User login
Fillers: Past, Present, and Future
Summer hair care
Daily and weekly hair care for black women may include styling, relaxing, perming, coloring, braiding, or hot ironing. Moisture compromises the integrity of the hairstyles, which may lead some women to avoid contact with water, humidity, and sweat, all ingredients of summer for many people.
In my clinic, many black women are seen for scalp disorders such as scarring alopecia, folliculitis, hair breakage, and seborrhea. However, I also make a point of asking each of these patients about her hair care practices. If concerns for hair make them less inclined to swim or sweat, I remind them that proper hair care practices can minimize scalp diseases and hair loss, and that they need not avoid outdoor exercise when the weather heats up.
Summer hair care guidelines that I recommend to skin of color patients are mainly the same as at other times of the year, including proper moisturizing of the hair before and after treatments, minimizing time between chemical treatments, not coloring and chemically relaxing the hair at the same time, avoiding hot combs and hot styling tools, and treating any scalp inflammation early and aggressively.
However, summer is a great time to cut and style the hair with natural curls if possible, because beating the heat and humidity with harsh styling practices can break the hair and lead to irreversible hair shaft damage.
Other tips to help your patients manage their hair in the summer months include recommending sulfate-free shampoos in place of regular shampoos. Between washes, a dry shampoo is best used at the root of the hair, and is a great alternative to hair washing after the beach or after exercise. Dry shampoos are widely available and when used daily absorb dirt, oil, and hair products applied to the hair. After washing, I advise patients to apply a leave-in conditioner to damp or dry hair. These conditioners help protect the hair shaft from styling damage.
Prior to workouts, styling hair into a ponytail or French twist can help protect the hair from sweat. If patients report that their hair is starting to break, advise them to minimize the relaxing and heat styling, and to choose loose twists and gentle, loose braids. Finally, applying a serum or "smoothing lotion" with ingredients such as argan oil or mineral oil to the hair before styling can help to smooth strands, mask fly-aways, and prevent summer frizz.
Dr. Talakoub is in private practice in McLean, Va.
Daily and weekly hair care for black women may include styling, relaxing, perming, coloring, braiding, or hot ironing. Moisture compromises the integrity of the hairstyles, which may lead some women to avoid contact with water, humidity, and sweat, all ingredients of summer for many people.
In my clinic, many black women are seen for scalp disorders such as scarring alopecia, folliculitis, hair breakage, and seborrhea. However, I also make a point of asking each of these patients about her hair care practices. If concerns for hair make them less inclined to swim or sweat, I remind them that proper hair care practices can minimize scalp diseases and hair loss, and that they need not avoid outdoor exercise when the weather heats up.
Summer hair care guidelines that I recommend to skin of color patients are mainly the same as at other times of the year, including proper moisturizing of the hair before and after treatments, minimizing time between chemical treatments, not coloring and chemically relaxing the hair at the same time, avoiding hot combs and hot styling tools, and treating any scalp inflammation early and aggressively.
However, summer is a great time to cut and style the hair with natural curls if possible, because beating the heat and humidity with harsh styling practices can break the hair and lead to irreversible hair shaft damage.
Other tips to help your patients manage their hair in the summer months include recommending sulfate-free shampoos in place of regular shampoos. Between washes, a dry shampoo is best used at the root of the hair, and is a great alternative to hair washing after the beach or after exercise. Dry shampoos are widely available and when used daily absorb dirt, oil, and hair products applied to the hair. After washing, I advise patients to apply a leave-in conditioner to damp or dry hair. These conditioners help protect the hair shaft from styling damage.
Prior to workouts, styling hair into a ponytail or French twist can help protect the hair from sweat. If patients report that their hair is starting to break, advise them to minimize the relaxing and heat styling, and to choose loose twists and gentle, loose braids. Finally, applying a serum or "smoothing lotion" with ingredients such as argan oil or mineral oil to the hair before styling can help to smooth strands, mask fly-aways, and prevent summer frizz.
Dr. Talakoub is in private practice in McLean, Va.
Daily and weekly hair care for black women may include styling, relaxing, perming, coloring, braiding, or hot ironing. Moisture compromises the integrity of the hairstyles, which may lead some women to avoid contact with water, humidity, and sweat, all ingredients of summer for many people.
In my clinic, many black women are seen for scalp disorders such as scarring alopecia, folliculitis, hair breakage, and seborrhea. However, I also make a point of asking each of these patients about her hair care practices. If concerns for hair make them less inclined to swim or sweat, I remind them that proper hair care practices can minimize scalp diseases and hair loss, and that they need not avoid outdoor exercise when the weather heats up.
Summer hair care guidelines that I recommend to skin of color patients are mainly the same as at other times of the year, including proper moisturizing of the hair before and after treatments, minimizing time between chemical treatments, not coloring and chemically relaxing the hair at the same time, avoiding hot combs and hot styling tools, and treating any scalp inflammation early and aggressively.
However, summer is a great time to cut and style the hair with natural curls if possible, because beating the heat and humidity with harsh styling practices can break the hair and lead to irreversible hair shaft damage.
Other tips to help your patients manage their hair in the summer months include recommending sulfate-free shampoos in place of regular shampoos. Between washes, a dry shampoo is best used at the root of the hair, and is a great alternative to hair washing after the beach or after exercise. Dry shampoos are widely available and when used daily absorb dirt, oil, and hair products applied to the hair. After washing, I advise patients to apply a leave-in conditioner to damp or dry hair. These conditioners help protect the hair shaft from styling damage.
Prior to workouts, styling hair into a ponytail or French twist can help protect the hair from sweat. If patients report that their hair is starting to break, advise them to minimize the relaxing and heat styling, and to choose loose twists and gentle, loose braids. Finally, applying a serum or "smoothing lotion" with ingredients such as argan oil or mineral oil to the hair before styling can help to smooth strands, mask fly-aways, and prevent summer frizz.
Dr. Talakoub is in private practice in McLean, Va.
Major finding: Key numerical finding (e.g., number needed to treat to prevent one death/event; number lived or died as result of intervention). Maximum 10 words/1 sentence.
Data source: Include type of study (e.g., randomized, placebo controlled trial; retrospective case-control study). Include number in the study.
Disclosures: Sponsor of study, funding source, relevant disclosures. If author has no relevant disclosures, "Dr. X reported having no financial disclosures." If necessary, "Meeting Y did not require reports of financial disclosures." Check meeting website because many list disclosures. Written in sentence form.

Product News: 05 2013
PDL Versus PDT for Port-wine Stains

In the May 2013 issue of the British Journal of Dermatology (2013;168:1040-1046) Gao et al reported on a side-by-side comparison of the use of photodynamic therapy (PDT) versus the pulsed dye laser (PDL) for the treatment of 9 red and 6 purple port-wine stains (PWSs). Fifteen patients (age range, 11–36 years) with PWSs were chosen and 2 adjacent areas of the lesion were randomly assigned to receive either a single PDL treatment or a single PDT session. Eleven lesions were on the neck area, 3 on the upper arm, and 1 on the upper leg. The PDL had a wavelength of 585 nm, and PDT was performed with intravenous hematoporphyrin monomethyl ether and a low-power copper vapor laser (510.6 and 578.2 nm, respectively). The PDT-treated area was done 30 minutes after the PDL-treated area with the other areas being covered. The clinical outcome was measured colorimetrically (blanching rates) and visually.
For the red PWSs the blanching rates at 2 months with the PDL were 11% to 24% and 22% to 55% with PDT (P=.006). For the purple PWSs, blanching rates ranged from 8% to 33% with PDL and 30% to 45% with PDT (P=.0313). Two patients with purple PWSs showed no response to either PDT or PDL. All PDT sites developed localized edema, and all PDL sites developed edema, blistering, purpura, and crusts. Four patients with red PWSs developed hyperpigmentation at the PDL sites.
What’s the issue?
Although there have been studies showing that PDT is an effective treatment of PWSs, this study is a side-by-side quantitative comparison of PDL versus PDT. This study showed that PDT is as effective and as safe as PDL and possibly superior for the treatment of red and purple flat PWSs. This study represents promising steps forward in PDT treatment of dermatologic conditions.
Even though PDL therapy is considered the current standard for treatment of PWSs, this study does show good clearance with PDT. Pulsed dye laser therapy has been more readily available in North America and Europe, though in China, where this study took place, it is not common. The PDT in this study utilized an intravenous photosensitizer, which may not be suitable for all patients. Other limitations of this study include the small sample size and the possibility that treating the lesion halves in close proximity to each other may compound adverse effects. Because each half of the lesion (close proximity to one another) was treated, the effects of each treatment may have been compounded.
Could PDT become an adjuvant treatment in the armamentarium for resistant port-wine stains?
In the May 2013 issue of the British Journal of Dermatology (2013;168:1040-1046) Gao et al reported on a side-by-side comparison of the use of photodynamic therapy (PDT) versus the pulsed dye laser (PDL) for the treatment of 9 red and 6 purple port-wine stains (PWSs). Fifteen patients (age range, 11–36 years) with PWSs were chosen and 2 adjacent areas of the lesion were randomly assigned to receive either a single PDL treatment or a single PDT session. Eleven lesions were on the neck area, 3 on the upper arm, and 1 on the upper leg. The PDL had a wavelength of 585 nm, and PDT was performed with intravenous hematoporphyrin monomethyl ether and a low-power copper vapor laser (510.6 and 578.2 nm, respectively). The PDT-treated area was done 30 minutes after the PDL-treated area with the other areas being covered. The clinical outcome was measured colorimetrically (blanching rates) and visually.
For the red PWSs the blanching rates at 2 months with the PDL were 11% to 24% and 22% to 55% with PDT (P=.006). For the purple PWSs, blanching rates ranged from 8% to 33% with PDL and 30% to 45% with PDT (P=.0313). Two patients with purple PWSs showed no response to either PDT or PDL. All PDT sites developed localized edema, and all PDL sites developed edema, blistering, purpura, and crusts. Four patients with red PWSs developed hyperpigmentation at the PDL sites.
What’s the issue?
Although there have been studies showing that PDT is an effective treatment of PWSs, this study is a side-by-side quantitative comparison of PDL versus PDT. This study showed that PDT is as effective and as safe as PDL and possibly superior for the treatment of red and purple flat PWSs. This study represents promising steps forward in PDT treatment of dermatologic conditions.
Even though PDL therapy is considered the current standard for treatment of PWSs, this study does show good clearance with PDT. Pulsed dye laser therapy has been more readily available in North America and Europe, though in China, where this study took place, it is not common. The PDT in this study utilized an intravenous photosensitizer, which may not be suitable for all patients. Other limitations of this study include the small sample size and the possibility that treating the lesion halves in close proximity to each other may compound adverse effects. Because each half of the lesion (close proximity to one another) was treated, the effects of each treatment may have been compounded.
Could PDT become an adjuvant treatment in the armamentarium for resistant port-wine stains?
In the May 2013 issue of the British Journal of Dermatology (2013;168:1040-1046) Gao et al reported on a side-by-side comparison of the use of photodynamic therapy (PDT) versus the pulsed dye laser (PDL) for the treatment of 9 red and 6 purple port-wine stains (PWSs). Fifteen patients (age range, 11–36 years) with PWSs were chosen and 2 adjacent areas of the lesion were randomly assigned to receive either a single PDL treatment or a single PDT session. Eleven lesions were on the neck area, 3 on the upper arm, and 1 on the upper leg. The PDL had a wavelength of 585 nm, and PDT was performed with intravenous hematoporphyrin monomethyl ether and a low-power copper vapor laser (510.6 and 578.2 nm, respectively). The PDT-treated area was done 30 minutes after the PDL-treated area with the other areas being covered. The clinical outcome was measured colorimetrically (blanching rates) and visually.
For the red PWSs the blanching rates at 2 months with the PDL were 11% to 24% and 22% to 55% with PDT (P=.006). For the purple PWSs, blanching rates ranged from 8% to 33% with PDL and 30% to 45% with PDT (P=.0313). Two patients with purple PWSs showed no response to either PDT or PDL. All PDT sites developed localized edema, and all PDL sites developed edema, blistering, purpura, and crusts. Four patients with red PWSs developed hyperpigmentation at the PDL sites.
What’s the issue?
Although there have been studies showing that PDT is an effective treatment of PWSs, this study is a side-by-side quantitative comparison of PDL versus PDT. This study showed that PDT is as effective and as safe as PDL and possibly superior for the treatment of red and purple flat PWSs. This study represents promising steps forward in PDT treatment of dermatologic conditions.
Even though PDL therapy is considered the current standard for treatment of PWSs, this study does show good clearance with PDT. Pulsed dye laser therapy has been more readily available in North America and Europe, though in China, where this study took place, it is not common. The PDT in this study utilized an intravenous photosensitizer, which may not be suitable for all patients. Other limitations of this study include the small sample size and the possibility that treating the lesion halves in close proximity to each other may compound adverse effects. Because each half of the lesion (close proximity to one another) was treated, the effects of each treatment may have been compounded.
Could PDT become an adjuvant treatment in the armamentarium for resistant port-wine stains?

Maximize cosmetic procedures for men
MIAMI BEACH – More men are seeking cosmetic dermatologic procedures and products, and successfully engaging and treating this segment of the population require recognition of a number of gender-specific differences with respect to skin biology, skin aging, behaviors, and rejuvenation goals, according to Dr. Ivan Camacho.
"We need to be able to understand all of these the differences in order to be able to provide tailored treatments for our patients, so they can get the best results possible," Dr. Camacho said during a focus session on men’s aesthetics at the annual meeting of the American Academy of Dermatology.
Skin biology
When it comes to skin biology, men and women share a number of characteristics, but there are important differences driven by genetic or hormonal specificity that can affect treatment outcomes, Dr. Camacho said. For example, although the number of cell layers and thickness of the stratum corneum is similar in men and women, the dermis is about 20% thicker in men than in women, across the age spectrum and in all anatomic locations, he noted.
Men also have higher collagen density early in life, but they experience skin thinning at a younger age than women. For women, skin thickness generally remains constant until menopause, and then the skin begins to thin rapidly. This difference is most likely because of the role of testosterone in maintaining collagen content, said Dr. Camacho of the University of Miami.
Men also have less subcutaneous fat, greater distribution of body fat in the abdomen and trunk, and higher facial bone density mass than women, Dr. Camacho explained. In addition, men tend to have higher transepidermal water loss because of the lack of estrogen, which has positive effects in the stratum corneum, he said.
Dr. Camacho described other functional differences in men’s skin compared with women’s skin, including:
• A fourfold increase in sebum generation.
• A 30% overall increase in sweating.
• Different hair distribution as determined by androgens, but also by genetics.
• Stronger skin tone.
• Greater sensitivity to ultraviolet radiation, and thus a lower minimal erythema dose threshold and increased rate of skin cancers.
• Greater susceptibility to bacterial and viral infections and slower healing rates as a result of the inhibitory effects of testosterone and hydrotestosterone with respect to wound healing.
• Greater susceptibility to stress-induced immunosuppression, which may explain the higher skin cancer rates and delayed wound healing.
Skin aging
As for the aging process, men age differently from women in that their higher collagen density leads to better maintenance of elasticity, and their higher facial bone density provides better overall support, said Dr. Camacho.
However, thicker skin and stronger muscles make men more prone to develop deeper expression lines, as opposed to the "superficial wrinkles that women complain about," Dr. Camacho noted.
Also, the reduced level of subcutaneous fat in men can lead to more dramatic volume loss.
"Men are ‘sinkers.’ We sink more than wrinklers or saggers, because we have good elasticity, but we actually tend to lose quite a bit of subcutaneous fat," Dr. Camacho explained.
As a result of other differences related to skin aging, he said, men’s skin may be:
• More prone to acne and enlarged pores due to the higher sebaceous gland count.
• More prone to darker and/or redder complexions because of the increased tone and vascularity.
• More likely to have dull areas due to the epidermal water loss.
• Less prone to perioral lines and wrinkles due to facial hair distribution, which acts as a structural support.
• More likely to have unwanted fat in the abdominal and trunk region.
• More likely to develop both melanoma and nonmelanoma skin cancers and to experience photoaging because of greater sensitivity to ultraviolet radiation.
Behavior
In Dr. Camacho’s experience, men tend to be very goal oriented, and that carries over to cosmetic procedures.
"Men are very results-oriented, so we want to have a very clear purpose of what we want to achieve with a given treatment or product," he added, noting that male patients often prefer a lot of detail about procedures and processes.
Providing the extra details requires a greater educational effort on the part of the physician, he said, but "that’s a great thing, because they are going to be well informed about the pros and cons of a given treatment."
Male patients also want fast results. For these reasons, injectables and laser therapies are probably a good fit, he noted.
Men also tend to prefer simplicity, minimal discomfort, and minimal downtime, making noninvasive procedures and multifunctional skin care products ideal, he added.
Rejuvenation goals
Men often have rejuvenation goals that are different from those of women, Dr. Camacho said.
The most common reason that men seek cosmetic treatment is for a "tired, sinking face"; they want to look refreshed and confident, but they want subtle, natural-looking results, he said.
And, of course, there’s hair.
"Hair, hair, hair. Hair is a huge concern for men," Dr. Camacho said.
Sometimes men think they have too much hair, sometimes they have too little. Men drive the market for hair loss treatments, and also are increasingly seeking hair removal treatments, Dr. Camacho noted. Since traditional methods for hair removal, such as waxing, shaving, and epilation, are temporary and can cause irritation, laser hair removal is increasing in popularity among men. In fact, according to the American Society of Aesthetic Plastic Surgery, it was the second most common nonsurgical cosmetic intervention for men in 2011, Dr. Camacho said.
Other useful cosmetic procedures
One of the most popular noninvasive cosmetic interventions for both men and women is neuromodulation injections, for softening of expression lines and treating areas including the glabella, forehead, and periocular area, that can contribute to an angry-, tired-, or sad-looking face, Dr. Camacho said.
In 2011, men accounted for 9.1% of botulinum toxin treatment patients, and this represented a 258% increase from the year 2000, he noted.
Skin resurfacing treatments are increasing in popularity among men as well. In 2011, men accounted for 7.3% of skin resurfacing treatments, making skin resurfacing the fourth most common nonsurgical cosmetic intervention in men, Dr. Camacho said.
Other treatments for skin issues of concern to men include laser and light therapies to improve the complexion, and skin-tightening procedures, such as radiofrequency and ultrasound, to help improve skin laxity
In addition, data from 2011 showed that men accounted for about 20% of patients undergoing CoolSculpting, which is both effective and appealing to men seeking treatment for abdominal and trunk fat deposits, Dr. Camacho said.
Treatment pearls
When providing facial treatments for men, preservation of a masculine appearance is essential, Dr. Camacho said.
"The last thing we want to do is have a man’s face looking like a woman’s face; we need to be able to preserve the masculine appearance," Dr. Camacho said, noting that in his experience, a combination of neurotoxins and dermal fillers is excellent for achieving desired results.
For neurotoxins, remember that men require doses at about 1.5 to 2 times as much as women, he said
"But also remember that men want to preserve some animation, so it’s always important to keep a balance between being effective with our treatment, but also keeping the patient happy with what they want," he said.
In Dr. Camacho’s experience, most men are less concerned with periocular lines, but some are, so be sure to ask them exactly what they want at a treatment session.
"You can’t assume they want three areas treated at a time as we usually do with women," he said.
Be sure to preserve the masculine position of the brow, which in men is very subtle, located right at the supraorbital rim, and has no major arching, said Dr. Camacho.
By avoiding injecting at the superior portion of the orbicularis ocular muscle, the subtle arch at the supraorbital rim can be maintained, and feminization of the brow avoided, he said.
"Also, when treating the frontalis major make sure to go all the way lateral, because you don’t want a little bit of frontalis pulling and giving some arching to the eyebrows," he added.
As for fillers, keep in mind that men probably will require higher volumes, which is an important consideration when discussing finances during the initial consultation.
Fillers are particularly useful in the tear trough area for men seeking treatment of tired-looking sunken eyes.
"Very easily, we can create a smooth transition between the lower eyelid and cheek. We can also use (fillers) for prominent nasolabial folds," Dr. Camacho explained.
Before filling the lines, however, consider restoring the cheek to correct for the midfacial fat loss common in men, he noted.
Also, if treatment involves the lip area, avoid overfilling the vermilion border – this will feminize the lips, he said.
Breaking into the men’s market
Consider developing a marketing strategy that shows your practice’s appeal to both genders – by launching a website and developing marketing materials that feature both male and female models and patients, and by offering cosmeceutical product lines developed for men, Dr. Camacho suggested.
"The modern man is here, and the modern man is actively looking for advice on cosmetic procedures and recommendations for skin care. Dermatologists will have a very important role in male aesthetics," he said, noting that a dermatologist’s role can include enhancing awareness and cultural acceptance of cosmetic interventions for men.
"We have every day in our practices, an opportunity to educate our male patients on the multiple treatment options available for them. We also have a responsibility for being knowledgeable about the specificities of male skin ... to be able to formulate tailored treatments, and to be able to, therefore, obtain the best results for our male patients," he said.
Dr. Camacho reported having no disclosures.
MIAMI BEACH – More men are seeking cosmetic dermatologic procedures and products, and successfully engaging and treating this segment of the population require recognition of a number of gender-specific differences with respect to skin biology, skin aging, behaviors, and rejuvenation goals, according to Dr. Ivan Camacho.
"We need to be able to understand all of these the differences in order to be able to provide tailored treatments for our patients, so they can get the best results possible," Dr. Camacho said during a focus session on men’s aesthetics at the annual meeting of the American Academy of Dermatology.
Skin biology
When it comes to skin biology, men and women share a number of characteristics, but there are important differences driven by genetic or hormonal specificity that can affect treatment outcomes, Dr. Camacho said. For example, although the number of cell layers and thickness of the stratum corneum is similar in men and women, the dermis is about 20% thicker in men than in women, across the age spectrum and in all anatomic locations, he noted.
Men also have higher collagen density early in life, but they experience skin thinning at a younger age than women. For women, skin thickness generally remains constant until menopause, and then the skin begins to thin rapidly. This difference is most likely because of the role of testosterone in maintaining collagen content, said Dr. Camacho of the University of Miami.
Men also have less subcutaneous fat, greater distribution of body fat in the abdomen and trunk, and higher facial bone density mass than women, Dr. Camacho explained. In addition, men tend to have higher transepidermal water loss because of the lack of estrogen, which has positive effects in the stratum corneum, he said.
Dr. Camacho described other functional differences in men’s skin compared with women’s skin, including:
• A fourfold increase in sebum generation.
• A 30% overall increase in sweating.
• Different hair distribution as determined by androgens, but also by genetics.
• Stronger skin tone.
• Greater sensitivity to ultraviolet radiation, and thus a lower minimal erythema dose threshold and increased rate of skin cancers.
• Greater susceptibility to bacterial and viral infections and slower healing rates as a result of the inhibitory effects of testosterone and hydrotestosterone with respect to wound healing.
• Greater susceptibility to stress-induced immunosuppression, which may explain the higher skin cancer rates and delayed wound healing.
Skin aging
As for the aging process, men age differently from women in that their higher collagen density leads to better maintenance of elasticity, and their higher facial bone density provides better overall support, said Dr. Camacho.
However, thicker skin and stronger muscles make men more prone to develop deeper expression lines, as opposed to the "superficial wrinkles that women complain about," Dr. Camacho noted.
Also, the reduced level of subcutaneous fat in men can lead to more dramatic volume loss.
"Men are ‘sinkers.’ We sink more than wrinklers or saggers, because we have good elasticity, but we actually tend to lose quite a bit of subcutaneous fat," Dr. Camacho explained.
As a result of other differences related to skin aging, he said, men’s skin may be:
• More prone to acne and enlarged pores due to the higher sebaceous gland count.
• More prone to darker and/or redder complexions because of the increased tone and vascularity.
• More likely to have dull areas due to the epidermal water loss.
• Less prone to perioral lines and wrinkles due to facial hair distribution, which acts as a structural support.
• More likely to have unwanted fat in the abdominal and trunk region.
• More likely to develop both melanoma and nonmelanoma skin cancers and to experience photoaging because of greater sensitivity to ultraviolet radiation.
Behavior
In Dr. Camacho’s experience, men tend to be very goal oriented, and that carries over to cosmetic procedures.
"Men are very results-oriented, so we want to have a very clear purpose of what we want to achieve with a given treatment or product," he added, noting that male patients often prefer a lot of detail about procedures and processes.
Providing the extra details requires a greater educational effort on the part of the physician, he said, but "that’s a great thing, because they are going to be well informed about the pros and cons of a given treatment."
Male patients also want fast results. For these reasons, injectables and laser therapies are probably a good fit, he noted.
Men also tend to prefer simplicity, minimal discomfort, and minimal downtime, making noninvasive procedures and multifunctional skin care products ideal, he added.
Rejuvenation goals
Men often have rejuvenation goals that are different from those of women, Dr. Camacho said.
The most common reason that men seek cosmetic treatment is for a "tired, sinking face"; they want to look refreshed and confident, but they want subtle, natural-looking results, he said.
And, of course, there’s hair.
"Hair, hair, hair. Hair is a huge concern for men," Dr. Camacho said.
Sometimes men think they have too much hair, sometimes they have too little. Men drive the market for hair loss treatments, and also are increasingly seeking hair removal treatments, Dr. Camacho noted. Since traditional methods for hair removal, such as waxing, shaving, and epilation, are temporary and can cause irritation, laser hair removal is increasing in popularity among men. In fact, according to the American Society of Aesthetic Plastic Surgery, it was the second most common nonsurgical cosmetic intervention for men in 2011, Dr. Camacho said.
Other useful cosmetic procedures
One of the most popular noninvasive cosmetic interventions for both men and women is neuromodulation injections, for softening of expression lines and treating areas including the glabella, forehead, and periocular area, that can contribute to an angry-, tired-, or sad-looking face, Dr. Camacho said.
In 2011, men accounted for 9.1% of botulinum toxin treatment patients, and this represented a 258% increase from the year 2000, he noted.
Skin resurfacing treatments are increasing in popularity among men as well. In 2011, men accounted for 7.3% of skin resurfacing treatments, making skin resurfacing the fourth most common nonsurgical cosmetic intervention in men, Dr. Camacho said.
Other treatments for skin issues of concern to men include laser and light therapies to improve the complexion, and skin-tightening procedures, such as radiofrequency and ultrasound, to help improve skin laxity
In addition, data from 2011 showed that men accounted for about 20% of patients undergoing CoolSculpting, which is both effective and appealing to men seeking treatment for abdominal and trunk fat deposits, Dr. Camacho said.
Treatment pearls
When providing facial treatments for men, preservation of a masculine appearance is essential, Dr. Camacho said.
"The last thing we want to do is have a man’s face looking like a woman’s face; we need to be able to preserve the masculine appearance," Dr. Camacho said, noting that in his experience, a combination of neurotoxins and dermal fillers is excellent for achieving desired results.
For neurotoxins, remember that men require doses at about 1.5 to 2 times as much as women, he said
"But also remember that men want to preserve some animation, so it’s always important to keep a balance between being effective with our treatment, but also keeping the patient happy with what they want," he said.
In Dr. Camacho’s experience, most men are less concerned with periocular lines, but some are, so be sure to ask them exactly what they want at a treatment session.
"You can’t assume they want three areas treated at a time as we usually do with women," he said.
Be sure to preserve the masculine position of the brow, which in men is very subtle, located right at the supraorbital rim, and has no major arching, said Dr. Camacho.
By avoiding injecting at the superior portion of the orbicularis ocular muscle, the subtle arch at the supraorbital rim can be maintained, and feminization of the brow avoided, he said.
"Also, when treating the frontalis major make sure to go all the way lateral, because you don’t want a little bit of frontalis pulling and giving some arching to the eyebrows," he added.
As for fillers, keep in mind that men probably will require higher volumes, which is an important consideration when discussing finances during the initial consultation.
Fillers are particularly useful in the tear trough area for men seeking treatment of tired-looking sunken eyes.
"Very easily, we can create a smooth transition between the lower eyelid and cheek. We can also use (fillers) for prominent nasolabial folds," Dr. Camacho explained.
Before filling the lines, however, consider restoring the cheek to correct for the midfacial fat loss common in men, he noted.
Also, if treatment involves the lip area, avoid overfilling the vermilion border – this will feminize the lips, he said.
Breaking into the men’s market
Consider developing a marketing strategy that shows your practice’s appeal to both genders – by launching a website and developing marketing materials that feature both male and female models and patients, and by offering cosmeceutical product lines developed for men, Dr. Camacho suggested.
"The modern man is here, and the modern man is actively looking for advice on cosmetic procedures and recommendations for skin care. Dermatologists will have a very important role in male aesthetics," he said, noting that a dermatologist’s role can include enhancing awareness and cultural acceptance of cosmetic interventions for men.
"We have every day in our practices, an opportunity to educate our male patients on the multiple treatment options available for them. We also have a responsibility for being knowledgeable about the specificities of male skin ... to be able to formulate tailored treatments, and to be able to, therefore, obtain the best results for our male patients," he said.
Dr. Camacho reported having no disclosures.
MIAMI BEACH – More men are seeking cosmetic dermatologic procedures and products, and successfully engaging and treating this segment of the population require recognition of a number of gender-specific differences with respect to skin biology, skin aging, behaviors, and rejuvenation goals, according to Dr. Ivan Camacho.
"We need to be able to understand all of these the differences in order to be able to provide tailored treatments for our patients, so they can get the best results possible," Dr. Camacho said during a focus session on men’s aesthetics at the annual meeting of the American Academy of Dermatology.
Skin biology
When it comes to skin biology, men and women share a number of characteristics, but there are important differences driven by genetic or hormonal specificity that can affect treatment outcomes, Dr. Camacho said. For example, although the number of cell layers and thickness of the stratum corneum is similar in men and women, the dermis is about 20% thicker in men than in women, across the age spectrum and in all anatomic locations, he noted.
Men also have higher collagen density early in life, but they experience skin thinning at a younger age than women. For women, skin thickness generally remains constant until menopause, and then the skin begins to thin rapidly. This difference is most likely because of the role of testosterone in maintaining collagen content, said Dr. Camacho of the University of Miami.
Men also have less subcutaneous fat, greater distribution of body fat in the abdomen and trunk, and higher facial bone density mass than women, Dr. Camacho explained. In addition, men tend to have higher transepidermal water loss because of the lack of estrogen, which has positive effects in the stratum corneum, he said.
Dr. Camacho described other functional differences in men’s skin compared with women’s skin, including:
• A fourfold increase in sebum generation.
• A 30% overall increase in sweating.
• Different hair distribution as determined by androgens, but also by genetics.
• Stronger skin tone.
• Greater sensitivity to ultraviolet radiation, and thus a lower minimal erythema dose threshold and increased rate of skin cancers.
• Greater susceptibility to bacterial and viral infections and slower healing rates as a result of the inhibitory effects of testosterone and hydrotestosterone with respect to wound healing.
• Greater susceptibility to stress-induced immunosuppression, which may explain the higher skin cancer rates and delayed wound healing.
Skin aging
As for the aging process, men age differently from women in that their higher collagen density leads to better maintenance of elasticity, and their higher facial bone density provides better overall support, said Dr. Camacho.
However, thicker skin and stronger muscles make men more prone to develop deeper expression lines, as opposed to the "superficial wrinkles that women complain about," Dr. Camacho noted.
Also, the reduced level of subcutaneous fat in men can lead to more dramatic volume loss.
"Men are ‘sinkers.’ We sink more than wrinklers or saggers, because we have good elasticity, but we actually tend to lose quite a bit of subcutaneous fat," Dr. Camacho explained.
As a result of other differences related to skin aging, he said, men’s skin may be:
• More prone to acne and enlarged pores due to the higher sebaceous gland count.
• More prone to darker and/or redder complexions because of the increased tone and vascularity.
• More likely to have dull areas due to the epidermal water loss.
• Less prone to perioral lines and wrinkles due to facial hair distribution, which acts as a structural support.
• More likely to have unwanted fat in the abdominal and trunk region.
• More likely to develop both melanoma and nonmelanoma skin cancers and to experience photoaging because of greater sensitivity to ultraviolet radiation.
Behavior
In Dr. Camacho’s experience, men tend to be very goal oriented, and that carries over to cosmetic procedures.
"Men are very results-oriented, so we want to have a very clear purpose of what we want to achieve with a given treatment or product," he added, noting that male patients often prefer a lot of detail about procedures and processes.
Providing the extra details requires a greater educational effort on the part of the physician, he said, but "that’s a great thing, because they are going to be well informed about the pros and cons of a given treatment."
Male patients also want fast results. For these reasons, injectables and laser therapies are probably a good fit, he noted.
Men also tend to prefer simplicity, minimal discomfort, and minimal downtime, making noninvasive procedures and multifunctional skin care products ideal, he added.
Rejuvenation goals
Men often have rejuvenation goals that are different from those of women, Dr. Camacho said.
The most common reason that men seek cosmetic treatment is for a "tired, sinking face"; they want to look refreshed and confident, but they want subtle, natural-looking results, he said.
And, of course, there’s hair.
"Hair, hair, hair. Hair is a huge concern for men," Dr. Camacho said.
Sometimes men think they have too much hair, sometimes they have too little. Men drive the market for hair loss treatments, and also are increasingly seeking hair removal treatments, Dr. Camacho noted. Since traditional methods for hair removal, such as waxing, shaving, and epilation, are temporary and can cause irritation, laser hair removal is increasing in popularity among men. In fact, according to the American Society of Aesthetic Plastic Surgery, it was the second most common nonsurgical cosmetic intervention for men in 2011, Dr. Camacho said.
Other useful cosmetic procedures
One of the most popular noninvasive cosmetic interventions for both men and women is neuromodulation injections, for softening of expression lines and treating areas including the glabella, forehead, and periocular area, that can contribute to an angry-, tired-, or sad-looking face, Dr. Camacho said.
In 2011, men accounted for 9.1% of botulinum toxin treatment patients, and this represented a 258% increase from the year 2000, he noted.
Skin resurfacing treatments are increasing in popularity among men as well. In 2011, men accounted for 7.3% of skin resurfacing treatments, making skin resurfacing the fourth most common nonsurgical cosmetic intervention in men, Dr. Camacho said.
Other treatments for skin issues of concern to men include laser and light therapies to improve the complexion, and skin-tightening procedures, such as radiofrequency and ultrasound, to help improve skin laxity
In addition, data from 2011 showed that men accounted for about 20% of patients undergoing CoolSculpting, which is both effective and appealing to men seeking treatment for abdominal and trunk fat deposits, Dr. Camacho said.
Treatment pearls
When providing facial treatments for men, preservation of a masculine appearance is essential, Dr. Camacho said.
"The last thing we want to do is have a man’s face looking like a woman’s face; we need to be able to preserve the masculine appearance," Dr. Camacho said, noting that in his experience, a combination of neurotoxins and dermal fillers is excellent for achieving desired results.
For neurotoxins, remember that men require doses at about 1.5 to 2 times as much as women, he said
"But also remember that men want to preserve some animation, so it’s always important to keep a balance between being effective with our treatment, but also keeping the patient happy with what they want," he said.
In Dr. Camacho’s experience, most men are less concerned with periocular lines, but some are, so be sure to ask them exactly what they want at a treatment session.
"You can’t assume they want three areas treated at a time as we usually do with women," he said.
Be sure to preserve the masculine position of the brow, which in men is very subtle, located right at the supraorbital rim, and has no major arching, said Dr. Camacho.
By avoiding injecting at the superior portion of the orbicularis ocular muscle, the subtle arch at the supraorbital rim can be maintained, and feminization of the brow avoided, he said.
"Also, when treating the frontalis major make sure to go all the way lateral, because you don’t want a little bit of frontalis pulling and giving some arching to the eyebrows," he added.
As for fillers, keep in mind that men probably will require higher volumes, which is an important consideration when discussing finances during the initial consultation.
Fillers are particularly useful in the tear trough area for men seeking treatment of tired-looking sunken eyes.
"Very easily, we can create a smooth transition between the lower eyelid and cheek. We can also use (fillers) for prominent nasolabial folds," Dr. Camacho explained.
Before filling the lines, however, consider restoring the cheek to correct for the midfacial fat loss common in men, he noted.
Also, if treatment involves the lip area, avoid overfilling the vermilion border – this will feminize the lips, he said.
Breaking into the men’s market
Consider developing a marketing strategy that shows your practice’s appeal to both genders – by launching a website and developing marketing materials that feature both male and female models and patients, and by offering cosmeceutical product lines developed for men, Dr. Camacho suggested.
"The modern man is here, and the modern man is actively looking for advice on cosmetic procedures and recommendations for skin care. Dermatologists will have a very important role in male aesthetics," he said, noting that a dermatologist’s role can include enhancing awareness and cultural acceptance of cosmetic interventions for men.
"We have every day in our practices, an opportunity to educate our male patients on the multiple treatment options available for them. We also have a responsibility for being knowledgeable about the specificities of male skin ... to be able to formulate tailored treatments, and to be able to, therefore, obtain the best results for our male patients," he said.
Dr. Camacho reported having no disclosures.
AT THE AAD ANNUAL MEETING
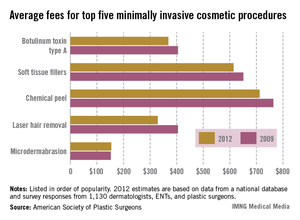
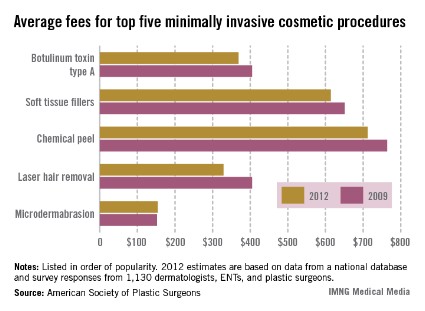
Doctor fees drop for Botox, hair removal
The average physician fee for the most popular form of minimally invasive cosmetic surgery, the injection of botulinum toxin type A, dropped nearly 9% from 2009 to 2012, according to data from the American Society of Plastic Surgeons.
The average fees for four of the five most popular minimally invasive surgeries fell during that period. Laser hair removal showed the greatest decline (18.7%), followed by botulinum toxin A (8.9%). Average fees also fell for chemical peels (6.8%) and soft tissue fillers (5.7%). However, the average fee for microdermabrasion went up 1.3%, the ASPS data showed.
The average physician fees for 2012 were $369 for botulinum injection, $614 for soft tissue fillers, $712 for chemical peels, $329 for laser hair removal, and $154 for microdermabrasion.
An estimated 6.1 million botulinum toxin A injections were performed in 2012, which was almost half of the 13 million minimally invasive procedures performed for the year. The next-most-popular procedure was soft tissue filler injections, which accounted for almost 2 million procedures, the ASPS reported.
The average physician fee for the most popular form of minimally invasive cosmetic surgery, the injection of botulinum toxin type A, dropped nearly 9% from 2009 to 2012, according to data from the American Society of Plastic Surgeons.
The average fees for four of the five most popular minimally invasive surgeries fell during that period. Laser hair removal showed the greatest decline (18.7%), followed by botulinum toxin A (8.9%). Average fees also fell for chemical peels (6.8%) and soft tissue fillers (5.7%). However, the average fee for microdermabrasion went up 1.3%, the ASPS data showed.
The average physician fees for 2012 were $369 for botulinum injection, $614 for soft tissue fillers, $712 for chemical peels, $329 for laser hair removal, and $154 for microdermabrasion.
An estimated 6.1 million botulinum toxin A injections were performed in 2012, which was almost half of the 13 million minimally invasive procedures performed for the year. The next-most-popular procedure was soft tissue filler injections, which accounted for almost 2 million procedures, the ASPS reported.
The average physician fee for the most popular form of minimally invasive cosmetic surgery, the injection of botulinum toxin type A, dropped nearly 9% from 2009 to 2012, according to data from the American Society of Plastic Surgeons.
The average fees for four of the five most popular minimally invasive surgeries fell during that period. Laser hair removal showed the greatest decline (18.7%), followed by botulinum toxin A (8.9%). Average fees also fell for chemical peels (6.8%) and soft tissue fillers (5.7%). However, the average fee for microdermabrasion went up 1.3%, the ASPS data showed.
The average physician fees for 2012 were $369 for botulinum injection, $614 for soft tissue fillers, $712 for chemical peels, $329 for laser hair removal, and $154 for microdermabrasion.
An estimated 6.1 million botulinum toxin A injections were performed in 2012, which was almost half of the 13 million minimally invasive procedures performed for the year. The next-most-popular procedure was soft tissue filler injections, which accounted for almost 2 million procedures, the ASPS reported.
More men seek skin care products
MIAMI BEACH – American men are showing an increased interest in skin care products, according to Dr. Ivan Camacho.
Men are becoming more aware of the importance of skin care, and they are actively seeking information and products. In fact, the men’s skin care market increased 9% from 2009 to 2010, and is expected to grow 16% by 2014, Dr. Camacho said at the annual meeting of the American Academy of Dermatology.
One point for dermatologists to keep in mind when it comes to introducing men to a skin care routine is that simple is best. Using multipurpose products, keeping regimens to one or two steps – three at most – and incorporating new products into an established routine, such as shaving, will likely improve compliance and results, said Dr. Camacho of the University of Miami.
Dr. Camacho’s additional tips for better skin care for men include:
• Recommend multifunctional products, such as those that combine antioxidants and botanicals, as well as other cosmeceuticals that can enhance anti-aging, provide anti-inflammatory effects, and hydrate the skin.
• Suggest fragrance-free or subtly scented products.
• Incorporate a broad-spectrum sunscreen (also unscented or subtly scented) with a sun protection factor (SPF) of at least 30. A product with botanical and other cosmeceutical ingredients or with anti-inflammatory properties may be a good choice, especially in patients with inflammatory conditions like acne or rosacea.
• Incorporate a moisturizer, which is very important for restoring facial hydration and improving the skin barrier. A moisturizer can be included in the sunscreen or other products.
"Tell patients to moisturize, moisturize, moisturize," Dr. Camacho said, noting: "If you tell them they need to do it three times a day, they will probably do it once a day, because this is a practice very neglected by many men. As we know, moisturizers will benefit all skin types."
For men with oily skin, recommend an oil-absorbing or mattifying formulation; for those with drier skin, recommend a lipid-based formulation. Given that more men are seeking information about skin care, dermatologists would do well to become knowledgeable about the various products available that may be most appealing to and effective for men, said Dr. Camacho.
Products currently attracting attention include moisturizers with topical caffeine, which has been shown to reduce the transepidermal water loss that is greater in men than in women, he noted.
Also, glycerin-based and niacinamide-based moisturizers have been shown in several studies to reduce transepidermal water loss, which may increase after shaving, he said.
In addition, many men can benefit from cleansers and toners developed for their particular skin types, shaving products that prevent or relieve irritation, oil-absorbing primers to provide temporary relief for skin oiliness, and exfoliating products and retinoids to improve an uneven complexion, said Dr. Camacho.
In addition, antiaging formulations containing alpha-hydroxy acids, retinoids, growth factors, antioxidants, peptides, and/or botanicals can be used to help reverse ultraviolet-related damage and help improve the appearance of fine lines, he said.
Dr. Camacho reported having no disclosures.
MIAMI BEACH – American men are showing an increased interest in skin care products, according to Dr. Ivan Camacho.
Men are becoming more aware of the importance of skin care, and they are actively seeking information and products. In fact, the men’s skin care market increased 9% from 2009 to 2010, and is expected to grow 16% by 2014, Dr. Camacho said at the annual meeting of the American Academy of Dermatology.
One point for dermatologists to keep in mind when it comes to introducing men to a skin care routine is that simple is best. Using multipurpose products, keeping regimens to one or two steps – three at most – and incorporating new products into an established routine, such as shaving, will likely improve compliance and results, said Dr. Camacho of the University of Miami.
Dr. Camacho’s additional tips for better skin care for men include:
• Recommend multifunctional products, such as those that combine antioxidants and botanicals, as well as other cosmeceuticals that can enhance anti-aging, provide anti-inflammatory effects, and hydrate the skin.
• Suggest fragrance-free or subtly scented products.
• Incorporate a broad-spectrum sunscreen (also unscented or subtly scented) with a sun protection factor (SPF) of at least 30. A product with botanical and other cosmeceutical ingredients or with anti-inflammatory properties may be a good choice, especially in patients with inflammatory conditions like acne or rosacea.
• Incorporate a moisturizer, which is very important for restoring facial hydration and improving the skin barrier. A moisturizer can be included in the sunscreen or other products.
"Tell patients to moisturize, moisturize, moisturize," Dr. Camacho said, noting: "If you tell them they need to do it three times a day, they will probably do it once a day, because this is a practice very neglected by many men. As we know, moisturizers will benefit all skin types."
For men with oily skin, recommend an oil-absorbing or mattifying formulation; for those with drier skin, recommend a lipid-based formulation. Given that more men are seeking information about skin care, dermatologists would do well to become knowledgeable about the various products available that may be most appealing to and effective for men, said Dr. Camacho.
Products currently attracting attention include moisturizers with topical caffeine, which has been shown to reduce the transepidermal water loss that is greater in men than in women, he noted.
Also, glycerin-based and niacinamide-based moisturizers have been shown in several studies to reduce transepidermal water loss, which may increase after shaving, he said.
In addition, many men can benefit from cleansers and toners developed for their particular skin types, shaving products that prevent or relieve irritation, oil-absorbing primers to provide temporary relief for skin oiliness, and exfoliating products and retinoids to improve an uneven complexion, said Dr. Camacho.
In addition, antiaging formulations containing alpha-hydroxy acids, retinoids, growth factors, antioxidants, peptides, and/or botanicals can be used to help reverse ultraviolet-related damage and help improve the appearance of fine lines, he said.
Dr. Camacho reported having no disclosures.
MIAMI BEACH – American men are showing an increased interest in skin care products, according to Dr. Ivan Camacho.
Men are becoming more aware of the importance of skin care, and they are actively seeking information and products. In fact, the men’s skin care market increased 9% from 2009 to 2010, and is expected to grow 16% by 2014, Dr. Camacho said at the annual meeting of the American Academy of Dermatology.
One point for dermatologists to keep in mind when it comes to introducing men to a skin care routine is that simple is best. Using multipurpose products, keeping regimens to one or two steps – three at most – and incorporating new products into an established routine, such as shaving, will likely improve compliance and results, said Dr. Camacho of the University of Miami.
Dr. Camacho’s additional tips for better skin care for men include:
• Recommend multifunctional products, such as those that combine antioxidants and botanicals, as well as other cosmeceuticals that can enhance anti-aging, provide anti-inflammatory effects, and hydrate the skin.
• Suggest fragrance-free or subtly scented products.
• Incorporate a broad-spectrum sunscreen (also unscented or subtly scented) with a sun protection factor (SPF) of at least 30. A product with botanical and other cosmeceutical ingredients or with anti-inflammatory properties may be a good choice, especially in patients with inflammatory conditions like acne or rosacea.
• Incorporate a moisturizer, which is very important for restoring facial hydration and improving the skin barrier. A moisturizer can be included in the sunscreen or other products.
"Tell patients to moisturize, moisturize, moisturize," Dr. Camacho said, noting: "If you tell them they need to do it three times a day, they will probably do it once a day, because this is a practice very neglected by many men. As we know, moisturizers will benefit all skin types."
For men with oily skin, recommend an oil-absorbing or mattifying formulation; for those with drier skin, recommend a lipid-based formulation. Given that more men are seeking information about skin care, dermatologists would do well to become knowledgeable about the various products available that may be most appealing to and effective for men, said Dr. Camacho.
Products currently attracting attention include moisturizers with topical caffeine, which has been shown to reduce the transepidermal water loss that is greater in men than in women, he noted.
Also, glycerin-based and niacinamide-based moisturizers have been shown in several studies to reduce transepidermal water loss, which may increase after shaving, he said.
In addition, many men can benefit from cleansers and toners developed for their particular skin types, shaving products that prevent or relieve irritation, oil-absorbing primers to provide temporary relief for skin oiliness, and exfoliating products and retinoids to improve an uneven complexion, said Dr. Camacho.
In addition, antiaging formulations containing alpha-hydroxy acids, retinoids, growth factors, antioxidants, peptides, and/or botanicals can be used to help reverse ultraviolet-related damage and help improve the appearance of fine lines, he said.
Dr. Camacho reported having no disclosures.
AT THE AAD ANNUAL MEETING
Skin of Color - A tasty twist on sun protection
In an effort to improve sun protection and curb skin cancer, dermatologists are doing a better job of educating patients of all skin types about the consequences of UV damage. Sunscreen manufacturers also continue to develop more elegant formulations of both chemical and physical blockers that do not leave a whitish hue on darker skin.
But what about some other, lesser-known innovative ways we can protect ourselves without looking chalky?
Just in time for summer, here’s some food for thought.
Strawberries, as well as other darker-colored berries, are known to contain polyphenols that are antioxidants. Researchers in Italy and Spain tested a strawberry extract on cultured human fibroblasts to see whether there was a photoprotective effect. They added strawberry extract in different concentrations (0.05, 0.25, and 0.5 mg/mL) to all but the control group. They then exposed the samples to a dose of UV light "equivalent to 90 minutes of midday summer sun in the French Riviera," said lead investigator Maurizio Battino. Strawberry extract, especially at a concentration of 0.5 mg/mL, provided UVA protection, and not only boosted cell survival and viability, but also minimized DNA damage, compared with the effects on control cells (J. Agric. Food Chem. 2012;60:2322-70). Perhaps there will be topical sunscreens that contain strawberry extract in the future.
Other foods high in antioxidants that have been considered to have potential sun-protective benefits include bell peppers (red, yellow, green) and yellow squash (high in carotenoids); tomatoes and watermelon (high in lycopene); dark berries such as blueberries, acai, blackberries, and cranberries (rich in anthocyanin); turmeric root (curcumin); pomegranate (ellagic acid); green and black tea (catechins); dark cocoa (flavenols); green leafy vegetables such as spinach and kale (xanthophylls, oxygenated carotenoids); and fish such as mackerel, salmon, trout, herring, and sardines (omega-3 fatty acids).
Of course, just because certain foods have protective benefits does not mean we can advise patients to eat some fruits and veggies and then go lie in the sun sans sunscreen. These foods are not a replacement for the more common methods of sun protection, but they certainly contribute to overall health and, by extension, to healthy skin of all types.
This column, "Skin of Color," appears regularly in Skin & Allergy News, a publication of Frontline Medical Communications. Dr. Wesley practices dermatology in Beverly Hills, Calif. Scan the QR code to read this column online at edermatologynews.com.
Do you have questions about treating patients with dark skin? If so, send them to sknews@frontlinemedcom.com.
In an effort to improve sun protection and curb skin cancer, dermatologists are doing a better job of educating patients of all skin types about the consequences of UV damage. Sunscreen manufacturers also continue to develop more elegant formulations of both chemical and physical blockers that do not leave a whitish hue on darker skin.
But what about some other, lesser-known innovative ways we can protect ourselves without looking chalky?
Just in time for summer, here’s some food for thought.
Strawberries, as well as other darker-colored berries, are known to contain polyphenols that are antioxidants. Researchers in Italy and Spain tested a strawberry extract on cultured human fibroblasts to see whether there was a photoprotective effect. They added strawberry extract in different concentrations (0.05, 0.25, and 0.5 mg/mL) to all but the control group. They then exposed the samples to a dose of UV light "equivalent to 90 minutes of midday summer sun in the French Riviera," said lead investigator Maurizio Battino. Strawberry extract, especially at a concentration of 0.5 mg/mL, provided UVA protection, and not only boosted cell survival and viability, but also minimized DNA damage, compared with the effects on control cells (J. Agric. Food Chem. 2012;60:2322-70). Perhaps there will be topical sunscreens that contain strawberry extract in the future.
Other foods high in antioxidants that have been considered to have potential sun-protective benefits include bell peppers (red, yellow, green) and yellow squash (high in carotenoids); tomatoes and watermelon (high in lycopene); dark berries such as blueberries, acai, blackberries, and cranberries (rich in anthocyanin); turmeric root (curcumin); pomegranate (ellagic acid); green and black tea (catechins); dark cocoa (flavenols); green leafy vegetables such as spinach and kale (xanthophylls, oxygenated carotenoids); and fish such as mackerel, salmon, trout, herring, and sardines (omega-3 fatty acids).
Of course, just because certain foods have protective benefits does not mean we can advise patients to eat some fruits and veggies and then go lie in the sun sans sunscreen. These foods are not a replacement for the more common methods of sun protection, but they certainly contribute to overall health and, by extension, to healthy skin of all types.
This column, "Skin of Color," appears regularly in Skin & Allergy News, a publication of Frontline Medical Communications. Dr. Wesley practices dermatology in Beverly Hills, Calif. Scan the QR code to read this column online at edermatologynews.com.
Do you have questions about treating patients with dark skin? If so, send them to sknews@frontlinemedcom.com.
In an effort to improve sun protection and curb skin cancer, dermatologists are doing a better job of educating patients of all skin types about the consequences of UV damage. Sunscreen manufacturers also continue to develop more elegant formulations of both chemical and physical blockers that do not leave a whitish hue on darker skin.
But what about some other, lesser-known innovative ways we can protect ourselves without looking chalky?
Just in time for summer, here’s some food for thought.
Strawberries, as well as other darker-colored berries, are known to contain polyphenols that are antioxidants. Researchers in Italy and Spain tested a strawberry extract on cultured human fibroblasts to see whether there was a photoprotective effect. They added strawberry extract in different concentrations (0.05, 0.25, and 0.5 mg/mL) to all but the control group. They then exposed the samples to a dose of UV light "equivalent to 90 minutes of midday summer sun in the French Riviera," said lead investigator Maurizio Battino. Strawberry extract, especially at a concentration of 0.5 mg/mL, provided UVA protection, and not only boosted cell survival and viability, but also minimized DNA damage, compared with the effects on control cells (J. Agric. Food Chem. 2012;60:2322-70). Perhaps there will be topical sunscreens that contain strawberry extract in the future.
Other foods high in antioxidants that have been considered to have potential sun-protective benefits include bell peppers (red, yellow, green) and yellow squash (high in carotenoids); tomatoes and watermelon (high in lycopene); dark berries such as blueberries, acai, blackberries, and cranberries (rich in anthocyanin); turmeric root (curcumin); pomegranate (ellagic acid); green and black tea (catechins); dark cocoa (flavenols); green leafy vegetables such as spinach and kale (xanthophylls, oxygenated carotenoids); and fish such as mackerel, salmon, trout, herring, and sardines (omega-3 fatty acids).
Of course, just because certain foods have protective benefits does not mean we can advise patients to eat some fruits and veggies and then go lie in the sun sans sunscreen. These foods are not a replacement for the more common methods of sun protection, but they certainly contribute to overall health and, by extension, to healthy skin of all types.
This column, "Skin of Color," appears regularly in Skin & Allergy News, a publication of Frontline Medical Communications. Dr. Wesley practices dermatology in Beverly Hills, Calif. Scan the QR code to read this column online at edermatologynews.com.
Do you have questions about treating patients with dark skin? If so, send them to sknews@frontlinemedcom.com.
Major finding: Key numerical finding (e.g., number needed to treat to prevent one death/event; number lived or died as result of intervention). Maximum 10 words/1 sentence.
Data source: Include type of study (e.g., randomized, placebo controlled trial; retrospective case-control study). Include number in the study.
Disclosures: Sponsor of study, funding source, relevant disclosures. If author has no relevant disclosures, "Dr. X reported having no financial disclosures." If necessary, "Meeting Y did not require reports of financial disclosures." Check meeting website because many list disclosures. Written in sentence form.

Pulley stitch: A go-to for defects under tension
EDITOR'S NOTE: August 26, 2013: This article has been amended since it was first published to make it clear that Dr. Kelley Pagliai Redbord's description of the pulley stitch procedure was taken directly from an article published by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg.2011;37:1503-5). In her presentation, Dr. Redbord credited Dr. Yag-Howard and her article. However, this credit and attribution to Dr. Yag-Howard was not included in the article published.
WASHINGTON – The pulley stitch "is my go-to stitch for defects under tension," said Dr. Kelley Pagliai Redbord.
The pulley stitch allows for considerable reduction in the surface area of a large defect that can’t be closed by side-to-side stitches alone, making it an excellent choice for use on the scalp and legs, Dr. Redbord said at the Atlantic Dermatological Conference.
"When the tension across the wound is decreased, buried dermal sutures can be placed more easily and accurately," she said. "I use it a lot as an intraoperative tissue expander."
Dr. Redbord said that her description of the pulley stitch was taken from an article by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg. 2011; 37:1503-5).*
The pulley stitch can serve as a temporary suture that can be left in place or removed, said Dr. Redbord, a dermatologist in group practice in Rockville, Md.

The technique follows a far-near-near-far pattern, starting the stitch 8 mm from the wound edge (far), then bringing it to the opposite side just 4 mm from the wound edge (near). Dr. Redbord then reenters the stitch 4 mm from the wound edge on the initial side (near), and makes another pass to the opposite side 8 mm from the wound edge (far).
Multiple passes through the tissue create resistance that keeps the suture from slipping. "The loops of the stitch are placed at an oblique angle so that the inner and outer loops are offset and do not override each other," she noted. This technique minimizes potential skin damage from pressure necrosis caused by overriding loop sutures. The pulley stitch has a 2:1 mechanical advantage over an interrupted suture, and the additional friction of a second loop prevents the knot from slipping.
A modification of the pulley stitch is to loop the suture through an external loop on the opposite side of the incision, and pull across. "This new loop functions as a pulley and directs the tension away from the other strands," she said.
Another stitch with excellent eversion, in which the pulley stitch plays a key role, is the subcutaneous inverted cross mattress stitch (SICM). The SCIM is entirely subcutaneous, and combines the buried vertical mattress stitch and the buried pulley stitch.
The SCIM "uses the buried vertical mattress’s ability to evert wound edges and combines it with the pulley stitch’s ability to decrease tension at the wound edge," she said.
The four-step process is as follows:
• 1. Insert the needle into the dermis 3-5 mm lateral to the wound edge. Advance the needle into the upper reticular dermis, and then curve down to exit through the lower reticular dermis.
• 2. Insert the needle into the opposite edge of the wound at the lower reticular dermis and advance into the upper reticular dermis, then curve down and exit intradermally.
• 3. Insert the needle across the defect using an intradermal approach 1-2 mm lateral to the initial needle insertion point. Then, create a second buried vertical mattress stitch.
• 4. Pull the two stitches to close, which "creates a pulley effect with minimal recoil, and tie off," Dr. Redbord said.
"The pulley system locks the wound edges so that a knot can be tied without slipping," she added.
Dr. Redbord said she had no relevant financial disclosures.
EDITOR'S NOTE: August 26, 2013: This article has been amended since it was first published to make it clear that Dr. Kelley Pagliai Redbord's description of the pulley stitch procedure was taken directly from an article published by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg.2011;37:1503-5). In her presentation, Dr. Redbord credited Dr. Yag-Howard and her article. However, this credit and attribution to Dr. Yag-Howard was not included in the article published.
WASHINGTON – The pulley stitch "is my go-to stitch for defects under tension," said Dr. Kelley Pagliai Redbord.
The pulley stitch allows for considerable reduction in the surface area of a large defect that can’t be closed by side-to-side stitches alone, making it an excellent choice for use on the scalp and legs, Dr. Redbord said at the Atlantic Dermatological Conference.
"When the tension across the wound is decreased, buried dermal sutures can be placed more easily and accurately," she said. "I use it a lot as an intraoperative tissue expander."
Dr. Redbord said that her description of the pulley stitch was taken from an article by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg. 2011; 37:1503-5).*
The pulley stitch can serve as a temporary suture that can be left in place or removed, said Dr. Redbord, a dermatologist in group practice in Rockville, Md.
The technique follows a far-near-near-far pattern, starting the stitch 8 mm from the wound edge (far), then bringing it to the opposite side just 4 mm from the wound edge (near). Dr. Redbord then reenters the stitch 4 mm from the wound edge on the initial side (near), and makes another pass to the opposite side 8 mm from the wound edge (far).
Multiple passes through the tissue create resistance that keeps the suture from slipping. "The loops of the stitch are placed at an oblique angle so that the inner and outer loops are offset and do not override each other," she noted. This technique minimizes potential skin damage from pressure necrosis caused by overriding loop sutures. The pulley stitch has a 2:1 mechanical advantage over an interrupted suture, and the additional friction of a second loop prevents the knot from slipping.
A modification of the pulley stitch is to loop the suture through an external loop on the opposite side of the incision, and pull across. "This new loop functions as a pulley and directs the tension away from the other strands," she said.
Another stitch with excellent eversion, in which the pulley stitch plays a key role, is the subcutaneous inverted cross mattress stitch (SICM). The SCIM is entirely subcutaneous, and combines the buried vertical mattress stitch and the buried pulley stitch.
The SCIM "uses the buried vertical mattress’s ability to evert wound edges and combines it with the pulley stitch’s ability to decrease tension at the wound edge," she said.
The four-step process is as follows:
• 1. Insert the needle into the dermis 3-5 mm lateral to the wound edge. Advance the needle into the upper reticular dermis, and then curve down to exit through the lower reticular dermis.
• 2. Insert the needle into the opposite edge of the wound at the lower reticular dermis and advance into the upper reticular dermis, then curve down and exit intradermally.
• 3. Insert the needle across the defect using an intradermal approach 1-2 mm lateral to the initial needle insertion point. Then, create a second buried vertical mattress stitch.
• 4. Pull the two stitches to close, which "creates a pulley effect with minimal recoil, and tie off," Dr. Redbord said.
"The pulley system locks the wound edges so that a knot can be tied without slipping," she added.
Dr. Redbord said she had no relevant financial disclosures.
EDITOR'S NOTE: August 26, 2013: This article has been amended since it was first published to make it clear that Dr. Kelley Pagliai Redbord's description of the pulley stitch procedure was taken directly from an article published by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg.2011;37:1503-5). In her presentation, Dr. Redbord credited Dr. Yag-Howard and her article. However, this credit and attribution to Dr. Yag-Howard was not included in the article published.
WASHINGTON – The pulley stitch "is my go-to stitch for defects under tension," said Dr. Kelley Pagliai Redbord.
The pulley stitch allows for considerable reduction in the surface area of a large defect that can’t be closed by side-to-side stitches alone, making it an excellent choice for use on the scalp and legs, Dr. Redbord said at the Atlantic Dermatological Conference.
"When the tension across the wound is decreased, buried dermal sutures can be placed more easily and accurately," she said. "I use it a lot as an intraoperative tissue expander."
Dr. Redbord said that her description of the pulley stitch was taken from an article by Dr. Cyndi Yag-Howard in Dermatologic Surgery (Dermatol. Surg. 2011; 37:1503-5).*
The pulley stitch can serve as a temporary suture that can be left in place or removed, said Dr. Redbord, a dermatologist in group practice in Rockville, Md.
The technique follows a far-near-near-far pattern, starting the stitch 8 mm from the wound edge (far), then bringing it to the opposite side just 4 mm from the wound edge (near). Dr. Redbord then reenters the stitch 4 mm from the wound edge on the initial side (near), and makes another pass to the opposite side 8 mm from the wound edge (far).
Multiple passes through the tissue create resistance that keeps the suture from slipping. "The loops of the stitch are placed at an oblique angle so that the inner and outer loops are offset and do not override each other," she noted. This technique minimizes potential skin damage from pressure necrosis caused by overriding loop sutures. The pulley stitch has a 2:1 mechanical advantage over an interrupted suture, and the additional friction of a second loop prevents the knot from slipping.
A modification of the pulley stitch is to loop the suture through an external loop on the opposite side of the incision, and pull across. "This new loop functions as a pulley and directs the tension away from the other strands," she said.
Another stitch with excellent eversion, in which the pulley stitch plays a key role, is the subcutaneous inverted cross mattress stitch (SICM). The SCIM is entirely subcutaneous, and combines the buried vertical mattress stitch and the buried pulley stitch.
The SCIM "uses the buried vertical mattress’s ability to evert wound edges and combines it with the pulley stitch’s ability to decrease tension at the wound edge," she said.
The four-step process is as follows:
• 1. Insert the needle into the dermis 3-5 mm lateral to the wound edge. Advance the needle into the upper reticular dermis, and then curve down to exit through the lower reticular dermis.
• 2. Insert the needle into the opposite edge of the wound at the lower reticular dermis and advance into the upper reticular dermis, then curve down and exit intradermally.
• 3. Insert the needle across the defect using an intradermal approach 1-2 mm lateral to the initial needle insertion point. Then, create a second buried vertical mattress stitch.
• 4. Pull the two stitches to close, which "creates a pulley effect with minimal recoil, and tie off," Dr. Redbord said.
"The pulley system locks the wound edges so that a knot can be tied without slipping," she added.
Dr. Redbord said she had no relevant financial disclosures.
EXPERT ANALYSIS FROM THE ATLANTIC DERMATOLOGICAL CONFERENCE
Major finding: Key numerical finding (e.g., number needed to treat to prevent one death/event; number lived or died as result of intervention). Maximum 10 words/1 sentence.
Data source: Include type of study (e.g., randomized, placebo controlled trial; retrospective case-control study). Include number in the study.
Disclosures: Sponsor of study, funding source, relevant disclosures. If author has no relevant disclosures, "Dr. X reported having no financial disclosures." If necessary, "Meeting Y did not require reports of financial disclosures." Check meeting website because many list disclosures. Written in sentence form.

Microwave therapy zaps hyperhidrosis long-term
MAUI, HAWAII – The future of hyperhidrosis therapy may be microwave ablation, a Food and Drug Administration–cleared method of destroying sweat glands noninvasively.
"We’ve seen that it’s effective in about 90% of patients, the patients are really satisfied, and the side effects are transient," Dr. Nazanin Saedi said at the Hawaii Dermatology Seminar, sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Larger patient numbers and more long-term data are needed before the therapy becomes common in clinical practice, but it shouldn’t take long to accumulate such data, because the proprietary miraDry microwave treatment system (marketed by Miramar Labs) is much in demand by patients, noted Dr. Saedi of Thomas Jefferson University, Philadelphia.
An estimated 4.3 million Americans have axillary hyperhidrosis, Dr. Saedi said. Numerous treatment options are available, but most have significant drawbacks, she noted. First-line therapy is topical aluminum chloride, with or without salicylic acid; irritant dermatitis is a common complaint.
Second-line options include iontophoresis, which requires treatments two or three times per week and can be quite painful, Dr. Saedi said. Botulinum toxin A injections are highly effective, but they must be repeated every 4-6 months, and can cause weakness of the underlying muscles. Oral medications include anticholinergic agents and alpha2-adrenergic drugs, all with side effects many patients find problematic.
Before microwave therapy, surgical procedures were the only means of destroying sweat glands, and surgery is considered third-line therapy, Dr. Saedi said.
"Now that we have the newer technologies, I think surgery will become even more rare," she predicted.
The study that earned the miraDry device its Food and Drug Administration marketing clearance was a blinded trial in which 120 patients were randomized 2:1 to microwave therapy or a sham procedure. At baseline, all participants were rated 3 or 4 on the 1-4 Hyperhidrosis Disease Severity Scale (HDSS). At a follow-up point of 30 days, 89% of patients in the treatment group met the primary endpoint – an HDSS score of 1 or 2 – compared with 54% of controls. Roughly 70% of patients in the microwave treatment group still had an HDSS score of 1-2 at 12 months (Dermatol. Surg. 2012;38:185-91).
However, that study involved an earlier-generation, less efficient device, Dr. Saedi noted. In an open-label study of 31 patients treated with the current-generation, commercially available miraDry device, all subjects had a baseline HDSS score of 3 or 4. Twelve months after patients received 1-3 treatment sessions, 90% had an HDSS score of 1 or 2. In addition, 90% of patients had at least a 50% reduction in gravimetrically measured axillary sweat, and 85% had at least a 5-point improvement on the Dermatologic Life Quality Index (Dermatol. Surg. 2012;38:728-35).
In the microwave treatment procedure, an applicator is placed on the skin surface to deliver focused energy to the dermal-fat interface, where sweat glands are located. Microwaves are preferentially absorbed by tissues with high water content, such as sweat glands, and poorly absorbed by fat. A cooling system keeps the heat at the lower skin layer. A heat dome at about 60° C is created along the dermal-fat junction, resulting in sweat gland thermolysis, Dr. Saedi explained.
Two hours prior to treatment, the patient takes 800 mg of ibuprofen. A grid of temporary markings is placed over the area to be treated, and the dermis is anesthetized with injections of a 1:1 mix of 1% plain lidocaine and 1% lidocaine plus epinephrine at 1-cm intervals.
Microwave therapy entails two treatment sessions roughly 3 months apart. The first typically takes 60-90 minutes, the second 30-60 minutes.
Dr. Saedi said swelling, bruising, discomfort, and altered sensation in and around the treatment area are all common side effects of microwave therapy, but all are short-term. Less common side effects include swelling extending beyond the treatment area, a tight banding sensation in the axilla, and arm and hand numbness lasting less than 24 hours, she said.
One audience member who has treated 130 patients via microwave therapy reported that one of them developed a significant brachial nerve palsy that has lasted for 5 months. As a consequence, the commenter said he now routinely employs tumescent anesthesia in an effort to steer clear of the axillary nerve bundles. But Dr. Suzanne L. Kilmer said she doubts that will prevent the occasional case of brachial nerve palsy, which she believes is the result of variant anatomy.
"We’ve done the procedure on many thin people, and not had brachial nerve palsy be an issue, so I’m not sure that tumescent anesthesia will make a difference," said Dr. Kilmer of the University of California, Davis.
Pulsed ultrasound is currently under investigation as a means of treating hyperhidrosis through destruction of sweat glands, session moderator Dr. Christopher B. Zachary said in response to an audience question. "This would be an off-label indication right now, but you can absolutely hit that region with an ultrasound device and cause heating. It’s quite likely that ultrasound will be used extensively in exactly the same way as microwave, and probably with the same efficacy," predicted Dr. Zachary of the University of California, Irvine.
Dr. Zachary is a consultant to and has received research funding from numerous laser and other medical device companies, as has Dr. Kilmer. Dr. Saedi had no financial conflicts to disclose. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – The future of hyperhidrosis therapy may be microwave ablation, a Food and Drug Administration–cleared method of destroying sweat glands noninvasively.
"We’ve seen that it’s effective in about 90% of patients, the patients are really satisfied, and the side effects are transient," Dr. Nazanin Saedi said at the Hawaii Dermatology Seminar, sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Larger patient numbers and more long-term data are needed before the therapy becomes common in clinical practice, but it shouldn’t take long to accumulate such data, because the proprietary miraDry microwave treatment system (marketed by Miramar Labs) is much in demand by patients, noted Dr. Saedi of Thomas Jefferson University, Philadelphia.
An estimated 4.3 million Americans have axillary hyperhidrosis, Dr. Saedi said. Numerous treatment options are available, but most have significant drawbacks, she noted. First-line therapy is topical aluminum chloride, with or without salicylic acid; irritant dermatitis is a common complaint.
Second-line options include iontophoresis, which requires treatments two or three times per week and can be quite painful, Dr. Saedi said. Botulinum toxin A injections are highly effective, but they must be repeated every 4-6 months, and can cause weakness of the underlying muscles. Oral medications include anticholinergic agents and alpha2-adrenergic drugs, all with side effects many patients find problematic.
Before microwave therapy, surgical procedures were the only means of destroying sweat glands, and surgery is considered third-line therapy, Dr. Saedi said.
"Now that we have the newer technologies, I think surgery will become even more rare," she predicted.
The study that earned the miraDry device its Food and Drug Administration marketing clearance was a blinded trial in which 120 patients were randomized 2:1 to microwave therapy or a sham procedure. At baseline, all participants were rated 3 or 4 on the 1-4 Hyperhidrosis Disease Severity Scale (HDSS). At a follow-up point of 30 days, 89% of patients in the treatment group met the primary endpoint – an HDSS score of 1 or 2 – compared with 54% of controls. Roughly 70% of patients in the microwave treatment group still had an HDSS score of 1-2 at 12 months (Dermatol. Surg. 2012;38:185-91).
However, that study involved an earlier-generation, less efficient device, Dr. Saedi noted. In an open-label study of 31 patients treated with the current-generation, commercially available miraDry device, all subjects had a baseline HDSS score of 3 or 4. Twelve months after patients received 1-3 treatment sessions, 90% had an HDSS score of 1 or 2. In addition, 90% of patients had at least a 50% reduction in gravimetrically measured axillary sweat, and 85% had at least a 5-point improvement on the Dermatologic Life Quality Index (Dermatol. Surg. 2012;38:728-35).
In the microwave treatment procedure, an applicator is placed on the skin surface to deliver focused energy to the dermal-fat interface, where sweat glands are located. Microwaves are preferentially absorbed by tissues with high water content, such as sweat glands, and poorly absorbed by fat. A cooling system keeps the heat at the lower skin layer. A heat dome at about 60° C is created along the dermal-fat junction, resulting in sweat gland thermolysis, Dr. Saedi explained.
Two hours prior to treatment, the patient takes 800 mg of ibuprofen. A grid of temporary markings is placed over the area to be treated, and the dermis is anesthetized with injections of a 1:1 mix of 1% plain lidocaine and 1% lidocaine plus epinephrine at 1-cm intervals.
Microwave therapy entails two treatment sessions roughly 3 months apart. The first typically takes 60-90 minutes, the second 30-60 minutes.
Dr. Saedi said swelling, bruising, discomfort, and altered sensation in and around the treatment area are all common side effects of microwave therapy, but all are short-term. Less common side effects include swelling extending beyond the treatment area, a tight banding sensation in the axilla, and arm and hand numbness lasting less than 24 hours, she said.
One audience member who has treated 130 patients via microwave therapy reported that one of them developed a significant brachial nerve palsy that has lasted for 5 months. As a consequence, the commenter said he now routinely employs tumescent anesthesia in an effort to steer clear of the axillary nerve bundles. But Dr. Suzanne L. Kilmer said she doubts that will prevent the occasional case of brachial nerve palsy, which she believes is the result of variant anatomy.
"We’ve done the procedure on many thin people, and not had brachial nerve palsy be an issue, so I’m not sure that tumescent anesthesia will make a difference," said Dr. Kilmer of the University of California, Davis.
Pulsed ultrasound is currently under investigation as a means of treating hyperhidrosis through destruction of sweat glands, session moderator Dr. Christopher B. Zachary said in response to an audience question. "This would be an off-label indication right now, but you can absolutely hit that region with an ultrasound device and cause heating. It’s quite likely that ultrasound will be used extensively in exactly the same way as microwave, and probably with the same efficacy," predicted Dr. Zachary of the University of California, Irvine.
Dr. Zachary is a consultant to and has received research funding from numerous laser and other medical device companies, as has Dr. Kilmer. Dr. Saedi had no financial conflicts to disclose. SDEF and this news organization are owned by the same parent company.
MAUI, HAWAII – The future of hyperhidrosis therapy may be microwave ablation, a Food and Drug Administration–cleared method of destroying sweat glands noninvasively.
"We’ve seen that it’s effective in about 90% of patients, the patients are really satisfied, and the side effects are transient," Dr. Nazanin Saedi said at the Hawaii Dermatology Seminar, sponsored by Global Academy for Medical Education/Skin Disease Education Foundation.
Larger patient numbers and more long-term data are needed before the therapy becomes common in clinical practice, but it shouldn’t take long to accumulate such data, because the proprietary miraDry microwave treatment system (marketed by Miramar Labs) is much in demand by patients, noted Dr. Saedi of Thomas Jefferson University, Philadelphia.
An estimated 4.3 million Americans have axillary hyperhidrosis, Dr. Saedi said. Numerous treatment options are available, but most have significant drawbacks, she noted. First-line therapy is topical aluminum chloride, with or without salicylic acid; irritant dermatitis is a common complaint.
Second-line options include iontophoresis, which requires treatments two or three times per week and can be quite painful, Dr. Saedi said. Botulinum toxin A injections are highly effective, but they must be repeated every 4-6 months, and can cause weakness of the underlying muscles. Oral medications include anticholinergic agents and alpha2-adrenergic drugs, all with side effects many patients find problematic.
Before microwave therapy, surgical procedures were the only means of destroying sweat glands, and surgery is considered third-line therapy, Dr. Saedi said.
"Now that we have the newer technologies, I think surgery will become even more rare," she predicted.
The study that earned the miraDry device its Food and Drug Administration marketing clearance was a blinded trial in which 120 patients were randomized 2:1 to microwave therapy or a sham procedure. At baseline, all participants were rated 3 or 4 on the 1-4 Hyperhidrosis Disease Severity Scale (HDSS). At a follow-up point of 30 days, 89% of patients in the treatment group met the primary endpoint – an HDSS score of 1 or 2 – compared with 54% of controls. Roughly 70% of patients in the microwave treatment group still had an HDSS score of 1-2 at 12 months (Dermatol. Surg. 2012;38:185-91).
However, that study involved an earlier-generation, less efficient device, Dr. Saedi noted. In an open-label study of 31 patients treated with the current-generation, commercially available miraDry device, all subjects had a baseline HDSS score of 3 or 4. Twelve months after patients received 1-3 treatment sessions, 90% had an HDSS score of 1 or 2. In addition, 90% of patients had at least a 50% reduction in gravimetrically measured axillary sweat, and 85% had at least a 5-point improvement on the Dermatologic Life Quality Index (Dermatol. Surg. 2012;38:728-35).
In the microwave treatment procedure, an applicator is placed on the skin surface to deliver focused energy to the dermal-fat interface, where sweat glands are located. Microwaves are preferentially absorbed by tissues with high water content, such as sweat glands, and poorly absorbed by fat. A cooling system keeps the heat at the lower skin layer. A heat dome at about 60° C is created along the dermal-fat junction, resulting in sweat gland thermolysis, Dr. Saedi explained.
Two hours prior to treatment, the patient takes 800 mg of ibuprofen. A grid of temporary markings is placed over the area to be treated, and the dermis is anesthetized with injections of a 1:1 mix of 1% plain lidocaine and 1% lidocaine plus epinephrine at 1-cm intervals.
Microwave therapy entails two treatment sessions roughly 3 months apart. The first typically takes 60-90 minutes, the second 30-60 minutes.
Dr. Saedi said swelling, bruising, discomfort, and altered sensation in and around the treatment area are all common side effects of microwave therapy, but all are short-term. Less common side effects include swelling extending beyond the treatment area, a tight banding sensation in the axilla, and arm and hand numbness lasting less than 24 hours, she said.
One audience member who has treated 130 patients via microwave therapy reported that one of them developed a significant brachial nerve palsy that has lasted for 5 months. As a consequence, the commenter said he now routinely employs tumescent anesthesia in an effort to steer clear of the axillary nerve bundles. But Dr. Suzanne L. Kilmer said she doubts that will prevent the occasional case of brachial nerve palsy, which she believes is the result of variant anatomy.
"We’ve done the procedure on many thin people, and not had brachial nerve palsy be an issue, so I’m not sure that tumescent anesthesia will make a difference," said Dr. Kilmer of the University of California, Davis.
Pulsed ultrasound is currently under investigation as a means of treating hyperhidrosis through destruction of sweat glands, session moderator Dr. Christopher B. Zachary said in response to an audience question. "This would be an off-label indication right now, but you can absolutely hit that region with an ultrasound device and cause heating. It’s quite likely that ultrasound will be used extensively in exactly the same way as microwave, and probably with the same efficacy," predicted Dr. Zachary of the University of California, Irvine.
Dr. Zachary is a consultant to and has received research funding from numerous laser and other medical device companies, as has Dr. Kilmer. Dr. Saedi had no financial conflicts to disclose. SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
