User login
VIDEO: Asthma meds’ safety data reassuring in pregnancy
SAN DIEGO – How safe are asthma medications during pregnancy? And how adherent are pregnant women to asthma medications? Dr. Jennifer A. Namazy of Scripps Clinic, La Jolla, Calif., summarizes the reassuring data on use of asthma medications by pregnant women, and she outlines her own approach to ensure pregnant women with asthma remain healthy and medication adherent.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – How safe are asthma medications during pregnancy? And how adherent are pregnant women to asthma medications? Dr. Jennifer A. Namazy of Scripps Clinic, La Jolla, Calif., summarizes the reassuring data on use of asthma medications by pregnant women, and she outlines her own approach to ensure pregnant women with asthma remain healthy and medication adherent.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
SAN DIEGO – How safe are asthma medications during pregnancy? And how adherent are pregnant women to asthma medications? Dr. Jennifer A. Namazy of Scripps Clinic, La Jolla, Calif., summarizes the reassuring data on use of asthma medications by pregnant women, and she outlines her own approach to ensure pregnant women with asthma remain healthy and medication adherent.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
ANALYSIS FROM 2014 AAAAI ANNUAL MEETING

Laboring women preferred epidural to patient-controlled remifentanil analgesia
NEW ORLEANS – Laboring women had better overall pain relief satisfaction from epidurals than from remifentanil patient-controlled analgesia, according to results presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Although Dr. Liv Freeman, of Leiden (the Netherlands) University Medical Center, and her colleagues expected to find that the two pain relief methods would be equivalent, the results of their multisite, randomized controlled study instead showed a significantly higher pain appreciation (pain relief satisfaction) score in women who received epidural analgesia during delivery.

"This should be taken into account when pain relief is offered to women in labor," said Dr. Freeman, who noted that the study’s intention was to provide more definitive data about the two pain relief methods because previous studies were underpowered – with some data showing the two methods were comparable.
An advantage to using remifentanil, an opioid similar to pethidine, is that it is fast-acting, typically cycling within 3 minutes. This attribute allows the drug to be self-administered and lowers costs, said Dr. Freeman. There are maternal side effects, however, including respiratory depression, nausea and vomiting, and sedation.
Placental transfer also occurs with remifentanil, although "the drug is so short acting, it is cleared once the baby is born when discontinued in the second stage of labor," Dr. Freeman said.
As for the potential risks of using an epidural, Dr. Freeman said that although rare, epidural hematomas can occur, and that "about 1 in 100 women experience postspinal headache, and between 10% and 20% of mothers develop a fever during labor."
Before active labor began, 709 women were randomly assigned to the remifentanil patient-controlled analgesia (PCA) group, and 705 were assigned to the epidural group. The maternal age was about 31 years in each group, and other demographic baseline data also were similar. Nearly one-third more of the remifentanil PCA group, 402 women in all, opted to use the pain medication during labor, and 296 assigned to the epidural group chose to use it.
All women across the cohorts were asked hourly to rate their pain relief on a visual analog scale.
The total time-weighted pain appreciation score for the remifentanil PCA group was 25.7, versus 36.8 in the epidural group (P = .001).
Although the analysis was based on intention to treat, Dr. Freeman noted that 53 of the women in the self-administered pain relief group requested epidurals while in labor. Three women converted from an epidural to the self-administered pain medication.
The epidurals were performed according to local procedures across the 15 Dutch sites where the trial was conducted. Remifentanil PCA was 30 mcg administered intravenously with a 3-minute lockout time. The women had the option of increasing their dose to 40 mcg or decreasing it to 20 mcg.
The duration of analgesia was notably shorter in the remifentanil PCA group than in the epidural group: 236 minutes (interquartile range, 128-376 minutes) vs. 309 minutes (IQR, 181-454 minutes).
There were 22 elective cesarean deliveries in the remifentanil group and 29 in the epidural group. Three women in the epidural cohort were lost to follow-up, and two withdrew their consent.
There were no significant differences in important maternal and fetal outcomes, said Dr. Freeman. Because the safety profiles of remifentanil and epidural analgesia are essentially the same, physicians should counsel women about the pros and cons of each, she said.
This study was funded by ZonMw, the Netherlands Organisation for Health Research and Development. Dr. Freeman did not report any relevant financial disclosures.
NEW ORLEANS – Laboring women had better overall pain relief satisfaction from epidurals than from remifentanil patient-controlled analgesia, according to results presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Although Dr. Liv Freeman, of Leiden (the Netherlands) University Medical Center, and her colleagues expected to find that the two pain relief methods would be equivalent, the results of their multisite, randomized controlled study instead showed a significantly higher pain appreciation (pain relief satisfaction) score in women who received epidural analgesia during delivery.
"This should be taken into account when pain relief is offered to women in labor," said Dr. Freeman, who noted that the study’s intention was to provide more definitive data about the two pain relief methods because previous studies were underpowered – with some data showing the two methods were comparable.
An advantage to using remifentanil, an opioid similar to pethidine, is that it is fast-acting, typically cycling within 3 minutes. This attribute allows the drug to be self-administered and lowers costs, said Dr. Freeman. There are maternal side effects, however, including respiratory depression, nausea and vomiting, and sedation.
Placental transfer also occurs with remifentanil, although "the drug is so short acting, it is cleared once the baby is born when discontinued in the second stage of labor," Dr. Freeman said.
As for the potential risks of using an epidural, Dr. Freeman said that although rare, epidural hematomas can occur, and that "about 1 in 100 women experience postspinal headache, and between 10% and 20% of mothers develop a fever during labor."
Before active labor began, 709 women were randomly assigned to the remifentanil patient-controlled analgesia (PCA) group, and 705 were assigned to the epidural group. The maternal age was about 31 years in each group, and other demographic baseline data also were similar. Nearly one-third more of the remifentanil PCA group, 402 women in all, opted to use the pain medication during labor, and 296 assigned to the epidural group chose to use it.
All women across the cohorts were asked hourly to rate their pain relief on a visual analog scale.
The total time-weighted pain appreciation score for the remifentanil PCA group was 25.7, versus 36.8 in the epidural group (P = .001).
Although the analysis was based on intention to treat, Dr. Freeman noted that 53 of the women in the self-administered pain relief group requested epidurals while in labor. Three women converted from an epidural to the self-administered pain medication.
The epidurals were performed according to local procedures across the 15 Dutch sites where the trial was conducted. Remifentanil PCA was 30 mcg administered intravenously with a 3-minute lockout time. The women had the option of increasing their dose to 40 mcg or decreasing it to 20 mcg.
The duration of analgesia was notably shorter in the remifentanil PCA group than in the epidural group: 236 minutes (interquartile range, 128-376 minutes) vs. 309 minutes (IQR, 181-454 minutes).
There were 22 elective cesarean deliveries in the remifentanil group and 29 in the epidural group. Three women in the epidural cohort were lost to follow-up, and two withdrew their consent.
There were no significant differences in important maternal and fetal outcomes, said Dr. Freeman. Because the safety profiles of remifentanil and epidural analgesia are essentially the same, physicians should counsel women about the pros and cons of each, she said.
This study was funded by ZonMw, the Netherlands Organisation for Health Research and Development. Dr. Freeman did not report any relevant financial disclosures.
NEW ORLEANS – Laboring women had better overall pain relief satisfaction from epidurals than from remifentanil patient-controlled analgesia, according to results presented at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
Although Dr. Liv Freeman, of Leiden (the Netherlands) University Medical Center, and her colleagues expected to find that the two pain relief methods would be equivalent, the results of their multisite, randomized controlled study instead showed a significantly higher pain appreciation (pain relief satisfaction) score in women who received epidural analgesia during delivery.
"This should be taken into account when pain relief is offered to women in labor," said Dr. Freeman, who noted that the study’s intention was to provide more definitive data about the two pain relief methods because previous studies were underpowered – with some data showing the two methods were comparable.
An advantage to using remifentanil, an opioid similar to pethidine, is that it is fast-acting, typically cycling within 3 minutes. This attribute allows the drug to be self-administered and lowers costs, said Dr. Freeman. There are maternal side effects, however, including respiratory depression, nausea and vomiting, and sedation.
Placental transfer also occurs with remifentanil, although "the drug is so short acting, it is cleared once the baby is born when discontinued in the second stage of labor," Dr. Freeman said.
As for the potential risks of using an epidural, Dr. Freeman said that although rare, epidural hematomas can occur, and that "about 1 in 100 women experience postspinal headache, and between 10% and 20% of mothers develop a fever during labor."
Before active labor began, 709 women were randomly assigned to the remifentanil patient-controlled analgesia (PCA) group, and 705 were assigned to the epidural group. The maternal age was about 31 years in each group, and other demographic baseline data also were similar. Nearly one-third more of the remifentanil PCA group, 402 women in all, opted to use the pain medication during labor, and 296 assigned to the epidural group chose to use it.
All women across the cohorts were asked hourly to rate their pain relief on a visual analog scale.
The total time-weighted pain appreciation score for the remifentanil PCA group was 25.7, versus 36.8 in the epidural group (P = .001).
Although the analysis was based on intention to treat, Dr. Freeman noted that 53 of the women in the self-administered pain relief group requested epidurals while in labor. Three women converted from an epidural to the self-administered pain medication.
The epidurals were performed according to local procedures across the 15 Dutch sites where the trial was conducted. Remifentanil PCA was 30 mcg administered intravenously with a 3-minute lockout time. The women had the option of increasing their dose to 40 mcg or decreasing it to 20 mcg.
The duration of analgesia was notably shorter in the remifentanil PCA group than in the epidural group: 236 minutes (interquartile range, 128-376 minutes) vs. 309 minutes (IQR, 181-454 minutes).
There were 22 elective cesarean deliveries in the remifentanil group and 29 in the epidural group. Three women in the epidural cohort were lost to follow-up, and two withdrew their consent.
There were no significant differences in important maternal and fetal outcomes, said Dr. Freeman. Because the safety profiles of remifentanil and epidural analgesia are essentially the same, physicians should counsel women about the pros and cons of each, she said.
This study was funded by ZonMw, the Netherlands Organisation for Health Research and Development. Dr. Freeman did not report any relevant financial disclosures.
AT THE PREGNANCY MEETING
Major finding: Time-weighted, overall satisfaction scores for women who received an epidural were 36.8, compared with 25.7 for women using remifentanil, a significant difference.
Data source: Multisite, randomized controlled equivalence trial of 705 women who were administered an epidural vs. 709 women using patient-controlled remifentanil.
Disclosures: This study was funded by ZonMw, the Netherlands Organisation for Health Research and Development. Dr. Freeman did not report any relevant financial disclosures.

Obesity does not interfere with accuracy of noninvasive preterm birth monitoring
NEW ORLEANS – Maternal obesity does not lessen the predictive value of noninvasive uterine electromyography monitoring, according to a poster presentation at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"We wanted to see if in this subset of pregnant women, the noninvasive method was as effective as in other pregnant women," said Dr. Miha Lucovnik, a perinatologist at the University Medical Center, Ljubljana, Slovenia.
"Uterine contractions, at term or preterm, are one of the most common reasons for visits to obstetrical triage, but determining which patient with contractions is in true labor and needs to be admitted is, however, difficult," said Dr. Lucovnik. "The inability to accurately diagnose preterm labor leads to missed opportunities to improve outcomes of premature neonates, and also to unnecessary costs and side effects of treatments in women who would not deliver preterm regardless of intervention."

One of the more common monitoring methods – tocodynamometry – measures length and frequency of contractions but is often ineffective at detecting these signals in women with a BMI of 30 kg/m2 and above, he said.
Electromyography (EMG) is more effective at monitoring the progression of true labor, because it can detect "the changes in cell excitability and coupling necessary for effective contractions," said Dr. Lucovnik.
To detect uterine activity, electrodes are placed on the patient’s abdomen with vertical and horizontal axes parallel to the patient’s vertical and horizontal axes, respectively, and with center-to-center distances between adjacent electrodes set about 5.0-5.5 cm apart. The uterine EMG is then measured for 30 minutes.
For the study, Dr. Lucovnik and his colleagues reviewed the predictive values of uterine EMG for preterm delivery in 88 women divided into three cohorts: 20 with a BMI of 30 or greater; 64 with a BMI of 25-29.9; and 4 with a BMI of 18.5-24.9.
The investigators did not find any significant difference between the cohorts in the area under the curve prediction of preterm delivery within 7 days (AUC was 0.95 in the normal and overweight cohorts, and 1 in the obese group; P = .08).
Six patients with low uterine EMG scores delivered prematurely within 7 days from the EMG measurement. No significant differences in BMI were reported between this false negative group (range, 26.13 plus or minus 1.03) and the combined true positive and true negative preterm labor groups (range, 28.04 plus or minus 3.77; P = .32).
"We know that predictive values of currently used methods to diagnose preterm labor are even lower in women with high BMI," said Dr. Lucovnik. "Our study showed that the accuracy of uterine EMG monitoring and its predictive value for preterm delivery are not affected by obesity in pregnant patients."
Dr. Lucovnik reported that he did not have any relevant disclosures.
NEW ORLEANS – Maternal obesity does not lessen the predictive value of noninvasive uterine electromyography monitoring, according to a poster presentation at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"We wanted to see if in this subset of pregnant women, the noninvasive method was as effective as in other pregnant women," said Dr. Miha Lucovnik, a perinatologist at the University Medical Center, Ljubljana, Slovenia.
"Uterine contractions, at term or preterm, are one of the most common reasons for visits to obstetrical triage, but determining which patient with contractions is in true labor and needs to be admitted is, however, difficult," said Dr. Lucovnik. "The inability to accurately diagnose preterm labor leads to missed opportunities to improve outcomes of premature neonates, and also to unnecessary costs and side effects of treatments in women who would not deliver preterm regardless of intervention."
One of the more common monitoring methods – tocodynamometry – measures length and frequency of contractions but is often ineffective at detecting these signals in women with a BMI of 30 kg/m2 and above, he said.
Electromyography (EMG) is more effective at monitoring the progression of true labor, because it can detect "the changes in cell excitability and coupling necessary for effective contractions," said Dr. Lucovnik.
To detect uterine activity, electrodes are placed on the patient’s abdomen with vertical and horizontal axes parallel to the patient’s vertical and horizontal axes, respectively, and with center-to-center distances between adjacent electrodes set about 5.0-5.5 cm apart. The uterine EMG is then measured for 30 minutes.
For the study, Dr. Lucovnik and his colleagues reviewed the predictive values of uterine EMG for preterm delivery in 88 women divided into three cohorts: 20 with a BMI of 30 or greater; 64 with a BMI of 25-29.9; and 4 with a BMI of 18.5-24.9.
The investigators did not find any significant difference between the cohorts in the area under the curve prediction of preterm delivery within 7 days (AUC was 0.95 in the normal and overweight cohorts, and 1 in the obese group; P = .08).
Six patients with low uterine EMG scores delivered prematurely within 7 days from the EMG measurement. No significant differences in BMI were reported between this false negative group (range, 26.13 plus or minus 1.03) and the combined true positive and true negative preterm labor groups (range, 28.04 plus or minus 3.77; P = .32).
"We know that predictive values of currently used methods to diagnose preterm labor are even lower in women with high BMI," said Dr. Lucovnik. "Our study showed that the accuracy of uterine EMG monitoring and its predictive value for preterm delivery are not affected by obesity in pregnant patients."
Dr. Lucovnik reported that he did not have any relevant disclosures.
NEW ORLEANS – Maternal obesity does not lessen the predictive value of noninvasive uterine electromyography monitoring, according to a poster presentation at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"We wanted to see if in this subset of pregnant women, the noninvasive method was as effective as in other pregnant women," said Dr. Miha Lucovnik, a perinatologist at the University Medical Center, Ljubljana, Slovenia.
"Uterine contractions, at term or preterm, are one of the most common reasons for visits to obstetrical triage, but determining which patient with contractions is in true labor and needs to be admitted is, however, difficult," said Dr. Lucovnik. "The inability to accurately diagnose preterm labor leads to missed opportunities to improve outcomes of premature neonates, and also to unnecessary costs and side effects of treatments in women who would not deliver preterm regardless of intervention."
One of the more common monitoring methods – tocodynamometry – measures length and frequency of contractions but is often ineffective at detecting these signals in women with a BMI of 30 kg/m2 and above, he said.
Electromyography (EMG) is more effective at monitoring the progression of true labor, because it can detect "the changes in cell excitability and coupling necessary for effective contractions," said Dr. Lucovnik.
To detect uterine activity, electrodes are placed on the patient’s abdomen with vertical and horizontal axes parallel to the patient’s vertical and horizontal axes, respectively, and with center-to-center distances between adjacent electrodes set about 5.0-5.5 cm apart. The uterine EMG is then measured for 30 minutes.
For the study, Dr. Lucovnik and his colleagues reviewed the predictive values of uterine EMG for preterm delivery in 88 women divided into three cohorts: 20 with a BMI of 30 or greater; 64 with a BMI of 25-29.9; and 4 with a BMI of 18.5-24.9.
The investigators did not find any significant difference between the cohorts in the area under the curve prediction of preterm delivery within 7 days (AUC was 0.95 in the normal and overweight cohorts, and 1 in the obese group; P = .08).
Six patients with low uterine EMG scores delivered prematurely within 7 days from the EMG measurement. No significant differences in BMI were reported between this false negative group (range, 26.13 plus or minus 1.03) and the combined true positive and true negative preterm labor groups (range, 28.04 plus or minus 3.77; P = .32).
"We know that predictive values of currently used methods to diagnose preterm labor are even lower in women with high BMI," said Dr. Lucovnik. "Our study showed that the accuracy of uterine EMG monitoring and its predictive value for preterm delivery are not affected by obesity in pregnant patients."
Dr. Lucovnik reported that he did not have any relevant disclosures.
AT THE PREGNANCY MEETING 2014
Major finding: No significant differences in BMI were found in the false negative group (range, 26.13 plus or minus 1.03) and the combined true positive and true negative preterm labor groups combined (range, 28.04 plus or minus 3.77) (P = .32).
Data source: Retrospective analysis of 88 women, including 20 women with BMI greater than 30 kg/m2, noninvasively monitored for preterm birth.
Disclosures: Dr. Lucovnik reported that he did not have any relevant disclosures.

Eight tools for improving obstetric patient safety and unit performance
Obstetricians, obstetric nurses, nurse managers, and obstetric department heads are almost always well-trained, hard working, highly motivated individuals dedicated to providing the best possible care for their patients. Nevertheless, errors in the provision of care are all too common.1–3 Even though these errors are confined to a small percentage of patient interactions, they engender profound consequences: injuries to mothers or their babies, higher costs to treat associated complications, and medical-legal suits that can entangle both clinicians and plaintiffs for years.
Why do such errors occur when it is the goal of well-trained and dedicated practi-tioners to provide error-free care? There are several reasons:
- The provision of medical care in the early 21st Century is an enormously complex endeavor.
- Physicians and nurses are human beings and, therefore, do not—and never will—perform perfectly all the time, in every situation, with every patient.
- The systems within which care providers work and the tools with which they work are often suboptimal and inefficient and are not designed to maximize patient safety.
- Financial constraints on hospital systems and physician practices dictate that obstetricians and obstetric nurses care for as many patients as possible in limited periods of time.
How then can obstetrics professionals seek to eradicate or at least decrease the number of medical errors that occur during the provision of maternity care?
To accomplish this, we must address the core issues at the root of these medical errors. Solutions must be implemented to 1) simplify the often unnecessary complexity of delivering medical care and 2) create systems and tools that minimize errors and catch those that do occur before they can cause harm.
Yet, how is this to be accomplished? In this article, I describe eight tools developed over time by clinicians who have worked in the field of obstetric patient safety. These tools provide some answers and concrete starting points.
TOOL 1: CONTINUING EDUCATION
William Osler once said, “It is astonishing with how little reading a doctor can practice medicine, but it is not astonishing how badly he may do it.”
As the years out of residency and nursing school accumulate, clinicians—both obstetricians and obstetric nurses—find it all too easy to continue to practice pretty much the way they did during training. However, medical science changes, new protocols improve on the old, and new techniques and medications are introduced yearly into the practice arena. If a clinician is to deliver the best possible care, he or she has to keep abreast of these developments in obstetrics and refresh his or her memory from time to time about things learned long ago. Such acquisition of new and review of old obstetric knowledge can be achieved only through ongoing study.
There are many ways continuing education can be accomplished. You can read new editions of textbooks when they are published or follow an obstetric journal through its yearly cycle. Cutting-edge, clinically oriented, interactive courses in all major areas of obstetrics are available to clinicians online. The recertification criteria of the American College of Obstetricians and Gynecologists (ACOG), state licensing requirements, and individual obstetric department recredentialing requirements often mandate such continuing education.
TOOL 2: SIMULATION PROGRAMS
Most obstetric emergencies, especially the most dangerous ones, occur infrequently, making it difficult for the many members of any labor and delivery unit to have their skills sharply honed to best deal with them. This is less of a problem at busy institutions where, simply due to the numbers of patients cared for, such emergencies are encountered on a regular basis. But at smaller facilities they are, fortunately, rare. The only way a unit can maintain its competency to handle such situations when they do arise—and they will—is to practice them in simulation mode.
There is now an increasing amount of literature demonstrating that simulation programs are effective not only at improving the knowledge base of obstetrics providers but also at improving Apgar scores, reducing admissions to neonatal intensive care units (NICUs), and preventing brachial plexus injuries.4
An effective simulation program should contain the following features:
- a thorough, didactic review of the clinical aspects of emergency care for all of the major obstetric emergencies (postpartum hemorrhage, shoulder dystocia, eclamptic seizure, maternal collapse, and urgent cesarean section)
- practice drills for the above
- training in teamwork and communication skills
- frequent repetition, ideally with each major obstetric emergency being covered twice per year.
Many institutions have developed simulation training centers. While these can be excellent teaching facilities, something is lost if simulation training is not done on the actual unit where obstetricians and obstetric nurses will encounter emergencies. Simulation programs also should be time-efficient and should be scheduled to make it easy for obstetrics personnel to participate. For greater convenience and knowledge retention, it is better to have short simulation programs at frequent intervals than day-long programs once per year or every other year.
Related Article: How simulation can train, and refresh, physicians for critical OB events Robert Gherman, MD; Andrew Satin, MD; Roxane Gardner, MD, MPH
TOOL 3: INTERNAL AUDITS
It is a mantra in business that you can’t fix what you can’t measure. And while obstetric units usually keep track of such things as rates of cesarean section, elective induction at less than 39 weeks, and admission to the NICU, it is rare that data are kept on other extremely important information. For instance, how often is an induction started with no indication for it written in the admission note? How often is the vacuum or forceps applied with no note documenting the reason or the discussion of risks and benefits with the patient? How often does estimated fetal weight go unnoted in the medical record of a mother with gestational diabetes?
An audit program, either in computer format or with manual collection on paper, is a vital tool for each labor and delivery unit to use in assessing the quality of the care it provides. Such an audit, by covering a sufficiently large number of clinical data points, can give tremendous insight into the specifics of the unit’s performance over the range of obstetric care situations. It will show where things are being done well and where they are not. The audit becomes even more valuable if it is designed so that each of the measured data points can be evaluated for individual clinician performance as well as for the labor and delivery unit as a whole.
Similar audits also should be conducted in individual physician offices and obstetric clinics. Many of the errors that occur in providing obstetric care occur prenatally: tests not performed, lack of follow-up of known problems, or poor communication with patients or with the labor and delivery unit.
One of the major benefits of audit programs that are conducted on a regular basis—every 6 months or annually are common intervals—is that trends in performance in each area of care can be evaluated. As deficiencies are pointed out to providers, their compliance with best care practices should improve from cycle to cycle.
TOOL 4: BEST PRACTICE PROTOCOLS
Medicine is now well past the point where protocols are seen as “restrictive” or “advocating cookbook medicine.” Well-designed protocols summarize best practices derived from evidence-based studies and the consensus of obstetric experts. They serve as convenient reminders to physicians in various clinical situations so that these clinicians do not have to rely solely on what they happen to remember about caring for a given condition. Protocols also provide a certain uniformity of care, which in itself decreases the likelihood of errors being made.
Each obstetric department should have a set of protocols to cover the most common obstetric situations, such as:
- premature rupture of membranes
- instrumental vaginal deliveries
- oxytocin administration.
Each unit does not have to devise its own protocols; ACOG and nearby academic institutions are excellent sources for protocols that can be replicated and implemented so that they do not have to be created de novo.
Related Article: More strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD; Alexis C. Gimovsky, MD (January 2011)
TOOL 5: SAFETY CHECKLISTS
Just as well-designed protocols can serve as convenient reminders of best practices, low-tech physical checklists can be kept at nursing stations and in labor and delivery rooms to serve as reminders of best practices during obstetric emergencies. For instance, having a laminated set of easy-to-read protocols for postpartum hemorrhage, eclamptic seizure, maternal collapse, and shoulder dystocia in a delivery room can allow a charge nurse or other supervisor to check to make sure all proper procedures are being performed by the team actually administering care to a patient in crisis, with nothing important overlooked.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
TOOL 6: COMPLETE DOCUMENTATION
Almost as many lawsuits are lost because of poor documentation as are lost because of inappropriate medical care. The obstetric literature,1 and my own experience with the medical-legal system, clearly demonstrate the need for appropriate, careful documentation of the events that transpire during patient care. Notes do not have to be especially long or verbose—but they must contain all relevant information and describe the obstetrician’s thinking at various decision points.
Documentation can be inadequate because of time constraints, poor understanding of the events that transpired, or simply a lack of remembering to include salient points that should be covered in a clinical note.
Clinicians can be prompted to include key aspects of care in the medical record by using prepared templates. Such templates are easy to fill out, remind clinicians to document information that would otherwise not get recorded, and result in a much more complete patient chart. By using a template, a clinician would never forget to record the head-to-body delivery interval after a shoulder dystocia or whether a fetal heart rate was obtained in the operating room just prior to starting a cesarean section.
Related Article: Sound strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010)
TOOL 7: SMART MEDICAL RECORDS
In obstetrics we are fortunate that there is a limited range of issues that recur repeatedly, such as gestational hypertension, placental abruption, and fetal distress. One soon gains experience in managing these conditions and, with the help of best-practice protocols, optimal care almost always can be provided.
Still, many clinical presentations can pose diagnostic challenges, especially in atypical cases. Moreover, clinicians managing a patient’s care may not immediately remember the best means of evaluating and treating a certain condition in specific circumstances. For example, at 3:00 am it may be difficult to recall whether it is nifedipine or labetalol that should be avoided with asthmatic patients or which antibiotic formulation is currently recommended for prophylaxis in a patient with premature rupture of membranes at 30 weeks’ gestation who is allergic to penicillin.
Smart medical records, already widely used in other fields of medicine, are an antidote to this problem. When certain diagnoses, physical findings, clinical details, or laboratory data are entered into specific fields in an electronic medical record, templates that have been added to the record automatically appear to show relevant information, such as tests that should be performed, treatments that should be administered, and alternative diagnoses that should be considered. Such reminders are not presented as obligations or “hard stops”; they are usually displayed in the form of easily dismissible pop-ups or “reminder bubbles” that appear on the screen and serve solely to jog memory and provide information.
Such smart electronic medical record features can be provided either by the main electronic medical record vendor or added as subprograms by other providers.
Related Article: EHRs and medicolegal risk: How they help, when they could hurt Martin L. Gimovsky, MD; Baohuong N. Trans, DO (March 2013)
TOOL 8: MATERNITY UNIT ON-SITE CONSULTATIONS
Every labor and delivery unit has its own culture, a combination of institutional history and the personality of the doctors and nurses working there. Some units function efficiently, have the most modern equipment, and provide superb medical care. Other units have less than adequate facilities, remain entrenched in older practices, and have disruptive or uncooperative personnel that interfere with the smooth running of the unit. Moreover, each maternity unit, based on its resources, patient population, and staff skills, devises its own solutions to the same sorts of problems that all other obstetric units share. Unfortunately, there is little collaboration between units to discuss common problems and trade best practices. The result is that all too often each unit invents its own “wheel” when many excellent “wheels” already have been developed for the same issues around the country.
An on-site visit by an outside consultant—an obstetrician, an obstetric nurse, or both—can identify ongoing institutional problems, point out care deficiencies the unit may not be aware of, and provide resources and ideas to help solve the issues identified. Moreover, an outside consultant can offer unbiased and authoritative opinions to help move initiatives that may be stalled by local personalities or institutional politics.
Some features that a well-conducted on-site consultation will evaluate are:
- adequacy of obstetric triage
- capacity to perform stat cesarean sections 24/7
- 24-hour availability of obstetricians, anesthesiologists, pediatricians, and operating room teams
- preparation for handling various obstetric emergencies
- oxytocin administration protocols and compliance
- adequacy of physician and nurse charting
- ongoing skills assessment of fetal heart-rate monitor interpretation
- presence of practitioners whose disruptive behavior compromises the safety of the unit
- preparation for nonmedical emergencies, such as infant abduction, natural disaster; fire; shooter; or disruptive patients, visitors, or staff.
IMPLEMENTATION CAN EQUAL SAFER CARE
As long as people have babies, less than desirable outcomes will occasionally occur. As long as care providers are human beings, the provision of obstetric care will continue to be imperfect.
It is up to those entrusted with the responsibility of caring for mothers and their babies to provide as much support and backup as possible to obstetricians and obstetric nurses, all of whom sincerely desire to do everything possible to deliver safe care to their patients.
Tools for providing such support and backup are available and can be implemented fairly easily on most obstetric units. They do involve an expenditure of both time and money. However, the most important requirement for success is an institutional willingness to 1) acknowledge that the care a given unit provides can be improved, 2) perform an in-depth evaluation of the quality of care currently being administered, and 3) move ahead with the sorts of tools discussed in this article that will enable clinicians to provide optimal care for mothers and babies.
SHARE YOUR EXPERIENCE!
Did implementation of a tool described in this article solve a problem or improve performance for your obstetric unit? Tell us about it by emailing to: obg@frontlinemedcom.com Please include your name, city, and state.
- Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008;112(6):1279–1283.
- Gluck PA. Medical error theory. Obstet Gynecol Clin North Am. 2008;35(1):11–17, vii.
- Anakiraman V, Ecker J. Quality in obstetric care: measuring what matters. Obstet Gynecol. 2010;116(3):728–732.
- Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177–182.

Henry M. Lerner, MD, is Assistant Clinical Professor of Obstetrics & Gynecology at Harvard Medical School in Boston, Massachusetts. He has been in private practice of obstetrics and gynecology for 35 years, has served on the board of a major medical malpractice carrier for 14 years, and has helped defend more than 300 obstetricians in medical malpractice cases across the country.
Dr. Lerner reports that he is a consultant to The Sullivan Group, a patient safety education provider.
Henry M. Lerner, MD, is Assistant Clinical Professor of Obstetrics & Gynecology at Harvard Medical School in Boston, Massachusetts. He has been in private practice of obstetrics and gynecology for 35 years, has served on the board of a major medical malpractice carrier for 14 years, and has helped defend more than 300 obstetricians in medical malpractice cases across the country.
Dr. Lerner reports that he is a consultant to The Sullivan Group, a patient safety education provider.
Henry M. Lerner, MD, is Assistant Clinical Professor of Obstetrics & Gynecology at Harvard Medical School in Boston, Massachusetts. He has been in private practice of obstetrics and gynecology for 35 years, has served on the board of a major medical malpractice carrier for 14 years, and has helped defend more than 300 obstetricians in medical malpractice cases across the country.
Dr. Lerner reports that he is a consultant to The Sullivan Group, a patient safety education provider.
Obstetricians, obstetric nurses, nurse managers, and obstetric department heads are almost always well-trained, hard working, highly motivated individuals dedicated to providing the best possible care for their patients. Nevertheless, errors in the provision of care are all too common.1–3 Even though these errors are confined to a small percentage of patient interactions, they engender profound consequences: injuries to mothers or their babies, higher costs to treat associated complications, and medical-legal suits that can entangle both clinicians and plaintiffs for years.
Why do such errors occur when it is the goal of well-trained and dedicated practi-tioners to provide error-free care? There are several reasons:
- The provision of medical care in the early 21st Century is an enormously complex endeavor.
- Physicians and nurses are human beings and, therefore, do not—and never will—perform perfectly all the time, in every situation, with every patient.
- The systems within which care providers work and the tools with which they work are often suboptimal and inefficient and are not designed to maximize patient safety.
- Financial constraints on hospital systems and physician practices dictate that obstetricians and obstetric nurses care for as many patients as possible in limited periods of time.
How then can obstetrics professionals seek to eradicate or at least decrease the number of medical errors that occur during the provision of maternity care?
To accomplish this, we must address the core issues at the root of these medical errors. Solutions must be implemented to 1) simplify the often unnecessary complexity of delivering medical care and 2) create systems and tools that minimize errors and catch those that do occur before they can cause harm.
Yet, how is this to be accomplished? In this article, I describe eight tools developed over time by clinicians who have worked in the field of obstetric patient safety. These tools provide some answers and concrete starting points.
TOOL 1: CONTINUING EDUCATION
William Osler once said, “It is astonishing with how little reading a doctor can practice medicine, but it is not astonishing how badly he may do it.”
As the years out of residency and nursing school accumulate, clinicians—both obstetricians and obstetric nurses—find it all too easy to continue to practice pretty much the way they did during training. However, medical science changes, new protocols improve on the old, and new techniques and medications are introduced yearly into the practice arena. If a clinician is to deliver the best possible care, he or she has to keep abreast of these developments in obstetrics and refresh his or her memory from time to time about things learned long ago. Such acquisition of new and review of old obstetric knowledge can be achieved only through ongoing study.
There are many ways continuing education can be accomplished. You can read new editions of textbooks when they are published or follow an obstetric journal through its yearly cycle. Cutting-edge, clinically oriented, interactive courses in all major areas of obstetrics are available to clinicians online. The recertification criteria of the American College of Obstetricians and Gynecologists (ACOG), state licensing requirements, and individual obstetric department recredentialing requirements often mandate such continuing education.
TOOL 2: SIMULATION PROGRAMS
Most obstetric emergencies, especially the most dangerous ones, occur infrequently, making it difficult for the many members of any labor and delivery unit to have their skills sharply honed to best deal with them. This is less of a problem at busy institutions where, simply due to the numbers of patients cared for, such emergencies are encountered on a regular basis. But at smaller facilities they are, fortunately, rare. The only way a unit can maintain its competency to handle such situations when they do arise—and they will—is to practice them in simulation mode.
There is now an increasing amount of literature demonstrating that simulation programs are effective not only at improving the knowledge base of obstetrics providers but also at improving Apgar scores, reducing admissions to neonatal intensive care units (NICUs), and preventing brachial plexus injuries.4
An effective simulation program should contain the following features:
- a thorough, didactic review of the clinical aspects of emergency care for all of the major obstetric emergencies (postpartum hemorrhage, shoulder dystocia, eclamptic seizure, maternal collapse, and urgent cesarean section)
- practice drills for the above
- training in teamwork and communication skills
- frequent repetition, ideally with each major obstetric emergency being covered twice per year.
Many institutions have developed simulation training centers. While these can be excellent teaching facilities, something is lost if simulation training is not done on the actual unit where obstetricians and obstetric nurses will encounter emergencies. Simulation programs also should be time-efficient and should be scheduled to make it easy for obstetrics personnel to participate. For greater convenience and knowledge retention, it is better to have short simulation programs at frequent intervals than day-long programs once per year or every other year.
Related Article: How simulation can train, and refresh, physicians for critical OB events Robert Gherman, MD; Andrew Satin, MD; Roxane Gardner, MD, MPH
TOOL 3: INTERNAL AUDITS
It is a mantra in business that you can’t fix what you can’t measure. And while obstetric units usually keep track of such things as rates of cesarean section, elective induction at less than 39 weeks, and admission to the NICU, it is rare that data are kept on other extremely important information. For instance, how often is an induction started with no indication for it written in the admission note? How often is the vacuum or forceps applied with no note documenting the reason or the discussion of risks and benefits with the patient? How often does estimated fetal weight go unnoted in the medical record of a mother with gestational diabetes?
An audit program, either in computer format or with manual collection on paper, is a vital tool for each labor and delivery unit to use in assessing the quality of the care it provides. Such an audit, by covering a sufficiently large number of clinical data points, can give tremendous insight into the specifics of the unit’s performance over the range of obstetric care situations. It will show where things are being done well and where they are not. The audit becomes even more valuable if it is designed so that each of the measured data points can be evaluated for individual clinician performance as well as for the labor and delivery unit as a whole.
Similar audits also should be conducted in individual physician offices and obstetric clinics. Many of the errors that occur in providing obstetric care occur prenatally: tests not performed, lack of follow-up of known problems, or poor communication with patients or with the labor and delivery unit.
One of the major benefits of audit programs that are conducted on a regular basis—every 6 months or annually are common intervals—is that trends in performance in each area of care can be evaluated. As deficiencies are pointed out to providers, their compliance with best care practices should improve from cycle to cycle.
TOOL 4: BEST PRACTICE PROTOCOLS
Medicine is now well past the point where protocols are seen as “restrictive” or “advocating cookbook medicine.” Well-designed protocols summarize best practices derived from evidence-based studies and the consensus of obstetric experts. They serve as convenient reminders to physicians in various clinical situations so that these clinicians do not have to rely solely on what they happen to remember about caring for a given condition. Protocols also provide a certain uniformity of care, which in itself decreases the likelihood of errors being made.
Each obstetric department should have a set of protocols to cover the most common obstetric situations, such as:
- premature rupture of membranes
- instrumental vaginal deliveries
- oxytocin administration.
Each unit does not have to devise its own protocols; ACOG and nearby academic institutions are excellent sources for protocols that can be replicated and implemented so that they do not have to be created de novo.
Related Article: More strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD; Alexis C. Gimovsky, MD (January 2011)
TOOL 5: SAFETY CHECKLISTS
Just as well-designed protocols can serve as convenient reminders of best practices, low-tech physical checklists can be kept at nursing stations and in labor and delivery rooms to serve as reminders of best practices during obstetric emergencies. For instance, having a laminated set of easy-to-read protocols for postpartum hemorrhage, eclamptic seizure, maternal collapse, and shoulder dystocia in a delivery room can allow a charge nurse or other supervisor to check to make sure all proper procedures are being performed by the team actually administering care to a patient in crisis, with nothing important overlooked.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
TOOL 6: COMPLETE DOCUMENTATION
Almost as many lawsuits are lost because of poor documentation as are lost because of inappropriate medical care. The obstetric literature,1 and my own experience with the medical-legal system, clearly demonstrate the need for appropriate, careful documentation of the events that transpire during patient care. Notes do not have to be especially long or verbose—but they must contain all relevant information and describe the obstetrician’s thinking at various decision points.
Documentation can be inadequate because of time constraints, poor understanding of the events that transpired, or simply a lack of remembering to include salient points that should be covered in a clinical note.
Clinicians can be prompted to include key aspects of care in the medical record by using prepared templates. Such templates are easy to fill out, remind clinicians to document information that would otherwise not get recorded, and result in a much more complete patient chart. By using a template, a clinician would never forget to record the head-to-body delivery interval after a shoulder dystocia or whether a fetal heart rate was obtained in the operating room just prior to starting a cesarean section.
Related Article: Sound strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010)
TOOL 7: SMART MEDICAL RECORDS
In obstetrics we are fortunate that there is a limited range of issues that recur repeatedly, such as gestational hypertension, placental abruption, and fetal distress. One soon gains experience in managing these conditions and, with the help of best-practice protocols, optimal care almost always can be provided.
Still, many clinical presentations can pose diagnostic challenges, especially in atypical cases. Moreover, clinicians managing a patient’s care may not immediately remember the best means of evaluating and treating a certain condition in specific circumstances. For example, at 3:00 am it may be difficult to recall whether it is nifedipine or labetalol that should be avoided with asthmatic patients or which antibiotic formulation is currently recommended for prophylaxis in a patient with premature rupture of membranes at 30 weeks’ gestation who is allergic to penicillin.
Smart medical records, already widely used in other fields of medicine, are an antidote to this problem. When certain diagnoses, physical findings, clinical details, or laboratory data are entered into specific fields in an electronic medical record, templates that have been added to the record automatically appear to show relevant information, such as tests that should be performed, treatments that should be administered, and alternative diagnoses that should be considered. Such reminders are not presented as obligations or “hard stops”; they are usually displayed in the form of easily dismissible pop-ups or “reminder bubbles” that appear on the screen and serve solely to jog memory and provide information.
Such smart electronic medical record features can be provided either by the main electronic medical record vendor or added as subprograms by other providers.
Related Article: EHRs and medicolegal risk: How they help, when they could hurt Martin L. Gimovsky, MD; Baohuong N. Trans, DO (March 2013)
TOOL 8: MATERNITY UNIT ON-SITE CONSULTATIONS
Every labor and delivery unit has its own culture, a combination of institutional history and the personality of the doctors and nurses working there. Some units function efficiently, have the most modern equipment, and provide superb medical care. Other units have less than adequate facilities, remain entrenched in older practices, and have disruptive or uncooperative personnel that interfere with the smooth running of the unit. Moreover, each maternity unit, based on its resources, patient population, and staff skills, devises its own solutions to the same sorts of problems that all other obstetric units share. Unfortunately, there is little collaboration between units to discuss common problems and trade best practices. The result is that all too often each unit invents its own “wheel” when many excellent “wheels” already have been developed for the same issues around the country.
An on-site visit by an outside consultant—an obstetrician, an obstetric nurse, or both—can identify ongoing institutional problems, point out care deficiencies the unit may not be aware of, and provide resources and ideas to help solve the issues identified. Moreover, an outside consultant can offer unbiased and authoritative opinions to help move initiatives that may be stalled by local personalities or institutional politics.
Some features that a well-conducted on-site consultation will evaluate are:
- adequacy of obstetric triage
- capacity to perform stat cesarean sections 24/7
- 24-hour availability of obstetricians, anesthesiologists, pediatricians, and operating room teams
- preparation for handling various obstetric emergencies
- oxytocin administration protocols and compliance
- adequacy of physician and nurse charting
- ongoing skills assessment of fetal heart-rate monitor interpretation
- presence of practitioners whose disruptive behavior compromises the safety of the unit
- preparation for nonmedical emergencies, such as infant abduction, natural disaster; fire; shooter; or disruptive patients, visitors, or staff.
IMPLEMENTATION CAN EQUAL SAFER CARE
As long as people have babies, less than desirable outcomes will occasionally occur. As long as care providers are human beings, the provision of obstetric care will continue to be imperfect.
It is up to those entrusted with the responsibility of caring for mothers and their babies to provide as much support and backup as possible to obstetricians and obstetric nurses, all of whom sincerely desire to do everything possible to deliver safe care to their patients.
Tools for providing such support and backup are available and can be implemented fairly easily on most obstetric units. They do involve an expenditure of both time and money. However, the most important requirement for success is an institutional willingness to 1) acknowledge that the care a given unit provides can be improved, 2) perform an in-depth evaluation of the quality of care currently being administered, and 3) move ahead with the sorts of tools discussed in this article that will enable clinicians to provide optimal care for mothers and babies.
SHARE YOUR EXPERIENCE!
Did implementation of a tool described in this article solve a problem or improve performance for your obstetric unit? Tell us about it by emailing to: obg@frontlinemedcom.com Please include your name, city, and state.
Obstetricians, obstetric nurses, nurse managers, and obstetric department heads are almost always well-trained, hard working, highly motivated individuals dedicated to providing the best possible care for their patients. Nevertheless, errors in the provision of care are all too common.1–3 Even though these errors are confined to a small percentage of patient interactions, they engender profound consequences: injuries to mothers or their babies, higher costs to treat associated complications, and medical-legal suits that can entangle both clinicians and plaintiffs for years.
Why do such errors occur when it is the goal of well-trained and dedicated practi-tioners to provide error-free care? There are several reasons:
- The provision of medical care in the early 21st Century is an enormously complex endeavor.
- Physicians and nurses are human beings and, therefore, do not—and never will—perform perfectly all the time, in every situation, with every patient.
- The systems within which care providers work and the tools with which they work are often suboptimal and inefficient and are not designed to maximize patient safety.
- Financial constraints on hospital systems and physician practices dictate that obstetricians and obstetric nurses care for as many patients as possible in limited periods of time.
How then can obstetrics professionals seek to eradicate or at least decrease the number of medical errors that occur during the provision of maternity care?
To accomplish this, we must address the core issues at the root of these medical errors. Solutions must be implemented to 1) simplify the often unnecessary complexity of delivering medical care and 2) create systems and tools that minimize errors and catch those that do occur before they can cause harm.
Yet, how is this to be accomplished? In this article, I describe eight tools developed over time by clinicians who have worked in the field of obstetric patient safety. These tools provide some answers and concrete starting points.
TOOL 1: CONTINUING EDUCATION
William Osler once said, “It is astonishing with how little reading a doctor can practice medicine, but it is not astonishing how badly he may do it.”
As the years out of residency and nursing school accumulate, clinicians—both obstetricians and obstetric nurses—find it all too easy to continue to practice pretty much the way they did during training. However, medical science changes, new protocols improve on the old, and new techniques and medications are introduced yearly into the practice arena. If a clinician is to deliver the best possible care, he or she has to keep abreast of these developments in obstetrics and refresh his or her memory from time to time about things learned long ago. Such acquisition of new and review of old obstetric knowledge can be achieved only through ongoing study.
There are many ways continuing education can be accomplished. You can read new editions of textbooks when they are published or follow an obstetric journal through its yearly cycle. Cutting-edge, clinically oriented, interactive courses in all major areas of obstetrics are available to clinicians online. The recertification criteria of the American College of Obstetricians and Gynecologists (ACOG), state licensing requirements, and individual obstetric department recredentialing requirements often mandate such continuing education.
TOOL 2: SIMULATION PROGRAMS
Most obstetric emergencies, especially the most dangerous ones, occur infrequently, making it difficult for the many members of any labor and delivery unit to have their skills sharply honed to best deal with them. This is less of a problem at busy institutions where, simply due to the numbers of patients cared for, such emergencies are encountered on a regular basis. But at smaller facilities they are, fortunately, rare. The only way a unit can maintain its competency to handle such situations when they do arise—and they will—is to practice them in simulation mode.
There is now an increasing amount of literature demonstrating that simulation programs are effective not only at improving the knowledge base of obstetrics providers but also at improving Apgar scores, reducing admissions to neonatal intensive care units (NICUs), and preventing brachial plexus injuries.4
An effective simulation program should contain the following features:
- a thorough, didactic review of the clinical aspects of emergency care for all of the major obstetric emergencies (postpartum hemorrhage, shoulder dystocia, eclamptic seizure, maternal collapse, and urgent cesarean section)
- practice drills for the above
- training in teamwork and communication skills
- frequent repetition, ideally with each major obstetric emergency being covered twice per year.
Many institutions have developed simulation training centers. While these can be excellent teaching facilities, something is lost if simulation training is not done on the actual unit where obstetricians and obstetric nurses will encounter emergencies. Simulation programs also should be time-efficient and should be scheduled to make it easy for obstetrics personnel to participate. For greater convenience and knowledge retention, it is better to have short simulation programs at frequent intervals than day-long programs once per year or every other year.
Related Article: How simulation can train, and refresh, physicians for critical OB events Robert Gherman, MD; Andrew Satin, MD; Roxane Gardner, MD, MPH
TOOL 3: INTERNAL AUDITS
It is a mantra in business that you can’t fix what you can’t measure. And while obstetric units usually keep track of such things as rates of cesarean section, elective induction at less than 39 weeks, and admission to the NICU, it is rare that data are kept on other extremely important information. For instance, how often is an induction started with no indication for it written in the admission note? How often is the vacuum or forceps applied with no note documenting the reason or the discussion of risks and benefits with the patient? How often does estimated fetal weight go unnoted in the medical record of a mother with gestational diabetes?
An audit program, either in computer format or with manual collection on paper, is a vital tool for each labor and delivery unit to use in assessing the quality of the care it provides. Such an audit, by covering a sufficiently large number of clinical data points, can give tremendous insight into the specifics of the unit’s performance over the range of obstetric care situations. It will show where things are being done well and where they are not. The audit becomes even more valuable if it is designed so that each of the measured data points can be evaluated for individual clinician performance as well as for the labor and delivery unit as a whole.
Similar audits also should be conducted in individual physician offices and obstetric clinics. Many of the errors that occur in providing obstetric care occur prenatally: tests not performed, lack of follow-up of known problems, or poor communication with patients or with the labor and delivery unit.
One of the major benefits of audit programs that are conducted on a regular basis—every 6 months or annually are common intervals—is that trends in performance in each area of care can be evaluated. As deficiencies are pointed out to providers, their compliance with best care practices should improve from cycle to cycle.
TOOL 4: BEST PRACTICE PROTOCOLS
Medicine is now well past the point where protocols are seen as “restrictive” or “advocating cookbook medicine.” Well-designed protocols summarize best practices derived from evidence-based studies and the consensus of obstetric experts. They serve as convenient reminders to physicians in various clinical situations so that these clinicians do not have to rely solely on what they happen to remember about caring for a given condition. Protocols also provide a certain uniformity of care, which in itself decreases the likelihood of errors being made.
Each obstetric department should have a set of protocols to cover the most common obstetric situations, such as:
- premature rupture of membranes
- instrumental vaginal deliveries
- oxytocin administration.
Each unit does not have to devise its own protocols; ACOG and nearby academic institutions are excellent sources for protocols that can be replicated and implemented so that they do not have to be created de novo.
Related Article: More strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD; Alexis C. Gimovsky, MD (January 2011)
TOOL 5: SAFETY CHECKLISTS
Just as well-designed protocols can serve as convenient reminders of best practices, low-tech physical checklists can be kept at nursing stations and in labor and delivery rooms to serve as reminders of best practices during obstetric emergencies. For instance, having a laminated set of easy-to-read protocols for postpartum hemorrhage, eclamptic seizure, maternal collapse, and shoulder dystocia in a delivery room can allow a charge nurse or other supervisor to check to make sure all proper procedures are being performed by the team actually administering care to a patient in crisis, with nothing important overlooked.
Related Article: Develop and use a checklist for 3rd- and 4th-degree perineal lacerations Robert L. Barbieri, MD (Editorial, August 2013)
TOOL 6: COMPLETE DOCUMENTATION
Almost as many lawsuits are lost because of poor documentation as are lost because of inappropriate medical care. The obstetric literature,1 and my own experience with the medical-legal system, clearly demonstrate the need for appropriate, careful documentation of the events that transpire during patient care. Notes do not have to be especially long or verbose—but they must contain all relevant information and describe the obstetrician’s thinking at various decision points.
Documentation can be inadequate because of time constraints, poor understanding of the events that transpired, or simply a lack of remembering to include salient points that should be covered in a clinical note.
Clinicians can be prompted to include key aspects of care in the medical record by using prepared templates. Such templates are easy to fill out, remind clinicians to document information that would otherwise not get recorded, and result in a much more complete patient chart. By using a template, a clinician would never forget to record the head-to-body delivery interval after a shoulder dystocia or whether a fetal heart rate was obtained in the operating room just prior to starting a cesarean section.
Related Article: Sound strategies to avoid malpractice hazards on labor and delivery Martin L. Gimovsky, MD, and Alexis C. Gimovsky, MD (December 2010)
TOOL 7: SMART MEDICAL RECORDS
In obstetrics we are fortunate that there is a limited range of issues that recur repeatedly, such as gestational hypertension, placental abruption, and fetal distress. One soon gains experience in managing these conditions and, with the help of best-practice protocols, optimal care almost always can be provided.
Still, many clinical presentations can pose diagnostic challenges, especially in atypical cases. Moreover, clinicians managing a patient’s care may not immediately remember the best means of evaluating and treating a certain condition in specific circumstances. For example, at 3:00 am it may be difficult to recall whether it is nifedipine or labetalol that should be avoided with asthmatic patients or which antibiotic formulation is currently recommended for prophylaxis in a patient with premature rupture of membranes at 30 weeks’ gestation who is allergic to penicillin.
Smart medical records, already widely used in other fields of medicine, are an antidote to this problem. When certain diagnoses, physical findings, clinical details, or laboratory data are entered into specific fields in an electronic medical record, templates that have been added to the record automatically appear to show relevant information, such as tests that should be performed, treatments that should be administered, and alternative diagnoses that should be considered. Such reminders are not presented as obligations or “hard stops”; they are usually displayed in the form of easily dismissible pop-ups or “reminder bubbles” that appear on the screen and serve solely to jog memory and provide information.
Such smart electronic medical record features can be provided either by the main electronic medical record vendor or added as subprograms by other providers.
Related Article: EHRs and medicolegal risk: How they help, when they could hurt Martin L. Gimovsky, MD; Baohuong N. Trans, DO (March 2013)
TOOL 8: MATERNITY UNIT ON-SITE CONSULTATIONS
Every labor and delivery unit has its own culture, a combination of institutional history and the personality of the doctors and nurses working there. Some units function efficiently, have the most modern equipment, and provide superb medical care. Other units have less than adequate facilities, remain entrenched in older practices, and have disruptive or uncooperative personnel that interfere with the smooth running of the unit. Moreover, each maternity unit, based on its resources, patient population, and staff skills, devises its own solutions to the same sorts of problems that all other obstetric units share. Unfortunately, there is little collaboration between units to discuss common problems and trade best practices. The result is that all too often each unit invents its own “wheel” when many excellent “wheels” already have been developed for the same issues around the country.
An on-site visit by an outside consultant—an obstetrician, an obstetric nurse, or both—can identify ongoing institutional problems, point out care deficiencies the unit may not be aware of, and provide resources and ideas to help solve the issues identified. Moreover, an outside consultant can offer unbiased and authoritative opinions to help move initiatives that may be stalled by local personalities or institutional politics.
Some features that a well-conducted on-site consultation will evaluate are:
- adequacy of obstetric triage
- capacity to perform stat cesarean sections 24/7
- 24-hour availability of obstetricians, anesthesiologists, pediatricians, and operating room teams
- preparation for handling various obstetric emergencies
- oxytocin administration protocols and compliance
- adequacy of physician and nurse charting
- ongoing skills assessment of fetal heart-rate monitor interpretation
- presence of practitioners whose disruptive behavior compromises the safety of the unit
- preparation for nonmedical emergencies, such as infant abduction, natural disaster; fire; shooter; or disruptive patients, visitors, or staff.
IMPLEMENTATION CAN EQUAL SAFER CARE
As long as people have babies, less than desirable outcomes will occasionally occur. As long as care providers are human beings, the provision of obstetric care will continue to be imperfect.
It is up to those entrusted with the responsibility of caring for mothers and their babies to provide as much support and backup as possible to obstetricians and obstetric nurses, all of whom sincerely desire to do everything possible to deliver safe care to their patients.
Tools for providing such support and backup are available and can be implemented fairly easily on most obstetric units. They do involve an expenditure of both time and money. However, the most important requirement for success is an institutional willingness to 1) acknowledge that the care a given unit provides can be improved, 2) perform an in-depth evaluation of the quality of care currently being administered, and 3) move ahead with the sorts of tools discussed in this article that will enable clinicians to provide optimal care for mothers and babies.
SHARE YOUR EXPERIENCE!
Did implementation of a tool described in this article solve a problem or improve performance for your obstetric unit? Tell us about it by emailing to: obg@frontlinemedcom.com Please include your name, city, and state.
- Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008;112(6):1279–1283.
- Gluck PA. Medical error theory. Obstet Gynecol Clin North Am. 2008;35(1):11–17, vii.
- Anakiraman V, Ecker J. Quality in obstetric care: measuring what matters. Obstet Gynecol. 2010;116(3):728–732.
- Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177–182.
- Clark SL, Belfort MA, Dildy GA, Meyers JA. Reducing obstetric litigation through alterations in practice patterns. Obstet Gynecol. 2008;112(6):1279–1283.
- Gluck PA. Medical error theory. Obstet Gynecol Clin North Am. 2008;35(1):11–17, vii.
- Anakiraman V, Ecker J. Quality in obstetric care: measuring what matters. Obstet Gynecol. 2010;116(3):728–732.
- Draycott T, Sibanda T, Owen L, et al. Does training in obstetric emergencies improve neonatal outcome? BJOG. 2006;113(2):177–182.

Does maternal obesity increase the risk of preterm delivery?
The developed world is in the midst of an unprecedented increase in human body mass. This increase can be attributed to widespread access to large amounts of inexpensive calories—particularly carbohydrates—and diminishing physical exertion. We have “evolved” from creatures struggling to get enough food to survive to vertebrates drowning in an ocean of calories and ease.
Although obesity clearly lies on the causal pathway for diseases such as diabetes and endometrial cancer, it also is associated with many other unhealthy behaviors and exposures. For example, obese women tend to earn less money, achieve less in school, smoke, and live farther away from markets and playgrounds—and the list of confounders goes on and on. We can measure height and weight with ease and precision, but we can’t assess and quantify most of these other confounders.
Related Article: Should you start prescribing lorcaserin or orlistat to your overweight or obese patients? Robert L. Barbieri, MD (Editorial, October 2013)
Cnattingius and colleagues give us another “obesity is bad” paper, this time with the outcome of preterm delivery. They found not only an association between obesity and preterm delivery but also a “mass response effect”—that is, the association increased along with maternal BMI.
The magnitude of the associations was small (odds ratios <3.0 for preterm delivery among overweight and obese women, compared with women of normal weight), and despite valiant efforts by the investigators to control for confounding, the imprecision I mentioned above limits their findings.
I declared a personal moratorium on reading “obesity is bad” papers a few years back. Even if obesity is a real risk factor for poor perinatal outcomes and not a proxy for residual confounding, we still have no idea, short of invasive surgery, how to modify that risk. Real progress will require effective lifestyle intervention—and we know so little about how to get people to lead healthy lives. It is difficult enough to modify our own behavior (recall your New Year’s resolutions), even harder to motivate our patients to lose weight and exercise.
What this evidence means for practice
Obesity is at best a weak risk factor for preterm delivery. Unless you are more successful than I have been at getting women to modify their diet and exercise, I would not make heavy mothers feel any worse.
John M. Thorp Jr., MD
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: obg@frontlinemedcom.com Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
The developed world is in the midst of an unprecedented increase in human body mass. This increase can be attributed to widespread access to large amounts of inexpensive calories—particularly carbohydrates—and diminishing physical exertion. We have “evolved” from creatures struggling to get enough food to survive to vertebrates drowning in an ocean of calories and ease.
Although obesity clearly lies on the causal pathway for diseases such as diabetes and endometrial cancer, it also is associated with many other unhealthy behaviors and exposures. For example, obese women tend to earn less money, achieve less in school, smoke, and live farther away from markets and playgrounds—and the list of confounders goes on and on. We can measure height and weight with ease and precision, but we can’t assess and quantify most of these other confounders.
Related Article: Should you start prescribing lorcaserin or orlistat to your overweight or obese patients? Robert L. Barbieri, MD (Editorial, October 2013)
Cnattingius and colleagues give us another “obesity is bad” paper, this time with the outcome of preterm delivery. They found not only an association between obesity and preterm delivery but also a “mass response effect”—that is, the association increased along with maternal BMI.
The magnitude of the associations was small (odds ratios <3.0 for preterm delivery among overweight and obese women, compared with women of normal weight), and despite valiant efforts by the investigators to control for confounding, the imprecision I mentioned above limits their findings.
I declared a personal moratorium on reading “obesity is bad” papers a few years back. Even if obesity is a real risk factor for poor perinatal outcomes and not a proxy for residual confounding, we still have no idea, short of invasive surgery, how to modify that risk. Real progress will require effective lifestyle intervention—and we know so little about how to get people to lead healthy lives. It is difficult enough to modify our own behavior (recall your New Year’s resolutions), even harder to motivate our patients to lose weight and exercise.
What this evidence means for practice
Obesity is at best a weak risk factor for preterm delivery. Unless you are more successful than I have been at getting women to modify their diet and exercise, I would not make heavy mothers feel any worse.
John M. Thorp Jr., MD
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: obg@frontlinemedcom.com Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!
The developed world is in the midst of an unprecedented increase in human body mass. This increase can be attributed to widespread access to large amounts of inexpensive calories—particularly carbohydrates—and diminishing physical exertion. We have “evolved” from creatures struggling to get enough food to survive to vertebrates drowning in an ocean of calories and ease.
Although obesity clearly lies on the causal pathway for diseases such as diabetes and endometrial cancer, it also is associated with many other unhealthy behaviors and exposures. For example, obese women tend to earn less money, achieve less in school, smoke, and live farther away from markets and playgrounds—and the list of confounders goes on and on. We can measure height and weight with ease and precision, but we can’t assess and quantify most of these other confounders.
Related Article: Should you start prescribing lorcaserin or orlistat to your overweight or obese patients? Robert L. Barbieri, MD (Editorial, October 2013)
Cnattingius and colleagues give us another “obesity is bad” paper, this time with the outcome of preterm delivery. They found not only an association between obesity and preterm delivery but also a “mass response effect”—that is, the association increased along with maternal BMI.
The magnitude of the associations was small (odds ratios <3.0 for preterm delivery among overweight and obese women, compared with women of normal weight), and despite valiant efforts by the investigators to control for confounding, the imprecision I mentioned above limits their findings.
I declared a personal moratorium on reading “obesity is bad” papers a few years back. Even if obesity is a real risk factor for poor perinatal outcomes and not a proxy for residual confounding, we still have no idea, short of invasive surgery, how to modify that risk. Real progress will require effective lifestyle intervention—and we know so little about how to get people to lead healthy lives. It is difficult enough to modify our own behavior (recall your New Year’s resolutions), even harder to motivate our patients to lose weight and exercise.
What this evidence means for practice
Obesity is at best a weak risk factor for preterm delivery. Unless you are more successful than I have been at getting women to modify their diet and exercise, I would not make heavy mothers feel any worse.
John M. Thorp Jr., MD
TELL US WHAT YOU THINK!
Share your thoughts on this article or on any topic relevant to ObGyns and women’s health practitioners. Tell us which topics you’d like to see covered in future issues, and what challenges you face in daily practice. We will consider publishing your letter and in a future issue.
Send your letter to: obg@frontlinemedcom.com Please include the city and state in which you practice.
Stay in touch! Your feedback is important to us!

How I avoid open power morcellation
How I avoid open power morcellation
Several gynecologic surgeons at my hospital (I am one of them) have developed approaches to hysterectomy and myomectomy that avoid open power morcellation.
For laparoscopic hysterectomy, we place two or three 5-mm ports and use a retroperitoneal approach. We identify the ureters in the retroperitoneal space and trace them into the pelvis. They often need to be lateralized in cases involving endometriosis or large fibroids. We then coagulate the uterine artery where it crosses over the ureter, as the vessel is smaller and straighter in this location. This strategy reduces blood loss and lessens the need to fulgurate the vessels at the cervix, where the ureter is vulnerable to injury.
When the uterus is large, we morcellate it transvaginally or through a 3-cm transverse suprapubic incision after placing a retractor. Be aware that 60% of women with fibroids can have coexisting adenomyosis. As Dr. Barbieri noted in his editorial, use of an internal morcellator can disperse small tissue fragments throughout the peritoneal cavity, where they may “re-implant” and undergo malignant transformation.
For laparoscopic myomectomy, I place 600 µg of misoprostol—a very potent drug used to contract the uterus, with a large safety margin—in the rectum before starting the surgery, to help reduce blood loss. I also place atraumatic vascular clips on the uterine vessels in the retroperitoneum and on the utero-ovarian ligaments. Along with the use of vasopressin, these techniques markedly reduce blood loss. A 3-cm transverse suprapubic incision then is used, with fibroids removed through a retractor and the uterus then repaired.
Traditional laparoscopy enables the surgeon to change the degree of Trendelenburg, which is very helpful.
Our patients almost always go home within several hours. On postoperative day 2, most of them report needing only nonsteroidal anti-inflammatory drugs for pain and say they are eating and ambulating well. In my experience, these patients appear to have much less postoperative pain than those who undergo vaginal hysterectomy.
In 2012, 97% of major gynecologic surgical cases at my hospital were minimally invasive, with a very low complication rate. The procedures included resection of severe endometriosis, removal of very large uteri, myomectomy, and treatment of endometrial cancer, including node dissection.
Ray Wertheim, MD
Director of the AAGL Center of Excellence Minimally Invasive Gynecology Program,
Inova Fair Oaks Hospital, Fairfax, Virginia
Morcellated leiomyosarcoma is a very real risk
As a gynecologic oncologist at the University of Miami, I saw at least three cases (referred to us) of morcellated leiomyosarcomas. Within 1 or 2 months of the original surgery, each patient had to be returned to the operating room (OR) for an exploration, and disseminated tumor was found. No patient survived beyond 1 year. Therefore, I was surprised at the 5-year survival rate of 46% presented in Dr. Barbieri’s editorial.
Karen Nishida, MD
Miramar, Florida
Dr. Barbieri responds
I appreciate Dr. Wertheim’s excellent surgical pearls. Clinicians at the Inova hospitals are national leaders in advancing women’s health.
I agree with Dr. Nishida that open power morcellation of an occult leiomyosarcoma likely worsens the prognosis of the patient. Even with intensive treatment some of these patients will die within 2 years from sarcomatosis.
Related Articles:
Benefits and pitfalls of open power morcellation of uterine fibroids Robert L. Barbieri, MD (Editorial, February 2014)
Options for reducing the use of open power morcellation of uterine tumors Robert L. Barbieri, MD (Editorial, March 2014)
A likely case of encephalitis linked to teratoma
I enjoyed the interesting case presented by Dr. Barbieri and Dr. Clark in their editorial on ovarian teratoma and encephalitis. A few months ago a neurologist called me about a similar case. The patient was experiencing seizures and had a 17-cm mass beneath the umbilicus. I agreed to resect the mass, which was suspicious for an immature teratoma, and the patient recovered slowly.
I am glad to see this reference in the literature now. I am sure the editorial by Dr. Barbieri and Dr. Clark will prove handy to our colleagues.
Courtney Ridley, MD
Sacramento, California
Dr. Barbieri responds
I appreciate Dr. Ridley taking time from her busy practice to write about her experience with an ovarian tumor and encephalitis. The practice of obstetrics and gynecology is very rewarding because we are always encountering new ideas and constantly evolving our approaches to patient care. The link between encephalitis and ovarian teratoma was discovered only in 2007. It is regrettable that many women likely died before 2007 because they did not undergo timely removal of an ovarian teratoma, a simple operation.
Trend toward longer labors is not progress
I would like to mention several points not raised in Dr. Barbieri’s editorial on 21st Century labor “norms.” First, the question is not how long the labor is but whether it involves continuous descent. If the fetus does not come down, it won’t come out. Guidelines are useful only for those obstetric care providers who lack the experience to make that judgment.
When cesarean delivery follows a long second stage, the surgery is difficult and dangerous because the anatomy is distorted, and tissues are friable and often infected.
Further, a long second stage is associated with increased rates of stress urinary incontinence, uterine and vaginal prolapse, and even postpartum fistula.
Long labors also are associated with an increased risk of postpartum hemorrhage. All of the postpartum hysterectomies I have seen performed in the past few years have followed long labors.
Long labors—especially a long second stage—are associated with increased rates of fetal infection and birth trauma and, therefore, an increased risk of cerebral palsy and NICU admission.
I strongly suspect that if one calculated the costs correctly, a very long labor (>24 hr) would be much more expensive than a scheduled cesarean delivery.
In my opinion, this trend toward longer labors is not progress. Approaching it as such is, in many ways, misguided.
Robert D. Dyson, MD, PhD
Portland, Oregon
Dr. Barbieri responds
I appreciate Dr. Dyson’s wise warnings. In my editorial, I did not focus adequately on the potential pitfalls of permitting long labors. I agree that the longer the second stage, the more likely that fetal and maternal complications will ensue. More information is needed to assess the safety of permitting a prolonged second stage.
In the past, I felt very uncomfortable permitting a second stage lasting longer than 3 hours. However, based on recent reports, my current practice is to be patient and permit the second stage to continue for up to 4 hours or longer.
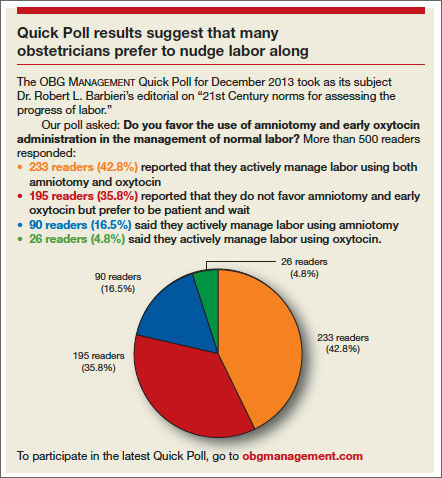
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com Please include your name, city and state.
How I avoid open power morcellation
Several gynecologic surgeons at my hospital (I am one of them) have developed approaches to hysterectomy and myomectomy that avoid open power morcellation.
For laparoscopic hysterectomy, we place two or three 5-mm ports and use a retroperitoneal approach. We identify the ureters in the retroperitoneal space and trace them into the pelvis. They often need to be lateralized in cases involving endometriosis or large fibroids. We then coagulate the uterine artery where it crosses over the ureter, as the vessel is smaller and straighter in this location. This strategy reduces blood loss and lessens the need to fulgurate the vessels at the cervix, where the ureter is vulnerable to injury.
When the uterus is large, we morcellate it transvaginally or through a 3-cm transverse suprapubic incision after placing a retractor. Be aware that 60% of women with fibroids can have coexisting adenomyosis. As Dr. Barbieri noted in his editorial, use of an internal morcellator can disperse small tissue fragments throughout the peritoneal cavity, where they may “re-implant” and undergo malignant transformation.
For laparoscopic myomectomy, I place 600 µg of misoprostol—a very potent drug used to contract the uterus, with a large safety margin—in the rectum before starting the surgery, to help reduce blood loss. I also place atraumatic vascular clips on the uterine vessels in the retroperitoneum and on the utero-ovarian ligaments. Along with the use of vasopressin, these techniques markedly reduce blood loss. A 3-cm transverse suprapubic incision then is used, with fibroids removed through a retractor and the uterus then repaired.
Traditional laparoscopy enables the surgeon to change the degree of Trendelenburg, which is very helpful.
Our patients almost always go home within several hours. On postoperative day 2, most of them report needing only nonsteroidal anti-inflammatory drugs for pain and say they are eating and ambulating well. In my experience, these patients appear to have much less postoperative pain than those who undergo vaginal hysterectomy.
In 2012, 97% of major gynecologic surgical cases at my hospital were minimally invasive, with a very low complication rate. The procedures included resection of severe endometriosis, removal of very large uteri, myomectomy, and treatment of endometrial cancer, including node dissection.
Ray Wertheim, MD
Director of the AAGL Center of Excellence Minimally Invasive Gynecology Program,
Inova Fair Oaks Hospital, Fairfax, Virginia
Morcellated leiomyosarcoma is a very real risk
As a gynecologic oncologist at the University of Miami, I saw at least three cases (referred to us) of morcellated leiomyosarcomas. Within 1 or 2 months of the original surgery, each patient had to be returned to the operating room (OR) for an exploration, and disseminated tumor was found. No patient survived beyond 1 year. Therefore, I was surprised at the 5-year survival rate of 46% presented in Dr. Barbieri’s editorial.
Karen Nishida, MD
Miramar, Florida
Dr. Barbieri responds
I appreciate Dr. Wertheim’s excellent surgical pearls. Clinicians at the Inova hospitals are national leaders in advancing women’s health.
I agree with Dr. Nishida that open power morcellation of an occult leiomyosarcoma likely worsens the prognosis of the patient. Even with intensive treatment some of these patients will die within 2 years from sarcomatosis.
Related Articles:
Benefits and pitfalls of open power morcellation of uterine fibroids Robert L. Barbieri, MD (Editorial, February 2014)
Options for reducing the use of open power morcellation of uterine tumors Robert L. Barbieri, MD (Editorial, March 2014)
A likely case of encephalitis linked to teratoma
I enjoyed the interesting case presented by Dr. Barbieri and Dr. Clark in their editorial on ovarian teratoma and encephalitis. A few months ago a neurologist called me about a similar case. The patient was experiencing seizures and had a 17-cm mass beneath the umbilicus. I agreed to resect the mass, which was suspicious for an immature teratoma, and the patient recovered slowly.
I am glad to see this reference in the literature now. I am sure the editorial by Dr. Barbieri and Dr. Clark will prove handy to our colleagues.
Courtney Ridley, MD
Sacramento, California
Dr. Barbieri responds
I appreciate Dr. Ridley taking time from her busy practice to write about her experience with an ovarian tumor and encephalitis. The practice of obstetrics and gynecology is very rewarding because we are always encountering new ideas and constantly evolving our approaches to patient care. The link between encephalitis and ovarian teratoma was discovered only in 2007. It is regrettable that many women likely died before 2007 because they did not undergo timely removal of an ovarian teratoma, a simple operation.
Trend toward longer labors is not progress
I would like to mention several points not raised in Dr. Barbieri’s editorial on 21st Century labor “norms.” First, the question is not how long the labor is but whether it involves continuous descent. If the fetus does not come down, it won’t come out. Guidelines are useful only for those obstetric care providers who lack the experience to make that judgment.
When cesarean delivery follows a long second stage, the surgery is difficult and dangerous because the anatomy is distorted, and tissues are friable and often infected.
Further, a long second stage is associated with increased rates of stress urinary incontinence, uterine and vaginal prolapse, and even postpartum fistula.
Long labors also are associated with an increased risk of postpartum hemorrhage. All of the postpartum hysterectomies I have seen performed in the past few years have followed long labors.
Long labors—especially a long second stage—are associated with increased rates of fetal infection and birth trauma and, therefore, an increased risk of cerebral palsy and NICU admission.
I strongly suspect that if one calculated the costs correctly, a very long labor (>24 hr) would be much more expensive than a scheduled cesarean delivery.
In my opinion, this trend toward longer labors is not progress. Approaching it as such is, in many ways, misguided.
Robert D. Dyson, MD, PhD
Portland, Oregon
Dr. Barbieri responds
I appreciate Dr. Dyson’s wise warnings. In my editorial, I did not focus adequately on the potential pitfalls of permitting long labors. I agree that the longer the second stage, the more likely that fetal and maternal complications will ensue. More information is needed to assess the safety of permitting a prolonged second stage.
In the past, I felt very uncomfortable permitting a second stage lasting longer than 3 hours. However, based on recent reports, my current practice is to be patient and permit the second stage to continue for up to 4 hours or longer.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com Please include your name, city and state.
How I avoid open power morcellation
Several gynecologic surgeons at my hospital (I am one of them) have developed approaches to hysterectomy and myomectomy that avoid open power morcellation.
For laparoscopic hysterectomy, we place two or three 5-mm ports and use a retroperitoneal approach. We identify the ureters in the retroperitoneal space and trace them into the pelvis. They often need to be lateralized in cases involving endometriosis or large fibroids. We then coagulate the uterine artery where it crosses over the ureter, as the vessel is smaller and straighter in this location. This strategy reduces blood loss and lessens the need to fulgurate the vessels at the cervix, where the ureter is vulnerable to injury.
When the uterus is large, we morcellate it transvaginally or through a 3-cm transverse suprapubic incision after placing a retractor. Be aware that 60% of women with fibroids can have coexisting adenomyosis. As Dr. Barbieri noted in his editorial, use of an internal morcellator can disperse small tissue fragments throughout the peritoneal cavity, where they may “re-implant” and undergo malignant transformation.
For laparoscopic myomectomy, I place 600 µg of misoprostol—a very potent drug used to contract the uterus, with a large safety margin—in the rectum before starting the surgery, to help reduce blood loss. I also place atraumatic vascular clips on the uterine vessels in the retroperitoneum and on the utero-ovarian ligaments. Along with the use of vasopressin, these techniques markedly reduce blood loss. A 3-cm transverse suprapubic incision then is used, with fibroids removed through a retractor and the uterus then repaired.
Traditional laparoscopy enables the surgeon to change the degree of Trendelenburg, which is very helpful.
Our patients almost always go home within several hours. On postoperative day 2, most of them report needing only nonsteroidal anti-inflammatory drugs for pain and say they are eating and ambulating well. In my experience, these patients appear to have much less postoperative pain than those who undergo vaginal hysterectomy.
In 2012, 97% of major gynecologic surgical cases at my hospital were minimally invasive, with a very low complication rate. The procedures included resection of severe endometriosis, removal of very large uteri, myomectomy, and treatment of endometrial cancer, including node dissection.
Ray Wertheim, MD
Director of the AAGL Center of Excellence Minimally Invasive Gynecology Program,
Inova Fair Oaks Hospital, Fairfax, Virginia
Morcellated leiomyosarcoma is a very real risk
As a gynecologic oncologist at the University of Miami, I saw at least three cases (referred to us) of morcellated leiomyosarcomas. Within 1 or 2 months of the original surgery, each patient had to be returned to the operating room (OR) for an exploration, and disseminated tumor was found. No patient survived beyond 1 year. Therefore, I was surprised at the 5-year survival rate of 46% presented in Dr. Barbieri’s editorial.
Karen Nishida, MD
Miramar, Florida
Dr. Barbieri responds
I appreciate Dr. Wertheim’s excellent surgical pearls. Clinicians at the Inova hospitals are national leaders in advancing women’s health.
I agree with Dr. Nishida that open power morcellation of an occult leiomyosarcoma likely worsens the prognosis of the patient. Even with intensive treatment some of these patients will die within 2 years from sarcomatosis.
Related Articles:
Benefits and pitfalls of open power morcellation of uterine fibroids Robert L. Barbieri, MD (Editorial, February 2014)
Options for reducing the use of open power morcellation of uterine tumors Robert L. Barbieri, MD (Editorial, March 2014)
A likely case of encephalitis linked to teratoma
I enjoyed the interesting case presented by Dr. Barbieri and Dr. Clark in their editorial on ovarian teratoma and encephalitis. A few months ago a neurologist called me about a similar case. The patient was experiencing seizures and had a 17-cm mass beneath the umbilicus. I agreed to resect the mass, which was suspicious for an immature teratoma, and the patient recovered slowly.
I am glad to see this reference in the literature now. I am sure the editorial by Dr. Barbieri and Dr. Clark will prove handy to our colleagues.
Courtney Ridley, MD
Sacramento, California
Dr. Barbieri responds
I appreciate Dr. Ridley taking time from her busy practice to write about her experience with an ovarian tumor and encephalitis. The practice of obstetrics and gynecology is very rewarding because we are always encountering new ideas and constantly evolving our approaches to patient care. The link between encephalitis and ovarian teratoma was discovered only in 2007. It is regrettable that many women likely died before 2007 because they did not undergo timely removal of an ovarian teratoma, a simple operation.
Trend toward longer labors is not progress
I would like to mention several points not raised in Dr. Barbieri’s editorial on 21st Century labor “norms.” First, the question is not how long the labor is but whether it involves continuous descent. If the fetus does not come down, it won’t come out. Guidelines are useful only for those obstetric care providers who lack the experience to make that judgment.
When cesarean delivery follows a long second stage, the surgery is difficult and dangerous because the anatomy is distorted, and tissues are friable and often infected.
Further, a long second stage is associated with increased rates of stress urinary incontinence, uterine and vaginal prolapse, and even postpartum fistula.
Long labors also are associated with an increased risk of postpartum hemorrhage. All of the postpartum hysterectomies I have seen performed in the past few years have followed long labors.
Long labors—especially a long second stage—are associated with increased rates of fetal infection and birth trauma and, therefore, an increased risk of cerebral palsy and NICU admission.
I strongly suspect that if one calculated the costs correctly, a very long labor (>24 hr) would be much more expensive than a scheduled cesarean delivery.
In my opinion, this trend toward longer labors is not progress. Approaching it as such is, in many ways, misguided.
Robert D. Dyson, MD, PhD
Portland, Oregon
Dr. Barbieri responds
I appreciate Dr. Dyson’s wise warnings. In my editorial, I did not focus adequately on the potential pitfalls of permitting long labors. I agree that the longer the second stage, the more likely that fetal and maternal complications will ensue. More information is needed to assess the safety of permitting a prolonged second stage.
In the past, I felt very uncomfortable permitting a second stage lasting longer than 3 hours. However, based on recent reports, my current practice is to be patient and permit the second stage to continue for up to 4 hours or longer.
WE WANT TO HEAR FROM YOU!
Drop us a line and let us know what you think about this or other current articles, which topics you'd like to see covered in future issues, and what challenges you face in daily practice. Tell us what you think by emailing us at: obg@frontlinemedcom.com Please include your name, city and state.
Obesity a driving factor in stillbirth
NEW ORLEANS – Almost 20% of the stillbirths that occurred over an 8-year period appeared to be associated with obesity.
A database review of nearly 3 million births found that the risk of stillbirth increased along with body mass index and gestational age. For women with the highest BMI – 50 kg/m2 – the incidence of a stillbirth jumped from 1.8/1,000 pregnancies at 39 weeks to 3/1,000 at 40 weeks and to more than 5/1,000 by 41 weeks, Dr. Ruofan Yao reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"There is a dose-response relationship where the greater the BMI, the higher the risk of stillbirth. Obesity is a major contributing risk for stillbirth, where 20% of all stillbirths happen to women who are obese, and 1 in 4 stillbirths after 37 weeks is associated with obesity," said Dr. Yao of Drexel University, Philadelphia. "This is significantly higher than the population-attributable risk for chronic hypertension or pregestational diabetes."
Dr. Yao used birth and death records from Texas and Washington to determine the associations between weight and stillbirth. The Texas cohort included data on about 2 million births that occurred from 2006 to 2011. The Washington cohort included data on about 1 million from 2003 to 2011. Of the nearly 3 million births analyzed, about 9,000 were stillbirths. Fetuses with severe congenital anomalies were excluded from the analysis, as were pregnancies with a gestational age of less than 20 weeks.
Overall, 51% of the mothers in the analysis were of normal weight. About a quarter were overweight. Class I obesity was present in 13%, class II in 6%, and class III in 3.5%. The remaining 0.5% had a BMI of 50 or higher.
Although the risk of stillbirth rose with BMI and gestational age, overweight women were at no significantly increased risk of stillbirth compared with normal-weight women.
Women in class I were about twice as likely to have a stillbirth at both 37-39 weeks and 40-42 weeks. For women in class II, the risk was about 2.5 times higher at 37-39 weeks and twice as high at 40-42 weeks. In class III, the risk of stillbirth was three times higher at both time points.
The risk was sharply elevated for women with a BMI of 50 or more. At 37-39 weeks, they had a threefold increased risk. That jumped to a ninefold increased risk by 40-42 weeks, Dr. Yao said.
A separate analysis quantified population-attributable risk (PAR) for obesity and stillbirth. For all obesity (30 or higher), the risk was almost 20% overall. The PAR was 24% for early-term pregnancies and 28% for late-term pregnancies.
"Furthermore, over 5% of stillbirths from 37-39 weeks were associated with the much smaller subset of women who are morbidly obese, and this number jumps to 8% from 40-42 weeks," he said.
"Our data pointed to 39 weeks as a pivotal point in the pregnancy where the risk of stillbirth increases at a dramatic pace for women with BMI more than 50," Dr. Yao said in an interview. "I believe it is reasonable to have a discussion with patients in this BMI group regarding their maternal and fetal risks for expectant management verses delivery at 39 weeks. Whether to extend this recommendation to other obese women is unclear until more studies can delineate the risks and benefits more clearly."
The pathophysiology behind the association of obesity and preterm birth isn’t yet clear, he added.
"It is known in endocrine and medicine literature that obesity increases the baseline inflammatory response, and this may lead to abnormal placental growth and the development of uteroplacental insufficiency," Dr. Yao said.
"Obesity is also commonly associated with sleep apnea, which often worsens in pregnancy and can lead to transient hypoxic state, hindering normal fetal growth, and increase the risk of preeclampsia. Obesity also leads to glucose intolerance and increased serum lipid and triglyceride levels, leading to accelerated fetal growth velocity, and may contribute to the development of uteroplacental insufficiency. Additionally, the dietary habits of many obese women tend to exacerbate that problem."
Dr. Yao reported that he had no financial disclosures.
NEW ORLEANS – Almost 20% of the stillbirths that occurred over an 8-year period appeared to be associated with obesity.
A database review of nearly 3 million births found that the risk of stillbirth increased along with body mass index and gestational age. For women with the highest BMI – 50 kg/m2 – the incidence of a stillbirth jumped from 1.8/1,000 pregnancies at 39 weeks to 3/1,000 at 40 weeks and to more than 5/1,000 by 41 weeks, Dr. Ruofan Yao reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"There is a dose-response relationship where the greater the BMI, the higher the risk of stillbirth. Obesity is a major contributing risk for stillbirth, where 20% of all stillbirths happen to women who are obese, and 1 in 4 stillbirths after 37 weeks is associated with obesity," said Dr. Yao of Drexel University, Philadelphia. "This is significantly higher than the population-attributable risk for chronic hypertension or pregestational diabetes."
Dr. Yao used birth and death records from Texas and Washington to determine the associations between weight and stillbirth. The Texas cohort included data on about 2 million births that occurred from 2006 to 2011. The Washington cohort included data on about 1 million from 2003 to 2011. Of the nearly 3 million births analyzed, about 9,000 were stillbirths. Fetuses with severe congenital anomalies were excluded from the analysis, as were pregnancies with a gestational age of less than 20 weeks.
Overall, 51% of the mothers in the analysis were of normal weight. About a quarter were overweight. Class I obesity was present in 13%, class II in 6%, and class III in 3.5%. The remaining 0.5% had a BMI of 50 or higher.
Although the risk of stillbirth rose with BMI and gestational age, overweight women were at no significantly increased risk of stillbirth compared with normal-weight women.
Women in class I were about twice as likely to have a stillbirth at both 37-39 weeks and 40-42 weeks. For women in class II, the risk was about 2.5 times higher at 37-39 weeks and twice as high at 40-42 weeks. In class III, the risk of stillbirth was three times higher at both time points.
The risk was sharply elevated for women with a BMI of 50 or more. At 37-39 weeks, they had a threefold increased risk. That jumped to a ninefold increased risk by 40-42 weeks, Dr. Yao said.
A separate analysis quantified population-attributable risk (PAR) for obesity and stillbirth. For all obesity (30 or higher), the risk was almost 20% overall. The PAR was 24% for early-term pregnancies and 28% for late-term pregnancies.
"Furthermore, over 5% of stillbirths from 37-39 weeks were associated with the much smaller subset of women who are morbidly obese, and this number jumps to 8% from 40-42 weeks," he said.
"Our data pointed to 39 weeks as a pivotal point in the pregnancy where the risk of stillbirth increases at a dramatic pace for women with BMI more than 50," Dr. Yao said in an interview. "I believe it is reasonable to have a discussion with patients in this BMI group regarding their maternal and fetal risks for expectant management verses delivery at 39 weeks. Whether to extend this recommendation to other obese women is unclear until more studies can delineate the risks and benefits more clearly."
The pathophysiology behind the association of obesity and preterm birth isn’t yet clear, he added.
"It is known in endocrine and medicine literature that obesity increases the baseline inflammatory response, and this may lead to abnormal placental growth and the development of uteroplacental insufficiency," Dr. Yao said.
"Obesity is also commonly associated with sleep apnea, which often worsens in pregnancy and can lead to transient hypoxic state, hindering normal fetal growth, and increase the risk of preeclampsia. Obesity also leads to glucose intolerance and increased serum lipid and triglyceride levels, leading to accelerated fetal growth velocity, and may contribute to the development of uteroplacental insufficiency. Additionally, the dietary habits of many obese women tend to exacerbate that problem."
Dr. Yao reported that he had no financial disclosures.
NEW ORLEANS – Almost 20% of the stillbirths that occurred over an 8-year period appeared to be associated with obesity.
A database review of nearly 3 million births found that the risk of stillbirth increased along with body mass index and gestational age. For women with the highest BMI – 50 kg/m2 – the incidence of a stillbirth jumped from 1.8/1,000 pregnancies at 39 weeks to 3/1,000 at 40 weeks and to more than 5/1,000 by 41 weeks, Dr. Ruofan Yao reported at the annual Pregnancy Meeting sponsored by the Society for Maternal-Fetal Medicine.
"There is a dose-response relationship where the greater the BMI, the higher the risk of stillbirth. Obesity is a major contributing risk for stillbirth, where 20% of all stillbirths happen to women who are obese, and 1 in 4 stillbirths after 37 weeks is associated with obesity," said Dr. Yao of Drexel University, Philadelphia. "This is significantly higher than the population-attributable risk for chronic hypertension or pregestational diabetes."
Dr. Yao used birth and death records from Texas and Washington to determine the associations between weight and stillbirth. The Texas cohort included data on about 2 million births that occurred from 2006 to 2011. The Washington cohort included data on about 1 million from 2003 to 2011. Of the nearly 3 million births analyzed, about 9,000 were stillbirths. Fetuses with severe congenital anomalies were excluded from the analysis, as were pregnancies with a gestational age of less than 20 weeks.
Overall, 51% of the mothers in the analysis were of normal weight. About a quarter were overweight. Class I obesity was present in 13%, class II in 6%, and class III in 3.5%. The remaining 0.5% had a BMI of 50 or higher.
Although the risk of stillbirth rose with BMI and gestational age, overweight women were at no significantly increased risk of stillbirth compared with normal-weight women.
Women in class I were about twice as likely to have a stillbirth at both 37-39 weeks and 40-42 weeks. For women in class II, the risk was about 2.5 times higher at 37-39 weeks and twice as high at 40-42 weeks. In class III, the risk of stillbirth was three times higher at both time points.
The risk was sharply elevated for women with a BMI of 50 or more. At 37-39 weeks, they had a threefold increased risk. That jumped to a ninefold increased risk by 40-42 weeks, Dr. Yao said.
A separate analysis quantified population-attributable risk (PAR) for obesity and stillbirth. For all obesity (30 or higher), the risk was almost 20% overall. The PAR was 24% for early-term pregnancies and 28% for late-term pregnancies.
"Furthermore, over 5% of stillbirths from 37-39 weeks were associated with the much smaller subset of women who are morbidly obese, and this number jumps to 8% from 40-42 weeks," he said.
"Our data pointed to 39 weeks as a pivotal point in the pregnancy where the risk of stillbirth increases at a dramatic pace for women with BMI more than 50," Dr. Yao said in an interview. "I believe it is reasonable to have a discussion with patients in this BMI group regarding their maternal and fetal risks for expectant management verses delivery at 39 weeks. Whether to extend this recommendation to other obese women is unclear until more studies can delineate the risks and benefits more clearly."
The pathophysiology behind the association of obesity and preterm birth isn’t yet clear, he added.
"It is known in endocrine and medicine literature that obesity increases the baseline inflammatory response, and this may lead to abnormal placental growth and the development of uteroplacental insufficiency," Dr. Yao said.
"Obesity is also commonly associated with sleep apnea, which often worsens in pregnancy and can lead to transient hypoxic state, hindering normal fetal growth, and increase the risk of preeclampsia. Obesity also leads to glucose intolerance and increased serum lipid and triglyceride levels, leading to accelerated fetal growth velocity, and may contribute to the development of uteroplacental insufficiency. Additionally, the dietary habits of many obese women tend to exacerbate that problem."
Dr. Yao reported that he had no financial disclosures.
AT THE PREGNANCY MEETING
Major finding: Nearly 20% of stillbirths that occurred over an 8-year period were associated with obesity.
Data source: Population-based data with information on almost 3 million births.
Disclosures: Dr. Yao reported that he had no financial disclosures.
Delivery of identical twins near 33 weeks balances outcomes
NEW ORLEANS – The optimal time to deliver monoamniotic twins is right around 33 weeks, when the risks of intrauterine death and neonatal complications are both very low.
"Monoamniotic twin pregnancies are at extremely high risk of intrauterine death before 28 weeks’ gestation," Dr. Tim Van Mieghem said at the Pregnancy Meeting, sponsored by the Society for Maternal Fetal Medicine. "But with regular fetal monitoring and ultrasound, that risk is extremely low from 28 to 32 weeks."

At the same time, the risk of neonatal complications decreases as the pregnancy advances. The fulcrum that balances both optimal outcomes is 33 weeks, 4 days.
To determine this, Dr. Van Mieghem looked at a retrospective cohort of monoamniotic twin pregnancies followed during 2003-2013 in Canada and Europe. The group comprised 193 pregnancies (386 fetuses); the investigators excluded conjoined twins and cases of twin reversed arterial perfusion. The rate of twin-twin transfusion syndrome was low (3%).
The rate of fetal anomalies was quite high (53; 14%), said Dr. Van Mieghem of the University Hospital of Leuven, Belgium. Twelve of the pregnancies were terminated. There were 28 double intrauterine deaths and 14 single intrauterine deaths. Most of these were caused by cord events; seven were iatrogenic.
Most of the fetuses (76%) were born alive at an average of 32 weeks’ gestation. Most of the mothers received corticosteroids (91%), and most deliveries were by cesarean section (97%). The mean birth weight was 1,749 g. The neonatal death rate was 5.7%.
The most common neonatal complications were respiratory; 80% of the infants needed respiratory support and 40% had respiratory distress syndrome. The rate of nonrespiratory complications was about 15%. Sepsis occurred in about 10%. The remainder of the complications were necrotizing enterocolitis, intraventricular hemorrhage, and periventricular leukomalacia.
The risk of intrauterine death decreased as the pregnancy advanced. At 24 weeks, it was about 5%, but by 28 weeks had dropped to a low of 1.4%. Thereafter, the risk began to rise, reaching about 7% by week 35.
The risk of neonatal complications also decreased as the pregnancy advanced. It reached its nadir of about 2% at around 28 weeks and stayed low until about 33 weeks, when it began to rise. By 34 weeks it was near 7%, but dropped to close to 0 shortly after 35 weeks.
"The risk curves intersected at 32 weeks, 4 days," Dr. Van Mieghem said. "Based on these curves, it seems prudent to deliver these fetuses at 32 weeks, when the risk of both intrauterine demise and neonatal complications is about 3%."
He added that there were no significant differences in neonatal outcomes between pregnancies that were monitored on an inpatient and outpatient basis. The gestational age at delivery was about a week earlier in inpatients (32 vs. 33 weeks.) The rate of fetal distress was slightly higher among inpatients (21% vs. 23%). The outpatient pregnancies resulted in larger infants (mean 1,827 g vs. 1,776 g).
The rate of nonrespiratory neonatal complications was about 9% in each group. However, significantly more infants in the inpatient group needed ventilation (76% vs. 63%). They were also on ventilation about a day longer (5 days vs. 4 days).
There were one single and two double intrauterine deaths in the outpatient group, and one single intrauterine death in the inpatient group. But because all of the outpatient deaths occurred before 28 weeks, Dr. Van Mieghem said they probably could not have been averted by inpatient management.
"If you were looking at the rate of truly preventable deaths, it likely would have been 0 in both groups," he said.
Dr. Van Mieghem had no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – The optimal time to deliver monoamniotic twins is right around 33 weeks, when the risks of intrauterine death and neonatal complications are both very low.
"Monoamniotic twin pregnancies are at extremely high risk of intrauterine death before 28 weeks’ gestation," Dr. Tim Van Mieghem said at the Pregnancy Meeting, sponsored by the Society for Maternal Fetal Medicine. "But with regular fetal monitoring and ultrasound, that risk is extremely low from 28 to 32 weeks."
At the same time, the risk of neonatal complications decreases as the pregnancy advances. The fulcrum that balances both optimal outcomes is 33 weeks, 4 days.
To determine this, Dr. Van Mieghem looked at a retrospective cohort of monoamniotic twin pregnancies followed during 2003-2013 in Canada and Europe. The group comprised 193 pregnancies (386 fetuses); the investigators excluded conjoined twins and cases of twin reversed arterial perfusion. The rate of twin-twin transfusion syndrome was low (3%).
The rate of fetal anomalies was quite high (53; 14%), said Dr. Van Mieghem of the University Hospital of Leuven, Belgium. Twelve of the pregnancies were terminated. There were 28 double intrauterine deaths and 14 single intrauterine deaths. Most of these were caused by cord events; seven were iatrogenic.
Most of the fetuses (76%) were born alive at an average of 32 weeks’ gestation. Most of the mothers received corticosteroids (91%), and most deliveries were by cesarean section (97%). The mean birth weight was 1,749 g. The neonatal death rate was 5.7%.
The most common neonatal complications were respiratory; 80% of the infants needed respiratory support and 40% had respiratory distress syndrome. The rate of nonrespiratory complications was about 15%. Sepsis occurred in about 10%. The remainder of the complications were necrotizing enterocolitis, intraventricular hemorrhage, and periventricular leukomalacia.
The risk of intrauterine death decreased as the pregnancy advanced. At 24 weeks, it was about 5%, but by 28 weeks had dropped to a low of 1.4%. Thereafter, the risk began to rise, reaching about 7% by week 35.
The risk of neonatal complications also decreased as the pregnancy advanced. It reached its nadir of about 2% at around 28 weeks and stayed low until about 33 weeks, when it began to rise. By 34 weeks it was near 7%, but dropped to close to 0 shortly after 35 weeks.
"The risk curves intersected at 32 weeks, 4 days," Dr. Van Mieghem said. "Based on these curves, it seems prudent to deliver these fetuses at 32 weeks, when the risk of both intrauterine demise and neonatal complications is about 3%."
He added that there were no significant differences in neonatal outcomes between pregnancies that were monitored on an inpatient and outpatient basis. The gestational age at delivery was about a week earlier in inpatients (32 vs. 33 weeks.) The rate of fetal distress was slightly higher among inpatients (21% vs. 23%). The outpatient pregnancies resulted in larger infants (mean 1,827 g vs. 1,776 g).
The rate of nonrespiratory neonatal complications was about 9% in each group. However, significantly more infants in the inpatient group needed ventilation (76% vs. 63%). They were also on ventilation about a day longer (5 days vs. 4 days).
There were one single and two double intrauterine deaths in the outpatient group, and one single intrauterine death in the inpatient group. But because all of the outpatient deaths occurred before 28 weeks, Dr. Van Mieghem said they probably could not have been averted by inpatient management.
"If you were looking at the rate of truly preventable deaths, it likely would have been 0 in both groups," he said.
Dr. Van Mieghem had no financial disclosures.
On Twitter @alz_gal
NEW ORLEANS – The optimal time to deliver monoamniotic twins is right around 33 weeks, when the risks of intrauterine death and neonatal complications are both very low.
"Monoamniotic twin pregnancies are at extremely high risk of intrauterine death before 28 weeks’ gestation," Dr. Tim Van Mieghem said at the Pregnancy Meeting, sponsored by the Society for Maternal Fetal Medicine. "But with regular fetal monitoring and ultrasound, that risk is extremely low from 28 to 32 weeks."
At the same time, the risk of neonatal complications decreases as the pregnancy advances. The fulcrum that balances both optimal outcomes is 33 weeks, 4 days.
To determine this, Dr. Van Mieghem looked at a retrospective cohort of monoamniotic twin pregnancies followed during 2003-2013 in Canada and Europe. The group comprised 193 pregnancies (386 fetuses); the investigators excluded conjoined twins and cases of twin reversed arterial perfusion. The rate of twin-twin transfusion syndrome was low (3%).
The rate of fetal anomalies was quite high (53; 14%), said Dr. Van Mieghem of the University Hospital of Leuven, Belgium. Twelve of the pregnancies were terminated. There were 28 double intrauterine deaths and 14 single intrauterine deaths. Most of these were caused by cord events; seven were iatrogenic.
Most of the fetuses (76%) were born alive at an average of 32 weeks’ gestation. Most of the mothers received corticosteroids (91%), and most deliveries were by cesarean section (97%). The mean birth weight was 1,749 g. The neonatal death rate was 5.7%.
The most common neonatal complications were respiratory; 80% of the infants needed respiratory support and 40% had respiratory distress syndrome. The rate of nonrespiratory complications was about 15%. Sepsis occurred in about 10%. The remainder of the complications were necrotizing enterocolitis, intraventricular hemorrhage, and periventricular leukomalacia.
The risk of intrauterine death decreased as the pregnancy advanced. At 24 weeks, it was about 5%, but by 28 weeks had dropped to a low of 1.4%. Thereafter, the risk began to rise, reaching about 7% by week 35.
The risk of neonatal complications also decreased as the pregnancy advanced. It reached its nadir of about 2% at around 28 weeks and stayed low until about 33 weeks, when it began to rise. By 34 weeks it was near 7%, but dropped to close to 0 shortly after 35 weeks.
"The risk curves intersected at 32 weeks, 4 days," Dr. Van Mieghem said. "Based on these curves, it seems prudent to deliver these fetuses at 32 weeks, when the risk of both intrauterine demise and neonatal complications is about 3%."
He added that there were no significant differences in neonatal outcomes between pregnancies that were monitored on an inpatient and outpatient basis. The gestational age at delivery was about a week earlier in inpatients (32 vs. 33 weeks.) The rate of fetal distress was slightly higher among inpatients (21% vs. 23%). The outpatient pregnancies resulted in larger infants (mean 1,827 g vs. 1,776 g).
The rate of nonrespiratory neonatal complications was about 9% in each group. However, significantly more infants in the inpatient group needed ventilation (76% vs. 63%). They were also on ventilation about a day longer (5 days vs. 4 days).
There were one single and two double intrauterine deaths in the outpatient group, and one single intrauterine death in the inpatient group. But because all of the outpatient deaths occurred before 28 weeks, Dr. Van Mieghem said they probably could not have been averted by inpatient management.
"If you were looking at the rate of truly preventable deaths, it likely would have been 0 in both groups," he said.
Dr. Van Mieghem had no financial disclosures.
On Twitter @alz_gal
AT THE PREGNANCY MEETING
Major finding: For monoamniotic twins, the risks of intrauterine death and neonatal complications are both about 3% at 33 weeks’ gestation, making that the best time to deliver these babies.
Data source: The retrospective study comprised 193 monoamniotic twin pregnancies during 2003-2013.
Disclosures: Dr. Tim Van Mieghem had no financial disclosures.

Low-risk prenatal testing gives 12 times more false positives than cell-free DNA testing
The current prenatal screening standard of care for Down syndrome and other trisomies in low-risk pregnancies is more than three times as likely to return a false positive, compared with false positive rates from noninvasive, cell-free DNA testing, according to a new study.
The findings likely will strengthen public demand for the novel testing to become routine, according to Dr. Diana W. Bianchi, lead author of the CARE (Comparison of Aneuploidy Risk Evaluation) study.
"The pregnant women social media groups are very aware of the false positives. I think everybody knows somebody who has had one, since there’s 1 in 20 chance of that [happening]," Dr. Bianchi said in an interview.
Surprising results
Also revealed in the study was cell-free DNA testing’s essentially 100% negative predictive value for aneuploidies in low-risk populations.
The results are "very impressive," said Dr. Michael F. Greene, associate editor of the New England Journal of Medicine, in an interview. "I do think this is going to sweep the table in terms of what is offered to pregnant women," particularly if other studies demonstrate the same level of efficacy, he said. The study was published online (N. Engl. J. Med. 2014;370:799-808).

To compare false positive rates in the two methods of screening, Dr. Bianchi and her team analyzed test results from 1,914 women (average age, 30 years) enrolled from the general obstetrical population across 21 centers in 14 states. Participants either had or planned to have standard aneuploidy serum screening. All women were risk classified according to standard screening and had a singleton fetus without aneuploidy and a gestational age of at least 8 weeks. A second serum sample was taken from each woman, and massively parallel sequencing was used by laboratory personnel blinded to fetal karyotype to determine the chromosome dosage. Birth outcomes or karyotypes were used as the reference standard.
For trisomies 21 and 18, the false positive rates returned by cell-free DNA testing were significantly lower than those returned by standard screening: 6 patients vs. 69 out of 1,909 for trisomy 21 (0.3% vs. 3.6%; P less than .001), and 3 vs. 11 out of 1,905 for trisomy 18 (0.2% vs. 0.6%, P = .03).
The positive detection rate for cell-free DNA testing of all aneuploidies (5 for trisomy 21, 2 for trisomy 18, and 1 for trisomy 13) was 100% (95% confidence interval, 99.8-100). The positive predictive values for the cell-free DNA testing, compared with standard screening, were 45.5% vs. 4.2% for trisomy 21, and 40.0% vs. 8.3% for trisomy 18.
These positive predictive values, Dr. Greene and Dr. Elizabeth G. Phimister wrote in an accompanying editorial, "underscore the conclusion that assaying fetal DNA is a screening tool and not a diagnostic intervention." However, they concluded, "the observed negative predictive values of 100% with 95% confidence limits down to 99.8%, combined with the significantly and substantively lower false positive rates with cell-free DNA screening than with standard screening, augur well for pregnant women and their fetuses" (N. Engl. J. Med. 2014;370:874-5).
"I think it is going to surprise people when they see that the current standard of care has such a low positive predictive value in a general obstetrical population," said Dr. Bianchi, who also directs the Mother Infant Research Institute at Tufts Medical Center, Boston.

The primary outcome was determined by newborn physical examination in 1,857 patients (97.0%) and by karyotype in 57 patients (3.0%). Of these, chorionic villus sampling was performed in 10 patients, amniocentesis in 38, testing of the products of conception in 3, and postnatal evaluation in 6. The women whose cell-free DNA tests came back with false positive readings all had live births with normal physical examinations.
The secondary endpoint was a similar comparison of detection rates for trisomy 13 (Patau syndrome). There was one false positive result for trisomy 13 with cell-free DNA testing, as compared with six false positive results on standard screening, thus showing a trend toward significance (P = .059) in the 899 patients who underwent standard screening for trisomy 13.
Fetal fraction not maternal age–related
The researchers found that cell-free DNA testing had the same high-sensitivity detection rates in low-risk obstetrical populations as has been previously established in high-risk ones. Generally considered at higher risk for trisomy 21, women 35 years and older who were tested in either the first or second trimesters had results that were nearly identical to results from women under age 35 in terms of both their mean percentage of free fetal DNA and their standard screening results and/or cell-free DNA results (11.3% and 11.6%, respectively). For women tested in the third trimester, the fetal fraction was higher (mean, 24.6%).
This finding further strengthens the argument that the technology should be available to the general obstetric population. "The amount of the DNA was the same when we stratified the relatively high risk from the relatively low risk," said Dr. Bianchi. "That will be a surprise to some people who postulated that the high-risk women would have more DNA circulating. They don’t."
The consistent fetal fraction also lends itself to greater flexibility when prenatal screening occurs, allowing women to be screened anytime between 10 and 40 weeks gestational age. This could mean better prenatal care for women who do not have their first prenatal visit until late in the second trimester, for example. Because the current screening methods are specific to certain gestational times, if a woman is erratic with her prenatal visits, testing may be impossible.
Regarding its utility in women carrying multiple fetuses, Dr. Bianchi said that about 10% of the time, the fetal fraction per fetus tends to be too low to get an accurate reading.
‘Throwing down the gauntlet’
The test’s unparalleled accuracy could give greater peace of mind to women who might have had difficulty getting pregnant and so are wary of the miscarriage risks posed by invasive diagnostic testing, according to Dr. Bianchi. Fewer invasive diagnostic tests could also lower costs across the system.
When all results for trisomies 21 and 18 were combined, the researchers found that the false positive rates for standard screening were 4.2%, compared with 0.5% for cell-free DNA testing. "If all pregnant women had undergone cell-free DNA testing as a primary screening method and if all women with positive results had undergone post-test counseling and had decided to undergo an invasive procedure," wrote the authors, "there would have been a relative reduction of 89% in the number of diagnostic invasive procedures required to confirm a positive screening result."
The data should move professional societies to take action, according to Dr. Bianchi. "That’s kind of the gauntlet that we’re throwing down." More data are on the way, she said, which will "enable the professional societies to take a cumulative look and decide what their recommendations are going to be."
As it stands, the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists state that the testing be used only in women at higher risk for giving birth to children with aneuploidies, such as women aged 35 years or older or those with a history of pregnancy with trisomy, and that positive cell-free DNA results should be confirmed by invasive diagnostic testing.
For now, because the tests are not considered routine prenatal care, low-risk patients usually pay out of pocket for these tests, which Dr. Bianchi said many women are willing to do. The cost of the test ranges anywhere from $1,200 to upward of $2,700, although some careful Internet searching for deals can net tests at substantially lower prices, she said.
Market pressures
For some physicians in the field, this public demand for a screening test not subject to Food and Drug Administration (FDA) regulation has not outweighed the level of proof it offers in the clinical setting. One of these critics was, until recently, Dr. Greene.
"Companies have been free to build consumer demand for cell-free DNA testing by aggressively marketing the tests, emphasizing data that do not answer key questions," wrote Dr. Greene in July 2013, in an editorial he coauthored (N. Engl. J. Med. 2013;369:499-501). "As a result, cell-free DNA testing seems to be drifting into routine practice ahead of the evidence," stated Dr. Greene, who is also chief of obstetrics at Massachusetts General Hospital in Boston, and who wrote with his colleagues that the test’s positive predictive value, largely unreported by manufacturers, was still in question.
"The problem is that the proof-of-principle studies that all these companies have published to date have been with ratios of ‘Down’s’ to ‘normals’ ranging from 1 to 7, 1 to 13, or 1 to 20," said Dr. Greene in an interview. "All were done in retrospective populations at extraordinarily high risk."
However, with the CARE study, "what’s impressive is the positive predictive value in a low-incidence group of patients," he said.
Sponsored by Illumina/Verinata, the study puts pressure on other companies to publish their own data in peer-reviewed journals, said Dr. Greene. "Once this paper appears in print, [Verinata] will get a leg up, and the other companies won’t want to let them get too far ahead of them."
According to Dr. Bianchi, Verinata is now seeking FDA approval to market the testing as an in vitro diagnostic product. She expects demand for the testing to be led not by physicians but by patients. "People often ask me why the DNA testing took off so quickly," said Dr. Bianchi. "I think a factor is social media. I find there is a discrepancy between what the average patient knows and the general obstetrician knows because of the discussions [online]. "
Although some women will still need an invasive procedure to resolve a screen positive test, Dr. Bianchi said most pregnant women, including older women, are going to be reassured with the 100% negative predictive value.
"The younger woman’s benefit will primarily be the reduced false positive rate, because overwhelmingly, she is going to have a normal fetus, so her major benefit is not being made anxious and being sent for all the subsequent testing."
Dr. Bianchi and her coauthors disclosed relationships with Verinata/Illumina, maker of the Verifi cell-free DNA prenatal test. Dr. Bianchi is also on the clinical advisory board of Verinata. Dr. Greene stated that he had no conflict of interest disclosures. The study was sponsored by Illumina, ClinicalTrials.gov number NCT01663350.
The good news out of this is the much lower rate of false positives compared with traditional screening. But what I think is important here is that it’s potentially so easy and accurate to do this testing, that I hope it will continue to be done with full discussion and informed consent regarding the implications, and without judgment about whether or not women ought to pursue this testing. What’s in the background of decisions about testing is the question of abortion, which is as personal and value-laden a decision as anyone can make. As a result, discussion of the fact that testing may lead inevitably to decisions about abortion has to be a part of the conversation from the beginning.
 |
|
The concepts of prenatal screening and diagnostic testing have been around for a long time, so in principle they are not new to obstetricians and their patients. Prenatal screening should be performed only with full consent, and with discussion of the potential downstream implications and questions that women and their partners may need to confront, similar to chess where you are thinking three moves ahead. The discussion should address what will happen at the point of the first test, including the possibility of a further diagnostic test, and then where things will go if the fetus is found to have one of these trisomies.
My concern is that because this new testing technology is easy and accurate, and greatly reduces the potential for anxiety caused by false positives, there might be the assumption that it’s a good thing to do for all women. My own view is that it will be good for some, and not for others. You want to be sure where your patient stands before you embark on this pathway. You want to be sure of the woman’s and her partner’s values before you offer this testing as something that will inform decisions about whether to bring the pregnancy to term.
In addition, I suspect it is inevitable that we will move in the direction of using this technology to test or screen for a whole list of other genetic conditions. We should be talking about whether or not that’s a good thing. For example, some women know that they are BRCA1 carriers, and they will ask their obstetricians if they can use this technology to test for conditions like that. Clinicians will need to start expanding their resources for patient education about genetics, and for genetic counseling of these patients, in order to be prepared for these kinds of questions.
Dr. Steven Joffe, a pediatric oncologist and bioethicist, is vice chair of medical ethics at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, and an attending physician at the Children’s Hospital of Philadelphia. Dr. Joffe had no conflict of interest disclosures.
The good news out of this is the much lower rate of false positives compared with traditional screening. But what I think is important here is that it’s potentially so easy and accurate to do this testing, that I hope it will continue to be done with full discussion and informed consent regarding the implications, and without judgment about whether or not women ought to pursue this testing. What’s in the background of decisions about testing is the question of abortion, which is as personal and value-laden a decision as anyone can make. As a result, discussion of the fact that testing may lead inevitably to decisions about abortion has to be a part of the conversation from the beginning.
|
|
The concepts of prenatal screening and diagnostic testing have been around for a long time, so in principle they are not new to obstetricians and their patients. Prenatal screening should be performed only with full consent, and with discussion of the potential downstream implications and questions that women and their partners may need to confront, similar to chess where you are thinking three moves ahead. The discussion should address what will happen at the point of the first test, including the possibility of a further diagnostic test, and then where things will go if the fetus is found to have one of these trisomies.
My concern is that because this new testing technology is easy and accurate, and greatly reduces the potential for anxiety caused by false positives, there might be the assumption that it’s a good thing to do for all women. My own view is that it will be good for some, and not for others. You want to be sure where your patient stands before you embark on this pathway. You want to be sure of the woman’s and her partner’s values before you offer this testing as something that will inform decisions about whether to bring the pregnancy to term.
In addition, I suspect it is inevitable that we will move in the direction of using this technology to test or screen for a whole list of other genetic conditions. We should be talking about whether or not that’s a good thing. For example, some women know that they are BRCA1 carriers, and they will ask their obstetricians if they can use this technology to test for conditions like that. Clinicians will need to start expanding their resources for patient education about genetics, and for genetic counseling of these patients, in order to be prepared for these kinds of questions.
Dr. Steven Joffe, a pediatric oncologist and bioethicist, is vice chair of medical ethics at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, and an attending physician at the Children’s Hospital of Philadelphia. Dr. Joffe had no conflict of interest disclosures.
The good news out of this is the much lower rate of false positives compared with traditional screening. But what I think is important here is that it’s potentially so easy and accurate to do this testing, that I hope it will continue to be done with full discussion and informed consent regarding the implications, and without judgment about whether or not women ought to pursue this testing. What’s in the background of decisions about testing is the question of abortion, which is as personal and value-laden a decision as anyone can make. As a result, discussion of the fact that testing may lead inevitably to decisions about abortion has to be a part of the conversation from the beginning.
|
|
The concepts of prenatal screening and diagnostic testing have been around for a long time, so in principle they are not new to obstetricians and their patients. Prenatal screening should be performed only with full consent, and with discussion of the potential downstream implications and questions that women and their partners may need to confront, similar to chess where you are thinking three moves ahead. The discussion should address what will happen at the point of the first test, including the possibility of a further diagnostic test, and then where things will go if the fetus is found to have one of these trisomies.
My concern is that because this new testing technology is easy and accurate, and greatly reduces the potential for anxiety caused by false positives, there might be the assumption that it’s a good thing to do for all women. My own view is that it will be good for some, and not for others. You want to be sure where your patient stands before you embark on this pathway. You want to be sure of the woman’s and her partner’s values before you offer this testing as something that will inform decisions about whether to bring the pregnancy to term.
In addition, I suspect it is inevitable that we will move in the direction of using this technology to test or screen for a whole list of other genetic conditions. We should be talking about whether or not that’s a good thing. For example, some women know that they are BRCA1 carriers, and they will ask their obstetricians if they can use this technology to test for conditions like that. Clinicians will need to start expanding their resources for patient education about genetics, and for genetic counseling of these patients, in order to be prepared for these kinds of questions.
Dr. Steven Joffe, a pediatric oncologist and bioethicist, is vice chair of medical ethics at the Perelman School of Medicine, University of Pennsylvania, Philadelphia, and an attending physician at the Children’s Hospital of Philadelphia. Dr. Joffe had no conflict of interest disclosures.
The current prenatal screening standard of care for Down syndrome and other trisomies in low-risk pregnancies is more than three times as likely to return a false positive, compared with false positive rates from noninvasive, cell-free DNA testing, according to a new study.
The findings likely will strengthen public demand for the novel testing to become routine, according to Dr. Diana W. Bianchi, lead author of the CARE (Comparison of Aneuploidy Risk Evaluation) study.
"The pregnant women social media groups are very aware of the false positives. I think everybody knows somebody who has had one, since there’s 1 in 20 chance of that [happening]," Dr. Bianchi said in an interview.
Surprising results
Also revealed in the study was cell-free DNA testing’s essentially 100% negative predictive value for aneuploidies in low-risk populations.
The results are "very impressive," said Dr. Michael F. Greene, associate editor of the New England Journal of Medicine, in an interview. "I do think this is going to sweep the table in terms of what is offered to pregnant women," particularly if other studies demonstrate the same level of efficacy, he said. The study was published online (N. Engl. J. Med. 2014;370:799-808).
To compare false positive rates in the two methods of screening, Dr. Bianchi and her team analyzed test results from 1,914 women (average age, 30 years) enrolled from the general obstetrical population across 21 centers in 14 states. Participants either had or planned to have standard aneuploidy serum screening. All women were risk classified according to standard screening and had a singleton fetus without aneuploidy and a gestational age of at least 8 weeks. A second serum sample was taken from each woman, and massively parallel sequencing was used by laboratory personnel blinded to fetal karyotype to determine the chromosome dosage. Birth outcomes or karyotypes were used as the reference standard.
For trisomies 21 and 18, the false positive rates returned by cell-free DNA testing were significantly lower than those returned by standard screening: 6 patients vs. 69 out of 1,909 for trisomy 21 (0.3% vs. 3.6%; P less than .001), and 3 vs. 11 out of 1,905 for trisomy 18 (0.2% vs. 0.6%, P = .03).
The positive detection rate for cell-free DNA testing of all aneuploidies (5 for trisomy 21, 2 for trisomy 18, and 1 for trisomy 13) was 100% (95% confidence interval, 99.8-100). The positive predictive values for the cell-free DNA testing, compared with standard screening, were 45.5% vs. 4.2% for trisomy 21, and 40.0% vs. 8.3% for trisomy 18.
These positive predictive values, Dr. Greene and Dr. Elizabeth G. Phimister wrote in an accompanying editorial, "underscore the conclusion that assaying fetal DNA is a screening tool and not a diagnostic intervention." However, they concluded, "the observed negative predictive values of 100% with 95% confidence limits down to 99.8%, combined with the significantly and substantively lower false positive rates with cell-free DNA screening than with standard screening, augur well for pregnant women and their fetuses" (N. Engl. J. Med. 2014;370:874-5).
"I think it is going to surprise people when they see that the current standard of care has such a low positive predictive value in a general obstetrical population," said Dr. Bianchi, who also directs the Mother Infant Research Institute at Tufts Medical Center, Boston.
The primary outcome was determined by newborn physical examination in 1,857 patients (97.0%) and by karyotype in 57 patients (3.0%). Of these, chorionic villus sampling was performed in 10 patients, amniocentesis in 38, testing of the products of conception in 3, and postnatal evaluation in 6. The women whose cell-free DNA tests came back with false positive readings all had live births with normal physical examinations.
The secondary endpoint was a similar comparison of detection rates for trisomy 13 (Patau syndrome). There was one false positive result for trisomy 13 with cell-free DNA testing, as compared with six false positive results on standard screening, thus showing a trend toward significance (P = .059) in the 899 patients who underwent standard screening for trisomy 13.
Fetal fraction not maternal age–related
The researchers found that cell-free DNA testing had the same high-sensitivity detection rates in low-risk obstetrical populations as has been previously established in high-risk ones. Generally considered at higher risk for trisomy 21, women 35 years and older who were tested in either the first or second trimesters had results that were nearly identical to results from women under age 35 in terms of both their mean percentage of free fetal DNA and their standard screening results and/or cell-free DNA results (11.3% and 11.6%, respectively). For women tested in the third trimester, the fetal fraction was higher (mean, 24.6%).
This finding further strengthens the argument that the technology should be available to the general obstetric population. "The amount of the DNA was the same when we stratified the relatively high risk from the relatively low risk," said Dr. Bianchi. "That will be a surprise to some people who postulated that the high-risk women would have more DNA circulating. They don’t."
The consistent fetal fraction also lends itself to greater flexibility when prenatal screening occurs, allowing women to be screened anytime between 10 and 40 weeks gestational age. This could mean better prenatal care for women who do not have their first prenatal visit until late in the second trimester, for example. Because the current screening methods are specific to certain gestational times, if a woman is erratic with her prenatal visits, testing may be impossible.
Regarding its utility in women carrying multiple fetuses, Dr. Bianchi said that about 10% of the time, the fetal fraction per fetus tends to be too low to get an accurate reading.
‘Throwing down the gauntlet’
The test’s unparalleled accuracy could give greater peace of mind to women who might have had difficulty getting pregnant and so are wary of the miscarriage risks posed by invasive diagnostic testing, according to Dr. Bianchi. Fewer invasive diagnostic tests could also lower costs across the system.
When all results for trisomies 21 and 18 were combined, the researchers found that the false positive rates for standard screening were 4.2%, compared with 0.5% for cell-free DNA testing. "If all pregnant women had undergone cell-free DNA testing as a primary screening method and if all women with positive results had undergone post-test counseling and had decided to undergo an invasive procedure," wrote the authors, "there would have been a relative reduction of 89% in the number of diagnostic invasive procedures required to confirm a positive screening result."
The data should move professional societies to take action, according to Dr. Bianchi. "That’s kind of the gauntlet that we’re throwing down." More data are on the way, she said, which will "enable the professional societies to take a cumulative look and decide what their recommendations are going to be."
As it stands, the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists state that the testing be used only in women at higher risk for giving birth to children with aneuploidies, such as women aged 35 years or older or those with a history of pregnancy with trisomy, and that positive cell-free DNA results should be confirmed by invasive diagnostic testing.
For now, because the tests are not considered routine prenatal care, low-risk patients usually pay out of pocket for these tests, which Dr. Bianchi said many women are willing to do. The cost of the test ranges anywhere from $1,200 to upward of $2,700, although some careful Internet searching for deals can net tests at substantially lower prices, she said.
Market pressures
For some physicians in the field, this public demand for a screening test not subject to Food and Drug Administration (FDA) regulation has not outweighed the level of proof it offers in the clinical setting. One of these critics was, until recently, Dr. Greene.
"Companies have been free to build consumer demand for cell-free DNA testing by aggressively marketing the tests, emphasizing data that do not answer key questions," wrote Dr. Greene in July 2013, in an editorial he coauthored (N. Engl. J. Med. 2013;369:499-501). "As a result, cell-free DNA testing seems to be drifting into routine practice ahead of the evidence," stated Dr. Greene, who is also chief of obstetrics at Massachusetts General Hospital in Boston, and who wrote with his colleagues that the test’s positive predictive value, largely unreported by manufacturers, was still in question.
"The problem is that the proof-of-principle studies that all these companies have published to date have been with ratios of ‘Down’s’ to ‘normals’ ranging from 1 to 7, 1 to 13, or 1 to 20," said Dr. Greene in an interview. "All were done in retrospective populations at extraordinarily high risk."
However, with the CARE study, "what’s impressive is the positive predictive value in a low-incidence group of patients," he said.
Sponsored by Illumina/Verinata, the study puts pressure on other companies to publish their own data in peer-reviewed journals, said Dr. Greene. "Once this paper appears in print, [Verinata] will get a leg up, and the other companies won’t want to let them get too far ahead of them."
According to Dr. Bianchi, Verinata is now seeking FDA approval to market the testing as an in vitro diagnostic product. She expects demand for the testing to be led not by physicians but by patients. "People often ask me why the DNA testing took off so quickly," said Dr. Bianchi. "I think a factor is social media. I find there is a discrepancy between what the average patient knows and the general obstetrician knows because of the discussions [online]. "
Although some women will still need an invasive procedure to resolve a screen positive test, Dr. Bianchi said most pregnant women, including older women, are going to be reassured with the 100% negative predictive value.
"The younger woman’s benefit will primarily be the reduced false positive rate, because overwhelmingly, she is going to have a normal fetus, so her major benefit is not being made anxious and being sent for all the subsequent testing."
Dr. Bianchi and her coauthors disclosed relationships with Verinata/Illumina, maker of the Verifi cell-free DNA prenatal test. Dr. Bianchi is also on the clinical advisory board of Verinata. Dr. Greene stated that he had no conflict of interest disclosures. The study was sponsored by Illumina, ClinicalTrials.gov number NCT01663350.
The current prenatal screening standard of care for Down syndrome and other trisomies in low-risk pregnancies is more than three times as likely to return a false positive, compared with false positive rates from noninvasive, cell-free DNA testing, according to a new study.
The findings likely will strengthen public demand for the novel testing to become routine, according to Dr. Diana W. Bianchi, lead author of the CARE (Comparison of Aneuploidy Risk Evaluation) study.
"The pregnant women social media groups are very aware of the false positives. I think everybody knows somebody who has had one, since there’s 1 in 20 chance of that [happening]," Dr. Bianchi said in an interview.
Surprising results
Also revealed in the study was cell-free DNA testing’s essentially 100% negative predictive value for aneuploidies in low-risk populations.
The results are "very impressive," said Dr. Michael F. Greene, associate editor of the New England Journal of Medicine, in an interview. "I do think this is going to sweep the table in terms of what is offered to pregnant women," particularly if other studies demonstrate the same level of efficacy, he said. The study was published online (N. Engl. J. Med. 2014;370:799-808).
To compare false positive rates in the two methods of screening, Dr. Bianchi and her team analyzed test results from 1,914 women (average age, 30 years) enrolled from the general obstetrical population across 21 centers in 14 states. Participants either had or planned to have standard aneuploidy serum screening. All women were risk classified according to standard screening and had a singleton fetus without aneuploidy and a gestational age of at least 8 weeks. A second serum sample was taken from each woman, and massively parallel sequencing was used by laboratory personnel blinded to fetal karyotype to determine the chromosome dosage. Birth outcomes or karyotypes were used as the reference standard.
For trisomies 21 and 18, the false positive rates returned by cell-free DNA testing were significantly lower than those returned by standard screening: 6 patients vs. 69 out of 1,909 for trisomy 21 (0.3% vs. 3.6%; P less than .001), and 3 vs. 11 out of 1,905 for trisomy 18 (0.2% vs. 0.6%, P = .03).
The positive detection rate for cell-free DNA testing of all aneuploidies (5 for trisomy 21, 2 for trisomy 18, and 1 for trisomy 13) was 100% (95% confidence interval, 99.8-100). The positive predictive values for the cell-free DNA testing, compared with standard screening, were 45.5% vs. 4.2% for trisomy 21, and 40.0% vs. 8.3% for trisomy 18.
These positive predictive values, Dr. Greene and Dr. Elizabeth G. Phimister wrote in an accompanying editorial, "underscore the conclusion that assaying fetal DNA is a screening tool and not a diagnostic intervention." However, they concluded, "the observed negative predictive values of 100% with 95% confidence limits down to 99.8%, combined with the significantly and substantively lower false positive rates with cell-free DNA screening than with standard screening, augur well for pregnant women and their fetuses" (N. Engl. J. Med. 2014;370:874-5).
"I think it is going to surprise people when they see that the current standard of care has such a low positive predictive value in a general obstetrical population," said Dr. Bianchi, who also directs the Mother Infant Research Institute at Tufts Medical Center, Boston.
The primary outcome was determined by newborn physical examination in 1,857 patients (97.0%) and by karyotype in 57 patients (3.0%). Of these, chorionic villus sampling was performed in 10 patients, amniocentesis in 38, testing of the products of conception in 3, and postnatal evaluation in 6. The women whose cell-free DNA tests came back with false positive readings all had live births with normal physical examinations.
The secondary endpoint was a similar comparison of detection rates for trisomy 13 (Patau syndrome). There was one false positive result for trisomy 13 with cell-free DNA testing, as compared with six false positive results on standard screening, thus showing a trend toward significance (P = .059) in the 899 patients who underwent standard screening for trisomy 13.
Fetal fraction not maternal age–related
The researchers found that cell-free DNA testing had the same high-sensitivity detection rates in low-risk obstetrical populations as has been previously established in high-risk ones. Generally considered at higher risk for trisomy 21, women 35 years and older who were tested in either the first or second trimesters had results that were nearly identical to results from women under age 35 in terms of both their mean percentage of free fetal DNA and their standard screening results and/or cell-free DNA results (11.3% and 11.6%, respectively). For women tested in the third trimester, the fetal fraction was higher (mean, 24.6%).
This finding further strengthens the argument that the technology should be available to the general obstetric population. "The amount of the DNA was the same when we stratified the relatively high risk from the relatively low risk," said Dr. Bianchi. "That will be a surprise to some people who postulated that the high-risk women would have more DNA circulating. They don’t."
The consistent fetal fraction also lends itself to greater flexibility when prenatal screening occurs, allowing women to be screened anytime between 10 and 40 weeks gestational age. This could mean better prenatal care for women who do not have their first prenatal visit until late in the second trimester, for example. Because the current screening methods are specific to certain gestational times, if a woman is erratic with her prenatal visits, testing may be impossible.
Regarding its utility in women carrying multiple fetuses, Dr. Bianchi said that about 10% of the time, the fetal fraction per fetus tends to be too low to get an accurate reading.
‘Throwing down the gauntlet’
The test’s unparalleled accuracy could give greater peace of mind to women who might have had difficulty getting pregnant and so are wary of the miscarriage risks posed by invasive diagnostic testing, according to Dr. Bianchi. Fewer invasive diagnostic tests could also lower costs across the system.
When all results for trisomies 21 and 18 were combined, the researchers found that the false positive rates for standard screening were 4.2%, compared with 0.5% for cell-free DNA testing. "If all pregnant women had undergone cell-free DNA testing as a primary screening method and if all women with positive results had undergone post-test counseling and had decided to undergo an invasive procedure," wrote the authors, "there would have been a relative reduction of 89% in the number of diagnostic invasive procedures required to confirm a positive screening result."
The data should move professional societies to take action, according to Dr. Bianchi. "That’s kind of the gauntlet that we’re throwing down." More data are on the way, she said, which will "enable the professional societies to take a cumulative look and decide what their recommendations are going to be."
As it stands, the Society for Maternal-Fetal Medicine and the American College of Obstetricians and Gynecologists state that the testing be used only in women at higher risk for giving birth to children with aneuploidies, such as women aged 35 years or older or those with a history of pregnancy with trisomy, and that positive cell-free DNA results should be confirmed by invasive diagnostic testing.
For now, because the tests are not considered routine prenatal care, low-risk patients usually pay out of pocket for these tests, which Dr. Bianchi said many women are willing to do. The cost of the test ranges anywhere from $1,200 to upward of $2,700, although some careful Internet searching for deals can net tests at substantially lower prices, she said.
Market pressures
For some physicians in the field, this public demand for a screening test not subject to Food and Drug Administration (FDA) regulation has not outweighed the level of proof it offers in the clinical setting. One of these critics was, until recently, Dr. Greene.
"Companies have been free to build consumer demand for cell-free DNA testing by aggressively marketing the tests, emphasizing data that do not answer key questions," wrote Dr. Greene in July 2013, in an editorial he coauthored (N. Engl. J. Med. 2013;369:499-501). "As a result, cell-free DNA testing seems to be drifting into routine practice ahead of the evidence," stated Dr. Greene, who is also chief of obstetrics at Massachusetts General Hospital in Boston, and who wrote with his colleagues that the test’s positive predictive value, largely unreported by manufacturers, was still in question.
"The problem is that the proof-of-principle studies that all these companies have published to date have been with ratios of ‘Down’s’ to ‘normals’ ranging from 1 to 7, 1 to 13, or 1 to 20," said Dr. Greene in an interview. "All were done in retrospective populations at extraordinarily high risk."
However, with the CARE study, "what’s impressive is the positive predictive value in a low-incidence group of patients," he said.
Sponsored by Illumina/Verinata, the study puts pressure on other companies to publish their own data in peer-reviewed journals, said Dr. Greene. "Once this paper appears in print, [Verinata] will get a leg up, and the other companies won’t want to let them get too far ahead of them."
According to Dr. Bianchi, Verinata is now seeking FDA approval to market the testing as an in vitro diagnostic product. She expects demand for the testing to be led not by physicians but by patients. "People often ask me why the DNA testing took off so quickly," said Dr. Bianchi. "I think a factor is social media. I find there is a discrepancy between what the average patient knows and the general obstetrician knows because of the discussions [online]. "
Although some women will still need an invasive procedure to resolve a screen positive test, Dr. Bianchi said most pregnant women, including older women, are going to be reassured with the 100% negative predictive value.
"The younger woman’s benefit will primarily be the reduced false positive rate, because overwhelmingly, she is going to have a normal fetus, so her major benefit is not being made anxious and being sent for all the subsequent testing."
Dr. Bianchi and her coauthors disclosed relationships with Verinata/Illumina, maker of the Verifi cell-free DNA prenatal test. Dr. Bianchi is also on the clinical advisory board of Verinata. Dr. Greene stated that he had no conflict of interest disclosures. The study was sponsored by Illumina, ClinicalTrials.gov number NCT01663350.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Major finding: Cell-free DNA testing bested standard prenatal screening false positive rates for trisomy 21 (0.3% vs. 3.6%; P less than .001) and for trisomy 18 (0.2% vs. 0.6%; P = .03). Positive predictive values for cell-free DNA were 45.5% vs. 4.2% for trisomy 21 and 40.0% vs. 8.3% for trisomy 18.
Data source: Prospective, blinded, multisite observational study of blood samples from 1,914 women with low-risk singleton pregnancies.
Disclosures: Dr. Bianchi and all her coauthors disclosed relationships with Verinata/Illumina, maker of the Verifi cell-free DNA prenatal test. Dr. Bianchi is also on the clinical advisory board of Verinata. The study was sponsored by Illumina, ClinicalTrials.gov number NCT01663350.

Antiphospholipid, thrombosis histories differently affect pregnancy antithrombotic needs
SNOWMASS, COLO. – Whether a woman with antiphospholipid antibodies meets diagnostic criteria for antiphospholipid syndrome makes a huge difference in her risk of pregnancy failure.
Having antiphospholipid antibodies alone confers only a modest increase in the risks of thrombosis and/or pregnancy mishap, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium, sponsored by the American College of Rheumatology.
"You don’t have to jump all over these patients and get them worked up into a tizzy that they’re going to have blood clots or major pregnancy problems if they’ve never had them before," said Dr. Clowse, director of the Duke University Autoimmunity in Pregnancy registry in Durham, N.C.
The published experience indicates that women with antiphospholipid antibodies (aPL) but not antiphospholipid syndrome (APS) have roughly a 15% rate of pregnancy loss in their first pregnancy, not much different than the 11% rate in the general population. In contrast, women with untreated APS have up to a 90% pregnancy loss rate. With aspirin at 81 mg/day, this rate drops to 50%, and with dual therapy of low-dose aspirin plus either low-molecular-weight (LMW) or unfractionated heparin, the risk falls further to 25%, still twice that of the general population.

Thus, the distinction between aPL and APS is key. In addition to its implications for pregnancy outcome, it also guides the duration of anticoagulation following thrombosis. Anticoagulation needs to continue indefinitely in patients with APS because of their high risk of another clotting event. Indeed, patients with APS, if left untreated after a thrombotic event, have a 25% chance of another event within the next year, the rheumatologist noted.
"The diagnosis of APS is actually straightforward, but in patients referred to our lupus clinic from outside I see the term being used pretty fast and loose, and I think it’s somewhat inappropriate to do so. There are many patients with antiphospholipid antibodies who don’t have APS," she continued.
The current diagnostic criteria for APS – the so-called Sydney criteria (J. Thromb. Haemost. 2006;4:295-306) – require both laboratory and clinical findings. The laboratory criteria require a finding of lupus anticoagulant, medium- or high-titer IgG or IgM anticardiolipin antibodies, and/or medium- or high-titer anti-beta2-glycoprotein-1 antibody. The test results need to be positive on two occasions 12 weeks apart, although treatment for presumptive APS can start after tentative diagnosis based upon the first positive test.
To meet the vascular criteria for APS, a patient simply has to have had an arterial, venous, or small vessel thrombosis in any tissue or organ. The pregnancy criteria are more elaborate. To qualify, a woman must have had spontaneous abortions at less than 10 weeks’ gestation in at least three or more consecutive pregnancies, or a second- or third-trimester pregnancy loss of a normal fetus, or premature birth of a morphologically normal fetus before week 34 due to preeclampsia or placental insufficiency.
In women with full-blown APS, antibody titers matter quite a bit in terms of pregnancy outcome. In a study of 51 women with APS who were treated with LMW heparin and aspirin throughout 55 pregnancies, the 20 women with antibody titers greater than four times the upper limit of normal had a 35% rate of delivering an appropriately grown baby after 32 weeks’ gestation. The 35 antibody-positive women with titers less than four times the upper limit of normal had a 77% rate of normal delivery (Acta Obstet. Gynecol. Scand. 2011;90:1428-33).
In women with aPL only, the risk of pregnancy loss may be so low that aspirin isn’t protective. In an intriguing Italian study of 139 pregnancies in 114 women with aPL but not APS, the pregnancy loss rate in 104 pregnancies treated throughout with low-dose aspirin was 7.7%, while in 35 untreated pregnancies the rate was 2.9% (J. Rheumatol. 2013;40:425-9).
"The conclusion here is you can go ahead and use aspirin, but we don’t know that it’s doing a whole lot. Maybe we’re really just treating ourselves," Dr. Clowse mused.
Evidence from the PROMISSE trial, the largest-ever U.S. study of pregnancy loss in lupus patients, points to lupus anticoagulant as the main driver of pregnancy morbidity in patients with aPL. Thirty-nine percent of lupus anticoagulant–positive patients had adverse pregnancy outcomes, compared with just 3% of those without lupus anticoagulant. Unfortunately, treatment with heparin, aspirin, prednisone, or hydroxychloroquine didn’t mitigate the risk (Arthritis Rheum. 2012;64:2311-8).
While pregnancy loss is the biggest concern among most women with APS, it’s important to watch for maternal complications, including early severe preeclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and thrombotic events.
"It’s worth talking to the woman before pregnancy and explaining that, unfortunately, pregnancy loss is not necessarily the worst thing that can happen. Her health can also be at risk," Dr. Clowse observed.
In her own practice, everybody with APS goes on aspirin at 81 mg/day throughout pregnancy, even if there has been no prior pregnancy loss. With a history of three or more consecutive pregnancy losses, the treatment is low-dose LMW heparin plus low-dose aspirin. In women with a history of pregnancy loss that doesn’t reach that level, there is no good evidence to provide guidance as to whether to use low-dose LMW heparin plus aspirin or aspirin alone; however, she tends to be more aggressive in women with lupus anticoagulant or very high titers of the other aPLs. Women with a history of thrombosis, whether arterial or venous, are encouraged to remain on full-dose LMW heparin plus low-dose aspirin throughout pregnancy.
Dr. Clowse reported serving as a consultant to UCB.
SNOWMASS, COLO. – Whether a woman with antiphospholipid antibodies meets diagnostic criteria for antiphospholipid syndrome makes a huge difference in her risk of pregnancy failure.
Having antiphospholipid antibodies alone confers only a modest increase in the risks of thrombosis and/or pregnancy mishap, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium, sponsored by the American College of Rheumatology.
"You don’t have to jump all over these patients and get them worked up into a tizzy that they’re going to have blood clots or major pregnancy problems if they’ve never had them before," said Dr. Clowse, director of the Duke University Autoimmunity in Pregnancy registry in Durham, N.C.
The published experience indicates that women with antiphospholipid antibodies (aPL) but not antiphospholipid syndrome (APS) have roughly a 15% rate of pregnancy loss in their first pregnancy, not much different than the 11% rate in the general population. In contrast, women with untreated APS have up to a 90% pregnancy loss rate. With aspirin at 81 mg/day, this rate drops to 50%, and with dual therapy of low-dose aspirin plus either low-molecular-weight (LMW) or unfractionated heparin, the risk falls further to 25%, still twice that of the general population.
Thus, the distinction between aPL and APS is key. In addition to its implications for pregnancy outcome, it also guides the duration of anticoagulation following thrombosis. Anticoagulation needs to continue indefinitely in patients with APS because of their high risk of another clotting event. Indeed, patients with APS, if left untreated after a thrombotic event, have a 25% chance of another event within the next year, the rheumatologist noted.
"The diagnosis of APS is actually straightforward, but in patients referred to our lupus clinic from outside I see the term being used pretty fast and loose, and I think it’s somewhat inappropriate to do so. There are many patients with antiphospholipid antibodies who don’t have APS," she continued.
The current diagnostic criteria for APS – the so-called Sydney criteria (J. Thromb. Haemost. 2006;4:295-306) – require both laboratory and clinical findings. The laboratory criteria require a finding of lupus anticoagulant, medium- or high-titer IgG or IgM anticardiolipin antibodies, and/or medium- or high-titer anti-beta2-glycoprotein-1 antibody. The test results need to be positive on two occasions 12 weeks apart, although treatment for presumptive APS can start after tentative diagnosis based upon the first positive test.
To meet the vascular criteria for APS, a patient simply has to have had an arterial, venous, or small vessel thrombosis in any tissue or organ. The pregnancy criteria are more elaborate. To qualify, a woman must have had spontaneous abortions at less than 10 weeks’ gestation in at least three or more consecutive pregnancies, or a second- or third-trimester pregnancy loss of a normal fetus, or premature birth of a morphologically normal fetus before week 34 due to preeclampsia or placental insufficiency.
In women with full-blown APS, antibody titers matter quite a bit in terms of pregnancy outcome. In a study of 51 women with APS who were treated with LMW heparin and aspirin throughout 55 pregnancies, the 20 women with antibody titers greater than four times the upper limit of normal had a 35% rate of delivering an appropriately grown baby after 32 weeks’ gestation. The 35 antibody-positive women with titers less than four times the upper limit of normal had a 77% rate of normal delivery (Acta Obstet. Gynecol. Scand. 2011;90:1428-33).
In women with aPL only, the risk of pregnancy loss may be so low that aspirin isn’t protective. In an intriguing Italian study of 139 pregnancies in 114 women with aPL but not APS, the pregnancy loss rate in 104 pregnancies treated throughout with low-dose aspirin was 7.7%, while in 35 untreated pregnancies the rate was 2.9% (J. Rheumatol. 2013;40:425-9).
"The conclusion here is you can go ahead and use aspirin, but we don’t know that it’s doing a whole lot. Maybe we’re really just treating ourselves," Dr. Clowse mused.
Evidence from the PROMISSE trial, the largest-ever U.S. study of pregnancy loss in lupus patients, points to lupus anticoagulant as the main driver of pregnancy morbidity in patients with aPL. Thirty-nine percent of lupus anticoagulant–positive patients had adverse pregnancy outcomes, compared with just 3% of those without lupus anticoagulant. Unfortunately, treatment with heparin, aspirin, prednisone, or hydroxychloroquine didn’t mitigate the risk (Arthritis Rheum. 2012;64:2311-8).
While pregnancy loss is the biggest concern among most women with APS, it’s important to watch for maternal complications, including early severe preeclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and thrombotic events.
"It’s worth talking to the woman before pregnancy and explaining that, unfortunately, pregnancy loss is not necessarily the worst thing that can happen. Her health can also be at risk," Dr. Clowse observed.
In her own practice, everybody with APS goes on aspirin at 81 mg/day throughout pregnancy, even if there has been no prior pregnancy loss. With a history of three or more consecutive pregnancy losses, the treatment is low-dose LMW heparin plus low-dose aspirin. In women with a history of pregnancy loss that doesn’t reach that level, there is no good evidence to provide guidance as to whether to use low-dose LMW heparin plus aspirin or aspirin alone; however, she tends to be more aggressive in women with lupus anticoagulant or very high titers of the other aPLs. Women with a history of thrombosis, whether arterial or venous, are encouraged to remain on full-dose LMW heparin plus low-dose aspirin throughout pregnancy.
Dr. Clowse reported serving as a consultant to UCB.
SNOWMASS, COLO. – Whether a woman with antiphospholipid antibodies meets diagnostic criteria for antiphospholipid syndrome makes a huge difference in her risk of pregnancy failure.
Having antiphospholipid antibodies alone confers only a modest increase in the risks of thrombosis and/or pregnancy mishap, Dr. Megan E.B. Clowse said at the Winter Rheumatology Symposium, sponsored by the American College of Rheumatology.
"You don’t have to jump all over these patients and get them worked up into a tizzy that they’re going to have blood clots or major pregnancy problems if they’ve never had them before," said Dr. Clowse, director of the Duke University Autoimmunity in Pregnancy registry in Durham, N.C.
The published experience indicates that women with antiphospholipid antibodies (aPL) but not antiphospholipid syndrome (APS) have roughly a 15% rate of pregnancy loss in their first pregnancy, not much different than the 11% rate in the general population. In contrast, women with untreated APS have up to a 90% pregnancy loss rate. With aspirin at 81 mg/day, this rate drops to 50%, and with dual therapy of low-dose aspirin plus either low-molecular-weight (LMW) or unfractionated heparin, the risk falls further to 25%, still twice that of the general population.
Thus, the distinction between aPL and APS is key. In addition to its implications for pregnancy outcome, it also guides the duration of anticoagulation following thrombosis. Anticoagulation needs to continue indefinitely in patients with APS because of their high risk of another clotting event. Indeed, patients with APS, if left untreated after a thrombotic event, have a 25% chance of another event within the next year, the rheumatologist noted.
"The diagnosis of APS is actually straightforward, but in patients referred to our lupus clinic from outside I see the term being used pretty fast and loose, and I think it’s somewhat inappropriate to do so. There are many patients with antiphospholipid antibodies who don’t have APS," she continued.
The current diagnostic criteria for APS – the so-called Sydney criteria (J. Thromb. Haemost. 2006;4:295-306) – require both laboratory and clinical findings. The laboratory criteria require a finding of lupus anticoagulant, medium- or high-titer IgG or IgM anticardiolipin antibodies, and/or medium- or high-titer anti-beta2-glycoprotein-1 antibody. The test results need to be positive on two occasions 12 weeks apart, although treatment for presumptive APS can start after tentative diagnosis based upon the first positive test.
To meet the vascular criteria for APS, a patient simply has to have had an arterial, venous, or small vessel thrombosis in any tissue or organ. The pregnancy criteria are more elaborate. To qualify, a woman must have had spontaneous abortions at less than 10 weeks’ gestation in at least three or more consecutive pregnancies, or a second- or third-trimester pregnancy loss of a normal fetus, or premature birth of a morphologically normal fetus before week 34 due to preeclampsia or placental insufficiency.
In women with full-blown APS, antibody titers matter quite a bit in terms of pregnancy outcome. In a study of 51 women with APS who were treated with LMW heparin and aspirin throughout 55 pregnancies, the 20 women with antibody titers greater than four times the upper limit of normal had a 35% rate of delivering an appropriately grown baby after 32 weeks’ gestation. The 35 antibody-positive women with titers less than four times the upper limit of normal had a 77% rate of normal delivery (Acta Obstet. Gynecol. Scand. 2011;90:1428-33).
In women with aPL only, the risk of pregnancy loss may be so low that aspirin isn’t protective. In an intriguing Italian study of 139 pregnancies in 114 women with aPL but not APS, the pregnancy loss rate in 104 pregnancies treated throughout with low-dose aspirin was 7.7%, while in 35 untreated pregnancies the rate was 2.9% (J. Rheumatol. 2013;40:425-9).
"The conclusion here is you can go ahead and use aspirin, but we don’t know that it’s doing a whole lot. Maybe we’re really just treating ourselves," Dr. Clowse mused.
Evidence from the PROMISSE trial, the largest-ever U.S. study of pregnancy loss in lupus patients, points to lupus anticoagulant as the main driver of pregnancy morbidity in patients with aPL. Thirty-nine percent of lupus anticoagulant–positive patients had adverse pregnancy outcomes, compared with just 3% of those without lupus anticoagulant. Unfortunately, treatment with heparin, aspirin, prednisone, or hydroxychloroquine didn’t mitigate the risk (Arthritis Rheum. 2012;64:2311-8).
While pregnancy loss is the biggest concern among most women with APS, it’s important to watch for maternal complications, including early severe preeclampsia, HELLP (hemolysis, elevated liver enzymes, and low platelet count) syndrome, and thrombotic events.
"It’s worth talking to the woman before pregnancy and explaining that, unfortunately, pregnancy loss is not necessarily the worst thing that can happen. Her health can also be at risk," Dr. Clowse observed.
In her own practice, everybody with APS goes on aspirin at 81 mg/day throughout pregnancy, even if there has been no prior pregnancy loss. With a history of three or more consecutive pregnancy losses, the treatment is low-dose LMW heparin plus low-dose aspirin. In women with a history of pregnancy loss that doesn’t reach that level, there is no good evidence to provide guidance as to whether to use low-dose LMW heparin plus aspirin or aspirin alone; however, she tends to be more aggressive in women with lupus anticoagulant or very high titers of the other aPLs. Women with a history of thrombosis, whether arterial or venous, are encouraged to remain on full-dose LMW heparin plus low-dose aspirin throughout pregnancy.
Dr. Clowse reported serving as a consultant to UCB.
EXPERT ANALYSIS FROM THE WINTER RHEUMATOLOGY SYMPOSIUM
