User login
Self-worth training boosts ketamine’s effects in severe depression

The double-blind, randomized clinical trial is the first to assess combining ketamine with a low-cost protective learning program, researchers note.
They add that the findings are an important step toward long-lasting depression treatment for millions of patients whose depression does not improve following first-line therapies.
“One of the biggest challenges in psychiatry and psychology is seeing evidence of longer-term benefits and longer-term compliance,” lead investigator Rebecca B. Price, PhD, associate professor of psychiatry and psychology, University of Pittsburgh, told this news organization.

“Anything that can get somebody well quickly and keep them well for some length of time is really exciting – and a whole paradigm shift for how things have been done up to now,” Dr. Price said.
The findings were published online in the American Journal of Psychiatry.
Promoting self-worth
About one-third of patients with depression remain treatment-resistant even after trying different medications at different doses and at different combinations, the investigators note.
Ketamine and esketamine, a nasal spray formulation of the drug, have been shown previously to improve symptoms in patients with TRD. While the benefits are evident within a few hours of treatment, the effects often wane after just a few weeks.
Ketamine and esketamine must be administered in a clinical setting and patients must be monitored for at least 2 hours after treatment. Repeat dosing is costly, both in time and expense, so clinical researchers have been studying ways to extend the drug’s effects without additional treatments.
The new study combined ketamine treatment with a computer-based active automated self-association training (ASAT) program that the researchers developed. It uses positive words and imagery to promote positive self-image and self-worth.
The trial included 154 adults with treatment-resistant unipolar depression whose symptoms persisted after therapy with at least two medications. Participants received an IV infusion of ketamine 0.5 mg/kg plus active ASAT (n = 53), saline plus active ASAT (n = 51), or ketamine plus sham ASAT (n = 50).
The active program used words like “sweet,” “lovable,” and “worthy” that appeared on the screen interspersed with images of people smiling and the patient’s own photo. Participants were also asked to complete certain mouse-tracking tasks during the session.
The sham ASAT was similar but included neutral words and images. ASAT and sham ASAT were delivered twice daily over 4 consecutive days for 20 minutes.
Clear benefit
Results showed that ketamine rapidly and significantly reduced depression scores within 24 hours of treatment (group-by-time interaction: standardized beta, –1.30; 95% confidence interval, –1.89 to –0.70).
Depression scores in the ketamine-plus-ASAT group remained low and stable over a 30-day period, compared with the saline-plus-ASAT group (standardized beta, –0.61; 95% CI, –0.95 to –0.28).
Participants who received ketamine plus sham ASAT saw initial improvement in symptoms immediately following infusion, but depression symptoms returned after a few weeks.
While researchers hoped to see positive effects from ASAT, “I certainly did not expect to see something so clear to jump right out,” Dr. Price said.
The investigators are now examining whether the computer program can be administered effectively remotely and whether its effects are equally beneficial following treatment with esketamine.
Greatest unmet need
Gerard Sanacora, MD, PhD, professor of psychiatry, and director, Yale Depression Research Program, Yale University, New Haven, Conn., said that extending the effects of ketamine or esketamine without additional dosing is “probably the greatest unmet need in relation to treatments with ketamine and esketamine.”
He added that there are large economic, time, and access burdens associated with the treatment of ketamine.
“Anything we can do to reduce the number of treatments needed or increase the sustainability or the duration of effect would be a tremendous benefit,” said Dr. Sanacora, who was not involved with the research.
Adding an easily accessible, nonpharmacological therapeutic approach to ketamine treatment could be valuable, he said – but more research is needed.
“I’m not sure that this specific associated positive thinking is really the critical component. I think we still have some work to do there. But it does demonstrate that we can use ancillary or augmenting nonpharmacological treatments to extend the effect,” Dr. Sanacora said.
The study was funded by the National Institute of Mental Health and Clinical and Translational Science Institute at the University of Pittsburgh. Dr. Price is the named inventor on a University of Pittsburgh–owned provisional patent filing related to the combination intervention described in this report. Dr. Sanacora reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The double-blind, randomized clinical trial is the first to assess combining ketamine with a low-cost protective learning program, researchers note.
They add that the findings are an important step toward long-lasting depression treatment for millions of patients whose depression does not improve following first-line therapies.
“One of the biggest challenges in psychiatry and psychology is seeing evidence of longer-term benefits and longer-term compliance,” lead investigator Rebecca B. Price, PhD, associate professor of psychiatry and psychology, University of Pittsburgh, told this news organization.
“Anything that can get somebody well quickly and keep them well for some length of time is really exciting – and a whole paradigm shift for how things have been done up to now,” Dr. Price said.
The findings were published online in the American Journal of Psychiatry.
Promoting self-worth
About one-third of patients with depression remain treatment-resistant even after trying different medications at different doses and at different combinations, the investigators note.
Ketamine and esketamine, a nasal spray formulation of the drug, have been shown previously to improve symptoms in patients with TRD. While the benefits are evident within a few hours of treatment, the effects often wane after just a few weeks.
Ketamine and esketamine must be administered in a clinical setting and patients must be monitored for at least 2 hours after treatment. Repeat dosing is costly, both in time and expense, so clinical researchers have been studying ways to extend the drug’s effects without additional treatments.
The new study combined ketamine treatment with a computer-based active automated self-association training (ASAT) program that the researchers developed. It uses positive words and imagery to promote positive self-image and self-worth.
The trial included 154 adults with treatment-resistant unipolar depression whose symptoms persisted after therapy with at least two medications. Participants received an IV infusion of ketamine 0.5 mg/kg plus active ASAT (n = 53), saline plus active ASAT (n = 51), or ketamine plus sham ASAT (n = 50).
The active program used words like “sweet,” “lovable,” and “worthy” that appeared on the screen interspersed with images of people smiling and the patient’s own photo. Participants were also asked to complete certain mouse-tracking tasks during the session.
The sham ASAT was similar but included neutral words and images. ASAT and sham ASAT were delivered twice daily over 4 consecutive days for 20 minutes.
Clear benefit
Results showed that ketamine rapidly and significantly reduced depression scores within 24 hours of treatment (group-by-time interaction: standardized beta, –1.30; 95% confidence interval, –1.89 to –0.70).
Depression scores in the ketamine-plus-ASAT group remained low and stable over a 30-day period, compared with the saline-plus-ASAT group (standardized beta, –0.61; 95% CI, –0.95 to –0.28).
Participants who received ketamine plus sham ASAT saw initial improvement in symptoms immediately following infusion, but depression symptoms returned after a few weeks.
While researchers hoped to see positive effects from ASAT, “I certainly did not expect to see something so clear to jump right out,” Dr. Price said.
The investigators are now examining whether the computer program can be administered effectively remotely and whether its effects are equally beneficial following treatment with esketamine.
Greatest unmet need
Gerard Sanacora, MD, PhD, professor of psychiatry, and director, Yale Depression Research Program, Yale University, New Haven, Conn., said that extending the effects of ketamine or esketamine without additional dosing is “probably the greatest unmet need in relation to treatments with ketamine and esketamine.”
He added that there are large economic, time, and access burdens associated with the treatment of ketamine.
“Anything we can do to reduce the number of treatments needed or increase the sustainability or the duration of effect would be a tremendous benefit,” said Dr. Sanacora, who was not involved with the research.
Adding an easily accessible, nonpharmacological therapeutic approach to ketamine treatment could be valuable, he said – but more research is needed.
“I’m not sure that this specific associated positive thinking is really the critical component. I think we still have some work to do there. But it does demonstrate that we can use ancillary or augmenting nonpharmacological treatments to extend the effect,” Dr. Sanacora said.
The study was funded by the National Institute of Mental Health and Clinical and Translational Science Institute at the University of Pittsburgh. Dr. Price is the named inventor on a University of Pittsburgh–owned provisional patent filing related to the combination intervention described in this report. Dr. Sanacora reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The double-blind, randomized clinical trial is the first to assess combining ketamine with a low-cost protective learning program, researchers note.
They add that the findings are an important step toward long-lasting depression treatment for millions of patients whose depression does not improve following first-line therapies.
“One of the biggest challenges in psychiatry and psychology is seeing evidence of longer-term benefits and longer-term compliance,” lead investigator Rebecca B. Price, PhD, associate professor of psychiatry and psychology, University of Pittsburgh, told this news organization.
“Anything that can get somebody well quickly and keep them well for some length of time is really exciting – and a whole paradigm shift for how things have been done up to now,” Dr. Price said.
The findings were published online in the American Journal of Psychiatry.
Promoting self-worth
About one-third of patients with depression remain treatment-resistant even after trying different medications at different doses and at different combinations, the investigators note.
Ketamine and esketamine, a nasal spray formulation of the drug, have been shown previously to improve symptoms in patients with TRD. While the benefits are evident within a few hours of treatment, the effects often wane after just a few weeks.
Ketamine and esketamine must be administered in a clinical setting and patients must be monitored for at least 2 hours after treatment. Repeat dosing is costly, both in time and expense, so clinical researchers have been studying ways to extend the drug’s effects without additional treatments.
The new study combined ketamine treatment with a computer-based active automated self-association training (ASAT) program that the researchers developed. It uses positive words and imagery to promote positive self-image and self-worth.
The trial included 154 adults with treatment-resistant unipolar depression whose symptoms persisted after therapy with at least two medications. Participants received an IV infusion of ketamine 0.5 mg/kg plus active ASAT (n = 53), saline plus active ASAT (n = 51), or ketamine plus sham ASAT (n = 50).
The active program used words like “sweet,” “lovable,” and “worthy” that appeared on the screen interspersed with images of people smiling and the patient’s own photo. Participants were also asked to complete certain mouse-tracking tasks during the session.
The sham ASAT was similar but included neutral words and images. ASAT and sham ASAT were delivered twice daily over 4 consecutive days for 20 minutes.
Clear benefit
Results showed that ketamine rapidly and significantly reduced depression scores within 24 hours of treatment (group-by-time interaction: standardized beta, –1.30; 95% confidence interval, –1.89 to –0.70).
Depression scores in the ketamine-plus-ASAT group remained low and stable over a 30-day period, compared with the saline-plus-ASAT group (standardized beta, –0.61; 95% CI, –0.95 to –0.28).
Participants who received ketamine plus sham ASAT saw initial improvement in symptoms immediately following infusion, but depression symptoms returned after a few weeks.
While researchers hoped to see positive effects from ASAT, “I certainly did not expect to see something so clear to jump right out,” Dr. Price said.
The investigators are now examining whether the computer program can be administered effectively remotely and whether its effects are equally beneficial following treatment with esketamine.
Greatest unmet need
Gerard Sanacora, MD, PhD, professor of psychiatry, and director, Yale Depression Research Program, Yale University, New Haven, Conn., said that extending the effects of ketamine or esketamine without additional dosing is “probably the greatest unmet need in relation to treatments with ketamine and esketamine.”
He added that there are large economic, time, and access burdens associated with the treatment of ketamine.
“Anything we can do to reduce the number of treatments needed or increase the sustainability or the duration of effect would be a tremendous benefit,” said Dr. Sanacora, who was not involved with the research.
Adding an easily accessible, nonpharmacological therapeutic approach to ketamine treatment could be valuable, he said – but more research is needed.
“I’m not sure that this specific associated positive thinking is really the critical component. I think we still have some work to do there. But it does demonstrate that we can use ancillary or augmenting nonpharmacological treatments to extend the effect,” Dr. Sanacora said.
The study was funded by the National Institute of Mental Health and Clinical and Translational Science Institute at the University of Pittsburgh. Dr. Price is the named inventor on a University of Pittsburgh–owned provisional patent filing related to the combination intervention described in this report. Dr. Sanacora reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AMERICAN JOURNAL OF PSYCHIATRY
‘Disturbing’ lack of follow-up care after psychiatric crises
There is a concerning lack of follow-up care for young people who experience a mental health crisis, new research suggests.
The follow-up rate was less than 30% for those who had visited an ED.
The strongest predictor of follow-up was having received both primary and mental health care during the 6 months prior to using the acute service.
“For people discharging folks after a psychiatric crisis, whether it be in a hospital or emergency room setting, connecting them with their outpatient provider to ensure the transfer of care and continuity of care is vitally important to reduce risks for this population,” coinvestigator Brian Skehan, MD, PhD, assistant professor and psychiatrist, University of Massachusetts, Worcester, said during a press briefing.
If these discharged patients do not have a provider, “make sure they get one,” Lisa Dixon, MD, editor-in-chief of Psychiatric Services, added during the same briefing. “That’s the gift of life potentially for these young people.”
The findings were published online in Psychiatric Services.
Alarming trends
The alarming suicide trends among youths were exacerbated by the COVID-19 pandemic, Dr. Skehan noted.
He cited a 2021 study that showed more than 44% of high school students experienced persistent sadness or hopelessness over the previous year, 1 in 5 seriously considered suicide, and almost 1 in 10 actually attempted suicide.
“When we look at the number of young adults and adolescents struggling with behavioral health issues, the data trend is disturbing nationwide,” Dr. Skehan said.
The current study included participants aged 12-27 years who had private insurance. Many youth in this age category are experiencing significant changes, such as moving from high school to college and from pediatric providers to adult providers – and some “get lost in this transition,” said Dr. Skehan.
He noted many inpatient psychiatric units are not geared to young adults. “They may miss out on some aspects of inpatient care because it’s not geared to their developmental stage,” he said.
Assessing U.S. patient data in the IBM MarketScan commercial database (2013-2018), the researchers created two study samples: 95,153 inpatients and 108,576 patients who used the ED. All had an acute event stemming from a mental health condition.
The investigators explored the role of “established” outpatient care, defined as having had at least one visit with a provider of primary or mental health care in the 6 months prior to the acute psychiatric event.
Covariates included age at time of service (aged 12-17 years or 18-27 years), gender, health care plan type, psychiatric diagnosis, whether the acute event was self-harm or suicide related, and medical complexity.
Low follow-up rates
In the inpatient group, the average age was 18.9 years, the most common length of hospital stay was 4-6 days, and 1.5% left against medical advice. The most common primary diagnosis was major depression (53.7%), followed by bipolar disorder (22.3%). The least common disorders were PTSD, comorbid eating disorders, and disruptive disorders.
About one-third of participants had used both primary and mental health care during the 6 months before hospitalization, whereas 22.8% had no established outpatient care. Established care was most common among those with comorbid eating disorders and least common among those with psychotic disorders.
Results showed 42.7% of the hospitalized patients received follow up within 7 days and 67.4% received follow up within 30 days.
The strongest predictor of mental health follow-up care was established outpatient care. Compared with those who had no such care, those who had received both primary care and mental health care before the acute event had the highest odds of receiving follow-up (within 7 days, adjusted odds ratio, 2.81; 95% confidence interval, 2.68-2.94).
Older age and leaving against medical advice were associated with decreased likelihood of follow-up. Female sex, hospitalizations related to self-harm or suicidality, and longer length of stay were associated with increased likelihood of mental health follow-up care.
Compared with those hospitalized for major depression, those hospitalized for schizophrenia, bipolar disorder, PTSD, disruptive disorders, or comorbid substance use disorder were less likely to receive mental health follow-up. For example, only 23.7% of youth with comorbid substance use discharged from the hospital had follow-up within 7 days.
Similar patterns were observed for 30-day follow-up care.
‘Accessible and appealing’ options needed
In the ED-visit group, the average age was 19.5 years (58% female). Most (70.4%) had no chronic health conditions other than a psychiatric disorder. The primary diagnoses were anxiety disorders or phobias (44.1%) and major depression (23%).
One in four visits included a code for self-harm, suicidal ideation, or suicide attempt. And almost one third lacked established outpatient care before the ED visit.
Results showed 28.6% of the ED group received mental health care follow-up within 7 days and 46.4% received it within 30 days.
Again, the strongest predictor of mental health follow-up was prior outpatient care. For example, compared with participants with no established outpatient care, those with both primary care and mental health care were the most likely to receive follow-up within 7 days (aOR, 4.06; 95% CI, 3.72-4.42).
These numbers “are far from the goal of making sure everybody is getting follow-up care within 7 days of an acute psychiatric event,” Dr. Skehan said.
He stressed the need for “accessible and appealing options for youth.” These could include telehealth services, improved communication among health care providers in the ED, and reducing barriers to access follow-up care.
“This probably highlights the need to have more case management and referral services, and maybe make sure patients have a follow-up appointment before they leave the emergency room,” said Dr. Skehan. “This doesn’t necessarily guarantee they’ll get there but hopefully it makes it more likely they will have that access should they need it.”
The study was funded by grants from the National Institute of General Medical Sciences and the National Center for Advancing Translational Sciences, from the National Institutes of Health. The investigators reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There is a concerning lack of follow-up care for young people who experience a mental health crisis, new research suggests.
The follow-up rate was less than 30% for those who had visited an ED.
The strongest predictor of follow-up was having received both primary and mental health care during the 6 months prior to using the acute service.
“For people discharging folks after a psychiatric crisis, whether it be in a hospital or emergency room setting, connecting them with their outpatient provider to ensure the transfer of care and continuity of care is vitally important to reduce risks for this population,” coinvestigator Brian Skehan, MD, PhD, assistant professor and psychiatrist, University of Massachusetts, Worcester, said during a press briefing.
If these discharged patients do not have a provider, “make sure they get one,” Lisa Dixon, MD, editor-in-chief of Psychiatric Services, added during the same briefing. “That’s the gift of life potentially for these young people.”
The findings were published online in Psychiatric Services.
Alarming trends
The alarming suicide trends among youths were exacerbated by the COVID-19 pandemic, Dr. Skehan noted.
He cited a 2021 study that showed more than 44% of high school students experienced persistent sadness or hopelessness over the previous year, 1 in 5 seriously considered suicide, and almost 1 in 10 actually attempted suicide.
“When we look at the number of young adults and adolescents struggling with behavioral health issues, the data trend is disturbing nationwide,” Dr. Skehan said.
The current study included participants aged 12-27 years who had private insurance. Many youth in this age category are experiencing significant changes, such as moving from high school to college and from pediatric providers to adult providers – and some “get lost in this transition,” said Dr. Skehan.
He noted many inpatient psychiatric units are not geared to young adults. “They may miss out on some aspects of inpatient care because it’s not geared to their developmental stage,” he said.
Assessing U.S. patient data in the IBM MarketScan commercial database (2013-2018), the researchers created two study samples: 95,153 inpatients and 108,576 patients who used the ED. All had an acute event stemming from a mental health condition.
The investigators explored the role of “established” outpatient care, defined as having had at least one visit with a provider of primary or mental health care in the 6 months prior to the acute psychiatric event.
Covariates included age at time of service (aged 12-17 years or 18-27 years), gender, health care plan type, psychiatric diagnosis, whether the acute event was self-harm or suicide related, and medical complexity.
Low follow-up rates
In the inpatient group, the average age was 18.9 years, the most common length of hospital stay was 4-6 days, and 1.5% left against medical advice. The most common primary diagnosis was major depression (53.7%), followed by bipolar disorder (22.3%). The least common disorders were PTSD, comorbid eating disorders, and disruptive disorders.
About one-third of participants had used both primary and mental health care during the 6 months before hospitalization, whereas 22.8% had no established outpatient care. Established care was most common among those with comorbid eating disorders and least common among those with psychotic disorders.
Results showed 42.7% of the hospitalized patients received follow up within 7 days and 67.4% received follow up within 30 days.
The strongest predictor of mental health follow-up care was established outpatient care. Compared with those who had no such care, those who had received both primary care and mental health care before the acute event had the highest odds of receiving follow-up (within 7 days, adjusted odds ratio, 2.81; 95% confidence interval, 2.68-2.94).
Older age and leaving against medical advice were associated with decreased likelihood of follow-up. Female sex, hospitalizations related to self-harm or suicidality, and longer length of stay were associated with increased likelihood of mental health follow-up care.
Compared with those hospitalized for major depression, those hospitalized for schizophrenia, bipolar disorder, PTSD, disruptive disorders, or comorbid substance use disorder were less likely to receive mental health follow-up. For example, only 23.7% of youth with comorbid substance use discharged from the hospital had follow-up within 7 days.
Similar patterns were observed for 30-day follow-up care.
‘Accessible and appealing’ options needed
In the ED-visit group, the average age was 19.5 years (58% female). Most (70.4%) had no chronic health conditions other than a psychiatric disorder. The primary diagnoses were anxiety disorders or phobias (44.1%) and major depression (23%).
One in four visits included a code for self-harm, suicidal ideation, or suicide attempt. And almost one third lacked established outpatient care before the ED visit.
Results showed 28.6% of the ED group received mental health care follow-up within 7 days and 46.4% received it within 30 days.
Again, the strongest predictor of mental health follow-up was prior outpatient care. For example, compared with participants with no established outpatient care, those with both primary care and mental health care were the most likely to receive follow-up within 7 days (aOR, 4.06; 95% CI, 3.72-4.42).
These numbers “are far from the goal of making sure everybody is getting follow-up care within 7 days of an acute psychiatric event,” Dr. Skehan said.
He stressed the need for “accessible and appealing options for youth.” These could include telehealth services, improved communication among health care providers in the ED, and reducing barriers to access follow-up care.
“This probably highlights the need to have more case management and referral services, and maybe make sure patients have a follow-up appointment before they leave the emergency room,” said Dr. Skehan. “This doesn’t necessarily guarantee they’ll get there but hopefully it makes it more likely they will have that access should they need it.”
The study was funded by grants from the National Institute of General Medical Sciences and the National Center for Advancing Translational Sciences, from the National Institutes of Health. The investigators reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There is a concerning lack of follow-up care for young people who experience a mental health crisis, new research suggests.
The follow-up rate was less than 30% for those who had visited an ED.
The strongest predictor of follow-up was having received both primary and mental health care during the 6 months prior to using the acute service.
“For people discharging folks after a psychiatric crisis, whether it be in a hospital or emergency room setting, connecting them with their outpatient provider to ensure the transfer of care and continuity of care is vitally important to reduce risks for this population,” coinvestigator Brian Skehan, MD, PhD, assistant professor and psychiatrist, University of Massachusetts, Worcester, said during a press briefing.
If these discharged patients do not have a provider, “make sure they get one,” Lisa Dixon, MD, editor-in-chief of Psychiatric Services, added during the same briefing. “That’s the gift of life potentially for these young people.”
The findings were published online in Psychiatric Services.
Alarming trends
The alarming suicide trends among youths were exacerbated by the COVID-19 pandemic, Dr. Skehan noted.
He cited a 2021 study that showed more than 44% of high school students experienced persistent sadness or hopelessness over the previous year, 1 in 5 seriously considered suicide, and almost 1 in 10 actually attempted suicide.
“When we look at the number of young adults and adolescents struggling with behavioral health issues, the data trend is disturbing nationwide,” Dr. Skehan said.
The current study included participants aged 12-27 years who had private insurance. Many youth in this age category are experiencing significant changes, such as moving from high school to college and from pediatric providers to adult providers – and some “get lost in this transition,” said Dr. Skehan.
He noted many inpatient psychiatric units are not geared to young adults. “They may miss out on some aspects of inpatient care because it’s not geared to their developmental stage,” he said.
Assessing U.S. patient data in the IBM MarketScan commercial database (2013-2018), the researchers created two study samples: 95,153 inpatients and 108,576 patients who used the ED. All had an acute event stemming from a mental health condition.
The investigators explored the role of “established” outpatient care, defined as having had at least one visit with a provider of primary or mental health care in the 6 months prior to the acute psychiatric event.
Covariates included age at time of service (aged 12-17 years or 18-27 years), gender, health care plan type, psychiatric diagnosis, whether the acute event was self-harm or suicide related, and medical complexity.
Low follow-up rates
In the inpatient group, the average age was 18.9 years, the most common length of hospital stay was 4-6 days, and 1.5% left against medical advice. The most common primary diagnosis was major depression (53.7%), followed by bipolar disorder (22.3%). The least common disorders were PTSD, comorbid eating disorders, and disruptive disorders.
About one-third of participants had used both primary and mental health care during the 6 months before hospitalization, whereas 22.8% had no established outpatient care. Established care was most common among those with comorbid eating disorders and least common among those with psychotic disorders.
Results showed 42.7% of the hospitalized patients received follow up within 7 days and 67.4% received follow up within 30 days.
The strongest predictor of mental health follow-up care was established outpatient care. Compared with those who had no such care, those who had received both primary care and mental health care before the acute event had the highest odds of receiving follow-up (within 7 days, adjusted odds ratio, 2.81; 95% confidence interval, 2.68-2.94).
Older age and leaving against medical advice were associated with decreased likelihood of follow-up. Female sex, hospitalizations related to self-harm or suicidality, and longer length of stay were associated with increased likelihood of mental health follow-up care.
Compared with those hospitalized for major depression, those hospitalized for schizophrenia, bipolar disorder, PTSD, disruptive disorders, or comorbid substance use disorder were less likely to receive mental health follow-up. For example, only 23.7% of youth with comorbid substance use discharged from the hospital had follow-up within 7 days.
Similar patterns were observed for 30-day follow-up care.
‘Accessible and appealing’ options needed
In the ED-visit group, the average age was 19.5 years (58% female). Most (70.4%) had no chronic health conditions other than a psychiatric disorder. The primary diagnoses were anxiety disorders or phobias (44.1%) and major depression (23%).
One in four visits included a code for self-harm, suicidal ideation, or suicide attempt. And almost one third lacked established outpatient care before the ED visit.
Results showed 28.6% of the ED group received mental health care follow-up within 7 days and 46.4% received it within 30 days.
Again, the strongest predictor of mental health follow-up was prior outpatient care. For example, compared with participants with no established outpatient care, those with both primary care and mental health care were the most likely to receive follow-up within 7 days (aOR, 4.06; 95% CI, 3.72-4.42).
These numbers “are far from the goal of making sure everybody is getting follow-up care within 7 days of an acute psychiatric event,” Dr. Skehan said.
He stressed the need for “accessible and appealing options for youth.” These could include telehealth services, improved communication among health care providers in the ED, and reducing barriers to access follow-up care.
“This probably highlights the need to have more case management and referral services, and maybe make sure patients have a follow-up appointment before they leave the emergency room,” said Dr. Skehan. “This doesn’t necessarily guarantee they’ll get there but hopefully it makes it more likely they will have that access should they need it.”
The study was funded by grants from the National Institute of General Medical Sciences and the National Center for Advancing Translational Sciences, from the National Institutes of Health. The investigators reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PSYCHIATRIC SERVICES
‘Not in our lane’: Physicians rebel at idea they should discuss gun safety with patients
The latest NPR/PBS NewsHour/Marist poll shows that that the margin of public opinion in the United States is the widest that it has been during the past 10 years in favor of taking steps to control gun violence; 59% of U.S. adults said it’s more important to control gun violence than to protect gun rights, and 35% said the opposite.
Have physicians’ opinions about gun issues in our country shifted meaningfully during that period? That’s a complex question that can be informed with the basic snapshot provided by doctors› comments to New York University (and Medscape blogger) bioethicist Arthur L. Caplan’s four video blogs on whether physicians should discuss gun safety with their patients. Dr. Caplan’s video blogs appeared on the Medscape website in 2014, 2016, 2018, and 2022.
Hundreds of physicians have posted comments to Dr. Caplan’s arguments that doctors should bring up gun safety when talking to their patients. The great majority of comments opposed his position in 2014, and that remained the case through 2022, regardless of incidents of gun-related violence. Supportive comments have been a small minority that has grown only slightly over his four video blogs.
Physicians’ lack of qualifications
The most prevalent counterarguments expressed against Dr. Caplan’s position are that physicians lack the proper knowledge to discuss gun safety with patients; and the responsibility falls on family members, certified firearms instructors, teachers, and others – but not doctors – to educate people about firearm safety.
“Then there’s a third group that says, ‘I don’t want to do this because I am too busy trying to figure out what is wrong with the patient,’ ” Dr. Caplan says.
Here are a few on-point comments that were posted to his video blogs:
- “Unless physicians become certified firearms instructors like myself, they are not qualified to talk to patients on the subject and should advise patients to find a program and take a course.” – Dr. Ken Long, March 31, 2014
- “Gun safety should be taught in school, just like health and sex education.” – Patricia L., Feb. 11, 2016
- “None of my medical or surgical training or experience qualifies me as a policy expert on gun laws or regulations.” – Dr. Kelly Hyde, Dec. 23, 2018
- “I have the Constitution hanging in my office with an NRA plaque next to it. Most MDs can’t mow their own yard.” – Dr. Brian Anseeuw, June 21, 2022
Do mental health issues trump gun talks?
Another counterargument to discussing gun safety with patients involves mental health issues that many physicians may not be trained to address. Mental health entered comments to Dr. Caplan’s video blogs in 2016 and has shaped much of the discussion since.
- “First of all, two-thirds of gun deaths are suicides. It is foolish to talk about counseling patients about gun safety, etc, and ignore the mental health issues.” – Dr. Jeffrey Jennings, Jan. 25, 2016
- “Suicide victims and those committing mass shootings are mentally ill. ... Blame society, drugs, mental illness, easy access to illegal firearms, and poor recognition of SOS (signs of suicide).” – Dr. Alan DeCarlo, Dec. 24, 2018
- “Yes, we have gun violence, but what is the underlying problem? Bullying? Mental issues? Not enough parental supervision? These and others are the issues I feel need to be discussed.” – T. Deese, June 24, 2022
- “The causes of increased gun violence are mental health, problems with bullying, social media, and normalization of deviant behavior.” – Julie Johng, 2022
Added responsibility is too much
Another theme that has grown over time is that talks of gun safety just heap issues onto physicians’ treatment plates that are already too full.
- “Oh, for God’s sake, is there anything else I can do while I›m at it? Primary care has gotten to be more headache than it’s worth. Thanks for another reason to think about retiring.” – Dr. Kathleen Collins, March 31, 2014
- “THE JOB OF POLICE, COURTS, AND LAW-EDUCATED PROSECUTORS SHOULD NOT BE HANDLED BY PHYSICIANS.” – Dr. Sudarshan Singla, Jan. 25, 2016
- “This is a debate that only those at the academic/ivory tower–level of medicine even have time to lament. The frontline medical providers barely have enough time to adequately address the pertinent.” – Tobin Purslow, Jan. 15, 2016
Other ways to communicate
For his part, Dr. Caplan believes there is a variety of ways physicians can effectively discuss gun safety with patients to help minimize the potential of injury or death.
Acknowledging that other aspects of treatment are often more pressing, he suggested that the gun safety education could be done through educational videos that are shown in waiting rooms, through pamphlets available at the front desk, or throuigh a newsletter sent to patients.
“Everything doesn’t have to happen in conversation. The doctor’s office should become more of an educational site.
“I am 100% more passionate about this than when I first started down this road.”
A version of this article first appeared on Medscape.com.
The latest NPR/PBS NewsHour/Marist poll shows that that the margin of public opinion in the United States is the widest that it has been during the past 10 years in favor of taking steps to control gun violence; 59% of U.S. adults said it’s more important to control gun violence than to protect gun rights, and 35% said the opposite.
Have physicians’ opinions about gun issues in our country shifted meaningfully during that period? That’s a complex question that can be informed with the basic snapshot provided by doctors› comments to New York University (and Medscape blogger) bioethicist Arthur L. Caplan’s four video blogs on whether physicians should discuss gun safety with their patients. Dr. Caplan’s video blogs appeared on the Medscape website in 2014, 2016, 2018, and 2022.
Hundreds of physicians have posted comments to Dr. Caplan’s arguments that doctors should bring up gun safety when talking to their patients. The great majority of comments opposed his position in 2014, and that remained the case through 2022, regardless of incidents of gun-related violence. Supportive comments have been a small minority that has grown only slightly over his four video blogs.
Physicians’ lack of qualifications
The most prevalent counterarguments expressed against Dr. Caplan’s position are that physicians lack the proper knowledge to discuss gun safety with patients; and the responsibility falls on family members, certified firearms instructors, teachers, and others – but not doctors – to educate people about firearm safety.
“Then there’s a third group that says, ‘I don’t want to do this because I am too busy trying to figure out what is wrong with the patient,’ ” Dr. Caplan says.
Here are a few on-point comments that were posted to his video blogs:
- “Unless physicians become certified firearms instructors like myself, they are not qualified to talk to patients on the subject and should advise patients to find a program and take a course.” – Dr. Ken Long, March 31, 2014
- “Gun safety should be taught in school, just like health and sex education.” – Patricia L., Feb. 11, 2016
- “None of my medical or surgical training or experience qualifies me as a policy expert on gun laws or regulations.” – Dr. Kelly Hyde, Dec. 23, 2018
- “I have the Constitution hanging in my office with an NRA plaque next to it. Most MDs can’t mow their own yard.” – Dr. Brian Anseeuw, June 21, 2022
Do mental health issues trump gun talks?
Another counterargument to discussing gun safety with patients involves mental health issues that many physicians may not be trained to address. Mental health entered comments to Dr. Caplan’s video blogs in 2016 and has shaped much of the discussion since.
- “First of all, two-thirds of gun deaths are suicides. It is foolish to talk about counseling patients about gun safety, etc, and ignore the mental health issues.” – Dr. Jeffrey Jennings, Jan. 25, 2016
- “Suicide victims and those committing mass shootings are mentally ill. ... Blame society, drugs, mental illness, easy access to illegal firearms, and poor recognition of SOS (signs of suicide).” – Dr. Alan DeCarlo, Dec. 24, 2018
- “Yes, we have gun violence, but what is the underlying problem? Bullying? Mental issues? Not enough parental supervision? These and others are the issues I feel need to be discussed.” – T. Deese, June 24, 2022
- “The causes of increased gun violence are mental health, problems with bullying, social media, and normalization of deviant behavior.” – Julie Johng, 2022
Added responsibility is too much
Another theme that has grown over time is that talks of gun safety just heap issues onto physicians’ treatment plates that are already too full.
- “Oh, for God’s sake, is there anything else I can do while I›m at it? Primary care has gotten to be more headache than it’s worth. Thanks for another reason to think about retiring.” – Dr. Kathleen Collins, March 31, 2014
- “THE JOB OF POLICE, COURTS, AND LAW-EDUCATED PROSECUTORS SHOULD NOT BE HANDLED BY PHYSICIANS.” – Dr. Sudarshan Singla, Jan. 25, 2016
- “This is a debate that only those at the academic/ivory tower–level of medicine even have time to lament. The frontline medical providers barely have enough time to adequately address the pertinent.” – Tobin Purslow, Jan. 15, 2016
Other ways to communicate
For his part, Dr. Caplan believes there is a variety of ways physicians can effectively discuss gun safety with patients to help minimize the potential of injury or death.
Acknowledging that other aspects of treatment are often more pressing, he suggested that the gun safety education could be done through educational videos that are shown in waiting rooms, through pamphlets available at the front desk, or throuigh a newsletter sent to patients.
“Everything doesn’t have to happen in conversation. The doctor’s office should become more of an educational site.
“I am 100% more passionate about this than when I first started down this road.”
A version of this article first appeared on Medscape.com.
The latest NPR/PBS NewsHour/Marist poll shows that that the margin of public opinion in the United States is the widest that it has been during the past 10 years in favor of taking steps to control gun violence; 59% of U.S. adults said it’s more important to control gun violence than to protect gun rights, and 35% said the opposite.
Have physicians’ opinions about gun issues in our country shifted meaningfully during that period? That’s a complex question that can be informed with the basic snapshot provided by doctors› comments to New York University (and Medscape blogger) bioethicist Arthur L. Caplan’s four video blogs on whether physicians should discuss gun safety with their patients. Dr. Caplan’s video blogs appeared on the Medscape website in 2014, 2016, 2018, and 2022.
Hundreds of physicians have posted comments to Dr. Caplan’s arguments that doctors should bring up gun safety when talking to their patients. The great majority of comments opposed his position in 2014, and that remained the case through 2022, regardless of incidents of gun-related violence. Supportive comments have been a small minority that has grown only slightly over his four video blogs.
Physicians’ lack of qualifications
The most prevalent counterarguments expressed against Dr. Caplan’s position are that physicians lack the proper knowledge to discuss gun safety with patients; and the responsibility falls on family members, certified firearms instructors, teachers, and others – but not doctors – to educate people about firearm safety.
“Then there’s a third group that says, ‘I don’t want to do this because I am too busy trying to figure out what is wrong with the patient,’ ” Dr. Caplan says.
Here are a few on-point comments that were posted to his video blogs:
- “Unless physicians become certified firearms instructors like myself, they are not qualified to talk to patients on the subject and should advise patients to find a program and take a course.” – Dr. Ken Long, March 31, 2014
- “Gun safety should be taught in school, just like health and sex education.” – Patricia L., Feb. 11, 2016
- “None of my medical or surgical training or experience qualifies me as a policy expert on gun laws or regulations.” – Dr. Kelly Hyde, Dec. 23, 2018
- “I have the Constitution hanging in my office with an NRA plaque next to it. Most MDs can’t mow their own yard.” – Dr. Brian Anseeuw, June 21, 2022
Do mental health issues trump gun talks?
Another counterargument to discussing gun safety with patients involves mental health issues that many physicians may not be trained to address. Mental health entered comments to Dr. Caplan’s video blogs in 2016 and has shaped much of the discussion since.
- “First of all, two-thirds of gun deaths are suicides. It is foolish to talk about counseling patients about gun safety, etc, and ignore the mental health issues.” – Dr. Jeffrey Jennings, Jan. 25, 2016
- “Suicide victims and those committing mass shootings are mentally ill. ... Blame society, drugs, mental illness, easy access to illegal firearms, and poor recognition of SOS (signs of suicide).” – Dr. Alan DeCarlo, Dec. 24, 2018
- “Yes, we have gun violence, but what is the underlying problem? Bullying? Mental issues? Not enough parental supervision? These and others are the issues I feel need to be discussed.” – T. Deese, June 24, 2022
- “The causes of increased gun violence are mental health, problems with bullying, social media, and normalization of deviant behavior.” – Julie Johng, 2022
Added responsibility is too much
Another theme that has grown over time is that talks of gun safety just heap issues onto physicians’ treatment plates that are already too full.
- “Oh, for God’s sake, is there anything else I can do while I›m at it? Primary care has gotten to be more headache than it’s worth. Thanks for another reason to think about retiring.” – Dr. Kathleen Collins, March 31, 2014
- “THE JOB OF POLICE, COURTS, AND LAW-EDUCATED PROSECUTORS SHOULD NOT BE HANDLED BY PHYSICIANS.” – Dr. Sudarshan Singla, Jan. 25, 2016
- “This is a debate that only those at the academic/ivory tower–level of medicine even have time to lament. The frontline medical providers barely have enough time to adequately address the pertinent.” – Tobin Purslow, Jan. 15, 2016
Other ways to communicate
For his part, Dr. Caplan believes there is a variety of ways physicians can effectively discuss gun safety with patients to help minimize the potential of injury or death.
Acknowledging that other aspects of treatment are often more pressing, he suggested that the gun safety education could be done through educational videos that are shown in waiting rooms, through pamphlets available at the front desk, or throuigh a newsletter sent to patients.
“Everything doesn’t have to happen in conversation. The doctor’s office should become more of an educational site.
“I am 100% more passionate about this than when I first started down this road.”
A version of this article first appeared on Medscape.com.
Teens with diagnosed and undiagnosed ADHD report similar quality of life
The results align with findings from other studies suggesting lower quality of life (QOL) in teens with ADHD, but the current study is the first known to focus on the association between ADHD diagnosis itself vs. ADHD symptoms, and QOL, the researchers wrote. The findings show that at least some of the reduced QOL is associated with the diagnosis itself, they explained.
The researchers directly compared 393 teens with a childhood ADHD diagnosis to 393 matched teens with no ADHD diagnosis but who had hyperactive/inattentive behaviors.
The researchers reviewed self-reports from individuals who were enrolled in a population-based prospective study in Australia. The primary outcome was quality of life at age 14-15, which was measured with Child Health Utility 9D (CHU9D), a validated quality of life measure.
Study results
Overall, teens with and without an ADHD diagnosis reported similar levels of overall quality of life; the mean difference in the primary outcome CHU9D score was –0.03 (P = .10). Teens with and without an ADHD diagnosis also showed similar scores on measures of general health, happiness, and peer trust, the researchers noted.
The researchers also reviewed eight other prespecified, self-reported measures: academic self-concept, global health, negative social behaviors, overall happiness, peer trust, psychological sense of school membership, self-efficacy, and self-harm.
Teens diagnosed with ADHD in childhood were more than twice as likely to report self-harm (odds ratio 2.53, P less than .001) and displayed significantly more negative social behaviors (mean difference 1.56, P = .002), compared with teens without an ADHD diagnosis.
Teens diagnosed with ADHD in childhood also scored significantly worse on measures of sense of school membership (mean difference −2.58, P less than .001), academic self-concept (mean difference, −0.14; P = .02), and self-efficacy (mean difference −0.20; P = .007), compared to teens without an ADHD diagnosis.
The average age at ADHD diagnosis was 10 years, and 72% of the ADHD-diagnosed group were boys. No significant differences were noted for levels of hyperactive/inattentive behaviors and between girls and boys, but girls overall and children with the highest levels of hyperactive and inattentive behaviors reported generally worse outcomes, regardless of ADHD diagnosis, the researchers noted.
Don’t rush to diagnosis
Although rates of ADHD diagnosis in children continue to rise, the prevalence of hyperactivity and inattentive behaviors appears stable, which suggests a problem with diagnosis, senior author Alexandra Barratt, MBBS, MPH, PhD, professor of public health at the University of Sydney, Australia, said in an interview.
“Our hypothesis was that children who had been diagnosed, and we assume treated for, ADHD would have better outcomes, compared to children matched for hyperactivity/inattention behaviors who were left undiagnosed and untreated, but we were surprised to find that, at best, outcomes were unchanged, and for some outcomes, worse,” Dr. Barratt said.
“Our study provides evidence that diagnosing ADHD may lead, inadvertently, to long-term harms, particularly for children with mild or borderline hyperactivity and inattention behaviors,” she emphasized.
“We can’t say from this study what to do instead, but previously one of our team has looked at stepped diagnosis as an alternative option for children with mild or borderline hyperactivity and inattention behaviors,” she said.
The stepped diagnosis includes such actions as gathering behavior data from multiple sources, and conducting a period of watchful waiting without presumption of a diagnosis or active treatment.
Given the findings of the new study, “I would ask that health professionals considering a child who may have ADHD be aware that there is an evidence gap around the long-term impact of an ADHD diagnosis on children, and to proceed cautiously,” Dr. Barratt said. As for additional research, independent, high-quality, randomized controlled trials of ADHD diagnosis in children with mild or borderline hyperactivity/inattention behaviors are urgently needed, with long-term, patient-centered outcomes including quality of life she noted.
ADHD screening needs improvement
The incidence and prevalence of ADHD is on the rise, but much of the perceived increase in ADHD may be due to overdiagnosis, “and a lack of robust thorough psychological testing as standard of care for diagnosis,” Peter Loper, MD, a pediatrician and psychiatrist at the University of South Carolina, Columbia, said in an interview.
The current study “reinforces the necessity of consistent screening for comorbid mental health problems, and specifically for thoughts of self-harm, in those children who are diagnosed with ADHD,” he said.
Expressing his lack of astonishment about the study findings, Dr. Loper said: “Previous data indicates that while following initial diagnosis of a medical or mental health problem, patients may experience a sense of relief; however, this is followed shortly thereafter by feelings of insufficiency or anxiety related to their specific diagnosis.”
“As it stands now, ADHD is often diagnosed in children and adolescents using basic screening questionnaires,” said Dr. Loper. “The findings of this study may bolster calls for more robust and thorough psychological testing for supporting the diagnosis of ADHD,” he said.
Individuals diagnosed with ADHD can sometimes have difficulty with social skills and relating to others, said Dr. Loper. “They may be more prone to internalize their poor school performance as due to being ‘stupid’ or ‘dumb,’ ” he said. Children and teens with ADHD should, whenever possible, be involved in extracurricular activities that support the development of social skills, he said. Parents’ praise of the process/effort, rather than focusing only on outcomes such as grades, is very important for the esteem of children and teens with ADHD, he added.
The study limitations included the use of observational data vs. data from randomized trials, and the potential for confounding factors in propensity scoring, the researchers wrote. Additional limitations include the size of the sample, which may have been too small to detect additional differences between diagnosed teens and matched controls, they noted.
“As the study authors appropriately cite, a large, randomized trial would be very helpful in supporting additional understanding of this issue,” Dr. Loper added.
The study was supported by the National Health and Medical Research Council The researchers and Dr. Loper had no financial conflicts to disclose.
The results align with findings from other studies suggesting lower quality of life (QOL) in teens with ADHD, but the current study is the first known to focus on the association between ADHD diagnosis itself vs. ADHD symptoms, and QOL, the researchers wrote. The findings show that at least some of the reduced QOL is associated with the diagnosis itself, they explained.
The researchers directly compared 393 teens with a childhood ADHD diagnosis to 393 matched teens with no ADHD diagnosis but who had hyperactive/inattentive behaviors.
The researchers reviewed self-reports from individuals who were enrolled in a population-based prospective study in Australia. The primary outcome was quality of life at age 14-15, which was measured with Child Health Utility 9D (CHU9D), a validated quality of life measure.
Study results
Overall, teens with and without an ADHD diagnosis reported similar levels of overall quality of life; the mean difference in the primary outcome CHU9D score was –0.03 (P = .10). Teens with and without an ADHD diagnosis also showed similar scores on measures of general health, happiness, and peer trust, the researchers noted.
The researchers also reviewed eight other prespecified, self-reported measures: academic self-concept, global health, negative social behaviors, overall happiness, peer trust, psychological sense of school membership, self-efficacy, and self-harm.
Teens diagnosed with ADHD in childhood were more than twice as likely to report self-harm (odds ratio 2.53, P less than .001) and displayed significantly more negative social behaviors (mean difference 1.56, P = .002), compared with teens without an ADHD diagnosis.
Teens diagnosed with ADHD in childhood also scored significantly worse on measures of sense of school membership (mean difference −2.58, P less than .001), academic self-concept (mean difference, −0.14; P = .02), and self-efficacy (mean difference −0.20; P = .007), compared to teens without an ADHD diagnosis.
The average age at ADHD diagnosis was 10 years, and 72% of the ADHD-diagnosed group were boys. No significant differences were noted for levels of hyperactive/inattentive behaviors and between girls and boys, but girls overall and children with the highest levels of hyperactive and inattentive behaviors reported generally worse outcomes, regardless of ADHD diagnosis, the researchers noted.
Don’t rush to diagnosis
Although rates of ADHD diagnosis in children continue to rise, the prevalence of hyperactivity and inattentive behaviors appears stable, which suggests a problem with diagnosis, senior author Alexandra Barratt, MBBS, MPH, PhD, professor of public health at the University of Sydney, Australia, said in an interview.
“Our hypothesis was that children who had been diagnosed, and we assume treated for, ADHD would have better outcomes, compared to children matched for hyperactivity/inattention behaviors who were left undiagnosed and untreated, but we were surprised to find that, at best, outcomes were unchanged, and for some outcomes, worse,” Dr. Barratt said.
“Our study provides evidence that diagnosing ADHD may lead, inadvertently, to long-term harms, particularly for children with mild or borderline hyperactivity and inattention behaviors,” she emphasized.
“We can’t say from this study what to do instead, but previously one of our team has looked at stepped diagnosis as an alternative option for children with mild or borderline hyperactivity and inattention behaviors,” she said.
The stepped diagnosis includes such actions as gathering behavior data from multiple sources, and conducting a period of watchful waiting without presumption of a diagnosis or active treatment.
Given the findings of the new study, “I would ask that health professionals considering a child who may have ADHD be aware that there is an evidence gap around the long-term impact of an ADHD diagnosis on children, and to proceed cautiously,” Dr. Barratt said. As for additional research, independent, high-quality, randomized controlled trials of ADHD diagnosis in children with mild or borderline hyperactivity/inattention behaviors are urgently needed, with long-term, patient-centered outcomes including quality of life she noted.
ADHD screening needs improvement
The incidence and prevalence of ADHD is on the rise, but much of the perceived increase in ADHD may be due to overdiagnosis, “and a lack of robust thorough psychological testing as standard of care for diagnosis,” Peter Loper, MD, a pediatrician and psychiatrist at the University of South Carolina, Columbia, said in an interview.
The current study “reinforces the necessity of consistent screening for comorbid mental health problems, and specifically for thoughts of self-harm, in those children who are diagnosed with ADHD,” he said.
Expressing his lack of astonishment about the study findings, Dr. Loper said: “Previous data indicates that while following initial diagnosis of a medical or mental health problem, patients may experience a sense of relief; however, this is followed shortly thereafter by feelings of insufficiency or anxiety related to their specific diagnosis.”
“As it stands now, ADHD is often diagnosed in children and adolescents using basic screening questionnaires,” said Dr. Loper. “The findings of this study may bolster calls for more robust and thorough psychological testing for supporting the diagnosis of ADHD,” he said.
Individuals diagnosed with ADHD can sometimes have difficulty with social skills and relating to others, said Dr. Loper. “They may be more prone to internalize their poor school performance as due to being ‘stupid’ or ‘dumb,’ ” he said. Children and teens with ADHD should, whenever possible, be involved in extracurricular activities that support the development of social skills, he said. Parents’ praise of the process/effort, rather than focusing only on outcomes such as grades, is very important for the esteem of children and teens with ADHD, he added.
The study limitations included the use of observational data vs. data from randomized trials, and the potential for confounding factors in propensity scoring, the researchers wrote. Additional limitations include the size of the sample, which may have been too small to detect additional differences between diagnosed teens and matched controls, they noted.
“As the study authors appropriately cite, a large, randomized trial would be very helpful in supporting additional understanding of this issue,” Dr. Loper added.
The study was supported by the National Health and Medical Research Council The researchers and Dr. Loper had no financial conflicts to disclose.
The results align with findings from other studies suggesting lower quality of life (QOL) in teens with ADHD, but the current study is the first known to focus on the association between ADHD diagnosis itself vs. ADHD symptoms, and QOL, the researchers wrote. The findings show that at least some of the reduced QOL is associated with the diagnosis itself, they explained.
The researchers directly compared 393 teens with a childhood ADHD diagnosis to 393 matched teens with no ADHD diagnosis but who had hyperactive/inattentive behaviors.
The researchers reviewed self-reports from individuals who were enrolled in a population-based prospective study in Australia. The primary outcome was quality of life at age 14-15, which was measured with Child Health Utility 9D (CHU9D), a validated quality of life measure.
Study results
Overall, teens with and without an ADHD diagnosis reported similar levels of overall quality of life; the mean difference in the primary outcome CHU9D score was –0.03 (P = .10). Teens with and without an ADHD diagnosis also showed similar scores on measures of general health, happiness, and peer trust, the researchers noted.
The researchers also reviewed eight other prespecified, self-reported measures: academic self-concept, global health, negative social behaviors, overall happiness, peer trust, psychological sense of school membership, self-efficacy, and self-harm.
Teens diagnosed with ADHD in childhood were more than twice as likely to report self-harm (odds ratio 2.53, P less than .001) and displayed significantly more negative social behaviors (mean difference 1.56, P = .002), compared with teens without an ADHD diagnosis.
Teens diagnosed with ADHD in childhood also scored significantly worse on measures of sense of school membership (mean difference −2.58, P less than .001), academic self-concept (mean difference, −0.14; P = .02), and self-efficacy (mean difference −0.20; P = .007), compared to teens without an ADHD diagnosis.
The average age at ADHD diagnosis was 10 years, and 72% of the ADHD-diagnosed group were boys. No significant differences were noted for levels of hyperactive/inattentive behaviors and between girls and boys, but girls overall and children with the highest levels of hyperactive and inattentive behaviors reported generally worse outcomes, regardless of ADHD diagnosis, the researchers noted.
Don’t rush to diagnosis
Although rates of ADHD diagnosis in children continue to rise, the prevalence of hyperactivity and inattentive behaviors appears stable, which suggests a problem with diagnosis, senior author Alexandra Barratt, MBBS, MPH, PhD, professor of public health at the University of Sydney, Australia, said in an interview.
“Our hypothesis was that children who had been diagnosed, and we assume treated for, ADHD would have better outcomes, compared to children matched for hyperactivity/inattention behaviors who were left undiagnosed and untreated, but we were surprised to find that, at best, outcomes were unchanged, and for some outcomes, worse,” Dr. Barratt said.
“Our study provides evidence that diagnosing ADHD may lead, inadvertently, to long-term harms, particularly for children with mild or borderline hyperactivity and inattention behaviors,” she emphasized.
“We can’t say from this study what to do instead, but previously one of our team has looked at stepped diagnosis as an alternative option for children with mild or borderline hyperactivity and inattention behaviors,” she said.
The stepped diagnosis includes such actions as gathering behavior data from multiple sources, and conducting a period of watchful waiting without presumption of a diagnosis or active treatment.
Given the findings of the new study, “I would ask that health professionals considering a child who may have ADHD be aware that there is an evidence gap around the long-term impact of an ADHD diagnosis on children, and to proceed cautiously,” Dr. Barratt said. As for additional research, independent, high-quality, randomized controlled trials of ADHD diagnosis in children with mild or borderline hyperactivity/inattention behaviors are urgently needed, with long-term, patient-centered outcomes including quality of life she noted.
ADHD screening needs improvement
The incidence and prevalence of ADHD is on the rise, but much of the perceived increase in ADHD may be due to overdiagnosis, “and a lack of robust thorough psychological testing as standard of care for diagnosis,” Peter Loper, MD, a pediatrician and psychiatrist at the University of South Carolina, Columbia, said in an interview.
The current study “reinforces the necessity of consistent screening for comorbid mental health problems, and specifically for thoughts of self-harm, in those children who are diagnosed with ADHD,” he said.
Expressing his lack of astonishment about the study findings, Dr. Loper said: “Previous data indicates that while following initial diagnosis of a medical or mental health problem, patients may experience a sense of relief; however, this is followed shortly thereafter by feelings of insufficiency or anxiety related to their specific diagnosis.”
“As it stands now, ADHD is often diagnosed in children and adolescents using basic screening questionnaires,” said Dr. Loper. “The findings of this study may bolster calls for more robust and thorough psychological testing for supporting the diagnosis of ADHD,” he said.
Individuals diagnosed with ADHD can sometimes have difficulty with social skills and relating to others, said Dr. Loper. “They may be more prone to internalize their poor school performance as due to being ‘stupid’ or ‘dumb,’ ” he said. Children and teens with ADHD should, whenever possible, be involved in extracurricular activities that support the development of social skills, he said. Parents’ praise of the process/effort, rather than focusing only on outcomes such as grades, is very important for the esteem of children and teens with ADHD, he added.
The study limitations included the use of observational data vs. data from randomized trials, and the potential for confounding factors in propensity scoring, the researchers wrote. Additional limitations include the size of the sample, which may have been too small to detect additional differences between diagnosed teens and matched controls, they noted.
“As the study authors appropriately cite, a large, randomized trial would be very helpful in supporting additional understanding of this issue,” Dr. Loper added.
The study was supported by the National Health and Medical Research Council The researchers and Dr. Loper had no financial conflicts to disclose.
FROM JAMA NETWORK OPEN
Dementia signs detected years before diagnosis
offering hope for interventions to reduce the risk of the disease developing.
To date it has been unclear whether it might be possible to detect changes in brain function before the onset of symptoms, so researchers at the University of Cambridge and Cambridge University Hospitals NHS Foundation Trust set out to determine whether people who developed a range of neurodegenerative diagnoses demonstrated reduced cognitive function at their baseline assessment.
The authors explained: “The pathophysiological processes of neurodegenerative diseases begin years before diagnosis. However, prediagnostic changes in cognition and physical function are poorly understood, especially in sporadic neurodegenerative disease.”
Prediagnostic cognitive and functional impairment identified
The researchers analyzed data from the UK Biobank and compared cognitive and functional measures, including problem solving, memory, reaction times and grip strength, as well as data on weight loss and gain and on the number of falls, in individuals who subsequently developed a number of dementia-related diseases (Alzheimer’s disease, Parkinson’s disease, frontotemporal dementia, progressive supranuclear palsy, dementia with Lewy bodies, and multiple system atrophy), with those who did not have a neurodegenerative diagnosis. After adjustment for the effects of age, the same measures were regressed against time to diagnosis. The study was published in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association.
The researchers found evidence of prediagnostic cognitive impairment and decline with time, particularly in Alzheimer’s disease where those who went on to develop the disease scored more poorly compared with healthy individuals when it came to problem solving tasks, reaction times, remembering lists of numbers, prospective memory, and pair matching. This was also the case for people who developed frontotemporal dementia, the authors said.
Nol Swaddiwudhipong, MB, of the University of Cambridge, and first author, said: “When we looked back at patients’ histories, it became clear that they were showing some cognitive impairment several years before their symptoms became obvious enough to prompt a diagnosis. The impairments were often subtle, but across a number of aspects of cognition.”
Prediagnostic functional impairment and decline was also observed in multiple diseases, the authors said. People who went on to develop Alzheimer’s disease were more likely than were healthy adults to have had a fall in the previous 12 months, with those patients who went on to develop progressive supranuclear palsy (PSP) being more than twice as likely as healthy individuals to have had a fall.
The time between baseline assessment and diagnosis varied between 4.7 years for dementia with Lewy bodies and 8.3 years for Alzheimer’s disease.
“For every condition studied – including Parkinson’s disease and dementia with Lewy bodies – patients reported poorer overall health at baseline,” said the authors.
Potential for new treatments
The study findings that cognitive and functional decline occurs “years before symptoms become obvious” in multiple neurodegenerative diseases, raises the possibility that in the future at-risk patients could be screened to help select those who would benefit from interventions to reduce their risk of developing one of the conditions, or to help identify patients suitable for recruitment to clinical trials for new treatments.
Dr Swaddiwudhipong emphasized: “This is a step towards us being able to screen people who are at greatest risk – for example, people over 50 or those who have high blood pressure or do not do enough exercise – and intervene at an earlier stage to help them reduce their risk.”
There are currently very few effective treatments for dementia or other forms of neurodegeneration, the authors pointed out, in part because these conditions are often only diagnosed once symptoms appear, whereas the underlying neurodegeneration may have “begun years, even decades, earlier.” This means that by the time patients take part in clinical trials, it may already be too late in the disease process to alter its course, they explained.
Timothy Rittman, BMBS, PhD, department of clinical neurosciences, University of Cambridge, and senior author, explained that the findings could also help identify people who can participate in clinical trials for potential new treatments. “The problem with clinical trials is that by necessity they often recruit patients with a diagnosis, but we know that by this point they are already some way down the road and their condition cannot be stopped. If we can find these individuals early enough, we’ll have a better chance of seeing if the drugs are effective,” he emphasized.
Commenting on the new research, Richard Oakley, PhD, associate director of research at Alzheimer’s Society, said: “Studies like this show the importance in continued investment in dementia research to revolutionize diagnosis and drive new treatments, so one day we will beat dementia.”
The research was funded by the Medical Research Council with support from the NIHR Cambridge Biomedical Research Centre. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape UK.
offering hope for interventions to reduce the risk of the disease developing.
To date it has been unclear whether it might be possible to detect changes in brain function before the onset of symptoms, so researchers at the University of Cambridge and Cambridge University Hospitals NHS Foundation Trust set out to determine whether people who developed a range of neurodegenerative diagnoses demonstrated reduced cognitive function at their baseline assessment.
The authors explained: “The pathophysiological processes of neurodegenerative diseases begin years before diagnosis. However, prediagnostic changes in cognition and physical function are poorly understood, especially in sporadic neurodegenerative disease.”
Prediagnostic cognitive and functional impairment identified
The researchers analyzed data from the UK Biobank and compared cognitive and functional measures, including problem solving, memory, reaction times and grip strength, as well as data on weight loss and gain and on the number of falls, in individuals who subsequently developed a number of dementia-related diseases (Alzheimer’s disease, Parkinson’s disease, frontotemporal dementia, progressive supranuclear palsy, dementia with Lewy bodies, and multiple system atrophy), with those who did not have a neurodegenerative diagnosis. After adjustment for the effects of age, the same measures were regressed against time to diagnosis. The study was published in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association.
The researchers found evidence of prediagnostic cognitive impairment and decline with time, particularly in Alzheimer’s disease where those who went on to develop the disease scored more poorly compared with healthy individuals when it came to problem solving tasks, reaction times, remembering lists of numbers, prospective memory, and pair matching. This was also the case for people who developed frontotemporal dementia, the authors said.
Nol Swaddiwudhipong, MB, of the University of Cambridge, and first author, said: “When we looked back at patients’ histories, it became clear that they were showing some cognitive impairment several years before their symptoms became obvious enough to prompt a diagnosis. The impairments were often subtle, but across a number of aspects of cognition.”
Prediagnostic functional impairment and decline was also observed in multiple diseases, the authors said. People who went on to develop Alzheimer’s disease were more likely than were healthy adults to have had a fall in the previous 12 months, with those patients who went on to develop progressive supranuclear palsy (PSP) being more than twice as likely as healthy individuals to have had a fall.
The time between baseline assessment and diagnosis varied between 4.7 years for dementia with Lewy bodies and 8.3 years for Alzheimer’s disease.
“For every condition studied – including Parkinson’s disease and dementia with Lewy bodies – patients reported poorer overall health at baseline,” said the authors.
Potential for new treatments
The study findings that cognitive and functional decline occurs “years before symptoms become obvious” in multiple neurodegenerative diseases, raises the possibility that in the future at-risk patients could be screened to help select those who would benefit from interventions to reduce their risk of developing one of the conditions, or to help identify patients suitable for recruitment to clinical trials for new treatments.
Dr Swaddiwudhipong emphasized: “This is a step towards us being able to screen people who are at greatest risk – for example, people over 50 or those who have high blood pressure or do not do enough exercise – and intervene at an earlier stage to help them reduce their risk.”
There are currently very few effective treatments for dementia or other forms of neurodegeneration, the authors pointed out, in part because these conditions are often only diagnosed once symptoms appear, whereas the underlying neurodegeneration may have “begun years, even decades, earlier.” This means that by the time patients take part in clinical trials, it may already be too late in the disease process to alter its course, they explained.
Timothy Rittman, BMBS, PhD, department of clinical neurosciences, University of Cambridge, and senior author, explained that the findings could also help identify people who can participate in clinical trials for potential new treatments. “The problem with clinical trials is that by necessity they often recruit patients with a diagnosis, but we know that by this point they are already some way down the road and their condition cannot be stopped. If we can find these individuals early enough, we’ll have a better chance of seeing if the drugs are effective,” he emphasized.
Commenting on the new research, Richard Oakley, PhD, associate director of research at Alzheimer’s Society, said: “Studies like this show the importance in continued investment in dementia research to revolutionize diagnosis and drive new treatments, so one day we will beat dementia.”
The research was funded by the Medical Research Council with support from the NIHR Cambridge Biomedical Research Centre. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape UK.
offering hope for interventions to reduce the risk of the disease developing.
To date it has been unclear whether it might be possible to detect changes in brain function before the onset of symptoms, so researchers at the University of Cambridge and Cambridge University Hospitals NHS Foundation Trust set out to determine whether people who developed a range of neurodegenerative diagnoses demonstrated reduced cognitive function at their baseline assessment.
The authors explained: “The pathophysiological processes of neurodegenerative diseases begin years before diagnosis. However, prediagnostic changes in cognition and physical function are poorly understood, especially in sporadic neurodegenerative disease.”
Prediagnostic cognitive and functional impairment identified
The researchers analyzed data from the UK Biobank and compared cognitive and functional measures, including problem solving, memory, reaction times and grip strength, as well as data on weight loss and gain and on the number of falls, in individuals who subsequently developed a number of dementia-related diseases (Alzheimer’s disease, Parkinson’s disease, frontotemporal dementia, progressive supranuclear palsy, dementia with Lewy bodies, and multiple system atrophy), with those who did not have a neurodegenerative diagnosis. After adjustment for the effects of age, the same measures were regressed against time to diagnosis. The study was published in Alzheimer’s & Dementia: The Journal of the Alzheimer’s Association.
The researchers found evidence of prediagnostic cognitive impairment and decline with time, particularly in Alzheimer’s disease where those who went on to develop the disease scored more poorly compared with healthy individuals when it came to problem solving tasks, reaction times, remembering lists of numbers, prospective memory, and pair matching. This was also the case for people who developed frontotemporal dementia, the authors said.
Nol Swaddiwudhipong, MB, of the University of Cambridge, and first author, said: “When we looked back at patients’ histories, it became clear that they were showing some cognitive impairment several years before their symptoms became obvious enough to prompt a diagnosis. The impairments were often subtle, but across a number of aspects of cognition.”
Prediagnostic functional impairment and decline was also observed in multiple diseases, the authors said. People who went on to develop Alzheimer’s disease were more likely than were healthy adults to have had a fall in the previous 12 months, with those patients who went on to develop progressive supranuclear palsy (PSP) being more than twice as likely as healthy individuals to have had a fall.
The time between baseline assessment and diagnosis varied between 4.7 years for dementia with Lewy bodies and 8.3 years for Alzheimer’s disease.
“For every condition studied – including Parkinson’s disease and dementia with Lewy bodies – patients reported poorer overall health at baseline,” said the authors.
Potential for new treatments
The study findings that cognitive and functional decline occurs “years before symptoms become obvious” in multiple neurodegenerative diseases, raises the possibility that in the future at-risk patients could be screened to help select those who would benefit from interventions to reduce their risk of developing one of the conditions, or to help identify patients suitable for recruitment to clinical trials for new treatments.
Dr Swaddiwudhipong emphasized: “This is a step towards us being able to screen people who are at greatest risk – for example, people over 50 or those who have high blood pressure or do not do enough exercise – and intervene at an earlier stage to help them reduce their risk.”
There are currently very few effective treatments for dementia or other forms of neurodegeneration, the authors pointed out, in part because these conditions are often only diagnosed once symptoms appear, whereas the underlying neurodegeneration may have “begun years, even decades, earlier.” This means that by the time patients take part in clinical trials, it may already be too late in the disease process to alter its course, they explained.
Timothy Rittman, BMBS, PhD, department of clinical neurosciences, University of Cambridge, and senior author, explained that the findings could also help identify people who can participate in clinical trials for potential new treatments. “The problem with clinical trials is that by necessity they often recruit patients with a diagnosis, but we know that by this point they are already some way down the road and their condition cannot be stopped. If we can find these individuals early enough, we’ll have a better chance of seeing if the drugs are effective,” he emphasized.
Commenting on the new research, Richard Oakley, PhD, associate director of research at Alzheimer’s Society, said: “Studies like this show the importance in continued investment in dementia research to revolutionize diagnosis and drive new treatments, so one day we will beat dementia.”
The research was funded by the Medical Research Council with support from the NIHR Cambridge Biomedical Research Centre. The authors reported no conflicts of interest.
A version of this article first appeared on Medscape UK.
FROM ALZHEIMER’S & DEMENTIA
FDA confirms nationwide Adderall shortage
The U.S. Food and Drug Administration which are approved for treating attention deficit hyperactivity disorder and narcolepsy.
The FDA announcement follows weeks of reports of a shortage of the drug by pharmacy chains and Adderall users.
The agency said it is in “frequent” contact with all manufacturers of Adderall – and reported that one of those companies, Teva, is experiencing ongoing intermittent manufacturing delays.
Other manufacturers continue to produce amphetamine mixed salts, but there is not enough supply to continue to meet U.S. market demand through those producers, the FDA noted.
“Until supply is restored, there are alternative therapies, including the extended-release version of amphetamine mixed salts, available to health care professionals and their patients for amphetamine mixed salts’ approved indications,” the agency said.
Patients should work with their health care provider to determine their best treatment option, it added.
The organization is continuing to monitor the supply of Adderall and to help manufacturers resolve the shortage.
Its Drug Shortage webpage has additional information about the situation and is updated regularly.
“We continue to use all the tools we have available to help keep supply available for patients and will provide public updates regarding the Adderall shortage,” the FDA said.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration which are approved for treating attention deficit hyperactivity disorder and narcolepsy.
The FDA announcement follows weeks of reports of a shortage of the drug by pharmacy chains and Adderall users.
The agency said it is in “frequent” contact with all manufacturers of Adderall – and reported that one of those companies, Teva, is experiencing ongoing intermittent manufacturing delays.
Other manufacturers continue to produce amphetamine mixed salts, but there is not enough supply to continue to meet U.S. market demand through those producers, the FDA noted.
“Until supply is restored, there are alternative therapies, including the extended-release version of amphetamine mixed salts, available to health care professionals and their patients for amphetamine mixed salts’ approved indications,” the agency said.
Patients should work with their health care provider to determine their best treatment option, it added.
The organization is continuing to monitor the supply of Adderall and to help manufacturers resolve the shortage.
Its Drug Shortage webpage has additional information about the situation and is updated regularly.
“We continue to use all the tools we have available to help keep supply available for patients and will provide public updates regarding the Adderall shortage,” the FDA said.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration which are approved for treating attention deficit hyperactivity disorder and narcolepsy.
The FDA announcement follows weeks of reports of a shortage of the drug by pharmacy chains and Adderall users.
The agency said it is in “frequent” contact with all manufacturers of Adderall – and reported that one of those companies, Teva, is experiencing ongoing intermittent manufacturing delays.
Other manufacturers continue to produce amphetamine mixed salts, but there is not enough supply to continue to meet U.S. market demand through those producers, the FDA noted.
“Until supply is restored, there are alternative therapies, including the extended-release version of amphetamine mixed salts, available to health care professionals and their patients for amphetamine mixed salts’ approved indications,” the agency said.
Patients should work with their health care provider to determine their best treatment option, it added.
The organization is continuing to monitor the supply of Adderall and to help manufacturers resolve the shortage.
Its Drug Shortage webpage has additional information about the situation and is updated regularly.
“We continue to use all the tools we have available to help keep supply available for patients and will provide public updates regarding the Adderall shortage,” the FDA said.
A version of this article first appeared on Medscape.com.
Poor visual acuity linked to depression, changes in brain structure
After multiple adjustments, analysis of data from more than 114,000 participants in the UK Biobank Study showed that visual impairment was linked to a 19% higher risk for depression.
In addition, imaging results showed a significant link between deteriorating brain structures and depression in those with poor visual acuity.

“Our findings highlight the value of visual health in association with mental health,” Xiayin Zhang, PhD, Guangdong Eye Institute, department of ophthalmology, Guangdong Provincial People’s Hospital, Guangzhou, China, and colleagues write.
“Screening of vision at an early stage should be embedded in the middle-aged and older population to stratify the vulnerable population at risk for depression,” the investigators add.
The findings were published online in JAMA Network Open.
UK biobank analyses
The analysis included 114,583 participants (54.5% women; mean age, 56.8 years) from the UK Biobank who completed standardized questionnaires and underwent ocular examinations.
To test distance visual acuity, all were asked to read letters on lines from the top to the bottom of a chart while wearing prescribed optical correction. Visual impairment was defined as visual acuity worse than 0.3 logarithm of the minimum angle of resolution (LogMAR) units.
Depressive symptoms were self-reported using the two-item Patient Health Questionnaire (PHQ-2), in which a score of 3 or more indicates depression. As well, a medical practitioner conducted an assessment of depression at baseline.
Among the participants, 87.2% had no visual impairment or depression and acted as the healthy control group. In addition, 3.2% showed visual impairment, 10% reported a diagnosis of depression, and 0.4% had both.
Researchers adjusted for age, sex, race, ethnicity, education, smoking, alcohol consumption, physical activity, family history of severe depression, obesity, hypertension, diabetes, hyperlipidemia, and deprivation on the Townsend index.
Among those with visual impairment, 12.4% had depression, compared with 9.9% without visual impairment.
Structure deterioration
After adjusting for potential confounders, visual impairment was associated with a 19% higher risk for depression (odds ratio, 1.19; 95% confidence interval, 1.05-1.34; P = .003). In addition, 1-line–worse visual acuity was associated with 5% higher odds of depression (OR, 1.05; 95% CI, 1.04-1.07; P < .001).
The association between visual acuity and depression was found in both younger (39-58 years) and older (59-72 years) groups, as well as in both men and women.
The researchers also explored the association between depressive symptoms and brain structure using MRI scans from a subset of 7,844 individuals (51% women; 2% with visual impairment).
Results showed linear associations between PHQ-2 scores and the left volume of gray matter in the supracalcarine cortex (coefficient, 7.61; 95% CI, 3.9-11.3; adjusted P = .006).
The investigators note that the supracalcarine cortex is spatially connected to the primary visual cortex, suggesting the visual cortex may be involved in the pathogenesis of depression.
PHQ-2 scores were also associated with mean isotropic volume fraction (ISOVF) in the right fornix (cres) and/or stria terminalis (coefficient, .003; 95% CI, 0.001-0.004; adjusted P = .01).
The links “could be moderated by visual acuity, whereby increased PHQ score was associated with higher ISOVF levels only among those with poorer visual acuity (P = .02 for interaction),” the investigators report.
These results “suggest that poorer visual acuity was associated with greater depressive symptoms and may have contributed to the related deterioration of the fornix and stria terminalis,” they add.
They note that previous studies have supported the hypothesis that the fornix and stria terminalis are involved in the pathophysiology of other brain-related conditions, including schizophrenia, bipolar disorder, and autism spectrum disorder.
However, the investigators did not have information on how long the participants had experienced visual impairment, so they couldn’t investigate whether results were affected by time. Additional study limitations cited were that depression may affect vision and that a large proportion of the participants (89.3%) were White.
Study ‘adds nuance’
Commenting on the study, Ipsit V. Vahia, MD, of the department of psychiatry at Harvard Medical School, Boston, and associate chief of geriatric psychiatry at McLean Hospital, Belmont, Mass., said the study “adds nuance to our understanding” of the well-established relationship between vision deficits and depression.
“It indicates that even mild visual deficits may be associated with depression,” said Dr. Vahia, who was not involved with the research.
The investigators validated this association by showing that visual acuity was also associated with neuroimaging markers of depression, he added.
Although the study was not designed to demonstrate causal relationships between mood and vision and its findings do not confirm that correcting visual acuity deficits will resolve depressive symptoms, “the large study sample and high quality of data should give clinicians confidence in the study’s findings,” Dr. Vahia said.
“Correcting visual acuity deficits can be considered standard care for older adults worldwide, and this study suggests that providing this standard care could also benefit mental health,” he concluded.
The study was supported by the National Natural Science Foundation of China, the China Postdoctoral Science Foundation, the Outstanding Young Talent Trainee Program of Guangdong Provincial People’s Hospital, the Guangdong Provincial People’s Hospital Scientific Research Funds for Leading Medical Talents and Distinguished Young Scholars in Guangdong Province, the Talent Introduction Fund of Guangdong Provincial People’s Hospital, the Science and Technology Program of Guangzhou, China, the Project of Special Research on Cardiovascular Diseases, the Research Foundation of Medical Science and Technology of Guangdong Province, the University of Melbourne at Research Accelerator Program, and the CERA (Centre for Eye Research Australia) Foundation and Victorian State Government for the Centre for Eye Research Australia. The investigators and Dr. Vahia have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After multiple adjustments, analysis of data from more than 114,000 participants in the UK Biobank Study showed that visual impairment was linked to a 19% higher risk for depression.
In addition, imaging results showed a significant link between deteriorating brain structures and depression in those with poor visual acuity.
“Our findings highlight the value of visual health in association with mental health,” Xiayin Zhang, PhD, Guangdong Eye Institute, department of ophthalmology, Guangdong Provincial People’s Hospital, Guangzhou, China, and colleagues write.
“Screening of vision at an early stage should be embedded in the middle-aged and older population to stratify the vulnerable population at risk for depression,” the investigators add.
The findings were published online in JAMA Network Open.
UK biobank analyses
The analysis included 114,583 participants (54.5% women; mean age, 56.8 years) from the UK Biobank who completed standardized questionnaires and underwent ocular examinations.
To test distance visual acuity, all were asked to read letters on lines from the top to the bottom of a chart while wearing prescribed optical correction. Visual impairment was defined as visual acuity worse than 0.3 logarithm of the minimum angle of resolution (LogMAR) units.
Depressive symptoms were self-reported using the two-item Patient Health Questionnaire (PHQ-2), in which a score of 3 or more indicates depression. As well, a medical practitioner conducted an assessment of depression at baseline.
Among the participants, 87.2% had no visual impairment or depression and acted as the healthy control group. In addition, 3.2% showed visual impairment, 10% reported a diagnosis of depression, and 0.4% had both.
Researchers adjusted for age, sex, race, ethnicity, education, smoking, alcohol consumption, physical activity, family history of severe depression, obesity, hypertension, diabetes, hyperlipidemia, and deprivation on the Townsend index.
Among those with visual impairment, 12.4% had depression, compared with 9.9% without visual impairment.
Structure deterioration
After adjusting for potential confounders, visual impairment was associated with a 19% higher risk for depression (odds ratio, 1.19; 95% confidence interval, 1.05-1.34; P = .003). In addition, 1-line–worse visual acuity was associated with 5% higher odds of depression (OR, 1.05; 95% CI, 1.04-1.07; P < .001).
The association between visual acuity and depression was found in both younger (39-58 years) and older (59-72 years) groups, as well as in both men and women.
The researchers also explored the association between depressive symptoms and brain structure using MRI scans from a subset of 7,844 individuals (51% women; 2% with visual impairment).
Results showed linear associations between PHQ-2 scores and the left volume of gray matter in the supracalcarine cortex (coefficient, 7.61; 95% CI, 3.9-11.3; adjusted P = .006).
The investigators note that the supracalcarine cortex is spatially connected to the primary visual cortex, suggesting the visual cortex may be involved in the pathogenesis of depression.
PHQ-2 scores were also associated with mean isotropic volume fraction (ISOVF) in the right fornix (cres) and/or stria terminalis (coefficient, .003; 95% CI, 0.001-0.004; adjusted P = .01).
The links “could be moderated by visual acuity, whereby increased PHQ score was associated with higher ISOVF levels only among those with poorer visual acuity (P = .02 for interaction),” the investigators report.
These results “suggest that poorer visual acuity was associated with greater depressive symptoms and may have contributed to the related deterioration of the fornix and stria terminalis,” they add.
They note that previous studies have supported the hypothesis that the fornix and stria terminalis are involved in the pathophysiology of other brain-related conditions, including schizophrenia, bipolar disorder, and autism spectrum disorder.
However, the investigators did not have information on how long the participants had experienced visual impairment, so they couldn’t investigate whether results were affected by time. Additional study limitations cited were that depression may affect vision and that a large proportion of the participants (89.3%) were White.
Study ‘adds nuance’
Commenting on the study, Ipsit V. Vahia, MD, of the department of psychiatry at Harvard Medical School, Boston, and associate chief of geriatric psychiatry at McLean Hospital, Belmont, Mass., said the study “adds nuance to our understanding” of the well-established relationship between vision deficits and depression.
“It indicates that even mild visual deficits may be associated with depression,” said Dr. Vahia, who was not involved with the research.
The investigators validated this association by showing that visual acuity was also associated with neuroimaging markers of depression, he added.
Although the study was not designed to demonstrate causal relationships between mood and vision and its findings do not confirm that correcting visual acuity deficits will resolve depressive symptoms, “the large study sample and high quality of data should give clinicians confidence in the study’s findings,” Dr. Vahia said.
“Correcting visual acuity deficits can be considered standard care for older adults worldwide, and this study suggests that providing this standard care could also benefit mental health,” he concluded.
The study was supported by the National Natural Science Foundation of China, the China Postdoctoral Science Foundation, the Outstanding Young Talent Trainee Program of Guangdong Provincial People’s Hospital, the Guangdong Provincial People’s Hospital Scientific Research Funds for Leading Medical Talents and Distinguished Young Scholars in Guangdong Province, the Talent Introduction Fund of Guangdong Provincial People’s Hospital, the Science and Technology Program of Guangzhou, China, the Project of Special Research on Cardiovascular Diseases, the Research Foundation of Medical Science and Technology of Guangdong Province, the University of Melbourne at Research Accelerator Program, and the CERA (Centre for Eye Research Australia) Foundation and Victorian State Government for the Centre for Eye Research Australia. The investigators and Dr. Vahia have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
After multiple adjustments, analysis of data from more than 114,000 participants in the UK Biobank Study showed that visual impairment was linked to a 19% higher risk for depression.
In addition, imaging results showed a significant link between deteriorating brain structures and depression in those with poor visual acuity.
“Our findings highlight the value of visual health in association with mental health,” Xiayin Zhang, PhD, Guangdong Eye Institute, department of ophthalmology, Guangdong Provincial People’s Hospital, Guangzhou, China, and colleagues write.
“Screening of vision at an early stage should be embedded in the middle-aged and older population to stratify the vulnerable population at risk for depression,” the investigators add.
The findings were published online in JAMA Network Open.
UK biobank analyses
The analysis included 114,583 participants (54.5% women; mean age, 56.8 years) from the UK Biobank who completed standardized questionnaires and underwent ocular examinations.
To test distance visual acuity, all were asked to read letters on lines from the top to the bottom of a chart while wearing prescribed optical correction. Visual impairment was defined as visual acuity worse than 0.3 logarithm of the minimum angle of resolution (LogMAR) units.
Depressive symptoms were self-reported using the two-item Patient Health Questionnaire (PHQ-2), in which a score of 3 or more indicates depression. As well, a medical practitioner conducted an assessment of depression at baseline.
Among the participants, 87.2% had no visual impairment or depression and acted as the healthy control group. In addition, 3.2% showed visual impairment, 10% reported a diagnosis of depression, and 0.4% had both.
Researchers adjusted for age, sex, race, ethnicity, education, smoking, alcohol consumption, physical activity, family history of severe depression, obesity, hypertension, diabetes, hyperlipidemia, and deprivation on the Townsend index.
Among those with visual impairment, 12.4% had depression, compared with 9.9% without visual impairment.
Structure deterioration
After adjusting for potential confounders, visual impairment was associated with a 19% higher risk for depression (odds ratio, 1.19; 95% confidence interval, 1.05-1.34; P = .003). In addition, 1-line–worse visual acuity was associated with 5% higher odds of depression (OR, 1.05; 95% CI, 1.04-1.07; P < .001).
The association between visual acuity and depression was found in both younger (39-58 years) and older (59-72 years) groups, as well as in both men and women.
The researchers also explored the association between depressive symptoms and brain structure using MRI scans from a subset of 7,844 individuals (51% women; 2% with visual impairment).
Results showed linear associations between PHQ-2 scores and the left volume of gray matter in the supracalcarine cortex (coefficient, 7.61; 95% CI, 3.9-11.3; adjusted P = .006).
The investigators note that the supracalcarine cortex is spatially connected to the primary visual cortex, suggesting the visual cortex may be involved in the pathogenesis of depression.
PHQ-2 scores were also associated with mean isotropic volume fraction (ISOVF) in the right fornix (cres) and/or stria terminalis (coefficient, .003; 95% CI, 0.001-0.004; adjusted P = .01).
The links “could be moderated by visual acuity, whereby increased PHQ score was associated with higher ISOVF levels only among those with poorer visual acuity (P = .02 for interaction),” the investigators report.
These results “suggest that poorer visual acuity was associated with greater depressive symptoms and may have contributed to the related deterioration of the fornix and stria terminalis,” they add.
They note that previous studies have supported the hypothesis that the fornix and stria terminalis are involved in the pathophysiology of other brain-related conditions, including schizophrenia, bipolar disorder, and autism spectrum disorder.
However, the investigators did not have information on how long the participants had experienced visual impairment, so they couldn’t investigate whether results were affected by time. Additional study limitations cited were that depression may affect vision and that a large proportion of the participants (89.3%) were White.
Study ‘adds nuance’
Commenting on the study, Ipsit V. Vahia, MD, of the department of psychiatry at Harvard Medical School, Boston, and associate chief of geriatric psychiatry at McLean Hospital, Belmont, Mass., said the study “adds nuance to our understanding” of the well-established relationship between vision deficits and depression.
“It indicates that even mild visual deficits may be associated with depression,” said Dr. Vahia, who was not involved with the research.
The investigators validated this association by showing that visual acuity was also associated with neuroimaging markers of depression, he added.
Although the study was not designed to demonstrate causal relationships between mood and vision and its findings do not confirm that correcting visual acuity deficits will resolve depressive symptoms, “the large study sample and high quality of data should give clinicians confidence in the study’s findings,” Dr. Vahia said.
“Correcting visual acuity deficits can be considered standard care for older adults worldwide, and this study suggests that providing this standard care could also benefit mental health,” he concluded.
The study was supported by the National Natural Science Foundation of China, the China Postdoctoral Science Foundation, the Outstanding Young Talent Trainee Program of Guangdong Provincial People’s Hospital, the Guangdong Provincial People’s Hospital Scientific Research Funds for Leading Medical Talents and Distinguished Young Scholars in Guangdong Province, the Talent Introduction Fund of Guangdong Provincial People’s Hospital, the Science and Technology Program of Guangzhou, China, the Project of Special Research on Cardiovascular Diseases, the Research Foundation of Medical Science and Technology of Guangdong Province, the University of Melbourne at Research Accelerator Program, and the CERA (Centre for Eye Research Australia) Foundation and Victorian State Government for the Centre for Eye Research Australia. The investigators and Dr. Vahia have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
E-health program improves perinatal depression
Patients with perinatal depression who used a specialized online tool showed improvement in symptoms, compared with controls who received routine care, based on data from 191 individuals.
Although perinatal depression affects approximately 17% of pregnant women and 13% of postpartum women, the condition is often underrecognized and undertreated, Brian Danaher, PhD, of Influents Innovations, Eugene, Ore., and colleagues wrote. Meta-analyses have shown that e-health interventions based on cognitive-behavioral therapy (CBT) can improve depression in general and perinatal depression in particular.
An e-health program known as the MomMoodBooster has demonstrated effectiveness at reducing postpartum depression, and the researchers evaluated the effectiveness of a perinatal version.
In a study published in the American Journal of Obstetrics & Gynecology, the researchers randomized 95 pregnant women and 96 postpartum women who met screening criteria for depression to routine care for perinatal depression, which included a 24/7 crisis hotline and a referral network or PDP plus a version of the MomMoodBooster with a perinatal depression component (MMB2). Participants were aged 18 and older, with no active suicidal ideation. The average age was 32 years; 84% were non-Hispanic, 67% were White, and 94% were married or in a long-term relationship. During the 12 weeks, each of six sessions became accessible online in sequence.
The primary endpoint was the change in outcomes at 12 weeks after the start of the program, with depressive symptom severity measured using the Patient Health Questionnaire (PHQ-9). Anxiety was assessed as a secondary outcome by using the Depression Anxiety Stress Scale. The minimal clinically important difference (MCID) was used to evaluate clinical significance, and was defined as a reduction in PHQ-9 of at least 5 points from baseline.
After controlling for perinatal status at baseline and assessment time, the MMB2 group had significantly greater decreases in depression severity and stress compared with the routine care group. In addition, based on MCID, significantly more women in the MMB2 group showed improvements in depression, compared with the routine care group (43% vs. 26%; odds ratio, 2.12; P = .015).
A total of 88 of the 89 women in the MMB2 group accessed the sessions, and approximately half (49%) viewed all six sessions.
Of the women who used the MMB2 program, 96% said that it was easy to use, 93% said they would recommend it, and 83% said it was helpful to them.
The study findings were limited by several factors including the lack of long-term follow-up data and inability to determine the durability of the treatment effects, the researchers noted. Another key limitation is the demographics of the study population (slightly older and a greater proportion of White individuals than the national average), which may not be representative of all perinatal women in the United States.
However, the results are consistent with findings from previous studies, including meta-analyses of CBT-based programs, the researchers wrote.
“When used in a largely self-directed approach, MMB2 could fill the gap when in-person treatment options are limited as well as for women whose circumstances (COVID) and/or concerns (stigma, costs) reduce the acceptability of in-person help,” they said. Use of e-health programs such as MMB2 could increase the scope of treatment for perinatal depression.
Expanding e-health options may improve outcomes and reduce disparities
Perinatal and postpartum depression is one of the most common conditions affecting pregnancy, Lisette D. Tanner, MD, of Emory University, Atlanta, said in an interview. “Depression can have serious consequences for both maternal and neonatal well-being, including preterm birth, low birth weight, and poor bonding, as well as delayed emotional and cognitive development of the newborn.
“While clinicians are encouraged to screen patients during and after pregnancy for signs and symptoms of depression, once identified, the availability of effective treatment is limited. Access to mental health resources is a long-standing disparity in medicine, and therefore research investigating readily available e-health treatment strategies is critically important,” said Dr. Tanner, who was not involved in the study.
In the current study, “I was surprised by the number of patients who saw a clinically significant improvement in depression scores in such a short period of time. An average of only 20 days elapsed between baseline and post-test scores and almost 43% of patients showed improvement. Mental health interventions typically take longer to demonstrate an effect, both medication and talk therapies,” she said.
“The largest barrier to adoption of any e-health modality into clinical practice is often the cost of implementation and maintaining infrastructure,” said Dr. Tanner. “A cost-effectiveness analysis of this intervention would be helpful to better delineate the value of such of program in comparison to more traditional treatments.”
More research is needed on the effectiveness of the intervention for specific populations, such as groups with lower socioeconomic status and patients with chronic mood disorders, Dr. Tanner said. “Additionally, introducing the program in locations with limited access to mental health resources would support more widespread implementation.”
The study was supported by the National Institutes of Mental Health. The researchers had no financial conflicts to disclose. Dr. Tanner had no financial conflicts to disclose.
Patients with perinatal depression who used a specialized online tool showed improvement in symptoms, compared with controls who received routine care, based on data from 191 individuals.
Although perinatal depression affects approximately 17% of pregnant women and 13% of postpartum women, the condition is often underrecognized and undertreated, Brian Danaher, PhD, of Influents Innovations, Eugene, Ore., and colleagues wrote. Meta-analyses have shown that e-health interventions based on cognitive-behavioral therapy (CBT) can improve depression in general and perinatal depression in particular.
An e-health program known as the MomMoodBooster has demonstrated effectiveness at reducing postpartum depression, and the researchers evaluated the effectiveness of a perinatal version.
In a study published in the American Journal of Obstetrics & Gynecology, the researchers randomized 95 pregnant women and 96 postpartum women who met screening criteria for depression to routine care for perinatal depression, which included a 24/7 crisis hotline and a referral network or PDP plus a version of the MomMoodBooster with a perinatal depression component (MMB2). Participants were aged 18 and older, with no active suicidal ideation. The average age was 32 years; 84% were non-Hispanic, 67% were White, and 94% were married or in a long-term relationship. During the 12 weeks, each of six sessions became accessible online in sequence.
The primary endpoint was the change in outcomes at 12 weeks after the start of the program, with depressive symptom severity measured using the Patient Health Questionnaire (PHQ-9). Anxiety was assessed as a secondary outcome by using the Depression Anxiety Stress Scale. The minimal clinically important difference (MCID) was used to evaluate clinical significance, and was defined as a reduction in PHQ-9 of at least 5 points from baseline.
After controlling for perinatal status at baseline and assessment time, the MMB2 group had significantly greater decreases in depression severity and stress compared with the routine care group. In addition, based on MCID, significantly more women in the MMB2 group showed improvements in depression, compared with the routine care group (43% vs. 26%; odds ratio, 2.12; P = .015).
A total of 88 of the 89 women in the MMB2 group accessed the sessions, and approximately half (49%) viewed all six sessions.
Of the women who used the MMB2 program, 96% said that it was easy to use, 93% said they would recommend it, and 83% said it was helpful to them.
The study findings were limited by several factors including the lack of long-term follow-up data and inability to determine the durability of the treatment effects, the researchers noted. Another key limitation is the demographics of the study population (slightly older and a greater proportion of White individuals than the national average), which may not be representative of all perinatal women in the United States.
However, the results are consistent with findings from previous studies, including meta-analyses of CBT-based programs, the researchers wrote.
“When used in a largely self-directed approach, MMB2 could fill the gap when in-person treatment options are limited as well as for women whose circumstances (COVID) and/or concerns (stigma, costs) reduce the acceptability of in-person help,” they said. Use of e-health programs such as MMB2 could increase the scope of treatment for perinatal depression.
Expanding e-health options may improve outcomes and reduce disparities
Perinatal and postpartum depression is one of the most common conditions affecting pregnancy, Lisette D. Tanner, MD, of Emory University, Atlanta, said in an interview. “Depression can have serious consequences for both maternal and neonatal well-being, including preterm birth, low birth weight, and poor bonding, as well as delayed emotional and cognitive development of the newborn.
“While clinicians are encouraged to screen patients during and after pregnancy for signs and symptoms of depression, once identified, the availability of effective treatment is limited. Access to mental health resources is a long-standing disparity in medicine, and therefore research investigating readily available e-health treatment strategies is critically important,” said Dr. Tanner, who was not involved in the study.
In the current study, “I was surprised by the number of patients who saw a clinically significant improvement in depression scores in such a short period of time. An average of only 20 days elapsed between baseline and post-test scores and almost 43% of patients showed improvement. Mental health interventions typically take longer to demonstrate an effect, both medication and talk therapies,” she said.
“The largest barrier to adoption of any e-health modality into clinical practice is often the cost of implementation and maintaining infrastructure,” said Dr. Tanner. “A cost-effectiveness analysis of this intervention would be helpful to better delineate the value of such of program in comparison to more traditional treatments.”
More research is needed on the effectiveness of the intervention for specific populations, such as groups with lower socioeconomic status and patients with chronic mood disorders, Dr. Tanner said. “Additionally, introducing the program in locations with limited access to mental health resources would support more widespread implementation.”
The study was supported by the National Institutes of Mental Health. The researchers had no financial conflicts to disclose. Dr. Tanner had no financial conflicts to disclose.
Patients with perinatal depression who used a specialized online tool showed improvement in symptoms, compared with controls who received routine care, based on data from 191 individuals.
Although perinatal depression affects approximately 17% of pregnant women and 13% of postpartum women, the condition is often underrecognized and undertreated, Brian Danaher, PhD, of Influents Innovations, Eugene, Ore., and colleagues wrote. Meta-analyses have shown that e-health interventions based on cognitive-behavioral therapy (CBT) can improve depression in general and perinatal depression in particular.
An e-health program known as the MomMoodBooster has demonstrated effectiveness at reducing postpartum depression, and the researchers evaluated the effectiveness of a perinatal version.
In a study published in the American Journal of Obstetrics & Gynecology, the researchers randomized 95 pregnant women and 96 postpartum women who met screening criteria for depression to routine care for perinatal depression, which included a 24/7 crisis hotline and a referral network or PDP plus a version of the MomMoodBooster with a perinatal depression component (MMB2). Participants were aged 18 and older, with no active suicidal ideation. The average age was 32 years; 84% were non-Hispanic, 67% were White, and 94% were married or in a long-term relationship. During the 12 weeks, each of six sessions became accessible online in sequence.
The primary endpoint was the change in outcomes at 12 weeks after the start of the program, with depressive symptom severity measured using the Patient Health Questionnaire (PHQ-9). Anxiety was assessed as a secondary outcome by using the Depression Anxiety Stress Scale. The minimal clinically important difference (MCID) was used to evaluate clinical significance, and was defined as a reduction in PHQ-9 of at least 5 points from baseline.
After controlling for perinatal status at baseline and assessment time, the MMB2 group had significantly greater decreases in depression severity and stress compared with the routine care group. In addition, based on MCID, significantly more women in the MMB2 group showed improvements in depression, compared with the routine care group (43% vs. 26%; odds ratio, 2.12; P = .015).
A total of 88 of the 89 women in the MMB2 group accessed the sessions, and approximately half (49%) viewed all six sessions.
Of the women who used the MMB2 program, 96% said that it was easy to use, 93% said they would recommend it, and 83% said it was helpful to them.
The study findings were limited by several factors including the lack of long-term follow-up data and inability to determine the durability of the treatment effects, the researchers noted. Another key limitation is the demographics of the study population (slightly older and a greater proportion of White individuals than the national average), which may not be representative of all perinatal women in the United States.
However, the results are consistent with findings from previous studies, including meta-analyses of CBT-based programs, the researchers wrote.
“When used in a largely self-directed approach, MMB2 could fill the gap when in-person treatment options are limited as well as for women whose circumstances (COVID) and/or concerns (stigma, costs) reduce the acceptability of in-person help,” they said. Use of e-health programs such as MMB2 could increase the scope of treatment for perinatal depression.
Expanding e-health options may improve outcomes and reduce disparities
Perinatal and postpartum depression is one of the most common conditions affecting pregnancy, Lisette D. Tanner, MD, of Emory University, Atlanta, said in an interview. “Depression can have serious consequences for both maternal and neonatal well-being, including preterm birth, low birth weight, and poor bonding, as well as delayed emotional and cognitive development of the newborn.
“While clinicians are encouraged to screen patients during and after pregnancy for signs and symptoms of depression, once identified, the availability of effective treatment is limited. Access to mental health resources is a long-standing disparity in medicine, and therefore research investigating readily available e-health treatment strategies is critically important,” said Dr. Tanner, who was not involved in the study.
In the current study, “I was surprised by the number of patients who saw a clinically significant improvement in depression scores in such a short period of time. An average of only 20 days elapsed between baseline and post-test scores and almost 43% of patients showed improvement. Mental health interventions typically take longer to demonstrate an effect, both medication and talk therapies,” she said.
“The largest barrier to adoption of any e-health modality into clinical practice is often the cost of implementation and maintaining infrastructure,” said Dr. Tanner. “A cost-effectiveness analysis of this intervention would be helpful to better delineate the value of such of program in comparison to more traditional treatments.”
More research is needed on the effectiveness of the intervention for specific populations, such as groups with lower socioeconomic status and patients with chronic mood disorders, Dr. Tanner said. “Additionally, introducing the program in locations with limited access to mental health resources would support more widespread implementation.”
The study was supported by the National Institutes of Mental Health. The researchers had no financial conflicts to disclose. Dr. Tanner had no financial conflicts to disclose.
FROM THE AMERICAN JOURNAL OF OBSTETRICS & GYNECOLOGY
Suicide notes offer ‘unique window’ into motives, risks in the elderly
A new analysis of notes penned by seniors who died by suicide reveals several common themes. These include feeling as if they were a burden, feelings of guilt, experiencing mental illness, loneliness, or isolation, as well as poor health and/or disability.
“The most important message [in our findings] is that there is hope,” study investigator Ari B. Cuperfain, MD, Temerty Faculty of Medicine, University of Toronto, told this news organization.
“Suicide risk is modifiable, and we encourage that care providers sensitively explore thoughts of suicide in patients expressing depressive thoughts or difficulty coping with other life stressors,” he said.
The study was published online in The American Journal of Geriatric Psychiatry.
Opportunity for intervention
Most previous studies of late-life suicide have focused on risk factors rather than the themes and meaning underlying individuals’ distress.
Dr. Cuperfain’s group had previously analyzed suicide notes to “explore the relationship between suicide and an individual’s experience with mental health care in all age groups,” he said. For the current study, the investigators analyzed the subset of notes written exclusively by older adults.
The researchers “hypothesized that suicide notes could provide a unique window into the thought processes of older adults during a critical window for mental health intervention,” he added.
Although effective screening for suicidality in older adults can mitigate suicide risk, the frequency of suicide screening decreases with increasing age, the authors noted.
In addition, suicide attempts are typically more often fatal in older adults than in the general population. Understanding the motivations for suicide in this vulnerable population can inform potential interventions.
The researchers used a constructivist grounded theory framework to analyze suicide notes available from their previous study and notes obtained from the Office of the Coroner in Toronto from adults aged 65 years and older (n = 29; mean [SD], age 76.2 [8.3] years; 79% men).
The investigators began with open coding of the notes, “specifying a short name to a segment of data that summarizes and accounts for each piece of data.” They then used a series of techniques to identify terms and themes (repeated patterns of ideas reflected in the data).
Once themes had been determined, they identified “pathways between these themes and the final act of suicide.”
Common themes
Four major themes emerged in the analysis of the suicide notes.
Recurring terms included “pain,” “[poor] sleep,” or “[wakeful] nights,” as well as “sorry” (either about past actions or about the suicide), and “I just can’t” (referring to the inability to carry on).
The suicide notes “provided the older writers’ conceptual schema for suicide, elucidating the cognitive process linking their narratives to the acts of suicide.” Examples included the following:
- Suicide as a way out or solution to an insoluble problem.
- Suicide as the final act in a long road of suffering.
- Suicide as the logical culmination of life (the person “lived a good life”).
“Our study enriches the understanding of ‘why’ rather than just ‘which’ older adults die by suicide,” the authors noted.
“Care providers can help older adults at risk of suicide through a combination of treatment options. These include physician involvement to manage depression, psychosis, or pain, psychotherapy to reframe certain ways of thinking, or social activities to reduce isolation,” Dr. Cuperfain said.
“By understanding the experiences of older adults and what is underlying their suicidal thoughts, these interventions can be tailored specifically for the individual experiencing distress,” he added.
Untangling suicide drivers
Commenting on the study, Yeates Conwell, MD, professor and vice chair, department of psychiatry, University of Rochester (N.Y.) Medical Center, said that “by analyzing the suicide notes of older people who died by suicide, the paper lends a unique perspective to our understanding of why they may have taken their lives.”

Dr. Conwell, director of the geriatric psychiatry program and codirector of the Center for the Study and Prevention of Suicide, University of Rochester, and author of an accompanying editorial, said that “by including the decedent’s own voice, the analysis of notes is a useful complement to other approaches used for the study of suicide in this age group”.
However, “like all other approaches, it is subject to potential biases in interpretation. The meaning in the notes must be derived with careful consideration of context, both what is said and what is not said, and the likelihood that both overt and covert messages are contained in and between their lines,” cautioned Dr. Conwell.
“Acknowledging the strength and limitations of each approach to the study of suicide death, together they can help untangle its drivers and support the search for effective, acceptable, and scalable prevention interventions. No one approach alone, however, will reveal the ‘cause’ of suicide,” Dr. Conwell wrote.
No source of study funding was provided. Dr. Cuperfain reports no relevant financial relationships. The other authors’ disclosures are listed on the original article. Dr. Conwell reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new analysis of notes penned by seniors who died by suicide reveals several common themes. These include feeling as if they were a burden, feelings of guilt, experiencing mental illness, loneliness, or isolation, as well as poor health and/or disability.
“The most important message [in our findings] is that there is hope,” study investigator Ari B. Cuperfain, MD, Temerty Faculty of Medicine, University of Toronto, told this news organization.
“Suicide risk is modifiable, and we encourage that care providers sensitively explore thoughts of suicide in patients expressing depressive thoughts or difficulty coping with other life stressors,” he said.
The study was published online in The American Journal of Geriatric Psychiatry.
Opportunity for intervention
Most previous studies of late-life suicide have focused on risk factors rather than the themes and meaning underlying individuals’ distress.
Dr. Cuperfain’s group had previously analyzed suicide notes to “explore the relationship between suicide and an individual’s experience with mental health care in all age groups,” he said. For the current study, the investigators analyzed the subset of notes written exclusively by older adults.
The researchers “hypothesized that suicide notes could provide a unique window into the thought processes of older adults during a critical window for mental health intervention,” he added.
Although effective screening for suicidality in older adults can mitigate suicide risk, the frequency of suicide screening decreases with increasing age, the authors noted.
In addition, suicide attempts are typically more often fatal in older adults than in the general population. Understanding the motivations for suicide in this vulnerable population can inform potential interventions.
The researchers used a constructivist grounded theory framework to analyze suicide notes available from their previous study and notes obtained from the Office of the Coroner in Toronto from adults aged 65 years and older (n = 29; mean [SD], age 76.2 [8.3] years; 79% men).
The investigators began with open coding of the notes, “specifying a short name to a segment of data that summarizes and accounts for each piece of data.” They then used a series of techniques to identify terms and themes (repeated patterns of ideas reflected in the data).
Once themes had been determined, they identified “pathways between these themes and the final act of suicide.”
Common themes
Four major themes emerged in the analysis of the suicide notes.
Recurring terms included “pain,” “[poor] sleep,” or “[wakeful] nights,” as well as “sorry” (either about past actions or about the suicide), and “I just can’t” (referring to the inability to carry on).
The suicide notes “provided the older writers’ conceptual schema for suicide, elucidating the cognitive process linking their narratives to the acts of suicide.” Examples included the following:
- Suicide as a way out or solution to an insoluble problem.
- Suicide as the final act in a long road of suffering.
- Suicide as the logical culmination of life (the person “lived a good life”).
“Our study enriches the understanding of ‘why’ rather than just ‘which’ older adults die by suicide,” the authors noted.
“Care providers can help older adults at risk of suicide through a combination of treatment options. These include physician involvement to manage depression, psychosis, or pain, psychotherapy to reframe certain ways of thinking, or social activities to reduce isolation,” Dr. Cuperfain said.
“By understanding the experiences of older adults and what is underlying their suicidal thoughts, these interventions can be tailored specifically for the individual experiencing distress,” he added.
Untangling suicide drivers
Commenting on the study, Yeates Conwell, MD, professor and vice chair, department of psychiatry, University of Rochester (N.Y.) Medical Center, said that “by analyzing the suicide notes of older people who died by suicide, the paper lends a unique perspective to our understanding of why they may have taken their lives.”
Dr. Conwell, director of the geriatric psychiatry program and codirector of the Center for the Study and Prevention of Suicide, University of Rochester, and author of an accompanying editorial, said that “by including the decedent’s own voice, the analysis of notes is a useful complement to other approaches used for the study of suicide in this age group”.
However, “like all other approaches, it is subject to potential biases in interpretation. The meaning in the notes must be derived with careful consideration of context, both what is said and what is not said, and the likelihood that both overt and covert messages are contained in and between their lines,” cautioned Dr. Conwell.
“Acknowledging the strength and limitations of each approach to the study of suicide death, together they can help untangle its drivers and support the search for effective, acceptable, and scalable prevention interventions. No one approach alone, however, will reveal the ‘cause’ of suicide,” Dr. Conwell wrote.
No source of study funding was provided. Dr. Cuperfain reports no relevant financial relationships. The other authors’ disclosures are listed on the original article. Dr. Conwell reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new analysis of notes penned by seniors who died by suicide reveals several common themes. These include feeling as if they were a burden, feelings of guilt, experiencing mental illness, loneliness, or isolation, as well as poor health and/or disability.
“The most important message [in our findings] is that there is hope,” study investigator Ari B. Cuperfain, MD, Temerty Faculty of Medicine, University of Toronto, told this news organization.
“Suicide risk is modifiable, and we encourage that care providers sensitively explore thoughts of suicide in patients expressing depressive thoughts or difficulty coping with other life stressors,” he said.
The study was published online in The American Journal of Geriatric Psychiatry.
Opportunity for intervention
Most previous studies of late-life suicide have focused on risk factors rather than the themes and meaning underlying individuals’ distress.
Dr. Cuperfain’s group had previously analyzed suicide notes to “explore the relationship between suicide and an individual’s experience with mental health care in all age groups,” he said. For the current study, the investigators analyzed the subset of notes written exclusively by older adults.
The researchers “hypothesized that suicide notes could provide a unique window into the thought processes of older adults during a critical window for mental health intervention,” he added.
Although effective screening for suicidality in older adults can mitigate suicide risk, the frequency of suicide screening decreases with increasing age, the authors noted.
In addition, suicide attempts are typically more often fatal in older adults than in the general population. Understanding the motivations for suicide in this vulnerable population can inform potential interventions.
The researchers used a constructivist grounded theory framework to analyze suicide notes available from their previous study and notes obtained from the Office of the Coroner in Toronto from adults aged 65 years and older (n = 29; mean [SD], age 76.2 [8.3] years; 79% men).
The investigators began with open coding of the notes, “specifying a short name to a segment of data that summarizes and accounts for each piece of data.” They then used a series of techniques to identify terms and themes (repeated patterns of ideas reflected in the data).
Once themes had been determined, they identified “pathways between these themes and the final act of suicide.”
Common themes
Four major themes emerged in the analysis of the suicide notes.
Recurring terms included “pain,” “[poor] sleep,” or “[wakeful] nights,” as well as “sorry” (either about past actions or about the suicide), and “I just can’t” (referring to the inability to carry on).
The suicide notes “provided the older writers’ conceptual schema for suicide, elucidating the cognitive process linking their narratives to the acts of suicide.” Examples included the following:
- Suicide as a way out or solution to an insoluble problem.
- Suicide as the final act in a long road of suffering.
- Suicide as the logical culmination of life (the person “lived a good life”).
“Our study enriches the understanding of ‘why’ rather than just ‘which’ older adults die by suicide,” the authors noted.
“Care providers can help older adults at risk of suicide through a combination of treatment options. These include physician involvement to manage depression, psychosis, or pain, psychotherapy to reframe certain ways of thinking, or social activities to reduce isolation,” Dr. Cuperfain said.
“By understanding the experiences of older adults and what is underlying their suicidal thoughts, these interventions can be tailored specifically for the individual experiencing distress,” he added.
Untangling suicide drivers
Commenting on the study, Yeates Conwell, MD, professor and vice chair, department of psychiatry, University of Rochester (N.Y.) Medical Center, said that “by analyzing the suicide notes of older people who died by suicide, the paper lends a unique perspective to our understanding of why they may have taken their lives.”
Dr. Conwell, director of the geriatric psychiatry program and codirector of the Center for the Study and Prevention of Suicide, University of Rochester, and author of an accompanying editorial, said that “by including the decedent’s own voice, the analysis of notes is a useful complement to other approaches used for the study of suicide in this age group”.
However, “like all other approaches, it is subject to potential biases in interpretation. The meaning in the notes must be derived with careful consideration of context, both what is said and what is not said, and the likelihood that both overt and covert messages are contained in and between their lines,” cautioned Dr. Conwell.
“Acknowledging the strength and limitations of each approach to the study of suicide death, together they can help untangle its drivers and support the search for effective, acceptable, and scalable prevention interventions. No one approach alone, however, will reveal the ‘cause’ of suicide,” Dr. Conwell wrote.
No source of study funding was provided. Dr. Cuperfain reports no relevant financial relationships. The other authors’ disclosures are listed on the original article. Dr. Conwell reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF GERIATRIC PSYCHIATRY
Mental Health Outcomes Among Transgender Veterans and Active-Duty Service Members in the United States: A Systematic Review
According to the United States Transgender Survey, 39% of respondents reported experiencing serious psychological distress (based on the Kessler 6 Psychological Distress Scale) in the past 30 days compared with 5% in the general population.1 Additionally, 40% of respondents attempted suicide in their lifetime, compared with 5% in the general population.1 Almost half of respondents reported being sexually assaulted at some time in their life, and 10% reported being sexually assaulted in the past year.1
Studies have also shown that veterans and active-duty service members experience worse mental health outcomes and are at increased risk for suicide than civilians and nonveterans.2-5 About 1 in 4 active-duty service members meet the criteria for diagnosis of a mental illness.4 Service members were found to have higher rates of probable anxiety and posttraumatic stress disorder (PTSD) compared with the general population.2,6 In 2018, veteran suicide deaths accounted for about 13% of all deaths by suicide in the US even though veterans only accounted for about 7% of the adult population in that year.5,7 Also in 2018, about 17 veterans committed suicide per day.5 According to the Health Related Behaviors Survey of active-duty service members, about 18% reported thinking about attempting suicide some time in their lives compared with 4% of the general population.2,3 Additionally, 5% of service members reported previous suicide attempts compared with 0.5% in the general population.2,3 It is clear that transgender individuals, veterans, and service members have certain mental health outcomes that are worse than that of the general population.1-7
Transgender individuals along with LGB (lesbian, gay, bisexual) individuals have long faced discrimination and unfair treatment in the military.8-11 In the 1920s, the first written policies were established that banned gay men from serving in the military.9 The US Department of Defense (DoD) continued these policies until in 1993, the “Don’t Ask Don’t Tell” policy was established, which had the façade of being more inclusive for LGB individuals but forced LGB service members to hide their sexual identity and continued the anti-LGBTQ messages that previous policies had created.8,10,11 In 2010, “Don’t Ask Don’t Tell” was repealed, which allowed LGB individuals to serve in the military without concealing their sexual orientation and without fear of discharge based on their sexual identity.11 This repeal did not allow transgender individuals to serve their country as the DoD categorized transgender identity as a medical and mental health disorder.8,11
In 2016, the ban on transgender individuals serving in the military was lifted, and service members could no longer be discharged or turned away from joining the military based on gender identity.8,12 However, in 2018, this order was reversed. The new policy stated that new service members must meet requirements and standards of their sex assigned at birth, and individuals with a history of gender dysphoria or those who have received gender-affirming medical or surgical treatment were prohibited to serve in the military.8,13 This policy did not apply to service members who joined before it took effect. Finally, in April 2021, the current policy took effect, permitting transgender individuals to openly serve in the military. The current policy states that service members cannot be discharged or denied reenlistment based on their gender identity and provides support to receive gender-affirming medical care.14 Although transgender individuals are now accepted in military service, there is still much progress needed to promote equity among transgender service members.
In 2015, according to the Health Related Behaviors Survey of active-duty service members, 0.6% of service members identified as transgender, the same percentage as US adults who identify as transgender.2,15 Previous research has shown that the prevalence of gender identity disorder among veterans is higher than that among the general US population.16 Many studies have shown that worse mental health outcomes exist among LGBTQ veterans and service members compared with heterosexual, cisgender veterans and service members.17-24 However, fewer studies have focused solely on mental health outcomes among transgender veterans and active-duty service members, and there exists no current literature review on this topic. In this article, we present data from the existing literature on mental health outcomes in transgender veterans and active-duty service members. We hypothesize, based on the current literature, that transgender veterans and service members have worse mental health outcomes than their cisgender counterparts. Key terms used in this paper are defined in the Key Definitions.25-27
Methods
We conducted a systematic review of articles presenting data on mental health outcomes in transgender veterans and active-duty service members. The National Library of Medicine PubMed database was searched using the following search terms in various combinations: mental health outcomes, transgender, veterans, military, active duty, substance use, and sexual trauma. The literature search was performed in August 2021 and included articles published through July 31, 2021. Methodology, size, demographics, measures, and main findings were extracted from each article. All studies were eligible for inclusion regardless of sample size. Studies that examined the LGBTQ population without separating transgender individuals were excluded. Studies that examined mental health outcomes including, but not limited to, PTSD, depression, suicidality, anxiety, and substance use disorders (SUDs) in addition to sexual trauma were included. Studies that only examined physical health outcomes were excluded. Qualitative studies, case reports, and papers that did not present original data were excluded (Figure).
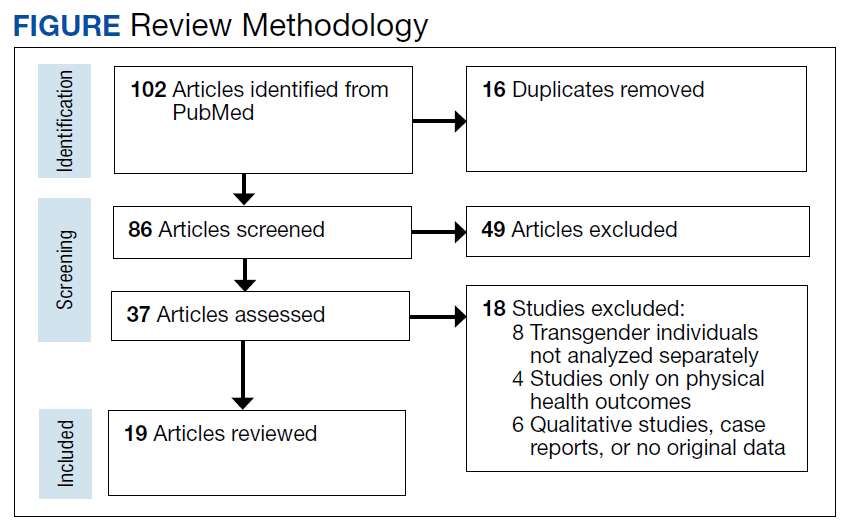
Results
Our search resulted in 86 publications. After excluding 65 articles that did not meet the inclusion criteria, 19 studies were included in this review. The Appendix shows the summary of findings from each study, including the study size and results. All studies were conducted in the United States. Most papers used a cross-sectional study design. Most of the studies focused on transgender veterans, but some included data on transgender active-duty service members.
We separated the findings into the following categories based on the variables measured: mental health, including depression, anxiety, PTSD, and serious mental illness; suicidality and self-harm; substance use; and military sexual trauma (MST). Many studies overlapped multiple categories.
Mental Health
Most of the studies included reported that transgender veterans have statistically significant worse mental health outcomes compared with cisgender veterans.28-30 In addition, transgender active-duty service members were found to have worse mental health outcomes than cisgender active-duty service members.31 MST and discrimination were associated with worse mental health outcomes among transgender veterans.32,33 One study showed a different result than others and found that transgender older adults with prior military service had higher psychological health-related quality of life and lower depressive symptoms than those without prior military service (P = .02 and .04, respectively).34 Another study compared transgender veterans with active-duty service members and found that transgender veterans reported higher rates of depression (64.6% vs 30.9%; χ2 = 11.68; P = .001) and anxiety (41.3% vs 18.2%; χ2 = 6.54; P = .01) compared with transgender service members.35
Suicidality and Self-harm
Eleven of the 19 studies included measured suicidality and/or self-harm as an outcome. Transgender veterans and active-duty service members were found to have higher odds of suicidality than their cisgender counterparts.16,28,29,31 In addition, transgender veterans may die by suicide at a younger age than cisgender veterans.36 Stigma and gender-related discrimination were found to be associated with suicidal ideation.33,37-39 Transgender veterans were less likely than transgender nonveterans to report nonsuicidal self-injury (NSSI).40
Substance Use
Two studies focused on substance use, while 5 other studies included substance use in their measures. One of these 2 studies that focused only on substance use outcomes found that transgender veterans were more likely than cisgender veterans to have any SUD (7.2% vs 3.9%; P < .001), in addition to specifically cannabis (3.4% vs 1.5%; P < .001), amphetamine (1.1% vs 0.3%; P < .001), and cocaine use disorders (1.5% vs 1.1%; P < .001).41
Another study reported that transgender veterans had lower odds of self-reported alcohol use but had greater odds of having alcohol-related diagnoses compared with cisgender veterans.42 Of the other studies, it was found that a higher percentage of transgender veterans were diagnosed with an SUD compared with transgender active-duty service members, and transgender veterans were more likely than cisgender veterans to be diagnosed with alcohol use disorder.29,31 Additionally, rural transgender veterans had increased odds of tobacco use disorder compared with transgender veterans who lived in urban areas.43
Military Sexual Trauma
Five of the studies included examined MST, defined as sexual assault or sexual harassment that is experienced during military service.44 Studies found that 15% to 17% of transgender veterans experienced MST.32,45 Transgender veterans were more likely to report MST than cisgender veterans.28,29 MST was found to be consistently associated with depression and PTSD.32,45 A high percentage (83.9%) of transgender active-duty service members reported experiencing sexual harassment and almost one-third experienced sexual assault.46
Discussion
Outcomes examined in this review included MST, substance use, suicidality, and symptoms of depression, anxiety, and PTSD among transgender active-duty service members and veterans. To our knowledge, no other review on this topic exists. There is a review of the health and well-being of LGBTQ veterans and service members, but a majority of the included studies did not separate transgender individuals from LGB persons.17 This review of transgender individuals showed similar results to the review of LGBTQ individuals.17 This review also presented similar results to previous studies that indicated that transgender individuals in the general population have worse mental health outcomes compared with their cisgender counterparts, in addition to studies that showed that veterans and active-duty service members have worse mental health outcomes compared with civilians and nonveterans.1-5 The population of focus in this review faced a unique set of challenges, being that they belonged to both of these subsets of the population, both of which experienced worse mental health outcomes, according to the literature.
Studies included in our review found that transgender veterans and service members have worse mental health outcomes than cisgender veterans and service members.28-31 This outcome was predicted based on previous data collection among transgender individuals, veterans, and active-duty service members. One of the studies included found different results and concluded that prior military service was a protective factor against poorer mental health outcomes.34 This could be, in part, due to veterans’ access to care through the US Department of Veterans Affairs (VA) system. It has been found that transgender veterans use VA services at higher rates than the general population of veterans and that barriers to care were found more for medical treatment than for mental health treatment.47 One study found that almost 70% of transgender veterans who used VA services were satisfied with their mental health care.48 In contrast, another study included in our review found that transgender veterans had worse mental health outcomes than transgender service members, possibly showing that even with access to care, the burden of stigma and discrimination worsens mental health over time.31 Although it has been shown that transgender veterans may feel comfortable disclosing their gender identity to their health care professional, many barriers to care have been identified, such as insensitivity and lack of knowledge about transgender care among clinicians.49-51 With this information, it would be useful to ensure proper training for health care professionals on providing gender-affirming care.
Most of the studies also found that transgender veterans and service members had greater odds of suicidal thoughts and events than cisgender veterans and service members.16,28,29,35 On the contrary, transgender veterans were less likely than transgender nonveterans to report NSSI, which could be for various reasons.40 Transgender veterans may report less NSSI but experience it at similar rates, or veteran status may be a protective factor for NSSI.
Very few studies included SUDs in their measurements, but it was found that transgender veterans were more likely than cisgender veterans to have any drug and alcohol use disorder.29,41 In addition, transgender veterans were more likely than transgender service members to be diagnosed with an SUD, again showing that over time and after time of service, mental health may worsen due to the burden of stigma and discrimination.31 Studies that examined MST found that transgender veterans were more likely than cisgender veterans to report MST, which replicates previous data that found high rates of sexual assault experienced among transgender individuals.1,28,29
There is a lack of literature surrounding transgender veterans and active-duty service members, especially with regard to gender-affirming care provided to these populations. To the best of our knowledge, there exists only one original study that examines the effect of gender-affirming hormone therapy and surgery on mental health outcomes among transgender veterans.52 Further research in this area is needed, specifically longitudinal studies examining the effects of gender-affirming medical care on various outcomes, including mental health. Few longitudinal studies exist that examine the mental health effects of gender-affirming hormone therapy on transgender individuals in the general population.53-60 Most of these studies have shown a significant improvement in parameters of depression and anxiety following hormonal treatment, although long-term large follow-up studies to understand whether these improvements persist over time are missing also in the general population. However, as previously described, transgender veterans and service members are a unique subset of the transgender population and require separate data collection. Hence, further research is required to provide optimal care for this population. In addition, early screening for symptoms of mental illness, substance use, and MST is important to providing optimal care.
Limitations
This review was limited due to the lack of data collected from transgender veterans and service members. The studies included did not allow for standardized comparisons and did not use identical measures. Some papers compared transgender veterans with transgender nonveterans, some transgender veterans and/or service members with cisgender veterans and/or service members, and some transgender veterans with transgender service members. There were some consistent results found across the studies, but some studies showed contradictory results or no significant differences within a certain category. It is difficult to compare such different study designs and various participant populations. Additional research is required to verify and replicate these results.
Conclusions
Although this review was limited due to the lack of consistent study designs in the literature examining the mental health of transgender veterans and active-duty service members, overall results showed that transgender veterans and service members experience worse mental health outcomes than their cisgender counterparts. With this knowledge and exploring the history of discrimination that this population has faced, improved systems must be put into place to better serve this population and improve health outcomes. Additional research is required to examine the effects of gender-affirming care on mental health among transgender veterans and service members.
1. James SE, Herman JL, Rankin S, Keisling M, Mottet L, Anafi M. The Report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality. December 2016. Accessed August 22, 2022. https://www.ustranssurvey.org
2. Meadows SO, Engel CC, Collins RL, et al. 2015 Department of Defense Health Related Behaviors Survey (HRBS). Rand Health Q. 2018;8(2):434.
3. Lipari R, Piscopo K, Kroutil LA, Miller GK. Suicidal thoughts and behavior among adults: results from the 2014 National Survey on Drug Use and Health. NSDUH Data Review. 2015:1-14. https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR2-2014/NSDUH-FRR2-2014.pdf
4. Kessler RC, Heeringa SG, Stein MB, et al. Thirty-day prevalence of DSM-IV mental disorders among nondeployed soldiers in the US Army: results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). JAMA Psychiatry. 2014;71(5):504-513. doi:10.1001/jamapsychiatry.2014.28
5. U.S. Department of Veterans Affairs Office of Mental Health and Suicide Prevention. 2020 National Veteran Suicide Prevention Annual Report. November 2020. Accessed August 22, 2022. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
6. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602. doi:10.1001/archpsyc.62.6.593
7. Vespa J. Those who SERVED: America’s veterans from World War II to the war on terror. The United States Census Bureau. June 2, 2020. Accessed August 22, 2022. https://www.census.gov/library/publications/2020/demo/acs-43.html
8. Seibert DC, Keller N, Zapor L, Archer H. Military transgender care. J Am Assoc Nurse Pract. 2020;32(11):764-770. doi:10.1097/JXX.0000000000000519
9. Rigby WC. Military penal law: A brief survey of the 1920 revision of the Articles of War. J Crim Law Criminol. 1921;12(1):84.
10. Department of Defense Directive Number 1332.14: Enlisted Administrative Separations. December 21, 1993. Accessed August 22, 2022. https://biotech.law.lsu.edu/blaw/dodd/corres/pdf/d133214wch1_122193/d133214p.pdf
11. Aford B, Lee SJ. Toward complete inclusion: lesbian, gay, bisexual, and transgender military service members after repeal of Don’t Ask, Don’t Tell. Soc Work. 2016;61(3):257-265. doi:10.1093/sw/sww033
12. Department of Defense Instruction 1300.28: In-Service Transition for Transgender Service Members. June 30, 2016. Accessed August 22, 2022. https://dod.defense.gov/Portals/1/features/2016/0616_policy/DoD-Instruction-1300.28.pdf
13. Department of Defense. Directive-type Memorandum (DTM)-19-004 - Military Service by Transgender Persons and Persons with Gender Dysphoria. March 12. 2019. Accessed August 22, 2022. https://health.mil/Reference-Center/Policies/2020/03/17/Military-Service-by-Transgender-Persons-and-Persons-with-Gender-Dysphoria
14. US Department of Defense Instruction 1300.28: In-Service Transition for Transgender Service Members. April 30, 2021. Accessed August 22, 2022. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/130028p.pdf
15. Flores AR, Herman JL, Gates GJ, Brown TNT. How many adults identify as transgender in the United States? The Williams Institute; 2016. Accessed August 22, 2022. https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/
16. Blosnich JR, Brown GR, Shipherd Phd JC, Kauth M, Piegari RI, Bossarte RM. Prevalence of gender identity disorder and suicide risk among transgender veterans utilizing veterans health administration care. Am J Public Health. 2013;103(10):e27-e32. doi:10.2105/AJPH.2013.301507
17. Mark KM, McNamara KA, Gribble R, et al. The health and well-being of LGBTQ serving and ex-serving personnel: a narrative review. Int Rev Psychiatry. 2019;31(1):75-94. doi:10.1080/09540261.2019.1575190
18. Blosnich J, Foynes MM, Shipherd JC. Health disparities among sexual minority women veterans. J Womens Health (Larchmt). 2013;22(7):631-636. doi:10.1089/jwh.2012.4214
19. Blosnich JR, Bossarte RM, Silenzio VM. Suicidal ideation among sexual minority veterans: results from the 2005-2010 Massachusetts Behavioral Risk Factor Surveillance Survey. Am J Public Health. 2012;102(suppl 1):S44-S47. doi:10.2105/AJPH.2011.300565
20. Blosnich JR, Gordon AJ, Fine MJ. Associations of sexual and gender minority status with health indicators, health risk factors, and social stressors in a national sample of young adults with military experience. Ann Epidemiol. 2015;25(9):661-667. doi:10.1016/j.annepidem.2015.06.001
21. Cochran BN, Balsam K, Flentje A, Malte CA, Simpson T. Mental health characteristics of sexual minority veterans. J Homosex. 2013;60(2-3):419-435. doi:10.1080/00918369.2013.744932
22. Lehavot K, Browne KC, Simpson TL. Examining sexual orientation disparities in alcohol misuse among women veterans. Am J Prev Med. 2014;47(5):554-562. doi:10.1016/j.amepre.2014.07.002
23. Scott RL, Lasiuk GC, Norris CM. Depression in lesbian, gay, and bisexual members of the Canadian Armed Forces. LGBT Health. 2016;3(5):366-372. doi:10.1089/lgbt.2016.0050
24. Wang J, Dey M, Soldati L, Weiss MG, Gmel G, Mohler-Kuo M. Psychiatric disorders, suicidality, and personality among young men by sexual orientation. Eur Psychiatry. 2014;29(8):514-522. doi:10.1016/j.eurpsy.2014.05.001
25. American Psychological Association. Gender. APA Style. September 2019. Updated July 2022. Accessed August 22, 2022. https://apastyle.apa.org/style-grammar-guidelines/bias-free-language/gender
26. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed., American Psychiatric Association; 2013.
27. Deutsch MB. Overview of gender-affirming treatments and procedures. UCSF Transgender Care. June 17, 2016. Accessed August 22, 2022. https://transcare.ucsf.edu/guidelines/overview
28. Brown GR, Jones KT. Health correlates of criminal justice involvement in 4,793 transgender veterans. LGBT Health. 2015;2(4):297-305. doi:10.1089/lgbt.2015.0052
29. Brown GR, Jones KT. Mental health and medical health disparities in 5135 transgender veterans receiving healthcare in the Veterans Health Administration: a case-control study. LGBT Health. 2016;3(2):122-131. doi:10.1089/lgbt.2015.0058
30. Downing J, Conron K, Herman JL, Blosnich JR. Transgender and cisgender US veterans have few health differences. Health Aff (Millwood). 2018;37(7):1160-1168. doi:10.1377/hlthaff.2018.0027
31. Holloway IW, Green D, Pickering C, et al. Mental health and health risk behaviors of active duty sexual minority and transgender service members in the United States military. LGBT Health. 2021;8(2):152-161. doi:10.1089/lgbt.2020.0031
32. Beckman K, Shipherd J, Simpson T, Lehavot K. Military sexual assault in transgender veterans: results from a nationwide survey. J Trauma Stress. 2018;31(2):181-190. doi:10.1002/jts.22280
33. Blosnich JR, Marsiglio MC, Gao S, Gordon AJ, Shipherd JC, Kauth M, Brown GR, Fine MJ. Mental health of transgender veterans in US states with and without discrimination and hate crime legal protection. Am J Public Health. 2016;106(3):534-540. doi:10.2105/AJPH.2015.302981
34. Hoy-Ellis CP, Shiu C, Sullivan KM, Kim HJ, Sturges AM, Fredriksen-Goldsen KI. Prior military service, identity stigma, and mental health among transgender older adults. Gerontologist. 2017;57(suppl 1):S63-S71. doi:10.1093/geront/gnw173
35. Hill BJ, Bouris A, Barnett JT, Walker D. Fit to serve? Exploring mental and physical health and well-being among transgender active-duty service members and veterans in the U.S. military. Transgend Health. 2016;1(1):4-11. Published 2016 Jan 1. doi:10.1089/trgh.2015.0002
36. Blosnich JR, Brown GR, Wojcio S, Jones KT, Bossarte RM. Mortality among veterans with transgender-related diagnoses in the Veterans Health Administration, FY2000-2009. LGBT Health. 2014;1(4):269-276. doi:10.1089/lgbt.2014.0050
37. Carter SP, Allred KM, Tucker RP, Simpson TL, Shipherd JC, Lehavot K. Discrimination and suicidal ideation among transgender veterans: the role of social support and connection. LGBT Health. 2019;6(2):43-50. doi:10.1089/lgbt.2018.0239
38. Lehavot K, Simpson TL, Shipherd JC. Factors associated with suicidality among a national sample of transgender veterans. Suicide Life Threat Behav. 2016;46(5):507-524. doi:10.1111/sltb.12233
39. Tucker RP, Testa RJ, Reger MA, Simpson TL, Shipherd JC, Lehavot K. Current and military-specific gender minority stress factors and their relationship with suicide ideation in transgender veterans. Suicide Life Threat Behav. 2019;49(1):155-166. doi:10.1111/sltb.12432
40. Aboussouan A, Snow A, Cerel J, Tucker RP. Non-suicidal self-injury, suicide ideation, and past suicide attempts: Comparison between transgender and gender diverse veterans and non-veterans. J Affect Disord. 2019;259:186-194. doi:10.1016/j.jad.2019.08.046
41. Frost MC, Blosnich JR, Lehavot K, Chen JA, Rubinsky AD, Glass JE, Williams EC. Disparities in documented drug use disorders between transgender and cisgender U.S. Veterans Health Administration patients. J Addict Med. 2021;15(4):334-340. doi:10.1097/ADM.0000000000000769
42. Williams EC, Frost MC, Rubinsky AD, et al. Patterns of alcohol use among transgender patients receiving care at the Veterans Health Administration: overall and relative to nontransgender patients. J Stud Alcohol Drugs. 2021;82(1):132-141. doi:10.15288/jsad.2021.82.132
43. Bukowski LA, Blosnich J, Shipherd JC, Kauth MR, Brown GR, Gordon AJ. Exploring rural disparities in medical diagnoses among veterans with transgender-related diagnoses utilizing Veterans Health Administration care. Med Care. 2017;55(suppl 9):S97-S103. doi:10.1097/MLR.0000000000000745
44. U.S. Department of Veterans Affairs. Military Sexual Trauma. Updated August 1, 2022. Accessed August 22, 2022. https://www.mentalhealth.va.gov/mentalhealth/msthome/index.asp
45. Lindsay JA, Keo-Meier C, Hudson S, Walder A, Martin LA, Kauth MR. Mental health of transgender veterans of the Iraq and Afghanistan conflicts who experienced military sexual trauma. J Trauma Stress. 2016;29(6):563-567. doi:10.1002/jts.22146
46. Schuyler AC, Klemmer C, Mamey MR, et al. Experiences of sexual harassment, stalking, and sexual assault during military service among LGBT and Non-LGBT service members. J Trauma Stress. 2020;33(3):257-266. doi:10.1002/jts.22506
47. Shipherd JC, Mizock L, Maguen S, Green KE. Male-to-female transgender veterans and VA health care utilization. Int J Sexual Health. 2012;24(1):78-87. doi:10.1080/19317611.2011.639440
48. Lehavot K, Katon JG, Simpson TL, Shipherd JC. Transgender veterans’ satisfaction with care and unmet health needs. Med Care. 2017;55(suppl 9):S90-S96. doi:10.1097/MLR.0000000000000723
49. Kauth MR, Barrera TL, Latini DM. Lesbian, gay, and transgender veterans’ experiences in the Veterans Health Administration: positive signs and room for improvement. Psychol Serv. 2019;16(2):346-351. doi:10.1037/ser0000232

50. Rosentel K, Hill BJ, Lu C, Barnett JT. Transgender veterans and the Veterans Health Administration: exploring the experiences of transgender veterans in the Veterans Affairs Healthcare System. Transgend Health. 2016;1(1):108-116. Published 2016 Jun 1. doi:10.1089/trgh.2016.0006
51. Dietert M, Dentice D, Keig Z. Addressing the needs of transgender military veterans: better access and more comprehensive care. Transgend Health. 2017;2(1):35-44. Published 2017 Mar 1. doi:10.1089/trgh.2016.0040
52. Tucker RP, Testa RJ, Simpson TL, Shipherd JC, Blosnich JR, Lehavot K. Hormone therapy, gender affirmation surgery, and their association with recent suicidal ideation and depression symptoms in transgender veterans. Psychol Med. 2018;48(14):2329-2336. doi:10.1017/S0033291717003853
53. Colizzi M, Costa R, Todarello O. Transsexual patients’ psychiatric comorbidity and positive effect of cross-sex hormonal treatment on mental health: results from a longitudinal study. Psychoneuroendocrinology. 2014;39:65-73. doi:10.1016/j.psyneuen.2013.09.029
54. Heylens G, Verroken C, De Cock S, T’Sjoen G, De Cuypere G. Effects of different steps in gender reassignment therapy on psychopathology: a prospective study of persons with a gender identity disorder. J Sex Med. 2014;11(1):119-126. doi:10.1111/jsm.12363
55. Fisher AD, Castellini G, Ristori J, et al. Cross-sex hormone treatment and psychobiological changes in transsexual persons: two-year follow-up data. J Clin Endocrinol Metab. 2016;101(11):4260-4269. doi:10.1210/jc.2016-1276
56. Aldridge Z, Patel S, Guo B, et al. Long-term effect of gender-affirming hormone treatment on depression and anxiety symptoms in transgender people: a prospective cohort study. Andrology. 2021;9(6):1808-1816. doi:10.1111/andr.12884
57. Costantino A, Cerpolini S, Alvisi S, Morselli PG, Venturoli S, Meriggiola MC. A prospective study on sexual function and mood in female-to-male transsexuals during testosterone administration and after sex reassignment surgery. J Sex Marital Ther. 2013;39(4):321-335. doi:10.1080/0092623X.2012.736920
58. Keo-Meier CL, Herman LI, Reisner SL, Pardo ST, Sharp C, Babcock JC. Testosterone treatment and MMPI-2 improvement in transgender men: a prospective controlled study. J Consult Clin Psychol. 2015;83(1):143-156. doi:10.1037/a0037599
59. Turan S‚ , Aksoy Poyraz C, Usta Sag˘lam NG, et al. Alterations in body uneasiness, eating attitudes, and psychopathology before and after cross-sex hormonal treatment in patients with female-to-male gender dysphoria. Arch Sex Behav. 2018;47(8):2349-2361. doi:10.1007/s10508-018-1189-4
60. Oda H, Kinoshita T. Efficacy of hormonal and mental treatments with MMPI in FtM individuals: cross-sectional and longitudinal studies. BMC Psychiatry. 2017;17(1):256. Published 2017 Jul 17. doi:10.1186/s12888-017-1423-y
According to the United States Transgender Survey, 39% of respondents reported experiencing serious psychological distress (based on the Kessler 6 Psychological Distress Scale) in the past 30 days compared with 5% in the general population.1 Additionally, 40% of respondents attempted suicide in their lifetime, compared with 5% in the general population.1 Almost half of respondents reported being sexually assaulted at some time in their life, and 10% reported being sexually assaulted in the past year.1
Studies have also shown that veterans and active-duty service members experience worse mental health outcomes and are at increased risk for suicide than civilians and nonveterans.2-5 About 1 in 4 active-duty service members meet the criteria for diagnosis of a mental illness.4 Service members were found to have higher rates of probable anxiety and posttraumatic stress disorder (PTSD) compared with the general population.2,6 In 2018, veteran suicide deaths accounted for about 13% of all deaths by suicide in the US even though veterans only accounted for about 7% of the adult population in that year.5,7 Also in 2018, about 17 veterans committed suicide per day.5 According to the Health Related Behaviors Survey of active-duty service members, about 18% reported thinking about attempting suicide some time in their lives compared with 4% of the general population.2,3 Additionally, 5% of service members reported previous suicide attempts compared with 0.5% in the general population.2,3 It is clear that transgender individuals, veterans, and service members have certain mental health outcomes that are worse than that of the general population.1-7
Transgender individuals along with LGB (lesbian, gay, bisexual) individuals have long faced discrimination and unfair treatment in the military.8-11 In the 1920s, the first written policies were established that banned gay men from serving in the military.9 The US Department of Defense (DoD) continued these policies until in 1993, the “Don’t Ask Don’t Tell” policy was established, which had the façade of being more inclusive for LGB individuals but forced LGB service members to hide their sexual identity and continued the anti-LGBTQ messages that previous policies had created.8,10,11 In 2010, “Don’t Ask Don’t Tell” was repealed, which allowed LGB individuals to serve in the military without concealing their sexual orientation and without fear of discharge based on their sexual identity.11 This repeal did not allow transgender individuals to serve their country as the DoD categorized transgender identity as a medical and mental health disorder.8,11
In 2016, the ban on transgender individuals serving in the military was lifted, and service members could no longer be discharged or turned away from joining the military based on gender identity.8,12 However, in 2018, this order was reversed. The new policy stated that new service members must meet requirements and standards of their sex assigned at birth, and individuals with a history of gender dysphoria or those who have received gender-affirming medical or surgical treatment were prohibited to serve in the military.8,13 This policy did not apply to service members who joined before it took effect. Finally, in April 2021, the current policy took effect, permitting transgender individuals to openly serve in the military. The current policy states that service members cannot be discharged or denied reenlistment based on their gender identity and provides support to receive gender-affirming medical care.14 Although transgender individuals are now accepted in military service, there is still much progress needed to promote equity among transgender service members.
In 2015, according to the Health Related Behaviors Survey of active-duty service members, 0.6% of service members identified as transgender, the same percentage as US adults who identify as transgender.2,15 Previous research has shown that the prevalence of gender identity disorder among veterans is higher than that among the general US population.16 Many studies have shown that worse mental health outcomes exist among LGBTQ veterans and service members compared with heterosexual, cisgender veterans and service members.17-24 However, fewer studies have focused solely on mental health outcomes among transgender veterans and active-duty service members, and there exists no current literature review on this topic. In this article, we present data from the existing literature on mental health outcomes in transgender veterans and active-duty service members. We hypothesize, based on the current literature, that transgender veterans and service members have worse mental health outcomes than their cisgender counterparts. Key terms used in this paper are defined in the Key Definitions.25-27
Methods
We conducted a systematic review of articles presenting data on mental health outcomes in transgender veterans and active-duty service members. The National Library of Medicine PubMed database was searched using the following search terms in various combinations: mental health outcomes, transgender, veterans, military, active duty, substance use, and sexual trauma. The literature search was performed in August 2021 and included articles published through July 31, 2021. Methodology, size, demographics, measures, and main findings were extracted from each article. All studies were eligible for inclusion regardless of sample size. Studies that examined the LGBTQ population without separating transgender individuals were excluded. Studies that examined mental health outcomes including, but not limited to, PTSD, depression, suicidality, anxiety, and substance use disorders (SUDs) in addition to sexual trauma were included. Studies that only examined physical health outcomes were excluded. Qualitative studies, case reports, and papers that did not present original data were excluded (Figure).
Results
Our search resulted in 86 publications. After excluding 65 articles that did not meet the inclusion criteria, 19 studies were included in this review. The Appendix shows the summary of findings from each study, including the study size and results. All studies were conducted in the United States. Most papers used a cross-sectional study design. Most of the studies focused on transgender veterans, but some included data on transgender active-duty service members.
We separated the findings into the following categories based on the variables measured: mental health, including depression, anxiety, PTSD, and serious mental illness; suicidality and self-harm; substance use; and military sexual trauma (MST). Many studies overlapped multiple categories.
Mental Health
Most of the studies included reported that transgender veterans have statistically significant worse mental health outcomes compared with cisgender veterans.28-30 In addition, transgender active-duty service members were found to have worse mental health outcomes than cisgender active-duty service members.31 MST and discrimination were associated with worse mental health outcomes among transgender veterans.32,33 One study showed a different result than others and found that transgender older adults with prior military service had higher psychological health-related quality of life and lower depressive symptoms than those without prior military service (P = .02 and .04, respectively).34 Another study compared transgender veterans with active-duty service members and found that transgender veterans reported higher rates of depression (64.6% vs 30.9%; χ2 = 11.68; P = .001) and anxiety (41.3% vs 18.2%; χ2 = 6.54; P = .01) compared with transgender service members.35
Suicidality and Self-harm
Eleven of the 19 studies included measured suicidality and/or self-harm as an outcome. Transgender veterans and active-duty service members were found to have higher odds of suicidality than their cisgender counterparts.16,28,29,31 In addition, transgender veterans may die by suicide at a younger age than cisgender veterans.36 Stigma and gender-related discrimination were found to be associated with suicidal ideation.33,37-39 Transgender veterans were less likely than transgender nonveterans to report nonsuicidal self-injury (NSSI).40
Substance Use
Two studies focused on substance use, while 5 other studies included substance use in their measures. One of these 2 studies that focused only on substance use outcomes found that transgender veterans were more likely than cisgender veterans to have any SUD (7.2% vs 3.9%; P < .001), in addition to specifically cannabis (3.4% vs 1.5%; P < .001), amphetamine (1.1% vs 0.3%; P < .001), and cocaine use disorders (1.5% vs 1.1%; P < .001).41
Another study reported that transgender veterans had lower odds of self-reported alcohol use but had greater odds of having alcohol-related diagnoses compared with cisgender veterans.42 Of the other studies, it was found that a higher percentage of transgender veterans were diagnosed with an SUD compared with transgender active-duty service members, and transgender veterans were more likely than cisgender veterans to be diagnosed with alcohol use disorder.29,31 Additionally, rural transgender veterans had increased odds of tobacco use disorder compared with transgender veterans who lived in urban areas.43
Military Sexual Trauma
Five of the studies included examined MST, defined as sexual assault or sexual harassment that is experienced during military service.44 Studies found that 15% to 17% of transgender veterans experienced MST.32,45 Transgender veterans were more likely to report MST than cisgender veterans.28,29 MST was found to be consistently associated with depression and PTSD.32,45 A high percentage (83.9%) of transgender active-duty service members reported experiencing sexual harassment and almost one-third experienced sexual assault.46
Discussion
Outcomes examined in this review included MST, substance use, suicidality, and symptoms of depression, anxiety, and PTSD among transgender active-duty service members and veterans. To our knowledge, no other review on this topic exists. There is a review of the health and well-being of LGBTQ veterans and service members, but a majority of the included studies did not separate transgender individuals from LGB persons.17 This review of transgender individuals showed similar results to the review of LGBTQ individuals.17 This review also presented similar results to previous studies that indicated that transgender individuals in the general population have worse mental health outcomes compared with their cisgender counterparts, in addition to studies that showed that veterans and active-duty service members have worse mental health outcomes compared with civilians and nonveterans.1-5 The population of focus in this review faced a unique set of challenges, being that they belonged to both of these subsets of the population, both of which experienced worse mental health outcomes, according to the literature.
Studies included in our review found that transgender veterans and service members have worse mental health outcomes than cisgender veterans and service members.28-31 This outcome was predicted based on previous data collection among transgender individuals, veterans, and active-duty service members. One of the studies included found different results and concluded that prior military service was a protective factor against poorer mental health outcomes.34 This could be, in part, due to veterans’ access to care through the US Department of Veterans Affairs (VA) system. It has been found that transgender veterans use VA services at higher rates than the general population of veterans and that barriers to care were found more for medical treatment than for mental health treatment.47 One study found that almost 70% of transgender veterans who used VA services were satisfied with their mental health care.48 In contrast, another study included in our review found that transgender veterans had worse mental health outcomes than transgender service members, possibly showing that even with access to care, the burden of stigma and discrimination worsens mental health over time.31 Although it has been shown that transgender veterans may feel comfortable disclosing their gender identity to their health care professional, many barriers to care have been identified, such as insensitivity and lack of knowledge about transgender care among clinicians.49-51 With this information, it would be useful to ensure proper training for health care professionals on providing gender-affirming care.
Most of the studies also found that transgender veterans and service members had greater odds of suicidal thoughts and events than cisgender veterans and service members.16,28,29,35 On the contrary, transgender veterans were less likely than transgender nonveterans to report NSSI, which could be for various reasons.40 Transgender veterans may report less NSSI but experience it at similar rates, or veteran status may be a protective factor for NSSI.
Very few studies included SUDs in their measurements, but it was found that transgender veterans were more likely than cisgender veterans to have any drug and alcohol use disorder.29,41 In addition, transgender veterans were more likely than transgender service members to be diagnosed with an SUD, again showing that over time and after time of service, mental health may worsen due to the burden of stigma and discrimination.31 Studies that examined MST found that transgender veterans were more likely than cisgender veterans to report MST, which replicates previous data that found high rates of sexual assault experienced among transgender individuals.1,28,29
There is a lack of literature surrounding transgender veterans and active-duty service members, especially with regard to gender-affirming care provided to these populations. To the best of our knowledge, there exists only one original study that examines the effect of gender-affirming hormone therapy and surgery on mental health outcomes among transgender veterans.52 Further research in this area is needed, specifically longitudinal studies examining the effects of gender-affirming medical care on various outcomes, including mental health. Few longitudinal studies exist that examine the mental health effects of gender-affirming hormone therapy on transgender individuals in the general population.53-60 Most of these studies have shown a significant improvement in parameters of depression and anxiety following hormonal treatment, although long-term large follow-up studies to understand whether these improvements persist over time are missing also in the general population. However, as previously described, transgender veterans and service members are a unique subset of the transgender population and require separate data collection. Hence, further research is required to provide optimal care for this population. In addition, early screening for symptoms of mental illness, substance use, and MST is important to providing optimal care.
Limitations
This review was limited due to the lack of data collected from transgender veterans and service members. The studies included did not allow for standardized comparisons and did not use identical measures. Some papers compared transgender veterans with transgender nonveterans, some transgender veterans and/or service members with cisgender veterans and/or service members, and some transgender veterans with transgender service members. There were some consistent results found across the studies, but some studies showed contradictory results or no significant differences within a certain category. It is difficult to compare such different study designs and various participant populations. Additional research is required to verify and replicate these results.
Conclusions
Although this review was limited due to the lack of consistent study designs in the literature examining the mental health of transgender veterans and active-duty service members, overall results showed that transgender veterans and service members experience worse mental health outcomes than their cisgender counterparts. With this knowledge and exploring the history of discrimination that this population has faced, improved systems must be put into place to better serve this population and improve health outcomes. Additional research is required to examine the effects of gender-affirming care on mental health among transgender veterans and service members.
According to the United States Transgender Survey, 39% of respondents reported experiencing serious psychological distress (based on the Kessler 6 Psychological Distress Scale) in the past 30 days compared with 5% in the general population.1 Additionally, 40% of respondents attempted suicide in their lifetime, compared with 5% in the general population.1 Almost half of respondents reported being sexually assaulted at some time in their life, and 10% reported being sexually assaulted in the past year.1
Studies have also shown that veterans and active-duty service members experience worse mental health outcomes and are at increased risk for suicide than civilians and nonveterans.2-5 About 1 in 4 active-duty service members meet the criteria for diagnosis of a mental illness.4 Service members were found to have higher rates of probable anxiety and posttraumatic stress disorder (PTSD) compared with the general population.2,6 In 2018, veteran suicide deaths accounted for about 13% of all deaths by suicide in the US even though veterans only accounted for about 7% of the adult population in that year.5,7 Also in 2018, about 17 veterans committed suicide per day.5 According to the Health Related Behaviors Survey of active-duty service members, about 18% reported thinking about attempting suicide some time in their lives compared with 4% of the general population.2,3 Additionally, 5% of service members reported previous suicide attempts compared with 0.5% in the general population.2,3 It is clear that transgender individuals, veterans, and service members have certain mental health outcomes that are worse than that of the general population.1-7
Transgender individuals along with LGB (lesbian, gay, bisexual) individuals have long faced discrimination and unfair treatment in the military.8-11 In the 1920s, the first written policies were established that banned gay men from serving in the military.9 The US Department of Defense (DoD) continued these policies until in 1993, the “Don’t Ask Don’t Tell” policy was established, which had the façade of being more inclusive for LGB individuals but forced LGB service members to hide their sexual identity and continued the anti-LGBTQ messages that previous policies had created.8,10,11 In 2010, “Don’t Ask Don’t Tell” was repealed, which allowed LGB individuals to serve in the military without concealing their sexual orientation and without fear of discharge based on their sexual identity.11 This repeal did not allow transgender individuals to serve their country as the DoD categorized transgender identity as a medical and mental health disorder.8,11
In 2016, the ban on transgender individuals serving in the military was lifted, and service members could no longer be discharged or turned away from joining the military based on gender identity.8,12 However, in 2018, this order was reversed. The new policy stated that new service members must meet requirements and standards of their sex assigned at birth, and individuals with a history of gender dysphoria or those who have received gender-affirming medical or surgical treatment were prohibited to serve in the military.8,13 This policy did not apply to service members who joined before it took effect. Finally, in April 2021, the current policy took effect, permitting transgender individuals to openly serve in the military. The current policy states that service members cannot be discharged or denied reenlistment based on their gender identity and provides support to receive gender-affirming medical care.14 Although transgender individuals are now accepted in military service, there is still much progress needed to promote equity among transgender service members.
In 2015, according to the Health Related Behaviors Survey of active-duty service members, 0.6% of service members identified as transgender, the same percentage as US adults who identify as transgender.2,15 Previous research has shown that the prevalence of gender identity disorder among veterans is higher than that among the general US population.16 Many studies have shown that worse mental health outcomes exist among LGBTQ veterans and service members compared with heterosexual, cisgender veterans and service members.17-24 However, fewer studies have focused solely on mental health outcomes among transgender veterans and active-duty service members, and there exists no current literature review on this topic. In this article, we present data from the existing literature on mental health outcomes in transgender veterans and active-duty service members. We hypothesize, based on the current literature, that transgender veterans and service members have worse mental health outcomes than their cisgender counterparts. Key terms used in this paper are defined in the Key Definitions.25-27
Methods
We conducted a systematic review of articles presenting data on mental health outcomes in transgender veterans and active-duty service members. The National Library of Medicine PubMed database was searched using the following search terms in various combinations: mental health outcomes, transgender, veterans, military, active duty, substance use, and sexual trauma. The literature search was performed in August 2021 and included articles published through July 31, 2021. Methodology, size, demographics, measures, and main findings were extracted from each article. All studies were eligible for inclusion regardless of sample size. Studies that examined the LGBTQ population without separating transgender individuals were excluded. Studies that examined mental health outcomes including, but not limited to, PTSD, depression, suicidality, anxiety, and substance use disorders (SUDs) in addition to sexual trauma were included. Studies that only examined physical health outcomes were excluded. Qualitative studies, case reports, and papers that did not present original data were excluded (Figure).
Results
Our search resulted in 86 publications. After excluding 65 articles that did not meet the inclusion criteria, 19 studies were included in this review. The Appendix shows the summary of findings from each study, including the study size and results. All studies were conducted in the United States. Most papers used a cross-sectional study design. Most of the studies focused on transgender veterans, but some included data on transgender active-duty service members.
We separated the findings into the following categories based on the variables measured: mental health, including depression, anxiety, PTSD, and serious mental illness; suicidality and self-harm; substance use; and military sexual trauma (MST). Many studies overlapped multiple categories.
Mental Health
Most of the studies included reported that transgender veterans have statistically significant worse mental health outcomes compared with cisgender veterans.28-30 In addition, transgender active-duty service members were found to have worse mental health outcomes than cisgender active-duty service members.31 MST and discrimination were associated with worse mental health outcomes among transgender veterans.32,33 One study showed a different result than others and found that transgender older adults with prior military service had higher psychological health-related quality of life and lower depressive symptoms than those without prior military service (P = .02 and .04, respectively).34 Another study compared transgender veterans with active-duty service members and found that transgender veterans reported higher rates of depression (64.6% vs 30.9%; χ2 = 11.68; P = .001) and anxiety (41.3% vs 18.2%; χ2 = 6.54; P = .01) compared with transgender service members.35
Suicidality and Self-harm
Eleven of the 19 studies included measured suicidality and/or self-harm as an outcome. Transgender veterans and active-duty service members were found to have higher odds of suicidality than their cisgender counterparts.16,28,29,31 In addition, transgender veterans may die by suicide at a younger age than cisgender veterans.36 Stigma and gender-related discrimination were found to be associated with suicidal ideation.33,37-39 Transgender veterans were less likely than transgender nonveterans to report nonsuicidal self-injury (NSSI).40
Substance Use
Two studies focused on substance use, while 5 other studies included substance use in their measures. One of these 2 studies that focused only on substance use outcomes found that transgender veterans were more likely than cisgender veterans to have any SUD (7.2% vs 3.9%; P < .001), in addition to specifically cannabis (3.4% vs 1.5%; P < .001), amphetamine (1.1% vs 0.3%; P < .001), and cocaine use disorders (1.5% vs 1.1%; P < .001).41
Another study reported that transgender veterans had lower odds of self-reported alcohol use but had greater odds of having alcohol-related diagnoses compared with cisgender veterans.42 Of the other studies, it was found that a higher percentage of transgender veterans were diagnosed with an SUD compared with transgender active-duty service members, and transgender veterans were more likely than cisgender veterans to be diagnosed with alcohol use disorder.29,31 Additionally, rural transgender veterans had increased odds of tobacco use disorder compared with transgender veterans who lived in urban areas.43
Military Sexual Trauma
Five of the studies included examined MST, defined as sexual assault or sexual harassment that is experienced during military service.44 Studies found that 15% to 17% of transgender veterans experienced MST.32,45 Transgender veterans were more likely to report MST than cisgender veterans.28,29 MST was found to be consistently associated with depression and PTSD.32,45 A high percentage (83.9%) of transgender active-duty service members reported experiencing sexual harassment and almost one-third experienced sexual assault.46
Discussion
Outcomes examined in this review included MST, substance use, suicidality, and symptoms of depression, anxiety, and PTSD among transgender active-duty service members and veterans. To our knowledge, no other review on this topic exists. There is a review of the health and well-being of LGBTQ veterans and service members, but a majority of the included studies did not separate transgender individuals from LGB persons.17 This review of transgender individuals showed similar results to the review of LGBTQ individuals.17 This review also presented similar results to previous studies that indicated that transgender individuals in the general population have worse mental health outcomes compared with their cisgender counterparts, in addition to studies that showed that veterans and active-duty service members have worse mental health outcomes compared with civilians and nonveterans.1-5 The population of focus in this review faced a unique set of challenges, being that they belonged to both of these subsets of the population, both of which experienced worse mental health outcomes, according to the literature.
Studies included in our review found that transgender veterans and service members have worse mental health outcomes than cisgender veterans and service members.28-31 This outcome was predicted based on previous data collection among transgender individuals, veterans, and active-duty service members. One of the studies included found different results and concluded that prior military service was a protective factor against poorer mental health outcomes.34 This could be, in part, due to veterans’ access to care through the US Department of Veterans Affairs (VA) system. It has been found that transgender veterans use VA services at higher rates than the general population of veterans and that barriers to care were found more for medical treatment than for mental health treatment.47 One study found that almost 70% of transgender veterans who used VA services were satisfied with their mental health care.48 In contrast, another study included in our review found that transgender veterans had worse mental health outcomes than transgender service members, possibly showing that even with access to care, the burden of stigma and discrimination worsens mental health over time.31 Although it has been shown that transgender veterans may feel comfortable disclosing their gender identity to their health care professional, many barriers to care have been identified, such as insensitivity and lack of knowledge about transgender care among clinicians.49-51 With this information, it would be useful to ensure proper training for health care professionals on providing gender-affirming care.
Most of the studies also found that transgender veterans and service members had greater odds of suicidal thoughts and events than cisgender veterans and service members.16,28,29,35 On the contrary, transgender veterans were less likely than transgender nonveterans to report NSSI, which could be for various reasons.40 Transgender veterans may report less NSSI but experience it at similar rates, or veteran status may be a protective factor for NSSI.
Very few studies included SUDs in their measurements, but it was found that transgender veterans were more likely than cisgender veterans to have any drug and alcohol use disorder.29,41 In addition, transgender veterans were more likely than transgender service members to be diagnosed with an SUD, again showing that over time and after time of service, mental health may worsen due to the burden of stigma and discrimination.31 Studies that examined MST found that transgender veterans were more likely than cisgender veterans to report MST, which replicates previous data that found high rates of sexual assault experienced among transgender individuals.1,28,29
There is a lack of literature surrounding transgender veterans and active-duty service members, especially with regard to gender-affirming care provided to these populations. To the best of our knowledge, there exists only one original study that examines the effect of gender-affirming hormone therapy and surgery on mental health outcomes among transgender veterans.52 Further research in this area is needed, specifically longitudinal studies examining the effects of gender-affirming medical care on various outcomes, including mental health. Few longitudinal studies exist that examine the mental health effects of gender-affirming hormone therapy on transgender individuals in the general population.53-60 Most of these studies have shown a significant improvement in parameters of depression and anxiety following hormonal treatment, although long-term large follow-up studies to understand whether these improvements persist over time are missing also in the general population. However, as previously described, transgender veterans and service members are a unique subset of the transgender population and require separate data collection. Hence, further research is required to provide optimal care for this population. In addition, early screening for symptoms of mental illness, substance use, and MST is important to providing optimal care.
Limitations
This review was limited due to the lack of data collected from transgender veterans and service members. The studies included did not allow for standardized comparisons and did not use identical measures. Some papers compared transgender veterans with transgender nonveterans, some transgender veterans and/or service members with cisgender veterans and/or service members, and some transgender veterans with transgender service members. There were some consistent results found across the studies, but some studies showed contradictory results or no significant differences within a certain category. It is difficult to compare such different study designs and various participant populations. Additional research is required to verify and replicate these results.
Conclusions
Although this review was limited due to the lack of consistent study designs in the literature examining the mental health of transgender veterans and active-duty service members, overall results showed that transgender veterans and service members experience worse mental health outcomes than their cisgender counterparts. With this knowledge and exploring the history of discrimination that this population has faced, improved systems must be put into place to better serve this population and improve health outcomes. Additional research is required to examine the effects of gender-affirming care on mental health among transgender veterans and service members.
1. James SE, Herman JL, Rankin S, Keisling M, Mottet L, Anafi M. The Report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality. December 2016. Accessed August 22, 2022. https://www.ustranssurvey.org
2. Meadows SO, Engel CC, Collins RL, et al. 2015 Department of Defense Health Related Behaviors Survey (HRBS). Rand Health Q. 2018;8(2):434.
3. Lipari R, Piscopo K, Kroutil LA, Miller GK. Suicidal thoughts and behavior among adults: results from the 2014 National Survey on Drug Use and Health. NSDUH Data Review. 2015:1-14. https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR2-2014/NSDUH-FRR2-2014.pdf
4. Kessler RC, Heeringa SG, Stein MB, et al. Thirty-day prevalence of DSM-IV mental disorders among nondeployed soldiers in the US Army: results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). JAMA Psychiatry. 2014;71(5):504-513. doi:10.1001/jamapsychiatry.2014.28
5. U.S. Department of Veterans Affairs Office of Mental Health and Suicide Prevention. 2020 National Veteran Suicide Prevention Annual Report. November 2020. Accessed August 22, 2022. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
6. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602. doi:10.1001/archpsyc.62.6.593
7. Vespa J. Those who SERVED: America’s veterans from World War II to the war on terror. The United States Census Bureau. June 2, 2020. Accessed August 22, 2022. https://www.census.gov/library/publications/2020/demo/acs-43.html
8. Seibert DC, Keller N, Zapor L, Archer H. Military transgender care. J Am Assoc Nurse Pract. 2020;32(11):764-770. doi:10.1097/JXX.0000000000000519
9. Rigby WC. Military penal law: A brief survey of the 1920 revision of the Articles of War. J Crim Law Criminol. 1921;12(1):84.
10. Department of Defense Directive Number 1332.14: Enlisted Administrative Separations. December 21, 1993. Accessed August 22, 2022. https://biotech.law.lsu.edu/blaw/dodd/corres/pdf/d133214wch1_122193/d133214p.pdf
11. Aford B, Lee SJ. Toward complete inclusion: lesbian, gay, bisexual, and transgender military service members after repeal of Don’t Ask, Don’t Tell. Soc Work. 2016;61(3):257-265. doi:10.1093/sw/sww033
12. Department of Defense Instruction 1300.28: In-Service Transition for Transgender Service Members. June 30, 2016. Accessed August 22, 2022. https://dod.defense.gov/Portals/1/features/2016/0616_policy/DoD-Instruction-1300.28.pdf
13. Department of Defense. Directive-type Memorandum (DTM)-19-004 - Military Service by Transgender Persons and Persons with Gender Dysphoria. March 12. 2019. Accessed August 22, 2022. https://health.mil/Reference-Center/Policies/2020/03/17/Military-Service-by-Transgender-Persons-and-Persons-with-Gender-Dysphoria
14. US Department of Defense Instruction 1300.28: In-Service Transition for Transgender Service Members. April 30, 2021. Accessed August 22, 2022. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/130028p.pdf
15. Flores AR, Herman JL, Gates GJ, Brown TNT. How many adults identify as transgender in the United States? The Williams Institute; 2016. Accessed August 22, 2022. https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/
16. Blosnich JR, Brown GR, Shipherd Phd JC, Kauth M, Piegari RI, Bossarte RM. Prevalence of gender identity disorder and suicide risk among transgender veterans utilizing veterans health administration care. Am J Public Health. 2013;103(10):e27-e32. doi:10.2105/AJPH.2013.301507
17. Mark KM, McNamara KA, Gribble R, et al. The health and well-being of LGBTQ serving and ex-serving personnel: a narrative review. Int Rev Psychiatry. 2019;31(1):75-94. doi:10.1080/09540261.2019.1575190
18. Blosnich J, Foynes MM, Shipherd JC. Health disparities among sexual minority women veterans. J Womens Health (Larchmt). 2013;22(7):631-636. doi:10.1089/jwh.2012.4214
19. Blosnich JR, Bossarte RM, Silenzio VM. Suicidal ideation among sexual minority veterans: results from the 2005-2010 Massachusetts Behavioral Risk Factor Surveillance Survey. Am J Public Health. 2012;102(suppl 1):S44-S47. doi:10.2105/AJPH.2011.300565
20. Blosnich JR, Gordon AJ, Fine MJ. Associations of sexual and gender minority status with health indicators, health risk factors, and social stressors in a national sample of young adults with military experience. Ann Epidemiol. 2015;25(9):661-667. doi:10.1016/j.annepidem.2015.06.001
21. Cochran BN, Balsam K, Flentje A, Malte CA, Simpson T. Mental health characteristics of sexual minority veterans. J Homosex. 2013;60(2-3):419-435. doi:10.1080/00918369.2013.744932
22. Lehavot K, Browne KC, Simpson TL. Examining sexual orientation disparities in alcohol misuse among women veterans. Am J Prev Med. 2014;47(5):554-562. doi:10.1016/j.amepre.2014.07.002
23. Scott RL, Lasiuk GC, Norris CM. Depression in lesbian, gay, and bisexual members of the Canadian Armed Forces. LGBT Health. 2016;3(5):366-372. doi:10.1089/lgbt.2016.0050
24. Wang J, Dey M, Soldati L, Weiss MG, Gmel G, Mohler-Kuo M. Psychiatric disorders, suicidality, and personality among young men by sexual orientation. Eur Psychiatry. 2014;29(8):514-522. doi:10.1016/j.eurpsy.2014.05.001
25. American Psychological Association. Gender. APA Style. September 2019. Updated July 2022. Accessed August 22, 2022. https://apastyle.apa.org/style-grammar-guidelines/bias-free-language/gender
26. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed., American Psychiatric Association; 2013.
27. Deutsch MB. Overview of gender-affirming treatments and procedures. UCSF Transgender Care. June 17, 2016. Accessed August 22, 2022. https://transcare.ucsf.edu/guidelines/overview
28. Brown GR, Jones KT. Health correlates of criminal justice involvement in 4,793 transgender veterans. LGBT Health. 2015;2(4):297-305. doi:10.1089/lgbt.2015.0052
29. Brown GR, Jones KT. Mental health and medical health disparities in 5135 transgender veterans receiving healthcare in the Veterans Health Administration: a case-control study. LGBT Health. 2016;3(2):122-131. doi:10.1089/lgbt.2015.0058
30. Downing J, Conron K, Herman JL, Blosnich JR. Transgender and cisgender US veterans have few health differences. Health Aff (Millwood). 2018;37(7):1160-1168. doi:10.1377/hlthaff.2018.0027
31. Holloway IW, Green D, Pickering C, et al. Mental health and health risk behaviors of active duty sexual minority and transgender service members in the United States military. LGBT Health. 2021;8(2):152-161. doi:10.1089/lgbt.2020.0031
32. Beckman K, Shipherd J, Simpson T, Lehavot K. Military sexual assault in transgender veterans: results from a nationwide survey. J Trauma Stress. 2018;31(2):181-190. doi:10.1002/jts.22280
33. Blosnich JR, Marsiglio MC, Gao S, Gordon AJ, Shipherd JC, Kauth M, Brown GR, Fine MJ. Mental health of transgender veterans in US states with and without discrimination and hate crime legal protection. Am J Public Health. 2016;106(3):534-540. doi:10.2105/AJPH.2015.302981
34. Hoy-Ellis CP, Shiu C, Sullivan KM, Kim HJ, Sturges AM, Fredriksen-Goldsen KI. Prior military service, identity stigma, and mental health among transgender older adults. Gerontologist. 2017;57(suppl 1):S63-S71. doi:10.1093/geront/gnw173
35. Hill BJ, Bouris A, Barnett JT, Walker D. Fit to serve? Exploring mental and physical health and well-being among transgender active-duty service members and veterans in the U.S. military. Transgend Health. 2016;1(1):4-11. Published 2016 Jan 1. doi:10.1089/trgh.2015.0002
36. Blosnich JR, Brown GR, Wojcio S, Jones KT, Bossarte RM. Mortality among veterans with transgender-related diagnoses in the Veterans Health Administration, FY2000-2009. LGBT Health. 2014;1(4):269-276. doi:10.1089/lgbt.2014.0050
37. Carter SP, Allred KM, Tucker RP, Simpson TL, Shipherd JC, Lehavot K. Discrimination and suicidal ideation among transgender veterans: the role of social support and connection. LGBT Health. 2019;6(2):43-50. doi:10.1089/lgbt.2018.0239
38. Lehavot K, Simpson TL, Shipherd JC. Factors associated with suicidality among a national sample of transgender veterans. Suicide Life Threat Behav. 2016;46(5):507-524. doi:10.1111/sltb.12233
39. Tucker RP, Testa RJ, Reger MA, Simpson TL, Shipherd JC, Lehavot K. Current and military-specific gender minority stress factors and their relationship with suicide ideation in transgender veterans. Suicide Life Threat Behav. 2019;49(1):155-166. doi:10.1111/sltb.12432
40. Aboussouan A, Snow A, Cerel J, Tucker RP. Non-suicidal self-injury, suicide ideation, and past suicide attempts: Comparison between transgender and gender diverse veterans and non-veterans. J Affect Disord. 2019;259:186-194. doi:10.1016/j.jad.2019.08.046
41. Frost MC, Blosnich JR, Lehavot K, Chen JA, Rubinsky AD, Glass JE, Williams EC. Disparities in documented drug use disorders between transgender and cisgender U.S. Veterans Health Administration patients. J Addict Med. 2021;15(4):334-340. doi:10.1097/ADM.0000000000000769
42. Williams EC, Frost MC, Rubinsky AD, et al. Patterns of alcohol use among transgender patients receiving care at the Veterans Health Administration: overall and relative to nontransgender patients. J Stud Alcohol Drugs. 2021;82(1):132-141. doi:10.15288/jsad.2021.82.132
43. Bukowski LA, Blosnich J, Shipherd JC, Kauth MR, Brown GR, Gordon AJ. Exploring rural disparities in medical diagnoses among veterans with transgender-related diagnoses utilizing Veterans Health Administration care. Med Care. 2017;55(suppl 9):S97-S103. doi:10.1097/MLR.0000000000000745
44. U.S. Department of Veterans Affairs. Military Sexual Trauma. Updated August 1, 2022. Accessed August 22, 2022. https://www.mentalhealth.va.gov/mentalhealth/msthome/index.asp
45. Lindsay JA, Keo-Meier C, Hudson S, Walder A, Martin LA, Kauth MR. Mental health of transgender veterans of the Iraq and Afghanistan conflicts who experienced military sexual trauma. J Trauma Stress. 2016;29(6):563-567. doi:10.1002/jts.22146
46. Schuyler AC, Klemmer C, Mamey MR, et al. Experiences of sexual harassment, stalking, and sexual assault during military service among LGBT and Non-LGBT service members. J Trauma Stress. 2020;33(3):257-266. doi:10.1002/jts.22506
47. Shipherd JC, Mizock L, Maguen S, Green KE. Male-to-female transgender veterans and VA health care utilization. Int J Sexual Health. 2012;24(1):78-87. doi:10.1080/19317611.2011.639440
48. Lehavot K, Katon JG, Simpson TL, Shipherd JC. Transgender veterans’ satisfaction with care and unmet health needs. Med Care. 2017;55(suppl 9):S90-S96. doi:10.1097/MLR.0000000000000723
49. Kauth MR, Barrera TL, Latini DM. Lesbian, gay, and transgender veterans’ experiences in the Veterans Health Administration: positive signs and room for improvement. Psychol Serv. 2019;16(2):346-351. doi:10.1037/ser0000232
50. Rosentel K, Hill BJ, Lu C, Barnett JT. Transgender veterans and the Veterans Health Administration: exploring the experiences of transgender veterans in the Veterans Affairs Healthcare System. Transgend Health. 2016;1(1):108-116. Published 2016 Jun 1. doi:10.1089/trgh.2016.0006
51. Dietert M, Dentice D, Keig Z. Addressing the needs of transgender military veterans: better access and more comprehensive care. Transgend Health. 2017;2(1):35-44. Published 2017 Mar 1. doi:10.1089/trgh.2016.0040
52. Tucker RP, Testa RJ, Simpson TL, Shipherd JC, Blosnich JR, Lehavot K. Hormone therapy, gender affirmation surgery, and their association with recent suicidal ideation and depression symptoms in transgender veterans. Psychol Med. 2018;48(14):2329-2336. doi:10.1017/S0033291717003853
53. Colizzi M, Costa R, Todarello O. Transsexual patients’ psychiatric comorbidity and positive effect of cross-sex hormonal treatment on mental health: results from a longitudinal study. Psychoneuroendocrinology. 2014;39:65-73. doi:10.1016/j.psyneuen.2013.09.029
54. Heylens G, Verroken C, De Cock S, T’Sjoen G, De Cuypere G. Effects of different steps in gender reassignment therapy on psychopathology: a prospective study of persons with a gender identity disorder. J Sex Med. 2014;11(1):119-126. doi:10.1111/jsm.12363
55. Fisher AD, Castellini G, Ristori J, et al. Cross-sex hormone treatment and psychobiological changes in transsexual persons: two-year follow-up data. J Clin Endocrinol Metab. 2016;101(11):4260-4269. doi:10.1210/jc.2016-1276
56. Aldridge Z, Patel S, Guo B, et al. Long-term effect of gender-affirming hormone treatment on depression and anxiety symptoms in transgender people: a prospective cohort study. Andrology. 2021;9(6):1808-1816. doi:10.1111/andr.12884
57. Costantino A, Cerpolini S, Alvisi S, Morselli PG, Venturoli S, Meriggiola MC. A prospective study on sexual function and mood in female-to-male transsexuals during testosterone administration and after sex reassignment surgery. J Sex Marital Ther. 2013;39(4):321-335. doi:10.1080/0092623X.2012.736920
58. Keo-Meier CL, Herman LI, Reisner SL, Pardo ST, Sharp C, Babcock JC. Testosterone treatment and MMPI-2 improvement in transgender men: a prospective controlled study. J Consult Clin Psychol. 2015;83(1):143-156. doi:10.1037/a0037599
59. Turan S‚ , Aksoy Poyraz C, Usta Sag˘lam NG, et al. Alterations in body uneasiness, eating attitudes, and psychopathology before and after cross-sex hormonal treatment in patients with female-to-male gender dysphoria. Arch Sex Behav. 2018;47(8):2349-2361. doi:10.1007/s10508-018-1189-4
60. Oda H, Kinoshita T. Efficacy of hormonal and mental treatments with MMPI in FtM individuals: cross-sectional and longitudinal studies. BMC Psychiatry. 2017;17(1):256. Published 2017 Jul 17. doi:10.1186/s12888-017-1423-y
1. James SE, Herman JL, Rankin S, Keisling M, Mottet L, Anafi M. The Report of the 2015 U.S. Transgender Survey. National Center for Transgender Equality. December 2016. Accessed August 22, 2022. https://www.ustranssurvey.org
2. Meadows SO, Engel CC, Collins RL, et al. 2015 Department of Defense Health Related Behaviors Survey (HRBS). Rand Health Q. 2018;8(2):434.
3. Lipari R, Piscopo K, Kroutil LA, Miller GK. Suicidal thoughts and behavior among adults: results from the 2014 National Survey on Drug Use and Health. NSDUH Data Review. 2015:1-14. https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR2-2014/NSDUH-FRR2-2014.pdf
4. Kessler RC, Heeringa SG, Stein MB, et al. Thirty-day prevalence of DSM-IV mental disorders among nondeployed soldiers in the US Army: results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). JAMA Psychiatry. 2014;71(5):504-513. doi:10.1001/jamapsychiatry.2014.28
5. U.S. Department of Veterans Affairs Office of Mental Health and Suicide Prevention. 2020 National Veteran Suicide Prevention Annual Report. November 2020. Accessed August 22, 2022. https://www.mentalhealth.va.gov/docs/data-sheets/2020/2020-National-Veteran-Suicide-Prevention-Annual-Report-11-2020-508.pdf
6. Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602. doi:10.1001/archpsyc.62.6.593
7. Vespa J. Those who SERVED: America’s veterans from World War II to the war on terror. The United States Census Bureau. June 2, 2020. Accessed August 22, 2022. https://www.census.gov/library/publications/2020/demo/acs-43.html
8. Seibert DC, Keller N, Zapor L, Archer H. Military transgender care. J Am Assoc Nurse Pract. 2020;32(11):764-770. doi:10.1097/JXX.0000000000000519
9. Rigby WC. Military penal law: A brief survey of the 1920 revision of the Articles of War. J Crim Law Criminol. 1921;12(1):84.
10. Department of Defense Directive Number 1332.14: Enlisted Administrative Separations. December 21, 1993. Accessed August 22, 2022. https://biotech.law.lsu.edu/blaw/dodd/corres/pdf/d133214wch1_122193/d133214p.pdf
11. Aford B, Lee SJ. Toward complete inclusion: lesbian, gay, bisexual, and transgender military service members after repeal of Don’t Ask, Don’t Tell. Soc Work. 2016;61(3):257-265. doi:10.1093/sw/sww033
12. Department of Defense Instruction 1300.28: In-Service Transition for Transgender Service Members. June 30, 2016. Accessed August 22, 2022. https://dod.defense.gov/Portals/1/features/2016/0616_policy/DoD-Instruction-1300.28.pdf
13. Department of Defense. Directive-type Memorandum (DTM)-19-004 - Military Service by Transgender Persons and Persons with Gender Dysphoria. March 12. 2019. Accessed August 22, 2022. https://health.mil/Reference-Center/Policies/2020/03/17/Military-Service-by-Transgender-Persons-and-Persons-with-Gender-Dysphoria
14. US Department of Defense Instruction 1300.28: In-Service Transition for Transgender Service Members. April 30, 2021. Accessed August 22, 2022. https://www.esd.whs.mil/Portals/54/Documents/DD/issuances/dodi/130028p.pdf
15. Flores AR, Herman JL, Gates GJ, Brown TNT. How many adults identify as transgender in the United States? The Williams Institute; 2016. Accessed August 22, 2022. https://williamsinstitute.law.ucla.edu/publications/trans-adults-united-states/
16. Blosnich JR, Brown GR, Shipherd Phd JC, Kauth M, Piegari RI, Bossarte RM. Prevalence of gender identity disorder and suicide risk among transgender veterans utilizing veterans health administration care. Am J Public Health. 2013;103(10):e27-e32. doi:10.2105/AJPH.2013.301507
17. Mark KM, McNamara KA, Gribble R, et al. The health and well-being of LGBTQ serving and ex-serving personnel: a narrative review. Int Rev Psychiatry. 2019;31(1):75-94. doi:10.1080/09540261.2019.1575190
18. Blosnich J, Foynes MM, Shipherd JC. Health disparities among sexual minority women veterans. J Womens Health (Larchmt). 2013;22(7):631-636. doi:10.1089/jwh.2012.4214
19. Blosnich JR, Bossarte RM, Silenzio VM. Suicidal ideation among sexual minority veterans: results from the 2005-2010 Massachusetts Behavioral Risk Factor Surveillance Survey. Am J Public Health. 2012;102(suppl 1):S44-S47. doi:10.2105/AJPH.2011.300565
20. Blosnich JR, Gordon AJ, Fine MJ. Associations of sexual and gender minority status with health indicators, health risk factors, and social stressors in a national sample of young adults with military experience. Ann Epidemiol. 2015;25(9):661-667. doi:10.1016/j.annepidem.2015.06.001
21. Cochran BN, Balsam K, Flentje A, Malte CA, Simpson T. Mental health characteristics of sexual minority veterans. J Homosex. 2013;60(2-3):419-435. doi:10.1080/00918369.2013.744932
22. Lehavot K, Browne KC, Simpson TL. Examining sexual orientation disparities in alcohol misuse among women veterans. Am J Prev Med. 2014;47(5):554-562. doi:10.1016/j.amepre.2014.07.002
23. Scott RL, Lasiuk GC, Norris CM. Depression in lesbian, gay, and bisexual members of the Canadian Armed Forces. LGBT Health. 2016;3(5):366-372. doi:10.1089/lgbt.2016.0050
24. Wang J, Dey M, Soldati L, Weiss MG, Gmel G, Mohler-Kuo M. Psychiatric disorders, suicidality, and personality among young men by sexual orientation. Eur Psychiatry. 2014;29(8):514-522. doi:10.1016/j.eurpsy.2014.05.001
25. American Psychological Association. Gender. APA Style. September 2019. Updated July 2022. Accessed August 22, 2022. https://apastyle.apa.org/style-grammar-guidelines/bias-free-language/gender
26. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. 5th ed., American Psychiatric Association; 2013.
27. Deutsch MB. Overview of gender-affirming treatments and procedures. UCSF Transgender Care. June 17, 2016. Accessed August 22, 2022. https://transcare.ucsf.edu/guidelines/overview
28. Brown GR, Jones KT. Health correlates of criminal justice involvement in 4,793 transgender veterans. LGBT Health. 2015;2(4):297-305. doi:10.1089/lgbt.2015.0052
29. Brown GR, Jones KT. Mental health and medical health disparities in 5135 transgender veterans receiving healthcare in the Veterans Health Administration: a case-control study. LGBT Health. 2016;3(2):122-131. doi:10.1089/lgbt.2015.0058
30. Downing J, Conron K, Herman JL, Blosnich JR. Transgender and cisgender US veterans have few health differences. Health Aff (Millwood). 2018;37(7):1160-1168. doi:10.1377/hlthaff.2018.0027
31. Holloway IW, Green D, Pickering C, et al. Mental health and health risk behaviors of active duty sexual minority and transgender service members in the United States military. LGBT Health. 2021;8(2):152-161. doi:10.1089/lgbt.2020.0031
32. Beckman K, Shipherd J, Simpson T, Lehavot K. Military sexual assault in transgender veterans: results from a nationwide survey. J Trauma Stress. 2018;31(2):181-190. doi:10.1002/jts.22280
33. Blosnich JR, Marsiglio MC, Gao S, Gordon AJ, Shipherd JC, Kauth M, Brown GR, Fine MJ. Mental health of transgender veterans in US states with and without discrimination and hate crime legal protection. Am J Public Health. 2016;106(3):534-540. doi:10.2105/AJPH.2015.302981
34. Hoy-Ellis CP, Shiu C, Sullivan KM, Kim HJ, Sturges AM, Fredriksen-Goldsen KI. Prior military service, identity stigma, and mental health among transgender older adults. Gerontologist. 2017;57(suppl 1):S63-S71. doi:10.1093/geront/gnw173
35. Hill BJ, Bouris A, Barnett JT, Walker D. Fit to serve? Exploring mental and physical health and well-being among transgender active-duty service members and veterans in the U.S. military. Transgend Health. 2016;1(1):4-11. Published 2016 Jan 1. doi:10.1089/trgh.2015.0002
36. Blosnich JR, Brown GR, Wojcio S, Jones KT, Bossarte RM. Mortality among veterans with transgender-related diagnoses in the Veterans Health Administration, FY2000-2009. LGBT Health. 2014;1(4):269-276. doi:10.1089/lgbt.2014.0050
37. Carter SP, Allred KM, Tucker RP, Simpson TL, Shipherd JC, Lehavot K. Discrimination and suicidal ideation among transgender veterans: the role of social support and connection. LGBT Health. 2019;6(2):43-50. doi:10.1089/lgbt.2018.0239
38. Lehavot K, Simpson TL, Shipherd JC. Factors associated with suicidality among a national sample of transgender veterans. Suicide Life Threat Behav. 2016;46(5):507-524. doi:10.1111/sltb.12233
39. Tucker RP, Testa RJ, Reger MA, Simpson TL, Shipherd JC, Lehavot K. Current and military-specific gender minority stress factors and their relationship with suicide ideation in transgender veterans. Suicide Life Threat Behav. 2019;49(1):155-166. doi:10.1111/sltb.12432
40. Aboussouan A, Snow A, Cerel J, Tucker RP. Non-suicidal self-injury, suicide ideation, and past suicide attempts: Comparison between transgender and gender diverse veterans and non-veterans. J Affect Disord. 2019;259:186-194. doi:10.1016/j.jad.2019.08.046
41. Frost MC, Blosnich JR, Lehavot K, Chen JA, Rubinsky AD, Glass JE, Williams EC. Disparities in documented drug use disorders between transgender and cisgender U.S. Veterans Health Administration patients. J Addict Med. 2021;15(4):334-340. doi:10.1097/ADM.0000000000000769
42. Williams EC, Frost MC, Rubinsky AD, et al. Patterns of alcohol use among transgender patients receiving care at the Veterans Health Administration: overall and relative to nontransgender patients. J Stud Alcohol Drugs. 2021;82(1):132-141. doi:10.15288/jsad.2021.82.132
43. Bukowski LA, Blosnich J, Shipherd JC, Kauth MR, Brown GR, Gordon AJ. Exploring rural disparities in medical diagnoses among veterans with transgender-related diagnoses utilizing Veterans Health Administration care. Med Care. 2017;55(suppl 9):S97-S103. doi:10.1097/MLR.0000000000000745
44. U.S. Department of Veterans Affairs. Military Sexual Trauma. Updated August 1, 2022. Accessed August 22, 2022. https://www.mentalhealth.va.gov/mentalhealth/msthome/index.asp
45. Lindsay JA, Keo-Meier C, Hudson S, Walder A, Martin LA, Kauth MR. Mental health of transgender veterans of the Iraq and Afghanistan conflicts who experienced military sexual trauma. J Trauma Stress. 2016;29(6):563-567. doi:10.1002/jts.22146
46. Schuyler AC, Klemmer C, Mamey MR, et al. Experiences of sexual harassment, stalking, and sexual assault during military service among LGBT and Non-LGBT service members. J Trauma Stress. 2020;33(3):257-266. doi:10.1002/jts.22506
47. Shipherd JC, Mizock L, Maguen S, Green KE. Male-to-female transgender veterans and VA health care utilization. Int J Sexual Health. 2012;24(1):78-87. doi:10.1080/19317611.2011.639440
48. Lehavot K, Katon JG, Simpson TL, Shipherd JC. Transgender veterans’ satisfaction with care and unmet health needs. Med Care. 2017;55(suppl 9):S90-S96. doi:10.1097/MLR.0000000000000723
49. Kauth MR, Barrera TL, Latini DM. Lesbian, gay, and transgender veterans’ experiences in the Veterans Health Administration: positive signs and room for improvement. Psychol Serv. 2019;16(2):346-351. doi:10.1037/ser0000232
50. Rosentel K, Hill BJ, Lu C, Barnett JT. Transgender veterans and the Veterans Health Administration: exploring the experiences of transgender veterans in the Veterans Affairs Healthcare System. Transgend Health. 2016;1(1):108-116. Published 2016 Jun 1. doi:10.1089/trgh.2016.0006
51. Dietert M, Dentice D, Keig Z. Addressing the needs of transgender military veterans: better access and more comprehensive care. Transgend Health. 2017;2(1):35-44. Published 2017 Mar 1. doi:10.1089/trgh.2016.0040
52. Tucker RP, Testa RJ, Simpson TL, Shipherd JC, Blosnich JR, Lehavot K. Hormone therapy, gender affirmation surgery, and their association with recent suicidal ideation and depression symptoms in transgender veterans. Psychol Med. 2018;48(14):2329-2336. doi:10.1017/S0033291717003853
53. Colizzi M, Costa R, Todarello O. Transsexual patients’ psychiatric comorbidity and positive effect of cross-sex hormonal treatment on mental health: results from a longitudinal study. Psychoneuroendocrinology. 2014;39:65-73. doi:10.1016/j.psyneuen.2013.09.029
54. Heylens G, Verroken C, De Cock S, T’Sjoen G, De Cuypere G. Effects of different steps in gender reassignment therapy on psychopathology: a prospective study of persons with a gender identity disorder. J Sex Med. 2014;11(1):119-126. doi:10.1111/jsm.12363
55. Fisher AD, Castellini G, Ristori J, et al. Cross-sex hormone treatment and psychobiological changes in transsexual persons: two-year follow-up data. J Clin Endocrinol Metab. 2016;101(11):4260-4269. doi:10.1210/jc.2016-1276
56. Aldridge Z, Patel S, Guo B, et al. Long-term effect of gender-affirming hormone treatment on depression and anxiety symptoms in transgender people: a prospective cohort study. Andrology. 2021;9(6):1808-1816. doi:10.1111/andr.12884
57. Costantino A, Cerpolini S, Alvisi S, Morselli PG, Venturoli S, Meriggiola MC. A prospective study on sexual function and mood in female-to-male transsexuals during testosterone administration and after sex reassignment surgery. J Sex Marital Ther. 2013;39(4):321-335. doi:10.1080/0092623X.2012.736920
58. Keo-Meier CL, Herman LI, Reisner SL, Pardo ST, Sharp C, Babcock JC. Testosterone treatment and MMPI-2 improvement in transgender men: a prospective controlled study. J Consult Clin Psychol. 2015;83(1):143-156. doi:10.1037/a0037599
59. Turan S‚ , Aksoy Poyraz C, Usta Sag˘lam NG, et al. Alterations in body uneasiness, eating attitudes, and psychopathology before and after cross-sex hormonal treatment in patients with female-to-male gender dysphoria. Arch Sex Behav. 2018;47(8):2349-2361. doi:10.1007/s10508-018-1189-4
60. Oda H, Kinoshita T. Efficacy of hormonal and mental treatments with MMPI in FtM individuals: cross-sectional and longitudinal studies. BMC Psychiatry. 2017;17(1):256. Published 2017 Jul 17. doi:10.1186/s12888-017-1423-y