User login
Team documentation—the good, the surprising
The clerical work involved in managing the electronic health record (EHR) is clearly not at the top of the skill set for physicians, yet many office-based clinicians find themselves bogged down in this work with no easy way out.
However, practices that are adopting team-based care—where each team member works at the top of his or her skill set—are finding a solution in the form of scribing or team documentation. This approach can ease that burden and perhaps even help to curb physician burnout in the process. But many questions still surround this approach, notably: What do we know about the quality of this documentation?
A recent study published by Misra-Hebert and colleagues reported on this issue.1 It provides some insight—and reason for optimism, especially because the study authors found that outpatient notes from trained staff stack up quite well when compared to those of physicians. Having worked myself with this approach to documentation, I can attest to its benefits, as well.
Team documented notes compare well
There are 2 different ways that physicians can get help with documentation. One involves the use of trained scribes, who come from a variety of backgrounds and are charged with writing down, or scribing, what the physician says. The other involves training staff, usually certified medical assistants (CMAs) or licensed practical nurses (LPNs), to take on a wide variety of additional duties including refill management, care gap closure, and most of the duties concerning the EHR—including documentation.
Misra-Hebert and colleagues studied the second approach in a retrospective chart review of ambulatory progress notes written before and after 8 practice sites transitioned to using medical assistants as scribes. Comparing notes relating to diabetes encounters and same-day appointments, the study authors found important evidence that using staff in this way does not adversely affect—and may even enhance—documentation previously done entirely by physicians. For diabetes encounters, scribed notes were rated higher in overall quality, as well as more up to date, thorough, useful, and comprehensible, than unscribed notes.1
Scribing versus team documentation: terminology can be important
A person who is serving in a medical scribe role is a "personal assistant to the physician; performing documentation in the [electronic health record], gathering information for the patient's visit, and partnering with the physician to deliver the pinnacle of efficient patient care," according to Scribe America, the largest US company that employs scribes, providing their services to hospitals, emergency departments, and outpatient care and urgent care facilities, etc.1
Scribes versus team-based care
Scribe America mainly employs medical students, offering students a way to become exposed to physicians, mentors, and medical care. In fact, they note on their website that "a background in medical scribing is quickly becoming the standard for premedical experience, and is suggested by medical school acceptance committees across the country."2
Bellin Health, and many practices transitioning to team-based care, do not use medical students as scribes but rather "train up" employed certified medical assistants and licensed practical nurses to perform what they call "team documentation." This is the model described by Misra-Hebert and colleagues.3 The advantage is that these licensed health care workers can perform many other aspects of patient care, such as agenda setting and basic health coaching, and can perform additional work in the electronic health record, such as order entry and pending refills.
References
- What is a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/what_is_medical_scribe.html. Accessed June 20, 2016. .
- Why be a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/why_be_a_medical_scribe.html. Accessed June 20, 2016.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
In my experience
This change in the way we approach EHRs involves commitment, as I have seen first hand. There needs to be significant training to make this work and there needs to be more staff, since physicians require 2 of these valuable team members to function effectively. (At least that has been our experience.)
How has the physician’s role changed? Prior to team-based care, I would try to enter information into the EHR in the room while seeing the patient. After the visit, I would go to the computer at my station and use voice recognition software to add information. Now, the CMA/LPN does the initial documentation and other EHR work, while I am able to focus on the patient without the distraction of the computer. When I leave the room, the CMA/LPN stays with the patient, arranging necessary tests or consults, scheduling future labs and appointments, and reviewing the chart, all before seeing the next patient.
We are in the process of implementing team-based care throughout our 32-location health care system and have found that using CMAs and LPNs to assist with documentation is a “win” for everyone. And since the problems with burnout and all of the other reasons for making this transformation to team-based care applies to all office-based specialties, we plan to have our entire system adopt this model.
An ObGyn group was the first specialty group to pilot this model in our system. In fact, the American College of Obstetricians and Gynecologists’ interprofessional Task Force of Collaborative Practice published in March 2016 a strong recommendation that all practices across all specialties adopt team-based care.2 Among the aims of this care are that it should “respond to emerging demands and reduce undue burdens on health care providers.”
In order for this transformation to teambased care to be successful and sustainable at Bellin Health, we realized that we had to achieve 3 wins:
A win for the patient. Patients immediately notice that their physicians are now able to focus on them during the office visit, since the physicians no longer have to tend to the demands of the computer. In addition, since the CMAs/LPNs are with patients during the entire visit, the patients bond with them and feel the extra support from this relationship.
A win for the care team. Physician satisfaction has never been higher. Charts are usually closed at the end of each half-day. There is no need to take work home at night. CMAs/LPNs feel empowered and meaningfully involved in patient care. Their increase in satisfaction mirrors that of the physicians.
A win for the system. Not only are quality measures improving, but access improves since this team support increases efficiency. We are able to see more patients per day and are billing at a higher level of service, since there is more time to attend to more of the patient’s needs, thanks to the additional team support.
Team documentation can help bring the joy back
There is much talk about putting joy back into the practice of medicine. But the benchmark of any change needs to be whether it helps our patients. I believe that team documentation does. Happier, less burned-out physicians are able to better focus on patients during their visit. As one patient recently said to me at the end of a visit, “I feel like I’ve got my doctor back.” That is something that patients, and doctors alike, can feel good about.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
- Jennings J, Nielson P, Buck, ML, et al. Executive summary: Collaboration in Practice: Implementing Team-Based Care: Report of the American College of Obstetricians and Gynecologists’ Task Force on Collaborative Practice. Obstet Gynecol. 2016;127(3):612−627.
James Jerzak, MD
Dr. Jerzak is a practicing family physician, Bellin Health, Green Bay, Wisconsin.
The author reports no financial relationships relevant to this article.
James Jerzak, MD
Dr. Jerzak is a practicing family physician, Bellin Health, Green Bay, Wisconsin.
The author reports no financial relationships relevant to this article.
James Jerzak, MD
Dr. Jerzak is a practicing family physician, Bellin Health, Green Bay, Wisconsin.
The author reports no financial relationships relevant to this article.
The clerical work involved in managing the electronic health record (EHR) is clearly not at the top of the skill set for physicians, yet many office-based clinicians find themselves bogged down in this work with no easy way out.
However, practices that are adopting team-based care—where each team member works at the top of his or her skill set—are finding a solution in the form of scribing or team documentation. This approach can ease that burden and perhaps even help to curb physician burnout in the process. But many questions still surround this approach, notably: What do we know about the quality of this documentation?
A recent study published by Misra-Hebert and colleagues reported on this issue.1 It provides some insight—and reason for optimism, especially because the study authors found that outpatient notes from trained staff stack up quite well when compared to those of physicians. Having worked myself with this approach to documentation, I can attest to its benefits, as well.
Team documented notes compare well
There are 2 different ways that physicians can get help with documentation. One involves the use of trained scribes, who come from a variety of backgrounds and are charged with writing down, or scribing, what the physician says. The other involves training staff, usually certified medical assistants (CMAs) or licensed practical nurses (LPNs), to take on a wide variety of additional duties including refill management, care gap closure, and most of the duties concerning the EHR—including documentation.
Misra-Hebert and colleagues studied the second approach in a retrospective chart review of ambulatory progress notes written before and after 8 practice sites transitioned to using medical assistants as scribes. Comparing notes relating to diabetes encounters and same-day appointments, the study authors found important evidence that using staff in this way does not adversely affect—and may even enhance—documentation previously done entirely by physicians. For diabetes encounters, scribed notes were rated higher in overall quality, as well as more up to date, thorough, useful, and comprehensible, than unscribed notes.1
Scribing versus team documentation: terminology can be important
A person who is serving in a medical scribe role is a "personal assistant to the physician; performing documentation in the [electronic health record], gathering information for the patient's visit, and partnering with the physician to deliver the pinnacle of efficient patient care," according to Scribe America, the largest US company that employs scribes, providing their services to hospitals, emergency departments, and outpatient care and urgent care facilities, etc.1
Scribes versus team-based care
Scribe America mainly employs medical students, offering students a way to become exposed to physicians, mentors, and medical care. In fact, they note on their website that "a background in medical scribing is quickly becoming the standard for premedical experience, and is suggested by medical school acceptance committees across the country."2
Bellin Health, and many practices transitioning to team-based care, do not use medical students as scribes but rather "train up" employed certified medical assistants and licensed practical nurses to perform what they call "team documentation." This is the model described by Misra-Hebert and colleagues.3 The advantage is that these licensed health care workers can perform many other aspects of patient care, such as agenda setting and basic health coaching, and can perform additional work in the electronic health record, such as order entry and pending refills.
References
- What is a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/what_is_medical_scribe.html. Accessed June 20, 2016. .
- Why be a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/why_be_a_medical_scribe.html. Accessed June 20, 2016.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
In my experience
This change in the way we approach EHRs involves commitment, as I have seen first hand. There needs to be significant training to make this work and there needs to be more staff, since physicians require 2 of these valuable team members to function effectively. (At least that has been our experience.)
How has the physician’s role changed? Prior to team-based care, I would try to enter information into the EHR in the room while seeing the patient. After the visit, I would go to the computer at my station and use voice recognition software to add information. Now, the CMA/LPN does the initial documentation and other EHR work, while I am able to focus on the patient without the distraction of the computer. When I leave the room, the CMA/LPN stays with the patient, arranging necessary tests or consults, scheduling future labs and appointments, and reviewing the chart, all before seeing the next patient.
We are in the process of implementing team-based care throughout our 32-location health care system and have found that using CMAs and LPNs to assist with documentation is a “win” for everyone. And since the problems with burnout and all of the other reasons for making this transformation to team-based care applies to all office-based specialties, we plan to have our entire system adopt this model.
An ObGyn group was the first specialty group to pilot this model in our system. In fact, the American College of Obstetricians and Gynecologists’ interprofessional Task Force of Collaborative Practice published in March 2016 a strong recommendation that all practices across all specialties adopt team-based care.2 Among the aims of this care are that it should “respond to emerging demands and reduce undue burdens on health care providers.”
In order for this transformation to teambased care to be successful and sustainable at Bellin Health, we realized that we had to achieve 3 wins:
A win for the patient. Patients immediately notice that their physicians are now able to focus on them during the office visit, since the physicians no longer have to tend to the demands of the computer. In addition, since the CMAs/LPNs are with patients during the entire visit, the patients bond with them and feel the extra support from this relationship.
A win for the care team. Physician satisfaction has never been higher. Charts are usually closed at the end of each half-day. There is no need to take work home at night. CMAs/LPNs feel empowered and meaningfully involved in patient care. Their increase in satisfaction mirrors that of the physicians.
A win for the system. Not only are quality measures improving, but access improves since this team support increases efficiency. We are able to see more patients per day and are billing at a higher level of service, since there is more time to attend to more of the patient’s needs, thanks to the additional team support.
Team documentation can help bring the joy back
There is much talk about putting joy back into the practice of medicine. But the benchmark of any change needs to be whether it helps our patients. I believe that team documentation does. Happier, less burned-out physicians are able to better focus on patients during their visit. As one patient recently said to me at the end of a visit, “I feel like I’ve got my doctor back.” That is something that patients, and doctors alike, can feel good about.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The clerical work involved in managing the electronic health record (EHR) is clearly not at the top of the skill set for physicians, yet many office-based clinicians find themselves bogged down in this work with no easy way out.
However, practices that are adopting team-based care—where each team member works at the top of his or her skill set—are finding a solution in the form of scribing or team documentation. This approach can ease that burden and perhaps even help to curb physician burnout in the process. But many questions still surround this approach, notably: What do we know about the quality of this documentation?
A recent study published by Misra-Hebert and colleagues reported on this issue.1 It provides some insight—and reason for optimism, especially because the study authors found that outpatient notes from trained staff stack up quite well when compared to those of physicians. Having worked myself with this approach to documentation, I can attest to its benefits, as well.
Team documented notes compare well
There are 2 different ways that physicians can get help with documentation. One involves the use of trained scribes, who come from a variety of backgrounds and are charged with writing down, or scribing, what the physician says. The other involves training staff, usually certified medical assistants (CMAs) or licensed practical nurses (LPNs), to take on a wide variety of additional duties including refill management, care gap closure, and most of the duties concerning the EHR—including documentation.
Misra-Hebert and colleagues studied the second approach in a retrospective chart review of ambulatory progress notes written before and after 8 practice sites transitioned to using medical assistants as scribes. Comparing notes relating to diabetes encounters and same-day appointments, the study authors found important evidence that using staff in this way does not adversely affect—and may even enhance—documentation previously done entirely by physicians. For diabetes encounters, scribed notes were rated higher in overall quality, as well as more up to date, thorough, useful, and comprehensible, than unscribed notes.1
Scribing versus team documentation: terminology can be important
A person who is serving in a medical scribe role is a "personal assistant to the physician; performing documentation in the [electronic health record], gathering information for the patient's visit, and partnering with the physician to deliver the pinnacle of efficient patient care," according to Scribe America, the largest US company that employs scribes, providing their services to hospitals, emergency departments, and outpatient care and urgent care facilities, etc.1
Scribes versus team-based care
Scribe America mainly employs medical students, offering students a way to become exposed to physicians, mentors, and medical care. In fact, they note on their website that "a background in medical scribing is quickly becoming the standard for premedical experience, and is suggested by medical school acceptance committees across the country."2
Bellin Health, and many practices transitioning to team-based care, do not use medical students as scribes but rather "train up" employed certified medical assistants and licensed practical nurses to perform what they call "team documentation." This is the model described by Misra-Hebert and colleagues.3 The advantage is that these licensed health care workers can perform many other aspects of patient care, such as agenda setting and basic health coaching, and can perform additional work in the electronic health record, such as order entry and pending refills.
References
- What is a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/what_is_medical_scribe.html. Accessed June 20, 2016. .
- Why be a medical scribe? ScribeAmerica website. http://www.scribeamerica.com/why_be_a_medical_scribe.html. Accessed June 20, 2016.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
In my experience
This change in the way we approach EHRs involves commitment, as I have seen first hand. There needs to be significant training to make this work and there needs to be more staff, since physicians require 2 of these valuable team members to function effectively. (At least that has been our experience.)
How has the physician’s role changed? Prior to team-based care, I would try to enter information into the EHR in the room while seeing the patient. After the visit, I would go to the computer at my station and use voice recognition software to add information. Now, the CMA/LPN does the initial documentation and other EHR work, while I am able to focus on the patient without the distraction of the computer. When I leave the room, the CMA/LPN stays with the patient, arranging necessary tests or consults, scheduling future labs and appointments, and reviewing the chart, all before seeing the next patient.
We are in the process of implementing team-based care throughout our 32-location health care system and have found that using CMAs and LPNs to assist with documentation is a “win” for everyone. And since the problems with burnout and all of the other reasons for making this transformation to team-based care applies to all office-based specialties, we plan to have our entire system adopt this model.
An ObGyn group was the first specialty group to pilot this model in our system. In fact, the American College of Obstetricians and Gynecologists’ interprofessional Task Force of Collaborative Practice published in March 2016 a strong recommendation that all practices across all specialties adopt team-based care.2 Among the aims of this care are that it should “respond to emerging demands and reduce undue burdens on health care providers.”
In order for this transformation to teambased care to be successful and sustainable at Bellin Health, we realized that we had to achieve 3 wins:
A win for the patient. Patients immediately notice that their physicians are now able to focus on them during the office visit, since the physicians no longer have to tend to the demands of the computer. In addition, since the CMAs/LPNs are with patients during the entire visit, the patients bond with them and feel the extra support from this relationship.
A win for the care team. Physician satisfaction has never been higher. Charts are usually closed at the end of each half-day. There is no need to take work home at night. CMAs/LPNs feel empowered and meaningfully involved in patient care. Their increase in satisfaction mirrors that of the physicians.
A win for the system. Not only are quality measures improving, but access improves since this team support increases efficiency. We are able to see more patients per day and are billing at a higher level of service, since there is more time to attend to more of the patient’s needs, thanks to the additional team support.
Team documentation can help bring the joy back
There is much talk about putting joy back into the practice of medicine. But the benchmark of any change needs to be whether it helps our patients. I believe that team documentation does. Happier, less burned-out physicians are able to better focus on patients during their visit. As one patient recently said to me at the end of a visit, “I feel like I’ve got my doctor back.” That is something that patients, and doctors alike, can feel good about.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
- Jennings J, Nielson P, Buck, ML, et al. Executive summary: Collaboration in Practice: Implementing Team-Based Care: Report of the American College of Obstetricians and Gynecologists’ Task Force on Collaborative Practice. Obstet Gynecol. 2016;127(3):612−627.
- Misra-Hebert AD, Amah L, Rabovsky A, et al. Medical scribes: how do their notes stack up? J Fam Pract. 2016;65(3):155−159.
- Jennings J, Nielson P, Buck, ML, et al. Executive summary: Collaboration in Practice: Implementing Team-Based Care: Report of the American College of Obstetricians and Gynecologists’ Task Force on Collaborative Practice. Obstet Gynecol. 2016;127(3):612−627.
In this Article
- Scribing vs team documentation
- How has the physician’s role changed?

Public speaking fundamentals. Preparation: Tips that lead to a solid, engaging presentation

Public speaking is one of the best ways to market and promote your skills as a physician. It is an ethical way of communicating and showcasing your areas of interest and expertise to professional or lay audiences. Most physicians and health care professionals take pride in their ability to communicate. After all, that is how we take a history, discuss our findings with patients, and educate individuals on restoring or maintaining their health. Public speaking, though, for the most part is a learned skill. Except for presentations to faculty at bedside or at grand rounds, we have received little training in public speaking.
Few of us are naturally comfortable in front of a live audience or a TV or video camera. But with a little practice and diligent preparation, we can become good or even excellent, confident public speakers. This article—the first in a series of 3—provides you with preparatory tips and techniques to enhance your public speaking skills.
First, know your audience
Whether you are presenting to a group of 20 or 200, you can do certain things in advance to ensure that your presentation achieves the desired response. Most important: Know your audience. Don’t assume the audience is like you. To connect with them, you need to understand why your topic is important to them. What do they expect to learn from the presentation? Each attendee will be asking, “What’s in it for me?”
To keep listeners interested and engaged, you also must know their level of knowledge about the topic. If you are speaking to a group of residents about pelvic organ prolapse, you would use different language and content than if you were speaking to practicing primary care doctors; and these elements would be different again if you were speaking to a group of practicing urogynecologists. It’s insulting to recite basic information to highly knowledgeable physicians, or to present sophisticated technical content and complicated slides to novice physicians or lay people.
When presenting in a foreign country, learn how the culture of the audience differs from yours. How do they dress? What style of humor do they favor? How do they typically communicate? What gestures are appropriate or inappropriate? Are there religious influences to consider?
Practical steps. Before the meeting or event, speak to the organizer or meeting planner and find out the audience’s level of knowledge on the topic. Ask about audience expectations as well as demographics (such as age and background). If you are speaking at an industry event, research the event’s website and familiarize yourself with the mission of the event and who are the typical attendees. If you are presenting to a corporation, learn as much as you can about it by visiting its website, reading news reports, and reviewing associated blogs.
In addition to knowing the needs of the audience, ask the meeting planner about the goals and objectives for the program to make certain you can deliver on the requests.
Know your talk stem to stern
Review your slide material thoroughly. Understand each slide in the presentation and be comfortable with its content.
Avoid reading from slides. Reciting content that viewers can read for themselves breeds boredom and makes them lose interest. Further, when you are looking at the slides, you are not making eye contact with the audience and risk losing their attention. Good speakers are so comfortable with their slides that they can discuss each one without having to look at it.
Rehearse. The best way to achieve the foregoing is to rehearse. Your audience will be able to tell if you took the slide deck directly from a CD and loaded it into a computer and are giving the talk for the first time. You’ll need to know how long the program is to last and how long you are to speak. We suggest you practice with a timer to be certain you do not exceed the allotted time. Rehearse your talk aloud several times with all the props and audiovisual equipment you plan to use. This practice will help to curb filler words such as “ah” and “um.” It is also helpful to practice slide transitions, pauses, and even your breathing.
Prepare for the unexpected, too. Dinner meetings, for instance, may not start on time due to office or hospital delays for attending physicians, possibly resulting in a need to shorten your presentation.
Ask about the meeting agenda. If a meal is to be served, will you be speaking beforehand? This is the least favorable time slot, as you are holding people hostage before they can eat. Our preference is to speak after the appetizer is served and the orders have been taken by the wait staff. This way, attendees are not starving and they have something to drink. You can assure the waiters they won’t be disturbing you, and you can ask them to avoid walking in front of the projector. Ideally, you should end your presentation before dessert arrives and use the remaining time to field questions.
We suggest that you prepare a handout to be distributed at the end of the program, not before. You want your audience focused on you and your slides as you are speaking. Tell the audience you will be providing a handout of your presentation, which will minimize note-taking during your talk.
Your speech opening
The first and last 30 seconds of any speech probably have the most impact.1 Give extra thought, time, and effort to your opening and closing remarks. Do not open with “Good evening, it is a pleasure to be here tonight.” That wastes precious seconds.
While opening a speech with a joke or funny story is the conventional wisdom, ask yourself1:
- Is my selection appropriate to the occasion and for this audience?
- Is it in good taste?
- Does it relate to me (my service) or to the event or the group? Does it support my topic or its key points?
A humorous story or inspirational vignette that relates to your topic or audience can grab the audience’s attention. If you feel that demands more presentation skill than you possess at the outset of your public-speaking career, give the audience what you know and what they most want to hear. You know the questions that you have heard most at cocktail receptions or professional society meetings. So, put the answers to those questions in your speech.
For example. A scientist working with a major corporation was preparing a speech for a lay audience. Since most of the audience did not know what scientists do, he offered the following analogy: “Being a scientist is like doing a jigsaw puzzle in a snowstorm at night...you don’t have all the pieces...and you don’t have the picture on the front of the box to work from.” You can say more with less.1
Your closing
The closing is an important aspect of your speech. Summarize the key elements to your presentation. If you are going to take questions, a good approach is to say, “Before my closing remarks, are there any questions?” Following the questions, finish with a takeaway message that ties into your theme.1
Prepare an autobiographical introduction
We suggest that you write your own introduction and e-mail it to the person who will be introducing you. Let them know it is a suggestion that they are welcome to modify. We have found that most emcees or meeting planners are delighted to have the introduction and will use it just as you have written it. Also bring hard copy with you; many emcees will have forgotten to download what you sent. The figure shows an example of the introduction that one of us (NHB) uses, and you are welcome to modify it for your own use.
Ask about and confirm audiovisual support
Ask the meeting planner ahead of time if they will be providing the computer, projector, and screen. And if, for instance, they will provide a projector but not a computer, make sure the computer you will bring is compatible with their projector. Also, you will probably not require a microphone for a small group, but if you are speaking in a loud restaurant, a portable microphone-speaker system may be helpful.
Arrive early at the program venue to make sure the computers, projector, screen placement, and seating arrangement are all in order. Nothing can sidetrack a speaker (even a seasoned one) like a problem with the computer or equipment setup—for example, your flash drive requiring a USB port cannot connect to the sponsor’s computer, or your program created on a Mac does not run on the sponsor’s PC.
Show time: Getting ready
Another benefit in arriving early, besides being able to check on the equipment, is the chance to greet the audience members as they enter. It is easier to speak to a group of friends than strangers. And if you can remember their names, you can call on them and ask their opinion or how they might manage a patient who has the condition you are discussing. You also could suggest to the meeting planner that name tags for attendees would be helpful.
Warming up. A public speaker, like an athlete, needs to warm up physically before the event. If the facility has an anteroom available, use it for the following exercises suggested by public speaking coach Patricia Fripp1:
- Stand on one leg and shake the other (remove high heels first). When you place your raised foot back on the floor, it will feel lighter than the other one. Repeat the exercise using the other leg. Imagine your energy going down through the floor and up out of your head. While this sounds quite comical, it is not. It is a practical technique used by actors.
- Shake your hands vigorously. Hold them above your head, bending your wrists and elbows, then return your arms to your sides. This will make your hand movements more natural.
- Warm up your facial muscles by chewing in a highly exaggerated way. Do shoulder and neck rolls. Imagine you are at eye level with a clock. As you look at 12 o’clock, pull as much of your face up to the 12 as you can; move your eyes to 3 and repeat, then down to 6, and finally over to 9.
Not only do these exercises warm you up but they also relax you. The exaggerated movements help your movements to flow more naturally.1
This is just the start
Thorough preparation is key to making a solid presentation. But other factors are important too. Your goal is for the audience to take action or to implement suggestions from your presentation. In part 2 of this series, we will share tips on elements of the presentation itself that will encourage audience engagement and message retention. We will discuss how to make your message “stick” and how to make a dynamic, effective presentation that holds your audience’s attention for your entire talk.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Reference
- Fripp P. Add credibility to your business reputation through public speaking. Patricia Fripp website. http://www.fripp.com/add-credibility-to-your-business-reputation-through-public-speaking/. Accessed June 15, 2016.
Mickey M. Karram, MD, and Neil H. Baum, MD

Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.

Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
The authors report no financial relationships relevant to this article.
Mickey M. Karram, MD, and Neil H. Baum, MD
Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.
Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
The authors report no financial relationships relevant to this article.
Mickey M. Karram, MD, and Neil H. Baum, MD
Dr. Karram is Professor of Obstetrics and Gynecology and Urology, University of Cincinnati School of Medicine, and Director, Urogynecology, The Christ Hospital, Cincinnati, Ohio.
Dr. Baum practices urology in New Orleans, Louisiana, and is Associate Clinical Professor of Urology, Tulane Medical School and Louisiana State University School of Medicine, New Orleans. Dr. Baum is an OBG Management Contributing Editor.
The authors report no financial relationships relevant to this article.
Public speaking is one of the best ways to market and promote your skills as a physician. It is an ethical way of communicating and showcasing your areas of interest and expertise to professional or lay audiences. Most physicians and health care professionals take pride in their ability to communicate. After all, that is how we take a history, discuss our findings with patients, and educate individuals on restoring or maintaining their health. Public speaking, though, for the most part is a learned skill. Except for presentations to faculty at bedside or at grand rounds, we have received little training in public speaking.
Few of us are naturally comfortable in front of a live audience or a TV or video camera. But with a little practice and diligent preparation, we can become good or even excellent, confident public speakers. This article—the first in a series of 3—provides you with preparatory tips and techniques to enhance your public speaking skills.
First, know your audience
Whether you are presenting to a group of 20 or 200, you can do certain things in advance to ensure that your presentation achieves the desired response. Most important: Know your audience. Don’t assume the audience is like you. To connect with them, you need to understand why your topic is important to them. What do they expect to learn from the presentation? Each attendee will be asking, “What’s in it for me?”
To keep listeners interested and engaged, you also must know their level of knowledge about the topic. If you are speaking to a group of residents about pelvic organ prolapse, you would use different language and content than if you were speaking to practicing primary care doctors; and these elements would be different again if you were speaking to a group of practicing urogynecologists. It’s insulting to recite basic information to highly knowledgeable physicians, or to present sophisticated technical content and complicated slides to novice physicians or lay people.
When presenting in a foreign country, learn how the culture of the audience differs from yours. How do they dress? What style of humor do they favor? How do they typically communicate? What gestures are appropriate or inappropriate? Are there religious influences to consider?
Practical steps. Before the meeting or event, speak to the organizer or meeting planner and find out the audience’s level of knowledge on the topic. Ask about audience expectations as well as demographics (such as age and background). If you are speaking at an industry event, research the event’s website and familiarize yourself with the mission of the event and who are the typical attendees. If you are presenting to a corporation, learn as much as you can about it by visiting its website, reading news reports, and reviewing associated blogs.
In addition to knowing the needs of the audience, ask the meeting planner about the goals and objectives for the program to make certain you can deliver on the requests.
Know your talk stem to stern
Review your slide material thoroughly. Understand each slide in the presentation and be comfortable with its content.
Avoid reading from slides. Reciting content that viewers can read for themselves breeds boredom and makes them lose interest. Further, when you are looking at the slides, you are not making eye contact with the audience and risk losing their attention. Good speakers are so comfortable with their slides that they can discuss each one without having to look at it.
Rehearse. The best way to achieve the foregoing is to rehearse. Your audience will be able to tell if you took the slide deck directly from a CD and loaded it into a computer and are giving the talk for the first time. You’ll need to know how long the program is to last and how long you are to speak. We suggest you practice with a timer to be certain you do not exceed the allotted time. Rehearse your talk aloud several times with all the props and audiovisual equipment you plan to use. This practice will help to curb filler words such as “ah” and “um.” It is also helpful to practice slide transitions, pauses, and even your breathing.
Prepare for the unexpected, too. Dinner meetings, for instance, may not start on time due to office or hospital delays for attending physicians, possibly resulting in a need to shorten your presentation.
Ask about the meeting agenda. If a meal is to be served, will you be speaking beforehand? This is the least favorable time slot, as you are holding people hostage before they can eat. Our preference is to speak after the appetizer is served and the orders have been taken by the wait staff. This way, attendees are not starving and they have something to drink. You can assure the waiters they won’t be disturbing you, and you can ask them to avoid walking in front of the projector. Ideally, you should end your presentation before dessert arrives and use the remaining time to field questions.
We suggest that you prepare a handout to be distributed at the end of the program, not before. You want your audience focused on you and your slides as you are speaking. Tell the audience you will be providing a handout of your presentation, which will minimize note-taking during your talk.
Your speech opening
The first and last 30 seconds of any speech probably have the most impact.1 Give extra thought, time, and effort to your opening and closing remarks. Do not open with “Good evening, it is a pleasure to be here tonight.” That wastes precious seconds.
While opening a speech with a joke or funny story is the conventional wisdom, ask yourself1:
- Is my selection appropriate to the occasion and for this audience?
- Is it in good taste?
- Does it relate to me (my service) or to the event or the group? Does it support my topic or its key points?
A humorous story or inspirational vignette that relates to your topic or audience can grab the audience’s attention. If you feel that demands more presentation skill than you possess at the outset of your public-speaking career, give the audience what you know and what they most want to hear. You know the questions that you have heard most at cocktail receptions or professional society meetings. So, put the answers to those questions in your speech.
For example. A scientist working with a major corporation was preparing a speech for a lay audience. Since most of the audience did not know what scientists do, he offered the following analogy: “Being a scientist is like doing a jigsaw puzzle in a snowstorm at night...you don’t have all the pieces...and you don’t have the picture on the front of the box to work from.” You can say more with less.1
Your closing
The closing is an important aspect of your speech. Summarize the key elements to your presentation. If you are going to take questions, a good approach is to say, “Before my closing remarks, are there any questions?” Following the questions, finish with a takeaway message that ties into your theme.1
Prepare an autobiographical introduction
We suggest that you write your own introduction and e-mail it to the person who will be introducing you. Let them know it is a suggestion that they are welcome to modify. We have found that most emcees or meeting planners are delighted to have the introduction and will use it just as you have written it. Also bring hard copy with you; many emcees will have forgotten to download what you sent. The figure shows an example of the introduction that one of us (NHB) uses, and you are welcome to modify it for your own use.
Ask about and confirm audiovisual support
Ask the meeting planner ahead of time if they will be providing the computer, projector, and screen. And if, for instance, they will provide a projector but not a computer, make sure the computer you will bring is compatible with their projector. Also, you will probably not require a microphone for a small group, but if you are speaking in a loud restaurant, a portable microphone-speaker system may be helpful.
Arrive early at the program venue to make sure the computers, projector, screen placement, and seating arrangement are all in order. Nothing can sidetrack a speaker (even a seasoned one) like a problem with the computer or equipment setup—for example, your flash drive requiring a USB port cannot connect to the sponsor’s computer, or your program created on a Mac does not run on the sponsor’s PC.
Show time: Getting ready
Another benefit in arriving early, besides being able to check on the equipment, is the chance to greet the audience members as they enter. It is easier to speak to a group of friends than strangers. And if you can remember their names, you can call on them and ask their opinion or how they might manage a patient who has the condition you are discussing. You also could suggest to the meeting planner that name tags for attendees would be helpful.
Warming up. A public speaker, like an athlete, needs to warm up physically before the event. If the facility has an anteroom available, use it for the following exercises suggested by public speaking coach Patricia Fripp1:
- Stand on one leg and shake the other (remove high heels first). When you place your raised foot back on the floor, it will feel lighter than the other one. Repeat the exercise using the other leg. Imagine your energy going down through the floor and up out of your head. While this sounds quite comical, it is not. It is a practical technique used by actors.
- Shake your hands vigorously. Hold them above your head, bending your wrists and elbows, then return your arms to your sides. This will make your hand movements more natural.
- Warm up your facial muscles by chewing in a highly exaggerated way. Do shoulder and neck rolls. Imagine you are at eye level with a clock. As you look at 12 o’clock, pull as much of your face up to the 12 as you can; move your eyes to 3 and repeat, then down to 6, and finally over to 9.
Not only do these exercises warm you up but they also relax you. The exaggerated movements help your movements to flow more naturally.1
This is just the start
Thorough preparation is key to making a solid presentation. But other factors are important too. Your goal is for the audience to take action or to implement suggestions from your presentation. In part 2 of this series, we will share tips on elements of the presentation itself that will encourage audience engagement and message retention. We will discuss how to make your message “stick” and how to make a dynamic, effective presentation that holds your audience’s attention for your entire talk.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Public speaking is one of the best ways to market and promote your skills as a physician. It is an ethical way of communicating and showcasing your areas of interest and expertise to professional or lay audiences. Most physicians and health care professionals take pride in their ability to communicate. After all, that is how we take a history, discuss our findings with patients, and educate individuals on restoring or maintaining their health. Public speaking, though, for the most part is a learned skill. Except for presentations to faculty at bedside or at grand rounds, we have received little training in public speaking.
Few of us are naturally comfortable in front of a live audience or a TV or video camera. But with a little practice and diligent preparation, we can become good or even excellent, confident public speakers. This article—the first in a series of 3—provides you with preparatory tips and techniques to enhance your public speaking skills.
First, know your audience
Whether you are presenting to a group of 20 or 200, you can do certain things in advance to ensure that your presentation achieves the desired response. Most important: Know your audience. Don’t assume the audience is like you. To connect with them, you need to understand why your topic is important to them. What do they expect to learn from the presentation? Each attendee will be asking, “What’s in it for me?”
To keep listeners interested and engaged, you also must know their level of knowledge about the topic. If you are speaking to a group of residents about pelvic organ prolapse, you would use different language and content than if you were speaking to practicing primary care doctors; and these elements would be different again if you were speaking to a group of practicing urogynecologists. It’s insulting to recite basic information to highly knowledgeable physicians, or to present sophisticated technical content and complicated slides to novice physicians or lay people.
When presenting in a foreign country, learn how the culture of the audience differs from yours. How do they dress? What style of humor do they favor? How do they typically communicate? What gestures are appropriate or inappropriate? Are there religious influences to consider?
Practical steps. Before the meeting or event, speak to the organizer or meeting planner and find out the audience’s level of knowledge on the topic. Ask about audience expectations as well as demographics (such as age and background). If you are speaking at an industry event, research the event’s website and familiarize yourself with the mission of the event and who are the typical attendees. If you are presenting to a corporation, learn as much as you can about it by visiting its website, reading news reports, and reviewing associated blogs.
In addition to knowing the needs of the audience, ask the meeting planner about the goals and objectives for the program to make certain you can deliver on the requests.
Know your talk stem to stern
Review your slide material thoroughly. Understand each slide in the presentation and be comfortable with its content.
Avoid reading from slides. Reciting content that viewers can read for themselves breeds boredom and makes them lose interest. Further, when you are looking at the slides, you are not making eye contact with the audience and risk losing their attention. Good speakers are so comfortable with their slides that they can discuss each one without having to look at it.
Rehearse. The best way to achieve the foregoing is to rehearse. Your audience will be able to tell if you took the slide deck directly from a CD and loaded it into a computer and are giving the talk for the first time. You’ll need to know how long the program is to last and how long you are to speak. We suggest you practice with a timer to be certain you do not exceed the allotted time. Rehearse your talk aloud several times with all the props and audiovisual equipment you plan to use. This practice will help to curb filler words such as “ah” and “um.” It is also helpful to practice slide transitions, pauses, and even your breathing.
Prepare for the unexpected, too. Dinner meetings, for instance, may not start on time due to office or hospital delays for attending physicians, possibly resulting in a need to shorten your presentation.
Ask about the meeting agenda. If a meal is to be served, will you be speaking beforehand? This is the least favorable time slot, as you are holding people hostage before they can eat. Our preference is to speak after the appetizer is served and the orders have been taken by the wait staff. This way, attendees are not starving and they have something to drink. You can assure the waiters they won’t be disturbing you, and you can ask them to avoid walking in front of the projector. Ideally, you should end your presentation before dessert arrives and use the remaining time to field questions.
We suggest that you prepare a handout to be distributed at the end of the program, not before. You want your audience focused on you and your slides as you are speaking. Tell the audience you will be providing a handout of your presentation, which will minimize note-taking during your talk.
Your speech opening
The first and last 30 seconds of any speech probably have the most impact.1 Give extra thought, time, and effort to your opening and closing remarks. Do not open with “Good evening, it is a pleasure to be here tonight.” That wastes precious seconds.
While opening a speech with a joke or funny story is the conventional wisdom, ask yourself1:
- Is my selection appropriate to the occasion and for this audience?
- Is it in good taste?
- Does it relate to me (my service) or to the event or the group? Does it support my topic or its key points?
A humorous story or inspirational vignette that relates to your topic or audience can grab the audience’s attention. If you feel that demands more presentation skill than you possess at the outset of your public-speaking career, give the audience what you know and what they most want to hear. You know the questions that you have heard most at cocktail receptions or professional society meetings. So, put the answers to those questions in your speech.
For example. A scientist working with a major corporation was preparing a speech for a lay audience. Since most of the audience did not know what scientists do, he offered the following analogy: “Being a scientist is like doing a jigsaw puzzle in a snowstorm at night...you don’t have all the pieces...and you don’t have the picture on the front of the box to work from.” You can say more with less.1
Your closing
The closing is an important aspect of your speech. Summarize the key elements to your presentation. If you are going to take questions, a good approach is to say, “Before my closing remarks, are there any questions?” Following the questions, finish with a takeaway message that ties into your theme.1
Prepare an autobiographical introduction
We suggest that you write your own introduction and e-mail it to the person who will be introducing you. Let them know it is a suggestion that they are welcome to modify. We have found that most emcees or meeting planners are delighted to have the introduction and will use it just as you have written it. Also bring hard copy with you; many emcees will have forgotten to download what you sent. The figure shows an example of the introduction that one of us (NHB) uses, and you are welcome to modify it for your own use.
Ask about and confirm audiovisual support
Ask the meeting planner ahead of time if they will be providing the computer, projector, and screen. And if, for instance, they will provide a projector but not a computer, make sure the computer you will bring is compatible with their projector. Also, you will probably not require a microphone for a small group, but if you are speaking in a loud restaurant, a portable microphone-speaker system may be helpful.
Arrive early at the program venue to make sure the computers, projector, screen placement, and seating arrangement are all in order. Nothing can sidetrack a speaker (even a seasoned one) like a problem with the computer or equipment setup—for example, your flash drive requiring a USB port cannot connect to the sponsor’s computer, or your program created on a Mac does not run on the sponsor’s PC.
Show time: Getting ready
Another benefit in arriving early, besides being able to check on the equipment, is the chance to greet the audience members as they enter. It is easier to speak to a group of friends than strangers. And if you can remember their names, you can call on them and ask their opinion or how they might manage a patient who has the condition you are discussing. You also could suggest to the meeting planner that name tags for attendees would be helpful.
Warming up. A public speaker, like an athlete, needs to warm up physically before the event. If the facility has an anteroom available, use it for the following exercises suggested by public speaking coach Patricia Fripp1:
- Stand on one leg and shake the other (remove high heels first). When you place your raised foot back on the floor, it will feel lighter than the other one. Repeat the exercise using the other leg. Imagine your energy going down through the floor and up out of your head. While this sounds quite comical, it is not. It is a practical technique used by actors.
- Shake your hands vigorously. Hold them above your head, bending your wrists and elbows, then return your arms to your sides. This will make your hand movements more natural.
- Warm up your facial muscles by chewing in a highly exaggerated way. Do shoulder and neck rolls. Imagine you are at eye level with a clock. As you look at 12 o’clock, pull as much of your face up to the 12 as you can; move your eyes to 3 and repeat, then down to 6, and finally over to 9.
Not only do these exercises warm you up but they also relax you. The exaggerated movements help your movements to flow more naturally.1
This is just the start
Thorough preparation is key to making a solid presentation. But other factors are important too. Your goal is for the audience to take action or to implement suggestions from your presentation. In part 2 of this series, we will share tips on elements of the presentation itself that will encourage audience engagement and message retention. We will discuss how to make your message “stick” and how to make a dynamic, effective presentation that holds your audience’s attention for your entire talk.
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
Reference
- Fripp P. Add credibility to your business reputation through public speaking. Patricia Fripp website. http://www.fripp.com/add-credibility-to-your-business-reputation-through-public-speaking/. Accessed June 15, 2016.
Reference
- Fripp P. Add credibility to your business reputation through public speaking. Patricia Fripp website. http://www.fripp.com/add-credibility-to-your-business-reputation-through-public-speaking/. Accessed June 15, 2016.
In this Article
- Preparing a presentation
- Your speech opening
- AV equipment and support
ObGyn salaries jumped in the last year
The mean income for ObGyns rose by 10% in 2015 over 2014 ($277,000 compared with $249,000), according to a recent report from Medscape.1 This jump follows a gradual increase over the last few years ($243,000 in 2013; $242,000 in 2012; $220,000 in 2011).1−3 The report included responses from 19,183 physicians across 26 specialties, 5% (nearly 1,000) of whom were ObGyns.1
The highest earners among all physician specialties were orthopedists ($443,000), cardiologists, and dermatologists. The lowest earners were pediatricians ($204,000), endocrinologists, and family physicians. The highest ObGyn earners lived in the Southwest ($307,000), the North Central region, and the West.1
Merritt Hawkins & Associates, a national physician search and consulting firm, recently evaluated the annual starting salaries and year-over-year increases of 3,342 of its physician and advanced practitioner recruiting assignments. They found that ObGyns had the second greatest increase in starting salaries among specialties, at 16%. They also found obstetrics and gynecology to be among the top 5 specialties most in demand.4
The gender picture
As in past years, male ObGyns reported higher earnings than their female counterparts: full-time male ObGyns earned $304,000 while full-time female ObGyns earned $256,000.1
According to a report published in the British Medical Journal in June 2016, there are drastic differences between the incomes of white and black male and female physicians in the United States.5 White male physicians had an adjusted median annual income of $253,042 (95% confidence interval [CI], $248,670−$257,413), compared with $188,230 ($170,844−$205,616) for black male physicians, $163,234 (95% CI, $159,912−$166,557) for white female physicians, and $152,784 (95% CI, $137,927−$167,641) for black female physicians.
How does employment status factor in? Of the self-employed, men earn $310,000 while women earn $285,000. Men who are employed report earning $293,000, with women reporting $244,000.5 (This includes full-time workers but does not control for the number of hours worked.) When Medscape evaluated full- versus part-time work (<40 hours per week), results indicated that, among primary care and most other specialties, more female physicians (25%) are part-timers than males (12%).6 However, among ObGyns, 13% of women report part-time employment versus 16% of men.1
Time with patients. Medscape reports that, among all physicians, 41% of men spent 17 minutes or more with their patients, compared with 49% of women. For office-based ObGyns, 31% of men and 39% of women spent 17 minutes or more with patients.1
Can disparity in leadership positions explain gender-related salary discrepancy?
In 2015, 48% of all medical students were female.7 In residency, the ratio of men to women is similar: For 2013−2014, the Association of American Medical Colleges (AAMC) reported that 46% of all residents were female.8 For ObGyn residency, however, the AMA’s FREIDA Online specialty training search (detailing 2014 general program information) indicates that, of the 5,018 active residents and fellows in ObGyn, 81.4% are female.9
Although the ObGyn field is becoming female-dominated, leadership within the specialty remains male dominated, points out Laura E. Baecher-Lind, MD, MPH, Director of the Division of General Obstetrics & Gynecology at Tufts Medical Center, Boston, Massachusetts. Dr. Baecher-Lind authored a study in 2012 in which she explored whether the proportions of ObGyn leadership positions held by women reflect the proportion of women who entered the field at the same time as current leaders.10 She found that very few academic department chair positions in ObGyn are held by women, although that number is gradually increasing.10 In addition, her study results indicated that women should hold 71 of the total of 194 ObGyn leadership positions. In actuality, 41 of the leadership positions were held by women (21.1%, P<.001) when based on the proportion of women entering residency programs. When considering only leaders who graduated during the years in which residency matching data were available, she found that women should hold 28 of 74 leadership positions, but they actually held 20 (27.0%, P = .05).10
Could the salary discrepancy disappear if more women held leadership positions? OBG <scaps>Management</scaps> posed this question to Dr. Baecher-Lind. “I suspect that the gender pay gap would persist,” she said. “Studies indicate that women hold implicit gender bias as strongly as men. This bias leads to devaluing women’s skills and accomplishments compared with men’s and is a strong contributor to the leadership and pay gaps in this country and in our specialty. We need to be mindful of this implicit bias and work against it with policies such as salary transparency and salary audits to encourage parity.”11
Do patients have a gender preference for their ObGyn?
Although multiple surveys have been published regarding patient gender preference when choosing an ObGyn, overall results have not been analyzed. To address this literature gap, Kyle J. Tobler, MD, and colleagues at the Womack Army Medical Center in Fort Bragg, North Carolina, and Uniformed Services University of the Health Sciences in Bethesda, Maryland, searched multiple sources to provide a conglomerate analysis of patients' gender preference when choosing an ObGyn. An abstract describing their study was published in Obstetrics & Gynecology in May 2016 and presented at the American College of Obstetricians and Gynecologists 2016 Annual Clinical and Scientific Meeting, May 14−17, in Washington, DC.1
A personal impetus for studying gender preference
The impetus for this project truly was initiated for Dr. Tobler when he was a 4th-year medical student. "I was trying to decide if Obstetrics and Gynecology was the right field for me," he said. "I was discouraged by many people around me, who told me that men in ObGyn would not have a place, as female patients only wanted female ObGyns. And with the residency match at 60% to 70% women for ObGyn, it did seem that men would not have a place. Thus, I began searching the literature to verify if the question for gender preference for their ObGyn provider had been evaluated previously, and I found mixed results." After medical school Dr. Tobler pursued this current meta-analysis to address the conflict-ing results.
Details of the study
Dr. Tobler and his colleagues explored PubMed, Embase, PsycINFO (American Psychological Association's medical literature database), Cumulative Index to Nursing and Allied Health Literature (EBSCO Health's database), Scopus (Elsevier's abstract and citation database of peer-reviewed literature), and references of relevant articles. Included were 4,822 electronically identified citations of English-language studies, including surveys administered to patients that specifically asked for gender preference of their ObGyn provider.
The researchers found that 23 studies met their inclusion criteria, comprising 14,736 patients. Overall, 8.3% (95% confidence interval [CI], 0.08-0.09) of ObGyn patients reported a preference for a male provider, 50.2% (95% CI, 0.49-0.51) preferred a female provider, and 41.3% (95% CI, 0.40-0.42) reported no gender preference when choosing an ObGyn.1
What about US patients?
A subanalysis of studies (n = 9,861) conducted in the United States from 1999 to 2008 (with the last search undertaken in April 2015) showed that 8.4% (95% CI, 0.08-0.09) preferred a male ObGyn, 53.2% (95% CI, 0.52-0.54) preferred a female ObGyn, and 38.5% (95% CI, 0.38-0.39) had no gender preference.1
"We were surprised by the numbers," comments Dr. Tobler. "The general trend demonstrated a mix between no preference or a preference for female providers, but not by a large margin."
"We considered analyzing for age," he said, "but most of the studies gave a mean or median age value and were widely distributed. We were able, however, to break our analysis down into regions where one would expect a very strong preference for female providers--the Middle East and Africa. But, in fact, results were not much different than for Western countries. Our results for this subanalysis of Middle Eastern countries and Nigeria (n = 1,951) demonstrated that 8.7% of women (95% CI, 4.1-13.3) preferred a male provider, 51.2% (95% CI, 17.2-85.1) preferred a female provider, and 46.9% (95% CI, 9.3-84.5) had no gender preference."1
References
- Tobler KJ, Wu J, Khafagy AM, et al. Gender preference of the obstetrician gynecologist provider: a systematic review and meta-analysis. Obstet Gynecol. 2016;127(5)(suppl):43S. http://journals.lww.com/greenjournal/page/results.aspx?txtkeywords=Gender+preference+of+the+obstetrician+gynecologist+provider. Accessed May 18, 2016.
What are ObGyns’ greatest practice concerns?
The Medicus Firm reported in its 2016 Physician Practice Preference and Relocation Survey that the top 3 major practice concerns for practicing physicians were compensation, work-life balance, and work-related burnout and stress.12 They found that physicians in general were slightly more satisfied with their 2015 income than their 2014 income, but less optimistic about the future. Only 29% projected that their 2016 income would increase over their 2015 earnings.
With ObGyn salaries on the up in 2015, less than half (46%) of ObGyns reported to Medscape that they feel fairly compensated; these physicians made $62,000 more than those who believed their pay was unfair.1 Fifty-four percent of employed male ObGyns and 64% of employed female ObGyns reported feeling fairly compensated, compared with 43% and 32%, respectively, who were self-employed.
ObGyns indicated in the 2016 Medscape report that the prime causes of stress were bureaucratic tasks and spending too many hours at work. More than half (52%) of ObGyns spend 30 to 45 hours per week seeing patients, and 40% spend more time than that.1 According to employment status, 56% of those who are self-employed and 58% of those who are employed spend 10 hours or more per week on administrative tasks.1
Lucia DiVenere, MA, Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists (ACOG) in Washington, DC, offers a brief look, with an in-depth focus to come in an upcoming issue, at the growing concern of burnout among physicians and how it can affect both ObGyns and their patients. She outlines ACOG’s efforts to help ObGyns maintain work-life balance in “ObGyn burnout: ACOG takes aim.”
ObGyn burnout: ACOG takes aim

Lucia DiVenere, MA
The good news: More women have access to coverage for health care than ever before--better insurance coverage for pregnancy, contraceptives, and well-woman care.
The bad news: America faces a shortage of ObGyns to provide that care, a shortage not likely to go away soon.
One of the imperatives of this dynamic is that we need to help every practicing ObGyn perform at his or her very best: your highest level of quality care, your best productivity, and your best ability to survive and thrive in an always changing and often challenging work environment.
This imperative is undermined when ObGyns are so stressed, overworked, overworried, and undersupported that you experience the very real effects of physician burnout.
Studies show that:
- ObGyns experience high rates of burnout
- rates of burnout are increasing over time
- women, the majority gender in obstetrics and gynecology, experience higher rates of burnout than their male counterparts.
Between 2011 and 2014, rates of physician burnout increased from 45.5% to 54.4%.1 Fifty-one percent of ObGyns reported experiencing burnout in 2015, with women reporting 55% compared to 46% for men.2
This insert is a quick look at this important issue, which can seriously erode an ObGyn's ability to provide high-quality care and continue enjoying practice. It can take a real toll on your personal health and well-being, too. In an upcoming issue of OBG Management, I will take a deeper dive, previewing the American College of Obstetricians and Gynecologists (ACOG) and American Medical Association resources to help you avoid burnout, plus highlighting ObGyns who provide insight and inspiration. I also will interview ACOG President Tom Gellhaus, MD, who is dedicating his presidency to providing you with opportunities to experience new and meaningful aspects of the ObGyn specialty. I will discuss ACOG's programs to help you combat burnout, as well as how you can:
- help underserved women around the globe through medical missions
- bring your leadership and passion for women's health to your state and national capitals
- explore your artistic side.
ObGyn burnout amounts to a public health challenge in women's health care. ACOG takes your well-being seriously, so that you can continue to ensure the well-being of women.
Lucia DiVenere, MA, is Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists in Washington, DC.
Ms. DiVenere reports no financial relationships relevant to this article. .
References
- Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clinic Proceedings. 2015;90(12):1600-1613.
- Peckham C. Medscape Lifestyle Report 2016: Bias and Burnout. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview. Published January 13, 2016. Accessed June 14, 2016.
Effects of the ACA on ObGyns
As of February 2016, 12.7 million Americans selected plans through the Health Insurance Marketplace of the Affordable Care Act (ACA).1 Physicians often have no choice in whether or not they participate in Health Insurance Exchanges; however, in 2016, 24% of ObGyns said they plan to participate in exchanges, 25% do not, and the rest are unsure.1
It is still unclear how the ACA affects physician income.1 When ObGyns who participated in Health Insurance Exchanges in 2015 were asked whether their income was affected, approximately 60% reported no change, 30% reported a decrease, and 9% said it increased.1
Medicus reported that physicians’ approval of the ACA has declined since last year. In their 2016 report, 71% of respondents gave the ACA a passing grade (A, B, C, or D), compared with 83% in 2015 and 77% in 2014. Fewer than 3% of 2016 respondents gave the ACA an “A.”12
Medscape reported that 36% of ObGyns have seen an increase in the number of patients due to the ACA.1 A 2015 report from the Kaiser Family Foundation and The Commonwealth Fund assessing the experiences and attitudes of primary care providers after the first year of ACA coverage found no association with lower- and higher-quality care whether or not patient load had increased.13 Among those in the Medscape report who said that quality of care had worsened, 21% had a greater patient load; 18% reported no increase in patient load. Seventy-eight percent of physicians whose patient load increased said that quality had stayed the same or improved; 82% of those who experienced no increase in patient load reported that quality had stayed the same or improved.1
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Peckham C. Medscape Ob/Gyn Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/womenshealth. Published April 1, 2016. Accessed June 8, 2016.
- Reale D, Yates J. ObGyn salaries continue gradual improvement. OBG Manag. 2015;27(7):34−37.
- Peckham C. Medscape Ob/Gyn Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 14, 2014. Accessed June 8, 2016.
- Merritt Hawkins. Survey: Starting salaries for physicians spiking. http://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Pdf/Merritt_Hawkins_Starting_Salaries_For_Physicians_Spiking.pdf. Published June 7, 2016. Accessed June 17, 2016.
- Ly DP, Seabury SA, Jena AB, Newhouse RL. Differences in incomes of physicians in the United States by race and sex: observational study [published online ahead of print June 7, 2016]. BMJ. 2016;353:i2923. http://dx.doi.org/10.1136/bmj.i2923. Accessed June 8, 2016.
- Peckham C. Medscape Physician Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/public/overview#page=1. Published April 1, 2016. Accessed June 15, 2016.
- Kaiser Family Foundation. Distribution of medical school graduates by gender. http://kff.org/other/state-indicator/medical-school-graduates-by-gender/. Published 2016. Accessed June 22, 2016.
- Lautenberger DM, Dandar VM, Raezer CL, Sloane RA. The state of women in academic medicine, 2013-2014. Association of American Medical Colleges. 2014. https://members.aamc.org/eweb/upload/The%20State%20of%20Women%20in%20Academic%20Medicine%202013-2014%20FINAL.pdf. Accessed June 17, 2016.
- American Medical Association. FREIDA Online specialty training search: Obstetrics and Gynecology, 2014. https://freida.ama-assn.org/Freida/user/specStatisticsSearch.do?method=viewDetail&pageNumber=2&spcCd=220. Accessed June 17, 2016.
- Baecher-Lind L. Women in leadership positions within obstetrics and gynecology. Obstet Gynecol. 2012;120(6):1415−1418.
- Email correspondence with Laura E. Baecher-Lind, June 19, 2016.
- Medicus Firm. The Medicus Firm releases annual Physician Practice Preference Survey for 2016. http://www .themedicusfirm.com/the-medicus-firm-releases-annual-physician-practice-preference-survey-for-2016. Published May 4, 2016. Accessed June 10, 2016.
- Hamel L, Doty MM, Norton M, et al; Kaiser Family Foundation and The Commonwealth Fund. Experiences and attitudes of primary care providers under the first year of ACA coverage expansion. http://www.commonwealthfund.org/publications/issue-briefs/2015/jun/primary-care-providers-first-year-aca. Published June 18, 2015. Accessed June 15, 2016.
The mean income for ObGyns rose by 10% in 2015 over 2014 ($277,000 compared with $249,000), according to a recent report from Medscape.1 This jump follows a gradual increase over the last few years ($243,000 in 2013; $242,000 in 2012; $220,000 in 2011).1−3 The report included responses from 19,183 physicians across 26 specialties, 5% (nearly 1,000) of whom were ObGyns.1
The highest earners among all physician specialties were orthopedists ($443,000), cardiologists, and dermatologists. The lowest earners were pediatricians ($204,000), endocrinologists, and family physicians. The highest ObGyn earners lived in the Southwest ($307,000), the North Central region, and the West.1
Merritt Hawkins & Associates, a national physician search and consulting firm, recently evaluated the annual starting salaries and year-over-year increases of 3,342 of its physician and advanced practitioner recruiting assignments. They found that ObGyns had the second greatest increase in starting salaries among specialties, at 16%. They also found obstetrics and gynecology to be among the top 5 specialties most in demand.4
The gender picture
As in past years, male ObGyns reported higher earnings than their female counterparts: full-time male ObGyns earned $304,000 while full-time female ObGyns earned $256,000.1
According to a report published in the British Medical Journal in June 2016, there are drastic differences between the incomes of white and black male and female physicians in the United States.5 White male physicians had an adjusted median annual income of $253,042 (95% confidence interval [CI], $248,670−$257,413), compared with $188,230 ($170,844−$205,616) for black male physicians, $163,234 (95% CI, $159,912−$166,557) for white female physicians, and $152,784 (95% CI, $137,927−$167,641) for black female physicians.
How does employment status factor in? Of the self-employed, men earn $310,000 while women earn $285,000. Men who are employed report earning $293,000, with women reporting $244,000.5 (This includes full-time workers but does not control for the number of hours worked.) When Medscape evaluated full- versus part-time work (<40 hours per week), results indicated that, among primary care and most other specialties, more female physicians (25%) are part-timers than males (12%).6 However, among ObGyns, 13% of women report part-time employment versus 16% of men.1
Time with patients. Medscape reports that, among all physicians, 41% of men spent 17 minutes or more with their patients, compared with 49% of women. For office-based ObGyns, 31% of men and 39% of women spent 17 minutes or more with patients.1
Can disparity in leadership positions explain gender-related salary discrepancy?
In 2015, 48% of all medical students were female.7 In residency, the ratio of men to women is similar: For 2013−2014, the Association of American Medical Colleges (AAMC) reported that 46% of all residents were female.8 For ObGyn residency, however, the AMA’s FREIDA Online specialty training search (detailing 2014 general program information) indicates that, of the 5,018 active residents and fellows in ObGyn, 81.4% are female.9
Although the ObGyn field is becoming female-dominated, leadership within the specialty remains male dominated, points out Laura E. Baecher-Lind, MD, MPH, Director of the Division of General Obstetrics & Gynecology at Tufts Medical Center, Boston, Massachusetts. Dr. Baecher-Lind authored a study in 2012 in which she explored whether the proportions of ObGyn leadership positions held by women reflect the proportion of women who entered the field at the same time as current leaders.10 She found that very few academic department chair positions in ObGyn are held by women, although that number is gradually increasing.10 In addition, her study results indicated that women should hold 71 of the total of 194 ObGyn leadership positions. In actuality, 41 of the leadership positions were held by women (21.1%, P<.001) when based on the proportion of women entering residency programs. When considering only leaders who graduated during the years in which residency matching data were available, she found that women should hold 28 of 74 leadership positions, but they actually held 20 (27.0%, P = .05).10
Could the salary discrepancy disappear if more women held leadership positions? OBG <scaps>Management</scaps> posed this question to Dr. Baecher-Lind. “I suspect that the gender pay gap would persist,” she said. “Studies indicate that women hold implicit gender bias as strongly as men. This bias leads to devaluing women’s skills and accomplishments compared with men’s and is a strong contributor to the leadership and pay gaps in this country and in our specialty. We need to be mindful of this implicit bias and work against it with policies such as salary transparency and salary audits to encourage parity.”11
Do patients have a gender preference for their ObGyn?
Although multiple surveys have been published regarding patient gender preference when choosing an ObGyn, overall results have not been analyzed. To address this literature gap, Kyle J. Tobler, MD, and colleagues at the Womack Army Medical Center in Fort Bragg, North Carolina, and Uniformed Services University of the Health Sciences in Bethesda, Maryland, searched multiple sources to provide a conglomerate analysis of patients' gender preference when choosing an ObGyn. An abstract describing their study was published in Obstetrics & Gynecology in May 2016 and presented at the American College of Obstetricians and Gynecologists 2016 Annual Clinical and Scientific Meeting, May 14−17, in Washington, DC.1
A personal impetus for studying gender preference
The impetus for this project truly was initiated for Dr. Tobler when he was a 4th-year medical student. "I was trying to decide if Obstetrics and Gynecology was the right field for me," he said. "I was discouraged by many people around me, who told me that men in ObGyn would not have a place, as female patients only wanted female ObGyns. And with the residency match at 60% to 70% women for ObGyn, it did seem that men would not have a place. Thus, I began searching the literature to verify if the question for gender preference for their ObGyn provider had been evaluated previously, and I found mixed results." After medical school Dr. Tobler pursued this current meta-analysis to address the conflict-ing results.
Details of the study
Dr. Tobler and his colleagues explored PubMed, Embase, PsycINFO (American Psychological Association's medical literature database), Cumulative Index to Nursing and Allied Health Literature (EBSCO Health's database), Scopus (Elsevier's abstract and citation database of peer-reviewed literature), and references of relevant articles. Included were 4,822 electronically identified citations of English-language studies, including surveys administered to patients that specifically asked for gender preference of their ObGyn provider.
The researchers found that 23 studies met their inclusion criteria, comprising 14,736 patients. Overall, 8.3% (95% confidence interval [CI], 0.08-0.09) of ObGyn patients reported a preference for a male provider, 50.2% (95% CI, 0.49-0.51) preferred a female provider, and 41.3% (95% CI, 0.40-0.42) reported no gender preference when choosing an ObGyn.1
What about US patients?
A subanalysis of studies (n = 9,861) conducted in the United States from 1999 to 2008 (with the last search undertaken in April 2015) showed that 8.4% (95% CI, 0.08-0.09) preferred a male ObGyn, 53.2% (95% CI, 0.52-0.54) preferred a female ObGyn, and 38.5% (95% CI, 0.38-0.39) had no gender preference.1
"We were surprised by the numbers," comments Dr. Tobler. "The general trend demonstrated a mix between no preference or a preference for female providers, but not by a large margin."
"We considered analyzing for age," he said, "but most of the studies gave a mean or median age value and were widely distributed. We were able, however, to break our analysis down into regions where one would expect a very strong preference for female providers--the Middle East and Africa. But, in fact, results were not much different than for Western countries. Our results for this subanalysis of Middle Eastern countries and Nigeria (n = 1,951) demonstrated that 8.7% of women (95% CI, 4.1-13.3) preferred a male provider, 51.2% (95% CI, 17.2-85.1) preferred a female provider, and 46.9% (95% CI, 9.3-84.5) had no gender preference."1
References
- Tobler KJ, Wu J, Khafagy AM, et al. Gender preference of the obstetrician gynecologist provider: a systematic review and meta-analysis. Obstet Gynecol. 2016;127(5)(suppl):43S. http://journals.lww.com/greenjournal/page/results.aspx?txtkeywords=Gender+preference+of+the+obstetrician+gynecologist+provider. Accessed May 18, 2016.
What are ObGyns’ greatest practice concerns?
The Medicus Firm reported in its 2016 Physician Practice Preference and Relocation Survey that the top 3 major practice concerns for practicing physicians were compensation, work-life balance, and work-related burnout and stress.12 They found that physicians in general were slightly more satisfied with their 2015 income than their 2014 income, but less optimistic about the future. Only 29% projected that their 2016 income would increase over their 2015 earnings.
With ObGyn salaries on the up in 2015, less than half (46%) of ObGyns reported to Medscape that they feel fairly compensated; these physicians made $62,000 more than those who believed their pay was unfair.1 Fifty-four percent of employed male ObGyns and 64% of employed female ObGyns reported feeling fairly compensated, compared with 43% and 32%, respectively, who were self-employed.
ObGyns indicated in the 2016 Medscape report that the prime causes of stress were bureaucratic tasks and spending too many hours at work. More than half (52%) of ObGyns spend 30 to 45 hours per week seeing patients, and 40% spend more time than that.1 According to employment status, 56% of those who are self-employed and 58% of those who are employed spend 10 hours or more per week on administrative tasks.1
Lucia DiVenere, MA, Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists (ACOG) in Washington, DC, offers a brief look, with an in-depth focus to come in an upcoming issue, at the growing concern of burnout among physicians and how it can affect both ObGyns and their patients. She outlines ACOG’s efforts to help ObGyns maintain work-life balance in “ObGyn burnout: ACOG takes aim.”
ObGyn burnout: ACOG takes aim
Lucia DiVenere, MA
The good news: More women have access to coverage for health care than ever before--better insurance coverage for pregnancy, contraceptives, and well-woman care.
The bad news: America faces a shortage of ObGyns to provide that care, a shortage not likely to go away soon.
One of the imperatives of this dynamic is that we need to help every practicing ObGyn perform at his or her very best: your highest level of quality care, your best productivity, and your best ability to survive and thrive in an always changing and often challenging work environment.
This imperative is undermined when ObGyns are so stressed, overworked, overworried, and undersupported that you experience the very real effects of physician burnout.
Studies show that:
- ObGyns experience high rates of burnout
- rates of burnout are increasing over time
- women, the majority gender in obstetrics and gynecology, experience higher rates of burnout than their male counterparts.
Between 2011 and 2014, rates of physician burnout increased from 45.5% to 54.4%.1 Fifty-one percent of ObGyns reported experiencing burnout in 2015, with women reporting 55% compared to 46% for men.2
This insert is a quick look at this important issue, which can seriously erode an ObGyn's ability to provide high-quality care and continue enjoying practice. It can take a real toll on your personal health and well-being, too. In an upcoming issue of OBG Management, I will take a deeper dive, previewing the American College of Obstetricians and Gynecologists (ACOG) and American Medical Association resources to help you avoid burnout, plus highlighting ObGyns who provide insight and inspiration. I also will interview ACOG President Tom Gellhaus, MD, who is dedicating his presidency to providing you with opportunities to experience new and meaningful aspects of the ObGyn specialty. I will discuss ACOG's programs to help you combat burnout, as well as how you can:
- help underserved women around the globe through medical missions
- bring your leadership and passion for women's health to your state and national capitals
- explore your artistic side.
ObGyn burnout amounts to a public health challenge in women's health care. ACOG takes your well-being seriously, so that you can continue to ensure the well-being of women.
Lucia DiVenere, MA, is Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists in Washington, DC.
Ms. DiVenere reports no financial relationships relevant to this article. .
References
- Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clinic Proceedings. 2015;90(12):1600-1613.
- Peckham C. Medscape Lifestyle Report 2016: Bias and Burnout. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview. Published January 13, 2016. Accessed June 14, 2016.
Effects of the ACA on ObGyns
As of February 2016, 12.7 million Americans selected plans through the Health Insurance Marketplace of the Affordable Care Act (ACA).1 Physicians often have no choice in whether or not they participate in Health Insurance Exchanges; however, in 2016, 24% of ObGyns said they plan to participate in exchanges, 25% do not, and the rest are unsure.1
It is still unclear how the ACA affects physician income.1 When ObGyns who participated in Health Insurance Exchanges in 2015 were asked whether their income was affected, approximately 60% reported no change, 30% reported a decrease, and 9% said it increased.1
Medicus reported that physicians’ approval of the ACA has declined since last year. In their 2016 report, 71% of respondents gave the ACA a passing grade (A, B, C, or D), compared with 83% in 2015 and 77% in 2014. Fewer than 3% of 2016 respondents gave the ACA an “A.”12
Medscape reported that 36% of ObGyns have seen an increase in the number of patients due to the ACA.1 A 2015 report from the Kaiser Family Foundation and The Commonwealth Fund assessing the experiences and attitudes of primary care providers after the first year of ACA coverage found no association with lower- and higher-quality care whether or not patient load had increased.13 Among those in the Medscape report who said that quality of care had worsened, 21% had a greater patient load; 18% reported no increase in patient load. Seventy-eight percent of physicians whose patient load increased said that quality had stayed the same or improved; 82% of those who experienced no increase in patient load reported that quality had stayed the same or improved.1
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
The mean income for ObGyns rose by 10% in 2015 over 2014 ($277,000 compared with $249,000), according to a recent report from Medscape.1 This jump follows a gradual increase over the last few years ($243,000 in 2013; $242,000 in 2012; $220,000 in 2011).1−3 The report included responses from 19,183 physicians across 26 specialties, 5% (nearly 1,000) of whom were ObGyns.1
The highest earners among all physician specialties were orthopedists ($443,000), cardiologists, and dermatologists. The lowest earners were pediatricians ($204,000), endocrinologists, and family physicians. The highest ObGyn earners lived in the Southwest ($307,000), the North Central region, and the West.1
Merritt Hawkins & Associates, a national physician search and consulting firm, recently evaluated the annual starting salaries and year-over-year increases of 3,342 of its physician and advanced practitioner recruiting assignments. They found that ObGyns had the second greatest increase in starting salaries among specialties, at 16%. They also found obstetrics and gynecology to be among the top 5 specialties most in demand.4
The gender picture
As in past years, male ObGyns reported higher earnings than their female counterparts: full-time male ObGyns earned $304,000 while full-time female ObGyns earned $256,000.1
According to a report published in the British Medical Journal in June 2016, there are drastic differences between the incomes of white and black male and female physicians in the United States.5 White male physicians had an adjusted median annual income of $253,042 (95% confidence interval [CI], $248,670−$257,413), compared with $188,230 ($170,844−$205,616) for black male physicians, $163,234 (95% CI, $159,912−$166,557) for white female physicians, and $152,784 (95% CI, $137,927−$167,641) for black female physicians.
How does employment status factor in? Of the self-employed, men earn $310,000 while women earn $285,000. Men who are employed report earning $293,000, with women reporting $244,000.5 (This includes full-time workers but does not control for the number of hours worked.) When Medscape evaluated full- versus part-time work (<40 hours per week), results indicated that, among primary care and most other specialties, more female physicians (25%) are part-timers than males (12%).6 However, among ObGyns, 13% of women report part-time employment versus 16% of men.1
Time with patients. Medscape reports that, among all physicians, 41% of men spent 17 minutes or more with their patients, compared with 49% of women. For office-based ObGyns, 31% of men and 39% of women spent 17 minutes or more with patients.1
Can disparity in leadership positions explain gender-related salary discrepancy?
In 2015, 48% of all medical students were female.7 In residency, the ratio of men to women is similar: For 2013−2014, the Association of American Medical Colleges (AAMC) reported that 46% of all residents were female.8 For ObGyn residency, however, the AMA’s FREIDA Online specialty training search (detailing 2014 general program information) indicates that, of the 5,018 active residents and fellows in ObGyn, 81.4% are female.9
Although the ObGyn field is becoming female-dominated, leadership within the specialty remains male dominated, points out Laura E. Baecher-Lind, MD, MPH, Director of the Division of General Obstetrics & Gynecology at Tufts Medical Center, Boston, Massachusetts. Dr. Baecher-Lind authored a study in 2012 in which she explored whether the proportions of ObGyn leadership positions held by women reflect the proportion of women who entered the field at the same time as current leaders.10 She found that very few academic department chair positions in ObGyn are held by women, although that number is gradually increasing.10 In addition, her study results indicated that women should hold 71 of the total of 194 ObGyn leadership positions. In actuality, 41 of the leadership positions were held by women (21.1%, P<.001) when based on the proportion of women entering residency programs. When considering only leaders who graduated during the years in which residency matching data were available, she found that women should hold 28 of 74 leadership positions, but they actually held 20 (27.0%, P = .05).10
Could the salary discrepancy disappear if more women held leadership positions? OBG <scaps>Management</scaps> posed this question to Dr. Baecher-Lind. “I suspect that the gender pay gap would persist,” she said. “Studies indicate that women hold implicit gender bias as strongly as men. This bias leads to devaluing women’s skills and accomplishments compared with men’s and is a strong contributor to the leadership and pay gaps in this country and in our specialty. We need to be mindful of this implicit bias and work against it with policies such as salary transparency and salary audits to encourage parity.”11
Do patients have a gender preference for their ObGyn?
Although multiple surveys have been published regarding patient gender preference when choosing an ObGyn, overall results have not been analyzed. To address this literature gap, Kyle J. Tobler, MD, and colleagues at the Womack Army Medical Center in Fort Bragg, North Carolina, and Uniformed Services University of the Health Sciences in Bethesda, Maryland, searched multiple sources to provide a conglomerate analysis of patients' gender preference when choosing an ObGyn. An abstract describing their study was published in Obstetrics & Gynecology in May 2016 and presented at the American College of Obstetricians and Gynecologists 2016 Annual Clinical and Scientific Meeting, May 14−17, in Washington, DC.1
A personal impetus for studying gender preference
The impetus for this project truly was initiated for Dr. Tobler when he was a 4th-year medical student. "I was trying to decide if Obstetrics and Gynecology was the right field for me," he said. "I was discouraged by many people around me, who told me that men in ObGyn would not have a place, as female patients only wanted female ObGyns. And with the residency match at 60% to 70% women for ObGyn, it did seem that men would not have a place. Thus, I began searching the literature to verify if the question for gender preference for their ObGyn provider had been evaluated previously, and I found mixed results." After medical school Dr. Tobler pursued this current meta-analysis to address the conflict-ing results.
Details of the study
Dr. Tobler and his colleagues explored PubMed, Embase, PsycINFO (American Psychological Association's medical literature database), Cumulative Index to Nursing and Allied Health Literature (EBSCO Health's database), Scopus (Elsevier's abstract and citation database of peer-reviewed literature), and references of relevant articles. Included were 4,822 electronically identified citations of English-language studies, including surveys administered to patients that specifically asked for gender preference of their ObGyn provider.
The researchers found that 23 studies met their inclusion criteria, comprising 14,736 patients. Overall, 8.3% (95% confidence interval [CI], 0.08-0.09) of ObGyn patients reported a preference for a male provider, 50.2% (95% CI, 0.49-0.51) preferred a female provider, and 41.3% (95% CI, 0.40-0.42) reported no gender preference when choosing an ObGyn.1
What about US patients?
A subanalysis of studies (n = 9,861) conducted in the United States from 1999 to 2008 (with the last search undertaken in April 2015) showed that 8.4% (95% CI, 0.08-0.09) preferred a male ObGyn, 53.2% (95% CI, 0.52-0.54) preferred a female ObGyn, and 38.5% (95% CI, 0.38-0.39) had no gender preference.1
"We were surprised by the numbers," comments Dr. Tobler. "The general trend demonstrated a mix between no preference or a preference for female providers, but not by a large margin."
"We considered analyzing for age," he said, "but most of the studies gave a mean or median age value and were widely distributed. We were able, however, to break our analysis down into regions where one would expect a very strong preference for female providers--the Middle East and Africa. But, in fact, results were not much different than for Western countries. Our results for this subanalysis of Middle Eastern countries and Nigeria (n = 1,951) demonstrated that 8.7% of women (95% CI, 4.1-13.3) preferred a male provider, 51.2% (95% CI, 17.2-85.1) preferred a female provider, and 46.9% (95% CI, 9.3-84.5) had no gender preference."1
References
- Tobler KJ, Wu J, Khafagy AM, et al. Gender preference of the obstetrician gynecologist provider: a systematic review and meta-analysis. Obstet Gynecol. 2016;127(5)(suppl):43S. http://journals.lww.com/greenjournal/page/results.aspx?txtkeywords=Gender+preference+of+the+obstetrician+gynecologist+provider. Accessed May 18, 2016.
What are ObGyns’ greatest practice concerns?
The Medicus Firm reported in its 2016 Physician Practice Preference and Relocation Survey that the top 3 major practice concerns for practicing physicians were compensation, work-life balance, and work-related burnout and stress.12 They found that physicians in general were slightly more satisfied with their 2015 income than their 2014 income, but less optimistic about the future. Only 29% projected that their 2016 income would increase over their 2015 earnings.
With ObGyn salaries on the up in 2015, less than half (46%) of ObGyns reported to Medscape that they feel fairly compensated; these physicians made $62,000 more than those who believed their pay was unfair.1 Fifty-four percent of employed male ObGyns and 64% of employed female ObGyns reported feeling fairly compensated, compared with 43% and 32%, respectively, who were self-employed.
ObGyns indicated in the 2016 Medscape report that the prime causes of stress were bureaucratic tasks and spending too many hours at work. More than half (52%) of ObGyns spend 30 to 45 hours per week seeing patients, and 40% spend more time than that.1 According to employment status, 56% of those who are self-employed and 58% of those who are employed spend 10 hours or more per week on administrative tasks.1
Lucia DiVenere, MA, Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists (ACOG) in Washington, DC, offers a brief look, with an in-depth focus to come in an upcoming issue, at the growing concern of burnout among physicians and how it can affect both ObGyns and their patients. She outlines ACOG’s efforts to help ObGyns maintain work-life balance in “ObGyn burnout: ACOG takes aim.”
ObGyn burnout: ACOG takes aim
Lucia DiVenere, MA
The good news: More women have access to coverage for health care than ever before--better insurance coverage for pregnancy, contraceptives, and well-woman care.
The bad news: America faces a shortage of ObGyns to provide that care, a shortage not likely to go away soon.
One of the imperatives of this dynamic is that we need to help every practicing ObGyn perform at his or her very best: your highest level of quality care, your best productivity, and your best ability to survive and thrive in an always changing and often challenging work environment.
This imperative is undermined when ObGyns are so stressed, overworked, overworried, and undersupported that you experience the very real effects of physician burnout.
Studies show that:
- ObGyns experience high rates of burnout
- rates of burnout are increasing over time
- women, the majority gender in obstetrics and gynecology, experience higher rates of burnout than their male counterparts.
Between 2011 and 2014, rates of physician burnout increased from 45.5% to 54.4%.1 Fifty-one percent of ObGyns reported experiencing burnout in 2015, with women reporting 55% compared to 46% for men.2
This insert is a quick look at this important issue, which can seriously erode an ObGyn's ability to provide high-quality care and continue enjoying practice. It can take a real toll on your personal health and well-being, too. In an upcoming issue of OBG Management, I will take a deeper dive, previewing the American College of Obstetricians and Gynecologists (ACOG) and American Medical Association resources to help you avoid burnout, plus highlighting ObGyns who provide insight and inspiration. I also will interview ACOG President Tom Gellhaus, MD, who is dedicating his presidency to providing you with opportunities to experience new and meaningful aspects of the ObGyn specialty. I will discuss ACOG's programs to help you combat burnout, as well as how you can:
- help underserved women around the globe through medical missions
- bring your leadership and passion for women's health to your state and national capitals
- explore your artistic side.
ObGyn burnout amounts to a public health challenge in women's health care. ACOG takes your well-being seriously, so that you can continue to ensure the well-being of women.
Lucia DiVenere, MA, is Officer, Government and Political Affairs, at the American Congress of Obstetricians and Gynecologists in Washington, DC.
Ms. DiVenere reports no financial relationships relevant to this article. .
References
- Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general US working population between 2011 and 2014. Mayo Clinic Proceedings. 2015;90(12):1600-1613.
- Peckham C. Medscape Lifestyle Report 2016: Bias and Burnout. Medscape website. http://www.medscape.com/features/slideshow/lifestyle/2016/public/overview. Published January 13, 2016. Accessed June 14, 2016.
Effects of the ACA on ObGyns
As of February 2016, 12.7 million Americans selected plans through the Health Insurance Marketplace of the Affordable Care Act (ACA).1 Physicians often have no choice in whether or not they participate in Health Insurance Exchanges; however, in 2016, 24% of ObGyns said they plan to participate in exchanges, 25% do not, and the rest are unsure.1
It is still unclear how the ACA affects physician income.1 When ObGyns who participated in Health Insurance Exchanges in 2015 were asked whether their income was affected, approximately 60% reported no change, 30% reported a decrease, and 9% said it increased.1
Medicus reported that physicians’ approval of the ACA has declined since last year. In their 2016 report, 71% of respondents gave the ACA a passing grade (A, B, C, or D), compared with 83% in 2015 and 77% in 2014. Fewer than 3% of 2016 respondents gave the ACA an “A.”12
Medscape reported that 36% of ObGyns have seen an increase in the number of patients due to the ACA.1 A 2015 report from the Kaiser Family Foundation and The Commonwealth Fund assessing the experiences and attitudes of primary care providers after the first year of ACA coverage found no association with lower- and higher-quality care whether or not patient load had increased.13 Among those in the Medscape report who said that quality of care had worsened, 21% had a greater patient load; 18% reported no increase in patient load. Seventy-eight percent of physicians whose patient load increased said that quality had stayed the same or improved; 82% of those who experienced no increase in patient load reported that quality had stayed the same or improved.1
Share your thoughts! Send your Letter to the Editor to rbarbieri@frontlinemedcom.com. Please include your name and the city and state in which you practice.
- Peckham C. Medscape Ob/Gyn Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/womenshealth. Published April 1, 2016. Accessed June 8, 2016.
- Reale D, Yates J. ObGyn salaries continue gradual improvement. OBG Manag. 2015;27(7):34−37.
- Peckham C. Medscape Ob/Gyn Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 14, 2014. Accessed June 8, 2016.
- Merritt Hawkins. Survey: Starting salaries for physicians spiking. http://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Pdf/Merritt_Hawkins_Starting_Salaries_For_Physicians_Spiking.pdf. Published June 7, 2016. Accessed June 17, 2016.
- Ly DP, Seabury SA, Jena AB, Newhouse RL. Differences in incomes of physicians in the United States by race and sex: observational study [published online ahead of print June 7, 2016]. BMJ. 2016;353:i2923. http://dx.doi.org/10.1136/bmj.i2923. Accessed June 8, 2016.
- Peckham C. Medscape Physician Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/public/overview#page=1. Published April 1, 2016. Accessed June 15, 2016.
- Kaiser Family Foundation. Distribution of medical school graduates by gender. http://kff.org/other/state-indicator/medical-school-graduates-by-gender/. Published 2016. Accessed June 22, 2016.
- Lautenberger DM, Dandar VM, Raezer CL, Sloane RA. The state of women in academic medicine, 2013-2014. Association of American Medical Colleges. 2014. https://members.aamc.org/eweb/upload/The%20State%20of%20Women%20in%20Academic%20Medicine%202013-2014%20FINAL.pdf. Accessed June 17, 2016.
- American Medical Association. FREIDA Online specialty training search: Obstetrics and Gynecology, 2014. https://freida.ama-assn.org/Freida/user/specStatisticsSearch.do?method=viewDetail&pageNumber=2&spcCd=220. Accessed June 17, 2016.
- Baecher-Lind L. Women in leadership positions within obstetrics and gynecology. Obstet Gynecol. 2012;120(6):1415−1418.
- Email correspondence with Laura E. Baecher-Lind, June 19, 2016.
- Medicus Firm. The Medicus Firm releases annual Physician Practice Preference Survey for 2016. http://www .themedicusfirm.com/the-medicus-firm-releases-annual-physician-practice-preference-survey-for-2016. Published May 4, 2016. Accessed June 10, 2016.
- Hamel L, Doty MM, Norton M, et al; Kaiser Family Foundation and The Commonwealth Fund. Experiences and attitudes of primary care providers under the first year of ACA coverage expansion. http://www.commonwealthfund.org/publications/issue-briefs/2015/jun/primary-care-providers-first-year-aca. Published June 18, 2015. Accessed June 15, 2016.
- Peckham C. Medscape Ob/Gyn Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/womenshealth. Published April 1, 2016. Accessed June 8, 2016.
- Reale D, Yates J. ObGyn salaries continue gradual improvement. OBG Manag. 2015;27(7):34−37.
- Peckham C. Medscape Ob/Gyn Compensation Report 2014. Medscape website. http://www.medscape.com/features/slideshow/compensation/2014/womenshealth. Published April 14, 2014. Accessed June 8, 2016.
- Merritt Hawkins. Survey: Starting salaries for physicians spiking. http://www.merritthawkins.com/uploadedFiles/MerrittHawkins/Pdf/Merritt_Hawkins_Starting_Salaries_For_Physicians_Spiking.pdf. Published June 7, 2016. Accessed June 17, 2016.
- Ly DP, Seabury SA, Jena AB, Newhouse RL. Differences in incomes of physicians in the United States by race and sex: observational study [published online ahead of print June 7, 2016]. BMJ. 2016;353:i2923. http://dx.doi.org/10.1136/bmj.i2923. Accessed June 8, 2016.
- Peckham C. Medscape Physician Compensation Report 2016. Medscape website. http://www.medscape.com/features/slideshow/compensation/2016/public/overview#page=1. Published April 1, 2016. Accessed June 15, 2016.
- Kaiser Family Foundation. Distribution of medical school graduates by gender. http://kff.org/other/state-indicator/medical-school-graduates-by-gender/. Published 2016. Accessed June 22, 2016.
- Lautenberger DM, Dandar VM, Raezer CL, Sloane RA. The state of women in academic medicine, 2013-2014. Association of American Medical Colleges. 2014. https://members.aamc.org/eweb/upload/The%20State%20of%20Women%20in%20Academic%20Medicine%202013-2014%20FINAL.pdf. Accessed June 17, 2016.
- American Medical Association. FREIDA Online specialty training search: Obstetrics and Gynecology, 2014. https://freida.ama-assn.org/Freida/user/specStatisticsSearch.do?method=viewDetail&pageNumber=2&spcCd=220. Accessed June 17, 2016.
- Baecher-Lind L. Women in leadership positions within obstetrics and gynecology. Obstet Gynecol. 2012;120(6):1415−1418.
- Email correspondence with Laura E. Baecher-Lind, June 19, 2016.
- Medicus Firm. The Medicus Firm releases annual Physician Practice Preference Survey for 2016. http://www .themedicusfirm.com/the-medicus-firm-releases-annual-physician-practice-preference-survey-for-2016. Published May 4, 2016. Accessed June 10, 2016.
- Hamel L, Doty MM, Norton M, et al; Kaiser Family Foundation and The Commonwealth Fund. Experiences and attitudes of primary care providers under the first year of ACA coverage expansion. http://www.commonwealthfund.org/publications/issue-briefs/2015/jun/primary-care-providers-first-year-aca. Published June 18, 2015. Accessed June 15, 2016.
In this Article
- ACOG takes aim at burnout
- Considering salary and leadership disparities
- ObGyns’ greatest practice concerns

Detecting cancer: Pearls for the primary care physician
According to the Surveillance, Epidemiology, and End Results database, 5-year overall survival rates have improved for nearly all tumor types during the past 40 years.1 This has been accomplished with better treatment and earlier detection of the most common cancers, as well as the uncommon but highly curable tumor types.
Primary care physicians play a vital role in detecting cancers at earlier stages and synthesizing information from a patient’s presentation, vital signs, physical examination, and results of laboratory and radiographic testing. Yet cancers can be easily overlooked, and highly curable cancers such as Hodgkin lymphoma and testicular cancer, with 5-year survival rates above 85%, can have unusual presentations. Aside from the obvious health consequences, missed cancer diagnoses are often the subject of malpractice suits.
This paper reviews cancers that are easily missed and provides clinically relevant pearls from an oncologic perspective for primary care physicians, who are generally the first point of contact for patients.
BREAST CANCER DETECTION AND SCREENING
Breast cancer is the second most common cause of cancer death in US women and the most common cause of death in US women ages 20 to 59 (Table 1).2–4
Screening mammography has had a significant impact on early detection rates, and this has translated into a 20% to 30% decrease in the breast cancer mortality rate.5,6 But despite national screening guidelines, up to 15% of cases are diagnosed on the basis of a palpable breast mass not detected on mammography, and 30% are diagnosed with a breast mass during the interval between mammograms.5,6 Moreover, delay in breast cancer diagnosis is one of the most common reasons for malpractice suits.7,8
Warning signs
Breast cancer can present clinically as a single, dominant, indurated mass with irregular borders. The mass can have associated ecchymosis, erythema, nipple discharge, nipple retraction, and nipple eczema.9,10 Pay close attention to any history of breast trauma, pain, signs or symptoms suggestive of local infection, and the lesion’s relationship to the patient’s menstrual cycle. Locally advanced disease typically presents with axillary adenopathy, as well as skin findings such as erythema, thickening, and dimpling.
Initial imaging workup for a breast mass
Women presenting with a breast mass should undergo breast imaging, followed by core needle biopsy of any suspicious abnormality. Depending on the clinical breast examination and the interpretation of the mammogram, as reported as a Breast Imaging Reporting and Data System (BIRADS) score, ultrasonography, magnetic resonance imaging, or biopsy may be the next course of action. Ultrasonography is recommended in evaluating masses in women who are under age 30 (who are more likely to have dense breasts that make standard mammography difficult to interpret) or who are pregnant (because it does not involve radiation).
For patients with a borderline or indeterminate clinical examination (eg, asymmetric skin-thickening or discoloration, nipple discharge or inversion, nodularity, finding on imaging [ie, BIRADS 3 lesion]), closer follow-up with repeat or additional imaging or biopsy, or both, is strongly recommended.
Screening recommendations vary
The age at which to start breast cancer screening has been a matter of debate in recent years, and different organizations have different recommendations (Table 2).11–13 According to the American Cancer Society (ACS), women should begin screening mammography at age 45 and should continue it indefinitely as long as they are in good health.11 This guideline is in line with those of the National Comprehensive Cancer Network (NCCN)12 but differs from those of the US Preventive Services Task Force (USPSTF).13
One reason for the controversy is that although starting screening at a younger age may allow for earlier detection, it also leads to overdiagnosis and to unnecessary tests and procedures. However, the NCCN noted limitations in studies looking at the overdiagnosis of breast cancer, including their use of incidence data from the 1970s, which not only underestimated the annual incidence of breast cancer in the United States, but also neglected to differentiate invasive cancer from ductal carcinoma in situ.12 Additionally, by detecting breast cancer lesions 2 years before they are discovered by clinical breast examination, mammography has been found to reduce the mortality rate from breast cancer.14
The frequency of mammography should be individualized and should involve not only an assessment of the patient’s risk factors (eg, age, family history, genetic predisposition, history of precancerous lesions, history of radiation exposure) but also a discussion of the benefits, limitations, and potential harms of screening. Both the ACS and the NCCN recommend yearly mammography for women ages 45 to 54. For those age 55 and older, the ACS recommends screening mammography every 2 years until the patient’s life expectancy is less than 10 years, whereas the NCCN recommends yearly screening mammography indefinitely. Meanwhile, the USPSTF recommends mammograms every 2 years for women ages 50 to 74.
Pearls
- Pay close attention to a history of breast trauma, pain, and signs of infection.
- Consider ultrasonography for women under age 30, who are more likely to have dense breasts.
COLORECTAL CANCER
With an estimated annual incidence of 132,700 cases diagnosed in the United States in 2015, colorectal cancer is the third most common cancer.
National guidelines that recommend colonoscopy (starting at age 50 for people at standard risk) have had a significant impact on early detection rates and have translated into a significant decrease in mortality rates.2,15,16 However, a missed diagnosis of colorectal cancer is one of the most common reasons for malpractice suits, typically because the patient was not referred for colonoscopy according to national guidelines.17–19
Symptoms depend on tumor location
In symptomatic cases, clinical manifestations differ depending on tumor location.
Left-sided tumors can present with hematochezia, colicky abdominal pain, and a change in bowel habits. And because the descending (left) colon has a smaller lumen than the right and tumors typically are annular in shape, left-sided cancers may present with abdominal distention with or without bowel obstruction or nausea and vomiting.
Right-sided tumors typically present with iron deficiency anemia from unrecognized blood loss.
Tumors near the rectum can cause tenesmus, rectal pain, and diminished caliber of stools.
In the United States, 20% of colorectal cancer patients have distant metastases at the time of diagnosis, and the most common sites are the lymph nodes, liver, lungs, and peritoneum.17
Uncommon presentations of colorectal cancer include pneumaturia, fecaluria or recurrent urinary tract infection from a fistula, bacteremia with Streptococcus bovis or Clostridium septicum, and intra-abdominal abscess from a localized bowel perforation.20,21
Initial workup
Once cancer is suspected, colonoscopy is the most accurate and versatile diagnostic test. It not only permits localization and biopsy of lesions throughout the large bowel, but also detects synchronous neoplasms and permits removal of polyps. Computed tomographic (CT) colonography is an alternative if colonoscopy is contraindicated, but it can only detect larger (ie, > 6-mm) tumors.22
According to the ACS,23 men and women at average risk should undergo colorectal cancer screening beginning at age 50. ACS screening recommendations for polyps and colorectal cancer include flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, double-contrast barium enema every 5 years, or CT colonography every 5 years. Tests that detect cancer but not polyps include guaiac-based fecal occult blood test (every year), fecal immunochemical test (every year), stool DNA test (every 3 years). These recommendations are fairly consistent with those of the NCCN12 and USPSTF24 (Table 3).12,23,24
Pearls
- Uncommon presentations include urinary tract problems and intra-abdominal abscess.
- CT colonography can only detect larger tumors.
PROSTATE CANCER
With an estimated 220,800 cases and 27,540 deaths in 2015, prostate cancer is the most common cancer and the second most common cause of cancer-related death in US men.2 Widespread use of serum prostate-specific antigen (PSA) testing has increased the rate of detection of prostate cancer.
Signs and symptoms
Most men with early-stage prostate cancer have no symptoms directly attributable to the disease.
Obstructive symptoms such as hesitancy, decreased stream, retention, and nocturia are common but are usually related to concomitant benign prostatic hypertrophy. As in prostatitis, patients with prostate cancer may present with irritative symptoms such as urinary frequency, dysuria, and urgency.
Patients who present with locally advanced prostate cancer may have symptoms secondary to local invasion, such as hematuria, hematospermia, and new-onset erectile dysfunction.
Prostate cancer usually metastasizes to bone, most commonly to the vertebrae and sternum, and the associated pain can be acute or insidious.
Diagnosis
Prostate cancer is most often diagnosed after biopsy prompted by an elevated PSA level or an abnormal digital rectal examination. The most common abnormal laboratory findings in patients with metastatic prostate cancer are an elevated serum PSA level (typically > 10 ng/mL), an elevated serum alkaline phosphatase level, and anemia, which are all proportional to the extent of bone involvement.
Screening is still controversial
There has been considerable controversy in recent years with regard to PSA screening because of the lack of significant benefit and the potential for harm to the patient, with an overdiagnosis rate ranging from 23% to 42%.25
According to the ACS,26 certain groups of men should make an informed decision with their physician about whether to undergo screening: men over age 50 at average risk of prostate cancer and with at least a 10-year life expectancy, men over age 45 at high risk, and men over age 40 at an even higher risk. These ACS guidelines are consistent with those of the NCCN12 but differ from those of the USPSTF27 (Table 4).12,26,27
The patient should fully understand the risks and benefits of prostate cancer screening, as well as why it is controversial: ie, while the lifetime risk of being diagnosed with prostate cancer has increased, the lifetime risk of dying from it has remained the same after the advent of PSA testing.
Adverse effects of biopsy and treatment
Prostate biopsy is associated with infectious and bleeding complications, in addition to anxiety and physical discomfort.28 Treatment-related adverse effects include urinary incontinence, sexual dysfunction, and bowel problems.
Could these potential harms be overstated and the benefit be greater than currently thought? The NCCN12 noted that some of the landmark prostate cancer screening studies found a potential benefit in screening high-risk patients such as black men. Moreover, the studies used the sextant prostate biopsy technique, whereas now the extended core biopsy technique is the standard of care. And the studies may have underestimated the benefit of screening because the trial patients were relatively old (age 60) when their first PSA measurement was done, they were screened at long intervals (every 4 years), and the treatment options available at the time were not as good as those available today.12
Pearls
- Laboratory findings in metastatic prostate cancer are proportional to the extent of bone involvement.
- Most men with early-stage prostate cancer have no symptoms attributable to the disease.
LUNG CANCER
Lung cancer is the second most common type of cancer in men and women but has the highest mortality rate. In the United States, in 2015, an estimated 221,200 new cases of lung cancer and 158,040 deaths were expected.2 Lung cancer deaths have begun to decline in both men and women, and this is due to the decline in smoking. The impact of lung cancer screening may not be seen for another 5 to 10 years.29
A wide range of symptoms, presentations
Many patients with squamous cell carcinoma and small-cell lung carcinoma present with symptoms related to tumor involvement of the central airways,30 including cough, hemoptysis, and postobstructive pneumonia. Partial obstruction of a bronchus may cause localized wheezing, heard by the patient or by the clinician on auscultation, whereas obstruction of larger airways can cause stridor.
Patients with advanced disease present with dull, aching, persistent chest pain from mediastinal, pleural, or chest wall extension, dyspnea from lymphangitic tumor spread, tumor emboli, pneumothorax, pleural effusion, or pericardial effusion with tamponade. Less commonly, patients may present with unilateral paralysis of the diaphragm from phrenic nerve damage or with hoarseness from recurrent laryngeal nerve compression.31
Bronchorrhea—production of large volumes of thin, mucoid secretions resulting in cough—may be a feature of bronchoalveolar cell carcinoma, a rare subtype of non-small-cell lung carcinoma.
Patients uncommonly present with superior vena cava syndrome, an oncologic emergency that most often causes facial and arm swelling, dyspnea, cough, and headache.
Non-small-cell lung carcinoma arising in the superior sulcus may in rare cases cause Pancoast syndrome (manifested by shoulder pain and atrophy of the hand muscles from brachial plexus involvement), Horner syndrome (manifested by ptosis, miosis, and anhidrosis), or rib destruction.
If metastasis occurs, lung cancer commonly metastasizes to the liver and adrenal glands. At the time of diagnosis, 20% to 30% of patients with small-cell lung carcinoma have symptoms of central nervous system metastasis.
The screening controversy
Lung cancer screening is controversial because previous large studies have failed to show a clinical benefit (ie, improved survival rates) of CT screening in smokers. However, based on the results of a later large randomized trial,32 the ACS33 now recommends that patients ages 55 to 74 who are in fairly good health, have at least a 30-pack-year smoking history, and are currently smoking or have quit smoking within the last 15 years should discuss with their physician the benefits, limitations, and potential harms of lung cancer screening. These recommendations are similar to those of the NCCN12,34 and USPSTF35 (Table 5).12,33–35 The ACS guidelines also emphasize that screening should be done only at facilities with extensive experience with low-dose CT.
Follow-up evaluation
If imaging detects a lung nodule, its size and consistency are crucial in determining the course of action.33 If an endobronchial growth or solid nodule larger than 8 mm is discovered, the primary care physician should consider ordering either a repeat low-dose CT scan after 1 month or a positron-emission tomography CT scan.34 The diagnosis should be confirmed by biopsy or by surgical removal of the nodule if localized and accessible, with sites of metastasis typically taking priority.
Pearl
- At diagnosis, 20% to 30% of patients with small-cell lung cancer have symptoms of central nervous system metastasis.
HIGHLY CURABLE CANCERS WITH UNUSUAL PRESENTATIONS
Hodgkin lymphoma
With 9,190 new cases in the United States annually and a 5-year overall survival rate over 85%, Hodgkin lymphoma is one of the least common but most curable cancers.1,2 In the United States, there are two diagnostic peaks, one around age 20 and one around age 65.36 In patients with human immunodeficiency virus infection, the rate is 15 to 30 times higher than in the general population, regardless of disease status or compliance with highly active retroviral therapy.37
Hodgkin lymphoma typically presents as a nontender painless mass with rubbery consistency. The involved lymph node is typically cervical or supraclavicular. Although not detectable on physical examination, enlarged mediastinal nodes and retroperitoneal nodes are often present. Less commonly, patients may present with enlarged axillary and inguinal nodes.38
A second common presentation is the discovery of a mediastinal mass on routine chest radiography. A large percentage of patients present with at least one systemic symptom, which may include fever, night sweats, and unintentional weight loss. Generalized pruritus occurs early in the disease course in 10% to 15% of patients and is occasionally severe enough to cause intense scratching and excoriations.
A more unusual presentation of Hodgkin lymphoma is severe pain at areas of involvement after alcohol ingestion.
Most patients present with overt disease, but the presenting symptoms and signs may be relatively nonspecific and subtle and more consistent with an infectious process.
Hodgkin disease has a variable tempo, but overt symptoms typically occur after several months rather than years. As a general rule, it starts at a single site within the lymphatic system, usually a lymph node, and then spreads to adjacent nodes via lymphatic channels before disseminating to distant nonadjacent sites and organs. With this in mind, it is unusual to have bilateral axillary involvement without disease in the lower neck, and extremely unusual to have hepatic or bone marrow infiltration without disease in the spleen.
The diagnosis is established by whole lymph node tissue biopsy. Due to the high rate of inflammation in the area, inguinal nodes should not be biopsied if other equally suspicious peripheral nodes are present elsewhere. When the diagnosis of Hodgkin lymphoma is made from biopsy of an extranodal site, such as the stomach, spleen, Waldeyer ring, central nervous system, lung, bone, or skin, lymph node biopsy is also desirable for diagnostic confirmation.
Testicular cancer
Although accounting for only about 1% of all cancers in men, testicular cancer is the most common solid tumor affecting males between ages 15 and 35.1,2 With a 5-year survival rate of over 95%, testicular cancer is also one of the most curable cancers.
Testicular tumors usually present as a painless nodule or swelling of one testicle. Uncommonly, patients have metastatic disease at diagnosis, with the most common sites being lymph nodes, lung, bone, and the brain. Gynecomastia, associated with the production of human chorionic gonadotropin, occurs in about 5% of men with testicular germ cell tumors and 20% to 30% of men with Leydig cell tumors.39 Rarely, patients may present with paraneoplastic hyperthyroidism, which is secondary to thyroid-stimulating hormone and human chorionic gonadotropin sharing a common homologous alpha and beta subunit.40
Prompt diagnosis and treatment of testicular cancer provides the best opportunity for cure. Therefore, any testicular mass, even a painful scrotal lesion, should be evaluated as if it is testicular cancer until it is proven otherwise. The diagnostic evaluation of suspected testicular cancer includes scrotal ultrasonography. Radiographic testing, as deemed clinically necessary by the consulting urologist and medical oncologist, may include chest radiography, CT (chest, abdomen, pelvis), brain magnetic resonance imaging, or bone scan.
The primary care laboratory evaluation should include a complete metabolic profile and measurements of lactate dehydrogenase and serum tumor markers such as alpha fetoprotein and human chorionic gonadotropin. In nonseminomatous germ cell tumors, alpha fetoprotein or human chorionic gonadotropin, or both, can be elevated in 80% to 85% of patients. However, in seminoma, alpha fetoprotein is never elevated, and the serum human chorionic gonadotropin is elevated in only 20% to 25% of patients.41
Patients with a suspicious testicular mass should be referred promptly to a urologist for consideration of radical inguinal orchiectomy and, in some cases, retroperitoneal lymph node dissection. Testicular biopsy is not part of the evaluation as it may result in tumor seeding into the scrotal sac or metastatic spread of tumor to the inguinal nodes. Inguinal biopsy of the contralateral testis is considered if ultrasonography raises suspicion of an intratesticular abnormality, cryptorchid testis, or marked testicular atrophy. Discussing sperm banking with the patient is part of the diagnostic workup, as cumulative cisplatin doses greater than 400 mg/m2 can result in permanent infertility in 50% of men.42
Pearls
- In Hodgkin lymphoma, bilateral axillary involvement without disease in the lower neck is unusual.
- Discussing sperm banking is part of the diagnostic workup for testicular cancer.
- National Cancer Institute (NIH). Surveillance, Epidemiology and End Results (SEER) Program. SEER Cancer Statistics Review, 1975–2010. http://seer.cancer.gov/csr/1975_2010/. Accessed May 9, 2016.
- American Cancer Society. Cancer Facts & Figures 2015.
www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2015/. Accessed May 9, 2016. - Tabár L, Vitak B, Chen HH, Yen MF, Duffy SW, Smith RA. Beyond randomized controlled trials: organized mammographic screening substantially reduces breast carcinoma mortality. Cancer 2001; 91:1724–1731.
- Tabar L, Fagerberg G, Chen HH, et al. Efficacy of breast cancer screening by age. New results from the Swedish two-county trial. Cancer 1995; 75:2507–2517.
- Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med 2002; 137:347–360.
- Esserman LJ, Shieh Y, Rutgers EJ, et al. Impact of mammographic screening on the detection of good and poor prognosis breast cancers. Breast Cancer Res Treat 2011; 130:725–734.
- Wallace E, Lowry J, Smith SM, Fahey T. The epidemiology of malpractice claims in primary care: a systematic review. BMJ Open 2013; 3:pii:e002929.
- Gandhi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med 2006; 145:488–496.
- Morrow M. The evaluation of common breast problems. Am Fam Physician 2000; 61:2371–2378, 2385.
- Santen RJ, Mansel R. Benign breast disorders. N Engl J Med 2005; 353:275–285.
- American Cancer Society. Breast cancer prevention and early detection. www.cancer.org/cancer/breastcancer/moreinformation/breastcancerearlydetection/breast-cancer-early-detection-acs-recs. Accessed May 17, 2016.
- National Comprehensive Cancer Network (NCCN). NCCN Guidelines. www.nccn.org/professionals/physician_gls/f_guidelines.asp#site. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Breast cancers Screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/breast-cancer-screening. Accessed May 17, 2016.
- Mandelblatt JS, Cronin KA, Bailey S, et al; Breast Cancer Working Group of the Cancer Intervention and Surveillance Modeling Network. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann Intern Med 2009; 151:738–747.
- Newcomb PA, Norfleet RG, Storer BE, Surawicz TS, Marcus PM. Screening sigmoidoscopy and colorectal cancer mortality. J Natl Cancer Inst 1992; 84:1572–1575.
- Bressler B, Paszat LF, Chen Z, Rothwell DM, Vinden C, Rabeneck L. Rates of new or missed colorectal cancers after colonoscopy and their risk factors: a population-based analysis. Gastroenterology 2007; 132:96–102.
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014; 64:9–29.
- Feld AD. Malpractice risks associated with colon cancer and inflammatory bowel disease. J Gastroenterol 2004; 99:1641–1644.
- Goodman D, Irvin TT. Delay in the diagnosis and prognosis of carcinoma of the right colon. Br J Surg 1993; 80:1327–1329.
- Alvarez JA, Baldonedo RF, Bear IG, Alvarez P, Jorge JL. Anaerobic liver abscesses as initial presentation of silent colonic cancer. HPB (Oxford) 2004; 6:41–42.
- Tsai HL, Hsieh JS, Yu FJ, et al. Perforated colonic cancer presenting as intra-abdominal abscess. Int J Colorectal Dis 2007; 22:15–19.
- Levin B, Lieberman DA, McFarland B, et al; American Cancer Society Colorectal Cancer Advisory Group; US Multi-Society Task Force; American College of Radiology Colon Cancer Committee. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 2008; 134:1570–1595.
- American Cancer Society. Colorectal cancer prevention and early detection. www.cancer.org/cancer/colonandrectumcancer/moreinformation/colonandrectumcancerearlydetection/colorectal-cancer-early-detection-acs-recommendations. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Colorectal cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/colorectal-cancer-screening. Accessed May 17, 2016.
- Schröder FH, Hugosson J, Roobol MJ, et al; ERSPC Investigators. Screening and prostate cancer mortality: results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet 2014; 384:2027–2035.
- American Cancer Society. Prostate cancer prevention and early detection. www.cancer.org/cancer/prostatecancer/moreinformation/prostatecancerearlydetection/index. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Prostate cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/prostate-cancer-screening. Accessed June 1, 2016.
- Essink-Bot ML, de Koning HJ, Nijs HG, Kirkels WJ, van der Maas PJ, Schröder FH. Short-term effects of population-based screening for prostate cancer on health-related quality of life. J Natl Cancer Inst 1998; 90:925–931.
- Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. BMJ (Clin Res Ed) 2000; 321:323–329.
- Chute CG, Greenberg ER, Baron J, Korson R, Baker J, Yates J. Presenting conditions of 1,539 population-based lung cancer patients by cell type and stage in New Hampshire and Vermont. Cancer 1985; 56:2107–2111.
- Ramadan HH, Wax MK, Avery S. Outcome and changing cause of unilateral vocal cord paralysis. Otolaryngol Head Neck Surg 1998;118:199–202.
- Church TR, Black WC, Aberle DR, et al. Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med 2013; 368:1980–1991.
- American Cancer Society. Lung cancer prevention and early detection. www.cancer.org/cancer/lungcancer-non-smallcell/moreinformation/lungcancerpreventionandearlydetection/index. Accessed May 17, 2016.
- Lung Cancer Screening. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. www.nccn.org/professionals/physician_gls/pdf/lung_screening.pdf. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Lung cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/lung-cancer-screening. Accessed May 17, 2016.
- National Cancer Institute (NIH). Surveillance, Epidemiology, and End Results (SEER) Program. SEER Cancer Statistics Review: 1973-1994. http://seer.cancer.gov/archive/csr/1973_1994/. Accessed May 17, 2016.
- Mauch PM, Kalish LA, Kadin M, Coleman CN, Osteen R, Hellman S. Patterns of presentation of Hodgkin disease. Implications for etiology and pathogenesis. Cancer 1993; 71:2062–2071.
- Gobbi PG, Cavalli C, Gendarini A, et al. Reevaluation of prognostic significance of symptoms in Hodgkin’s disease. Cancer 1985; 56:2874–2880.
- Einhorn LH. Treatment of testicular cancer: a new and improved model. J Clin Oncol 1990; 8:1777–1781.
- Tseng A Jr, Horning SJ, Freiha FS, Resser KJ, Hannigan JF Jr, Torti FM. Gynecomastia in testicular cancer patients. Prognostic and therapeutic implications. Cancer 1985; 56:2534–2538.
- Gilligan TD, Seidenfeld J, Basch EM, et al; American Society of Clinical Oncology. American Society of Clinical Oncology clinical practice guideline on uses of serum tumor markers in adult males with germ cell tumors. J Clin Oncol 2010; 28:3388–3404.
- Brydøy M, Fosså SD, Klepp O, et al. Paternity following treatment for testicular cancer. J Natl Cancer Inst 2005; 97:1580–1588.
According to the Surveillance, Epidemiology, and End Results database, 5-year overall survival rates have improved for nearly all tumor types during the past 40 years.1 This has been accomplished with better treatment and earlier detection of the most common cancers, as well as the uncommon but highly curable tumor types.
Primary care physicians play a vital role in detecting cancers at earlier stages and synthesizing information from a patient’s presentation, vital signs, physical examination, and results of laboratory and radiographic testing. Yet cancers can be easily overlooked, and highly curable cancers such as Hodgkin lymphoma and testicular cancer, with 5-year survival rates above 85%, can have unusual presentations. Aside from the obvious health consequences, missed cancer diagnoses are often the subject of malpractice suits.
This paper reviews cancers that are easily missed and provides clinically relevant pearls from an oncologic perspective for primary care physicians, who are generally the first point of contact for patients.
BREAST CANCER DETECTION AND SCREENING
Breast cancer is the second most common cause of cancer death in US women and the most common cause of death in US women ages 20 to 59 (Table 1).2–4
Screening mammography has had a significant impact on early detection rates, and this has translated into a 20% to 30% decrease in the breast cancer mortality rate.5,6 But despite national screening guidelines, up to 15% of cases are diagnosed on the basis of a palpable breast mass not detected on mammography, and 30% are diagnosed with a breast mass during the interval between mammograms.5,6 Moreover, delay in breast cancer diagnosis is one of the most common reasons for malpractice suits.7,8
Warning signs
Breast cancer can present clinically as a single, dominant, indurated mass with irregular borders. The mass can have associated ecchymosis, erythema, nipple discharge, nipple retraction, and nipple eczema.9,10 Pay close attention to any history of breast trauma, pain, signs or symptoms suggestive of local infection, and the lesion’s relationship to the patient’s menstrual cycle. Locally advanced disease typically presents with axillary adenopathy, as well as skin findings such as erythema, thickening, and dimpling.
Initial imaging workup for a breast mass
Women presenting with a breast mass should undergo breast imaging, followed by core needle biopsy of any suspicious abnormality. Depending on the clinical breast examination and the interpretation of the mammogram, as reported as a Breast Imaging Reporting and Data System (BIRADS) score, ultrasonography, magnetic resonance imaging, or biopsy may be the next course of action. Ultrasonography is recommended in evaluating masses in women who are under age 30 (who are more likely to have dense breasts that make standard mammography difficult to interpret) or who are pregnant (because it does not involve radiation).
For patients with a borderline or indeterminate clinical examination (eg, asymmetric skin-thickening or discoloration, nipple discharge or inversion, nodularity, finding on imaging [ie, BIRADS 3 lesion]), closer follow-up with repeat or additional imaging or biopsy, or both, is strongly recommended.
Screening recommendations vary
The age at which to start breast cancer screening has been a matter of debate in recent years, and different organizations have different recommendations (Table 2).11–13 According to the American Cancer Society (ACS), women should begin screening mammography at age 45 and should continue it indefinitely as long as they are in good health.11 This guideline is in line with those of the National Comprehensive Cancer Network (NCCN)12 but differs from those of the US Preventive Services Task Force (USPSTF).13
One reason for the controversy is that although starting screening at a younger age may allow for earlier detection, it also leads to overdiagnosis and to unnecessary tests and procedures. However, the NCCN noted limitations in studies looking at the overdiagnosis of breast cancer, including their use of incidence data from the 1970s, which not only underestimated the annual incidence of breast cancer in the United States, but also neglected to differentiate invasive cancer from ductal carcinoma in situ.12 Additionally, by detecting breast cancer lesions 2 years before they are discovered by clinical breast examination, mammography has been found to reduce the mortality rate from breast cancer.14
The frequency of mammography should be individualized and should involve not only an assessment of the patient’s risk factors (eg, age, family history, genetic predisposition, history of precancerous lesions, history of radiation exposure) but also a discussion of the benefits, limitations, and potential harms of screening. Both the ACS and the NCCN recommend yearly mammography for women ages 45 to 54. For those age 55 and older, the ACS recommends screening mammography every 2 years until the patient’s life expectancy is less than 10 years, whereas the NCCN recommends yearly screening mammography indefinitely. Meanwhile, the USPSTF recommends mammograms every 2 years for women ages 50 to 74.
Pearls
- Pay close attention to a history of breast trauma, pain, and signs of infection.
- Consider ultrasonography for women under age 30, who are more likely to have dense breasts.
COLORECTAL CANCER
With an estimated annual incidence of 132,700 cases diagnosed in the United States in 2015, colorectal cancer is the third most common cancer.
National guidelines that recommend colonoscopy (starting at age 50 for people at standard risk) have had a significant impact on early detection rates and have translated into a significant decrease in mortality rates.2,15,16 However, a missed diagnosis of colorectal cancer is one of the most common reasons for malpractice suits, typically because the patient was not referred for colonoscopy according to national guidelines.17–19
Symptoms depend on tumor location
In symptomatic cases, clinical manifestations differ depending on tumor location.
Left-sided tumors can present with hematochezia, colicky abdominal pain, and a change in bowel habits. And because the descending (left) colon has a smaller lumen than the right and tumors typically are annular in shape, left-sided cancers may present with abdominal distention with or without bowel obstruction or nausea and vomiting.
Right-sided tumors typically present with iron deficiency anemia from unrecognized blood loss.
Tumors near the rectum can cause tenesmus, rectal pain, and diminished caliber of stools.
In the United States, 20% of colorectal cancer patients have distant metastases at the time of diagnosis, and the most common sites are the lymph nodes, liver, lungs, and peritoneum.17
Uncommon presentations of colorectal cancer include pneumaturia, fecaluria or recurrent urinary tract infection from a fistula, bacteremia with Streptococcus bovis or Clostridium septicum, and intra-abdominal abscess from a localized bowel perforation.20,21
Initial workup
Once cancer is suspected, colonoscopy is the most accurate and versatile diagnostic test. It not only permits localization and biopsy of lesions throughout the large bowel, but also detects synchronous neoplasms and permits removal of polyps. Computed tomographic (CT) colonography is an alternative if colonoscopy is contraindicated, but it can only detect larger (ie, > 6-mm) tumors.22
According to the ACS,23 men and women at average risk should undergo colorectal cancer screening beginning at age 50. ACS screening recommendations for polyps and colorectal cancer include flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, double-contrast barium enema every 5 years, or CT colonography every 5 years. Tests that detect cancer but not polyps include guaiac-based fecal occult blood test (every year), fecal immunochemical test (every year), stool DNA test (every 3 years). These recommendations are fairly consistent with those of the NCCN12 and USPSTF24 (Table 3).12,23,24
Pearls
- Uncommon presentations include urinary tract problems and intra-abdominal abscess.
- CT colonography can only detect larger tumors.
PROSTATE CANCER
With an estimated 220,800 cases and 27,540 deaths in 2015, prostate cancer is the most common cancer and the second most common cause of cancer-related death in US men.2 Widespread use of serum prostate-specific antigen (PSA) testing has increased the rate of detection of prostate cancer.
Signs and symptoms
Most men with early-stage prostate cancer have no symptoms directly attributable to the disease.
Obstructive symptoms such as hesitancy, decreased stream, retention, and nocturia are common but are usually related to concomitant benign prostatic hypertrophy. As in prostatitis, patients with prostate cancer may present with irritative symptoms such as urinary frequency, dysuria, and urgency.
Patients who present with locally advanced prostate cancer may have symptoms secondary to local invasion, such as hematuria, hematospermia, and new-onset erectile dysfunction.
Prostate cancer usually metastasizes to bone, most commonly to the vertebrae and sternum, and the associated pain can be acute or insidious.
Diagnosis
Prostate cancer is most often diagnosed after biopsy prompted by an elevated PSA level or an abnormal digital rectal examination. The most common abnormal laboratory findings in patients with metastatic prostate cancer are an elevated serum PSA level (typically > 10 ng/mL), an elevated serum alkaline phosphatase level, and anemia, which are all proportional to the extent of bone involvement.
Screening is still controversial
There has been considerable controversy in recent years with regard to PSA screening because of the lack of significant benefit and the potential for harm to the patient, with an overdiagnosis rate ranging from 23% to 42%.25
According to the ACS,26 certain groups of men should make an informed decision with their physician about whether to undergo screening: men over age 50 at average risk of prostate cancer and with at least a 10-year life expectancy, men over age 45 at high risk, and men over age 40 at an even higher risk. These ACS guidelines are consistent with those of the NCCN12 but differ from those of the USPSTF27 (Table 4).12,26,27
The patient should fully understand the risks and benefits of prostate cancer screening, as well as why it is controversial: ie, while the lifetime risk of being diagnosed with prostate cancer has increased, the lifetime risk of dying from it has remained the same after the advent of PSA testing.
Adverse effects of biopsy and treatment
Prostate biopsy is associated with infectious and bleeding complications, in addition to anxiety and physical discomfort.28 Treatment-related adverse effects include urinary incontinence, sexual dysfunction, and bowel problems.
Could these potential harms be overstated and the benefit be greater than currently thought? The NCCN12 noted that some of the landmark prostate cancer screening studies found a potential benefit in screening high-risk patients such as black men. Moreover, the studies used the sextant prostate biopsy technique, whereas now the extended core biopsy technique is the standard of care. And the studies may have underestimated the benefit of screening because the trial patients were relatively old (age 60) when their first PSA measurement was done, they were screened at long intervals (every 4 years), and the treatment options available at the time were not as good as those available today.12
Pearls
- Laboratory findings in metastatic prostate cancer are proportional to the extent of bone involvement.
- Most men with early-stage prostate cancer have no symptoms attributable to the disease.
LUNG CANCER
Lung cancer is the second most common type of cancer in men and women but has the highest mortality rate. In the United States, in 2015, an estimated 221,200 new cases of lung cancer and 158,040 deaths were expected.2 Lung cancer deaths have begun to decline in both men and women, and this is due to the decline in smoking. The impact of lung cancer screening may not be seen for another 5 to 10 years.29
A wide range of symptoms, presentations
Many patients with squamous cell carcinoma and small-cell lung carcinoma present with symptoms related to tumor involvement of the central airways,30 including cough, hemoptysis, and postobstructive pneumonia. Partial obstruction of a bronchus may cause localized wheezing, heard by the patient or by the clinician on auscultation, whereas obstruction of larger airways can cause stridor.
Patients with advanced disease present with dull, aching, persistent chest pain from mediastinal, pleural, or chest wall extension, dyspnea from lymphangitic tumor spread, tumor emboli, pneumothorax, pleural effusion, or pericardial effusion with tamponade. Less commonly, patients may present with unilateral paralysis of the diaphragm from phrenic nerve damage or with hoarseness from recurrent laryngeal nerve compression.31
Bronchorrhea—production of large volumes of thin, mucoid secretions resulting in cough—may be a feature of bronchoalveolar cell carcinoma, a rare subtype of non-small-cell lung carcinoma.
Patients uncommonly present with superior vena cava syndrome, an oncologic emergency that most often causes facial and arm swelling, dyspnea, cough, and headache.
Non-small-cell lung carcinoma arising in the superior sulcus may in rare cases cause Pancoast syndrome (manifested by shoulder pain and atrophy of the hand muscles from brachial plexus involvement), Horner syndrome (manifested by ptosis, miosis, and anhidrosis), or rib destruction.
If metastasis occurs, lung cancer commonly metastasizes to the liver and adrenal glands. At the time of diagnosis, 20% to 30% of patients with small-cell lung carcinoma have symptoms of central nervous system metastasis.
The screening controversy
Lung cancer screening is controversial because previous large studies have failed to show a clinical benefit (ie, improved survival rates) of CT screening in smokers. However, based on the results of a later large randomized trial,32 the ACS33 now recommends that patients ages 55 to 74 who are in fairly good health, have at least a 30-pack-year smoking history, and are currently smoking or have quit smoking within the last 15 years should discuss with their physician the benefits, limitations, and potential harms of lung cancer screening. These recommendations are similar to those of the NCCN12,34 and USPSTF35 (Table 5).12,33–35 The ACS guidelines also emphasize that screening should be done only at facilities with extensive experience with low-dose CT.
Follow-up evaluation
If imaging detects a lung nodule, its size and consistency are crucial in determining the course of action.33 If an endobronchial growth or solid nodule larger than 8 mm is discovered, the primary care physician should consider ordering either a repeat low-dose CT scan after 1 month or a positron-emission tomography CT scan.34 The diagnosis should be confirmed by biopsy or by surgical removal of the nodule if localized and accessible, with sites of metastasis typically taking priority.
Pearl
- At diagnosis, 20% to 30% of patients with small-cell lung cancer have symptoms of central nervous system metastasis.
HIGHLY CURABLE CANCERS WITH UNUSUAL PRESENTATIONS
Hodgkin lymphoma
With 9,190 new cases in the United States annually and a 5-year overall survival rate over 85%, Hodgkin lymphoma is one of the least common but most curable cancers.1,2 In the United States, there are two diagnostic peaks, one around age 20 and one around age 65.36 In patients with human immunodeficiency virus infection, the rate is 15 to 30 times higher than in the general population, regardless of disease status or compliance with highly active retroviral therapy.37
Hodgkin lymphoma typically presents as a nontender painless mass with rubbery consistency. The involved lymph node is typically cervical or supraclavicular. Although not detectable on physical examination, enlarged mediastinal nodes and retroperitoneal nodes are often present. Less commonly, patients may present with enlarged axillary and inguinal nodes.38
A second common presentation is the discovery of a mediastinal mass on routine chest radiography. A large percentage of patients present with at least one systemic symptom, which may include fever, night sweats, and unintentional weight loss. Generalized pruritus occurs early in the disease course in 10% to 15% of patients and is occasionally severe enough to cause intense scratching and excoriations.
A more unusual presentation of Hodgkin lymphoma is severe pain at areas of involvement after alcohol ingestion.
Most patients present with overt disease, but the presenting symptoms and signs may be relatively nonspecific and subtle and more consistent with an infectious process.
Hodgkin disease has a variable tempo, but overt symptoms typically occur after several months rather than years. As a general rule, it starts at a single site within the lymphatic system, usually a lymph node, and then spreads to adjacent nodes via lymphatic channels before disseminating to distant nonadjacent sites and organs. With this in mind, it is unusual to have bilateral axillary involvement without disease in the lower neck, and extremely unusual to have hepatic or bone marrow infiltration without disease in the spleen.
The diagnosis is established by whole lymph node tissue biopsy. Due to the high rate of inflammation in the area, inguinal nodes should not be biopsied if other equally suspicious peripheral nodes are present elsewhere. When the diagnosis of Hodgkin lymphoma is made from biopsy of an extranodal site, such as the stomach, spleen, Waldeyer ring, central nervous system, lung, bone, or skin, lymph node biopsy is also desirable for diagnostic confirmation.
Testicular cancer
Although accounting for only about 1% of all cancers in men, testicular cancer is the most common solid tumor affecting males between ages 15 and 35.1,2 With a 5-year survival rate of over 95%, testicular cancer is also one of the most curable cancers.
Testicular tumors usually present as a painless nodule or swelling of one testicle. Uncommonly, patients have metastatic disease at diagnosis, with the most common sites being lymph nodes, lung, bone, and the brain. Gynecomastia, associated with the production of human chorionic gonadotropin, occurs in about 5% of men with testicular germ cell tumors and 20% to 30% of men with Leydig cell tumors.39 Rarely, patients may present with paraneoplastic hyperthyroidism, which is secondary to thyroid-stimulating hormone and human chorionic gonadotropin sharing a common homologous alpha and beta subunit.40
Prompt diagnosis and treatment of testicular cancer provides the best opportunity for cure. Therefore, any testicular mass, even a painful scrotal lesion, should be evaluated as if it is testicular cancer until it is proven otherwise. The diagnostic evaluation of suspected testicular cancer includes scrotal ultrasonography. Radiographic testing, as deemed clinically necessary by the consulting urologist and medical oncologist, may include chest radiography, CT (chest, abdomen, pelvis), brain magnetic resonance imaging, or bone scan.
The primary care laboratory evaluation should include a complete metabolic profile and measurements of lactate dehydrogenase and serum tumor markers such as alpha fetoprotein and human chorionic gonadotropin. In nonseminomatous germ cell tumors, alpha fetoprotein or human chorionic gonadotropin, or both, can be elevated in 80% to 85% of patients. However, in seminoma, alpha fetoprotein is never elevated, and the serum human chorionic gonadotropin is elevated in only 20% to 25% of patients.41
Patients with a suspicious testicular mass should be referred promptly to a urologist for consideration of radical inguinal orchiectomy and, in some cases, retroperitoneal lymph node dissection. Testicular biopsy is not part of the evaluation as it may result in tumor seeding into the scrotal sac or metastatic spread of tumor to the inguinal nodes. Inguinal biopsy of the contralateral testis is considered if ultrasonography raises suspicion of an intratesticular abnormality, cryptorchid testis, or marked testicular atrophy. Discussing sperm banking with the patient is part of the diagnostic workup, as cumulative cisplatin doses greater than 400 mg/m2 can result in permanent infertility in 50% of men.42
Pearls
- In Hodgkin lymphoma, bilateral axillary involvement without disease in the lower neck is unusual.
- Discussing sperm banking is part of the diagnostic workup for testicular cancer.
According to the Surveillance, Epidemiology, and End Results database, 5-year overall survival rates have improved for nearly all tumor types during the past 40 years.1 This has been accomplished with better treatment and earlier detection of the most common cancers, as well as the uncommon but highly curable tumor types.
Primary care physicians play a vital role in detecting cancers at earlier stages and synthesizing information from a patient’s presentation, vital signs, physical examination, and results of laboratory and radiographic testing. Yet cancers can be easily overlooked, and highly curable cancers such as Hodgkin lymphoma and testicular cancer, with 5-year survival rates above 85%, can have unusual presentations. Aside from the obvious health consequences, missed cancer diagnoses are often the subject of malpractice suits.
This paper reviews cancers that are easily missed and provides clinically relevant pearls from an oncologic perspective for primary care physicians, who are generally the first point of contact for patients.
BREAST CANCER DETECTION AND SCREENING
Breast cancer is the second most common cause of cancer death in US women and the most common cause of death in US women ages 20 to 59 (Table 1).2–4
Screening mammography has had a significant impact on early detection rates, and this has translated into a 20% to 30% decrease in the breast cancer mortality rate.5,6 But despite national screening guidelines, up to 15% of cases are diagnosed on the basis of a palpable breast mass not detected on mammography, and 30% are diagnosed with a breast mass during the interval between mammograms.5,6 Moreover, delay in breast cancer diagnosis is one of the most common reasons for malpractice suits.7,8
Warning signs
Breast cancer can present clinically as a single, dominant, indurated mass with irregular borders. The mass can have associated ecchymosis, erythema, nipple discharge, nipple retraction, and nipple eczema.9,10 Pay close attention to any history of breast trauma, pain, signs or symptoms suggestive of local infection, and the lesion’s relationship to the patient’s menstrual cycle. Locally advanced disease typically presents with axillary adenopathy, as well as skin findings such as erythema, thickening, and dimpling.
Initial imaging workup for a breast mass
Women presenting with a breast mass should undergo breast imaging, followed by core needle biopsy of any suspicious abnormality. Depending on the clinical breast examination and the interpretation of the mammogram, as reported as a Breast Imaging Reporting and Data System (BIRADS) score, ultrasonography, magnetic resonance imaging, or biopsy may be the next course of action. Ultrasonography is recommended in evaluating masses in women who are under age 30 (who are more likely to have dense breasts that make standard mammography difficult to interpret) or who are pregnant (because it does not involve radiation).
For patients with a borderline or indeterminate clinical examination (eg, asymmetric skin-thickening or discoloration, nipple discharge or inversion, nodularity, finding on imaging [ie, BIRADS 3 lesion]), closer follow-up with repeat or additional imaging or biopsy, or both, is strongly recommended.
Screening recommendations vary
The age at which to start breast cancer screening has been a matter of debate in recent years, and different organizations have different recommendations (Table 2).11–13 According to the American Cancer Society (ACS), women should begin screening mammography at age 45 and should continue it indefinitely as long as they are in good health.11 This guideline is in line with those of the National Comprehensive Cancer Network (NCCN)12 but differs from those of the US Preventive Services Task Force (USPSTF).13
One reason for the controversy is that although starting screening at a younger age may allow for earlier detection, it also leads to overdiagnosis and to unnecessary tests and procedures. However, the NCCN noted limitations in studies looking at the overdiagnosis of breast cancer, including their use of incidence data from the 1970s, which not only underestimated the annual incidence of breast cancer in the United States, but also neglected to differentiate invasive cancer from ductal carcinoma in situ.12 Additionally, by detecting breast cancer lesions 2 years before they are discovered by clinical breast examination, mammography has been found to reduce the mortality rate from breast cancer.14
The frequency of mammography should be individualized and should involve not only an assessment of the patient’s risk factors (eg, age, family history, genetic predisposition, history of precancerous lesions, history of radiation exposure) but also a discussion of the benefits, limitations, and potential harms of screening. Both the ACS and the NCCN recommend yearly mammography for women ages 45 to 54. For those age 55 and older, the ACS recommends screening mammography every 2 years until the patient’s life expectancy is less than 10 years, whereas the NCCN recommends yearly screening mammography indefinitely. Meanwhile, the USPSTF recommends mammograms every 2 years for women ages 50 to 74.
Pearls
- Pay close attention to a history of breast trauma, pain, and signs of infection.
- Consider ultrasonography for women under age 30, who are more likely to have dense breasts.
COLORECTAL CANCER
With an estimated annual incidence of 132,700 cases diagnosed in the United States in 2015, colorectal cancer is the third most common cancer.
National guidelines that recommend colonoscopy (starting at age 50 for people at standard risk) have had a significant impact on early detection rates and have translated into a significant decrease in mortality rates.2,15,16 However, a missed diagnosis of colorectal cancer is one of the most common reasons for malpractice suits, typically because the patient was not referred for colonoscopy according to national guidelines.17–19
Symptoms depend on tumor location
In symptomatic cases, clinical manifestations differ depending on tumor location.
Left-sided tumors can present with hematochezia, colicky abdominal pain, and a change in bowel habits. And because the descending (left) colon has a smaller lumen than the right and tumors typically are annular in shape, left-sided cancers may present with abdominal distention with or without bowel obstruction or nausea and vomiting.
Right-sided tumors typically present with iron deficiency anemia from unrecognized blood loss.
Tumors near the rectum can cause tenesmus, rectal pain, and diminished caliber of stools.
In the United States, 20% of colorectal cancer patients have distant metastases at the time of diagnosis, and the most common sites are the lymph nodes, liver, lungs, and peritoneum.17
Uncommon presentations of colorectal cancer include pneumaturia, fecaluria or recurrent urinary tract infection from a fistula, bacteremia with Streptococcus bovis or Clostridium septicum, and intra-abdominal abscess from a localized bowel perforation.20,21
Initial workup
Once cancer is suspected, colonoscopy is the most accurate and versatile diagnostic test. It not only permits localization and biopsy of lesions throughout the large bowel, but also detects synchronous neoplasms and permits removal of polyps. Computed tomographic (CT) colonography is an alternative if colonoscopy is contraindicated, but it can only detect larger (ie, > 6-mm) tumors.22
According to the ACS,23 men and women at average risk should undergo colorectal cancer screening beginning at age 50. ACS screening recommendations for polyps and colorectal cancer include flexible sigmoidoscopy every 5 years, colonoscopy every 10 years, double-contrast barium enema every 5 years, or CT colonography every 5 years. Tests that detect cancer but not polyps include guaiac-based fecal occult blood test (every year), fecal immunochemical test (every year), stool DNA test (every 3 years). These recommendations are fairly consistent with those of the NCCN12 and USPSTF24 (Table 3).12,23,24
Pearls
- Uncommon presentations include urinary tract problems and intra-abdominal abscess.
- CT colonography can only detect larger tumors.
PROSTATE CANCER
With an estimated 220,800 cases and 27,540 deaths in 2015, prostate cancer is the most common cancer and the second most common cause of cancer-related death in US men.2 Widespread use of serum prostate-specific antigen (PSA) testing has increased the rate of detection of prostate cancer.
Signs and symptoms
Most men with early-stage prostate cancer have no symptoms directly attributable to the disease.
Obstructive symptoms such as hesitancy, decreased stream, retention, and nocturia are common but are usually related to concomitant benign prostatic hypertrophy. As in prostatitis, patients with prostate cancer may present with irritative symptoms such as urinary frequency, dysuria, and urgency.
Patients who present with locally advanced prostate cancer may have symptoms secondary to local invasion, such as hematuria, hematospermia, and new-onset erectile dysfunction.
Prostate cancer usually metastasizes to bone, most commonly to the vertebrae and sternum, and the associated pain can be acute or insidious.
Diagnosis
Prostate cancer is most often diagnosed after biopsy prompted by an elevated PSA level or an abnormal digital rectal examination. The most common abnormal laboratory findings in patients with metastatic prostate cancer are an elevated serum PSA level (typically > 10 ng/mL), an elevated serum alkaline phosphatase level, and anemia, which are all proportional to the extent of bone involvement.
Screening is still controversial
There has been considerable controversy in recent years with regard to PSA screening because of the lack of significant benefit and the potential for harm to the patient, with an overdiagnosis rate ranging from 23% to 42%.25
According to the ACS,26 certain groups of men should make an informed decision with their physician about whether to undergo screening: men over age 50 at average risk of prostate cancer and with at least a 10-year life expectancy, men over age 45 at high risk, and men over age 40 at an even higher risk. These ACS guidelines are consistent with those of the NCCN12 but differ from those of the USPSTF27 (Table 4).12,26,27
The patient should fully understand the risks and benefits of prostate cancer screening, as well as why it is controversial: ie, while the lifetime risk of being diagnosed with prostate cancer has increased, the lifetime risk of dying from it has remained the same after the advent of PSA testing.
Adverse effects of biopsy and treatment
Prostate biopsy is associated with infectious and bleeding complications, in addition to anxiety and physical discomfort.28 Treatment-related adverse effects include urinary incontinence, sexual dysfunction, and bowel problems.
Could these potential harms be overstated and the benefit be greater than currently thought? The NCCN12 noted that some of the landmark prostate cancer screening studies found a potential benefit in screening high-risk patients such as black men. Moreover, the studies used the sextant prostate biopsy technique, whereas now the extended core biopsy technique is the standard of care. And the studies may have underestimated the benefit of screening because the trial patients were relatively old (age 60) when their first PSA measurement was done, they were screened at long intervals (every 4 years), and the treatment options available at the time were not as good as those available today.12
Pearls
- Laboratory findings in metastatic prostate cancer are proportional to the extent of bone involvement.
- Most men with early-stage prostate cancer have no symptoms attributable to the disease.
LUNG CANCER
Lung cancer is the second most common type of cancer in men and women but has the highest mortality rate. In the United States, in 2015, an estimated 221,200 new cases of lung cancer and 158,040 deaths were expected.2 Lung cancer deaths have begun to decline in both men and women, and this is due to the decline in smoking. The impact of lung cancer screening may not be seen for another 5 to 10 years.29
A wide range of symptoms, presentations
Many patients with squamous cell carcinoma and small-cell lung carcinoma present with symptoms related to tumor involvement of the central airways,30 including cough, hemoptysis, and postobstructive pneumonia. Partial obstruction of a bronchus may cause localized wheezing, heard by the patient or by the clinician on auscultation, whereas obstruction of larger airways can cause stridor.
Patients with advanced disease present with dull, aching, persistent chest pain from mediastinal, pleural, or chest wall extension, dyspnea from lymphangitic tumor spread, tumor emboli, pneumothorax, pleural effusion, or pericardial effusion with tamponade. Less commonly, patients may present with unilateral paralysis of the diaphragm from phrenic nerve damage or with hoarseness from recurrent laryngeal nerve compression.31
Bronchorrhea—production of large volumes of thin, mucoid secretions resulting in cough—may be a feature of bronchoalveolar cell carcinoma, a rare subtype of non-small-cell lung carcinoma.
Patients uncommonly present with superior vena cava syndrome, an oncologic emergency that most often causes facial and arm swelling, dyspnea, cough, and headache.
Non-small-cell lung carcinoma arising in the superior sulcus may in rare cases cause Pancoast syndrome (manifested by shoulder pain and atrophy of the hand muscles from brachial plexus involvement), Horner syndrome (manifested by ptosis, miosis, and anhidrosis), or rib destruction.
If metastasis occurs, lung cancer commonly metastasizes to the liver and adrenal glands. At the time of diagnosis, 20% to 30% of patients with small-cell lung carcinoma have symptoms of central nervous system metastasis.
The screening controversy
Lung cancer screening is controversial because previous large studies have failed to show a clinical benefit (ie, improved survival rates) of CT screening in smokers. However, based on the results of a later large randomized trial,32 the ACS33 now recommends that patients ages 55 to 74 who are in fairly good health, have at least a 30-pack-year smoking history, and are currently smoking or have quit smoking within the last 15 years should discuss with their physician the benefits, limitations, and potential harms of lung cancer screening. These recommendations are similar to those of the NCCN12,34 and USPSTF35 (Table 5).12,33–35 The ACS guidelines also emphasize that screening should be done only at facilities with extensive experience with low-dose CT.
Follow-up evaluation
If imaging detects a lung nodule, its size and consistency are crucial in determining the course of action.33 If an endobronchial growth or solid nodule larger than 8 mm is discovered, the primary care physician should consider ordering either a repeat low-dose CT scan after 1 month or a positron-emission tomography CT scan.34 The diagnosis should be confirmed by biopsy or by surgical removal of the nodule if localized and accessible, with sites of metastasis typically taking priority.
Pearl
- At diagnosis, 20% to 30% of patients with small-cell lung cancer have symptoms of central nervous system metastasis.
HIGHLY CURABLE CANCERS WITH UNUSUAL PRESENTATIONS
Hodgkin lymphoma
With 9,190 new cases in the United States annually and a 5-year overall survival rate over 85%, Hodgkin lymphoma is one of the least common but most curable cancers.1,2 In the United States, there are two diagnostic peaks, one around age 20 and one around age 65.36 In patients with human immunodeficiency virus infection, the rate is 15 to 30 times higher than in the general population, regardless of disease status or compliance with highly active retroviral therapy.37
Hodgkin lymphoma typically presents as a nontender painless mass with rubbery consistency. The involved lymph node is typically cervical or supraclavicular. Although not detectable on physical examination, enlarged mediastinal nodes and retroperitoneal nodes are often present. Less commonly, patients may present with enlarged axillary and inguinal nodes.38
A second common presentation is the discovery of a mediastinal mass on routine chest radiography. A large percentage of patients present with at least one systemic symptom, which may include fever, night sweats, and unintentional weight loss. Generalized pruritus occurs early in the disease course in 10% to 15% of patients and is occasionally severe enough to cause intense scratching and excoriations.
A more unusual presentation of Hodgkin lymphoma is severe pain at areas of involvement after alcohol ingestion.
Most patients present with overt disease, but the presenting symptoms and signs may be relatively nonspecific and subtle and more consistent with an infectious process.
Hodgkin disease has a variable tempo, but overt symptoms typically occur after several months rather than years. As a general rule, it starts at a single site within the lymphatic system, usually a lymph node, and then spreads to adjacent nodes via lymphatic channels before disseminating to distant nonadjacent sites and organs. With this in mind, it is unusual to have bilateral axillary involvement without disease in the lower neck, and extremely unusual to have hepatic or bone marrow infiltration without disease in the spleen.
The diagnosis is established by whole lymph node tissue biopsy. Due to the high rate of inflammation in the area, inguinal nodes should not be biopsied if other equally suspicious peripheral nodes are present elsewhere. When the diagnosis of Hodgkin lymphoma is made from biopsy of an extranodal site, such as the stomach, spleen, Waldeyer ring, central nervous system, lung, bone, or skin, lymph node biopsy is also desirable for diagnostic confirmation.
Testicular cancer
Although accounting for only about 1% of all cancers in men, testicular cancer is the most common solid tumor affecting males between ages 15 and 35.1,2 With a 5-year survival rate of over 95%, testicular cancer is also one of the most curable cancers.
Testicular tumors usually present as a painless nodule or swelling of one testicle. Uncommonly, patients have metastatic disease at diagnosis, with the most common sites being lymph nodes, lung, bone, and the brain. Gynecomastia, associated with the production of human chorionic gonadotropin, occurs in about 5% of men with testicular germ cell tumors and 20% to 30% of men with Leydig cell tumors.39 Rarely, patients may present with paraneoplastic hyperthyroidism, which is secondary to thyroid-stimulating hormone and human chorionic gonadotropin sharing a common homologous alpha and beta subunit.40
Prompt diagnosis and treatment of testicular cancer provides the best opportunity for cure. Therefore, any testicular mass, even a painful scrotal lesion, should be evaluated as if it is testicular cancer until it is proven otherwise. The diagnostic evaluation of suspected testicular cancer includes scrotal ultrasonography. Radiographic testing, as deemed clinically necessary by the consulting urologist and medical oncologist, may include chest radiography, CT (chest, abdomen, pelvis), brain magnetic resonance imaging, or bone scan.
The primary care laboratory evaluation should include a complete metabolic profile and measurements of lactate dehydrogenase and serum tumor markers such as alpha fetoprotein and human chorionic gonadotropin. In nonseminomatous germ cell tumors, alpha fetoprotein or human chorionic gonadotropin, or both, can be elevated in 80% to 85% of patients. However, in seminoma, alpha fetoprotein is never elevated, and the serum human chorionic gonadotropin is elevated in only 20% to 25% of patients.41
Patients with a suspicious testicular mass should be referred promptly to a urologist for consideration of radical inguinal orchiectomy and, in some cases, retroperitoneal lymph node dissection. Testicular biopsy is not part of the evaluation as it may result in tumor seeding into the scrotal sac or metastatic spread of tumor to the inguinal nodes. Inguinal biopsy of the contralateral testis is considered if ultrasonography raises suspicion of an intratesticular abnormality, cryptorchid testis, or marked testicular atrophy. Discussing sperm banking with the patient is part of the diagnostic workup, as cumulative cisplatin doses greater than 400 mg/m2 can result in permanent infertility in 50% of men.42
Pearls
- In Hodgkin lymphoma, bilateral axillary involvement without disease in the lower neck is unusual.
- Discussing sperm banking is part of the diagnostic workup for testicular cancer.
- National Cancer Institute (NIH). Surveillance, Epidemiology and End Results (SEER) Program. SEER Cancer Statistics Review, 1975–2010. http://seer.cancer.gov/csr/1975_2010/. Accessed May 9, 2016.
- American Cancer Society. Cancer Facts & Figures 2015.
www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2015/. Accessed May 9, 2016. - Tabár L, Vitak B, Chen HH, Yen MF, Duffy SW, Smith RA. Beyond randomized controlled trials: organized mammographic screening substantially reduces breast carcinoma mortality. Cancer 2001; 91:1724–1731.
- Tabar L, Fagerberg G, Chen HH, et al. Efficacy of breast cancer screening by age. New results from the Swedish two-county trial. Cancer 1995; 75:2507–2517.
- Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med 2002; 137:347–360.
- Esserman LJ, Shieh Y, Rutgers EJ, et al. Impact of mammographic screening on the detection of good and poor prognosis breast cancers. Breast Cancer Res Treat 2011; 130:725–734.
- Wallace E, Lowry J, Smith SM, Fahey T. The epidemiology of malpractice claims in primary care: a systematic review. BMJ Open 2013; 3:pii:e002929.
- Gandhi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med 2006; 145:488–496.
- Morrow M. The evaluation of common breast problems. Am Fam Physician 2000; 61:2371–2378, 2385.
- Santen RJ, Mansel R. Benign breast disorders. N Engl J Med 2005; 353:275–285.
- American Cancer Society. Breast cancer prevention and early detection. www.cancer.org/cancer/breastcancer/moreinformation/breastcancerearlydetection/breast-cancer-early-detection-acs-recs. Accessed May 17, 2016.
- National Comprehensive Cancer Network (NCCN). NCCN Guidelines. www.nccn.org/professionals/physician_gls/f_guidelines.asp#site. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Breast cancers Screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/breast-cancer-screening. Accessed May 17, 2016.
- Mandelblatt JS, Cronin KA, Bailey S, et al; Breast Cancer Working Group of the Cancer Intervention and Surveillance Modeling Network. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann Intern Med 2009; 151:738–747.
- Newcomb PA, Norfleet RG, Storer BE, Surawicz TS, Marcus PM. Screening sigmoidoscopy and colorectal cancer mortality. J Natl Cancer Inst 1992; 84:1572–1575.
- Bressler B, Paszat LF, Chen Z, Rothwell DM, Vinden C, Rabeneck L. Rates of new or missed colorectal cancers after colonoscopy and their risk factors: a population-based analysis. Gastroenterology 2007; 132:96–102.
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014; 64:9–29.
- Feld AD. Malpractice risks associated with colon cancer and inflammatory bowel disease. J Gastroenterol 2004; 99:1641–1644.
- Goodman D, Irvin TT. Delay in the diagnosis and prognosis of carcinoma of the right colon. Br J Surg 1993; 80:1327–1329.
- Alvarez JA, Baldonedo RF, Bear IG, Alvarez P, Jorge JL. Anaerobic liver abscesses as initial presentation of silent colonic cancer. HPB (Oxford) 2004; 6:41–42.
- Tsai HL, Hsieh JS, Yu FJ, et al. Perforated colonic cancer presenting as intra-abdominal abscess. Int J Colorectal Dis 2007; 22:15–19.
- Levin B, Lieberman DA, McFarland B, et al; American Cancer Society Colorectal Cancer Advisory Group; US Multi-Society Task Force; American College of Radiology Colon Cancer Committee. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 2008; 134:1570–1595.
- American Cancer Society. Colorectal cancer prevention and early detection. www.cancer.org/cancer/colonandrectumcancer/moreinformation/colonandrectumcancerearlydetection/colorectal-cancer-early-detection-acs-recommendations. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Colorectal cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/colorectal-cancer-screening. Accessed May 17, 2016.
- Schröder FH, Hugosson J, Roobol MJ, et al; ERSPC Investigators. Screening and prostate cancer mortality: results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet 2014; 384:2027–2035.
- American Cancer Society. Prostate cancer prevention and early detection. www.cancer.org/cancer/prostatecancer/moreinformation/prostatecancerearlydetection/index. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Prostate cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/prostate-cancer-screening. Accessed June 1, 2016.
- Essink-Bot ML, de Koning HJ, Nijs HG, Kirkels WJ, van der Maas PJ, Schröder FH. Short-term effects of population-based screening for prostate cancer on health-related quality of life. J Natl Cancer Inst 1998; 90:925–931.
- Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. BMJ (Clin Res Ed) 2000; 321:323–329.
- Chute CG, Greenberg ER, Baron J, Korson R, Baker J, Yates J. Presenting conditions of 1,539 population-based lung cancer patients by cell type and stage in New Hampshire and Vermont. Cancer 1985; 56:2107–2111.
- Ramadan HH, Wax MK, Avery S. Outcome and changing cause of unilateral vocal cord paralysis. Otolaryngol Head Neck Surg 1998;118:199–202.
- Church TR, Black WC, Aberle DR, et al. Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med 2013; 368:1980–1991.
- American Cancer Society. Lung cancer prevention and early detection. www.cancer.org/cancer/lungcancer-non-smallcell/moreinformation/lungcancerpreventionandearlydetection/index. Accessed May 17, 2016.
- Lung Cancer Screening. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. www.nccn.org/professionals/physician_gls/pdf/lung_screening.pdf. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Lung cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/lung-cancer-screening. Accessed May 17, 2016.
- National Cancer Institute (NIH). Surveillance, Epidemiology, and End Results (SEER) Program. SEER Cancer Statistics Review: 1973-1994. http://seer.cancer.gov/archive/csr/1973_1994/. Accessed May 17, 2016.
- Mauch PM, Kalish LA, Kadin M, Coleman CN, Osteen R, Hellman S. Patterns of presentation of Hodgkin disease. Implications for etiology and pathogenesis. Cancer 1993; 71:2062–2071.
- Gobbi PG, Cavalli C, Gendarini A, et al. Reevaluation of prognostic significance of symptoms in Hodgkin’s disease. Cancer 1985; 56:2874–2880.
- Einhorn LH. Treatment of testicular cancer: a new and improved model. J Clin Oncol 1990; 8:1777–1781.
- Tseng A Jr, Horning SJ, Freiha FS, Resser KJ, Hannigan JF Jr, Torti FM. Gynecomastia in testicular cancer patients. Prognostic and therapeutic implications. Cancer 1985; 56:2534–2538.
- Gilligan TD, Seidenfeld J, Basch EM, et al; American Society of Clinical Oncology. American Society of Clinical Oncology clinical practice guideline on uses of serum tumor markers in adult males with germ cell tumors. J Clin Oncol 2010; 28:3388–3404.
- Brydøy M, Fosså SD, Klepp O, et al. Paternity following treatment for testicular cancer. J Natl Cancer Inst 2005; 97:1580–1588.
- National Cancer Institute (NIH). Surveillance, Epidemiology and End Results (SEER) Program. SEER Cancer Statistics Review, 1975–2010. http://seer.cancer.gov/csr/1975_2010/. Accessed May 9, 2016.
- American Cancer Society. Cancer Facts & Figures 2015.
www.cancer.org/research/cancerfactsstatistics/cancerfactsfigures2015/. Accessed May 9, 2016. - Tabár L, Vitak B, Chen HH, Yen MF, Duffy SW, Smith RA. Beyond randomized controlled trials: organized mammographic screening substantially reduces breast carcinoma mortality. Cancer 2001; 91:1724–1731.
- Tabar L, Fagerberg G, Chen HH, et al. Efficacy of breast cancer screening by age. New results from the Swedish two-county trial. Cancer 1995; 75:2507–2517.
- Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med 2002; 137:347–360.
- Esserman LJ, Shieh Y, Rutgers EJ, et al. Impact of mammographic screening on the detection of good and poor prognosis breast cancers. Breast Cancer Res Treat 2011; 130:725–734.
- Wallace E, Lowry J, Smith SM, Fahey T. The epidemiology of malpractice claims in primary care: a systematic review. BMJ Open 2013; 3:pii:e002929.
- Gandhi TK, Kachalia A, Thomas EJ, et al. Missed and delayed diagnoses in the ambulatory setting: a study of closed malpractice claims. Ann Intern Med 2006; 145:488–496.
- Morrow M. The evaluation of common breast problems. Am Fam Physician 2000; 61:2371–2378, 2385.
- Santen RJ, Mansel R. Benign breast disorders. N Engl J Med 2005; 353:275–285.
- American Cancer Society. Breast cancer prevention and early detection. www.cancer.org/cancer/breastcancer/moreinformation/breastcancerearlydetection/breast-cancer-early-detection-acs-recs. Accessed May 17, 2016.
- National Comprehensive Cancer Network (NCCN). NCCN Guidelines. www.nccn.org/professionals/physician_gls/f_guidelines.asp#site. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Breast cancers Screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/breast-cancer-screening. Accessed May 17, 2016.
- Mandelblatt JS, Cronin KA, Bailey S, et al; Breast Cancer Working Group of the Cancer Intervention and Surveillance Modeling Network. Effects of mammography screening under different screening schedules: model estimates of potential benefits and harms. Ann Intern Med 2009; 151:738–747.
- Newcomb PA, Norfleet RG, Storer BE, Surawicz TS, Marcus PM. Screening sigmoidoscopy and colorectal cancer mortality. J Natl Cancer Inst 1992; 84:1572–1575.
- Bressler B, Paszat LF, Chen Z, Rothwell DM, Vinden C, Rabeneck L. Rates of new or missed colorectal cancers after colonoscopy and their risk factors: a population-based analysis. Gastroenterology 2007; 132:96–102.
- Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin 2014; 64:9–29.
- Feld AD. Malpractice risks associated with colon cancer and inflammatory bowel disease. J Gastroenterol 2004; 99:1641–1644.
- Goodman D, Irvin TT. Delay in the diagnosis and prognosis of carcinoma of the right colon. Br J Surg 1993; 80:1327–1329.
- Alvarez JA, Baldonedo RF, Bear IG, Alvarez P, Jorge JL. Anaerobic liver abscesses as initial presentation of silent colonic cancer. HPB (Oxford) 2004; 6:41–42.
- Tsai HL, Hsieh JS, Yu FJ, et al. Perforated colonic cancer presenting as intra-abdominal abscess. Int J Colorectal Dis 2007; 22:15–19.
- Levin B, Lieberman DA, McFarland B, et al; American Cancer Society Colorectal Cancer Advisory Group; US Multi-Society Task Force; American College of Radiology Colon Cancer Committee. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guideline from the American Cancer Society, the US Multi-Society Task Force on Colorectal Cancer, and the American College of Radiology. Gastroenterology 2008; 134:1570–1595.
- American Cancer Society. Colorectal cancer prevention and early detection. www.cancer.org/cancer/colonandrectumcancer/moreinformation/colonandrectumcancerearlydetection/colorectal-cancer-early-detection-acs-recommendations. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Colorectal cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/colorectal-cancer-screening. Accessed May 17, 2016.
- Schröder FH, Hugosson J, Roobol MJ, et al; ERSPC Investigators. Screening and prostate cancer mortality: results of the European Randomised Study of Screening for Prostate Cancer (ERSPC) at 13 years of follow-up. Lancet 2014; 384:2027–2035.
- American Cancer Society. Prostate cancer prevention and early detection. www.cancer.org/cancer/prostatecancer/moreinformation/prostatecancerearlydetection/index. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Prostate cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/prostate-cancer-screening. Accessed June 1, 2016.
- Essink-Bot ML, de Koning HJ, Nijs HG, Kirkels WJ, van der Maas PJ, Schröder FH. Short-term effects of population-based screening for prostate cancer on health-related quality of life. J Natl Cancer Inst 1998; 90:925–931.
- Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smoking, smoking cessation, and lung cancer in the UK since 1950: combination of national statistics with two case-control studies. BMJ (Clin Res Ed) 2000; 321:323–329.
- Chute CG, Greenberg ER, Baron J, Korson R, Baker J, Yates J. Presenting conditions of 1,539 population-based lung cancer patients by cell type and stage in New Hampshire and Vermont. Cancer 1985; 56:2107–2111.
- Ramadan HH, Wax MK, Avery S. Outcome and changing cause of unilateral vocal cord paralysis. Otolaryngol Head Neck Surg 1998;118:199–202.
- Church TR, Black WC, Aberle DR, et al. Results of initial low-dose computed tomographic screening for lung cancer. N Engl J Med 2013; 368:1980–1991.
- American Cancer Society. Lung cancer prevention and early detection. www.cancer.org/cancer/lungcancer-non-smallcell/moreinformation/lungcancerpreventionandearlydetection/index. Accessed May 17, 2016.
- Lung Cancer Screening. National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology. www.nccn.org/professionals/physician_gls/pdf/lung_screening.pdf. Accessed May 17, 2016.
- US Preventive Services Task Force (USPSTF). Lung cancer: screening. www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/lung-cancer-screening. Accessed May 17, 2016.
- National Cancer Institute (NIH). Surveillance, Epidemiology, and End Results (SEER) Program. SEER Cancer Statistics Review: 1973-1994. http://seer.cancer.gov/archive/csr/1973_1994/. Accessed May 17, 2016.
- Mauch PM, Kalish LA, Kadin M, Coleman CN, Osteen R, Hellman S. Patterns of presentation of Hodgkin disease. Implications for etiology and pathogenesis. Cancer 1993; 71:2062–2071.
- Gobbi PG, Cavalli C, Gendarini A, et al. Reevaluation of prognostic significance of symptoms in Hodgkin’s disease. Cancer 1985; 56:2874–2880.
- Einhorn LH. Treatment of testicular cancer: a new and improved model. J Clin Oncol 1990; 8:1777–1781.
- Tseng A Jr, Horning SJ, Freiha FS, Resser KJ, Hannigan JF Jr, Torti FM. Gynecomastia in testicular cancer patients. Prognostic and therapeutic implications. Cancer 1985; 56:2534–2538.
- Gilligan TD, Seidenfeld J, Basch EM, et al; American Society of Clinical Oncology. American Society of Clinical Oncology clinical practice guideline on uses of serum tumor markers in adult males with germ cell tumors. J Clin Oncol 2010; 28:3388–3404.
- Brydøy M, Fosså SD, Klepp O, et al. Paternity following treatment for testicular cancer. J Natl Cancer Inst 2005; 97:1580–1588.
KEY POINTS
- By detecting breast cancer lesions 2 years before they are discovered by clinical breast examination, mammography has been found to reduce the mortality rate from breast cancer.
- In the United States, 20% of colorectal cancer patients have distant metastases at the time of diagnosis. The most common sites are the lymph nodes, liver, lungs, and peritoneum.
- The patient should fully understand the risks and benefits of prostate-specific antigen (PSA) screening and that it is controversial because, since the advent of PSA testing, the lifetime risk of being diagnosed with prostate cancer has increased, but the lifetime risk of dying from it has remained the same.
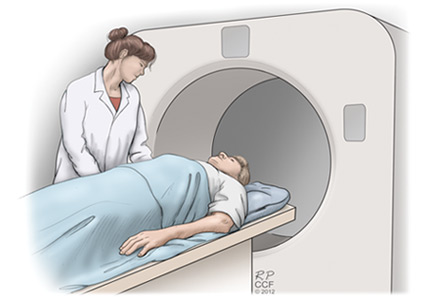
Premature ventricular contractions: Reassure or refer?
Doctor, my heart ______.” Fill in the blank with: skips, flip-flops, hiccups, stops, beats in my throat or chest, or any of the various ways patients describe palpitations. One cannot practice clinical medicine and not see patients with some variation of this chief complaint.1–3 Not every patient who complains of palpitations will be found to have premature ventricular contractions (PVCs), but PVCs are often part of the clinical problem.
This review focuses on the initial evaluation and management of PVCs in the primary care setting (Figure 1). It is not intended to be a comprehensive review of the pathophysiology, electrophysiology, or localization and ablation of PVCs. We will discuss approaches to the initial therapy of symptomatic PVCs. We will not discuss catheter-based therapy in detail except for which patients might benefit from referral to a clinical cardiac electrophysiologist.
Findings that should prompt consideration for referral to a specialist (“red flags”) are summarized at the end of each section. The type of specialist depends to a degree on the cardiology practice available to the referring physician. In our practice, such patients are typically seen by an electrophysiologist. In other practices, a general cardiologist might see such patients initially.
INITIAL EVALUATION
A primary concern of any patient presenting with a new symptom is whether the symptom is a marker of serious risk to health or life. In a patient with palpitations, the answer depends in large part on whether he or she has underlying structural heart disease—and that is the focus of the initial evaluation.
History: Information to ascertain
- When did the patient first notice the palpitations?
- Had there been any significant life events, either illness or emotional stress, at the time the palpitations began?
- Does the patient have a known history of heart disease (myocardial infarction, heart surgery, valvular heart disease, heart failure)?
- What medications is the patient taking?
- Does the patient take any dietary or health supplements? Ask specifically about any supplements taken to help with weight loss or increase energy levels. Almost all of them contain caffeine or other “natural” sympathomimetic agents. Also ask specifically about illicit drug use. If the patient is accompanied by a parent or partner, this question can be challenging.
- When do the palpitations occur? At random? At rest? With exercise? Time of day? In relation to the menstrual cycle? (More about this later.)
- Does anything make the palpitations better? If they occur at rest, does activity make them better or worse?
- Are there symptoms of heart failure, such as dyspnea on exertion, early fatigue, decline in exercise or exertional capacity, orthopnea, or paroxysmal nocturnal dyspnea?
- Are there symptoms suggesting cardiac ischemia, such as substernal chest pain or discomfort, chest pain or discomfort brought on by or made worse by exertion, or chest pain relieved with rest or sublingual nitroglycerin?
- Have the palpitations ever been associated with syncope? Keep in mind that syncope is transient loss of consciousness that spontaneously resolves with no features to suggest seizures.4 Thus, a patient who reports he or she “blacks out” with the palpitations but never falls or slumps has not had loss of consciousness and therefore has not had syncope.5
- Is there any history of unexplained death in the family, especially in younger people? Is there a history of unexplained accidental death in young family members?
Red flags obtained from the history
- Syncope related to palpitations
- Palpitations triggered by activity or exertion
- Known significant heart disease, congenital heart disease, or history of heart surgery
- Family history of premature unexplained sudden death in a first-degree relative.
Physical examination
The physical examination should focus on detecting any signs of underlying heart or vascular disease, eg:
- Significant murmurs
- Abnormal S3 or S4
- Displaced and diffuse point of maximal impulse or precordial heave
- Signs of right or left heart failure, or both, eg, peripheral edema, elevation of jugular venous pulse, rales, S3, S4.
Electrocardiography
We consider 12-lead electrocardiography (ECG) a part of the initial examination and assessment, not an ancillary test. One cannot evaluate a patient’s complaint of palpitations without ECG. Ideally, ECG should include a long 12-lead rhythm strip. The clinician should look for any evidence of underlying structural heart disease, eg:
- Pathologic Q waves
- Long QT interval
- ST-segment elevation in leads V1 and V2 consistent with a Brugada pattern
- Epsilon waves (seen in right ventricular arrhythmogenic cardiomyopathy).
Examples of the above can be found at sites such as ecgpedia.org.
Red flags in the physical examination and ECG
Any of the above findings on physical examination or ECG should prompt consideration of early referral, even though we have yet to establish that the palpitations are due to PVCs. Early consultation is suggested not for treatment of the palpitations but for further evaluation of structural heart disease.
Assuming the history, physical examination, and electrocardiography do not demonstrate any reasons for early cardiology or electrophysiology consultation, what’s next?
FURTHER EVALUATION: EXTENDED MONITORING
With luck, the patient’s typical palpitations will occur during ECG, in which case the palpitations can reasonably be attributed to PVCs. If not, monitoring is required to establish the cause of the patient’s symptoms.
The type of monitoring to order depends on the frequency of the palpitations. If the patient reports several episodes per day, then a 24- or 48-hour Holter monitor should both allow for a diagnosis and document the PVC burden (ie, the percent of the patient’s heartbeats that are PVCs), or the burden of whatever is the cause of the patient’s palpitations.
If the palpitations are less frequent, a 14-to-30-day monitor should be considered. A standard event recorder can confirm that the palpitations are due to PVCs but does not tell you the PVC burden. For that, a system capable of mobile outpatient cardiac telemetry is needed. Several such systems are commercially available.
A Holter monitor or other monitoring system is useful in determining whether the PVCs are unifocal (all look the same) or multifocal (have more than one morphology) and whether, in addition to PVCs, the patient has nonsustained ventricular tachycardia or sustained ventricular tachycardia (by definition lasting longer than 30 seconds or associated with symptoms of hemodynamic compromise such as near-syncope). Even if the patient has nonsustained ventricular tachycardia, if the heart is structurally normal the prognosis remains excellent.
Given the importance of knowing whether the patient has structural heart disease, we have a low threshold for ordering echocardiography, especially if nonsustained ventricular tachycardia has been documented. The finding of significant systolic dysfunction on echocardiography should prompt a cardiology consultation even if the physical examination is normal. In patients who have a high PVC burden, echocardiography is used to monitor for arrhythmia-induced cardiomyopathy.6
If the patient’s symptoms occur with activity, an exercise study can be helpful. It is important to either supervise the study oneself or, at the least, alert the exercise laboratory staff that the study is being performed to evaluate for exercise-induced arrhythmias. If the exercise study induces sustained ventricular tachycardia, the patient is almost invariably admitted to the hospital and inpatient consultation with an electrophysiologist is obtained.
Red flags on extended monitoring
- Multifocal PVCs or nonsustained ventricular tachycardia
- Polymorphic nonsustained ventricular tachycardia
- Sustained ventricular tachycardia; this still may be idiopathic and have a benign prognosis but generally should prompt referral.
If at this point no red flags have been uncovered, monitoring has established the patient’s symptoms are due to PVCs, and our examination and ancillary testing have established the patient has a structurally normal heart, what is the next step?
IDIOPATHIC PVCs
PVCs in a patient with a structurally normal heart are called “idiopathic.” Often, these patients will also be found to have nonsustained ventricular tachycardia, and may also be classified as having “idiopathic ventricular tachycardia.” Regardless of whether the patient has PVCs, nonsustained ventricular tachycardia, or both, the management approach is the same.
Roughly 60% to 80% of idiopathic PVCs originate from the right ventricle, in particular the right ventricular outflow tract.7 Patients with outflow tract PVCs typically present between the ages of 30 and 50 but range from adolescents to elders. More women than men are affected.
Outflow tract PVCs often occur only, or at much greater frequency, within a range of heart rates.8 Individual patients may have different ranges of heart rates at which their PVCs are more frequent. Patients may complain that their palpitations are more frequent at rest, early in exercise, at a peak of exercise, or early in recovery from exercise. It is not unusual for patients with outflow tract PVCs to report that activity reduces the frequency of their palpitations. Women might note an increase in their symptoms during menstruation.9 It is not clear, however, that this perceived increase in palpitations is in fact due to an increase in the number of PVCs.10
If the patient’s PVCs have not been captured on 12-lead ECG (ie, if it is not seen in all 12 leads), 12-lead Holter monitoring, if available, can be helpful. Examination of the morphology of the PVC on 12-lead ECG is extremely helpful. Outflow tract PVCs are the most common cause of idiopathic PVCs and nonsustained ventricular tachycardia and are easily recognizable with 12-lead ECG.
ECG points to the origin of the PVCs
A PVC arising on the right side of the heart will activate the right ventricle first and then the left ventricle. This is analogous to the sequence of ventricular activation in a patient with left bundle-branch block. Not surprisingly, on ECG a right-sided PVC looks similar to the QRS complex seen in left bundle-branch block—similar, but not identical.
When describing PVCs or the morphology of nonsustained ventricular tachycardia, the terms “left bundle-branch block pattern” and “right bundle-branch block pattern” refer to lead V1. If the PVC is negative (or mostly negative) in V1, the PVC has a left bundle-branch block pattern. A PVC that is positive in V1 is said to have a right bundle-branch block pattern and by implication arises from the left side of the heart.
A PVC originating from the top of the heart will move from top to bottom. The electrical axis of the PVC will be directed inferiorly. This means the PVC will be strongly positive in the inferior leads, ie, II, aVF, and III.
The electrocardiogram shown in Figure 2 demonstrates the typical appearance of a right ventricular outflow tract PVC.
If the PVC arises from the left ventricular outflow tract, the axis will still be inferiorly directed. However, the further to the left the origin of the PVC, the earlier the precordial transition will occur (the point at which the PVC is more positive than negative in the precordial leads). A PVC origin far enough to the left will result in a right bundle-branch block pattern PVC.
Not all idiopathic PVCs arise from the outflow tracts. A right bundle branch block pattern PVC does not imply the presence of underlying structural heart disease. PVCs may arise from both the tricuspid and mitral valve annuli, the left ventricular fascicles, or from the epicardium.
Multiple methods have been proposed to locate the origin of the PVC. For example, Park et al reviewed the use of surface ECG in locating the site of origin of ventricular tachycardia.11 All such algorithms should be applied with care, and with awareness of the caveats associated with their use.
Arrhythmogenic right ventricular cardiomyopathy is not benign
Arrhythmogenic right ventricular cardiomyopathy may give rise to PVCs or nonsustained ventricular tachycardia with morphologies similar to those of right ventricular outflow tract PVCs and ventricular tachycardia. The ventricular tachycardia complicating arrhythmogenic cardiomyopathy is, like PVCs arising from the right ventricular outflow tract, commonly associated with exercise or activity.
Unlike right ventricular outflow tract tachycardia, ventricular tachycardia related to arrhythmogenic cardiomyopathy is not benign.12 Distinguishing right ventricular outflow tract tachycardia from tachycardia secondary to arrhythmogenic cardiomyopathy is therefore critical.
Good-quality ECG demonstrating normal right ventricular size and function is reassuring, and if echocardiography is not conclusive, cardiovascular magnetic resonance imaging may provide additional diagnostic and prognostic data, especially when arrhythmogenic cardiomyopathy, cardiac sarcoidosis, or cardiac amyloidosis is suspected.6
Recently, magnetic resonance imaging has been used most for infiltrative diseases as the imaging modality of choice due to its superior tissue characterization and noninvasive morphological and functional evaluation. Magnetic resonance imaging findings in patients with arrhythmogenic cardiomyopathy correlate well with those of endomyocardial biopsy, angiography, and echocardiography and have been associated with incremental arrhythmic risk in the setting of electrical abnormalities. The increasing use of magnetic resonance imaging is leading to the recognition that left ventricular involvement (left-dominant arrhythmogenic right ventricular cardiomyopathy) is more common than previously recognized, with some suggesting that arrhythmogenic right ventricular cardiomyopathy should be simply called “arrhythmogenic cardiomyopathy.”
Although endomyocardial biopsy can establish the diagnosis of arrhythmogenic right ventricular cardiomyopathy, it is rarely performed because it has a high false-negative rate owing to the patchy, epicardial nature of this disorder.13
Red flags for cardiomyopathy
- Multifocal PVCs, or nonsustained ventricular tachycardia of more than one morphology on monitoring
- Syncope associated with active exercise
- Abnormal imaging findings that are consistent with arrhythmogenic right ventricular cardiomyopathy, cardiac sarcoidosis, or amyloidosis.
WHEN TO TREAT IDIOPATHIC PVCs
In our practice we explain to patients that there are two primary indications for treating idiopathic PVCs: (1) to relieve symptoms or (2) in asymptomatic patients with presumed arrhythmia-induced cardiomyopathy, to try to reverse the cardiomyopathy by eliminating the PVCs.
Some patients report severe symptoms due to their PVCs. Other patients appear to have no symptoms whatsoever, while still others are not overly bothered by the PVCs but are concerned that they may indicate they are at increased risk of cardiac events. In this last group, an evaluation such as outlined above that discloses no evidence of structural heart disease and reassurance by the physician may be all the treatment needed.
Even if they have no symptoms or only minimal symptoms, patients with a high PVC burden require follow-up because of the association between frequent PVCs and arrhythmia-induced cardiomyopathy.14,15 What constitutes a “high” PVC burden remains a matter of debate. Left ventricular dysfunction has generally been reported at PVC burdens above 15% to 25% of the total cardiac beats, though this percentage can be as low as 10%.14
Eliminating the high burden of PVCs in patients with left ventricular dysfunction may significantly improve left ventricular systolic function.15 It is likely, however, that more than PVC burden alone contributes to the development of the cardiomyopathy.14
Given these complexities, it is reasonable to request an electrophysiology consultation for patients who have more than rare PVCs. What is rare? There is no defined standard, but a PVC burden less than 1% is reasonable.
Treatment of the PVCs may be indicated in patients with systolic heart failure receiving cardiac resynchronization therapy, ie, a biventricular pacemaker. For cardiac resynchronization therapy to be clinically beneficial, close to 100% of heartbeats need to be paced, and frequent PVCs, even at a burden less than 10%, may undermine its effectiveness.16
HOW TO INTERVENE?
Beta-blockers and nondihydropyridine calcium channel blockers have both been used to treat symptomatic PVCs. If the patient is found to have systolic dysfunction as part of the evaluation, a beta-blocker is indicated, irrespective of any desire to treat the PVCs. Beta-blockers and calcium channel blockers both have low adverse effect profiles. They are available in once-a-day formulations and are inexpensive. Their efficacy is variable. The use of these medications is well within the purview of the primary care physician.
Selective beta-blockers are the first choice in treatment, and metoprolol is commonly used in clinical practice. We start with a low dose and increase it based on symptom relief.
As noted, only nondihydropyridine calcium channel blockers should be used for treatment of PVCs. As with beta-blockers, we start at a low dose and increase as needed based on the response to therapy.
Antiarrhythymic drugs are classified according to the Vaughan-Williams system. The ones most frequently used for PVCs are the class Ic drugs propafenone and flecainide and the class III drugs sotalol, amiodarone, and dofetalide. However, in our experience, if first-line agents (ie, beta-blockers and nondihydropyridine calcium channel blockers) are unsuccessful in controlling the patient’s symptoms, most primary care physicians are uncomfortable prescribing class Ic and class III drugs. Failure of a beta-blocker, a calcium channel blocker, or both often results in referral to a cardiologist or electrophysiologist.
The consultation should include a careful discussion with the patient regarding the risk of treatment with a type I or a type III drug vs catheter ablation. Treatment with class I or class III antiarrhythmic drugs always entails a small risk of proarrhythmia. The choice between drug therapy or ablation therapy is highly individualized. However, if elimination of the PVCs is of paramount importance, such as in cases of arrhythmia-induced cardiomyopathy, ablation therapy is more effective at eliminating the PVCs, although at the cost of an invasive procedure. Fortunately, the risk of complications with ablation therapy is quite low.
No drugs are approved by the US Food and Drug Administration for treating PVCs or nonsustained ventricular tachycardia. The drugs that do have an indication for treatment of ventricular arrhythmias are labeled as being indicated for “sustained” or “life-threatening” ventricular arrhythmias. The use of drugs for the treatment of PVCs or nonsustained ventricular tachycardia represents off-label usage.
Referral to discuss catheter ablation of the PVCs6 should be considered for patients who:
- Have undergone unsuccessful attempts at drug therapy for either symptoms or PVC-related cardiomyopathy
- Refuse drug therapy but have severe symptoms, or
- Do not respond to cardiac resynchronization therapy due to suboptimal pacing due to PVCs.
- Kennedy HL, Underhill SJ. Frequent or complex ventricular ectopy in apparently healthy subjects: a clinical study of 25 cases. Am J Cardiol 1976; 38:141–148.
- Brodsky M, Wu D, Denes P, Kanakis C, Rosen KM. Arrhythmias documented by 24 hour continuous electrocardiographic monitoring in 50 male medical students without apparent heart disease. Am J Cardiol 1977; 39:390–395.
- Sobotka PA, Mayer JH, Bauernfeind RA, Kanakis C Jr, Rosen KM. Arrhythmias documented by 24-hour continuous ambulatory electrocardiographic monitoring in young women without apparent heart disease. Am Heart J 1981; 101:753–759.
- Sheldon RS, Grubb BP 2nd, Olshansky B, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm 2015;12:e41–e63.
- Benditt DG, Adkisson WO. Approach to the patient with syncope: venues, presentations, diagnoses. Cardiol Clin 2013; 31:9–25.
- Pedersen CT, Kay GN, Kalman J, et al. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm 2014; 11:e166–e196.
- Iwai S, Cantillon DJ, Kim RJ, et al. Right and left ventricular outflow tract tachycardias: evidence for a common electrophysiologic mechanism. Cardiovasc Electrophysiol 2006; 17:1052–1058.
- Buxton AE, Waxman HL, Marchlinski FE, Simson MB, Cassidy D, Josephson ME. Right ventricular tachycardia: clinical and electrophysiologic characteristics. Circulation 1983; 68:917–927.
- Marchlinski FE, Deely MP, Zado ES. Sex-specific triggers for right ventricular outflow tract tachycardia. Am Heart J 2000; 139:1009–1013.
- Fuenmayor AJ, Araujo X, Fuenmayor AM. Cardiac arrhythmias during two different stages of the menstrual cycle. Int J Cardiol 1998; 63:267–270.
- Park KM, Kim YH, Marchlinski FE. Using the surface electrocardiogram to localize the origin of idiopathic ventricular tachycardia. Pacing Clin Electrophysiol 2012; 35:1516–1527.
- Te Riele AS, Hauer RN. Arrhythmogenic right ventricular dysplasia/cardiomyopathy: clinical challenges in a changing disease spectrum. Trends Cardiovasc Med 2015; 25:191–198.
- Philips B, Cheng A. 2015 update on the diagnosis and management of arrhythmogenic right ventricular cardiomyopathy. Curr Opin Cardiol 2016; 31:46–56.
- Del Carpio Munoz F, Syed FF, Noheria A, et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J Cardiovasc Electrophysiol 2011; 22:791–798.
- Yarlagadda RK, Iwai S, Stein KM, et al. Reversal of cardiomyopathy in patients with repetitive monomorphic ventricular ectopy originating from the right ventricular outflow tract. Circulation 2005; 112:1092–1097.
- Zhang Q, Zhou Y, Yu CM. Incidence, definition, diagnosis, and management of the cardiac resynchronization therapy nonresponder. Curr Opin Cardiol 2015; 30:40–49.
Doctor, my heart ______.” Fill in the blank with: skips, flip-flops, hiccups, stops, beats in my throat or chest, or any of the various ways patients describe palpitations. One cannot practice clinical medicine and not see patients with some variation of this chief complaint.1–3 Not every patient who complains of palpitations will be found to have premature ventricular contractions (PVCs), but PVCs are often part of the clinical problem.
This review focuses on the initial evaluation and management of PVCs in the primary care setting (Figure 1). It is not intended to be a comprehensive review of the pathophysiology, electrophysiology, or localization and ablation of PVCs. We will discuss approaches to the initial therapy of symptomatic PVCs. We will not discuss catheter-based therapy in detail except for which patients might benefit from referral to a clinical cardiac electrophysiologist.
Findings that should prompt consideration for referral to a specialist (“red flags”) are summarized at the end of each section. The type of specialist depends to a degree on the cardiology practice available to the referring physician. In our practice, such patients are typically seen by an electrophysiologist. In other practices, a general cardiologist might see such patients initially.
INITIAL EVALUATION
A primary concern of any patient presenting with a new symptom is whether the symptom is a marker of serious risk to health or life. In a patient with palpitations, the answer depends in large part on whether he or she has underlying structural heart disease—and that is the focus of the initial evaluation.
History: Information to ascertain
- When did the patient first notice the palpitations?
- Had there been any significant life events, either illness or emotional stress, at the time the palpitations began?
- Does the patient have a known history of heart disease (myocardial infarction, heart surgery, valvular heart disease, heart failure)?
- What medications is the patient taking?
- Does the patient take any dietary or health supplements? Ask specifically about any supplements taken to help with weight loss or increase energy levels. Almost all of them contain caffeine or other “natural” sympathomimetic agents. Also ask specifically about illicit drug use. If the patient is accompanied by a parent or partner, this question can be challenging.
- When do the palpitations occur? At random? At rest? With exercise? Time of day? In relation to the menstrual cycle? (More about this later.)
- Does anything make the palpitations better? If they occur at rest, does activity make them better or worse?
- Are there symptoms of heart failure, such as dyspnea on exertion, early fatigue, decline in exercise or exertional capacity, orthopnea, or paroxysmal nocturnal dyspnea?
- Are there symptoms suggesting cardiac ischemia, such as substernal chest pain or discomfort, chest pain or discomfort brought on by or made worse by exertion, or chest pain relieved with rest or sublingual nitroglycerin?
- Have the palpitations ever been associated with syncope? Keep in mind that syncope is transient loss of consciousness that spontaneously resolves with no features to suggest seizures.4 Thus, a patient who reports he or she “blacks out” with the palpitations but never falls or slumps has not had loss of consciousness and therefore has not had syncope.5
- Is there any history of unexplained death in the family, especially in younger people? Is there a history of unexplained accidental death in young family members?
Red flags obtained from the history
- Syncope related to palpitations
- Palpitations triggered by activity or exertion
- Known significant heart disease, congenital heart disease, or history of heart surgery
- Family history of premature unexplained sudden death in a first-degree relative.
Physical examination
The physical examination should focus on detecting any signs of underlying heart or vascular disease, eg:
- Significant murmurs
- Abnormal S3 or S4
- Displaced and diffuse point of maximal impulse or precordial heave
- Signs of right or left heart failure, or both, eg, peripheral edema, elevation of jugular venous pulse, rales, S3, S4.
Electrocardiography
We consider 12-lead electrocardiography (ECG) a part of the initial examination and assessment, not an ancillary test. One cannot evaluate a patient’s complaint of palpitations without ECG. Ideally, ECG should include a long 12-lead rhythm strip. The clinician should look for any evidence of underlying structural heart disease, eg:
- Pathologic Q waves
- Long QT interval
- ST-segment elevation in leads V1 and V2 consistent with a Brugada pattern
- Epsilon waves (seen in right ventricular arrhythmogenic cardiomyopathy).
Examples of the above can be found at sites such as ecgpedia.org.
Red flags in the physical examination and ECG
Any of the above findings on physical examination or ECG should prompt consideration of early referral, even though we have yet to establish that the palpitations are due to PVCs. Early consultation is suggested not for treatment of the palpitations but for further evaluation of structural heart disease.
Assuming the history, physical examination, and electrocardiography do not demonstrate any reasons for early cardiology or electrophysiology consultation, what’s next?
FURTHER EVALUATION: EXTENDED MONITORING
With luck, the patient’s typical palpitations will occur during ECG, in which case the palpitations can reasonably be attributed to PVCs. If not, monitoring is required to establish the cause of the patient’s symptoms.
The type of monitoring to order depends on the frequency of the palpitations. If the patient reports several episodes per day, then a 24- or 48-hour Holter monitor should both allow for a diagnosis and document the PVC burden (ie, the percent of the patient’s heartbeats that are PVCs), or the burden of whatever is the cause of the patient’s palpitations.
If the palpitations are less frequent, a 14-to-30-day monitor should be considered. A standard event recorder can confirm that the palpitations are due to PVCs but does not tell you the PVC burden. For that, a system capable of mobile outpatient cardiac telemetry is needed. Several such systems are commercially available.
A Holter monitor or other monitoring system is useful in determining whether the PVCs are unifocal (all look the same) or multifocal (have more than one morphology) and whether, in addition to PVCs, the patient has nonsustained ventricular tachycardia or sustained ventricular tachycardia (by definition lasting longer than 30 seconds or associated with symptoms of hemodynamic compromise such as near-syncope). Even if the patient has nonsustained ventricular tachycardia, if the heart is structurally normal the prognosis remains excellent.
Given the importance of knowing whether the patient has structural heart disease, we have a low threshold for ordering echocardiography, especially if nonsustained ventricular tachycardia has been documented. The finding of significant systolic dysfunction on echocardiography should prompt a cardiology consultation even if the physical examination is normal. In patients who have a high PVC burden, echocardiography is used to monitor for arrhythmia-induced cardiomyopathy.6
If the patient’s symptoms occur with activity, an exercise study can be helpful. It is important to either supervise the study oneself or, at the least, alert the exercise laboratory staff that the study is being performed to evaluate for exercise-induced arrhythmias. If the exercise study induces sustained ventricular tachycardia, the patient is almost invariably admitted to the hospital and inpatient consultation with an electrophysiologist is obtained.
Red flags on extended monitoring
- Multifocal PVCs or nonsustained ventricular tachycardia
- Polymorphic nonsustained ventricular tachycardia
- Sustained ventricular tachycardia; this still may be idiopathic and have a benign prognosis but generally should prompt referral.
If at this point no red flags have been uncovered, monitoring has established the patient’s symptoms are due to PVCs, and our examination and ancillary testing have established the patient has a structurally normal heart, what is the next step?
IDIOPATHIC PVCs
PVCs in a patient with a structurally normal heart are called “idiopathic.” Often, these patients will also be found to have nonsustained ventricular tachycardia, and may also be classified as having “idiopathic ventricular tachycardia.” Regardless of whether the patient has PVCs, nonsustained ventricular tachycardia, or both, the management approach is the same.
Roughly 60% to 80% of idiopathic PVCs originate from the right ventricle, in particular the right ventricular outflow tract.7 Patients with outflow tract PVCs typically present between the ages of 30 and 50 but range from adolescents to elders. More women than men are affected.
Outflow tract PVCs often occur only, or at much greater frequency, within a range of heart rates.8 Individual patients may have different ranges of heart rates at which their PVCs are more frequent. Patients may complain that their palpitations are more frequent at rest, early in exercise, at a peak of exercise, or early in recovery from exercise. It is not unusual for patients with outflow tract PVCs to report that activity reduces the frequency of their palpitations. Women might note an increase in their symptoms during menstruation.9 It is not clear, however, that this perceived increase in palpitations is in fact due to an increase in the number of PVCs.10
If the patient’s PVCs have not been captured on 12-lead ECG (ie, if it is not seen in all 12 leads), 12-lead Holter monitoring, if available, can be helpful. Examination of the morphology of the PVC on 12-lead ECG is extremely helpful. Outflow tract PVCs are the most common cause of idiopathic PVCs and nonsustained ventricular tachycardia and are easily recognizable with 12-lead ECG.
ECG points to the origin of the PVCs
A PVC arising on the right side of the heart will activate the right ventricle first and then the left ventricle. This is analogous to the sequence of ventricular activation in a patient with left bundle-branch block. Not surprisingly, on ECG a right-sided PVC looks similar to the QRS complex seen in left bundle-branch block—similar, but not identical.
When describing PVCs or the morphology of nonsustained ventricular tachycardia, the terms “left bundle-branch block pattern” and “right bundle-branch block pattern” refer to lead V1. If the PVC is negative (or mostly negative) in V1, the PVC has a left bundle-branch block pattern. A PVC that is positive in V1 is said to have a right bundle-branch block pattern and by implication arises from the left side of the heart.
A PVC originating from the top of the heart will move from top to bottom. The electrical axis of the PVC will be directed inferiorly. This means the PVC will be strongly positive in the inferior leads, ie, II, aVF, and III.
The electrocardiogram shown in Figure 2 demonstrates the typical appearance of a right ventricular outflow tract PVC.
If the PVC arises from the left ventricular outflow tract, the axis will still be inferiorly directed. However, the further to the left the origin of the PVC, the earlier the precordial transition will occur (the point at which the PVC is more positive than negative in the precordial leads). A PVC origin far enough to the left will result in a right bundle-branch block pattern PVC.
Not all idiopathic PVCs arise from the outflow tracts. A right bundle branch block pattern PVC does not imply the presence of underlying structural heart disease. PVCs may arise from both the tricuspid and mitral valve annuli, the left ventricular fascicles, or from the epicardium.
Multiple methods have been proposed to locate the origin of the PVC. For example, Park et al reviewed the use of surface ECG in locating the site of origin of ventricular tachycardia.11 All such algorithms should be applied with care, and with awareness of the caveats associated with their use.
Arrhythmogenic right ventricular cardiomyopathy is not benign
Arrhythmogenic right ventricular cardiomyopathy may give rise to PVCs or nonsustained ventricular tachycardia with morphologies similar to those of right ventricular outflow tract PVCs and ventricular tachycardia. The ventricular tachycardia complicating arrhythmogenic cardiomyopathy is, like PVCs arising from the right ventricular outflow tract, commonly associated with exercise or activity.
Unlike right ventricular outflow tract tachycardia, ventricular tachycardia related to arrhythmogenic cardiomyopathy is not benign.12 Distinguishing right ventricular outflow tract tachycardia from tachycardia secondary to arrhythmogenic cardiomyopathy is therefore critical.
Good-quality ECG demonstrating normal right ventricular size and function is reassuring, and if echocardiography is not conclusive, cardiovascular magnetic resonance imaging may provide additional diagnostic and prognostic data, especially when arrhythmogenic cardiomyopathy, cardiac sarcoidosis, or cardiac amyloidosis is suspected.6
Recently, magnetic resonance imaging has been used most for infiltrative diseases as the imaging modality of choice due to its superior tissue characterization and noninvasive morphological and functional evaluation. Magnetic resonance imaging findings in patients with arrhythmogenic cardiomyopathy correlate well with those of endomyocardial biopsy, angiography, and echocardiography and have been associated with incremental arrhythmic risk in the setting of electrical abnormalities. The increasing use of magnetic resonance imaging is leading to the recognition that left ventricular involvement (left-dominant arrhythmogenic right ventricular cardiomyopathy) is more common than previously recognized, with some suggesting that arrhythmogenic right ventricular cardiomyopathy should be simply called “arrhythmogenic cardiomyopathy.”
Although endomyocardial biopsy can establish the diagnosis of arrhythmogenic right ventricular cardiomyopathy, it is rarely performed because it has a high false-negative rate owing to the patchy, epicardial nature of this disorder.13
Red flags for cardiomyopathy
- Multifocal PVCs, or nonsustained ventricular tachycardia of more than one morphology on monitoring
- Syncope associated with active exercise
- Abnormal imaging findings that are consistent with arrhythmogenic right ventricular cardiomyopathy, cardiac sarcoidosis, or amyloidosis.
WHEN TO TREAT IDIOPATHIC PVCs
In our practice we explain to patients that there are two primary indications for treating idiopathic PVCs: (1) to relieve symptoms or (2) in asymptomatic patients with presumed arrhythmia-induced cardiomyopathy, to try to reverse the cardiomyopathy by eliminating the PVCs.
Some patients report severe symptoms due to their PVCs. Other patients appear to have no symptoms whatsoever, while still others are not overly bothered by the PVCs but are concerned that they may indicate they are at increased risk of cardiac events. In this last group, an evaluation such as outlined above that discloses no evidence of structural heart disease and reassurance by the physician may be all the treatment needed.
Even if they have no symptoms or only minimal symptoms, patients with a high PVC burden require follow-up because of the association between frequent PVCs and arrhythmia-induced cardiomyopathy.14,15 What constitutes a “high” PVC burden remains a matter of debate. Left ventricular dysfunction has generally been reported at PVC burdens above 15% to 25% of the total cardiac beats, though this percentage can be as low as 10%.14
Eliminating the high burden of PVCs in patients with left ventricular dysfunction may significantly improve left ventricular systolic function.15 It is likely, however, that more than PVC burden alone contributes to the development of the cardiomyopathy.14
Given these complexities, it is reasonable to request an electrophysiology consultation for patients who have more than rare PVCs. What is rare? There is no defined standard, but a PVC burden less than 1% is reasonable.
Treatment of the PVCs may be indicated in patients with systolic heart failure receiving cardiac resynchronization therapy, ie, a biventricular pacemaker. For cardiac resynchronization therapy to be clinically beneficial, close to 100% of heartbeats need to be paced, and frequent PVCs, even at a burden less than 10%, may undermine its effectiveness.16
HOW TO INTERVENE?
Beta-blockers and nondihydropyridine calcium channel blockers have both been used to treat symptomatic PVCs. If the patient is found to have systolic dysfunction as part of the evaluation, a beta-blocker is indicated, irrespective of any desire to treat the PVCs. Beta-blockers and calcium channel blockers both have low adverse effect profiles. They are available in once-a-day formulations and are inexpensive. Their efficacy is variable. The use of these medications is well within the purview of the primary care physician.
Selective beta-blockers are the first choice in treatment, and metoprolol is commonly used in clinical practice. We start with a low dose and increase it based on symptom relief.
As noted, only nondihydropyridine calcium channel blockers should be used for treatment of PVCs. As with beta-blockers, we start at a low dose and increase as needed based on the response to therapy.
Antiarrhythymic drugs are classified according to the Vaughan-Williams system. The ones most frequently used for PVCs are the class Ic drugs propafenone and flecainide and the class III drugs sotalol, amiodarone, and dofetalide. However, in our experience, if first-line agents (ie, beta-blockers and nondihydropyridine calcium channel blockers) are unsuccessful in controlling the patient’s symptoms, most primary care physicians are uncomfortable prescribing class Ic and class III drugs. Failure of a beta-blocker, a calcium channel blocker, or both often results in referral to a cardiologist or electrophysiologist.
The consultation should include a careful discussion with the patient regarding the risk of treatment with a type I or a type III drug vs catheter ablation. Treatment with class I or class III antiarrhythmic drugs always entails a small risk of proarrhythmia. The choice between drug therapy or ablation therapy is highly individualized. However, if elimination of the PVCs is of paramount importance, such as in cases of arrhythmia-induced cardiomyopathy, ablation therapy is more effective at eliminating the PVCs, although at the cost of an invasive procedure. Fortunately, the risk of complications with ablation therapy is quite low.
No drugs are approved by the US Food and Drug Administration for treating PVCs or nonsustained ventricular tachycardia. The drugs that do have an indication for treatment of ventricular arrhythmias are labeled as being indicated for “sustained” or “life-threatening” ventricular arrhythmias. The use of drugs for the treatment of PVCs or nonsustained ventricular tachycardia represents off-label usage.
Referral to discuss catheter ablation of the PVCs6 should be considered for patients who:
- Have undergone unsuccessful attempts at drug therapy for either symptoms or PVC-related cardiomyopathy
- Refuse drug therapy but have severe symptoms, or
- Do not respond to cardiac resynchronization therapy due to suboptimal pacing due to PVCs.
Doctor, my heart ______.” Fill in the blank with: skips, flip-flops, hiccups, stops, beats in my throat or chest, or any of the various ways patients describe palpitations. One cannot practice clinical medicine and not see patients with some variation of this chief complaint.1–3 Not every patient who complains of palpitations will be found to have premature ventricular contractions (PVCs), but PVCs are often part of the clinical problem.
This review focuses on the initial evaluation and management of PVCs in the primary care setting (Figure 1). It is not intended to be a comprehensive review of the pathophysiology, electrophysiology, or localization and ablation of PVCs. We will discuss approaches to the initial therapy of symptomatic PVCs. We will not discuss catheter-based therapy in detail except for which patients might benefit from referral to a clinical cardiac electrophysiologist.
Findings that should prompt consideration for referral to a specialist (“red flags”) are summarized at the end of each section. The type of specialist depends to a degree on the cardiology practice available to the referring physician. In our practice, such patients are typically seen by an electrophysiologist. In other practices, a general cardiologist might see such patients initially.
INITIAL EVALUATION
A primary concern of any patient presenting with a new symptom is whether the symptom is a marker of serious risk to health or life. In a patient with palpitations, the answer depends in large part on whether he or she has underlying structural heart disease—and that is the focus of the initial evaluation.
History: Information to ascertain
- When did the patient first notice the palpitations?
- Had there been any significant life events, either illness or emotional stress, at the time the palpitations began?
- Does the patient have a known history of heart disease (myocardial infarction, heart surgery, valvular heart disease, heart failure)?
- What medications is the patient taking?
- Does the patient take any dietary or health supplements? Ask specifically about any supplements taken to help with weight loss or increase energy levels. Almost all of them contain caffeine or other “natural” sympathomimetic agents. Also ask specifically about illicit drug use. If the patient is accompanied by a parent or partner, this question can be challenging.
- When do the palpitations occur? At random? At rest? With exercise? Time of day? In relation to the menstrual cycle? (More about this later.)
- Does anything make the palpitations better? If they occur at rest, does activity make them better or worse?
- Are there symptoms of heart failure, such as dyspnea on exertion, early fatigue, decline in exercise or exertional capacity, orthopnea, or paroxysmal nocturnal dyspnea?
- Are there symptoms suggesting cardiac ischemia, such as substernal chest pain or discomfort, chest pain or discomfort brought on by or made worse by exertion, or chest pain relieved with rest or sublingual nitroglycerin?
- Have the palpitations ever been associated with syncope? Keep in mind that syncope is transient loss of consciousness that spontaneously resolves with no features to suggest seizures.4 Thus, a patient who reports he or she “blacks out” with the palpitations but never falls or slumps has not had loss of consciousness and therefore has not had syncope.5
- Is there any history of unexplained death in the family, especially in younger people? Is there a history of unexplained accidental death in young family members?
Red flags obtained from the history
- Syncope related to palpitations
- Palpitations triggered by activity or exertion
- Known significant heart disease, congenital heart disease, or history of heart surgery
- Family history of premature unexplained sudden death in a first-degree relative.
Physical examination
The physical examination should focus on detecting any signs of underlying heart or vascular disease, eg:
- Significant murmurs
- Abnormal S3 or S4
- Displaced and diffuse point of maximal impulse or precordial heave
- Signs of right or left heart failure, or both, eg, peripheral edema, elevation of jugular venous pulse, rales, S3, S4.
Electrocardiography
We consider 12-lead electrocardiography (ECG) a part of the initial examination and assessment, not an ancillary test. One cannot evaluate a patient’s complaint of palpitations without ECG. Ideally, ECG should include a long 12-lead rhythm strip. The clinician should look for any evidence of underlying structural heart disease, eg:
- Pathologic Q waves
- Long QT interval
- ST-segment elevation in leads V1 and V2 consistent with a Brugada pattern
- Epsilon waves (seen in right ventricular arrhythmogenic cardiomyopathy).
Examples of the above can be found at sites such as ecgpedia.org.
Red flags in the physical examination and ECG
Any of the above findings on physical examination or ECG should prompt consideration of early referral, even though we have yet to establish that the palpitations are due to PVCs. Early consultation is suggested not for treatment of the palpitations but for further evaluation of structural heart disease.
Assuming the history, physical examination, and electrocardiography do not demonstrate any reasons for early cardiology or electrophysiology consultation, what’s next?
FURTHER EVALUATION: EXTENDED MONITORING
With luck, the patient’s typical palpitations will occur during ECG, in which case the palpitations can reasonably be attributed to PVCs. If not, monitoring is required to establish the cause of the patient’s symptoms.
The type of monitoring to order depends on the frequency of the palpitations. If the patient reports several episodes per day, then a 24- or 48-hour Holter monitor should both allow for a diagnosis and document the PVC burden (ie, the percent of the patient’s heartbeats that are PVCs), or the burden of whatever is the cause of the patient’s palpitations.
If the palpitations are less frequent, a 14-to-30-day monitor should be considered. A standard event recorder can confirm that the palpitations are due to PVCs but does not tell you the PVC burden. For that, a system capable of mobile outpatient cardiac telemetry is needed. Several such systems are commercially available.
A Holter monitor or other monitoring system is useful in determining whether the PVCs are unifocal (all look the same) or multifocal (have more than one morphology) and whether, in addition to PVCs, the patient has nonsustained ventricular tachycardia or sustained ventricular tachycardia (by definition lasting longer than 30 seconds or associated with symptoms of hemodynamic compromise such as near-syncope). Even if the patient has nonsustained ventricular tachycardia, if the heart is structurally normal the prognosis remains excellent.
Given the importance of knowing whether the patient has structural heart disease, we have a low threshold for ordering echocardiography, especially if nonsustained ventricular tachycardia has been documented. The finding of significant systolic dysfunction on echocardiography should prompt a cardiology consultation even if the physical examination is normal. In patients who have a high PVC burden, echocardiography is used to monitor for arrhythmia-induced cardiomyopathy.6
If the patient’s symptoms occur with activity, an exercise study can be helpful. It is important to either supervise the study oneself or, at the least, alert the exercise laboratory staff that the study is being performed to evaluate for exercise-induced arrhythmias. If the exercise study induces sustained ventricular tachycardia, the patient is almost invariably admitted to the hospital and inpatient consultation with an electrophysiologist is obtained.
Red flags on extended monitoring
- Multifocal PVCs or nonsustained ventricular tachycardia
- Polymorphic nonsustained ventricular tachycardia
- Sustained ventricular tachycardia; this still may be idiopathic and have a benign prognosis but generally should prompt referral.
If at this point no red flags have been uncovered, monitoring has established the patient’s symptoms are due to PVCs, and our examination and ancillary testing have established the patient has a structurally normal heart, what is the next step?
IDIOPATHIC PVCs
PVCs in a patient with a structurally normal heart are called “idiopathic.” Often, these patients will also be found to have nonsustained ventricular tachycardia, and may also be classified as having “idiopathic ventricular tachycardia.” Regardless of whether the patient has PVCs, nonsustained ventricular tachycardia, or both, the management approach is the same.
Roughly 60% to 80% of idiopathic PVCs originate from the right ventricle, in particular the right ventricular outflow tract.7 Patients with outflow tract PVCs typically present between the ages of 30 and 50 but range from adolescents to elders. More women than men are affected.
Outflow tract PVCs often occur only, or at much greater frequency, within a range of heart rates.8 Individual patients may have different ranges of heart rates at which their PVCs are more frequent. Patients may complain that their palpitations are more frequent at rest, early in exercise, at a peak of exercise, or early in recovery from exercise. It is not unusual for patients with outflow tract PVCs to report that activity reduces the frequency of their palpitations. Women might note an increase in their symptoms during menstruation.9 It is not clear, however, that this perceived increase in palpitations is in fact due to an increase in the number of PVCs.10
If the patient’s PVCs have not been captured on 12-lead ECG (ie, if it is not seen in all 12 leads), 12-lead Holter monitoring, if available, can be helpful. Examination of the morphology of the PVC on 12-lead ECG is extremely helpful. Outflow tract PVCs are the most common cause of idiopathic PVCs and nonsustained ventricular tachycardia and are easily recognizable with 12-lead ECG.
ECG points to the origin of the PVCs
A PVC arising on the right side of the heart will activate the right ventricle first and then the left ventricle. This is analogous to the sequence of ventricular activation in a patient with left bundle-branch block. Not surprisingly, on ECG a right-sided PVC looks similar to the QRS complex seen in left bundle-branch block—similar, but not identical.
When describing PVCs or the morphology of nonsustained ventricular tachycardia, the terms “left bundle-branch block pattern” and “right bundle-branch block pattern” refer to lead V1. If the PVC is negative (or mostly negative) in V1, the PVC has a left bundle-branch block pattern. A PVC that is positive in V1 is said to have a right bundle-branch block pattern and by implication arises from the left side of the heart.
A PVC originating from the top of the heart will move from top to bottom. The electrical axis of the PVC will be directed inferiorly. This means the PVC will be strongly positive in the inferior leads, ie, II, aVF, and III.
The electrocardiogram shown in Figure 2 demonstrates the typical appearance of a right ventricular outflow tract PVC.
If the PVC arises from the left ventricular outflow tract, the axis will still be inferiorly directed. However, the further to the left the origin of the PVC, the earlier the precordial transition will occur (the point at which the PVC is more positive than negative in the precordial leads). A PVC origin far enough to the left will result in a right bundle-branch block pattern PVC.
Not all idiopathic PVCs arise from the outflow tracts. A right bundle branch block pattern PVC does not imply the presence of underlying structural heart disease. PVCs may arise from both the tricuspid and mitral valve annuli, the left ventricular fascicles, or from the epicardium.
Multiple methods have been proposed to locate the origin of the PVC. For example, Park et al reviewed the use of surface ECG in locating the site of origin of ventricular tachycardia.11 All such algorithms should be applied with care, and with awareness of the caveats associated with their use.
Arrhythmogenic right ventricular cardiomyopathy is not benign
Arrhythmogenic right ventricular cardiomyopathy may give rise to PVCs or nonsustained ventricular tachycardia with morphologies similar to those of right ventricular outflow tract PVCs and ventricular tachycardia. The ventricular tachycardia complicating arrhythmogenic cardiomyopathy is, like PVCs arising from the right ventricular outflow tract, commonly associated with exercise or activity.
Unlike right ventricular outflow tract tachycardia, ventricular tachycardia related to arrhythmogenic cardiomyopathy is not benign.12 Distinguishing right ventricular outflow tract tachycardia from tachycardia secondary to arrhythmogenic cardiomyopathy is therefore critical.
Good-quality ECG demonstrating normal right ventricular size and function is reassuring, and if echocardiography is not conclusive, cardiovascular magnetic resonance imaging may provide additional diagnostic and prognostic data, especially when arrhythmogenic cardiomyopathy, cardiac sarcoidosis, or cardiac amyloidosis is suspected.6
Recently, magnetic resonance imaging has been used most for infiltrative diseases as the imaging modality of choice due to its superior tissue characterization and noninvasive morphological and functional evaluation. Magnetic resonance imaging findings in patients with arrhythmogenic cardiomyopathy correlate well with those of endomyocardial biopsy, angiography, and echocardiography and have been associated with incremental arrhythmic risk in the setting of electrical abnormalities. The increasing use of magnetic resonance imaging is leading to the recognition that left ventricular involvement (left-dominant arrhythmogenic right ventricular cardiomyopathy) is more common than previously recognized, with some suggesting that arrhythmogenic right ventricular cardiomyopathy should be simply called “arrhythmogenic cardiomyopathy.”
Although endomyocardial biopsy can establish the diagnosis of arrhythmogenic right ventricular cardiomyopathy, it is rarely performed because it has a high false-negative rate owing to the patchy, epicardial nature of this disorder.13
Red flags for cardiomyopathy
- Multifocal PVCs, or nonsustained ventricular tachycardia of more than one morphology on monitoring
- Syncope associated with active exercise
- Abnormal imaging findings that are consistent with arrhythmogenic right ventricular cardiomyopathy, cardiac sarcoidosis, or amyloidosis.
WHEN TO TREAT IDIOPATHIC PVCs
In our practice we explain to patients that there are two primary indications for treating idiopathic PVCs: (1) to relieve symptoms or (2) in asymptomatic patients with presumed arrhythmia-induced cardiomyopathy, to try to reverse the cardiomyopathy by eliminating the PVCs.
Some patients report severe symptoms due to their PVCs. Other patients appear to have no symptoms whatsoever, while still others are not overly bothered by the PVCs but are concerned that they may indicate they are at increased risk of cardiac events. In this last group, an evaluation such as outlined above that discloses no evidence of structural heart disease and reassurance by the physician may be all the treatment needed.
Even if they have no symptoms or only minimal symptoms, patients with a high PVC burden require follow-up because of the association between frequent PVCs and arrhythmia-induced cardiomyopathy.14,15 What constitutes a “high” PVC burden remains a matter of debate. Left ventricular dysfunction has generally been reported at PVC burdens above 15% to 25% of the total cardiac beats, though this percentage can be as low as 10%.14
Eliminating the high burden of PVCs in patients with left ventricular dysfunction may significantly improve left ventricular systolic function.15 It is likely, however, that more than PVC burden alone contributes to the development of the cardiomyopathy.14
Given these complexities, it is reasonable to request an electrophysiology consultation for patients who have more than rare PVCs. What is rare? There is no defined standard, but a PVC burden less than 1% is reasonable.
Treatment of the PVCs may be indicated in patients with systolic heart failure receiving cardiac resynchronization therapy, ie, a biventricular pacemaker. For cardiac resynchronization therapy to be clinically beneficial, close to 100% of heartbeats need to be paced, and frequent PVCs, even at a burden less than 10%, may undermine its effectiveness.16
HOW TO INTERVENE?
Beta-blockers and nondihydropyridine calcium channel blockers have both been used to treat symptomatic PVCs. If the patient is found to have systolic dysfunction as part of the evaluation, a beta-blocker is indicated, irrespective of any desire to treat the PVCs. Beta-blockers and calcium channel blockers both have low adverse effect profiles. They are available in once-a-day formulations and are inexpensive. Their efficacy is variable. The use of these medications is well within the purview of the primary care physician.
Selective beta-blockers are the first choice in treatment, and metoprolol is commonly used in clinical practice. We start with a low dose and increase it based on symptom relief.
As noted, only nondihydropyridine calcium channel blockers should be used for treatment of PVCs. As with beta-blockers, we start at a low dose and increase as needed based on the response to therapy.
Antiarrhythymic drugs are classified according to the Vaughan-Williams system. The ones most frequently used for PVCs are the class Ic drugs propafenone and flecainide and the class III drugs sotalol, amiodarone, and dofetalide. However, in our experience, if first-line agents (ie, beta-blockers and nondihydropyridine calcium channel blockers) are unsuccessful in controlling the patient’s symptoms, most primary care physicians are uncomfortable prescribing class Ic and class III drugs. Failure of a beta-blocker, a calcium channel blocker, or both often results in referral to a cardiologist or electrophysiologist.
The consultation should include a careful discussion with the patient regarding the risk of treatment with a type I or a type III drug vs catheter ablation. Treatment with class I or class III antiarrhythmic drugs always entails a small risk of proarrhythmia. The choice between drug therapy or ablation therapy is highly individualized. However, if elimination of the PVCs is of paramount importance, such as in cases of arrhythmia-induced cardiomyopathy, ablation therapy is more effective at eliminating the PVCs, although at the cost of an invasive procedure. Fortunately, the risk of complications with ablation therapy is quite low.
No drugs are approved by the US Food and Drug Administration for treating PVCs or nonsustained ventricular tachycardia. The drugs that do have an indication for treatment of ventricular arrhythmias are labeled as being indicated for “sustained” or “life-threatening” ventricular arrhythmias. The use of drugs for the treatment of PVCs or nonsustained ventricular tachycardia represents off-label usage.
Referral to discuss catheter ablation of the PVCs6 should be considered for patients who:
- Have undergone unsuccessful attempts at drug therapy for either symptoms or PVC-related cardiomyopathy
- Refuse drug therapy but have severe symptoms, or
- Do not respond to cardiac resynchronization therapy due to suboptimal pacing due to PVCs.
- Kennedy HL, Underhill SJ. Frequent or complex ventricular ectopy in apparently healthy subjects: a clinical study of 25 cases. Am J Cardiol 1976; 38:141–148.
- Brodsky M, Wu D, Denes P, Kanakis C, Rosen KM. Arrhythmias documented by 24 hour continuous electrocardiographic monitoring in 50 male medical students without apparent heart disease. Am J Cardiol 1977; 39:390–395.
- Sobotka PA, Mayer JH, Bauernfeind RA, Kanakis C Jr, Rosen KM. Arrhythmias documented by 24-hour continuous ambulatory electrocardiographic monitoring in young women without apparent heart disease. Am Heart J 1981; 101:753–759.
- Sheldon RS, Grubb BP 2nd, Olshansky B, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm 2015;12:e41–e63.
- Benditt DG, Adkisson WO. Approach to the patient with syncope: venues, presentations, diagnoses. Cardiol Clin 2013; 31:9–25.
- Pedersen CT, Kay GN, Kalman J, et al. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm 2014; 11:e166–e196.
- Iwai S, Cantillon DJ, Kim RJ, et al. Right and left ventricular outflow tract tachycardias: evidence for a common electrophysiologic mechanism. Cardiovasc Electrophysiol 2006; 17:1052–1058.
- Buxton AE, Waxman HL, Marchlinski FE, Simson MB, Cassidy D, Josephson ME. Right ventricular tachycardia: clinical and electrophysiologic characteristics. Circulation 1983; 68:917–927.
- Marchlinski FE, Deely MP, Zado ES. Sex-specific triggers for right ventricular outflow tract tachycardia. Am Heart J 2000; 139:1009–1013.
- Fuenmayor AJ, Araujo X, Fuenmayor AM. Cardiac arrhythmias during two different stages of the menstrual cycle. Int J Cardiol 1998; 63:267–270.
- Park KM, Kim YH, Marchlinski FE. Using the surface electrocardiogram to localize the origin of idiopathic ventricular tachycardia. Pacing Clin Electrophysiol 2012; 35:1516–1527.
- Te Riele AS, Hauer RN. Arrhythmogenic right ventricular dysplasia/cardiomyopathy: clinical challenges in a changing disease spectrum. Trends Cardiovasc Med 2015; 25:191–198.
- Philips B, Cheng A. 2015 update on the diagnosis and management of arrhythmogenic right ventricular cardiomyopathy. Curr Opin Cardiol 2016; 31:46–56.
- Del Carpio Munoz F, Syed FF, Noheria A, et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J Cardiovasc Electrophysiol 2011; 22:791–798.
- Yarlagadda RK, Iwai S, Stein KM, et al. Reversal of cardiomyopathy in patients with repetitive monomorphic ventricular ectopy originating from the right ventricular outflow tract. Circulation 2005; 112:1092–1097.
- Zhang Q, Zhou Y, Yu CM. Incidence, definition, diagnosis, and management of the cardiac resynchronization therapy nonresponder. Curr Opin Cardiol 2015; 30:40–49.
- Kennedy HL, Underhill SJ. Frequent or complex ventricular ectopy in apparently healthy subjects: a clinical study of 25 cases. Am J Cardiol 1976; 38:141–148.
- Brodsky M, Wu D, Denes P, Kanakis C, Rosen KM. Arrhythmias documented by 24 hour continuous electrocardiographic monitoring in 50 male medical students without apparent heart disease. Am J Cardiol 1977; 39:390–395.
- Sobotka PA, Mayer JH, Bauernfeind RA, Kanakis C Jr, Rosen KM. Arrhythmias documented by 24-hour continuous ambulatory electrocardiographic monitoring in young women without apparent heart disease. Am Heart J 1981; 101:753–759.
- Sheldon RS, Grubb BP 2nd, Olshansky B, et al. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm 2015;12:e41–e63.
- Benditt DG, Adkisson WO. Approach to the patient with syncope: venues, presentations, diagnoses. Cardiol Clin 2013; 31:9–25.
- Pedersen CT, Kay GN, Kalman J, et al. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Heart Rhythm 2014; 11:e166–e196.
- Iwai S, Cantillon DJ, Kim RJ, et al. Right and left ventricular outflow tract tachycardias: evidence for a common electrophysiologic mechanism. Cardiovasc Electrophysiol 2006; 17:1052–1058.
- Buxton AE, Waxman HL, Marchlinski FE, Simson MB, Cassidy D, Josephson ME. Right ventricular tachycardia: clinical and electrophysiologic characteristics. Circulation 1983; 68:917–927.
- Marchlinski FE, Deely MP, Zado ES. Sex-specific triggers for right ventricular outflow tract tachycardia. Am Heart J 2000; 139:1009–1013.
- Fuenmayor AJ, Araujo X, Fuenmayor AM. Cardiac arrhythmias during two different stages of the menstrual cycle. Int J Cardiol 1998; 63:267–270.
- Park KM, Kim YH, Marchlinski FE. Using the surface electrocardiogram to localize the origin of idiopathic ventricular tachycardia. Pacing Clin Electrophysiol 2012; 35:1516–1527.
- Te Riele AS, Hauer RN. Arrhythmogenic right ventricular dysplasia/cardiomyopathy: clinical challenges in a changing disease spectrum. Trends Cardiovasc Med 2015; 25:191–198.
- Philips B, Cheng A. 2015 update on the diagnosis and management of arrhythmogenic right ventricular cardiomyopathy. Curr Opin Cardiol 2016; 31:46–56.
- Del Carpio Munoz F, Syed FF, Noheria A, et al. Characteristics of premature ventricular complexes as correlates of reduced left ventricular systolic function: study of the burden, duration, coupling interval, morphology and site of origin of PVCs. J Cardiovasc Electrophysiol 2011; 22:791–798.
- Yarlagadda RK, Iwai S, Stein KM, et al. Reversal of cardiomyopathy in patients with repetitive monomorphic ventricular ectopy originating from the right ventricular outflow tract. Circulation 2005; 112:1092–1097.
- Zhang Q, Zhou Y, Yu CM. Incidence, definition, diagnosis, and management of the cardiac resynchronization therapy nonresponder. Curr Opin Cardiol 2015; 30:40–49.
KEY POINTS
- The focus of the initial evaluation is to determine whether there is underlying structural heart disease. If there is, early referral to a specialist is probably warranted.
- Idiopathic PVCs (in which there is no structural heart disease) have a benign prognosis.
- Treatment of PVCs is indicated for relief of symptoms if reassurance is not sufficient.
- Patients who have a high PVC burden (> 10% of total heartbeats, though this is a subject of debate) should have an evaluation of their systolic function. If it is normal at baseline, periodic follow-up echocardiograms should be considered.
- Patients with a very high burden (> 20%) are at high risk of arrhythmia-induced cardiomyopathy. In these patients, referral is prudent, as some patients may opt for more aggressive treatment of their PVCs.
- In patients with severe symptoms for whom medical management has failed, referral for consideration of catheter ablation is reasonable.

The evolution of office notes and the electronic medical record: The CAPS note
Until the advent of the electronic medical record (EMR), patient charts were filled with handwritten notes documenting visits to the office and read in linear fashion, starting with the patient’s perspective of the problem, then the objective findings of the physical examination, supporting objective data, and finally, the physician’s assessment and treatment plan.
The reliable subjective, objective, assessment, plan (SOAP) approach to notes first advocated by Lawrence Weed in the 1960s did a remarkable job of conveying the physician’s thought process, supporting data, and conclusions.1,2 The notes were brief by necessity, as the physician did not want to spend time writing extraneous information.
In the age of the EMR, large quantities of data are included in the patient notes that have no connection to or do not clearly convey the physician’s thought process. In 2013, 78% of office-based physicians were using EMRs, an increase from 18% in 2001 and an adoption rate accelerated by federal government policies.3,4 But many physicians still do not feel competent reading or writing notes in an EMR and still prefer to read succinct narrative notes.5
This problem is not unique to seasoned physicians. Medical students are also failing to learn how to appropriately document office visits in the EMR, as 52% of medical schools prohibit them from writing in patient charts.6
As a result, we believed that a reassessment of Dr. Weed’s problem-oriented approach to the medical record was required to streamline the EMR and facilitate the way information is conveyed between providers of the patient’s care. Too often, large quantities of laboratory, radiographic, and pathology results are dumped into the record, burying pertinent information about the physician’s thought process, assessment, and evaluation and treatment plan and making it difficult to quickly and efficiently determine the plan.
We recently adopted an approach to office notes that is a modification of the SOAP note. While physicians often gather subjective, objective, and laboratory information to deductively formulate a diagnosis, it is not necessary to document it in the traditional deductive format in the EMR when the information is readily accessible in other areas of the record. Furthermore, a deductive format in the modern EMR produces excessively lengthy notes that require pages of screen scrolling to find the key elements required for effective patient care. This is time-consuming and is a daily obstruction to patient care.
The format that we have been using for almost 10 years still allows the physician to adhere to the problem-oriented medical note philosophy. We call it the CAPS note, which stands for concern, assessment, plan, and supporting data. This approach allows others involved in the patient’s care to efficiently extract critical components (assessment and plan for a specifically stated problem) while still allowing the inclusion of supporting data for reference and for coding and billing.
The structure of the CAPS note is:
- Concern: The primary purpose of the patient’s visit, including the history of the present illness, as conveyed by the patient, and the current status of the concern.
- Assessment: A succinct definition of the patient’s concern along with an accompanying medical diagnosis.
- Plan: The clinician’s immediate and long-term intentions for addressing the patient’s concern or condition.
- Supporting objective and subjective information: All supporting objective data, starting with the physical examination, then the results of laboratory and radiographic tests, and any other information that contributed to the clinician’s medical reasoning. Then, subjective information is included, such as the patient’s past medical, surgical, family, and social histories; current medications; allergies; and a comprehensive review of systems.
This structure keeps the most important information at the top when the encounter is opened on the computer screen and eliminates the need for unnecessary scrolling and searching, not to mention frustration and delays in patient care. Other less pertinent information appears toward the bottom of the record.
THE APSO NOTE VS THE SOAP NOTE
Frustration over the difficulty of finding the most pertinent information in the EMR—the assessment and the plan—has led others to propose a rearrangement of the traditional SOAP note. The APSO (assessment, plan, subjective, objective) note7,8 was created for inpatient daily progress notes, a situation in which the patient’s concern is unlikely to change dramatically on a daily basis and was not intended for use in outpatient clinics.8 While the APSO format does allow colleagues rapid access to the physician’s assessment and plan, it abandons the patient-centered approach of Dr. Weed’s problem-oriented medical record in that it makes it more difficult to find why the patient initially sought care, how long the patient has had the problem, or if there were prior attempts to treat it. These critical details are buried in the bowels of the note.
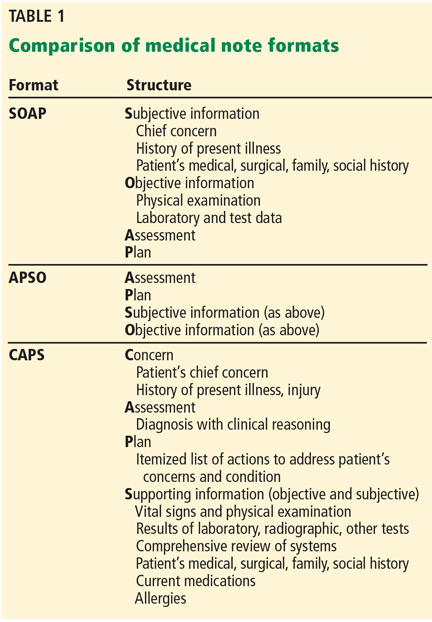
The advantage of the CAPS note (Table 1) is that it retains the patient-centered, problem-oriented spirit of the SOAP format, while moving potentially supportive yet distracting data fields to later in the note. Thus it is applicable to inpatient and outpatient settings.
In the inpatient setting, the fields remain in the same order, but the chief complaint is often the admitting diagnosis or surgical procedure, followed by a quick line on the interval history. The assessment and plan can then follow in much the same way as it would in the outpatient setting, and below that are the patient’s daily laboratory results, radiographic studies, physical examination findings, and any other relevant supporting data. This format allows rapid access to critical information needed by either consultants or cross-covering practitioners who primarily want to know why the patient was admitted, the status, and the primary team’s plan.
ANY TEMPLATE HAS LIMITATIONS
Any standardized template for progress notes in the EMR has limitations. The CAPS format would be easier for a hospital-based physician, who typically addresses one or a small number of concerns, than for an office-based general practitioner who may have to address a multitude of comorbidities in a single visit.
Also, different physicians use the EMR differently. For example, a survey of 1,088 physicians found that 60% of primary care physicians used templates (60%) vs only 34% of specialists, and that 38% of specialists relied mainly on dictation.9
The CAPS approach to the office visit note offers a blend of a template and free text, either typed or dictated, while keeping a structured format that permits others participating in the patient’s care to easily extract desired information. The template can easily be brought up in the patient’s chart, then by either typing or using voice-recognition software, the patient’s chief complaint, history of the present illness, assessment, and plan can be easily completed.
The CAPS format should continue to allow notes to fulfill medicolegal and billing obligations, but without cluttering true clinical reasoning. As more institutions adopt an open-notes policy, permitting patients to freely browse their own medical records, patients will benefit from a clearly structured clinical note that focuses on their problem and the practitioner’s solution. This provides patients a sense of validation and reassurance that the note starts with their concern and history, followed by the practitioner’s assessment and plan, so they can easily affirm that they were accurately heard and can identify the diagnosis given to them by the medical practitioner and the plan moving forward.
Since a return to succinct, albeit often illegible, handwritten clinic notes is impossible, our proposed method of documenting a clinic visit embraces the EMR with a concise yet comprehensive clinic note.
- Jacobs L. Interview with Lawrence Weed, MD—the father of the problem-oriented medical record looks ahead. Perm J 2009; 13:84–89.
- Cameron S, Turtle-Son I. Learning to write case notes using the SOAP format. JCD 2002; 80:286–292.
- Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2013. NCHS Data Brief 2014; 143:1–8.
- Centers for Medicare & Medicaid Services (CMS). EHR incentive program. www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html. Accessed April 28, 2016.
- Han H, Lopp L. Writing and reading in the electronic health record: an entirely new world. Med Educ Online 2013; 18:1–7.
- Hammoud MM, Dalrymple JL, Christner JG, et al. Medical student documentation in electronic health records: a collaborative statement from the Alliance for Clinical Education. Teach Learn Med 2012; 24:257–266.
- Shoolin J, Ozeran L, Hamann C, Bria W 2nd. Association of Medical Directors of Information Systems consensus on inpatient electronic health record documentation. Appl Clin Inform 2013; 4:293–303.
- Hahn JS, Bernstein JA, McKenzie RB, King BJ, Longhurst CA. Rapid implementation of inpatient electronic physician documentation at an academic hospital. Appl Clin Inform 2012; 3:175–185.
- Pollard SE, Neri PM, Wilcox AR, et al. How physicians document outpatient visit notes in an electronic health record. Int J Med Inform 2013; 82:39–46.
Until the advent of the electronic medical record (EMR), patient charts were filled with handwritten notes documenting visits to the office and read in linear fashion, starting with the patient’s perspective of the problem, then the objective findings of the physical examination, supporting objective data, and finally, the physician’s assessment and treatment plan.
The reliable subjective, objective, assessment, plan (SOAP) approach to notes first advocated by Lawrence Weed in the 1960s did a remarkable job of conveying the physician’s thought process, supporting data, and conclusions.1,2 The notes were brief by necessity, as the physician did not want to spend time writing extraneous information.
In the age of the EMR, large quantities of data are included in the patient notes that have no connection to or do not clearly convey the physician’s thought process. In 2013, 78% of office-based physicians were using EMRs, an increase from 18% in 2001 and an adoption rate accelerated by federal government policies.3,4 But many physicians still do not feel competent reading or writing notes in an EMR and still prefer to read succinct narrative notes.5
This problem is not unique to seasoned physicians. Medical students are also failing to learn how to appropriately document office visits in the EMR, as 52% of medical schools prohibit them from writing in patient charts.6
As a result, we believed that a reassessment of Dr. Weed’s problem-oriented approach to the medical record was required to streamline the EMR and facilitate the way information is conveyed between providers of the patient’s care. Too often, large quantities of laboratory, radiographic, and pathology results are dumped into the record, burying pertinent information about the physician’s thought process, assessment, and evaluation and treatment plan and making it difficult to quickly and efficiently determine the plan.
We recently adopted an approach to office notes that is a modification of the SOAP note. While physicians often gather subjective, objective, and laboratory information to deductively formulate a diagnosis, it is not necessary to document it in the traditional deductive format in the EMR when the information is readily accessible in other areas of the record. Furthermore, a deductive format in the modern EMR produces excessively lengthy notes that require pages of screen scrolling to find the key elements required for effective patient care. This is time-consuming and is a daily obstruction to patient care.
The format that we have been using for almost 10 years still allows the physician to adhere to the problem-oriented medical note philosophy. We call it the CAPS note, which stands for concern, assessment, plan, and supporting data. This approach allows others involved in the patient’s care to efficiently extract critical components (assessment and plan for a specifically stated problem) while still allowing the inclusion of supporting data for reference and for coding and billing.
The structure of the CAPS note is:
- Concern: The primary purpose of the patient’s visit, including the history of the present illness, as conveyed by the patient, and the current status of the concern.
- Assessment: A succinct definition of the patient’s concern along with an accompanying medical diagnosis.
- Plan: The clinician’s immediate and long-term intentions for addressing the patient’s concern or condition.
- Supporting objective and subjective information: All supporting objective data, starting with the physical examination, then the results of laboratory and radiographic tests, and any other information that contributed to the clinician’s medical reasoning. Then, subjective information is included, such as the patient’s past medical, surgical, family, and social histories; current medications; allergies; and a comprehensive review of systems.
This structure keeps the most important information at the top when the encounter is opened on the computer screen and eliminates the need for unnecessary scrolling and searching, not to mention frustration and delays in patient care. Other less pertinent information appears toward the bottom of the record.
THE APSO NOTE VS THE SOAP NOTE
Frustration over the difficulty of finding the most pertinent information in the EMR—the assessment and the plan—has led others to propose a rearrangement of the traditional SOAP note. The APSO (assessment, plan, subjective, objective) note7,8 was created for inpatient daily progress notes, a situation in which the patient’s concern is unlikely to change dramatically on a daily basis and was not intended for use in outpatient clinics.8 While the APSO format does allow colleagues rapid access to the physician’s assessment and plan, it abandons the patient-centered approach of Dr. Weed’s problem-oriented medical record in that it makes it more difficult to find why the patient initially sought care, how long the patient has had the problem, or if there were prior attempts to treat it. These critical details are buried in the bowels of the note.
The advantage of the CAPS note (Table 1) is that it retains the patient-centered, problem-oriented spirit of the SOAP format, while moving potentially supportive yet distracting data fields to later in the note. Thus it is applicable to inpatient and outpatient settings.
In the inpatient setting, the fields remain in the same order, but the chief complaint is often the admitting diagnosis or surgical procedure, followed by a quick line on the interval history. The assessment and plan can then follow in much the same way as it would in the outpatient setting, and below that are the patient’s daily laboratory results, radiographic studies, physical examination findings, and any other relevant supporting data. This format allows rapid access to critical information needed by either consultants or cross-covering practitioners who primarily want to know why the patient was admitted, the status, and the primary team’s plan.
ANY TEMPLATE HAS LIMITATIONS
Any standardized template for progress notes in the EMR has limitations. The CAPS format would be easier for a hospital-based physician, who typically addresses one or a small number of concerns, than for an office-based general practitioner who may have to address a multitude of comorbidities in a single visit.
Also, different physicians use the EMR differently. For example, a survey of 1,088 physicians found that 60% of primary care physicians used templates (60%) vs only 34% of specialists, and that 38% of specialists relied mainly on dictation.9
The CAPS approach to the office visit note offers a blend of a template and free text, either typed or dictated, while keeping a structured format that permits others participating in the patient’s care to easily extract desired information. The template can easily be brought up in the patient’s chart, then by either typing or using voice-recognition software, the patient’s chief complaint, history of the present illness, assessment, and plan can be easily completed.
The CAPS format should continue to allow notes to fulfill medicolegal and billing obligations, but without cluttering true clinical reasoning. As more institutions adopt an open-notes policy, permitting patients to freely browse their own medical records, patients will benefit from a clearly structured clinical note that focuses on their problem and the practitioner’s solution. This provides patients a sense of validation and reassurance that the note starts with their concern and history, followed by the practitioner’s assessment and plan, so they can easily affirm that they were accurately heard and can identify the diagnosis given to them by the medical practitioner and the plan moving forward.
Since a return to succinct, albeit often illegible, handwritten clinic notes is impossible, our proposed method of documenting a clinic visit embraces the EMR with a concise yet comprehensive clinic note.
Until the advent of the electronic medical record (EMR), patient charts were filled with handwritten notes documenting visits to the office and read in linear fashion, starting with the patient’s perspective of the problem, then the objective findings of the physical examination, supporting objective data, and finally, the physician’s assessment and treatment plan.
The reliable subjective, objective, assessment, plan (SOAP) approach to notes first advocated by Lawrence Weed in the 1960s did a remarkable job of conveying the physician’s thought process, supporting data, and conclusions.1,2 The notes were brief by necessity, as the physician did not want to spend time writing extraneous information.
In the age of the EMR, large quantities of data are included in the patient notes that have no connection to or do not clearly convey the physician’s thought process. In 2013, 78% of office-based physicians were using EMRs, an increase from 18% in 2001 and an adoption rate accelerated by federal government policies.3,4 But many physicians still do not feel competent reading or writing notes in an EMR and still prefer to read succinct narrative notes.5
This problem is not unique to seasoned physicians. Medical students are also failing to learn how to appropriately document office visits in the EMR, as 52% of medical schools prohibit them from writing in patient charts.6
As a result, we believed that a reassessment of Dr. Weed’s problem-oriented approach to the medical record was required to streamline the EMR and facilitate the way information is conveyed between providers of the patient’s care. Too often, large quantities of laboratory, radiographic, and pathology results are dumped into the record, burying pertinent information about the physician’s thought process, assessment, and evaluation and treatment plan and making it difficult to quickly and efficiently determine the plan.
We recently adopted an approach to office notes that is a modification of the SOAP note. While physicians often gather subjective, objective, and laboratory information to deductively formulate a diagnosis, it is not necessary to document it in the traditional deductive format in the EMR when the information is readily accessible in other areas of the record. Furthermore, a deductive format in the modern EMR produces excessively lengthy notes that require pages of screen scrolling to find the key elements required for effective patient care. This is time-consuming and is a daily obstruction to patient care.
The format that we have been using for almost 10 years still allows the physician to adhere to the problem-oriented medical note philosophy. We call it the CAPS note, which stands for concern, assessment, plan, and supporting data. This approach allows others involved in the patient’s care to efficiently extract critical components (assessment and plan for a specifically stated problem) while still allowing the inclusion of supporting data for reference and for coding and billing.
The structure of the CAPS note is:
- Concern: The primary purpose of the patient’s visit, including the history of the present illness, as conveyed by the patient, and the current status of the concern.
- Assessment: A succinct definition of the patient’s concern along with an accompanying medical diagnosis.
- Plan: The clinician’s immediate and long-term intentions for addressing the patient’s concern or condition.
- Supporting objective and subjective information: All supporting objective data, starting with the physical examination, then the results of laboratory and radiographic tests, and any other information that contributed to the clinician’s medical reasoning. Then, subjective information is included, such as the patient’s past medical, surgical, family, and social histories; current medications; allergies; and a comprehensive review of systems.
This structure keeps the most important information at the top when the encounter is opened on the computer screen and eliminates the need for unnecessary scrolling and searching, not to mention frustration and delays in patient care. Other less pertinent information appears toward the bottom of the record.
THE APSO NOTE VS THE SOAP NOTE
Frustration over the difficulty of finding the most pertinent information in the EMR—the assessment and the plan—has led others to propose a rearrangement of the traditional SOAP note. The APSO (assessment, plan, subjective, objective) note7,8 was created for inpatient daily progress notes, a situation in which the patient’s concern is unlikely to change dramatically on a daily basis and was not intended for use in outpatient clinics.8 While the APSO format does allow colleagues rapid access to the physician’s assessment and plan, it abandons the patient-centered approach of Dr. Weed’s problem-oriented medical record in that it makes it more difficult to find why the patient initially sought care, how long the patient has had the problem, or if there were prior attempts to treat it. These critical details are buried in the bowels of the note.
The advantage of the CAPS note (Table 1) is that it retains the patient-centered, problem-oriented spirit of the SOAP format, while moving potentially supportive yet distracting data fields to later in the note. Thus it is applicable to inpatient and outpatient settings.
In the inpatient setting, the fields remain in the same order, but the chief complaint is often the admitting diagnosis or surgical procedure, followed by a quick line on the interval history. The assessment and plan can then follow in much the same way as it would in the outpatient setting, and below that are the patient’s daily laboratory results, radiographic studies, physical examination findings, and any other relevant supporting data. This format allows rapid access to critical information needed by either consultants or cross-covering practitioners who primarily want to know why the patient was admitted, the status, and the primary team’s plan.
ANY TEMPLATE HAS LIMITATIONS
Any standardized template for progress notes in the EMR has limitations. The CAPS format would be easier for a hospital-based physician, who typically addresses one or a small number of concerns, than for an office-based general practitioner who may have to address a multitude of comorbidities in a single visit.
Also, different physicians use the EMR differently. For example, a survey of 1,088 physicians found that 60% of primary care physicians used templates (60%) vs only 34% of specialists, and that 38% of specialists relied mainly on dictation.9
The CAPS approach to the office visit note offers a blend of a template and free text, either typed or dictated, while keeping a structured format that permits others participating in the patient’s care to easily extract desired information. The template can easily be brought up in the patient’s chart, then by either typing or using voice-recognition software, the patient’s chief complaint, history of the present illness, assessment, and plan can be easily completed.
The CAPS format should continue to allow notes to fulfill medicolegal and billing obligations, but without cluttering true clinical reasoning. As more institutions adopt an open-notes policy, permitting patients to freely browse their own medical records, patients will benefit from a clearly structured clinical note that focuses on their problem and the practitioner’s solution. This provides patients a sense of validation and reassurance that the note starts with their concern and history, followed by the practitioner’s assessment and plan, so they can easily affirm that they were accurately heard and can identify the diagnosis given to them by the medical practitioner and the plan moving forward.
Since a return to succinct, albeit often illegible, handwritten clinic notes is impossible, our proposed method of documenting a clinic visit embraces the EMR with a concise yet comprehensive clinic note.
- Jacobs L. Interview with Lawrence Weed, MD—the father of the problem-oriented medical record looks ahead. Perm J 2009; 13:84–89.
- Cameron S, Turtle-Son I. Learning to write case notes using the SOAP format. JCD 2002; 80:286–292.
- Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2013. NCHS Data Brief 2014; 143:1–8.
- Centers for Medicare & Medicaid Services (CMS). EHR incentive program. www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html. Accessed April 28, 2016.
- Han H, Lopp L. Writing and reading in the electronic health record: an entirely new world. Med Educ Online 2013; 18:1–7.
- Hammoud MM, Dalrymple JL, Christner JG, et al. Medical student documentation in electronic health records: a collaborative statement from the Alliance for Clinical Education. Teach Learn Med 2012; 24:257–266.
- Shoolin J, Ozeran L, Hamann C, Bria W 2nd. Association of Medical Directors of Information Systems consensus on inpatient electronic health record documentation. Appl Clin Inform 2013; 4:293–303.
- Hahn JS, Bernstein JA, McKenzie RB, King BJ, Longhurst CA. Rapid implementation of inpatient electronic physician documentation at an academic hospital. Appl Clin Inform 2012; 3:175–185.
- Pollard SE, Neri PM, Wilcox AR, et al. How physicians document outpatient visit notes in an electronic health record. Int J Med Inform 2013; 82:39–46.
- Jacobs L. Interview with Lawrence Weed, MD—the father of the problem-oriented medical record looks ahead. Perm J 2009; 13:84–89.
- Cameron S, Turtle-Son I. Learning to write case notes using the SOAP format. JCD 2002; 80:286–292.
- Hsiao CJ, Hing E. Use and characteristics of electronic health record systems among office-based physician practices: United States, 2001-2013. NCHS Data Brief 2014; 143:1–8.
- Centers for Medicare & Medicaid Services (CMS). EHR incentive program. www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Basics.html. Accessed April 28, 2016.
- Han H, Lopp L. Writing and reading in the electronic health record: an entirely new world. Med Educ Online 2013; 18:1–7.
- Hammoud MM, Dalrymple JL, Christner JG, et al. Medical student documentation in electronic health records: a collaborative statement from the Alliance for Clinical Education. Teach Learn Med 2012; 24:257–266.
- Shoolin J, Ozeran L, Hamann C, Bria W 2nd. Association of Medical Directors of Information Systems consensus on inpatient electronic health record documentation. Appl Clin Inform 2013; 4:293–303.
- Hahn JS, Bernstein JA, McKenzie RB, King BJ, Longhurst CA. Rapid implementation of inpatient electronic physician documentation at an academic hospital. Appl Clin Inform 2012; 3:175–185.
- Pollard SE, Neri PM, Wilcox AR, et al. How physicians document outpatient visit notes in an electronic health record. Int J Med Inform 2013; 82:39–46.
KEY POINTS
- The CAPS format provides an advantage over the traditional approach by transferring potentially note-cluttering data that is available elsewhere in the EMR to the bottom of the note, allowing more efficient communication of the true purpose for the patient’s visit, the diagnosis, and the physician’s approach to resolving the patient’s concern.
- As healthcare systems allow patients to browse their electronic charts, the CAPS format shows them that their concern was heard accurately and clearly states the diagnosis and plan of care.

Alpha-1 antitrypsin deficiency: An underrecognized, treatable cause of COPD
Alpha-1 antitrypsin deficiency is a common but underrecognized genetic condition that increases the risk of chronic obstructive pulmonary disease (COPD) and liver disease. Primary care providers can play a critical role in detecting it and managing patients who have it.
RECOGNIZED CASES ARE THE TIP OF THE ICEBERG
First described in 1963,1 alpha-1 antitrypsin deficiency is estimated to affect 100,000 Americans, fewer than 15,000 of whom have received a clinical diagnosis. As further evidence of its underrecognition,2–7 many patients experience long delays between their first symptoms and the diagnosis. Early studies indicated that the average diagnostic delay was 7.2 years,4 and the latest studies, as recent as 2013, indicate a similar diagnostic delay.7
Furthermore, many patients see multiple healthcare providers before receiving the correct diagnosis. A 1994 survey by this author4 found that 43.7% of patients who had severe deficiency of alpha-1 antitrypsin saw at least three physicians before the correct diagnosis was made.
Why is the disease underrecognized?
Several reasons may account for underrecognition of this disease. Many clinicians—including, unfortunately, many pulmonologists—do not know much about it,7,8 do not adhere to clinical guidelines,9,10 or harbor the misperception that there is no therapy available and, therefore, no compelling reason to make a diagnosis.7
Regarding inadequate knowledge, in a study by Taliercio, Chatburn, and this author,8 internal medicine residents scored only 63% correct on a 10-question quiz on diagnostic features of alpha-1 antitrypsin deficiency. There was no evidence of a training effect—senior residents scored no higher than interns.
Similarly, when Greulich et al7 surveyed German and Italian internists, general practitioners, and pulmonologists, one-fourth to one-half of them (depending on specialty and country) stated that they knew either very little or nothing at all about alpha-1 antitrypsin deficiency. In addition, 7% to 8% agreed with the statement, “There is no treatment available for this disease.”7
Nonadoption of clinical guidelines has been widely recognized in medicine and is evident in the failure to implement various recommended practices,9,10 such as low-stretch ventilation for acute respiratory distress syndrome and prophylaxis against deep vein thrombosis.
Finding the rest of the iceberg
Efforts to enhance compliance with guidelines on testing for alpha-1 antitrypsin deficiency have included using the electronic medical record to prompt physicians to test appropriate candidates.11–13
Jain et al13 examined the effect of installing such a prompting system to remind physicians to test for alpha-1 antitrypsin deficiency in patients with airflow obstruction that does not reverse with a bronchodilator—a recognized indication for testing for this disease according to standards endorsed by the American Thoracic Society and European Respiratory Society.14 At baseline, only 4.7% of appropriate candidates were being tested; after a prompt was installed in the electronic medical record, the rate rose to 15.1%, still a minority of candidates.
Another strategy is to empower respiratory therapists who perform pulmonary function tests to invite patients to be tested if their pulmonary function tests show postbronchodilator airflow obstruction. Rahaghi et al15 showed that using this strategy, 20 (0.63%) of 3,152 patients who were found to have fixed airflow obstruction when they underwent pulmonary function testing were newly diagnosed with severe deficiency of alpha-1 antitrypsin. Other targeted detection studies in patients with COPD estimated the prevalence of alpha-1 antitrypsin deficiency at up to 12%.3
PHYSIOLOGY AND PATHOPHYSIOLOGY OF ALPHA-1 ANTITRYPSIN DEFICIENCY
Alpha-1 antitrypsin is a single-chain, 394-amino acid glycoprotein with three carbohydrate side chains found at asparagine residues along the primary structure.16
A major physiologic function of this molecule is to bind neutrophil elastase, which it does avidly. In a “mousetrap-like” mechanism,16 an active site on the alpha-1 antitrypsin molecule captures the neutrophil elastase and is cleaved, releasing steric energy in the molecule, catapulting the neutrophil elastase to the opposite side of the alpha-1 antitrypsin molecule, and inactivating it (Figure 1).
MM is normal, ZZ is not
Alpha-1 antitrypsin deficiency is inherited as an autosomal-codominant condition.17
The SERPINA1 gene, which codes for alpha-1 antitrypsin, is located on the long arm of the 14th chromosome, and more than 150 alleles of this gene have been identified to date. The normal allele is denoted M, and the allele most commonly associated with severe deficiency is denoted Z. People who are homozygous for the M allele (ie, normal) are called PI*MM (PI stands for “protease inhibitor”), and those who are homozygous for the Z allele are PI*ZZ. More than 90% of patients with severe alpha-1 antitrypsin deficiency are PI*ZZ.18
The Z allele has a single amino acid substitution (glutamic acid-to-lysine at position 342), which results in abnormal folding and formation of polymers of the Z molecule within hepatocytes.19,20 These polymers are recognized on liver biopsy as periodic acid-Schiff diastase-resistant eosinophilic inclusion bodies on histologic staining (Figure 2).
With alpha-1 antitrypsin trapped as Z-molecule polymers in the liver, the amount in the bloodstream falls, and there is a consequent decrease in the amount available in the lung to oppose the proteolytic burden of neutrophil elastase, especially in people who smoke or work in dusty environments.21
Tan et al22 have shown that some of the polymerized Z protein can escape the liver and circulate in the blood and that alveolar macrophages may also produce Z polymers. These Z polymers are chemotactic for neutrophils,23 so that their presence in the lung fuels the inflammatory cascade by recruiting more neutrophils to the lung, thereby increasing the proteolytic burden to the lung and increasing the risk of emphysema. Z monomers that do circulate can bind neutrophil elastase, but their binding avidity to neutrophil elastase is substantially lower than that of M-type alpha-1 antitrypsin.
CLINICAL MANIFESTATIONS
Alpha-1 antitrypsin deficiency of the PI*ZZ type is associated with two major clinical manifestations:
- Emphysema, resulting from the loss of proteolytic protection of the lung by alpha-1 antitrypsin (a toxic loss of function), and
- Liver diseases such as cirrhosis and chronic hepatitis, which result from abnormal accumulation of alpha-1 antitrypsin within hepatocytes (a toxic gain of function), and hepatoma.17
Other clinical manifestations of PI*ZZ alpha-1 antitrypsin deficiency include panniculitis and an association with cytoplasmic antineutrophil cytoplasmic antibody-positive vasculitis.17
Some uncertainty exists regarding the risk associated with the PI*MZ heterozygous state because there has been no systematic longitudinal study of people with this genotype. However, the weight of available experience suggests that PI*MZ individuals who have never smoked are not at increased risk of developing emphysema.24
Findings from a national registry: PI*ZZ COPD resembles ‘usual’ COPD
Distinguishing patients with alpha-1 antitrypsin deficiency from those with “usual” COPD (ie, without alpha-1 antitrypsin deficiency) can be difficult, as shown in data from the National Heart, Lung, and Blood Institute’s Alpha-1 Antitrypsin Deficiency Registry study.18 This multicenter, longitudinal, observational study contains the largest well-characterized cohort with severe deficiency of alpha-1 antitrypsin (PI*ZZ, PI*ZNull, etc), with 1,129 patients.
Pulmonary function test results were consistent with emphysema in most of the patients in the registry. Mean postbronchodilator pulmonary function values (± standard error of the mean) were:
- Forced expiratory volume in 1 second (FEV1) 46.7% of predicted (± 30%)
- Ratio of FEV1 to forced vital capacity 42.9% (± 20.4% )
- Mean diffusing capacity for carbon monoxide 50.3% of predicted (± 22.5%).
Like many patients with usual COPD, 60% of the registry patients demonstrated a component of airway reactivity, with significant reversal of airflow obstruction over three spirometries after receiving a dose of an inhaled bronchodilator (characterized by a 12% and 200-mL postbronchodilator rise in FEV1). Moreover, 78 patients had normal lung function.
Symptoms also resembled those in patients with usual emphysema, chronic bronchitis, or both. On enrollment in the registry, 83.9% of the patients had shortness of breath on exertion, 75.5% had wheezing with upper respiratory infections, 65.3% had wheezing without upper respiratory infection, 67.6% had recent debilitating chest illness, 42.4% had “usual” cough, and 49.6% had annual cough and phlegm episodes.
Imaging findings. Although the classic teaching is that emphysema due to alpha-1 antitrypsin deficiency produces lower-lobe hyperlucency on plain films, relying on this sign would lead to underrecognition, as 36% of PI*ZZ patients have apical-predominant emphysema on chest computed tomography,24 which resembles the usual centriacinar emphysema pattern. Figure 3 shows axial computed tomographic scans through the apices and the bases of the lungs of a patient with alpha-1 antitrypsin deficiency.
In view of these difficulties, guidelines from the American Thoracic Society and European Respiratory Society14 endorse testing for alpha-1 antitrypsin deficiency in all adults who have symptoms and fixed airflow obstruction (Table 1).
CONSEQUENCES OF ALPHA-1 ANTITRYPSIN DEFICIENCY
Two large screening studies2,3,25,26 followed people who were identified at birth as having alpha-1 antitrypsin deficiency to examine the natural course of the disease.
The larger of the two studies27 tested 200,000 Swedish newborns. Follow-up of this cohort to age 35 indicated that 35-year-old never-smoking PI*ZZ individuals have normal lung function and no excess emphysema on computed tomography compared with normal peers matched for age and sex.27 In contrast, the few PI*ZZ ever-smokers demonstrated a lower level of transfer factor and significantly more emphysema on computed tomography than normal (PI*MM) never-smokers.
Faster decline in lung function
Data from the National Heart, Lung, and Blood Institute registry indicate that, on average, people with severe alpha-1 antitrypsin deficiency lose lung function faster than people without the disease.28 Specifically, in never-smokers in the registry, the average rate of FEV1 decline was 67 mL/year, and among ex-smokers, it was 54 mL/year. Both of these values exceed the general age-related rate of FEV1 decline of approximately 20 to 25 mL/year in never-smoking, normal adults. Among current smokers in the registry with severe alpha-1 antitrypsin deficiency, the rate of FEV1 decline was 109 mL/year.
Rates of FEV1 decline over time vary among groups with differing degrees of airflow obstruction. For example, PI*ZZ patients with moderate COPD (stage II of the four-stage Global Initiative for Chronic Obstructive Lung Disease classification system) lose lung function faster than patients with either milder or more severe degrees of airflow obstruction.29
As with COPD in general, exacerbations of COPD in people with severe deficiency of alpha-1 antitrypsin are associated with worsened clinical status. In one series,30 54% of 265 PI*ZZ patients experienced an exacerbation in the first year of follow-up, and 18% experienced at least three. Such exacerbations occurred in December and January in 32% of these individuals, likely due to a viral precipitant.
Increased mortality
Severe deficiency of alpha-1 antitrypsin is associated not only with severe morbidity but also death. In the national registry, the overall rate of death was 18.6% at 5 years of follow-up, or approximately 3% per year.28
A low FEV1 at entry was a bad sign. Patients entering the registry with FEV1 values below 15% of predicted had a 36% mortality rate at 3 years, compared with 2.6% in those whose baseline FEV1 exceeded 50% of predicted.
Underlying causes of death in registry participants included emphysema (accounting for 72% of deaths) and cirrhosis (10%),31 which were the only causes of death more frequent than in age- and sex-matched controls. In a series of never-smokers who had PI*ZZ alpha-1 antitrypsin deficiency,32 death was less frequently attributed to emphysema than in the national registry (46%) and more often attributed to cirrhosis (28%), indicating that never-smokers may more frequently escape the ravages of emphysema but experience a higher rate of developing cirrhosis later in life.33
DIAGNOSING ALPHA-1 ANTITRYPSIN DEFICIENCY
Available blood tests for alpha-1 antitrypsin deficiency include:
The serum alpha-1 antitrypsin level, most often done by nephelometry. Normal serum levels generally range from 100 to 220 mg/dL.
Phenotyping, usually performed by isoelectric focusing, which can identify different band patterns associated with different alleles.
Genotyping involves determining which alpha-1 antitrypsin alleles are present, most often using polymerase chain reaction testing targeting the S and Z alleles and occasionally set up to detect less common alleles such as F and I.17
Gene sequencing is occasionally necessary to achieve an accurate, definitive diagnosis.
Free, confidential testing is available
Clinical testing most often involves checking both a serum level and a phenotype or genotype. Such tests are often available in hospital laboratories and commercial laboratories, with testing also facilitated by the availability of free testing kits from several manufacturers of drugs for alpha-1 antitrypsin deficiency.
The Alpha-1 Foundation (www.alpha1.org)34 also offers a free, home-based confidential testing kit through a research protocol at the Medical University of South Carolina (alphaone@musc.edu) called the Alpha-1 Coded Testing (ACT) study. Patients can receive a kit and lancet at home, submit the dried blood-spot specimen, and receive in the mail a confidential serum level and genotype.
The availability of such home-based confidential testing allows patients to seek testing without a physician’s order and makes it easier for facilitated allied health providers, such as respiratory therapists, to recommend testing in appropriate clinical circumstances.15
TREATMENT OF ALPHA-1 ANTITRYPSIN DEFICIENCY
The treatment of patients with severe deficiency of alpha-1 antitrypsin and emphysema generally resembles that of patients with usual COPD. Specifically, smoking cessation, bronchodilators, occasionally inhaled steroids, supplemental oxygen, preventive vaccinations, and pulmonary rehabilitation are indicated as per usual clinical assessment.
Lung volume reduction surgery, which is beneficial in appropriate subsets of COPD patients, is generally less effective in those with severe alpha-1 antitrypsin deficiency,35 specifically because the magnitude of FEV1 increase and the duration of such a rise are lower than in usual COPD patients.
Augmentation therapy
Specific therapy for alpha-1 antitrypsin deficiency currently involves weekly intravenous infusions of purified, pooled human-plasma-derived alpha-1 antitrypsin, so-called augmentation therapy. Four drugs have been approved for use in the United States:
- Prolastin-C (Grifols, Barcelona, Spain)
- Aralast NP (Baxalta, Bonneckborn, IL)
- Zemaira (CSL Behring, King of Prussia, PA)
- Glassia (Baxalta, Bonneckborn, IL, and Kamada, Ness Ziona, Israel).
All of these were approved for use in the United States on the basis of biochemical efficacy. Specifically, infusion of these drugs has been shown to raise serum levels above a protective threshold value (generally considered 57 mg/dL, the value below which the risk of developing emphysema increases beyond normal).
Randomized controlled trials36,37 have addressed the efficacy of intravenous augmentation therapy, and although no single trial has been definitive, the weight of evidence shows that augmentation therapy can slow the progression of emphysema. For example, in a study by Dirksen et al,37 augmentation therapy was associated with a slower progression of emphysema as assessed by the rate of loss of lung density on computed tomography.
On the basis of the available evidence, the American Thoracic Society and European Respiratory Society14 have recommended augmentation therapy in individuals with “established airflow obstruction from alpha-1 antitrypsin deficiency.”14 Their guidelines go on to say that the evidence that augmentation therapy is beneficial “is stronger for individuals with moderate airflow obstruction (eg, FEV1 35%–60% of predicted) than for those with severe airflow obstruction. Augmentation therapy is not currently recommended for individuals without emphysema.”
The guidelines recognize that although augmentation therapy does not satisfy the usual criteria for cost-effectiveness (< $50,000 per quality-adjusted life year) due to its high cost (approximately $100,000 per year if paid for out of pocket),38 it is recommended for appropriate candidates because it is the only available specific therapy for severe deficiency of alpha-1 antitrypsin.
Novel therapies
In addition to current treatment approaches of augmentation therapy, a number of novel treatment strategies are being investigated, several of which hold much promise.
Gene therapy, using adeno-associated virus to transfect the normal human gene into individuals with severe deficiency of alpha-1 antitrypsin, has been undertaken and is currently under study. In addition, a variety of approaches to interdict production of abnormal Z protein from the liver are being examined, as well as inhaled hyaluronic acid to protect the lung.
- Laurell C, Eriksson A. The electrophoretic alpha-1 globulin pattern of serum in alpha-1 antitrypsin deficiency. Scand J Clin Lab Invest 1963; 15:132–140.
- Aboussouan LS, Stoller JK. Detection of alpha-1 antitrypsin deficiency: a review. Respir Med 2009; 103:335–341.
- Stoller JK, Brantly M. The challenge of detecting alpha-1 antitrypsin deficiency. COPD 2013; 10(suppl 1):26–34.
- Stoller JK, Smith P, Yang P, Spray J. Physical and social impact of alpha 1-antitrypsin deficiency: results of a survey. Cleve Clin J Med 1994; 61:461–467.
- Stoller JK, Sandhaus RA, Turino G, Dickson R, Rodgers K, Strange C. Delay in diagnosis of alpha1-antitrypsin deficiency: a continuing problem. Chest 2005; 128:1989–1994.
- Campos MA, Wanner A, Zhang G, Sandhaus RA. Trends in the diagnosis of symptomatic patients with alpha1-antitrypsin deficiency between 1968 and 2003. Chest 2005; 128:1179–1186.
- Greulich T, Ottaviani S, Bals R, et al. Alpha1-antitrypsin deficiency—diagnostic testing and disease awareness in Germany and Italy. Respir Med 2013; 107:1400–1408.
- Taliercio RM, Chatburn RL, Stoller JK. Knowledge of alpha-1 antitrypsin deficiency among internal medicine house officers and respiratory therapists: results of a survey. Respir Care 2010; 55:322–327.
- Rubenfeld GD, Cooper C, Carter G, Thompson BT, Hudson LD. Barriers to providing lung-protective ventilation to patients with acute lung injury. Crit Care Med 2004; 32:1289–1293.
- Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282:1458–1465.
- Rahaghi F, Ortega I, Rahaghi N, et al. Physician alert suggesting alpha-1 antitrypsin deficiency testing in pulmonary function test (PFT) results. COPD 2009; 6:26–30.
- Campos M, Hagenlocker B, Martinez N, et al. Impact of an electronic medical record clinical reminder to improve detection of COPD and alpha-1 antitrypsin deficiency in the Veterans Administration (VA) system (abstract). Am J Respir Crit Care Med 2011;183:A5356. www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2011.183.1_MeetingAbstracts.A5356. Accessed May 24, 2016.
- Jain A, McCarthy K, Xu M, Stoller JK. Impact of a clinical decision support system in an electronic health record to enhance detection of alpha(1)-antitrypsin deficiency. Chest 2011;140:198–204.
- American Thoracic Society, European Respiratory Society. American Thoracic Society/European Respiratory Society statement: standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med 2003; 168:818–900.
- Rahaghi FF, Sandhaus RA, Brantly ML, et al. The prevalence of alpha-1 antitrypsin deficiency among patients found to have airflow obstruction. COPD 2012; 9:352–358.
- Carrell RW, Lomas DA. Alpha1-antitrypsin deficiency—a model for conformational diseases. N Engl J Med 2002; 346:45–53.
- Stoller JK, Aboussouan LS. A review of alpha1-antitrypsin deficiency. Am J Respir Crit Care Med 2012; 185:246–259.
- McElvaney NG, Stoller JK, Buist AS, et al. Baseline characteristics of enrollees in the National Heart, Lung and Blood Institute Registry of Alpha 1-Antitrypsin Deficiency. Alpha 1-Antitrypsin Deficiency Registry Study Group. Chest 1997; 111:394–403.
- Lomas DA, Evans DL, Finch JT, Carrell RW. The mechanism of Z alpha 1-antitrypsin accumulation in the liver. Nature 1992; 357:605–607.
- Lomas DA, Finch JT, Seyama K, Nukiwa T, Carrell RW. Alpha 1-antitrypsin Siiyama (Ser53-->Phe). Further evidence for intracellular loop-sheet polymerization. J Biol Chem 1993; 268:15333–15335.
- Mayer AS, Stoller JK, Bucher Bartelson B, James Ruttenber A, Sandhaus RA, Newman LS. Occupational exposure risks in individuals with PI*Z alpha(1)-antitrypsin deficiency. Am J Respir Crit Care Med 2000; 162:553–558.
- Tan L, Dickens JA, Demeo DL, et al. Circulating polymers in alpha1-antitrypsin deficiency. Eur Respir J 2014; 43:1501–1504.
- Parmar JS, Mahadeva R, Reed BJ, et al. Polymers of alpha(1)-antitrypsin are chemotactic for human neutrophils: a new paradigm for the pathogenesis of emphysema. Am J Respir Cell Mol Biol 2002; 26:723–730.
- Molloy K, Hersh CP, Morris VB, et al. Clarification of the risk of chronic obstructive pulmonary disease in alpha1-antitrypsin deficiency PiMZ heterozygotes. Am J Respir Crit Care Med 2014; 189:419–427.
- Parr DG, Stoel BC, Stolk J, Stockley RA. Pattern of emphysema distribution in alpha1-antitrypsin deficiency influences lung function impairment. Am J Respir Crit Care Med 2004; 170:1172–1178.
- Sveger T. Liver disease in alpha1-antitrypsin deficiency detected by screening of 200,000 infants. N Engl J Med 1976; 294:1316–1321.
- O’Brien ML, Buist NR, Murphey WH. Neonatal screening for alpha1-antitrypsin deficiency. J Pediatr 1978; 92:1006–1010.
- Piitulainen E, Montero LC, Nystedt-Duzakin M, et al. Lung function and CT densitometry in subjects with alpha-1-antitrypsin deficiency and healthy controls at 35 years of age. COPD 2015; 12:162–167.
- The Alpha-1-Antitrypsin Deficiency Registry Study Group. Survival and FEV1 decline in individuals with severe deficiency of alpha1-antitrypsin. Am J Respir Crit Care Med 1998; 158:49–59.
- Dawkins PA, Dawkins CL, Wood AM, Nightingale PG, Stockley JA, Stockley RA. Rate of progression of lung function impairment in alpha1-antitrypsin deficiency. Eur Respir J 2009; 33:1338–1344.
- Needham M, Stockley RA. Alpha 1-antitrypsin deficiency. 3: clinical manifestations and natural history. Thorax 2004; 59:441–445.
- Tomashefski JF Jr, Crystal RG, Wiedemann HP, Mascha E, Stoller JK. The bronchopulmonary pathology of alpha-1 antitrypsin (AAT) deficiency: findings of the Death Review Committee of the National Registry for Individuals with Severe Deficiency of Alpha-1 Antitrypsin. Hum Pathol 2004; 35:1452–1461.
- Tanash HA, Nilsson PM, Nilsson JA, Piitulainen E. Clinical course and prognosis of never-smokers with severe alpha-1-antitrypsin deficiency (PiZZ). Thorax 2008; 63:1091–1095.
- Walsh JW, Snider GL, Stoller JK. A review of the Alpha-1 Foundation: its formation, impact, and critical success factors. Respir Care 2006; 51:526–531.
- Rokadia HK, Stoller JK. Surgical and bronchoscopic lung volume reduction treatment for a-1 antitrypsin deficiency. Clin Pulm Med 2015; 22:279–285.
- Dirksen A, Piitulainen E, Parr DG, et al. Exploring the role of CT densitometry: a randomised study of augmentation therapy in alpha1-antitrypsin deficiency. Eur Respir J 2009; 33:1345–1353.
- Dirksen A, Dijkman JH, Madsen F, et al. A randomized clinical trial of alpha(1)-antitrypsin augmentation therapy. Am J Respir Crit Care Med 1999; 160:1468–1472.
- Gildea TR, Shermock KM, Singer ME, Stoller JK. Cost-effectiveness analysis of augmentation therapy for severe alpha1-antitrypsin deficiency. Am J Respir Crit Care Med 2003; 167:1387–1392.
Alpha-1 antitrypsin deficiency is a common but underrecognized genetic condition that increases the risk of chronic obstructive pulmonary disease (COPD) and liver disease. Primary care providers can play a critical role in detecting it and managing patients who have it.
RECOGNIZED CASES ARE THE TIP OF THE ICEBERG
First described in 1963,1 alpha-1 antitrypsin deficiency is estimated to affect 100,000 Americans, fewer than 15,000 of whom have received a clinical diagnosis. As further evidence of its underrecognition,2–7 many patients experience long delays between their first symptoms and the diagnosis. Early studies indicated that the average diagnostic delay was 7.2 years,4 and the latest studies, as recent as 2013, indicate a similar diagnostic delay.7
Furthermore, many patients see multiple healthcare providers before receiving the correct diagnosis. A 1994 survey by this author4 found that 43.7% of patients who had severe deficiency of alpha-1 antitrypsin saw at least three physicians before the correct diagnosis was made.
Why is the disease underrecognized?
Several reasons may account for underrecognition of this disease. Many clinicians—including, unfortunately, many pulmonologists—do not know much about it,7,8 do not adhere to clinical guidelines,9,10 or harbor the misperception that there is no therapy available and, therefore, no compelling reason to make a diagnosis.7
Regarding inadequate knowledge, in a study by Taliercio, Chatburn, and this author,8 internal medicine residents scored only 63% correct on a 10-question quiz on diagnostic features of alpha-1 antitrypsin deficiency. There was no evidence of a training effect—senior residents scored no higher than interns.
Similarly, when Greulich et al7 surveyed German and Italian internists, general practitioners, and pulmonologists, one-fourth to one-half of them (depending on specialty and country) stated that they knew either very little or nothing at all about alpha-1 antitrypsin deficiency. In addition, 7% to 8% agreed with the statement, “There is no treatment available for this disease.”7
Nonadoption of clinical guidelines has been widely recognized in medicine and is evident in the failure to implement various recommended practices,9,10 such as low-stretch ventilation for acute respiratory distress syndrome and prophylaxis against deep vein thrombosis.
Finding the rest of the iceberg
Efforts to enhance compliance with guidelines on testing for alpha-1 antitrypsin deficiency have included using the electronic medical record to prompt physicians to test appropriate candidates.11–13
Jain et al13 examined the effect of installing such a prompting system to remind physicians to test for alpha-1 antitrypsin deficiency in patients with airflow obstruction that does not reverse with a bronchodilator—a recognized indication for testing for this disease according to standards endorsed by the American Thoracic Society and European Respiratory Society.14 At baseline, only 4.7% of appropriate candidates were being tested; after a prompt was installed in the electronic medical record, the rate rose to 15.1%, still a minority of candidates.
Another strategy is to empower respiratory therapists who perform pulmonary function tests to invite patients to be tested if their pulmonary function tests show postbronchodilator airflow obstruction. Rahaghi et al15 showed that using this strategy, 20 (0.63%) of 3,152 patients who were found to have fixed airflow obstruction when they underwent pulmonary function testing were newly diagnosed with severe deficiency of alpha-1 antitrypsin. Other targeted detection studies in patients with COPD estimated the prevalence of alpha-1 antitrypsin deficiency at up to 12%.3
PHYSIOLOGY AND PATHOPHYSIOLOGY OF ALPHA-1 ANTITRYPSIN DEFICIENCY
Alpha-1 antitrypsin is a single-chain, 394-amino acid glycoprotein with three carbohydrate side chains found at asparagine residues along the primary structure.16
A major physiologic function of this molecule is to bind neutrophil elastase, which it does avidly. In a “mousetrap-like” mechanism,16 an active site on the alpha-1 antitrypsin molecule captures the neutrophil elastase and is cleaved, releasing steric energy in the molecule, catapulting the neutrophil elastase to the opposite side of the alpha-1 antitrypsin molecule, and inactivating it (Figure 1).
MM is normal, ZZ is not
Alpha-1 antitrypsin deficiency is inherited as an autosomal-codominant condition.17
The SERPINA1 gene, which codes for alpha-1 antitrypsin, is located on the long arm of the 14th chromosome, and more than 150 alleles of this gene have been identified to date. The normal allele is denoted M, and the allele most commonly associated with severe deficiency is denoted Z. People who are homozygous for the M allele (ie, normal) are called PI*MM (PI stands for “protease inhibitor”), and those who are homozygous for the Z allele are PI*ZZ. More than 90% of patients with severe alpha-1 antitrypsin deficiency are PI*ZZ.18
The Z allele has a single amino acid substitution (glutamic acid-to-lysine at position 342), which results in abnormal folding and formation of polymers of the Z molecule within hepatocytes.19,20 These polymers are recognized on liver biopsy as periodic acid-Schiff diastase-resistant eosinophilic inclusion bodies on histologic staining (Figure 2).
With alpha-1 antitrypsin trapped as Z-molecule polymers in the liver, the amount in the bloodstream falls, and there is a consequent decrease in the amount available in the lung to oppose the proteolytic burden of neutrophil elastase, especially in people who smoke or work in dusty environments.21
Tan et al22 have shown that some of the polymerized Z protein can escape the liver and circulate in the blood and that alveolar macrophages may also produce Z polymers. These Z polymers are chemotactic for neutrophils,23 so that their presence in the lung fuels the inflammatory cascade by recruiting more neutrophils to the lung, thereby increasing the proteolytic burden to the lung and increasing the risk of emphysema. Z monomers that do circulate can bind neutrophil elastase, but their binding avidity to neutrophil elastase is substantially lower than that of M-type alpha-1 antitrypsin.
CLINICAL MANIFESTATIONS
Alpha-1 antitrypsin deficiency of the PI*ZZ type is associated with two major clinical manifestations:
- Emphysema, resulting from the loss of proteolytic protection of the lung by alpha-1 antitrypsin (a toxic loss of function), and
- Liver diseases such as cirrhosis and chronic hepatitis, which result from abnormal accumulation of alpha-1 antitrypsin within hepatocytes (a toxic gain of function), and hepatoma.17
Other clinical manifestations of PI*ZZ alpha-1 antitrypsin deficiency include panniculitis and an association with cytoplasmic antineutrophil cytoplasmic antibody-positive vasculitis.17
Some uncertainty exists regarding the risk associated with the PI*MZ heterozygous state because there has been no systematic longitudinal study of people with this genotype. However, the weight of available experience suggests that PI*MZ individuals who have never smoked are not at increased risk of developing emphysema.24
Findings from a national registry: PI*ZZ COPD resembles ‘usual’ COPD
Distinguishing patients with alpha-1 antitrypsin deficiency from those with “usual” COPD (ie, without alpha-1 antitrypsin deficiency) can be difficult, as shown in data from the National Heart, Lung, and Blood Institute’s Alpha-1 Antitrypsin Deficiency Registry study.18 This multicenter, longitudinal, observational study contains the largest well-characterized cohort with severe deficiency of alpha-1 antitrypsin (PI*ZZ, PI*ZNull, etc), with 1,129 patients.
Pulmonary function test results were consistent with emphysema in most of the patients in the registry. Mean postbronchodilator pulmonary function values (± standard error of the mean) were:
- Forced expiratory volume in 1 second (FEV1) 46.7% of predicted (± 30%)
- Ratio of FEV1 to forced vital capacity 42.9% (± 20.4% )
- Mean diffusing capacity for carbon monoxide 50.3% of predicted (± 22.5%).
Like many patients with usual COPD, 60% of the registry patients demonstrated a component of airway reactivity, with significant reversal of airflow obstruction over three spirometries after receiving a dose of an inhaled bronchodilator (characterized by a 12% and 200-mL postbronchodilator rise in FEV1). Moreover, 78 patients had normal lung function.
Symptoms also resembled those in patients with usual emphysema, chronic bronchitis, or both. On enrollment in the registry, 83.9% of the patients had shortness of breath on exertion, 75.5% had wheezing with upper respiratory infections, 65.3% had wheezing without upper respiratory infection, 67.6% had recent debilitating chest illness, 42.4% had “usual” cough, and 49.6% had annual cough and phlegm episodes.
Imaging findings. Although the classic teaching is that emphysema due to alpha-1 antitrypsin deficiency produces lower-lobe hyperlucency on plain films, relying on this sign would lead to underrecognition, as 36% of PI*ZZ patients have apical-predominant emphysema on chest computed tomography,24 which resembles the usual centriacinar emphysema pattern. Figure 3 shows axial computed tomographic scans through the apices and the bases of the lungs of a patient with alpha-1 antitrypsin deficiency.
In view of these difficulties, guidelines from the American Thoracic Society and European Respiratory Society14 endorse testing for alpha-1 antitrypsin deficiency in all adults who have symptoms and fixed airflow obstruction (Table 1).
CONSEQUENCES OF ALPHA-1 ANTITRYPSIN DEFICIENCY
Two large screening studies2,3,25,26 followed people who were identified at birth as having alpha-1 antitrypsin deficiency to examine the natural course of the disease.
The larger of the two studies27 tested 200,000 Swedish newborns. Follow-up of this cohort to age 35 indicated that 35-year-old never-smoking PI*ZZ individuals have normal lung function and no excess emphysema on computed tomography compared with normal peers matched for age and sex.27 In contrast, the few PI*ZZ ever-smokers demonstrated a lower level of transfer factor and significantly more emphysema on computed tomography than normal (PI*MM) never-smokers.
Faster decline in lung function
Data from the National Heart, Lung, and Blood Institute registry indicate that, on average, people with severe alpha-1 antitrypsin deficiency lose lung function faster than people without the disease.28 Specifically, in never-smokers in the registry, the average rate of FEV1 decline was 67 mL/year, and among ex-smokers, it was 54 mL/year. Both of these values exceed the general age-related rate of FEV1 decline of approximately 20 to 25 mL/year in never-smoking, normal adults. Among current smokers in the registry with severe alpha-1 antitrypsin deficiency, the rate of FEV1 decline was 109 mL/year.
Rates of FEV1 decline over time vary among groups with differing degrees of airflow obstruction. For example, PI*ZZ patients with moderate COPD (stage II of the four-stage Global Initiative for Chronic Obstructive Lung Disease classification system) lose lung function faster than patients with either milder or more severe degrees of airflow obstruction.29
As with COPD in general, exacerbations of COPD in people with severe deficiency of alpha-1 antitrypsin are associated with worsened clinical status. In one series,30 54% of 265 PI*ZZ patients experienced an exacerbation in the first year of follow-up, and 18% experienced at least three. Such exacerbations occurred in December and January in 32% of these individuals, likely due to a viral precipitant.
Increased mortality
Severe deficiency of alpha-1 antitrypsin is associated not only with severe morbidity but also death. In the national registry, the overall rate of death was 18.6% at 5 years of follow-up, or approximately 3% per year.28
A low FEV1 at entry was a bad sign. Patients entering the registry with FEV1 values below 15% of predicted had a 36% mortality rate at 3 years, compared with 2.6% in those whose baseline FEV1 exceeded 50% of predicted.
Underlying causes of death in registry participants included emphysema (accounting for 72% of deaths) and cirrhosis (10%),31 which were the only causes of death more frequent than in age- and sex-matched controls. In a series of never-smokers who had PI*ZZ alpha-1 antitrypsin deficiency,32 death was less frequently attributed to emphysema than in the national registry (46%) and more often attributed to cirrhosis (28%), indicating that never-smokers may more frequently escape the ravages of emphysema but experience a higher rate of developing cirrhosis later in life.33
DIAGNOSING ALPHA-1 ANTITRYPSIN DEFICIENCY
Available blood tests for alpha-1 antitrypsin deficiency include:
The serum alpha-1 antitrypsin level, most often done by nephelometry. Normal serum levels generally range from 100 to 220 mg/dL.
Phenotyping, usually performed by isoelectric focusing, which can identify different band patterns associated with different alleles.
Genotyping involves determining which alpha-1 antitrypsin alleles are present, most often using polymerase chain reaction testing targeting the S and Z alleles and occasionally set up to detect less common alleles such as F and I.17
Gene sequencing is occasionally necessary to achieve an accurate, definitive diagnosis.
Free, confidential testing is available
Clinical testing most often involves checking both a serum level and a phenotype or genotype. Such tests are often available in hospital laboratories and commercial laboratories, with testing also facilitated by the availability of free testing kits from several manufacturers of drugs for alpha-1 antitrypsin deficiency.
The Alpha-1 Foundation (www.alpha1.org)34 also offers a free, home-based confidential testing kit through a research protocol at the Medical University of South Carolina (alphaone@musc.edu) called the Alpha-1 Coded Testing (ACT) study. Patients can receive a kit and lancet at home, submit the dried blood-spot specimen, and receive in the mail a confidential serum level and genotype.
The availability of such home-based confidential testing allows patients to seek testing without a physician’s order and makes it easier for facilitated allied health providers, such as respiratory therapists, to recommend testing in appropriate clinical circumstances.15
TREATMENT OF ALPHA-1 ANTITRYPSIN DEFICIENCY
The treatment of patients with severe deficiency of alpha-1 antitrypsin and emphysema generally resembles that of patients with usual COPD. Specifically, smoking cessation, bronchodilators, occasionally inhaled steroids, supplemental oxygen, preventive vaccinations, and pulmonary rehabilitation are indicated as per usual clinical assessment.
Lung volume reduction surgery, which is beneficial in appropriate subsets of COPD patients, is generally less effective in those with severe alpha-1 antitrypsin deficiency,35 specifically because the magnitude of FEV1 increase and the duration of such a rise are lower than in usual COPD patients.
Augmentation therapy
Specific therapy for alpha-1 antitrypsin deficiency currently involves weekly intravenous infusions of purified, pooled human-plasma-derived alpha-1 antitrypsin, so-called augmentation therapy. Four drugs have been approved for use in the United States:
- Prolastin-C (Grifols, Barcelona, Spain)
- Aralast NP (Baxalta, Bonneckborn, IL)
- Zemaira (CSL Behring, King of Prussia, PA)
- Glassia (Baxalta, Bonneckborn, IL, and Kamada, Ness Ziona, Israel).
All of these were approved for use in the United States on the basis of biochemical efficacy. Specifically, infusion of these drugs has been shown to raise serum levels above a protective threshold value (generally considered 57 mg/dL, the value below which the risk of developing emphysema increases beyond normal).
Randomized controlled trials36,37 have addressed the efficacy of intravenous augmentation therapy, and although no single trial has been definitive, the weight of evidence shows that augmentation therapy can slow the progression of emphysema. For example, in a study by Dirksen et al,37 augmentation therapy was associated with a slower progression of emphysema as assessed by the rate of loss of lung density on computed tomography.
On the basis of the available evidence, the American Thoracic Society and European Respiratory Society14 have recommended augmentation therapy in individuals with “established airflow obstruction from alpha-1 antitrypsin deficiency.”14 Their guidelines go on to say that the evidence that augmentation therapy is beneficial “is stronger for individuals with moderate airflow obstruction (eg, FEV1 35%–60% of predicted) than for those with severe airflow obstruction. Augmentation therapy is not currently recommended for individuals without emphysema.”
The guidelines recognize that although augmentation therapy does not satisfy the usual criteria for cost-effectiveness (< $50,000 per quality-adjusted life year) due to its high cost (approximately $100,000 per year if paid for out of pocket),38 it is recommended for appropriate candidates because it is the only available specific therapy for severe deficiency of alpha-1 antitrypsin.
Novel therapies
In addition to current treatment approaches of augmentation therapy, a number of novel treatment strategies are being investigated, several of which hold much promise.
Gene therapy, using adeno-associated virus to transfect the normal human gene into individuals with severe deficiency of alpha-1 antitrypsin, has been undertaken and is currently under study. In addition, a variety of approaches to interdict production of abnormal Z protein from the liver are being examined, as well as inhaled hyaluronic acid to protect the lung.
Alpha-1 antitrypsin deficiency is a common but underrecognized genetic condition that increases the risk of chronic obstructive pulmonary disease (COPD) and liver disease. Primary care providers can play a critical role in detecting it and managing patients who have it.
RECOGNIZED CASES ARE THE TIP OF THE ICEBERG
First described in 1963,1 alpha-1 antitrypsin deficiency is estimated to affect 100,000 Americans, fewer than 15,000 of whom have received a clinical diagnosis. As further evidence of its underrecognition,2–7 many patients experience long delays between their first symptoms and the diagnosis. Early studies indicated that the average diagnostic delay was 7.2 years,4 and the latest studies, as recent as 2013, indicate a similar diagnostic delay.7
Furthermore, many patients see multiple healthcare providers before receiving the correct diagnosis. A 1994 survey by this author4 found that 43.7% of patients who had severe deficiency of alpha-1 antitrypsin saw at least three physicians before the correct diagnosis was made.
Why is the disease underrecognized?
Several reasons may account for underrecognition of this disease. Many clinicians—including, unfortunately, many pulmonologists—do not know much about it,7,8 do not adhere to clinical guidelines,9,10 or harbor the misperception that there is no therapy available and, therefore, no compelling reason to make a diagnosis.7
Regarding inadequate knowledge, in a study by Taliercio, Chatburn, and this author,8 internal medicine residents scored only 63% correct on a 10-question quiz on diagnostic features of alpha-1 antitrypsin deficiency. There was no evidence of a training effect—senior residents scored no higher than interns.
Similarly, when Greulich et al7 surveyed German and Italian internists, general practitioners, and pulmonologists, one-fourth to one-half of them (depending on specialty and country) stated that they knew either very little or nothing at all about alpha-1 antitrypsin deficiency. In addition, 7% to 8% agreed with the statement, “There is no treatment available for this disease.”7
Nonadoption of clinical guidelines has been widely recognized in medicine and is evident in the failure to implement various recommended practices,9,10 such as low-stretch ventilation for acute respiratory distress syndrome and prophylaxis against deep vein thrombosis.
Finding the rest of the iceberg
Efforts to enhance compliance with guidelines on testing for alpha-1 antitrypsin deficiency have included using the electronic medical record to prompt physicians to test appropriate candidates.11–13
Jain et al13 examined the effect of installing such a prompting system to remind physicians to test for alpha-1 antitrypsin deficiency in patients with airflow obstruction that does not reverse with a bronchodilator—a recognized indication for testing for this disease according to standards endorsed by the American Thoracic Society and European Respiratory Society.14 At baseline, only 4.7% of appropriate candidates were being tested; after a prompt was installed in the electronic medical record, the rate rose to 15.1%, still a minority of candidates.
Another strategy is to empower respiratory therapists who perform pulmonary function tests to invite patients to be tested if their pulmonary function tests show postbronchodilator airflow obstruction. Rahaghi et al15 showed that using this strategy, 20 (0.63%) of 3,152 patients who were found to have fixed airflow obstruction when they underwent pulmonary function testing were newly diagnosed with severe deficiency of alpha-1 antitrypsin. Other targeted detection studies in patients with COPD estimated the prevalence of alpha-1 antitrypsin deficiency at up to 12%.3
PHYSIOLOGY AND PATHOPHYSIOLOGY OF ALPHA-1 ANTITRYPSIN DEFICIENCY
Alpha-1 antitrypsin is a single-chain, 394-amino acid glycoprotein with three carbohydrate side chains found at asparagine residues along the primary structure.16
A major physiologic function of this molecule is to bind neutrophil elastase, which it does avidly. In a “mousetrap-like” mechanism,16 an active site on the alpha-1 antitrypsin molecule captures the neutrophil elastase and is cleaved, releasing steric energy in the molecule, catapulting the neutrophil elastase to the opposite side of the alpha-1 antitrypsin molecule, and inactivating it (Figure 1).
MM is normal, ZZ is not
Alpha-1 antitrypsin deficiency is inherited as an autosomal-codominant condition.17
The SERPINA1 gene, which codes for alpha-1 antitrypsin, is located on the long arm of the 14th chromosome, and more than 150 alleles of this gene have been identified to date. The normal allele is denoted M, and the allele most commonly associated with severe deficiency is denoted Z. People who are homozygous for the M allele (ie, normal) are called PI*MM (PI stands for “protease inhibitor”), and those who are homozygous for the Z allele are PI*ZZ. More than 90% of patients with severe alpha-1 antitrypsin deficiency are PI*ZZ.18
The Z allele has a single amino acid substitution (glutamic acid-to-lysine at position 342), which results in abnormal folding and formation of polymers of the Z molecule within hepatocytes.19,20 These polymers are recognized on liver biopsy as periodic acid-Schiff diastase-resistant eosinophilic inclusion bodies on histologic staining (Figure 2).
With alpha-1 antitrypsin trapped as Z-molecule polymers in the liver, the amount in the bloodstream falls, and there is a consequent decrease in the amount available in the lung to oppose the proteolytic burden of neutrophil elastase, especially in people who smoke or work in dusty environments.21
Tan et al22 have shown that some of the polymerized Z protein can escape the liver and circulate in the blood and that alveolar macrophages may also produce Z polymers. These Z polymers are chemotactic for neutrophils,23 so that their presence in the lung fuels the inflammatory cascade by recruiting more neutrophils to the lung, thereby increasing the proteolytic burden to the lung and increasing the risk of emphysema. Z monomers that do circulate can bind neutrophil elastase, but their binding avidity to neutrophil elastase is substantially lower than that of M-type alpha-1 antitrypsin.
CLINICAL MANIFESTATIONS
Alpha-1 antitrypsin deficiency of the PI*ZZ type is associated with two major clinical manifestations:
- Emphysema, resulting from the loss of proteolytic protection of the lung by alpha-1 antitrypsin (a toxic loss of function), and
- Liver diseases such as cirrhosis and chronic hepatitis, which result from abnormal accumulation of alpha-1 antitrypsin within hepatocytes (a toxic gain of function), and hepatoma.17
Other clinical manifestations of PI*ZZ alpha-1 antitrypsin deficiency include panniculitis and an association with cytoplasmic antineutrophil cytoplasmic antibody-positive vasculitis.17
Some uncertainty exists regarding the risk associated with the PI*MZ heterozygous state because there has been no systematic longitudinal study of people with this genotype. However, the weight of available experience suggests that PI*MZ individuals who have never smoked are not at increased risk of developing emphysema.24
Findings from a national registry: PI*ZZ COPD resembles ‘usual’ COPD
Distinguishing patients with alpha-1 antitrypsin deficiency from those with “usual” COPD (ie, without alpha-1 antitrypsin deficiency) can be difficult, as shown in data from the National Heart, Lung, and Blood Institute’s Alpha-1 Antitrypsin Deficiency Registry study.18 This multicenter, longitudinal, observational study contains the largest well-characterized cohort with severe deficiency of alpha-1 antitrypsin (PI*ZZ, PI*ZNull, etc), with 1,129 patients.
Pulmonary function test results were consistent with emphysema in most of the patients in the registry. Mean postbronchodilator pulmonary function values (± standard error of the mean) were:
- Forced expiratory volume in 1 second (FEV1) 46.7% of predicted (± 30%)
- Ratio of FEV1 to forced vital capacity 42.9% (± 20.4% )
- Mean diffusing capacity for carbon monoxide 50.3% of predicted (± 22.5%).
Like many patients with usual COPD, 60% of the registry patients demonstrated a component of airway reactivity, with significant reversal of airflow obstruction over three spirometries after receiving a dose of an inhaled bronchodilator (characterized by a 12% and 200-mL postbronchodilator rise in FEV1). Moreover, 78 patients had normal lung function.
Symptoms also resembled those in patients with usual emphysema, chronic bronchitis, or both. On enrollment in the registry, 83.9% of the patients had shortness of breath on exertion, 75.5% had wheezing with upper respiratory infections, 65.3% had wheezing without upper respiratory infection, 67.6% had recent debilitating chest illness, 42.4% had “usual” cough, and 49.6% had annual cough and phlegm episodes.
Imaging findings. Although the classic teaching is that emphysema due to alpha-1 antitrypsin deficiency produces lower-lobe hyperlucency on plain films, relying on this sign would lead to underrecognition, as 36% of PI*ZZ patients have apical-predominant emphysema on chest computed tomography,24 which resembles the usual centriacinar emphysema pattern. Figure 3 shows axial computed tomographic scans through the apices and the bases of the lungs of a patient with alpha-1 antitrypsin deficiency.
In view of these difficulties, guidelines from the American Thoracic Society and European Respiratory Society14 endorse testing for alpha-1 antitrypsin deficiency in all adults who have symptoms and fixed airflow obstruction (Table 1).
CONSEQUENCES OF ALPHA-1 ANTITRYPSIN DEFICIENCY
Two large screening studies2,3,25,26 followed people who were identified at birth as having alpha-1 antitrypsin deficiency to examine the natural course of the disease.
The larger of the two studies27 tested 200,000 Swedish newborns. Follow-up of this cohort to age 35 indicated that 35-year-old never-smoking PI*ZZ individuals have normal lung function and no excess emphysema on computed tomography compared with normal peers matched for age and sex.27 In contrast, the few PI*ZZ ever-smokers demonstrated a lower level of transfer factor and significantly more emphysema on computed tomography than normal (PI*MM) never-smokers.
Faster decline in lung function
Data from the National Heart, Lung, and Blood Institute registry indicate that, on average, people with severe alpha-1 antitrypsin deficiency lose lung function faster than people without the disease.28 Specifically, in never-smokers in the registry, the average rate of FEV1 decline was 67 mL/year, and among ex-smokers, it was 54 mL/year. Both of these values exceed the general age-related rate of FEV1 decline of approximately 20 to 25 mL/year in never-smoking, normal adults. Among current smokers in the registry with severe alpha-1 antitrypsin deficiency, the rate of FEV1 decline was 109 mL/year.
Rates of FEV1 decline over time vary among groups with differing degrees of airflow obstruction. For example, PI*ZZ patients with moderate COPD (stage II of the four-stage Global Initiative for Chronic Obstructive Lung Disease classification system) lose lung function faster than patients with either milder or more severe degrees of airflow obstruction.29
As with COPD in general, exacerbations of COPD in people with severe deficiency of alpha-1 antitrypsin are associated with worsened clinical status. In one series,30 54% of 265 PI*ZZ patients experienced an exacerbation in the first year of follow-up, and 18% experienced at least three. Such exacerbations occurred in December and January in 32% of these individuals, likely due to a viral precipitant.
Increased mortality
Severe deficiency of alpha-1 antitrypsin is associated not only with severe morbidity but also death. In the national registry, the overall rate of death was 18.6% at 5 years of follow-up, or approximately 3% per year.28
A low FEV1 at entry was a bad sign. Patients entering the registry with FEV1 values below 15% of predicted had a 36% mortality rate at 3 years, compared with 2.6% in those whose baseline FEV1 exceeded 50% of predicted.
Underlying causes of death in registry participants included emphysema (accounting for 72% of deaths) and cirrhosis (10%),31 which were the only causes of death more frequent than in age- and sex-matched controls. In a series of never-smokers who had PI*ZZ alpha-1 antitrypsin deficiency,32 death was less frequently attributed to emphysema than in the national registry (46%) and more often attributed to cirrhosis (28%), indicating that never-smokers may more frequently escape the ravages of emphysema but experience a higher rate of developing cirrhosis later in life.33
DIAGNOSING ALPHA-1 ANTITRYPSIN DEFICIENCY
Available blood tests for alpha-1 antitrypsin deficiency include:
The serum alpha-1 antitrypsin level, most often done by nephelometry. Normal serum levels generally range from 100 to 220 mg/dL.
Phenotyping, usually performed by isoelectric focusing, which can identify different band patterns associated with different alleles.
Genotyping involves determining which alpha-1 antitrypsin alleles are present, most often using polymerase chain reaction testing targeting the S and Z alleles and occasionally set up to detect less common alleles such as F and I.17
Gene sequencing is occasionally necessary to achieve an accurate, definitive diagnosis.
Free, confidential testing is available
Clinical testing most often involves checking both a serum level and a phenotype or genotype. Such tests are often available in hospital laboratories and commercial laboratories, with testing also facilitated by the availability of free testing kits from several manufacturers of drugs for alpha-1 antitrypsin deficiency.
The Alpha-1 Foundation (www.alpha1.org)34 also offers a free, home-based confidential testing kit through a research protocol at the Medical University of South Carolina (alphaone@musc.edu) called the Alpha-1 Coded Testing (ACT) study. Patients can receive a kit and lancet at home, submit the dried blood-spot specimen, and receive in the mail a confidential serum level and genotype.
The availability of such home-based confidential testing allows patients to seek testing without a physician’s order and makes it easier for facilitated allied health providers, such as respiratory therapists, to recommend testing in appropriate clinical circumstances.15
TREATMENT OF ALPHA-1 ANTITRYPSIN DEFICIENCY
The treatment of patients with severe deficiency of alpha-1 antitrypsin and emphysema generally resembles that of patients with usual COPD. Specifically, smoking cessation, bronchodilators, occasionally inhaled steroids, supplemental oxygen, preventive vaccinations, and pulmonary rehabilitation are indicated as per usual clinical assessment.
Lung volume reduction surgery, which is beneficial in appropriate subsets of COPD patients, is generally less effective in those with severe alpha-1 antitrypsin deficiency,35 specifically because the magnitude of FEV1 increase and the duration of such a rise are lower than in usual COPD patients.
Augmentation therapy
Specific therapy for alpha-1 antitrypsin deficiency currently involves weekly intravenous infusions of purified, pooled human-plasma-derived alpha-1 antitrypsin, so-called augmentation therapy. Four drugs have been approved for use in the United States:
- Prolastin-C (Grifols, Barcelona, Spain)
- Aralast NP (Baxalta, Bonneckborn, IL)
- Zemaira (CSL Behring, King of Prussia, PA)
- Glassia (Baxalta, Bonneckborn, IL, and Kamada, Ness Ziona, Israel).
All of these were approved for use in the United States on the basis of biochemical efficacy. Specifically, infusion of these drugs has been shown to raise serum levels above a protective threshold value (generally considered 57 mg/dL, the value below which the risk of developing emphysema increases beyond normal).
Randomized controlled trials36,37 have addressed the efficacy of intravenous augmentation therapy, and although no single trial has been definitive, the weight of evidence shows that augmentation therapy can slow the progression of emphysema. For example, in a study by Dirksen et al,37 augmentation therapy was associated with a slower progression of emphysema as assessed by the rate of loss of lung density on computed tomography.
On the basis of the available evidence, the American Thoracic Society and European Respiratory Society14 have recommended augmentation therapy in individuals with “established airflow obstruction from alpha-1 antitrypsin deficiency.”14 Their guidelines go on to say that the evidence that augmentation therapy is beneficial “is stronger for individuals with moderate airflow obstruction (eg, FEV1 35%–60% of predicted) than for those with severe airflow obstruction. Augmentation therapy is not currently recommended for individuals without emphysema.”
The guidelines recognize that although augmentation therapy does not satisfy the usual criteria for cost-effectiveness (< $50,000 per quality-adjusted life year) due to its high cost (approximately $100,000 per year if paid for out of pocket),38 it is recommended for appropriate candidates because it is the only available specific therapy for severe deficiency of alpha-1 antitrypsin.
Novel therapies
In addition to current treatment approaches of augmentation therapy, a number of novel treatment strategies are being investigated, several of which hold much promise.
Gene therapy, using adeno-associated virus to transfect the normal human gene into individuals with severe deficiency of alpha-1 antitrypsin, has been undertaken and is currently under study. In addition, a variety of approaches to interdict production of abnormal Z protein from the liver are being examined, as well as inhaled hyaluronic acid to protect the lung.
- Laurell C, Eriksson A. The electrophoretic alpha-1 globulin pattern of serum in alpha-1 antitrypsin deficiency. Scand J Clin Lab Invest 1963; 15:132–140.
- Aboussouan LS, Stoller JK. Detection of alpha-1 antitrypsin deficiency: a review. Respir Med 2009; 103:335–341.
- Stoller JK, Brantly M. The challenge of detecting alpha-1 antitrypsin deficiency. COPD 2013; 10(suppl 1):26–34.
- Stoller JK, Smith P, Yang P, Spray J. Physical and social impact of alpha 1-antitrypsin deficiency: results of a survey. Cleve Clin J Med 1994; 61:461–467.
- Stoller JK, Sandhaus RA, Turino G, Dickson R, Rodgers K, Strange C. Delay in diagnosis of alpha1-antitrypsin deficiency: a continuing problem. Chest 2005; 128:1989–1994.
- Campos MA, Wanner A, Zhang G, Sandhaus RA. Trends in the diagnosis of symptomatic patients with alpha1-antitrypsin deficiency between 1968 and 2003. Chest 2005; 128:1179–1186.
- Greulich T, Ottaviani S, Bals R, et al. Alpha1-antitrypsin deficiency—diagnostic testing and disease awareness in Germany and Italy. Respir Med 2013; 107:1400–1408.
- Taliercio RM, Chatburn RL, Stoller JK. Knowledge of alpha-1 antitrypsin deficiency among internal medicine house officers and respiratory therapists: results of a survey. Respir Care 2010; 55:322–327.
- Rubenfeld GD, Cooper C, Carter G, Thompson BT, Hudson LD. Barriers to providing lung-protective ventilation to patients with acute lung injury. Crit Care Med 2004; 32:1289–1293.
- Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282:1458–1465.
- Rahaghi F, Ortega I, Rahaghi N, et al. Physician alert suggesting alpha-1 antitrypsin deficiency testing in pulmonary function test (PFT) results. COPD 2009; 6:26–30.
- Campos M, Hagenlocker B, Martinez N, et al. Impact of an electronic medical record clinical reminder to improve detection of COPD and alpha-1 antitrypsin deficiency in the Veterans Administration (VA) system (abstract). Am J Respir Crit Care Med 2011;183:A5356. www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2011.183.1_MeetingAbstracts.A5356. Accessed May 24, 2016.
- Jain A, McCarthy K, Xu M, Stoller JK. Impact of a clinical decision support system in an electronic health record to enhance detection of alpha(1)-antitrypsin deficiency. Chest 2011;140:198–204.
- American Thoracic Society, European Respiratory Society. American Thoracic Society/European Respiratory Society statement: standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med 2003; 168:818–900.
- Rahaghi FF, Sandhaus RA, Brantly ML, et al. The prevalence of alpha-1 antitrypsin deficiency among patients found to have airflow obstruction. COPD 2012; 9:352–358.
- Carrell RW, Lomas DA. Alpha1-antitrypsin deficiency—a model for conformational diseases. N Engl J Med 2002; 346:45–53.
- Stoller JK, Aboussouan LS. A review of alpha1-antitrypsin deficiency. Am J Respir Crit Care Med 2012; 185:246–259.
- McElvaney NG, Stoller JK, Buist AS, et al. Baseline characteristics of enrollees in the National Heart, Lung and Blood Institute Registry of Alpha 1-Antitrypsin Deficiency. Alpha 1-Antitrypsin Deficiency Registry Study Group. Chest 1997; 111:394–403.
- Lomas DA, Evans DL, Finch JT, Carrell RW. The mechanism of Z alpha 1-antitrypsin accumulation in the liver. Nature 1992; 357:605–607.
- Lomas DA, Finch JT, Seyama K, Nukiwa T, Carrell RW. Alpha 1-antitrypsin Siiyama (Ser53-->Phe). Further evidence for intracellular loop-sheet polymerization. J Biol Chem 1993; 268:15333–15335.
- Mayer AS, Stoller JK, Bucher Bartelson B, James Ruttenber A, Sandhaus RA, Newman LS. Occupational exposure risks in individuals with PI*Z alpha(1)-antitrypsin deficiency. Am J Respir Crit Care Med 2000; 162:553–558.
- Tan L, Dickens JA, Demeo DL, et al. Circulating polymers in alpha1-antitrypsin deficiency. Eur Respir J 2014; 43:1501–1504.
- Parmar JS, Mahadeva R, Reed BJ, et al. Polymers of alpha(1)-antitrypsin are chemotactic for human neutrophils: a new paradigm for the pathogenesis of emphysema. Am J Respir Cell Mol Biol 2002; 26:723–730.
- Molloy K, Hersh CP, Morris VB, et al. Clarification of the risk of chronic obstructive pulmonary disease in alpha1-antitrypsin deficiency PiMZ heterozygotes. Am J Respir Crit Care Med 2014; 189:419–427.
- Parr DG, Stoel BC, Stolk J, Stockley RA. Pattern of emphysema distribution in alpha1-antitrypsin deficiency influences lung function impairment. Am J Respir Crit Care Med 2004; 170:1172–1178.
- Sveger T. Liver disease in alpha1-antitrypsin deficiency detected by screening of 200,000 infants. N Engl J Med 1976; 294:1316–1321.
- O’Brien ML, Buist NR, Murphey WH. Neonatal screening for alpha1-antitrypsin deficiency. J Pediatr 1978; 92:1006–1010.
- Piitulainen E, Montero LC, Nystedt-Duzakin M, et al. Lung function and CT densitometry in subjects with alpha-1-antitrypsin deficiency and healthy controls at 35 years of age. COPD 2015; 12:162–167.
- The Alpha-1-Antitrypsin Deficiency Registry Study Group. Survival and FEV1 decline in individuals with severe deficiency of alpha1-antitrypsin. Am J Respir Crit Care Med 1998; 158:49–59.
- Dawkins PA, Dawkins CL, Wood AM, Nightingale PG, Stockley JA, Stockley RA. Rate of progression of lung function impairment in alpha1-antitrypsin deficiency. Eur Respir J 2009; 33:1338–1344.
- Needham M, Stockley RA. Alpha 1-antitrypsin deficiency. 3: clinical manifestations and natural history. Thorax 2004; 59:441–445.
- Tomashefski JF Jr, Crystal RG, Wiedemann HP, Mascha E, Stoller JK. The bronchopulmonary pathology of alpha-1 antitrypsin (AAT) deficiency: findings of the Death Review Committee of the National Registry for Individuals with Severe Deficiency of Alpha-1 Antitrypsin. Hum Pathol 2004; 35:1452–1461.
- Tanash HA, Nilsson PM, Nilsson JA, Piitulainen E. Clinical course and prognosis of never-smokers with severe alpha-1-antitrypsin deficiency (PiZZ). Thorax 2008; 63:1091–1095.
- Walsh JW, Snider GL, Stoller JK. A review of the Alpha-1 Foundation: its formation, impact, and critical success factors. Respir Care 2006; 51:526–531.
- Rokadia HK, Stoller JK. Surgical and bronchoscopic lung volume reduction treatment for a-1 antitrypsin deficiency. Clin Pulm Med 2015; 22:279–285.
- Dirksen A, Piitulainen E, Parr DG, et al. Exploring the role of CT densitometry: a randomised study of augmentation therapy in alpha1-antitrypsin deficiency. Eur Respir J 2009; 33:1345–1353.
- Dirksen A, Dijkman JH, Madsen F, et al. A randomized clinical trial of alpha(1)-antitrypsin augmentation therapy. Am J Respir Crit Care Med 1999; 160:1468–1472.
- Gildea TR, Shermock KM, Singer ME, Stoller JK. Cost-effectiveness analysis of augmentation therapy for severe alpha1-antitrypsin deficiency. Am J Respir Crit Care Med 2003; 167:1387–1392.
- Laurell C, Eriksson A. The electrophoretic alpha-1 globulin pattern of serum in alpha-1 antitrypsin deficiency. Scand J Clin Lab Invest 1963; 15:132–140.
- Aboussouan LS, Stoller JK. Detection of alpha-1 antitrypsin deficiency: a review. Respir Med 2009; 103:335–341.
- Stoller JK, Brantly M. The challenge of detecting alpha-1 antitrypsin deficiency. COPD 2013; 10(suppl 1):26–34.
- Stoller JK, Smith P, Yang P, Spray J. Physical and social impact of alpha 1-antitrypsin deficiency: results of a survey. Cleve Clin J Med 1994; 61:461–467.
- Stoller JK, Sandhaus RA, Turino G, Dickson R, Rodgers K, Strange C. Delay in diagnosis of alpha1-antitrypsin deficiency: a continuing problem. Chest 2005; 128:1989–1994.
- Campos MA, Wanner A, Zhang G, Sandhaus RA. Trends in the diagnosis of symptomatic patients with alpha1-antitrypsin deficiency between 1968 and 2003. Chest 2005; 128:1179–1186.
- Greulich T, Ottaviani S, Bals R, et al. Alpha1-antitrypsin deficiency—diagnostic testing and disease awareness in Germany and Italy. Respir Med 2013; 107:1400–1408.
- Taliercio RM, Chatburn RL, Stoller JK. Knowledge of alpha-1 antitrypsin deficiency among internal medicine house officers and respiratory therapists: results of a survey. Respir Care 2010; 55:322–327.
- Rubenfeld GD, Cooper C, Carter G, Thompson BT, Hudson LD. Barriers to providing lung-protective ventilation to patients with acute lung injury. Crit Care Med 2004; 32:1289–1293.
- Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999; 282:1458–1465.
- Rahaghi F, Ortega I, Rahaghi N, et al. Physician alert suggesting alpha-1 antitrypsin deficiency testing in pulmonary function test (PFT) results. COPD 2009; 6:26–30.
- Campos M, Hagenlocker B, Martinez N, et al. Impact of an electronic medical record clinical reminder to improve detection of COPD and alpha-1 antitrypsin deficiency in the Veterans Administration (VA) system (abstract). Am J Respir Crit Care Med 2011;183:A5356. www.atsjournals.org/doi/pdf/10.1164/ajrccm-conference.2011.183.1_MeetingAbstracts.A5356. Accessed May 24, 2016.
- Jain A, McCarthy K, Xu M, Stoller JK. Impact of a clinical decision support system in an electronic health record to enhance detection of alpha(1)-antitrypsin deficiency. Chest 2011;140:198–204.
- American Thoracic Society, European Respiratory Society. American Thoracic Society/European Respiratory Society statement: standards for the diagnosis and management of individuals with alpha-1 antitrypsin deficiency. Am J Respir Crit Care Med 2003; 168:818–900.
- Rahaghi FF, Sandhaus RA, Brantly ML, et al. The prevalence of alpha-1 antitrypsin deficiency among patients found to have airflow obstruction. COPD 2012; 9:352–358.
- Carrell RW, Lomas DA. Alpha1-antitrypsin deficiency—a model for conformational diseases. N Engl J Med 2002; 346:45–53.
- Stoller JK, Aboussouan LS. A review of alpha1-antitrypsin deficiency. Am J Respir Crit Care Med 2012; 185:246–259.
- McElvaney NG, Stoller JK, Buist AS, et al. Baseline characteristics of enrollees in the National Heart, Lung and Blood Institute Registry of Alpha 1-Antitrypsin Deficiency. Alpha 1-Antitrypsin Deficiency Registry Study Group. Chest 1997; 111:394–403.
- Lomas DA, Evans DL, Finch JT, Carrell RW. The mechanism of Z alpha 1-antitrypsin accumulation in the liver. Nature 1992; 357:605–607.
- Lomas DA, Finch JT, Seyama K, Nukiwa T, Carrell RW. Alpha 1-antitrypsin Siiyama (Ser53-->Phe). Further evidence for intracellular loop-sheet polymerization. J Biol Chem 1993; 268:15333–15335.
- Mayer AS, Stoller JK, Bucher Bartelson B, James Ruttenber A, Sandhaus RA, Newman LS. Occupational exposure risks in individuals with PI*Z alpha(1)-antitrypsin deficiency. Am J Respir Crit Care Med 2000; 162:553–558.
- Tan L, Dickens JA, Demeo DL, et al. Circulating polymers in alpha1-antitrypsin deficiency. Eur Respir J 2014; 43:1501–1504.
- Parmar JS, Mahadeva R, Reed BJ, et al. Polymers of alpha(1)-antitrypsin are chemotactic for human neutrophils: a new paradigm for the pathogenesis of emphysema. Am J Respir Cell Mol Biol 2002; 26:723–730.
- Molloy K, Hersh CP, Morris VB, et al. Clarification of the risk of chronic obstructive pulmonary disease in alpha1-antitrypsin deficiency PiMZ heterozygotes. Am J Respir Crit Care Med 2014; 189:419–427.
- Parr DG, Stoel BC, Stolk J, Stockley RA. Pattern of emphysema distribution in alpha1-antitrypsin deficiency influences lung function impairment. Am J Respir Crit Care Med 2004; 170:1172–1178.
- Sveger T. Liver disease in alpha1-antitrypsin deficiency detected by screening of 200,000 infants. N Engl J Med 1976; 294:1316–1321.
- O’Brien ML, Buist NR, Murphey WH. Neonatal screening for alpha1-antitrypsin deficiency. J Pediatr 1978; 92:1006–1010.
- Piitulainen E, Montero LC, Nystedt-Duzakin M, et al. Lung function and CT densitometry in subjects with alpha-1-antitrypsin deficiency and healthy controls at 35 years of age. COPD 2015; 12:162–167.
- The Alpha-1-Antitrypsin Deficiency Registry Study Group. Survival and FEV1 decline in individuals with severe deficiency of alpha1-antitrypsin. Am J Respir Crit Care Med 1998; 158:49–59.
- Dawkins PA, Dawkins CL, Wood AM, Nightingale PG, Stockley JA, Stockley RA. Rate of progression of lung function impairment in alpha1-antitrypsin deficiency. Eur Respir J 2009; 33:1338–1344.
- Needham M, Stockley RA. Alpha 1-antitrypsin deficiency. 3: clinical manifestations and natural history. Thorax 2004; 59:441–445.
- Tomashefski JF Jr, Crystal RG, Wiedemann HP, Mascha E, Stoller JK. The bronchopulmonary pathology of alpha-1 antitrypsin (AAT) deficiency: findings of the Death Review Committee of the National Registry for Individuals with Severe Deficiency of Alpha-1 Antitrypsin. Hum Pathol 2004; 35:1452–1461.
- Tanash HA, Nilsson PM, Nilsson JA, Piitulainen E. Clinical course and prognosis of never-smokers with severe alpha-1-antitrypsin deficiency (PiZZ). Thorax 2008; 63:1091–1095.
- Walsh JW, Snider GL, Stoller JK. A review of the Alpha-1 Foundation: its formation, impact, and critical success factors. Respir Care 2006; 51:526–531.
- Rokadia HK, Stoller JK. Surgical and bronchoscopic lung volume reduction treatment for a-1 antitrypsin deficiency. Clin Pulm Med 2015; 22:279–285.
- Dirksen A, Piitulainen E, Parr DG, et al. Exploring the role of CT densitometry: a randomised study of augmentation therapy in alpha1-antitrypsin deficiency. Eur Respir J 2009; 33:1345–1353.
- Dirksen A, Dijkman JH, Madsen F, et al. A randomized clinical trial of alpha(1)-antitrypsin augmentation therapy. Am J Respir Crit Care Med 1999; 160:1468–1472.
- Gildea TR, Shermock KM, Singer ME, Stoller JK. Cost-effectiveness analysis of augmentation therapy for severe alpha1-antitrypsin deficiency. Am J Respir Crit Care Med 2003; 167:1387–1392.
KEY POINTS
- Only about 15% of people who have alpha-1 antitrypsin disease have received a diagnosis of it.
- The disease is genetic. People who are homozygous for the Z allele of the gene that codes for alpha-1 antitrypsin are at increased risk of lung and liver disease.
- Chronic obstructive pulmonary disease (COPD) due to alpha-1 antitrypsin deficiency is difficult to distinguish from “usual” COPD on a clinical basis, but blood tests are available.
- The basic care of a patient with COPD due to alpha-1 antitrypsin disease is the same as for any patient with COPD, ie, with bronchodilators, inhaled steroids, supplemental oxygen, preventive vaccinations, and pulmonary rehabilitation as indicated. Specific treatment consists of weekly infusions of alpha-1 antitrypsin (augmentation therapy).
Best practices in LGBT care: A guide for primary care physicians
Primary care physicians are very likely to encounter lesbian, gay, bisexual, and transgender (LGBT) patients in their practice, and must be able to provide informed, appropriate, and culturally sensitive care.
Approximately 9 million people in the United States identify as lesbian, gay, or bisexual, and 700,000 adults are transgender.1 In the 2013 National Health Interview Survey,2 which queried 34,557 adults about their sexual orientation, 2.3% reported being lesbian, gay, or bisexual, with only slight differences according to age or sex: of those ages 18 through 44, 1.9% were gay or lesbian and 1.1% were bisexual; of those ages 65 and over, 0.7% were gay or lesbian and 0.2% were bisexual. By sex, 0.9% of women vs 0.4% of men identified as bisexual.2
This article identifies and corrects common myths about LGBT care, addresses disparities in healthcare access, and outlines a step-by-step approach for delivering comprehensive care to LGBT patients.
MYTHS ABOUT LGBT CARE
Myth #1: L = G = B = T
Although LGBT is a commonly used term, each group described by the abbreviation has its own unique healthcare needs. For example, lesbian and bisexual women are more likely than heterosexual women to smoke, and gay men are at increased risk for human immunodeficiency virus (HIV) and other sexually transmitted infections.3,4 Transgender persons have high rates of suicide.5
Primary care of the LGBT patient needs to be individualized but also informed by the knowledge of distinct risks and behaviors associated with particular groups.
Myth #2: Sexual orientation = sexual activity
Sexual identity correlates closely but not completely with sexual behavior; individuals may engage in same-sex behavior but not identify as lesbian, gay, or bisexual.6,7 Many women who identify as lesbian have previously had sex with men, and men may have had same-sex encounters but consider themselves heterosexual.8,9
Since the risk of certain infections is related to sexual activity, providers should query patients about their sexual partners and practices in an open, nonjudgmental way, and avoid labeling patients solely according to sexual orientation. Table 1 suggests questions to use when interviewing patients.
Myth #3: Sexual orientation = gender identity
Gender identity describes a person’s inherent sense of being a woman, man, or of neither gender, whereas sexual orientation refers to how a person identifies their physical and emotional attraction to others.10,11 Conflating the two concepts can alienate patients, lead to incorrect assumptions, and result in an underestimation of an individual’s risk of sexually transmitted diseases.
Using questions such as “Are you sexually active with men, women, or both?” or “When you are sexually active, what parts of your body do you use?” with all patients, regardless of gender identity, will facilitate open and honest conversations that allow for appropriate counseling and risk assessment. Table 2 lists commonly used gender-identity terms.
Myth #4: LGBT people have the same access to healthcare as heterosexual people
People who identify as lesbian, gay, bisexual, or transgender experience significant disparities in access to healthcare compared with cisgender heterosexual people. For example, lesbian women are less likely to receive the human papillomavirus vaccine, cervical cancer screening, and mammograms, and men in same-sex relationships are twice as likely to have unmet medical needs.8,12 In a national survey,5 19% of transgender individuals reported that they had been refused healthcare. Among 152 transgender adults who described their experiences with the healthcare system, 7% reported receiving substandard care.13
We can eliminate these disparities by creating a welcoming environment for all patients (Table 3), and also by being aware of the specific services that should be offered to LGBT individuals.
ADDRESSING THE NEEDS OF LGBT PATIENTS
Outlined here is an office-based approach for addressing the unique clinical concerns of adult LGBT patients. Not all of these issues need to or should be addressed at the first visit, and the sequence in which these steps are accomplished may vary.
Step #1: Screen for mental health disorders
Lesbian, bisexual, and gay people are more likely to experience depression and anxiety. According to the results of a large meta-analysis,14 the prevalence of these conditions is 1.5 times higher in this population than in heterosexual people. Risk may vary according to group, with gay and bisexual men experiencing a higher lifetime prevalence of anxiety and depression than lesbian and bisexual women.15 Suicidal attempts are also more common in gay and bisexual men, who have a lifetime risk four times higher than that of heterosexual men.14
The risk of suicide is even higher among transgender people: 41% of surveyed transgender adults reported that they had attempted suicide, with higher rates in younger individuals.5 Risk factors include experiences of harassment or physical or sexual violence, as well as poverty, low education level, and unemployment.5 The risk of suicide in transgender people who served in the military is 20 times higher than that in the general veteran population.16
It is imperative to routinely screen LGBT patients for anxiety, depression, and suicidality and to refer them to mental health providers who are sensitive to LGBT patients’ needs and concerns. Screening tools such as the Patient Health Questionnaire-2 (PHQ2), PHQ9A, PHQ9, and Generalized Anxiety Disorder 7-item scale (GAD7) are useful in screening patients for depression and anxiety in addition to mnemonics such as SIGECAPS (sleep, interest, guilt, energy, concentration, appetite, psychomotor, suicidal thoughts or ideation).17
Although the same screening tools are used in cisgender heterosexual patients, factors contributing to the experience of depression or anxiety may be directly related to gender identity, gender expression, or sexual orientation. In a 2001 study, more lesbian, gay, and bisexual people reported lifetime and day-to-day experiences with discrimination than heterosexual people, and approximately 42% attributed this in part or in total to their sexual orientation.18
Step #2: Assess for substance use
Substance use is also more common in LGBT people. Lesbian and bisexual women have higher rates of tobacco abuse, exposure to second-hand smoke, and alcohol and drug dependence.3,14 In one study, compared with heterosexual individuals, the odds of lifetime alcohol and substance use disorder was three times higher in lesbian women, and the odds of lifetime drug-use disorder was 1.6 times higher in gay men.19
In a survey of transgender people, 30% reported using tobacco compared with 20% of the US adult population, and 8% reported using alcohol or drugs to cope with mistreatment and bias.5 In a study of transgender women in San Francisco, 58% used alcohol and 43% used substances, including marijuana, methamphetamine, and crack cocaine. Substance use significantly increased the odds of testing positive for HIV.20
Clinicians should carefully question LGBT patients about their use of alcohol, tobacco, and other substances and provide counseling and assistance with cessation. Several LGBT-specific resources can be used to aid patients in their efforts, and referral to substance abuse groups that are welcoming to LGBT people may increase cessation rates.19,21
Step #3: Offer appropriate screening services
Human papillomavirus (HPV). Like heterosexual women, lesbian and bisexual women are at risk of HPV infection, which is associated with cervical cancer and genital warts.8 HPV can be transmitted in several ways, including skin-to-skin and digital-to-genital contact, as well as penile-vaginal intercourse. Lesbian and bisexual women may have acquired HPV from previous male sexual partners or from female-to-female transmission.8 In a study comparing cervical cancer screening results among lesbian, bisexual, and heterosexual women, there was no significant difference in the odds for Papanicolaou (Pap) test abnormalities and only a minor decrease in the odds of HPV infection.22 Lesbian and bisexual women should receive Pap and HPV testing according to current guidelines.
Other sexually transmitted infections, including herpes simplex virus 1, herpes simplex virus 2, Trichomonas vaginalis, syphilis, and hepatitis A, can be passed between female partners; risk may vary according to sexual practices.23 Thus, providers should not assume that lesbian women are at low risk of these infections and should screen according to current guidelines.
The US Centers for Disease Control and Prevention (CDC) recommends annual screening for Chlamydia infection for all women under age 25, as well as those at increased risk for this infection (ie, those with a new sex partner or multiple sex partners).24
Breast cancer. Studies reveal that lesbian and bisexual women are less likely to receive mammograms, and they may have several risk factors that increase their risk for breast cancer, including overweight, obesity, and excessive alcohol intake.12,18,25 Providers should discuss the risks and benefits of mammography and offer this screening service at appropriate intervals.
Screening in men who have sex with men
Men who have sex with men are at increased risk for several sexually transmitted infections, including HIV, syphilis, gonorrhea, Chlamydia, anal HPV, and hepatitis B and C.4,9 The CDC recommends annual sexual health screening that includes serologic testing for HIV and syphilis, and urine, rectal, or pharyngeal testing for gonorrhea and Chlamydia according to sexual practices.24
In contrast, routine screening for anal HPV is not currently recommended because we lack data demonstrating that screening reduces mortality rates from anal carcinoma.24,26 Nevertheless, the CDC acknowledges that some clinicians may choose to perform anal Pap testing in patients who are at high risk, and guidelines from the New York City Department of Health and Mental Hygiene suggest annual anal Pap testing in HIV-positive men who have sex with men.27
According to the results of a systematic review,28 a significant proportion of transgender women reported sexual practices that increased their risk for sexually transmitted infections, and 27.7% tested positive for HIV infection. In contrast, rates of HIV and risk behaviors were much lower among transgender men. Risk may be heightened in transgender women who have not had sexual reassignment surgery and who engage in insertive anal, vaginal, or oral intercourse.28 An awareness of an individual patient’s current anatomy and sexual practices is essential for providing appropriate counseling about sexually transmitted infections.
‘Screen what you have’
When considering screening for breast, cervical, and prostate cancer, providers should consider an individual patient’s surgical history and hormonal status. “Screen what you have” is an easy rule to help both patients and providers remember which services to consider.
Transgender men who have not had a mastectomy should discuss the risks and benefits of breast cancer screening and consider mammography as recommended by the American Cancer Society.29 Similarly, cervical cancer screening should be performed according to current guidelines, although providers should be aware that this examination can cause significant anxiety and emotional distress for the patient.30
In transgender women, guidelines for breast cancer screening for those who were previously or currently treated with hormones are lacking. The University of California-San Francisco Center of Excellence for Transgender Health recommends mammography for patients over age 50 with additional risk factors (family history, obesity, estrogen and progestin use for more than 5 years).31 Transgender women should be counseled about the risks and benefits of prostate cancer screening.
Step #4: Immunize, and promote healthy behaviors
Table 4 outlines the screening services, immunizations, and health behavior promotions that should be offered to LGBT patients.
Vaccinations. LGBT individuals should be routinely offered HPV vaccination through age 26, according to current guidelines.24 Immunization against hepatitis A and B is also recommended for men who have sex with men, if they are not already immune.24 Meningococcal vaccine should be given to men who have sex with men if they have an additional medical, occupational, or lifestyle risk factor.32
Physical activity should be encouraged, especially in lesbian and bisexual women, who are more likely to be overweight and obese.25 In a recent study,33 gay, lesbian, and bisexual youths (ages 12–22) reported 1.21 to 2.62 fewer hours of moderate or vigorous physical activity per week than their “completely heterosexual” counterparts, and were 46% to 76% less likely to participate in team sports, in part due to concerns about gender nonconformity. On the other hand, results from a recent national survey of adults ages 18 through 64 found no significant differences in physical activity according to sexual orientation.
Providers should address patients’ perceived barriers to participating in exercise programs.2
Preexposure prophylaxis against HIV. A growing number of patients and health providers are asking about preexposure prophylaxis for HIV infection. The initial CDC recommendations for the daily use of emtricitabine-tenofovir were restricted to gay and bisexual men and men who have sex with men in serodiscordant relationships or in situations where the HIV status of the patient’s partner was unknown.34 Since then, the CDC has expanded the groups who may benefit from preexposure prophylaxis.35 Assessment of the patient’s ability to adhere to a daily oral medication regimen is central to its success. Patients should be screened for hepatitis, HIV, and renal and liver function before starting emtricitabine-tenofovir and should have these tests repeated at 3-month intervals if pre-exposure prophylaxis is continued.
Step #5: Initiate or continue hormone therapy for transgender individuals
Hormone therapy often improves the quality of life for patients who desire to have their physical appearance align more closely with their gender identity.29 Moreover, abruptly stopping hormone therapy can have significant psychological consequences.36
Clinicians should feel comfortable starting hormone therapy for patients who have been diagnosed with gender dysphoria by a mental health professional, can demonstrate knowledge about and outcomes of hormone therapy, and have lived as a member of the desired gender (“real-life experience”) for at least 3 months, and preferably 12 months.29 More recently, some practitioners have advocated prescribing hormone therapy for patients without the requirement for real-life experience or a formal letter from a mental health professional recommending hormonal therapy.37 However, mental healthcare is recommended for any patient with moderate to severe mental health conditions, especially if not treated at the time of presentation.37
Providers should continue hormone therapy for patients who are already receiving it, while being aware of the appropriate treatment goals and monitoring parameters. The two main principles of hormone therapy for transgender patients are to reduce endogenous hormone levels and their associated sex characteristics and replace with hormones of the preferred sex.29 Doses and formulations are similar to those used for treatment of hypogonadism. This topic has been reviewed by Spack.10
The only absolute contraindications to hormone therapy are estrogen- or testosterone-responsive tumors. Otherwise, hormone therapy can be initiated or continued with the patient’s informed consent about its benefits and risks.
Estrogen therapy may increase the risk of thromboembolic disease, coronary artery disease, cerebrovascular disease, severe migraine headaches, liver dysfunction, and macroprolactinoma.29 In a cross-sectional study of 100 transgender patients receiving hormone therapy, 12% of transgender women experienced a thromboembolic or cardiovascular event after an average of 11 years of treatment.38 However, many of these patients had additional risk factors for these events, such as smoking. In contrast, results from a recent systematic review39 indicated a much lower rate of venous thromboembolism among transgender women receiving estrogen therapy (1.7%–6.3%). Use of transdermal estrogen may minimize the likelihood of thromboembolic disease, and cessation of hormonal care in the perioperative period is advisable, especially for procedures with greater risk of venous thromboembolism.39
Transgender men are at risk of erythrocytosis (hematocrit > 50%) as a result of testosterone therapy. Although current guidelines indicate that testosterone may increase the risk of breast or uterine cancer, results from a recent systematic review40 indicate that the overall cancer incidence in transgender men is not higher than in natal controls. Both estrogen and testosterone therapy increase insulin resistance and fasting glucose levels, whereas only estrogen increases triglyceride concentrations.40
For transgender women, estrogen levels should be maintained in the normal range for cisgender women of reproductive age (< 200 pg/mL), and testosterone levels should be suppressed to less than 55 ng/dL. Goal testosterone levels for transgender men are between 320 and 1,000 ng/dL and should be measured at intervals specific to the preparation used (ie, measured midway between injections for individuals treated with testosterone cypionate). Estradiol levels should be less than 50 ng/dL.29 Transgender women and men should have estradiol and testosterone levels measured quarterly during the first year of treatment, and then every 6 to 12 months thereafter once goal levels are achieved.
Additional monitoring for transgender women includes measuring serum prolactin at baseline and after 12 months of therapy, and serum electrolytes for those taking spironolactone as antiandrogen therapy. Complete blood cell counts and liver function tests should be done every 3 months during the first year of testosterone therapy for transgender men, and then one to two times per year.29 Reference laboratory values for the patient’s affirmed gender should be used to assess response to therapy as well as effects on end-organ function.
The marked suppression of endogenous hormone levels that occurs during therapy may have adverse effects on the bone mineral density of both transgender women and men. Clinicians should assess patients’ baseline risk for osteoporotic fracture at the time hormone therapy is started and consider bone mineral density testing if appropriate. For those at low risk for fracture, current guidelines recommend screening for osteoporosis starting at age 60.29
Providers should counsel patients who have recently initiated hormone therapy that some changes may occur gradually over time. While transgender women will notice a decrease in libido and spontaneous erections within the first 3 months of therapy, breast growth begins approximately 3 to 6 months after treatment is started. Similarly, for transgender men, fat redistribution occurs during the first 6 months of treatment, but facial and body hair growth occur more slowly and are at maximum 4 to 5 years after starting hormone therapy.29 Amenorrhea typically occurs 1 to 6 months after starting hormonal therapy for transgender men.
Some patients may be interested in surgery to continue their physical transformation to the desired sex. Patients who have used hormone therapy and participated in a real-life experience or otherwise completed social transition by living as the affirmed gender for 12 months are considered eligible for surgery if they can demonstrate a good understanding of the cost, potential complications, and expected recovery time of the procedure. Guidelines also recommend that the patient demonstrate progress in work, family, and interpersonal issues regarding their new gender.29 Available surgical options include breast augmentation, orchiectomy and penectomy, and vaginoplasty, clitoroplasty, and vulvoplasty for transgender women. Feminizing procedures include voice surgery, thyroid cartilage reduction, and facial feminization surgery. Transgender men may choose to have mastectomy, hysterectomy and salpingo-oophorectomy, vaginectomy, scrotoplasty and testicular implant placement, and implantation of a penile prosthesis. Additional virilizing surgeries include voice surgery and pectoral implants.41
Step #6: Screen for intimate partner violence
Intimate partner violence refers to physical, sexual, and psychological harm by a current or former partner or spouse, and it can occur in gay and lesbian relationships. In 2000, a National Violence Against Women survey found that 21.5% of men and 35.4% of women who reported living with a same-sex partner had experienced physical abuse.42 More recent studies confirm rates similar to those in heterosexual relationships. In an online study,43 11.8% of men who have sex with men reported physical violence from a current male partner, and about 4% reported experiencing coerced sex.
Intimate partner violence is uniquely challenging for LGBT people. In addition to the commonly described methods an abuser uses to maintain power and control, forced disclosure or “outing”—publicly revealing someone’s sexual orientation or gender identity—may result in additional psychological violence and harm. Survivors of intimate partner violence who are in same-gender intimate relationships often find that obtaining services through the police, judicial, and social services systems is challenging. Survivors may be required to disclose their sexual orientation or gender identity as part of filing a report or judicial order to obtain help or protection from the abuser. Many male and transgender survivors of intimate partner violence are unable to access traditional shelters. Female survivors may find that their same-sex abusers have the same access to resources and shelters that they do.
Intimate partner violence is associated with negative physical and mental health outcomes. Physical injuries such as bruises, fractures, and burns are some of the more obvious harms survivors sustain. However, the negative psychological impact on survivors cannot be overstated. LGBT individuals are at greater risk of depression and substance abuse as a result of intimate partner violence than their cisgender heterosexual counterparts. The stress resulting from stigmatization and discrimination can be exacerbated by intimate partner violence.44 This can be seen in health outcomes of HIV-positive men who have sex with men, in whom abuse predicts interruptions in care, more advanced HIV disease, and HIV-associated hospitalizations.45
We recommend that providers screen all LGBT patients for intimate partner violence. One commonly used tool is the Partner Violence Screen, which consists of three gender-neutral questions:
- Have you been hit, kicked, punched, or otherwise hurt by someone in the past year? If so, by whom?
- Do you feel safe in your current relationship?
- Is there a partner from a previous relationship who is making you feel unsafe now?
Like other screening tools for intimate partner violence, the Partner Violence Screen is more specific than sensitive.46 Screening and discussions about intimate partner violence should be performed in a private, confidential manner while the patient is alone.
Providers who care for LGBT patients need to be aware of not only the medical and mental health sequelae of intimate partner violence but also the social and legal issues facing survivors. Familiarity with the available community resources and their limitations can better facilitate trust and patient care for those affected by intimate partner violence. In one study, the most frequent requests for assistance from sexual and gender minority survivors were for counseling, safe housing, legal assistance, and assistance navigating the medical system.47 Providers should refer patients to LGBT-focused resources in their community as available, and when no such resources exist, initiate contact with standard domestic violence services, with patient consent, to ask about a program’s ability to assist survivors of LGBT intimate partner violence.
IN A NUTSHELL
Optimizing the care of LGBT patients requires developing both clinical and cultural competency.
Initial steps for creating an inclusive and welcoming clinical environment include becoming familiar with local resources for LGBT patients (support groups, substance and alcohol cessation groups, mental health providers; see sidebar), providing education and training for support staff and nurses, and establishing gender-neutral bathrooms. Waiting areas should include literature relevant to LGBT patients and signage that is relevant to all patients, including gender-nonconforming individuals. Providers should offer all patients universal HIV screening initially and at clinically appropriate intervals and discuss preexposure prophylaxis with emtricitabine-tenofovir for at-risk individuals.
For transgender patients, addressing them by their preferred name and pronouns is central to building rapport. General health maintenance is the same for transgender patients as for cisgender patients and can be guided by the adage “screen what you have.” Hormonal care can be offered using an informed consent method consistent with the World Professional Association for Transgender Health Standards of Care.48 Guidelines exist to assist providers in initiation and maintenance of hormonal care. Cross-gender hormonal therapy is initiated with low-dose medication that is gradually increased over time, with a goal of approximating the pubertal changes of the desired gender over a 2- to 3-year period. Some, but not all, patients may pursue various surgical procedures as part of their gender affirmation process.
- Gates GJ. How many people are lesbian, gay, bisexual, or transgender? Williams Institute. 2011. http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Accessed May 19, 2016.
- Ward BW, Dahlhamer JM, Galinsky AM, Joesti SS. Sexual orientation and health among U.S. Adults: National Health Interview Survey, 2013. Natl Health Stat Report 2014; 77:1–10.
- Cochran SD, Bandiera FC, Mays VM. Sexual orientation-related differences in tobacco use and secondhand smoke exposure among US adults aged 20-59 years: 2003–2010 National Health and Nutrition Examination surveys. Am J Publ Health 2013; 103:1837–1844.
- Mayer KH. Sexually transmitted diseases in men who have sex with men. Clin Infect Disease 2011; 53:S79–S83.
- Grant JM, Mottet LA, Tanis J, Herman JL, Harrison J, Keisling M. National transgender discrimination survey report on health and health care. www.thetaskforce.org/static_html/downloads/reports/reports/ntds_report_on_health.pdf. Accessed May 19, 2016.
- Pathela P, Hajat A, Schillinger J, Blank S, Sell R, Mostashari F. Discordance between sexual behavior and self-reported sexual identity: a population-based survey of New York City men. Ann Intern Med 2006; 145:416–425.
- Chandra A, Mosher WD, Copen C, Sionean C. Sexual behavior, sexual attraction, and sexual identity in the United States: data from the 2006–2009 National Survey of Family Growth. Natl Health Stat Report 2011; 36:1–36.
- Agenor M, Peitzmeier S, Gordon AR, Haneuse S, Potter JE, Austin SB. Sexual orientation identity disparities in awareness and initiation of the human papillomavirus vaccine among U.S. women and girls: a national survey. Ann Intern Med 2015; 163:99–106.
- Ard KL, Makadon HJ. Improving the health care of lesbian, gay, bisexual and transgender (LGBT) people: understanding and eliminating health disparities. www.lgbthealtheducation.org/wp-content/uploads/12-054_LGBTHealtharticle_v3_07-09-12.pdf. Accessed May 19, 2016.
- Spack NP. Management of transgenderism. JAMA 2013; 309:474–484.
- National LGBT Health Education Center. Achieving health equity for lesbian, gay, bisexual, and transgender (LGBT) people, Module 1. www.lgbthealtheducation.org/wp-content/uploads/Achieving-Health-Equity-for-LGBT-People-1.pdf. Accessed May 19, 2016.
- Buchmueller T, Carpenter CS. Disparities in health Insurance coverage, access, and outcomes for individuals in same-sex versus different-sex relationships, 2000–2007. Am J Public Health 2010; 100:489–496.
- Kosenko K, Rintamaki L, Raney S, Maness K. Transgender patient perceptions of stigma in health care contexts. Med Care 2013; 51:819–822.
- King M, Semlyen J, Tai SS, et al. A systematic review of mental disorder, suicide, and deliberate self-harm in lesbian, gay, and bisexual people. BMC Psychiatry 2008; 8:70.
- Bostwick WB, Boyd CJ, Hughes TL, McCabe SE. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. Am J Public Health 2010; 100:468–475.
- Blosnich JR, Brown GR, Shipherd JC, Kauth M, Piegari RI, Bossarte RM. Prevalence of gender identity disorder and suicide risk among transgender veterans utilizing Veterans Health Administration care. Am J Public Health 2013: 103:e27–e32.
- Maurer DM. Screening for depression. Am Fam Physician 2012; 85:139–144.
- Mays VM, Cochran SD. Mental health correlates of perceived discrimination among lesbian, gay, and bisexual adults in the United States. Am J Pub Health 2001; 91:1869–1875.
- McCabe SE, West BT, Hughes TL, Boyd CJ. Sexual orientation and substance abuse treatment utilization in the United States: results from a national survey. J Subst Abuse Treat 2013; 44:4–12.
- Santos GM, Rapues J, Wilson EC, et al. Alcohol and substance use among transgender women in San Francisco: prevalence and association with human immunodeficiency virus infection. Drug Alcohol Rev 2014; 33:287–295.
- National LGBT Tobacco Control Network. www.lgbttobacco.org. Accessed May 19, 2016.
- Massad LS, Xie X, Minkoff H, et al. Abnormal Pap tests and human papillomavirus infections among HIV infected and uninfected women who have sex with women. J Low Genit Tract Dis 2014; 18:50–56.
- Gorgos LM, Marrazzo JM. Sexually transmitted infections among women who have sex with women. Clin Infect Dis 2011; 53:S84–S91.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR 2015; 64(3):1–138.
- Boehmer U, Bowen DJ, Bauer GR. Overweight and obesity in sexual-minority women: evidence from population-based data. Am J Public Health 2007; 97:1134–1140.
- Smyczek P, Singh AE, Romanowski B. Anal intraepithelial neoplasia: review and recommendations for screening and management. Int J STD AIDS 2013; 24:843–851.
- New York City Department of Health and Mental Hygiene. Preventing sexually transmitted infections. 2013; 32(4):19–27. www.nyc.gov/html/doh/html/data/chi32-4_screening.html. Accessed May 19, 2016.
- Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav 2008; 12:1–17.
- Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, et al. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2009; 94:3132–3133.
- Peitzmeier SM, Reisner SL, Harigopal P, Potter J. Female-to-male patients may have high prevalence of unsatisfactory paps compared to non-transgender females: implications for cervical cancer screening. J Gen Intern Med 2014; 29:778–784.
- UCSF Center of Excellence for Transgender Health. Primary care protocol for transgender patient care. http://transhealth.ucsf.edu/protocols. Accessed May 19, 2016.
- Centers for Disease Control and Prevention. Recommended adult immunization schedule United States—2015. www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf. Accessed May 19, 2016.
- Calzo JP, Roberts AL, Corliss HL, Blood EA, Kroshus E, Austin SB. Physical activity disparities in heterosexual and sexual minority youth ages 12–22 years old: roles of childhood gender nonconformity and athletic self-esteem. Ann Behav Med 2014; 47:17–27.
- Centers for Disease Control and Prevention. Interim guidance for clinicians considering the use of preexposure prophylaxis for the prevention of HIV infection in heterosexually active adults. MMWR 2012; 61:586–589.
- Centers for Disease Control and Prevention and US Public Health Service. Preexposure prophlyaxis for the prevention of HIV infection in the United States—2014. A clinical practice guideline. www.cdc.gov/hiv/pdf/PrEPguidelines2014.pdf. Accessed May 19, 2016.
- Feldman JL, Goldberg J. Transgender primary medical care: suggested guidelines for clinicians in British Columbia. www.cwhn.ca/en/node/27567. Accessed May 19, 2016.
- Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-noncomforming people, version 7. Int J Transgenderism 2011; 13:165–232.
- Wierckx K, Mueller S, Weyers S, et al. Long-term evaluation of cross-sex hormone treatment in transsexual persons. J Sex Med 2012; 9: 2641–2651.
- Asscheman H, T’Sjoen G, Lemaire A, et al. Venous thrombo-embolism as a complication of cross-sex hormone treatment of male-to-female transsexual subjects: a review. Andrologia 2014; 46:791–795.
- Weinand JD, Safer JD. Hormone therapy in transgender adults is safe with provider supervision. A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol 2015; 2:55–60.
- Unger CA. Care of the transgender patient: the role of the gynecologist. Am J Obstet Gynecol 2014; 210:16–26.
- Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. Washington, DC: US Department of Justice, National Institute of Justice; 2000. P. 29–31. Report No.: NCJ 181867.
- Stephenson R, Khosropour C, Sullivan P. Reporting of intimate partner violence among men who have sex with men in an online survey. West J Emerg Med 2010; 11:242–246.
- Chen PH, Jacobs A, Rovi SL. Intimate partner violence: IPV in the LGBT community. FP Essent 2013; 412:28–35.
- Siemieniuk R, Miller P, Woodman K, et al. Prevalence, clinical associations, and impact of intimate partner violence among HIV infected gay and bisexual men: a population based study. HIV Med 2013; 14:293–302.
- Rabin RF, Jennings JM, Campbell JC, Bair-Merritt MH. Intimate partner violence screening tools: a systematic review. Am J Prev Med 2009; 36:439–445.
- Ford CL, Slavin T, Hilton KL, Holt SL. Intimate partner violence prevention services and resources in Los Angeles: issues, needs, and challenges for assisting lesbian, gay, bisexual, and transgender clients. Health Promot Pract 2013; 14:841–849.
- World Professional Association for Transgender Health. www.wpath.org/site_page.cfm?pk_association_webpage_menu=1351. Accessed May 19, 2016.
Primary care physicians are very likely to encounter lesbian, gay, bisexual, and transgender (LGBT) patients in their practice, and must be able to provide informed, appropriate, and culturally sensitive care.
Approximately 9 million people in the United States identify as lesbian, gay, or bisexual, and 700,000 adults are transgender.1 In the 2013 National Health Interview Survey,2 which queried 34,557 adults about their sexual orientation, 2.3% reported being lesbian, gay, or bisexual, with only slight differences according to age or sex: of those ages 18 through 44, 1.9% were gay or lesbian and 1.1% were bisexual; of those ages 65 and over, 0.7% were gay or lesbian and 0.2% were bisexual. By sex, 0.9% of women vs 0.4% of men identified as bisexual.2
This article identifies and corrects common myths about LGBT care, addresses disparities in healthcare access, and outlines a step-by-step approach for delivering comprehensive care to LGBT patients.
MYTHS ABOUT LGBT CARE
Myth #1: L = G = B = T
Although LGBT is a commonly used term, each group described by the abbreviation has its own unique healthcare needs. For example, lesbian and bisexual women are more likely than heterosexual women to smoke, and gay men are at increased risk for human immunodeficiency virus (HIV) and other sexually transmitted infections.3,4 Transgender persons have high rates of suicide.5
Primary care of the LGBT patient needs to be individualized but also informed by the knowledge of distinct risks and behaviors associated with particular groups.
Myth #2: Sexual orientation = sexual activity
Sexual identity correlates closely but not completely with sexual behavior; individuals may engage in same-sex behavior but not identify as lesbian, gay, or bisexual.6,7 Many women who identify as lesbian have previously had sex with men, and men may have had same-sex encounters but consider themselves heterosexual.8,9
Since the risk of certain infections is related to sexual activity, providers should query patients about their sexual partners and practices in an open, nonjudgmental way, and avoid labeling patients solely according to sexual orientation. Table 1 suggests questions to use when interviewing patients.
Myth #3: Sexual orientation = gender identity
Gender identity describes a person’s inherent sense of being a woman, man, or of neither gender, whereas sexual orientation refers to how a person identifies their physical and emotional attraction to others.10,11 Conflating the two concepts can alienate patients, lead to incorrect assumptions, and result in an underestimation of an individual’s risk of sexually transmitted diseases.
Using questions such as “Are you sexually active with men, women, or both?” or “When you are sexually active, what parts of your body do you use?” with all patients, regardless of gender identity, will facilitate open and honest conversations that allow for appropriate counseling and risk assessment. Table 2 lists commonly used gender-identity terms.
Myth #4: LGBT people have the same access to healthcare as heterosexual people
People who identify as lesbian, gay, bisexual, or transgender experience significant disparities in access to healthcare compared with cisgender heterosexual people. For example, lesbian women are less likely to receive the human papillomavirus vaccine, cervical cancer screening, and mammograms, and men in same-sex relationships are twice as likely to have unmet medical needs.8,12 In a national survey,5 19% of transgender individuals reported that they had been refused healthcare. Among 152 transgender adults who described their experiences with the healthcare system, 7% reported receiving substandard care.13
We can eliminate these disparities by creating a welcoming environment for all patients (Table 3), and also by being aware of the specific services that should be offered to LGBT individuals.
ADDRESSING THE NEEDS OF LGBT PATIENTS
Outlined here is an office-based approach for addressing the unique clinical concerns of adult LGBT patients. Not all of these issues need to or should be addressed at the first visit, and the sequence in which these steps are accomplished may vary.
Step #1: Screen for mental health disorders
Lesbian, bisexual, and gay people are more likely to experience depression and anxiety. According to the results of a large meta-analysis,14 the prevalence of these conditions is 1.5 times higher in this population than in heterosexual people. Risk may vary according to group, with gay and bisexual men experiencing a higher lifetime prevalence of anxiety and depression than lesbian and bisexual women.15 Suicidal attempts are also more common in gay and bisexual men, who have a lifetime risk four times higher than that of heterosexual men.14
The risk of suicide is even higher among transgender people: 41% of surveyed transgender adults reported that they had attempted suicide, with higher rates in younger individuals.5 Risk factors include experiences of harassment or physical or sexual violence, as well as poverty, low education level, and unemployment.5 The risk of suicide in transgender people who served in the military is 20 times higher than that in the general veteran population.16
It is imperative to routinely screen LGBT patients for anxiety, depression, and suicidality and to refer them to mental health providers who are sensitive to LGBT patients’ needs and concerns. Screening tools such as the Patient Health Questionnaire-2 (PHQ2), PHQ9A, PHQ9, and Generalized Anxiety Disorder 7-item scale (GAD7) are useful in screening patients for depression and anxiety in addition to mnemonics such as SIGECAPS (sleep, interest, guilt, energy, concentration, appetite, psychomotor, suicidal thoughts or ideation).17
Although the same screening tools are used in cisgender heterosexual patients, factors contributing to the experience of depression or anxiety may be directly related to gender identity, gender expression, or sexual orientation. In a 2001 study, more lesbian, gay, and bisexual people reported lifetime and day-to-day experiences with discrimination than heterosexual people, and approximately 42% attributed this in part or in total to their sexual orientation.18
Step #2: Assess for substance use
Substance use is also more common in LGBT people. Lesbian and bisexual women have higher rates of tobacco abuse, exposure to second-hand smoke, and alcohol and drug dependence.3,14 In one study, compared with heterosexual individuals, the odds of lifetime alcohol and substance use disorder was three times higher in lesbian women, and the odds of lifetime drug-use disorder was 1.6 times higher in gay men.19
In a survey of transgender people, 30% reported using tobacco compared with 20% of the US adult population, and 8% reported using alcohol or drugs to cope with mistreatment and bias.5 In a study of transgender women in San Francisco, 58% used alcohol and 43% used substances, including marijuana, methamphetamine, and crack cocaine. Substance use significantly increased the odds of testing positive for HIV.20
Clinicians should carefully question LGBT patients about their use of alcohol, tobacco, and other substances and provide counseling and assistance with cessation. Several LGBT-specific resources can be used to aid patients in their efforts, and referral to substance abuse groups that are welcoming to LGBT people may increase cessation rates.19,21
Step #3: Offer appropriate screening services
Human papillomavirus (HPV). Like heterosexual women, lesbian and bisexual women are at risk of HPV infection, which is associated with cervical cancer and genital warts.8 HPV can be transmitted in several ways, including skin-to-skin and digital-to-genital contact, as well as penile-vaginal intercourse. Lesbian and bisexual women may have acquired HPV from previous male sexual partners or from female-to-female transmission.8 In a study comparing cervical cancer screening results among lesbian, bisexual, and heterosexual women, there was no significant difference in the odds for Papanicolaou (Pap) test abnormalities and only a minor decrease in the odds of HPV infection.22 Lesbian and bisexual women should receive Pap and HPV testing according to current guidelines.
Other sexually transmitted infections, including herpes simplex virus 1, herpes simplex virus 2, Trichomonas vaginalis, syphilis, and hepatitis A, can be passed between female partners; risk may vary according to sexual practices.23 Thus, providers should not assume that lesbian women are at low risk of these infections and should screen according to current guidelines.
The US Centers for Disease Control and Prevention (CDC) recommends annual screening for Chlamydia infection for all women under age 25, as well as those at increased risk for this infection (ie, those with a new sex partner or multiple sex partners).24
Breast cancer. Studies reveal that lesbian and bisexual women are less likely to receive mammograms, and they may have several risk factors that increase their risk for breast cancer, including overweight, obesity, and excessive alcohol intake.12,18,25 Providers should discuss the risks and benefits of mammography and offer this screening service at appropriate intervals.
Screening in men who have sex with men
Men who have sex with men are at increased risk for several sexually transmitted infections, including HIV, syphilis, gonorrhea, Chlamydia, anal HPV, and hepatitis B and C.4,9 The CDC recommends annual sexual health screening that includes serologic testing for HIV and syphilis, and urine, rectal, or pharyngeal testing for gonorrhea and Chlamydia according to sexual practices.24
In contrast, routine screening for anal HPV is not currently recommended because we lack data demonstrating that screening reduces mortality rates from anal carcinoma.24,26 Nevertheless, the CDC acknowledges that some clinicians may choose to perform anal Pap testing in patients who are at high risk, and guidelines from the New York City Department of Health and Mental Hygiene suggest annual anal Pap testing in HIV-positive men who have sex with men.27
According to the results of a systematic review,28 a significant proportion of transgender women reported sexual practices that increased their risk for sexually transmitted infections, and 27.7% tested positive for HIV infection. In contrast, rates of HIV and risk behaviors were much lower among transgender men. Risk may be heightened in transgender women who have not had sexual reassignment surgery and who engage in insertive anal, vaginal, or oral intercourse.28 An awareness of an individual patient’s current anatomy and sexual practices is essential for providing appropriate counseling about sexually transmitted infections.
‘Screen what you have’
When considering screening for breast, cervical, and prostate cancer, providers should consider an individual patient’s surgical history and hormonal status. “Screen what you have” is an easy rule to help both patients and providers remember which services to consider.
Transgender men who have not had a mastectomy should discuss the risks and benefits of breast cancer screening and consider mammography as recommended by the American Cancer Society.29 Similarly, cervical cancer screening should be performed according to current guidelines, although providers should be aware that this examination can cause significant anxiety and emotional distress for the patient.30
In transgender women, guidelines for breast cancer screening for those who were previously or currently treated with hormones are lacking. The University of California-San Francisco Center of Excellence for Transgender Health recommends mammography for patients over age 50 with additional risk factors (family history, obesity, estrogen and progestin use for more than 5 years).31 Transgender women should be counseled about the risks and benefits of prostate cancer screening.
Step #4: Immunize, and promote healthy behaviors
Table 4 outlines the screening services, immunizations, and health behavior promotions that should be offered to LGBT patients.
Vaccinations. LGBT individuals should be routinely offered HPV vaccination through age 26, according to current guidelines.24 Immunization against hepatitis A and B is also recommended for men who have sex with men, if they are not already immune.24 Meningococcal vaccine should be given to men who have sex with men if they have an additional medical, occupational, or lifestyle risk factor.32
Physical activity should be encouraged, especially in lesbian and bisexual women, who are more likely to be overweight and obese.25 In a recent study,33 gay, lesbian, and bisexual youths (ages 12–22) reported 1.21 to 2.62 fewer hours of moderate or vigorous physical activity per week than their “completely heterosexual” counterparts, and were 46% to 76% less likely to participate in team sports, in part due to concerns about gender nonconformity. On the other hand, results from a recent national survey of adults ages 18 through 64 found no significant differences in physical activity according to sexual orientation.
Providers should address patients’ perceived barriers to participating in exercise programs.2
Preexposure prophylaxis against HIV. A growing number of patients and health providers are asking about preexposure prophylaxis for HIV infection. The initial CDC recommendations for the daily use of emtricitabine-tenofovir were restricted to gay and bisexual men and men who have sex with men in serodiscordant relationships or in situations where the HIV status of the patient’s partner was unknown.34 Since then, the CDC has expanded the groups who may benefit from preexposure prophylaxis.35 Assessment of the patient’s ability to adhere to a daily oral medication regimen is central to its success. Patients should be screened for hepatitis, HIV, and renal and liver function before starting emtricitabine-tenofovir and should have these tests repeated at 3-month intervals if pre-exposure prophylaxis is continued.
Step #5: Initiate or continue hormone therapy for transgender individuals
Hormone therapy often improves the quality of life for patients who desire to have their physical appearance align more closely with their gender identity.29 Moreover, abruptly stopping hormone therapy can have significant psychological consequences.36
Clinicians should feel comfortable starting hormone therapy for patients who have been diagnosed with gender dysphoria by a mental health professional, can demonstrate knowledge about and outcomes of hormone therapy, and have lived as a member of the desired gender (“real-life experience”) for at least 3 months, and preferably 12 months.29 More recently, some practitioners have advocated prescribing hormone therapy for patients without the requirement for real-life experience or a formal letter from a mental health professional recommending hormonal therapy.37 However, mental healthcare is recommended for any patient with moderate to severe mental health conditions, especially if not treated at the time of presentation.37
Providers should continue hormone therapy for patients who are already receiving it, while being aware of the appropriate treatment goals and monitoring parameters. The two main principles of hormone therapy for transgender patients are to reduce endogenous hormone levels and their associated sex characteristics and replace with hormones of the preferred sex.29 Doses and formulations are similar to those used for treatment of hypogonadism. This topic has been reviewed by Spack.10
The only absolute contraindications to hormone therapy are estrogen- or testosterone-responsive tumors. Otherwise, hormone therapy can be initiated or continued with the patient’s informed consent about its benefits and risks.
Estrogen therapy may increase the risk of thromboembolic disease, coronary artery disease, cerebrovascular disease, severe migraine headaches, liver dysfunction, and macroprolactinoma.29 In a cross-sectional study of 100 transgender patients receiving hormone therapy, 12% of transgender women experienced a thromboembolic or cardiovascular event after an average of 11 years of treatment.38 However, many of these patients had additional risk factors for these events, such as smoking. In contrast, results from a recent systematic review39 indicated a much lower rate of venous thromboembolism among transgender women receiving estrogen therapy (1.7%–6.3%). Use of transdermal estrogen may minimize the likelihood of thromboembolic disease, and cessation of hormonal care in the perioperative period is advisable, especially for procedures with greater risk of venous thromboembolism.39
Transgender men are at risk of erythrocytosis (hematocrit > 50%) as a result of testosterone therapy. Although current guidelines indicate that testosterone may increase the risk of breast or uterine cancer, results from a recent systematic review40 indicate that the overall cancer incidence in transgender men is not higher than in natal controls. Both estrogen and testosterone therapy increase insulin resistance and fasting glucose levels, whereas only estrogen increases triglyceride concentrations.40
For transgender women, estrogen levels should be maintained in the normal range for cisgender women of reproductive age (< 200 pg/mL), and testosterone levels should be suppressed to less than 55 ng/dL. Goal testosterone levels for transgender men are between 320 and 1,000 ng/dL and should be measured at intervals specific to the preparation used (ie, measured midway between injections for individuals treated with testosterone cypionate). Estradiol levels should be less than 50 ng/dL.29 Transgender women and men should have estradiol and testosterone levels measured quarterly during the first year of treatment, and then every 6 to 12 months thereafter once goal levels are achieved.
Additional monitoring for transgender women includes measuring serum prolactin at baseline and after 12 months of therapy, and serum electrolytes for those taking spironolactone as antiandrogen therapy. Complete blood cell counts and liver function tests should be done every 3 months during the first year of testosterone therapy for transgender men, and then one to two times per year.29 Reference laboratory values for the patient’s affirmed gender should be used to assess response to therapy as well as effects on end-organ function.
The marked suppression of endogenous hormone levels that occurs during therapy may have adverse effects on the bone mineral density of both transgender women and men. Clinicians should assess patients’ baseline risk for osteoporotic fracture at the time hormone therapy is started and consider bone mineral density testing if appropriate. For those at low risk for fracture, current guidelines recommend screening for osteoporosis starting at age 60.29
Providers should counsel patients who have recently initiated hormone therapy that some changes may occur gradually over time. While transgender women will notice a decrease in libido and spontaneous erections within the first 3 months of therapy, breast growth begins approximately 3 to 6 months after treatment is started. Similarly, for transgender men, fat redistribution occurs during the first 6 months of treatment, but facial and body hair growth occur more slowly and are at maximum 4 to 5 years after starting hormone therapy.29 Amenorrhea typically occurs 1 to 6 months after starting hormonal therapy for transgender men.
Some patients may be interested in surgery to continue their physical transformation to the desired sex. Patients who have used hormone therapy and participated in a real-life experience or otherwise completed social transition by living as the affirmed gender for 12 months are considered eligible for surgery if they can demonstrate a good understanding of the cost, potential complications, and expected recovery time of the procedure. Guidelines also recommend that the patient demonstrate progress in work, family, and interpersonal issues regarding their new gender.29 Available surgical options include breast augmentation, orchiectomy and penectomy, and vaginoplasty, clitoroplasty, and vulvoplasty for transgender women. Feminizing procedures include voice surgery, thyroid cartilage reduction, and facial feminization surgery. Transgender men may choose to have mastectomy, hysterectomy and salpingo-oophorectomy, vaginectomy, scrotoplasty and testicular implant placement, and implantation of a penile prosthesis. Additional virilizing surgeries include voice surgery and pectoral implants.41
Step #6: Screen for intimate partner violence
Intimate partner violence refers to physical, sexual, and psychological harm by a current or former partner or spouse, and it can occur in gay and lesbian relationships. In 2000, a National Violence Against Women survey found that 21.5% of men and 35.4% of women who reported living with a same-sex partner had experienced physical abuse.42 More recent studies confirm rates similar to those in heterosexual relationships. In an online study,43 11.8% of men who have sex with men reported physical violence from a current male partner, and about 4% reported experiencing coerced sex.
Intimate partner violence is uniquely challenging for LGBT people. In addition to the commonly described methods an abuser uses to maintain power and control, forced disclosure or “outing”—publicly revealing someone’s sexual orientation or gender identity—may result in additional psychological violence and harm. Survivors of intimate partner violence who are in same-gender intimate relationships often find that obtaining services through the police, judicial, and social services systems is challenging. Survivors may be required to disclose their sexual orientation or gender identity as part of filing a report or judicial order to obtain help or protection from the abuser. Many male and transgender survivors of intimate partner violence are unable to access traditional shelters. Female survivors may find that their same-sex abusers have the same access to resources and shelters that they do.
Intimate partner violence is associated with negative physical and mental health outcomes. Physical injuries such as bruises, fractures, and burns are some of the more obvious harms survivors sustain. However, the negative psychological impact on survivors cannot be overstated. LGBT individuals are at greater risk of depression and substance abuse as a result of intimate partner violence than their cisgender heterosexual counterparts. The stress resulting from stigmatization and discrimination can be exacerbated by intimate partner violence.44 This can be seen in health outcomes of HIV-positive men who have sex with men, in whom abuse predicts interruptions in care, more advanced HIV disease, and HIV-associated hospitalizations.45
We recommend that providers screen all LGBT patients for intimate partner violence. One commonly used tool is the Partner Violence Screen, which consists of three gender-neutral questions:
- Have you been hit, kicked, punched, or otherwise hurt by someone in the past year? If so, by whom?
- Do you feel safe in your current relationship?
- Is there a partner from a previous relationship who is making you feel unsafe now?
Like other screening tools for intimate partner violence, the Partner Violence Screen is more specific than sensitive.46 Screening and discussions about intimate partner violence should be performed in a private, confidential manner while the patient is alone.
Providers who care for LGBT patients need to be aware of not only the medical and mental health sequelae of intimate partner violence but also the social and legal issues facing survivors. Familiarity with the available community resources and their limitations can better facilitate trust and patient care for those affected by intimate partner violence. In one study, the most frequent requests for assistance from sexual and gender minority survivors were for counseling, safe housing, legal assistance, and assistance navigating the medical system.47 Providers should refer patients to LGBT-focused resources in their community as available, and when no such resources exist, initiate contact with standard domestic violence services, with patient consent, to ask about a program’s ability to assist survivors of LGBT intimate partner violence.
IN A NUTSHELL
Optimizing the care of LGBT patients requires developing both clinical and cultural competency.
Initial steps for creating an inclusive and welcoming clinical environment include becoming familiar with local resources for LGBT patients (support groups, substance and alcohol cessation groups, mental health providers; see sidebar), providing education and training for support staff and nurses, and establishing gender-neutral bathrooms. Waiting areas should include literature relevant to LGBT patients and signage that is relevant to all patients, including gender-nonconforming individuals. Providers should offer all patients universal HIV screening initially and at clinically appropriate intervals and discuss preexposure prophylaxis with emtricitabine-tenofovir for at-risk individuals.
For transgender patients, addressing them by their preferred name and pronouns is central to building rapport. General health maintenance is the same for transgender patients as for cisgender patients and can be guided by the adage “screen what you have.” Hormonal care can be offered using an informed consent method consistent with the World Professional Association for Transgender Health Standards of Care.48 Guidelines exist to assist providers in initiation and maintenance of hormonal care. Cross-gender hormonal therapy is initiated with low-dose medication that is gradually increased over time, with a goal of approximating the pubertal changes of the desired gender over a 2- to 3-year period. Some, but not all, patients may pursue various surgical procedures as part of their gender affirmation process.
Primary care physicians are very likely to encounter lesbian, gay, bisexual, and transgender (LGBT) patients in their practice, and must be able to provide informed, appropriate, and culturally sensitive care.
Approximately 9 million people in the United States identify as lesbian, gay, or bisexual, and 700,000 adults are transgender.1 In the 2013 National Health Interview Survey,2 which queried 34,557 adults about their sexual orientation, 2.3% reported being lesbian, gay, or bisexual, with only slight differences according to age or sex: of those ages 18 through 44, 1.9% were gay or lesbian and 1.1% were bisexual; of those ages 65 and over, 0.7% were gay or lesbian and 0.2% were bisexual. By sex, 0.9% of women vs 0.4% of men identified as bisexual.2
This article identifies and corrects common myths about LGBT care, addresses disparities in healthcare access, and outlines a step-by-step approach for delivering comprehensive care to LGBT patients.
MYTHS ABOUT LGBT CARE
Myth #1: L = G = B = T
Although LGBT is a commonly used term, each group described by the abbreviation has its own unique healthcare needs. For example, lesbian and bisexual women are more likely than heterosexual women to smoke, and gay men are at increased risk for human immunodeficiency virus (HIV) and other sexually transmitted infections.3,4 Transgender persons have high rates of suicide.5
Primary care of the LGBT patient needs to be individualized but also informed by the knowledge of distinct risks and behaviors associated with particular groups.
Myth #2: Sexual orientation = sexual activity
Sexual identity correlates closely but not completely with sexual behavior; individuals may engage in same-sex behavior but not identify as lesbian, gay, or bisexual.6,7 Many women who identify as lesbian have previously had sex with men, and men may have had same-sex encounters but consider themselves heterosexual.8,9
Since the risk of certain infections is related to sexual activity, providers should query patients about their sexual partners and practices in an open, nonjudgmental way, and avoid labeling patients solely according to sexual orientation. Table 1 suggests questions to use when interviewing patients.
Myth #3: Sexual orientation = gender identity
Gender identity describes a person’s inherent sense of being a woman, man, or of neither gender, whereas sexual orientation refers to how a person identifies their physical and emotional attraction to others.10,11 Conflating the two concepts can alienate patients, lead to incorrect assumptions, and result in an underestimation of an individual’s risk of sexually transmitted diseases.
Using questions such as “Are you sexually active with men, women, or both?” or “When you are sexually active, what parts of your body do you use?” with all patients, regardless of gender identity, will facilitate open and honest conversations that allow for appropriate counseling and risk assessment. Table 2 lists commonly used gender-identity terms.
Myth #4: LGBT people have the same access to healthcare as heterosexual people
People who identify as lesbian, gay, bisexual, or transgender experience significant disparities in access to healthcare compared with cisgender heterosexual people. For example, lesbian women are less likely to receive the human papillomavirus vaccine, cervical cancer screening, and mammograms, and men in same-sex relationships are twice as likely to have unmet medical needs.8,12 In a national survey,5 19% of transgender individuals reported that they had been refused healthcare. Among 152 transgender adults who described their experiences with the healthcare system, 7% reported receiving substandard care.13
We can eliminate these disparities by creating a welcoming environment for all patients (Table 3), and also by being aware of the specific services that should be offered to LGBT individuals.
ADDRESSING THE NEEDS OF LGBT PATIENTS
Outlined here is an office-based approach for addressing the unique clinical concerns of adult LGBT patients. Not all of these issues need to or should be addressed at the first visit, and the sequence in which these steps are accomplished may vary.
Step #1: Screen for mental health disorders
Lesbian, bisexual, and gay people are more likely to experience depression and anxiety. According to the results of a large meta-analysis,14 the prevalence of these conditions is 1.5 times higher in this population than in heterosexual people. Risk may vary according to group, with gay and bisexual men experiencing a higher lifetime prevalence of anxiety and depression than lesbian and bisexual women.15 Suicidal attempts are also more common in gay and bisexual men, who have a lifetime risk four times higher than that of heterosexual men.14
The risk of suicide is even higher among transgender people: 41% of surveyed transgender adults reported that they had attempted suicide, with higher rates in younger individuals.5 Risk factors include experiences of harassment or physical or sexual violence, as well as poverty, low education level, and unemployment.5 The risk of suicide in transgender people who served in the military is 20 times higher than that in the general veteran population.16
It is imperative to routinely screen LGBT patients for anxiety, depression, and suicidality and to refer them to mental health providers who are sensitive to LGBT patients’ needs and concerns. Screening tools such as the Patient Health Questionnaire-2 (PHQ2), PHQ9A, PHQ9, and Generalized Anxiety Disorder 7-item scale (GAD7) are useful in screening patients for depression and anxiety in addition to mnemonics such as SIGECAPS (sleep, interest, guilt, energy, concentration, appetite, psychomotor, suicidal thoughts or ideation).17
Although the same screening tools are used in cisgender heterosexual patients, factors contributing to the experience of depression or anxiety may be directly related to gender identity, gender expression, or sexual orientation. In a 2001 study, more lesbian, gay, and bisexual people reported lifetime and day-to-day experiences with discrimination than heterosexual people, and approximately 42% attributed this in part or in total to their sexual orientation.18
Step #2: Assess for substance use
Substance use is also more common in LGBT people. Lesbian and bisexual women have higher rates of tobacco abuse, exposure to second-hand smoke, and alcohol and drug dependence.3,14 In one study, compared with heterosexual individuals, the odds of lifetime alcohol and substance use disorder was three times higher in lesbian women, and the odds of lifetime drug-use disorder was 1.6 times higher in gay men.19
In a survey of transgender people, 30% reported using tobacco compared with 20% of the US adult population, and 8% reported using alcohol or drugs to cope with mistreatment and bias.5 In a study of transgender women in San Francisco, 58% used alcohol and 43% used substances, including marijuana, methamphetamine, and crack cocaine. Substance use significantly increased the odds of testing positive for HIV.20
Clinicians should carefully question LGBT patients about their use of alcohol, tobacco, and other substances and provide counseling and assistance with cessation. Several LGBT-specific resources can be used to aid patients in their efforts, and referral to substance abuse groups that are welcoming to LGBT people may increase cessation rates.19,21
Step #3: Offer appropriate screening services
Human papillomavirus (HPV). Like heterosexual women, lesbian and bisexual women are at risk of HPV infection, which is associated with cervical cancer and genital warts.8 HPV can be transmitted in several ways, including skin-to-skin and digital-to-genital contact, as well as penile-vaginal intercourse. Lesbian and bisexual women may have acquired HPV from previous male sexual partners or from female-to-female transmission.8 In a study comparing cervical cancer screening results among lesbian, bisexual, and heterosexual women, there was no significant difference in the odds for Papanicolaou (Pap) test abnormalities and only a minor decrease in the odds of HPV infection.22 Lesbian and bisexual women should receive Pap and HPV testing according to current guidelines.
Other sexually transmitted infections, including herpes simplex virus 1, herpes simplex virus 2, Trichomonas vaginalis, syphilis, and hepatitis A, can be passed between female partners; risk may vary according to sexual practices.23 Thus, providers should not assume that lesbian women are at low risk of these infections and should screen according to current guidelines.
The US Centers for Disease Control and Prevention (CDC) recommends annual screening for Chlamydia infection for all women under age 25, as well as those at increased risk for this infection (ie, those with a new sex partner or multiple sex partners).24
Breast cancer. Studies reveal that lesbian and bisexual women are less likely to receive mammograms, and they may have several risk factors that increase their risk for breast cancer, including overweight, obesity, and excessive alcohol intake.12,18,25 Providers should discuss the risks and benefits of mammography and offer this screening service at appropriate intervals.
Screening in men who have sex with men
Men who have sex with men are at increased risk for several sexually transmitted infections, including HIV, syphilis, gonorrhea, Chlamydia, anal HPV, and hepatitis B and C.4,9 The CDC recommends annual sexual health screening that includes serologic testing for HIV and syphilis, and urine, rectal, or pharyngeal testing for gonorrhea and Chlamydia according to sexual practices.24
In contrast, routine screening for anal HPV is not currently recommended because we lack data demonstrating that screening reduces mortality rates from anal carcinoma.24,26 Nevertheless, the CDC acknowledges that some clinicians may choose to perform anal Pap testing in patients who are at high risk, and guidelines from the New York City Department of Health and Mental Hygiene suggest annual anal Pap testing in HIV-positive men who have sex with men.27
According to the results of a systematic review,28 a significant proportion of transgender women reported sexual practices that increased their risk for sexually transmitted infections, and 27.7% tested positive for HIV infection. In contrast, rates of HIV and risk behaviors were much lower among transgender men. Risk may be heightened in transgender women who have not had sexual reassignment surgery and who engage in insertive anal, vaginal, or oral intercourse.28 An awareness of an individual patient’s current anatomy and sexual practices is essential for providing appropriate counseling about sexually transmitted infections.
‘Screen what you have’
When considering screening for breast, cervical, and prostate cancer, providers should consider an individual patient’s surgical history and hormonal status. “Screen what you have” is an easy rule to help both patients and providers remember which services to consider.
Transgender men who have not had a mastectomy should discuss the risks and benefits of breast cancer screening and consider mammography as recommended by the American Cancer Society.29 Similarly, cervical cancer screening should be performed according to current guidelines, although providers should be aware that this examination can cause significant anxiety and emotional distress for the patient.30
In transgender women, guidelines for breast cancer screening for those who were previously or currently treated with hormones are lacking. The University of California-San Francisco Center of Excellence for Transgender Health recommends mammography for patients over age 50 with additional risk factors (family history, obesity, estrogen and progestin use for more than 5 years).31 Transgender women should be counseled about the risks and benefits of prostate cancer screening.
Step #4: Immunize, and promote healthy behaviors
Table 4 outlines the screening services, immunizations, and health behavior promotions that should be offered to LGBT patients.
Vaccinations. LGBT individuals should be routinely offered HPV vaccination through age 26, according to current guidelines.24 Immunization against hepatitis A and B is also recommended for men who have sex with men, if they are not already immune.24 Meningococcal vaccine should be given to men who have sex with men if they have an additional medical, occupational, or lifestyle risk factor.32
Physical activity should be encouraged, especially in lesbian and bisexual women, who are more likely to be overweight and obese.25 In a recent study,33 gay, lesbian, and bisexual youths (ages 12–22) reported 1.21 to 2.62 fewer hours of moderate or vigorous physical activity per week than their “completely heterosexual” counterparts, and were 46% to 76% less likely to participate in team sports, in part due to concerns about gender nonconformity. On the other hand, results from a recent national survey of adults ages 18 through 64 found no significant differences in physical activity according to sexual orientation.
Providers should address patients’ perceived barriers to participating in exercise programs.2
Preexposure prophylaxis against HIV. A growing number of patients and health providers are asking about preexposure prophylaxis for HIV infection. The initial CDC recommendations for the daily use of emtricitabine-tenofovir were restricted to gay and bisexual men and men who have sex with men in serodiscordant relationships or in situations where the HIV status of the patient’s partner was unknown.34 Since then, the CDC has expanded the groups who may benefit from preexposure prophylaxis.35 Assessment of the patient’s ability to adhere to a daily oral medication regimen is central to its success. Patients should be screened for hepatitis, HIV, and renal and liver function before starting emtricitabine-tenofovir and should have these tests repeated at 3-month intervals if pre-exposure prophylaxis is continued.
Step #5: Initiate or continue hormone therapy for transgender individuals
Hormone therapy often improves the quality of life for patients who desire to have their physical appearance align more closely with their gender identity.29 Moreover, abruptly stopping hormone therapy can have significant psychological consequences.36
Clinicians should feel comfortable starting hormone therapy for patients who have been diagnosed with gender dysphoria by a mental health professional, can demonstrate knowledge about and outcomes of hormone therapy, and have lived as a member of the desired gender (“real-life experience”) for at least 3 months, and preferably 12 months.29 More recently, some practitioners have advocated prescribing hormone therapy for patients without the requirement for real-life experience or a formal letter from a mental health professional recommending hormonal therapy.37 However, mental healthcare is recommended for any patient with moderate to severe mental health conditions, especially if not treated at the time of presentation.37
Providers should continue hormone therapy for patients who are already receiving it, while being aware of the appropriate treatment goals and monitoring parameters. The two main principles of hormone therapy for transgender patients are to reduce endogenous hormone levels and their associated sex characteristics and replace with hormones of the preferred sex.29 Doses and formulations are similar to those used for treatment of hypogonadism. This topic has been reviewed by Spack.10
The only absolute contraindications to hormone therapy are estrogen- or testosterone-responsive tumors. Otherwise, hormone therapy can be initiated or continued with the patient’s informed consent about its benefits and risks.
Estrogen therapy may increase the risk of thromboembolic disease, coronary artery disease, cerebrovascular disease, severe migraine headaches, liver dysfunction, and macroprolactinoma.29 In a cross-sectional study of 100 transgender patients receiving hormone therapy, 12% of transgender women experienced a thromboembolic or cardiovascular event after an average of 11 years of treatment.38 However, many of these patients had additional risk factors for these events, such as smoking. In contrast, results from a recent systematic review39 indicated a much lower rate of venous thromboembolism among transgender women receiving estrogen therapy (1.7%–6.3%). Use of transdermal estrogen may minimize the likelihood of thromboembolic disease, and cessation of hormonal care in the perioperative period is advisable, especially for procedures with greater risk of venous thromboembolism.39
Transgender men are at risk of erythrocytosis (hematocrit > 50%) as a result of testosterone therapy. Although current guidelines indicate that testosterone may increase the risk of breast or uterine cancer, results from a recent systematic review40 indicate that the overall cancer incidence in transgender men is not higher than in natal controls. Both estrogen and testosterone therapy increase insulin resistance and fasting glucose levels, whereas only estrogen increases triglyceride concentrations.40
For transgender women, estrogen levels should be maintained in the normal range for cisgender women of reproductive age (< 200 pg/mL), and testosterone levels should be suppressed to less than 55 ng/dL. Goal testosterone levels for transgender men are between 320 and 1,000 ng/dL and should be measured at intervals specific to the preparation used (ie, measured midway between injections for individuals treated with testosterone cypionate). Estradiol levels should be less than 50 ng/dL.29 Transgender women and men should have estradiol and testosterone levels measured quarterly during the first year of treatment, and then every 6 to 12 months thereafter once goal levels are achieved.
Additional monitoring for transgender women includes measuring serum prolactin at baseline and after 12 months of therapy, and serum electrolytes for those taking spironolactone as antiandrogen therapy. Complete blood cell counts and liver function tests should be done every 3 months during the first year of testosterone therapy for transgender men, and then one to two times per year.29 Reference laboratory values for the patient’s affirmed gender should be used to assess response to therapy as well as effects on end-organ function.
The marked suppression of endogenous hormone levels that occurs during therapy may have adverse effects on the bone mineral density of both transgender women and men. Clinicians should assess patients’ baseline risk for osteoporotic fracture at the time hormone therapy is started and consider bone mineral density testing if appropriate. For those at low risk for fracture, current guidelines recommend screening for osteoporosis starting at age 60.29
Providers should counsel patients who have recently initiated hormone therapy that some changes may occur gradually over time. While transgender women will notice a decrease in libido and spontaneous erections within the first 3 months of therapy, breast growth begins approximately 3 to 6 months after treatment is started. Similarly, for transgender men, fat redistribution occurs during the first 6 months of treatment, but facial and body hair growth occur more slowly and are at maximum 4 to 5 years after starting hormone therapy.29 Amenorrhea typically occurs 1 to 6 months after starting hormonal therapy for transgender men.
Some patients may be interested in surgery to continue their physical transformation to the desired sex. Patients who have used hormone therapy and participated in a real-life experience or otherwise completed social transition by living as the affirmed gender for 12 months are considered eligible for surgery if they can demonstrate a good understanding of the cost, potential complications, and expected recovery time of the procedure. Guidelines also recommend that the patient demonstrate progress in work, family, and interpersonal issues regarding their new gender.29 Available surgical options include breast augmentation, orchiectomy and penectomy, and vaginoplasty, clitoroplasty, and vulvoplasty for transgender women. Feminizing procedures include voice surgery, thyroid cartilage reduction, and facial feminization surgery. Transgender men may choose to have mastectomy, hysterectomy and salpingo-oophorectomy, vaginectomy, scrotoplasty and testicular implant placement, and implantation of a penile prosthesis. Additional virilizing surgeries include voice surgery and pectoral implants.41
Step #6: Screen for intimate partner violence
Intimate partner violence refers to physical, sexual, and psychological harm by a current or former partner or spouse, and it can occur in gay and lesbian relationships. In 2000, a National Violence Against Women survey found that 21.5% of men and 35.4% of women who reported living with a same-sex partner had experienced physical abuse.42 More recent studies confirm rates similar to those in heterosexual relationships. In an online study,43 11.8% of men who have sex with men reported physical violence from a current male partner, and about 4% reported experiencing coerced sex.
Intimate partner violence is uniquely challenging for LGBT people. In addition to the commonly described methods an abuser uses to maintain power and control, forced disclosure or “outing”—publicly revealing someone’s sexual orientation or gender identity—may result in additional psychological violence and harm. Survivors of intimate partner violence who are in same-gender intimate relationships often find that obtaining services through the police, judicial, and social services systems is challenging. Survivors may be required to disclose their sexual orientation or gender identity as part of filing a report or judicial order to obtain help or protection from the abuser. Many male and transgender survivors of intimate partner violence are unable to access traditional shelters. Female survivors may find that their same-sex abusers have the same access to resources and shelters that they do.
Intimate partner violence is associated with negative physical and mental health outcomes. Physical injuries such as bruises, fractures, and burns are some of the more obvious harms survivors sustain. However, the negative psychological impact on survivors cannot be overstated. LGBT individuals are at greater risk of depression and substance abuse as a result of intimate partner violence than their cisgender heterosexual counterparts. The stress resulting from stigmatization and discrimination can be exacerbated by intimate partner violence.44 This can be seen in health outcomes of HIV-positive men who have sex with men, in whom abuse predicts interruptions in care, more advanced HIV disease, and HIV-associated hospitalizations.45
We recommend that providers screen all LGBT patients for intimate partner violence. One commonly used tool is the Partner Violence Screen, which consists of three gender-neutral questions:
- Have you been hit, kicked, punched, or otherwise hurt by someone in the past year? If so, by whom?
- Do you feel safe in your current relationship?
- Is there a partner from a previous relationship who is making you feel unsafe now?
Like other screening tools for intimate partner violence, the Partner Violence Screen is more specific than sensitive.46 Screening and discussions about intimate partner violence should be performed in a private, confidential manner while the patient is alone.
Providers who care for LGBT patients need to be aware of not only the medical and mental health sequelae of intimate partner violence but also the social and legal issues facing survivors. Familiarity with the available community resources and their limitations can better facilitate trust and patient care for those affected by intimate partner violence. In one study, the most frequent requests for assistance from sexual and gender minority survivors were for counseling, safe housing, legal assistance, and assistance navigating the medical system.47 Providers should refer patients to LGBT-focused resources in their community as available, and when no such resources exist, initiate contact with standard domestic violence services, with patient consent, to ask about a program’s ability to assist survivors of LGBT intimate partner violence.
IN A NUTSHELL
Optimizing the care of LGBT patients requires developing both clinical and cultural competency.
Initial steps for creating an inclusive and welcoming clinical environment include becoming familiar with local resources for LGBT patients (support groups, substance and alcohol cessation groups, mental health providers; see sidebar), providing education and training for support staff and nurses, and establishing gender-neutral bathrooms. Waiting areas should include literature relevant to LGBT patients and signage that is relevant to all patients, including gender-nonconforming individuals. Providers should offer all patients universal HIV screening initially and at clinically appropriate intervals and discuss preexposure prophylaxis with emtricitabine-tenofovir for at-risk individuals.
For transgender patients, addressing them by their preferred name and pronouns is central to building rapport. General health maintenance is the same for transgender patients as for cisgender patients and can be guided by the adage “screen what you have.” Hormonal care can be offered using an informed consent method consistent with the World Professional Association for Transgender Health Standards of Care.48 Guidelines exist to assist providers in initiation and maintenance of hormonal care. Cross-gender hormonal therapy is initiated with low-dose medication that is gradually increased over time, with a goal of approximating the pubertal changes of the desired gender over a 2- to 3-year period. Some, but not all, patients may pursue various surgical procedures as part of their gender affirmation process.
- Gates GJ. How many people are lesbian, gay, bisexual, or transgender? Williams Institute. 2011. http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Accessed May 19, 2016.
- Ward BW, Dahlhamer JM, Galinsky AM, Joesti SS. Sexual orientation and health among U.S. Adults: National Health Interview Survey, 2013. Natl Health Stat Report 2014; 77:1–10.
- Cochran SD, Bandiera FC, Mays VM. Sexual orientation-related differences in tobacco use and secondhand smoke exposure among US adults aged 20-59 years: 2003–2010 National Health and Nutrition Examination surveys. Am J Publ Health 2013; 103:1837–1844.
- Mayer KH. Sexually transmitted diseases in men who have sex with men. Clin Infect Disease 2011; 53:S79–S83.
- Grant JM, Mottet LA, Tanis J, Herman JL, Harrison J, Keisling M. National transgender discrimination survey report on health and health care. www.thetaskforce.org/static_html/downloads/reports/reports/ntds_report_on_health.pdf. Accessed May 19, 2016.
- Pathela P, Hajat A, Schillinger J, Blank S, Sell R, Mostashari F. Discordance between sexual behavior and self-reported sexual identity: a population-based survey of New York City men. Ann Intern Med 2006; 145:416–425.
- Chandra A, Mosher WD, Copen C, Sionean C. Sexual behavior, sexual attraction, and sexual identity in the United States: data from the 2006–2009 National Survey of Family Growth. Natl Health Stat Report 2011; 36:1–36.
- Agenor M, Peitzmeier S, Gordon AR, Haneuse S, Potter JE, Austin SB. Sexual orientation identity disparities in awareness and initiation of the human papillomavirus vaccine among U.S. women and girls: a national survey. Ann Intern Med 2015; 163:99–106.
- Ard KL, Makadon HJ. Improving the health care of lesbian, gay, bisexual and transgender (LGBT) people: understanding and eliminating health disparities. www.lgbthealtheducation.org/wp-content/uploads/12-054_LGBTHealtharticle_v3_07-09-12.pdf. Accessed May 19, 2016.
- Spack NP. Management of transgenderism. JAMA 2013; 309:474–484.
- National LGBT Health Education Center. Achieving health equity for lesbian, gay, bisexual, and transgender (LGBT) people, Module 1. www.lgbthealtheducation.org/wp-content/uploads/Achieving-Health-Equity-for-LGBT-People-1.pdf. Accessed May 19, 2016.
- Buchmueller T, Carpenter CS. Disparities in health Insurance coverage, access, and outcomes for individuals in same-sex versus different-sex relationships, 2000–2007. Am J Public Health 2010; 100:489–496.
- Kosenko K, Rintamaki L, Raney S, Maness K. Transgender patient perceptions of stigma in health care contexts. Med Care 2013; 51:819–822.
- King M, Semlyen J, Tai SS, et al. A systematic review of mental disorder, suicide, and deliberate self-harm in lesbian, gay, and bisexual people. BMC Psychiatry 2008; 8:70.
- Bostwick WB, Boyd CJ, Hughes TL, McCabe SE. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. Am J Public Health 2010; 100:468–475.
- Blosnich JR, Brown GR, Shipherd JC, Kauth M, Piegari RI, Bossarte RM. Prevalence of gender identity disorder and suicide risk among transgender veterans utilizing Veterans Health Administration care. Am J Public Health 2013: 103:e27–e32.
- Maurer DM. Screening for depression. Am Fam Physician 2012; 85:139–144.
- Mays VM, Cochran SD. Mental health correlates of perceived discrimination among lesbian, gay, and bisexual adults in the United States. Am J Pub Health 2001; 91:1869–1875.
- McCabe SE, West BT, Hughes TL, Boyd CJ. Sexual orientation and substance abuse treatment utilization in the United States: results from a national survey. J Subst Abuse Treat 2013; 44:4–12.
- Santos GM, Rapues J, Wilson EC, et al. Alcohol and substance use among transgender women in San Francisco: prevalence and association with human immunodeficiency virus infection. Drug Alcohol Rev 2014; 33:287–295.
- National LGBT Tobacco Control Network. www.lgbttobacco.org. Accessed May 19, 2016.
- Massad LS, Xie X, Minkoff H, et al. Abnormal Pap tests and human papillomavirus infections among HIV infected and uninfected women who have sex with women. J Low Genit Tract Dis 2014; 18:50–56.
- Gorgos LM, Marrazzo JM. Sexually transmitted infections among women who have sex with women. Clin Infect Dis 2011; 53:S84–S91.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR 2015; 64(3):1–138.
- Boehmer U, Bowen DJ, Bauer GR. Overweight and obesity in sexual-minority women: evidence from population-based data. Am J Public Health 2007; 97:1134–1140.
- Smyczek P, Singh AE, Romanowski B. Anal intraepithelial neoplasia: review and recommendations for screening and management. Int J STD AIDS 2013; 24:843–851.
- New York City Department of Health and Mental Hygiene. Preventing sexually transmitted infections. 2013; 32(4):19–27. www.nyc.gov/html/doh/html/data/chi32-4_screening.html. Accessed May 19, 2016.
- Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav 2008; 12:1–17.
- Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, et al. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2009; 94:3132–3133.
- Peitzmeier SM, Reisner SL, Harigopal P, Potter J. Female-to-male patients may have high prevalence of unsatisfactory paps compared to non-transgender females: implications for cervical cancer screening. J Gen Intern Med 2014; 29:778–784.
- UCSF Center of Excellence for Transgender Health. Primary care protocol for transgender patient care. http://transhealth.ucsf.edu/protocols. Accessed May 19, 2016.
- Centers for Disease Control and Prevention. Recommended adult immunization schedule United States—2015. www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf. Accessed May 19, 2016.
- Calzo JP, Roberts AL, Corliss HL, Blood EA, Kroshus E, Austin SB. Physical activity disparities in heterosexual and sexual minority youth ages 12–22 years old: roles of childhood gender nonconformity and athletic self-esteem. Ann Behav Med 2014; 47:17–27.
- Centers for Disease Control and Prevention. Interim guidance for clinicians considering the use of preexposure prophylaxis for the prevention of HIV infection in heterosexually active adults. MMWR 2012; 61:586–589.
- Centers for Disease Control and Prevention and US Public Health Service. Preexposure prophlyaxis for the prevention of HIV infection in the United States—2014. A clinical practice guideline. www.cdc.gov/hiv/pdf/PrEPguidelines2014.pdf. Accessed May 19, 2016.
- Feldman JL, Goldberg J. Transgender primary medical care: suggested guidelines for clinicians in British Columbia. www.cwhn.ca/en/node/27567. Accessed May 19, 2016.
- Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-noncomforming people, version 7. Int J Transgenderism 2011; 13:165–232.
- Wierckx K, Mueller S, Weyers S, et al. Long-term evaluation of cross-sex hormone treatment in transsexual persons. J Sex Med 2012; 9: 2641–2651.
- Asscheman H, T’Sjoen G, Lemaire A, et al. Venous thrombo-embolism as a complication of cross-sex hormone treatment of male-to-female transsexual subjects: a review. Andrologia 2014; 46:791–795.
- Weinand JD, Safer JD. Hormone therapy in transgender adults is safe with provider supervision. A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol 2015; 2:55–60.
- Unger CA. Care of the transgender patient: the role of the gynecologist. Am J Obstet Gynecol 2014; 210:16–26.
- Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. Washington, DC: US Department of Justice, National Institute of Justice; 2000. P. 29–31. Report No.: NCJ 181867.
- Stephenson R, Khosropour C, Sullivan P. Reporting of intimate partner violence among men who have sex with men in an online survey. West J Emerg Med 2010; 11:242–246.
- Chen PH, Jacobs A, Rovi SL. Intimate partner violence: IPV in the LGBT community. FP Essent 2013; 412:28–35.
- Siemieniuk R, Miller P, Woodman K, et al. Prevalence, clinical associations, and impact of intimate partner violence among HIV infected gay and bisexual men: a population based study. HIV Med 2013; 14:293–302.
- Rabin RF, Jennings JM, Campbell JC, Bair-Merritt MH. Intimate partner violence screening tools: a systematic review. Am J Prev Med 2009; 36:439–445.
- Ford CL, Slavin T, Hilton KL, Holt SL. Intimate partner violence prevention services and resources in Los Angeles: issues, needs, and challenges for assisting lesbian, gay, bisexual, and transgender clients. Health Promot Pract 2013; 14:841–849.
- World Professional Association for Transgender Health. www.wpath.org/site_page.cfm?pk_association_webpage_menu=1351. Accessed May 19, 2016.
- Gates GJ. How many people are lesbian, gay, bisexual, or transgender? Williams Institute. 2011. http://williamsinstitute.law.ucla.edu/wp-content/uploads/Gates-How-Many-People-LGBT-Apr-2011.pdf. Accessed May 19, 2016.
- Ward BW, Dahlhamer JM, Galinsky AM, Joesti SS. Sexual orientation and health among U.S. Adults: National Health Interview Survey, 2013. Natl Health Stat Report 2014; 77:1–10.
- Cochran SD, Bandiera FC, Mays VM. Sexual orientation-related differences in tobacco use and secondhand smoke exposure among US adults aged 20-59 years: 2003–2010 National Health and Nutrition Examination surveys. Am J Publ Health 2013; 103:1837–1844.
- Mayer KH. Sexually transmitted diseases in men who have sex with men. Clin Infect Disease 2011; 53:S79–S83.
- Grant JM, Mottet LA, Tanis J, Herman JL, Harrison J, Keisling M. National transgender discrimination survey report on health and health care. www.thetaskforce.org/static_html/downloads/reports/reports/ntds_report_on_health.pdf. Accessed May 19, 2016.
- Pathela P, Hajat A, Schillinger J, Blank S, Sell R, Mostashari F. Discordance between sexual behavior and self-reported sexual identity: a population-based survey of New York City men. Ann Intern Med 2006; 145:416–425.
- Chandra A, Mosher WD, Copen C, Sionean C. Sexual behavior, sexual attraction, and sexual identity in the United States: data from the 2006–2009 National Survey of Family Growth. Natl Health Stat Report 2011; 36:1–36.
- Agenor M, Peitzmeier S, Gordon AR, Haneuse S, Potter JE, Austin SB. Sexual orientation identity disparities in awareness and initiation of the human papillomavirus vaccine among U.S. women and girls: a national survey. Ann Intern Med 2015; 163:99–106.
- Ard KL, Makadon HJ. Improving the health care of lesbian, gay, bisexual and transgender (LGBT) people: understanding and eliminating health disparities. www.lgbthealtheducation.org/wp-content/uploads/12-054_LGBTHealtharticle_v3_07-09-12.pdf. Accessed May 19, 2016.
- Spack NP. Management of transgenderism. JAMA 2013; 309:474–484.
- National LGBT Health Education Center. Achieving health equity for lesbian, gay, bisexual, and transgender (LGBT) people, Module 1. www.lgbthealtheducation.org/wp-content/uploads/Achieving-Health-Equity-for-LGBT-People-1.pdf. Accessed May 19, 2016.
- Buchmueller T, Carpenter CS. Disparities in health Insurance coverage, access, and outcomes for individuals in same-sex versus different-sex relationships, 2000–2007. Am J Public Health 2010; 100:489–496.
- Kosenko K, Rintamaki L, Raney S, Maness K. Transgender patient perceptions of stigma in health care contexts. Med Care 2013; 51:819–822.
- King M, Semlyen J, Tai SS, et al. A systematic review of mental disorder, suicide, and deliberate self-harm in lesbian, gay, and bisexual people. BMC Psychiatry 2008; 8:70.
- Bostwick WB, Boyd CJ, Hughes TL, McCabe SE. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. Am J Public Health 2010; 100:468–475.
- Blosnich JR, Brown GR, Shipherd JC, Kauth M, Piegari RI, Bossarte RM. Prevalence of gender identity disorder and suicide risk among transgender veterans utilizing Veterans Health Administration care. Am J Public Health 2013: 103:e27–e32.
- Maurer DM. Screening for depression. Am Fam Physician 2012; 85:139–144.
- Mays VM, Cochran SD. Mental health correlates of perceived discrimination among lesbian, gay, and bisexual adults in the United States. Am J Pub Health 2001; 91:1869–1875.
- McCabe SE, West BT, Hughes TL, Boyd CJ. Sexual orientation and substance abuse treatment utilization in the United States: results from a national survey. J Subst Abuse Treat 2013; 44:4–12.
- Santos GM, Rapues J, Wilson EC, et al. Alcohol and substance use among transgender women in San Francisco: prevalence and association with human immunodeficiency virus infection. Drug Alcohol Rev 2014; 33:287–295.
- National LGBT Tobacco Control Network. www.lgbttobacco.org. Accessed May 19, 2016.
- Massad LS, Xie X, Minkoff H, et al. Abnormal Pap tests and human papillomavirus infections among HIV infected and uninfected women who have sex with women. J Low Genit Tract Dis 2014; 18:50–56.
- Gorgos LM, Marrazzo JM. Sexually transmitted infections among women who have sex with women. Clin Infect Dis 2011; 53:S84–S91.
- Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR 2015; 64(3):1–138.
- Boehmer U, Bowen DJ, Bauer GR. Overweight and obesity in sexual-minority women: evidence from population-based data. Am J Public Health 2007; 97:1134–1140.
- Smyczek P, Singh AE, Romanowski B. Anal intraepithelial neoplasia: review and recommendations for screening and management. Int J STD AIDS 2013; 24:843–851.
- New York City Department of Health and Mental Hygiene. Preventing sexually transmitted infections. 2013; 32(4):19–27. www.nyc.gov/html/doh/html/data/chi32-4_screening.html. Accessed May 19, 2016.
- Herbst JH, Jacobs ED, Finlayson TJ, McKleroy VS, Neumann MS, Crepaz N. Estimating HIV prevalence and risk behaviors of transgender persons in the United States: a systematic review. AIDS Behav 2008; 12:1–17.
- Hembree WC, Cohen-Kettenis P, Delemarre-van de Waal HA, et al. Endocrine treatment of transsexual persons: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2009; 94:3132–3133.
- Peitzmeier SM, Reisner SL, Harigopal P, Potter J. Female-to-male patients may have high prevalence of unsatisfactory paps compared to non-transgender females: implications for cervical cancer screening. J Gen Intern Med 2014; 29:778–784.
- UCSF Center of Excellence for Transgender Health. Primary care protocol for transgender patient care. http://transhealth.ucsf.edu/protocols. Accessed May 19, 2016.
- Centers for Disease Control and Prevention. Recommended adult immunization schedule United States—2015. www.cdc.gov/vaccines/schedules/downloads/adult/adult-combined-schedule.pdf. Accessed May 19, 2016.
- Calzo JP, Roberts AL, Corliss HL, Blood EA, Kroshus E, Austin SB. Physical activity disparities in heterosexual and sexual minority youth ages 12–22 years old: roles of childhood gender nonconformity and athletic self-esteem. Ann Behav Med 2014; 47:17–27.
- Centers for Disease Control and Prevention. Interim guidance for clinicians considering the use of preexposure prophylaxis for the prevention of HIV infection in heterosexually active adults. MMWR 2012; 61:586–589.
- Centers for Disease Control and Prevention and US Public Health Service. Preexposure prophlyaxis for the prevention of HIV infection in the United States—2014. A clinical practice guideline. www.cdc.gov/hiv/pdf/PrEPguidelines2014.pdf. Accessed May 19, 2016.
- Feldman JL, Goldberg J. Transgender primary medical care: suggested guidelines for clinicians in British Columbia. www.cwhn.ca/en/node/27567. Accessed May 19, 2016.
- Coleman E, Bockting W, Botzer M, et al. Standards of care for the health of transsexual, transgender, and gender-noncomforming people, version 7. Int J Transgenderism 2011; 13:165–232.
- Wierckx K, Mueller S, Weyers S, et al. Long-term evaluation of cross-sex hormone treatment in transsexual persons. J Sex Med 2012; 9: 2641–2651.
- Asscheman H, T’Sjoen G, Lemaire A, et al. Venous thrombo-embolism as a complication of cross-sex hormone treatment of male-to-female transsexual subjects: a review. Andrologia 2014; 46:791–795.
- Weinand JD, Safer JD. Hormone therapy in transgender adults is safe with provider supervision. A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol 2015; 2:55–60.
- Unger CA. Care of the transgender patient: the role of the gynecologist. Am J Obstet Gynecol 2014; 210:16–26.
- Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. Washington, DC: US Department of Justice, National Institute of Justice; 2000. P. 29–31. Report No.: NCJ 181867.
- Stephenson R, Khosropour C, Sullivan P. Reporting of intimate partner violence among men who have sex with men in an online survey. West J Emerg Med 2010; 11:242–246.
- Chen PH, Jacobs A, Rovi SL. Intimate partner violence: IPV in the LGBT community. FP Essent 2013; 412:28–35.
- Siemieniuk R, Miller P, Woodman K, et al. Prevalence, clinical associations, and impact of intimate partner violence among HIV infected gay and bisexual men: a population based study. HIV Med 2013; 14:293–302.
- Rabin RF, Jennings JM, Campbell JC, Bair-Merritt MH. Intimate partner violence screening tools: a systematic review. Am J Prev Med 2009; 36:439–445.
- Ford CL, Slavin T, Hilton KL, Holt SL. Intimate partner violence prevention services and resources in Los Angeles: issues, needs, and challenges for assisting lesbian, gay, bisexual, and transgender clients. Health Promot Pract 2013; 14:841–849.
- World Professional Association for Transgender Health. www.wpath.org/site_page.cfm?pk_association_webpage_menu=1351. Accessed May 19, 2016.
KEY POINTS
- Lesbian and bisexual women are at increased risk for overweight, obesity, tobacco use, and drug and alcohol use disorders. Clinicians should screen for these conditions regularly and provide appropriate referral.
- Annual screening for HIV, syphilis, Chlamydia, and gonorrhea should be offered to men who have sex with men.
- Pre-exposure prophylaxis against HIV infection may be appropriate for some at-risk individuals who can adhere to daily therapy.
- “Screen what you have” is a rule that can help physicians to consider the appropriate screening services for transgender individuals.
- Hormone therapy (estrogen and testosterone) can benefit transgender individuals who are changing their physical appearance to their affirmed gender.
