoracic Surgeons. ACC/AHA/HRS 2008 guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: executive summary. Heart Rhythm 2008; 5:934–955.
Solomon SD, Zile M, Pieske B, et al; Prospective comparison of ARNI with ARB on Management Of Heart Failure with Preserved Ejection Fraction (PARAMOUNT) Investigators. The angiotensin receptor neprilysin inhibitor LCZ696 in heart failure with preserved ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet 2012; 380:1387–1395.
Neprilysin is an endogenous enzyme that degrades vasoactive peptides such as bradykinin and natriuretic peptides. Inhibition of neprilysin raises the levels of these peptides, leading to less cardiac remodeling, less sodium retention, and less vasoconstriction.
Neprilysin inhibition must be combined with inhibition of the renin-angiotensin-aldosterone system, optimally with an angiotensin II receptor blocker.
PARADIGM-HF showed a 20% reduction in the primary outcome of death from cardiovascular causes or hospitalization for heart failure with sacubitril-valsartan 200 mg twice daily vs enalapril 10 mg twice daily at a median follow-up of 27 months.
The ultimate role of combined neprilysin and angiotensin receptor inhibitors remains to be determined.
Many patients who have osteoarthritis of the knee and a torn meniscus can defer having the meniscus repaired and undergo physical therapy instead. If a trial of physical therapy does not help, they can opt for surgery later.
This seems to be the take-home message from the recent Meniscal Tear in Osteoarthritis Research (METEOR) trial,1 which compared the efficacy of arthroscopic partial meniscectomy plus physical therapy vs physical therapy alone for patients with knee symptoms, a meniscal tear, and mild to moderate osteoarthritis of the knee.1
In brief, patients improved to a roughly similar degree with either approach, and although many patients assigned to physical therapy eventually underwent surgery anyway by 6 months, the delay did not adversely affect outcomes.
In this article, we review the background, design, and findings of the METEOR trial, and their implications for clinical practice.
SURGERY: HIGH VOLUME, BUT LITTLE EVIDENCE
Magnetic resonance imaging (MRI) often incidentally reveals meniscal lesions in middle-aged and older patients who have osteoarthritis and knee pain.2 Should these patients undergo arthroscopic meniscal repair? The decision is difficult, since it is hard to distinguish the symptoms of a meniscal tear from those of osteoarthritis.3
Current evidence suggests that, for symptomatic knee osteoarthritis by itself, arthroscopic surgery is no more effective than conservative management.4,5 But what about surgery for a torn meniscus in addition to osteoarthritis?
Osteoarthritis is the most common joint disease, accounting for many physician visits.6 More than 26 million Americans over age 25 have some form of it, and the prevalence of symptomatic, radiographically confirmed osteoarthritis of the knee was 12.1% in the third National Health and Nutrition Examination Survey.7
We used to consider osteoarthritis a “wear-and-tear” disease—thus the term “degenerative joint disease.” But today, we know that it is an active response to injury, involving inflammatory and metabolic pathways.8 Moreover, the risk of osteoarthritis and its progression seems to be higher in those who have had meniscal injury and total or arthroscopic partial meniscectomy.9,10
MRI is not commonly used in managing knee osteoarthritis, but it has been used diagnostically in patients with symptoms of a meniscal tear, such as clicking, locking, popping, giving way, and pain with pivoting or twisting. Traumatic meniscal tears (a longitudinal or radial tear pattern) most often occur in active younger people and often lead to meniscal surgery.11,12 In contrast, degenerative meniscal tears (horizontal, oblique, or complex tear pattern or meniscal maceration) tend to occur in older people,11,12 but how to manage them is not widely agreed upon.
Of note, most patients with osteoarthritis of the knee have torn, macerated, or heavily damaged menisci.13,14 Meniscal lesions are also common in middle-aged people in the general population, with a higher prevalence in people who are older, heavier, or female, or who have a family history of osteoarthritis.15
These abnormalities are only weakly associated with symptoms.2 However, when a patient has knee symptoms and a torn meniscus is detected on MRI, the tear is often assumed to be the source of the symptoms, and meniscal tears are the most common reason for arthroscopy.16
Since we have no way to prevent the progression of joint damage from osteoarthritis with drugs or by any other means, the goal is to alleviate the symptoms. Many patients report pain relief or functional improvement after arthroscopic surgery. But arthroscopic lavage or debridement for osteoarthritis has not been found to be better than conservative treatment or placebo in randomized controlled trials.4,5
In contrast, the current standard treatment for a symptomatic degenerative meniscal tear is arthroscopic partial meniscectomy. Nearly 500,000 of these procedures are performed annually in the United States.16 But based on the best evidence, arthroscopic partial meniscectomy does not result in better pain relief and functional improvement than does physical therapy alone in patients who have a torn meniscus and knee osteoarthritis.17,18
OVERVIEW OF THE METEOR TRIAL
The METEOR trial was a randomized controlled trial conducted at seven US tertiary referral centers. Its aim was to compare the short-term (6-month) and long-term (12-month) efficacy of arthroscopic partial meniscectomy and physical therapy in patients with symptomatic meniscal tear and osteoarthritis of the knee.19 It was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases.1
Patients were age 45 and older
METEOR patients had to be at least 45 years old and have symptomatic meniscal tears and knee osteoarthritis detected on MRI or radiography.1
Osteoarthritis was defined broadly, given that it begins well before the appearance of radiographic evidence such as an osteophyte or joint-space narrowing.19 Patients with cartilage defects on MRI were also enrolled, as were patients with radiographically documented osteoarthritis.19
Patients were considered to have a symptomatic meniscal tear if they had had at least 4 weeks of symptoms (such as episodic pain and pain that was acute and localized to one spot on the knee, as well as typical mechanical pain suggesting a meniscal tear, such as clicking, catching, popping, giving way, or pain with pivoting or twisting) in addition to evidence of a meniscal tear on MRI.19
Patients were excluded if they had a chronically locked knee (a clear-cut indication for arthroscopic partial meniscectomy), advanced osteoarthritis (Kellgren-Lawrence grade 4), inflammatory arthritis, clinically symptomatic chondrocalcinosis, or bilateral symptomatic meniscal tears.19 Patients who had undergone surgery or injection of a viscosupplement in the index knee during the past 4 weeks were also excluded.19
Of 1,330 eligible patients, 351 (26.4%) were enrolled and randomly assigned in a 1:1 ratio to a treatment group by means of a secure program on the trial website.1,19 Of those who were eligible but did not enroll, 195 (14.6%) were not referred and 784 (58.9%) declined to participate. Of those who declined, more preferred surgery than physical therapy (36.1% vs 21%). No information is available on any differences in baseline characteristics between the enrolled patients and the eligible patients who declined.
Randomization was done in blocks of varying size within each site, stratified according to sex and the extent of osteoarthritis on baseline radiography. The extent of osteoarthritis was categorized either as Kellgren-Lawrence grade 0 (normal, no features of osteoarthritis) to grade 2 (definite osteoarthritis, a definite osteophyte without joint-space narrowing) or as Kellgren-Lawrence grade 3 (moderate osteoarthritis, < 50% joint-space narrowing).1,19 The two treatment groups were similar with respect to age, sex, race or ethnicity, baseline Kellgren-Lawrence grade, and baseline Western Ontario and McMaster Universities Arthritis Index (WOMAC) physical function score.1
The mean age of the participants was 58, and 85% were white. Sixty-three percent had Kellgren-Lawrence grade 0 to 2 osteoarthritis, and 27% had grade 3.1
Surgery plus physical therapy vs physical therapy alone
The surgery group underwent arthroscopic partial meniscectomy, which involved trimming the damaged meniscus back to a stable rim1,19 and trimming loose fragments of cartilage and bone.
After the procedure, patients were scheduled for physical therapy. Although there is no consensus on the need for or the effectiveness of postoperative physical therapy in this setting, the investigators believed that including it in both study groups would help to isolate the independent effects of surgery. The physical therapy regimen after surgery was similar to that provided in the nonoperative group.1,19
Physical therapy was designed to address inflammation, range of motion, muscle strength, muscle-length restriction, functional mobility, and proprioception and balance.1,19 There were three stages; criteria for advancing from one phase to the next included the level of self-reported pain, observed strength, range of knee motion, knee effusion, and functional mobility.1,18
The duration of participation varied depending on the pace of improvement. Generally, the program lasted about 6 weeks.1,19
Crossover and other therapies were allowed
Crossover from physical therapy alone to surgery was allowed during the trial if the patient and surgeon thought it was clinically indicated.
Participants in both groups were permitted to take acetaminophen and nonsteroidal anti-inflammatory drugs as needed. Intra-articular injections of glucocorticoids were also allowed during the trial.
OUTCOMES MEASURED
WOMAC physical function score
The primary outcome of the METEOR trial was the difference between the study groups in the change in WOMAC physical function score from baseline to 6 months, at which point participants were expected to have achieved maximum improvement.1,19 Questionnaires were also administered at 3 months to assess the early response to surgery or physical therapy and again at 12 months.
The complete WOMAC also measures pain and stiffness in addition to physical function, with separate subscales for each. The change in WOMAC score is one of the most widely endorsed outcome measures in assessing interventions in osteoarthritis or other conditions of the lower extremities.20 The METEOR trial authors considered the WOMAC scale to be highly valid and reliable, with a Cronbach alpha value of 0.97 (maximum value = 1; the higher the better).
No ceiling or floor effects were observed in the WOMAC physical function score in patients with osteoarthritis and a meniscal tear in a pilot study for METEOR.19
In the main METEOR study, WOMAC physical function was scored on a scale of 0 to 100, with a higher score indicating worse physical function.1 Changes in the score were also measured as a yes-or-no question, defined a priori as whether the score declined by at least 8 points, which is considered the minimal clinically important difference in osteoarthritis patients.1,19
KOOS and MOS SF-36 scores
Secondary outcomes were measured in several domains, including pain, generic functional status, quality of life, and health care utilization.1,19
The KOOS (Knee Injury and OA Outcome Scale) is specific for knee pain, being designed to evaluate short-term and long-term symptoms and function in patients with knee injury and associated problems.21 It has five subscales, which are scored separately: pain, other symptoms, activities of daily living, sport and recreation, and knee-related quality of life.21 Since the WOMAC pain scale showed a ceiling effect in the pilot study in patients undergoing surgery, the authors chose the KOOS pain scale as a pain measure.19 Scores were transformed to a 0–100 scale, with a higher score indicating more pain.1
The MOS SF-36 (Medical Outcomes Study 36-item short form) was used to measure general health status and function.1,19
STATISTICAL ANALYSIS: INTENTION-TO-TREAT AND AS-TREATED
The study was powered to detect a 10-point difference in WOMAC physical function scores at 6 months of follow-up between the operative and nonoperative groups, anticipating losses to follow-up and crossover, with preplanned subgroup (Kellgren–Lawrence grade 0–2 vs grade 3) analysis.1,19
The primary analysis used a modified intention-to-treat approach and was implemented with an analysis of covariance with changes in the WOMAC score from baseline to 6 months as the dependent variable, treatment as the independent variable of interest, and study site as a covariate. Other covariates, such as age, sex, and baseline Kellgren-Lawrence grade, were balanced across groups and were therefore not included in the analysis.1,19
Secondary analyses used an “as-treated” approach, ie, according to the treatment actually received.1,19 Secondary intention-to-treat analysis—using binary outcome measures in which treatment failure was defined as improvement in the WOMAC score of less than 8 points or crossing over to the other treatment—was also performed to estimate efficacy at the level of the patient rather than at the group level.1,19
BOTH GROUPS IMPROVED
In the intention-to-treat analyses at 6 months and 12 months after randomization, both groups improved, with no clinically important or statistically significant differences between the groups in functional status (WOMAC score, MOS SF-36 score) or pain (KOOS score).1 The mean improvement (decline) in the WOMAC score from baseline to 6 months was 20.9 points in the surgery group vs 18.5 points in the physical therapy group, a difference of 2.4 points (95% confidence interval [CI], −1.8 to 6.5).1
35% of physical therapy patients underwent surgery by 12 months
Of the 177 patients randomized to physical therapy alone, by 6 months 1 had died, 1 had undergone total knee replacement, 4 had withdrawn, and 2 were lost to follow-up. Of the 169 remaining, 51 (30%) had undergone arthroscopic partial meniscectomy. An additional 8 patients who were assigned to physical therapy crossed over to surgery between 6 and 12 months.1,19
Of the 174 patients randomized to surgery, by 6 months 1 had died, 3 had undergone total knee replacement, 7 had withdrawn, and 2 were ineligible. Of the 161 remaining, 9 (6%) had not undergone the procedure.
Other outcomes
Subgroup analysis based on the baseline radiographic grade (Kellgren-Lawrence grade 0 to 2 vs grade 3) did not show a difference between groups in functional improvement at 6 months (P = .13 for interaction).1
No statistically significant difference was noted in rates of overall or specific adverse events between the two groups over the first 12 months.1 Adverse events rated as mild or moderate in severity occurred in 15 participants in the surgery group and 13 participants in the physical therapy group.1 Long-term risks associated with these interventions are being assessed, and longitudinal assessment of imaging studies is planned to address this question but is not yet available.1,18
In the physical therapy group, 21 patients (12%) received intra-articular glucocorticoid injections, as did 9 patients (6%) in the surgery group.1,19
TRANSLATING THE METEOR RESULTS TO EVERYDAY PRACTICE
There are many challenges in designing surgical trials. Indeed, by one estimate,22 only about 40% of treatment questions involving surgical procedures can be evaluated by a randomized controlled trial.
Although the METEOR trial was not blinded, it was the first large, multicenter, randomized controlled trial to compare arthroscopic partial meniscectomy vs standardized physical therapy by using high-quality methodology such as careful sample-size calculation, balancing the groups according to known prognostic factors with block randomization, and intention-to-treat analysis. Moreover, the outcome measures were obtained from validated self-reporting questionnaires (WOMAC for function and KOOS for pain), reducing the possibility of observer bias.19 In addition, analyses were performed with the analysts blinded to the randomization assignment.
Limitations of the trial
A few limitations of the study are worth noting.
Patients age 45 or older with both symptomatic meniscal tear and osteoarthritis were the target population of this study. However, it is important to distinguish between the study population and the target population in a physician’s practice.
The investigators adopted broad definitions of osteoarthritis and symptoms of meniscal tear. Twenty-one percent of participants had normal findings on plain radiography, with cartilage defects visible only on MRI. Further, episodic pain or acute pain localized to a joint line was regarded as a symptom consistent with a torn meniscus.
In practice, arthroscopic partial meniscectomy is usually considered when a patient with a long history of tolerable osteoarthritis presents with a sudden onset of intolerable pain after a squatting or twisting injury.
In addition, the study population was predominantly white (85%), and the study was performed in tertiary referral academic medical centers. Therefore, the outcomes achieved with surgery or physical therapy may not translate to the community setting. Clinicians must be careful to account for these types of differences in extrapolating to patients in their own practice.
Potential enrollment bias
Although randomization is a rigorous method that eliminates selection bias in assigning individuals to study and control groups, selective enrollment could have created bias.1 As the authors mentioned, only 26% of eligible patients were enrolled, possibly reflecting patients’ or surgeons’ strong preferences for one treatment or the other. Because the study and control groups were hardly random samples of eligible populations, we must be careful in generalizing the efficacy of physical therapy.1
Crossover may have obscured the benefit of surgery
During the first 6 months, 30% of patients crossed over from physical therapy to surgery. High crossover rates in surgical trials are common, especially when comparing surgery with medical therapy.23 Given that most of the patients assigned to only physical therapy who crossed over to surgery did not have substantial improvement in functional status, it seems that crossover occurred by nonrandom factors, potentially biasing the study results. With the high degree of crossover from the nonoperative group to the surgical group, intention-to-treat analysis may have given an inflated estimate of the effect of physical therapy.
To account for crossovers, researchers defined a binary outcome a priori: patients were considered to have had a successful treatment response if they improved by at least 8 points on the WOMAC scale (a clinically important difference) and did not cross over from their assigned treatment. At 6 months, 67.1% of patients assigned to surgery showed a successful treatment response, compared with 43.8% of patients assigned to physical therapy alone (P = .001).1
In patients who crossed over, the last scores before crossover were carried over, and primary analysis of the WOMAC score at 6 months was repeated to estimate the effect of crossovers from the nonoperative to the surgery group. This exploratory analysis showed a 13.0-point improvement in WOMAC score at 6 months with physical therapy alone vs a 20.9-point improvement with surgery, suggesting that the similarity in outcomes between the two groups may be explained in part by additional improvements from surgery for those who crossed over from physical therapy alone.1
Implications for functional improvement
Lacking a comparison group that underwent a sham surgical procedure, one cannot conclude that surgery after crossover improved functional status in those patients. However, there was no significant difference in WOMAC physical function scores at 12 months between the 30% of patients in the physical therapy group who crossed over and underwent surgery during the first 6 months and patients initially assigned to surgery. This finding suggests that physical therapy can be recommended as a first-line therapy, although we must be cautious, given that the physical therapy group required more background therapy (eg, intra-articular glucocorticoid injections), and that this study was not powered to detect such differences at 12 months.
Also, a patient may need to get better quickly, to get back to work, for example. Although the data were not definitive, at 3 months the patients in the surgery group seemed to have better pain control and function than those in the physical therapy group. A cost-benefit analysis of physical therapy compared with surgery for short-term outcomes may be helpful before generalizing these findings.
SURGERY VS SHAM PROCEDURE: THE FIDELITY GROUP RESULTS
In a later publication from the Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group,24 146 patients with symptoms consistent with degenerative meniscal tear but no knee osteoarthritis were randomized to undergo arthroscopic partial meniscectomy or a sham procedure. At 12 months, no differences were noted between the groups in terms of change of symptoms from baseline to 12 months.
The authors concluded that the outcomes with meniscectomy were no better than with a sham procedure.24
SURGERY FIRST, OR PHYSICAL THERAPY FIRST?
The use of knee arthroscopy has increased sharply in middle-aged patients in recent years. Indeed, this demographic group accounts for nearly half of the knee arthroscopic procedures performed for meniscal tears, although the increase may be due in part to issues with surgeons’ coding and insurance authorization.16
The METEOR trial showed that a structured physical therapy program can be as effective as surgery as a first-line therapy in many patients with symptomatic meniscal tears and mild to moderate osteoarthritis. These results should inform clinical practice in that most such patients need not be immediately referred for surgical intervention.
However, a subset of these patients may benefit from surgery rather than nonoperative therapy. Given the potential risks and public health implications of arthroscopic surgery for meniscal tears, further study is needed to better characterize these patients. A randomized sham-controlled trial is under way25 with the goal of assessing the efficacy of arthroscopic partial meniscectomy for medial meniscus tears in patients with or without knee osteoarthritis, and it is hoped this study will shed further light on this issue.
Based on the results of the METEOR trial, the physical therapy regimen that was used may be reasonable before referring patients with knee osteoarthritis and symptomatic meniscal tears for surgery.
References
Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med2013; 368:1675–1684.
Englund M, Guermazi A, Gale D, et al. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med2008; 359:1108–115.
Englund M, Guermazi A, Lohmander SL. The role of the meniscus in knee osteoarthritis: a cause or consequence?Radiol Clin North Am2009; 47:703–712.
Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med2002; 347:81–68.
Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med2008; 359:1097–1107.
Quintana JM, Escobar A, Arostegui I, et al. Prevalence of symptoms of knee or hip joints in older adults from the general population. Aging Clin Exp Res2008; 20:329–336.
Lawrence RC, Felson DT, Helmick CG, et al; National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum2008; 58:26–35.
Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum2012; 64:1697–1707.
Englund M, Lohmander LS. Risk factors for symptomatic knee osteoarthritis fifteen to twenty-two years after meniscectomy. Arthritis Rheum2004; 50:2811–2819.
Papalia R, Del Buono A, Osti L, Denaro V, Maffulli N. Meniscectomy as a risk factor for knee osteoarthritis: a systematic review. Br Med Bull2011; 99:89–106.
Englund M, Guermazi A, Roemer FW, et al. Meniscal tear in knees without surgery and the development of radiographic osteoarthritis among middle-aged and elderly persons: The Multicenter Osteoarthritis Study. Arthritis Rheum2009; 60:831–839.
Poehling GG, Ruch DS, Chabon SJ. The landscape of meniscal injuries. Clin Sports Med1990; 9:539–549.
Bhattacharyya T, Gale D, Dewire P, et al. The clinical importance of meniscal tears demonstrated by magnetic resonance imaging in osteoarthritis of the knee. J Bone Joint Surg Am2003; 85-A:4–9.
Sowers M, Karvonen-Gutierrez CA, Jacobson JA, Jiang Y, Yosef M. Associations of anatomical measures from MRI with radiographically defined knee osteoarthritis score, pain, and physical functioning. J Bone Joint Surg Am2011; 93:241–251.
Ding C, Martel-Pelletier J, Pelletier JP, et al. Meniscal tear as an osteoarthritis risk factor in a largely non-osteoarthritic cohort: a cross-sectional study. J Rheumatol2007; 34:776–784.
Kim S, Bosque J, Meehan JP, Jamali A, Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am2011; 93:994–1000.
Herrlin S, Hållander M, Wange P, Weidenhielm L, Werner S. Arthroscopic or conservative treatment of degenerative medial meniscal tears: a prospective randomised trial. Knee Surg Sports Traumatol Arthrosc2007; 15:393–401.
Herrlin SV, Wange PO, Lapidus G, Hållander M, Werner S, Weidenhielm L. Is arthroscopic surgery beneficial in treating non-traumatic, degenerative medial meniscal tears? A five year follow-up. Knee Surg Sports Traumatol Arthrosc2013; 21:358–364.
Katz JN, Chaisson CE, Cole B, et al. The MeTeOR trial (Meniscal Tear in Osteoarthritis Research): rationale and design features. Contemp Clin Trials2012; 33:1189–1196.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol1988; 15:1833–1840.
Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes2003; 1:64.
Solomon MJ, McLeod RS. Should we be performing more randomized controlled trials evaluating surgical operations?Surgery1995; 118:459–467.
Farrokhyar F, Karanicolas PJ, Thoma A, et al. Randomized controlled trials of surgical interventions. Ann Surg2010; 251:409–416.
Sihvonen R, Paavola M, Malmivaara A. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med2013; 369:2515–2524.
Hare KB, Lohmander LS, Christensen R, Roos EM. Arthroscopic partial meniscectomy in middle-aged patients with mild or no knee osteoarthritis: a protocol for a double-blind, randomized sham-controlled multicentre trial. BMC Musculoskelet Disord2013; 14:71.
Yong Gil Hwang, MD Assistant Professor of Medicine, Division of Rheumatology, Department of Medicine, University of Pittsburgh, PA
C. Kent Kwoh, MD Professor of Medicine and Medical Imaging, The Charles A. L. and Suzanne M. Stephens Chair of Rheumatology; Chief, Division of Rheumatology; and Director, University of Arizona Arthritis Center, Department of Medicine, University of Arizona, Tucson; Member, Treatment Guidelines Committee, Osteoarthritis Research Society International
Address: C. Kent Kwoh, MD, The University of Arizona Arthritis Center, 1501 North Campbell Avenue, PO Box 245093, Tucson, AZ 85724-5093; e-mail: kwoh@arthritis.arizona.edu
Yong Gil Hwang, MD Assistant Professor of Medicine, Division of Rheumatology, Department of Medicine, University of Pittsburgh, PA
C. Kent Kwoh, MD Professor of Medicine and Medical Imaging, The Charles A. L. and Suzanne M. Stephens Chair of Rheumatology; Chief, Division of Rheumatology; and Director, University of Arizona Arthritis Center, Department of Medicine, University of Arizona, Tucson; Member, Treatment Guidelines Committee, Osteoarthritis Research Society International
Address: C. Kent Kwoh, MD, The University of Arizona Arthritis Center, 1501 North Campbell Avenue, PO Box 245093, Tucson, AZ 85724-5093; e-mail: kwoh@arthritis.arizona.edu
Author and Disclosure Information
Yong Gil Hwang, MD Assistant Professor of Medicine, Division of Rheumatology, Department of Medicine, University of Pittsburgh, PA
C. Kent Kwoh, MD Professor of Medicine and Medical Imaging, The Charles A. L. and Suzanne M. Stephens Chair of Rheumatology; Chief, Division of Rheumatology; and Director, University of Arizona Arthritis Center, Department of Medicine, University of Arizona, Tucson; Member, Treatment Guidelines Committee, Osteoarthritis Research Society International
Address: C. Kent Kwoh, MD, The University of Arizona Arthritis Center, 1501 North Campbell Avenue, PO Box 245093, Tucson, AZ 85724-5093; e-mail: kwoh@arthritis.arizona.edu
Many patients who have osteoarthritis of the knee and a torn meniscus can defer having the meniscus repaired and undergo physical therapy instead. If a trial of physical therapy does not help, they can opt for surgery later.
This seems to be the take-home message from the recent Meniscal Tear in Osteoarthritis Research (METEOR) trial,1 which compared the efficacy of arthroscopic partial meniscectomy plus physical therapy vs physical therapy alone for patients with knee symptoms, a meniscal tear, and mild to moderate osteoarthritis of the knee.1
In brief, patients improved to a roughly similar degree with either approach, and although many patients assigned to physical therapy eventually underwent surgery anyway by 6 months, the delay did not adversely affect outcomes.
In this article, we review the background, design, and findings of the METEOR trial, and their implications for clinical practice.
SURGERY: HIGH VOLUME, BUT LITTLE EVIDENCE
Magnetic resonance imaging (MRI) often incidentally reveals meniscal lesions in middle-aged and older patients who have osteoarthritis and knee pain.2 Should these patients undergo arthroscopic meniscal repair? The decision is difficult, since it is hard to distinguish the symptoms of a meniscal tear from those of osteoarthritis.3
Current evidence suggests that, for symptomatic knee osteoarthritis by itself, arthroscopic surgery is no more effective than conservative management.4,5 But what about surgery for a torn meniscus in addition to osteoarthritis?
Osteoarthritis is the most common joint disease, accounting for many physician visits.6 More than 26 million Americans over age 25 have some form of it, and the prevalence of symptomatic, radiographically confirmed osteoarthritis of the knee was 12.1% in the third National Health and Nutrition Examination Survey.7
We used to consider osteoarthritis a “wear-and-tear” disease—thus the term “degenerative joint disease.” But today, we know that it is an active response to injury, involving inflammatory and metabolic pathways.8 Moreover, the risk of osteoarthritis and its progression seems to be higher in those who have had meniscal injury and total or arthroscopic partial meniscectomy.9,10
MRI is not commonly used in managing knee osteoarthritis, but it has been used diagnostically in patients with symptoms of a meniscal tear, such as clicking, locking, popping, giving way, and pain with pivoting or twisting. Traumatic meniscal tears (a longitudinal or radial tear pattern) most often occur in active younger people and often lead to meniscal surgery.11,12 In contrast, degenerative meniscal tears (horizontal, oblique, or complex tear pattern or meniscal maceration) tend to occur in older people,11,12 but how to manage them is not widely agreed upon.
Of note, most patients with osteoarthritis of the knee have torn, macerated, or heavily damaged menisci.13,14 Meniscal lesions are also common in middle-aged people in the general population, with a higher prevalence in people who are older, heavier, or female, or who have a family history of osteoarthritis.15
These abnormalities are only weakly associated with symptoms.2 However, when a patient has knee symptoms and a torn meniscus is detected on MRI, the tear is often assumed to be the source of the symptoms, and meniscal tears are the most common reason for arthroscopy.16
Since we have no way to prevent the progression of joint damage from osteoarthritis with drugs or by any other means, the goal is to alleviate the symptoms. Many patients report pain relief or functional improvement after arthroscopic surgery. But arthroscopic lavage or debridement for osteoarthritis has not been found to be better than conservative treatment or placebo in randomized controlled trials.4,5
In contrast, the current standard treatment for a symptomatic degenerative meniscal tear is arthroscopic partial meniscectomy. Nearly 500,000 of these procedures are performed annually in the United States.16 But based on the best evidence, arthroscopic partial meniscectomy does not result in better pain relief and functional improvement than does physical therapy alone in patients who have a torn meniscus and knee osteoarthritis.17,18
OVERVIEW OF THE METEOR TRIAL
The METEOR trial was a randomized controlled trial conducted at seven US tertiary referral centers. Its aim was to compare the short-term (6-month) and long-term (12-month) efficacy of arthroscopic partial meniscectomy and physical therapy in patients with symptomatic meniscal tear and osteoarthritis of the knee.19 It was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases.1
Patients were age 45 and older
METEOR patients had to be at least 45 years old and have symptomatic meniscal tears and knee osteoarthritis detected on MRI or radiography.1
Osteoarthritis was defined broadly, given that it begins well before the appearance of radiographic evidence such as an osteophyte or joint-space narrowing.19 Patients with cartilage defects on MRI were also enrolled, as were patients with radiographically documented osteoarthritis.19
Patients were considered to have a symptomatic meniscal tear if they had had at least 4 weeks of symptoms (such as episodic pain and pain that was acute and localized to one spot on the knee, as well as typical mechanical pain suggesting a meniscal tear, such as clicking, catching, popping, giving way, or pain with pivoting or twisting) in addition to evidence of a meniscal tear on MRI.19
Patients were excluded if they had a chronically locked knee (a clear-cut indication for arthroscopic partial meniscectomy), advanced osteoarthritis (Kellgren-Lawrence grade 4), inflammatory arthritis, clinically symptomatic chondrocalcinosis, or bilateral symptomatic meniscal tears.19 Patients who had undergone surgery or injection of a viscosupplement in the index knee during the past 4 weeks were also excluded.19
Of 1,330 eligible patients, 351 (26.4%) were enrolled and randomly assigned in a 1:1 ratio to a treatment group by means of a secure program on the trial website.1,19 Of those who were eligible but did not enroll, 195 (14.6%) were not referred and 784 (58.9%) declined to participate. Of those who declined, more preferred surgery than physical therapy (36.1% vs 21%). No information is available on any differences in baseline characteristics between the enrolled patients and the eligible patients who declined.
Randomization was done in blocks of varying size within each site, stratified according to sex and the extent of osteoarthritis on baseline radiography. The extent of osteoarthritis was categorized either as Kellgren-Lawrence grade 0 (normal, no features of osteoarthritis) to grade 2 (definite osteoarthritis, a definite osteophyte without joint-space narrowing) or as Kellgren-Lawrence grade 3 (moderate osteoarthritis, < 50% joint-space narrowing).1,19 The two treatment groups were similar with respect to age, sex, race or ethnicity, baseline Kellgren-Lawrence grade, and baseline Western Ontario and McMaster Universities Arthritis Index (WOMAC) physical function score.1
The mean age of the participants was 58, and 85% were white. Sixty-three percent had Kellgren-Lawrence grade 0 to 2 osteoarthritis, and 27% had grade 3.1
Surgery plus physical therapy vs physical therapy alone
The surgery group underwent arthroscopic partial meniscectomy, which involved trimming the damaged meniscus back to a stable rim1,19 and trimming loose fragments of cartilage and bone.
After the procedure, patients were scheduled for physical therapy. Although there is no consensus on the need for or the effectiveness of postoperative physical therapy in this setting, the investigators believed that including it in both study groups would help to isolate the independent effects of surgery. The physical therapy regimen after surgery was similar to that provided in the nonoperative group.1,19
Physical therapy was designed to address inflammation, range of motion, muscle strength, muscle-length restriction, functional mobility, and proprioception and balance.1,19 There were three stages; criteria for advancing from one phase to the next included the level of self-reported pain, observed strength, range of knee motion, knee effusion, and functional mobility.1,18
The duration of participation varied depending on the pace of improvement. Generally, the program lasted about 6 weeks.1,19
Crossover and other therapies were allowed
Crossover from physical therapy alone to surgery was allowed during the trial if the patient and surgeon thought it was clinically indicated.
Participants in both groups were permitted to take acetaminophen and nonsteroidal anti-inflammatory drugs as needed. Intra-articular injections of glucocorticoids were also allowed during the trial.
OUTCOMES MEASURED
WOMAC physical function score
The primary outcome of the METEOR trial was the difference between the study groups in the change in WOMAC physical function score from baseline to 6 months, at which point participants were expected to have achieved maximum improvement.1,19 Questionnaires were also administered at 3 months to assess the early response to surgery or physical therapy and again at 12 months.
The complete WOMAC also measures pain and stiffness in addition to physical function, with separate subscales for each. The change in WOMAC score is one of the most widely endorsed outcome measures in assessing interventions in osteoarthritis or other conditions of the lower extremities.20 The METEOR trial authors considered the WOMAC scale to be highly valid and reliable, with a Cronbach alpha value of 0.97 (maximum value = 1; the higher the better).
No ceiling or floor effects were observed in the WOMAC physical function score in patients with osteoarthritis and a meniscal tear in a pilot study for METEOR.19
In the main METEOR study, WOMAC physical function was scored on a scale of 0 to 100, with a higher score indicating worse physical function.1 Changes in the score were also measured as a yes-or-no question, defined a priori as whether the score declined by at least 8 points, which is considered the minimal clinically important difference in osteoarthritis patients.1,19
KOOS and MOS SF-36 scores
Secondary outcomes were measured in several domains, including pain, generic functional status, quality of life, and health care utilization.1,19
The KOOS (Knee Injury and OA Outcome Scale) is specific for knee pain, being designed to evaluate short-term and long-term symptoms and function in patients with knee injury and associated problems.21 It has five subscales, which are scored separately: pain, other symptoms, activities of daily living, sport and recreation, and knee-related quality of life.21 Since the WOMAC pain scale showed a ceiling effect in the pilot study in patients undergoing surgery, the authors chose the KOOS pain scale as a pain measure.19 Scores were transformed to a 0–100 scale, with a higher score indicating more pain.1
The MOS SF-36 (Medical Outcomes Study 36-item short form) was used to measure general health status and function.1,19
STATISTICAL ANALYSIS: INTENTION-TO-TREAT AND AS-TREATED
The study was powered to detect a 10-point difference in WOMAC physical function scores at 6 months of follow-up between the operative and nonoperative groups, anticipating losses to follow-up and crossover, with preplanned subgroup (Kellgren–Lawrence grade 0–2 vs grade 3) analysis.1,19
The primary analysis used a modified intention-to-treat approach and was implemented with an analysis of covariance with changes in the WOMAC score from baseline to 6 months as the dependent variable, treatment as the independent variable of interest, and study site as a covariate. Other covariates, such as age, sex, and baseline Kellgren-Lawrence grade, were balanced across groups and were therefore not included in the analysis.1,19
Secondary analyses used an “as-treated” approach, ie, according to the treatment actually received.1,19 Secondary intention-to-treat analysis—using binary outcome measures in which treatment failure was defined as improvement in the WOMAC score of less than 8 points or crossing over to the other treatment—was also performed to estimate efficacy at the level of the patient rather than at the group level.1,19
BOTH GROUPS IMPROVED
In the intention-to-treat analyses at 6 months and 12 months after randomization, both groups improved, with no clinically important or statistically significant differences between the groups in functional status (WOMAC score, MOS SF-36 score) or pain (KOOS score).1 The mean improvement (decline) in the WOMAC score from baseline to 6 months was 20.9 points in the surgery group vs 18.5 points in the physical therapy group, a difference of 2.4 points (95% confidence interval [CI], −1.8 to 6.5).1
35% of physical therapy patients underwent surgery by 12 months
Of the 177 patients randomized to physical therapy alone, by 6 months 1 had died, 1 had undergone total knee replacement, 4 had withdrawn, and 2 were lost to follow-up. Of the 169 remaining, 51 (30%) had undergone arthroscopic partial meniscectomy. An additional 8 patients who were assigned to physical therapy crossed over to surgery between 6 and 12 months.1,19
Of the 174 patients randomized to surgery, by 6 months 1 had died, 3 had undergone total knee replacement, 7 had withdrawn, and 2 were ineligible. Of the 161 remaining, 9 (6%) had not undergone the procedure.
Other outcomes
Subgroup analysis based on the baseline radiographic grade (Kellgren-Lawrence grade 0 to 2 vs grade 3) did not show a difference between groups in functional improvement at 6 months (P = .13 for interaction).1
No statistically significant difference was noted in rates of overall or specific adverse events between the two groups over the first 12 months.1 Adverse events rated as mild or moderate in severity occurred in 15 participants in the surgery group and 13 participants in the physical therapy group.1 Long-term risks associated with these interventions are being assessed, and longitudinal assessment of imaging studies is planned to address this question but is not yet available.1,18
In the physical therapy group, 21 patients (12%) received intra-articular glucocorticoid injections, as did 9 patients (6%) in the surgery group.1,19
TRANSLATING THE METEOR RESULTS TO EVERYDAY PRACTICE
There are many challenges in designing surgical trials. Indeed, by one estimate,22 only about 40% of treatment questions involving surgical procedures can be evaluated by a randomized controlled trial.
Although the METEOR trial was not blinded, it was the first large, multicenter, randomized controlled trial to compare arthroscopic partial meniscectomy vs standardized physical therapy by using high-quality methodology such as careful sample-size calculation, balancing the groups according to known prognostic factors with block randomization, and intention-to-treat analysis. Moreover, the outcome measures were obtained from validated self-reporting questionnaires (WOMAC for function and KOOS for pain), reducing the possibility of observer bias.19 In addition, analyses were performed with the analysts blinded to the randomization assignment.
Limitations of the trial
A few limitations of the study are worth noting.
Patients age 45 or older with both symptomatic meniscal tear and osteoarthritis were the target population of this study. However, it is important to distinguish between the study population and the target population in a physician’s practice.
The investigators adopted broad definitions of osteoarthritis and symptoms of meniscal tear. Twenty-one percent of participants had normal findings on plain radiography, with cartilage defects visible only on MRI. Further, episodic pain or acute pain localized to a joint line was regarded as a symptom consistent with a torn meniscus.
In practice, arthroscopic partial meniscectomy is usually considered when a patient with a long history of tolerable osteoarthritis presents with a sudden onset of intolerable pain after a squatting or twisting injury.
In addition, the study population was predominantly white (85%), and the study was performed in tertiary referral academic medical centers. Therefore, the outcomes achieved with surgery or physical therapy may not translate to the community setting. Clinicians must be careful to account for these types of differences in extrapolating to patients in their own practice.
Potential enrollment bias
Although randomization is a rigorous method that eliminates selection bias in assigning individuals to study and control groups, selective enrollment could have created bias.1 As the authors mentioned, only 26% of eligible patients were enrolled, possibly reflecting patients’ or surgeons’ strong preferences for one treatment or the other. Because the study and control groups were hardly random samples of eligible populations, we must be careful in generalizing the efficacy of physical therapy.1
Crossover may have obscured the benefit of surgery
During the first 6 months, 30% of patients crossed over from physical therapy to surgery. High crossover rates in surgical trials are common, especially when comparing surgery with medical therapy.23 Given that most of the patients assigned to only physical therapy who crossed over to surgery did not have substantial improvement in functional status, it seems that crossover occurred by nonrandom factors, potentially biasing the study results. With the high degree of crossover from the nonoperative group to the surgical group, intention-to-treat analysis may have given an inflated estimate of the effect of physical therapy.
To account for crossovers, researchers defined a binary outcome a priori: patients were considered to have had a successful treatment response if they improved by at least 8 points on the WOMAC scale (a clinically important difference) and did not cross over from their assigned treatment. At 6 months, 67.1% of patients assigned to surgery showed a successful treatment response, compared with 43.8% of patients assigned to physical therapy alone (P = .001).1
In patients who crossed over, the last scores before crossover were carried over, and primary analysis of the WOMAC score at 6 months was repeated to estimate the effect of crossovers from the nonoperative to the surgery group. This exploratory analysis showed a 13.0-point improvement in WOMAC score at 6 months with physical therapy alone vs a 20.9-point improvement with surgery, suggesting that the similarity in outcomes between the two groups may be explained in part by additional improvements from surgery for those who crossed over from physical therapy alone.1
Implications for functional improvement
Lacking a comparison group that underwent a sham surgical procedure, one cannot conclude that surgery after crossover improved functional status in those patients. However, there was no significant difference in WOMAC physical function scores at 12 months between the 30% of patients in the physical therapy group who crossed over and underwent surgery during the first 6 months and patients initially assigned to surgery. This finding suggests that physical therapy can be recommended as a first-line therapy, although we must be cautious, given that the physical therapy group required more background therapy (eg, intra-articular glucocorticoid injections), and that this study was not powered to detect such differences at 12 months.
Also, a patient may need to get better quickly, to get back to work, for example. Although the data were not definitive, at 3 months the patients in the surgery group seemed to have better pain control and function than those in the physical therapy group. A cost-benefit analysis of physical therapy compared with surgery for short-term outcomes may be helpful before generalizing these findings.
SURGERY VS SHAM PROCEDURE: THE FIDELITY GROUP RESULTS
In a later publication from the Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group,24 146 patients with symptoms consistent with degenerative meniscal tear but no knee osteoarthritis were randomized to undergo arthroscopic partial meniscectomy or a sham procedure. At 12 months, no differences were noted between the groups in terms of change of symptoms from baseline to 12 months.
The authors concluded that the outcomes with meniscectomy were no better than with a sham procedure.24
SURGERY FIRST, OR PHYSICAL THERAPY FIRST?
The use of knee arthroscopy has increased sharply in middle-aged patients in recent years. Indeed, this demographic group accounts for nearly half of the knee arthroscopic procedures performed for meniscal tears, although the increase may be due in part to issues with surgeons’ coding and insurance authorization.16
The METEOR trial showed that a structured physical therapy program can be as effective as surgery as a first-line therapy in many patients with symptomatic meniscal tears and mild to moderate osteoarthritis. These results should inform clinical practice in that most such patients need not be immediately referred for surgical intervention.
However, a subset of these patients may benefit from surgery rather than nonoperative therapy. Given the potential risks and public health implications of arthroscopic surgery for meniscal tears, further study is needed to better characterize these patients. A randomized sham-controlled trial is under way25 with the goal of assessing the efficacy of arthroscopic partial meniscectomy for medial meniscus tears in patients with or without knee osteoarthritis, and it is hoped this study will shed further light on this issue.
Based on the results of the METEOR trial, the physical therapy regimen that was used may be reasonable before referring patients with knee osteoarthritis and symptomatic meniscal tears for surgery.
Many patients who have osteoarthritis of the knee and a torn meniscus can defer having the meniscus repaired and undergo physical therapy instead. If a trial of physical therapy does not help, they can opt for surgery later.
This seems to be the take-home message from the recent Meniscal Tear in Osteoarthritis Research (METEOR) trial,1 which compared the efficacy of arthroscopic partial meniscectomy plus physical therapy vs physical therapy alone for patients with knee symptoms, a meniscal tear, and mild to moderate osteoarthritis of the knee.1
In brief, patients improved to a roughly similar degree with either approach, and although many patients assigned to physical therapy eventually underwent surgery anyway by 6 months, the delay did not adversely affect outcomes.
In this article, we review the background, design, and findings of the METEOR trial, and their implications for clinical practice.
SURGERY: HIGH VOLUME, BUT LITTLE EVIDENCE
Magnetic resonance imaging (MRI) often incidentally reveals meniscal lesions in middle-aged and older patients who have osteoarthritis and knee pain.2 Should these patients undergo arthroscopic meniscal repair? The decision is difficult, since it is hard to distinguish the symptoms of a meniscal tear from those of osteoarthritis.3
Current evidence suggests that, for symptomatic knee osteoarthritis by itself, arthroscopic surgery is no more effective than conservative management.4,5 But what about surgery for a torn meniscus in addition to osteoarthritis?
Osteoarthritis is the most common joint disease, accounting for many physician visits.6 More than 26 million Americans over age 25 have some form of it, and the prevalence of symptomatic, radiographically confirmed osteoarthritis of the knee was 12.1% in the third National Health and Nutrition Examination Survey.7
We used to consider osteoarthritis a “wear-and-tear” disease—thus the term “degenerative joint disease.” But today, we know that it is an active response to injury, involving inflammatory and metabolic pathways.8 Moreover, the risk of osteoarthritis and its progression seems to be higher in those who have had meniscal injury and total or arthroscopic partial meniscectomy.9,10
MRI is not commonly used in managing knee osteoarthritis, but it has been used diagnostically in patients with symptoms of a meniscal tear, such as clicking, locking, popping, giving way, and pain with pivoting or twisting. Traumatic meniscal tears (a longitudinal or radial tear pattern) most often occur in active younger people and often lead to meniscal surgery.11,12 In contrast, degenerative meniscal tears (horizontal, oblique, or complex tear pattern or meniscal maceration) tend to occur in older people,11,12 but how to manage them is not widely agreed upon.
Of note, most patients with osteoarthritis of the knee have torn, macerated, or heavily damaged menisci.13,14 Meniscal lesions are also common in middle-aged people in the general population, with a higher prevalence in people who are older, heavier, or female, or who have a family history of osteoarthritis.15
These abnormalities are only weakly associated with symptoms.2 However, when a patient has knee symptoms and a torn meniscus is detected on MRI, the tear is often assumed to be the source of the symptoms, and meniscal tears are the most common reason for arthroscopy.16
Since we have no way to prevent the progression of joint damage from osteoarthritis with drugs or by any other means, the goal is to alleviate the symptoms. Many patients report pain relief or functional improvement after arthroscopic surgery. But arthroscopic lavage or debridement for osteoarthritis has not been found to be better than conservative treatment or placebo in randomized controlled trials.4,5
In contrast, the current standard treatment for a symptomatic degenerative meniscal tear is arthroscopic partial meniscectomy. Nearly 500,000 of these procedures are performed annually in the United States.16 But based on the best evidence, arthroscopic partial meniscectomy does not result in better pain relief and functional improvement than does physical therapy alone in patients who have a torn meniscus and knee osteoarthritis.17,18
OVERVIEW OF THE METEOR TRIAL
The METEOR trial was a randomized controlled trial conducted at seven US tertiary referral centers. Its aim was to compare the short-term (6-month) and long-term (12-month) efficacy of arthroscopic partial meniscectomy and physical therapy in patients with symptomatic meniscal tear and osteoarthritis of the knee.19 It was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases.1
Patients were age 45 and older
METEOR patients had to be at least 45 years old and have symptomatic meniscal tears and knee osteoarthritis detected on MRI or radiography.1
Osteoarthritis was defined broadly, given that it begins well before the appearance of radiographic evidence such as an osteophyte or joint-space narrowing.19 Patients with cartilage defects on MRI were also enrolled, as were patients with radiographically documented osteoarthritis.19
Patients were considered to have a symptomatic meniscal tear if they had had at least 4 weeks of symptoms (such as episodic pain and pain that was acute and localized to one spot on the knee, as well as typical mechanical pain suggesting a meniscal tear, such as clicking, catching, popping, giving way, or pain with pivoting or twisting) in addition to evidence of a meniscal tear on MRI.19
Patients were excluded if they had a chronically locked knee (a clear-cut indication for arthroscopic partial meniscectomy), advanced osteoarthritis (Kellgren-Lawrence grade 4), inflammatory arthritis, clinically symptomatic chondrocalcinosis, or bilateral symptomatic meniscal tears.19 Patients who had undergone surgery or injection of a viscosupplement in the index knee during the past 4 weeks were also excluded.19
Of 1,330 eligible patients, 351 (26.4%) were enrolled and randomly assigned in a 1:1 ratio to a treatment group by means of a secure program on the trial website.1,19 Of those who were eligible but did not enroll, 195 (14.6%) were not referred and 784 (58.9%) declined to participate. Of those who declined, more preferred surgery than physical therapy (36.1% vs 21%). No information is available on any differences in baseline characteristics between the enrolled patients and the eligible patients who declined.
Randomization was done in blocks of varying size within each site, stratified according to sex and the extent of osteoarthritis on baseline radiography. The extent of osteoarthritis was categorized either as Kellgren-Lawrence grade 0 (normal, no features of osteoarthritis) to grade 2 (definite osteoarthritis, a definite osteophyte without joint-space narrowing) or as Kellgren-Lawrence grade 3 (moderate osteoarthritis, < 50% joint-space narrowing).1,19 The two treatment groups were similar with respect to age, sex, race or ethnicity, baseline Kellgren-Lawrence grade, and baseline Western Ontario and McMaster Universities Arthritis Index (WOMAC) physical function score.1
The mean age of the participants was 58, and 85% were white. Sixty-three percent had Kellgren-Lawrence grade 0 to 2 osteoarthritis, and 27% had grade 3.1
Surgery plus physical therapy vs physical therapy alone
The surgery group underwent arthroscopic partial meniscectomy, which involved trimming the damaged meniscus back to a stable rim1,19 and trimming loose fragments of cartilage and bone.
After the procedure, patients were scheduled for physical therapy. Although there is no consensus on the need for or the effectiveness of postoperative physical therapy in this setting, the investigators believed that including it in both study groups would help to isolate the independent effects of surgery. The physical therapy regimen after surgery was similar to that provided in the nonoperative group.1,19
Physical therapy was designed to address inflammation, range of motion, muscle strength, muscle-length restriction, functional mobility, and proprioception and balance.1,19 There were three stages; criteria for advancing from one phase to the next included the level of self-reported pain, observed strength, range of knee motion, knee effusion, and functional mobility.1,18
The duration of participation varied depending on the pace of improvement. Generally, the program lasted about 6 weeks.1,19
Crossover and other therapies were allowed
Crossover from physical therapy alone to surgery was allowed during the trial if the patient and surgeon thought it was clinically indicated.
Participants in both groups were permitted to take acetaminophen and nonsteroidal anti-inflammatory drugs as needed. Intra-articular injections of glucocorticoids were also allowed during the trial.
OUTCOMES MEASURED
WOMAC physical function score
The primary outcome of the METEOR trial was the difference between the study groups in the change in WOMAC physical function score from baseline to 6 months, at which point participants were expected to have achieved maximum improvement.1,19 Questionnaires were also administered at 3 months to assess the early response to surgery or physical therapy and again at 12 months.
The complete WOMAC also measures pain and stiffness in addition to physical function, with separate subscales for each. The change in WOMAC score is one of the most widely endorsed outcome measures in assessing interventions in osteoarthritis or other conditions of the lower extremities.20 The METEOR trial authors considered the WOMAC scale to be highly valid and reliable, with a Cronbach alpha value of 0.97 (maximum value = 1; the higher the better).
No ceiling or floor effects were observed in the WOMAC physical function score in patients with osteoarthritis and a meniscal tear in a pilot study for METEOR.19
In the main METEOR study, WOMAC physical function was scored on a scale of 0 to 100, with a higher score indicating worse physical function.1 Changes in the score were also measured as a yes-or-no question, defined a priori as whether the score declined by at least 8 points, which is considered the minimal clinically important difference in osteoarthritis patients.1,19
KOOS and MOS SF-36 scores
Secondary outcomes were measured in several domains, including pain, generic functional status, quality of life, and health care utilization.1,19
The KOOS (Knee Injury and OA Outcome Scale) is specific for knee pain, being designed to evaluate short-term and long-term symptoms and function in patients with knee injury and associated problems.21 It has five subscales, which are scored separately: pain, other symptoms, activities of daily living, sport and recreation, and knee-related quality of life.21 Since the WOMAC pain scale showed a ceiling effect in the pilot study in patients undergoing surgery, the authors chose the KOOS pain scale as a pain measure.19 Scores were transformed to a 0–100 scale, with a higher score indicating more pain.1
The MOS SF-36 (Medical Outcomes Study 36-item short form) was used to measure general health status and function.1,19
STATISTICAL ANALYSIS: INTENTION-TO-TREAT AND AS-TREATED
The study was powered to detect a 10-point difference in WOMAC physical function scores at 6 months of follow-up between the operative and nonoperative groups, anticipating losses to follow-up and crossover, with preplanned subgroup (Kellgren–Lawrence grade 0–2 vs grade 3) analysis.1,19
The primary analysis used a modified intention-to-treat approach and was implemented with an analysis of covariance with changes in the WOMAC score from baseline to 6 months as the dependent variable, treatment as the independent variable of interest, and study site as a covariate. Other covariates, such as age, sex, and baseline Kellgren-Lawrence grade, were balanced across groups and were therefore not included in the analysis.1,19
Secondary analyses used an “as-treated” approach, ie, according to the treatment actually received.1,19 Secondary intention-to-treat analysis—using binary outcome measures in which treatment failure was defined as improvement in the WOMAC score of less than 8 points or crossing over to the other treatment—was also performed to estimate efficacy at the level of the patient rather than at the group level.1,19
BOTH GROUPS IMPROVED
In the intention-to-treat analyses at 6 months and 12 months after randomization, both groups improved, with no clinically important or statistically significant differences between the groups in functional status (WOMAC score, MOS SF-36 score) or pain (KOOS score).1 The mean improvement (decline) in the WOMAC score from baseline to 6 months was 20.9 points in the surgery group vs 18.5 points in the physical therapy group, a difference of 2.4 points (95% confidence interval [CI], −1.8 to 6.5).1
35% of physical therapy patients underwent surgery by 12 months
Of the 177 patients randomized to physical therapy alone, by 6 months 1 had died, 1 had undergone total knee replacement, 4 had withdrawn, and 2 were lost to follow-up. Of the 169 remaining, 51 (30%) had undergone arthroscopic partial meniscectomy. An additional 8 patients who were assigned to physical therapy crossed over to surgery between 6 and 12 months.1,19
Of the 174 patients randomized to surgery, by 6 months 1 had died, 3 had undergone total knee replacement, 7 had withdrawn, and 2 were ineligible. Of the 161 remaining, 9 (6%) had not undergone the procedure.
Other outcomes
Subgroup analysis based on the baseline radiographic grade (Kellgren-Lawrence grade 0 to 2 vs grade 3) did not show a difference between groups in functional improvement at 6 months (P = .13 for interaction).1
No statistically significant difference was noted in rates of overall or specific adverse events between the two groups over the first 12 months.1 Adverse events rated as mild or moderate in severity occurred in 15 participants in the surgery group and 13 participants in the physical therapy group.1 Long-term risks associated with these interventions are being assessed, and longitudinal assessment of imaging studies is planned to address this question but is not yet available.1,18
In the physical therapy group, 21 patients (12%) received intra-articular glucocorticoid injections, as did 9 patients (6%) in the surgery group.1,19
TRANSLATING THE METEOR RESULTS TO EVERYDAY PRACTICE
There are many challenges in designing surgical trials. Indeed, by one estimate,22 only about 40% of treatment questions involving surgical procedures can be evaluated by a randomized controlled trial.
Although the METEOR trial was not blinded, it was the first large, multicenter, randomized controlled trial to compare arthroscopic partial meniscectomy vs standardized physical therapy by using high-quality methodology such as careful sample-size calculation, balancing the groups according to known prognostic factors with block randomization, and intention-to-treat analysis. Moreover, the outcome measures were obtained from validated self-reporting questionnaires (WOMAC for function and KOOS for pain), reducing the possibility of observer bias.19 In addition, analyses were performed with the analysts blinded to the randomization assignment.
Limitations of the trial
A few limitations of the study are worth noting.
Patients age 45 or older with both symptomatic meniscal tear and osteoarthritis were the target population of this study. However, it is important to distinguish between the study population and the target population in a physician’s practice.
The investigators adopted broad definitions of osteoarthritis and symptoms of meniscal tear. Twenty-one percent of participants had normal findings on plain radiography, with cartilage defects visible only on MRI. Further, episodic pain or acute pain localized to a joint line was regarded as a symptom consistent with a torn meniscus.
In practice, arthroscopic partial meniscectomy is usually considered when a patient with a long history of tolerable osteoarthritis presents with a sudden onset of intolerable pain after a squatting or twisting injury.
In addition, the study population was predominantly white (85%), and the study was performed in tertiary referral academic medical centers. Therefore, the outcomes achieved with surgery or physical therapy may not translate to the community setting. Clinicians must be careful to account for these types of differences in extrapolating to patients in their own practice.
Potential enrollment bias
Although randomization is a rigorous method that eliminates selection bias in assigning individuals to study and control groups, selective enrollment could have created bias.1 As the authors mentioned, only 26% of eligible patients were enrolled, possibly reflecting patients’ or surgeons’ strong preferences for one treatment or the other. Because the study and control groups were hardly random samples of eligible populations, we must be careful in generalizing the efficacy of physical therapy.1
Crossover may have obscured the benefit of surgery
During the first 6 months, 30% of patients crossed over from physical therapy to surgery. High crossover rates in surgical trials are common, especially when comparing surgery with medical therapy.23 Given that most of the patients assigned to only physical therapy who crossed over to surgery did not have substantial improvement in functional status, it seems that crossover occurred by nonrandom factors, potentially biasing the study results. With the high degree of crossover from the nonoperative group to the surgical group, intention-to-treat analysis may have given an inflated estimate of the effect of physical therapy.
To account for crossovers, researchers defined a binary outcome a priori: patients were considered to have had a successful treatment response if they improved by at least 8 points on the WOMAC scale (a clinically important difference) and did not cross over from their assigned treatment. At 6 months, 67.1% of patients assigned to surgery showed a successful treatment response, compared with 43.8% of patients assigned to physical therapy alone (P = .001).1
In patients who crossed over, the last scores before crossover were carried over, and primary analysis of the WOMAC score at 6 months was repeated to estimate the effect of crossovers from the nonoperative to the surgery group. This exploratory analysis showed a 13.0-point improvement in WOMAC score at 6 months with physical therapy alone vs a 20.9-point improvement with surgery, suggesting that the similarity in outcomes between the two groups may be explained in part by additional improvements from surgery for those who crossed over from physical therapy alone.1
Implications for functional improvement
Lacking a comparison group that underwent a sham surgical procedure, one cannot conclude that surgery after crossover improved functional status in those patients. However, there was no significant difference in WOMAC physical function scores at 12 months between the 30% of patients in the physical therapy group who crossed over and underwent surgery during the first 6 months and patients initially assigned to surgery. This finding suggests that physical therapy can be recommended as a first-line therapy, although we must be cautious, given that the physical therapy group required more background therapy (eg, intra-articular glucocorticoid injections), and that this study was not powered to detect such differences at 12 months.
Also, a patient may need to get better quickly, to get back to work, for example. Although the data were not definitive, at 3 months the patients in the surgery group seemed to have better pain control and function than those in the physical therapy group. A cost-benefit analysis of physical therapy compared with surgery for short-term outcomes may be helpful before generalizing these findings.
SURGERY VS SHAM PROCEDURE: THE FIDELITY GROUP RESULTS
In a later publication from the Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group,24 146 patients with symptoms consistent with degenerative meniscal tear but no knee osteoarthritis were randomized to undergo arthroscopic partial meniscectomy or a sham procedure. At 12 months, no differences were noted between the groups in terms of change of symptoms from baseline to 12 months.
The authors concluded that the outcomes with meniscectomy were no better than with a sham procedure.24
SURGERY FIRST, OR PHYSICAL THERAPY FIRST?
The use of knee arthroscopy has increased sharply in middle-aged patients in recent years. Indeed, this demographic group accounts for nearly half of the knee arthroscopic procedures performed for meniscal tears, although the increase may be due in part to issues with surgeons’ coding and insurance authorization.16
The METEOR trial showed that a structured physical therapy program can be as effective as surgery as a first-line therapy in many patients with symptomatic meniscal tears and mild to moderate osteoarthritis. These results should inform clinical practice in that most such patients need not be immediately referred for surgical intervention.
However, a subset of these patients may benefit from surgery rather than nonoperative therapy. Given the potential risks and public health implications of arthroscopic surgery for meniscal tears, further study is needed to better characterize these patients. A randomized sham-controlled trial is under way25 with the goal of assessing the efficacy of arthroscopic partial meniscectomy for medial meniscus tears in patients with or without knee osteoarthritis, and it is hoped this study will shed further light on this issue.
Based on the results of the METEOR trial, the physical therapy regimen that was used may be reasonable before referring patients with knee osteoarthritis and symptomatic meniscal tears for surgery.
References
Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med2013; 368:1675–1684.
Englund M, Guermazi A, Gale D, et al. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med2008; 359:1108–115.
Englund M, Guermazi A, Lohmander SL. The role of the meniscus in knee osteoarthritis: a cause or consequence?Radiol Clin North Am2009; 47:703–712.
Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med2002; 347:81–68.
Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med2008; 359:1097–1107.
Quintana JM, Escobar A, Arostegui I, et al. Prevalence of symptoms of knee or hip joints in older adults from the general population. Aging Clin Exp Res2008; 20:329–336.
Lawrence RC, Felson DT, Helmick CG, et al; National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum2008; 58:26–35.
Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum2012; 64:1697–1707.
Englund M, Lohmander LS. Risk factors for symptomatic knee osteoarthritis fifteen to twenty-two years after meniscectomy. Arthritis Rheum2004; 50:2811–2819.
Papalia R, Del Buono A, Osti L, Denaro V, Maffulli N. Meniscectomy as a risk factor for knee osteoarthritis: a systematic review. Br Med Bull2011; 99:89–106.
Englund M, Guermazi A, Roemer FW, et al. Meniscal tear in knees without surgery and the development of radiographic osteoarthritis among middle-aged and elderly persons: The Multicenter Osteoarthritis Study. Arthritis Rheum2009; 60:831–839.
Poehling GG, Ruch DS, Chabon SJ. The landscape of meniscal injuries. Clin Sports Med1990; 9:539–549.
Bhattacharyya T, Gale D, Dewire P, et al. The clinical importance of meniscal tears demonstrated by magnetic resonance imaging in osteoarthritis of the knee. J Bone Joint Surg Am2003; 85-A:4–9.
Sowers M, Karvonen-Gutierrez CA, Jacobson JA, Jiang Y, Yosef M. Associations of anatomical measures from MRI with radiographically defined knee osteoarthritis score, pain, and physical functioning. J Bone Joint Surg Am2011; 93:241–251.
Ding C, Martel-Pelletier J, Pelletier JP, et al. Meniscal tear as an osteoarthritis risk factor in a largely non-osteoarthritic cohort: a cross-sectional study. J Rheumatol2007; 34:776–784.
Kim S, Bosque J, Meehan JP, Jamali A, Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am2011; 93:994–1000.
Herrlin S, Hållander M, Wange P, Weidenhielm L, Werner S. Arthroscopic or conservative treatment of degenerative medial meniscal tears: a prospective randomised trial. Knee Surg Sports Traumatol Arthrosc2007; 15:393–401.
Herrlin SV, Wange PO, Lapidus G, Hållander M, Werner S, Weidenhielm L. Is arthroscopic surgery beneficial in treating non-traumatic, degenerative medial meniscal tears? A five year follow-up. Knee Surg Sports Traumatol Arthrosc2013; 21:358–364.
Katz JN, Chaisson CE, Cole B, et al. The MeTeOR trial (Meniscal Tear in Osteoarthritis Research): rationale and design features. Contemp Clin Trials2012; 33:1189–1196.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol1988; 15:1833–1840.
Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes2003; 1:64.
Solomon MJ, McLeod RS. Should we be performing more randomized controlled trials evaluating surgical operations?Surgery1995; 118:459–467.
Farrokhyar F, Karanicolas PJ, Thoma A, et al. Randomized controlled trials of surgical interventions. Ann Surg2010; 251:409–416.
Sihvonen R, Paavola M, Malmivaara A. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med2013; 369:2515–2524.
Hare KB, Lohmander LS, Christensen R, Roos EM. Arthroscopic partial meniscectomy in middle-aged patients with mild or no knee osteoarthritis: a protocol for a double-blind, randomized sham-controlled multicentre trial. BMC Musculoskelet Disord2013; 14:71.
References
Katz JN, Brophy RH, Chaisson CE, et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med2013; 368:1675–1684.
Englund M, Guermazi A, Gale D, et al. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med2008; 359:1108–115.
Englund M, Guermazi A, Lohmander SL. The role of the meniscus in knee osteoarthritis: a cause or consequence?Radiol Clin North Am2009; 47:703–712.
Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med2002; 347:81–68.
Kirkley A, Birmingham TB, Litchfield RB, et al. A randomized trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med2008; 359:1097–1107.
Quintana JM, Escobar A, Arostegui I, et al. Prevalence of symptoms of knee or hip joints in older adults from the general population. Aging Clin Exp Res2008; 20:329–336.
Lawrence RC, Felson DT, Helmick CG, et al; National Arthritis Data Workgroup. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum2008; 58:26–35.
Loeser RF, Goldring SR, Scanzello CR, Goldring MB. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum2012; 64:1697–1707.
Englund M, Lohmander LS. Risk factors for symptomatic knee osteoarthritis fifteen to twenty-two years after meniscectomy. Arthritis Rheum2004; 50:2811–2819.
Papalia R, Del Buono A, Osti L, Denaro V, Maffulli N. Meniscectomy as a risk factor for knee osteoarthritis: a systematic review. Br Med Bull2011; 99:89–106.
Englund M, Guermazi A, Roemer FW, et al. Meniscal tear in knees without surgery and the development of radiographic osteoarthritis among middle-aged and elderly persons: The Multicenter Osteoarthritis Study. Arthritis Rheum2009; 60:831–839.
Poehling GG, Ruch DS, Chabon SJ. The landscape of meniscal injuries. Clin Sports Med1990; 9:539–549.
Bhattacharyya T, Gale D, Dewire P, et al. The clinical importance of meniscal tears demonstrated by magnetic resonance imaging in osteoarthritis of the knee. J Bone Joint Surg Am2003; 85-A:4–9.
Sowers M, Karvonen-Gutierrez CA, Jacobson JA, Jiang Y, Yosef M. Associations of anatomical measures from MRI with radiographically defined knee osteoarthritis score, pain, and physical functioning. J Bone Joint Surg Am2011; 93:241–251.
Ding C, Martel-Pelletier J, Pelletier JP, et al. Meniscal tear as an osteoarthritis risk factor in a largely non-osteoarthritic cohort: a cross-sectional study. J Rheumatol2007; 34:776–784.
Kim S, Bosque J, Meehan JP, Jamali A, Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Joint Surg Am2011; 93:994–1000.
Herrlin S, Hållander M, Wange P, Weidenhielm L, Werner S. Arthroscopic or conservative treatment of degenerative medial meniscal tears: a prospective randomised trial. Knee Surg Sports Traumatol Arthrosc2007; 15:393–401.
Herrlin SV, Wange PO, Lapidus G, Hållander M, Werner S, Weidenhielm L. Is arthroscopic surgery beneficial in treating non-traumatic, degenerative medial meniscal tears? A five year follow-up. Knee Surg Sports Traumatol Arthrosc2013; 21:358–364.
Katz JN, Chaisson CE, Cole B, et al. The MeTeOR trial (Meniscal Tear in Osteoarthritis Research): rationale and design features. Contemp Clin Trials2012; 33:1189–1196.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol1988; 15:1833–1840.
Roos EM, Lohmander LS. The Knee injury and Osteoarthritis Outcome Score (KOOS): from joint injury to osteoarthritis. Health Qual Life Outcomes2003; 1:64.
Solomon MJ, McLeod RS. Should we be performing more randomized controlled trials evaluating surgical operations?Surgery1995; 118:459–467.
Farrokhyar F, Karanicolas PJ, Thoma A, et al. Randomized controlled trials of surgical interventions. Ann Surg2010; 251:409–416.
Sihvonen R, Paavola M, Malmivaara A. Arthroscopic partial meniscectomy versus sham surgery for a degenerative meniscal tear. N Engl J Med2013; 369:2515–2524.
Hare KB, Lohmander LS, Christensen R, Roos EM. Arthroscopic partial meniscectomy in middle-aged patients with mild or no knee osteoarthritis: a protocol for a double-blind, randomized sham-controlled multicentre trial. BMC Musculoskelet Disord2013; 14:71.
METEOR trial was a randomized controlled trial comparing the short-term and long-term efficacy of arthroscopic partial meniscectomy vs physical therapy in patients with a symptomatic meniscal tear and knee osteoarthritis.
Both treatment groups in the METEOR trial received physical therapy in order to determine the incremental benefit of surgery and physical therapy compared with physical therapy alone.
The trial investigators used specific definitions of osteoarthritis and symptoms of meniscal tear.
Meniscectomy is often performed for patients with symptoms consistent with a meniscal tear and evidence of a meniscal tear on magnetic resonance imaging, but the benefits of this procedure are unclear.
Many patients with diabetes mellitus develop complex, accelerated, multifocal coronary artery disease. Moreover, if they undergo revascularization with either coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI), their risk of morbidity and death afterward is higher than in those without diabetes.1,2
Over the last 2 decades, CABG and PCI have advanced significantly, as have antithrombotic therapy and drug therapies to modify cardiovascular risk factors such as hyperlipidemia, hypertension, and diabetes.
Several earlier studies showed CABG to be more beneficial than PCI in diabetic patients with multivessel coronary artery disease.3–5 However, the topic has been controversial, and a substantial proportion of these patients continue to undergo PCI rather than CABG.
There are two main reasons for the continued use of PCI in this population. First, PCI is evolving, with new adjuvant drugs and drugeluting stents. Many cardiologists believe that earlier trials, which did not use contemporary PCI techniques, are outdated and that current, state-of-the-art PCI may be equivalent to—if not superior to—CABG.
Second, PCI is often performed on an ad hoc basis immediately after diagnostic angiography, leaving little time for discussion with the patient about alternative treatments. In this scenario, patients are inclined to undergo PCI immediately, while they are already on the table in the catheterization suite, rather than CABG at a later date.6
In addition, although the current joint guide-lines of the American College of Cardiology and the American Heart Association state that CABG is preferable to PCI for patients with diabetes and multivessel coronary artery disease, they give it only a level IIa recommendation.7
The much-anticipated Future Revascularization Evaluation in Patients With Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM) trial8 was designed to settle the CABG-vs-PCI debate, thereby leading to a stronger guideline recommendation for the preferred revascularization strategy in this patient population.
WHY ARE DIABETIC PATIENTS DIFFERENT?
Diabetes mellitus is a major risk factor for premature and aggressive coronary artery disease. Several mechanisms have been proposed to explain this association.
Diabetic patients have higher concentrations of several inflammatory proteins than those without diabetes, including C-reactive protein, tumor necrosis factor, and platelet-derived soluble CD40 ligand. They also have higher levels of adhesion molecules such as vascular cell adhesion molecule-1 and intercellular adhesion molecule.9,10 In addition, when blood sugar levels are high, platelets express more glycoprotein IIb/IIIa receptors and are therefore more prone to aggregate.11
These prothrombotic and proinflammatory cytokines, in conjunction with endothelial dysfunction and metabolic disorders such as hyperglycemia, hyperlipidemia, obesity, insulin resistance, and oxidative stress, lead to accelerated atherosclerosis in patients with diabetes.12 Also, because diabetes is a systemic disease, the atherosclerotic process is diffuse, and many patients with diabetes have left main coronary artery lesions and diffuse multivessel coronary artery disease.13,14
Although the short-term outcomes of revascularization by any means are comparable in patients with and without diabetes, diabetic patients have lower long-term survival rates and higher rates of myocardial infarction and need for repeat procedures.15 Diabetic patients who undergo PCI have a high rate of stent thrombosis and restenosis.16,17 Similarly, those undergoing CABG have higher rates of postoperative infection and renal and neurologic complications.18,19
BEFORE THE FREEDOM TRIAL
The question of CABG vs PCI has plagued physicians ever since PCI came to the forefront in the 1980s. Before stents were widely used, PCI with balloon angioplasty was known to be comparable to CABG for single-vessel disease, but whether it was beneficial in patients with multivessel disease or left main disease was not entirely evident. Randomized clinical trials were launched to answer the question.
Studies of balloon angioplasty vs CABG
The BARI trial (Bypass Angioplasty Revascularization Investigation),5,20 published in 1996, compared PCI (using balloon angioplasty without a stent) and CABG in patients with multivessel coronary artery disease (Table 120–29).
Between 1988 and 1991, the trial randomly assigned 1,829 patients with multivessel disease to receive either PCI or CABG and compared their long-term outcomes. Although there was no difference in mortality rates between the two groups overall, the diabetic subgroup had a significantly better survival rate with CABG than with PCI, which was sustained over a follow-up period of 10 years.5
BARI had a significant clinical impact at the time and led to a clinical alert by the National Heart, Lung, and Blood Institute recommending CABG over PCI for patients with diabetes. However, not everyone accepted the results, because they were based on a small number of patients (n = 353) in a retrospectively determined subgroup. Further, the BARI trial was conducted before the advent of coronary stents, which were later shown to improve outcomes after PCI. Also, optimal medical therapy after revascularization was not specified in the protocol, which likely affected outcomes.
EAST (Emory Angioplasty Versus Surgery Trial)21 and CABRI (Coronary Angioplasty Versus Bypass Revascularization Investigation) 22 were similar randomized trials comparing angioplasty and CABG in patients with multivessel coronary artery disease. These showed better outcomes after CABG in patients with diabetes. However, lack of statistical significance because of small sample sizes limited their clinical impact.
Studies of PCI with bare-metal stents vs CABG
The ARTS trial (Arterial Revascularization Therapy Study) compared PCI (with bare-metal stents) and CABG in 1,205 patients with multivessel coronary artery disease.23 The mortality rate did not differ significantly between two treatment groups overall or in the diabetic subgroup. However, the repeat revascularization rate was higher with PCI than with CABG.
The SoS trial (Stenting or Surgery)24 had similar results.
The ERACI II trial (Argentine Randomized Study: Coronary Angioplasty With Stenting Versus Coronary Bypass Surgery in Multi-Vessel Disease)25 found no difference in mortality rates at 5 years with CABG vs PCI.
These trials were criticized, as none of them routinely used glycoprotein IIb/IIIa inhibitors with PCI, which by then had been shown to reduce mortality rates.30 However, these trials made it clear that restenosis requiring repeat revascularization was a major disadvantage of PCI with bare-metal stents compared with CABG in patients with diabetes. Drug-eluting stents, which significantly reduced the rates of in-stent restenosis and target-lesion revascularization, were expected to overcome this major disadvantage.
Studies of PCI with drug-eluting stents vs CABG
ARTS II was the first trial to compare PCI with drug-eluting stents vs CABG. This was a nonrandomized single-arm study of 607 patients (including 159 with diabetes) who were treated with drug-eluting stents; the outcomes were compared with the CABG group from the earlier ARTS trial.31
At 3 years, in the diabetic subgroup, the rates of death, myocardial infarction, and stroke were not significantly different between treatments, although a trend favored PCI. However, this comparison was limited by selection bias, as ARTS II was a nonrandomized trial in which operators chose patients for drug-eluting stents in an attempt to match already known outcomes from the CABG cohort of ARTS.
SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery) was the first randomized trial comparing PCI with drug-eluting stents (in this trial, paclitaxel-eluting) vs CABG in patients with three-vessel or left main coronary artery disease.26,27 Subgroup analysis in patients with diabetes mellitus revealed a higher rate of major adverse cardiac and cerebrovascular events (death, myocardial infarction, stroke, or repeat revascularization) in the PCI group than in the CABG patients, largely driven by higher rates of repeat revascularization after PCI.32,33 SYNTAX was not designed to assess significant differences in rates of death.
The CARDIa trial (Coronary Artery Revascularization in Diabetes) randomized patients with diabetes and multivessel coronary artery disease to PCI (about one-third with bare-metal stents and two-thirds with drug-eluting stents) or CABG. Rates of major adverse cardiac and cerebrovascular events were higher in the PCI group, again largely driven by higher rates of repeat revascularization.4 CARDIa was stopped early because of a lack of enrollment and could not provide sufficient evidence to endorse one strategy over the other.
VA-CARDS (Veteran Affairs Coronary Artery Revascularization in Diabetes) randomized patients with diabetes and proximal left anterior descending artery or multivessel coronary artery disease to receive PCI with drug-eluting stents or CABG.28 Although the rate of death was lower with CABG than with PCI at 2 years, the trial was underpowered and was terminated at 25% of the initial intended patient enrollment. In addition, only 9% of diabetic patients screened were angiographically eligible for the study.29
Registry data. Analysis of a large data set from the National Cardiovascular Disease Registry and the Society of Thoracic Surgeons revealed a survival advantage of CABG over PCI for a follow-up period of 5 years.34 However, this was a nonrandomized study, so its conclusions were not definitive.
THE FREEDOM TRIAL
Given the limitations of the trials described above, the National Heart, Lung, and Blood Institute sponsored the FREEDOM trial—an appropriately powered, randomized comparison of PCI (with drug-eluting stents) and CABG (using arterial grafting) in patients with diabetes and multivessel coronary artery disease using contemporary techniques and concomitant optimal medical therapy.8
FREEDOM study design
The FREEDOM trial enrolled 1,900 patients with diabetes and angiographically confirmed multivessel coronary artery disease (83% with three-vessel disease) with stenosis of more than 70% in two or more major epicardial vessels involving at least two separate coronary-artery territories. The main exclusion criteria were severe left main coronary artery stenosis (≥ 50% stenosis), class III or IV congestive heart failure, and previous CABG or valve surgery. For CABG surgery, arterial revascularization was encouraged.
Dual antiplatelet therapy was recommended for at least 12 months in patients receiving a drug-eluting stent, and optimal medical management for diabetes, hypertension, and hyperlipidemia was strongly advocated.
Between April 2005 and April 2010, 32,966 patients were screened, of whom 3,309 were eligible for the trial and 1,900 consented and were randomized (953 to the PCI group and 947 to the CABG group). The patients were followed for a minimum of 2 years and had a median follow-up time of 3.8 years. Outcomes were measured with an intention-to-treat analysis.
Study results
Patients. The groups were comparable with regard to baseline demographics and cardiac risk factors.
The mean age was 63; 29% of the patients were women, and 83% had three-vessel coronary artery disease. The mean hemoglobin A1c was 7.8%, and the mean ejection fraction was 66%. The mean SYNTAX score, which defines the anatomic complexity of lesions, was 26 (≤ 22 is mild, 23–32 is intermediate, and ≥ 33 is high). The mean EURO score, which defines surgical risk, was 2.7 (a score ≥ 5 being associated with a lower rate of survival).
The primary composite outcome (death, nonfatal myocardial infarction, or nonfatal stroke) occurred less frequently in the CABG group than in the PCI group (Table 2). CABG was also associated with significantly lower rates of death from any cause and of myocardial infarction. Importantly, survival curves comparing the two groups diverged at 2-year follow-up. In contrast to other outcomes assessed, stroke occurred more often in the CABG group. The 5-year rates in the CABG group vs the PCI group were:
Primary outcome—18.7% vs 26.6%, P = .005
Death from any cause—10.9% vs 16.3%, P = .049
Myocardial infarction—6% vs 13.9%, P < .0001
Stroke—5.2% vs 2.4%, P = .03.
The secondary outcome (death, nonfatal myocardial infarction, nonfatal stroke, or repeat revascularization at 30 days or 12 months) had occurred significantly more often in the PCI group than in the CABG group at 1 year (16.8% vs 11.8%, P = .004), with most of the difference attributable to a higher repeat revascularization rate in the PCI group (12.6% vs 4.8%, P < .001).
Subgroup analysis. CABG was superior to PCI across all prespecified subgroups, covering the complexity of the coronary artery disease. Event rates with CABG vs PCI, by tertiles of the SYNTAX score:
SYNTAX scores ≤ 22: 17.2% vs 23.2%
SYNTAX scores 23–32: 17.7% vs 27.2%
SYNTAX scores ≥ 33: 22.8% vs 30.6%.
Cost-effectiveness. Although up-front costs were higher with CABG, at $34,467 for the index hospitalization vs $25,845 for PCI (P < .001), when the in-trial results were extended to a lifetime horizon, CABG had an incremental cost-effectiveness ratio of $8,132 per quality-adjusted life-year gained vs PCI.35 Traditionally, therapies are considered costeffective if the incremental cost-effectiveness ratio is less than $50,000 per quality-adjusted life-year gained.
WHY MAY CABG BE SUPERIOR IN DIABETIC PATIENTS?
Figure 1.
The major advantage of CABG over PCI is the ability to achieve complete revascularization. Diabetic patients with coronary artery disease tend to have diffuse, multifocal disease with several stenotic lesions in multiple coronary arteries. While stents only treat the focal area of most significant occlusion, CABG may bypass all proximal vulnerable plaques that could potentially develop into culprit lesions over time, truly bypassing the diseased segments (Figure 1).
In addition, heavy calcification may not allow optimal stenting in these patients.
Use of multiple stents increases the risk of restenosis, which could lead to a higher incidence of myocardial infarction and need for repeat revascularization. This was evident in the FREEDOM trial, in which the mean number of stents per patient was 4.2. Also, some lesions need to be left untreated because of the complexity involved.
The major improvement in outcomes after CABG has resulted from using arterial conduits such as the internal mammary artery rather than the saphenous vein.36 The patency rates of internal mammary artery grafts exceed 80% over 10 years.37 Internal mammary artery grafting was done in 94% of patients receiving CABG in the FREEDOM trial.
WHAT DOES THIS MEAN?
FREEDOM was a landmark trial that confirmed that CABG provides significant benefit compared with contemporary PCI with drug-eluting stents in patients with diabetes mellitus and multivessel coronary artery disease. It was a large multicenter trial that was adequately powered, unlike most of the earlier trials of this topic.
Unlike previous trials in which the benefit of CABG was driven by reduction in repeat revascularizations alone, FREEDOM showed lower incidence rates of all-cause mortality and myocardial infarction with CABG than with PCI. CABG was better regardless of SYNTAX score, number of diseased vessels, ejection fraction, race, or sex of the patient, indicating that it leads to superior outcomes across a wide spectrum of patients.
An argument that cardiologists often cite when recommending PCI is that it can save money due to lower length of index hospital stay and lower procedure costs of with PCI than with CABG. However, in FREEDOM, CABG also appeared to be highly cost-effective.
FREEDOM had limitations
While FREEDOM provided robust data proving the superiority of CABG, the study had several limitations.
Although there was an overall survival benefit with CABG compared with PCI, the difference in incidence of cardiovascular deaths (which accounted for 64% of all deaths) was not statistically significant.
The trial included only patients who were eligible for both PCI and CABG. Hence, the results may not be generalizable to all diabetic patients with multivessel coronary artery disease—indeed, only 10% of those screened were considered eligible for the trial. However, it is likely that several patients screened in the FREEDOM trial may not have been eligible for PCI or CABG at the time of screening, since the revascularization decision was made by a multidisciplinary team and a more appropriate decision (either CABG or PCI) was then made.
Other factors limiting the general applicability of the results were low numbers of female patients (28.6%), black patients (6.3%), patients with an ejection fraction of 40% or less (2.5%), and patients with a low SYNTAX score (35%).
There were several unexplained observations as well. The difference in events between the treatment groups was much higher in North America than in other regions. The number of coronary lesions in the CABG group was high (mean = 5.74), but the average numbers of grafts used was only 2.9, and data were not provided regarding use of sequential grafting. Similarly, an average of only 3.5 of the six stenotic lesions per patient in the PCI group were revascularized; whether this was the result of procedural limitations with PCI was not entirely clear.
In addition, while the investigators mention that an average patient received four stents, a surprising finding was that the mean total length of the stents used was only 26 mm. This appears too small, as the usual length of one drug-eluting stent is about 20 to 30 mm.
Since only high-volume centers with good outcome data were included in the trial, the results may lack validity for patients undergoing revascularization at low-volume community centers.
It remains to be seen if the benefits of CABG will be sustained over 10 years and longer, when saphenous vein grafts tend to fail and require repeat revascularization, commonly performed with PCI. Previous data suggest that the longer the follow-up, the better the results with CABG. However, long-term results (> 10 years) in studies comparing drugeluting stents and CABG are not available.
Despite limitations, FREEDOM may change clinical practice
Despite these limitations, the FREEDOM trial has the potential to change clinical practice and strengthen current recommendations for CABG in these patients.
The trial underscored the importance of a multidisciplinary heart team approach in managing patients with complex coronary artery disease, similar to that being used in patients with severe aortic stenosis since transcatheter aortic valve replacement became available.
It should also bring an end to the practice of ad hoc PCI, especially in patients with diabetes and multivessel coronary artery disease. It is now imperative that physicians discuss current evidence for therapeutic options with the patients and their families before performing diagnostic angiography rather than immediately afterward, to give the patients ample time to make an informed decision. This is important, as most patients are likely to choose PCI in the same setting over CABG unless there is extensive discussion about the risks and benefits of both strategies done in an unbiased manner before angiography.
The fear of open heart surgery, a longer hospital stay, and a higher risk of stroke with CABG may lead some patients to choose PCI instead. In addition, factors that may preclude CABG in otherwise-eligible patients include anatomic considerations (diffuse distal vessel disease, poor conduits), individual factors (frailty, poor renal function, poor pulmonary function, patient preference), and local expertise.
Nevertheless, the patient should be presented with current evidence, and discussions regarding the optimal procedure should be held with a heart team, which should include an interventional cardiologist, a cardiothoracic surgeon, and a noninvasive cardiologist to facilitate an unbiased decision.
Regardless of the strategy chosen, the importance of compliance with optimal medical therapy (statins, antiplatelet agents, diabetes treatment) should be continuously emphasized to the patient.
WHAT DOES THE FUTURE HOLD?
Despite unequivocal evidence that CABG is superior to PCI in eligible patients with diabetes mellitus in the current era, PCI technologies continue to evolve rapidly. Newer second-generation drug-eluting stents have shown lower rates of restenosis38,39 and may shorten the duration of post-PCI dual-antiplatelet therapy, a nuisance that has negatively affected outcomes with drug-eluting stents (because of problems of cost, poor compliance, and increased bleeding risk).
At the same time, CABG has also improved, with more extensive use of complete arterial conduits and use of an off-pump bypass technique that in theory poses a lower risk of stroke, although this has not yet been shown in a randomized trial.40
Alternative approaches are being investigated. One of them is a hybrid procedure in which minimally invasive off-pump arterial grafting is combined with drug-eluting stents, which may reduce the risk of stroke and speed postoperative recovery.
References
Flaherty JD, Davidson CJ. Diabetes and coronary revascularization. JAMA2005; 293:1501–1508.
Nicholls SJ, Tuzcu EM, Kalidindi S, et al. Effect of diabetes on progression of coronary atherosclerosis and arterial remodeling: a pooled analysis of 5 intravascular ultrasound trials. J Am Coll Cardiol2008; 52:255–262.
Mack MJ, Banning AP, Serruys PW, et al. Bypass versus drug-eluting stents at three years in SYNTAX patients with diabetes mellitus or metabolic syndrome. Ann Thorac Surg2011; 92:2140–2146.
Kapur A, Hall RJ, Malik IS, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol2010; 55:432–440.
The final 10-year follow-up results from the BARI randomized trial. J Am Coll Cardiol2007; 49:1600–1606.
Hlatky MA. Compelling evidence for coronary-bypass surgery in patients with diabetes. N Engl J Med2012; 367:2437–2438.
Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation2011; 124:2574–2609.
Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med2012; 367:2375–2384.
Moreno PR, Murcia AM, Palacios IF, et al. Coronary composition and macrophage infiltration in atherectomy specimens from patients with diabetes mellitus. Circulation2000; 102:2180–2184.
Bluher M, Unger R, Rassoul F, et al. Relation between glycaemic control, hyperinsulinaemia and plasma concentrations of soluble adhesion molecules in patients with impaired glucose tolerance or type II diabetes. Diabetologia2002; 45:210–216.
Creager MA, Luscher TF, Cosentino F, Beckman JA. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Circulation2003; 108:1527–1532.
Biondi-Zoccai GG, Abbate A, Liuzzo G, Biasucci LM. Atherothrombosis, inflammation, and diabetes. J Am Coll Cardiol2003; 41:1071–1077.
Waller BF, Palumbo PJ, Lie JT, Roberts WC. Status of the coronary arteries at necropsy in diabetes mellitus with onset after age 30 years. Analysis of 229 diabetic patients with and without clinical evidence of coronary heart disease and comparison to 183 control subjects. Am J Med1980; 69:498–506.
Morrish NJ, Stevens LK, Head J, et al. A prospective study of mortality among middle-aged diabetic patients (the London Cohort of the WHO Multinational Study of Vascular Disease in Diabetics) I: causes and death rates. Diabetologia1990; 33:538–541.
Laskey WK, Selzer F, Vlachos HA, et al. Comparison of in-hospital and one-year outcomes in patients with and without diabetes mellitus undergoing percutaneous catheter intervention (from the National Heart, Lung, and Blood Institute Dynamic Registry). Am J Cardiol2002; 90:1062–1067.
Mathew V, Gersh BJ, Williams BA, et al. Outcomes in patients with diabetes mellitus undergoing percutaneous coronary intervention in the current era: a report from the Prevention of REStenosis with Tranilast and its Outcomes (PRESTO) trial. Circulation2004; 109:476–480.
Glaser R, Selzer F, Faxon DP, et al. Clinical progression of incidental, asymptomatic lesions discovered during culprit vessel coronary intervention. Circulation2005; 111:143–149.
Morricone L, Ranucci M, Denti S, et al. Diabetes and complications after cardiac surgery: comparison with a non-diabetic population. Acta Diabetologica1999; 36:77–84.
Hogue CW, Murphy SF, Schechtman KB, Davila-Roman VG. Risk factors for early or delayed stroke after cardiac surgery. Circulation1999; 100:642–647.
The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med1996; 335:217–225.
King SB, Kosinski AS, Guyton RA, Lembo NJ, Weintraub WS. Eightyear mortality in the Emory Angioplasty versus Surgery Trial (East). J Am Coll Cardiol2000; 35:1116–1121.
Kurbaan AS, Bowker TJ, Ilsley CD, Sigwart U, Rickards AF; CABRI Investigators (Coronary Angioplasty versus Bypass Revascularization Investigation). Difference in the mortality of the CABRI diabetic and nondiabetic populations and its relation to coronary artery disease and the revascularization mode. Am J Cardiol2001; 87:947–950.
Serruys PW, Ong AT, van Herwerden LA, et al. Five-year outcomes after coronary stenting versus bypass surgery for the treatment of multivessel disease: the final analysis of the Arterial Revascularization Therapies Study (ARTS) randomized trial. J Am Coll Cardiol2005; 46:575–581.
Booth J, Clayton T, Pepper J, et al. Randomized, controlled trial of coronary artery bypass surgery versus percutaneous coronary intervention in patients with multivessel coronary artery disease: six-year follow-up from the Stent or Surgery Trial (SoS). Circulation2008; 118:381–388.
Rodriguez AE, Baldi J, Fernandez Pereira C, et al. Five-year follow-up of the Argentine randomized trial of coronary angioplasty with stenting versus coronary bypass surgery in patients with multiple vessel disease (ERACI II). J Am Coll Cardiol2005; 46:582–588.
Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med2009; 360:961–972.
Mohr FW, Morice MC, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet2013; 381:629–638.
Kamalesh M, Sharp TG, Tang XC, et al. Percutaneous coronary intervention versus coronary bypass surgery in United States veterans with diabetes. J Am Coll Cardiol2013; 61:808–816.
Ellis SG. Coronary revascularization for patients with diabetes: updated data favor coronary artery bypass grafting. J Am Coll Cardiol2013; 61:817–819.
Bhatt DL, Marso SP, Lincoff AM, et al. Abciximab reduces mortality in diabetics following percutaneous coronary intervention. J Am Coll Cardiol2000; 35:922–928.
Serruys PW, Ong AT, Morice MC, et al. Arterial Revascularisation Therapies Study Part II - Sirolimus-eluting stents for the treatment of patients with multivessel de novo coronary artery lesions. EuroIntervention2005; 1:147–156.
Kappetein AP, Head SJ, Morice MC, et al. Treatment of complex coronary artery disease in patients with diabetes: 5-year results comparing outcomes of bypass surgery and percutaneous coronary intervention in the SYNTAX trial. Eur J Cardiothorac Surg2013; 43:1006–1013.
Banning AP, Westaby S, Morice MC, et al. Diabetic and nondiabetic patients with left main and/or 3-vessel coronary artery disease: comparison of outcomes with cardiac surgery and paclitaxel-eluting stents. J Am Coll Cardiol2010; 55:1067–1075.
Weintraub WS, Grau-Sepulveda MV, Weiss JM, et al. Comparative effectiveness of revascularization strategies. N Engl J Med2012; 366:1467–1476.
Magnuson EA, Farkouh ME, Fuster V, et al; FREEDOM Trial Investigators. Cost-effectiveness of percutaneous coronary intervention with drug eluting stents versus bypass surgery for patients with diabetes and multivessel coronary artery disease: results from the FREEDOM trial. Circulation2013; 127:820–831.
Loop FD, Lytle BW, Cosgrove DM, et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med1986; 314:1–6.
Tector AJ, Schmahl TM, Janson B, et al. The internal mammary artery graft. Its longevity after coronary bypass. JAMA1981; 246:2181–2183.
Stone GW, Rizvi A, Newman W, et al. Everolimus-eluting versus paclitax-eleluting stents in coronary artery disease. N Engl J Med2010; 362:1663–1674.
Serruys PW, Silber S, Garg S, et al. Comparison of zotarolimus-eluting and everolimus-eluting coronary stents. N Engl J Med2010; 363:136–146.
Lamy A, Devereaux PJ, Prabhakaran D, et al. Off-pump or on-pump coronary-artery bypass grafting at 30 days. N Engl J Med2012; 366:1489–1497.
Bhuvnesh Aggarwal, MD Department of Internal Medicine, Cleveland Clinic
Sachin S. Goel, MD Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Joseph F. Sabik, MD Chair, Department of Thoracic and Cardiovascular Surgery; Staff, Critical Care Center, Heart and Vascular Institute, Cleveland Clinic; and Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Mehdi H. Shishehbor, DO, MPH, PhD Director, Endovascular Services, Interventional Cardiology and Vascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, PhD, Interventional Cardiology and Vascular Medicine, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: shishem@ccf.org
Bhuvnesh Aggarwal, MD Department of Internal Medicine, Cleveland Clinic
Sachin S. Goel, MD Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Joseph F. Sabik, MD Chair, Department of Thoracic and Cardiovascular Surgery; Staff, Critical Care Center, Heart and Vascular Institute, Cleveland Clinic; and Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Mehdi H. Shishehbor, DO, MPH, PhD Director, Endovascular Services, Interventional Cardiology and Vascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, PhD, Interventional Cardiology and Vascular Medicine, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: shishem@ccf.org
Author and Disclosure Information
Bhuvnesh Aggarwal, MD Department of Internal Medicine, Cleveland Clinic
Sachin S. Goel, MD Cardiovascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Joseph F. Sabik, MD Chair, Department of Thoracic and Cardiovascular Surgery; Staff, Critical Care Center, Heart and Vascular Institute, Cleveland Clinic; and Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH
Mehdi H. Shishehbor, DO, MPH, PhD Director, Endovascular Services, Interventional Cardiology and Vascular Medicine, Heart and Vascular Institute, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, PhD, Interventional Cardiology and Vascular Medicine, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: shishem@ccf.org
Many patients with diabetes mellitus develop complex, accelerated, multifocal coronary artery disease. Moreover, if they undergo revascularization with either coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI), their risk of morbidity and death afterward is higher than in those without diabetes.1,2
Over the last 2 decades, CABG and PCI have advanced significantly, as have antithrombotic therapy and drug therapies to modify cardiovascular risk factors such as hyperlipidemia, hypertension, and diabetes.
Several earlier studies showed CABG to be more beneficial than PCI in diabetic patients with multivessel coronary artery disease.3–5 However, the topic has been controversial, and a substantial proportion of these patients continue to undergo PCI rather than CABG.
There are two main reasons for the continued use of PCI in this population. First, PCI is evolving, with new adjuvant drugs and drugeluting stents. Many cardiologists believe that earlier trials, which did not use contemporary PCI techniques, are outdated and that current, state-of-the-art PCI may be equivalent to—if not superior to—CABG.
Second, PCI is often performed on an ad hoc basis immediately after diagnostic angiography, leaving little time for discussion with the patient about alternative treatments. In this scenario, patients are inclined to undergo PCI immediately, while they are already on the table in the catheterization suite, rather than CABG at a later date.6
In addition, although the current joint guide-lines of the American College of Cardiology and the American Heart Association state that CABG is preferable to PCI for patients with diabetes and multivessel coronary artery disease, they give it only a level IIa recommendation.7
The much-anticipated Future Revascularization Evaluation in Patients With Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM) trial8 was designed to settle the CABG-vs-PCI debate, thereby leading to a stronger guideline recommendation for the preferred revascularization strategy in this patient population.
WHY ARE DIABETIC PATIENTS DIFFERENT?
Diabetes mellitus is a major risk factor for premature and aggressive coronary artery disease. Several mechanisms have been proposed to explain this association.
Diabetic patients have higher concentrations of several inflammatory proteins than those without diabetes, including C-reactive protein, tumor necrosis factor, and platelet-derived soluble CD40 ligand. They also have higher levels of adhesion molecules such as vascular cell adhesion molecule-1 and intercellular adhesion molecule.9,10 In addition, when blood sugar levels are high, platelets express more glycoprotein IIb/IIIa receptors and are therefore more prone to aggregate.11
These prothrombotic and proinflammatory cytokines, in conjunction with endothelial dysfunction and metabolic disorders such as hyperglycemia, hyperlipidemia, obesity, insulin resistance, and oxidative stress, lead to accelerated atherosclerosis in patients with diabetes.12 Also, because diabetes is a systemic disease, the atherosclerotic process is diffuse, and many patients with diabetes have left main coronary artery lesions and diffuse multivessel coronary artery disease.13,14
Although the short-term outcomes of revascularization by any means are comparable in patients with and without diabetes, diabetic patients have lower long-term survival rates and higher rates of myocardial infarction and need for repeat procedures.15 Diabetic patients who undergo PCI have a high rate of stent thrombosis and restenosis.16,17 Similarly, those undergoing CABG have higher rates of postoperative infection and renal and neurologic complications.18,19
BEFORE THE FREEDOM TRIAL
The question of CABG vs PCI has plagued physicians ever since PCI came to the forefront in the 1980s. Before stents were widely used, PCI with balloon angioplasty was known to be comparable to CABG for single-vessel disease, but whether it was beneficial in patients with multivessel disease or left main disease was not entirely evident. Randomized clinical trials were launched to answer the question.
Studies of balloon angioplasty vs CABG
The BARI trial (Bypass Angioplasty Revascularization Investigation),5,20 published in 1996, compared PCI (using balloon angioplasty without a stent) and CABG in patients with multivessel coronary artery disease (Table 120–29).
Between 1988 and 1991, the trial randomly assigned 1,829 patients with multivessel disease to receive either PCI or CABG and compared their long-term outcomes. Although there was no difference in mortality rates between the two groups overall, the diabetic subgroup had a significantly better survival rate with CABG than with PCI, which was sustained over a follow-up period of 10 years.5
BARI had a significant clinical impact at the time and led to a clinical alert by the National Heart, Lung, and Blood Institute recommending CABG over PCI for patients with diabetes. However, not everyone accepted the results, because they were based on a small number of patients (n = 353) in a retrospectively determined subgroup. Further, the BARI trial was conducted before the advent of coronary stents, which were later shown to improve outcomes after PCI. Also, optimal medical therapy after revascularization was not specified in the protocol, which likely affected outcomes.
EAST (Emory Angioplasty Versus Surgery Trial)21 and CABRI (Coronary Angioplasty Versus Bypass Revascularization Investigation) 22 were similar randomized trials comparing angioplasty and CABG in patients with multivessel coronary artery disease. These showed better outcomes after CABG in patients with diabetes. However, lack of statistical significance because of small sample sizes limited their clinical impact.
Studies of PCI with bare-metal stents vs CABG
The ARTS trial (Arterial Revascularization Therapy Study) compared PCI (with bare-metal stents) and CABG in 1,205 patients with multivessel coronary artery disease.23 The mortality rate did not differ significantly between two treatment groups overall or in the diabetic subgroup. However, the repeat revascularization rate was higher with PCI than with CABG.
The SoS trial (Stenting or Surgery)24 had similar results.
The ERACI II trial (Argentine Randomized Study: Coronary Angioplasty With Stenting Versus Coronary Bypass Surgery in Multi-Vessel Disease)25 found no difference in mortality rates at 5 years with CABG vs PCI.
These trials were criticized, as none of them routinely used glycoprotein IIb/IIIa inhibitors with PCI, which by then had been shown to reduce mortality rates.30 However, these trials made it clear that restenosis requiring repeat revascularization was a major disadvantage of PCI with bare-metal stents compared with CABG in patients with diabetes. Drug-eluting stents, which significantly reduced the rates of in-stent restenosis and target-lesion revascularization, were expected to overcome this major disadvantage.
Studies of PCI with drug-eluting stents vs CABG
ARTS II was the first trial to compare PCI with drug-eluting stents vs CABG. This was a nonrandomized single-arm study of 607 patients (including 159 with diabetes) who were treated with drug-eluting stents; the outcomes were compared with the CABG group from the earlier ARTS trial.31
At 3 years, in the diabetic subgroup, the rates of death, myocardial infarction, and stroke were not significantly different between treatments, although a trend favored PCI. However, this comparison was limited by selection bias, as ARTS II was a nonrandomized trial in which operators chose patients for drug-eluting stents in an attempt to match already known outcomes from the CABG cohort of ARTS.
SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery) was the first randomized trial comparing PCI with drug-eluting stents (in this trial, paclitaxel-eluting) vs CABG in patients with three-vessel or left main coronary artery disease.26,27 Subgroup analysis in patients with diabetes mellitus revealed a higher rate of major adverse cardiac and cerebrovascular events (death, myocardial infarction, stroke, or repeat revascularization) in the PCI group than in the CABG patients, largely driven by higher rates of repeat revascularization after PCI.32,33 SYNTAX was not designed to assess significant differences in rates of death.
The CARDIa trial (Coronary Artery Revascularization in Diabetes) randomized patients with diabetes and multivessel coronary artery disease to PCI (about one-third with bare-metal stents and two-thirds with drug-eluting stents) or CABG. Rates of major adverse cardiac and cerebrovascular events were higher in the PCI group, again largely driven by higher rates of repeat revascularization.4 CARDIa was stopped early because of a lack of enrollment and could not provide sufficient evidence to endorse one strategy over the other.
VA-CARDS (Veteran Affairs Coronary Artery Revascularization in Diabetes) randomized patients with diabetes and proximal left anterior descending artery or multivessel coronary artery disease to receive PCI with drug-eluting stents or CABG.28 Although the rate of death was lower with CABG than with PCI at 2 years, the trial was underpowered and was terminated at 25% of the initial intended patient enrollment. In addition, only 9% of diabetic patients screened were angiographically eligible for the study.29
Registry data. Analysis of a large data set from the National Cardiovascular Disease Registry and the Society of Thoracic Surgeons revealed a survival advantage of CABG over PCI for a follow-up period of 5 years.34 However, this was a nonrandomized study, so its conclusions were not definitive.
THE FREEDOM TRIAL
Given the limitations of the trials described above, the National Heart, Lung, and Blood Institute sponsored the FREEDOM trial—an appropriately powered, randomized comparison of PCI (with drug-eluting stents) and CABG (using arterial grafting) in patients with diabetes and multivessel coronary artery disease using contemporary techniques and concomitant optimal medical therapy.8
FREEDOM study design
The FREEDOM trial enrolled 1,900 patients with diabetes and angiographically confirmed multivessel coronary artery disease (83% with three-vessel disease) with stenosis of more than 70% in two or more major epicardial vessels involving at least two separate coronary-artery territories. The main exclusion criteria were severe left main coronary artery stenosis (≥ 50% stenosis), class III or IV congestive heart failure, and previous CABG or valve surgery. For CABG surgery, arterial revascularization was encouraged.
Dual antiplatelet therapy was recommended for at least 12 months in patients receiving a drug-eluting stent, and optimal medical management for diabetes, hypertension, and hyperlipidemia was strongly advocated.
Between April 2005 and April 2010, 32,966 patients were screened, of whom 3,309 were eligible for the trial and 1,900 consented and were randomized (953 to the PCI group and 947 to the CABG group). The patients were followed for a minimum of 2 years and had a median follow-up time of 3.8 years. Outcomes were measured with an intention-to-treat analysis.
Study results
Patients. The groups were comparable with regard to baseline demographics and cardiac risk factors.
The mean age was 63; 29% of the patients were women, and 83% had three-vessel coronary artery disease. The mean hemoglobin A1c was 7.8%, and the mean ejection fraction was 66%. The mean SYNTAX score, which defines the anatomic complexity of lesions, was 26 (≤ 22 is mild, 23–32 is intermediate, and ≥ 33 is high). The mean EURO score, which defines surgical risk, was 2.7 (a score ≥ 5 being associated with a lower rate of survival).
The primary composite outcome (death, nonfatal myocardial infarction, or nonfatal stroke) occurred less frequently in the CABG group than in the PCI group (Table 2). CABG was also associated with significantly lower rates of death from any cause and of myocardial infarction. Importantly, survival curves comparing the two groups diverged at 2-year follow-up. In contrast to other outcomes assessed, stroke occurred more often in the CABG group. The 5-year rates in the CABG group vs the PCI group were:
Primary outcome—18.7% vs 26.6%, P = .005
Death from any cause—10.9% vs 16.3%, P = .049
Myocardial infarction—6% vs 13.9%, P < .0001
Stroke—5.2% vs 2.4%, P = .03.
The secondary outcome (death, nonfatal myocardial infarction, nonfatal stroke, or repeat revascularization at 30 days or 12 months) had occurred significantly more often in the PCI group than in the CABG group at 1 year (16.8% vs 11.8%, P = .004), with most of the difference attributable to a higher repeat revascularization rate in the PCI group (12.6% vs 4.8%, P < .001).
Subgroup analysis. CABG was superior to PCI across all prespecified subgroups, covering the complexity of the coronary artery disease. Event rates with CABG vs PCI, by tertiles of the SYNTAX score:
SYNTAX scores ≤ 22: 17.2% vs 23.2%
SYNTAX scores 23–32: 17.7% vs 27.2%
SYNTAX scores ≥ 33: 22.8% vs 30.6%.
Cost-effectiveness. Although up-front costs were higher with CABG, at $34,467 for the index hospitalization vs $25,845 for PCI (P < .001), when the in-trial results were extended to a lifetime horizon, CABG had an incremental cost-effectiveness ratio of $8,132 per quality-adjusted life-year gained vs PCI.35 Traditionally, therapies are considered costeffective if the incremental cost-effectiveness ratio is less than $50,000 per quality-adjusted life-year gained.
WHY MAY CABG BE SUPERIOR IN DIABETIC PATIENTS?
Figure 1.
The major advantage of CABG over PCI is the ability to achieve complete revascularization. Diabetic patients with coronary artery disease tend to have diffuse, multifocal disease with several stenotic lesions in multiple coronary arteries. While stents only treat the focal area of most significant occlusion, CABG may bypass all proximal vulnerable plaques that could potentially develop into culprit lesions over time, truly bypassing the diseased segments (Figure 1).
In addition, heavy calcification may not allow optimal stenting in these patients.
Use of multiple stents increases the risk of restenosis, which could lead to a higher incidence of myocardial infarction and need for repeat revascularization. This was evident in the FREEDOM trial, in which the mean number of stents per patient was 4.2. Also, some lesions need to be left untreated because of the complexity involved.
The major improvement in outcomes after CABG has resulted from using arterial conduits such as the internal mammary artery rather than the saphenous vein.36 The patency rates of internal mammary artery grafts exceed 80% over 10 years.37 Internal mammary artery grafting was done in 94% of patients receiving CABG in the FREEDOM trial.
WHAT DOES THIS MEAN?
FREEDOM was a landmark trial that confirmed that CABG provides significant benefit compared with contemporary PCI with drug-eluting stents in patients with diabetes mellitus and multivessel coronary artery disease. It was a large multicenter trial that was adequately powered, unlike most of the earlier trials of this topic.
Unlike previous trials in which the benefit of CABG was driven by reduction in repeat revascularizations alone, FREEDOM showed lower incidence rates of all-cause mortality and myocardial infarction with CABG than with PCI. CABG was better regardless of SYNTAX score, number of diseased vessels, ejection fraction, race, or sex of the patient, indicating that it leads to superior outcomes across a wide spectrum of patients.
An argument that cardiologists often cite when recommending PCI is that it can save money due to lower length of index hospital stay and lower procedure costs of with PCI than with CABG. However, in FREEDOM, CABG also appeared to be highly cost-effective.
FREEDOM had limitations
While FREEDOM provided robust data proving the superiority of CABG, the study had several limitations.
Although there was an overall survival benefit with CABG compared with PCI, the difference in incidence of cardiovascular deaths (which accounted for 64% of all deaths) was not statistically significant.
The trial included only patients who were eligible for both PCI and CABG. Hence, the results may not be generalizable to all diabetic patients with multivessel coronary artery disease—indeed, only 10% of those screened were considered eligible for the trial. However, it is likely that several patients screened in the FREEDOM trial may not have been eligible for PCI or CABG at the time of screening, since the revascularization decision was made by a multidisciplinary team and a more appropriate decision (either CABG or PCI) was then made.
Other factors limiting the general applicability of the results were low numbers of female patients (28.6%), black patients (6.3%), patients with an ejection fraction of 40% or less (2.5%), and patients with a low SYNTAX score (35%).
There were several unexplained observations as well. The difference in events between the treatment groups was much higher in North America than in other regions. The number of coronary lesions in the CABG group was high (mean = 5.74), but the average numbers of grafts used was only 2.9, and data were not provided regarding use of sequential grafting. Similarly, an average of only 3.5 of the six stenotic lesions per patient in the PCI group were revascularized; whether this was the result of procedural limitations with PCI was not entirely clear.
In addition, while the investigators mention that an average patient received four stents, a surprising finding was that the mean total length of the stents used was only 26 mm. This appears too small, as the usual length of one drug-eluting stent is about 20 to 30 mm.
Since only high-volume centers with good outcome data were included in the trial, the results may lack validity for patients undergoing revascularization at low-volume community centers.
It remains to be seen if the benefits of CABG will be sustained over 10 years and longer, when saphenous vein grafts tend to fail and require repeat revascularization, commonly performed with PCI. Previous data suggest that the longer the follow-up, the better the results with CABG. However, long-term results (> 10 years) in studies comparing drugeluting stents and CABG are not available.
Despite limitations, FREEDOM may change clinical practice
Despite these limitations, the FREEDOM trial has the potential to change clinical practice and strengthen current recommendations for CABG in these patients.
The trial underscored the importance of a multidisciplinary heart team approach in managing patients with complex coronary artery disease, similar to that being used in patients with severe aortic stenosis since transcatheter aortic valve replacement became available.
It should also bring an end to the practice of ad hoc PCI, especially in patients with diabetes and multivessel coronary artery disease. It is now imperative that physicians discuss current evidence for therapeutic options with the patients and their families before performing diagnostic angiography rather than immediately afterward, to give the patients ample time to make an informed decision. This is important, as most patients are likely to choose PCI in the same setting over CABG unless there is extensive discussion about the risks and benefits of both strategies done in an unbiased manner before angiography.
The fear of open heart surgery, a longer hospital stay, and a higher risk of stroke with CABG may lead some patients to choose PCI instead. In addition, factors that may preclude CABG in otherwise-eligible patients include anatomic considerations (diffuse distal vessel disease, poor conduits), individual factors (frailty, poor renal function, poor pulmonary function, patient preference), and local expertise.
Nevertheless, the patient should be presented with current evidence, and discussions regarding the optimal procedure should be held with a heart team, which should include an interventional cardiologist, a cardiothoracic surgeon, and a noninvasive cardiologist to facilitate an unbiased decision.
Regardless of the strategy chosen, the importance of compliance with optimal medical therapy (statins, antiplatelet agents, diabetes treatment) should be continuously emphasized to the patient.
WHAT DOES THE FUTURE HOLD?
Despite unequivocal evidence that CABG is superior to PCI in eligible patients with diabetes mellitus in the current era, PCI technologies continue to evolve rapidly. Newer second-generation drug-eluting stents have shown lower rates of restenosis38,39 and may shorten the duration of post-PCI dual-antiplatelet therapy, a nuisance that has negatively affected outcomes with drug-eluting stents (because of problems of cost, poor compliance, and increased bleeding risk).
At the same time, CABG has also improved, with more extensive use of complete arterial conduits and use of an off-pump bypass technique that in theory poses a lower risk of stroke, although this has not yet been shown in a randomized trial.40
Alternative approaches are being investigated. One of them is a hybrid procedure in which minimally invasive off-pump arterial grafting is combined with drug-eluting stents, which may reduce the risk of stroke and speed postoperative recovery.
Many patients with diabetes mellitus develop complex, accelerated, multifocal coronary artery disease. Moreover, if they undergo revascularization with either coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI), their risk of morbidity and death afterward is higher than in those without diabetes.1,2
Over the last 2 decades, CABG and PCI have advanced significantly, as have antithrombotic therapy and drug therapies to modify cardiovascular risk factors such as hyperlipidemia, hypertension, and diabetes.
Several earlier studies showed CABG to be more beneficial than PCI in diabetic patients with multivessel coronary artery disease.3–5 However, the topic has been controversial, and a substantial proportion of these patients continue to undergo PCI rather than CABG.
There are two main reasons for the continued use of PCI in this population. First, PCI is evolving, with new adjuvant drugs and drugeluting stents. Many cardiologists believe that earlier trials, which did not use contemporary PCI techniques, are outdated and that current, state-of-the-art PCI may be equivalent to—if not superior to—CABG.
Second, PCI is often performed on an ad hoc basis immediately after diagnostic angiography, leaving little time for discussion with the patient about alternative treatments. In this scenario, patients are inclined to undergo PCI immediately, while they are already on the table in the catheterization suite, rather than CABG at a later date.6
In addition, although the current joint guide-lines of the American College of Cardiology and the American Heart Association state that CABG is preferable to PCI for patients with diabetes and multivessel coronary artery disease, they give it only a level IIa recommendation.7
The much-anticipated Future Revascularization Evaluation in Patients With Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM) trial8 was designed to settle the CABG-vs-PCI debate, thereby leading to a stronger guideline recommendation for the preferred revascularization strategy in this patient population.
WHY ARE DIABETIC PATIENTS DIFFERENT?
Diabetes mellitus is a major risk factor for premature and aggressive coronary artery disease. Several mechanisms have been proposed to explain this association.
Diabetic patients have higher concentrations of several inflammatory proteins than those without diabetes, including C-reactive protein, tumor necrosis factor, and platelet-derived soluble CD40 ligand. They also have higher levels of adhesion molecules such as vascular cell adhesion molecule-1 and intercellular adhesion molecule.9,10 In addition, when blood sugar levels are high, platelets express more glycoprotein IIb/IIIa receptors and are therefore more prone to aggregate.11
These prothrombotic and proinflammatory cytokines, in conjunction with endothelial dysfunction and metabolic disorders such as hyperglycemia, hyperlipidemia, obesity, insulin resistance, and oxidative stress, lead to accelerated atherosclerosis in patients with diabetes.12 Also, because diabetes is a systemic disease, the atherosclerotic process is diffuse, and many patients with diabetes have left main coronary artery lesions and diffuse multivessel coronary artery disease.13,14
Although the short-term outcomes of revascularization by any means are comparable in patients with and without diabetes, diabetic patients have lower long-term survival rates and higher rates of myocardial infarction and need for repeat procedures.15 Diabetic patients who undergo PCI have a high rate of stent thrombosis and restenosis.16,17 Similarly, those undergoing CABG have higher rates of postoperative infection and renal and neurologic complications.18,19
BEFORE THE FREEDOM TRIAL
The question of CABG vs PCI has plagued physicians ever since PCI came to the forefront in the 1980s. Before stents were widely used, PCI with balloon angioplasty was known to be comparable to CABG for single-vessel disease, but whether it was beneficial in patients with multivessel disease or left main disease was not entirely evident. Randomized clinical trials were launched to answer the question.
Studies of balloon angioplasty vs CABG
The BARI trial (Bypass Angioplasty Revascularization Investigation),5,20 published in 1996, compared PCI (using balloon angioplasty without a stent) and CABG in patients with multivessel coronary artery disease (Table 120–29).
Between 1988 and 1991, the trial randomly assigned 1,829 patients with multivessel disease to receive either PCI or CABG and compared their long-term outcomes. Although there was no difference in mortality rates between the two groups overall, the diabetic subgroup had a significantly better survival rate with CABG than with PCI, which was sustained over a follow-up period of 10 years.5
BARI had a significant clinical impact at the time and led to a clinical alert by the National Heart, Lung, and Blood Institute recommending CABG over PCI for patients with diabetes. However, not everyone accepted the results, because they were based on a small number of patients (n = 353) in a retrospectively determined subgroup. Further, the BARI trial was conducted before the advent of coronary stents, which were later shown to improve outcomes after PCI. Also, optimal medical therapy after revascularization was not specified in the protocol, which likely affected outcomes.
EAST (Emory Angioplasty Versus Surgery Trial)21 and CABRI (Coronary Angioplasty Versus Bypass Revascularization Investigation) 22 were similar randomized trials comparing angioplasty and CABG in patients with multivessel coronary artery disease. These showed better outcomes after CABG in patients with diabetes. However, lack of statistical significance because of small sample sizes limited their clinical impact.
Studies of PCI with bare-metal stents vs CABG
The ARTS trial (Arterial Revascularization Therapy Study) compared PCI (with bare-metal stents) and CABG in 1,205 patients with multivessel coronary artery disease.23 The mortality rate did not differ significantly between two treatment groups overall or in the diabetic subgroup. However, the repeat revascularization rate was higher with PCI than with CABG.
The SoS trial (Stenting or Surgery)24 had similar results.
The ERACI II trial (Argentine Randomized Study: Coronary Angioplasty With Stenting Versus Coronary Bypass Surgery in Multi-Vessel Disease)25 found no difference in mortality rates at 5 years with CABG vs PCI.
These trials were criticized, as none of them routinely used glycoprotein IIb/IIIa inhibitors with PCI, which by then had been shown to reduce mortality rates.30 However, these trials made it clear that restenosis requiring repeat revascularization was a major disadvantage of PCI with bare-metal stents compared with CABG in patients with diabetes. Drug-eluting stents, which significantly reduced the rates of in-stent restenosis and target-lesion revascularization, were expected to overcome this major disadvantage.
Studies of PCI with drug-eluting stents vs CABG
ARTS II was the first trial to compare PCI with drug-eluting stents vs CABG. This was a nonrandomized single-arm study of 607 patients (including 159 with diabetes) who were treated with drug-eluting stents; the outcomes were compared with the CABG group from the earlier ARTS trial.31
At 3 years, in the diabetic subgroup, the rates of death, myocardial infarction, and stroke were not significantly different between treatments, although a trend favored PCI. However, this comparison was limited by selection bias, as ARTS II was a nonrandomized trial in which operators chose patients for drug-eluting stents in an attempt to match already known outcomes from the CABG cohort of ARTS.
SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery) was the first randomized trial comparing PCI with drug-eluting stents (in this trial, paclitaxel-eluting) vs CABG in patients with three-vessel or left main coronary artery disease.26,27 Subgroup analysis in patients with diabetes mellitus revealed a higher rate of major adverse cardiac and cerebrovascular events (death, myocardial infarction, stroke, or repeat revascularization) in the PCI group than in the CABG patients, largely driven by higher rates of repeat revascularization after PCI.32,33 SYNTAX was not designed to assess significant differences in rates of death.
The CARDIa trial (Coronary Artery Revascularization in Diabetes) randomized patients with diabetes and multivessel coronary artery disease to PCI (about one-third with bare-metal stents and two-thirds with drug-eluting stents) or CABG. Rates of major adverse cardiac and cerebrovascular events were higher in the PCI group, again largely driven by higher rates of repeat revascularization.4 CARDIa was stopped early because of a lack of enrollment and could not provide sufficient evidence to endorse one strategy over the other.
VA-CARDS (Veteran Affairs Coronary Artery Revascularization in Diabetes) randomized patients with diabetes and proximal left anterior descending artery or multivessel coronary artery disease to receive PCI with drug-eluting stents or CABG.28 Although the rate of death was lower with CABG than with PCI at 2 years, the trial was underpowered and was terminated at 25% of the initial intended patient enrollment. In addition, only 9% of diabetic patients screened were angiographically eligible for the study.29
Registry data. Analysis of a large data set from the National Cardiovascular Disease Registry and the Society of Thoracic Surgeons revealed a survival advantage of CABG over PCI for a follow-up period of 5 years.34 However, this was a nonrandomized study, so its conclusions were not definitive.
THE FREEDOM TRIAL
Given the limitations of the trials described above, the National Heart, Lung, and Blood Institute sponsored the FREEDOM trial—an appropriately powered, randomized comparison of PCI (with drug-eluting stents) and CABG (using arterial grafting) in patients with diabetes and multivessel coronary artery disease using contemporary techniques and concomitant optimal medical therapy.8
FREEDOM study design
The FREEDOM trial enrolled 1,900 patients with diabetes and angiographically confirmed multivessel coronary artery disease (83% with three-vessel disease) with stenosis of more than 70% in two or more major epicardial vessels involving at least two separate coronary-artery territories. The main exclusion criteria were severe left main coronary artery stenosis (≥ 50% stenosis), class III or IV congestive heart failure, and previous CABG or valve surgery. For CABG surgery, arterial revascularization was encouraged.
Dual antiplatelet therapy was recommended for at least 12 months in patients receiving a drug-eluting stent, and optimal medical management for diabetes, hypertension, and hyperlipidemia was strongly advocated.
Between April 2005 and April 2010, 32,966 patients were screened, of whom 3,309 were eligible for the trial and 1,900 consented and were randomized (953 to the PCI group and 947 to the CABG group). The patients were followed for a minimum of 2 years and had a median follow-up time of 3.8 years. Outcomes were measured with an intention-to-treat analysis.
Study results
Patients. The groups were comparable with regard to baseline demographics and cardiac risk factors.
The mean age was 63; 29% of the patients were women, and 83% had three-vessel coronary artery disease. The mean hemoglobin A1c was 7.8%, and the mean ejection fraction was 66%. The mean SYNTAX score, which defines the anatomic complexity of lesions, was 26 (≤ 22 is mild, 23–32 is intermediate, and ≥ 33 is high). The mean EURO score, which defines surgical risk, was 2.7 (a score ≥ 5 being associated with a lower rate of survival).
The primary composite outcome (death, nonfatal myocardial infarction, or nonfatal stroke) occurred less frequently in the CABG group than in the PCI group (Table 2). CABG was also associated with significantly lower rates of death from any cause and of myocardial infarction. Importantly, survival curves comparing the two groups diverged at 2-year follow-up. In contrast to other outcomes assessed, stroke occurred more often in the CABG group. The 5-year rates in the CABG group vs the PCI group were:
Primary outcome—18.7% vs 26.6%, P = .005
Death from any cause—10.9% vs 16.3%, P = .049
Myocardial infarction—6% vs 13.9%, P < .0001
Stroke—5.2% vs 2.4%, P = .03.
The secondary outcome (death, nonfatal myocardial infarction, nonfatal stroke, or repeat revascularization at 30 days or 12 months) had occurred significantly more often in the PCI group than in the CABG group at 1 year (16.8% vs 11.8%, P = .004), with most of the difference attributable to a higher repeat revascularization rate in the PCI group (12.6% vs 4.8%, P < .001).
Subgroup analysis. CABG was superior to PCI across all prespecified subgroups, covering the complexity of the coronary artery disease. Event rates with CABG vs PCI, by tertiles of the SYNTAX score:
SYNTAX scores ≤ 22: 17.2% vs 23.2%
SYNTAX scores 23–32: 17.7% vs 27.2%
SYNTAX scores ≥ 33: 22.8% vs 30.6%.
Cost-effectiveness. Although up-front costs were higher with CABG, at $34,467 for the index hospitalization vs $25,845 for PCI (P < .001), when the in-trial results were extended to a lifetime horizon, CABG had an incremental cost-effectiveness ratio of $8,132 per quality-adjusted life-year gained vs PCI.35 Traditionally, therapies are considered costeffective if the incremental cost-effectiveness ratio is less than $50,000 per quality-adjusted life-year gained.
WHY MAY CABG BE SUPERIOR IN DIABETIC PATIENTS?
Figure 1.
The major advantage of CABG over PCI is the ability to achieve complete revascularization. Diabetic patients with coronary artery disease tend to have diffuse, multifocal disease with several stenotic lesions in multiple coronary arteries. While stents only treat the focal area of most significant occlusion, CABG may bypass all proximal vulnerable plaques that could potentially develop into culprit lesions over time, truly bypassing the diseased segments (Figure 1).
In addition, heavy calcification may not allow optimal stenting in these patients.
Use of multiple stents increases the risk of restenosis, which could lead to a higher incidence of myocardial infarction and need for repeat revascularization. This was evident in the FREEDOM trial, in which the mean number of stents per patient was 4.2. Also, some lesions need to be left untreated because of the complexity involved.
The major improvement in outcomes after CABG has resulted from using arterial conduits such as the internal mammary artery rather than the saphenous vein.36 The patency rates of internal mammary artery grafts exceed 80% over 10 years.37 Internal mammary artery grafting was done in 94% of patients receiving CABG in the FREEDOM trial.
WHAT DOES THIS MEAN?
FREEDOM was a landmark trial that confirmed that CABG provides significant benefit compared with contemporary PCI with drug-eluting stents in patients with diabetes mellitus and multivessel coronary artery disease. It was a large multicenter trial that was adequately powered, unlike most of the earlier trials of this topic.
Unlike previous trials in which the benefit of CABG was driven by reduction in repeat revascularizations alone, FREEDOM showed lower incidence rates of all-cause mortality and myocardial infarction with CABG than with PCI. CABG was better regardless of SYNTAX score, number of diseased vessels, ejection fraction, race, or sex of the patient, indicating that it leads to superior outcomes across a wide spectrum of patients.
An argument that cardiologists often cite when recommending PCI is that it can save money due to lower length of index hospital stay and lower procedure costs of with PCI than with CABG. However, in FREEDOM, CABG also appeared to be highly cost-effective.
FREEDOM had limitations
While FREEDOM provided robust data proving the superiority of CABG, the study had several limitations.
Although there was an overall survival benefit with CABG compared with PCI, the difference in incidence of cardiovascular deaths (which accounted for 64% of all deaths) was not statistically significant.
The trial included only patients who were eligible for both PCI and CABG. Hence, the results may not be generalizable to all diabetic patients with multivessel coronary artery disease—indeed, only 10% of those screened were considered eligible for the trial. However, it is likely that several patients screened in the FREEDOM trial may not have been eligible for PCI or CABG at the time of screening, since the revascularization decision was made by a multidisciplinary team and a more appropriate decision (either CABG or PCI) was then made.
Other factors limiting the general applicability of the results were low numbers of female patients (28.6%), black patients (6.3%), patients with an ejection fraction of 40% or less (2.5%), and patients with a low SYNTAX score (35%).
There were several unexplained observations as well. The difference in events between the treatment groups was much higher in North America than in other regions. The number of coronary lesions in the CABG group was high (mean = 5.74), but the average numbers of grafts used was only 2.9, and data were not provided regarding use of sequential grafting. Similarly, an average of only 3.5 of the six stenotic lesions per patient in the PCI group were revascularized; whether this was the result of procedural limitations with PCI was not entirely clear.
In addition, while the investigators mention that an average patient received four stents, a surprising finding was that the mean total length of the stents used was only 26 mm. This appears too small, as the usual length of one drug-eluting stent is about 20 to 30 mm.
Since only high-volume centers with good outcome data were included in the trial, the results may lack validity for patients undergoing revascularization at low-volume community centers.
It remains to be seen if the benefits of CABG will be sustained over 10 years and longer, when saphenous vein grafts tend to fail and require repeat revascularization, commonly performed with PCI. Previous data suggest that the longer the follow-up, the better the results with CABG. However, long-term results (> 10 years) in studies comparing drugeluting stents and CABG are not available.
Despite limitations, FREEDOM may change clinical practice
Despite these limitations, the FREEDOM trial has the potential to change clinical practice and strengthen current recommendations for CABG in these patients.
The trial underscored the importance of a multidisciplinary heart team approach in managing patients with complex coronary artery disease, similar to that being used in patients with severe aortic stenosis since transcatheter aortic valve replacement became available.
It should also bring an end to the practice of ad hoc PCI, especially in patients with diabetes and multivessel coronary artery disease. It is now imperative that physicians discuss current evidence for therapeutic options with the patients and their families before performing diagnostic angiography rather than immediately afterward, to give the patients ample time to make an informed decision. This is important, as most patients are likely to choose PCI in the same setting over CABG unless there is extensive discussion about the risks and benefits of both strategies done in an unbiased manner before angiography.
The fear of open heart surgery, a longer hospital stay, and a higher risk of stroke with CABG may lead some patients to choose PCI instead. In addition, factors that may preclude CABG in otherwise-eligible patients include anatomic considerations (diffuse distal vessel disease, poor conduits), individual factors (frailty, poor renal function, poor pulmonary function, patient preference), and local expertise.
Nevertheless, the patient should be presented with current evidence, and discussions regarding the optimal procedure should be held with a heart team, which should include an interventional cardiologist, a cardiothoracic surgeon, and a noninvasive cardiologist to facilitate an unbiased decision.
Regardless of the strategy chosen, the importance of compliance with optimal medical therapy (statins, antiplatelet agents, diabetes treatment) should be continuously emphasized to the patient.
WHAT DOES THE FUTURE HOLD?
Despite unequivocal evidence that CABG is superior to PCI in eligible patients with diabetes mellitus in the current era, PCI technologies continue to evolve rapidly. Newer second-generation drug-eluting stents have shown lower rates of restenosis38,39 and may shorten the duration of post-PCI dual-antiplatelet therapy, a nuisance that has negatively affected outcomes with drug-eluting stents (because of problems of cost, poor compliance, and increased bleeding risk).
At the same time, CABG has also improved, with more extensive use of complete arterial conduits and use of an off-pump bypass technique that in theory poses a lower risk of stroke, although this has not yet been shown in a randomized trial.40
Alternative approaches are being investigated. One of them is a hybrid procedure in which minimally invasive off-pump arterial grafting is combined with drug-eluting stents, which may reduce the risk of stroke and speed postoperative recovery.
References
Flaherty JD, Davidson CJ. Diabetes and coronary revascularization. JAMA2005; 293:1501–1508.
Nicholls SJ, Tuzcu EM, Kalidindi S, et al. Effect of diabetes on progression of coronary atherosclerosis and arterial remodeling: a pooled analysis of 5 intravascular ultrasound trials. J Am Coll Cardiol2008; 52:255–262.
Mack MJ, Banning AP, Serruys PW, et al. Bypass versus drug-eluting stents at three years in SYNTAX patients with diabetes mellitus or metabolic syndrome. Ann Thorac Surg2011; 92:2140–2146.
Kapur A, Hall RJ, Malik IS, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol2010; 55:432–440.
The final 10-year follow-up results from the BARI randomized trial. J Am Coll Cardiol2007; 49:1600–1606.
Hlatky MA. Compelling evidence for coronary-bypass surgery in patients with diabetes. N Engl J Med2012; 367:2437–2438.
Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation2011; 124:2574–2609.
Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med2012; 367:2375–2384.
Moreno PR, Murcia AM, Palacios IF, et al. Coronary composition and macrophage infiltration in atherectomy specimens from patients with diabetes mellitus. Circulation2000; 102:2180–2184.
Bluher M, Unger R, Rassoul F, et al. Relation between glycaemic control, hyperinsulinaemia and plasma concentrations of soluble adhesion molecules in patients with impaired glucose tolerance or type II diabetes. Diabetologia2002; 45:210–216.
Creager MA, Luscher TF, Cosentino F, Beckman JA. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Circulation2003; 108:1527–1532.
Biondi-Zoccai GG, Abbate A, Liuzzo G, Biasucci LM. Atherothrombosis, inflammation, and diabetes. J Am Coll Cardiol2003; 41:1071–1077.
Waller BF, Palumbo PJ, Lie JT, Roberts WC. Status of the coronary arteries at necropsy in diabetes mellitus with onset after age 30 years. Analysis of 229 diabetic patients with and without clinical evidence of coronary heart disease and comparison to 183 control subjects. Am J Med1980; 69:498–506.
Morrish NJ, Stevens LK, Head J, et al. A prospective study of mortality among middle-aged diabetic patients (the London Cohort of the WHO Multinational Study of Vascular Disease in Diabetics) I: causes and death rates. Diabetologia1990; 33:538–541.
Laskey WK, Selzer F, Vlachos HA, et al. Comparison of in-hospital and one-year outcomes in patients with and without diabetes mellitus undergoing percutaneous catheter intervention (from the National Heart, Lung, and Blood Institute Dynamic Registry). Am J Cardiol2002; 90:1062–1067.
Mathew V, Gersh BJ, Williams BA, et al. Outcomes in patients with diabetes mellitus undergoing percutaneous coronary intervention in the current era: a report from the Prevention of REStenosis with Tranilast and its Outcomes (PRESTO) trial. Circulation2004; 109:476–480.
Glaser R, Selzer F, Faxon DP, et al. Clinical progression of incidental, asymptomatic lesions discovered during culprit vessel coronary intervention. Circulation2005; 111:143–149.
Morricone L, Ranucci M, Denti S, et al. Diabetes and complications after cardiac surgery: comparison with a non-diabetic population. Acta Diabetologica1999; 36:77–84.
Hogue CW, Murphy SF, Schechtman KB, Davila-Roman VG. Risk factors for early or delayed stroke after cardiac surgery. Circulation1999; 100:642–647.
The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med1996; 335:217–225.
King SB, Kosinski AS, Guyton RA, Lembo NJ, Weintraub WS. Eightyear mortality in the Emory Angioplasty versus Surgery Trial (East). J Am Coll Cardiol2000; 35:1116–1121.
Kurbaan AS, Bowker TJ, Ilsley CD, Sigwart U, Rickards AF; CABRI Investigators (Coronary Angioplasty versus Bypass Revascularization Investigation). Difference in the mortality of the CABRI diabetic and nondiabetic populations and its relation to coronary artery disease and the revascularization mode. Am J Cardiol2001; 87:947–950.
Serruys PW, Ong AT, van Herwerden LA, et al. Five-year outcomes after coronary stenting versus bypass surgery for the treatment of multivessel disease: the final analysis of the Arterial Revascularization Therapies Study (ARTS) randomized trial. J Am Coll Cardiol2005; 46:575–581.
Booth J, Clayton T, Pepper J, et al. Randomized, controlled trial of coronary artery bypass surgery versus percutaneous coronary intervention in patients with multivessel coronary artery disease: six-year follow-up from the Stent or Surgery Trial (SoS). Circulation2008; 118:381–388.
Rodriguez AE, Baldi J, Fernandez Pereira C, et al. Five-year follow-up of the Argentine randomized trial of coronary angioplasty with stenting versus coronary bypass surgery in patients with multiple vessel disease (ERACI II). J Am Coll Cardiol2005; 46:582–588.
Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med2009; 360:961–972.
Mohr FW, Morice MC, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet2013; 381:629–638.
Kamalesh M, Sharp TG, Tang XC, et al. Percutaneous coronary intervention versus coronary bypass surgery in United States veterans with diabetes. J Am Coll Cardiol2013; 61:808–816.
Ellis SG. Coronary revascularization for patients with diabetes: updated data favor coronary artery bypass grafting. J Am Coll Cardiol2013; 61:817–819.
Bhatt DL, Marso SP, Lincoff AM, et al. Abciximab reduces mortality in diabetics following percutaneous coronary intervention. J Am Coll Cardiol2000; 35:922–928.
Serruys PW, Ong AT, Morice MC, et al. Arterial Revascularisation Therapies Study Part II - Sirolimus-eluting stents for the treatment of patients with multivessel de novo coronary artery lesions. EuroIntervention2005; 1:147–156.
Kappetein AP, Head SJ, Morice MC, et al. Treatment of complex coronary artery disease in patients with diabetes: 5-year results comparing outcomes of bypass surgery and percutaneous coronary intervention in the SYNTAX trial. Eur J Cardiothorac Surg2013; 43:1006–1013.
Banning AP, Westaby S, Morice MC, et al. Diabetic and nondiabetic patients with left main and/or 3-vessel coronary artery disease: comparison of outcomes with cardiac surgery and paclitaxel-eluting stents. J Am Coll Cardiol2010; 55:1067–1075.
Weintraub WS, Grau-Sepulveda MV, Weiss JM, et al. Comparative effectiveness of revascularization strategies. N Engl J Med2012; 366:1467–1476.
Magnuson EA, Farkouh ME, Fuster V, et al; FREEDOM Trial Investigators. Cost-effectiveness of percutaneous coronary intervention with drug eluting stents versus bypass surgery for patients with diabetes and multivessel coronary artery disease: results from the FREEDOM trial. Circulation2013; 127:820–831.
Loop FD, Lytle BW, Cosgrove DM, et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med1986; 314:1–6.
Tector AJ, Schmahl TM, Janson B, et al. The internal mammary artery graft. Its longevity after coronary bypass. JAMA1981; 246:2181–2183.
Stone GW, Rizvi A, Newman W, et al. Everolimus-eluting versus paclitax-eleluting stents in coronary artery disease. N Engl J Med2010; 362:1663–1674.
Serruys PW, Silber S, Garg S, et al. Comparison of zotarolimus-eluting and everolimus-eluting coronary stents. N Engl J Med2010; 363:136–146.
Lamy A, Devereaux PJ, Prabhakaran D, et al. Off-pump or on-pump coronary-artery bypass grafting at 30 days. N Engl J Med2012; 366:1489–1497.
References
Flaherty JD, Davidson CJ. Diabetes and coronary revascularization. JAMA2005; 293:1501–1508.
Nicholls SJ, Tuzcu EM, Kalidindi S, et al. Effect of diabetes on progression of coronary atherosclerosis and arterial remodeling: a pooled analysis of 5 intravascular ultrasound trials. J Am Coll Cardiol2008; 52:255–262.
Mack MJ, Banning AP, Serruys PW, et al. Bypass versus drug-eluting stents at three years in SYNTAX patients with diabetes mellitus or metabolic syndrome. Ann Thorac Surg2011; 92:2140–2146.
Kapur A, Hall RJ, Malik IS, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol2010; 55:432–440.
The final 10-year follow-up results from the BARI randomized trial. J Am Coll Cardiol2007; 49:1600–1606.
Hlatky MA. Compelling evidence for coronary-bypass surgery in patients with diabetes. N Engl J Med2012; 367:2437–2438.
Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation2011; 124:2574–2609.
Farkouh ME, Domanski M, Sleeper LA, et al. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med2012; 367:2375–2384.
Moreno PR, Murcia AM, Palacios IF, et al. Coronary composition and macrophage infiltration in atherectomy specimens from patients with diabetes mellitus. Circulation2000; 102:2180–2184.
Bluher M, Unger R, Rassoul F, et al. Relation between glycaemic control, hyperinsulinaemia and plasma concentrations of soluble adhesion molecules in patients with impaired glucose tolerance or type II diabetes. Diabetologia2002; 45:210–216.
Creager MA, Luscher TF, Cosentino F, Beckman JA. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I. Circulation2003; 108:1527–1532.
Biondi-Zoccai GG, Abbate A, Liuzzo G, Biasucci LM. Atherothrombosis, inflammation, and diabetes. J Am Coll Cardiol2003; 41:1071–1077.
Waller BF, Palumbo PJ, Lie JT, Roberts WC. Status of the coronary arteries at necropsy in diabetes mellitus with onset after age 30 years. Analysis of 229 diabetic patients with and without clinical evidence of coronary heart disease and comparison to 183 control subjects. Am J Med1980; 69:498–506.
Morrish NJ, Stevens LK, Head J, et al. A prospective study of mortality among middle-aged diabetic patients (the London Cohort of the WHO Multinational Study of Vascular Disease in Diabetics) I: causes and death rates. Diabetologia1990; 33:538–541.
Laskey WK, Selzer F, Vlachos HA, et al. Comparison of in-hospital and one-year outcomes in patients with and without diabetes mellitus undergoing percutaneous catheter intervention (from the National Heart, Lung, and Blood Institute Dynamic Registry). Am J Cardiol2002; 90:1062–1067.
Mathew V, Gersh BJ, Williams BA, et al. Outcomes in patients with diabetes mellitus undergoing percutaneous coronary intervention in the current era: a report from the Prevention of REStenosis with Tranilast and its Outcomes (PRESTO) trial. Circulation2004; 109:476–480.
Glaser R, Selzer F, Faxon DP, et al. Clinical progression of incidental, asymptomatic lesions discovered during culprit vessel coronary intervention. Circulation2005; 111:143–149.
Morricone L, Ranucci M, Denti S, et al. Diabetes and complications after cardiac surgery: comparison with a non-diabetic population. Acta Diabetologica1999; 36:77–84.
Hogue CW, Murphy SF, Schechtman KB, Davila-Roman VG. Risk factors for early or delayed stroke after cardiac surgery. Circulation1999; 100:642–647.
The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med1996; 335:217–225.
King SB, Kosinski AS, Guyton RA, Lembo NJ, Weintraub WS. Eightyear mortality in the Emory Angioplasty versus Surgery Trial (East). J Am Coll Cardiol2000; 35:1116–1121.
Kurbaan AS, Bowker TJ, Ilsley CD, Sigwart U, Rickards AF; CABRI Investigators (Coronary Angioplasty versus Bypass Revascularization Investigation). Difference in the mortality of the CABRI diabetic and nondiabetic populations and its relation to coronary artery disease and the revascularization mode. Am J Cardiol2001; 87:947–950.
Serruys PW, Ong AT, van Herwerden LA, et al. Five-year outcomes after coronary stenting versus bypass surgery for the treatment of multivessel disease: the final analysis of the Arterial Revascularization Therapies Study (ARTS) randomized trial. J Am Coll Cardiol2005; 46:575–581.
Booth J, Clayton T, Pepper J, et al. Randomized, controlled trial of coronary artery bypass surgery versus percutaneous coronary intervention in patients with multivessel coronary artery disease: six-year follow-up from the Stent or Surgery Trial (SoS). Circulation2008; 118:381–388.
Rodriguez AE, Baldi J, Fernandez Pereira C, et al. Five-year follow-up of the Argentine randomized trial of coronary angioplasty with stenting versus coronary bypass surgery in patients with multiple vessel disease (ERACI II). J Am Coll Cardiol2005; 46:582–588.
Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med2009; 360:961–972.
Mohr FW, Morice MC, Kappetein AP, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet2013; 381:629–638.
Kamalesh M, Sharp TG, Tang XC, et al. Percutaneous coronary intervention versus coronary bypass surgery in United States veterans with diabetes. J Am Coll Cardiol2013; 61:808–816.
Ellis SG. Coronary revascularization for patients with diabetes: updated data favor coronary artery bypass grafting. J Am Coll Cardiol2013; 61:817–819.
Bhatt DL, Marso SP, Lincoff AM, et al. Abciximab reduces mortality in diabetics following percutaneous coronary intervention. J Am Coll Cardiol2000; 35:922–928.
Serruys PW, Ong AT, Morice MC, et al. Arterial Revascularisation Therapies Study Part II - Sirolimus-eluting stents for the treatment of patients with multivessel de novo coronary artery lesions. EuroIntervention2005; 1:147–156.
Kappetein AP, Head SJ, Morice MC, et al. Treatment of complex coronary artery disease in patients with diabetes: 5-year results comparing outcomes of bypass surgery and percutaneous coronary intervention in the SYNTAX trial. Eur J Cardiothorac Surg2013; 43:1006–1013.
Banning AP, Westaby S, Morice MC, et al. Diabetic and nondiabetic patients with left main and/or 3-vessel coronary artery disease: comparison of outcomes with cardiac surgery and paclitaxel-eluting stents. J Am Coll Cardiol2010; 55:1067–1075.
Weintraub WS, Grau-Sepulveda MV, Weiss JM, et al. Comparative effectiveness of revascularization strategies. N Engl J Med2012; 366:1467–1476.
Magnuson EA, Farkouh ME, Fuster V, et al; FREEDOM Trial Investigators. Cost-effectiveness of percutaneous coronary intervention with drug eluting stents versus bypass surgery for patients with diabetes and multivessel coronary artery disease: results from the FREEDOM trial. Circulation2013; 127:820–831.
Loop FD, Lytle BW, Cosgrove DM, et al. Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med1986; 314:1–6.
Tector AJ, Schmahl TM, Janson B, et al. The internal mammary artery graft. Its longevity after coronary bypass. JAMA1981; 246:2181–2183.
Stone GW, Rizvi A, Newman W, et al. Everolimus-eluting versus paclitax-eleluting stents in coronary artery disease. N Engl J Med2010; 362:1663–1674.
Serruys PW, Silber S, Garg S, et al. Comparison of zotarolimus-eluting and everolimus-eluting coronary stents. N Engl J Med2010; 363:136–146.
Lamy A, Devereaux PJ, Prabhakaran D, et al. Off-pump or on-pump coronary-artery bypass grafting at 30 days. N Engl J Med2012; 366:1489–1497.
Patients with diabetes have a higher prevalence of multivessel coronary artery disease and often have complex, diffuse lesions.
Bypass surgery is the preferred method of revascularization in appropriately selected patients with diabetes and multivessel coronary artery disease.
In the FREEDOM trial, only about 10% of the screened patients were eligible for the study, limiting its generalizability; however, this is comparable to exclusion rates in previous large randomized trials.
When choosing a revascularization method, the physician team needs to discuss the options with the patient before performing diagnostic angiography. The team should include a cardiac surgeon and a cardiologist.
Some members of the public may have noticed the conclusions of a recent study1 that said that if an older postmenopausal woman has her bone mineral density measured to screen for osteoporosis and has a normal or only mildly low result, she does not need to come back for another measurement for approximately 15 years.
We believe this interpretation of the study’s findings is overly simplistic and may have the unfortunate result of causing some people to neglect their bone health. Moreover, the study looked mainly at baseline T scores as the determinant of the subsequent screening interval. However, clinicians must carefully consider a variety of clinical risk factors when deciding how often to obtain bone mineral density measurements. The ultimate goal is to not miss the window of opportunity for early detection and treatment when it would matter the most (ie, before fractures develop).
Here, we will review this recent study, its findings, and its implications.
OSTEOPOROSIS POSES AN ENORMOUS PUBLIC HEALTH PROBLEM
If we consider only the hip, an estimated 10 million people in the United States have osteoporosis (T score ≤ −2.5 or a preexisting fragility fracture), and 33.6 million have osteopenia (T score −1.01 to −2.49).2 The number of people with osteopenia can be assumed to be much higher if other skeletal sites are considered.
By increasing the risk of fragility fractures, osteoporosis poses an enormous public health problem. The surgeon general’s report points out that one of every two white women over age 50 will experience an osteoporosis-related fracture in her lifetime.3 Of all osteoporosis-related fractures, those of the hip carry the worse clinical outcome. Approximately one in five elderly people who experience an osteoporosis-related hip fracture need long-term nursing home care, and as many as 20% die within 1 year.3
In recognition of the burden of osteoporosis, the US Preventive Services Task Force (USPSTF)4 and other scientific bodies2,3 recommend an initial bone mineral density test for all women age 65 and older. Dual-energy x-ray absorptiometry (DXA) is considered the gold standard for bone mineral density testing. Although the patient population that should receive an initial bone mineral density test has been clearly identified (see below), guidelines on the optimal frequency of testing do not exist, as data have been lacking. Recognizing this knowledge gap, Gourlay et al1 attempted to answer the question of how often elderly postmenopausal women should be retested.
WHEN DO 10% OF ELDERLY POSTMENOPAUSAL WOMEN REACH A T SCORE OF −2.5?
Gourlay et al1 analyzed data from 4,957 women in the Study of Osteoporotic Fractures. These women were predominantly white, were at least 67 years old and ambulatory, and had normal bone mineral density or osteopenia and no history of hip or clinical vertebral fracture at baseline. They had been recruited between 1986 and 1988 at sites in Baltimore, MD, Minneapolis, MN, the Monongahela Valley near Pittsburgh, PA, and Portland, OR.
DXA of the hip had been performed at baseline and at multiple times thereafter. The average follow-up time was 8 years.
The primary outcome measured was how long it took for 10% of the patients to reach a T score of −2.5 or less at the femoral neck or total hip as they progressed from having normal bone mineral density to osteoporosis or from osteopenia to osteoporosis and before they developed a fracture or needed treatment for osteoporosis.
Clinical risk factors such as age, body mass index, estrogen use at baseline, fracture after age 50, current smoking, current or past use of glucocorticoids, and self-reported rheumatoid arthritis were included as covariates in time-to-event analyses.
ANSWER: 16.8 YEARS (IF NORMAL AT BASELINE)
The authors estimated that 10% of women would make the transition to osteoporosis before having a hip or clinical vertebral fracture in the following intervals:
16.8 years in women whose bone mineral density was normal at baseline (T score at femoral neck and total hip of −1.00 or higher)
17.3 years in women who had mild osteopenia at baseline (T score −1.01 to −1.49)
4.7 years in women with moderate osteopenia at baseline (T score −1.5 to −1.99)
1.1 years in women with advanced osteopenia at baseline (T score −2.00 to −2.49).
The authors also found that body mass index and current estrogen use were the only clinical risk factors that influenced these intervals; other clinical factors such as a fracture after age 50, current smoking, previous or current use of oral glucocorticoids, and self-reported rheumatoid arthritis did not.
They concluded that osteoporosis would develop in fewer than 10% of women if the rescreening interval was lengthened to 15 years for women with normal density or mild osteopenia, 5 years for women with moderate osteopenia, and 1 year for women with advanced osteopenia.
WHAT DOES THIS MEAN FOR THE PRACTICING CLINICIAN?
Who needs an initial DXA test according to current guidelines?
The USPSTF,4 the National Osteoporosis Foundation (NOF),5 the International Society for Clinical Densitometry (ISCD),6 and the American Association of Clinical Endocrinologists (AACE)7 propose that the following groups should undergo DXA:
All women age 65 and older
All postmenopausal women who have had a fragility fracture or who have one or more risk factors for osteoporosis (height loss, body mass index < 20 kg/m2, family history of osteoporosis, active smoking, excessive alcohol consumption)
Adults who have a condition (eg, rheumatoid arthritis) or are taking a medication (eg, glucocorticoids in a daily dose ≥ 5 mg of prednisone or its equivalent for ≥ 3 months) associated with low bone mass or bone loss
Anyone being considered for drug therapy for osteoporosis, discontinuing therapy for osteoporosis (including estrogen), or being treated for osteoporosis, to monitor the effect of treatment.
Assessing fracture risk. Although clinicians have traditionally relied on bone mineral density obtained by DXA to estimate fracture risk, the World Health Organization has developed a computer-based algorithm that calculates an individual’s 10-year fracture probability from easily obtained clinical risk factors with or without adding femoral-neck bone mineral density. The Fracture Risk Assessment tool, or FRAX, has attracted intense interest since its introduction in 2007 and has been endorsed by the USPSTF4 and by other scientific societies, including the NOF5 and the ISCD.8 In fact, the most recent USPSTF guidelines,4 which recommend screening all women age 65 and older, call for using FRAX to identify younger women at higher risk of fracture.
According to FRAX, a 65-year-old white woman who has no risk factors has a 9.3% chance of developing a major osteoporotic fracture in the next 10 years. And if a younger woman (between the ages of 50 and 64) has a fracture risk as high or higher than a 65-year-old white woman who has no risk factors, then she too should be screened by DXA.
What are the current recommendations about follow-up DXA testing?
In eligible patients, the Centers for Medicare and Medicaid Services will pay for a DXA scan every 2 years. This interval is based on the concept that in an otherwise healthy person, it takes a minimum of 2 years to see a significant change in bone mineral density that can be attributed to a biological change in the bone and not just chance. The USPSTF4 and scientific societies such as the NOF5 generally agree with the Medicare guidelines of retesting every 2 years but recognize certain clinical situations that may warrant more frequent retesting (see below).
But the real question is how long the DXA screening interval can be extended so that meaningful information can still be obtained to help make management decisions and before a complication such as a fracture occurs. While there is convincing evidence to support the recommendations for an initial DXA test, data to answer the question of how long the resting interval should be are lacking.
Before the study by Gourlay et al,1 the only data on repeat DXA came from work by Hillier et al.9 But those investigators asked a different question. They were interested in how well repeated measurements predicted fractures. They used the same population that Gourlay et al did but evaluated fractures, not T scores. They concluded that in healthy, adult postmenopausal women, repeating the bone mineral density measurement up to 8 years later adds little value to initial measurement for predicting incident fractures.
Clinical factors also count
The T score should not be the only major factor determining the interval for bone mineral density testing in elderly women; clinical risk factors also should be kept in mind.
Gourlay et al concluded that age and T scores are the key predictive factors in determining the bone mineral density testing interval in elderly, postmenopausal women for screening purposes.1 In their statistical model, clinical risk factors such as fracture after age 50, current smoking, previous or current use of glucocorticoids, and self-reported rheumatoid arthritis did not influence the testing interval. They say that clinicians should not feel compelled to shorten the testing interval when these risk factors are present.
Readers may take this to mean that if these results were strictly applied to a 70-year-old white woman receiving oral glucocorticoids for rheumatoid arthritis and who has a baseline T score of −1.45, then her next test may be postponed by 15 years (given that both these factors did not influence the testing interval). Readers may also conclude that if this patient’s T score were −1.51, then her screening interval would be 5 years and not 15 years.
However, Gourlay et al say1 that clinicians can choose to shorten the testing interval if there is evidence of decreased activity or mobility, weight loss, or other risk factors not considered in their analysis.
Soon after this study1 was published, Lewiecki et al10 and others11–13 published critical commentaries addressing controversial issues surrounding the study. They highlighted the importance of considering clinical risk factors for fracture in addition to the femoral neck and total hip T scores. In response to these comments, Gourlay et al clarified that their results were not generalizable to patients with secondary osteoporosis, such as those taking glucocorticoids or those who have rheumatic diseases.14
Figure 1. The effects of several clinical risk factors on the 10-year probability of a major osteoporotic fracture occurring in 65-year-old white men and women in the United States.
Readers should keep in mind that clinical risk factors make independent contributions to fracture risk (Figure 1).15
Readers should also recognize the following groups in whom the results of the study by Gourlay et al are not applicable since they were not included in their study:
Men
Women other than white women
Women already diagnosed with osteoporosis and on bisphosphonates or any other osteoporosis treatment (except for estrogen). The findings also do not apply to:
Patients who experience a significant decline in health status or who develop new clinical conditions (such as hyperparathyroidism, paraproteinemias, or type 2 diabetes) or who use medications such as glucocorticoids that cause rapid bone loss. Changes in clinical situations such as these may necessitate more frequent bone mineral density testing in spite of a “good” baseline T score.
Perimenopausal women or women who received their first bone mineral density test before age 65. Perimenopause and menopause may trigger rapid bone loss, which may be as much as one T-score point (ie, 1 standard deviation) at the spine and femoral neck.16 Therefore, testing done during this time cannot be used as the basis of future monitoring.
The study did not address asymptomatic vertebral fractures and lumbar spine density
Gourlay et al1 did not take into account asymptomatic spinal fractures; they used only clinical vertebral fractures in their risk estimates of spinal fractures. Ascertainment of morphometric spinal fractures may be methodologically challenging, but if the study had included these fractures, the outcomes and conclusions could have been very different.
Vertebral fractures are present in as many as 14% to 33% of postmenopausal women17 and indicate osteoporosis (regardless of the bone mineral density). Moreover, most vertebral fractures are clinically silent and escape detection, and approximately only one in three radiographically defined vertebral fractures is reported clinically.18,19 Given the prevalence of these fractures, we and others10 have noted that the results of the Gourlay study may be biased toward longer screening intervals because they did not account for morphometric vertebral fractures.
Gourlay et al used T scores only of the femoral neck and total hip and not those of the lumbar spine. Some studies have found that hip measurements may be superior to spine measurements for overall osteoporotic fracture prediction.20,21 However, lumbar spine bone mineral density is predictive of fracture at other skeletal sites,22,23 is a widely accepted skeletal site measurement, and is used to diagnose osteoporosis. Moreover, the lumbar spine T score can be −2.5 or higher even if the total hip or femoral neck T score is lower than −2.5.
More fractures occur in people with osteopenia than with osteoporosis
Osteoporosis imparts a much higher risk of fracture than does osteopenia. However, if one recognizes the much greater prevalence of osteopenia (33.6 million people) compared with osteoporosis (10 million),2 it is not hard to appreciate that the number of fractures is higher in the osteopenic group than in those with osteoporosis based on T scores. Siris et al24 point out that at least half of osteoporotic fractures are in patients with osteopenia, who comprise a larger segment of the population than those with osteoporosis.
Some clinical trials have shown that bisphosphonates are not effective in preventing clinical fractures in women who do not have osteoporosis.25,26 However, clinicians must recognize that while bisphosphonates may not be as effective in preventing fractures in the osteopenic group with no other clinical risk factors, the presence of multiple clinical risk factors incrementally increases the fracture risk (which can be assessed via FRAX) and may require starting drug therapy earlier.
Women with vertebral fractures are considered to have clinical osteoporosis even if they have T scores in the osteopenic range, and must be considered for drug therapy.
The public health burden of fractures will not decrease unless individuals with low bone mineral density who are at an increased risk of fracture are identified and treated.24
Is DXA testing overused or underused? does it decrease the rate of fractures?
The study of Gourlay et al1 captured a lot of media attention, with many newspapers and blogs claiming that women may be getting tested too often.27,28 However, in reality, this test is highly underutilized. The 2011 Healthcare Effectiveness Data and Information Set report noted that 71.0% of women in Medicare health maintenance organizations and 75.0% of women in Medicare preferred provider organizations ever had a bone mineral density test for osteoporosis.29 While these numbers may not appear to be too far from the target, they are a poor gauge of DXA use as they include all types of bone mineral density tests in a woman’s lifetime, including even heel tests at health fairs.
Central DXA is used far less than one might expect. King and Fiorentino, in a recent analysis, showed that only about 14% of fee-for-service Medicare beneficiaries 65 years and older had one or more DXA tests in 2010.30 DXA retesting also does not seem to be an issue, with only 1 in 10 elderly women reporting having had a repeat test at 2-year intervals, and fewer than 1 in 100 tested reported testing more frequently.30
References
Gourlay ML, Fine JP, Preisser JS, et al; Study of Osteoporotic Fractures research group. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med2012; 366:225–233.
National Osteoporosis Foundation (NOF). America’s Bone Health: The State of Osteoporosis and Low Bone Mass in Our Nation. Washington, DC: National Osteoporosis Foundation; 2002.
US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Office of the Surgeon General; 2004.
US Preventive Services Task Force. Screening for osteoporosis: US preventive services task force recommendation statement. Ann Intern Med2011; 154:356–364.
National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington, DC: National Osteoporosis Foundation; 2010.
Baim S, Binkley N, Bilezikian JP, et al. Official Positions of the International Society for Clinical Densitometry and executive summary of the 2007 ISCD Position Development Conference. J Clin Densitom2008; 11:75–91.
Watts NB, Bilezikian JP, Camacho PM, et al; AACE Osteoporosis Task Force. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the diagnosis and treatment of postmenopausal osteoporosis. Endocr Pract2010; 16(suppl 3):1–37.
The International Society for Clinical Densitometry (ISCD); the International Osteoporosis Foundation (IOF). 2010 Official Positions on FRAX. www.iscd.org/official-positions. Accessed February 1, 2013.
Hillier TA, Stone KL, Bauer DC, et al. Evaluating the value of repeat bone mineral density measurement and prediction of fractures in older women: the study of osteoporotic fractures. Arch Intern Med2007; 167:155–160.
Lewiecki EM, Laster AJ, Miller PD, Bilezikian JP. More bone density testing is needed, not less. J Bone Miner Res2012; 27:739–742.
Leslie WD, Morin SN, Lix LM. Bone-density testing interval and transition to osteoporosis. N Engl J Med2012; 366:1547.
Gourlay ML, Preisser JS, Lui LY, Cauley JA, Ensrud BeStudy of Osteoporotic Fractures Research Group. BMD screening in older women: initial measurement and testing interval. J Bone Miner Res2012; 27:743–746.
Kanis JA, Oden A, Johansson H, Borgström F, Ström O, McCloskey E. FRAX and its applications to clinical practice. Bone2009; 44:734–743.
Recker RR. Early postmenopausal bone loss and what to do about it. Ann NY Acad Sci2011; 1240:E26–E30.
Genant HK, Jergas M, Palermo L, et al. Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J Bone Miner Res1996; 11:984–996.
Black DM, Cummings SR, Karpf DB, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet1996; 348:1535–1541.
Nevitt MC, Ettinger B, Black DM, et al. The association of radiographically detected vertebral fractures with back pain and function: a prospective study. Ann Intern Med1998; 128:793–800.
Leslie WD, Tsang JF, Caetano PA, Lix LM; Manitoba Bone Density Program. Effectiveness of bone density measurement for predicting osteoporotic fractures in clinical practice. J Clin Endocrinol Metab2007; 92:77–81.
Leslie WD, Lix LM, Tsang JF, Caetano PA; Manitoba Bone Density Program. Single-site vs multisite bone density measurement for fracture prediction. Arch Intern Med2007; 167:1641–1647.
Stone KL, Seeley DG, Lui LY, et al; Osteoporotic Fractures Research Group. BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res2003; 18:1947–1954.
Black DM, Cummings SR, Genant HK, Nevitt MC, Palermo L, Browner W. Axial and appendicular bone density predict fractures in older women. J Bone Miner Res1992; 7:633–638.
Siris ES, Baim S, Nattiv A. Primary care use of FRAX: absolute fracture risk assessment in postmenopausal women and older men. Postgrad Med2010; 122:82–90.
Cummings SR, Black DM, Thompson DE, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA1998; 280:2077–2082.
McClung MR, Geusens P, Miller PD, et al; Hip Intervention Program Study Group. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med2001; 344:333–340.
King AB, Fiorentino DM. Medicare payment cuts for osteoporosis testing reduced use despite tests’ benefit in reducing fractures. Health Aff (Millwood)2011; 30:2362–2370.
Angelo A. Licata, MD, PhD Director, Endocrine Calcium Clinic, Department of Endocrinology, Diabetes, and Metabolism, and Director, Center for Space Medicine, Department of Biomedical Engineering, Cleveland Clinic; Clinical Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
Address: Angelo A. Licata, MD, PhD, Department of Endocrinology, Diabetes, and Metabolism, F20, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: licataa@ccf.org.
Angelo A. Licata, MD, PhD Director, Endocrine Calcium Clinic, Department of Endocrinology, Diabetes, and Metabolism, and Director, Center for Space Medicine, Department of Biomedical Engineering, Cleveland Clinic; Clinical Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
Address: Angelo A. Licata, MD, PhD, Department of Endocrinology, Diabetes, and Metabolism, F20, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: licataa@ccf.org.
Author and Disclosure Information
Krupa B. Doshi, MD, CCD Department of Endocrinology, Diabetes, and Metabolism, Cleveland Clinic
Leila Z. Khan, MD, CCD Department of Endocrinology, Diabetes, and Metabolism, Cleveland Clinic
Angelo A. Licata, MD, PhD Director, Endocrine Calcium Clinic, Department of Endocrinology, Diabetes, and Metabolism, and Director, Center for Space Medicine, Department of Biomedical Engineering, Cleveland Clinic; Clinical Assistant Professor, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University
Address: Angelo A. Licata, MD, PhD, Department of Endocrinology, Diabetes, and Metabolism, F20, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail: licataa@ccf.org.
Some members of the public may have noticed the conclusions of a recent study1 that said that if an older postmenopausal woman has her bone mineral density measured to screen for osteoporosis and has a normal or only mildly low result, she does not need to come back for another measurement for approximately 15 years.
We believe this interpretation of the study’s findings is overly simplistic and may have the unfortunate result of causing some people to neglect their bone health. Moreover, the study looked mainly at baseline T scores as the determinant of the subsequent screening interval. However, clinicians must carefully consider a variety of clinical risk factors when deciding how often to obtain bone mineral density measurements. The ultimate goal is to not miss the window of opportunity for early detection and treatment when it would matter the most (ie, before fractures develop).
Here, we will review this recent study, its findings, and its implications.
OSTEOPOROSIS POSES AN ENORMOUS PUBLIC HEALTH PROBLEM
If we consider only the hip, an estimated 10 million people in the United States have osteoporosis (T score ≤ −2.5 or a preexisting fragility fracture), and 33.6 million have osteopenia (T score −1.01 to −2.49).2 The number of people with osteopenia can be assumed to be much higher if other skeletal sites are considered.
By increasing the risk of fragility fractures, osteoporosis poses an enormous public health problem. The surgeon general’s report points out that one of every two white women over age 50 will experience an osteoporosis-related fracture in her lifetime.3 Of all osteoporosis-related fractures, those of the hip carry the worse clinical outcome. Approximately one in five elderly people who experience an osteoporosis-related hip fracture need long-term nursing home care, and as many as 20% die within 1 year.3
In recognition of the burden of osteoporosis, the US Preventive Services Task Force (USPSTF)4 and other scientific bodies2,3 recommend an initial bone mineral density test for all women age 65 and older. Dual-energy x-ray absorptiometry (DXA) is considered the gold standard for bone mineral density testing. Although the patient population that should receive an initial bone mineral density test has been clearly identified (see below), guidelines on the optimal frequency of testing do not exist, as data have been lacking. Recognizing this knowledge gap, Gourlay et al1 attempted to answer the question of how often elderly postmenopausal women should be retested.
WHEN DO 10% OF ELDERLY POSTMENOPAUSAL WOMEN REACH A T SCORE OF −2.5?
Gourlay et al1 analyzed data from 4,957 women in the Study of Osteoporotic Fractures. These women were predominantly white, were at least 67 years old and ambulatory, and had normal bone mineral density or osteopenia and no history of hip or clinical vertebral fracture at baseline. They had been recruited between 1986 and 1988 at sites in Baltimore, MD, Minneapolis, MN, the Monongahela Valley near Pittsburgh, PA, and Portland, OR.
DXA of the hip had been performed at baseline and at multiple times thereafter. The average follow-up time was 8 years.
The primary outcome measured was how long it took for 10% of the patients to reach a T score of −2.5 or less at the femoral neck or total hip as they progressed from having normal bone mineral density to osteoporosis or from osteopenia to osteoporosis and before they developed a fracture or needed treatment for osteoporosis.
Clinical risk factors such as age, body mass index, estrogen use at baseline, fracture after age 50, current smoking, current or past use of glucocorticoids, and self-reported rheumatoid arthritis were included as covariates in time-to-event analyses.
ANSWER: 16.8 YEARS (IF NORMAL AT BASELINE)
The authors estimated that 10% of women would make the transition to osteoporosis before having a hip or clinical vertebral fracture in the following intervals:
16.8 years in women whose bone mineral density was normal at baseline (T score at femoral neck and total hip of −1.00 or higher)
17.3 years in women who had mild osteopenia at baseline (T score −1.01 to −1.49)
4.7 years in women with moderate osteopenia at baseline (T score −1.5 to −1.99)
1.1 years in women with advanced osteopenia at baseline (T score −2.00 to −2.49).
The authors also found that body mass index and current estrogen use were the only clinical risk factors that influenced these intervals; other clinical factors such as a fracture after age 50, current smoking, previous or current use of oral glucocorticoids, and self-reported rheumatoid arthritis did not.
They concluded that osteoporosis would develop in fewer than 10% of women if the rescreening interval was lengthened to 15 years for women with normal density or mild osteopenia, 5 years for women with moderate osteopenia, and 1 year for women with advanced osteopenia.
WHAT DOES THIS MEAN FOR THE PRACTICING CLINICIAN?
Who needs an initial DXA test according to current guidelines?
The USPSTF,4 the National Osteoporosis Foundation (NOF),5 the International Society for Clinical Densitometry (ISCD),6 and the American Association of Clinical Endocrinologists (AACE)7 propose that the following groups should undergo DXA:
All women age 65 and older
All postmenopausal women who have had a fragility fracture or who have one or more risk factors for osteoporosis (height loss, body mass index < 20 kg/m2, family history of osteoporosis, active smoking, excessive alcohol consumption)
Adults who have a condition (eg, rheumatoid arthritis) or are taking a medication (eg, glucocorticoids in a daily dose ≥ 5 mg of prednisone or its equivalent for ≥ 3 months) associated with low bone mass or bone loss
Anyone being considered for drug therapy for osteoporosis, discontinuing therapy for osteoporosis (including estrogen), or being treated for osteoporosis, to monitor the effect of treatment.
Assessing fracture risk. Although clinicians have traditionally relied on bone mineral density obtained by DXA to estimate fracture risk, the World Health Organization has developed a computer-based algorithm that calculates an individual’s 10-year fracture probability from easily obtained clinical risk factors with or without adding femoral-neck bone mineral density. The Fracture Risk Assessment tool, or FRAX, has attracted intense interest since its introduction in 2007 and has been endorsed by the USPSTF4 and by other scientific societies, including the NOF5 and the ISCD.8 In fact, the most recent USPSTF guidelines,4 which recommend screening all women age 65 and older, call for using FRAX to identify younger women at higher risk of fracture.
According to FRAX, a 65-year-old white woman who has no risk factors has a 9.3% chance of developing a major osteoporotic fracture in the next 10 years. And if a younger woman (between the ages of 50 and 64) has a fracture risk as high or higher than a 65-year-old white woman who has no risk factors, then she too should be screened by DXA.
What are the current recommendations about follow-up DXA testing?
In eligible patients, the Centers for Medicare and Medicaid Services will pay for a DXA scan every 2 years. This interval is based on the concept that in an otherwise healthy person, it takes a minimum of 2 years to see a significant change in bone mineral density that can be attributed to a biological change in the bone and not just chance. The USPSTF4 and scientific societies such as the NOF5 generally agree with the Medicare guidelines of retesting every 2 years but recognize certain clinical situations that may warrant more frequent retesting (see below).
But the real question is how long the DXA screening interval can be extended so that meaningful information can still be obtained to help make management decisions and before a complication such as a fracture occurs. While there is convincing evidence to support the recommendations for an initial DXA test, data to answer the question of how long the resting interval should be are lacking.
Before the study by Gourlay et al,1 the only data on repeat DXA came from work by Hillier et al.9 But those investigators asked a different question. They were interested in how well repeated measurements predicted fractures. They used the same population that Gourlay et al did but evaluated fractures, not T scores. They concluded that in healthy, adult postmenopausal women, repeating the bone mineral density measurement up to 8 years later adds little value to initial measurement for predicting incident fractures.
Clinical factors also count
The T score should not be the only major factor determining the interval for bone mineral density testing in elderly women; clinical risk factors also should be kept in mind.
Gourlay et al concluded that age and T scores are the key predictive factors in determining the bone mineral density testing interval in elderly, postmenopausal women for screening purposes.1 In their statistical model, clinical risk factors such as fracture after age 50, current smoking, previous or current use of glucocorticoids, and self-reported rheumatoid arthritis did not influence the testing interval. They say that clinicians should not feel compelled to shorten the testing interval when these risk factors are present.
Readers may take this to mean that if these results were strictly applied to a 70-year-old white woman receiving oral glucocorticoids for rheumatoid arthritis and who has a baseline T score of −1.45, then her next test may be postponed by 15 years (given that both these factors did not influence the testing interval). Readers may also conclude that if this patient’s T score were −1.51, then her screening interval would be 5 years and not 15 years.
However, Gourlay et al say1 that clinicians can choose to shorten the testing interval if there is evidence of decreased activity or mobility, weight loss, or other risk factors not considered in their analysis.
Soon after this study1 was published, Lewiecki et al10 and others11–13 published critical commentaries addressing controversial issues surrounding the study. They highlighted the importance of considering clinical risk factors for fracture in addition to the femoral neck and total hip T scores. In response to these comments, Gourlay et al clarified that their results were not generalizable to patients with secondary osteoporosis, such as those taking glucocorticoids or those who have rheumatic diseases.14
Figure 1. The effects of several clinical risk factors on the 10-year probability of a major osteoporotic fracture occurring in 65-year-old white men and women in the United States.
Readers should keep in mind that clinical risk factors make independent contributions to fracture risk (Figure 1).15
Readers should also recognize the following groups in whom the results of the study by Gourlay et al are not applicable since they were not included in their study:
Men
Women other than white women
Women already diagnosed with osteoporosis and on bisphosphonates or any other osteoporosis treatment (except for estrogen). The findings also do not apply to:
Patients who experience a significant decline in health status or who develop new clinical conditions (such as hyperparathyroidism, paraproteinemias, or type 2 diabetes) or who use medications such as glucocorticoids that cause rapid bone loss. Changes in clinical situations such as these may necessitate more frequent bone mineral density testing in spite of a “good” baseline T score.
Perimenopausal women or women who received their first bone mineral density test before age 65. Perimenopause and menopause may trigger rapid bone loss, which may be as much as one T-score point (ie, 1 standard deviation) at the spine and femoral neck.16 Therefore, testing done during this time cannot be used as the basis of future monitoring.
The study did not address asymptomatic vertebral fractures and lumbar spine density
Gourlay et al1 did not take into account asymptomatic spinal fractures; they used only clinical vertebral fractures in their risk estimates of spinal fractures. Ascertainment of morphometric spinal fractures may be methodologically challenging, but if the study had included these fractures, the outcomes and conclusions could have been very different.
Vertebral fractures are present in as many as 14% to 33% of postmenopausal women17 and indicate osteoporosis (regardless of the bone mineral density). Moreover, most vertebral fractures are clinically silent and escape detection, and approximately only one in three radiographically defined vertebral fractures is reported clinically.18,19 Given the prevalence of these fractures, we and others10 have noted that the results of the Gourlay study may be biased toward longer screening intervals because they did not account for morphometric vertebral fractures.
Gourlay et al used T scores only of the femoral neck and total hip and not those of the lumbar spine. Some studies have found that hip measurements may be superior to spine measurements for overall osteoporotic fracture prediction.20,21 However, lumbar spine bone mineral density is predictive of fracture at other skeletal sites,22,23 is a widely accepted skeletal site measurement, and is used to diagnose osteoporosis. Moreover, the lumbar spine T score can be −2.5 or higher even if the total hip or femoral neck T score is lower than −2.5.
More fractures occur in people with osteopenia than with osteoporosis
Osteoporosis imparts a much higher risk of fracture than does osteopenia. However, if one recognizes the much greater prevalence of osteopenia (33.6 million people) compared with osteoporosis (10 million),2 it is not hard to appreciate that the number of fractures is higher in the osteopenic group than in those with osteoporosis based on T scores. Siris et al24 point out that at least half of osteoporotic fractures are in patients with osteopenia, who comprise a larger segment of the population than those with osteoporosis.
Some clinical trials have shown that bisphosphonates are not effective in preventing clinical fractures in women who do not have osteoporosis.25,26 However, clinicians must recognize that while bisphosphonates may not be as effective in preventing fractures in the osteopenic group with no other clinical risk factors, the presence of multiple clinical risk factors incrementally increases the fracture risk (which can be assessed via FRAX) and may require starting drug therapy earlier.
Women with vertebral fractures are considered to have clinical osteoporosis even if they have T scores in the osteopenic range, and must be considered for drug therapy.
The public health burden of fractures will not decrease unless individuals with low bone mineral density who are at an increased risk of fracture are identified and treated.24
Is DXA testing overused or underused? does it decrease the rate of fractures?
The study of Gourlay et al1 captured a lot of media attention, with many newspapers and blogs claiming that women may be getting tested too often.27,28 However, in reality, this test is highly underutilized. The 2011 Healthcare Effectiveness Data and Information Set report noted that 71.0% of women in Medicare health maintenance organizations and 75.0% of women in Medicare preferred provider organizations ever had a bone mineral density test for osteoporosis.29 While these numbers may not appear to be too far from the target, they are a poor gauge of DXA use as they include all types of bone mineral density tests in a woman’s lifetime, including even heel tests at health fairs.
Central DXA is used far less than one might expect. King and Fiorentino, in a recent analysis, showed that only about 14% of fee-for-service Medicare beneficiaries 65 years and older had one or more DXA tests in 2010.30 DXA retesting also does not seem to be an issue, with only 1 in 10 elderly women reporting having had a repeat test at 2-year intervals, and fewer than 1 in 100 tested reported testing more frequently.30
Some members of the public may have noticed the conclusions of a recent study1 that said that if an older postmenopausal woman has her bone mineral density measured to screen for osteoporosis and has a normal or only mildly low result, she does not need to come back for another measurement for approximately 15 years.
We believe this interpretation of the study’s findings is overly simplistic and may have the unfortunate result of causing some people to neglect their bone health. Moreover, the study looked mainly at baseline T scores as the determinant of the subsequent screening interval. However, clinicians must carefully consider a variety of clinical risk factors when deciding how often to obtain bone mineral density measurements. The ultimate goal is to not miss the window of opportunity for early detection and treatment when it would matter the most (ie, before fractures develop).
Here, we will review this recent study, its findings, and its implications.
OSTEOPOROSIS POSES AN ENORMOUS PUBLIC HEALTH PROBLEM
If we consider only the hip, an estimated 10 million people in the United States have osteoporosis (T score ≤ −2.5 or a preexisting fragility fracture), and 33.6 million have osteopenia (T score −1.01 to −2.49).2 The number of people with osteopenia can be assumed to be much higher if other skeletal sites are considered.
By increasing the risk of fragility fractures, osteoporosis poses an enormous public health problem. The surgeon general’s report points out that one of every two white women over age 50 will experience an osteoporosis-related fracture in her lifetime.3 Of all osteoporosis-related fractures, those of the hip carry the worse clinical outcome. Approximately one in five elderly people who experience an osteoporosis-related hip fracture need long-term nursing home care, and as many as 20% die within 1 year.3
In recognition of the burden of osteoporosis, the US Preventive Services Task Force (USPSTF)4 and other scientific bodies2,3 recommend an initial bone mineral density test for all women age 65 and older. Dual-energy x-ray absorptiometry (DXA) is considered the gold standard for bone mineral density testing. Although the patient population that should receive an initial bone mineral density test has been clearly identified (see below), guidelines on the optimal frequency of testing do not exist, as data have been lacking. Recognizing this knowledge gap, Gourlay et al1 attempted to answer the question of how often elderly postmenopausal women should be retested.
WHEN DO 10% OF ELDERLY POSTMENOPAUSAL WOMEN REACH A T SCORE OF −2.5?
Gourlay et al1 analyzed data from 4,957 women in the Study of Osteoporotic Fractures. These women were predominantly white, were at least 67 years old and ambulatory, and had normal bone mineral density or osteopenia and no history of hip or clinical vertebral fracture at baseline. They had been recruited between 1986 and 1988 at sites in Baltimore, MD, Minneapolis, MN, the Monongahela Valley near Pittsburgh, PA, and Portland, OR.
DXA of the hip had been performed at baseline and at multiple times thereafter. The average follow-up time was 8 years.
The primary outcome measured was how long it took for 10% of the patients to reach a T score of −2.5 or less at the femoral neck or total hip as they progressed from having normal bone mineral density to osteoporosis or from osteopenia to osteoporosis and before they developed a fracture or needed treatment for osteoporosis.
Clinical risk factors such as age, body mass index, estrogen use at baseline, fracture after age 50, current smoking, current or past use of glucocorticoids, and self-reported rheumatoid arthritis were included as covariates in time-to-event analyses.
ANSWER: 16.8 YEARS (IF NORMAL AT BASELINE)
The authors estimated that 10% of women would make the transition to osteoporosis before having a hip or clinical vertebral fracture in the following intervals:
16.8 years in women whose bone mineral density was normal at baseline (T score at femoral neck and total hip of −1.00 or higher)
17.3 years in women who had mild osteopenia at baseline (T score −1.01 to −1.49)
4.7 years in women with moderate osteopenia at baseline (T score −1.5 to −1.99)
1.1 years in women with advanced osteopenia at baseline (T score −2.00 to −2.49).
The authors also found that body mass index and current estrogen use were the only clinical risk factors that influenced these intervals; other clinical factors such as a fracture after age 50, current smoking, previous or current use of oral glucocorticoids, and self-reported rheumatoid arthritis did not.
They concluded that osteoporosis would develop in fewer than 10% of women if the rescreening interval was lengthened to 15 years for women with normal density or mild osteopenia, 5 years for women with moderate osteopenia, and 1 year for women with advanced osteopenia.
WHAT DOES THIS MEAN FOR THE PRACTICING CLINICIAN?
Who needs an initial DXA test according to current guidelines?
The USPSTF,4 the National Osteoporosis Foundation (NOF),5 the International Society for Clinical Densitometry (ISCD),6 and the American Association of Clinical Endocrinologists (AACE)7 propose that the following groups should undergo DXA:
All women age 65 and older
All postmenopausal women who have had a fragility fracture or who have one or more risk factors for osteoporosis (height loss, body mass index < 20 kg/m2, family history of osteoporosis, active smoking, excessive alcohol consumption)
Adults who have a condition (eg, rheumatoid arthritis) or are taking a medication (eg, glucocorticoids in a daily dose ≥ 5 mg of prednisone or its equivalent for ≥ 3 months) associated with low bone mass or bone loss
Anyone being considered for drug therapy for osteoporosis, discontinuing therapy for osteoporosis (including estrogen), or being treated for osteoporosis, to monitor the effect of treatment.
Assessing fracture risk. Although clinicians have traditionally relied on bone mineral density obtained by DXA to estimate fracture risk, the World Health Organization has developed a computer-based algorithm that calculates an individual’s 10-year fracture probability from easily obtained clinical risk factors with or without adding femoral-neck bone mineral density. The Fracture Risk Assessment tool, or FRAX, has attracted intense interest since its introduction in 2007 and has been endorsed by the USPSTF4 and by other scientific societies, including the NOF5 and the ISCD.8 In fact, the most recent USPSTF guidelines,4 which recommend screening all women age 65 and older, call for using FRAX to identify younger women at higher risk of fracture.
According to FRAX, a 65-year-old white woman who has no risk factors has a 9.3% chance of developing a major osteoporotic fracture in the next 10 years. And if a younger woman (between the ages of 50 and 64) has a fracture risk as high or higher than a 65-year-old white woman who has no risk factors, then she too should be screened by DXA.
What are the current recommendations about follow-up DXA testing?
In eligible patients, the Centers for Medicare and Medicaid Services will pay for a DXA scan every 2 years. This interval is based on the concept that in an otherwise healthy person, it takes a minimum of 2 years to see a significant change in bone mineral density that can be attributed to a biological change in the bone and not just chance. The USPSTF4 and scientific societies such as the NOF5 generally agree with the Medicare guidelines of retesting every 2 years but recognize certain clinical situations that may warrant more frequent retesting (see below).
But the real question is how long the DXA screening interval can be extended so that meaningful information can still be obtained to help make management decisions and before a complication such as a fracture occurs. While there is convincing evidence to support the recommendations for an initial DXA test, data to answer the question of how long the resting interval should be are lacking.
Before the study by Gourlay et al,1 the only data on repeat DXA came from work by Hillier et al.9 But those investigators asked a different question. They were interested in how well repeated measurements predicted fractures. They used the same population that Gourlay et al did but evaluated fractures, not T scores. They concluded that in healthy, adult postmenopausal women, repeating the bone mineral density measurement up to 8 years later adds little value to initial measurement for predicting incident fractures.
Clinical factors also count
The T score should not be the only major factor determining the interval for bone mineral density testing in elderly women; clinical risk factors also should be kept in mind.
Gourlay et al concluded that age and T scores are the key predictive factors in determining the bone mineral density testing interval in elderly, postmenopausal women for screening purposes.1 In their statistical model, clinical risk factors such as fracture after age 50, current smoking, previous or current use of glucocorticoids, and self-reported rheumatoid arthritis did not influence the testing interval. They say that clinicians should not feel compelled to shorten the testing interval when these risk factors are present.
Readers may take this to mean that if these results were strictly applied to a 70-year-old white woman receiving oral glucocorticoids for rheumatoid arthritis and who has a baseline T score of −1.45, then her next test may be postponed by 15 years (given that both these factors did not influence the testing interval). Readers may also conclude that if this patient’s T score were −1.51, then her screening interval would be 5 years and not 15 years.
However, Gourlay et al say1 that clinicians can choose to shorten the testing interval if there is evidence of decreased activity or mobility, weight loss, or other risk factors not considered in their analysis.
Soon after this study1 was published, Lewiecki et al10 and others11–13 published critical commentaries addressing controversial issues surrounding the study. They highlighted the importance of considering clinical risk factors for fracture in addition to the femoral neck and total hip T scores. In response to these comments, Gourlay et al clarified that their results were not generalizable to patients with secondary osteoporosis, such as those taking glucocorticoids or those who have rheumatic diseases.14
Figure 1. The effects of several clinical risk factors on the 10-year probability of a major osteoporotic fracture occurring in 65-year-old white men and women in the United States.
Readers should keep in mind that clinical risk factors make independent contributions to fracture risk (Figure 1).15
Readers should also recognize the following groups in whom the results of the study by Gourlay et al are not applicable since they were not included in their study:
Men
Women other than white women
Women already diagnosed with osteoporosis and on bisphosphonates or any other osteoporosis treatment (except for estrogen). The findings also do not apply to:
Patients who experience a significant decline in health status or who develop new clinical conditions (such as hyperparathyroidism, paraproteinemias, or type 2 diabetes) or who use medications such as glucocorticoids that cause rapid bone loss. Changes in clinical situations such as these may necessitate more frequent bone mineral density testing in spite of a “good” baseline T score.
Perimenopausal women or women who received their first bone mineral density test before age 65. Perimenopause and menopause may trigger rapid bone loss, which may be as much as one T-score point (ie, 1 standard deviation) at the spine and femoral neck.16 Therefore, testing done during this time cannot be used as the basis of future monitoring.
The study did not address asymptomatic vertebral fractures and lumbar spine density
Gourlay et al1 did not take into account asymptomatic spinal fractures; they used only clinical vertebral fractures in their risk estimates of spinal fractures. Ascertainment of morphometric spinal fractures may be methodologically challenging, but if the study had included these fractures, the outcomes and conclusions could have been very different.
Vertebral fractures are present in as many as 14% to 33% of postmenopausal women17 and indicate osteoporosis (regardless of the bone mineral density). Moreover, most vertebral fractures are clinically silent and escape detection, and approximately only one in three radiographically defined vertebral fractures is reported clinically.18,19 Given the prevalence of these fractures, we and others10 have noted that the results of the Gourlay study may be biased toward longer screening intervals because they did not account for morphometric vertebral fractures.
Gourlay et al used T scores only of the femoral neck and total hip and not those of the lumbar spine. Some studies have found that hip measurements may be superior to spine measurements for overall osteoporotic fracture prediction.20,21 However, lumbar spine bone mineral density is predictive of fracture at other skeletal sites,22,23 is a widely accepted skeletal site measurement, and is used to diagnose osteoporosis. Moreover, the lumbar spine T score can be −2.5 or higher even if the total hip or femoral neck T score is lower than −2.5.
More fractures occur in people with osteopenia than with osteoporosis
Osteoporosis imparts a much higher risk of fracture than does osteopenia. However, if one recognizes the much greater prevalence of osteopenia (33.6 million people) compared with osteoporosis (10 million),2 it is not hard to appreciate that the number of fractures is higher in the osteopenic group than in those with osteoporosis based on T scores. Siris et al24 point out that at least half of osteoporotic fractures are in patients with osteopenia, who comprise a larger segment of the population than those with osteoporosis.
Some clinical trials have shown that bisphosphonates are not effective in preventing clinical fractures in women who do not have osteoporosis.25,26 However, clinicians must recognize that while bisphosphonates may not be as effective in preventing fractures in the osteopenic group with no other clinical risk factors, the presence of multiple clinical risk factors incrementally increases the fracture risk (which can be assessed via FRAX) and may require starting drug therapy earlier.
Women with vertebral fractures are considered to have clinical osteoporosis even if they have T scores in the osteopenic range, and must be considered for drug therapy.
The public health burden of fractures will not decrease unless individuals with low bone mineral density who are at an increased risk of fracture are identified and treated.24
Is DXA testing overused or underused? does it decrease the rate of fractures?
The study of Gourlay et al1 captured a lot of media attention, with many newspapers and blogs claiming that women may be getting tested too often.27,28 However, in reality, this test is highly underutilized. The 2011 Healthcare Effectiveness Data and Information Set report noted that 71.0% of women in Medicare health maintenance organizations and 75.0% of women in Medicare preferred provider organizations ever had a bone mineral density test for osteoporosis.29 While these numbers may not appear to be too far from the target, they are a poor gauge of DXA use as they include all types of bone mineral density tests in a woman’s lifetime, including even heel tests at health fairs.
Central DXA is used far less than one might expect. King and Fiorentino, in a recent analysis, showed that only about 14% of fee-for-service Medicare beneficiaries 65 years and older had one or more DXA tests in 2010.30 DXA retesting also does not seem to be an issue, with only 1 in 10 elderly women reporting having had a repeat test at 2-year intervals, and fewer than 1 in 100 tested reported testing more frequently.30
References
Gourlay ML, Fine JP, Preisser JS, et al; Study of Osteoporotic Fractures research group. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med2012; 366:225–233.
National Osteoporosis Foundation (NOF). America’s Bone Health: The State of Osteoporosis and Low Bone Mass in Our Nation. Washington, DC: National Osteoporosis Foundation; 2002.
US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Office of the Surgeon General; 2004.
US Preventive Services Task Force. Screening for osteoporosis: US preventive services task force recommendation statement. Ann Intern Med2011; 154:356–364.
National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington, DC: National Osteoporosis Foundation; 2010.
Baim S, Binkley N, Bilezikian JP, et al. Official Positions of the International Society for Clinical Densitometry and executive summary of the 2007 ISCD Position Development Conference. J Clin Densitom2008; 11:75–91.
Watts NB, Bilezikian JP, Camacho PM, et al; AACE Osteoporosis Task Force. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the diagnosis and treatment of postmenopausal osteoporosis. Endocr Pract2010; 16(suppl 3):1–37.
The International Society for Clinical Densitometry (ISCD); the International Osteoporosis Foundation (IOF). 2010 Official Positions on FRAX. www.iscd.org/official-positions. Accessed February 1, 2013.
Hillier TA, Stone KL, Bauer DC, et al. Evaluating the value of repeat bone mineral density measurement and prediction of fractures in older women: the study of osteoporotic fractures. Arch Intern Med2007; 167:155–160.
Lewiecki EM, Laster AJ, Miller PD, Bilezikian JP. More bone density testing is needed, not less. J Bone Miner Res2012; 27:739–742.
Leslie WD, Morin SN, Lix LM. Bone-density testing interval and transition to osteoporosis. N Engl J Med2012; 366:1547.
Gourlay ML, Preisser JS, Lui LY, Cauley JA, Ensrud BeStudy of Osteoporotic Fractures Research Group. BMD screening in older women: initial measurement and testing interval. J Bone Miner Res2012; 27:743–746.
Kanis JA, Oden A, Johansson H, Borgström F, Ström O, McCloskey E. FRAX and its applications to clinical practice. Bone2009; 44:734–743.
Recker RR. Early postmenopausal bone loss and what to do about it. Ann NY Acad Sci2011; 1240:E26–E30.
Genant HK, Jergas M, Palermo L, et al. Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J Bone Miner Res1996; 11:984–996.
Black DM, Cummings SR, Karpf DB, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet1996; 348:1535–1541.
Nevitt MC, Ettinger B, Black DM, et al. The association of radiographically detected vertebral fractures with back pain and function: a prospective study. Ann Intern Med1998; 128:793–800.
Leslie WD, Tsang JF, Caetano PA, Lix LM; Manitoba Bone Density Program. Effectiveness of bone density measurement for predicting osteoporotic fractures in clinical practice. J Clin Endocrinol Metab2007; 92:77–81.
Leslie WD, Lix LM, Tsang JF, Caetano PA; Manitoba Bone Density Program. Single-site vs multisite bone density measurement for fracture prediction. Arch Intern Med2007; 167:1641–1647.
Stone KL, Seeley DG, Lui LY, et al; Osteoporotic Fractures Research Group. BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res2003; 18:1947–1954.
Black DM, Cummings SR, Genant HK, Nevitt MC, Palermo L, Browner W. Axial and appendicular bone density predict fractures in older women. J Bone Miner Res1992; 7:633–638.
Siris ES, Baim S, Nattiv A. Primary care use of FRAX: absolute fracture risk assessment in postmenopausal women and older men. Postgrad Med2010; 122:82–90.
Cummings SR, Black DM, Thompson DE, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA1998; 280:2077–2082.
McClung MR, Geusens P, Miller PD, et al; Hip Intervention Program Study Group. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med2001; 344:333–340.
King AB, Fiorentino DM. Medicare payment cuts for osteoporosis testing reduced use despite tests’ benefit in reducing fractures. Health Aff (Millwood)2011; 30:2362–2370.
References
Gourlay ML, Fine JP, Preisser JS, et al; Study of Osteoporotic Fractures research group. Bone-density testing interval and transition to osteoporosis in older women. N Engl J Med2012; 366:225–233.
National Osteoporosis Foundation (NOF). America’s Bone Health: The State of Osteoporosis and Low Bone Mass in Our Nation. Washington, DC: National Osteoporosis Foundation; 2002.
US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Office of the Surgeon General; 2004.
US Preventive Services Task Force. Screening for osteoporosis: US preventive services task force recommendation statement. Ann Intern Med2011; 154:356–364.
National Osteoporosis Foundation. Clinician’s Guide to Prevention and Treatment of Osteoporosis. Washington, DC: National Osteoporosis Foundation; 2010.
Baim S, Binkley N, Bilezikian JP, et al. Official Positions of the International Society for Clinical Densitometry and executive summary of the 2007 ISCD Position Development Conference. J Clin Densitom2008; 11:75–91.
Watts NB, Bilezikian JP, Camacho PM, et al; AACE Osteoporosis Task Force. American Association of Clinical Endocrinologists Medical Guidelines for Clinical Practice for the diagnosis and treatment of postmenopausal osteoporosis. Endocr Pract2010; 16(suppl 3):1–37.
The International Society for Clinical Densitometry (ISCD); the International Osteoporosis Foundation (IOF). 2010 Official Positions on FRAX. www.iscd.org/official-positions. Accessed February 1, 2013.
Hillier TA, Stone KL, Bauer DC, et al. Evaluating the value of repeat bone mineral density measurement and prediction of fractures in older women: the study of osteoporotic fractures. Arch Intern Med2007; 167:155–160.
Lewiecki EM, Laster AJ, Miller PD, Bilezikian JP. More bone density testing is needed, not less. J Bone Miner Res2012; 27:739–742.
Leslie WD, Morin SN, Lix LM. Bone-density testing interval and transition to osteoporosis. N Engl J Med2012; 366:1547.
Gourlay ML, Preisser JS, Lui LY, Cauley JA, Ensrud BeStudy of Osteoporotic Fractures Research Group. BMD screening in older women: initial measurement and testing interval. J Bone Miner Res2012; 27:743–746.
Kanis JA, Oden A, Johansson H, Borgström F, Ström O, McCloskey E. FRAX and its applications to clinical practice. Bone2009; 44:734–743.
Recker RR. Early postmenopausal bone loss and what to do about it. Ann NY Acad Sci2011; 1240:E26–E30.
Genant HK, Jergas M, Palermo L, et al. Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis The Study of Osteoporotic Fractures Research Group. J Bone Miner Res1996; 11:984–996.
Black DM, Cummings SR, Karpf DB, et al. Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention Trial Research Group. Lancet1996; 348:1535–1541.
Nevitt MC, Ettinger B, Black DM, et al. The association of radiographically detected vertebral fractures with back pain and function: a prospective study. Ann Intern Med1998; 128:793–800.
Leslie WD, Tsang JF, Caetano PA, Lix LM; Manitoba Bone Density Program. Effectiveness of bone density measurement for predicting osteoporotic fractures in clinical practice. J Clin Endocrinol Metab2007; 92:77–81.
Leslie WD, Lix LM, Tsang JF, Caetano PA; Manitoba Bone Density Program. Single-site vs multisite bone density measurement for fracture prediction. Arch Intern Med2007; 167:1641–1647.
Stone KL, Seeley DG, Lui LY, et al; Osteoporotic Fractures Research Group. BMD at multiple sites and risk of fracture of multiple types: long-term results from the Study of Osteoporotic Fractures. J Bone Miner Res2003; 18:1947–1954.
Black DM, Cummings SR, Genant HK, Nevitt MC, Palermo L, Browner W. Axial and appendicular bone density predict fractures in older women. J Bone Miner Res1992; 7:633–638.
Siris ES, Baim S, Nattiv A. Primary care use of FRAX: absolute fracture risk assessment in postmenopausal women and older men. Postgrad Med2010; 122:82–90.
Cummings SR, Black DM, Thompson DE, et al. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: results from the Fracture Intervention Trial. JAMA1998; 280:2077–2082.
McClung MR, Geusens P, Miller PD, et al; Hip Intervention Program Study Group. Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med2001; 344:333–340.
King AB, Fiorentino DM. Medicare payment cuts for osteoporosis testing reduced use despite tests’ benefit in reducing fractures. Health Aff (Millwood)2011; 30:2362–2370.
The criteria for who should undergo bone mineral density measurement are well established, but data on repeat testing are scarce.
Gourlay et al concluded that age and T scores are the key predictive factors in determining the bone mineral density testing interval, while clinical risk factors such as fracture after age 50, current smoking, previous or current use of glucocorticoids, and self-reported rheumatoid arthritis are not.
The Fracture Risk Assessment tool (FRAX) is a useful clinical tool that calculates an individual’s 10-year risk of fracture. It is available at www.shef.ac.uk/FRAX
The recent publication of the AIM-HIGH trial (Atherothrombosis Intervention in Metabolic Syndrome With Low HDL/High Triglycerides: Impact on Global Health Outcomes)1 has thrown the use of niacin as a lipid-modifying therapy into question. The trial was stopped early because an interim analysis found that the patients who took extended-release niacin had no clinical benefit. In addition, it found a trend toward more ischemic strokes, though this finding was later found not to be statistically significant.
Complicating the interpretation, while both the treatment group and the control group in the study received statin therapy, the researchers attempted to keep low-density lipoprotein cholesterol (LDL-C) levels equal, meaning that patients in the control group received more intensive statin therapy than those in the treatment group. And the placebo that the control patients received was actually a low dose of niacin, to induce flushing and thus to blind study participants and their physicians to which drug they were taking.
In the article that follows, I will explore the background, design, findings, and implications of this key trial and try to untangle the many questions about how to interpret it.
LOWERING LDL-C REDUCES RISK, BUT DOES NOT ELIMINATE IT
Large randomized controlled trials have consistently shown that lowering the level of LDL-C reduces cardiovascular event rates by 25% to 45% both in people who are known to have coronary artery disease and in those who are not.2–4 As a result, guidelines for preventing cardiovascular disease have increasingly emphasized maintaining low LDL-C levels. This has led to a proliferation in the use of inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A reductase (statins) in patients at high cardiovascular risk.
However, these agents only reduce the risk—they do not eliminate it. Needed are additional therapies to complement existing LDL-C-lowering approaches to lower the cardiovascular risk even further.
Raising HDL-C: The next frontier
One such strategy for further lowering cardiovascular risk that has received considerable interest is to promote the biological activity of the “good” cholesterol.
Studies have consistently shown that the higher the plasma level of high-density lipoprotein cholesterol (HDL-C), the lower the risk of cardiovascular events, suggesting that raising HDL-C may be beneficial.5 Studies in animals with atherosclerosis show that raising HDL-C via genetic modification of the animal or direct infusion of the molecule has a favorable impact on both the size and the structure of experimental plaque.6,7
Accordingly, much activity has focused on developing new therapies that raise HDL-C more effectively than current ones.
Why niacin should protect the heart
For more than 50 years, niacin has been used to manage dyslipidemia.
In addition to raising HDL-C levels more effectively than any other agent available today, niacin also lowers the levels of LDL-C, triglycerides, and lipoprotein (a).8 Before statins were available, the Coronary Drug Project found that niacin reduced the rate of nonfatal myocardial infarction and the 15-year mortality rate.9 In addition, niacin has been shown to slow the progression of carotid intimal-medial thickness and coronary atherosclerosis, and even to reverse these processes in some trials.10–12
However, a number of issues remain about using niacin to prevent cardiovascular events. Nearly all patients who take it experience flushing, which limits its tolerability and, thus, our ability to titrate doses to levels needed for adequate lipid changes. While a number of modifications of niacin administration have been developed (eg, extended-release formulations and products that inhibit flushing), no large study has tested the clinical efficacy of these strategies. Furthermore, until AIM-HIGH, no large-scale trial had directly evaluated the impact of niacin therapy on a background of statin therapy.
AIM-HIGH STUDY DESIGN
The intent of the AIM-HIGH trial was to determine whether extended-release niacin (Niaspan) would reduce the risk of cardiovascular events when added to therapy with a statin—in this case, simvastatin (Zocor) supplemented with ezetimibe (Zetia).1
The trial was funded by the National Heart, Lung, and Blood Institute (NHLBI) and by Abbott Laboratories, which also supplied the extended-release niacin and the ezetimibe. Merck donated the simvastatin.
Patient characteristics
The patients were all at least 45 years of age with established, stable coronary heart disease, cerebrovascular or carotid arterial disease, or peripheral arterial disease. They also had to have low levels of HDL-C (< 40 mg/dL in men, < 50 mg/dL in women), elevated triglycerides (150–400 mg/dL), and LDL-C levels lower than 180 mg/dL if they were not taking a statin at entry.
The mean age of the patients was 64 years, 85% were men, and 92% were white. They had a high prevalence of cardiovascular risk factors: 34% had diabetes, 71% had hypertension, and 81% had metabolic syndrome. Nearly all (94%) of the patients were taking a statin at entry; 76% had been taking one for more than 1 year, and 40% had been taking one for more than 5 years.1
Simvastatin, ezetimibe, and either niacin or placebo
All lipid-modifying agents except statins and ezetimibe were stopped for least 4 weeks after enrollment.
All patients then entered a 4- to 8-week open-label period, during which they took simvastatin 40 mg daily and extended-release niacin starting at 500 mg and increased weekly up to 2,000 mg daily. Patients who could tolerate at least 1,500 mg daily were randomly assigned to treatment with either niacin 1,500 to 2,000 mg or matching placebo. Both groups continued to receive simvastatin. The placebo contained a small dose of immediate-release niacin (50 mg) in each tablet to induce flushing and to maintain blinding of treatment.
Given that niacin also lowers LDL-C, an algorithm was used to try to keep LDL-C levels roughly the same in both treatment groups. This involved adjusting the simvastatin dose and permitting the use of ezetimibe 10 mg to keep the LDL-C level between 40 and 80 mg/dL. Accordingly, participating physicians were told their patients’ LDL-C levels but were blinded to their HDL-C and triglyceride levels throughout the study.
Every 6 months, patients had a follow-up visit in the clinic, and midway through each 6-month interval they received a phone call from the investigators.1
AIM-HIGH end points
The primary end point was the composite of the first event of death due to coronary heart disease, nonfatal myocardial infarction, ischemic stroke, hospitalization for acute coronary syndrome, or symptom-driven revascularization of the coronary or cerebral arteries.
Secondary end points were:
Death from coronary heart disease, nonfatal myocardial infarction, ischemic stroke, or hospitalization for acute coronary syndrome
Death from coronary heart disease, nonfatal myocardial infarction, or ischemic stroke
Death from cardiovascular causes.
Tertiary end points included:
Death from any cause
Individual components of the primary end point
Prespecified subgroups according to sex, history or no history of diabetes, and presence or absence of the metabolic syndrome.1
All clinical events were adjudicated by a central committee.
STUDY HALTED EARLY
The study was planned to run for a mean of 4.6 years, during which 800 primary end point events were expected. With these numbers, the investigators calculated that the study had 85% power to detect a 25% reduction in the primary end point, at a one-sided alpha level of 0.025.
The plan called for an interim analysis when 50% of the anticipated events had occurred, with prespecified stopping boundaries based on either efficacy or futility. The boundary for lack of efficacy required an observed hazard ratio of at least 1.02 with a probability of less than .001.
In the interim analysis, after a median follow-up of only 3 years, the data and safety monitoring board recommended stopping the study early because the boundary for futility had been crossed and, unexpectedly, the rate of ischemic stroke was higher in the niacin-treated patients than in those receiving placebo.
MAJOR FINDINGS OF AIM-HIGH
Of 4,273 patients who began open-label treatment with niacin, 3,414 were randomized to treatment with niacin or placebo.1
HDL-C levels went up in both groups
At 2 years:
HDL-C levels had increased by 25.0% (to 42 mg/dL) in the niacin group and by 9.8% (to 38 mg/dL) in the placebo group
Triglycerides had decreased by 28.6% with niacin and by 8.1% with placebo
LDL-C had decreased by 12.0% with niacin and by 5.5% with placebo.
Patients in the placebo group were more likely to have subsequently received the maximum dose of simvastatin, ie, 80 mg/day (24.7% vs 17.5%), and to have received ezetimibe (21.5% vs 9.5%). More patients in the niacin group required either dose reduction of the study drug (6.3% vs 3.4%) or drug discontinuation (25.4% vs 20.1%).1
No difference in the primary end point
There was no difference between the two treatment groups in the rate of the primary end point, which occurred in 282 (16.4%) of the 1,718 patients in the niacin group and 272 (16.2%) of the 1,696 patients in the placebo group (P = .79; hazard ratio 1.02, 95% confidence interval 0.87–1.21).1
However, more patients in the niacin group than in the placebo group who reached the primary end point did so by having a first ischemic stroke: 27 patients (1.6%) vs 15 patients (0.9%). Eight of these patients, all in the niacin group, had their stroke between 2 months and 4 years after they had stopped taking the study drug.
Further analysis that included all ischemic strokes revealed the same trend: 29 vs 18 patients (P = .11).1
No benefit was observed for niacin-treated patients in terms of any of the secondary or tertiary end points.
Subgroup analysis revealed no evidence of statistical heterogeneity: ie, niacin seemed to lack efficacy in all the prespecified subgroups studied (age 65 and older vs younger, men vs women, and those with or without diabetes, metabolic syndrome, prior myocardial infarction, or statin use at entry).
In general, niacin was well tolerated in the active-treatment group, with a low incidence of liver and muscle abnormalities.
PUTTING AIM-HIGH IN CONTEXT
How should practicing clinicians interpret these outcomes?
Ever since the NHLBI reported (in an urgent press release) that it was stopping the study early due to futility and a potential excess of strokes,13 there has been considerable debate as to which factors contributed to these outcomes. In the wake of the publication of more detailed information about the trial,1 this debate is likely to continue.
The AIM-HIGH results can be interpreted in several ways:
Perhaps niacin is no good as a preventive agent
Perhaps raising HDL-C is flawed as a preventive strategy
Perhaps AIM-HIGH had methodologic flaws, such as looking at the wrong patient cohort or using a treatment protocol that set itself up for failure
Perhaps statins are so good that, once you prescribe one, anything else you give provides no additional benefit.
Which of these is correct?
Is niacin no good?
In its most simple form, AIM-HIGH has always been seen as a clinical trial of niacin. While the early trials of immediate-release niacin were encouraging in terms of its effects on lipids, atherosclerotic plaque, and cardiovascular outcomes, using it in clinical practice has always been challenging, largely because many patients cannot tolerate it in doses high enough to be effective. A number of developments have improved niacin’s tolerability, but its clinical impact in the statin era has not been evaluated.
Niacin’s lack of efficacy in this trial will ultimately be viewed as a failure of the drug itself, but is this the case?
AIM-HIGH was not simply a direct comparison of niacin vs placebo on top of standard medical practice. The investigators recognized that niacin has additional effects—in particular, lowering levels of atherogenic lipids—and they attempted to control for these effects by titrating the other LDL-C-lowering therapies during the study. As a result, the trial was actually a comparison between niacin plus low-dose simvastatin on the one hand, and placebo plus high-dose simvastatin (and, more often, also ezetimibe) on the other.
Furthermore, the placebo-treated patients received small doses of immediate-release niacin to induce flushing and maintain blinding. It is therefore hard to conclude that this clinical trial was a direct evaluation of the impact of niacin.
In contrast, the Heart Protection Study 2-Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2-THRIVE) study is currently evaluating extended-release niacin in combination with laropiprant, a prostaglandin receptor antagonist, vs placebo in more than 24,000 statin-treated patients.14 Without any in-trial titration of lipids, this study provides a more direct comparison of the effects of niacin in the statin era.
Niacin continues to attract interest, largely because it can raise HDL-C by 20% to 30% when given at doses of 1,500 mg or more. Also, consistent observations from population studies of an inverse relationship between HDL-C levels and cardiovascular risk5 have stimulated interest in developing novel agents that substantially raise HDL-C.
Is raising HDL-C a flawed strategy?
The failure of HDL-C-raising therapies in clinical trials15,16 has fueled concern that HDL may not be the magic elixir that many have sought. Given that niacin is the most effective HDL-C-raising agent currently available, its lack of efficacy in AIM-HIGH could be perceived as another nail in the coffin of the hypothesis that raising the HDL-C level with pharmacologic agents is beneficial.
AIM-HIGH was designed to examine the effects of raising HDL-C. To this end, it was performed exclusively in patients with low HDL-C levels, and the investigators tried to isolate the potential effects of raising HDL-C by equalizing the LDL-C levels in the treatment groups.
However, the HDL-C changes observed in AIM-HIGH are likely to have undermined the study objective. While niacin predictably increased HDL-C levels by 25%, an unexpected increase in HDL-C of 9.8% in the placebo-treated patients resulted in a difference in achieved HDL-C levels of only 4 mg/dL between the groups. This was far less than anticipated, and it likely had a major impact on an already underpowered study.
AIM-HIGH was designed to have 85% power to demonstrate a 25% reduction in clinical events, which was an optimistic estimate. On the basis of population studies, a difference of 4 mg/dL in HDL-C would be anticipated to result in no more than a 10% lower rate of clinical events, far beyond AIM-HIGH’s limit of detection.
The reasons for the increase in HDL-C in the placebo group are unknown, but they likely reflect the use of higher doses of simvastatin, some regression to the mean, and, possibly, the small doses of immediate-release niacin that the placebo contained. (Contrary to the belief of the investigators, there have been some reports of lipid changes with such doses,17 which may have contributed to the observed HDL-C-raising.)
Given that the HDL-C difference between the groups was relatively small and that niacin has additional effects beyond raising HDL-C and lowering LDL-C, it is unlikely that the futility of AIM-HIGH reflects a major indictment of HDL-C-raising. For the time being, the jury is still out on this question.
Was AIM-HIGH methodologically flawed?
A number of methodologic issues may have affected AIM-HIGH’s ability to adequately address its objectives.
The wrong cohort? In planning a study such as AIM-HIGH, the need for a relatively small sample size and the need to detect the greatest relative risk reduction with niacin would require enrollment of patients at the highest risk of cardiovascular events despite the use of statins. These needs were satisfied by only including patients who had atherosclerotic cardiovascular disease and low HDL-C levels. The inclusion of patients with low levels of HDL-C was also expected to promote greater increases in this lipid, and potentially event reduction, with niacin.
But no benefit was observed. It remains to be determined whether the inclusion of a high proportion of patients with the metabolic syndrome adversely affected the ability to detect a benefit with niacin. While post hoc analyses of studies of carotid intimal-medial thickness demonstrated no relationship between raising HDL-C with niacin and slowing of disease progression in patients with the metabolic syndrome,18 it remains to be determined whether this would translate to any effect on cardiovascular event rates.
Inadequate statistical power? An underpowered study would leave very little room for error, a pertinent point given the variability in therapeutic response in both actively treated and placebo-treated patients typically encountered in clinical trials. Giving low doses of immediate-release niacin and titrating the simvastatin dose to control LDL-C, resulting in imbalances in lipid-modifying therapies, represent additional flaws in the study design.
Stopped too soon? The early cessation of the study was somewhat questionable. The study crossed the prespecified boundary for lack of efficacy at the time of the interim analysis, and initial review by the data and safety monitoring board suggested an excess rate of ischemic stroke with niacin. The inclusion of this latter finding in the press release prompted considerable speculation regarding potential mechanisms and also concern among patients currently taking niacin. The subsequent finding that this signal was not statistically significant serves as an important warning for those conducting clinical trials not to prematurely overstate preliminary observations.
The implications for agents used in clinical practice are considerable: negative findings should not be overemphasized without robust evidence.
Do statins make everything else irrelevant?
The final factor to consider is the relative modifiability of residual clinical risk in statin-treated patients.
While residual risk is often cited as the reason to develop new antiatherosclerotic therapies, it is unknown how many of these ongoing events can be prevented. Several nonmodifiable factors such as age and concomitant disease are likely to contribute to these clinical events, which may limit our ability to further reduce event rates in patients who have already achieved low LDL-C levels with statin therapy. This may underscore the observation that no major clinical trial has demonstrated clinical benefit of an antiatherosclerotic agent on top of background medical care that included statins.
The finding that atherosclerosis continues to progress in many patients even though they take statins in high doses or achieve low LDL-C levels suggests that there is still room for improvement.
WHAT FUTURE FOR NIACIN?
So what does the future hold for niacin? The ongoing HPS2-THRIVE study provides another opportunity to evaluate the potential clinical efficacy of niacin in statin-treated patients. For now, we must wait for the results of this study.
In the meantime, it would seem reasonable to continue treatment with niacin in patients who need it for its multiple lipid-modifying effects. Whether clinicians will be less likely to initiate niacin therapy until there is clear evidence of clinical benefit remains uncertain. As for HDL-C, it remains to be determined whether any therapy targeting either quantitative or qualitative changes will be beneficial.
Over the last 3 decades, clinical trials have provided important insights into the prevention of cardiovascular events and have had a profound impact on clinical practice. Such studies simply evaluate whether one strategy is better or worse than the existing standard of care. They do not provide mechanistic insights, and when attempts have been made to address mechanisms in the study design, the trial, as in the case of AIM-HIGH, leaves more questions than answers.
Future trials will provide more clarity as to the optimal way to treat patients, but they must be based on a robust design that permits the study question to be adequately addressed.
References
The AIM-HIGH Investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med2011; 365:2255–2267.
Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet1994; 344:1383–1389.
MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet2002; 360:7–22.
Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med2008; 359:2195–2207.
Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med1977; 62:707–714.
Rubin EM, Krauss RM, Spangler EA, Verstuyft JG, Clift SM. Inhibition of early atherogenesis in transgenic mice by human apolipoprotein AI. Nature1991; 353:265–267.
Nicholls SJ, Cutri B, Worthley SG, et al. Impact of short-term administration of high-density lipoproteins and atorvastatin on atherosclerosis in rabbits. Arterioscler Thromb Vasc Biol2005; 25:2416–2421.
deLemos AS, Wolfe ML, Long CJ, Sivapackianathan R, Rader DJ. Identification of genetic variants in endothelial lipase in persons with elevated high-density lipoprotein cholesterol. Circulation2002; 106:1321–1326.
Canner PL, Berge KG, Wenger NK, et al. Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin. J Am Coll Cardiol1986; 8:1245–1255.
Taylor AJ, Sullenberger LE, Lee HJ, Lee JK, Grace KA. Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol (ARBITER) 2: a double-blind, placebo-controlled study of extended-release niacin on atherosclerosis progression in secondary prevention patients treated with statins. Circulation2004; 110:3512–3517.
Taylor AJ, Lee HJ, Sullenberger LE. The effect of 24 months of combination statin and extended-release niacin on carotid intima-media thickness: ARBITER 3. Curr Med Res Opin2006; 22:2243–2250.
Brown BG, Zhao X-Q, Chait A, et al. Simvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary disease. N Engl J Med2001; 345:1583–1592.
Brown BG, Zhao XQ. Nicotinic acid, alone and in combinations, for reduction of cardiovascular risk. Am J Cardiol2008; 101:58B–62B.
Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med2007; 357:2109–2122.
Ginsberg HN, Elam MB, Lovato LC, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med2010; 362:1563–1574.
Luria MH, Sapoznikov D. Raising HDL cholesterol with low-dose nicotinic acid and bezafibrate: preliminary experience. Postgrad Med J1993; 69:296–299.
Taylor AJ, Zhu D, Sullenberger LE, Lee HJ, Lee JK, Grace KA. Relationship between glycemic status and progression of carotid intima-media thickness during treatment with combined statin and extended-release niacin in ARBITER 2. Vasc Health Risk Manag2007; 3:159–164.
Stephen J. Nicholls, MBBS, PhD Assistant Professor of Molecular Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University; Cardiovascular Director, Cleveland Clinic Coordinating Center for Clinical Research, Heart and Vascular Institute, Cleveland Clinic
Address: Stephen Nicholls, Department of Cardiovascular Medicine, JJ65, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH, 44195; email: nichols1@ccf.org
The author has disclosed that he receives honoraria from AstraZeneca, Merck, Roche, and Takeda; is a consultant to Anthera, AstraZeneca, Merck, NovoNordisk, Pfizer, and Takeda; and receives research support from Anthera, AstraZeneca, Eli Lilly, Novartis, and Resverlogix.
Stephen J. Nicholls, MBBS, PhD Assistant Professor of Molecular Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University; Cardiovascular Director, Cleveland Clinic Coordinating Center for Clinical Research, Heart and Vascular Institute, Cleveland Clinic
Address: Stephen Nicholls, Department of Cardiovascular Medicine, JJ65, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH, 44195; email: nichols1@ccf.org
The author has disclosed that he receives honoraria from AstraZeneca, Merck, Roche, and Takeda; is a consultant to Anthera, AstraZeneca, Merck, NovoNordisk, Pfizer, and Takeda; and receives research support from Anthera, AstraZeneca, Eli Lilly, Novartis, and Resverlogix.
Author and Disclosure Information
Stephen J. Nicholls, MBBS, PhD Assistant Professor of Molecular Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University; Cardiovascular Director, Cleveland Clinic Coordinating Center for Clinical Research, Heart and Vascular Institute, Cleveland Clinic
Address: Stephen Nicholls, Department of Cardiovascular Medicine, JJ65, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH, 44195; email: nichols1@ccf.org
The author has disclosed that he receives honoraria from AstraZeneca, Merck, Roche, and Takeda; is a consultant to Anthera, AstraZeneca, Merck, NovoNordisk, Pfizer, and Takeda; and receives research support from Anthera, AstraZeneca, Eli Lilly, Novartis, and Resverlogix.
The recent publication of the AIM-HIGH trial (Atherothrombosis Intervention in Metabolic Syndrome With Low HDL/High Triglycerides: Impact on Global Health Outcomes)1 has thrown the use of niacin as a lipid-modifying therapy into question. The trial was stopped early because an interim analysis found that the patients who took extended-release niacin had no clinical benefit. In addition, it found a trend toward more ischemic strokes, though this finding was later found not to be statistically significant.
Complicating the interpretation, while both the treatment group and the control group in the study received statin therapy, the researchers attempted to keep low-density lipoprotein cholesterol (LDL-C) levels equal, meaning that patients in the control group received more intensive statin therapy than those in the treatment group. And the placebo that the control patients received was actually a low dose of niacin, to induce flushing and thus to blind study participants and their physicians to which drug they were taking.
In the article that follows, I will explore the background, design, findings, and implications of this key trial and try to untangle the many questions about how to interpret it.
LOWERING LDL-C REDUCES RISK, BUT DOES NOT ELIMINATE IT
Large randomized controlled trials have consistently shown that lowering the level of LDL-C reduces cardiovascular event rates by 25% to 45% both in people who are known to have coronary artery disease and in those who are not.2–4 As a result, guidelines for preventing cardiovascular disease have increasingly emphasized maintaining low LDL-C levels. This has led to a proliferation in the use of inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A reductase (statins) in patients at high cardiovascular risk.
However, these agents only reduce the risk—they do not eliminate it. Needed are additional therapies to complement existing LDL-C-lowering approaches to lower the cardiovascular risk even further.
Raising HDL-C: The next frontier
One such strategy for further lowering cardiovascular risk that has received considerable interest is to promote the biological activity of the “good” cholesterol.
Studies have consistently shown that the higher the plasma level of high-density lipoprotein cholesterol (HDL-C), the lower the risk of cardiovascular events, suggesting that raising HDL-C may be beneficial.5 Studies in animals with atherosclerosis show that raising HDL-C via genetic modification of the animal or direct infusion of the molecule has a favorable impact on both the size and the structure of experimental plaque.6,7
Accordingly, much activity has focused on developing new therapies that raise HDL-C more effectively than current ones.
Why niacin should protect the heart
For more than 50 years, niacin has been used to manage dyslipidemia.
In addition to raising HDL-C levels more effectively than any other agent available today, niacin also lowers the levels of LDL-C, triglycerides, and lipoprotein (a).8 Before statins were available, the Coronary Drug Project found that niacin reduced the rate of nonfatal myocardial infarction and the 15-year mortality rate.9 In addition, niacin has been shown to slow the progression of carotid intimal-medial thickness and coronary atherosclerosis, and even to reverse these processes in some trials.10–12
However, a number of issues remain about using niacin to prevent cardiovascular events. Nearly all patients who take it experience flushing, which limits its tolerability and, thus, our ability to titrate doses to levels needed for adequate lipid changes. While a number of modifications of niacin administration have been developed (eg, extended-release formulations and products that inhibit flushing), no large study has tested the clinical efficacy of these strategies. Furthermore, until AIM-HIGH, no large-scale trial had directly evaluated the impact of niacin therapy on a background of statin therapy.
AIM-HIGH STUDY DESIGN
The intent of the AIM-HIGH trial was to determine whether extended-release niacin (Niaspan) would reduce the risk of cardiovascular events when added to therapy with a statin—in this case, simvastatin (Zocor) supplemented with ezetimibe (Zetia).1
The trial was funded by the National Heart, Lung, and Blood Institute (NHLBI) and by Abbott Laboratories, which also supplied the extended-release niacin and the ezetimibe. Merck donated the simvastatin.
Patient characteristics
The patients were all at least 45 years of age with established, stable coronary heart disease, cerebrovascular or carotid arterial disease, or peripheral arterial disease. They also had to have low levels of HDL-C (< 40 mg/dL in men, < 50 mg/dL in women), elevated triglycerides (150–400 mg/dL), and LDL-C levels lower than 180 mg/dL if they were not taking a statin at entry.
The mean age of the patients was 64 years, 85% were men, and 92% were white. They had a high prevalence of cardiovascular risk factors: 34% had diabetes, 71% had hypertension, and 81% had metabolic syndrome. Nearly all (94%) of the patients were taking a statin at entry; 76% had been taking one for more than 1 year, and 40% had been taking one for more than 5 years.1
Simvastatin, ezetimibe, and either niacin or placebo
All lipid-modifying agents except statins and ezetimibe were stopped for least 4 weeks after enrollment.
All patients then entered a 4- to 8-week open-label period, during which they took simvastatin 40 mg daily and extended-release niacin starting at 500 mg and increased weekly up to 2,000 mg daily. Patients who could tolerate at least 1,500 mg daily were randomly assigned to treatment with either niacin 1,500 to 2,000 mg or matching placebo. Both groups continued to receive simvastatin. The placebo contained a small dose of immediate-release niacin (50 mg) in each tablet to induce flushing and to maintain blinding of treatment.
Given that niacin also lowers LDL-C, an algorithm was used to try to keep LDL-C levels roughly the same in both treatment groups. This involved adjusting the simvastatin dose and permitting the use of ezetimibe 10 mg to keep the LDL-C level between 40 and 80 mg/dL. Accordingly, participating physicians were told their patients’ LDL-C levels but were blinded to their HDL-C and triglyceride levels throughout the study.
Every 6 months, patients had a follow-up visit in the clinic, and midway through each 6-month interval they received a phone call from the investigators.1
AIM-HIGH end points
The primary end point was the composite of the first event of death due to coronary heart disease, nonfatal myocardial infarction, ischemic stroke, hospitalization for acute coronary syndrome, or symptom-driven revascularization of the coronary or cerebral arteries.
Secondary end points were:
Death from coronary heart disease, nonfatal myocardial infarction, ischemic stroke, or hospitalization for acute coronary syndrome
Death from coronary heart disease, nonfatal myocardial infarction, or ischemic stroke
Death from cardiovascular causes.
Tertiary end points included:
Death from any cause
Individual components of the primary end point
Prespecified subgroups according to sex, history or no history of diabetes, and presence or absence of the metabolic syndrome.1
All clinical events were adjudicated by a central committee.
STUDY HALTED EARLY
The study was planned to run for a mean of 4.6 years, during which 800 primary end point events were expected. With these numbers, the investigators calculated that the study had 85% power to detect a 25% reduction in the primary end point, at a one-sided alpha level of 0.025.
The plan called for an interim analysis when 50% of the anticipated events had occurred, with prespecified stopping boundaries based on either efficacy or futility. The boundary for lack of efficacy required an observed hazard ratio of at least 1.02 with a probability of less than .001.
In the interim analysis, after a median follow-up of only 3 years, the data and safety monitoring board recommended stopping the study early because the boundary for futility had been crossed and, unexpectedly, the rate of ischemic stroke was higher in the niacin-treated patients than in those receiving placebo.
MAJOR FINDINGS OF AIM-HIGH
Of 4,273 patients who began open-label treatment with niacin, 3,414 were randomized to treatment with niacin or placebo.1
HDL-C levels went up in both groups
At 2 years:
HDL-C levels had increased by 25.0% (to 42 mg/dL) in the niacin group and by 9.8% (to 38 mg/dL) in the placebo group
Triglycerides had decreased by 28.6% with niacin and by 8.1% with placebo
LDL-C had decreased by 12.0% with niacin and by 5.5% with placebo.
Patients in the placebo group were more likely to have subsequently received the maximum dose of simvastatin, ie, 80 mg/day (24.7% vs 17.5%), and to have received ezetimibe (21.5% vs 9.5%). More patients in the niacin group required either dose reduction of the study drug (6.3% vs 3.4%) or drug discontinuation (25.4% vs 20.1%).1
No difference in the primary end point
There was no difference between the two treatment groups in the rate of the primary end point, which occurred in 282 (16.4%) of the 1,718 patients in the niacin group and 272 (16.2%) of the 1,696 patients in the placebo group (P = .79; hazard ratio 1.02, 95% confidence interval 0.87–1.21).1
However, more patients in the niacin group than in the placebo group who reached the primary end point did so by having a first ischemic stroke: 27 patients (1.6%) vs 15 patients (0.9%). Eight of these patients, all in the niacin group, had their stroke between 2 months and 4 years after they had stopped taking the study drug.
Further analysis that included all ischemic strokes revealed the same trend: 29 vs 18 patients (P = .11).1
No benefit was observed for niacin-treated patients in terms of any of the secondary or tertiary end points.
Subgroup analysis revealed no evidence of statistical heterogeneity: ie, niacin seemed to lack efficacy in all the prespecified subgroups studied (age 65 and older vs younger, men vs women, and those with or without diabetes, metabolic syndrome, prior myocardial infarction, or statin use at entry).
In general, niacin was well tolerated in the active-treatment group, with a low incidence of liver and muscle abnormalities.
PUTTING AIM-HIGH IN CONTEXT
How should practicing clinicians interpret these outcomes?
Ever since the NHLBI reported (in an urgent press release) that it was stopping the study early due to futility and a potential excess of strokes,13 there has been considerable debate as to which factors contributed to these outcomes. In the wake of the publication of more detailed information about the trial,1 this debate is likely to continue.
The AIM-HIGH results can be interpreted in several ways:
Perhaps niacin is no good as a preventive agent
Perhaps raising HDL-C is flawed as a preventive strategy
Perhaps AIM-HIGH had methodologic flaws, such as looking at the wrong patient cohort or using a treatment protocol that set itself up for failure
Perhaps statins are so good that, once you prescribe one, anything else you give provides no additional benefit.
Which of these is correct?
Is niacin no good?
In its most simple form, AIM-HIGH has always been seen as a clinical trial of niacin. While the early trials of immediate-release niacin were encouraging in terms of its effects on lipids, atherosclerotic plaque, and cardiovascular outcomes, using it in clinical practice has always been challenging, largely because many patients cannot tolerate it in doses high enough to be effective. A number of developments have improved niacin’s tolerability, but its clinical impact in the statin era has not been evaluated.
Niacin’s lack of efficacy in this trial will ultimately be viewed as a failure of the drug itself, but is this the case?
AIM-HIGH was not simply a direct comparison of niacin vs placebo on top of standard medical practice. The investigators recognized that niacin has additional effects—in particular, lowering levels of atherogenic lipids—and they attempted to control for these effects by titrating the other LDL-C-lowering therapies during the study. As a result, the trial was actually a comparison between niacin plus low-dose simvastatin on the one hand, and placebo plus high-dose simvastatin (and, more often, also ezetimibe) on the other.
Furthermore, the placebo-treated patients received small doses of immediate-release niacin to induce flushing and maintain blinding. It is therefore hard to conclude that this clinical trial was a direct evaluation of the impact of niacin.
In contrast, the Heart Protection Study 2-Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2-THRIVE) study is currently evaluating extended-release niacin in combination with laropiprant, a prostaglandin receptor antagonist, vs placebo in more than 24,000 statin-treated patients.14 Without any in-trial titration of lipids, this study provides a more direct comparison of the effects of niacin in the statin era.
Niacin continues to attract interest, largely because it can raise HDL-C by 20% to 30% when given at doses of 1,500 mg or more. Also, consistent observations from population studies of an inverse relationship between HDL-C levels and cardiovascular risk5 have stimulated interest in developing novel agents that substantially raise HDL-C.
Is raising HDL-C a flawed strategy?
The failure of HDL-C-raising therapies in clinical trials15,16 has fueled concern that HDL may not be the magic elixir that many have sought. Given that niacin is the most effective HDL-C-raising agent currently available, its lack of efficacy in AIM-HIGH could be perceived as another nail in the coffin of the hypothesis that raising the HDL-C level with pharmacologic agents is beneficial.
AIM-HIGH was designed to examine the effects of raising HDL-C. To this end, it was performed exclusively in patients with low HDL-C levels, and the investigators tried to isolate the potential effects of raising HDL-C by equalizing the LDL-C levels in the treatment groups.
However, the HDL-C changes observed in AIM-HIGH are likely to have undermined the study objective. While niacin predictably increased HDL-C levels by 25%, an unexpected increase in HDL-C of 9.8% in the placebo-treated patients resulted in a difference in achieved HDL-C levels of only 4 mg/dL between the groups. This was far less than anticipated, and it likely had a major impact on an already underpowered study.
AIM-HIGH was designed to have 85% power to demonstrate a 25% reduction in clinical events, which was an optimistic estimate. On the basis of population studies, a difference of 4 mg/dL in HDL-C would be anticipated to result in no more than a 10% lower rate of clinical events, far beyond AIM-HIGH’s limit of detection.
The reasons for the increase in HDL-C in the placebo group are unknown, but they likely reflect the use of higher doses of simvastatin, some regression to the mean, and, possibly, the small doses of immediate-release niacin that the placebo contained. (Contrary to the belief of the investigators, there have been some reports of lipid changes with such doses,17 which may have contributed to the observed HDL-C-raising.)
Given that the HDL-C difference between the groups was relatively small and that niacin has additional effects beyond raising HDL-C and lowering LDL-C, it is unlikely that the futility of AIM-HIGH reflects a major indictment of HDL-C-raising. For the time being, the jury is still out on this question.
Was AIM-HIGH methodologically flawed?
A number of methodologic issues may have affected AIM-HIGH’s ability to adequately address its objectives.
The wrong cohort? In planning a study such as AIM-HIGH, the need for a relatively small sample size and the need to detect the greatest relative risk reduction with niacin would require enrollment of patients at the highest risk of cardiovascular events despite the use of statins. These needs were satisfied by only including patients who had atherosclerotic cardiovascular disease and low HDL-C levels. The inclusion of patients with low levels of HDL-C was also expected to promote greater increases in this lipid, and potentially event reduction, with niacin.
But no benefit was observed. It remains to be determined whether the inclusion of a high proportion of patients with the metabolic syndrome adversely affected the ability to detect a benefit with niacin. While post hoc analyses of studies of carotid intimal-medial thickness demonstrated no relationship between raising HDL-C with niacin and slowing of disease progression in patients with the metabolic syndrome,18 it remains to be determined whether this would translate to any effect on cardiovascular event rates.
Inadequate statistical power? An underpowered study would leave very little room for error, a pertinent point given the variability in therapeutic response in both actively treated and placebo-treated patients typically encountered in clinical trials. Giving low doses of immediate-release niacin and titrating the simvastatin dose to control LDL-C, resulting in imbalances in lipid-modifying therapies, represent additional flaws in the study design.
Stopped too soon? The early cessation of the study was somewhat questionable. The study crossed the prespecified boundary for lack of efficacy at the time of the interim analysis, and initial review by the data and safety monitoring board suggested an excess rate of ischemic stroke with niacin. The inclusion of this latter finding in the press release prompted considerable speculation regarding potential mechanisms and also concern among patients currently taking niacin. The subsequent finding that this signal was not statistically significant serves as an important warning for those conducting clinical trials not to prematurely overstate preliminary observations.
The implications for agents used in clinical practice are considerable: negative findings should not be overemphasized without robust evidence.
Do statins make everything else irrelevant?
The final factor to consider is the relative modifiability of residual clinical risk in statin-treated patients.
While residual risk is often cited as the reason to develop new antiatherosclerotic therapies, it is unknown how many of these ongoing events can be prevented. Several nonmodifiable factors such as age and concomitant disease are likely to contribute to these clinical events, which may limit our ability to further reduce event rates in patients who have already achieved low LDL-C levels with statin therapy. This may underscore the observation that no major clinical trial has demonstrated clinical benefit of an antiatherosclerotic agent on top of background medical care that included statins.
The finding that atherosclerosis continues to progress in many patients even though they take statins in high doses or achieve low LDL-C levels suggests that there is still room for improvement.
WHAT FUTURE FOR NIACIN?
So what does the future hold for niacin? The ongoing HPS2-THRIVE study provides another opportunity to evaluate the potential clinical efficacy of niacin in statin-treated patients. For now, we must wait for the results of this study.
In the meantime, it would seem reasonable to continue treatment with niacin in patients who need it for its multiple lipid-modifying effects. Whether clinicians will be less likely to initiate niacin therapy until there is clear evidence of clinical benefit remains uncertain. As for HDL-C, it remains to be determined whether any therapy targeting either quantitative or qualitative changes will be beneficial.
Over the last 3 decades, clinical trials have provided important insights into the prevention of cardiovascular events and have had a profound impact on clinical practice. Such studies simply evaluate whether one strategy is better or worse than the existing standard of care. They do not provide mechanistic insights, and when attempts have been made to address mechanisms in the study design, the trial, as in the case of AIM-HIGH, leaves more questions than answers.
Future trials will provide more clarity as to the optimal way to treat patients, but they must be based on a robust design that permits the study question to be adequately addressed.
The recent publication of the AIM-HIGH trial (Atherothrombosis Intervention in Metabolic Syndrome With Low HDL/High Triglycerides: Impact on Global Health Outcomes)1 has thrown the use of niacin as a lipid-modifying therapy into question. The trial was stopped early because an interim analysis found that the patients who took extended-release niacin had no clinical benefit. In addition, it found a trend toward more ischemic strokes, though this finding was later found not to be statistically significant.
Complicating the interpretation, while both the treatment group and the control group in the study received statin therapy, the researchers attempted to keep low-density lipoprotein cholesterol (LDL-C) levels equal, meaning that patients in the control group received more intensive statin therapy than those in the treatment group. And the placebo that the control patients received was actually a low dose of niacin, to induce flushing and thus to blind study participants and their physicians to which drug they were taking.
In the article that follows, I will explore the background, design, findings, and implications of this key trial and try to untangle the many questions about how to interpret it.
LOWERING LDL-C REDUCES RISK, BUT DOES NOT ELIMINATE IT
Large randomized controlled trials have consistently shown that lowering the level of LDL-C reduces cardiovascular event rates by 25% to 45% both in people who are known to have coronary artery disease and in those who are not.2–4 As a result, guidelines for preventing cardiovascular disease have increasingly emphasized maintaining low LDL-C levels. This has led to a proliferation in the use of inhibitors of 3-hydroxy-3-methylglutaryl coenzyme A reductase (statins) in patients at high cardiovascular risk.
However, these agents only reduce the risk—they do not eliminate it. Needed are additional therapies to complement existing LDL-C-lowering approaches to lower the cardiovascular risk even further.
Raising HDL-C: The next frontier
One such strategy for further lowering cardiovascular risk that has received considerable interest is to promote the biological activity of the “good” cholesterol.
Studies have consistently shown that the higher the plasma level of high-density lipoprotein cholesterol (HDL-C), the lower the risk of cardiovascular events, suggesting that raising HDL-C may be beneficial.5 Studies in animals with atherosclerosis show that raising HDL-C via genetic modification of the animal or direct infusion of the molecule has a favorable impact on both the size and the structure of experimental plaque.6,7
Accordingly, much activity has focused on developing new therapies that raise HDL-C more effectively than current ones.
Why niacin should protect the heart
For more than 50 years, niacin has been used to manage dyslipidemia.
In addition to raising HDL-C levels more effectively than any other agent available today, niacin also lowers the levels of LDL-C, triglycerides, and lipoprotein (a).8 Before statins were available, the Coronary Drug Project found that niacin reduced the rate of nonfatal myocardial infarction and the 15-year mortality rate.9 In addition, niacin has been shown to slow the progression of carotid intimal-medial thickness and coronary atherosclerosis, and even to reverse these processes in some trials.10–12
However, a number of issues remain about using niacin to prevent cardiovascular events. Nearly all patients who take it experience flushing, which limits its tolerability and, thus, our ability to titrate doses to levels needed for adequate lipid changes. While a number of modifications of niacin administration have been developed (eg, extended-release formulations and products that inhibit flushing), no large study has tested the clinical efficacy of these strategies. Furthermore, until AIM-HIGH, no large-scale trial had directly evaluated the impact of niacin therapy on a background of statin therapy.
AIM-HIGH STUDY DESIGN
The intent of the AIM-HIGH trial was to determine whether extended-release niacin (Niaspan) would reduce the risk of cardiovascular events when added to therapy with a statin—in this case, simvastatin (Zocor) supplemented with ezetimibe (Zetia).1
The trial was funded by the National Heart, Lung, and Blood Institute (NHLBI) and by Abbott Laboratories, which also supplied the extended-release niacin and the ezetimibe. Merck donated the simvastatin.
Patient characteristics
The patients were all at least 45 years of age with established, stable coronary heart disease, cerebrovascular or carotid arterial disease, or peripheral arterial disease. They also had to have low levels of HDL-C (< 40 mg/dL in men, < 50 mg/dL in women), elevated triglycerides (150–400 mg/dL), and LDL-C levels lower than 180 mg/dL if they were not taking a statin at entry.
The mean age of the patients was 64 years, 85% were men, and 92% were white. They had a high prevalence of cardiovascular risk factors: 34% had diabetes, 71% had hypertension, and 81% had metabolic syndrome. Nearly all (94%) of the patients were taking a statin at entry; 76% had been taking one for more than 1 year, and 40% had been taking one for more than 5 years.1
Simvastatin, ezetimibe, and either niacin or placebo
All lipid-modifying agents except statins and ezetimibe were stopped for least 4 weeks after enrollment.
All patients then entered a 4- to 8-week open-label period, during which they took simvastatin 40 mg daily and extended-release niacin starting at 500 mg and increased weekly up to 2,000 mg daily. Patients who could tolerate at least 1,500 mg daily were randomly assigned to treatment with either niacin 1,500 to 2,000 mg or matching placebo. Both groups continued to receive simvastatin. The placebo contained a small dose of immediate-release niacin (50 mg) in each tablet to induce flushing and to maintain blinding of treatment.
Given that niacin also lowers LDL-C, an algorithm was used to try to keep LDL-C levels roughly the same in both treatment groups. This involved adjusting the simvastatin dose and permitting the use of ezetimibe 10 mg to keep the LDL-C level between 40 and 80 mg/dL. Accordingly, participating physicians were told their patients’ LDL-C levels but were blinded to their HDL-C and triglyceride levels throughout the study.
Every 6 months, patients had a follow-up visit in the clinic, and midway through each 6-month interval they received a phone call from the investigators.1
AIM-HIGH end points
The primary end point was the composite of the first event of death due to coronary heart disease, nonfatal myocardial infarction, ischemic stroke, hospitalization for acute coronary syndrome, or symptom-driven revascularization of the coronary or cerebral arteries.
Secondary end points were:
Death from coronary heart disease, nonfatal myocardial infarction, ischemic stroke, or hospitalization for acute coronary syndrome
Death from coronary heart disease, nonfatal myocardial infarction, or ischemic stroke
Death from cardiovascular causes.
Tertiary end points included:
Death from any cause
Individual components of the primary end point
Prespecified subgroups according to sex, history or no history of diabetes, and presence or absence of the metabolic syndrome.1
All clinical events were adjudicated by a central committee.
STUDY HALTED EARLY
The study was planned to run for a mean of 4.6 years, during which 800 primary end point events were expected. With these numbers, the investigators calculated that the study had 85% power to detect a 25% reduction in the primary end point, at a one-sided alpha level of 0.025.
The plan called for an interim analysis when 50% of the anticipated events had occurred, with prespecified stopping boundaries based on either efficacy or futility. The boundary for lack of efficacy required an observed hazard ratio of at least 1.02 with a probability of less than .001.
In the interim analysis, after a median follow-up of only 3 years, the data and safety monitoring board recommended stopping the study early because the boundary for futility had been crossed and, unexpectedly, the rate of ischemic stroke was higher in the niacin-treated patients than in those receiving placebo.
MAJOR FINDINGS OF AIM-HIGH
Of 4,273 patients who began open-label treatment with niacin, 3,414 were randomized to treatment with niacin or placebo.1
HDL-C levels went up in both groups
At 2 years:
HDL-C levels had increased by 25.0% (to 42 mg/dL) in the niacin group and by 9.8% (to 38 mg/dL) in the placebo group
Triglycerides had decreased by 28.6% with niacin and by 8.1% with placebo
LDL-C had decreased by 12.0% with niacin and by 5.5% with placebo.
Patients in the placebo group were more likely to have subsequently received the maximum dose of simvastatin, ie, 80 mg/day (24.7% vs 17.5%), and to have received ezetimibe (21.5% vs 9.5%). More patients in the niacin group required either dose reduction of the study drug (6.3% vs 3.4%) or drug discontinuation (25.4% vs 20.1%).1
No difference in the primary end point
There was no difference between the two treatment groups in the rate of the primary end point, which occurred in 282 (16.4%) of the 1,718 patients in the niacin group and 272 (16.2%) of the 1,696 patients in the placebo group (P = .79; hazard ratio 1.02, 95% confidence interval 0.87–1.21).1
However, more patients in the niacin group than in the placebo group who reached the primary end point did so by having a first ischemic stroke: 27 patients (1.6%) vs 15 patients (0.9%). Eight of these patients, all in the niacin group, had their stroke between 2 months and 4 years after they had stopped taking the study drug.
Further analysis that included all ischemic strokes revealed the same trend: 29 vs 18 patients (P = .11).1
No benefit was observed for niacin-treated patients in terms of any of the secondary or tertiary end points.
Subgroup analysis revealed no evidence of statistical heterogeneity: ie, niacin seemed to lack efficacy in all the prespecified subgroups studied (age 65 and older vs younger, men vs women, and those with or without diabetes, metabolic syndrome, prior myocardial infarction, or statin use at entry).
In general, niacin was well tolerated in the active-treatment group, with a low incidence of liver and muscle abnormalities.
PUTTING AIM-HIGH IN CONTEXT
How should practicing clinicians interpret these outcomes?
Ever since the NHLBI reported (in an urgent press release) that it was stopping the study early due to futility and a potential excess of strokes,13 there has been considerable debate as to which factors contributed to these outcomes. In the wake of the publication of more detailed information about the trial,1 this debate is likely to continue.
The AIM-HIGH results can be interpreted in several ways:
Perhaps niacin is no good as a preventive agent
Perhaps raising HDL-C is flawed as a preventive strategy
Perhaps AIM-HIGH had methodologic flaws, such as looking at the wrong patient cohort or using a treatment protocol that set itself up for failure
Perhaps statins are so good that, once you prescribe one, anything else you give provides no additional benefit.
Which of these is correct?
Is niacin no good?
In its most simple form, AIM-HIGH has always been seen as a clinical trial of niacin. While the early trials of immediate-release niacin were encouraging in terms of its effects on lipids, atherosclerotic plaque, and cardiovascular outcomes, using it in clinical practice has always been challenging, largely because many patients cannot tolerate it in doses high enough to be effective. A number of developments have improved niacin’s tolerability, but its clinical impact in the statin era has not been evaluated.
Niacin’s lack of efficacy in this trial will ultimately be viewed as a failure of the drug itself, but is this the case?
AIM-HIGH was not simply a direct comparison of niacin vs placebo on top of standard medical practice. The investigators recognized that niacin has additional effects—in particular, lowering levels of atherogenic lipids—and they attempted to control for these effects by titrating the other LDL-C-lowering therapies during the study. As a result, the trial was actually a comparison between niacin plus low-dose simvastatin on the one hand, and placebo plus high-dose simvastatin (and, more often, also ezetimibe) on the other.
Furthermore, the placebo-treated patients received small doses of immediate-release niacin to induce flushing and maintain blinding. It is therefore hard to conclude that this clinical trial was a direct evaluation of the impact of niacin.
In contrast, the Heart Protection Study 2-Treatment of HDL to Reduce the Incidence of Vascular Events (HPS2-THRIVE) study is currently evaluating extended-release niacin in combination with laropiprant, a prostaglandin receptor antagonist, vs placebo in more than 24,000 statin-treated patients.14 Without any in-trial titration of lipids, this study provides a more direct comparison of the effects of niacin in the statin era.
Niacin continues to attract interest, largely because it can raise HDL-C by 20% to 30% when given at doses of 1,500 mg or more. Also, consistent observations from population studies of an inverse relationship between HDL-C levels and cardiovascular risk5 have stimulated interest in developing novel agents that substantially raise HDL-C.
Is raising HDL-C a flawed strategy?
The failure of HDL-C-raising therapies in clinical trials15,16 has fueled concern that HDL may not be the magic elixir that many have sought. Given that niacin is the most effective HDL-C-raising agent currently available, its lack of efficacy in AIM-HIGH could be perceived as another nail in the coffin of the hypothesis that raising the HDL-C level with pharmacologic agents is beneficial.
AIM-HIGH was designed to examine the effects of raising HDL-C. To this end, it was performed exclusively in patients with low HDL-C levels, and the investigators tried to isolate the potential effects of raising HDL-C by equalizing the LDL-C levels in the treatment groups.
However, the HDL-C changes observed in AIM-HIGH are likely to have undermined the study objective. While niacin predictably increased HDL-C levels by 25%, an unexpected increase in HDL-C of 9.8% in the placebo-treated patients resulted in a difference in achieved HDL-C levels of only 4 mg/dL between the groups. This was far less than anticipated, and it likely had a major impact on an already underpowered study.
AIM-HIGH was designed to have 85% power to demonstrate a 25% reduction in clinical events, which was an optimistic estimate. On the basis of population studies, a difference of 4 mg/dL in HDL-C would be anticipated to result in no more than a 10% lower rate of clinical events, far beyond AIM-HIGH’s limit of detection.
The reasons for the increase in HDL-C in the placebo group are unknown, but they likely reflect the use of higher doses of simvastatin, some regression to the mean, and, possibly, the small doses of immediate-release niacin that the placebo contained. (Contrary to the belief of the investigators, there have been some reports of lipid changes with such doses,17 which may have contributed to the observed HDL-C-raising.)
Given that the HDL-C difference between the groups was relatively small and that niacin has additional effects beyond raising HDL-C and lowering LDL-C, it is unlikely that the futility of AIM-HIGH reflects a major indictment of HDL-C-raising. For the time being, the jury is still out on this question.
Was AIM-HIGH methodologically flawed?
A number of methodologic issues may have affected AIM-HIGH’s ability to adequately address its objectives.
The wrong cohort? In planning a study such as AIM-HIGH, the need for a relatively small sample size and the need to detect the greatest relative risk reduction with niacin would require enrollment of patients at the highest risk of cardiovascular events despite the use of statins. These needs were satisfied by only including patients who had atherosclerotic cardiovascular disease and low HDL-C levels. The inclusion of patients with low levels of HDL-C was also expected to promote greater increases in this lipid, and potentially event reduction, with niacin.
But no benefit was observed. It remains to be determined whether the inclusion of a high proportion of patients with the metabolic syndrome adversely affected the ability to detect a benefit with niacin. While post hoc analyses of studies of carotid intimal-medial thickness demonstrated no relationship between raising HDL-C with niacin and slowing of disease progression in patients with the metabolic syndrome,18 it remains to be determined whether this would translate to any effect on cardiovascular event rates.
Inadequate statistical power? An underpowered study would leave very little room for error, a pertinent point given the variability in therapeutic response in both actively treated and placebo-treated patients typically encountered in clinical trials. Giving low doses of immediate-release niacin and titrating the simvastatin dose to control LDL-C, resulting in imbalances in lipid-modifying therapies, represent additional flaws in the study design.
Stopped too soon? The early cessation of the study was somewhat questionable. The study crossed the prespecified boundary for lack of efficacy at the time of the interim analysis, and initial review by the data and safety monitoring board suggested an excess rate of ischemic stroke with niacin. The inclusion of this latter finding in the press release prompted considerable speculation regarding potential mechanisms and also concern among patients currently taking niacin. The subsequent finding that this signal was not statistically significant serves as an important warning for those conducting clinical trials not to prematurely overstate preliminary observations.
The implications for agents used in clinical practice are considerable: negative findings should not be overemphasized without robust evidence.
Do statins make everything else irrelevant?
The final factor to consider is the relative modifiability of residual clinical risk in statin-treated patients.
While residual risk is often cited as the reason to develop new antiatherosclerotic therapies, it is unknown how many of these ongoing events can be prevented. Several nonmodifiable factors such as age and concomitant disease are likely to contribute to these clinical events, which may limit our ability to further reduce event rates in patients who have already achieved low LDL-C levels with statin therapy. This may underscore the observation that no major clinical trial has demonstrated clinical benefit of an antiatherosclerotic agent on top of background medical care that included statins.
The finding that atherosclerosis continues to progress in many patients even though they take statins in high doses or achieve low LDL-C levels suggests that there is still room for improvement.
WHAT FUTURE FOR NIACIN?
So what does the future hold for niacin? The ongoing HPS2-THRIVE study provides another opportunity to evaluate the potential clinical efficacy of niacin in statin-treated patients. For now, we must wait for the results of this study.
In the meantime, it would seem reasonable to continue treatment with niacin in patients who need it for its multiple lipid-modifying effects. Whether clinicians will be less likely to initiate niacin therapy until there is clear evidence of clinical benefit remains uncertain. As for HDL-C, it remains to be determined whether any therapy targeting either quantitative or qualitative changes will be beneficial.
Over the last 3 decades, clinical trials have provided important insights into the prevention of cardiovascular events and have had a profound impact on clinical practice. Such studies simply evaluate whether one strategy is better or worse than the existing standard of care. They do not provide mechanistic insights, and when attempts have been made to address mechanisms in the study design, the trial, as in the case of AIM-HIGH, leaves more questions than answers.
Future trials will provide more clarity as to the optimal way to treat patients, but they must be based on a robust design that permits the study question to be adequately addressed.
References
The AIM-HIGH Investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med2011; 365:2255–2267.
Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet1994; 344:1383–1389.
MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet2002; 360:7–22.
Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med2008; 359:2195–2207.
Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med1977; 62:707–714.
Rubin EM, Krauss RM, Spangler EA, Verstuyft JG, Clift SM. Inhibition of early atherogenesis in transgenic mice by human apolipoprotein AI. Nature1991; 353:265–267.
Nicholls SJ, Cutri B, Worthley SG, et al. Impact of short-term administration of high-density lipoproteins and atorvastatin on atherosclerosis in rabbits. Arterioscler Thromb Vasc Biol2005; 25:2416–2421.
deLemos AS, Wolfe ML, Long CJ, Sivapackianathan R, Rader DJ. Identification of genetic variants in endothelial lipase in persons with elevated high-density lipoprotein cholesterol. Circulation2002; 106:1321–1326.
Canner PL, Berge KG, Wenger NK, et al. Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin. J Am Coll Cardiol1986; 8:1245–1255.
Taylor AJ, Sullenberger LE, Lee HJ, Lee JK, Grace KA. Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol (ARBITER) 2: a double-blind, placebo-controlled study of extended-release niacin on atherosclerosis progression in secondary prevention patients treated with statins. Circulation2004; 110:3512–3517.
Taylor AJ, Lee HJ, Sullenberger LE. The effect of 24 months of combination statin and extended-release niacin on carotid intima-media thickness: ARBITER 3. Curr Med Res Opin2006; 22:2243–2250.
Brown BG, Zhao X-Q, Chait A, et al. Simvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary disease. N Engl J Med2001; 345:1583–1592.
Brown BG, Zhao XQ. Nicotinic acid, alone and in combinations, for reduction of cardiovascular risk. Am J Cardiol2008; 101:58B–62B.
Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med2007; 357:2109–2122.
Ginsberg HN, Elam MB, Lovato LC, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med2010; 362:1563–1574.
Luria MH, Sapoznikov D. Raising HDL cholesterol with low-dose nicotinic acid and bezafibrate: preliminary experience. Postgrad Med J1993; 69:296–299.
Taylor AJ, Zhu D, Sullenberger LE, Lee HJ, Lee JK, Grace KA. Relationship between glycemic status and progression of carotid intima-media thickness during treatment with combined statin and extended-release niacin in ARBITER 2. Vasc Health Risk Manag2007; 3:159–164.
References
The AIM-HIGH Investigators. Niacin in patients with low HDL cholesterol levels receiving intensive statin therapy. N Engl J Med2011; 365:2255–2267.
Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet1994; 344:1383–1389.
MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet2002; 360:7–22.
Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med2008; 359:2195–2207.
Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med1977; 62:707–714.
Rubin EM, Krauss RM, Spangler EA, Verstuyft JG, Clift SM. Inhibition of early atherogenesis in transgenic mice by human apolipoprotein AI. Nature1991; 353:265–267.
Nicholls SJ, Cutri B, Worthley SG, et al. Impact of short-term administration of high-density lipoproteins and atorvastatin on atherosclerosis in rabbits. Arterioscler Thromb Vasc Biol2005; 25:2416–2421.
deLemos AS, Wolfe ML, Long CJ, Sivapackianathan R, Rader DJ. Identification of genetic variants in endothelial lipase in persons with elevated high-density lipoprotein cholesterol. Circulation2002; 106:1321–1326.
Canner PL, Berge KG, Wenger NK, et al. Fifteen year mortality in Coronary Drug Project patients: long-term benefit with niacin. J Am Coll Cardiol1986; 8:1245–1255.
Taylor AJ, Sullenberger LE, Lee HJ, Lee JK, Grace KA. Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol (ARBITER) 2: a double-blind, placebo-controlled study of extended-release niacin on atherosclerosis progression in secondary prevention patients treated with statins. Circulation2004; 110:3512–3517.
Taylor AJ, Lee HJ, Sullenberger LE. The effect of 24 months of combination statin and extended-release niacin on carotid intima-media thickness: ARBITER 3. Curr Med Res Opin2006; 22:2243–2250.
Brown BG, Zhao X-Q, Chait A, et al. Simvastatin and niacin, antioxidant vitamins, or the combination for the prevention of coronary disease. N Engl J Med2001; 345:1583–1592.
Brown BG, Zhao XQ. Nicotinic acid, alone and in combinations, for reduction of cardiovascular risk. Am J Cardiol2008; 101:58B–62B.
Barter PJ, Caulfield M, Eriksson M, et al. Effects of torcetrapib in patients at high risk for coronary events. N Engl J Med2007; 357:2109–2122.
Ginsberg HN, Elam MB, Lovato LC, et al. Effects of combination lipid therapy in type 2 diabetes mellitus. N Engl J Med2010; 362:1563–1574.
Luria MH, Sapoznikov D. Raising HDL cholesterol with low-dose nicotinic acid and bezafibrate: preliminary experience. Postgrad Med J1993; 69:296–299.
Taylor AJ, Zhu D, Sullenberger LE, Lee HJ, Lee JK, Grace KA. Relationship between glycemic status and progression of carotid intima-media thickness during treatment with combined statin and extended-release niacin in ARBITER 2. Vasc Health Risk Manag2007; 3:159–164.
The study was stopped early because of the concerns raised by the interim analysis.
The AIM-HIGH results can be interpreted in several ways: perhaps niacin is no good as a preventive agent; perhaps raising levels of high-density lipoprotein cholesterol (HDL-C) is flawed as a preventive strategy; perhaps AIM-HIGH had methodologic flaws; or perhaps statins are so good that, once you prescribe one, anything else you do will not make much of a difference.
It seems reasonable to continue niacin treatment in patients who need its multiple lipid-modifying effects. It is uncertain if clinicians will be less likely to prescribe niacin therapy until we have clear evidence of clinical benefit. As for HDL-C, it remains to be determined whether any therapy targeting quantitative or qualitative changes will be beneficial.
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail shishem@gmail.com
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail shishem@gmail.com
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
Author and Disclosure Information
Olcay Aksoy, MD Department of Cardiovascular Medicine, Cleveland Clinic
Samir R. Kapadia, MD Department of Cardiovascular Medicine, Cleveland Clinic
Christopher Bajzer, MD Department of Cardiovascular Medicine, Cleveland Clinic
Wayne M. Clark, MD Department of Neurology, Oregon Health & Science University, Portland; Investigator, Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)
Mehdi H. Shishehbor, DO, MPH, PhD Department of Cardiovascular Medicine, Cleveland Clinic
Address: Mehdi H. Shishehbor, DO, MPH, Heart & Vascular Institute, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail shishem@gmail.com
Dr. Shishehbor has disclosed teaching and speaking for Abbott Vascular.
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
For patients with carotid artery stenosis, percutaneous intervention with stenting is as good as surgery (carotid endarterectomy). This was the major finding of the recently completed Carotid Revascularization Endarterectomy Versus Stenting Trial (CREST)1—with some qualifications.
CREST is the latest in a series of clinical trials of treatment of carotid stenosis that have generated reams of numbers and much debate. The topic of surgery vs percutaneous intervention is a moving target, as techniques evolve and improve. We believe the CREST results are valuable and should help inform decisions about treatment in the “real world.”
In this article, we offer a critical review of CREST, with a careful evaluation of its methods, results, and conclusions.
AN EVOLVING FIELD
Despite improvements in diagnosis and management, stroke remains one of the leading causes of morbidity and death in the United States, with an annual incidence of 780,000 cases and 270,000 deaths.2,3
Figure 1. Carotid endarterectomy has long been an established treatment in selected patients with symptomatic carotid artery stenosis of 50% or greater or asymptomatic stenosis of 60% or greater. However, percutaneous carotid artery angioplasty with stenting and placement of an embolic protection device is gaining ground as a reasonable, safe, less invasive alternative.From 10% to 30% of ischemic strokes are due to emboli from the carotid arteries.4–6 Carotid endarterectomy is an established treatment in selected patients with symptomatic carotid stenosis of 50% or greater or asymptomatic stenosis of 60% or greater.7,8 However, percutaneous techniques such as carotid artery angioplasty with stenting have improved, making them a viable, less invasive option (Figure 1).
Randomized trials of stenting have had mixed results, leading the Centers for Medicare and Medicaid Services (CMS) to adopt strict reimbursement policies. Currently, CMS reimburses for stenting only in symptomatic cases with at least 50% carotid artery stenosis. It also reimburses for stenting in asymptomatic cases in patients at high risk with 80% or greater stenosis, but only if the patients are enrolled in ongoing clinical trials or registries.
CREST compared stenting with endarterectomy and provided important insights into each approach.1
BEFORE CREST
Endarterectomy is superior to medical therapy for symptomatic stenosis
First described in 1953, carotid endarterectomy became the most widely used invasive treatment for significant carotid stenosis.9 Several studies have described patient subsets that benefit from this procedure.
NASCET (the North American Symptomatic Carotid Endarterectomy Trial)10 assigned 2,226 patients with symptomatic stenosis (transient ischemic attack or stroke within the past 180 days) to medical management or endarterectomy.
Surgery was associated with a 65% lower rate of ipsilateral cerebral events in patients with 70% or greater stenosis.10 Surgery was also found to be superior in patients with moderate disease (50% to 69% stenosis), but the difference only approached statistical significance. In patients with stenosis of less than 50%, the outcomes were similar with endarterectomy and medical management.11
ECST (the European Carotid Surgery Trial)12 included a similar population of 3,024 patients. Those with high-grade disease (stenosis ≥ 80%) had significantly better outcomes with endarterectomy, but in those with stenosis less than 70%, surgery was no better than drug therapy.
Comment. NASCET and ECST taught us that endarterectomy is clearly superior to medical therapy in patients with severe symptomatic carotid disease. However, both trials excluded patients at high surgical risk, eg, those with severe coronary artery disease, kidney disease, or heart failure. Additionally, medical management was not aggressive by today’s standards in terms of control of blood pressure and hyperlipidemia, and this could have skewed the results in favor of carotid endarterectomy.
The case for carotid endarterectomy for asymptomatic stenosis
Endarterectomy has also been compared with drug therapy for asymp tomatic carotid artery stenosis in several trials.13–15
ACAS (the Asymptomatic Carotid Atherosclerosis Study)15 assigned 1,662 patients who had no symptoms and had at least 60% carotid artery stenosis to endarterectomy or to medical management, and found a relative risk reduction of 53% in favor of surgery.15
The Veterans Affairs Cooperative Study Group14 corroborated these results in 444 patients with asymptomatic stenosis of greater than 50%. Endarterectomy was associated with a 61% lower risk of transient ischemic attack, transient monocular blindness, or stroke compared with medical therapy. However, there was no statistically significant difference in rates of stroke or death at 30 days.14
ACST (the Asymptomatic Carotid Surgery Trial),13 the largest study to compare carotid endarterectomy with drug therapy for asymptomatic stenosis, randomized 3,120 patients to surgery or drug therapy. The net 5-year risk of stroke was 6.4% with endarterectomy vs 11.8% with drug therapy (P < .0001). The rate of fatal stroke was also lower with endarterectomy: 2.1% vs 4.2% (P = .006).13
Comment. The results of these and other studies of endarterectomy vs medical therapy may not be applicable to current practice, since medical therapy has evolved and the risks with current drug therapy are likely much lower than seen in these trials, some of which began 2 decades ago. Another problem with interpreting these trials is that they excluded surgically “high-risk” patients, which limits the generalizability of the findings to this particular patient population.
The American Heart Association and the American Stroke Association have, on the basis of these trials, recommended carotid endarterectomy in patients with7,8,16:
Ipsilateral, symptomatic carotid artery stenosis of 70% to 99% (class I, level of evidence A)
Symptomatic stenosis of 50% to 69%, depending on patient-specific factors such as age, sex, and comorbidities
High-grade asymptomatic carotid stenosis, if the patients are carefully selected and the surgery is performed by surgeons with procedural morbidity and mortality rates of less than 3% (class I, level of evidence A).
In all cases, treatment should be individualized according to the patient’s comorbid conditions and preferences, with a thorough discussion of risks and benefits (Table 1).7,8,16
The case for percutaneous intervention
While carotid endarterectomy is proven to be more efficacious than medical management in certain patient subsets, studies favoring surgery over medical therapy have been criticized because they excluded patients with significant comorbidities. In addition, surgery has been associated with significant cardiovascular events, wound complications, and cranial nerve damage, and it requires general anesthesia in most cases.12,17–19 These and other factors spurred the development of less invasive, percutaneous approaches for patients with substantial comorbidities.
So far, several trials have investigated carotid angioplasty with or without stents and with or without devices to capture distal emboli. This interest set the stage for CREST.20,21
Initial attempts at angioplasty without distal protection were not very successful. A meta-analysis of nonrandomized trials that included 714 patients from the initial 13 studies of angioplasty (with or without stenting) and 6,970 patients from 20 studies of carotid endarterectomy found angioplasty to be possibly associated with higher rates of stroke within 30 days of the procedure.20
With improvements in technology, routine use of embolic protection devices, more experience, and better selection of patients, the outcome of carotid stenting has improved. In fact, a meta-analysis comparing stenting without an embolic protection device (26 trials with 2,357 patients) vs stenting with an embolic protection device (11 trials with 839 patients) showed that embolic protection led to significantly better outcomes with fewer strokes—outcomes arguably similar to those of carotid endarterectomy.21
SAPPHIRE (the Stenting and Angioplasty With Protection in Patients at High Risk for Endarterectomy trial)22 was the only completed US trial until CREST that compared carotid artery stenting with distal protection against surgery. It included 334 high-risk patients with either symptomatic stenosis of 50% or greater or asymptomatic stenosis of 80% or greater.
The results suggested that the outcomes with stenting with embolic protection were in fact similar to those of endarterectomy, with possibly fewer complications.23 The benefit persisted up to 2 years.22
The US Food and Drug Administration (FDA), on the basis of these data, approved the use of stenting with distal protection for high-risk patients, and the CMS reimburses for symptomatic stenosis of 50% or greater and for asymptomatic stenosis of 80% or greater as long as the patient is enrolled in a registry.
SPACE (the Stent-Protected Angioplasty Versus Carotid Endarterectomy in Symptomatic Patients trial),24 conducted in Germany, included 1,214 patients with symptomatic stenosis of at least 50%. Results were similar in terms of the combined primary end point of stroke or death at 30 days. However, the results were not similar enough to prove that stenting is not inferior to surgery, according to preset study criteria.
EVA-3S (the Endarterectomy Versus Stenting in Patients With Symptomatic Severe Carotid Stenosis trial),25 in France, evaluated 527 patients with symptomatic carotid disease (stenosis ≥ 60%), but was terminated early due to significantly higher rates of death or stroke at 30 days in the stenting group.
Comment. SPACE and EVA-3S have been widely criticized for not mandating the use of an embolic protection device (used in 27% of cases in SPACE and in 91.9% of cases in EVA-3S). Questions were also raised about the experience level of the operators who performed the carotid stenting: up to 39% of the primary operators involved in stent placement were trainees.26 Also, myocardial infarction (MI), an important complication of carotid endarterectomy, was not included in the primary end point.
ICSS (the International Carotid Stenting Study)27 compared stenting with endarterectomy in 1,713 patients with symptomatic carotid stenosis of greater than 50%. The primary end point was the rate of fatal or disabling stroke at 3 years.
An interim safety analysis at 120 days of follow-up showed the primary end point had occurred in 4.0% of stenting cases vs 3.2% of endarterectomy cases, a difference that was not statistically significant (hazard ratio [HR] 1.28, 95% confidence interval [CI] 0.77–2.11). However, the risk of any stroke was higher with stenting, with a rate of 7.7% vs 4.1% in the surgical group—a statistically significant difference (HR 1.92, 95% CI 1.27–2.89).
In a substudy of ICSS,28 the investigators corroborated these findings, using magnetic resonance imaging to evaluate for new ischemic brain lesions periprocedurally. They found more new ischemic brain lesions in patients who underwent stenting than in patients who underwent surgery—a statistically significant finding.
Comment. ICSS had limitations: eg, it included only patients with symptoms, and the training for the stenting procedure was not standardized. Furthermore, the use of embolic protection devices was not mandated in stenting procedures.
Because of the controversial and incongruous findings of the above trials, there has been much anticipation for further large, appropriately conducted, randomized controlled trials such as CREST.
CREST STUDY DESIGN
CREST was a prospective, multicenter randomized controlled trial with blinded end point adjudication. Assignment to stenting or surgery occurred in a one-to-one fashion, and patients were stratified by medical center and symptomatic status.
Conducted at 108 sites in the United States and nine sites in Canada, CREST was supported by a grant from the National Institutes of Health and by the manufacturer of the catheter and stent delivery and embolic protection systems. The manufacturer’s representative held a nonvoting position on the executive committee and reviewed the manuscript of the results before submission.
CREST included patients with or without symptoms
CREST was initially designed to compare carotid artery stenting vs carotid endarterectomy in patients with symptoms, but enrollment was later extended to patients without symptoms.
Patients with symptoms were included if they had stenosis of at least 50% on angiography, at least 70% on ultrasonography, or at least 70% on computed tomographic angiography or magnetic resonance angiography if stenosis on ultrasonography was 50% to 69%. Carotid artery stenosis was considered symptomatic if the patient had a transient ischemic attack, amaurosis fugax, or minor disabling stroke in the hemisphere supplied by the target vessel within 180 days of randomization.
Patients without symptoms were eligible if they had at least 60% stenosis on angiography, at least 70% stenosis on ultrasonography, or at least 80% stenosis on computed tomographic angiography or magnetic resonance angiography if the stenosis was 50% to 69% on ultrasonography.
Other eligibility criteria included favorable anatomy and clinical stability for both stenting and surgical procedures.
Exclusion criteria were evolving stroke, history of major stroke, chronic or paroxysmal atrial fibrillation on anticoagulation therapy, MI within the previous 30 days, and unstable angina.
Patients received antiplatelet agents
Patients undergoing stenting received aspirin and clopidogrel (Plavix) before and up to 30 days after the procedure. Continuation of antiplatelet therapy was recommended beyond 1 month.
Patients undergoing endarterectomy received aspirin before surgery and continued to receive aspirin for at least 1 year.
Alternatives to aspirin in both groups were ticlopidine (Ticlid), clopidogrel, or aspirin with extended-release dipyridamole (Aggrenox).
End points: Stroke, MI, death
The primary end point was a composite of periprocedural clinical stroke (any type), MI, or death, and of ipsilateral stroke up to 4 years after the procedure. Secondary analyses were also planned for evaluation of treatment modification by age, symptom status, and sex.
Stroke was defined as any acute neurologic ischemic event lasting at least 24 hours with focal signs and symptoms.
Two separate definitions were applied to distinguish major stroke from nonmajor stroke. Major stroke was defined as a National Institutes of Health Stroke Scale (NIHSS) score greater than 9 or records suggesting that the event was a disabling stroke if admitted to another facility. Nonmajor stroke included an event that did not fit these criteria. The stroke review process was initiated with a significant neurologic event, a positive transient ischemia attack or stroke questionnaire, or a two-point or greater increase in the NIHSS score.
MI was defined as a combination of an elevation of cardiac enzymes to at least twice the laboratory upper limit of normal, as well as clinical signs suggesting MI or electrocardiographic evidence of ischemia.29
Stroke was adjudicated by two independent neurologists, and MI was adjudicated by two independent cardiologists blinded to treatment group assignment.
The Rankin scale, the transient ischemic attack and stroke questionnaire, and the Medical Outcomes Survey were also used to assess for disability and quality of life in long-term follow-up.
Intention-to-treat analysis
Intention-to-treat survival analysis was used along with time-to-event statistical modeling with adjustment for major baseline covariates. Differences in outcomes were assessed, and a noninferiority analysis was performed. Kaplan-Meier estimates were constructed of the proportion of patients remaining free of the composite end point at 30 days, 6 months, 1 year, and annually thereafter, and of the associated confidence intervals. The hazard ratios between groups were estimated after adjustment for important covariates.
Most patients enrolled were available for analysis
From December 2000 to July 2008, 2,522 patients were enrolled; 1,271 were assigned to stenting, and 1,251 were assigned to surgery. After randomization, 2.8% of the patients assigned to stenting withdrew consent, 5.7% underwent surgery, and 2.6% were lost to follow-up. Of those assigned to surgery, 5.1% withdrew consent, 1.0% underwent stenting, and 3.8% were lost to follow-up.
A ‘conventional-risk’ patient population
The trial sought to include a “conventional-risk” patient population to make the study more applicable to real-world practice. The mean age was 69 years in both groups. Of the 2,522 patients enrolled:
35% were women
47% had asymptomatic carotid disease
86% had carotid stenosis of 70% or greater
86% had hypertension
30% had diabetes mellitus
83% had hyperlipidemia
26% were current smokers
42% had a history of cardiovascular disease
21% had undergone coronary artery bypass grafting surgery.
The only statistically significant difference in measured baseline variables between the two treatment groups was a slightly higher rate of dyslipidemia in the group undergoing surgery.
The interventionalists and surgeons were highly experienced
Operators performing stenting underwent a lead-in phase of training, with close supervision and scrutiny before eligibility. Of patients undergoing stenting, 96.1% also received an embolic protection device. Antiplatelet therapy was continued in 99% of the patients.
The surgeons performing endarterectomy were experienced and had documented low complication rates. General anesthesia was used in 90% of surgical patients. Shunts were used during surgery in 57%, and patches were used in 62%. After endarterectomy, 91% of the patients received antiplatelet therapy.
CREST STUDY RESULTS: STENTING WAS AS GOOD AS SURGERY
Periprocedural outcomes
Stroke, MI, or death: 5.2% with stenting vs 4.5% with surgery, HR 1.18, 95% CI 0.82–1.68, P = .38
Stroke: 4.1% vs 2.3%, HR 1.79, 95% CI 1.14–2.82, P = .01
Major ipsilateral stroke: 0.9% vs 0.3%, HR 2.67, 95% CI 0.85–8.40, P = .09.
MI: 1.1% vs 2.3%, HR 0.50, 95% CI 0.26–0.94, P = .03
Cranial nerve palsy: 0.3% vs 4.8%, HR 0.07, 95% CI 0.02–0.18, P < .0001 (Table 2).
Outcomes at 4 years
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Figure 2. Kaplan-Meier analysis of the primary outcome (stroke, myocardial infarction, or death during the periprocedural period or any ipsilateral stroke within 4 years after randomization) for patients undergoing carotid artery stenting or carotid endarterectomy.The primary end point (periprocedural stroke, MI, or death, or ipsilateral stroke within 4 years after the procedure): 7.2% with stenting vs 6.8% with surgery, HR 1.11, 95% CI 0.81–1.51, P = .51. A Kaplan-Meier analysis showed similar findings with statistically similar outcomes (Figure 2).
Ipsilateral stroke: 2.0% vs 2.4%, HR 0.94, 95% CI 0.50–1.76, P = .85.
The primary outcome was analyzed for interactions of baseline variables, and no effect was detected for symptomatic status or sex. There was a suggestion of an interaction with age, with older patients (over age 70) benefiting more from endarterectomy.
Quality-of-life indices showed that both major and minor strokes were likely to produce long-term physical limitations, with minor stroke associated with worse mental and physical health at 1 year. The effect of periprocedural MI on long-term physical and mental health was less certain. The increased incidence of cranial nerve palsy noted with endarterectomy has been found before and has had no effect on quality of life.
WHAT DO THE CREST FINDINGS MEAN?
CREST is the largest trial to date to compare stenting and surgery. It is an important addition to the literature, not only because of its size, but also because it focused on a real-world patient population. For this reason, its results are more applicable to patients seen in primary care clinics, ie, with peripheral vascular disease, coronary artery disease, diabetes mellitus, hypertension, and smoking.
As noted, previous studies of endarterectomy had strict inclusion and exclusion criteria, which selected against patients at high surgical risk. Therefore, the CREST findings are of greater relevance when comparing stenting and endarterectomy.
Periprocedural and long-term neurologic outcomes
CREST showed similar findings for the composite end point of periprocedural stroke, death, or MI (ie, within 30 days of the procedure) and long-term stroke, establishing similar outcomes in patients undergoing stenting and surgery.
However, an analysis of the individual components of the composite end point showed significant differences between the two treatments. The risk of ipsilateral periprocedural stroke was higher with stenting; these events were defined as nonmajor by NIHSS criteria. The risk of contralateral stroke was similar and low with each treatment.
While the increased risk of periprocedural ipsilateral stroke was not synonymous with an increased risk of major stroke, post hoc analysis showed that any stroke was associated with decreased physical and mental health at 1 year. Therefore, patients who had even a minor stroke did worse from a physical and mental standpoint, a finding that argues for the superiority of surgery in selected patients at risk of periprocedural stroke.
If periprocedural stroke is excluded, the risk of long-term ipsilateral stroke was similar for each treatment, and extremely low (2% for stenting, 2.4% for surgery). Despite this, given the importance of periprocedural minor and major stroke, better predictive models are needed to identify patients at risk of procedural neurologic events. These prediction models will allow better patient selection.
The CREST data and medical therapy
The rates of stroke in this trial were similar to those observed with current medical treatment (approximately 1% per year), especially for patients with asymptomatic disease. Such findings introduce fresh controversy in the necessity of performing either procedure for this patient subset and may lead to further studies evaluating current medical therapy vs intervention.
Periprocedural myocardial infarction
Vascular surgery has long been associated with high cardiovascular risk, especially an increased risk of periprocedural MI.30 Findings from CREST provide further evidence of the risk of MI with endarterectomy in a real-world patient population. Given the evidence of a strong correlation between periprocedural cardiac enzyme elevations and adverse outcomes, the increased incidence of periprocedural MI is worrisome.31 As with risk assessment for periprocedural stroke, better predictive models are needed for patients at risk of cardiovascular events during endarterectomy.
Procedural complications
Carotid endarterectomy entails incisions in the neck with disruption of tissue planes, as opposed to catheter entry site wounds with stenting. The more invasive nature of endarterectomy thus carries a higher risk of wound complications. In fact, in the NASCET trial, the risk of wound complications was 9.3%.10,19 In CREST, surgery carried a higher risk of wound complications compared with stenting (42 vs 0 cases), although stenting involved more periprocedural transfusions, presumably due to retroperitoneal bleeding in four patients.
Use of general anesthesia is also associated with adverse outcomes.17,18 In CREST, 90% of endarterectomy procedures required general anesthesia, whereas none of the stenting procedures required this.
Cranial nerve palsy is an often overlooked but real complication after these procedures. Cranial nerve palsies can lead to vocal, swallowing, and sensory problems that can have a transient or permanent impact on quality of life. In CREST, as in EVA-3S, SAPPHIRE, and ICSS, this risk was substantially higher with surgery,23,25,27 although the long-term consequences of these palsies were not found to affect quality of life at 1 year of follow-up.
HOW CREST FINDINGS COMPARE WITH PREVIOUS STUDIES
Patients in CREST enjoyed overall better outcomes than in previous studies. In earlier trials of surgery vs medical therapy, the rates of adverse outcomes were higher than in CREST. In NASCET, the risk of ipsilateral stroke was 9% with surgery, with 2.5% being fatal or disabling strokes.10 In the ECST, rates of major stroke or death with endarterectomy were 7.0% within 30 days of surgery and 37.0% at a mean follow-up of 6.1 years.12
In earlier studies of surgery vs stenting, outcomes at 30 days were also substantially worse than those in CREST. In the EVA-3S trial, the 30-day incidence of stroke or death was 3.9% after surgery and 9.6% after stenting. These findings were similar at 6 months in EVA-3S, with a 6.1% rate of adverse events after surgery and 11.7% after stenting.25 In the SAPPHIRE trial, the cumulative incidence of stroke and death at 1 year was 21.4% for surgery and 13.6% for stenting.23
Overall, the CREST results show better outcomes than in previous trials. This may be due to improvements in technical aspects of the interventions and to more aggressive drug therapy. Also, because of the high number of patients enrolled in CREST, surgeons and interventionalists were required to meet eligibility criteria, which could have contributed to the improved outcomes.32
CREST was also unique in that stenting was done with an embolic protection device whenever possible, and this also likely had an impact on outcomes.
The CREST data suggest that interventions for carotid artery stenosis should only be performed by rigorously trained, experienced personnel at high-volume centers, as this provided lower event rates compared with previous studies. Additional data should also help identify those at risk of periprocedural stroke and MI, thereby helping to match the patient to the most appropriate procedure. The pros and cons of surgery and stenting are shown in Table 3.1,10,23,25,27
CREST vs ICSS
CREST and ICSS, published within a few months of each other, seem to have arrived at entirely different conclusions. As both studies are well-designed randomized controlled trials, these distinct results have yielded much controversy. However, closer scrutiny sheds light as to why the results may be different.
While ICSS focused only on patients with symptoms, CREST also included those without symptoms. The difference in patient populations is itself enough to account for the different outcomes.
Also, the interim analysis of ICSS was at 120 days, which makes periprocedural events a more dominant factor in outcomes, whereas these events likely do not last into the long term, as was the case in CREST. Analysis of the ICSS data at a later follow-up date may show results more similar to those of CREST.
The design of ICSS was also different than CREST. In ICSS, the use of an embolic protection device in stenting was not mandated, and the study lacked a lead-in phase of intensive training for those performing stenting. Furthermore, MI was adjudicated only when clinically recognized, which is different than the more rigorous method used in CREST.
Yet despite these differences, CREST and ICSS shed light on a controversial area of carotid stenosis management, and both studies boasted low rates of periprocedural complications. Clinicians should keep in mind the inclusion criteria and the technical specificities of these trials in order to explain to patients the risks and benefits of stenting and surgery, and to arrive at a decision together.
Limitations
The results of CREST should also be reviewed carefully due to a number of limitations. The study began in 2000 with symptomatic patients only, and began enrolling asymptomatic patients in 2005, so that the methodology of the study was changed midway. However, the investigators performed a subgroup analysis to distinguish between outcomes of the symptomatic and the asymptomatic groups and found no statistical interaction for the primary end point based on symptom status.
Despite careful patient selection, many of the predictors of adverse outcomes with stenting, such as lesion length, level of calcification, and lesion location, were not accounted for in the earlier days of enrollment. This may have had an impact on the incidence of stroke in patients enrolled in the early years of the trial. We await the analysis of predictors of perioperative stroke from CREST.
TAKE-HOME POINTS AND FUTURE DIRECTIONS
The CREST findings show that outcomes with stenting are similar to those with surgery in both the short term and the long term, and that the choice of management should be individualized. Each patient’s risk of MI and stroke should be considered based on a variety of factors, including the severity of coronary artery disease, the length of the carotid lesion, the level of calcification, the location of the lesion, and aortic atheroma. The treatment should be selected after also taking into account the patient’s preference and the available expertise, and only after a comprehensive discussion with the patient.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
References
Brott TG, Hobson RW, Howard G, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med2010; 363:11–23.
Thom T, Haase N, Rosamond W, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation2006; 113:e85–e151.
Rosamond WD, Folsom AR, Chambless LE, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke1999; 30:736–743.
Chaturvedi S, Bruno A, Feasby T, et al; Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Carotid endarterectomy—an evidence-based review: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology2005; 65:794–801.
Howell GM, Makaroun MS, Chaer RA. Current management of extracranial carotid occlusive disease. J Am Coll Surg2009; 208:442–453.
Barnett HJ, Gunton RW, Eliasziw M, et al. Causes and severity of ischemic stroke in patients with internal carotid artery stenosis. JAMA2000; 283:1429–1436.
Biller J, Feinberg WM, Castaldo JE, et al. Guidelines for carotid endarterectomy: a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Circulation1998; 97:501–509.
Goldstein LB, Adams R, Alberts MJ, et al; American Heart Association; American Stroke Association Stroke Council. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council: cosponsored by the Atherosclerotic Peripheral Vascular Disease Interdisciplinary Working Group; Cardiovascular Nursing Council; Clinical Cardiology Council; Nutrition, Physical Activity, and Metabolism Council; and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation2006; 113:e873–e923.
Strully KJ, Hurwitt ES, Blankenberg HW. Thrombo-endarterectomy for thrombosis of the internal carotid artery in the neck. J Neurosurg1953; 10:474–482.
Beneficial effect of carotid endarterectomy in symptomatic patients with high-grade carotid stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1991; 325:445–453.
Barnett HJ, Taylor DW, Eliasziw M, et al. Benefit of carotid endarterectomy in patients with symptomatic moderate or severe stenosis. North American Symptomatic Carotid Endarterectomy Trial Collaborators. N Engl J Med1998; 339:1415–1425.
Randomised trial of endarterectomy for recently symptomatic carotid stenosis: final results of the MRC European Carotid Surgery Trial (ECST). Lancet1998; 351:1379–1387.
Halliday A, Mansfield A, Marro J, et al; MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group. Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet2004; 363:1491–1502.
Hobson RW, Weiss DG, Fields WS, et al. Efficacy of carotid endarterectomy for asymptomatic carotid stenosis. The Veterans Affairs Cooperative Study Group. N Engl J Med1993; 328:221–227.
Endarterectomy for asymptomatic carotid artery stenosis. Executive Committee for the Asymptomatic Carotid Atherosclerosis Study. JAMA1995; 273:1421–1428.
Sacco RL, Adams R, Albers G, et al; American Heart Association/American Stroke Association Council on Stroke; Council on Cardiovascular Radiology and Intervention; American Academy of Neurology. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Circulation2006; 113:e409–e449.
Watts K, Lin PH, Bush RL, et al. The impact of anesthetic modality on the outcome of carotid endarterectomy. Am J Surg2004; 188:741–747.
Weber CF, Friedl H, Hueppe M, et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: GALA Study Subgroup Analysis. World J Surg2009; 33:1526–1532.
Ferguson GG, Eliasziw M, Barr HW, et al. The North American Symptomatic Carotid Endarterectomy Trial: surgical results in 1415 patients. Stroke1999; 30:1751–1758.
Golledge J, Mitchell A, Greenhalgh RM, Davies AH. Systematic comparison of the early outcome of angioplasty and endarterectomy for symptomatic carotid artery disease. Stroke2000; 31:1439–1443.
Kastrup A, Gröschel K, Krapf H, Brehm BR, Dichgans J, Schulz JB. Early outcome of carotid angioplasty and stenting with and without cerebral protection devices: a systematic review of the literature. Stroke2003; 34:813–819.
Gurm HS, Yadav JS, Fayad P, et al; SAPPHIRE Investigators. Long-term results of carotid stenting versus endarterectomy in high-risk patients. N Engl J Med2008; 358:1572–1579.
Yadav JS, Wholey MH, Kuntz RE, et al; Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators. Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med2004; 351:1493–1501.
Eckstein HH, Ringleb P, Allenberg JR, et al. Results of the Stent-Protected Angioplasty versus Carotid Endarterectomy (SPACE) study to treat symptomatic stenoses at 2 years: a multinational, prospective, randomised trial. Lancet Neurol2008; 7:893–902.
Mas JL, Chatellier G, Beyssen B, et al; EVA-3S Investigators. Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med2006; 355:1660–1771.
Roffi M, Sievert H, Gray WA, et al. Carotid artery stenting versus surgery: adequate comparisons?Lancet Neurol2010; 9:339–341.
International Carotid Stenting Study Investigators; Ederle J, Dobson J, Featherstone RL, et al. Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet2010; 375:985–997.
Bonati LH, Jongen LM, Haller S, et al; ICSS-MRI study group. New ischaemic brain lesions on MRI after stenting or endarterectomy for symptomatic carotid stenosis: a sub-study of the International Carotid Stenting Study (ICSS). Lancet Neurol2010; 9:353–362.
Sheffet AJ, Roubin G, Howard G, et al. Design of the Carotid Revascularization Endarterectomy vs. Stenting Trial (CREST). Int J Stroke2010; 5:40–46.
Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines on Perioperative Cardiovascular Evaluation for Noncardiac Surgery) developed in collaboration with the American Society of Echocardiography, American Society of Nuclear Cardiology, Heart Rhythm Society, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, and Society for Vascular Surgery. J Am Coll Cardiol2007; 50:e159–e241.
Bhatt DL, Topol EJ. Does creatinine kinase-MB elevation after percutaneous coronary intervention predict outcomes in 2005? Periprocedural cardiac enzyme elevation predicts adverse outcomes. Circulation2005; 112:906–915.
Hobson RW, Howard VJ, Roubin GS, et al; CREST. Credentialing of surgeons as interventionalists for carotid artery stenting: experience from the lead-in phase of CREST. J Vasc Surg2004; 40:952–957.
In CREST, stenting and surgery had similar combined rates of stroke, MI, and death when performed by highly qualified interventionalists and surgeons in carefully selected patients.
The risk of periprocedural stroke was higher with stenting; most of those strokes were nonmajor. Both major and nonmajor strokes were associated with decreased quality of life in long-term follow-up.
Endarterectomy was associated with higher rates of periprocedural MI than stenting.
Endarterectomy carried a significantly higher rate of cranial nerve damage than stenting.
A major placebo-controlled trial has found that a statin can reduce the risk of venous thromboembolism (VTE).1
We do not recommend prescribing this class of drugs for this purpose until much more research has been done, and we certainly do not recommend substituting a statin for anticoagulant therapy in a patient at risk of VTE.
Nevertheless, we are excited by the latest findings, and we find comfort in knowing that if a patient is taking a statin for an approved indication, ie, reducing the risk of cardiovascular disease in a patient with hyperlipidemia or a previous cardiovascular event, the drug will also reduce the risk of VTE.
In the pages that follow, we describe and comment on what is known about the effect of statins on the risk of VTE.
ARTERIAL AND VENOUS THROMBOSIS: HOW ARE THEY LINKED?
The causes of arterial thrombosis may not be entirely distinct from those of deep vein thrombosis and pulmonary embolism, collectively referred to as VTE. Some studies have found that risk factors for arterial thrombosis overlap with those for VTE.2–4 However, other studies have shown no association between venous and arterial events.5–10
Hyperlipidemia, in particular, has been evaluated to see if it is a risk factor for VTE. As with other risk factors for arterial thrombosis, the data have been mixed, with some reports favoring an association with VTE and others not.4,5,11 Even so, preventive strategies targeting arterial risk factors have shown promise in reducing VTE events.12
Although commonly used to treat hyperlipidemia, statins (3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors) are believed to reduce the incidence of thrombosis by a number of mechanisms13:
Decreasing platelet aggregation
Inhibiting expression of tissue factor and plasminogen activator inhibitor 1
Increasing expression of tissue plasminogen activator
Increasing expression of thrombomodulin, which can activate protein C and prevent thrombin-induced platelet and factor V activation and fibrinogen clotting.
STATINS AND VTE IN OBSERVATIONAL AND CASE-CONTROL STUDIES
In view of the multiple effects of statins, several studies have looked at whether these drugs reduce the occurrence of both arterial thrombosis and VTE.14–19
Two prospective observational studies and four case-control studies found that statins reduced the risk of VTE by 20% to 60%.14–19 Interestingly, two of the case-control studies found that antiplatelet therapy did not reduce the risk of VTE.18,19
However, retrospective studies published in 200220 and 200921 found no statistically significant reduction in the incidence of VTE in statin users vs nonusers (Table 1). Observational and case-control studies, though, can have biases and confounders that may go unrecognized without rigorous prospective investigation.
THE JUPITER STUDY
The Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) study primarily sought to determine if rosuvastatin (Crestor) 20 mg/day, compared with placebo, would reduce the rate of first major cardiovascular events.22 A prespecified secondary end point of the trial was VTE, making JUPITER the first randomized, placebo-controlled trial to specifically test whether statins prevent VTE.1
Inclusion criteria: Normal LDL, high CRP
The study included men age 50 and older and women age 60 and older with no history of cardiovascular disease. In addition, their lowdensity lipoprotein (LDL) cholesterol levels had to be lower than 130 mg/dL (3.4 mmol/L), their triglyceride levels had to be lower than 500 mg/dL (5.6 mmol/L), and their highsensitivity C-reactive protein (hs-CRP) levels had to be 2.0 mg/L or higher.
Since high levels of hs-CRP, a marker of inflammation, predict cardiovascular events and since statins lower hs-CRP levels, the investigators hypothesized that people with elevated hs-CRP but without hyperlipidemia might benefit from statin treatment.21
Patients were excluded if they had received lipid-lowering therapy within 6 weeks of the trial screening, had diabetes mellitus or uncontrolled hypertension, were currently using postmenopausal hormone-replacement therapy, or had had cancer within the previous 5 years, except for certain skin cancers.
Candidates who complied well during a 4-week placebo run-in phase were randomly assigned to receive either rosuvastatin 20 mg daily (an intermediate dose) or a matching placebo. In all, 17,802 people were randomized. The two assigned groups appeared to be well matched.
Patients were to come in for visits twice a year for 60 months after randomization to be assessed for symptomatic deep venous thrombosis and pulmonary embolism. New cases of VTE were confirmed by imaging studies, by the initiation of anticoagulation therapy, or by death ascribed to pulmonary embolism.
Idiopathic VTE was classified as unprovoked if it occurred in the absence of trauma, hospitalization, or surgery within 3 months before the event, and in the absence of any diagnosed cancer within 3 months before and after the event. Provoked VTE events were those that occurred in a participant with cancer or when a precipitating event was associated with trauma, hospitalization, or surgery.
Rosuvastatin prevents heart attack, stroke
On the recommendation of the trial’s independent data and safety monitoring board, JUPITER was stopped early because the trial drug showed evidence of efficacy in preventing the combined primary end point of a first major cardiovascular event—ie, nonfatal myocardial infarction, nonfatal stroke, hospitalization for unstable angina, an arterial revascularization procedure, or confirmed death from a cardiovascular cause.22 (The cardiovascular outcomes of the JUPITER study were reviewed by Shishehbor and Hazen23 in the January 2009 issue of the Cleveland Clinic Journal of Medicine; see doi:10.3949/ccjm.75a.08105).
Formal follow-up for the trial's primary and secondary efficacy end points ended then, but data on VTE continued to be collected until each patient’s closeout visit as part of a safety monitoring protocol. The last closeout visit occurred on August 20, 2008. The primary analysis focused on events occurring up to March 30, 2008, the date the study was stopped.
Secondary end point results: Rosuvastatin prevents VTE
At a median follow-up of 1.9 years, an episode of VTE had occurred in 94 (0.53%) of the 17,802 patients—34 in the rosuvastatin group and 60 in the placebo group.1 This translates to 0.18 and 0.32 events per 100 person-years of follow-up in the rosuvastatin and placebo groups, respectively (hazard ratio for the rosuvastatin group 0.57, 95% confidence interval [CI] 0.37–0.86, P = .007).
Forty-four cases of VTE were classified as provoked and 50 cases were categorized as unprovoked. The risk reduction was statistically significant for provoked cases (hazard ratio 0.52, 95% CI 0.28–0.96, P = .03), but not for unprovoked events (hazard ratio 0.61, 95% CI 0.35–1.09, P = .09).
Subgroup analysis revealed no significant association between patient characteristics and the impact of rosuvastatin on the risk of a VTE event, but, as expected, more benefit was associated with higher baseline lipid levels.
STILL TOO SOON TO ADVISE ROUTINE STATIN USE TO PREVENT VTE
While the JUPITER trial data show an apparent benefit of statin use on the rate of VTE events, advising routine use of statins to prevent VTE is premature, for three main reasons.
Many must be treated to prevent one case of VTE. The number needed to treat (NNT) with rosuvastatin for 5 years to prevent either a case of VTE or a cardiovascular event was 21, and the NNT to prevent one cardiovascular event was 25. In a review of the two most recent case-control studies investigating the effects of statins on VTE,18,19 Cushman24 calculated that the NNT to prevent one VTE event each year was 333 for those age 75 and older. Though the Jupiter data did not provide the specific incidence of VTE at 1 year, except graphically, we can estimate that the NNT to prevent one VTE event at 1 year in the study is also very high.
Practically speaking, the perceived benefits of VTE prevention require large numbers to be treated, and the net clinical gain is still largely in preventing arterial events such as heart attack and stroke rather than VTE.
Statins, though safe, can still have adverse effects. The JUPITER study found a trend (albeit nonsignificant) toward more muscle complaints and elevations on liver function testing in apparently healthy persons taking a statin.22 Although severe complications of statin therapy such as rhabdomyolysis and elevations of creatine phosphokinase are rare, patients taking a statin have a 39% higher risk of an adverse event, most commonly myalgias or abnormalities on liver function testing.25 Were statins to be given routinely to even more people than they are now, more adverse outcomes would be likely.
More study is needed. The JUPITER study did not address a high risk of VTE. In fact, the investigators provided no information as to the VTE history of those enrolled.
Clearly, statins should not be substituted for proven prophylaxis and anticoagulation without further investigation, especially for patients with recurrent deep venous thrombosis, hospitalized patients, postoperative patients, and other patients prone to VTE.
OUR VIEW
The JUPITER study is an important leap forward in adding to our knowledge of how to prevent VTE. For people with another indication for taking a statin (eg, a previous cardiovascular event, hyperlipidemia), it is helpful to know that their risk of VTE may be reduced without exposure to the risks of other kinds of conventional thromboprophylaxis.
We look forward to additional studies to elaborate on the benefits of statins in both the prevention and treatment of VTE for averagerisk and VTE-prone populations.
References
Glynn RJ, Danielson E, Fonseca FA, et al. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med2009; 360:1851–1861.
Prandoni P, Bilora F, Marchiori A, et al. An association between atherosclerosis and venous thrombosis. N Engl J Med2003; 348:1435–1441.
Prandoni P, Ghirarduzzi A, Prins MH, et al. Venous thromboembolism and the risk of subsequent symptomatic atherosclerosis. J Thromb Haemost2006; 4:1891–1896.
Braekkan SK, Mathiesen EB, Njolstad I, Wilsgaard T, Stormer J, Hansen JB. Family history of myocardial infarction is an independent risk factor for venous thromboembolism: the Tromso study. J Thromb Haemost2008; 6:1851–1857.
Tsai AW, Cushman M, Rosamond WD, Heckbert SR, Polak JF, Folsom AR. Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology. Arch Intern Med2002; 162:1182–1189.
van der Hagen PB, Folsom AR, Jenny NS, et al. Subclinical atherosclerosis and the risk of future venous thrombosis in the Cardiovascular Health Study. J Thromb Haemost2006; 4:1903–1908.
Reich LM, Folsom AR, Key NS, et al. Prospective study of subclinical atherosclerosis as a risk factor for venous thromboembolism. J Thromb Haemost2006; 4:1909–1913.
Huerta C, Johansson S, Wallander MA, Rodriguez LA. Risk of myocardial infarction and overall mortality in survivors of venous thromboembolism. Thromb J2008; 6:10.
Linnemann B, Schindewolf M, Zgouras D, Erbe M, Jarosch-Preusche M, Lindhoff-Last E. Are patients with thrombophilia and previous venous thromboembolism at higher risk to arterial thrombosis?Thromb Res2008; 121:743–750.
Schwaiger J, Kiechl S, Stockner H, et al. Burden of atherosclerosis and risk of venous thromboembolism in patients with migraine. Neurology2008; 71:937–943.
Linnemann B, Zgouras D, Schindewolf M, Schwonberg J, Jarosch-Preusche M, Lindhoff-Last E. Impact of sex and traditional cardiovascular risk factors on the risk of recurrent venous thromboembolism: results from the German MAISTHRO Registry. Blood Coagul Fibrinolysis2008; 19:159–165.
Steffen LM, Folsom AR, Cushman M, Jacobs DR, Rosamond WD. Greater fish, fruit, and vegetable intakes are related to lower incidence of venous thromboembolism: the Longitudinal Investigation of Thromboembolism Etiology. Circulation2007; 115:188–195.
Arslan F, Pasterkamp G, de Kleijn DP. Unraveling pleiotropic effects of statins: bit by bit, a slow case with perspective. Circ Res2008; 103:334–336.
Grady D, Wenger NK, Herrington D, et al. Postmenopausal hormone therapy increases risk for venous thromboembolic disease. The Heart and Estrogen/progestin Replacement Study. Ann Intern Med2000; 132:689–696.
Ray JG, Mamdani M, Tsuyuki RT, Anderson DR, Yeo EL, Laupacis A. Use of statins and the subsequent development of deep vein thrombosis. Arch Intern Med2001; 161:1405–1410.
Doggen CJ, Lemaitre RN, Smith NL, Heckbert SR, Psaty BM. HMG CoA reductase inhibitors and the risk of venous thrombosis among postmenopausal women. J Thromb Haemost2004; 2:700–701.
Lacut K, Oger E, Le Gal G, et al. Statins but not fibrates are associated with a reduced risk of venous thromboembolism: a hospitalbased case-control study. Fundam Clin Pharmacol2004; 18:477–482.
Ramcharan AS, Van Stralen KJ, Snoep JD, Mantel-Teeuwisse AK, Rosendaal FR, Doggen CJ. HMG-CoA reductase inhibitors, other lipid-lowering medication, antiplatelet therapy, and the risk of venous thrombosis. J Thromb Haemost2009; 7:514–520.
Sørensen HT, Horvath-Puho E, Sogaard KK, et al. Arterial cardiovascular events, statins, low-dose aspirin and subsequent risk of venous thromboembolism: a population-based case-control study. J Thromb Haemost2009; 7:521–528.
Yang CC, Jick SS, Jick H. Statins and the risk of idiopathic venous thromboembolism. Br J Clin Pharmacol2002; 53:101–105.
Smeeth L, Douglas I, Hall AJ, Hubbard R, Evans S. Effect of statins on a wide range of health outcomes: a cohort study validated by comparison with randomized trials. Br J Clin Pharmacol2009; 67:99–109.
Ridker PM, Danielson E, Fonseca FA, et al; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med2008; 359:2195–2207.
Shishehbor MH, Hazen SL. JUPITER to Earth: A statin helps peole with normal LDL-C and high hs-CRP, but what does it mean?Cleve Clin J Med2009; 76:37–44.
Cushman M. A new indication for statins to prevent venous thromboembolism? Not yet. J Thromb Haemost2009; 7:511–513.
Silva MA, Swanson AC, Gandhi PJ, Tataronis GR. Statin-related adverse events: a meta-analysis. Clin Ther2006; 28:26–35.
Alejandro Perez, MD Section of Vascular Medicine, Department of Cardiovascular Medicine, Cleveland Clinic
John R. Bartholomew, MD, FACC Head, Section of Vascular Medicine; Professor of Medicine, Department of Cardiovascular Medicine; and Department of Hematologic Oncology and Blood Disorders, Cleveland Clinic
Address: John R. Bartholomew, MD, FACC, Department of Cardiovascular Medicine, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail barthoj@ccf.org
Alejandro Perez, MD Section of Vascular Medicine, Department of Cardiovascular Medicine, Cleveland Clinic
John R. Bartholomew, MD, FACC Head, Section of Vascular Medicine; Professor of Medicine, Department of Cardiovascular Medicine; and Department of Hematologic Oncology and Blood Disorders, Cleveland Clinic
Address: John R. Bartholomew, MD, FACC, Department of Cardiovascular Medicine, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail barthoj@ccf.org
Author and Disclosure Information
Alejandro Perez, MD Section of Vascular Medicine, Department of Cardiovascular Medicine, Cleveland Clinic
John R. Bartholomew, MD, FACC Head, Section of Vascular Medicine; Professor of Medicine, Department of Cardiovascular Medicine; and Department of Hematologic Oncology and Blood Disorders, Cleveland Clinic
Address: John R. Bartholomew, MD, FACC, Department of Cardiovascular Medicine, J3-5, Cleveland Clinic, 9500 Euclid Avenue, Cleveland, OH 44195; e-mail barthoj@ccf.org
A major placebo-controlled trial has found that a statin can reduce the risk of venous thromboembolism (VTE).1
We do not recommend prescribing this class of drugs for this purpose until much more research has been done, and we certainly do not recommend substituting a statin for anticoagulant therapy in a patient at risk of VTE.
Nevertheless, we are excited by the latest findings, and we find comfort in knowing that if a patient is taking a statin for an approved indication, ie, reducing the risk of cardiovascular disease in a patient with hyperlipidemia or a previous cardiovascular event, the drug will also reduce the risk of VTE.
In the pages that follow, we describe and comment on what is known about the effect of statins on the risk of VTE.
ARTERIAL AND VENOUS THROMBOSIS: HOW ARE THEY LINKED?
The causes of arterial thrombosis may not be entirely distinct from those of deep vein thrombosis and pulmonary embolism, collectively referred to as VTE. Some studies have found that risk factors for arterial thrombosis overlap with those for VTE.2–4 However, other studies have shown no association between venous and arterial events.5–10
Hyperlipidemia, in particular, has been evaluated to see if it is a risk factor for VTE. As with other risk factors for arterial thrombosis, the data have been mixed, with some reports favoring an association with VTE and others not.4,5,11 Even so, preventive strategies targeting arterial risk factors have shown promise in reducing VTE events.12
Although commonly used to treat hyperlipidemia, statins (3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors) are believed to reduce the incidence of thrombosis by a number of mechanisms13:
Decreasing platelet aggregation
Inhibiting expression of tissue factor and plasminogen activator inhibitor 1
Increasing expression of tissue plasminogen activator
Increasing expression of thrombomodulin, which can activate protein C and prevent thrombin-induced platelet and factor V activation and fibrinogen clotting.
STATINS AND VTE IN OBSERVATIONAL AND CASE-CONTROL STUDIES
In view of the multiple effects of statins, several studies have looked at whether these drugs reduce the occurrence of both arterial thrombosis and VTE.14–19
Two prospective observational studies and four case-control studies found that statins reduced the risk of VTE by 20% to 60%.14–19 Interestingly, two of the case-control studies found that antiplatelet therapy did not reduce the risk of VTE.18,19
However, retrospective studies published in 200220 and 200921 found no statistically significant reduction in the incidence of VTE in statin users vs nonusers (Table 1). Observational and case-control studies, though, can have biases and confounders that may go unrecognized without rigorous prospective investigation.
THE JUPITER STUDY
The Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) study primarily sought to determine if rosuvastatin (Crestor) 20 mg/day, compared with placebo, would reduce the rate of first major cardiovascular events.22 A prespecified secondary end point of the trial was VTE, making JUPITER the first randomized, placebo-controlled trial to specifically test whether statins prevent VTE.1
Inclusion criteria: Normal LDL, high CRP
The study included men age 50 and older and women age 60 and older with no history of cardiovascular disease. In addition, their lowdensity lipoprotein (LDL) cholesterol levels had to be lower than 130 mg/dL (3.4 mmol/L), their triglyceride levels had to be lower than 500 mg/dL (5.6 mmol/L), and their highsensitivity C-reactive protein (hs-CRP) levels had to be 2.0 mg/L or higher.
Since high levels of hs-CRP, a marker of inflammation, predict cardiovascular events and since statins lower hs-CRP levels, the investigators hypothesized that people with elevated hs-CRP but without hyperlipidemia might benefit from statin treatment.21
Patients were excluded if they had received lipid-lowering therapy within 6 weeks of the trial screening, had diabetes mellitus or uncontrolled hypertension, were currently using postmenopausal hormone-replacement therapy, or had had cancer within the previous 5 years, except for certain skin cancers.
Candidates who complied well during a 4-week placebo run-in phase were randomly assigned to receive either rosuvastatin 20 mg daily (an intermediate dose) or a matching placebo. In all, 17,802 people were randomized. The two assigned groups appeared to be well matched.
Patients were to come in for visits twice a year for 60 months after randomization to be assessed for symptomatic deep venous thrombosis and pulmonary embolism. New cases of VTE were confirmed by imaging studies, by the initiation of anticoagulation therapy, or by death ascribed to pulmonary embolism.
Idiopathic VTE was classified as unprovoked if it occurred in the absence of trauma, hospitalization, or surgery within 3 months before the event, and in the absence of any diagnosed cancer within 3 months before and after the event. Provoked VTE events were those that occurred in a participant with cancer or when a precipitating event was associated with trauma, hospitalization, or surgery.
Rosuvastatin prevents heart attack, stroke
On the recommendation of the trial’s independent data and safety monitoring board, JUPITER was stopped early because the trial drug showed evidence of efficacy in preventing the combined primary end point of a first major cardiovascular event—ie, nonfatal myocardial infarction, nonfatal stroke, hospitalization for unstable angina, an arterial revascularization procedure, or confirmed death from a cardiovascular cause.22 (The cardiovascular outcomes of the JUPITER study were reviewed by Shishehbor and Hazen23 in the January 2009 issue of the Cleveland Clinic Journal of Medicine; see doi:10.3949/ccjm.75a.08105).
Formal follow-up for the trial's primary and secondary efficacy end points ended then, but data on VTE continued to be collected until each patient’s closeout visit as part of a safety monitoring protocol. The last closeout visit occurred on August 20, 2008. The primary analysis focused on events occurring up to March 30, 2008, the date the study was stopped.
Secondary end point results: Rosuvastatin prevents VTE
At a median follow-up of 1.9 years, an episode of VTE had occurred in 94 (0.53%) of the 17,802 patients—34 in the rosuvastatin group and 60 in the placebo group.1 This translates to 0.18 and 0.32 events per 100 person-years of follow-up in the rosuvastatin and placebo groups, respectively (hazard ratio for the rosuvastatin group 0.57, 95% confidence interval [CI] 0.37–0.86, P = .007).
Forty-four cases of VTE were classified as provoked and 50 cases were categorized as unprovoked. The risk reduction was statistically significant for provoked cases (hazard ratio 0.52, 95% CI 0.28–0.96, P = .03), but not for unprovoked events (hazard ratio 0.61, 95% CI 0.35–1.09, P = .09).
Subgroup analysis revealed no significant association between patient characteristics and the impact of rosuvastatin on the risk of a VTE event, but, as expected, more benefit was associated with higher baseline lipid levels.
STILL TOO SOON TO ADVISE ROUTINE STATIN USE TO PREVENT VTE
While the JUPITER trial data show an apparent benefit of statin use on the rate of VTE events, advising routine use of statins to prevent VTE is premature, for three main reasons.
Many must be treated to prevent one case of VTE. The number needed to treat (NNT) with rosuvastatin for 5 years to prevent either a case of VTE or a cardiovascular event was 21, and the NNT to prevent one cardiovascular event was 25. In a review of the two most recent case-control studies investigating the effects of statins on VTE,18,19 Cushman24 calculated that the NNT to prevent one VTE event each year was 333 for those age 75 and older. Though the Jupiter data did not provide the specific incidence of VTE at 1 year, except graphically, we can estimate that the NNT to prevent one VTE event at 1 year in the study is also very high.
Practically speaking, the perceived benefits of VTE prevention require large numbers to be treated, and the net clinical gain is still largely in preventing arterial events such as heart attack and stroke rather than VTE.
Statins, though safe, can still have adverse effects. The JUPITER study found a trend (albeit nonsignificant) toward more muscle complaints and elevations on liver function testing in apparently healthy persons taking a statin.22 Although severe complications of statin therapy such as rhabdomyolysis and elevations of creatine phosphokinase are rare, patients taking a statin have a 39% higher risk of an adverse event, most commonly myalgias or abnormalities on liver function testing.25 Were statins to be given routinely to even more people than they are now, more adverse outcomes would be likely.
More study is needed. The JUPITER study did not address a high risk of VTE. In fact, the investigators provided no information as to the VTE history of those enrolled.
Clearly, statins should not be substituted for proven prophylaxis and anticoagulation without further investigation, especially for patients with recurrent deep venous thrombosis, hospitalized patients, postoperative patients, and other patients prone to VTE.
OUR VIEW
The JUPITER study is an important leap forward in adding to our knowledge of how to prevent VTE. For people with another indication for taking a statin (eg, a previous cardiovascular event, hyperlipidemia), it is helpful to know that their risk of VTE may be reduced without exposure to the risks of other kinds of conventional thromboprophylaxis.
We look forward to additional studies to elaborate on the benefits of statins in both the prevention and treatment of VTE for averagerisk and VTE-prone populations.
A major placebo-controlled trial has found that a statin can reduce the risk of venous thromboembolism (VTE).1
We do not recommend prescribing this class of drugs for this purpose until much more research has been done, and we certainly do not recommend substituting a statin for anticoagulant therapy in a patient at risk of VTE.
Nevertheless, we are excited by the latest findings, and we find comfort in knowing that if a patient is taking a statin for an approved indication, ie, reducing the risk of cardiovascular disease in a patient with hyperlipidemia or a previous cardiovascular event, the drug will also reduce the risk of VTE.
In the pages that follow, we describe and comment on what is known about the effect of statins on the risk of VTE.
ARTERIAL AND VENOUS THROMBOSIS: HOW ARE THEY LINKED?
The causes of arterial thrombosis may not be entirely distinct from those of deep vein thrombosis and pulmonary embolism, collectively referred to as VTE. Some studies have found that risk factors for arterial thrombosis overlap with those for VTE.2–4 However, other studies have shown no association between venous and arterial events.5–10
Hyperlipidemia, in particular, has been evaluated to see if it is a risk factor for VTE. As with other risk factors for arterial thrombosis, the data have been mixed, with some reports favoring an association with VTE and others not.4,5,11 Even so, preventive strategies targeting arterial risk factors have shown promise in reducing VTE events.12
Although commonly used to treat hyperlipidemia, statins (3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors) are believed to reduce the incidence of thrombosis by a number of mechanisms13:
Decreasing platelet aggregation
Inhibiting expression of tissue factor and plasminogen activator inhibitor 1
Increasing expression of tissue plasminogen activator
Increasing expression of thrombomodulin, which can activate protein C and prevent thrombin-induced platelet and factor V activation and fibrinogen clotting.
STATINS AND VTE IN OBSERVATIONAL AND CASE-CONTROL STUDIES
In view of the multiple effects of statins, several studies have looked at whether these drugs reduce the occurrence of both arterial thrombosis and VTE.14–19
Two prospective observational studies and four case-control studies found that statins reduced the risk of VTE by 20% to 60%.14–19 Interestingly, two of the case-control studies found that antiplatelet therapy did not reduce the risk of VTE.18,19
However, retrospective studies published in 200220 and 200921 found no statistically significant reduction in the incidence of VTE in statin users vs nonusers (Table 1). Observational and case-control studies, though, can have biases and confounders that may go unrecognized without rigorous prospective investigation.
THE JUPITER STUDY
The Justification for the Use of Statins in Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER) study primarily sought to determine if rosuvastatin (Crestor) 20 mg/day, compared with placebo, would reduce the rate of first major cardiovascular events.22 A prespecified secondary end point of the trial was VTE, making JUPITER the first randomized, placebo-controlled trial to specifically test whether statins prevent VTE.1
Inclusion criteria: Normal LDL, high CRP
The study included men age 50 and older and women age 60 and older with no history of cardiovascular disease. In addition, their lowdensity lipoprotein (LDL) cholesterol levels had to be lower than 130 mg/dL (3.4 mmol/L), their triglyceride levels had to be lower than 500 mg/dL (5.6 mmol/L), and their highsensitivity C-reactive protein (hs-CRP) levels had to be 2.0 mg/L or higher.
Since high levels of hs-CRP, a marker of inflammation, predict cardiovascular events and since statins lower hs-CRP levels, the investigators hypothesized that people with elevated hs-CRP but without hyperlipidemia might benefit from statin treatment.21
Patients were excluded if they had received lipid-lowering therapy within 6 weeks of the trial screening, had diabetes mellitus or uncontrolled hypertension, were currently using postmenopausal hormone-replacement therapy, or had had cancer within the previous 5 years, except for certain skin cancers.
Candidates who complied well during a 4-week placebo run-in phase were randomly assigned to receive either rosuvastatin 20 mg daily (an intermediate dose) or a matching placebo. In all, 17,802 people were randomized. The two assigned groups appeared to be well matched.
Patients were to come in for visits twice a year for 60 months after randomization to be assessed for symptomatic deep venous thrombosis and pulmonary embolism. New cases of VTE were confirmed by imaging studies, by the initiation of anticoagulation therapy, or by death ascribed to pulmonary embolism.
Idiopathic VTE was classified as unprovoked if it occurred in the absence of trauma, hospitalization, or surgery within 3 months before the event, and in the absence of any diagnosed cancer within 3 months before and after the event. Provoked VTE events were those that occurred in a participant with cancer or when a precipitating event was associated with trauma, hospitalization, or surgery.
Rosuvastatin prevents heart attack, stroke
On the recommendation of the trial’s independent data and safety monitoring board, JUPITER was stopped early because the trial drug showed evidence of efficacy in preventing the combined primary end point of a first major cardiovascular event—ie, nonfatal myocardial infarction, nonfatal stroke, hospitalization for unstable angina, an arterial revascularization procedure, or confirmed death from a cardiovascular cause.22 (The cardiovascular outcomes of the JUPITER study were reviewed by Shishehbor and Hazen23 in the January 2009 issue of the Cleveland Clinic Journal of Medicine; see doi:10.3949/ccjm.75a.08105).
Formal follow-up for the trial's primary and secondary efficacy end points ended then, but data on VTE continued to be collected until each patient’s closeout visit as part of a safety monitoring protocol. The last closeout visit occurred on August 20, 2008. The primary analysis focused on events occurring up to March 30, 2008, the date the study was stopped.
Secondary end point results: Rosuvastatin prevents VTE
At a median follow-up of 1.9 years, an episode of VTE had occurred in 94 (0.53%) of the 17,802 patients—34 in the rosuvastatin group and 60 in the placebo group.1 This translates to 0.18 and 0.32 events per 100 person-years of follow-up in the rosuvastatin and placebo groups, respectively (hazard ratio for the rosuvastatin group 0.57, 95% confidence interval [CI] 0.37–0.86, P = .007).
Forty-four cases of VTE were classified as provoked and 50 cases were categorized as unprovoked. The risk reduction was statistically significant for provoked cases (hazard ratio 0.52, 95% CI 0.28–0.96, P = .03), but not for unprovoked events (hazard ratio 0.61, 95% CI 0.35–1.09, P = .09).
Subgroup analysis revealed no significant association between patient characteristics and the impact of rosuvastatin on the risk of a VTE event, but, as expected, more benefit was associated with higher baseline lipid levels.
STILL TOO SOON TO ADVISE ROUTINE STATIN USE TO PREVENT VTE
While the JUPITER trial data show an apparent benefit of statin use on the rate of VTE events, advising routine use of statins to prevent VTE is premature, for three main reasons.
Many must be treated to prevent one case of VTE. The number needed to treat (NNT) with rosuvastatin for 5 years to prevent either a case of VTE or a cardiovascular event was 21, and the NNT to prevent one cardiovascular event was 25. In a review of the two most recent case-control studies investigating the effects of statins on VTE,18,19 Cushman24 calculated that the NNT to prevent one VTE event each year was 333 for those age 75 and older. Though the Jupiter data did not provide the specific incidence of VTE at 1 year, except graphically, we can estimate that the NNT to prevent one VTE event at 1 year in the study is also very high.
Practically speaking, the perceived benefits of VTE prevention require large numbers to be treated, and the net clinical gain is still largely in preventing arterial events such as heart attack and stroke rather than VTE.
Statins, though safe, can still have adverse effects. The JUPITER study found a trend (albeit nonsignificant) toward more muscle complaints and elevations on liver function testing in apparently healthy persons taking a statin.22 Although severe complications of statin therapy such as rhabdomyolysis and elevations of creatine phosphokinase are rare, patients taking a statin have a 39% higher risk of an adverse event, most commonly myalgias or abnormalities on liver function testing.25 Were statins to be given routinely to even more people than they are now, more adverse outcomes would be likely.
More study is needed. The JUPITER study did not address a high risk of VTE. In fact, the investigators provided no information as to the VTE history of those enrolled.
Clearly, statins should not be substituted for proven prophylaxis and anticoagulation without further investigation, especially for patients with recurrent deep venous thrombosis, hospitalized patients, postoperative patients, and other patients prone to VTE.
OUR VIEW
The JUPITER study is an important leap forward in adding to our knowledge of how to prevent VTE. For people with another indication for taking a statin (eg, a previous cardiovascular event, hyperlipidemia), it is helpful to know that their risk of VTE may be reduced without exposure to the risks of other kinds of conventional thromboprophylaxis.
We look forward to additional studies to elaborate on the benefits of statins in both the prevention and treatment of VTE for averagerisk and VTE-prone populations.
References
Glynn RJ, Danielson E, Fonseca FA, et al. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med2009; 360:1851–1861.
Prandoni P, Bilora F, Marchiori A, et al. An association between atherosclerosis and venous thrombosis. N Engl J Med2003; 348:1435–1441.
Prandoni P, Ghirarduzzi A, Prins MH, et al. Venous thromboembolism and the risk of subsequent symptomatic atherosclerosis. J Thromb Haemost2006; 4:1891–1896.
Braekkan SK, Mathiesen EB, Njolstad I, Wilsgaard T, Stormer J, Hansen JB. Family history of myocardial infarction is an independent risk factor for venous thromboembolism: the Tromso study. J Thromb Haemost2008; 6:1851–1857.
Tsai AW, Cushman M, Rosamond WD, Heckbert SR, Polak JF, Folsom AR. Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology. Arch Intern Med2002; 162:1182–1189.
van der Hagen PB, Folsom AR, Jenny NS, et al. Subclinical atherosclerosis and the risk of future venous thrombosis in the Cardiovascular Health Study. J Thromb Haemost2006; 4:1903–1908.
Reich LM, Folsom AR, Key NS, et al. Prospective study of subclinical atherosclerosis as a risk factor for venous thromboembolism. J Thromb Haemost2006; 4:1909–1913.
Huerta C, Johansson S, Wallander MA, Rodriguez LA. Risk of myocardial infarction and overall mortality in survivors of venous thromboembolism. Thromb J2008; 6:10.
Linnemann B, Schindewolf M, Zgouras D, Erbe M, Jarosch-Preusche M, Lindhoff-Last E. Are patients with thrombophilia and previous venous thromboembolism at higher risk to arterial thrombosis?Thromb Res2008; 121:743–750.
Schwaiger J, Kiechl S, Stockner H, et al. Burden of atherosclerosis and risk of venous thromboembolism in patients with migraine. Neurology2008; 71:937–943.
Linnemann B, Zgouras D, Schindewolf M, Schwonberg J, Jarosch-Preusche M, Lindhoff-Last E. Impact of sex and traditional cardiovascular risk factors on the risk of recurrent venous thromboembolism: results from the German MAISTHRO Registry. Blood Coagul Fibrinolysis2008; 19:159–165.
Steffen LM, Folsom AR, Cushman M, Jacobs DR, Rosamond WD. Greater fish, fruit, and vegetable intakes are related to lower incidence of venous thromboembolism: the Longitudinal Investigation of Thromboembolism Etiology. Circulation2007; 115:188–195.
Arslan F, Pasterkamp G, de Kleijn DP. Unraveling pleiotropic effects of statins: bit by bit, a slow case with perspective. Circ Res2008; 103:334–336.
Grady D, Wenger NK, Herrington D, et al. Postmenopausal hormone therapy increases risk for venous thromboembolic disease. The Heart and Estrogen/progestin Replacement Study. Ann Intern Med2000; 132:689–696.
Ray JG, Mamdani M, Tsuyuki RT, Anderson DR, Yeo EL, Laupacis A. Use of statins and the subsequent development of deep vein thrombosis. Arch Intern Med2001; 161:1405–1410.
Doggen CJ, Lemaitre RN, Smith NL, Heckbert SR, Psaty BM. HMG CoA reductase inhibitors and the risk of venous thrombosis among postmenopausal women. J Thromb Haemost2004; 2:700–701.
Lacut K, Oger E, Le Gal G, et al. Statins but not fibrates are associated with a reduced risk of venous thromboembolism: a hospitalbased case-control study. Fundam Clin Pharmacol2004; 18:477–482.
Ramcharan AS, Van Stralen KJ, Snoep JD, Mantel-Teeuwisse AK, Rosendaal FR, Doggen CJ. HMG-CoA reductase inhibitors, other lipid-lowering medication, antiplatelet therapy, and the risk of venous thrombosis. J Thromb Haemost2009; 7:514–520.
Sørensen HT, Horvath-Puho E, Sogaard KK, et al. Arterial cardiovascular events, statins, low-dose aspirin and subsequent risk of venous thromboembolism: a population-based case-control study. J Thromb Haemost2009; 7:521–528.
Yang CC, Jick SS, Jick H. Statins and the risk of idiopathic venous thromboembolism. Br J Clin Pharmacol2002; 53:101–105.
Smeeth L, Douglas I, Hall AJ, Hubbard R, Evans S. Effect of statins on a wide range of health outcomes: a cohort study validated by comparison with randomized trials. Br J Clin Pharmacol2009; 67:99–109.
Ridker PM, Danielson E, Fonseca FA, et al; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med2008; 359:2195–2207.
Shishehbor MH, Hazen SL. JUPITER to Earth: A statin helps peole with normal LDL-C and high hs-CRP, but what does it mean?Cleve Clin J Med2009; 76:37–44.
Cushman M. A new indication for statins to prevent venous thromboembolism? Not yet. J Thromb Haemost2009; 7:511–513.
Silva MA, Swanson AC, Gandhi PJ, Tataronis GR. Statin-related adverse events: a meta-analysis. Clin Ther2006; 28:26–35.
References
Glynn RJ, Danielson E, Fonseca FA, et al. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med2009; 360:1851–1861.
Prandoni P, Bilora F, Marchiori A, et al. An association between atherosclerosis and venous thrombosis. N Engl J Med2003; 348:1435–1441.
Prandoni P, Ghirarduzzi A, Prins MH, et al. Venous thromboembolism and the risk of subsequent symptomatic atherosclerosis. J Thromb Haemost2006; 4:1891–1896.
Braekkan SK, Mathiesen EB, Njolstad I, Wilsgaard T, Stormer J, Hansen JB. Family history of myocardial infarction is an independent risk factor for venous thromboembolism: the Tromso study. J Thromb Haemost2008; 6:1851–1857.
Tsai AW, Cushman M, Rosamond WD, Heckbert SR, Polak JF, Folsom AR. Cardiovascular risk factors and venous thromboembolism incidence: the longitudinal investigation of thromboembolism etiology. Arch Intern Med2002; 162:1182–1189.
van der Hagen PB, Folsom AR, Jenny NS, et al. Subclinical atherosclerosis and the risk of future venous thrombosis in the Cardiovascular Health Study. J Thromb Haemost2006; 4:1903–1908.
Reich LM, Folsom AR, Key NS, et al. Prospective study of subclinical atherosclerosis as a risk factor for venous thromboembolism. J Thromb Haemost2006; 4:1909–1913.
Huerta C, Johansson S, Wallander MA, Rodriguez LA. Risk of myocardial infarction and overall mortality in survivors of venous thromboembolism. Thromb J2008; 6:10.
Linnemann B, Schindewolf M, Zgouras D, Erbe M, Jarosch-Preusche M, Lindhoff-Last E. Are patients with thrombophilia and previous venous thromboembolism at higher risk to arterial thrombosis?Thromb Res2008; 121:743–750.
Schwaiger J, Kiechl S, Stockner H, et al. Burden of atherosclerosis and risk of venous thromboembolism in patients with migraine. Neurology2008; 71:937–943.
Linnemann B, Zgouras D, Schindewolf M, Schwonberg J, Jarosch-Preusche M, Lindhoff-Last E. Impact of sex and traditional cardiovascular risk factors on the risk of recurrent venous thromboembolism: results from the German MAISTHRO Registry. Blood Coagul Fibrinolysis2008; 19:159–165.
Steffen LM, Folsom AR, Cushman M, Jacobs DR, Rosamond WD. Greater fish, fruit, and vegetable intakes are related to lower incidence of venous thromboembolism: the Longitudinal Investigation of Thromboembolism Etiology. Circulation2007; 115:188–195.
Arslan F, Pasterkamp G, de Kleijn DP. Unraveling pleiotropic effects of statins: bit by bit, a slow case with perspective. Circ Res2008; 103:334–336.
Grady D, Wenger NK, Herrington D, et al. Postmenopausal hormone therapy increases risk for venous thromboembolic disease. The Heart and Estrogen/progestin Replacement Study. Ann Intern Med2000; 132:689–696.
Ray JG, Mamdani M, Tsuyuki RT, Anderson DR, Yeo EL, Laupacis A. Use of statins and the subsequent development of deep vein thrombosis. Arch Intern Med2001; 161:1405–1410.
Doggen CJ, Lemaitre RN, Smith NL, Heckbert SR, Psaty BM. HMG CoA reductase inhibitors and the risk of venous thrombosis among postmenopausal women. J Thromb Haemost2004; 2:700–701.
Lacut K, Oger E, Le Gal G, et al. Statins but not fibrates are associated with a reduced risk of venous thromboembolism: a hospitalbased case-control study. Fundam Clin Pharmacol2004; 18:477–482.
Ramcharan AS, Van Stralen KJ, Snoep JD, Mantel-Teeuwisse AK, Rosendaal FR, Doggen CJ. HMG-CoA reductase inhibitors, other lipid-lowering medication, antiplatelet therapy, and the risk of venous thrombosis. J Thromb Haemost2009; 7:514–520.
Sørensen HT, Horvath-Puho E, Sogaard KK, et al. Arterial cardiovascular events, statins, low-dose aspirin and subsequent risk of venous thromboembolism: a population-based case-control study. J Thromb Haemost2009; 7:521–528.
Yang CC, Jick SS, Jick H. Statins and the risk of idiopathic venous thromboembolism. Br J Clin Pharmacol2002; 53:101–105.
Smeeth L, Douglas I, Hall AJ, Hubbard R, Evans S. Effect of statins on a wide range of health outcomes: a cohort study validated by comparison with randomized trials. Br J Clin Pharmacol2009; 67:99–109.
Ridker PM, Danielson E, Fonseca FA, et al; JUPITER Study Group. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med2008; 359:2195–2207.
Shishehbor MH, Hazen SL. JUPITER to Earth: A statin helps peole with normal LDL-C and high hs-CRP, but what does it mean?Cleve Clin J Med2009; 76:37–44.
Cushman M. A new indication for statins to prevent venous thromboembolism? Not yet. J Thromb Haemost2009; 7:511–513.
Silva MA, Swanson AC, Gandhi PJ, Tataronis GR. Statin-related adverse events: a meta-analysis. Clin Ther2006; 28:26–35.
Risk factors for VTE overlap with those for arterial thrombosis, although the data are mixed.
The statin drugs have a number of effects on factors other than lipid levels, notably on markers of inflammation and on clotting factors.
In the JUPITER trial, the incidence of VTE in people taking rosuvastatin (Crestor) 20 mg/day was about half that in people taking placebo. This was a relatively healthy population, and the incidence in both groups was low.
Further study is needed in patients at risk of VTE.
Should patients with poorly controlled asthma be treated empirically for gastroesphageal reflux disease (GERD)?
Current guidelines1 indicate that trying a proton pump inhibitor may be worthwhile. However, the results of a recent multicenter trial2 indicate that this does not help control asthma symptoms and that we need to reevaluate the guidelines and focus on other factors that can worsen asthma control.
REFLUX DISEASE IS LINKED TO ASTHMA
GERD’s association with asthma has long been recognized. Asthma patients have a higher prevalence of GERD than the general population, with reported rates of 20% to 80%.3–8
GERD may worsen asthma via several mechanisms. If stomach acid gets into the airway, it can induce bronchoconstriction, vagal reflexes, and chronic airway inflammation, all of which can increase airway reactivity.9–16 Chronic reflux can also cause inflammation of the esophagus, which can exacerbate cough and possibly bronchospasm via neurogenic mechanisms.17
In turn, asthma may worsen GERD. Airway restriction can lead to hyperinflation and increased negative inspiratory pleural pressure, both of which may reduce the effectiveness of the lower esophageal sphincter.18 In addition, the beta-agonists and methylxanthines used to treat asthma may impair function of the lower esophageal sphincter and exacerbate reflux.18–20
CURRENT GUIDELINES ARE BASED ON LIMITED INFORMATION
The symptoms of GERD and asthma are nonspecific and can be similar (chest tightness, chest discomfort), which can make it challenging for clinicians or patients to distinguish asthma from GERD.2 Moreover, in asthma patients, GERD often presents without classic symptoms such as heartburn, and thus has been labeled “silent” GERD.
Earlier studies21–29 (Table 1) suggested that treating GERD may improve asthma control. Based on this information, the most recent asthma guidelines from the National Institutes of Health (NIH) recommend trying GERD treatment in patients with poorly controlled asthma, even if they do not have classic GERD symptoms.1
However, these studies all had significant limitations, such as small sample size. Also, the definitions of asthma and GERD differed from study to study. In some cases, the definition of GERD included self-reported GERD, which often fails to correlate with GERD documented with esophageal pH monitoring in asthma patients.1 These limitations were highlighted in a Cochrane review,30 which found that asthma patients with GERD showed no overall improvement in asthma after treatment of reflux. It concluded that small groups of patients may benefit, but that predicting who will respond is difficult.
Larger randomized controlled trials28,29 attempted to address some of these limitations, with varying results.
Littner et al29 gave lansoprazole (Prevacid) 30 mg twice daily or placebo to 207 patients with moderate to severe asthma and symptomatic GERD and saw no improvement in daily asthma symptoms, ie, asthma control in the active-treatment group. While these patients had an improvement in symptoms of severe reflux, their overall quality-of-life scores were similar to those of the placebo group. Of note, patients needing more than one type of drug for asthma control had a lower rate of asthma exacerbations.
Kiljander et al28 gave esomeprazole (Nexium) 40 mg twice daily or placebo to 770 patients who had mild to moderate asthma and symptoms of nocturnal asthma with or without symptoms of GERD. The only benefit was a slight improvement in peak expiratory flow in those with symptoms of both GERD and nocturnal asthma, and this was most significant in patients taking long-acting beta-agonists. Other measures—eg, the forced expiratory volume in the first second (FEV1), use of a beta-agonist, symptom scores, and nocturnal awakenings—did not improve.
In both of these studies,28,29 patients reported symptoms of GERD, so they did not have silent GERD.
THE DESIGN OF SARA
To address the limitations of the studies discussed above and evaluate the effect on asthma control of treating silent GERD, the American Lung Association and the National Heart, Lung, and Blood Institute funded the multicenter Study of Acid Reflux in Asthma (SARA) (Table 2).2
In SARA, 412 patients age 18 and older with inadequately controlled asthma were randomized to receive esomeprazole 40 mg twice a day or placebo for 24 weeks. Inadequate control was defined as a score of 1.5 or higher on the Juniper Asthma Control Questionnaire31 despite treatment with inhaled corticosteroids. Patients had no symptoms of GERD. The 40-mg twice-daily dosage of esomeprazole was chosen because it is known to suppress more than 90% of acid reflux.24,32
All patients completed a baseline asthma diary, recording peak expiratory flow rates, asthma symptoms, nighttime symptoms, and beta-agonist use. This information was collected every 4 weeks throughout the trial.
All participants also underwent esophageal pH monitoring for an objective confirmation of GERD. Patients were randomized independently of the results of the pH probe; in fact, investigators and patients were blinded to these results.
The primary outcome measure was the rate of episodes of poor asthma control, with poor control defined as any of the following:
A decrease of 30% or more in the morning peak expiratory flow rate on 2 consecutive days, compared with the patient’s best rate during the run-in period
An urgent visit, defined as an unscheduled health care visit, for asthma symptoms
The need for a course of oral prednisone for treatment of asthma.
Asthma was defined as doctor-diagnosed, plus either a positive methacholine challenge test (a concentration of methacholine causing a 20% reduction in FEV1 [PC20] < 16 mg/mL) or a positive bronchodilator response (a 12% increase in FEV1) to an inhaled beta-agonist. Participants had no other indication for acid suppression, including symptoms of GERD or previously diagnosed erosive esophageal or gastric disease.
Acid reflux was evaluated by ambulatory pH monitoring, which had to last at least 16 hours and span one meal and 2 hours in the recumbent position. Reflux was present if the pH was less than 4.0 for more than 5.8% of total time, 8.2% of time upright, or 3.5% of time lying down.33 Episodes and severity were measured by the Gastroesophageal Reflux Disease Symptom Assessment Scale.34
SARA RESULTS: NO IMPROVEMENT IN ASTHMA WITH GERD TREATMENT
The SARA treatment and control groups had similar baseline characteristics, with similar asthma symptoms. Most of the patients were women: 72% of the placebo group and 64% of the esomeprazole group. Most had baseline spirometric results at the lower end of normal (the mean FEV1 was 76% ± 16 SD in the treatment group and 78% ± 15 in the placebo group) and had very poor asthma control, with an average Juniper Asthma Control Questionnaire score of 1.9 (> 1.5 is considered poor control).31 GERD was documented with esophageal pH monitoring in 40% of patients, showing that a significant number had silent GERD.
Episodes of poor asthma control occurred with similar frequency in the esomeprazole and placebo groups (2.5 vs 2.3 events per personyear, P = .66). Treatment made no difference in this end point regardless of the baseline results of pH monitoring. No treatment effect was noted in the individual components of the episodes of poor asthma control or in secondary outcomes, including pulmonary function, airway reactivity, asthma control, symptom scores, nocturnal awakening, or quality of life.
In addition, subgroup analysis failed to identify any group—including those with documented reflux on pH probe testing or those receiving a long-acting beta-agonist—who benefited from proton pump inhibitor therapy.
The investigators concluded that these data suggest treatment of silent GERD does not improve asthma control and thus that a reevaluation of current guidelines and clinical practice is warranted.2
ISSUES REMAIN
This large clinical trial, in which asthma and GERD were well defined and objectively measured, was robustly negative in terms of showing any benefit of treatment of silent GERD on asthma control. The study population was representative of those for whom such a treatment is recommended in the current NIH guidelines, which are based on data published prior to SARA.
However, while SARA was well designed and had clear results, it had some limitations, and some issues regarding GERD and asthma remain unanswered.
Is acid the only problem in GERD? SARA focused on acidic GERD. Aspiration of substances such as pancreatic enzymes, pepsin, and bile has also been shown to induce symptoms in asthma patients.2,32,35 In addition, distention of the esophagus and stimulation of neurogenically mediated reflexes can cause symptoms or neurogenic airway inflammation that is not mitigated by drugs that target acid reflux.32
Indirectly supporting this theory is evidence that surgical interventions such as fundoplication can improve asthma symptoms. 36 However, this evidence is only from small studies with significant limitations.
Is proximal GERD worse than distal GERD? SARA did not address whether proximal and distal reflux may affect asthma differently. The importance of proximal reflux in asthma has not been clearly established, but there is evidence that patients with proximal GERD have a higher incidence of nocturnal cough than patients who have only distal reflux. 37
Dimango et al38 recently reported additional data from SARA in which patients with poorly controlled asthma underwent both proximal and distal esophageal pH monitoring to see if proximal GERD was associated with poor asthma control: 304 patients underwent dual pH-probe assessment and 38% of them had proximal reflux. The authors found no difference between those with and without proximal GERD with regard to nocturnal awakenings, need to use a rescue inhaler, inhaled controller medication dose, lung function, or airway reactivity by methacholine challenge. However, they did find that those with proximal GERD had worse asthma quality-of-life scores, and worse health-related quality-of-life scores and were more likely to complain of cough.
Thus, it appears that proximal GERD may worsen quality of life in asthmatic patients but does not worsen asthma control.
SARA RESULTS: IMPLICATIONS FOR MANAGEMENT
The SARA results suggest that patients with poorly controlled asthma who are on adequate controller medications should not be treated empirically for silent GERD in the expectation that the asthma will improve. Rather, they suggest that the focus should be on other factors that can worsen asthma control, such as the ability to properly use an inhaler, the ability to afford medications, compliance with drug treatment, and adequate control of other significant comorbidities such as allergic bronchopulmonary aspergillosis, sinusitis, allergic rhinitis, vocal cord dysfunction, and occult heart disease. The most recent NIH guidelines also suggest considering referral to an asthma specialist if symptoms persist despite adequate controller therapy.
References
National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J Allergy Clin Immunol2007; 120( suppl 5):S94–S138.
Mastronarde JG, Anthonisen NR, Castro M, et al., American Lung Association Asthma Clinical Research CentersEfficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med2009; 360:1487–1499.
Sontag SJ, O’Connell S, Khandelwal S, et al Most asthmatics have gastroesophageal reflux with or without bronchodilator therapy. Gastroenterology1990; 99:613–620.
Harding SM, Guzzo MR, Richter JE. The prevalence of gastroesophageal reflux in asthma patients without reflux symptoms. Am J Respir Crit Care Med2000; 162:34–39.
Vincent D, Cohen-Jonathan AM, Leport J, et al Gastro-oesophageal reflux prevalence and relationship with bronchial reactivity in asthma. Eur Respir J1997; 10:2255–2259.
Simpson WG. Gastroesophageal reflux disease and asthma. Diagnosis and management. Arch Intern Med1995; 155:798–803.
Irwin RS, Curley FJ, French CL. Difficult-to-control asthma. Contributing factors and outcome of a systematic management protocol. Chest1993; 103:1662–1669.
Harding SM, Richter JE. The role of gastroesophageal reflux in chronic cough and asthma. Chest1997; 111:1389–1402.
Richter JE. Asthma and gastroesophageal reflux disease: the truth is difficult to define. Chest1999; 116:1150–1152.
Ekstrom T, Tibbling L. Esophageal acid perfusion, airway function, and symptoms in asthmatic patients with marked bronchial hyperreactivity. Chest1989; 96:995–998.
Herve P, Denjean A, Jian R, Simonneau G, Duroux P. Intraesophageal perfusion of acid increases the bronchomotor response to methacholine and to isocapnic hyperventilation in asthmatic subjects. Am Rev Respir Dis1986; 134:986–989.
Wu DN, Tanifuji Y, Kobayashi H, et al Effects of esophageal acid perfusion on airway hyperresponsiveness in patients with bronchial asthma. Chest2000; 118:1553–1556.
Cuttitta G, Cibella F, Visconti A, Scichilone N, Bellia V, Bonsignore G. Spontaneous gastroesophageal reflux and airway patency during the night in adult asthmatics. Am J Respir Crit Care Med2000; 161:177–181.
Jack CI, Calverley PM, Donnelly RJ, et al Simultaneous tracheal and oesophageal pH measurements in asthmatic patients with gastrooesophageal reflux. Thorax1995; 50:201–204.
Harding SM, Schan CA, Guzzo MR, Alexander RW, Bradley LA, Richter JE. Gastroesophageal reflux-induced bronchoconstriction. Is microaspiration a factor?Chest1995; 108:1220–1227.
Irwin RS, Madison JM, Fraire AE. The cough reflex and its relation to gastroesophageal reflux. Am J Med2000; 108( suppl 4a):73S–78S.
Choy D, Leung R. Gastro-oesophageal reflux disease and asthma. Respirology1997; 2:163–168.
Zerbib F, Guisset O, Lamouliatte H, Quinton A, Galmiche JP, Tunon-De-Lara JM. Effects of bronchial obstruction on lower esophageal sphincter motility and gastroesophageal reflux in patients with asthma. Am J Respir Crit Care Med2002; 166:1206–1211.
Lacy BE, Mathis C, DesBiens J, Liu MC. The effects of nebulized albuterol on esophageal function in asthmatic patients. Dig Dis Sci2008; 53:2627–2633.
Ford GA, Oliver PS, Prior JS, Butland RJ, Wilkinson SP. Omeprazole in the treatment of asthmatics with nocturnal symptoms and gastrooesophageal reflux: a placebo-controlled cross-over study. Postgrad Med J1994; 70:350–354.
Teichtahl H, Kronborg IJ, Yeomans ND, Robinson P. Adult asthma and gastro-oesophageal reflux: the effects of omeprazole therapy on asthma. Aust N Z J Med1996; 26:671–676.
Meier JH, McNally PR, Punja M, et al Does omeprazole (Prilosec) improve respiratory function in asthmatics with gastroesophageal reflux? A double-blind, placebo-controlled crossover study. Dig Dis Sci1994; 39:2127–2133.
Harding SM, Richter JE, Guzzo MR, Schan CA, Alexander RW, Bradley LA. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med1996; 100:395–405.
Levin TR, Sperling RM, McQuaid KR. Omeprazole improves peak expiratory flow rate and quality of life in asthmatics with gastroesophageal reflux. Am J Gastroenterol1998; 93:1060–1063.
Boeree MJ, Peters FT, Postma DS, Kleibeuker JH. No effects of highdose omeprazole in patients with severe airway hyperresponsiveness and (a)symptomatic gastro-oesophageal reflux. Eur Respir J1998; 11:1070–1074.
Kiljander TO, Salomaa ER, Hietanen EK, Terho EO. Gastroesophageal reflux in asthmatics: a double-blind, placebo-controlled crossover study with omeprazole. Chest1999; 116:1257–1264.
Kiljander TO, Harding SM, Field SK, et al Effects of eso-meprazole 40 mg twice daily on asthma: a randomized placebo-controlled trial. Am J Respir Crit Care Med2006; 173:1091–1097.
Littner MR, Leung FW, Ballard ED, Huang B, Samra NKLansoprazole Asthma Study Group. Effects of 24 weeks of lansoprazole therapy on asthma symptoms, exacerbations, quality of life, and pulmonary function in adult asthmatic patients with acid reflux symptoms. Chest2005; 128:1128–1135.
Gibson PG, Henry R, Coughlan JJL. Gastro-oesophageal reflux treatment for asthma in adults and children. Coch-rane Database Syst Rev2000;CD001496. Also available online at www.cochrane.org/reviews/en/ab001496.html. Accessed January 28, 2010.
Juniper EF, Bousquet J, Abetz L, Bateman EDGOAL Committee. Identifying ‘well-controlled’ and ‘not well-controlled’ asthma using the Asthma Control Questionnaire. Respir Med2006; 100:616–621.
Canning BJ, Mazzone SB. Reflex mechanisms in gastro-esophageal reflux disease and asthma. Am J Med2003; 115( suppl 3A):45S–48S.
Richter JE, Bradley LA, DeMeester TR, Wu WC. Normal 24-hr ambulatory esophageal pH values. Influence of study center, pH electrode, age, and gender. Dig Dis Sci1992; 37:849–856.
Damiano A, Handley K, Adler E, Siddique R, Bhattacharyja A. Measuring symptom distress and health-related quality of life in clinical trials of gastroesophageal reflux disease treatment: further validation of the Gastroesophageal Reflux Disease Symptom Assessment Scale (GSAS). Dig Dis Sci2002; 47:1530–1537.
Asano K, Suzuki H. Silent acid reflux and asthma control [editorial]. N Engl J Med2009; 360:1551–1553.
Rakita S, Villadolid D, Thomas A, et al Laparoscopic Nissen fundoplication offers high patient satisfaction with relief of extraesophageal symptoms of gastroesophageal reflux disease. Am Surg2006; 72:207–212.
Tomonaga T, Awad ZT, Filipi CJ, et al Symptom predictability of reflux-induced respiratory disease. Dig Dis Sci2002; 47:9–14.
Dimango E, Holbrook JT, Simpson E, et al., American Lung Association Asthma Clinical Research Centers. Effects of asymptomatic proximal and distal gastroesophageal reflux on asthma severity. Am J Respir Crit Care Med2009; 180:809–816.
Brent P. Riscili, MD Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus
Jonathan P. Parsons, MD, MSc Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus, and Investigator in the Study of Acid Reflux in Asthma (SARA)
John G. Mastronarde, MD, MSc Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus, and Principal Investigator in the Study of Acid Reflux in Asthma (SARA)
Address: John G. Mastronarde, MD, The Ohio State University Medical Center, 201 Davis Heart/Lung Research Institute, 473 W. 12th Avenue, Columbus, OH 43210; e-mail john.mastronarde@osumc.edu
Dr. Parsons has received honoraria from GlaxoSmithKline, Merck, and AstraZeneca.
Brent P. Riscili, MD Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus
Jonathan P. Parsons, MD, MSc Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus, and Investigator in the Study of Acid Reflux in Asthma (SARA)
John G. Mastronarde, MD, MSc Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus, and Principal Investigator in the Study of Acid Reflux in Asthma (SARA)
Address: John G. Mastronarde, MD, The Ohio State University Medical Center, 201 Davis Heart/Lung Research Institute, 473 W. 12th Avenue, Columbus, OH 43210; e-mail john.mastronarde@osumc.edu
Dr. Parsons has received honoraria from GlaxoSmithKline, Merck, and AstraZeneca.
Author and Disclosure Information
Brent P. Riscili, MD Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus
Jonathan P. Parsons, MD, MSc Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus, and Investigator in the Study of Acid Reflux in Asthma (SARA)
John G. Mastronarde, MD, MSc Division of Pulmonary, Allergy, Critical Care, and Sleep Medicine, The Ohio State University Medical Center, Columbus, and Principal Investigator in the Study of Acid Reflux in Asthma (SARA)
Address: John G. Mastronarde, MD, The Ohio State University Medical Center, 201 Davis Heart/Lung Research Institute, 473 W. 12th Avenue, Columbus, OH 43210; e-mail john.mastronarde@osumc.edu
Dr. Parsons has received honoraria from GlaxoSmithKline, Merck, and AstraZeneca.
Should patients with poorly controlled asthma be treated empirically for gastroesphageal reflux disease (GERD)?
Current guidelines1 indicate that trying a proton pump inhibitor may be worthwhile. However, the results of a recent multicenter trial2 indicate that this does not help control asthma symptoms and that we need to reevaluate the guidelines and focus on other factors that can worsen asthma control.
REFLUX DISEASE IS LINKED TO ASTHMA
GERD’s association with asthma has long been recognized. Asthma patients have a higher prevalence of GERD than the general population, with reported rates of 20% to 80%.3–8
GERD may worsen asthma via several mechanisms. If stomach acid gets into the airway, it can induce bronchoconstriction, vagal reflexes, and chronic airway inflammation, all of which can increase airway reactivity.9–16 Chronic reflux can also cause inflammation of the esophagus, which can exacerbate cough and possibly bronchospasm via neurogenic mechanisms.17
In turn, asthma may worsen GERD. Airway restriction can lead to hyperinflation and increased negative inspiratory pleural pressure, both of which may reduce the effectiveness of the lower esophageal sphincter.18 In addition, the beta-agonists and methylxanthines used to treat asthma may impair function of the lower esophageal sphincter and exacerbate reflux.18–20
CURRENT GUIDELINES ARE BASED ON LIMITED INFORMATION
The symptoms of GERD and asthma are nonspecific and can be similar (chest tightness, chest discomfort), which can make it challenging for clinicians or patients to distinguish asthma from GERD.2 Moreover, in asthma patients, GERD often presents without classic symptoms such as heartburn, and thus has been labeled “silent” GERD.
Earlier studies21–29 (Table 1) suggested that treating GERD may improve asthma control. Based on this information, the most recent asthma guidelines from the National Institutes of Health (NIH) recommend trying GERD treatment in patients with poorly controlled asthma, even if they do not have classic GERD symptoms.1
However, these studies all had significant limitations, such as small sample size. Also, the definitions of asthma and GERD differed from study to study. In some cases, the definition of GERD included self-reported GERD, which often fails to correlate with GERD documented with esophageal pH monitoring in asthma patients.1 These limitations were highlighted in a Cochrane review,30 which found that asthma patients with GERD showed no overall improvement in asthma after treatment of reflux. It concluded that small groups of patients may benefit, but that predicting who will respond is difficult.
Larger randomized controlled trials28,29 attempted to address some of these limitations, with varying results.
Littner et al29 gave lansoprazole (Prevacid) 30 mg twice daily or placebo to 207 patients with moderate to severe asthma and symptomatic GERD and saw no improvement in daily asthma symptoms, ie, asthma control in the active-treatment group. While these patients had an improvement in symptoms of severe reflux, their overall quality-of-life scores were similar to those of the placebo group. Of note, patients needing more than one type of drug for asthma control had a lower rate of asthma exacerbations.
Kiljander et al28 gave esomeprazole (Nexium) 40 mg twice daily or placebo to 770 patients who had mild to moderate asthma and symptoms of nocturnal asthma with or without symptoms of GERD. The only benefit was a slight improvement in peak expiratory flow in those with symptoms of both GERD and nocturnal asthma, and this was most significant in patients taking long-acting beta-agonists. Other measures—eg, the forced expiratory volume in the first second (FEV1), use of a beta-agonist, symptom scores, and nocturnal awakenings—did not improve.
In both of these studies,28,29 patients reported symptoms of GERD, so they did not have silent GERD.
THE DESIGN OF SARA
To address the limitations of the studies discussed above and evaluate the effect on asthma control of treating silent GERD, the American Lung Association and the National Heart, Lung, and Blood Institute funded the multicenter Study of Acid Reflux in Asthma (SARA) (Table 2).2
In SARA, 412 patients age 18 and older with inadequately controlled asthma were randomized to receive esomeprazole 40 mg twice a day or placebo for 24 weeks. Inadequate control was defined as a score of 1.5 or higher on the Juniper Asthma Control Questionnaire31 despite treatment with inhaled corticosteroids. Patients had no symptoms of GERD. The 40-mg twice-daily dosage of esomeprazole was chosen because it is known to suppress more than 90% of acid reflux.24,32
All patients completed a baseline asthma diary, recording peak expiratory flow rates, asthma symptoms, nighttime symptoms, and beta-agonist use. This information was collected every 4 weeks throughout the trial.
All participants also underwent esophageal pH monitoring for an objective confirmation of GERD. Patients were randomized independently of the results of the pH probe; in fact, investigators and patients were blinded to these results.
The primary outcome measure was the rate of episodes of poor asthma control, with poor control defined as any of the following:
A decrease of 30% or more in the morning peak expiratory flow rate on 2 consecutive days, compared with the patient’s best rate during the run-in period
An urgent visit, defined as an unscheduled health care visit, for asthma symptoms
The need for a course of oral prednisone for treatment of asthma.
Asthma was defined as doctor-diagnosed, plus either a positive methacholine challenge test (a concentration of methacholine causing a 20% reduction in FEV1 [PC20] < 16 mg/mL) or a positive bronchodilator response (a 12% increase in FEV1) to an inhaled beta-agonist. Participants had no other indication for acid suppression, including symptoms of GERD or previously diagnosed erosive esophageal or gastric disease.
Acid reflux was evaluated by ambulatory pH monitoring, which had to last at least 16 hours and span one meal and 2 hours in the recumbent position. Reflux was present if the pH was less than 4.0 for more than 5.8% of total time, 8.2% of time upright, or 3.5% of time lying down.33 Episodes and severity were measured by the Gastroesophageal Reflux Disease Symptom Assessment Scale.34
SARA RESULTS: NO IMPROVEMENT IN ASTHMA WITH GERD TREATMENT
The SARA treatment and control groups had similar baseline characteristics, with similar asthma symptoms. Most of the patients were women: 72% of the placebo group and 64% of the esomeprazole group. Most had baseline spirometric results at the lower end of normal (the mean FEV1 was 76% ± 16 SD in the treatment group and 78% ± 15 in the placebo group) and had very poor asthma control, with an average Juniper Asthma Control Questionnaire score of 1.9 (> 1.5 is considered poor control).31 GERD was documented with esophageal pH monitoring in 40% of patients, showing that a significant number had silent GERD.
Episodes of poor asthma control occurred with similar frequency in the esomeprazole and placebo groups (2.5 vs 2.3 events per personyear, P = .66). Treatment made no difference in this end point regardless of the baseline results of pH monitoring. No treatment effect was noted in the individual components of the episodes of poor asthma control or in secondary outcomes, including pulmonary function, airway reactivity, asthma control, symptom scores, nocturnal awakening, or quality of life.
In addition, subgroup analysis failed to identify any group—including those with documented reflux on pH probe testing or those receiving a long-acting beta-agonist—who benefited from proton pump inhibitor therapy.
The investigators concluded that these data suggest treatment of silent GERD does not improve asthma control and thus that a reevaluation of current guidelines and clinical practice is warranted.2
ISSUES REMAIN
This large clinical trial, in which asthma and GERD were well defined and objectively measured, was robustly negative in terms of showing any benefit of treatment of silent GERD on asthma control. The study population was representative of those for whom such a treatment is recommended in the current NIH guidelines, which are based on data published prior to SARA.
However, while SARA was well designed and had clear results, it had some limitations, and some issues regarding GERD and asthma remain unanswered.
Is acid the only problem in GERD? SARA focused on acidic GERD. Aspiration of substances such as pancreatic enzymes, pepsin, and bile has also been shown to induce symptoms in asthma patients.2,32,35 In addition, distention of the esophagus and stimulation of neurogenically mediated reflexes can cause symptoms or neurogenic airway inflammation that is not mitigated by drugs that target acid reflux.32
Indirectly supporting this theory is evidence that surgical interventions such as fundoplication can improve asthma symptoms. 36 However, this evidence is only from small studies with significant limitations.
Is proximal GERD worse than distal GERD? SARA did not address whether proximal and distal reflux may affect asthma differently. The importance of proximal reflux in asthma has not been clearly established, but there is evidence that patients with proximal GERD have a higher incidence of nocturnal cough than patients who have only distal reflux. 37
Dimango et al38 recently reported additional data from SARA in which patients with poorly controlled asthma underwent both proximal and distal esophageal pH monitoring to see if proximal GERD was associated with poor asthma control: 304 patients underwent dual pH-probe assessment and 38% of them had proximal reflux. The authors found no difference between those with and without proximal GERD with regard to nocturnal awakenings, need to use a rescue inhaler, inhaled controller medication dose, lung function, or airway reactivity by methacholine challenge. However, they did find that those with proximal GERD had worse asthma quality-of-life scores, and worse health-related quality-of-life scores and were more likely to complain of cough.
Thus, it appears that proximal GERD may worsen quality of life in asthmatic patients but does not worsen asthma control.
SARA RESULTS: IMPLICATIONS FOR MANAGEMENT
The SARA results suggest that patients with poorly controlled asthma who are on adequate controller medications should not be treated empirically for silent GERD in the expectation that the asthma will improve. Rather, they suggest that the focus should be on other factors that can worsen asthma control, such as the ability to properly use an inhaler, the ability to afford medications, compliance with drug treatment, and adequate control of other significant comorbidities such as allergic bronchopulmonary aspergillosis, sinusitis, allergic rhinitis, vocal cord dysfunction, and occult heart disease. The most recent NIH guidelines also suggest considering referral to an asthma specialist if symptoms persist despite adequate controller therapy.
Should patients with poorly controlled asthma be treated empirically for gastroesphageal reflux disease (GERD)?
Current guidelines1 indicate that trying a proton pump inhibitor may be worthwhile. However, the results of a recent multicenter trial2 indicate that this does not help control asthma symptoms and that we need to reevaluate the guidelines and focus on other factors that can worsen asthma control.
REFLUX DISEASE IS LINKED TO ASTHMA
GERD’s association with asthma has long been recognized. Asthma patients have a higher prevalence of GERD than the general population, with reported rates of 20% to 80%.3–8
GERD may worsen asthma via several mechanisms. If stomach acid gets into the airway, it can induce bronchoconstriction, vagal reflexes, and chronic airway inflammation, all of which can increase airway reactivity.9–16 Chronic reflux can also cause inflammation of the esophagus, which can exacerbate cough and possibly bronchospasm via neurogenic mechanisms.17
In turn, asthma may worsen GERD. Airway restriction can lead to hyperinflation and increased negative inspiratory pleural pressure, both of which may reduce the effectiveness of the lower esophageal sphincter.18 In addition, the beta-agonists and methylxanthines used to treat asthma may impair function of the lower esophageal sphincter and exacerbate reflux.18–20
CURRENT GUIDELINES ARE BASED ON LIMITED INFORMATION
The symptoms of GERD and asthma are nonspecific and can be similar (chest tightness, chest discomfort), which can make it challenging for clinicians or patients to distinguish asthma from GERD.2 Moreover, in asthma patients, GERD often presents without classic symptoms such as heartburn, and thus has been labeled “silent” GERD.
Earlier studies21–29 (Table 1) suggested that treating GERD may improve asthma control. Based on this information, the most recent asthma guidelines from the National Institutes of Health (NIH) recommend trying GERD treatment in patients with poorly controlled asthma, even if they do not have classic GERD symptoms.1
However, these studies all had significant limitations, such as small sample size. Also, the definitions of asthma and GERD differed from study to study. In some cases, the definition of GERD included self-reported GERD, which often fails to correlate with GERD documented with esophageal pH monitoring in asthma patients.1 These limitations were highlighted in a Cochrane review,30 which found that asthma patients with GERD showed no overall improvement in asthma after treatment of reflux. It concluded that small groups of patients may benefit, but that predicting who will respond is difficult.
Larger randomized controlled trials28,29 attempted to address some of these limitations, with varying results.
Littner et al29 gave lansoprazole (Prevacid) 30 mg twice daily or placebo to 207 patients with moderate to severe asthma and symptomatic GERD and saw no improvement in daily asthma symptoms, ie, asthma control in the active-treatment group. While these patients had an improvement in symptoms of severe reflux, their overall quality-of-life scores were similar to those of the placebo group. Of note, patients needing more than one type of drug for asthma control had a lower rate of asthma exacerbations.
Kiljander et al28 gave esomeprazole (Nexium) 40 mg twice daily or placebo to 770 patients who had mild to moderate asthma and symptoms of nocturnal asthma with or without symptoms of GERD. The only benefit was a slight improvement in peak expiratory flow in those with symptoms of both GERD and nocturnal asthma, and this was most significant in patients taking long-acting beta-agonists. Other measures—eg, the forced expiratory volume in the first second (FEV1), use of a beta-agonist, symptom scores, and nocturnal awakenings—did not improve.
In both of these studies,28,29 patients reported symptoms of GERD, so they did not have silent GERD.
THE DESIGN OF SARA
To address the limitations of the studies discussed above and evaluate the effect on asthma control of treating silent GERD, the American Lung Association and the National Heart, Lung, and Blood Institute funded the multicenter Study of Acid Reflux in Asthma (SARA) (Table 2).2
In SARA, 412 patients age 18 and older with inadequately controlled asthma were randomized to receive esomeprazole 40 mg twice a day or placebo for 24 weeks. Inadequate control was defined as a score of 1.5 or higher on the Juniper Asthma Control Questionnaire31 despite treatment with inhaled corticosteroids. Patients had no symptoms of GERD. The 40-mg twice-daily dosage of esomeprazole was chosen because it is known to suppress more than 90% of acid reflux.24,32
All patients completed a baseline asthma diary, recording peak expiratory flow rates, asthma symptoms, nighttime symptoms, and beta-agonist use. This information was collected every 4 weeks throughout the trial.
All participants also underwent esophageal pH monitoring for an objective confirmation of GERD. Patients were randomized independently of the results of the pH probe; in fact, investigators and patients were blinded to these results.
The primary outcome measure was the rate of episodes of poor asthma control, with poor control defined as any of the following:
A decrease of 30% or more in the morning peak expiratory flow rate on 2 consecutive days, compared with the patient’s best rate during the run-in period
An urgent visit, defined as an unscheduled health care visit, for asthma symptoms
The need for a course of oral prednisone for treatment of asthma.
Asthma was defined as doctor-diagnosed, plus either a positive methacholine challenge test (a concentration of methacholine causing a 20% reduction in FEV1 [PC20] < 16 mg/mL) or a positive bronchodilator response (a 12% increase in FEV1) to an inhaled beta-agonist. Participants had no other indication for acid suppression, including symptoms of GERD or previously diagnosed erosive esophageal or gastric disease.
Acid reflux was evaluated by ambulatory pH monitoring, which had to last at least 16 hours and span one meal and 2 hours in the recumbent position. Reflux was present if the pH was less than 4.0 for more than 5.8% of total time, 8.2% of time upright, or 3.5% of time lying down.33 Episodes and severity were measured by the Gastroesophageal Reflux Disease Symptom Assessment Scale.34
SARA RESULTS: NO IMPROVEMENT IN ASTHMA WITH GERD TREATMENT
The SARA treatment and control groups had similar baseline characteristics, with similar asthma symptoms. Most of the patients were women: 72% of the placebo group and 64% of the esomeprazole group. Most had baseline spirometric results at the lower end of normal (the mean FEV1 was 76% ± 16 SD in the treatment group and 78% ± 15 in the placebo group) and had very poor asthma control, with an average Juniper Asthma Control Questionnaire score of 1.9 (> 1.5 is considered poor control).31 GERD was documented with esophageal pH monitoring in 40% of patients, showing that a significant number had silent GERD.
Episodes of poor asthma control occurred with similar frequency in the esomeprazole and placebo groups (2.5 vs 2.3 events per personyear, P = .66). Treatment made no difference in this end point regardless of the baseline results of pH monitoring. No treatment effect was noted in the individual components of the episodes of poor asthma control or in secondary outcomes, including pulmonary function, airway reactivity, asthma control, symptom scores, nocturnal awakening, or quality of life.
In addition, subgroup analysis failed to identify any group—including those with documented reflux on pH probe testing or those receiving a long-acting beta-agonist—who benefited from proton pump inhibitor therapy.
The investigators concluded that these data suggest treatment of silent GERD does not improve asthma control and thus that a reevaluation of current guidelines and clinical practice is warranted.2
ISSUES REMAIN
This large clinical trial, in which asthma and GERD were well defined and objectively measured, was robustly negative in terms of showing any benefit of treatment of silent GERD on asthma control. The study population was representative of those for whom such a treatment is recommended in the current NIH guidelines, which are based on data published prior to SARA.
However, while SARA was well designed and had clear results, it had some limitations, and some issues regarding GERD and asthma remain unanswered.
Is acid the only problem in GERD? SARA focused on acidic GERD. Aspiration of substances such as pancreatic enzymes, pepsin, and bile has also been shown to induce symptoms in asthma patients.2,32,35 In addition, distention of the esophagus and stimulation of neurogenically mediated reflexes can cause symptoms or neurogenic airway inflammation that is not mitigated by drugs that target acid reflux.32
Indirectly supporting this theory is evidence that surgical interventions such as fundoplication can improve asthma symptoms. 36 However, this evidence is only from small studies with significant limitations.
Is proximal GERD worse than distal GERD? SARA did not address whether proximal and distal reflux may affect asthma differently. The importance of proximal reflux in asthma has not been clearly established, but there is evidence that patients with proximal GERD have a higher incidence of nocturnal cough than patients who have only distal reflux. 37
Dimango et al38 recently reported additional data from SARA in which patients with poorly controlled asthma underwent both proximal and distal esophageal pH monitoring to see if proximal GERD was associated with poor asthma control: 304 patients underwent dual pH-probe assessment and 38% of them had proximal reflux. The authors found no difference between those with and without proximal GERD with regard to nocturnal awakenings, need to use a rescue inhaler, inhaled controller medication dose, lung function, or airway reactivity by methacholine challenge. However, they did find that those with proximal GERD had worse asthma quality-of-life scores, and worse health-related quality-of-life scores and were more likely to complain of cough.
Thus, it appears that proximal GERD may worsen quality of life in asthmatic patients but does not worsen asthma control.
SARA RESULTS: IMPLICATIONS FOR MANAGEMENT
The SARA results suggest that patients with poorly controlled asthma who are on adequate controller medications should not be treated empirically for silent GERD in the expectation that the asthma will improve. Rather, they suggest that the focus should be on other factors that can worsen asthma control, such as the ability to properly use an inhaler, the ability to afford medications, compliance with drug treatment, and adequate control of other significant comorbidities such as allergic bronchopulmonary aspergillosis, sinusitis, allergic rhinitis, vocal cord dysfunction, and occult heart disease. The most recent NIH guidelines also suggest considering referral to an asthma specialist if symptoms persist despite adequate controller therapy.
References
National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J Allergy Clin Immunol2007; 120( suppl 5):S94–S138.
Mastronarde JG, Anthonisen NR, Castro M, et al., American Lung Association Asthma Clinical Research CentersEfficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med2009; 360:1487–1499.
Sontag SJ, O’Connell S, Khandelwal S, et al Most asthmatics have gastroesophageal reflux with or without bronchodilator therapy. Gastroenterology1990; 99:613–620.
Harding SM, Guzzo MR, Richter JE. The prevalence of gastroesophageal reflux in asthma patients without reflux symptoms. Am J Respir Crit Care Med2000; 162:34–39.
Vincent D, Cohen-Jonathan AM, Leport J, et al Gastro-oesophageal reflux prevalence and relationship with bronchial reactivity in asthma. Eur Respir J1997; 10:2255–2259.
Simpson WG. Gastroesophageal reflux disease and asthma. Diagnosis and management. Arch Intern Med1995; 155:798–803.
Irwin RS, Curley FJ, French CL. Difficult-to-control asthma. Contributing factors and outcome of a systematic management protocol. Chest1993; 103:1662–1669.
Harding SM, Richter JE. The role of gastroesophageal reflux in chronic cough and asthma. Chest1997; 111:1389–1402.
Richter JE. Asthma and gastroesophageal reflux disease: the truth is difficult to define. Chest1999; 116:1150–1152.
Ekstrom T, Tibbling L. Esophageal acid perfusion, airway function, and symptoms in asthmatic patients with marked bronchial hyperreactivity. Chest1989; 96:995–998.
Herve P, Denjean A, Jian R, Simonneau G, Duroux P. Intraesophageal perfusion of acid increases the bronchomotor response to methacholine and to isocapnic hyperventilation in asthmatic subjects. Am Rev Respir Dis1986; 134:986–989.
Wu DN, Tanifuji Y, Kobayashi H, et al Effects of esophageal acid perfusion on airway hyperresponsiveness in patients with bronchial asthma. Chest2000; 118:1553–1556.
Cuttitta G, Cibella F, Visconti A, Scichilone N, Bellia V, Bonsignore G. Spontaneous gastroesophageal reflux and airway patency during the night in adult asthmatics. Am J Respir Crit Care Med2000; 161:177–181.
Jack CI, Calverley PM, Donnelly RJ, et al Simultaneous tracheal and oesophageal pH measurements in asthmatic patients with gastrooesophageal reflux. Thorax1995; 50:201–204.
Harding SM, Schan CA, Guzzo MR, Alexander RW, Bradley LA, Richter JE. Gastroesophageal reflux-induced bronchoconstriction. Is microaspiration a factor?Chest1995; 108:1220–1227.
Irwin RS, Madison JM, Fraire AE. The cough reflex and its relation to gastroesophageal reflux. Am J Med2000; 108( suppl 4a):73S–78S.
Choy D, Leung R. Gastro-oesophageal reflux disease and asthma. Respirology1997; 2:163–168.
Zerbib F, Guisset O, Lamouliatte H, Quinton A, Galmiche JP, Tunon-De-Lara JM. Effects of bronchial obstruction on lower esophageal sphincter motility and gastroesophageal reflux in patients with asthma. Am J Respir Crit Care Med2002; 166:1206–1211.
Lacy BE, Mathis C, DesBiens J, Liu MC. The effects of nebulized albuterol on esophageal function in asthmatic patients. Dig Dis Sci2008; 53:2627–2633.
Ford GA, Oliver PS, Prior JS, Butland RJ, Wilkinson SP. Omeprazole in the treatment of asthmatics with nocturnal symptoms and gastrooesophageal reflux: a placebo-controlled cross-over study. Postgrad Med J1994; 70:350–354.
Teichtahl H, Kronborg IJ, Yeomans ND, Robinson P. Adult asthma and gastro-oesophageal reflux: the effects of omeprazole therapy on asthma. Aust N Z J Med1996; 26:671–676.
Meier JH, McNally PR, Punja M, et al Does omeprazole (Prilosec) improve respiratory function in asthmatics with gastroesophageal reflux? A double-blind, placebo-controlled crossover study. Dig Dis Sci1994; 39:2127–2133.
Harding SM, Richter JE, Guzzo MR, Schan CA, Alexander RW, Bradley LA. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med1996; 100:395–405.
Levin TR, Sperling RM, McQuaid KR. Omeprazole improves peak expiratory flow rate and quality of life in asthmatics with gastroesophageal reflux. Am J Gastroenterol1998; 93:1060–1063.
Boeree MJ, Peters FT, Postma DS, Kleibeuker JH. No effects of highdose omeprazole in patients with severe airway hyperresponsiveness and (a)symptomatic gastro-oesophageal reflux. Eur Respir J1998; 11:1070–1074.
Kiljander TO, Salomaa ER, Hietanen EK, Terho EO. Gastroesophageal reflux in asthmatics: a double-blind, placebo-controlled crossover study with omeprazole. Chest1999; 116:1257–1264.
Kiljander TO, Harding SM, Field SK, et al Effects of eso-meprazole 40 mg twice daily on asthma: a randomized placebo-controlled trial. Am J Respir Crit Care Med2006; 173:1091–1097.
Littner MR, Leung FW, Ballard ED, Huang B, Samra NKLansoprazole Asthma Study Group. Effects of 24 weeks of lansoprazole therapy on asthma symptoms, exacerbations, quality of life, and pulmonary function in adult asthmatic patients with acid reflux symptoms. Chest2005; 128:1128–1135.
Gibson PG, Henry R, Coughlan JJL. Gastro-oesophageal reflux treatment for asthma in adults and children. Coch-rane Database Syst Rev2000;CD001496. Also available online at www.cochrane.org/reviews/en/ab001496.html. Accessed January 28, 2010.
Juniper EF, Bousquet J, Abetz L, Bateman EDGOAL Committee. Identifying ‘well-controlled’ and ‘not well-controlled’ asthma using the Asthma Control Questionnaire. Respir Med2006; 100:616–621.
Canning BJ, Mazzone SB. Reflex mechanisms in gastro-esophageal reflux disease and asthma. Am J Med2003; 115( suppl 3A):45S–48S.
Richter JE, Bradley LA, DeMeester TR, Wu WC. Normal 24-hr ambulatory esophageal pH values. Influence of study center, pH electrode, age, and gender. Dig Dis Sci1992; 37:849–856.
Damiano A, Handley K, Adler E, Siddique R, Bhattacharyja A. Measuring symptom distress and health-related quality of life in clinical trials of gastroesophageal reflux disease treatment: further validation of the Gastroesophageal Reflux Disease Symptom Assessment Scale (GSAS). Dig Dis Sci2002; 47:1530–1537.
Asano K, Suzuki H. Silent acid reflux and asthma control [editorial]. N Engl J Med2009; 360:1551–1553.
Rakita S, Villadolid D, Thomas A, et al Laparoscopic Nissen fundoplication offers high patient satisfaction with relief of extraesophageal symptoms of gastroesophageal reflux disease. Am Surg2006; 72:207–212.
Tomonaga T, Awad ZT, Filipi CJ, et al Symptom predictability of reflux-induced respiratory disease. Dig Dis Sci2002; 47:9–14.
Dimango E, Holbrook JT, Simpson E, et al., American Lung Association Asthma Clinical Research Centers. Effects of asymptomatic proximal and distal gastroesophageal reflux on asthma severity. Am J Respir Crit Care Med2009; 180:809–816.
References
National Asthma Education and Prevention Program. Expert Panel Report 3 (EPR-3): Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J Allergy Clin Immunol2007; 120( suppl 5):S94–S138.
Mastronarde JG, Anthonisen NR, Castro M, et al., American Lung Association Asthma Clinical Research CentersEfficacy of esomeprazole for treatment of poorly controlled asthma. N Engl J Med2009; 360:1487–1499.
Sontag SJ, O’Connell S, Khandelwal S, et al Most asthmatics have gastroesophageal reflux with or without bronchodilator therapy. Gastroenterology1990; 99:613–620.
Harding SM, Guzzo MR, Richter JE. The prevalence of gastroesophageal reflux in asthma patients without reflux symptoms. Am J Respir Crit Care Med2000; 162:34–39.
Vincent D, Cohen-Jonathan AM, Leport J, et al Gastro-oesophageal reflux prevalence and relationship with bronchial reactivity in asthma. Eur Respir J1997; 10:2255–2259.
Simpson WG. Gastroesophageal reflux disease and asthma. Diagnosis and management. Arch Intern Med1995; 155:798–803.
Irwin RS, Curley FJ, French CL. Difficult-to-control asthma. Contributing factors and outcome of a systematic management protocol. Chest1993; 103:1662–1669.
Harding SM, Richter JE. The role of gastroesophageal reflux in chronic cough and asthma. Chest1997; 111:1389–1402.
Richter JE. Asthma and gastroesophageal reflux disease: the truth is difficult to define. Chest1999; 116:1150–1152.
Ekstrom T, Tibbling L. Esophageal acid perfusion, airway function, and symptoms in asthmatic patients with marked bronchial hyperreactivity. Chest1989; 96:995–998.
Herve P, Denjean A, Jian R, Simonneau G, Duroux P. Intraesophageal perfusion of acid increases the bronchomotor response to methacholine and to isocapnic hyperventilation in asthmatic subjects. Am Rev Respir Dis1986; 134:986–989.
Wu DN, Tanifuji Y, Kobayashi H, et al Effects of esophageal acid perfusion on airway hyperresponsiveness in patients with bronchial asthma. Chest2000; 118:1553–1556.
Cuttitta G, Cibella F, Visconti A, Scichilone N, Bellia V, Bonsignore G. Spontaneous gastroesophageal reflux and airway patency during the night in adult asthmatics. Am J Respir Crit Care Med2000; 161:177–181.
Jack CI, Calverley PM, Donnelly RJ, et al Simultaneous tracheal and oesophageal pH measurements in asthmatic patients with gastrooesophageal reflux. Thorax1995; 50:201–204.
Harding SM, Schan CA, Guzzo MR, Alexander RW, Bradley LA, Richter JE. Gastroesophageal reflux-induced bronchoconstriction. Is microaspiration a factor?Chest1995; 108:1220–1227.
Irwin RS, Madison JM, Fraire AE. The cough reflex and its relation to gastroesophageal reflux. Am J Med2000; 108( suppl 4a):73S–78S.
Choy D, Leung R. Gastro-oesophageal reflux disease and asthma. Respirology1997; 2:163–168.
Zerbib F, Guisset O, Lamouliatte H, Quinton A, Galmiche JP, Tunon-De-Lara JM. Effects of bronchial obstruction on lower esophageal sphincter motility and gastroesophageal reflux in patients with asthma. Am J Respir Crit Care Med2002; 166:1206–1211.
Lacy BE, Mathis C, DesBiens J, Liu MC. The effects of nebulized albuterol on esophageal function in asthmatic patients. Dig Dis Sci2008; 53:2627–2633.
Ford GA, Oliver PS, Prior JS, Butland RJ, Wilkinson SP. Omeprazole in the treatment of asthmatics with nocturnal symptoms and gastrooesophageal reflux: a placebo-controlled cross-over study. Postgrad Med J1994; 70:350–354.
Teichtahl H, Kronborg IJ, Yeomans ND, Robinson P. Adult asthma and gastro-oesophageal reflux: the effects of omeprazole therapy on asthma. Aust N Z J Med1996; 26:671–676.
Meier JH, McNally PR, Punja M, et al Does omeprazole (Prilosec) improve respiratory function in asthmatics with gastroesophageal reflux? A double-blind, placebo-controlled crossover study. Dig Dis Sci1994; 39:2127–2133.
Harding SM, Richter JE, Guzzo MR, Schan CA, Alexander RW, Bradley LA. Asthma and gastroesophageal reflux: acid suppressive therapy improves asthma outcome. Am J Med1996; 100:395–405.
Levin TR, Sperling RM, McQuaid KR. Omeprazole improves peak expiratory flow rate and quality of life in asthmatics with gastroesophageal reflux. Am J Gastroenterol1998; 93:1060–1063.
Boeree MJ, Peters FT, Postma DS, Kleibeuker JH. No effects of highdose omeprazole in patients with severe airway hyperresponsiveness and (a)symptomatic gastro-oesophageal reflux. Eur Respir J1998; 11:1070–1074.
Kiljander TO, Salomaa ER, Hietanen EK, Terho EO. Gastroesophageal reflux in asthmatics: a double-blind, placebo-controlled crossover study with omeprazole. Chest1999; 116:1257–1264.
Kiljander TO, Harding SM, Field SK, et al Effects of eso-meprazole 40 mg twice daily on asthma: a randomized placebo-controlled trial. Am J Respir Crit Care Med2006; 173:1091–1097.
Littner MR, Leung FW, Ballard ED, Huang B, Samra NKLansoprazole Asthma Study Group. Effects of 24 weeks of lansoprazole therapy on asthma symptoms, exacerbations, quality of life, and pulmonary function in adult asthmatic patients with acid reflux symptoms. Chest2005; 128:1128–1135.
Gibson PG, Henry R, Coughlan JJL. Gastro-oesophageal reflux treatment for asthma in adults and children. Coch-rane Database Syst Rev2000;CD001496. Also available online at www.cochrane.org/reviews/en/ab001496.html. Accessed January 28, 2010.
Juniper EF, Bousquet J, Abetz L, Bateman EDGOAL Committee. Identifying ‘well-controlled’ and ‘not well-controlled’ asthma using the Asthma Control Questionnaire. Respir Med2006; 100:616–621.
Canning BJ, Mazzone SB. Reflex mechanisms in gastro-esophageal reflux disease and asthma. Am J Med2003; 115( suppl 3A):45S–48S.
Richter JE, Bradley LA, DeMeester TR, Wu WC. Normal 24-hr ambulatory esophageal pH values. Influence of study center, pH electrode, age, and gender. Dig Dis Sci1992; 37:849–856.
Damiano A, Handley K, Adler E, Siddique R, Bhattacharyja A. Measuring symptom distress and health-related quality of life in clinical trials of gastroesophageal reflux disease treatment: further validation of the Gastroesophageal Reflux Disease Symptom Assessment Scale (GSAS). Dig Dis Sci2002; 47:1530–1537.
Asano K, Suzuki H. Silent acid reflux and asthma control [editorial]. N Engl J Med2009; 360:1551–1553.
Rakita S, Villadolid D, Thomas A, et al Laparoscopic Nissen fundoplication offers high patient satisfaction with relief of extraesophageal symptoms of gastroesophageal reflux disease. Am Surg2006; 72:207–212.
Tomonaga T, Awad ZT, Filipi CJ, et al Symptom predictability of reflux-induced respiratory disease. Dig Dis Sci2002; 47:9–14.
Dimango E, Holbrook JT, Simpson E, et al., American Lung Association Asthma Clinical Research Centers. Effects of asymptomatic proximal and distal gastroesophageal reflux on asthma severity. Am J Respir Crit Care Med2009; 180:809–816.
Acid reflux is more prevalent in patients with asthma, and it often occurs without classic symptoms such as heartburn.
Current guidelines, based on data from older studies with significant limitations, recommend considering treatment for reflux disease, even without the classic symptoms, in patients with uncontrolled asthma.
The recent Study of Acid Reflux in Asthma found not only that treating silent acid reflux does not improve asthma control, but also that esophageal pH monitoring does not detect a subgroup of asthma patients who might respond to a proton pump inhibitor. These data suggest that we should reconsider clinical practice based on current guidelines.

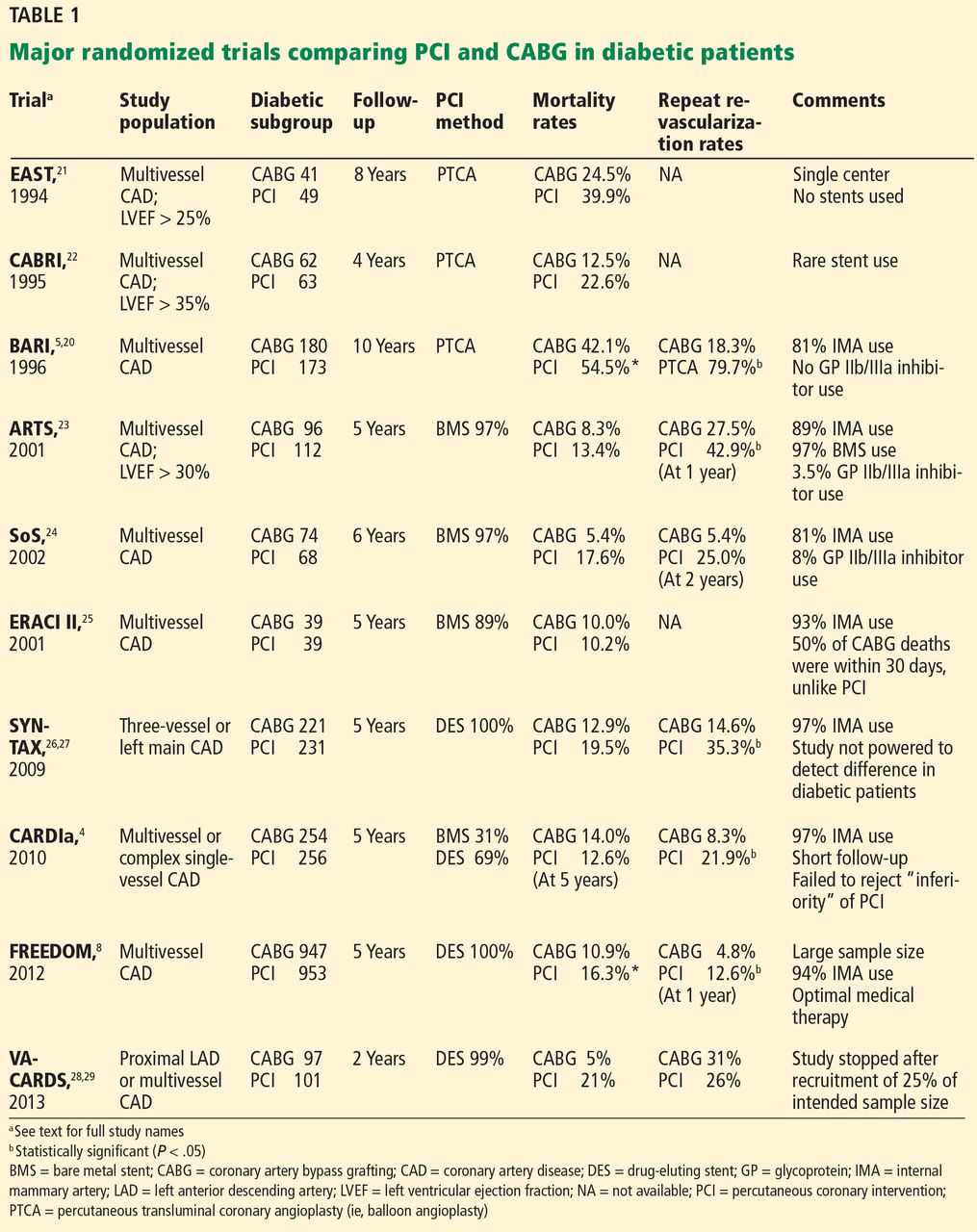
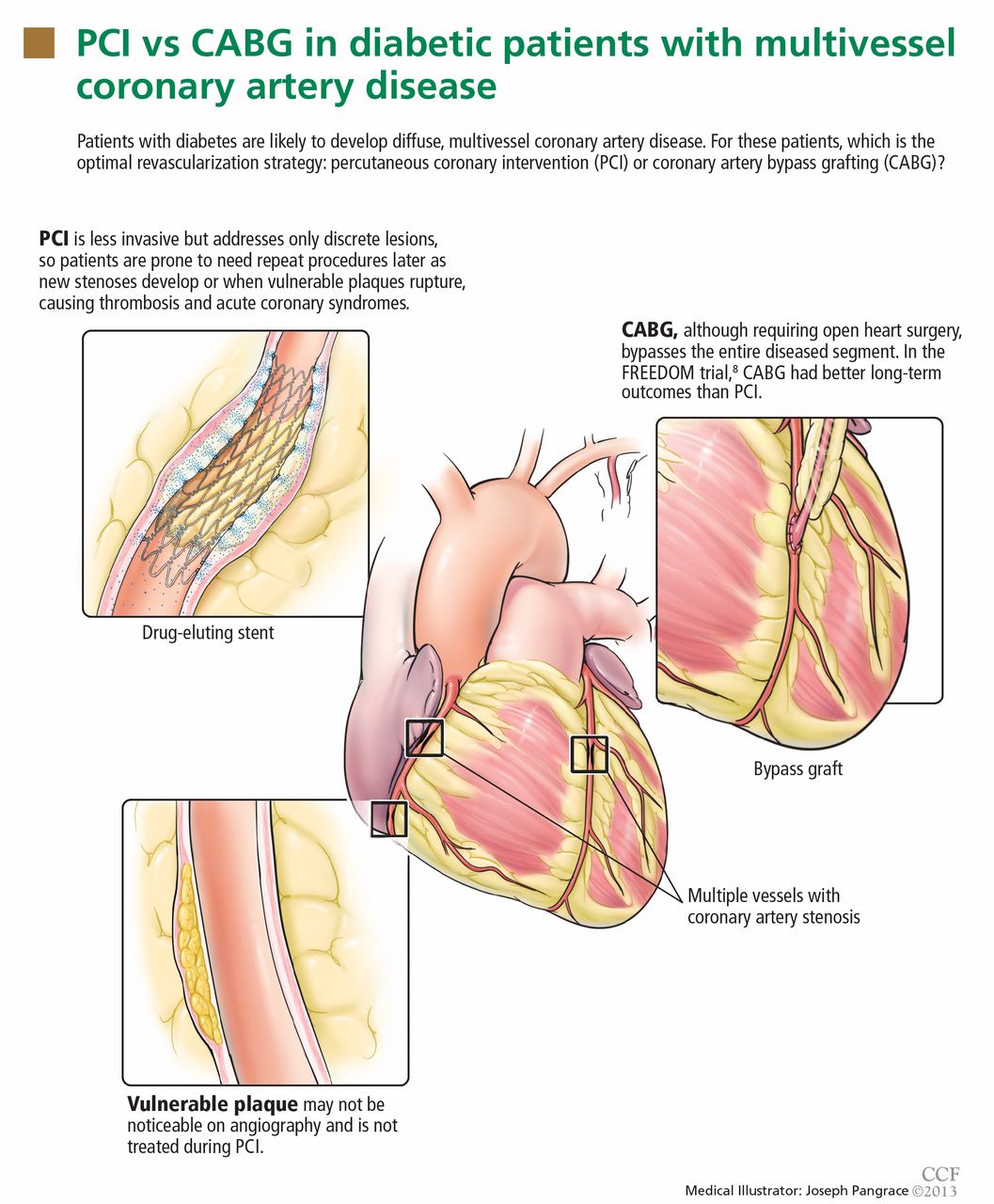
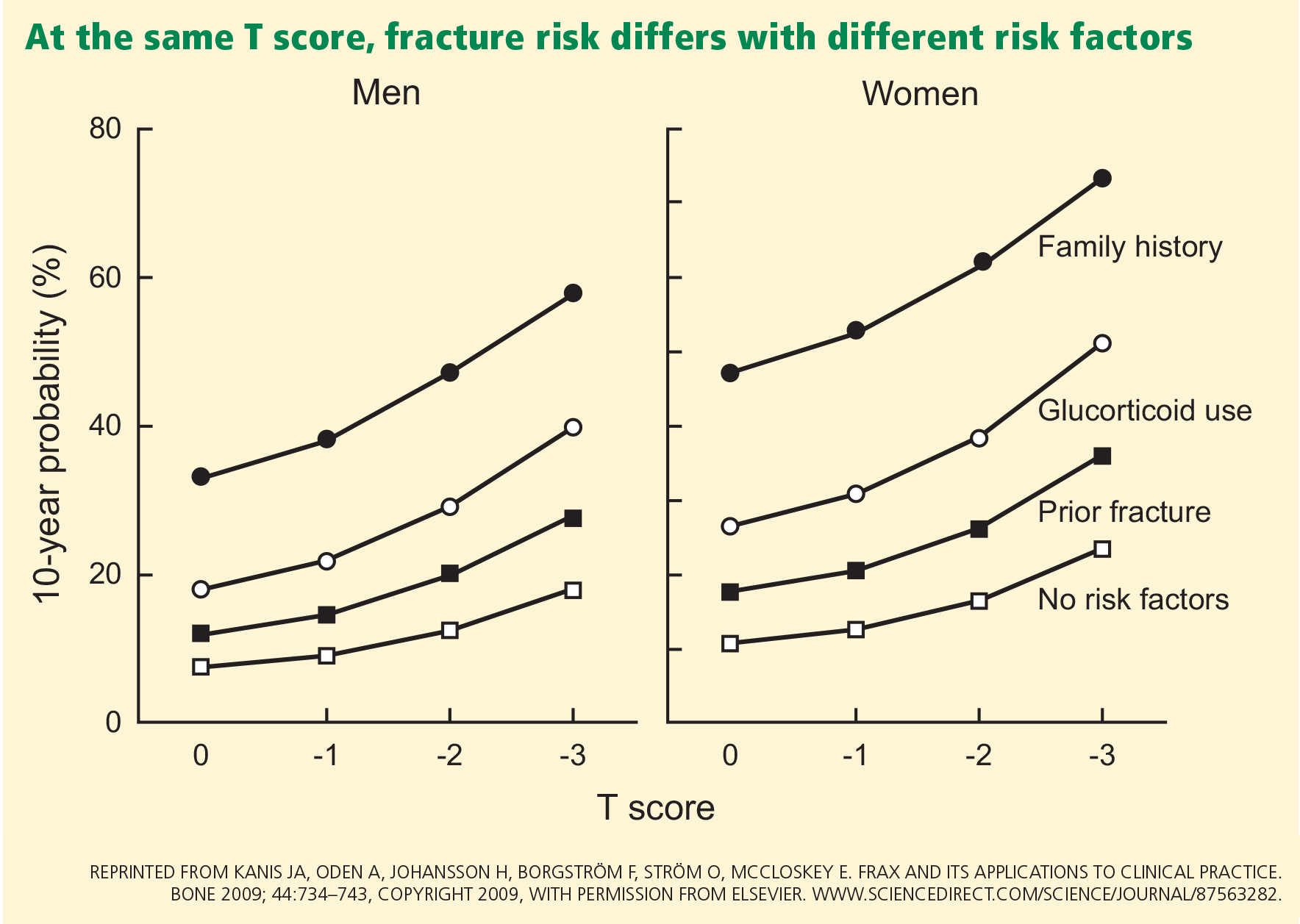
 Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.
Brott TG, et al; CREST Investigators. Stenting versus endarterectomy for treatment of carotid-artery stenosis. N Engl J Med 2010; 363:11–23. Copyright 2010, Massachusetts Medical Society. All rights reserved.