User login
Decline in ambulatory function
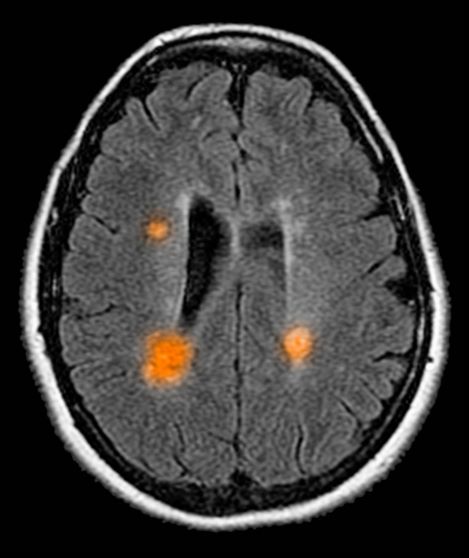
Based on this patient's history and presentation, the likely diagnosis is primary progressive multiple sclerosis (PPMS). PPMS represents around 10% of MS cases and tends to develop about a decade later than relapsing MS. Unlike other forms of MS, this phenotype progresses steadily instead of in an episodic fashion like relapsing forms of MS. Most patients with PPMS present with gait difficulty because lesions often develop on the spinal cord. While relapsing-remitting MS (RRMS) is much more common among women than men, men with MS are more likely to have the progressive form.
Although this patient's MRI ultimately points to multiple sclerosis, his functional deficits may initially suggest other conditions in the differential diagnosis. Brainstem gliomas typically manifest in unsteady gait, weakness, double vision, difficulty swallowing, dysarthria, headache, drowsiness, nausea, and vomiting. Transverse myelitis often presents with rapid-onset weakness, sensory deficits, and bowel/bladder dysfunction. Musculoskeletal and neurologic symptoms are common in Lyme disease. B12 deficiency can present with worsening weakness and a sensory ataxia that can present as balance difficulties, but it would not cause focal lesions on the MRI, nor would it present with bladder symptoms. In addition, the patient's steady decline in function rules out RRMS.
PPMS is diagnosed with confirmation of gradual change in functional ability (often ambulation) over time without remission or relapse. These criteria include 1 full year of worsening neurologic function without asymptomatic periods as well as two of these signs of disease: brain lesion, two or more spinal cord lesions, and oligoclonal bands or elevated Immunoglobulin G index. These timing-specific criteria can delay diagnosis, as seen here.
Ocrelizumab is the only FDA-approved disease-modifying therapy (DMT) proven to alter disease progression in ambulatory patients with PPMS. American Academy of Neurology guidelines recommend ocrelizumab for patients with PPMS who are likely to benefit from this therapy. While it is thought that DMTs are more effective at targeting inflammation in RRMS than nerve degeneration in PPMS, these agents may show benefit for patients with active PPMS (relapse and/or evidence of new MRI activity) rather than inactive disease. A recent PPMS study concluded that among patients with relapse or disease activity, DMTs were associated with a significant reduction of long-term disability risk. Together with immunomodulatory therapy, rehabilitation can help manage symptoms.
Krupa Pandey, MD, Director, Multiple Sclerosis Center, Department of Neurology & Neuroscience Institute, Hackensack University Medical Center; Neurologist, Department of Neurology, Hackensack Meridian Health, Hackensack, NJ.
Krupa Pandey, MD, has serve(d) as a speaker or a member of a speakers bureau for: Bristol-Myers Squibb; Biogen; Alexion; Genentech; Sanofi-Genzyme.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Based on this patient's history and presentation, the likely diagnosis is primary progressive multiple sclerosis (PPMS). PPMS represents around 10% of MS cases and tends to develop about a decade later than relapsing MS. Unlike other forms of MS, this phenotype progresses steadily instead of in an episodic fashion like relapsing forms of MS. Most patients with PPMS present with gait difficulty because lesions often develop on the spinal cord. While relapsing-remitting MS (RRMS) is much more common among women than men, men with MS are more likely to have the progressive form.
Although this patient's MRI ultimately points to multiple sclerosis, his functional deficits may initially suggest other conditions in the differential diagnosis. Brainstem gliomas typically manifest in unsteady gait, weakness, double vision, difficulty swallowing, dysarthria, headache, drowsiness, nausea, and vomiting. Transverse myelitis often presents with rapid-onset weakness, sensory deficits, and bowel/bladder dysfunction. Musculoskeletal and neurologic symptoms are common in Lyme disease. B12 deficiency can present with worsening weakness and a sensory ataxia that can present as balance difficulties, but it would not cause focal lesions on the MRI, nor would it present with bladder symptoms. In addition, the patient's steady decline in function rules out RRMS.
PPMS is diagnosed with confirmation of gradual change in functional ability (often ambulation) over time without remission or relapse. These criteria include 1 full year of worsening neurologic function without asymptomatic periods as well as two of these signs of disease: brain lesion, two or more spinal cord lesions, and oligoclonal bands or elevated Immunoglobulin G index. These timing-specific criteria can delay diagnosis, as seen here.
Ocrelizumab is the only FDA-approved disease-modifying therapy (DMT) proven to alter disease progression in ambulatory patients with PPMS. American Academy of Neurology guidelines recommend ocrelizumab for patients with PPMS who are likely to benefit from this therapy. While it is thought that DMTs are more effective at targeting inflammation in RRMS than nerve degeneration in PPMS, these agents may show benefit for patients with active PPMS (relapse and/or evidence of new MRI activity) rather than inactive disease. A recent PPMS study concluded that among patients with relapse or disease activity, DMTs were associated with a significant reduction of long-term disability risk. Together with immunomodulatory therapy, rehabilitation can help manage symptoms.
Krupa Pandey, MD, Director, Multiple Sclerosis Center, Department of Neurology & Neuroscience Institute, Hackensack University Medical Center; Neurologist, Department of Neurology, Hackensack Meridian Health, Hackensack, NJ.
Krupa Pandey, MD, has serve(d) as a speaker or a member of a speakers bureau for: Bristol-Myers Squibb; Biogen; Alexion; Genentech; Sanofi-Genzyme.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
Based on this patient's history and presentation, the likely diagnosis is primary progressive multiple sclerosis (PPMS). PPMS represents around 10% of MS cases and tends to develop about a decade later than relapsing MS. Unlike other forms of MS, this phenotype progresses steadily instead of in an episodic fashion like relapsing forms of MS. Most patients with PPMS present with gait difficulty because lesions often develop on the spinal cord. While relapsing-remitting MS (RRMS) is much more common among women than men, men with MS are more likely to have the progressive form.
Although this patient's MRI ultimately points to multiple sclerosis, his functional deficits may initially suggest other conditions in the differential diagnosis. Brainstem gliomas typically manifest in unsteady gait, weakness, double vision, difficulty swallowing, dysarthria, headache, drowsiness, nausea, and vomiting. Transverse myelitis often presents with rapid-onset weakness, sensory deficits, and bowel/bladder dysfunction. Musculoskeletal and neurologic symptoms are common in Lyme disease. B12 deficiency can present with worsening weakness and a sensory ataxia that can present as balance difficulties, but it would not cause focal lesions on the MRI, nor would it present with bladder symptoms. In addition, the patient's steady decline in function rules out RRMS.
PPMS is diagnosed with confirmation of gradual change in functional ability (often ambulation) over time without remission or relapse. These criteria include 1 full year of worsening neurologic function without asymptomatic periods as well as two of these signs of disease: brain lesion, two or more spinal cord lesions, and oligoclonal bands or elevated Immunoglobulin G index. These timing-specific criteria can delay diagnosis, as seen here.
Ocrelizumab is the only FDA-approved disease-modifying therapy (DMT) proven to alter disease progression in ambulatory patients with PPMS. American Academy of Neurology guidelines recommend ocrelizumab for patients with PPMS who are likely to benefit from this therapy. While it is thought that DMTs are more effective at targeting inflammation in RRMS than nerve degeneration in PPMS, these agents may show benefit for patients with active PPMS (relapse and/or evidence of new MRI activity) rather than inactive disease. A recent PPMS study concluded that among patients with relapse or disease activity, DMTs were associated with a significant reduction of long-term disability risk. Together with immunomodulatory therapy, rehabilitation can help manage symptoms.
Krupa Pandey, MD, Director, Multiple Sclerosis Center, Department of Neurology & Neuroscience Institute, Hackensack University Medical Center; Neurologist, Department of Neurology, Hackensack Meridian Health, Hackensack, NJ.
Krupa Pandey, MD, has serve(d) as a speaker or a member of a speakers bureau for: Bristol-Myers Squibb; Biogen; Alexion; Genentech; Sanofi-Genzyme.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
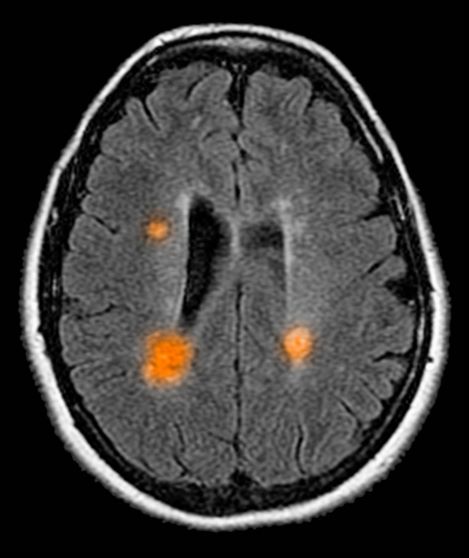
A 59-year-old man presents with worsening decline in ambulatory function and worsening bladder function. He reports "difficulty getting around" for the past year and a half, which he theorized might be because of arthritis, aging, or many years of biking. He presented to his primary care physician 2 months ago and was referred to rheumatology. His height is 5 ft 11 in and his weight is 166 lb (BMI 23.1). The patient subsequently reported a decreased attention span to the rheumatologist. He has no other significant medical or surgical history, though his brother has psoriatic arthritis. MRI shows multiple brain lesions without gadolinium enhancement and multiple spinal cord lesions.
Even mild MS relapses may signal faster disability accumulation
Nondisabling relapses that occur early in the course of relapsing-remitting multiple sclerosis (RRMS) signal faster accumulation of disability relative to no early relapses, new research suggests. However, in the large registry study, this association was not found in patients treated with high-efficacy, disease-modifying therapies (DMTs) early on.
The results suggest that ,” said lead author Cyrus Daruwalla, MD, department of clinical neurosciences at the University of Cambridge, and Addenbrooke’s Hospital, Cambridge, England.
Dr. Daruwalla presented the findings at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Questioning EMA restrictions
“We designed this project because regulators, including EMA [European Medicines Agency], restrict the use of certain DMTs to only those with disabling relapses. In particular, natalizumab [Tysabri] and fingolimod [Gilenya] can only be used as the first-line therapy for people with rapidly evolving, severe MS – which includes having two disabling relapses in a year,” Dr. Daruwalla noted.
“In clinic, when we see somebody who has a nondisabling relapse, we’re left with the question of what is the prognostic significance of that relapse, and how should it influence treatment decisions,” he added.
Using prospectively collected data from the MSBase international registry, the researchers examined data on individuals with RRMS and complete early relapse severity information.
They compared patients with exclusively nondisabling relapses in the 2 years after definitive RRMS diagnosis with peers with no relapses within this time frame.
To mitigate the confounding effect of DMT use, the investigators performed analyses in participants untreated during follow-up, and then in those who received only older or “platform” therapies (interferon-beta, glatiramer acetate, dimethyl fumarate, or teriflunomide) during follow-up.
In the untreated cohort, 285 patients had nondisabling relapses and 4,717 had no relapses during the 2 years after diagnosis. Those with early nondisabling relapses had a significantly increased risk for disability accumulation (adjusted hazard ratio [aHR], 1.29; 95% confidence interval [CI], 1.00-1.68).
In the treated cohort, 1,074 patients had nondisabling early relapses and 7,262 did not.
In this cohort, those treated with “platform” DMTs who had nondisabling relapses showed a significantly increased risk for disability accumulation compared with treated peers who had no relapses (aHR, 1.33; 95% CI, 1.15-1.54).
Notably, said Dr. Daruwalla, in patients treated at any point during follow-up with high-efficacy DMTs, including monoclonal antibodies, sphingosphine-1 phosphate modulators, and hematopoietic stem cell transplantation, there was no difference in disability accumulation between patients who did and did not experience nondisabling relapses (aHR, 0.90; 95% CI, 0.71-1.13).
The data clearly show that early nondisabling relapses are associated with a higher risk of disability accumulation than no early relapses in people with relapsing remitting MS,” Dr. Daruwalla said.
However, he noted, treatment with high-efficacy DMTs offers protection against disability accumulations.
“Therefore, contrary to EMA guidance, nondisabling relapses should be considered in decisions to initiate or escalate treatment, including with high-efficacy therapies,” he added.
Valuable, confirmatory data
Patricia Coyle, MD, professor of neurology and director of the MS Comprehensive Care Center at Stony Brook (N.Y.) University, called the study “valuable.”
“It confirms prior data that having relapses is bad in MS even if they are mild, and provides additional modest data in support of high-efficacy versus moderate-efficacy DMT,” said Dr. Coyle, who was not involved with the research.
“Although certainly not definitive, it adds to data supporting high-efficacy as preferred treatment [and] addresses a completely arbitrary governmental limitation to DMT use in Europe,” she added.
The study had no commercial funding. Dr. Daruwalla has reported no relevant financial relationships. Dr. Coyle reports having received consulting fees from Accordant, Biogen, Bristol-Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio; and grant funding from Actelion, Alkermes, Bristol-Myers Squibb, CorEvitas, Genentech/Roche, Sanofi Genzyme, MedDay, and Novartis.
A version of this article first appeared on Medscape.com.
Nondisabling relapses that occur early in the course of relapsing-remitting multiple sclerosis (RRMS) signal faster accumulation of disability relative to no early relapses, new research suggests. However, in the large registry study, this association was not found in patients treated with high-efficacy, disease-modifying therapies (DMTs) early on.
The results suggest that ,” said lead author Cyrus Daruwalla, MD, department of clinical neurosciences at the University of Cambridge, and Addenbrooke’s Hospital, Cambridge, England.
Dr. Daruwalla presented the findings at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Questioning EMA restrictions
“We designed this project because regulators, including EMA [European Medicines Agency], restrict the use of certain DMTs to only those with disabling relapses. In particular, natalizumab [Tysabri] and fingolimod [Gilenya] can only be used as the first-line therapy for people with rapidly evolving, severe MS – which includes having two disabling relapses in a year,” Dr. Daruwalla noted.
“In clinic, when we see somebody who has a nondisabling relapse, we’re left with the question of what is the prognostic significance of that relapse, and how should it influence treatment decisions,” he added.
Using prospectively collected data from the MSBase international registry, the researchers examined data on individuals with RRMS and complete early relapse severity information.
They compared patients with exclusively nondisabling relapses in the 2 years after definitive RRMS diagnosis with peers with no relapses within this time frame.
To mitigate the confounding effect of DMT use, the investigators performed analyses in participants untreated during follow-up, and then in those who received only older or “platform” therapies (interferon-beta, glatiramer acetate, dimethyl fumarate, or teriflunomide) during follow-up.
In the untreated cohort, 285 patients had nondisabling relapses and 4,717 had no relapses during the 2 years after diagnosis. Those with early nondisabling relapses had a significantly increased risk for disability accumulation (adjusted hazard ratio [aHR], 1.29; 95% confidence interval [CI], 1.00-1.68).
In the treated cohort, 1,074 patients had nondisabling early relapses and 7,262 did not.
In this cohort, those treated with “platform” DMTs who had nondisabling relapses showed a significantly increased risk for disability accumulation compared with treated peers who had no relapses (aHR, 1.33; 95% CI, 1.15-1.54).
Notably, said Dr. Daruwalla, in patients treated at any point during follow-up with high-efficacy DMTs, including monoclonal antibodies, sphingosphine-1 phosphate modulators, and hematopoietic stem cell transplantation, there was no difference in disability accumulation between patients who did and did not experience nondisabling relapses (aHR, 0.90; 95% CI, 0.71-1.13).
The data clearly show that early nondisabling relapses are associated with a higher risk of disability accumulation than no early relapses in people with relapsing remitting MS,” Dr. Daruwalla said.
However, he noted, treatment with high-efficacy DMTs offers protection against disability accumulations.
“Therefore, contrary to EMA guidance, nondisabling relapses should be considered in decisions to initiate or escalate treatment, including with high-efficacy therapies,” he added.
Valuable, confirmatory data
Patricia Coyle, MD, professor of neurology and director of the MS Comprehensive Care Center at Stony Brook (N.Y.) University, called the study “valuable.”
“It confirms prior data that having relapses is bad in MS even if they are mild, and provides additional modest data in support of high-efficacy versus moderate-efficacy DMT,” said Dr. Coyle, who was not involved with the research.
“Although certainly not definitive, it adds to data supporting high-efficacy as preferred treatment [and] addresses a completely arbitrary governmental limitation to DMT use in Europe,” she added.
The study had no commercial funding. Dr. Daruwalla has reported no relevant financial relationships. Dr. Coyle reports having received consulting fees from Accordant, Biogen, Bristol-Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio; and grant funding from Actelion, Alkermes, Bristol-Myers Squibb, CorEvitas, Genentech/Roche, Sanofi Genzyme, MedDay, and Novartis.
A version of this article first appeared on Medscape.com.
Nondisabling relapses that occur early in the course of relapsing-remitting multiple sclerosis (RRMS) signal faster accumulation of disability relative to no early relapses, new research suggests. However, in the large registry study, this association was not found in patients treated with high-efficacy, disease-modifying therapies (DMTs) early on.
The results suggest that ,” said lead author Cyrus Daruwalla, MD, department of clinical neurosciences at the University of Cambridge, and Addenbrooke’s Hospital, Cambridge, England.
Dr. Daruwalla presented the findings at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Questioning EMA restrictions
“We designed this project because regulators, including EMA [European Medicines Agency], restrict the use of certain DMTs to only those with disabling relapses. In particular, natalizumab [Tysabri] and fingolimod [Gilenya] can only be used as the first-line therapy for people with rapidly evolving, severe MS – which includes having two disabling relapses in a year,” Dr. Daruwalla noted.
“In clinic, when we see somebody who has a nondisabling relapse, we’re left with the question of what is the prognostic significance of that relapse, and how should it influence treatment decisions,” he added.
Using prospectively collected data from the MSBase international registry, the researchers examined data on individuals with RRMS and complete early relapse severity information.
They compared patients with exclusively nondisabling relapses in the 2 years after definitive RRMS diagnosis with peers with no relapses within this time frame.
To mitigate the confounding effect of DMT use, the investigators performed analyses in participants untreated during follow-up, and then in those who received only older or “platform” therapies (interferon-beta, glatiramer acetate, dimethyl fumarate, or teriflunomide) during follow-up.
In the untreated cohort, 285 patients had nondisabling relapses and 4,717 had no relapses during the 2 years after diagnosis. Those with early nondisabling relapses had a significantly increased risk for disability accumulation (adjusted hazard ratio [aHR], 1.29; 95% confidence interval [CI], 1.00-1.68).
In the treated cohort, 1,074 patients had nondisabling early relapses and 7,262 did not.
In this cohort, those treated with “platform” DMTs who had nondisabling relapses showed a significantly increased risk for disability accumulation compared with treated peers who had no relapses (aHR, 1.33; 95% CI, 1.15-1.54).
Notably, said Dr. Daruwalla, in patients treated at any point during follow-up with high-efficacy DMTs, including monoclonal antibodies, sphingosphine-1 phosphate modulators, and hematopoietic stem cell transplantation, there was no difference in disability accumulation between patients who did and did not experience nondisabling relapses (aHR, 0.90; 95% CI, 0.71-1.13).
The data clearly show that early nondisabling relapses are associated with a higher risk of disability accumulation than no early relapses in people with relapsing remitting MS,” Dr. Daruwalla said.
However, he noted, treatment with high-efficacy DMTs offers protection against disability accumulations.
“Therefore, contrary to EMA guidance, nondisabling relapses should be considered in decisions to initiate or escalate treatment, including with high-efficacy therapies,” he added.
Valuable, confirmatory data
Patricia Coyle, MD, professor of neurology and director of the MS Comprehensive Care Center at Stony Brook (N.Y.) University, called the study “valuable.”
“It confirms prior data that having relapses is bad in MS even if they are mild, and provides additional modest data in support of high-efficacy versus moderate-efficacy DMT,” said Dr. Coyle, who was not involved with the research.
“Although certainly not definitive, it adds to data supporting high-efficacy as preferred treatment [and] addresses a completely arbitrary governmental limitation to DMT use in Europe,” she added.
The study had no commercial funding. Dr. Daruwalla has reported no relevant financial relationships. Dr. Coyle reports having received consulting fees from Accordant, Biogen, Bristol-Myers Squibb, Celgene, Genentech/Roche, GlaxoSmithKline, Horizon, Janssen, Novartis, Sanofi Genzyme, and Viela Bio; and grant funding from Actelion, Alkermes, Bristol-Myers Squibb, CorEvitas, Genentech/Roche, Sanofi Genzyme, MedDay, and Novartis.
A version of this article first appeared on Medscape.com.
FROM ECTRIMS 2022
Stem cell therapy strikes out in progressive MS
In two retrospective studies that drew from the international MSBase registry, . One study looked at progressive MS and found no evidence of superiority. Another study in relapsing-remitting MS showed a reduction in relapses compared with treatment with the immune reconstitution therapies alemtuzumab and cladribine, though the results were not definitive.
Scant evidence supporting AHSCT for progressive MS
Some previous, small retrospective studies had suggested that AHSCT could benefit progressive MS. For example, a study published in Neurology looked at outcomes following AHSCT in 210 patients with MS and found a disability worsening–free survival of 85.5% at 5 years in relapsing-remitting MS and 71.0% in progressive MS. However, such studies are prone to bias, according to Bruce Cree, MD, PhD, who was asked to comment on the progressive MS study. Both studies were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
AHSCT has attracted interest as a treatment for both relapsing-remitting and progressive MS, and some retrospective studies have reported signals of efficacy for both. Despite that, the biology of progressive MS is inconsistent with an expectation of success, said Tomas Kalincik, MD, PhD, who presented the two studies. “AHSCT is primarily a very potent anti-inflammatory therapy. Therefore, it is assumed that where localized, episodic inflammation is not part of the clinical picture, such as nonactive progressive MS forms, AHSCT should not be more effective than standard DMTs. In fact, in these scenarios, the potent DMTs also show at best marginal effect on disability outcomes. Therefore, the lack of evidence for superiority of the effectiveness of AHSCT over natalizumab in progressive MS is not surprising. The clinical implications of our study therefore are that the use of AHSCT in inactive progressive MS cannot be justified based on the presently available data,” said Dr. Kalincik, who is head of neuroimmunology at Royal Melbourne Hospital and head of the Clinical Outcomes Research Unit at the University of Melbourne, in an email exchange.
Dr. Cree agreed. “Right now, based on this very, very large data set that MSBase can afford, there really doesn’t seem to be a basis for this presumption that you’re going to get the therapeutic bang for the buck that you want to see with HSCT,” he said.
Despite the scientific attention that AHSCT has received, Dr. Cree has never been convinced that AHSCT is likely to be broadly useful in MS. “The simple concept is that MS is an autoimmune disease, so if you can reset the immune system, that you would eradicate MS in that individual, and then that individual would be fine thereafter. It’s a bit naive, but nonetheless, it’s an OK concept to begin a series of studies for investigation. I think there’s a potential place for this in relapsing disease, but when it comes to a cure for progressive MS, everything that we understand about this disease is pointing away from a peripheral immune system inflammatory etiology as the driver for what is causing progression, and so we have to, in my opinion, think about other possible etiologies for what might be driving and underlying disability worsening in progressive MS,” said Dr. Cree.
Two studies
In the progressive MS study, the researchers conducted a propensity-matched analysis of 39 patients treated with AHSCT and 65 who were treated with natalizumab. There were no significant differences between the two groups in overall annualized relapse rate or annual relapse rate by year. Disability outcomes were also similar, with no differences in worsening or improvement.
In the relapsing-remitting MS study, Dr. Kalincik’s group drew on data from 6 centers as well as the MSBase registry. They compared outcomes following AHSCT with outcomes of patients taking the immune-reconstitution DMTs mitoxantrone, alemtuzumab, and cladribine. The study included matched cohorts of 135 patients treated with AHSCT versus 312 treated with alemtuzumab, 72 treated with AHSCT versus 164 treated with cladribine, and 30 treated with AHSCT versus 100 treated with mitoxantrone. All groups had similar outcomes, with the exception of a greater likelihood of confirmed disability improvement in treatment with AHSCT versus alemtuzumab (hazard ratio, 1.63; P = .02). The cumulative probability of improvement was higher in the AHSCT group both at year 2 (28% versus 19%) and year 4 (30% versus 22%).
“The analysis suggested trends that may favor the effectiveness AHSCT over alemtuzumab, cladribine, and mitoxantrone, but the analysis was not fully powered. More research with larger cohorts is needed,” said Dr. Kalincik.
Dr. Cree has consulted for Biogen. Dr. Kalincik has financial relationships with Merck, BMS, Roche, Janssen, Sanofi Genzyme, Novartis, Biogen, Eisai, Teva, BioCSL, and Celgene.
In two retrospective studies that drew from the international MSBase registry, . One study looked at progressive MS and found no evidence of superiority. Another study in relapsing-remitting MS showed a reduction in relapses compared with treatment with the immune reconstitution therapies alemtuzumab and cladribine, though the results were not definitive.
Scant evidence supporting AHSCT for progressive MS
Some previous, small retrospective studies had suggested that AHSCT could benefit progressive MS. For example, a study published in Neurology looked at outcomes following AHSCT in 210 patients with MS and found a disability worsening–free survival of 85.5% at 5 years in relapsing-remitting MS and 71.0% in progressive MS. However, such studies are prone to bias, according to Bruce Cree, MD, PhD, who was asked to comment on the progressive MS study. Both studies were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
AHSCT has attracted interest as a treatment for both relapsing-remitting and progressive MS, and some retrospective studies have reported signals of efficacy for both. Despite that, the biology of progressive MS is inconsistent with an expectation of success, said Tomas Kalincik, MD, PhD, who presented the two studies. “AHSCT is primarily a very potent anti-inflammatory therapy. Therefore, it is assumed that where localized, episodic inflammation is not part of the clinical picture, such as nonactive progressive MS forms, AHSCT should not be more effective than standard DMTs. In fact, in these scenarios, the potent DMTs also show at best marginal effect on disability outcomes. Therefore, the lack of evidence for superiority of the effectiveness of AHSCT over natalizumab in progressive MS is not surprising. The clinical implications of our study therefore are that the use of AHSCT in inactive progressive MS cannot be justified based on the presently available data,” said Dr. Kalincik, who is head of neuroimmunology at Royal Melbourne Hospital and head of the Clinical Outcomes Research Unit at the University of Melbourne, in an email exchange.
Dr. Cree agreed. “Right now, based on this very, very large data set that MSBase can afford, there really doesn’t seem to be a basis for this presumption that you’re going to get the therapeutic bang for the buck that you want to see with HSCT,” he said.
Despite the scientific attention that AHSCT has received, Dr. Cree has never been convinced that AHSCT is likely to be broadly useful in MS. “The simple concept is that MS is an autoimmune disease, so if you can reset the immune system, that you would eradicate MS in that individual, and then that individual would be fine thereafter. It’s a bit naive, but nonetheless, it’s an OK concept to begin a series of studies for investigation. I think there’s a potential place for this in relapsing disease, but when it comes to a cure for progressive MS, everything that we understand about this disease is pointing away from a peripheral immune system inflammatory etiology as the driver for what is causing progression, and so we have to, in my opinion, think about other possible etiologies for what might be driving and underlying disability worsening in progressive MS,” said Dr. Cree.
Two studies
In the progressive MS study, the researchers conducted a propensity-matched analysis of 39 patients treated with AHSCT and 65 who were treated with natalizumab. There were no significant differences between the two groups in overall annualized relapse rate or annual relapse rate by year. Disability outcomes were also similar, with no differences in worsening or improvement.
In the relapsing-remitting MS study, Dr. Kalincik’s group drew on data from 6 centers as well as the MSBase registry. They compared outcomes following AHSCT with outcomes of patients taking the immune-reconstitution DMTs mitoxantrone, alemtuzumab, and cladribine. The study included matched cohorts of 135 patients treated with AHSCT versus 312 treated with alemtuzumab, 72 treated with AHSCT versus 164 treated with cladribine, and 30 treated with AHSCT versus 100 treated with mitoxantrone. All groups had similar outcomes, with the exception of a greater likelihood of confirmed disability improvement in treatment with AHSCT versus alemtuzumab (hazard ratio, 1.63; P = .02). The cumulative probability of improvement was higher in the AHSCT group both at year 2 (28% versus 19%) and year 4 (30% versus 22%).
“The analysis suggested trends that may favor the effectiveness AHSCT over alemtuzumab, cladribine, and mitoxantrone, but the analysis was not fully powered. More research with larger cohorts is needed,” said Dr. Kalincik.
Dr. Cree has consulted for Biogen. Dr. Kalincik has financial relationships with Merck, BMS, Roche, Janssen, Sanofi Genzyme, Novartis, Biogen, Eisai, Teva, BioCSL, and Celgene.
In two retrospective studies that drew from the international MSBase registry, . One study looked at progressive MS and found no evidence of superiority. Another study in relapsing-remitting MS showed a reduction in relapses compared with treatment with the immune reconstitution therapies alemtuzumab and cladribine, though the results were not definitive.
Scant evidence supporting AHSCT for progressive MS
Some previous, small retrospective studies had suggested that AHSCT could benefit progressive MS. For example, a study published in Neurology looked at outcomes following AHSCT in 210 patients with MS and found a disability worsening–free survival of 85.5% at 5 years in relapsing-remitting MS and 71.0% in progressive MS. However, such studies are prone to bias, according to Bruce Cree, MD, PhD, who was asked to comment on the progressive MS study. Both studies were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
AHSCT has attracted interest as a treatment for both relapsing-remitting and progressive MS, and some retrospective studies have reported signals of efficacy for both. Despite that, the biology of progressive MS is inconsistent with an expectation of success, said Tomas Kalincik, MD, PhD, who presented the two studies. “AHSCT is primarily a very potent anti-inflammatory therapy. Therefore, it is assumed that where localized, episodic inflammation is not part of the clinical picture, such as nonactive progressive MS forms, AHSCT should not be more effective than standard DMTs. In fact, in these scenarios, the potent DMTs also show at best marginal effect on disability outcomes. Therefore, the lack of evidence for superiority of the effectiveness of AHSCT over natalizumab in progressive MS is not surprising. The clinical implications of our study therefore are that the use of AHSCT in inactive progressive MS cannot be justified based on the presently available data,” said Dr. Kalincik, who is head of neuroimmunology at Royal Melbourne Hospital and head of the Clinical Outcomes Research Unit at the University of Melbourne, in an email exchange.
Dr. Cree agreed. “Right now, based on this very, very large data set that MSBase can afford, there really doesn’t seem to be a basis for this presumption that you’re going to get the therapeutic bang for the buck that you want to see with HSCT,” he said.
Despite the scientific attention that AHSCT has received, Dr. Cree has never been convinced that AHSCT is likely to be broadly useful in MS. “The simple concept is that MS is an autoimmune disease, so if you can reset the immune system, that you would eradicate MS in that individual, and then that individual would be fine thereafter. It’s a bit naive, but nonetheless, it’s an OK concept to begin a series of studies for investigation. I think there’s a potential place for this in relapsing disease, but when it comes to a cure for progressive MS, everything that we understand about this disease is pointing away from a peripheral immune system inflammatory etiology as the driver for what is causing progression, and so we have to, in my opinion, think about other possible etiologies for what might be driving and underlying disability worsening in progressive MS,” said Dr. Cree.
Two studies
In the progressive MS study, the researchers conducted a propensity-matched analysis of 39 patients treated with AHSCT and 65 who were treated with natalizumab. There were no significant differences between the two groups in overall annualized relapse rate or annual relapse rate by year. Disability outcomes were also similar, with no differences in worsening or improvement.
In the relapsing-remitting MS study, Dr. Kalincik’s group drew on data from 6 centers as well as the MSBase registry. They compared outcomes following AHSCT with outcomes of patients taking the immune-reconstitution DMTs mitoxantrone, alemtuzumab, and cladribine. The study included matched cohorts of 135 patients treated with AHSCT versus 312 treated with alemtuzumab, 72 treated with AHSCT versus 164 treated with cladribine, and 30 treated with AHSCT versus 100 treated with mitoxantrone. All groups had similar outcomes, with the exception of a greater likelihood of confirmed disability improvement in treatment with AHSCT versus alemtuzumab (hazard ratio, 1.63; P = .02). The cumulative probability of improvement was higher in the AHSCT group both at year 2 (28% versus 19%) and year 4 (30% versus 22%).
“The analysis suggested trends that may favor the effectiveness AHSCT over alemtuzumab, cladribine, and mitoxantrone, but the analysis was not fully powered. More research with larger cohorts is needed,” said Dr. Kalincik.
Dr. Cree has consulted for Biogen. Dr. Kalincik has financial relationships with Merck, BMS, Roche, Janssen, Sanofi Genzyme, Novartis, Biogen, Eisai, Teva, BioCSL, and Celgene.
FROM ECTRIMS 2022
More evidence for EBV’s role in MS
In 2022, two studies received quite a bit of attention. One showed that EBV seroconversion occurs in the years prior to MS diagnosis in virtually every patient, and that serum levels of the neuronal damage biomarker neurofilament light (NfL) rose following EBV infection. Another paper showed anti-EBNA (Epstein-Barr nuclear antigen) antibodies in the cerebrospinal fluid cross-react with the central nervous system antigen GlialCAM in some MS patients.
Based on those studies, “it’s tempting to speculate that primary EBV infection could be a trigger to the autoimmune process suspected for MS,” said Tilman Schneider-Hohendorf, PhD, during a presentation at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Dr. Schneider-Hohendorf, who is a postdoctoral fellow at the University of Münster, Germany, presented a new study that added more evidence that EBV may be a key player in MS pathogenesis. He and colleagues conducted a genetic analysis of patient T cells and found evidence that EBV viral activity may be occurring during MS.
A viral pathway to MS
Asked for comment, Bruce Cree, MD, PhD, said: “I think it is a very interesting one, because what we know about EBV is that it’s a risk factor for MS. So many studies performed over the last 20 years have shown a very strong association between EBV infection and the occurrence of MS. Studies have shown quite conclusively that EBV infection precedes MS in almost every patient, and that EBV infection is followed by a rise in serum NfL, which is a biomarker of neuronal damage. You have EBV infection, and then typically several years later a rise in serum concentrations of this marker of neuronal injury, and this is all in a presymptomatic state. Then that is followed by the onset of clinical symptoms in MS. That temporal sequence, I think, is very convincing,” said Dr. Cree, who is a professor of clinical neurology at the University of California, San Francisco.
He pointed out that EBV is not the sole causal pathway of MS, since genetic and environmental factors are known to be involved. “Nonetheless, it’s very strong evidence to indicate that this virus is involved in disease pathogenesis,” said Dr. Cree.
The new research takes the work a step further by revealing a population of T cells in MS patients that appear to be responding directly to EBV during active viral disease. That could be telling because most people who experience an EBV infection and experience mononucleosis recover, and some never even realize they have been infected. As a herpes virus, EBV remains in a latent state in B cells and other immune cells. “We know that you need an EBV infection (to trigger MS), but is EBV in some way continuing to be active in MS?” said Dr. Cree.
Other groups have looked for such evidence, but results have been mixed. Dr. Cree’s own group looked for evidence of EBV in spinal fluid of MS patients when they first present with symptoms, and could find no evidence. On the other hand, an autopsy study of MS patients has found evidence of chronic EBV infection in and around the brain, including the meninges, which could implicate the B cells found in that region. Another study found EBV-targeting antibodies that cross react with neuronal antigens in the cerebral spinal fluid of MS patients. “So depending on the assay used and the types of investigation, there is variable evidence to indicate that EBV has a role in ongoing MS pathogenesis – that it isn’t just a risk factor for MS that triggers the disease but potentially has a role in determining the course of MS,” said Dr. Cree.
IS EBV part of MS pathogenesis?
The new study presented at ECTRIMS by Dr. Schneider-Hohendorf offered evidence that MS patients have excess CD8-positive T cells that recognize EBV antigens typically shed during active viral infection. The results suggest “that the immune system is responding to that chronic infection,” said Dr. Cree.
The findings have some implications for a clinical study now in progress, called EMBOLD, which is looking at whether a heterologous infusion of T cells that have been primed to attack EBV could improve symptoms of progressive MS. “The hypothesis there is that chronically infected cells within the body are causing progressive MS and that if we could eradicate those cells, both within the central nervous system and within the periphery, perhaps we could see improvement in MS functional outcomes,” said Dr. Cree, who is a co-investigator for the EMBOLD study. The trial is using T cells from donors that are matched for the human leukocyte antigen complex, which is hoped will target and kill EBV-infected cells.
The study presented by Dr. Schneider-Hohendorf supports the approach. “There is an implication from this study that the trial that that’s currently being conducted might actually possibly have a benefit in the sense that there’s now another piece of evidence to indicate that EBV is not only a risk factor for MS, but may actually participate during the course of the disease as part of the pathogenesis,” said Dr. Cree.
In the new study, the researchers sequenced the T-cell receptor variable beta-chain (TRBV) peripheral repertoire among three cohorts of MS patients: A discovery cohort with 1,336 patients with MS and 229 controls; a validation cohort with 59 patients with MS and 51 controls; and 35 monozygotic twins who were discordant for MS. They identified sequences known to bind to EBV, SARS-CoV-2, cytomegalovirus, and influenza A, and used the latter three viruses as a proof of concept to demonstrate the validity of the approach. EBV-specific MHC-1 restricted CD8 TRBV in the serum of MS patients, with large effect sizes in the discovery (+2.2), validation (+2.1), and MS twin (+1.6) populations. The findings in the twin population rule out a genetic or environmental explanation for the findings in the discovery and validation cohorts, according to Dr. Schneider-Hohendorf.
The researchers also sequenced CSF among six healthy donors and five patients with MS and found significant differences. The T-cell populations had more lytic properties that suggested ongoing immune surveillance. “We can conclude that we found a broader response that could indicate an aberrant immune response. This could be a remnant of disease triggering an event or it could indicate an ongoing immune response to EBV. Is this EBV activity? We really don’t know. To find out, we would expand our pathogen-specific sequences, we would assess CNS tissue and lesions, and we would define the primary response in pediatric cohorts to better understand what might go wrong,” Dr. Schneider-Hohendorf concluded.
Dr. Cree has a financial relationship with Biogen and is a co-investigator for the EMBOLD trial. Dr. Schneider-Hohendorf has financial relationships with Biogen, Novartis, and Roche.
In 2022, two studies received quite a bit of attention. One showed that EBV seroconversion occurs in the years prior to MS diagnosis in virtually every patient, and that serum levels of the neuronal damage biomarker neurofilament light (NfL) rose following EBV infection. Another paper showed anti-EBNA (Epstein-Barr nuclear antigen) antibodies in the cerebrospinal fluid cross-react with the central nervous system antigen GlialCAM in some MS patients.
Based on those studies, “it’s tempting to speculate that primary EBV infection could be a trigger to the autoimmune process suspected for MS,” said Tilman Schneider-Hohendorf, PhD, during a presentation at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Dr. Schneider-Hohendorf, who is a postdoctoral fellow at the University of Münster, Germany, presented a new study that added more evidence that EBV may be a key player in MS pathogenesis. He and colleagues conducted a genetic analysis of patient T cells and found evidence that EBV viral activity may be occurring during MS.
A viral pathway to MS
Asked for comment, Bruce Cree, MD, PhD, said: “I think it is a very interesting one, because what we know about EBV is that it’s a risk factor for MS. So many studies performed over the last 20 years have shown a very strong association between EBV infection and the occurrence of MS. Studies have shown quite conclusively that EBV infection precedes MS in almost every patient, and that EBV infection is followed by a rise in serum NfL, which is a biomarker of neuronal damage. You have EBV infection, and then typically several years later a rise in serum concentrations of this marker of neuronal injury, and this is all in a presymptomatic state. Then that is followed by the onset of clinical symptoms in MS. That temporal sequence, I think, is very convincing,” said Dr. Cree, who is a professor of clinical neurology at the University of California, San Francisco.
He pointed out that EBV is not the sole causal pathway of MS, since genetic and environmental factors are known to be involved. “Nonetheless, it’s very strong evidence to indicate that this virus is involved in disease pathogenesis,” said Dr. Cree.
The new research takes the work a step further by revealing a population of T cells in MS patients that appear to be responding directly to EBV during active viral disease. That could be telling because most people who experience an EBV infection and experience mononucleosis recover, and some never even realize they have been infected. As a herpes virus, EBV remains in a latent state in B cells and other immune cells. “We know that you need an EBV infection (to trigger MS), but is EBV in some way continuing to be active in MS?” said Dr. Cree.
Other groups have looked for such evidence, but results have been mixed. Dr. Cree’s own group looked for evidence of EBV in spinal fluid of MS patients when they first present with symptoms, and could find no evidence. On the other hand, an autopsy study of MS patients has found evidence of chronic EBV infection in and around the brain, including the meninges, which could implicate the B cells found in that region. Another study found EBV-targeting antibodies that cross react with neuronal antigens in the cerebral spinal fluid of MS patients. “So depending on the assay used and the types of investigation, there is variable evidence to indicate that EBV has a role in ongoing MS pathogenesis – that it isn’t just a risk factor for MS that triggers the disease but potentially has a role in determining the course of MS,” said Dr. Cree.
IS EBV part of MS pathogenesis?
The new study presented at ECTRIMS by Dr. Schneider-Hohendorf offered evidence that MS patients have excess CD8-positive T cells that recognize EBV antigens typically shed during active viral infection. The results suggest “that the immune system is responding to that chronic infection,” said Dr. Cree.
The findings have some implications for a clinical study now in progress, called EMBOLD, which is looking at whether a heterologous infusion of T cells that have been primed to attack EBV could improve symptoms of progressive MS. “The hypothesis there is that chronically infected cells within the body are causing progressive MS and that if we could eradicate those cells, both within the central nervous system and within the periphery, perhaps we could see improvement in MS functional outcomes,” said Dr. Cree, who is a co-investigator for the EMBOLD study. The trial is using T cells from donors that are matched for the human leukocyte antigen complex, which is hoped will target and kill EBV-infected cells.
The study presented by Dr. Schneider-Hohendorf supports the approach. “There is an implication from this study that the trial that that’s currently being conducted might actually possibly have a benefit in the sense that there’s now another piece of evidence to indicate that EBV is not only a risk factor for MS, but may actually participate during the course of the disease as part of the pathogenesis,” said Dr. Cree.
In the new study, the researchers sequenced the T-cell receptor variable beta-chain (TRBV) peripheral repertoire among three cohorts of MS patients: A discovery cohort with 1,336 patients with MS and 229 controls; a validation cohort with 59 patients with MS and 51 controls; and 35 monozygotic twins who were discordant for MS. They identified sequences known to bind to EBV, SARS-CoV-2, cytomegalovirus, and influenza A, and used the latter three viruses as a proof of concept to demonstrate the validity of the approach. EBV-specific MHC-1 restricted CD8 TRBV in the serum of MS patients, with large effect sizes in the discovery (+2.2), validation (+2.1), and MS twin (+1.6) populations. The findings in the twin population rule out a genetic or environmental explanation for the findings in the discovery and validation cohorts, according to Dr. Schneider-Hohendorf.
The researchers also sequenced CSF among six healthy donors and five patients with MS and found significant differences. The T-cell populations had more lytic properties that suggested ongoing immune surveillance. “We can conclude that we found a broader response that could indicate an aberrant immune response. This could be a remnant of disease triggering an event or it could indicate an ongoing immune response to EBV. Is this EBV activity? We really don’t know. To find out, we would expand our pathogen-specific sequences, we would assess CNS tissue and lesions, and we would define the primary response in pediatric cohorts to better understand what might go wrong,” Dr. Schneider-Hohendorf concluded.
Dr. Cree has a financial relationship with Biogen and is a co-investigator for the EMBOLD trial. Dr. Schneider-Hohendorf has financial relationships with Biogen, Novartis, and Roche.
In 2022, two studies received quite a bit of attention. One showed that EBV seroconversion occurs in the years prior to MS diagnosis in virtually every patient, and that serum levels of the neuronal damage biomarker neurofilament light (NfL) rose following EBV infection. Another paper showed anti-EBNA (Epstein-Barr nuclear antigen) antibodies in the cerebrospinal fluid cross-react with the central nervous system antigen GlialCAM in some MS patients.
Based on those studies, “it’s tempting to speculate that primary EBV infection could be a trigger to the autoimmune process suspected for MS,” said Tilman Schneider-Hohendorf, PhD, during a presentation at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Dr. Schneider-Hohendorf, who is a postdoctoral fellow at the University of Münster, Germany, presented a new study that added more evidence that EBV may be a key player in MS pathogenesis. He and colleagues conducted a genetic analysis of patient T cells and found evidence that EBV viral activity may be occurring during MS.
A viral pathway to MS
Asked for comment, Bruce Cree, MD, PhD, said: “I think it is a very interesting one, because what we know about EBV is that it’s a risk factor for MS. So many studies performed over the last 20 years have shown a very strong association between EBV infection and the occurrence of MS. Studies have shown quite conclusively that EBV infection precedes MS in almost every patient, and that EBV infection is followed by a rise in serum NfL, which is a biomarker of neuronal damage. You have EBV infection, and then typically several years later a rise in serum concentrations of this marker of neuronal injury, and this is all in a presymptomatic state. Then that is followed by the onset of clinical symptoms in MS. That temporal sequence, I think, is very convincing,” said Dr. Cree, who is a professor of clinical neurology at the University of California, San Francisco.
He pointed out that EBV is not the sole causal pathway of MS, since genetic and environmental factors are known to be involved. “Nonetheless, it’s very strong evidence to indicate that this virus is involved in disease pathogenesis,” said Dr. Cree.
The new research takes the work a step further by revealing a population of T cells in MS patients that appear to be responding directly to EBV during active viral disease. That could be telling because most people who experience an EBV infection and experience mononucleosis recover, and some never even realize they have been infected. As a herpes virus, EBV remains in a latent state in B cells and other immune cells. “We know that you need an EBV infection (to trigger MS), but is EBV in some way continuing to be active in MS?” said Dr. Cree.
Other groups have looked for such evidence, but results have been mixed. Dr. Cree’s own group looked for evidence of EBV in spinal fluid of MS patients when they first present with symptoms, and could find no evidence. On the other hand, an autopsy study of MS patients has found evidence of chronic EBV infection in and around the brain, including the meninges, which could implicate the B cells found in that region. Another study found EBV-targeting antibodies that cross react with neuronal antigens in the cerebral spinal fluid of MS patients. “So depending on the assay used and the types of investigation, there is variable evidence to indicate that EBV has a role in ongoing MS pathogenesis – that it isn’t just a risk factor for MS that triggers the disease but potentially has a role in determining the course of MS,” said Dr. Cree.
IS EBV part of MS pathogenesis?
The new study presented at ECTRIMS by Dr. Schneider-Hohendorf offered evidence that MS patients have excess CD8-positive T cells that recognize EBV antigens typically shed during active viral infection. The results suggest “that the immune system is responding to that chronic infection,” said Dr. Cree.
The findings have some implications for a clinical study now in progress, called EMBOLD, which is looking at whether a heterologous infusion of T cells that have been primed to attack EBV could improve symptoms of progressive MS. “The hypothesis there is that chronically infected cells within the body are causing progressive MS and that if we could eradicate those cells, both within the central nervous system and within the periphery, perhaps we could see improvement in MS functional outcomes,” said Dr. Cree, who is a co-investigator for the EMBOLD study. The trial is using T cells from donors that are matched for the human leukocyte antigen complex, which is hoped will target and kill EBV-infected cells.
The study presented by Dr. Schneider-Hohendorf supports the approach. “There is an implication from this study that the trial that that’s currently being conducted might actually possibly have a benefit in the sense that there’s now another piece of evidence to indicate that EBV is not only a risk factor for MS, but may actually participate during the course of the disease as part of the pathogenesis,” said Dr. Cree.
In the new study, the researchers sequenced the T-cell receptor variable beta-chain (TRBV) peripheral repertoire among three cohorts of MS patients: A discovery cohort with 1,336 patients with MS and 229 controls; a validation cohort with 59 patients with MS and 51 controls; and 35 monozygotic twins who were discordant for MS. They identified sequences known to bind to EBV, SARS-CoV-2, cytomegalovirus, and influenza A, and used the latter three viruses as a proof of concept to demonstrate the validity of the approach. EBV-specific MHC-1 restricted CD8 TRBV in the serum of MS patients, with large effect sizes in the discovery (+2.2), validation (+2.1), and MS twin (+1.6) populations. The findings in the twin population rule out a genetic or environmental explanation for the findings in the discovery and validation cohorts, according to Dr. Schneider-Hohendorf.
The researchers also sequenced CSF among six healthy donors and five patients with MS and found significant differences. The T-cell populations had more lytic properties that suggested ongoing immune surveillance. “We can conclude that we found a broader response that could indicate an aberrant immune response. This could be a remnant of disease triggering an event or it could indicate an ongoing immune response to EBV. Is this EBV activity? We really don’t know. To find out, we would expand our pathogen-specific sequences, we would assess CNS tissue and lesions, and we would define the primary response in pediatric cohorts to better understand what might go wrong,” Dr. Schneider-Hohendorf concluded.
Dr. Cree has a financial relationship with Biogen and is a co-investigator for the EMBOLD trial. Dr. Schneider-Hohendorf has financial relationships with Biogen, Novartis, and Roche.
FROM ECTRIMS 2022
New research confirms recommendations on COVID-19 boosters in MS
, as currently recommended.
“We have shown that even MS patients whose B cells were depleted from circulation with ocrelizumab can mount immune responses to COVID-19 vaccines,” said lead study author Ilya Kister, MD, of NYU Langone’s Multiple Sclerosis Comprehensive Care Center in New York.
The findings were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
VIOLA study
The data stem from VIOLA, an ongoing prospective study of humoral and cellular immune responses to COVID-19 vaccines in 60 patients with MS receiving ocrelizumab at MS care centers at NYU Langone and the University of Colorado Denver.
The mean age of participants was 38 years, 73% were women, all had been taking ocrelizumab for a mean of 1.7 years, and 45% had had COVID-19 prior to vaccination.
The researchers examined antibody and cellular responses to the two-dose series of mRNA COVID-19 vaccine (80% received the Pfizer-BioNTech vaccine, 18% the Moderna vaccine, and 2% unknown) over 24 weeks. In addition, 57% of the participants received the third dose/booster.
Results showed that antibody and cellular responses to SARS-CoV-2 spike protein significantly increased after the two-dose mRNA COVID-19 vaccination, though antibody responses tended to peak between 4 and 12 weeks and declined thereafter. There was no significant decline in cellular responses at week 24.
“The third dose ‘booster’ again significantly increased antibody and cellular responses compared with the pre–third dose levels,” Dr. Kister said.
“Importantly, cellular responses remained elevated or even increased from 4 weeks to 12 weeks after third dose/booster. Overall, these data strongly support the need for a third dose in MS patients on ocrelizumab,” Dr. Kister added.
Participants with “hybrid immunity” (those who had been infected with SARS-CoV-2 and who had also been vaccinated for COVID) had markedly higher SARS-CoV-2–specific antibody and cellular responses than those of peers with vaccine-only immunity.
CDC recs
Looking ahead, Dr. Kister said the VIOLA investigators plan to present data on the durability of COVID-19 vaccines in ocrelizumab-treated patients up to 48 weeks after the third dose.
For immunocompromised patients, such as those taking ocrelizumab, the Centers for Disease Control and Prevention considers the third dose of mRNA vaccine not as a “booster” but as part of the regular vaccine series.
“In other words, all these patients should receive three doses as part of their ‘primary’ series,” Dr. Kister noted.
The CDC also recommends receiving the updated booster for COVID-19 that became available in September 2022 (the fourth dose of the vaccine).
“Our study did not evaluate the efficacy of this fourth dose; but based on our results, it is reasonable to suppose that the fourth dose would also lead to a further increase in immune defenses,” Dr. Kister said.
The VIOLA study is an investigator-initiated collaboration supported by F. Hoffmann-La Roche Ltd/Genentech Inc. Dr. Kister has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, as currently recommended.
“We have shown that even MS patients whose B cells were depleted from circulation with ocrelizumab can mount immune responses to COVID-19 vaccines,” said lead study author Ilya Kister, MD, of NYU Langone’s Multiple Sclerosis Comprehensive Care Center in New York.
The findings were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
VIOLA study
The data stem from VIOLA, an ongoing prospective study of humoral and cellular immune responses to COVID-19 vaccines in 60 patients with MS receiving ocrelizumab at MS care centers at NYU Langone and the University of Colorado Denver.
The mean age of participants was 38 years, 73% were women, all had been taking ocrelizumab for a mean of 1.7 years, and 45% had had COVID-19 prior to vaccination.
The researchers examined antibody and cellular responses to the two-dose series of mRNA COVID-19 vaccine (80% received the Pfizer-BioNTech vaccine, 18% the Moderna vaccine, and 2% unknown) over 24 weeks. In addition, 57% of the participants received the third dose/booster.
Results showed that antibody and cellular responses to SARS-CoV-2 spike protein significantly increased after the two-dose mRNA COVID-19 vaccination, though antibody responses tended to peak between 4 and 12 weeks and declined thereafter. There was no significant decline in cellular responses at week 24.
“The third dose ‘booster’ again significantly increased antibody and cellular responses compared with the pre–third dose levels,” Dr. Kister said.
“Importantly, cellular responses remained elevated or even increased from 4 weeks to 12 weeks after third dose/booster. Overall, these data strongly support the need for a third dose in MS patients on ocrelizumab,” Dr. Kister added.
Participants with “hybrid immunity” (those who had been infected with SARS-CoV-2 and who had also been vaccinated for COVID) had markedly higher SARS-CoV-2–specific antibody and cellular responses than those of peers with vaccine-only immunity.
CDC recs
Looking ahead, Dr. Kister said the VIOLA investigators plan to present data on the durability of COVID-19 vaccines in ocrelizumab-treated patients up to 48 weeks after the third dose.
For immunocompromised patients, such as those taking ocrelizumab, the Centers for Disease Control and Prevention considers the third dose of mRNA vaccine not as a “booster” but as part of the regular vaccine series.
“In other words, all these patients should receive three doses as part of their ‘primary’ series,” Dr. Kister noted.
The CDC also recommends receiving the updated booster for COVID-19 that became available in September 2022 (the fourth dose of the vaccine).
“Our study did not evaluate the efficacy of this fourth dose; but based on our results, it is reasonable to suppose that the fourth dose would also lead to a further increase in immune defenses,” Dr. Kister said.
The VIOLA study is an investigator-initiated collaboration supported by F. Hoffmann-La Roche Ltd/Genentech Inc. Dr. Kister has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, as currently recommended.
“We have shown that even MS patients whose B cells were depleted from circulation with ocrelizumab can mount immune responses to COVID-19 vaccines,” said lead study author Ilya Kister, MD, of NYU Langone’s Multiple Sclerosis Comprehensive Care Center in New York.
The findings were presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
VIOLA study
The data stem from VIOLA, an ongoing prospective study of humoral and cellular immune responses to COVID-19 vaccines in 60 patients with MS receiving ocrelizumab at MS care centers at NYU Langone and the University of Colorado Denver.
The mean age of participants was 38 years, 73% were women, all had been taking ocrelizumab for a mean of 1.7 years, and 45% had had COVID-19 prior to vaccination.
The researchers examined antibody and cellular responses to the two-dose series of mRNA COVID-19 vaccine (80% received the Pfizer-BioNTech vaccine, 18% the Moderna vaccine, and 2% unknown) over 24 weeks. In addition, 57% of the participants received the third dose/booster.
Results showed that antibody and cellular responses to SARS-CoV-2 spike protein significantly increased after the two-dose mRNA COVID-19 vaccination, though antibody responses tended to peak between 4 and 12 weeks and declined thereafter. There was no significant decline in cellular responses at week 24.
“The third dose ‘booster’ again significantly increased antibody and cellular responses compared with the pre–third dose levels,” Dr. Kister said.
“Importantly, cellular responses remained elevated or even increased from 4 weeks to 12 weeks after third dose/booster. Overall, these data strongly support the need for a third dose in MS patients on ocrelizumab,” Dr. Kister added.
Participants with “hybrid immunity” (those who had been infected with SARS-CoV-2 and who had also been vaccinated for COVID) had markedly higher SARS-CoV-2–specific antibody and cellular responses than those of peers with vaccine-only immunity.
CDC recs
Looking ahead, Dr. Kister said the VIOLA investigators plan to present data on the durability of COVID-19 vaccines in ocrelizumab-treated patients up to 48 weeks after the third dose.
For immunocompromised patients, such as those taking ocrelizumab, the Centers for Disease Control and Prevention considers the third dose of mRNA vaccine not as a “booster” but as part of the regular vaccine series.
“In other words, all these patients should receive three doses as part of their ‘primary’ series,” Dr. Kister noted.
The CDC also recommends receiving the updated booster for COVID-19 that became available in September 2022 (the fourth dose of the vaccine).
“Our study did not evaluate the efficacy of this fourth dose; but based on our results, it is reasonable to suppose that the fourth dose would also lead to a further increase in immune defenses,” Dr. Kister said.
The VIOLA study is an investigator-initiated collaboration supported by F. Hoffmann-La Roche Ltd/Genentech Inc. Dr. Kister has reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
From ECTRIMS 2022
GFAP may complement NfL as MS biomarker
Neurofilament light chain (NfL) is a biomarker for both disease progression and treatment response in multiple sclerosis (MS), but the search continues for additional biomarkers to distinguish between disease activity and progression.
At a session of the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), researchers presented evidence that Acceptance of NfL wasn’t universal, either.
Patients with MS follow wide-ranging disease courses, and disability arises due to two partially independent mechanisms, according to Stephanie Meier, who presented results suggests from a study of two cohorts. “Firstly, the acute disease activity leading to relapse associated worsening or RAW (relapse-associated worsening), and secondly the chronic deterioration of neurologic functions leading to progression independent of relapse activity,” said Ms. Meier, a PhD student at University of Basel, Switzerland.
GFAP and NfL may be complementary biomarkers
NfL is a structural protein of neurons, while GFAP is a structure protein of astrocytes. NfL therefore reflects neuronal damage, while GFAP is an indicator of astrogliosis and astrocytic damage. GFAP has been shown to be increased in progressive MS and has been applied in traumatic brain injury and neuromyelitis optica spectrum disorder, according to Ms. Meier.
Her group examined data from two cohorts with “extreme” phenotypes. One cohort included 169 patients with stable MS and 184 with worsening disease progression but no sign of relapses. The other was a focal inflammation cohort that comprised paired samples from 66 patients: One sample from an active time point characterized by a relapse or at least one contrast-enhancing lesion (CEL) detected in the previous 30 days, and one remission sample when there was no relapse in the past year and no CEL in the previous 6 months.
The focal inflammation cohort demonstrated an association between raised NfL levels, with a 53% increase in predicted serum NfL during the active state after a multivariate analysis (P < .0001). GFAP values, on the other hand, were nearly identical.
In the progression cohort, there was more total yearly brain loss in the worsening group (0.42% vs. 0.14%; P = .0005). Baseline GFAP predicted gray matter atrophy (–0.24% per year, P < .0001) but NfL did not. The reverse was true for white matter atrophy, with NfL being predictive (–0.26% per year; P < .0001) but not GFAP.
“The use of biomarkers such as NfL and GFAP could be useful to understand the MS disease course by detecting disease activity that is not usually measurable with standard methods,” said Ms. Meier.
“We found that NfL was strongly associated with acute inflammation and prognosticated white matter volume loss, while GFAP has a potential as a prognostic biomarker for disease worsening, including progression independent of relapse activity, and baseline GFAP also prognosticated gray matter volume loss. From this we can conclude that serum GFAP is a promising biomarker reflecting progression in MS and it is complementary to NfL, as NfL is more strongly associated with acute inflammatory activity,” said Ms. Meier.
A biomarker of disease progression
In another presentation, Mark Wessels, MD, PhD, discussed use of GFAP as a biomarker of disease progression among patients treated with natalizumab. He noted that heightened levels of GFAP are found in astrocytes in chronic MS lesions. Serum GFAP also has been linked to lesion load and clinical outcomes in relapsing-remitting MS.
“The overall aim of our study was to evaluate the value of serum GFAP to monitor disability progression and treatment response in a natalizumab-treated cohort in which disease activity is effectively suppressed, and we did this by investigating GFAP as biomarker for progression despite suppression of inflammation,” said Dr. Wessels, a neurologist at Amsterdam University Medical Center.
The researchers evaluated data from an observational cohort at their institution in Amsterdam. GFAP decreased significantly after 3 months of treatment in both groups, then stabilized, but there was no difference between the groups. GFAP correlated with ventricle fraction at all time points with the exception of the last follow-up. It also correlated with lesion volume. However, GFAP did not correlate with whole brain parenchyma volume over time. There was no difference in GFAP among treatment responders and nonresponders.
Baseline serum GFAP predicted the annualized rate of ventricle volume change (P = .009). At 12 months it predicted both annualized rate of ventricle volume change (P = .009) and thalamus volume (P = .025).
“We’ve been struggling with how to interpret this data. We did see that GFAP and inflammation appear to be associated with each other. What supports this interpretation is that the GFAP decreased significantly after starting high efficacy treatments, namely natalizumab. We also found some clues that GFAP and brain atrophy may have a relationship with each other. Our conclusions weren’t entirely conclusive, possibly due to our smaller cohort sizes, and the use of various MRI scans over the years. And then the question of today was whether GFAP should be implemented in the clinic. Unfortunately, we couldn’t find evidence for use of GFAP as a disease progression biomarker, but we did find some clues of its use as both monitoring lesion volume and monitoring brain atrophy, making it still an interesting biomarker,” said Dr. Wessels.
What does it all mean?
In the Q&A session following the talks, one audience member challenged some of the assumptions behind the use of NfL and GFAP. “We don’t really know what these proteins actually do, and what they truly measure,” he said. Another criticism voiced by the commenter was that the platforms used to measure high and low values may be inconsistent. Finally, there are questions about the underlying theory. “I think our simplistic model for thinking that these are all just measurements of damage is potentially something that we have to reassess … or the assumption that these measures have to correlate to brain atrophy, as if that’s a gold standard. We all know that brain atrophy has totally failed us in the clinic and been incapable of giving us anything that’s useful for monitoring our patients,” said the questioner.
Elias Sotirchos, MD, who presented on NfL values and brain atrophy MS patients, agreed that it’s important to compare values across platforms to ensure consistency. He also cited potential issues with reference populations, since there may be a variety of contributors to neurotoxicity based on behaviors such as smoking, drinking, or comorbidities. “The selection of the reference population is important to be a representative of the MS population in which we are trying to apply that measurement of that normative value,” said Dr. Sotirchos, assistant professor of neurology at Johns Hopkins Medicine, Baltimore.
Ms. Basel and Dr. Wessels have no relevant financial disclosures. Dr. Sotirchos has financial relationships with Alexion, Viela Bio, Horizon Therapeutics, Genentech, Biogen, and Ad Scientiam.
Neurofilament light chain (NfL) is a biomarker for both disease progression and treatment response in multiple sclerosis (MS), but the search continues for additional biomarkers to distinguish between disease activity and progression.
At a session of the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), researchers presented evidence that Acceptance of NfL wasn’t universal, either.
Patients with MS follow wide-ranging disease courses, and disability arises due to two partially independent mechanisms, according to Stephanie Meier, who presented results suggests from a study of two cohorts. “Firstly, the acute disease activity leading to relapse associated worsening or RAW (relapse-associated worsening), and secondly the chronic deterioration of neurologic functions leading to progression independent of relapse activity,” said Ms. Meier, a PhD student at University of Basel, Switzerland.
GFAP and NfL may be complementary biomarkers
NfL is a structural protein of neurons, while GFAP is a structure protein of astrocytes. NfL therefore reflects neuronal damage, while GFAP is an indicator of astrogliosis and astrocytic damage. GFAP has been shown to be increased in progressive MS and has been applied in traumatic brain injury and neuromyelitis optica spectrum disorder, according to Ms. Meier.
Her group examined data from two cohorts with “extreme” phenotypes. One cohort included 169 patients with stable MS and 184 with worsening disease progression but no sign of relapses. The other was a focal inflammation cohort that comprised paired samples from 66 patients: One sample from an active time point characterized by a relapse or at least one contrast-enhancing lesion (CEL) detected in the previous 30 days, and one remission sample when there was no relapse in the past year and no CEL in the previous 6 months.
The focal inflammation cohort demonstrated an association between raised NfL levels, with a 53% increase in predicted serum NfL during the active state after a multivariate analysis (P < .0001). GFAP values, on the other hand, were nearly identical.
In the progression cohort, there was more total yearly brain loss in the worsening group (0.42% vs. 0.14%; P = .0005). Baseline GFAP predicted gray matter atrophy (–0.24% per year, P < .0001) but NfL did not. The reverse was true for white matter atrophy, with NfL being predictive (–0.26% per year; P < .0001) but not GFAP.
“The use of biomarkers such as NfL and GFAP could be useful to understand the MS disease course by detecting disease activity that is not usually measurable with standard methods,” said Ms. Meier.
“We found that NfL was strongly associated with acute inflammation and prognosticated white matter volume loss, while GFAP has a potential as a prognostic biomarker for disease worsening, including progression independent of relapse activity, and baseline GFAP also prognosticated gray matter volume loss. From this we can conclude that serum GFAP is a promising biomarker reflecting progression in MS and it is complementary to NfL, as NfL is more strongly associated with acute inflammatory activity,” said Ms. Meier.
A biomarker of disease progression
In another presentation, Mark Wessels, MD, PhD, discussed use of GFAP as a biomarker of disease progression among patients treated with natalizumab. He noted that heightened levels of GFAP are found in astrocytes in chronic MS lesions. Serum GFAP also has been linked to lesion load and clinical outcomes in relapsing-remitting MS.
“The overall aim of our study was to evaluate the value of serum GFAP to monitor disability progression and treatment response in a natalizumab-treated cohort in which disease activity is effectively suppressed, and we did this by investigating GFAP as biomarker for progression despite suppression of inflammation,” said Dr. Wessels, a neurologist at Amsterdam University Medical Center.
The researchers evaluated data from an observational cohort at their institution in Amsterdam. GFAP decreased significantly after 3 months of treatment in both groups, then stabilized, but there was no difference between the groups. GFAP correlated with ventricle fraction at all time points with the exception of the last follow-up. It also correlated with lesion volume. However, GFAP did not correlate with whole brain parenchyma volume over time. There was no difference in GFAP among treatment responders and nonresponders.
Baseline serum GFAP predicted the annualized rate of ventricle volume change (P = .009). At 12 months it predicted both annualized rate of ventricle volume change (P = .009) and thalamus volume (P = .025).
“We’ve been struggling with how to interpret this data. We did see that GFAP and inflammation appear to be associated with each other. What supports this interpretation is that the GFAP decreased significantly after starting high efficacy treatments, namely natalizumab. We also found some clues that GFAP and brain atrophy may have a relationship with each other. Our conclusions weren’t entirely conclusive, possibly due to our smaller cohort sizes, and the use of various MRI scans over the years. And then the question of today was whether GFAP should be implemented in the clinic. Unfortunately, we couldn’t find evidence for use of GFAP as a disease progression biomarker, but we did find some clues of its use as both monitoring lesion volume and monitoring brain atrophy, making it still an interesting biomarker,” said Dr. Wessels.
What does it all mean?
In the Q&A session following the talks, one audience member challenged some of the assumptions behind the use of NfL and GFAP. “We don’t really know what these proteins actually do, and what they truly measure,” he said. Another criticism voiced by the commenter was that the platforms used to measure high and low values may be inconsistent. Finally, there are questions about the underlying theory. “I think our simplistic model for thinking that these are all just measurements of damage is potentially something that we have to reassess … or the assumption that these measures have to correlate to brain atrophy, as if that’s a gold standard. We all know that brain atrophy has totally failed us in the clinic and been incapable of giving us anything that’s useful for monitoring our patients,” said the questioner.
Elias Sotirchos, MD, who presented on NfL values and brain atrophy MS patients, agreed that it’s important to compare values across platforms to ensure consistency. He also cited potential issues with reference populations, since there may be a variety of contributors to neurotoxicity based on behaviors such as smoking, drinking, or comorbidities. “The selection of the reference population is important to be a representative of the MS population in which we are trying to apply that measurement of that normative value,” said Dr. Sotirchos, assistant professor of neurology at Johns Hopkins Medicine, Baltimore.
Ms. Basel and Dr. Wessels have no relevant financial disclosures. Dr. Sotirchos has financial relationships with Alexion, Viela Bio, Horizon Therapeutics, Genentech, Biogen, and Ad Scientiam.
Neurofilament light chain (NfL) is a biomarker for both disease progression and treatment response in multiple sclerosis (MS), but the search continues for additional biomarkers to distinguish between disease activity and progression.
At a session of the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS), researchers presented evidence that Acceptance of NfL wasn’t universal, either.
Patients with MS follow wide-ranging disease courses, and disability arises due to two partially independent mechanisms, according to Stephanie Meier, who presented results suggests from a study of two cohorts. “Firstly, the acute disease activity leading to relapse associated worsening or RAW (relapse-associated worsening), and secondly the chronic deterioration of neurologic functions leading to progression independent of relapse activity,” said Ms. Meier, a PhD student at University of Basel, Switzerland.
GFAP and NfL may be complementary biomarkers
NfL is a structural protein of neurons, while GFAP is a structure protein of astrocytes. NfL therefore reflects neuronal damage, while GFAP is an indicator of astrogliosis and astrocytic damage. GFAP has been shown to be increased in progressive MS and has been applied in traumatic brain injury and neuromyelitis optica spectrum disorder, according to Ms. Meier.
Her group examined data from two cohorts with “extreme” phenotypes. One cohort included 169 patients with stable MS and 184 with worsening disease progression but no sign of relapses. The other was a focal inflammation cohort that comprised paired samples from 66 patients: One sample from an active time point characterized by a relapse or at least one contrast-enhancing lesion (CEL) detected in the previous 30 days, and one remission sample when there was no relapse in the past year and no CEL in the previous 6 months.
The focal inflammation cohort demonstrated an association between raised NfL levels, with a 53% increase in predicted serum NfL during the active state after a multivariate analysis (P < .0001). GFAP values, on the other hand, were nearly identical.
In the progression cohort, there was more total yearly brain loss in the worsening group (0.42% vs. 0.14%; P = .0005). Baseline GFAP predicted gray matter atrophy (–0.24% per year, P < .0001) but NfL did not. The reverse was true for white matter atrophy, with NfL being predictive (–0.26% per year; P < .0001) but not GFAP.
“The use of biomarkers such as NfL and GFAP could be useful to understand the MS disease course by detecting disease activity that is not usually measurable with standard methods,” said Ms. Meier.
“We found that NfL was strongly associated with acute inflammation and prognosticated white matter volume loss, while GFAP has a potential as a prognostic biomarker for disease worsening, including progression independent of relapse activity, and baseline GFAP also prognosticated gray matter volume loss. From this we can conclude that serum GFAP is a promising biomarker reflecting progression in MS and it is complementary to NfL, as NfL is more strongly associated with acute inflammatory activity,” said Ms. Meier.
A biomarker of disease progression
In another presentation, Mark Wessels, MD, PhD, discussed use of GFAP as a biomarker of disease progression among patients treated with natalizumab. He noted that heightened levels of GFAP are found in astrocytes in chronic MS lesions. Serum GFAP also has been linked to lesion load and clinical outcomes in relapsing-remitting MS.
“The overall aim of our study was to evaluate the value of serum GFAP to monitor disability progression and treatment response in a natalizumab-treated cohort in which disease activity is effectively suppressed, and we did this by investigating GFAP as biomarker for progression despite suppression of inflammation,” said Dr. Wessels, a neurologist at Amsterdam University Medical Center.
The researchers evaluated data from an observational cohort at their institution in Amsterdam. GFAP decreased significantly after 3 months of treatment in both groups, then stabilized, but there was no difference between the groups. GFAP correlated with ventricle fraction at all time points with the exception of the last follow-up. It also correlated with lesion volume. However, GFAP did not correlate with whole brain parenchyma volume over time. There was no difference in GFAP among treatment responders and nonresponders.
Baseline serum GFAP predicted the annualized rate of ventricle volume change (P = .009). At 12 months it predicted both annualized rate of ventricle volume change (P = .009) and thalamus volume (P = .025).
“We’ve been struggling with how to interpret this data. We did see that GFAP and inflammation appear to be associated with each other. What supports this interpretation is that the GFAP decreased significantly after starting high efficacy treatments, namely natalizumab. We also found some clues that GFAP and brain atrophy may have a relationship with each other. Our conclusions weren’t entirely conclusive, possibly due to our smaller cohort sizes, and the use of various MRI scans over the years. And then the question of today was whether GFAP should be implemented in the clinic. Unfortunately, we couldn’t find evidence for use of GFAP as a disease progression biomarker, but we did find some clues of its use as both monitoring lesion volume and monitoring brain atrophy, making it still an interesting biomarker,” said Dr. Wessels.
What does it all mean?
In the Q&A session following the talks, one audience member challenged some of the assumptions behind the use of NfL and GFAP. “We don’t really know what these proteins actually do, and what they truly measure,” he said. Another criticism voiced by the commenter was that the platforms used to measure high and low values may be inconsistent. Finally, there are questions about the underlying theory. “I think our simplistic model for thinking that these are all just measurements of damage is potentially something that we have to reassess … or the assumption that these measures have to correlate to brain atrophy, as if that’s a gold standard. We all know that brain atrophy has totally failed us in the clinic and been incapable of giving us anything that’s useful for monitoring our patients,” said the questioner.
Elias Sotirchos, MD, who presented on NfL values and brain atrophy MS patients, agreed that it’s important to compare values across platforms to ensure consistency. He also cited potential issues with reference populations, since there may be a variety of contributors to neurotoxicity based on behaviors such as smoking, drinking, or comorbidities. “The selection of the reference population is important to be a representative of the MS population in which we are trying to apply that measurement of that normative value,” said Dr. Sotirchos, assistant professor of neurology at Johns Hopkins Medicine, Baltimore.
Ms. Basel and Dr. Wessels have no relevant financial disclosures. Dr. Sotirchos has financial relationships with Alexion, Viela Bio, Horizon Therapeutics, Genentech, Biogen, and Ad Scientiam.
FROM ECTRIMS 2022
Can MS be stopped early in its tracks?
, the earliest detected preclinical phase of multiple sclerosis (MS). Researchers found that dimethyl fumarate reduced the risk of a first acute or progressive event related to CNS demyelination by more than 80%, compared with placebo.
Patients with RIS have incidental MRI abnormalities typical of MS but have no symptoms of the disease. The condition is usually detected when a patient seeks treatment for another issue, such as migraines or head trauma.
The study is the first randomized clinical trial to examine efficacy of a disease-modifying therapy in delaying symptoms in RIS. “It really supports the concept of the benefit of early treatment intervention within this given MS disease spectrum,” lead investigator Darin Okuda, MD, professor of neurology at the University of Texas Southwestern Medical Center in Dallas, told delegates attending the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis.
Topic of debate
RIS was first identified by Dr. Okuda in 2008. Increased use of brain imaging led to the detection of patients with incidental white-matter pathology in the central nervous system on MRI. Some of the findings were nonspecific, but others were highly suggestive of demyelinating pathology based on their location and morphology in the central nervous system.
Although the prevalence of RIS is unknown, incidentally discovered white matter lesions resembling demyelination occur in an estimated 0.1%-0.7% of the general population. Up to half of patients with RIS experience a first clinical MS event within 10 years.
Diagnostic criteria and whether to treat patients with RIS prophylactically has long been a topic of debate among neurologists and radiologists.
Researchers conducted the multicenter, randomized, double-blinded, placebo-controlled ARISE study in 2016, recruiting 87 patients with RIS. The majority of participants were women, and most were diagnosed in their early 40s.
Patients received oral dimethyl fumarate at 240 mg twice daily or placebo and were followed for 96 weeks (1 year, 10 months). Clinical assessments were completed at baseline, at weeks 48 and 96, and at the time of the first clinical event. MRI scans were performed only at the beginning and end of the study.
Those who received dimethyl fumarate had a significantly lower risk of experiencing a first clinical demyelinating event during the study period (adjusted hazard ratio, 0.07; P = .005).
After adjusting for the number of gadolinium-enhancing lesions at baseline, there was a significant reduction in the number of new or newly enlarged T2-weighted hyperintense lesions, a secondary endpoint, in the dimethyl fumarate group, compared with those on placebo (HR, 0.20; P = .042).
“In the future we’d like to see further studies performed to assess the impact on disability outcome measures following treatment for a meaningful amount of time,” Dr. Okuda said.
‘Striking’ findings
Barbara Giesser, MD, a neurologist at Pacific Neuroscience Institute in Santa Monica, Calif., called the results “striking,” but noted that questions remain.
“Up until this study we haven’t had anything like it to guide us in determining whether we should treat RIS or not,” she said. “Obviously, larger studies are needed, but I think this is a very important and well-done study.”
In addition to the small sample size, Dr. Giesser noted that the study lacked data on the presence of risk factors that are known to increase RIS patients’ risk of developing MS, such as evidence of spinal cord lesions. That issue was also raised during discussion of the paper in Amsterdam.
“I don’t think this means you should treat everybody with RIS necessarily,” Dr. Giesser said. “But I think it suggests that in people with RIS, particularly if they do have risk factors, you could consider treatment with dimethyl fumarate.”
The study was funded by Biogen. Dr. Okuda has received support from Biogen and EMD Serono/Merck; and consulting fees from Alexion, Biogen, EMD Serono, Genzyme, Novartis, RVL Pharmaceuticals, TG Therapeutics, Viela Bio, Celgene/Bristol Myers Squibb, Genentech, Janssen Pharmaceuticals, and Osmotica Pharmaceuticals. Dr. Giesser reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, the earliest detected preclinical phase of multiple sclerosis (MS). Researchers found that dimethyl fumarate reduced the risk of a first acute or progressive event related to CNS demyelination by more than 80%, compared with placebo.
Patients with RIS have incidental MRI abnormalities typical of MS but have no symptoms of the disease. The condition is usually detected when a patient seeks treatment for another issue, such as migraines or head trauma.
The study is the first randomized clinical trial to examine efficacy of a disease-modifying therapy in delaying symptoms in RIS. “It really supports the concept of the benefit of early treatment intervention within this given MS disease spectrum,” lead investigator Darin Okuda, MD, professor of neurology at the University of Texas Southwestern Medical Center in Dallas, told delegates attending the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis.
Topic of debate
RIS was first identified by Dr. Okuda in 2008. Increased use of brain imaging led to the detection of patients with incidental white-matter pathology in the central nervous system on MRI. Some of the findings were nonspecific, but others were highly suggestive of demyelinating pathology based on their location and morphology in the central nervous system.
Although the prevalence of RIS is unknown, incidentally discovered white matter lesions resembling demyelination occur in an estimated 0.1%-0.7% of the general population. Up to half of patients with RIS experience a first clinical MS event within 10 years.
Diagnostic criteria and whether to treat patients with RIS prophylactically has long been a topic of debate among neurologists and radiologists.
Researchers conducted the multicenter, randomized, double-blinded, placebo-controlled ARISE study in 2016, recruiting 87 patients with RIS. The majority of participants were women, and most were diagnosed in their early 40s.
Patients received oral dimethyl fumarate at 240 mg twice daily or placebo and were followed for 96 weeks (1 year, 10 months). Clinical assessments were completed at baseline, at weeks 48 and 96, and at the time of the first clinical event. MRI scans were performed only at the beginning and end of the study.
Those who received dimethyl fumarate had a significantly lower risk of experiencing a first clinical demyelinating event during the study period (adjusted hazard ratio, 0.07; P = .005).
After adjusting for the number of gadolinium-enhancing lesions at baseline, there was a significant reduction in the number of new or newly enlarged T2-weighted hyperintense lesions, a secondary endpoint, in the dimethyl fumarate group, compared with those on placebo (HR, 0.20; P = .042).
“In the future we’d like to see further studies performed to assess the impact on disability outcome measures following treatment for a meaningful amount of time,” Dr. Okuda said.
‘Striking’ findings
Barbara Giesser, MD, a neurologist at Pacific Neuroscience Institute in Santa Monica, Calif., called the results “striking,” but noted that questions remain.
“Up until this study we haven’t had anything like it to guide us in determining whether we should treat RIS or not,” she said. “Obviously, larger studies are needed, but I think this is a very important and well-done study.”
In addition to the small sample size, Dr. Giesser noted that the study lacked data on the presence of risk factors that are known to increase RIS patients’ risk of developing MS, such as evidence of spinal cord lesions. That issue was also raised during discussion of the paper in Amsterdam.
“I don’t think this means you should treat everybody with RIS necessarily,” Dr. Giesser said. “But I think it suggests that in people with RIS, particularly if they do have risk factors, you could consider treatment with dimethyl fumarate.”
The study was funded by Biogen. Dr. Okuda has received support from Biogen and EMD Serono/Merck; and consulting fees from Alexion, Biogen, EMD Serono, Genzyme, Novartis, RVL Pharmaceuticals, TG Therapeutics, Viela Bio, Celgene/Bristol Myers Squibb, Genentech, Janssen Pharmaceuticals, and Osmotica Pharmaceuticals. Dr. Giesser reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, the earliest detected preclinical phase of multiple sclerosis (MS). Researchers found that dimethyl fumarate reduced the risk of a first acute or progressive event related to CNS demyelination by more than 80%, compared with placebo.
Patients with RIS have incidental MRI abnormalities typical of MS but have no symptoms of the disease. The condition is usually detected when a patient seeks treatment for another issue, such as migraines or head trauma.
The study is the first randomized clinical trial to examine efficacy of a disease-modifying therapy in delaying symptoms in RIS. “It really supports the concept of the benefit of early treatment intervention within this given MS disease spectrum,” lead investigator Darin Okuda, MD, professor of neurology at the University of Texas Southwestern Medical Center in Dallas, told delegates attending the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis.
Topic of debate
RIS was first identified by Dr. Okuda in 2008. Increased use of brain imaging led to the detection of patients with incidental white-matter pathology in the central nervous system on MRI. Some of the findings were nonspecific, but others were highly suggestive of demyelinating pathology based on their location and morphology in the central nervous system.
Although the prevalence of RIS is unknown, incidentally discovered white matter lesions resembling demyelination occur in an estimated 0.1%-0.7% of the general population. Up to half of patients with RIS experience a first clinical MS event within 10 years.
Diagnostic criteria and whether to treat patients with RIS prophylactically has long been a topic of debate among neurologists and radiologists.
Researchers conducted the multicenter, randomized, double-blinded, placebo-controlled ARISE study in 2016, recruiting 87 patients with RIS. The majority of participants were women, and most were diagnosed in their early 40s.
Patients received oral dimethyl fumarate at 240 mg twice daily or placebo and were followed for 96 weeks (1 year, 10 months). Clinical assessments were completed at baseline, at weeks 48 and 96, and at the time of the first clinical event. MRI scans were performed only at the beginning and end of the study.
Those who received dimethyl fumarate had a significantly lower risk of experiencing a first clinical demyelinating event during the study period (adjusted hazard ratio, 0.07; P = .005).
After adjusting for the number of gadolinium-enhancing lesions at baseline, there was a significant reduction in the number of new or newly enlarged T2-weighted hyperintense lesions, a secondary endpoint, in the dimethyl fumarate group, compared with those on placebo (HR, 0.20; P = .042).
“In the future we’d like to see further studies performed to assess the impact on disability outcome measures following treatment for a meaningful amount of time,” Dr. Okuda said.
‘Striking’ findings
Barbara Giesser, MD, a neurologist at Pacific Neuroscience Institute in Santa Monica, Calif., called the results “striking,” but noted that questions remain.
“Up until this study we haven’t had anything like it to guide us in determining whether we should treat RIS or not,” she said. “Obviously, larger studies are needed, but I think this is a very important and well-done study.”
In addition to the small sample size, Dr. Giesser noted that the study lacked data on the presence of risk factors that are known to increase RIS patients’ risk of developing MS, such as evidence of spinal cord lesions. That issue was also raised during discussion of the paper in Amsterdam.
“I don’t think this means you should treat everybody with RIS necessarily,” Dr. Giesser said. “But I think it suggests that in people with RIS, particularly if they do have risk factors, you could consider treatment with dimethyl fumarate.”
The study was funded by Biogen. Dr. Okuda has received support from Biogen and EMD Serono/Merck; and consulting fees from Alexion, Biogen, EMD Serono, Genzyme, Novartis, RVL Pharmaceuticals, TG Therapeutics, Viela Bio, Celgene/Bristol Myers Squibb, Genentech, Janssen Pharmaceuticals, and Osmotica Pharmaceuticals. Dr. Giesser reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ECTRIMS 2022
Is MRI a viable alternative to lumbar puncture for MS diagnosis?
, a new study indicates.
The presence of oligoclonal bands is “very specific for MS and is obtained by lumbar puncture, which is invasive and can be unpleasant, so it is not an ideal test,” said study investigator Daniel Ontaneda, MD, PhD, with the Mellen Center for MS Treatment and Research at the Cleveland Clinic.
In a pilot study, the central vein sign was “highly correlated with the presence of oligoclonal bands and in many cases could serve to prove that a person has MS without the need for a spinal tap,” Dr. Ontaneda said.
The study was presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Reducing the need for lumbar puncture
Oligoclonal bands in cerebrospinal fluid are commonly used as a diagnostic biomarker for MS and can serve to meet the requirement for dissemination in time in the 2017 McDonald criteria. Central vein sign is an emerging neuroimaging biomarker for MS that may improve diagnostic accuracy and reduce the need for lumbar puncture.
For the study, the investigators compared the sensitivity, specificity, and positive predictive value of central vein sign on MRI with that of oligoclonal bands in cerebrospinal fluid for MS diagnosis.
Among the 53 participants, 24 (45%) met 2017 McDonald criteria for dissemination in space and time at baseline, and 27 (51%) met the criteria at 12-month follow-up.
At initial presentation, sensitivity for MS diagnosis was 75% for oligoclonal bands, 83% for central vein sign “Select-3” (3 central vein sign–positive lesions per scan), and 71% for central vein sign “Select-6” (6 central vein sign–positive lesions per scan).
The point estimate of sensitivity of central vein sign was higher than of oligoclonal bands, but there was no significant difference in sensitivities across methods.
Specificity at initial presentation was 76% for oligoclonal bands, 48% for Select-3, and 86% for Select-6.
The presence of oligoclonal bands was more specific than Select-3 for diagnosis of MS at initial presentation (P = .03), as was Select-6 (P = .001). There was no significant difference when comparing cerebrospinal fluid oligoclonal bands with central vein sign Select-6.
At 12-month follow-up, the positive predictive value was 84% for oligoclonal bands and 95% for Select-6; combining oligoclonal bands and Select-6 gave a positive predictive value of 100%.
Dr. Ontaneda said that on the basis of these promising pilot data, the researchers have secured funding from the National Institutes of Health for a prospective study to further investigate the central vein sign as a potential biomarker for MS.
He also said there is “active discussion as to whether central vein sign should be added to the diagnostic criteria for MS.
“We think that it’s probably about time that we have diagnostic biomarkers that are sensitive and specific and can help us do away with complicated criteria to make the diagnosis, in favor of an imaging biomarker,” Dr. Ontaneda said.
A green light for further research
Commenting on the study, Shaheen Lakhan, MD, a neurologist and researcher from Boston, said that, “if an imaging finding on an otherwise routinely done MRI for patients with MS is just as good as analyses from the fluid from a spinal tap, of course, neurologists, and for sure patients, would go for the former.
“However, this study doesn’t fully support that argument just yet. It is retrospective with a tiny sample size, and the full way they standardized assessments and reporting hasn’t been fully reported,” said Dr. Lakhan, who was not involved in the study.
The study does, however, offer a “solid signal to green-light further exploration of a noninvasive assessment that may replace the dreaded spinal tap.
“In general, these principles need to be applied to all our invasive diagnostic criteria from biopsies to risky procedures, and also the incorporation of artificial intelligence/machine learning to aid in standardizing and scaling these assessments – and, frankly, reduce human error in readings,” said Dr. Lakhan.
Funding for the study was provided by the Race to Erase MS Foundation and the NIH. Dr. Ontaneda has received research support from the NIH, the National MS Society, the Patient Centered Outcomes Research Institute, the Race to Erase MS Foundation, Genentech, Sanofi, and Novartis and has consulted for Biogen, Genentech, Sanofi, Janssen, Novartis, and Merck. Dr. Lakhan has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study indicates.
The presence of oligoclonal bands is “very specific for MS and is obtained by lumbar puncture, which is invasive and can be unpleasant, so it is not an ideal test,” said study investigator Daniel Ontaneda, MD, PhD, with the Mellen Center for MS Treatment and Research at the Cleveland Clinic.
In a pilot study, the central vein sign was “highly correlated with the presence of oligoclonal bands and in many cases could serve to prove that a person has MS without the need for a spinal tap,” Dr. Ontaneda said.
The study was presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Reducing the need for lumbar puncture
Oligoclonal bands in cerebrospinal fluid are commonly used as a diagnostic biomarker for MS and can serve to meet the requirement for dissemination in time in the 2017 McDonald criteria. Central vein sign is an emerging neuroimaging biomarker for MS that may improve diagnostic accuracy and reduce the need for lumbar puncture.
For the study, the investigators compared the sensitivity, specificity, and positive predictive value of central vein sign on MRI with that of oligoclonal bands in cerebrospinal fluid for MS diagnosis.
Among the 53 participants, 24 (45%) met 2017 McDonald criteria for dissemination in space and time at baseline, and 27 (51%) met the criteria at 12-month follow-up.
At initial presentation, sensitivity for MS diagnosis was 75% for oligoclonal bands, 83% for central vein sign “Select-3” (3 central vein sign–positive lesions per scan), and 71% for central vein sign “Select-6” (6 central vein sign–positive lesions per scan).
The point estimate of sensitivity of central vein sign was higher than of oligoclonal bands, but there was no significant difference in sensitivities across methods.
Specificity at initial presentation was 76% for oligoclonal bands, 48% for Select-3, and 86% for Select-6.
The presence of oligoclonal bands was more specific than Select-3 for diagnosis of MS at initial presentation (P = .03), as was Select-6 (P = .001). There was no significant difference when comparing cerebrospinal fluid oligoclonal bands with central vein sign Select-6.
At 12-month follow-up, the positive predictive value was 84% for oligoclonal bands and 95% for Select-6; combining oligoclonal bands and Select-6 gave a positive predictive value of 100%.
Dr. Ontaneda said that on the basis of these promising pilot data, the researchers have secured funding from the National Institutes of Health for a prospective study to further investigate the central vein sign as a potential biomarker for MS.
He also said there is “active discussion as to whether central vein sign should be added to the diagnostic criteria for MS.
“We think that it’s probably about time that we have diagnostic biomarkers that are sensitive and specific and can help us do away with complicated criteria to make the diagnosis, in favor of an imaging biomarker,” Dr. Ontaneda said.
A green light for further research
Commenting on the study, Shaheen Lakhan, MD, a neurologist and researcher from Boston, said that, “if an imaging finding on an otherwise routinely done MRI for patients with MS is just as good as analyses from the fluid from a spinal tap, of course, neurologists, and for sure patients, would go for the former.
“However, this study doesn’t fully support that argument just yet. It is retrospective with a tiny sample size, and the full way they standardized assessments and reporting hasn’t been fully reported,” said Dr. Lakhan, who was not involved in the study.
The study does, however, offer a “solid signal to green-light further exploration of a noninvasive assessment that may replace the dreaded spinal tap.
“In general, these principles need to be applied to all our invasive diagnostic criteria from biopsies to risky procedures, and also the incorporation of artificial intelligence/machine learning to aid in standardizing and scaling these assessments – and, frankly, reduce human error in readings,” said Dr. Lakhan.
Funding for the study was provided by the Race to Erase MS Foundation and the NIH. Dr. Ontaneda has received research support from the NIH, the National MS Society, the Patient Centered Outcomes Research Institute, the Race to Erase MS Foundation, Genentech, Sanofi, and Novartis and has consulted for Biogen, Genentech, Sanofi, Janssen, Novartis, and Merck. Dr. Lakhan has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a new study indicates.
The presence of oligoclonal bands is “very specific for MS and is obtained by lumbar puncture, which is invasive and can be unpleasant, so it is not an ideal test,” said study investigator Daniel Ontaneda, MD, PhD, with the Mellen Center for MS Treatment and Research at the Cleveland Clinic.
In a pilot study, the central vein sign was “highly correlated with the presence of oligoclonal bands and in many cases could serve to prove that a person has MS without the need for a spinal tap,” Dr. Ontaneda said.
The study was presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Reducing the need for lumbar puncture
Oligoclonal bands in cerebrospinal fluid are commonly used as a diagnostic biomarker for MS and can serve to meet the requirement for dissemination in time in the 2017 McDonald criteria. Central vein sign is an emerging neuroimaging biomarker for MS that may improve diagnostic accuracy and reduce the need for lumbar puncture.
For the study, the investigators compared the sensitivity, specificity, and positive predictive value of central vein sign on MRI with that of oligoclonal bands in cerebrospinal fluid for MS diagnosis.
Among the 53 participants, 24 (45%) met 2017 McDonald criteria for dissemination in space and time at baseline, and 27 (51%) met the criteria at 12-month follow-up.
At initial presentation, sensitivity for MS diagnosis was 75% for oligoclonal bands, 83% for central vein sign “Select-3” (3 central vein sign–positive lesions per scan), and 71% for central vein sign “Select-6” (6 central vein sign–positive lesions per scan).
The point estimate of sensitivity of central vein sign was higher than of oligoclonal bands, but there was no significant difference in sensitivities across methods.
Specificity at initial presentation was 76% for oligoclonal bands, 48% for Select-3, and 86% for Select-6.
The presence of oligoclonal bands was more specific than Select-3 for diagnosis of MS at initial presentation (P = .03), as was Select-6 (P = .001). There was no significant difference when comparing cerebrospinal fluid oligoclonal bands with central vein sign Select-6.
At 12-month follow-up, the positive predictive value was 84% for oligoclonal bands and 95% for Select-6; combining oligoclonal bands and Select-6 gave a positive predictive value of 100%.
Dr. Ontaneda said that on the basis of these promising pilot data, the researchers have secured funding from the National Institutes of Health for a prospective study to further investigate the central vein sign as a potential biomarker for MS.
He also said there is “active discussion as to whether central vein sign should be added to the diagnostic criteria for MS.
“We think that it’s probably about time that we have diagnostic biomarkers that are sensitive and specific and can help us do away with complicated criteria to make the diagnosis, in favor of an imaging biomarker,” Dr. Ontaneda said.
A green light for further research
Commenting on the study, Shaheen Lakhan, MD, a neurologist and researcher from Boston, said that, “if an imaging finding on an otherwise routinely done MRI for patients with MS is just as good as analyses from the fluid from a spinal tap, of course, neurologists, and for sure patients, would go for the former.
“However, this study doesn’t fully support that argument just yet. It is retrospective with a tiny sample size, and the full way they standardized assessments and reporting hasn’t been fully reported,” said Dr. Lakhan, who was not involved in the study.
The study does, however, offer a “solid signal to green-light further exploration of a noninvasive assessment that may replace the dreaded spinal tap.
“In general, these principles need to be applied to all our invasive diagnostic criteria from biopsies to risky procedures, and also the incorporation of artificial intelligence/machine learning to aid in standardizing and scaling these assessments – and, frankly, reduce human error in readings,” said Dr. Lakhan.
Funding for the study was provided by the Race to Erase MS Foundation and the NIH. Dr. Ontaneda has received research support from the NIH, the National MS Society, the Patient Centered Outcomes Research Institute, the Race to Erase MS Foundation, Genentech, Sanofi, and Novartis and has consulted for Biogen, Genentech, Sanofi, Janssen, Novartis, and Merck. Dr. Lakhan has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ECTRIMS 2022
NfL levels might presage MS disability
Neurofilament light chain (NfL) is a well-known and useful biomarker for multiple sclerosis (MS) disease activity, but its association with disease progression is not well understood. A new analysis of MS patients in California’s EPIC cohort suggests that
“We see evidence for accelerated neuroaxonal damage in the year preceding the first diagnosis of the progression events, [but] only if they were associated with evidence of focal inflammatory activity – that can be either clinical or imaging evidence,” said Ahmed Abdelhak, MD, during a presentation of the study at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
“By the time we diagnose the EDSS progression, it’s already too late. Every damage or any accelerated neuroaxonal damage that has happened in association with this event already took place around a year ago. I think [this has] huge implications for the designing of clinical trials,” said Dr. Abdelhak, who is a postdoctoral researcher at the University of California, San Francisco.
In the study, researchers analyzed data from 609 MS cases, with a total of 3,906 office visits. The median age was 42 years, and 69.6% were female. Median disease duration was 6 years.
They examined the association between NfL scores and confirmed disease worsening, as recorded by an increase in EDSS score. There was an increase in NfL age-adjusted z score about 12 months in advance among patients with a progression association with a relapse in the past year, compared with individuals who did not experience disease progression. There was also a more modest increase among individuals who had disease progression without a recent relapse, but this was not statistically significant.
“Our findings suggest that the association between NfL levels and EDSS worsening is most prominent in the setting of relapse-associated events,” said Dr. Abdelhak.
Clinical implications and audience skepticism
During the Q&A following the talk, session moderator Charlotte Teunissen, PhD, professor of neurochemistry at Amsterdam University Medical Center, asked about the clinical implication of the finding. “It seems that you concluded that axonal damage has been done before the progression starts. Is that your conclusion? So it means that there is no option to interfere anymore, consequently.”
Dr. Abdelhak responded: “I think that’s a very important interpretation of the data, which I’m sure is a relatively new way of thinking about it. That means, indeed, that when we see these patients, measuring NfL wouldn’t deliver any additional value because they don’t differ between the groups at the time of EDSS worsening. And there is probably nothing more we can do about this event. But it’s still very important to know that any therapeutic intervention has also the need to prevent future disability progression, future neuroaxonal damage, but regarding what has happened already, I’m a little bit skeptical if we will be able to change anything.”
Dr. Teunissen expressed skepticism that there was no further neurodegeneration following the spike in NfL, and pointed out an important caveat, which was the study’s reliance on NfL. “You base your conclusions on what you observe for NfL, and it’s a far-fetched conclusion that there is no further axonal damage ongoing. Maybe NfL is just one marker, and it’s not the best biomarker to measure progression,” she said.
Dr. Abdelhak conceded that it will be necessary to confirm the findings with other biomarkers of neurological injury. Even different subunits of the NfL protein have been shown to have different dynamics in other neurological conditions. “So the data we have give definitely an incomplete picture because we [know] nothing about the other biomarkers of neuroaxonal injury, including the other subunits of NfL,” he said.
Later in the Q&A, Alasdair Coles, MD, professor of neurology at University of Cambridge (England), spoke from the audience. He suggested that the findings could be seen as dispiriting for clinicians. “Would the panel agree that actually for a clinician this is all rather disappointing, because none of these markers are telling us anything that we don’t otherwise know by examining the patient and doing scans?”
“I can attempt to tackle that provocative question,” replied Elias Sotirchos, MD, who also presented on an association between NfL and brain atrophy research during the session. He pointed out that all clinical tests are imperfect, and suggested that NfL isn’t something to be used in isolation. It could be useful when patients are experiencing new symptoms, or worsening symptoms, and in combination with MRI results. “My interpretation of NfL is that it does have incremental value, telling us which patients have lesions that are more destructive, potentially, given all of these consistent associations with brain atrophy and disability progression over time,” said Dr. Sotirchos, who is an assistant professor of neurology at Johns Hopkins Medicine, Baltimore.
Dr. Abdelhak and Dr. Teunissen have no relevant financial disclosures. Dr. Sotirchos has financial relationships with Alexion, Viela Bio, Horizon Therapeutics, Genentech, and Ad Scientiam.
Neurofilament light chain (NfL) is a well-known and useful biomarker for multiple sclerosis (MS) disease activity, but its association with disease progression is not well understood. A new analysis of MS patients in California’s EPIC cohort suggests that
“We see evidence for accelerated neuroaxonal damage in the year preceding the first diagnosis of the progression events, [but] only if they were associated with evidence of focal inflammatory activity – that can be either clinical or imaging evidence,” said Ahmed Abdelhak, MD, during a presentation of the study at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
“By the time we diagnose the EDSS progression, it’s already too late. Every damage or any accelerated neuroaxonal damage that has happened in association with this event already took place around a year ago. I think [this has] huge implications for the designing of clinical trials,” said Dr. Abdelhak, who is a postdoctoral researcher at the University of California, San Francisco.
In the study, researchers analyzed data from 609 MS cases, with a total of 3,906 office visits. The median age was 42 years, and 69.6% were female. Median disease duration was 6 years.
They examined the association between NfL scores and confirmed disease worsening, as recorded by an increase in EDSS score. There was an increase in NfL age-adjusted z score about 12 months in advance among patients with a progression association with a relapse in the past year, compared with individuals who did not experience disease progression. There was also a more modest increase among individuals who had disease progression without a recent relapse, but this was not statistically significant.
“Our findings suggest that the association between NfL levels and EDSS worsening is most prominent in the setting of relapse-associated events,” said Dr. Abdelhak.
Clinical implications and audience skepticism
During the Q&A following the talk, session moderator Charlotte Teunissen, PhD, professor of neurochemistry at Amsterdam University Medical Center, asked about the clinical implication of the finding. “It seems that you concluded that axonal damage has been done before the progression starts. Is that your conclusion? So it means that there is no option to interfere anymore, consequently.”
Dr. Abdelhak responded: “I think that’s a very important interpretation of the data, which I’m sure is a relatively new way of thinking about it. That means, indeed, that when we see these patients, measuring NfL wouldn’t deliver any additional value because they don’t differ between the groups at the time of EDSS worsening. And there is probably nothing more we can do about this event. But it’s still very important to know that any therapeutic intervention has also the need to prevent future disability progression, future neuroaxonal damage, but regarding what has happened already, I’m a little bit skeptical if we will be able to change anything.”
Dr. Teunissen expressed skepticism that there was no further neurodegeneration following the spike in NfL, and pointed out an important caveat, which was the study’s reliance on NfL. “You base your conclusions on what you observe for NfL, and it’s a far-fetched conclusion that there is no further axonal damage ongoing. Maybe NfL is just one marker, and it’s not the best biomarker to measure progression,” she said.
Dr. Abdelhak conceded that it will be necessary to confirm the findings with other biomarkers of neurological injury. Even different subunits of the NfL protein have been shown to have different dynamics in other neurological conditions. “So the data we have give definitely an incomplete picture because we [know] nothing about the other biomarkers of neuroaxonal injury, including the other subunits of NfL,” he said.
Later in the Q&A, Alasdair Coles, MD, professor of neurology at University of Cambridge (England), spoke from the audience. He suggested that the findings could be seen as dispiriting for clinicians. “Would the panel agree that actually for a clinician this is all rather disappointing, because none of these markers are telling us anything that we don’t otherwise know by examining the patient and doing scans?”
“I can attempt to tackle that provocative question,” replied Elias Sotirchos, MD, who also presented on an association between NfL and brain atrophy research during the session. He pointed out that all clinical tests are imperfect, and suggested that NfL isn’t something to be used in isolation. It could be useful when patients are experiencing new symptoms, or worsening symptoms, and in combination with MRI results. “My interpretation of NfL is that it does have incremental value, telling us which patients have lesions that are more destructive, potentially, given all of these consistent associations with brain atrophy and disability progression over time,” said Dr. Sotirchos, who is an assistant professor of neurology at Johns Hopkins Medicine, Baltimore.
Dr. Abdelhak and Dr. Teunissen have no relevant financial disclosures. Dr. Sotirchos has financial relationships with Alexion, Viela Bio, Horizon Therapeutics, Genentech, and Ad Scientiam.
Neurofilament light chain (NfL) is a well-known and useful biomarker for multiple sclerosis (MS) disease activity, but its association with disease progression is not well understood. A new analysis of MS patients in California’s EPIC cohort suggests that
“We see evidence for accelerated neuroaxonal damage in the year preceding the first diagnosis of the progression events, [but] only if they were associated with evidence of focal inflammatory activity – that can be either clinical or imaging evidence,” said Ahmed Abdelhak, MD, during a presentation of the study at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
“By the time we diagnose the EDSS progression, it’s already too late. Every damage or any accelerated neuroaxonal damage that has happened in association with this event already took place around a year ago. I think [this has] huge implications for the designing of clinical trials,” said Dr. Abdelhak, who is a postdoctoral researcher at the University of California, San Francisco.
In the study, researchers analyzed data from 609 MS cases, with a total of 3,906 office visits. The median age was 42 years, and 69.6% were female. Median disease duration was 6 years.
They examined the association between NfL scores and confirmed disease worsening, as recorded by an increase in EDSS score. There was an increase in NfL age-adjusted z score about 12 months in advance among patients with a progression association with a relapse in the past year, compared with individuals who did not experience disease progression. There was also a more modest increase among individuals who had disease progression without a recent relapse, but this was not statistically significant.
“Our findings suggest that the association between NfL levels and EDSS worsening is most prominent in the setting of relapse-associated events,” said Dr. Abdelhak.
Clinical implications and audience skepticism
During the Q&A following the talk, session moderator Charlotte Teunissen, PhD, professor of neurochemistry at Amsterdam University Medical Center, asked about the clinical implication of the finding. “It seems that you concluded that axonal damage has been done before the progression starts. Is that your conclusion? So it means that there is no option to interfere anymore, consequently.”
Dr. Abdelhak responded: “I think that’s a very important interpretation of the data, which I’m sure is a relatively new way of thinking about it. That means, indeed, that when we see these patients, measuring NfL wouldn’t deliver any additional value because they don’t differ between the groups at the time of EDSS worsening. And there is probably nothing more we can do about this event. But it’s still very important to know that any therapeutic intervention has also the need to prevent future disability progression, future neuroaxonal damage, but regarding what has happened already, I’m a little bit skeptical if we will be able to change anything.”
Dr. Teunissen expressed skepticism that there was no further neurodegeneration following the spike in NfL, and pointed out an important caveat, which was the study’s reliance on NfL. “You base your conclusions on what you observe for NfL, and it’s a far-fetched conclusion that there is no further axonal damage ongoing. Maybe NfL is just one marker, and it’s not the best biomarker to measure progression,” she said.
Dr. Abdelhak conceded that it will be necessary to confirm the findings with other biomarkers of neurological injury. Even different subunits of the NfL protein have been shown to have different dynamics in other neurological conditions. “So the data we have give definitely an incomplete picture because we [know] nothing about the other biomarkers of neuroaxonal injury, including the other subunits of NfL,” he said.
Later in the Q&A, Alasdair Coles, MD, professor of neurology at University of Cambridge (England), spoke from the audience. He suggested that the findings could be seen as dispiriting for clinicians. “Would the panel agree that actually for a clinician this is all rather disappointing, because none of these markers are telling us anything that we don’t otherwise know by examining the patient and doing scans?”
“I can attempt to tackle that provocative question,” replied Elias Sotirchos, MD, who also presented on an association between NfL and brain atrophy research during the session. He pointed out that all clinical tests are imperfect, and suggested that NfL isn’t something to be used in isolation. It could be useful when patients are experiencing new symptoms, or worsening symptoms, and in combination with MRI results. “My interpretation of NfL is that it does have incremental value, telling us which patients have lesions that are more destructive, potentially, given all of these consistent associations with brain atrophy and disability progression over time,” said Dr. Sotirchos, who is an assistant professor of neurology at Johns Hopkins Medicine, Baltimore.
Dr. Abdelhak and Dr. Teunissen have no relevant financial disclosures. Dr. Sotirchos has financial relationships with Alexion, Viela Bio, Horizon Therapeutics, Genentech, and Ad Scientiam.
FROM ECTRIMS 2022
A better way to predict fall risk in patients with MS?
Compared with patients with MS who didn’t fall, those who did fall had worse neuromuscular function as evidenced by a reduced rate of force development.
“Our study suggests that instead of looking at reduced maximum muscle strength, perhaps we should start looking at reduced rate of force development when trying to identify potential fallers,” said Laurits Taul-Madsen, PhD student, Aarhus University, Denmark.
The study was presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Explosive strength
In contrast to maximal muscle strength, the rate of force development is a measure of explosive strength, or simply the amount of force that an individual can produce over a given time period. When a patient is about to fall, what’s most important is not how strong the person is, but how quickly they can produce enough force to counteract the balance perturbation, thus avoid falling, said Dr. Taul-Madsen.
“If a person is very slow to produce this force, [that person] will have fallen before he or she has produced enough force to counteract the balance perturbation that the person is experiencing,” he added.
Research has shown a reduced rate of force development (RFD) in patients with MS, compared with healthy controls. However, little is known about the impact of RFD on falls in those with MS.
To investigate, researchers studied 53 adults with MS: Twenty-four had no fall history in the prior year, 16 had one to two prior falls, and 13 had three or more falls. The two groups of fallers were both slightly older and had a slightly higher Expanded Disability Status Scale (EDSS) scores, “which may not be so surprising,” Dr. Taul-Madsen said.
Knee extensor neuromuscular function, including maximum muscle strength and RFD at 50 and 200 milliseconds, was assessed via isokinetic dynamometry.
A high RFD is “good and the non-fallers had the highest RFD at 50 ms.” On this measure, “we saw quite a big difference between the non-fallers and the two groups of fallers,” Dr. Taul-Madsen reported.
At 200 ms, the RFD was again highest in the group of non-fallers but the difference was somewhat smaller. Non-fallers also had greater maximum muscle strength than that of the fallers.
There was “good” correlation between these neuromuscular measurements and falls, Dr. Taul-Madsen said.
He noted that RFD, which can be improved with resistance training, “seems like a specialized and difficult measurement, but it doesn’t have to be. It can be measured with just a linear encoder and a chair to perform the sit-to-stand test, so in clinical practice, it’s quite easily measured.”
‘Highly promising’ approach
“There are some data on predictors of falls in persons with MS, but not yet on neuromuscular function, as has been done in other populations,” said Brian Sandroff, PhD, senior research scientist, Kessler Foundation, West Orange, N.J.
This study is “interesting in that recurrent fallers were distinguished based on having worse neuromuscular function,” said Dr. Sandroff, who was not part of the research team.
“Although this relationship is somewhat intuitive,” RFD provides a “potentially sensitive measure that can be addressed via specific resistance exercise programs as a highly promising approach for reducing fall risk and falls themselves in persons with MS,” Dr. Sandroff said.
More generally, he said this study provides “more evidence on the multisystemic benefits of exercise training and having better physical fitness in persons with MS.
“The evidence seems to be converging more and more on this, as research groups across countries and continents are reporting on similar themes,” said Dr. Sandroff.
The study had no specific funding. Dr. Taul-Madsen and Dr. Sandroff report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with patients with MS who didn’t fall, those who did fall had worse neuromuscular function as evidenced by a reduced rate of force development.
“Our study suggests that instead of looking at reduced maximum muscle strength, perhaps we should start looking at reduced rate of force development when trying to identify potential fallers,” said Laurits Taul-Madsen, PhD student, Aarhus University, Denmark.
The study was presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Explosive strength
In contrast to maximal muscle strength, the rate of force development is a measure of explosive strength, or simply the amount of force that an individual can produce over a given time period. When a patient is about to fall, what’s most important is not how strong the person is, but how quickly they can produce enough force to counteract the balance perturbation, thus avoid falling, said Dr. Taul-Madsen.
“If a person is very slow to produce this force, [that person] will have fallen before he or she has produced enough force to counteract the balance perturbation that the person is experiencing,” he added.
Research has shown a reduced rate of force development (RFD) in patients with MS, compared with healthy controls. However, little is known about the impact of RFD on falls in those with MS.
To investigate, researchers studied 53 adults with MS: Twenty-four had no fall history in the prior year, 16 had one to two prior falls, and 13 had three or more falls. The two groups of fallers were both slightly older and had a slightly higher Expanded Disability Status Scale (EDSS) scores, “which may not be so surprising,” Dr. Taul-Madsen said.
Knee extensor neuromuscular function, including maximum muscle strength and RFD at 50 and 200 milliseconds, was assessed via isokinetic dynamometry.
A high RFD is “good and the non-fallers had the highest RFD at 50 ms.” On this measure, “we saw quite a big difference between the non-fallers and the two groups of fallers,” Dr. Taul-Madsen reported.
At 200 ms, the RFD was again highest in the group of non-fallers but the difference was somewhat smaller. Non-fallers also had greater maximum muscle strength than that of the fallers.
There was “good” correlation between these neuromuscular measurements and falls, Dr. Taul-Madsen said.
He noted that RFD, which can be improved with resistance training, “seems like a specialized and difficult measurement, but it doesn’t have to be. It can be measured with just a linear encoder and a chair to perform the sit-to-stand test, so in clinical practice, it’s quite easily measured.”
‘Highly promising’ approach
“There are some data on predictors of falls in persons with MS, but not yet on neuromuscular function, as has been done in other populations,” said Brian Sandroff, PhD, senior research scientist, Kessler Foundation, West Orange, N.J.
This study is “interesting in that recurrent fallers were distinguished based on having worse neuromuscular function,” said Dr. Sandroff, who was not part of the research team.
“Although this relationship is somewhat intuitive,” RFD provides a “potentially sensitive measure that can be addressed via specific resistance exercise programs as a highly promising approach for reducing fall risk and falls themselves in persons with MS,” Dr. Sandroff said.
More generally, he said this study provides “more evidence on the multisystemic benefits of exercise training and having better physical fitness in persons with MS.
“The evidence seems to be converging more and more on this, as research groups across countries and continents are reporting on similar themes,” said Dr. Sandroff.
The study had no specific funding. Dr. Taul-Madsen and Dr. Sandroff report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Compared with patients with MS who didn’t fall, those who did fall had worse neuromuscular function as evidenced by a reduced rate of force development.
“Our study suggests that instead of looking at reduced maximum muscle strength, perhaps we should start looking at reduced rate of force development when trying to identify potential fallers,” said Laurits Taul-Madsen, PhD student, Aarhus University, Denmark.
The study was presented at the annual meeting of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS).
Explosive strength
In contrast to maximal muscle strength, the rate of force development is a measure of explosive strength, or simply the amount of force that an individual can produce over a given time period. When a patient is about to fall, what’s most important is not how strong the person is, but how quickly they can produce enough force to counteract the balance perturbation, thus avoid falling, said Dr. Taul-Madsen.
“If a person is very slow to produce this force, [that person] will have fallen before he or she has produced enough force to counteract the balance perturbation that the person is experiencing,” he added.
Research has shown a reduced rate of force development (RFD) in patients with MS, compared with healthy controls. However, little is known about the impact of RFD on falls in those with MS.
To investigate, researchers studied 53 adults with MS: Twenty-four had no fall history in the prior year, 16 had one to two prior falls, and 13 had three or more falls. The two groups of fallers were both slightly older and had a slightly higher Expanded Disability Status Scale (EDSS) scores, “which may not be so surprising,” Dr. Taul-Madsen said.
Knee extensor neuromuscular function, including maximum muscle strength and RFD at 50 and 200 milliseconds, was assessed via isokinetic dynamometry.
A high RFD is “good and the non-fallers had the highest RFD at 50 ms.” On this measure, “we saw quite a big difference between the non-fallers and the two groups of fallers,” Dr. Taul-Madsen reported.
At 200 ms, the RFD was again highest in the group of non-fallers but the difference was somewhat smaller. Non-fallers also had greater maximum muscle strength than that of the fallers.
There was “good” correlation between these neuromuscular measurements and falls, Dr. Taul-Madsen said.
He noted that RFD, which can be improved with resistance training, “seems like a specialized and difficult measurement, but it doesn’t have to be. It can be measured with just a linear encoder and a chair to perform the sit-to-stand test, so in clinical practice, it’s quite easily measured.”
‘Highly promising’ approach
“There are some data on predictors of falls in persons with MS, but not yet on neuromuscular function, as has been done in other populations,” said Brian Sandroff, PhD, senior research scientist, Kessler Foundation, West Orange, N.J.
This study is “interesting in that recurrent fallers were distinguished based on having worse neuromuscular function,” said Dr. Sandroff, who was not part of the research team.
“Although this relationship is somewhat intuitive,” RFD provides a “potentially sensitive measure that can be addressed via specific resistance exercise programs as a highly promising approach for reducing fall risk and falls themselves in persons with MS,” Dr. Sandroff said.
More generally, he said this study provides “more evidence on the multisystemic benefits of exercise training and having better physical fitness in persons with MS.
“The evidence seems to be converging more and more on this, as research groups across countries and continents are reporting on similar themes,” said Dr. Sandroff.
The study had no specific funding. Dr. Taul-Madsen and Dr. Sandroff report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ECTRIMS 2022